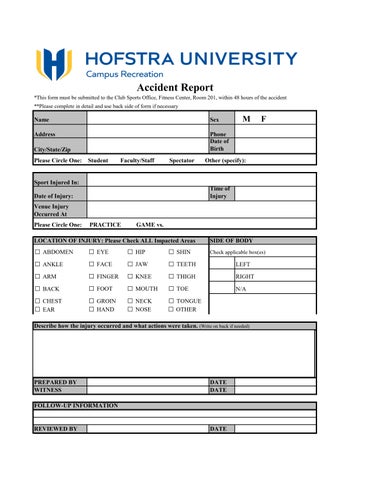
Accident Report
*This form must be submitted to the Club Sports Office, Fitness Center, Room 201, within 48 hours of the accident
**Please complete in detail and use back side of form if necessary
Name Sex M F
Address Phone
City/State/Zip
Date of Birth
Please Circle One: Student Faculty/Staff Spectator Other (specify):
Sport Injured In:
Date of Injury: Time of Injury
Venue Injury
Occurred At
Please Circle One:
REVIEWED