The business journal for doctors in private practice
Cleaning up
Our resident accountant looks at ways you can spring-clean your finances P10
Tie-up with NHS is boundless
The outlook for private patient units is bright. Our new series
Cat
The seven medico-legal sins
An expert looks at the areas where private doctors run into ethical difficulties P20 monitors their progress P18
Doctors facing a £1m+ claim surge
By Robin Stride
A surge in £1m+ claims against self-employed doctors has prompted a renewed plea for a fairer and more affordable compensation system.
New figures given to Independent Practitioner Today also brought a warning that if nothing is done, then rising indemnity costs could force more specialists out of private practice.
According to the Medical Defence Union (MDU), multi-millionpound damages in clinical negligence claims are no longer rare.
The defence body’s Dr Mike Devlin said: ‘Some of the largest compensation payments we have made have been on behalf of MDU members in independent practice.
‘For example, our highest payment to date was £9.2m plus legal costs to compensate a patient rendered tetraplegic following spinal surgery.
‘Another example was £6.2m in damages with £3m in legal costs to a female patient who suffered nerve damage after plastic surgery.
‘In the first claim, the damages were so high because of the cost of providing future care and accommodation for a young person with a long life expectancy. In the sec-
ond, the claimant’s loss of earnings made up most of the award.’
The MDU said multi-millionpound compensation claims against consultants in private practice, and GPs, had risen threefold over the last decade.
Last year, it settled 12 compensation claims for more than £1m on behalf of consultant and GP members. In the last three years, it has paid over £100m to compensate patients and pay legal costs in 36 negligence claims exceeding £1m.
The MDU said payments were no reflection on clinical standards, which remain high, but rather a result of a combination of economic pressure ‘and an outdated legal system meaning compensation costs are calculated on the basis of private, rather than NHS care’.
By contrast, in 2005, just four settled claims exceeded the £1m mark and, in 1995, the union gave only one patient £1m compensation.
Dr Devlin, head of professional standards and liaison, warned that clinical negligence claims inflation was doubling every seven years. A claim costing £9m if settled today was likely to cost at least £18m by 2022.
Organisations indemnifying
doctors in the independent sector had ‘no option’ but to reflect the cost of these claims in their subscriptions.
He said another factor was the different risks faced by individual specialties in independent practice: ‘For example, surgeons in certain specialties like plastic and orthopaedics are relatively more likely to be sued than ophthalmologists and general surgeons.
‘Not only is this unsustainable for doctors, but more widely it affects all taxpayers who are funding public liabilities such as the NHS Litigation Authority’s, which were estimated to be £28.3bn in April 2015.
‘It is possible that if awards were to continue to rise unchecked, practice in the independent sector might decline because of the rising costs of indemnity. This could result in more patients seeking treatment in the NHS who might otherwise have sought private care, resulting in more pressure on an already-stretched public service.’
The MDU is calling for legal reform so patients are compensated appropriately but in a fairer and more affordable way. You can find out more at www.themdu. com/faircomp.
HCA may not have to divest with cream
Hospital group HCA may not have to sell off some of its hospitals after all following a change of heart by the Competition and Markets Authority (CMA) in its latest provisional report.
The body said its view came after hearing new evidence about the likelihood of more private hospitals opening in London.
Roger Witcomb, chairman of the CMA’s Private Healthcare Market Remittal Group, explained: ‘We still believe the market requires more competition, but the new information we have received in the course of the remittal means that we now believe that divestment is no longer a proportionate remedy.’
He said any benefits to ‘consumers’ of a divestment would be shortlived and not large enough to outweigh the cost of selling. The group had found no other remedy which was both effective and proportionate.
The decision was ‘finely balanced’ and not unanimous. ‘We will of course consider responses to this provisional decision before making a final decision on remedies.’
Parties were given only until 13 April to respond.
n See page 4
your guide to case history marketing lessons from the aesthetics industry on what not to do when marketing P12
confidence in what you do
How to overcome your ‘fear of sales’ which is holding back your aesthetics clinic P14
beating the competition
Just how worried should you be about your competitors in private practice? P26
avoid risk of being accused of assault advice on how to avoid patient complaints following an intimate examination P30
Protecting your goodwill legal briefing on how to restrict leaving partners so they don’t damage you P33
beware of financial sharks
Why you should be wary of investment offers that look too good to be true P38
Plus our regular
ediTorial commenT
We rightly hear much about protecting patients but, as we are your business journal, this issue has some useful articles aimed at protecting you, the doctor.
There are more threats to the unwary than ever before.
As ever, independent practitioners need preserving from the mounting cost of claims (see our cover story).
Sadly, £1m+ pay-outs are no longer unusual. Surely there needs to be a change in the legal system before more excellent consultants and GPs decide the cost of protection in private practice is unaffordable?
Our expert writers this month
are also giving some useful advice on a number of fronts: medico-legal areas that could potentially cause complaints or claims (page 20), tips to help you avoid being accused of assault (page 30) and a warning of financial sharks out to consume doctors (page 38).
Lots of specialties could also benefit from our guide to protecting them from badly displayed case history reports on their websites (page 12).
And for the increasing number of doctors in groups, the need to protect your goodwill, and your practice, is brilliantly covered by our legal writers (page 33).
Tell us your news Editorial director Robin Stride at robin@ip-today.co.uk Phone: 07909 997340 @robinstride
To adverTise Contact advertising manager Margaret Floate at margifloate@btinternet.com Phone: 01483 824094
To subscribe lisa@marketingcentre.co.uk Phone 01752 312140
Publisher: Gillian Nineham at gill@ip-today.co.uk Phone: 07767 353897
Head of design: Jonathan Anstee chief sub-editor: Vincent Dawe 12,450 circulation figures verified by the Audit Bureau of Circulations
No sour taste for pensions in the Budget
by edie bourne
Chancellor George Osborne’s ‘sugar tax’ Budget gave senior doctors a rare taste of sweetness after it left their pensions unscathed.
Retirement nest-eggs escaped being crunched further from more radical changes that were feared in the run-up to his speech last month.
Many high earners were expecting a pocket-hitting reduction in tax relief on pension contributions in Mr Osborne’s eighth Budget speech – but this failed to materialise.
Instead, his plans included several measures to support private consultants and GPs who are investors and long-term savers.
The ISA saving rate will be increased to £20,000 a year from April 2017 – up from £15,240.
At the same time, individuals under 40 can save up to £4,000 annually under a new ‘Lifetime ISA’.
Every £4 saved will be matched by £1 from the Government, up to the age of 50. The savings can be withdrawn tax-free if used towards a deposit on a first home worth up to £450,000 or if they remain in the account until after the holder’s 60th birthday.
The money can be withdrawn at any other stage but the Government bonus, and any interest or growth on this, would then be lost. There is also a 5% charge for doing so.
Capital gains tax (CGT) due on investments will be cut from 28% to 20% cent for higher-rate tax payers and from 18% down to 10% for basic-rate tax payers from this month.
Patrick Convey, technical director of specialist financial planners Cavendish Medical, told Independent Practitioner Today the CGT
announcements brought good news for those making a sale on assets.
But he said it should be noted that this did not include second homes or buy-to-let properties –another blow for landlords.
He added: ‘Overall, we are pleased that savers are being rewarded and we are certainly relieved the Chancellor has decided not to bring in further changes to the pensions system at this time.
‘However, please remember that the lifetime allowance for pension savings is still being reduced to £1m in April – which is likely to catch every senior doctor.
‘Furthermore, the annual allowance will be reduced for those with an annual income of more than £150k.’
Accountant Susan Hutter, of Shelley Stock Hutter, said: ‘There was good news on pensions, as it was expected that all or part of the tax-free lump sum, currently a maximum of 25% from a private pension scheme, would become taxable.
‘It was also expected that tax relief on premiums paid into a pension scheme would be limited to basic-rate tax. The Chancellor did not introduce either of these measures.’
Accountant James Gransby, of MHA MacIntyre Hudson, added: ‘The lack of further changes gives a welcome respite, although the changes already announced will adversely affect a large number of people in the NHS scheme.’
Mr Osborne also granted a welcome change to tax bands – the threshold at which people pay 40% will rise from £42,385 to £45,000 in April 2017. The tax-free personal allowance will rise from £11,000 to £11,500 next year.
What’s in the Budget for you? See page 6
by a staff reporter
Budget plans to make it more costly for many patients to see a private doctor have been fiercely criticised by insurers and the private medical insurance salesforce.
Bupa UK managing director Richard Bowden said the 0.5 percentage point insurance premium tax rise from 9.5% to 10% made ‘no sense’, while an industry leader warned it would put more pressure on the NHS.
The rise to 10%, due in October, will be the second rise in the tax in just a few months – it went up from 6% to 9.5% only last November.
Stuart Scullion, chairman of the
Association of Medical Insurers and Intermediaries, said the industry was disappointed to note how this tax would impact on private medical insurance as well as cash plans, and subsequently the NHS.
He said: ‘We do believe more support is needed to improve flood defences in the UK and we express great sympathy for those who have been affected by the flooding. However, it does not make sense to fund this through penalising those people who are choosing to prioritise their health through private medical insurance and health cash plans.
‘As the second increase in six months, in a market where premi-
ums are on the increase already, this new change could be the difference between someone maintaining their health insurance or leaving the market and going back into the NHS.’
Mr Scullion said the rise was a ‘double hit’ for employees in companies with health insurance or health cash plan benefits. They would effectively be taxed twice and, rather than incentivising employers to offer health benefits to staff, this would further discourage this type of support and increase the burden on the NHS.
The AMII is campaigning for health-related insurance to be exempt from the tax.
Richard Bowden, managing director Bupa UK, said: ‘Even a small increase adds to the unfair penalty on those individuals and employers who pay extra towards their healthcare, on top of the tax they already pay to fund the state system.
‘It makes no sense to tax a service that reduces the burden on an increasingly strained NHS. Health insurance should be zero-rated like it is in many other countries, and like life or critical illness insurance in the UK.
‘The UK now has one of the highest rates of tax on health insurance out of 28 European countries.’
Insurance tax rise slated Meeting falls victim to doctors’ strike
The BMA’s fight over the junior doctors’ contract has scuppered one of the year’s biggest private practice events – its annual private practice conference.
It cancelled the 6 April meeting weeks in advance because of a clash with industrial strike action by juniors in England.
There was also concern that going ahead could potentially create ‘difficulties’ for doctors leaving their trusts to attend the conference.
Association leaders feared the annual meeting, covering essential business topics* for more than 100 new and established independent practitioner consultants
* wHy waiT a year?
and GPs, would backfire with adverse publicity for its Private Practice Committee and the BMA.
Private Practice Committee
chairman Mr Derek Machin told Independent Practitioner Today: ‘We were very disappointed to have to cancel the private practice conference this year, but when the Junior Doctors Committee announced that it was having industrial action on the same day, it became apparent that the BMA and conference attenders were very likely to be subjected to criticism and we would be handing the Government a club to beat as with.
‘There was also the issue that doctors intending to come to the conference might be put under pressure to remain in their trust.
‘We certainly saw a dramatic fall in attendance at the staff, associate specialists and specialty doctors committee when their meeting coincided with industrial action.’
Mr Machin said the BMA considered trying to re-arrange the conference for a later date this year, but the short notice and uncertainty of speakers’ availability made that impractical.
He added: ‘We will be having a conference in 2017.’
stay up to date on the essential business topics for independent practitioners by taking up Independent Practitioner Today’s direct debit subscription offer for our annual ten issues. see page 22 for details
Private patients seek more powerful voice
The Private Patients Forum (PPF) plans to increase its impact as the private patients’ voice.
Director Don Grocott, who is leaving the post, said: ‘We’ve made an excellent start with much-appreciated support primar-
ily from key hospital groups and now we must build momentum to be the champion that patients need, delivering in a way that all the industry can support.’
Matt James, chief executive of the Private Healthcare Information
Network (PHIN), said: ‘Our experience suggests that to build trust among patients you first have to build trust within the industry. I hope that the private hospitals and insurers will get behind PPF’s mission and new leader.’
derek machin: said attenders at the conference would be criticised
don grocott matt James
New player forces CMA into a U-turn
By Robin Stride
The entry of American hospital operator the Cleveland Clinic into the London healthcare arena ( Independent Practitioner Today , Nov 2015) is a key reason why Competition and Markets Authority (CMA) investigators have had a change of heart (see p1).
Initially last Autumn, the group, with 15 hospitals in Ohio, Florida, Nevada, Canada and Abu Dhabi, told us there had been no decision on whether its lease on a 200,000+ft2 building at 33 Grosvenor Place would even be used as a medical facility. An administration building was mentioned as a possibility.
However the CMA’s latest report, Private healthcare remittal –provisional decision on remedies, has every confidence that Cleveland Clinic will go ahead with a large private hospital in the city with around 215 beds. Specialties would include cardiology, orthopaedics, urology, vascular and neurology treatments.
This would bring more competition to the capital and could relieve HCA of a requirement to sell either The Wellington and Platinum Medical Centre, or The London Bridge Hospital and the Princess Grace Hospital.
A CMA suggestion to force HCA to rent out some of its facilities to
a rival has been widely considered unworkable.
Meanwhile, Cleveland Clinic has revealed to the CMA that it has detailed business plans –which could evolve as it learns more about the market. These set out its strategy for entering the private hospital arena in central London, writes the CMA, ‘through the acquisition of the site in Grosvenor Place’.
combination with other nonHCA hospitals) within two years of it opening its inpatient facility, i.e. by the beginning of 2022, assuming that the facility opens in late 2019/early 2020.’
Other developments include a large European group’s intention to open a 65,000ft2 private hospital in London’s Wigmore Street. It would specialise in spinal treatments and neurology.
THE cma’S cHanging viEw
Statement from Roger witcomb, chairman of the Private Healthcare market
Remittal group:
‘In the course of our reconsideration of the central London market, we have received a substantial number of submissions and heard a great deal of new evidence.
‘In our final report in the original investigation and again in our provisional findings on the remittal, we identified that customers of privately-funded healthcare in central London were paying too much, largely because of HCA’s strong market position.
Some of our medical consultant readers have already been retained in an advisory capacity for the project. The company told the CMA it was working with them to develop its plans. These could include another site if the Grosvenor Place building failed to get planning permission.
The CMA says Cleveland Clinic has a strong reputation for quality and innovation in the US, which is likely to help it establish a reputation in the market, initially among consultants, but also insurers, patients and private medical insurance corporate clients.
