• Begin to engage governments as a creditable organization, speaking with one voice for better access to more patients
An idea…..
Myeloma Action Month is a global social awareness campaign that takes place every March to raise awareness of multiple myeloma. We urge the community to champion Myeloma Action Month to help make a positive impact on those suffering from this blood cancer.
Will you take action for the myeloma community?
MAM: 2025 Results & 5 Year Growth
2025 MAM Results:
•Social Reach: 53.6M
•Social Interactions: 51k
•Social Mentions: 9.6k
•Total Countries Reached: 52
MAM Growth 2020 –> 2025
•From 5.6m to 53.6m reach!
•74 Countries Engaged!
Let's join together to make a truly global campaign in March 2026! Here’s how…
MAM + GMAN: Partner Personalization Examples
2026 MAM + GMAN: Campaign Idea
Each country can work on having a key point of interest in their territory light up in red supporting MAM for the month of March. Would it be great if….Paris, Rio, Niagara Falls, Toronto, San Francisco, New York could have a landmark lit in red!!!
MAM + GMAN: Next Steps
MAM + GMAN: How Do We Align & Work Together?
• IMF MarCom team in conjunction with Christine, Martine and Serdar worked on a concept to include all countries.
• To personalize the campaign, the IMF will provide the MAM Logo to support creation of aligning country branding colors with the Logo (as you will see on the next slide).
• Each country will utilize the MAM Logo and associated graphics and video assets to show their support.
o For those countries that need help aligning the MAM logo with their brand, IMF MarCom are happy to help.
• To effectively track the campaign, ALL will use the hashtag #MyelomaActionMonth
• To effectively communicate the campaign, ALL will not use Myeloma Awareness Month, rather ALL need to use Myeloma Action Month in any of their associated text in posting and communicating the campaign.
• IMF will share all assets for the campaign in an easily accessible content collection on their Digital Asset Management Database.
• IMF will share their posting schedule to help others devise their campaign
RESEARCH
Global Scientific update
Joseph Mikhael, MD, Med, FRCPC, FACP, FASCO Chief Medical Officer, International Myeloma Foundation
STATE OF MYELOMA RESEARCH IN 2025
GMAN 2025
JOSEPH MIKHAEL, MD, MED, FRCPC
CHIEF MEDICAL OFFICER, IMF PROFESSOR, CITY OF HOPE CANCER CENTER
WE ARE LIVING IN THE GOLDEN AGE OF MYELOMA WITH IMPROVING QUANTITY AND QUALITY OF LIFE!
BUT WE ARE ALSO LIVING IN A DAY OF UNPRECEDENTED DISPARITIES
Research is essentially based on answering important questions
I will describe the “state” of myeloma research by proposing 10 critical unanswered questions in myeloma
1. SHOULD WE BE SCREENING FOR MYELOMA?
Iceland Screens, Treats, or Prevents Multiple Myeloma
Inclusion criteria:
-Born ≤1975
-Icelandic resident
Exclusion criteria:
-Previous lymphoproliferative disease
Only arm 2 and 3:
-Previously known MGUS (excluded for this analysis)
Psychiatric health: Assessed at registration, after MGUS notification, and annually
Rögnvaldsson S et al. (2021) Blood Cancer Journal; 11, 94
Dr. Joe’s Take on Screening
This is a MASSIVE and critical study to educate us about the feasibility and usefulness of screening
We have to remember Iceland does not represent the whole planet but is an important place to start (especially due to genetic information there)
All screening programs are focused by age, gender, family history, etc and we should expect the same in MM –especially as it is twice as common in patients of African descent
The ISTOPMM trial will likely answer the key question of whether or not screening saves lives in the next 2 years...
2. SHOULD WE TREAT SMOLDERING MYELOMA?
AQUILA: Study Design
AQUILA enrollment period: December 2017 to May 2019 at 124 sites in 23 countries
Screening
Key eligibility criteria:
• ≥18 years of age
• Confirmed SMM diagnosis (per IMWG criteria) for ≤5 years
• ECOG PS score of 0 or 1
• Clonal BMPCs ≥10% and ≥1 of the following risk factors:
- Serum M-protein ≥30 g/L
- IgA SMM
- Immunoparesis with reduction of 2 uninvolved Ig isotypes
- Serum involved:uninvolved FLC ratio ≥8 and <100
- Clonal BMPCs >50% to <60%
All patients were required to have CT/PET-CT and MRI imaging during screening
Treatment/active monitoring phase Follow-up phase
DARA monotherapy
1800 mg SCb QW Cycles 1-2, Q2W Cycles 3-6, Q4W thereafter in 28-day cycles until 39 cycles/36 months*
Active monitoring
No disease-specific treatment, with AE monitoring up to 36 months*
• Efficacy follow-up until progression by SLiM-CRAB
• Survival follow-up every 6 months until end of study
Primary endpoint:
• PFS by IRC per IMWG SLiM-CRAB criteriac Key secondary endpoints:
IMWG, International Myeloma Working Group; ECOG PS, Eastern Cooperative Oncology Group performance status; BMPC, bone marrow plasma cell; FLC, free light chain; CT, computed tomography; MRI, magnetic resonance imaging; QW, weekly; Q2W, every 2 weeks; Q4W, every 4 weeks; AE, adverse event; IRC, independent review committee; ORR, overall response rate. aRisk factors included involved:uninvolved FLC ratio
30 g/L (yes vs no), IgA SMM (yes vs no), immunoparesis (reduction of 2 uninvolved immunoglobulins vs other), or clonal BMPCs (>50% to <60% vs 50%). bDARA SC (1800 mg co-formulated with recombinant human hyaluronidase PH20 [rHuPH20; 2,000 U/mL; ENHANZE® drug delivery technology; Halozyme, Inc.]). cPFS was defined as duration from randomization to
AQUILA: Progression to MM by IMWG SLiM-CRAB Criteria (IRC Assessment)
follow-up: 65.2 months
AQUILA: Overall Survival
*Deaths due to an event occurring after the AE reporting window (ie, events that happened after patient started subsequent therapy or >30 days after last dose) or deaths with unknown reason.
Early intervention with fixed duration DARA extended overall survival versus active monitoring
AQUILA: Safety Overview
Dr. Joe’s Take on Smoldering Myeloma
• Wow this is a VERY important study and may well change the way we think about and treat high risk smoldering myeloma
• The study was critical to really prove we can delay the progression to active myeloma and even improve survival with 3 years of daratumumab
• It underscores the important of a DISCUSSION with the health care team as many options can be offered to patients with high risk smoldering MM
• There will me MANY more trials coming in this area, with even more intense therapies like combinations and even CAR T Cell therapy...
Discontinue DARA therapy only after 24 months of D-R maintenance for patients with CR and 12 months of sustained MRD negativity
Restart DARA therapy upon confirmed loss of CR without PD or recurrence of MRD
ECOG PS, Eastern Cooperative Oncology Group performance status; V, bortezomib; SC, subcutaneous; PO, oral; d, dexamethasone; IV, intravenous; QW, weekly; Q2W, every 2 weeks; PD, progressive disease; Q4W, every 4 weeks; MRD, minimal residual disease; CR, complete response; OS, overall survival; ISS, International Staging System; rHuPH20, recombinant human hyaluronidase PH20; IMWG, International Myeloma Working Group; VGPR, very good partial response. aStratified by ISS stage and cytogenetic risk. bDARA 1,800 mg co-formulated with rHuPH20 (2,000 U/mL; ENHANZE drug delivery technology, Halozyme, Inc., San Diego, CA, USA). cResponse and disease progression were assessed using a computerized algorithm based on IMWG response criteria. dMRD was assessed using the clonoSEQ assay (v.2.0; Adaptive Biotechnologies, Seattle, WA, USA) in patients with VGPR post consolidation and at the time of suspected CR. Overall MRD-negativity rate was defined as the proportion of patients who achieved both MRD negativity (10 –5 threshold) and CR at any time.
Isa-VRD vs VRD: Study design – Part 1
Stratification for randomization prior to:
1. Induction: R-ISS stage (I/II versus III versus not classified)
2. Maintenance: R-ISS stage at study entry (I/II versus III versus not classified) and MRD– after last HDM (no versus yes versus unknown)
Induction (3 x 6-week cycles)
Maintenance (4-week cycles) Days 1, 8, 15, and 22 Days 1 and 15 Day 1 Days 1, 8, 15, 22, and 29 Days 1, 15, 29
R: 10/15/25 mg PO; Days 1-14 and 22-35 V: 1.3 mg/m2 SC; Days 1, 4, 8, 11, 22, 25, 29, and 32
d: 20 mg POb; Days 1-2, 4-5, 8-9, 11-12, 15, 22-23, 25-26, 29-30, and 32-33
d: 20 mg PO; Days 1, 8, 15, and 22 R: 10 mg (up to 15 mg, if tolerated) PO; continuously Treatment for 3 years or until PD
Primary end pointsc: Post-induction MRD– (NGF, 10–5); PFS after second randomization
Key secondary end points: PFS (whole study); OS (whole study and from second randomization); post-induction CR; CR and MRD– after HDM and during and after maintenance therapy
Selected secondary end point: PFS after first randomization
Study design: Isa-VRd vs VRd in transplant-ineligible NDMM
Treatment until PD, unacceptable toxicities, patient withdrawal
9+ DARA: 1,800 mg SC Q4W Rd: schedule as above 28-day cycles until disease progression or unacceptable toxicity
Primary endpoint:
• Overall MRD (≥CR) negativity
Key secondary endpoints:
• PFS
• Sustained MRD (≥CR) negativity (≥12 months)
• ≥CR rate
• OS
DARA SC, daratumumab and recombinant human hyaluronidase for subcutaneous injection; ECOG PS, Eastern Cooperative Oncology Group performance status; V, bortezomib; SC, subcutaneous; R, lenalidomide; PO, oral; d, dexamethasone; DARA, daratumumab; QW, weekly; Q3W, every 3 weeks; Q4W, every 4 weeks; CR, complete response.
