The IMF InfoLine team is here to support you and your loved ones with the most up-to-date information about myeloma
Call the IMF InfoLine at 1.800.452.CURE (toll-free in the U.S. & Canada) or 1.818.487.7455 (worldwide), or email InfoLine@myeloma.org with your questions, or if you wish to discuss the contents of this booklet.
Want answers and don’t want to wait?
Get the answers you need anytime from Myelo® , your 24/7 generative AI assistant that is designed to support you on your journey with myeloma. Ask Myelo your questions at myeloma.org.
Join the Myeloma Knowledge Platform
Visit myprofile.myeloma.org and create your personal online IMF account to receive the most helpful content recommendations tailored to support your unique myeloma journey.
You are not alone
The International Myeloma Foundation (IMF) is here to help you. We are committed to providing information and support for patients with multiple myeloma (which we refer to simply as “myeloma”) and their care partners, friends, and family members.
The IMF supports the myeloma community with a broad range of resources available on our website myeloma.org, and through numerous programs and services such as publications, seminars, webinars, workshops, and the IMF InfoLine.
Contact the IMF InfoLine with your myeloma-related questions and concerns by calling 1.818.487.7455, emailing InfoLine@myeloma.org, or scheduling a convenient time to talk with an IMF InfoLine Coordinator at mmsm.link/infoline. You will receive the most up-to-date information about myeloma in a compassionate and caring manner.
IMF publications
The IMF’s Patient Handbook offers an overview of myeloma, from its precursor conditions to diagnosis, staging and risk stratification, myeloma’s effects on the body, when to begin treatment and the therapies approved by the U.S. Food and Drug Administration (FDA), as well as supportive care measures that may help you manage the symptoms and side effects of both myeloma and its treatments. This booklet will also direct you to other resources that may be relevant in your particular case.
The IMF’s Understanding-series publications offer more detailed information about a broad range of myeloma-specific topics. Words in bold+blue used in this and in other IMF publications are explained in the IMF’s companion booklet, Understanding Myeloma Vocabulary, which you can access directly at glossary.myeloma.org. Another helpful reference booklet is Understanding Your Test Results.
If you prefer to read any of the IMF’s publications in electronic format, the light blue links will take you to the corresponding resources. All IMF publications are free-of-charge and can be read, downloaded, or requested in printed format at publications.myeloma.org.
What to keep in mind
¡ Myeloma is treatable and many patients live long and productive lives after being diagnosed. Myeloma research is a robust field that is evolving at an unprecedented pace and the treatment options for patients are expanding like never before.
¡ Effective communication between the patient and the healthcare team is essential. You should feel empowered to share your goals,
preferences, experiences, and concerns, as well as to ask questions or to seek another opinion. This leads to better outcomes.
¡ Keep an organized record of your comprehensive medical history as well as all aspects of your myeloma journey. This is made easier by today’s electronic medical records systems or “portals.” Your doctors must have access to your medical records, too.
¡ While myeloma is a cancer that is not known to most patients at the time of their diagnosis, you can learn about it and have an active role in your own medical care, making good decisions in partnership with your doctor. The IMF can help you become a well-informed patient who keeps up-to-date with the latest developments in the field.
Precursors to myeloma
All people who eventually develop active myeloma have previously had a benign condition called monoclonal gammopathy of undetermined significance (MGUS, pronounced “EM-gus”), followed by smoldering multiple myeloma (SMM, pronounced “ess-em-EM”).
The risk of progression from MGUS to active myeloma is 1% per year, and only 20% of people with MGUS eventually develop myeloma. The risk of progression from SMM to active myeloma is 10% per year for the first 5 years, 3% per year for the next 5 years, and 1%–2% per year for the next 10 years.
Not everyone with MGUS or SMM will develop active myeloma. However, if you have been diagnosed with MGUS or SMM, you should be monitored for a possible change in status at regular intervals by an experienced hematologist-oncologist (specialist in blood and bone marrow cancers), preferably by a myeloma specialist. For more information, read the IMF’s publication Understanding MGUS and Smoldering Multiple Myeloma.
Clonal plasma cells in bone marrow
Presence of myeloma defining events no no yes
Likelihood of progression ~1% per year ~10% per year not applicable
Management observation only observation, clinical trials, or treatment if high-risk SMM treatment
Table 1. Differences between MGUS, SMM, and active myeloma
Incidence of myeloma and other factors
In the United States, according to data from the Surveillance, Epidemiology, and End Results (SEER) program of the National Cancer Institute (NCI), there were an estimated 36,110 new cases of myeloma diagnosed in 2025, representing 1.8% of all new cancer cases. Based on the latest data available at the time of this publication, there were an estimated 192,144 people living with myeloma in the U.S. in 2022. See seer.cancer.gov/statfacts/html/mulmy.html.
Men are more likely than women to develop myeloma. Myeloma is most frequently diagnosed in individuals who are 65–74 years old, but it is also being diagnosed in people younger than 50. Only 5%–10% of myeloma patients are under the age of 40. Myeloma in children is extremely rare. The incidence of myeloma is increasing in several parts of the world, especially in Asia.
In the U.S. and worldwide, there are significant myeloma survival disparities due to delayed diagnosis and reduced access to treatment. Myeloma is the most common blood cancer in individuals of African descent, who have twice the risk of developing myeloma when compared to White individuals. Mortality from myeloma is twice as high in Black individuals as it is in White individuals. On average, Black and Hispanic individuals are diagnosed with myeloma at a younger age and with more advanced disease than when White individuals are diagnosed.
When barriers to early diagnosis and treatment are removed, Black and Hispanic patients with myeloma have survival rates similar to those of White patients. In all myeloma patients, earlier diagnosis can result in earlier treatment and better outcomes. The IMF is committed to improving patient outcomes by breaking down barriers to healthcare equity and raising myeloma awareness. For information about the IMF’s M-Power initiative, visit mpower.myeloma.org.
Myeloma is not considered to be hereditary. However, approximately 5%–7% of myeloma diagnoses occur in individuals with a close relative diagnosed with MGUS, SMM, or myeloma. If you have a close relative with such a diagnosis, tell your primary care doctor to include this information in your medical record. Conversely, tell your relatives to inform their doctors to include your diagnosis in their medical history if you have MGUS, SMM, or myeloma.
In the majority of patients, a cause of myeloma is unknown. Theories include changes in the immune system that occur with advancing age. There are some associations that put patients at higher risk of developing myeloma, including exposure to toxins, pesticides, and herbicides (e.g., Agent Orange). Myeloma is more common in first responders, particularly in firefighters.
The basics of myeloma disease
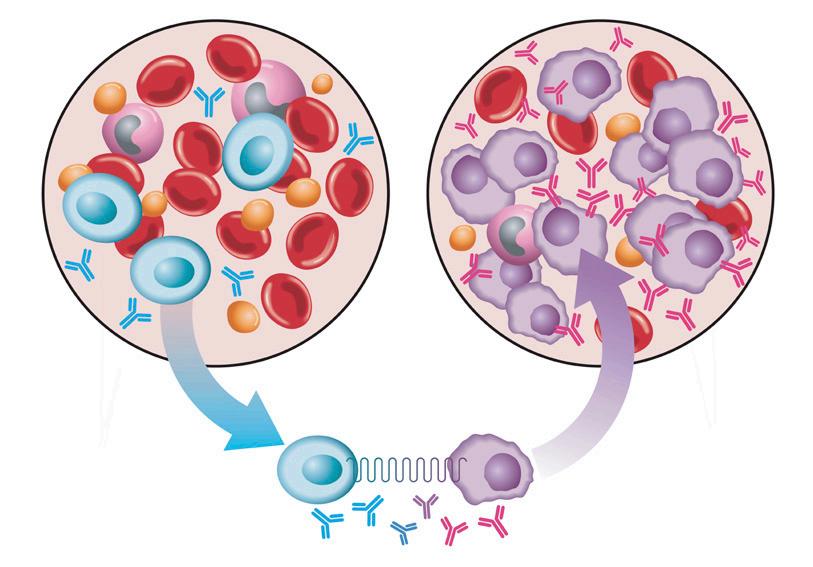
Myeloma is a cancer of the plasma cells. Normal plasma cells live in the bone marrow and produce normal polyclonal (many types) antibodies that can fight many types of infections. For example, when you are vaccinated, the plasma cells learn to produce the antibodies needed to protect you against a specific illness.
