Dr. Keith Jarvi’s Exploration of Male Infertility Reveals Broader Implications for Men’s Health
Restrictions Beyond Legality Stop Thinking and Just Start Doing
Access to Abortion Combining Academia, Industry, and Clinical Practice with Dr. Paul Kudlow
INNOVATION IN ACTION
THE CONFERENCE INTEGRATING ARTS AND SCIENCE TO INNOVATE
HEALTHCARE
AUG 30, 2025
10 AM - 4 PM
7 HART HOUSE CIR, TORONTO, ON M5S 3H3
ATTENDEES
IN THIS ISSUE
DESIGN EDITORS:
Stefanie Jinyin Wang (CoDirector)
Nichole Zhou (Co-Director)
Emily Huang
Yu-Wen Jan
Lauren Jones
Jeah Kim
Anaiah Reyes
Incoming Team:
Ravneet Jaura (Co-Director)
Jinny Moon (Co-Director)
Qingyue Guo
Athena Li
Vicky Lin
Josip Petrusa
Raymond Zhang
EDITORS-IN-CHIEF:
Kristen Ashworth
Suraiya Mangra
Nayaab Punjani
Kyla Trkulja
SOCIAL MEDIA TEAM:
Lizabeth Teshler (Director)
Emily Huang, MScBMC
JOURNALISTS & EDITORS:
Aria Afsharian
Tesam Ahmed
Gabriela Blaszczyk
Ilakkiah Chandran
Tiffany Chien
Agustina Crespi
Anthaea-Grace Patricia Dennis
Clarize Donato
Kanak Gupta
Omar Hassan
Rachel Lebovic
Josephine Machado
Sabeeka Malik
Caroline Marr
Madeleine Matthews
Gharaza Nasir
Christina Pereira
Steven Shen
Selina Tang
Kowsar Teymouri
Priya van Oosterhout
Saleena Zedan
Lielle Ronen
Abigail Wolfensohn
PHOTOGRAPHERS:
Katherine Guo
Nancy Kim
Anaiah Reyes, MScBMC
Letter from the EDITORS
Summer 2025 is here, and so is the newest issue of the IMS Magazine!
This issue is dedicated to the complex and evolving world of reproductive health. Our viewpoint articles offer a versatile array of perspectives highlighting some of the most pressing and pertinent challenges in the field. From the “morality tax” of emergency contraception, to the global crisis in abortion accessibility, to the underdiagnosis and undertreatment of women’s reproductive conditions, and the past and current landscape of embryonic stem cell research–all topics encompass both the tensions and breakthroughs changing reproductive science as we know it.
We also explore research in reproductive health currently underway here at the Institute of Medical Science. For this issue, we feature the research of Dr. Mrinalini Balki, an obstetric anesthesiologist at Mount Sinai Hospital, who is exploring the use of oxytocin to train myometrial contractility and ultimately improve maternal outcomes during childbirth. In addition, we highlight the work of Dr. Keith Jarvi, Chief of Urology at Mount Sinai Hospital, whose research is transforming the diagnosis and treatment of male infertility by uncovering its genetic foundations.
Meanwhile, the start of the summer in graduate school is often signalled by thesis defenses and some bittersweet goodbyes to graduating lab mates. At the IMS Magazine, we too must say some longing farewells. Suraiya Mangra, Co-Editor-in-Chief for 2024–2025, and Kiko Huang, Executive Editor, will both be dearly missed as they go on to defend their Master’s this summer. We wish them the absolute best as they embark on exciting new chapters.
As the outgoing Editor-in-Chief, Suraiya leaves behind an enduring legacy at the IMS Magazine–one shaped by dedicated leadership and a deep passion for the work we do. Suraiya had some heartfelt parting words to share:
“At the beginning of my graduate school journey, I never imagined I would have the privilege of sharing my passion for science communication and leading such a talented team of journalists, editors, and designers as IMS Magazine’s Editor-in-Chief. From our record-breaking student and reader engagement to our first successful Fall launch party and OGS workshop, I am thrilled to have contributed to the magazine’s most exciting and impactful year thus far. Most of all, I want to express my gratitude directly to my fellow Co-Editors-in-Chief, Kyla and Kristen, our executive team, contributors, event collaborators, and our IMS faculty: we’ve built such a strong sense of community, and working with you all has truly been the highlight of my IMS experience. Although it feels bittersweet to be closing this chapter as both a graduate student and as an Editor-in-Chief, I’m proud of everything our team has accomplished and I’m excited to see how the IMS Magazine flourishes going forward!” – Suraiya Mangra
With some departures comes an exciting addition to the Editor-in-Chief team: we’re thrilled to welcome Nayaab Punjani, who has been a key member of the IMS Magazine for the past several years. She had some words to share as she steps into this new role:
“When I joined the Institute of Medical Science back in 2020, it was the height of the COVID-19 pandemic—an era of scientific miscommunication and confusion. The IMS Magazine provided an opportunity for me to contribute towards enhancing the lay delivery of research, while also building my scientific writing skills. Starting off as a copy editor, then journalist for feature and spotlight articles, it has been an amazing journey. Watching the IMS Magazine team grow, while also being able to connect with faculty and students and learn about the amazing, diverse translational research we have here at the IMS has been invaluable. I joined the executive team as the Features Executive Editor last year in 2024, having had a taste for the work that goes on behind the scenes to produce each magazine issue. I am excited to be joining Kyla and Kristen as a Co-Editor-in-Chief for the upcoming 2025-2026 academic year and I look forward to seeing the team continue to flourish and grow!” – Nayaab Punjani
Good luck Suraiya! We will miss you so much, but your future is so bright. And welcome Nayaab to the EIC team, we are so lucky to have you.
As always, thank you to all of our journalists and editors for their unwavering hard work on the Summer issue, and to our Design team, for their creativity and care in bringing it to life. We hope you enjoy this issue!
Sincerely,
Suraiya Mangra
Suraiya is a 2nd year MSc student investigating the effects of neuromodulation interventions on brain morphology in patients with neurodegenerative disorders at the Krembil Research Institute under the supervision of Dr. Andres Lozano.
Nayaab Punjani
Nayaab is a PhD student examining a neuroprotective drug therapy for cervicallevel traumatic spinal cord injury at the Krembil Research Institute under the supervision of Dr. Michael Fehlings.
@nayaab_punjani
Kristen Ashworth
Kristen is a PhD student studying the use of a human-based retinal organoid model to investigate cell therapies for genetic eye disease under the supervision of Dr. Brian Ballios at the Krembil Research Institute.
@K_Ashworth01
Kyla Trkulja
Kyla is a PhD student studying the mechanism of action of novel therapies for lymphoma under the supervision of Dr. Armand Keating, Dr. John Kuruvilla, and Dr. Rob Laister.
@kylatrkulja
DIRECTOR’S MESSAGE
CDR. MINGYAO LIU
Director, Institute of Medical Science Professor, Department of Surgery
Senior Scientist, Toronto General Hospital Research Institute, University Health Network
ongratulations to our IMS community on another successful academic year. With the warm summer months comes a time for reflection on the accomplishments of our students, staff, and faculty, and on behalf of IMS, I would like to extend a heartfelt congratulations to everyone for their hard work and achievements. It brings me great excitement to think about what the upcoming year holds for our community—and the prospect of reproducing this year’s success aligns nicely with the Summer 2025 theme of the IMS Magazine on Reproductive Health.
This edition features two IMS faculty members whose research is focused on improving reproductive health for both males and females alike. Dr. Mrinalini Balki is investigating ways of making childbirth safer and more patient-centered, while Dr. Keith Jarvi is striving to uncover treatments for male infertility. It is our pleasure to share their accomplishments with the community in this issue.
We are also pleased to put the spotlight on three outstanding individuals within the IMS community that have made impacts beyond their research. Dr. Jennifer Rabin shares her journey into academia as a female scientist and the initiatives she has pioneered to foster support among women in the field. Dr. Paul Kudlow, an IMS alum, discusses how he strategically combined his passions for medicine and investment banking to become CEO of a venture capital firm. Lastly, Shaghayegh (Feri) Boroojeni underlines her journey into IMS as an international student and how she found community through student-led initiatives, eventually leading to her winning the Jay Keystone Memorial Award for IMS MedDash.
Additionally, this issue shares the highlights of our annual IMS Scientific Day, the community’s favourite celebration of the hard work and accomplishments of our students, faculty, and alumni. On behalf of the IMS community, I extend my warmest congratulations to the new faculty joining IMS and members who have received promotions this year.
This edition also marks my final Director’s Message for the IMS Magazine. It has been an honour and a privilege to be a part of such a talented community here at the IMS, and I have enjoyed using each issue of the IMS Magazine to highlight the incredible people that make our department so impactful in the lab and beyond. I have been involved with the Magazine since 2012 as Associate Director of IMS, 2014 as Interim Director, and 2015 as Director, and have enjoyed reading every issue—especially the IMS50 Special Edition in 2018 and Student Life Special Edition in 2024. I have cherished working with the students that make up the IMS Magazine team, and it has been a delight to recognize their hard work in the letters of support I have written as part of their scholarship and medical school applications over the years. It has been a treasured experience to witness their great success in graduate school and throughout their career development, and I am incredibly proud to be a part of the team here at the IMS Magazine.
I would like to thank Suraiya Mangra for her contributions to the IMS Magazine as Editor-in-Chief as she transitions into her career, and welcome Nayaab Punjani as incoming Editor-in-Chief. As well, I would like to thank our returning Editors-in-Chief, Kristen and Kyla, as well as the dedicated journalists, editors, photographers, and design team for their exceptional work in bringing this issue of the IMS Magazine to life.
Lastly, I would like to thank our talented students, faculty, and staff that make up the IMS community for making my last 10 years as Director so memorable and full of pride. It has been an honour, and I look forward to seeing what’s next for our incredible members.
Sincerely,
Dr. Mingyao Liu Director, Institute of Medical Science
Photo Credit: Mikaeel Valli
Contributors Summer 2025
Beatrice Acheson is a first-year MSc student working under the supervision of Dr. Peter St George-Hyslop at the Tanz Centre for Research in Neurodegenerative Disease (CRND), where she investigates the genetic and molecular mechanisms underlying microglial dysfunction in Alzheimer’s Disease. When she is not in the lab, Beatrice is likely reading a book, attending a yoga class, or playing beach volleyball. bea.acheson
Aria Afsharian a first-year MSc student at St. Michael’s Hospital under Dr. Andras Kapus. His research focuses on cell biology, specifically the role of signalling proteins in the antiviral immune response. Apart from the lab, Aria enjoys drawing, reading and working out.
Jasmine Amini is a first-year MSc student working under the supervision of Drs. Daphne Korczak and Samantha
Anthony at the Hospital for Sick Children. Her research interests lie in social media use and family functioning among youth with an acute self-harm or suiciderelated concern. Outside of academia, Jasmine enjoys reading, volunteering, and exploring Toronto.
Tiffany Chien is a PhD student in the Department of Medical Biophysics working at the Mouse Imaging Centre. Under the supervision of Dr. John Sled & Dr. Jason Lerch, her research aims to investigate how maternal autoantibodies affect offspring brain and behavior development. She is also a science writer for RawTalk Podcast. In her free time, she enjoys reading, baking, solving puzzles & board games, and being outdoors with her husband and golden retriever. tiffanycblum
working under the supervision of Dr. Daniel Felsky at the Centre for Addiction
structural and functional brain changes and genetic factors to influence trajectories of psychosis in youth. Outside of the lab, Tesam loves to read, enjoy nature, and spend time with friends.
and Dr. Jiwon Oh at
the end goal of understanding early disease and the development of a prognostic test to
time, Gabriela volunteers as a ski patroller and loves to try new foods around the city. gabi.blaszczyk
Ilakkiah Chandran is a 3rd year PhD Candidate at IMS, supervised by Dr. Danielle Andrade at the Adult Genetic Epilepsy Program. Her research explores the genotype and phenotype of rare genetic epilepsies in adults, focusing on how their features evolve with age. In her free time, she enjoys reading, going on impromptu adventures and tuning into some true crime!
Kevan Clifford is a PhD student in the IMS program, working under the supervision of Dr. Yuliya Nikolova at the Centre for Addiction and Mental Health. His research combines bioinformatics and neuroimaging approaches to characterize shared risk pathways between brain aging and psychiatric illnesses. Outside of the lab, Kevan enjoys trail running, photography, and a good book (preferably while curled up with his cat, Rauru).
Omar I. Hassan is a MSc student transferring to PhD in the laboratory of Dr. Michael Fehlings. He studies neuromodulatory and regenerative strategies in spinal cord injury and has a particular focus on translation from laboratory to clinic. Currently his work is focused on restoring chloride homeostasis through repurposed pharmacological agents. Outside of the lab, he enjoys horology, falconry and yapping over election politics. omar_hassan1535
Graphic design by Nichole Zhou
jasmine_amini9
Kiko Huang is a second-year MSc student, currently studying glaucoma through an epidemiological lens under the supervision of Dr. Yaping Jin. Her work aims to investigate various trends in ophthalmology and vision care to gain a better understanding of the health landscape and guide policy. During her free time, she’s likely out exploring all the food that the city has to offer (recommendations appreciated)!
kikohuangs
Alyona Ivanova is a PhD student investigating the molecular signature of glioblastoma using spatial -omics technologies at the Hospital for Sick Children under the supervision of Dr. Sunit Das. Alyona is a professional figure skater and a model. Alyona is a creative content manager of Panoramics - A Vision. She enjoys traveling, cooking, and reading.
_alyonaivanova_
Josephine Machado is a first-year MSc student working under the supervision of Dr. Andrea Knight at The Hospital for Sick Children. Her research is focused on examining the neuropsychiatric impacts of childhood-onset systemic lupus erythematosus (cSLE) through the study of brain-aging in children with the condition. Outside of research, Josephine enjoys reading, playing the piano, nature walks, and volunteering.
Sabeeka Malik is a first-year MSc student at the SickKids Research Institute, working under the supervision of Dr. Andreas Schulze. Her research aims to determine effective substrate reduction therapy drug candidates for Mucopolysaccharidosis III (Sanfilippo Syndrome), a lysosomal storage disease. Outside of the lab, Sabeeka enjoys reading and playing card games with her friends.
Gharaza Nasir is a first-year MSc student at the Toronto General Hospital Research Institute, working under the supervision of Dr. Arndt Vogel. Her research utilizes patient-derived xenograft (PDX) models to investigate tumour dynamics and evaluate potential therapeutic strategies for Cholangiocarcinoma. In her free time, Gharaza enjoys working out, playing video games, and spending time with friends and family.
g.harazanasir
Kowsar Teymouri is a third-year PhD student working under the supervision of Dr. James Kennedy at the Centre for Addiction and Mental Health (CAMH). Kowsar is investigating the role of the immune system genes in schizophrenia and how they are associated with different subgroups of schizophrenia. If not at CAMH, you can find Kowsar running along the lakeshore, creating content for her travel blog, hiking in new trails or painting.
kowsar_teymouri
Priya van Oosterhout is a firstyear MSc student working under the supervision of Dr. Yuliya Nikolova at the Centre for Addiction and Mental Health (CAMH). Priya is investigating how substance use disorders affect the way in which the brain ages, as measured by MRI data. In her free time, she enjoys trying new food, watching movies, or going on hikes.
priya.vo
Photography Team
Katherine Guo is a first-year MSc student working under the supervision of Dr. Shannon Lange at the Centre for Addiction and Mental Health. Her work focuses on patterns of alcohol consumption and its related harms, aiming to better-understand the association between alcohol consumption and suicide mortality. Outside of her academics, Katherine spends her time working on various graphic design projects, taking photos, and exploring the wildlife in and outside of the city.
Copy Editors
Agustina Crespi
Anthaea-Grace Patricia Dennis
Clarize Donato
Kanak Gupta
Rachel Lebovic
Caroline Marr
Madeleine Matthews
Christina Pereira
Steven Shen
Selina Tang
Saleena Zedan
Nancy Kim is a first-year MSc student under the supervision of Dr. Amanda Boyle at the Center of Addiction and Mental Health. Her research focuses on neuroinflammation in different brain tumours originating from glial cells. She uses PET neuroimaging and histology studies to quantify neuroinflammation for early diagnosis and staging of these tumours. Outside of her research, she enjoys playing volleyball, exploring restaurants (mostly ramen places) and cafes (especially for matcha) near campus.
Social Media Team
Lizabeth Teshler (Lead) is a PhD student supervised by Dr. Brian Feldman at The Hospital for Sick Children. Her research investigates how to improve the clinical examination of musculoskeletal health for people with Hemophilia. Outside of research, she loves biking, spending time outdoors, and exploring new cities.
Lielle Ronen is a first-year MSc student in Dr. Andrew Sage’s Lab at the Latner Thoracic Surgery Research Labs in PMCRT. Her research investigates smoking damage in donor lungs to improve post-transplant outcomes using Ex-Vivo Lung Perfusion (EVLP). Aside from research, she loves painting, baking, running and trying local restaurants in Toronto.