Dr. Joe’s Take on Quadruplets
• It is very clear that combining more mechanisms of action controls the disease better
• With these newer agents, it is feasible to give quadruplets to most patients with newly diagnosed myeloma
• There is an art in dosing these agents to maximize the synergy and minimize the toxicity
• dose of lenalidomide
• dose and frequency of bortezomib
• dosing and tapering of dexamethasone
• We are still working on the ideal duration of agents in frontline and how to de-escalate or even discontinue therapy
4. WHAT IS THE OPTIMAL MAINTENANCE STRATEGY IN MYELOMA?
PERSEUS: Study Design
Maintenance
Key eligibility criteria
• Transplanteligible NDMM
• Age 18‒70 years
• ECOG PS ≤2
Continue DR until PD Stop Dara and Restart Dara continue R per criteria
• MRD-negativityc rate was defined as the proportion of patients achieving MRD negativity and ≥CR in the ITT population
– Patients who were not evaluable or had indeterminate results were considered MRD positive
– MRD was evaluated post consolidationd at the time of suspected CR/sCR; at 12, 18, 24, 30, and 36 months after cycle 1 day 1; and yearly thereaftere
aStratified by ISS stage and cytogenetic risk. bDara 1800 mg co-formulated with rHuPH20 (2000 U/mL; ENHANZE ® drug delivery technology, Halozyme, Inc., San Diego, CA, USA); VRd administered as in the VRd group. cMRD was assessed using the clonoSEQ assay (v.2.0; Adaptive Biotechnologies, Seattle, WA, USA) in patients with ≥VGPR post consolidation and at the time of suspected ≥CR. dIn patients with ≥VGPR. eIn patients who achieved CR/sCR and remained on study.
CR, complete response; Dara, daratumumab; DR, daratumumab and lenalidomide; DVRd, daratumumab, bortezomib, lenalidomide, and dexamethasone; ECOG PS, Eastern Cooperative Oncology Group performance status; ISS, International Staging System; ITT, intent-to-treat; MRD, minimal residual disease; NDMM, newly diagnosed multiple myeloma; PD, progressive disease; rHuPH20, recombinant human hyaluronidase PH20; R, lenalidomide; sCR, stringent
PERSEUS: Sustained
MRD-Negativity (10‒5) ≥CR Rates
Presented by P Moreau at the American Society of Clinical Oncology (ASCO) Annual Meeting; May 30–June 3, 2025; Chicago, IL, USA & Virtual
Sustained MRD-negativitya (10–5) ≥CR rate
Dr. Joe’s Take on Maintenance
• Historically we know that lenalidomide maintenance prolongs PFS and even improves survival
• Other approaches have added agents to lenalidomide to improve outcomes, especially in higher risk patients
• Due to its convenience and emerging data, there has been a trend to use daratumumab in maintenance
• The recent results from the PERSEUS is quite convincing for its use for up to 2 years
• Several ongoing studies are evaluating the potential to STOP maintenance primarily based on MRD status
5. CAN MRD STATUS GUIDE THERAPY?
The Evolution of Response Assessment in Myeloma
Courtesy of Rafael Fonseca
Dr. Joe’s Take on MRD
• MRD is an incredibly powerful biomarker
• MRD is diagnostic and prognostic currently and will be more ”therapeutic” very soon
• It may help reduce the need of certain more intense therapies like stem cell transplant
• It is a particularly important goal in high risk myeloma
• It is now an accepted endpoint in clinical trials
• I believe it will become standard practice in myeloma to guide escalation and de-escalation of therapy....
6. HOW DO WE OVERCOME HIGH RISK MM?
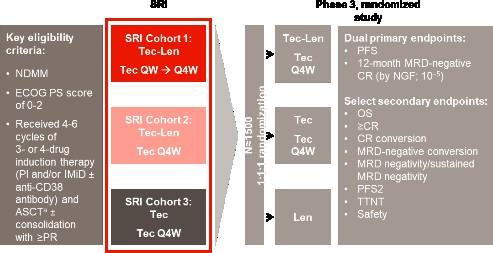
GMMG-CONCEPT Trial design
Stem cell mobilization after cycle 3
Isa: 10 mg/kg D1,8,15,22 in C1; D1,15 in C2+; K: 20 mg/m² D1,2 of C1; 36 mg/m² D8,9,15,16 of C1 and D1,2,8,9,15,16 in C2+; from 2021 onwards: 56 mg/m² on D1,8,15 and 70 mg/m² on D1,15 in maintenance; R: 25 mg D1-21 all Cycles; d: 40 mg D1,8,15,22 all Cycles (20 mg age >75).
Arm A: app. 15-18 months after inclusion
Arm B: app. 12 months after inclusion
HRMM criteria: ISS stage II or III PLUS ≥1 of: del(17p), t(4;14), t(14;16) and/or ≥3 copies 1q21 (amp1q21)
Primary objective: MRD negativity after consolidation (NGF, 10-5)
Secondary objective: PFS; Selected tertiary objectives: ORR, OS
ASCT, autologous stem-cell transplant; d, dexamethasone; HDT, high-dose therapy; HRMM, high-risk multiple myeloma; Isa, isatuximab; ISS, International Staging System; K, carfilzomib; MRD, minimal residual disease; ND, newly-diagnosed; NGF, next-generation flow; ORR, overall response rate; OS, overall survival; PFS, progression-free survival; R, lenalidomide; TE, transplant-eligible; TNE, transplant-ineligible. Following a protocol amendment in 2021, carfilzomib application was switched to once weekly 56 mg/m 2 .
Progression-free and Overall Survival
• Median follow-up of 43 months (0-90.2 months)
1st cohort: 69 months (0-90.2 months)
2nd cohort: 33 months (5.5-43.3 months)
5Y-OS-rate: 72% (65.0-78.9%)
6Y-OS-rate: 69% (61.2-76.8%)
Lisa B. Leypoldt, MD
Results
Sustaining MRD-negativity was associated with increased PFS
CI, confidence interval; HR: hazard ratio; MRD, minimal residual disease. Clinical data cut-off: April 28, 2025.
Multivariable time-dependent Coxregression analysis showed a prognostic PFS benefit for remaining in MRD negativity versus non–MRD negativity with a hazard ratio of 0.15 (95% CI, 0.07-0.29, p<0.0001)
Results for TE patients. Figure shows a Simon-Makuch plot illustrating the estimated survival while staying in the state of MRD-negativity compared to the estimated survival while staying in the state of MRD-positivity. Patients may switch between the two states under therapy.
PRESENTED BY:
Lisa B. Leypoldt, MD
Dr. Joe’s Take on High Risk Myeloma
• A NEW definition is soon to be released to truly identify those patients at highest risk
• It is genuinely an unmet need in MM, as sadly some still succumb to their disease in the first year of diagnosis
• Patients require combination therapies, given continuously and with MRD negativity as the goal
• It is possible that CAR T Cell therapy may change this approach as even high risk patients can have deep and durable responses to CAR T
7. CAN WE MORE EFFECTIVELY, SAFELY AND CONVENIENTLY GIVE BISPECIFIC ANTIBODIES?
Cytokine Release Syndrome (CRS)
Severity for BsAbs and CAR T Ranges From Mild to Life-Threatening
CAR T: Need to Manufacture
Monitoring for CRS, Neurotoxicity
• Vital signs (eg, temperature, O2 saturation)
• Review of systems and physical exam
– Focus on cardiovascular, pulmonary, and neurologic systems
• Rule out infection
• Laboratory monitoring
– CRP
– Cytokines
– Ferritin
– LDH
• Mental status scoring
RESPIRATORY
Hypoxia
Dyspnea
Capillary leak syndrome
HEPATIC
Transaminitis
ALP
Hyperbilirubinemia
RENAL
Serum creatinine
Renal insufficiency
TLS
HEMATOLOGIC
Anemia
Thrombocytopenia
Neutropenia
CONSTITUTIONAL
Fever
Fatigue, malaise
Headache
NEUROLOGIC
Delirium
Somnolence
Dysphagia
CARDIOVASCULAR
Sinus tachycardia
Hypotension
Arrhythmias
GASTROINTESTINAL
Nausea
Vomiting
Diarrhea
MUSCULOSKELETAL
CPK
Myalgia
Weakness
Neurotoxicity in Immunotherapy
Monitoring for Immune Effector CellAssociated Neurotoxicity Syndrome (ICANS)1,2
ICE screening tool
Review of systems and physical examination
– Focus on neurologic systems
Rule out infection
If ICANS suspected – Neuroimaging (ideally MRI)
– Diagnostic lumbar puncture for opening pressure and infection tests
Corticosteroids are typically indicated for ICANS ≥ grade 2
• Every treatment in myeloma goes through an evolution after approval to increase efficacy and reduce toxicity
• We are in the midst of that evolution now
• working towards outpatient management
• understanding side effects
• developing strategies to prevent and treat them rapidly
• sharing information between experts to speed up the process
• The IMF Immune Therapy Registry was designed to do this!
