The business journal for doctors in private practice
In this issue
What does living with Covid entail for private doctors?
troubleshooter Jane Braithwaite advises on this thorny issue n Page 16
Earth isn’t the only one suffering Climate change affects health, so we need to grasp this to better support patients, says Bupa’s James Sherwood P20
Dawn Hodgkins examines the Government's latest Covid plan P12 Panic doesn’t help your investment Dr Ben Holdsworth on why taking a long-term investment is key P32
Poaching war for staff harming private care
By Robin Stride
Mounting staff recruitment and retention problems in private hospitals are hitting crisis point and threatening consultants’ support.
According to the former chief executive of the UK’s largest private hospital, HCA’s The Wellington, it is all-out war as independent sector bosses scramble to keep posts filled. He revealed some are paying golden handshakes worth thousands of pounds to attract nurses to join them.
Bosses are fighting even within the same hospital group to sign up targeted individual.
Other managers face huge problems keeping staff, whose loyalty has been financially ignored, working alongside new people given £5,000 signing-on fees.
The current state of play was unveiled at the private healthcare sector’s major annual conference, Private Healthcare Summit 2022, run by market analysts LaingBuisson.
Keith Hague – at the Wellington Hospital for 12 years before orchestrating the development of the new Cleveland Clinic in London
In association with
which opened this month –warned that some private hospitals were ‘fighting to survive’.
He said: ‘I know there are some huge problems in terms of recruitment and retention in the NHS, but in the private sector it is absolutely killing the way the private sector works.’
in their own group. That’s how tense this situation is.’
One in the Midlands found a rival group offering a senior nurse £9,000 more to join them.
The employer said it could only afford to pay £5,000 extra, but the incumbent was persuaded to stay when it offered to send her on a course she had hoped to go on for years.
If bosses needed more nurses preCovid, they might look to central Europe or chat with an agent in Australasia, but recruitment was now far more complex.
Mr Hague, now with associate Peter Goddard and running a new venture in executive healthcare recruitment called Goddard and Hague, said a chief executive at a London tertiary private hospital closed it down at the start of Covid.
‘A small portion were furloughed. The rest were made redundant and we were sat in front of this chief executive this week and he was saying "Why the hell did we do that?"’
rybody else they could find purely for one thing – more money.
‘From my days in private hospital management, we made lots of mistakes, probably more than anyone in this room, but one thing we did learn, Peter and I, was that retention is not always about more money.
‘Certainly, in terms of the highend clinical staff and the tertiary staff, critical care nurses, cardiac technologists and so on, it’s not about money there.
‘It is about development, skills, opportunity and the chance for people to grow within their own company and feel empowered by their company.
‘That’s all gone. It’s all gone; it’s dog eat dog out there and actually you wouldn’t think it, but it’s worse outside London. Small private hospitals are struggling to maintain their numbers.’
Private independent healthcare consultants had been decimated. ‘A lot of them have gone – they have made themselves redundant because they have no volume. A big London cardiologist with 20 people laid off all his staff. A lot of them retired early.’
Chief executives were ‘killing one another to try to get hold of staff and not only are they competing against competitor hospitals, they are competing with hospitals ➱ continued on page 5
Hospitals were all grabbing eve-
Healthcare recruiter Keith Hague
TELL US YOUR NEWS. Contact editorial director Robin Stride
ADVERTISE WITH US. To advertise in the digital journal, on our website or in our business and lifestyle directories, contact Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT
£90 independent practitioners. £210 organisations. £90 GPs and practice managers (private & NHS).
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE
Email karen@marketingcentre.co.uk Or phone 01752 312140.
Retention and recruitment of healthcare staff has been a huge challenge for as long as many of us can remember.
Nursing shortages were with us long before Covid-19, but now they and other staff patients and doctors rely on are becoming harder to find by the day.
Frustrated private hospital bosses are at loggerheads with one another (see our page 1 story) and it looks like a ward war out there.
Some are fighting rival local hospitals – and even others in their own group – to persuade targeted individuals to swap allegiance and work for them.
Others are throwing thousands of pounds at the problem to try and attract people with golden handshakes or prevent them from leaving.
Presumably, that will only add to their management problems as loyal existing staff get to hear they are not worth as much as their new colleagues.
In a candid presentation to the LaingBuisson Private Healthcare Summit 2022, hospital chief executive turned recruiter Keith Hague revealed the situation was so bad it was like bosses were ‘killing one another to try to get hold of staff’.
Staffing levels were helped through the pandemic when people returned to help out, but now many have gone again. And so have others who worked tirelessly through it and now want ‘out’ and more flexibility.
The work-life balance increasingly sought by many doctors in recent years is being followed by those in other professions too. And employers in healthcare are also paying the price of not looking after people as well as they could have done in the past.
As inflation surges and stimulates more itchy feet, the message to any doctor who employs staff they value is: ‘Don’t you dare risk losing them.’
The elements of a service to emulate Prof Paul Robinson of the Orri Clinic explains the success of this eating disorder service, praised by the CQC as an example for others to follow P14
Make it easier for patients to pay Richard Gregory follows his introduction to point-of-sale finance last month to explain how it contributes to greater self-pay sales growth P18
Handling complaints in private care
The MDU’s Dr Ellie Mein explains the new Code of Practice from the Independent Sector Complaints Adjudication Service P22
Get the message out
Marketing expert Simon Marett reveals why more independent practitioners are turning to promoting their services after the Covid pandemic. P24
A group confident in turning out hits 2022: the difficult second album for Circle Health Group? Its chief medical officer Dr Paul Manning reflects on successes and plans for the future P26
Make it easy to get the money Simon Brignall begins his series in which he highlights 30 key areas for practices to consider to overcome their billing and collection challenges P28
PLUS
OUR REGULAR COLUMNS
Doctor on the Road: Worthy successor to hot-hatch genre
The Ford Focus ST is a nimble hot-hatch that takes our reviewer Dr Tony Rimmer back to his SHO days P40
Starting a private practice: You can’t afford to simply ignore VAT
Accountant Ian Tongue presents a recap on ValueAdded Tax and how this may affect your practice P42
Profits Focus: A lucky 13% profit hike
Urologists typically enjoyed some healthy profit rises in our latest unique benchmarking survey P45
Donations to new NHS pensions to go ahead
By Edie Bourne
Doctors who are part of the NHS Pension Scheme will pay revised contribution rates following the Government consultation which ended in January – but the new rules have been delayed for six months until October 2022.
One of the main updates is that doctors’ contribution rates will be based on pensionable pay rather than their notional whole-time equivalent pay. Part-time members would therefore pay reduced pension contribution sums in the future.
The changes, initially proposed in a consultation launched last October, are part of moving all members to the 2015 pension scheme from April 2022. The 2015 scheme is a career average revalued earnings (CARE) pension scheme unlike the former final-salary schemes of 1995 and 2008.
New contributions – which will also be decreased from seven to six tiers – will be phased in over two years. The full amendments can be seen in the chart below, but, in general, higher earners will be contributing less into their pension. For example, the highest contri-
bution tier would be lowered to 12.5% rather than the current 13.5% and 14.5%.
Patrick Convey, technical director at specialist financial planners Cavendish Medical, said: ‘The new contribution rates may be positive for those in higher income brackets – but facing further changes can make it difficult for NHS members to ascertain their true pension position, particularly when the full McCloud remedy has not yet been introduced.
‘We always assumed the new rates would be delayed, as it seemed unfathomable to introduce this
major overhaul just two months after the consultation concluded.
‘The extension will give everyone more time to adjust to the new rates as well as the significant changes caused by moving everyone to the 2015 scheme. After all, we are still not due to receive official McCloud regulations until October 2023, which could make matters even more complicated.’
The McCloud remedy sets out how and when those deemed to have suffered age discrimination by moving to the 2015 NHS pension scheme originally will be compensated.
PROPOSED CHANGES TO THE CURRENT MEMBER CONTRIBUTIONS STRUCTURE
Free webinar on pensions attracts doctors
Independent Practitioner Today readers are registering for a free webinar to help guide them through a host of financial issues facing them in the year ahead.
‘NHS Pensions and Tax – what you need to know’ is being run by specialist financial planners Cavendish Medical, on Wednesday 27 April 2022 at 6.30pm.
Dr Benjamin Holdsworth, a director of the company, said:
‘Every year, the rules surrounding pay, pensions and taxation become ever more complex. This year is set to be even more challenging if you’re trying to get an accurate idea of your own financial position.
‘Not only are we awaiting the finer details of how the McCloud remedy will work in practice, but, from April, all members will move to the 2015 pension scheme.
‘You could be accruing benefits in the new pension, as well as maintaining your benefits in your former scheme. That means understanding two different growth rates and two different sets of rules – at the same time as trying to unravel the last seven years of activity in your current pension scheme because of the McCloud judgment.
‘We are hosting the webinar to
explain some of the key issues to consider and the actions to take now.’
Cavendish Medical provides specialist financial planning advice to medical professionals covering pensions, tax planning, savings and investments.
To register your attendance, go to https://cavendishmedical.com/ webinar-nhs-pensions-and-taxwednesday-27th-april/
Self-pay rise continues
Robin Stride reports from this year’s lively conference at the Queen Elizabeth II Conference Centre, Westminster
Promising self-pay market growth last year looks set to continue in the months ahead, the conference heard.
LaingBuisson self-pay consultant Liz Heath forecasted growth of 10% a year might be achievable.
Most of the 200-plus audience indicated they were very positive about self-pay’s potential, with 56% predicting growth of 15% or more in the next 12 months.
Mrs Heath called on the private healthcare industry to understand and respond to what appeared to be fundamental shifts in consumer attitudes to independent treatment.
But she cautioned that the potential for self-pay could be hit by economic factors, capacity or staffing issues. Interest needed to be converted into activity and people helped to understand how to obtain private treatment.
She said the over-55s were the
key demographic but younger age groups should not be forgotten. Many needed guidance and support because the private sector was new to them.
Around a fifth of private hospital revenues have been coming from self-pay, but new figures are expected to show a big increase as people seek to avoid the 6.1m+ NHS waiting lists.
Speakers agreed people were looking for information on cost, prices and affordability – but there
was criticism that hospitals were not making this easy.
Finding this information on some hospital websites takes too many clicks – meaning hospitals and consultants lose business.
Pricing clarity was criticised by freelance healthcare consultant Aileen Morrison who warned: ‘The whole experience for the patient can be tainted when they get the final bill.’
She said the industry now had the chance to treat self-pay as a long-term opportunity where people would return as self-payers or see the value of private medical insurance. It was time providers thought more about the customer.
David Hare, chief executive of the Independent Healthcare Providers Network, said there was ‘a huge opportunity for the sector to go out and help people navigate their way into private treatment.’
Speaking of his experience,
‘patient John’ described a tiresome mountain of red tape, phone calls and conversations to finally secure treatment through his private medical insurance policy. This contrasted markedly with what happened when finally at the hospital – treatment to discharge was excellent.
On another occasion, he made phone calls to four hospitals about an operation for his young son. Only one bothered to get back to him – and that one got the business.
Rachel Power, Patients’ Association boss, said patients complained about bad communication all the time.
Dr Gajan Srikanthan, medical director at digital solutions company Lumeon, said three key problems faced everyone in healthcare: staff shortages and burnout, reducing margins and higher expectations from digitally experienced patients.
Flexibility is cure for staff shortages
Demand for staff has never been so high – nor the number of candidates so low, reported Kate Shoesmith, deputy chief executive of the Recruitment and Employment Organisation.
Two months ago, demand was double that of February 2021. Retention was the big problem with, for instance a 5% increase in nurse vacancies arising in just one week in March. Nursing vacancies totalled 77,000.
She said while pay was important to people during inflationary times, the career agenda was too.
It was imperative to have pay increments, reward and loyalty packages. Just because someone had been with you five to ten years did not mean they would stay forever.
Employers should ask how they
were rewarding those existing staff as well as those to whom they were giving golden handshakes who come in from overseas or relocated.
Ms Shoesmith warned that people were now choosing to work in a very different way to the past, with work-life balance especially important.
A global shortage of healthcare workers meant employers will have to compete for staff wherever they went.
Mr Suhail Mirza, author of LaingBuisson’s Healthcare Workforce UK 2021 report, agreed salary increases were not necessarily the answer: people were looking for flexibility.
Paul Scandrett, director of international health at rostering solutions company Allocate Software, said very few organisations either
corporately or at board level had written down what a good roster looked like.
Those in the UK who were getting their rosters out four to six weeks early were using half as much agency as those who did not. ‘It’s startling. If there’s one thing –get your rosters out on time and with some thought about what good can look like. It can be an absolute transformation.’
Flexibility paid dividends. A lot of staff post-Covid would be looking to work part-time or indeed not at all. His company’s experience was that organisations who allowed staff to self-book their shifts and choose when they wanted to work were, on average, using 25% less agency than those that did not.
Mr Scandrett challenged emp -
loyers to ask staff how they were feeling, not necessarily every six months or a year but at the end of every shift, so they had as close a feedback loop as possible –‘because the reality is how the last shift felt like is the way they feel about the organisation’.
He asked them to consider what they had really had a pool or bank for: short-term sickness, long-term absence, cover, an increase with activity? It might be for all those reasons, but comprehending this helped people who would work for them to understand the rules of the game when they were asked to work.
For many staff coming back to the service, or returning temporarily, when they worked was more important than what they were going to earn.
Liz Heath of LaingBuisson
Talking to your staff is best way to keep them
Hospitals with visible leadership and who truly care for their people will have better retention rates, according to recruitment specialist Keith Hague.
He said leaders walked around their hospitals in the past to talk to people, but he questioned how many now went down to the catering department and spoke to the person emptying the bins every day.
Many bosses hid away in their office. ‘Just try it yourself. Ring the private hospital and say can you give me the name of the chief executive?’
Retention was more than just putting an advert in the paper or going on local radio. ‘It’s about leadership and general management and actually showing that you care for people.’
Ops done by employed surgeons set to rise
A huge rise in the number of private operations performed by consultant surgeons who are directly employed by independent hospitals is predicted by 2027.
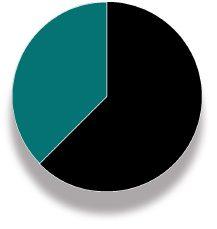
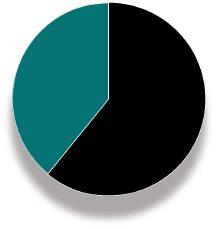
Over 200 delegates, including doctors, hospital bosses and healthcare organisations were asked to vote:
As many as 42% said a quarter to half of operations in the next five years would be done by surgeons on an employment contract.
Just over a third believed it would be 10%-25% while 15% of delegates thought these surgeons would account for more than 50% of procedures.
Only 8% thought less than 10% of operations would be done by these consultants.
‘High salaries are not sustainable’
The future prospect of high salaries for consultants employed in a small number of private hospitals was thrown into question during a debate on specialists’ working arrangements.
Consultant anaesthetist Dr Aubrey Bristow, a founder and director of the Phoenix Hospital Group in London and Chelmsford, said he thought the jury was out as to what would be feasible for the independent hospitals.
‘Some of the salaries, from my perspective, appear to be quite generous that people tell me they’ve been offered and it will be interesting to see whether in five or ten-years’ time those hospital providers are still able to provide that level of salary for that level of work – and I don’t think we’ve actually got the answer to that.’
He doubted many consultants would want to move from full-time NHS work to employment in the private sector. The younger generation of consultants coming up had an affinity with the NHS.
Schoen Clinic London hospital director Steve Smith said consultants wanting to join were a mix of younger doctors wanting to dabble in the independent sector and experienced consultants who had become disillusioned with the NHS.
