The business journal for doctors in private practice
Packed with news, views, tips and articles to support you in your private practice
What patients really want Consumerism in healthcare is on the rise. But do we know what patients want? P16
New inspection rules
The CQC has published draft rules for private practices. Have your say before 19 October P22
Top-class private nursing
An experienced matron outlines the top ten qualities to look for in a private nurse P34
Fraudsters’ target is YOU
By Robin Stride
Private consultants and GPs are being put on red alert over rising threats to their practice finances from fraudsters.
Independent practitioners and their staff are seen as potential easy targets from criminals responsible for conning the cash from over 40% of businesses in the UK last year alone.
Doctors face attacks from an arsenal of sophisticated stings including:
n Phone scams;
n Malicious software;
n Phishing;
n Mandate fraud;
n Cheque cheats.
Now Lloyds Bank has joined with Independent Practitioner Today in this issue to help readers beat the maze of trickery being used by criminal gangs to try and steal their money.
Head of healthcare banking services, Ian Crompton, warned: ‘An independent practitioner, or any healthcare professional, is likely to be a target. They are high earners and there is probably a perception they move money around and have large amounts, and that’s what fraudsters target.
Calling all new
‘I would advise any independent practitioner to advise their staff to be extra careful because there is such a lot of this fraud going on at this present time.
‘The fraudsters don’t care about the business – all they care about is an opening. We are keen to get this message across to independent practitioners and the staff working for them.
‘Anyone could be a target and they could lose many thousands of pounds – it can be tens of thousands. People think it won’t happen to them, and it does.’
Lloyds Bank said a spate of large cases recently affected veterinary surgeons. But once target groups knew they were being attacked, they increased their defences, so criminals moved to other businesses where they thought there was money.
The trusting nature of the medical profession also makes many
doctors and staff vulnerable to attack.
Mr Crompton warned: ‘These guys will try and defraud whomever they think they can. Everybody should be on their guard, especially if they have credit balances.
‘What fraudsters try and do is to get someone to release their codes and even while you are speaking to them, they are taking money out of your account. They are very clever in what they do and it is effective.
It’s a bit like opening your wallet to them; they are so credible that people get drawn into it.’
Lloyds Bank is also warning of a recent escalation in employee fraud, most commonly when corrupt staff present cheques drawn on a business account for personal gain. This is usually done by forging signatures.
n See page 32
independent practitioners
Don’t miss our seven-page ‘Starting a private practice’ section featuring three articles from experts to help you in the early days and beyond n See pages 24-31
map out your marketing plan advice on creating a marketing strategy for your aesthetics medicine business P20
make sure you get paid Why it’s vital to consider the management of billing and collection at the outset P26
lock out the scammers stop fraudsters using scams to get their hands on the funds in your practice P32
it’s how you tell ‘em that counts a pr expert explains what the media looks for and how to use it to get publicity P38
don’t put all your eggs in one basket our resident investment advisers explain why it’s important to spread your risk P44
lessons learned from the 2015 budget a specialist medical accountant analyses how the budget affects private doctors P54
our regular columns
Dilemmas:
PMI salesmen devise plan to fight tax rises
by robin stride
The professional body that helps bring insured patient business to consultants’ doors has hit back at Government plans to hoist insurance premium tax by a shock 58% from November.
According to the Association of Medical Insurers and Intermediaries (AMII), the Budget’s ‘unrealistic and unacceptable’ rise ( Independent Practitioner Today , July August) will represent the final straw for some customers who will now cancel their cover.
due consideration of the wider impact.’
He claimed the Chancellor and his department had shown a distinct lack of consideration about the wider impact of the ‘illconceived’ decision.
Mr Scullion said cost was one of the single biggest considerations for both employers and consumers as to whether they continued with private medical insurance cover.
It was the single biggest factor in his own business as to why they had cancelled their policies.
Don’t fall victim to fraud
It’s time to get your personal and business chequebooks out. Have a look and see if any cheques have been removed from the back or the middle.
Hopefully, everything is as it should be. But if any pages are missing then, sadly, you could be one of the rising number of people being targeted by fraudsters aiming to make your bank balance less healthy.
Chequebook fraud is just one of the armoury of weapons being used against successful businesses. And stealing blank cheques is only the tip of the iceberg, as Lloyds Bank reveals in this issue of Independent
Practitioner Today (page one and page 32).
Amazingly, over 40% of UK businesses experienced fraud in the last year, so we are confident we will help many readers by highlighting some of the more sophisticated scams.
A number of doctors we have heard about got the shock of their lives when they realised their practices were being milked of thousands of pounds, often over long periods of time.
Doctors are trusted and trusting. And with many having no business background, they could be more vulnerable targets than most.
Tell us your news Editorial director Robin Stride at robin@ip-today.co.uk Phone: 07909 997340 @robinstride
To adverTise Contact advertising manager Margaret Floate at margifloate@btinternet.com Phone: 01483 824094
To subscribe lisa@marketingcentre.co.uk Phone 01752 312140
Publisher: Gillian Nineham at gill@ip-today.co.uk Phone: 07767 353897
Head of design: Jonathan Anstee chief sub-editor: Vincent Dawe 12,450 circulation figures verified by the Audit Bureau of Circulations ediTorial commenT
It has produced a four point plan (see below) to help companies who buy private medical insurance for their employees to limit the damage and reduce costs ahead of the tax rise from 6% to 9.5%.
AMII chairman Stuart Scullion said: ‘While I think many of us expected there to be an increase, we are both surprised and disappointed at the size and scale of such an increase, which appears to have been announced without
Mr Sculllion, managing director of PHP, said tax relief on premiums for subscribers who were either aged over 60 or retired would have been a better way to stimulate demand and release the pressure on the NHS.
He told Independent Practitioner Today: ‘The Government should be encouraging subscribers to private medical insurance as a means of releasing some of the current pressures being felt throughout all sectors of the NHS.’
figHTing Talk – wHaT
THe amii advises
1 if your renewal date is prior to the 1 november and you currently pay monthly, consider switching to annual payment. This will save the 3.5% insurance premium tax uplift and could provide a further saving of between 4-5% as a result of the monthly payment premium.
2 if you are considering introducing private medical insurance as a new staff benefit – do it before the 1 november 2015 and pay annually. This will delay the impact of the increase until november 2016.
3 consider introducing or increasing a policy excess. £100 excess applied to all plan members would typically reduce premiums by between 8-10%. These are estimates not specific to any provider.
4 company schemes with more than 100 staff covered should consider a non-insured/self-funded option under a health care trust which does not attract the tax.
Call to stop insurance fall
by leslie berry
Latest figures showing a further drop in the number of patients with private health cover serve as a ‘wake up call for us all’ in the sector, a Bupa boss has warned.
UK general manager Alex Perry claimed more people would not take up medical insurance unless it became more affordable – but November’s insurance premium tax rise (see story opposite) would be a blow to affordability.
He said: ‘The need for fundamental reform is more pressing than ever – the whole sector must work together to improve affordability, demonstrate the quality we deliver and improve the customer experience.
‘If we increase the number of people accessing private health
care, we can start to take some pressure off an overloaded NHS.’
Market analyst LaingBuisson puts the number of UK private medical cover policies (insured and selfinsured) at 3.94m at the start of 2015, down from 3.97m in 2014.
It said policy numbers were now 9% below a 4.32m peak seven years ago, with 10.5% of the population covered compared to 12.3% in 2009.
There were similar falls of around 14,000 for both companypaid policies and individualpaid policies last year.
Report author and economist Philip Blackburn said the insurance premium tax rise was needed ‘like a hole in the head’ and medical cover was at a crossroads.
‘A lack of growth in volume
demand when the UK economic cycle is at a strong point, suggests there are barriers to a wider market which need to be addressed.
‘While tackling high costs of cover needs to be an ongoing priority for everyone within the
private healthcare industry, demonstrating the financial benefit of private healthcare to employers would appear imperative for longterm market prosperity.
‘To this end, investment in the value of private healthcare is required from insurers, hospitals and doctors alike.’
He said longterm growth of corporate medical cover depended on the tangible financial and nonfinancial payoffs to employers as a core part of health and wellbeing spend. Insurers were making progress to quantify these.
Health Cover UK Market Report 12th edition. Cost: £1,335 for individual package (£3,235 office package) including printed copy, PDF and Microsoft Excel data files. www. laingbuisson.co.uk
Group’s big fine is warning to all
An opthalmologists’ membership group fined a six figure sum for breaching competition law is taking steps to ensure members and staff are fully aware of legal requirements in future.
Consultant Eye Surgeons Partnership (CESP) Ltd said its board was putting a ‘comprehensive competition law compliance programme’ in place and was committed to ensuring compliance.
It declined to add to a prepared statement until at least after board members meet next month.
CESP was fined £500,000, reduced to £382,000, by the Competition and Markets Authority (CMA) after admitting liability for a number of infringements:
Recommending its members refuse to accept lower fees offered by an insurer, and that they charge insured patients higher selfpay fees.
Circulating among members detailed price lists for ophthalmic procedures such as cataract surgery to be used with insurers. These collectively set prices did not pass on lower local costs –such as cheaper hospital fees – and
made it harder for insurers and patients to obtain lower prices.
Facilitating the sharing of consultants’ future pricing and business intentions such as whether to sign up to a private hospital group’s package price, which enabled members to align their responses.
CMA’s reduced fine involved discounts for adopting a compliance programme and settlement.
CESP, representing interests of 37 limited liability partnerships (LLPs) and their 200 consultant members, said it cooperated with the CMA throughout.
It provides members with a number of services including access to CESP negotiated contracts with insurers. Each LLP has a board representative.
The CMA’s Ann Pope said this was the first time formal competition law enforcement action had been taken against medical professionals in the UK.
She said: ‘This case demonstrates the CMA’s commitment to taking action in specialised and regulated sectors including the professions and makes it clear that
membership organisations and their members are not outside the scope of competition law or its penalties.’
The CMA hoped other professional membership organisations
would note the case and ensure they operated without infringing competition law.
It will work with businesses in the sector to ensure they understand how to comply.
fiPo takes competition case to court of
appeal
The federation of independent Practitioner organisations (fiPo) is pressing ahead with its legal challenge arising from the competition and markets authority (cma) inquiry into private healthcare. after taking legal advice, it is due to take its case against the competition appeal Tribunal (caT) to The court of appeal. last april, the caT dismissed fiPo’s appeal on all seven grounds of its challenge (independent Practitioner Today, may 2015).
The doctors’ body is challenging the cma finding that the power of private medical insurers has no adverse effect on competition. it was ‘disappointed’ with a two-to-one caT majority judgment backing the cma’s view that private medical insurers’ power had no adverse effect on competition.
fiPo vowed then to pursue ‘all options available’. it has been buoyed by the strong dissenting opinion from the tribunal’s non-lawyer member, economist dermot glynn.
The organisation has told consultants that it has also made representations to the cma to reconsider some issues due to developments arising since the authority’s report last year that threaten private practice livelihoods.
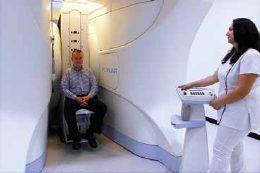
Beaming rays of hope
By Edie Bourne
The healthcare company behind plans for a new 150-bed hospital offering proton beam therapy in London aims to bring in existing UK clinicians and support staff as well as physicians from the United Arab Emirates for visiting programmes.
Billion-dollar Abu Dhabi-based VPS Healthcare aims to open its cancer centre in 2017 at the site of the historic grade II listed Royal
Masonic Hospital in Hammersmith, which closed in 2006.
It has 12 hospitals plus medical centres, pharmaceutical manufacturing operations, an international pharmacy retail chain and medical support services spread throughout the Middle East, Europe and India.
Founder and managing director
Dr Shamsheer Vayalil said entering the UK was ‘a long-held personal dream of mine’.
Although proton beam therapy is
not yet available in the UK, work has started on a new centre in Newport, Wales, due to open next year. Proton Partners plans others in Northumberland and London by 2017.
These will be available for NHS patients from England, Scotland and Wales, medically-insured private patients and self-payers.
Proton’s chief medical adviser, Prof Karol Sikora, said there was ‘a pressing need’ to make the treatment more accessible worldwide.
‘Proton beam therapy can be
Hospital’s charitable act for soccer fan
things are really kicking off for chelsea fan Jude Liversage, aged seven. He can now walk flat-footed for the first time after a selective dorsal rhizotomy (sdr) performed by consultant neurosurgeon Mr Kristian Aquilina (pictured, inset) at the Portland Hospital, London.
the hospital’s sdr unit, the first of its kind in the uK private sector, waived much of its bill after hearing his story.
Amazed dad tony Liversage, who works on a football team of children with cerebral palsy, said: ‘it really is remarkable and gives us hope that, after a period of rehabilitation, Jude will be able to be more mobile and more independent and eventually be able to kick a ball around like other kids.’
only about 25% of children between the ages of four and ten with cerebral palsy may be able to benefit from sdr, designed to reduce spasticity in the legs and ankles.
A few sdr cases have been seen at a handful of
nHs specialist centres, but the us option for the operation can cost three times as much. the Liversage family’s hopes of treatment were almost dashed after realising they could raise less than half of what they needed –despite a high-profile fund-raising programme.
Plans for helping sick doctors
Key principles for improving services for doctors with mental health and addiction problems were highlighted at a roundtable discussion of interested parties hosted by the GMC.
Talks considered one of the recommendations outlined in an independent review of doctors who take their own lives while under investigation by the GMC, published last December.
This was to set up a national support service for doctors with mental health or addiction problems.
Principles highlighted by the ‘talking shop’ for the development of services in this area included:
All such services should be separate from the GMC and seen to be separate;
There must be liaison with the GMC where there is a risk to patient safety;
Clear rules are needed around information disclosure and the relationship with the GMC so that doctors are not discouraged from accessing help;
Systems need to be in place
within organisations to encourage early awareness and early intervention, as well as making sure there are support services for doctors with complex issues;
Services must be accessible and confidential. This is vital if doctors are to have the confidence to selfrefer and disclose.
The GMC said it would work with experts in this area to encourage better support as well as seeking their help as it reformed the way it dealt with this group of doctors.
See ‘Doctors’ stress revealed’, p10
used to treat a diverse range of cancers. It damages less of the surrounding tissue and gives patients a greater chance of avoiding longterm side-effects,’ Prof Sikora said.
Figures from the company said, in 2012, 140 patients from the UK were sent abroad for treatment at a cost of £114,000 each to the Department of Health. And it is anticipated NHS demand for the therapy will reach 1,500 patients by 2017 at an estimated cost of £171m – based on 2012 cost data.
App-licable to all your CPD needs
Doctors can manage their continuous professional development on the new app: ‘GMC My CPD’.
Aimed at everyone on the medical register, it allows doctors to record learning activities on the go at the click of a button on a mobile device.
Whether on the way back from a seminar or when they have received some good advice from a colleague, the app aims to provide a useful way for doctors to store learning points.
It also allows them to set a reminder to ask them later if changes to their practice have been effective.
The app will allow doctors to record all aspects of their work wherever they are, so long as they have their mobile with them.
Many already have a system for managing their continuing professional development, although not necessarily a portable one. The GMC said the app can complement those systems or act as a single way of recording learning for those who do not yet have one.
In addition, the app will allow them to photograph learning certificates and voice record their ideas and thoughts.
The app can be downloaded via Android and Apple app stores.
‘don’t walk blindly into this tax charge’
Patrick Convey (left) of Cavendish Medical
Doctors miss out by lack of website
Thousands of independent practitioners are losing potential patients because they have no website presence.
According to a report from website specialists, only 50% of private doctors have a website.
Beware of tax grab on saving for pensions
By Leslie Berry
Senior doctors are being advised to seek help now rather than risk losing huge sums unnecessarily from an imminent pension ‘tax grab’.
Financial advisers warned this month that the Government has already increased the tax it has collected from people breaching the pensions lifetime allowance (LTA) by a staggering 276% since George Osborne became Chancellor of the Exchequer.
Under the LTA, the amount savers can pay into their pensions free of tax is limited. The current limit is £1.25m – but this will be cut to £1m in April 2016.
And those who breach the allowance are subject to tax on the excess charged at up to 55%.
The LTA has been chopped many times since its introduction in 2006. It was cut to £1.5m in April 2012 from its peak of £1.8m in 2011.
In 2009-10, HM Revenue and Customs collected almost £25m from people breaching their pension contributions limits. However, in 2014-15, the tax receipts rose dramatically to £94m.
Another less-publicised effect of the cut in the LTA is that in return the amount individuals can draw out free of tax is also reduced.
When the LTA was £1.8m, individuals could draw a pension lump sum of up to £450,000. This was normally paid tax-free, subject to certain rules. With an LTA of £1m, that amount has been reduced to £250,000.
Patrick Convey, technical director at financial planning specialists Cavendish Medical, told Independent Practitioner Today : ‘This substantial increase in tax revenue shows that with the constant reductions to the LTA limit, more professionals are being caught out.
‘The rate is being cut again next year, meaning many senior doctors could trigger an extra tax charge.’
He warned: ‘This also proves that the Government’s pension protection schemes are often too complicated for many savers to use effectively. We have seen many new clients who come to us having previously been poorly advised in this area.
‘Do not walk blindly into this tax charge. Your tax liabilities could be minimised with careful planning. Seek help without delay.’
HMRC has yet to confirm details of new protection schemes to coincide with the cut to the LTA in 2016. These are expected by the end of the year.
A quarter have a minor listing or nothing at all online, while the remaining 25% appear only as a biography on a private hospital or clinic website.
Smart Medical Web claims its research shows the industry is falling behind patients’ expectations.
Co-founder Chris John said that private doctors had been slow to meet online expectation despite the fact that it was widely understood that a successful online presence drives retention and business growth.
He said: ‘Not only did only 50% of the UK private medical practitioners not have a website, but just having one isn’t enough. Ninety-one per cent of private patients said their choice is influenced by its look and feel.
‘Being complacent with an outdated biography on a clinic or hospital website or a personal site
created a decade ago isn’t an option.’
Fifteen-hundred current and pro spective UK private patients were surveyed on the process of seeking an independent practitioner by OnePoll.
The report uncovers a number of areas that it says require attention to support the business retention and growth of independent practitioners.
Smart Medical Web, which puts the average website quality score for the private medical sector at 35%, said: ‘Ultimately, a lack of online presence or a “dated” and unprofessional website can cause a patient to look elsewhere.’
Mr John added: ‘Private medical practitioners are notoriously busy, often juggling the dual role of supporting both NHS and private patients. But neglecting to meet the expectations of today’s digital consumer may negatively impact the opportunity for business growth in the future.’
To register to receive the report, go to www.smartmedicalweb. com/pre-register-for-the-privatepatient-survey-report.
BiggEst wEBsitE turn-offs incLudE:
45.2% of private patients are negatively influenced by the lack of information available to explain treatments
the general look and feel of a website being outdated is the second biggest turnoff (23.47%)
only 30% of private practitioner websites can be viewed by mobiles
75% of private medical practitioner sites are not equipped for search engine optimisation
Offshore tax evaders and those enabling it will face even tougher sanctions under a new crackdown.
