Surgeon Mr David Sellu relives his court case resulting from a patient’s death P14
The business journal for doctors in private practice
Don’t be scammed How to protect your practice from the growing use of social engineering techniques P30
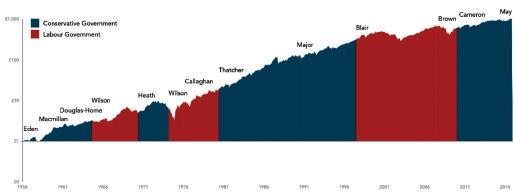
Timing the market
An expert explains why political dramas are not a basis for investment success P44
Plan to help private doctors with stress
By Robin Stride
Independent practitioners will have access to their own ‘well-being guardians’ in private surgeries, clinics and hospitals under plans being promoted this month by a doctors’ defence body.
These posts are being developed in the NHS and now the Medical Protection Society (MPS) is pushing to have them mirrored in the private healthcare sector to help rising numbers of doctors facing mental health issues.
Earlier this year, the BMA called for more mental health support for NHS staff after a report found only half of doctors were aware of any services to help them with physical and mental health problems at their workplace. One-in-five respondents said no support services were provided.
An MPS spokesperson told Independent Practitioner Today : ‘There is still work to be done on how this role can be developed in private practice, particularly among smaller stand-alone clinics and practices who we would encourage to join up to and form a cluster.
‘We want to ensure doctors have a
dedicated person who makes their health and well-being a core priority and is trained to recognise and support them when they are experiencing difficulties and will look to work with the industry to see how this could be best implemented.’
The MPS warns that private healthcare, NHS organisations, the Care Quality Commission (CQC), and the Government must act to tackle the ‘burn-out endemic’ in healthcare and support doctors to stay in practice, rather than quit or move abroad.
In a new report, Breaking the burnout cycle, it says only organisationwide interventions will safeguard the well-being of doctors and avoid them becoming burnt out and disillusioned in ever greater numbers.
An MPS survey of 275 UK doctors revealed that 35% of respondents have considered moving abroad due to personal well-being concerns, 45% have considered leaving the profession for the same reasons, and 44% said they do not feel encouraged by managers or partners to discuss well-being issues.
The Society is calling for:
A named well-being guardian in all NHS organisations by 2022, with
the same principle applied to private healthcare and GP practices, ensuring access to someone trained to recognise and support them when they are experiencing difficulties;
Governments to fund a confidential counselling service for all healthcare professionals across England, Wales, Scotland and in Northern Ireland;
The CQC to assess the extent to which healthcare providers look after the well-being of their doctors as a key line of inquiry.
MPS president Prof Dame Jane Dacre said: ‘It is perhaps one of the great paradoxes of our age, that modern medicine allows doctors to do more for their patients than ever before, yet increasing evidence shows doctors feel burnt out and disillusioned in ever greater numbers.
‘The causes of burn-out have been widely debated and include the growing demands and complexity of the job, a faster pace of work and tighter financial constraints.
‘The problem is also not unique to the UK, to the NHS or to any one specialty. It is a global phenomenon affecting all clinicians.’
MAC CHAIRS TO BE PAID
Specialists are for the first time going to be paid to chair medical advisory committees (MACs) in private hospitals.
In a break with tradition in the sector, which has seen doctors do this work on a voluntary basis, they are to be paid a salary of £12,000 a year.
See our fully story on page 4
MPS president Prof Dame Jane Dacre
TELL US YOUR NEWS Contact editorial director Robin Stride
Take stock of your marketing
Jane Braithwaite considers how best to analyse your results of your marketing so you can learn from your successes and failures and reduce its costs P16
ADVERTISE WITH US Contact advertising manager Margaret Floate at margifloate@btinternet.com Phone: 01483 824094
GET A SUBSCRIPTION DISCOUNT
£90 independent practitioners.
£90 GPs and practice managers (private & NHS). £210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE – USE SUBSCRIPTION FORM ON PAGE 25
Or email karen@marketingcentre.co.uk Or phone 01752 312140. Or go to the ‘Subscribe’ page of our website www.independent-practitioner-today.co.uk
Chief sub-editor: Vincent Dawe
Head of design: Jonathan Anstee
Publisher: Gillian Nineham at gill@ip-today.co.uk Phone: 07767 353897
EDITORIAL COMMENT
Stress battle plan welcome
Burnout is affecting more and more doctors and often goes unreported and undetected, so people suffer in silence or hit the buffers.
Traditionally, it has been hard for victims to know where to turn and, for that reason, we are glad to be able to highlight the problem in our lead story today.
Private doctors of all ages can have well-being problems, whether these arise from a variety of business worries surrounding their independent work, increased pressures within the NHS or personal circumstances such as divorce. For some, it’s all three.
So we are delighted to back current efforts to extend moves towards a welfare guardian system in the NHS into private healthcare too (see story on page one).
As Medical Protection Society president Prof Dame Jane Dacre says in the defence body’s new
report, Breaking the burnout cycle: ‘As leaders, managers and peers, we are all responsible for identifying signs of burnout in ourselves and others and in working together to develop strategies to enhance personal resilience.’
The World Health Organization (WHO) has now recognised burnout as a syndrome brought about by unsuccessfully managed chronic workplace stress. It will be working on evidence-based guidelines on mental well-being in the workplace.
Work needs doing on how the wellness guardian role can be developed in private practice, but why not consider how you can take things forward?
It will be interesting to see what the MPS’s talks with the industry come up with to progress the idea, and what both small practices and larger organisations do. Let us know.
Reconnecting with nature aids health
Our series on how to create a great user experience continues as our authors delve into the world of biophilic design P20
Five ways to success with property
Dr Lafina Diamandis outlines the five big investment strategies that doctors need to know when it comes to bricks and mortar P22
Reflecting well on you
Get revalidation sorted! This month’s analysis of the requirements for a successful appraisal and revalidation looks at dealing with feedback P26
Unearthing buried treasure
Data can be difficult to access in private healthcare, but Fiona Booth argues that we must all work together to make the most of this asset P34
Ever-rising cost of being sued
Solicitor Niloo Bozorgi looks at the costs of clinical negligence claims for private doctors and upcoming changes that will affect them P38
PLUS OUR REGULAR COLUMNS
Start a private practice: Are benefits in kind always really kind?
Ian Tongue highlights some of the more common taxable benefits that doctors might come across P48
Doctor on the Road: A very rewarding experience
It’s a doctor’s favourite, but can the latest version of the iconic Porsche 911 live up to expectations? P50
Profits Focus: Thirteen: lucky for some
Our unique benchmarking series looks at the financial fortunes of ENT surgeons P53
Pension pain continues
By Edie Bourne
Doctors will be able to choose their own NHS pension contribution rate in a bid to avoid substantial tax bills under new Government proposals launched last month.
If approved, the changes would mean increased flexibility for doctors, who would receive the same pension accrual as the contribution rate chosen.
Before 1 April each year, doctors would need to decide their desired accrual level and pay the corresponding contributions.
This will be in 10% increments; for example, 30% accrual with 30% contributions or 40% accrual with 40% contributions.
In a further boost, individuals could also review their pension growth towards the end of the scheme year when their likely total earnings for the period are more accurate.
They could then adjust their
accrual/contribution level accordingly.
Also, if a lower accrual level is chosen, employers could opt to pay the scheme member any unused contributions as a lump sum at the end of the year.
Patrick Convey, technical director of specialist financial planners Cavendish Medical, explained:
‘The tax implications caused by the tapered annual allowance have had a significant impact on the NHS workforce with consultants taking the logical step to adjust their workloads accordingly.
‘News that the Government is finally listening to those who have been penalised for saving into a fixed contribution pension scheme will come as a relief to many.
‘However, these proposals will add extra levels of convolution to already difficult calculations. Even the consultation document states “the department is concerned that the complex interaction of tax,
Patrick Convey: Says the proposals will ‘add extra levels of convolution to already difficult calculations’
pay and pensions can take considerable amounts of individual time and resources to manage’’.’
Mr Convey added: ‘You will need to ensure you are in possession of all the facts before attempting to calculate your own preferred contribution or accrual rate in order to minimise tax liabilities.
‘This is a decision which can only be made with the help of detailed financial modelling, taking into account factors such as your trading structure, likely future income and even lifestyle choices for retirement.
‘For example, opting for a much lower accrual will mean a significantly reduced pension in retirement.
‘We would advise that your first step is to request your annual pension statement from the NHS Pensions Agency.
‘Do this as soon as you can, as lengthy delays can occur and we have known many of the statements to contain computer-generated errors, so they must be thoroughly checked.
‘You can then use this statement as a basis for discussions with your financial planner to ascertain your current position and the likely tax implications going forward.’
The consultation is due to close on 1 November 2019.
Will tax ‘cure’ stop doctors cutting hours?
Doctors with a private practice have welcomed the Government’s response following strong pressure from medical bodies to come up with a cure for the pension tax problem.
Mr Richard Packard, chairman of the Federation of Independent Practitioner Organisations (FIPO), said: ‘As far as the independent sector is concerned, these measures should make consultants less worried about their tax status relative to their pension cap, allowing them to take on work to complement their NHS activity.’
The options (see story above), aimed at enabling senior medical staff to minimise the effect of the complex pension changes brought in by former Chancellor George Osborne, are currently out for consultation.
But FIPO said it remained to be seen if the measures would be sufficiently practical to allow
Our September issue reported doctors’ drive against the punitive pension tax system
consultants to return to their previous hours.
Mr Packard said: ‘This current problem for the NHS is a prime example of the law of unintended consequences and a misunderstanding of the levels of professionalism and commitment
that have allowed the NHS to provide the service that it does.’
Private doctors organisation the London Consultants Association was pleased to see that the Government’s latest consultation last month had reacted to doctors’ criticism of earlier plans.
Dr Mark Vanderpump, chairman of the London Consultants Association
Chairman Dr Mark Vanderpump told Independent Practitioner Today that the association hoped the Government’s formal response to the consultation would address the ‘tax, facility and ability to practise implication’ concerns raised by many of his members and FIPO.
Advice committee heads to be paid
By Robin Stride
Consultants are for the first time to be paid to chair medical advisory committees (MACs) in private hospitals.
In a break with tradition in the sector, which has seen doctors do this work on a voluntary basis, specialists at Spire Healthcare’s 39 hospitals will be paid £12,000 a year each to head its MACs.
Each post holder will now be appointed, rather than voted for, and will serve in the role for a fixed term of four years.
Spire group medical director Dr JeanJacques de Gorter told Independent Practitioner Today: ‘It’s going to be interesting to see if they can walk the tightrope of representing the doctors’ views, but acting in accordance with patient safety and good governance and oversight.’
He said the company wanted to communicate the importance of
good medical governance and assurance, and recognise that the burden on MAC chairmens’ time was increasing.
Dr de Gorter, who has subsequently left Spire, said it also wanted to attract the ‘right sort of person –someone not after the kudos but someone really interested in the job.’
He said the previous voting system ‘didn’t always bring the best to the surface’.
Independent Doctors Federation chief executive Sue Smith commented: ‘The well established providers have for many years sustained multi disc iplinary med ical advisory committees. This has traditionally relied on consultant users giving of their own time to provide an advisory role to management.
‘As regulation and compliance tighten, the governance agenda is no longer just clinical but also corporate. This now recognises that the consultant straddles all sides of the equation.
‘The news from Spire that MAC chairs would now be a paid consultancy role begged a few questions.
‘But if placed in a non executive context, it recognises the significant time commitment required from this imp o rtant role and the leadership of a critical oversight group of clinicians.
‘It certainly is an improvement on outdated payments in kind and will be reliant on good management and governance from the provider and the clinician.
Look abroad to boost earnings
Private healthcare operators have ‘significant opportunities’ for growth outside of private medical insurance if they look to the Middle East and put effort into these markets.
Healthcare consultancy company boss
Elizabeth Boultbee said the main government purchasers of treatment abroad – Kuwait, Qatar, The United Arab Emirates and Kingdom of Saudi Arabia – had spent on 80% more patients since 2012; a rise from 9,738 to 17,742
The small national populations in each country cannot support the development and maintenance of tertiary level services and treatment is mainly bought from the UK, Germany and the US.
But she warned that developing the potential required a longterm strategy that influences all the decision m akers involved in the patient pathway – local doctors, hospital specialty boards, overseas treatment boards, the patient and their family, and the relevant embassy or health office in the UK.
Ms Boultbee said about 85% of sponsored patients would already have a named hospital/consultant before they left their home country, so most activities needed to take place in the local country.
Speaking at the LaingBuission
Private Acute Healthcare Conference, she recommended providers:
Concentrate on tertiary specialties where there is capacity and will
To win more self-payers, give them what they want
Independent practitioners could have more self pay business if their operators were properly up to speed, according to an independent healthcare consultant.
He told the LaingBuisson Private Acute Healthcare Conference that ‘mystery shopping’ demonstrated there were pockets of good practice ‘but there are still a lot of operators out there that I would suggest are not fully fit for purpose’.
Richard Gregory, ( right ) formerly director of market engagement at BMI Healthcare, said these doctors were not responding to what the self pay customer was expecting.
Patients in the private sector wanted clear, consistent and competitive pricing, plus a high level of quality service and safety delivered in comfortable surroundings. The service had to be flexible and delivered at pace. But any perceived weakness meant the supplier would not be considered.
ingness of consultants and teams to treat international patients;
Raise awareness of their brand including social media campaigns;
Market themselves at exhibitions and major healthcare events;
Get consultants to participate at specialty specific conferences/ workshops, and their involvement in visiting doctor programmes;
Publish quality and outcome data.
Andrew Coombs, HCA Healthcare commercial director, reported ‘enormous demand’ from international markets and he was ‘bullish’ about the UK market’s outlook.
People were very much focused on private medical insurance earnings but they needed to be much bolder.
HCA China deal – see story opposite
Mr Gregory said patients also expected ‘swift and timely’ access to a highly personalised service. A combination of those factors would lead to greater business. He told a mixed audience of doctors, providers, insurers and providers that operators needed to concentrate on consumer expectations and tailor the service to exceed these.
Jean-Jacques de Gorter
Elizabeth Boultbee
Private sector brought into national audit
A pilot study has launched to enable health procedures provided by independent healthcare providers in England to be included in future national clinical audits.
Jointly led by the Healthcare Quality Improvement Partnership (HQIP) and t he Independent Healthcare Providers Network, the project will focus on procedures relating to breast cancer in older people and cataract surgery, with the study anticipated to be completed in summer 2020.
While independent providers can contribute to a few programmes to improve standards, including the National Joint Registry, they are not currently included within the national clinical audit and patient outcomes programme (NCAPOP), commissioned and managed by HQIP.
HQIP medical director Dr Danny Keenan said the results of the pilot should help ensure independent providers got the right support to take part in all relevant national clinical audits. This would give a more comprehensive and reliable picture of the quality of care in the English health system.
HCA link to China to expand market
By Douglas Shepherd
Consultants working at HCA
Healthcare UK hospitals are being offered new private practice opportunities to see patients from China.
International patients based there now have access to oncology expertise and treatment by HCA UK under a partnership with Circle Harmony.
The deal enables Circle Harmony patients to have virtual consultations and get their case reviewed by HCA UK doctors via virtual multidisciplinar y team (MDT) meetings. Patients from China will also come to the UK for treatment in the UK, where they can access medicines unavailable in their own country.
HCA UK said the arrangement reflected how advances in technology were creating new ways to provide access to care and expertise in the international market.
Around 500,000 Chinese patients
travelled oversees for treatment last year, with 100,000 travelling outside of Asia.
HCA commercial director Andrew Coombs said:
‘We have seen an increasingly diversified international patient base over the past five years and this, combined with advances in technology, creates new opportunities for growth and partnership globally.
‘By working with Circle Harmony, we are bringing together leading doctors in the UK and China to provide patients with the best possible medical care and expertise.
‘Through virtual MDTs and consultations, patients will be able to access expertise without boarding a plane, and for those who need treatment in the UK, we are able to provide a seamless patient pathway into our network of hospitals in London and Manchester.’
Digestive unit goes down well with inspectors Compensation costs
London Digestive Centre at HCA UK’s Princess Grace Hospital has been rated ‘outstanding’ by the CQC.
The purpose built outpatient and diagnostics centre treating upper and lowergastrointestinal diseases, liver and pancreatic disorders, neurogastroenterology and ENT conditions was singled out for its strong leadership and its vision, ‘centred on providing highquality care’.
CQC inspectors also highlighted the ‘outstanding’ contribution of staff who ‘worked together quickly to coordinate care in urgent cases and this had a demonstrable impact on patient outcomes’.
higher for Scotland
Doctors in Scotland are set to face higher costs following a Government actuary decision to leave the personal injury discount rate unchanged.
According to the Medical Defence Union (MDU), this has dashed hopes of a more balanced personal injury compensation system.
The actuary’s review of the Personal Injury Discount Rate (PIDR) in Scotland concluded that it should remain at –0.75% with effect from 1 October, in line with the retail price index.
PIDR is the mechanism used to calculate personal injury awards for future care and loss of earnings: the lower the rate set, the higher the cost of compensation.
MDU legal services and Scottish affairs director Dr Hugh Stewart said when the rate was cut by 3.25% in 2017, it had a dramatic effect on compensation claims for Scottish doctors and for the NHS in Scotland.
This led to an increase in the provision for claims against Scottish NHS Health Boards of £160m of public money. It was hoped a review of the way the rate was set would produce a result that better balanced the needs of injured patients against the cost of compensation to doctors
Scotland’s discount rate is 0.5% lower than that recently set in England and Wales, meaning higher costs for doctors.
Circle Harmony chief executive Hua Bai added: ‘Harmony’s signing of the contract paved the way for Circle Harmony and HCA to join hands in building an international health service network that provides the best clinical resources and consultants from both countries.
‘Especially in oncology and more complicated cases, Circle Harmony strives to offer customers integrated total care by using innovative technologies and collaborating with academic leaders, specialists and medical institution partners.’
