The business journal for doctors in private practice
Avoid property funding pitfalls
A financing expert shows you how to navigate the borrowing maze when financing a building project P14
A litmus test for financial well-being
How internal audit can help private practice businesses assess the accuracy of internal controls P18
Need I spell it out for you?
Outsourcing secretarial services may be all the rage, but doctors must remember to remain clear in their dictation P28
Help stop tax rise
By Robin Stride
Independent practitioners are being urged to sign a petition aimed at protecting private patients from further increases in the insurance premium tax they pay on health cover.
Supporters of a new campaign, launched by the professional body representing companies who sell an estimated 70% of the UK’s private medical insurance, fear the tax element on policies could otherwise be the same as VAT.
But they warn thousands of policyholders could not afford a 20% tax level and would cancel their cover – leading to more pressures on an already overloaded NHS. Insurance premium tax rose from 6% to 9.5% in November 2015 and went up to 10% last November. In June, it is due to increase to 12%.
Following the Government’s Spring Budget U-turn on a planned National Insurance increase for the self-employed, Chancellor Philip Hammond will look to make up the shortfall and there are concerns insurance premium tax will be targeted this Autumn.
Now the Association of Medical Insurers and Intermediaries (AMII) has asked Independent Practitioner Today readers for their help.
Its chairman Stuart Scullion said: ‘We need the backing of the consultants who do private prac-
tice to support the insurance premium tax petition. It is in the interests of everybody – especially the consumer.
‘We want them to sign up to the petition and talk about the campaign. I don’t think doctors have been near enough to the insurance premium coalface to be thinking of it.
‘But we need to try and get them to have a better understanding of how insurance premium tax increases do impact on the market.’
The campaign wants to collect at least 100,000 signatures within six months so the whole issue can be debated in parliament.
Intermediaries at the AMII annual meeting reported individuals and companies cancelling private medical insurance policies due to the rising tax element.
Some insured people who have just paid more for policies have seen the tax rise absorbed by their provider. But Mr Scullion claimed this was unhelpful as it made Govern ment think the industry was fair game for further attacks.
Mr Scullion told the meeting: ‘If we do not stand up and make our voice heard, there is a worry that the Government will continue to nudge insurance premium tax up, and this could have a potentially catastrophic impact on industry.
‘I’m concerned that if we don’t speak up now, insurance premium
tax could reach 20% by 2020, if not sooner.’
He said there was a complete lack of understanding and appreciation of the value the private healthcare sector adds to the UK economy, let alone how it could support an overstretched NHS.
‘We should be encouraging usage of the private sector, not penalising us at every opportunity.
‘We need to fight our corner and lobby anyone and everyone to enlist support in getting this message out.’
Alex Perry, chief executive of Bupa Insurance Ltd, told the meeting in Whittlebury, Northamptonshire: ‘The independent healthcare sector needs to continue to focus on delivering the
best possible outcomes for our customers and the best value for money. We must also speak up for a fairer tax environment.
‘Insurance premium tax on health insurance is unfair and counter-productive. The Government’s loading of tax onto health insurance has already seen the number of people who pay for health insurance themselves shrink by a third since 1997.’
STUART SCULLION, chairman of the AMII
‘I am concerned that if we don’t speak up now, insurance premium tax could reach 20% by 2020, if not sooner’ ➱ continued on page 2
when gmc says to involve a Pc
Protecting confidentiality kicks off a series by the MdU on doctors questions P10
be a smart talker with patients
A look at the options for private practices to communicate with their patients P12
you can promote yourself cheaply
Marketing your practice need not cost the earth, argues surgeon dev Lall P21
Freelancers beware
A new tax law is causing anxiety for those working for hospitals and via agencies P24
take a leaf out of a successful book doctors can boost patient satisfaction by taking cues from the business world P34
mind your contract language
Legal advice on contractual terms and conditions you need for your business P38
Let’s fight iniquitous tax
Private doctors are being asked to sign a petition lobbying Government to get its hands off health insurance premiums (see story on page one) and we hope you give it strong support.
Successive rises in insurance premium tax on private medical cover means policies are being cancelled. People go instead to an overstretched NHS.
The tax is due to go up to 12% in June and could increase again in the autumn. It has already risen by 66%, up from 6% to 10%, in just over a year.
HM Treasury sees it as lowhanging fruit for generating revenue and some medical
insurance industry leaders fear 20% is possible.
For years, the biggest inflationary factor on premiums was medical costs. But now taxation is becoming one of the biggest drivers of premium rises.
A petition supported by enough doctors and private healthcare insurance/health cash plan customers will send a clear message to Government and raise public awareness of the impact of these tax hikes. Health is different. It’s not the same as general insurance products or other employee benefits. And it should not be taxed in the same way either.
tell US yoUr newS Editorial director Robin Stride at robin@ip-today.co.uk Phone: 07909 997340 @robinstride to advertiSe Contact advertising manager Margaret Floate at margifloate@btinternet.com Phone: 01483 824094
to SUbScribe lisa@marketingcentre.co.uk Phone 01752 312140
Publisher: Gillian Nineham at gill@ip-today.co.uk Phone: 07767 353897
Head of design: Jonathan Anstee chief sub-editor: Vincent Dawe Circulation figures verified by the Audit Bureau of Circulations
Inheritance tax rules shift
Family homeowners will benefit from inheritance tax (IHT) rule changes from this month.
A new allowance, the residence nil rate band (RNRB), will add £100,000 to an individual’s own nil rate band of £325,000 on condition the main residence is passed upon death to direct descendants such as children, grandchildren and step-children.
The allowance, being phased in over four years, will rise £25,000 each tax year until 2020 when an extra £175,000 allowance per person will be available. The new band, also known as the family home allowance, is transferable between spouses and civil partners, permitting them to pass on up to £1m wealth without incurring tax.
Patrick Convey, technical director of specialist financial planners Cavendish Medical, said the increased IHT allowance was good news for doctors, but there were vital issues to consider. The new allowance will be unavailable to the childless or those with £2m+
estates, where the RNRB will fall by £1 for every £2 the estate exceeds this figure.
He said this might seem a substantial headline sum, but many families had seen significant growth in their property’s value since buying.
A couple each with property and investments worth £1.5m would be hit if the first spouse died leaving everything to the other.
‘The surviving partner suddenly has a £3m estate – far exceeding the family home allowance. This is where careful will planning can be so important.
‘We meet a surprising number of high-achieving individuals who have not reviewed their will in the last ten years, when new regulations, tax considerations and personal circumstances have changed considerably. It is imperative you check if your will and subsequent IHT plans are still fitfor-purpose.’
The basic IHT nil rate band has been frozen at £325,000 until the end of 2020-21 tax year.
Public backs tax-free private health cover
Bupa research reported in Independent Practitioner Today in February found 58% of the wider public believes health insurance should be tax-free like life or critical illness cover.
Bupa’s Mr Perry said as the challenges for the UK healthcare system became more urgent, a full and open debate on future funding was needed – including the role that insurance can play in the system.
Fiona Booth, chief executive of the Association of independent Healthcare Organisations, said: ‘The UK independent hospital sector wants to help alleviate pressure on the NHS by encouraging patients to use their private medical insurance.
‘Increases in insurance premium tax may disincentivise people to take up or continue with private medical insurance, which will only serve to increase the pressure on an already overstretched NHS.’ add yoUr SignatUre to tHe camPaign at amii.org.uk/ipt-petition
continued from front page
Software that banishes red tape is a hit with doctors
Over 1,500 independent practitioners have so far joined Healthcode’s new online register – billed as the definitive source of information about private doctors.
Private Practice Register (PPR), launched last summer, is free and aims to help doctors build their practice.
Doctors can complete a single online form covering the minimum information required by different insurers.
They can select those they want to register with, including some smaller providers they may not have previously considered, potentially helping them to attract new patients.
Healthcode’s managing director Peter Connor said the response showed there was a real appetite for a service that banished private healthcare red tape, starting with the insurer recognition process.
‘Healthcode’s long-term ambition is to connect independent practitioners, private medical insurers and hospital providers through our secure online services so that all can work more effectively together.
‘The PPR is a critical element in this project: it showcases practitioners to other stakeholders, establishes secure lines of communication and it’s fully integrated with our ePractice solution, so practitioners can easily manage their profile and practice in one location.’
Healthcode said PPR had received an early vote of confidence from private medical insurers including AXA PPP healthcare and Aviva, who recognised its potential to streamline their provider recognition processes.
A PPR profile gives free access to Healthcode’s secure messaging service, enabling the sending of encrypted confidential and sensitive information such as financial and patient data to insurer and hospital contacts.
Action to tackle indemnity subs
by leslie berry
A defence body has acted to try and halt further heavy increases in medical indemnity costs arising from a change in the formula courts use to decide compensation payments.
Last month, Independent Practitioner Today reported the future of potentially thousands of consultants and GPs in private practice was threatened by a lowering of the discount rate from 2.5% to -0.75%.
As doctors waited to find out the impact on their subscriptions the Medical and Dental Defence Union of Scotland (MDDUS) said it was exploring ‘all necessary action’ to protect members.’
It challenged the Lord Chancellor Liz Truss to stay implementation while showing her reasoning in greater detail and said legal advice suggested she had erred legally in the process and substance of her decision-making.
The union added: ‘We do not discount further action once we have studied her response.’
It gave a cautious welcome to a Ministry of Justice consultation document on how the discount rate should be set in future. The MDDUS claims the solutions are
‘Calamity’ looms for defence fees
tort reform, cost-capping and clearer, more transparent and broadly-based tests for setting the discount rate.
Scotland has followed England with the same discount rate cut. MDDUS chief executive Chris Kenny called it ‘good news for lawyers’, adding that it was disappointing Scottish ministers followed England ‘in this potentially legally flawed decision’.
The Medical Defence Union (MDU) said it was doing all it could to try and minimise the impact on members.
It warned in March of a ‘calamitous’ impact on members. But there was a pleasant surprise for some consultants when their 2017-18 subscription notifications arrived later, as the projected
increase caused by the changed discount rate was not factored in.
The MDU said most had not risen, or increased slightly on last year, and these were already committed to before the rate decision announcement.
A spokeswoman said: ‘These subscriptions, which take effect for members renewing on 1 April 2017, reflect the claims experience in each specialty. However, we are assessing whether further changes are needed as a result of the discount change and will keep members informed.’
Examples of costs given were:
Anaesthetics: £100k nonindemnified income (NII); £6,815, no change;
Urology: £100k NII; £24,970, no change;
Orthopaedics, excluding spinal: £75k NII; £30,750, down 2.5%; Gynaecology: £75k NII; £33,913, down 1.9%.
Medical Protection Society chief executive Simon Kayll said the impact on consultants depended on the amount of private work they did and their specialty.
‘We will communicate any changes to subscription rates to members directly as they approach their renewal dates.’
Get updated in your specialty
‘Independents’ Day’ – The London Healthcare Conference – has announced speakers for its Royal Society of Medicine event on 4 July.
Keynote speaker is Dr Kevin Fong, a consultant anaesthetist at University College London Hospital and expert on space medicine and extreme environment physiology.
Lead speakers (see below) have also been announced for 12 specialty areas. Many of them have a strong academic position as
well as NHS and private practices. The conference, promising ‘cutting-edge academic and clinical insight from leading consultants’, is supported by the Independent Doctors Federation Education Trust and is accredited for continuing professional development.
Cardiology: Dr Julian Jarman;
Dementia/neurology: Dr Ben Turner;
Diabetes: Dr Mark Vanderpump;
Fertility: Mr Michel Dooley;
Imaging: Dr Simon Padley;
Mental health: Dr Michael Craig;
Neurorehabilitation: Dr Richard Greenwood;
Oncology: Dr Peter Harper;
Orthopaedics: Prof Justin Cobb;
Paediatric allergies: Prof Gideon Lack;
Advances in surgery: Mr Charles Imber;
Spinal surgery: Mr Peter Hamlyn. For further details, go to the website www.londonhealthcareconference.org.
Private GPs to rise Salary plan unpopular
By Robin Stride
Private GP numbers could be swelled due to the number of fedup NHS doctors who want to leave their jobs, according to an Independent Doctors Federation (IDF) leader.
Dr Neil Haughton, chairman of the body’s GP Committee, said: ‘The way that NHS practice is heading could well push NHS GPs into more independent or mixed practices.
‘Our colleagues’ morale is at rock bottom and a third of NHS GPs are due to retire in the next five years.’
Private GPs push to get NHS listing
The Royal College of General Practitioners will lobby to get private GPs onto NHS databases so their practices are recognised by hospital computing systems.
IDF GP Committee chairman Dr Neil Haughton said: ‘We should then finally receive discharge summaries and other communication when care is shared between the NHS and private sectors.’
He reported that the Care Quality Commission (CQC) was keen to promote this connection, which was a basic patient safety issue.
Doctors thanked for trialist role
Private GP practices who volunteered for pilot inspections from the Care Quality Commission were thanked by IDF GP Committee chairman Dr Neil Haughton.
He said the inspections ‘emphasised the problem that guidelines from head office have to filter down to the actual inspectors on the ground’.
New chairman
Consultant gastroenterologist Dr Sean Preston is the new chairman of the IDF Specialists’ Committee.
In his annual report, he pledged the IDF’s help for any GP wanting to provide private care or go fully private.
The federation could offer advice networks, seminars, online help and the ‘vast experience’ of private GP members.
Dr Haughton told the IDF AGM:
‘The more entrepreneurial practices are seeking to make their work more efficient and rewarding by privatising certain services such as minor surgery or joint injections.
‘This would not compromise NHS service, but would complement it and attract more doctors
Dr
Neil Haughton, head of the IDF’s GP Committee
into primary care, which is essential for the future of the health service.’
He said the IDF’s mission was to attract more members and be more representative of private medicine nationally. But he expected new members would mainly be consultants, as most private GPs, especially London full-timers, had already joined.
GPs still free to refer
Private GPs’ concerns about ‘managed care’ – where GPs are bypassed in specialist referrals – are now better understood by private medical insurers, the IDF believes.
GP Committee chairman Dr Neil Haughton said the group had continued to engage with insurers, although the insurers had pointed out that many NHS GPs did not know which consultant to refer to, either privately or on the NHS, as links between primary and secondary care had been ‘sadly eroded’.
For the most part, private GPs could still refer to their preferred specialist.
Dr Haughton added: ‘Bupa has been especially responsive and acknowledge that GP-initiated investigation could actually save them money by avoiding unnecessary referral, and we shall be pursuing this in the year to come as well as other initiatives.’
Continuing difficulties faced by private GPs when trying to make referrals to NHS hospitals for NHSregistered patients are being taken up by the IDF.
Health authorities and NHS England have admitted there is no statutory reason why this should not be possible.
New president’s challenge
IDF new president Dr Brian O’Connor said it was ‘a privilege and a challenge’ to be in post at a time of big change in the private medical sector.
He looked forward to the profession ‘gaining lost ground’ and said
without doctors’ contribution and engagement in the independent care sector, private practice would cease to flourish.
The IDF had enjoyed some successful negotiations with private medical insurers, he said.
Ideas to attract younger members
IDF chief executive Sue Smith aims to encourage more younger members to step forward and help the body build a stronger voice.
The federation plans a wide range of activities including break-
fast tutorials, basic life support training, child protection training, a sailing day, a golf day and a musical evening.
Members are welcome to suggest other activities.
Salaried consultant jobs in private practice are in the offing from at least two hospital groups, as Independent Practitioner Today has previously reported, but they don’t look like attracting IDF members.
President Dr Brian O’Connor asked for a show of hands at the AGM from anyone who would contemplate the idea.
Only one consultant put his hand up, and then explained to quizical colleagues: ‘I’d contemplate it – but would then reject it.’
The straw poll came after Mark Rainey, director of Phy sician Services at HCA Healthcare UK, gave observations on the London market and outlined physician employment by his firm in the US. He highlighted ten reasons why consultants might favour employment: practice management demands, economic pressures, technology and IT investments, work/life balance, focus on quality and pay-for-performance, physician shortages, insurers’ financial pressures, succession planning, indemnity insurance and growth of hospital-based physician programmes.
Fees publishing body ‘unknown’
The Private Healthcare Information Network (PHIN) is charged with publishing fee and outcome information on consultants’ and hospitals – but still has to make some headway in publicising its role to private doctors.
Dr Brian O’Connor, outgoing specialist committee chairman, said he did a straw poll of independent practitioners and people did not know what it stood for.
