Advancements in cancer treatment and prevention have significantly improved survival rates, with approximately two million Australians now living with or beyond cancer.1,2 However, one third will develop cardiovascular disease, a rate 40% higher than the general population, making it the leading cause of morbidity and mortality in cancer survivors.2
Cardio-oncology is an emerging interdisciplinary field that focuses on the intersection of cardiovascular health and cancer care. It aims to identify risk factors, improve early detection, and develop strategies for the prevention and management of heart problems in cancer patients.3 The field also explores how pre-existing cardiovascular conditions can influence cancer treatment outcomes and plays a vital role in improving both quality of life and long-term outcomes for cancer survivors.1
Cardiovascular implications of cancer therapy
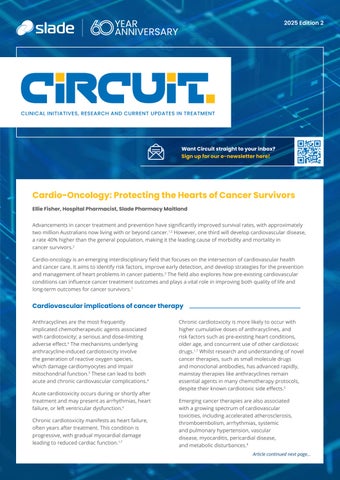
Anthracyclines are the most frequently implicated chemotherapeutic agents associated with cardiotoxicity; a serious and dose-limiting adverse effect.4 The mechanisms underlying anthracycline-induced cardiotoxicity involve the generation of reactive oxygen species, which damage cardiomyocytes and impair mitochondrial function.5 These can lead to both acute and chronic cardiovascular complications.4
Acute cardiotoxicity occurs during or shortly after treatment and may present as arrhythmias, heart failure, or left ventricular dysfunction.6
Chronic cardiotoxicity manifests as heart failure, often years after treatment. This condition is progressive, with gradual myocardial damage leading to reduced cardiac function.1,7
Chronic cardiotoxicity is more likely to occur with higher cumulative doses of anthracyclines, and risk factors such as pre-existing heart conditions, older age, and concurrent use of other cardiotoxic drugs.1,7 Whilst research and understanding of novel cancer therapies, such as small molecule drugs and monoclonal antibodies, has advanced rapidly, mainstay therapies like anthracyclines remain essential agents in many chemotherapy protocols, despite their known cardiotoxic side effects.5
Emerging cancer therapies are also associated with a growing spectrum of cardiovascular toxicities, including accelerated atherosclerosis, thromboembolism, arrhythmias, systemic and pulmonary hypertension, vascular disease, myocarditis, pericardial disease, and metabolic disturbances.8
Article continued next page...
Cardiovascular risk-mitigation strategies
Effective management of cardiovascular risk in cancer patients requires early identification and ongoing monitoring of patients at increased risk of cardiotoxicity. A personalised approach is essential, balancing the therapeutic benefits of cancer treatment against the potential for cardiovascular harm.1 In patients with potentially curable malignancies and longer life expectancy, cardiotoxicity may become a significant source of long-term morbidity and mortality.1
Baseline cardiovascular risk assessments utilising cardiovascular risk calculators6,8,9 are recommended for all cancer patients prior to initiation of therapy. Example tools such as the Heart Failure Association–International Cardio-Oncology Society baseline cardiovascular toxicity risk stratification tool help to determine a patient’s cancer therapy-related cardiovascular toxicity (CTR-CVT) score to guide the cardio-oncology approach.6
Patients with cancer who have coexisting cardiovascular risk factors, established cardiovascular disease, are receiving potentially cardiotoxic cancer treatments or mediastinal radiation, or have a history of such treatments, are more likely to have an elevated CTR-CVT score.8 A high or very high risk score recommends that patients receive referral to a cardio-oncology program or cardiologist, are provided with the risk/benefit balance of cardiotoxic anticancer treatment and early intervention of cardioprotective strategies, such as lifestyle modifications and medications.7
Cardio-oncology care pathways recommend cardiovascular risk is regularly reviewed throughout the patient journey to optimise identification and appropriate management of potential cardiovascular complications.7
International guidelines and risk stratification tools, e.g. European Society of Cardiology Guidelines on Cardio-oncology 2022 for managing cardiovascular risk in cancer patients7 are supported by Australian clinicians, however further research is required to understand their applicability to personalise care locally and may not meet the needs of underrepresented populations such as Aboriginal and Torres Strait Islander peoples.3
