The business journal for doctors in private practice
In this issue
Be extra careful using social media
Social media is a great tool to promote your practice, but you need to follow some rules P22
Selling this city’s expertise London’s leading private healthcare providers have united to champion it to international patients P24
Don’t sit back and wait for patients
Reflections on the UK’s self-pay prospects from the author of LaingBuisson’s latest market report. n Page 18
Understand what patients want
A medico-legal adviser shows what to do if a patient is dissatisfied with their consultation P34
Private docs’ view of CQC:
Outstanding Good Requires Inadequate improvement
By Robin Stride
New and seasoned independent doctors are counting the cost of being stuck on a costly waiting list to get the official nod to set up and grow their private practices.
Problems with the Care Quality Commission (CQC) have led to a stream of complaints brought to the attention of the Independent Doctors Federation (IDF) which has pledged a desire to work with the inspectorate to fix problems.
According to the independent CQC adviser to the doctors’ body, many are asking why the watchdog has not invested time and money spent on its new Single Assessment Framework (SAF) and portal into reducing ‘an ever-growing waiting time’ for decisions on applications from those starting up and others changing location or expanded regulated activities.
Reporting in the IDF News journal this summer, Martha Walker said: ‘Currently there is around a 28-30 week waiting time for submission of applications to obtaining a decision.
‘Understandably, this is causing
Our sponsors
considerable frustration amongst members, as it is paralysing their ability to start and expand their practices.’
She appealed for affected members to contact the group’s regulation committee, which she said had a healthy working relationship with the CQC, so it could explore solutions to reducing the ‘unacceptable waiting period’.
The IDF welcomed a ‘clear and honest’ statement issued by the CQC’s interim chief executive Kate Terroni about ‘the current state of disarray the regulator is in’ that culminated in the departure this summer of its chief executive Ian Trenholm.
Regulation committee chair Dr Laila Kaikavoosi said most IDF members were affected by at least one of three areas of concern Ms Terroni spoke about.
She told Independent Practitioner Today : ‘Accessing the new portal has proved very problematic for many members, especially for colleagues who are registering new clinics, adding services to their existing clinics, or relocating.
‘A waiting time of 30 weeks for processing an application is unacceptable and can cause significant disruption and distress to service providers.
‘The priority of our members is to provide excellence in patient care. Therefore, it is important that the regulatory process of registration and inspection does not take away the clinician’s attention from their main role as a provider of excellent care.’
IDF chief executive officer Ken Mackness added: ‘The IDF understands the problems the CQC are encountering and welcomes the opportunity to work with them in any way to resolve the issues to meet the demands of an ever-growing group of private patients.’
The IDF hosts an event on 19 November welcoming CQC representatives to talk openly and honestly to IDF members.
It will be held at the Royal College of Nursing’s HQ near Harley Street and will delve into the CQC’s new regulatory approach, including the SAF launched in November 2023.
Dr Tim Ballard, its national professional adviser for primary medical services and integrated care, and Dr Janet Ortega, deputy director of primary and community care, are due to participate and face a Q&A session.
CQC interim chief executive Kate Terroni has apologised in a statement to registered providers saying: ‘We’ve got things wrong in the implementation of our new regulatory approach.
'I know that the changes we’ve delivered so far are not what we promised. It’s made things more difficult than they should be. We’re not where we want to be and we’re determined to put things right.’
She recognised ‘technical issues and challenges’ with the provider portal meant some providers had not had a good experience and many suffered registration delays.
She outlined three urgent and immediate areas of action: improving the CQC’s regulatory approach, fixing and improving the provider portal and rethinking the organisation’s ways of working.
➱ continued on page 5
TELL US YOUR NEWS.
Contact editorial director Robin Stride (right)
Email: robin@ip-today.co.uk
How to plan a new clinic building
Our Troubleshooters Sue O’Gorman and Hannah Browning give advice on how to turn your dream for a private practice clinic into reality P14
Phone: 07909 997340 @robinstride
ADVERTISE WITH US. To advertise in the digital journal, on our website or in our business and lifestyle directories, contact Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Email: andrew@spotonmedia.co.uk
Chief sub-editor: Vincent Dawe
Head of design: Jonathan Anstee
Follow Independent Practitioner Today on
Get the best out of your virtual PA
Teaming with ideas
David Hare explains the new toolkit on multidisciplinary team working which has been developed by his Independent Healthcare Providers Network P27
Care-givers need help in their jobs
We need to reframe how we think about support for carers, argues Bupa’s Dr Tim Woodman, as younger people increasingly step into this role P30
Effective collaboration between healthcare professionals and your virtual secretarial team is vital. Stacey Burrows gives some more tips P16 NEWS
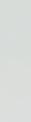
Doctors’ data to be issued by default
The Private Healthcare Information Network is changing the way doctors are required to publish their data in order to inform patient choice P36
Should I outsource my billing?
Efficient management of medical billing is crucial for the financial health and operational efficiency of practices. Derek Kelly of Medserv shows how P38
Business Dilemmas: Treating a patient with anorexia
The MDU’s Dr Kathy Leask advises a private GP anxious about treating a patient with an eating disorder P44
Start a private practice:
Understanding your accounts
Accountant Alec James gives a back-to-basics lesson on making accounts clearer to the new private doctor P46
Doctor on the Road:
New MINI remains great fun to drive
Dr Tony Rimmer found the whole revised MINI range has something to offer every medic P48 www.independent-practitioner-today.co.uk
Ditch the emotion when you invest
All investors are tempted to act on irrational impulses. But Guy Beck of Cavendish Medical reveals the evidence that we should do otherwise P40
Fall-out of failure to protect data
New Data Protection Fining Guidance has been published. Solicitor Philippa Doyle explains what this means for independent healthcare providers P42
Doctors face threat of tax trap after pay rise
Salary increase could push doctors into high taxation rates
By Edie Bourne
Some independent practitioners who work as NHS doctors will be hit by various tax traps following the 6% pay rise declared at the end of July.
The new Government announced it would accept the recommendations of the independent Doctors’ and Dentists’ Review Body (DDRB), which had recommended the increase to salaries, backdated to April.
But the pay rise could mean some doctors falling into an effective 60% income tax rate, according to specialist financial planners Cavendish Medical.
This is because those earning between £100,000 and £125,140 suffer from an increased rate of tax due to an anomaly in the tax sys-
tems of England, Wales and Northern Ireland.
Guy Beck, senior financial planner with Cavendish Medical, told Independent Practitioner Today : ‘Although the additional rate of income tax of 45% applies to earnings above £125,140, those with salaries just behind this level can pay 60%.
‘This is because for every £2 that you earn above £100,000, you lose £1 of your £12,570 personal allowance.
‘At the same time, senior doctors with earnings above £260,000 could be hit by the tapered annual allowance which limits the amount of tax-free growth on their pension to £60,000 a year. This is not an easy calculation, as the sums depend on pension growth rather than contributions.
‘So, along with the obvious positives of receiving a pay rise, we have to consider the implications that any increase in salary can push doctors into less-than-ideal tax positions.
‘Experts have warned that doctors may once again feel they need
to reduce hours or overtime, as we saw when the tapered allowance was at its most punitive a few years ago.’
Mr Beck continued: ‘We have an interesting couple of months ahead as we await the first fiscal measures, and the first Budgetary announcement, of the new Government.
‘It may be that the rates of income tax and/or pensions taxation could be amended in the future, but, for now, doctors must consider the tax they might be paying on their hard-earned income.’
He said any doctors with queries about the pay rise, the impact on their finances or their wider financial plan should speak to advisers who completely understood their NHS salary and pension details.
Doctors cut NHS commitment due to stress
Doctors are not just reducing their NHS commitments to take up private practice – there is an increasing trend to step back to ease workload and capacity pressures.
Years of worsening levels of satisfaction plus burnout are leading doctors to ‘take matters into their own hands’ to improve their wellbeing and reduce potential risk to patient care, according to a GMC report.
Its latest annual report into doctors’ workplace experiences found that higher proportions of medics are reducing their hours (19% in 2023 and 18% in 2022, compared with 8% in 2021) and declining to take on additional work – 41% in 2023 and 42% in 2022, compared with 23% in 2021.
Now the regulator is calling for urgent solutions and warning that, if the trend continues unad-
dressed, the capacity of already stretched health services could be reduced even more, putting patients at risk.
One-in-three doctors were found to be ‘struggling’, meaning they were regularly working beyond their rostered hours and feeling unable to cope with their workload.
Nearly a quarter of doctors (23%) took a leave of absence due to stress in the previous year, consistent with 2022 (22%), but up from 17% in 2021.
The Council said concerning patterns are seen across all groups, with 48% of GPs struggling and consistently having worse experiences than others since the report began in 2019.
Doctors with disabilities also continue to report worse experiences, being more likely to be dis-
satisfied in their work (44% vs 38%) and consider retiring early (13% vs 7%).
GMC chief executive Charlie Massey said: ‘We must be clear that doctors protecting their wellbeing is essential, but they shouldn’t feel their only option is to reduce their working hours.
‘This presents challenges in capacity planning, adding further pressure to services that are already stretched.’
The regulator wants employers to do more to support doctors now, while longer-term solutions are developed by workforce planners to improve conditions.
Its report says employers should focus on developing more compassionate leadership, create more supportive and inclusive environments, demonstrate doctors and other healthcare professionals are properly valued, and ensure doctors feel empowered and listened to.
See www.gmc-uk.org/about/ what-we-do-and-why/data-andresearch/the-state-of-medicaleducation-and-practice-in-theuk
Support for doctors, page 5
Guy Beck of Cavendish Medical
Nuffield brings in warning system
By a staff reporter
The UK’s largest healthcare charity, Nuffield Health, is implementing a standardised national paediatric early-warning system in its hospitals to help clinicians spot and treat a deteriorating child patient quickly and act on concerns.
NHS England announced last November that its hospitals were rolling out a new early warning system for doctors and nurses treating children to quickly identify deterioration, escalate care and act on parental concerns.
The system, called the National Paediatric Early Warning System (PEWS), is a collaboration between NHS England, The Royal College of Paediatrics and Child Health and The Royal College of Nursing.
It allows doctors to track possible deterioration in a child’s condition on a chart, measuring blood pressure, heart rate, oxygen levels and levels of consciousness, with different scores representing the level of concern.
A FIRST FOR A PRIVATE HOSPITAL GROUP
Nuffield Health believes it is the first independent hospital group to standardise a national paediatric early-warning system across its hospitals.
The National Paediatric Early Warning System (PEWS), which is also being implemented across NHS hospitals in England, tracks for vital signs such as blood pressure, heart rate and oxygen levels.
If there are concerns that the child is sicker than the tracker chart suggests, care will be rapidly escalated – for example, if the child has sepsis.
Patient safety commissioner Dr Henrietta Hughes recommended ‘Martha’s rule’ is implemented across hospitals in England after Martha Mills, aged 13, died in 2021 following failure in treating her sepsis in an NHS hospital.
Thirty of Nuffield Health’s 37 hospitals see children and young people with a variety of conditions.
The operator said while these already had paediatric early-warning systems in place, this change would provide a single, national standardised process for patients, families and staff to have a clear way of ensuring issues are detected and escalated rapidly.
Ophthalmic services provider
Optegra has opened a new clinic in Hounslow dedicated to NHS cataract surgery for patients in west London and surrounding area.
Optegra Eye Clinic West London is part the company’s network of specialist eye hospitals and clinics across the UK and Europe providing cataract and vision correction
procedures. Consultant surgeon Mr Nick Glover will be leading cataract surgery at the venue, supported by clinic manager Nikki Kaur and optometrist Amardeep Bans.
The new clinic, opened by Hounslow mayor Cllr Karen Smith –pictured being tested – is committed to treatment within four-six weeks of referral.
healthcare systems and ensuring our early warning systems are consistent with the new national rollout in the NHS will positively impact the care journey of our younger patients, their families and our clinical teams.’
Clinical services director Alison McCourt said: ‘We owe our younger patients and their families the highest standards of quality and safety. If a parent or carer raises a concern that their child is getting ill or sicker than the score shows, this will immediately escalate the child’s care regardless of other clinical observations.
‘Nuffield Health hospitals are key parts of local connected
Experienced non-execs appointed at Genesis
Private cancer care provider
GenesisCare UK has appointed the former chief executive of BMI Healthcare, the UK’s largest private hospital provider between 2011 and 2014, as one of two new non-executive directors on its UK board.
Stephen Collier, chair of national community services provider HCRG Care Group, is chairing its quality assurance committee.
He is joined by David Young, formerly Global chief executive at
Jamie Crew, Nuffield’s national lead for children and young people, said: ‘This is an important turning point in child health within the independent sector, mirroring the approach in the NHS.
‘We believe we are the first independent provider to implement this standardised change. It provides improved working methods and safety, supporting doctors and nurses to do the very best for the children and young people in their care.’
GenesisCare, who led the global restructuring of the business between 2023 and 2024.
Genesis boss Justin Hely said: ‘Their combined strategic and sector-based experience will be invaluable as we continue to focus on growing our network and delivering the highest possible standards of care to patients with a suspected or confirmed cancer diagnosis.’
Alison McCourt, Nuffield Health’s clinical services director
Stephen Collier and David Young
Patients retain dim view of NHS waits
Results of the latest annual survey of NHS hospital inpatients are largely unchanged since 2022 but remain significantly worse than before the pandemic, according to a new report from the national healthcare watchdog.
The Care Quality Commission (CQC) study – which excluded the health service’s private patient units (PPUs) – highlighted continued frustration with waiting times and an increase in the number who felt their health deteriorated while waiting for elective care admissions.
Nicola Wise, the watchdog’s director of secondary and specialist healthcare, called it ‘disappointing’ not to have seen more improvement in patient experience since the last survey.
‘Overall, satisfaction rates remain far lower than they were pre-Covid, with delays in accessing care and poorly co-ordinated discharge from hospital, both real factors impacting on the quality of people’s hospital stay.
‘It’s also concerning that we’ve seen an increase in the number of people who feel their health deteriorated while they waited for elective care – further evidence that
DOCTORS AND NURSES SCORE HIGHLY
Most respondents remained positive about their interactions with doctors and nurses – as has been the case in previous years.
75% said they ‘always’ felt included by doctors in conversations about their care – up from 74% in 2022
82% felt they were ‘always’ treated with dignity and respect by hospital staff – unchanged from 2022
78% said they were given the right amount of information about their care and treatment
90% felt they were able to talk to hospital staff about their worries and fears – 59% ‘always’ and 31% ‘sometimes’.
51% gave a score of nine or higher out of ten for their overall patient experience.
the current imbalance between patient demand and treatment capacity is putting people at risk.’
The 2023 adult inpatient survey captures the views and experience of over 63,500 people who stayed in one of 131 acute and specialist NHS trusts in England for at least one night during November last year.
Carried out annually since 2002, the survey asked patients for their opinions on the care they received. This included quality of information and communication with staff, whether they were given enough privacy, the amount of
support given to help them eat and drink, and on their discharge arrangements.
42% of respondents who were in hospital for elective care in 2023 said they would have liked to have been admitted sooner – compared to 39% who said this in 2022.
43% said their health deteriorated while waiting to be admitted – up from 41% in 2022.
Of those who reported a decline in their condition, 25% said it got ‘a bit worse’ and 18% said it got ‘much worse’.
The CQC said: ‘People’s experience of being discharged from hos-
IHPN REACTION
Reacting to the report, the Independent Healthcare Providers Network (IHPN) said it would encourage anyone seeking rapid access to highquality healthcare to consider private healthcare.
It is suggesting three avenues: using private medical insurance schemes, self-pay options and exploring the possibilities of choosing a private provider to deliver their NHS-funded care.
Chief executive David Hare told Independent Practitioner
Today: ‘The CQC’s latest inpatient survey demonstrates yet again that NHS patients are waiting far too long to get the care they need to live productive and fulfilling lives.’
pital also remained poor. Only 33% of respondents said they were involved ‘a great deal’ in decisions about their discharge – a notable drop from the 37% who said this in 2022.
‘Less than half (44%) said they “definitely” knew what would happen next in their care after leaving hospital (down from 45% in 2022) and fewer people said that staff discussed the need for further support from health and social care services with them before they were discharged (77% in 2023 compared to 79% in 2022 and 81% in 2020).’
Private providers ready to fix CQC’s faults
Private healthcare providers aim to be at the forefront of discussions about improving the sector’s experiences with the Care Quality Commission (CQC).
Dawn Hodgkins, director of regulation at the Independent Health care Providers Network (IHPN), said a strong commission was vital to provide patients and the health system as a whole with an independent assessment of services.