‘Get involved’
New blood and fresh minds are being invited to bring their skills to the IDF’s committees. Outgoing IDF president, private GP Dr Peter King-Lewis, appealed to them to get involved to help shape their careers and their futures.
independent doctors federation (idf) annual general meeting
Review pricing terms
By Robin Stride
Doctor expert witnesses have been advised to revise their terms and conditions if these have not been updated in the last three years.
Lynden Alexander, who leads an expert witness training programme at Professional Solutions, said updates were needed to cater for many changes in the market. Talking at a BMA conference for doctor expert witnesses, he warned experts were now required
to assess time and cost commitments for their involvement at the outset of the case. In tandem, there was a drive to increase quality.
He advised doctors to be wary of quoting prices without having a very clear understanding of what a particular case would involve.
Doctors needed to be sensitive as to how they could increase efficiency in their work and, if asked if they could do something about the price, they needed to know whether they could cut their fee
and still have a profitable business.
He warned that some doctors quoted for a job thinking they would need one lever file for the paperwork and had then ended up with ten.
Mr Alexander suggested expert witnesses would find it useful to submit an early draft of a report and prevent them spending much time honing the wording, only to find on completion that the instructing solicitor came back wanting lots of changes.
Advice for expert witnesses
A solicitor warned consultants and GPs that expert witness work can be lucrative and rewarding –but it carried some real risks. If they were going to take up this type of specialist private work, then they needed to be committed and do it properly, he said.
Alex Leslie, of Radcliffe LeBrasseur, said some doctors had come unstuck when solicitors occasionally discovered their expertise was not as expert as they claimed.
They should take care with their CV, stay within their area of expertise and be certain they knew the rules they were working under. Law teams looked out for publica-
tions the doctor had put into the public domain to see if their CV was accurate.
Listing ‘dos and don’ts’, Mr Leslie advised doctors to be sure to set out details of the literature or other information they relied on, something many experts didn’t do.
They should also consider whether they would be seen as partial if they failed to set out literature that did not back their opinion.
If they had been previously criticised by a judge, then they should tell the solicitor engaging them and should avoid appearing to decide the ultimate question or disputed facts.
When writing reports, they should use short and simple sentences. These really helped because nothing could be made too simple for lawyers, he said.
The expert witness should also watch their demeanour in the witness box. A judge, jury or panel would be assessing how they gave their evidence and how they reacted to searching and informed cross-examination.
Doctors should also check they were covered for their work in case things went wrong. If that happened and a judge criticised the doctor, then that would affect the witness’s future credibility and potential work opportunities.
AReAS to CoveR IN youR teRmS AND CoNDItIoNS
Acceptance of instructions
Producing the report: advisory/ court reports
Answering questions
Further reports
experts’ meetings
Preparation for trial: conference with counsel
Attending trial: cancellation charges
Disbursements: payment terms
Lawyer
tells how to get witness work
Getting paid for expert witness work can be a big problem, according to a solicitor and marketing expert.
Mark Solon, whose firm Bond Solon trains expert witnesses, said doctors’ marketing involved four ‘Ps’: Price – getting it right; Product – defining the expert witness’s service; Place – how you reach your customer; Promotion – marketing strategy.
Only half of the 150 doctors in the audience admitted to having done any marketing. Of those that did, directories were the most popular avenue.
Mr Solon advised doctors to have a good website and said solicitors found expert witness doctors from the following sources:
The legal firm’s database; Appearances in court on other cases;
Doctors doing expert witness work should make sure their fees reflect their expertise, according to consultant neurologist Mr Michael Gross, of the Neurology Clinic.
He advised the BMA conference audience to take on this sort of work only if they enjoyed the heat of combat. They needed to be resilient and
to be successful they had to remember the slogan ‘preparation, preparation, preparation’. Giving a host of tips in a talk about cross-examination, he warned that barristers were paid to make expert witness doctors look less than competent. But the more aggressive the questioning, the more points the expert witness would be scoring.
Recommendations from clients; Expert agencies;
Directories, databases and professional bodies.
Other marketing ideas for doctors included mailshots, advertisements in journals, articles, meetings and seminars, universities and other academic institutions and internet or literature searches.
bma medico-legal conference
Homes tax catch for going abroad
By Charles King
Doctors who are living overseas and sell a home in the UK should beware of being caught out by changes to the capital gains tax rules, specialist medical accountants warn.
The changes, which came into force on 6 April 2015, mean nonUK residents must pay tax on any increase in the property’s value from that date until the date of the sale, and to submit a capital gains tax return within 30 days of completion.
Melanie Thomas, of Manchesterbased firm Hall Liddy, said there had been a number of cases where doctors had unwittingly fallen foul of the rules.
‘Many doctors who go to live or work overseas are unaware of the changes. If they decide to sell their property while they are out of the country, it often doesn’t occur to them to tell their accountant until it’s time to do their annual tax return, when it may be too late.
‘One client has been hit by a heavy penalty for failing to submit a return within the 30-day period – even though there was no capital gains tax payable. He didn’t inform us of the sale at the time and the solicitors which carried out the conveyancing failed to advise him of the rules.’
The rules apply to non-UK residents selling UK residential property, whether it is their home or a rental property.
They must submit an online capital gains tax return within 30 days of the sale, whether there is any tax to pay or not, and even if they have made a loss on the property. To calculate capital gains due, they will have to have a valuation of property as at 6 April 2015.
Ms Thomas said any tax due must also be paid within 30 days of the sale, although those registered for UK tax can choose to pay it at the same time as tax due for their normal self-assessment – by 31 January 2018 for gains realised in the 2016-17 year.
If the property is held jointly, then each non-resident person must file a return and pay their share of any charge. There are daily penalties for not filing a return.
Expanded knee centre re-opens
GPs and former celebrity patient model Jodie Kidd ( right ) joined surgeons to celebrate The Wellington Hospital’s newly refurbished Knee Unit in St John’s Wood and its 25th anniversary.
The HCA Unit, London’s only dedicated knee surgery unit, reopened following extensive refurbishment and has expanded to ten surgeons.
Unit director and consultant orthopaedic surgeon Mr Howard Ware said: ‘This new refurbish -
ment was a necessary step for us to take to continue providing highquality, cuttingedge treatment and provide the best standard of care for our patients. Our philosophy is very much about providing patients with individual care and joint expertise.’
Surgeons have seen a steady increase in demand for their services with over 2,000 patients
R&D credits easier to get but admin burden rises
One of the few business-friendly announcements in the Budget was the Chancellor’s confirmation that research and development tax credits will be easier to claim in the future, according to a tax adviser.
Gary Telford, director of tax services at medical accountants Shelley Stock Hutter told Independent Practitioner Today this would be good news for doctors in a position to benefit by getting some relief from the hike in business rates.
Chancellor Philip Hammond also delayed the quarterly reporting for businesses with turnover under £85,000. This will be deferred for one year to April 2019, giving them more time to prepare. But Mr Telford warned it would still be ‘an unacceptable burden’ when it arrived. He said it would mean having to buy approved software to be able to run the system and would add to the administrative burden.
Joint enterPrise: (from left)
Mr Michael neeb, HCA international chief executive and president; Dr roger Wolman, rheumatology, sports and exercise medicine; consultant orthopaedic surgeons Mr rahul Patel, Mr robin Pollock, Mr sam oussedik, unit director Mr Howard Ware, Mr Matthew Bartlett, Mr richard Carrington, Mr William Aston, Mr David sweetnam and Mr Chinmay Gupte (knee trauma). Missing from picture – Mr Jonathan Miles.
seen last year and record numbers expected in 2017. Appointments are now available at weekends.
Hospital chief executive Sarah Fisher said the Knee Unit was a real asset for The Wellington Hospital.
‘The multidisciplinary team have always dedicated themselves to providing innovative, comprehensive care to all patients and this refurbishment allows them to continue to provide world-leading care.’
James Gransby, head of healthcare at MHA MacIntyre Hudson, warned the fall in the tax-free dividend allowance from £5,000 to £2,000 a year from April 2018 would be ‘a blow’ for doctors operating through a limited company. It followed hot on the heels of a 7.5% rise to dividend rates that they were already reeling from. See lead story to the right
Bupa wins award for commitment to customer care
Bupa has been recognised for excellent service by winning the Customer Commitment award at the 2017 UK Customer Satisfaction Awards.
Alex Perry, Bupa Insurance Ltd chief executive, said: ‘Winning this accolade is a recognition that the team always works hard to put the customer at the heart of what they do.’
Dividends threatened
By Leslie Berry
Self-employed doctors and those who take dividends from their own limited companies came off badly in the Chancellor’s first –and last – Spring Budget.
However, within hours of announcing tax rises in the form of National Insurance contributions for the self-employed –dubbed a ‘tax on ambition’ – the Prime Minister was quick to push formal proposals back to the autumn.
One week later, amid a backlash from both sides of the political divide, the plans were scrapped altogether.
But independent practitioners running their business as a limited company will still have to pay more tax as plans to dramatically reduce the new dividend tax allowance were announced, just one year after it was created.
From April 2018, the new allow-
ance will be cut from £5,000 to £2,000, affecting doctors who pay themselves in the form of dividends as well as those who hold shares in portfolios outside of ISAs or pensions.
The Government estimates that this move will impact around 2.27m individuals in 2018-19.
Currently, dividend income above the £5,000 threshold is taxed at 7.5% for basic-rate taxpayers, 32.5% for higher-rate taxpayers and 38.1% for additional-rate taxpayers.
Simon Bruce, managing director of specialist financial planners Cavendish Medical, explained: ‘The changes in company dividend taxation announced just last year had already increased tax payments for many doctors running their practices as limited companies. Facing another tax rise so soon will be a further blow.
‘The modest 1% cut in corporation tax previously announced to
New cancer centre to be built in Liverpool
Proton Partners International has announced plans for a new £35m cancer treatment centre in Liverpool.
The Rutherford Cancer Centre North West, to be built in the new £1bn Paddington Village, part of the city’s Knowledge Quarter (KQ), will offer radiotherapy, chemotherapy and imaging from 2018, and proton beam therapy in 2019.
City mayor Joe Anderson said: ‘We are delighted KQ Liverpool has been able to attract another prestigious development to Paddington Village.
Proton’s chief executive Mike Moran said the quarter would be a world-class destination for science, innovation, education and technology.
The centre, one of four being built by the company in the UK, is expected to treat up to 500 patients a year.
Others are being built in Newport, Northumberland and Reading, and other sites are being considered.
start in April 2017 will offer little comfort to high-achieving doctors working long hours to create a competitive and client-focused practice.
‘Investors with shares held outside ISAs or pensions should also take note. With harsh reductions to the lifetime and annual allowances for tax-free pension savings, ISAs are already an important consideration for the successful professional – particularly with the increased limit of £20,000 per annum available from this April.’
The income tax personal allowance rises from £11,000 to £11,500 from April. The higher-rate tax band will rise from £43,000 to £45,000 and the additional rate tax band will remain unchanged, at £150,000.
From this autumn, a new National Savings & Investments bond will be available, paying 2.2% on deposits up to £3,000.
However, Mr Hammond had
earlier announced that inflation is forecast to rise to 2.4% this year –already above the bond’s return. The bond is still likely to be popular given the poor returns available on other cash accounts and the security of a governmentbacked product.
The Chancellor will no longer prepare a Spring Budget, preferring to declare his financial intentions in the Autumn Statement.
Mr Bruce continued: ‘We are unable to control the ever-changing financial landscape, but we can ensure our own finances are in the best possible position to react to opportunities and challenges as they arise.
‘If you are facing higher tax on profits, increased tax from oversaving into your pension – both annually and overall – and reduced tax relief on any buy-to-let properties you own, you should check without delay that your own financial plan is still fit for purpose.’
‘Momentum is really beginning to build for KQ Liverpool and we can expect more exciting announcements like Proton Partners International’s, which will further cement its reputation as a world-leading hub in medical and life sciences research.’
Proton is also building a genomics research centre at the Life Sciences Accelerator building in Liverpool, which will be the first part of a health campus set to surround the £335m new Royal Liverpool Hospital.
The genomics programme will support the firm’s broader research work with the University of Liverpool’s Physics Department. Architects’ impressions of the new cancer treatment centre in Liverpool
Proton’s boss Mike Moran
AccoUnTAnT’s clinic: HEAlTHy cAsH FloW
Cash flow is lifeblood of your practice
Cash is vital to all firms, but some private practices are not doing enough to ensure their business is operating at optimum health. Without a healthy cash flow in your business, you could face problems paying staff, taxes, overheads and fall short of paying yourself a salary. Susan Hutter (right) sets out some useful pointers
Forecasting
Make sure you prepare by having a simple annual forecast of income and expenditure, which is then updated when the actual figures are available and/or when things change.
Forecasting expenditure is relatively easy, as most consultants know what their practice overheads are and the date when payment needs to be made. Important dates to bear in mind include PAYE tax – which is due on the 19th of the month following the salary payment.
For example, PAYE on salaries which are paid in May is due to be paid to HM Revenue and Customs on 19 June.
If you trade as a limited company, corporation tax is due nine months after the yearend date. For example, if the practice has a financial yearend of 31 December, the tax will be due on the 1 October in the following year.
If you trade as an unincorporated business, practice profits will be subject to income tax,
partly due on 31 January in the tax year and partly due on the 31 July following the tax year. For the tax year 201718, part of the tax will be due on 31 January 2018 and part on 31 July 2018.
Income is much more difficult to predict. Generally, it is best practice to base the forecast of future monthly income on the basis of the previous 12 months of business.
Working capital
Working capital is the recurring running expenses of the practice – for example, rent and salaries, including your own drawings –and you should aim to have at least three months of funds in the practice accounts.
Once the forecast has been prepared, you will be able to gauge the monthly working capital requirement. If the practice bank account dips below the three months, you may have to dip into your private funds.
Someone senior in the practice should check invoices from third
parties and it may well be that you, as the consultant, have to do this before passing them to the necessary person for payment wherever possible.
Do make sure, wherever possible, they keep within the payment times stipulated.
Debt collection
It is vital to get out invoices to insurers as soon as possible after the treatment – and make sure this is no longer than a week.
As most consultants are aware, you are in the insurer’s hands with payment times and some are not always the fastest to settle. Someone within your practice should be chasing up insurance companies at least on a monthly basis.
For uninsured patients, it is advisable they settle on the day of the treatment, regardless of how long you have been treating them.
Susan Hutter is a specialist medical accountant and partner at Shelley Stock Hutter
Diplomatic DiSputeS
many consultants have huge difficulties in getting paid for their work done for embassies. if you are not getting paid, you must make sure you do not do any more work for the patients until you are paid for work already outstanding.
i know some consultants who continue to carry on with work despite being owed thousands of pounds. make sure you impress upon them your terms and conditions, otherwise this could impact on your cash flow considerably.
the good news is there are a number of agencies which specialise in helping you collect agency money. While they take a percentage, it is worth it and will undoubtedly reduce the hassle in your working life.
When GMC says to
In the first of a new series for independent practitioners, addressing topics in new GMC Confidentiality guidance, Dr Catherine Wills (below) looks at one of the most common questions to the MDU’s advice line: when to disclose information to the police
DISCloSING INforMATIoN to the police can raise difficult dilemmas for independent practitioners.
If in doubt, ask your medical defence organisation for expert advice before passing on information.
Disclosing patient information without consent can only be justified in limited circumstances. Even if a request is from the police, your legal and ethical duties of confidentiality still apply.
The GMC’s new Confidentiality guidance, 1 which comes into effect on 25 April 2017, says you must not disclose personal information to a third party such as a
police officer without the patient’s explicit consent unless it is required by law, ordered by a court, or justifiable in the public interest.
legally required disclosures
There are limited circumstances when you are legally obliged to disclose or volunteer information to the police, and the guidance says: ‘You must disclose information if it is required by statute or if ordered to by a judge or presiding officer of the court’ (paragraph 17).
Examples include:
➲ The road Traffic Act 1988 allows the police, under certain circumstances, to require information from anyone, which may lead to the identification of a driver alleged to have committed a road traffic offence. It is an offence to fail to comply.
➲ Under the Terrorism Act 2000, it is an offence not to disclose as soon as reasonably practicable information which you believe might be of ‘material assistance’ in preventing an act of terrorism or in apprehending a person who has committed, has prepared or has instigated an act of terrorism.