The CMA adds: ‘On this basis, although it is not possible to identify reliably the precise timing of when a competitive constraint will emerge, we consider that Cleveland Clinic is likely to exert such a competitive constraint (in
BUPa STiLL UnHaPPy
alex Perry, general manager of Bupa UK customer, said: ‘The cma has confirmed again that there isn’t enough competition in central London, with Hca dominating the private hospital market and charging higher prices. This means our customers have been paying more than they need to for treatment at Hca hospitals in central London and this will continue until potentially 2022.
‘while it suggests that a probable new entrant will bring more competition to the London market, customers won’t see a benefit for up to six years. meanwhile, they’ll continue to be penalised by higher prices. we ask the cma to act now to address this gap.
‘we will continue to do all we can to improve affordability and choice for London customers.’
The hospital, whose owners are impressed by London’s attraction to overseas patients, is expected to take 15 months to establish following planning permission, but will see self pay and insured patients too.
The CMA has already brought in changes following its initial investigation, including:
A crackdown on benefits and incentive schemes given to referring clinicians by private hospital operators;
The appointment of the Private Healthcare Information Network to provide independent information for private patients on healthcare performance. Its website will carry data on, among other things, private hospitals’ performance;
The ability for the CMA to be able to review future arrangements where private hospital operators team up with NHS private patient units and to prohibit any arrangements that might substantially lessen competition.
‘In our original investigation, we sought to address that problem by requiring HCA to sell one or two of its central London hospitals. We still believe the market requires more competition, but the new information we have received in the course of the remittal means that we now believe that divestment is no longer a proportionate remedy.
‘This new information has included evidence of probable entry into the central London market, which we consider will provide a competitive constraint on HCA within the next four to six years.
‘This means that benefits to consumers of a divestment would be short-lived and not large enough to outweigh the cost of divestment, and we have found no other remedy which is both effective and proportionate.
‘This was a finely balanced decision, and the group was not unanimous. We will, of course, consider responses to this provisional decision before making a final decision on remedies.’
a Hca spokesman said: ‘London offers an open, accessible and competitive market for private healthcare providers.
‘Over the past six years, it has continued to grow and diversify, with existing players expanding and new entrants investing in the opportunities the capital has to offer.
‘Hca welcomes the cma’s recognition that the competitive landscape in London will continue to evolve and we will engage with the cma for the remainder of the consultation process.’
Londonbound: our front page from november 2014
NHS spurs private boost
By a staff reporter
Independent sector growth last year was led by private acute healthcare, up 8% to £7.8bn, according to a new report from market analysts LaingBuisson.
It said this was driven by recovering private demand as well as NHS ‘Choose and Book’ patients opting to receive NHSpaid treatment in independent hospitals.
LaingBuisson chairman William Laing, speaking at the report launch, reflected that the private acute medical care market grew strongly during most of the 2000s. It was then driven by a combination of modest increases in the number of people with private medical cover, new medical technology which increased the use of private health cover among subscribers, rising prices, and outsourcing of NHS surgical activity to the independent sector.
Growth stalled after the 2009 recession, falling to close to zero in real terms in 2010 and 2011. The principal cause was the 8% cumulative fall in the number of people with private medical cover during 2009–11.
But Mr Laing said the last three
years from 2012 had witnessed the reestablishment of growth in the private acute medical care market – but not through any recovery of demand for private medical cover which had traditionally been the engine of growth for private healthcare provision.
‘Rather, the main driver of renewed growth has been NHS outsourcing, particularly through the ‘Choose and Book’ system, which gives NHS patients access to independent hospitals for elective surgery.
‘It is this, together with strengthening selfpay demand and a surge in overseas demand that accounts for the re establishment of realterms growth in the private acute medical care market from 2012 to date. Meanwhile, demand funded by private medical cover continues to be stagnant.’
LaingBuisson said that, in 2015 in the UK, sources of funding for independent acute medical surgical hospitals and clinics came from:
Private medical cover, £2,383m;
NHS, £1,524m;
UK private selfpay, £844m;
Overseas, £386m.
Private payment remained the largest source of funding, account
HCA begins menu of fixed-price treatment
HCA Healthcare UK has for the first time launched fixed price treatment on over 40 procedures across all of its hospitals after seeing an average 12% annual growth in selfpay revenue.
The scheme offers a fixed consultation price, upfront guaranteed bill with no hidden costs or extra fees, and all pretreatment tests except MRI and CT scanning.
HCA research suggests that while people put a premium on quality when making healthcare decisions, the ability to put a fixed price on care from the outset can provide extra confidence and reassurance for patients to go
ahead with proposed private treatment.
Procedures include knee and hip replacement, diagnostic colonoscopy, hysterectomy and varicose vein removal. Paediatric treatment is also available on some procedures including hernia repair. Other procedures will be added later.
Chief executive Mike Neeb said: ‘The self pay market is growing and it is important that HCA offers patients the flexibility to access different payment methods.’
Eligibility, procedures and pricing are shown on the HCA website https://hcafixedprice.co.uk.
ing for 70% of private acute hospital revenue, predominantly through ‘private medical cover’ –the umbrella term for ordinary private medical insurance (PMI) together with noninsured medical expenses schemes which some employers prefer to run as an alternative PMI.
But the NHS had been rapidly increasing its share, which now stands at 30%, having risen from less than 5% a decade ago.
Further outsourcing of NHS activity was now being driven by the Any Qualified Provider policy,
which gave people in England free choice to use either an NHS or an independent sector hospital for elective surgery, paid for by the NHS.
LaingBuisson said a key challenge facing the private acute hospital sector was how to respond to a situation where the share of funding derived from traditional private medical insurance had dropped and been replaced by NHS funding.
‘While welcome, NHS funded activity brings with it significantly lower margins, and the challenge to providers’ profitability is further exacerbated by costcontainment pressures from the major insurers, in particular Bupa, which stated publicly during 2014 that it is seeking a 20% reduction in provider prices as a prerequisite for containing medical insurance prices, which it views as essential to stimulate consumer demand for private medical insurance once again.’
LaingBuisson’s Healthcare Market Review – 28th edition, from £805. Available from www. laingbuisson.co.uk See ‘Tie-up with NHS is boundless’, page 18
Nuffield tests system of patient e-records
Nuffield Health has agreed with software provider InterSystems to implement TrakCare, an integrated electronic health record system for clinicians and patients.
Nuffield’s chief digital and information officer Alan Payne said its ambition was to create integrated healthcare with the patient at the centre of everything it did, and its partnership with InterSystems would help it achieve this.
Mr Payne said: ‘Better use of data and technology has the power to improve health and transform the quality of care.
‘By joining up an individual’s healthcare journey, we can not
only provide an enhanced experience, but give the consumer more control over their health and wellbeing.’
Nuffield said it would work with InterSystems initially on a proof of concept solution which will be deployed into pilot sites, before a full rollout across its 31 hospitals.
In parallel, the use of TrakCare and other technology from InterSystems will be progressed in wider areas of Nuffield Health’s business with the aim of providing a single consistent health record accessible by clinicians and patients inside and outside of a clinical setting.
budget speciAl
Small changes all adding up
Doctors’ pensions thankfully escaped further fiddling in the Budget – as we report on page two – but James Gransby finds many aspects of independent practitioners’ businesses and finances will be affected in the months and years ahead
corporation tax rates
Corporation tax is 20% and will fall to 19% on 1 April 2017 and then to 17% on 1 April 2020 rather than the previously announced 18%. This will benefit doctors operating their private fee work through a limited company.
Using a limited company for private fee work can still be a taxefficient option, despite the increase to dividend taxation.
Involving a spouse and saving money in the company are key ingredients to making this work to maximum advantage.
Taking the example of a 40% taxpayer, the box below shows a rough and ready comparison between sole trader and limited company structures where all profits are extracted as dividends in a sole name.
When the rate falls to 17%,
then for every £100 earned, £83 will remain as profits after tax in the company for later withdrawal, versus £53 for the Additional Rate personal taxpayers (45% + 2% NIC).
Effect on you: For those operating through a limited company, the fall to 17% will take some of the sting out of the increase in dividend taxation and, for some, it could lead to an overall tax saving compared to being a sole trader, depending on income levels.
class 2 nic
This is being scrapped from April 2018, so will save some admin and a small amount of tax for those operating their private fee work as a sole trader or in partnership.
Effect on you: If you are a sole trader, then this will result in a small saving and less bureaucracy.
capital gains tax (cgt)
This is to fall from 28% to 20% for higher-rate taxpayers, but not for the sale of second properties.
The reduction came in on 6 April 2016 and will also benefit trusts in the same way.
Effect on you: If you buy and sell shares outside of an ISA or have trust tax exposure, this may benefit you.
personal tax
No real changes here, although the increase in the personal allowance to £11,000 from 6 April 2016 means that the band in which the personal allowance is withdrawn is widened to between £100,000 and £122,000. Here there is an effective tax rate of 60% on earned income. The 40% tax band rises to £45,000 from 6 April 2017.
Effect on you: Beware of the widened effective 60% tax band.
isAs
There are two changes – the annual limit will rise from £15,240 to £20,000 from 6 April 2017 and a new Lifetime ISA is coming in for the under-40s.
Full details of the Lifetime ISA are awaited, but we do know they are available to those who are under the age of 40 on 1 April 2017. Contributions made up to
the age of 50, up to a maximum of £4,000 a year, will be topped up by the Government by 25% for either buying a first home or reaching age 60. The topped-up ISA can be drawn down when either the person buys their first home (up to £450k value), reaches age 60 or is diagnosed with a terminal illness. If funds are withdrawn before these events, then the annual topups will be clawed back along with the associated interest.
First homes: This may give a welcome boost for parents helping their adult children onto the property ladder if up to £4,000 a year is deposited in the offspring’s name.
The minimum age to open such an ISA is 18 and so there may be a few years where the £4,000 limit can be taken advantage of before a first home is bought. In this case, £4,000 is turned into £5,000 each year courtesy of the Government.
The Government top-up does not count towards the overall £20k ISA limit but the £4k invested does.
Age 60: It can be seen as a type of retirement saving which can be used alongside the NHS and private pension schemes and not affect the pension annual allowances or lifetime allowances. Some commentators have
mooted that this is a Trojan horse heralding a new type of pension saving for the future.
Effect on you: Helping children or yourself get on the property ladder has a new boost, or you may want to consider it as an alternative form of retirement saving for those under 40.
new allowances from April 2017
Some will benefit from two brandnew allowances. Each are £1,000. The first is for selling goods and services, the second is on income from property. Those who trade occasionally or earn income from renting their driveway, for example, will not need to pay tax on that income or declare it to HMRC if it is below the limits.
Effect on you: If you have income below £1,000 from these sources, then up to £470 tax a year will be saved on each source.
changes to entrepreneurs’ Relief on cessation
A consultation was undertaken in February 2016 on the future of Entrepreneurs’ Relief and the circumstances in which a 10% rate of tax may be obtained on liquidation of a company at the end of its life.
The conclusion reached essentially means that the preferential rate will only be available on retirement, not if the trade is carried on again after liquidation.
Effect on you: If you were thinking about extracting company funds in one lump sum before retirement, then you may have extra tax to pay on withdrawal.
Entrepreneurs’ relief becomes available to shareholders who are not officers or employees of the company.
This may be relevant where a shareholder – for instance, a spouse – is not a director of the company or on the payroll.
The shares will have to have been held for three years and the minimum holding of 5%, which is currently the case, will also disappear. Effect on you: If your spouse has shares but is not a director, then they could benefit from 10% tax on liquidation if they have held the shares for three years.
Entrepreneurs relief available on an associated disposal to a relative.
Where an asset has been used for the purposes of a trade, then if the asset is sold within three years of retirement and the retirement met the qualifying criteria for Entrepreneurs Relief, then there is a three-year window when the asset can be sold and also qualify for the 10% tax rate.
Extending this to allow a sale to a relative will offer tax-planning opportunities, especially at the three year mark if the asset has not been sold by then.
Effect on you: Only relevant if you own relevant trading assets; for example, consulting rooms.
company car tax rates
These continue to rise, meaning that only the most very efficient cars will give any sort of taxation advantage.
For the most fuel-efficient cars the 100% first-year allowance for electric cars is extended to April 2021 from 2018.
Effect on you: You will pay more tax on your company car and for electric cars you will have more time to benefit from 100% tax write-off – subject to private use restrictions.
directors’ loans
Where a director – or connected party – borrows money from their limited company, there is an increase in the ‘section 455’ tax due if the loan is not repaid within nine months of the company’s year-end.
The rate rises from 25% tax to 32.5% in line with dividend rate for a 40% taxpayer. This may be relevant where ‘dividend hopping’ – declaring a low dividend one tax year in anticipation of a larger dividend the following year – is used as a tax-planning exercise.
If you operate via a company, it may make it more important to repay directors’ loans within nine months of the year-end.
Effect on you: Only if you have a loan from your company which is not repaid within nine months of the year-end.
preventing the use of personal service companies in the public sector
This does not apply to fees earned from private patients whether direct or via insurance companies, so unless you undertake work direct for NHS trusts or the like, then you will be unaffected by this change.
This seems at odds with the reduction in corporation tax mentioned at the start, as with one hand the Government is encouraging the use of a limited company, but then restricting who can do so.
Other changes
Changes such as a rise in the VAT threshold to £83k, the ability to declare your tax digitally and ‘pay as you go’ quarterly, and an increase in the penalty to 60% for using tax schemes caught by general anti-avoidance legislation were also announced, but will affect only a very few people. On the face of it, the Budget did not bring many fundamental changes, but a number of the above changes will affect a large volume of practitioners.
James Gransby is a partner at MHA MacIntyre Hudson
Independent practitioners with property interests will be affected by the Budget in a number of ways. Accountant Susan Hutter reports
Annual tax on envelope dwellings (Ated)
My clients who work in the medical profession have been asking me regularly about investing in a residential property. From this month, limited companies that own a residential property with a value of over £500,000 on 1 April 2016 will be subject to an ATED tax.
But if the property is let out at a commercial rate to a non-connected person, it will be exempt from this. For properties between £500,000 and £1m, the annual tax is £3,500. For properties between £1m and £2m, it is £7,000. For non-exempt properties, there will be another sting in the tail as Stamp Duty will increase from this month, April 2016, to 15% on the purchase of these properties. However, once again, if the property is let out commercially to unconnected persons, then the normal Stamp Duty rates will apply. If the
property is let out initially but for less than three years, the Stamp Duty relief will be clawed back.
An ATED tax return is required, even if the property is exempt. This must be filed by 30 April following the year of assessment. So for 2015-16 the return has to be filed by 30 April 2016.
business rates
For consultants and private GPs who rent commercial premises and have to pay business rates there is good news, as the rates are being reduced for lower-value properties.
