INDEPENDENT PRACTITIONER




An explosive and detailed analysis for Independent Practitioner Today by leading specialist medical accountants Stanbridge Associates has identified 11 ground-changers doctors can expect to see in private practice over the next five years



October 2015 www.independent-practitioner-today.co.uk
measurement is key to success anyone can start a company, but making it profitable requires expertise. aesthetics business expert pam Underdown explains what you need to do to be sustainable P14


in quality straits as the care Quality commission analyses private doctors’ responses to its consultation, Martha Walker (left) asks whether independent doctors should stay within its remit P22


time to take shelter as employee? the current private healthcare system may not be sustainable, warns private healthcare entrepreneur Keith Hague. it may be time for specialists to consider the benefits of being an employee P32
Clearly, there will be some massive issues facing independent practitioners over the next five years and this month we highlight 11 big ones that could be game changers.
The ‘Stanbridge Report’ featured on our cover and starting on page 28 gives a fascinating insight into what your world could be like by 2020. It is a scary future for some – but happy for others.
But, with the pace of change so fast, we’d expect to see many of the 11 lining up sooner than predicted.
Controversy is inevitable –especially with a salaried service option – and there will inevitably be winners and losers.
Consultants need to consider how their practice could be affected by fast-moving events and many will have to take business advice to find their own winning formula.
As the fastest-growing medi-
cal publication, Independent Practitioner Today will continue to help give you the news you need to know, and useful articles from an array of experts, to help you tackle the future.
There are many other longrunning topics facing independent practitioners right now and, in this issue, our writers cover a varied selection including self-pay, profits, patients’ complaints, staff matters, regulation, marketing, and buying and selling a practice.
Thanks for all your positive comments you brought to our stand at recent events, especially at Olympia’s CCR Expo earlier this month, where the clinical, cosmetic and reconstructive worlds came together.
Business is certainly booming in this largely self-pay sector and there is much for many practice businesses to learn from the non-clinical operations of doctors in aesthetics.
the art of the gentle reminder
Self-pay patients are on the rise, but that means your non-payers could be on the increase too. Gary nials set out his tips and template letters to help chase up what you are owed P38
the whole world in your hand
Spreading your wings abroad? dr andrew Vallance-owen explains the ‘fixer’ agency that helps UK healthcare providers overcome challenges of international expansion P42

market turmoil in china our resident investment adviser Simon bruce explains why it’s important to keep global events in perspective and to hold your nerve when it comes to investment strategy P46



Business dilemmas: avoid being accused of assault With more doctors facing allegations of sexual assault in recent years, dr bev Ward answers your questions P48
doctor on the road: Home within range if you are a doctor who gets excited by the latest electronic equipment, then the bMW i3 could be for you P50
Profits Focus: ticking over very nicely
Finances are ticking over nicely for cardiologists featured in our unique benchmarking series P56
tell US yoUr newS Editorial director Robin Stride at robin@ip-today.co.uk Phone: 07909 997340 @robinstride to advertiSe Contact advertising manager Margaret Floate at margifloate@btinternet.com Phone: 01483 824094 to SUBScriBe lisa@marketingcentre.co.uk Phone 01752 312140
Publisher: Gillian Nineham at gill@ip-today.co.uk Phone: 07767 353897
Head of design: Jonathan Anstee chief sub-editor: Vincent Dawe 12,450 circulation figures verified by the Audit Bureau of Circulations

By robin Stride
A salaried service is beckoning for increasing numbers of consultants who want to do private work in independent hospitals.
Self-employed status has been passionately championed by generations of independent practitioners – but employment is now being seen as an increasingly attractive option for many younger specialists.
Just months ago, consultants were given strong advice against taking salaried posts during the Independent Doctors Federation annual general meeting.
Specialists’ committee chairman Dr Brian O’Connor warned: ‘Ultimately, a system of salaried consultants in private hospitals would diminish if not abolish the influence of doctors, whose independence would be sacrificed in the interests of their employer, which may be at variance with best clinical practice.’
However an analysis for Independent Practitioner Today on the future of private practice, by specialist medical accountants Stanbridge Associates, sees a second salaried job for consultants in private hospitals as one of 11 big likely changes in the next five years.
The Stanbridge Report’s view is backed by Mr Keith Hague, former chief executive of the UK’s largest private hospital, The Wellington Hospital, in London. He is now suggesting consultants think seriously about the possibility.
Writing in this issue of Independent Practitioner Today , he says: ‘Some will argue otherwise and

the time has come for the consultant to consider his or her practice under a different organisational structure. employment within the private sector may well be worthy of consideration
KeitH HagUe
some may be right, but I think the time has come for the consultant to consider his or her practice under a different organisational structure. Employment within the private sector may well be worthy of consideration.’
Mr Hague, who is now chairman of Worldwide Healthcare Assoc iates – which helps independent practitioners ‘start, trans-
form and grow’ their practice businesses – admits: ‘As little as five years ago, had I mentioned to any consultant group that they should consider being employed by a private hospital organisation, I would most likely have been turfed out of the room.
‘But things are different now and time has moved on and one may wish to consider that the
long-honoured practice in existence for over 50 years, whereby consultants bill a fee for service alongside the hospital facility fee, is more than likely not fit for purpose.’
According to the Stanbridge Report, the employed private consultant phenomenon has happened in the US and some private hospital groups in the UK are considering the option.
Author Ray Stanbridge says: ‘With the NHS already accounting for close to 30% of the spend in the private sector, there will be an increasing number of consultants who choose to take a second salaried job with a private hospital.
‘The potential advantages for them are many. If they undertake NHS work alone, they do not have to incur the cost of indemnity insurance. Secretarial and other costs will be borne by private hospitals and they will not have total patient responsibility.’
Big changes in the private healthcare sector are seen as likely to put pressure on consultants to seriously consider a salaried option.
These include spiralling costs –with defence fees making it impossible for some to practise –falling income and the withdrawal of free rooms and secretarial support following the Competition and Markets Authority investigation into private healthcare.
Others are being enticed by the attraction of being able to escape administration and the management side of running a business and spending more time with their young families.
See pages 28 and 32
By Leslie Berry
Senior doctors are being warned they will face a new limit to the amount they can receive in redundancy pay from the NHS if a new Parliament Bill is passed.
Greg Hands, the Chief Secretary to the Treasury, has announced a £95,000 cap for public sector workers in order to end what he called ‘golden goodbyes’.
The limit will apply to all forms of severance compensation including redundancy payments, pension top-ups and exit payments.
Patrick Convey, technical director at specialist financial planners Cavendish Medical, told Independent Practitioner Today: ‘Currently, high-achieving NHS consultants are entitled to exit payments of up to two years’ pay. This new move will bring about a significant reduction to their exit benefits.
‘Crucially, the option to take their pension early – where the compensation is used to buy out the actuarial reduction and the shortfall is topped up by the employer – will be lost.
‘This could be a substantial dis-
advantage to many doctors. We are already receiving calls from clients considering their positions.’
At present, no date has been set for the introduction of these changes.
At the same time, further reforms are being introduced via the Small Business, Enterprise and Employment Act 2015 to allow NHS employers to recover exit payments made to high-earners who return to the same part of the organisation within 12 months.
These regulations are expected to come into force in April 2016.
Steve Gray will be the new Nuffield Health Group chief executive following David Mobbs’s decision to step down at the end of 2015 after 14 years in order ‘to explore new opportunities’.
Mr Gray was previously group international healthcare director for Superdrug parent company AS Watson.
Mr Mobbs repositioned Nuffield
Health from a hospital operator to a health and well-being business including 31 hospitals, 77 fitness and wellbeing centres.
The charity said: ‘He has transformed Nuffield Health by bringing together private hospitals, clinics, fitness and

well-being centres, diagnostic units and an extensive range of healthcare services into one complete health and well-being service.’
The group is the largest single employer of physiotherapists outside of the NHS.
Deregulating private doctors from the long arm of Care Quality Commission (CQC) inspectors could do them a disservice, according to a private practice adviser.
According to medical management consultant Martha Walker, most independent doctors want to demonstrate that, in the words of the CQC, the service they offer is safe, effective, caring, responsive and well-led.
Writing in this month’s edition, she says: ‘By removing themselves from regulation, I believe that doctors are laying themselves open to criticism and the question “What have they got to hide?”
The CQC is currently analysing independent doctors’ responses to its recent consultation, including the question ‘Should independent doctors remain within the scope of regulation by CQC?’
Dr James MacKay, chairman of the Independent Doctors Federation’s Regulation Committee, aims to continue work with the CQC to drive independent healthcare standards even higher. He hopes all IDF members have replied to the consultation paper, seen as probably the most important of its kind that the CQC had issued.
IDF GP committee chair Dr Neil Haughton said most of the IDF’s suggestions were taken on board in the CQC consultation paper. See page 22
Surgeons at The Harley Street Clinic Children’s Hospital in London have enabled a 13-yearold boy to walk again, nine months after he was shot four times and left for dead.
Almost 150 children and school staff were massacred by Taliban gunmen in Peshawar, Pakistan, last December. Muhammed Khan survived but lost all bodily functions below the waist because his spine was so badly damaged. Doctors from several countries said nothing could be done for him and predicted he would be

confined to a wheelchair for life. But his parents refused to give up hope. They launched an appeal, answered by two donors, and the schoolboy’s medical notes were
Muhammed and his parents pictured with spinal surgeon Mr Irfan Malik (right) of the London Neurosurgery Partnership, part of The Harley Street Clinic
sent to nerve surgeon Prof Thomas Carlstedt and spinal surgeon Mr
The family flew to the UK and Muhammed underwent a six-hour
operation to rebuild his shattered spine and reconnect nerves.
After a few days, he began to regain feeling in his legs and then, to doctors’ and physiotherapists’ amazement, asked for a support frame and began to walk about a week after surgery.
Mr Malik, a member of the London Neurosurgery Partnership, said: ‘We were amazed and we started to see a “miraculous” recovery; much more progress than we had dared hope for.’
By Edie Bourne
Tighter NHS procedures covering the acceptance of gifts by doctors have brought a warning to independent practitioners too.
The Government recently announ ced the introduction of the ‘sunshine rule’, meaning that doctors and other NHS staff must declare gifts, payments or hospitality received from pharmaceutical companies.
From next year, it will be mandatory for them to keep a register of gifts. Anyone failing to declare this information will face sanctions and disciplinary action under the Bribery Act 2010.
According to defence body MDDUS medical adviser Dr Naeem Nazem, transparency and
caution is also required when it comes to accepting patients’ presents too.
He urged doctors to exercise caution when offered gifts from both patients or drug firms.
Said Dr Naeem Nazem: ‘Private doctors should probably be even more cautious, as patients do not have the right to refer their concerns to the Parliamentary and Health Service Ombudsman, as it does not fall under the NHS complaints procedures.
‘They should also check whether the private hospital they are working under has any contractual requirements on the receipt of gifts for private doctors working in them.
‘Finally, they have a direct contractual relationship with their patient and should make sure that


singer Paula Sides, aged 32, from Yorkshire, has been able to continue her career with the English Touring Opera after laser surgery. She is among private patients featured in a ‘Live A Fuller Life’ television advertising campaign by Optegra Eye Health Care. Before treatment, she had struggled to see scripts, the conductor or fellow singers’ facial expressions. Patients featured in the campaign capture the diversity of surgeons’ skills. Jemma Durbridge, UK marketing manager for Optegra, said: ‘With the powerful imagery and personal stories, this is a highly emotive advertising campaign which Optegra is proud to be launching.’
Most patients would share data with their GP from wearable devices like fitness bands to help them monitor their health, according to a survey of 1,000 UK adults by KPMG.
Nearly three-quarters (74%) said they would be happy to wear a device that monitors their health and reports it back to their GP. But most were cautious about how their health data is processed – with just 8% saying they were happy for a private firm to do so.
a gift can’t be considered as being influencing the bargaining powers of each side, as that could be considered as breaching an implied term of the contract.’
The new Government measures relate to gifts from pharmaceutical representatives and medical device makers. But MDDUS advises doctors to adopt the spirit of the legislation and also keep a register of gifts from patients.
Dr Nazem said in many cases it might be entirely reasonable to accept a small token or recognition of gratitude from a patient, but there were times when a gift could represent something more.
He added: ‘The offer of larger gifts can be particularly uncomfortable for doctors and it is probably best to try and discourage

these without causing the patient offence. Doctors should carefully consider the size of any gift, the patient’s potential motive and any possible impact on their professional judgement.’
The GMC advises doctors not to ‘encourage patients to give, lend or bequeath money or gifts that will directly or indirectly benefit you’.
Avebury Computing, the company behind practice management software MidexPRO, says its new Cloud version launched last month follows 15 months of development and testing.
It said the version is compatible with MAC, tablets and smart phones, as well as the traditional Windows platform and allows
seamless online billing of Bupa and other insurers’ invoices.
A select group of users have been trialling the new software, which has been instrumental in polishing the system to its final release state. Managing director Gary Parker said he believed the new software would prove even more popular than its predecessor.
BMI is to offer oncology e-prescribing across all its 30 facilities providing chemotherapy services.
It said this would offer significant benefits, including maximising patient safety and improved medicines management, a more attractive proposition for oncology consultants, a single standard prescribing model for chemother-
apy and wider business opportunities for its hospitals.
The move also paves the way for e-prescribing in other specialties, using Knowledge Medical Systems’ iQemo browser-based prescribing.
BMI Healthcare boss Jill Watts said consultants, insurers and commissioners recognised the patient safety benefits of e-prescribing.
Future growth in the healthcare industry will centre around ten technologies, according to growth partnership company Frost & Sullivan.
It says these are: surgical robots,
digital pathology, neuroprosthetics, surgical laser, smart pills, optical imaging, health informatics, integrated vital signs monitoring, artificial organs and four-dimensional (4D) ultrasound imaging.
By Robin Stride
Private healthcare is poised for strong growth if it works to harness a variety of emerging opportunities, according to the boss of the Association of Independent Healthcare Organisations (AIHO).
Chief executive Fiona Booth told the LaingBuisson Private Acute Healthcare Conference in London there were openings through collaboration with the Government, NHS and private medical insurance (PMI) stakeholders.
She said: ‘Steady growth in selfpay gives a strong indication that people are increasingly willing to pay for healthcare, yet uptake of PMI has stagnated. AIHO believes that, through collaboration with stakeholders, we need to look at what products are on offer and work collaboratively to develop products that are attractive and valued by consumers.
‘I am absolutely positive that, through collaboration and with the right product, we can grow the PMI market together.’
Ms Booth said the new Conservative Government’s willingness to engage with businesses and to support private-public partnerships meant there was a real opportunity to start engaging pro-actively.
She continued: ‘The Spending Review is also underway and I have found the door is open to discuss what the sector can do to support
the NHS, and the nation’s health, more widely.
‘We know the sector can deliver a greater range of services and to more insured and self-paying patients alike. We need to be discussing how an invigorated and incentivised PMI market can make a real difference to the economy and the public purse.’
The sector grew by almost £4bn last year, she said, largely through its partnership with the NHS at a time when the population’s needs were growing and intensifying in complexity.
Independent hospitals were continuing to invest annually in innovative and cutting-edge care. This was often used to benefit NHS trusts and patients.
Evidence of contribution
Ms Booth said with the Government focused on delivering largescale efficiencies and productivity gains, the sector needed to effectively evidence its contribution.
As a result, AIHO – which represents over 250 hospitals – had partnered with health economists to look at the sector’s provision of elective orthopaedic treatments.
‘Specifically, we a looking at hip and knee surgery and the social and economic contribution this makes in terms of value and outcomes. We will have the results of this work soon and look forward to sharing them with you.’
Turning to the new Care Quality