➲ You must inform the police if, in the course of your work, you discover an act of female genital mutilation (fGM) appears to have been carried out on a girl under the age of 18 in England and Wales.*
➲ You must disclose information if required to do so by a valid and lawful court order. It is important to note that a court may not ordinarily order the disclosure of medical records where criminal proceedings have not yet begun.
In practice, it is a good idea to ask your medical defence organisation to help you check the validity and lawful basis of a court order and understand exactly what it requires, as soon as you receive it.
While you must disclose information required by law, the GMC expects you to satisfy yourself that personal information is needed and required and to disclose only relevant information in the way legally required.
You should also ‘tell patients about such disclosures, wherever practicable, unless it would undermine the purpose’ (paragraph 88).
disclosures in the public interest
In practice, most police requests for information will require you to judge whether disclosing the information is in the best interests of the patient or the wider public interest.
Sometimes, police requests for information without patient consent come with an assurance that the request is made in relation to Section 29 of the Data Protection Act 1998 (DPA).
It is important to keep in mind that, while the DPA may permit disclosure of information without consent, the DPA does not mandate disclosure.
lawfully permitted disclosures of information within the terms of the DPA are not always justifiable on an ethical basis. So, if in doubt, it’s a good idea to get advice from your medical defence organisation about whether disclosure is likely to be justifiable in the public interest.
The GMC’s guidance says that confidential information may be disclosed in the public interest, without the patient’s consent, or exceptionally where consent has
Most police requests for information will require you to judge whether disclosing the information is in the best interests of the patient or the wider public interest
involve a PC
been withheld, if ‘the benefits to an individual or to society outweigh both the public and the patient’s interest in keeping the information confidential’ (paragraph 22).
In other words, you must balance the potential harm to the patient, and to the overall trust between patients and doctors, against the benefit to be gained from releasing the information.
You will need to judge each case individually, considering whether failure to disclose ‘may expose others to a risk of death or serious harm’ (paragraph 64).
In the MDU’s experience, examples of when disclosure will generally be appropriate include if a patient has confessed to a serious crime such as child abuse or has expressed an intention to attack someone.
Another example is if you are concerned a patient poses a risk to the public such as when the patient has made threats of violence.
Examples of serious crime
The GMC does not define serious crime in the guidance but refers to examples given in the NHS’s Confidentiality Code of Practice , 2 including murder, manslaughter, rape, kidnapping and child abuse or neglect causing significant harm.
These decisions are not always straightforward and you should get medico-legal advice if you are unsure.
You should record your reasons for disclosing, or withholding, information, in case you are called upon later to justify your decision. If you do decide to pass on information to the police in the public interest, the GMC says you should ‘disclose relevant information promptly to an appropriate person or authority’ and if it is safe and practicable, you should
inform the patient first, even if you intend to disclose the information without consent (paragraph 68).
It may be appropriate to clarify with the police whether seeking patient consent or informing the patient would prejudice their investigation. You should record the steps taken to obtain consent and your justifications for disclosing information without consent.
other requests
The GMC also says you ‘must participate in procedures set up to protect the public from violent and sex offenders, such as multiagency public protection arrange-
ments (MAPPA) in England, Wales and Scotland and public protection arrangements in Northern Ireland (PPANI)’.
You must also seriously consider requests for information for formal reviews established to learn lessons or improved systems such as inquests, inquiries, significant case reviews and domestic homicide reviews (paragraph 71).
References:
1. Confidentiality: good practice in handling patient information, GMC, 2017. www.gmc-uk.org/Confidentiality2017. pdf_69037815.pdf
2. Confidentiality: NHS Code of Practice; Supplementary Guidance: Public Interest
Disclosures, Department of Health, November 2010. www.gov.uk/government/uploads/system/uploads/attachment_data/file/216476/dh_122031.pdf
* The mandatory duty to report FGM only applies to doctors working in England and Wales. But, of course, FGM is illegal throughout the UK and there may be an ethical duty to report cases for doctors in Scotland and Northern Ireland under safeguarding duties.
The GMC also has guidance which refers to an FGM action plan in Scotland and guidelines in Northern Ireland. www. gmc-uk.org/guidance/27723.asp?dm_ i=OUY,3NFNX,JWQ6LB,D4L9E,1
Dr Catherine Wills is MDU deputy head of advisory services
kEEPing in TOUcH WiTH PATiEnTs
Be a smart talker
Communications between many practices and their patients in this digital age need improving. Jane Braithwaite (right) says it is important for all of us to learn about the options now available and to take a view on which system might best suit our practice and our patients
Communi C ation with patients is key to all medical practices and there is an abundance of technology available to assist.
in a previous article about how to get more patients (‘Be more attractive’, September 2016, and on our website www.independent-practitioner-today.co.uk), we considered ways to use technology to communicate from a marketing perspective.
t his month, i discuss how we communicate with our existing patients to increase loyalty and improve their level of satisfaction with our service.
Before we think about technologies to improve communication, we need to start by focusing on
what our patients want, then we can have a sensible discussion about the right technology to fulfil those needs.
Let’s start by asking ‘What do patients want?’ we know what patients want when they visit their doctor. they want good eye contact, undivided attention and time to have a full discussion about their concerns and worries.
Patients also demand privacy and to be treated with respect. in the private medical world, these face-to-face interactions are critical, but we need to think carefully about the other aspects of the service we provide.
How does a patient want to book an appointment?
is phoning the medical secretary the best option for them? i f a patient has read an article in the press, how can they check out their concerns with their doctor? arranging follow-up treatment, getting a repeat prescription and dealing with the demands of the insurance companies are aspects that patients consider part of the service you provide as a doctor, so your team’s performance in these matters affects your reputation. as a doctor, your reputation will be built on the overall service you provide and not just the treatment you give.
i n their personal lives, our patients are using apps to do their banking, email to ask questions of their children’s school-teachers and online booking systems to schedule yoga classes.
i n business, conference calls and Skype are used daily to communicate and avoid travel. it follows that these same people want and expect to have these options when communicating with their doctor as a patient.
What do doctors want?
Doctors want to maximise the time they have available to attend to patients. most doctors do not want to spend time booking appointments, dealing with random questions and the ongoing demands of insurance companies. these tasks are delegated to the medical secretary, who is a key
member of the team and is building a good reputation with patients by delivering the services the practice’s patients need. we also want to run our practices on a cost-effective basis. to do this, we need to ensure that practices are resourced well, but we need to take care that the resources are employed wisely. most practices still consider the phone to be the key method of patients communicating with them.
But handling large volumes of calls is difficult and some practices regularly have a voicemail message stating that the phones are so busy that patients should leave a message which will be replied to by the end of the day. m any practice emails also return an automatic ‘out of office’ message to patients’ emails asking them to call, as the email may not be answered promptly. So the problem is exacerbated.
Research shows that most patients aged 50 and above prefer to use the phone to call their doctor, but younger patients would prefer to use email or book online. we should aim to meet both demands and at the same time reduce the administrative burden on our teams.
t he benefits of using digital communications to communicate can be summarised as:
➀ to deliver the high-quality service our patients demand; ➁ to enable us to achieve number 1 in a cost-effective manner. So we start by deciding which aspects of our service need to be improved and then consider how to achieve this.
Day-to-day communications many patients prefer email communications to phone and we should embrace this.
Email is convenient to patients, as they can write a quick note
with patients
We should stop seeing emails as annoying and embrace this communication method
10
tips to improve your practice’s
communication
❶ use email and online booking to relieve the pressure on phone answering
❷ utilise text messaging and emails to send reminder emails and confirmations
❸ provide new patients with a guide to your practice that covers communication and the options open to them
❹ investigate using an online booking system
❺ prepare patient guides to answer frequently asked questions and post them on your website
❻ use your website to support your efforts. your patient guide should be available on your website
❼ consider a monthly newsletter to patients keeping them updated about your practice and covering any recent press articles that may have caused undue concern
❽ consider making videos to answer frequently asked questions and post them on your website
❾ respond to press articles on your website
❿ investigate using a patient portal and keep abreast of developments in this area
while on the tube or in the evening when they have spare time. it is also more private than making a phone call.
managing emails is much easier and cost-effective than managing phone calls, which are real time and intrusive. we should stop seeing emails as annoying and embrace this communication method. written communications also have the benefit of providing a documented trail of the conversation.
So, i would advise you to cancel the ‘out of office’ encouraging patients to call you and replace it with one stating that a response will be provided within a certain time-frame so that expectations are set.
then develop an email strategy with your team. Perhaps agree a process with your medical secre tary so that all emails are responded to within four hours to ensure a timely response and avoid a follow-up call.
Online appointment booking m any patients are familiar with using online booking systems. For example, the mind Body Connect app is used by 35m active con sumers in 130 countries to book wellness services from fitness classes, beauty treatments to physiotherapy. users can book an appointment, which is then auto matically updated into their online calendar with address details and other information.
i t is only natural that these same patients will expect this technology from their doctors in the very near future.
most practice management sys tems offer an online booking sys tem, and Doctify is continuing to develop this as a key benefit of its system.
You can, of course, develop your own facility on your website, but it is worth considering the pros
and cons of this approach, especially the costs involved.
Dealing with ad-hoc questions
Between appointments, many patients ask question relating to their symptoms, medication and treatment plans. t hese can be time-consuming and often very repetitive for doctors to answer.
i f you have embraced email, you have already made this more manageable and these queries can be answered in a standardised
Patient guides can be prepared to answer the more frequently asked questions relating to medication and treatment plans.
t hese can be emailed out to patients to answer their question more fully. t hese same guides could also be used as blog articles or factsheets on your website.
Patient portals
there is much discussion about patient-centric care: patients taking more control over their own health information. Patient portals are a great way to enable this and there are various systems available. i t is important for all of us to learn about the options available and to take a view on which system might suit our practice and our patients best.
How to keep patients satisfied, page 34
Jane Braithwaite is managing direc-
Property Finance for the Independent Healthcare Sector
Avoid property funding pitfalls
AS your practice grows, you will invariably require more space or new space.
This may mean converting newly acquired premises or extending your existing property.
u nderstanding lenders’ concerns and how they approach a funding proposal will help independent practitioners manage the process of borrowing money and ultimately allow them to be better placed to succeed in raising the funds for their project.
A look at a recent case based in the Home Counties will help to illustrate some of the issues that arise.
development funding case study
A private healthcare practitioner bought a high street commercial unit and successfully secured planning permission to refurbish and extend the property, creating several hundred square feet of modern consultancy D1 space. D1 is a category of land use under the Town and Country Planning ( u se Classes) o rder 1987 – as amended. It covers several non-residential institutions including clinics, health centres, crèches and day nurseries among others. The practitioner’s intention is to provide lettable serviced
Lenders in the market are keen to finance private practices looking to refurbish or develop their premises. Maurice Citron (right) maps out the risks in the lending process and how best to navigate the borrowing maze
space to other private consultants.
Commercially, the business plan makes good sense. The area in question is affluent and there is a lack of local and accessible space to support growing private healthcare demand. As traditional retail use continues to decline on the high street, there is an opportunity for alternative uses and D1 is one of these.
However, from a lending perspective, a case like this can fall between two stools and possibly more.
lender’s classification
The works to the premises were substantial enough to be classified by most lenders as development. However, the client is not a developer. Their experience and knowledge is healthcare.
An important prerequisite for development finance is the ability to evidence a solid track-record of previous successful projects. Notwithstanding the borrower being considered a very credible candidate, the application stalled with several lenders because the case couldn’t be classified into their lending criteria.
The healthcare team couldn’t take it on because the works constituted development and the development team turned it
down because the client wasn’t a developer.
Any lending proposal has to meet the lender’s criteria to be successful and it is worth considering the process from their perspective.
Lenders continually analyse their loan book to develop lending strategy. Lending criteria puts this strategy into practice. It enables the lender to decide the levels of debt they are prepared to lend and uses defined parameters applied to the borrower, the property and the track-record of the business.
The criteria set out loan-tovalue limits, debt servicing ratios and the returns required for the actual and perceived risks taken. The criteria and strategy are continually responding to the market and the wider economic context.
In our case study, lenders found it difficult to classify the proposal into their existing criteria and this can be a frequent problem with small-to-medium healthcare development projects.
Some lenders had issues with the status of the end user. The vast majority of practices are classified as owner-occupiers.
Lenders like healthcare occupiers for one very simple reason. Historical analysis over the years
l British company comprising experienced specialist medical and medico-legal report transcribers.
l Information Governance and Patient Confidentiality adhered to at all times.
l Familiar with DGL/PMMS/Mosaiq as well as bespoke template provision.
Same lead typist with back-up always available. Your own dedicated Medical Account Manager. Recommended by Clinicians and Expert Witnesses nationwide because . . .
l Set up an OutSec account today and have total flexibility with no contract or monthly fees.
SSL secure data transfer (as used by all the major online banks). Record and send your audio files using an iPhone, Android or digital dictaphone from anywhere in the world.
– and property cycles – show healthcare owner-occupiers are less likely to default on their obligations compared to other property borrowers. As a sector, healthcare carries less risk and lenders will offer higher loan to values and more competitive debt pricing as a result.
In our case study, the business plan was based on receiving rent for serviceable space, and some lenders considered this investment.
Investment lending terms can be more onerous then those offered to owner-occupiers and again a seemingly good match was derailed.
Healthcare development is usually considered as commercial development, which can be disadvantageous. residential development, on the other hand, is the primary focus for many lenders given the well-established undersupply of housing nationally.
However, there is a strong case for lenders to take a nuanced approach to healthcare development. on the whole, developers are focused on the exit. Their commitment to the project ends when the finished product is sold.
In contrast, healthcare commitment continues past the point of practical completion because the intention is to occupy the prop-
kEY FACtORS In thE LEnDInG PROCESS
VALUAtIOn
the loan as a percentage of the property’s value is one key criteria for lenders and determines the limits of what they will lend.
the lender will want to know the open market value of the property as it currently is. this may be difficult to establish if there are not many comparable properties in the local area that are being used for the same purpose.
the estimated end value of the completed property is also necessary.
At the start of the funding process, it could save time and be costeffective to instruct a chartered surveyor with experience in the healthcare sector and request a valuation report.
this will provide real substance to the figures and will give confidence to both the borrower and the lender. Any offer of funding will ultimately be subject to valuation, so having a handle on the values at the start of the process will be very useful.
tRADInG PERFORMAnCE
Lenders want to see your financial forecast or track-record, which will show them there are enough earnings in the business to service the debt. this will probably include interest payments and capital repayments with a certain amount of additional capacity to protect against interest rate volatility. there are different ways of measuring performance, but ‘earnings before interest tax depreciation and amortisation’ (EBItDA) is one measure preferred by many lenders.
As a sector, healthcare carries less risk and lenders will offer higher loan to values and more competitive debt pricing as a result
erty. The intention is critical. It will define the commercial attitude to the project from the outset.
solutions are out there
Fortunately, there is a plethora of property financiers in the uK who can provide a solution for most problems and, in the right hands, there are means and ways to mitigate the risks that concern lenders.
The practitioner in our case study succeeded in obtaining several offers of funding relating to different stages of the project. For example, short-term funds were offered for the construction phase up to practical completion.
These funds would then be re financed to a different lender providing a 20-year amortising term loan. The lender was provided with additional comfort by leveraging supporting assets.
With funds in place, construc-
Earnings will be considered in terms of how resilient and predictable they are. A resilient turnover is key now that we are in the Brexit process.
Lenders will want comfort that the business cash flow will be able to repel recessionary factors as the Uk adjusts to being apart from the EU. that said, the healthcare sector has historically proved to be relatively resilient to downturns, which is why many lenders are keen on the sector.
tion is due to start early this spring, with the opening set for the middle of summer.
Having the benefit of experience will make a difference to securing development funds. A comprehensive appraisal is necessary to ensure every possible funding route has been considered and explored.
Practitioners would also do well to ensure they have full unrestricted access to the entire lending market before they commit to a lender.
of course, all lenders will have their specific lending criteria in place, but solutions will be more forthcoming with those lenders –and particularly the people in their team – who are less processdriven.
Process lending usually works well where there is a high volume of transactions and cases can be easily pigeon-holed. However, pri-
vate healthcare development is a deviation from the norm and a more borrower-focused attitude will help deliver results.
In summary, lenders are keen on the private healthcare sector because of the sector’s track record. They understand private healthcare demand is traveling in one direction given population trends and the stresses on the NHS.
There is finance out there for healthcare development. The lending process should become easier as demand in the market grows and more projects are delivered raising confidence generally.