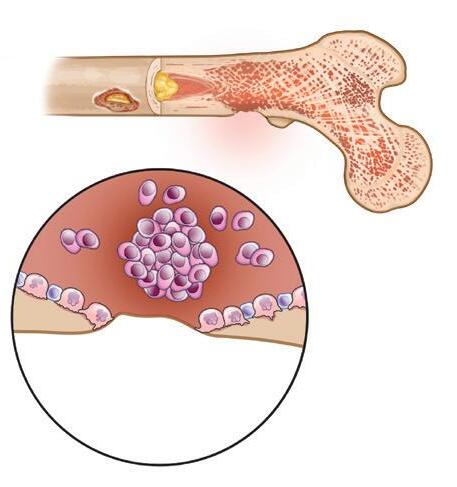
Myeloma cells are monoclonal (duplicates of a single cell) cancerous plasma cells that proliferate (grow) out of control in such a large number that they crowd the bone marrow – see Figure 1. Myeloma cells produce an abnormal protein known as monoclonal protein (myeloma protein, M-protein), which damages bone and bone marrow. M-protein is found in large amounts in the blood or urine of myeloma patients and is a way of measuring the disease.
Antibodies are also called immunoglobulins (Ig). They are composed of a molecule that has both “heavy” and “light” chains. The M-protein is commonly measured as the heavy and light chains together, but some patients only have measurable light chains. Furthermore, in some patients M-protein can only be measured in the urine. A very small percentage of myeloma patients have no measurable M-protein at all.
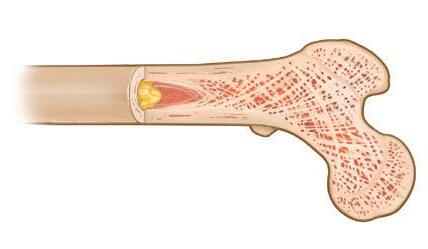
Myeloma is called “multiple” because it usually involves multiple areas in the body. Myeloma most often grows in the bone marrow within the spine, skull, pelvis, rib cage, shoulders, and hips. Myeloma can appear as a lesion,
healthy bone marrow
regular number of healthy plasma cells and normal antibodies
plasma cells transform into myeloma cells
myeloma
uncontrolled proliferation of myeloma cells and abnormal antibodies
Figure 1. Healthy plasma cells transform into myeloma cells
which can be tumor or an area of bone loss. The bones of the hands, feet, and lower parts of the arms and legs are usually unaffected.
Myeloma is a cancer of the immune system, and you may wish to read the following IMF publication for more information, Understanding the Immune System in Myeloma.
Early diagnosis is key to best outcomes
Most myeloma patients are diagnosed by a primary care doctor or internist. Some myeloma patients are diagnosed by doctors with other medical specialties, such as nephrologists, neurologists, rheumatologists, or orthopedic surgeons. If you or your doctor suspect that you might have myeloma, a prompt consultation with a myeloma specialist is highly recommended.
Myeloma specialists at large “high-volume” treatment centers or academic institutions care for hundreds of myeloma patients, conduct clinical trials with novel myeloma therapies, and develop the expertise needed to help guide you in making decisions about your overall treatment strategy.
Warning signs of myeloma
Any ONE of these early warning signs could indicate myeloma:
¡ Bone pain (persistent or recurrent)
¡ Back pain (persistent or recurrent)
¡ Fatigue (unexplained progressive tiredness)
A correct diagnosis of myeloma that is made earlier in the disease course can result in earlier treatment and fewer secondary complications. A study
SLiMCRAB myeloma-de ning events (MDE):
Sixty percent (60%) or more plasma cells in the bone marrow.
Light chains ratio (monoclonal to normal) of 100 or more.
MRI imaging of 2 or more focal lesions in bone marrow.
Calcium level in the blood elevated above normal.
Renal damage (kidneys).
Anemia (low hemoglobin in red blood cell count).
Bone damage.
myeloma
monoclonal gammopathy of undetermined signi cance
Figure 2. Possible evolution from MGUS to active myeloma
found that when a patient is diagnosed by a primary care doctor, the typical diagnostic interval is more than 6 months. When a patient is diagnosed by a hematologist-oncologist, the typical diagnostic interval is less than 3 months. Myeloma is a highly individual disease. It can be slow-moving or aggressive. A local hematologist-oncologist might see a few myeloma patients or none at all. This is why it has become commonplace for a local doctor to collaborate with a myeloma specialist in administering the care of a patient with myeloma.
Diagnostic criteria
The IMF International Myeloma Working Group (IMWG), the research arm of the IMF, is one of the most prestigious organizations for myeloma experts. IMWG members conduct collaborative basic, clinical, and translational research to improve outcomes for patients while providing scientifically validated, critically appraised consensus guidelines for healthcare providers, including criteria on myeloma diagnosis, treatment, supportive care, testing, and more.
In 2003, the IMWG first published the CRAB criteria. Any ONE of the CRAB criteria can indicate the presence of end-organ damage due to myeloma:
¡ Calcium – elevated level in the serum (blood) more than 11 mg/dL (higher than the upper limit of normal).
¡ Renal (kidney) impairment – creatinine clearance < 40 mL per minute or serum creatinine > 2 mg/dL.
¡ Anemia (low red blood cell count) – hemoglobin value < 10 g/dL.
¡ Bone damage (at least one osteolytic lesion) – if bone marrow has < 10% clonal plasma cells, more than one bone lesion is required to distinguish myeloma from a solitary plasmacytoma.
In 2014, the IMWG expanded the CRAB criteria by adding 3 new SLiM biomarkers that indicate active myeloma before end-organ damage occurs.
¡ Sixty percent (60%) monoclonal plasma cells present in the bone marrow.
¡ Light chains ratio of involved-to-uninvolved sFLC of 100 or more. Involved FLC level must be ≥ 100 mg/L. Uninvolved light chains are those that are not made by myeloma cells.
¡ MRI imaging of 2 or more focal lesions in bone marrow.
In brief, the current IMWG guidelines state that the diagnosis of active myeloma must include BOTH of the following:
1. Presence of monoclonal plasma cells in the bone marrow ≥ 10% or biopsy-proven bony or extramedullary plasmacytoma (a tumor of monoclonal plasma cells that is found in soft tissue outside of the bone marrow and separate from bone).
2. Evidence of at least one SLiMCRAB myeloma-defining event (MDE).
Start with these THREE screening tests
Efficient testing can save myeloma patients from delayed diagnosis and secondary complications. When ALL three of these low-cost and accurate tests are used together, they will identify 99% of myeloma cases:
1. Serum free light-chain (sFLC) test,
2. Serum protein electrophoresis (SPEP), and
3. Immunofixation electrophoresis (IFE).
When the SPEP test is used alone (without sFLC and IFE), 1 out of 8 cases of myeloma will not be detected. Be sure to get all THREE of these accurate and cost-effective screening tests if myeloma is suspected.
Table 2. Effects of increased myeloma cells in bone marrow
C – Calcium levels in the blood are increased
Release of calcium from damaged bone into the bloodstream.
R – Renal problems –kidney damage
A – Anemia
B – Bone damage Osteoporosis (thinning) or more severe damage
(e.g., lytic lesions, fractures, collapse of a vertebra)
Other types of organ dysfunction
Abnormal immune function
M-proteins can pass from the bloodstream into the urine, causing kidney damage. High blood calcium, infections, and other factors can also cause or increase kidney damage.
Decrease in number and activity of red blood cell-producing cells in the bone marrow.
Local or systemic effects of myeloma, other than CRAB features.
The myeloma cells reduce the number and activity of normal plasma cells capable of producing antibodies against infection.
• Mental confusion
• Dehydration
• Constipation
• Fatigue
• Weakness
• Renal (kidney) damage
• Impaired circulation
• Fatigue
• Mental confusion
• Fatigue
• Weakness
• Bone pain
• Fracture or collapse of a bone
• Nerve or spinal cord damage
• Neuropathy
• Recurrent infections
• Bleeding problems
• Other individual problems
• Susceptibility to infection
• Delayed recovery from infection
• Reduced response to vaccination
Important testing in myeloma
Many tests and techniques are used to diagnose, monitor, and assess myeloma status throughout the disease course. Test results best reflect a myeloma patient’s status when followed and reviewed over time. No single test is adequate to tell the whole story of a patient’s current myeloma status.
A trend or pattern reveals more than a single test result or study. Each test can be thought of as a piece of a puzzle; only when the pieces are assembled correctly can a patient and an experienced myeloma specialist make the proper inferences and decisions.
Baseline (initial) testing of a newly diagnosed myeloma patient must be gathered so that it can be used for comparison with later data. Baseline testing should include the sFLC test, bone marrow biopsy, and MRI scan. Do NOT compare your test results to those of other patients. Each case of myeloma is unique.