She told Independent Practitioner Today: ‘We are committed to work-
Dawn Hodgkins of the IHPN
ing closely with the CQC’s new leadership to ensure it is fit for purpose, both in terms of “getting the basics right” around ensuring
swift registration of much needed new health and care provision and timely inspections of services – as well as developing new and more innovative ways of assessing health and care services.’
NHS providers will also be working with the CQC to restore confidence in the future regulation of services following an interim report on the regulator’s failings by Dr Penny Dash, chair of the North-West London Integrated Care Board.
NHS Confederation chief executive Matthew Taylor said: ‘Health
leaders recognise that there have been a number of failings, already acknowledged by the interim Care Quality Commission chief executive, in rolling out the new regulatory assessment regime and they and the teams they manage often report feeling overloaded and dissatisfied with the state of the present model of regulation.
‘NHS leaders frequently say they feel the current system is out of step with the parameters in which they are operating and doesn’t recognise the full extent of the pressures they are working under.’
Promote yourself to win self-payers
By Olive Carterton
Individual consultants, groups, chambers and clinics offering a range of services are being advised to take a proactive approach to developing the self-pay side of the business.
Self-pay expert Liz Heath warns that while promotion to GPs by consultants, clinics and larger providers is still important, the developing digital world means engaging with potential patients and referrers now requires a more refined approach.
She says: ‘Simply having a website that is updated occasionally is not sufficient. All recent research suggests a heavy bias towards seeking online information for all forms of healthcare, so visibility and proactive presence online is becoming increasingly important.’
Patients have told researchers that consultants should invest in their ‘shop windows’, including participation in legally-mandated processes such as the Private Healthcare Information Network (PHIN), and provide information
Liz Heath of LaingBuisson
that adds a human touch to their clinical information.
She advises readers in this issue of Independent Practitioner Today : ‘It is often the human touch and ensuring that language used is patient-friendly that can make the difference.
‘The difference between simply providing information and genuinely seeking to engage with potential patients is subtle but very important.’
Ms Heath, author of market analyst LaingBuisson’s latest self-pay report, quotes a survey by the company showing a significant proportion of marketing and promotional spend in the private healthcare sector is now being committed to self-pay.
This acknowledges that ‘engaging with consumers and potential patients proactively around selfpay is increasingly important’.
Turning to the outlook for self-
pay, she says the general feeling is that self-pay growth in percentage terms will be in the low to midsingle digits for the remainder of 2024 and into next year.
But she adds: ‘This does not mean that for individual consultants and some providers the bubble has burst – indeed we know that there are pockets of high selfpay growth with continuing demand for services across the board.’
LaingBuisson’s research found that no provider expected the market overall would fall in the next three years. Thirty per cent believe it will grow by more than 10%, 30% by 5-10%, 10% by up to 5% and 30% felt it would remain static.
Optimists are advised to realise the self-pay market is ‘not immune to economic uncertainty’.
Self-pay average price increases are around 5% up on the 2022-23 average prices, suggesting providers are ‘keen to absorb some cost pressures’.
The author continues to find significant differences in guide prices, with the difference between the highest and lowest often more than 100%.
LaingBuisson Private Healthcare Self-Pay Report 6th edition is available at https://go.laingbuisson. com/selfpay6.
Reflections on the UK self-pay market – can we be optimistic about growth prospects? See page 18
Figures reveal boom in overseas patients
An 800% increase in the number of non-UK patient admissions for private medical treatment and diagnosis since 2016 has been logged by the Private Healthcare Information Network (PHIN).
There were 10,640 patients admissions reported for non-UK patient in 2023, but the biggest single year-on-year increase (144%) came between 2021 (3,305 admissions) and 2022 (8,075) when travel restrictions were eased following the Covid-19 pandemic. Private treatment accounted for 20,980 (63%) of elective admissions for non-UK patients, with NHS private patient units responsible for the remaining 12,105 (37%).
Patients from countries on the Arabian Peninsula made up 46% of private admissions for patients from outside the UK.
The most common treatments to travel for were therapeutic chemotherapy, diagnostic upper GI endoscopy, therapeutic drug therapy and therapeutic intravenous drug infusion. These are also highvolume procedures for UK patients using private healthcare.
PHIN chief executive Dr Ian Gargan said: ‘We work with the UK’s 650+ private hospitals, including NHS PPUs, and the data they submit to us appears to show that patients – especially those from the Middle East – increasingly
value the private healthcare sector in the UK. More and more are coming each year, leading to a recordbreaking number in 2023.
‘As well as ensuring these patients receive the care they need, the growing number of international patients allows private providers to maximise capacity and brings a boost to the UK economy.
‘Studies have shown a significant link between spending on healthcare and wider gross value-added benefits.
‘For those travelling for healthcare, this could include spending on hotels, restaurants and retail, for example.’
He said the ‘medical tourism
market’ commonly made people think about Brits going abroad for treatment rather than patients travelling to the UK.
But research for PHIN found 86% of respondents who had either had private treatment in the past three years – or would consider it in the next three years – had not thought of going abroad and did or would remain in the UK for diagnosis and treatment.
Cost was a major factor for twothirds of patients who had considered or travelled for treatment outside the UK.
People mostly travelled for dental treatment and Turkey was the most popular destination.
LaingBuisson’s report on self-pay
Clinic acquisition part of Bupa’s growth plans
By Douglas Shepherd
Bupa Health Services has announced a new partnership and the acquisition of specialist outpatient clinic London Medical in Marylebone High Street.
The companies say the latter’s specialist services from 96 consultants working at the centre will complement Bupa Health Services’ existing portfolio and, most importantly, create a seamless and speedy pathway for patients from diagnosis to treatment.
Dr Ralph Abraham, founder of London Medical and the awardwinning London Diabetes Centre, said: ‘We’re delighted to join Bupa Health Services. Our partnership with Bupa will create significant new opportunities for us.
‘The Bupa name is well recognised globally as a standard-bearer of high-quality care, enabling us to work with world renowned doctors and offer our patients access
PPU WATCH
Compiled by Philip Housden
NHS PPUs showing 20% growth and record private patient incomes
NHS trusts are now starting to publish their 2023-24 annual reports and accounts and although gaps remain, private patient incomes are clearly showing significant growth.
And they may be reaching a record high.
Five of the top ten central London NHS trusts have released their accounts as I write and these show a forecast revenue of £197m. This represents an average growth rate of 24% – in 2022-23 it was 23%.
The five trusts are:
to the very best specialist care. Our patients will continue to access the high-quality care they currently enjoy from London Medical.’
London Medical primarily specialises in diabetes treatment and management. As diabetes can cause a breadth of other condi -
Guy’s and St Thomas’ (17% increase);
Great Ormond Street Hospital (44%);
Chelsea and Westminster (12%);
Royal Free (24%);
Barts Health (29%).
These five trusts represented 37% of the central London total in 2022-23 and so the final figure is forecast to be £518m once accounts are published by Royal Marsden, Moorfields, Imperial College, King’s College and UCL.
Strong growth is not just in the capital
Outside London, three of the top ten earning trusts have also published their 2023-24 accounts.
These show a 20% increase, with the growth rates being similar:
Oxford University at £9m income with 22% growth;
tions, it has extended its specialist services to include endocrinology, cardiology, paediatrics, ophthalmology, sexual health and weight management, as well as provide access to private GP services.
Sarah Melia, general manager at Bupa Health Services, said: ‘London Medical’s specialist dia-
Hampshire Hospitals at £7.3m and 22% growth;
Bedfordshire Hospitals at £7m and 16% growth.
A 20% increase in income across the whole NHS PPU sector would deliver an unprecedented sum of £773m total private patient earnings.
That is up £129m from £644m in 2022-23. This would be a new record, surpassing the pre-Covid level of £675m in 2019-20.
A more detailed review of the overall NHS trust private patient performance will be featured in a future issue of Independent Practitioner Today.
Philip Housden is director of Housden Group commercial healthcare consultancy
betes services and expertise will offer customers fast access to diagnosis, treatment and support when they need it, as well as onward pathways to high-quality care at Cromwell Hospital.
‘This acquisition is part of our long-term strategy to provide more Bupa services directly to customers. We’re looking forward to expanding our specialist services into diabetes care with the London Medical team to provide more valued customers with fast and worry-free access to their healthcare needs.’
Bupa Health Services comprises 71 health clinics and the Cromwell Hospital.
This acquisition is part of its long-term strategy to provide more Bupa services directly to customers and follows Bupa Health Clinics’ successful acquisition of Blackberry Clinics in January 2024 and the Smart Clinics in December 2023, plus the current expansion of facilities at Cromwell Hospital.
Online tool helps to calculate VAT
Independent practitioners considering cosmetic, aesthetic of medico-legal work can now use a digital tool available from HMRC to find out what registering for VAT may mean for them.
The free VAT Registration Estimator has been developed after feedback from small businesses suggested an online tool would be helpful to show when their turnover could require them to register for VAT and its effect on profits.
It should take around 20 minutes to complete on first use and is accessed through GOV.UK guidance pages, rather than the Government Gateway. HMRC said it would not record the details you input.
London Medical’s premises in Marylebone and Dr Ralph Abraham (inset)
Harley St robotic pharmacy grows
By Agnes Rose
Leading private e-prescription app and delivery service Pharmacierge plans to expand its reach to benefit more independent practitioners after relocating to a cutting-edge 5,500 sq ft dispensary featuring a 30-foot multi-arm dispensing robot.
The device is the largest of its kind in the Harley Street Medical Area and will assist a UK-wide expansion to also serve more hospitals and private patient units.
Machine learning-driven robotic stock management allows staff to focus on complex tasks, enhancing efficiency and minimising medication wastage.
Backed by 85 leading private GPs and consultants across all medical specialties, the new Wimpole Street premises extend the company’s operations to 8,000 sq ft – ten times the size of its original 2015 location.
The multi-arm dispensing robot, occupying one wing of the new premises, improves efficiency and ensures rapid availability of a wide range of medications for Pharmacierge’s 4,500-plus GP and consultant users.
It said: ‘Over 90% of clinicians surveyed report that Pharmacierge ePrescribing saves their practice five to 15 minutes per prescription, reducing the need for multiple car journeys and pharmacy visits for patients.
‘Institutional benefits include centralised administration, real-
time tracking and simplified preop medication pathways.’
The project involved transforming two 18th-century Georgian properties into a streamlined clinical space, integrating cutting-edge software and pharmacy design.
This transformation aims ‘to revolutionise the private pharmacy pathway by combining advanced technology with traditional pharmacy values’. The facility includes areas dedicated to controlled, refrigerated and biological medications.
Independent Doctors Federation president Dr Phil Batty said: ‘Pharmacierge’s integration of advanced technology with trusted healthcare practices sets a new benchmark in the industry.’
Pharmacierge’s co-founders are Robert and Edward Ungar, whose father Leon was a founding member of The Royal Pharmaceutical Society. The family has a long history in London pharmacy, having also co-founded The Doctor’s Laboratory and other pharmacies in the Marylebone and Mayfair.
Pharmacierge’s new 5,500 sq ft premises were opened by Mark Kildea, chief executive of the Howard De Walden Estate (left), and Dr Phil Batty (right) and co-founders Edward (centre left) and Robert Ungar
Researchers to examine fairness of AI
fairness
by
is being
It is hoped the findings will highlight what areas need to be addressed in the design and use of AI tools and help shape future developments in the field.
Pressure group the Patients Association said the researchers
AI set to cut healthcare workforce hours by 15%
Fifteen per cent of the current healthcare workforce hours will be subject to automation by 2030, according to the latest analysis by retail investors’ website Stocklytics.com.
The growing reliance on artificial intelligence (AI) will be primarily due to the swelling patient population and a shorter pool of health specialists, it says.
Edith Reads, the site’s financial analyst, said the Covid-19 pandemic’s impact on patient volumes served as a critical wake-up call, underscoring the urgent need to modernise and upgrade the healthcare system.
‘The adoption of AI is expected to alleviate the workload on healthcare providers, potentially reducing burnout rates and improving job satisfaction,’ she said.
‘By automating mundane tasks, healthcare professionals can dedicate more time to patient care, research and specialised medical procedures, thereby enhancing the overall quality of healthcare services.’
Nearly 90% of healthcare workers, life science companies and tech vendors are said to use AI in some capacity.
AI implementation in healthcare systems can be categorised into machine learning, natural language processing, computer vision and context-aware computing.
Machine learning has taken the lead in most AI-driven solutions by integrating AI and robotics in diagnosis and treatment.
were particularly keen to hear from people suffering from multiple long-term conditions who have interacted with the healthcare service, and people from underrepresented and discriminated communities.
The analysts say: ‘The secondlargest region in the AI healthcare market – after north America – is Europe. The European market will grow at a robust rate of around 10.3% from 2023 to 2030, driven by the intense focus on R&D activities and advancements in biotechnology drug discovery, particularly in key markets like Germany and the UK.’
The
of artificial intelligence (AI) in healthcare
researched
the national institute for data science the Alan Turing Institute, Queen Mary University London, and the Turing-Roche partnership.
Inside Pharmacierge’s £10m multi-arm dispensing robot in Wimpole Street
Our Tuesday news e-alerts have been busy with some important stories during the holiday period since our last digital issue. So here and on the next two pages is a round-up for readers who may have missed out while they were away
Call for action on negligence costs
The Government is being urged by the Medical Defence Union to consult on proposals to address the rocketing cost of clinical negligence.
According to the MDU’s annual report and accounts, the current situation is ‘unsustainable’.
Last year, the defence body settled several claims where claimant costs were disproportionately high. One claimant received £1,000 but the legal costs were £30,000. Another claimant received £23,000 – and their legal costs were a whopping £140,000.
MDU chief executive Dr Matthew Lee warned that the entire clinical negligence system was ‘crying out for reform’. He said: ‘Nowhere is that more evident than in the disproportionate legal costs awarded in lowervalue clinical negligence claims. We regularly see legal costs eclipse
the amount of compensation awarded to a patient.’
Dr Lee has written to Health and Social Care Secretary Wes Streeting urging him to take action.
He said: ‘Every pound the NHS pays out in a settlement for clinical negligence is a pound less that cannot be spent on innovation and improving patient care for all.
‘We have been seeing a steady increase in claims costs and, in 2023, we paid out the highest amount in indemnity and legal costs for over ten years. The MDU paid out £99m for settled claims –up from £78m the previous year. This shows the substantial amounts involved in clinical negligence litigation and why reform is warranted.
‘That is why the MDU has been campaigning for reform for decades. The prompt introduction of fixed recoverable costs – the
amount of legal costs that the winning party can claim back from the losing party – in clinical negligence claims up to £25,000 would be a start, shortly followed by a commitment to extend that regime to claims valued up to £250,000.’
Dr Lee also called for the repeal of S2(4) of the Law Reform (Personal Injuries) Act 1948, requiring the courts to disregard the existence of the NHS when making a compensation award, and instead doing so on the basis of the cost of private care.
The defence body reported that during 2023, it closed 80% of medical claims and 59% of dental claims without a payment of damages.
Where cases proceeded to trial and concluded in 2023, the MDU’s annual report shows that 71% were successfully defended.
Dr Lee added: ‘When a clinical negligence claim arises, it can be one of the most stressful episodes of a healthcare professional’s career. The MDU supports members every step of the way, and our success rate in defending claims demonstrates this.’
Additionally, in recognition of the difficulties healthcare professionals can experience during a medico-legal event, the MDU’s annual report explains how the organisation has launched a new partnership with the independent charity: Doctors in Distress. The charity now provides MDU members with access to health and well-being services to support positive mental health.
Meeting to explore advances in patient pathways
Doctors in private practice are being invited to register for a free conference bringing together leading experts, innovators and policymakers to explore revolutionary advances in patient pathways through innovation.
Howard de Walden Estate, the major landlord for the Harley Street Medical Area, is hosting the event for its biennial Healthcare Conference 2024 at the Royal Society of Medicine on Thursday 31 October.
The conference will showcase expert panels and keynote addresses from industry leaders.
Howard de Walden Estate chief
executive Mark Kildea said: ‘We are thrilled to bring together such a distinguished group of speakers and attendees to discuss the future of healthcare.
‘This conference will demonstrate how sharing knowledge, enhanced collaboration and driving innovation can revolutionise patient pathways and healthcare delivery.’
Farhad Karim, chief operating officer of Blackstone, will discuss investment opportunities in the UK healthcare sector and Prof Dame Molly Stevens from the University of Oxford’s Institute of Biomedical Engineering will give insights into how innovation will shape the future of healthcare.
The conference is chaired by the Rt Hon Lord Kakkar, president of the Thrombosis Research Institute
and chairman of King’s Health Partners Academic Health Sciences, who will deliver opening and closing remarks, chair panels and host question and answer sessions.
Registration is now open and, with limited spaces available, the organisers said registering interest to attend is essential. The event is certified for continuing professional development points..