• IMWG guidelines for bispecific antibodies and CAR T Cell therapy
• now with a “living” component by keeping them up to date online
8. IS THERE AN IDEAL SEQUENCING APPROACH
IN RELAPSED MYELOMA?
Don’t Save the Best for Last!
In every new LOT, ~15-35% of patients are lost
Figure adapted from: Yong, K et al. Br J Haematol 2016;175(2):252-264
Shared Decision-Making Strategies
Patients and providers should make individualized decisions together regarding treatment
SHARE approach
Seek patient participation
Help the patient explore and compare treatment options
Assess patient’s values and preferences
Reach a decision with the patient
Evaluate the patient’s decision
Noonan K, et al. J Adv Pract Oncol. 2022;13:15-21; Faiman B, et al. Clin J Oncol Nurs. 2019;23:540-42;
International Myeloma Foundation. https://www.myeloma.org/resource-library/tip-card-myeloma-treatment-discussion-tool.
Dr. Joe’s Take on Sequencing
• There really is no IDEAL sequence that we know of in myeloma
Key Principles include:
• Use the most effective therapies as early as possible in the disease course
• in eligible patients sequence CAR T prior to other immunotherapies
• The BCMA target can be used more than once
•
Shared decision making is critical to matching the right therapy to the patient
9. HOW CAN WE ADDRESS THE GLOBAL DISPARITIES IN MYELOMA?
Reference:
Liu, X., Zhuang, H., Li, F. et al. Trends and projections of the global and regional burden of multiple myeloma in adults aged 40 and over, 1990–2044. Sci Rep 15, 13595 (2025). https://doi.org/10.1038/s41598-025-96981-w
M-Power = Myeloma Power
The facts are sobering:
• Myeloma is twice as common in African Americans
• Survival in African Americans in HALF that of White Americans
• The disparity is multifactorial
The core vision of this initiative is to improve the short- and long-term outcomes of African American and Latino patients with myeloma. We want to empower patients and communities to change the course of myeloma…
Enhance access to optimal care by educating myeloma providers about the disparity and how to reduce it
Engage the community to increase awareness and provide support
Shorten the time to diagnosis by educating primary care providers to recognize the disease and order the right tests
Dr. Joe’s Take on Disparities
• There is no greater problem in myeloma worldwide!
• It is a combination of multiple factors
• Social determinant of Health
• Delayed Diagnosis
• Reduced Access to Novel therapies
• It is not an easily solved problem but critical advances can be made
• The IMF M-Power program is an example of a strategy that can be applied more broadly with short and long term goals
• GMAN is uniquely positioned to be a part of the solution!
10. ARE WE CURING MYELOMA?
Survival in multiple myeloma has improved over time
1. Puertas B, et al. Cancers (Basel). 2023;15(5):1558
Long-Term (≥5 Year) Remission and Survival After Treatment With Ciltacabtagene Autoleucel in CARTITUDE-1
Patients With Relapsed/Refractory Multiple Myeloma
1Atrium Health/Levine Cancer Institute, Wake Forest University School of Medicine, Charlotte, NC, USA; 2University of California, San Francisco, CA, USA; 3Mayo Clinic, Rochester, MN, USA; 4Abramson Cancer Center, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA; 5Massachusetts General Hospital Cancer Center, Boston, MA, USA; 6City of Hope Comprehensive Cancer Center, Duarte, CA, USA; 7Karmanos Cancer Institute, Wayne State University, Detroit, MI, USA; 8UPMC Hillman Cancer Center, Pittsburgh, PA, USA; 9Tennessee Oncology, Nashville, TN, USA; 10Medical College of Wisconsin, Milwaukee, WI, USA; 11University of Chicago, Chicago, IL, USA; 12Icahn School of Medicine at Mount Sinai, New York, NY, USA; 13Johnson & Johnson, Shanghai, China; 14Johnson & Johnson, Spring House, PA, USA; 15Johnson & Johnson, Raritan, NJ, USA; 16Legend Biotech USA Inc., Somerset, NJ, USA Presented by PM Voorhees at the American Society of Clinical Oncology (ASCO) Annual Meeting; May 30–June 3, 2025; Chicago, IL, USA & Virtual
Copies of this presentation obtained through Quick Response (QR) Codes are for personal use only and may not be reproduced without permission from ASCO® or the author of this presentation.
CARTITUDE-1 Long-Term Remission:
One-Third of Patients Were Progression-Free for ≥5 Years
Overall population (N=97); median follow-up: 61.3 months
Progression-free survival
Presented by PM Voorhees at the American Society of Clinical Oncology (ASCO) Annual Meeting; May 30–June 3, 2025; Chicago, IL, USA & Virtual
32 of 97 (33%) patients were treatment- and progression-free at ≥5 years
cilta-cel, ciltacabtagene autoleucel.
Dr. Joe’s Take on Cure
• I like to define cure in the way someone on the street would likely define it... someone is given limited therapy then no longer has to think about the disease
• We have always had a very small fraction of patients who with limited therapy have particularly long remissions
• I believe that fraction continues to grow with the novel approaches we are providing
• It will not happen overnight – but will be the result of a global coalition against myeloma bringing together the best science, clinical trials, experts and motivated patients...
Bonus Topic – Down with Dex!
Dr. Joe’s Approach to Dex
Dexamethasone Dose De-escalation Protocol
1. Assess 40 mg versus 20 mg weekly starting dose
2. Limit starting dose to 2 to 3 months
3. Then taper dose each month over the course of 3 to 4 months
4. Plan to stop dexamethasone at 6 months
5. Regular assessments for toxicity and de-escalate sooner if clinically indicated Join the DOWN with DEX movement!
FFinal Thoughts...
• There are still MANY more unanswered questions!
• But the future for myeloma patients is genuinely bright
• We must all be a
part of the solution!
OUR VISION:
A world where every myeloma patient can live life to the fullest, unburdened by the disease.
OUR MISSION:
Improving the quality of life of myeloma patients while working toward prevention and a cure.
Stop DARA therapy after ≥24 months of DR maintenance for patients with ≥CR and 12 months of sustained MRD negativity (10–5)
Restart DARA therapy upon confirmed loss of CR without PD or recurrence of MRD
PERSEUS: NCT03710603
aStratified by ISS stage and cytogenetic risk. bDARA 1,800 mg co-formulated with rHuPH20 (2,000 U/mL; ENHANZE drug delivery technology, Halozyme, Inc., San Diego, CA, USA). cResponse and disease progression were assessed using a computerized algorithm based on IMWG response criteria. dMRD was assessed using the clonoSEQ assay (v.2.0; Adaptive Biotechnologies, Seattle, WA, USA) in patients with ≥VGPR post-consolidation and at the time of suspected ≥CR. Overall, the MRD-negativity rate was defined as the proportion of patients who achieved both MRD negativity (10 –5 threshold) and ≥CR at any time. CR, complete response; d, dexamethasone; DARA, daratumumab; DR, daratumumab and lenalidomide; DVRd, daratumumab, bortezomib, lenalidomide, and dexamet hasone; ECOG PS, Eastern Cooperative Oncology Group performance status; IMWG, International Myeloma Working Group; ISS, International Staging System; IV, intravenous; MRD, minimal residual disease; NDMM, newly diagnosed multiple myeloma; OS, overall survival; PD, progressive disease; PFS, progression-free survival; PO, oral; QW, weekly; Q2W, every 2 weeks; Q4W, every 4 weeks; R, lenalidomide; rHuPH20, recombinant human hyaluronidase PH20; SC, subcut aneous; V, bortezomib; VGPR, very good partial response; VRd, bortezomib, lenalidomide, and dexamet hasone.
CEPHEUS: Study Design
Key eligibility criteria:
• NDMM (TIE or transplant deferred)
• ECOG PS score of 0-2
• Frailty score of 0-1
VRd
V: 1.3 mg/m2 SC Days 1, 4, 8, 11
R: 25 mg PO Days 1-14
d: 20 mg PO Days 1, 2, 4, 5, 8, 9, 11, 12
9+
R: 25 mg PO Days 1-21
d: 40 mg PO Days 1, 8, 15, 22
Primary endpoint:
• Overall MRD (≥CR) negativity
DVRd
DARA: 1,800 mg SCa QW Cycles 1-2, Q3W Cycles 3-8
VRd: schedule as above 21-day cycles
8 cycles of bortezomib treatment
DRd Cycle 9+
DARA: 1,800 mg SCa Q4W
Key secondary endpoints:
• ≥CR rate 1 :
Rd: schedule as above 28-day cycles until disease progression or unacceptable toxicity
aDara 1800 mg co-formulated with recombinant human hyaluronidase PH20 ([rHuPH20; 2000 U/mL; ENHANZE® drug delivery technology; Halozyme, Inc., San Diego, CA, USA).
Nonfrail patients had longer PFS than frail patients
The PFS benefit of the addition of daratumumab was maintained across frailty subgroups
Facon. Leukemia. 2022;36:1066.