Commission (CQC) inspections of independent hospitals, she said being inspected against the same fundamental standards as NHS hospitals would help counter the misplaced view that private sector standards were less rigorous than those in the health service.
Early indications from members suggested the new inspection regime was more credible and robust than in the past, but there was still ‘some way to go’ in ensuring that all inspectors understood independent hospitals and that the CQC recognised the sector’s model of provision rather than trying to fit it in to an NHS model.
She said some of the CQC’s new standards on effectiveness and leadership would highlight best practice within the sector. ‘This will give us more to showcase to policymakers, patients and the media.’
the private hospitals’ trade body is calling for the country-wide shortage of nurses to be addressed. aIho says the shortage is caused by a lack of training places and slow registration for staff from overseas.
aIho chief executive Fiona Booth said the health Secretary had made a number of interventions on the costly use of agency staff by the nhS, but this was avoiding the root causes of the issue.
She told the meeting: ‘I believe the nhS can learn a lot from how our sector has adapted quickly and innovatively to these circumstances. Independent hospitals are maximising staffing levels through better use of skill-mix and many aIho members are reporting spending up to 30% less on agency staff than the nhS.’
Private acute medical hospitals’ income has been boosted by a surge in overseas patients.
LaingBuisson economist Philp Blackburn said the international sector accounted for 3.4% of the funding mix just six years ago, but by last year had nearly doubled. Self pay patients – who are
tipped to become increasingly important to the market – rose from 15.8% to 16.7% in the same period.
Rising incomes among consultants doing NHS work in the private sector was reflected in an increase from 23.4% in 2009 to 28.9% in 2014.
Six years ago, the private medical insurance (PMI) market accounted for 57.4%, but by last year was down to under half the funding, at 47.9%.
Looking to the future, Mr Blackburn forecasted good scope for growth both in London and outside. Private hospitals, NHS
hospitals and Harley Street were ‘upping’ their marketing to attract demand, he claimed.
But he warned demand might become vulnerable later due to the rise in global medical tourism and more competing countries. He predicted good growth was likely to feature under NHS choice
New quality data on private consultants’ and hospitals’ performance is needed urgently to help win more business for the sector, according to Bupa UK’s general manager.
Mr Alex Perry told the LaingBuisson conference: ‘We need to objectively and comparably demonstrate the quality of care and outcomes that we can deliver in the private sector.’
He believed the creation of the Private Healthcare Information Network (PHIN) was one of the best things to come out of the Competition and Markets Authority (CMA) inquiry into the sector. But he stressed: ‘This needs to become established quickly and start to collect and report outcome data soon.
‘We need to push it to go as far as it can as a sector. In the longer term, we need PHIN on steroids so that we can demonstrate worldclass levels of quality to customers in the UK and overseas.’
Mr Perry said he could not exaggerate the importance of this in changing the insurance proposition to customers, so that it became about accessing the best quality healthcare.
Customers needed easy online booking for appointments with doctors and therapists so that they could do this when and where they wanted and not have to spend ages calling around on the

phone. Bupa was working with providers to deliver this.
He warned: ‘At the moment, our market is going absolutely nowhere. LaingBuisson recorded a small decrease in PMI subscribers in 2014 in the market – and this comes at a time of record numbers in employment and record population. This is on the back of several years of stagnation. And we are slowly building to a crisis.’
Now came a new threat with the more than 50% rise to insurance premium tax, going up to 9.5% from 1 November ( Independent Practitioner Today, September 2015).
But Mr Perry was optimistic of a healthier future for the private healthcare sector if effort was put into demonstrating quality, being willing to change ways of working and cutting costs.
‘We asked LaingBuisson in 2014 to estimate how the market could grow if we in the industry could deliver new ways of working and demonstrate greater quality in the private sector along with better value for money. They estimated we could bring in £2.2bn of extra funding by 2020, which would be a significant help to the NHS.’
This would mean full patient lists for the many consultants, who told the CMA they wanted to do more private work, while hospitals could use their spare capacity and spread their costs over more patients to give better value.
The sector needed to make a compelling case as to why it could offer part of the solution to the current NHS crisis if more and not fewer people were encouraged to take up PMI.
Mr Perry said Bupa had been very demanding of its own business. ‘Last year, we delivered cost savings of £30m and we are going after more this year by streamlining some of our processes.’
➲ PHIN boss Matt James welcomed Mr Perry’s comments. He said everything was geared towards meeting the CMA’s requirements for better published information from April 2017.
‘The leading private hospitals are fully engaged in preparing to meet the challenge and dozens of new member hospitals, including many
and the ongoing need to clear waiting lists.
But he said the number of players in the market was certain to increase, including possible overseas providers, and the NHS would try to lower the average tariff over time. Some providers could struggle to make return at tariff.
With strong growth in UK employment in recent years, many more employees could be covered by private medical cover and accessing private hospitals.
Mr Blackburn said economic trends looked favourable but next month’s insurance premium tax hike was a blow and almost cer
tain to dampen demand. It was likely to affect the small to mediumsized enterprises (SMEs) most – and LaingBuisson analysis suggested SMEs were particularly sensitive to price changes.
Selfpay healthcare was likely to be well supported by a favourable economy and cracks in NHS per
‘every day, thousands of skilful experienced consultants and therapists deliver great care and outcomes to customers who have PMI. But we do not show this.
‘In fact, we are unable to clearly demonstrate this. Furthermore, there are many aspects to our customers’ experience that could be a lot better.
‘this means that in a world that moved on some time ago, we are still trading off the 1980s’ value proposition of fast access to treatment and care by an experienced consultant. now, don’t get me wrong; these are still a good feature of PMI, but the world has moved on significantly and we need to catch up. or we risk becoming an irrelevance – a Yellow Pages in the age of Google.’
alex PeRRY
General manager for Bupa uK Customer
NHS private patient units, are now also coming on board. Together we are working hard to implement the collection of an enhanced minimum data set from the beginning of 2016 that will see private healthcare broadly align to NHS information standards. This is vital to enable comparability and proper risk adjustment.’
PHIN was planning the process for sharing data for quality assurance with 12,500 doctors and was engaging with the professions to ensure published data was ‘complete, robust and fair’.
formance more likely to widen than narrow.
A priority was to show employers that PMI as part of a wellbeing package had tangible financial value and could help improve productivity. He believed insurers were doing good work towards this and future developments were promising.
By Robin Stride
Doctors in aesthetics would have even more competition if the cos metic surgery arena had a cleaner profile, a survey shows.
Nine in ten non-cosmetic prac titioners polled, such as GPs and dentists, admitted they had at one time or another considered offer ing aesthetic treatments.
But a third were put off over concerns about lax regulation and horror stories emerging from the sector.
Other reasons for not moving forward included not understand ing legal frameworks or the mar keting involved.
The survey, run by OnePoll for the CCR Expo trade event earlier this month, was also widened to quiz 70 cosmetic practitioners, including surgeons and derma tologists.
A third said their colleagues probably saw the field as lucrative but were scared to enter it because of a lack of knowledge.
Nearly 10% felt too many untrained providers – even those medically qualified – were ‘having a go’ at offering aesthetic procedures and damaging the reputation of credible and properly qualified clinicians.
Flying the flag: CCR Expo surveyed doctors and cosmetic practitioners
Outside of cost, the top reason cited was fear stemming from horror stories about botched treatment, followed by wariness of the results looking ‘unnatural’, and not knowing which practitioners are qualified to perform the procedures.
CCR Expo, at Olympia, this year also played host to the annual meetings for the British Association of Aesthetic Plastic Surgeons (BAAPS), the British Cosmetic Dermatology Group and the Journal of Aesthetic Nursing
Doctors are increasingly likely to be investigated for criminal offences such as sexual assault, manslaughter or the new offence of wilful neglect, a defence organisation has warned.
The Medical Defence Union (MDU) is advising doctors of the importance of seeking legal help early on if they think they might be facing a criminal investigation.
World Class International Faculty already includes: Dr Raj Acquilla, Dr Raina Zarb Adami, Dr John Ashworth, Mr Jonathan Britto, Dr Erri Cippini, Mr Alex D. Karidis, Dr Nick Lowe, Dr Vishal Madan, Miss Joy Odili and Dr Raffaele Rauso 10-11 OCTOBER 2014 LONDON OLYMPIA
Just over a third felt the biggest problem was newbies lacking specialist expertise – such as highlevel training in facial anatomy.
other medical colleagues’ – those not practising aesthetics – opinion might be of the sector, a third said it was seen with strong prejudice and as ‘beneath them’.
CCR Expo is a major scale, multidisciplinary meeting packed with CPD accredited content for doctors, surgeons, nurses, clinic owners and other health professionals with an interest in aesthetic medicine.
From scalpel to syringe, CCR Expo provides a professional platform for the exchange of ideas, the pursuit of best practice and the sharing of knowledge, insight and expertise. Visit www.ccr-expo.com/ipt4 to discover more.
In another study of 500 women commissioned by CCR Expo, 38% confided that they had considered cosmetic surgery procedures such as facial injectables or liposuction, but only half of them had ever gone through with it.
For the first time, it held a ‘Getting Started in Aesthetics’ allday theatre jam-packed with workshops and lectures aimed at medics who wish to know more about the arena.
The agenda included advice from lawyers and top cosmetic exponents including doctors, surgeons and industry experts offering input on operating a practice legally, ethically and successfully.
Peter Jones, chief executive of conference organisers Nineteen Events, said: ‘We don’t necessarily encourage more clinicians to join the aesthetics arena, but our research clearly shows there is a strong desire for more clarity in the sector, alongside some understandable concerns.’
Our regular series ‘Breaking Into The Aesthetics Business’ starts on page 14
Negligence claims alleging doctors failed to diagnose diabetes or manage it properly rose significantly over a ten-year period, the Medical Defence Union (MDU) has found.
Official Charity:
@ccr_expo #CCR2014 www.facebook.com/ccrexpo1 REGISTER NOW AT www.ccr-expo.com
The number of patients suing doctors increased by 28% from 162 claims from 2003-07 to 207 cases from 2008-12, although the
CCR6660
vast majority of cases did not lead to compensation being paid.
In total, 92 negligence claims were settled for just over £8.2m plus legal costs of around £1.2m over the decade.
More than 1,215 incidents involved diabetes over the decade to 2012. There were 489 complaints, 123 coroner’s inquiries and
44 GMC investigations. The MDU’s Dr Caroline Fryar said: ‘With the announcement by Diabetes UK that the number of UK adults living with diabetes has reached 3.3m – a 60% increase over the past decade, it is perhaps not surprising that doctors have also seen an increase in claims and complaints involving diabetes.’
Senior solicitor Ian Barker, one of a team of three lawyers employed by the defence body to work on criminal cases, said crim inal convictions were still very rare, but there was a greater chance of a doctor being subject to criminal investigation than five years ago.
Mr Barker said such cases were often very complex, demanding specialist knowledge and tenacity to achieve a successful outcome.
‘One factor behind the increase in cases is the climate following the Jimmy Savile scandal which has led to a spike in sexual assault allegations. Manslaughter allegations are less common, but there has also been an increase in the number of cases being investigated by police in recent years.
‘Add to that the new criminal offence of wilful neglect, which applies to individual doctors and other healthcare professionals who ill-treat or neglect someone in their care, regardless of the harm this caused.’
The MDU said while the Department of Health had indicated that only the most serious departures from acceptable standards should be prosecuted, there was no clear threshold for investigation, so it was difficult to predict numbers.
Mr Barker added: ‘Only about one-in-four prosecutions for manslaughter handled by the MDU’s in-house team have resulted in a conviction overall and the incidence of conviction in sexual cases is very much lower. This is despite the fact that the Crown Prosecution Service’s overall conviction rate is around 80%.’


“Since












We live in an ever-changing digital age. every day, people see the creation of new products and services which they can comment about instantly on social media.
There have also been tremendous medical advances over the past decades, but the way the healthcare sector provides its services has not kept pace with modern lifestyle changes.
Many patients still have to phone the doctor’s secretary for appointments or receive handwritten bills. And while 66% of Britons use technology to manage their personal banking, only 16% use it to manage their healthcare.1
People’s lives are becoming even busier and they are increasingly looking for instant solutions to suit their lifestyles and make life easier.
This opens up a huge opportunity for our sector if we work together.
There has been a decline in individual spending on healthcare since the recession started in 2009, and the latest analysis from l aingBuisson highlighted the scale of the issue. At the start of 2015, the number of private medical cover policies in the UK –both insured and self-insured – was 3.94m, down from 3.97m in 2014.2
However, we know that people value private healthcare. They just want it to suit their modern lifestyles, be more affordable and with proven higher quality.
One way which we can bring more people into the sector is by offering customers options that meet their different budgets.
We know that affordability is a key concern for increasingly savvy consumers. For half of Generation X (32 to 55-year-olds) the barrier to having private health insurance is that they cannot afford it.
Furthermore, 37% said they would be more likely to have it if it was more affordable. 3 This is why we launched Bupa Fundamental Health i nsurance, an entry-level product to meet

By DR Steve Iley Medical director at Bupa UK
demand for more affordable healthcare and reach more potential customers.
Secondly, we need to prove the quality of our care – and that means sharing quality outcomes to our customers and demonstrating the expertise of the private sector.
Bupa’s Finder website is the biggest online private healthcare directory and is helping doctors, clinics and hospitals to grow their businesses.
i t’s an opportunity for private consultants to demonstrate their
Bupa’s Finder website an opportunity for private consultants to demonstrate their expertise and experience, prove they provide high-quality care, and better connect with patients

expertise and experience, prove they provide high-quality care, and better connect with patients. With 50,000 visits a month, is your private practice making the most of this gateway?
At Bupa, we continue to invest heavily in developing new products and service, but we know there is still a long way to go. That is why it’s essential that the entire private healthcare sector continues to challenge itself to think innovatively, and that we all work together to create new ways to meet our customers’ changing lifestyles. n
ReFeReNCeS
1. Figures from YouGov Plc. Total sample size was 2,011 adults. Fieldwork was undertaken between 25-26 March 2015. The survey was carried out online. The figures have been weighted and are representative of all GB adults (aged 18+).
2. LaingBuisson’s Health Cover report –released August 2015.
3. Generation X has been taken as those born 1959 to 1982. Figures are from YouGov Plc. Total sample size was 2,005 adults. Fieldwork was undertaken between 2-3 July 2014. The survey was carried out online. The figures have been weighted and are representative of all UK adults (aged 18+).
For the last 18 years, we have been helping healthcare organisations manage and transform their operations, both in the UK and abroad.
We exist to help independent practitioners start, transform and grow their practices and businesses. We help to plan and develop medical facilities and to market healthcare services using all available communications channels and technologies. While you concentrate on caring for patients, we aim to take away the burden of managing your practice or business.
We build unique teams for every situation and change that team as your needs change and, uniquely, we have experts who can deal with crises who are available 24x7. We combine clinical expertise with commercial sense; we see the full picture and we provide support when and where it’s needed most.
We work with both public and private sector healthcare providers, and we have an enviable track record in operations management, clinical advice, consultancy and development.
For an introductory discussion, please call Keith Hague CEO on +44 (0)20 3356 9699 or mobile +44 (0)7577 414038 www.worldwidehealthcare.co.uk
With more consultants expanding their business through groups or teaming up with those offering complementary services, such as physio- and psychotherapists, Susan Hutter explores the different ways of incentivising staff and providing a career path
How you incentivise staff will depend on the structure in which doctors operate.
Those trading as a limited company can consider passing over shares in some way to key employees.
They could sell shares to coworkers at market value. However, the employees may or may not relish this thought, particularly if they do not have the wherewithal to pay for the shares.
Some consultants will allow employees to pay for shares in instalments. However, the consultant will still have to pay the relevant capital gains tax (CGT) based on the date of the transfer of the shares, whether or not the money has been received.
Most consultants who trade as limited companies will qualify for ‘Entrepreneurs’ Relief’, which means that the CGT on the sale of the shares would be at an effective rate of 10%.
w hile it is not expensive, no one wants to pay tax on money that they have not received. unfortunately, offering shares to employees ‘free of charge’ causes income tax problems.
Effectively, this is a gift and has to be reported to HM Revenue and Customs (HMRC).
It is likely to say that the gift was related to the employment and is therefore taxable as employ ment income. The employee would then have to pay income tax on the market value of the shares – ouch!
Unfortunately, offering shares to employees ‘free of charge’ causes income tax problems. Effectively, this is a gift and has to be reported to HM Revenue and Customs
How to avoid this
Issue ‘share options’ as opposed to shares. A share option is valued at the market value at the date of the grant of the option, but the recipient of the option does not have to pay for the option at that time.
The option gives the employee a right to exercise the option in the future, under certain preagreed circumstances.
This is usually on the sale to a third party, or management buyout. o f course, it is hoped that
between the date of the grant and the date of the exercise the value of the shares will go up. In fact, the options would only be exercised if the company had gone up in value.
Anyone considering this route will need to take legal and financial advice as a ‘share option agreement’ needs to be drawn up. Also, the valuation has to be agreed with HMRC.
Those not trading as a limited company could consider incorpo-
rating and, at the date of incorporation, gift the key employees a small percentage of the share capital in the new entity.
At that stage, the shares will not have a value for income tax purposes and therefore there will not be an income tax charge. Alternatively, they could explore the possibility of setting up a partnership and bringing in the key employees as junior partners. It will probably be best to do this as a limited liability partnership (LLP), which offers similar kind of protections to a limited company. The main advantage of an LLP – or any partnership – is that profit shares can be adjusted each year without any concerns for extra income tax or CGT.
A limited company does not offer this kind of flexibility. The downside of an LLP compared to a limited company is that income tax is payable by the partners on their total profit share whether or not all of this has been drawn from the business.
So it is much more difficult to mitigate higher-rate tax and thereby retain cash in the business – for example, to re-invest – as easily as within a limited company.
A limited company’s top rate of tax is 20% and the owners/ employees only pay income tax on what they draw.
Susan Hutter is a partner at specialist medical accountants Shelley Stock Hutter
is continuously updated based on the latest medical research to bring you current evidence-based recommendations.
Our unparalleled team of physicians and editors places new research in the context of the existing body of medical knowledge using their professional expertise and first-hand clinical experience.
This combination of Evidence & Experience is invaluable in crafting point-of-care recommendations trusted by more than one million clinicians worldwide.
Plus, you may earn RCGP CPD learning credits while researching topics in UpToDate.
To learn more or to subscribe risk-free, visit learn.uptodate.com/UK15 or call +1-800-998-6374 | +1-781-392-2000 7a.m. – 9p.m. (GMT-5).
Anyone can start a company. But making it profitable and sustainable in a competitive economy requires skills and expertise. Pam Underdown (right) explains what you need to do