‘Where do I put my money going forward? I think there is a hybrid there, I think the future, at least for
the Schoen, is going to be a mix of employed and traditional practising privilege models.’
He said that during a Care Quality Commission visit to the clinic the week before, an inspector expressed strong support for the employed model.
‘So I questioned him on that because I’m sitting here sort of looking down both sides of the road. Their view was that the outcomes of the employed model, clinically, they felt was superior. I think that’s an interesting ask and it’s certainly a discussion I’ve flagged to the inspector. I want to pick up that thread and flesh it out more.’
Recruitment specialist Keith Hague said large private hospital groups could not afford the payroll to compete with The Cleveland’s deep pockets.
‘HCA would say they are employing doctors – they are not. They are employing doctors to stop them from leaving.’ It was an opportunistic way of keeping them, he said.
Call to put an end to solo doctors Watchdog ‘not interested in solution to retention’
The president-elect of the Independent Doctors Federation called for an end to the lone private doctor.
Dr Philip Batty, one of 300 doctors on an employment contract at the just-opened Cleveland Clinic in London, told the conference sole practitioners should be phased out.
He said: ‘I worry about people working independently. Some will be excellent, I don’t doubt that, but it just leaves an opportunity for a maverick, for a Shipman, for a Paterson or something of that nature and I seriously worry about that.’
Mr Hague said his company went to the Competition and Markets Authority (CMA) and requested some relief for private consultants so they could have free hospital consulting rooms and some medical staff costs paid through the hospital group.
But it was ‘just like you were asking the CMA if they would support drug dealers on the street because they had gone out of business. They were not interested.’
He said healthcare had not cared for its lower-paid workers as it should. ‘I as a CEO used to say to the HR director: “Look, just get them from The Philippines, India,
Pakistan, maybe Portugal, central Europe.” And we were all guilty of bringing cheap labour in and we didn’t take care of them.
‘So what happened when Covid hit and when we came out of the EU was they walked away. I can’t tell you how complex recruitment is now in the independent sector. There are no retention strategies; nobody thinking clever about retention.
‘Their only retention strategy is “I’ll call the Nuffield hospital and we will offer this great lady another ten grand. And we will keep her. And did you say X was thinking about leaving? Let’s give her another five grand and send her on a course”.’
Dr Aubrey Bristow
➱ continued from front page
Stress toll due to GMC probe shown
By a staff reporter
A GMC report ‘Doctors who have died while under investigation or during a period of monitoring’ is a further reminder of the need for reforms to the medical regulator to be implemented without delay, according to a defence body.
The report shows that between 1 January 2018 and 31 December 2020, of the 29 doctors who sadly died during the course of a GMC investigation or programme
Tenth doctor joins OCL Vision clinic
Ophthalmic surgeon Miss Rabia Bourkiza has become the tenth consultant to join the growing team of eye experts at London’s independent OCL Vision clinic.
A vitreoretinal specialist, she joins the clinic’s three-strong consultant retina team and also works at London North West University Healthcare NHS Trust.
Her appointment comes as OCL Vision expands its operations. It
of monitoring, five died by suicide.
Dr Caroline Fryar, head of advisory services at the Medical Defence Union (MDU), called the report ‘sombre reading’.
She said: ‘Members tell us time and again that undergoing a GMC investigation is one of the most difficult experiences of their professional lives. To learn that, over a period of three years, five doctors died by suicide while they were involved in the process is truly heart-breaking. Our first thoughts
are with their families, friends and colleagues.’
The Government has committed to bring forward legislation to fundamentally reform the GMC –including the fitness-to-practise process.
Dr Fryar said: ‘Today’s report is a further reminder why that reform is urgently needed, so the GMC can take a more flexible and responsive approach. We urge the Government to deliver that legislative change without delay.’
has appointed seven new support staff, including three patient coordinators following more than 3,000 recent patient inquiries.
Opened in 2018, the independent clinic has seen demand for pri-
Ophthalmic surgeon Miss Rabia Bourkiza, a vitreoretinal specialist
She said the MDU worked closely with the GMC to communicate the doctors’ perspective of investigations. While the GMC was not complacent, the investigation process in many instances still took far too long and added to doctors’ stress.
Doctors experiencing health and well-being issues can find information on sources of support, such as its peer support network, on the MDU’s dedicated webpage.
Care
group offers jobs to Ukrainian refugees
vate care soar as the NHS wrestles with huge backlogs of patients after the pandemic forced hospitals to cancel thousands of ‘nonessential’ ophthalmic operations such as cataract surgery.
‘No blame’ inquiries re-inforced
The Medical Defence Union has welcomed a House of Lords vote to strengthen the ‘safe-space’ provisions under which healthcare professionals can take part in investigations that take place following a patient safety incident.
Chief executive Dr Matthew Lee said: ‘The need to move away from a culture of blame to one of openness and learning has been widely recognised for some time.
‘With this in mind, the Health and Care Bill includes important provisions so that healthcare pro-
fessionals can engage with the Health Services Safety Investigations Body (HSSIB) in a so-called safe space.’
The House of Lords voted in favour of an amendment to remove coroners from the list of exemptions to the prohibition on the HSSIB disclosing information from the safe-space.
Dr Lee said his union had made a strong case for this since the bill was published. The change would prevent coroners from being able to routinely request material provided
to HSSIB investigations naming individual healthcare professionals.
He added: ‘This vote is a victory for all those who want to see the new HSSIB and its investigations yield results, with improvements identified in the interests of patient safety.
‘For that to happen, it is essential to enable healthcare professionals to engage with its investigations without fear of blame. That’s why we are urging the Government to agree to the amendment staying in the bill.’
Circle Health Group says it hopes to sponsor up to 500 visas for Ukrainian refugees and their families, creating jobs in its 54 sites across England, Scotland and Wales. It announced the move ahead of the Government’s new sponsorship programme for businesses to provide visas and employment opportunities for Ukrainian refugees.
As well as clinical roles, Circle sites will offer administrative, engineering, logistics and project management positions.
Chief executive Paolo Pieri said: ‘As one of the UK’s big employers, we want to offer jobs and a fresh start to Ukrainian refugees forced to flee from their homeland. We are eager to help in some small way and stand with the Ukrainian people in this moment of unspeakable suffering.’
Circle said it would partner with the Government and third-sector organisations to remove bureaucratic barriers and move rapidly to offer a lifeline to individuals and families in need.
Dr Caroline Fryar of the MDU
Orthopaedic and sports medicine group Fortius Clinic has joined forces with Spire St Anthony’s Hospital, Cheam, to launch its second Joint Replacement Centre.
Fortius and Spire create joint clinic Data issued on serious injuries in private care
The centre provides hip and knee replacements using the latest robotic technology for patients in and around Wimbledon, South London and Surrey.
Fortius consultant hip and knee surgeon Mr Simon Bridle performed the first total hip replacement using the Stryker Mako at Spire St Anthony’s Hospital and praised the system for allowing greater ability to tailor the operation to the patient’s individual needs.
Consultant knee surgeon Mr Giles Heilpern ( right ) called the Mako robot ‘a game changer’.
He said: ‘It allows far greater accuracy of implantation compared to conventional nonrobotic joint replacement, leading to accelerated recovery and excellent outcomes.
‘It also very importantly allows bespoke implantation of the joint replacement in a position best suited to that individual rather than the more traditional onesize-fits-all approach typical with conventional instrumentation. The more I do, the more convinced I am.’
Fortius Clinic chief executive Jim McAvoy said: ‘We are delighted to have partnered with Spire St Anthony’s Hospital to provide this technology to our patients who live in south-west London.
‘The hospital is close to our recently opened diagnostic and outpatient clinic in Wimbledon and working with the team at Spire St Anthony’s allows us to offer our world-class care and first-class service to a wider network of patients.’
Fortius opened its first Joint Replacement Centre at Cromwell Hospital, London, in 2017, also with a Mako robot and enhanced recovery pathway.
By Agnes Rose
People considering private healthcare now have more information than ever before following the publication of new data about serious injuries incurred by patients in the sector.
The Private Healthcare Information Network (PHIN) figures reveal there were 22 instances where patients sustained serious injuries while receiving private treatment across the UK during the 12-months up to the end of September 2021.
A total of 734,000 people received private healthcare treatment in this time.
The injuries relate to the most serious incidents which are reportable by law to health regulators such as the Care Quality Commission (CQC).
PHIN said these are defined as permanent injuries to bodily, sensory, motor, physiologic or intel-
PPU WATCH
Compiled by Philip Housden
Surrey-Berkshire NHS trust expands its private brand
Frimley Health has expanded its Parkside private care brand into the NHS trust’s new Heather wood Hospital, Ascot, which is providing planned care services to Frimley Health NHS Trust’s 900,000 catchment across Berkshire, Hampshire, Surrey and south Buckinghamshire. Reported to cost £99m, the 11,500m 2 Heatherwood Hospital includes six operating theatres, outpatient and diagnostic facilities, 48 inpatient beds plus 24 day-
PHIN chief executive Matt James
lectual functions and may include permanent damage to vision or nerves, removal of the wrong limb or organ or brain damage.
Patients can now search for this information on PHIN’s website, alongside support and guides to help them decide which provider is best for their care.
PHIN chief executive Matt James
said: ‘The availability of good data is vital to learning and improvement, and this publication represents another step toward real transparency on safety and outcomes.
‘It is too early to draw any meaningful conclusions from comparisons between providers or with the NHS.
‘We applaud those hospitals that have provided complete data and encourage those who have not to do so.
‘As a patient, I would insist on being treated in a hospital that reports openly on its care and can show how data is used to improve safety and quality. It is easy to find those hospitals on PHIN’s website.’
PHIN published the information as part of its role to support people considering private healthcare with details about safety, quality and costs.
case cubicles with integrated private patient facilities.
Parkside Suite Heatherwood comprises a purpose-built private patient unit inpatient ward of ten en-suite single rooms for elective surgical patients on the third floor of the new build and an outpatient department with five consulting rooms and two minor ops treatment rooms.
The trust’s successful private patient brand and footprint already includes dedicated facilities for private patients at both Frimley Park and Wexham Park hospitals.
Frimley Health earned a record £10.7m in 2019-20 at 1.61% of turnover, and has for several years been a leading NHS trust provider of private patient services, in most years ranking 11th across the whole NHS in England and number one outside of London.
In 2020-21, trust income fell to £4.4m revenues, down 58.6% due to Covid, and Frimley fell to the fourth highest earning trust behind Cambridge, Oxford and The Christie Hospital, Manchester. Philip Housden is a director of Housden Group. See ‘How to boost PPUs’, page 44
Training boosted in private sector
By Leslie Berry
The Royal College of Surgeons of England (RCS) has welcomed a successful national effort to train hundreds of NHS junior doctors in the independent healthcare sector over the last 18 months.
Figures from the Independent Healthcare Providers Network (IHPN) show more than 4,000 have been trained in private hospitals since 2020 under the Doctors In Training initiative – and now it is hoped to considerably increase the number.
The college has long called for all elective NHS operations to include a surgical trainee, including those procedures delivered in the independent sector.
According to RCS vice-president
Miss Fiona Myint, this is vital because a substantial volume of NHS work, such as hip and knee replacements, now takes place in private units.
She said: ‘We appreciate the considerable amount of work that has been done to establish guidance to support an increase in surgical training in the independent sector. We are keen to ensure that the national guidance is implemented as fully as possible at the local level.
‘We are committed to working with the NHS and the independent sector to overcome the barriers to accessing training, so that opportunities are offered consistently across the country.’
CHANCELLOR’S SPRING STATEMENT
Dismay at failure to grow private cover
Chancellor Rishi Sunak’s Spring Statement has left insurers disappointed at his failure to provide tax incentives to help attract more patients to take up private medical insurance.
The Association of Medical Insurers and Intermediaries (AMII) said the Chancellor should have used the opportunity to incentivise private medical insurance take-up to help tackle the record-breaking NHS treatment backlog.
David Middleton, its chairman, said: ‘The Chancellor’s Spring Budget Statement gave the perfect opportunity for the Government to help alleviate the huge care and treatment backlogs in the NHS by introducing tax incentives for those who wish to, and already have, purchased private medical insurance.
David Middleton of the Association of Medical Insurers and Intermediaries
‘The Government’s delivery plan for tackling the Covid-19 backlog of elective care published in February made positive noises about how the private medical market can work with the NHS.
‘Calls for tax incentives have already been made from the Conservative backbenches in Parliament and this would have been the ideal time to announce this policy initiative.’
He said the AMII regretted the Chancellor had chosen not to act and was asking: if not now, when?
The surge in junior training in independent healthcare facilities followed a landmark agreement to increase training opportunities in the sector.
An IHPN report last month reflects on progress made since it reached agreement in September 2020 with the Confederation of Postgraduate Schools of Surgery, Health Education England (HEE), and NHS England to ensure the independent healthcare sector plays its part in training the next generation of doctors.
Cancellation of many elective procedures in the NHS due to the pandemic meant independent providers were able to ensure juniors’ training was not disrupted –particularly as part of its delivery of
Budget does nothing for pensions, BMA protests
The BMA has expressed concerns over the Spring statement’s failure to take any steps to ease senior doctors’ problems with pension payments taxation.
Council chairman Dr Chaand Nagpaul said: ‘It is deeply disappointing that the Chancellor has failed to heed the BMA’s call to address the punitive pension taxation rules, which is resulting in many doctors being unable to take on extra work or forced to retire early.
‘This comes at a time of when severe staffing shortages threatens the very sustainability of the NHS and compromises patients care.’
He also criticised the absence of a costed plan to deliver a longterm workforce strategy to ensure the NHS has the doctors, nurses and staff it needs to meet current and future healthcare demands.
routine orthopaedic and ophthalmology treatment.
IHPN’s report sets out the cultural shift around medical training in the last 18 months, with a recognition of the widespread benefits of having the independent sector as a training provider and the need for all parts of the healthcare system to work together.
With a commitment to building on the progress made since 2020, the report also makes recommendations to ensure NHS junior doctors can more easily access the high-quality training in the independent sector.
Newmedica’s medical boss looking for new recruits
Mr Nigel Kirkpatrick, consultant ophthalmologist and partner at the Newmedica eye health clinics and surgical centres in Gloucester, is now the company’s new medical director.
He said he was spending a lot of time recruiting new consultants for its network of clinics nationwide, ‘making sure we pick the right people’ to give patients the best possible experience.
‘I get bored with doing the same thing all the time, so balancing the medical director role with working in my own clinics is perfect for me. And I know the NHS needs a lot of help to deliver what patients need –it’s one of the reasons I haven’t even thought of retirement,’ he said.
‘If we all work together, we can make the system better for patients, which is all that matters.’
Miss Fiona Myint of the RCS
Mind health clinic expands to Bristol
By Douglas Shepherd
Re:Cognition Health is expanding its UK business with a new clinic in Bristol, scheduled for opening next month.
The 3,500 square foot site will be the company’s first clinic combining clinical trials, private practice and medico-legal services under one roof.
Re:Cognition Health Bristol will offer a range of brain and mind services to optimise cognitive health and performance, comprising:
Clinical trials: specialising in Alzheimer’s and other conditions affecting the brain and mind;
Children’s services: gold-standard ADHD and autism assessments plus other mental health conditions;
Memory clinic: specialist assessments, blood test panel, brain scans and clinical management plans;
Founder and chief executive Dr Emer MacSweeney said: ‘It is an exciting time for Re:Cognition Health as we continue to expand
not only our clinical services but also our clinics in the UK and US.
‘We are proud to invest in research through international clinical trials and to be making a positive impact on the lives of patients, their families and also on society.’
The clinic will serve as a model for all Re:Cognition Health clinics due to open as part of the business’s expansion plans.
