The business journal for doctors in private practice
In this issue
Where cardiologists err A medico-legal analysis of clinical negligence claims notified to the MDU P18
It’s time to take off like the travel industry Healthcode is set to make online appointment booking a reality P24
Avoid going to the dogs Thinking long term is key when it comes to investing and trying to pick instant winners is just gambling P38
How best to get nabbed by the taxman
Ten ways to make sure you get investigated by HM Revenue and Customs n Page 44
Tax year set to change
By Robin Stride
Independent practitioners are being warned they face an administrative ‘nightmare’ under plans which could confront them with a change of tax year alongside the move to Making Tax Digital (MTD).
The Office of Tax Simplification (OTS) is suggesting two options for the Treasury to replace the date of the end of the fiscal year from 5 April – and most businesses back a change to bring the UK in line with other countries, according to a study by accounting firm BDO.
With MTD’s obligation to keep records digitally and report information quarterly being extended from VAT-registered businesses to all unincorporated income taxpayers from April 2023, it is feared solo practitioners particularly will struggle to cope.
Specialist medical accountant Vanessa Sanders, of Stanbridge Associates, said: ‘The administrative burden of operating all this alone is so overwhelming that doing it as a group will be much more time and cost-effective.
‘Some doctors may think this is too much of a headache and it will bring forward the retirements of those towards the end of their careers.
‘We’ve seen this already. Fewer doctors are going it alone. Most are joining together; it has been a trend for a while.’
In association with
The OTS’s year-end proposals are either:
31 March: The end of a calendar quarter and the UK financial year-end date used by the UK Government for its own accounts, or;
31 December: The calendar year end adopted by other large jurisdictions such as the US, Canada, Germany and France.
Mrs Sanders said: ‘Consultants and private GPs are going to face having to change the way they do business because things will have to be in real time. They are already going to have to do so with MTD.
‘But changing the year-end will impact on when they will have to retrieve information; for example, if they are non-UK residents and have overseas income, they will have to get that in real time and process the information correctly.
‘There are financial and administrative burdens for those who are self-employed and who enjoy rental income already because they will have to change their accounting systems to cope with MTD. Altering these systems again will cause more headaches.
‘It may mean they have to pay tax earlier than when they are used to. It will mean changes to inquiries and how they are conducted – although this is not a massive problem for consultants because they are not an HM Revenue and Customs [HMRC] target anymore. Dentists and private GPs are the main target in our experience.
‘Some doctors doing medicolegal work could be left strapped for cash because they are going to have to pay their tax earlier and there are a lot of time lags between doing the work and receiving payment.
‘There’s going to be greater reliance on their adviser for ensuring they are compliant, because the penalty structure is changing too.
‘Doctors may see their tax codes being altered more often as their information is given more frequently to HMRC. It will be a short-term nightmare – but with longer-term benefits. The positive is they will be able to plan better.
‘Their accountant will be able to help them plan with more certainty, not just for paying tax but
It will be a short-term nightmare – but with longer-term benefits VANESSA SANDERS
to achieve their future financial goals.’
More change is likely to increase pressure on HMRC staff whose extra work due to Covid grants, loans and VAT/income tax payments extensions have put correspondence six weeks behind.
Accountants warned that delays could be expected for getting references to pay tax, register for selfassessment or setting up new payroll schemes.
David Redfern, of DSR Tax Refunds Ltd, said the UK’s tax year beginning on 6 April had long been an international anomaly. He has told clients the UK is the oddone out, not only because of its April start but also for splitting that month between two tax years, adding to tax accounting complexity. He said the last thing business needed right now was additional administrative burden. But a change, although a complex process, would ultimately make things simpler for small businesses and make it easier for companies with an international foothold.
Accountant Vanessa Sanders
TELL US YOUR NEWS. Contact editorial director Robin Stride
ADVERTISE WITH US. To advertise in the journal or our website business and lifestyle directories, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT
£90 independent practitioners. £210 organisations. £90 GPs and practice managers (private & NHS).
Save £15 paying by direct debit: individuals £75 (organisations £180).
The way things are going, the answer may be ‘No’ much quicker than we could have imagined.
Not only is the weather system fast changing, the business climate around independent practitioners is moving on apace too.
You are not alone if you are feeling how nice it would be to just have a couple of years to get on with the job and not have to worry about the endless rule changes underpinning your work.
Pensions and tax shake-ups present small business entrepreneurs like doctors with a constant stream of moving deadlines and requirements governing the pensions and tax system. With this and other factors hitting the solo doctor hardest, no wonder we are seeing a growth in groups.
Now more costly and time-
consuming upheaval is on the way, as highlighted on page one.
Making Tax Digital (MTD) is something those doctors who charge VAT, on medico-legal work for example, have done for some time. Now it’s getting ever nearer for all self-employed consultants and GPs.
On the horizon, meanwhile, is a seemingly inescapable change to the tax year and our lead story outlines just some of the ways it could affect you.
Your tax official will be standing over you saying: ‘This procedure may be a bit painful – but you should find things much easier in the long run.’
Some accountants privately predict chaos.
They have been pretty much left alone to assist taxpayers through MTD, which has forced businesses and individuals to adopt and pay for new software approved by . . . HM Revenue and Customs.
Devices are to be better monitored
David Hare explains what the Government’s response to the Medicines and Medical Devices Safety Review will mean for the independent sector P12
What the court expects of you
Lord Hodge, deputy president of the Supreme Court, gives the keynote address at this year’s Expert Witness Institute online conference P16
Safe
messaging
Can you guarantee the safety and confidentiality of patients when using messaging apps? Joost Bruggeman shows what to look for in an app P26
Ensure you get paid
Simon Brignall discusses five common themes arising from his conversations with consultants wanting to address their medical billing issues P28
Know the limits of your experience
What happens when you take on procedures that fall out of your usual practice yet within your expected skill set? Dr Emma Green advises P34
Are you selling a private practice?
Solicitor Kirsty Odell outlines the necessary advance preparations a doctor needs to take before selling their private practice P36
PLUS OUR REGULAR COLUMNS
Business Dilemmas: When asked to be an influencer
Dr Ellie Mein discusses the issues to consider if you are asked to partner with health and sporting brands P40
Doctor on the Road: Lots of life left in the petrol engine
Dr Tony Rimmer takes a spin in the new Skoda Octavia whose petrol engine is refined and economical P42
Profits Focus: Ticking over quite nicely
Our series benchmarking the financial performance of private specialists this month looks at cardiologists P47
Ask for pension statement now
By Edie Bourne
Independent practitioners with an NHS position are being advised not to wait to discover if they will receive an annual pension statement from the NHS Pensions Agency.
Specialist medical financial advisers Cavendish Medical is telling doctors they should actively request a statement now for 202021 to establish whether they are likely to be paying substantial tax charges on their pension savings.
The ‘annual allowance’ limits the amount of tax-free pension savings which can be accrued each year to £40,000.
Every autumn the NHS Pensions Agency issues statements detailing doctors’ annual pension contributions for the preceding tax year but only if the doctor has ‘deemed growth’ in their pension pot of more than £40,000.
Those who breach the harsher ‘tapered’ allowance may not get a statement, as the agency is not duty bound to issue them to individuals breaching this particular cap.
The ‘tapered’ annual allowance applies to pension savers with a ‘threshold income’ of over £200,000 and reduces the limit on a sliding scale to as low as £4,000 for the highest earners.
Doctors’ threshold income includes earnings from all sources, so this might include NHS salary, private practice or academic work, investment income and buy-to-let incomes.
The NHS Pensions Agency is not duty bound to issue statements to individuals breaching this particular cap.
Patrick Convey, technical director at Cavendish Medical, exp lained: ‘People can wrongly assume that if they do not receive a statement, they have not breached the annual allowance. This can cause significant issues.
allowance can apply for the NHS to pay the tax charge under the Scheme Pays system in exchange for reduced future benefits.
The application for Scheme Pays is normally 31 July each year, but for the 2019-20 tax year, this has been extended to 31 March 2022.
There have not been any announcements regarding the deadline for 2020-21, which currently remains as 31 July 2022. There are also other payments options which should be considered.
‘There are several reasons for not receiving a statement – firstly, you may not have breached the standard allowance or the NHS Pensions Agency has not received your correct data.
‘Remember also that the agency is not monitoring the contributions to any private pensions, which will also count towards the level of allowance relevant to you.
‘To ensure you have a complete picture of your current position, we would urge you to request a statement as soon as possible.’
Those breaching the annual
Mr Convey told Independent Practitioner Today: ‘Pensions are not getting any less complex. There are new rules and regulations every few months and each one can have an impact on your calculations and your future plans.
‘Please give yourself enough time to ask for a statement – there can be lengthy delays at the agency – and have the figures thoroughly checked by experts well versed in examining the fine detail.
‘Every year, we witness statements with small errors such as wrong pay levels that can cause large mistakes if left unchallenged.’
Fix pensions to retain doctors
Fixing the pensions tax fiasco, which has cost specialists many thousands of pounds, is crucial to retain consultants, a doctors’ leader has warned.
BMA consultants committee chairman Dr Vishal Sharma urged the Government to not simply focus on recruiting staff but, more importantly, to concentrate on retaining existing highly skilled clinicians who have kept the NHS afloat during its most challenging period.
He said: ‘This means prioritising their health, well-being and fair pay and working conditions, while fixing longstanding pension taxation problems that limit the amount of work doctors can do and leave many considering early retirement.’
NHS waiting list figures for England show a record 5.45m patients waiting to start treatment at the end of June but the BMA estimates that England has 50,000 too few doctors to meet demand.
Complaints service joins larger body to secure future
The Independent Sector Complaints Adjudication Service (ISCAS) believes it has assured its future role in supporting private practice by moving under the umbrella of dispute resolution experts.
It is linking with mediation specialist the Centre for Effective Dispute Resolution (CEDR), an internationally recognised leader in the field with experience across all sectors, from small claims to disputes valued billions of pounds.
ISCAS director Sally Taber said she would be consulting with specialists’ bodies such as the London Consultants’ Association and the Federation of Independent Practitioner Organisations (FIPO) about how the change could assist private practice.
She told Independent Practitioner Today: ‘One of the indicators of a reputable private medical practice is candour and fairness in its discourse with its patients, particularly in response to any concerns about treatment.
‘A recognised indicator of this quality in UK private practice is using the ISCAS code of practice for the handling of patient complaints, with its ultimate provision for independent resolution. (https://iscas.cedr.com ).
‘The Paterson Inquiry has recommended (Recommendation 6) that this fact should be made more generally known among those in private medical practice and their patients, including those in NHS private patient units.’
She said the attachment to the charity CEDR would support its aim of giving ISCAS’s subscribing private doctors, clinics and hospitals high standards of complaint handling.
Patrick Convey
Consultants’ leader Dr Vishal Sharma ISCAS director Sally Taber
By Olive Carterton
Calls for greater transparency about doctors’ interests, particularly payments from the pharmaceutical and medical device industry, are being backed by ministers and private healthcare operators.
In a longawaited response to last year’s Independent Medicines and Medical Devices Safety Review, the Government has rejected a recommendation for the GMC’s register to be expanded to include a list of
financial and nonpecuniary interests for all doctors.
But it does want the publication of interests to be held by local healthcare providers.
This includes making it a regulatory requirement that doctors and all other healthcare professionals declare their relevant interests to their employer/organisation where they are providing services.
Writing in Independent Practitioner Today’s digital page turn issue, and the feature section of this website this month, the boss
of the Independent Healthcare Providers Network (IHPN) says the information would be publicly available for patients to see.
Chief executive David Hare warns these changes will also cover independent providers and his trade body will work with the Department of Health and Social Care ‘to ensure there is appropriate implementation, governance and enforcement of this approach’.
He said later: ‘Increasing transparency around healthcare professionals’ financial and nonpecuniary
Consultants with Circle Health Group have given a thumbs up to the roll out of ‘The Circle Philosophy’ across its combined network of over 53 independent hospitals.
The company, which has invested £100m so far this year in new technology, regeneration, hospital expansion and theatres, says this underlines its commitment to its people and patients and combines the culture at its three hospitals and BMI Healthcare’s 50 that it took over last year.
It prioritises ‘essential values of selflessness and compassion, reflected in how the company’s workforce serves patients and one another’ and is a culmination of what healthcare professionals and other members of staff have stated they want for their workplace.
Circle Health Group’s core mission is to become ‘the UK’s most innovative and patient focused healthcare organisation’.
Its philosophy spells out its principles: patients come first, belief in its people, good enough never is, being open minded and innovative, and its values: those who are
selfless and compassionate, collaborative and committed, agile and brave, tenacious and creative.
Asked what the new philosophy meant to him and his practice, specialist hip and knee surgeon Mr Rhodri Llywelyn Williams, who is is based at BMI Werndale, Carmarthenshire, said: ‘To be a good surgeon, you need to care about what you do and the way you do it.
‘As surgeons, the knowledge that the culture we work in supports us is reassuring. I know I and other consultants are valued by the organisation. The innovation and direction the group has taken has benefitted my practice.’
Mr Ben Gooding, a shoulder and elbow consultant at BMI The Park Hospital in Nottingham, said: ‘The Circle Health Group philosophy is a combination of two tried and tested philosophies that have been built over ten years.
‘In combining the scale of BMI with Circle’s clinical led innovation, we can guarantee that patient care continues to be the foremost priority.’
Circle’s ‘operating system’ aims to encourage staff, whatever their
role or status, to raise patient safety concerns. This celebrates those who ‘stop the line’, a term borrowed from Japanese manufacturing, which it says has proved to help staff speak up.
It also prioritises fixing systems and processes at their core rather than implementing workarounds. Staff are encouraged to ‘swarm’ problems and fix them fully.
Circle’s chief people officer David Cooper said the philosophy had been enthusiastically adopted across the company and was one way to ensure Circle became the hospital of choice for private consultants.
Massoud Fouladi, co founder and group clinical chairman, said: ‘We are committed to delivering the very best patient care. Key to this is developing and protecting the culture. It is clear that staff, whether they originally came from Circle or BMI, want the same things from where they work.’
interests is a key way of ensuring the highest possible patient confidence in the care they receive and we welcome the Government’s commitment to strengthening oversight in this area across both NHS and independent healthcare provision.’
The IHPN believes rapid growth in implantable medical devices makes it vital for a more joined up approach to recording and regulating their use to keep patients safe.
Important implications for private doctors – see David Hare’s feature on page 12
Clarity on sponsor deals Surgeons back Circle Health’s safety-first tenet
A new, noninvasive technique for the application of Xen stent into the eye to treat acute glaucoma, developed by The London Ophthalmology Centre, was used to save the sight of former Children’s Laureate Michael Rosen.
Clinical director, consultant ophthalmologist Mr Vik Sharma, said: ‘Michael woke from a coma in hospital and the first thing he noticed was he had a distinct fogginess in his left eye.
‘I knew that if he was not treated in the next week or two, he could go blind. I used the Xen stent combined with a new technique to fit which creates a new pathway for the fluid to drain out of, but without the cuts and stitches, making it quicker and safer giving greater likelihood of a successful outcome for the patient.’
Michael Rosen with glaucoma specialist Mr Vik Sharma
Orthopaedic surgeons Mr Ben Gooding (inset) and Mr Rhodri Llywelyn Williams
Group offers help to cope with gripes
The London Consultants’ Association (LCA) expressed concern at patient behaviour towards consultants in private and NHS practice and said it recognised the impact on morale.