From 1 April 2017, the Small Business Rate Relief will be permanently doubled from 50% to 100%. Also, the thresholds will be increased so that practices with a property with a rateable value of £12,000 and below will receive 100% relief.
Practices with a property with a rateable value between £12,000 and £15,000 will receive tapered relief.
stamp duty on commercial property
For those who wish to buy or have bought commercial property as an investment, there is good news – since the 16 March Budget, Stamp Duty rates have been reduced on lower-priced commercial property.
There is now no charge on properties costing up to £150,000, 2% on the next £150,000 and 5% above this.
Susan Hutter is a partner at accountancy firm Shelley Stock Hutter (SSH) and a specialist business adviser for the medical profession
‘second homes under attack’, page 46
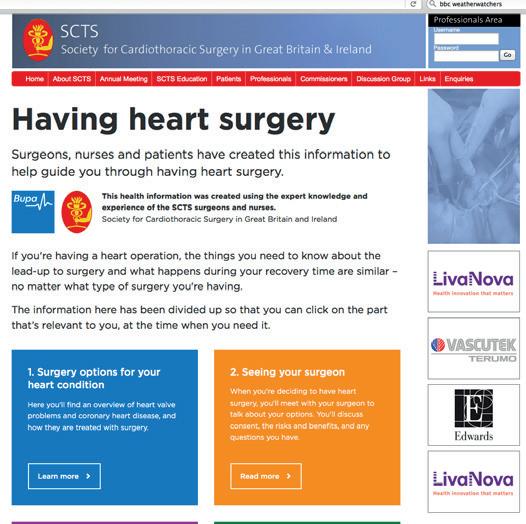
Help for heart patients
By Charles King
A new website launched by Bupa and The Society for Cardiothoracic Surgery (SCTS) aims to give peace of mind to those facing heart surgery.
The online hub has been developed for patients, families and carers and is relevant for all types of heart surgery, with videos of a surgeon, cardiothoracic nurse and patient following their surgical journey all the way through from the first appointment to their eventual recovery.
It gives advice and reassurance from trusted SCTS experts, with
Apology is best way to prevent a complaint
Apologies to patients tend to prevent formal complaints rather than the reverse, according to Dr Rob Hendry, medical director at Medical Protection.
He said: ‘It is important that a meaningful apology should be offered as soon as it becomes apparent that an adverse incident has occurred or the patient is unhappy with their care.
information they know is reliable and medicallyevidenced.
Bupa research found four in five UK adults turn to the internet for health advice, yet many admit
‘It may be some time before all the facts, and perhaps the reasons why and how the events occurred, are understood. Until these are established, speculation should be avoided, as this is unhelpful to all involved. However, this consideration should not hinder a prompt apology being forthcoming.’
The defence body has long advised members that an apology is not an admission of liability; rather, it is an acknowledgment that something has gone wrong and a way of expressing empathy.
Dr Hendry said Medical Protection always advocated a full and objective review of the event, with the patient being informed of any lessons that could be learnt.
NHS pain is private GP gain
Increasing numbers of GPs could be available for private practice work as a result of the NHS general practice crisis.
finding conflicting health information, leading to confusion and frustration.
Dr Steve Iley, Bupa UK medical director, said: ‘This website will be a great resource for anyone wanting a human approach to what can be a difficult procedure to understand, with evidencebased information in one place, taking people from their first appointment through to surgery and recovery.
SCTS presidentelect Mr Graham Cooper said: ‘We saw a clear need for an online resource that patients could rely on for information about heart surgery. This website is the product of years of hard
work in partnership with Bupa.
‘We know it will be a valuable tool for the thousands of patients in the UK who are faced with heart surgery each year. It’s also a great hub for surgeons, carers and the wider healthcare industry, who can use the information to engage with patients and provide real life examples of treatment and recovery.’
The website is free for anyone to access through the Bupa or SCTS websites:
www.bupa.co.uk/SCTS heartsurgery
http://scts.org/patients/having_heart_surgery/
Patients get more technology-savvy
Six in ten Britons have used technology to access healthcare, according to a study of 1,014 British adults carried out by ondemand video GP consultation service, PushDoctor.co.uk.
One in five have communicated with a GP online, 27% would do so if it meant they could have an immediate or same day appointment, and 26% if they couldn’t travel to their GP surgery.
Ordering repeat prescriptions (29%), is the most popular way of using technology to access healthcare services and 17% have used video consultation services to speak to a GP.
officer at PushDoctor.co.uk, said:
‘Clearly, there is significant demand among patients for new pathways to healthcare which work better for them, and are more in keeping with the ways they manage other areas of their lives.
‘Such technologies are being gradually introduced into the healthcare industry in the UK, but, looking at this data, there is a need to speed up this process.
More than 900 GP practices are in a weak financial position, with 294 believing they are financially ‘unsustainable’.
A BMA survey found nearly 300 practices facing closure and half of those in England reporting GPs planning to desert the NHS.
Convenience is leading this step change, with 30% claiming they would consult a GP via video if it meant they could have an appointment when they wanted.
Dr Adam Simon, chief medical
Unit revamps due to rise in demand
‘In introducing this greater level of convenience and choice, providers will be better equipped to help a greater number of patients, while bringing access to healthcare more in line with the ways other industries have modernised over the past five to ten years.’
Company founder Eren Ozagir said most patients appreciated the need for innovations to get quicker and more convenient advice.
Lead child and adolescent consultant Dr Alex Horne (pictured
London’s Nightingale Hospital has launched a renovated Young Person’s Unit in its Marylebone base following a 30% increase in demand for services, which include treatment for inpatients with eating disorders and depression.
right) said: ‘The earlier any problems are identified and understood, the earlier an appropriate diagnosis and treatment programme can begin.’
PRACTiCeS MAde PeRFeCT
Are you really doing the job you do best? That you enjoy most?
For 18 years we’ve helped large and small healthcare organisations across the world transform, grow, and improve the way they manage their businesses. Making your life better. And your patients.
While you concentrate on caring for your patients, our role is to help remove the yoke of management.
Not just the day-to-day logistics, but strategically, short and long term. Over the years we’ve transformed and grown countless practices and business. Planning and developing medical facilities. Marketing your healthcare services professionally, by knowing and employing the technology and media that deliver results.
Our teams are tailored to your needs. And if those needs change, so does our team. We have crisis management experts available 24 x 7. We combine clinical expertise with commercial sense and experience. We see the full picture, providing support when and where you need it most.
We work with both public and private sector healthcare providers. Our case histories in operations management, clinical advice, consultancy and development are outstanding.
To give it a thorough examination, call Peter Goddard on +44 (0)203 356 9699 or mobile +44 (0)780 314 4954
www.worldwidehealthcare.co.uk
Charles Rifkind Property
Neil Huband Communications
Peter Goddard Performance
Keith Hague CEO
Howard Ware Medical
Dr.Danny McGuigan Leadership
Scott Hague Technology
ACCOUNTANT’S CLINIC
Cleaning up
Springtime not only marks the beginning of better weather – hopefully – but also the beginning of a new tax year. Susan Hutter looks at different ways to spring-clean your finances
As much as you may not wish to do so, now is a good time to get your records up to date and pass them to your accountants, so that they can prepare not only the practice accounts but also your personal tax return.
The sooner you do it after the beginning of the tax year, the better, as everything will be fresher in your memory.
Also, your accountant will be able to work on the tax return sooner rather than later and you will know exactly where you stand for payment of tax on 31 January 2017 and 31 July 2017.
The beginning of the tax year is also a good time to look at your personal finances and decide whether or not any changes need to be made. The sooner you take advantage of tax breaks in the tax year the higher the tax saving.
Aspects to consider are:
Transfer of assets to lowerearning spouse
For independent practitioners who are married and whose spouse either has no income or very little income, it is worth
transferring income earning assets to the lower-earning spouse to take advantage of personal allowances and the nil rate-band of tax.
You can earn up to about £42,000 before the higher rateband of tax comes into play.
The assets that you could consider transferring are bank and building society cash deposit accounts, stocks and shares where the dividend yield is fairly high and investment properties that give rise to rental income.
There are no capital gains tax or inheritance tax consequences of transfers of assets between spouses.
Cash and/or Stocks & Shares
ISAs for the tax year 2016-17 m aximise your savings into an IsA. however, instead of paying a lump sum into a stocks & shares IsA, it may be worth considering paying a monthly payment over the tax year which spreads the risk, as you are buying units at all different prices.
In a volatile stock market, this is something worth considering and you should take the advice of an independent financial adviser.
Sending your children out to work . . . for you
For doctors who run their own practices, either via a company or as a sole trader or partnership, you might consider employing your children – as long as the role would be considered a proper one within the practice.
children have the same allowances and basic rate-bands as their parents, but hm Revenue and customs will look very carefully into such arrangements and therefore it is imperative that the salary is commensurate with work carried out.
many specialists’ children help them with IT, as they are usually better at dealing with this than their parents!
But the duties have to be clearly noted, so that if an inquiry is raised, the consultant is able to substantiate the claim.
By diverting, say, £3,000 a year to an offspring’s salary, as long as they have no other income, there will be no tax on this.
Therefore, for a consultant who is a 40% or 45% taxpayer, the tax saving is between £600 and £675.
Dividends v director’s salary
For private doctors who operate as a limited company, the tax rates on company dividends have increased since 6 April last year. In most cases, dividends are still more tax-efficient than a salary, but it is recommended you take advice about this, as the mix between the two might not be quite the same under the new regime.
Susan Hutter is a specialist accountant for the medical profession and a partner at Shelley Stock Hutter
ESMYA® (ULIPRISTAL ACETATE) TRANSFORMS THE MANAGEMENT OF UTERINE FIBROIDS
ESMYA® is the first medical treatment for the long-term management of moderate to severe symptoms of uterine fibroids.1
O Licensed for intermittent use1
O Fast, reliable and sustained control of bleeding2
O Significant and sustained reductions in fibroid volume from baseline2
O Improved quality of life compared to baseline2 O Well-tolerated2
PRESCRIBING INFORMATION
Esmya (ulipristal acetate) Please refer to the SmPC before prescribing. Presentation: 5mg tablet. Indication: Pre-operative or intermittent treatment of moderate to severe symptoms of uterine fibroids in adult women of reproductive age. Dose and administration: One tablet of 5mg to be taken orally once a day for a maximum of 3 months, starting during first week of menstrual cycle. This 3 month treatment course can be repeated. Re-treatment courses should start at the earliest during the first week of the second menstruation following the previous treatment course completion. Each treatment course should not exceed 3 months. Treatment free intervals are required between courses. Repeated intermittent treatment has been studied for up to 4 intermittent treatment courses. Please refer to SmPC for missed dose information. Patients with renal or hepatic impairment: No dose adjustment in mild to moderate renal impairment or mild hepatic impairment. Not recommended for patients with severe renal impairment and moderate or severe hepatic impairment unless patient is closely monitored. Children and adolescent under 18 years: No relevant use. Contraindications: Pregnancy, Breastfeeding, Genital bleeding of unknown aetiology. Uterine, Cervical, Ovarian or Breast cancer. Hypersensitivity to active substance or any excipients. Pregnancy and lactation: Contraindicated during pregnancy and lactation. Warnings and Precautions: Should only be prescribed after careful diagnosis and pregnancy should be precluded prior to treatment. Use in women with severe asthma insufficiently controlled by oral glucocorticoids is not recommended. Concomitant use of hormonal contraceptives are not recommended hence a non-hormonal contraceptive method should be used. Reversible histological changes of the endometrium: ‘Progesterone Receptor Modulator Associated Endometrial Changes’ (PAEC) may be observed in patients. Also, reversible thickening of the
endometrium may occur during treatment. If it persists beyond 3 months following the end of treatment and return of menstruations, and/or an altered bleeding pattern is noted, this may need to be investigated as per usual clinical practice. Please refer to SmPC for further details on endometrial changes and management of the same. In case of repeated intermittent treatment, periodic monitoring of the endometrium is recommended. This includes an annual ultrasound to be performed after resumption of menstruation during off-treatment period. Treatment leads to significant reduction in menstrual blood loss within 10 days and patients should notify their physician if heavy bleeding persists. Drug interactions: Hormonal contraceptives and progestogens are likely to reduce the efficacy of ulipristal acetate by competitive action on progesterone receptors, hence co-administration is not recommended. Not recommended for patients receiving moderate or potent CYP3A4 inhibitors or potent CYP3A4 inducers (e.g. rifampicin, carbamazepine, phenytoin, St John’s wort). Co-administration of P-gp substrates (e.g. dabigatran etexilate, digoxin) should be separated in time by at least 1.5 hours. Undesirable effects: The following adverse reactions have been reported during first treatment courses: Very Common (>1/10) Amenorrhea, Endometrial thickening; Common (>1/100 to <1/10) Headache, Vertigo, Abdominal pain, Nausea, Acne, Musculoskeletal pain, Hot flush, Pelvic pain, Ovarian cyst, Breast tenderness/pain, Fatigue, Weight gain.; Uncommon (>1/1000 to <1/100) Anxiety, Emotional disorder, Dizziness, Dry mouth, Constipation, Alopecia, Dry skin, Hyperhidrosis, Back pain, Urinary incontinence, Uterine haemorrhage, Metrorrhagia, Genital discharge, Breast discomfort, Oedema, Asthenia, Increase in cholesterol level Increased triglycerides, Rare (≥1/10,000 to <1/1,000) Epistaxis, Dyspepsia, Flatulence, Rupture of ovarian cyst, Breast swelling. When comparing repeated treatment courses, overall adverse reaction rates were less frequent in subsequent
treatment courses than during the first one and each adverse reaction was less frequent or remained in the same frequency category (except dyspepsia which was classified as uncommon). Overdose: Limited experience. Single doses of up to 200mg and daily doses of 50mg for 10 consecutive days administered to a limited number of subjects, and no severe or serious adverse reactions were reported. Special precautions for storage: Keep the blisters in the outer carton to protect from light. Legal Category: POM Basic UK NHS cost: £114.13 per pack of 28 tabs. Marketing Authorisation Numbers: EU/1/12/750/001, EU/1/12/750/002, EU/1/12/750/003, EU/1/12/750/004, EU/1/12/750/005. Marketing Authorisation Holder: Gedeon Richter Plc., Gyömrői út 19-21., 1103 Budapest, Hungary. Further information is available from: Gedeon Richter UK Ltd, 127 Shirland Road, London W9 2EP. Tel: 0207 604 8800. Email: info.uk@gedeonrichter.eu Date of Authorisation: 27th of May 2015. Date of Preparation: 16th of June 2015.