Abigail Wolfensohn is a first-year MSc student in Dr. Mojgan Hodaie’s lab at Toronto Western Hospital. She is researching how the brain’s wasteclearance system functions in people with trigeminal neuralgia, a chronic facial pain condition. In her free time, she enjoys outdoor activities, puzzles, trying new restaurants, and playing the piano. abbywolfen
IMS Design Team
The IMS Design Team is a group of second year MSc students in the Biomedical Communications (BMC) program. Turning scientific research into compelling and effective visualizations is their shared passion, and they are thrilled to contribute to the IMS Magazine.
Exploring Myometrial Function to Improve Maternal Outcomes
By Gharaza Nasir and Sabeeka Malik
Every year, thousands of women around the world experience life threatening bleeding following the birth of their children. In 2023, an estimated 260,000 women worldwide died from childbirth, with the leading cause of death being postpartum hemorrhaging (PPH).1 PPH is defined as more than 500 mL of maternal blood loss in the first 24 hours after childbirth.2 One of the main causes of PPH is uterine atony, which refers to the failure of the uterus to contract. Normally during childbirth, following delivery of the placenta, the uterus contracts to compress the blood vessels that are left at the utero-placental interface. If the uterus fails to contract, these blood vessels remain open and bleed freely, potentially leading to severe hemorrhage.2
To combat this, uterotonic medications are administered to stimulate uterine contraction and are critical in the prevention and treatment of PPH. However, large doses of uterotonics, such as oxytocin and carbetocin, can lead to adverse side effects, including nausea, hypotension, and myocardial ischemia.2,3,4 This raises a key question: what is the optimal dosage of uterotonics that effectively manages PPH while minimizing the risk of adverse effects?
This is what Dr. Mrinalini Balki aims to answer through her research. Dr. Balki moved to Canada to pursue fellowships in Toronto, after completing her medical training in India. She is now a professor in the Departments of Anesthesia, Obstetrics and Gynaecology, and Physiology at
the Temerty Faculty of Medicine at the University of Toronto and is a staff anesthesiologist at Mount Sinai Hospital.
While doing her obstetric anesthesia fellowship, Dr. Balki came across a triennial report from the Confidential Enquiries into Maternal Deaths in the United Kingdom, which documented two deaths following an excessive administration of oxytocin.5 Through preliminary clinical research, Dr. Balki and her team determined that only 0.5 units of oxytocin were needed to elicit a uterine response–significantly lower than the then-standard dose of 10 units. Their findings played a monumental role in decreasing the standard dosage of oxytocin to 0.5-1 units for scheduled cesarean deliveries.6 This pivotal study further prompted her team to investigate the potential negative effects associated with higher doses of oxytocin.
One adverse effect of administering excessive dosage of oxytocin during labour is a phenomenon known as desensitization.2,3 This oxytocin-induced desensitization typically occurs following prolonged use of oxytocin for labour augmentation and can lead to labour arrest, often necessitating an emergency C-section. Through clinical investigation, Dr. Balki found that patients who had become desensitized to oxytocin bled excessively, posing a barrier to further study this phenomenon in a clinical setting. Her team moved their research to the lab to better study this occurrence and the relationship between uterotonics and uterine contractility.
At first, Dr. Balki worked with animal models and successfully showed how rodent myometrial tissue (muscular layer of the uterus) responded best to oxytocin in comparison to other utertonics.7 Building on these findings, Dr. Balki and her team then moved to study human uterine muscle contractility using an organ bath system.7,8 This technique involves immersing small pieces of myometrium in a warm oxygenrich solution that replicates the natural environment of the human body.9 Based on insights from these pre-clinical studies, Dr. Balki proposed uterotonic dosing strategies tailored to different patient groups. She also developed the standardized “Rule of Threes” protocol, now widely used worldwide in the clinical management of PPH.10
The “Rule of Threes” protocol guides clinicians in determining the appropriate amount of uterotonics for the prevention and treatment of PPH, particularly in high stress clinical situations. Physicians rely on two clinical measures to determine the best course of action for patients as outlined in the protocol. The first is determining the uterine contractility, which is assessed by physically examining the uterine tone in response to the drug. The second measure is the extent of uterine bleeding, which is determined by a decrease in hematocrit levels (red blood cell count) or by direct measurement of blood loss. These factors, when considered together, allow Dr. Balki and other clinicians to determine the appropriate dosage of uterotonics to meet each patient’s specific needs.
Dr. Balki has been a pioneer in translating her research findings into clinical practice, and particularly, in shaping clinical guidelines involving oxytocin dosing.3,11 “As much research as we do, it holds little value unless it leads to changes in clinical practice,” Dr. Balki highlights. Her work has not only influenced protocols at Mount Sinai Hospital but has also had an international impact.
Obstetrics has advanced significantly from decades ago, when labour pain was considered a natural burden, and women had no access to pain relief during childbirth. Now, it is a prioritized focus of maternal care. Building on this progress, Dr. Balki envisions a future where women’s health is prioritized globally. Despite strides made in recent years, she emphasizes that there is still lots of work to be done, particularly in uncovering the mechanisms behind oxytocin-induced desensitization
and addressing other complex challenges in women’s health. In addition to her work on PPH and oxytocin desensitization, she and her team also pioneered the use of procedural spinal ultrasound to more accurately identify the epidural space. This enhances both the safety and success rate of epidural placement for patients with a high body mass index or challenging spinal anatomy requesting labour analgesia.12 Her team also supports highly specialized fetal surgery programs that allow fetuses to be treated in utero. These procedures can correct or prevent complications early in development, providing the fetus with a better chance at a healthy outcome.
Dr. Balki’s work impacts various facets of obstetrics, and she hopes to continue exploring other ways to improve both fetal and maternal health outcomes.
As the only lab in Canada dedicated to myometrial contractility, Dr. Balki hopes to collaborate with experts nationally and globally to expand the scope of her research. She aims to incorporate more proteomics in her pre-clinical work to begin uncovering the molecular pathways involved in uterine muscle function and desensitization. Beyond reproductive health, her team’s desensitization model may be adapted to study contractility of smooth muscle in other systems, expanding the impact of their work beyond obstetrics. Aside from research, Dr. Balki is deeply committed to knowledge translation and is actively involved in obstetric anesthesia education at Mount Sinai Hospital and the University of Toronto.
Overall, Dr. Balki’s work exemplifies how deeply rooted scientific inquiry can lead to meaningful improvements in maternal care. By bridging the gap between bench research and bedside practice, her lab continues to shape the future of obstetrics. As her team pushes the boundaries of knowledge, the potential for broader impact across women’s reproductive health is only just beginning to unfold.
References
1. World Health Organization. Maternal mortality. 2025. Available from https://www.who.int/news-room/fact-sheets/detail/maternal-mortality#:~:text=Overview,most%20could%20have%20 been%20prevented
2. Gallos I, Williams H, Price M, et al. Uterotonic drugs to prevent postpartum haemorrhage: a network meta-analysis. Health Technology Assessment. 2019; 23(9).
3. Carvalho JC, Balki M, Kingdom M, et al. Oxytocin Requirements at Elective Cesarean Delivery: A Dose-Finding Study. Obstetrics and Gynecology. 2004; 104(5): 1005-1010.
4. Moran C, Bhuinneain M, Geary M, et al. Myocardial ischaemia in normal patients undergoing elective Caesarean section: a peripartum assessment. Anaesthesia. 2008; 56(11): 1051-1058.
5. Crowhurst JA, Plaat F. Why mothers die-report on confidential enquiries into maternal deaths in the United Kingdom 1994-96. Anaesthesia. 1999; 54(3): 207-9.
6. Osilla EV, Patel P, Sharma S. Oxytocin. In: StatPearls [Internet]. 2025 Jan. Available from https://www.ncbi.nlm.nih.gov/books/ NBK507848/
7. Balki M, Cristian AL, Kingdom J. Oxytocin pretreatment of pregnant rat myometrium reduces the efficacy of oxytocin but not of ergonovine maleate or prostaglandin F2 alpha. Reprod Sci. 2010; 17(3): 269-77.
8. Balki M, Ramachandran N, Lee S, et al. The Recovery Time of Myometrial Responsiveness After Oxytocin-Induced Desensitization in Human Myometrium In Vitro. Anesth Analg. 2016: 122(5): 1508-15
9. Upchurch WJ, Iaizzo PA. In vitro contractile studies within isolated tissue baths: Translational research from Visible Heart Laboratories. Exp Biol Med. 2022: 247(7): 584-597.
10. Balki M, Tsen L. Oxytocin Protocols for Cesarean Delivery. International Anesthesiology Clinics. Spring. 2014: 52(2): 48-66.
11. Balki M, Ronayne M, Davies S, et al. Minimum oxytocin dose requirement after cesarean delivery for lavor arrest. Obstet Gynecol. 2006: 107(1): 45-50.
12. Balki M. Locating the epidural space in obstetric patients - ultrasounds a useful tool: continuing professional development. Can J Anaesth. 2010: 57(12): 1111-26.
Dr. Mrinalini Balki Senior Clinician Scientist, Lunenfeld Tenenbaum Research Institute, Sinai Health System
Photo Credit: Dr. Mrinalini Balki
Through the Looking Glass:
Dr. Keith Jarvi’s Exploration of Male Infertility Reveals Broader Implications for Men’s Health
By Beatrice Acheson
Infertility, like many other reproductive health topics, tends to centre around female issues, but recent statistics compel us to think otherwise. Infertility affects around 15 to 20% of couples, and male factors account for nearly a third of these cases.1 Despite the prevalence of male infertility, it is often neglected, with most resources directed toward female treatments, leaving men underdiagnosed and undertreated. Dr. Keith Jarvi, a clinician scientist at Mount Sinai Hospital and professor at the Institute of Medical Science, has devoted his career to addressing this disparity by developing male-focused diagnostics and treatments while also uncovering how infertility may serve as an indicator of overall health.
“There are a vast number of resources for women with infertility, and large numbers of clinics, but there are fewer doctors offering fertility care for men,” says Dr. Jarvi. “Care for infertility is skewed toward female treatments.” This skew has prompted the development of malefocused fertility programs. In collaboration with urologists Dr. Kirk Lo and Dr. Ethan Grober, Dr. Jarvi directs The Murray Koffler Urologic Wellness Centre. The centre, which operates between Mount Sinai and Women’s College Hospital in Toronto, provides nearly all services available for the diagnosis and treatment of male infertility.
Dr. Jarvi is not only working to improve access to care; he is transforming the way infertility is diagnosed and treated in
male patients. He describes the current treatment landscape, explaining that there are two avenues available: “you can treat the men with infertility, or you can manage the couple’s infertility,” Dr. Jarvi says. Treatments, such as corrective surgeries or hormonal therapies, address the root cause of male infertility in hopes of improving sperm quality or other parameters. Management, in contrast, focuses on helping couples conceive through assisted reproductive technologies like in vitro fertilization and sperm banking.2
Choosing between “treating” or “managing” male infertility depends largely on its underlying cause, which is not always easy to identify. Male infertility may result from acquired factors, like testicular trauma, infection, and exposure to toxins; or, it may be attributable to congenital factors, including developmental alterations, genetic abnormalities, and hormonal imbalances.3 Adding to the complexity, acquired and congenital factors do not produce uniform changes across individuals, and may have variable effects on sperm parameters like motility, morphology, or number.4
Dr. Jarvi is working with this heterogeneity, rather than against it, to develop personalized treatment paradigms. Dr. Jarvi has identified testicular proteins in semen that may predict the underlying cause of male infertility, simplifying diagnoses and eliminating the need for invasive procedures like testicular biopsies.5 With collaborators at the
Cleveland Clinic, Dr. Jarvi developed a model to predict changes in semen parameters following surgical repair of varicocele, an enlarged vein in the scrotum affecting sperm production.6 The tool is now widely used in clinics and helps determine which patients will benefit from surgical intervention, meaning fewer invasive procedures and more hopeful outcomes. Dr. Jarvi is committed to shifting the treatment and diagnostic landscape for male infertility toward personalized approaches.
Dr. Jarvi isn’t stopping there; he intends to build on his work with biomarkers and propel the field of male infertility into a new era of precision medicine. To do so, he is studying the genetic contributions underlying male infertility. Like many conditions, male infertility is attributable to both environmental and genetic factors. Further elucidating the genetic underpinnings of male infertility will provide opportunities for more precise diagnoses, personalized treatment options, and predictive medicine aiding in early intervention and preventive health planning.
Dr. Jarvi’s fascination with the genetic etiology of male infertility began over 20 years ago, when Dr. Lap-Chee Tsui, discoverer of the genetic defect that causes cystic fibrosis (CF), asked Dr. Jarvi to examine his patients for a missing vas deferens—the duct that transports sperm to the urethra. Its absence is an irreversible cause of male infertility.
Dr. Keith Jarvi, Clinician Scientist at Mount Sinai Hospital, IMS professor, and Director of the Murray Koffler Urologic Wellness Centre
Dr. Keith Jarvi is turning to genetics to understand the link between male infertility and other men’s health issues.
Dr. Jarvi agreed on the condition that Dr. Tsui also sequence the genes of his patients, suspecting his patients with no vas deferens may be carriers of the CF mutation. An unlikely collaboration was born. In 1998, they published an article demonstrating the association between CF mutations and the absence of the vas deferens. The findings transformed clinical practice and prompted increased genetic screening and counseling for men with infertility.7 For the first time, infertility was used as a window into broader implications for men’s health.
CF is not the only genetic condition related to male infertility. Dr. Jarvi and others have identified potential associations between male infertility and other common men’s health problems, including prostate cancer, colon cancer, and melanomas.8-10 In his latest project, Dr. Jarvi is collaborating with geneticists Dr. Steve Scherer and Dr. Christian Marshall to uncover the genetic link underlying these associations. By integrating seminal biomarker data with genetic analysis, Dr. Jarvi hopes to identify predictors of infertility and related hereditary conditions, like cancer.
According to Dr. Jarvi, “examining genetic predisposition is probably the best shot we have at understanding the longterm risks of infertility… [and] the other health risks that men with infertility or their children may experience.” Dr. Jarvi is harnessing his own expertise and the expertise of his collaborators to promote a more comprehensive approach to treating male infertility and the diseases that often arise with it.
The benefits of understanding the genetic link between male infertility and other conditions are two-fold. First, the knowledge will enhance our current understanding of the pathways and mechanisms that underly male infertility, potentially unlocking novel pharmacological strategies for treatment and management. Second, it will provide crucial insight that may reshape the current standard of care for male infertility
and related health issues. Through decoding the relationships between male infertility and other hereditary conditions, Dr. Jarvi is laying the groundwork for precision medicine that extends beyond reproduction. To do so, he is leveraging his expertise and capitalizing on his propensity for collaboration, thereby ushering in a more informed and holistic approach to treating male infertility and related conditions.
References
1. Witherspoon L, Flannigan R. Male factor infertility: Initial workup and diagnosis in primary care. Can Fam Physician. 2021;67(4):248–54.
2. Agarwal A, Baskaran S, Parekh N, et al. Male infertility. The Lancet. 2021;397(10271):319–33.
3. Brannigan RE, Hermanson L, Kaczmarek J, Kim SK, Kirkby E, Tanrikut C. Updates to Male Infertility: AUA/ASRM Guideline (2024). J Urol. 2024 Dec;212(6):789–99.
4. Eisenberg ML, Esteves SC, Lamb DJ, et al. Male infertility. Nat Rev Dis Primer. 2023;9(1):1–22.
5. Drabovich AP, Jarvi K, Diamandis EP. Verification of male infertility biomarkers in seminal plasma by multiplex selected reaction monitoring assay. Mol Cell Proteomics MCP. 2011;10(12):M110.004127.
6. Samplaski MK, Yu C, Kattan MW, et al. Nomograms for predicting changes in semen parameters in infertile men after varicocele repair. Fertil Steril. 2014;102(1):68–74.
7. Jarvi K, McCallum S, Zielenski J, Durie P, Tullis E, Wilchanski M, et al. Heterogeneity of reproductive tract abnormalities in men with absence of the vas deferens: role of cystic fibrosis transmembrane conductance regulator gene mutations. Fertility and Sterility. 1998 Oct 1;70(4):724–8.
8. Eisenberg ML, Li S, Brooks JD, et al. Increased Risk of Cancer in Infertile Men: Analysis of U.S. Claims Data. J Urol. 2015;193(5):1596–601.
9. Walsh TJ, Croughan MS, Schembri M, et al. Increased Risk of Testicular Germ Cell Cancer Among Infertile Men. Arch Intern Med. 2009;169(4):351–6.
10. 10. Walsh TJ, Schembri M, Turek PJ, et al. Increased risk of high-grade prostate cancer among infertile men. Cancer. 2010;116(9):2140–7.