IFM-2017-03
PFS
Transplant NON eligible NDMM:
Anti-CD38 plus VRd induction and anti-CD38-R maintenance
IMROZ CEPHEUS
Median follow-up: 59.7 mo
CARTITUDE 5
Frontline Treatment 2025
Eligibility for ASCT
200 mg/m2 melphalan (I, A) followed by ASCT (I, A) First
LEN, Dara-Len maintenance
ASCT, autologous stem cell transplant; C, cyclophosphamide; D, daratumumab; d, dexamethasone; M, melphalan; NDMM, newly diagnosed multiple myeloma; P, prednisone; R, lenalidomide; T, thalidomide; TE, transplant eligible; V, bortezomib. Sonneveld P, et al NEJM 2024; Gay F, et al. ASH 2023 (Abstract No. 4 – oral presentation); Goldschmidt H, et al. Lancet Haematol. 2022;9(11):e810–e821; Leypoldt LB, et al. J Clin Oncol. 2023; Perrot A. Et al
SEQUENCING AND TREATMENT AT RELAPSE: DO WE HAVE TO WAIT RELAPSE FOR ALL?
Treatment landscape for triple-class exposed MM patients in 2026 and beyond
1° line 2° line 3° line
Anti-CD38 MoAbs
Bortezomib and lenalidomide
Carfilzomib/ixazomib/ pomalidomide, elotuzumab/selinexor/Bela maf 4° line 5° line and beyond
• Cilta-cel
• Teclistamab
• Elranatamab
• Talquetamab
• Ide-cel
• Selinexor
• Melflufen
Study design
MIDAS = MInimal residual Disease Adapted Strategy
(G-CSF+/- plerixafor) Induction
MRD evaluation
Standard risk (MRD <10-5)
IsaKRD x 6 (28d cycles) MRD
Stem cell collection after cycle 3
High risk (MRD >10-5)
Risk-adapted consolidation and maintenance
x 6
+ IsaKRD x 2
ASCT + IsaKRD x 2
(3 years) Isa - Iberdomide (3 years)
ASCT
Key Takeaway Points
In MRD-positive patients, tandem ASCT did not provide additional benefit in terms of MRD-negativity compared to single ASCT.
Can We APPLY novel approaches early on?
Baseline Vs Dynamic RISK
CAR-T cells in patients with suboptimal response to ASCT
CARTITUDE 2 cohort D N=17
DRUG AVAILABILITY ACCESS AFFORDABILITY
THESE ARE EXCITING TIMES FOR MM RESEARCH GREAT IMPROVEMENT
IN SURVIVAL MORE QUESTION THEN ANSWERS BUT…
If I had an hour to solve a problem and my life depended on the solution, I would spend the first 55 minutes determining the proper question to ask, for once I know the proper question, I could solve the problem in less than five minutes
A. Einstein
Thank you
Division of Hematology, Department of Molecular Biotechnology and Health Sciences, University of Torino
Azienda Ospedaliero-Universitaria Città della Salute e della
Scienza di Torino, Torino, Italy
Prof . Benedetto Bruno
Clinical trial and multiple myeloma Unit
Dr. Sara Bringhen
Dr. Alessandra Larocca
Dr. Roberto Mina
Dr. Giulia Benevolo
Dr. Stefania Oliva
Dr. Mattia D’Agostino
Dr. Giuseppe Bertuglia
Dr. Lorenzo Cani
Dr. Andrea Casson
Dr. Tommaso Picardi
Dr. Edoardo Marchetti
European Myeloma Network
Prof Mario Boccadoro
Prof Pieter Sonneveld EMN team
Laboratory Staff Transplant Unit Nurses Data Managing Staff
COFFEE BREAK / POSTER SESSION
CANADA, CROATIA, CZECHIA, DENMARK, NORWAY, PORTUGAL
THANK YOU TO OUR SUMMIT SPONSORS
ADVOCACY
GLOBAL POWER OF PATIENT ADVOCACY
FOCUSED ON MYELOMA RESEARCH AND POLICY
Moderator: Mira Armour
Panelists: Joseph Mikhael, Christine Battistini, Francesca Gay, Jungsook Park, Martine Elias
INDUSTRY PARTNER PRESENTATION
LUNCH
VERANDA RESTAURANT
THANK YOU TO OUR SUMMIT SPONSORS
INDUSTRY PARTNER PRESENTATION
JOHNSON & JOHNSON
ACCESS
HEALTH TECHNOLOGY ASSESSMENT & EQUITABLE ACCESS
Neil Grubert
Overcoming Access Barriers for Cancer Therapies
7th June 2025
Variations in time to national launch and public reimbursement
Average time from global first launch to national launch and public reimbursement (months)
Source: Based on PhRMA analysis of IQVIA MIDAS and country regulatory data * Data for Canada relate to public plans only
A new Access to Medicine Index
Approaches used by companies to provide access in different markets
• Pharmaceutical companies are taking steps to address access in low-income countries, but significant gaps remain.
• Patients in LMICs are largely excluded from clinical trials, limiting their access to new treatments.
• Efforts to expand local availability of medicines through voluntary licensing and technology transfers are limited.
Availability of new cancer drugs in Europe
Source: EFPIA Patients WAIT Indicator 2024 Survey
Time to availability of new cancer drugs in Europe
Source: EFPIA Patients WAIT Indicator 2024 Survey
What pricing methods are used in Europe?
What factors are considered in value assessment?
Source: Delivering the Triple Win: A Value-Based Approach to Pricing, Office of Health Economics
HTA challenges for multiple myeloma therapies
Challenge Features
Complexity of treatment landscape Clinical trials for MM are designed based on exposure to prior therapies, often meaning that trial data is incompatible with HTA requirements to conduct evaluations based on the line of therapy
Generalisability of evidence The generalisability of trial results to real-world settings is relatively low for MM owing to the heterogeneity of the patient populations
Clinical trial design As a rare disease, MM clinical trials are often designed as single-arm studies, making it difficult to identify appropriate comparators
Equity of patient access MM occurs twice as frequently in black people as white and Asian people, yet black people are under-represented in clinical trials and may reap fewer benefits from novel therapies
Combination therapies & indication expansions Many new therapies for MM are combination therapies, increasing costs and making it difficult to achieve cost-effectiveness
Surrogate endpoints HTA bodies are slow to accept such endpoints—owing partly to limited evidence of their validity in MM
Patient-relevant outcomes HTA agencies differ in their acceptance of HRQoL tools
EU joint HTA—the biggest development in international HTA history
Joint HTA will be restricted to four clinical domains:
• Identification of a health problem and current technology
• Examination of technical characteristics of the technology
• Relative safety
• Relative clinical effectiveness
The scope of JCAs should reflect all member states’ requirements in terms of data and analyses.
The reports shall not contain any value judgement or conclusions on overall clinical added value of the assessed health technology and shall be limited to a description of (1) relative effects and (2) degree of certainty of the relative effects.
Germany’s AMNOG system—a model for the world?
• Germany is unusual in allowing manufacturers to launch drugs as soon as they receive marketing authorisation at a price of their choosing and with full reimbursement.
• HTA and rebate negotiation follow over the next year, with agreed rebates then being backdated by six months.
• Orphan drugs with projected annual sales in Germany of ≤ €30 million undergo a streamlined benefit assessment.
Source: Based on data from the Gemeinsamer Bundesausschuß der Ärzte, Zahnärzte, Krankenhäuser und Krankenkassen (GBA).
NICE is the gatekeeper to market access in England
Source: NHS Commercial Framework for Medicines.
Three main objectives of managed entry
Objective
Control budget impact
Managed entry approach
Financially-based agreements
Level of activity
Tackle uncertainty
Coverage with evidence development
Population/patient
Population
Manage variable drug response rates
Outcomes-based agreements
Patient
Managed entry for cancer drugs in EU/OECD
Use of managed entry, post-marketing studies and other approaches to regulate access to cancer drugs
• 25 countries use financially based managed entry agreements (MEAs), including rebates/discounts, pricevolumeagreements,orexpenditurecaps.
• 17 nations use performance-based MEAs, which include arrangements such as coveragewith evidencedevelopmentand payment-by-resultsagreements.
• 8 countries sometimes require marketing authorisation holders to conduct postmarketing studies to provide confirmatoryevidenceofclinicalbenefit.
• Financially based approaches are generallyfavouredfortheir simplicity and predictability, with a relatively limited administrative burden on healthcare systems.
Cancer Drugs Fund in England
104,267
• Earlier access for patients to the promising treatments while uncertainty is assessed through real-world data collection.
• Interim funding for all newly recommended cancer drugs.
• Fixed budget and cost controls.
• A new fast-track NICE process for companies to apply for appraisals.
• Clearer and faster decision making.
• More flexible deals to encourage responsible pricing.
Improving access to combination oncology therapies in Europe
• Value assessment frameworks adapted to combination therapies.
• Ways to comply with anti-trust regulations.
• Responding to demands for price cuts to meet payers’ value expectations.
Combination therapy pricing breakthrough
• UK Competition and Markets Authority (CMA) will not prioritise investigations into certain engagements between companies “carried out in good faith” to make combination therapies available to NHS patients.
• ABPI’s negotiation framework will play a key role in ensuring compliance with terms of concession.
• Information exchanged must be limited to what is strictly necessary and should not include confidential net prices.
