The business journal for doctors in private practice
In this issue
How to lose media coverage
PR guru Tingy Simoes gives some tongue-in-cheek advice about keeping journalists happy P16
Drilling down on claims
The MDU’s negligence files reveal what private orthopods are being sued for P28
In this issue
What does a billing firm do for me?
Billing expert Simon Brignall answer the most common questions he is asked by consultants n See page 32
Keep up to date as a doctor employer
An update to employment law changes in response to the Covid-19 pandemic P34
London market stalls
By Robin Stride
Consultants’ private practice in central London is likely to be quiet for the next three months due to patients becoming ‘jittery again’ in the third lockdown, analysts warn.
LaingBuisson’s 7th edition of its Private Acute Healthcare Central London Market Report finds the area’s private acute healthcare market in the year running up to Covid-19 was its strongest in revenue growth since 2014.
But its author Ted Townsend admits: ‘What 2021 will hold for the central London independent hospital sector is anyone’s guess.
‘While pent-up demand led to a noted rise in the number of patients through their doors in the later months of 2020, the third lockdown has made patients nervous and the first half of 2021 is expected to be quiet as a result.
‘Nevertheless, central London private hospitals should continue to benefit from the restrictions being placed on NHS PPUs as well as lack of private capacity in hospitals outside of London, not to mention the ongoing backlog of private patients and the potential for new self-pay patients.’
He said the pandemic had obscured Brexit’s potential impact.
‘Whether this emerges as an issue, either through a loss of those jobs which offer health insurance as a
CENTRAL LONDON’S PRIVATE CARE IN FIGURES
Consultants
perk to other counties, or through difficulties in staff recruitment, remains to be seen.’
A return of international and embassy patients plus higher private medical insurance spending and oncology revenues drove growth of more than 7% during 2019. Hospitals are broadly expected to maintain 2019 revenues, but the report warns profits ‘may be a different story’.
NHS contracts kept the sector going during the pandemic when they might have closed, but the analysis says it is hard to predict when overseas patients will return.
On the upside, the financial, insurance and legal services sector, with many insured patients, seems to have survived well and the report sees benefits for central London from NHS PPU restrictions, lack of private capacity in hospitals elsewhere and a backlog of private patients and potential new self-payers.
Source: LaingBuisson TRANSFORMERS:
LaingBuisson estimates private medical insurance revenues grew by 4.6% in 2019, from £922m to
£964m, generating 56.4% of hospital revenue, following previous year falls.
This was partially reflected in the zone’s strength in complex care areas like oncology. Insurers tried to manage costs in the face of ‘flat demand’ for their products and growing claims from oncology patients, who account for 4% of patient volumes but 25% of total spend.
The most successful insurance
cost management policies included: n Call centres directing patients to cheaper hospitals and consultants; n More pathway management, such as recommending physiotherapy and pain management before or instead of orthopaedic surgery; n Price negotiation, such as putting out tenders on a specialty basis and inviting hospitals to bid, plus offering patients cash payments for being treated by the NHS. Self-pay revenue estimates rose by only 1.4% in 2019 to £354m, or 20.7% of total revenues, and apparently fell for some hospitals and groups despite high marketing budgets, ‘suggesting there is some sort of impediment to growing revenue from this source beyond some initial “easy wins”’.
➱ continued on page 3
TELL US YOUR NEWS. Contact editorial director Robin Stride
ADVERTISE WITH US. To advertise in the journal or our website business and lifestyle directories, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT
£90 independent practitioners. £210 organisations. £90 GPs and practice managers (private & NHS).
Save £15 paying by direct debit: individuals £75 (organisations £180).
The profession has waited well over a year for the Government’s response to the Paterson Report, the long-running inquiry that the former Bishop of Norwich led into rogue surgeon Ian Paterson.
This, you may recall, provoked – among many other issues –fears among some leading independent practitioner representatives of a widespread drift away from self-employment to a salaried service for doctors in private practice.
expected was missing. Even after all this time.
The resulting story, which we carried on our website the same day on 23 March, made barely 1,000 words because the response had only scratched the surface of the issues raised and dealt with only a third of the 15 recommendations made in the Paterson Report.
We are told a full response to the report of the inquiry, set up in 2017, ‘will come later in 2021’ and that can’t come too soon.
Monitoring doctors where they work
David Hare of the Independent Healthcare Providers Network reports on how the Medical Practitioners Assurance Framework is going P14
You can learn leadership
Jane Braithwaite explores the ways in which leadership skills can be enhanced and highlights the support available to help achieve this P20
Single spot for doctors’ data
How do you maintain control over all your information and use it to advance your practice? The Private Practice Register is the answer P24
Tricks to make your website shine Marketing experts Simon Marett and Michael Sullivan look at website design and the key apsect you need to think about before launching a new site P30
Ignore the siren song of the markets
Don’t keep checking your portfolio. Dr Benjamin Holdsworth of financial advisers Cavendish Medical explains it’s mad to try following markets P36
Re-opening is not that simple Dr Sara Sreih and Lucy Hannington of the MPS highlight some important consderations for private doctors trying to get back to ‘open for business’ P42
PLUS OUR REGULAR COLUMNS
Survive a private practice: Help you need to carry on
Accountant Ian Tongue recaps on the financial support measures for private practices hit by the pandemic P44
Covid-19 then got in the way of any progress, so when we heard the long-expected retort was on its way late last month, we were ready to give it some big coverage and reaction.
When it arrived, in the form of a statement from patient safety minister Nadine Dorries, we were – like many others in the private health sector – disappointed that much of what was
Last month’s updates are welcome and their content no surprise. But as Matt James, chief executive of the Private Healthcare Information Network (PHIN) has observed, most telling is what remains to be addressed – most notably wholepractice information and better information for patients, which are the report’s recommendations one and three.
Doctor on the Road: A hatchback to give Tesla a run for its money
Dr Tony Rimmer is impressed by the Polestar 2, an all-electric hatchback by the makers of Volvo P46
Profits Focus: Dwindling income stream
Our unique benchmarking survey reveals a disappointing year for many urologists’ businesses P51
New law to rectify pension inequity
By Edie Bourne
Doctors who found out last month they can decide which benefits they should take to remedy the age discrimination caused by moving to the 2015 pension scheme have been told that new legislation is being drafted – but will not be in place for several years.
NHS Employers has confirmed that the Government is working on the legislation and hopes to have this in place by October 2023, so that all members can make their choice of pension scheme benefits ‘with confidence’.
New processes to help the decision will also be introduced.
The ‘McCloud’ consultation concluded that affected doctors have the right to make a ‘deferred choice’ of which remedy benefits
to take – the pension benefits from their previous 1995/2008 pension scheme or those from the 2015 scheme.
By making this decision at retirement, doctors will be able to calculate which set of benefits are the most valuable to them. The Government has confirmed that full information will be provided to members at this time.
However, if members have already retired before the new legislation has been introduced, they will be contacted and asked to make their choice retrospectively. Payments will then be backdated to the time when benefits became payable.
Patrick Convey, technical director at specialist financial advisers Cavendish Medical, said: ‘It has been useful to get some clarity on
how the “McCloud” ruling will work in practice, but we need to wait another two-and-a-half years for the full legislation to be produced.
‘Doctors retiring before then –and we have witnessed many seeking early retirement because of the harsh tax rules and the impact of the last year – might be confused as to what this means for them.
‘The Government has said that in some cases, it might be possible for the choice to be made sooner, but that the legislation that would allow schemes to do this is “limited”.’
NHS Employers also confirmed that from 1 April 2022, all members of former NHS pensions such as 1995 and 2008 will be moved to the new scheme, regardless of their age, and the old schemes will subsequently be closed.
Patrick Convey: ‘Even the tiniest of errors can have big impacts on pay and pension figures further down the line’
Mr Convey explained: ‘If you are a member of one of the legacy schemes, you will keep any service that you earned up until 1 April 2022 and be able to access your benefits normally. Going forward, any benefits you earn after this date will be in the 2015 scheme.
‘As ever with all things relating to the NHS pension, keep all your records handy and please ensure that your pay and pensions details are kept up to date. We often see mistakes on payslips and even the tiniest of errors can have big impacts on pay and pension figures further down the line.’
Public is ‘ready to spend on private care’
Most of the public are ready to spend their money on going to a private doctor if they think it necessary, according to a survey.
As many as 54% of those taking part in the study, by private doctor specialist company Ellerton Marketing, would pay for private healthcare if the need arose.
For the 46% who would not, 20%
Digital tech to greatly change care, insurance expert says
Digital technology and wearable devices will see the delivery of healthcare in the private sector and NHS ‘change beyond comprehension’ over the coming years, according to a leading insurance expert.
might consider paying in the event of extended NHS waiting times, poor NHS treatment or for faster referral to specialists (19%).
When asked about post-pandemic healthcare services, a quarter of participants felt that telephone or online consultations should continue.
The survey received over 500
Stuart Scullion, who is standing down as chairman of the Association of Medical Insurers and Inter mediaries (AMII), said the organisation wanted to be involved in that change and play its part to improve things for the better.
He described interest in health and well-being, including private medical insurance, as buoyant due to the impact of Covid 19, particularly in relation to mental health, and resulting increases in NHS waiting times.
responses and is broadly reflective of UK demography, a company spokesman said.
Overall, 44% of participants had paid to access healthcare at some time and 14% had private health insurance.
Asked what a private health insurance provider could do to encourage them to consider mov-
ing their policy, responses included:
Lower premiums;
Less red tape;
Make things as easy as possible;
Cashback for healthy lifestyle;
Include pre-existing conditions;
Fewer exclusions;
Offer an incentive to join;
No NHS GP referral.
Shoots of recovery visible
There is optimism of a rise in selfpay revenues as NHS waiting times encourage more people to go private.
Some hospitals are improving marketing and targeting individual patients effectively rather than relying on private consultants to bring them the work
The study notes that established consultants in large practices often
feel they do not need to attract work by offering lower prices through a hospital self-pay package, so deals are agreed with specialists who need the work, rather than those who can bring it in.
Revenues from embassy work grew by 20.3% to £374m in 2019. But travel and visa restrictions are predicted to slow patients’ return and home countries have their own economic and pandemic issues.
➱ continued from front page
Rise in phone calls indicates recovery
By Leslie Berry
‘Private practice is bouncing back’ is the message from private practice management services company Designated Medical.
It reports a ‘buzz in the air’ in recent weeks following its busiest time for many months as consultants’ practices experience more inquiries and bookings.
Greater patient confidence as more people get vaccinated against the pandemic are one reason for the upturn. They are happier about making their long-awaited medical appointments.
Designated Medical believes the most obvious indicator of a bounceback in the private healthcare sec-
tor was the number of calls received from patients inquiring about appointments.
In a message to clients, it said: ‘The increase in call volumes during February and the early part of March has reassured us that we are starting to see an increase in the confidence of patients who are now looking to book their medical appointments after many months of waiting.
‘During the last week of February, our call volumes were 40% higher than in the first week of February and the first week of March has been our busiest week this year.’
It added: ‘Our experience definitely supports the view expressed in the Independent Practitioner
Today on 2 March which reported optimism of a significant bounceback in private practice this year.
‘They quoted statistics from a survey poll recently undertaken by the MDDUS, stating that six in ten of the private clinicians who responded to the survey expected to see their volume of work increase in 2021.
‘This positive view is welcomed, particularly as 52% of the clinicians reported that their private work had dropped by more than half because of Covid-19.
‘This is encouraging news for everyone in private healthcare and most importantly for patients who will be able to source the expertise and care they need.’
SECTOR’S SUPPORT FOR NHS REVEALED
Independent hospitals in England delivered over three million NHS procedures in England under national arrangements during the Covid-19 pandemic, new figures have shown.
A year on from the historic partnership between the health service and independent hospitals, which made nearly all private capacity available to the NHS ‘at cost’, new figures show the sector’s major contribution.
Marking the first anniversary of the NHS and private partnership, the Independent Healthcare Providers Network (IHPN) has launched a new report showcasing some of the many partnerships between independent and NHS providers. Independent providers also played a key role in supporting NHS junior doctors – hosting over 2,000 medical trainees throughout 2020.
While the agreement concluded at the end of March, IHPN said independent providers remained committed to supporting the Covid-19 recovery and would continue to play a key role working with local NHS partners to deal with the significant backlog of delayed care.
Data published last month showed the largest ever official waiting list on record at 4.6m, with over 300,000 people now waiting over a year for treatment.
IHPN boss David Hare said: ‘Independent providers remain committed to supporting the NHS as part of the post-Covid recovery and this partnership will continue to evolve in the months and years ahead with a renewed focus on clearing the significant backlog of NHS operations, while also ensuring private patients can access the care they need.’
Nearly six million people in England may be on a hidden waiting list, having not come forward or been referred for treatment yet due to the significant disruption during the pandemic, NHS leaders fear.
Analysis commissioned by the NHS Confederation suggests the true demand for elective care could be much larger when referrals for treatment, such as from GPs, begin to increase again, following a 30% drop last year.
It says that 5.9m fewer referrals for elective treatment were made in 2020 compared to 2019 –14.25m compared to 20.18m.
The difference is believed to be due to the disruption of the pandemic and the public not coming forward despite the NHS being ‘open for business’.
The NHS Confederation said the exact size of this hidden list was unknown, as some people might have sought care elsewhere, while others might never come forward. It added: ‘However, if a sizeable majority did present, it could significantly add to the total. One of the modelling projections in the analysis suggests the backlog could therefore reach 6.9m by the end of 2021.’
Chief executive Danny Mortimer said: ‘Health leaders are concerned that we may be scratching the surface of this waiting list if further referrals come through at a time when coronavirus pressures are still high, the workforce is in a very fragile state and when capacity is still so constrained.
‘For their part, NHS organisations are making substantial changes to how they work to improve access and maximise the capacity that is available to them.
‘They are working together to organise treatment between different organisations and they are applying best practice at a scale and pace that have not been seen before. But this will not be enough to address the problems our patients face.’
A poster produced by the Independent Healthcare Providers Network illustrates the work that the private sector has done to support the NHS
Advice follows email scam strike on doctor
By Douglas Shepherd
Smart thinking thwarted a phishing scam that could have resulted in a hefty financial loss for one doctor.
Accountants who are members of the Association of Independent Specialist Medical Accountants (AISMA) were tipped off about the incident by a colleague so that they could make their doctor clients aware of it.
The doctor was using an NHS email address to conduct business with the accountant. At the end of the day on the Friday, the doctor emailed a query about a tax payment.
On the following Monday, the accountant received the exact same email again, apparently from the doctor, word for word. But it was not a forwarded message. This arose his suspicions and he called the client to discuss.
The doctor then said he had been
in contact with the accountant via email over the previous few days about submitting payment to a different bank account. He recognised that the sort code and account number were unfamiliar, so did not proceed with the payment.
AISMA reports: ‘Having checked the email records, it transpired that the client was having an email conversation with a cybercriminal masquerading as the accountant.
‘The hacker had created a very convincing email, replicating the layout of the accountant’s email, including his personal signature.
‘The email address looked the same as the accountant’s email address, but on closer inspection an ‘O’ had been replaced with a zero, a very subtle change that was hard to spot at first glance.
‘So, it is likely that the client’s email account had been compromised in some way, this could be via redirecting messages, or the password was leaked and the hack-
The rise of the robots at King Edward VII unit
Four colorectal surgeons from Precision Surgery Group are delivering a new robotics surgery service at London’s independent King Edward VII’s Hospital. The team includes two of the UK’s most experienced surgeons in the field of colorectal robotics, Mr Danilo Miskovic and Mr Charles Evans, with Mr Alexander von Roon and Mr James Kinross. Between them, the team has performed more than 500 major robotic colorectal procedures and will now work exclusively at the hospital.
The hacker created a very convincing email, replicating the layout of the accountant’s email
ers had full access to the client’s inbox.
‘Fortunately, in this scenario, both the client and the accountant spotted the ruse and were not fooled by this elaborate attempt to steal money.’
The association issued some tips to help you stay alert and spot
phishing attempts like the one described here:
➲ Be wary of any requests to pay into a new or different account. This is known as a ‘call to action’ and is a common trait in phishing emails. If you are unsure, phone and speak to the person involved.
➲ Look at the tone of the email: is it like a normal email you would receive from this contact? In this scenario, the requests from the hacker had grammatical and spelling errors.
➲ Never email personal or confidential information like bank account details or any personal identifiable information that can be used by cyber criminals. Use a secure method to transfer sensitive information like password protected attachments or use secure online portals.
➲ Protect your online accounts with a strong password and enable two-factor authentication wherever possible.
Mr Von Roon, clinical director for general surgery at King Edward VII’s, said: ‘Coming together as a team to deliver this service provides specific advantages. Not only does it improve the quality of care, but it allows us to collect important outcomes data using new digital technologies.
‘This is a key teaching tool that not only aids us in driving innovation safely forward, but it standardises best practice and, most importantly, improves the quality of our patients’ lives as well as their outcomes.’
will improve patient outcomes and further enhance quality and safety.
‘The new service is part of a broader plan for the hospital, strengthening King Edward VII’s Hospital’s reputation as a centre of excellence in key clinical specialties.’
(Left to right) Surgeons Danilo Miskovic, Charles Evans, Alexander von Roon and James Kinross
PHIN’s data study will help doctors
By Olive Carterton
A new research project aims to give consultants more meaningful feedback about the work they do in private practice.
It will initially focus on three projects: patient reported outcome measures (PROMs), adverse events and the substitution of care between the public and private healthcare sector.
The work is being carried out under a partnership between the Private Healthcare Information Network (PHIN) and the Department of Health Policy, London School of Economics and Political Science (LSE).
PHIN chief medical officer Dr Jon Fistein told Independent Practitioner Today : ‘Our partnership with LSE will allow us to adopt an academic approach and understanding to our data insights.
‘This will strengthen our work, providing meaningful insights and feedback to consultants from their private practice data, as well
as supporting the publication of fair and accurate performance measures on our website.’
The partnership – one of the first academic partnerships focusing on private provision of healthcare in the UK – will look at maximising the use of PHIN data for understanding the quality of care within sector.