Adverse events should be reported. Reporting forms and information can be found at www.mhra.gov.uk/yellowcard. Adverse events should also be reported to Women’s Health Division of Gedeon Richter (UK) Ltd on 0207 604 8806 or drugsafety.uk@gedeonrichter.eu
References 1. ESMYA® SmPC. May 2015. 2. Donnez, J; Hudecek, R; Donnez, 0, et al. Efficacy and safety of repeated use of ulipristal acetate in uterine fibroids. Fertil Steril 2015; 103(2):519-27.
mARkETing yoUR clinic
Make your case studies attract
Julia Kendrick outlines key learnings from the aesthetics industry and how to maximise your business potential with simple case study strategies
Across All areas of medicine, high-quality case studies can showcase clinical skills and persuade patients of the benefits of a particular treatment.
For cash-pay business such as those in medical aesthetics, case studies can optimise the patient decision-making process and ultimately boost business by expanding your existing customer base while still attracting those allimportant new patients.
Yet, time and again, we see poor-quality examples that do not truly reflect clinical skill nor treatment benefits and are ultimately damaging your business by failing to convert ‘considerers’ into patients.
This easy step-by-step guide should help you avoid the five most common case study mistakes and ultimately capitalise on your greatest assets: positive patient experiences and strong clinical results.
misTAkE 1: Poor quality
How often have you been at a congress presentation or browsing someone’s website and seen a grainy, poorly-lit ‘before and after’ photograph, in which the subject has been shot from completely different angles?
Whether you are looking at rhinoplasty or burns treatment –nobody will be convinced of your
clinical skill or the efficacy of a procedure or treatment if they can’t easily compare like for like.
This really is the most common mistake – but the easiest to fix.
Firstly, invest in the right equipment: a bridge or digital singlelens reflex (Dslr) camera won’t cost the earth and are convenient, relatively easy to use and deliver good-quality shots.
A tripod helps give you a standardised set-up for steady, consistent shots that capture the fine details and a continuous light unit is particularly useful for showing up finer details.
Take a variety of shots, including: x4-5 larger area and focused area shots; Full frontal, 3/4 and side views;
‘Dynamic’ and ‘at rest’ expressions or movements.
For ‘before and afters’, consistency is paramount: ensure the patient is photographed in exactly the same position, with the same lighting and camera settings.
The only differences we want to see are those as a result of treatment. Backgrounds should be plain white or black and, if possible, the patient should wear the same clothes at each shoot.
For facial close-up shoots – and especially for any kind of cosmetic or aesthetic procedure – make sure all make-up and jewellery are removed, and hair is kept well back from the face to avoid distracting from the actual results.
misTAkE 2: Unrealistic results
This is a particular bugbear in aesthetics, where ‘above average’ case studies have often resulted in unrealistic treatment expectations.
This situation is not limited to aesthetics and tars all practitioners with the same brush – damaging trust and credibility among patients.
My advice is to take a clear, ethical approach: use images of an ‘average’ result to set expectations, but make a separate note of the ‘best’ results achieved so far.
Eye-tracking studies have also shown that people skip over images which look ‘too perfect’ or ‘over-done’, so steer clear of any case studies which show a high
‘How often have you been at a congress presentation and seen a grainy, poorly-lit “before and after” photograph?’
degree of augmentation or an ‘extreme’ make-over.
When it comes to Photoshop or any kind of digital manipulation, my advice is don’t.
The aesthetic industry has learned the hard way about how air-brushed images can impact trust and is now dealing with an ever-increasing scepticism about the accuracy of treatment claims.
Quality and integrity are fundamental in building trust, therefore it is vital that your images are a true reflection of the treatment and procedure effect.
It is a huge advantage to provide images which you can publicly profile as being ‘unretouched’.
misTAkE 3: lack of consent
This is a big one and can potentially land you in very hot legal water. This is particularly so when case study images have been used in your Pr and marketing efforts, as these can take on a life of their own online and become virtually impossible to eradicate.
It is very important to provide a clear overview to patients on what is involved in being a case study – including how their images and testimonials may be used for both clinical and marketing purposes.
If patients agree, they should sign a comprehensive consent form which outlines all these details and gives you the rights to use the materials as stipulated.
Patients should also be made aware of how to withdraw their consent and be encouraged to
Strong testimonials bring to life the emotion behind a treatment decision and help us to imagine how we would feel after having treatment ourselves
contact you with any questions in the interim.
Always ensure you adhere to Association of the British Pharmaceutical Industry’s or other relevant professional codes of practice regarding case study use with consumer audiences – there can be no promotion of prescription-only medicines among the public.
misTAkE 4: no testimonial Images are powerful, but they don’t tell the whole story. Whether you are presenting trial results at a clinical symposium or presenting potential treatment options to a patient, the biggest ‘convincer’ to your audience will still be rooted in emotion.
strong testimonials bring to life the emotion behind a treatment decision and help us to imagine how we would feel after having treatment ourselves.
Work with your case studies to tell the story of their experience, but in a succinct bite-sized format – 250 words or a one- to two-minute video.
Make sure you cover:
How they felt before treatment? What questions did they have? How were these handled?
What motivated them to have the treatment in the first place?
What was the treatment experience like? Focus on key concerns such as pain, downtime, recovery;
How does it make them feel now? What can they do now that they couldn’t before?
How have other people responded to their experience?
Your patients are your walking, talking examples of success –make sure you are mobilising them as advocates for you and capitalise on the power of word of mouth
misTAkE 5: Blocked channels
In my experience, nine times out of ten practitioners do not use their case studies effectively across all their available educational, P r and marketing channels.
some rely just on bombarding their website full of ‘before and after’ images, others rely on a coffee-table book – or worse, a ringbinder folder – in the waiting room to do the talking for them.
Your patients are your walking, talking examples of success – make sure you are mobilising them as advocates for you and capitalise on the power of word of mouth.
Incorporate your ‘before and after’ photos, videos and written testimonials across as many of the following channels as possible:
clinic marketing materials;
Patient newsletters;
clinical posters/podium presentations;
Website and blog;
Pr materials;
Waiting room content.
Go for quality over quantity and use a variety of media – photos, written quotes, videos – to maximise interest and attention.
Powerful personal recommendations
It is well known that when someone we trust tells us something, we are instantly more likely to believe and buy.
For every treatment pathway, product or service, you must overcome this ‘tipping point’ in order for patients to switch from consideration to action.
one way to take control of this powerful process is to literally let your work speak for you by avoiding the pitfalls above and developing impactful case studies. By effectively highlighting reallife clinical results and mobilising positive patient experiences through multiple marketing channels, you will have a highly persuasive tool to convince both new and existing patients to make that decision and ultimately boost your business potential.
scared of marketing your aesthetic clinic? see page 14
Julia Kendrick (left) is an award-winning communicator with a passion for medical aesthetics and more than 11 years of industry experience
Unrealistic expectations: People skip over images which look too perfect or appear ‘over-done’
bREAkinG inTo ThE AEsThETics bUsinEss
Confidence in. . .
.
‘Fear’
of sales and marketing could be holding back your business. But Pam Underdown believes you could really learn to overcome your concerns – forever
. .what you do
After tAlking to many medical aesthetic practitioners, i ’ve learned that nearly all of them wish they never had to do any marketing – let alone any selling. let’s be honest; you are trained to be a doctor, nurse or dentist and not a sales and marketing expert.
So if you feel completely out of your comfort zone when trying to promote yourself, you are not alone.
But if your goal is to serve as many of your ideal patients as possible, then sales and marketing are two of the main skills that will take you there.
So, what are the differences between the two skills?
Marketing – increasing the number of people who know about you and your service;
Sales – actively helping someone to decide if they want to work with you and how they can. the goal of effective marketing is to attract your preferred patients to you, then educate them so they understand if and how you can help them.
Getting your message across
An important part of your role is to position you and your clinic by communicating the key unique benefits of working with you in a way that matters to the patient.
You need to be able to describe your value and why you are different from the competition, then make sure that the patient feels comfortable they are making a good choice and will not regret their decision.
i t is difficult for prospective patients – on their own – to determine the objective professional skill and quality of a given aesthetic professional.
i nstead, they typically determine who is right for them based on their perception of your professional brand, personal recommendations and pricing.
One of the quickest ways to get really clear on this is to identify what you would like to be known for.
getting clear on your message is the foundation of any business. today, we only get very small windows of opportunity to reach out and connect with our target market simply because, as con➱ p16
sumers, we are all inundated with media messages.
So it’s important to make sure that all of your messaging sounds compelling by building potential customers’ trust and liking at the same time as stimulating their interest, simply because you are talking their language.
One of the key foundational principles is to remember what it is your patient is actually buying from you: confidence, safety, quality, hope and results.
Make sure you use ‘patientfocused language’ that is talking directly to the pains, problems and concerns that they wish to resolve. Use the word ‘you’ on your marketing and website –even on your ‘About Us’ page.
Before creating your copy –think about the following:
What are the top three biggest problems they face?
What three things do they want more than anything?
What is the number-one result you can help your patient achieve?
What other benefits will they get as a result of working with you?
What will the higher emotional benefits be?
i f you are like the majority of practitioners, you likely cringe hearing the word ‘sales’, as it conjures up images of aggressive and pushy promotional tactics that are totally misaligned with your values and personality.
selling = helping
However, the word ‘sell’ is derived from the i celandic word ‘Selja’ and the Anglo-Saxon word ‘Syllan’; both mean ‘to serve’ or ‘to give’.
Ultimately, selling is about helping people who already want and need your services to make their decision more easily.
People don’t always understand that you can help them – particularly if they have a skin condition they have struggled with for many years and they don’t know that there is help available for them.
t herefore, to not serve them when you know you can help them is doing both the patient and you a disservice.
We all have images in our mind about sales and selling that have
One of the key foundational principles is to remember what it is your patient is actually buying from you: confidence, safety, quality, hope and results
been built up over the years. there are often bad images in our mind of the pushy car sales person with the greasy hair or the aggressive double-glazing sales person that interrupted our evening meal.
Whatever the image is for you, it’s very hard to shake this idea that ‘sales’ is an icky word. So if you do have a problem with it –then the key is to think about it differently and use different words.
Popular misconceptions there is still a misconception that you have to have the ‘gift of the gab’ or to be really smooth or charming to get the sale, but that’s not the case.
think about your own experiences – have you ever won over by someone who was a ‘gift of the gab’ smoothie’? i expect not. However, if you did, there is a high chance you regretted it quickly afterwards.
Another serious misconception is that you must have a patter or a sales spiel or script. But if we hear a sales spiel in parrot-fashion, we all know we are being sold to, don’t we?
Just like the people who coldcall us during an evening to sell us insurance or get us to change energy suppliers, or the charity workers in a busy shopping centre – they all have their spiel. And nine times out of ten, we know we are being sold to and we don’t like it.
So why is that? it’s because the majority of people actually like buying – but they don’t like being sold to.
the goal of effective selling is to determine whether you have the right product or service to actually solve your patients’ problems. instead of selling, the key is educate your patients about what you do and how it can help them,
while keeping patient safety at the forefront of everything you do. Build trust by listening and asking questions to discover and understand your patient’s feelings, concerns and motives. You must show genuine interest with intention to serve and educate your patients and not just sell to them. engage with your patients in a way that shows your priority is to take care of them. taking the time to really understand your patient before you educate them will ensure they only go ahead with a treatment if it is right for them and right for you.
➲ Don’t forget that sales is all about asking questions in order for the patient to be able to identify whether what you can offer is right for them or not.
➲ i t’s not about you telling them; it’s about you really listening, asking lots of questions, providing education and advice and then allowing them time to make an informed decision.
➲ i t is a matching process: are you right for them? Are they right for you? Will this be a win-win for both parties?
i f someone decides that they aren’t going to go ahead, you can still help them to come to that decision and ultimately leave your clinic in a better place than they were before they found you. Do this by offering them some free skincare advice, knowledge or tips that will help them along their way.
Two types of people
What is interesting is that there are two different types of people out there: there are the people who worry too much that they may come across as pushy, but they don’t at all.
t hen there are those who say they are very comfortable with sales and selling, but they are often over-confident, which means that they often come across as pushy and aggressive. the key is to find a balance. When we worry about being pushy, there are certain types of people we are all thinking about. t hey are the ones that push things on you: they talk at you and don’t listen.
they are really only interested in pushing their agenda on you, they don’t respect your time, they
aren’t sensitive to your body language, they don’t leave you alone. But when you try as politely as you can to get rid of them, they don’t see or hear you. these are the people we worry about when we have a fear of being too pushy. At the other end of the scale are the under-confident people, who are always backing away from the patient. if you fear being pushy, there is a reasonable likelihood that you are naturally coming across as under-confident.
You could be doing and saying everything right, but subconsciously this means that something just doesn’t feel quite right for the patient. t hey won’t be able to articulate why, but there is a feeling that is giving them a lack of safety, reassurance and confidence in you.
if you are worried about being pushy, i can almost guarantee that you aren’t, simply because pushy people aren’t very sensitive
The goal of effective selling is to determine whether you have the right product or service to actually solve your patients’ problems
to other people and they are not very good at picking up signals or reading people. if you are subconsciously backing away, your prospective patient doesn’t feel safe, because you haven’t led them to a decision –yes or no. even though they may have felt that you had understood their needs, they may have noticed that something just didn’t feel right.
show conviction
i f you didn’t ask them if they wanted to go ahead (or not), then not only would they have felt rejected but they would have sensed that there was an element of safety missing from the conversation.
it’s very important to show conviction during the whole conversation, not only when you are talking about your treatments and the results you can provide, but also when you ask whether they
are happy to proceed after being fully informed and educated. the end result of not educating (selling) is that the patient is going to lose out in other ways: they didn’t get the results they were looking for and they didn’t get the help they needed. Or perhaps they did get it a week later when they went to your competitors – but perhaps your competitors didn’t do a very good job and the patient’s safety and wellbeing was compromised? t hen who lost out? Both of you.
Next month: I will explain why the team you surround yourself with can make or break your business, how you can find the right team players and how to ensure they produce a consistent experience for your patients every time they visit.
Pam Underdown (pictured left) is chief executive at Aesthetic Business Transformations
PRivATE PATiEnT UniTs
Tie-up with NHS is boundless
The outlook for private patient units in NHS hospitals looks bright. Philip Housden (below) explains why in the first of a new series monitoring their progress in the year ahead
What exactly are private patient units (PPUs) and what is it like to provide a private patient service within an NhS trust?
are they only a pale imitation of private hospitals – or are they, in fact, something different and the ‘best of both worlds’? and how can these services be better made to work – for patients, for consultants and trusts – right across the NhS?