Chairman Dr Mark Vanderpump said: ‘The pandemic has resulted in new ways of working, with an increased risk of breakdown in communication. It is noted that there was a significant increase in complaints in the Independent Sector Complaints Adjudication Service’s annual report. The LCA is available to provide mentoring to any members who require support.’
A straw poll of the Federation of Independent Practitioner Organisations’ board produced the general consensus that abuse episodes are infrequent.
According to one consultant, complaints had increased from selfpay patients who he believed never intended to pay anyway and were just trying to avoid the NHS waiting lists.
Chairman Mr Richard Packard said: ‘I am sure most of the issues during the lockdowns where private access was restricted were down to patients not understanding why they could not have their procedure when they wanted.
‘I certainly found that if suitable explanations were in place and a remote consultation with appropriate investigations was done there were no issues.’
GMC guidance on ending a professional relationship with a patient acknowledges doctors may wish to stop treating patients who have been violent or abusive.
Mayo expands
Mayo Clinic Healthcare at Portland Place, London, is adding new medical specialties.
A cardiology team includes Dr Elijah Behr, Dr Sanjay Prasad, and Dr Gosia Wamil. Gastroenterologists include Dr James East and Dr Bobby Prasad, while Dr John Costello leads pulmonology.
How to deal with abusive patients
We reported last month on a joint survey by Independent Practitioner Today and the Medical Defence Union (MDU) revealing that as many as one-in-five private doctors have suffered abuse from their private patients during the pandemic. Dr Caroline Fryar, head of advisory services, gives her view on abusive patients and how independent practitioners should respond
There are various reasons why patients or their carers may demonstrate challenging or abusive behaviour.
They may be in pain or in distress, they may have previously had a poor medical experience or they may have unrealistic expectations about their or a relative’s treatment. Such behaviours can take the form of demanding or controlling behaviour, an unwillingness to listen/lack of co operation, verbal abuse or threats and even physical violence against people or property. The pandemic will undoubtedly
have exacerbated feelings of stress, anxiety and distress for many.
There are actions independent practitioners can take. Observe a patient’s manner, what they say and how they say it.
Acknowledging that a patient appears unhappy or frustrated, and indicating you wish to understand why and help if possible, may help deescalate the situation.
Showing a willingness to listen, asking open ended questions and avoiding encroaching on the person’s personal space may also calm the situation.
If a patient becomes aggressive or violent despite these steps, then you should consider what followup action is required. In some cases, this may require police involvement.
It is a good idea to have a clear policy setting out that abusive and threatening behaviour from patients will not be tolerated. This should be readily available; for example, a notice in the waiting room or on your website. The MDU can offer specific advice tailored to your circumstances. Full survey results, page 20
COVID STRESS HAS LED TO SOCIETY’S FRUSTRATION
Mr Ian McDermott (right), consultant orthopaedic surgeon at London Sports Orthopaedics and honorary professor associate at Brunel University, responds to the survey
In my practice, I’ve noticed a much higher than normal level of general stress and tension, from hospital staff, our own staff in our own practice, from other doctors and from patients – i.e. from everyone!
I think an enormous amount of psychological damage has been done to everyone, worldwide, and frustration at ’the virus’ and/or ‘the Government’ –depending on one’s perspective – is now, purposely I believe, spilling out into stress and tension between individuals; for example ’the masked’ vs ’the nonmasked’ and ’the vaccinated’ vs ’the nonvaccinated’.
And for many, who perhaps struggle to make any sense at all about everything that’s going on, their reaction may simply be one of general stress and angst, with a shorter fuse, quicker tempers and a greater likelihood of anger.
I don’t think this is actually unique in any way to medicine within the private sector. I think it’s a much wider and broader thing across the whole of society, including how some people are driving.
I suspect that there might well be a lot more stress/ anger directed by some people now towards the NHS because of the deep frustrations that so many people have suffered with reference to almost all nonCovid
healthcare being stopped because of just one specific pathogen/condition, and with every other illness being treated as if it is unimportant by comparison.
People can’t get to see a GP in person. They struggle to even get a phonecall or video consult with a GP.
They’re ’told off’ if they attend A&E for nonemergency problems. They’re told they’ll have to wait two years to see a consultant specialist or a dentist. They’re told that there are literally millions of people on NHS waiting lists now and that they’ll have to wait umpteen months or even years for any elective surgery.
And yet they’re still being subjected to the ‘Save the NHS’ mantra, to videos of nurses and doctors doing TikTok dances and to adverts for free pizzas and coffees for NHS staff.
I’m just very, very glad and relieved that I’m not still practising within the NHS myself anymore.
My friends who still do are all saying that it’s even more stressful and difficult than it was preCovid and how they simply can’t get anything done anymore.
My personal perspective of the independent sector is that, at present, there’s still a lot of stress, uncertainty and inefficiency when it comes to getting patients booked in for surgery, because of all the many everchanging, arbitrary and ofttimes illogical rules and restrictions.
However, otherwise, I’ve thankfully not noticed or suffered any significant level of increased abuse from anyone. Yet!
Consultant sells practice to HCA
By Charles King
A practice set up by an entrepreneurial consultant to look after pregnant mothers and women with fertility problems has celebrated its 21st year by being sold to hospital group HCA.
The Birth Company in Harley Street, and more recently in Alderley Edge, Cheshire, has been acquired to enhance the work of The Portland Hospital for Women and Children.
It was founded in 2000 by obstetrician and gynaecologist Dr Donald Gibb, who left the NHS in 1999 in the month he was 50.
He shared his tips for a successful practice in an Independent Practitioner Today article (July-August 2013) called ‘A labour of love’.
The business offers 3D and 4D pregnancy scans, NIPT screening and complementary services, such as reflexology, pregnancy massage and psychotherapy counselling.
HCA said as The Portland Hospital was the only private hos-
pital in the UK solely dedicated to the healthcare of women and children, the acquisition of The Birth Company – which performs over 8,000 ultrasound scans annually –would expand its capacity to offer ‘exceptional care’ to mums-to-be.
Every year, the hospital’s maternity unit delivers over 1,200 babies and its team of over 600 consultants diagnose and treat more than 40,000 children.
Jane Whitney-Smith, its chief executive, called the acquisition a ‘strategic partnership’.
She said: ‘We are positive that this acquisition will create exciting new opportunities for The Portland Hospital, while further enhancing our obstetrics services and the high-quality maternity care and support we provide for all women.
‘Not only will The Birth Company extend our offer to mums-to-be, but it will also increase choice, which, alongside clinical excellence, is at the heart of what we strive to provide for our patients.
‘This partnership will form a natu-
ral pathway into the hospital for delivery and the onward care needs of both mum and baby in the years to come.’
Kate Richardson, managing director of The Birth Company, said: ‘By working alongside the expert team at The Portland Hospital, we will be able to provide a seamless care for mums-to-be from pregnancy and beyond.’
Dr Donald Gibb and the entrance to his Harley Street practice
THE BIRTH PANGS OF A PRIVATE PRACTICE
Setting up a company called The Birth Company at Companies House was ‘the most inspirational thing I did’, according to its founder consultant obstetrician and gynaecologist Dr Donald Gibb.
In a previous article for Independent Practitioner Today, he said his plans originally included setting up a website called DonaldGibb.co.uk.
‘I then realised that people would have to know my name in order to access this, but if they knew my name, then they knew about me already.’
He added: ‘It has been an interesting journey to a successful practice. It needs vision, investment, dedication, hard work and courage. Taking calculated risks is an essential part of this.
‘Even if an initiative fails, we will learn from it. I do not believe in luck: it is all about positioning and seizing opportunities.’
Share your successful practice’s story with Independent Practitioner Today. Contact robin@ip-today.co.uk
Private sector welcomes care contracting reforms
Private providers have welcomed the Government’s new Health and Care Bill, saying it signals the start of an important debate about the NHS’s future direction.
David Furness, director of policy at the Independent Healthcare Providers Network (IHPN), said it supported a move towards more integrated services, but the legislation should also be judged on whether it ensured patients had quick access to diagnosis and treatment.
He said the Health and Social Care Committee had rightly
argued it was vital that new integrated care systems drew on the experience and expertise of all parts of the healthcare system, including the independent sector.
He called for a new procurement regime ‘that encourages innovation rather than incumbency’.
BMA deputy chairman Dr David Wrigley commented: ‘The BMA has long supported collaboration and called for the removal of enforced competition through Section 75, which the bill would achieve.
‘However, the Government has
to go further if the NHS is going to be truly protected from unnecessary and costly private sector involvement. The most effective way of doing that is to make the NHS the default option for NHS contracts and to only tender competitively where this is not possible.
‘This is also vital to avoid the awarding of contracts without scrutiny to private providers at huge expense to the taxpayer, as was seen with the procurement of PPE and Test and Trace during the pandemic.’
The Independent Healthcare Providers Network (IHPN) has ensured new NHS England boss Amanda Pritchard is up to speed on what the private sector can offer.
Chief executive David Hare said: ‘Independent healthcare providers have played a pivotal role in supporting the NHS through the pandemic and we look forward to working with Amanda to build on these successful partnerships and ensure the health service is fully equipped to tackle the key challenges it faces post-Covid.’
By Robin Stride
Over eight-in-ten medical claims against doctor members of the Medical Defence Union (MDU) were successfully defended last year, its annual report reveals.
Some 82% of medical claims and 56% of dental claims brought against members were successfully defended.
The defence body said 83% of GMC cases involving MDU members at the case examiner stage were resolved without referral to a hearing at the Medical Practitioner Tribunal Service. The equivalent figure for GDC cases is 82%.
Writing in the report, MDU chief executive Dr Christine Tomkins says: ‘Settlement rates for our cases in 2020 were just 17% for medical claims and 44% for dental – meaning claimants did not succeed in demonstrating they had been negligently damaged, and should therefore be financially compensated, in 83% of medical
Breast cancer repair innovation offered by King Edward VII unit MDU’s defence success
Independent charitable hospital King Edward VII’s is incorporating two new innovations to combat some damaging long-term side effects of breast cancer surgeries.
The lymphatic microsurgical healing approach (LYMPHA) reduces the risk of secondary breast cancer-related lymphedema (BCRL).
It redirects waste products from the lymphatic system into the veins, enabling waste products to flow away and reducing the risk of lymphedema.
LYMPHA uses a combination of a paramagnetic tracer and fluorescent imaging (Endomagnetics and Stryker) to identify the extremely small lymphatics (<1mm) draining from the arm, and guide the surgical team at the time of operating. Consultant breast and recon -
claims and 56% of dental claims against our members.
‘The MDU’s claims team’s excellent outcomes also reflect our recognition that claims against individual members can affect reputations. We know how much your professional reputation matters to you.
‘We never settle claims for expediency’s sake and members are always involved in decisions about their claims.’
Dr Tomkins, who is retiring this month after 35 years with the organisation, also highlighted a key topic which she has fought hard to try get reformed: the cost of clinical negligence in the UK.
She said the extent of the problem was laid bare last November when HM Treasury analysis showed provision for clinical negligence claims was now worth £3,600 per household in England, compared to £700 per household ten years ago.
The scale of the rise in clinical negligence costs did not reflect a
decline in clinical standards; the issue was that the medical negligence system was both ‘unfair and unsustainable’.
Dr Tomkins highlighted disproportionate legal costs as just one notable defect of the current system.
For example, a significant proportion of the cases the MDU settled for below £25,000 in 2020 saw legal costs paid to the claimants’ lawyers exceed the damages payment paid to claimants by over 500%.
Dr Tomkins warned: ‘This system cannot remain unreformed any
longer. It has multiple defects. We have campaigned for many years for legal reform to address these.
‘As the true cost of Covid-19 on the healthcare system and the economy becomes clear, the impetus for change grows stronger. I can assure you that the MDU will continue to champion positive reform and encourage the Government to take ambitious action to change and improve the current system, which is destructive and outdated.’
The report shows almost all the requests received from its healthcare professional members for help with medico-legal issues were supported. It provided full assistance, which can include legal defence and claims indemnity, in over 99% of cases in the last five years.
Its expert advisers, who are doctors and dentists themselves, helped with record demand – over 35,000 requests for assistance or advice from members in 2020.
structive surgeon Mr Paul Thiruchelvam leads the team and works very closely with his colleagues, consultant plastic and microsurgical surgeons Mr Navid Jallali and Miss Judith Hunter, to do the complex procedure.
The technique has been introduced alongside deep inferior epigastric artery perforator (DIEP) flap reconstruction, a complex type of microsurgical breast reconstructive surgery.
Miss Hunter said: ‘Lymphoedema can be very debilitating and has traditionally been a challenge to treat.
‘Recently there has been renewed interest in microsurgical approaches to address this condition, but as with anything, prevention has turned out to be better than cure.
‘Paul, Navid and I had the privilege to travel to Genoa a few years ago to learn from the pioneer of the LYMPHA technique and have been delighted with our early results back in London.
‘If a patient is having a lymph node dissection along with a mastectomy, and we are already there with the skills and equipment to
perform an immediate breast reconstruction, it makes sense to offer them the LYMPHA procedure too’.
Mr Thiruchelvam said: ‘It is incredibly rewarding to be able to work so closely with my outstanding microsurgical colleagues to reduce women’s risk of suffering from this long-term condition.’
Chief executive Dr Christine Tomkins
(Below) the SPY-PHI portable fluorescence imaging system
Sports group starts mobile cardiac lab Surgeons blind to their eco damage
By Leslie Berry
Nearly three-quarters (74%) of surgeons say they have received no guidance to improve the sustainability of their practice.
A global survey by the European Society of Coloproc tology (ESCP) found only 6% of respondents had received direction on sustainable surgery at a national level.
The colorectal surgeons’ organisation said: ‘Surgery is the most energy and wasteintensive specialty in hospitals, contributing significantly to climate change.
‘According to a Lancet study [‘Countdown on health and climate change 2020’], the healthcare sector is responsible for 4.6% of global carbon emissions, with a single operation releasing an average of 200kg CO2 into the atmosphere.
‘Nine in ten surgeons agreed there is an urgent need for sustainability guidelines (79%) and further research (92%) to address issues with sustainability in surgery.’
The survey, which received 392 online responses from 56 countries, highlights a greater need for healthcare leaders to instigate sector-wide change from the top. Hospital leadership (39%) and policymakers (20%) were identified as having the greatest responsibility to influence the sustainability of surgery.
And while only 13% felt the responsibility lay with the surgeon or the individual themselves, respondents were eager to consider using fully re-usable or partly re-usable equipment, forgoing nonsterile gloves and reducing the use of anaesthetic gases during surgery.
The ESCP has made a commitment to conduct new research into sustainable surgery practices to build up the evidence base required to inform clinical guidance.
Its general secretary Prof Antonino Spinelli said: ‘It is time for surgeons to wake up to the sustainability crisis we are facing.
‘While saving lives must always be our priority, the waste-intensive nature of our practice is harming the environment at an alarming rate and putting our patients’ future health at risk.’
Over half (56%) of those surveyed felt a key barrier to improving sustainability in colorectal surgery was a lack of understanding across the profession, with over half of respondents unaware of the scale of surgery’s carbon footprint.
MPs call for changes to compensation payment
MPs’ proposals to reform the way compensation costs are calculated in England have been welcomed by a defence body.