PHIN said the link-up would produce ‘high-quality and impactful research that will benefit patients and demonstrate the potential of the unique data PHIN holds to a wider audience.’
The partnership has begun with
Pancreas cancer first for The London Clinic
The London Clinic has announced it is the first independent hospital in the UK to employ OncoSil, a ‘breakthrough’ new treatment for pancreatic cancer.
This is a single-use brachytherapy device (internal radiation) that delivers a pre-determined dose of beta-radiation directly into cancerous tissue.
It is used in combination with chemotherapy to treat patients with locally advanced pancreatic cancer.
The hospital said the new nuclear medicine therapy was an option for treating locally
advanced pancreatic cancer where the tumour is unresectable.
Beta particles emitted by OncoSil cause damage to cancer cell DNA, which renders them incapable of further cell division which can ultimately shrink the tumour mass.
The treatment has been shown in clinical studies to increase overall survival and lead to downstaging, allowing patients to undergo surgery to remove their tumours. This surgery statistically improves the five-year survival rate from ~7% to >20%.
Implantation is an outpatient
This will strengthen our work providing meaningful insights and feedback to consultants from their private practice data
DR JON FISTEIN, PHIN CHIEF MEDICAL OFFICER
PHIN’S LATEST FIGURES
19 the number of serious safety incidents (‘never events’) reported across 272 independent and NHS hospitals treating private patients from 1 October 2019 to 30 September 2020. This compares with 20 between 1 July 2019 to 30 June 2020.
247 The number of reported healthcare associated infections in the year across 1.1m bed days at sites where PHIN could calculate a rate.
49 The number of reported surgical site infections (SSI) across 21,452 patients undergoing hip and knee replacement procedures.
the secondment of a research officer from LSE to PHIN, Dr Michael Anderson, who is also a practising NHS GP and currently undertaking a PhD in health economics and health policy.
Dr Anderson said: ‘There are only a few pre-existing studies which explore quality issues in the private healthcare sector in the UK, so this remains a gap in the literature and a relatively untapped area for health policy research.
‘We are therefore very grateful to be one of the first research institutions granted access to PHIN data for this purpose.’
539,720 The total number of private spells in the UK, down from 605,110 in the earlier period. PHIN has also published statistics on NHS volumes in facilities which treat private patients – including all independent and NHS hospitals which treat private patients. This was to ensure that people using its website could get a more complete understanding of the scale and nature of treatment offered at hospitals where they might be considering private care.
Oncosil delivers radio-active microparticles straight to the pancreatic tumour. Dr Zarni Win (right)
procedure which takes around 60 minutes.
Dr Zarni Win, radiologist and nuclear medicine physician at The London Clinic, said: ‘I am particularly excited about this new therapy, as it now offers a much higher chance for pancreatic cancer patients with locally advanced disease to undergo curative surgery
following OncoSil therapy, compared to a pessimistic outcome with conventional treatment.’
Nigel Lange, chief executive and managing director at the makers, said: ‘This provides patients and their clinicians with an encouraging new approach and hope in a disease where there has been little advancement for decades.’
Points system for late payers of tax
By Vanessa Sanders
New rules are being introduced for late filing and late payment penalties for income tax self-assessment.
It will apply with effect from 6 April 2023 for taxpayers within the Making Tax Digital regime – those with business or property turnover of more than £10,000 per year –and 6 April 2024 for other selfassessment taxpayers.
Late filing or submission penalties
A points-based system is being introduced, meaning each time a taxpayer misses a submission deadline, they incur a point.
The taxpayer becomes liable to a fixed penalty of £200 upon reaching the points threshold.
The threshold depends on the submission frequency: annual accrual = two points; quarterly = four points; and monthly = five points.
The points incurred will expire after 24 months, providing the
taxpayer remains below the threshold.
Once the threshold is reached, all points will expire if the taxpayer meets their return obligations for a set period.
This period is based on their submission frequency: annually, 24 months; quarterly, 12 months; monthly, six months.
If the taxpayer continues to miss deadlines after they reach the points threshold and has been issued with a penalty, they will become liable for further fixed-rate penalties as additional obligations are missed.
But a taxpayer will not be liable if a reasonable excuse for not submitting on time is provided, and there is a right of appeal against both points and penalties.
Late payment penalties
There will be no penalty for tax paid late but within 15 days of the due date.
The first penalty thereafter is set at 2% of the outstanding amount if
payment is made between 16 and 30 days after the due date.
This rises to 4% of the outstanding amount if tax is left outstanding 30 days after the due date. A second penalty is charged at 4% a year, calculated on a daily basis on the total amount outstanding after day 30.
To avoid or reduce penalties, the taxpayer can approach HM Revenue and Customs (HMRC) to agree a Time to Pay Arrangement. The approach is likely to have to be made in person and usually involves discussion of affordability.
But our experience shows that HMRC has little sympathy for what it may consider to be extravagant lifestyle choices, such as private school fees, expensive vehicle lease payments and an unwillingness to cash in ISAs.
Vanessa Sanders is a partner with accountancy, finance and tax advisory medical specialists, Stanbridge Associates Ltd
Oncology equipment firm gears up for expansion
Global oncology provider GenesisCare has appointed Justin Hely as its new UK general manager.
The company said Mr Hely would help guide the expansion of the organisation’s clinics and treatment centres across the UK.
In the past 24 months, the company has added two new centres to its network with the opening of an advanced radiotherapy centre in Bristol and the launch of ‘Europe’s most advanced radiotherapy centre’ at London Cromwell Hospital.
This offers patients access to the MRIdian MR-Linac, Gamma Knife Icon and Varian Edge Linac treatments.
It has introduced several innovative oncology services and technology, including ViewRay’s MRIdian MR-Guided Linac, Stereotactic Radiosurgery (SRS), Theranostics and the national roll out of spacing gel which is provided as standard for all our prostate patients.
GenesisCare said it had strong relationships with major healthcare insurers and would be launching digital innovations to streamline clinical referral processes.
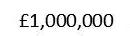
Compiled by Philip Housden
Oxford hospitals considering options to develop private patient business
Oxford University Hospitals Trust (OUH) is considering another partnership with a private hospital operator.
The £960m-turnover trust earned £8.1m in private patient income in 2019-20 – 0.84% of all patient income. This ranks it 13th in the NHS and third outside London and enjoying growth of 18% in 2019-20.
Now it is sounding out the market for expressions of interest to learn if UK and international private hospital groups are potentially interested in a partnership to jointly develop a long-term private
patient business across some or all OUH’s clinical specialties and four main sites.
The trust’s private patient growth plans have previously involved the joint venture approach.
However, a partnership with the Mayo Clinic to open an outpatient and ambulatory London base, which led to the development of a six-story diagnostic and outpatient clinic in Portland Place, was abandoned last year when, just five months after opening, the Mayo Clinic bought out the trust to become sole owner.
Might PHIN support changes to PPU data submissions?
PPU Watch has learned that the Private Healthcare Information Network (PHIN) is working with NHS Digital on a project aiming to
simplify the data submission process.
The ADAPt project pilot studies will start later this year aimed at achieving the creation of a single, national dataset for private and NHS elective activity that incorporates PHIN’s private data into NHS Digital’s systems.
Any NHS private patient units interested should contact hospitals@phin.org.uk.
What a difference a year makes . . .
More than 100 delegates attended the sixth annual NHS Private Patient Units national conference just over a year ago, held at St Thomas’ Hospital, London.
The message from speaker after speaker was that PPUs are growing and should be confident of longterm success.
However, we all know what happened next. As this column has reported, the last year has been a tough one for PPUs, with an average of perhaps 75% reduction in incomes from private patients for NHS trusts.
But I am pleased to say that, looking ahead, optimism is now returning and many PPUs with continued restrictions are aiming to re-open their capacity and services for private patients in the summer.
In response, this year’s national conference is now to be rescheduled to late 2021. PPU Watch will be reporting on all these developments and more in the coming months.
Philip Housden is a director of the Housden Group. See his feature article on PPUs in the northern home counties on page 38
By a staff reporter
Menopause Plan, a new product from Bupa Health Clinics, gives women 45 minutes with a trained menopause GP who will develop a personalised care programme for managing their symptoms.
Customers will then have a follow-up appointment 12 weeks later and a year’s access to Bupa’s Anytime Healthline, a 24/7 nurseled service.
It is thought that many women miss out on more support from their GPs because training in identifying and managing the menopause is not a compulsory part of GP training. NICE guidelines only came into place in 2015.
Bupa Health Clinics commercial director Alaana Woods said: ‘A 45-minute appointment with a GP who is trained in this area is invaluable, especially for women who find it difficult to open up or are embarrassed by symptoms they’re experiencing.
‘We’re also incredibly proud to partner with the charity Wellbeing of Women and will be giving 5% of each Menopause Plan sold to them to help fund vital research into women’s health.’
Wellbeing of Women invest in pioneering research which helps find cures and develops new tests and treatments that will change the lives of women, girls and babies.
Janet Lindsay, chief executive of Wellbeing of Women, added: ‘The menopause directly affects half the population, yet it has remained a stubbornly taboo topic.
‘Supporting women through this stage provides opportunities to help them manage any symptoms, promote healthy lifestyles and prevent diseases such as osteoporosis and cardiovascular disease.’
Bupa has also launched its new women’s health hub, which is accessible to everyone and aims to be a go-to source of information and guidance on topics covering women’s health events, from periods to menopause.
New Bupa service for menopause Get defence body help quickly
Doctors are being urged to seek support early on if they are aware of a potential complaint.
All doctors are likely to face a complaint at some point in their career, but it is feared the pandemic may result in an influx of patient complaints resulting from issues such as delays in diagnosis, treatment and referrals.
Dr Caroline Fryar, head of advisory services at the Medical Defence Union (MDU), said this was of particular concern, as many complaints had the potential to
become claims for compensation in the years ahead, which was worrying for many doctors.
‘Consequently, the stress of dealing with complaints and claims far into the future could push many doctors to breaking point.’
She was speaking as the MDU revealed results of a survey of 741 doctors in partnership with the Healthcare Leadership Academy.
Among the 40% who were GPs, nearly half of complaints were made within the last five years and a similar percentage were related to
an alleged delayed or missed diagnosis. But 40% of complaints were resolved locally within the individual’s own clinical team.
GPs stated that the commonest reasons for a patient complaint included increased waiting times for treatments, delays in accessing screening and tests, communication difficulties and consulting with patients online.
In the last year, consultants were the most likely to face a complaint due to treatment complications (30%) compared to 5% of GPs.
Proton beam training expanded
Proton beam therapy services provider Rutherford Health has expanded its proton training programme for oncologists to meet rising demand.
The course was designed with the University of Pennsylvania and IBA Worldwide, the largest maker of proton therapy machines.
It gives oncologists certification to administer high-energy proton beam therapy in cancer patients. Thirty-five oncologists have become certified in proton beam therapy since the training began three years ago and 20 more begin the programme in the next two months.
The two-part programme involves an e-learning module called Oncolink, delivered by IBA Worldwide, followed by a course with Pennsylvania University, currently done virtually due to the pandemic. The course takes two weeks to complete depending on the flexibility of trainee oncologists.
How to care for staff when your clinic opens again
Employers are being encouraged by The Regenerative Clinic, based in London’s Harley Street medical area, to foster an open dialogue with staff to make all team members feel safe and well looked after as they adapt to new ways of working.
Guidelines it has issued for businesses stress the importance of looking after their staff’s general well-being and keeping in touch with them.
They suggest: ‘You should show concern for their physical and mental well-being whether they are in the office or working remotely.
‘Facilitate a culture of holistic care by encouraging them to take time away from their desks, create walking meetings and encouraging physical activity and a good diet.’
The clinic said every business would have a view on what is right for them culturally. ‘Some businesses will return to work flexibly, giving their people the opportunity to work from home on a more permanent basis. But that is not right for every company.’
It warned that the need for testing and flexibility was likely to continue in some version for the next 12 months at least.
The Regenerative Clinic has its own Covid-19 testing facility with a 24 hour on-site laboratory, plus a clinic in Manchester Piccadilly.
The Regenerative Clinic chief executive Simon Checkley said: ‘There is much to be optimistic about in the coming months, but businesses should be realistic that risks still remain.
‘There is a balance to be made in re-activating your teams, having face-to-face to meetings and in returning to the social working norms that are so productive and often enjoyable for staff.’
See our feature on ‘How to be a flexible working winner’ on p20 in our February issue and online
By Robin Stride
Calls are mounting to begin the task of planning a huge defence cover shake-up for independent practitioners.
Leaders from a range of interests in the private healthcare sector are keen to see discretionary defence cover replaced by a much fairer system.
Their views were aired at a digital conference attended by an audience of 200 interested parties, including consultants.
The LaingBuisson event considered three key questions:
Is there a growing problem of identifying where liability sits?
Is there a fix?
Does the sector want to take control and implement a fix?
The consensus of the conference was a ‘yes’ to all.
Meeting chairman Stephen Collier, who was an independent adviser to the Paterson inquiry and is chairman of NHS Professionals, said the private sector in the UK had generally sorted out the liability question for employed consultants and for NHS caseload. But a gap remained where a patient suffers harm and a consultant is not an employee. To
Cyber attacks in pandemic surge Reform urged for medical defence
The pandemic saw a surge in ransomware attacks.
During this period, data extortion become the most used attack method – with 1,430 incidents reported globally in 2020.
The healthcare sector ranked in the top five most targeted by ransomware data extortion last year, reporting 97 incidents, according to data from cybersecurity tech -
whom should the patient direct themselves ?
Some medical malpractice policies side-stepped this by writing cover where the private hospital was legally liable to pay.
But the challenge created then was that only a law court could give a definite answer on whether in any particular circumstance the hospital was legally liable to pay. This then forced parties back into litigation.
The former BMI Hospitals boss said any resolution would need a sector-wide approach. It could wait for regulators or government to impose a resolution or it could take the initiative and design something that worked. This was the challenge the sector really faced.
Key speaker Cathy Vickery, vicepresident of legal services at HCA Healthcare UK, told the seminar that hospitals recognised this as a difficult area and wanted to do the right thing for their patients.
She added: ‘I personally think unregulated discretionary cover has had its time.
‘I think it’s been fantastic in the past, but the instances where the provider is exercising discretion effectively to pull it are becoming
more frequent and that’s often at a time when patients need it the most.’
David Hare, chief executive of the Independent Healthcare Providers Network, agreed that discretionary cover had served consultants well over the years, and much of the medical defence organisations’ work had been effective.
But he, too, believed the time had come to look at an alternative, warning: ‘If we don’t, it will be imposed upon us.’
He hoped in the next few months the various parties could be brought round the table to take things further.
Mr Hare said it would not be enough for the sector to come together and propose what it wanted to do. It would need to work collaboratively with others, including the NHS. The Government would expect that.
Discretionary cover’s differences from insurance mean it is not contractual, there is no ombudsman, and it is not regulated.
Recommendations in the Paterson Report a month before the pandemic’s first lockdown last year included a call for an urgent review of medical indemnity to
Surgeons start same-day clinic for retinal detachment
prevent discretionary withdrawal of cover.
From the defence body side, Dr Rob Hendry, medical director at MPS partnerships, agreed the discretionary model had worked well in the past and had given medical defence organisations (MDOs) flexibility to address some ‘unusual situations’. It had largely been used to the benefit of doctors and patients.
But he agreed the world was changing and the Government had issued discussion documents about the future of medical indemnity.
He said he would like to see the best bits of insurance and indemnity in some way combined in an integrated approach that was to everyone’s advantage.
Asked if there was still a role for MDOs, he argued there was. They had an insurance capability and a main reason doctors joined them was for the wider protection available, including help with regulators, coroners, support if charged with criminal offences, risk management and prevention work.
mature babies at Great Ormond Street Hospital, the vitreoretinal clinic offers a full range of elective treatments for conditions including eye floaters, epiretinal membrane and macular hole.
nology company CrowdStrike Intelligence services
A growing trend in ransomware actors targeting countries’ healthcare organisations began to form early last year as nations worldwide declared public health emergencies and hackers tried to access sensitive information relating to Covid-19 positive cases and scientific research into possible treatments.
Independent eye clinic Ophthalmic Consultants of London (OCL) has launched a new vitreoretinal service that includes emergency, same-day surgical treatment for patients suffering retinal detachment.
Led by surgeon Mr Chien Wong, who is head of the UK national retinal detachment centre for pre-
The team has been joined by Mr Lorenzo Motta, a vitreoretinal surgeon at East Kent Hospitals University NHS Trust.
OCL reports a surge in demand following the dramatic lengthening of NHS wait times due to the pandemic.
In January, 36.5% of NHS patients referred for eye surgery in England had been waiting more than 18 weeks for treatment.
Conference chair Stephen Collier
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2011
Bupa claims clients back its reforms
Eighty-six per cent of Bupa customers thought the insurer should negotiate the best prices with consultants and hospitals to manage costs on their behalf.
An independent ICM poll of the insurers’ customers found:
87% expected the insurer to pursue value for money on their behalf;
74% thought some consultants charged too much for treatment;
87% agreed consultants should inform patients of the consultation cost and likely cost of any subsequent procedure or treatments before an initial appointment;
84% thought that consultants should ensure patients were aware of outcome data for their treatment and the consultants’ success rate with that treatment;
76% believe health insurers should use medical evidence to help prevent members from undergoing unnecessary and ineffective treatments;
84% of Bupa members thought health insurers should monitor consultants and hospitals to ensure high-quality care was given and that costs were managed.
More people ask about self-pay
Two-in-five GPs reported a rise in the number of patients asking about self-pay treatment options compared to the year before.
Half of the GPs responding to a Spire Healthcare survey said they believed the private sector offered good value for money for patients who seek self-pay treatment or use their private medical insurance.
MDU’s U-turn on indemnity cover
Doctors facing subscription rises with the MDU were saved even bigger increases because the body reverted to discretionary cover rather than insurance, it said.
The defence body said many private doctors would pay around 9% more for cover but they could have been hit with hefty doubledigit subscription rises without its U-turn.