• CMA believes the change “will have a real, positive impact now and in the future, and will benefit patients, innovating businesses and the UK economy at large.”
CAR-T-cell therapy infrastructure
Source: Achieving CAR-T-Cell Therapy Health System Readiness, IQVIA
CAR-T-cell treatment rates
Source: Strengthening Pathways for Cell and Gene Therapies: Current State And Future Scenarios, IQVIA
Global interest in Spain’s academic CAR-T-cell therapies
• More than 500 patients in Spain have received one of three “academic” CAR-T-cell therapies developed by the Clínic-Idibaps in Barcelona.
• ARI-0002 is indicated for multiple myeloma.
• Academic CAR-T-cell therapies offer faster and more local production, substantially lower costs and the flexibility to prescribe them off label, leading to more frequent use than commercial treatments.
• The Dutch government has donated €35mn for a trial comparing ARI-0001 with commercial CAR-T-cell therapies in lymphoma.
• The drug has PRIME status and is one of three academic CAR-T-cell therapies approved by EMA in a pilot project to support the development of non-commercial ATMPs.
• In India, ARI-0001 is marketed as Qartemi by Immuneel Therapeutics at a cost of INR 3.5-5mn (€37,354-53,362).
• A global alliance of 50 hospitals is interested in Spain’s academic pharmaceuticals.
Regional cross-border collaborations
• Beneluxa Initiative has focused largely on ATMPs. Belgium andtheNetherlandshavebeenthemainusersofoutputs.
• Joint Nordic HTA Bodies (formerly FINOSE) and Nordic Pharmaceutical Forum work closely together and have regular interaction with Beneluxa. Working Group on Exchange of Information and Experience in the Medicines Area(WGEMA)hasamorestrategicfocus.
• Valletta Declaration Group has kept a relatively low profile, serving as a platform for information exchange, but a “resurgence”ofactivityisexpected.
• SUSTAIN-HTA will support the HTA Coordination Group and its Subgroup on Methodology and “aims to assist in the alignmentofHTAmethodologies.”
• Eight countries have expressed interest in voluntary cooperationonjointHTA.
• NICE has worked closely with the Danish Medicines Council. SpainandPortugalarealsolookingtocollaborate.
Transcontinental cross-border collaborations
Name Participants Key objectives
Project Orbis Australia, Brazil, Canada, Israel, Singapore, Switzerland, UK, US
Access Consortium Australia, Canada, Singapore, Switzerland, UK
Accelerated regulatory approval of cancer therapies
UK Int’l Recognition Framework
UK, Australia, Canada, EU, Japan, Switzerland, Singapore and US*
Accelerated regulatory approval of nononcology drugs
• Project Orbis approved 10 new cancer drugs and 8 new oncology indications from May 2021 to December 2023 and has shown “exceptional worth in clinical situations where time reallydoesmatter.”
AUS-CAN-NZ-UK Collaboration Arrangement
Health Economics Methods
Australia, Canada, New Zealand, UK
UK recognition and lighter-touch evaluation of marketing authorisations of cutting-edge drugs from 7 other regulatory authorities
8 “like-minded” HTA bodies will share information on best practice and conduct a pilot JCA
Advisory group US, Canada, UK Will explore dynamic efficiency and dynamic pricing in economic models, use of novel or non-traditional value elements, and integration of health equity considerations
- Canada, Belgium, Denmark, Iceland, Ireland, Netherlands, Norway, Portugal, Sweden
Canada will work with members of Beneluxa Initiative, Nordic Pharmaceutical Forum and Portugal to share experiences on dealing with lack of evidence and negotiating prices for high-priced drugs
* UK MHRA recognises decisions of other designated regulatory agencies
• Access Consortium “creates a market of some 160 million people”andwillexplorecollaborationwithHTAagencies.
• AUS-CAN-NZ-UK Collaboration Arrangement will conduct at leastonepilotjointclinicalassessment.
• NICE International is increasingly active, especially in APAC and LatinAmerica(includingabilateralagreementwithTaiwan).
• HEMA plans to engage regularly with the international HTA community to discuss new value elements, health equity, dynamicpricing.
• Pan-American Health Organization (PAHO) participated in a recentmeetingofthe NovelMedicinesPlatform.
Outlook
• Profound changes in the US market will have global repercussions. Will US pharmaceutical tariffs be implemented? Will “Most-Favored Nation” pricing become a reality?
• HTA is becoming increasingly complex and nuanced, reflecting changes in healthcare systems, health technologies, data sources (including real-world data), availability of information from other agencies, collaboration and the use of AI and machine learning for data analysis and modelling.
• HTA could shift to health technology management for some drugs.
• EU joint clinical assessment will produce a common report for all EU Member States but will not replace national appraisal and non-clinical elements of HTA.
• What role will China play in the global market in coming years?
• Cross-border collaboration is likely to grow in importance.
• Non-traditional value elements will become more influential.
• What will reshoring of production and MEAT criteria mean for prices and budgets?
IMF Senior VP, Global Advocacy Access, Policy & Research
MRD @ EMA Project Update (i2TEAMM Europe)
Mimi Choon-Quinones
HTA Consortium Collaborators
The Heads of HTA Agencies is an independent group of 32 European healthcare agencies working together to advance strategic collaboration on HTA.
Health Technology Assessment international is a collaboration of HTA professionals who are dedicated to shaping the future of health systems and improving health outcomes for all people.
ISPOR is the leading global scientific and educational organization for health economics and outcomes research ( #HEOR)
The Institute for Clinical and Economic Review (ICER) is an independent, non-profit research institute that conducts evidence-based reviews of health care interventions, including prescription drugs, other treatments, and diagnostic tests.
HTA EU Country Collaborators
Country Insights: HTA Partners
Austria Austrian Institute for Health Technology Assessment (AIHTA), Ludwig Boltzmann Institute (LBI-HTA), UMIT – University for Health Sciences, Medical Informatics and Technology
Belgium Belgian Health Care Knowledge Centre (KCE), Scientific Institute of Public Health (IPH)
Bulgaria National Center of Public Health and Analyses (NCPHA)
Croatia Croatian Institute of Public Health (CIPH), Agency for Quality and Accreditation in Health Care and Social Welfare (AAZ)
Cyprus Ministry of Health of the Republic of Cyprus
Czech Republic Ministry of Health of the Czech Republic, State Institute for Drug Control (SÚKL)
Denmark DEFACTUM – Department of Public Health Research and Development (Central Denmark Region)
Estonia University of Tartu, Institute of Family Medicine and Public Health (UTA)
Finland Finnish Medicines Agency (FIMEA), Finnish Coordinating Center for Health Technology Assessment (FinCCHTA), National Institute for Health and Welfare (THL)
France Haute Autorité de Santé (HAS)
Germany Institute for Quality and Efficiency in Health Care (IQWiG), Federal Joint Committee (G-BA), German Institute for Medical Documentation and Information (DIMDI)
Greece Ministry of Health HTA Committee, supported by National Organization for Medicines (EOF), Institute of Pharmaceutical Research and Technology (IFET)
Hungary National Institute of Pharmacy and Nutrition (NIPN), Health Services Management Training Centre, Semmelweis University
Ireland Health Information and Quality Authority (HIQA), National Centre for Pharmacoeconomics (NCPE)
Italy Italian Medicines Agency (AIFA), National Agency for Regional Health Services (Agenas), Regional HTA centers (e.g., CRUF, UCSC Gemelli)
Lithuania Institute of Hygiene (HI), State Health Care Accreditation Agency (VASPVT), State Medicines Control Agency (VVKT)
Malta Directorate for Pharmaceutical Affairs (DPA), Ministry for Health
Netherlands Zorginstituut Nederland (ZIN – National Health Care Institute)
Norway Norwegian Directorate of Health (Hdir), Norwegian Institute of Public Health (NIPHNO), Norwegian Medicines Agency (NoMA)
Poland Agency for Health Technology Assessment and Tariff System (AOTMiT)
Spain Spanish Network of Agencies for Health Technology Assessment and Benefits of the National Health System (RedETS), coordinated by the Ministry of Health
LMICs HTA Collaborators
Country
HTA Body/Institution
Notes
Thailand Health Intervention and Technology Assessment Program (HITAP) One of the most mature HTA bodies in LMICs
India Health Technology Assessment India (HTAIn)
Indonesia INA-HTAC
Philippines HTA Unit, Department of Health
Brazil CONITEC
South Africa National Essential Medicines List Committee (NEMLC)
Kenya Ministry of Health’s HTA Technical Working Group
Pakistan Health Planning, Systems Strengthening & Information Analysis Unit (HPSIU)
Supports evidence-based resource allocation
Established to support the national health insurance program
Institutionalized by Universal Health Care Act
Advises Ministry of Health on incorporation of technologies
Uses HTA principles for formulary decisions
Emerging HTA system in development
Moving toward institutionalization
Research Results
1: Generating MRD evidence needed for market entry agreements
2: The Power of Partnerships
EMA Timeline Overview
On 10/06/2024 and again on 15/11/2024, i2TEAMM Europe requested Qualification Advice, pursuant to Article 57(1)(n) of Regulation (EC) 726/2004 of the European Parliament and of the Council, on the use of Minimal Residual Disease (MRD) as an early endpoint in clinical trials conducted in patients with Multiple Myeloma (MM) in order to support regulatory decisions.