Ev E ry larg E business in the world today started out as a small one. In fact, the average Fortune 500 Company began with an initial investment of less than $25,000.
Heinz started with horseradish and a horse-drawn buggy. Sony started with rice cookers. Marriott started with a root beer stand. Proctor and gamble started with selling candles door to door. They all started small.
The real reason they are among the largest businesses in the world today has nothing to do with the ‘idea’ or the product the founder created and everything to do with the skills they had to grow it.
Success in business has nothing to do with the idea, the product or the service being sold and everything to do with the skills necessary to execute.
Sadly, most businesses fail before their fifth birthday, and the reason has little to do with the idea.
Knowing what you’re doing
We all know the great business owners out there who are rich and successful in business because they know how to run the business side of their business.
They understand and use the critical business skills and tools that are essential in order to create sustainable financial success. Of course, there are the lucky ones, but even they must find a way to sustain their good fortune before their luck runs out.
long-term sustainability always comes from knowing what you are doing and measuring your progress. Businesses don’t run ➱ p16




themselves and, tragically, there are many business owners who don’t know how to run them either.
Many jump around from the next shiny new technology or equipment to the next ‘new’ marketing campaign in an attempt to just get rich.
This is ultimately a shortsighted goal, as the goal of running a business should be about creating a sustainable financial asset for the long haul and not just about getting rich quickly.
There are far too many books and experts out there who claim you can get rich in a ‘four-hour week’ but this is nonsense and a shortsighted attitude which can eventually mean that the business owner either quits or is just too exhausted to carry on.
Many business owners believe that the key to increasing profits is just to increase the sales, but that is not the only requirement.
It is only by acquiring the skills and tools you need to understand and measure all of your activities and results – financial, marketing and business – that you will own the key to knowing which activities need to change in order to produce superior profits and sustainable cash flow.
a s Charlie Munger – Warren
Buffet’s business partner – says: ‘Business is highly complex and anyone who says it’s easy is stupid’. as a health professional, you know that staying good at anything requires learning and executing the right skills and tools and then practising them over and over.
When you first start your medical aesthetic training, you will need models and free patients to practice on before you feel competent and confident in your skills and abilities.
Even though you will, no doubt, have your many years of medical experience and years of injecting, you will still need to go through this steep learning curve and continue to practise your new skills over and over again.
Business is no different. Every skill is learnable and mastering the business of aesthetics will take time, effort and patience.
Succeeding in business is highly complex and anyone who tells you otherwise is trying to sell you something.
Business is an intellectual sport and anyone who plays the game with their emotions and guts does not win.
There is simply not a way to ‘get lucky’ sustainably. Napoleon Hill’s best-selling book is called
when it comes to business and financial analysis, it starts with the numbers and you can’t understand the numbers if you can’t speak the language
You will need to have a good computer system that can easily provide reports to tell you:
revenues
number of new patients/number of existing patients
percentage of revenues to overhead costs
Average order size per patient
Average number of return visits per year
revenue streams broken down by procedures and treatments
marketing source
return of investment (roi) for each promotional effort
Cost per patient: determining the cost to acquire and maintain a medical aesthetic patient is key to maximising practice profitability
THINK and Grow Rich not Use your Gut and Grow Rich or Do What you Love and Grow Rich
Too many people make the mistake of believing they can get rich and stay rich just by doing what they love. Of course, doing what you love may leave you feeling fulfilled and leaves you feeling energised and excited, but in many cases, it will not create long-term financial success.
Business is a game and, like any game, there are winners and losers. There is fierce competition and a set of rules. There is not one competitive sport out there that has an announcer who says ‘Don’t worry. We don’t have a scoreboard, as no one looks at it anyway’.
Read the scoreboard
But, yet, that is how the majority of people play the game of business. There are bad moves and good moves, but it is the strategy and the ability to read and understand your business ‘scoreboards’ that is critical.
‘If you can’t read the scoreboard, you don’t know the score. If you don’t know the score, you can’t tell the winners from the losers.’ Warren Buffet. you must know your facts and this means your numbers. Numbers don’t lie. Ignorance is not bliss and facts won’t cease to
exist just because you ignore them. anyone who hates to measure does not want to be held accountable.
Think about it. If you started to measure the most critical aspects of your business right now, not only are you more aware of what is actually happening – hourly, daily and weekly – but those numbers will improve just by the simple act of measuring them.
When it comes to business and financial analysis, it starts with the numbers and you can’t understand the numbers if you can’t speak the language.
Is your clinic profitable? While a review of accounting statements or tax returns will tell you if your operation is in the red or the black, you need to know an awful lot more than that.
For example: is each patient you treat profitable? and did the new dermal filler campaign you just completed bring the return on
investment you originally estimated? For many practices, these questions are more difficult to answer.
go through your database and study your accounts receivable carefully. you’ll see certain pockets of positive results that you can get more of, if you simply put some effort into promoting them. look for trends.
Which are your most popular procedures performed? Which procedures are the most profitable, taking into account how much of your own time is involved? The fastest and easiest way to increase your revenues is to replicate your successes again and again.
Study your patient demographics. you will see trends in age, gender, marital status, home ownership, children, education level, occupation and income. y ou’re not judging your
patients. you’re simply learning the type of person who is most likely to be attracted to you for certain procedures.
By the way, if you don’t like the trends you come up with, you need to change your marketing to attract those whom you do want as your preferred patient. you will need to have a good computer system that can easily provide reports to tell you vital information – see box to the left.
Taking the time to determine the cost of acquiring new patients, as well as the potential long-term profit margin for specific patients groups can help you fine-tune your pricing.
It can also streamline operations and zero in on your most successful marketing avenues, culminating in increased profitability.
This data will help you determine where to spend your time, money and resources to put more
efforts in certain areas such as patient flow and staff training and less in areas that are not helping you or your bottom line.
Ensure you keep great records again this year so you can compare your numbers to last year, because these numbers are either getting better or worse but definitely not the same.
Better yet, compare week by week, rather than by month or quarter, so you can change course mid-week if you need to.
Measuring and managing the critical aspects of your business is the key to sustainability. you can’t sustain something unless you know what is working and what isn’t.
next month: how to create a compelling patient experience and watch your profits grow overnight
Pam Underdown is chief executive at Aesthetic Business Transformation

A guide to being ‘froogle’ with your publicity campaigns. Tingy
Simoes (below) shares the secrets of how to keep your keyword spend down through the sneaky medium of promotional integration

There is no way of running a private practice – indeed, a private or public anything – and remain unaware of the implications of online searchability.
The importance of having a strong internet presence is, these days, simply inescapable. i can already sense the eyerolls. But fear not – this is not an article trying to convince you of the wisdom of having a website and optimising it.
You know this already. What i will do is to give you some shortcuts – video-gamers would call a ‘hack’ – to ripping up Google’s rate cards, through the sneaky medium of integration.
Businesses today, in healthcare or otherwise, will be peddled every thing from search-engine optimisation and pay-per-click services to print advertising, public relations, social media, you name it.
Horses for courses
There is a place for all formats and don’t believe anyone who tells you that one is ‘better’ than the other. it really boils down to who your audience is, where they are, what they’re looking for and, ultimately, your budget. A lot of this defines the mix of promotional channels likely to work for you.
But, in a world of so many options, it can become a neverending fight between each for their ‘share’ of the budget, with different and competing entities insisting that what they have to sell will solve all your problems.
You may recall from my previous
article that i stressed the importance of identifying innovations and trends and ‘packaging’ them under a catchy name or concept. Doing this well can have much farther-reaching effects than simply securing the attention of a busy journalist through a humorous pun or intriguing headline. in the big bad world wide web, the keyword is king.
The value of a keyword is entirely dependent on its popularity, the size of the companies chasing it, the number of products and the depth of the pockets involved. Google knows this. Google is wise and charges accordingly.
if you’re a company that has a great product and, say, for example, it’s soap – then poor you. ‘ s oap’ can be picked up in search by washing powders, soap operas, hair products, detergents; the list is endless.
The competition is equally fierce when it comes to terms such as cosmetic surgery, flu, heartburn, cataracts, tennis elbow, piles. i’ve had to manage campaigns in all of these areas –and they say Pr isn’t glamorous! The little guys are always going up against the Goliaths of pharma companies, medical device manufacturers, clinic chains, multi➱ p20




national brands, all with staggeringly big budgets.
s o, not unreasonably, many independent clinics and private practitioners feel they have no choice but to pour every last penny of their budgets into this particular format. Yet how can you possibly compete and come out on top?
You need to be smart to carve out your own space, where ‘your’ keyword becomes king. The sneakiest way is to use other channels to turn the process on its head.

The downside of Pr is the lack of control you have over the final product. The upside is its costeffectiveness. You can’t have both total control over what runs and low costs: that’s called advertising and it’s why it can be eye-wateringly expensive. You’re paying for a guaranteed insertion to appear before an audited, proven audience.
As mentioned in my previous articles – and proven by my career – good Pr does work. And by good Pr i mean well-researched stories, skilfully crafted to be irresistible to the media.
The biggest asset a Pr company has is how well they can work with the client to produce something with a real edge. We know Pr can’t offer guarantees – again, refer to ad agencies for this – but a package that has all the necessary ingredients and is sold by a capable Pr professional can dramati-
Use the best aspects of the PR and social media formats to eliminate the worst aspects of the others –expense and competition
cally increase the chances of pick-up to near certainty.
s o how can P r and its conjoined twin, social media, mix well in a world where buying success is possible but outside the realm of most budgets?
You use them to create your own keywords and phrases. if you come up with terms that no one else is using, Google won’t get upset. Why? Because they have little value.
i t must mean that no one is actually typing these words, so why would you want them? Clearly, Google doesn’t place a high value on anything that isn’t being searched for.
clever campaign
This is where integration comes in. You can achieve some of this through well-built websites and organic visibility, but don’t forget that if your stories are running in the mainstream media, you have the ability to tell people what to look for.
You can achieve it with clever campaign themes, hashtags, catchphrases and new concepts. Clearly, people aren’t familiar with the term – they won’t be or it would have a high value and you couldn’t afford it, if you see what i mean – so introduce it.
Use the best aspects of the P r and social media formats to eliminate the worst aspects of the others – expense and competition.
A ‘gold standard’ example is the recent ice Bucket Challenge. The
concept was promoted mainly through social media hashtags and Pr, which took off, with evergrowing coverage giving more and more credence to the term, ranking it higher on the search, making it unique to the ALs charity (amyotrophic lateral sclerosis). it became a viral, global phenomenon, but it only started with telling people new words to search for.
several years ago, when scouring plastic surgery conference abstracts to find something that might appeal to the mainstream (hmm, ‘ h ow to empty a liposuction syringe without spatter’ . . . might give that one a miss), i came across one about buttock enhancement by a Florida surgeon.
It became a viral, global phenomenon, but it only started with telling people new words to search for
The miami Thong lift h e explained that, historically, these procedures would leave scars at the top of the buttocks, but these were simply incompatible with the G-string bikinis favoured by the women of south Beach, so he came up with a modified technique.
i asked if he would mind if, for the purposes of media interest in the conference, i christened his procedure ‘The Miami Thong Lift’.
From UK national newspapers to U s TV programmes such as Good Morning America, the Miami Thong Lift took the world by storm. i f you search for it even now, at least the first 20 pages of Google – close to half-a-million hits – are dedicated entirely to that one specific procedure and the surgeon who invented it.
No one searched for it before; now patients all over the world do. The term would have had no value before, but the creator now owns a brand, a searched-for industry term.
More recently, i launched a lens implant for age-related macular degeneration.
One of the things that caught our eye (sorry!) was that the technology had been inspired by a glitch in the h ubble space telescope. The media loved our angle that NAsA was helping grannies knit again, and everywhere people were calling it ‘the h ubble implant’ .
i t spread like wildfire. No one would have searched this term
before; now it had astronomical value.
so if you’re offering a skincare product, make it unique and encapsulate the benefits in a catchy concept. You will always get slaughtered by the big manufacturers’ budgets for buying ads and keywords, but they do not have a monopoly on campaign creativity.
This is where P r and social media can be magical: to prep the themes to be introduced and direct the audience to search.
#Unique hashtag
s earch means find, find means share, share means sales. so your product? Create a unique hashtag or a fun social media challenge. release news about its most unexpected features, conduct unusual surveys that prove it’s needed and christen the problem it’s solving. For readers of my previous piece, think Manolonoma!
Whatever the angle is, stay relentlessly integrated. Place the concept in the press, spread it on social media to imbue it with value . . . then own the keyword. so the ‘lack of control’ of Pr can actually work in your favour, because news travels fast and cheap keywords gather power as your theme is shared.
A good P r and social media strategy will see the people of Twitter and readers of The Mail become your voice. The weakness of keywords – cost – is overcome because you have something unique and Google’s rate card can be torn to strips.
i ntegration eliminates the weaknesses of individual marketing channels, because their characteristics complement each other, turning you into a force to be reckoned with.
integration is the keyword.
Next month: The reluctant celeb – a more academic look at the personalities in surgery/medicine and why these traits can make for either a hellish or heavenly relationship with journalists
Tingy Simoes is owner/managing director of Wavelength Marketing Communications (www.wavelengthgroup.com) and author of the firstever PR manual for doctors and surgeons How to Cut it in the Media by CRC Press