For more information about the Healthcare Conference 2024, including registration details and a full schedule of events, please visit www.hdwe.co.uk/healthcare-conference.
The MDU’s Dr Matthew Lee
What patients look for when choosing
By Robin Stride
New research compiled from contacts with hundreds of patients provides a unique insight into what they want to know about consultants before considering approaching them for private treatment.
Findings of the unprecedented survey commissioned by the Private Healthcare Information Network (PHIN) give specialists a useful marketing check-list to help turn potential inquiries into business.
The data collection body said feedback from focus groups and a YouGov survey, gathering opinions from over 2,000 people, showed patients do substantial research into their private healthcare.
Reporting on the results, it says: ‘For focus group participants, this was particularly about their consultants. Therefore, how consultants first present themselves to
potential patients – for example, on PHIN’s website – is critical.
‘If a patient wants to meaningfully compare several consultants before proceeding, this will require time and expense; so really exercising “choice” at this stage is
challenging, reinforcing the importance of the information available online.
‘Patients primarily want to know up-to-date information on how good a consultant is, how many procedures they’ve carried out, their outcomes and patient satisfaction ratings.’
Survey participants urged consultants to invest in their ‘shop windows’, including participation in legally mandated processes like PHIN and providing information to add a human touch to their clinical presentation.
What patients consider desirable details for consultants to include in their marketing material include:
Career history and training;
How long they have practised;
Their areas of specialisation;
Any societies they belong to;
What organisations they currently work with;
Their involvement in clinical
research and use of the latest technologies.
But patients also think it is important to see details telling them more about the consultant as a whole person, such as their out-of-work life.
PHIN’s 54-page report arising from the research – Patient priorities: research into patient confidence and choice in the UK’s private healthcare sector – advises: ‘Patients want any indications of ‘how relatable’ the consultant is, whether they are sincere and genuinely care.’
Patients said they would always prefer a consultant who cared enough to present all their relevant profile information – this was seen as a proxy for caring more generally.
PHIN said it was told multiple times that any gaps – especially the lack of a photo – ‘creates uncertainty’.
‘For reassurance, some patients seek out information on the GMC’s website to see if there are any complaints about consultants, restrictions on their practice or any suggestions of malpractice.
‘Patients also like to know that the consultants are supported by a safe working environment and can call on reliable, modern facilities and effective teams to help them in their work.’
Clients still confused by unclear fees
Efforts to improve fee information for patients seeking private healthcare have a long way to go, according to findings of major research from the Private Healthcare Information Network (PHIN).
It says participants reported a lack of clarity and completeness in how private healthcare costs are represented, particularly the full set of in-hospital fees, as well as financing options.
‘This prevents patients from making an informed choice and managing trade-offs. This was especially true for self-pay patients who felt that costs often seemed opaque, if not misleading,’ it warns.
The data body’s new publication, Patient priorities: research into patient confidence and choice in the UK’s private health-
care sector, was compiled following research among hundreds of patients.
PHIN reports: ‘The clear request from patients to hospitals was for much greater transparency about the full set of costs, and what factors might affect them, so that meaningful comparisons can be made.
‘Patients recognise that a precise figure may not be possible where there are several variables – such as having multiple health conditions – but ‘even a ballpark number would be helpful’.
PHIN chief executive Dr Ian Gargan revealed: ‘Although cost can be a barrier to using the private sector, some of our focus group participants were surprised that it was not as expensive as initially thought.
‘They wanted more guidance on base prices and factors that might affect the full cost, which could allow them to make more informed decisions weighing up the health cost against the financial cost.’
People searching for treatment also want easy-to-access information about financing, such as interest-free loans, payment plans or other options to help.
Information about safety and clinical outcomes was also welcome while patients experiencing previous problems with their care particularly wanted to know from hospitals whether special facilities, such as intensive care units, were frequently used and how well-trained their staff were in their use.
Turning to insurers, patients asked for reminders at the begin-
ning of their healthcare journeys that they should inform their GPs they had private healthcare. NHS GPs are thought to rarely ask about this unless prompted and PHIN says this information can significantly affect the direction of the process.
Insurers were also asked to provide more clarity about what procedures qualified for self-referrals and which did not; what was considered as a ‘pre-existing’ condition, plus exclusions such as any hospitals not covered by policies, or where ‘hidden costs’ might be likely.
People needing aftercare – especially chemotherapy patients in one of PHIN’s focus groups –wanted to know if insurers would still be there for them after their treatment and for how long.
Private doctors playing big role in NHS recovery
New figures show the private healthcare sector is now delivering nearly one in five of all NHS operations.
Independent providers were responsible for removing nearly three-quarters of a million people from the NHS waiting list in the first five months of 2024 alone.
Quarterly NHS data analysis from the Independent Healthcare Providers Network (IHPN) shows independent sector providers are on average delivering over 100,000 patient care episodes weekly so far this year.
This is an average rise of around one third (30,000 patients a week) since the NHS Independent Sector Weekly Activity Return (WAR) dataset began publication in 2021. In the first half of 2024, independent providers had increased NHS activity by more than 30% compared with pre-pandemic levels in 2019.
Analysis of the official NHS Referral to Treatment (RTT) figures show a steady rise in the independent sector’s role in tackling the NHS backlog over the last few years.
The IHPN reports trauma and orthopaedics and ophthalmology as the biggest contributors to the overall increase in independent sector activity since 2019.
In May 2024, trauma and orthopaedics activity was up by over one fifth (20.9%) compared with the same month in 2019, while ophthalmology, driven by a significant increase in capacity for delivering cataract replacement procedures, was up over 190% in the same period.
The providers’ body said: ‘In total, the independent sector now
delivers over one quarter (26.3%) of all NHS trauma and orthopaedics elective activity and over one fifth (23.6%) of all NHS ophthalmology activity, helping ophthalmology to be the only major specialty where median NHS waiting times are now lower than before the pandemic.
‘The most recent NHS RTT data also shows that waiting times for NHS treatment continue to be shorter in the independent sector. Patients seen by independent providers had waited an average of under 13 weeks – compared with an average of 18 weeks for those seen by NHS providers.’
All NHS planned care services delivered by the independent sector are paid at NHS prices and delivered to NHS patients free at the point of use, with 92% of independent acute hospitals rated good or outstanding by the Care Quality Commission.
Patients can cut months off NHS waits
The private healthcare sector is alerting patients in England they could cut months off their wait for care by exercising their right to choose a different provider for their NHS treatment.
New analysis from the Independent Healthcare Providers Network (IHPN) has found that, across the country, patients need to travel just 12 miles – around 25 minutes by car – to cut three months off their waiting time. In the North-west, for example, a patient waiting for treatment in a hospital with a long average waiting time for the region would only need to travel 8.5 miles to a hospital with lower waiting times and see their average waiting time go from 21 weeks down to below seven weeks – a saving of over 14 weeks.
There are also significant variations in waiting times for different patient treatments across regions:
➲ Patients waiting for trauma and orthopaedics treatment in hospitals with the longest waits in the South-west, wait on average 23 weeks, while patients waiting in the providers with the shortest, wait just over nine weeks – a disparity of 14 weeks (3.5 months).
➲ Waits for ophthalmic care in the East of England vary from over 17 weeks, down to just over three
weeks – a range of over 14 weeks.
➲ Waits for gynaecology care in the North-west vary from 23.5 weeks, down to just over 10.9 weeks – a range of over 12 weeks.
According to polling conducted by Savanta for the IHPN, almost three-quarters (73%) of the public believe they should have a right to choose where they receive their NHS treatment.
Over seven-in-ten people (71%) would be happy to travel more than 30 minutes outside of their local area to get treatment more quickly.
Only 5% of people said they would not travel outside their local area to get quicker treatment from the NHS. For patients travelling outside their area for treatment, their travel and accommodation costs can be covered by the NHS.
NHS patients can choose to receive their treatment at an independent provider and new data in the report shows that 96% of people in England live within a 30 minute drive of an independent provider, with people living in the most deprived areas of England just as likely to live near an independent provider as the general population.
IHPN chief executive David Hare said: ‘These new figures show just how much quicker patients can be treated when they are given a choice over where they receive their NHS care.
‘This “right to choose” has been in place since the last Labour government was in office, but too few people are aware that the power is in their hands when choosing a healthcare provider.’
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2014
Doctors’ fears over insurer’s fee shifts
The Federation of Independent Practitioner Organisations (FIPO) expressed ‘serious concerns’ over an AXA PPP bid to cut many consultants’ fees by around 20% and persuade more specialists to agree tie-in contracts.
Letters from the previous month to an initial batch of doctors who had no formal agreements with the insurer invited them to sign up.
More specialists were expected to be contacted in the following months with wording customised to their circumstances.
The insurer also announced a new fee schedule from 1 October 2015, which meant lower fees overall, although it said some
would rise and others would be frozen.
There would be two consultant categories recognised by the insurer:
Fee-approved (contracted);
Fee-limited (not contracted –and so subject to the new schedule).
FIPO’s deputy chairman Mr Richard Packard (right) said: ‘According to AXA PPP, the first group is being offered potentially better access to patients through a so-called “fast track” referral system.
However, if the majority of consultants sign up to AXA PPP’s fee-approved contract, this will cease to be of any added benefit, as the pool of private patients is finite.
‘Fee-limited consultants will still be able to charge at their normal rates, but reimbursement from AXA PPP will be limited, meaning patients will have to make up the shortfall.’
FIPO advised consultants to ‘be wary of engaging with insurers and losing their contract with the patient, for what may be shortterm, if any, gain.’
AXA PPP refused to say how many specialists it had agreements with or was writing to, calling this information ’commercially sensitive.’
It claimed its initiative would secure cost-effective, quality treatment for members for the foreseeable future.
Fee-approved specialists would enjoy the reassurance that their fees would be paid in full in
accordance with their contract, ‘removing any financial consideration from their relationship with their patients’.
‘Doctors Ltd’ talks are proving taxing
Specialist medical accountants are continuing talks with the taxman aimed at preserving independent practitioners’ right to incorporate their businesses.
Nearly 30 accountancy firms backed plans to form a special interest group to represent consultants’ and private GPs’ financial interests in talks with HM Revenue and Customs.
The group was set up informally after a wing of HM Revenue and Customs claimed independent practitioners were reaping unfair tax advantages by incorporating their businesses and, additionally, selling goodwill.
PMI costs are ‘a bar to growth’
Four-in-ten business leaders claimed the main barrier to offering their staff private healthcare was the expense.
But 28% would be more likely to pay for it if it was cheaper and
17% would do so if they believed it was better value, according to a survey.
Over half (55%) of the 1,081 decision-makers surveyed told the YouGov online research for Bupa that the sector lacked transparency, such as on quality.
The findings followed a call by the Competition and Markets Authority for more information on the quality and value provided by the private healthcare sector.
A Bupa boss urged everyone to play their part to demonstrate to more customers that the private healthcare sector offered good value and quality healthcare.
He said: ‘Doctors in private practice and other clinicians have a key role in driving quality and value.
‘Many medical innovations and procedures can be cost-reducing or cost-neutral, and I urge clinicians to take a lead on finding creative ways to promote efficient medical practice that maintains excellence and reasonable clinical freedom.’
Private care
set to tackle NHS queues
Consultants and private hospitals were hoping to benefit from a £250m NHS cash injection aimed at clearing the NHS backlog for knee, hip and cataract operations.
Some observers believed that independent practitioners could also benefit from self-payers because to achieve the target would mean a temporary rise in patients waiting over 18 weeks.
GROWING YOUR PRACTICE: SETTING UP A NEW CLINIC
How to plan a new clinic building
With increasing numbers of consultants considering how to turn their dreams for a private practice clinic into reality, our troubleshooters Sue O’Gorman and Hannah Browning give some warnings – and encouragement
QI am thinking about setting up a new clinic with a few consultant colleagues, but we don’t know where to start. What areas would we need to think about and how would we go about it?
AMore and more consultants are making the move to setting up their own independent clinics and facilities. The idea of practising in a way that is driven by the clinician rather than the hospital is very appealing to many. However, this is not an easy route. Setting up a healthcare facility takes huge amounts of time, effort, expertise, energy and more money than you realise.
This type of project will be allconsuming for many months, even if you have a team of expert support. Be realistic with yourself whether you have the time and bandwidth, especially if you have a busy NHS and/or private practice.
There will be points in the project when you may need to be onsite or make several decisions quickly; therefore, if your availability is limited, this could impact the delivery and could add additional cost.
Despite these warnings, consultants do set up clinics. It certainly is possible and they can be very successful.
Where to start?
Understanding the type of facility you are looking to create is a good starting point. This is particularly relevant if there are a number of consultants coming together. You all need to be on the same page with a very clear vision and end goal.
All the questions below will help you to understand the type of building you need in terms of space and layout, the potential investment for equipment, staffing requirements and the regulatory requirements with the Care Quality Commission:
What types of specialties would you like to perform?
Roughly how many consultants/clinicians will be using the facility?
What diagnostic procedures will you need access to?
Will you perform minor procedures and what types of potential equipment are needed?
Unless you have a large group of busy consultants setting up the clinic, it is unlikely that you will be able to generate enough revenue to offset the costs with your group alone
sultants with regular clinics so that they become familiar with the clinic, staff and your ways of working.
Diagnostics
Not all diagnostics need to be available on site. Most providers won’t have the budget or space for an MRI scanner, for example. You do, however, need to think about your patient pathways and where patients may be able to access the diagnostics you don’t provide.
Understanding the process for enabling consultants to join and having a robust practicing privileges process will be required
Will any surgery be performed? If so, what procedures?
If surgery is going to be on site, what sort of recovery is needed?
Will you see and treat children?
The specialties
Depending on the group of consultants, you may have a singlespecialty focus or a diversity across a range of specialties.
There is also an option that you start with fewer services with a plan to grow and develop more over time. If this is the case, do keep this in mind at the initial stages, as you will need to understand where the growth can happen within the physical location.
Having just one service line to set up will be simpler than multiple specialties and it will enable you to focus on the ultimate pathway for this patient group.
Consultants and clinicians
Understanding who will be using your facility is important. Are you just creating a clinic for the partners or will other consultants be able to see patients?
Unless you have a large group of busy consultants setting up the clinic, it is unlikely that you will be able to generate enough revenue to offset the costs with your group alone. Understanding the process for enabling consultants to join and having a robust practising privileges process will be required. There will also be a balance between having enough consultants with clinics to build revenue and not too many on your practising privileges that you are not able to safely manage your consultant body.
In an ideal world, you need con-
Are there certain diagnostics that are critical to your pathway? If the pathway becomes too disjointed, then your service may not be viable.
Diagnostics all come with their own regulatory requirements, especially if you are using radiation. Also, think about who will report the scans and the systems you will need to process and store images.
Minor ops
As healthcare progresses, there are a greater number of procedures able to be performed in a walk-inwalk-out setting. This will extend the revenue opportunities for clinics.
Look within the specialties as to what is safe and appropriate to perform in outpatients.
From a facility perspective, you will need a room with the required air changes, a sink, washable floor and walls and so on.
Surgery
If you are looking at performing surgery, this will take your venture from a clinic set-up to an acute surgical provider.
There are a number of regulations about the correct and safe set-up of a theatre and expert support should be sought to get these aspects right.
A new build will have some different requirements to an existing building, so it is important you understand what regulations are relevant to your project.
Having surgery within the facility can, however, dramatically change the revenue potential, so it is worth considering.
Children
There is demand for the provision of children’s services in private healthcare. This is due to a num-
ber of providers reducing or removing these services over the last few years.
The regulatory requirements for treating children are much more complex than adults. As a clinic, you will not receive any more money from an insurer for treating a child, but you will have higher staffing costs and risk.
If you would like to see children, you will need dedicated areas within the clinic and to recruit a paediatric nurse.
These questions are just a few to consider as part of your initial discussions; however, it is just the tip of the iceberg. Getting the right experts on board at the start of the project will help you to navigate the complexities of setting up.
If you get the foundations of your new business right, then you will ultimately save yourself time and money later on.
Sue O’Gorman is director of Medici Healthcare Consultancy. Website: www.medicihealthcareconsultancy. co.uk. Email: sue@medicihealthcareconsultancy.co.uk.
Hannah Browning is director of Beyond Excellence Healthcare Consultancy. Website: www.beyondexcellenceconsultancy.co.uk. Email: info@beyondexcellenceconsultancy. co.uk.
Sue O’Gorman & Hannah Browning
Get the best out of your virtual PA
Effective collaboration between healthcare professionals and your virtual secretarial team is vital. Stacey Burrows backs up her July-August article in Independent Practitioner Today with five more top tips
THE TRANSITION from an inhouse secretary to a virtual secretarial team can generate doubts and uncertainties, especially for healthcare professionals accustomed to physical interaction.