Patients will be able to access innovative treatment such as CART cell t herapy. HCA also has a clinical trials facility in Sarah Cannon Research Institute UK, offering patients access to cuttingedge cancer therapies at the earliest opportunity.
Merger means occupational health boost
Doctors Clinic Group (DCG) has acquired Maitland Medical, enabling it to offer broader occupational health services, such as absence management and ‘fitness for task’ medicals, to corporations.
Chief executive Dave Mezher said the company now offered 35 services, ranging from standard GP appointments, screenings for women, dermatology, cardiology and minor surgery.
DCG, a GP chain launched in 2014 as London Doctors Clinic, is adding to its 15 outlets by opening in Birmingham and aims to add more soon.
Prices start at £59 for 15 minutes. Maitland Medical will continuing trading under its own brand.
Andrew Coombs
Health clinics top hackers’ hit list
By Edie Bourne
The need for private practices to give close attention to data security has been underlined by a report naming healthcare as the most breached industry in the US.
Cyber-attack prevention specialists SecurityScorecard said although the industry recognised that reported incidents of data breaches were rising, and had stringent data security compliance and reporting requirements, it continued to be targeted by ‘malicious actors’.
It believes the reason for the bullseye placed on the healthcare industry is the detailed information that healthcare providers and their business associates collect, process, transmit and store.
The company said: ‘Electronic
HCA recruits top insurance executive to advise it
AXA PPP chief executive Keith Gibbs has joined HCA Healthcare UK’s advisory board.
The hospital group said he had an outstanding track record in leading a commercially successful business and brought a wealth of experience and knowledge of the private health insurance market and how best to serve individual and corporate customers.
HCA UK’s Advisory Board, set up to support the company’s agenda around quality care and sectorwide collaboration, provides strategic insights and guidance to the leadership team.
Chief executive John Reay said: ‘He joins an outstanding group of board members who, with their
Personal Health Information (ePHI) and Electronic Medical Records (EMR) contain all the most valuable information that a malicious actor can sell on the dark web.
‘Name, birth date, social security number are only the tip of the iceberg; even low-skilled fraud actors are able to easily monetise such information.
‘However, the additional data points of EMR and ePHI include financial records, health insurance information and all the aggregate information needed to exponentially increase the value of the data. Everything from low-level identity theft to advanced insurance fraud is made possible with the prolific amount of hacked data available on the internet underground.’
Data breaches in the healthcare
range of expertise, are challenging us to think about the new and different ways we can continue to provide the highest-quality care and experience to our patients.’
Mr Gibbs said it was a great opportunity to take part in discussions focused on driving quality care for patients and looking at how the sector could collaborate and improve its offering.
industry cost more than those in any other industry analysed and when it comes to compromised organisations, size does not matter.
SecurityScorecard said private practices and local clinics found themselves more vulnerable than larger organisations, as smaller practices could not afford a fulltime security team and relied solely on a third-party IT consultant.
‘A common breach scenario would involve the third-party IT consultant being compromised, zzand since that person services multiple clients – all the clients would be compromised as well.’
Last year, a US health department report highlighted the impact of data breaches on small practices. Four out of five US physicians’ offices experienced a data breach and a single compromised
orthopaedic practice led to 500 patient profiles being sold on the dark web.
SecurityScorecard said: ‘Increases across the board in every category for the healthcare industry indicate that malicious actors target every potential vulnerability to obtain the valuable records stored by providers.
‘Attacks against smaller healthcare clinics are on the rise compared to insurance companies, pharmacies, hospitals and colleges.
‘Malicious actors increasingly target small networks for the purposes of staying under the radar and having more success, as larger enterprises are looking for malicious activity.’
How fraudsters use social engineering techniques to target your practice. See page 30
High rate of sex pests in healthcare shown
One-in-five doctors say they have either experienced or witnessed sexual harassment in the workplace within the last three years.
Seventeen per cent said they had been sexually harassed by a patient and 3% by a colleague.
Of those, three-quarters said the harassment came from another doctor, and one in ten cited harassment from a nurse.
These are among the findings of a report* investigating sexual harassment among doctors in the UK, conducted by health information firm Medscape, and responded to by over 1,300 doctors.
The most common types of harassment from colleagues reported by respondents included deliberately infringing on personal space/ standing too close, unwanted groping, hugging, patting or other physical contact and sexual com-
ments about body parts, leering or sexually looking at body parts.
Regarding harassment from patients, the most common type was patients acting in an overtly sexual manner (53%), asking the doctor on a date (29%) or trying to grope or rub against the doctor (24%).
Report author GP Dr Rob Hicks said: ‘Doctors have a right to a safe workplace, yet this report shows that many are still experiencing or witnessing unacceptable behaviour by colleagues and by patients.’
Over half of those who experienced sexual harassment did not report it. Forty-three per cent of all doctors surveyed believed that successful or senior staff were more likely to be granted greater leeway over inappropriate conduct.
Sexual Harassment of UK Doctors: Report 2019
Keith Gibbs, former boss of AXA PPP
Former
Plastic surgeons face drop in cosmetic ops
By Olive Carterton
Brexit could bring a further drop in business for many plastic surgeons, a major report from industry analysts warns.
According to LaingBuisson, the cosmetic surgery market is likely to be hit ‘particularly hard’ if there is an economic downturn as a result of Britain leaving the EU.
It says the market suffered between 2009 and 2012 and there is every reason to believe that what is essentially a discretionary spend will fare no better if household budgets are squeezed.
The analysts’ comments came following a British Association of Aesthetic Plastic Surgeons (BAAPS) report that the only significant areas of growth in 2017 were in breast augmentation and breast reduction.
Liz Heath, author of the Cosmetic Surgery Market Report first edition , said: ‘While cosmetic procedures have lost their stigma and are increasingly part of the beauty and well-being programme of many women, it is still a remarkably price-sensitive market.
‘It is, of course, one in which
PPU WATCH
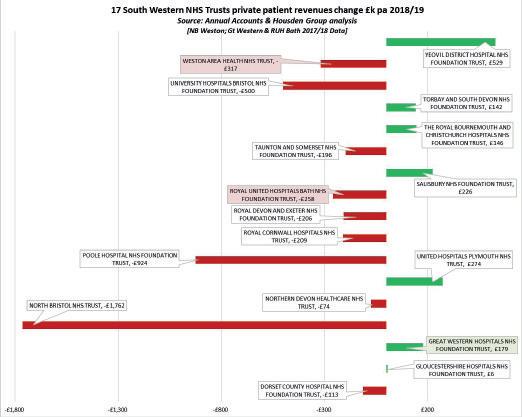
Compiled by Philip Housden
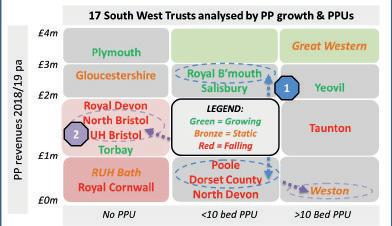
The future of PPUs?
The future for NHS private patient units (PPUs) is to offer the ‘best of both worlds’, according to Shams Maladwala, managing director of Marsden Private Care.
PPUs could provide the scale of an NHS hospital, a specialist service, world-leading research and the very best governance, delivered with private sector service standards, he told LaingBuisson’s Private Acute Healthcare conference.
Mr Maladwala told the London meeting that NHS PPUs should collaborate, perhaps in networks,
many people pay personally for their procedures, so the fact that they are looking for value for money is understandable.
‘At the same time, the PIP [poly implant prostheses] scandal has given people pause, though a price-driven and poorly regulated non-surgical cosmetic procedures market suggests there are scandals ahead, as patients do not always grasp the risks run in cost-cutting.
‘It also makes the market especially vulnerable in downturns and with the uncertainty of Brexit around the corner, there may be interesting times ahead for the cosmetic surgery market.’
Her findings cover cosmetic surgery, non-surgical cosmetic treatment and cosmetic dentistry and show the cosmetic surgery market has grown little in the last five years.
But it is not all bad news. The report reveals the non-surgical cosmetic treatment market is strong and is expected to be worth more than £3bn in five years’ time.
LaingBuisson said: ‘Whereas private hospitals appear to view cosmetic surgery as a “nice to have”, there are specialist providers and clinics who are actively developing
linking up centres of excellence such as The Marsden with other trusts who did not have the infrastructure or know-how to make the most of their own local market opportunities.
He said: ‘The research focus of The Royal Marsden is a key driver of quality across all areas and enables the trust to attract world-leading clinicians, while the robust system of governance of an NHS hospital ensures maximum safety and effectiveness for all patients.’
Private care at The Royal Marsden has grown significantly over the past five years, resulting in many benefits for the whole hospital.
Revenue generated by private care is reinvested into the hospital
LaingBuisson’s report warns that consumer spending in cosmetic surgery may drop in a recession
business by looking for new ways to engage existing and potential clients.
‘As the report finds, it is no doubt greatly to their benefit that nonsurgical treatments frequently lead to full surgical interventions later.
‘While cosmetic surgery has lost much of its previous stigma, the influence of social media is a key driver for growth.
and allows development in leading-edge services for both private, and NHS patients.
Tunbridge Wells to reopen
The Wells Suite
Maidstone and Tunbridge Wells NHS Trust is to reopen inpatient capacity for private patients.
The trust has identified ten inpatient rooms to be located within the original PPU, The Wells Suite, that was closed for private patients over a year ago.
It earned £1.4m private patient income in 2018-19, which was a fall of £967,000 and 40% on the previous year, but as recently as 2015-16 it earned £6.9m private patient revenues.
‘Not only is this about marketing and promotion, but it is a forum for the capturing and sharing of patient experiences, including by celebrities who are increasingly open about the work they have had done.’
LaingBuisson said price was a key driver, especially among young women seeking non-surgical procedures.
It added: ‘This is worrying in a market which currently lacks regulation, as patients may not fully understand the risks or implications for poor clinical practice.
‘It may take a public health or medical malpractice scandal to trigger much-needed regulatory reform in this area.’
In the cosmetic surgery market, prices have risen in the past four years. For example, the marketleading procedure, breast augmentation, has become 8% more expensive between 2014 and 2018.
The report said there was evidence to suggest that overseas travel for cosmetic surgery, especially to Europe, was declining slightly due to a weaker pound and more aggressive marketing by UK providers.
Lynn Gray, deputy chief operating officer at the Kent trust, said: ‘The trust has identified that a significant number of patients admitted to the hospital hold private health insurance and so these patients will again be offered the option of being admitted to the private ward.
‘The beds will be made available from late October/early November, in time to help ease the NHS demand pressures through the winter and all surpluses from The Wells Suite will also be used for the benefit of NHS patients.’
Philip Housden is a director of Housden Group. See his feature article on page 41
One-stop-shop dermatology clinic opens
Consultants at a new private dermatology clinic launched this month in south London aim to provide a one-stop shop for patients.
Stratum Clinic Wimbledon and Raynes Park said it opened the facility in Lambton Road to offer all forms of dermatology, including skin cancer and mole checks, under one roof.
The company has a range of investors including some, but not all, of its consultants.
Lead consultant dermatologist Dr Janakan Natkunarajah said their clinic was designed to deliver a full patient pathway from investigation, diagnosis and treatment, so patients should not need to go anywhere else.
‘Too often, skincare patients are passed from pillar to post and we think that is unhelpful. As a centre of excellence, we have a number of consultants specialising in all areas of dermatology,’ Dr Nathunarajah said.
‘By integrating everything under one roof, it is less disruptive for the patient and puts their needs first as they embark on their personalised treatment programme. They can see the same dermatologist and get immediate access to treatment if that is required.’
Dr Natkunarajah said a key focus area was Mohs micrographic surgery for treating the two most common types of skin cancer.
The clinic, with five consultation rooms and situated above an NHS medical practice, said it picked the area because it was becoming a magnet and destination location for innovative health and skincare facilities and treatments.
Treatments offered include skin cancer surgery, hair and nail disorders, acne, rosacea, birthmarks, cosmetic dermatology, injectables, peels and skin rejuvenation, laser hair removal,
(L-R) Dr Janakan Natkunarajah with Wimbledon MP Stephen Hammond and Stratum Clinics chief executive Allan Johnson
tattoo removal and intense pulsed light (IPL) treatment.
Stratum Clinic Wimbledon and Raynes Park is the latest addition to the company’s clinics network. Last year it joined The Dermatology Partnership to be part of a group including the Harley Street Dermatology Clinic and the Canterbury Skin and Laser Clinic.
Stratum has a dermatology clinic in Oxford and expects to open another soon in Cheltenham, Gloucestershire. Non-investor consultants work under practising privileges.
Care complaints continue to rise
By Robin Stride
Official complaints from patients about consultant care in private practice are continuing to rise year on year, with 59% of complaints including this element in 2017-18. This compares to 52% the year before and 33% in 2016-17, according to the Independent Healthcare Sector Complaints Adjudication Service (ISCAS).
Its annual report said how complaints are handled remains one of the most frequent concerns raised by patients, although this issue decreased against the previous year.
Gripes about complaints-handling appeared in 64% of cases and administration/information complaints in nearly a quarter of cases. Clinical outcome complaints featured in a quarter of cases, while
TYPES OF HEADS OF COMPLAINTS
discharge and aftercare issues featured in one in five.
The total number of complaints that went on to be adjudicated rose from 101 to 107, with a third upheld, 36% partially upheld and 31% not upheld.
Of the 107, adjudicators
fied 275 heads of complaint – the individual elements of the complaint on which the adjudication is made.
ISCAS director Sally Taber said: ‘It has been another busy year for ISCAS, with the independent sector continuing to innovate and
diversify, while at the same time coming under greater scrutiny regarding transparency of information.’
Private hospitals subscribe to the organisation, but this is not compulsory in the independent sector.
The service reported it had increased the number and range of subscribers, including those providing innovative digital healthcare platforms.
But it said some private patients still had no access to independent adjudication, either because the provider was not a subscriber or where the NHS private patient unit (PPU) did not realise that the Parliamentary and Health Service Ombudsman was unable to help private patients, even when treated in the NHS.
A minority of PPUs currently subscribe to the scheme, which ISCAS says leaves most of their patients without recourse to an independent review stage to their complaint.
It aims to increase the number of NHS PPU subscribers in the year ahead. Individual ISCAS subscribers paid an average cost of £2,833 for adjudication cases. Goodwill payments to patients, averaging £758, were made in 82% of cases.
Pets’ health takes sway
By Leslie Berry
Patients are more likely to pay for the healthcare of their pet than go for a private healthcare check-up, a study has found.
Research commissioned by Bluecrest Health Screening found that half of UK adults (48%) pay for health checks and appointments for their pets, but just one in ten (11%) said they would invest in a medical check for themselves.
Those polled spent twice as much money getting their pet’s health examined, spending £90 on average, compared to just an average of £46 getting their own health checked out, over a period of five years.
This is despite the majority of people (58%) saying they worry about their health on a daily basis.
Structure of London’s huge new private unit is finished
The final external piece of the eight-story 185-bed Cleveland Clinic at 33 Grosvenor Place, London, has been put in place.
Opening in Spring 2021, it will have eight operating rooms, a neurological suite with rehabilitation, and focus on heart and vascular, orthopaedics, digestive diseases, neurosciences and general surgery.
The company’s first facility in in Europe will produce its own heat and power.
Three-quarters of those who worry about their health confessed to spending up to half an hour every day concerned about health issues.
The research also found that more than half (51%) of British adults are reluctant to invest in their health unless there is something noticeably wrong.
Many say they feel anxious about what the tests might reveal, while others claim to not have the time to be checked out by a health professional.
One in five said they were not willing to pay for a health test.
Bluecrest managing director Peter Blencowe commented: ‘Our health is our most precious asset, but this research shows just how low it is in many adults’ priorities.
‘Most of us don’t think twice when asked to spend £100 to service our vehicle or boiler, or to pay for annual health check-ups for
App-based access to private doctors
Employee benefits provider Unum has launched a new app-based service to give employees fast, easy and remote access to private GPs and health support.
Help@hand is a range of appbased services giving employees and their families improved access to medical support at the touch of a screen. Four key services are available to employees and families:
Remote GP – Aims to provide access to a remote GP within two hours of requesting an appointment. Unlimited face-to-face video consultations with a UK-based GP, 24 hours a day, 365 days a year.
Second opinion – Two consultations available a year, face-to-face or via video and provided by a UK-based specialist following a diagnosis from a treating doctor.
Mental health support – Up to eight consultations annually including an initial assessment.
Physiotherapy – Up to eight consultations a year including an initial assessment.
The service, available with Unum’s group income protection policies at no additional cost, is offered in partnership with specialist provider Square Health.
Founded by doctors, Square Health has over 20 years of experience within the healthcare sector, with access to over 5,000 medical specialists across the UK.
Company founder Dr Bippon Vinayak said: ‘Based on our wellestablished “Clinic in a Pocket” concept, we have placed an easily accessible “clinic” in the hands of employees for use by themselves and their families.
‘The service provides access to a UK GP at any time and from anywhere in the world. In addition, it provides help with two of the most common causes of workplace absence – musculoskeletal and mental health.
‘We’ve been working closely with employers and these services are cited as best at addressing the biggest challenges to employee
our pets. But the fact we rarely check our own health shows how little we are willing to invest in ourselves.’
well-being, and we know how much an insurance product that also helps employees manage their health will be valued.’
Peter O’Donnell, Unum UK chief executive, said: ‘We know that access to convenient medical support can be a major challenge for workers and their families.
‘By partnering with Square Health, we’re providing employees with direct access to an expansive medical network to help with diagnosis and treatment as and when necessary.
‘Employers want to support the health of their workforce and we wanted to offer a service that made a tangible difference.
‘Early treatment can often result in a quicker resolution to a medical condition or problem and bring added peace of mind.’
A poll shows people spend much more on their pets’ health than their own
Dr Bippon Vinayak of Square Health
ACCOUNTANT’S CLINIC: THE BUILDING BLOCKS OF ACCOUNTANCY
Susan Hutter continues with her A–Z of top tips. This month, she turns to ‘D’…
to of is for ‘Drawings’ top tips
THE AMOUNT consultants and GPs draw from their practice is obviously one of the most important issues for them.