In the meantime, the current funding pitfalls can be managed to secure finance for private practice projects.
Maurice Citron is director of Citron Singer Finance, a property finance broker specialising in the healthcare sector
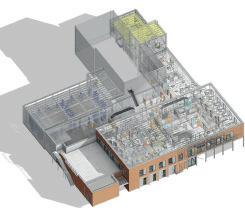
An architect’s impression of the rear of completed high street development of a private practice clinic in the case study
mEdicAl TAlEs
American dreaming
Cosmetic surgeons loved to be invited to Californian babe parties. It was where they did most of their recruitment. TV doctor and fulltime writer Dr Michael O’Donnell (left) draws from his new book,
Medicine’s Strangest Cases
Some 40 years ago, many of the strangest cases in American medicine – strange to european eyes, that is – regularly put themselves on display at cocktail parties in southern California.
During the 1970s, plastic surgeons took over from psychiatrists as purveyors of the American Dream, as many Americans decided that what was holding them back were not inhibitions but baggy eyelids, baldness or sagging boobs.
Suddenly, physical image became as important as mental cleanliness, and personal fulfilment was not so much a matter of letting it all hang out as having it all tucked in.
The parties were the surgical equivalent of Tupperware parties. In southern California, a woman who’d had a face job, a nose job, a chin job or a boob job would give a cocktail party for her plastic surgeon just as soon as the scars had healed and invite her friends round so they could see what he had done for her.
The women had no inhibitions about their operations. Damn it all: the surgery was so expensive, you wanted folks to know you could afford it.
The surgeons, whose role hovered uneasily between doctor and gigolo, were delighted to attend, because the show-off parties were where they recruited most of their future customers.
In october 1977, when I visited the annual convention of American cosmetic surgeons, the high seriousness of the scientific programme was undermined by the whispered observations in the cor-
ridors. ‘Guess whose nose he just got … There goes the Boob King of San Diego … That guy’s re-slung half the asses in Beverly Hills.’
The length of the limousines that queued to collect their owners at the end of each day fuelled the suspicion expressed by other American physicians that cosmetic surgeons were doctors who trained to do good, then learned to do well.
The stands in the exhibition hall did a brisk trade in aids to selfadvertisement. one offered ‘customised visiting cards’. What on earth is a non-customised visiting card?
o n the back of his cards, the purchaser could have a cartoon of an ape-faced man saying, ‘Don’t envy a good complexion, buy one’, or of a woman – blonde, of course – sitting en negligée before her dressing table saying, ‘mirror, mirror on the wall … lie to me’.
cosmetic overkill
Convention hotels offered plentiful evidence of cosmetic overkill. one evening, I happened upon a hotel lobby filled with tuxedoed surgeons and their wives and girlfriends. The women looked stunning and I realised that, when a girl hitches up to a cosmetic surgeon, she becomes a walking, talking advertisement of his skill.
There wasn’t a wrinkle in sight, not even on the petite blonde whose ball gown seemed fashioned from a fisherman’s net of none too narrow a mesh, presumably to show off her guy’s overall competence.
yet the scene was surprisingly unarousing, as unarousing as those
aloof ladies who, when I was an adolescent, posed in their underwear on London u nder ground posters and whose breasts and thighs seemed sculpted from ice.
In 1977, it wasn’t just breasts and thighs. When I got into conversation with a couple of the surgeons’ ‘accompanying persons’, I discovered that their faces were also frozen: hoisted into place so often that, like Nancy reagan ten years later, they were stuck with the same expression whether they confronted tragedy or comedy. Their faces, thanks to their surgeon boyfriends, had become closed books.
The carefree Californian attitude to cosmetic surgery derived naturally from the cult of youth that then prevailed in the southern end of the state.
In Santa m onica, for instance, you qualified for a senior citizen’s pass at the age of 50, but few citizens applied.
on my way home, I discovered that the cult didn’t travel well. o ne of the more depressing features of New york evenings in 1977 was the sight of men in manhattan mid-town bars, weary after a day in the office, striving dangerously to live up – or, more accurately, down – to the age of their hair transplants. Strange cases indeed.
Medicine’s Strangest Cases, recommended price £7.99, ISBn 9781910232941.
Published by Portico, an imprint of Pavilion Books
A litmus test for financial well-being
Every business should have controls to ensure good records and accurate financial reporting. Ebert Hyman (below) explains how an internal audit can help small private practice businesses assess the suitability and accuracy of their internal controls
Audit
to keep your business on track
If you run a small business, you are likely to be exempt by HM Rev enue and Customs (HMRC) from needing to audit your annual limited company accounts.
This said, I would advise you think carefully about introducing some basic controls to help ensure good records and accurate financial reporting.
The size, diversity and complexity of your business are all factors to consider in deciding on action. You may be in complete control or you may be relying on others such as a secretary or bookkeeper to ensure that records are kept and everything is declared.
Regular audits are a very helpful tool to assess progress and accuracy of your controls. The process of audit involves checking transactions, records and systems in order to assure suitability and accuracy.
By conducting these audits, you effectively test your internal controls – to make sure things are happening as they should with the desired outcome.
The key consideration is that the audit needs to be independent and objective in order to be useful. Audit activities can be managed internally or outsourced to your accountant or a specialist thirdparty organisation and you will have to decide which option fits best.
Smaller businesses very often make use of internal audit. Internal audits are perfectly reasonable, provided they are objective and there is a degree of separation between the operator and auditor.
Why audit?
There are several reasons why you should consider auditing your activities.
Audit allows you to:
Assess specific activities to establish whether your business conforms with predetermined contractual, regulatory or statutory requirements. For instance, are you keeping good records in line with HMRC’s guidance?
Assess and regularly review the economy, effectiveness and efficiency in the use of your resources. Are your suppliers giving you value for money?
Determine whether the current management structure and internal controls are fit for purpose. For example, are they effective in achieving company policies and objectives?
Determine whether you have safeguards in place to mitigate potential fraud against the company by employees or management. For example, do you reconcile your takings to what is deposited into your bank account and are they completed accurately?
The list continues.
CASE STUdiES
1. Poor record-keeping
Doctor X trades through a limited company and relies on an employee to file and keep records and receipts of all the businessrelated income and expenses.
The doctor received a tax compliance check letter from HMRC, requesting additional information pertaining to their accounts and tax calculation.
A disorganised process of filing and errors meant that Dr X had to spend several days to help find the necessary receipts and documents.
This resulted in a complete overhaul of the filing process and implementation of a regular audit to ensure that the system remains robust and effective.
2. missed income
Employee Y, an experienced secretary, is also responsible for billing all the patient episodes in a medical practice. Internal controls dictate that she compares invoices with the doctors’ diaries to ensure the billing is accurate and complete.
Dr W keeps a record of the number of patients seen on each day, and decides to audit a small sample of patient files to establish whether the billing has been completed correctly.
It transpires that employee Y missed the billing of some patient episodes, even though there were internal controls which were meant to protect against this.
Dr W and employee Y agree that, in future, there should be a separation between the person billing and the person checking for errors.
3. Unallocated cash receipts
Employee Z is responsible for receipting, recording and banking of cash payments. She is also responsible for reconciling the daily takings against sales reports. She had an inordinate amount of responsibility in relation to receipts and it was noted that the practice was at a high risk of error and potential fraud.
A recent concern over a patient’s payment resulted in an audit to compare the daily reconciliations with money banked.
It transpired that cash had been received and banked, but that the patient account had not been updated.
Regular audits are a very helpful tool to assess progress and accuracy of your controls
Preparing for an audit
The potential scope of an internal audit is wide and there are no mandatory standards to dictate what your approach should be.
Every business will have its own criteria based on its company-specific factors and you therefore have the opportunity to tailor this to suit your needs.
You will need a plan and this should focus on the key risk areas of your business to help you prioritise your efforts. Consider the biggest threats first and the areas where the business is more likely to make errors.
Once you have identified the key areas of your audit, you will need to allocate the audit assignment to the relevant auditor and explain the scope as well as the evidence required to achieve the objective.
Ideally, you should choose someone who has adequate knowledge and experience about the internal processes being audited. This will ensure a more effective and timely audit.
Audit tests
There are several different tests which can be used and the audit plan can include both your financial and non-financial goals.
If you want to make sure that a predefined process is actually being followed, the auditor may perform a ‘walkthrough test’ to confirm that the process does indeed operate in the way that you believe it does.
It may not always be practical to check every single transaction that takes place in an organisation. For this reason, the auditor may decide to test a sample of items to establish whether controls are, in fact, being implemented, tracing each item through the various steps in the process.
Another very useful tool is to check the accounting audit trail, to substantiate transactions by finding the evidence to prove them. This may be looking for corresponding receipts to prove expenses or activity logs associated with declared income.
A good accounting software package will create an electronic audit trial which will help speed up audit checks by producing reports and analysis. Some packages will also give you the option
Ensure you are aware of any big changes in your figures year on year, which may signal attention from the tax authorities
to electronically store documents as evidence of transactions.
The auditor may also use analytical tools such as spreadsheets to compare datasets to identify ratios and key variances. Ratio and variance analyses are then used to identify unusual movements or irregularities which can be investigated as they occur.
The audit findings should be documented and then reviewed by the responsible person. The findings may indicate the need to update internal controls and processes where failings have been identified.
Considerations
Consider and regularly review your process of recording transactions to ensure accurate reporting of your operations. At the same time, make sure you have a process to file, organise and store associated documentation.
While audits are periodic, internal controls govern the day-today activities of the business. You should not have to wait for the result of your audit to recommend and, indeed, adjust internal controls if you are concerned about their effectiveness.
When selecting the relevant auditor, do try to ensure that they have appropriate authority or status within the organisation to obtain the applicable information from various departments as well as being able to access the necessary areas of audit.
The auditor should be appropriately qualified, ideally a qualified accountant if leading on a financial audit. This may not be possible to arrange internally and so ask your external accountant for advice and guidance, where possible.
Ensure you are aware of any big changes in your figures year on year, which may signal attention from the tax authorities. You should always be in a position to verify and explain such changes or anomalies.
The audit will undoubtedly be more successful if activities are planned, supervised and reviewed.
Ebert Hyman is a chartered global management accountant and general manager at London Urology Group and 101 Diagnostics
Dear Reader,
Subscribing to Independent Practitioner Today is the only way you can be sure you will see every issue and have the option of reading us online using our special page-turnable edition. Don’t risk missing out. Our personal subscription for doctors and managers is only £90 a year and £210 for organisations. But you can cut this to just £75 and £180 respectively if you pay by direct debit. So take advantage of this offer now for our unique business journal dedicated to supporting you in your private practice. We’re confident your subscription will repay itself many times over!
Editorial director
Amex/Diners
Doctors, please give GMC No. (See rates listed above)
indicates this item must be
Instructions to your Bank or Building Society to pay Direct Debits
Name and full address of your bank/Building Society Banks and Building Societies may not accept Direct Debit instructions for some types of account To: The Manager
Banks and Building Societies may not accept direct debit instructions for some types of account Signature(s) date
post your application (no postage required – UK only) to: independent practitioner today Subscriptions department, FreepoSt, po Box 36, plymouth, pL1 1Br
phone: 01752 312140 Fax: 01752 313162 email: lisa@marketingcentre.co.uk or subscribe online at www.independent-practitioner-today.co.uk if you want to pay by card
the payment dates change, The Independent Practitioner Limited will notify you 10 working days in advance of your account being debited or as otherwise agreed.
If an error is made by The Independent Practitioner Limited or your Bank or Building Society, you are guaranteed a full and immediate refund from your branch of the amount paid.
You can cancel a Direct Debit at any time, by writing to your
You can promote yourself cheaply
Marketing your practice need not cost the earth, argues surgeon Mr Dev Lall (below). A lot of it can be done for free
One miscOnceptiOn so many consultants have about marketing their private practices is that it has to cost a lot of money.
sure, if you engage the services of a marketing consultancy, that can certainly be the case. expertise doesn’t come cheap and neither does the labour in actually putting that expertise to work on your behalf.
if you have been following my articles for any length of time, you will know that, of the plethora of ways of growing your practice, all vary wildly in terms of expertise and effort required to implement as well as cost to set up and maintain.
For example, to get started in pay-per-click advertising, you’re going to need a website, landing pages, have adverts created and to pay up front for ‘clicks’ directing traffic to those landing pages. i f you have a decent website already – as you certainly should – then great; you’re more than half way there. i f not, you’re going to have to factor in the cost of getting a website sorted before
you can even think about starting pay-per-click advertising. similarly with print advertising. creating the advert – if you don’t have the skill to do it yourself –will cost money and the cost of actually running the advert varies from publication to publication. so can you really promote your practice at low – or no – cost? t he answer is: yes, it can be done. But, first, i think we should pause for a moment.
A
word of warning
Whatever you think about our rate of pay in the n H s or remuneration for private work, none of us would consider ourselves poor. Yet one issue i see arise time and again is that consultants are reluctant to invest in their practices and pay others for their expertise, be that in marketing, website design or anything else. While a tight control of the bottom line is vital in any business,
reluctance to spend and invest in your business is very bad news. t he outcome is slow, if any, growth and an inability to keep up with your competitor colleagues. so while you can save money by doing many things yourself – i have seen consultants design their own websites or run their own pay-per-click adverts, for example – the price of that is twofold. Firstly, your time. time which ➱ p22
might be better spent doing other things – seeing patients or just having fun with the family, for that matter. secondly, the risk of doing a substandard job.
so, by all means, check out one or more of these free ways of marketing your private practice. But always ask yourself if you’re better off paying someone else to do some of them for you.
Gp networking events
i f there’s one way consultants approach growing their private practices, it is by holding educational or networking meetings with Gps.
i’ve talked at length about how to approach them in a previous article, so i won’t go into detail here, except to say that the success of these meetings revolve around prior planning, your own personality – how warm and fuzzy you are – and, most importantly, regular follow-up with attendees.
Referrals from consultant colleagues closely related to networking with Gps is networking with your consultant colleagues. For almost all of us, consultants in other specialties are an important source of referrals.
For example, gastroenterologists frequently refer patients to general surgeons; care of the elderly consultants and diabetologists refer to ophthalmologists; rheumatologists to orthopaedic surgeons –and vice versa – and so on.
t hink also of paramedical specialties such as optometrists and physiotherapists too.
s o look at the conditions you treat and ask yourself who – other than G p s – could send those patients your way. then it’s a matter of forging a relationship with those colleagues and making sure you do a superlative job when they refer patients in your direction.
pR – paper/radio TV p ublic relations ( p R) is all about getting free publicity in exchange for providing content or a story of value to readership/viewers of different media outlets. Quid pro quo in the truest sense.
Free pR can be astonishingly easy to get and can provide you with many tens of thousands of poundsworth of exposure – and often even exposure that would be impossible to otherwise achieve.
t he trick is to remember that the newspaper, magazine, radio or even tV station has not the slightest interest in promoting you. their interest is in having content for their newspaper, magazine or programme that is of interest to their readership and so keeps them buying. in that way, they make money through sales of the magazine as well as attracting advertisers.
s o when it comes to putting together your press release, make
sure the story you tell is of genuine interest to the readership of that publication. Do that and the editor will bite your hand off to run your piece. they’ve got bills to pay too, you know.
Guest blogging marketing is all about getting in front of your target market.
t here are now innumerable websites dedicated to people with conditions you treat, so approaching the webmaster of one or more of these sites and providing content is a great way to become more visible to potential patients. in many ways, this is similar to pR but even easier to get exposure.
Forum marketing
this is very similar to guest blogging, but the difference is that you join a forum that provides support to people with a particular condition and when a question comes up, you make a comment.
this is not about offering a clinical opinion without having seen a patient, but providing useful general advice. in this way, you provide value, many relevant people will see your post – and often share it –and the link back to your website will generate targeted traffic.
Under no circumstances post spammy ‘come and see me i’ll fix you up’-type posts. t his is crass and will rapidly see you banished from the forum.
build your own website
i t is perfectly possible to build your own website, at minimal cost. All you need to do is buy a domain name, sort out hosting and get cracking on building your own website.
One of the best software platforms is Wordpress and this is completely free. Alternatively, many hosting companies provide their own website building software which you can use.