Blood and urine tests
¡ Complete blood count (CBC) testing is used to measure the three key blood cells:
¡ Red blood cells (RBC) that carry oxygen,
¡ White blood cells (WBC) that form part of the immune system, and
¡ Platelets that help with blood clotting.
¡ The chemistry panel blood test is part of a routine physical exam. The individual tests recommended for myeloma patients by both the IMWG and the NCCN are blood urea nitrogen (BUN), serum creatinine, creatinine clearance, estimated glomerular filtration rate (eGFR), calcium, and total protein.
¡ The serum albumin (sALB) test measures normal protein in the blood.
¡ The beta-2 microglobulin (β2-microglobulin, β2M, or β2M) test measures a small protein that is a tumor marker in myeloma. It is detected in the blood by the serum β2M test (sβ2M).
¡ The serum lactate dehydrogenase (sLDH) test measures the level of an enzyme used to monitor myeloma activity.
¡ The serum protein electrophoresis (SPEP) and the urine protein electrophoresis (UPEP) tests are used in both diagnosing and monitoring myeloma. These tests enable both the calculation of M-protein amount and the identification of the type of monoclonal spike for each patient. The M-spike, a sharp pattern that occurs on protein electrophoresis tests, is a marker for the activity of myeloma cells – see Figure 3.
¡ The immunofixation electrophoresis (IFE) test of the serum (sIFE) or urine (uIFE) identifies the types of the M-protein: heavy chain (G, A, D, E, or M) and the light chain (kappa or lambda).
¡ The serum free light-chain (sFLC) test assesses the kappa light-chain level, the lambda light-chain level, and the kappa/lambda ratio produced by the myeloma cells. Measuring the output of myeloma cells is an indirect but effective way to assess the amount and activity of the cancer.
¡ C-reactive protein (CRP) is made in the liver. It increases in amount when there is inflammation throughout the body.
Cytogenetics
Cytogenetics testing detects missing, rearranged, or extra chromosomes (strands of DNA and proteins in the nucleus of a cell).
Cytogenetic tests do not measure your inherent genetics. These tests assess the chromosomes in your plasma cells and provide important information about your myeloma.
Figure 3. SPEP test results albumin
Normal SPEP result
Abnormal result with myeloma cells producing the M-protein, creating an M-spike in the beta-2 zone
Abnormal result with myeloma cells producing the M-protein, creating an M-spike in the gamma zone
The fluorescence in situ hybridization (FISH) testing is the assessment of the chromosomes of all myeloma cells in a bone marrow sample. FISH testing can detect the presence of translocations, missing pieces, extra pieces, and loss of chromosomes. FISH can detect changes regardless of whether myeloma cells are growing or not. Special gene probes that fluoresce (glow) are added to the bone marrow sample. These probes track genetic material after cell division and signal the presence or absence of chromosomal abnormalities (CA) that are known to occur in myeloma.
Each chromosome is given probes of a different color. For example, if genetic material from chromosome 4 is wrongly connected to chromosome 14, then
the differently colored dots of genetic material from these chromosomes appear together, indicating the high-risk abnormality t(4;14), which stands for “translocation of genetic material between chromosomes 4 and 14.”
Other abnormalities that are considered high-risk in myeloma are t(14;16) and t(14;20), del(17p) which stands for “deletion of the short arm (upper part) of chromosome 17,” and +1q which stands for “a gain in the long arm (lower part) of chromosome 1” – see Figure 4.
Bone marrow testing
Myeloma is a cancer of the bone marrow, so it is critical to test the bone marrow to make the diagnosis. This testing helps assess the percentage of plasma cells in the bone marrow and the general marrow function. Bone marrow testing is repeated again when myeloma relapses.
Bone marrow aspiration is the removal, by a needle, of a sample of fluid and cells from the bone marrow for examination under a microscope. Bone marrow biopsy is the removal, by a hollow-bore needle, of a sample of tissue from the bone itself. Both the bone marrow aspiration and the bone marrow biopsy are usually done at the same time.
Bone testing
Bone testing techniques are:
¡ X-rays were used in years past to assess myeloma bone disease, often with a test called the “skeletal survey,” but X-rays are no longer recommended in myeloma because they cannot detect damage until it has become extensive.
Figure 4. Chromosomal abnormalities in high-risk myeloma
¡ Bone density testing is a method of assessing bone integrity, osteopenia, and osteoporosis.
¡ Computed axial tomography (CAT or CT) scanning is commonly used in myeloma to assess the bones. A whole-body low-dose CT (WBLDCT) scan is preferred due to reduced radiation exposure.
¡ Positron emission tomography (PET) scanning is a very sensitive technique that uses the technology of CT scans but adds the ability to assess for cellular activity. This can be particularly helpful in patients with extramedullary disease (EMD), whose myeloma is outside of the bone or bone marrow.
¡ Magnetic resonance imaging (MRI) is a sensitive test that can assess anatomy very precisely and is particularly helpful in myeloma for assessing spinal or bone marrow involvement.
For a more in-depth discussion of tests used in myeloma, read the IMF’s publication Understanding Your Test Results.
Staging
Staging was first used in diseases like breast cancer and colon cancer by measuring the size of a solid tumor. The staging system used for solid tumors does not apply to blood-based cancers like myeloma.
In 1975, the Durie-Salmon Staging System became the first to classify patients with myeloma based on the correlation between the amount of myeloma and the damage caused by it. Dr. Brian G.M. Durie (1942–2025) co-founded the IMF in 1990 together with Susie Durie and myeloma patient Brian D. Novis.
Risk stratification
The staging system for myeloma continues to evolve as a prognostication tool to provide guidance to clinicians in the evaluation and treatment of patients – see Table 3. Approximately 20% of patients with myeloma have a more aggressive form of disease that tends to relapse more quickly after treatment. This is known as high-risk multiple myeloma (HRMM).
In 2005, the IMWG developed the International Staging System (ISS) to reflect the spectrum of risk of myeloma by using two simple blood tests: albumin and β2M.
In 2015, the IMWG published the Revised International Staging System (R-ISS), combining the ISS with two tests performed on bone marrow samples taken at the time of diagnosis to measure lactate dehydrogenase (LDH) and look for chromosomal abnormalities del(17p), t(4;14), and t(14;16) by fluorescence in situ hybridization (FISH).
In 2022, the IMWG updated the R-ISS to R2-ISS by including additional biomarkers and dividing patients into four risk groups instead of three: Low Risk (Score 0), Low-Intermediate (Score 0.5–1.0), Intermediate-High (Score 1.5–2.5), and High Risk (Score 3.0–5.0).
In June 2025, the IMWG and the International Myeloma Society (IMS) published a new consensus, a biologically-informed classification of risk that uses recent research data and advances in treatment. To assess treatment intensity, treatment duration, and clinical trial enrollment, patients are divided into two groups: Standard-Risk and High-Risk.
The presence of high-risk features doesn’t always correlate with real-world outcomes or current treatment standards, and does not necessarily mean that a patient’s myeloma will be aggressive.
The IMF has a support group for patients with HRMM that meets virtually. Please contact HRMM@imfsupport.org.
Table 3. Risk stratification of myeloma
PROGNOSTIC FACTOR
CRITERIA
ISS Stage I sβ2M < 3.5 mg/L, sALB ≥ 3.5 g/dL
Stage II
Stage III
R-ISS
Stage I
Stage II
Stage III
Not ISS stage I or III
sβ2M ≥ 5.5 mg/L
• ISS stage I,
• standard-risk chromosomal abnormalities by FISH, and
• LDH is lower than the upper limit of normal
Not R-ISS stage I or III
• ISS stage III plus
• either high-risk chromosomal abnormalities by FISH or LDH is higher than the upper limit of normal
High-Risk One or more chromosomal abnormality: del(17p), t(4;14), t(14;16)
R2-ISS Low-Intermediate Score 0.5: 1q+ (gain or amplification of chromosome 1).
Score 1 (each): del(17p), t(4;14), high LDH, ISS stage II
Intermediate-High Score 1.5: ISS stage III
IMWG-IMS classification
Standard-Risk All high-risk factors listed below are absent.
High-Risk
• del(17p) if present in at least 20% of myeloma cells.
• TP53 mutations.
• t(4;14) or t(4;16) or t(14;20) with 1q+ or del(1p32), or both.
• monoallelic del(1p32) with 1q+ or biallelic del(1p32).