As the Care Quality Commission (CQC) analyses independent doctors’ responses to its recent consultation, addresses one big outstanding question: doctors remain within the scope of regulation by CQC?
The deadline for responses to the CQC consultation document asking independent doctors for their opinions on the proposed way that regulation will take place in their sector has just closed.
The paper was comprehensive and five of the six questions were straightforward asking:
1. Where the CQC should find out about the services provided (Key lines of enquiry);
2. What sort of intelligence/evidence should CQC look at?
3. Should CQC rate independent doctor services?
5. h ow can CQC recognise and encourage notable practice?
6. h ow can they gather views from all stakeholders about the service?
however, tucked in the middle was Question 4, the curved ball: ‘do you agree that independent doctors should remain within the scope of regulation by CQC?’
i t’s not clear if the question relates only to single-handed GPs who work out of a couple of rooms with a secretary or includes group practices with a team of support staff and extensive accommodation.
and then there are the practices owned by non-medics who employ doctors to be the face of the practice or clinic.
a t this stage, there are more questions than answers. So whatever the general response to this question, i think it will be open to further discussion and comment in the coming months before any final decision is made.
i am sure there are many valid reasons why independent doctors
get out of CQC regulation’, it may be worth considering reasons why independent doctors should contemplate remaining within scope of CQC regulation.
The CQC has, justifiably, received bad press in the past and been charged with not being fit for purpose.
But it is now widely recognised by the general public as the watchdog for health care in this country, both nhS and private.
i n many ways, CQC is about public perception. By removing independent doctors from regulation but not the independent hospitals or dentists, it is giving a very mixed message about private
PMP, one of the largest insured professional indemnity practice surgeons.
PMP believe this to be unique within the UK market discretionary cover through a professional membership
The benefit to surgeons being that they are covered than a discretion based cover offered by some of the
Why occurrence based v usual contractual
But an increasing number want to register even if they fall outside of scope. When asked why, the answer is simple – to have the CQC logo on their website gives them a certain amount of credibility as a recognised provider of healthcare.
line with the dentists.
With occurrence coverage, the surgeon receives a separate policy limits remain in place after the end of the policy surgeon complete reassurance that they are covered
With PMP there is further reassurance that the cover discretionary membership cover.
Talking to doctors and their managers once the registration process is completed, i find in general that comments are positive.
(Required for Claims Made coverage when retiring
Most repeated include:
CQC regulation is by no means perfect, but i think the consultation paper was constructive and demonstrated a willingness on behalf of the CQC to understand how our diverse sector works. i just wonder if deregulating independent doctors would be doing a disservice to them.
a s i say, there are more questions than answers.
With run off coverage, the surgeon agrees a fixed limit claims made in any year of the coverage and based occurrence took place.
‘ i t has made us sharpen up in areas we were lacking in’;
‘ i t stopped us resting on our laurels’;
Reference 1. CQC estimates that as many as 60,000 doctors are doing private work, but less than 1% are directly regulated by CQC.
Claims made policies do not cover claims made after required to secure “run off” cover when they move practicing (either retirement or permanent illness/disability),
‘ e nsured staff are properly trained and appraised’;
This can be expensive and limited to the one Limit run off cover.
Source: CQC Consultation 2015 What do you think? Write to robin@ip-today.co.uk



Obstetrics and Gynaecology in Cuba
9 – 30 November 2015
Ecuador and the Galapagos Islands
14 – 27 November 2015
Ophthalmology in South India
16 – 29 November 2015
Occupational Therapy in Sri Lanka
10 – 23 January 2016
Medicine and Society in Sri Lanka
17 – 30 January 2016
Medicine and Society in Cuba
4 – 15 February 2016
Eastern Cuba
15 – 25 February 2016
Malabar Journey – South India
28 February – 13 March 2016
Palliative and Cancer Care in China
12 – 25 March 2016
Physiotherapy in India
4 – 17 April 2016
In the Footsteps of the Knights of St John 15 April – 1 May 2016
Obstetrics, Gynaecology and Fertility in China
8 – 21 May 2016
Veterinary Medicine in South Africa 11 – 23 May 2016
East of Java - Java, Bali, Komodo
3 – 17 June 2016
Anaesthesia in China
3 – 11 September 2016
Medical History Cruise in the Eastern Mediterranean 5 – 16 September 2016
Dental Study Tour to Indonesia 9 – 22 September 2016
Dental Cruise along the Rhine 12 – 19 September 2016
Future Tours:
Medical History in Italy: October 2016
Ophthalmology in Japan: October 2016
Paediatrics in North India: November 2016
Pushkar Camel Fair, N.India: November 2016
We also organise private groups and tailor-made tours. Please contact us for further details.
For full details please contact:
JON BAINES TOURS LIMITED
1A Salcott Road, London, SW11 6DQ info@jonbainestours.co.uk
Tel: 0207 223 5618 / 9485
Fax: 020 7228 7290 www.jonbainestours.co.uk
Dear Reader,
Subscribing to Independent Practitioner Today is the only way you can be sure you will see every issue. Don’t risk missing out. Our personal subscription for doctors and managers is only £85 a year and £200 for organisations. But you can cut this to just £70 and £175 respectively if you pay by direct debit.
So take advantage of this offer now for our unique business journal dedicated to supporting you in your private practice. We’re confident your subscription will repay itself many times over!
Editorial director

I encose a cheque made payable to The Independent Practitioner Ltd
Please debit my Mastercard/Visa/ Amex/Diners Card No Expiry Date Security No ***
Instructions to your Bank or Building Society to pay Direct Debits

Instructions to your Bank or Building Society to pay Direct Debits Name and full address of your bank/Building Society
your application (no postage required – UK only) to: independent practitioner Today Subscriptions department, FREEpOST, pO Box 36, plymouth, pL1 1BR
third parties – for example, either to assign or extend a lease? If you have a mortgage, are there any penalties for early redemption? Is the legal use of the property –based on both the title and the planning requirements – compliant with the practical use?
If you intend to retain ownership of your premises, tell your lawyer to prepare a draft lease with a minimum ten-year term –the minimum requirement of a buyer and their funder.
a lso ask your lawyer to check your staff contracts and ensure you have a complete set available to disclose to the buyer.
Collation of information required by a buyer
There are certain steps a buyer will expect you to take. These include:
‘Due diligence’ inquiries
a ccounts, employment contracts, hire purchase agreements, leases, waste contracts, practice insurance, confirmation of Care Quality Commission registration.
Premises
energy performance certificates and asbestos reports;
Completion of commercial property standard inquiries.
Whether
you are buying or selling a private practice,
it is essential you make the necessary advance preparations which will
place you in pole positon for taking this forward.
Lynne Abbess and Puja Solanki
say this means you can ensure time is not wasted later nor opportunities lost
Here are some tips in buying and selling a practice to help you get started:
Preliminaries
There is nothing more likely to rock the confidence of a prospective buyer than to discover, midway through the process,that their seller has ‘failed to get all their ducks lined up’. a n early approach to your accountant and lawyer are essential to avoid this.
Your accountant
Liaise with your accountant to ensure your affairs are completely up to date and that your business is structured in the most appropriate way to enable you to maximise the value from it.
Check also any relevant timing issues which may impact upon your decision to sell and the timing of it – for example, with regard to tax allowances and so on.
Your lawyer a sk your lawyer to check your title documents to identify any steps that need to be taken to enable you to pass on the property to your buyer. Do you have a complete set of title documents? are any consents required from
Your
To ensure you achieve the full market value for your practice, you should consult professional valuers/agents. They will initially provide you with a valuation, together with market evidence of what you may expect to achieve.
e ssentially, your practice is worth ‘what someone is prepared to pay for it’ – but as the majority of buyers will adopt a similar approach towards evaluating a business, your valuers will be able to advise you on what to expect.
They should also be familiar with what has been achieved in other similar transactions, which may be relevant to your specialty or your locality.
That said, you may be lucky enough to receive an offer from a ‘special interest purchaser’ which is higher than you anticipate, as they may not be constrained by the requirement for bank finance, and may have a ‘vision’ for the development of the business in the future.
Market evidence from a specialist valuer/agent can prove invaluable in these circumstances – and it would be most unwise simply to rely on the written-down ‘valuation’ of the business shown in your accounts.
This may be too low or may even be too high, allowing false expectations to develop. For example, an implantologist who was trying to sell his business in the Harley Street area was shocked to be told it was valueless – as he had no ‘hold’ over his premises, and the cost of relocating elsewhere would, in the circumstances of his particular practice, have outweighed any value.
Once a buyer has been found and a price agreed, there are three significant steps to consider:
Your buyer will want to raise questions ‘formally’ – that is to say, through your lawyer. Your replies will be treated as ‘representations’ – meaning anything which is subsequently discovered to be untrue or misleading will give rise to a claim against you for misrepresentation.
The extent of the inquiries raised will vary – but be prepared to have to tackle a long list. and rely on your lawyer to phrase the replies in appropriate legal language to limit your exposure to a claim.
This is the document which demonstrates the passing of the legal interest in your business from you to your buyer.
You should ensure the agreement is prepared by a specialist lawyer and that it is specifically tailored to the regulatory and operational regime under which your practice operates. a sale agreement for a general business would not contain all the safeguards sensibly required.
There may also be a preliminary contract entered into between you and the buyer to create a commitment for both parties to proceed at a date in the future, allowing
time for other essential steps to be put in place in the meantime.
But don’t be tempted to agree to an exchange which leaves too many issues to be resolved, as you might find yourself tied into a deal which has no realistic chance of proceeding – while, in the meantime, you are prevented from marketing your business to anyone else.
3. Transfer of Undertakings/ Protection of Employment (TUPE) rules
You will have obligations under TUP e legislation to inform and consult with your employees on the transfer of their employment to the buyer.
e ssentially, the position of the buyer will be a reflection of all that is required of the seller.
Once again, preparation is key – and if you fail to prepare yourself and a seller is let down at the last minute, your reputation as a
While the process may, at first, appear complicated, you should be able to achieve your objectives with the minimum disruption with support from the appropriate specialist advisers
credible buyer will be damaged in the marketplace.
Your accountant
Take specialist accountancy and tax advice to ensure that you acquire and operate the business in the most tax-efficient way.
Failure to obtain a funding offer at an early stage, or failing to make a decision regarding funding, causes the majority of delays in a transaction.
Discuss ‘in principle’ funding with your bank/financial adviser as early as possible to place you in the best position to process the application as soon as your offer is accepted by the seller.
Your lawyer engage with your lawyer to clarify the time – and other aspects – of setting up any legal structure required to enable you to contract with a seller
business transfer agreement
ensure this reflects any practical implications thrown up as a consequence of the due diligence exercise that are necessary to protect your position.
e nsure sufficient warranties and indemnities are included in respect of the key aspects of the business to protect any liabilities that may arise after completion
Negotiate appropriate restrictive covenants to protect the goodwill that you are purchasing from the seller (which may also be a requirement of your lender)
ensure you are familiar with the staff arrangements – including any practicalities which flow from this.
engage with the staff to provide reassurance and continuity relating to your takeover of the business.
Compulsory registration is needed which can take up to eight weeks, so an early approach is vital. a CQC-countersigned check by the Disclosure and Barring Service is required, which can take four to six weeks to obtain, so factor this into your timetable. Note that this will not be necessary if you are acquiring shares in a company, as the company should already be CQC-registered.
Negotiate appropriate restrictive covenants to protect the goodwill that you are purchasing from the seller – which may also be a requirement of your lender.
e nsure sufficient warranties and indemnities are included in respect of the key aspects of the medical business to protect any liabilities that may arise after completion.
You will want to agree with the seller the best means of announcing your take-over of the business in order to best secure patient/ client loyalty
Your specialist advisers, such as valuers, agents, lawyers and accountants, should be approached at an early stage in the process to present you with the best opportunity of achieving a smooth transaction. They will know the questions to ask and will advise you on the most appropriate course of action as and when issues arise – as well as generally supporting you throughout the process.
While the process may, at first, appear complicated, you should be able to achieve your objectives with the minimum disruption with support from the appropriate specialist advisers who are already familiar with these complexities.
Independent Practitioner Today has joined forces with leading niche healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes’ of free legal advice.







and
An explosive and detailed analysis for Independent Practitioner Today by leading specialist medical accountants Stanbridge Associates has identified 11 big changes doctors can expect to see in private practice over the next five years
Will your business be able to convert – or run out of time?
Whatever happens, those practising in 2020 will be working in a vastly different environment than those today. PRivATE PRACTiCE iN FivE yEARS’ TimE
Independent pract I t I oners and the private practice market in the UK are facing a period of unprecedented change. the impact of this year’s general election results, changes in organisation and practice in the n H s , the impact of the c ompetition and Markets a uthority’s ( c M a’s) october 2014 ruling, and the aggressive fee reducing strategies of some insurers are just a few of the pressures for changes affecting the sector.

CHANGE 1:

SEvEN-dAy woRkiNG iN THE NHS will bE THE NoRm
MANy SecTorS in the community now have to work a sevenday week. The old days of a nine-to-five environment, Monday to Friday, for a professional have gone for many.
By 2020, consultants with an NHS appointment will have to work on a ‘five days in seven’ contract, effectively on a rotational basis.
This increased flexibility will make it harder for many to plan and organise their private practices. Private clinics will have to become more flexible – and, in turn, could be carried out at weekends.
This will introduce more flexibility in the market place and, as a result will result, paradoxically, in an increase in the number of private patients for many consultants.
The proposed changes in the NHS will have positive long-term tax benefits in the private sector.

CHANGE 2: moRE CoNSUlTANTS will HAvE A SECoNd Job wiTH A PRivATE HoSPiTAl
WITH THe NHS already accounting for close to 30% of the spend in the private sector, there will be an increasing number of consult-
ants who choose to take a second salaried job with a private hospital.
The potential advantages for them are many. If they do NHS work alone, they do not have to incur the huge cost of indemnity insurance.
Secretarial and other costs will be borne by private hospitals and they will not have total patient responsibility.
This phenomenon has happened in the US and some private hospital groups are known to be looking at strategies as how best to take advantage of this trend over here.
CHANGE 3: PRivATE PRACTiCE will bE CoNFiNEd iNCREASiNGly To loNdoN ANd THE SoUTH-EAST
Alre A dy IT is estimated that more than 50% of private practice is conducted in this area. The proportion of self-pay is much higher in the South-east than elsewhere.
In addition, overseas patients, with one or two notable exceptions, do not venture out of london and are seen by londonbased consultants.
There will be obvious exceptions to this trend, but it will be increasingly difficult to find consultants engaged in private practice in the rural shires of england and in the extremities of the UK.
Patients will increasingly be seen to travel to the South-east for their treatment. A return to the glory of Harley Street?

CHANGE 4: GRoUPS will
Acc U r AT e INF or MATI o N is very hard to find, but groups now appear to account for between 15-20% of the patient spend on consultancy fees in the UK.
Groups have been shown to increase disposable income of their members. Patients like groups, consultants like them, and hospitals feel comfortable with them.
At Stanbridge Associates, we anticipate that insurers – despite AXA PPP’s challenge to the cMA rulings – will increasingly see the merits of doing business with groups and negotiating group rates.
As a result of this, we would expect to see a new breed of professional group practice managers emerging.
CHANGE 5: THERE will bE SHARP GRowTH iN SElF-PAy
F IGU re S SUGG e ST that an increasing number of people are establishing their own private savings schemes to meet the cost of future medical bills.
Published data suggests that the number of insured individual patients has declined in recent years as a result of recessionary pressures, rising premiums and increasing confusion as to what personal private medical insurance actually offers.
With the anticipated recovery in the economy and increase in disposable income, we anticipate that people will save themselves rather than return to insurers.
The situation will, of course change drastically if tax relief were ever to be introduced on private medical insurance premiums.
e vidence from around the world is mixed, although it suggests that tax relief does stimulate demand.
If the economy improves, there is increasing pressure on the NHS and the l abour party falls in to disarray, we could possibly see the introduction of tax relief on medical insurance premiums by 2020.
The odds, however, at this stage are still pretty long.
A lArGe
of consultants will have tales of alleged bad treatment and bullying by some insurers.
Some consultants have had their recognition removed by insurers for the flimsiest or very dubious reasons.
Individual efforts can reverse such decisions, and some insurers are sympathetic to consultant views when errors are made. However, there is no formal system of arbitration or redress.
This situation will change by 2020. Some doctor groups, such as the Independent d octors Federation, are already in negotiations with insurers.
By 2020, it is believed that a proper independent system will be in place to formally assess disputes between consultants and insurers.
There will be more openness and consultants will generally feel less aggrieved. Some of the worst insurer behaviour over the past five years will be a thing of distant memories.
whatever happens, those practising in 2020 will be working in a vastly different environment than those today
CHANGE 7: THERE will bE A RiSE iN REAl TERmS iN CoNSUlTANT FEES FRom iNSURERS
do need consultants on board if they are to grow their market.
over the next few years, we can expect to see a number of charm offensives from insurers reversing pressures over the past five to ten years.
There will be a difference. All consultants believe they provide a ‘quality’ service. Insurers take this for granted.
We can expect to see an increasing interest in remuneration packages for consultants linked into their economic and financial efficiency. This means the more efficient they are and the more they save insurers money, the better they will be rewarded.
The science of measurement in economic terms of consultant quality is still very young.
By 2020, it will be commonplace and insurers will use the vast amount of data they have to differentially reward consultants.
We can also expect to see the formal introduction of part payment, top-up fees or partial insurance cover.
CHANGE 8:
WHIle SoMe of the cMA rulings in its october 2014 directive are theor etically sound, there are practical implications.
Already, for example, its ruling that consultants cannot have in excess of 5% shares in certain undertakings is resulting in some