According to one defence body chief, the report into maternity safety from a House of Commons Health and Social Care Select Committee should be a wake-up call.
Michael Devlin, head of professional standards and liaison at the Medical Defence Union (MDU), hoped the report would foster improvements and a learning culture where incidents are thor -
oughly investigated and lessons learned and shared.
He said: ‘We are particularly pleased to see the Committee recommend the Department of Health and Social Care removes “the need to compensate on the basis of private healthcare provision where appropriate NHS care is available; and that compensation is standardised against the national average wage”.’
This means repealing Section 2(4) of the 1948 Law Reform Act. The MDU has long advocated for these reforms which it argues
Devlin of the MDU
would help restore much needed balance to the system of clinical claims litigation.
The Institute of Sport, Exercise and Health (ISEH), in partnership with HCA Healthcare UK and Canon Medical Systems Ltd, has launched a mobile cardiac laboratory in a drive to protect the cardiovascular health of elite athletes.
Available to attend any sporting venue in Europe, it is the brainchild of ISEH consultant sports cardiologist Prof Guido Pieles. He said the service aimed to identify pre-existing cardiac abnormalities and ensure optimal management and follow-up. ‘This will help to provide athletes and their families with peace of mind and offer valuable time and cost efficiencies for sporting organisations.’
GenesisCare invests in new technology
Private cancer care provider GenesisCare has invested in new technology to increase patient access to diagnostics and radiotherapy services after securing eight-figure funding from HSBC Equipment Finance (UK) Ltd.
With 14 specialist cancer treatment centres operating across the UK, the provider is committed to investing early in the latest evidence-based technologies that hold the greatest potential for improved life outcomes.
UK general manager Justin Hely said: ‘This investment follows a number of significant steps we’ve taken to ensure timely and highquality cancer care for our patients during the pandemic and beyond.
‘As people regain confidence to visit their GP and enter a cancer care treatment pathway, we are committed to being there to provide world-class cancer services.’
Prof Guido Pieles
Michael
Imperial College Healthcare NHS Trust’s private patient arm has established an international network with a first member, Aman Hospital, Qatar.
This 100-bed facility offers a wide range of medical and surgical services across numerous specialties, including cardiology, ophthalmology and obstetrics. It is expected to open next month.
Multidisciplinary teams from the trust will work collaboratively with network members to help them make improvements to their clinical care and services while also establishing processes to enable members to transfer patients to
Compiled by Philip Housden
and from Imperial Private Healthcare’s London facilities if more complex care is needed.
This may enable patients to return to their ‘home’ hospital sooner than with a standard overseas referral.
The International Affiliate Network will also provide trust staff with unique work experience and development opportunities, helping to improve care for the trust’s patients and local communities.
Alistair Russell, director of business development at Imperial Private Healthcare, said: ‘We’re really excited to launch the International Affiliate Network
and welcome the first member.
‘We’re looking forward to building a referral network on a global scale, to share knowledge and expertise and advance patient care at a local level.’
The trust has been supported in the development of the network by Healthcare UK and the newly formed NHS Export Collaborative, a joint initiative between NHS England, NHS Improvement, the Department of Health and Social Care and the Department for International Trade.
In 2019-20 Imperial’s private patient income was £53.8m, third highest in the NHS.
On the move...
UCLH upgrades private ward at neurology unit London PPU starts overseas network
The private ward at the National Hospital for Neurology and Neurosurgery, closed since June, is due to re-open this month after undergoing a major transformation as part of a refurbishment programme across University College
London Hospital Private Healthcare. Its project includes general improvements to ward infrastructure, a complete refurbishment of all 18 bedrooms, redesigned bathrooms to make them more accessible for patients with neurological
Concierge service boasts global reach
A rapid response referral service, offering premier, bespoke medical pathways for people with complex and often time-critical care needs via The HCA UK Concierge Centre is proving to be a lifeline for patients from all over the world. The Marylebone service provides a single point of contact where all healthcare needs can be addressed no matter how complex or difficult, including ICU to ICU transfers. So far, the service has supported patients coming to HCA’s hospitals
from over 30 countries, including six ‘red’ nations while abiding by Government Covid regulations. They have been repatriated following trauma or illness when overseas. In one case, the team worked with an embassy after an eastern Europe earthquake to medivac a critically ill pregnant patient to London to receive specialist care and ultimately give birth safely.
There has also been a rising demand from NHS inpatients want-
conditions, the adaption of a bedroom and en suite bathrooms for bariatric patients.
Kerensa Heffron, director of UCLH Private Healthcare, said: ‘We believe all of these changes will vastly improve the experience
Annabelle Neame, HCA’s business development director
ing to transfer to the private sector who often require complex care.
HCA’s business development director Annabelle Neame said: ‘With HCA UK’s unmatched resources and pool of consultants,
Kim Foord-Paton, private patient services manager at Guy’s and St Thomas’, has left the trust to join BMI The Sloane Hospital, Beckenham, London, as executive director from this month.
It is understood that following the merger between the trust and Royal Brompton and Harefield Hospitals, the latter’s specialist care managing director David Shrimpton will take on the leadership of private patient services across the whole enlarged trust.
In 2019-20, the two trusts, ranked fourth and sixth in the NHS, reported combined private patient incomes of £67m, which, if sustained, should take the merged trust to second only to The Royal Marsden and above Great Ormond Street.
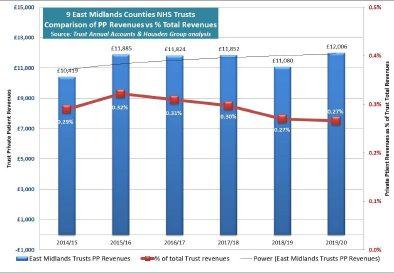
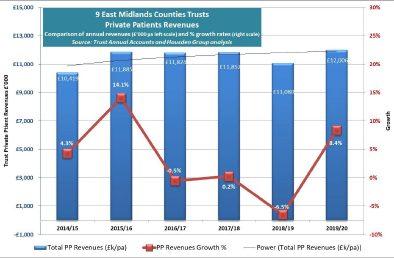
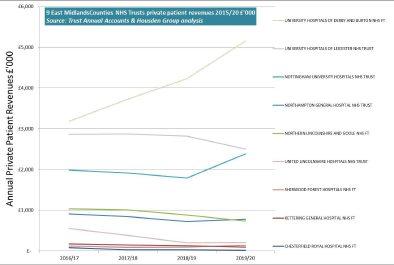
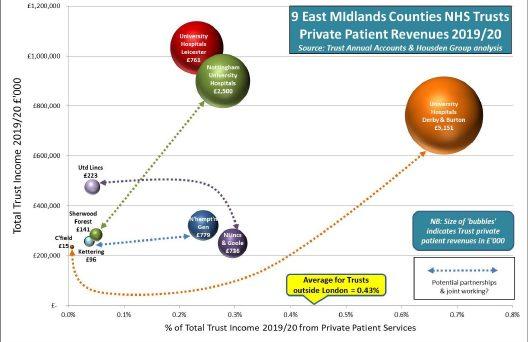
Philip Housden is a director of Housden Group. See his feature article on PPUs in East Midlands on page 31
we will be able to offer our patients.’
The trust reported private patient income of £5.8m in the 2020-21 accounts, down 73% due to Covid-19 from £21.7m the year before. a decline from 2.21% to 0.53% of total income.
we are able to ensure clients can access the best possible care, quickly – covering everything from ICU transfers to neurorehabilitation right through to lifesaving complex surgery and care.’
The service, open 24 hours 365 days a year and aiming to respond to all requests within two hours, has partnered with Charles Taylor Assistance (formerly Cega) to arrange patients’ international travel.
HCA said this was the first direct partnership in the UK between a direct healthcare provider and a medivac aviation transfer specialist, meaning the service can arrange global transfers which are not reliant on private medical insurance.
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2011
A levy for private work
Doctors in private practice should have their profits capped and repay NHS funds used to train them, according to a survey of patients.
Fifty-seven per cent of adults questioned claimed specialists –who were widely appalled at the findings – should pay back at least some training costs.
Just a third of the 2,059 polled online by Populus thought doctors should pay back nothing – as long as they continued to do their ‘fair share’ of NHS work.
Just 12% told the study for Benenden Healthcare that, as doctors were taxed on private earnings, they should not be expected to pay back anything.
Three-quarters believed NHSemployed doctors should be allowed to see private patients too, but 69% agreed private profits should be regulated.
Keep your pension from taxman
Independent practitioners were being urged to safeguard their tax-free pensions under a new protection scheme.
Using HM Revenue and Customs (HMRC) application forms could save them up to £165,000. But advisers warned that failure to act would cause some doctors to forfeit some of this from their pension plan.
The then lifetime allowance, limiting how much an individual could build tax-free in pension funds, was set to drop from £1.8m to £1.5m from the following April and there would be a 55% penalty tax rate above this allowance.
If applied to the Government’s £300,000 reduction, this equated to handing over a £165,000 ‘present’ to HM Treasury.
But the new protection gave individuals a personalised lifetime allowance of £1.8m, provided certain criteria were met.
Doctors with pension savings above £1.5m or who expected to rise above this – perhaps due to salary rises – were being advised to consider applying for the new ‘fixed protection scheme’.
Specialist financial planners Cavendish Medical warned: ‘Anyone with a current or projected future NHS pension of £50,000 and/or significant private pensions should urgently seek advice. It is imperative to act now, as using the ostrich approach could be very expensive.’
Sloppy ways cost dear
Failure to make some simple checks was costing consultants thousands of pounds worth in cheques, business advisers warned.
Doctors were said to be losing money because they were not running their business along normal commercial lines.
Losses were arising from:
Billing for too little;
Forgetting to bill at all;
Failure to chase up debts;
Lack of processes to spot errors;
Insufficient staff training.
BMA steps up fight against pension cuts
Independent practitioners faced yet another ‘assault’ on their pensions under planned NHS reforms and were being urged by the BMA to register their opposition.
The rallying cry came after actuaries advised the association that the Department of Health’s latest pension proposals could leave doctors £200,000 worse of over their careers in return for a worse retirement deal.
Doctors then giving 8.5% of salary would pay 10.9% the
following year rising to 14.5% by 2014, the association warned.
We reported that doctors would also be hammered under Lord Hutton’s public sector pensions review due to a rise in the normal retirement age and moving consultants from final salary to career average schemes.
BMA modelling indicated a 25-year-old doctor retiring as a consultant at 60 could receive a £19,000 lower pension than under their existing deal. GPs would take a similar hit.
Private healthcare surviving recession
The private healthcare market was forecast to grow by 15.7% between 2011 and 2015, reaching £35.9bn by the end of the forecast period.
TELL US YOUR NEWS
Share your experience of what has and has not worked in your private practice. Even if it’s bad news, let us know and we can spread the word to stop others falling into the same pitfalls.
Contact editorial director Robin Stride at robin@ip-today.co.uk
Devices are to be better monitored
Devising a new strategy – David Hare (right) explains what the Government’s response to the Medicines and Medical Devices Safety Review will mean for the independent sector
IMPROVING HOW the health system responds to patients’ concerns and ‘putting patient voice at the centre of patient safety’ is currently a key focus for both Government and healthcare providers.
This is especially pertinent due to the ongoing work around responding to the former Bishop of Norwich’s inquiry into rogue surgeon Ian Paterson.
And in July we finally saw the long-awaited Government response to last year’s Independent Med -
icines and Medical Devices Safety Review (IMMDS).
This sets out what action it is taking to support patients who have suffered because of Primodos, sodium valproate and pelvic mesh implants – and what more can be done to reduce the risk of avoidable harm from medicines and medical devices in the future.
The Government’s response sets out several key reforms:
Improving how the system listens to and responds to concerns raised by patients;
Strengthening the evidence base on which decisions are made;
Improving the safety of medicines and devices.
The response will have important implications for doctors and others working in the independent healthcare sector.
One of the biggest recommendations the Government has accepted from the IMMDS is the introduction of a new Patient Safety Commissioner.
The incumbent will ‘champion the value of listening to patients
BEWARE IF YOU ARE BEING SPONSORED
In addition to greater information and auditing of medical devices, the Government has also recognised the need for greater transparency around doctors’ interests and particularly payments from the pharmaceutical and medical device industry.
While it rejected a recommendation for the GMC register to be expanded to include a list of financial and non-pecuniary interests for all doctors – and opted instead for publications of interests to be held by healthcare providers at the local level – the Government aims to make progress in this area.
This includes making it a regulatory requirement that all registered healthcare professionals, not just doctors, must declare their relevant interests to their employer/ organisation where they are providing services, with information publicly available for patients to access.
These changes will also cover independent providers and the IHPN will be working with the Department of Health and Social Care to ensure there is appropriate implementation, governance, and enforcement of this approach.
and promoting users’ perspectives in seeking improvements to patient safety around the use of medicines and medical devices’.
The remit, critically, will cover care in both the NHS and independent sector.
It is intended for the Commissioner to be in post in the second half of 2022 and we at the Independent Healthcare Providers Network (IHPN) will be looking to engage with them early on and work together to further support patient safety in the sector.
Monitoring implants
This ‘whole systems’ approach to safety is also replicated in the Government’s commitment to establishing a patient identifiable database to ensure that implantable devices are effectively monitored and any issues affecting patient safety are responded to. It will apply to devices being used across the healthcare system.
This more joined-up approach to recording and regulating the use of medical devices across the whole healthcare system to keep patients safe is to be welcomed
The Government plans to hold a public consultation on a new UK-wide Medical Device Information System (MDIS), with £11m set-aside for 2021-22 to scope, test and cost options for MDIS and other medical devices patient safety workstreams.
This more joined-up approach to recording and regulating the use of medical devices across the whole healthcare system to keep patients safe is to be welcomed –particularly at a time of rapid growth of implantable medical
devices both in the UK and internationally.
IHPN is working to ensure that independent providers are fully linked with the new networks of specialist centres that the review recommended should be set up to provide comprehensive treatment, care and advice for those affected by implanted mesh.
Eight specialist centres have already been set up around the country and the Government has also committed to the development of a patient-reported outcome measure (PROM) for pelvic mesh procedures which will be commissioned through the National Institute of Health Research in 2022.
Manditory reporting
With regards the thornier issue around reporting payments from the pharmaceutical and medical device industry, the Government has committed to looking into
this further, including whether there is a need to make reporting mandatory through legislation.
The IMMDS, along with the ongoing response to the Paterson inquiry, demonstrates the real need to ensure patients are listened to when it comes to safety.
Healthcare providers across the whole system must be open, responsive and transparent about the care they deliver. And note that women comprised the vast majority of patients involved in these two inquiries.
There is still much to do on this agenda, but we welcome the Government’s ‘whole systems’ approach which reflects the key role independent providers – and those that work in the sector –have in making sure all patients receive the safest possible treat
ment.