Under successive h ealthcare acts, NhS trusts are able to provide private patient services. Indeed, the 2012 health and Social care act lifted the so-called ‘PP cap’ –restricting private patient revenues to those of 2003-04 levels – to a theoretical ceiling of 49% of revenues for foundation trusts. at the last count, 84 of the 136 N h S trusts providing acute services in england had a PPU. these vary in style and size and commercial success. In central l ondon, Royal Marsden and Imperial c ollege lead the way with revenues of £77m and £43m respectively reported last year.
Total private patient revenues are now worth £526m to the NHS, a reported growth of almost 30% over the last five years
however, more typically, most trust PPUs outside l ondon in non-metropolitan areas have revenues of £1m-£5m a year.
total private patient revenues are now worth £526m to the NhS, a reported growth of almost 30% over the last five years.
If taken together, NhS PPUs represent the third largest provider of private care to most major insurers.
But, as we know, PPUs cannot be ‘taken together’, as they vary so
much in style, capacity, offering and, of course, there is no united brand or co-ordinated commercial approach. I will explore these issues in future articles.
Range of benefits
t he reason PPUs are a growing feature of the UK healthcare landscape is that they continue to offer a range of benefits.
For insured and self-pay patients, they can provide access to services that are backed up by 24/7 infrastructure that most private hospitals cannot match: for example, intensive care or robotic surgery.
For consultants, the same patient safety agenda is the prompt for them choosing to use the PPU for their patients with complex needs and co-morbidities.
t he sheer convenience of onsite, ad hoc access makes a difference, too, for experienced consultants and also those just starting out in private practice that perhaps cannot get access to
boundless
wHy I THINk PPus are oN To a wINNer
Following my popular 2013 series on PPus in Independent Practitioner
Today, I have continued to work with many NHS trusts to help develop and grow profitable private patient services, writes Philip Housden
This has enabled a real insight into the day-to-day challenges of delivering a private service within a public sector environment.
I am passionate about how PPus can be part of the answer to the strategic and financial challenges the NHS faces, and so in this new series, I will be sharing learned practical insights. and I will comment on how PPus can best respond to changing policy issues and healthcare industry current affairs.
The single most important ingredient for future growth is to prepare the ground to ensure there is leadership from the senior executive team who are overtly supporting the PPu. yes, overtly, prepared to declare that private patient services are a normal part of the work of the trust. without such support the game will be lost. How clear is such support in your trust?
I was dismayed by the lack of any reference by Lord Carter in his recent report and 15 recommendations to the potential for income generation and commercial activities to make fuller use of expensive NHS assets.
This surely is a trick missed and ignores the tangible gains that have been made in recent years by PPus.
crowded theatre space at the local private hospital.
For the host N h S trust, a PPU should be delivering a positive commercial return achieved on the marginal cost provision of leveraging estate and assets. this all should add up to a winwin-win. Where it does, then the PPU works very well – but healthcare being what it is means that there are many challenges along the way.
Practical suggestions
In the months ahead, I will be exploring those issues and seeking to provide practical suggestions on how to help get trusts on track to deliver that win-win-win.
So, as we start the new financial year, I am optimistic about growth and achieving increased surpluses from private patient activities for the trusts I work with.
What brings that optimism? a pril is always a fresh start and brings optimism to even the most cynical – the lighter evenings, the opportunity to rest from winter
pressures, a pause perhaps from weekly reporting on spend to the turnaround team …
But I see something more: pressures that are enabling change. t he burning platform of N h S finances is opening up management to income generation, not just cost control.
t hat private hospitals treat so many NhS patients has inadvertently created a much more mixed market. and the move to regular three-session days and seven-day working is encouraging a more commercial examination of the potential capacity inherent in a trust.
For these reasons, I am optimistic about the year ahead and I will be sharing how the year is going, and suggesting how PPUs can best respond to the financial and other NhS challenges that will undoubtedly present.
Philip Housden is a director of Housden Group, a management consultancy specialising in commercial support in the healthcare sector
Seven medico-legal
There are many advantages to working in private practice for doctors who successfully establish themselves. However, there are potential medico-legal ‘snakes’ that doctors need to be aware of and take steps to avoid. Dr Marika Davies looks at some common areas in which independent practitioners can run into difficulties
medico-legal sins
1 patient expectations
Patients may have unrealistic expectations of what can be achieved from medical intervention, which may lead to an unhappy patient and a complaint or claim.
If you are concerned that a patient has not appreciated the limitations of treatment, it is important to document the discussions in as much detail as possible within the medical record. It may be helpful to suggest that they return with family members for further discussions. You may want to offer them a second opinion or simply conclude that you are unable to treat them going forward.
Do not be pressurised into providing treatment you do not think is in the patient’s best interests.
2
Keeping up to date and revalidation
GMC guidance says: ‘You must keep your professional knowledge and skills up to date.’
The GMC also expects you to regularly take part in activities that maintain and develop your competence and performance, and to be familiar with guidelines and developments that affect your work.
It can be challenging to show evidence of this at yearly appraisals, particularly for doctors who work solely in private practice, who may have fewer opportunities for continuing professional development (CPD), audit and peer feedback. Identifying and addressing this early is key to a smooth appraisal and revalidation process.
3 communication and confidentiality
Keeping clear and accurate medical records is essential for good
You should not make unjustifiable claims about the quality of service you provide, and should not hand out business cards to your NHS patients
Indemnity arrangements for waiting-list initiatives in private hospitals may not be straightforward, so be sure to clarify this with the trust or your defence organisation before undertaking this type of work.
5
Financial conflicts of interest and promoting your services
You must not allow any financial or commercial interests to affect the way you prescribe for, treat or refer patients.
6 legal
requirements
Documentation and storage of information relating to private patients should be comparable to that provided in the NHS. Under the Data Protection Act 1998, doctors who carry out private practice are required to register with the Information Commissioner.
continuity of care, and invaluable should a complaint or claim arise.
It is good practice to keep those with overall responsibility for the patient’s care informed – such as the patient’s GP – provided your patient does not object.
If a patient will not allow you to contact their GP, then you are responsible for their care until their treatment and any aftercare is completed.
The rules of confidentiality are no different in private practice and you must be careful of any inadvertent breaches; for example, by reception staff in waiting areas.
4 indemnity
There is now a legal obligation on doctors to have adequate insurance or indemnity in place. In order to ensure you are protected for the work you do, you must keep your defence body informed of the scope of your practice and must declare the extent of your income.
Doctors who fail to do so, or who provide incorrect or incomplete information, may find they are not covered if an incident arises.
The GMC says: ‘You must be honest in financial and commercial dealings with patients, employers, insurers and other organisations or individuals.’
Do not ask for or accept any inducement that may affect, or be seen to affect, the way you prescribe for, treat or refer patients. And tell patients about your fees, if possible before seeking their consent to treatment.
If you wish to use rooms in an NHS hospital to carry out private practice, be aware that you will need formal approval from the hospital authorities.
The BMA advises that ancillary NHS staff cannot be used for free, and NHS secretaries or receptionists should not be asked to work privately without payment.
Be sure not to undertake private practice at times when you have NHS commitments.
If you choose to advertise your services, the GMC says you must make sure the information you publish is factual and can be checked. And the information you give out must not exploit patients’ vulnerability or lack of medical knowledge.
You should not make unjustifiable claims about the quality of service you provide, and should not hand out business cards to your NHS patients.
You should also check whether you are required to register with the Care Quality Commission (CQC), which regulates the independent healthcare sector in England. A failure to register may result in a fine or referral to the GMC.
7 if things go wrong
You have a professional duty to be open and honest with patients when things go wrong. You should respond promptly to complaints and provide a full explanation and apology where appropriate.
Be aware that care providers registered with the CQC now have a legal obligation to inform any patient harmed by the provision of a healthcare service, regardless of whether a complaint has been made or a question asked about it. Although the ‘duty of candour’ applies to organisations, the responsibility of informing the patient may fall to you as the treating doctor
Dr Marika Davies (below) is a medicolegal adviser at Medical Protection
subsCribe to get every issue!
Dear Reader,
Subscribing to Independent Practitioner Today is the only way you can be sure you will see every issue. Don’t risk missing out. Our personal subscription for doctors and managers is only £90 a year and £210 for organisations. But you can cut this to just £75 and £180 respectively if you pay by direct debit.
So take advantage of this offer now for our unique business journal dedicated to supporting you in your private practice. We’re confident your subscription will repay itself many times over!
Editorial director
Instructions to your Bank or Building Society to pay Direct Debits
Name and full address of your bank/Building Society
Banks and Building Societies may not accept direct debit instructions for some types of account
Banks and Building Societies may not accept Direct Debit instructions for some types of account
post your application (no postage required – UK only) to: independent practitioner today Subscriptions department, FreepoSt, po Box 36, plymouth, pl1 1Br
phone: 01752 312140 Fax: 01752 313162 email: lisa@marketingcentre.co.uk or subscribe online at www.independent-practitioner-today.co.uk if you
You can cancel a Direct Debit at any time, by writing to your
How to choose a private hospital
In a four-part series for Independent Practitioner Today, Malcolm McCoskery (right) examines key issues facing doctors as they look to build their practice
He is looking at four different topics aiming to help consultants as they aim to build their practice. Last month, he covered teamwork and whether to work as part of a multi-disciplinary team or, indeed, whether single-handed practice is still relevant in today’s market.
Here he looks at choosing a private hospital.
Each article is aimed at consultants who may be at different stages of their career. They may be taking their first steps in private practice. Or it may be that they started their practice some time ago and wish to take their business a stage further either by themselves or as part of a group.
So, having decided if you are wishing to go it alone or as part of a team, you now need to decide where you wish to practise.
Location, location, location obviously, location is important. For hospitals outside central London, the position of the chosen hospital in relation to the local nhS trust campus where you or your team already work will mean that many gPs will already know of you.
in central London, this will be less important but still very relevant. although other means of private hospital marketing have been used in recent years, ➱ p24
the most important referral route remains from the gP direct.
The hospital’s brand
Secondly, i do think that the hospital’s brand is important. i shall be discussing branding from the perspective of the doctor and the multi-disciplinary team in the next issue, but there may be corporate values and judgements that you already have in your mind that influence you.
Some of these may include charity or not-for-profit; nhS private unit; foreign ownership; private equity-owned models. or it could simply be that you have personally had good or bad service previously at one or another hospital.
The cQc report
a third consideration – and one that has not featured in the past – is the hospital’s Care Quality Commission (CQC) report.
Private hospitals are now in the
process of being reviewed and reported on by the CQC. Whether the report has foundation or not, insurers and patients will be guided by its findings.
The CQC considers five key questions that each hospital is measured by: is the service safe, effective, caring, responsive and well-led?
But it also needs to be satisfied if other fundamental patient standards are being met.
These cover dignity and respect; safeguarding from abuse/duty of candour; sufficient food and drink; suitable premises and proper equipment; complaints procedures; governance; and that staffing is adequate in terms of numbers, their training and in their fitness to practise.
i f the hospital has been reviewed by the CQC, its report should be in the hospital’s reception and on the home page of their website.
Whether the CQC report has foundation or not, insurers and patients will be guided by its findings
competitors
Fourthly, you need to think of your competitors and you will need to look at the types of surgery and treatments already offered at each hospital.
i t may be, for example, that h ospital 1 already has a similar team in place and you may not get the service nor potential revenue you require.
hospital 2 may want to expand into your market and although it may not have all the attributes that you need, it may be willing to invest to help you increase your business.
n ot all equipment, of course, has to be bought outright and many pieces of, say, theatre kit can be rented with a view to purchase later.
Don’t forget though – the fact that hospital 1 is already geared up in your discipline could be an advantage. it already has all the jigsaw pieces in place. There is a good reason why all the jewellers are based in hatton garden.
The hospital team at the end of the day, you want to further your private practice and the hospital wishes to develop its services for private patients. The relationship is symbiotic.
Which takes me to the fifth and potentially the most important consideration, that of the management, business development and – crucially – clinical teams that each potential hospital has to offer.
Crosscare - providing private practices with efficient paperless working
Crosscare is a proven clinical system used within private practices and specialist clinics in and around Harley Street and across the UK.
Alongside the standard clinical record keeping and prescribing systems, Crosscare’s appointments, reporting and integrated accounting modules make the tracking of workload, invoices and revenues simple and user friendly.
We understand that each practice works in their own unique way, so being a fully customisable system, Crosscare can be easily tailored to fit your individual needs.
For further information on how our Crosscare solution can help your practice call us now on 01233 722670 or visit www.advancedcomputersoftware.com/ahc
Depending on the complexity of what you or your team is providing, you will need help, guidance, support and energy, whether it be from the group’s head office, the hospital’s chief executive, the business development and marketing teams and the clinical and non-clinical teams who will assist your practice. The hospital ‘needs to not only say what it does, but do what it says’.
Support should be consistent throughout the hospital at all times. Will the ward and reception teams offer you uniform levels of support late on a Saturday night?
and what is the senior doctor or resident medical officer (RM o ) cover? i f the hospital does not have iCU facilities, the definition
of ‘RMo cover’ needs to be investigated.
You may know of a colleague or colleagues who already work at the proposed hospital. They may be able to give you some advice of any potential negatives, if any. a lso, the chosen hospital should be able to offer the diagnostic capability and technology you and your patients require onsite. i f the 3T MR i is elsewhere, your patients are going to be inconvenienced and the reporting potentially delayed.
if you are going to operate as a multi-disciplinary team – and as i discussed in the first article in this series, this model is becoming increasingly prevalent especially in central London and other large cities – then you may wish to assess the hospital’s ability to support your team with appropriate senior clinical staff. For example, a clinical nurse specialist could be a vital cog for all concerned.
The provision of both Level 2 and Level 3 critical care may also be important to you or your team.
Marketing and business development
Finally, with Competition and Markets authority inquiries and the Bribery act still high on the agenda, hospitals are unable to make generous gestures to encourage business as perhaps they might have done in the past.
But there may still be ways that hospital groups can help doctors develop their practice and you should obtain the chief executive’s pledge about the availability of various marketing initiatives.
For example, it may be that the hospital could help the team of doctors to put together an educational seminar for gPs.
o r practice visits can be arranged if there is a g P liaison team in place. it is also vital that you feature on the hospital website and, if produced, any directory that is given out to gPs and other primary care personnel. if you have your own website, then you would want to ensure that the hospital’s policy lets potential patients link to it. not every hospital allows this.
it may also suit the doctors to develop their services under the umbrella brand of the chosen hospital.
if you have your own website, then you would want to ensure that the hospital’s policy lets potential patients link to it. Not every hospital allows this
Yet, if the team wishes to expand into other geographical or indeed ‘competitor’ hospitals, then this might be a short-sighted decision and you may want to retain the strength of your own brand. i shall consider this in more detail in the next issue.