Photo Credit: Susan Lau
Master of Science in Biomedical Communications
Master’s Research Project
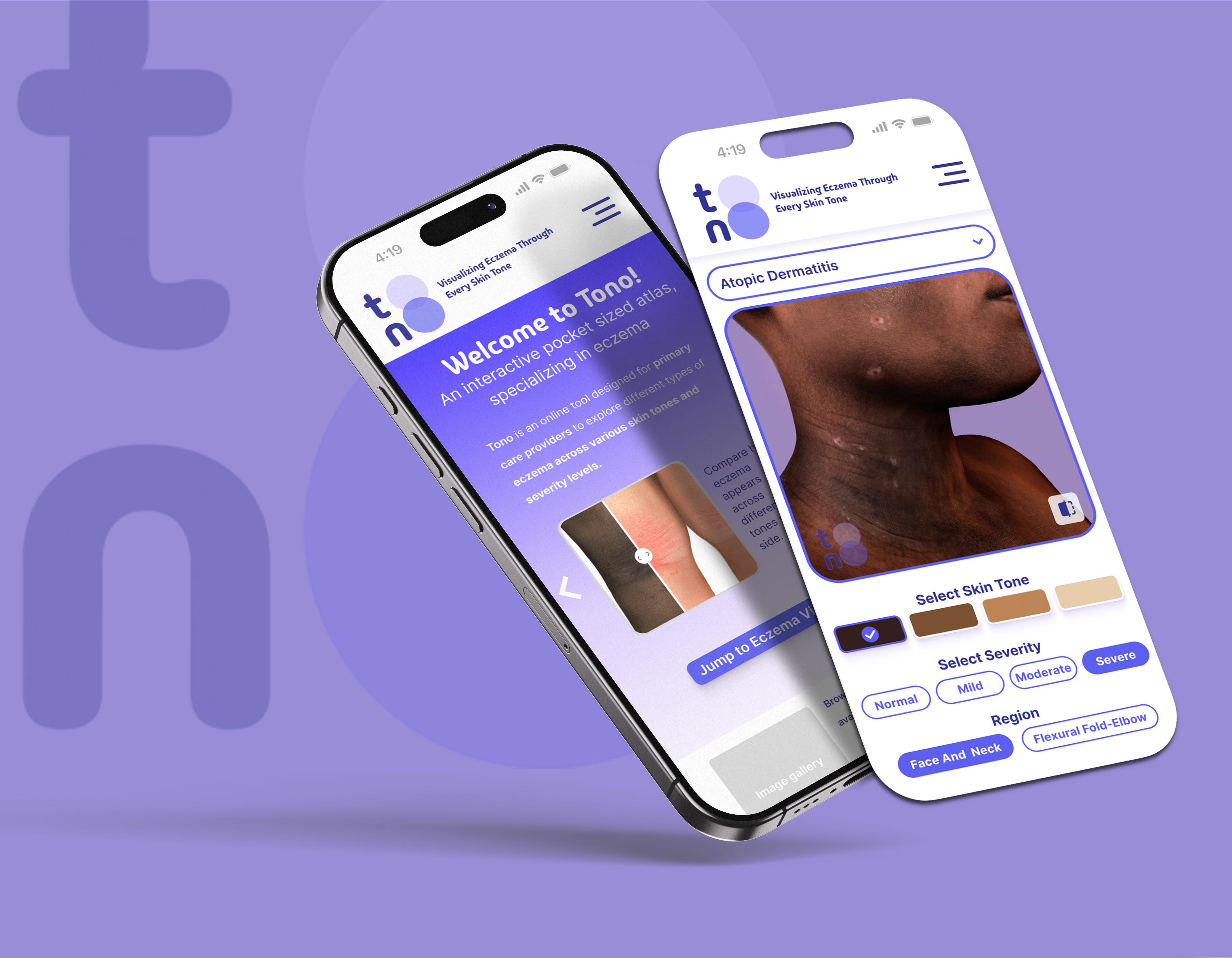
Tono: Visualizing Eczema Through Every Skin Tone
In dermatology, there is an urgent need for diverse dermatological resources, as traditional medical references often lack adequate representation of conditions on darker skin. TONO is a mobileaccessible virtual reference, designed to help primary care practitioners recognize eczema across all skin tones and severities. Where photography falls short, due to lighting, variability, or limited image availability, TONO uses consistent, medically accurate illustrations to depict key features across a spectrum of presentations, helping to fill a critical gap in medical education and support more equitable care.
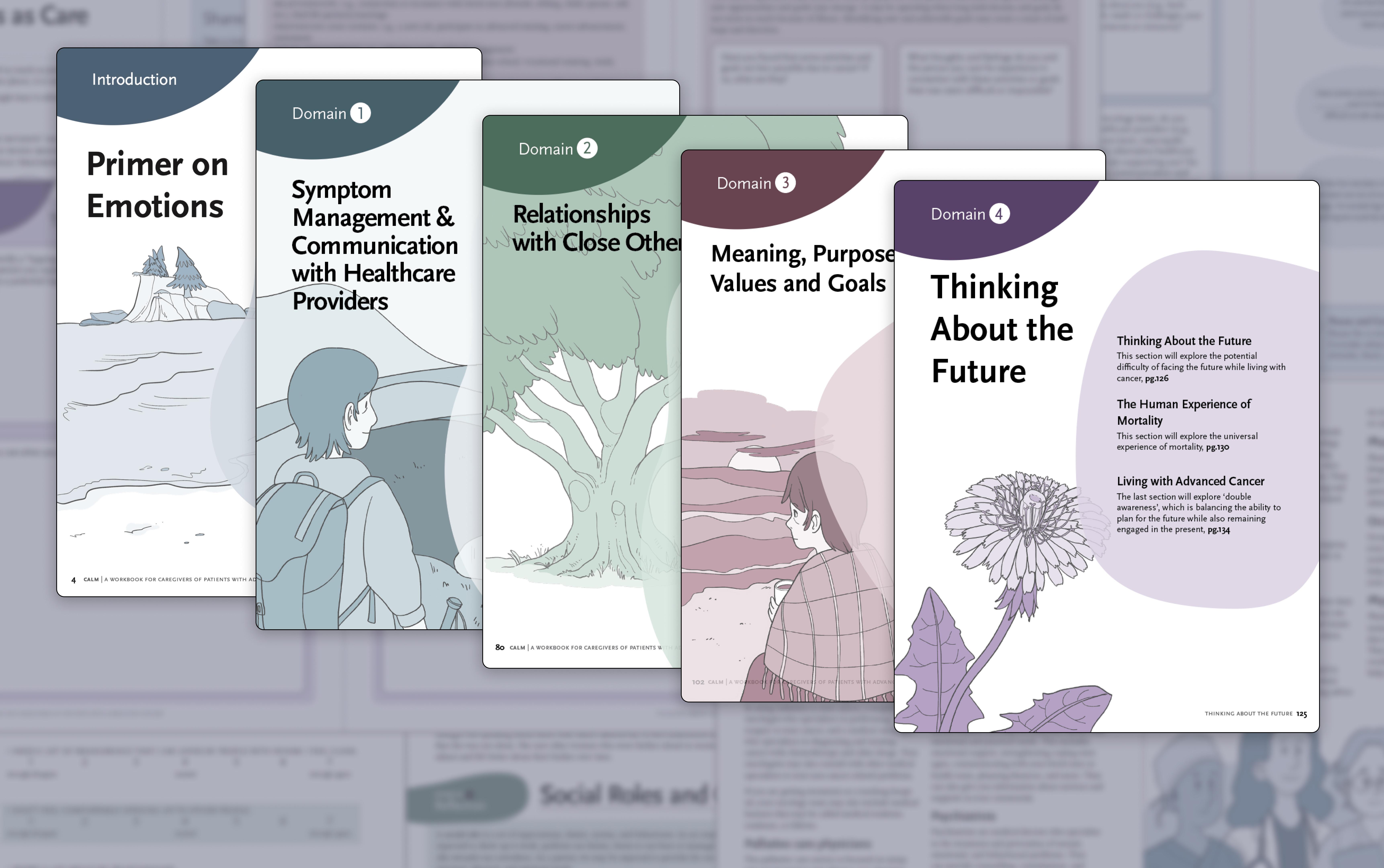
Master’s Research Project CALM for Caregivers: A Workbook for Caregivers of Patients with Advanced Cancer
The mental and physical impact of a cancer diagnosis on the patient’s caregiver is often overlooked. CALM for Caregivers is a comic-based workbook that will facilitate greater caregiver awareness, knowledge, and confidence in themselves and their care. Through the use of empathetic and carefully crafted comics and illustrations, this workbook serves to support caregivers of patients with advanced cancer.
Emily Huang
Naomi Clay Rodríguez
Master’s Research Project
The Family/Friends of Individuals at Risk of Suicide Training (FIRST) Program: An Explanatory 2D Animation
This 2D animation follows the journey of three character pairings, to communicate the need for and benefits of the FIRST Program—a novel gatekeeper training (GKT) initiative tailored for the family and friends of individuals at risk of suicide. Unlike traditional GKT programs, FIRST addresses the emotional and practical needs of caregivers, whose specific needs are left
unmet by existing suicide prevention training programs. The video aims to engage potential funders, securing support for implementation
while highlighting the program’s potential to reduce healthcare strain through communitybased suicide prevention.
Yu-Wen Jan is a graduate student in Biomedical Communications at the University of Toronto, with a background in Life Sciences and two years of plant science research experience at Academia Sinica in Taiwan. Her interest in visual storytelling grew during her lab work, where she was motivated to bridge scientific knowledge gaps through visuals. Now specializing in biomedical visualization, Yu-Wen transforms complex concepts into clear, engaging content using 2D/3D illustration, motion graphics, and interactive media. She is passionate about collaborating with scientists to communicate research effectively, making science more accessible to both expert and general audiences.
Coursework
Island Micro-Heroes: How mycorrhizal fungi help repair coastal ecosystems
Shubhreet Kaur Johal
Yu-Wen Jan
Graphic design by Nichole Zhou
From Diagnostic Challenges to Medical Gaslighting:
The Difficult Reality is that Women’s Reproductive Conditions are Underdiagnosed
By Kyla Trkulja
Intense, throbbing abdominal pain filled my winter holiday in 2024. It was a strange kind of pain that I’ve never experienced, despite having menstrual cramps nearly every month. After almost fainting at Christmas dinner one week after the pain started, my fiancé took me to the emergency room. When the doctor came in, he didn’t even try to hide that he felt like I was wasting his time. He said my bloodwork looked normal, and these were just menstrual cramps, despite me insisting that I’ve experienced those cramps for 12 years and I knew that this was something different.
After advocating for myself, he reluctantly ordered an ultrasound and CT scan, which revealed that I had an infection in my upper reproductive tract known as pelvic inflammatory disease (PID). The doctor told me this was usually caused by a sexually transmitted infection (STI), which confused me given that my screening panel came back clean, but he barely stayed in the room long enough to prescribe me antibiotics, let alone answer my questions. I got my prescription and was told I would feel better in a few days.
I was in pain for over four months. I visited the emergency room five times during this period, as the doctors said to return “if the pain didn’t go away.” Each time I went, I had to answer the same questions, get another ultrasound, and undergo bloodwork, eventually
culminating to doctors telling me they didn’t know why I was still in pain before sending me home. Four months later, I finally saw a gynecologist who made everything make sense. A small portion of cases of PID are simply due to chance, not STIs,1 and women are often in chronic pain for weeks to months. Although I wasn’t thrilled that I had some bad luck, I was relieved to finally be validated and to get some assurance that the symptoms I was experiencing were legitimate. However, this quickly turned to anger when I thought about that first doctor’s dismissal who so brazenly told me this was nothing, and all the subsequent doctors who made me believe that the pain was all in my head when the imaging came back normal.
Unfortunately, situations like these are far too common among women, with conditions affecting the reproductive tract frequently being under- or misdiagnosed. Overlapping symptoms and imaging limitations make their diagnosis challenging,1 while medical gaslighting from physicians and other healthcare professionals can result in symptoms not being taken seriously. In addition to the negative impact on a woman’s quality of life, underdiagnosis can have serious, longterm consequences. In the case of PID, letting inflammation go untreated can lead to ectopic pregnancies, infertility, and chronic pelvic pain due to reproductive organs adhering to each other, or other
organs such as the liver.1,2 Misdiagnosis can therefore have severe consequences that can permanently worsen a patient’s life, making it even more frustrating when medical professionals are quick to dismiss the symptoms.
PID is just one of many reproductive conditions that can result in a delayed or misdiagnosis. Polycystic ovarian syndrome (PCOS) is another, characterized by excessive androgen (male-dominant) hormones, menstrual irregularities, and polycystic ovaries.3 This condition is the most common chronic reproductive and metabolic endocrine disorder affecting women of childbearing age, with an estimated prevalence of 4-21% of women worldwide,3 and is a major cause of infertility.4 The causes and clinical presentation of PCOS are complex, involving multiple physiological systems4–as a result, the condition is underdiagnosed, with diagnosis frequently being delayed.4,5 A recent study including almost 1400 women with PCOS worldwide found that half of these patients saw at least three healthcare professionals before being diagnosed with the condition, and for a third of them, this took over two years.5 The vast majority of women were unsatisfied with their diagnostic experience and the information provided to them at the time of diagnosis, with only 35.2% and 15.6% being satisfied with each of these respective aspects of their healthcare.5
Due to the metabolic-related features of PCOS, the consequences of underdiagnosis go far beyond discomfort and infertility. PCOS can lead to serious complications such as metabolic syndrome, type 2 diabetes, endometrial cancer, and cardiovascular disease.3,4 Treatments to manage the symptoms of PCOS and increase fertility are available, so a timely diagnosis is critical for managing the condition and preventing future complications.3 Unfortunately, similar to other reproductive health conditions, symptom heterogeneity, differences in diagnostic methods and criteria, and the dismissal by healthcare providers pose obstacles to timely diagnosis and can lead to catastrophic long-term consequences in millions of women worldwide.5
Perhaps the most distressing stories, however, come from women with endometriosis–a chronic condition characterized by the presence of endometrial-like tissue outside of the uterus. Although the causes of this condition remain poorly understood, its symptoms often include pelvic pain, fatigue, bowel and bladder symptoms, and infertility.6 Endometriosis is estimated to affect about 10% of reproductiveage women, and has been identified in almost 50% of women with persistent pelvic pain and 40% of women living with infertility.7 Despite its serious long-term complications and associated reduced quality of life, there is currently no cure.6
However, medications and surgery help manage the symptoms, especially in the early stages, making a timely diagnosis imperative in minimizing disruptions to a woman’s life.
The delay in diagnosing endometriosis even exceeds that of PCOS, with the median time from symptom onset to diagnosis being over 10 years, and 74% of patients receiving at least one false diagnosis, such as PCOS, before endometriosis is correctly identified.8 These delays can deprive patients of timely treatments and proper management of their condition, leading to depression, adverse effects on intimate relationships, missed school and work, and frequent visits to urgent and nonurgent medical centres.9 This diagnostic delay can also have serious medical consequences. A recent meta-analysis including almost 2 million women with endometriosis found that the condition was associated with gestational and obstetric complications such as increased risk of preterm birth and miscarriage.9
The disheartening reality is that underdiagnosis of reproductive conditions in women can have lasting, life-altering impacts, ranging from chronic pain, infertility, secondary diseases, and pregnancy complications. However, complex symptoms, diagnostic challenges, and the unfortunate dismissal and normalization of these symptoms by society–including healthcare
providers–results in women frequently being misdiagnosed and left isolated as they navigate their symptoms and well-being. Increasing awareness of these conditions coupled with improved methods of diagnosis are resulting in some improvements, but considerable progress is still required before timely, compassionate, and informed diagnosis becomes commonplace. In the meantime, the most important thing an individual can do is advocate for yourself–you know your body best and can tell when something is wrong. Listen to those instincts and ensure you are getting the proper testing and information to take care of your health and quality of life. Hopefully, better medical practices will eventually follow.
References
1. Edward M, Ernest A, Christopher TY, et al. Timely diagnosis of PID: Leveraging ultrasound for Effective Management. Health Science Reports. 2025 Mar;8(3).
2. Basit H, Pop A, Malik A, et al. Fitz-Hugh-Curtis Syndrome. In: StatPearls. Florida: StatPearls; 2025.
3. Rababa’h AM, Matani BR, Yehya A. An update of polycystic ovary syndrome: Causes and therapeutics options. Heliyon. 2022 Oct;8(10).
4. Jiang B. The global burden of polycystic ovary syndrome in women of reproductive age: Findings from the GBD 2019 Study. International Journal of Women’s Health. 2025 Jan;17.
5. Gibson-Helm M, Teede H, Dunaif A, et al. Delayed diagnosis and a lack of information associated with dissatisfaction in women with polycystic ovary syndrome. The Journal of Clinical Endocrinology & Metabolism. 2016 Dec;102(2).
6. Allaire C, Bedaiwy MA, Yong PJ. Diagnosis and management of endometriosis. Canadian Medical Association Journal. 2023 Mar;195(10).
7. Giudice LC. Endometriosis. New England Journal of Medicine. 2010 Jun;362(25).
8. Hudelist G, Fritzer N, Thomas A, et al. Diagnostic delay for endometriosis in Austria and Germany: Causes and possible consequences. Human Reproduction. 2012 Sep;27(12).
9. Agarwal SK, Chapron C, Giudice LC, et al. Clinical diagnosis of endometriosis: A call to action. American Journal of Obstetrics and Gynecology. 2019 Apr;220(4).