But virtual secretaries have proven to be invaluable allies, bringing multiple benefits by streamlining workflow and maximising outcomes in medical practices.
This collaboration between healthcare professionals and virtual secretaries can be a resounding success, especially if a strong and effective relationship is established, creating a positive experience for all.
Here are five more practical tips that healthcare professionals can implement to establish a good working dynamic with virtual secretaries, ranging from communication and roles to administrative tasks.
TIP 1: Optimise dictations for better understanding
In the world of medicine, accuracy and efficiency in recording information are fundamental pillars for quality of care, correct billing and regulatory compliance.
Virtual secretaries, as key allies in practice management, play a crucial role in this process. However, in order to optimise dictation and facilitate transcription, the collaboration of the healthcare professional is essential in aspects such as:
Pace of speech;
Avoidance of unnecessary noise in the recording;
Clear pronunciation of words. In addition, the healthcare pro-
BONUS TIP: WORK WITH A TEAM RATHER THAN AN INDIVIDUAL
For a more effective and efficient collaboration, consider working with a team of virtual secretaries instead of one individual.
This will provide you with yearround coverage, as there will always be someone available to attend to your needs.
A team can work together to handle multiple patients or calls simultaneously, which increases efficiency and reduces waiting time for your patients.
By implementing these ten strategies, healthcare professionals will be able to free up valuable time to focus on attending to their patients and providing the best possible care.
And virtual secretaries, in turn, will contribute significantly to the success of the practice by taking on administrative and support tasks efficiently and professionally.
fessional must make it clear to the virtual secretary that medical information is highly sensitive, so important issues such as where the information will be stored and how it will be protected must be discussed from the outset to ensure compliance with all General Data Protection Regulations (GDPR)
TIP 2: Define a clear system for file storage
Clarity in the storage of medical information is crucial. It is important to let the virtual secretary know the software or platform where different types of patient documents will be filed – for example registration forms, clinical letters and appointment forms.
Some doctors use Healthcode for transcripts of clinical letters, dropbox for patient registration forms and other platforms for results and reports.
It is important to keep in mind:
Store information in accordance with medical privacy and security regulations;
Ensure that the virtual secretary is fully aware of the storage system and platforms used;
Regularly review and update the
Maintaining consistent patient care and administrative support requires a well-structured plan to manage absences due to holidays, sick days or unforeseen events
storage system to ensure its efficiency;
Use secure and obscure password formats
It is also important to follow the law on GDPR and ensure all files are stored and secured with this in mind and never shared to a third party without permission – for example, the patient may give permission for a GP to be sent a clinic letter.
TIP 3: Remind the virtual secretary to prioritise prompt response to calls to improve the patient experience
Communication is paramount to patient satisfaction and the effectiveness of the entire patient journey.
To ensure calls are answered quickly and professionally, consider the following strategies:
➲ Establish a clear call handling policy: Define the expected response time for incoming calls, aiming to answer every call in three rings or less.
➲ Train your virtual secretary: Provide your virtual secretary with the knowledge and resources necessary to handle common patient queries, such as making appointments, providing general information or directing calls to the appropriate staff.
➲ Periodically review call handling performance: Monitor call handling metrics, such as average response time and call resolution rates, to identify areas for improvement and optimise patient satisfaction.
TIP 4: Ensure uninterrupted service coverage
Maintaining consistent patient care and administrative support requires a well-structured plan to manage absences due to holidays, sick days or unforeseen events.
To ensure uninterrupted coverage and minimise interruptions, a primary dedicated virtual secretary from the team can be assigned for day-to-day tasks and a secondary secretary to provide support during planned or unplanned absences.
Both primary and secondary secretaries are familiar with all aspects of the practice’s operations, allowing them to manage a wide range of tasks effectively.
Additionally, clear communication protocols should be established to transfer patient information, manage urgent matters, and maintain continuity of care during absences.
TIP 5: Take advantage of virtual secretaries to proactively manage late payments
Bad debt can significantly impact the financial health of a medical practice.
To minimise financial losses and maintain healthy cash flow, the healthcare professional should work in collaboration with the virtual secretaries to:
☛ Implement a system to identify and address potential bad debt cases early on;
☛ Provide the virtual secretary with access to relevant tools and resources, such as patient billing software and debt collection templates, to streamline the process;
☛ Regularly monitor debt collection metrics, such as collection rates and insurer payment polices, to evaluate the effectiveness of implemented strategies.
Each payor type requires its own processes in order to collect efficiently and in a timely manner.
Stacey Burrows is manager at Virtual Medsec Direct. Website: www.virtualmedsecdirect.co.uk. Email: sales@virtualmedsecdirect. co.uk
www.litfieldhouse.co.uk
ANALYSIS OF SELF-PAY MARKET
Don’t sit back and wait for patients
Reflections on the UK self-pay market – can we be optimistic about growth prospects?
Liz Heath (below), author of market analyst LaingBuisson’s latest selfpay report, shares some thoughts
WHILE THERE is a continued sense of optimism about the future of the self-pay market, we must acknowledge that it is not immune to economic uncertainty.
Improved information about all forms of private healthcare has been important in raising awareness of choice and, for some, ways to spread the cost and make it more affordable.
It is no surprise that there remains a direct correlation between the well-publicised and lengthening NHS waiting lists for elective procedures and diagnostics and inquiries around self-pay.
But other factors are at play, such as the wider economy and economic confidence at an individual level.
The
balance of these factors and the role of NHS waiting times in driving demand for private treatment has not always been easy to determine in the past and while other factors remain, access to –and maybe loss of confidence in –NHS services does now seem to be the primary driver.
Future projections
While future projections appear sound, the scale of growth is difficult to estimate, as there are constraints on the private sector’s ability to expand – primarily related to capacity, staffing and resourcing.
Innovation and efficiency are becoming important factors that are driving shorter hospital stays
and an increasing shift to ambulatory and day surgery.
Providers are optimistic about the future and assuming inflation levels begin to stabilise and fall and economic confidence begins to return, demand looks set to continue at current levels for the foreseeable future.
Consumer confidence is key to discretionary healthcare spending, whether this be for an MRI scan, a knee replacement or a facelift. Some of the key demographics for self-pay and some cosmetic surgery appear to be choosing to spend money on health and well-being if they can, despite the financial pressures on household spending.
Elective providers often view the
Providers are optimistic about the future and assuming inflation levels begin to stabilise and fall and economic confidence begins to return, demand looks set to continue at current levels for the foreseeable future
over-60s market as their core selfpay market. The continuing growth of the ‘baby boomer’ generation and, to a degree, their insulation from some of the impacts of the financial crisis, suggests a sustainable market in some of the core specialties such as orthopaedics, general surgery and ophthalmology.
Greater demand
For the first time in recent years, interest in private medical insurance has also grown markedly, suggesting there is greater demand for private healthcare overall and, for some, a desire to protect themselves in case of healthcare need and ensure rapid access to cancer treatment, for example.
The double-digit annual self-pay growth predicted some years ago was achieved but growth then stalled slightly, with high singledigit growth reported subsequently
THE PRICING CONUNDRUM
LaingBuisson analyses self-pay guide prices from across the UK. One of the challenges for the sector, and for individual consultants, is keeping prices reasonable and accessible while managing inflationary pressures and increases in the costs of healthcare delivery.
This year, LaingBuisson collected and analysed guide prices for the highest demand procedures from across the UK.
The results were interesting in that, overall, average price increases seem to have been around 5% on the 2022-23 average prices, suggesting providers are keen to absorb some cost pressures. Medical inflation has been running at around 6% over the same period.
We continue to find significant differences in guide prices with the difference between the highest and lowest often more than 100%.
We know that patients rate local access more highly than other factors and therefore it may not be an issue if a local price is much higher – the patient may not want to travel further afield, anyway.
Looking back, the double-digit annual self-pay growth predicted some years ago was achieved but growth then stalled slightly, with high single-digit growth reported subsequently.
This year, the general feeling is that self-pay growth will be in the low to mid-single digits as we look forward through the rest of 2024 and into 2025.
This does not mean that for individual consultants and some providers the bubble has burst – indeed we know that there are pockets of high self-pay growth with continuing demand for services across the board.
In LaingBuisson’s provider survey, carried out as part of the report’s research, no respondent felt the market overall would decrease in the next three years. 30% believe it will grow by more than 10%, 30% by 5-10%, 10% by up to 5% and 30% felt it would remain static.
This is quite a shift over the last 18 months but perhaps reflects a more realistic view of the shortterm market.
Additional feedback from those within the industry suggests sustainable low-to-middle singledigit growth over the next two years, which fits with the pattern of activity noted by the Private Healthcare Information Network (PHIN) and others – and still reflects higher self-pay activity than in 2019.
What about cosmetic surgery?
LaingBuisson’s self-pay report also focuses on the cosmetic surgery and hair restoration surgery markets. The latter has shown signs of expansion in recent years and a small part of the overall cosmetic surgery and self-pay market, appears reasonably robust.
An example of the differences in guide prices is well-illustrated in the table below.
SUMMARY OF GUIDE PRICES FOR HIGH-VOLUME SELF-PAY PROCEDURES AND DIAGNOSTICS
Source: LaingBuisson, June 2024
During the year, Practice Plus Group has publicised its Wellsoon self-pay offer much more widely and its prices are frequently at the lower end of the spectrum. One of its key messages is that the price promoted is the price the patient will pay, with no hidden extras or uncertainty.
This approach is certainly innovative and may provide a healthy challenge in local markets. If patients are saying they want predictable, guaranteed costs, then this type of clarity and transparency is to be welcomed.
The transparency in self-pay consultant fees and visibility via the PHIN website is a positive development that allows comparisons across the UK in a way not previously possible for both initial and follow-up consultations and for procedures.
It does not appear that there is inherent competitiveness with consultant fees, rather that there is a ‘market level’ with little variation.
The same cannot be said for demand for cosmetic surgery, which, according to the British Association of Aesthetic Plastic Surgeons (BAAPS) annual audits, has dipped after the post-Covid bounce-back.
This is at odds with the global picture, with growth seen in all the most popular cosmetic surgery procedures.
Even the non-surgical aesthetics market has seen a slight recent slow-down in the UK. Does this mean the aesthetics and cosmetic surgery market has peaked or, more likely, found its level?
It is difficult to be sure, but we do know that economic pressures can influence discretionary spend and maybe consumers are being more
cautious in their approach to treatments.
Of course, there is always a twist, and we are still seeing many patients choosing treatment abroad, primarily for cost reasons and some non-UK providers becoming more active in their patient acquisition strategies in the UK.
➱ continued on page 20
Is there evidence of consumers making different choices?
PROVIDERS WE spoke with all felt that many consumers were making conscious and informed choices in seeking private healthcare options.
We know from recent research from PHIN and earlier research from the Independent Healthcare Providers Network that this is a consistent theme but not yet fully embedded as a consumer behaviour.
What emerged very clearly from the PHIN research, however, was that information to make those choices – particularly for those new to private healthcare – can be lacking. And we must not forget that self-pay spans a vast range from a low-cost private GP appointment right through to complex and costly cancer care.
Mix and match
PHIN noted that increasingly, consumers are adopting a ‘mix and match’ approach to private healthcare and the NHS, opting to seek the best ‘fit’ for their needs at the time, whether this be consultation, diagnostics or treatment. This too is a trend LaingBuisson has identified.
Elements of choice are not just about which hospital or consultant but may also involve reassurance and certainty around pricing and ways to spread the cost of treatment.
LaingBuisson has found that different elements of the patient pathway before committing to treatment are sometimes disconnected and do not always support the patient sufficiently from first inquiry through to treatment.
Ironically, this is something the cosmetic surgery sector generally does well, so perhaps there is some learning here. The surge in selfpay demand outside of the ‘traditional’ geographic private healthcare hotspots also means that it is far less likely that patients will have existing knowledge of how to navigate the sometimes complex entry points and pathways into private healthcare.
In terms of specialties, consumers are making different choices sometimes because they feel there is no alternative. The highest demand for self-pay procedures remains in hip and knee replace-
ments and cataract surgery. However, other specialties such as general surgery and gynaecology have also seen growth.
Growth in areas such as gynaecology are also leading to younger patients seeking self-pay options as they weigh up the long NHS waits and their own well-being and lifestyle circumstances.
What can private practitioners take from this research?
AS WELL as LaingBuisson’s research, recent research from the Private Healthcare Information Network (PHIN) also provides a strong steer for practitioners. The passive approach and hoping that patients will somehow find their way to you is very much a thing of the past.
Whether it is individual consultants, groups or chambers or clinics offering a range of services, a proactive approach needs to be a strong feature in business development.
PHIN noted that not all patients have a ‘consumer mindset’ when navigating private healthcare, although there has been a clear shift over recent years.
One of the key findings from the PHIN research was around patient journeys, something LaingBuisson has also reflected on.
Patient journeys are very diverse because of their priorities and circumstances. So too their appetites for information, which can depend on their physical or emotional state, confidence in handling such information and previous experience in the private sector.
This has been described to LaingBuisson in the past as the difference between the ‘desperate and the discerning’ – the former just wanting to get treatment as quickly and affordably as possible and the latter taking time to consider options and choices.
Perhaps most importantly, as confirmed by LaingBuisson’s research, PHIN was told by
patients that ‘consultants should invest in their ‘shop windows’, including participation in legallymandated processes like PHIN, and provide information that adds a human touch to their clinical information.
It is often the human touch and ensuring that language used is patient friendly that can make the difference. The difference between simply providing information and genuinely seeking to engage with potential patients is subtle but very important.
In LaingBuisson’s own survey, it was clear that a significant proportion of marketing and promotional spend is being committed to self-pay, as shown below.
This acknowledges that engaging with consumers and potential patients proactively around selfpay is increasingly important.
The highest spend areas within marketing budgets were digital, online and social media. Promotion to GPs by consultants, clinics and larger providers is still deemed important, but our digital world means that engaging with potential patients and referrers now needs a more refined approach. Simply having a website that is updated occasionally is not sufficient. All recent research suggests a heavy bias towards seeking online information for all forms of healthcare, so visibility and proactive presence online is becoming increasingly important.
Source: LaingBuisson survey 2024
➪ For more information about the LaingBuisson Private Healthcare Self-Pay Report 6th edition, follow this link: https:// go.laingbuisson.com/selfpay6
OF MARKETING BUDGET
MEDICO-LEGAL: USING SOCIAL MEDIA TO PROMOTE YOUR PRACTICE
Be extra careful using
THERE ARE an estimated 56.2 million active users of social media in the UK.
And according to the latest Digital 2024 Report, the UK is in the top ten countries for social media use as a percentage of the population – 83% compared with 78% in France and 70% in the US.
With such a large potential audience, it makes sense for your practice to have a presence on social media platforms and many doctors also find it useful for networking or to discuss healthcare topics with colleagues.
But while social media can be a great asset to build your brand and advertise, it is not without professional risks.
Doctors are not like regular members of the online community – you can be held accountable by the GMC and other regulators for things you post, like or share, even if they do not relate directly to your practice.
So, if you want to be a social media supremo and avoid difficulties, we have some useful advice:
Keep control of your content
Take a moment to review content before posting to ensure you have not written anything that could be seen as inadvertently misleading, made claims about a service that cannot be objectively justified or omitted relevant information.
You must also ensure that you are not straying into areas outside of your expertise.
You might need to take more care about the precision of your posts than when using social media with friends or family.
The GMC’s new guidance on Using social media as a medical professional emphasises that doctors’ conduct should justify patients’ trust in you and the public’s trust in the profession.
If you are posting about medical issues, it’s important to be clear
Social media can be a great tool to promote your independent practice – provided you follow a few simple rules, says Dr Udvitha Nandasoma (right)
using social media
about your credentials and be able to substantiate and justify what you say.
If advertising your practice or promoting other services or products, the GMC says you must ‘comply with relevant law, guidance and regulatory codes including those from the Committee of Advertising Practice (CAP), the Advertising Standards Authority (ASA) and the Competition and Markets Authority’.
There are strict rules in place to regulate social media promotions from the ASA.
It needs to be made clear if any account, including but not limited to a social media influencer and/or celebrity, has been paid to promote your services.
Paid promotions must be clearly defined as such at the start of the post caption, and clearly visible on posts such as Instagram Stories, with the hashtag #AD or #Advertisement. In-platform ‘Paid promotion’ labels may be used in addition, but aren’t sufficient on their own.
Even if a post does declare it is a paid-for advert, it can still be problematic if the information is inaccurate or biased.
Using social media to promote cosmetic services can be especially problematic and you should ensure content is in line with the relevant CAP guidance as well as avoiding promotional tactics such as competitions – prohibited by the GMC – that could encourage people to make an ill-considered decision.
In addition, prescription-only medicines (POMs), including botulinum toxin, cannot be advertised directly to the general public on social media under the Human Medicines Regulations 2012. Even using hashtags like #botox could amount to promotion of a POM and might fall foul of those regulations.