Whichever trading structure you operate under, the overriding question is: How much you should draw and, in the case of limited companies, how the money should be drawn?
The trading structures used by doctors cover the whole gamut fom sole trader, partnership, limited liability partnership (LLP) to limited companies.
Sole traders, partnerships and LLPs
If you are a sole trader, work in a partnership or in a LLP, then your tax status will be self-employed. Whatever you draw, it is not regarded as an expense of the practice. The income tax on the practice profit is calculated on the figure before deducting drawings.
The drawings themselves are not subject to income tax. Therefore, it is imperative to ensure that you either leave enough money in the practice bank account to pay income tax on the profit or, alternatively, reserve it in a personal account out of the drawings you take from the practice.
Limited companies
Many consultants and GPs trade as limited companies, where they are both owners and directors.
One of the most important tax planning points is where the consultant/GP has a non-earning spouse or a lower-earning spouse. In which case, from a tax point of view, it is advisable to pass some of the share capital to the spouse so that they can share in the company income via a dividend.
This mitigates higher-rate tax, as the spouse will have their own personal allowances and the 20% rate band which takes them to £50,000, before entering the higher tax bands of 40% and 50%.
Doctors can draw money from their company either as a dividend (also a ‘D’) or a salary or a mixture of the two. If you are going to be able to divide the share capital between yourself and a lower-earning spouse, then it is sensible to take the majority of your drawings as a dividend.
A small, but useful tax break is that the first £2,000 a year dividend is tax-free. The company does not receive tax relief on the dividends drawn, the corporation tax is charged on profits before the dividend.
The shareholders will have to pay income tax on the dividends depending on their rate of tax.
A 20% taxpayer pays 7.5%, a 40% taxpayer pays 32.5% and a 45% taxpayer pays 38.1%.
As with the drawings from a selfemployed business, it is vital to ensure that you reserve enough money to pay the tax on the dividend, so be careful not to spend it all.
One would be tempted to assume that due to the fact the tax rates of dividends are lower than tax rates on salaries – which are 20%, 40% and 45% respectively – it is far more tax-efficient to take a dividend than a salary.
However, unlike a dividend, a salary is deductible from profit
before calculating the corporation tax liability. Also, tax is deducted at source under PAYE, so that you do not have to worry about setting money aside from the tax.
The sting in the tail is the National Insurance liability, paid by the employer, which is 13.8% of the gross salary. This in itself is taxdeductible, but nevertheless is expensive.
Additionally, there is employees’ National Insurance, also deducted at source. The rates of National Insurance are 12% at the first £50,000 and 2% thereafter. Overall, it is usually marginally better to take a dividend. It is advisable to ask your accountant to work out what is best for you.
In addition to putting aside income tax, take care to reserve for corporation tax, which is at 19% on the company profit.
Working capital
Whatever the trading structure –sole trader, partnership, LLP or limited company – it is vital to leave enough money in the practice to cover its working capital requirement. As a rule of thumb, try to make sure there is a least three months’ overheads left in the practice.
DUE DILIGENCE is usually only required in the medical profession if one is either buying or selling a practice. If a practice is being bought, then all aspects of the practice will need to be reviewed, not only financial.
As far as financial due diligence is concerned, you should request the last three years’ practice accounts and if they are out of date – that is to say, more than three months old – you should seek upto-date figures showing a summary of trading and also assets and liabilities.
At this point, it is wise to show the figures to your accountant,
is also for ‘Due diligence’
who then may wish to raise further questions. It is also sensible to take legal advice at this juncture.
The best people to carry out a review of the quality of the practice are the consultants themselves and their practice managers. This would include examining patient lists and practice procedures.
If you are selling your practice, the due diligence work carried out on your practice records will be done by the purchaser.
However, if you are going to get paid by instalments – that is to say, you are not going to receive all the money on completion – then it is often worth doing some financial due diligence on the purchaser to ensure that they are likely to have enough money to pay each instalment.
Many deals are structured with
an agreed consideration, with, say, 50% payable on completion and then something like two further payments a year and two years after completion for 25% each. Sometimes the later payments are dependent on results.
This means that the vendors could be at risk if the purchaser does not have a sufficient financial covenant to be able to make the subsequent instalments. Once again, it is worth enlisting your accountant’s help in this connection.
In all cases, and as always, it is important to take professional advice before proceeding with any of the above suggestions.
Susan Hutter (left) is a partner at Blick Rothenberg and part of the team that advises doctors
Innovative property developers
ON TRIAL
David Sellu (right) was a surgeon with a distinguished record extending over 40 years. In 2010, a patient died under his care in a private hospital.
Surgeon’s manslaughter
THE OLD BAILEY, November 2013
‘Would the defendant stand up . . .’
It took a few seconds to accept who the defendant was. I rose slowly to my feet.
The trial had lasted nearly six weeks. Each morning, as my family and I walked from the tube station to the court, we were mobbed by photographers walking backwards ahead of us with their cameras pointed in our direction.
There was an even bigger crowd of paparazzi standing outside the only public entrance into the court and the whirring noise of their cameras was unmistakable. We had been advised to comport ourselves normally, with dignity, and not attempt to hide our faces.
‘They will get their pictures anyway, and if not outside the court, it will be on the doorsteps outside your home,’ my medico-legal adviser told me.
right was the public gallery on two floors.
I sat in a cage flanked by two prison officers, one of whom was armed with a pair of handcuffs.
A nurse was on stand-by. The archaic court rituals were well rehearsed. Two loud taps had announced the judge’s entrance into the courtroom, which he made through a huge door. He was dressed in garb that would not have looked out of place two centuries ago; we had all stood up and watched him bow to the lawyers, and they in turn bowed back; then we waited for him to sit down, before we did.
I cast a quick glance at my wife and family before facing the judge. I felt frightened and humiliated in equal measure, but tried to show no outward signs of my distress.
Unprecidented publicity
There followed a sequence of extraordinary events that led to him being prosecuted and convicted for the patient’s death and sent to prison. His licence to practise was suspended, his career cut short.
Events that took place later showed that this was an unfair trial with tinges of racism. He won an appeal against his conviction and is now a free man. But the damage had already been done.
He tells his story….
If I thought events outside were intimidating, I found the interior of the Old Bailey even more daunting, with its wooden panels covering the walls, high ceilings with their ornate linings, the massive corridors, the cavernous courtroom.
Despite my beta-blocker drug, prescribed to control my high blood pressure, each heartbeat resounded through my chest like a gong.
In a cage
Sitting low down, across from the judge, I was forced to look up at him on his raised platform. I knew he was in his early sixties from his Wikipedia entry, but he looked older in his wig and glasses. He took all his notes on his laptop and at the beginning of their interrogation, each witness was instructed to speak slowly.
The jury were seated on two levels to my left, and between them and the judge was the witness box where I had given evidence for nearly three days. In the well between us sat the prosecuting and defence lawyers and to my
There were now more people in the courtroom than at any time during the six weeks of the trial. I was aware of the intense medical, legal, press and public interest in my case. It had received unprecedented publicity in the press. A surgeon on trial for manslaughter.
‘David Sellu, for the offence of unlawfully killing Mr James Hughes, I sentence you to twoand-a-half-years in prison…’
I could hear low rumblings from all sides of the court and louder voices from the public gallery. The prison warder, who had been standing next to me, took my hand and locked me in handcuffs.
As he led me out of the dock, I looked up towards my family, who I could hear crying. I recalled my barrister cross-examining a consultant anaesthetist with whom I had worked closely for nearly 20 years; she had witnessed my work at close quarters.
Defence barrister: ‘You said you have known Mr Sellu as a colleague since 1994. You have frequently worked with him in the NHS and in private practice. You have worked with him in the operating theatre?’
manslaughter ordeal
Witness: ‘Correct.’
Defence barrister: ‘Many of these cases were complex and high risk?’
Witness: ‘Yes.’
Defence barrister: ‘In relation to clinical work in theatre, has that involved Mr Sellu operating on colleagues referred to him?’
Witness: ‘Yes.’
Defence barrister: ‘Has Mr Sellu been frequently called upon by clinicians in the intensive therapy unit for his opinion?’
Witness: ‘Yes. He is the first port of call for patients with abdominal pain, such is the level of trust of my intensive care colleagues in Mr Sellu.’
Defence barrister: ‘How would you describe him as a clinician?’
Witness: ‘He is a very good doctor and a very good surgeon. He is meticulous in his planning and diagnostics. He is a very caring doctor. I have seen him talk in a sensitive manner to patients with cancer.’
Defence barrister: ‘Has he saved lives?’ The answer had been a resounding ‘Yes’.
Looking after sheep I do not know my date of birth. Born in Sierra Leone at a time when there were no records of births in my village, I began life in
rural Africa where I was destined to find work cultivating rice and looking after a small flock of sheep and goats. I was the first of ten children.
My parents never went to school and could neither read nor write English. They were subsistence farmers and even by African standards this was a lowly occupation.
When I was older, my parents could remember the name of the farm where they worked when I was born and could recall that it was about the start of the harvest season, which was typically November. The best calculations placed my year of birth as between 1948 and 1950.
After many years of infertility, my aunt, who was in her early 40s, had decided that the time had come to look for an opportunity to raise a child born to her sisters’ families; she was handed me.
My aunt, also illiterate, lived in the provincial capital, Bo, which was where I now found myself. She never discussed sending me to school.
Over time, I made friends with the older children who lived a few doors down from us; I would wait for them to get home from school, then go to their house to play.
I did not speak English, but entreated them to teach me how
My school friends and I would huddle under lamp posts on the streets to do our homework until we were forced by tiredness or mosquitoes to go to bed
ter than my son who is much older and has been going to school for nearly two years.’
to read and write, in return for helping launder their school uniforms and serving as goalkeeper in the street football team. I was good in goal but not much use anywhere else on the pitch.
Good progress
I didn’t wear shoes before my teens and went everywhere barefoot. Only children from rich families wore shoes.
My friends said I was making good progress with reading and writing. One day, one of my uncle’s friends, a policeman, came to the house and placed the newspaper he was carrying on a table. By now, I could read whole sentences, despite not knowing what they meant. I recognised many of the words in the newspaper and read them aloud.
He urged my uncle to get me sent to school: ‘Can you not see how well he can read? He can read bet-
I discovered years later that when the headmaster met up with my aunt on my first day at school, between them they determined that my date of birth would be 22 November 1946. As we did not celebrate birthdays, it would be several years before I was to recognise the significance of this date, soon to be inscribed in my passport.
In the evenings, my school friends and I would huddle under lamp posts on the streets to do our homework until we were forced by tiredness or mosquitoes to go to bed. Electricity was in short supply and expensive. I gained eight subjects at ‘O’-level and five at ‘A’-level. I won a scholarship to study medicine in Manchester after taking a gap year to work as a science teacher in my old school, to earn additional money to subsidise my studies.
In September 1968, I arrived in the UK to start a medical degree. It was my first time on an aeroplane.
Adapted from Did He Save Lives?
A Surgeon’s Story, £9.99, Sweetcroft Publishing ISBN 9781912892327 from Amazon. His story continues in Independent Practitioner Today next month
Take stock of your marketing drives
ANALYSING YOUR results can be a tricky thing to do in marketing because certain aspects are difficult, if not impossible, to quantify.
WHETHER YOU ARE AN EXPERIENCED PRIVATE DOCTOR OR FINDING YOUR FEET, THIS SERIES WILL SERVE AS A HELPFUL GUIDE TO THE EXCITING, AND SOMETIMES CONFUSING, WORLD OF HEALTHCARE MARKETING.
In the final feature in this series, Jane Braithwaite (right) considers how best to analyse your results so you can learn from your successes and failures – and continue to improve outcomes and reduce costs
Many factors may influence a patient to make an appointment with your practice.
And these factors will grow exponentially if you have been running marketing campaigns across multiple channels such as print advertising, social media, and email.
How then can you accurately measure the success of your marketing efforts?
Establishing
a baseline
The best place to start is by establishing a baseline measurement that you can use to compare preand post-campaign changes over a select period.
ure is the number of new patient appointments in a given month. You may also wish to measure the number of follow-up appointments, prescriptions, procedures and diagnostic tests ordered, depending on your specialty.
Most practice management software packages will allow you to compile appointment reports over a given period and we recommend you get into the habit of producing monthly, quarterly and annual reports, depending on how detailed you want your analysis to be.
Define your channels
Once you have established your baseline, it is time to consider what other information to record and measure.
Increasing patient numbers is the end game, but there is much more to medical marketing than THE PRIVATE PRACTICE GROWTH GUIDE IS DESIGNED TO GIVE INDEPENDENT PRACTITIONERS THE KNOWLEDGE AND TOOLS THEY NEED TO DEVELOP THEIR PRIVATE PRACTICE.
For most private doctors, the fundamental baseline you will meas-
immediate ‘sales’ and you need to ensure that you are monitoring all the aspects of a successful practice.
These include the:
Number of phone and email inquiries you receive;
General number of visitors to your website or to a specific page;
Percentage of patients who would recommend your practice to their friends and family;
Number of followers, likes and shares you have on social media platforms.
This process is referred to as ‘defining your channels’ and can be as big or small a list as you need.
If you and your team are struggling to compile all of the information you want to analyse into a periodic report, consider whether you really need to have this information or whether reports can be divided into smaller, more manageable ones for digital marketing, traditional marketing and friend and family recommendations.
Being objective
Throughout this medical marketing series, setting clear objectives has been a consistent theme when planning your marketing activity. Clear objectives will not only help you to determine what you should be doing; it will help you to determine if you were successful in doing it.
Marketing, like medicine, is always moving forward with new techniques, methods and underlying theory and you should always be aiming to improve and refocus your activity.
Whenever you analyse the results of your marketing activity, be mindful of the information you have and what you wish you had and be creative in ways you can obtain this as part of your next campaign.
Measuring the unmeasurable
As I have said, certain things just can’t be sensibly measured, how-
ever hard you might try. Marketing is as much about brand awareness – how many people know about you and your practice – as it is about final sales – the number of patients you see – and one does not always mirror the other.
Practical example
This practical example demonstrates what might be considered unmeasurable or unquantifiable data for market analysis:
Miss Smith, consultant orthopaedic surgeon, has recently launched a rapid care service for the diagnosis and treatment of broken bones in a single visit. The service is new and so her current baseline of patients is zero.
To promote the service, she has invested in an email marketing campaign and has sent service information to 100 private GPs and 100 physiotherapists.
Our defined channel then is
email marketing and we can measure the number of emails sent, how many were opened (open rate) and how many interactions there were (click rate).
A month on, Miss Smith is pleased to see that the email campaign received a 75% open rate and a 50% click rate. But she is disappointed to find that none of the recipients of her email have referred any patients to the rapid care service, keeping her baseline of patients at zero.
A week later, she attends a medical conference and bumps into a physiotherapist who was included on the original email campaign. The physiotherapist comments that he recommended the service to a patient, but was unsure of the cost of treatment and whether patients could be seen at weekends. As a result, the patient went to their local A&E.
In the above example, it would be easy to brand the email market-
l Tax structuring to suit personal circumstances (LLP, limited companies)
l Solvent liquidations
l Consultant groups and consortia
l Assessment of pension contributions in light of tapering annual allowances
l Ad hoc assistance with HMRC investigations and reviews.
ing campaign a failure, as it has had no quantifiable impact on our baseline, despite positive open and click rates within our defined channel of email marketing.
Miss Smith might well decide to abandon the campaign, or even the service, as a result of the poor results of our analysis.
However, the email marketing campaign has been successful in informing GPs and physiotherapists about her rapid care service, although it didn’t anticipate or answer certain questions.
Turning failure into success
Let’s revisit Miss Smith and her email marketing campaign to see how we can take the disappointing results and use these to define our objectives for future campaigns.
The original campaign yielded no increase to our baseline of patients but did suggest an increase to wider brand awareness with potential referrers.
Our objective for the next marketing campaign should then be to provide referral and fee information in order to grow our baseline.
Miss Smith decides that email marketing works well for referrers and plans to send a follow-up email out with clear instructions of how to refer to the service as well as concise information covering service hours and associated costs.
She also anticipates that her referrers may see insured patients and so details the various providers that recognise her rapid care service.
Understanding that this is important information, Miss Smith also ensures that these questions are answered on a dedicated page of her website and that her admin team are fully aware of the details.
A month on, Miss Smith is delighted to see that the second email campaign received the same 75% open rate and a 50% click rate and has been referred several patients, raising her baseline to ten.
In this very simple example, we have identified and learned from past mistakes and used these to help improve our next campaign.
The analysis could be further improved in future by monitoring the number of visits to the updated website page, as well as
the number of calls received by her admin team.
Conclusion
Analysing your marketing activity can be a never-ending process of questions and answers, and it is important to maintain clear objectives so you can cut through all the information and make positive changes to your marketing activity.
Obtaining quantifiable information through the establishment of baselines and defined channels will help focus your activity and provides good metrics of success. But it is important to pay due consideration to the unquantifiable aspects of marketing, including brand awareness, perception and reputation.
There will be months when your results appear disappointing and periods where your numbers skyrocket and you may be tempted to be reactive with your marketing campaigns as a point of need. Always try to remain objective and consistent with your marketing and don’t let a good or bad month distract or divert your attention.
We hope that The Private Practice Growth Guide has helped you to better understand the various marketing methods and tools available to medics and that you now feel equipped to plan, implement and analyse some truly fantastic marketing campaigns for your practice.
Medical marketing is a growing specialty and there is no right or wrong way to approach it.
Some private practitioners will use clever marketing to cement their position as being the go-to for a specialised treatment or procedure.
Others may make a name for themselves as a generalist or someone who is always available in a pinch.
The best marketing follows the best products and, cliché as it may be, placing the patient experience at the heart of all you do is the greatest recipe for success.