unforeseen effects – discrimination against doctors, more power to hospitals and a reduction in competition.
Given that many consultants charge the same fees – they have to under the Bupa open referral and similar schemes – much of the investment into obtaining fees comparative data may prove to be irrelevant. In any event, many patients do not choose their consultants on price alone. overall, we would expect that some of the rulings will be reversed or overtaken by events, since they are not necessarily appropriate to the natural pace of market changes.
CHANGE 9: THERE will bE lESS
oN e o F the phenomena of the past few years has been a significant growth in medico-legal work. This has followed the American pattern of behaviour in an increasing litigious environment.
Many NHS trusts are facing increasing claims and these are becoming very expensive. Some indeed are spurious and the days of the ambulance-chasing solicitor have not totally been eliminated in practice.
o ver the next five years, we would expect an increasing debate on the concept of a ‘no fault’ culture as evidenced by countries such as New Zealand.
Insurers will use the vast amount of data they have to differentially reward consultants
The introduction of changes along this model will have the effect of reducing claim costs on both the NHS and private sector.
There will be, in time, a decline in the inexorable rise of premium costs on the one hand. o n the other hand, there will be a decline in incomes for those who have increasingly turned to medicolegal work.
CHANGE 10: THERE will bE A dECliNE iN NUmbERS oF CoNSUlTANT ‘CHARACTERS’
T H e d Ay S of the mega-practice are already probably in decline, save in london.
younger consultants have more sub-specialisation than their elder colleagues and have been trained in an era of e U working time directives and human rights.
For many younger consultants, family life is more important than their private practice potential and the hard work it entails.
As a result of these changes in work-life balance in society in general, we would expect to see a gradual decline in the number of large practices run by ‘characters’, who satisfy the three ‘A’s – affability, availability and ability, in that order.
The consultants of the future will generally be less ambitious and will work fewer hours than their predecessors. As a result, private practice delivery will become more regimented.
CHANGE 11: THE ElECTRoNiC REvolUTioN will TAkE oFF
IN BUSINeSS terms, perhaps the most dynamic expected change in the market will be the result of the electronic revolution.
This is already being eagerly embraced by younger consultants. We can expect to see consultants using Skype from home, greater use of social media, Facebook as a measure of quality and very fast interchange of information that will be totally alien to many practices.
Personal contact and recommendation will increasingly be succeeded by machine recommendation.
Conclusion of course, it may be that not everything discussed above will happen. other changes will force their way in too. But at the very least, all those involved in the private medical sector market in the UK will have a fascinating, if not bumpy, ride over the next five years.
is the current private healthcare system sustainable? See page 32
Ray Stanbridge (right) is a specialist medical accountant with Stanbridge Associates



The current private healthcare system may not be sustainable, warns Keith Hague (right). It could be time for consultants to think about the benefits of a huge change – being employed by a private hospital
After A lifetime in healthcare, both in the public and private sectors, i never really thought the time was coming when i would see that fundamental change is needed in the way the private sector handles the application of private consultant practice.

Since the Harold Shipman debacle, consultants in the UK have been subject to a wave of change, at times bordering on significant criticism of the way they practise, both in the NHS and in the private sector.
i t’s hard to think of another group of healthcare professionals who have endured the onslaught from government, the regulators, their NHS masters and indeed anyone that feels criticism would be appropriate.

And yet some of those critics have little understanding of what consultant practice really entails and the pressure and responsibility that goes with the job. in the UK, private sector things are becoming complex for the consultant. His or her practice costs are spiralling and practice revenues are falling.
medical defence costs have spiralled out of all proportion over the last three years.
A consultant in spinal surgery, for instance, will more than likely have seen defence costs triple to well over six figures in the last few years.
t hose who specialise in complex surgery will have seen the same happen. And, right now, some consultants are being
refused defence cover, as their practice is judged to be risky. Or in other words, costly. this, combined with the rising costs of practice facilities, the costs of administration of a practice and the fact that the Competition and m arkets Authority (CmA) has removed the support opportunities available from private operators, makes the lot of the consultant pretty miserable at present.
Added to this cost pressure, there is a decided trend from the health insurers towards lowering reimbursement. the topline revenue for any consultant practice is under significant pressure and the relationship between some of the major UK insurers and consultants could be argued to be at an alltime low.
Unattractive proposition
i was speaking to a group of young surgeons recently who were close to moving into the consultant grade. When asked if they were considering developing private practice alongside their NHS work, the response was a definite ‘no’. Simply, they said they could not afford the cost of private practice and the reimbursement for new consultants from one UK insurer was deemed to be too low to make this an attractive proposition. So it looks at least from my straw poll of young doctors that the new feedstock of consultants into the private sector will diminish. Not a good sign, really, for those of us who wish to have ourselves and our families cared for in the independent sector.
Some fundamental questions need to be asked:
i s there an alternative for the application of private practice?
i s there an opportunity for a consultant to still practise privately but without the cost pressures and the trend towards diminishing revenues?
is this the time for a consultant to consider ‘employment’ in the private sector?

As little as five years ago, had mentioned to any consultant group that they should consider being employed by a private hos pital organisation, i would most likely have been turfed out of the room.
not fit for purpose
But things are different now and time has moved on and one may wish to consider that the longhonoured practice in existence for over 50 years, whereby consultants bill a fee for service alongside the hospital facility fee, is more than likely ‘not fit for purpose’.
Private patient episodes can generate multiple bills for the insurer to settle.
But under a system whereby the consultant is employed by the hospital, the insurer gets one bill.
Good for the insurers, that’s true.
But those rising practice costs currently borne by the consultant, especially defence costs, disappear and become a cost to be borne by the hospital.
i n a similar vein, the hospital will assume responsibility for the application of medical governance concerning the practice of the consultant.
And surely any consultant in singlehanded practice – and even those working in groups – will welcome the support of such a change.
So is it time for the consultant to move under the protective umbrella of the private hospital organisation by obtaining employment?
Some will argue otherwise and some may be right. But i think the time has come for the specialist to consider his or her practice under a different organisational structure.
employment within the private sector may well be worthy of consideration.
Keith
Hague is chairman of Worldwide Healthcare Associates
Should consultants be employed by private hospitals? Would that suit you? or would you say ‘never!’ Let independent Practitioner today know your views by emailing robin@ip-today.co.uk


Having just a website is not enough. As Chris John (below) reports, it has got to be mobile-friendly

A consider A ble number of private medical practitioners are relying on the website of the private hospital or clinic from which they base their surgery. They hope that a biography – which is quite often dry – is enough.
i n fact, the result of analysis into 100 private medical practitioners and their online presence revealed that only 50% had a website to showcase their business. incredibly, 25% had nothing at all, as Independent Practitioner Today reported last month. but with 91% of 1,500 patient respondents to a survey we carried out citing that their choice of private medical practitioner is influenced by the look and feel of a website, what of those who have
taken the right step to showcase their business directly?
According to o fcom’s annual communications market report, more than a quarter (28%) of those aged over 55 now own a tablet and many use it as their main computing device.
i n addition, the take-up of smartphones is almost on a par with that of laptops (63%) among uK households, while desktop Pc ownership has dropped, from 44% in 2012 to 35% in 2014.
disappointing figures
Yet our survey found only 30% of private medical practitioner websites could be viewed across mobile devices.
c onsidering the increase in
smartphone and tablet use, the fact that so few websites could be viewed away from a desktop was disappointing.
With more than two-thirds of websites not being mobileresponsive, the sector is not responding quickly enough to the expectations of patients and that of search engines.
our private patient survey identified that nearly one-third of people between 25 and 45 are turned off by not being able to view a website on a mobile device. And with search engines like Google launching special algorithms to prioritise websites that are mobile-friendly when a search is conducted on a mobile device, practitioners with outdated
With more than two-thirds of websites not being mobileresponsive, the sector is not responding quickly enough to the expectations of patients
websites may just start falling behind.
How a website performs during a search is most important at those times when prospective patients are directly seeking a practitioner. only a quarter of the websites analysed had been optimised effectively for search engines – which is great for them, as the competition isn’t exactly strong right now.
The overall Average Quality score compared websites against five criteria. The most important one is the ability to build trust quickly and effectively.
There is no point in being found via a search engine if the prospective patient landing on the website homepage can’t easily tell that it is relevant to what they are looking for.
smart medical Web’s trust criteria included whether:
There were clear validation cues in the form of testimonials or badges from affiliated companies;
The practitioner showed membership of professional bodies;
Whether there was a landline number and contact address;
The pricing was clear;
There were photos of the team, building and/or office to enable the prospective patient to understand what to expect.
Although private doctor websites performed best overall in the ‘trust’ category, 57% of websites still underperformed.
Chris John is a co-founder of Smart Medical Web

only 30% of private medical practitioner websites could be viewed across mobile devices
75% of private medical practitioner sites are not equipped for search engine optimisation
Private medical sector websites received an average quality score of 34.85%
the following table details the five criteriabenchmarking results: total websites reviewed 100 Mobile-friendly websites


























One of the most underused methods of attracting patients to private practice has to be through using video. Dev Lall (right) believes independent practitioners could do better

Think abou T it: if there’s one thing almost everyone in the western world spends hours every night doing, it is watching the television.
i t is the single most popular method of relaxation of an evening for the vast majority of the population. and this behaviour is mirrored online. People watch vast amounts of online video too. in fact, according to alexa, the company that ranks websites in terms of traffic, the top three websites for traffic globally are:
1. Google
2. Facebook
3. YouTube
Founded in 2005, YouTube basically allows anyone to upload video to the internet, where you can choose to share it with whoever you like according to the privacy settings you select.
The great thing is that these videos are indexed and the entire library is searchable. Visitors can go to YouTube and search for content of interest to them. a nd while the majority of searches are for music – and, of all things, Minecraft! – plenty of people also search for medical information.
The other thing to recognise is that YouTube is owned by Google, the world’s biggest search engine with over 1.1 billion unique visitors monthly. So when you search on Google, the results you get are not only web pages with relevant content, but also relevant videos it finds on YouTube.
Go to www.google.co.uk and type in ‘hernia operation’. although the results you get will be slightly different to mine (i’m in London), you will see something akin to the top picture on the right.
Scroll down the screen and at position 12 you will see this see the picture at right, middle. if you then click on the link, you will be taken to YouTube and you will see what is shown in the third screengrab image down on the right.
Why this is a big deal
First of all, understand that the entire point of marketing is to be seen and found by people who could benefit from your expertise. if you perform the search as i did, you will see that in the top 100 ‘hits’ that Google serves up, there is only one video.
That video is highly visible among the other search results –just look at second image down on the right. better yet, perform the search for yourself and see how eye-catching it is.
That in itself, regardless of the position it is served on the page, makes it highly likely to be clicked on. This, in turn, means that if you ‘owned’ that video, you could direct traffic – in other words potential patients – to your own website. in this case, the video is simply one a patient has put up himself – not a clinician looking to promote his or her expertise.
The third screenshot picture is particularly telling: it shows that since the video was uploaded in December 2012, it has been viewed 177,269 times.
Yes, those visitors will be from around the world, not just the uk but even so, it clearly demonstrates how powerful a traffic-generating strategy it is to have video online for people to see. People are interested in even mundane surgical procedures such as open inguinal hernia repair.
opportunity knocks online video is a huge opportunity for a consultant in private practice because virtually no one is doing this. a nd i ’ve not been impressed by many that are.



Rather than go into a long discussion about how to present yourself on camera, the most instructive thing is to view the video yourself and see what the narrator is both doing and not doing.
The first and perhaps most important point is not to allow yourself to be intimidated by the camera or worry about making it ‘professional’.
i f you view the hernia video, you will see that it is wobbly, in places out of focus, with poor lighting and occasional dodgy audio. The narrator ‘ums’ and ‘ahs’. h e repeats himself. h e’s unshaven. he talks about the fact he ‘hasn’t taken a shit’ (3:10 seconds) and needs laxatives.
he walks, talks and speaks in an ordinary way. he’s not some charismatic, media-trained personality; he’s just an ordinary guy, talking about a simple, common medical problem and his experience of being on the receiving end of treatment for it.
he’s not using jargon. he’s not going into any kind of technical
i would always recommend you script your video. not word for word, but have a 6x4 card with a few bullet points to refer to. that will help keep you focused and relevant.
Duration: 5-7 minutes is good. Much longer and people will get bored and click away. not good.
casual yet smart and professional. you should aim to look accessible to the viewer – not intimidating or standoffish. it is obviously possible to be underdressed in jeans and t-shirt, but equally possible to look too stuffy and remote by wearing a pinstripe suit with a flower in your buttonhole and a plum in your mouth.
think friendly, knowledgeable uncle and you’ll be about right. you want the viewer to feel at ease in confiding their medical problems in you.
three computer screenshots of a google search on ‘hernia operation’ – the third showing a click through to the youtube website
discussion. h e’s talking about pain and his stitches. he’s someone any patient could relate to. in short, he’s human. and he’s describing the typical patient experience after an elective open inguinal hernia repair.
getting started with online video
So how do you go about recording your video? and what should you talk about?
The cardinal sin in any marketing approach is to be boring and fail to engage the interest of people with conditions you treat.
That is why the vast majority of consultants’ websites are so bad at generating patients for them. They are, at best, glossy brochures or CVs and that’s all.
So when it comes to producing your videos, you need to really put yourself in your patients’ shoes and make sure everything you say is relevant and of interest to them.
and the best way to do that is to think back and make sure your video answers all the questions
Jargon is the kiss of death in all marketing. it is occasionally important to use some medical terminology – for example, ‘hip resurfacing’ – because the patient may have heard of it and be looking to find out more about it. But this is the exception rather than the rule.
use vocabulary a 10-year-old would understand with simple sentence structure – think sun reader and avoid jargon whenever possible.
this is a big problem. i have never yet met a clinician who has got this one right. Because the problem is that, as an expert, you know far more about every condition you treat than any patient – with extremely rare exception –possibly needs to know. and if you don’t reign yourself in very carefully, you will end up either confusing the hell out of the viewer or boring them to tears.
you and your juniors get asked about the care, treatment and management of conditions in your specialty.
The approach i recommend is to sit down and write down any and every question you get asked about the condition you want to talk about and to answer that question in the video. no matter how seemingly trite or irrelevant it may seem to you, it matters to patients, so address each point. in addition, ask yourself what questions people don’t ask you but should – then answer that ‘question’ too.
online video is a huge opportunity for the smart and forwardthinking consultant to grow their private practice if only they would try. Too many are intimidated by the technology and by the thought of appearing on camera.
The rewards are enormous and the field is wide open – hardly anyone is doing this, and those few who are, are making a mess of it.
i t doesn’t require expensive equipment – your smartphone will record perfectly good video –or for you to have a glittering media personality. o n the contrary, it simply requires an ability to communicate with the viewer like a human being.
i n the example i have shown, the video Patrick Schwerdtfeger put up of his hernia repair comes up at position 12 in a Google search for ‘hernia operation’.
i magine what it would do for your practice if you had a video relevant to your specialty in position 12?
a nd taking it a little further, imagine if you had six or a dozen videos all relevant to your specialty on YouTube, with half a dozen coming up on page one when people search for experts in your field.
What would that do for your private practice, do you think?
Mr Dev Lall is an upper-GI surgeon and runs specialist private practice consultancy www.PrivatePracticeExpert.co.uk
Self-pay patients are on the rise – as Independent Practitioner Today reported in our July-August issue – but that means your non-payers could be on the increase too. Gary Nials (right) suggests you get prepared using his tips and template letters to help chase up what you are owed