Medical tourists quit
Private doctors in the UK were risking losing out on a medical tourism boom because they were not harnessing marketing opportunities, we warned.
A survey of the international medical travel sector found widespread optimism about the future of medical tourism, despite the economic downturn, with travel for beauty surgery expected to be the biggest growth area.
But it was feared that other countries were likely to cream off much of the overseas patient potential.
Medical travel expert Keith Pollard warned the UK ‘continues to sit back on its laurels’ when it comes to the medical travel sector.
He had just returned from Monaco where the International Medical Travel Exhibition and Conference featured 24 countries with a significant representation. But UK presence was ‘zero’.
Another rise in pension contribution
Private doctors who paid into an NHS pension were feeling the pinch after being hit by the second contribution hike in 13 months.
Some saw deductions of up to 13.3% of their pay from this month at a time when they were hurting from a one-year extension to an NHS salary pay freeze.
The Department of Health implemented the first of its annual pension rises in April 2012, when the average consultant’s contributions rose from 8.5% to 9.9%
Private patients boost NHS
Private patient income of NHS trusts rose by 5.3% to £471m in 2011-12.
According to market analysts LaingBuisson, growth was stronger in London, with the top five private earners seeing combined revenues climb by 15%. These were Royal Marsden, Royal Brompton & Harefield, Guy’s & St Thomas’, Moorfields and King’s College.
Revalidation is IDF’s gain
A 26% membership rise for the Independent Doctors Federation (IDF) saw its numbers increase to 1,140. Much of the membership rise resulted from doctors joining for appraisal and revalidation, using the IDF’s designated body status.
Share your experience of what has and has not worked in your private practice. Even if it’s bad news, let us know and we can spread the word to stop others falling into the same pitfalls.. Contact editorial director Robin Stride at
ACCOUNTANT’S CLINIC: THE BUILDING BLOCKS OF ACCOUNTANCY
Julia Burn continues with her A-Z of top tips. This month she turns to the letter T
is for tax to of top tips
An update following the Budget and how it may affect you and your business
DESPITE ALL the leaks, last month’s Budget still contained some surprises. My review at that time on Independent Practitioner Today’s website summarised the key points affecting doctors in private practice.
Now the dust has settled, here is more detail about the practical aspects of these new measures.
Support measures
During the pandemic, the Govern-
ment has offered various support for businesses.
The following changes to the key support measures were noted in the Budget speech:
Coronavirus Job Retention Scheme (Furlough)
The furlough scheme which was due to come to an end has now been extended again to September 2021.
This is a welcome measure for
businesses who have had to close their doors and continues to give assistance to businesses allowing them to be flexible while lockdown eases.
Businesses will be asked to contribute 10% of the furlough amount in July and 20% in August and September.
Now that lockdown is gradually easing, businesses can start to return to some normality and hopefully begin to take staff off fur-
lough as and when normal services can resume.
Rates
The business rates holiday has now been extended to the end of June, followed by a six-month period where the discount will be twothirds. Relief is capped at £2m per business.
This is a welcome measure for practices who have had to close their doors to face-to-face consul-
tations and goes a little way to sheltering the losses they may have encountered.
Funding
Additional funding may also be available through the Recovery Loan Scheme, but we await the details of eligibility criteria and how to apply.
The previous Coronavirus Business Interrup tion Loan Scheme (CBIL) and bounce-back loan schemes closed to applications at the end of March 2021.
TAX
Income tax
The tax-free personal allowance at £12,570 has been frozen from April 2021 to 2026. While not strictly a tax rate rise – allowing manifesto promises to be honoured – in real terms, people’s take-home pay will reduce, as these allowances have not kept pace with inflation.
Likewise, the higher rate income tax threshold of £50,270 has been frozen from April 2021 to 2026. Income tax rates also remain unchanged.
Businesses should start to regenerate now that lockdown is easing, but it will take the economy a long time to recover. There will still be an element of inflation expected between now and 2026, so people will feel the pinch of this with the cash they have available to spend.
The pension lifetime allowance has been frozen until 2026.
This measure could have a real impact on long-term pension savings and may actually encourage those people on attractive defined benefit pension schemes – for example, NHS consultants – to retire earlier than planned so that they can avoid the punitive 25% surcharge tax associated with pension savings in excess of the lifetime allowance threshold.
This point is highly relevant to doctors who have a substantial amount of funds tied up in the NHS defined benefits scheme.
The current pensions lifetime allowance is £1,073,100. This is a limit on the amount of accumulated pension savings which can be held without triggering a pension charge.
Now would be an appropriate time to consider your options and discuss the best way forward for
A super deduction for investment in innovation of 130% of expenditure has been introduced which may be accessible for medical practitioners involved in clinical research or planning significant capital expenditure
The Chancellor announced that companies will be able to carry back losses of up to £2m against profits made in the prior three years.
This can be a welcome relief to businesses who have made large losses due to the pandemic but have been previously profit-making and would create a cash injection at a potentially crucial time.
It is, though, worth careful consideration where companies are going to enter the higher corporation tax band of 25% in 2023, whether to carry back any losses, therefore saving taxes at 19% and receive cash now or carrying them forward to make savings in the future at 25%.
Super deduction
you with your independent financial adviser.
Corporation tax
The Government had re-introduced a tiered rate of corporation tax. The rate for small companies, with profits chargeable to corporation tax of less that £50,000 a year will remain at 19%.
For companies generating profits of £250,000 or more a year, the corporation tax rate will rise to 25%, which is a huge jump in tax rates.
Companies generating profits of between £50,000 and £250,000 will receive an element of taper relief, so only those earning profits of over £250,000 will be taxed at the full 25% rate.
Thankfully, these measures are not coming into effect until April 2023.
Where the pension lifetime allowance has not been reached, it may be worth considering companies making a pension contribution on behalf of its employees as part of their remuneration package.
The pension payment is an allowable deduction from profits chargeable to corporation tax and could therefore mitigate some of the additional tax suffered by those companies falling under the new 25% charge.
to Business Asset Disposal Relief –previously known as Entrepreneurs Relief – which currently has a lifetime allowance of £1m.
This is likely to be welcome news for those practitioners looking to dispose of their companies in the near future and wanting to take advantage of this relief.
Stamp Duty Land Tax
The Stamp Duty Land Tax (SDLT) holiday has been extended to the end of June. After that, property sale completions occurring before 1 October 2021 will benefit from a reduced nil rate band.
This will mean that the first £250,000 of the price of a property will not attract SDLT. Currently, no SDLT is payable on the first £500,000 of the price.
A super deduction for investment in innovation of 130% of expenditure has been introduced which may be accessible for medical practitioners involved in clinical research or planning significant capital expenditure.
Companies that acquire new plant and machinery assets qualifying for capital allowances will be entitled to a tax deduction of either 50% or 130% for expenditure incurred between 1 April 2021 and 31 March 2023, with the 130% rate expected to apply to the majority of qualifying assets.
Where companies have made future plans to invest in new capital equipment, it is a good time to consider whether it is possible to bring this investment forward to enable them to benefit from these enhanced reliefs.
Careful consideration needs to be made if it is likely that these assets will be disposed of in the future as this would create an additional tax charge.
Inheritance tax
There have been no changes here and the inheritance tax threshold remains at £325,000, meaning more estates will be captured, as the threshold has not increased in line with inflation.
Capital gains tax
There have been no changes –even though these were expected to change. The annual exemption, which is currently £12,300, remains frozen until April 2026.
Also, there have been no changes
The second holiday is up to £12,500 less generous to buyers, which will encourage people to complete on properties before 1 July 2021.
This will be especially relevant to practitioners who currently own properties that they are looking to dispose of.
The future
The cost to the economy of the pandemic cannot be underestimated, and the measures Rishi Sunak has put in place will start to compensate for the shortfall, but there will inevitably need to be additional measures in the future.
He also noted the cost of interest on these borrowings, acknowledging that this had become more expensive for the Government in recent weeks.
Undoubtedly, further tax rises are coming, but some of the predictions that have been made about other tax rises did not happen in this Budget – for example, the muted increase in Capital Gains Tax.
But surely this will be revisited in future Budgets.
Julia Burn (below) is a director at Blick Rothenberg and part of the team that advises medical practitioners
Monitoring doctors wherever they work
Independent Practitioner Today readers will know the Independent Healthcare Providers Network (IHPN) is committed to playing its role in supporting all our members and the people that work with them, says David Hare (right)
AS THE trade association representing healthcare providers across the independent sector, we also want to deliver the best possible care to patients and drive continuous improvement of safety and quality in the sector.
A key part of this is around improving consistency in safety and medical governance, something the Care Quality Commission has highlighted as an area for improvement in recent years. The subject is a key issue raised by the Paterson case.
In 2018, the IHPN therefore began the development of a Medical Practitioners Assurance Framework (MPAF) led by former NHS England national medical director Sir Bruce Keogh.
The framework’s aim is to support improvement and consistency in the oversight of medical practitioners in the independent acute sector.
It seeks to identify expected practice and set out clearly where responsibility lies for ensuring the best available care possible for patients across the following areas:
Creating an effective clinical governance structure for medical practitioners;
Monitoring patient safety, clinical quality and encouraging continuous improvement;
Supporting whole practice appraisal and raising and responding to concerns.
Critically, the framework was designed to be a ‘live’ document and provide a contemporary consensus view of expected practice,
How we reported on the impact of the Medical Practitioners Assurance Framework in November 2019
giving confidence to patients and regulators over ‘what good looks like’.
Over one year on from its launch, IHPN is pleased to have finished an independent assessment of how the framework is being used by independent providers and practitioners and how it can be further improved on.
Tangible changes
Despite the impact of Covid 19 on the independent sector and wider healthcare system, the framework has been wholeheartedly embraced.
There are high levels of awareness and support for the principles contained in it among independent sector medical directors, registered managers and medical advisory committee chairmen.
And critically, it has led to some tangible changes and improvements in providers’ governance processes and frameworks.
We were pleased to hear from
independent practitioners about the benefits they felt the MPAF had brought to their organisations.
These included ‘much clearer understanding of roles and responsibilities for individual practitioners and awareness of proper engagement with governance and assurance processes’ and greater importance given to ‘peertopeer working, with emphasis on multidisciplinary team (MDT) approach to practice and management of complex cases’.
Our review did, however, highlight the importance of ongoing engagement with practitioners about the MPAF.
Making
relevance clear
In particular,targeted communications for those working in the sector were suggested, including how the MPAF relates to other safety and governance frameworks so that its relevance and impact on the practitioner’s practice is clear.
Further communication about the MPAF from independent providers to all medical practitioners with practising privileges, including potentially incorporating knowledge of the MPAF principles into the annual or biannual review of practising privileges, was also suggested. IHPN will look into supporting both of these suggestions.
Our review also found that those working in the sector are keen to build on the MPAF. In some key areas there is appetite to develop the framework’s principles even further.
This includes more clarity
around standards and best practice for MDTs; obtaining data on a practitioner’s whole scope of practice; and clarity about how medical appraisal outputs are used to support medical governance.
IHPN is also looking into how it can further embed the framework in the medical practitioner community and particularly with smaller independent providers.
Greater collaboration
Responding to the coronavirus pandemic has undoubtedly been the focus for the whole of the healthcare system in the year following the MPAF’s launch.
But with much greater collaboration between independent and NHS providers as part of the Covid response, it is even more crucial to ensure the full implementation of the MPAF and a genuine ‘wholesystems’ approach to safety and governance, particularly evaluating scope of practice.
We thank all practitioners working in the sector for their engagement with this issue and we look forward to working with them over the coming months and years to further embed the MPAF. This will help continually improve the safety and quality of care delivered by independent sector providers to both NHS and private patients.
See how MPAF is working in practice in ‘Single spot for doctor’s data’, page 24
David Hare is chief executive of the IHPN
MAKE YOUR MONEY WORK HARDER
No ordinary account
Paul Forder, senior area manager at the Wesleyan Group, explains how independent practitioners can get the most out of money they have saved in growing commercial
accounts
AS THEIR practices have flourished, many independent practitioners have been saving their profits into standard commercial bank accounts.
Faced with the risk of large tax charges for withdrawing funds from their businesses, doctors often leave these untouched.
However, by doing so, they could be risking their capital losing real term value and missing out on opportunities to put their money to work in support of their own goals.
With this in mind, it’s essential that doctors consider how they can get the most from the money they’ve worked so hard to earn –including commercial investments and pension saving.
Beating inflation
The top commercial account providers in the UK are currently paying 0% interest.
With inflation at 0.7%, 1 this means those keeping their money in low interest commercial accounts will see their funds gradually lose value in ‘real terms’ –effectively reducing their buying power as the price of goods and services rise.
It may sound like an extreme example, but £100,000 left in an account earning 0% interest for the past five years with 2% inflation would now be worth just £90,573 in today’s terms.2
Investing, however, can offer the chance to achieve real term growth by outpacing inflation. There is a range of investment options available. The right one for each doctor will largely depend on their appetite for risk.
For example, investing in stocks and shares may involve more risk
than investing in government bonds – government ‘IOUs’ that pay interest on investors’ money for a fixed period of time, but could bring higher returns in the long run.
Investments are typically held for at least five years, but often longer. If practitioners are likely to need the money sooner, it might not be right for them.
A financial adviser can help assess whether investing aligns with individuals’ financial plans. Potential investors should always remember that the value of investments can go down as well as up, and they may get back less than they invest.
Pension saving
It is never too early to grow pension savings.
While dependent on individual
circumstances, redirecting business savings into pensions could deliver significant benefits for the business as a whole, while providing a taxefficient way for doctors to extract value from their businesses towards their future goals.
For example, businesses can claim Corporation Tax relief against employer pension contributions.
By making an employer contribution to their pension pot –where appropriate – a business owner could grow their retirement funds while reducing the amount of tax their business has to pay.
Meanwhile, saving into pensions can provide inheritance tax benefits and can help to safeguard money earmarked for retirement should a business face liquidation.
Putting funds into a pension might not be appropriate for those
It’s essential that doctors consider how they can get the most from the money they’ve worked so hard to earn –including commercial investments and pension saving
who will need access to the money before the normal minimum pension age of 55 – or 57 when the rules change in 2028.
Practitioners will also need to ensure that they have enough headroom in their annual allowance and lifetime annual allowance to avoid potentially punitive tax charges.
Again, a financial adviser will be able to help assess each individual’s options.
At Wesleyan Financial Services, we understand the unique financial needs of independent practitioners. Our specialist financial consultants can advise on how to get the most out of the money you have saved.
To arrange an initial 30-minute ‘Quickstart’ conversation to discuss your finances , email financialreview@wesleyan.co.uk
References
1. ONS Consumer Prices Index including owner occupiers’ housing costs (CPIH) = 0.7% in February 2021
2. Assuming the lump sum deposit of £100,000 earned 0% interest in an environment of 2% inflation for the last five years
How best to lose
Hate the idea of being a meedja darling and want to know how to alienate journalists? Here we show you some top tips you can implement if – God forbid – you are ever asked to comment on a case or a news story. Tingy Simoes (right) shares the inside knowledge to ensure you’re never asked again
media coverage
WHY WOULD you want to foster close relations with journalists? A lot of the time doctors wonder why the media don’t come knocking more often.
‘But I’m the foremost expert in this area,’ they declare in shocked, hurt accents. ‘Why use *that* guy?’
Journalists have a wide network of experts and publicists that they contact when they’re working on a story.
Like most people, they’ll ring those who they like the best: the friendliest, the ones they’ve known the longest or even the one who is most likely to give them what they want; in other words, they will say anything to get into the newspaper – aka, rent-a-quotes.
See also Clarke’s 4th Law: For every expert there is an equal and opposite expert – known in the legal world as Gibson’s Law: for every PhD there is an equal and opposite PhD!
Let’s posit that you have somehow accidentally stumbled into the realm of being considered a valuable expert by the press, but having positive publicity and growing your practice is the last thing you want on Earth.
Top tips
Never fear! I have a selection of top tips to ensure you can entirely alienate journalists and are able to retreat to the peace and quiet of Mount Olympus.
Firstly, do not be appreciative of the gesture of being called upon. The most ideal scenario is to act indignant that your life has been irreparably damaged by a lowly journalist daring to contact you for comment about Meghan Markle’s bunions.
Make sure you strongly convey they clearly do not know who you are and that you’re doing the Lord’s orthopaedic work and you simply do not know or care who Meghan Markle is.
I have a selection of top tips to ensure you can entirely alienate journalists and are able to retreat to the peace and quiet of Mount Olympus
editing for style rather than accuracy, and don’t hold back on critiquing their word choices.
You got through medical school, so writing for a national newspaper should come entirely naturally to you, duh. Ideally, you should return a piece that reads like something out of a peer-reviewed journal.
Crucially, never forget to criticise their ‘other’ sources. What’s that: the article is quoting more than one expert? Someone other than you? You trained that other clinician – they’re a nobody!
Insider tip
Make this absolutely clear. Whinge about this rival who criticised your Sacred Juvederm technique and threaten to report the outlet to their regulator.
Another good insider tip is to contact the journalist on a daily, or even hourly, basis, demanding to know when the story will run and why hasn’t it run yet. Preferably late in the afternoon, when it’s copy filing time.
Journalists simply don’t get enough emails during the day, and surely you will be making them feel important by flooding their inbox. Their time is not as valuable as your own, of course. You are busy saving the world one nose
job at a time (see above: Lord’s work).
Ultimately, remember that journalists are not normal people like you, with feelings or integrity –and that they are all the same, no matter what their background or how long their career has been.
While some might claim they take their responsibilities seriously – legendary US journalist Joan Kron of Allure’s Scalpel News fame once said to me ‘Every time I mention a doctor, I know I’m putting someone on their operating table’, she probably wasn’t serious.
Media interest will continue in your work, sadly, because you are so truly magnificent. But hopefully by following some of these recommendations, you can alienate enough of the press to make your life bearable.