But i would advise most people against building their own website. You need to have not only a bent for coding html/css, but also an artistic streak to create something that looks professional. You need to also be willing to invest the time to learn how to set things up correctly for search engine optimisation, Google analytics, remarketing and all the rest of it. Yes, you can learn how to do it, but unless you know this kind of stuff already – or are desperate to learn – just pay someone to do it for you. it’ll be done to a higher standard and far quicker than you could likely do it.
youTube videos
Online video is a great way to grow your practice. All modern smartphones come equipped with perfectly good video cameras and all you need is a tripod and microphone and away you go. i deally, you would invest in
video editing software, but there are plenty of free versions out there you can use too. Record as many videos as you like about the conditions you want, create your own You tube channel and away you go.
practice ‘open days’ Holding an open day for patients with given conditions or symptoms is a great way to grow your practice.
Like G p meetings, the event needs to be thought through carefully. However, this can not only successfully generate a stream of new patients for you but also give you exposure in the press, either as a newsworthy event in itself or through pR.
patient referral programmes patients with certain conditions, particularly cancer and chronic conditions, often congregate, either physically or in the virtual
online world. i t’s a good idea to ask them if they are willing to send any friends or relatives they think you could help your way –and costs you nothing.
Get your private hospital to promote you
many private hospitals have their own marketing departments and they will help promote you if you ask them. You seeing more patients is in the hospitals’ interests, too, of course.
so there you have it: ten free or virtually free ways anyone can grow their private practice.
With the exception of building a website, everyone could and should put as many of these strategies to work in their practice as possible.
c ost is not the issue – only a willingness to give it a go.
Dev Lall is a surgeon who runs a specialist private practice consultancy www.privatepracticeexpert.co.uk
nEw TAx RUlEs
Freelancers beware
New IR35 legislation from 5 April 2017 has caused much anxiety for doctors working for hospital trusts, including via an agency. James Gransby reports
whom does it affect?
The legislation affects anyone providing personal services to a ‘public sector body’ (PSB) through a limited company, including NHS trusts, GP practices and other health bodies. And it applies where services are given via agencies.
If your contract is caught by IR35, then the trust or other end client will deduct income tax at the 20% basic rate and employees’ National Insurance contribution (NIC) at the appropriate rate for the size of payment and withhold these amounts from the payment made to your company.
They will have also paid over 13.8% employers’ NIC. This will be done by setting you up on the payroll as a special class of employee, albeit one without the usual employment rights.
why is the law changing?
IR35 rules became law in 2000 and were revised in 2011 to remove tax advantages for individuals operating through limited companies where the nature of the relationship was more akin to an employee’s. Before then, such workers commonly took most of their pay in dividends, so avoiding National Insurance.
Until now, the onus was on the worker’s company to decide if IR35 rules applied. But this made it difficult for HM Revenue and Customs (HMRC) to identify which firms should be within the rules and, following some well-publicised public sector cases – the BBC’s own director general was not an employee –the Government acted.
So, from April 2017, it has been the PSB’s responsibility to decide if IR35 applies and, if so, to operate PAYE on payments made as if the PSB was the direct employer.
what are trusts doing?
Even as late as mid-March, many NHS trusts were refusing to give details of any reviews undertaken to contractors, merely saying they had not fully assessed the legislation’s impact and would release no further information until they had done so. It did not help that an HMRC online review tool was unavailable until then.
Some trusts are taking the not unexpected but potentially penal decision to remove any sort of risks from themselves and apply IR35 in blanket fashion to all contracts. This is particularly unwelcome, as it means higher tax costs for the trust and worker, and also allows HMRC to challenge the contractor’s company on why it never applied the legislation itself in the past.
Importantly, the IR35 legislation itself has not changed, only the responsibility for its application. As trusts now have to report IR35 payments through payroll reporting, HMRC will be able to identify large numbers of companies previously thought to have been outside IR35.
This opens up the possibility of inquiries into earlier tax years, potentially leading to back-payments of tax plus interest and penalties for incorrect tax returns.
Is there a way around it?
HMRC has made it clear it will penalise any attempt to side-step the legislation by changing the nature of the relationship between the PSB and the worker. It has already issued warnings regarding a number of ‘schemes’ claiming to avoid the new rules. So proper analysis of existing relationships will be required to assess the effect of the new rules.
Those operating via an umbrella
firm are unlikely to be caught, as PAYE should already be applied. Surgical groups formed of multiple individuals are also likely to be outside of the legislation thanks to the ability to substitute one group member for another to perform the role.
what do I need to do?
If you have had money withheld, then ensure the trust has correctly reviewed your contract. If the trust or agency has mistakenly deducted the tax when it should not have or not deducted it when it should, this will affect your finances.
How do I check?
On an online tool you can enter your contract details via a series of questions to determine your contract’s IR35 status. Go to www.tax. service.gov.uk/check-employment-status-for-tax/setup
If you disagree with the trust’s decision, you should discuss this with it and compare where your answers differ from ones they used to assess you.
How do I get this tax back?
If tax has been deducted at source from your income, it needs to be claimed back against your tax return as tax deducted at source.
so if I claim the tax back, am I worse off as a result?
Apart from the cash flow loss, you will be further disadvantaged, as IR35 rules aim to ensure HMRC does not allow those operating through a limited company to benefit from the lower tax and dividend rates available. Only the tax, not the NI, will be refundable. The trust will face an additional 13.8% charge for Employer’s NI and the amounts paid to you will also increase the
payroll costs to be taken into account when applying the Apprenticeship Levy (0.5%). The trust may therefore want to renegotiate contract rates to take the increased costs into account.
But the dividend rates raised last year and worsened in the Budget: wasn’t that enough? Apparently not. The Chancellor thinks IR35 legislation has been incorrectly applied by those operating through a ltd company. Hence the change of reporting responsibility to the public sector to try to solve this perceived problem.
Does this affect my private practice work?
In short, no. Work undertaken directly for patients or via insurance companies falls outside the new rules, for two reasons:
❶ Firstly, the new rules only apply to those entities classed as public authorities. These are identified as being any body to which the 2000 (2002 in Scotland); Freedom Of Information Act applies.
❷ Also, the nature of private fee work does not involve a potential employer-employee relationship. It is rumoured the rules may apply to private sector contracts in future, but that would lead to widespread change and has not been announced by Government. Yet.
what should I do now?
Next time you work for an NHS trust or GP practice, check your payment carefully to see if tax has been deducted. You should ask the trust what stance it is taking on these payments. Talk to your specialist medical accountant about this for further advice.
James Gransby is a partner with MHA MacIntyre Hudson accountants
Outpatients are a delicate balance
When asking ‘how big is the private patient unit (PPU)?’, most of us could be forgiven for responding with an answer stating how many beds there are on the designated private patient ward.
But that is a very ‘bed-centric’ view of what makes up a PPU. it may be the ward that is most visible to the patient, but we all know there is a wide-ranging team effort required to deliver a safe, high-quality, clinical service.
s o, it is time to look at the choices and the compromises that private patient managers in nhs trusts have to consider and grap-
ple with when trying to make the best of their local situation.
Let’s start with the question of private outpatients and their place in a PPU. The patient journey usually starts with a referral from their g P or consultant and the patient is then offered an appointment in an outpatient clinic.
To meet this demand, independent hospitals offer a comprehensive outpatient service – but PPUs generally much less so. Why is this?
For independent hospitals, the outpatients offer consultants a place of ‘capture’ of the private patient and the outpatient pool is
In case you mIssed It…
Last month’s article in our ongoing series highlighted the interface between the PPu and the rest of the nHs trust, and how getting this right can drive growth in financial surpluses from the trust’s investment in the PPu
the benefits that flow from treating the relationship between the PPu and the rest of the hospital as a ‘trading’ one were discussed, and these included the financial and service gains made from offering nHs patients a private room product.
these ‘amenity beds’ give patients a choice, and bring commercial and customer service thinking into the trust.
the source of the inpatient activity, mainly surgical, that drives the use of theatres and – at least traditionally – is the ‘engine of the hospital’.
Operating theatres are expensive, but insurer surgical codes typically deliver the most value. Consultants expect – and independent hospitals generally require, at least tacitly – that patients seen in outpatients on campus are then admitted to that same hospital in due course. in simplistic terms, outpatients are the feeder of inpatient work for independent hospitals. This is best understood by looking at it from the provider’s point of view.
Cinderella department
The caricature of this can be summarised like this: ‘as consultants charge their outpatients’ fees based on time and the host hospital only charges the consultant for room hire, the profit lies with the consultant, and the organisational effort and costs mainly with the hospital.’
For this reason, it used to be the case that outpatients were the Cinderella department: a ‘loss leader’ generally required only to ensure that the profitable inpatient activity was protected.
This is no longer really true, but the legacy of that long-standing imbalance still has an impact on PPUs today.
in reality, of course, this has all changed now.
The increasing range of outpatient and ambulatory procedures and diagnostic tests have revolutionised outpatient settings and the patient experience.
Investment has delivered outpatient services that are now clearly profit centres in their own right
What started with diagnostic imaging investment in MRi and CT scanners has developed into therapeutic techniques that are blending imaging and pathology and significantly reducing admission rates and lengths of stay and extending the range of treatable conditions.
Profit centres
The local independent hospital was once the sole option of when it came to patients’ choice of private outpatients. h owever, patients now have the choice of h igh s treet providers, new focused specialty brands and ‘super-centres’ such as h C a’s Platinum and s hard centres, which have taken private outpatient services to a new level.
For these providers, investment has delivered outpatient services that are now clearly profit centres in their own right.
s o, what is the right place for outpatient services within nhs PPUs?
Previous articles in this Independent Practitioner Today series have demonstrated how, most typically, nhs PPUs cater for the activities that independent hospitals cannot support: the most complex, the semi-urgent, the techniques dependent on specific equipment and staff skills.
This work is what PPUs do best and it is, generally, not cannibalising the local private healthcare market but instead stimulating it. almost by definition, therefore, this is not a market of commoditised high-volume, lower-margin cases, but the reverse: lower volume and higher margin.
This suits busy nhs hospitals, of course, as they are already managing high and variable demand in their day job, and the ‘1% private patient tail cannot wag the 99% nhs dog’.
Translate that into outpatient settings and it can be better understood why diagnostic imaging for private inpatients can be supported as routine.
But, for many nhs trusts, the setting up of diagnostic imaging to support significant private outpatients puts too great a strain on the system, particularly for the relative rewards.
Space and time
a nother way to understand the dilemma facing nhs PPU managers regarding the extent to which they should support outpatients is the use of space and time.
Outpatient services can take up a lot of space, such as:
Consulting rooms and the size of inpatient ensuite bedrooms;
Waiting areas and reception, where the environment should be welcoming, probably refurbished at some cost;
i n an accessible location on what might be a spread-out, confusing campus.
Then there is equipment to house and administration to complete. These challenges, and the compromises that have to be made to overcome them in most trusts, mean that the ratios for ‘earnings per private patient car parking visit’ and ‘returns per risk of private patient complaint’ are just not worth it.
This will not be true everywhere – these have been sweeping gener-
alisations, of course – but they are true-isms nevertheless.
indeed, there are lots of examples of where outpatients can work, provided the local service design solutions have grappled with the challenges of location, timing, staffing, capacity and the commercial enterprises, and knowingly the mix achieves a reasonable return for the effort.
such examples include: 3T MRi, cardiac CT, non-interventional cardiology, dermatology clinics; and vary site by site.
But a general private outpatient service that provides what an independent hospital provides and is open to volume traffic? You don’t see many of those outside of the London teaching trusts, and for good reasons.
Consultants looking to work with their nhs PPU that has an outpatient-based service would be well advised to think through the commercial constraints and opportunities from the PPU manager’s point of view.
a PPU should and can be more than just beds – but the bar is rightly set quite high for private outpatients.
Next month: a summary of the past year, lessons learned and positive suggestions for how the NHS should be revitalising PPU services nationwide
Philip Housden (right) is a director of Housden Group, a management consultancy specialising in commercial support in the healthcare sector
HARLEY STREET LAWYERS
37 HARLEY STREET, LONDON, W1G 8QG
l medical and health specialists
l established for over 22 years in Harley street
l Recovery of doctors’ and clinics’ outstanding fees
l Fast, friendly and professional
l Free initial 30-minute legal consultations with one of our specialist lawyers to assess your legal needs
RIPPon PateL & FRencH LLP
contact: emma Patel or sian mcKay tel: 020 7323 0404 email: info@rpfsolicitors.com Web: www.rpfsolicitors.com
Need I spell it out to
Doctors, of course, know all about the need to be clear, accurate and understandable. But please do also remember that fact when dictating to your medical secretary, pleads Stephanie Carmichael-Drage (left)
Wi T h T he growing use of outsourced and online services in healthcare, the relationship between the clinician and their secretarial support is often more distant and can seem impersonal when compared to the past.
There is less opportunity now for each side to learn the ways of the other and adapt to their needs and those of the practice.
This may be less than ideal in some respects, but it is, in fact, a consequence of modern healthcare, so we had better get used to it. And with the tightening of budgets and the Competition and Markets Authority imposing charges direct to the clinician for an on-site hospital secretarial service, outsourced support can be the most simple and cost-effective way forward for many clinicians. So it is imperative to keep the potential pitfalls in mind at all times. Being presented with an audio file containing ambiguous, confusing or partially dictated information is the equivalent of the ‘heart-sink’ consultation for a medical secretary.
A common scenario goes like this:
The medical secretary starts her day and prioritises her workload accordingly. She is progressing well with the dictations until she hears ‘Letter to Mrs Jones. No, actually, letter to, well, the chap she saw last before coming to me; i think his name was Smith. Dear Mr, put the right name in here and look up his address, please.’ This is the despair of a medical secretary’s daily life and also raises the potential of a breach of information governance and patient confidentiality.
So, is this a letter to Mrs Jones or on Mrs Jones? We will take it that it is a letter on Mrs Jones, but which Mrs
you?
Jones is it? There is no Christian name, no date of birth and no identifying reference number such as a hospital number. Then, of course, who is the letter to: Mr Smith?
Another scenario, that will have all medical secretaries nodding their head in recognition is the clinic letter that has been typed up on, shall we say, a Mr Paul Smith – a complex letter that has taken time for the clinician to dictate and the secretary to type. But, at the end of the dictation comes the following words: ‘ i
have made a mistake. i told you that this was dictation on Paul Smith. it is absolutely not. it is on Andrew Jones.’
The medical secretary will, at this point, be reaching for the coffee pot. But if the doctor had simply had the correct set of notes in front of him when he started the dictation and had not dictated from memory with the wrong set of notes in front of him, then this relatively simply error could have been avoided. The consequences of this not having been noticed are, of course, monumental.
Expensive implications
For the most part, the impact is merely time-consuming and can be relatively easily resolved by a little digging and cross-referencing by the medical secretary. h owever, anyone who uses a secretarial service, whether inhouse or outsourced, needs to be aware of the possible implications.
if each medical secretary spends just a relatively little amount of extra time on resolving such issues, it still ultimately means the service ends up costing more.
An outsourced secretarial service relies more readily on the information as dictated by the clinician.
A remote typist, albeit who may work within a case management system, will not have access to clinic data, patient notes, test results or hand-written summaries, so will rely solely on the information dictated by the clinician with regards to which patient the letter is on and whom the letter is to.
With the cost-savings of outsourcing secretarial typing, which can be substantial, it is imperative to dictate clear, detailed and concise information on each and every sound file.
A seemingly small slip could create all sorts of problems in these days of heightened aware-
ness of issues such as confidentiality, information governance and duty of care.
Obviously, if patients receive wrong or inaccurate information, it can be extremely worrying and distressing. A referral being sent to urology rather than neurology could lead to a delay in urgent treatment, with devastating consequences for the patient.
When communicating with an in-house medical secretary or with outsourced or online secretarial support, we would urge all clinicians to use the same skills and thoughtfulness they display when carrying out their daily professional duties.
Be clear, accurate and plain. That will make life easier for your medical secretary, so they, in turn, can make life easier for you.
Stephanie Carmichael-Drage is head of the medical department at www. outsec.co.uk
prActisiNG privileGes Now AvAilAble
CollECTing pAymEnTs
Make your chasing easier
You’ve earned it – so make sure you get it! Gary Nials (below) presents ten checks and balances to improve your billing
your
1
Terms and conditions
As part of your billing process, it is important to make sure the patient/payer understands your terms and conditions and they are kept informed of any changes (see page 38).
Make sure therefore the patient knows clearly their obligations for payment of your fees, even if they are insured.
Embassies should be comfortable with your fees and any changes due to complex work will need to be supported by a medical report.
Also, set out clearly your terms and conditions for medico-legal work which should be clear on payment terms.