Other clinics are in London, Guildford, Plymouth, Birmingham, Winchester and Washington DC in America.
Clinical services director Dustin Reibe said: ‘Our team is passionate about providing an early and accurate diagnosis, using the very latest diagnostics to optimise patient outcomes and we are thrilled to be offering this service to the Gloucestershire community.’
Re:Cognition Health Bristol is at Unit 240, Phase 200 Ground Floor, Aztec West.
‘Give public chance to go private’
Less than half of the public know they can choose where they receive their NHS treatment, including in the independent sector, according to the Independent Healthcare Providers Network.
The organisation’s policy director David Furness urged the NHS to make a big drive to ensure the public are given all the information so they can make the best decisions about their care.
Figures last month showed yet another record NHS waiting list of over 6.1m.
Now it was vital that Health Secretary Sajid Javid’s commitment to give patients more choice and control of their care was translated into concrete action to improve access to treatment, said Mr Furness.
‘Tackling the elective backlog is
the public’s number-one priority for the NHS and people will now want to see the Government delivering on its promises and doing all it can to put power in the hands of patients and stop waiting lists getting out of control.’
Meanwhile the Royal College of Surgeons of England has urged for a national effort to level up access to surgery, as figures show nearly 24,000 patients wait two years or more for consultant-led hospital treatment.
The Government asked the NHS to contact every patient who has waited two years or more by the end of March, to offer them a choice of an independent provider or a different hospital they could travel to.
College vice-president and consultant ENT surgeon Mr Tim
Mr Tim Mitchell, vice-president of the Royal College of Surgeons of England
Mitchell said: ‘If someone is left waiting years for a planned hip or knee operation, for example, it’s not surprising they will now be struggling to walk or work.
‘We must find a way to get these patients treated, even if it means paying for them to travel to a part of the country that’s less afflicted or paying for treatment in the independent sector.’
But he warned that success depended on sorting the longstanding issue of staff vacancies and improved workforce planning.
Harley Street unit starts pain clinic
The Harley Street Specialist Hospital (HSSH) is opening a pain management clinic with 14 pain consultants available to treat specialist areas.
Patients can be cross-referred within the hospital for a range of treatments for spinal, headaches, neck, pelvic, dental, back, shoulder, upper limb, hand, knee, hip, foot and ankle conditions.
Chief operating officer Marcus Whiteley said: ‘Creating proper whole-body solutions for alleviating and managing pain is critical for a person’s emotional wellbeing. Pain is prevalent in our times with one third of all adults in the UK suffering with lower back pain.
‘Around 20% of these people seek advice from their GP. This equates to around 2.6m patients every year. Our goal is to assist people in taking action to manage a pain-free life with treatment and the correct strategies. The breadth of experience that we have in the team is unparalleled and we hope to help a lot of people.’
HSSH pain consultants: Pain injections and management: Dr Fariborz Neirami, Dr Stephen Humble, Dr Roman Cregg, Dr Stefanos Palmisani, Dr Norman Kufakwaro; Pain injections and spinal surgery: Mr Fady Sedra, Mr Mohamed Ahmed, Mr Wai Weng Yoon; Wisdom tooth extraction and oral pain: Mr Luke Cascarini, Mr Spencer Hodges, Miss Natasha Berridge, Mr Mustansir Alibhai, Mr Ravinder Pabla, Mr Tamer Theodossy.
Dr Emer MacSweeney
The Harley Street Specialist Hospital
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2012
50p tax cut is too late for doctors
Chancellor George Osborne’s cut in the 50p top tax rate came too late for hundreds of independent practitioners who said they had been forced to abandon business plans.
Scores of smaller practices were opting to see fewer patients, 250 others were known to be shutting completely, and many were cutting down on NHS work in a bid to contain taxable incomes.
Accountants said, despite warnings, many doctors were unprepared for the extra tax they needed to pay after losing their personal allowance the previous year on earnings over £100,000. This meant they were effectively taxed at a 60% marginal rate.
The 2012 Budget cut the top tax rate to 45p from April 2013.
Accountants Stanbridge Associates said the winners were the 2,000 consultants in the UK who had incorporated their businesses. Most had avoided the 50% rate.
Seek the self-pay market
The boss of the UK’s biggest private hospital group advised would-be and existing private doctors that they needed to capitalise on the potential of the self-pay market.
Stephen Collier, chief executive of General Healthcare Group, said the industry needed to go after self-payers following an 18-month period when it had received ‘a hell of a kicking’.
He warned delegates at a BMA private practice conference: ‘You can’t wait for patients to come to you through traditional channels.’
The private sector is too disjointed
A leading commentator on private healthcare criticised a ‘remarkable absence’ of a joint approach by doctors, hospitals and insurers to promote the sector.
Economist William Laing said that, as an independent observer, it seemed there was ‘an awful lot of bickering going on but very
little presentation of the case for private health’.
Laing & Buisson’s [now called LaingBuisson] chief executive claimed this demonstrated a degree of immaturity in the sector, since all players depended on one another. Mr Laing said there was a need for the various groups to speak more and with one voice.
The costs of private care drive people abroad
Private doctors in the UK were losing millions of pounds worth of potential custom because patients were opting to travel abroad.
Nearly three-quarters of patients in a survey of over 1,000 said they had saved more than £2,000 by travelling overseas.
12.7% said they had saved more than £10,000 by having their treatment outside the UK.
Thanks a million!
HM Revenue and Customs (HMRC) signalled no let-up in its campaign to squeeze every last drop of tax owed by doctors.
One of its senior officials told a doctors’ conference that 1,000 civil investigations had started against medics who should have come forward but chose not to, and
criminal investigations were being considered.
Of 1,500 disclosures raising £10m, one included a doctor who paid the tax department ‘over £1m’, and six who handed over £100,000.
She warned: ‘It’s better to come to us before we come to you.’
Check your indemnity if volunteering abroad
Doctors volunteering to give their services free abroad were being warned to check their indemnity arrangements.
The MDU said doctors should check whether indemnity could be sourced in the destination country – if not, then they should ensure they were covered under arrangements with their defence body.
They should also see if they needed to register with the local regulator to work in the country. This could be a slow, process so they should allow plenty of time.
TELL US YOUR NEWS
Share your experience of what has and has not worked in your private practice. Even if it’s bad news, let us know and we can spread the word to stop others falling into the same pitfalls.
Contact editorial director Robin Stride at robin@ip-today.co.uk
Spending too much time on billing instead of patient care?
Let Medical Billing & Collection do the hard work for you.
With 30 years’ experience helping over 1,500 private consultants, groups, clinics and hospitals.
• Dedicated account manager
• Reduce bad debts to less than 0.5%
• Increase net income by up to 25%
• 24/7 online access to your data
• Faster payments through e-billing for insurers and patients.
Discover more at medbc.co.uk or 01494 763999
What does living with Covid mean?
The Government recently set out its plan for ‘Living with Covid19’. Dawn Hodgkins examines what this means for independent practitioners
THE GOVERNMENT’S ‘Living with Covid-19’ document sets out how it will balance the competing aims of removing Covid restrictions, while also continuing to protect people most vulnerable to the virus and ‘maintaining contingency capabilities to deal with a range of possible scenarios relating to the pandemic’.
But for independent healthcare practitioners and providers, what does ‘living with Covid’ mean in terms of their ability to deliver vital healthcare services and keep patients safe?
While there are many unknowns about how testing, self-isolation and infection prevention and control (IPC) guidance will continue to develop in the coming months, here is a rundown of what we know so far and some of the issues practitioners and providers will need to grapple with.
Requirement to self-isolate
One of the key commitments in the Government’s ‘Living with Covid-19’ strategy is removing the legal requirement to self-isolate following a positive test – though adults and children who test positive will continue to be advised to stay at home and avoid contact with other people.
This is a notable change in the policy around testing and self-isolation. Given the importance of keeping healthcare settings Covidfree, both NHS England and the UK Health Security Agency (UKHSA) have stated clearly that healthcare staff who test positive for Covid should not attend work
until they have had two negative lateral flow test results taken 24 hours apart, with the first test not taken before day five after their initial positive test.
Of course, in practice, ensuring that both staff and patients are clear that they should not access or use healthcare premises if they have tested positive or think they have Covid will be a challenge with this more liberal testing and isolation policy.
Perhaps one of the most controversial elements of the Government’s plan is the intention to end the provision of free universal symptomatic and asymptomatic testing for the general public from 1 April.
This is a significant change and while the Government’s report states that limited symptomatic testing will be available for a ‘small number of at-risk groups’ as well as for social care staff, as I write, it remains unclear what testing will be available for healthcare staff delivering both NHS and private care as well as those needing treatment.
Further clarity
Getting further clarity of this will be key, as access to Covid testing by both patients and healthcare staff will be critical both in stopping the spread of the virus as well as providing reassurance to patients and giving them confidence that everything is being done to ensure their care is as safe as possible.
While these two changes were a key plank of the Government’s ‘Living with Covid-19’ strategy, there do, however, remain a number of other key questions healthcare practitioners and providers will need answers to in the coming months.
For patients requiring treatment, both the pre- and post-surgery protocols will need to be considered.
Currently, best practice states that, where possible, surgery should be delayed for at least seven weeks following a Covid infection, with the exception of those needing urgent treatment or where the risk of delaying surgery are particularly great.
But with both NHS and independent healthcare providers facing a significant increase in
Perhaps one of the most controversial elements of the Government’s plan is the intention to end the provision of free universal symptomatic and asymptomatic testing for the general public from 1 April
health and social care providers registered with the Care Quality Commission.
As part of that consultation, the Government will also be looking to strengthen requirements for healthcare professionals to be vaccinated for Covid.
Compulsory vaccination
While the Government has revoked regulations making vaccination a condition of deployment (VCOD) for health and care professionals, the issue has not gone away and there will remain a real focus both from organisations and from professional regulators to encourage as many healthcare workers as possible to get vaccinated.
Coronavirus has shown itself to be particularly unpredictable, producing many twists and turns over the last two years.
It is vital that all healthcare providers and practitioners remain
vigilant in keeping it at bay. But with cases firmly on the downward trajectory at the time of writing, we are definitely moving into a new phase – balancing both the need to keep patients safe and ensuring as many people are treated as possible, given the growing backlog of care.
This will not always be easy to navigate, but the Independent Healthcare Providers Network (IHPN) will be working hard to ensure the views of independent providers and practitioners are fully plugged into conversations so the sector can continue to do its best for the millions of patients they treat every year.
Dawn Hodgkins (right) is director of regulation at the Independent Healthcare Providers Network (IHPN)
complexity and demand, and growing backlogs of patients – not to mention Covid variants becoming less severe – there are questions over whether this approach remains appropriate.
With testing and self-isolation regimes being eased for the wider populations, which make it more challenging to understand the numbers of patients who have had Covid, ensuring clear guidance is in place for patients on what precautions they need to take before and after treatment will be vital.
This is particularly important for those who are older and more vulnerable.
Infection control
Looking at broader infection and prevention control measures, with the retreat of the virus, it its likely that guidance will increasingly be made at more local and regional levels.
Independent providers and practitioners should make sure they are plugged into local discussions about this.
Reflecting the new ‘Living with Covid-19’ environment we will be working in, the Government has also announced it intends to consult on updating the code of practice on the prevention and control of infections which applies to all
The elements of a service to emulate
Orri, an independent specialist eating disorder service in Central London, won an outstanding rating from the Care Quality Commission following its very first inspection.
It went down so well with the inspectors that, as we reported last month, the watchdog’s head of hospital inspection praised it as ‘an excellent example to other providers who should look to learn from this report’. Prof Paul Robinson (left), consultant psychiatrist at Orri, tells more
How we reported on the CQC’s opinion of the Orri Clinic last month
HAVING BEEN associated with Orri from the outset, I was delighted to read this very positive report from the Care Quality Commission (CQC).
I have long been convinced that most patients with severe eating disorders do not require admission to inpatient care.
And I have also considered that – for those who are admitted –some could have avoided admission with intensive community care and some, perhaps most, could be discharged early when medically stable, to such care.
That was the basis for the service I developed at the Royal Free Hospital in the 1990s and I was so pleased when Orri’s founder and chief executive Kerrie Jones, who is a leading psychotherapist in the eating disorder sector, invited me to be part of the Orri project in 2019.
Elements of success
The idea that one can treat people with severe eating disorders in day care has been supported by the eating disorder charity BEAT and NICE but unfortunately not taken up universally, for reasons that escape me. Thankfully, Orri has now shown that it can be done effectively and safely.
What are the elements that have contributed to the success of Orri?
They are many, and the CQC has recognised them, but I would like to point to a few key areas that I believe to be essential.
The first is effective leadership, and I am referring here not only to our excellent chief executive, but also to the whole senior clinical and management team.
Their belief in the Orri model and their high professional standards allow the rest of the staff to participate in what some in the eating disorders field regard as a risky enterprise.
It is only when the leadership are able to convey a sense of professionalism, adherence to safety and to outcome monitoring, that more junior staff, as well as clients, can feel confident enough to get on with the difficult task of client recovery.
A second key area is adherence to effective professional practice, backed by research evidence, where that exists, and to professional standards where it does not.
The fact that this is universal at Orri means that the quality of care provided is as high as it can be.
Building relationships
I believe the third area that contributes hugely to Orri’s success is the relationships built up between staff and clients. People with eating disorders can experience criticism and rejection when it comes to their beliefs about eating and the body.
They can be dismissed as seeming ‘self-absorbed’. At Orri, a compassionate approach from staff recognises that our clients are in the grip of a compulsion they cannot control and getting alongside the client in this way is an essential part of helping them move on to a healthier way of life.
Could Orri, with five stars, do any better? Of course, the answer is ‘yes’. The model needs to be made available to all NHS patients using both face-to-face and online therapy.
And as well as thinking of expanding existing Orri in a new location, and perhaps establishing Orri 2, we might consider whether other community approaches such as home care might be within our reach.
Whatever the future holds, Orri has, through its successful CQC inspection, become established as a beacon service to be used and emulated by other services. For Orri and its model, the future looks very promising.
Prof Paul Robinson is research and development director at Orri and professor (Teaching) Division of Medicine, University College London
The free digital prescribing platform for all private prescribers.
CloudRx take care of the dispensing, payment and delivery of medicines direct to your patients, wherever in the country they may be, for more convenient access to their medicines.
TRANSFORMATIONAL
Order prescriptions at the touch of a button to support all consultations and add a whole new level of convenience for your patients.
SIMPLE, CONVENIENT AND SECURE
Simple and fast digital prescribing.
Legal paperless prescriptions, repeat prescriptions and controlled drugs.
Prescriber fees can be charged to the patient if requested.
INTEGRATED
Our API enables frictionless integration with healthcare brands & clinical software including Heydoc, MidexPRO, eClinic and YouClinic
“We were struggling to keep up with the admin side of the prescriptions, not to mention storage for medication to cope with a huge increase in prescriptions. CloudRx immediately took away the strain. Since our partnership we have grown by more than 200% in size. We could not have done that without their support.”
– Dr Louise Newson, Newson Health
Can I charge a fee for emails?
Our troubleshooter Jane Braithwaite (right) answers independent practitioners’ questions on business matters
Should I charge patients for phone calls and answering their questions sent by email? These take up a lot of my time
THE TRADITIONAL model of seeing patients face to face has been challenged over the last couple of years and patients have become more accustomed to talking to their doctor by video, phone and emailing questions.
Many private GPs and consultants were challenged by the number of patient phone calls and emails prior to Covid, but we have definitely seen a marked increase.
Being able to provide patient care in a number of different manners brings advantages, and a mix of approaches can be adopted to improve patient experience.