Financial Secretary to the Treasury, David Gauke, warned: ‘Time’s up for people who don’t pay their fair share of tax by hiding their money offshore.
‘People who evade tax, facilitate or turn a blind eye to tax evasion
will now face powerful criminal and civil sanctions under our tough new regime.’
HMRC is consulting on:
A new criminal offence for offshore evasion – so you can no longer plead ignorance;
Increasing financial penalties including a penalty to the value of the asset hidden offshore; Publicly naming evaders.
Help to expand business
By Robin Stride
New and experienced independent practitioners are beefing up their business with help from leading experts in the healthcare sector who have joined to recreate a unique consultancy.
Led by Keith Hague, former chief executive of the UK’s largest private hospital, The Wellington, Worldwide Healthcare Associates (WHA) is helping healthcare organisations manage and transform their businesses, both in the UK and overseas.
Mr Hague told Independent Practitioner Today: ‘All clinicians aim to serve their patients at the highest standards and, to many, starting or running a practice or
business can be a daunting and distracting burden.
‘We exist to help independent practitioners start, transform and grow their practices and businesses, conceive, plan and develop medical facilities and to market their services using all available communications channels and technologies.
‘We can take away the burden of managing that business.’
WHA, based in Hanover Square, London, was originally formed by Mr Hague and Mike Hall 18 years ago. Its ten associates have proven track-records in their own area of expertise within the healthcare sector, ranging from clinical care to all aspects of business management.
The company has access to potential investors and helps with planning, recruitment, staff development, technology, operations and crisis management and clinical advice.
It also liaises with healthcare stakeholders in the private and public sectors here and abroad.
Mr Hague said WHA built unique teams for every situation and changed that team as clients’ needs changed.
He added: ‘We combine clinical expertise with commercial sense, and we know where technology fits in – we see the full picture and provide support where it’s needed most.’
www.worldwidehealthcare.
co.uk
Rise in sexual assault gripes prompts advice
A rise in sexual assault allegations against doctors has prompted new guidance from the Medical Defence Union (MDU).
The medical defence body said allegations against members rose 66% over a recent 11-year period with 12 allegations in 2003 compared to 20 cases in 2013.
There were 167 cases of doctors being accused of sexual assault over the 11-year period, with most being cleared after investigation.
Medico-legal adviser Dr Beverley Ward said: ‘Allegations of sexual assault against doctors are increasing, although overall the number of cases remains very small – averaging around 15 cases per year, in our experience.
‘While, in the vast majority of cases, the doctor is cleared of any wrong-doing, the investigations into the incident can be prolonged, damaging for the doctor’s career and is distressing for all involved.
‘If the media pick up on the story, it can be very upsetting, as
even if the doctor is later cleared, he may feel his reputation has been tainted.’
She said cases usually arose from misunderstandings such as a patient not understanding why a
symptom in one part of the body might require an examination elsewhere.
A chaperone was not present for any of the sexual assault allegation cases notified to the MDU in 2013.
To Avoid miSundeRSTAndingS:
Follow gmC advice on intimate examinations and be aware of policies such as offering a chaperone
ensure the patient knows what is involved in the examination when getting their consent.
Be aware that some patients may consider routine touching or even being close to them – such as performing ophthalmoscopy in a darkened room – as intimate and requiring a chaperone
give patients privacy to dress and undress and avoid lighthearted or personal comments
Stop examining if the patient asks; for example, if they are experiencing discomfort
Keep records of the discussion with the patient, why the examination was clinically indicated, that a chaperone was offered and whether the patient accepted or declined
From ‘Protecting yourself from a sexual assault allegations’ ☞ www.themdu.com/guidance-and-advice
Healthcode’s electronic billing boost
Hospital providers at group and local level are being helped to resolve any e-billing difficulties under a new initiative from Healthcode.
The company has appointed Sam Hobbs to lead on optimising electronic billing for insured patients.
It is hoped to improve the proportion of submitted e-bills which are complete, correct and can be validated first time.
She will work with hospitals on things like staff training and system changes to help them meet industry billing standards.
Ms Hobbs said e-billing was one of the most effective ways to cut administration costs and boost cash flow. Simple errors and omissions could cause bills to be rejected and lead to frustrating delays. But problems could often be quickly resolved.
Managing director Peter Connor said the main insurers expected to receive bills electronically but this was in providers’ interests too, as it was quicker and more secure.
‘We can take away the burden of managing that business’ Keith Hague, chief executive officer Worldwide Healthcare Associates
One in five self-diagnose on web
One-in-five people admit to self-diagnosing illnesses rather than make time to see a doctor.
Research in the UK Digital Health Report, from on-demand video GP service PushDoctor.co.uk, reveals 21.8% of people have chosen to try and diagnose their symptoms on the web because:
They were unable to get a doctor’s appointment (11%) or;
Their GP wasn’t available quickly enough (10.8%).
When asked what they would not be prepared to cancel in order to fit in a doctor’s appointment for a health issue causing them
‘moderate concern’, 47% were not even prepared to get out of bed, saying they would not miss the chance of a lie-in.
The internet was the first place all age groups under 65 went for advice when starting to feel unwell.
Analysis of data from 61m UK internet searches for 160 leading health issues reveals the trend for self-diagnoses is on the rise, up 19% over the last 12 months – an average of an extra 848,000 searches monthly.
PushDoctor chief medical officer Dr Adam Simon said: ‘As well as health searches being
on the rise, 58% of people now actively use technology to manage their health and wellbeing on a daily basis.
‘Twenty-two per cent use devices to monitor exercise and activity, 15% use tech to track their daily calorie intake and 12% to monitor sleep quality.
‘People feel good about how technology is helping them keep track of their health. Seventy per cent of people say that new technology helps them feel more in control or more aware of how to manage their health and well-being.’
See ‘What patients really want’, page 16
Physio plan’s fast relief
By a staff reporter
Patients with musculoskeletal (MSK) pain are getting fast-track access to the help they need using a physiotherapy self-referral service run by Bupa.
The insurer’s UK medical director Dr Steve Iley said the service helps customers get advice and any treatment needed quickly.
He said: ‘Historically, the options available for supporting and treating patients with musculoskeletal conditions were more limited to face-to-face appointments with physiotherapists and orthopaedic surgeons.
‘These types of treatments and the time they require may not suit busy lifestyles and can put some people off seeing their GP about MSK pain. This could delay them getting the necessary treatment, particularly if they don’t think any of these options fit their condition.’
The self-referral service also provides access to self-help videos, physiotherapists, orthopaedic physicians and surgeons – offering a range of self-help and assisted options to support the best possible outcome.
Bupa said 10% of customers ringing the physiotherapy selfreferral phone service did not need to see a physiotherapist at all following specialist advice, such as to rest or do exercises, and there was an average 30% reduction in the need for surgery.
Although over half of British adults say they have suffered from muscle, bone or joint pain, new findings from Bupa reveal that 23% people are taking a ‘grin and bear it’ approach – admitting they would wait at least a month before seeing their GP about their pain.
And 20% say it is unlikely they would speak to a GP about the condition at all.
A Bupa survey of 2,010 British adults reveals people who are choosing not to see their GP about musculoskeletal conditions make this decision for a number of reasons:
23% worry it would be a waste of time;
11% claim that they would not have enough time in their day to see a doctor about their condition;
30% do not believe muscle, bone or joint pain is a serious medical problem.
The insurer found the British public is seeking other ways of treating muscle, bone or joint pain:
37% would consider alternative therapies, such as yoga or going to the gym;
33% of people say that they would manage their condition with painkillers rather than see their GP;
25% would recommend treating muscle, bone or joint pain with home remedies, such as hot baths.
Katherine Cran, physiotherapist at Bupa’s Basinghall Health Centre, east London, said: ‘In these cases, quick access to professional advice and treatment is key, which is why we support customers to get immediate advice over the phone through our physio therapy self-referral service, helping people to recover sooner and prevent recurring long-term problems.’
The survey found that women
in particular are reluctant to seek GP advice about muscle, bone or joint pain. Twenty-eight per cent said they would wait over a month or more to see a GP about these conditions, compared to only 18% of men.
Women are also more likely to turn to painkillers, with 38% saying they feel they could manage muscle, bone and joint pain with painkillers, versus 27% of men.
Almost half (42%) of women also believe that those suffering from muscle, bone and joint pain should seek alternative ways to get better, such as practising yoga or going to the gym, compared to 32% of men.
A further 10% of women would choose to treat this type of pain with natural home remedies, such as a hot bath, heat wrap or massage, versus just 5% of men.
ComRes online survey of 2,010 adults, 22-25 May 2015. Figures have been weighted and are representative of all GB adults aged 18+. Thirty per cent of Bupa claims are for MSK treatment and services
Tell uS youR SToRy
Share your experience of what has and has not worked in your private practice. even if it’s bad news, let us know and we can spread the word to prevent other independent practitioners falling into the same pitfalls.
Contact editorial director Robin Stride at robin@ip-today.co.uk
Bupa medical director dr Steve iley
Limit to GMC raps
By Charles King
New time limits for how long sanctions on a doctor’s registration are published online or made available to the public could be on the way.
Under current rules, when a doctor receives a sanction, the outcome is published on the GMC website and disclosed to anyone who asks. It remains online indefinitely, even after any restrictions have been lifted.
This includes details of doctors who have been suspended, had restrictions on their practice, agreed undertakings such as retraining or been erased from the medical register.
But now the council proposes new time limits depending on the sanction imposed and whether the doctor is still practising.
A suspended but still registered
NEWS IN BRIEF
doctor would have their sanction published for 20 years under these proposals. After then, it would no longer be made available online or disclosed to the public.
The GMC’s website includes sanctions placed on a doctor’s registration following fitness-to-practise investigations from 2005 onwards, when electronic records were introduced. Older sanctions, while not published online, are available on request.
Now it is proposed to give patients more information by transferring online all sanctions given to still-registered doctors for complaints arising from 19942005.
Publication of these sanctions will also be subject to time limits to make sure that they are only published for as long as it is in the public interest to do so.
The consultation also includes
NHS waits get longer
NHS patients are waiting longer than ever for surgery, according to new research from the Patients Association.
It said the average waiting times for hip replacement, knee replacement, operations on hernias, adenoids, gallstones, cataracts and tonsillectomies were all above 90 days.
Plastic surgery support
The British Association of Plastic, Reconstructive and Aesthetic Surgeons (BAPRAS) is calling for greater provision for plastic surgery patients to access psychological support during or following reconstructive treatment.
Ninety-three per cent of members surveyed said access to specialist psychological assessment and treatment was important for their patient group. Sixty-four per cent saw patients in need of psychological support every week.
Manchester scan suite
Nuffield Health, in partnership with Manchester Science Partnerships (MSP), has announced details of its plan to open a ‘five-star’ diagnostic suite at Citylabs in Manchester city centre in November.
It will deliver MRI, X-ray, mammography, CT and cardiac and ultrasound services plus
proposals to make decisions clearer in cases where a doctor has appealed a sanction or agreed undertakings.
GMC chief executive Niall Dickson said: ‘Under Human Rights law, we have to be proportionate and we have also reflected on changes in the law around the disclosure of criminal convictions.
‘As a result, we have concluded that publishing sanctions indefinitely in some situations could be disproportionate, if it happened a long time ago or if the doctor is no longer practising.
‘We want to strike the correct balance between the rights of patients to know and a doctor’s right to privacy.’
The GMC was ‘keen’ to hear from doctors so that it could get this balance right. The deadline is 23 September and the new policy is due next August.
private GP appointments, health assessments, and physiotherapy.
Formerly the Royal Eye Hospital, Citylabs is Manchester’s new centre for biotech businesses including laboratories and medical research facilities, as well as a retail and teaching space.
Call for fertility checks
Mr Michael Dooley, consultant gynaecologist at the Poundbury Clinic at King Edward VII’s Hospital Sister Agnes, is calling for fertility checks for women from the age of 25 to maximise their chances of successfully having a child.
He said: ‘We get our cars checked once a year, yet why don’t we get our fertility regularly checked? For a couple trying for a family, a fertility check can be life-changing.’
Post-travel clinic opens
Dr Sharon Marlowe (right), a specialist consultant in infectious diseases, has opened what is billed as the ‘South-west’s only post-travel clinic’ at Spire The Glen Hospital Bristol.
The Post-Travel Clinic for Tropical and Infectious
New Nuffield unit opens
Fifty consultants went on an unusual ward round – inspecting Nuffield Health’s new £30m Cambridge Hospital before the official opening next to its old building, which continued to function throughout the works. Space and the deliberate design to allow as much natural light into the building as possible was particularly well received.
Consultant orthopaedic surgeon Mr Graham Keene said: ‘It is amazing to see how much light floods into the new operating theatres – quite a unique offering nowadays. That, coupled with the fantastic technology is a recipe for success.’
Diseases is for those feeling unwell after returning from an exotic travel destination. Test specimens are sent directly to the National Parasitology Reference Laboratory at the Hospital of Tropical Diseases or to the Rare and Imported Pathogens Laboratory.
Bowel screening first
The London Clinic has announced it is the first UK private hospital to introduce Endocuff Vision (pictured above), a new device to help increase the detection of pre-cancerous polyps as part of bowel cancer screening.
Aspen’s safety accolade
Aspen Healthcare Group hospitals have been awarded AfPP (Association for Perioperative Practice) accreditation for theatre safety, effective risk management strategies and ongoing commitment to patient safety.
For the last 18 years, we have been helping healthcare organisations manage and transform their operations, both in the UK and abroad.
YOUR BUSINESS SUCCESS BEGINS HERE.
We exist to help independent practitioners start, transform and grow their practices and businesses. We help to plan and develop medical facilities and to market healthcare services using all available communications channels and technologies. While you concentrate on caring for patients, we aim to take away the burden of managing your practice or business.
We build unique teams for every situation and change that team as your needs change and, uniquely, we have experts who can deal with crises who are available 24x7. We combine clinical expertise with commercial sense; we see the full picture and we provide support when and where it’s needed most.
We work with both public and private sector healthcare providers, and we have an enviable track record in operations management, clinical advice, consultancy and development.
For an introductory discussion, please call Keith Hague CEO on +44 (0)3356 9699. www.worldwidehealthcare.co.uk
Doctors’ stress revealed
By a staff reporter
A defence body survey of more than 600 UK members reveals that 85% have experienced mental health issues, with common issues being stress (75%), anxiety (49%) and low self-esteem (36%).
A third of respondents told MPS they have had depression during their medical career, while one in ten (13%) stated they had experienced suicidal feelings.
Of those who had experienced mental health issues, they cited heavy workload (76%) and long
working hours (70%) as factors that had a high or moderate impact on their mental health.
Additionally, high levels of regulation and scrutiny affected half of respondents’ mental health, and experience of a negligence claim had an impact on a quarter of them.
The effect on their professional life is striking, as 60% believe their mental health issues had an impact on their concentration and 36% felt it impacted on their empathy towards patients.
Four in ten of those affected did
EYE ACHIEVERS
Optegra Eye Health Care has selected Fight For Sight as its corporate charity.
It said the charity’s focus on eye research was ‘a perfect synergy’ with its notfor-profit research and development division, Optegra Eye Sciences. The company’s hospitals in the UK will host fundraising events in October.
Optegra’s new chief to raise firm’s profile
The new UK boss of Optegra Eye Health Care UK has spoken of his aim to increase awareness of the broader scope of the company’s expertise.
Managing director Rory Passmore said: ‘Refractive surgery is vital to our business and continues to be a core part of our service, but we also offer so much more.
‘Our first-class surgeons have a wealth of experience and knowledge to diagnose and treat the most complex of eye conditions. Our UK focus is to drive awareness in the market to ensure that patients understand that we can treat the full range of A to Z of eye health.’
Next year sees a new phase for
the company when it opens the multi-million-pound Optegra Eye Hospital London just off Harley Street at 25 Queen Anne Street.
It said the purpose-built facility was designed to give patients ‘an exceptional experience’ and would be a leading location for technology and expertise.
Mr Passmore has held previous senior healthcare roles in South Africa before moving to the UK seven years ago to work for BMI Healthcare as regional director.
Optegra has also given itself a new brand identity to help raise its profile in its hospitals’ local areas and build closer relationships with optometrists, opticians and GPs.
not discuss their issues with anyone, with 58% of those believing they did not need support and a quarter (24%) feeling there was a stigma attached to mental health issues.
MPS senior medico-legal adviser Dr Pallavi Bradshaw said: ‘Doctors help their patients with mental health problems but they often suffer alone. The experience can be isolating and can have a negative impact on professional confidence.
‘Medical Protection urges colleagues of doctors to look out for
signs of mental health problems and offer support, such as talking through issues or helping to balance their workload.
‘It is important that doctors know that seeking help will not automatically lead to a referral to the General Medical Council or put their careers at risk.
‘Colleagues should provide support to those who may be vulnerable and in the interests of providing the best care to their patients.
Doctors must seek help as soon as they experience mental health difficulties.’
Live demos top bill at aesthetic expo
Europe’s largest medical aesthetic showcase, CCR Expo, says it will offer the sector’s most exciting live demonstrations and seminars completely free with registration for its third annual event on 8-9 October at the London Olympia Grand Hall.
The Expo has been hailed as leading the way for a new era of collaboration between the surgi cal and non-surgical disciplines, despite historically disparate branches of the aesthetic sector.
Live demonstrations will offer the latest in lasers, thread lifts, micro-need ling, nutra- and cos mecuticals, showcase how cryo lipolysis meets radiofrequency, and offer up-to-the-minute tech niques for non-surgical body con touring, dermal fillers and hair-removal.
The seminar programme includes ‘Getting Started in Aesthetics’ workshops with presentations including setting up, trendsetting promotion and marketing techniques, how to optimise digital media, introducing cosmeceutical lines, and futureproofing your business.
Other topics are training, how to stand out from the crowd while adhering to best practice guide-
lines and insurance claims unique to cosmetic surgery and non-surgical treatment.
Show chief executive Peter Jones said last year’s feedback showed doctors wanted to know how to start out in aesthetics, not how to manage an already thriving practice.
‘Our strapline for the Getting Started in Aesthetics Theatre is “If you’re going to do it, do it right” and this is exactly what we are hoping to achieve with this exciting programme of speakers, discussions and demonstrations.’
The event offers 200 exhibitors and presentations from clinicians worldwide. To register, go to www. ccr-expo.com.
See aesthetics medicine feature on page 20
Rory Passmore, MD of Optegra, welcomes Catherine Woodhead, director of fundraising at Fight For Sight, to Optegra Eye Hospital Surrey in Guildford
TRAINING DATES
WIGMORE medical TRAINING
SEPTEMBER
OCTOBER
NOVEMBER
2 Non-Surgical Rhinoplasty NEW
6 Mini-Thread Lift & Dermal Filler*
7 Advanced Toxins* (am)
7 Advanced Fillers-LF* (pm)
Mini-Thread Lift & Dermal Filler*
DECEMBER
Skinrölla Dermal Roller (pm)
Skincare & Peels
ZO Medical Basic (Dublin)
ZO Medical Adv. (Dublin)
Intro to Toxins*
Intro to Fillers*
26 ZO Medical Basic
27 ZO Medical Interm.
28 ZO Medical Adv.
‘Accept that patients want to record you’
By Edie Bourne
Doctors may not like the idea of patients secretly recording consultations, but the law offers them little or no protection against it, a defence body has warned.