PMDD: Misdiagnosed, & Misunderstood
By Josephine Machado
Somehow, the sunlight seeping through Katie’s linen curtains brings on feelings of disdain. She reaches for her phone to find text messages that cause her to feel a profound sense of loneliness and isolation that she herself cannot understand. She then snaps at her partner for uttering a simple “good morning” and spends the remainder of her day failing to concentrate on her experiments in the lab. She lacks the energy to take her dog on his evening walk, experiences intense joint pain, and has lost all interest in the book she has been reading. To the average person, these symptoms would be alarming, but to Katie, it is a recurring monthly experience; she suffers from premenstrual dysphoric disorder (PMDD).
PMDD is a chronic, cyclical mood disorder that affects an individual’s emotional and physical health in the days that lead up to their menstrual cycle.1 The symptoms of PMDD are much more extreme than commonly experienced premenstrual symptoms. Though tied to reproductive health and hormonal changes, PMDD is classified as a mental health disorder.2 A recent meta-analysis found the prevalence of PMDD to be 1.6%—affecting 31 million girls and women globally; however, this statistic is restricted to community-based studies that followed strict Diagnostic and Statistical Manual of Mental Disorders (DSM) diagnostic criteria and does not reflect provisional diagnoses.3 According to the DSM-5, diagnosing PMDD requires that symptoms (1) occur in the luteal phase of one’s cycle (the final
week before the onset of menstruation), (2) interfere with the individual’s work, school, or social life, and (3) should not be considered an exacerbation of an underlying psychiatric disorder.1 The individual must also experience at least five hallmark symptoms in most menstrual cycles over a single year, including at least one of the “core symptoms” pertaining to emotional distress.1 Core symptoms include marked (1) affective lability, (2) irritability, (3) depressed mood, and (4) anxiety. Additional hallmark symptoms include decreased interest in usual activities, poor concentration, lethargy, marked change in appetite, sleep changes, a sense of feeling overwhelmed, and physical symptoms such as joint pains.1 Diagnosis should also be confirmed with daily symptom tracking throughout at least two symptomatic cycles.1
PMDD significantly impacts an individual’s physical, psychological, social, and economic well-being, underscoring why underdiagnosis is such a pressing issue. In 2013, the American Psychiatric Association made the decision to include PMDD as an official stand-alone diagnosis in the depressive disorders section of the DSM-5. This decision has led to an influx of research, interest, and research funding for the condition over the last decade.1
A globally distributed, survey-based study conducted between January and March 2020 reported that individuals with PMDD experience serious distress in various aspects of daily life. Of the 3600 participants, 47% were reported to have
engaged in self-harm at least once during a PMDD crisis; 82% experienced suicidal thoughts during their luteal phase at least once, with 40% experiencing suicidal thoughts at some point monthly.4 Moreover, 26% of participants reported attempting suicide during a PMDD crisis.4 Additional burdens include depressive episodes, which can include feelings of hopelessness and worthlessness, alongside self-critical thoughts, and frequent or sudden tearfulness. These symptoms can exist alongside anxiety, irritability, and difficulties with concentration.1 As a result of studies such as this one, the serious nature of this condition is becoming increasingly evident.
Despite its severe consequences, PMDD remains underdiagnosed, undertreated, and misunderstood—both in practice and at a societal level. A study by Osborn et al. which interviewed 17 women diagnosed with PMDD found that an average of 20 years elapsed between initial PMDD symptom onset and obtaining a correct diagnosis and treatment, exemplifying the difficulty of diagnosis.5 The ramifications of PMDD on an individual’s social functionality and quality of life are similarly profound and extensive. A 2025 study based in the United Kingdom examined the impact of PMDD on life and relationship quality. The study found that PMDD patients had a significantly lower perceived quality of life across all World Health Organization (WHO) domains including physical health, psychological health, social relationships, and environment, in comparison to controls. Partners of PMDD
patients also reported a significantly lower quality of life in most of the Adult Carer’s Quality of Life Questionnaire domains (support for caring, caring choice, caring stress, personal growth, sense of value, ability to care, and carer satisfaction), when compared to the partners of healthy controls. Both patients and partners also reported significantly lower relationship quality in their romantic relationships compared to healthy controls and their respective partners.6
According to individuals diagnosed with PMDD, one of their most life-altering experiences includes enduring the barriers to diagnosis.7 A study exploring diagnosis and treatment of PMDD in 32 patients who identified as having PMDD in the U.S. healthcare system reported that almost 30% of participants experienced misdiagnoses including those of bipolar disorder, borderline personality disorder, and post-traumatic stress disorder, in addition to adverse effects from inappropriate treatments and medications.7 Pre-existing medical and structural barriers to diagnosis alone include limited health-provider knowledge, nonadherence to diagnosis and treatment guidelines, a lack of insurance, and limited access to healthcare services. For example, an 87-participant surveybased study of physicians by Craner et al. found that most physicians (98.9%) used clinical interviews as a component of their practice when diagnosing PMDD, yet only 11.5% of these physicians reported adhering to diagnostic guidelines.8
Some individuals have even reported instances of medical gaslighting, and dismissal of symptoms. The aforementioned medical barriers can further manifest in the form of internalized individual obstructions such as medical trauma, mistrust, fear, and shame, as well as cultural barriers such as reproductive and mental health stigma, gender and cultural norms, and cultural preferences for alternative medicine.8 In terms of cultural norms, the stigma surrounding the psychotropic and hormonal interventions that are often used to treat PMDD led to a decreased utilization in many non-Western contexts.8 These factors can lead to diagnostic delay, ultimately leading to an increasingly negative experience for this group of individuals.
The stigma surrounding women’s reproductive health can be debilitating. Many PMDD patients internalize their condition as a personal flaw4 when it is simply a medical diagnosis. Individuals with PMDD have described a deep sense of shame and worthlessness, which was reinforced by repeated dismissal from professionals and society.7 Many patients delay seeking help due to internalized stigma and the belief that menstrual suffering is “normal.”6
Treatment options are available to alleviate such suffering including selective serotonin reuptake inhibitors (SSRIs), hormonal therapies (e.g. oral contraceptives), and surgical options in severe and treatmentresistant cases. Complementary therapies such as cognitive behavioral therapy,
mindfulness-based interventions, as well as lifestyle modifications can also be of benefit, but are often underutilized.1 Routine screening for cycle-related mood symptoms in gynecological and primary care settings may also help identify PMDD cases earlier.
Overall, PMDD is a serious and commonly misunderstood condition that highlights critical gaps in the diagnosis, recognition, and treatment of conditions surrounding women’s reproductive health. Addressing women’s health concerns requires not only a systemic shift towards improved diagnosis and treatment, but a socio-cultural shift in the prioritization of women’s mental health as a crucial component of healthcare.
References
1. Cary E, Simpson P. Premenstrual disorders and PMDD - a review. Best Practice & Research Clinical Endocrinology & Metabolism 2024;38:101858. https://doi.org/10.1016/j.beem.2023.101858.
2. Mishra S, Elliott H, Marwaha R. Premenstrual Dysphoric Disorder. StatPearls, Treasure Island (FL): StatPearls Publishing; 2025.
3. Reilly TJ, Patel S, Unachukwu IC, et al. The prevalence of premenstrual dysphoric disorder: Systematic review and meta-analysis. Journal of Affective Disorders 2024;349:534–40. https://doi.org/10.1016/j. jad.2024.01.066.
4. Brown D, Smith DM, Osborn E, et al. Women with Premenstrual Dysphoric Disorder experiences of suicidal thoughts and behaviours: a mixed methods study. Front Psychiatry 2024;15:1442767. https:// doi.org/10.3389/fpsyt.2024.1442767.
5. Osborn E, Wittkowski A, Brooks J, et al.. Women’s experiences of receiving a diagnosis of premenstrual dysphoric disorder: a qualitative investigation. BMC Women’s Health 2020;20:242. https://doi. org/10.1186/s12905-020-01100-8.
6. Hodgetts S, Kinghorn A. Examining the impact of premenstrual dysphoric disorder (PMDD) on life and relationship quality: An online cross-sectional survey study. PLoS ONE 2025;20:e0322314. https:// doi.org/10.1371/journal.pone.0322314.
7. Chan K, Rubtsova AA, Clark CJ. Exploring diagnosis and treatment of premenstrual dysphoric disorder in the U.S. healthcare system: a qualitative investigation. BMC Women’s Health 2023;23:272. https:// doi.org/10.1186/s12905-023-02334-y.
8. Nayak A, Wood SN, Hantsoo L. Barriers to Diagnosis and Treatment for Premenstrual Dysphoric Disorder (PMDD): A Scoping Review. Reprod Sci 2025. https://doi.org/10.1007/s43032-025-01861-3.
The Morality Tax:
Exploring Price Gouging Practices on Emergency Contraceptive Pills
By Jasmine Amini
$36.99 CAD for brand name, $24.99 CAD for generic—these are prices for the two emergency contraceptive pills offered at Shoppers Drug Mart.1 Emergency contraceptive pills (ECPs), colloquially known as “the morning after pill”, are safe, effective medications that help prevent unwanted pregnancies.2 Despite their efficacy, low production cost, and availability, significant barriers hinder widely accessible ECP use among Canadians. Given that ECPs like Plan B cost approximately $0.51 CAD3 to produce, one question looms: why are ECPs so prohibitively expensive?
Perhaps unsurprisingly, mark-ups and service fees are the primary components of the whopping $30+ price tag associated with common ECPs. In Canada, ECPs are kept behind the counter of pharmacies. This means a portion of their cost is allocated to dispensing and counselling services; dispensing fees are charged at the discretion of the individual pharmacy, but in regions like British Columbia, dispensing fees for ECP prescriptions can reach up to $20.3 ECP mark-ups are further evident when comparing their cost at pharmacies to community clinics. For example, at community-based clinic Planned Parenthood Toronto, Plan B is available for only $13 CAD; however, patients must consult with a peer health educator or clinician to obtain an ECP prescription. The bulk of ECP cost, however, comes directly from the pharmaceutical companies producing these medications. A recent investigation
by the New York Times found that companies like Barr Pharmaceuticals sold Plan B prescriptions at a staggering 85% profit margin,4 which is above the average profit margin of ~76.5% among large pharmaceutical companies, according to a recent meta-analysis.5 These exorbitant profit margins have enabled the continual growth of companies producing ECPs.
To underscore the importance of equitable ECP access, it is critical to understand how these medications work. The active ingredient in ECPs is typically levonorgestrel, a synthetic form of female sex hormone progestogen.2 Levonorgestrel works to prevent ovulation of a mature egg (the female gamete), thus inhibiting fertilization by sperm. Timing of ECP use is essential, which underscores the importance of removing cost barriers. Specifically, ECPs must be used within five days of unprotected sex; however, the sooner they are taken, the more effective they are at preventing pregnancy.6 The urgency around ECP use further emphasizes the harms of prohibitive cost and lacking accessibility of these medications.
Although corporate profit-seeking is an important factor affecting ECP prices, public attitudes towards ECP use may also be a barrier to reducing costs and enacting key policy changes. In one qualitative study of postsecondary students in Ontario, several participants described traveling to distant pharmacies or pretending to purchase
ECPs for another individual due to their discomfort around procuring ECPs.7 Strategies to maintain secrecy and avoid confrontation among study participants betrays a sense of shame around the use of ECPs, or of being the “type of person” who uses them. The stigma around ECP use serves not only to belittle affected individuals—it also impedes them from recognizing and confronting the ways in which companies that produce and supply ECPs exploit them. Without public rallying, the impetus to enact policy change protecting Canadians from ECP price gouging is effectively zero.
Larger organizations also perpetuate stigma around ECP use. In 2017, United Kingdom pharmacy giant, Boots, refused to reduce the price of their brand-name and generic ECP (then 44.50 CAD) over fears that doing so would “incentivize inappropriate use” among consumers.8 Although Boots eventually did walk back their stance, following suit with other major competitors, their original statement is telling of the ethos around ECP use in the Western world. In taking a traditionalist stance to disincentivize “inappropriate use”, companies like Boots are making moral judgments on consumer’s sex lives, an area over which they should have no claim, and are using said judgements to justify extortionate ECP prices.
Notwithstanding that people use ECPs for various reasons that are not “their fault”, such as broken condoms or sexual assault, justifications of ECP pricing by private
entities, like Boots, on the basis of moral “wrongdoing” by consumers should raise concern. It is important to consider and scrutinize the messages that potentially underlie corporate justifications for price gouging on ECPs, which may centre around punishing “risky” sexual behaviours. It is not the role of a healthcare provider or pharmaceutical company to determine how an individual should exert their autonomy, nor is it their role to enforce what they consider as appropriate “punishment” for “inappropriate use” of ECPs. In the same way that we should continue offering care to a patient with lung cancer who smokes, we should be offering ECPs at low cost to whoever needs them, when they need them.
Concerns around access to ECPs are even more pressing in the context of Roe v. Wade, a supreme court ruling protecting abortion access in the USA, being overturned in 2022.9 With abortions being banned in 12 states, and gestational limits enforced in 29 states10, demand for ECPs skyrocketed. In the week following Roe v. Wade being overturned, one pharmaceutical company, Wisp, reported a 3000% increase in sales, and suppliers like CVS and Rite Aid implemented policies limiting the number of ECPs consumers could buy at a given time.11 Although these buying behaviours are understandable, they highlight concerning truths regarding the ECP industry, namely that ECP producers can capitalize on consumer fear and lack of choice, and that they stand to gain from legislation restricting reproductive health care.
The main challenge now is determining how we move forward. Without governmental pressure, companies are not incentivized to reduce ECP costs. This is particularly troubling due to the timesensitive nature of these medications and that they are often the last option to prevent unwanted pregnancy, aside from the less common copper intrauterine devices. Encouragingly, our government may partner with ECP producers to subsidize ECP cost for Canadian consumers. Bill C-64, or the Pharmacare Act, aims to do just that. Specifically, Bill C-64 proposes to enhance pre-existing provincial and territorial drug benefit programs, offering single-payer coverage for a variety of prescription medications.12 Alongside diabetes medication, contraceptive devices and medications will be the first prescriptions covered under Bill C-64.
Although recent legislative action is promising, the fight to ensure stigma-free access to ECPs, and contraceptive care broadly, remains ever-present. As the overturning of Roe v. Wade has shown, access to reproductive healthcare is tenuous and can be rescinded with changing political landscapes. In an era where reproductive healthcare is continually threatened, it is critical to be vocal against restrictions to ECP access. Far from being a source of shame, access to ECPs and reproductive care should be viewed as an important cornerstone of the Canadian healthcare system, one that values and upholds individual autonomy for all.
References
1. Buy Contraceptives Products Online | Shoppers Drug Mart, https:// www.shoppersdrugmart.ca/shop/categories/health/sexual-wellness-and-family-planning/sexual-wellness/contraceptives/c/FS-HTS102?sort=trending&page=0&lang=en (accessed 26 April 2025).
2. Vrettakos C, Bajaj T. Levonorgestrel. In: StatPearls. Treasure Island (FL): StatPearls Publishing, http://www.ncbi.nlm.nih.gov/books/ NBK539737/ (2025, accessed 19 April 2025).
3. CFP Services Chart: Services, fees and claims data for government-sponsored pharmacy programs.
4. Sorkin AR, Giang V, Gandel S, et al. Who’s Profiting From Demand for Plan B? The New York Times, 28 June 2022, https://www. nytimes.com/2022/06/28/business/dealbook/plan-b-contraception-pills-profit.html (28 June 2022, accessed 19 April 2025).
5. Ledley FD, McCoy SS, Vaughan G, et al. Profitability of Large Pharmaceutical Companies Compared With Other Large Public Companies. JAMA 2020; 323: 834–843.
6. Gemzell-Danielsson K, Berger C, P.g.l. L. Emergency contraception — mechanisms of action. Contraception 2013; 87: 300–308.
7. Szajbely K, Neiterman E. Exploring the experiences of Ontario post-secondary students with the emergency contraception pill. J Obstet Gynaecol Can 2025; 102825.
8. Boots “ends grossly sexist surcharge” and lowers the price of emergency contraception following years of campaigning by charities and MPs. BPAS Campaigns, https://bpas-campaigns.org/news/ boots-ends-grossly-sexist-surcharge-and-lowers-the-price-of-emergency-contraception-following-years-of-campaigning-by-charitiesand-mps/ (accessed 20 April 2025).
9. Totenberg N. Supreme Court overturns Roe v. Wade, ending right to abortion upheld for decades. NPR, 24 June 2022, https://www. npr.org/2022/06/24/1102305878/supreme-court-abortion-roe-vwade-decision-overturn (24 June 2022, accessed 5 May 2025).
10. U.S. Abortion Policies. KFF, https://www.kff.org/interactive/womens-health-profiles/united-states/ (accessed 5 May 2025).
11. Pharmacy sees 3,000% jump in emergency contraceptive sales after Roe ruling - CBS News, https://www.cbsnews.com/news/emergency-contraception-roe-v-wade-plan-b-spike-in-sales-wisp/ (2022, accessed 5 May 2025).
12. Canada H. Universal Access to Contraception, https://www.canada. ca/en/health-canada/news/2024/02/backgrounder-universal-access-to-contraception.html (2024, accessed 22 April 2025).