The level of support that a hospital offers could depend on:
Whether you are going to use one hospital alone;
The complexity of the treatments you offer – and hence, if intensive care is involved, the revenue you will generate;
if you offer something new or different;
The synergy between you and the hospital.
all of these considerations will affect your decision as to whether you are going to be loyal to one hospital or whether you wish to spread your favours across competing private healthcare groups, if there are other options available.
You or your team must make the right choice(s) when looking to select a private hospital . . . or two . . . or three.
i t is not a simple or cut-anddried decision. The hospital’s location, brand, CQC report, competitors, management and staffing, and marketing are all, as i have explained, important considerations.
o bjective, rather than subjective decisions do have to be taken. The future success of you and your team and, most importantly, the appropriate care of your patients, is at stake.
next time: The importance of branding your practice
Malcolm McCoskery is a chartered marketer and consultant in marketing, whose recent 20-year private hospital career included senior management posts at four different private hospitals/groups. Email him at: m.mccoskery@yahoo.co.uk
Getting ahead of
So
just how worried should you be about competition in private practice? Dev Lall gives his views and suggestions
If you run a business, there’s always one thing that is tickling away at the back of your mind. And that is … the competition.
Who they are, what they might be up to, whether they are doing any better than you, the pressure of keeping one step ahead of them. All these factors prey on the businessman’s mind.
And consultants in private practice are no different in that
respect at least. They, too, are always looking over their shoulder and wondering what their colleagues are up to and how well or otherwise they are doing.
Now, on the face of it, this seems reasonable. After all, there are only so many private patients out there, and if your colleagues’ practice is doing well or growing, then, in all likelihood, they are doing that by taking patients –
‘market share’ – away from you, aren’t they?
Well, maybe. But maybe not. But before I get into that, a word about what competition is and what it is not, because many consultants appear to have got this confused.
If two consultants are both, say, orthopaedic surgeons with expertise in hip replacement surgery, they work in the same private hospital and draw patients from the same catchment area, with the same conditions and see patients at the same times, then, yes, they are competitors.
There are good reasons to suppose they are competing with each other for patients. It is understandable why there might be some friendly rivalry or even jealousy between the two. on the other hand, if one is a general surgeon and the other an orthopaedic surgeon, clearly they are not competing for the same patients. There is no overlap –they treat different conditions entirely.
Consultants in this scenario
could not be considered competitors. yet, frequently, jealousy and rivalry still exists between them over their private practices. That is not real competition. It is rivalry. And while sometimes rivalry is a healthy spur to greater success, other times it is not.
In any case, I contend that wondering how ‘the other guy’ is doing – real competitor or not – is a waste of time and head space. It is far, far better for you to focus your energies and efforts on your own practice. So forget about them. How well or otherwise they are doing is irrelevant. All you need to keep an eye on is your own bottom line. How you are doing.
And decide how you can do better to achieve your own income goals. Worrying about the competition – real or imagined – is pointless. It doesn’t change anything.
The myth of competition first, let’s deal with a myth about competition. In many geographic areas – not all, but many more
the competition
I contend that wondering how ‘the other guy’ is doing –real competitor or not – is a waste of time and head space
than you might think – demand for private care is greater than the local availability of consultants to satisfy that demand.
Not only that, the numbers of people who want to be looked after privately is rising – particularly self-pay patients.
So, in these locations, one consultant growing his practice does not mean that another practice in the same area has to shrink. There are plenty of patients to go around.
Managing competition
So you look around and see that there are several consultants doing similar things on your ‘patch’. What should you do about it? What can you do about it? And how do you maintain and ideally grow your practice?
Although all consultants feel the heat from their colleagues, I think the most sensitive is the new consultant: the new appointee in a department with one or two senior, well-established colleagues.
It can be quite difficult getting started in private practice. Not
only is it financially stressful but it can also be quite demoralising to see the lion’s share of the private work go elsewhere despite your efforts.
A consultant new to private practice often finds their NHS income subsidises the obligatory costs of private practice – rooms, indemnity and so on – until their private income exceeds these costs.
And unless you make concerted efforts to grow your practice quickly, you can find yourself continuing to make a loss for many months or even years.
But whether you’re a new consultant just starting out or an established consultant looking to grow your practice, how do you grow despite the competition cramping your style?
A two-day fully inclusive residential medical management course for senior SPRs and new consultants covering leadership and negotiation, private practice, business planning and appraisal. Only £250. To be held in Balliol College, Oxford, on 13th and 14th September 2016. For more details, see:
www.oxbridgecourses.com
The obvious solution to competition
The obvious way of dealing with competition is to proactively and effectively market your practice. Because the guy with the biggest private practice – all other things being equal – is always the guy who is best known in that specialty.
Best known to potential patients and best known to professionals that can refer patients his way: GPs, other consultants, optometrists and so on.
Now, you might say: ‘Hold on, what about Mr XyZ? He doesn’t do any of this marketing stuff, yet he still has a great private practice.’
To which I would reply: how do you know how good his practice is? Sure, you might get the impression of busy clinics, but you don’t know the numbers. What are his costs? What is his case mix? Two consultants in the same specialty
If
seeing the exact same numbers of patients can have wildly different incomes depending upon the case mix of conditions they see.
Secondly, you can’t take what people say at face value. Not everyone likes talking about their income.
Those that do so may exaggerate to look good; we’re all human, after all. And, then again, they may not even know – except just before the accounts are due, and even then the numbers are a year out of date – so they guess.
So how do you know he is not marketing his practice? Many consultants make a point of socialising with GPs on a regular basis and this too is marketing and you may not be aware of it going on in the background.
But all that aside, even if your colleague is not doing any marketing at all, the fact he has a busier practice than you will be because he is better known among
potential patients and those who can refer him patients.
So if you increase awareness about you and your expertise among potential patients and those that can refer patients to you, your practice will grow too. That’s the whole point of marketing, after all. To be seen by potential patients and those who can refer patients to you. And as you will have seen from this series, you are very much spoilt for choice in terms of ways of doing precisely that.
The not-so-obvious solution to competition
I said earlier that ‘the guy with the biggest practice – all other things being equal – is always the guy who is best known in that specialty’. So as well as marketing your practice to become more visible to potential patients, there is something else you could – and should – do. Make things unequal. Tip
the scales in your favour. And the wonderful thing about this is that it eliminates your competition entirely.
Eliminating the competition Competitors are only competitors if you share the same category. In other words, if you do the same thing in the same way for the same people. Change one or more of those elements and you will find yourself in your own category with no competition.
To illustrate with an example, take two general surgeons. Both have exactly the same expertise but one focuses all his time and effort on looking for and treating sportsmen and women with groin pain.
That surgeon now operates in a category of one. He has no competition. This strategy – eliminating all competition and placing yourself into a category of one – is an approach that anyone can take. And there are a whole host
Why worry about the competition when you can eliminate it entirely?
of ways of doing it, not just by focusing on particular conditions. for example by:
Providing a service that your local colleagues do not – for example, hip/ankle arthroscopy;
Providing the same service a different (and better) way – for example, day-case surgery rather than overnight stay;
Providing a more convenient service – for example, late evening or weekend clinics and theatre lists;
Homing in on a specific ‘niche’, such as promoting yourself as a female specialist who only treats men or women. Depending upon specialty, this could work particularly well – a female breast surgeon, gynaecologist or fertility expert, for example;
Providing extraordinary service and convenience. for example, a new patient with a painful knee gets seen and assessed by you in the morning, an MRI and the
result that afternoon and an arthroscopy later that same evening, if required.
your imagination really is the only limit. one simple approach is to put yourself in the patients’ shoes and ask yourself what you would like to happen if you had a given condition.
Another way is to write down a list of the top ten things patients complain about and promote your practice as one in which those things don’t happen.
yet another way is to look at how things are done in other specialties, countries or even other industries entirely and see what you can emulate.
After all, why worry about the competition when you can eliminate it entirely?
Dev Lall (left) is an upper-GI surgeon who runs specialist private practice consultancy www.PrivatePracticeExpert.co.uk
Avoid risk of being accused of assault
Large numbers of doctors continue to seek advice after receiving complaints following an intimate examination. Dr Richard Brittain (below) offers some useful advice
Contact: nick Brecker. Tel: 020 7253 0030
Email: nbrecker@caldwellandbraham.co.uk
Web: www.caldwellandbraham.co.uk
Doctors are routinely required to examine the most intimate areas of a patient’s body. While this may be an everyday occurrence for private practitioners, these procedures can, of course, often be embarrassing or distressing for patients.
No doctor wishes to be on the receiving end of an allegation of inappropriate behaviour or, worse, sexual assault. so it is crucial to approach these examinations in the right way to ensure the patient is as comfortable as they can be and that they fully understand what to expect.
Unfortunately, medical defence
bodies handle a large number of calls regarding consent and intimate examinations: from alleged inappropriate conduct to concerns about patients who refuse a chaperone.
Patient complaints in this regard are not uncommon and if examinations of an intimate nature are not approached in the right way, they can result in GMc referrals or, even in extreme cases, reports to the police, with potentially catastrophic consequences for a doctor’s career.
Gaining informed patient consent is essential in clinical exami➱ p32
nation. Before carrying out intimate examinations, private practitioners must first fully explain to the patient how and why the examination will be conducted and be satisfied that the patient clearly understands what is involved.
disturbing case
one recent and disturbing case in France highlighted how the consenting process is not always adhered to. BB c News reported last october that trainee doctors at a hospital in Lyon had allegedly been advised by senior staff to carry out certain procedures on patients without their consent.
It emerged that some trainees were alleged to have practised vaginal examinations on sleeping patients and conducted a smear test on a pregnant patient during a routine pelvic examination – all without prior consent. While this was denied by the hospital, a number of trainee doctors have since spoken out on social media to verify the allegations.
the principle that ‘every person has the right to have their body integrity protected against invasion by others’ has long been recognised in common law.
It has also been defined in case law in many jurisdictions, perhaps most classically by Justice Benjamin cardoza in his 1914 ruling in New York: ‘every human being of adult years and sound mind has a right to determine what shall be done with their body; and a surgeon who performs an operation without the patient’s consent commits an assault.’
When considered in these terms, it is clear why the process of securing informed consent is so vitally important in medicine, not only for the patient’s benefit but also to protect the doctor from any accusations of wrongdoing.
the legal position of informed consent was clarified with last year’s highprofile supreme court ruling in the case Montgomery v Lanarkshire Health Board, which involved allegations surrounding birthrelated injuries and attracted a lot of publicity because of the £5.25m payout.
this case was highly significant, as it crystallised the law in relation to consent – more specifically, issues around the amount of
it is conceivable that a patient may perceive an intimate examination to be one where the doctor touches them or perhaps even where the doctor is simply close to them
Key poinTs
consider what the patient may perceive to be an intimate examination
fully explain to patients how an intimate examination will be conducted in a way that the patient can understand
for consent to be valid, it must be informed, competent and freely given
consent protects the patient but also helps to safeguard the doctor from any accusations of wrong-doing
patients should be offered a chaperone for intimate examinations, even where the doctor and the patient are the same gender
chaperones reduce risk of complaint or allegations against doctors
information a patient is entitled to be told before making a treatment decision.
In summary, the ruling underlined the need for all doctors involved in treatment discussions with patients to be sufficiently wellinformed and trained in how to obtain fully informed consent.
t hey must be able to identify when a patient may need more information and a greater understanding in order to make a decision about any proposed treatment.
the patient does not have to ask specific questions, but if they express concerns, then the questions which would naturally flow from these concerns must be explored and answered fully.
there are some exceptions, such as where the patient has made it clear they do not wish to be informed of risks of injury, where disclosure would be seriously detrimental to the patient’s health and in urgent or emergency situations.
In short, for consent to be valid, it must be informed, competent and freely given. Furthermore, it should be clearly and accurately recorded in the patient’s records.
So what constitutes an intimate examination?
While examination of breasts, genitalia and rectum would clearly fall into that category, definitions can vary from patient to patient. It is conceivable that a patient may perceive an intimate examination to be one where the doctor touches them or perhaps even where the doctor is simply close to them.
Doctors have a duty to explain why the examination is required in a way that the patient can
understand. It is important the patient knows what to expect, including any possible pain or discomfort.
Patients should be given an opportunity to ask questions before the examination begins and doctors should be prepared to stop the examination if asked. Factors such as cultural or religious attitudes can have a bearing on how comfortable patients are when being examined.
Patients should be given privacy when undressing – it is not appropriate to help them undress unless they have specifically asked for your assistance.
importance of chaperones
Before carrying out an intimate examination, it is important to ask the patient if they would like a chaperone present during the consultation.
the role of the chaperone is to reassure patients and offer emotional support, as intimate examinations can be an embarrassing and sometimes uncomfortable experience.
It is recommended that even where the doctor and patient are of the same gender, the offer of a chaperone is still made.
the chaperone does not have to be medically qualified but should have received appropriate training and must be sensitive and respectful of the patient’s dignity and confidentiality.
an appropriately trained member of healthcare staff is usually preferable to a patient’s friend or relative, who would not be considered an impartial observer. He or she should be prepared to reassure the patient if they show signs of distress or discomfort and be familiar with the procedures
involved in a routine intimate examination.
any discussion about a chaperone should be noted in the medical record. Where one is present, this should be noted alongside their name. If the patient does not want a chaperone and you are happy to proceed, then it should be noted that a chaperone was offered and declined.
We have encountered cases where doctors have been accused of inappropriately touching a patient after a chaperone has left the consultation. t herefore, where a chaperone is requested, they should be present for the whole examination and, if practicable, be able to see what the doctor is doing. the chaperone must be prepared to raise concerns about a doctor’s behaviour, where necessary.
If a patient refuses a chaperone, GM c guidance encourages doctors to explain clearly why there is a need for one to be present. If this fails, then, in the patient’s best interests, doctors should: ‘consider referring the patient to a colleague who would be willing to examine them without a chaperone, as long as a delay would not adversely affect the patient’s health’.
It is worth remembering the presence of a chaperone can minimise the risk of allegations of inappropriate behaviour during intimate examinations, benefitting both the patient and the doctor too.
Private practitioners should be familiar with the GMc guidance Intimate examinations and chaperones (2013)
Dr Richard Brittain is a medical adviser for MDDUS
Protecting your
Private practice owners must strike the right balance between dissuading any leaver from breaching a restrictive covenant while at the same time ensuring the wording is not so wide as to risk being seen as unreasonable – and therefore unenforceable. lynne abbess and puja solanki report
IN receNt years, there have been a number of high profile cases in the High c ourt dealing with the protection of goodwill and the enforceability of restrictive covenants.