Jane Braithwaite is managing director of Designated Medical, which offers business services for private consultants, including medical secretary support, book-keeping and digital marketing
CREATING A GREAT CONSUMER EXPERIENCE: BIOPHILIC DESIGN
Reconnecting with nature aids health
Independent Practitioner Today’s series on how to create a great user experience continues as Nick Butcher and Dr Nick Hayward delve into the world of biophilic design
BIOPHILIC DESIGN is a concept being increasingly incorporated into stores, offices, homes and healthcare.
With the word ‘well-being’ considered so much more than just a buzzword of the past 12 months, American biologist Edward O. Wilson’s theory of biophilia is being implemented in many types of environments.
Wilson described biophilia as ‘an innate and genetically determined affinity of human beings with the natural world’. But despite this, we far too often exile ourselves from nature in favour of our manmade settings.
We repeatedly alienate ourselves from the natural environment
that we supposedly share an inherent bond with. Historically, and especially since the industrial revolution, society has shown habits that destroy our natural world as technology progresses.
Healing power
Therefore, to reconnect with nature, we can embrace biophilic design not only to create health benefits for patients, but also to help the employees of your clinic, practice or hospital.
Lexicon Medicum by Robert Hooper spoke of the ‘healing powers of nature’ in 1839, arguing that many illnesses could be cured without the aid of medicine, but by paying attention to air quality, the food
At the heart of medical finance
or by using
Biophilic designs: Bluewater Shopping Centre, Kent, shows what can be done
Biophilic design can be achieved through artificial plants
wall graphics
we eat, how much physical activity we do and the rest we receive along with our state of mind.
So, even in the 1800s, our environment was considered to be therapeutic and capable of supporting our health and recovery.1
Stress and anxiety are major issues for patients during hospitalisation and are known to hinder patient recovery.2
This can be caused by all variety of factors, including anxieties related to illness and recovery, shared rooms, unfamiliar surrounding or worries at home.
If these fears are stunting patient recovery or in some cases making the patient worse, then any efforts to make their experience easier is important to consider.
Further research has shown the significant healing benefits, particularly for hospital inpatients, of immersion in environments that include the principles of biophilia within their design.
As with certain colours and textures, our minds are programmed to feel most at ease in organic surroundings. Of course, we acknowledge that certain clinical spaces must be kept clean and free from live plants and flowers.
But many clinical areas such as outpatient waiting rooms, meeting points, restaurants and corridors may be suitable for safe biophilic additions.
The great outdoors
As well, there are many creative alternatives that allow us to integrate inpatient locations with aspects of nature. For example, we can use design that mimics natural environments or bring plants into view from inpatient rooms while ensuring their safe separation for infection control requirements.
Biophilic design does not simply mean adding plants to a room, but natural sunlight, natural colours and textures or even a distant view of the great outdoors can improve patient well-being.
It has been found that hospital inpatients with a window view of nature reportedly had shorter stays than those without such views. There are cases where, as well as a shorter length of stay, there was also less pain medication dispensed and an overall improvement in patient well-being in biophilic healthcare environments.
A great way to incorporate biophilic design in a medical setting is through embracing natural light. With large windows, we can achieve sky views, views of natural environments and allow in warm sunlight too. These additions are a huge improvement over the sterile brightness of flat panels with medical strip lighting, which can feel alien and uncomfortable to most patients and guests.
An American study was carried out between 1972 and 1981 in a Pennsylvania hospital that observed the recovery of patients after cholecystectomy. The study looked to determine if the assignment of patient rooms had an effect on the speed of recovery.
Twenty-three surgical patients
were designated to rooms that had windows looking out over a view of nature. A further twenty-three surgical patients were given rooms where the window looked out towards brick walls.
The patients with a view of nature were found to have a shorter postoperative stay with more positive patient reported outcomes. They also had a much lower analgesic requirement than the group of patients without a view of nature.3
Wall graphics
Another way of including aspects of biophilic design is through artificial plants or by using wall graphics that depict the many qualities of nature. These may not have the added benefit of improved air quality that real plants provide, but the association can still create the effects of enhanced well-being.
The use of natural colour and materials, such as wood or stone can contribute to the way people are feeling, offering a more holistic healing process in a medical environment too. If these natural elements cannot be brought indoors, you can still represent naturally occurring patterns through art, furniture or architecture.
It could simply be the use of natural motifs such as leaves, trees or honeycomb shapes within furniture or walls that promotes wellness within a space.
Patient satisfaction can dramatically improve in biophilic healthcare settings. And let us not forget the potential benefits for our overstretched clinical staff too.
A series of studies run by Exeter University revealed that employees
were up to 15% more productive when working in an environment that had houseplants.4
Including elements of nature into a space occupied by employees, be it an office, a clinic room or the staff lounge, can provide a relaxing and restful environment for employees while proving to enhance productivity, creativity, reduce stress and increase mental well-being.
So why not incorporate biophilic design into your healthcare setting and note that even small creative additions can restore the natural connection for your patients, your colleagues and yourself.
Nick Butcher is creative director of branding and design agency Beyond London and Dr Nick Hayward an academic clinician in Southampton
INVESTING IN PROPERTY
Five ways to success
Dr Lafina Diamandis
HAVING A PLAN when it comes to property investment is vital. It’s like setting up a business or becoming a doctor – you’re unlikely to succeed if you set out without a plan or identifying the steps you need to take to achieve your goals.
You need to know as much as possible about the different ways you can invest in property, choose a strategy and focus on it. Here is an outline of different options:
1
Buy to let
Buy to let (BTL) is easily the most common property strategy known and the basic model implies buying a property to let it out, usually to a single tenant, long-term; for example, six to 12 months.
Technically speaking, any property purchased to let out is a buyto-let, but depending on the type and number of tenants and the duration of the tenancy, the name given to the type of letting differs.
For example, when you let a
property, you can choose to let it in one of the following ways – subject to local rules and regulations as well as your mortgage terms and conditions:
Single let;
Serviced accommodation;
Holiday let;
Multi-let;
Commercial let to shops or firms. These may be long lets – more than three months – or short let : anything up to 90 days. Different types of letting require different types of rental agreements, so make sure you check with a solicitor or relevant authority before going ahead.
You might want to consider investing in a BTL if life is too unstable for you to settle on investing in a property where you will live long-term. You might also consider BTL if you can’t afford to buy in the area you want to live yet.
So you buy a property and rent it out to make a profit. Simple, right? Wrong. Having taught and spoken to hundreds of doctors about prop-
erty, I’m shocked by how many doctors have bought a BTL property using few or zero criteria, and without knowing how to calculate whether a deal makes sense or not.
The result is that many more people than you might imagine own BLT properties which either yield little profit or, worse still, they make a loss every month. This can happen for various reasons including void periods, a drop in market rent and rise in interest rates.
2 Buy, refurbish, refinance (BRR)
This involves buying a property, refurbishing it to add value and therefore increasing the market value, and refinancing it – ideally, to extract all or most of the original funds invested and use them to invest again.
Investors like BRR, as it means they can keep recycling their funds from one project to another, which allows them to build up a portfolio of investment properties quite quickly. This method is also called momentum investing and works best with properties priced under £100,000 due to low stamp duty costs, although you can use this strategy on any project if the numbers work.
While you can use mortgages to buy properties under £100,000, bear in mind that you will have limited options in getting a mortgage for properties under £40,000,
and you may have to wait a minimum of six to 12 months before your lender will release further funds to you.
3
Rent to rent (R2R)
Rent to rent is a favourite strategy among many investors who have no cash to invest, as it allows you to use leverage to make massive cash flow from a property without buying it. It’s also known as let-to-let, let-to-multi-let, corporate letting, leasing and many other variations.
This strategy works by renting out a property for a period of three to five years or more and legally subletting it to a tenant/s to generate a positive cash flow after expenses. Naturally, the rent you receive from your tenant must be greater than the rent you pay to the property owner, just like when you have a mortgage, and any expenses you will be covering.
Why would a property owner consider allowing you to do this when they could do it themselves and keep the profits? Well, there are many landlords out there who are tired of dealing with tenants and maintenance issues and would love someone to look after things while still paying them a good rent.
Think about how you can best help the owner while creating a viable business for yourself. You may be wondering how you can make a profit if you are offering to
success with property
pay the market rent. This is where the skills you’ll develop in assessing how to maximise the potential of a property come in.
You might find that the landlord will be willing to rent it to you for a little below the market rent, given that the luxury of having a fully managed property with no vacant periods is far more valuable.
4
Houses of multiple occupation
HMOs (or multi-lets) have been around for a long time. At one point or another, you may have lived in a HMO yourself as a student or young doctor; the official definition of a HMO for licensing purposes under the Housing Act 2004 is a property occupied by five or more people, forming two or more separate households.
To maximise the potential of the HMO and create higher cash flow, an investor may let the property on a room-by-room basis with bills included, rather than having all tenants on the same contract splitting a single-let rent between them. This works well for people who don’t know each other, as it allows greater independence and flexibility than being tied into a contract with others.
In some HMOs, there are shared kitchens and bathrooms, while in others the rooms are more like bedsits with a kitchenette and even ensuite bathroom. Usually, these
sorts of rooms are priced at a premium, as most folk will pay extra for the luxury of their own bathroom.
The rental income generated from HMOs is much higher than you could achieve through letting the property out to a single tenant or family, but the amount you can charge per room or unit is very much driven by demand in your area. You can check demand and market room rents on websites such as spareroom. com.
The total rental income for the number of rooms let should be significantly higher than the market rent for letting the entire property on a single-let basis to make it worth running.
When comparing the profits on a single versus multi-let, don’t forget to include the expenses associated with running a HMO – for example, utility bills, mortgage, cleaner, insurance.
While HMOs generate a higher cash flow, they also generate higher tenant turnover and maintenance issues, so you need to make sure you set up a team to deal with this.
5 Purchase lease options (PLO)
This is a complicated topic and a commercial solicitor experienced in lease options is the best person to advise you.
A purchase option is a type of legal agreement that gives you the right to buy a property at a pre-agreed price
within an agreed time period but without the obligation to do so.
The fee for the privilege of doing this is usually £1, but depending on the type of property deal, it could be in the thousands. In other words, you can control a property without owning it, like in the R2R strategy.
If we go a step further and you want to use the property to generate profit – as you do in R2R – you need a purchase lease option contract which will allow you to use the property as you wish in return for a monthly payment (lease fee).
As with R2R, you can even refurbish the property if you have the owner’s consent to do so. This strategy suits people who either don’t have funds to invest or don’t want to invest large amounts of funds into property or those who for some reason can’t get a mortgage to buy at that time.
The PLO strategy is relatively unknown to the general public but it is widely used by property developers and commercial investors. Typically, they use a purchase option to control a piece of land or building while applying for planning permission.
A purchase option buys them time, minimises the risk of buying an asset where planning applications – which cost thousands – can be rejected and also temporarily eliminates competition, as the vendor isn’t permitted to sell to anyone else while under a PLO contract.
Next month: How to fund your deals
Dr Lafina Diamandis is co-founder of Eurekadoc, a start-up helping doctors to realise their full potential through diverse medical education and careers curation and is passionate about helping doctors to become financially independent through property –even with limited time, funds or experience.
She runs the only UK course specialising in property training for doctors, has delivered education and training to more than 1,000 doctors and is an advocate for portfolio careers in medicine.
In 2018, Lafina launched the first Learn While Investing crowdfunding project making it possible for doctors to get involved in property projects that are fully transparent and offer an opportunity for education and training.
Lafina and her business partner John Friis made a property development project available to the medical community through Simple Crowdfunding, overfunding it in just seven minutes
SUBSCRIBE TODAY TO GET EVERY ISSUE AND READ US ONLINE
Dear Reader,
Subscribing to Independent Practitioner Today is the only way you can be sure you will see every issue and have the option of reading us online using our special page-turnable edition. Don’t risk missing out. Our personal subscription for doctors and managers is only £90 a year and £210 for organisations. But you can cut this to just £75 and £180 respectively if you pay by direct debit.
So take advantage of this offer now for our unique business journal dedicated to supporting you in your private practice. We’re confident your subscription will repay itself many times over!
Editorial director
APPLICATION FOR SUBSCRIPTION
Instructions to your Bank or Building Society to pay Direct Debits
Name and full address of your bank/Building Society
To: The Manager Bank/Building Society Address Postcode Ref. No.
Banks and Building Societies may not accept Direct Debit instructions for some types of account
send a copy of your letter to us.
KEEPING UP TO DATE
Reflecting well on you
Get it sorted! Kate Lewis and Darren Wiggins look at the requirements for a successful appraisal and revalidation
THIS MONTH, we look at significant events, feedback and compliments and complaints.
This follows September’s article, where we looked at what happens if you fail to engage with revalidation requirements, the supporting information required and continuing professional development (CPD) needed.
Significant events
The GMC states: ‘A significant event is any unintended or unexpected event, which could or did lead to harm of one or more patients. This includes incidents which did not cause harm but could have done or where the event should have been prevented.’
It is a requirement of the revalidation process that you declare any significant event you have been involved with since your last appraisal and that you reflect upon it. It is probable that an involvement in a significant event and critical reflection upon that will lead to a change in your work behaviour and practice, and demonstrate your learning from such an event.
You should be able to explain to your appraiser the reasons why you have chosen these events and you should focus on the insight and learning from the event, rather than discussing the facts of the events or the number of events you have recorded.
The organisation that you work for may use different terminology such as serious untoward incident or serious incident requiring investigation.
Many organisations will have a process to formally record significant events and a procedure for responding to them. If you are working as a locum, you should find out what the local protocol is.
In most circumstances, if you are a locum involved in a significant event, the organisation will report to your designated body and Responsible Officer (RO) any details for investigation. If you are selfemployed, you should record any significant events or incidents and review them.
At appraisal, you should be able to demonstrate that you are aware of any correlation in the types of incidents that you have recorded
about your practice and discuss any actions you have taken to prevent such events or incidents recurring. You should reflect upon any areas that you have identified for further learning within your CPD and personal development plan (PDP).
We often get calls from doctors regarding what to include in this section on their appraisal form. The simple answer is any complaint, concern or compliment that you have been named in over the last 12 months.
To disclose that you have been the subject of a complaint, no matter how serious, shows your honesty and integrity. We are all human and mistakes are made. It is better to face things, review the occurrence and reflect upon how we could have done things differently so that we do not make the same mistakes again. Try to look at things positively and move forwards. If you were to not declare an event or incident and your appraiser or RO were to become aware of it, that would not look favourably for you. Honesty is by far the best policy.
Duty of candour
All healthcare professionals have a responsibility to be honest, open and transparent with patients, colleagues and employers if things go wrong. Healthcare professionals are also required to take part in reviews and investigations when requested to do so and to support and encourage colleagues to be honest and not stop someone from raising a concern.
The GMC and the Nursing and Midwifery Council have produced joint guidance on this subject. It is called: ‘Openness and honesty when things go wrong: the professional duty of candour.’ It can be found online at www.gmc uk. org/ /media/documents/openness and honesty when thingsgowrong theprofessionaldutyofcand____pdf61540594.pdf
Within this article, there are many more reading references which could be useful to read, reflect upon and use as part of your CPD.
Collecting feedback
All licensed doctors are expected to collect both colleague and patient feedback at least once within their
revalidation cycle (five years). Both negative and positive feedback are a valuable tool for you to reflect upon your practice.
Negative feedback should be a building block to aspire to learn from or change your practice accordingly. Judgements should not be made on any negative feedback in isolation from the entire process.
You will need to review the feedback and compare the feedback from patients and colleagues against your own self assessment scores. This should be discussed at appraisal.
It is easiest to use questionnaires to gather feedback from colleagues and patients. You can use an independent company to organise this for you or use the GMC questionnaires that it has available on its website as well as its self assessment questionnaire.
The GMC expects that any questionnaire will be administered independently of the doctor and the appraiser.
Please note that, for patient feedback questionnaires, they need to be collected back independently from the patient either by being handed back to a receptionist to post back to the administrator of your feedback or by providing a stamped addressed envelope for the patient to take the questionnaire home, complete it and post back to the administrator.
It may be that the organisation where you are working will have its own system and process for gathering patient and colleague feedback and you are responsible for engaging with it. If you practise in a setting that does not have such a system in place, you will need to contact an independent provider to assist you.
If you do not directly treat patients, then you would need to think in broader terms of who could give you feedback on your work as a doctor; for example, customers, medical students, people who receive reports from you and appraisees.
In all circumstances, you would need to discuss this with your appraiser or RO to see what is an acceptable alternative dependent upon your scope of work.
For colleague feedback, you will need to supply your survey company with a list of people whom they can contact to complete the
feedback questionnaire. Ideally, you should give ten medical and tennon medical colleagues who are able to give feedback on your professional performance.
Each colleague will be contacted by the survey company and invited to complete the feedback questionnaire and return it to the company directly. The company should monitor returns from your colleagues and send reminders when necessary.
It may be that insufficient questionnaires are returned and you will need to supply further details of other colleagues.
As previously stated, you need to complete a self assessment questionnaire which reflects on the results of the feedback which includes:
What the optimal results were of the feedback and how you intend to maintain this level of performance;
What were the suboptimal results of the feedback and how do you intend to improve on these areas of your practice?
The GMC recommends that, when using its questionnaires, a minimum of 15 colleagues and 34 patient questionnaires are to be collected.
Once these questionnaires are received by the organisation completing the survey, they will be analysed and you should receive a personalised report which summarises the results and compares these against the GMC benchmark tool.
We always advise doctors who use our revalidation and appraisal services not to leave feedback until the fifth year of the revalidation cycle. It is far better to collect feedback along the way so that you do not struggle with it at the end. It makes life so much easier.
Embrace complaints
At your appraisal, you must declare and reflect upon all formal complaints about you. You should select those complaints where, upon reflection, you have changed your practice.
You do not have to discuss every complaint. Focus on those that you have learned from the most.
You should explain to your appraiser why you have chosen to discuss these over others as part of your appraisal discussion and explain what you have learned
from these complaints and how they reflected upon the changes you have made in your practice or that you intend to make.