But in private healthcare we need to be mindful of how we charge for these different interactions, what the insurance companies allow and also how patients react to different fees.
Pre-covid, most private doctors charged for face-to-face consultations and accepted there might be a couple of phone calls or emails as follow-up, especially if surgery were needed, and there would be no charge for these follow-ups.
At no cost
I recently met a consultant who had seen a patient for one face-toface consultation and had received 28 follow-up emails from them in the following 12 months and had replied to each one at no cost.
Taking into account the amount of time invested in the care of this patient, the one-off consultation fee did not nearly cover the cost of care provided. So how do we charge patients appropriately for these new interactions?
There is a convincing argument to charge the same fee for a virtual/video consultation as for a face-to-face one.
The length of discussion is the same, as is the nature of the discussion, and so it follows that the fee should be equal. Some patients may prefer to meet via video either due to time or geographical con-
straints and see this option as advantageous to them.
Major insurance companies allow consultants to charge for consultations that are not face to face and they describe them as ‘remote’. Initially, the amount allowed was capped to a maximum limit, but this was challenged and it is now possible to charge the same fee for a virtual consultation as a face-to-face one.
Remote consultation
Bupa themselves run a virtual GP service where the fees are based on the meeting time. A 15-minute call with a GP will cost £49 and a 30-minute call will cost £89.
A remote consultation can also cover a consultation via phone call rather than video, and some patients prefer this, as they don’t like the perceived intrusion of video or they see no added benefit in being able to see their consultant’s face. I make no comment!
The big question is how will patients react to being charged for a phone call when they have come to expect these ad hoc calls as part of the overall service and thus free?
Some patients will feel that introducing a fee for these calls is too much and will object strongly. This is obviously less of an issue for insured patients, although many of them may incur an excess fee. For self-pay patients, we need to think very carefully about how these fees are introduced.
One tip I would offer is to ensure that phone calls are positioned as appointments rather than ad hoc interactions.
I would set up a process with your medical PA whereby phone calls are scheduled into your clinic even if your preference is to add them at the end of your face-toface clinics.
The message your medical PA delivers to the patient will feel different. The patient will under-
stand that they have a scheduled appointment within your clinic rather than a perception that you will call on a slightly ad hoc basis at the end of your clinic.
Time-consuming job
But how do patients feel about paying for emails and prescriptions? Replying to patients’ emails can be very time-consuming, especially if the patient is asking lots of detailed medical questions.
Most doctors I know do not charge for these responses, but maybe they should? It is far more common to see a charge for prescriptions, though. To the best of my knowledge, most insurance companies do not cover costs for emails or prescriptions.
As with all fees, it is essential that the patient knows in advance the cost of their care. When a patient books any appointment, they must receive confirmation of the likely cost of treatment.
Most medical PAs have a standard email they send to confirm an appointment, which also details the likely cost of treatment, and this should also be used when confirming a video consultation. If you are charging for email responses and prescriptions, these costs must be provided in advance too.
The ability to charge appropriately for the services offered in private healthcare will continue to be a challenge and it is important to continually review the actual cost of providing the care to our patients and attempt to recover these costs.
If you have any specific questions you would like answered in coming issues of Independent Practitioner Today, please get in touch.
Jane Braithwaite is managing director of Designated Medical, whose experts offer bespoke support across accountancy, marketing, medical PA and HR BOOK YOUR DEMO
Maybe you're completely happy with the software you use to run your practice. Perhaps you have everything in one place, routine tasks are automated, and reporting is accurate and insightful. If so, stop reading now.
However, if you think the day to day running of your practice could be improved, we'd love the chance to demonstrate e-clinic to you.
The number one choice for private practice
Future-proof your practice and offer everything a modern patient expects:
> iPad compatibility
> Online booking & payments with fully integrated card processing
> Electronic consent & treatment forms
> Integrated drugs database & digital prescribing with direct delivery
> Fast & easy patient communications by email or text
YOUR FREE 30 MINUTE DEMO
RETAIL FINANCE
By making it easier to pay you generate more sales
A new way of paying for healthcare is rapidly gaining pace and helping to fuel significant growth in self-pay business. Richard Gregory (right) follows his introduction to point-of-sale finance last month to explain how it contributes to greater self-pay sales growth
POINT-OF-SALE (POS) finance products have been used extensively in the cosmetic and dental markets for a long time.
Both have traditionally had a significantly larger proportion of business-to-consumer (B2C) work than the acute healthcare sector, whose business has historically and predominantly been based on relationships with private medical insurers and local NHS trusts and clinical commissioning groups.
The adoption of POS finance products in the acute sector has therefore been much slower to develop and was used mainly as a last resort for those patients who were struggling to afford upfront, private treatment.
There was little advertising, hardly any promotion and little mention of them early in the patient journey.
But this has all now started to change as the self-pay market has grown, mainly due to the deteriorat-
avoid using my savings? Do I want to spread over time to protect cash flow? Do I want to pay interest over longer or 0% over a shorter period? It provides fantastic flexibility.
➲ Patients are protected by Section 75 of the Consumer Credit Act, which means the lender is liable for the failure of the product or service.
ing state of NHS waiting lists. They have become a larger contributor to hospital revenues and profits.
Of course, the pandemic has exacerbated the wait times and pushed many more people down the self-funding route, making the offer of POS finance products even more important and pivotal.
The 2020 LaingBuisson self-pay survey showed that POS finance products were one of the top three drivers of self-pay according to those hospital operators who responded.
These are some ways that POS finance products benefit both selfpaying patients and hospital operators and consultants alike.
➲ Speed of treatment is being sought by those worried about waiting for NHS treatment and so seeing clearly that they can pay in different ways is essential.
➲ This is not about affordability. It’s about choice – how do I want to pay? Do I want to
➲ A patient thinks: ‘If you remove my uncertainty over how to pay, then I will see more value in your product. It feels more attainable and therefore more attractive and you have removed a fundamental objection.
➲
‘If, during my consideration stage, you have offered me greater clarity and choice of payment options, I am more likely to stick with you. I feel you are responding to my needs and helping me.’
➲ As in the retail sector, offering POS finance products in healthcare significantly boosts sales and conversion rates.
➲
Electing to pay using a POS finance product means the hospital operator and/or the consultant is instantly paid upfront in full. This mean no chasing, fewer patients changing their minds, no patients turning up for their treatment having not paid. There are much better processes and a not insignificant time saving
So, yes, POS finance products are growing as a key proposition in self-pay treatments. In fact, you would be hard pressed to find any hospital operator who does not now offer some form of POS finance product.
But the question still remains whether hospital operators are making the most of them, which means using them as an integral part of patient choice rather than as ‘deal clinchers’ as a last resort. If we accept that offering POS finance products extends choice to a patient, then how best can they be deployed to make self-pay more accessible?
There are four key things hospitals and consultants should do:
1Integrate any POS finance product application process into your customer relationship manage ment (CRM) system or contact management software. At the click of a button, the patient receives an instant email and SMS message with a payment option calculator and a pre-populated application to complete online.
The easier it is to apply, the quicker a patient can be accepted and the less time is spent re-entering personal data or having to access stand-alone systems and processes.
Richard Gregory explained the impact of POS finance in last month’s article
2
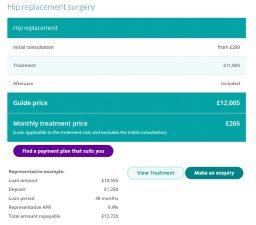
Use POS finance products to better promote the cost of treatment by presenting a treatment price as a monthly repayment.
As consumers, we are used to subscription-based payments. If this is promoted at the consideration stage, more patients will likely self-pay. A few hospital operators now have payment plan calculators embedded in their websites. See the examples above and below.
3
Ensure that patients can check whether they would be eligible for credit as early as possible in the pathway and allow them to apply online.
Once people know they can obtain credit and how they can spread the cost, they are more comfortable with the purchasing decision.
4
Ensure your self-pay advisers and practice team are fully conversant with your POS
finance products’ terms and conditions and are confident to introduce these early in the process without feeling that somehow, this is distasteful.
It is of mutual benefit for hospital operators, consultants and selfpaying patients alike if POS finance products are made available. Hospital operators and consultants will see their sales increase and patients can gain access to affordable treatment early. However, making POS finance products available is not the end game; it is just a start.
The way to unlock their full potential is to put them front and centre of self-pay propositions, make them prominent on marketing both on- and offline, make it easy to apply and integrate the process and products into the patient pathways wherever possible.
in self-pay
Secretary Supported Administrator access reduces workload for practitioners. mPrescribe® facilitates patient entry, status monitoring and preparation of prescriptions for mobile authorisation.
Clinical Governance
Co-founded and co-owned by leading private clinicians, our secure and encrypted technology is compliant with all GPhC, GDPR and e-Prescribing regulations. mPrescribe® app allows you to prescribe flexibly without a laptop, for same day or next day delivery to your patients nationwide
“Wonderful, seamless, easy to use service.” Dr Catrin Bevan, London General Practice
“Competitively priced.” Dr Sean White, Consultant in Pain Medicine
“Intuitive and secure.” Dr Tim Wigmore, Consultant Intensivist & Anaesthetist, Schoen Clinic
“Delivered the same day.... Outstanding!” Dr Elisa Astorri, Academic Physician Rheumatologist, Rheumatology
“Go the extra mile.” Dr John O’Donohue, Consultant Gastroenterologist
Richard Gregory runs an independent healthcare consultancy, specialising
BMI has teamed up with Chrysalis Finance to offer POS finance
THE IMPACT OF CLIMATE CHANGE
Our planet isn’t the
Climate change is inextricably linked to health – and its serious worldwide adverse health outcomes are undeniable. Its direct health cost burden globally is estimated at between $2bn and $4bn a year by 2030.1
Healthcare providers and insurers need to understand this relationship to better support patients and customers, says James Sherwood (right)
Climate change describes longterm alterations in the average weather patterns affecting the Earth’s local, regional, and global climates. It is commonly measured as the average increase in our global surface temperature.
The world has reached approximately 1°C of global warming above pre-industrial levels. Projections show with high confidence that temperatures will be likely to rise 1.5°C between 2030 and 2052 if they continue to increase at the current rate.2
In the long term, the goal is to keep the increase in global average temperature to well below 2°C above pre-industrial levels.
Climate change is rapidly shaping the environment around us, including through rising temperatures and extreme weather events.
It is primarily driven by human activities, particularly fossil fuel burning which increases heattrapping greenhouse gas levels in the Earth’s atmosphere causing surface temperatures to rise. These human-produced temperature increases are commonly referred to as global warming.3
The most significant impacts of climate change on health include:
Respiratory conditions and allergies
There is a direct link between the intensification of climate change and the worsening of existing respiratory conditions. Conditions of particular concern include asthma, respiratory allergic disease, chronic obstructive pulmonary disease (COPD) and respiratory tract infections.
only one suffering
Looking at current trends, we are likely to see more patients with these conditions, with the most vulnerable populations worst affected.
For example, the pollen season will get longer and more severe, meaning that patients may require medical assistance and treatment more frequently and for more extended periods of the year.
The growing incidence of wildfires may result in a local increase in disease burden after these events. Additionally, changes in the profile of respiratory conditions are expected to alter patterns of pharmaceutical use and result in greater use of medication.4
Cardiovascular conditions
Extreme and prolonged heat and air pollution as a result of burning fossil fuels will lead to an increased risk of cardiovascular conditions, such as ischaemic heart disease, strokes, heart failure, arrhythmias and cardiac death.5,6
High temperatures will result in increased hospitalisations due to cardiovascular conditions such as myocardial infarction.7
Mental health
Mental health can be impacted both directly through climate disasters and indirectly through the consequences of climate change. This can range from ecological anxiety to depression, post-traumatic stress and suicide.
It is estimated that, globally, as many as half of the people who survive extreme weather events experience adverse mental health outcomes.8
We need to recognise the impact that the overarching threat of climate change can have on mental health, leading to conditions such as ecological anxiety and ecological grief.
Infectious disease
Changes in temperature and rainfall have altered the distribution of
Viruses transmitted by mosquitos are anticipated to expand to North America and Europe as the continents become warmer, posing a threat to 49% of the world’s population by 2050
change and the associated increase in extreme temperatures and weather events. Both heat and cold exposure elevate their risk of cardiovascular and cerebrovascular deaths, as well as respiratory deaths and morbidity.
Extreme heat also has a negative impact on birth outcomes – length of gestation, birth weight, and stillbirth increase. Studies also present links between various pollutants and the development of autism and asthma in children.11
Next month: Fighting back –James Sherwood presents a round-up of the insurer’s efforts to become a net zero emissions business
References
1. Climate change and health; World Health Organization; February 2018.
2. Global warming of 1.5°C; Intergovernmental Panel on Climate Change, 2019.
3. Global warming vs Climate Change, NASA Global Climate Change, 2022.
some water-borne illnesses and disease vectors. Diseases traditionally associated with tropical and subtropical regions are reaching new areas of the world because of climate change.
For example, viruses transmitted by mosquitos are anticipated to expand to North America and Europe as the continents become warmer, posing a threat to 49% of the world’s population by 2050.9
As such, there is a need for accurate forecasting and monitoring of climate change and its impact on infectious diseases.
Dermatology
As the skin is exposed to the environment, it is especially vulnerable to increased heat and humidity.
Some of the impacts of climate change on the skin are directly linked to extreme weather events, which will lead to an increase in skin infections, inflammatory skin diseases, and traumatic skin disorders.
Skin cancer rates may be affected by changes in temperature. Poland predicts an increase of 10% of skin cancer morbidity and 3% mortality by 2080.10
Protecting the most vulnerable
Older people are one of the most vulnerable groups to climate
Understanding the scope and scale of impacts on pregnant women and new-born babies is an important first step to developing and implementing services designed to treat or prevent the impacts associated with climate change.
Compared with a future without climate change, the World Health Organization projected excess deaths for the year 2030: with 38,000 of these due to heat exposure in older people, 48,000 due to diarrhoea, 60,000 due to malaria, and 95,000 due to childhood undernutrition.12
Impact on healthcare delivery
The frequency and intensity of severe weather events will increase. In these circumstances, hospitals, clinics or care homes may be physically damaged or face power outages.
Roads may be flooded or destroyed, making it hard for emergency services to reach patients or for patients to come to healthcare professionals. Severe weather events anywhere around the globe can disrupt supply chains, thus impacting patient care and costs.
The longer-term migration and movement of people from regions affected by climate change may also pose a risk to healthcare systems in neighbouring countries which may not have sufficient capacity to support additional demand.
4. Potential Changes in Disease Patterns and Pharmaceutical Use in Response to Climate Change; Journal of Toxicology and Environmental Health; 2013.
5. Impact of climate and air pollution on acute coronary syndromes: an update from the European Society of Cardiology Congress 2017; Scandinavian Cardiovascular Journal; 2017.
6. The global threat of outdoor ambient air pollution to cardiovascular health: time for intervention; 2017.
7. Temporal trends of the association between ambient temperature and hospitalisations for cardiovascular diseases in Queensland, Australia from 1995 to 2016: A timestratified casecrossover study; PLOS; July 2020.
8. Global climate change and mental health; Current Opinion in Psychology; April 2020.
9. Global expansion and redistribution of Aedesborne virus transmission risk with climate change; PLOS; March 2019.
10. Climate Related Diseases. Current Regional Variability and Projections to the Year 2100; Quaestiones Geographicae 2018.
11. Towards a fuller assessment of benefits to children’s health of reducing air pollution and mitigating climate change due to fossil fuel combustion; Environ Res. 2019.
12. WHO – Quantitative risk assessment of the effects of climate change on selected causes of death, 2030s and 2050s; WHO report; 2014.