Finally, if you employ someone to manage social media content
for your practice, they should have clear guidelines and policies to follow and effective supervision.
There are obvious dangers in giving someone access to your own social media accounts to post on your behalf.
Maintain confidentiality
The GMC emphasises the importance of maintaining patient confidentiality and respecting their dignity and right to privacy when using any social media, including private forums and messaging groups.
Even if you have been careful not to disclose too much, be alert to the risk that information in several different posts might be enough to identify someone –known as jigsaw identification.
Before using testimonials or images of satisfied patients on social media sites like Instagram, you need to explain what information you intend to post, where it will be posted, for what purpose and to what audience and obtain their consent.
The need for explicit patient consent, ideally in writing, applies whether or not you think they are identifiable, as set out in the GMC’s Making and using visual and audio recordings of patients
Be transparent about your interests
In its social media guidance, the GMC also says: ‘If you use social media to advertise your services, or use your professional position to promote or endorse any other services or products, you must be open and honest about any interests you have that may influence –or could be seen to influence – the recommendations you make.’
Failing to be up-front about direct and indirect financial incentives can raise serious concerns about your probity.
In Identifying and managing conflicts of interest , the GMC gives
Doctors are not like regular members of the online community – you can be held accountable by the GMC and other regulators for things you post, like or share
for nuance or banter: even if you believe your words cannot be taken seriously, others might have an entirely different view of a light-hearted post and things can escalate quickly.
Maintain professional boundaries
Having a social media profile means there is a risk of unwanted approaches from patients and others seeking personal advice or reassurance.
examples of potential conflicts and states that ‘trust can be damaged by the perception that a medical professional may be prioritising their own interests above patient care, even if the medical professional is confident their interests have no influence over the way they practise’.
A social media policy should help pre-empt problems, but if in doubt, it’s better to check with a colleague first than rely on your own assessment.
Don’t be a keyboard warrior It is not just your posts that matter, but also your comments and interactions with others on social media.
The GMC’s social media guidance states that a doctor’s communication online should meet the same standards as would apply face to face: ‘You must not use social media to abuse, discriminate against, bully, harass or deliberately target any individual or group.’
The GMC states that doctors ‘have rights to freedom of belief, privacy and expression’ on social media, but you also need to take account of ‘the possible impact on other people’s rights and interests’.
For this reason, it is important to remain measured and professional and do not allow yourself to be caught in a war of words with another poster or organisation.
Social media is not really a place
Responding would be a mistake, as this is likely to establish a duty of care that could leave you vulnerable to a clinical negligence claim or complaint and it would be difficult to justify giving medical advice to an individual without access to all the relevant information.
Worse still, the patient might be based in a different jurisdiction where you are not registered or indemnified.
More generally, we recommend that you avoid communicating with patients through personal social networking sites, adjust the privacy settings of your social media accounts and do not give out personal information.
The GMC says that patients who contact you though your private social media accounts should be directed to an appropriate healthcare setting and points to its guidance on Maintaining personal and professional boundaries
Social media is a useful channel for promoting your practice and raising awareness, but it’s much better to have a plan and think about your posts rather than attempt damage limitation after a mistake has gone viral or attracted the attention of the GMC. Contact your medical defence organisation if you need specific advice.
Dr Udvitha Nandasoma is the head of advisory services at the Medical Defence Union (MDU)
Selling this city’s expertise abroad
Healthcare London is a unique collaborative of London’s leading private healthcare providers and teaching hospitals that have come together to serve as a global gateway to exceptional healthcare expertise. Its aim is to showcase why the capital is the destination of choice for international patients seeking to advance their complex care needs. Project director Michael Barker reports
LONDON IS known for having the highest concentration of top medical and surgical specialists globally, attracting talent from all around the world.
Its reputation as a hotspot for international medical tourism is only increasing, highlighting the growing importance of access to quality healthcare for patients from overseas.
More than 100,000 individuals based abroad annually choose England’s capital as their preferred destination for medical treatments.
What makes London such a clear destination for patients from abroad seeking the best in healthcare is the wide array of specialised medical treatments available, from cancer care to specialist surgery, cardiac interventions and major trauma in world-class healthcare facilities. It is also a truly diverse and multicultural city.
But London punches way below its weight. Research from market analysts LaingBuisson showed London is 15th on global rankings – by value – well below comparative western markets. Healthcare London is a platform to make London a global hub for medical excellence.
Enhancing patient care through collaboration
Health is one of the best investments you can make. To enable many more international patients to access the quality of treatment the city has, Healthcare London brings together several leading private healthcare providers, including prominent NHS teaching hospitals with private patient units.
Our collaborative comprises world-renowned clinics and hospitals, including Chelsea and Westminster Hospital Private Care (NHS unit), Cleveland Clinic London, Cromwell Hospital, HCA Healthcare UK, King Edward VII’s Hospital, Imperial College Healthcare Private Care (NHS unit), Phoenix Hospital Group, The London Clinic, and University College London Hospitals Private Healthcare (NHS unit).
Our purpose is to provide international patients with access to world-leading healthcare models and exceptional outcomes in London.
We help patients navigate the ➱ continued on page 26
The FREE and integrated digital prescribing platform used by almost 1000 private prescribers every month
CloudRx take care of the dispensing, payment and delivery of medicines direct to your patients for more convenient access their medicines.
Prescribe within your chosen clinical system via our frictionless integration with Semble, WriteUpp, MidexPRO, eClinic, Pabau, Jelly Software, and ClinicYou. Alternatively, simply register for free and prescribe directly at www.cloudrx.co.uk. Repeat prescriptions and controlled drugs. Prescriber fees can be charged if desired. Easy access to medicines not normally stocked by most pharmacies at great prices.
“We were struggling to keep up with the admin side of the prescriptions, not to mention storage for medication to cope with a huge increase in prescriptions. CloudRx immediately took away the strain. Since our partnership we have grown by over 200% in size. We could not have done that without their support. It has allowed for seamless scalability...”
– Dr Louise Newson, Newson Health
complexities of seeking healthcare abroad by offering a single portal for exploring various treatment options, making it easier to find the most suitable hospital for their needs while promoting safe, multidisciplinary, value-based and co-ordinated care services.
Our unique approach
Healthcare London’s distinctive approach values collaboration, transparency and operational excellence. This collaborative effort allows us to leverage the collective expertise of our partner institutions, providing patients with access to a comprehensive network of healthcare services.
Delivering this approach means ensuring we have the right systems and governance in place.
Fine-tuning processes, establishing clear communication channels and implementing effective decision-making structures are essential to ensuring co-ordination and collaboration between our diverse partner organisations.
For instance, each partner has a named operational lead. All operational leads meet monthly. These regular meetings drive our operational engine, refining processes, and developing crucial tools like performance measurement platforms to assess return on investment.
One significant development has been the creation of e-qualification questionnaires, which allow us to efficiently qualify new leads and opportunities, ensuring we can target and align with the right international markets – that is, where our services are most needed and where we can make the most impact.
Understanding the needs of different countries and healthcare markets is crucial for us. Each market has its own set of regulations, cultural expectations and healthcare challenges. To better understand these needs, we have conducted thorough analyses of specific markets.
Through this process, we have gained valuable insights into how patients in these areas seek healthcare and what attracts them to London for their healthcare needs.
This has allowed us to develop detailed briefing documents and practical strategies that align with the preferences and expectations
Together with our partners, we are on a mission to make London a global hub for medical excellence, and our journey in Saudi Arabia is just the beginning of this journey
Safe zones for discussion: We have established pathways for safe discussions on collaborative matters, keeping sensitive commercial details confidential. This ensures that our partners can collaborate without compromising their competitive positions.
Support and vision for the future
of the stakeholders within our target markets.
What drives us
Healthcare London unites various healthcare providers, each with their own unique approaches and expertise. Our ambition is to enhance these individual strengths, providing a platform for collaborative work to ensure the highest quality care for patients.
To achieve this, we have implemented a robust governance structure to guide our strategic decisions and foster a culture of inclusivity, transparency and open communication.
Our steering committee, consisting of chief executivess or equivalents from each partner organisation, meets quarterly to tackle critical issues such as budgeting, market strategies and the overarching direction of the project.
Their insight and leadership are instrumental in steering Healthcare London toward its goals. My role as the project director is to work closely with the partners to generate and maintain trusting relationships within which we can progress our objectives.
Inclusivity, transparency and the creation of safe zones for discussion are at the core of our collaborative efforts.
These values have been instrumental in enabling us to bring together prominent London clinics and hospitals and create synergy and partnership among diverse healthcare providers.
Inclusivity: We have eliminated high barriers to entry, so we can create an inclusive environment where all partners feel welcome.
Transparency: Clear and open communication about our goals, processes and standards has been instrumental in building trust among our partners.
Our collaboration has been greatly supported by the Indep endent Healthcare Providers Network (IHPN), which hosts Healthcare London, and the Department for Business and Trade (DBT).
The IHPN provides an independent platform that creates a safe and productive environment for collaboration.
The DBT has, in addition, played a crucial role in guiding, facilitating, and connecting Healthcare London with relevant embassies.
This has allowed us to successfully engage with key markets like Saudi Arabia. Building on these achievements, we are now looking to extend our offering and explore opportunities for collaboration in additional markets.
Looking ahead, we plan to expand our project team to include other skills sets which are needed for achieving our objectives for the next year.
Our focus will remain on building relationships in identified markets such as Saudi Arabia, Nigeria and India.
We aim for steady growth, learning from our experiences and nurturing the valuable relationships we’ve already established.
Understanding and adapting to the needs of different countries and healthcare markets allows us to support our partners more effectively and maximise our impact on a global scale.
Success in Saudi Arabia
We were incredibly proud to launch Healthcare London at the prestigious Health Tourism Future Forum in Saudi Arabia in April 2024.
It was a fantastic opportunity for us to showcase our collaboration on the global stage for the first time.
London has always been a magnet for international patients, particularly from the Middle East. With such a clear demand in the
market, our presence in Saudi Arabia felt like a natural fit.
During the forum, we had the privilege of engaging in many meaningful discussions on how we can best support patients in the region and work collaboratively to address unmet needs. Our message was simple: we are here to complement and contribute to the local healthcare ecosystem, not to compete.
Together with our partners, we strive to support healthcare development worldwide through a range of exciting initiatives. This includes teaching and education for in-country clinical teams, arranging visits for hands-on training and providing advisory services and staff exchanges. These initiatives enable us to invest back into the global healthcare community, ensuring that the benefits of our expertise and resources extend far beyond the borders of London.
The interest and enthusiasm we saw in Saudi Arabia have set the stage for exciting opportunities and partnerships in the region and beyond.
Together with our partners, we are on a mission to make London a global hub for medical excellence, and our journey in Saudi Arabia is just the beginning of this journey.
Looking ahead
Since being established, we’ve been proud to see our collaborative grow and evolve. As we enter our next phase, we are committed to maintaining our values of trust, collaboration and transparency, expanding our team and continuing to deliver exceptional healthcare to patients worldwide.
To keep up to date with Healthcare London, you can follow us on Linked In at www. linkedin.com/company/healthcare-london/
Michael Barker (right) trained as a physiotherapist and founded healthcare strategy business Saffron Steer. He started as Healthcare London project director in late 2022 and also works as a specialist adviser to the NHS’s New Hospital Programme
Teaming with ideas
News of a new toolkit to help consultants in private practice get the most of multidisciplinary team working was featured on the front page of our previous issue. David Hare reveals more about the Independent Healthcare Providers Network (IHPN) initiative and its aim to support them in utilising all the expertise of their clinical teams in the best interests of patients. ➱ See overleaf
AS INDEPENDENT Practitioner
Today readers know well – as a clinician, you are only ever as good as your team.
And in the independent health sector, we are lucky to have some of the best healthcare professionals in the world, from surgeons to pathologists, oncologists to radiologists, nurses to physios, radiographers to occupational therapists.
But the difference between delivering good care versus great care is how all these individual parts of the puzzle work together in the best interests of patients. This is where multidisciplinary team (MDT) working comes in.
At their most basic level, MDTs are where healthcare professionals work together alongside patients to make team-based clinical decisions. The value of MDT working is well established in the medical world and for cancer care in particular it is seen as the gold standard.
With each patient, of course, being unique, MDTs offer practitioners the opportunity to:
Explore all potential treatment options;
Hear perspectives from other professionals with their own specialisms and expertise;
Discuss ideas and potential challenges;
Ultimately find the approach giving the best outcome for the patient and their own individual circumstances.
As I talk to many of my clinical colleagues in the sector, MDTs are viewed as one of the most rewarding parts of the job, providing a chance to share experiences and discuss and debate with some of the best healthcare brains.
But the failure to establish appropriate MDT working can have a hugely detrimental impact on patients. This was demonstrated in both the NHS and independent sector in the case of the jailed surgeon Ian Paterson, where the failure to hold effective MDT meetings for his patients meant his criminal actions could not be adequately challenged by his colleagues.
Sharing best practice
As part of IHPN’s ongoing programme of work to identify and share best practice around clinical governance, we have worked with
MDT meetings boost
NHS England, the Care Quality
Com mission – which looks at MDT working as part of its inspection process – royal colleges, insurers, patients’ charities and independent providers to produce a new toolkit.
This aims to help those in the private healthcare sector develop, strengthen and improve its approaches to MDTs.
This is particularly important considering the growing use of technology and the move towards virtual and hybrid MDT meetings.
The toolkit is designed to be used by clinicians in independent
providers of all types, sizes and structures, and looks to support the use of MDTs beyond cancer care to a broader range of medical settings.
It provides key principles to support providers in identifying when MDT meetings should be carried out in patients’ best interest. This is important because MDT meetings are not necessary for all patients and depend on the patient’s diagnosis and the nature and complexity of the care.
Rather than provide a list of conditions where MDTs should be considered standard practice, which
would rapidly date, our resource provides two principles for independent providers to use to evaluate when patients being treated in their organisations should have an MDT review or could potentially benefit from one.
Firstly, is an MDT required by authoritative guidance – notably from a royal college, NHS England or GIRFT, the Getting It Right First Time benchmarking programme in the NHS? And secondly, is an MDT considered to be good practice?
This is particularly in the case where there is no clear standard treatment pathway or there is a range of different treatment options, including the use of an ‘innovative’ procedure and hence an MDT would be of significant value.
Effective chairperson
Our resource also looks at what clinicians and providers should consider when setting up and running MDT meetings.
This includes the team itself and the presence of an effective MDT chair, meeting infrastructure and logistics such as whether meetings are in a physical meeting room, are virtual/hybrid meetings or asynchronous MDTs run entirely online. Robust team governance processes and ensuring there is
Staff at London’s Prostate Centre attend a
patient-centred clinical decisionmaking are also key, with the need for clinicians to ensure patients are fully aware of any MDT meetings and understand their purpose, its members and their roles.
We highlighted some best practice examples in the toolkit from across the independent sector, as well as the wider health service, to stimulate and support independent providers to strengthen their MDT governance and develop innovative new approaches.
These include exemplars around the leadership and management of MDTs. For example, MDT chairs having a standardised role/job description and access to a training scheme to help improve chairing skills where necessary – and the use of dedicated MDT co-ordinators who work closely with the MDT chairs to ensure processes run smoothly.
There are also fantastic examples of the use of asynchronous MDT
JellyPx
platforms that are available to consultants doing complex spinal surgery.
Patients are added to the electronic platform by their consultant prior to surgery, and information on demographics and relevant clinical details are uploaded.
Virtual meeting
The digital platform is available for use 24 hours a day and can be accessed at the MDT panel member’s convenience and independently of other panel members. All members of the MDT review the patient details, proposed surgery and relevant imaging.
If there is any uncertainty over the surgery that requires further discussion, a virtual MDT meeting is scheduled with the panel and the listing consultant.
The platform has been well received by consultants and is recognised as an effective use of time,
with further MDTs being developed based on these principles.
A crucial factor in the MDT meeting process is also the quality of patient engagement. We highlight examples where consultants write to patients if they are to be discussed and are notified of the MDT outcome.
If mobility concerns are raised at the MDT meeting, the physiotherapists call the patient to discuss their home and social support situation for the patient to put practical solutions in place prior to surgery to enhance their recovery.
If required, the spinal nurse calls any complex patients and/or their care-givers to instigate conversations regarding realistic expectations of surgery.
This includes discussions about preparing physically and mentally for surgery and post-op recovery, and to initiate care planning and support for discharge.
Through engagement with the
Comprehensive diary management.
patient, a collaborative approach aims to proactively set the patient up for the best chance of success and a positive outcome from their surgery.
Patients feel more confident in their medical management plan as further expert clinical opinions have been sought and given.