Restrictions Beyond Legality: Access to Abortion
By Ilakkiah Chandranv
Imagine being wheelchair-bound inside a burning building. As smoke starts to fill the air, you and others in the building rush to the brightly lit emergency exit. When you get to it, you discover that the only way to reach the door is by climbing a steep staircase. There is no ramp, no elevator, and no alternate route. As people rush past you and exit out this door to safety, you become aware of the barrier in front of you, as, despite the door not being locked or blocked, you physically can’t access it. As the smoke grows thicker, even with the legal right to escape, and the door being right in front of you, the barrier of the stairs makes safety impossible for you.
With abortion existing within policy, but missing in practice, the inability to reach the emergency exit, is what access to abortion services feels like for many Canadians, with care being too far, the wait being too long, and the system being too hard to navigate. This gap reflects the limitations of our healthcare system, impacting those of marginalized communities to an even greater degree.
In Canada, abortion has been legal for over 55 years, meaning that at the federal level, there are no laws restricting a Canadian’s legal right to abortion access.1 However, the availability of abortion services is often impacted by geographic distance, longstanding medical discrimination, and policy gaps. In urban regions across Canada, accessing abortion services is typically straightforward, but this isn’t
the case in rural areas. For example, a Canada-wide national survey conducted in 2012 identified that, with the exception of Quebec and British Columbia, abortion services were largely concentrated within cities.2 Furthermore, even in the absence of geographic barriers, practitioners in rural regions of Canada were far more likely to describe hesitation from their colleagues that impacted their ability to provide surgical abortions.3 This means that individuals living in remote or rural areas are faced with the choice of experiencing stigma or ambiguity from their care team when seeking abortion services, or taking time off work, arranging travel, finding childcare, and navigating unfamiliar healthcare facilities—all while managing an experience that is overwhelming both physically and emotionally.
This issue goes beyond inconvenience; it is a growing public health concern that has been overlooked for decades. Limited availability of abortion care leads to increased wait times and delays in receiving medical attention. Delays in abortion care increase the physical and emotional toll on patients.4 In some cases, this may also lead to some people being forced to carry pregnancies they did not choose, which is associated with poor mental and physical health outcomes, increased exposure to domestic violence, and long-term financial insecurity.4–6
Although the impact of restricted abortion services on marginalized populations is better explored in
the United States, investigations of reproductive health in Canada suggest similar findings, with Indigenous women, racialized individuals, people with disabilities, individuals from the 2SLGBTQIA+ community, and immigrants facing disproportionate barriers to all forms of reproductive care, including abortion. With higher rates of medical discrimination and stigma experienced by these individuals when seeking healthcare, the impacts are compounded when receiving abortion services.7,8 For example, in Indigenous communities, abortion must be understood within the context of ongoing reproductive injustice. The legacy of forced sterilizations, persistent failures in culturally safe care with prioritization of Westernized practices, and the lack of post-abortion support has eroded trust in health institutions. This history limits not only the availability of abortion services, but also affects individuals’ willingness to seek out and trust the care they are offered, especially when faced with dismissal or stigma.9,10
Immigrant women face similar challenges, encountering a lack of culturally affirming care and often having to choose between Westernized practices or their own cultural values and beliefs when making decisions about their reproductive health.8 Furthermore, their experiences are often impacted by the lack of support available in their native languages, and restrictions based on their citizenship status.8 Moreover, many non-binary Canadians
report feeling pressured to conceal their gender identities when navigating reproductive care, to avoid denial and refusal in receiving medical attention.11 Labelling abortion facilities as “womenonly spaces” can create significant barriers to transgender inclusivity— frequently excluding trans women and girls, and trans men and boys who wish to use available services as a result of discrimination and stigma.12
Despite the long history of medical discrimination and its impacts on health outcomes, abortion continues to be treated as a politically sensitive topic rather than a medical necessity. This framing not only perpetuates limited access to services but also restricts the public’s exposure to accurate information, contributing to the growing infodemic of abortion misinformation.13 The exacerbation of misinformation—like that abortions exacerbate cancer risk or infertility, and pose psychological risks—underscores the importance of acting now.14,15
Abortion should be treated like any other essential healthcare service to be safe, evidence-based, timely, and accessible. Strategies explored in the US, such as dispensing mifepristone—a common medication used for abortion—through telemedicine and by pharmacists, have been associated with an increase in efficient and patient-oriented abortion care.16
In other cases, engaging directly with communities, expanding education on
traditional and Westernized practices of abortion care within medical teams, and acknowledging the role of remote abortion clinics can help address limited access while ensuring sensitivity around the topic. Moreover, recognizing that abortions are not simply a one-time procedure but one that requires follow-up care can support those accessing services in navigating their physical and mental health throughout the process.
There is no single solution that will fix every barrier. However, we need to stop pretending that legality is equivalent to accessibility. We need to recognize that abortion services in Canada are not equally distributed, with individuals who are already experiencing marginalization by other structures within Canada also being more likely to experience barriers limiting their ability to use abortion services.
Abortion is not just a private matter, nor is it an issue that only affects some individuals. Abortion services are integral to health and require consideration of health and equity, to ensure that every Canadian can receive the care they need.
References
1. Public Health Agency of Canada. Abortion in Canada. Government of Canada (2024).
2. Norman, W. V et al. Abortion health services in Canada: Results of a 2012 national survey. Can Fam Physician 62, e209–e217 (2016).
3. Norman, W. V., Soon, J. A., Maughn, N. & Dressler, J. Barriers to Rural Induced Abortion Services in Canada: Findings of the British Columbia Abortion Providers Survey (BCAPS). PLoS One 8, e67023 (2013).
4. Wasser, O., Ralph, L. J., Kaller, S. & Biggs, M. A. Experiences of delay-causing obstacles and mental health at the time of abortion seeking. Contracept X 6, 100105 (2024).
5. Wallace, M. E., Stoecker, C., Sauter, S. & Vilda, D. States’ Abortion Laws Associated With Intimate Partner Violence-Related Homicide Of Women And Girls In The US, 2014-20. Health Aff (Millwood) 43, 682–690 (2024).
6. Wisner, K. L. & Appelbaum, P. S. Abortion Restriction and Mental Health. JAMA Psychiatry 80, 285 (2023).
7. Coen-Sanchez, K. et al. Reproductive justice in patient care: tackling systemic racism and health inequities in sexual and reproductive health and rights in Canada. Reprod Health 19, 44 (2022).
8. Machado, S., Wiedmeyer, M., Watt, S., Servin, A. E. & Goldenberg, S. Determinants and Inequities in Sexual and Reproductive Health (SRH) Care Access Among Im/Migrant Women in Canada: Findings of a Comprehensive Review (2008–2018). J Immigr Minor Health 24, 256–299 (2022).
9. Monchalin, R. et al. “I would love for there not to be so many hoops ”: recommendations to improve abortion service access and experiences made by Indigenous women and 2SLGTBQIA+ people in Canada. Sex Reprod Health Matters 31, (2023).
10. Monchalin, R. et al. A qualitative study exploring access barriers to abortion services among Indigenous Peoples in Canada. Contraception 124, 110056 (2023).
11. Lowik, A. J. “I Gender Normed as Much as I Could”: Exploring Nonbinary People’s Identity Disclosure and Concealment Strategies in Reproductive Health Care Spaces. Women’s Reproductive Health 10, 531–549 (2023).
12. Prince Edward Island Abortion Rights Network. Trans-Inclusive Abortion Services Manual . (2021).
13. Pagoto, S. L., Palmer, L. & Horwitz-Willis, N. The Next Infodemic: Abortion Misinformation. J Med Internet Res 25, e42582 (2023).
14. Berglas, N. F. et al. State-Mandated (Mis)Information and Women’s Endorsement of Common Abortion Myths. Women’s Health Issues 27, 129–135 (2017).
15. Gill, R. & Norman, W. V. Telemedicine and medical abortion: dispelling safety myths, with facts. Mhealth 4, 3 (2018).
16. Rasmussen, K. N., Janiak, E., Cottrill, A. A. & Stulberg, D. B. Expanding access to medication abortion through pharmacy dispensing of mifepristone: Primary care perspectives from Illinois. Contraception 104, 98–103 (2021).
Blurring the Lines:
Differentiating the Roles of Embryonic Stem Cells in Biomedical Research
By Gabriela Blaszczyk
In an ideal world, there would not be thousands of people dying each year waiting for an organ transplant. In this ideal world, couples would not struggle with navigating the journey of infertility challenges. What potential solutions do both scenarios have in common? Human embryonic stem cells.
One needs to be careful with the exact definition of a stem cell. In popular culture, this is an umbrella term used to describe novel fad treatments to retain that “youthful glow”, or more bleakly, a strategy predatory companies use for selling a supposed “cure” for a debilitating disease that has not yet been rigorously tested. Biologically, a stem cell has the potential to generate multiple cell types in the body and self-renew indefinitely. However, there are various types of stem cells, each having different capacity. The stem cells found in a developing embryo are pluripotent, meaning they are unrestricted in their developmental potential. Stem cells found in the adult body, such as cells found in your blood or your brain, are restricted to becoming a defined cell type and serve the purpose of repairing an organ in case of damage, and these are multipotent.1
Since embryonic stem cells (ESCs) can generate any cell type in the body, ESC research has proven beneficial in the fields of human fertility and development, drug discovery (by supplying human cells for testing, circumventing the need for human experimentation), transplantation therapy,
and even in clinical trials to alleviate deficits following spinal cord injury.2 ESCs have been used for research from both human3 and rodent sources4,5 for over 30 years. These cells are harvested from leftover in vitro fertilization procedures and are kept in culture for further use. From there, they can be used indefinitely, generating a cell line. However, despite the promise of ESCs, there are legal and moral dilemmas to navigate, as well as several misconceptions, when it comes to effectively utilizing human embryonic material.
Current public misconceptions may have the potential to harm the scientific progress of human stem cell research, resulting in a reduction or complete ban of human stem cells.6 The primary concern of the public is that human embryos are destroyed every time a research lab requires access to ESCs. While ethically controversial, this is a misconception, as researchers use the same ESC lines for several decades, which were generated
in the early years of ESC research. The International Society for Stem Cell Research (ISSCR) is the main international governing body and provides guidelines on the use of human stem cells for academic research purposes. The ISSCR states that “all [forms of embryonic] research should have a compelling scientific rationale and necessitate the use of these materials rather than employ alternative models. The research should use the minimum number of embryos necessary to achieve the scientific objective”.7 Whether in a fertility clinic or in the lab, human embryos can only be kept in culture for 14 days (known as the 14-day rule), and this is governed into law in several countries. Furthermore, human embryos or synthetic material resembling human embryos cannot be implanted into a mammalian uterus under any circumstance.7 While there are regulatory guidelines outlining ESC use, public misconceptions about human ESC research undermine the scientific potential and impact of the findings.
Another current debate concerns the relevance of the 14-day rule. Scientists have never been able to observe the discrete developmental steps occurring between the 14- and 28-day period post-fertilization, and our knowledge of this time in human development is extrapolated from animal models. This is also known as the “black box” of human development. Mice are the most common model for comparison, however there are significant differences in development, namely their gestation period only being 21 days. This time frame is when many genetic and developmental disorders develop, as well as when many pregnancies fail,8 therefore with more studies into this developmental timepoint, there is the chance to help many individuals.
Are there reasonable alternatives? Induced pluripotent stem cells (iPSCs) are derived from any cell in the adult organism (most commonly from non-invasive tissues such as blood, skin, or urine) and are synthetically reverted to an embryonic-like state.9 These have been shown to mimic ESCs, and there have been many methods describing their use in the generation of various cells for study, and even embryolike structures. One key difference with iPSCs is that they do not have the capacity to form a human fetus. Beyond generating iPSCs, there are many discrete signatures and steps that simply cannot be replicated in a dish, rendering them nonviable (due to acquired damage, and residual “memory” of the adult cell type). This begs the question: are there still reasonable
instances where human embryos need to be used to answer a research question where an alternative, such as human iPSCs, will not suffice? iPSCs mimic ESCs biologically and even surpass their utility in instances such as transplantation or modelling genetic disorders. We can generate cells from iPSCs to use on the same patient and circumvent the need for matching with a different donor, or needs for genetic editing. However, there are still concerns on whether these cell types equal on a genetic level.10
The use of human embryonic material in research is easily misconstrued if the correct definitions are not used. A letter to the US President from congress argued for the cessation of government funding of human ESC research stating that adult stem cells (mostly mentioned to be sourced from bone marrow or umbilical cord blood) have been used to cure numerous disorders, and that transplantation therapies have not progressed quickly enough.6 However, they failed to acknowledge that these adult stem cells do not have the same pluripotent capacity as ESCs or iPSCs, and therefore cannot be used in the same manner for developmental research, regenerative therapies, or modelling disease in a human context.
To see progress in stem cell research, we will require an interdisciplinary approach. Basic researchers, engineers, and medical doctors will need to work together to develop new avenues for innovating the
approaches we have today. While we need to keep in mind that no scientific models are perfect replicas of what occurs within an organism, but rather an approximation, we should also celebrate the strong translational potential of ESCs for more directly exploring diseases in ways not possible with human experimentation. As scientists, we can strive to educate our peers and present both strengths and limitations as well as realities of human ESCs in research.
References
1. Stem cell glossary. [Internet]. International Society for Stem Cell Research; 2024. [cited: 2025 May 5]. Available from: https://www. aboutstemcells.org/info/glossary
2. Fessler RG, Ehsanian R, Liu CY, et al. A phase 1/2a dose-escalation study of oligodendrocyte progenitor cells in individuals with subacute cervical spinal cord injury. J Neurosurg Spine. 2022;37(6):812820. doi: 10.3171/2022.5.SPINE22167
3. Thomson JA, Itskovitz-Eldor J, Shapiro SS, et al. Embryonic stem cell lines derived from human blastocysts. Science. 1998;282(5391):1145-7. doi: 10.1126/science.282.5391.1145
4. Evans MJ, Kaufman MH. Establishment in culture of pluripotential cells from mouse embryos. Nature. 1981;292(5819):154-6. doi: 10.1038/292154a0
5. Martin GR. Isolation of a pluripotent cell line from early mouse embryos cultured in medium conditioned by teratocarcinoma stem cells. Proc Natl Acad Sci U S A. 1981;78(12):7634-8. doi: 10.1073/ pnas.78.12.7634
6. Smith, Chris. “Member letter to president trump on human embryonic stem cell research”. 04/07/2025. Congressman Chris Smith [chrissmith.house.gov]. Available from: https://chrissmith.house. gov/uploadedfiles/member_letter_to_president_trump_on_human_embryonic_stem_cell_research_april_7_2025.pdf
7. Lovell-Badge R, Anthony E, Barker RA, et al. ISSCR Guidelines for Stem Cell Research and Clinical Translation: The 2021 update. Stem Cell Reports. 2021;16(6):1398-1408. doi: 10.1016/j.stemcr.2021.05.012
8. Williams K, Johnson MH. Adapting the 14-day rule for embryo research to encompass evolving technologies. Reprod Biomed Soc Online. 2020;10:1-9. doi: 10.1016/j.rbms.2019.12.002
9. Takahashi K, Tanabe K, Ohnuki M, et al. Induction of pluripotent stem cells from adult human fibroblasts by defined factors. Cell. 2007;131(5):861-72. doi: 10.1016/j.cell.2007.11.019
10. Chin MH, Mason MJ, Xie W, et al. Induced pluripotent stem cells and embryonic stem cells are distinguished by gene expression signatures. Cell Stem Cell. 2009;5(1):111-123. doi:10.1016/j. stem.2009.06.008
Condoms to Cash: A Despot’s Guide to Financial and Political Success
A Satirical Critique of Aid Mismanagement and Population Politics
By Omar I. Hassan
In representative politics, especially within developing regions, population size determines your political clout. Like you, and many of your fellow ambitious politicians in the Global South, this is not a burden—it’s a strategy. Bloat your constituency for a louder voice—and in turn, control over more state resources. In a postcolonial world eager to cover past injustices, international donors rush to deliver humanitarian aid with few conditions and even fewer questions. For the politically savvy, this is not solely aid; it’s an opportunity. Among the most abundant and misunderstood of these gifts are contraceptives. You might wonder, why would you invite contraceptives at all if your population size determines your power?
That is precisely why you need to not only manage this aid, but leverage it as well. These foreign-sourced tools of reproductive control may be unfamiliar to your people and you—the benevolent yet enterprising representative—are best poised to hold this aid for the ‘public good’. When leveraged, contraceptives can easily become a vehicle for your political power and profit.
Step 1: Attract Aid
Begin by appealing to state and international donors such as the United Nations Population Fund, United States Agency for International Aid (USAID), or the Global Fund. Present the situation as alarming as possible with inflated public health statistics1–3—emphasizing maternal and child mortality, HIV prevalence, and adolescent pregnancies.
Pull those heartstrings enough and you will be rewarded with warehouses worth of implants, condoms, and DepoProvera (an injectable contraceptive). Romanus Pakure, former acting director of Papua New Guinea’s National AIDS council knew this game well. During the 2008 human immunodeficiency virus (HIV) and tuberculosis (TB) epidemics, Pakure secured millions of condoms— leaving two million of them to expire unused and undistributed, while others were sold to fund his administration’s trips abroad4 Papua New Guinea has the highest proportion of HIV cases in Oceania, accounting for more than 99% of Oceania’s HIV cases, when excluding Australia and New Zealand.5
Step 2: Direct the Flow
Having secured a steady flow of aid, centralize it. Fill key positions in Ministries of Health or Welfare Departments with loyalists—a common practice in Pakistan, where procurement of equipment is predominantly managed by political bodies instead of clinicians and hospitals.6 This allows you to strategically allocate (or misallocate) as you please. Kenya’s 2021 HIV report showed inflated demand and underreported supplies to extract more donor aid.7 Donors seem to trust local governments to “self-assess” and fulfill all their needs.8 After all, why wouldn’t they trust the loyal servant of the people that you are?