The purpose of recording complaints and compliments and reflecting upon them is key to improving the way you practise. It will help identify the things that you do well and your strengths and, conversely, those areas that you need to improve upon.
Showing self-awareness
Reviewing complaints and compliments information will indicate any changes that you need to make. It shows selfawareness and that you are willing to act upon any concerns or comments about your work and make changes in response to the feedback that you have received.
Compliments are important pieces of evidence to help you to reflect upon your practice. Collecting such evidence from colleagues and patients – letters, cards, emails – and discussing these with your appraiser gives you the opportunity to confirm areas where you have a positive influence on patient care.
Reflection upon the compliments should be discussed at your appraisal. However, please ensure that you remove any personal identifiable information from any correspondence used for data protection purposes.
If you do not have any complaints or compliments within which you are not named personally, then you should consider researching any complaints and compliments locally where you are working that may have resulted in a change of protocol or policy which has influenced your practice. This can be discussed at appraisal.
Kate Lewis and Darren Wiggins (below) are from ACI Training and Consult ancy Ltd, specialists in revalidation and appraisal services
What doctors
Independent practitioners have revealed
a survey what they really want from a practice management system. Kingsley Hollis (right) presents some key findings
• Completely open scanner that is well tolerated by claustrophobic patients
• Weight-bearing scans for spine and joints enable a more precise diagnosis
• Patients who are large or cannot lie down can be accommodated
BUSINESSES THAT take customer loyalty for granted are doomed to
When Jamie Oliver’s Italian restaurants called in the administrators last Spring, commentators lined-up to give their verdict on what had gone wrong.
While it was generally accepted that market conditions had got tougher for the casual dining brands, one of the most common criticisms was perhaps the most damning – in its drive for expansion, the business had lost touch with the people who mattered most.
The lesson applies to businesses across every sector, particularly in technology where the pace of change is usually quicker.
So it is important that companies like Healthcode are mindful of our customers’ priorities and needs when developing new products and services or the outcome could be a herd of unwanted white elephants.
At the end of last year, we surveyed 700 independent practitioner customers to get an insight into what mattered most to them and what they wanted from their practice management system.
Here are some of our findings:
☛ Ease of use is more important than breadth of functionality in a practice management system
On a scale of 1 to 5, where 1 was ‘not important and 5 ‘very important’, practitioners rated ease of use most highly (average 4.61). Breadth of functionality had an average score of 3.74, suggesting that practitioners valued new sys-
to
tem features but not for the sake of it. In short, technology had to be at the service of users and not the other way around.
☛ Data protection is now a key consideration when choosing a practice management provider
Unsurprisingly, doctors wanted a system provider who was capable of delivering a modern solution, but they also rated ‘managed data backup’ and ‘data security’ as important (4.31 and 4.07 respectively).
This is reassuring because practitioners are considered data controllers in law and thus accountable to the Information Commissioner’s Office for any failure to comply with the Data Protection Act 2018. That includes having appropriate security measures in place to protect personal data and ensuring the compliance of organisations that process data on their behalf.
☛ Electronic billing to patients was the most important feature in a new practice management system
Electronic billing to private medical insurers has been common practice for years, but the Private Healthcare Information Network estimates that around one-in-four private healthcare procedures in the UK are now self-funded. That is around 200,000 procedures a year.1 Rather than spending precious time and money issuing paper invoices to these patients, more than 68% of practices wanted a digital solution.
The next most important feature was a mobile app, which was rated as important by 41% of respondents, who want to take care of busi-
MANAGEMENT SYSTEMS
ness even if they are away from the office.
Healthcode surveyed 700 private doctor customers to get an insight into what they wanted from their practice management system
doctors really want PROBLEMS WITH THE TAX MAN?
This makes sense in the context of previous Healthcode analysis of our ePractice users, which showed that a growing number of practitioners see patients at more than one treatment site.2
☛ Invoicing is rated the most important aspect of practice management
Asked to rate five aspects of practice management from 1 to 5, invoicing was considered most important, with an average score of 4.5, slightly higher than data security compliance (4.3).
It shows that practitioners are well attuned to the demands of running a practice and the significance of maintaining a healthy cash flow position.
It contradicts the common misconception that doctors can’t also have a flair for business. In fact, in my experience, the ingrained habits of reflection and critical thinking actually give them a head start when they embark on independent practice.
Indeed, most of the practitioners I meet understand the business of running a practice and are open to new ideas. Of course, my role is to ensure they have access to the right support and technology, from invoicing to reporting tools so they can examine the financial health of their business.
The results of this survey have informed Healthcode’s product development strategy in recent months as we have focused on ensuring our services are aligned to practitioners’ needs. We will share news of these developments in the coming months.
More broadly, I think every business – including independent practices – can benefit from this kind of listening exercise, from surveys to inviting individual customers to share their experience or give anonymous feedback.
Such an approach helps to highlight what is going well and any problems that need to be addressed. And it is an important way to demonstrate to customers that they are respected and valued.
References
1. Private healthcare prices becoming more transparent but further progress needed, warns PHIN; PHIN website, 9 May 2019. https://media.phin.org.uk/news-private-healthcare-prices-becoming-moretransparent-but-further-progress-neededwarns-PHIN
2. Multi-site independent practices need remote control, says Healthcode; Healthcode website, 5 May 2015. www. healthcode.co.uk/latest-news/multi-siteindependent-practices-need-remote-control-says-healthcode
Kingsley Hollis is head of business development (ePractice) at Healthcode
HMRC tax investigations and disputes create difficult and stressful times.
As an award winning firm of tax experts, our highly experienced partners specialise in resolving problems relating to tax investigations and disputes with HMRC.
To find out, in confidence, how we can help call 0800 734 3333.
‘Here to help. Not to judge.’
Don’t be scammed
FRAUDSTERS NOW frequently use social engineering techniques to prepare for an attack, in which their ultimate aim is to successfully steal funds from medical practices run by private consultants and GPs. They use this approach knowing that it may be possible to get potential victims to divulge passwords or payment authorisation codes or to unwittingly remit funds. They do this by persuading victims that the situation presented to them is normal and the approach can be trusted.
As Dr David Modic, research associate at the Computer Laboratory, Cambridge University, said at the TranUnion Fraud Summit:1 ‘It’s easier and cheaper for fraudsters to exploit humans than it is machines, so of course this is an avenue they will continue to pursue.’
Fraudsters often start by finding out snippets of publicly available information about the practice and its employees. The internet is often a key enabler for fraudsters to be able to scour a number of records very quickly. A simple name search on an internet search engine can
With medical practices a favourite target for fraudsters, Vin Pandha (right) shows what you can do to protect yours from the growing use of social engineering techniques
reveal a great deal of personal information that is available online about an individual, some of which we may have forgotten was even there.
With social media profiles in professional and social capacities showing your current employment details, when you are on holiday or checked into a conference all day, together with information on the practice website and news articles, the fraudsters are well armed to carry out a fraud attack.
Once they have the background information, the fraudsters move on to more direct contact with the practice itself using social engineering techniques.
So, what are the key methods fraudsters use to carry out social engineering?
EMAIL: A deceitful attempt to obtain information by email is known as phishing. The email will appear to come from a genuine sender such as the bank, a government department or a supplier because fraudsters will make the email sending address look identical or extremely similar.
The email will ask for certain information or it will contain a link to a fake website or a malicious attachment.
P HONE : When criminals make their approach by phone to gather the information, it’s known as ‘vishing’ (voice phishing). They use technology to make a trusted phone number appear on the incoming caller display and this is known as ‘spoofing’.
It’s very convincing and can lead potential victims into believing that the call is from a genuine organisation or caller, and they are then tricked into divulging information sought by the fraudster.
T EXT: SMiShing (emphasising the SMS) is where fraudsters use a text message to carry out social engineering.
Again, they will use spoofing technology to make the text look like it has been sent from a
It’s easier and cheaper for fraudsters to exploit humans than it is machines, so of course this is an avenue they will continue to pursue genuine number and when they do this, the fake message actually falls into any previous string of text messages received from the genuine organisation or person owning that number.
MALWARE: Malware is short for ‘malicious software’ and is a type of computer virus. A fraudster’s aim is to get a victim to click on an attachment within an email or click on a hyperlink which infects the computer.
The malware then operates in the background without the computer user being aware, allowing the fraudster to capture data, record key strokes such as passwords or divert users to genuine looking websites which request the input of information.
IN PERSON: Carrying out social engineering face to face in person is less common. However, in surroundings frequented by the public, fraudsters may observe conversations, phone calls, look over the desk at documents or computer screens to capture any information which may help create a successful fraud attack.
For example, a conversation about the practice manager being away for a week while they move house could lead a fraudster to include this information in a fake payment email purporting to be from them.
Vin Pandha is commercial fraud manager at Lloyds Banking Group
References 1. TransUnion, June 2018. www. transunion.co.uk/press-office/ news/2018/06/uk-businessesunderestimate-the-threat-of-socialengineering-despite-increase-in-attacks
WHAT CAN YOUR PRACTICE DO TO GUARD AGAINST SOCIAL ENGINEERING?
1
Don’t click on links within emails or texts, or open email attachments unless it’s known who has sent the message and you can be sure it’s genuine.
2
Don’t give out sensitive or internal-only information via phone, email or text without verifying the person asking for that information. If necessary, call them back using a number you know to be correct.
3 Check your privacy settings on social media platforms to ensure you do not have private information openly available and only connect with individuals whom you genuinely know and trust.
4 Consider as a medical practice what information you want and don’t want to be public knowledge and ensure staff comply with this policy.
5
Be mindful of confidential conversations between colleagues and/or phone conversations with patients being overheard in the public space.
6
7
Only download software to your PC from sources you trust and delete it when no longer needed.
Ensure all PCs are protected by high-quality antivirus software and run frequent scans. Always ensure software updates are actioned promptly and keep firewalls switched on.
8
Never provide online banking passwords or online payment authorisation codes on the phone or in response to an email or text message. A genuine bank colleague will never ask you to divulge these.
CHENIES MEWS IMAGING CENTRE
SPECIALIST MRI IN THE HEART OF LONDON
• Advanced Cardiac MRI
• 3T Neuro MRI
• MRI for patients with cardiac pacemakers
T: 0203 887 0566
E: referrals@cheniesmews.com
W: www.cheniesmews.com
DRIVE TO IMPROVE SAFETY
Safely sewn together
Implications for independent doctors arising from the NHS Patient Safety Strategy are examined by David Hare
PATIENT SAFETY
once again hit the headlines this summer with the publication of a new NHS Patient Safety Strategy
This 80-page document was commissioned by Health Secre tary Matt Hancock to go alongside the NHS Long Term Plan and ensure that safety is the ‘golden thread’ running through the health system.
The strategy, which aims to save thousands of lives every year, was met with much approval across the healthcare system. But what will it mean for independent clinicians?
The Independent Healthcare Providers Network (IHPN) was pleased to be closely involved in the strategy’s development over the last year.
Our key priority was to ensure that a system-wide approach is taken to patient safety, with a recognition of the significant role the independent sector annually plays in providing care to millions of patients.
We were therefore pleased that the final document adopted this approach. With the tagline ‘Safer culture, safer systems, safer patients’, the strategy echoed IHPN’s view that the patient safety
agenda can only be progressed if the whole healthcare system is working together.
That means sharing data, sharing concerns, and sharing best practice and innovation.
Indeed, IHPN authored a section on the independent sector, arguing that alignment of patient safety standards between the NHS and independent sector has not always been effective.
And as I have made clear in previous columns in Independent Practitioner Today, key to changing this is ensuring independent sector providers can submit information to NHS safety databases and participate in clinical audits.
Greater transparency
This will help to drive continuous improvement and greater transparency. Ultimately, it will ensure that patients have access to information on the nature, quality and safety of services delivered by all healthcare providers.
What is known as The Acute Data Alignment Programme (ADAPt) is being developed under the joint leadership of the Private Healthcare Information Network (PHIN) and NHS Digital.
This will be critical in integrating data on privately-funded healthcare into NHS systems and standards for the first time, and IHPN is pleased to be supporting this work.
Looking more broadly at the strategy’s ‘system-wide’ approach to safety, IHPN welcomes the focus
The patient safety agenda can only be progressed if the whole healthcare system is working together. That means sharing data, sharing concerns, and sharing best practice and innovation
embedded across all regulatory bodies.
IHPN will be working with HEE to ensure this syllabus works for independent sector clinicians –both corporate and stand-alone providers – reflecting not only the significant numbers of clinicians who work both for the NHS and independently but also the importance of reassuring all patients about the quality of care they receive, regardless of where they receive it.
on ‘culture’ and its importance in laying the foundations for safe care.
As part of their work to foster a ‘patient safety culture’ across the health system and tackle the fear and blame that can happen when raising issues and concerns around safety, the strategy has committed to putting some clear metrics around measuring ‘culture’.
These are akin to those currently in the NHS Staff Survey: to understand different providers’ culture as well as staff perceptions of the fairness and effectiveness of dealing with patient safety incidents.
Independent healthcare providers, who were praised for having a strong leadership culture and staff engagement in the CQC’s State of Care report last year, are in line to benefit from metrics being put in place around this. There could be an opportunity to showcase the good work going on in the sector around safe and responsive culture.
Linked to this, the strategy also outlines the work the NHS will be doing in collaboration with Health Education England (HEE) to create a single patient safety syllabus and training programme for the whole of the healthcare system and to ensure that a shared understanding of patient safety is
Key announcements
Other key announcements in the strategy include the:
Introduction of a Patient Safety Incident Response Framework to improve the response to an investigation of incidents;
Implementation of a new medical examiner system to better scrutinise deaths;
Development of a new National Patient Safety Alerts Committee to improve the response to new and emerging risks.
Overall, the NHS Patient Safety Strategy and the explicit commitment to system-wide solutions is a positive recognition of the thousands of clinicians who work in the independent sector.
We will be working with the patient safety team at NHS Improvement to cement the sector’s contribution to the patient safety agenda to ensure the millions of patients treated in the independent sector can access the safest possible care.
David Hare (right) is chief executive of the Independent Healthcare Providers Network
Health Secretary Matt Hancock has described safety as the ‘golden thread’ running through the health system
Unearthing treasure
INFORMATION HAS become one of the most important currencies in the modern world, transforming the way organisations operate and the way consumers access goods and services.
Even in the healthcare sector, data is a prized asset. Professional services firm EY recently estimated the value of NHS patient records at nearly £10bn a year.1
It is an astonishing sum, based on the data’s value to commercial organisations and its potential to unlock operational savings within the NHS, improve health outcomes and thereby benefit the UK economy.
But as the EY report also makes clear, there would be significant costs involved in the ‘aggregation, cleaning, curating, hosting, analysing and protecting the transformation of these raw data records into a consolidated longitudinal patient-level dataset’.
In other words, simply accumulating and storing terabytes of unstructured data that lies buried within organisations is pointless. Information only has a real value if we can make sense of it and put it to a practical purpose. That means it has to be accurate, up to date, accessible, secure and shareable when appropriate.
The costly failure of the Connecting for Health project
Data can be difficult to access in the private healthcare sector, but Healthcode’s Fiona Booth (right) argues that we must all work together to make the most of this asset
shows that this is no easy task, but it is encouraging that the NHS’s digital strategy is now based on developing common information standards and interoperable systems, rather than imposing one technology solution from the top.
Matter of urgency
Of course, recording and sharing information is not only a challenge for the NHS, it has become a matter of growing urgency within the private health sector too.
This is something I have seen at first hand in recent years as head of the Assoc iation of Independent Healthcare Organisations and now at Healthcode.
It started with the publication of the Competition and Markets Authority report into the private healthcare market in 2014, which demanded greater transparency about both charges and quality and outcomes data so patients could make informed decisions.
Another huge watershed moment was the scandal of disgraced surgeon Ian Paterson who was jailed in 2017 after carrying out unnecessary breast operations, causing serious reputational damage to the NHS and private hospitals where he practised and prompting calls for better sharing of information –and concerns – about consultants’ performance.
An independent inquiry into the Paterson case, chaired by the Bishop of Norwich, is due to report its findings towards the end of this year and is likely to include recommendations for improving consultant oversight.
Compatible with NHS
Some progress is already being made. The Private Healthcare Inform ation Network (PHIN) is currently working with NHS Digital on the ADAPt Programme (Acute Data Alignment Programme) which aims to ensure that data on privately-funded healthcare is compatible with NHS systems and standards.
And, this month, the Independent Healthcare Providers Network (IHPN) is due to launch its Medical Practitioners Assurance Framework (MPAF), originally referenced as its consultant oversight framework, developed under the leadership of Sir Bruce Keogh to improve clinical governance.
IHPN’s chief executive David Hare has already said that this will require a single dataset about every consultant’s whole clinical practice which would then be available to all the hospitals where they work.2
Both these projects are significant because they put data front and centre. They require common
data standards and compatible systems so that information currently held in one place can be collated, shared and analysed securely and efficiently.
But, to work, they need different stakeholders to set aside any qualms and embrace the principle of data-sharing in the interests of good clinical governance and patient safety.
Healthcode’s Private Practice Register (PPR) shows what can be achieved. The company originally launched this back in 2016 to streamline the cumbersome private medical insurance recognition process.
The idea was that practitioners could create an online profile with all the information they need to apply to the insurers of their choice in one go.
Comprehensive directory
Practitioners would then manage their own profile to ensure the information held about them was accurate – such as contact details –and showcase their qualifications, clinical expertise and experience to insurers.
Fast forward to 2019 and The PPR has evolved into a comprehensive directory and register of consultants offering services in the independent sector, with more than 16,000 practitioner profiles on the system.
And it is also being rolled out to hospitals, who will be able to view the profiles of consultants with practising privileges, including details such as their scope of practice, indemnity cover and appraisal status.
We expect that consultants will be able to use the system to apply for practising privileges and grow their private practice, while hospitals will have an important tool to help them with clinical governance and identifying concerns.