MDDUS advised independent practitioners who find themselves in this situation to avoid defensive reactions and simply accept it as a product of the digital age.
Increasing smartphone use makes it easier for patients wishing to make an audio – or in some cases a video – recording of a medical appointment with their doctor.
MDDUS medical adviser Dr Mary Peddie said: ‘Patients don’t need a doctor’s consent to record the consultation, as section 36 of the Data Protection Act 1998 considers that the information in the recording belongs to them.
‘Some doctors may believe that recording consultations is intrusive, shows a lack of trust and is damaging to the doctor-patient relationship. However, patients
have the right to record a consultation and then use the information obtained as they choose.’
The MDDUS said, in its experience, the majority of recordings supported the actions of the doctor and confirmed they acted appropriately, both personally and clinically.
Dr Peddie said a recording may help avoiding misunderstandings. ‘We are all aware that patients often do not understand a doctor’s best attempts at explanations in layman’s terms. It is worth considering whether there may be a genuine and positive reason for the patient recording the appointment.
‘Doctors should discuss these reasons with their patient. Patients may not feel confident of remembering or fully understanding complex instructions from their doctor or they may wish to share the information with their family to help them reach a decision on treatment options.’
Even covert recordings can be admissible evidence in court.
Diagnostics clinic takes over Harley St premises
Nuada Group, the healthcare enterprise co-owned by a partnership of doctors, nurses and healthcare professionals, has acquired the lease of facilities at 19 Harley Street from Renaissance Healthcare.
These include a diagnostic and surgery centre with two operating theatres, a full imaging suite and over 12 consulting rooms.
The centre has been fitted with modern medical equipment, including a latest generation CT scanner, fluoroscopy, ultrasound and EOS X-ray machine.
Hospital is to move to new site nearby
South Wales’s independent hospital HMT Sancta Maria has won planning permission to develop a hospital at Parc Felindre, north of Swansea.
The new unit will replace the existing HMT Sancta Maria hospital in Uplands, Swansea, which is owned and operated by Healthcare Management Trust (HMT), a not-for-profit independent healthcare provider.
Bosses say the new hospital will be a flagship within HMT’s portfolio, incorporating some of the most up-to-date facilities.
They said it would be equipped to do a significantly enhanced range of services, including the latest-generation MRI scanner, digital X-ray room and diagnostic ultrasound and cardiology suite.
There will be 18 private en-suite patient rooms including a highdependency unit, a six-bed day ward, 13 consulting rooms including dedicated ophthalmology, ENT and plastic surgery rooms,
two ultra-clean, digitally integrated operating theatres and an endoscopy suite.
Work is scheduled to begin in early 2016 and is due for completion in Spring 2017.
HMT Sancta Maria hospital director Stuart Hammond said: ‘We are thrilled that our plans to build a new state-of-the-art hospital in a prime Swansea location have been approved. The location at Felindre, just off the M4 with parking for over 100 cars, will give our growing number of patients excellent access to the hospital and represents a significant investment in Swansea by HMT.’
HMT Sancta Maria works with over 150 of Wales’s leading consultants to provide a full range of healthcare services to south and Wales including cosmetic surgery, orthopaedic, cardiology and general surgery. It was founded in 1985 as a registered charity and has a portfolio of hospitals and care homes throughout the UK.
A spokesman said the group will further develop its partnerships in urology, gynaecology, spine, foetal medicine and medical imaging. These services will be offered at 19 Harley Street and 45 Queen Anne Street, which houses Nuada’s 3T MRI scanner.
The move into Harley Street follows the company’s entry into providing surgical services in gynaecology, urology and spine which began last January and builds on its strong base in prostate cancer imaging and diagnosis.
Doctors hit hard financially
Doctors are suffering from a financial treble whammy, according to a financial provider to the medical profession.
Alan Whiting, of Wesleyan, said doctors were reporting huge changes in their professional lives which were causing them uncertainty and stress.
‘They have seen a drop in income in real terms as pay rises
fail to keep pace with inflation. In addition, changes to the NHS Pension Scheme mean they are paying more to retire later and on less income. Then there are the pension tax changes which are hitting doctors at the latter stages of their career.’
But most doctors told a company survey they would go for the same job if they had their time again.
An artist’s impression of the new hospital to be built near Swansea
The future of eye health care is coming to Harley Street.
A home for pioneering treatments.
Harley Street will soon welcome a pioneering new addition to its clinical line-up: Optegra Eye Hospital London – a dedicated centre for eye care.
Opening December 2015, the new hospital will be the first ever facility on Harley Street to deliver the full spectrum of eye health care under one roof. Inside state-of-the-art facilities, our team of ophthalmic professionals will carry out leading-edge procedures, including laser eye surgery, lens replacement, cataract removal and medical eye treatments.
With a consultant-led approach that has helped to secure Optegra’s reputation as the UK’s most trusted eye health care specialist*, Optegra Eye Hospital London is set to push the boundaries of eye treatment possibilities.
A home for experts.
To learn how to refer patients to our new hospital, or to join the Optegra Eye Hospital London team in an administrative or clinical role, please visit optegra.com/london or call 0808 169 2192.
ACCOUNTANT’S CLINIC: TAx PRObeS
Keep calm when under
investigation
Private doctors have been involved in HMRC tax investigations along with many other businesses in the last few years. Susan Hutter summarises the main types of probe you are likely to be involved in and how these should be handled for the best outcome
There are three main types of inquiry:
1. General – subdivided into:
Full inquiry
This involves a comprehensive review of the underlying records supporting a particular tax return and can include a review of the private financial affairs of the taxpayer as well as the business.
Aspect inquiry
These concentrate on one or more aspects of a tax return. These inquiries cover most of the casework carried out by h M r evenue and Customs (hMrC) inspectors and are the most relevant to doctors.
2. Random inquiry
Only a very small proportion of tax returns will be taken up for a full inquiry on an entirely random basis. But once they have commenced, they will follow the same format as a general inquiry.
3. Compliance review
h M r C carries out compliance checks to make sure a specific tax return is correct. Starting a compliance check does not necessarily mean h M r C believes there are any serious problems.
Indeed, most of these types of checks are routine. But, generally, something will have triggered a check; for example, where the figures on a tax return vary wildly compared to previous years.
Obviously, there is usually a very good reason for this and
these cases are solved in a few weeks.
In all of the above cases, there is no need to be alarmed – unless, of course, you are aware of any wrongdoing, in which case you should ‘come clean’ immediately.
h M r C believes that most of their ‘customers’ are honest and aims to treat them all with respect.
It is obviously troubling to receive a letter out of the blue from hMrC raising inquiries, but if this happens, it is advisable to contact your accountant immediately. They will be used to dealing with such matters and will work with you to obtain the best result.
Professional
fee protection insurance (PFP)
I always recommend that my clients take out PFP insurance, which means that, in the event of a tax inquiry, professional fees are covered by the insurance policy, usually up to a limit of £50,000.
The fees for dealing with a tax inquiry are generally between £1,500 and £5,000 plus VaT.
Bearing in mind that the premiums are relatively inexpensive –between £200 and £300 a year – it is money well spent.
Most accountants will use a registered scheme that they recommend to their clients. If your accountant does not offer one, it is sensible to look at the specialist insurers and take one out directly.
If you do it this way, you should check with the insurer that it is willing to work with your accountant and not just accountants on its ‘list’, as obviously it is better for you if your own accountant can assist with an inquiry on your behalf.
The PFP policy should be put on risk immediately you receive an inquiry letter from hMrC, otherwise the initial charges may not be covered.
Inquiry process
Depending on the complexity, an inquiry usually takes between two to six months to be dealt with.
In most cases, the inquiry will involve an exchange of letters
between you/your accountant and hMrC, and it normally takes two to three letters before the matter has been resolved.
Towards the end of the inquiry, if there are one or two matters still outstanding, h M r C is usually prepared to negotiate and, in most cases, is reasonable. Sometimes it asks to meet the taxpayer, although this is rare. In most cases, the matter will be dealt with by correspondence and/or phone conversations between you, your accountant and hMrC. h owever, if you do have to attend a meeting, you don’t have to panic. It is obviously sensible to go with your accountant, but the reason for the meeting is usually so h M r C can understand a particularly complicated aspect of the case without the need for protracted correspondence.
Once the matter has been agreed, a ‘closure letter’ will be sent by h M r C to the taxpayer and their accountant.
at this point, any extra tax, plus interest, will need to be paid to hMrC. however, in some cases, investigations have shown that a tax refund is payable to the taxpayer and it will then be paid together with interest.
In all cases, try to treat a tax investigation as a business matter and not a personal one.
Susan Hutter is a partner at specialist medical accountants Shelley Stock Hutter
is continuously updated based on the latest medical research to bring you current evidence-based recommendations.
Our unparalleled team of physicians and editors places new research in the context of the existing body of medical knowledge using their professional expertise and first-hand clinical experience.
This combination of Evidence & Experience is invaluable in crafting point-of-care recommendations trusted by more than one million clinicians worldwide.
Plus, you may earn RCGP CPD learning credits while researching topics in UpToDate.
What patients
Independent Practitioner Today ran three stories last month highlighting the increasing case for consumerism in private healthcare. So what do patients really want? Aileen Morrison has researched the subject and reports here on her findings
CoNSumerISATIoN of healthcare means patients being active participants in their healthcare choices, having freedom of choice and a voice to express opinions and feedback just like they have with other purchases.
Consumers are exposed to more choice and voice in all areas of purchasing now, especially with the use of the internet and social media, so it is thought they expect the same in healthcare.
Crosscare - providing private practices with efficient paperless working
Crosscare is a proven clinical system used within private practices and specialist clinics in and around Harley Street and across the UK.
Alongside the standard clinical record keeping and prescribing systems, Crosscare’s appointments, reporting and integrated accounting modules make the tracking of workload, invoices and revenues simple and user friendly.
We understand that each practice works in their own unique way, so being a fully customisable system, Crosscare can be easily tailored to fit your individual needs.
For further information on how our Crosscare solution can help your practice call us now on 01233 722670 or visit www.advancedcomputersoftware.com/ahc
So I wanted to find out to what extent patients expect to be treated as healthcare consumers and if their expectations are being met.
As part of an mBA at Warwick Business School, I used an online questionnaire to survey over 400 people with a broad age range from across the uK.
Normally, patient feedback in healthcare comes from patient satisfaction surveys. But an important difference with this survey was that a large proportion of responses were from people who had not used private healthcare in the past year.
This gave a much broader view of expectations of both current and potential future customers.
Demand for ‘a voice’
The survey showed that patients did expect to have a voice. more
than 90% expected to be involved in decisions about their healthcare, but only about two-thirds felt this was happening.
The majority also felt they had enough information to be involved in decision-making, but despite this, it was not happening. So patients do have a voice but we are not giving them the opportunity to be heard.
Clearly, we need to engage with patients as consumers and involve them in decision-making rather than treating them as passive bystanders.
How to increase this engagement will inevitably depend on the nature of the service. f or some, it might be giving patients access to their medical records or test results to give them the information to help discuss next steps with their clinician.
for others, it might be to train doctors to make decision-making a collaborative process and to allow patients to have their voice heard.
We also need to make it easier for patients to let us know when they are not happy with a service, as more than 40% of those surveyed said they did not feel they could complain if they were unhappy with their medical service or treatment.
really want
Easy access
Another aspect I looked at was access to services. We know that people who use private healthcare want fast access to appointments.
That was also shown in the survey results as the main reason people choose to go private. But what is often not considered is when patients want to schedule appointments.
Appointments are often scheduled at the convenience of the hospital or doctor or to fit around NHS schedules – so at weekends. But that is not when patients want to see their doctor.
Patients would much rather schedule appointments and procedures in the working week and especially in the mornings.
Despite showing this preference, only 22% of people surveyed said they got their preferred appointment time. So we are often not meeting patient expectations of choice from the initial contact.
Thus, we need to think like other service providers. Hotel bars, for example, stay open until the last customer leaves. And there is a city law firm that responds to all emails within 30 minutes.
This is all done to meet the needs of the consumer – and the health consumer should be no different.
People expect value for money, too, whether they are paying for the service directly themselves or indirectly through an insurance policy. So we need to ensure they are getting access to a real choice of appointments to fit in with their needs.
By being flexible with appointment times, it is also much easier for patients to differentiate between the NHS and the private sector, which could help to attract more people to use private healthcare who have not used it in the past.
In fact, 45% of those surveyed said they would use the private sector if NHS waiting times increased. So being able to offer fast, flexible appointments is a clear advantage.
Influencers of choice
I also looked at what was considered when making choices in private healthcare.
Price is important in any sector and in a competitive environment like healthcare there is pressure for prices to decrease. What is really interesting from this survey is that patients said that price is of secondary importance. They are more interested in quality and convenience.
So, when marketing services, this is what we should be emphasising to help patients make informed choices. And because low prices can infer lower quality, we should not be tempted to slash prices to attract more customers.
A further aspect of pricing is that, of those who had used private healthcare in the past, a significant number were dissatisfied with the price they had paid after the event.
This suggests they did not feel they had received value for money or that the price was not made clear to them from the outset.
This is certainly something we can work to improve and some hospital groups have already taken steps to address this by offering fixed-price treatment packages to help improve clarity of pricing.
Patients said that quality is important to them when choosing a private hospital or doctor, but what do health consumers consider to be indicators of quality? We think of quality as outcome led – such as infection rates or the number of days for recovery from an operation.
But patients have a different view of quality. Things we might
consider incidental are seen as quality by patients; for example, the warmth of the greeting at reception and whether they are offered a cup of tea.
Patients said that the surroundings where the event takes place is not as important, but whom they interact with is. And this includes the doctors.
This means that you can have clinically the best surgeon in the world, but if they are not friendly to the patient, a significant proportion will not perceive this as a quality service.
Customer service
Publishing data on surgical and other clinical quality outcome measures is clearly important. But as far as patients as consumers are concerned, investing in customer service training for staff, including doctors, will have a significant impact on the patient perception of quality.
The word ‘perception’ is important here because this does not relate to clinical quality but rather the patients’ perception of service quality, because this is what defines their choices.
A further question raised by this is where do potential customers
you can have clinically the best surgeon in the world but if they are not friendly to the patient, a significant proportion will not perceive this as a quality service
whAt providers need to do
to meet patients’ expectations, there are a number of things independent practitioners need to do:
they need to learn to engage with patients to ensure they not only have a voice but have one that is heard
patients said they want choices when booking appointments, so doctors need to be flexible to their needs and show them that they are getting value for money
to help patients choose between private hospitals, healthcare providers and doctors, practitioners need to demonstrate quality indicators that are valuable to the patient as well as retaining a high quality of clinical care
if doctors can do these things, it will help patients to have the choice and voice they expect to have as healthcare consumers
As patients continue to adopt a more consumerist attitude, doctors need to keep asking them what patients expect from them, because what is clear from this study is that doctors can’t assume they know what patients want. they have to ask them
find out about the quality of a service provider in order to make a choice?
The internet is increasingly being used for health information, with one in 20 Google searches relating to health. more than 80% of the survey respondents said they used the internet to find health information and that they find this information useful. more people look to friends and family for recommendations for a doctor or healthcare provider, however. This may be because purchasing healthcare is a highrisk and often expensive purchase, but what is clear is that they rely on known and trusted individuals for recommendations.
So although it is useful to have good websites and promotional material, providing a good service will ensure patients will become ambassadors of the service and recommend to friends and family.
These are just a few of the insights from the survey, but, overall, what was found was that patients said that they do expect to be consumers of healthcare –they expect voice and choice.
But this is not always happening and where expectations are not met, then this makes for a disappointing experience.
Aileen Morrison (right) is head of private patient development at InHealth
breaking into the aesthetics business
Map out your marketing
In the fifth of her essential series for doctors in the aesthetics world, Pam Underdown (right) shows how to create a marketing strategy
A m A rketing str A tegy is essential for focusing your energy towards the right actions that will deliver on what you want to accomplish. t here’s no need to over-think it or over-do it.
t he focus should be making sure that your treatments and services meet patients’ needs and that you are able to develop longterm and profitable relationships with them.
you will need to create a flexible strategy that can respond to changes in the marketplace and your patients’ perceptions. keep it simple: often the simplest and best ideas can be overlooked. And keep it brief: 15 pages at the most.
Before you begin, establish a deadline for when you want to complete your plan and put it into action.
then establish your team’s roles and responsibilities. it is also critical to work out how much you have to spend, as that can have a major impact on the strategies you decide to implement. Once you have these items in hand, you’re ready to put your plan together.
Part 1: Discover where you are now. Where do you want to be? What is getting in the way?
Having a clear idea of what you want your business to be at the start means you are more likely to achieve your goals.
it is important to have a clear understanding of your ideal patients, your market place, your competition, the treatments and services you wish to offer, the way you want to market yourself, your brand and your image, the type of patients you wish to attract and how you are going to attract them.
Begin your marketing strategy document with an honest and rigorous s WO t (strengths, weaknesses, opportunities, threats) analysis.
then ask yourself:
What do i want to achieve? then set clear, realistic objectives.
What are my prospective patients really buying (hope, confidence)?
What motivates them to take action?
What is the buying journey
they will go on? How can i ensure my business is there, every step of the way?
Which treatments and services are the most profitable?
What’s the best way of communicating with my patients?
How can i continuously monitor and improve my customer service?
How will i price my treatments and services?
Could changing my products or services increase sales and profitability?
Part 2: Decide whom you are going to attract and how you will attract them your marketing needs to cut through the thousands of media messages that your prospective patients are seeing and hearing every single day. How will you cut through the noise? e nsure you are using patient-focused language that talks directly to the patient’s pains, wants and emotions. Don’t forget that your patients are looking for a transformation and results. t hey will only ever buy what they want and not what they need. so find out:
What are the top three biggest problems they face?
What do they want more than anything?
What is the No.1 ‘result’ you can help your patient achieve?
What will the higher emotional benefits be?
What will it cost them not to make the change?
m are sure your marketing is human, authentic and, above all, personal. A big brand will spend millions trying to get you to connect with their logo, but it’s far easier for humans to recognise a face. your prospective patients will use the web and mobile to instantly research a treatment, product or service anywhere, anytime. is your business visible in all of the places that your prospective patients are spending time? We live in a very transparent world and your prospective patients are forming powerful and quick impressions of your business after seeing pictures, videos, posts, and reviews. is everything they see and read about you giving them a positive impression?
marketing plan
Part 3: Define your vision, your goals and objectives and your competitive advantage.