• β2M 5.5 mg/L or higher, with creatinine less than 1.2 mg/dL.
Types of myeloma
The patient’s type of myeloma is identified by the IFE test. Knowing your myeloma type is helpful to understanding your disease and its treatment options.
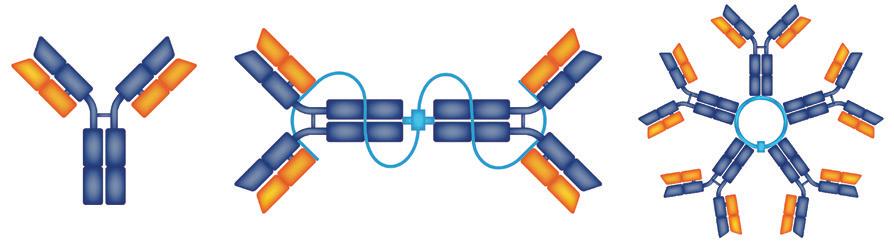
An immunoglobulin protein that is produced by the patient’s myeloma cells is made up of 2 heavy chains bound to 2 light chains – see Figure 5.
¡ There are 5 types of heavy chains. Each patient’s myeloma cells produce only 1 of these 5 types: IgG, IgA, IgD, IgE, and IgM.
¡ There are 2 types of light chains: kappa (κ) and lambda (λ). Each patient’s myeloma cells produce only 1 of these 2 types.
IgG
myeloma
Approximately 65% of myeloma patients have IgG myeloma with either kappa or lambda light chains. The behavior of IgG myeloma conforms to CRAB criteria features.
IgA myeloma
IgA myeloma is the second-most common type, also with either kappa or lambda light chains. Patients with IgA myeloma sometimes have tumors outside of the bone.
IgD, IgE, or IgM
myelomas
These three types of myeloma are rare. IgD myeloma can be accompanied by plasma cell leukemia (PCL).
Understanding light chains
More than half of myeloma patients produce free light chains, but most of these patients produce the complete molecule combination of light chains bound to heavy chains. About 20% of patients produce light chains only.
Light-chain M-proteins are smaller and weigh less than heavy chains, making it possible for them to fit through the tiny capillaries that send
Figure 5. Structures of immunoglobulins
blood to the kidneys. The light chains that arrive by blood to the kidneys may build up to the point of blocking the kidney’s tubules, causing reduced kidney function.
This is why patients with light-chain only myeloma are more likely to have kidney damage or deposits of light chains in/on nerves or other organs.
In the majority of patients with light-chain myeloma, their disease can be measured with the sFLC test. In some patients, their myeloma can be measured only in the urine.
Only 1%–2% of myeloma patients produce very little or no M-protein of any type. These patients may have to be assessed by other means (e.g., imaging, bone marrow testing).
The goal of treatment is to normalize the light-chain levels, especially the ratio, and to eliminate the M-protein.
Extramedullary disease (EMD)
Myeloma is primarily a disease of the bone marrow, but it can escape or grow outside of the bone and affect other parts of the body. Imaging studies are required to detect and monitor EMD. It may be higher risk and more aggressive than myeloma that is confined to the bone marrow.
See Table 4 for an overview of other plasma cell diseases related to myeloma.
Table 4. Other plasma cell diseases related or similar to myeloma
DISEASE TYPE
Waldenström Macroglobulinemia (WM)
Amyloidosis
Light Chain Deposition Disease (LCDD)
POEMS syndrome
DESCRIPTION
A hybrid-like disease between myeloma and lymphoma where there is an IgM monoclonal protein and bone marrow involvement of cells that are “lymphoplasmacytic.” WM must be differentiated from IgM myeloma.
Amyloidosis is a disease of damage to organs due to protein deposits. “AL amyloidosis” is related to myeloma (the L refers to light chains), is often treated similarly to myeloma, and can co-exist with myeloma (although one disease tends to be dominant over the other). Abnormal plasma cells produce light chains that undergo a conformational change and deposit in organs and/or tissues. Specialized testing is needed to assess the deposits.
Abnormal plasma cells produce light chains that are deposited into tissue, namely the kidney. The diagnosis is made on the kidney biopsy and patients are treated similarly to myeloma.
POEMS is an acronym for Polyneuropathy, Organomegaly, Endocrinopathy, Monoclonal gammopathy, and Skin changes.
Myeloma’s effects on the body Inside the bone marrow
All the blood cells – white blood cells, red blood cells, and platelets – are made in the bone marrow. When myeloma grows in the bone marrow, the effects include a reduction in blood cell production. Anemia, a low level of red blood cells or hemoglobin, is an early and common sign of myeloma.
Cells in healthy bone marrow maintain our skeletons in a balanced state of bone breakdown and bone buildup. The presence of myeloma cells in the bone marrow stimulates the cells that break down bone (osteoclasts) and suppresses cells that build new bone (osteoblasts). This lack of balance results in bone pain, fractures, and the release of calcium into the blood.
Outside the bone marrow
The release of calcium from bones into the bloodstream can result in hypercalcemia, a higher than normal level of calcium in the blood. Hypercalcemia can cause loss of appetite, nausea, thirst, fatigue, muscle weakness, restlessness, confusion, and other symptoms.
Both hypercalcemia and high levels of M-protein in the blood can seriously damage the kidneys, causing kidney failure. As myeloma cells build up in the bone marrow, M-protein is released into the circulating blood, which can cause tissue damage at distant sites (e.g., kidney damage).
M-protein can also interfere with blood clotting or circulation, potentially causing other organ or tissue damage (e.g., damage to nerve tissue).
Possible urgent problems at diagnosis
Upon diagnosis, the management of your myeloma is the top priority until remission has been achieved, except in cases of emergency medical problems. There are medical problems that require immediate attention before beginning systemic therapy for myeloma. These include compromised bony structures, nerve damage, infections, and kidney disease.
Along with the immediate management of the complications, a prompt consultation with a myeloma specialist is essential to ensure that any treatment of an urgent medical problem does not limit your options for the treatment of myeloma.
Bony complications and nerve damage
Bony areas of lytic lesions, fractures, or collapsed vertebrae can cause bone pain and nerve or spinal cord damage. The vertebrae are often affected by myeloma. Because the spinal cord runs through the vertebrae, painful vertebral fractures may occur. In addition, myeloma tumors growing in the vertebrae can press on spinal nerves. Nerve compression is not uncommon. Loss of motor nerves can cause paralysis.
Vertebral compression fractures (VCF) are a serious complication of myeloma. Treatments of VCFs include analgesics to relieve pain, bracing to provide temporary stability, and minimally invasive surgical procedures such as vertebral augmentation and balloon kyphoplasty. For more information about VCFs, read the IMF’s publication Understanding Treatment of Myeloma-Induced Vertebral Compression Fractures.
Infection
The growth of myeloma cells reduces the number and activity of normal plasma cells that produce antibodies against infection, leaving the patient susceptible to infection. Furthermore, as the marrow is taken over by myeloma cells, the production of normal cells, including infection-fighting white blood cells, can be reduced in number. Serious infections may occur, requiring immediate intervention.
Kidney damage or failure
Renal (kidney) damage or failure can cause dramatic fatigue and weakness, mental confusion, and decrease or lack of urination. Treatments range from hydration to dialysis.
Blood clots and thromboembolic events
Clotting events may be medical emergencies. Treatment is based on patient risk factors, location of the clot, and potential impact on local and distant tissues.
Your healthcare team
Studies have shown that a positive relationship between the patient and their healthcare team is associated with improved survival in cancer. Also, it has been demonstrated that optimal patient care occurs when there is effective communication among all members of the patient’s healthcare team. In myeloma, the central member of such a team is the myeloma specialist, but your healthcare team may also include your primary care physician, nurse or nurse practitioner, orthopedic surgeon (bone specialist), nephrologist (kidney specialist), dentist or oral surgeon, and pharmacist.
When to begin treatment of myeloma
The most important initial decision is when to begin treatment for your myeloma. The urgency of starting treatment depends upon the exact problems faced by an individual patient. This is why the experience and expertise of a myeloma specialist is of such importance.
Understanding the results of your baseline testing, as well as the staging and prognostic classification of your myeloma will help you make the decision about initiating treatment.
Selecting a myeloma treatment regimen
Discuss the overall treatment strategy with your myeloma doctor. It is important that you understand your options and engage in shared decision-making. The following questions may facilitate a conversation with your doctor.
¡ Age: Does my age affect treatment selection and treatment outcome?
¡ Other medical issues: Will my other diagnoses affect my myeloma treatment?