These are just some of the brilliant examples of how MDT working can benefit both clinicians and patients.
We hope all clinicians across the independent healthcare sector find this resource useful and that it supports them in their work to fully utilise all the expertise of their clinical teams in the best interests of patients.
David Hare (right) is the chief executive of the Independent Healthcare Providers Network (IHPN)
Automation reduces the admin of onboarding and your routine communications.
Patient data from your web site can generate actions in Jelly.
Online booking with portals for your patients and consultants.
A full range of clinical information can be collected on patients.
Integrates with SignatureRx, CloudRx for digital prescriptions, Viva Health labs, TDL for pathology, Healthcode for insurer billing, Stripe, Opayo for card payments, Zoom for telehealth, Xero for accounting.
Image library to track progress and upload images from any remote device.
Design your own specialist forms for use by patients and users.
Templated notes, documents, diagrams, auto generation of GP letters are available.
Handles complex billing requirements for self-funders, families or insured patients.
Care-givers need help in their jobs
As people are living longer, the demographic who care for family members is shifting. The latest Bupa Wellbeing Index findings reveal that increasingly younger people are stepping into this role, juggling their caring responsibilities with building a career and a life, so we need to reframe how we think about support for carers, argues Bupa’s Dr Tim Woodman (right)
MEDICAL
ADVANCES , better access to healthcare and a greater understanding of the importance of exercise and nutrition are leading to a rise in multigenerational families.
While this is a positive for many families, those caught between caring for their aging parents, elderly grandparents, siblings and their own children are feeling new pressures. They face the challenges of trying to juggle healthcare responsibilities with busy modern-day lives.
The Bupa Wellbeing Index reveals that millennials – people aged between 25 and 44 – are increasingly stepping into the role of caring for multiple generations in their families.
Millennials also represent the age group most significantly affected by care-giving responsibilities in their daily lives, facing the mounting pressures of caring at a time when they are building careers and transitioning through important life stages: growing families, buying homes and building their pensions.
This Missing Middle demographic – consisting of 6.2 million millennials – has replaced the original ‘sandwich generation’, those aged between 45 and 59, who were previously identified as primary care-givers.
Across all ages, women (38%) are more likely to look after the family than men (30%). And over a third (34%) of women who take on the role of primary care-giver feel a sense of responsibility to take care of the family’s health, compared to a quarter of men (26%).
The research identifies a number of reasons why people take on the role of caring for their family’s health.
Nearly one in five (18%) of those who become the primary caregiver say everyone else assumes they will, while almost as many (15%) say they had to step into the role because no one else in the family would take it on.
Over one in five (21%) millennials (25-44) who become the primary care-giver point to having the closest relationship to family members in need as a reason for looking after them. And overall, a greater proportion of women (26%) than men (19%) cite this as a reason.
Some people have also had to call in sick to fulfil their caring responsibilities, with an average of two sick days taken across all age groups
Types of caring support
When we think about carers, we often think about full-time caring responsibilities.
However, sometimes the most common acts of care are the smaller ones, such as regular phone calls with relatives (31%) or helping with tasks at home, such as cleaning, cooking, gardening (24%) or supporting them with regular chores such as food shopping (16%) and leisure activities (18%).
No matter how small the task may seem, every activity in caring for a family member takes time out of a person’s day when they have their own competing pressures to manage as well.
Additionally, 21% of respondents are responsible for supporting a family member with their mental health.
Overall, just 16% feel wellequipped to support family members who are struggling with their mental health. Those aged 25-34 are most confident in this regard (22%), with those over 55 least able to help (12%).
Impact on health and well-being
Our research shows that the UK is a nation of carers – 83% of those surveyed said that the health and well-being of the family is their greatest priority, 81% said over and above their own health and well-being, 48% said over their career and 68% said over their relationship with a spouse/partner. However, this responsibility isn’t without its toll on the carer. 35% of those surveyed said they had lost sleep due to anxiety or stress about a family member’s health, and this was highest
among older millennials, those aged 35 to 44 (44%).
Overall, one in seven (14%) survey respondents say that looking after their family has had a negative impact on their mental health, with millennials (19%) most likely to report mental health issues from their caregiving activities.
The weight of expectations on individuals may be a factor, with 35% feeling that they are expected to look after their family without concern for their own mental health and well-being.
This is highest among millennials (47%), who are also most likely to say they are struggling with their own mental health but have not told their family members (22%).
Worryingly, one in fourteen (7%) respondents report missing two of their own health appointments in the past year to look after a family member. Additionally, a significant number of respondents put off or delayed booking GP appointments.
Impact on personal and social lives
Millennials, in particular, report suffering with care-giving burnout, as nearly three-quarters (68%) say that looking after their family has impacted their daily life.
For example, 42% experienced loss of sleep worrying, 61% have missed out on social or leisure activities and 59% have missed out on social events with friends.
Half (50%) of millennials also say they have missed big events or life milestones, such as weddings, birthdays or holidays with friends, to look after their family members’ health. Despite this impact on their personal and social lives, many people view their responsibilities as positive.
One respondent said: ‘Caring for multiple generations has been hard, as I am a single mum, but I also do as much as possible to help my elderly grandparents. Splitting time to help both generations is hard but equally rewarding when I can make a difference.’
Impact on working life
Millennials are the backbone of the workplace and a crucial generation for the economy. But the anxiety and stress of caring for the family’s health can have a signifi-
cant effect on a person’s work-life and career.
Our research shows that a large proportion of people report that their work-life balance has been impacted by taking on responsibility for multigenerational health and wellness. Over half (51%) say that these responsibilities have impacted their working life at some stage.
Family care-givers also report missing days at work. In the past year alone, respondents have had to take an average of two days annual leave to fulfil these responsibilities, rising to almost three days in the case of 16-34 year-olds.
Some people have also had to call in sick to fulfil their caring responsibilities, with an average of two sick days taken across all age groups.
When it comes to career progression, 27% of respondents think this may have stunted their development, with more men (28%) than women (25%) believing this to be the case.
The figure is high for millennials (43%) at a time when many are looking to build prosperous careers for the future and save for retirement (30% of 44-54 year-olds and 14% of those aged over 55).
While some are finding that multigenerational health responsibilities are slowing their career progression, others are having to stop indefinitely.
One respondent commented: ‘I had to leave my job to look after my mother who has been diagnosed with a brain tumour. She needs constant supervision. My daughter suffers from anxiety and paranoia. It’s an effort to support both at the same time.
‘My relationship with my partner and social life are suffering badly. I’m just so tired.’
Any loss of talent, whether that is through sick days or losing staff permanently, has a direct impact on an organisation’s ability to grow. At Bupa, we are seeing increasing demand for family health support from employers to support those with multigenerational health responsibilities.
Impact on life at work
Caring responsibilities are also impacting life in the workplace, with one in seven (14%) care-givers
➱ continued on page 32
finding it hard to concentrate at work due to the worry of family health.
More women (16%) report this to be a problem than men (12%), while nearly one in five (18%) millennials are struggling to focus at work.
Missing out also extends to work social events, which can be key to forging good relationships with colleagues and enjoying the world of work. One in seven (14%) say they have had to miss out on work socials to care for their family, which rises to 20% for millennials.
Supporting multigenerational care-givers
Three in five of those surveyed (68%) would welcome more support when it comes to managing their care -giving responsibilities and maintaining their own wellbeing.
Overall, 58% of those employed say that having access to private healthcare for them and their family would improve their ability to do their current job.
Online health and well-being
Care-givers say that increased support from employers in the workplace would enable them to perform better in their daily work and careers
guidance is valued more highly by millennials (28%) than those aged 45-54 (20%) and 55+ (11%). When considering the benefits they would most value in looking for a new job, schemes that support care -givers in multigenerational families score highly.
Almost a third (31%) are looking for flexible working arrangements, which may help them to better balance their work-life and caring responsibilities.
Private healthcare (20%) and private medical insurance (20%)
are also important factors for people when looking for a new job.
Conclusion
The findings of this report show that the Missing Middle, those caught between caring for their aging parents, grandparents, siblings and their own children, are feeling new pressures as they miss out on more than ever before.
Millennials are increasingly stepping into this role as they age and they are feeling the impact in their daily lives, missing out on career opportunities, social activities and healthcare at a critical point in their lives.
Care-givers are spending hundreds of hours each year looking after their family’s emotional and physical needs.
While they often report that they do this because they feel responsible for these duties, they also feel that other family members should be doing more to help and that increased support from employers in the workplace would enable them to perform better in their daily work and careers.
This is important for both individuals and employers, with many care-givers reporting that they have missed out on chances for advancement and been forced to take sick days or holiday to care for family members.
As clinicians and employers, we should be cognisant that younger people are increasingly taking on this responsibility and of the impact it can have on their lives, health and well-being.
We need to make sure that this vital demographic is properly supported, whether that’s in our roles by offering remote and digital options, where clinically appropriate, to make our services more accessible or as employers offering flexible working arrangements and access to support for physical and mental health problems.
This will enable us to give the Missing Middle the support they need to fulfil their potential in the workplace and wider society.
Dr Tim Woodman is medical director for policy and cancer services at Bupa UK Insurance
*Results of 2023 Clinical Audit of Speech in Noise results C
Our Hearing Aid patients achieve an average improvement of 39% in Speech in Noise Scores, when measured pre and post hearing aid fitting!*
Diagnostic Audiology Including Paediatrics • Tinnitus Rehabilitation • Vestibular Testing • PTA & Tympanometry • Speech Audiometry • Speech In Noise Testing• Specialist Tests Including OAE, VEMP & ASSR • Ear Wax Removal • Independent Hearing Aid Provider
Sandison Easson is a firm of truly specialist medical accountants who provide personal and tailored advice to clients.
We act for medical professionals throughout all stages of their career with clients in almost every town in England, Scotland and Wales.
We cut through the complicated jargon and deliver practical, easy to understand advice. Call us
Accountants
TO LEARN MORE ABOUT US VISIT PINDROPHEARING.CO.UK
WE PROVIDE THE USUAL SERVICES YOU WOULD EXPECT FROM AN ACCOUNTANT SUCH AS PREPARATION OF YOUR ACCOUNTS AND TAX DECLARATIONS BUT OFFER SO MUCH MORE INCLUDING ADVICE ON:
• SETTING UP A NEW PRIVATE PRACTICE
• BUILDING AN EXISTING PRIVATE PRACTICE
• BUSINESS STRUCTURES TO PROTECT WEALTH
• BUSINESS STRUCTURES TO MAXIMISE TAX EFFICIENCY
• CLAIMING TAX REFUNDS INCLUDING OVERPAID ANNUAL ALLOWANCE TAX
• REMUNERATION PLANNING FOR YOU AND YOUR FAMILY
• UNDERSTAND ANNUAL ALLOWANCE TAX
• MAXIMISING LEGITIMATE EXPENSE CLAIMS
MEDICO-LEGAL: RESOLVING CONFLICT WITH PATIENTS
Understand what your patient wants
What can you do if a patient is unsatisfied with the outcome of their consultation and refuses to pay? Fin Wright discusses some steps you could take
IT CAN be frustrating for a private doctor when, after seeing a patient and writing a report detailing the consultation and your findings, the patient says this was not the outcome they hoped for and they no longer wish to pay your fee.
In some instances, their concerns may be easily remedied. For example, perhaps the history was not detailed as accurately as the patient felt it could have been. But when the patient challenges your conclusions and any diagnoses made, the way forward from here can be less obvious, even for more experienced clinicians.
In the GMC’s Good Medical Practice guidance, it emphasises the importance placed on your obligations when communicating information.
The guidance states: ‘You must be honest and trustworthy, and maintain patient confidentiality in all your professional written, verbal and digital communications. (Paragraph 88).
‘You must make sure any information you communicate as a medical professional is accurate, not false or misleading.’ (Paragraph 89)
This means you must take reasonable steps to check the information is accurate, you should not deliberately leave out relevant information or minimise or trivialise risks of harm and you should not present opinion as established fact.
Therefore, while a patient may not be happy with the outcome of a consultation, you are still dutybound to act in accordance with your obligations and to be open and honest with your conclusions.
Case study
It may be helpful to consider an example here for illustration:
Mrs A was concerned regarding their eight-year-old child and decided to approach a private consultant in child and adolescent psychiatry for a consultation to explore the child’s change in behaviour.
During the consultation, the psychiatrist spent some time exploring the child’s history and came to the diagnosis of depression and recommended that an ADHD assessment be considered.
Mrs A disagreed with the diagnosis of depression and felt the
psychiatrist should have been able to diagnose attention deficit hyperactivity disorder (ADHD) during that consultation, rather than potentially have to pay a fee for a further assessment.
She also felt time was wasted discussing the patient’s history when this could have been gleaned from reading a report they had previously submitted.
As a result, Mrs A either wanted the letter rectifying, the further assessment funded by the psychiatrist or to have the fee waived for the consultation already held.
The psychiatrist, already aware of their obligations and satisfied with the letter written, declined to alter the letter or accommodate Mrs A’s other demands.
recommendations, and answer any queries Mrs A may have.
It is helpful to follow-up meetings such as this with a written summary of what was discussed, and any conclusions drawn.
This is beneficial to ensure all parties are on the same page after the meeting, but also to demonstrate an audit trail of steps taken to remedy the situation, which would reflect well on the psychiatrist if the matter escalates.
Should Mrs A be reluctant to meet, this may well not be an option.
In line with the earlier mentioned guidance from the GMC, if the clinician feels their communications meet the thresholds outlined, then they are under no obligation to alter their letter.
C. To try and reach a shared understanding of the expectations and limitations of the available options.’
And paragraphs 18 and 19 of the guidance continues: ‘You must seek to explore your patient’s needs, values and priorities that influence their decision-making, their concerns and preferences about the options and their expectations about what treatment or care could achieve.
‘You should ask questions to encourage patients to express what matters to them, so you can identify what information about the options might influence their choice.’
What the patient wants
It is vital that a clinician establishes what it is that the patient is expecting from the consultation, what is important to them with regards to potential outcomes and to set their expectations as to how likely this may be
Feeling bullied
As a result, Mrs A sent several messages putting in a subject access request (SAR) and requesting the psychiatrist’s GMC number. The psychiatrist felt bullied by Mrs A and pressured into doing what she wanted.
In this scenario, when there is so much activity and pressure from Mrs A, it can feel overwhelming and difficult to navigate a way forward.
Putting the request for the psychiatrist’s GMC number and SAR aside – these would, of course, need to be considered and complied with – the crux of the matter is focusing on Mrs A’s dissatisfaction with the assessment received. In instances such as this, while this can be daunting, it can be worthwhile to consider offering a meeting with Mrs A.
Within this meeting, the psychiatrist could explore the concerns raised by Mrs A, explain how they came to their diagnosis and
While the fallout from the situation with Mrs A may be unpleasant and may unfortunately result in a complaint, the focus from the clinician’s point of view would need to be on conflict resolution and reflecting on the situation to ensure they are satisfied with the standard of care provided.
Set patient’s expectations
This situation is, of course, less than ideal for the clinician involved, and for the party seeking treatment.
One way to try and mitigate the risk of such a situation, and potential escalation, is for the clinician to have a candid discussion with the patient or responsible guardian before providing care to set their expectations about the possible outcome.
The GMC’s guidance on Decision-making and Consent reflects this. It says: ‘The exchange of information between doctor and patient is central to good decision making.
‘It’s during this process that you can find out what’s important to a patient, so you can identify the information they will need to make the decision.
‘The purpose of the dialogue is:
A. To help the patient understand their role in the process and their right to choose whether or not to have treatment or care.
B. To make sure the patient has the opportunity to consider relevant information that might influence their choice between the available options.
Based on this guidance, it is vital that a clinician establishes what it is that the patient is expecting from the consultation, what is important to them with regards to potential outcomes and to set their expectations as to how likely this may be.
For example, in Mrs A’s case, had the psychiatrist been aware she was seeking an ADHD diagnosis at the consultation, they could have set her expectations accordingly and explained the potential pathway from this consultation and the steps necessary to provide their child with appropriate care.
This would ideally have mitigated the risk of the subsequent behaviour from Mrs A and enabled a more positive and productive working relationship.
The psychiatrist may also wish to ensure they documented any conversation where expectations are set so there is a clear audit trail if any issues arise later.
Private practitioners can contact their medical defence organisation for medico-legal advice and support with handling a situation like the one described above.
If any assistance be needed on the financial aspect of a situation like this, then clinicians may wish to contact an organisation they belong to, such as the BMA, who may be able to assist.
Fin Wright (right) is a case manager at Medical Protection
Doctors’ data to be issued by default
The Private Healthcare Information Network (PHIN) works to support consultants and hospitals to comply with its requirements under the Private Healthcare Market Investigation Order as it looks to make the market more transparent and inform patient choice. Anne Coyne reports
PHIN IS introducing a process known as ‘presumed publication’ from the end of this month –September 2024 – in a bid to increase the amount of available data to meet its goals.