What are your goals? you need to define them very clearly. t hey may be financial or they may be aspirational, such as awards and recognition. Whatever your goals are, the key is to be very clear and time-specific. s etting bite-sized goals will keep you focused, motivated and on track.
if you don’t have a competitive advantage that matters to your prospective patients, they will only be able to tell the difference based on price alone.
to create a unique competitive advantage and to stand out from the crowd, you need to answer the following questions:
What do you do that is different to your competitors?
What do you offer that no one else does?
What do you do better than anyone else?
recruiting like-minded individuals is essential if you want to make sure your vision matters as much to your team as it does to you.
Part 4: Design your sales funnel and marketing plan
e nsure your marketing is useful and can be found. Write useful, educational articles that can be commented on and shared. there are two types of prospective patients: those in the market for a treatment immediately and those who are gathering information and aren’t ready to buy yet –which can take up to two years. What can you offer those who aren’t ready to go ahead yet?
Perhaps a taster session during ‘Love your skin Wednesdays’ or a free skincare guide. e ither way, ensure they are on your email database to build the relationship, trust, credibility and liking.
Part 5: Develop your tactical plan of action and your marketing skills
Once you have decided on your marketing strategy, draw up a tactical marketing plan to set out how you plan to execute and evaluate the success of that strategy. your plan sets out the aims, actions, dates, costs, resources and who is responsible for what. Decide which areas need monitoring and improving.
Will you measure based on emotional benchmarks, so you know the impact your clinic has emotionally on every patient? Or will you measure it by performance: how quickly your phone is answered?
Will you measure by financial targets or by patient feedback? Ask each new patient how they heard about your business and why they chose you over and above your competitors.
test small, spend small and fail small first, then scale up. test all of your marketing first before scaling. n othing is worse than launching a full-blown campaign and spending a fortune, if it doesn’t work. r egardless of the size of your campaign or available resources, there is no excuse not to test small first. By getting feedback from real patients early on, you can save yourself considerable time down the line by addressing any issues early.
m arketing plans shouldn’t be set in stone. And it’s not the end of the world if your marketing mix doesn’t work as well as you had hoped initially.
What’s important is to track every performance detail you can, not only with testing and statistical analysis but also with an oldfashioned ear to the ground.
Once you have knowledge about what works and what doesn’t – you can then refine your plan and your strategies as you go, learning and tweaking accordingly. it is impor-
tant to remain focused on the end goals: growth and profit.
Continuously develop your skills. every skill is learnable and your ability to master the marketing and the business side of your business is key to your survival.
Part 6. Deliver results if you look after your patients –they will look after your profits. return patients and referrals are what make a business successful. s tart by delivering a superior patient experience and establish
how you can maximise each patient in terms of return visits, average spend and referrals. Ask yourself how you will ringfence your loyal brand advocates to ensure they return and refer. What can you add to enhance the results for your patients? What can you offer that will encourage them to see you each month? What can you do to increase satisfaction? your loyal patients are your brand advocates and should be treated like gold. Don’t take them for granted.
reward for loyalty with points for every pound they spend. the key is to reward them with something they’ve never had before to introduce them to something new that will encourage regular returns. Be careful what you give away. Work out the figures and make sure it’s profitable.
Pam Underdown is chief executive at Aesthetic Business Transformations
regulating independent practitioners
New inspection rules
The future of your business is at stake! It is vital you respond to the Care Quality Commission’s draft handbook on its approach to regulating independent doctor
services, now out for consultation. But you only get until 19 October, warns Martha Walker
A new Care Quality Commission (CQC) handbook due later this year will guide independent doctor services on:
How an inspection will take place;
what information the CQC will collect before and during the inspection;
where it will gather it from;
what kind of evidence the service will need to provide for a successful inspection.
The CQC has acknowledged that ‘one size does not fit all’ within the private sector.
The draft is comprehensive and has been written following input from various stakeholders, including regular discussion with the Independent Doctors Federation.
The consultation consists of two documents: the draft handbook and the appendix.
A format for future inspections is clearly laid out. Here, it is particularly pleasing to see that the concerns about the short notice given for announced inspections and having to juggle appointments and staff has been listened to. In future, these inspections will have four weeks’ notice.
There have been many problematic areas for the CQC in how to regulate independent doctors because there are very few, if any, areas that can be measured and compared objectively across the sector.
notably, the much talked about Key Lines of enquiry (KLOes) that are standardised to a great extent in the nHS take on a very different format in the independent sector, which, by its very nature, is not standardised.
I think the KLOes listed in the Appendix are practical and, from my experience work
WhaT you neeD To KnoW
Deadline for response: 19 october
consultation documents:
ing with independent doctors, most would be able to provide extensive evidence to demonstrate their practice was safe, effective, caring, responsive and wellled.
The six questions being asked are constructive, inviting comments.
But, there is one curved ball that I wasn’t expecting.
The questions cover:
KLOes;
Information that CQC plans to look at;
Should independent doctors be rated;
How notable practices can be identified; Gathering information about the service from external sources.
And then there is the curved ball … should independent doctors remain within the scope of CQC regulation or should the GMC assume total responsibility for this through revalidation?
I would consider this consultation document to be the most important one the CQC has asked private doctors to comment on. So it is vital that every provider of independent doctor services responds to the CQC.
This consultation is open to the public, so it is likely colleagues in the nHS, among others, will have views on how the independent doctor services should be regulated.
Please take time to respond – it is the future of your business this consultation is about.
Martha Walker is medical management consultant at CQCConsultancy.co.uk and author of Independent Practitioner Today’s ‘The Essential Guide to CQC Registration’, December 2010
1. consultation – our approach to regulating: independent doctor services
2. how cqc regulates: appendix to the provider handbook
Do you agree that the Key lines of will enable us to comment on independent doctor services under the five key questions? is there anything else we should include?
We have provided examples of the evidence we may look for during our inspections. Do you agree that this will identify any areas of poor quality care?
q2 Do you agree that the examples of intelligence we plan to look at will identify both good practice and risks of poor-quality care?
q3 should cqc rate independent doctor services?
if cqc are granted the powers to rate independent doctor services in the future, which of the approaches below should we take?
inspect and rate across all of the five key questions in line with our current model for other services we rate?
inspect against all of the five key questions but only rate against certain key questions?
if you think we should only rate against some of the key questions, which key questions should we rate? l safe l effective l caring l responsive
l Well-led
if you think we should consider other options, please tell us what these are.
q4 Do you agree that independent doctors should remain within the scope of regulation by cqc?
if yes, please tell us why you think it should be cqc
q5 how can cqc recognise and encourage notable practice for independent doctor services?
q6 During our inspections of independent doctor services, we will use a number of methods to gather information from providers, the public and others about their views of the services provided. Do you agree that the proposed methods of doing this are the right ones to use?
Will they enable us to gather views from all of the people we need to hear from?
• setting up in Chambers/Groups
• limited companies and LLP’s
• financial planning
• record keeping schemes
• purchase of consulting rooms and surgeries
• inheritance tax and capital gains tax planning
• VAT
For more information please contact us by: Wilmslow
Phone: 01625 527351
Fax: 01625 539315 Harley Street
Phone: 020 7307 8759
Fax: 01625 539315
Email: info@sandisoneasson.co.uk
Website: www.sandisoneasson.co.uk
Think of your time – it counts a lot
You will need to build your own marketing machine if you want to avoid seeing patients effectively ‘for free’
Probably the biggest challenge when it comes to private practice is when you’re starting out for the first time. Surgeon Mr Dev Lall (right) has some wise words
Before you can even see your first private patient, there are, of course, a number of obligate costs: medical indemnity; consulting rooms; secretarial support fees.
And there’s little you can do about these expenses except take them on the chin, because until your cash flow exceeds your costs, you’re running at a loss.
This is why it’s so important to grow as quickly as you can as a new consultant in private practice. u ntil those costs are met, you’re losing money the same as any other business.
The reason doctors don’t always recognise this is that they have their NHS income, of course, which subsidises a low-earning private practice until income exceeds expenses.
u nless you crunch the numbers, it’s not always obvious what is happening.
But even then you are not in the clear. Because when private income = private expenses, you might be cost-neutral – the business is ‘paying for itself’ – but you remain very much time-negative. In other words, you’re investing
time in your private practice and getting no financial return for it at all. Probably large amounts of time; time you could spend elsewhere with family and friends. And, in a very real sense, you’re literally seeing patients for free.
So, certainly in the beginning, it makes a great deal of sense to see whatever private patients you can, and not to be too choosey about the clinical conditions –within your specialty of course –that you take on privately.
The advantage of this is that your private income will more rapidly rise to exceed your costs, and you become more visible among GPs and others who will refer patients your way.
Once you’ve met the first target of becoming cost-neutral, you’ve got to start making enough of a profit that you think it’s actually worthwhile spending the time you are in private practice.
This is, of course, subjective and will vary from consultant to consultant. What one consultant might feel worthwhile may not be to another.
But it bears careful thinking about, because the strategy that worked to get you cost neutral –to see all patients with whatever clinical conditions that they might have within your field – is not such a wise approach as you grow your practice.
Hassle factor
We’ve talked about this before, but it bears repeating again: not all clinical conditions within your specialty are equal in terms of time required to look after in terms of remuneration and in terms of sheer hassle factor.
After all, would you rather perform one Whipple’s procedure –with the ITU stay, prolonged recovery and significant opportunity for complications and so on – or a handful of hernia repairs on the same list which are mostly day-case procedures and seldom have any issues at all?
The thing is, while we all recognise this, few people will be selective in the cases they treat privately. They continue to take on all-comers. And while this increases their income, it disproportionately increases their time commitment.
So the smart approach once you
have covered your obligate costs is to start getting selective in the patients you treat privately. Astonishingly, few consultants will do this, worried that if they turn a single private patient away then the flow of patients will rapidly dry up; that GPs and others won’t refer patients to them and patients themselves will stop coming through their own volition. And it simply isn’t true.
The problem consultants don’t see
In the NHS, we are truly spoiled. It might not feel like it, but really we are. Because we find ourselves part of a gigantic, multifaceted machine that allows us to deliver healthcare. The first aspect of ‘the machine’ is perhaps the most obvious of the two.
This is the part that actually permits and facilitates the delivery of healthcare. The staff – the nurses, cooks, cleaners, porters, secretarial and operating department staff. The facilities and equipment – the wards, imaging equipment, operating theatres and so on –that are required to manage and treat patients.
In the NHS, it’s all there and, as a consultant – or junior for that matter, we just slot in and get on with the business of looking after our patients.
And, privately, it’s pretty easy to recreate this. We have our clinical expertise which we take with us and by gaining admission rights, rooms and so on at private hospitals, we gain access to the facilities required to provide treatment and care for private patients.
But there’s another, hidden aspect to ‘the machine’ that is far less obvious but equally important.
Because the unseen part of the NHS machine is the part that generates the patients to care for in the first place: the GPs, optometrists, physiotherapists, the publicity of health awareness and risk avoidance campaigns.
This vitally important part of the NHS ‘machine’ is monolithic yet hidden in plain sight.
The problem is that this is the bit that is missing when you start out in private practice for the first time.
This is the bit you don’t even know you need until it’s absent,
and you have all those empty slots in your private clinics, and hours of hanging around between patients.
This is the bit that doesn’t come with admitting rights to that private hospital.
The uncomfortable truth is that a private practice requires a private marketing machine. And you’re going to have to build it for yourself.
Few consultants understand –initially, at least – the problems I’ve highlighted above, especially the marketing machine within the NHS. They see the potential rewards of private practice but not the difficulties. With one exception: how to get patients.
The problem new consultants focus on
If there’s one question I’m asked more than any other, it’s how to get traction in your private practice when you’re just starting out.
How do you attract the referrals from GPs when it seems that, despite all your efforts, they continue to send patients to the more established, senior colleagues in your department?
The uncomfortable truth is that it’s not easy. There is no magic solution that will change things overnight. But it most certainly can be done.
Challenging the status quo
Marketing is not narrowly looking for more patients. Rather, it is all about making yourself more visible to those who could benefit your practice in some way. It’s not just a matter of putting yourself in front of more patients.
When framed this way, the solution becomes much clearer. Because there are two groups of people who could benefit your practice:
1
Potential patients – people with the conditions you treat;
2
Professionals who can refer patients to you, such as GPs, optometrists and so on.
And this, in turn, means there needs to be two arms to your marketing efforts: one aimed at potential patients, the other at those who might refer patients to you.
You see, when a patient consults a GP looking to see someone
privately, there are one of two approaches they will take.
Either they will have no idea who could treat their condition, in which case they will ask to be referred to ‘somebody’, in which case the GP will decide who that consultant should be.
Or, alternatively, they will have decided through their own research whom they want to see and ask to be sent to that particular consultant.
The trick is to make sure you are that particular consultant. This is why you need to proactively and enthusiastically market and promote your practice to potential patients every way you can.
That way, they will either make their own appointment to see you or, if they go through their GP, will ask to be referred to you specifically. So that is the first way of breaking down referral patterns to senior colleagues.
The second way is to promote yourself to the referrers themselves, so you gain visibility, authority and credibility in their eyes too, so that GPs don’t automatically think of your colleague but your name comes to mind too.
This is one of the reasons for holding GP educational meetings, of course. To increase our visibility to the very people who could send private patients our way.
Yet there is far more we could do to get and stay front of mind among GPs, not just hold the occasional educational meeting –although that is a discussion for another day.
This two-armed approach to marketing – systematically targeting both patients and referrers – is where the real gold lies. This is how you build a thriving practice in the shortest possible time, as well as overcome entrenched referral patterns to senior, more established colleagues.
Because not only does a successful private practice require its own marketing machine, without which you’re going to struggle to succeed, the responsibility for building the machine lies with you alone.
Mr Dev Lall is an upper-GI surgeon and runs a specialist private practice consultancy. He can be found online at www.PrivatePracticeExpert.co.uk
Make sure you get
It’s vital to consider your billing and collection management from the very beginning of private practice. Gary Nials reports
So you have decided to take the leap and gone into private practice. you have employed a secretary and organised a good location to see your patients. The practice has a name and you have set up a business bank account.
But one thing that you may have not yet given much thought to is the invoicing of your work.
This will be the one area that is most important and will require some time and effort.
Most of the patients you will see in the early days of your practice will, no doubt, be privately insured patients.
So you will need to register with the major private medical insurers such as Bupa and AXA PPP. They are the largest and will be where most of your first patients come from.
you should also consider Aviva, Simplyhealth, VitalityHealth (formerly PruHealth) and WPA to
name a few of the many others out there.
Most of the information required to register with them will be on each of their websites under the provider section.
once registered, it is very important that you understand their processes for invoicing. They all differ and not following their processes will inevitably delay payment.
Importance of pricing
your pricing is also key at this stage, and Bupa and AXA PPP will have set fees for procedures which will have to be adhered to.
The individual fee schedules for each insurer can also be found on their websites under their provider sections.
Attention to detail is vital when raising invoices for insurers. Always pay attention to the insurer’s rules and processes for invoic-
ing. For example, some set a maximum number of procedures that can be billed on any one invoice.
They have set pricing levels for more than one procedure. So, for example, the first procedure can be charged at 100% of the set fee, the second at 50% and so on.
And they also have rules about what procedures can be billed with each other, which is known as unbundling.
The invalid combinations can be found on the Clinical Coding and Schedule Development Group (CCSD) website at www.ccsd.org. uk. The CCSD schedules contain the standard codes for procedures and diagnostic tests for the u K private healthcare sector.
And as well as abiding by the pricing set out in the insurer’s fee schedule and pricing rules, using the correct codes for the procedures and ensuring the combina-
insurers have rules about what procedures can be billed with each other, known as unbundling
billing and collection is not as straightforward as it sounds. You could get your secretary to do it for you, but then you may need another to deal with your appointments and patients’ needs.
You could do all this yourself or you could outsource it to a professional company. the key thing is not to ignore this vital task, because its where all your income will be coming from.
paid
treatiNG patieNts from embassies
You may be considering treating embassy patients, depending on where your practice is based, and those patients must be easy to invoice for. but be aware that a new set of rules comes into play. every invoice sent to an embassy will require a Letter of Guarantee (LoG) from the embassy. these should be sourced before you see the patient and you must ensure the correct details are on them. Without a valid LoG, the invoice will take a very long time to get paid.
Details to check are the patient’s name, date and description of the procedure. always keep a copy, because the paperwork sometimes goes astray. it is often necessary to produce another copy of the LoG.
tions are right, you will also have to deliver the invoice correctly.
Bupa, for example, will require its invoicing sent electronically.
o nce you have invoiced, you must still remain vigilant. It is very important that you regularly check for when the insurers make that payment to you.
This payment must be reconciled with the original invoice because there may be a patient liability.
Patient liability results from policy excesses or patients exceeding their benefit limit. If this happens, you will have to raise another invoice to the patient for the remaining fee not paid by the insurer.
you will soon be dealing with self-pay patients, as they are known. unlike insurers, who usually pay via bank transfers, selfpay patients will want to pay you in a way that is most convenient to them.
Credit and debit cards are the most common forms of payment, so you will have to set up your practice to take them.
Chasing patients
But another element requiring your time and effort will be the chasing of the other self-pay patients either by phone, email or post.
Always ensure that you get contact details for each patient you see, even if they start out as insurance patients. A patient registration form comes in very handy here, so prepare one that captures contact and insurance details. you should also use the form to set out your terms and conditions so that the patient is fully aware of their liabilities if the insurance company does not cover all the fee.
Some self-pay patients will always pay on time, but some may require some prodding.
o f course, if your practice is entirely self-pay patients, then a lot of the rules and regulations of invoicing when dealing with insurers won’t be relevant.
Gary Nials (right) is managing director at Med ical Billing and Collection
Dear Reader,
Subscribing to Independent Practitioner Today is the only way you can be sure you will see every issue. Don’t risk missing out. Our personal subscription for doctors and managers is only £85 a year and £200 for organisations. But you can cut this to just £70 and £175 respectively if you pay by direct debit.
So take advantage of this offer now for our unique business journal dedicated to supporting you in your private practice. We’re confident your subscription will repay itself many times over!
Editorial director
rates listed above) post your application (no postage required – UK only) to: independent practitioner today subscriptions department, Freepost, po box 36, plymouth, pL1 1br
I encose a cheque made payable to The Independent Practitioner Ltd
Amex/Diners
Date
No
Instructions to your Bank or Building Society to pay Direct Debits
Instructions to your Bank or Building Society to pay Direct Debits Name and full address of your bank/Building Society
Name(s) of account holders
Name and full address of your bank/Building Society Banks and Building Societies may not accept Direct Debit instructions for some types of account
Or subscribe online at www.independent-practitioner-today.co.uk
branch of the amount paid.
staRtinG a pRivate pRaCtiCe 3: fORminG a GROup
It’s usually better to hang together
There is strength in numbers – Ian Tongue (right) presents a guide to the whys and the wherefores of independent practitioners working as a group
Working in a group can have a number of advantages and this approach is common among certain specialties.
it may seem straightforward to work as a group, but it requires significant planning and a commitment to each other. And that can take months or even years to get off the ground.
i f successful, a group can provide a great chance to increase revenues, cut costs and provide that all important support structure. This article explores some of the more common considerations.