¡ Treatment setting: Will I receive treatment at a clinic or take medication at home? What if I have a preference between inpatient or outpatient care?
¡ Transplant: Is an autologous transplant recommended in my case?
¡ Day-to-day functioning: How will treatment affect my daily activities, and my personal and professional obligations?
¡ Speed of response: How rapidly will the treatment work?
¡ Side effects: What are the possible treatment side effects? How can side effects be prevented or minimized?
¡ Financial considerations: Is my treatment covered by insurance? What will be my financial responsibility? Are there resources to help me pay for treatment?
FDA-approved drugs used to treat myeloma
Many highly effective therapies are approved for treatment of myeloma by the FDA. In addition, numerous clinical trials are currently investigating new drugs, new drug combinations, new drug classes, and other novel approaches to the treatment of patients with myeloma.
A drug class is a group of medications that have a similar chemical structure or a similar mechanism of action (MOA) that induces an effect in the body. Listed below in alphabetical order are the drug classes currently used in the treatment of myeloma, as well as the individual drugs in each class and their FDA-approved indications.
New drugs and drug combinations are typically first approved by the FDA to be used for relapsed or refractory multiple myeloma (RRMM). An approval by the FDA of a frontline therapy for newly diagnosed multiple myeloma (NDMM) typically requires clinical trial data that demonstrates the drug’s efficacy and safety after comparing it to standard of care (SOC) therapy, a benchmark treatment that is widely accepted by medical experts as the most appropriate. Frontline therapy is the initial treatment used in an effort to achieve response in a patient with NDMM.
Please note that if a particular therapy is not working for you, there may be other available treatment options. However, it is not advisable to rapidly skip from one treatment regimen to another.
Alkylating agents
Chemotherapy is any drug or combination of drugs used to kill cancer cells. An alkylating agent is a chemotherapeutic agent that crosslinks the DNA of myeloma cells and blocks cell division. Alkylating agents were the earliest effective drugs used in the treatment of myeloma, with melphalan first synthesized in 1953 and first used to treat myeloma in 1962. Cyclophosphamide and bendamustine are two other alkylating agents currently used in myeloma.
Antibody-drug conjugate (ADC)
An ADC is a combination of a monoclonal antibody and a chemotherapy agent. The first and only medication in the ADC drug class that has been approved by the FDA to treat myeloma is Blenrep® (belantamab mafodotinblmf), a combination of a monoclonal antibody that that binds to the B-cell maturation antigen (BCMA) protein on the surface of myeloma cells and a chemotherapy microtubule inhibitor. The monoclonal antibody delivers the chemotherapy agent directly to the myeloma cells to kill the myeloma cells. Blenrep is FDA-approved for the treatment of RRMM after at least 2 prior lines of therapy.
Immunomodulatory agents
An immunomodulatory agent is a drug that can modify, enhance, or suppress the functioning of the immune system. Thalidomide, an oral immunomodulatory agent that has been studied since at least the 1950s, was first used to treat myeloma in a 1997 clinical trial, ushering in the age of “novel therapies” in myeloma. Thalidomide is now infrequently used in the U.S., as it has given rise to a next generation of immunomodulatory agents with increased efficacy and reduced side effects.
¡ Pomalyst® (pomalidomide) is FDA-approved for the treatment of RRMM after at least 2 prior lines of therapy. For more information, read the IMF’s publication Understanding POMALYST® (pomalidomide).
¡ Revlimid® (lenalidomide) is FDA-approved for use throughout the myeloma disease course. For more information, read the IMF’s publication Understanding REVLIMID® (lenalidomide).
¡ Thalidomide is the generic drug name of this medication, which is also marketed under the brand name Thalomid®. Though used infrequently in the U.S., it is still sometimes used during the later stages of disease, in cases of renal failure, or when the patient has low blood counts. It is sometimes used in induction therapy and consolidation therapy. For more information, read the IMF’s publication Understanding Thalidomide Therapy in Myeloma.
Immunotherapies
Immunotherapies are treatments that enhance the body’s natural defenses to fight cancer.
Monoclonal antibodies (mAb)
Monoclonal antibodies are a type of immunotherapy. Manufactured in a lab rather than produced in the human body, monoclonal antibodies are specifically designed to find and bind to cancer cells or immune system cells for diagnostic or treatment purposes. Monoclonal antibodies can be used alone, or they can be used to deliver drugs, toxins, or radioactive material directly to tumor cells.
¡ Darzalex ® (daratumumab) and Darzalex Faspro® (daratumumab + hyaluronidase-fihj) are FDA-approved for use throughout the myeloma disease course, from HR SMM through RRMM. For more information, read the IMF’s publication Understanding DARZALEX® (daratumumab) and DARZALEX FASPRO® (daratumumab + hyaluronidase-fihj).
¡ Empliciti® (elotuzumab) is FDA-approved for the treatment of RRMM after at least 1 prior therapy. For more information, read the IMF’s publication Understanding EMPLICITI® (elotuzumab).
¡ Sarclisa® (isatuximab-irfc) is FDA-approved for use throughout the myeloma disease course. For more information, read the IMF’s publication Understanding SARCLISA® (isatuximab-irfc).
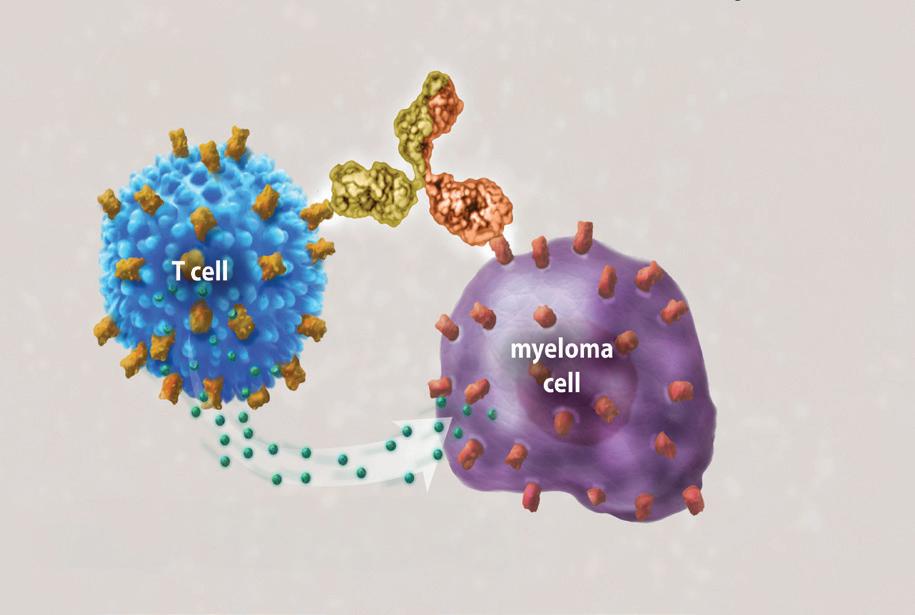
Figure 6. Bispecific antibody mechanism of action
bispecific antibody
bispecific antibody binds to CD3 CD3 on the surface of the T cell
bispecific antibody binds to tumor-specific antigen tumor-specific antigen on the surface of the myeloma cell
bispecific antibody activates the T cell to release cytotoxic granules that kill the myeloma cell
Bispecific antibodies (bsAb)
Bispecific antibodies are a type of immunotherapy. An artificial antibody that binds to two (“bi”) targeted cells, typically one antigen on the myeloma cell and another antigen on an immune cell, such as a T cell or natural killer (NK) cell – see Figure 6.
¡ Elrexfio® (elranatamab-bcmm) is FDA-approved for the treatment of RRMM after at least 4 prior lines of therapy. For more information, read the IMF’s publication Understanding ELREXFIO ® (elranatamab-bcmm).
¡ Lynozyfic™ (linvoseltamab-gcpt) is FDA-approved for the treatment of RRMM after at least 4 prior lines of therapy. For more information, visit mmsm.link/lin-gcpt .
¡ Talvey ® (talquetamab-tgvs) is FDA-approved for the treatment of RRMM after at least 4 prior lines of therapy. For more information, read the IMF’s publication Understanding TALVEY® (talquetamab-tgvs).
¡ Tecvayli® (teclistamab-cqyv) is FDA-approved for the treatment of RRMM after at least 4 prior lines of therapy. For more information, read the IMF’s publication Understanding TECVAYLI® (teclistmab-cqyv).