If self-pay is on the up in your practice, then you will now be dealing with more individuals as opposed to insurance companies. surely this would make life easier for the doctor?
No more bureaucracy or waiting on the phone to speak to another adviser who seems to know nothing about you or your practice.
Unfortunately, the reality of dealing with the general public is very different and potentially brings its own challenges.
a first step is to always invoice the patient as quickly as possible and ensure the invoice has clearly defined payment terms.
These terms should leave no doubt in the mind of the patient about when you are expecting payment.
after you have sent the invoice,
contact the patient preferably by phone to ensure they have received the invoice and they are going to pay. Most of the time, carrying out these simple first steps will ensure a prompt payment.
However, there will be the odd occasion where further reminders will be required. f or these, you should have a process ready for chasing payments. This needs to be consistent and robust and followed every time.
The best way is to have some chase letter templates ready.
The first chase letter should be a reminder and informs the patient that they have an outstanding invoice. Obviously, they know this, but it does not hurt to give people a little nudge.
your practice’s address patient’s name and address Today’s date
your practice’s address patient’s name and address
Today’s date
Dear Mr X
Ref: Outstanding Invoice XXXX dated 3rd July 2008 for £150: Despite sending several reminders to you in the past, your invoice still remains unpaid.
This is a fINal ReMINDeR before we take further action. If I do not receive payment or hear from you within seven working days, I will have no alternative but to pass your outstanding debt onto a debt collector. In order to cover the costs of pursuing this debt, there will be a surcharge of x% added to the invoice. This process will affect your credit rating.
To pay by cheque, please make payable to Dr y and send to the address above quoting the invoice number on the back.
Dear Mr X,
Ref: Outstanding Invoice XXXX dated 3rd July 2008 for £150:
I am writing to you because my records show your invoice is now overdue and I have been unable to contact you. I would be grateful if you could settle this by return.
To pay by cheque, please make payable to Dr y and send to the address above quoting the invoice number on the back.
I look forward to receiving your payment shortly. yours sincerely
Dr y
Typically, this letter would be sent once the invoice’s payments terms have expired and you have not been able to talk to the patient. even after you have sent the chase letter, you should still continue to try to contact the patient. There may be good reason for them being late with payment.
If, after a week, you have still not received a payment and the patient has not responded to any calls, you should now send a further chase letter and this should be a little more forceful in its language than the first.
again, you are pointing out that they owe money to your practice and you are expecting payment.
your practice’s address patient’s name and address
Today’s date
yours sincerely
Dr y
More often than not, a letter of this kind will induce the patient to pay. However, if they do not, then you must follow through and engage the services of a professional reputable debt collector.
These templates and having a consistent self-pay chase process should help keep you on top of your practice debt.
you should note, though, that dealing with individuals requires a lot of effort and time. If you lack the time, you should consider outsourcing this to a professional company. They will have processes in place and the resources to chase those payments.
Dear Mr X
Ref: Outstanding Invoice XXXX dated 3rd July 2008 for £150: I am writing to you because, despite repeated attempts to get you to settle the invoice, it still remains unpaid. I must now request that payment is sent by return.
To pay by cheque, please make payable to Dr y and send to the address above quoting the invoice number on the back.
I look forward to receiving your payment shortly. yours sincerely
Dr y
Hopefully, this should prompt the patient into paying but do not give up on phone calls to ensure they do.
finally, if you have still not received any payment or word from the patient, you should consider your next action. you have two choices, either to write the debt off or use a debt collection agency. Writing off the debt should be done under guidance from your accountant.
If you choose debt collection, then you must warn the patient that this will be your response to them not paying. The final chase letter (above right) should spell what you are willing to do next.
Gary Nials is the managing director of Medical Billing & Collection
• Completely open scanner that is well tolerated by claustrophobic patients
• Weight-bearing scans for spine and joints enable a more precise diagnosis
• Patients who are large or cannot lie down can be accommodated
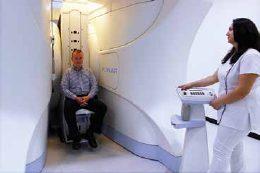
more information go online
Receiving
your first instructions is exciting. Michael R Young continues his series by showing how to respond
Solicitor S looking for an expert to help them with a clinical negligence case will either look on the appropriate register or database or have someone recommended to them.
if your name comes to the fore, they will usually make initial contact with you by letter. there is no interview or selection process. the letter may be no more than
the book costs £60, but independent practitioner today has secured discount of a third off for readers, so you pay only £40. listen to the audio content which accompanies the book at this website: www.otmoorpublishing.com/audio. For more information and to order, email stephen.bonner@ otmoorpublishing.com, quoting reference ‘Young/ipt’.

‘Are you able to help?’ or it may set out the background to the case, either briefly or in full.
Your letter of instructions will be very carefully worded and you should regard it as being akin to an examination question.
Read carefully
r ead it very carefully several times. Are you clear about what you are being asked to do? if the instructions are not clear, ask for clarification. Are you being instructed as the expert for the claimant of for the defendant or are you being instructed as a single joint expert, acting for both the claimant and the defendant?
Most of my work was for the claimant, but occasionally i was instructed to act as a single joint expert, probably because they

Your letter of instructions will be very carefully worded and you should regard it as being akin to an examination question
were low-value cases or because they were not very complex. Your responsibilities and duties as a single joint expert are exactly the same as if you were acting for the claimant or the defendant.
Also look at who are the claimant and defendant – would you have a conflict of interest if you accepted the case?
At this stage, it is worth speaking to the solicitor to find out as much as you can about the case. i used to make a point of speaking to solicitors as soon as i could.
Personal contact with the solicitor, even at this early stage, is invaluable. it helps develop rapport. i f it is something that is beyond your expertise, then say so.
Don’t fall into the trap of trying to please. You must always bear in mind your responsibilities under the civil Procedure rules Part 35 ( c P r 35) to give opinions only within your own area of expertise. But if you have to decline the work, remind the solicitor about the type of work you can undertake and ask him or her to bear you in mind in the future. if you are able to help, then ask the solicitor to send you a copy of the case file. once you have the
Review and evaluate letter of instructions – 30 mins
Check records and associated documents for completeness – 1 hour
Review records and documents and extract relevant and important information – 2 hours
Carry out a research of the literature, critically appraising evidence for positive and negative findings – 1 hour 30 mins
identify important issues and compare and contrast and crossreference them with issues raised in letter of instructions – 30 mins
prepare draft report and begin to break down the evidence into relevant and significant constituent parts – 3 hours
Review report; check for factual accuracy and cross-reference with letter of instructions – 1 hour
prepare final report – 1 hour
proof-read final report, check for factual accuracy and readability –30 mins
total anticipated time: 11 hours
case file, read everything through very carefully. initially, this is to confirm two things:
1 Has the solicitor sent you everything he or she says has been sent?
2 is there any additional information that you require before you can begin work on the report?
c ontact the solicitor sooner rather than later if anything is missing or if you need him or her to obtain additional records. if you believe that the solicitor has overlooked what you feel might be important aspects of the case, tell him or her. Do not be afraid of framing your own questions.
After you have reviewed the file, write back confirming your acceptance of the solicitor’s instructions, the likely fee and enclose a copy of your terms of business (see my previous article in the July-August issue of Independent Practitioner Today).
papeRwoRk tip
i would recommend you assign each case your own unique reference number and use this in all correspondence relating to that case.
the system i used was simple: My surname/client surname/a unique number i had given the case, then a full stop followed by the number of the letter and so forth i had written relating to the case. For example: Young/ SMitH213.3
For the avoidance of doubt, always make a point of not only accepting the solicitor’s instructions but also confirming your interpretation of the instructions; for example, if you think there is any ambiguity in what they are asking you to do. By doing this, you obviate possible future misunderstandings.
Whenever i accepted any instructions, and providing that my instructions were clear, i would copy them word for word into my acceptance letter. if the instructions were unclear, i would say what i thought i was being asked to do.
i f i got this wrong, then the solicitors would soon correct their mistake.
try to estimate how long you think it is going to take you to complete your report. i suggest you break down your time into the various elements of writing a report.
You could include a copy of this breakdown with your letter of acceptance – see example in box above.
By showing the solicitor how you have arrived at your fee, you demonstrate that you have thought about the case and that you have not just plucked a figure out of thin air.
i t also gives the solicitor an insight into the methodical way you work, which hopefully will impress him or her.
Adapted from The Effective and Efficient Clinical Negligence Expert Witness , by Michael r . Young, price £60 from otmoor Publishing










HMRC tax investigations and disputes create difficult and stressful times.
As an award winning firm of tax experts, our highly experienced partners specialise in resolving problems relating to tax investigations and disputes with HMRC.
To find out, in confidence, how we can help call 0800 734 3333.
‘Here to help. Not to judge.’



Amid the relentless media attention on the challenges facing the NhS, it is worth reminding ourselves that excellence in our healthcare system still attracts widespread international interest. there is a global need to deliver modern, cost-effective services to growing and ageing populations – and many countries are turning to the UK for solutions.
this demand for our expertise is growing in every area of healthcare delivery: primary care, education and training, infrastructure, healthcare systems and operational management are just some areas of British know-how that are being exported around the world. much of this overseas demand for British expertise is fulfilled with the help of healthcare UK. Launched in 2013, healthcare UK is a joint partnership between UK trade and investment (UKti), the d epartment of h ealth and NhS england.
t he partnership arose from UKti’s highly successful ‘Business is Great’ campaign, a spin-off from the ‘Britain is Great’ campaign that promoted the UK and showcased export opportunities in advance of the London Olympics.
essentially, healthcare UK is the ‘fixer’ between UK capabilities in the N h S, private, academic and third sectors and the overseas governments and organisations that need this expertise. in 2014-15, there were £749m of healthcare-related contracts signed from 26 projects fixed through us. And, as i write, we are already well on the way to that figure again now.
We are geared up to help British healthcare providers overcome the challenges of international expansion. Our high-level contacts in key markets mean we can facilitate introductions to overseas policy makers, healthcare commissioners and investors.
We can then use our local knowledge to provide bespoke support that boosts the chance of pitching successfully for contracts. this might include developing a compelling business case, advising on local business culture or brokering further meetings to improve partnership working.
support from embassies the cross-government nature of our work means that British providers enjoy the active support of the healthcare leads in our embassies and consulates around the world, plus the full range of expert international trade advice and practical help from UKti.
h ealthcare UK targets its resources carefully to bring maximum reward to British providers. there is a global need for better healthcare, but ongoing assessment of international opportunities enables us to identify priority markets with the biggest growth potential and a receptiveness to overseas expertise.
the Gulf States are a key area of interest, as are i ndia, Brazil and China. Opportunity is also growing in other South American countries and the ASeAN region, particularly indonesia, Singapore and malaysia. this approach has brought major rewards.
We decided from the outset that healthcare UK’s impact would be enhanced by focusing on specific sectors. We chose five aspects of healthcare for which there is both considerable international demand and a rich pool of experience and innovation in the UK.
these are:
Clinical services – including primary and elderly care;
training and education;
digital health and harnessing technology for patient benefit;
i nfrastructure design, including commissioning and operation of healthcare delivery;
health systems development.
notable successes there have been notable successes across all five sectors.
the partnership between Great Ormond Street hospital (GOSh) and the m inistry of h ealth in Kuwait to develop a cancer treatment programme will replicate the world-class clinical services provided at the well-known London institution.
this link-up includes a ‘visiting consultant’ programme, training and education modules, on-site attachments for Kuwaiti staff at GOSh and clinical service reviews
as well as on-going advice and remote support.
in the digital arena, computer software companies like tPP are successfully piloting their system solutions to improve delivery of healthcare in China and the Gulf region.
Specialist companies such as the Nine health Community interest Company have now signed agreements to develop intelligent clinic information at sites in Zhejiang Province, China. the biggest financial successes so ➱ p44



UK Top 20 accountants specialising in the healthcare sector
• National firm of the Year 2013
AISMA member (Maidstone and Leicester offices)
• 12 offices including London City
• Tax Structures for Hospital Consultants - dispelling myths
• Surgeon groups and consortia
GP Practices including mergers and federations
• Solvent liquidations (for companies at the end of their lives)
For more information please contact: South East
James Gransby FCA
E: james.gransby@mhllp.co.uk
T: +44 (0)1622 754033
M: +44 (0)7712321899
East Midlands


Robert Nelson DChA FCA
E: robert.nelson@mhllp.co.uk
T: +44 (0)1162 894289
M: +44 (0)7814009160
General email: healthcare@mhllp.co.uk www.macintyrehudson.co.uk




far have come via major infrastructure projects. Consulting companies like Arup and Aedas are finding that their design, engineering and other professional services are much in demand, often working in consortia with architects.
i nternational h ospital Group (ihG) is partnering with the China Railway and e ngineering Company and local government in Guizhou Province to co-develop and manage a 1,000-bed hospital.
opportunities out there
Large contracts have also been secured in the Gulf States. For example, the hugely complex design and production work for the new Cleveland Clinic in Abu d habi is being undertaken by Aedas and AhR Architecture.
the opportunities are out there. h ealthcare UK identified qualified leads with a value of more than £12bn in 2014-15. in China alone, our embassy and UK ti teams highlighted potential opportunities for the UK worth £7.5bn by the end of last year, and this now stands at over £9bn.
Finding leads, however, has not been the issue; it is more of a challenge to identify UK companies and organisations, including NhS trusts, ready to grab these opportunities.
We are particularly interested in working with UK providers for certain types of healthcare projects, especially for opportunities in China.
t hese include the need for expertise in:
developing and operating new private hospitals and care home complexes, including retirement villages;
training and education of healthcare professionals (at scale) and hospital managers;
t he design and operation of polyclinics to support primary care.
international expansion invol ves resources and some level of risk, of course. it usually requires at least one full-time member of staff, backed with the support and finance needed to research opportuni ties, travel and, hopefully, build the all-important relationships which can lead to contracts.
Many initiatives overseas start with consulting work. this helps build relationships and trust and enables assessment of potential longer-term opportunities.
A number of countries have solid routine secondary care but are ambitious to develop tertiary and higher-level specialist care.
experienced medical consultants can bring trusted advice on training, standards, operating protocols and supply chain; for example, which equipment to purchase to run a high-standard service.
there are also opportunities to be more directly involved in operating and training of specialists both abroad (preferable) but sometimes in the uk before appropriate facilities have been built.
the numbers to be trained can be significant, so groups or consortia may be necessary to develop a consistent professional offering.
there is also a need for consulting advice on clinical management and performance measurement. Consultants with clinical or medical director experience can be useful here.
Our message to healthcare providers is that there has never been a better time to look overseas for new income streams
Starting small has been the answer for some UK providers. Small-scale education and training contracts or the provision of consulting expertise on design or management/operations can be useful in building relationships which can lead to bigger opportunities.
Joining a trade mission is a great way to open doors to new business. Organised by healthcare UK and other government departments, participants benefit from an itinerary that maximises the exposure to potential business partners. Unfortunately, we do not usually have the budget to cover travel and accommodation.

ongoing support from the top of the office and the board.
t he reluctance of some N h S bodies to devote resources to the export market is understandable. We all know that funding is tight and the focus on efficiency savings will remain.
A requirement that returns on investment are made within the same budget year can be a further complication.
Our message to healthcare providers, however, is that there has never been a better time to look overseas for new income streams. his is especially true for some of the bigger N h S trusts which already have international reputations they can build on.

t he strategy will also require
t he rewards can be large – and one successful contract can often lead to another. By drawing on ealthcare UK’s support, whatever the size of the opportunity, organisations can mitigate risks by targeting business leads that offer the best chances of success.
these missions may be led by senior government figures or government-appointed business ambassadors, providing the political clout to reach top-level decisionmakers in our priority markets.
Political support for major contracts will always be needed, but building local relationships is vital too. h ealthcare UK also organises missions to reach decision-makers at the local level, allowing practical discussions to take place about the scope for UK expertise to meet community needs.
As we expand our network of contacts in the UK, we are confident that more providers will appreciate the value of these overseas opportunities – if only through exploratory consultancy in the first instance.
i t does take a certain size of organisation to invest enough money to develop an international development strategy. But with thorough research and business planning, backed by the support from h ealthcare UK, UK ti and our embassy teams, the longterm rewards can be significant.
Dr Andrew Vallance-Owen is specialist medical adviser at Healthcare UK
If you want to know more about the work of Healthcare UK, the business opportunities currently on the table or wish to join an exploratory trade mission, you can contact Dr Andrew Vallance-Owen by email at andrew. vallance-owen@uktispecialist.com.
An easy to use software system, which fully supports the clinician and office staff and makes the whole process of running a busy Practice a lot easier.
Call now for a chat and ask about a free, no obligation demonstration of our comprehensive system that has been designed to save your Practice time and money.
‘PPM’ – Private Practice Manager.
PERFECT FOR YOUR PRACTIC E
t: 01992 676162 www. ppmsoftware.com/ppm e: tomhunt@ppmsoftware.com
An independent firm offering one to one meetings anywhere in the UK giving advice and help with:
• how to start in private practice
• how to maximise private practice income
• ways to reduce tax payments
• setting up in Chambers/Groups
• limited companies and LLP’s
• financial planning
• record keeping