Please note: this article includes a short excerpt from my book How to Cut it in the Media
Tingy Simoes is an award-winning publicist with over 20 years’ experience, founder and managing director of Wavelength Marketing Communic ations (www.wavelengthgroup. com) and author of the first-ever PR manual for the plastic surgeons and aesthetic professionals, How to Cut it in the Media
For an extra bonus, make their job seem banal and worthless – everyone loves that! Don’t forget to be sniffy about the publication. Stress that neither you nor your patients would ever debase themselves by reading the Mail on Sunday
If, unfortunately, you have managed to be somehow entrapped into commenting because of your undisputed splendour in the particular area of expertise that is required, insist in the strongest terms that they will run their full article past your eagle eye before publication.
And if/when they do provide the copy, concentrate specifically on
Remote prescribing requires safeguards
Claire Garcia (right) discusses the GMC’s updated guidance on Good practice in prescribing and managing medicines and devices, which came into effect
from Monday 5 April
LONG BEFORE the NHS made changes, in response to the Covid19 pandemic, about how it delivered services to patients, the independent sector was pioneering the widespread use of remote consultations
The number of online healthcare providers registered in the UK rose from 14 to 47 between 2013 and 2021. This expansion may have been partly driven by demand from time-poor professionals needing quick access to medical advice, but now many more patients are accessing healthcare online due to Covid and the necessity to control the spread of infection.
So our updated guidance, Good practice in prescribing and managing medicines and devices, is timely and will, I hope, be welcomed by all doctors committed to ensuring a safe experience for their patients.
Digital revolution
Alongside our own call for evidence on remote consultations and prescribing, which we held in early 2020, we also took heed of the safety concerns, such as those in the Care Quality Commission’s report The state of care in independent sector primary care online services
Our call for evidence enabled us to listen to the views, experience, and expertise of more than 70 individuals and organisations. Their input helped us to fully understand how we could ensure our guidance could keep pace with the digital revolution taking place in our healthcare systems.
Since then, patient bodies, including Healthwatch, published
The doctor will Zoom you now: getting the most out of the virtual health and care experience , which sheds more light on experiences and learning from the widescale remote provision of healthcare during the pandemic.
While our prescribing guidance is about much more than remote healthcare, our updated version had to be structured to reflect the new reality that remote consultations are now as routine for many doctors and patients as face-to-face consultations.
But the one thing that remains crucial, as made clear in our guidance, is that doctors must meet our ethical standards regardless of the setting in which they work.
If it’s not possible for doctors to
meet those expectations via a remote consultation, they should switch to face-to-face or signpost to alternative services.
Many online healthcare providers have a business model which relies on digital patient questionnaires, sometimes designed to convert inquiries into sales. Such questionnaires may have a role in providing a satisfactory patient experience that enables quick and easy access to healthcare.
But, as our updated guidance makes clear, prescribing requires a sufficient understanding of the patient, and there is a risk if these systems do not provide that.
Questionnaires for patients should be designed to support a two-way dialogue and, by doing so, allow doctors to meet our professional ethical standards.
Keeping patients safe
One of the key findings from our call for evidence was the crucial role that effective information sharing plays in keeping patients safe – regardless of whether health advice is provided online or face to face. This is especially true when prescribing controlled drugs or other medicines liable to misuse, overuse or addiction.
Here, a failure to share information can mean the difference between life and death. Our updated guidance is clear that doctors must not prescribe these types of medicine without access to medical records unless it’s an emergency and no other suitably qualified practitioner is available without unsafe delay.
Remote consultations are now as routine for many doctors and patients as face-to-face consultations
The fragmented infrastructure of UK healthcare means that doctors in the independent sector are not always able to easily access NHS medical records.
That is why it is so important that independent prescribers should, where necessary for patient safety, seek patient consent to verify information with their GP before prescribing and share information afterwards. Eventually, I hope information sharing between all health professionals involved in a patient’s care will become easier.
But the fact is that each individual doctor is accountable for the prescriptions they sign. They also have a personal and professional ethical decision to make if they feel patient safety is compromised. Where this is the case, they have a duty to raise concerns. Doing so not only protects patients but also protects the reputation of healthcare businesses and maintains confidence in the profession. Good practice in prescribing and managing medicines and medical devices.
How we reported on the new GMC guidance last month
Claire Garcia is policy manager at the GMC
THE POWER OF PEOPLE
You can learn leadership
Jane Braithwaite (right) continues her ‘The power of people’ series by exploring the ways in which leadership skills can be enhanced and highlights the support and tools available to help achieve this
Some leaders make leadership look easy. They come across with both charm and sincerity, generating enthusiasm and support for their ideas and attracting a loyal following. We watch these impressive individuals in awe, admiring the seemingly natural ability they were lucky enough to be born with.
To a certain extent, it may be true that some people have personality traits well suited to a leadership role, but leadership skills can be learned, developed and improved both by experience and more formal training.
The statue of Britain’s wartime leader Sir Winston Churchill outside the Houses of Parliament
GOOD LEADERS energise their teams to succeed and, in every organisation, the ability to do this is an advantage, enabling them to achieve more and to progress at pace. A lack of leadership leads to slow decisions or, worse, no decisions and a lack of progress.
In the past, we have spoken about our three ‘C’s of leadership: Clarity – Clarity of purpose and a relentless determination to achieve that purpose; Communication – To communicate effectively with the team and generate enthusiasm to achieve the team’s purpose; Care – A genuine dedication to the well-being and development of the team.
When we consider the great leaders of our time – for example, Winston Churchill and Nelson Mandela – we see a consistently strong sense of purpose or cause and an absolute determination to achieve success.
And looking at the skills of business leaders such as Tim Cook of Apple and Sheryl Sandberg of Facebook, we recognise the same traits of a strong sense of purpose, but also a huge commitment to building the best team, empowering the team and recognising individuals for the success they achieve.
Great example
A leader who has taken centre stage in the last few months is Brigadier Phillip Prosser, who stepped up to the podium as part of the Government’s Covid campaign on 7 January.
Originally from Wales, Prosser was commissioned into the military in 1992 having completed a degree in engineering. He went on to serve on several occasions in Bosnia, Iraq and Afghanistan prior to serving on home soil as part of the PPE distribution campaign in 2020 and most recently taking lead of the logistics of the campaign to roll out the Covid vaccine.
In many businesses, if someone is good at doing their functional role, they are often promoted into a leadership role with very limited training
succeed is obvious and it is clear he has a very strong sense of purpose in his role as the leader of this cur rent campaign.
Strong, clear communications are demonstrated as he delivers key messages with absolute clarity, and while there are no wasted words, he commands trust and builds a belief that he can deliver as illustrated in the following statement.
‘It is my role to deliver combat supplies to UK forces in time of war. My team are used to complexity and building supply chains at speed in the most arduous and challenging conditions. We aim to deliver vaccine as soon after it is supplied as possible, not leaving vast quantities in the warehouse –it needs to be in arms not on shelves.’
When asked about achieving such ambitious targets, he describes three factors needed to succeed.
Noble purpose;
Dynamic plan;
Amazing teams.
In every conversation I have witnessed, Prosser raises the profile of the NHS team alongside his own team, referring to two world-class institutions and describing the ‘heroic efforts’ being made.
He appears to be a leader who would step back from congratula tions and deflect the compliments and recognition towards the team that he leads.
How does the military train such effective leaders? Most signifi cantly, they deliver extensive lead ership training that is very carefully planned and far more comprehensive than we typically see in business and other govern ment organisations.
A digital prescription platform to allow convenient prescribing from home
CloudRx is a digital prescription system that allows prescribers to create and send an electronic prescription to our fully licensed pharmacy for fast delivery direct to your patient. It can be used from home by doctors working away from their practices.
No cost to prescribers
Simple and quick prescription creation.
Legal paperless prescriptions, including repeat prescriptions and controlled drugs.
Patients receive text and email requesting secure payment. Alternatively, we can invoice the prescriber or clinic each month.
Prescriber Fees can be added if requested
Medicines are dispensed and dispatched by a variety of delivery options
Fully integrated into MidexPRO
Register for free by visiting cloudrx.co.uk
As he admitted himself, he has ‘never battled a virus before’ and so provides a great example of how strong leadership skills can be applied to very different situations. Prosser talks about his current role as a ‘noble purpose’ which marks ‘the beginning of the end of Covid’. This ‘noble purpose’ is his cause and his determination to ➱ p22
In many businesses, if someone is good at doing their functional role, they are often promoted into a leadership role with very limited
“We have worked with CloudRX to maintain a cold chain for the medication and direct delivery to patients at home.”
Dr Charlotte Norton, Medical Director of The Slimming Clinic, the UK’s largest chain of private doctor-led weight loss clinics
training and rely on their natural ability rather to lead.
The ethos of the military is to serve, and doing so is a duty that affects the style of their leaders. A military leader takes responsibility for the well-being of their team and their extended community and prioritises their need.
In a crisis, the team must be motivated and inspired by their leader and they must also have total trust and confidence in them. Often their lives will depend on their leader.
The style of leadership, exhibited by the military is known as transformational leadership, and was initially introduced by leadership expert James MacGregor Burns, who gives us this definition.
Transformational leadership occurs when one or more persons engage with others in such a way that leaders and followers raise one another to higher levels of motivation and morality.
Transformational leadership is widely believed to be the optimal style of leadership largely because most individuals want to experience this type of leadership in their professional lives. Transformational leaders inspire and motivate their team and trust them to make decisions, giving them a greater opportunity to be creative and make changes.
How do we develop our leadership skills?
The starting point for any leader must be self-knowledge and selfawareness. Understanding how we naturally behave as leaders and our strengths and weaknesses is the only sure-fire way to develop our skills and to become better.
Once we understand our current style, we can identify behaviours to improve, explore training and additional support to help us learn to improve.
There is an overwhelming amount of information regarding leadership development which is evidence in itself of how many of us value the development of these skills, but it is hard to fathom where to start.
Developing self-awareness
Most of us believe we have a strong awareness of how we come across as individuals and leaders, but,
Many of us have blind spots and being made aware of them is the basis for improvement
sadly, this is often not the case and how others see us is often quite different to how we perceive ourselves to be.
For example, you may believe you communicate regularly with your team and see yourself as a strong communicator, but your team may feel you are quite closed and need to communicate more.
This is very common feedback from teams when asked about their leader. Many of us have blind spots and being made aware of them is the basis for improvement. Improving self-awareness allows us to understand how others see us, identify any blind spots and allows us to choose to act in some way to improve.
Embarking on a journey to develop greater self-awareness is brave and it is important to remind ourselves that there is no perfect person, no perfect leader and no perfect behaviours. The aim is improvement overall and being the best leader possible for us.
Psychometric tests
One of the most commonly used tools for improving self-awareness in leadership are psychometric tools; for example the Myers Briggs Type Indicator (MBTI).
MBTI is widely recognised to be incredibly valuable and has been used for over 50 years. The tool divides everyone into 16 personality types represented by a combination of four letters as follows:
Extroverted (E) vs Introverted (I);
Sensing (S) vs Intuition(N);
Thinking (T) vs Feeling (F);
Judging (J) vs Perceiving (P).
I really like Myers Briggs, but the terminology used is hard to remember (am I ENTJ?) and so I prefer to use a tool called C-Me profiling.
The concept is similar, but the results are based on behaviours rather than personalities and four colours representing these different behaviours. It is therefore
much easier to remember, as it’s visual. I am a yellow and red.
One of the other benefits is that a team familiar with C-Me can use the colours as a ‘language’ to help them work well together and communicate more effectively.
360-degree feedback
The concept of 360-degree feedback is to gather comments from several sources to be assessed and analysed to identify recurring trends and therefore generate useful data to improve self-awareness and identify areas for personal development.
Ideally, you would include a good number of participants, preferably 15 people, with differing relationships to you.
Aim to choose some contributors who are senior to you, members of your peer group and members of your team so that you really get a 360-degree view. In some circumstances, you might also choose to invite patients to take part, although this is not always relevant when assessing leadership skills.
Many doctors will be familiar with the 360-degree feedback requirement of the GMC validation, which is indeed similar but focuses more on your behaviour as a doctor as opposed to as a leader.
There is no doubt that implementing 360-degree feedback is admin-heavy and you will need to find a good system to support this. There are numerous tools available and specialist companies available to help.
Coaching and development
Greater self-awareness will highlight personal development areas, and these will obviously differ for each individual.
Once you have a greater understanding of the leadership behaviours you would like to focus on developing, it is time to look for support to help you and there is a vast amount of support available.
The number of books and podcasts focusing on leadership is quite astounding and for anyone who is willing and motivated to invest time in reading and listening, so much can be learned in this way.
Most of us are time poor and we need motivation to keep us on track and may wish to consider
engaging a personal coach to support this journey.
Again, the number of coaches available is overwhelming and it is worth investing some serious time into finding the right person with the right skills for you.
Training programmes
Many universities and independent companies run leadership training programmes in a traditional classroom setting or on a virtual basis.
This formal approach can be valuable if you are motivated to gain a recognised qualification that may help you further your career or perhaps you would value the opportunity to step outside your normal environment and dedicate some time to learning.
These courses do require a significant investment in time attending the course itself and completing the set work and, of course, the cost of the course itself.
Summary
Becoming a better leader is an objective shared by many of us and there is definitely a lot of support to help us achieve this goal.
To progress requires an investment of our time to develop greater self-awareness, being honest with ourselves and being brave, potentially listening to feedback that opens blind spots that are unknown and unexpected.
Choosing to act and improve requires self-motivation and commitment but doing so not only improves individuals as leaders in the workplace, but potentially has benefits in our personal lives.
The best leaders, of course, appreciate that as well as developing their own behaviours and leadership skills, they also need to create and manage amazing teams and next month we will explore this topic, discussing tools and techniques to help leaders develop high-performing teams.
If you would like to share your comments regarding leadership or discuss support for you and your team, please do get in touch.
Jane Braithwaite is managing director of Designated Medical, which offers business services for private consultants, including medical secretary support, book-keeping and digital marketing
THE PRIVATE PRACTICE
Independent practice gives you control over the amount of time you spend with patients and the clinical treatments you provide, but how do you maintain control of all your information and use it to advance your practice?
This is where The Private Practice Register comes into its own, explains Fiona Booth (below)
Single spot for doctors’ data
DO YOU know where to find all the different documents you need to apply for private medical insurer recognition or renew your hospital practising privileges?
What about the appraisal information necessary to revalidate and maintain your licence to practise? Or evidence of your expertise such as published articles, qualifications and clinical interests that will help attract new referrals?
Locating that one, all-important certificate in time can become a bit of a scramble, while a change of address or bank might entail hours of calls and emails to ensure that these details are updated on all the relevant systems.
The Private Practice Register (The PPR) is Healthcode’s smart solution to this challenge. An efficient and secure way to collate information and share it when appropriate so that organisations have the correct details about your practice and you can continue to focus on patients.
The anatomy of the PPR
Put simply, The PPR is a secure online platform where you can control your practice information and documents in one place, ensuring they are up to date and accurate.
More than 24,000 practitioners now have a unique PPR profile, at zero cost, which provides a detailed picture of their clinical practice.
Each PPR profile has 11 sections which can hold a wealth of information. These are:
1. Main profile page: Your details and contact information – for example, practice name, correspondence and billing address –registration with one of the statutory health regulators, GMC
The Private Practice Register is an efficient and secure way to collate information and share it when appropriate so that organisations have the correct details about your practice and you can continue to focus on patients
IN A NUTSHELL: WITH A PPR PROFILE, YOU CAN:
Fast-track your private medical insurer recognition
Store essential private practice data in one place
Ensure private medical insurer and hospitals have access to accurate information
Save time when updating your details
Send secure messages to insurers and hospitals in your network
number (if applicable) and membership of professional bodies.
There is also an option to upload a photo and provide a short biography.
2. NHS Practice : The name and address of the NHS trust where you work, job title, start date, end date, uploaded NHS reference and NHS referee details.
3. Private practice : The facilities where you have practising privileges with start and end dates, the type of care provided, patient demographic and practice hours.
4. Scope of practice : The procedures that you are trained and competent to perform and permitted to undertake under your licence to practise. This section is currently being added to the PPR on a controlled basis for GMCregistered practitioners (see ‘what next’ overleaf).
5. Fitness to practise: Your licence to practise, certifications, appraisal information, Disclosure and Barring Service certificate and Information Commis sioner’s Officer registration.
Healthcode’s GMC republishing licence automatically updates The PPR with information from the List of Registered Medical Practitioners (LRMP), including revalidation status, designated body, Responsible Officer and annual retention fee due date.
6. Specialties and qualifications: Details of your primary medical qualification, specialty, sub-specialty and procedures undertaken by CCSD code and description.
7. Medical secretary: Name and contact details of your medical secretary/practice manager and their office hours.
8. Publications: Details of published papers where you are listed as author or co-author, including
Promote your expertise and credentials
Support the independent healthcare sector
the option to include a link or upload.
9. Banking: Payment information for insurers.
10. Indemnity: Your medical indemnity provider and documentation.
11. Insurer recognition: Overview of your recognition by private medical insurers (PMIs).
Make connections
The ability to store all this information securely in one place is convenient, but the real appeal of The PPR lies in the fact that it is a platform which connects all stakeholders in the independent healthcare sector: practitioners, PMIs and more than 300 private hospitals. This paves the way for more effective working practices and communication across the sector. For example:
Private medical insurers – If you have a PPR profile, you can use the platform as a one-stop shop to apply for recognition from the major insurers.
Those new to private practice can save a huge amount of time and avoid duplication by completing The PPR registration form and selecting the PMIs to whom they want to apply. These insurers then have access to all the data necessary to complete the recognition stage.
Nor will you need to inform all your insurer contacts when your details change because they automatically receive update notifications via the PPR, while you will
• Completely open scanner that is well tolerated by claustrophobic patients
• Weight-bearing scans for spine and joints enable a more precise diagnosis
• Patients who are large or cannot lie down can be accommodated
also be notified if your recognition status changes.
Hospitals – Private hospitals that subscribe to the standard PPR service can view the PPR profiles of their consultant population and are automatically notified of updates, saving you the trouble of informing each hospital individually.
You are notified if a hospital wants to amend information about your practice which it believes to be inaccurate, such as practice hours or the date you started seeing patients at the hospital.