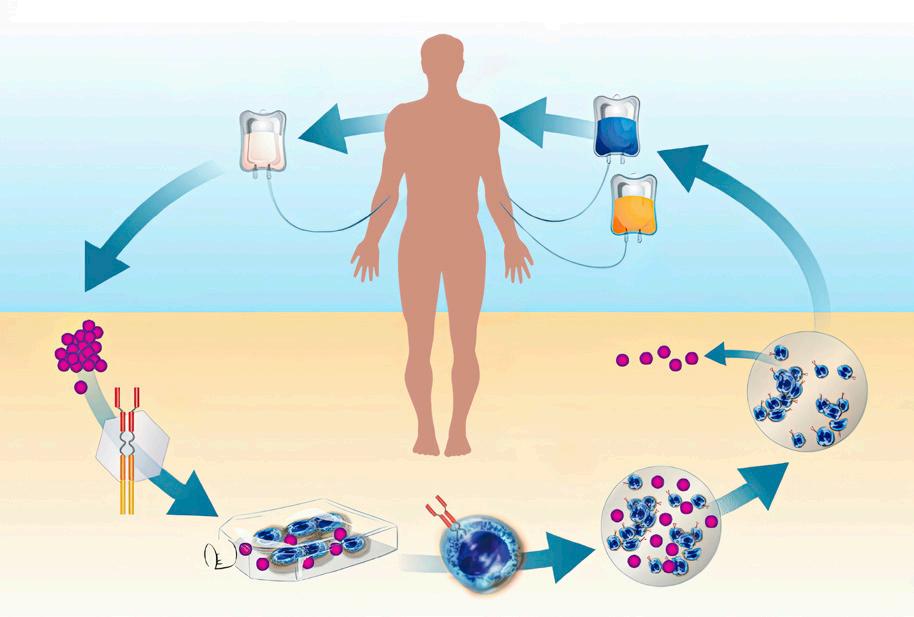
CAR T-cell therapy
Chimeric antigen receptor (CAR) T-cell therapy is a type of immunotherapy. The mechanism of action is as follows: (1) T cells are collected from the patient’s bloodstream, (2) these cells are modified to produce receptors
Figure 7. CAR T-cell therapy mechanism of action
that recognize the patient’s myeloma cells, (3) the engineered T cells are multiplied in a laboratory in large numbers, (4) they are re-infused into the patient, (5) the engineered T cells begin to destroy the patient’s myeloma cells – see Figure 7.
¡ Abecma® (idecabtagene vicleucel) is FDA-approved for the treatment of RRMM after at least 2 prior lines of therapy. For more information, read the IMF’s publication Understanding ABECMA® (idecabtagene vicleucel).
¡ Carvykti® (ciltacabtagene autoleucel) is FDA-approved for the treatment of RRMM after at least 1 prior line of therapy. For more information, read the IMF’s publication Understanding CARVYKTI® (ciltacabtagene autoleucel).
Proteasome inhibitors (PI)
A proteasome inhibitor is any drug that interferes with the normal function of the proteasome. A proteasome is a joined group (“complex”) of enzymes (“proteases”) that breaks down the damaged or unwanted proteins in both normal cells and cancer cells into smaller components. Proteasomes also carry out the regulated breakdown of undamaged proteins in the cell, a process that is necessary for the control of many critical cellular functions. These smaller protein components are then used to create new proteins required by the cell, which is important for maintaining balance within the cell and for regulating cell growth.
¡ Kyprolis® (carfilzomib) is FDA-approved for the treatment of RRMM after at least 1 prior therapy. For more information, read the IMF’s publication Understanding KYPROLIS® (carfilzomib).
¡ Ninlaro® (ixazomib) is FDA-approved for the treatment of RRMM after at least 1 prior therapy. For more information, read the IMF’s publication Understanding NINLARO® (ixazomib).
¡ Velcade® (bortezomib) is FDA-approved for use throughout the myeloma disease course. For more information, read the IMF’s publication Understanding VELCADE® (bortezomib).
Selective inhibitor of nuclear export (SINE)
The first and only medication in the SINE drug class that has been approved by the FDA to treat myeloma is Xpovio® (selinexor). It works by preventing myeloma cells from expelling tumor suppressor proteins that help protect the cell from cancer. The forced nuclear retention of these proteins can counteract the pathways that allow cancer cells to continue to grow and divide. Xpovio is FDA-approved for the treatment of RRMM after at least 1 prior therapy. For more information, read the IMF’s publication Understanding XPOVIO® (selinexor).
Steroids
A steroid is a type of hormone. Steroidal hormones are produced by the body, and the synthetic analogues (equivalents) of some steroids can be manufactured in a laboratory. Dexamethasone is a synthetic adrenocortical steroid that has multiple effects and is used for many conditions. Dexamethasone is the generic drug name of this medication, which is also marketed under multiple brand names. Dexamethasone is one of the most frequently used medications in the treatment of myeloma, typically given in combination with other agents. For more information, read the IMF’s publication Understanding Dexamethasone in the Treatment of Myeloma.
Autologous stem cell transplant (ASCT)
ASCT has been used as a treatment for myeloma for several decades. The medical term for ASCT is “high-dose therapy (HDT) with stem cell rescue.” In patients with myeloma, the myeloma cells are intermixed in the same bone marrow microenvironment as the normal stem cells.
HDT is more effective at killing myeloma cells in the bone marrow than standard-dose chemotherapy, but HDT is also capable of damaging your normal stem cells. In the ASCT procedure, your stem cells are harvested (collected) before HDT has been administered, then reinfused (transplanted) into you to “rescue” your bone marrow from the effects of HDT.
For more information, see Figure 8 and read the IMF’s publication Understanding Stem Cell Transplant in Myeloma.
1. Induction therapy is given to prepare patient for ASCT.
2. Stem cells are mobilized from the bone marrow into the bloodstream.
3. Stem cells are collected from the bloodstream, frozen, and stored in a laboratory.
4. Patient is treated with high-dose chemotherapy to kill remaining cancer cells.
5. Stem cells are thawed and infused back into the patient through a vein.
6. Stem cells travel to the bone marrow and begin producing new blood cells.
Figure 8. The ASCT procedure
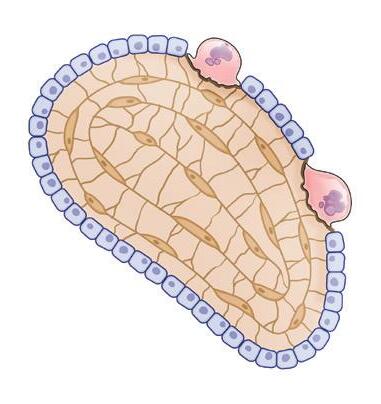
Treatment of myeloma bone disease
Approximately 70%–80% of patients with myeloma develop bone disease, which can cause bones to become thinner and weaker, and can create lytic lesions, which look like holes in the bone. The weakened bone is more likely to break due to minor pressures or injury. The bones most commonly affected are the spine, pelvis, ribs, skull, and the upper ends of the long bones of the arms and legs.
In a healthy skeleton, there is a balance between cells called osteoclasts (which break down bone tissue) and osteoblasts (which build new bone tissue) –see Figure 9. Myeloma cells cause osteoclasts to break down more bone tissue than is required for normal skeletal health while inhibiting the formation of osteoblasts and preventing the repair of bone loss.
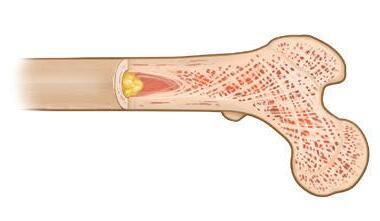
In addition to causing bone disease, the process of accelerated bone breakdown releases calcium from the bones into the bloodstream, causing a condition called hypercalcemia, an elevated level of calcium in the blood. See Figure 10 for a comparison of healthy bone to bone affected by myeloma.
Bone-modifying agents (BMA) help prevent bone damage and fractures, called skeletal-related events (SRE). BMAs have no antimyeloma effect and do not prevent progression of early myeloma. BMAs can be safely combined with
Figure 9. Osteoclasts and osteoblasts
yellow marrow compact bone spongy bone containing red marrow
osteoclast (breaks down bone)
osteoblast (builds new bone) - +
Figure 10. Healthy bone compared to myeloma bone
healthy bone
multiple myeloma
lytic lesion myeloma cells
most myeloma therapies, although your doctor may decide not to give an intravenous BMA on or close to the day you receive IV therapy for your myeloma. Confirm with your doctor that the BMA you are receiving is not being combined with another drug that can harm your kidneys.
BMAs include bisphosphonates and a monoclonal antibody. For more information, read the IMF’s publication Understanding Treatment of Myeloma Bone Disease.