James Sherwood is general manager, operations and healthcare management, Bupa
Handling complaints within the private sector
Dr Ellie Mein explains the complaints-handling process within the private sector and the introduction of the new Code of Practice from the Independent Sector Complaints Adjudication Service
AN ENT SURGEON contacted the MDU after he learnt that a complaint from one of his private patients was being ‘escalated to the ISCAS for independent adjudication’ despite him already responding via the private hospital.
He was unfamiliar with this organisation and the adjudication process the hospital had notified him of. Consequently, he wanted advice on what to expect, as he was also concerned about the confidentiality aspect of the request for patient records by this third party.
ISCAS – otherwise known as The Independent Sector Complaints Adjudication Service – sits within the Centre for Effective Dispute Resolution (CEDR). It provides independent adjudication on complaints for the private healthcare sector, specifically for those organisations that subscribe to it.
A recent significant development is that, as of the 1 February 2022, a new ISCAS Code of Practice for Complaints Management has been published that aligns with the Parliamentary and Health Service Ombudsman (PHSO) Complaint Handling Framework.
The PHSO provides an independent complaint-handling service for complaints that have not been resolved locally by the NHS in England.
Aligned
with NHS
While it has long been the case that the principles of good complaint handling in the NHS are broadly applicable to the private sector, this new ISCAS code will bring the approach to complaints about private care even more in line with the NHS complaints procedure.
In the NHS, the complaints process outlines two stages: local resolution followed by the PHSO if the complainant remains dissatisfied. The ISCAS code, however, sets out a three-stage process for addressing complaints.
The first is when the complaint is raised directly with the hospital or clinic and this is where the relevant clinician, such as our ENT surgeon, will contribute to a response.
If this does not resolve the concerns, stage two involves an internal review by someone who was not involved in responding at stage one.
This new ISCAS code will bring the approach to complaints about private care even more in line with the NHS complaints procedure
Thereafter, an unresolved complaint can be escalated to stage three, which involves ISCAS independent adjudication. The aim of this stage is to bring a final resolution of the complaint for all parties and there is no right of appeal against a decision reached.
Once ISCAS has accepted a complaint for adjudication, it asks the complainant for written confirmation that they wish to participate in the process and outlines the terms of this.
Patient’s
consent
The complainant’s/patient’s consent will also be obtained for the subscriber – the hospital or clinic – to provide ISCAS, the independent adjudicator and any instructed clinical experts with a copy of their clinical records and complaint correspondence to date.
Being aware of this step may reassure clinicians about ISCAS requests for medical records and letters.
As part of the adjudication process, the adjudicator compiles a timeline and identifies the key themes of the complaint. These are then shared with both the complainant and the subscriber and their response to these points of complaint are invited.
Following the complaint being defined and agreed, the adjudicator may, as part of their investigation, instruct an expert witness to opine on the clinical matters of the complaint.
If this is the case, the complainant and subscriber will be provided with a list of intended questions for this expert and invited to comment with any suggested amendments.
At the end of the investigation, the adjudicator writes to the subscriber, usually within three to six months for most cases, to communicate their final decision.
This letter will provide:
A summary of the case and decision;
Any learning points for the subscriber organisation;
Advice to support resolution, such as when an apology is necessary;
How to improve compliance with the ISCAS code.
Additionally, they have the authority to award a goodwill payment. Such payments may recognise shortcomings in the service but can also be made for poor complaint handling, distress or inconvenience up to a maximum limit of £5,000.
This illustrates why it is important to get the local complaint handling right before ISCAS becomes involved, as the handling of the complaint can be scrutinised as well as the incident which gave rise to the complaint.
Watchdog involvement ISCAS shares adjudication decisions with the Care Quality Commission (CQC) in England and the Healthcare Inspectorate Wales (HIW). Individual clinician details are anonymised, but the hospital/ organisation will remain identifiable.
The CQC considers issues arising from complaints as part of the repository of information it holds on each hospital/organisation and may use this to recommend improvements.
As an alternative to adjudication and following the agreement of both parties, mediation may be offered as an alternative route to resolution. However, if mediation is not successful, the complaint can still run through the adjudication process.
Go to https://iscas.cedr.com/ patients/provider-directory to learn more about ISCAS subscribers. Further information on the goodwill payment structure and managing unacceptable behaviour by complainants can be found at https://iscas.cedr.com/ healthcare-providers/subscribercontent.
Dr Ellie Mein (right) is a medico-legal adviser at the Medical Defence Union (MDU)
Get the message out
Simon Marett (right) reveals why more independent practitioners are turning to marketing themselves after the pandemic
about your practice
THE PANDEMIC has created the time and opportunity for many private practitioners to take a step back and reflect on where their practices are and where they would like to take them in the future.
This period has also seen a seismic shift in the way private healthcare is delivered to patients, with consumer behaviour changing quickly and new companies entering the market.
With NHS waiting lists growing in length and more patients than ever looking to the private healthcare sector for treatment, independent practitioners across the UK are now thinking about marketing and the difference it can make to their practices.
Marketing is an often misunderstood term in healthcare, and it can relate to several aspects of running a successful practice. Whether you are launching a new online clinic and need help finding new patients or looking to give your current clinic a facelift, having a strong brand and online presence has never been more important.
In the first of a series of articles, I will look at some of the most relevant aspects of healthcare marketing for you to think about.
Time for a brand refresh?
We often get asked by practitioners when the right time is for a brand refresh. Our response is always about ensuring that your clinic continues to remain relevant to your patients now and in the future.
There are several situations that would prompt serious consideration for having a brand refresh. These include a brand looking tired and outdated, internal discontent among partners or employees, or a clinic losing market share and patients to a new entrant to the market.
A brand refresh need not be expensive and can be an excellent
Word-of-mouth recommendations from colleagues, friends and family are the most powerful tool in marketing’s armoury and should be used at every opportunity: across your website, print, social channels and email marketing
resources need to go into a patient acquisition plan that clearly outlines how you are going to attract new patients with your proposition and the marketing channels you intend to use.
Social display advertising, paid search, PR, retargeting, direct mail and customer relationship management (CRM) are all channels that need to be explored, tested and assessed so you find the right blend that works for your clinic.
nels if patient reviews and recommendations are effectively managed.
Patient behaviour is changing quickly and constantly evolving. New healthcare start-ups are launching every week in the UK and technology continues to drive change across the sector. It is therefore vital that every healthcare business keeps in step with the market, its patients and their ever-changing needs.
way of reconnecting with patients, employees and breathing life into an existing clinic.
Digital transformation
Digital transformation has become a bit of a buzz-word in recent years, and it is one of the most common types of projects that we get involved with.
Technology is evolving at a rapid rate and the pandemic has accelerated a change in patient behaviour that could not have been foreseen only a few years ago. Clinics are now being forced by patients to adopt new technologies, which include allowing patients to manage their consultations, blood tests and medication online or via an app.
A failure to embrace these technological changes and adopt new technologies and transform working practices puts traditional clinics at risk of being left behind.
Finding new patients
Possibly the biggest challenge that a new clinic will face when they launch is attracting new patients. It is a common mistake to go through the Care Quality Commission application process, build the clinic website and create the operational set-up and just expect paying patients to turn up at the door.
Private healthcare just does not work like that. Time, effort and
Let your existing patients do your marketing Patient reviews are now mainstream in private healthcare, but there are still private practices who have yet to embrace the power of positive patient reviews. Word of mouth and recommendations from colleagues, friends and family are the most powerful tool in marketing’s armoury and should be used at every opportunity: across your website, print, social channels and email marketing.
In some cases, working hard on patient recommendations and reviews can drive an unprecedented volume of new patient enquiries. In some cases, clinics may not need to spend valuable budget on other acquisition chan-
A private healthcare clinic may not have had a need to explore marketing before, but it can be a powerful tool for any healthcare business and can help re-energise a company, lift new patient/customer numbers and motivate internal teams by bringing everyone together under a common vision.
If you think your brand or business might need a refresh and you are not sure where to start, get in touch with us first.
Ellerton Marketing provides a free 60-minute business ‘health check’ for all Independent Practitioner Today readers and can help guide you through some of the key steps you should be thinking about when it comes to marketing your clinic
Simon Marett is founder and director of Ellerton Marketing
IS IT TIME YOU DID SOME MARKETING?
Patient Satisfaction – When was the last time you asked your patients about their experience? What do they like about being a patient at your clinic and where can you improve?
Patient Retention – Are patients returning for treatment and help or are they going elsewhere? What are your patient reviews telling you?
Patient Pathway / Journey – Is the current patient journey where it needs to be? Carry out an audit across all touchpoints before, during and after consultation
New Patients – How many new patients are you attracting each month? Where are they coming from?
Your Brand – How does your clinic brand match up against the competition? Is your proposition still relevant or looking tired and dated? Compare websites, marketing, social media
The Competition – What is happening in the market? What are your competitors offering and how does that compare to your proposition?
A group confident in turning out hits
‘We want to give our consultants access to this brave new world with our new consumerfacing strategy and our multimillion-pound investment programme DR PAUL MANNING (left) PROFILE OF
2022: the difficult second album for Circle Health Group? Chief medical officer Dr Paul Manning reflects on recent award-winning successes and outlines plans for future releases
THE ARRIVAL of 2022 marks two years since Circle Health Group acquired BMI Healthcare and became the largest independent provider of hospital services in the UK.
Back then, none of us could, in our wildest dreams, have predicted how those two years would play out.
It was just days after the integration of BMI Healthcare into Circle Health Group’s network, that our chief executive Paolo Pieri put the group’s entire business plan on hold to support the NHS during the pandemic.
Alongside clinical and non-clinical staff alike, our consultants stepped in to support the NHS, see-
ing 700,000 NHS patients and carrying out more than 30,000 cancer operations.
In total last year, you, our consultants, helped us to see more than 1.8m patients and deliver over 255,000 theatre procedures.
Let’s pause and think about that for a second. It’s extraordinary and it doesn’t even include the tireless hours being put in by our consultants in the NHS. It’s no exaggeration to say yours was a crucial contribution to keeping the healthcare system running and saving countless lives in the process.
The increased number of complex surgical cases we took on at Circle meant hospital teams were
working at full capacity for months at a time.
The front line
There are so many stories of our colleagues working tirelessly to support what was a national effort. Circle’s Runnymede Hospital in Lyne, Surrey, for example, ran three operating theatres at capacity and routinely carried out up to six major trauma and cancer operations daily on behalf of Ashford and St Peter’s Hospital (ASPH). The paediatric ward at ASPH was also relocated to Runnymede –much to the delight of the team at the hospital who enjoyed caring for and supporting children and their parents.
While the pandemic raged and our staff provided this invaluable support to battle Covid, a huge effort was underway behind the scenes to make sure Circle and BMI came together as seamlessly as possible and these efforts were not derailed.
Corporate mergers are renowned for being fiendishly tricky to get right at the best of times, let alone during a pandemic.
There were thousands of staff to be taken on board – Circle’s headcount increased over 1,000% to 16,000 – and large-scale debt financing to be secured, not to mention the concurrent acquisition of 30 properties.
Taking a toll
The same colleagues organising this also had to support colleagues on whom the pandemic was inevitably taking its toll.
To help staff cope with the challenge of increased workloads and uncertainty, our people team swung into action, launching initiatives to help staff deal with these unprecedented working conditions, while also offering advice and support around anxiety, depression, talking to children about Covid-19, and working remotely while caring for family members.
We even launched Thrive Mental Health, an NHS-approved mental health app designed to provide users with preventative strategies and help for managing stress and anxiety.
Across Circle, our colleagues stepped into the breach to help one another.
Take the Hampshire Clinic, where the physiotherapy department began running pilates and hydrotherapy sessions for colleagues to help teams from a variety of departments de-stress and engage with each other.
Stories like this were legion and there really should have been a trophy for each and every one of our colleagues when, despite all the challenges thrown at us, Circle was named Private Hospital Group of the Year by HealthInvestor UK and LaingBuisson.
It was also a mark of everyone’s efforts when we were voted one of the Top 25 Big Companies to work for in the Sunday Times’s annual awards for 2020-21.
What comes next?
So, yes, it has been quite a couple of years. The big question is how can we follow up on this gargantuan effort?
It feels a little like a band trying to follow up on a blockbuster album. As if 2022 is time to release that difficult second album. Well, I’m pleased to say we are ready for that challenge – and I think we’ve got some big hits on our hands.
These all stem from a focus on the same core beliefs we’ve had since Circle Health’s foundation in 2004, namely a commitment to empowering people with the latest technology, modern facilities and an environment that supports them.
A lot has changed in the last 18 years and one thing that has become crystal clear is how important it is that we do not fall into the trap so many do in healthcare, which is to be analogue in a digital age.
Consumers are more unforgiving than ever; they expect the speed of Google, the design of Apple, the responsiveness of Uber and the convenience of Amazon.
We want to give our consultants access to this brave new world with our new consumer-facing strategy and our multi-millionpound investment programme.
Digital-first strategy
Our new consumer-facing strategy began in 2021 and it has been paying dividends over the first few months of 2022.
We were the first operator to introduce direct consumer booking online and the latest data shows that more than 80,000 consumers have now booked directly online.
In addition, we have moved the majority of our consultants’ diaries online to enable patients to book directly at a time of their choice with their doctor of choice. This is also unique within the industry and puts the consumer in the driving seat for the first time in sector’s history.
This consumer growth strategy has been underpinned by significant investment of £1.5m in our tech platforms and delivered by our in-house development team. This team have successfully rolled out a digital health platform across the group, with full e-health records.
Consumers are more unforgiving than ever; they expect the speed of Google, the design of Apple, the responsiveness of Uber and the convenience of Amazon
a wide range of medical equipment from across its extensive portfolio.
Over the course of the ten-year period, each of Circle’s 50 hospitals will be receiving different GE products from CT and MRI scanners to ultrasound and patient monitoring.
The partnership is also an opportunity to make use of GE’s expertise in servicing and consultancy. The deal provides an exclusive servicing contract to maintain all of Circle’s medical imaging equipment, including technology that has not been provided by GE.
In 2021, we invested £100m in facilities and services across our hospital network. This has seen the arrival of American-designed scanners, fully digitalised patient pathways and a partnership with Spanish-based Ribera Salud, who are widely acknowledged to have the most advanced hospital technology systems in the world.
In 2022, we continue to focus on investment and regeneration, with the next stage of our £165m programme of delivering new technology and infrastructure to hospitals across the group.
The focus has been increasing capacity, both in terms of patient numbers and in additional consulting space.
These projects will mirror some recently completed programmes, like the £6m investment at The Park Hospital in Nottingham to build new laminar flow theatre, outpatient reception and dedicated treatment rooms, alongside a new CT scanner, digital X-ray and fluoroscopy room.
Projects like this have been directed by consultants whom we always turn to in order to understand what they need to best serve their patients.
Landmark partnership
This focus on patient-centricity is what led to January’s announcement that Circle and GE Healthcare were entering into a landmark ten-year partnership deal to provide our hospitals with industry leading diagnostic equipment.
The agreement was set up to give our consultants the tech they needed to make faster, more targeted and more informed decisions.
GE Healthcare will be providing
In addition to the servicing, as part of Circle’s IT regeneration, GE will be providing a bespoke digital consultancy. They will be playing an important role in the continued process of integration taking place across the business as well as supporting the introduction of electronic patient records.
The objective is to give you the very best equipment and facilities possible to deliver the best patient outcomes.
Our sights have also been set overseas. The group became the first operator to enter China, successfully opening two highly profitable hospitals in Shanghai.
The first of these facilities, called Circle Harmony Xinyong Clinic, has a full suite of services including primary care, diagnostics, operating theatres, endoscopy and paediatrics.