Evidently, direct distribution to your constituency is an ill-advised goal.
Contraceptives marked “Not for Sale” are merely suggestions; they can be redirected quietly into black markets or resold through pharmacies that you hold stake in, generating a consistent and profitable form of revenue. Uganda has mastered this tactic, having an estimated 10% of public contraceptive stock regularly “falling off the boat” into private markets, generating a robust parallel economy.3 Similar criticisms were raised in a Department for International Development (DFID) report in Nigeria, where widespread diversion of aid-funded birth control were redirected into private sectors.3 The local business will thank you, as well as your loyal retainers. (Almost) Everyone wins.
Step 3: Monetize Morality
If the public starts to question the missing aid, rising accidental pregnancies, and worsening STI-related epidemics—don’t
panic.1–3,9 Instead, simply pivot. Denounce the contraceptives.10,11 They are foreign and immoral colonial impositions. Return to the embrace of tradition and faith, touting arguments against birth control while blaming strife on the misguided and insufficient aid that is being sent. Solidify the support of your conservative and rural communities. After all, these are foreign tools donated by outsiders. Who is to say they do so with your best interest in mind? Is it the supposed liberation that they tout or simply population control?11–14
Communist Romania’s 1966 ‘Anti-Abortion Decree’ (Decree 770) banned abortion outright and ran heavy slander campaigns
against IUDs, condoms, and hormonal birth control methods.15 The government also de facto banned almost all access to birth control and ensured population fertility through monthly gynecological exams.15 The resulting birthrates shot up from below average to 54 percent in excess over other Eastern European countries.15 The purpose? To bolster the Romanian Communist Party numbers.
Much like Romania, your public opposition of contraceptives can nurture both the growth of your population and political base. Larger families will depend on you through state provisions—education, food, and jobs. This makes them a more pliable electorate; willing to bend to your will through your tightly bound patronage. Each redirected condom, oral pill, contraceptive injection, and IUD translates into another future voter.
Step 4: Sustain the Cycle
By jeopardizing reproductive autonomy, population counts will rise, and so too will your aid shipments. Donors will be instilled with a sense of urgency to meet the needs of your rapidly growing constituency and worsening epidemics. Bangladesh, Malawi, Guinea, and the Central African Republic have all successfully employed this model of redirecting over-ordered reproductive health supplies into local markets.8 Multiple sub-Saharan African countries had contraceptives diverted by local officials for resale and were rarely penalized. Such corruptions are often chalked up to a mere consequence of weak supply chain
oversight, low salaries among health workers, and collusion between vendors and government employees.16 A harmonious cycle is created; as more contraceptive aid is misdirected, donors increase aid, and the opportunities to convert contraceptive supplies into monetary profit expand. Each link in the cycle is designed to feed the next phase of the swindle.
Step 5: Fight Reforms
Sadly, this eloquent system now faces grave threats from those who seek to undermine it. Donors are increasingly suspicious. Some are demanding increased transparency through third-party audits or whistle blower campaigns such as the Global Fund’s “I Speak Out Now!.”17 Even more threateningly, they have been shown to try and subvert your own civil society to oversee your actions.18,19 Foreigners stoking a betrayal from your own people! Still, this is not a cause for alarm. Keep a tight hold on the press and question the legitimacy of observers. Always remember: you alone know what the people need.
The Caution of Satire
Although fictitious in tone, this guide is grounded in very tangible patterns of aid theft and misuse, corruption, and political manipulation that stunts the development of many struggling countries. The redirection of contraceptive aid through unchecked donations is not only ineffective, but harmful to the very communities this aid seeks to serve. The result of exacerbated health crises and undermined reproductive autonomy remains insufficiently addressed.
With such little oversight, there are few tangible reports—other than those made by third-party observers. These observers are often impeded with restrictions by local governments, corruption, or coercion. The purpose of this piece is not to denounce donations or advocate for withholding them, but rather to increase conditions and enforcement as part of the emergency response. Here, satire seeks to reflect the very real detriments of perverse incentives, rampant institutional corruption, and weak oversight in turning critical aid supplies into tools of profit and power.
References
1. Noel S. US says it will reduce health aid to Zambia because medicines were stolen and sold. 2025 May 8.
2. Druce N & Oduwole Y. Reproductive Health Commodity Security Country Case study: Nigeria. 2005 October.
3. Republic of the Philippines. RA 10354 “RESPONSIBLE PARENTHOOD AND REPRODUCTIVE HEALTH ACT OF 2012”. January 1.
4. AlJazeera. People in Kenya say lives at risk as HIV drugs run short. 2021 24 Apr.
5. O’Brien J. Pope Francis Should Lift Abortion Bans to Fight Zika. 2016 February 10.
6. UNAIDS. AIDS Epidemic Update. 2009.
7. Talbot M. Is Contraception Under Attack? 2024 Dec 3;
8. UNHCR. Procurement of Medical Equipment for Hospitals in KPK-Pakistan. 2020; Available at: https://www.ungm.org/Public/ Notice/112194.
9. The Global Fund of the Inspect General. I Speak Out Now! Available at: https://www.ispeakoutnow.org/.
10. Tomlinson BAC. Working with Civil Society in Foreign Aid: Possibilities for South-South Cooperation? 2013 June.
11. Schoeberlein J. Corruption and the right to sexual and reproductive health in sub-Saharan Africa. 2021.
12. Philipovic J. How American Women Could Lose the Right to Birth Control. 2024 May 20.
13. Weber L. Conservative Attacks on Birth Control can Threaten Access. 2024 June 5.
14. Friedman W. Corruption and averting AIDS deaths. World Dev 2018;110:13–25.
15. Berelson B. Romania’s 1966 Anti-Abortion Decree: The Demographic Experience of the First Decàde. Population Studies 1979;33(2):209–222.
16. International Rescue Committee. How U.S. aid cuts impact public health. 2025 March 19.
17. CDC National Prevention Information Network. AIDS Explosion Warning for Papua New Guinea. 2002 Mar 13.
By Aria Afsharian
“Even though we as graduate students emphasize the love of our work, we can’t do it without support... Failure is inevitable but there are other things to reassure you that you are capable. That you can do it.”
This quote encapsulates Shaghayegh (Feri) Faroozan’s story as she reflects on the mountainous journey it took to get to where she is now: a sixth-year PhD student in Dr. Nigil Haroon’s lab at Toronto Western Hospital and recent Sara Al-Bader Memorial Award recipient. As an international student from Iran, Feri’s path to science took shape back when she was studying for the Iranian University Entrance Exam: “Though it was tough, it gave me the opportunity to think about my future,” she reflected. “I really enjoyed cell and molecular biology in high school, so I decided to go into that field for my bachelor’s and master’s degrees.” In line with her interest in cell biology, Feri studied cell death pathways and male infertility during her master’s. But it was after her master’s where Feri described a major turning point in her life: her supervisor offered her a job at his in vitro fertilization (IVF) clinic in the Iranian city of Isfahan, where she would work in the embryology lab. The job offer came at a critical time in Feri’s life, as this was also when she was supporting her father who was diagnosed with late-stage glioblastoma. As Feri put it, this experience helped to “anchor” herself during a highly frustrating and stressful time. Building on her experience
at the IVF clinic, Feri shifted focus to her overarching goal of pursuing a PhD abroad to branch out into more diverse areas of research in immunology.
It was not long after this that she came across a paper by Dr. Haroon on autophagy and spondyloarthritis, a disease which, at the time, she had no idea about. Fascinated by Dr. Haroon’s work, she reached out to him to learn more about his research and to potentially join his lab as a graduate student. With everything going on in her life, however, Feri gave little thought to her request, assuming that she would not hear back–which made it even more surprising when she got a response in the middle of the night. This was yet another invigorating moment in Feri’s life, as she received this email back from Dr. Haroon while she was with her father in the hospital emergency room. Despite missing the early bird deadline for applications, Feri recalls how supportive Dr. Haroon was of her situation, helping her to get an extension for applying, leading to her being offered a place at the Institute of Medical Science (IMS) to begin her PhD. “When I heard back from IMS that I was accepted, I felt like I was on cloud nine,” Feri explained when reminiscing her excitement of the good news. But this acceptance was bittersweet as her father’s condition was deteriorating, and she had to decide whether she should stay with him or leave and come to Canada. When asked what swayed her decision, she remembered the final push given to her by her mom: “She told
me to go. That I should go after my life and pursue my goals.” This was the final motivation that Feri needed to embark on her new journey in Canada as a graduate student in the summer of 2019.
But what was it like coming to Canada as a newcomer? When asked this question, Feri acknowledged the difficulties that international students face when they leave their homes to start a new life in another country, explaining that “usually [newcomers] can feel lost on what to do and where to go.” Having mentioned this, she then discussed how her own experience was smooth thanks to the wide support network she had upon her arrival. Her best friend was pursuing her master’s degree in Toronto at the time, and she helped her find a place to live and set up her student card, banking, and phone number. During our talk, Feri could not stress enough just how happy she was to join the IMS in Toronto, but that is not to say that she did not miss home as well, describing the “long rich history [of my home city] that I miss being a part of, compared to the relatively newer history of Canada. Not that it’s a bad thing, it’s just different.” With Feri’s move to Toronto being settled, I then asked more specifically about her current research.
Spondyloarthritis is a chronic inflammatory disease that mainly affects the spine and peripheral joints. Interestingly, this disease also manifests in regions outside of the joints, such as inflammation of the eyes, skin, and
gut.1 Feri is specifically focused on the relationship between the gut and the joints in the context of spondyloarthritis. She explains the importance of breaking away from the idea that inflammation is only a regional effect, but rather, “there are systemic connections between different parts of the body; inflammation in one region can spark inflammation in another.” For example, Feri explains, there is evidence that immune cells in the joints can express markers associated with the gut, and vice versa.1 While Feri’s love for research shines through her dedication and commitment from her master’s to her current work, she also emphasizes the importance of community involvement.
Feri became involved with extracurriculars from day one of her PhD, and has been a major contributor to student life at both
the University of Toronto (UofT) and IMS ever since. A lot of her time was spent with UofT Talks, a student-run symposium that discusses major breakthroughs in health research. Feri led the organizing committee from 2021 to 2023, and describes this as huge achievement for her since “2023 was the first time we held UofT Talks in-person after the pandemic, so I am very proud of my team and what we were able to accomplish.” Building off this success, Feri teamed up with her lab mates to create IMS MedDash, an Amazing Race-style competition for high-school students interested in learning more about research, which is currently set to host its inaugural event this July. The intention with MedDash, was to introduce biomedical science research to the youth in upper years of high school since they are in a critical point of deciding their future, specifically those from underserved communities, and present science in a fun, interactive way.
After her PhD, Feri hopes to work in industry, citing her desire to see the impact of her work faster as opposed to the slower-paced environment of academia. Looking back on her journey, Feri stressed the importance of extracurricular involvement, especially in graduate school, proclaiming that “achievements in graduate school can be slow, so getting involved in other activities can help remind you that you are not a failure, and that your potential can be realized in many different ways beyond just the lab.” Through this we arrive at the essence of
Feri’s story; the need to surround yourself with the right people. From her master’s supervisor helping her get a job at the IVF clinic, to Dr. Haroon helping with her graduate school application, to her friend helping her transition to Toronto life, we must realize that we are not in this alone. Graduate school should be a time to build and foster connections, enabling us to make an impact not only on ourselves but also on our community.
References
Shaghayegh (Feri) Faroozan PhD Candidate, Toronto Western Hospital.
Photo Credit: Feri Foroozan
Stop Thinking and Just Start Doing:
Combining Academia, Industry, and Clinical Practice
with Dr. Paul Kudlow
By Priya van Oosterhout
There are two universal truths in graduate school: first, that it is unpredictable, and second, no two students will share the same journey. Institute of Medical Science (IMS) alumni Dr. Paul Kudlow’s exceptional career has embodied these truths, combining the best of academia, clinical practice, and industry. Sitting down with Dr. Kudlow, a clinician-teacher at Sunnybrook Health Sciences Centre, assistant professor in the Department of Psychiatry at the University of Toronto, and founding partner of venture capital firm North South Ventures, I had the opportunity to discuss how his journey has led to where he is today, and how pulling from different areas of expertise has shaped his success thus far.
After completing his undergraduate degree in physiology and management, Dr. Kudlow faced a choice between the two worlds he was a part of: investment banking, or medicine. However, as fate would have it, the economic crash in 2008 pushed him towards the latter. Pursuing his fascination with human physiology, Dr. Kudlow began medical school at Western University, where he discovered his love of research while conducting a study on the use of cognitive enhancers (such as caffeine and stimulants) among Canadian medical students. With his newfound interest in medical research, Dr. Kudlow explains that psychiatry is “one of the fields with the most research opportunity, because it is very much at the frontier of medicine.” It was during
this first foray into research where he first encountered what he calls “the discovery problem in academia,” in which researchers often struggle to parse the literature to find the exact data or studies relevant to their work. To tackle that discovery gap, Dr. Kudlow co-founded TrendMD, a “recommended-for-you” bar for scholarly articles. When readers finish a paper online, TrendMD suggests links to other studies on related questions, helping researchers uncover useful work they might otherwise miss. The tool now appears on thousands of journals and delivers more than 150 million tailored recommendations each month. When discussing this transition from medical student to CEO, it almost sounded simple. At least at first.
How does one even start a company? What does it mean to be a CEO? “Honestly,” Dr. Kudlow laughs, “I’m still figuring that out.” In TrendMD’s early days he met his co-founder online, spent two years building the product and raising seed capital, and likens the experience to “stumbling through a dark basement—you spot one obstacle with a flashlight, solve it, then move on.” As TrendMD scaled, the demands of a growing startup and a psychiatry residency collided, so he took an academic leave, turned TrendMD data into a PhD in bibliometrics, divested his stake in 2019, and finished residency. During the first wave of COVID-19 he co-founded North South Ventures, a venture capital firm which backs earlystage health-tech and biotech teams
aiming to improve patient outcomes and make health systems run better. “After TrendMD,” he says, “it was my turn— let’s see if I can pick companies, not just build one.”
Breakthroughs in biotech and health-tech are rare, so NSV looks for discoveries that could meaningfully shift patient care even when the odds are long. One example is YourChoice Therapeutics, developer of the first non-hormonal, reversible male contraceptive pill. Seeing its potential to reshape family planning, NSV backed the company early, with Dr. Kudlow excitedly stating that it “could change the world.”
As NSV attracts more capital, he aims to write larger cheques sooner, pairing those investments with a network of clinicians, scientists, and operators who can speed a project’s path to patients. His goal, he says, is to “take science straight from the bench—or the bedside—to the people who need it.”
While his exploits in industry are certainly very impressive, when asked about what he’s most proud of, Dr. Kudlow unequivocally says that it is his clinical work. Working as an inpatient psychiatrist at Sunnybrook, he speaks about how important it is being a part of a patient’s care journey, stating, “working one-on-one with patients gives me a level of purpose no spreadsheet can match.” He also performs psychiatric interventions, treating individuals with severe depression and working closely with them to enhance their quality of life.
Fellow of the Royal College of Physicians and Surgeons of Canada
Clinician-Teacher at Sunnybrook Health Sciences Centre
Assistant Professor, Department of Psychiatry in the University of Toronto’s Temerty Faculty of Medicine
His clinical practice has also informed his work at NSV, giving him perspective on patient needs, and the challenges involved in administering healthcare. This led me to my next question: how does someone bridge the gap between academia, clinical practice, and industry?
Drawing on his graduate-school experience, Dr. Kudlow says academia, clinical medicine, and the startup world often feel like separate planets, each with its own gravity and ground rules. Business moves at sprint speed, powered by mottos like “move fast, break things.”
Medicine, by contrast, is guided by careful protocols that put patient safety first. As Dr. Kudlow puts it, “That mantra really doesn’t work in clinical medicine. You can’t move fast and break things, otherwise people get hurt.” However, not everything is different, and he mentions that there are a lot of similarities between good business, good science, and good medicine. The key to balancing everything, he explains, is being aware of how different the three worlds are and leveraging the strengths of each to mitigate the weaknesses of the others. Industry CEOs often trumpet products long before they work, whereas scientists wait for peer-reviewed results. If each side adopted a bit of the other’s culture—faster iteration in the lab, more openness in the boardroom—breakthroughs would reach patients sooner.
As we began to wrap up our conversation, I had one final question: what is your advice for people in academia or medicine, who are looking to start their own companies, or venture into industry? For this, Dr. Kudlow had one main point that he emphasized heavily: “stop thinking, just start doing.” He explains that for most people, the biggest challenge is simply getting started, and with the introduction of artificial intelligence (AI), the market is changing at breakneck speeds, and you won’t know what obstacles you will face until you’re there to shine a light on them.