Bisphosphonates
In 2018, the American Society of Clinical Oncology (ASCO) published updated guidelines on BMAs, recommending bisphosphonate therapy for all patients with myeloma that requires treatment, with or without evidence of lytic lesions or vertebral compression fractures (VCFs).
Bisphosphonates are particularly helpful for myeloma patients being treated with steroids, which reduce bone density. Bisphosphonates inhibit and destroy osteoclasts, thereby reducing bone breakdown. When myeloma is well controlled, bisphosphonates allow bone healing to occur.
¡ Aredia® (pamidronate) is administered monthly by means of an intravenous (IV) infusion. Findings from a large clinical trial by the Nordic Myeloma Study Group (NMSG) in 2010 compared Aredia given at 30 mg to Aredia given at 90 mg, and validated the efficacy of the reduced dose.
¡ Zometa® (zoledronate or zoledronic acid) is administered monthly by means of an IV infusion. Findings from the Z-MARK clinical trial in 2016 showed that the use of Zometa every 12 weeks instead of every 4 weeks did not result in an increased risk of skeletal events over 2 years.
Bisphosphonates are excreted via the kidneys and can cause kidney toxicity. Toxicities associated with bisphosphonates are related to dosage, frequency of administration, and duration of infusion – any or all of which may be modified by your doctor. The ASCO guidelines note that there are insufficient data to recommend a specific duration of bisphosphonate therapy beyond 2 years.
Monoclonal antibody for bone disease
Xgeva® (denosumab) was FDA-approved in 2018 based on a clinical trial that demonstrated the non-inferiority of Xgeva when compared to Zometa. Xgeva blocks the ability of osteoclasts to mature, function, and survive. Xgeva produces a low level of kidney-related side effects when compared to bisphosphonates. The ASCO guidelines indicate that Xgeva may be preferable to bisphosphonates in patients with kidney damage. Xgeva is given as a subcutaneous (SQ) injection, a method of administering medication under the skin by a short needle that injects a drug into the tissue layer between skin and muscle.
Solitary plasmacytoma of bone (SPB)
SPB is NOT myeloma. SPB is a rare cancer of unknown origin, a single mass of monoclonal plasma cells in a bone or bone marrow. SPB diagnosis requires a biopsy of the solitary bone lesion that shows infiltration by plasma cells, negative imaging results for other bone lesions, absence of clonal plasma cells in a sample of bone marrow, and no evidence of systemic myeloma.
SPB can be treated, and sometimes cured, with the use of radiation therapy or surgery. However, the majority of people with SPB are eventually diagnosed with myeloma.
Supportive care
Supportive care is an important part of managing myeloma. In addition to myeloma bone disease, supportive care addresses possible complications such as kidney damage, infections, thromboembolism, and peripheral neuropathy. The IMWG states the following: “Prompt intervention and appropriate management of these complications are crucial for optimizing patient outcomes. In addition to the management of specific symptoms, other supportive care measures may be beneficial to alleviating the physical and emotional impact of living with myeloma.”
Fatigue
According to the National Cancer Institute (NCI), fatigue is the most common side effect of cancer treatment. Fatigue can also be caused by the myeloma itself, as well as by other medical conditions and their treatment.
The most common causes of fatigue in myeloma patients include anemia and persistent pain, which can result in weight loss, decreased appetite, and a sense of weakness. When more than one issue is present at the same time, fatigue can be severe.
If your anemia is severe, your doctor may recommend treatment with erythropoietin or a blood transfusion. For more information, read the IMF’s publication Understanding Fatigue in Myeloma.
Neuropathy
Neuropathy occurs when the nerves are damaged or inflamed, or when degeneration of nerve tissue has occurred, leading to changes in the way nerves function. The symptoms of nerve damage depend on the type of nerves affected (sensory, motor, or autonomic).
Some individuals who develop myeloma may have neuropathy from pre-existing conditions, such as diabetes or autoimmune diseases. Others can develop neuropathy when they are in the precursor state of MGUS. Patients with myeloma can develop neuropathy in the course of their disease or as a side effect of myeloma therapies.
Peripheral neuropathy (PN) is the most common type of neuropathy in patients with myeloma. PN is a condition that affects nerves in the feet, lower legs, arms, hands, and/or fingers. It is always best to prevent problems from occurring or to treat them early if they do occur. In many patients with myeloma, neuropathy is at least partially reversible. For more information, read the IMF’s publication Understanding Neuropathy in Myeloma.
Infections
Infections are a common and recurrent problem in patients with cancer. It is essential to discuss with your doctor a strategy to promptly bring infections under control. Antibiotics or antivirals may be necessary for an active infection, and prophylactic use can be considered. Your doctor may prescribe medication to boost your white blood cell count. Intravenous immunoglobulin (IVIG) may be appropriate for severe infections.
Thromboembolism
Myeloma is a cancer that can put patients at risk of blood clots. In addition, some drugs used to treat myeloma further increase that risk. Patients are given blood thinners. It may be as simple as aspirin or a full anticoagulation drug regimen. The patient should discuss this with their myeloma doctor and be aware of the signs and symptoms of blood clots, especially if experiencing a solitary swollen leg.
Gastrointestinal side effects
Medications can treat nausea, vomiting, constipation, or diarrhea. Maintaining adequate fluid intake and nutrition is important. Severe symptoms may require hospitalization.
Diet
No specific diet has been developed for myeloma patients, although research has clearly demonstrated a link between obesity and myeloma. In general, a healthy diet emphasizes “real” foods like fruits, vegetables, fish and other lean animal proteins, and whole grains. Avoid processed foods, added sugars, and trans fats. Use caution in these areas:
¡ Herbal and vitamin supplements – Check with your doctor or pharmacist before taking supplements while receiving treatment for myeloma. Some interactions between drugs and supplements may prevent myeloma treatments from working effectively and some interactions can create serious medical problems. Pharmacies can help identify potential interactions.
¡ Vitamin C – Doses greater than 1000 mg per day may be counterproductive in myeloma and can increase the risk of kidney damage.
Mental health
Your mental health is critical. Talk with a mental health professional if you feel anxious or depressed or if others are concerned about you. This is a normal response to cancer and most patients will need some help at one time or another. Support among peers may be helpful, and engaging with a myeloma support group can add to your support network. Visit support.myeloma.org or email sgteam@myeloma.org for help with finding an in-person or virtual group.
Physical activity
Check with your doctor to clarify what type of physical activity is appropriate for you. Usually, some physical activity can be planned, such as walking or swimming, flexibility and strength exercises, and/or a personalized yoga program.
Your immune system
In myeloma, the patient’s immune system is compromised both by the disease and by its treatments. It is important for patients to remain current with their vaccinations, and to discuss this with their doctors. Wash your hands frequently, and be sure to get regular sleep!
Response or remission
Response and remission are interchangeable terms used to describe the complete or partial disappearance of the signs and symptoms of myeloma. Remission is not a cure. As of 2025, the depth of response to myeloma treatment is classified as follows:
¡ Stringent complete response (sCR) is CR as defined below, plus normal FLC ratio and absence of clonal cells in bone marrow by immunohistochemistry or immunofluorescence.
¡ Complete response (CR) is negative immunofixation on serum (blood) and urine, and disappearance of any soft tissue plasmacytomas, and ≤ 5% plasma cells in bone marrow.
¡ Very good partial response (VGPR) is serum M-protein and urine M-protein detectable by immunofixation but not on electrophoresis, or ≥ 90% reduction in serum M-protein, plus urine M-protein < 100 mg per 24 hours.
¡ Partial response (PR) is a ≥ 50% reduction in M-protein, and reduction in 24-hour urinary M-protein by ≥ 90% (or to < 200 mg per 24 hours).
¡ Minimal response (MR) is a 25%–49% reduction of serum M-protein and reduction in 24-hour urine M-protein by 50%–89%.
The efficacy of current myeloma therapies is assessed in terms of minimal residual disease (MRD). MRD-negative means that not even 1 myeloma
cell is found in 100,000 or 1,000,000 sampled bone marrow plasma cells (depending on the test used). MRD means that even after CR or sCR has been attained, a patient may still have myeloma cells remaining that can be verified with bone marrow testing.
A higher percent of regression in disease does not automatically confer longer survival. When there is residual disease, the characteristics of the remaining drug-resistant myeloma cells determine the outcome. These remaining myeloma cells may or may not have a tendency for immediate regrowth. If there is no regrowth, this is called “plateau phase” or “residual but stable disease.”