The operational model brought together leading doctors from the UK and Shanghai’s top teaching hospitals.
Building on this success is part of the group’s long-term vision, with an imminent pipeline for 20 further hospitals across China and, in turn, offering much greater opportunities to consultants to expand their experience and reach.
The next few years will be very different to the ones that followed the 2020 creation of Circle Health Group. Very different indeed.
But, as we come out of the pandemic, we do so with a story of dedication and selflessness by our consultants and wider staff that is quite humbling.
We are confident that in this post-pandemic era we can repay that effort and offer our consultants a very bright future indeed.
BILLING AND COLLECTION
This month and for the next two issues of Independent Practitioner Today, Simon Brignall (right) will highlight 30 key areas for practices to consider to overcome their billing and collection challenges. The first ten start here
Make it easy to get the money
BEST PRACTICE
1Do the splits
If you split the medical billing from the many other tasks your medical secretary carries out, then you will find it is a real benefit. Separating the billing process from the patient’s clinical journey allows your medical secretary to maintain a warm and engaging relationship with the patient, because they are no longer required to make those difficult segues into conversations about money.
By removing the burden of the billing process, this allows your secretary to respond to any new inquiries or patient queries more effectively – which, in turn, boosts revenue.
2
Focus on your skills
Many consultants and medical secretaries make the mistake of not focusing on their core skill set: treating patients and growing the practice.
Just because you can do something does not mean you should. I often meet consultants who are spending their weekends carrying out the medical billing and collection role for their practice.
This is not a valuable use of their time and experience, which could be much better employed if they opted to conduct an additional morning clinic and by choosing to outsource their billing.
A medical secretary’s time is better spent efficiently managing patient inquiries than being on hold on the phone with insurance companies or reconciling payments.
Billing companies are not only more experienced in this area but will often add functionality to improve the patient experience and allow the practice to grow.
IT’S ALL IN THE SET-UP
3 Boost cash flow
Many new consultants entering private practice find that, due to the reduced re-imbursement levels available to them from insurers, it is even more important to ensure the billing and collection is quick, accurate and efficient.
They face an array of fixed costs – such as medical indemnity premiums, medical secretary fees and possibly practice management
Consultants typically do not set their prices effectively because they have not done enough research when initially conducting this exercise or because it has been many years since they last looked at them
This means a consultant is paid based on either their activity or their longevity/hierarchy within the group. Some groups are more equitable and choose to make adjustments by granting time off.
We are very experienced with managing all these group structures and can accommodate whatever payment pathways they adopt.
As we replicate the group structure in our proprietary software, this means that access to their data can be provided at either the group or consultant level.
patient does not turn up or provide adequate notice of cancellation.
Remember, you need to ensure any potential charge is clearly detailed to your patient as part of your terms and conditions. By having a policy in place, you then have the option on whether you choose to enforce it or not.
TAKE A TIME-OUT TO REVIEW
9
Review your fees regularly
software – but enjoy a distinct advantage in choosing to outsource their billing.
This is because most billing companies’ fees are calculated against monies received and often billed in arrears. That comes as a welcome relief to the practice cash flow when you start out.
4 Use a medical accountant
Deciding on your practice structure is a conversation that needs to take place with your accountant. This is because the regulations and reporting requirements are subject to change that will dictate which option is best for you.
These options will include limited company or sole trader status.
Some independent practitioners, due to the nature of the services they provide, may be able to opt for a limited liability partnership (LLP) and a good medical accountant will be able to explore these options with you.
5 Group structure matters
Practice groups come in a range of structures and sizes.
Groups’ sizes can be organic in nature and their administration needs to be able to accommodate any fluctuations in size. This can often lead to difficult binary decisions around staffing.
Group structures can include virtual groups, which appear to the patient as one entity but, effectively, they are made up of a loose group of individual practices.
Other groups have more formal structures such as limited companies or LLPs, with a central bank account where funds and costs are allocated based on an agreed model.
Groups by their very nature can suffer from a range of problems that often arise from their volume of activity.
Pricing can vary between consultants and even by the location where the activity is conducted. This can make them hard to manage unless robust processes are put in place alongside accurate reporting.
THE DEVIL IS IN THE
DETAILS
6 Fee transparency
Make sure that your patients are aware of your fees up front.
This should also include notification of their liability for any outstanding balances that are not re-imbursed by their private medical insurer.
This is not only a Competition and Markets Authority requirement but it will also minimise the potential for disputes over payment.
7 Adopt a patient registration form
Your form should ideally be part of any new patient process in the practice.
It details all the patient demographics, including mobile number and email address as well as their insurance policy details and authorisation number.
It can also have disclaimers such as the patient liability discussed above.
8 Have a DNA policy
Did Not Attends (DNAs) are a frustrating fact of life. Some practices we partner with minimise this by asking us to collect money up front for new patients, especially for international patients.
It is important that you decide on your DNA policy and what charges will be applicable if a
I know from the many conversations I have had over the years that this has always been something that appears to give consultants the most stress.
It is a very difficult area, both within the insurance market as well as the self-pay sector.
In our experience, consultants typically do not set their prices effectively because they have not done enough research when initially conducting this exercise or because it has been many years since they last looked at them.
10
Do an annual assessment
Make a habit of annually reviewing your practice, because fees are not the only thing you should examine.
Access to accurate practice data detailing your activity at the various locations where you practise, or the type of patients you are seeing, allows you to spot trends over time and adjust accordingly.
It is easy to make assumptions about your practice that do not reflect its true position. This may lead you to open another clinic at a popular location or add functionality to better support a rise in selfpay activity you are seeing.
Our reporting dashboard at MBC provides reports on the type of procedures a practice is conducting and can track GP referral data. This allows a practice to engage with its referral network about new or popular treatments that will benefit their patients. We also conduct a practice review as part of our on-boarding process.
If any of these topics have highlighted areas of concern, I suggest you take steps to address to them.
Simon Brignall is director of business development at Medical Billing & Collection, which is celebrating 30 years of partnering with consultants in private practice
PREPARING FOR RETIREMENT
What you need to do when retiring
Dealing with medical records and the hand-over of patients are likely to be the most burdensome tasks when winding down your practice. Dr Lucy Hanington (right) looks at the rules and practicalities you need to consider
If you are planning to retain records beyond the recommended period, it is worth recording the reason for doing so
PRIVATE PRACTICE requires doctors to undertake a range of duties normally subsumed by the wider team within an NHS setting. Whether you are winding down in preparation for retirement or moving on to new pastures, advance planning is required to ensure compliance with regulatory and legal requirements. Thought needs to be given to the ongoing management of medical records. Ensuring the safe hand-over of patients can be a lengthy process. Moreover, the pandemic has highlighted the importance of contingency planning to ensure that patients’ needs can be met if the unexpected happens.
Medical records
The GMC’s Confidentiality guidance states at paragraph 128:1 ‘If you are responsible for managing patient records or other patient information, you must make sure the records you are responsible for are made, stored, transferred, protected and disposed of in line with data protection law and other relevant laws.
‘You should make use of professional expertise when selecting and developing systems to record, access and send electronic data.’ It may be necessary to make alternative arrangements for the secure storage of records on retirement, if you are unable to keep them in their current location.
While there are no specific guidelines dealing with how long private records need to be kept for,
paragraph 130 of the above GMC guidance states: ‘The UK health departments publish guidance on how long health records should be kept and how they should be disposed of. You should follow the guidance, even if you do not work in the NHS.’
Details of the guidance for each country can be found in the table.
A summary of recommendations has been included, but it will be important to review the guidance in each case, as there are a number of exceptions to the rules in addition to geographical variations. Special considerations apply in the case of electronic records. It is advisable to review records towards the end of the retention period, because if there has been an adverse incident or there is potential for a claim, it may be sensible to keep them for longer.
Defending yourself as a doctor is much harder in the absence of records. However, you should bear in mind the EU General Data Protection Regulations and the Data Protection Act 1988.
The latter states: ‘Personal data processed for any purpose or purposes shall not be kept longer than is necessary for that purpose or those purposes.’
If you are planning to retain records beyond the recommended period, it is worth recording the reason for doing so.
If you have decided that records should be destroyed, you will need to ensure this is done in an appropriate manner.
For example, you may wish to incinerate paper records, shred them using a cross-cut shredder or approach an appropriately accredited commercial company who can assist with this process on your behalf.
These companies will also issue a certificate of destruction for your own records, which testifies your compliance with the relevant legislation.
Given your ongoing obligations to our private patient records, you may wish to consider registering with the Office of the Information Commissioner as a data controller if you have not done so already.
Handover of patients
If patients are likely to require ongoing care, it will be necessary to discuss future arrangements
with them. And it will also be important to ensure you follow Good Medical Practice2 in handing patients over.
This guidance states that you must: ‘Check, where practical, that a named clinician or team has taken over responsibility when your role in providing a patient’s care has ended. This may be particularly important for patients with impaired capacity or who are vulnerable for other reasons.’
You will need to ask each patient whether they wish to continue with private care or return to the NHS.
Private patients may well have a view as to which practitioner they would prefer to see going forward. The doctor to whom you are to hand over should be someone who ‘has the appropriate qualifications, skills and experience to provide safe care for the patient’.
Identifying an individual who will take over your private practice on your retirement can significantly ease the administrative burden.
Dealing with medical records and the hand-over of patients are likely to be the most burdensome tasks when winding down your practice.
Contingency planning
These aspects of private practice should also be a focus of attention more generally during your career. The Covid pandemic has highlighted the uncertainties of life for all of us.
Ill health unfortunately becomes more likely with age, but all private practitioners should have plans in place to ensure patient needs can be addressed in the event of unexpected absence from work.
A range of materials are available to guide the development of business continuity planning and can be adapted to individual circumstances. It will be important to ensure that appropriate colleagues are able to access patient lists and medical records.
You may wish to consider whom patients should be signposted to in the event that you are not in a position to provide necessary care. How will this be done? Is there any useful information that can be placed on an ‘out of office’ email or website to assist patients if you are not available?
Ongoing activity and obligations
Retirement means different things to different people. Medicine is intricately woven into every aspect of our lives as doctors and can be hard to leave behind.
You may be considering new uses for your knowledge and experience, such as involvement with a medical charity.
If expert witness work has formed part of your practice, you should always take care to review instructions carefully prior to acceptance.
Legal cases can take many years to reach a conclusion and it is not uncommon for experts to be called upon in relation to a case long after
GUIDANCE BY HOME COUNTRY
ENGLAND
Records Management Code of Practice 2021 www.nhsx.nhs.uk/informationgovernance/guidance/recordsmanagement-code/recordsmanagement-code-ofpractice-2021/ Appendix 2 sets out the retention rules for each record type.
WALES
Reference is made to the guidance above and further information can be found on the Digital Health and Care Wales Website https://dhcw.nhs.wales/
SCOTLAND
Scottish Government Records Management Health and Social Care Code of Practice (Scotland) 2020 www.informationgovernance. scot.nhs.uk/rmcop2020/ See Section 6 for retention periods
NORTHERN IRELAND
Good Management, Good Records www.health-ni.gov.uk/ publications/good-managementgood-records-disposal-schedule See Disposal Schedule Section D
they have retired from clinical work.
Prior to winding down your private practice, you will need to review your indemnity arrangements and your GMC status; ongoing registration and cover may be required.
You may wish to seek specific advice from your medical defence organisation.
Dr Lucy Hanington is a medico-legal consultant at Medical Protection
SUMMARY
For GP records, the retention period generally extends for the lifetime of the patient and ten years after death in England, Wales and Northern Ireland. Three years after death in Scotland.
For hospital records of adult patients, the retention period is usually eight years from the end of treatment or after death. There are exceptions, though: in the case of prison notes and those relating to areas including oncology, maternity and mental health, the retention period is longer. Maternity notes, for example, should be retained for 25 years after the last child has been born.
The notes of paediatric patients should be kept until the 25th birthday unless the patient was 17 at the time treatment ended. In which case, they should be kept until the 26th birthday – or, if the patient has died, eight years after death in England, Wales and Northern Ireland, and three years after death in Scotland.
WHEN EVENTS CAUSE MARKET TURMOIL
One of the most important roles a financial planner takes on is that of behavioural coach –stopping investors from doing more damage than the markets can
Panic doesn’t help your investments
What to do when uncertainty abounds? Dr Benjamin Holdsworth (right) on why taking a long-term investment view is key
AT THE time of writing, authoritarian states are flexing their muscles: Russia violating Ukraine’s sovereignty and China’s ongoing subjugation of Hong Kong with the new National Security Law alongside its apparent support for Russia being cases in point.
The world is looking gloomy and we are rightly concerned when watching the humanitarian cost of such acts on the news.
The West continues to struggle with what is hopefully the backend of the Covid crisis as populations gather immunity through vaccination and infection as new drugs and treatments come online almost daily.
Economically, the greatest challenge is soaring inflation, hitting levels not seen for several decades. As a consequence, interest rates and yields on bonds have started to
rise and global equity markets have started the year down. This, too, can feel unsettling.
It is always easy to feel that the present is more uncertain than the past.
Armageddon scenarios
We have all but forgotten the Armageddon scenarios of events such as the Y2K software bug issues of 2000. Planes were expected to
fall out of the sky, nuclear power stations were thought to be potentially out of control, and so on.
Then there was the emotional and geopolitical impact of 9/11 or the fear many felt in 2008 when Lehman Brothers failed and the meltdown of the financial system was a real risk.
The chart on the opposite page shows the growth of £100 from
Material global events are ever present
Data source: Vanguard Global Stock Index ACC, 4/8/1998 to 14/2/2022 in GBP used as proxy for the performance of global equities. Its use in this chart does not constitute any form of recommendation and is provided for educational purposes only
NHS Pensions & Annual Allowance Tax
Get ready in advance of April 2022 when the proposed changes to the NHS Pensions will allow you to reclaim some or all of any Annual Allowance tax you may have suffered in the past.
With our knowledge and in-house calculators, we will be able to predict in advance and check statements produced by NHS Pensions and Scottish Public Pensions Agency for accuracy for any refunds due.
For further information contact us at aa@semail.co.uk or telephone 01625 527351.
1998 to 2022 and illustrates that over the longer-term, financial markets have ultimately absorbed the consequences of these events and delivered steady forward progress.
Worst mistake
Being shaken out of markets based on today’s news is about the worst mistake any long-term investor can make.
This is why one of the most important roles a financial planner takes on is that of behavioural coach – stopping investors from doing more damage than the markets can.
Feeling concerned by what geopolitical events might mean financially? As ever, all the news that we see and worry about –including the invasion of Ukraine by Russia – is already reflected in market prices.
‘New’ news, as it develops, will have an influence on those prices,
Feeling uncertain about markets is not a valid reason for seeking to get out of markets
but, by its very definition, this is a random process that is hard to benefit from unless you own a crystal ball.
It is likely that markets will be volatile as events develop. The US market actually rose on the day Russia invaded.
Market weight
In terms of direct portfolio exposure, it is worth noting that Russia represents around 0.35% of global equity markets, and that is before this is diluted down in any portfolio by bond holdings.
To put this in perspective, the global market weight of Apple is over 4%! In fact, Apple’s cash reserves alone are of a broadly similar magnitude to Russia’s entire market capitalisation.
No one has any real idea as to the wider impact of the Russian invasion, but even if markets fall, we need to remember the following points:
Equity markets can go down –sometimes materially – as part of their journey to delivering positive longer-term returns after inflation.
Unless you require immediate liquidity from your equity positions, you should not take action. Feeling uncertain about markets is not a valid reason for seeking to get out of markets.
Selling risk assets at a time of market uncertainty can ultimately prove ill-advised, unless your personal circumstances have changed to the extent that you need immediate liquidity from your portfolio.