Objectives of the group
This is probably the most important. Why is the group being proposed and what will members get from it?
Typical objectives are to:
Share costs to bring economies of scale;
Spread risk and workload from cross-cover;
increase revenues;
Bid for contracts – for example, under ‘any qualified provider’ or from clinical commissioning groups;
Provide greater strength with insurers and private hospitals;
Provide flexibility.
Cost sharing
This is the simplest form of working together and is sometimes referred to as a ‘chambers’ arrangement. i n these circumstances, doctors are coming together to share costs, which are duplicated across your private
If successful, a group can provide a great chance to increase revenues, cut costs and provide that all important support structure
practices to reduce the cost base collectively.
This can work particularly well where the private practices are smaller and growing, as rooms and secretarial costs in particular can usually be reduced.
Revenue sharing
A significantly more committed position is to share revenues between the group. This could be incremental revenues from new income streams, for example, or relate to existing private practices. For new revenues, it is important that the distribution of this profit is agreed from the outset to avoid problems later on.
With existing private practices, it is vital that the allocation of ➱ p30
this profit works for all group members.
often there is a disparity on private practice size that results in existing private work being retained outside the group or an ‘eat what you kill’ type of profit arrangement being in place to protect existing practices.
Agreeing the above is a key part of the set-up process and is one area where problems can arise if such matters are not agreed from the outset.
the hurdles
one of the hardest things is to get everyone committed to the venture. i t is not uncommon for groups to fall in numbers during the embryonic stages.
i nevitably, the arrangement won’t suit everyone and you could have some initial interest in the arrangement from colleagues who really want to see what you are up to.
The key obstacles to overcome are:
Whittling the group down to those who are committed;
Deciding what happens to members’ existing private practices;
Dealing with disparity in existing private practice earnings levels;
Assigning roles and establishing the ground rules;
Agreeing a financial commitment level;
gauging the anticipated size and entry criteria for future members;
getting everyone in one place for periodic meetings.
financial considerations
Aside from a chambers arrangement, which can be a loose association, the main types of trading structure for a group are either a limited company or a limited liability partnership.
A limited company has shareholders (owners) and it is normal for them to receive dividends or a
combination of salary and dividends.
So here lies the first barrier for a group trading as a limited company, as the ownership structure (shareholding percentage) may not be the same as the intended profit share, particularly if the ‘eat what you kill’ arrangement is in place.
Using a company in this context would normally involve a more complex share structure and possibly consultants subcontracting to the company. There are many factors to consider here and these should be discussed in detail with an accountant.
As a result of the potential inflexibility of using a company, many groups have historically chosen a limited liability partnership or LLP.
This structure can be viewed as a hybrid between a conventional partnership and a limited company. Profits are shared by refer-
ence to certain criteria and can be variable and you enjoy a degree of limited liability from the arrangement, unlike a conventional partnership.
Historically, those who trade through a limited company themselves have often made their limited company a partner in the LLP rather than themselves personally, as there can be potential commercial and financial benefits of doing so.
However, new rules came into force last year which target the use of LLPs with corporate members. These rules were not necessarily designed to prevent what is a commercial venture and structure, but nonetheless they need careful navigation. This is a complex area and advice needs to be sought from an accountant.
Ian Tongue is a partner with accountants Sandison Easson & Co. See his recipe for group success opposite ➱
An easy to use software system, which fully supports the clinician and office staff and makes the whole process of running a busy Practice a lot easier.
Call now for a chat and ask about a free, no obligation demonstration of our comprehensive system that has been designed to save your Practice time and money.
‘PPM’ – Private Practice Manager.
PaTHway TO success as a grOuP
assign roles
It is easy to fall into the trap of assuming that someone else will deal with things. clear roles need to be defined and, like it or not, if you are the main driving force behind things at the early stage, you are likely to be doing more than anyone else.
you will need a representative to liaise on behalf of the members with a variety of professionals, as dealing with lots of members is inefficient. These professionals will often need information from each consultant and a co-ordinator for this is essential.
roles will need to be assigned on clinical as well as financial matters. It is always a good idea to identify those strengths within the group and assign accordingly.
seek a commitment
you need to establish as soon as possible who is ‘in’.
One of the first stages where people remove themselves is when a financial commitment is required. you should discuss things with your accountant to see how much you are likely to need from each member.
Have a business plan
For any financial venture, a business plan is certainly best practice. If you are seeking finance of any sort, it will be essential to securing funding. business plans do not have to be literary masterpieces, but must identify the opportunity, how you will exploit it and forecast the financial position in a realistic manner.
Take pointers from the various guidance available and note how people are given short shrift by the Tv ‘dragons’ if your figures don’t stack up!
shareholder/members’ agreement
depending on structure, you will need a formal agreement to set things out legally. These agreements differ depending on which structure is adopted following professional advice.
The agreement will set out the ground rules for the arrangement and requires a reasonable amount of organisation, as the solicitor will ask questions requiring a collective answer on a timely basis to avoid costs rising. Most solicitors have a template to help with this process.
Forming or joining a group can be an effective way of increasing your private practice and provide you with the flexibility and support that you would not have on your own. as always, seek advice from an accountant to assess the venture.
Lock out out the scammers
Stop fraudsters getting their hands on the funds held in your medical practice.
Ian Crompton (below) shows the scams you and your staff are at risk of – and how to beat them
As with other sectors, the threat of fraudsters targeting your medical practice continues to evolve. Practices can be seen as attractive targets for fraudsters, due to the relatively high bank account balances which are needed to conduct day-to-day finances. taking some simple steps can make a real difference to fraud -
sters’ success rates, so here are five common scams, which all practice employees who deal with banking or finance should be aware of.
1. Scam phone calls
Fraudsters use phone scams to obtain online banking passwords, confidential details or persuade you to move money to a ‘safe account’.
they will tell you there is a problem with your bank account and ask you to call back on an official number, say, from your bank card. By holding the line open until you call back, they convince you that you have reached the bank.
t hey may alter the incoming number which appears on your phone’s caller display to one
WAVELENGTH
which you know is the genuine number for the bank.
If you are not absolutely certain that it is your bank calling, you should ☛
Call the bank on a number that you know is correct from a different phone.
if this is not possible, ensure the phone line is clear first by waiting at least five minutes before calling back.
Or test the line by calling a friend or colleague first.
Remember that the bank will never ask you to transfer funds to a ‘safe account’ and will never call you to ask you to divulge full passwords, PiNs or payment authentication codes.
Remember that the bank will never ask you to transfer funds to a ‘safe account’ and will never call you to ask you to divulge full passwords, PINs or payment authentication codes
Therefore you should ☛
watch out for emails that are grammatically poor or that begin with ‘Dear valued customer’ or similar. A genuine bank email will always contain your name.
h over your cursor over links within emails to see the true web address.
Use a s PAM filter to remove unwanted emails and opt out of marketing emails on websites.
4. Mandate fraud
2.
Malware
Malware (malicious software) is often hidden in email attachments and free downloads. it can interrupt your online banking sessions and present you with a fake, but seemingly genuine screen, prompting you to enter passwords and codes which fraudsters can capture.
this information can be used by fraudsters to access your online accounts, make fraudulent payments and also to access other confidential information on your PC.
To guard against malware ☛ Ensure all PCs are protected by high-quality anti-virus and antispy software. Update it regularly and run frequent scans.
Only download programmes to your PC from sources you trust. if possible, provide a designated workstation that is not used for web browsing, email or other activities that could bring malware onto the system, for processing financial transactions. when you’re using your online banking service, if you are asked to enter passwords or verification codes at an unusual stage, log out immediately and call your bank.
3. Phishing
Phishing is another name for Email scams when fraudsters masquerade as your bank or other trusted organisations to obtain confidential information such as personal information, bank details or passwords.
t he email will usually link through to a fake website, which looks almost identical to the legitimate one.
A message usually suggests that you need to act urgently – for example, to prevent your online access from being blocked.
Fraudsters might send an email or letter which appears to come from the beneficiary of a genuine pay ment which you make.
t hey ask to change the bank account details for where the pay ment is sent to and if you don’t check the authenticity of the request, the next payment made will go to the fraudsters, not the intended recipient.
Therefore you should ☛
Review existing processes for sending payments and ensure that there are strong authentica tion measures in place.
Establish a single point of con tact (sPOC) with each regular sup plier and confirm any requests to change payment details with them on a number you know is correct.
5. Cheque overpayment
Beware of payments to you for significantly more money than you were expecting. Fraudsters may tell you that they have sent too much money to your bank account, asking you to return the additional amount sent in error.
if you return the money with out realising that the payment into your account was a fraudu lent cheque, you will lose out on those funds when the fraudulent cheque gets returned unpaid.
Therefore you should ☛
Contact your bank and ask them to investigate the origin of any payment from a new client which is more than you expected. For further help and guidance on how to avoid being a victim of fraud, contact Action Fraud www. actionfraud.police.uk or your bank.
Ian Crompton
is
head of Healthcare Banking Services at Lloyds Bank
The hallmarks of a good private nurse
Private hospital matron Caroline Cassels (above) has witnessed some enormous changes in the fields of nursing and general medical care over the last 30 years. Training methods have evolved, technologies transformed and medicine has advanced light years. But, she says, many of the qualities that make a top-class nurse have not changed
The besT nurses are still the ones who are truly committed to their patients and to the discipline of nursing.
They are those who understand the importance of kindness and compassion in recovery.
The top ten qualities that I believe consultants should look for in a private hospital nurse are as follows:
1
Passion
As the guardians of patient care, nurses must be passionate about their role, about caring for others and about their patients’ recovery.
I am incredibly passionate about people, so my favourite part of my role as matron is that I get to meet new people each and every day. I make sure that I visit as many patients as I can. I find out how they are and what we can do to make their stay in the hospital more comfortable.
When nurses actively engage with their patients, it is far easier to pick up on the minute details that might be affecting their recovery, their mood and their overall well-being.
A nurse must also be passionate about finding solutions to problems, whether it’s a patient’s headache, a consultant needing specialised equipment or supporting a fellow nurse on a tough day.
And finally, a private hospital nurse should always be passionate about his or her place of work. I feel incredibly privileged to work at King edward VII’s hospital and very proud of its history, its values, and the high calibre of nursing care that we offer.
I hope that this passion and pride is reflected in my own work; I can certainly see it through my team’s work each and every day.
2 Courage
I believe nursing today is a highly pressurised role, requiring more decisions and greater efficiency than ever before. Nurses require courage to make these tough decisions in the best interest of their patients’ well-being. As nurses, we face a diverse mix of people and problems each day and the best nurses will have the courage to speak up when they have concerns. It certainly takes courage to stand up to consultants, to fellow staff and to patients to ensure that we achieve the best results.
Nurses also require the personal strength and vision to innovate and to embrace new ways of working. It takes courage to step away from your routine, your habits or what you know in order to take on new ideas that might be in the best interests of your patient.
3
Technical skills
Nursing now not only requires more decisions, but requires more technical skills, more extensive knowledge and a broader understanding of medical care.
When a nurse first comes to work at a private hospital, the ever-changing demands of the job can be daunting.
Nurses working in private hospitals in particular can find themselves working on any ward from the surgical ward to the ICU. They can find themselves taking blood
one minute and assisting a patient with rehabilitation the next. It is essential for a private hospital nurse to be equipped with a wide set of skills and a deep knowledge base across a range of specialties.
Nurses require technical proficiency to act as a support system for consultants and in order to aid patients throughout their journey from admission to recovery. Technical skills are at the core of what we do.
4 Communication
A nurse with sound communication skills is invaluable.
Communication is essential to providing effective care for our patients, and I believe listening is just as important as what we say and do. At King e dward VII’s hospital, we firmly believe in the saying ‘no decision about me without me’, which is central to our philosophy of patient care.
Consistent and clear communication with our patients ultimately allows for the best outcomes. The nurse-to-patient ratio at private hospitals generally means that nurses are afforded more time to communicate with the patients.
The nurse in charge of the ward at our hospital visits each patient
5 Compassion
Compassion is how care is given through relationships based on empathy, respect and dignity
at least twice every shift to monitor their results, to hear about how they’re feeling and to provide them with any updates.
Communication is also key to effective teamwork and a good workplace. A good nurse will regularly communicate with fellow nurses, consultants and other hospital staff about a patient’s needs.
Compassion is how care is given through relationships based on empathy, respect and dignity. It can also be described as intelligent kindness and is central to how people perceive their care.
A good nurse will seek to learn and understand about their patient’s life or state of mind beyond their immediate condition or reason for being in the hospital.
We must look beyond a patient’s test results and consider their history, their experience and how they’re feeling at this moment. It is so important for nurses to be able to empathise with their patients.
It is also essential that we work in partnership with the whole team to assist in a patient’s recovery, which includes their consultant, other doctors or nurses, their partner and their family.
A good nurse should be able to say ‘I don’t know’, which should swiftly be followed by ‘but I can find out’
At King edward VII’s hospital, compassion also extends beyond the patients. I believe it is primarily about showing respect and attempting to understand the personal challenges that each person faces, from our cleaners to the consultants to the chief executive. When we each show compassion, the hospital begins to work and feel like a family.
6
Adaptability
As nurses, each day we encounter patients from all walks of life who are facing a wide range of conditions or ailments, each with their own set of fears, ideas and beliefs. We therefore must be constantly thinking on our feet.
A hospital is not a sausage factory, so a good nurse will be able to effectively read his or her patients and adapt their approach, providing tailored care to facilitate the best outcome for the patient.
When I first began working as a staff nurse, over half of my patients were ex-servicemen. I soon learned that many of these men required a certain style of care; a no-nonsense and straightforward approach was vital to their recovery. I was forced to adapt my patient approach in order to provide these men with the best possible care.
The same can be said in dealing with consultants and doctors. A perceptive nurse will adapt her demeanour, knowing the right
balance of toughness and softness with her colleagues.
7 A can-do attitude
When recruiting nurses, we look carefully for those who find no challenge too great or too small.
I know how important it is to our consultants to work with nurses who are willing to help them out with anything and who can support them without always being asked.
As a nurse, we strive to understand each consultant’s way of working and how we can assist them to deliver the best results for our patients.
It is not about having all the answers; a good nurse should be able to say ‘I don’t know’, which should swiftly be followed by ‘but I can find out’.
A can-do attitude means that whether you are seeking certain test results, a piece of equipment or for more information about a patient, your nurse is always willing to lend a hand.
8 leadership
Another one of my favourite aspects of my role as matron is working closely with new staff and helping to train them into confident and competent nurses.
I have worked with many nurses over the years who begin as a staff nurse and worked their way up to become a senior and most valued
member of the team. I love the fact that we get to nurture and cultivate the leaders of the future.
When I was training, half of our time was spent in hospitals and the other half in classrooms.
Training today, however, has changed dramatically, with much more time being spent in the classroom, so many nurses when they first enter the workforce are equipped with all the theory but need guidance in applying this practically. It is our responsibility to show them how to use these tools on the job.
9 Embraces tradition
I take immense pride in working at King e dward VII’s hospital, an institution steeped in nursing tradition. In terms of nursing care and values, not much has changed since it was established in 1899 by two sisters, Agnes and Fanny Keyser.
The sisters converted their home into a hospital for sick and wounded officers returning from the b oer War. This rich history informs the way that we approach nursing every day.
I believe private hospital consultants really value the traditions behind nursing care and we place great emphasis on these.
Our nursing staff continue to wear traditional uniforms each day, we provide a continuity of care through matron’s office ward rounds and the staff work in a
good old-fashioned hierarchy, which provides a clear working structure.
The best nurses will embrace the traditions of nursing: discipline, service and care of the highest standard.
10 Team-player
And finally, every good nurse will recognise their role in supporting a team.
When I recruit nurses, one of the key things that I look for is whether or not they can fit in with the current team.
A nurse can be outstanding at what they do, but if he or she does not co-operate within a team, then they are not the right fit.
Many of our nurses have been working here for five, ten or 15 years and have become seasoned experts at listening, adapting and communicating with their team.
b eing a nurse is ultimately about working with the patient, their family and friends, their doctors and consultants, and their nursing colleagues to deliver the best possible care and experience for the patient.
Caroline Cassels is matron at King Edward VII’s Hospital, London, where she began as a staff nurse over 30 years ago. She has been matron for 21 years and was honoured last year to receive a letter from HM The Queen and from The Duke of Kent congratulating her on these anniversaries and on her three decades of service there
www.medbc.co.uk
• Bad debts of less than 0.5%
Come and join the hundreds of other consultants who use MBC and experience the following benefits:
• Increase in net income by up to 25%
• Bad debts of less than 0.5%
• Increase in net income by up to 25%
• Freedom for the consultant and secretary to focus on the medical side of the practice
• Having a service tailored to your needs with your own Account Manager
• Having a service tailored to your needs with your own Account Manager
• Our fees are only charged on the money that we collect for the practice and NOT on what we invoice which means we share the same objectives
• 24/7 online access to both your financial and practice management data
• Freedom for the consultant and secretary to focus on the medical side of the practice
• 24/7 online access to both and practice management data
• Our fees are only charged on the money that we collect for the practice and NOT on what we invoice which means we
It’s how you tell ’em that counts
For those clinicians and organisations who have recognised the importance of media relations and agreed to dip their delicate toes into its murky waters, the first hurdle tends to be acquiring comprehension of what the mainstream press is after. Tingy Simoes (right) reports
So just what will the media recognise as ‘a story’?
Most importantly, you will want it to be one that will actually result in something positive – either an increase in credibility and reputation, or a good old-fashioned rise in the number of bodies through the door.
In my article in Independent Practitioner Today last month, I touched upon the concept of news that journalists and the public will find of interest.
Yet even after identifying these themes, the content needs trans-
lating into ‘normal speak’ because we are referring to newspapers and telly, not medical journals.
So unless your prospective patients are your fellow clinicians, I’m afraid it’s time to shelve the nerd talk and explore a new language.
This month, I will provide a number of real-life case studies where, through converting credible scientific material into something the public finds palatable, I have secured massive exposure for clients of all sizes across a wide range of media spanning the most high-
brow broadsheets and respected news programmes through to the most populist ‘red-tops’.
Crafting a package that will make headlines is neither easy nor achieved by accident, which is why so many PR campaigns fail when those in charge – client and publicist – don’t know how to operate together.
Shocking headlines
Unlike surgery, PR is not generally a very rewarding career – indeed, I do often question my life choices. We face huge pressures to secure exposure, our success is measured in column inches and we are never off the clock. And there is certainly no resting on laurels – as soon as you secure a splash, even if it’s front-page news, you’re already expected to be producing the next.
This means that on occasion, out of ignorance or desperation, tasteless or irrelevant stories get thrown together and issued for the sake of a shocking headline, regardless of whether it ultimately does much good in terms of business or credibility.
Journalists are also under immense pressure – one reporter at the Mail website recently told
me they are expected to post as many as 30 articles a day – and PRs know this.