The future of cardio-oncology
Cardio-oncology offers significant opportunities to improve patient care, however gaps remain. To support decision-making at both the population and individual levels in Australia, access to high-quality data is essential. This requires well-designed and generalisable clinical research to further understand the cardiotoxic mechanisms of new anticancer therapies and strengthen the evidence base for current interventions.3 Expanding multidisciplinary models of care and fostering collaboration with consumers will further enhance both cardio-oncology care and research in Australia.3
Image 1: Mechanism of cardiotoxicity in commonly used cancer therapies1
Past Challenges and Latest Advances in Menopause Management: Enhancing Care for Australian Women
Courtney Lawrence, Pharmacist in Charge, Slade Pharmacy Forster
Menopause, defined as the final menstrual period, typically occurs around age 50 and marks the end of a woman’s reproductive years.1 The preceding transitional phase, perimenopause, can begin up to a decade earlier and often lasts around four years.1 Hormonal fluctuations during this time commonly lead to symptoms such as vasomotor instability (hot flushes, night sweats), mood disturbances, low libido, and genitourinary syndrome of menopause, including vaginal dryness and painful intercourse.1 These symptoms can significantly impair quality of life, yet up to 85% of symptomatic women do not receive appropriate treatment.2 Beyond symptom burden, menopause is associated with increased long-term risks of cardiovascular disease, type 2 diabetes, and osteoporosis—largely due to declining estrogen levels, which affect bone density, lipid metabolism, and body composition.3
Historical Barriers to Care
Historically, menopause care in Australia has been hindered by unresolved medication shortages, limited PBS options, social stigma, and misinformation around evidence-based treatments. Early studies linking menopause hormone therapy (MHT) to increased risks of breast cancer4 and cardiovascular events5 led to widespread fear and underutilisation of MHT. Subsequent analyses have clarified that these risks are lower than initially reported and depend on patient age, duration, and type of therapy.6 For example, estrogen-only MHT used for five years in women aged 60–69 is associated with three additional breast cancer cases per 1,000 women compared to nine cases with ten years of use.7 Despite this, outdated perceptions continue to deter many women from initiating or continuing treatment.
Current Treatment Landscape
MHT remains the most effective treatment for vasomotor and urogenital symptoms. This typically includes estrogen with the addition of progesterone for women with an intact uterus to prevent endometrial hyperplasia.7 Other forms of systemic MHT include tibolone and conjugated estrogens with bazedoxifene, however these are not suitable in perimenopause.7 There are risks and contraindications to MHT (Table 1), as such it may not be suitable for all women. To mitigate risks, alternative routes of administration may be considered (e.g. transdermal, vaginal). Non-hormonal options are also available, particularly for women with contraindications to MHT. These include off-label use of certain antidepressants (e.g. paroxetine, venlafaxine), clonidine, and gabapentin.7 Herbal supplements are commonly used but lack robust safety and efficacy data and may interact with other medications.1,7
A New Class of Therapy: NK3R Antagonists
A significant recent development is the approval of neurokinin 3 receptor (NK3R) antagonists for vasomotor symptom management. These agents target the thermoregulatory centre in the hypothalamus, where declining estrogen levels disrupt temperature control.8 Fezolinetant, the first NK3R antagonist approved in Australia, is available as a 45 mg once-daily oral tablet.8 In clinical trials, it reduced vasomotor symptoms by 63%, compared to 40% with placebo.8 Adverse effects are generally mild and include headache, nausea, fatigue, and diarrhoea.8 Fezolinetant is contraindicated in patients with moderate-to-severe hepatic impairment or those taking CYP1A2 inhibitors.8 While not yet PBS-listed, fezolinetant offers a promising alternative for women unable or unwilling to use MHT.