A secure network – You can use the PPR platform to access Healthcode’s Secure Messaging service in order to send encrypted messages to key contacts within hospitals and insurers.
Stay in control
You have control over your PPR profile and are responsible for keeping the information up to date.
Access is restricted to organisations that you have authorised within your network for specific purposes. Insurers have read-only access to the data necessary to recognise a practitioner or to validate bills.
Meanwhile, hospitals with a standard subscription have access to the profile with limited authority to correct inaccuracies concerning their own organisation, such as the practitioner’s start date.
When this happens, you are automatically notified so you can
We have just launched a newlook fitness-to-practise section where you can upload and store all your appraisal information in one place
either confirm the update or contact the hospital to query the change.
To protect your privacy, The PPR is fully encrypted and data is stored within a private dedicated infrastructure physically located in the UK.
A back-up copy of the data is taken daily and securely stored in a separate UK hosted disaster recovery facility. Access to your account is controlled by log-in ID and password.
What next?
While it has already become the definitive source of information about independent practitioners, The PPR is continually having its features and capabilities expanded by Healthcode to enhance operational efficiency, information governance and quality assurance within the sector.
We have just launched a newlook fitness-to-practise section where you can upload and store all your appraisal information in one place:
Details of your current appraiser;
The appraisal period;
Summary;
Personal development plan and your full appraisal.
And we are now in the process of aligning The PPR with the principles of the Medical Practitioner’s Assurance Framework (MPAF).
Already adopted by private hospitals and considered evidence of good governance by the Care Quality Commission, MPAF requires hospitals to collate and consider practitioners’ whole scope of practice when awarding or renewing practising privileges.
Whole scope of practice as defined by the GMC means all aspects of your private and NHS practice, not just the procedures carried out at that specific hospital.
This represents a huge undertaking for hospitals and for consultants whose practice will be subject to greater scrutiny, but the new scope of practice section on The PPR is a significant step in the right direction and being rolled out by specialty.
It will initially show CCSDcoded procedures performed by a consultant at private hospital and clinic sites, the number of times they were carried out at each site over a 12-month rolling period, and the last time the procedure was recorded.
This data can be automatically captured from validated hospital bills submitted through Healthcode’s Clearing Service where the consultant is identified as the controlling specialist. It will only be visible to the consultant and subscribing hospitals where they hold practising privileges.
A consultant’s ‘profile’ page on The Private Practice Register. The blue tabs lead to different areas such as ‘scope of practice’ and ‘fitness to practise’
The next phase will be to complete the scope of practice section to match the rest of the data requirements set out in MPAF, including the necessary information about practitioners’ NHS practice.
Developmental work for this is already underway and Healthcode is consulting across the sector to ensure we get it right for all stakeholders.
For example, representatives from the BMA Private Practice Committee, the Independent Doctors Federation and the London Consultants Association have joined our PPR Data Standards Group, which is considering what data should be included in each PPR profile and in what format.
Ultimately, we expect that consultants will be able to apply for practising privileges through The PPR and for this process to fully comply with MPAF principles.
Since Healthcode launched The PPR five years ago, it has evolved into a dynamic online platform that connects you with private medical insurers and hospitals and supports your practice by enabling many tasks to be managed more efficiently.
Most importantly, it helps you manage your practice information at a time when the independent healthcare sector is becoming increasingly reliant on accurate, secure and shareable data.
Fiona Booth is head of external affairs and stakeholder engagement, Healthcode
NHS Pensions & Annual Allowance Tax
Get ready in advance of April 2022 when the proposed changes to the NHS Pensions will allow you to reclaim some or all of any Annual Allowance tax you may have suffered in the past.
With our knowledge and in-house calculators, we will be able to predict in advance and check statements produced by NHS Pensions and Scottish Public Pensions Agency for accuracy for any refunds due.
For further information contact us at aa@semail.co.uk or telephone 01625 527351.
CHECK OUT OUR BUSINESS DIRECTORY
Independent Practitioner Today now features an online advertising directory to complement our journal and website.
Split into ‘business’ and ‘lifestyle’ directories, they list the services independent practitioners need to run their practices or spend their well-earned money on.
To be included, contact Andrew Schofield at Spot On Media Email: andrew@spotonmedia.co.uk.
Drilling down into orthopaedic claims
Clinical negligence claims against orthopaedic surgeons in private practice come under the spotlight here as Dr Gemma Taylor and Andy Norman advise on how to manage risk
THE MDU recently analysed more than 400 claims notified to us in a recent five-year period by members working in independent orthopaedic practice and the issues that lie behind such claims.
We successfully defended 78% of the cases in this review, without paying compensation to the patient.
However, a claim for clinical negligence can be brought many years after the incident occurred, often without warning. Our expert claims handlers and medico-legal advisers understand how stressful this can be and the importance of mounting a robust defence of your position. Compensation is awarded with the aim of returning the patient to the position that they would have been in had the negligence not occurred.
If the injury suffered is such that the person can no longer work and requires a significant level of care, then considerable damages will be paid. The size of damages does not reflect the magnitude of the clinical error, but the injury to the patient.
Reasons for claims
The majority of claims files that the MDU received were due to one of four reasons: postoperative complications, delayed diagnosis, intra-operative complications and consent. Below we look at some of the most common allegations for each area:
Postoperative complications
Postoperative complications featured in almost half of the claims examined. Allegations included:
➲ Long-term pain.
➲ Poor healing and wound infection.
➲ Radial nerve damage and significant loss of function due to inadequate nerve protection during surgical fixation of the humerus.
➲ Femoral nerve damage following knee surgery leading to reduced mobility.
➲ Non-union of fractures due to poor surgical technique; for example, malpositioning.
➲ The use of wrong-sized implants and the failure of surgical components post-surgery.
While orthopaedic claim numbers have not increased in recent years, the cost of claims has spiralled
➲ Inadequate postoperative wound management; for example, an above-knee amputation following total knee replacement.
➲ Postoperative wound infection. In some cases, this led to the failure of joint replacements leading to revision surgery.
Delayed diagnosis
Allegations of delayed diagnosis or referral featured in around 15% of cases. Diagnoses that were allegedly missed or delayed included:
Tendon ruptures;
Sarcoma;
Meningitis;
Vascular necrosis;
Ligament/cartilage tears;
Osteomyelitis;
Dislocations;
Nerve damage.
Intra-operative issues
Ten per cent of claims alleged poor operative technique, during the course of a procedure.
Such allegations included:
Equipment or other foreign body left in the patient after surgery.
Chemical or diathermy burns, scarring or nerve damage.
Incorrect equipment used or the lack of available equipment resulting in surgical procedures being abandoned, delayed treatment and additional procedures required.
Severe bleeding due to perforation or puncture injury.
Nerve damage due to poor operative technique; for example, damage to the sciatic nerve during a total hip replacement, resulting in foot drop.
Intraoperative fractures, such as a femoral neck fracture during hip resurfacing surgery.
Consent
Consent issues featured in many cases, but 10% of claims involved allegations centred on inadequate consent.
The consent process is paramount in managing the patient’s realistic expectations. Failure to either manage those expectations or adequately explain the risks and benefits of the procedure was a common theme across the cohort of claims.
In a number of cases, it was alleged the risk of a worse outcome or long-term damage, including nerve damage, wasn’t properly explained.
Consent cases are often difficult to defend and it is vital to be aware of the impact of recent judgments such as Montgomery v Lanarkshire Health Board (2015) and the GMC’s updated guidance on Decision Making and Consent.
Record-keeping is vital. Without a thorough contemporaneous record of the detailed discussion with the patient about potential risks and benefits, a surgeon can find it difficult to defend allegations of consent, even where their usual practice is to discuss such issues.
Managing risks
Claims involving orthopaedic surgeons are made for a variety of reasons, but there are some common risk factors, which, if managed appropriately, can help to reduce risks.
These include:
☛ Provide patients with detailed information on all treatment options verbally and in writing and ensure they have appropriate time to make a decision.
☛ Consider more conservative treatment options and whether all avenues have been exhausted before recommending invasive procedures to patients – particularly in spinal or joint replacement surgery.
☛ See the patient ‘as a whole’ not just the isolated issue at hand. This includes consideration of comorbidities and psychological factors.
☛ Give appropriate safety netting advice so the patient knows in what circumstances to return for further advice.
☛ Keep detailed records of your discussions with patients including any phone calls by you or your administrative team. Record discussions with other clinicians: GPs, out-of-hours clinicians and other consultants involved in the care process. Many claims are brought a considerable time after events in question, so records can be vital.
☛ Make sure that the full range of equipment and necessary components are available when operating in the private setting. Consider an urgent referral to an NHS hospital if necessary.
☛ Be aware of the increased difficulties when operating on morbidly obese patients. Have a lower threshold for closer postoperative follow-up and early investigation of possible complications and consider whether it is more appropriate for these patients to be treated in an NHS setting with high-dependency care available if needed.
☛ Ensure you have robust postoperative arrangements for patients in the private setting. Remember that you must be contactable or provide appropriate cover and must arrange for prompt assessment of the patient in the event of any issues.
☛ Consider your professional duty of candour. If something goes wrong, apologise and notify the patient and any necessary parties as soon as possible.
While orthopaedic claim numbers have not increased in recent years, the cost of claims has spiralled. This is not due to clinical standards but to a deteriorating legal environment which the MDU is campaigning to reform.
You can see more at www. themdu.com/faircomp
Dr Gemma Taylor and Andy Norman (below) are senior claims handlers at the Medical Defence Union (MDU)
MARKETING AND BRANDING: WEBSITE DESIGN
Tricks to make your website attractive
Last month, Simon Marett and Michael Sullivan delved into the detail behind good logo design and the pitfalls to avoid when you are devising a logo for your practice. Here they look at website design and the key aspects you need to think about before launching a new site
YOU WILL see from the points below that not all of them are design-related and there is a lot you can do in advance by planning properly.
By dedicating time and thought to planning at the start of the process, you will find you will save time, effort and money in the long run.
As with logo design, there are now some online tools and websites available that enable you to ‘do it yourself’, but unless you have the time and patience to learn how to use the software, it is always a good option to appoint a trusted designer or agency.
They will have designed and built dozens of websites and that experience will help guide you through the process.
Here are a few aspects for you to consider:
1
Define the purpose of your website
We get approached by many healthcare practitioners who want a new website. They are often starting their own practice or, in many cases, they have an existing website that they are unhappy with because it is looking tired, dated or needs a refresh.
The first question we always ask is ‘why’? Before you start investing money into website design and build, it is vital that you are clear about the purpose of your website and why you want one.
Is it just a shop front for you and your practice or do you want to enable patients to book appointments online?
Most of the practitioners we work with also want to educate and empower their patients so a blog or resources section of the website will be needed.
You may also want to consider how you are holding patient data and how you want your website to integrate with your patient management system and customer relationship management (CRM) system so you can send patient emails and newsletters.
There are endless possibilities, but the key takeaway here is the importance of planning and asking the right questions that will pay dividends down the line.
2 Use a sitemap
One of the most common mistakes is where time has not been used to think about the structure of content on a website.
An example of a nicely structured site with navigation and sitemap in contrast to an unstructured site
A good example of this is where all the content is placed on the homepage with little thought given to the visitor, the information they might be looking for and how to find it.
We always advise our clients to do some market research and find examples of websites that they like and dislike and look at how they have structured the text, video
and image content across their website.
Biographies of your practitioners, images of your staff, pricing information and the patient journey are all good examples of content you can place on a sitemap. This simple exercise will make it easier for patients to navigate through your website and discover the content relevant for them.
A nicely designed site with main navigation in contrast to one where everything is dumped on the homepage with no navigation
Avoid a mishmash of stock images that are different colours and styles
3
Get your imagery right
Good use of text or copy on your website is clearly important and we look at that in more detail in point 4 below. But never underestimate the power of good imagery on a website.
Imagery can often be the difference between having a good and great website, as it can help you connect emotionally with a prospective patient.
Spend some time researching the types of images you want on your website and remember to keep your target audience in mind. For example, if you are targeting patients in the age range of 40-60, then using lots of images of young people in their 20s is not going to help.
Another good tip is to ask a designer to put a colour filter or treatment on the images you have selected. This will help you achieve a consistent, premium feel across your website rather than a mishmash of stock images that are different colours and styles. Use a good selection of images with filters as opposed to small, stock imagery can make a site look cheap and under-designed
4
Pay close attention to copy
Striking a good balance between space, imagery and text will help you towards your goal of creating a great looking website.
Copywriting is a specific skill and two common mistakes we see
A site that looks great on a mobile as opposed to one where the navigation does not render well on mobile
are when the copy on a website is unstructured and where large amounts of text are placed on a dark background. This can be a major turn-off for visitors and makes it difficult to read.
So, before you copy and paste your copy onto your homepage, ask your designer about copywriting or break your paragraphs of text into blocks and think about headlines, sub-heads and calls to action to help future website visitors read your website.
5
Think responsivetablets and mobile
In today’s mobile-first world, the majority of websites are now viewed on mobile and tablets, so
spending hours proofing your new website on your laptop or desktop is not going to give you a true picture of the patient experience.
Most good website software tools like Wordpress now offer a Responsive Design tool that will allow you to view the website on different devices and test how it will look for future visitors.
So, before you sign off your website and send it live to the world, make sure you have gone through the site on your laptop, tablet and mobile and checked everything is working as it should.
To conclude
Designing and building a great looking website that you don’t
Text broken up into digestable blocks is better than large blocks of text on a dark background
have to refresh every 12 months is essential for any healthcare practices.
Some principles remain whether your website has five pages or 500 and it is vital that practitioners go through the right processes and dedicate time to planning before they start spending valuable budget.
Working with a recommended designer or marketing agency is often a smart move in the longterm. They will have been through the process many times before and established tried and tested frameworks and processes.
This can make the experience of designing and building a website a lot smoother and ultimately deliver you a better end-product that will be built to last.
Next month, we will take you on a journey into the use of colour in marketing and branding
Simon Marett (below, left) and Michael Sullivan (right) are managing director and creative director of Ellerton Marketing Ltd, a specialist strategic marketing consultancy for independent healthcare practitioners
BILLING AND COLLECTION
What does a billing
With outstanding
invoices
nudging
the £1m mark in some clinics, Simon
and how that compares to what was previously carried out.
Brignall (below) answers the most common questions he is asked by consultants when they finally act to get their money back
CONSULTANTS HAVE many questions for me when I meet up with them to discuss their payment problems.
But some occur again and again – so I thought I would share them and answer them here.
Outstanding debt
It will come as no surprise that many of the questions I am asked are about outstanding debt. These regularly include:
What is the most you have ever been given to chase?
How far can you go back?
What is your collection success rate?
Should I pass you all of my outstanding invoices?
We have been asked to assist practices with over £300,000 in outstanding invoices a few times. In two cases with clinics, it was close to £1m. We got nearly all of it back.
Legally, you can go back six years to try and recover unpaid debts.
Medical Billing and Collection (MBC) maintains bad debts across the life of the company of less than 0.5% when we have been responsible for the entire billing cycle.
The collection of outstanding debt depends on many factors, but it is quite common for us to collect over 90% of the backlog. We ensure that anything we are unable to collect is identified so that consultants can obtain the appropriate tax relief.
I always recommend doctors use
the transition to MBC as something of a spring clean, as it makes sense to pass us everything so we can run it through our chase process.
This is managed sensitively, as we explain to patients that we have recently taken on the billing role for the practice.
How can I grow my practice?
Without a doubt, this is one of the most frequently asked questions and it is not confined to those consultants who are new to private practice.
Of course, this a massive question and it has no simple answer. Your practice growth can be the result of many factors, such as location, specialty, experience and patient mix.
But one thing is universal: the most successful private practices take the time to review their activity and finances.
They make decisions based on data and not what they think they know about their practice.
It is easy to make assumptions, based on historical data and information, that do not reflect the current situation. To conduct a comprehensive review, a practice needs to access up-to-date accurate information about its business.
This should include:
1 How much the practice has invoiced.
This should be broken down into a range of criteria including loca-
tion, patient type – for example, self-pay, private medical insured and medico-legal – specific payment company, type of activity carried out and where patients are coming from.
2
How much is outstanding from the work you have carried out. It is obviously vital for you to be paid for the work you are doing.
MBC provides consultants with 24/7 access to its reporting platform, which includes an array of reports which can be used to analyse their practice data.
We use this information as part of a review process to see the patient mix at each hospital where the consultant does private practice or to analyse practice activity
This allows the practice to review how it markets its services to its patients, through its website and hospital consultants page, as well as its referral network of GPs and colleagues.
Even established consultants can benefit from taking the time to update their referral network with information about any new treatment they are offering.
We are able to input a referring doctor’s name or other marketing source to monitor where patients are coming from.
I am often asked to provide activity data to assist consultants when they carry out an annual review of their fees.
It is important that a consultant’s fee schedule should remain competitive and reflect both their expertise and the demand for their services.
Having activity data broken down by patient payment type enables a practice to calculate the impact of any fee changes it implements and ensure that these are targeted where they will derive the most benefit.
3
My medical secretary does the billing, so why do I need a billing company? Probably the most important, and often overlooked, benefit from using a medical billing company is that it ensures your medical secretary can maintain a clinical relationship with the patient, unhampered by the business side of the practice.
Outsourcing allows this relationship to remain warm and engaging by compartmentalising the two sides of the practice, leaving the billing company to focus on the business side and those difficult conversations about money. This improves the patient experience and benefits the practice, as
billing firm do for me?
the secretary can focus on responding to new and existing patient inquiries.
Often the medical secretary is responsible for many tasks, including patient engagement, diary management, medical letters and booking theatres and tests on top of the billing and chasing.
There are not many individuals who have the combined skill set required to complete all these tasks perfectly, as well as find the time to fit them all into a busy working week.
The explosion in email and other digital methods of communication from patients means they are often just running to keep up. It is an almost impossible task
for one person to cope with, especially as the practice continues to grow.
In our experience, once the practice reaches a certain size, the secretary is so busy dealing with the patients and the medical side of the practice that the billing and collection is the area that often gets neglected, leading to problems with cash flow and aged debt. Not all medical secretaries enjoy chasing outstanding debt, but for those that do, there is an associated opportunity cost.