David Hare is chief executive of the IHPN
Whether you are a GP or a consultant, Doctors’ Indemnity can provide you with appropriate cover for your private practice including, but not limited to:
• A–rated* Lloyd’s underwritten insurance cover: commercial contract-based cover for claims covered under your policy, and not discretionary-based cover
• Indemnity limits to suit the nature of your practice
• 24/7 access to a team of dedicated specialist medico-legal advisors and practising medical malpractice specialist lawyers to assist with any claim or potential claims you might have
• Indemnity for medico-legal work you carry out
• Where appropriate our underwriting partners will be pleased to consider retroactive cover
• 20+ years’ extended reporting period to offer peace of mind when you retire or cease clinical practice Professional
ACCOUNTANT’S CLINIC: THE BUILDING BLOCKS OF ACCOUNTANCY
to of top tips
is for eXit strategy
In our A-Z of top tips, Julia Burn reaches the letter ‘X’
THE LAST 19 months have been difficult for many businesses and several of them, sadly, had to cease their activities and consider an exit plan. Others, on the other hand, have decided to retire sooner.
Exiting a business is not a straightforward process and, once you are satisfied that it is the right time for you and your business, various matters need to be considered.
You could exit your business in different ways. If you are running a family business, you may consider passing it down to the younger generations in your family. If the business has run its course, you may decide to liquidate it. Or you may simply sell it.
Taxation issues
The taxation treatment will depend on how you wish to exit and you should discuss this and your exit route with your accountant.
Gifting shares in your business to your descendants could be an attractive form of inheritance tax (IHT) planning.
If your children are in the medical profession and you wish for the business to continue, this may be something to consider, as you could then still play some part in the business; for example, as a consultant.
Gifting shares could create immediate capital gains tax (CGT) consequences. Gifts to connected parties would be deemed to take place at market value. The capital gain would be calculated as the difference between the market value and what you paid for the shares. Assuming certain conditions are met, hold-over relief could be claimed to defer any gains. This
means that any gains made on the transfer would be held over and taxed on the recipients at some point in the future when they dispose of the shares.
Assets qualifying for hold-over relief would include gifts of unquoted shares in personal trading companies. They would not include unincorporated businesses, but assets used in a business – for example, land and property – could qualify.
These gifts could fall with the IHT regime if you do not survive seven years after your gift. But Business Property Relief (BPR) may still be available which would result in no or reduced IHT. BPR is not available on gifts of cash.
Liquidation
If your private practice business has run its course, you may wish to liquidate it, as some highly specialised consultants I know have done in the last few years.
You may need to engage services of a liquidator, especially if you have a valuable business, to help you secure the most efficient tax treatment. This is a complex area and you would need to consult your accountant.
Any cash drawn as a result of a formal liquidation would often be treated as a capital disposal and would be subject to CGT for higherand additional-rate taxpayers at 20%, instead of dividend tax at 32.5% or 38.1%, depending on pretax personal income.
Business Asset Disposal Relief (BADR), formerly known as Entrepreneurs’ Relief, may be available to private doctors if all qualifying conditions are met and you are
Due to the availability of various options, every exit will differ and not every strategy will suit everyone’s needs
making a material disposal of a business asset – including a liquidation – which you have owned for at least two years before the disposal/liquidation.
Different conditions apply to different assets – for example, shares v unincorporated businesses – and so you should seek professional advice if this a route that you decide to take.
As long as you have not previously used any of your BADR lifetime limit, any distributions of up to £1m would be taxed at 10% and 20% thereafter.
Assuming you have no other capital gains, you should be entitled to an annual exemption, currently £12,300, which could be offset against the gains, subject to 20% tax.
If no BADR is available to you, the liquidation distribution – less available annual exemption – will be taxed at 20% as normal.
In the case of an informal liquidation – that is to say, not using a professional liquidator – HM Revenue and Customs will seek to tax most of the distribution as a dividend. The dividend tax rates are 7.5%, 32.5% and 38.1% depending on the income tax band they fall into.
Selling your business would have similar consequences to a formal liquidation; that is to say, any gain made on the disposal would be subject to CGT and a claim for BADR may be available.
In the case of a sale of shares, the buyer would be liable to stamp duty calculated as 0.5% of the consideration they pay you.
Any exits would be reportable events for tax purposes and your accountant will be able to advise you on the reporting requirements. Generally, such transactions would need to be disclosed by 31 January following the end of the tax year of the transaction.
Conclusion
Some medical practitioners may have decided or been forced to exit their business sooner due to the pandemic and its effect on their business activities.
Due to the availability of various options, every exit will differ and not every strategy will suit everyone’s needs.
There are ways of minimising the tax exposure and deciding how to exit may play a big part in planning for the future.
Getting professional advice will help you consider pros and cons of your exit strategy and decide on how to structure your exit in the most tax-efficient manner.
Julia Burn (right) is a director at Blick Rothenberg and part of the team that advises medical practitioners
breathe
What the court expects of you
Lord Hodge (right), deputy president of the Supreme Court, gave the keynote address at this year’s Expert Witness Institute online conference
DURING HIS first year as the Expert Witness Institute (EWI) president, Lord Hodge has been encouraged to reflect on his own experience of expert witnesses, both as a judge and advocate. His address at the conference explored the critical role of the expert witness in the administration of justice, together with judicial expectation.
He also shared his thoughts on the impact of the pandemic on the courts and commented that the title of the conference, ‘Lawyers and experts: facing the future together’, felt particularly apt.
Lord Hodge cited examples from several cases, and in particular referred to the South Australian case of Bonython, when outlining the considerations governing the admissibility of expert evidence.
On impartiality, he endorsed Mr Justice Cresswell in the case of the ‘Ikarian Reefer’. In the same case, Mr Justice Cresswell laid out the judicial expectation of the expert witness, which is now codified in England and Wales in practice direction 35, supplementing CPR part 35.
Building on these foundations, he offered his own observation on
what the court expects of a competent expert witness. These were: Independence and impartiality. While this might seem obvious, he felt it was concerning that, in a 2019 survey, 25% of expert witnesses had felt pressurised to change their report in a way that damaged their impartiality.
And 41% indicated that they had come across other expert witnesses they considered to be a ‘hired gun’. Expert evidence must be ‘expert’. An expert witness has to undertake the task of ‘being an expert’, being aware and competent in their duties to the court.
Continual critical examination of their own work or opinion. Ownership or – as expressed by Lord Justice McFarlane in a 2018 speech in one word – Clarity
Both clarity of thought and clarity of expression or presentation of the evidence will assist the judge greatly. Lord Hodge stressed that it was imperative that an expert witness takes full responsibility throughout the process of preparation and presentation for his or her opinion evidence.
He then turned to the expert’s cooperation with other actors and the role of professional organisations.
Having quoted Judge Claire Evans: ‘There are plenty not very good experts around. Some soidisants experts are worse than not very good; they do great harm’, he proceeded to give some examples.
Lord Hodge praised specialist organisations and institutions such as the EWI for their role in minimising the occurrence of harmful expert witnesses by advocating for high standards in expert evidence.
Impart credibility
Membership of these bodies could give credibility to an expert witness, as it showed that he or she was taking the role seriously by signing up to a set of standards of behaviour and competence and is maintaining his or her continual professional development.
Lord Hodge pointed out that lawyers and instructing parties also played an important part, not just by ascertaining that an expert
did possess the necessary expertise and making them aware of their duty to the court, but by ensuring the expert was made aware of all the facts of the case, including material that did not support the client’s case.
Returning to the results of the 2019 survey, Lord Hodge said: ‘Lawyers must do better. They may obtain useful assistance on best practice on consulting experts in guidance issued by the Civil Justice Council.’
Also, just as expert witnesses must learn to grapple with the intricacies of law and court proceedings, so too should lawyers improve their scientific and technical literacy to do their job effectively in cases concerning experts and testimony.
The task of policing compliance with an expert’s duties falls to the court. The ‘judicial primers project’ presented a valuable opportunity to assist judges in their task.
Importantly, the primers were not intended to replace scientific evidence, but in assisting judges in understanding and assessing evidence.
Lord Hodge reflected on the impact of the Covid-19 pandemic on the courts.
He was very much aware that life had not been easy for expert witnesses during the pandemic, both in terms of carrying out physical site visits or examinations, and in the financial impact, be that through postponed trials or delays in payment. However, not all consequences of the pandemic were bad.
Time to reflect
The court’s operations during the pandemic were, as in the words of the Lord Chief Justice, ‘the biggest pilot project the justice system has ever seen’.
It was important to take time to reflect on what had worked well
and how this could be harnessed more broadly to improve the overall function of the justice system.
He felt some immediate improvements were bound to stay; for example, online filing had been introduced at the Supreme Court and that practice would continue. This would save money and have a positive environmental impact.
With modern technology having been adopted on a widespread basis, Lord Hodge expected that remote hearings were here to stay, particularly for incidental and case management business.
He believed there was scope for more radical changes within the judicial system in the coming years. And more widespread access to justice could be provided by the accelerated move to digital services.
The task of transforming our justice system required the input of all actors in the court system.
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment
Premises
Regulatory requirements and investigations
CLINICAL NEGLIGENCE: CARDIOLOGISTS
Where cardiologists
Clinical negligence claims notified by Medical Defence Union cardiology members are analysed by Dr Claire Wratten, (right) who advises on cutting risk
OF THE MDU’s consultant cardiologist members, around one third have needed to seek our assistance in the last ten years with a wide range of matters.
These include GMC complaints, coroner’s inquests, employers’ disciplinary processes and clinical negligence claims in both NHS and independent practice.
However, claims against cardiologists are less common compared to some other specialities – such as orthopaedic surgery – but the size of damages awards and claimants’ solicitors’ legal costs can be considerable.
This article explores medical negligence claims brought against cardiologists working in independent practice over a recent ten-year period.
Reasons for claims
The reasons for cardiology claims range from incorrect or inadequate treatment to procedural complications. Themes of cardiology claims include:
Incorrect treatment
Nearly 20% of notified cardiology claims related to alleged incorrect or inadequate treatment.
The conditions affected were wide-ranging and covered both outpatient and inpatient care.
Examples of cases involving outpatient care include incorrect advice given to a patient with valvular heart disease resulting in premature death, misinterpretation of exercise tolerance tests and inadequate treatment of ischaemic heart disease.
Cases involving inpatient care included inadequate cardiac monitoring resulting in delayed detection of cardiac arrest.
Delayed diagnosis or treatment
Seventeen per cent of cardiology claims notified to the MDU were due to an alleged delay in diagnosis or treatment.
These included delays related to cardiac conditions such as bacterial endocarditis and coronary artery disease, and delays for unrelated conditions including malignancies and berry aneurysm.
Angiography
Complications following angiography featured in 15% of claims. The complications were some -
times relatively minor, such as pseudo-aneurysm at the site of femoral artery puncture or complications following use of radial artery access.
In other cases, the consequences were much more serious, such as stroke following angiography.
Ablation
& transoesophageal echocardiography
A further 15% of claims followed ablation for arrhythmias. The concerns raised by patients included burns, a stroke following ablation, postoperative infection and cardiac tamponade.
Drug reactions
Just over 10% of claims involved drug reactions, including complications following treatment with
go wrong
gentamicin and amiodarone, as well as adverse reactions to flecainide.
Other claims alleged vasovagal episodes due to cardiac medication.
Pacemaker insertion
Just under 10% of claims were brought following complications associated with pacemaker insertion. The concerns raised included unnecessary pacemaker insertion, concerns about the lack of an adequate consenting procedure and faulty devices.
It can be very distressing to find out a patient is bringing a claim against you. While claims numbers have remained steady in recent years, the cost of claims has spiralled.
This is not due to clinical standards but to a deteriorating legal environment which the MDU is campaigning to reform.
You can find out more at www. themdu.com/faircomp.
Dr Claire Wratten is senior medical claims handler at the Medical Defence Union
HOW YOU CAN AVOID BEING SUED
There are steps cardiologists can take to manage risk factors and cut the risk of misunderstandings which can lead to a claim. These include:
Ensure you fully document your discussions with patients and the reasons for choosing a particular treatment pathway. It will help with continuity of the patient’s care and can be useful in defending claims
Remember to have a thorough consenting procedure. Ensure the patient is aware of the risks, benefits and complications of the proposed procedure as well other therapeutic options. These should be carefully documented
Supporting information such as patient leaflets and information sheets can help patient understanding. The use of these should be documented in the records
Consent should be obtained by an appropriate member of the team and, ideally, by the cardiologist undertaking the procedure
Keep your eyes open for non-cardiac conditions either presenting with cardiac-like symptoms or existing alongside cardiac pathology
To avoid adverse drug reactions, it is important to check and document any allergies and if a reaction occurs, take appropriate steps
If things go wrong, be open and honest with the patient by providing an explanation of what has happened and the likely short- and longterm effects of this. Say sorry and get advice from your medical defence organisation if you believe the incident triggers the organisation’s duty of candour requirements
PATIENT CENTRED HEARING CARE
Exceptional audiological care starts with the right referral. At Pindrop Hearing, we understand each case as unique, and our team of expert Audiologists will work with your patients to find the right solution for them
• Specialists in Diagnostic Audiology including Paediatrics and Tinnitus rehabilitation
• Cutting edge on site facilities, including purpose built sound proof rooms and audiovestibular diagnostic services
• Comprehensive range of diagnostic tests including PTA, tympanometry and specialist tests including OAE's and VEMPS
•A wide range of hearing devices, not available on the NHS
• Outstanding aftercare and patient services
• Fully GDPR compliant
• Medico-Legal Audiology service including gold standard objective Audiological testing using Cortical AEP and ASSR
• Full COVID protection measures in all clinics alongside a dedicated online consultant portal
For more information, visit https://pindrophearing.co.uk/healthcare-professionals I
INDEPENDENT
Abuse from patients no longer just NHS problem
By Robin Stride
Abuse from patients has increasingly been a working hazard for doctors in the NHS, but the problem is now rife in private practice too.
A joint survey by Independent Practitioner Today and the Medical Defence Union (MDU) reveals as many as one-in-five independent practitioners have suffered abuse from their private patients during the pandemic.
95% of doctors said patients had
been understanding about the changes they had to make, but 21% reported they had been abused by patients and 28% had been involved in a complaint.
Doctors reported their main medico-legal concerns centred around increased waiting times for treatments, use of remote consultations and communication difficulties.
Stressed doctors
Dr Caroline Fryar, MDU head of advisory services, called it ‘worry-
ing’ that half of the 227 respondents to the study felt stressed or anxious on a weekly basis.
A third admitted they were going to work when they do not feel fit to do so.
She said: ‘Unfortunately, some respondents told us that they decided to stop private practice or
worry they are going to be held responsible for issues they have no control over.
‘Consequently, it’s important for independent practitioners to be provided with the necessary support when dealing with the additional pressures.’
Unfortunately, some respondents told us that they decided to stop private practice or worry they are going to be held responsible for issue they have no control over
CAROLINE FRYAR, MDU
INDEPENDENT PRACTITIONER TODAY/ MEDICAL DEFENCE UNION SURVEY
The MDU operates a peer support network for its members who are facing medico-legal challenges, such as complaints, inquests, GMC investigations and claims.
This enables them to speak with a fellow member who has ‘been in their shoes’ and who can offer both practical and emotional support and guidance.
Over half (58%) of consultants working in independent practice provided additional NHS services to support colleagues and patients during the pandemic.
Over a third of respondents said they had provided additional NHS services for the duration of the pandemic, while 23% provided their support during the height of the crisis.
Just under 60% of consultants reported that private practice services had decreased during the pandemic, with just 28% saying they had increased.
Nearly three-quarters of consultants (72%) said they would feel reassured if the Government took action to shield healthcare staff from litigation against the NHS caused by the pandemic.