This is in line with its Strategic Roadmap and Plan agreed by the Competition and Markets Authority (CMA) and private healthcare sector in the summer of 2022.
As outlined in the plan, ‘presumed publication’ is one of the key enablers to improve the volume and accuracy of incoming data and ensure successful implementation of the Private Health Market Investigation Order. This will mark a stepchange in the information provided to patients and inform choices.
The data regarding consultants’ practice is supplied by hospitals and it is essential for that data to be accurate to reliably inform patients’ decisions about their treatment.
Since 2017, consultants have been invited to provide PHIN with information about their fees and also to engage with the data submitted by hospitals to ensure it accurately reflects their practice.
If they notice any issues, there is a process for hospitals to improve data quality.
New system
Until now, no activity data has been published on the website unless consultants have verified it. This process will be changing slightly later in the year with ‘presumed publication’.
Consultants will continue to be invited to verify data about their
practice, but activity data will be published automatically if they do not engage with the information or raise any issues with it.
They will, of course, continue to be able to remove data from publication if they find issues later.
PHIN will also continue to apply what is called Small Numbers Suppression and will not publish data where seven or fewer episodes of a procedure has been performed.
Working together
The implementation of the new process comes after collaboration with consultants’ representative bodies and private healthcare providers to ensure the right processes are in place to correct and improve the private activity data submitted.
PHIN has also been contacting consultants through various channels to inform them of the impending change.
The resulting ability to publish basic activity measures – volume and length of stay – at consultant level will lay the foundation for publication of more complex measures.
PHIN receives private data at least quarterly from hospitals. The data is refreshed on the website in April, June, September and December.
Publishing consultant activity
PHIN and stakeholders in the sector recognise the importance of being able to publish consultant activity volumes on a wholepractice basis. This remains a key component of the presumed publication process.
It acknowledges that data quality issues need to be considered and mitigated where possible and has developed tools within its portal to allow consultants to exclude erroneous data.
It is also exploring the ability for consultants to self declare their NHS activity volumes.
PHIN is also continuing to explore the utility of using Hospital Episode Statistics (HES) data to determine consultantlevel activity in the NHS.
When presumed publication is introduced – and as is currently the case – consultants who have verified their activity data (vol
ume of procedures performed and average length of stay) will continue to have this information published on PHIN’s website.
The new process means that, in addition, should a consultant not verify their data nor raise any data issues, PHIN will publish consultant data that has been submitted on the basis it is complete and accurate.
This will also help to raise compliance levels with the Order and reduce the need for the CMA to take enforcement action.
Data issues
PHIN is committed to highquality data and if a consultant raises an issue relating to the episode data that has been submitted by the private hospitals or private patient units where they work, information regarding these episodes will not be published.
Consultants may request PHIN to revoke any data published, but this will be on the basis that the specific issues regarding an episode are identified and raised using the processes available on the PHIN portal.
It is important that episode data used to calculate Order measures is accurate and that data appearing about a consultant reflects that consultant’s practice.
When presumed publication is implemented, PHIN will encourage hospitals and consultants to resolve these as quickly as possible and, exceptionally, within a 12month period.
Consultants will be notified
Consultants have the option to nominate a delegate to undertake activities on their behalf on the PHIN portal
‘PRESUMED PUBLICATION’ AT A GLANCE:
Consultants will be able to verify accurate episode data more easily
Consultants will be able to identify data issues more easily, select the episode data and provide hospitals with the information that is needed to support any investigation
All hospitals were be asked to review the data issues raised in respect of their hospitals and to update the status on the data issues report
Consultants will be able to review their data and either accept the revised changes or dispute the outcome and progress discussions with the hospital
when a query has been actioned and they have the option to accept the resolution or dispute the outcome.
Any query that has not been reviewed by a consultant or hospital within 18 months will be archived as the episode will no longer contribute toward the calculation of measures.
Nominating a delegate
Consultants have the option to nominate a delegate to undertake activities on their behalf on the portal. Consultants are responsible for any activities a delegate undertakes.
Steps to nominate a delegate:
1. Once in the portal, click on the
‘cog wheel’ at the top right of the screen (red circle in the image below).
2. Click on ‘add user’.
3. Read and accept terms of nominating a delegate.
4. Complete delegate account and click ‘save’.
Help is at hand
The PHIN Consultant Services Team will host virtual sessions to support consultants and their delegates with any questions or process issues.
Anne Coyne (right) is consultant services manager at the Private Healthcare Information Network (PHIN)
BILLING AND COLLECTION
Should I outsource my billing?
Efficient management of medical billing is crucial for the financial health and operational efficiency of practices. Derek Kelly (right) gives a guide to what you need to know
MEDICAL BILLING encompasses the entire process of submitting and following up on claims with health insurance companies to receive payment for services rendered by healthcare providers.
Five of the key elements are:
1. Patient registration and verification: Gathering accurate patient information and verifying insurance coverage prior to treatment.
2. Medical coding: Assigning specific codes to diagnoses and procedures using standard coding systems.
3. Claim submission: Transmitting claims to insurance companies or other payers.
4. Adjudication: The process by which insurance companies evaluate claims based on their policies and rules to determine coverage and payment.
5. Payment boosting and reconciliation: Recording payments received, adjusting patient accounts accordingly, and reconciling any discrepancies.
Doctors today face a host of challenges with their practices’ medical billing. These include:
Multiple payers: private practices deal with multiple insurance companies, each with different policies, coverage details and reimbursement rates. This requires meticulous tracking and management to ensure timely and accurate payments.
Regulatory compliance: Adhering to UKspecific healthcare regulations, including General Data Protection Regulations (GDPR).
Accurate coding: Ensuring accurate coding to avoid claim denials and delays, which can impact cash flow and patient care.
Detailed documentation: Thorough and accurate clinical documentation is necessary to support the codes used. Incomplete or inaccurate documentation can result in claim rejections.
High denial rates: Incorrect or incomplete information, coding errors and non compliance with payer policies can lead to high denial rates. This impacts cash flow and requires additional resources to address and resubmit claims.
Appeals process: Managing and appealing denied claims is timeconsuming and requires expertise to successfully overturn denials.
Delayed payments : Inefficient billing processes can lead to delays in payments, affecting the financial stability of the practice.
Cash flow management: Ensuring a steady cash flow is challenging when dealing with inconsistent payment timelines and outstanding patient balances.
Transparent billing: Providing clear and transparent billing information to patients is crucial to avoid confusion and disputes. Misunderstandings can lead to delays in payments and affect patient satisfaction.
Software and systems: Integrating billing software with electronic health records systems and other practice management tools is essential for seamless operations. However, choosing the right technology and ensuring proper implementation can be complex.
Data security : Protecting sensitive patient information from cyber threats and ensuring robust data security measures is a constant concern.
Training needs: Continuous training is required to keep billing staff updated with the latest coding practices, regulatory changes, and payer policies.
Staff turnover: High turnover rates can disrupt billing processes and lead to inefficiencies. Retaining experienced and welltrained staff is a challenge.
Overheads: Maintaining an inhouse billing department involves significant overhead costs, including salaries, training, technology, and infrastructure.
Outsourcing decisions: Deciding whether to outsource billing operations to specialised companies involves weighing the benefits against the costs and potential loss of control over the billing process.
Effective communication: Clear communication with patients
A multispecialty practice in Manchester reduced billingrelated administrative costs by 30% after outsourcing its billing operations regarding their billing and payment responsibilities is essential to avoid misunderstandings and dissatisfaction.
Maintaining relationships:
Balancing the need to collect payments while maintaining positive patient relationships requires tact and effective communication strategies.
Taking on a medical billing service has, however, proved highly successful with hundreds of practices. One Londonbased consultant clinic partnered with a medical billing company and improved its claim acceptance rates by as much as 25% through enhanced coding accuracy and timely claim submissions.
In another case, a multispecialty practice in Manchester reduced billing related administrative costs by 30% after outsourcing its billing operations, allowing for an increased focus on patient care and practice growth.
Effective medical billing is not just about financial transactions but also about maintaining operational efficiency and patient satisfaction.
Outsourcing medical billing to a third party company offers numerous benefits, addressing key challenges faced by private practices. By harnessing their expertise, technology and streamlined processes, practices can enhance their operational efficiency, ensure compliance, optimise revenue cycles and improve patient care.
If you are looking to alleviate your administrative burdens and enhance your practice’s financial health then it makes sense to consider the advantages of partnering with a medical billing company.
Derek Kelly is marketing manager at Medserv
TEN AREAS WHERE MEDICAL BILLING COMPANIES ADDRESS DOCTORS’ BIG CHALLENGES
1
Easing
insurance complexities
Their dedicated teams have an in-depth knowledge of private insurance systems, ensuring accurate and compliant billing practices.
They streamline the billing process by managing multiple payers and staying updated with varying insurance policies, reducing the administrative burden on your practice.
2 Regulatory compliance
Billing companies are well-versed in UK-specific healthcare regulations and the requirements of the General Data Protection Regulations, ensuring your practice remains compliant and avoids penalties. They provide continuous training to their staff, keeping them informed about the latest regulatory changes and compliance standards.
3 Coding and documentation
Billing companies employ certified coders who ensure the use of correct ICD-10 and CPT codes, reducing the risk of claim denials due to coding errors.
They work closely with your practice to ensure complete and accurate clinical documentation, supporting the codes used and improving claim approval rates.
4 Claim denials and rejections
With their expertise, billing companies can significantly reduce claim denials by ensuring accurate and complete claim submissions.
They also handle the appeals process for denied claims efficiently and increase the chances of successful appeals.
5
Revenue cycle management
Outsourcing ensures timely claim submissions and follow-ups, leading to faster reimbursements and a steadier cash flow. Professional billing services optimise the entire revenue cycle, from patient registration to final payment, enhancing overall financial performance.
6
Patient billing and collections
As well as providing clear and transparent billing information to patients, leading to less confusion and disputes, they implement effective collection strategies, including timely follow-ups and patient communication, improving the rate of successful collections.
7
Technological integration
Investment in state-of-the-art billing software and systems ensures seamless integration with electronic health records and practice management systems. They also implement robust data security measures to protect sensitive patient information, reducing the risk of data breaches.
8
Staff training and retention
Outsourcing eliminates the need for in-house training from the private practice because billing companies ensure their employees are continuously trained in the latest billing practices and regulations.
They provide a stable and experienced workforce, reducing the disruptions caused by staff turnover and ensuring consistent billing performance.
9
Cost management
Another plus is that billing companies reduce the practice’s overheads. Outsourcing lessens the need for in-house billing staff, cutting down on salaries, training and technology costs.
Cost-effective solutions are on offer, tailored to your practice’s needs to help provide high-quality services at a lower overall cost.
10
Patient communication and satisfaction
Billing companies handle patient communications about billing and payments in a professional way, ensuring clarity and reducing misunderstandings.
And by managing billing and collections effectively, they help maintain positive patient relationships, allowing your practice to focus on delivering quality care.
Ditch the emotion when you invest
Investing is not easy – particularly when all investors are tempted to act on irrational impulses. Guy Beck (right) highlights the overwhelming evidence that we should do otherwise
WHILE WE all like to think that we are capable of making rational decisions, it appears that when it comes to investing, a switch inside even the most sensible person seems to flick and rationality disappears in a cloud of emotion.
Being an investor is not easy. We have to contend not only with the erratic and unpredictable nature of markets but also the sometimes inconsistent way in which we will be tempted to think and behave.
All investors should try their best to make rational decisions and to make their head rule their heart. Yet for many, while understanding that being rational makes sense, putting it into practice can be exceedingly difficult.
Benjamin Graham, one of the great investment minds of the 20th century, famously stated:
‘The investor’s chief problem – and even his worst enemy – is likely to be himself.’
Irrational investing manifests itself in many different ways:
Chopping and changing one’s investment plan influenced by what has just happened to the markets;
Trading shares in an online brokerage account;
Trying to pick market turning points; for example, when to be in or out of different markets
Being tempted into buying flavour-of-the-month investment ideas or chasing fund performance.
The list of irrational decisionmaking opportunities is long and undistinguished.
John Bogle summed this up perfectly in an address to the Investment Analysts Society of Chicago (2003): ‘If I have learned anything in my 52 years in this marvellous field, it is that, for a given individual or institution, the emotions of investing have destroyed far more potential investment returns than the economics of investing have ever dreamed of destroying.’
The ‘emotional cost’ of investing can, at times, be extremely large. By emotional costs, we mean the impact on returns that are caused by our own actions or inactions –our behaviour – rather than the markets.
People’s temptation to try to get in – or out – at the right time is huge. Imagine if you could have avoided the 50% market fall during the global financial crisis of
By and large, investors have a woeful track record of timing when best to jump in and out of markets
2007-08, or the blink-and-youhave-missed-it Covid crash in early 2020 and bought in again at the bottom.
By and large, investors have a woeful track record of timing when best to jump in and out of markets. It is worth remembering that you have to get two decisions right when market timing. The first is when to get out. The second is when to get back in again. The problem is that markets
work pretty efficiently at reflecting new information into prices of company shares and bonds quickly and thus every decision you make is a bet against the aggregate view of all investors trading in the markets. Markets move on the release of new information which is, by its very nature, random.
The returns that a fund delivers are known as time-weighted returns. The return an investor in a fund actually receives is known as the money-weighted return and will be impacted by the magnitude and timing of cash flows into or out of the fund that they make.
A well-known piece of research from Morningstar’s ‘Mind The Gap (2023)’ report estimates this ‘behaviour gap’ to be around -1.7% per year on a large sample of US funds.
The solution to this behaviour gap? Own a sensibly diversified portfolio with sufficient higherquality, shorter-dated bonds to
provide protection from portfolio falls, allowing you to stay invested throughout these inevitable episodes of market turmoil that arise from time to time.
As John Bogle, the founder of Vanguard used to say: ‘This too shall pass!’
Guy Beck is a senior financial planner with Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions. Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment
Premises Regulatory requirements and investigations
Michael Rourke
Tania Francis m.rourke@hempsons.co.uk t.francis@hempsons.co.uk
Fall-out of failure to look after data
New Data Protection Fining Guidance has been published by The Information Commissioners Office. Philippa Doyle explains what this means for independent healthcare providers and offers some practical take-away tips
THE NEW guidance covers circumstances where the Information Commissioners Office (ICO) would consider it appropriate to issue a fine and how it determines the amount of any fine imposed. The maximum amount of fines has not changed.
Statutory background
Under the Data Protection Act 2018 (DPA), the ICO may impose a fine where a person has:
Failed to comply with certain provisions of the UK General Data Protection Regulations (GDPR), an amended version of the EU GDPR, and came into force on 1 January 2021, following Brexit.
Failed to comply with an information notice, assessment notice or enforcement notice given under Part 6 of the DPA 2018.
Failed to comply with certain provisions of the UK General Data Protection Regulations (GDPR).
There are two levels of maximum fines – the ‘standard maximum amount’ and the ‘higher maximum’ amount – both of which are large sums which could significantly impact the financial standing of a business. Annex 2 of the guidance sets out which level of maximum fine applies to the relevant provisions of the UK GDPR and the DPA 2018.
The standard maximum is the greater of either £8.7m or 2% of the total worldwide annual turnover. The higher maximum is the greater of either £17.5m or 4% of the total worldwide annual turnover.
If there are multiple infringements arising from the same or linked conduct – ICO will assess on a case-by-case basis whether the incidents are linked – the overall fine will not exceed the specified amount for the gravest infringement.
Consideration factors
When deciding whether to issue a fine, the office will assess each case on an individual basis. However, it must have regard to the factors listed in Article 83 UK GDPR, as well as ensuring the fine imposed is effective, proportionate and dissuasive.
Factors to consider include:
➲ The nature, gravity and duration of the infringement;
➲ The intentional or negligent character of the infringement;
Under extraordinary conditions, the Commissioner has the discretion to lower a penalty if a private healthcare provider or company cannot afford it due to their financial status
CASE STUDIES
There have been several examples in recent years of healthcare organisations and practitioners being fined by the ICO for data breaches:
➤ Lister Hospital, a private hospital owned by HCA International, was fined £200,000 after a patient discovered a confidential IVF recording online. This breach was a result of the company sending unencrypted audio files to an Indian transcribing company.
➤ Bayswater Medical Centre was fined £35,000 (reduced from £80,000) after it left highly sensitive patient data in an empty building, which was found after representatives from another GP surgery viewed the building while preparing to take over the lease.