Combined with an ever-growing thirst for celebrity gossip and horror stories, it’s no wonder that what’s out there can seem, well, a bit unsavoury.
Yet I am here to prove to you that publicity can be achieved ethically and, in fact, can grow to protect and enhance your professional image. It can help you secure space – ‘virtual’ property, if you will, just like a game of Monopoly – both online and in the mind of the public.
I recently attended a surgical congress, where junior doctors were given the opportunity to unveil small-scale research projects.
Now let me clarify that I am not medically trained; I went to business school. Half the time I might not exactly understand the posters or what is being said, but I’m interested enough to ask questions. I remember one trainee saying to me in awe – it may have been terror – ‘You’re the most excited person here!’
As mentioned in my previous piece, if I, as a layperson, am fascinated, surely others will be as well? I’ve never yet been proven wrong.
One of the audits I witnessed had to do with treatments for a specific metatarsal disorder, Morton’s Neuroma.
There was little in the study that could be classified as ‘news’, but what caught my eye was a single observation by the presenter, who said that the condition was mainly common in women
between 40 and 60, which could be due to the female penchant for high heels.
Inside my head, all I could hear was: Manolo-noma!
The resulting news release made huge waves in The Times , The Sunday Telegraph, The Independent, the Daily Mail and BBC Radio 4, to name but a few.
Post-mortem, we can see why it was such a hit: the study had credibility, I sourced official statistics to back it up, and there was a popular culture/fashion reference to tie it to the public consciousness. But this was no accident – it took weeks of hard work.
The success of ‘manolonoma’, which made headlines even internationally, provides unique insight into what is considered ‘news’.
You may no longer be a junior doc conducting research on how many blood tests are necessary in trauma ward admissions or how many ‘red flag’ referrals are accurate – other studies I identified which also made national headlines – but you can audit trends in your own practice.
Rising popularity
What procedures are rising in popularity, what are patients asking for, what conditions are becoming more common, what type of people are presenting and why now? How are they paying?
There were recent changes in pension laws: are folks drawing on their retirement funds earlier, for private treatment? Are they having anti-ageing procedures because of forays into dating in their 50s and 60s?
Are teens having more sports injuries because they spend so much time inside playing video games? Has there been a rise in temporo-mandibular disorders? Why? Believe me, the public wants to know.
These are not just ‘stories’; they are substantive, relevant and credible ones that will elevate your reputation. You are in a unique position to find them, and there’s no need to sell your soul.
Sometimes it’s about specific techniques you are using, which are innovative. At a recent aesthetic surgery conference, a presenter was expanding, so to speak, on an approach utilising fat graft-
ing combined with implants for breast augmentation.
We could hardly hand over a scientific abstract to the Daily Mail, as it would have been incomprehensible, so we explained it as ‘icing the cupcake’.
Famously quirky
Our press releases are famously quirky, but they are always factual. Journalists regularly compliment them – one producer from BBC Breakfast said that in a whole day receiving thousands of releases, ours was the only one he’d bothered reading in its entirety.
Most of you might be familiar with the mnemonic SBAR (Situation, Background, Assessment and Recommendation). Not a thrilling subject for mainstream media, but did you know that it evolved from the nuclear submarine industry?
That’s quirky! We researched studies – I really do spend an unhealthy amount of time on Pubmed – proving that the use of SBAR in hospital communication cuts deaths. That’s interesting and factual! This gave birth to ‘The Shunt for Red October: Giving Hospital Communication Errors Das Boot’.
All stories are still based on scientific fact, but just given the consumer treatment – what in PR terms we call a hook, something to ‘peg’ the story to. Despite what you might think, journalists aren’t stupid and they won’t
memory distortion, sourced one of the country’s leading clinical psychologists to check our ideas, and commissioned independent research polling social media users to check if what we were suggesting was true.
The resulting ‘Digital Amnesia’ syndrome made headlines globally – newspapers from New York to Italy to Peru ran the story. My dad, who was on holiday in Portugal at the time, saw it on TV!
blindly take whatever your publicist gives them, regardless of how close their relationships are.
One last example I’d like to highlight has to do with a nonhealthcare project. A client launched the world’s first-ever entirely anonymous social media platform, a site hosting tens of thousands of personal diaries where writers could tell the truth, confess their affairs or fantasies.
Eureka moment
In a Eureka moment, I woke up one morning with the headline ‘The way we weren’t’ in my mind. I thought to posit the theory that the sometimes dishonest way traditional social media is used (one-upmanship, showing off) could be affecting later recalling of events.
We spent weeks researching
Naturally, not all agencies are willing or able to take as thorough an investigative approach, but that doesn’t mean you can’t help by understanding what they need to be able to sell. In my case, I rarely have a choice, because surgery and PR is a relationship still in its infancy, each one still approaching the other like Bambi on the ice.
You have the information at your fingertips: despite how you might feel on a Monday morning, your work is interesting and the world is listening. So, are you ready to talk?
Tingy Simoes is owner/managing director of Wavelength Marketing Communications (www.wavelengthgroup.com) and author of the firstever PR manual for doctors and surgeons ‘ How to Cut it in the Media’ by CRC Press
Next issue: Making you ‘futureproof’: the big bad world-wide web and the implications of searchability. How clever PR and social media campaigns help you gain valuable and cost-effective space built to protect and enhance your reputation
Tribinal’s ruling is not to be sniffed at
An employment tribunal finding that an nHS trust unfairly dismissed an employee for smelling of alcohol on duty has some important implications for independent practitioners.
t he case is of particular relevance to healthcare providers, who have to balance the difficult issue of complying with their duties towards patients and their obligations to staff.
And it provides a helpful reminder for employers on the steps to take to avoid costly litigation when handling cases concerning staff behaviour.
summary of facts
the employee (mr m) had worked for an nHS trust as a healthcare assistant for around ten years.
His manager was informed that he had arrived at work smelling of alcohol. t he manager spoke to him and took the same view.
mr m advised that he had only consumed a few beers the night before, but was suspended pending an investigation. At the same time, he was referred to occupational health, which found him fit to work.
t he investigation found there were no issues with mr m’s performance on the day in question, or more generally, but it came to light that there had previously been concerns that he smelt of alcohol. n o action was taken at the time.
mr m stated during the investigation that he had not been drunk at work and that he thought colleagues might have smelt his aftershave or hospital alcohol gel.
So you’ve smelt alcohol on a member of staff? Fiona McLellan and Jeremy Coy report on a sobering case for doctor employers
Practitioners should try to take a measured approach to staff concerns and consider the following:
☞ speak to employees informally and give them an opportunity to rectify problems where appropriate by reference to:
the issue;
the employee’s role;
Patient care;
☞ when investigating allegations, clearly inform employees what those allegations consist of at the outset and ensure that the ‘charges’ are fully framed and issued to the employee before a disciplinary hearing;
☞ always consider the appropriateness of sanctions short of dismissal, which can potentially be relied upon if there are further conduct issues;
☞ Keep all policies, especially disciplinary policies, under review and avoid departing from them unless there is a compelling reason to do so;
☞ ensure the individuals hearing the disciplinary and, if necessary, appeal hearings are aware of all the relevant policies/ procedures and apply them reasonably and proportionately to the circumstances;
☞ if in doubt, take legal advice
His manager became aware that he had been admitted to hospital for oesophagitis, which can be associated with excessive alcohol consumption, and she therefore requested he attend another occupational health appointment, but he refused.
At a disciplinary hearing, mr m was dismissed for gross misconduct on two grounds, namely:
1
2
Being under the influence of alcohol at work;
Failing to follow a reasonable management instruction by not attending a further occupational health appointment.
Following an unsuccessful appeal, mr m raised proceedings in the employment tribunal for unfair dismissal – and it found in his favour.
Employment tribunal decision
It found that:
A public body with a statutory duty to provide proper care to its
Unfit for duty meant incapable of functioning effectively at work through alcohol consumption and there was no evidence to show Mr M was, in fact, unfit for work
patients needs to be vigilant in maintaining the appropriate standards of conduct;
there was no doubt mr m smelt of alcohol and, as such, his explanation of only having consumed a few beers was unlikely;
It was reasonable in the circumstances for a second occupational health referral and m r m acted unreasonably in refusing to attend;
Unfit for duty meant incapable of functioning effectively at work through alcohol consumption and there was no evidence to show mr m was, in fact, unfit for work/had been drunk at work;
In determining if smelling of alcohol was sufficient to constitute gross misconduct, a question had to be asked about why action had not been taken previously when there had been concerns;
the trust could not rely on mr m’s refusal to attend occupational health as a reason to dismiss, as he
the tribunal recognised that healthcare providers are entitled to be scrupulous in setting standards. But conclusions must be fully supported by evidence
was never told or aware that this matter was being considered as part of the disciplinary investigation process. the judge therefore concluded that a reasonable employer would not have treated the conduct as sufficient to justify dismissal.
Key lessons for practitioners t here is nothing wrong with being concerned about an employee smelling of alcohol at work or indeed having concerns about other matters that might impact on patient care/services.
Indeed, the employment tribunal recognised that healthcare providers are entitled to be scrupulous in setting standards. However, conclusions must be fully supported by evidence even in the healthcare context.
Fiona McLellan is head of the employment team and Jeremy Coy is a solicitor at Hempsons
Free legal advice for independent Practitioner Today readers Ipt
independent Practitioner Today has joined forces with leading niche healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
call Hempsons on 020 7839 0278 between 9am and 5pm monday to Friday for your ten minutes’ of free legal advice.
Advice is available on: business structures: Commercial contracts: ian Hempseed Faisal dhalla
Competition: disputes: lindsay draffan Hilary King
Our medico-legal work series continues with advice from michael r. young on getting your terms of business right from the start – especially your fee requirements
Terms of business are very important – this document is the contract between you and the instructing solicitor.
s olicitors will instruct you in accordance with the Practice Direction1 that supplements the Civil Procedure rules Part 35. If you have not already made yourself familiar with this, then you should do so before you formulate your terms of business.
sometimes law firms have their own terms of business that they will expect the expert to work under, but you will need to give some thought to having your own terms.
Travelling and accommodation rates;
You must make it absolutely clear from the outset the terms under which you are prepared to undertake a particular piece of work.
Never work without having signed terms of business in place, because if things go wrong – for example, a dispute over payment – you have nothing in writing to fall back on.
Your terms of business should include the following minimum information:
The name and address of the law firm;
Their reference and your reference;
The date;
The name of the solicitor’s client;
Whether you are being appointed as an adviser, a single expert or a single joint expert;
The obligations of the solicitor to you;
Your obligations as an expert;
Your hourly rate and the fee you will charge for your report and for any other service you may be asked to provide;
Payment of fees – for example, when they will fall due and the interest you will charge if they are late;
A space at the end for the solicitor’s signature and the date confirming his or her acceptance of your terms;
A sentence to the effect that if the solicitor does not return your terms of business, then you assume that he or she has accepted them by default.
m ost expert witness organisation have pro forma terms of business contracts for their members to use.
see the box on the right for an example of the fees section used by myself in my terms of business.
Fees challenged
Despite having agreed your fees with the instructing solicitor, you should be aware that the court may question your fees and that you might therefore have to accept a reduced fee as ordered by the court.
If you are working for the claimant, and despite winning the case,
AN exAmple from my terms of busiNess
my fees are based upon the degree of responsibility and skill involved and the time necessarily occupied on the work.
the fee, including disbursements, in response to your instructions is agreed at £x for the advice/report/attending case conference/attending experts’ meeting/attending court (delete as appropriate)
my hourly rate for the preparation of evidence is currently £x staff working under my direction will be charged at an hourly rate appropriate to their skill and experience. Details of the rates applicable will be supplied upon request.
my daily rate for attending a hearing or case conference or a trial is currently £x that is the equivalent of ten hours of my hourly rate for preparation and includes time spent travelling and waiting. if i am able to return to my office by 2pm, i will charge a half-day rate of £x
Where i am instructed to prepare for and attend a hearing or case conference, and for whatever reason those instructions are revoked, i reserve the right to make a cancellation charge calculated on a sliding scale according to the period of notice given and the amount of time reserved for the hearing or case conference.
my rate for examining a client is £x per appointment. there is a £x fee for a failed appointment or cancellation made less than 24 hours beforehand.
Never work without having signed terms of business in place, because if things go wrong, you have nothing in writing to fall back on
the defendant’s insurers might question your fees, this is all part and parcel of being an expert.
An important point to bear in mind about your fees is that you will not be paid for work carried out to correct typographical errors or other errors in your reports, or if you fail to address issues raised within the letter of instruction. make a mistake and it will cost you time and money. Get it right first time.
Next month: Your first instructions
Adapted from The Effective and Efficient Clinical Negligence Expert Witness , by m ichael r . Young, price £60 from otmoor Publishing reference 1. CPR 35 is available at www.justice. gov.uk/courts/procedure-rules/civil/ rules/part35/pd_part35. Practice Direction is one part of it and it is probably more important to your work than Part 35.
speciAl offer! buy the book AND sAve £20 the book costs £60, but independent practitioner today has secured discount of a third off for readers, so you pay only £40. listen to the audio content which accompanies the book at this website: www.otmoorpublishing.com/audio. for more information and to order, email stephen.bonner@ otmoorpublishing.com, quoting reference ‘young/ipt’.
PROBLEMS WITH THE TAX MAN?
HMRC tax investigations and disputes create difficult and stressful times.
As an award winning firm of tax experts, our highly experienced partners specialise in resolving problems relating to tax investigations and disputes with HMRC.
To find out, in confidence, how we can help call 0800 734 3333.
‘Here to help. Not to judge.’
Don’t put all your eggs
in one basket
Will your investment portfolio withstand any market conditions?
Simon Bruce looks at the most effective way to prepare for all eventualities
Owners Of 4x4 vehicles often appreciate them most when they leave smooth city roads for rough country lanes.
And in investment, highlydiversified portfolios can provide similar reassurance. In blue skies and open highways, streamlined city saloons might cruise along just as well as an all-road vehicle, but the real test occurs when the road and weather conditions deteriorate.
That’s why people who travel through different terrains often invest in a car that can accommodate a range of environments and conditions but without sacrificing too much in fuel economy, efficiency and performance.
structuring an appropriate portfolio involves similar decisions. You need an allocation that can withstand a range of investment climates while being mindful of fees and taxes.
when certain sectors or stocks are performing strongly, it can be tempting to chase returns in one area. But if the underlying condi-
tions deteriorate, you can end up like a motorist on a deserted road in the rain with a flat tyre and without a spare.
Missing out
Likewise, when the market performs badly, the temptation might be to batten down the hatches. But if the investment skies brighten and the roads improve, you could risk missing out on better returns elsewhere.
One common perceived solution is to shift strategies according to the weather forecast. This is a tough – and potentially costly –challenge. It is the equivalent of
keeping two cars in the garage when you only need one. You’re paying double the insurance, road tax and servicing.
An alternative is to build a single diversified portfolio. That means spreading risk in a way that helps ensure your portfolio captures what global markets have to offer while reducing unnecessary risks.
In any one period, some parts of the portfolio will do well. Others will do poorly. You can’t predict which, but that is the point of diversification.
It is important to remember that you can never completely remove risk in any investment. e ven a
well-diversified portfolio is not bulletproof; in 2008-09 there were broad losses in financial markets.
Long-time strategy
However, you can still work to minimise the risks you do not need to take. These include exposing your portfolio unduly to the influences of individual stocks or sectors or countries or relying on last year’s performance.
An example is those who made big bets on technology stocks in the late 1990s. These concentrated bets might pay off for a little while, but it is hard to build a consistent long-term strategy.
And the fads are not free – it is hard to get your timing right and costly if you are buying and selling in a hurry.
with a British summer, you can never be quite sure whether the sunshine will last. Listen to the wrong weather report if you are a classic sports car owner and there may not be enough time to get home and put the top up before the rain starts; something akin to listening to expert opinion on which particular markets are likely to outperform next.
Remove guesswork
By contrast, owning a diversified portfolio is a bit like having an allweather, all-road, fuel-efficient vehicle in your garage.
It allows you to remove some of the guesswork and increase your average chance of staying dry while still arriving in comfort with some time to spare.
This does, of course, need to be
adjusted according to your ‘risk profile’ – roughly translated as how much time you are prepared to allow your partner to get ready before losing your nerve!
Through diversification we can increase the reliability of the outcome or chance of arriving at your destination ahead of time. Add discipline and competent implementation to the mix and you get a structured solution that is both low-cost and tax-efficient.
Just as expert engineers can design fuel-efficient vehicles for all conditions, astute financial planners know how to construct globally-diversified portfolios to help you capture what the markets offer in an efficient way while reducing the influence of random forces.
There will be the odd rain shower, but with the right investment vehicle, the ride should prove to be a more comfortable one.
Owning a diversified portfolio is a bit like having an all-weather, all-road, fuelefficient vehicle in your garage
Simon Bruce (right) is managing director of Cavendish Medical, specialist financial planners helping senior consultants in private practice and the NHS.
The content of this article is for information only and must not be considered as financial advice.
Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
Be safe and sorry
Dr Michael Devlin answers some burning questions about how the statutory duty of candour will apply to independent practitioners
When something goes wrong during treatment, individual doctors have long had an ethical duty to be open and transparent with the patient and try to put things right.
But following the mid-staffordshire inquiry, a legal duty of candour has now been introduced for all organisations registered with the Care Quality Commission (CQC), including private providers. this has prompted mDU members to contact our helpline, asking what this means for them.
h ere are some of their mostasked questions and the m DU’s advice.
What
incidents
do i need to report?
Under the duty of candour, your organisation needs to report all notifiable patient safety incidents as defined by Regulation 20(9) of the h ealth and s ocial Care Act 2008 (Regulated Activities) Regulations 2014.
A patient safety incident is notifiable if it meets the following criteria ‘in the reasonable opinion of a healthcare professional’:
A) Appears to have resulted in:
i. Death;
ii. impairment of the patient’s sensory, motor or intellectual functions for a continuous period of at least 28 days;
iii. Changes to the structure of the patient’s body;
iv. Prolonged pain or psychological harm;
v. shortened life expectancy.
B) Requires treatment to prevent the patient’s death or any injury which would lead to one or more of the outcomes above.
the notification threshold for independent providers differs from that for nhs bodies to reflect the existing CQC notification system for reporting deaths and serious injuries.
What should i do if i make a mistake which could harm a patient?
Doctors have an important role to play in helping an organisation meet its legal obligations, so it is important to familiarise yourself with the procedures in place at your hospital or clinic and know the name of the person responsible for overseeing the statutory duty of candour.
Frank explanation
Whether or not a mistake is notifiable under the regulations, you have an ethical duty to give patients a full and frank explanation, tell them what you propose to do to put it right and offer an apology.
however, if you suspect that the incident meets the reporting threshold for the statutory duty of candour, you should report this to the relevant manager straight away.
t he organisation must then take the following steps as soon as reasonably practicable:
i nform the patient – or their representative – in person;
give them a full explanation of what is known at the time, including what further inquiries will be carried out;
offer an apology;
Keep a written record of the notification to the patient;
Provide reasonable support to the patient – for example, an interpreter to ensure discussions are understood or giving emotional support;
Follow notification in person with a written note of the discussion and keep copies of correspondence;
make a statutory notification to the CQC in line with the Care Quality Commission (Registration) Regulations 2009. the CQC has published guidance for non-
nhs trust providers on notifications.1
Bear in mind that, as the treating clinician, your organisation may expect you to represent them in meetings with the patient. if you have any concerns about this, contact your medical defence organisation for advice. You should still contribute to and comply with systems to protect patients, in line with gm C guidance.