See www.themdu.com/press-centre/press-releases/mdu-concernedabout-mental-health-impact-ofpandemic-related-litigation
Has abuse by private patients increased during the pandemic in your private practice? And what was your response? Write to robin@ip-today.co.uk. Your identity will remain confidential
Nearly three-quarters of consultants (72%) said they would feel reassured if the Government took action to shield healthcare staff from litigation against the NHS caused by the pandemic
We can take off like
Today, the appointment booking process in the private healthcare sector is so fragmented, inefficient and limited in scope that it is holding us all back.
Peter Connor (right) explains why a centralised online booking system is critical to the sector’s prosperity and how Healthcode’s technology is making this a reality with benefits for independent practitioners and for their patients
BOOKING A SUMMER break was a frustrating experience for many holidaymakers this year as plans were thrown into doubt or thwarted by sudden travel restrictions.
Perhaps the disruption and uncertainty were more difficult to take because we have all become used to travel being easy, convenient and accessible over the years.
Albeit for different reasons, the experience has been a throwback to the situation of a few decades ago when booking a holiday was a time-consuming and complicated business.
Back then, most people opted to outsource the work to travel agents who would themselves have to make multiple calls to suppliers to check availability, hold seats and then confirm reservations.
As well as being a sub-optimal
experience for consumers, this bureaucratic exercise was costly for the travel and tourism sector too in terms of staff resources, inefficiency and missed opportunities. In the 1990s, industry bosses turned to technology to bring order to the chaos. The growth of internet use encouraged some consumers to go their own way, but the process was still overly complex because of the huge amount of data and fractured lines of communication.
The real game-changer proved to be a Global Distribution System (GDS), which enabled diverse service providers to exchange information about services and availability in real time through a central hub.
Transformed experience
Adoption of GDS within the travel sector really transformed the experience for ordinary consumers, enabling them to view the latest options online and book their own
flights and hotels. And it was one factor which led to the rapid expansion of overseas travel in the last two decades.
You may be able to see where I am going with this already, but there are clear parallels between the travel industry back then and the private healthcare sector now. Like them, we have a booking process which is inefficient and labour-intensive. Like them, different providers – private medical insurers, hospitals and practitioners – are unable to exchange real time information about availability, which carries the risk of double booking or wasted slots. And like them, opportunities for growth are being missed.
We know that patients expect to be able to access healthcare services online – from GP apps to booking an NHS Covid-19 vaccination – but live booking is relatively rare in the private sector and requires human intervention. It is true that some patients can reserve a slot on a provider’s online booking application, but the details will still need to be sent to the provider’s admin team and they will need to check the diary to confirm the appointment by phone or email.
Overall, the booking process is sclerotic, fragmented, prone to failures and detracts from the patient experience.
Healthcode’s appointment booking solution
Healthcode has long believed a central appointment booking sys-
like the travel industry
tem is critical to the future prosperity of the private healthcare sector, enabling us to optimise the process for providers and meet patient expectations.
We grasped how a GDS could transform private healthcare as it transformed the travel and hospitality sectors and so started to develop our own bespoke version for the sector, which is in the final stages of development.
Put simply, our GDS-based appointment booking solution is a hidden engine room that is capable of powering the appointment booking process for private healthcare.
This is how it works.
1
Providers – practitioners, clinics and hospitals – link to Healthcode’s GDS through an Application Programming Interface (API), which enables them to connect with multiple different booking sites.
2 Providers publish information about their services and synchronise appointment availability through the GDS.
3
This information is shared in real-time with the booking websites.
4
Third-party users use the booking site of their choice to search for an available slot. There is the potential to have a range of search criteria such as specialty, venue location, time, service type or estimated fee.
5
Once users book an appointment, this information is transmitted in real-time to the provider through the GDS and their appointment/diary system is automatically updated.
Booking system benefits
Healthcode’s appointment booking solution has significant benefits:
Standards-based – Healthcode has built the solution to globally recognised and proven Fast Healthcare Interoperability Resources (FHIR) messaging standards for data exchange, which have previously been implemented by the NHS for its Electronic Referrals System (ERS).
Efficient – A truly automated and seamless booking process is more efficient because it removes the need for human intervention to check and confirm booking slots. Accurate – The availability of appointments is synchronised in
real-time, eliminating the possibility of double-booking.
Ensure a better patient experience – The booking experience is smoother and less prone to failure and patients will have the reassurance of being able to make an appointment there and then at a convenient time and location.
Patient details are automatically collected at the outset so the provider can provide a personalised service.
Attract more patients – Providers can link to many different booking applications, which extends their potential reach at a time when NHS waiting times are prompting more people to consider private health services. Quick and easy to implement – It is only necessary to build one interface to the system to reach multiple booking applications, rather than building interfaces for each one.
Flexible – As well as linking to third-party booking applications via the system, providers also have the option to build a branded front-end booking service to their own specifications.
Secure – like all Healthcode solutions, it meets stringent information security standards, including
Our GDS-based appointment booking solution is a hidden engine room that is capable of powering the appointment booking process for private healthcare
enterprise quality infrastructure and end-to-end encryption to protect sensitive data.
Scalable – there are no development costs for existing users when more practitioners, providers and booking applications interface with the system.
Increases convenience and choice for patients – The solution will be an invisible but revolutionary development that enables patients to search multiple healthcare organisations, using different criteria and filters, to find the service that meets their needs, either directly or through a referring organisation.
Healthcode has consulted with providers to ensure the appointment booking solution meets their needs and hopes to release the prototype version later this year.
It is time for the private healthcare sector to emulate the travel sector and ditch the fragmented and inefficient appointment booking process that is holding us back. I’m proud that Healthcode’s innovation and online technology is again making it possible.
Peter Connor is managing director at Healthcode
MESSAGING APPS IN HEALTHCARE
Can you guarantee the safety and confidentiality of your patients when using digital messaging apps? Security and compliance should be front of mind for healthcare professionals, says Joost Bruggeman (right)
Safe messaging
DIGITAL MESSAGING apps have become an important facet of every day life, enabling people to stay in touch quickly and easily with friends, family and colleagues anytime, anywhere.
This convenience, however, does not come without risk and we have all experienced messages being sent to the wrong people or groups.
When communicating with friends, a mistaken message may be amusing or, at worst, embarrassing, but in the workplace the consequences can be far more serious.
In the medical sphere in particular, the potential for such errors poses a significant risk to patient confidentiality and data protection.
However, many medical professionals are unacquainted with this issue. A recent survey by the European Heart Rhythm Assoc iation (EHRA) revealed that 88.3% of its
members regularly use instant messaging apps for sharing clinical information with medical colleagues, yet 29.3% admitted they were unaware of EU data protection regulations when sharing clinical data.
A further 46.7% indicated there were no regulations in place at their institution regarding the sharing of clinical data via instant messaging.
Huge benefits
This is worrying but not surprising. Technology moves at a rapid pace, so it stands to reason that it frequently advances more quickly than the Government and industry can create new standards and procedures to address it.
Instant messaging tools offer huge benefits to medical practitioners, so the demand for them is strong.
This was clearly illustrated at the height of the pandemic when
FIVE THINGS TO LOOK FOR IN YOUR MESSAGING SERVICE
1
Fingerprint/facial recognition and PIN code security: To keep your patient data confidential, make sure you can secure your conversations and data with a mandatory PIN code and Face- or Touch-ID.
2
Image-editing features: To guarantee patient anonymity, look for an app that allows you to blur or cover names and faces in a photo, as well as providing tools for pointing out critical aspects of an image for colleagues.
3
Processor agreements: To be compliant with the EU’s General Data Protection Regulations, the messenger service should take responsibility, on your behalf as a healthcare professional, as the processor of your patient’s sensitive information. This ensures data privacy and security compliance at the individual and, with wider implementation, at the organisational level.
4
Identity and medical verification: Apps that verify their users as individuals and medical professionals create environments that can be trusted. Make sure your messenger can guarantee you are sending information to the right contact.
5
Separation between personal/professional media: Prevent patient data from being uploaded to personal cloud services. Save photos, videos and files directly to the messenger app rather than your device’s photo gallery.
An example of a case study function in the Siilo medical messaging app
informationsharing and fast decision making was essential for helping healthcare professionals learn how to deal with a hitherto unknown virus.
In these circumstances, frontline staff came to appreciate the value of being able to share details about individual patient cases, including photographs and other sensitive medical data. This facilitated rapid knowledge sharing, without which many more lives would undoubtedly have been lost.
Fit for purpose
The answer, therefore, is not to simply banish messaging apps, just when they have proven themselves indispensable. The better solution is for technology providers to create messaging tools which are fit for purpose and which meet the demands of medical staff, all without the associated risks that come with universally available providers.
Data security challenges were recognised some time ago and were a key influence behind the development of specialist healthcare apps such as Siilo.
However, the importance of using specialist tools is not yet fully understood because there is a failure to differentiate between security and compliance.
The basic promise of ‘end toend’ encryption, which is offered by the best known messaging apps, certainly provides a strong element of security. It means the servers of the vendor cannot decrypt the message data even if they wanted to because they do not have access to the encryption keys that belong to this encrypted data.
However, this only applies to data while it is ‘in transit’ from one phone to another. What happens when the data is ‘at rest’ and delivered to a phone or other device? This is a question that even data
protection officers in healthcare cannot answer.
After a phone receives a message, several synchronisations take place with common messaging apps.
Photos and videos are synced automatically to the photo library of the phone, where the media is not encrypted. All conversations are backed up by default and automatically go onto the cloud services of the phone provider – where message data is also stored unencrypted.
As such, all these unencrypted conversations are exposed to unauthorised third parties.
This is a huge problem because it becomes impossible for any medical professional sending an instant message on most services to be able to guarantee patient confidentiality.
A way which is often used to get around this is to anonymise patient information within communications, but this also brings significant issues. If healthcare teams cannot clearly identify which patient they are communicating about, it will almost certainly lead to confusion and mistakes which could easily be prevented.
No guarantee
What this means is that off theshelf messaging apps are not suitable for use within healthcare. Using them offers no guarantee of patient confidentiality and, worse still, may compromise their welfare.
What’s more, a recent ransomware attack on the Irish Health Service’s IT system has again highlighted the importance of robust data security. Little wonder, perhaps, that Siilo experienced a 908% surge in app downloads in Ireland following the recent incident.
Digitalisation offers tremendous benefits to the healthcare sector, but it is essential that it is truly fit to meet the standards expected within the medical profession. For communications technologies, this means applying absolute rigour to ensure patient confidentiality cannot be compromised.
Joost Bruggeman is a former surgery resident at Amsterdam University Medical Centre and now chief executive and co-founder of Siilo
It becomes impossible for any medical professional sending an instant message on most services to be able to guarantee patient confidentiality
CASE STUDY
Philip Luce (right) is chief executive at Bupa’s Cromwell Hospital, London. The hospital started using Siilo as the pandemic took hold last year.
He says: ‘Technology has been crucial during the pandemic to enable medical professionals to continue to provide the very best patient care. Here at Cromwell Hospital, Siilo is a key digital tool we introduced early on, that has proved invaluable as the pandemic developed.
‘It has enabled consultants in multidisciplinary teams (MDTs) to safely and securely discuss patient cases, share notes, scans and test results remotely.
‘This has been key in supporting our rapid-access patient pathways, enabling patients’ test results to be reviewed and consultants to collaborate in real time to develop tailored treatment plans. This streamlines our patient pathways, helping to ensure our patients’ treatment has not been delayed.
‘The ease of use and the speed in which teams were able to access and start using the app meant we were able to keep up with the pace and demands of such a unique and fast-moving crisis.
‘It is really important that we have timely communication between our clinicians to enable speedy diagnosis and tailored treatment plans for our patients. It also means we don’t have to worry about breaching patient confidentiality, we’re able to communicate more efficiently and are able to ask questions to other medical professionals across organisational boundaries.’
EXAMPLE OF IMPROVED CARE
‘Our consultant clinicians used Siilo to review the future treatment of a 46-year-old-patient who had been advised to stop chemotherapy, in place of radiotherapy treatment.
‘The lead consultant created a new patient file, to review the information at hand, and subsequently the breast team collectively approved of the decision to pursue a different method of treatment.’
HOW CRUCIAL IS THIS TYPE OF TECHNOLOGY BEYOND COVID?
‘The pandemic has changed the way we all work, and this includes at our hospital. Technology such as Siilo enables our consultants to communicate securely with one another in real-time. This is a great benefit to the delivery of rapid, quality patient care during Covid-19 and beyond the pandemic.
‘Providing a platform for these conversations to take place virtually means consultants are able to ensure that patients are getting the right and best treatment for them and their condition.
‘For our patients, this means they don’t have any delays in their treatment plan and this can leave them with peace of mind during what can be a worrying time.’
An example of the blurring and arrow tools used in the Siilo app
BILLING AND COLLECTION
Ensure you get paid
In the first of two articles, Simon Brignall (right) discusses five common themes arising from his conversations with consultants wanting to address their issues around medical billing and collection
lists and unreconciled insurance remittances.
Even when these practices use some form of software programme to control their billing system, more often than not these software programmes are run on laptops, notebooks and personal computers which are not backed up.
This is far from ideal from a business recovery perspective, because if the device is lost or the software becomes corrupt or the hardware fails, then the consultant’s recordkeeping and finances are put at risk – with all that this entails.
When commencing private practice, one of the first things doctors should do is to ensure their set up is run on a sound financial basis with the appropriate infrastructure.
A vital element of this would involve having a robust auditable system to facilitate the financial processes of the practice. This should include the ability to:
Raise invoices;
Reconcile payments;
Employ a robust chase process, including the ability to follow up on outstanding invoices using a range of communication methods.
Irrespective of what system is chosen, it is important to ensure it is backed up daily to provide financial integrity and conform to best practice.
If you are already in private practice, but currently do not have the appropriate infrastructure in place, then I recommend you put it at the top of your list of action points. This is because the risk you
Our experience is that consultants typically do not set their prices effectively because they have not done enough research when initially conducting this exercise
(CCSD), and some prices can differ by up to 100% between PMIs.
On top of this, each consultant must decide what rate they are going to charge for their consultation fees. In some cases, the contract the consultant has signed with the insurer will dictate what rate they can charge for both the procedure codes and the consultation fees.
Where the consultant is not contractually restricted, then they need to determine their fee structure and this is also the case for all fees related to selfpay patients.
5 Speed
It is important that a practice raises their invoices promptly; however, it is not uncommon for the practice to delay this function by weeks and months.
The longest delay I have seen was with a surgeon who had not raised an invoice for over two years and the size of the problem had meant the practice had become paralysed in addressing the issue.
So why does practice invoicing fall behind? There can be a range of reasons:
run is growing every day that this is not addressed.
3
Pricing
I know from experience that pricing has always been the area that appears to give consultants the most stress. The reason for this is that it is a very difficult area, both within the insurance market as well as the selfpay sector.
Firstly, the consultant must decide, where they have the contractual option, whether they are going to adhere to each private medical insurance (PMI) company’s price schedule. Secondly, they must know the individual price schedule for each PMI, as each has their own specific price for each code.
There are over 2,000 codes provided by the Clinical Coding and Schedule Development group
These decisions are often made with minimal information, as quite often the consultant will find that while their peers will share medical knowledge, they are less likely to share commercial information.