The PPR demonstrates that the technology exists to create an online platform on which data can be accessed and shared securely by users from different organisations in both the private and NHS sectors.
It proves that different stakeholders will engage with an industry-wide data project when they can see the benefits. And it means that we already have a head start in establishing a consultant over-
sight network which enables effective clinical governance across all healthcare settings.
I’m pleased to say that the IHPN asked Healthcode to comment on its draft assurance framework and we are ready to work with it to explore how The PPR can support the goal of improving clinical governance by building on what exists, rather than creating unnecessary bureaucracy.
Uncomfortable at sharing
Overall, I am optimistic that consultants, hospitals and insurers recognise that the sector must show it is addressing the shortcomings highlighted by the Paterson case, in terms of effective communication and information sharing, if it is to regain public confidence.
And yet, there is still a long way to go before the industry is comfortable with data-sharing. For example, as I write, thousands of consultants have yet to submit fee
information to the PHIN online portal, while PHIN’s report on the state of private data reporting in May revealed that 228 hospitals had made little or no progress in submitting data on adverse events and health outcomes.3
And we are yet to see real progress on other cross-sector initiatives that require the pooling of data such as centralised appointment booking.
When I joined Healthcode, I was unaware of the wealth of data that the company processes and holds securely on behalf of every private healthcare stakeholder in order to provide its online services.
It has been inspiring to see how technology can enable us to use data effectively, from automating time-consuming processes like billing, to secure messaging so that different organisations can connect and exchange information without compromising patient confidentiality.
At the start of this article, I made the point that the private healthcare sector could only realise the value of its data if we make use of it to deliver high-quality care and services. Now, much of our data is like buried treasure, but if we are willing to collaborate, we can be architects of our own fortune.
Fiona Booth is head of provider programmes and strategy at Healthcode
References
1. How we can place a value on health care data?; EY, 19 July 2019. www.ey. com/en_gl/life-sciences/how-we-canplace-a-value-on-health-care-data
2. Keep NHS and private sector in the loop and Both sectors need to share care data by David Hare, chief executive of IHPN; Independent Practitioner Today, May and June 2019
3. PHIN outlines the state of private data reporting; PHIN, 30 May 2019. https://media.phin.org.uk/phin-outlinesthe-state-of-private-data-reporting/
GETTING THE MONEY IN
Collection complexity
THE HISTORY of private consultants, clinics and groups is littered with a long history of incorrect billing – and, sadly, it has been getting worse.
At Medical Billing and Collection (MBC) we have recorded many examples of practices getting things wrong over the last 27 years or experiencing some very difficult issues in this field.
But as a result of the many changes to billing processes, combined with the greater administrative workload that busy practices face daily, things are getting a lot tougher for more and more doctors.
Most private consultants are typically running both an NHS and private practice, so they have considerable demands on their time.
On top of this, our data reveals that consultants are working harder to maintain the same income – the average value of the invoices we raise has reduced by 25% over the past ten years.
We have seen how practice secretaries have had to manage a big increase in the volume of communication they receive from patients. In the past five years, this has rocketed.
At the same time, secretaries are organising the clinics and theatres, typing correspondence and managing practice schedules. They then need to try and find the time to raise your medical invoices, reconcile the payments and chase any shortfalls and aged debt.
So we can see that there are many reasons why it is often difficult to ensure that the billing is being done both correctly and in a timely fashion, and also that robust chasing procedures are adhered to.
If your practice does not want to lose money on a continual basis or worse – contravene insurance company regulations and risk being derecognised by them – then it does need to make plans to address this critical area.
Some of the problem areas we see regularly are highlighted below:
CCSD
CCSD stands for Clinical Coding and Schedule Development and there are over 2,000 CCSD codes covering both consultations and procedures as well as an additional schedule of diagnostic codes.
The CCSD schedule is updated monthly and can include: Rules on which codes can be
Read Simon Brignall’s roundup of the pressures on doctors’ practices to get their billing and collection right and you will see why so many lose money if they try and do it themselves
billed together and those which cannot – known as ‘unbundling’;
The narrative against a specific code;
Replacement codes;
Discontinued codes;
New codes.
Any of the above can cause billing errors, so it is important these updates are reviewed for problems that may impact your practice.
Insurers
The CCSD schedule is used by the medical insurers as the basis to create their own fee schedule. But this is complicated, as it is not mandatory to follow CCSD rules.
So this means that each insurer can choose to adopt the CCSD schedule in whole or part, resulting in some not recognising specific codes and some having their own rules about which code combinations are acceptable for billing purposes.
Here are the main exceptions :
Some insurers will only allow certain codes to be billed in conjunction with a followup consultation;
One insurer does not allow a followup consultation to be billed within ten days of an operation;
An insurer can restrict the amount of inpatient care that can be billed by including a set amount within the specific code used in surgery;
Different rules around the billing of a local anaesthetic.
Due to the above, there are many varied and complex rules regarding the use of the codes and, on top of this, you need to know the pricing schedule for each insurer.
Here are some examples:
Some have a fee for each CCSD code;
Some place each CCSD code
into different categories for pricing purposes;
Some do not publish a schedule – they will pay what they consider to be market rate.
Different formulas
The last point to understand is the different coding formulas used by the various insurers. It is dependent upon the number of codes used.
Example 1
➠ Some state that if you bill three codes together, then you multiply the highest value code by 40% and then add that figure to the price of the highestvalue code;
➠ Some say that when two codes are used, you multiply the price of the highest value code by 25% and then add that figure to the highestvalue code.
Example 2
➠ Some decree that if you bill three codes together, you take the highestvalue code and add to that 50% of the second highestvalue code; then add 25% of the lowestvalue code to the figure that you have already calculated;
➠ Some say that when two codes are used, you add 50% of the second highest value code to the price of the highest value code.
Example 3
➠ Some say that when three codes are used, you can only charge for two codes, as they do not recognise the use of three;
➠ Some insurers state that when two codes are used, you add 50% of the second highestvalue code to the price of the highestvalue code.
Payments and remittances
It still surprises me how often we come across practices where there
are issues around payments and/ or remittances.
Let us start with the most important of these two, which is when payments from an insurer are not being sent to the correct bank account.
This can happen for a range of reasons, including when a consultant moves into a group, switches from a sole trader to a limited company or even changes their marital status.
AXA requires that any changes to your bank or contact information must be implemented through the Private Practice Register (PPR). If you are not already set up on the PPR, then this involves completing an online process that requires uploading supportive documentation. This has meant that some practices have been slow to update their records. At MBC, we routinely confirm that this information is correct as part of our onboarding process.
Remittances are often not being sent to the correct address. This can happen when a consultant moves home or as a result of changes in their place of work or medical secretary.
This results in payments not being reconciled, which can lead to invoices being chased that have already been paid. This is critical for remittances from the insurance companies, as you would not realise that you had to raise an invoice for a shortfall or an excess that had occurred.
Any delay in this important task looks unprofessional from the patient perspective and naturally means that receipt of these funds is delayed.
We find that issues around the billing and chasing of shortfalls are one of the most common issues practices have.
So, as can be seen, it is often a challenge to manage the issues I have outlined and you can now see
how a busy practice can have so many difficulties in this area.
The most common errors we see are price related that impact the total value of an invoice and result in a potential loss of income that may have gone back years.
Simon Brignall (pictured right) is director of business development at Medical Billing and Collection
WHAT STEPS TO PUT IN PLACE
Make sure you understand the complexities of the CCSD schedule for your specialty including what coding combinations can be used
Make sure that you code correctly by understanding the narrative for each code and review the monthly updates
Know the formula used by each insurer for pricing multiple codes
Be aware of the different rules each insurer will have over and above the CCSD schedule
Make sure that bank details for payment and contact details for remittances are up to date
Maintaining all of the above steps can be a daunting task; it is our experience that as the practice continues to grow, the consultant and the secretary are so busy dealing with the medical side of the practice that this area is frequently overlooked.
If you are struggling doing all of the above, then you need to consider outsourcing your medical billing and collection, as this specialist knowledge will typically form part of the services provided.
Ever-rising cost of being sued
OVERALL
COSTS of clinical negligence claims are now widely acknowledged to be at an unsustainable level and the Government has commenced various consultations on developing a cross government strategy to control costs.
The background to this is, of course, the costshifting model on which the justice system in England and Wales operates. Since April 2013, all claims for clinical negligence are subject to qualified oneway costsshifting (QOCS), so that a successful defendant cannot recover their costs from the losing claimant, except in very rare circumstances.
Niloo Bozorgi (below) looks at the costs of clinical negligence claims for independent practitioners and upcoming changes that will affect them
This is a change from the previous position – which still applies to most non clinical claims – whereby the unsuccessful party in a civil action pays the costs of the successful party.
This model is not without exception and an award in costs is always at the discretion of the court, which will have regard to all the circumstances of the case, including how the parties have conducted their case.
High costs
Either model can lead to high legal costs for independent practitioners facing a claim. Conversely for claimants, QOCS has meant that the possibility of footing the legal costs of their successful opponent is now a lesser consideration when contemplating an action in negligence.
In lower value claims, it has been known for the claimant’s solicitors’ legal costs to exceed the compensation their client receives.
Coupled with the present personal injury discount rate – leading to damages awarded at £37m in some cases – it is not surprising that indemnity premiums for independent practitioners can be very expensive.
In December 2018, the Government launched a consultation on the introduction of mandatory clinical negligence insurance cover for all regulated independent healthcare practitioners. The consultation closed in February this year.
Dearer for doctors
The consultation paper acknowledged that insurance cover is likely to be more costly for doctors than the discretionary indemnity provided by the medical defence organisations (MDOs) and will be unlikely to provide cover for the legal costs of doctors facing regulatory and other proceedings – such as inquests and criminal cases.
Insurance cover is likely to be more costly for doctors than the discretionary indemnity provided by the medical defence organisations
However, the concern was that the cover provided by the MDOs is discretionary and therefore the Government’s favoured option is for changes in legislation making insurance cover mandatory.
The effect on practitioners of such a change may be that they will have to take out two types of insurance/indemnity policy in order to ensure full protection. Obtaining and maintaining
insurance cover with adequate limits that does not exclude relevant activities can be difficult.
Should a practitioner have an adverse history as a result of previous claims or regulatory proceedings, not only will their premiums be likely to increase but the chances of finding an alternative provider will decrease in direct correlation.
Another difficulty
Another difficulty is that ‘claims made’ policies will only cover the practitioner in respect of claims reported to the insurer in that year.
A practitioner who has received a letter that they do not recognise as a claim or precursor to a claim will often deal with the letter as a complaint and thus will fail to report it to their insurer in contravention of the agreed policy.
It has been argued that root and branch reform of clinical negli
gence claims is the only sensible option for sustainably – and affordably – protecting practitioners and patients alike.
The Civil Justice Council working group has been set up to devise a bespoke process and a Fixed Recoverable Costs (FRC) regime for clinical negligence cases valued up to £25,000. The working group is due to report later this year.
A FRC regime would provide both parties with certainty as to the maximum amount they could be liable for and help to ensure proportionality on costs. In time. FRC may be extended to highervalue cases, thus providing longawaited stability on premium prices.
While reform may not be on the horizon just yet, there are optimistic signs that welcome changes may not be too far distant.
Niloo Bozorgi is a trainee solicitor at Hempsons
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes’ of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment
Premises
Regulatory requirements and investigations
Michael Rourke
Tania Francis m.rourke@hempsons.co.uk t.francis@hempsons.co.uk
A look back through our journal’s archives of ten years ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2009
£300k p.a. is realistic aim
A £300,000 pre-tax profit is now a realistic target for increasing numbers of NHS consultants with a private practice, we reported.
Figures from accountants showed the top 5% part-time private consultants hit £300k –many of them much more.
Stanbridge Associates said that, in London, the proportion who had gone through the £300,000 barrier was twice as high.
Fees were said to be ‘pretty tight’ with most specialists not increasing them, blaming insurance company pressure.
Many had kept their prices the same for self-pay patients too.
Bad debts are rising
Increasing numbers of consultants’ private practices were risking huge financial losses after allowing bad debts to escalate during the credit crunch.
Many were chasing thousands of pounds, but in the worse case scenarios they were owed hundreds of thousands of pounds before acting.
According to Medical Billing and Collection, the problem was 24% greater than 18 months previously – and it warned that this was set to worsen in the year ahead on the back of the recession.
The company’s Garry Chapman advised: ‘If doctors are owed more than 10% of their turnover, then it’s
something they should be looking at. If they are owed that now, then it’s only going to get worse.’
The mounting debts crisis was not just confined to solo practitioners. The larger and more successful a practice was, the bigger the trouble could be.
Doctors lose favour
Hospital hygiene and clearnliness had overtaken choice of consultant in the list of top reasons why the over-50s bought private medical insurance.
Saga Health found the top reason they bought private medical insurance was still to avoid NHS waiting, lists, followed by freedom to choose when and where to receive medical treatment.
But the company said MRSA publicity over NHS hospitals seemed to have resulted in hospital cleanliness becoming the third most important factor.
Overseas beauty ops scandal
One-in-four surgeons were reporting a rise in the number of patients suffering complications after taking cosmetic surgery ‘holidays’ over the last 18 months.
A British Association of Aesthetic Plastic Surgeons’ (BAAPS) survey found one in ten surgeons had seen between seven and nine patients with problems resulting from holiday surgery during that time.
According to a survey of 1,002 patients commissioned by Key Note, a total of 14.3% of them said they had visited a private GP in the previous year.
To what extent this reflected patients’ dissatisfaction with an NHS general practice gradually being torn apart by shifting goals in its pay system – and a collapse of the traditional partnership structure in favour of cheaper salaried GPs – could only be guessed at.
BAAPS president, consultant plastic surgeon Mr Nigel Mercer (right) said: ‘It is a serious concern that despite the economic downturn – or perhaps even because of it – the public is swayed by the promise of cheap surgery without being given the appropriate information to make an informed decision.
‘I find it appalling that most of these companies do not even mention risks, nor do they appear to have in place any mechanism if complications do arise.’
Private GPs on the rise
Increasing numbers of patients in the UK were choosing to visit a private GP, according to research from a market intelligence company.
Because you are worth it
A BMA guide to setting fees advised that, when negotiating fees, doctors should factor in their time, knowledge/experience, opportunity cost, running costs, professional expenses, travel expenses and pensions.
Where fee settlement was the patient’s responsibility, doctors were advised to discuss and agree the fee before doing any work. They should also take into account the fact there would be no pay for sickness, family reasons, holiday or study.
SUBSCRIBE TODAY
Don’t miss out on what we report and advise in the future. Sign up for a £75 subscription today –consultants, GPs and practice managers can save £15 with a direct debit.
See page 24
PRIVATE PATIENT UNITS
Income down but potential remains
Our monthly analysis of how private patient units are faring turns its attention to the 17 NHS trusts delivering acute care services to the south-west counties of Dorset, Devon, Cornwall, Wiltshire, Somerset and Gloucestershire. Philip Housden reports
REGIONAL TOTAL private patient revenues in the South-west fell significantly last year after a static period of three years. Total revenues are estimated at £28.5m, down from £31m the year before.
The decline masks a wide range of individual trust performance (see Figure 2 on the following page) and represents 0.53% of these trusts’ total revenues, down from 0.61% last year.
The combined national average outside of London is 0.5%.
Updated accounts for 2018-19 were available for all but three trusts at the time of writing – Great Western, Weston Area and Royal United Hospital Bath – for which 2017-18 data has been used.
The two trusts that have revenues above £3m a year – Great Western, Swindon, and United Hospitals Plymouth – deliver private patient services through contrasting approaches.
Great Western operates a 20-bed dedicated PPU, branded Shalbourne Private Health Care. During the past year, changes of management and some weakening of ring-fencing of private bed capacity are expected to have impacted on revenues which were £3.4m in 2017-18.
At Plymouth, the trust grew private patient revenues by £274,000 (9.6%), 0.61% of turnover, without re-opening its previous ringfenced capacity, The Meavy Clinic. Offering specialist regional services, the trust catchment is for
complex activity, a market opportunity which may drive further growth.
Gloucestershire Hospitals remained unchanged at £2.97m revenues in 2018-19; an essentially unchanged position for several years.
Balanced solution
The trust offers limited bed access at Cheltenham General, but has no dedicated inpatient capacity for private patients on the Gloucester Royal site.
It continues to search for a balanced solution for delivering dedicated private inpatient capacity. The Cheltenham General site has
strong potential, which would be delivered if the 15-bed Knightsbridge Ward were still fully available for private patients.
Gloucester is not as strong a catchment area, but the Royal Infirm ary has the surgical infrastructure to offer the high-quality patient safety back-up that clinicians most value.
Royal Bournemouth has moved forward in the past year with revenues up £146,000 and 5.3%, achieved after recruiting an experienced manager and opening the Bournemouth Private Clinic with five dedicated inpatient beds.
The trust also hosts a cardiology joint venture with Regent’s Park,
called the Dorset Heart Clinic, and has plans to extend inpatient bed capacity.
Planned merger
Bournemouth and Poole are two trusts working towards merger –now delayed until at least October 2020 – and joint work before then may lead to a reverse of the steep decline in private patient revenues on the Poole site, down £924,000 and 49% last year, to under £1m a year for the first time.
This was the consequence of ending the ring-fencing of the Cornelia Suite in Poole, a dedicated six- bed PPU opened in 2013.
Figure 1
However, a change in trust leadership followed and the unit has not enjoyed the same support in recent years.
Figure 1 on the previous page highlights the future links between Bournemouth and Poole, but also suggests the potential for a countywide approach given that Dorset County in Dorchester is keen to develop private patient services.
But Dorset County has again lost ground to record revenues of £783,000 last year, down 14.4% and £113,000 on 2017-18, the third consecutive year of declining revenues.
Big winners
Salisbury and Yeovil are the other big winners. Although Salisbury’s four dedicated beds in the Clarendon Suite is small by PPU standards, the trust has achieved 10.6%
growth (£226,000) through diagnostic and other earnings on top of inpatient growth.