Managing patient inquiries is a more productive use of their time instead of being stuck on hold with an insurance company. We often see practice revenues rising
The most successful private practices take the time to review their activity and finances
after they join us because they can focus more on the clinical side of their work, leaving the finances to us.
A billing company can also add functionality that may not be available through your current medical secretary. We offer our clients the ability to:
Invoice both patients and pri -
vate medical insurers electronically;
Take payments 24/7 through our online payment portal;
Collect payment up front when required;
Access their practice financial data on a 24/7 basis;
Ability to settle multiple outstanding invoices at the same time.
Outsourcing to a medical billing and collection company also means that any issues around staffing no longer impact the practice finances.
Simon Brignall is director of business development at Medical Billing and Collection
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes’ of free legal advice.
is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
Regulatory requirements and investigations
Keep up to date as an employer
There have been notable changes to employment law in response to the Covid-19 pandemic and some other developments which doctor employers in private practice should be aware of. Lucy Miles (top) and Kalani Bogahalande (right) report
THREE EMPLOYMENT law changes that have occured in the past year are: ❶
In April 2020, all workers were given the right to receive a written statement of terms and conditions on the first day of work or before.
❷The Parental Bereavement (Leave and Pay) Act 2018 took effect in April 2020. Employees who lose a child under the age of 18 or suffer a stillbirth after 24 weeks are now entitled to two weeks’ statutory leave.
If an employee has over 26 weeks of service, they are entitled to Statutory Parental Bereavement Pay. ❸
For calculating holiday pay, regulation 16 of the Working Time Regulations 1998 was amended in April 2020 to increase the reference period for determining an average week’s pay for workers without fixed hours or pay, from 12 weeks to 52 weeks.
There were also a few notable decisions concerning employment status and self-employment.
In Community Based Care Health Ltd v Narayan, the Employment Appeal Tribunal (EAT) found that a GP registered with a company providing out-ofhours medical services to the NHS, who had worked regular shifts at a single establishment for 12 years, had been correctly characterised as a ‘worker’.
This was even though there was no mutuality of obligation between the parties and where she provided her services through a limited company.
The EAT determined that a limited company could not satisfy the strict qualification and performance requirements imposed by the NHS nationally. This decision, which is potentially significant across the healthcare sector, has been appealed to the Court of Appeal and is expected to be heard in 2021.
Uber BV and others v Aslam and others was heard by the Supreme Court in July 2020. The court held that Uber drivers are workers and are therefore entitled to holiday pay and the national minimum wage.
These cases demonstrate the general direction of travel towards staff being workers despite what the contractual documents say.
It is anticipated that the current protections against redundancy for pregnant women will be extended
Covid-19 pandemic
The Covid-19 pandemic featured at the front and centre of employment law changes in 2020, as the law had to evolve rapidly in line with the various Government decisions.
Private practice employers must be conscious of the legal requirements relating to self-isolation, because requiring staff to attend work while they are required to isolate can result in a fine of up to £10,000. It is important to ensure:
Staff are fully aware of their obligations;
They do not feel any pressure to attend the workplace;
Accurate records are kept about those who have displayed symptoms.
Employers are still able to furlough employees through the Coronavirus Job Retention Scheme (CJRS). Furloughed staff are entitled to receive 80% of their currently salary, capped at £2,500, provided that the employee was on the payroll on 30 October 2020.
Employers can now bring back employees who were previously furloughed on a part-time basis. Staff who are on maternity, paternity or long-term sick leave can also be furloughed.
When selecting individuals to be furloughed, objective criteria must be used to avoid any potential for discrimination.
Private medical practices are able to utilise the CJRS, although it is not available to self-employed individuals, who would need to use the Self-Employed Income Support Scheme.
Looking forward
We expect the Covid-19 pandemic and Brexit to continue to take centre stage for employment law.
From 1 January 2021, the transitional arrangements in the withdrawal agreement came to an end. The new immigration laws which apply to EU citizens are expected to have a significant effect on the
healthcare sector, and medical practices will need to ensure their recruitment processes are updated to ensure their pre-employment checks are compliant.
The ability to engage professionals from EU countries is likely to be impacted because EU nationals who want to come to the UK to practise but had not done so, nor had their professional qualifications recognised in the UK, before the end of December 2020, will now be subject to visa requirements under a new points-based system and their qualifications will no longer be automatically recognised.
Brexit and the impact of Covid are expected to financially impact most businesses for the foreseeable future. Ultimately, some organisations will need to make contingency plans if restructures and downsizing become necessary.
So it will be important for employers to keep up to date on the laws
around redundancy, as changes may be introduced this year.
For example, it is anticipated that the current protections against redundancy for pregnant women will be extended.
At present, those on maternity leave who are at risk of redundancy must be offered suitable alternative roles in advance of others, but this protection ends once the individual returns to work.
The anticipated changes will mean that the protection will start from the date the employee informs her employer that she is pregnant and will last for six months after she returns to work from maternity leave.
This extended protection is also anticipated to be available to those taking adoption leave and shared parental leave.
Lucy Miles is an associate and Kalani Bogahalande a trainee solicitor at Hempsons
INVESTMENT BEHAVIOUR
Don’t keep checking your portfolio.
Dr Benjamin Holdsworth (below) explains the madness of markets
Ignore the siren songs
AS AN investor, it is generally a good idea to ignore what is going on in your portfolio most of the time. At the very least, it can be distracting and, at worst, it can be a source of unnecessary anxiety.
That advice is as applicable today as it ever was. The markets feel like they have gone a bit mad.
Since the start of the pandemic, and despite a 25% or so fall in late February and early March 2020, global markets – developed and emerging combined – have gone up by more than 10%.
Some sectors and companies have delivered far higher returns. For example, the ‘FAANGs’ –Facebook, Apple, Amazon, Netflix,
and Google, all beneficiaries of global lockdowns – have risen collectively by 45% since the pre-pandemic market high.
In May 2020, Elon Musk, Tesla’s chief executive, tweeted that its share price was too high and it fell 10% overnight to $80, yet Tesla’s share price has, since then, grown almost ten-fold to $804 on 10 February 2021.
Fair prices?
Today Tesla’s market capitalisation is now larger than the next nine global car manufacturers combined, including Honda, VW, Renault-Nissan and GM. We have not even mentioned Bitcoin.
Are these fair prices or are they overvalued?
The rational investor would say that the market is simply looking beyond the pandemic to a time of global recovery and a more normal world and that the market is the best judge of prices.
Yet some investors may have concerns that markets are in a bubble and question whether they should reduce their equity holdings.
Others may see the extraordinary returns from certain sectors and companies and feel a sense of FOMO – fear of missing out – that they are not more heavily invested in tech stocks or Tesla, for example.
The problem is that the markets may be right . . . or wrong. The one thing we know for sure is that it is impossible to know which with any certainty and the evidence tells us that even professionals have little ability to time entry into or out of stocks, sectors or markets successfully.
Mad markets
Markets can remain seemingly ‘mad’ for a long time. As John Maynard Keynes famously once said: ‘Markets can remain irrational longer than you can remain solvent.’
Sensible investing is about remaining highly diversified
Markets can remain seemingly ‘mad’ for a long time. As John Maynard Keynes famously once said: ‘Markets can remain irrational longer than you can remain solvent’
songs of the markets
across markets, sectors and companies to avoid absolute losses and to try to smooth out returns as much as possible over time. To many, that is a great comfort and allows them to sleep at night.
Reap rewards
Rebalancing periodically and reminding yourself that you do not need to cash in your equity assets in the near term is worthwhile.
It may not be as exciting as punting – which is what it is – on Tesla or Bitcoin, but it will reap its rewards over time.
Remember, too, that being diversified means that you will
Sensible investing is about remaining highly diversified across markets, sectors and companies to avoid absolute losses and to try to smooth out returns as much as possible over time
benefit from being in the companies and sectors that do well.
In 2020, the developed global stock markets returned around 12% in terms of GB pounds. Of this 12%, half – or an absolute 6% – of this return was attributed to the top ten stocks. The FAANGs alone represented 30% – that is to say, around 4% of the 12%. That is surely enough exposure for most. Stick with the plan and try not to look at, or think about, your portfolio too much.
Dr Benjamin Holdsworth is director of Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decision.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
PRIVATE
PATIENT UNITS: NORTHERN HOME COUNTIES
In our third annual round of reviewing the NHS private patient unit sector in England, Philip Housden brings a focus to the eight NHS trusts delivering acute care services to Oxfordshire, Berkshire, Buckinghamshire, and Hertfordshire Figure 1
The demand is there
FIGURES FROM the published 2019-20 annual accounts for this group of trusts show that total private patient revenues grew by £451,000 (2.24%) to £20.5m (Figure 3). These statistics were published in autumn 2020 and partially impacted by the early months of the Covid pandemic.
This represents 0.61% of these trusts’ total revenues and is down from 0.65% last year. For comparison, the combined national average outside of London is 0.43%.
The top trust in this group by both overall earnings and percentage of turnover remains Oxford University Hospitals
Oxford has developed local success through utilising specialty capacity across its four main hospital sites. The trust’s private patient revenues grew by £1.2m and 18% in 2019-20 to £8.1m and Oxford remains ranked 13th highest private patient earners within the NHS, and third outside London. Further growth was to be achieved through a joint venture
partnership with the Mayo Clinic, announced in 2017, to open an outpatient and ambulatory London base.
The clinic was staffed from both organisations to offer a wide range of services, including diagnostic, genetic testing and endoscopy.
Partnership abandoned
But, as reported in Independent Practitioner Today, this partnership was abandoned last year when the Mayo Clinic bought out the trust five months after opening to become the sole owner of the sixstory healthcare clinic in Portland Place, London.
East and North Hertfordshire Hospitals uses the branding Hertfordshire Private Healthcare to offer a range of private outpatients, day case and a small range of inpatient services – including two private en-suite rooms for orthopaedic and urology procedures only – between the Lister in Stevenage, Mount Vernon in Northwood, Middlesex, Hertford
County Hospital and QEII Hospital, Welwyn.
The private patient earnings of the trust grew by 3.8% and £124,000 to £3.35m in 2019-20, representing 0.77% of total revenues. The trust also has a colocated BMI hospital, Bishop’s Wood, on the Mount Vernon site.
Mount Vernon cancer services, which deliver a significant proportion of private patient revenue for the trust, are due to transfer to UCL from April 2021.
Buckinghamshire Healthcare delivers a limited range of private patient services from both the High Wycombe and Stoke Mandeville sites.
At Wycombe Hospital, the trust provides private amenity rooms to NHS patients who wish to pay for extra comfort and privacy after surgery.
These are available to orthopaedic, general surgery, plastic surgery and urology patients.
At Wycombe, the trust works with the on-campus BMI
Shelburne Hospital and this arrangement has survived the most recent review of BMI’s estate in relation to NHS partnership/colocated sites.
In 2019-20, the trust’s private patient revenues were £2.5m, up £24,000 and 1% on the previous year and representing 0.6% of total revenues.
Fell back
Luton and Dunstable , now merged with Bedford to form Bedfordshire Hospitals NHS Foundation Trust, does have a 13-bed inpatient PPU, the Cobham Clinic, providing a range of surgical services including bariatric, ENT and orthopaedic surgery.
The trust grew revenues by 2.2% and £36,000 last year to £2.13m, which is 0.6% of turnover. However, Bedford Hospital fell back by 18% and £337,000 to a total of £1.55m last year after several consecutive years of private patient revenues growth in real terms since 2011-12.
The northern home counties are an attractive market for private patients, but competition with the established independent hospital provider groups is strong
Despite a lack of dedicated inpatient beds, the trust achieves this income through the capture of diagnostic and low-volume specialty activity through its branded outpatient offer, the Bridges Clinic.
This offers a range of medical specialties, including endoscopy, cosmetic procedures, diagnostic imaging and physiotherapy. The recent merger provides the enlarged trust with the opportunity for cross-site working and collaboration on private patient services to build on the combined income of nearly £3.7m.
Crowded market
Royal Berkshire’s private patient revenues also fell back significantly in 2019-20 by £779,000 (33%). The trust operates in a crowded local independent hospital market and without designated private patient beds and so concentrates on complex surgery and niche services that the local competitors cannot provide.
The West Hertfordshire Trust Hospitals, located across Watford, St Alban’s and Hemel Hempstead, sit well in an attractive market for private patients.
However, they face significant competition from Spire’s Bushey and Harpenden hospitals and a range of other providers. The trust has reversed a long period of decline with growth sustained over both 2018-19 and 2019-20 financial years.
Growth last year was 18% and £140,000 to reach a total of £903,000; the highest income for five years and 0.27% of turnover, principally based on cardiac and diagnostic imaging and ambulatory services.
The trust has from time to time developed plans to open on-site private patient inpatient capacity, but these have not yet come to fruition. Figure 3
Great platform
This growth is in part due to the trust launching in 2019 a physiotherapy service for private patients at the West Hertfordshire Therapy Unit in Abbots Langley, which provides specialist treatment, including women’s health, muscular treatments and care for sports injuries.
Looking ahead, the site and service redevelopment programme, including a new hospital development at Watford General due to open in 2025, provides a great platform for inclusion of a wider range of private patient capacity and service than is presently able to be offered.
Milton Keynes Hospital’s earnings are stuck at £0.5m turnover, flat on 2018-19, but a further decline of total trust revenues to a new low of 0.22%. The trust has not yet invested in the potential to break into the attractive growing private patient market despite Spire’s cancelling of plans to open a private hospital in the city.
The northern home counties are an attractive market for private patients, but competition with the established independent hospital provider groups is strong.
Most regional trusts do now provide branded outpatient and diagnostic facilities that offer a local, fast access to consultants. However, a majority still do not have any protected designated pri-
vate patient beds. This means that where the trust is the provider of choice for consultants when considering patient safety – typically the case as the local independent providers usually do not have full critical care facilities – the low volume of private inpatients must continue to be accommodated on NHS wards or these insured inpatients are treated as NHS and so their insurers are not charged. Overall, regional trust earnings show modest growth despite the competition, both local and from London, and given the strong underlying demand factors, the market potential post-Covid remains attractive for the future.
As the ageing population, increasing patient safety agenda and the service limits delivered by private hospitals are all driving complex insured activity into NHS trust sites, if these trust were minded to invest in capacity and capability, then there are several opportunities to develop new NHS private patient services in this region.
Next month: the Southwest
Philip Housden (right) is managing director of Housden Group commercial healthcare consultancy
Figure 2
BUSINESS DILEMMAS
Death certificate poser
A request to certifying the death of a patient from Covid-19 presents a difficulty for this doctor. Dr Sally Old (below) gives her advice
Dilemma 1 Can I sign death form for Covid?
QI have received a call from the wife of one of my private patients with advanced prostate cancer who tells me that her husband has died at home.
She said my patient would have wanted me to sign his death certificate, as he trusted me and didn’t have a good relationship with his GP.
She revealed he had been disappointed with the outcome of a phone consultation with that GP in the week before his death. The patient had tested positive for Covid-19 and was self-isolating but had declined the GP’s advice of an admission to hospital when his condition deteriorated.
I feel that the GP would be better placed to sign the certificate, as I have not seen the patient for many months, but when I called the practice, I was told he was off sick and the receptionist didn’t know when he would return.
I don’t want to let the family down, so would it be reasonable for me to complete and sign the death certificate in these circumstances?
AOrdinarily, the doctor who attended the deceased during their last illness should complete the medical certificate of cause of death (MCCD). However, death certification rules in England and Wales have been changed temporarily to recognise that this may not be possible during the pandemic.
Under the Coronavirus Act 2020, the MCCD can be completed by a doctor who has not seen the patient in their last illness if it is not practicable for the attending doctor to do so themselves – for example, if that doctor is unwell or self-isolating.
Under the Coronavirus Act 2020, the death certificate can be completed by a doctor who has not seen the patient in their last illness
It would be reasonable for you to agree to certify the patient’s death, even if you had not attended him in his final illness, provided you are ‘able to state to the best of [your] knowledge and belief the cause of death’.
Practically speaking, this means having access to relevant medical records and the results of investigations such as the patient’s positive test result.
Updated guidance
The updated temporary guidance for doctors on completing death certificates states that you would need to delete the words ‘last seen by me’ on the MCCD and – if applicable – should include the name of a doctor who saw the patient within the last 28 days.
In this context, ‘seen’ includes video consultations but not consultation by phone/audio only. So it’s important to check whether any doctor actually saw the patient in the previous 28 days so you can accurately complete the MCCD.
If you discover that the patient had not been seen by a doctor in the previous 28 days or after death, you need to talk to the coroner and obtain their agreement before you can complete and sign the MCCD and should only go
ahead if you are able to state the cause of death to the best of your knowledge and belief.
The guidance states that Covid19 is an acceptable direct or underlying cause of death for the purposes of completing the MCCD.
You should also enter any other diseases, injuries, conditions or events that contributed to the death, but were not part of the direct sequence, in part two of the certificate, such as the patient’s advanced prostate cancer.
The new arrangements also make it easier for the patient’s death to be registered if he was seen by a doctor within the last 28 days.
Registrars will now accept scanned or photographed copies of the MCCD forwarded from a secure email account, although the original, signed document should be securely retained for delivery to the registrar as soon as circumstances allow.
Where the patient had not been seen within the last 28 days, relatives should be able to register the death if the coroner agrees to the completion of the MCCD.
Dr Sally Old is a medico-legal adviser at the MDU
Notes on retirement
What should you do about retaining patient records when retiring from private practice? Dr Sissy Frank (right) explains how to manage things
Dilemma 2
How long should I retain notes?
QAt the beginning of the coronavirus pandemic, I was redeployed to support colleagues in the NHS. While I will continue to do this, I have decided to retire from private practice. What are the issues around patient records that I need to consider so that I retire in an ethical, yet timely manner?