For most owners of private medical practices, the goodwill in the practice is one of, if not the, most valuable financial assets they will own.
It is essentially the value of the reputation of the practice and is intrinsically linked to the patients.
Unlike NHs goodwill, which it remains a criminal offence to buy or sell, private medical goodwill can be bought and sold in much the same way as any other goodwill and therefore has quantifiable worth attached to it.
For this reason, the owner of a practice is likely to want to protect their goodwill and this may
be achieved by a restrictive covenant which, if necessary, can be enforced by the courts.
t here are two alternative circumstances in which a restrictive covenant would be necessary.
Firstly, those purchasing a practice will want to protect the goodwill they have bought by seeking to prevent the seller from setting up in competition immediately after the sale.
Rival business
secondly, those with established practices will want to prevent those engaged in the practice from seeking to take patients away with them if they depart and set up a rival business.
In either case, a carefully drafted restrictive covenant, contained within either the business transfer agreement (B ta ) in the former case or within the consultant’s
Without having a restrictive covenant in writing, the practice owner runs the risk of their good
7 agreement in the latter case, can ameliorate the risk.
The Association of Independent Specialist Medical Accountants is a national network of firms advising over 3,000 medical practices across the UK. For some of the best advice available on accounting, taxation and pensions, visit our website and find your nearest AISMA accountant.
will being diluted if the incumbent – be they the original owner or a consultant – leaves the practice and seeks to take advantage of
the relationships they have built up direct with the patients while at the practice, with the intent of poaching them.
the following principles should be considered for inclusion within either a Bta or a consultant’s contract:
a statement that the goodwill of the practice belongs to the practice owner;
a complete bar on the use of the practice name indefinitely;
anticompetitive restrictions on a timelimited basis (see below).
In drafting a restrictive covenant, it is essential to have regard to the specific business in question.
It should never be assumed that ‘one size fits all’, as that approach could risk the enforceability of the restriction.
Anti-competitive restrictions
It is essential to ensure a restrictive covenant is reasonable and no wider than necessary to pro
tect the practice’s legitimate business interests.
t he clause amounts to a restraint on an individual’s ability to work, coupled with a restraint on the ability of a patient to see the practitioner of their choice.
It may be construed as being contrary to public law if there is any suggestion the nature of the restrictions imposed is greater than is necessary to protect the interests of the specific business in question.
If challenged, the restrictive covenant could be found to be unreasonable in the circumstances and therefore unenforceable.
It is therefore essential to consider the following principles:
1. duration this must be reasonable in order to be enforceable and for this reason it should be limited.
In fact, the greatest risk to the
practice owner arises the day after the leaver departs the practice and the impact of setting up a rival business is likely to dilute over a period of time.
o n this basis, it is worth protecting the initial period at all costs, even if it seems this is compromising longerterm future protection.
t he duration is usually therefore limited, more so in the case of a consultant, when it is likely to be limited to – for example, between six months and one year – than in the case of a seller, when it may be extended to, for example, up to two years.
2. Solicitation
a restriction on taking the patients of the practice is likely to be considered sensible in almost all cases, as essentially this goes to the very heart of the requirement for the restriction.
It may also be considered wise
“Kay and her team provide a seamless outsourced switchboard service. The result? More enquiries, outstanding service levels.”
Moneypenny client since 2013
Moneypenny will support your existing team by looking after overflow calls, or by providing a fully outsourced switchboard facility. moneypenny.co.uk 0333 202 1005
to extend the non solicitation clause to key members of staff.
3. geographical area careful thought must be given to the area of the restriction – and indeed whether it is relevant to impose a geographical restriction at all.
In the case of a very specialist practice where patients are prepared to travel long distances to the practice – for example, in Harley street – it may be considered irrelevant and a nonsolicitation clause may be all that is necessary. But, beyond this, the extent of any geographical restriction should vary depending upon the specific circumstances of the practice.
For example, in central London, a restraint of just a few hundred yards or even a specific road might be all that is reasonable; whereas, in a more rural setting, a five mile radius or even more might be acceptable.
Kay,
Moneypenny
Receptionist
a restriction on taking the patients of the practice is likely to be considered sensible in almost all cases
4. Subject matter restraints of trade may be considered by the courts to be unenforceable purely because the field of business encompassed is too wide.
t he restriction should reflect what needs to be protected and no more than this.
For example, it would not be reasonable to seek to restrict a leaver from undertaking NH s medical work elsewhere if the practice owner’s business is 100% private.
5. Extent
Where relevant, a practice owner should be entitled to seek to limit the leaver from practising as a sole trader, in partnership with others as a director or shareholder of a body corporate or as a practitioner engaged or employed by others.
e xceptions can sometimes be agreed such as undertaking emergency treatment or treating immediate members of the leaver’s family.
6. Financial incentives as an added incentive to encourage compliance, a financial recompense may be built into the agreement for breach, thereby making it less likely the leaver would think it worthwhile taking the chance of breaching the covenant.
this would require careful drafting, reflecting the specific circumstances of the practice, as anything which could be construed as being a penalty would not be enforceable.
In conclusion, a practice owner needs to strike the right balance between dissuading any leaver from breaching a restrictive covenant while ensuring that the wording is not so wide as to risk being held unreasonable and therefore unenforceable.
Negotiation of the clauses will be part and parcel of agreeing the B ta or the consultancy agreement, as relevant and specialist legal advice should be taken to ensure the practice owner’s interests are protected.
Lynne Abbess (left) is a partner and head of professional services group, and Puja Solanki (right) is a senior solicitor, at Hempsons solicitors
a financial recompense may be built into the agreement for breach, thereby making it less likely the leaver would think it worthwhile taking the chance of breaching the covenant
PROBLEMS WITH THE TAX MAN?
HMRC tax investigations and disputes create difficult and stressful times.
As an award winning firm of tax experts, our highly experienced partners specialise in resolving problems relating to tax investigations and disputes with HMRC.
To find out, in confidence, how we can help call 0800 734 3333.
‘Here to help. Not to judge.’
bREAkiNg iNTo mEdico-lEgAl woRk
Screening report is really a ‘loss leader’
The fee may seem low for a screening report. But larger fees may follow. Michael R. Young continues his series with his tips on preparing the document
Law firms want to establish early on whether or not they have more than a 50% chance of winning a clinical negligence case.
They are not going to fund a case, or encourage anyone else to, that they are unlikely to win.
Therefore, they often ask an expert to uncover the strengths and weaknesses of a case, and to make an assessment of their client’s chances of success.
solicitors will usually want the expert to do this on the minimum number of sides of a4 and usually for a minimum fee.
There are several points to bear in mind when considering accepting instructions to write a screening report.
The first is that although the fee
may seem low, larger fees may follow if you are subsequently instructed to write a full liability and causation report, and even later, to write a current condition and prognosis report. Think of the fee for a screening report as a loss-leader.
also remember that the expert’s opinion as to whether the case has merit needs to be supported by solid evidence. Do not give the solicitor unrealistic expectations of winning. Getting this wrong can be a costly mistake and extremely damaging to your reputation.
Because screening reports are nearly always short, it is tempting to think that a letter will suffice. But it is worthwhile investing time and effort to produce a goodquality report, albeit just presenting the bare bones of the case.
if later you are asked to write a full CP r 35-compliant liability and causation report, then the time and effort invested at this early stage will not have been wasted.
i t may be possible for you to recoup some of the ‘lost’ fee when costing out the full report.
Next month: The liability and causation report
adapted from The Effective and Efficient Clinical Negligence Expert Witness , by m ichael r . Young, price £60 from Otmoor Publishing
Special offeR! BuY the Book and Save £20
the book costs £60, but independent practitioner today has secured discount of a third off for readers, so you pay only £40. listen to the audio content which accompanies the book at this website: www.otmoorpublishing.com/audio. for more information and to order, email stephen.bonner@ otmoorpublishing.com, quoting reference ‘Young/ipt’.
Set the ScReening RepoRt aS outlined heRe
1 introduction, setting the scene for the reader:
Why the report has been written; that is to say, its purpose
Your name and qualifications as the report’s author
the name of the firm of instructing solicitors – not the individual solicitors’ name
the name of the solicitor’s client
Whether the client is the claimant or the defendant
a summary of your instructions, including the date of the letter of instruction. this is the terms of reference; it is best not trying to paraphrase the instructions because, in doing so, you may unknowingly alter their meaning. therefore, it is advisable to copy the instructions word for word from the solicitor’s letter
the sources of the evidence. this should be comprehensive and must include where the evidence has come from, the dates the evidence relates to and, perhaps equally as important, what is missing
a list of the contents and page numbers. this helps the reader find the information quickly
2
3
Summary, which includes the strengths and weaknesses of the case
if the solicitor has set out the chronology and facts of the case in his or her letter, there is no need to regurgitate these in the synopsis. however, if the solicitor has not, present the significant evidence as succinctly as possible. You should always aim to produce a synopsis of the evidence without losing any of the important information. the report must be signed and dated.
i never took any short cuts when i was writing a screening report. although they were, by their very nature, often not very long documents, i made sure that they were written and presented with the same professionalism i would give to any other type of report.
An independent firm offering one to one meetings anywhere in the UK giving advice and help with:
• how to start in private practice
• how to maximise private practice income
• computer software
An independent firm offering one to one meetings anywhere in the UK giving advice and help with:
• tax and financial advice re: car purchases
• how to start in private practice
• ways to reduce tax payments
• computer software
• how to maximise private practice income
• setting up in Chambers/Groups
• ways to reduce tax payments
• limited companies and LLP’s
• setting up in Chambers/Groups
• financial planning
• record keeping
• limited companies and LLP’s
• tax and financial advice re: car purchases
• pensions: NHS, personal and employee schemes
• pensions: NHS, personal and employee schemes
• purchase of consulting rooms and surgeries
• inheritance tax and capital gains tax planning
• purchase of consulting rooms and surgeries
• VAT
• inheritance tax and capital gains tax planning
For more information please contact us by:
• VAT
Wilmslow
Harley Street
For more information please contact us by:
Phone: 01625 527351
Wilmslow
Fax: 01625 539315
Phone: 01625 527351
Phone: 020 7307 8759
Harley Street
Fax: 01625 539315
Phone: 020 7307 8759
Email: info@sandisoneasson.co.uk
Fax: 01625 539315
Fax: 01625 539315
Website: www.sandisoneasson.co.uk
Email: info@sandisoneasson.co.uk
Website: www.sandisoneasson.co.uk
Specialist Medical Accountants
Our prescription for healthy financial advice
Our prescription for healthy financial advice
Free legal advice for independent Practitioner Today readers
independent Practitioner Today has joined forces with leading niche healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes’ of free legal advice.
Advice is available on: business structures: commercial contracts: ian Hempseed Faisal dhalla disputes: Hilary king
Author A. J. Cronin warned against unscrupulous medical practices in his famous novel, but what parallels can be drawn within the financial services industry? Dr Mark Martin examines why you should be aware of anything which looks too good to be true
Cronin’s groundbreaking novel The Citadel was first published in 1937 and highlighted the controversial issue of corrupt medical ethics.
The scottish author and former doctor drew on his own experiences of practising medicine, both in the coal-mining towns of Wales and the comparatively luxe surrounds of Harley street.
The main character dr Manson becomes seduced by material success. He begins to prescribe unnecessary remedies while endorsing products he does not believe in and offering operations of little benefit.
He creates a lucrative medical practice by treating concerned, rich housewives who are perfectly well. His desire to make money sits at odds with the professional integrity he once held dear.
Cronin once stated in an interview: ‘ i have written in The Citadel all i feel about the medical profession: its injustices, its hidebound unscientific stubbornness, its humbug . . . The horrors and inequities detailed in the story i have personally witnessed. This is not an attack against individuals, but against a system.’
The book was first met by mixed reviews from within the medical profession, with some senior practitioners angry at the suggestion that prosperous doctors could be duping their own well-heeled patients.
salesman’s spiel
u nfortunately, Manson’s moral transformation after he is swayed by the thought of easy money is something we still see in the finan-
cial industry today. and just like his patients, there are clients willing to accept exaggerated claims rather than scientific reason.
some investors still believe that pursuing ‘actively managed’ funds – where a manager is paid to guess which assets will perform better than the market average –will give them a bigger return on their investment.
Yet decades of academic research have proved that while there might be some outperformance over time, active managers have been unable to demonstrate consistent enough outperformance to justify substantially higher fees.
in fact, before fees, the average manager will broadly match the market’s return and, after fees, inevitably lag this return.
Passive funds – which track an index, market or asset class –achieve similar returns with significantly lower costs. However, just like The Citadel’s enthusiastic patients keen to try the doctor’s magic elixir, some investors still want to believe in the salesman’s spiel.
mining gold
When talking about one of the wealthy hypochondrical ladies being treated in the novel, one of Manson’s fellow doctors declares: ‘You’ve no idea what a gold mine that old woman has been to us. We’ve taken nuggets out of her.’ in fairness, the active managers have a strong marketing advantage – they can peddle the idea of a ‘best fund’, ‘the fund of funds’ or a ‘star fund manager’ who will beat the odds.
financial sharks
This is a far easier sell than making the words passive and average sound exciting.
a nd yet anyone feeling confident in the ability of active managers should study the respected ‘scorecards’ for active versus passive returns produced by financial ratings agency standard & Poor’s.
The latest report shows that, as of december 2014, nearly 87% of large-cap fund managers underperformed their benchmark over a one-year period. This increases to nearly 89% over a five-year period and 82% over ten years.
scams increasing sadly, with interest rates failing to beat inflation, risk-averse investors can find their attentions turning to riskier alternatives. and to satisfy this growing appetite, there has been an influx of alternative investments coming onto the market – from virtual currencies and unmined gold to overseas land and vintage wines. a mong the genuine offers are bogus schemes which have proved dangerous for even seasoned investors.
Fraudulent investment schemes are on the up. i n the last two years, fraud in the City of London has increased significantly, with around £1.73bn reported lost in 5,000 uk cases of investment fraud in 2014. Police believe the real figure is much higher, but victims do not always want to come forward.
The duped investors are often highly intelligent, sophisticated professionals. The scammers are simply very good at what they do. Their fail-safe ‘opportunities’ are presented in top-priced offices in exclusive locations in the City with glossy brochures and even glossier employees.
s hareholders’ details are open to the public, which means it is very easy to target unsuspecting investors directly. u sing high-
pressure sales techniques, the stockbrokers offer free ‘secret’ stock tips or research reports into a company the investor already holds shares in. or they will offer to buy or sell shares with the promise of big returns – only for victims to discover the shares are worthless.