Yeovil is a small trust with a track record of successful commercial developments, including the 14-bed Kingston Wing.
The trust still enjoys the highest percentage of trust revenues in the South-west, now at 1.61% of turnover, and grew 27.3% and £529k in 2018-19, reversing the previous year’s decline.
Neighbouring Taunton fell back 8.1% and £196,000 last year, reversing previous gains through the trust’s 12-bed Parkside Unit PPU at Musgrove Park Hospital.
Private patient services within NHS trusts in Bristol are a broad outlier in the region, particularly when compared with many other specialist care centres.
Although the city and catchment
are well provided for by independent hospitals, many other large trusts across England are growing private activity essentially because of the increasing focus on patient safety and risk for complex patients and procedures (see Note 2 on Figure 1 on the previous page).
Slow decline
North Bristol was previously the highest-earning trust by revenues in the region, but a slow decline was evident in terms of percentage of trust incomes even before last year’s 55% fall of £1.76m to £1.44m.
The trust has had turnover in private patient services operational management and there are no published plans for investment in a dedicated PPU and, without this focus, future growth is likely to be limited.
Across the city, private patient revenue at University Hospitals Bristol also declined steeply last year. Revenues fell 29% from £1.7m to £1.2m. Again, the trust has no dedicated PPU.
Opportunity for growth
It will merge with Weston Area in April 2020, providing an opportunity for a re-think and opportunities to invest for growth. Although small, Weston’s 12-bed Waterside Suite could be the focus for a new city-wide approach with the three trusts jointly developing a stronger private patient ‘chain’ together.
Royal United Hospitals Bath operates in one of the most competitive private hospital markets outside London. The trust is growing revenues, but from a low base. Local market potential remains
new 12-bed PPU inpatient ward, but this will not be open until perhaps early 2020.
Across the region, most of the NHS trusts are in a good position to exploit the important market niches for services that the independent hospital provider groups cannot provide
due to the relative affluence and size of the drive-time catchment.
But I understand that, despite this potential, the trust presently has no plans to invest in dedicated private patient capacity.
In Devon, the Royal Devon and Exeter has firm plans to invest in dedicated new capacity, albeit the work programme has been delayed.
The trust announced last year investment of £1.8m to open a
It has ambitions to at least double present revenues through this investment, although in 2018-19 revenues fell £206,000 (11.4%) to £1.6m.
Along the coast, Torbay and South Devon was previously the lowest revenue earner in the region by percentage of trust income but grew 15.1% last year and £142,000 to achieve income of £1.1m.
Weak competition
The trust faces relatively weak local independent sector competition and faces opportunities for growth.
Across the county, Northern Devon fell 11.7% and £74,000 to £560,000 (0.3% of turnover).
It once had a PPU, but has for some time used the capacity for NHS activity and, despite local consultant support, the market seems too small and geographi -
cally isolated to achieve anything easily on its own.
Perhaps there is room for a future county-wide link between the new service in Exeter and the other Devon trusts.
Across the Tamar, Royal Cornwall has the lowest private patient earnings of any trust in the region by turnover, at 0.09%. Revenues fell in 2018-19 by £209,000 to £361,000 (37%).
Ramsay’s Duchy Hospital is situated adjacent to the trust’s main site at Truro, so is well placed to exploit NHS capacity constraints. There are no presently declared plans by the trust to develop a local private patient service.
So there was a mixed performance for the region in 2018-19.
The South-west is not the strongest market for private patients, but, across the region, most of the NHS trusts are in a good position to exploit the important market niches for services that the inde -
pendent hospital provider groups cannot provide.
Where trusts have invested in capacity and protect it, earnings are stronger.
Looking to the future, the ageing population, increasing patient safety agenda and increasing restrictions on NHS access and lengthening waiting times means that there remain opportunities for all these trusts to consider the benefits of private patient services.
The region is the home of the only surviving regional group of NHS PPU managers and this supportive network provides a base for strengthening city- and countywide networks/groups/chains of NHS PPUs to exploit these market opportunities.
Next month: West Midlands
Philip Housden (right) is a director of Housden Group
CALCULATE YOUR NHS ANNUAL ALLOWANCE
INVESTMENT STRATEGIES
Only time will tell with the stock market
Timing isn’t everything. Patrick Convey on why political dramas are not a basis for investment success
OVER THE course of the summer, it was not unusual for the stock market to be a topic of conversation at barbeques or other social gatherings.
A neighbour or relative might ask about which investments are ‘good’ at the moment. The lure of getting in at the right time or avoiding the next downturn may tempt even disciplined, long-term investors.
But the reality of successfully timing markets is not as straightforward as it sounds.
Outguessing the market is difficult
Attempting to buy individual stocks or make tactical asset allocation changes at exactly the ‘right’ time presents investors with substantial challenges.
First and foremost, markets are fiercely competitive and adept at processing information.
During 2018, a daily average of $462.8bn in equity trading took place around the world. The combined effect of all this buying and selling is that available information, from economic data to investor preferences and so on, is quickly incorporated into market prices.
Trying to time the market based on an article from this morning’s newspaper or a segment from financial television is futile. It is very likely that information is
already reflected in prices by the time an investor can react to it.
Dimensional Fund Advisors recently studied the performance of actively managed US-based mutual funds and found that even professional investors have difficulty beating the market. Over the last 20 years, 77% of equity funds and 92% of fixed-income funds failed to survive and outperform their benchmarks after costs.
The positive news is that investors do not need to be able to time markets to have a good investment experience. Over time, capital mar-
kets have rewarded investors who have taken a long-term perspective and remained disciplined in the face of short-term noise.
The effect of politics
In recent months, the ‘noise’ has been led by politics and it is easy to believe this can have a greater impact on investment than is factually correct. Studies prove that, over the long run, the market has provided substantial returns regardless of who lives at Number 10.
There has been no shortage of speculation about how politics,
and political leaders in particular, will impact the stock market. The graph below helps to explain why investors would be well served avoiding the temptation to make significant changes to a long-term investment plan based upon these sorts of predictions.
It shows the growth of £1 invested in the UK market over more than 60 years and 12 prime ministers from Anthony Eden to Theresa May.
This exhibit does not suggest an obvious pattern of long-term stock market performance based upon
GROWTH OF ONE POUND INVESTED IN THE DIMENSIONAL UK MARKET INDEX, JANUARY 1956 – DECEMBER 2016
SOURCE: DIMENSIONAL FUND ADVISORS
happen to the stock market after a political event.
Cloud-Based Electronic Patient Records and Patient Portal
The positive news is that investors do not need to be able to time markets to have a good investment experience
which party has the majority in the House of Commons. What it shows is that, over the long run, the market has provided substantial returns regardless of who is in power.
A losing game
Trying to outguess the market is often a losing game. Current market prices offer an up-to-the-minute snapshot of the aggregate expectations of market participants – including expectations about the outcome and impact of elections. While unanticipated future events – genuine surprises – may trigger price changes in the future, the nature of these events cannot be known by investors today. As a result, it is difficult, if not impossible, to systematically benefit from trying to identify mispriced securities. So it is unlikely that investors can gain an edge by attempting to predict what will
Equity markets can help investors grow their assets, but investing is a long-term endeavour.
By focusing on the things they can control – like having an appropriate asset allocation, diversification, and managing expenses, turnover and taxes – investors can better position themselves to make the most of what capital markets have to offer.
Patrick Convey (right) is technical director at Cavend
ish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice.
Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions. Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
eClinicalWorks is a leader among independent, ambulatory practices, covering primary care and more than 50 specialities.
• Integrated Electronic Patient Record (EPR) and Clinic Management
• Comprehensive documentation of patient encounters
• Data analytics to deepen your understanding of your patients
• Streamlined workflows improve the provider and patient experience
Call to arrange a demo to see how we can help meet your needs!
Stuart Tebbutt
07891 217313
A character reference
A consultant asks for help after being asked to provide a testimonial for a colleague.
Dr Ellie Mein (right) responds
Dilemma 1 What do I put in the testimonial?
QI’m a urologist in independent practice and I’ve had a solicitor’s letter asking me to provide a written testimonial for a colleague undergoing a disciplinary investigation.
I’ve never been approached for one before and I’m not sure whether I should provide the testimonial and, if I do, what to include.
AIt is not unusual for doctors to be asked to provide references for colleagues when they are applying for jobs. In fact, the GMC has issued specific guidance on this topic which can be found at: www.gmc-uk.org/ethical-guidance/ethical-guidance-for-doctors/writing-references/ writing-references.
What is less common is being asked to write a testimonial for a colleague who is being investigated. Whatever the reason for providing the document, there are some standard principles to consider when writing a testimonial.
The first point to make is that you are not obliged to provide a testimonial if you do not feel able to do so for whatever reason.
If you decide not to provide the testimonial, reply to the solicitor to let them know. However, if you are happy to do so, the framework below may be helpful:
➤ Start with your full name, qualifications and job title.
➤ Explain who has asked you to write the testimonial, who it is about, how long you have known the colleague, in what capacity and for what purpose the document is being provided – for example, for consideration by the GMC.
➤ Make sure the solicitor informs you of the allegations that are being made against your colleague and outline these in the report.
The substance of your testimonial may be vary depending on whether the colleague is facing allegations of poor clinical competence or sexual impropriety towards colleagues, for example.
➤ Check with the person requesting the testimonial which areas it would be helpful for you to comment on. However, if you do not feel able to cover all the suggested points, then you should not do so.
For example, you may feel able to comment on a colleague’s clinical ability but do not know them well enough to comment on their character, their interactions with junior colleagues or their probity.
➤ Be honest and do not omit information that is relevant to the allegations which may not be helpful to your colleague. It is open to the colleague and their solicitor to not submit a testimonial if they feel that, on balance, it will not be supportive to their case.
➤ You must be able to be objective in what you say and be able to justify it.
If you can provide specific examples or evidence it will make for a more effective statement. But bear patient confidentiality in mind.
➤ Above all, it is important that your statement is accurate, honest, and professional in keeping with your obligations set out in the GMC’s Good Medical Practice (2013).
This states that: ‘You must be honest and trustworthy when writing reports, and when completing or signing forms, reports and other documents. You must make sure that any documents you write or sign are not false or misleading.’
If you receive a request for a testimonial or character reference for use in an investigation into a colleague’s practice and you are unsure of how to proceed, contact the MDU or your own medical defence organisation for further support.
Dr Ellie Mein is a medico-legal adviser at the MDU
When parents accuse you
A solicitor’s letter brings concern to a doctor following a consultation with a child. Dr Ellie Mein gives her advice
Dilemma 2 What is a Finding of Fact hearing?
QI am a consultant paediatrician who has been asked to provide a report on a sevenyear-old child whom I have recently seen at my practice.
The parents initially told me that the child had sustained the injuries following a fall, but I was concerned that the injury may be non-accidental. I recorded the history and his examination findings carefully in the records.
Recently, I have been contacted by a solicitor acting for the child’s father in family court proceedings, as the court has ordered that I write a statement.
This letter explained that the court was being asked to decide what had happened to the child and in particular to decide upon the nature and causation of the injuries.
The court was also to determine whether the injuries were non-accidental and, if so, to identify the perpetrator(s).
I am familiar with writing reports in relation to child protection proceedings and am happy to do so on this occasion. However, I noticed that the let-
ter refers to the intention of the judge to consider whether I should be a witness or given leave to intervene in a Finding of Fact hearing.
I have not seen this in any previous letters from the courts before and am concerned as to what this might mean.
What should I do?
AAs you have been asked if you wish to intervene in a Finding of Fact hearing, it could suggest that the parents have made allegations against you – such as alleging that you have exacerbated the injuries when examining the child in your practice or have, in fact, caused them.
You are obliged to write a statement, as this has been requested by the court. However, if criminal allegations are made against you, it is important to contact your medical defence body who may be able to provide legal assistance and represent you at the hearing.
As care proceedings are usually undertaken in private, there is often limited information available when members receive notifications of this kind.
Depending on the information available, it may be that you are advised to be added as an intervenor to the court proceedings. Any statement you submit can be
reviewed by your medico-legal adviser to ensure it provides a comprehensive chronology of the facts of your involvement in the case. If necessary, a solicitor may also be instructed to help with your case.
Following this, an expert opinion may be sought by the court and if it is established that you did not cause any injuries, then you can be dropped as an intervenor.
In this case, you will likely not be privy to further details of the legal case, as you will no longer be party to the proceedings.
When you are asked to provide a witness statement for child protection cases, it is worth considering:
Establishing early what is required of you. Are you a witness called by a party to proceedings or are you subject to a Court Order?
Is there any scope for you to be accused of causing injuries?
Are you a witness or an intervenor?
Always consider confidentiality; Are you being asked to do something that may not be in the child’s best interests?
27-30 January 2020
Anaesthesia, Critical Care & Pain
Dermatology • Emergency Medicine
General Practice • Plastic Surgery Radiology • Trauma & Orthopaedics
• Hands-on workshops
• Multidisciplinary lectures
• Satellite and joint sessions
• Bedside ultrasound course
• Contribution from allied specialities
• Keynote lectures by invited speakers
Are benefits in kind always really kind?
Ian Tongue highlights some of the more common taxable benefits that private doctors might come across
WHEN IT comes to paying tax on earnings, most doctors are familiar with the Pay As You Earn (PAYE) system and how tax and National Insurance is deducted on your monthly income.
But running alongside this are other components of your earnings that may suffer a tax charge. These are referred to as benefits in kind and are basically something you receive other than your salary that the taxman wants to tax you on.
Company cars
The most common area that a consultant may encounter a taxable benefit is if they are provided with a car by their employer, commonly referred to as a company car.
This could be either through a salary sacrifice scheme such as the NHS Fleet scheme or perhaps through your own limited company.
Either way, the calculations of the taxable benefit is the same, although the consideration of whether to have a company car through your own company is more complicated due to the cost of purchasing or leasing the car coming out of your company funds.
If you are considering this, your accountant should prepare figures to estimate the true cost of having a company car through your own limited company.
Over many years, the government has sought to reduce car emissions and therefore came up
with a system whereby you not only pay more company car tax according to the value of the car that has been provided, but you also pay more tax as emissions on the car increase.
In many ways, this was to discourage higher-emission company cars and this largely worked, with few people now having high-emission cars as part of their remuneration package.
With the raft of fully electric cars now available and more being released, having a car as part of your package has become more popular and it can also reduce superannuable earnings, which, for some, may reduce annual allowance charges for pension tax.
Reducing superannuable income through salary sacrifice may, however, ultimately reduce your pension on retirement and therefore you should seek advice before committing to this.
Electric and hybrid vehicles
Additionally, proposals are in place to substantially reduce the tax payable on fully electric cars and hybrids with long electric range from April 2020.
These proposals were recently amended to provide a 0% rate on fully electric cars from 6 April 2020 following a consultation document. The rate will gradually increase from 2021-22.
Also relevant are the new WLTP emissions test – an easy anagram for ‘Worldwide Harmonised Light Vehicle Test Procedure’ – which is
more stringent and results in different tax bands for vehicles registered after 6 April 2020.
This is resulting in a significant uptake of electric vehicles from consultants and leads, no doubt, to consultant car parks starting to see many more electric vehicles.
EXAMPLE OF CAR BENEFIT
Fully electric car (zero emissions), list price
£75,000
The benefit in kind for the tax year ending 5 April 2020 on the above is 16% of the list price and therefore a benefit in kind of £12,000 arises.
For an additional-rate taxpayer, this would be £5,400 in income tax for the 2019-20 tax year.
Assuming the proposed reduced tax rate reduction in April 2020 takes place, for the 2020-21 tax year there would be no benefit in kind or tax to pay.
For 2021-22, the benefit in kind rate is proposed to be 1%, which would amount to a benefit in kind of £750, resulting in income tax of £338 being payable for an additional-rate taxpayer.
For 2022-23, the benefit in kind rate is proposed to be 2%, which would amount to a benefit in kind of £1,500, resulting in income tax of £675 being payable for an additional-rate taxpayer and thereafter, under current proposals.
Clearly, electric vehicles as a company car become very attractive from April 2020, with the main risk being that the reduced rates are removed/amended or are only in place for a short period.
However, given the push to remove petrol and diesel cars from sale, it will act as a strong incentive so, hopefully, will be around for a reasonable period.
Salary sacrifice schemes
As discussed above, a common scen ario is having a car through the NHS fleet scheme, but some trusts do not offer this for whatever reason.
The method of calculating the level of salary sacrifice is primarily by reference to the lease cost that the trust is paying on your behalf. Once calculated, you receive less gross pay and your net monthly income falls. In addition, you will pay the tax calculated above as a benefit in kind from your NHS salary.
So, when considering whether you want to go ahead, you should look at the effective cost and determine whether this represents good value for money. In other words, could you buy the vehicle personally for less per month?
Over the years, there have been many other salary sacrifice schemes to exchange salary for other non-cash benefits. However, due to recent changes, there are far fewer arrangements in place and are now generally limited to:
Cars – as discussed above;
Childcare vouchers;
Additional pension – unlikely with the NHS;
Cycle-to-work schemes.
One other common salary sacrifice scheme was in relation to
workplace parking. This was an area where changes have been made and will explain why many consultants now have to report a benefit in kind for workplace parking still being provided as a deduction against gross pay.
Outside of the NHS, most employers now deduct the cost of parking from net pay to avoid a taxable benefit arising.
Health insurance
For those with their own limited companies, you could consider paying private health insurance for you and the family and the cost of the premium would be a taxable benefit.
This can be a net saving if you already operate a PAYE scheme, as the additional work to report the taxable benefit is modest. But if your business is not operating a PAYE scheme, the additional costs of administering the PAYE scheme and reporting would largely outweigh the savings.
Mileage allowances
HM Revenue and Customs (HMRC) has an approved rate of 45 pence per mile for an employer to pay their employee for the first 10,000
You should look at the effective cost [of a company car] and determine whether this represents good value for money. In other words, could you buy the vehicle personally for less?
miles of business mileage without a taxable benefit arising. Thereafter, the rate is 25p per mile.