The high-quality bonds in your portfolio provide more stable values and the liquidity to meet any liabilities without having to sell equities when they are down.
While it is natural to be concerned by the dramatic events we see reported, your financial investments should not add to those worries.
If they do, it is time to lean on your adviser for support.
Dr Benjamin Holdsworth is a director of Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions. Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment
Premises
Regulatory requirements and investigations
Michael Rourke
Tania Francis m.rourke@hempsons.co.uk
What happens in the hearing itself
In her last of three articles about employment tribunals, which can cost doctor employers many thousands of pounds if they lose, solicitor Julia Gray (right) explains what to expect if you face a hearing
EMPLOYMENT TRIBUNALS (ETs) are based in regional centres across England and Wales and this article applies only to them, not Scotland where a slightly different system is in place.
Currently, some have significant backlogs of cases, which means that hearings are being listed up to two years into the future. Partly as a result of the Covid pandemic, many cases are now heard virtually.
The ET will determine the type of hearing in advance, but changes are sometimes made at short
notice. The three types of hearing are:
Traditional ‘in-person’ hearings, held in an employment tribunal or court room;
Remote/virtual hearings via HM Courts and Tribunal Service’s Cloud Video Platform (CVP). These are conducted remotely with participants using web-based software;
Hybrid hearings, which are a combination of in-person and CVP – some of the participants attend via CVP and others in person.
The length of the hearing
depends on the complexity of the case and the number of witnesses giving evidence. Straightforward cases with just a couple of witnesses can be heard in a single day.
Court room
Ideally, you will want all your witnesses to attend the full hearing, and not just the days when they give their evidence. Although that can lead to resourcing issues in the workplace, it means that the witnesses can listen and consider the rest of the evidence.
The type of claim also determines whether the case will be heard by a judge sitting alone, or by a judge accompanied by two ‘wing members’ to form a panel. The ET hearing room is set out like a court room. The judge sits at one end, usually on a raised platform, alongside any wing members. They should be addressed as ‘Sir’ or ‘Madam’.
ET hearings are usually conducted in public. This means you can attend in the capacity of an observer to help you prepare for
your own case. It also means that members of the public, and occasionally the press, may sit in on your case.
Giving evidence
Many respondents are represented by an advocate in the hearing – a solicitor or barrister. Claimants often cannot afford an advocate and present their case themselves.
If you are represented by an advocate, you will usually only speak in the hearing when you are giving your evidence. If the hearing is virtual, the judge sometimes asks everyone apart from the advocates to switch off their cameras and microphones when not speaking. It is an offence to record or broadcast any part of an ET hearing – whether virtual or inperson.
If you are a witness, you are allowed to listen to the evidence of the other witnesses before and after you give yours.
When it is your turn to give evidence, if the hearing is in-person, you will be called to the witness stand – which is often just a desk with a chair behind it.
You will be asked to swear an oath on a religious book of your choice, or ‘affirm’, depending on your personal preference and beliefs, that the evidence you will give is the truth.
You are allowed to refer to a copy of your witness statement and the bundle when you are giving evidence, but they must not be annotated or tabbed.
After some preliminary questions, you will be asked questions by the claimant or, if they have one, their advocate. This is called cross-examination.
You are also likely to be asked some questions by the judge or panel. Bear in mind that the ET may form a view of you, and the reliability of your evidence, based on the way you answer questions.
The purpose of cross examination is to test your evidence, expose any weaknesses and, potentially, undermine your evidence. The credibility and reliability of your evidence may be challenged.
Cross-examination can be demanding and witnesses should have support available before and after giving evidence.
When all witnesses for both
Bear in mind that the tribunal may form a view of you, and the reliability of your evidence, based on the way you answer questions
PREPARATION TIPS
Much of the preparation will take place weeks or months before the hearing, such as bundles and witness statements described in my earlier articles. But extra preparation is worthwhile in the days leading up to the hearing
sides have given evidence, the advocates will take it in turns to make closing submissions summarising the case and the legal arguments. If there is time, the judge will give a decision at the end of the hearing.
Liability and remedy
There are two elements to an ET hearing: liability and remedy. If it is determined that the respondent was ‘liable’ for any claim, the ET will need to go on to consider ‘remedy’, that is to say, what compensation, if any, to award the claimant.
Sometimes there is insufficient time at the end of the hearing for the judge or panel to make a decision, in which case a written decision will be sent to the parties by post or email. Depending on the outcome, a separate remedy hearing will then have to be arranged for a later date.
Damages for successful unfair dismissal claims are calculated using a combination of a formula based on the claimant’s age and length of service, plus compensation for their loss of earnings.
The total amount that the ET can award is capped at a level which is adjusted annually; the maximum that can currently be awarded for unfair dismissal is just under £106,000.
The cap can be exceeded where the case involves whistleblowing or discrimination.
Compensation for discrimination and whistleblowing is calculated differently and can take account of injury to feelings as well as lost earnings, which, in serious cases involving high-earning claimants, can extend to hundreds of thousands of pounds.
The most up-to-date figures currently available show that the average (mean) ET award for a successful unfair dismissal claim in
It is a good idea to hold a case conference with your advocate and everyone involved in the case in the days leading up to the hearing
Re-read all relevant documents and especially your own witness statement the day before the hearing
If the hearing is by video, make sure you have the log-in details and that your technology is compatible and functioning. Your solicitor or the ET can provide details of a website where you can test your equipment in advance
If your hearing is in person, make sure you know where to be and when, and what you need to bring with you
2019-20 was £10,812 and for a disability discrimination claim £27,043.
Unlike other parts of the civil court system, the loser in an ET does not usually pay the legal costs of the successful party.
The ET judgment will be published online. It will name the parties, include detail about the claim, witness evidence and any compensation awarded.
There is a right to appeal to the London-based Employment Appeal Tribunal, but appeals are only allowed against an ET’s findings of law rather than findings of fact. So, in practice, appeals are not commonplace.
The public nature of ET decisions along with the inevitable cost and risk of litigation incentivises many parties to settle.
Resolving employment issues and avoiding claims in the first place is clearly preferable to defending a claim, but not always possible. Get expert advice to help you to understand and navigate the tribunal process if a claim does come your way.
Julia Gray is an associate at Hempsons solicitors
ADVICE ON GIVING EVIDENCE
1
Listen carefully to make sure you understand the question before you start to answer. If you don’t understand or if you need a few moments to consider the question properly, say so.
2
Regardless of who asks the question, respond straightforwardly and honestly. Try to remain calm and polite, even if you feel you are being provoked. If you are evasive or cautious with your answers, it might look like you have something to hide.
3
If you can’t remember the answer or you don’t know it, say so. Everyone will recognise that your memory is not perfect –especially when you are being asked about things that happened some time ago.
4 Never refuse to answer a question, no matter how irrelevant or inappropriate it seems – your advocate or the judge will intervene if necessary.
5
Try not to go off on tangents or volunteer more information than is requested. If more information is required, you will be asked to elaborate.
6
7
If you are asked to answer with ‘yes’ or ‘no’, but you feel that kind of answer would be misleading, explain why.
If your evidence is interrupted – for example, it spans the lunch break or is not finished at the end of the day – you must not discuss the case or your evidence with anyone during the break. This ban includes talking to other witnesses and your advocate.
BUSINESS DILEMMAS
Dr Kathryn Leask (below) discusses what to do if a patient requests a fitnessto-drive letter
Gauging fitness to drive
Dilemma 1 Must I sign him as fit to drive?
QI am a private GP and have a patient in their 70s who has asked me to provide them with a letter to confirm they are fit to drive, pending renewal of their driving licence by the DVLA.
They have referred to section 88 of the 1988 Road Traffic Act. As such, the patient feels that this means they can have a letter from their doctor to allow them to continue to drive.
Is this the case? Please could you advise further?
AYour patient will be aware of the guidance issued by the DVLA which may allow them to continue driving even though they do not hold a current driving licence.
This can apply when a new
licence has been applied for – for example, once they are over the age of 70 – and the application is being processed. The guidance states that ‘Your doctor must have told you that you are fit to drive’.
When considering writing a letter for a patient with regards to their fitness to drive, you must act within the limits of your competency and expertise, as set out in the GMC’s Good Medical Practice guidance (paragraph 14), and any form that you complete or sign must be accurate and contain all relevant information (paragraph 71).
In general terms, it is for the DVLA medical assessors to assess a person’s fitness to drive, and for the patient’s doctor to provide relevant information for the assessors to do so.
However, due to the delays that have occurred in processing licences, applicants have been requesting letters from their doctor to confirm they are fit to drive. Occasionally, you may feel there are circumstances in which you
are able to confirm that you have no reason to believe, based on the information available to you, that a patient may not be fit to drive, as you are not aware of any medical condition that requires notification to the DVLA.
The DVLA document ‘Assessing fitness to drive – a guide for medical professionals’ is a useful resource for this purpose.
Complete picture
If appropriate, you can confirm that there is nothing in the medical records that would exclude the patient from driving or that would require notifying the DVLA.
But it is recommended that you state that the patient has not, however, been examined for the purposes of assessing their fitness to drive.
Additionally, consider whether you have a complete picture of their medical history, particularly if the patient is only seeing you for a specific medical problem and also has an NHS GP, as well as the
reason why they are having to reapply for their licence.
Patients also need to be aware that undeclared conditions could affect their ability to drive (listed in the above document) and they would need to seek further assessment.
Finally, think about whether you are the best person to write such a letter, based on the information you have about the patient’s health.
This would allow you to state, with confidence, that they do not have a condition that could affect their ability to drive.
Dr Kathryn Leask is a medico-legal adviser at the Medical Defence Union
Dilemma 2
Do I accede to mum’s request?
QI recently saw a young child who had attended my practice along with their mother. The child is asthmatic, and the mother wanted to discuss their regular medication.
However, the parents are divorced and the mother does not want the father to have access to the child’s medical records, as he has just been released from prison.
She is concerned that he will use the records to find out where she lives and she feels vulnerable to physical attack.
I’m not sure what I should do in this situation. Can you advise please?
AIn most instances, anyone with parental responsibility for a child has a right to seek access to that child’s medical records.
Parental responsibility is defined in The Children Act 1989 as ‘all the rights, duties, powers, responsibilities and authority which by law a parent of a child has in relation to the child and [their] property’.
Birth mothers automatically have parental responsibility, as do married fathers.
Parents do not lose parental responsibility if they divorce, but responsibility can be restricted by a court.
When one parent asks the practice to disclose information about the child, there is no obligation to
seek consent from the other parent or to tell the other parent that you have received the request.
Nevertheless, it may be wise to make sure the other parent is aware of the request, so that you can take into account any objection they may make and the reasons for it.
The GMC states that a doctor may allow someone with parental responsibility to access a child’s medical records if the child or young person consents or if they lack capacity and it doesn’t go against the child’s best interests.
Disclosing information
However, the guidance also says: ‘If the records contain information given by the child or young person in confidence, you should not normally disclose the information without their consent.’
It may also be justifiable to disclose confidential information about the child to a third party who does not hold parental responsibility, providing this is clearly in the child’s best interests.
As previously mentioned, a father with parental responsibility has a right to request disclosure of his child’s records.
But as information should be withheld if disclosure would be contrary to the best interests of the child or if disclosure could lead to serious harm or be unreasonable to a third party, it would be entirely reasonable in this situation to remove the registered address from any copy records disclosed in this situation.
Dr Sally Old is a medico-legal adviser at the Medical Defence Union
When mum wants dad excluded
A consultant’s concerns about potential problems disclosing records to a parent with parental responsibility are tackled by Dr Sally Old (right)
Now open on weekends
NEW SESSIONS ARE AVAILABLE FOR INDEPENDENT PRIVATE PRACTICE ON WEEKENDS.
Fully CQC-registered clinic
Nursing support
Appontment-making
Secretarial support
Billing service
In-house pharmacy
We are a leading private outpatient clinic and we are inviting new applications for practising privileges for our extended opening hours on weekends.
Contact: david.briggs@londonmedical.co.uk 49 Marylebone High Street, London W1U 5HJ
londonmedical.co.uk
DOCTOR ON THE ROAD: FORD FOCUS ST
Worthy successor to hot-hatch genre
This nimble hot-hatch from Ford, one of a dying breed, took our motoring correspondent tester Dr Tony Rimmer (right) back to the days when he was an SHO
CAN YOU remember the first car you bought? For many of us, it would have been an old banger; something to get us from hospital to hospital during our medical student days.
However, despite the lack of sophistication on offer, I bet you still have fond memories associated with your first car. Can you also remember the first brand-new car that you bought?
Perhaps you never have bought a new car, but for those of us who have, there is something very special about being the first and only owner of your perfect and shiny pride and joy.
In my case, being a petrol head at heart and having recently become married, I wanted to celebrate my SHO status with the purchase of a hot-hatchback. We had a puppy who needed space too.
Sadly, I was unable to justify the extra £300 expense of a Golf GTI, but I did buy Ford’s equivalent: the
Escort XR3i. I was so glad that I did. Over the next several years, it served our growing family well with its great combination of practicality and sportiness. It was a sad day when it was stolen by thieves – as many were – never to be seen again.
So what about the present day?
The Golf GTI is still on offer in Mark 8 form, but is there an equivalent contender from Ford?
Challenge the Golf?
Well, the Escort models morphed into the Focus range in 1998 and we currently have the fourth generation on sale. The XR3i equivalent is the ST model and I have been driving one for a week to see if any of its predecessors’ DNA remains in place and if it can challenge the current Golf GTI.
The ST is based on the very practical five-door Focus body, but there the similarity ends. A bespoke and adjustable suspen -
sion system and light 19-inch alloys makes the most of the sporty chassis.
Power comes courtesy of a 2.3litre turbo-petrol engine that produces a GTI- equaling 276bhp – my XR3i only had 105bhp – and drives the front wheels. More powerful brakes and a six-speed manual gearbox complete the package.
STs are offered, and often bought, in distinctive bright colours and my test car was finished in Azura Blue, which is certainly striking.
Something special
The additional vents and wings also mark the car out as something special and they are more subdued than those on the extrovert Honda Civic Type-R. The Focus is a goodlooking modern car and the lower stance of the ST only improves its appearance.
Slip into the standard partialleather Recaro sports seats and you immediately feel that this is a serious driver’s car.
The steering wheel, pedals and gearstick are perfectly placed. Equipment is very generous with all the electronic aids, sound and navigation systems that you wish for.
To specify a GTI to this level would cost a lot more. Like all Focuses, it is also a supremely practical car; we journeyed with two small children in their isofixed seats, a medium-sized dog and still had adequate luggage space in the boot.
However, you don’t buy an ST for its practicality; you buy it for the performance and driving experience. Does it deliver?
Well, Fords have always looked after the keen driver, even their base models tend to be fun, so it is really no surprise that this sporty Focus is rewarding for the keen driver on the UK’s fast A and B roads.
The steering is sharp, the gear-
There is more than adequate space for luggage in the boot. But you don’t buy an ST for its practicality
box is a joy to use and brakes are strong. Handling through the curves is equal to the GTI and even better if the surfaces are smooth. This would make a great occasional track-day car.
The ride, although firm, is resilient and the only feature that interferes with progress is the torque-steer on full power – albeit entertaining in an old-school sort of way.
Nimble hot-hatch
The manual gearbox makes you feel more connected to the driving experience; smooth changes at the right time are up to you, not an automated robotic system.
I had great fun on my own on some favourite roads and savoured the nimbleness of this properly sorted and nimble hot-hatch. It brought back memories of my XR3i.
The Focus ST is another exemplar of a dying breed; a light and sporty internal combustionengined manual sports hatchback that entertains and satisfies the keen driver.