APatient care must be at the forefront of your decisionmaking when deciding to retire or close your private practice. Think of your patients in one of three categories: those you have treated in the past but no longer see, those you see regularly and those who are likely to require further treatment. It will be important to discuss ongoing care well in advance, as well as preparing treatment plans, particularly for patients that fall in the last two categories.
The GMC in its guidance Delegation and Referral (2013) makes clear that you should explain to the patient that you plan to transfer their care and ensure the patient is informed about who is responsible for their future care and treatment.
The guidance also states that you should seek the patient’s consent to disclose relevant information about them and to pass their record to their new doctor .
As a private practitioner, you will be registered as a data controller with the Information Commissioner’s Office – a statutory duty – enabling you to collect and hold patient information. Even after stopping independent practice, you might need to respond to a Subject Access Request; that is, a request for access to the notes you hold about a patient.
When disposing of records, you should ensure that this is done using appropriate means
The request could be made for a number of different reasons, including complaints or clinical negligence claims. Consequently, it is vital that you securely retain your patients’ records and consider each patient’s record before disposing of it.
The GMC’s Confidentiality (2017) guidance states: ‘If you are responsible for managing patient records or other patient information, you must make sure the records you are responsible for are made, stored, transferred, protected and disposed of in line with data protection law and other relevant laws.’
Although the previous regulations relating to the retention of private records (schedule 3 of The Private and Voluntary Health Care [England] Regulations 2001) are no longer in force, the GMC also states that you should follow the guidance by the UK health departments, regardless of whether you work in the NHS or not.
Information on appropriate retention time-scales can be found in Records Management Code of Practice for Health and Social Care, which explains that records should be considered on an individual basis and retention schedules vary between different types of records.
Although it is imperative you check the retention schedule with reference to the types of records you hold, the following are a few examples of the time-scales:
Adult health records – not specified elsewhere in the schedule: Eight years after conclusion of treatment or death;
Oncology records: 30 years or eight years after the patient has died;
Contraception/sexual health: Eight years unless there is an implant or device, in which case ten years – unless it is the record of a child, in which case it should be treated as a child record;
Records relating to litigation: Ten years after closure of the case.
These should be viewed as a minimum period for record retention, especially if there has been an adverse event or complaint.
The benefit of retaining a record
from a medico-legal standpoint should be balanced against the requirements of data protection law, which states that records should not be kept for longer than necessary.
When disposing of records, you should ensure that this is done using appropriate means; for example, by crosscut shredding, incineration or by using a commercial company with the necessary accreditations.
Dr Sissy Frank is a medico-legal adviser at the MDU
NOW OPEN ON SATURDAYS
New sessions are available for independent private practice on Saturdays.
Fully CQC-registered clinic Nursing support
Appontment-making Secretarial support
Billing service In-house pharmacy
We are a leading private outpatient clinic and we are inviting new applications for practising privileges for our extended opening hours on Saturdays.
GETTING BACK TO WORK
There is a cost to financial recovery for independent practitioners trying to get back to ‘open for business’. Dr Sara Sreih and Dr Lucy Hanington (below) highlight some important considerations
Re-opening is not that simple
THE EFFECTS of the Covid-19 pandemic has impacted many patients but also the private practitioners who rely on this work to maintain their livelihoods.
In the first wave of the pandemic, the provision of privately funded healthcare fell by up to 84%.1 The impact of this hit varied between specialties, with fields such as trauma and orthopaedics and ophthalmology being relatively more affected.2
However, there is reason to believe that any detrimental effect on private practice should be short-lived.
The reduction in private practice income showed a rapid recovery to almost pre-pandemic levels by the second lockdown.3
A UK survey of over 1,000 individuals also found that, since the pandemic, 27% are now considering paying for treatment or taking out private medical insurance, compared to just 15% prior to Covid-19.4
As the pressure on the NHS gradually eases, and hopefully continues to do so, there may be a temptation for private practitioners to throw themselves into their private work.
This could be to recover from financial loss, meet the increase in demand from patients and futureproof their businesses. But there are key issues to bear in mind when navigating a return to, or increase in, private practice.
Ethical and medico-legal risks
It is likely that there will be pandemic-related disruption to patient pathways for some time to come.
Practitioners should review their services regularly in this changing environment.
Redeployment and shielding
It is likely that there will be pandemic-related disruption to patient pathways for some time to come may continue to mean that key team members are less available than before. There may be delays in accessing scans or in the processing of laboratory investigations. Patient expectations will need to be carefully managed if complaints are to be avoided.
More disruption
Potential delays should be factored into clinical decision-making and patients will need to be safety-netted appropriately. There remains the possibility that the emergence of a further wave of Covid-19 could result in yet more disruption to healthcare services and impact both existing patients currently receiving care, as well as any new patients who wish to be seen. Where possible, contingency plans should be made.
Independent practitioners may be keen to ramp up their clinical work as soon as they are able to, but should consider their capacity, that of their team and the service as a whole.
High workload
Attempting to undertake too high a workload can result in a drop in clinical standards and increase in clinical errors,5 leading to adverse clinical outcomes.
This, in turn, can also lead to an increased risk of complaints, claims and other investigatory processes, adding further pressure onto staff.
Patients may come to the private setting with a set idea of what investigations or treatment they require, particularly given the potentially significant wait they may have endured.
The wishes of patients and the reasoning behind them should be explored and it is essential to ensure that clinical objectivity is maintained and usual guidance or evidence is followed when providing clinical care.
If a patient is asking for treatment that the clinician does not believe would meet the patient’s needs, then this should not be offered. However, this should be explained, alternative options discussed and the patient reminded of their right to seek a second opinion.
Of course, it may be that the clinician chooses to seek a second opinion themselves to provide an objective viewpoint on the clinical reasoning.
Good communication and documentation, as well as adhering to the principles of informed consent – in line with the GMC’s guidance on shared decision-making – are key in such situations.6
Any potential conflicts of interests, or perceived conflicts of interests, should also be considered.
For example, clinicians working in both the NHS and private practice would need to be mindful of any conflicting commitments with regards to their time when taking on additional work and take care not to conduct any private work when scheduled to be working in the NHS.
Even if the time in the NHS is not being used to see NHS patients, conducting private clinical work during this time would be an issue of probity and fraud.
The potential for (perceived) conflict also exists when an NHS patient seeks privately funded treatment or follow-up.
There is detailed guidance from
the GMC on how to handle such issues and it advises that if there is doubt as to whether there is a conflict of interest, you should act as though there is one and seek advice on the implications of any potential conflicts.7
Health and well-being
The pandemic has taken its toll on many in society, not least healthcare staff who have worked relentlessly in challenging environments and witnessed great suffering firsthand.
Many healthcare professionals have spent time volunteering or have been redeployed in other clinical areas to assist in the most recent wave and so may be returning to their private work already exhausted.
Indeed, the BMA has reported that almost 60% of doctors in England, Wales and Northern Ireland are suffering from anxiety or depression and 46% reporting a worsening since the pandemic.8
It therefore becomes a balancing act between the wish to see and treat many private patients and needing to ensure that the workdays are not so long and stressful that they negatively impact one’s health.
Many clinicians will be familiar with the idea that poor well-being and burnout has been found to affect patient safety.9
Burnout was an issue globally among clinicians in the preCovid-19 world, with calls for policy changes to address the concerns high on Medical Protection’s agenda.10 The pressure of the pandemic will only have added to the toll on staff.
Being stressed, tired and short on time can also impact communication with patients during consultations.
A survey we commissioned in 2017 showed that manner and attitude was the top reason for GP complaints, with three out of the top five reasons relating to communication.11 Most complaints to the NHS between 2013 and 2014 related to poor communication.12
Many patients may begin their journeys having already waited to be seen or treated, enduring a prolonged period of suffering with symptoms, and so extra care and attentiveness to their experiences and needs is recommended.
How much is too much?
Care must be taken in considering what is a manageable, acceptable and safe workload in one’s private practice setting. Allowances must be made for the challenges created by the pandemic.
Robust clinical governance systems and regular service evaluations will help to ensure patient safety in ever-changing circumstances.
Clear communication with patients and the managing of expectations are key in avoiding adverse medico-legal consequences.
But most importantly of all, doctors must prioritise their own wellbeing and that of their teams, so that they are able to continue to meet the demands placed upon them effectively and safely.
See burnout in doctors –page 48
Dr Sara Sreih and Dr Lucy Hanington are medico -legal consultants at Medical Protection
Don’t miss out. Financial support measures for private practices hit by the pandemic are still available. Ian Tongue (left) gives a recap of the main ones to be aware of
COVID-19’ s IMPACT has been with us for over a year now and the majority of private practices have experienced a significant reduction in income.
The Government has brought in several measures of financial support since the pandemic that have evolved and therefore it is worth recapping on the current situation.
CORONAVIRUS JOB RETENTION SCHEME
(CJRS)
This is by far the most publicised and widely used financial measure and is often referred to as the ‘furlough scheme’.
It has been a lifeline for a huge
The bounce-bank loan has been a welcome lifeline for many consultants who have not been able to work privately or had their income substantially reduced since the pandemic started
number of businesses and is an incentive to retain your employees during a period of downturn or inactivity. This scheme in particular has evolved several times during the period it has been in place. Initially, the scheme prevented the employee working in pretty much any capacity for the business with the exception of directors carrying out statutory responsibilities.
It also added the complication of only being available to those on the payroll at the end of February 2020 and largely based on that month’s pay for the calculations.
From 1 July 2020, a more flexible arrangement was put in place whereby you can claim financial support for the hours that an employee does not work and pay them for the hours they do work.
At the same time, the Government announced a reduction to the level of financial support in an attempt to wean businesses off the scheme.
Due to the upsurge in the virus, the scheme has been extended several times but has seen little further changes aside from the level of support and eligibility to claim. It has, however, introduced strict time-scales to make a claim for the support, which may see employers miss out if they are not organised.
At the time of writing, the scheme is set to end on 30 September 2021 and can be summarised as follows:
For periods up to 30 April 2021
Employees must have been employed as at 30 October 2020;
Those employees must have been reported under a PAYE scheme at any time between 20 March 2020 and 30 October 2020;
The lower of 80% of the monthly salary or £2,500 can be claimed each month;
Employers’ National Insurance and pension contributions cannot be claimed.
For the period from 1 May to 30 June 2021
Employees must have been employed as at 2 March 2021;
Those employees must have been reported under a PAYE scheme at any time between 20 March 2020 and 2 March 2021;
The lower of 80% of the
From 6 April 2021, a new loan support scheme is available to ensure that businesses still have access to financial support from banks and other financial institutions
had 100% security from the Government.
This led to a streamlined process of loan applications, with the money often paid over within a few days following a simplified application process. The CBIL loans were generally for larger businesses and the bounce-back scheme for smaller operations.
DON’T MISS OUT
These are the most commonly used financial measures by consultants carrying out private practice but it is not exhaustive.
monthly salary or £2,500 can be claimed each month;
Employers’ National Insurance and pension contributions cannot be claimed.
From 1 July 2021
At the time of writing, it appears that the same eligibility criteria will apply as with the period 1 May-30 June 2021.
However, the level of support will reduce as follows:
Claim for July 2021: lower of 70% of salary or £2,187.50.
Claim for August 2021 and September 2021: lower of 60% of monthly salary or £1,875 per month.
It is important to note that the deadline to claim support under the scheme is largely 14 days after the month end.
Therefore, the claim for April 2021 has to be submitted to HM Revenue and Customs by 14 May 2021 and so on until the proposed final claim for September which is due by 14 October 2021.
If you are in any doubt regarding the eligibility of the scheme to your circumstances, speak with your accountant.
LOAN SUPPORT
At the outset of the pandemic, the Government unveiled support in the form of a loan that had Government backing, known as a Coronavirus Business Interruption Loan (CBIL).
These loans had 80% Government security and therefore the lenders still required full applications to approve the loans, which made access to this funding difficult, as the banks felt the 20% exposure to bad loans could harm their operations.
The Government then introduced the bounce-back loan, which was capped at the lower of 25% of income or £50,000, but
The benefit of both loans are favourable repayment periods, low interest rates and deferred payment start dates.
The bounce-bank loan has been a welcome lifeline for many consultants who have not been able to work privately or had their income substantially reduced since the pandemic started.
The CBIL and bounce-back loans were available until 31 March 2021, after which time new or extended applications will not be available.
From 6 April 2021, a new loan support scheme is available to ensure that businesses still have access to financial support from banks and other financial institutions. This new arrangement is referred to as the recovery loan scheme.
The new arrangement operates in a similar way to the CBIL scheme whereby the Government will provide 80% security on the loan. Applications can be made from 6 April and close on 31 December 2021.
The new scheme offers loans and overdrafts from £25,001£10m and also other types of invoice or asset finance from £1,000 to £10m.
For loans and asset finance, the repayment term is up to six years and for overdrafts and invoice facilities, this is three years. No personal guarantees will be taken on facilities up to £250,000 and the borrower’s main home will not be taken as security.
As with the original CBIL scheme, a full loan application will be required by the bank to ensure the viability of the business to repay the debt in the future.
SELF-EMPLOYED
Despite many consultants being self-employed, few will have been eligible to claim under this scheme due to having salaried or other sources of income.
It may, however, have been
Depending on your circumstances, you may be entitled to other financial help and support, so speak with your accountant to ensure that you are not missing out.
applicable to a spouse or family member if they are self-employed.
Unlike the CJRS, which is claimed monthly, the selfemployed income support scheme is claimed in quarters, with the maximum amount available being £7,500 per quarter.
In last month’s Budget, the Chancellor announced an extension to this scheme to allow a fourth claim to be made on the same terms as previous, but a fifth claim will be subject to a review of how the business has fared over the pandemic period.
If you or a family member are eligible for this scheme, it is important they speak to their accountant to understand their position.
VAT
The majority of consultants will not be VAT-registered, as the medical services that they provide are exempt from VAT. For those that are VAT-registered, they had an option to defer the VAT relating to payments due between 20 March 2020 and 30 June 2020.
For those that did defer the payment of VAT, if you have not paid the deferred amount by 31 March 2021 and want to pay by instalments, you will need to apply for this by 31 June 2021 and can take up to 11 months depending on when the application is made.
However, as the scheme has been open since 23 February, each month that goes by reduces the number of months that you can repay the amount over. If you are in this position, contact your accountant to ensure that this has been dealt with.
Next month: A recap of tax charges on your pension
Ian Tongue is a partner with Sandison Easson and Co, specialist medical accountants
DOCTOR ON THE ROAD: POLESTAR 2
Polestar models were originally souped-up Volvos, but now the brand is a standalone marque for premium electric cars. Dr Tony Rimmer (below) reports on its latest offering which has its sights on Tesla
A hatchback to give Tesla a run for its money
KNOWING WHAT your competitors in the health market are offering and at what cost is vital for long-term profitability.
If you start offering services that have been well established by others close by, then you know you must have unique selling points at similar cost levels for the client base. It is your job to break any monopoly advantage held by your rivals.
For car manufacturers, the brand rival to beat in the accelerating electric vehicle market is, of course, Tesla. Having been established in
the UK since 2014, it has a huge lead over other makers and it is they who are playing ‘catch-up’.
Hugely successful
Initially focusing on the upper premium market with the Model S, it now has the middle-sized premium Model 3, which has gone on to be hugely successful and made Elon Musk – briefly – the richest man in the world.
Enter Polestar, an offshoot of Swedish maker Volvo, which is owned by Chinese giant, Geely.
Polestar models were originally souped-up Volvos, but now the brand is a stand-alone marque for premium electric cars. Its first model, the imaginatively named Polestar 1, was a 2018 fast sports coupé model with 590bhp that cost £135,000 and was left-hand drive only.
Now we have the Polestar 2, a premium all-electric hatchback that has its sights firmly set on the class-leader, the Tesla model 3.
Based on a Volvo chassis shared with the XC40, the Polestar’s large
Based on a Volvo chassis shared with the XC40, the Polestar’s large 78kWh battery pack is cleverly packaged down the car’s spine and under the floor
78kWh battery pack is cleverly packaged down the car’s spine and under the floor.
This powers two electric motors, front and rear, giving four-wheel drive and 402bhp. Maximum range is claimed to be 292 miles.
The car is very well equipped and the only significant option available is the £5,000 Performance Pack.
This adds special Ohlin dampers, Brembo brakes, 20-inch forged alloys, gold valve-caps and gold seatbelts. It does not add a bigger battery or any more power.
The on-the-road price is almost identical to the Model 3 and, at £49,900, just scrapes in below the £50,000 threshold to qualify for the Government’s £3,000 ultra low emission grant.
Good-looking pose
So how does the Polestar 2 compare to the Tesla? Well, my test car was fitted with the optional Performance Pack and strikes a good-looking pose on the road. It has a front ‘grille’ which gives it a more normal look and its slightly raised stance – remember, it uses the XC40 SUV platform –gives it real road presence.
The greatest benefit over the Model 3 in my book is the fact that
it is a hatchback. This is much more useful than the Tesla and essential if you have, like I do, a dog.
You have to move to the Tesla Model Y to get this benefit, which is likely to be a lot more expensive when it arrives in the UK later this year.
If you do not like the minimalist interior of the Model 3, the Polestar’s dashboard is more a conventional take on the high-tech information and functions available on all electric cars.
It also works better in a more intuitive way. The vegan interior –leather is not an option – is supremely comfortable and the quality of materials is definitely a step above the Tesla.
Room in the back is fine for two or three passengers with particularly good leg room. Boot space, at 440 litres is similar to the Model 3, but the hatchback, as mentioned, makes it more convenient. The front load area is only really big enough for the charging cables.
On the road, the Polestar 2 is as swift as any sports car. Like the Tesla, the linear silent acceleration is an experience that becomes slightly addictive and something you never tire from.
The regenerative braking can be
POLESTAR 2
Body: Five-seat hatchback, four-wheel drive
Engine: Dual electric motors. 78kWh battery
Power: 402bhp
Torque: 660Nm
The vegan interior is supremely comfortable and the quality of materials is definitely a step above the Tesla altered to taste and, in its most powerful mode, allows one-pedal driving. The steering is sharp and the handling is impressive for a car weighing more than two tonnes.