If the consultant gets this area wrong, it can lead to them being incorrectly priced within the market and so they lose patients because their pricing is too high, or worse they lose thousands of pounds due to their pricing being too low.
Our experience is that consultants typically do not set their prices effectively because they have not done enough research when initially conducting this exercise.
Fee structures are often not routinely reviewed. Many consultants who tell me it has been over a decade since they last looked at their fees!
4
CCSD
Once a consultant has decided on their pricing policy, they need to ensure they keep abreast of all the CCSD changes to the codes that are applicable to their specialty.
Changes to the coding schedules are implemented monthly. There can be replacement codes, new codes, changes to descriptions and the ability to bill multiple codes together.
All of this can also impact on what can be charged to each insurer. Lack of knowledge in this area can often lead to undercharging for procedures or billing problems with the PMIs that can delay payment.
Continuing to incorrectly invoice insurers can result in punitive action in extreme cases.
➤ Consultants who invoice themselves often prioritise seeing patients and other work commitments;
➤ Support staff can find that other administrative tasks get in the way. This can especially be the case in busy practices;
➤ Holiday and sickness absences. Whatever the reason, this cannot be allowed to happen. Not only does it reflect badly on the practice, which can negatively impact the patients view of their treatment, but it also means the practice’s cash flow suffers.
Remember, the longer the delay in raising an invoice, the greater the risk it results in a bad debt.
Some insurance companies now have strict time limits – typically six months – in which they need to receive an invoice otherwise they will not pay. Effectively, you could end up treating these patients for free.
Another advantage of invoicing promptly is that you will be aware of any issues that may arise, which often improve your chances of these being resolved.
As a good rule of thumb, the practice should set the goal of billing within 24 hours of any treatment carried out, as this will ensure good cash flow and minimise bad debts.
In next month’s article, I will cover the remaining five billing topics. But, in the meantime, you may want to start addressing the billing aspects I have covered here. But, of course, often the best solution is to contact a medical billing and collection company that has years of experience in this field.
Simon Brignall is director of business development for Medical Billing and Collection
PRIVATE PATIENT UNITS: EAST MIDLANDS
A region that’s ripe for collaboration
Our regional round-up of PPUs’ progress continues with Philip Housden’s (right) look at the private patient services in the nine NHS trusts delivering acute care services across the East Midlands’ counties of Northamptonshire, Leicestershire, Nottinghamshire, Derbyshire and Lincolnshire
THIS REVIEW is based on the information published in the Trust Annual Accounts for 201920, which was partially adversely impacted by the early months of the Covid pandemic.
At the time of writing, University Hospitals Leicester has not published annual accounts for 202021 and so a judgement estimate has been made regarding private patient incomes for the trust.
For this group of trusts, the accounts show that total private patient revenues in the region increased by 8.4% from £11.1m to £12.0m over 201819 (Figure 1).
This represents 0.27% of these trusts total revenues, flat from 2019 20 and remains below the combined national average outside of London of 0.43% (Figure 2)
Closer working
A feature of the region is that, as strategic planning for NHS services is in line with county boundaries, there is potential for this to also be a basis for closer working between trusts for private patient services development.
The trust that is most active with regards to private patient services in the East Midlands is University Hospitals Derby and Burton. The combined trust operates private services from Derby Royal, branded Derby Private Health.
The dedicated private patient unit houses 11 ensuite inpatient
rooms, five consultation rooms, a private chemotherapy suite and minor procedures room. The wellrespected local manager Sue Searle recently retired, having led Derby Private Health for five years, during which time revenues grew from just over £2m a year to the £5.15m achieved in 2020 21 – up 21.8% and £973,000 in the last year.
The trust is ambitious for further growth and in 2021 opens a new
dedicated operating theatre for private patients at the Royal Derby Hospital after a £2m investment.
Possible tie-up
Perhaps Derby Private Health has the potential to support Chesterfield Royal – where private patient income is negligible at £15,000 in 2019 20, down from £28,000 in 201819 and only 0.01% of turnover? University Hospitals of Leicester
has no dedicated inpatient private patient accommodation, with services spread between three main campuses across the city, from which a range of private ambulatory and diagnostic services is offered, including the Leicester Fertility Centre.
The trust’s estimated private patient revenues in 201920 were £2.5m, which is 0.28% of turnover.
Figure 1
Nottingham University Hospitals did not have a separate PPU for many years but housed private patients on NHS wards. However, the trust has opened a dedicated private patient unit at The Nottingham NHS Treatment Centre, named Nottingham Hospitals Private Healthcare. This investment has enabled the trust to increase private patient incomes by 33.2% and £595k in 201920 to reach £2.35m.
Also in the county, Sherwood Forest Hospitals, Health Service Journal’s Trust of the Year, has plans to extend the present limited private patients service at the King’s Mill Hospital near Mansfield. The trust reported revenues of only £141,000 in 2019 20, up 50% on the £94,000 earned in 201819 (0.05% of turnover).
Greater collaboration
Northampton General Hospital increased private patient revenues by 8.5% in 2019 20 to reach £779,000, which is 0.24% of total trust income.
In January 2020, the trust announced a commitment to working closer with Kettering General Hospital by moving towards a group management model to strengthen health services across Northamptonshire. This shows a commitment to greater collaboration between the two hospitals. At Kettering, private patient income was only £96,000 – 0.04% of total trust income –down 25% in 201920 on £132,000 the year before. Will a joint approach to private patient services be part of the joint approach?
Northern Lincolnshire and Goole have developed their own multisite service or ‘chain’ across three hospital sites in Goole and District, Diana, Princess of Wales, Grimsby and Scunthorpe General.
This is branded Lindsey Private Patients. In the past year, the revenues remained flat at £1m and 0.33% of total turnover. All cosmetic surgery is carried out at Goole Hospital using the Lindsey Suite single room accommodation and a range of other procedures and treatments are available at all three sites.
In 201920, the trust reported private patient revenues of £736,000 at 0.3% of turnover, down £146,000 and 16.6% on the year before.
United Lincolnshire Hospitals operates from Boston, Lincoln, Grantham and Louth sites. Pilgrim Hospital, Boston, has a dedicated private patient unit, the Bostonian Wing, with capacity for 20 beds. However, in 2019 20 the trust delivered only £203,000 revenues from private patients – 0.04% of turnover.
There is an opportunity for crosstrust working with neighbouring North Lincs to share back office and commercial costs to reinvigorate the trust’s service.
The opportunity for growth exists for East Midlands, but private patient income performance varies greatly, with neighbouring hospitals covering broadly similar
catchments delivering markedly different revenues. Therefore, increased partnership working between trusts could be the key to unlocking growth. Next month: Yorkshire
Philip Housden is managing director of Housden Group commercial healthcare consultancy
Figure 3
Figure 2
NHS Pensions & Annual Allowance Tax
Get ready in advance of April 2022 when the proposed changes to the NHS Pensions will allow you to reclaim some or all of any Annual Allowance tax you may have suffered in the past.
With our knowledge and in-house calculators, we will be able to predict in advance and check statements produced by NHS Pensions and Scottish Public Pensions Agency for accuracy for any refunds due.
For further information contact us at aa@semail.co.uk or telephone 01625 527351.
Figure 4
Scope of practice and acting within your skill set is important as a doctor, but what happens when someone takes on procedures that fall out of their usual practice yet within their expected skill set? Dr Emma Green discusses the issue
Knowing the limits of your expertise
A DOCTOR’S DUTY to act within their expertise has its origins in the Hippocratic Oath, but knowing the boundaries of practice is not always as straightforward as one might anticipate.
With the development of hybrid specialties, breast surgery – for example – can be performed by both plastic surgeons and general surgeons with breast surgery training.
Some procedures may also fall within the purview of different specialties – for example, endovascular procedures may quite properly be undertaken by both
vascular surgeons and radiologists.
What matters is that the doctor concerned has undergone the necessary training and has the appropriate skills and knowledge to carry out the proposed role and that their background specialty is relevant.
In other circumstances, clinicians may have their boundary of practice limited by exposure.
Smears, cannulation, venepuncture, breast examination and vaginal examination, for example, are considered skills that most GPs would have acquired through their training.
However, resources and patient preferences mean that often male GPs may be less likely to perform intimate female examinations than their female counterparts. This therefore leaves the question of whether they are skilled enough to perform the procedure should the need arise.
Safety issues
The same issues arise within private practice whereby clinicians may be required to perform procedures that are not within their regular area of practice or are only performed relatively infrequently
on a small patient population. This raises the question of competence alongside important patient safety issues.
Career breaks including parental leave can also result in doctors becoming deskilled and the Covid19 pandemic has led to concerns from some clinicians over deskilling due to operating list cancellations and deployment to other clinical areas.
For more specific circumstances like Covid 19 and parental leave, returntowork courses and supervised clinical practice, for example, can be used to counteract these
periods of not practising, thus reducing risk.
More generally, however, can it be considered acceptable practice to become deskilled in procedures which you may be required to perform in the future?
And it is unacceptable to perform procedures in circumstances where limited exposure means a clinician has not performed the skill recently.
GMC guidance
The GMC guidance within Good Medical Practice states that you must keep your professional skills up to date, you must regularly take part in activities that maintain and develop your competence and performance and you must recognise and work within the limits of your competence.
Therefore, it is important that clinicians have insight into those areas where they may be competent but out of practice or those areas where competence could be questioned.
Domain 2 of the same guidance, which addresses safety and quality, states that you must take part
The same gut instinct that can influence a clinical diagnosis could also be critical in getting a clinician to pause before proceeding with an unfamiliar practice in systems of quality assurance and quality improvement to promote patient safety.
This includes:
a) Taking part in regular reviews and audits of your own work and that of your team, responding constructively to the outcomes, taking steps to address any problems and carrying out further training where necessary; b) Regularly reflecting on your standards of practice and the care you provide.
Role of appraisal and revalidation
Appraisal should cover the whole scope of practice and therefore offers an opportunity to identify areas of discordance between procedures being performed in different areas of practice
It should also identify remedial actions to ensure professional skills are up to date and that doctors are working in their area of competency.
The Royal College of General Practitioners gives specific revalidation advice for those whose scope of practice involves specific
clinical skills – such as minor surgery, joint injections, cervical smears, intrauterine contraceptive device/intrauterine system insertions.1
It says: ‘It is appropriate and necessary to maintain an ongoing log of personal outcome data and reflect on the outcomes at least once in the revalidation cycle.’
The Royal College of Surgeons of Edinburgh recommends that surgeons keep a logbook of their operating activity – whether through the surgeon’s portfolio or through a different mechanism – as part of demonstrating the scope of their work and as an adjunct to validated outcome data.2
Clinicians should consult their college to get specialty specific guidance for appraisal and also revalidation supporting documentation to reflect their scope of practice.
Examples of ways that doctors may be encouraged to identify or address areas where they may need to focus their practice include supervised practice, logbooks, courses and education.
Emergency care: Good Samaritan acts
Acing within competence levels also extends to the Good Samaritan situation. Although there is no legal duty for doctors to assist in an emergency, there is an ethical and professional obligation.
In this situation, doctors remain obliged to make the care of a patient their primary concern and should consider their own limitations, both physically and in the scope of their clinical competence.
Limitations should be made clear to the person being assisted and doctors should still consider best interest decisions where capacity is impaired.
What should I do if faced with an unfamiliar procedure?
Doctors should be aware of warning signs which may indicate that they are unfamiliar with a procedure or may be about to stray out of their usual area of practice.
The same gut instinct that can influence a clinical diagnosis could also be critical in getting a clinician to pause before proceeding with an unfamiliar practice.
Reassessing the clinical urgency of a procedure in light of potential
riskbenefit to the patient may prevent a clinician from straying outside their area of training.
For example, it may be preferable to wake a patient from anaesthetic, rather than to proceed with a risk of harm to the patient if the scope of a procedure changes intraoperatively.
Similarly, a smear could be delayed until another colleague can supervise or undertake the procedure.
Some clinical skills such as venepuncture may carry few adverse consequences if performed after a prolonged period and many patients, even when aware of the lack of experience, remain happy for doctors to perform the procedure.
When obtaining patient consent for procedures, if appropriate, they should be advised of any limitations of the procedure being offered, including those identified by the clinician in terms of their scope of practice.
Claims have arisen in the context of relative inexperience in a procedure, which on the basis of Montgomery would be valid in terms of risks the patient may consider important in their decision making.
Patients should be given options of seeking treatment elsewhere with another provider or delaying treatment whilst they consider their options.
Complaints, disciplinary processes and regulatory investigations could all be a consequence of a doctor acting outside of their usual scope of practice, but claims can also arise should a patient suffer harm.
Always contact your medical defence organisation, for advice if in doubt.
References
1. Royal College of General Practitioners: RCGP Guide to supporting information for appraisal and revalidation (updated 2018)
2. Royal College of Surgeons of Edinburgh: Supporting Information Guidance for Surgery
Dr Emma Green (right) is a medicolegal consultant at Medical Protection
Whether you’re looking to retire or planning your next venture, it is essential you make the necessary preparations before you start the process of selling a private practice. Kirsty Odell (right) sets out some of the key stages to any transaction which will keep you on the right track for a smooth transition
Five key steps to sell a private practice
STEP 1 – Valuation/agents
Professional and specialist valuers/ agents can help you achieve the full market value for your business.
Unlike with NHS medical practices, this will include valuing the goodwill in a private practice.
As with any sale, your practice is only worth ‘what someone is prepared to pay for it’. It may not be appropriate to rely on the writtendown valuation of the business shown in your accounts, which may too low or too high depending on other circumstances.
Your valuers/agents should share comparative market evidence with you, as they will be familiar with what sale prices have been
achieved in other similar transactions.
They will advise you how best to market your practice to help you secure an offer.
STEP 2 – Appointing advisers
As well as valuers/agents, you should also approach accountants and lawyers.
In terms of your accountant, this initial approach will be to ensure that the financial information for the business is completely up to date and that the business accounts are presented in the most appropriate way to show its highest value.
Reduce tax liability
Also, restructuring the business may enable you to maximise its value and reduce your tax liability. For example, if the business is operated through a company, the accountant will advise on whether it is best to proceed with a share or asset sale.
Your accountant will continue to play a vital role in the transaction.
As lawyers, we will be able to advise if there are any pre-sale requirements to get the business ready for sale. For example, we advise if you need to engage early with any third parties such as landlords or banks to avoid any delays in the transaction at a later stage.
We always recommend that you instruct specialist advisers, as they will have a better understanding of the requirements of a sale of a medical business and should therefore be able to offer a more efficient approach, even if it means changing from your previous advisers.
STEP 3 – Due diligence
This is perhaps one of the more onerous parts of the transaction and it may cause delays depending on how well organised your business matters are.
The buyer’s legal advisers will raise a whole host of questions about the business and you will need to respond to those and pro-
vide supporting documentation. A buyer will not proceed without receiving satisfactory answers. Your replies will be treated as ‘representations’ and this means that if anything is subsequently discovered to be untrue or misleading, the buyer may have a claim against you for misrepresentation. It is therefore essential for you to take your time in answering the questions as fully and as accurately as you can – and to provide all of the supporting documentation available. You should prepare yourself for a long list of questions – both on the corporate side and also about the property arrangements.
Maintain momentum
By instructing lawyers well ahead of the sale, you will be able to be prepared, which will ensure that the momentum of the sale is maintained, with less opportunity for the buyer to negotiate down the price.