The EMA Scientific Officer for the procedure was Myriam Chapelin.
Serena Marchetti, Hilke Zander and Elina Asikanius were appointed as Coordinators.
Lukas Aguirre Dávila, Michal Zwiewka, Macarena Gajardo Álvarez, Joerg Zinserling, Torsten Holm Nielsen, Odoardo Olimpieri, Johanna Lähteenvuo, Karri Penttila, Olli Tenhunen, Pierre Demolis and Filip Josephson were appointed as Qualification Team members.
The EMA procedure started on 25/11/2024 & virtual HTA Engagements
List of Issues Responses Requested on 19/02/2025
~ ETA June. Any day now!
Q1: Does the CHMP agree that the rate of MRDnegCR, at 10-5 or higher threshold and measured at 9±3 or 12±3 months, translates into clinically meaningful benefit in patients with NDTE, NDTinE, and RR MM?
HTA Predictions on Upcoming EMA Advice:
-80% probability on agreeing that MRD negativity at 10-5 or higher threshold has a prognostic value at patient level. - Our data presented most likely will appear to support positive effect
Q2: Does the CHMP agree that a new therapy or combination of therapies that increases MRDnegCR rate by approximately 10% to 20%, at 10-5 or higher threshold and measured at 9±3 or 12±3 months, provides a major therapeutic advantage over approved therapies for patients with MM?
HTA Predictions on Upcoming EMA Advice:
- Major therapeutic advantage (MTA) will be discussions on a case-by-case basis - Discussions should not be limited to the comparator arm employed in the clinical trial intended to support registration.
Q3: Does the CHMP agree with the context of use for MRDnegCR, classified at 10-5 or higher threshold and measured at 9±3 or 12±3 months, as an early clinical endpoint in clinical trials to support regulatory approval of new indications for MM while PFS and OS results are maturing?
HTA Predictions on Upcoming EMA Advice:
- MRDnegCR as an endpoint to support (conditional) approval of a compound while the obligation to demonstrate long-term benefit remains, “plausible”
Q4: The totality of data presented by the i2TEAMM Europe meta-analysis, and by the independent meta-analysis conducted by University of Miami (EVIDENCE), provides evidence for the use of MRDnegCR as an early endpoint to measure therapeutic benefit and support benefit-risk assessments for regulatory approval in MM. Does the CHMP agree?
HTA Predictions on Upcoming EMA Advice:
- MRDnegCR as an endpoint in clinical trials in specific settings, together with the totality of the available evidence, in the context of a CMA, is plausible.
- Available data is not sufficient to support the use of MRDnegCR rate as an early, stand alone, clinical endpoint in randomised controlled trials in multiple myeloma to establish, on its own, the benefit/risk of new treatments or combinations and support a full MAA.
HTA Insights & Considerations
Deliberations on Clinically Guided Decision-Making (CGDM) in this context refers to adaptive treatment choices based on MRDnegCR status, including early stopping, or therapeutic switch.
HTA bodies value CGDM when:
1) Based on validated or regulator-endorsed endpoints like MRDnegCR
2) Aligned with patient preferences and supports real-world decision-making
Conditional reimbursement recommended if:
1) MRDnegCR is used as a treatment and reimbursement decision trigger
2) A registry tracks MRDnegCR rates, survival, and patient outcomes
3) Cost-effectiveness is modelled based on adaptive treatment paths
4) Implementation is supported by clinical algorithms and shared decision tools
Scoping PICO(S) for i2TEAMM Including Patient Experience Data & Clinically Guided Decision-Making (CGDM)
Scoping PICO(S) framework aims to systematically define the key elements necessary to evaluate MRDguided interventions in MM through the lenses of clinical effectiveness, patient experience data, and health system impact.
P=Population
I= Intervention
C=Comparator(s)
O=Outcome(s)
S=Settings/Study Design
HTA bodies are slow to accept such endpoints—owing partly to limited evidence of their validity in MM.
Examples Of What Is Needed:
- Lasting and unprecedented improvement in benefit, especially a cure
- Substantial extension of survival
- Long-term freedom from severe symptoms
- Extensive avoidance of severe side effects
1. Clinical Researchers / Investigators
Initiate PICO scoping to define research questions for systematic reviews, clinical trials, or health technology assessments.
Bring clinical expertise to frame population, interventions, comparators, and relevant outcomes.
2. Patient Representatives / Advocates
Provide input on patient-relevant outcomes and acceptable comparators/interventions.
Ensure patient experience data (PED) is incorporated meaningfully through:
Use of disease-specific QoL tools: EORTC QLQ-MY20, FACT-MM
- Anxiety/reassurance metrics related to MRD testing (survey data).
- Qualitative interviews highlighting patient preference for MRD-informed shared decisions.
Validated PROs and qualitative data demonstrating impact of MRD testing and MRDnegCR-based decision-making on QoL and psychological well-being.
HTA Insights Summary on MRD reimbursibility:
Today, the are no treatment guidelines for MRD in real world clinical practice
Lots of work ahead of us:
Implementation & Real-World Evidence: Evidence on clinician adoption, decision support tools, and access to MRD assays:
- Surveys of hematologists’ willingness and barriers to MRD-guided CGDM
- Collect Insights on clinical adoption, feasibility of MRD testing, interpretation of MRDneg
- Conduct surveys/focus groups on MRD utility
- Collaborate on clinical decision support tools
- Educate on MRD assay standardization & CGDM protocols
Meeting @ EMA in Amsterdam with Juan Garcia Burgos, Head of Public and Stakeholder Engagement at European Medicines Agency
COFFEE BREAK / POSTER SESSION
CANADA, CROATIA, CZECHIA, DENMARK, NORWAY, PORTUGAL
THANK YOU TO OUR SUMMIT SPONSORS
REGULATORY LANDSCAPE FOR MYELOMA THERAPIES (EMA PERSPECTIVE)
Andreas Kouroumalis, Scientific Officer, European Medicines Agency
EMA Regulatory Landscape for Myeloma Therapies
Presented by Andreas Kouroumalis Scientific Officer, European Medicines Agency
Disclaimer
The owner of copyright and other intellectual property rights for this presentation is EMA. The information made available in this presentation may be reproduced in accordance with the EMA Legal Notice provided that the source and the author is acknowledged. The presenter does not have any conflict of interests.
Outline
The EU Regulatory Network for Medicines
The Centralised Procedure
Overview of authorised medicinal products for MM
A (complicated) example of the lifecycle of a product
The EU Regulatory Network for Medicines
CHMP Working Parties and Expert Groups
• Advice to CHMP
• in the context of the scientific evaluation of marketing authorisation applications / regulatory procedures
• drafting and revision of scientific guidance documents
• Four Domains: Quality, Non-clinical, Methodology, Clinical
• Working Parties (WPs) have expertise in specific scientific fields and provide advice to the Committees
• Operational Expert Groups (OEGs) provide advice on specific scientific topics and support operational activities of the domain (e.g. Clinical Scientific Advisory Groups – SAGs)
• European Specialised Expert Communities (ESECs) complement the knowledge within the domain by contributing to specific topics and are a source of expertise for the network.
What EMA is not responsible for
• Authorisation of clinical trials
• Pricing or availability of medicines
• Advertising of medicines
• Patents on medicines
• Homoeopathic medicines
• Food supplements and cosmetics
• Develop treatment guidelines or provide medical advice
Outline
The EU Regulatory Network for Medicines
The centralised procedure
Overview of authorised medicinal products for MM
A (complicated) example of the lifecycle of a product
Centralised Procedure – Eligibility
Mandatory Scope - Art. 3(1) Regulation (EC) No 726/2004
ADVANCED THERAPY MEDICINAL PRODUCTS:
Auto-immune diseases and
AIDS Cancer Neurodegenerative disorders
Other immune dysfunctions Viral diseases
Recombinant DNA technology
Controlled gene expression
Monoclonal AB
Since Jan 1995 Gene therapy products Somatic Cell therapy products
Diabetes Orphan medicines
Since Nov 2005
Since May 2008
Tissue engineered products
Optional Scope - Art. 3(2) Regulation (EC) No 726/2004
New Active Substances (as of 20 Nov 2005) Significant Innovation; - Therapeutic, - Scientific, - Technical Interest of Patients at Community Level Art. 3(2)(a) Art. 3(2)(b) “Known substances” OR
Automatic access – Art. 3(3) Regulation (EC) No 726/2004
Generics/hybrids/duplicate of a product authorised via CP
Since Dec 2008
Paediatric medicines - Regulation 1901/2006
MAA including paediatric indication in accordance with a PIP
Paediatric Use Marketing Authorisation (PUMA) Art. 28 Art. 31
Centralised procedure – key elements
• One single MA application to EMA
• Compulsory for most innovative medicines, including rare diseases.