What could happen to me if i don’t report a notifiable incident?
While the statutory duty applies to organisations, failure to report a patient safety incident could have serious consequences for a registered healthcare professional. the gmC has stressed that candour is an essential duty for all professionals working with patients and this includes being ‘open and honest with their colleagues, employers and relevant organisations, and taking part in reviews and investigations when requested’.2
Failure to meet the gm C’s standards could lead to a fitnessto-practise investigation and a hearing before the medical Practitioners tribunal s ervice, with career-threatening implications. m eanwhile, the CQC has said providers should have a system in place to deal with possible breaches of the professional duty of candour by staff, including an investigation and escalation process, which may lead to referral to their professional regulator. t here are potentially serious consequences for your organisation, which could face a criminal prosecution for a breach of regulation 20, particularly if is part of a pattern of persistent or recurrent behaviour.
–
own up to errors
Will being candid with patients about safety incidents make them more likely to sue me for negligence?
this is a common concern, but an open dialogue with patients is not something to be afraid of. in fact, mDU members have told us that apologising early to a patient or their family can help restore trust and prevent a complaint altogether or resolve one more quickly.
Remember that saying sorry for something that has happened to the patient is not an admission of liability. section 2 of the Compensation Act 2006 says ‘an apology, offer of treatment or other redress, shall not of itself amount to an admission of negligence or breach of statutory duty’.
i f you are unsure about the wording of an apology, contact your medical defence organisation for specific advice, but it is important that regret is sincerely expressed in clear, unambiguous, non-technical language.
i own a cQc-registered clinic. What can i do to ensure my staff understand the statutory duty and help my organisation meet its obligations?
if you are registered as a provider with the CQC, you will be legally
obliged to ensure your clinic’s policies and culture support openness and comply with the fundamental standards of care and safety that are required by law. the CQC expects organisations to have suitable governance procedures and systems in place such as incident reporting forms, which include the recording of a duty of candour notification. staff should be properly trained in how to recognise and report ‘notifiable’ incidents and receive appropriate support if they are asked by the organisation to notify a patient under the statutory duty.
members of the team should be encouraged to raise patient safety concerns without fear of bullying or undermining and be prepared to take disciplinary action if it emerges that someone has obstructed a colleague from exercising their professional duty of candour.
How will cQc inspectors check that we are complying with our obligations under the statutory duty?
i n m arch 2015, the CQC published guidance for providers on how it will oversee the statutory duty of candour through its inspection regime.3
Rather than checking whether providers meet the specific regulation, the CQC is using key lines of
enquiry (KLoes) to assess whether the standard of care is safe. As far as the statutory duty of candour is concerned, the relevant KL oe s are:
Are lessons learned and improvements made when things go wrong?
h ow does the leadership and culture reflect the vision and values, encourage openness and transparency and promote good quality care?
it makes sense to prepare examples of how you have addressed these points ahead of an announced inspection.
i f inspectors are not satisfied that a provider has met its fundamental standards, they will identify any shortcomings in their inspection report.
t he CQC has said it will take a proportionate approach to inspections, but if a provider falls short, it could face another focused inspection to check whether recommended improvements have been made.
the CQC has said it will use its enforcement powers where necessary ‘to protect patients and to hold providers and, in some cases, individuals to account’. t hese include warning notices, civil law enforcement action or even criminal proceedings.4
References:
1. Statutory notifications: guidance for non-NHS Trust providers, CQC; April 2015. www.cqc.org.uk/content/ notifications-non-nhs-trust-providers.
2. Joint statement from the chief executives of statutory regulators of healthcare professionals. Openness and honesty – the professional duty of candour. GMC website; 13 October 2014. www.gmc-uk.org/Joint_ statement_on_the_professional_duty_ of_candour_FINAL.pdf_58140142.pdf.
3. Regulation 20: duty of candour, information for all providers, CQC; March 2015. www.cqc.org.uk/sites/ default/files/20150327_duty_of_ candour_guidance_final.pdf.
4. Enforcement policy, CQC; February 2015. www.cqc.org.uk/sites/default/ files/20150327_duty_of_candour_ guidance_final.pdf.
Dr Michael Devlin is MDU head of professional standards and liaison
InvestIng In ProPerty aBroad
Buying in Por tugal
Following last month’s article on where to buy real estate in Portugal, Dylan Mitchell looks at how to go about buying your dream villa or apartment in this beautiful country
Holidaymakers and property investors have often overlooked Portugal – but this is changing. Through a combination of tough cutbacks on government spending and the introduction of incentives to attract investors to help revive the economy, the Portuguese government has succeeded in not only saving the country from financial ruin but has furthermore created a growing economy that is going from strength to strength.
a nd with property prices at close to 35% of 2007 prices, investors from around the world are
starting to take note of the opportunities to be had.
The Portuguese are hospitable and easygoing, creating a relaxed pace and comfortable quality of life with a low cost of living. more than two million Britons visit Portugal every year and an estimated 60,000 live and work there.
There is lots to keep you busy with plenty of world-class golf courses throughout the country, a coastline ideal for sailing and some of the best surfing conditions in europe.
The coastline seems to offer an endless supply of beautiful
The Portuguese government has succeeded in not only saving the country from financial ruin but has also created a growing economy
beaches and picturesque whitewashed fishing villages. The climate in most parts is warm to hot all year round, making it ideal for the summer holidays and for getting away from the Uk winters. and then there’s the food, the wine and, of course, the port wine … good times!
With easy borderless travel within europe, we are no longer restricted to one country. a s Portugal is quite a narrow country, you are never far from being able to explore western spain. in fact, s eville is only a two-hour drive from Faro.
aBoVe: Carvoeiro on the algarve coast
Property buying
process
1
The more prepared you are, the smoother the whole buying process will go. If you are going to apply for a mortgage, it makes sense to confirm your affordability with an experienced mortgage broker before you start looking at property.
The broker will be able to confirm how much deposit you will need and the monthly costs for the mortgage, which will be important for your budgeting.
2
The next step should be to appoint a lawyer to act for you. There will be a notario involved in transfer of ownership, but he or she acts on behalf of the state and will not be involved in completing all the checks on the property.
your lawyer, called an advogado, should speak e nglish and will perform detailed checks on the property with the l and r egistry (Conservatoria do registro Predial).
These include ensuring the property comes with its own title deeds and that these match the ownership, description and boundaries you have been given.
There should also be tax documents from the Portuguese inland revenue (repartição de Finanças), which confirm the vendor has paid all the annual property taxes and rates.
The local council must also confirm the property has a habitation licence. i f you are considering renovating or extending the property, this is the time to confirm if what you want to do is possible.
Wait for your lawyer’s report before transferring any money or paying a deposit.
This will help you avoid mistakes and could also highlight some issues that may make you decide to renegotiate the price.
3
The next step is to sign the sales agreement called the Contrato de Promessa de Compra e Venda (CPCV). This takes place in front of a notario, and you can grant your lawyer permission to sign on your behalf.
The CPCV includes the details of the purchaser, vendor and the property, as well as all the agreed conditions such as fixtures and fittings, mains services connec -
Typically, you should allow approximately 8% of the purchase price to cover all the property taxes and fees
MorTgages
Mortgages to buy property in Portugal can be arranged through some UK-based banks and with Portuguese banks
Depending on the type of property, type of mortgage and the value of the property, banks are currently lending between 60% to 80% of the purchase price
all mortgages are what are known as full status, which means that you will need to provide proof of income to show that you can afford the mortgage repayments, although the banks will take into consideration any rental income that the property will generate
Mortgage terms available range from ten to 30 years, with a maximum age at the end of the term of 80 years
Life insurance is mandatory
tions, all payments and, most importantly for a new build home, the completion date. it is at this point that you will pay a deposit of 10% to 25%, which is non-refundable. i f the vendor pulls out of the deal, they will have to reimburse you twice the deposit paid.
e ven though this is still the beginning of the purchase process, with a non-refundable deposit, it is clearly important to have your finances and legal searches in order before reaching this point.
4
5
Arrange your mortgage, if applicable.
The final stage of the purchase takes place when you sign the deed of transfer (Escritura de Compra e Venda), again in front of the notario.
The remaining payment is made for the property, or if you are buying with a mortgage, the funds will be drawn down from the bank and paid to the vendor.
The notario will ensure the title deeds are amended to reflect you as the new owner of the property. a ll taxes must be paid at this point or before.
6
Your lawyer will then register the title deeds with the land registry. This can take a few weeks. in Portugal, there are designated ‘tourist’ and ‘residential’ homes, so if you are looking for a rental income from the property, first ensure that this is permissible.
Buying costs
Typically, you should allow approximately 8% of the purchase price to cover all the prop-
erty taxes and fees. This is divided as follows:
Transfer Tax (IMT: Imposto Municipal sobre Transmissões) is the main expense. This is levied on a sliding scale. If the property is going to be your main residence, then the first €92,407 is 0%, but if it is an investment property or holiday home, then this first tier is levied at 1%. There are then different tiers with increasing rates of tax. The IMT is normally paid a couple of days before you complete on the purchase at the notario’s office.
Stamp Duty (Imposto do Selo) is calculated as a fixed rate of 0.8% of the purchase price.
Notary and Land Registry fees are normally around €500.
Independent lawyer’s fees can range from 1% to 3% of the purchase price, depending on the amount of work involved and the value of the property.
Bank arrangement fee, survey fee and additional notario and registration fees for the mortgage and stamp tax duty – if buying with a mortgage.
The seller pays the estate agency fees.
Portuguese tax number
This is similar to a National Insurance number in the UK. To be able to buy a property, open a bank and connect to the utilities, you will require a Portuguese tax number (Numero de Contribuinte). This can be obtained from the local tax office or through your lawyer.
If you are going to spend less than six months a year in Portugal, you must appoint a fiscal representative who will be responsible
for the payment of your annual property taxes – similar to council tax in the UK – and the payment of any income tax on rental income, if applicable.
Your lawyer should be able to recommend a local specialist. If you receive rental income from the property, then you will need to submit an annual income tax return. Rental income for nonresidents is taxed at a flat rate of 15%. Mortgage interest payments are not deductible, but repairs and maintenance expenses are.
Inheritance tax was abolished in Portugal in 2004 for transfers of assets to parents, spouses and children. UK inheritance tax may still apply even if you are living in Portugal.
Foreign exchange
When buying a property overseas, bank charges and fluctuating exchange rates could have a major impact on the overall cost.
Specialist foreign exchange dealers will typically save you around 4% compared to the exchange rates offered by the high street banks. Even if you are only looking to buy a property for €100,000 this would be a saving of €4,000!
A good foreign exchange dealer can also fix exchange rates, reducing the risk of fluctuations in the future. For example, say you know that you have a stage payment due in three months’ time and you feel the current exchange rate is really attractive, you can fix the current exchange rate today for your transfer in three months.
Dylan Mitchell is director of PortugalPropertyCo.com
Calling it a day
Winding down a private practice needs careful planning. Mr Jerard Ross (right) answers two of your medico-legal dilemmas
Dilemma 1 How do I go about telling patients?
Q I have a successful private practice, but as I near retirement, I am starting to put plans in place to close it down. I do not want my patients’ care to suffer and would like to tell them I will no longer be practising.
What is the best way of doing this?
UK Top 20 accountants specialising in the healthcare sector
• National firm of the Year 2013 AISMA member (Maidstone and Leicester offices)
• 12 offices including London City
• Tax Structures for Hospital Consultants - dispelling myths
• Surgeon groups and consortia GP Practices including mergers and federations
• Solvent liquidations (for companies at the end of their lives)
For more information please contact: South East
James Gransby FCA
E: james.gransby@mhllp.co.uk
T: +44 (0)1622 754033
M: +44 (0)7712321899 East Midlands General email: healthcare@mhllp.co.uk www.macintyrehudson.co.uk
Robert Nelson DChA FCA
E: robert.nelson@mhllp.co.uk
T: +44 (0)1162 894289
M: +44 (0)7814009160
A It is good that you are thinking ahead and that the care of your patients is your primary concern. The best way of looking at it may be to consider your patients in three categories:
1 Those you have treated but no longer see;
2 Those you review regularly;
3 Those who are likely to require further treatment. Patients you review regularly and who are likely to require further treatment will need to be told of your plans well in advance and
you should discuss their ongoing care with them.
By informing these patients of your plans early on, they will be able to express a preference for their care going forwards.
The GMC says that you should explain to the patient that you plan to transfer their care and pass on the relevant information about their condition and history.
In Delegation and Referral (2013), the GMC says that you should explain to the patient that you plan to transfer their care, and pass on the relevant information about their condition and history.
You will need to make sure that the patient knows who will be responsible for their future care.
You should also make the patient aware of the fact that in referring them, you will be disclosing confidential information and that you will not be able to refer them without this disclosure.
Dilemma 2
What do I do with patients’ notes?
QOver the years, I have treated many patients in my private practice and so have many medical records. What should I do with these when I close my private practice?
AAs a doctor working in private practice, you will hold a great deal of information about patients and have been registered as a data controller with the Information Commissioner’s Office.
Even after closing your practice, and for as long as you hold this information, you will have to fulfil your duties as a data controller under the Data Protection Act 1998 (DPA).
This includes responding to Subject Access Requests – requests for access to the records you hold about a patient. These could be made for a number of reasons, including if a patient wishes to make a clinical negligence claim against you.
With this in mind, you will need to make sure you keep your patients’ records. This is a legal responsibility under the DPA.
You will need to make sure that the patient knows who will be responsible for their future care
How long you need to keep them depends upon a number of factors and is outlined in the Department of Health’s NHS Code of Practice for Records Management.
As an independent practitioner, you are working outside the NHS and so are exempt from the Public Records Act.
However, the GMC makes it clear in Confidentiality (2009) that it expects all doctors to use the outlined retention schedule and that it does not distinguish between records for private and NHS patients.
It is important that you check the retention schedule to establish how long you must keep records for, as it varies depending on the patient and the type of treatment they received.
For example, if you treated a child or young person, the record must be kept:
Until the patient’s 25th birthday or;
Until the patient’s 26th birthday if they were 17 when the treatment was concluded or; Where the patient has died, eight years after their death, except if the illness or death could have potential relevance to adult conditions or genetic implications.
By comparison, family planning records for adults should be kept for ten years after the last entry on the record.
When planning to close your practice, you should also consider who would fulfil your duties as data controller in the event of your death.
Patients may still require access to their personal information even after you have passed away. We recommend you discuss this with your solicitor when drawing up your will.
Dr Jerard Ross is a medico-legal adviser at the MDU
Doctor on the roaD: caterham seven
Engine on wheels
Hold on to your hats! Independent Practitioner Today motoring correspondent
Dr Tony Rimmer (right) reckons there is nothing this side of a Porsche or Ferrari likely to thrill you on a rare weekend off as this stress-buster
There is something very satisfying about going back to basics. We are trained as doctors to assess, diagnose and treat our patients to the best of our ability using all available aids.
But what if we have to perform with nothing more than our own eyes and hands? We would need to concentrate and act with confidence. if we get it right and the patient recovers, the sense of achievement would be huge.
Of course, this is an unlikely scenario in the world of modern UK practice where our access to
blood tests, X-rays and scans is taken for granted.
But perhaps an occasional reminder of the basics would do us good and actually be enjoyable.
Ditching modern aids
so what if we extend this idea to our car-driving and get rid of all the modern aids that we have come to expect in our modern technically advanced vehicles?
Let us ditch cruise control, airconditioning, power steering, power brakes and automatic gearboxes.
Would we enjoy the experience of controlling a machine and guiding it along our highways a whole lot more?
Well, to test the theory, i have been driving a car that fulfills these minimalist requirements for the keen driver and has been doing so without great change to its basic formula for the last 50 years.
i t is the Caterham s even and started life as the Lotus seven in the 1950s. The brainchild of the supremely talented but flawed founder of Lotus, Colin Chapman,
it exemplified his core principles of sports car design: ‘simplify and then add lightness’.
Caterham bought the rights from Lotus in 1972 and has been building and selling the s even ever since.
Different options
The car is available with different engines and suspension options and many owners use them for both road and track outings. The model number signifies the power-to-weight ratio in BhP per tonne, and ranges from the 160
While the acceleration figures are not fast by modern car standards, it feels twice as fast in this sports car that sits a few centimetres above the tarmac
screens and a full windscreen; pretty essential items. You then have to add another £3,000 if you don’t want to spend the 80-100 hours it would take to build it yourself from a kit. so, for an on-the-road £21,995, you could get the excellent new Mazda MX5 as an alternative. But that would be missing the point. There is nothing this side of a Porsche or Ferrari that can thrill you in the same way as a Caterham seven. You will be spending much less of your hard earned income and much less likely to lose your licence in the process too.
Dr Tony Rimmer is a GP practising in Guildford, Surrey
through the 270, 360 and 420 up to the completely mad, supercarchasing 620 model.
i was most interested in trying the base 160 model that could be most suitable, at reasonable cost, in the role of occasional-use sports car to blow the cobwebs away for the petrol-head doctor on a sunday morning blast.
Caterham has recently relaunched the 160 with a threecylinder turbocharged 600cc engine made by suzuki that may only produce 80bhp but is plenty for a car weighing only 495kg
With its separate mud-guarded front wheels and headlights on pods, the seven looks like the closest thing to a single-seat racing car for the road that you can get.
The simple act of getting in is a challenge, particularly for drivers over six feet tall, but once behind the wheel, you feel like Lewis h amilton before you even start the engine.
A tiny thick-rimmed steering
wheel sits directly in front of you and the stubby short-throw gearlever sits naturally where your left hand rests on the transmission tunnel.
s tarting up produces a sporty exhaust note that belies the diminutive engine size and any thoughts of weak performance disappear by the time you get up to third gear.
Feels faster
While the acceleration figures are not fast by modern car standards, it feels twice as fast in this sports car that sits a few centimetres above the tarmac and is open to all the elements.
Although the standard steel wheels have skinny tyres and power goes through a live rear axle, the handling and grip is better than anything you can experience in even the hottest of hot hatches.
The steering responds to the tiniest of inputs and you really do
feel part of the car itself. B-roads are most suited to seven piloting and if you string a few bends together along a stretch of your favourite road, you will find yourself ‘thinking’ through them as much as driving them.
This is a sublime experience and guaranteed to put a smile on your face for the rest of the day. even the ride is more comfortable than expected, helped by the high-profile walls of those narrow tyres.
Owning such a pure driving machine naturally comes with some compromises. There is little room for luggage and you would not want to travel long distances, particularly in poor weather.