Looking back to the universal truths of graduate school, I think Dr. Kudlow is a fantastic example how unpredictable it can be. His career embodies the spirit of forging your own path during your studies, and not settling into just one box (or in this case, sector). He began his career deciding between medicine and investment banking, discovered a passion for research, and co-founded two separate companies, all the while continuing his work as a psychiatrist at Sunnybrook. Graduate school can often feel like a set pathway—masters, then PhD, then postdoc, and finally working in academia for the rest of your career. However, as Dr. Kudlow exemplifies, there are many ways to achieve success, and there is no reason why a person must choose between academia, clinical practice, and the business world. So, as Dr. Kudlow says, stop thinking and just start doing, because you never know where you may end up.
Dr. Paul Kudlow, MD, PhD, FRCPC
Photo Credit: Paul Kudlow
Feeling Settled in the Unsettled –Dr. Rabin’s Journey into Academia and Exploring Women’s Brain Health
By Nayaab Punjani
Dr. Jenny Rabin’s path to academia, and to the fields of women’s brain health and neuromodulation, was anything but linear. Originally from Toronto, she began her undergraduate studies in philosophy at the University of Kings College in Halifax, Nova Scotia, drawn by the appeal of a smaller campus community. Although she eventually realized that philosophy was not the right career path for her, the program’s strong emphasis on essay writing proved invaluable in developing the writing skills she would later rely on as a scientist.
Her academic focus shifted when a biology course piqued her interest in the brain, prompting her to take courses in neuroscience and psychology. Four years later, she graduated with a BSc in Psychology and a growing interest in cognition and dementia. She then worked as a research assistant at Baycrest under the mentorship of the late Dr. Don Stuss, a renowned neuropsychologist. Inspired by this formative experience, she pursued an MA/PhD in Clinical Psychology at York University, specializing in neuropsychology under the supervision of Dr. Shayna Rosenbaum.
Following her time at York University, she completed a clinical residency in neuropsychology at Massachusetts General Hospital (MGH) in Boston. Eager to bridge her academic training with real-world clinical challenges, she remained at MGH as a postdoctoral fellow, where her research focused on Alzheimer’s disease (AD). Specifically, she investigated the risk and
protective factors that influence the onset and progression of AD using multimodal imaging and sensitive cognitive tests. Throughout this period, she was fortunate to be mentored by several leading experts in the field, including Drs. Reisa Sperling, Jasmeer Chhatwal, and Trey Hedden.
Almost three years into her postdoctoral fellowship, Dr. Rabin learned of an exciting opportunity that would mark a turning point in her career. In 2019, Dr. Rabin joined the Sunnybrook Research Institute, as a scientist and the neuropsychology lead of the Harquail Centre for Neuromodulation. The following year, in 2020, she was appointed Assistant Professor in the Department of Medicine (Neurology) at the University of Toronto.
Reflecting on the early days of her role at Sunnybrook, Dr. Rabin recalls being told her position was “a blank slate”—a prospect that was both exciting and daunting. “There was no blueprint,” she explains. “The only guidance was to help move the neuromodulation research program forward.” “What I’ve come to understand,” she notes, “is that if you really listen to patients, they’ll point you toward the most important research questions.”
In addition to her work in neuromodulation, Dr. Rabin’s research program places a strong emphasis on addressing disparities in AD, particularly those related to racial/ethnic background. As part of this commitment, she launched the Canadian Multi-Ethnic Research on
Aging (CAMERA) Study, a longitudinal, observational study designed to investigate the risk and protective factors for dementia across three of Canada’s largest ethnic groups: individuals who identify as Chinese, South Asian, and White. By focusing on these diverse populations, the CAMERA study seeks to fill critical gaps in dementia research, which has historically underrepresented non-White communities. To date, the study has enrolled over 200 participants. A key feature of the study is its emphasis on reciprocity: participants receive personalized feedback, including their blood work results, cognitive testing outcomes, and MRI findings. The research team also maintains ongoing communication through newsletters and has established a community advisory board. This board plays an essential role in shaping the study’s direction—helping to ensure that the research questions are meaningful, relevant, and grounded in the needs and perspectives of the communities being studied.
Another aspect of her work focuses on women’s brain health, an area that has long been overlooked in neuroscience. Most brain research has been conducted on male participants and male animals, which has left critical gaps in understanding how brain conditions manifest, progress, and respond to treatment in women. One of the central questions Dr. Rabin investigates is why women are at greater risk of developing AD. Emerging evidence from her lab suggests that earlier onset of menopause—and the corresponding loss of ovarian hormones,
If something isn’t going well, don’t keep it to yourself— share it, so we can work together to find a solution. “ “
Dr. Jenny Rabin
Scientist, Evaluative Clinical Sciences, Hurvitz Brain Sciences Research Program, Sunnybrook Research Institute
Neuropsychology lead, Harquail Centre for Neuromodulation, Sunnybrook Health Sciences Centre
Associate Professor, Department of Medicine (Neurology), University of Toronto
particularly estradiol—may be a key factor. Estradiol helps protect the brain, supporting synaptic function, reducing inflammation, and promoting resilience against neurodegeneration.
Dr. Rabin is not only advancing impactful science but also shaping the next generation of scientists. Reflecting on her own experience as a graduate student, she is intentional about the kind of mentor she strives to be, one who creates space for curiosity, growth, and open communication. “I think there are
a lot of things grad students don’t ask for, but still need or want,” she reflects. “So, I try to think: how can I bring that into my supervision?” She makes a point of checking in regularly with her students— not just about their projects, but also their well-being and professional development. She encourages her trainees to ask questions, admit when they’re unsure, and view uncertainty as a normal part of scientific learning.
As a female scientist, Dr. Rabin recognizes the unique challenges women in academia continue to face. In response, she founded the Toronto Women in Science Talks (TWIST) initiative, a platform designed to foster a supporting and empowering community for women in science. TWIST events are held quarterly and aim to create space for open, solutionfocused conversations about navigating academic careers. The first TWIST event, held in February 2025, featured a panel of accomplished female scientists who candidly discussed their academic journeys, the challenges they encountered, how they overcame them, and the lessons they learned along the way. In June, they hosted their second event, focused on self-advocacy, as women are often less likely than men to ask for promotions, resources, or recognition. The discussion provided practical tools for speaking up, setting boundaries, and negotiating with confidence. Future events will focus on mentorship, imposter syndrome, and parenthood. Dr. Rabin emphasizes that allyship is essential to creating systemic
change. She hopes that more men will attend future TWIST events—not only to better understand the barriers their female colleagues face, but to play an active role in advancing equity within academia.
Dr. Rabin ends by sharing some advice for students. She reflects on the many points in her own career when the next step wasn’t clear. She encourages students to find peace in not having all the answers.
“I hope students can feel settled, even in times of uncertainty. I hope students can learn to feel grounded, even in times of uncertainty. I often see students so eager to figure out their next step—sometimes years in advance. But I’ve come to realize that it’s often pointless to plan too far ahead, because so much can change along the way. There’s a lot of luck, serendipity, and timing involved in finding the right path. As much as we try to plan, we simply can’t predict everything. That’s why it’s important to enjoy every step of the journey, not just focus on the finish line. A master’s or PhD is a long road—it’s far too long to spend just waiting for it to be over. You have to find value and joy in the process itself.”
Lastly, she shares this mantra with her students: “never worry alone.” She values openness and believes that fostering honest, early communication is essential to addressing challenges before they escalate. “If something isn’t going well,” she says, “don’t keep it to yourself—share it, so we can work together to find a solution.”
Photo Credit: Dr. Jenny Rabin
Blood (and Organs) on Your Hands: A Timeline of Blood and Organ Donation Deferral Policies for Men Who Have Sex with Men in Canada
By Jasmine Amini
Canadian Blood Services (CBS) currently requires 832 000 blood units (each of them 450mL) to be donated yearly to meet ongoing demand.1 The landscape for organ donation is similarly fraught with high demand; more than 3400 Canadians remained on an organ donation waitlist at the end of 2023, while over 200 patients died while waiting for a transplant throughout the year.2 Despite steady need for blood and organ donations, several health organizations, including CBS, bear a legacy of refusing or deferring donations from men who have sex with men (MSM). In addition to straining available resources, policies against donation from MSM perpetuate harmful stereotypes and fail to reflect modern advances in viral testing.
Blanket bans against blood donations from MSM were first introduced in Canada during the 1980s at the peak of the acquired immunodeficiency syndrome (AIDS) epidemic.3 The rationale for these bans was to limit the spread of AIDS, which at the time, predominantly affected MSM.3 Mystery shrouded AIDS during this period; although health officials noticed that AIDS was transmitted through blood inoculation and sexual activity, little was known about the cause, let alone the treatment, of the virus.
Uncertainty around AIDS’ etiology fueled stigma against MSM, who were often harassed and socially excluded over fears of contamination, regardless of illness status.4 Following 1200 accidental HIV infections through contaminated blood
donations supplied by the Canadian Red Cross, a ban against blood donations from MSM was enacted in Canada in 1983. 5 Similar policies were soon adopted worldwide for both blood and organ donation by MSM.6
In 1984, scientists determined human immunodeficiency virus (HIV) to be the cause of AIDS.3 Following this discovery, research on procedures to detect HIV in blood progressed rapidly, with the first generation of HIV antibody tests being released in 1985.7 HIV tests advanced greatly in precision over the course of 15-20 years. While the first HIV blood test could only detect a singular antibody (IgG), the third and fourth generation tests of the late 1990’s were equipped to detect HIV antibodies, proteins produced by the immune system in response to pathogen exposure, and HIV antigens, pathogenic molecules that cause immune response. Advances in testing greatly improved test sensitivity, which then lay between 99.5-99.8%. Despite progress made in blood testing, one limitation to HIV assays remained: the test-negative window.
The test-negative window refers to the period between initial infection to when markers of infection can be accurately detected. The test-negative window for third and fourth generation HIV assays was two weeks, meaning newly infected individuals could falsely screen negative for HIV during this period. Concerns over donor infection during the test-negative window fueled policy decisions to retain
the blanket ban on blood and organ donation from MSM.3 The lifetime ban on blood donation from MSM in Canada remained in place until 2013, when it was replaced by a five-year deferral period that restricted donations from men who had sex with men within the past five years.5 These policy amendments came years after similar changes in Australia, the UK, and Sweden, although these countries implemented one, rather than five, year deferral periods. Canada’s deferral period was shortened to one year in 2016.8
Following years of research, lobbying, and advocacy, CBS officially updated their policies around blood donation from MSM in 2022, ending the one-year donor deferral period.8 In its place, CBS implemented a sexual behaviour screen, completed by all donors, that assesses recent sexual activity. Donors who have had anal intercourse with a new partner or multiple partners within the last three months must wait three months from last instance of anal intercourse to donate blood.9 Organ and tissue donations by MSM, however, remain restricted. Specifically, MSM must abstain from anal intercourse with men for at least a year prior to donation. 6 Organ donations by MSM who do not meet the sexual behaviour criterion, termed “increased risk” donations, may be made under exceptional circumstances in case of high need, with recipient consent.
Discrepancies in blood and organ donation policies for MSM between
Canada and countries with similar risk profiles also raises concerns over the scientific validity of these guidelines. For example, the United States of America (USA) allows organ and tissue donation from MSM who abstain from sex with men for at least 30 days prior to donation.6 With otherwise similar testing procedures,6 it seems unlikely that the risk of HIV infection from organ donation is higher in Canada than the USA to warrant the stricter policies. With the advent of nucleic acid amplification tests for HIV, which can detect infections around seven days post-exposure, the seemingly arbitrary differences in donation policies between similar jurisdictions is even more confusing.10
Although policies to defer donations from MSM in Canada stem from an abundance of caution, justifications for past and current practices are lacking from both an equity and, at times, scientific standpoint. Foremost, HIV is not exclusive to MSM. In 2023, nearly a third of new HIV infections were among females,11 with the majority of those infections coming from heterosexual intercourse. CBS’ recent move to a sexual behaviour-based screening tool is positive; however, this screen fails to recognize the non-negligible, though lower, risk of HIV infection via oral or vaginal sex.12 As such, the stigma and restrictions associated with blood/organ donation policies still primarily affect individuals from the 2SLGBTQIA+ community.
Despite headway being made in the fight to improve equity for MSM seeking to donate blood and organs, there is still work to be done. Efforts to remove barriers for organ donation from MSM are continuing, with activists taking Health Canada to court for discriminatory organ donation policies.13 Calls to action, such as those being made by the CommunityBased Research Centre,10 are being heard by major bodies such as the Canadian societies for Transplantation and Critical Care, demonstrating growing support for equitable reform. With continuous demand for blood and organs in Canada, it is critical to capitalize on advanced HIV testing to develop safe, equitable policies that encourage, rather than deter, lifesaving donations.
References
1. Canadian Blood Services is rallying people across the country to shine a light on the need for new donors, https://www.blood.ca/en/ about-us/media/newsroom/canadian-blood-services-rallying-people-across-country-shine-light-need-new (accessed 27 April 2025).
2. Summary statistics on organ transplants, wait-lists and donors | CIHI, https://www.cihi.ca/en/summary-statistics-on-organ-transplants-wait-lists-and-donors (accessed 27 April 2025).
3. Wilson K, Atkinson K, Keelan J. Three decades of MSM donor deferral policies. What have we learned? Int J Infect Dis 2014; 18: 1–3.
4. Handlovsky I, Sidhu J, Amato AT, et al. The collective trauma of HIV/AIDS and contemporary constructions of health: Older gay men’s perspectives. SSM Qual Res Health 2024; 6: 100477.
5. Jubran B, Billick M, Devlin G, et al. Reevaluating Canada’s policy for blood donations from men who have sex with men (MSM). J Public Health Policy 2016; 37: 428–439.
6. Leeies M, Collister D, Christie E, et al. Sexual and gender minority relevant policies in Canadian and United States organ and tissue donation and transplantation systems: An opportunity to improve equity and safety. Am J Transplant 2024; 24: 11–19.
7. Alexander TS. Human Immunodeficiency Virus Diagnostic Testing: 30 Years of Evolution. Clin Vaccine Immunol CVI 2016; 23: 249–253.
8. Canada H. Health Canada authorizes Canadian Blood Services’ submission to eliminate donor deferral period for men who have sex with men, https://www.canada.ca/en/health-canada/ news/2022/04/health-canada-authorizes-canadian-blood-services-submission-to-eliminate-donor-deferral-period-for-men-who-have-sex-with-men.html (2022, accessed 4 May 2025).
9. Sexual behaviour-based screening | Blood.ca, https://www. blood.ca/en/blood/am-i-eligible-donate-blood/sexual-behaviour-based-screening (accessed 3 May 2025).
10. Leeies M, Ho J, Gruber J, et al. Ending discriminatory practices in organ and tissue donation and transplantation (OTDT), https:// www.cbrc.net/ending_discriminatory_practices_in_organ_and_tissue_donation_and_transplantation_otdt (2023).
11. Canada PHA of. HIV in Canada: 2023 surveillance highlights, https://www.canada.ca/en/public-health/services/publications/diseases-conditions/hiv-2023-surveillance-highlights-infographic.html (2024, accessed 3 May 2025).
12. Boily M-C, Baggaley RF, Wang L, et al. Heterosexual risk of HIV-1 infection per sexual act: systematic review and meta-analysis of observational studies. Lancet Infect Dis 2009; 9: 118–129.
13. Aiello R. Man taking Health Canada to court over ‘stigmatizing, and discriminatory’ organ donation policy. CTVNews, https://www. ctvnews.ca/health/article/canadian-government-facing-new-legal-challenge-from-a-gay-man-over-deeply-hurtful-organ-donation-policy/ (2025, accessed 4 May 2025).
Contraception Isn’t Just Her Job
By Tiffany Chien
While pills, implants, intrauterine devices, and barrier methods have provided women with reproductive autonomy for decades, the current contraceptive landscape places a disproportionate amount of the physical and mental burden for pregnancy prevention on women.1 But what about men? Beyond condoms, which has a failure rate of up to 16% with typical use2, and vasectomies, with concerns over their semi-permanency, male contraceptive options remain limited, and progress has been slow.2
The development of safe, efficacious male contraceptives has proven to be a significant challenge. Specifically, a male birth control pill would have to suppress sperm production and/or viability or, inhibit ejaculation in a way that would avoid adverse mood and sexual side effects.
What types of male contraceptive candidates are in the pipeline?