• One assessment procedure (scientific committee’s opinion) based on individual assessments by Member States
• Common decision-making process (one European Commission decision)
• One MA valid in all EU member states and EEA
• Transparent evaluation
Pre-submission activities for Centralised Procedure
Proof of concept
Non clinical studies
Clinical studies
CHMP Opinion on compassionate use (triggered by MSs) M-7
PIP Compliance check
Request for accelerated assessment
Presubmission interaction
Letter of intent to submit Appointment of Rapporteurs
Request Eligibility for Centralised Procedure
Request Invented name review
ATMP certification
Scientific Advice / protocol assistance
Pipeline information
PRIME Designation
SME designation
Paediatric requirements (PIP)
Innovation task force
Orphan designation
ATMP classification
Mandatory steps
Optional steps
Not applicable to all
Centralised Procedure – Overview of assessment process
Validation
List of Questions
Rap/Co-Rap Day 80 AR
Potential additional steps
GMP, GLP, GCP Inspections
Responses
List of Outstanding Issues
Responses
Opinion EC Decision
Pharmacovigilance
Variations
Rap/Co-Rap D150 AR of responses
Rap/Co-Rap D195 AR of responses
Extensions
Renewal
Consultation of Scientific Advisory Group (SAG) or ad hoc expert group, other committees or WP
Oral explanation
Centralised Procedure – Rapporteurs and EMA product team
(Co-)Rapporteurs
• Scientific assessment and evaluation
• Take into account input from Working Parties, SAGs, Ad-Hoc Expert Groups
• Represent the CHMP and PRAC in liaison with applicant
• Presentation to committees if need for discussion
EMA Product Lead
• Primary contact point for applicant, Rapporteurs and EMA team throughout the lifecycle
• Provides procedural, clinical and regulatory science input
• Supports consolidation of a Committees’ position
• Facilitates cross-committees discussions
Where are patients involved?
Public Summaries of Opinion
Designation & Classification
PRE-SUBMISSION
POST AUTHORISATION
Post Marketing procedures
Centralised Procedure – Early access tools
• Enable patients access earlier than usual to promising new medicines addressing public health needs
• EU pharmaceutical legislation provides for early access tools:
Accelerated assessment
Conditional MA
Compassionate use
• EMA initiatives:
PRIME
Rolling review and expedited assessment of COVID-19 treatments or vaccines (during public health emergency)
Accelerated assessment
• For products of major interest from the point of view of public health and in particular from the viewpoint of therapeutic innovation
• What are the unmet needs?
• How the product will address them?
• What is the strength of evidence?
• Request to be submitted and agreed in advance of submitting the MA application
• In accelerated assessment maximum active time 150 days
Impact on procedure
Phase I 120 days
Clock-stop 30 days [Oral explanation]
Phase II 30 days
• Active time reduced to 150 days (120 + 30)
• The CHMP can revert to standard timetable at any time
Conditional Marketing Authorisation (CMA)
Key tool for early access when comprehensive data not yet available
Commission Regulation (EC) No 507/2006
Scope (at least 1)
• Seriously debilitating or lifethreatening diseases
• Emergency situations
• Orphan products
CHMP Guideline on Conditional Marketing Authorisation ( EMA/CHMP/509951/2006, Rev.1 Feb 2016)
Criteria (all)
• Positive benefit-risk balance
• Comprehensive data can be provided after authorisation
• Unmet medical needs will be addressed
• Benefits of immediate availability outweigh the risks
‘unmet medical needs’ means a condition for which there exists no satisfactory method of diagnosis, prevention or treatment authorised in the Community or, even if such a method exists, in relation to which the medicinal product concerned will be of major therapeutic advantage to those affected
CMA framework
Early and temporary authorisation awaiting comprehensive available clinical data* that target seriously debilitating or life-threatening diseases
To balance this temporary uncertainty additional scrutiny
• 1-year validity - Annual renewal
• 6-monthly PSUR cycle
• Information to the public (Summary of Product Characteristics / Package Leaflet)
• MA subject to Specific Obligations (SOBs)
* In emergency situations, also pre-clinical or pharmaceutical data may be less comprehensive
Specific Obligations (SOBs))
• Substantive element -> grant of MA and post-MA
• Feasibility
• Onus on the applicant
• Annual reports on the progress of the SOBs, confirm the B/R based on new available data
• Final objective (average 4 years): get a comprehensive dossier – support the switch to standard MA
• Examples of SOBs:
– Submission of final results from (ongoing) clinical studies:
• Mainly phase 3 studies
• Objectives include efficacy and safety
- Interim results of ongoing clinical studies
- Additional analyses
Orphan Drug Designation: criteria and incentives
RARITY
(prevalence)
SERIOUSNESS
Medical condition affecting not more than 5 in 10,000 persons in the Community
Pre-authorisation incentives
Protocol assistance: Scientific Advice with fee reductions
Extended incentives for small and medium sized enterprises (SMEs)
ALTERNATIVE METHODS
Life –threatening or chronically debilitating
No satisfactory method of diagnosis prevention or treatment of the condition authorised in the Community or, if such method exists, new medicine will be of significant benefit to those affected
Post-authorisation incentives
Priority Access to Parallel Scientific Advice with FDA
Fee reduction / exemption at Marketing
Authorisation Stage (annually reviewed)
Market exclusivity (10 years) (+ 2 if paediatric indication)
Automatic access to EU wide marketing authorisation
What is assessed?
Orphan designation Marketing authorisation
• The condition
• The chronically debilitating and lifethreatening nature of the condition
• The intention to treat the condition (medical plausibility)
• The prevalence <5 in 10,000, see guidance on website
• The significant benefit (if applicable)
• Quality / Safety / Efficacy
• Authorisation within designated condition
• The prevalence
• The significant benefit (if applicable)
Significant benefit
• Unique to the European Orphan Regulation
• Defined as: - a clinically relevant advantage - a major contribution to patient care
Clinically relevant advantage example
Carvykti for treatment of multiple myeloma:
“improved and sustained complete response rates after treatment with Carvykti as compared to Abecma in adult patients with relapsed and refractory multiple myeloma” Based on indirect comparisons.
PRIME scheme - Goals & Scope
Supporting patient access to innovative medicines
Medicinal products of major public health interest and in particular from the viewpoint of therapeutic innovation.
Potential to address to a significant extent an unmet medical need
Reinforce scientific and regulatory advice
Foster and facilitate early interaction
Raise awareness of requirements earlier in development
Optimise development for robust data generation
Focus efficient development
Promote generation of robust and high-quality data
Enable accelerated assessment
Promote generation of high-quality data
Facilitated by knowledge gained throughout development
Multiple Myeloma Medicines Previously in PRIME Scheme
Medicine
JCAR125 ATMP Relapsed/refractory MM after multiple therapies Withdrawn (development discontinued)
CARVYKTI ATMP Adult patients with relapsed/refractory MM Authorised
Blenrep Biological Relapsed/refractory MM with prior treatments Authorised (expired)
CT053 ATMP Relapsed/refractory MM Withdrawn (at applicant's request)
Abecma ATMP Relapsed/refractory MM with prior treatments
Authorised
Elrexfio Biological Multiple myeloma Authorised
Talvey Biological Relapsed/refractory MM (≥3 prior lines)
Authorised
Tecvayli Biological Relapsed/refractory MM (≥3 prior lines) Authorised
EMA regulatory pathways in recent MM approvals
-Full marketing authorisation (FMA): Usually based on RCT against SOC
Rare in recent MM approvals: initial clinical development has focused in late-line SATs
-Conditional marketing authorisation (CMA): Usually based on SAT, renewable yearly until the specific obligation(s) (SOBs) for conversion to FMA are met
SOBs for conditionally approved products can be found in Annex II.E of the SmPC
Most recent approvals in 4L+/5L+ MM are conditional, with the final CSR of the SAT as SOB (to confirm efficacy and provide longer safety follow-up) and/or also a confirmatory RCT vs. SOC in the same or an earlier line
Elrexfio SmPC
The EU Regulatory Network for Medicines
The centralised procedure
Overview of authorised medicinal products for MM
A (complicated) example of the lifecycle of a product
• First multiple myeloma product to be granted PRIME (10/2017)
• Accelerated assessment also granted (11/2019)
• CMA application for the treatment of adult patients with relapsed or refractory multiple myeloma whose prior therapy included a proteasome inhibitor, an immunomodulatory agent, and an anti-CD38 antibody (12/2019)
• DREAMM-2, Phase II interim results: Two dose cohorts, n=221 (97 patients with the applied for 2.5 mg/kg dose)
The initial approval
Favourable Effects
ORR (%) Percentage of participants with a confirmed partial response (PR) or better (i.e., PR, VGPR, CR and sCR, according to the 2016 IMWG Response Criteria by IRC.
DOR, (median, months)
Unfavourable Effects
Time from first documented evidence of PR or better until the earliest date of documented PD per IMWG, or death due to PD
mg/kg
= 97 32 No control arm other than another dose cohort
Median follow up of 12.35 months
95% CI: 4.2, NR
= 97
Risk Management
Healthcare professionals educational materials:
The Summary of Product Characteristics
Corneal adverse reaction guides
Training material including anatomy and physiology of the eye and description of eye exams
Eye care screening sheet to ensure coordinated communication between the haematologist/oncologist and eye care professional
Patient education materials:
The Summary of Product Characteristics and Package Leaflet
Corneal adverse reaction guides
Patient and pharmacy eye drop wallet cards
• Study population: previously treated with at least 2 prior lines of therapy, including 2 consecutive cycles of lenalidomide and a PI (median # of prior lines 4 Blenrep / 3 pom/dex)
• Enrollment for the main study was completed on 25 March 2022
• The cut-off date for the primary analysis of the DREAMM-3 study was 12 September 2022
data was included in Annual re-assessment of the CMA
DREAMM-3
Progression Free Survival
PRIMARY ANALYSIS
HR 1.03 (0.72, 1.47)
Median 11.2 (6.4, 14.5) vs. 7.0 (4.6, 10.6)
Update July 2023
HR 0.90 (0.65, 1.24)
Median 11.2 (6.6, 14.5) vs. 7.0 (4.6, 10.6)
Overall Survival
Planned interim analysis
HR 1.14 (0.72, 1.47)
Median 21.2 (18.7, NE) vs. 21.1 (15.1, NE)
37.5% overall maturity
Update July 2023
HR 1.03 (0.74, 1.43)
Median 22.7 (19, NE) vs. 22.9 (15.9, NE)
48.6% overall maturity
Grounds for refusal of the renewal
Evidence for the use of Blenrep in its approved indication was based on the objective response rate observed in a trial without a reference treatment arm allowing for the isolation of effects on PFS and OS.