Maintenance therapy
Maintenance therapy prolongs remission after the patient has achieved maximum response to treatment. The benefit of continuous therapy until disease progression has been demonstrated to improve survival, but it may be possible to receive maintenance therapy for a shorter time, depending on the patient’s response to treatment.
The choice of maintenance therapy usually depends on the patient’s depth of response and if the patient has high-risk disease. It is critical to promptly report any side effects from maintenance therapy to the treating doctor so that the therapy can be adjusted.
Relapsing myeloma
Relapse is the reappearance of signs and symptoms of myeloma after a period of improvement. Patients with relapsed disease have been treated, then developed signs and symptoms of myeloma at least 60 days after this treatment ended. There can be multiple periods of response and remission following treatment. Fortunately, a growing number of effective treatment protocols has significantly expanded therapy options for relapsing patients.
Relapse is a key time to discuss with a myeloma specialist the overall strategy that is most appropriate for you and your myeloma. The aim of treatment at each relapse is to achieve optimal response with the least toxicity. This is what leads to the best long-term outcome possible for each patient with myeloma. Therapy for relapsed disease should be based on underlying disease biology and patient characteristics.
If risk factors were identified when you were newly diagnosed and the initial treatment choice was made, this knowledge will have an impact on the choice of treatment when myeloma relapses. Additional risk factors may also become evident at the time of relapse.
Important terms to know include the following:
¡ Progression-free survival (PFS) is the length of time during and after the treatment that a patient’s myeloma does not get worse.
¡ Time-to-progression (TTP) is the time from start of treatment until myeloma relapses.
¡ Progressive disease is myeloma that is becoming worse or relapsing.
Duration and depth of initial therapy
After achieving their first remission, myeloma patients experience their first relapse at variable intervals. The duration and depth of a patient’s response to frontline therapy is often predictive of long-term efficacy in managing myeloma, and helps guide the selection of the next course of treatment. Patients who achieve MRD-negativity status tend to have better PFS.
Biochemical relapse
Biochemical relapse means there is disease progression based on increase in M-protein levels, but no myeloma-related symptoms of organ dysfunction. Biochemical relapse requires monitoring of M-protein levels to catch disease progression if or when it occurs.
In high-risk myeloma, treatment should be initiated early after biochemical relapse is diagnosed to avoid progression to symptomatic disease. Treatment of biochemical relapse is indicated in cases where there is an abnormal ratio by 2 measurements taken 2 months apart: M-spike shows an absolute rise of 0.5 gm/dL or the light chains measured by sFLC show an increase of 10 mg/dL or more.
Clinical relapse
Clinical relapse interventions vary depending upon the factors that are present. For example, if there are new soft-tissue plasmacytomas or bone lesions, your doctor may suggest radiation as a potentially satisfactory way to manage the relapse. Treatment of clinical relapse is indicated if there is any evidence of worsening CRAB criteria.
Relapse with extramedullary disease
Relapse in patients with extramedullary myeloma is addressed following the same principles as the management of high-risk disease with chromosomal abnormalities. Limited data is available on relapse with extramedullary disease as few clinical trials include such patients at this time. However, treatment with immunomodulatory agents and proteasome inhibitors has demonstrated efficacy. Local radiation for local disease control and pain relief, as well as surgical intervention should be considered. PET/CT imaging is key to evaluating and monitoring extramedullary myeloma.
Sequence of regimens after relapse
There is no ideal sequence of treatment regimens for a relapsing patient. Primarily, treatment options depend on the drugs to which the patient is no longer responsive. However, given the many new and emerging therapies, many patients have unexplored treatment options, including in the context of clinical trials.
Refractory myeloma
Myeloma is considered to be refractory in patients who have had progressive disease either during treatment or within 60 days following treatment. Patients who have short remissions or who become refractory to their initial therapy are considered to have high-risk disease.
A subset of patients may develop refractory disease that is no longer responsive to standard treatments, but myeloma that is refractory to one drug may be responsive to another drug in the same drug class or in a different class. The efficacy of a treatment protocol is dependent on the patient’s prior exposure to a specific myeloma drug, as well as to other drugs in the same class.
Patients with refractory myeloma must select from a narrower range of FDA-approved therapy options. The number of regimens a patient has been exposed to and the length of time for a regimen to lose efficacy are predictive of the outcome of therapy. The development of drug resistance may emerge over time.
In late-stage relapse and with refractory disease, attaining stable disease can have clinical benefits for the patient. This is another key time to discuss with your doctor the risks and benefits of clinical trial participation, which may offer access to new drugs and new therapies not yet approved by the FDA.
Clinical trials
A clinical trial is a medical research study with people who volunteer to test scientific approaches to preventing, detecting, diagnosing, or treating cancer, or to answer scientific questions. A clinical trial is launched only after laboratory studies have demonstrated the potential of a treatment or procedure to be more effective and/or less harmful than previously existing methods. The goal of clinical trials is to improve patient care.
For patients with myeloma, clinical trials are part of normal care that can offer earlier access to new drugs and new therapies that are not yet available outside of a study. If you have an interest in participating in a clinical trial, be sure to discuss with the doctor treating your myeloma all the potential risks and benefits that may apply to your particular case.
Clinical research in myeloma has become a robust field, with many studies enrolling patients at any given time. To help myeloma patients with personalized support for identifying and exploring clinical trial options across the U.S., the IMF has partnered with SparkCures. Visit myeloma.org/sparkcures or contact the IMF InfoLine for more information.
The U.S. government maintains the website clinicaltrials.gov, an online database of thousands of research studies from around the world. You may wish to also explore this resource. However, the U.S. government does not review or approve the safety and science of all the studies listed on this website.
For more information about what’s involved in study participation, read the IMF’s publication Understanding Clinical Trials in Myeloma.
In closing
This booklet is not meant to replace the advice of your doctors and nurses who are best able to answer questions about your specific healthcare management plan. The IMF intends only to provide you with information that will guide you in discussions with your healthcare team.
To help ensure a good quality of life through effective treatment, you must play an active role in your own medical care. We encourage you to visit myeloma.org for more information and to join the Myeloma Knowledge Platform at myprofile.myeloma.org.
To receive the most up-to-date information about myeloma in a caring and compassionate manner, call the IMF InfoLine at 1.818.487.7455, email InfoLine@myeloma.org, or visit mmsm.link/infoline to schedule a convenient time to talk with an IMF InfoLine Coordinator.
To get answers to your questions without having to wait, ask Myelo® anytime 24/7 at myeloma.org. This generative AI assistant is designed to help you find the right resources.
Use the hyperlinks and web addresses included in this publication for quick access to resources from the IMF. Sign up at subscribe.myeloma.org for our quarterly journal Myeloma Today and weekly e-newsletter Myeloma Minute, as well as alerts about IMF news, events, and actions.
The International Myeloma Foundation (IMF) is the global leader in myeloma. Our mission is to improve the quality of life of myeloma patients while working toward prevention and a cure. Since 1990, the IMF has been serving the myeloma community through the following four pillars:
RESEARCH At the IMF, finding a cure for myeloma is our top priority. The IMF Scientific Advisory Board (SAB) of leading myeloma experts identifies key opportunities to drive research forward. The IMF Black Swan Research Initiative® (BSRI®) is pushing the boundaries with early screening for a precursor condition of myeloma as well as cure-focused myeloma clinical trials. The IMF International Myeloma Working Group (IMWG) provides trusted guidelines for diagnosing, treating, and managing myeloma. We also fund innovative research through the IMF Brian D. Novis Research Grants.
EDUCATION Myeloma is a complex and unique journey for each patient. The IMF offers hundreds of videos and free publications in multiple languages to inform and empower patients and care partners to navigate their myeloma journey. All IMF seminars, webinars, and workshops are free-of-charge and designed to directly connect the patient community with expert myeloma clinicians. The IMF Nurse Leadership Board (NLB) provides recommendations for the management of myeloma. The IMF M-Power Project works to break down barriers and ensure health equity in underserved populations.
SUPPORT Studies show that social support can greatly improve the quality of life of people with cancer. The IMF offers more than 160 myeloma support groups across North America, including specialized groups for Spanish-speakers, people with smoldering myeloma, care partners of patients with myeloma, and patients who do not have care partners. The IMF InfoLine answers myeloma-related questions. Myelo®, the IMF’s generative AI assistant, is available 24/7 to help you find the right resources.
ADVOCACY In the U.S., the IMF Advocacy team represents your interests at the federal and state levels. Internationally, the IMF Global Myeloma Action Network (GMAN) works to improve patient access to treatments.