Although quick enough on the road, the 160 would feel out of its depth on a race-track, but there are much more powerful variants available, albeit at extra cost.
The £15,995 price-tag is a bit misleading as you then have to add £3,000 for the ‘s’ road pack that gives you carpets, hood, side
caTeRham seven 160S
Body: Two-seat sports car engine: 660cc three-cylinder turbo-charged
Power: 80bhp
Torque: 107nm
Top speed: 100mph
acceleration: 0-60mph in 6.9 secs
Fuel economy: 57.6mpg (combined)
On-the-road price: £21,995 (£18,995 self-build)
The model number signifies the power-to-weight ratio in BhP per tonne, and ranges from the 160 through the 270, 360 and 420 up to the 620 model
Lessons learned from the
2015 Budget
In the wake of the Budget, we asked specialist medical accountant Vanessa Sanders to wade through the small print and provide a detailed analysis of the key areas affecting independent practitioners in the months to come
The Tories’ first Budget for nearly two decades, back in July, was surprising in its further attack on those who already support the economy with their own business.
Big corporations are sitting pretty as we head to one of the lowest corporation tax rates in europe at 19% in 2017, reducing to 18% by 2020. But small companies are facing increased taxes with the proposed changes to the taxation of dividends.
This really is a blow for those of us working hard to shoulder the burden of growing the economy, provide real jobs and pay taxes.
Changes from 6 April 2016
The notional 10% tax credit on dividends will be abolished for individuals.
A £5,000 tax-free dividend allowance is being introduced.
Dividends above this level will be taxed at:
7.5% (basic rate);
32.5% (higher rate);
38.1% (additional rate).
But for those independent practitioners who have incorporated there are still distinct advantages. These include the limited liability, evening out profits over periods of uncertain times and changing
rates of personal taxation, allowing investment within the corporate environment and sharing the family business.
s hareholders with access to a basic rate band for 2016-17 –which has increased to £43,000 and is set to reach £50,000 – are still in a similar position to preBudget because of the £5,000 taxfree allowance.
A higher-rate taxpayer will pay tax at 32.5% on any dividend income in excess of the basic rate threshold, and an additional-rate payer will be taxed at an eyewatering 38.1% rate, but both
receive the tax-free dividend allowance.
That said, the cost comparison is always between sole trader and company. if we look at a typical consultant with profits of £100,000 and Nhs salary of £80,000, and a spouse who does not work outside of the home, we can see the results in table 1 on the right.
The employers’ allowance will negate the employers’ National insurance (Ni) on increases in salary beyond the Ni threshold.
But it is important to ensure the salary packages are commercially justifiable and that the non-fee earner does not benefit to a greater extent than the other director. This includes the whole package including pension contributions and gym memberships.
But let us have a look at where both spouses are in the higher rates (see table 2).
The typical consultant is married with a spouse also earning a higher salary; for example, spouse 1 earning £150,000 and spouse 2 earning £80,000 and private practices of equal size.
The big ‘but’ to be aware of here is that the dividends do not have to be paid out in the year in which the profits are earned, unlike the profits of a sole trade.
if the company did not pay out all of its profits, this is acceptable, as it allows for future planning such as to ensure continuity of the business in the event of a downturn.
or if the trade wished to invest in some equipment or a property or stocks and shares, then the company could still declare a lower amount – say, £150,000 of dividend – but keep the lower earner under the additional rate limit. This would save £5,330 in tax, thus managing personal taxes at these punitive rates of tax.
This flexibility is not available within a sole trader, as the individual pays taxes on the profits as they are earned at the rate of tax applicable during that period.
As you can see, while the effects of the Budget are not helpful to those of us who earn our living through our own efforts, they are certainly not disastrous. if you leave some of the profits as reserves in the company to invest in the longevity of the company, then these reserves can be maintained in the lower tax environment and invested for future growth.
The company can continue beyond its natural trading life and the growth and income be distributed when you and other shareholders are not paying such large percentages in personal tax; for example, when you retire.
The use of a company is particularly helpful when there are fluctuations in trading income, as profits are not subject to differing rates of personal taxation and Ni unnecessarily.
And there are also other potential shareholders to be considered. Do not forget anyone can own shares in their own right provided they are at least 18 years old. if you wish to let your views be known, there is a petition you can sign at www.ipetitions.com/petition/no-dividend-tax-for-smallbusiness-owners.
Pensions
The maximum level of contributions which attracts tax relief –including the basic-rate top-up – is currently £40,000 for a pension input period (PIP).
But this is to be reduced significantly for those earning in excess of £150,000, as reported in Independent Practitioner Today, JulyAugust 2015, page 2.
From April 2016, this allowance will be tapered by £1 for every £2 exceeding £150,000, subject to a maximum reduction of £30,000.
For those independent practitioners who have incorporated there are still distinct advantages
s o those earning in excess of £210,000 will receive tax relief on only £10,000 of contributions.
Tax relief is given by reference to contributions in the tax year, but the maximum amount attracting contributions is capped by reference to the PiP date.
This can be confusing if calculating unused allowances and it may be an issue for consultants with an Nhs pension which fluctuates when new salaries or merit awards affect their pension pots. Those affected may need to consult their adviser.
Introduction
non-domiciled individuals
Welcome to the BVRLA – I’m delighted that you’ve decided to join the trade association that provides a face for the vehicle rental and leasing industry, communicating its messages to customers, the media and government.
From the fiscal year 2018, any non-domiciled individuals (NDi) resident for 15 years out of the last 20 will be deemed domiciled for all UK taxes.
so why not turn to the experts in the field to help you find the vehicle that suits your needs?
The BVRLA’s corporate identity, particularly its logo, forms part of that message.
anthony K associates are vehicle leasing brokers specialising in providing vehicle contracts for doctors and all associated professions in the medical sector.
The BVRLA has three categories of membership, each with a logo that members are entitled to use (and, in some situations, are obliged to use). Appropriate use of our logo tells your customers, your suppliers, and the rest of the world that you adhere to the high standards that come with BVRLA membership.
o nce deemed domiciled, an individual will need to leave the UK for at least five consecutive tax years, including UK residents who wish to alter their status. This applies after 6 April 2017. if you have returned to the UK and your original status was as UK domiciled, you will re-acquire that status as soon as you acquire a UK residence, regardless of your intention to remain.
This brief guide explains how we expect our logos to be displayed – and how they should not be displayed. These are not hard-and-fast rules, and we sometimes depart from them ourselves, but we do expect our members to respect them and to gain our prior approval before using our logo in any way other than described here.
testimonials from our very many happy customers are proof of our attention to customer service and our practised ability to help clients get the vehicle they want quickly and easily.
If you need a copy of our logo, for use on your printed marketing material, or to go on a page of your website, please contact our communications team, who will be happy to send you an EPS or JPEG version appropriate for your purposes.
If you have any queries about use of the BVRLA logo that are not addressed in this guide, they will also be able to help
Doctors who own property also come in for a battering... ➱ p56
Gerry Keaney Chief executive, BVRLA
Anthony K. Associates Limited is authorised and regulated by the Financial Conduct Authority
Using the BVRLA Logo
renting out property
Mortgage interest is to be restricted. Currently, mortgage interest is deducted as an expense before the rental profits are charged to tax. Thus tax relief is given at the marginal rate of tax.
s o, for higher-rate taxpayers, this is at 40%. The Chancellor proposes to restrict mortgage interest relief to the basic rate, and given as a tax.
The change will be introduced gradually from April 2017 by 25% of finance costs available as a basic-rate deduction over the following four years.
r ent-a-room relief applies to private landlords, the owners of guest houses, B&Bs and similar small establishments, provided that they use the property as their main or only home.
From April 2016, the exemption increases from £4,250 to £7,500 per household. This is particularly useful where you have a univer-
This means tax which HM Revenue and Customs believes is owing can be accessed from personal accounts and investments
sity let owned by your offspring living in the property.
The ‘wear and tear allowance’, currently allowing relief on a 10% deduction of adjusted gross rents is to be replaced by tax relief claims only when furnishings are actually renewed.
For those of you heaving a sigh of relief or suppressing a sob as you wave off your offspring to university, the maintenance grants have been replaced by loans (increased to £8,200 with effect from 6 April 2016) to be repaid as the student reaches earnings of £21,000.
Considering the average earnings of graduates tabled in the Sunday Times University Guide, this should be immediately they get a job, so you may wish to consider alternative funding via employment or shareholding ownership.
But those who want to leave their homes…
Principal private pesidence
There is to be an additional nilrate band (NrB) for those leaving an interest in residential property, which was their principal private residence, to direct descendants. some flexibility will be built in where people have chosen to downsize their property before their demise, but this is subject to consultation.
travel and subsistence
Proposed changes mean that employment intermediaries, such as agencies and umbrella companies will no longer be able to claim tax relief for travel and subsistence if they are considered subject to the supervision, direction or control of any person (‘the sDC condition’).
Typically, this will affect locum assignments where the intermediary – whether your own company or via an agency – sends you as a temporary worker to supply a personal service or your labour.
This does not affect professional service firms because, as a consultant in private practice, you are not supplying your labour but a medical treatment or opinion. h owever, if you are working directly for the N hs in, say, Glasgow for two weeks of your holiday, but you live in London normally, then the travel between home and the temporary place of work will not be claimable against the income before it is taxed.
And woe betide if you owe any taxes…
recovery of debts
Legislation permitting the direct recovery of debts (D r D) will be introduced in the Finance Bill 2015.
• Completely open scanner that is well tolerated by claustrophobic patients
• Weight-bearing scans for spine and joints enable a more precise diagnosis
• Patients who are large or cannot lie down can be accommodated
For more information go online at: www.mri-london.com or call 020 7370 6003
The amount of the additional NrB will be the lower of: The value of the interest in the property (after mortgage charges); The ‘maximum amount’ of the band.
The band is to rise at a rate of £25,000 a year between 2018 (£100,000) to 2021 (£175,000) and thereafter linked to the Consumer Price index. The existing NrB of £325,000 will remain frozen until 2021.
of course, there is a restriction for those with more valuable estates. The new allowance will be removed at the rate of £1 for every £2 of the total net estate before allowances and exemptions – for example, Business Property relief – exceed £2m.
There are also to be anti-avoidance measures in place primarily around non-domiciled individuals using other vehicles to own their properties.
And there is bad news for those earning fees as locums...
This means tax which h M r evenue and Customs ( h M r C) believes is owing can be accessed from personal accounts and investments. hMrC will be able to recover debts of £1,000 or more from persistent non-payers, but has to guarantee to leave at least £5,000 in aggregate.
hMrC has promised to ensure that every debtor under DrD will have a face-to-face meeting before action is taken, but that funds will be frozen for 30 days to allow for the debtor to appeal. This will stop the debtor removing the funds. Apparently, there will be the right of appeal to the County Court and there will be a dedicated helpline to allow for ease of access. however, i would not recommend holding your breath, as the dedicated agent helpline can take in excess of 50 minutes to reply. if at all.
Vanessa Sanders is a director of specialist medical accountants
Stanbridge Associates
DO YOU FIND OUR PROFITS FOCUS SERIES USEFUL? Please let us know if it helps you or not. And if it doesn’t, what other data would you like to see presented?
Email robin@ip-today.co.uk
Working hard to keep up
Costs are up, but so are profits for ENT specialists in our latest unique benchmarking survey. But can it continue? Ray Stanbridge reports, with additional material from Martin Murray
rePreseNTATive FiGUres in our latest survey for Independent Practitioner Today reveal that the average private practice gross income of eNT surgeons has gone up by 4.5% from £132,000 in 2012 to £138,000 in 2013. Costs meanwhile have increased more – by 5.6%. They went up from £53,000 to £56,000.
Taxable profit has therefore risen by 3.8% from £79,000 to £82,000. There has been a slight decrease in the ratio of net margins/sales from 59.8% to 59.4%.
AVERAgE INCOME
Given the pressure on fees from insurers and market conditions, it is perhaps a little surprising that income rose.
working harder it appears that in certain areas of the country there has been a significant increase in Choose and Book work. But, clearly, some consultants appear to be working harder to earn the same as in previous years.
There have been a number of cost changes. staff costs and pen-
Clearly, some consultants appear to be working harder to earn the same as in previous years
sions have shown a small increase, from £16,000 to £17,000.
These average figures are distorted, as they may include elements of professional secretarial fees – at much higher costs – and family members assisting a consultant – at a lower cost.
The rise in personal allowance figures has again, it seems, stimulated some growth.
s ubscriptions and indemnity insurance costs have continued to rise a little. There are new entrants to the market and, on average, we are thankfully seeing a slowdown in the rate of growth of indemnity insurance costs.
o ther costs have shown some increase. These relate primarily to expenditure on marketing costs. i ncreasingly, practitioners are continuing to turn to marketing expertise to assist them in the growth of their practices.
WHO OUR ENT SURgEONS ARE
Our core sample refers to those who:
Have had a least five years’ private practice experience
Hold either a maximum part-time or new consultant NHS contract
Are seriously interested in pursuing private practice as a business
Are earning at least £5,000 a year in the private sector
May or may not have incorporated or be a member of a group
Source: Stanbridge Associates Ltd. Additional information: Sandison Easson and Co
it seems medical supplies/assistants fees fell slightly in the year to 5 April 2013, for reasons which are not immediately apparent.
What then of the future? Given the general election results, our view is that there is likely to be a growth in Choose and Book work over the next few years, rather than insured work.
indeed, some consultants have chosen to focus exclusively on this work – and in the process are saving indemnity cover costs.
There are also signs that younger
consultants are seeking a better work/leisure/lifestyle balance than their older contemporaries. As a result, through choice, they are tending to earn less.
Lack of growth
We do not see significant longterm growth in average incomes, although obviously the ‘super’ e NT practices will remain and continue to do well.
i f market conditions improve, and the number of insured patients rises, then obviously our
neutral assessment will be reviewed.
There is much pressure on the insurers to increase their customer base, and squeezing consultant fees may not necessarily be the best approach.
i t should be noted that it is increasingly difficult to effect any sort of statistically valid comparison of consultant e NT surgeon earnings.
This is because of fundamental changes in the market – some consultants have incorporated, others have joined groups, yet others have chosen to focus their activities almost exclusively on Choose and Book work.
All these factors make it extremely difficult to make any kind of consistent and fair comparison and our results are not statistically significant. Nonetheless, we have tried to give an idea of how well a typical consultant in this specialty is doing.
Actual figures vary enormously as in other specialties – and the small table on page 57 demonstrates this only too well.
next month: Cardiologists
Ray Stanbridge runs an accountancy, finance and tax advisory service specialising in the medical profession. Martin Murray is a partner at Sandison Easson and Co, specialist medical accountants
How Are you doing?
Use
Years ending 5 April
Jon Baines Tours
Escorted Medical and Cultural Tours and Cruises
Obstetrics and Gynaecology in Cuba
9 – 30 November 2015
Ecuador and the Galapagos Islands
14 – 27 November 2015
Ophthalmology in South India
16 – 29 November 2015
Occupational Therapy in Sri Lanka
10 – 23 January 2016
Medicine and Society in Sri Lanka
17 – 30 January 2016
Medicine and Society in Cuba
4 – 15 February 2016
Eastern Cuba
15 – 25 February 2016
Malabar Journey – South India
28 February – 13 March 2016
Palliative and Cancer Care in China
12 – 25 March 2016
Physiotherapy in India
4 – 17 April 2016
In the Footsteps of the Knights of St John 15 April – 1 May 2016
Obstetrics, Gynaecology and Fertility in China
8 – 21 May 2016
Veterinary Medicine in South Africa 11 – 23 May 2016
East of Java - Java, Bali, Komodo
3 – 17 June 2016
Anaesthesia in China
3 – 11 September 2016
Medical History Cruise in the Eastern Mediterranean 5 – 16 September 2016
Dental Study Tour to Indonesia 9 – 22 September 2016
Dental Cruise along the Rhine 12 – 19 September 2016
Future Tours:
Medical History in Italy: October 2016
Ophthalmology in Japan: October 2016
Paediatrics in North India: November 2016
Pushkar Camel Fair, N.India: November 2016
We also organise private groups and tailor-made tours. Please contact us for further details.
Uniting both the Surgical and Non-Surgical Communities
@ccr_expo #CCR2015 www.facebook.com/ccrexpo1
what’s coming in our october edition
Make sure you don’t miss our next issue, published on 22 October. Only subscribers to the journal are guaranteed to receive every copy and we don’t think anybody who is serious about continuing private practice in the future, when there is so much happening that will affect them, can afford to miss any issue.
Coming up next month:
Where is private practice going and what are the consequences for your business? We look at the changes to expect in the next five years
Improving the patient experience and your business admin at the same time. What a big doctors’ clinic learned from sending staff to see how a top hotel operates
Breaking Into Medico-Legal Work: Your first instructions
Hempsons laywers Puja Solanki and Lynne Abbess give tips on buying and selling a private practice
A medico-legal expert answers doctors’ concerns over the rise of sex assault allegations against practitioners
Practical video marketing for consultants
Big charge! Our motoring correspondent reviews the electric BMW i3 (right)
Dr Andrew Vallance-Owen gives an introduction to the ‘fixer’ agency that helps British healthcare providers overcome the challenges of international expansion
Our monthly series ‘Starting A Private Practice’ gives the key points to consider after your first year in practice
Some different ways of incentivising staff and providing them with a career path
In our ‘Breaking Into The Aesthetics Business’ series, Pamela Underdown explains the essential financial metrics needed to monitor, measure and improve to build a profitable and sustainable business
Consultants need to work together with private hospitals to manage patient complaints. Disa Young of the Independent Sector Complaints Adjudication Service (ISCAS) shows how
The big, bad world wide web and the implications of searchability: how clever PR and social media campaigns help specialists gain valuable, and more importantly, cost-effective space built to protect and enhance your reputation
Suffering from non-payers? Some template letters for you to send out will help
Profits Focus, our unique benchmarking series, looks at the income of consultant cardiologists in private practice
Plus all the latest news and views
ADVERTISERS: The deadline for booking advertising for our October issue falls on 25 September
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution.
Printed by Pepper Communications Ltd Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
£85 GPs and practice managers (private & NHS). £200 organisations.
But if you pay by direct debit, individuals pay only £70, and organisations £175. Call Proact Ltd on 01752 312140 Email: lisa@marketingcentre.co.uk
gUARAnTEE YOUR COPY
To guarantee your copy of Independent Practitioner Today by taking out a subscription (at the rates shown on the left), phone 01752 312140 or send off a subscription form on page 28 or email lisa@marketingcentre.co.uk. www.independent-practitioner-today.co.uk
If you pay by direct debit, individuals pay only £70 for a subscription. Just fill in the form on page 28 and send it to the Freepost address shown at the bottom of the form.
BACk ISSUES: £12.50 including post & packaging
CHAngIng ADDRESS OR SUBSCRIPTIOn DETAILS?
Phone 01752 312140 or Email lisa@marketingcentre.co.uk
Robin Stride, editorial director
12,450 circulation figures verified by the Audit Bureau of Circulations
The business journal for doctors in private practice