2 international patients
If you are treating international patients, it is good policy to get payment before you treat the patient or, at the very least, on the day.
Your practice should have the facility to either take payment online, on the phone or at point of sale. At Medical Billing and Collec tion, we receive over half our payments online from selfpayers at the weekend. So to ensure good cash flow, you should offer this facility.
3 sending the invoices
You should aim to send an invoice out within 24 hours.
But if this isn’t possible, for whatever reason, make sure you monitor each invoice and aim to send it out as soon as possible.
Only once the invoice is sent can it be paid. For self-payers, the sooner they receive the invoice, the sooner they are likely to pay.
For insurers, they are increasingly putting time limits in place, after which they will not accept invoices.
4 Checking the invoice
Before invoices are sent, you should ensure invoices are checked. This is particularly important because you do not want to give the payer any reason not to pay or have to resend the invoice.
Insurers often want pre-authorisation codes and correct patient membership numbers. If you use electronic billing, only correct information will be accepted.
With embassies in London, letters of guarantee (LOGs) will have to be included and details must ➱ p32
match with the invoice or they will be rejected.
5 Ensure receipt of invoice
If you send the invoice by post, it is a good idea to make contact with the patient/patient’s payer to ensure the invoice has been received.
When sending an invoice electronically, it is easier to have a paper trail. But when registering a patient, always try to obtain a mobile and email address to make follow-up communication easier and quicker.
6
Chasing invoices
Once you send an invoice, you need to keep a record of the invoice and when it was sent.
That way, you can reconcile payments once they are received and also diarise to chase them. This should be done systematically, although timing can vary based on the type of payer.
For example, you could chase self-payers every 14 days and private medical insurers every 28 days. This could vary again for embassies – normally every three months – and with medico-legal the same, if not longer.
7 Regular patients should pay regularly
If you are seeing a patient on an ongoing basis, it is a good idea to get paid your outstanding invoices before you treat them again.
Each practice is different and will set its own policy on this; however, it is not a good idea to build up a lot of outstanding debt with any one patient/payer. This is the same in any business and it is no different in private practice.
8
Chase invoices, not an invoice
It might seem straightforward, but when you are chasing a
patient or client for an invoice, check to see what other invoices are outstanding and chase for those as well.
If you are a practice manager or secretary managing a number of consultants, use the same principle. This is likely to be the case if you are doing medico-legal work as a practice or your practice is in London doing embassy work.
9 pricing
It is important to review your pricing on a regular basis –ideally every 12 months – otherwise you can lose out on revenue.
Clinical Coding and Schedule Development (CCSD) codes, which form the basis of insurance company’s benefits, change monthly (see page 48), so again your pricing should be monitored.
You also need to review your embassy fees, which have been squeezed in recent months, as well as your charges for medico-legal
reports. The busier you are can be a good indicator of whether you could consider increasing your medico-legal charges.
10 Bad debts
There will be occasions when invoices are not paid. This is a problem because tax is payable on the raising of the invoice, not payment.
Sometimes invoices will not be paid for some time. This could be many months and, at times, years. If it gets to the stage you decide to declare an invoice a bad debt, then advice from an accountant should be sought to do this.
Showing you have actively chased the invoice is important, as it will allow you to declare the invoice officially as a bad debt and, as a result, reclaim the tax paid.
Gary Nials is managing director of Medical Billing and Collection
Don’t miss our Wealth management guide 2017, published free with our June issue
This supplement will give details of professionals who can help you manage your wealth by supporting you with a wide range of services.
To advertise in this supplement, please phone Margaret Floate on 01483 824094 or email her at margifloate@ btinternet.com
To take out a subscription to independent practitioner Today, contact lisa Richardson by phone on 01752 312140 or email her at lisa@marketingcentre.co.uk
“ Kay looks after calls when our team is busy. The result? More appointments, outstanding service levels.”
Moneypenny client since 2015
Moneypenny will support your existing team by looking after overflow calls whenever you need – sending detailed messages back to your practice.
moneypenny.co.uk 0333 202 1005
Kay, Moneypenny Receptionist.
Take a leaf out of a successful book
Independent practitioners can take some useful cues from the business world to improve their patient satisfaction, says Stephanie Vaughan-Jones
DElivEring CustomEr satisfaction is vital for success throughout the business world.
Companies will go to great lengths to meet and exceed the expectations of their clients to ensure they become repeat customers. Without customers, there is no business. the same goes for private practitioners too. Without patients, there is no practice. And patient
satisfaction matters like never before.
We have never lived in a time where there has been so much choice for patients. this is great news for those who work in this sector but, of course, this means there is increased competition between practices too.
Just as in the business world, competition can be a very good thing. it makes an organisation
sharpen itself up, inspires marketing ideas and improves the look and feel of its clinics for patients.
Outsource client-facing roles Businesses are always looking for ways to trim their outgoings. the bottom line is the bottom line. But there is a fine line between keeping costs down and getting rid of vital business components. You still want to look profes
sional, but not at the expense of the patient experience and service you offer. t his is why an increasing number of businesses outsource tasks to improve their professional front and efficiency. o ne area they look to outsource is their phone calls. With customer service in mind, having a trained, professional and wellmannered person answer a call instantly improves the
service offered by that business. It’s the equivalent of polishing shoes and straightening a tie.
This is something private healthcare practices can hugely benefit from.
Getting through to the doctor’s business can be problematic and everyone has an anecdote to share:
Patients never getting through first time;
Getting lost in a labyrinthine phone system;
The receptionist answering the call falling short of good phone manners.
A call answered properly and promptly reassures the patient that their call matters and all is in hand. This is regardless of whether the person handling the call is able to give them the information they are wanting.
The fact a real person answered their call and informed them that the most appropriate person will be back in touch goes a long way to achieve outstanding patient service.
Outsourcing this task frees up reception and front-line staff to better handle the patients and visitors in the clinic, as well as giving them more time to complete administrative duties.
Hiring the right people
Many businesses believe exceptional customer service begins with whom they hire. It can make or break the customer service offering, and the same thing applies to private healthcare.
Having the right team of people in place is the first step to delivering patient service. It doesn’t matter how good you are at your practice, its future is in the hands of the people you hire, as it is they who are representing your clinic. But how do you know if you are hiring the right people for your practice?
Luckily, many businesses have already figured this out and share what they do, so healthcare practitioners can learn from this.
There is a saying: attitude over aptitude. That is to say, it is preferable to hire a person who has the right ‘can-do’, positive personality for the practice, but may not yet have the skills necessary to undertake the job fully.
In business, these people would be snapped up and trained to the
It doesn’t matter how good you are at your practice, its future is in the hands of the people you hire, as it is they who are representing your clinic
➲Willingness to serve: They are happy and keen to serve your patients, going above and beyond, if necessary.
Listening to customers’ feedback
Reading or listening to a customer’s feedback will do one of two things. You will delight in the praise and compliments being rained down on you or you will be filled with dread at what your customers may say.
It may be a difficult task to do, but the rewards of getting this feedback are enormous. They will show you a picture of your practice that you otherwise wouldn’t see.
receive many compliments, so make sure these are passed on to the team too.
Building a brand through customer service
A brand is so much more than a logo and website. It’s how a person feels about a business long after they’ve dealt with it, regardless of what it is: a soft drink, a car company or an energy supplier.
All have left their imprints on their customers and these people may not have even realised it. But there is a reason they will go back and choose their favourite product or service, time and time again.
appropriate level. They have been hired because they are ripe to be trained and are willing to learn.
The business invests a little in that person and gets a lot of hard work in return. Let’s compare this scenario with a business that hires a person with most of the skills required for the job, but lacks the ‘soft skills’ with which to fit into the company properly. The result is a culture-clash, one that often results in that employee being fired or leaving.
This is never more important than when hiring people who are patient-facing; for instance, your reception staff.
All of the skills necessary to carry out the work can be taught, but fantastic personality cannot. These are the people that patients notice when they visit a clinic, so getting the reception team right is vital to delivering outstanding customer service.
When interviewing candidates, ask yourself: ‘How would I feel if this person greeted me at a front desk?’ and ‘Would I like to sit next to this person on a plane?’
some factors to look out for
➲ Excellent communication skills: They listen more than they talk, which means they will give the appropriate amount of focus on your patients.
➲ Collaborative nature: They build a strong rapport with their colleagues and patients. This achieves results quicker and makes the practice a more harmonious place to be.
Businesses go to great lengths to encourage, read and review their customers’ feedback. As such, it’s almost an industry in itself, with many sites such as Trustpilot and Yelp dedicated to presenting honest opinions of businesses to the public. You may well ask: ‘Where is the value to a private healthcare practitioner?’
Well, before people become patients, they will often ask around for a recommendation from their friends and peers for the best practitioner they can find before making a judgement.
Think of the level of detail people go to before making a purchase of any kind. It’s natural that they will do the same when it comes to their health.
The most honest businesses are never afraid to ask a patient directly for their thoughts. Private healthcare practitioners could benefit from the same approach.
Asking for feedback on how a treatment went or their general opinion of the practice will equip you with information you may have remained ignorant of, such as:
Their calls not being answered;
The rude front desk staff;
Their consultation feeling a little short.
All of this you would never had known without asking.
But information garnered is useless until you put it into action. Use this as valuable checkpoints to improve your clinic, staff, even your own approach to patients.
As they are genuine concerns from patients, you know they are issues that must be addressed. And there is the chance you will
It’s because successful companies have woven excellent customer service into every aspect of their branding.
It’s also where we see so many smaller businesses lose out. They fail to include customer service when building their brand. The same applies to private healthcare practices too.
The most obvious – and often most ignored – aspects when brand-building are all of the touchpoints patients have with a practice.
A practice may look the part and offer excellent healthcare services, but when it comes to communications with their patients, they fall short.
Here is where practices can take a leaf out of businesses’ book. Every communication channel must reflect the service that practice wishes to give.
For instance, the tone of voice in an email or letter, the manner in which a phone call is handled or how friendly and caring the staff are.
All go into creating a brand with built on a solid foundation of patient care. This can be the difference between a patient returning and thinking highly of a practice, long after they have dealt with it, and one that has little or no impact.
Stephanie Vaughan-Jones (pictured above) is channel manager at phone answering specialist Moneypenny
bREAkiNG iNTo mEdico-lEGAl woRk: coURT AppEARANcEs
See you in court?
Lawyers play a tactical game of brinkmanship while doctor expert witnesses wait to see if they will be needed in court. In Michael R. Young’s experience, they rarely will be
Very few claims actually proceed to trial. A court appearance is therefore a rare event, so, at this stage, I would not give it too much thought.
During my many years as an expert, and despite the large number of cases in which I was involved, I only actually had to attend court once, and even then the two sides settled before the case proceeded to the court room.
Barristers and solicitors play a tactical game of brinkmanship and so the majority of cases never get as far as trial.
Having said that, the following is what currently happens at a trial. The claimant and defendant’s expert(s) are not in court at the same time; they give their oral evidence sequentially.
One expert is examined and then cross-examined by the other side’s barrister and then leaves the witness box. The next expert is then examined.
However, in his recent review of civil litigation costs, Lord Justice Jackson carried out research into the practice of concurrent expert evidence in court. The lawyers
have dubbed this ‘hot-tubbing’ and it is used in the Australian courts, although the Australians prefer to call it ‘concurrent evidence’.
Lord Justice Jackson suggested that ‘hot tubbing’ be piloted in the UK in cases where all parties and the judge agree to it. w hat happens in ‘hot tubbing’ is that the experts are sworn in together and sit in front of the judge, who puts the same questions to each expert in turn, so that the whole thing is more of a debate and less of a partisan adversarial process.
There are books that offer advice on what to expect if and when you are ever called to court. There are several organisations
that run courses on the expert witness in court and courtroom skills.
My advice is: by all means, read the books, but unless there is a real possibility of you actually having to go to court, don’t bother with the courses – at least not in the early part of your career.
Defence bodies may be able to help with a fact sheet on giving evidence in court and solicitors and barristers should also be able to give you guidance.
Next month: Getting paid
Adapted from The Effective and Efficient Clinical Negligence Expert Witness , by Michael r young, price £60 from Otmoor Publishing
SpeciAL offeR! BuY tHe
Book And SAve £20
the book costs £60, but independent practitioner today has secured discount of a third off for readers, so you pay only £40.
Listen to the audio content which accompanies the book at this website: www.otmoorpublishing.com/audio. for more information and to order, email stephen.bonner@ otmoorpublishing.com, quoting reference ‘Young/ipt’.
nice woRk
if You get it
court appearances are a rarity, but one court appearance that i almost had to make was memorable.
i received a phone call at home one Saturday afternoon from an instructing solicitor saying that the barrister in this particular case had dropped out and would i mind if the replacement barrister called me over the weekend to discuss the case, as it was going to trial. the barrister phoned me at midday on the Sunday just as i was about to go out for a prearranged lunch. we discussed the case and then, almost as an afterthought, i asked him when the case was likely to go to trial. He replied: ‘tomorrow! And we need you there.’ the trial was scheduled for 10am at a court 200 miles away near London. i kept my lunch appointment and then packed my suitcase while also phoning the solicitor to confirm that i would be paid for all of this. i booked a room at my club in London and then got the train. i had to be up early the following day to be at court in good time. i arrived only to find that the two parties were locked in negotiations in a side room. After an hour or so, a settlement was reached. i returned to London, did a bit of shopping, and then caught the train home that evening.
i received payment for two days’ work, plus all of my expenses.
An independent firm offering one to one meetings anywhere in the UK giving advice and help with:
• how to start in private practice
• how to maximise private practice income
• computer software
An independent firm offering one to one meetings anywhere in the UK giving advice and help with:
• tax and financial advice re: car purchases
• how to start in private practice
• ways to reduce tax payments
• computer software
• how to maximise private practice income
• setting up in Chambers/Groups
• ways to reduce tax payments
• limited companies and LLP’s
• setting up in Chambers/Groups
• financial planning
• record keeping
• limited companies and LLP’s
• tax and financial advice re: car purchases
• pensions: NHS, personal and employee schemes
• pensions: NHS, personal and employee schemes
purchase of consulting rooms and surgeries
• inheritance tax and capital gains tax planning
• purchase of consulting rooms and surgeries
• VAT
• inheritance tax and capital gains tax planning
For more information please contact us by:
• VAT
Wilmslow
Harley Street
For more information please contact us by:
Phone: 01625 527351
Wilmslow
Fax: 01625 539315
Phone: 01625 527351
Phone: 020 7307 8759
Harley Street
Fax: 01625 539315
Phone: 020 7307 8759
Email: info@sandisoneasson.co.uk
Fax: 01625 539315
Fax: 01625 539315
Website: www.sandisoneasson.co.uk
Email: info@sandisoneasson.co.uk
Website: www.sandisoneasson.co.uk
• Completely open scanner that is well tolerated by claustrophobic patients
• Weight-bearing scans for spine and joints enable a more precise diagnosis
• Patients who are large or cannot lie down can be accommodated
LEgAL BRIEFIng: yoUR TERMs AnD ConDITIons
Mind your Ts & Cs
Building on the previous articles in this series looking at key legal issues which doctors need to consider when starting up a healthcare business, Simon Lee (above) now turns to the contractual terms and conditions
a number of people have noted that legal terms and conditions on websites and in mobile apps play a key role in what has been called ‘the biggest lie on the internet’.
Let’s be honest here. How many of us, when faced with what looks like 300 pages of legal jargon that stand in our way, have simply ticked the box which reads ‘I confirm that I have read and accept these terms and conditions’, hoping that they didn’t contain anything too nasty?
I have to hold my hand up along with everyone else to this one because, while solicitors might like to think that contracts are as good a read as a bestseller, the truth is that many of them are long, often written in a form of legalese and, frankly, a bit boring. but this doesn’t mean that they are not important. It also doesn’t mean that there aren’t consequences for getting them wrong. for example, back in 2010 – and hopefully just to prove the point –
GameStation temporarily changed their T&Cs to say that, by accepting them, consumers were agreeing to sell their souls to the company, and around 7,500 people were said to have consented.
So, what type of terms and conditions might you need in setting up a healthcare business and what do you need to know about them?
What you will need
I have assumed here we are talking about some form of online business. See also our previous article in the series (‘Don’t get snared in your own web’, f ebruary 2017) and also on the Independent Practitioner Today website.