• computer software
• tax and financial advice re: car purchases
• pensions: NHS, personal and employee schemes
• purchase of consulting rooms and surgeries
• inheritance tax and capital gains tax planning
• VAT
For more information please contact us by:
Wilmslow
Phone: 01625 527351
Fax: 01625 539315
Harley Street
Phone: 020 7307 8759
Fax: 01625 539315
Email: info@sandisoneasson.co.uk
Website: www.sandisoneasson.co.uk
Simon Bruce explains why it’s important to keep global events in perspective and to hold your nerve
‘The hardesT work in investing is not intellectual, it’s emotional. Being rational in an emotional environment is not easy. The hardest work is not figuring out the optimal investment policy; it’s sustaining a long-term focus at market highs or market lows and staying committed to a sound investment policy.’
These are the wise words of american investment consultant Charles d e llis in his book Winning the Loser’s Game Experienced investors will be familiar with the scenario that has been playing out over the past couple of weeks in the global markets and familiar, too, with the feelings of uncertainty that can accompany such times.
specific events – in this case a falling Chinese equity market coupled with a broader reassessment of the prospects for the Chinese economy – often act as a trigger for a major movement in global equity markets. That is how equity markets work; the current value of the markets reflects the aggregate of the estimated current value of firms within it, based on the market’s view of their future earnings.
Markets move when new information becomes available. If this news is bad for company earnings, markets will fall; if it is positive they will rise. In this case, the Chinese government’s desperate attempts to shore up the Chinese equity market, combined with its recent devaluations of the Yuan,

was taken by the market as a sign that the Chinese economy –which represents around 15% of global GdP – was perhaps slowing at a faster rate than was previously thought.
The Chinese equity market rose dramatically by over 70% over the 12 months to May this year, fuelled by rampant speculation.
In the last week of May alone, 4.4 million online retail brokerage accounts were opened. Chinese investors had borrowed a record U s $232bn to invest in the market. The subsequent fall that we have seen has simply given back the previous rampant and unrealistic returns.
For those less familiar with investing, the temptation is to be concerned in the face of uncertainty and when faced with headline-grabbing BBC news reports, to worry about how their own hard-earned assets might be affected.
There are some important things to remember at times like these:
These market gyrations are an inevitable consequence of owning equity assets; markets go up, down and sideways from time to time.
Two steps forward and one step back is a reasonable way to think about owning equities. It is the very uncertainty of short-term market returns that delivers the
longer-term incremental returns that equities offer, above owning bonds or cash.
In investing, you do not make a financial loss unless you sell out of a position – for instance, selling equities when they are down.
Long-term investors have the luxury of being able to hold assets until the storm passes.
The allocation of equities in your portfolio should be linked to your emotional tolerance for risk, your financial capacity to suffer losses and your need to take risk in the first place.
Most investors own a balance between bonds and equities. Your portfolio should not have suffered anything like the headline falls of the Chinese market. If you are
concerned, then the balance may not be correct.
If you own a well-diversified portfolio made up predominantly of developed market equities and high-quality bonds, then your direct exposure to the Chinese market may be very small.
Investing in ‘emerging markets’ has provided stellar returns in the past, but an overexposure to these funds will have been very painful in recent times.
If you own high-quality bonds, then they will be undertaking their defensive duties at this time.
For example, since the start of a ugust, short-dated gilts have risen by around 0.5%, while the developed equity markets and the FTse all share Index have fallen a little over 10%.
To keep these short-term events in perspective, even with recent falls, the UK market is up around 45% over the past five years and the global developed markets are up around 60% over the same
time-frame. The UK market was last at its current level as recently as mid- d ecember 2014, but few were alarmed at that time, as the market was gradually rising.
The Us and UK economies are growing strongly – it is not all doom and gloom.
A dose of reality even considering the above, not everyone receives the best investment advice. Many are also their own investment managers. When the tide is rising, there is significant temptation to chase returns from fashionable sectors or fund managers. This can quickly lead to a lack of balance in your portfolio, which magnifies losses when there is an unexpected correction.
Frequently, we will meet investors who have either drifted away from their stockbroker or wealth manager or who simply have not had time to keep up to speed with their online investment accounts. Portfolio drift will happen over
time and increase the inherent level of risk you are taking without you even realising. Fund managers are taken over by other fund managers, funds are merged or close. even with dedication and time, keeping track of it all is no mean feat for any doctor.
Good structure and real diversification will protect you against broad-based equity market declines to some degree, but only if you have first taken the decision to get to grips with your portfolio.
a n unbalanced portfolio will not only be more volatile at times of market stress but will also fail to capture the full market recovery.
A portfolio is not a plan d o you know why you have an Isa and sIPP in the first place and what you are investing for? If it is just a general notion of future financial security, you may wish to get more specific. What will it actually take to maintain your current standard of living for the
rest of your life and still have assets to pass on to the family?
Summary r emember that investing is a long-term game that requires both patience and discipline. Once you realise that you can’t control the markets – and that nobody can – and that knee-jerk decisions almost always result in the wealth destruction strategy of buying high, selling low, then all you have left is structure, patience and discipline. Time heals most investment wounds.
Simon Bruce is managing director of Cavendish Medical, specialist financial planners helping senior consultants in private practice and the NHS.
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.


With more doctors – including those in private practice – facing allegations of sexual assault in recent years, Dr Bev Ward (left) answers your topical questions

QI am a physician working in private practice and was worried to read recently that sexual assault allegations have risen. I sometimes have to carry out intimate examinations on patients and am worried that my actions could be misinterpreted. What can I do to minimise this risk?
AA recent MDU report revealed that alleged sexual assault cases increased by 66% from 2003 to 2013, with 167 doctors being accused during that period ( Independent Practitioner Today, September 2015).
In the vast majority of cases, the doctor is cleared of any wrongdoing, but these accusations can still be very distressing for all involved and may leave the doctor feeling that their reputation has been damaged.
With this in mind, it is important that you take steps to mini-
mise the risk of a complaint. Familiarise yourself with the GMC’s guidance, Intimate examinations and chaperones (2013), which highlights how doctors should behave when conducting an intimate examination.
You should always obtain consent for any examination, but for intimate ones you need to make sure the patient understands exactly what is involved.
An intimate examination is one of the breast, genitalia and rectum. However, it is important to remember that some patients may regard any examination in which the doctor needs to touch or be very close to them as intimate.
Always consider what the patient might think of as intimate, even if it doesn’t seem so to you.
Some patients may feel a chaperone is needed for routine physical contact, or even if you just need to get very close without actually touching them.
Use professional judgement
In these circumstances, doctors are expected to use their professional judgment about whether a chaperone should be offered, depending upon the patient’s previously expressed views and level of anxiety.
A patient can withdraw their consent for a procedure at any time. If they ask you to stop, then do so.
When a patient is dressing or undressing, give them privacy and avoid making any light-hearted or personal comments, which may easily be misconstrued.
There may also be a misconception among some doctors that male patients do not require a chaperone. In fact, the gender of the doctor and the patient is irrelevant to whether a chaperone should be offered.
Although a chaperone’s principal responsibility is to protect patients from abuse, they can also reassure or comfort patients dur-
ing examinations that they might find embarrassing or distressing.
This is reflected in the criteria listed by the GMC, which says that doctors must be satisfied that their chaperone will:
Be sensitive and respect the patient’s dignity and confidentiality;
Reassure the patient, if necessary;
Be familiar with the procedure involved in a routine examination;
Stay throughout the examination and be able to see what the doctor is doing;
Be prepared to raise concerns about a doctor’s behaviour or actions.
As always, it is important to keep full and contemporaneous notes. Include details of any discussions you have with the patient, such as why the examination was clinically indicated and that a chaperone was offered, along with whether the patient accepted or declined your offer.
If an accusation of improper behaviour is made several years later and there is no record of who acted as a chaperone, it may be difficult to recall who witnessed the examination.
Q
With this increase in allegations of sexual assault, it seems wise to insist that all patients have a chaperone. Can I do this?
A It should be noted that despite the increase in allegations of sexual assault, the figures are still relatively small, with an average of 15 cases a year. Although patients have the right to a chaperone, they can also decline the offer if they would rather not have someone else in the room. In such situations, doc-
tors should explain why they would prefer a chaperone present.
If you are not comfortable treating the patient without a chaperone, you may need to refer them to another doctor who would be prepared to proceed without a chaperone, but only if their clinical needs allow it.
However, if the delay would adversely affect the patient’s health, then this would not be an appropriate solution.
If the examination does go ahead without a chaperone, the doctor should make a note that a chaperone was offered but the patient declined.
Occasionally, there may be no chaperone available or the patient may be unhappy with the chaperone offered.
For example, the patient may only want a chaperone of the same gender. If this happens, you can ask the patient to return at a different time – providing this is not against their clinical needs.
But asking a patient to return at a later date may make them feel under pressure to proceed without a chaperone now, which may lead to a complaint.
Publishing a chaperone policy will allow you to define in advance what will happen if a patient refuses a chaperone when offered.
This can help manage patient expectations and encourage them to make their wishes known at an early stage.
Dr Bev Ward is a medico-legal adviser at the MDU


If you are a doctor who loves your smartphone, gets excited by the latest electronic and robotic medical equipment, and has strong environmental interests, then this could be the car for you, says Dr Tony Rimmer (right)



I W ould S u GGEST that any independent practitioner, particularly those involved in a surgical specialty, has an intrinsic interest in all things technologically advanced.
o ur medical education is science-based and we continue to have a thirst for knowledge and follow the latest medical advances throughout our careers. I would also propose that most of us are also concerned about global warming and our over-reliance on fossil fuels.
We also like our cars and, with this in mind, many of us are intrigued by the advances that are being made in the motoring world.
Every large car manufacturer is spending millions of pounds researching and developing alternative-fueled cars with more efficient engines.
But the latest and most advanced petrol or diesel reciprocating engines are no more than 30% efficient. Electric motors are at least 90% efficient and have the added benefit of delivering maximum torque from rest.
This is why electric vehicles (EVs) have such appeal. They are only compromised by the size and weight of their batteries, their range and the national infrastructure available to re-charge them. despite these limitations, many of us are taking the plunge and buying into the whole EV idea. But is being a first-adopter too risky? Can you live with an electric vehicle as a daily drive? There are a handful of vehicles to choose from. At the entry level is the well established Nissan leaf and the small Renault Zoe hatch-

back and at the top end is the fantastic but pricey Tesla model S and BMW’s i8 supercar.
In the middle rank, and a car I think fits well with the independent practitioner buyer, is the premium BMW i3. The German maker has been really brave with the styling of its electric car and the i3 looks smart, stylish and futuristic.
Extensive use of carbon fibre and aluminium with a plastic body shell keeps the all-important total weight down and the lithium-ion batteries are under the cabin floor. This gives the i3 a tall and narrow appearance that is more like an MPV than a hatchback.
The electric motor produces 168bhp and can power the car for a claimed 80 to 120 miles on a full charge, depending on your driving style. This, of-course, is the Achilles heel of EV motoring.
In the real world, the useable range of any electric car is much less than the manufacturers’ quoted figures. I can tell you from experience, range anxiety is a real emotion.
BMW has gone some way to alleviate this by offering, for an extra £3,000, the Range Extender model. This has a two-cylinder 650cc motorcycle engine in the boot that kicks in to re-charge the batteries when they are running low.
It does not power the wheels at all. It has a tiny nine-litre fuel tank and extends the range by about 80 miles. This certainly reduces range anxiety, but long


Entry to the back seats is easy, as the rear doors are coach doors that open backwards – but only if the front doors are open too
trips are still not to be recommended: filling up every 80 miles is, at the very least, inconvenient. However, driving the i3 should all be about battery-powered driving and an overnight seven-hour charge from a domestic socket will give an 80% charge and this should be enough for most urban trips and commuting.
It is also supplied with connection leads for free power points out of town and also fast-charging points that are available at a few sites nationwide.
u nfortunately, the charging point infrastructure is also in its early stages of development and there aren’t that many and they are often occupied by other EVs when you get there.
The Ford Fiesta-sized interior is very different from all other cars, with a dual-screen dashboard and straightforward controls. Seats and carpets are made of sustainable materials and there is a real light and airy feel to the car helped by the raised seating positions and huge windscreen.
A major saving grace of the i3 is to be found in the driving. This is a really entertaining car to nip through urban traffic
body: Four-seat hatchback
Engine: One electric motor – plus 650cc petrol engine to recharge batteries in the Range Extender model
Power: 168bhp
Torque: 250Nm
Top speed: 93mph
Acceleration: 0-60mph in 7.8 secs
Claimed range: Up to 120 miles (up to 190 with Range Extender)
On-the-road price: £ 30,680 (£33,830 – Range Extender model)
It is quite roomy and cleverly packaged with space for two adults in the back and a flat but high-floored boot.
Entry to the back seats is easy, as the rear doors are coach doors that open backwards – but only if the front doors are open too. Although this feature is novel, it could be a bit of pain on the school run.
But a major saving grace of the i3 is to be found in the driving. This is a really entertaining car to nip through urban traffic.
Sharp steering, instant-response throttle and a super-tight turning circle gives it real dodgem qualities. What is even more addictive is the regenerative braking.
A few pre-set levels allow braking from the motor to top up the batteries and on its highest setting you can almost do away with touching the left pedal with your foot at all; a most satisfying challenge and great fun.
Even though you probably won’t hit the motorway very often, the i3 is a quiet, smooth and accomplished cruising companion.
The i3 has cutting-edge design, innovative engineering and strong performance. If you are an independent practitioner who loves your smartphone, gets excited by the latest electronic and robotic medical equipment and has strong green and environmental interests, this impressive BMW could be the car for you.
Dr Tony Rimmer is a GP practising in Guildford, Surrey
So you’ve been in private practice for a year now? Happy Anniversary! A year after starting your practice is a great time to take stock of things. Ian Tongue (right) looks at some of the areas that should be revisited 12 months on
A key part of running any successful private practice is periodically reviewing your business, making improvements and ensuring you are best placed in the ever changing world of private medicine. My tips outlined below are also relevant for those independent practitioners who are more established
Irrespective of trading structure, after your first anniversary you are likely to be facing your first large tax liability.
Your accountant should have advised from the outset how much to save for tax, but knowing your actual figures to pay can be a big relief.
Check that your accountant sends you a comprehensive request for information soon after your financial year-end and you should supply your information as soon as possible to allow the maximum time to prepare for your tax payments.
Thereafter, with – hopefully –rising profits, it can take some time for your tax payments to settle down.
Therefore, it is important you continue to provide your accountant with accounting records on a timely basis to ensure that there are no surprises.
It is often the case that your first year estimate of earnings is lower than what you actually achieved. Depending on the difference between them, you may be required to pay an extra premium to ensure that you are insured for all of the work performed. It is a false economy to not pay the cor rect premium and it could also land you in hot water with the GMC. Many consultants are considering alternative providers of indemnity and, in some cases, the premiums can vary significantly, so it is worth shopping around. Some of the newer entrants have been around for several years, so you draw on actual experiences of their claims handling by speaking with colleagues.
to charge more, but often the premium can be difficult to recover from the patient. The success of this will depend on how much the patient wants a specific surgeon or physician.