Many consultants work at multiple hospitals and may be paid more than the above or it may be part of your contract that you are based at multiple sites. Under each scenario, you will have a taxable benefit each year where you pay tax on the excess allowable.
Beneficial loans
Another area where a benefit in kind may arise is if your own limited company has loaned money to you via your directors’ loan account at a beneficial rate; that is to say, less than the HMRC official rate. In these circumstances, the interest saved is regarded as a taxable benefit, assuming the loan exceeds a certain level.
The system of reporting and collection of tax
The form which summarises all of your benefits in kind is called a P11d. This form is prepared by your employer after the tax year to which it relates and needs to be submitted to HMRC in early July each year.
A copy is provided to the
employee and it is important that this document is passed to your accountant, otherwise it is likely to trigger a tax inquiry.
Following the submission of your tax return, your NHS tax code is likely to change, which will increase the level of tax paid through your salary collecting the tax due. As always, ensure that you send your accountant any tax coding notices that you receive to ensure that you are paying the right amount of tax.
It is becoming more common for consultants to have taxable benefits other than their salary.
Before entering into any arrangements, it is advisable to discuss matters with your accountants to ensure you understand the implications and true cost of having taxable benefits.
Next month:
Reducing your risk of an HM Revenue and Customs inquiry
Tongue (right) is a partner with Sandison Easson accountants
Ian
The most common area that a doctor may encounter a taxable benefit is if they are provided with a car by their employer or by their own limited company
DOCTOR ON THE ROAD: PORSCHE 992
A very rewarding driver
It’s
a doctor’s
favourite – but can the latest version of the iconic 911 live up to expectations? Dr Tony Rimmer (right) couldn’t wait to find out…
As
IF, AS a private medical practitioner, you can create something groundbreaking and unique – a treatment, a service or a luxury clinic – then you and your practice will benefit both professionally and financially.
Every business strives to reach the point where their brand is iconic. At that point, on-going demand from clients ensures fiscal stability and the potential to increase profit margins.
As far as cars go, there are few real icons. There are even fewer that have remained in continuous production for over 50 years, albeit with constant updates.
The Porsche 911 is one such icon and a favourite with us medics. So, can the latest iteration, the 992, live up to its exalted status?
The newest 911 is a thorough development of the previous 991 version. The body is slightly larger and the chassis and body construction uses more aluminium and so the car is now lighter.
The engine is the same twinturbo 3.0 litre flat-six as used in
the later 991 models, but now has bigger turbochargers. In this S model, it produces 444bhp.
There will be a base Carrera model in due course with slightly less power. As standard is a new eight-speed Porsche ‘double clutch’ (PDK) gearbox, although Porsche is promising the future availability of a manual box.
Modernised interior
Perhaps the most obvious change for new owners will be the modernised interior. Apart from the driver-centred analogue tachometer, all the other instrumentation is now digital.
The latest generation Porsche Communication Management (PCM) touchscreen infotainment system is accessed via a large and clear 10.9-inch central screen. The leather interior also gives the new 911 more of an up-market luxury feel, particularly as it has neat stitching that extends to the door trims.
You will need £93,110 to match the starting list price of the Carrera
S, but the price will easily rise past the £100k barrier with a few choice options. The four-wheeldrive Carrera 4S costs an extra £5,300 and the S Cabriolet an extra £9,600. Competitors include the Audi R8, the Aston Martin Vantage and the McClaren 540C
As you approach the new 911, it does look wider at the front, but the extra length gives it a sleekness that looks more sophisticated. It looks great in lighter colours. The latest model is easily identifiable by the vertical third brake lights at the rear.
Luxury car
The up-to-date interior is a bit of a revelation. The digital instruments are very smart and work really well. High-quality materials used across the cabin make this new 911 feel like a real luxury car, justifying its lofty price.
As ever, luggage capacity is better than you think; the spacious front boot is complemented by useful space behind the front seats.
The folding rear seats may be small, but no rival can boast the ability to carry two small children or an occasional adult as rear passengers.
Special driving experience
A huge part of the 911’s iconic status has been determined by the very special and rewarding driving experience it has always delivered. The 992 model updates would be pointless if there were any new compromises.
So how does it perform? Well, like all good sports cars, it makes you feel good just sitting in the driver’s seat. The steering wheel is a perfect size and all the dials, analogue and digital, are perfectly placed.
The start-up is surprisingly subdued in the cabin and this is due to improved noise suppression.
My test car had the optional switchable sports exhaust, which is a must if you like to hear that wonderful flat-six when you are on the move.
Initial driving at low speeds is
you approach the new 911, it does look wider at the front, but the extra length gives it a sleekness that looks more sophisticated
driver experience
really easy and helped by excellent all-round visibility and a compliant ride. The gearbox changes are almost imperceptible in automatic mode.
But if you clear the urban sprawl and find some decent ‘A’ and ‘B’ roads, the 911 changes character. And what a character it becomes.
Select Sport or Sport + on the steering-wheel gear selector and the chassis tightens, the gearbox allows higher rev changes and the steering comes alive.
Safe and controlled
The claimed 0-62mph time of 3.5 seconds becomes entirely believable and you can cover cross-country routes at a pace that is super-swift but always feels safe and controlled.
Corners are confidently dispatched with aplomb and the ride actually improves with speed.
As you go faster, the 911 shrinks around you. Any concerns about its increased dimensions disappear and you really feel at one with this superb driving machine.
Switching to manual mode on the PDK gear selector gives you extra control that is closer to a manual gearbox than anything else I have driven, but you will need a race track to explore the car’s real dynamic limits.
Most importantly, though; can you have fun with the new 911 on normal roads? The answer is a resounding yes.
Every time that Porsche updates the 911, there is a worry that the recipe will be spoiled.
This eighth and latest iteration, the 992, is a superb high-quality sports car. It has advanced several aspects of the car to bring it right up to date and appeal to all of us who appreciate great cars.
It continues to be capable of being used as a daily drive but able to serve up thrills in abundance on demand.
It seems that Porsche has done it again. The 911’s iconic status is safe.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
Porsche has advanced several apsects of the car to bring it right up to date and appeal to all of us who appreciate great cars
PORSCHE 911 CARRERA S
Body: Two-plus-two coupé
Engine: 3.0 litre six-cylinder twin turbo
Power: 444bhp
Torque: 530Nm
Top speed: 191mph
Acceleration: 0-62mph in 3.5 seconds
Claimed economy: 31.7mpg combined cycle
CO2 emissions: 205g/km
On-the-road price: from £93,110
The steering wheel is a perfect size and all the dials are perfectly placed. The spacious front boot is complemented by useful space behind the front seats
The latest model is identifiable by the vertical third brake lights at the rear
MEDICO-LEGAL ADVICE
Facing a tricky ‘sickie’
Being asked by a patient to issue an ‘unfit for court’ certificate is a complex and emotive area that can lead to difficulties if doctors are unaware of the possible pitfalls, warns Gabrielle Pendlebury (right)
‘UNFIT FOR COURT’ certificates are normally submitted by defendants in criminal proceedings as justification for not answering bail.
If a medical certificate is accepted by the court, then cases, including contested hearings and trials, get adjourned rather than the court issuing a warrant for the defendant’s arrest without bail.
Certificates will also provide the defendant with enough evidence to defend a charge of failure to surrender to bail.
They may also be submitted by witnesses who are due to give evidence and by jurors. But doctors can find themselves colluding with reluctant witnesses and jurors if they are not careful.
attend court or the expiry date of the certificate.
were adjourned as the doctor issued repeat certificates.
To ensure you follow best practice, heed the relevant guidance.
The cost of adjourning trials to accommodate defendants and jurors can be very high, so certificates are carefully scrutinised.
Doctors should be aware that, when issuing a certificate in criminal proceedings, they make themselves liable to being summonsed to court to give evidence about the content of the certificate and may be asked to justify their statements.
So when writing a certificate, consider the Crown Prosecution Service guidance, which states that a certificate should contain enough detail for the court to decide, including:
The date the doctor examined the defendant;
The exact nature of the defendant’s ailment;
If it is not self-evident, why the ailment prevents the defendant from attending;
An indication as to when the defendant is likely to be able to
Circumstances where a court may find a medical certificate to be unsatisfactory include:
1
Where the certificate indicates that the defendant is unfit to work – rather than to attend court;
2 Where the nature of the defendant’s ailment – for example, a broken arm – does not appear to be capable of preventing his attendance at court;
3
Where the defendant is certified as suffering from stress/anxiety/depression and there is no indication of the defendant recovering within a realistic time-scale.
Stressed patient
In the case of R v Ealing Magistrates Court Ex p Burgess (2001), a man was due to be tried for harassment. He obtained a certificate from his doctor stating he was unfit to attend court, due to stress.
This resulted in the hearing being adjourned at significant cost and inconvenience to those involved and subsequent hearings
Eventually, the court lost patience and, on learning the patient had been attending another court as a claimant, it decided to exercise its discretion to disregard a certificate and heard the case in his absence.
The patient challenged this in the High Court, where the judges agreed with the magistrates. They said: ‘The court has a discretion which has to be exercised with proper regard to the principle that the defendant is entitled to a fair trial. That includes a fair opportunity to be present at his trial.
Enough is enough
‘However, the words are “fair opportunity”, not “unlimited opportunity”, otherwise it would never be possible to proceed in a defendant’s absence and a defendant would be able to postpone trials indefinitely without the risk that the court would eventually be able to say “enough is enough; we will proceed in his absence”.’
When writing a certificate, make clear you are giving an opinion and this is to help the court decide
Doctors should be aware that, when issuing a certificate in criminal proceedings, they make themselves liable to being summonsed to court to give evidence about the content of the certificate and may be asked to justify their statements
whether to require the patient to attend.
It might also be sensible to clearly state if the patient is truly incapable of attending court due to illness, either physical or psychiatric, or whether it would be inadvisable due to the risk of discomfort or exacerbation of a condition.
Careful consideration of requests for certificates, and careful wording of the certificate, should limit the risk of having to appear in court to justify the contents and limit the risk of criticism for being too ready to adhere to the patient’s request.
Gabrielle Pendlebury is a medicolegal consultant at Medical Protection
PROFITS FOCUS: ENT SURGEONS
Thirteen: lucky for some
It has been an excellent year for ENT surgeons profits. Ray Stanbridge examines the reasons in our latest benchmarking survey of NHS doctors’ earnings in private practice
THIS HAS been a very interesting and profitable year for many ENT surgeons.
Their average gross incomes rose by 4% between 2016 and 2017, going up from £168,000 to £175,000.
Costs fell by about 9%, for reasons which we explain below, dropping from £75,000 to £68,000 on average.
As a result, taxable profits have increased by about 14% from £93,000 to £107,000. All in all, a very satisfactory outcome.
Insurers continue to put ENT
Expenditure
fees under pressure but we have noticed two strong trends between 2016 and 2017.
Firstly, for some consultants there has been considerable growth in Choose and Book work. This work seems to ‘come and go’, but certainly in 2017 it seems to have been strong.
Market trend
Secondly, there has been continuing growth in self-pay. ENT surgeons are well placed to take advantage of this market trend.
I admit being a little surprised to
Taxable profits have increased by about 13% from £93,000 to £107,000. All in all, a very satisfactory outcome
find that costs for the typical surgeon in this specialty fell in 2017 against 2016.
A few consultants have taken advantage of managed service arrangements offered by hospital groups, which are compliant with Competition and Market Authority (CMA) rules. This means that secretarial and office costs may fall with an increase in room hire costs. Often there are cost savings, and this seems to be what has happened.
There was a small fall in medical supplies/assistant costs for reasons which we cannot fully explain.
Business base
Use of home costs have shown a slight rise and an increasing number of ENT consultants now use their home as a second business base.
Other costs have remained broadly like 2016 except for marketing/promotion. Reviewing this figure, it seems there was heavy expenditure by some consultants in 2016 on marketing/promotion. This was not repeated in 2017, with the result that average figures fell. Again, for those who had taken up managed service arrangements with hospitals, marketing services were provided directly by
RISING INCOME AND LOWERING COSTS HAVE LEAD TO A ENT SURGEON’S BUMPER PROFITS
HOW ARE YOU DOING?
them rather than paid for by consultants.
What then of the future? The trend for self-pay continues and we would expect gross incomes to exhibit continuing growth, albeit slower than in 2017 as the market has slowed down.
continue to perform satisfactorily in the coming year.
We were surprised at the extent of cost reductions, on average, we would expect costs to rise in 2018. Nonetheless, ENT surgeons should
As readers will be aware, however, our sample of consultants includes those who:
Have at least five years’ private practice experience;
Hold either a maximum parttime or a new consultant NHS contract;
Are seriously interested in pursuing private practice as a business;
Are earning at least £5,000 a year in the private sector;
May or may not have been incorporated, or be a member of a group.
A number of factors affect the results and may lead to distortions, such as the significant rise in the number of consultants incorporating, the growth of groups, pressures from insurers, the rise in self-pay and the effect of the CMA rulings on how consultants undertake their practices.
Next month: Orthopaedic surgeons
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists, Stanbridge Associates
Years ending 5 April
WHAT’S COMING IN OUR NOVEMBER ISSUE...
Make sure you don’t miss our next issue, published on 28 November. You may not receive every issue if you have not yet subscribed to the journal. Don’t risk missing out on vital topics we tackle next time:
Protect your private practice! Independent Practitioner Today has a trio of articles to help safeguard you and your business from data attack:
1. Vin Pandha reveals how criminals are attempting to obtain funds fraudulently, by targeting surgeries and medical practices using phishing and vishing techniques
2. Get it sorted: why you need to establish a data privacy and security awareness culture in your practice
3. The perils of posting on private social media groups. Information from these groups can become publicly accessible
Are your financial records up to date? Simon Brignall of Medical Billing and Collection highlights the difficulties of records being behind the times, which can even lead to problems with the tax inspectors.
Are you considering taking on staff, but unsure about the basis on which to engage them? Should you opt for a freelancer or offer an employment contract? Hempsons lawyer Julia Gray looks at the risks and benefits of self-employment
Orthopaedic surgeons – check out our Profits Focus to see how others in your specialty have been doing
How you can reduce the chances of an HMRC investigation
INDEPENDENT PRACTITIONER
TODAY
The
TELL US YOUR NEWS
Robin Stride, editorial director
Email: robin@ip-today.co.uk
@robinstride Circulation figures verified by the Audit Bureau of Circulations
Phone: 07909 997340
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution.
Printed by Pepper Communications Ltd Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Registered office: 7 Lindum Terrace, Lincoln LN2 5RP
Write to Independent Practitioner Today PO Box 198, Cranleigh GU6 9BB
Property investing for doctors – how to fund your deals
Business Dilemmas answers a query from a surgeon whose patient later died and now he’s worried a letter of claim from solicitors means he will have to go to court
Our accountant’s A-Z of top tips considers the letter E – for ‘expenses’, the ‘enterprise investment scheme’ and ‘expanding’
Many doctor investors question taking a ‘long-term’ approach of investing in the stock market. Dr Benjamin Holdsworth of Cavendish Medical considers a prudent investment horizon, whatever your age
The power of our senses and how to use these to create a positive visitor experience to our practice
Practising in the West Midlands? See our latest analysis of private patient unit earnings there
Our motoring correspondent finds the seven-seat SEAT Tarraco equals the class leaders
Plaudits for audits: the independent sector pilots the National Clinical Audits Programme
Surgeon Mr David Sellu, wrongly jailed for gross negligence manslaughter after a patient died in his private hospital, continues his amazing story in Independent Practitioner Today
Plus all the latest news and views
ADVERTISERS: The deadline for booking adverts in our November issue is 1 November
ADVERTISE WITH US
Margaret Floate, advertising manager Email: margifloate@btinternet.com Phone: 01483 824094
GET A SUBSCRIPTION DISCOUNT! £90 independent practitioners. £90 GPs and practice managers (private & NHS). £210 organisations. Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE – USE SUBSCRIPTION FORM ON PAGE 25 or EMAIL: karen@marketingcentre.co.uk or phone 01752 312140 or go to the ‘Subscribe’ page of our website www. independent-practitioner-today.co.uk
Publisher Gillian Nineham
Phone: 07767 353897. Email: gill@ip-today.co.uk
SAVE £15 WITH DIRECT DEBIT!
Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.
BACK ISSUES: £12.50 including post & packaging
Phone 01752 312140 or Email karen@marketingcentre.co.uk
Giving voice to the private sector
INDEPENDENT PRACTITIONER
Thanks to Healthcode for helping us to reduce the use of plastic
The new president of the Independent Doctors Federation, private GP Dr Neil Haughton, reveals his plans and hopes for the organisation in the years ahead n See page 18
business journal for doctors in private practice
Make access to self-pay easy
The private healthcare sector needs to do much more to make it easier for patients to access. And clearing up price confusion would be a good place to start, argues Keith Pollard n See page 21
What are you doing to attract patients
ADDRESS LABEL
Jane Braithwaite shows you how to choose the right marketing strategy to attract new patients and grow your practice
n See page 26
If undelivered, please return to: The Marketing Centre, 12 Mary Seacole Road, The Millfields, Plymouth, PL1 3JY
What are you doing sector
Integrated online solutions on one platform built to give customers time efficiency, compliance, robust data security and ability to connect seamlessly
Your financial and practice management on one secure platform
Improve:
• cash flow
• operational efficiency
Peace of mind knowing:
• your data is held securely and backed up
• your data is hosted in the UK
• no additional back office costs
A cost-effective integrated toolkit on one platform that:
• is scalable
return to: The Marketing Centre, 12 Mary Seacole Road, The Millfields, Plymouth, PL1 3JY
• includes key tools to manage both your financial and administrative tasks and processes
• allows you to manage your practice bookings for one or multiple locations
• maintains and manages your patient records and their associated transactions
• gives you the ability to communicate securely with other organisations such as hospitals and insurers
For more information and a demo of the system: ( 01784 263 150