➲ Any action taken by the controller or processor to mitigate the damage suffered by data subjects;
➲ The degree of responsibility of the controller or processor taking into account technical and organisational measures implemented by them;
➲ Any relevant previous infringements;
➲ The degree of co-operation with the ICO in order to remedy the infringement and mitigate the possible adverse effects of the infringement;
➲ The categories of personal data affected by the infringement;
➲ The manner in which the infringement became known to the ICO;
➲ Where measures referred to in
Article 58(2) UK GDPR have previously been ordered against the controller or processor concerned with regard to the same subjectmatter;
➲ Adherence to approved codes of conduct pursuant to Article 40 UK GDPR or approved certification mechanisms pursuant to Article 42 UK GDPR;
➲ Any other aggravating or mitigating factor applicable to the circumstances of the case, such as financial benefits gained or losses avoided, directly or indirectly, from the infringement.
Determining amount
If the ICO decides to issue a fine, then the amount is calculated using the following five-step approach:
Step 1: Assessment of the seriousness of the infringement;
Step 2: Accounting for turnover –where the controller or processor is part of an undertaking;
Step 3: Calculation of the starting point having regard to the seriousness of the infringement and, where relevant, the turnover of the undertaking;
Step 4: Adjustment to take into account any aggravating or mitigating factors;
Step 5: Assessment of whether the fine is effective, proportionate and dissuasive.
Under extraordinary conditions, the Commissioner has the discretion to lower a penalty if a private healthcare provider or company cannot afford it due to their financial status.
The practitioner or business concerned needs to make a claim of financial hardship. They will bear the responsibility of demonstrating that their circumstances warrant such a decrease.
Where appropriate, the Commissioner may enter an agreement providing additional time to pay a fine or to allow for the payment of the fine in instalments.
Take-aways
The updated guidance has helped provide clarity on both how the ICO reaches its decision and how it subsequently calculates any potential fine.
It is also worth bearing in mind that aside from the potential financial consequence, there may
also be reputational damage as a result of a breach.
Therefore, it makes for a timely reminder to independent healthcare providers to:
1
Check their data protection policies are in order, ensuring that they are complying with the latest ICO and UK GDPR requirements;
2
Ensure they have an effective response plan if there is a breach;
3
Ensure staff understand their obligations and what is expected of them. This could be via staff training or even regular internal risk assessments.
If you would like to read the full guidance, visit the ICO website https://ico.org.uk/ about-the-ico/our-information/ policies-and-procedures/dataprotection-fining-guidance/
If you have any queries around any aspect of this article or the ICO guidance, please don’t hesitate to contact Philippa Doyle (below), a partner in Hempson’s healthcare advisory team, by email at p.doyle@hempsons.co.uk
Dr Kathryn Leask
(below)
Treating patient with anorexia
shares her views with a private GP on treating a patient with an eating disorder
Dilemma 1 What is the best way to treat this?
QI’m a private GP who has recently seen a patient with an eating disorder. I am extremely concerned about this patient and want to provide support to maximise the chances of successful treatment. What would you advise?
AAccording to the charity Beat , at any given time, around 1.25m people in the UK are struggling with an eating disorder. Primarily eating disorders are mental illnesses that sometimes, but not always, have visible physical symptoms. Stereotypically associated with younger women, eating disorders can affect anyone of any age, gender, race, sexual orientation or socio-economic background.
While more research is needed to explore the exact causes of eating disorders, it is thought that genetic, cultural and biological factors may all play a role.
Identifying and treating people with an eating disorder can be a difficult area for GPs because of the sensitive nature of these conditions and the many ethical considerations that can arise, particularly in relation to consent and confidentiality.
Having said that, there are a number of ways in which you can support this patient.
Firstly, it is significant that the patient has decided to reach out to you for support and treatment.
Beat estimates that it takes people an average of three-and-a-half years for someone to get treatment after their symptoms first begin –quite often this is because people do not realise how ill they are.
Open mind
With this in mind, it is important to keep an open mind and be understanding of their concerns.
It is also important to consider other health factors, as people with eating disorders can sometimes have co-morbidities which may impact upon their eating disorder.
Next, it is worth making yourself aware of NICE guidance on eating disorders, which states that GPs
should offer a physical and mental health review at least annually to people with anorexia nervosa who are not receiving ongoing treatment for their eating disorder. The review should include:
Weight or BMI – adjusted for age if appropriate;
Blood pressure;
Relevant blood tests;
Any problems with daily functioning;
Assessment of risk related to both physical and mental health;
An ECG, for people with purging behaviours and/or significant weight changes;
A discussion of treatment options.
Often, the prolonged nature of an eating disorder can result in patients presenting with complex management dilemmas which, unfortunately, can lead to a complaint if patients and/or their carers feel that care has been unsatisfactory.
Reasons for complaints can include a delay in diagnosis or delayed referral to a specialist centre, the GP’s behaviour and attitude and a breakdown in communication, particularly when a patient’s
care is being shared between primary and secondary care.
Concerns about confidentiality can occur such as whether to disclose the patient’s information to third parties – for example, to other clinicians, employers or insurers – when the patient does not want their diagnosis divulged.
Patients may also refuse treatment, and this can be a difficult dilemma for GPs to deal with. When assessing a patient’s capacity to reach a decision regarding treatment, remember that the patient’s capacity is time- and decision-specific.
Keep these matters under review and consider whether the patient should be assessed under the Mental Health Act.
Although as a GP you may only occasionally see a patient who is presenting with an eating disorder, you do have a significant part to play in the early detection of these debilitating and life-threatening disorders.
As such, management of patients can be complex and challenging. When questions arise, get specific advice from your medical defence organisation.
When you think one of your patients is not fit enough to drive, what should you do? Dr Kathryn Leask gives her advice
Dilemma 2
Do I tell the DVLA about patient?
QI am a private GP who has been asked by the DVLA to assess one of my patient’s fitness to drive.
Unfortunately, I believe that the patient is not fit to drive, due to a previous health condition which has recently been exacerbated due to old age.
However, I am aware that the patient wishes to remain independent and, as such, they refuse to notify the DVLA of this issue. What should I do?
ALegally, it is the patient’s responsibility to inform the DVLA (or DVA in Northern Ireland) of any condition that might affect safe driving.
This can be via the gov.uk website in England, Scotland and Wales or nidirect.gov.uk in Northern Ireland and it is a criminal offence not to do this.
Ultimately, the decision as to whether the patient has their licence withdrawn lies with the DVLA, not you as their doctor.
Having said that, doctors have an ethical obligation to ensure the patient contacts the agency when their medical condition raises concerns about their fitness to drive.
Consequently, it is important for all doctors to be aware of the DVLA’s guidance on assessing patients’ fitness to drive, which includes information about which conditions and treatments impact fitness to drive and must therefore be reported.
Additionally, the GMC’s guidance outlines your duty of confidentiality and the actions you
When a patient is unfit to drive
should take if your patient is at risk of endangering public safety.
For example, if you believe a patient’s condition or treatment may impair their fitness to drive, you should explain this to the patient and tell them of their legal duty to inform the DVLA.
If the patient has capacity but does not accept this, then you can suggest they obtain a second opinion, but if they continue to drive when they’re not fit to do so, you may be obliged to disclose their information to the DVLA.
Patient consent should be sought before disclosing information about them, unless you can justify disclosing information in the public interest.
According to the GMC, you should not ask for consent if you have already decided to disclose information in the public interest, but you should tell the patient about your intention to disclose information about them, if it is safe to do so.
You can contact the DVLA to discuss your patient in confidence with a DVLA doctor (medical adviser) via email at medadviser@ dvla.gov.uk or by post. Under no circumstances does the DVLA reveal the source of any notification to the licence-holder.
If you do decide to contact the DVLA, you should confirm this with the patient in writing and also keep a written record of what – and to whom – you have disclosed, as, unfortunately, the patient may make a complaint or a claim against you.
Should the patient make a complaint, then it is wise to inform your medical defence organisation which can provide you with guidance and support.
Dr Kathryn Leask is a medico-legal adviser at the Medical Defence Union
Understanding your accounts
Unless your private income is only a very modest amount, then you should receive a set of financial statements – accounts – each year summarising the financial activity of your business over a period of time. Usually, these statements cover a 12-month period, but can be longer or shorter.
But the figures and terminology used within the accounts can make them difficult to understand when you first come across them. In a two-part article continuing next month, Alec James (right) runs through the key parts of the accounts to help make things clearer
THE BASICS
Accounts can follow various different formats, largely depending on if your private practice is declared as self-employed profits or via a partnership or limited company.
Limited companies and limited liability partnerships (LLPs) are bound by prescribed formats dictated by the Companies Act and accounting standards. Certain elements of the accounts are filed on public record.
For sole traders and partnerships, there are no prescribed formats but, again, principles for the policies used in their preparation exist and must be adhered to.
Whatever the business structure, the minimum information contained with a set of accounts will include a profit and loss account – also known as an income statement.
Larger businesses also include a balance sheet, various notes providing a breakdown of certain figures within the accounts and, on occasion, a cash flow statement. These additional pages are not always required but many businesses choose to voluntarily include them.
CASH BASIS vs ACCRUALS BASIS
There are two ways of recognising the income and expenditure within the financial statements: on a cash basis or by using the accruals basis.
The cash basis, as the name suggests, recognises the income and expenditure based on the amounts physically received or paid within the financial period.
This method is available to those working on a self-employed basis, either as a sole trader or a partnership. From 6 April 2024, this became the default method of accounting with HM Revenue and Customs (HMRC), however you can opt to continue on the accruals basis.
The traditional method of preparing accounts is called the accruals basis. This is where the accounts include the income and expenditure based on the dates that they relate to, rather than the amounts that have been physically received or paid in the accounting period.
This is the required basis for incorporated businesses, but is
also more suitable for larger unincorporated private practices. Larger businesses require more upto-date information and the cash basis can lead to less focus on the collection of debts.
PROFIT AND LOSS ACCOUNT/ INCOME STATEMENT
The profit and loss account summarises the income and expenditure within the accounting period. It will usually also show the comparative period’s figures, assuming, of course, that this is not your first year of trade.
This can be helpful in identifying how your business is performing financially in comparison to the previous year.
Comparing costs to the previous year is common practice and something you should review annually.
While you would expect certain costs to increase each year as your practice grows, there are a number
Comparing costs to the previous year is common practice and something you should review annually
ACCOUNTING AND TAXABLE PROFITS
A commonly asked question to an accountant is why the profits declared on a tax return – personal, partnership or company –do not agree to the accounts.
This is because there are adjustments which need to be made to the accounting profits to arrive at the figure that you or your business will pay tax on.
A common example of this is the purchase of equipment. A piece of purchased equipment to be used within your business is likely to have a longer life than 12 months.
In these scenarios, the piece of equipment is ‘capitalised’ and treated as what is referred to as a ‘fixed asset’. Fixed assets are recognised in the balance sheet (see my article next month) rather than the profit and loss account.
Each year the asset is used, business will recognise a proportion of the purchase cost. This is called depreciation, an accounting exercise which spreads the cost over its useful economic life which is determined by the business.
of fixed costs you will incur. You should review your costs in line with your own expectations.
In owner-managed businesses, it is very common for the owners to incur costs personally that relate to the business.
You should provide your accountant with details of these costs. This is to ensure you obtain the tax relief you are entitled to and reduce the amount of tax paid.
Because of this, depreciation is not an allowable cost for tax purposes. Instead, HMRC allows businesses to claim ‘capital allowances’ on the purchase of the equipment.
Capital allowances are a prescribed amount of relief which can be claimed, depending on the amount and type of equipment purchased, ranging from 6% per year to 100% in the first year.
There are also other costs which are an allowable business cost but are not allowable for tax purposes. These include things such as entertaining and certain legal and professional fees.
Because of the above, it is not uncommon for the accounting profit to differ to the taxable profit.
Some accounts will include a ‘tax computation’ which reconciles the accounting profit to the taxable profit, allowing you to clearly see the difference between the two figures.
Next month: Getting to grips with debtors and creditors, the balance sheet, the statement of financial position, key balance sheet terminology and fixed assets
Alec James is a partner at Sandison Easson
DOCTOR ON THE ROAD: MINI COOPER S
New MINI remains great fun to drive
The MINI remains a fun car at heart – just as it should – and Independent
Practitioner Today’s motoring correspondent Dr Tony Rimmer found the whole revised range has something to offer every medic
IT DOESN’T take long for a good idea to become normal and familiar. We are used to this in our medical practice.
The first MRI scanner to be used in the UK, for instance, was when one was installed in the Hammersmith Hospital in London in 1982. That was over 40 years ago but it still seems, to many of
us, quite a modern and innovative development.
In the automotive world, the Mini was a great idea and of groundbreaking design when launched in 1959.
After 20 years in production, you may think that its successor, the BMW MINI, has now been around for a long
time, but you must remember that the original BMC Mini was in production for twice as long.
Also, the original Mini was fundamentally of the same design during the whole of that time whereas the new MINI is now entering its fourth generation and, despite looking similar, is a
very different car under the skin compared to the 2001 original.
Despite the success of the allelectric MINI, there is still plenty of appetite among us buyers to stay with petrol-driven variants.
The step to EV ownership is still significantly more expensive and the electric MINI’s range has always been compromised by a relatively small 32kWh battery providing a real-world range of around only 100 miles.
The latest fourth-generation electric MINI has a bigger 40kWh battery, but this makes it heavier which could affect the handling.
Real essence
To get back to the real essence of what the MINI should be all about – go-kart-like handling, sharp steering and nippy performance –I have been testing the latest threedoor Cooper S petrol variant.
The normal Cooper model has a 1.5litre three-cylinder motor producing 154bhp, but the ‘S’ has a 2.0litre four-cylinder unit producing a healthy 201bhp. The power is delivered to the wheels via a sevenspeed dual-clutch automatic gearbox and, surprisingly, there is no option of a manual gearbox in any of the new MINIs.
The styling of the latest car has been smoothed out and there are new lights front and rear, but it is still unmistakably a modern MINI.
There are various trim levels available and the Cooper S gets heated seats, auto-folding and auto-dimming mirrors, adaptive LED headlights and a head-up display.
Seventeen-inch wheels are standard and my advice would be to resist upgrading to large 18inch wheels – they may look sportier but they stiffen the already firm ride too much.
The biggest changes to this latest MINI are to the interior. The dashboard is covered with a fabric that has a coarse knitted texture and, despite it sounding a bit odd, works really well to keep the MINI modern and stylish.
A huge centrally placed 9.4inch circular infotainment screen dominates the driver’s environment and, despite seeming a little bit overwhelming at first glance, works really well. All of the trim materials ooze quality and give this small car a real premium feel.
As with all previous versions of the MINI, the driver and front-seat passenger have plenty of space and comfort, but the rear passengers are not quite so lucky.
Although there is enough space to accommodate two average adults in the back, entry and exit can be a bit of a challenge.
If you regularly carry passengers or use a rear child seat, then you might want to consider the bigger but heavier five-door variant for an extra £1,750.
Boot space, as always, is very limited in this three-door classic model. You do not buy a MINI for its practicality.
Driving zest
It was with great relief that I found that, on the road, this latest version really drives with all the zest that a MINI should. The steering is sharper than most other cars and the way it handles the bends will never fail to put a smile on your face.
The performance is certainly in junior hot-hatch territory and is accompanied by a sporty roar from the exhaust and the occasional pop and crackle on the over-run.
The ride is certainly firm but never uncomfortable and suits the character of the car perfectly. The MINI remains a fun car at heart –just as it should be.
I found the whole revised MINI
Dr Tony Rimmer
is a former NHS GP practising in Guildford, Surrey
range has something to offer every medic.
There is a five- door version, the bigger Countryman SUV, and the new electric three-door.
I have always liked MINIs and owned a 2002 Cooper for many years.
This latest version of the petrol Cooper S ticks all the same boxes in all the right ways.
Body: Four-seat, three-door hatchback
Engine: 2.0litre four-cylinder turbo petrol
Power: 201bhp
Torque: 300Nm
Top speed: 150mph
Acceleration: 0-62mph in 6.6 seconds
Fuel consumption: 45.6mpg overall
CO2 emissions: 141g/km
On-the-road price: £26,700
As with all previous versions of the MINI, the driver and front-seat passenger have plenty of space and comfort
MINI COOPER S classic
(above)
A huge centrally placed 9.4inch circular infotainment screen dominates the driver’s environment
CHECK OUT OUR BUSINESS DIRECTORY
Independent Practitioner Today features an online advertising directory to complement our
and
Split into ‘business’ and ‘lifestyle’ directories, they list the services private doctors need to run their practices or spend their well-earned money on.
ADVERTISERS: The deadline for booking adverts in our October issue is 27 September
or for reprints, we would be happy to discuss licensing the copyright to you.
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent.
Material is governed by copyright.
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites
Robin Stride, editorial director Email: robin@ip-today.co.uk Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the digital journal, on our website or in our business directory, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912