offer a comprehensive demonstration and trial. Speak to colleagues about their experiences and ask your secretary if they have used any of them previously.
The key thing that comes up repeatedly by consultants with successful private practices is the top quality of their secretarial support.
This may be a self-employed secretary or business providing secretarial services. Either way, you must evaluate their performance to ensure that they are doing everything expected of them and to see that any areas where improvement is needed are communicated.
If you are having to get involved in the admin side a lot, then this is usually a sign of something not functioning correctly. The best use of your time is with patients.
Welcome to the BVRLA – I’m delighted that you’ve decided to join the trade association that provides a face for the vehicle rental and leasing industry, communicating its messages to customers, the media and government. The BVRLA’s corporate identity, particularly its logo, forms part of that message.
As your practice grows, the demands on your time become ever greater as does the responsibility level. Working in a group can provide additional support as well as more revenues in a lot of cases.
The BVRLA has three categories of membership, each with a logo that members are entitled to use (and, in some situations, are obliged to use). Appropriate use of our logo tells your customers, your suppliers, and the rest of the world that you adhere to the high standards that come with BVRLA membership.
For insured work, the tariff rates form a framework for charging, with some consultants choosing
For self-payers, the pricing structure is more flexible, particularly for certain specialties. Often the rates charged when you are starting out are lower than those of more established colleagues because you want to get your name out there. Once you are at a stage where you are known, you should consider your prices at least annually.
This brief guide explains how we expect our logos to be displayed – and how they should not be displayed. These are not hard-and-fast rules, and we sometimes depart from them ourselves, but we do expect our members to respect them and to gain our prior approval before using our logo in any way other than described here.
In the early stages of private practice, simple spreadsheets will be more than adequate. But as volume increases, the benefits of investing in bespoke practice management software become greater.
If you have the opportunity to join a group, then consider it and always involve your accountant with the financial aspects to ensure that the opportunity is a viable one.
If you need a copy of our logo, for use on your printed marketing material, or to go on a page of your website, please contact our communications team, who will be happy to send you an EPS or JPEG version appropriate for your purposes. If you have any queries about use of the BVRLA logo that are not addressed in this guide, they will also be able to help
Introduction Gerry Keaney Chief executive, BVRLA
There are a number of quality packages on the market and most
As you practice grows, your wealth will inevitably increase. Often the path from here involves moving home, school fees and
generally enjoying the benefit of all that additional hard work.
It is important that you consider the stability of your practice if taking on large financial commitments, as you could easily find yourself in a difficult position if the work dried up.
Where you have spare money, consider investing it wisely. Tax schemes and investment products that seem too good to be true are often just that.
Always appoint advisers who are part of a recognised professional body, where you can reasonably assume that they should act ethically and are answerable to someone for the advice and service provided.
From a tax perspective, the trading structure adopted for your private practice can have a significant impact.
Over the last ten years or so, lim-
ited companies have become very popular and, for the most part, are more tax-efficient, together with giving you more flexibility.
The recent Budget has changed the way in which dividends are taxed and the policy was ultimately to raise more tax revenues from those using a company to trade rather than the given explanation of simplification.
The new taxation rates are applicable from 6 April 2016 and increase the tax on dividends by 7.5% but give you a tax-free amount of £5,000 a year.
For those with smaller private practices, this can be of benefit; but, for the average consultant, it is likely that more tax will be due. Reductions in corporation tax rates to 19% then 18% scheduled for 2017 and 2020 respectively will, however, help offset some of this increase.
It is anticipated that most consultants can still operate as a com-
pany without being worse off compared to self-employment and there are numerous other benefits of this structure.
One benefit of trading as a company is potentially retaining more of your pension annual tax allowance, currently £40,000. This year’s Budget announced a new measure to restrict the annual allowance down to a minimum of £10,000 on a sliding scale for those earning between £150,000£210,000.
Dividends are classified as ‘earnings’ for this calculation, so involving a spouse will mean that the dividends are split and potentially the annual allowance preserved. In the right circumstances, this could potentially save £13,500 in tax a year.
As always, your individual circumstances will determine the most appropriate trading structure and you should discuss matters with your accountant.
Meet with your accountant Meeting with your accountant after your first anniversary and periodically after that is important to ensure that you are best placed from a financial perspective.
Your accountant should be discussing topics including the above and if they are not, you should look elsewhere for an accountant with medical knowledge.
Reviewing your private practice on your one-year anniversary is a great opportunity to revisit the key components of a successful and profitable private practice. Many of these areas require involvement from your accountant, so make an appointment to go through things with them.
Next month: A recap on the taxation of pensions
Ian Tongue is a partner with accountants Sandison Easson and Co
So why not turn to the experts in the field to help you find the vehicle that suits your needs?
anthony K associates are vehicle leasing brokers specialising in providing vehicle contracts for doctors and all associated professions in the medical sector.
Testimonials from our very many happy customers are proof of our attention to customer service and our practised ability to help clients get the vehicle



Care Quality Commission (CQC) regulations specify that independent hospitals have an independent review stage for complaints.
Ninety-eight per cent of independent hospitals in e ngland choose the i ndependent Sector Complaints adjudication Service (iSCaS) to provide this independent review.
Following the Francis r eport, hospitals are facing even greater scrutiny around complaints handling and this will, in turn, have an impact on your hospital-based private practice.
as part of your practising privileges at an iSCaS-member hospital, you agree to co-operate with the hospital’s complaints policy.
For i SC a S-member hospitals, this is a three-stage process:
1. t he registered manager is responsible for Stage 1;
2. Stage 2 is conducted by the corporate head office – in the case of group hospitals – or by the chairman of the board or appointed non-executive director in the case of individual hospitals;
3. i SC a S independent adjudication is the third and final stage for complaints that the provider has not been able to resolve. as such, a framework exists for the management of complaints and if a complaint is made about
you, you are the start of the process.
Having this structure in place is particularly beneficial for those complaints that you are unable to personally resolve.
What type of complaints does the iscAs code cover?
the code covers complaints made about clinical issues, but it does not deal with matters of clinical negligence. it also addresses nonclinical issues such as administration, fees and complaints handling itself.
Complaints are sometimes solely about consultant care, but they often involve more than one professional and it is important to fully co-operate with the process if the care you provided is part of a broader complaint.
What are your responsibilities?
it is vital to share information in a timely fashion with the registered manager about any complaints
made against you and to involve them if you are finding the complaint difficult to resolve.
Co-operate with any requests to meet with the patient. i SC a S encourages registered managers to offer to meet with patients to discuss their complaint and the vast majority of complaints are resolved through this means.
i t is also important that you make your consultant notes available to i SC a S if requested, with the appropriate consents, without delay.
ensure you have a copy of the hospital’s complaints policy and are familiar with its contents, particularly around time-scales within which to respond to complaints and how to signpost complainants on if you are not able to resolve their complaint.
learning lessons from complaints against consultants the iSCaS code places an emphasis on hospitals learning from complaints and it is important
that consultants take this on board too.
in 2014, 17% of all complaints that reached iSCaS independent adjudication (Stage 3) concerned consultants.
t he main issues complained about were:
l ack of informed consent around risk;
Consultant attitude and behaviour;
l ack of transparency around consultant fees – and linked to this, hospital fees. i n fact, complaints concerning fees is a growing area and will be covered in a future Independent Practitioner Today article.
making goodwill payments i SC a S adjudicators have developed a useful document setting out a decision-making structure for the awarding of goodwill payments to complainants.
t hese payments are not intended to be compensation or an admission of liability but rather a recognition of the inconvenience and distress caused to a patient.
the Goodwill Payments Guide is available to download on the i SC a S website at www.iscas.org. uk and is a structure you might choose to consider when making your own judgements.
in summary, patient complaints are an inevitable aspect of a consultant’s professional career and the i SC a S Code of Practice provides an invaluable framework for you to manage them.
Consultants and hospitals should not be responding to complaints independently of each other; instead they need to work in partnership and respond in a joined-up fashion.
Disa Young (right) is senior adviser at ISCAS


www.medbc.co.uk
• Bad debts of less than 0.5%
Come and join the hundreds of other consultants who use MBC and experience the following benefits:
• Increase in net income by up to 25%
• Bad debts of less than 0.5%
• Increase in net income by up to 25%
• Freedom for the consultant and secretary to focus on the medical side of the practice
• Having a service tailored to your needs with your own Account Manager
• Having a service tailored to your needs with your own Account Manager
• Our fees are only charged on the money that we collect for the practice and NOT on what we invoice which means we share the same objectives
• 24/7 online access to both your financial and practice management data
• Freedom for the consultant and secretary to focus on the medical side of the practice
• 24/7 online access to both and practice management data
• Our fees are only charged on the money that we collect for the practice and NOT on what we invoice which means we


DO yOU FIND OUR PROFITS FOCUS SeRIeS USeFUL?
Please let us know if it helps you or not. and if it doesn’t, what other data would you like to see presented?
email robin@ip-today.co.uk
Finances
are ticking over nicely for cardiologists featured in our unique benchmarking series, reports Ray Stanbridge. Additional material from Martin Murray
Consultant Cardiologists overall have some good news: they have continued to do well. our figures show average gross earnings have risen by about 2.9% between 2012 and 2013, from £138,000 to £142,000. inevitably costs have gone up –by 4% from £49,000 to £51,000. a s a result, taxable profits have increased by 2.2% from £89,000 to £91,000. so why has income increased? s ome cardiologists have mentioned increased patient (and gP) awareness of potential heart problems, and an increased interest in lifestyle/heart management.
other consultants, particularly out of london, have reported an increase in Choose and Book work, paid as self-employed.
What we are also hearing is that cardiologists are having to work harder for the same incomes. Paradoxically, this could be one effect of the cut in fees from insurers from about april 2012, following introduction of the Bupa open referral system and similar schemes. l ooking at costs, we see that there has been movement in several areas.
Firstly, staff costs and the con-
tributions for their pensions have shown some increase. a gain, as previously reported, this figure is influenced by the rise in the personal allowance for employees.
s ome family employee members are also receiving business pensions, particularly when the consultant is approaching his or her pension pot limit under the legislation. Following the July Budget, this trend is likely to continue further.
Consulting room hire costs have shown some increase. these figures pre-date the Competition and Markets authority rulings – effective from april 2015 – and we will
expect to see some steep rises in consulting room costs in future. there seems to have been some slowdown in the rate of growth of professional indemnity insurance premiums.
a relatively small number of cardiologists seem to have embraced the non-traditional insurers. other colleges, such as surgeons, have been much keener to review alternative providers. Bad debts/professional fees seem to have shown a slight decline on average, for reasons which are not immediately obvious. Finally, we would comment

Year ending 5 April. Figures rounded to nearest £1,000 (percentage is also rounded up)
Source: Stanbridge Associates Ltd. Additional information: Sandison Easson and Co
Patient First is the UK’s largest patient safety conference and exhibition supporting those looking for solutions to prevent harm and improve care.
n Extensive case study-driven seminar content, delivered by an expert faculty of speakers
n Learn how to improve patient safety standards and quality
n Practical solutions & best practise from industry leaders and organisations
n Choose from over 40 hours of CPD within six conference streams
n Get advice from over 100 product & service providers







that ‘other costs’ continue to remain at a fairly high level.
Cardiologists, as with other consultant colleagues, are continuing to invest in marketing, promotion and, in some cases, Pr
What of the future? in october 2014, we commented: ‘looking at more recent figures, it does seem that cardiologists have continued to do reasonably well.’
We have no reason, a year on, to change this assessment. We are glad to say prospects look reasonable for all cardiologists in private practice.
a s we said in Independent Practitioner Today in october 2014, our survey is not statistically significant but it is a representative
selection of income and expenditure incurred by cardiologists working around the country. as with other many specialties, it is increasingly difficult to come up with an ‘average’ consultant in this specialty due to the variability of what they do.
Earnings comparisons also become more complex due to the formation of groups and the take up of incorporation.
increase in NHs work
We are also increasingly seeing some cardiology consultants focus on Choose and Book work and taking extra nHs sessions rather than private practice.
i n some cases, their private practice income actually falls, with a rise in nHs income, even though they are undertaking similar work levels.
We have tried to make some compensatory adjustments to obtain reasonable trends. However, this is more difficult and we fear that market structure changes will, in the end, make comparisons almost meaningless. But we shall see.
our definition for consultants in the survey remains as in previous years. the survey is restricted to those consultant cardiologists who are not in full-time practice. they will:
Have had at least five years’ private practice experience;
Have held either a maximum part-time or a ‘new’ consultant contract in the nHs;
Be seriously interested in private practice as a business;
Be earning at least £5,000 in the private sector including Choose and Book work not paid through PaYE;
May or may not have incorporated or be a member of a group.
Next issue: orthopaedic surgeons
Ray Stanbridge runs an accountancy, finance and tax advisory service specialising in the medical profession. Martin Murray is a partner at Sandison Easson and Co, specialist medical accountants
years ending 5 april Source: Stanbridge Associates Ltd
Make sure you don’t miss our next issue, published on 26 November. Only subscribers to the journal are guaranteed to receive every copy and we don’t think anybody who is serious about continuing private practice in the future, when there is so much happening that will affect them, can afford to miss any issue.
Coming up next month:
When relationships between doctors break down. Plastic surgeon and Medical Women’s Federation honorary secretary Ms Beryl De Souza (right) writes about professionalism in medicine, particularly when doctors get into conflict with their colleagues.
Filing a tax return is one of the most hated jobs for private doctors. accountant’s Clinic presents some tips for speeding up the process

How to create a compelling patient experience and watch your profits grow overnight. Pam Underdown continues her ‘Breaking Into The aesthetics Business’ series and shows how to review the business from a patient’s perspective to ensure constant improvement
as more and more patients take to covert recording, MDDUS medical adviser Dr Mary Peddie reports that, surprisingly, the law offers you little or no protection
Dr Beverley Ward, MDU medico-legal adviser, looks at business dilemmas you might face when dealing with patients’ relatives
Independent practitioners should think again about using their NHS secretary, claims surgeon Dev Lall
eDITORIaL INqUIRIeS
Mental health and doctors: where can doctors turn for help? Dr Pallavi Bradshaw, senior medico-legal adviser at the Medical Protection Society, examines the issues
Improving the patient experience and your business at the same time. What a big doctors’ clinic learned from sending staff to a hotel
So a patient is complaining about your fees? Disa young, of the Independent Sector Complaints adjudication Service, has some advice to help prevent hassles
Inter-generational planning – Cavendish Medical sets out how to make the most of the financial assets of the whole family
Our ‘Doctor on the Road’ columnist Dr Tony Rimmer got his hands on a McLaren 650S. We’ve not seen him since…
For doctors starting a private practice, Ian Tongue gives a recap on the taxation of pensions
Smile please! Tingy Simoes hopes you will learn from the past mistakes of Doctors in the (Broadcasting) House
The threat in a letter of claim. a top lawyer describes how the increasingly complex world of indemnity insurance contains ‘problems that may threaten the stability of many practitioners’ state of mind’
aDveRTISeRS: The deadline for booking advertising for our November issue falls on 30 October
Robin Stride, editorial director
Email: robin@ip-today.co.uk Tel: 07909 997340
aDveRTISINg INqUIRIeS
Margaret Floate, advertising manager
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution.
Printed by Pepper Communications Ltd
Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
© The Independent Practitioner Ltd 2015
Registered office: 7 Lindum Terrace, Lincoln LN2 5RP
Write to
PO Box 198, Cranleigh GU6 9BB
Email: margifloate@btinternet.com Tel: 01483 824094
Publisher Gillian Nineham Tel: 07767 353897.
Email: gill@ip-today.co.uk
SUBSCRIPTIONS
£85 independent practitioners.
£85 GPs and practice managers (private & NHS). £200 organisations. But if you pay by direct debit, individuals pay only £70, and organisations £175. Call Proact Ltd on 01752 312140 Email: lisa@marketingcentre.co.uk

Robin Stride, editorial director @robinstride

To guarantee your copy of Independent Practitioner Today by taking out a subscription (at the rates shown on the left), phone 01752 312140 or send off a subscription form on page 24 or email lisa@marketingcentre.co.uk or go to the ‘about’ page of our website www.independent-practitioner-today.co.uk
If you pay by direct debit, individuals pay only £70 for a subscription. Just fill in the form on page 24 and send it to the Freepost address shown at the bottom of the form.
BaCk ISSUeS: £12.50 including post & packaging CHaNgINg aDDReSS OR
DeTaILS?
Phone 01752 312140 or email lisa@marketingcentre.co.uk