MHT Contraindications
• Undiagnosed vaginal bleeding
• Breast or endometrial cancers (current or past)
• Acute cardiovascular or thromboembolic events
• Severe liver disease
MHT Precautions
MHT Risks
MHT Adverse Effects
• Myocardial infarction, transient ischaemic attack or stroke
• High risk of venous thromboembolism
• Active liver disease
• Migraine with aura
• High risk of breast cancer
• Increased risk of:
• Blood clots
• Stroke
• Endometrial cancer (estrogen alone)
• Breast cancer
• Headache
• Nausea
• Fluid retention
• Vaginal bleeding
• Sore breasts
Continued next page...
Table 1: MHT Contraindications, Risks and Adverse Events7
Continued from page 3...
Policy and System-Level Improvements
In March 2025, the Australian Government announced a landmark investment in women’s health. Key initiatives included:9
• First menopause treatments on PBS in 20 years: Oestrogel® (transdermal estrogen), Prometrium® (oral micronised progesterone), and Oestrogel Pro® (combination pack)
• Medicare rebates for dedicated menopause health assessments from GPs, commencing 1 July 2025
• Funding for clinician training, public awareness campaigns, and national clinical guidelines
• Additional endometriosis and pelvic pain clinics equipped to support menopause9
Drug Updates for Endometriosis
These changes are expected to improve access, reduce out-of-pocket costs, and provide evidence-based care for women experiencing menopause and perimenopause.
Looking Ahead
While recent advances in treatment options and policy are encouraging, further progress is needed. Ongoing education for healthcare providers, public awareness, and broad accessibility to care is essential to ensure that all Australian women receive appropriate support during menopause. By adopting a holistic, evidence-based approach to menopause management, health professionals can play a pivotal role in improving the health and wellbeing of midlife women across the country.
Scan QR code for references
Justine Forbes, Hospital Pharmacist, Slade Pharmacy Hollywood
Endometriosis is a chronic disease in which endometrial tissue grows outside the uterus.1,2 Symptoms vary and can be severe (painful periods, pelvic pain, pain with sex, heavy menstrual bleeding, infertility); affecting quality of life, and limiting participation in education, work, and social activities.2-4 Endometriosis affects up to 10% of women, and contributes to over 40,000 hospitalisations annually.1,5
Managing endometriosis-associated pain may involve hormonal treatments, analgesics, surgery, physiotherapy or psychological interventions.3,4 Hormonal treatments aim to reduce pain and growth of ectopic endometrial tissue by inhibiting or suppressing estrogen activity.1,2 The RANZCOG Living Evidence Guideline recommends combined-oral-contraceptives (COC) and progestogens as first-line hormonal options, with gonadotrophin-releasing hormone (GnRH) agonists or antagonists considered if symptoms are not adequately managed.2,4
Two medications have recently been added to the PBS for the management of endometriosis - Ryeqo® and Dienogest.6 Ryeqo® (relugolix 40mg, estradiol 1mg, norethisterone 0.5mg) contains a COC in combination with a GnRH antagonist that supresses the release of estrogen and progesterone.2,7 Clinical trials show it significantly reduced period pain, pelvic pain, and pain during sex, lowered the need for analgesics, and improved health-related quality of life.3,4,8 The COC component helps to reduce GnRH-related side effects, like vasomotor symptoms and bone mineral density loss.4,8 Ryeqo® is a once-daily oral therapy.9
Dienogest, a fourth-generation progestin, is now available as a single ingredient 2mg tablet for endometriosis.2 It has been shown to decrease mean pelvic pain scores compared to placebo, and the need for pain medication.10
The addition of Ryeqo® and Dienogest to the PBS improves equitable access to treatment options for women with endometriosis-associated pain.