In this case, you are likely to need:
Ø Website and/or mobile app terms and conditions of use –Likely to be linked with the acceptable use policy;
Ø a cceptable use policy – How people use the site or app, including, but not limited to, leaving of comments and other interaction;
Ø Privacy policy – Crucial, given the sensitivities about use of patient data. It is really closely linked to data protection and you need to understand what data you are proposing to use in order to write it properly. Please see our forthcoming article in the series which covers data protection law in more detail;
Ø Cookies policy. This is a requirement to show what information is being gathered from users using these small bits of data sent from your computer to theirs.
Depending on what kind of activities you are undertaking and the way you model your business, you might well also need:
➲ a contract with patients –where this goes beyond what is covered in the terms of use for website and/or mobile app; ➲ a contract with other doctors or medical practitioners – such as where you are offering medical services using a network of people; ➲ o ther contracts such as contracts of employment for staff or a lease for occupation of premises.
Distance selling
While all of these contracts are important, we will concentrate on the patient terms and conditions and, within that, two important areas to get right. one relates to ‘distance selling’ and the other is the Consumer rights act 2015. Distance selling is relevant because of The Consumer Contracts (Information, Cancellation and a dditional Charges) r egulations 2013, in force from June 2014.
In this context, ‘consumer’ means ‘an individual acting for purposes which are wholly or mainly outside that individual’s trade, business craft or profession’ and ‘trader’ is someone acting for purposes which do relate to their trade or business.
So distance selling needs to be considered in the context of an online contract with patients or other users of your website or app, but is likely not to apply in the context of a contract with a doctor for the provision of medical services.
‘Distance selling’ covers a contract for goods, services, and/or digital content which is not concluded facetoface on the business premises of the trader or in a shop.
Therefore, it covers all contracts made online where goods or services are being sold which would, in turn, relate to online healthcare businesses in the uK. an important aspect of the regulations is the provision of certain information by the trader to the consumer.
This includes information on:
The total price payable;
Details of rights to cancel;
Information about the trader.
The right to cancel in respect of services allows a person at least 14
Many contracts are long, often written in a form of legalese and, frankly, a bit boring. But this doesn’t mean that they are not important
days to cancel after entering in to the contract with you. This means that you should not start providing the service in the cancellation period unless the consumer has specifically asked that you do.
In this case, while cancellation can still apply for any unperformed services, the consumer would still have to pay for any services they have asked you to perform. often, of course, in online businesses, people do want things done quicker than 14 days and so you would need to make sure
your contract is clear about how all this would work in practice.
The Consumer rights act 2015 consolidates a lot of previous consumer protection law and brings in some new areas too.
It covers the provision of goods, digital downloads, and – most likely to be relevant in the context of this series – the provision of services. one aspect that it covers is the terms and conditions which appear in your contract with each consumer/patient.
Some terms appear in a ‘blacklist’. They are automatically unenforceable in a contract and so it is better not to write them in to a contract in the first place.
These broadly are the same as in previous legislation, such as not permitting exclusion or limitation of liability for personal injury or death caused by negligence.
o ther items appear in a ‘greylist’. These are not automatically unenforceable, but will be subject
to a ‘fairness’ test and so caution should be used in applying them. e xamples here might be a disproportionately high charge in the event of cancellation or a clause limiting liability to less than the value of the services provided. Transparency is key in contracts with patients.
In conclusion, it is important you understand both what types of contracts you need and also how to get the content of them right. remember, any claims or legal challenges you face will still cost you valuable time – and potentially also money – to put right, even if they are ultimately unsuccessful. So working to get it right first time is key.
even if those using your products or services end up engaging in ‘the biggest lie on the internet’, do make sure that you don’t.
Simon Lee is an associate at Hempsons Solicitors
Free legal advice for Independent Practitioner Today readers IPT
Independent Practitioner Today has joined forces with leading niche healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes’ of free legal advice.
Hempseed Faisal Dhalla
Balancing tax vs.
Is your trading structure maximising opportunities for pension growth?
Simon Bruce (right) shows why you should ensure your practice and your pension are working together
Over the last decade, we have seen a drive for doctors to set up limited companies for their practices. this is mainly because it was assumed that small businesses would pay less tax than sole traders or partnerships.
In reality, this was not always the case and the commercial benefits of running the practice as a sole trader could sometimes outweigh marginal tax differences.
When the additional income tax rate fell from 50% to 45% in 2013-14, there seemed less incentive to form limited companies, and partnerships became popular again.
Last year, the Government introduced a new ‘dividend allowance’ in a bid to equalise the playing field between limited companies and sole traders.
the former dividend tax credit of 10% was scrapped and the new allowance means that an individual’s first £5,000 of dividends are tax-free.
But in the Budget last month, the Chancellor announced that, from April 2018, the allowance would fall to just £2,000.
Over and above this limit, dividends for basic taxpayers will incur a tax charge of 7.5%, higher-rate taxpayers will pay 32.5% and in the upper tax bracket, excess dividends will be charged at 38.1%.
is your private practice income causing you to pay more tax on your nhs pension growth?
One factor that is often overlooked by accountants is the impact your trading structure can have on NhS pension funding.
t here is an annual allowance which limits pension savings attracting income tax relief to £40,000.
Many senior doctors breach this rate just by being in the N h S Pension Scheme for another year,
Given the overlap between many of the key finance areas and a constantly changing financial landscape, there is a greater need than ever before to have a united source of advice
even before a new clinical excellence award or contractual pay increment is considered.
In addition, from April 2016, those who are deemed to have total income of £150,000 face an annual allowance which is reduced further by £1 for every £2 over this.
Note that total income is not just salary; it includes dividends, N h S pension contributions and other income from rental properties and so on.
For most senior doctors, this means an annual allowance of just £10,000.
t he result is that deemed ‘excesses’ above the annual allowance are considered in the same way as income and taxed at your highest marginal rate. t his can come as a big shock for the unprepared or unwary.
the new tapered annual allowance should be a key factor in business planning.
how it works in practice
As an example, let us look at Dr Smith. Dr Smith runs his medical practice in partnership with his spouse, who is also medically qualified.
h is income is £100K from the N h S and £200K from private practice, which is then split 70/30 between them as part of the partnership agreement. his income is
pension
now £240K and his wife earns £60K.
While the partnership may be efficient from an income tax point of view, this is not the case for pension planning.
the tapered annual allowance for someone earning £240K is now just £10,000, so his pension input above this sum may be taxed at his highest marginal rate of income tax of 45% – if he has no unused allowance to carry forward from previous years.
As a limited company
If Dr Smith now has a limited company with his wife as codirector and shareholder, his private practice income of £200K is all billed through the company.
Dr Smith and his wife can choose how to draw salary and dividends. If they do not need to draw, his official earnings remain at £100K – his NhS salary only.
So Dr Smith retains the full annual allowance of £40K – provided he has no other earnings from other sources.
h is wife can draw a salary appropriate for her role and any profits within the company would be subject to corporation tax.
A limited company can also contribute ‘pre-taxed’ company income to a pension. higher-rate taxpayers can put practice income straight into a personal pension rather than taking the income as a dividend.
this can be particularly useful for a spouse who will also have an annual allowance and may not be as concerned about the lifetime allowance.
however, care needs to be taken that any remuneration package and company pension contributions are appropriate to the role being performed.
Furthermore, if there are residential mortgages that need to be
repaid from income, this route may be less attractive, as there is less flexibility to retain profits in the company for withdrawal in the future.
Are you sure your practice structure is working as hard as you for your future?
Ideally, your accountant and financial adviser will be working together to ensure that opportunities for pension planning via your practice are not missed.
Given the overlap between many of the key finance areas and a constantly changing financial landscape, there is a greater need than ever before to have a united source of advice.
When dealing with large sums of money and critical life choices, doctors need to ensure their professional advisers have the complete picture of their financial interests and competence in the NhS pension.
Make sure your adviser and accountant have the same objectives – the decisions you take now will have a big effect on your future income.
Simon Bruce is managing director of Cavendish Medical, specialist financial planners helping senior consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor.
The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
PROBLEMS WITH THE TAX MAN?
HMRC tax investigations and disputes create difficult and stressful times.
As an award winning firm of tax experts, our highly experienced partners specialise in resolving problems relating to tax investigations and disputes with HMRC.
To find out, in confidence, how we can help call 0800 734 3333.
‘Here to help. Not to judge.’
Answers to your ethical conundrums
Report writing and confidentiality dilemmas facing independent practitioners are addressed this month by Dr Nicola Lennard (right)
UK Top 20 accountants specialising in the healthcare sector
• AISMA member (Maidstone and Leicester offices)
• 15 offices including London City
• Tax structures for Hospital Consultants - dispelling myths
• Surgeon groups and consortia
• GP Practices including mergers and federations
• Solvent liquidations (for companies at the end of their lives)
For more information please contact:
South East
James Gransby FCA
E: james.gransby@mhllp.co.uk
T: +44 (0)1622 754033
M: +44 (0)7712321899
East Midlands General email: healthcare@mhllp.co.uk www.macintyrehudson.co.uk
Robert Nelson DChA FCA
E: robert.nelson@mhllp.co.uk
T: +44 (0)1162 894289
M: +44 (0)7814009160
Dilemma 1 Can I pull out as expert witness?
QI am a senior neurologist and provide medico-legal reports for clinical negligence claims.
I’ve received a request from a solicitor asking additional questions on a particularly complex case on which I previously provided a report.
In addition, the solicitor has asked for an updated prognosis report and explained that I may be expected to attend court next year.
You could even face an adverse costs order if you refuse to give evidence or to provide the additional report
If the solicitors do not agree to release you from your obligations, you could be criticised by the court – or even face an adverse costs order – if you refuse to give evidence or to provide the additional report.
I am semi-retired and have made plans to travel abroad. I’m concerned that if I provide the additional report, I may not be in the country when the court case takes place. Can I decline to provide the additional report?
AThe responsibilities of experts in civil claims are governed by the Civil Procedure Rules and the expert has an overriding duty to the court, which continues even though you are semi-retired.
Bear in mind that there are likely to be significant costs incurred by a party in instructing a new expert for a case and, in particularly complex cases, there may be very few clinicians who feel able to provide an expert opinion.
Discuss your difficulties with the solicitors to see whether a new expert could be instructed. However, since you have not yet fully retired, this argument may not be judged as valid.
Doctors who undertake expert work should plan ahead carefully. Cases can remain open for many years and when approaching retirement, doctors would be well advised to inquire of the instructing solicitors about time-scales and make clear any limits on the commitment they can offer.
The GMC offers guidance on ‘Acting as a witness in legal proceedings’ and the Civil Justice Council sets out best practice in terms of experts’ duties.
Although neither document specifically addresses the effect of retirement on the duties of experts, the Civil Justice Council’s best practice guidance states that if experts withdraw, they must give formal and adequate written notice to those instructing them and provide reasons for withdrawing.
Doctors who act as experts must make sure they have appropriate indemnity in place and they maintain their GMC licence to practise if it is required for the work they do.
Dilemma 2
Should I report the gun-holder?
QI am a private GP and I received a request from the police some time ago for information about a patient applying for a shotgun certificate.
At the time, I responded to the police indicating that I had no concerns about the man’s health.
In addition, I added a clinical code to the notes to indicate that he was a firearms certificate holder.
The patient has recently been to see me, as he has been going through a significant period of stress at work and is also experiencing relationship difficulties – his wife is also a patient.
I am concerned the man is clinically depressed and have just begun to prescribe him antidepressants and referred him to a counsellor.
Should I report this father’s clinical condition to the police?
AThe national policy on the interpretation and application of UK firearms licensing law
is contained in the Home Office guidance ‘Guide on Firearms Licencing Law’, which was updated in April 2016.
This indicates that the doctor’s role is to assist the police, by providing any relevant information they are aware of to enable them to make a decision on an individual’s suitability to own a shotgun or firearms.
It is the police who take the ultimate responsibility for granting, renewing or revoking a firearms certificate, not the GP.
The firearms certification process does not impose any duty on GPs to proactively follow-up patients with gun certificates.
Doctors’ duty
The only duty on doctors is the one which already exists: to consider reporting to the police any serious concerns which come to their attention in the course of their normal clinical practice.
When a patient with a firearms certificate presents with new symptoms of depression, doctors should consider whether the patient is at increased risk of suicide or if he poses a risk to others. If so, the doctor should consider what actions might be needed to mitigate such risks, including, for example, contacting the police.
All doctors are under a professional obligation to consider disclosing to the proper authorities any information which, if not disclosed, might expose people to a risk of serious harm or death (GMC’s latest Confidentiality guidance, paragraphs 63-70).
Before disclosing the information, you should still seek the patient’s consent to disclosure, if possible.
If the patient refuses, you should consider their reasons for refusal, but if you judge that disclosure is justified in the public interest, you should inform the patient if it is possible and safe to do so, what information you intend to disclose and to whom.
The disclosure should be the minimum necessary to achieve the purpose and you should document your justification for disclosure in the patient’s records.
Dr Nicola Lennard is a medico-legal adviser at the MDU
How making tax digital
We now know more about the taxman’s plans for making tax digital. Ian Tongue outlines how this will affect independent practitioners
HM Revenue and Customs (HMRC) is determined to embrace digital technology and use this to increase tax revenues. It calls this measure ‘making tax digital’ or MTD for short.
It believes it loses around £8bn in tax revenues from inaccurate tax returns that the current tax inquiry system could never address.
MTD is therefore designed to force taxpayers into having more robust accounting records and systems and to report to HMRC more frequently, thereby increasing accuracy. Well, in theory at least.
My experience of dealing with medics over the last decade leads me to conclude that not much of the £8bn extra revenues will come from them.
So the important factor for doctors is managing the additional
burden of these changes so that MTD does not become ‘making tax difficult’.
This article recaps on some of the changes – first outlined in Independent Practitioner Today October 2016 – and looks at things from a practical perspective.
Recap on the changes
HMRC set out its vision in August 2016 by issuing six consultation papers with its proposed framework. This gave the accountancy profession and other interested parties the opportunity to respond to the changes.
On 31 January 2017, it issued the response to the changes which involved some concessions. But, as expected, the majority of the taxman’s wish list remains intact, with minimal ground being given.
On the whole, the response was disappointing, as it has left many
uncertainties in relation to the implementation of MTD, particularly for smaller businesses. So HMRC still needs to consider a number of areas further and more changes to the implementation are likely.
As things stand, by 2020 all businesses will be affected by MTD and the system of reporting tax information to HMRC periodically will be the norm.
Due to the speed at which the changes are being forced through, HMRC has staggered the implementation of MTD based on your business structure.
Following March’s Budget, the proposed timetable and most likely groups for doctors carrying out private work is as follows:
u nincorporated businesses (self-employed, partnerships and landlords) with income above the vAT threshold (£85,000 from 1
April 2017) but not registered for vAT – from April 2018; unincorporated businesses (as above) with income below the vAT threshold – from April 2019; unincorporated businesses (as above) who are vAT registered –from April 2019; Companies and large partnerships (>£10m income) – from 2020.
The dates are not clear in terms of whether this applies to accounting periods commencing after the dates above or whether you may have to apply the new rules ‘in year’. How this will operate in practice will be cleared up later in the year.
Your accountant should liaise with you on this once this issue has been addressed and advise you on your timetable for change. For many trading as selfemployed or in partnership with
digital affects you
a March accounting year, you have a little under 12 months to prepare for these changes. Don’t panic, though, as no doubt your accountant will be working behind the scenes to suggest the best option for you.
What is required?
HMRC has indicated that it wants your accounting figures quarterly and an ‘end of period statement’ of the annual figures, which is to be submitted by the sooner of ten months after the accounting year end or 31 January.
For someone with a 31 March year-end for their private practice, the usual date of 31 January of the following year will apply. But, for others, a new deadline will become the norm and this will be specific to your circumstances.
In the longer run, the tax return as we know it will die, but the annual reconciliation process will be akin to a lot of the work performed when a self-assessment tax return is produced.
HMRC’s systems are looking to integrate more fully such that they have more information in advance of this new annual process.
This sounds good, but the 201516 tax return tried to align income tax and n ational Insurance and has been a failure for many taxpayers who have anything but the simplest affairs.
Those with multiple salaries and private work have been particularly let down by the taxman, as HMRC’s computations are wrong, but it doesn’t stop them sending demand letters for payments.
Hopefully, HMRC will have its house in order for April 2018. But it does not have the best track record for making significant changes to systems, so watch this space.
To try and alleviate this, HMRC
has businesses performing a beta test of the MTD systems from April 2017.
What does it mean for me?