We will review your responses before sharing them with the buyer and their legal team, and help you to phrase the replies in appropriate legal language that will seek to limit your exposure. Try to avoid causing delays in replying to inquiries raised in due diligence by being prepared, so that you are able to keep the pressure on the buyer, who should be obtaining satisfactory funding and Care Quality Commission registration – if required.
STEP 4 – Sale documents
The buyer’s legal team will draft the sale documentation and negotiate the terms with your legal advisers. The key document will be a business transfer agreement or, in the case of a sale of shares in a company, a share purchase agreement.
A buyer will include clauses to seek to limit their liability post completion – where such liability relates to your acts prior to completion or relates to anything that you should have but didn’t disclose prior to completion.
The buyer will also, no doubt, include restrictive covenants to protect the goodwill of the practice. Depending on your intentions post sale, you may wish to negotiate the terms of these restrictions. When negotiating for you, we
would seek to limit your liability with financial caps and time limits on claims against you.
Another important document we will prepare is a Disclosure Letter.
This goes hand in hand with the warranties that are included in the sale document. Warranties are statements of fact about the business.
If any of those statements are untrue, you should disclose against them. The Disclosure Letter is the document by which you make specific disclosures against the warranties, and includes all the information you provided in reply to the due diligence inquiries.
Depending on the structure of the transaction, there may be a number of other ancillary documents to agree as part of the process.
This could include, for example, any property documentation to transfer an interest – such as a lease – in the premises, employment/ associate contracts where you are staying on at the practice after completion and company-related documents if any entity involved in the transaction is a company.
STEP 5 – Staff
It is most common that the Transfer of Undertakings [Protection of Employment] Regulations (TUPE) will apply where you are selling a practice.
This means that you will need to inform and possibly consult with the employees about the sale. We will be able to guide you on this process and advise you what your legal requirements are under TUPE.
If you are selling the shares in a company, then the staff will just continue to be employed by the company, so TUPE will not be applicable.
This short summary provides you with some guidance of the process of selling a private practice.
If you prepare well ahead and have specialist advisers to guide you through the transaction process, you should sell your business at the best price available without any unexpected comeback afterwards.
Kirsty Odell is an associate at Hempsons solicitors
A digital prescription platform to allow convenient prescribing from home
CloudRx is a digital prescription system that allows prescribers to create and send an electronic prescription to our fully licensed pharmacy for fast delivery direct to your patient. It can be used from home by doctors working away from their practices.
No cost to prescribers
Simple and quick prescription creation.
Legal paperless prescriptions, including repeat prescriptions and controlled drugs.
Patients receive text and email requesting secure payment. Alternatively, we can invoice the prescriber or clinic each month.
Prescriber Fees can be added if requested
Medicines are dispensed and dispatched by a variety of delivery options
Fully integrated into MidexPRO
Register for free by visiting cloudrx.co.uk
“We have worked with CloudRX to maintain a cold chain for the medication and direct delivery to patients at home.”
Dr Charlotte Norton, Medical Director of The Slimming Clinic, the UK’s largest chain of private doctor-led weight loss clinics
Avoid going to the
dogs
INVESTING IS simple, but not easy. The decision to invest in the first place requires foresight as well as the discipline to deny oneself spending today so that you do not have to eat own-brand baked beans out of the tin in retirement.
The second is deciding how much you want, need and can invest in equities that will act as the drivers of positive portfolio returns, above inflation, which will help fund future spending goals. Getting this right is key and where good advisers can add value. Next, an investor needs to decide the broad structure of the equity and bond components of their portfolio. A good place to start for equities is the structure of the global markets, which defines the basic country, sector and company weights and offers broad diversification.
As Eugene Fama, who won the Nobel Memorial Prize in Economic Sciences, said recently: ‘You need to be able to talk your way out of a market cap-weighted portfolio’. By this, he means that any decision to move away from this structure needs to be based on evidence and provide a good chance –although never the certainty – to improve the risk and return characteristics of this portfolio.
Simplest answer
That is a bit trickier and requires a reasonable degree of investment knowledge. ‘Occam’s razor’ suggests that the simplest answer to a complex problem is often the most effective. It certainly is in investing. Start with market capitalisation.
The final step is picking funds to
Thinking long term is key when it comes to investing.
Dr Benjamin Holdsworth (right) on why the noise of short-term performance is unhelpful
implement the strategy. Yet for many DIY investors, this is one of the first steps they take, heading to the ‘best buy’ fund lists in the Sunday papers or some investment website. Here is where the fun and danger start.
Some funds – usually measured over short time-frames such as three years – can have great looking track records. At this point many investors’ decisions are driven by common behavioural biases.
Hindsight bias is the most obvious – it is easy to identify a fund that has done well in the past, but difficult to pick one that will do well in the years ahead. Extrapolating the past into the future is rarely a successful strategy.
The fear of missing out is strong but needs to be resisted. Over -
confidence in the ability to pick a ‘market-beating’ fund manager goes against the grain of the bulk of the evidence we have to hand.
Over the past 20 years, for example, over 85% of all US equity funds failed to beat the market index and only around one third survived the whole period.1
Different parts of the market do well at different times, but no one really knows who the future winners are, not even the professionals. Naive investors take good short-term performance as a sign of skill.
Yet the reality is that much of the seemingly ‘good’ performance may be down to the part of the market that has performed well that happens to gel with the style of a specific fund.
There is an old industry saying
that markets pick managers, not the other way around.
‘Good’ performance may also simply be luck. You need at least 16 years of performance data to be 95% certain that skill rather than luck is the driver of outperformance, even for highly skilled managers.2
Three- or five-year performance records are largely worthless in identifying good funds. Yet that is where best-buy lists and many independent financial advisers tend to focus.
Spot the ‘dog’
One example of the noise investors face is the ‘Spot the dog’ report published by Bestinvest (owned by Tilney) every six months – and often highlighted in the Sunday papers – naming and shaming a list of funds, coined ‘dogs’, that have performed poorly relative to a broad market benchmark over three years.
Simultaneously, ‘pedigree’ funds are celebrated based on strong recent outperformance. By and large the ‘dogs’ were value funds made up of cheaper
stocks relative to some fundamental company metric, like book value or earnings, and the ‘pedigree’ funds were growth-oriented – more expensive companies – in their latest report.
Over the three years, growth stocks in general outperformed value stocks. Without this context, investors risk making decisions based on hindsight, picking investment styles that have done well and potentially lucky managers within those styles.
So far this year, many of the UK ‘dogs’ have outperformed the ‘pedigree’ funds, as value stocks have performed better than growth stocks.
‘Expert’ picks Investors Chronicle also tends to provide an annual Top 100 Funds list by broad investment category. Its 2012 global growth list identified nine funds and investment trusts.
Over the past ten years, only two out of the nine selected funds beat the market index, but did so handsomely. They are both highly concentrated, high conviction funds
One example of the noise investors face is the ‘Spot the dog’ report published by Bestinvest every six months naming and shaming a list of funds, coined ‘dogs’, that have performed poorly
holding just a handful of companies.
One of the funds suffered a fund-specific 50% fall within the period, which would have taken a strong stomach to live with. The other has experienced a couple of years of explosive growth, driven by a handful of companies and one electric car manufacturer.
Will they continue to do so well in the future? No one knows, not even the managers of these funds and certainly not the pundits creating best buy lists.
And that is the point. Basing an investment strategy on ‘I don’t really know’ seems a bit like gambling.
Capturing the market return with a well-diversified, low cost, systematic fund makes good sense and allows investors to ignore the best-buy and fund tips tables noise.
Thank goodness for Occam and his razor.
Dr Benjamin Holdsworth is a director of Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS.
References
1. S&P Dow Jones Indices – US SPIVA Report Year end 2020. http://us.spindices. com/resource-center/thought-leadership/ spiva/
2. An information ratio measures how much skill-based return a manager delivers relative to a representative benchmark and how much relative risk they took to achieve this. A ratio of 0.5 (i.e. half a unit of return for each unit of additional risk taken on) is deemed to be outstanding.
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
BUSINESS
Dilemma 1 Is it OK to be paid for a webinar?
QI am a consultant cardiologist who has recently been approached by a high-profile exercise brand to participate in a series of webinars on the benefits of exercise on heart health and future trends in healthcare.
They have stated that this is a paid opportunity, but is it appropriate for me to appear in these webinars? Please could you advise?
AIt is becoming increasingly common for medical professionals to utilise social channels to increase their professional presence online; for example, to advertise their services, to help disseminate specialist knowledge to the wider public and to form professional networks with other clinicians.
As such, in recent years there has been a rise in medical ‘influencers’.
Broadly speaking, this is an individual who is an expert in their chosen field who has access to a huge audience and can influence others to act based on their recommendations. While influencers are most commonly associated with Instagram, they also produce content on Facebook, TikTok and YouTube among others.
Many medical influencers use social media platforms to inform and educate the general public on various health topics. Consequently, many have been approached
When asked to be an influencer
Dr Ellie Mein (right) discusses the issues to consider if you are approached to partner with well-known health, exercise or sporting brands
by medical, health, fitness and lifestyle brands to become brand ambassadors or to participate in brand events, webinars and so on.
The advantage of medical professionals becoming prominent on social media and/or aligning with highprofile brands is that it can be an invaluable method of raising awareness of health campaigns/ conditions and connecting the public with health education from those who have the appropriate knowledge to give it.
Encouraging engagement
If done right, it can enhance the image of the profession, making it more accessible and encouraging people to engage with medical professionals.
Without qualified medical professionals, health misinformation and quackery would go unchallenged on social media, so it is important that the medical profession should have some presence in these spheres to temper pseudoscience and bad medical advice.
However, it is important to exercise caution if asked for specific
medical advice by an individual, as doing so is likely to establish a duty of care and could allow a patient to pursue a clinical negligence claim if they were dissatisfied with any advice received.
Also, it is important to be upfront and honest regarding any payment you receive as a result of a brand event or any social media activity that you undertake.
In its guidance focusing on financial dealings and conflicts of interest, the GMC says ‘conflicts of interest may arise in a range of situations. They are not confined to financial interests, and may also include other personal interests’.
Additionally, the GMC’s Doctors use of social media (2013) explains that ‘when you post material online, you should be open about any conflict of interest and declare any financial or commercial interests in healthcare organisations or pharmaceutical and biomedical companies’.
Advertisements must be clearly defined as such at the start of the post, commonly with the hashtag #AD or similar.
The Advertising Standards Authority also states that ‘if a brand gives an influencer a payment, free item or other “perk”, any resulting posts referencing the brand or their products become subject to consumer protection law, enforced by the Competition and Markets Authority and others, such as Trading Standards’. Depending on the webinars’ content, it may be that you would wish to relay anecdotes or examples from your clinical practice. But the principles of confidentiality would apply whether you are communicating offline or online.
Get consent
It is important not to discuss individual patients, living or dead. Posting details of a clinical case, however heavily anonymised, without patient consent would constitute a breach of confidentiality – as would sharing a photograph of a patient’s condition. It may also be possible for someone to identify a patient even when discussing a case anonymously.
Also, remember to consider how any comments you make either at an event or on social media may be perceived by colleagues, patients or the general public and be mindful about whether you are revealing confidential information. Most breaches of confidentiality happen inadvertently.
Finally, it is important to ensure that you have appropriate indemnity in place for any work done in your capacity as a doctor.
Dr Ellie Mein is a medico-legal adviser at the Medical Defence Union
Dilemma 2
Must I sign their exemption note?
QI am a private GP and have been contacted by a patient to provide them with a letter exempting them from having a PCR test for Covid when travelling to and from the UK. They have family abroad and travel quite frequently. I appreciate that this will have financial implications for the patient, as they are having to have the tests done on a regular basis.
The patient is finding the tests uncomfortable and states that the anticipation of having to have these done is causing them anxiety. The patient has also made reference to their diagnosis of asthma and how the anxiety of having to have a test done is making this worse.
I have reviewed the patient’s notes and the only reference to a respiratory problem I can find is a post-viral wheeze ten years ago. They did not require any specialist follow up.
The patient has been travelling for a number of months, but I have not personally seen them during this time. I have previously refused to provide them with an exemption letter for mask-wearing, as I did not believe there was a clinical indication to provide this.
The patient was very unhappy with this decision and made a complaint at the time. The patient says they have seen a doctor in the other country about their asthma and anxiety and has threatened to complain to the GMC if I don’t comply with their request. What should I do?
AAs the patient has expressed their dissatisfaction, their concerns should be dealt with in line with your complaints process. This should include an explanation for the decisions you have made so that the patient understands your reasoning.
You can make reference to the Government’s advice on the wearing of face coverings, PCR tests and quarantining during travel to and from the UK, which is available on its website. This page refers
Trying to avoid PCR test
A patient requests a letter exempting them from a PCR test before travel. Dr Kathryn Leask advises what to do
to those who may be exempt from having to have a Covid test for medical reasons, which include:
For urgent medical treatment or are accompanying someone who is travelling for urgent treatment, and it is not reasonably practical for you to obtain a negative Covid test in the three days before leaving; If you have a medical condition which means you cannot take a test – you must present a note from a doctor at checkin and to Border Force staff on arrival in England.
In its guidance Good Medical Practice (2013) , the GMC states that you must take reasonable steps to check information is correct when you complete or sign documents and must not deliberately leave out relevant information (paragraph 71).
If you provided a letter for the patient, you need to be in a position to justify your decision bearing in mind the wider public interest in travellers complying with the Government’s advice.
The patient has mentioned referring their concerns to the GMC and, therefore, it would be important to explain to the patient that you would need to be able to rely on supporting evidence from their records in order to provide such a letter, which does not appear to be available.
It is possible that you could be criticised if you provided an opinion that the patient should be exempt from having a test without any evidence to support this.
As you have not seen the patient or been in a position to examine
them, you may feel that the doctor whom the patient has seen abroad would be better placed to provide such an exemption letter, if they felt this was appropriate.
Dr Kathryn Leask (right) is a medicolegal adviser at the Medical Defence Union
DOCTOR ON THE ROAD: SKODA OCTAVIA
The latest Octavia proves that there is still much to be said for the internal combustion engine and it is with good reason that it has just been voted as Auto Express’s 2021
Family Car of the Year, says Dr Tony Rimmer (right)
Lots of life left in the petrol engine
NOW THAT the major drive towards electric power replacing the internal combustion engine (ICE) is in full flow, this may be a good time to review an example of a highly developed and efficient petrol-engined car which will do everything a family asks of it, but costs significantly less than an equivalent battery powered vehicle.
A recent study done by Volvo showed that it takes over 50,000 miles of use to break even on the total CO2 release into the atmosphere when comparing an electric car to an ICE car, considering the manufacturing processes and fuel use.
So it would seem that there is obviously a lot of life left in the older technology. More precise combustion and emission control is leading to less wasted energy and less harmful exhaust gases being released.
Volkswagen Group, the largest car manufacturer in the world, is still investing in cleaner and more efficient ICEs.
It has made great advances since the hugely embarrassing ‘Dieselgate’ fiasco and currently one of its most versatile and efficient ICE is the 148bhp 1.5 litre four-cylinder petrol TSi engine.
Probably the best value and most practical family hatchback that uses this engine is the awardwinning Skoda Octavia, whose latest model is its fourth iteration.