Yes, it is a bit noisy and the ride is a bit stiff, but this type of car will soon disappear for ever, so if you have any petrol in your veins or arteries, then it is worth your consideration.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
FORD FOCUS ST
Body: Five-door hatchback.
Front-wheel drive
Engine: 2.3litre four-cylinder turbo-petrol
Power: 276bhp
Top speed: 155mph
Acceleration:
Partial leather Recaro sport seats make it feel this is a serious driver’s car
A PRIVATE PRACTICE – Our series for doctors embarking on the independent journey
You can’t afford to simply ignore VAT
Ian Tongue presents a recap on Value-Added Tax (VAT) and how this may affect your private practice
VAT IS a tax we are all familiar with, as it is paid on the majority of the goods and services we buy.
Sometimes an invoice will separate out VAT, but in much of our day-to-day expenditure the price we pay is inclusive of VAT, particularly in the retail world.
When running a business, it is normal to have to be VATregistered, but within the medical profession it is less common for private practices.
The reason for this is that medical services are usually exempt from VAT, meaning that VAT does not need to be considered. But there are some exceptions which this article considers further.
VAT registration
VAT registration can be compulsory by law or on a voluntary basis for the smaller business.
For compulsory registration, you have to be making VAT-able supplies in excess of £85,000. However, for voluntary registration, there is no minimum, but you have to be making taxable supplies.
Taxable supplies are supplies (sales/fees) that are subject to VAT. VAT is usually charged at 20%, but there are lower rates and even a zero rate where VAT is charged but at 0%.
New house building is an example of a zero-rated activity whereby VAT is charged at 0% when you buy the property, but the builder can claim back the VAT suffered on the build costs.
For private practices, it is rare to register voluntarily and those medics who are registered have done so, as the compulsory registration limit has been reached.
Supplies
The process of looking at your supplies is very important, as this determines your VAT status and whether you have any compulsory obligations.
Another key factor is that you are required to consider VAT registration monthly by looking back 12 months each time and determine whether you have breached the registration threshold cumulatively in that 12-month period.
Supplies of medical services are generally exempt from VAT, meaning that you could have a high income but, as your supplies are
exempt, you will not breach the £85,000 compulsory VAT registration threshold.
In order to treat your supplies as medical, you must meet all of the following criteria:
1
2
Be a registered health professional;
Provide services within the profession in which you are registered to practice;
3
The primary purpose of the services is the protection, maintenance or restoration of the health of the person concerned.
The vast majority of clinical medical services carried out by consultants and GPs satisfies the above criteria.
The most common areas where the above is not met is medicolegal work and purely cosmetic procedures.
Medico-legal work
This type of work is common for consultants and, under the VAT legislation, is not regarded as a supply of medical services.
The reason for this is that the primary purpose of the work is not the protection, maintenance or restoration of the health of the person concerned, despite the fact that treatment recommendations may be considered as part of the report.
The primary purpose of medico-legal work is for a third party – a court – to make a decision and hence why this type of work is regarded as standard-rated for VAT purposes.
Therefore, if you are carrying out more than £85,000 of medicolegal work on a 12-month rolling basis, you must register for VAT and add 20% to your fee.
Cosmetic work
VAT and cosmetic work have been a contentious area for some time and, in many respects, it is due to the lack of understanding by HM Revenue and Customs (HMRC) of the work carried out.
HMRC has often sought to label a procedure as cosmetic rather than looking at the reasons why a patient is having treatment, whether this be for their physical or mental health.
It remains to be seen whether there will be any changes going forward, but, at present, the rules were set when the UK was part of
VAT and cosmetic work have been a contentious area for some time and, in many respects, it is due to the lack of understanding by HM Revenue and Customs of the work carried out
the EU and, for a cosmetic procedure to be regarded as subject to VAT, it must be purely cosmetic.
Therefore, it is important that if you operate in the aesthetic/cosmetic sector, you keep records of the medical condition that the patient is suffering on a case-bycase basis.
Where no medical condition is being treated, you will need to identify this work separately and track the level undertaken to ensure that you do not go over the £85,000 VAT threshold on a 12-month rolling basis. If you do, VAT registration will be required.
This is a complex area and the use of a specialist medical accountant is essential if you are in this position.
Other supplies
As doctors, you may be involved in other activities that could be taxsensitive for VAT purposes. The more common ones are:
Training;
Research;
Pharmaceutical work;
Royalties.
The rules for the above can vary, as do the rules if the work is undertaken in another country.
Accounting for VAT
One important thing to remember when you are VAT-registered is that you are acting as a collector of tax for HMRC.
As a result, you are placed under more scrutiny to ensure that your systems accurately record VAT payable and promptly pay this over to HMRC.
The penalties for not registering
or accounting for VAT correctly can be severe and therefore your systems need to be robust. And you can expect them to be reviewed by HMRC periodically via its compliance visits.
Medico-legal work usually takes some time to be paid and therefore it is beneficial to consider some of the VAT schemes available to help you manage the payment of VAT to HMRC.
Accounting for the VAT when you are paid is an important concession for this type of work, as are schemes to reduce the administration required, such as annual accounting of VAT.
Costs on which you suffer VAT are usually deductible against the VAT collected so that you pay over the net amount. However, if you are making a combination of exempt and standard-rated supplies, the calculations are more complex and you may not be able to recover all of the VAT on costs.
Another scheme which is available allows you to pay over a flat rate of VAT which is less than the 20% charged, which can be advantageous if you suffer low amounts of costs with VAT on them.
However, care must be taken here, as the flat rate is payable on all supplies and therefore if you are undertaking clinical and medicolegal work, this scheme is not usually appropriate.
The different VAT schemes have criteria that must be met. Your accountant should discuss with you to determine the most appropriate for your individual circumstances.
VAT can be a complex area and being VAT-registered can be a burden to your private practice. But it is an essential aspect to manage if you are undertaking work that is not exempt from VAT.
Help is at hand to prevent any risk of not registering, and using an accountant who understands the rules and practicalities around the medical sector is essential.
Next month:
The importance of paperwork including contracts
Ian Tongue (right) is a partner with Sandison Easson accountants
PRIVATE
PATIENT UNITS: FIXING THE PROBLEMS
How to boost PPUs
1WHAT IS needed is the development of a cohesive national framework, which has been missing for some years.
NHS trusts do not need the dead hand of the centre taking over. It is local responsiveness to the market that is required in such a hands-on business.
However, central leadership could reset the tone with clear messages to trust boards and a steer to support and align private patient services in support of core NHS provision.
A national working group, with input from sector leaders, could provide the narrative to help describe how trusts can reasonably work towards private patient services being ‘something that all trusts do’ and also create the structures to ensure best practice can be rolled out.
Perhaps there is room even for a single NHS private patient brand?
2
There needs to be encouragement for increasing local collaboration, and this could build on the national foundation to help leading trusts support their neighbours and those facing similar market conditions.
The south-west private patient managers group provides a template that could be strengthened, extended and embraced.
National leadership to support such groups engaging with private medical insurers could also reduce the administrative contracting burden and simplify and make more transparent the tariffs which vary so much across the NHS.
It would be possible for trusts to form local ‘chains’ of private patient services that reduce their back-office costs.
These could also give more choice and access for consultants working across the ‘chain’ and potentially be co-branded to offer a more visible market presence.
PPU expert Philip Housden (right) last month reviewed NHS private patient services development over the past four years and highlighted what has been learned. Here he suggests how to tackle three of the main challenges and opportunities now facing the PPU sector
of what is possible by working with independent provider partners.
There are many present and past examples of this, such as Birmingham University Hospitals with HCA, with others being explored.
It is possible to envisage most NHS trusts developing an on-site unit that could embrace private and NHS patients, ebbing and flowing with the changing demands of healthcare over the days, seasons and years.
These opportunities could be attractive to new market entrant providers with flexibility in where they invest and what they invest in.
Large independent hospital groups could also be of interest because this would facilitate closer working with the NHS.
Any closer alignment of private patient services and activities within NHS trusts is likely to create a range of benefits for the wider NHS, individual trusts, integrated care systems, local healthcare economies, consultants and their patients.
3
The third challenge and opportunity is finding capacity in the post-Covid world.
Most, if not all, trusts are looking at their own capacity in the light of increasing demands, driven by ageing population and other factors and also the need for transformation in service delivery.
The challenges of the ageing estate and pressure on beds and theatres leaves many NHS trusts unable or unwilling to assign footprint to and built estate for private patient services.
That is even though this comes at the likely expense of paying for insured patients ‘in the system’, probably those complex high-acuity patients that the local independent hospitals cannot provide for, rather than charging these costs to the insurers.
What is required on the ground
is flexible ‘ebb and flow’ ward space that can be rebadged as private without any need for new capacity. That ward admits the insured patients already in the trust first, then is topped-up with NHS patients to ensure efficient high throughput, flow and occupancy.
Private sector partnerships
Another route to achieve increased capacity is through private sector partnerships that embrace the mixed-service model of providing flexible capacity able to be accessed by private patients and NHS patients.
As the national NHS hospital rebuilding programme develops and community diagnostic services are built, there is the option to consider partnership arrangements to extend the range and size
There would even be benefits for the private healthcare sector, with insurers gaining more choice and boosting insurance take-up.
Although independent hospitals could face more competition, they would benefit from increased robustness to the critical care/ higher acuity pathways infrastructure and opportunities to develop on-site/coterminous partnership private healthcare capacity on trust campuses.
My single most powerful insight from the four years of reviewing NHS trusts’ private patient services in Independent Practitioner Today is that a ‘win-win-win-win’ is achievable for all key stakeholders.
Not enabling this is costly to the NHS and the whole sector.
Philip Housden is managing director of Housden Group commercial healthcare consultancy
A lucky 13% profit hike
Consultant urologists typically enjoyed some healthy profit rises in our latest benchmarking survey. Ray Stanbridge reports
I AM PLEASED to report that urologists came out winners in the profitability stakes in 2019-20.
Turnover increased by £20,0000 from £154,000 in 2018-19 to £174,000 in 2019-20. That is a 13 % rise.
Operating costs went up by 8.3% from £60,000 to £65,000. As a result, margins before tax rose by £15,000, or 16%, from £94,000 to £109,000.
There was a real growth in net income and consultant urologists’ private practices have flourished. There was still a lot of Choose and Book work, although this was cur-
AVERAGE
Expenditure
tailed as the first effects of Covid19 on the market began to be felt from February 2020.
Consultants experienced continuing ongoing pressure on fees from insurers, although we did notice that some urologists did well in focusing on self-pay or some subspecialties.
Costs growth
Costs continued to grow in some areas. The expense of consulting room hire rose probably in line with increasing patient volumes.
We noticed a relatively large growth in use of home costs.
Increasing numbers of urologists established their homes as being their primary office base to undertake administrative and research work
Increasing numbers of urologists established their homes as being their primary office base to undertake administrative and research work and some even used their homes to see patients before the pandemic.
There was some growth in attendance on courses and conferences and a number of urologists attended meetings at exotic venues.
Accounting and professional costs showed some increase, presumably a function of increased activity.
Other costs seemed to be fairly constant. All in all, it seems that costs were kept under control for 2019-20.
Very positive
What then of the future? Prior to Covid-19, the long-term trends for urologists seemed to be very positive income-wise. The sector was not materially affected by the pandemic in 2019-20.
However, there were significant effects of the pandemic on consultants’ earnings in the first half of 2020-21. We shall report on this next year.
Trying to portray reasonable year-on-year financial comparisons in a fast-changing market, that was also hit by Covid-19 in 2020-21, remains a challenge.
There are a variety of reasons. Urologists, as we have previously reported, have formed groups. Others have chosen to incorporate through a limited liability company or become members of a limited liability partnership.
A number have focused their pri vate business activities almost entirely on Choose and Book work.
Employment option
A small but increasing number of urologists have decided to take up
employment options with leading hospitals to do their private work.
As a result, these factors have made it more and more difficult to make year-on-year comparisons in our surveys.
Consultant urologists now have to earn at least £10,000 a year in the private sector to be included in this survey and they must also:
Hold either an old-style or a new-style employment contract with the NHS – they do not work exclusively in the private sector;
Have been in private practice for at least five years;
Be trading either as a sole trader, through a limited liability company or LLP or as a member of some other formal or informal group.
While our analysis of incomes and expenditures is not statistically significant, it is an attempt to record what a typical consultant urologist in private practice earns and spends on their business.
Next time: Anaesthetists
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists, Stanbridge Associates Limited
HOW ARE YOU DOING?
Use
HEALTHCODE ACADEMY
FREE 1-2-1 training for our customers
Healthcode is the UK’s official medical bill clearing company and has provided secure and encrypted systems to healthcare professionals since 2000. Pre-pandemic we processed around 27,000 electronic medical bills to insurers daily.
The Healthcode Academy provides:
FREE 1-2-1 online training available to anyone with a Healthcode user ID
Training sessions lasting between 30–60 minutes
Shorter bitesize options available
Training tailored to your needs using your own site and data
Certificate awarded on completion
We want to make sure you and your team have the tools on hand to make those important work tasks quicker and easier – and, ultimately, make your practice more efficient.
To find out more and book your training simply click here and select the module you require!
To find out more about our solutions visit our website www.healthcode.co.uk
Coming in our May issue, published on 10 May.
Staff retention problems in private healthcare are in Independent Practitioner Today’s headlines at the moment. Our Troubleshooter Jane Braithwaite responds to this consultant’s question which will strike a chord with many readers: ‘How do I improve staff retention and ensure my team is stable? Recently, I have lost members of staff and it will take me a long time to recruit and train new team members.’
Dr Kathryn Leask answers a doctor’s request for help dealing with a troubling scenario with a patient. Should the police be told? Her Business Dilemmas article also explains how to support a noncompliant patient
Often the biggest challenge that a clinic faces is finding or acquiring new patients. Simon Marett of Ellerton Marketing covers some of the main considerations and marketing ‘channels’ that are open to practitioners when they are looking to grow their patient base
Bupa’s James Sherwood follows his analysis on the impact of climate change on our health with a round-up of the insurer’s efforts to become a net zero emissions business
Pent up demand – a medical tourism opportunity? Medical travel expert Keith Pollard gives his view
INDEPENDENT PRACTITIONER
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution.
Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
So do you know the risks of being a company director? Hempsons solicitors Justin Cumberlege and Alison Oliver give a legal viewpoint
Doctors and nurses worldwide point to a roadmap to future-proof healthcare. Elsevier Health’s first ‘Clinician of the Future’ global report reveals current pain points, predictions for the future and how the industry can come together to address gaps
Good communication when interacting with patients is vital –particularly the more challenging ones
As Medical Billing and Collection celebrates 30 years of helping consultants, Simon Brignall continues with the next ten tips from 30 key areas to consider for practices aiming to overcome their medical billing and collection challenges
The importance of paperwork, including contracts – Sandison Easson specialist medical accountant Ian Tongue has some words of warning
Ray Stanbridge’s Profits Focus series examines the earnings of consultant anaesthetists
Plus all the latest news and views
And don’t forget to check out our additional news updates every week online
ADVERTISERS: The deadline for booking adverts in our May issue is 22 April
Write to Independent Practitioner Today 7 Lindum Terrace, Lincoln LN2 5RP
CHANGING ADDRESS, EMAIL ADDRESS OR SUBSCRIPTION DETAILS?
Phone 01752 312140 or email karen@marketingcentre.co.uk
To advertise in the digital journal, on our website or in our business directory, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912 Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners.
£90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180). TO SUBSCRIBE
Email karen@marketingcentre.co.uk or phone 01752 312140
Publisher Gillian Nineham Phone: 07767 353897.
Email: gillian.nineham@gmail.com
SAVE £15 WITH DIRECT DEBIT!
Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.