Therefore, efficacy was expected to be confirmed in a randomised controlled trial with a relevant reference regimen (DREAMM-3).
However, the primary analysis of the confirmatory study for Blenrep failed to demonstrate clinical benefit in terms of progression free survival or overall survival. Thus, the favourable benefit/risk balance of Blenrep in its approved indication has not been confirmed as required in the setting of a CMA.
Therefore, the CHMP has recommended not to renew the conditional marketing authorisation.
But…
INDUSTRY PARTNER PRESENTATION
REGENERON
WORLD CAFÉ
Myeloma Australia: Patient or Carer Administration of Subcutaneous Therapies – Hayley Beer
Myeloma Canada: Phase 0 – Michelle Oana
AF3M – France: HeMaVie – Eric Battini
Myeloma Australia:
Patient or Carer Administration of Subcutaneous Therapies
Lead, Stakeholder Engagement and Advocacy
Hayley Beer,
World Cafe Subcutaneous therapy self-administration in Australia
GMAN 7 June 2025 - Milan Hayley Beer Myeloma Australia
• Survival rates for myeloma are improving (56% survive years)1
• ~22,000 Australians living with myeloma at any one time2
• 50 new diagnoses each week
• People living with myeloma report financial toxicity and the highest symptom burden3
• Most costly cancer to treat in Australia4
• Significant carer burden
BORTEZOMIB@HOME
• Proteasome inhibitor used in many treatment regimens for MM
• Administration is by 20 second subcutaneous injection
• Average wait time from appointment to delivery was 85 min (range 50 -285)
• A survey of 20 patients in 2015 found that 80% would welcome a home-based program
• Bortezmib@Home program developed incorporating self-administration or GP administration
PATIENT ELIGIBILITY
• Is the patient interested? Or do they have a carer who is happy to learn?
• Does the consultant endorse their entry to the program
TRAINING, RESOURCES &
PETER MAC PROGRAM OUTLINE
Week 1
• Dr review
• Zometa
• Self-admin training
Week 1
Week 1
• Dr review
• Drreview
• Zometa
• Zometa
• Self-admin
• Self-admin training
Week 2
• Self-admin training with nurse
Week 3
• Self-admin training with nurse
Week 4
• Self-admin training with nurse
Week 2
• Phone call review with nurse
• Self-admin
Week 3
• Phone call review with nurse
Week 4
• Phone call review with nurse
• Self-admin
Week 5
• Week off treatment
Week 5
• Week off treatment
WEEKLY NURSE-LED TOXICITY CHECKS
Side effects
Blood result monitoring
Skin reactions
Injection technique
Medication supply
BORTEZOMIB@HOME ACTIVITY
70 patients
~1400 injections = ~1400 hours chair time saved
~$71,000 savings for the hospital
Average 6min per injection vs 4.5 hours in CDU
Reduced costs to patient in parking, petrol and food
et al. The development of a home-based therapeutic platform for multiple myeloma. Expert review of hematology.
doi:10.1080/17474086.2021.2022471
Beer H, Routledge D, Joyce T,
DARA@HOME
• A phase 2 study of the feasibility and efficacy of at home patient administered subcutaneous daratumumab in patients with relapsed multiple myeloma
• Study team: Dr Shafqat Inam, Professor Simon Harrison, Hayley Beer
• Pending micro-costing sub study
PUBLISHED PROGRAMS
PhD STUDY
Establishing barriers and enablers to nurse-enabled, subcutaneous therapy self-administration programs for myeloma patients to inform the development of a national implementation roadmap
Myeloma Canada: Phase 0
Michelle Oana, Chief Mission Officer
Building partnerships beyond the Myeloma Cmmunity
PHASE 0: Enhancing Blood Cancer
Clinical Trial Accrual and EDI in Canada
Changing the Face of Myeloma Research
Myeloma Canada
June 7, 2025 Milan Presented by GMAN
The Big Picture Problem:
How do we get more trials for myeloma patients in Canada, and how can we improve health equity (EDI) and access to them?
Clinical Trials in Canada Portfolio: Trending downward
Canada claims 4% of global trials, ranks 4th in trial sites, leads the G7 in productivity, and is known for skilled researchers and diverse study populations.
Yet….
• In 2022, Canada hosted only 3.1% of global clinical trials (down from 6% in 2010).
• Trials in Canada dropped 19% in 2023 vs. 2022, and 37% vs. 2021.
• Canada is the only G7 country with declining R&D spending as a share of GDP over 20 years.
Operating Costs New Clinical trials in Canada
The clinical trial landscape is changing
The competition is fierce, and the pressure is on
Clinical research is expanding at and exponential rate, creating a global competitive pressure cooker
….and we’re small fish in a big pond
If we don’t adapt, we’ll be left behind.
How do we fix this?
It’s not that simple… and where do we even start?
How it Started….
An idea, sparked by a question
Where it headed…. Building
a powerful network beyond the myeloma walls
Health eMatters IMPACT 2024
Who attended? Everyone who is impacted.
• Key researchers
• Industry partners
• Clinical trial nurses
• Patient advocates
• Hospital administrators
• Clinical Research Organizations
• Research Ethics Boards from key centres
• Health Canada
• Non-profits
• Clinical research coordinators
The outcome?
Then what happened? Phase 0 happened in March 2025
Where are we now?
Initiating a real-world Phase 0 pilot project in myeloma!
Bottom Line…
Broadening partnerships beyond your own community can:
• help everyone achieve shared goals, including your own
• amplify your impact and accelerate your mission
• move farther than you could alone —especially when resources are limited.
AF3M - FRANCE HeMaVie
Eric Battini, Member of the Board
Association Française des Malades du Myélome Multiple
GMAN Summit June 2025
Eric BATTINI Member of the Board
Introduction to AF3M
The French Association of Myeloma Patients
Support
Founded in 2007
Over 2900 members
Partners with IFM
French-speaking Myeloma
Intergroup
A Scientific Committee of 11 members
Awareness
Advocacy
Research
Partnerships
Personalized Phone Support
What is HémaVie™?
A personalized phone support by a nurse for all patients undergoing treatment and their caregivers
10 phone calls over 6 months
Why HémaVie™?
99 % of the time, patients experience the disease at home.
Patients need to be listened and reassured Objectives
Provide psychological and medical support
Development
Methodology
Launched with Celgene in 2016
Pilot phase in 4 hospitals extended to 17 centers
An operator specialized in support to patients outside hospitals
Coordination platform with the medical team
The nurse provides a structured report of the call
The hematologist receives the report and an alert if necessary
600 beneficiairies as of end of 2024
External qualitative analysis
Real emotional and psychological support
Patients are less anxious when meeting their hematologist
Patients are more educated, more active
Lessons learned
Key Takeaways
Introduce time frame flexibility according to the patient’s need (6 month is not always enough)
Allow direct application by patients
Success factors
Develop the project with an operator experienced in this type of support
Communication with hematologists is key: short pitch, meetings with the nurse…
AF3M helps patients become actors of their life with myeloma
DAY 1 CLOSE
Hayley Beer,
Lead, Stakeholder Engagement and Advocacy
Group Photo
Please join us for the 2025 GMAN Group Photo
Michiel Ton will organize the shot
Transportation for Dinner
Please Meet in the Quark Hotel Milano Lobby for Group Transportation to El Brellin Restaurant
If you are planning to transport yourself, please let our team know
Vicolo Privato Lavandai, 20144 Milano MI, Italy
THANK YOU TO OUR SUMMIT SPONSORS
OUR VISION:
A world where every myeloma patient can live life to the fullest, unburdened by the disease.
OUR MISSION:
Improving the quality of life of myeloma patients while working toward prevention and a cure.
IMF Core Values:
These are the core values we bring to accomplishing our mission each day.
Patient Centric
The patient experience is the focus of everything we do. Every interaction is an opportunity to establish a personal connection built on care and compassion which is the basis for continued support.
Respect All
As a team, we value honesty and transparency while creating a culture of mutual respect. We foster a myeloma community built on sincerity, authenticity, and kindness.
Excellence and Innovation
We value accountability, personal responsibility, and a steadfast commitment to excellence. We respect the legacy and reputation of our organization while seeking new solutions and advancements to improve outcomes, quality of life, and access to the best available resources for everyone impacted by myeloma.
Honor differences
We recognize each team member's skills and talents through collaboration and cooperation. Our programs aim to celebrate and support the diversity of our patients and their communities.