Top speed: 127mph
Acceleration: 0-60mph in 4.7 seconds
Claimed range (WLTP): 282 miles
CO2 emissions: 0g/km
On-the-road price: £49,900
So the Polestar 2 would be a great start for any of you ready to enter the electric car marketplace.
I am sure this is helped by the special Ohlin dampers, but the trade-off has become the Polestar 2’s Achilles heel – an overly firm ride. For a car that should be comfortable and smooth to make the most of its electric attributes, it disappoints.
The little Honda e I drove recently has a better ride. I would therefore recommend avoiding the Performance Pack option and enjoy more comfortable journeys and, at the same time, save significant money.
If you do not do many long journeys – where the Tesla Supercharger infrastructure wins hands down – then it is a classy alternative to the Model 3.
It drives really well, has sporty performance and has a real range of over 230 miles.
Also, look out for the new Volvo C40 crossover. Due in the UK early next year, it uses the same platform and drivetrain as the Polestar 2 and will have predictably solid Swedish build quality.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
The Polestar’s dashboard is more a conventional take on the high-tech information and functions available on all electric cars
BURNOUT IN DOCTORS
An unavoidable side-effect
With 58% of doctors now suffering from some form of anxiety or depression – and 46% saying their condition has worsened since last March – we are serialising sections of a new book edited by Dr Clare Gerada (right). This month: Burnout in doctors
Today readers can save 20% on Routledge.com with discount code BWC21. Offer ends 31 August 2021. Order now at: www.bit.ly/ Routledge_IPT
side-effect of caring
BURNOUT IS now a public health crisis. It is the single most prevalent psychological complaint found in those who work in the caring professions, with doctors, nurses and counsellors all at high risk.
It is formally defined and subjectively experienced as a state of physical, emotional and mental exhaustion caused by long term involvement in demanding situations.
People lose their joy and zest for work. It becomes mundane, routine and a burden. Burnout strikes those who have been most idealistic, enthusiastic and engaged.
Burnout is thought to be distinct from depression, but I think of them as part of the same process. There is a considerable overlap between symptoms – in particular around hopelessness, poor selfesteem, sleep disturbance – and it might be more acceptable to call oneself ‘burnt out’ than ‘depressed’.
Compassion fatigue is also closely linked to burnout and again the two could be considered to be part and parcel of the same thing.
Burnout is a psychological and behavioural syndrome where emotional exhaustion is a major feature. It was first described in 1974 by psychologist Herbert Freudenberger in his work looking at why those working with drug addicts experienced a gradual depletion in energy and loss of motivation and commitment.
While linked, stress and burnout are not the same. Stress is a general term referring to temporary adaptation – with positive as well as negative connotations – accompanied by physical and mental symptoms. In contrast, burnout is the final stage in a breakdown of the person’s ability to adapt, which results from the longterm imbalance between demands and resources.
Burnout has been described as the ‘painful realisation that we have failed to make the world a better place, to help the needy, to have a real impact in the organisation, that all of our efforts are for nothing’
Studying burnout
Despite thousands of studies, the exact prevalence of burnout is hard to pin down. It is probably as hard to measure as nostalgia, stoicism, fear, hate or love.
We cannot answer basic questions such as who gets it, who is more at risk, how much of it is there, let alone what interventions work in reducing it. Even the impact of burnout is not clearly known.
Of course, the cause is known: chronic, unremitting emotionally stressful jobs. But this does not really help in studying it.
Burnout has been described as the ‘painful realisation that we have failed to make the world a better place, to help the needy, to have a real impact in the organisation, that all of our efforts are for nothing’.
For me, this feels a much better, more honest and a less clinical definition to describe that hopeless feeling, when you know –hopefully temporarily – that you cannot go on caring for others and when you realise you cannot make a difference to your patients’ lives or to the system you work in.
I have had experience of losing interest in the well being of my patients, of becoming bored and,
worse still, of losing my compassion for them. Exhausted from juggling work and two young children, I felt an overwhelming desire to resign, to pack it all in and leave medicine completely.
It came to a head after a particularly busy and stressful morning surgery. I felt washed out, didn’t want to return for the evening clinic and resented patients having more of my time than my own family.
Many were my regulars; patients with longstanding, intractable problems and I felt disillusioned. What could I do to help them? I couldn’t find them jobs or rehousing. I couldn’t repair their broken relationships.
I couldn’t fix their lives. Medicine had lost its spark. I knew I needed a break from clinical practice. These emotions are so much harder to quantify than the multiple questions in burnout questionnaires and studies would imply.
Although the intensity, duration and consequences of burnout may vary between different individuals and across time in the same person, it always has the combination of the three components: physical, emotional and mental exhaustion.
Almost all research studies into
burnout rely on self report and largely poorly constructed crosssectional surveys. I worry that, by constantly measuring burnout, we might be perpetuating the problem rather than finding solutions.
We might also risk exaggerating the level of distress through contagion of misery. Furthermore, by measuring individual burnout we risk shifting the focus away from where it truly resides, the organisation.
Common feeling
What can be gleaned from these studies is that:
➤ Burnout is common.
➤ Prevalence reduces with better designed and larger studies.
➤ It is probably more prevalent in younger versus older doctors, though this is not entirely clear.
➤ It is probably more prevalent and more intense in those specialities working with patients who present with undifferentiated problems – general practice, accident and emergency – or where workload is harder to control, such as general medicine.
➤ Rates tend to be lower in those specialities that have less oncall commitments and are more containable in terms of hours and workload – and are more highly remunerated – such as plastic surgery and dermatology.
➤ It is probably increasing in the medical workforce.
In the main, those who are most at risk of burnout share three characteristics. The first is that their work is emotionally demanding. The second, that the individual has certain personality characteristics that draws them to ‘public’ service as a career and, finally, these individuals share a ‘patientcentred’ approach to their work. All three are equally important. Looking at the emotionally demanding nature of our work, in public service professions, people
Our February issue showed Covid has increased burnout in doctors
are exposed to emotionally demanding situations over a long period of time. Doctors have to deal with pain, helplessness, despair, death and accept the limits of science.
It is important to keep reminding myself, being a doctor is not easy. Even after 40 years, I am amazed at the trust patients give me, how they open up unconditionally and believe that I can ‘sort them out’. This is hard, emotional work.
This is not the same as saying the job is ‘stressful’. All jobs are stressful and many of us thrive on stress – and remember the opposite of no stress is boredom. It is the emotional aspect of our work that makes us most at risk of burnout.
Working long hours, seeing many patients in a single session, having no time between patients, working double shifts in highly emotionally charged or uncertain areas of medicine such as cancer care, general practice magnifies the risk because they act to increase our exposure to this emotional toil.
Personality characteristics
The second characteristic common in professional groups with burnout is that individuals share a common set of personality characteristics, attitudes and values that has drawn them to their role and which makes them more at risk.
We become doctors because we think we can make a difference to people’s lives and are willing to sacrifice parts of ourselves to do this.
The third factor is that of having a patient or person centred approach to one’s work. This means making others one’s first concern – as in the GMC’s Good Medical Practice . Most relationships are reciprocal, but the therapeutic relationship is not: the professional gives, the patient receives. This asymmetry is a source of stress.
On top of these three factors, we each bring our own vulnerabilities derived from our unique experiences, supports and personalities. Burnout is present in younger and older doctors, men and women, those in training and those who have achieved final accreditation status, those who work in hospital or general practice.
Anyone working so close to human suffering will, at some point in their career, develop some aspects of it
Addressing burnout
I do not believe we can prevent burnout; rather, we have to manage it, recognise it, minimise it and deal with it when it occurs.
Anyone working so close to human suffering will, at some point in their career, develop some aspects of it.
What is important is recognising when:
We can go on no longer;
Negative attitudes turn to loss of compassion;
Our sense of futility becomes a feeling of hopelessness and helplessness;
Our work loses its sparkle day in, day out;
We need to remove ourselves from the stressor.
The best place to start is in the workplace and in particular reduce the pressured environment in which staff work.
Environments where excessive workload, long work hours, fatigue, intense emotional interactions, restricted autonomy and where constant structural and organisational changes become the norm, lead to increased risk of burnout.
At a population level, the most important interventions should be at addressing the workplace stressors, including work pressure, resources – time, people and money – and creating the opportunities for teamworking.
On a larger scale, it means amending external factors, such as regulatory requirements, political influences and media pressures, which all contribute to chronic workplace distress.
Treating burnout as a public health crisis might mean we use the same prevention strategies as with any other threat to the public’s health. These would include:
➲ Primary prevention – preventing the problem arising in the first place. This largely needs to involve modifying the working environment in which doctors work, especially reducing direct patient contact.
What is needed is not to provide doctors with more resilience training but instead to address the environment in which they work. Just as mine owners have a responsibility to ensure a safe working mine for miners, so too do those who employ doctors have a responsibility to create a physical and psychological safe place to work.
A dangerous coal mine is not made less so by teaching miners how to relax. The leading drivers for burnout include excessive workload, chronic work stress and a lack of control over one’s daytoday work.
It is a problem of the healthcare organisation as a whole, rooted in issues related to the working environment and organisational culture.
➲ Secondary prevention aimed at reducing the impact of environmental or individual stressors. This might include addressing resilience, providing time out for doctors, improving the systems in the organisation to release time to think, providing group work, improving rest periods and so on.
➲ Tertiary prevention aimed at those with burnout. This is about improving the quality of life and reducing the impact of burnout on the individual. It means providing easy access to confidential services, a culture where it is ‘OK’ to admit you have had enough and opportunities to take time out.
No measure to prevent burnout will be effective unless attention is paid to enhancing a positive work
environment. Thus strategies directed at individuals will be of limited benefit.
I have created a short, easy mnemonic to help me remember what I need to do:
BBalance my work and play times;
U Understand my limitations – I am not a superhero;
RRecognise , prevent and treat burnout in myself and my teams;
N
Nurture the next generation – bring the fun back into work;
TTeamwork – rest, play and reflect together.
Finally, burnout can be a trigger for change and personal growth. The experience of burnout always involves pain and suffering, but it can then force someone, as it did for me, to examine priorities, learn and be more aware of one’s vulnerabilities.
I was lucky – my sympathetic and progressive partnership and opportunities outside the consulting room meant I could take time out, return when ready and restructure my working life to refresh my psychological self.
I modified my working practices, especially decreasing the time spent on facetoface clinical work.
My experience of burnout led to growth, change and further challenges that sustained me for the years to come.
Next month: Doctors as patients
Dr Clare Gerada is medical director of the Practitioner Health Programme, London, and a former RCGP chairman
Dwindling income stream
Our unique benchmarking survey reveals a disappointing year for many consultant urologists’ businesses. Ray Stanbridge reports
PROFITS FOR urologists in private practice reflected a year of little real change in our latest earnings study.
Gross incomes rose on average by £9,000, or 6.2%, from £145,000 to £154,000 in 2019.
But costs increased by about 13% from £53,000 to £60,000. As a result, taxable profits went up by around £2,000, or 2.2%, from £92,000 to £94,000. These consultants only broadly kept pace with inflation.
What then are the major reasons for the changes we have observed?
Consultant urologists’ fees for
private practice work have continued to rise. There is a lot of Choose and Book work in this area of medicine and many consultants have taken advantage of the opportunities in this area.
Growth in selfpay work seems to be lower than in other specialties and, as with all other disciplines, there is constant insurance pressure on fees.
Staff costs fall
Costs have shown a general increase over the 2018 19 year with one major exception. We have noticed a fall in staff costs. AVERAGE INCOME AND EXPENDITURE
This seems to be the result of urologists taking up offers of fully managed services with the various private hospitals they work from. Where consultants employ family members, there has been little change.
Consulting room hire costs have shown some increase, particularly where services are provided. As a result of the Competition and Markets Authority (CMA) rulings, as long ago as 2014, there are relatively few ‘deals’ available now to most consultants.
Indemnity loyalty
Professional indemnity costs have again shown some increase. Consultant urologists as a group seem to be more reluctant to shop around for indemnity cover than some of their colleagues in other disciplines. Many seem to be remarkably loyal to their existing providers.
But there is considerable pent-up demand and we would expect firm growth in income from 2021-22 and beyond
Expenditure
Use of home costs have shown some increase as more consultants do more of their administrative work at home. We expect to see these costs rise in future years, particularly because of changing work patterns as result of the Covid restrictions.
Motor costs, travel and conference expenses and other costs –primarily marketing – all seem to
have shown inflationary increases in the year.
We have noticed a slight increase in the bad debt rate for reasons we cannot currently explain.
The future
Without the hindsight knowledge of the impact of the Covid19 outbreak from March 2020, we would have said that we would expect to see further steady growth.
The Covid outbreak will generate some very strange figures for the next two years. But there is considerable pentup demand and we would expect firm growth in income from 202122 and beyond.
As we stated in our 2020 report in Independent Practitioner Today, it is difficult to effect reasonable year on year comparisons in a fastchanging market. Some urologists, as we have previously stated, have formed groups.
Others have chosen to incorporate through a limited company or have become members of a limited liability partnership.
Some have focused their activities almost exclusively on Choose and Book work while others have pursued private patients.
A small number of urologists have taken up an employment option with leading hospitals to undertake their private work. We expect this trend to continue in the next few years.
All these factors make comparisons, year on year, increasingly dif
ficult. We have also changed the criteria for eligibility in our survey. Consultant urologists now must earn at least £10,000 a year gross in the private sector – previously £5,000.
Our other criteria for entry are that consultant urologists must:
Hold either an old style or a new style employment contract with the NHS. Consultants in this survey do not work exclusively in the private sector;
Have been in private practice for at least five years;
Have been earning at least £10,000 a year from private practice;
Trade either as a sole trader, through a limited liability com
pany or limited liability partnership or as a member of some other group;
Note that although our samples may not be statistically significant, they do try to represent what is happening to a typical consultant urologist’s private practice in the UK.
Next month: Anaesthetists
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists, Stanbridge Associates Limited
HOW ARE YOU DOING?
THE PPR
(THE PRIVATE PRACTICE REGISTER)
Healthcode is the UK’s official medical bill clearing company and has provided secure and encrypted systems to healthcare professionals since 2001. Pre-pandemic we processed around 27,000 electronic medical bills to insurers daily.
What does The PPR mean for practitioners?
out and continuing, in private practice to maintain and market their practice profiles.
The PPR is a solution that unites the sector. It is a secure online platform where practitioners can control their practice information and documents in one place, ensuring they are up to date and accurate. More than 24,000 practitioners now have a PPR profile, at zero cost, which provides a detailed picture of their clinical practice.
One centralised record to increase transparency
Easily keep up-to-date information in one central location and provide visibility to the organisations you have a relationship with.
Remain in control, build and maintain your profile
Once you have a PPR profile, you can build on it as your capabilities and/or qualifications expand, ensuring practice rights are easy to maintain.
Alignment with the Medical Practitioners Assurance Framework (MPAF)
Ongoing development to support the requirements of the industry-adopted framework.
Fast-track your application for Private Medical Insurer recognition
Easy application for recognition with multiple insurers.
YOU’LL
Coming in our May issue, published on 11 May.
Tax charges on your pension – and what you can do about them.
Specialist medical accountant Ian Tongue reports
Are private doctors’ social media stunts worth the reputation risk?
Self-pay. Our analysis looks at the latest trends and the outlook for the months ahead
Learning lessons from urology claims – Dr Shabbir Choudhury, medico-legal adviser at the Medical Defence Union, analyses clinical negligence claims affecting urologists and provides advice on managing risk
Clinical codes are widely used in independent healthcare, but making sense of all those letters and numbers can feel like trying to master a foreign language. Jess Donelan looks at the growing significance of coding and offers practical advice on using codes when submitting bills
Our serialisation from Dr Clare Gerada’s book ‘Beneath The White Coat – doctors, their minds and mental health’ delves into the issue of doctors as patients. It is often said doctors make the worst patients. But she says once services can offer confidentiality, containment and skill in managing their problems, doctors are willing to present to care
Creating high-performing teams: As leaders, doctors want to lead high-performing teams and, as team members, they want to be working as part of them. But how do we establish a great team, how do we lead one and how do we play our part in contributing to the success of the team? Jane Braithwaite presents some interesting ideas that you can apply in your daily work
INDEPENDENT PRACTITIONER
TODAY
The business
Published by The Independent Practitioner
Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution.
Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Lisa Davison, real estate partner from specialist healthcare law firm Hempsons, looks at the merits of using a Declaration of Trust as a tool to protect valuable property investments
High-profile cases have put the spotlight on the consent process and clinicians are increasingly aware of the risks; however, data shows a number of claims alleging that a clinician failed to explain alternative treatment options. Medical Protection’s Dr Emma Green looks at the case law surrounding therapeutic options, GMC guidance on consent and how these impact on the information provided to patients
Dr Kathryn Leask discusses the GMC’s updated prescribing guidance and its impact on private practitioners
Our Business Dilemmas series advises on the role of the doctor as an expert witness and also tackles a query from a psychiatrist asked by the police for a patient’s medical records to help investigate a crime
Branding your practice: how smart use of colour helps you close the gap between good and bad branding
If you work in a private patients unit in the South-west, then don’t miss Philip Housden’s special report
Anaesthetists, check out our latest earnings survey in your specialty
Our motoring correspondent Dr Tony Rimmer tests the all-electric Volkswagen iD3
Plus all the latest news and views.
Don’t forget – you can find more news on our website throughout the month
ADVERTISERS: The deadline for booking adverts in our May issue is 23 April
Write to Independent Practitioner Today 7 Lindum Terrace, Lincoln LN2 5RP
CHANGING ADDRESS, EMAIL ADDRESS OR SUBSCRIPTION DETAILS? Phone 01752 312140 or email karen@marketingcentre.co.uk
To advertise in the journal or our website business and lifestyle directories, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912 Email: andrew@spotonmedia.co.uk
Follow Independent Practitioner Today on
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners.
£90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE
Email karen@marketingcentre.co.uk or phone 01752 312140
Publisher Gillian Nineham
Phone: 07767 353897.
Email: gillian.nineham@gmail.com
SAVE £15 WITH DIRECT DEBIT!
Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.