Promising research is being conducted for various hormonal and non-hormonal pharmaceuticals, and medical devices that could provide men with a diversity of contraceptive options. Birth control methods need to be dependable and, ideally, reversible; these methods should also have minimal side effects, be easy to take or use, and be affordable. 3
One hormonal method that has been successful as a long-acting reversible method for men is the NES-T (Nesterone/ Testosterone) gel.4 The gel is applied to each shoulder topically to prevent sperm production while maintaining testosterone at healthy levels to minimize side effects and sustain sexual function. This product is currently in phase 2b clinical trials to evaluate dosage and efficacy, and researchers are hopeful that it will be the first male contraceptive product to reach phase 3 (confirmation of safety and efficacy in a larger cohort) and hopefully become readily available within the next five to six years.4
While hormonal methods will likely be first to hit the market, alternative, nonhormonal options are still needed. In addition to having fewer side effects, non-hormonal contraceptives provide the potential for more diverse drug profiles compared to hormonal counterparts that are limited to early-stage sperm inhibition.5 There are several reversible non-hormonal pills currently in clinical trials. YCT-529 is a retinoic-acid receptor alpha inhibitor that works by blocking vitamin A access in the testes, thereby inhibiting sperm production.6 Additionally, a fast-acting, short-term male birth control pill using a soluble adenylyl cyclase (sAc) inhibitor, which has been shown to slow sperm motility and prevent sperm maturation in mice7, is currently in preclinical testing, with plans to initiate clinical trials sometime in 2025 for market release by 2031 if shown to be effective in humans.8
The last category of male birth control involves medical devices. In contrast to pharmaceutical methods, which on average have a research and development period of 12 years, medical devices benefit from a shorter timeline—approximately seven years to regulatory approval.9 These devices are typically referred to as vas-occlusive contraception, as they involve implanting a device or material (i.e. hydrogel) that blocks the transport of sperm through the vas deferens, the tube that carries sperm to the ejaculatory ducts.10 Unlike a vasectomy, which doesn’t always guarantee reversibility, vasocclusive methods are easily reversible through the natural degradation of the material, allowing users to restore their fertility if desired.10 One company developing occlusion gel contraceptives is Contraline, with its product ADAM, which is in phase 1 safety trials.10
Why has the production of male contraceptives taken so long?
Beyond scientific challenges, there are significant financial, regulatory, and cultural barriers to the use of male contraceptives. Once the drugs have been shown to be effective, there remains several safety requirements that must be met to ensure the side effects are minimal. Part of the drug approval process requires assessing the risk and benefits to the individual taking the drug.11 Unfortunately, for male contraceptives, the risk-benefit criteria are higher than female
contraceptives. For men, birth control offers no direct health benefits, so these medications must meet exceptionally high levels of safety—with no risks and side effects—to receive approval. In contrast, female birth control typically causes a range of side effects, including irregular bleeding, mood changes, weight gain, headaches, and nausea.12 However, these risks are generally deemed acceptable by the Food and Drug Administration, given that the potential morbidity and mortality of pregnancy and childbirth far exceed those associated with contraceptive use.
In our interview with Dr. Stephanie Page, endocrinologist and a professor of medicine at University of Washington, she is hopeful that the regulatory approval criteria for male contraceptives will evolve because “we should be thinking about the risk as a [couple], not just the man, since both [parties] are responsible for the pregnancy, and both should be responsible for the outcome of the pregnancy [...] because we’re trying to prevent a health consequence in the partnership.”
Bringing male contraceptives to market requires substantial investments, beyond grants available through government funding. Unfortunately, pharmaceutical companies that could provide funding for male contraceptives do not perceive a demand for these medications. Moreover, recent federal funding cuts by the Trump administration to reproductive health research terminated many studies previously funded by the United States
Agency for International Development (USAID)13, including a study on female sAC-based contraceptive.
Another key challenge lies in cultural barriers to male contraceptive uptake. Despite the growing interest in male contraceptives, many couples may still rely on female contraceptives due to the lack of awareness of, and education about, the alternative options for men. That doesn’t mean couples are satisfied with female contraceptives, especially since these existing methods have been associated with several adverse side effects.14
Experts believe that a shift in mindset would promote the uptake of male contraceptives. In our conversation with Dr. Logan Nickels, Chief Research Officer at Male Contraceptive Initiative, he emphasized that “the conversation has to shift away from thinking about male and female contraceptives as mutually exclusive landscapes with two separate populations demanding them… male contraception [is] women’s health.” The advancement of male contraceptives will more equitably distribute the benefits and burdens of pregnancy prevention, promoting a sense of shared responsibility for all involved.
Acknowledgements
References
1. Kimport K. More than a physical burden: Women’s mental and emotional work in preventing pregnancy [Internet]. U.S. National Library of Medicine; 2018 [cited 2025 May 28]. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC6115298/
2. How effective is male contraception? [Internet]. https://www.nichd. nih.gov/. Available from: https://www.nichd.nih.gov/health/topics/ menshealth/conditioninfo/effective
3. Contraception and birth control methods [Internet]. Centers for Disease Control and Prevention; [cited 2025 May 28]. Available from: https://www.cdc.gov/contraception/about/index.html
4. Population Council. Nestorone®/Testosterone Transdermal Gel for Male Contraception – Population Council [Internet]. popcouncil. org. 2022. Available from: https://popcouncil.org/project/nestorone-testosterone-transdermal-gel-for-male-contraception/
5. Nickels L, Yan W. Nonhormonal Male Contraceptive Development—Strategies for Progress. Pharmacological Reviews [Internet]. 2023 Nov 30;76(1):37–48. Available from: https://www.ncbi.nlm. nih.gov/pmc/articles/PMC10759220/
6. A non-hormonal pill could soon expand men’s birth control options [Internet]. American Chemical Society. 2022. Available from: https://www.acs.org/pressroom/newsreleases/2022/march/non-hormonal-pill-could-soon-expand-mens-birth-control-options.html
7. Balbach M, Rossetti T, Ferreira J, Ghanem L, Ritagliati C, Myers RW, et al. On-demand male contraception via acute inhibition of soluble adenylyl cyclase. Nature Communications [Internet]. 2023 Feb 14;14(1):637. Available from: https://www.nature.com/articles/ s41467-023-36119-6#citeas
8. SACYL Pharmaceuticals FAQs [Internet]. [cited 2025 May 28]. Available from: https://www.sacylpharma.com/faqs
9. Van Norman GA. Drugs, devices, and the FDA: Part 1: An overview of approval processes for drugs [Internet]. Elsevier; 2016 [cited 2025 May 28]. Available from: https://www.sciencedirect.com/science/ article/pii/S2452302X1600036X
10. Matsumoto NM, Chiartas TG, Paysour BR, Barry TJ, Ott LE, Tropsha Y, et al. Preclinical development of a novel injectable hydrogel for vas-occlusion. Contraception [Internet]. 2025 Feb 10;145:110839. Available from: https://www.sciencedirect.com/ science/article/pii/S0010782425000307
11. FDA draft guidance outlines criteria for conducting benefit/risk assessments [Internet]. Raps.org. 2025. Available from: https://www. raps.org/news-and-articles/news-articles/2021/10/fda-draft-guidance-outlines-criteria-for-conductin
12. Smith L. Birth control pill: Side effects, risks, alternatives, and the shot [Internet]. www.medicalnewstoday.com. 2020. Available from: https://www.medicalnewstoday.com/articles/290196#summary
13. Tanis F. The Trump administration kills nearly all USAID programs [Internet]. NPR. 2025. Available from: https://www.npr.org/sections/goats-and-soda/2025/02/26/nx-s1-5310673/usaid-trump-administration-global-health
14. Tumwesigye R, Kigongo E, Nakiganga S, Mbyariyehe G, Nabeshya J, Kabunga A, et al. Uptake and associated factors of male contraceptive method use: A community-based cross-sectional study in northern Uganda [Internet]. U.S. National Library of Medicine; 2023 [cited 2025 May 28]. Available from: https://pmc.ncbi.nlm.nih. gov/articles/PMC10353552/
The Immortal Life of Henrietta Lacks Exposes the Quiet Violence that Underlies Scientific Progress
By Beatrice Acheson
In 1951, in the “Colored Ward” of Johns Hopkins Hospital, Henrietta Lacks was diagnosed with cervical cancer after undergoing a routine tissue biopsy. Unknowingly and without consent, Henrietta had started a scientific revolution. Her cells, termed “HeLa” cells, would divide continuously and robustly in a petri dish, becoming the first immortal human cell line. In the decades following, her cells would enable the development of the polio vaccine, gene therapies for hemophilia, and chemotherapies for leukemia. This unprecedented advancement was accompanied by immense financial gain, as companies like Thermo Fisher Scientific made billions in profit through the commercialization of Henrietta’s cells. Henrietta died later that year, unaware of the immense impact of her contribution and the exploitation that would follow.1
For over 50 years, Henrietta Lacks’ identity was reduced to four letters: HeLa. In her biography, The Immortal Life of Henrietta Lacks, Rebecca Skloot reckons with Henrietta’s near erasure and restores her story in over 300 pages. Skloot’s desire to tell Henrietta’s story began in her high school biology classroom, when a teacher briefly mentioned the HeLa cells and the research they enabled. Years later, still curious, Skloot searched for Henrietta online, only to discover a disjointed collection of conflicting facts. Henrietta’s cells laid the groundwork for unprecedented scientific discovery, but no one knew who Henrietta really was. Skloot uncovers Henrietta’s legacy and
situates it amongst a larger conversation about ethics, autonomy, and consent in medical research.
Using news stories, medical records, and interviews, Skloot humanizes Henrietta, painting a portrait of her life from birth to diagnosis to death—and beyond. Throughout the book, Skloot deliberately retains the native dialects of the people she interviews, a decision made when Henrietta’s daughter, Deborah, said, “If you pretty up the way people spoke and change the things they said, that’s dishonest. It’s taking away their experiences, and theirselves.”1 Through meticulous storytelling, Skloot preserves the humanity of Henrietta and her family members, a consideration that was not offered in 1951.
Skloot also reminds the reader that while Henrietta’s story was unique, it does not exist in isolation and is rather a part of a longstanding pattern of injustice specifically experienced by Black communities. Skloot tells Henrietta’s story but also references other ethical violations that have occurred at the hands of scientists, including the Tuskegee trials and the forced sterilization of Black women. In doing so, Skloot establishes Henrietta’s story as part of a larger, systemic pattern of oppression and exploitation and exposes the injustices that arise in the absence of medical ethics.
The objectification and dehumanization of Black women take many forms, and Henrietta’s story serves as a reminder of the quieter, more insidious violence that occurs under the guise of science. The Immortal Life of Henrietta Lacks is a
stringent reminder that our responsibility as scientists extends beyond the test tube. We are accountable for the samples that we use and upholding the dignity of those who have provided them. Skloot reminds us that Henrietta’s story is not just one of scientific discovery, but also one of the ethical responsibilities that we owe to the “stories” that underlie the science.
In 2023, 13 years following the publication of the Immortal Life of Henrietta Lacks—and nearly 70 years after the first use of Henrietta’s cells—the Lacks family reached a settlement with Thermo Fisher Scientific.2 Decades following her cancer diagnosis, Henrietta’s family was finally compensated for the years of commercialization that occurred in the absence of her informed consent. Multiple avenues of justice are available to reckon with erasure such as Henrietta’s, whether through financial compensation or literary reclamation. As scientists we ought to engage with both to view our research through a more humanistic and ethical lens. Reading stories like the one Skloot so gracefully tells in The Immortal Life of Henrietta Lacks is an important step in this process.
1. Rebecca Skloot. The Immortal Life of Henrietta Lacks. New York, NY: Crown Publishers; 2010. 381 p.
Meredith Wadman. Science. 2023 [cited 2025 May 2]. What does the historic settlement won by Henrietta Lacks’s family mean for others? Available from:
Learning and Exploring at the
AACR Annual Meeting
Springtime in the Windy City
By Kyla Trkulja & Alyona Ivanova
This spring, two IMS Magazine team members, Kyla and Alyona, journeyed to Chicago for the American Association for Cancer Research (AACR) Annual Meeting. Every year, over 25 000 cancer researchers from around the world convene to share advancements across all areas of cancer research, from drug discovery to survivorship.
The conference was held at McCormick Place, a massive convention centre spanning four buildings. The week was filled with talks, posters, and networking sessions that allowed attendees to connect and celebrate the exciting new research from the past year. Princess Margaret Cancer Centre even hosted a fun Vegasthemed mixer at a rooftop bar, bringing the Toronto community together for a night of yummy food, casino games, and skyline views.
The days were packed with learning, but that didn’t stop attendees from taking some breaks to explore. Kyla took an architecture tour on a boat that cruised through the river in the heart of the city. Guests on the boat sipped refreshing
cocktails while learning about the history of Chicago’s beautiful skyscrapers—some of which are over 100 years old.
At night, Alyona embarked on a sunset cruise. Dazzled by the sparkle of the city at night, the boat took Alyona from the heart of the Magnificent Mile through the flood gate and into Lake Michigan. Watching the sun set behind the stunning skyline of Chicago from the open-air deck—it was a night to remember. A fun fact Alyona learned was that Chicago’s “Windy City” nickname originated from the frigid breezes that sweep from Lake Michigan through the narrow streets of the city, but also from Chicago’s reputation for verbose politicians.
Chicago’s food scene was unmatched; no matter where you were in the city, delicious eats were always close by. At the recommendation of her supervisor, Kyla visited The Dearborn to try their legendary fish and chips that beat Bobby Flay during his cooking show challenge—and the dish definitely lived up to the hype!
Alyona opted to try one of Chicago’s specialties – the deep-dish pizza. Instead of
a thin, crisp crust, deep-dish pizza is more like a pie with its thick, buttery base. The pizza’s pie structure is filled with layers of melty cheese and delicious tomato sauce. Alyona recommends Labriola Ristorante.
Between the thrilling cancer research breakthroughs and memorable tourism experiences, the week in Chicago flew by, leaving everyone inspired, optimistic, and looking forward to the next meeting in sunny San Diego!
The sunset cruise provided beautiful views of the Chicago skyline across Lake Michigan
Views of old and modern skyscrapers during the architecture boat tour
McCormick Place Convention Center spans four buildings and five floors to fit over 25 000 conference attendees
Photo Credit: Alyona Ivanova
Photo Credit: Kyla Trkulja
Photo Credit: Alyona Ivanova
Legendary fish and chips at The Dearborn and Chicago’s signature deep-dish pizza at Labriola Ristorante
Photos Credit: Kyla Trkulja
IMS Scientific Day 2025: Bridging Science and Community
By Kowsar Teymouri
On the morning of Friday, April 25th, 2025, among the hustle and bustle of the city, Hart House–the beautiful, gothic-style building at the heart of the University of Toronto–was housing a rush of its own. Preparations were underway for another successful annual Institute of Medical Science (IMS) Scientific Day. What began as a small gathering in 2006 has now grown into a full-day conference celebrating the academic excellence of students and faculty through events like the Bernard Langer keynote lecture, the Laidlaw manuscript competition, and the Alan Wu poster competition.
This year’s event kicked off with the morning session of the Alan Wu poster competition, showcasing students’ research across a wide variety of disciplines and methodologies, reflective of the vast reach of the IMS. Following this, Drs. Nadia Minian and Brian Ballios delivered a warm welcome through their opening remarks. Dr. Mingyao Liu then delivered a heartfelt report to conclude his remarkable tenyear tenure as the director of IMS, which was received with a standing ovation–a
Dr. Mingyao Liu delivers a 10-year leadership report on his term as the director of IMS
testament to the deep appreciation of his work by the IMS community. Dr. Liu has been an integral part of the students’ experience at the IMS, and he will be dearly missed by students and faculty alike.
Dr. Liu then introduced this year’s keynote lecturer, Dr. Sonia Anand, Professor of Medicine and Epidemiology at McMaster University. She discussed her groundbreaking research evaluating the genetic and environmental determinants of vascular health for women and participants of varying ancestral origin, inspiring the next generation of health equity researchers.
To make the lunch hour more lively, the IMS Scientific Day planning committee had organized a speed dating-style mentoring event, which provided students the opportunity to connect with six IMS faculty members—asking questions and receiving career advice in a dynamic setting.
The day continued with the Laidlaw manuscript competition, during which four students presented their published manuscripts to a panel of judges. This
session offered attendees a chance to learn about the impactful work that students have carried out throughout their graduate program.
Following a coffee break, the most anticipated event of the day took place: the award ceremony. Now an annual tradition, IMS students, staff, and faculty are recognized for their academic achievements, impacts on the education of the student body, and contributions to the IMS community. The IMS Scientific Day award ceremony reflects the culture of support, recognition, and mentorship at the core of our values. We would like to congratulate all of this year’s award winners!
The closing remarks by the co-leads of the planning committee concluded another successful and memorable IMS Scientific Day. We would like to thank the IMS planning committee for their amazing work in organizing this event. Last but certainly not least, we would like to thank Dr. Liu for the lasting impact he has had on the IMS community, and warmly welcome Dr. Lucy Osborne as the new interim director of IMS!
Photo Credit: Emily Yeung
Dr. Sonia Anand delivers the Bernard Langer keynote lecture
Photo Credit: Emily Yeung
Graduate students showcased their research during the Alan Wu poster competition
Photo Credit: Emily Yeung
To read the full comic, visit emilyhuang.ca
Author and Illustrator: Emily Huang
Mother Tongue
METHODS Community of Practice
A new student-led initiative connecting IMS students with peer advisors for specialized research support.
Become an advisor
Share your expertise in study design, research methodologies, and data analysis. Provide personalized guidance to help inform peers’ projects.
Find out more:
What you'll gain:
Make a lasting impact
Enhance the IMS graduate student experience
Help others navigate similar challenges
Improve leadership and problem-solving skills
Valuable teaching experience
Expand your network and build connections
READ IT ONLINE issuu.com/imsmagazine imsmagazine.com