Most consultants do not have a powerful accounting package, as it is simply not necessary.
More commonly, practice management software with billing and expense recording or simple spreadsheets are used. It largely depends on the size of your private practice and experience of the team around you.
Most of the practice management package providers are working on these changes, as inaction could render their product obsolete pretty quickly.
The difficulty is the cost involved in building direct links from these packages to HMRC’s submission gateway.
So I expect the solution for a number of packages is some form of integration into another software package that is compliant with the new changes. We are aware of such links and are advising clients based on their circumstances.
One concession that HMRC gave in the response to the consultation documents is to allow small businesses to continue using spreadsheets – without clearly defining ‘small’.
However, you cannot submit the required information from a spreadsheet directly and therefore some other software will need to be used.
HMRC has indicated that it will provide this free of charge for certain businesses, but, at the time of going to press, it is not certain what format this will be.
And I suspect that using spreadsheets and HMRC’s software is likely to be the least efficient way of managing your new obligations.
Those with multiple salaries and private work have been particularly let down by the taxman, as HMRC’s computations are wrong, but it doesn’t stop them sending demand letters for payments
Cash basis
Most businesses will have been used to declaring their accounting figures on an ‘accruals’ or due basis. HMRC accepts that to prepare the figures on this basis four times a year would be particularly onerous, so it is extending the cash accounting basis under MTD. This results in businesses declaring income received and payments made as they happen rather than when due/payable. The threshold will be £150,000, but there are a number of uncertainties with this approach which HMRC will respond to later.
The next steps for doctors are to discuss things with your accountant, who will, no doubt, be in touch over the coming months for those affected in April 2018. There are a number or uncertainties requiring a response from HMRC, so keep an eye out for further articles on this important topic in the coming months as new information clarifies your exact implementation timetable. Next month: A guide to expenses
Ian Tongue (left) is a partner with Sandison Easson accountants
doCToR on ThE RoAd: volvo v90
Estate car that boxes
Going big? Independent practitioners who need a large estate car should certainly consider this one, says our motoring correspondent Dr Tony Rimmer (right)
If prIvate practice is to flourish, there has to be growth. a successful group of independent practitioners who run efficient clinics may well look at expanding their skills and premises.
a merger with another clinic that has a good reputation but offers different services could be a smart move.
However, what would not be so clever would be to ignore and change the established ‘brand’ of that clinic. a loyal client base and good relationships with the local community has immense business value.
the value and power of established and respected brands is clearly demonstrated in the commercial world of motoring.
When the Chinese business group Geely bought volvo from
Volvo’s adaptive cruise control is another step towards autonomous driving and I have to say that I am very impressed
f ord in 2010, it knew exactly what it was getting and has been investing heavily in new models to build on the solid reputation of this iconic Swedish brand.
Most of us have a mental image of a volvo that takes the form of a boxy but practical estate car with excellent safety features and rocksolid build quality.
Sold well the 240 from the 1970s and the 740 from the 1980s were popular choices for professional middleclass families in a pre-SU v era. volvo estate cars have always sold well to the medical profession, so does the very latest model still have relevance and appeal?
Well, the first volvo product to emerge as a result of Geely’s heavy investment was the technologi -
cally innovative, all-new XC90 SUv, which I tested for Independent Practitioner Today (December 2015) and was highly impressed. Now we have their latest offering – the v90 – a large estate car to continue decades of established history.
t o compete directly with Mercedes’s e -class estate, a udi’s a 6 a vant and BMW’s 5-series touring, the new v90 has its work cut out. Like the new XC90, it is only available with a choice of two four-cylinder diesel engines; the 187bhp 2.0litre D4 and the 235bhp 2.4litre D5. there are three trim levels and a choice of two- or four-wheel drive. there is also a cross-country version. I have been testing the midrange D4 Inscription model that is likely to be the biggest seller.
The styling of modern estate cars avoids the boxy looks of previous generations and the steeply raked tailgate of the new V90 follows this trend
boxes clever
t he styling of modern estate cars avoids the boxy looks of previous generations and the steeply raked tailgate of the new v90 follows this trend.
a lthough you may lose out slightly on interior space, the result is far more pleasing to the eye.
Car-park appeal
With volvo’s signature ‘ t hor’s hammer’ running lights and an imposing front grille, there is great car-park appeal. It looks thoroughly modern, smart and upmarket.
Step inside and the light interior feels really contemporary with a 12.3 inch touchscreen that links the driver to a wide selection of cutting-edge technology.
Comfortable seats and the use
of high-quality materials completes the business-class feel. Generous head and knee room similarly spoil rear seat passengers. f or an extra £400 you can specify the f amily p ack, which adds a pair of integrated child booster seats to the rear bench. the standard powered tailgate opens a cavernous boot with automatically retracting load cover – another neat touch.
So the v90 has all the practical attributes to impress as a family car, but how does it drive? Well, you rarely notice that the diesel engine has four cylinders and is only 2.0 litres.
When cold, it can be a bit clattery, but at all other times the noise is subdued and the power output is always strong and immediate. Wind noise is also
VolVo V90 d4 inscription
Body: Five-seat estate car
Engine: 2.0 litre four-cylinder turbo diesel
Power: 187bhp
Top speed: 140mph
Acceleration: 0-60mph in 8.2 secs
Claimed economy: Combined 62.8mpg
Claimed Co2: 119g/km
on-the-road price: From £37,995
minimal and this, with the excellent smooth ride, makes the big volvo a great motorway cruiser.
Autonomous driving
Handling on twisty roads is better than you would imagine; the use of lighter materials has made the v90 more agile.
all versions are fitted with the latest version of volvo’s p ilot assist adaptive cruise control.
t his system is another step towards autonomous driving and I have to say that I am very impressed. It pretty much drives the car for you at speeds of up to 70mph. It accelerates, brakes and can even steer for you – as long as you keep a hand on the steering wheel – in light or dense traffic.
I tried it in a typical south-east of e ngland rush hour and it
worked without fault and certainly reduced the stress of a journey like this.
although I, like all petrol heads, love the freedom and enjoyment of driving on a clear road, when our increasingly busy traffic conditions do have to be tackled on a regular basis, I welcome such a feature. Well done, volvo; this is the future.
t he new v 90, like the XC90 before it, shows that volvo’s new owners are doing great things for the brand. If you need a large estate car, it deserves your consideration. Look out for other new volvos too. a new XC60 SU v is due in the UK before the end of 2017.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
Comfortable seats and the use of high-quality materials completes the business-class feel. Generous head and knee room similarly spoil rear seat passengers
PrIvAte medIcAL InSurAnce work In PrIvAte
PrActIce IS bIg buSIneSS, So Let CODe BUSTeR!
keeP You In the know every month, the clinical coding and Schedule development group (ccSd) reviews its 2,000-plus procedure codes, and more than 3,000-plus diagnostic codes, that form the basis of private medical insurance. It is crucial for independent practitioners and their practices to know these codes, so they bill correctly. If they don’t, then it could cost them money
Crack the code and get the money
coDE BUsTER!
CHaNgeS TO NOTe THIS MONTH
Specialties recently affected include: spine, spinal cord and peripheral nerves (Code a & V), breast (Code B), eye and orbital contents (Code C), ear, face, mouth, salivary and thyroid (Code F), radiotherapy (Code h), thorax and intra-thoracic organs (Code k), vascular system (Code L), urinary system and male reproductive organs (Code m), female reproductive organs (Code Q), skin and subcutaneous tissue (Code S).
there are 15 new proCedure Codes
F1090 – e xtraction of a tooth under general anaesthetic;
F1151 – Dental implant stage I –surgical placement of implants;
F1152 – Dental implant stage II –surgical exposure of buried implants;
F1153 – Dental implant stage III –placing of the prosthesis;
Q1281 – removal and/or replacement of an embedded/migrated mirena coil (as sole procedure);
H4685 – Insertion of biodegradable perirectal spacer under image guidance;
V2151 – arthrocentesis of temporomandibular joint – unilateral;
V2152 – arthrocentesis of temporomandibular – bilateral;
K6310 – CT coronary angiogram; Q2330 – Salpingectomy, including bilateral, as sole procedure;
C8688 – Thermal pulsation treatment for dry eyes caused by blocked meibomian glands;
A5751 – Facet joint injection, under X-ray control, 1 to 2 joints;
A5761 – Facet joint injection,
under X-ray control, 3 to 4 joints;
A5771 – Facet joint injection, under X-ray control, 5 or more joints;
C6720 – Laser treatment for glaucoma: e.g. Cyclodiode.
there are eight narrative Changes
A5750, A5760, A5770, M6192, L8880, B2986, B2990, M7940 and one inactivation: T7983
there are 81 unaCCeptaBle CoMBinations (also known as unBundling)
Of special note this month, there has been a code and price change for Bupa. Under surgeon’s category, code W8240 – meniscal allograft transplantation, has been increased from £548 to £1,040. Under anaesthetist’s category, the same code has been increased from £195 to £447.
also, common codes for spinal injection A5750 , A5760 and A5770 have been redefined, removing the facet joint injection part of the narrative, activating new codes for this part of the procedure: A5751, A5761 and A5771
Please remember, however, that codes are not mandatory for the insurers.
In other words, the inclusion of procedure codes within the Clinical Coding and Schedule Development Group list does not indicate the automatic agreement of individual insurers to provide benefit for this procedure.
You need to contact each insurer directly to find out whether benefit is provided.
Code Buster data is provided B y Medi C al Billing and ColleCtion. For Full details, go to the Clini C al Coding sChedule developMent we B site at www. CC sd. org.uk
No stopping urologists
Income prospects for urologists look good after a healthy profits rise – but groups continue to take an increasing share of the market. Ray Stanbridge reports
The marke T environment has changed significantly since 2008, as readers will be well aware.
Sole-trader urologists are no longer the norm. Groups continue to grow and flourish, and many urologists have chosen incorporation as a route forward.
We have also seen the dramatic growth of ‘Choose and Book’ work, which, for many in the country, is now the mainstream of their practices.
The impact of Bupa’s ‘open referral’ and other insurers’ programmes has had the impact of distorting fee patterns away from
the established to new consultants.
and finally, we are now seeing the results of the Competition and markets authority (Cma) orders from October 2015, which are having the effect of increasing consultant costs. all of these factors detract from the objectives of obtaining a reasonable trend in formulating this earnings analysis.
In my april 2016 report, I stated that I was hoping to restyle the format of Profit Focus. however, I have yet to find a better formula for presenting information in this benchmarking series, so am con-
aveRage INCOMe aND eXPeNDITURe
tinuing with the current basis of reporting, notwithstanding the significant problems.
It should be noted that our sample of consultant urologists is restricted to those:
Who have either had an oldstyle or a new-style NhS contract;
h ave been in practice for at least five years;
h ave been earning at least £5,000 a year gross from private practice;
may be trading as a sole practitioner or as a member of a group;
may or may not have incorporated;
Will continue to do some NhS work – meaning they are not in full-time private practice.
continue to prosper
Despite all the caveats, our headline figures suggest that, on average, private practice incomes have risen by 6.2% between 2014 and 2015, from £127,000 to £135,000.
Costs have gone up by 4.3% from £46,000 to £48,000 on average.
as a result, pre-tax profits have increased by about 7.4% from £81,000 to £87,000. a nd actual results are in line with my predictions.
Last year I stated: ‘Overall, we feel that urologists in private
RaNge OF gROSS INCOMeS
Year ending 5 April. Figures rounded to nearest £1,000 (percentage is also rounded up)
Source: Stanbridge Associates Ltd.
RaTIO ReMaINeD SIMILaR DeSPITe
practice will, on average, continue to prosper, though they may have to work harder to achieve the same income levels as their elders did and are doing.’
We have noticed that for conventional private practice work –insured and self-pay patients – groups seem to be taking an increasing market share.
Conventional sole-trader con -
sultants in the country appear to be doing more ‘Choose and Book’ work. Nonetheless, there does seem to be some strength generally in the private practice urology market.
impact of competition ruling
We have noticed some cost increases with respect to staff – a combination of increasing per -
sonal allowances for family staff members and the first effects of the Cma rulings.
Consulting room costs generally have increased, and this is almost certainly the impact of the Cma’s intervention.
There has been some increase in professional indemnity costs. We have noticed that some consultants are now using alternative suppliers, although the full extent of cover, in certain instances, is still difficult to determine.
With the exception of travel and conferences, most other costs have remained constant. These costs vary with the propensity for consultants to attend exotic conferences.
What then of the future? early indications of performance for the year to 5 april 2016, suggest that urology private practice is still robust and prospects still continue to look good.
as reported above, we are seeing some major structural changes with groups taking an increasing share of the market. In this respect urology is not unique.
next month: Anaesthetists
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists Stanbridge Accountants
UROLOgISTS’ PROFIT-eXPeNSeS
what’S coMing in oUr MaY iSSUe
Make sure you don’t miss our next issue, published on 18 May. you may not receive every issue if you have not yet subscribed to the journal. Don’t risk missing out on vital topics we tackle next time, including:
So what should you do if a private hospital wants to investigate your practice or suspend practising privileges? Dr Oliver Lord, a medico-legal adviser for the MDU, sets out some sound advice
Our legal briefing tackles the pitfalls of prescribing medication online. We review the key issues that any healthcare business will need to consider if they wish to develop a remote prescribing interface
Ten commandments for successful billing and collection in your practice. Be sure to show these tablets to the person/s responsible for getting the money in to your practice
Know your profit from your profitability when measuring financial performance. Increased profits do not necessarily result in increased profitability, so read the signs to avoid working harder for less.
How private practitioners are streamlining their multidisciplinary team meetings and becoming more efficient
Reports from expert talks at the BMa’s private practice conference
Breaking into medico legal work – your terms of business should always make it clear to solicitors when you expect to be paid
HMRC pressure is mounting on private doctors. Our accountant’s Clinic advises on the best ways to keep on the right side of the taxman
Our Strange Medical Tales series continues with the story of a doctor who was surprised to read his own obituary
Our new series on the gMC’s latest confidentiality guidance focuses on disclosures to a patient’s family and carers
Ray Stanbridge’ Profits Focus series examines the latest earnings of anaesthetists and finds a growth area is pain management. For those entering into this speciality, income has grown and future prospects also look bright, he reports
grr! Our Doctor On The Road columnist Dr Tony Rimmer takes the Jaguar F-Pace for a spin
Start a private practice gives doctors starting out in the independent sector a guide to expenses – established independent practitioners will want to read it too
Code Buster! brings you the latest changes to the codes independent practices need to know so they bill correctly
Plus all the latest news and views
aDveRTISeRS: The deadline for booking advertising for our May issue falls on 24 april
Published by the Independent Practitioner Ltd. Independent Practitioner today is editorially independent and thanks bupa for its assistance with distribution.
£90 gPs and practice managers (private & nhS). £210 organisations. but if you pay by direct debit, individuals pay only £75, and organisations £180 call Proact Ltd on 01752 312140 email: lisa@marketingcentre.co.uk
Stride, editorial director
To guarantee your copy of Independent Practitioner Today by taking out a subscription (at the rates shown on the left), phone 01752 312140 or send off a subscription form on page 20 or email lisa@marketingcentre.co.uk or go to the ‘about’ page of our website www.independent-practitioner-today.co.uk
If you pay by direct debit, individuals pay only £75 for a subscription. Just fill in the form on page 20 and send it to the Freepost address shown at the bottom of the form.
BaCK ISSUeS: £12.50 including post & packaging
CHaNgINg aDDReSS OR SUBSCRIPTION DeTaILS?
Phone 01752 312140 or email lisa@marketingcentre.co.uk
Robin
When we established our medical billing service, an e-billing capability was essential. Healthcode’s system has all the benefits: ease-of-use, efficiency and minimising our postage costs.
”
Rebecca Deering, Nuada Group
Securely manage your patient billing
As the UK’s official medical bill clearing company, Healthcode’s ePractice solution incorporates electronic billing to all major insurers and paper billing for self-pay patients, allowing you to have both paper and electronic bills under one system.
Using ePractice to bill, you can:
• Raise electronic or paper invoices
• Receive payment quicker for ebills
• Improve cash flow
• Ensure fewer errors
• Confirm your ebill is with the insurer
Healthcode’s ePractice solution offers:
Patient Billing
Patient Management
Payment Tracking & Financial Reporting
Appointments
Membership Enquiry
Complimentary ePractice App
Experts in Online Solutions for Smarter Healthcare... ‘code for success.