Using the chassis of the latest VW Golf Mk 8, the Octavia offers a roomier body with lots of individual and clever Skoda features. I have been driving a premium trim SE L model with manual gearbox. A styling update gives the Octavia a cleaner and modern
look. Still instantly recognisable, it has a wider and more purposeful stance. However, the biggest changes are inside the cabin.
Premium feel
Standard microsuede upholstery and a leather steering wheel together with higher-quality trim throughout the cabin give the car an almost premium feel – very close to the Golf.
In-car tech is the same as the latest Golf 8, which means an impressive 10.25-inch infotainment screen with wireless Apple CarPlay and Android Auto connectivity.
Most impressive though, is the interior space – always a great selling point for the Octavia. Spacious rear legroom for three adults and a truly cavernous 600litre boot is unrivalled by any competitor in this sector.
Supreme practicality is what the Skoda brand is all about. Idiosyncratic brand features like the umbrella in the driver’s door jamb and the ice-scraper in the fuel filler cap are welcome signs that Skoda continue to think of everything to help the owner use the car with minimal fuss.
Out on the road, the premium feel continues. The ride is smooth and noise levels are well suppressed. The steering and gearchange are precise and the engine has plenty of grunt while going about its business in a quiet and refined manner.
Impressive economy
We took the Octavia on a long trip to the Lake District and, on the motorway, it was as smooth, subdued and comfortable as any Audi or BMW rival. It also returned over 50mpg, which is hugely impressive and reflects the clever advanced tech to improve efficiency.
This is no wallowy cruiser and there is enough feedback from the chassis on twisty ‘B’ roads to interest if not entertain the keen driver.
It is not as engaging as, say, a Ford Focus, but it performs and handles well for a family hatchback.
The engine’s lack of capacity and outright power goes unnoticed 95% of the time and you cannot argue with the impressive fuel economy and reduced emissions.
So the new Octavia SE L is an impressive family hatchback and at a purchase price of £25,405, represents really good value. So why not go electric instead?
Although many independent practitioners may be tempted by Skoda’s new VW iD4-based electric brother, the Enyaq, you would have to justify driving around in a car that weighs an extra 600kg and costs £10,000 more.
The latest Octavia proves that there is still a lot to be said for the ICE and it is with good reason that it has just been voted as Auto Express’s 2021 Family Car of the year.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
SKODA OCTAVIA SE L 1.5 TSI
Body: Five-seat hatchback
The latest Octavia proves that there is still a lot to be said for the internal combustion engine
Engine: 1.5litre four-cylinder petrol
Power: 148bhp
Torque: 250Nm
Top speed: 144mph
Acceleration: 0-60mph in 8.2 secs
Economy – WLTP combined mpg: 47.9–52.3mpg
CO2 emissions: 123–133g/km
On-the-road price: From £25,405
In-car tech is the same as the latest Golf 8: a 10.25-inch infotainment screen
A cavernous 600litre boot is unrivalled by any competitor in this sector
A PRIVATE PRACTICE
– Our series for doctors embarking on the independent journey
How best to get nabbed by the
taxman
There have been countless situations where taxpayers are hauled over the coals for entering into an arrangement that they did not fully understand where the only beneficiary was the promoter
Ten ways to make sure you increase your chances of getting investigated… a list of dos
No one wants to attract the attention of HM Revenue and Customs (HMRC), but there is certainly a list of actions that can increase your chances of an inquiry. Ian Tongue looks at some of the key actions that would set you up to be a target
1 Engage in aggressive tax avoidance schemes
An almost sure-fire way to be subjected to a tax inquiry is to be involved in a tax avoidance scheme.
Many people do not realise that an investment or trading structure can be regarded as aggressive tax avoidance because, no doubt, the promoter of the scheme or structure will be downplaying the risks and criticise anyone who questions it.
There have been countless situations where taxpayers are hauled over the coals for entering into an arrangement that they did not fully understand where the only beneficiary was the promoter.
If it sounds too good to be true, then the chances are it will fail under scrutiny and it will be extremely stressful to be in that situation. Remember that the difference between tax avoid -
ance and evasion can be the thickness of a cell wall.
2 Choose tax-efficient investments poorly Sadly, many tax incentivised investments have proved fraudulent or unable to meet the criteria set out by HMRC.
These investments are often introduced by the government with good intentions to boost, for example, the film industry or offer start-up businesses essential capital from investors.
The spirit of these tax incentives is often abused and this can lead to investors being denied tax relief or having to pay it back potentially years later with interest and penalties.
Many film partnerships, Enterprise Zone Trust investments and Enterprise Investment Schemes have met this fate, so it is important that any such investments are made only following thorough investigation together with financial advice and ensure you inquire about any potential insurances available in case of failure.
3 Don’t declare your foreign earnings
Many doctors come from overseas or have spent time overseas and have financial interests abroad.
The rules around tax residency can be complicated and differ for those people who were born in the UK and those that enter the UK from another country.
It is important that you make your accountant aware of your worldwide financial interests for them to advise you on what needs to be disclosed. HMRC now have information-sharing agreements with most countries and are often provided with information to show that you may have foreign earnings.
In recent years, there have been several amnesties to disclose foreign earnings, so HMRC is likely to be less lenient for non-disclosure and ignorance of the rules is not a valid defence.
4 Don’t declare your property income
It is surprising how many times I have heard someone say that they do not make a profit because the mortgage payment is more than the rent received.
With most buy-to-let mortgages now requiring a repayment vehicle, it is more common for payments to be a mixture of capital and interest. Additionally, interest is now given less favourable treatment for higher-rate taxpayers, which often increases the taxable income from letting out a property.
Always provide your accountant with the full details of your costs and mortgage type to ensure the figures are accurate.
5 Claim excessive costs against your employment earnings
Employees are generally not required to incur too much by way of expenses to carry out their job. Because of this, HMRC only provides a narrow window to claim costs against a salary, citing that the cost must be wholly, exclusively and necessarily for the performance of the job.
In simple terms, it effectively means that you are contractually obligated to incur the cost as part of your employment contract.
If you are claiming for lots of costs under this heading, be aware that HMRC is likely to challenge the figures if it relates to items beyond the usual professional subscriptions and certain exam fees.
It is always best to run a payroll through a PAYE scheme, as it ensures full disclosure and usually reduces the risk of an inquiry
6
Claim excessive costs in your accounts
When it comes to being selfemployed or trading through a company, the wholly and exclusively rule still applies but the ‘necessarily’ part drops off.
This means that most costs that are incurred for a business purpose should be tax-deductible.
However, HMRC collects data for all professions and it is able to compare costs between businesses of the same type, so if your costs are excessive to the norm, it can often trigger an inquiry from HMRC.
7 Ignore VAT
We all pay VAT as we spend our hard-earned money, but for most doctors their business does not have to worry about being VAT-registered.
However, for those carrying out medico-legal work, consultancy or purely cosmetic work, you can only carry out £85,000 of this per year on a 12-month rolling basis, that is to say, you need to look back 12 months every month.
Failure to register for VAT can be very costly indeed both in terms of the VAT payable and penalties that HMRC levies.
If you are carrying out these types of work or anything nonclinical, you should discuss your circumstances with your accountant.
8
Do not operate a PAYE scheme
Often in small family-run businesses, there is no need to have a formal PAYE scheme, as the criteria to mandate a scheme is not reached.
However, there is a disclosure of the combined wages and salaries figure within your accounts, so if you are employing several people, you may receive some attention from HMRC.
It is always best to run a payroll through a PAYE scheme, as it ensures full disclosure and usually reduces the risk of an inquiry.
9 Wait until the last minute to prepare and file your tax return
Waiting until the last minute is never a good idea, as it puts additional pressure on whoever is preparing the tax return which can lead to error.
Depending on the nature of the potential error, it could lead to significant penalties and interest.
10 Don’t pay your taxes
This one is somewhat obvious, but if you do not pay your taxes, HMRC will almost certainly come knocking.
Historically, some taxpayers avoided filing returns so that HMRC did not know how much was owed, but the filing penalty system for non-submission of a tax return is so punitive that this can be very costly indeed.
Inquiries that you receive from HMRC are how the self-assessment system is policed and is just part of the process.
As these are normally opened from HMRC having information that an error/omission may have occurred, make sure you spend sufficient time preparing your accounts and tax information to ensure full disclosure.
Next month: Getting the most from your accounting systems
Ian Tongue (right) is a partner with Sandison Easson accountants
PROFITS FOCUS: CARDIOLOGISTS
Ticking over quite nicely
Profits have dropped for cardiologists in our latest unique benchmarking survey – but only slightly. Ray Stanbridge reports
IN MY report on this specialty’s business results last year, I commented that my initial view of figures to April 2019 suggested that cardiologists continued to do reasonably well.
A superficial review of some of the limited figures available to April 2020 suggested ongoing growth early in the financial year, but later, of course, there was an impact of the Covid-19 pandemic. Well, 2019 proved to be a ‘steady as she goes’ year for many consultant cardiologists.
Our headline figures show there was a slight fall in average private
practice earnings of 2.6% from £156,000 to £152,000 between 2018 and 2019.
Costs fell by 4% from £50,000 to £48,000. As a result, taxable profit showed a small fall on average of 1.9% from £106,00 to £104,000.
Balancing out
While we have noticed continuing insurance company pressure on fees, this was in a number of cases offset by growth in high margin self-pay patients. The two conflicting trends broadly balanced each other in 2019.
Staff costs rose in 2019 for many
cardiologists. To some extent, this was the effect of paying ‘home help’ higher salaries in line with the growth of personal allowances for tax. In others, it reflected higher secretarial salaries generally.
Perhaps surprisingly, room hire costs fell a little, perhaps reflecting a small reduction in volume or, perhaps more charitably, increased efficiency and usage of consulting rooms – that is to say, more patients per session.
Professional indemnity costs again showed a modest correction, with some insurers offering more competitive products.
Marketing costs
Other costs broadly remained the same as in 2018, save the reduction in ‘other costs’, which fell on average from £4,000 to £2,000. This largely reflected the reduction in marketing and website construction costs. By 2019, most consultants had developed their websites. What then of the future?
Rolling forward to 2021, many cardiologists have had a good period of trading reflecting significant pent-up demand arising from lack of activity at the peak of the lockdown.
In the previous year, 2020, it does seem that many cardiolo -
Many cardiologists have had a good period of trading reflecting significant pent-up demand arising from lack of activity at the peak of the lockdown
gist’s private practice incomes were hard hit – more details will follow when we prepare our 2020 figures.
As regular readers will be well aware, although our survey is not statistically significant, it does attempt to represent a picture at a moment of time of what a typical cardiologist in the UK may expect to earn and spend in his or her practice.
Choose and Book
There has been a growth in Choose and Book, which in some cases now represents a significant part of a consultant’s practice. The growth of self -pay has also had an impact. The appearance of employment models for consultants is also starting to have some effect on earnings.
HOW ARE YOU DOING?
The ebbs and flows of overseas patients, particularly in London, has also impacted on consultants’ year to year income.
In addition, we have seen that the growth of groups, offering a range of services including diagnostic tests, may have distorted figures.
pany or limited liability partnership.
An increasing number of cardiologists now trade through the vehicle of a limited liability com-
Put all these developments together and it makes it increasingly difficult to make realistic comparisons on a year-to-year basis.
With one significant change, our criteria for entry into our survey remains much as always. Our sample includes those who:
Have had at least five years’ private practice experience;
Have had or currently hold either a maximum part-time or a new consultant contract in the NHS – i.e. not completely private;
Are seriously interested in developing their private practice as a business;
Earn at least £10,000 in the private sector including Choose and Book work not paid through PAYE (previously £5,000);
May or may not have incorporated or be a member of a group.
Next month: ENT surgeons
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists, Stanbridge Associates Ltd
Years ending 5 April
ONLINE SOLUTIONS
INNOVATIVE ONLINE SOLUTIONS AT THE HEART OF THE HEALTHCARE SECTOR.
Our Online Solutions
Trusted by leading hospitals, independent practitioners and insurers to deliver high quality, secure and cost-effective IT systems. Seamlessly connect key stakeholders to support transparency within the sector and enhance patient safety.
Healthcode is the UK’s official medical bill clearing company and has provided secure and encrypted systems to healthcare professionals since 2000. Pre-pandemic we processed around 27,000 electronic medical bills to insurers daily.
To find out more about our solutions visit our website www.healthcode.co.uk
Coming in our October issue, published on 12 October.
Multiple jeopardy for doctors! We all know that we live in an increasingly regulated world, but have you ever thought about just how many sets of proceedings a doctor may face out of one incident? How about a complaint from a patient that results in i) police investigation and possible criminal trial; ii) GMC investigation; iii) Performers list proceedings/CQC investigation/inquest; iv) a civil claim for damages. Hempsons’ lawyer Tania Francis gives tips to avoid them
Tax nightmare on the way for independent practitioners? Stanbridge Associates’ specialist medical accountant and partner Vanessa Sanders follows up this month’s page-one story with more details and advice
The ‘online scams industry’ is booming as fraudsters take advantage of the pandemic to steal people’s personal information and their money. Healthcode looks at how you can protect your practice from data breaches and explains the measures it takes to keep your, and its, customers safe
Focus on ophthalmology claims: Dr Shabbir Choudhury, medico-legal advisor at the MDU, looks at clinical negligence claims against ophthalmologists and offers advice on managing risk in this specialty
Workplace health and well-being in private practice – Bupa commercial director Mark Allan draws on the lessons from the business clients he and his team work with
Medical Billing and Collection’s Simon Brignall resumes his twoparter by highlighting five more key areas to get right to ensure billing runs smoothly
INDEPENDENT PRACTITIONER
for doctors in private practice
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution.
Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Selling your practice. A leading consultant shares his personal experience
Private doctors are increasingly innovative and seeking new, effective ways to promote their clinic and stay ahead of the competition. But they should be mindful of how they present themselves and their services to the public and ensure compliance with relevant guidance and regulation, warns Dr Clare Devlin of Medical Protection
Our Business Dilemmas series discusses how to remotely manage a patient’s lithium prescription and answers a private GP’s concerns arising from a a solicitor’s request for assistance
ENT surgeons come under the spotlight in our unique benchmarking series, Profits Focus
If you work in a private patient unit in Yorkshire, then don’t miss Philip Housden’s financial update on what is going on there
Are you getting the most from your accounting systems? See Ian Tongue’s report
Our motoring correspondent Dr Tony Rimmer thinks he’s found the perfect second car for a young family with children: the Mazda MX-30
Plus Accountant’s Clinic, the latest from the Independent Healthcare Providers Network, more from the doctors’ specialist financial planning company Cavendish Medical, a focus on what was happening in private practice ten years ago and all the latest news and views
Don’t forget – you can find more news on our website throughout the month
ADVERTISERS: The deadline for booking adverts in our October issue is 24 September
Write to Independent Practitioner Today 7 Lindum Terrace, Lincoln LN2 5RP
CHANGING ADDRESS, EMAIL ADDRESS OR SUBSCRIPTION DETAILS?
Phone 01752 312140 or email karen@marketingcentre.co.uk
TELL US YOUR NEWS
Robin Stride, editorial director Email: robin@ip-today.co.uk Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the journal or our website business and lifestyle directories, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912 Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners.
£90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE
Email karen@marketingcentre.co.uk or phone 01752 312140
Publisher Gillian Nineham Phone: 07767 353897.
Email: gillian.nineham@gmail.com
Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.