The Financial Conduct a uthority (FCa) said it receives almost 5,000 calls a year from investors who believe they are victims of share scams, by which point around 10% have already handed over their money. o ften the scammers demand cash immediately, warning that the ‘brilliant’ opportunity will otherwise be lost.
The companies may even have links – real or otherwise – to credible organisations.
e very investor would like a product that offers a fail-safe high return with a minimum level of risk.
b ut the truth is that product does not exist. returns cannot be guaranteed and you should walk away if offered such an opportunity. You must conduct due diligence on any company or individual offering to invest your money and if it sounds too good to be true, it probably is.
Dr Mark Martin is chairman of Cavendish Medical, specialist financial planners helping senior consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
UK Top 20 accountants specialising in the healthcare sector
National firm of the Year 2013
• AISMA member (Maidstone and Leicester offices)
12 offices including London City
Tax Structures for Hospital Consultants - dispelling myths
Surgeon groups and consortia
GP Practices including mergers and federations
Solvent liquidations (for companies at the end of their lives)
For more information please contact:
South East
James Gransby FCA
E: james.gransby@mhllp.co.uk
T: +44 (0)1622 754033
M: +44 (0)7712321899
East Midlands
Robert Nelson DChA FCA
E: robert.nelson@mhllp.co.uk
T: +44 (0)1162 894289
M: +44 (0)7814009160
General email: healthcare@mhllp.co.uk www.macintyrehudson.co.uk
ChAsing dEbTs
The inside story of collecting debts
Many doctors labour under the impression that debt collectors operate the same way we see bailiffs at work on the television or in films. Gary Nials shows how it is really done
Debt collection? that means large, tough people visiting a debtor’s home and removing valuable items to recover the cost of the debt, doesn’t it?
er, well, no. nothing could be further from the truth.
t he debt collection process starts when a doctor hands over the outstanding invoice to a professional agency. b efore doing this, it is advisable that the doctor has made every effort to recover the debt themselves.
An agency will usually com -
mence the debt recovery cycle with an initial letter of claim to the debtor explaining that they have been instructed to collect the debt on behalf of the doctor. t he agency staff would then follow this up with daily phone calls.
Letter before action
if the agency has not received a positive response to their initial letter, they will follow the first letter with a solicitor’s ‘letter before action’ or lbA.
t he lb A will advise that a
summons could shortly be served upon them. Again, this will be followed up with daily phone calls.
i t will give the debtor a fixed number of days to respond to the lbA. An lbA from a solicitor can be the simple nudge that triggers the debtor to pay; for this reason, lbAs can be a very cost-effective method of debt recovery.
if they still have not received an assurance of payment, the sequence will be concluded with their final letter indicating that solicitors are now issuing a sum-
mons and giving details of the associated costs.
At any point the process will stop if:
A query or dispute is raised; Payment is received or acceptable terms are offered;
the doctor requests to put the chase on hold or wants it closed.
The summons o nce the file is passed to the agency’s appointed solicitors, a summons will be issued.
After 21 days from the summons being issued, if no response has been received from the defendant, the doctor, now known as the claimant in legal terms, is at liberty to apply for Judgment in Default. the Judgment order secures the debt and, at this stage, enforcement proceedings may begin.
Depending on the value of the debt, it will usually be enforced with the c ounty c ourt b ailiff (below £650) or the High court enforcement officer (above £650). in any matter where the debtor owns their property, a charging order will be considered.
if an acknowledgement is filed, the defendant will be granted a further seven days in which to file a defence, offer instalments or pay in full.
i f an offer of repayment is received during this period and if that offer is accepted, the court will enter ‘Judgment in terms’ and the defendant will be ordered
to pay the agreed instalments on a certain day of the month. t his day will be decided by the court. if, after the summons has been issued, a defence is filed, then the doctor will be asked for instructions with regard to whether or not they wish to proceed and oppose the defence.
the court will specify a date by which instructions are required and this request must be adhered to, because if a response is not received in time, the case will be ‘stayed’ (stopped).
if the doctor’s instructions are to oppose the defence, the file will be passed to the agency’s appointed solicitors’ litigation department, where the matter will be assigned to a solicitor who will then take instructions from the doctor with regard to how the defence should be responded to. the court will specify the dates by which paperwork must be filed. these dates must again be
The debt collection process starts when a doctor hands over the outstanding invoice to a professional agency
adhered to, because if they are not, the court is at liberty to strike out (dismiss) a claim.
t he doctor will be asked to name a representative to act as witness in the case.
t he witness need not attend court – an agent will do this on their behalf – but they will be required to sign a witness statement which will be drafted by the solicitor prior to the court hearing.
Mediation process
before a date is set for the court hearing, both sides are encouraged to come to an agreement to settle.
this process is known as mediation and is a free-of-charge service provided by the court.
it is advisable to try and reach a settlement at this stage, as the court will take this into consideration if a figure can’t be agreed and the matter proceeds to hearing.
Before a date is set for the court hearing, both sides are encouraged to come to an agreement to settle
if a resolution is not reached as a result of mediation, a court date will be allocated and the matter will proceed to a hearing.
the doctor can choose to attend or not, but, in any case, the solicitor will have arranged legal representation also.
b oth parties will be given the opportunity to present their case and once all evidence has been heard, the judge will make his or her ruling.
When judgment is awarded in favour of the doctor, the defendant will have to settle by a date specified by the court or the judgment can then be enforced.
As you can see, the process is complex and can be lengthy, so it is important to get professionals to help. Most debtors do, in fact, pay up after the first letter from an agency or the lbA.
Gary Nials is the managing director of Medical Billing and Collection
When plastic is not all fantastic
Dr Nicola Lennard answers plastic surgeons’ questions about being notified of a complaint – one from the GMC and another from a newspaper
Dilemma 1 What should I do with this gripe?
QI work as a consultant plastic surgeon. I recently carried out a breast augmentation on a 27-year-old woman. She seemed very happy about my care and the outcome and did not express any concerns at the time.
However, today I received a letter from the GMC which stated that the patient has made a complaint that she was not happy with the way I spoke to her.
I am shocked that this has happened – I always try to communicate clearly and openly with patients and have never had a complaint of this nature before.
The letter from the GMC says that the complaint is being referred back to the hospital that I work for and have asked for their details.
What does this means and what should I do?
AIt is always distressing to hear that a patient is unhappy with the treatment you have provided, especially if the first you hear about it is in a letter from the GMC.
It is important that you contact your medical defence organisation as soon as possible so that you are fully supported throughout the GMC investigation.
When the GMC receives a complaint, there are three routes it can take with it. These are set out below:
1 The complaint can be closed without further investigation;
2 If the complaint relates to serious concerns that could potential ly call the doctor’s fitness to practise into question, an investigation is commenced. This was formerly known as a stream 1 investigation;
3 Complaints which the GMC does not feel raise a question about the doctor’s fitness to practise and where they feel local investigation – for example, through the hospital complaints procedure –would be more appropriate are passed back to the doctor’s Responsible Officer. This was formerly known as a stream 2 investigation.
As the GMC has indicated that it is passing the concern back to your Responsible Officer and not investigating itself, this would indicate that at this stage the GMC does not believe there is a concern about your fitness to practise.
The GMC will want to communicate with your hospital and any others you work for – such as private hospitals, other NHS trusts or university posts – about the matter. You are obliged by law to give them these details.
You may be asked by your hospital about the complaint and what you think went wrong on this occasion. If so, you should explain the situation as well as any steps you have taken to make sure that the same situation does not happen again.
The complaint should also be discussed at your next annual appraisal in line with the GMC’s requirements for revalidation.
Once the hospital has carried out its investigation, it will report back to the GMC that the matter has been resolved.
The GMC is unlikely to take the matter further at this stage and will contact both you and the patient to let them know that the matter has been closed with no further action.
However, there is potential that if several similar concerns have been raised locally, then this may lead the GMC to reconsider the need for it to investigate.
Dilemma 2
What do I say to
nosy reporter?
QIn my work as a consultant plastic surgeon, I have built up quite a celebrity client base and have treated several sports stars, musicians and actors.
I recently performed a rhinoplasty on a popular television star. At the time, the patient seemed very happy with the result and she even recommended me to a friend of hers whom I have since had a consultation with.
story, it is important not to be tempted.
Most experienced journalists will understand that doctors have a duty of confidentiality and so if you contact them to say this, they will usually accept it.
Some journalists may be a bit more persistent and insist they just want to give you a chance to ‘put your side of the story across’, but you would be wise not to respond further.
In some cases, the journalist may not have enough information to make a story, but by giving them even a small amount of information, it may just be enough to make their piece.
It is also never wise to escalate a story into a war of words between you and a patient.
The GMC would certainly not look kindly upon this happening and you may find that you inflame the situation with the patient further.
It is understandable to be worried about the impact that a story like this could have upon your practice. However, if you were to comment on something like this, it could inflame things further, whereas not commenting can diffuse the situation.
You may find that the story is not published or that the patient does not chose to take things further.
Having heard from the journalist about the patient’s complaint, you may wish to write to the patient directly explaining that you are sorry to hear that they are unhappy with the outcome of their treatment and inviting them to get in touch with you directly so that you can address their concerns.
Dr Nicola Lennard (right) is a MDU medico-legal adviser
However, this morning, I received a telephone call from a journalist at a national newspaper, who says that the patient was unhappy with the result and is considering suing.
I really am surprised, as this is the first I have heard of this. I’m also upset about the impact this could have on my reputation. What should I do?
AWhen journalists get in touch about patient care, it can be a worrying time.
Even if it isn’t about a complaint, it can be difficult to know what to say, given your duty of confidentiality. Before doing anything, contact your medical defence organisation for advice on how best to respond.
It is important to remember that although your famous patient has chosen to speak publically about their medical treatment, it does not mean that you can do the same.
As with any patient, it is vital that you maintain your duty of confidentiality and remember that even confirming that you have treated someone could be seen as a breach of that duty.
Although it is frustrating that you cannot give your side of the
Upright Positional MRI
• Completely open scanner that is well tolerated by claustrophobic patients
• Weight-bearing scans for spine and joints enable a more precise diagnosis
• Patients who are large or cannot lie down can be accommodated
For more information go online at: www.mri-london.com or call 020 7370 6003 Medserena Upright MRI Centre 114a Cromwell Road, Kensington, London, SW7 4ES
The XE could quite easily become the default executive saloon choice for the successful independent practitioner, believes Independent Practitioner Today’s motoring correspondent Dr Tony Rimmer (below) DocToR
The cat with cream
IF THERE is a single car make that over the years became synonymous with the successful independent practitioner, it has to be Jaguar.
This quintessentially British brand has been the personal transport of choice for successful private doctors for decades.
I remember working as a junior doctor for a general surgeon who took delivery of a brand-new XJ6. He was very proud of it and was happy to show it off to his petrolhead junior colleague. I was impressed.
This was a time when Jaguar,
like most of the British motor industry, was at its peak but resting on its laurels.
Poor-quality manufacturing, lack of investment in new products and a blind denial of the threat from better foreign products ultimately had disastrous consequences. We lost Triumph, Austin, Rover and very nearly Jaguar.
Rescued by Ford
The company was rescued by Ford in the 1990s and, under its control, released the S-type mediumsized saloon and the smaller X-type.
Unfortunately, the X-type had Ford Mondeo underpinnings and never really felt like the sports saloon it was supposed to be.
Poor products contributed to Jaguar never making a profit during the Ford ownership period and in 2008 the firm was sold alongside Land Rover to Indian giant Tata.
It now had to be make or break for the brand.
Fortunately, Tata invested heavily and over eight short years completely turned the fortunes of the company around. Over the last five years, Jaguar Land Rover
has doubled the workforce and doubled vehicle sales.
Top players
They are now profitable and underlying the success is a range of great products. The new F-type sports two-seater and the XF saloon are top players in their market segments. Other premium brands now have serious home-grown competition. However, as in private practice where the biggest profits are to be made in the popular higher-volume treatments, the most profitable premium car segment is the
3-series BMW/Audi A4/Mercedes C-class sector.
Jaguar has not had a product to compete in this group since the lacklustre X-type, so now, not before time, it has released the XE saloon.
Given its importance, Jaguar has thrown everything it can into getting the XE just right. A new chassis, new engines and a new factory for assembly show just how serious they are. Available with two versions of the latest four-cylinder two-litre Ingenium diesel engine producing either 161bhp or 178bhp, they claim top-notch fuel efficiency and low emissions.
There are also two petrol models on offer: the two-litre fourcylinder with 197 or 237 bhp and the flagship V6 three-litre model which is straight out of the F-type and produces a rather sporty 355bhp.
I have been testing the R-Sport model with the 178bhp diesel engine which is likely to be the optimum version and the biggest seller.
Visually, the XE is like a smaller XF and it shares the bigger car’s good looks. The low stance is more balanced, better proportioned and more sporty than its big brother.
This is helped by the coupé-like roofline and means that it looks
like BMW’s 4-series Gran Coupé rather than the regular 3-series saloon. Showroom appeal is therefore assured.
The interior is bang up to date with clear instruments, comfortable seats and a great driving position. The infotainment system is state of the art with a massive centre screen.
All models get touch sat-nav, cruise control and parking sensors as standard. My test car had leather seats and the general trim quality is excellent.
You sit low which helps accentuate the sporty feel and although there is plenty of room up front, tall rear seat passengers might feel a little compromised by the limited headroom on offer.
Delivers superbly
To maintain the Jaguar marque’s reputation, the driving experience should satisfy the sporty needs of the keen driver as well as the comfort of passengers.
This is a big ask, but with the use of modern engine and gearbox technology linked to adaptive suspension, I am pleased to report that the XE delivers; superbly.
A smooth eight-speed automatic gearbox controlled by the wonderfully tactile rotary gear selector, which rises theatrically from the centre console on start-
Jaguar has hit the bull’s eye with the XE. It has taken on the most competitive sector in the premium car market and produced a car that beats its German competitors in nearly all areas
ing the engine, ensures that you are always in the right gear and changes are seamless.
The new diesel engine is powerful, subdued and the steering is well weighted and direct.
Jaguar has hit the bull’s eye with the XE. It has taken on the most competitive sector in the premium car market and produced a car that beats its German competitors in nearly all areas.
Great refinement with an excellent ride/handling balance and a sporty drive for keen drivers.
I think that for Jaguar, the XE could quite easily reclaim its crown to become the default executive saloon choice for the successful independent practitioner.
My old surgical boss would approve.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
Visually, the XE is like a smaller XF and it shares the bigger car’s good looks. The interior is bang up to date with clear instruments
STARTiNg A pRivATE pRAcTicE
Second homes come
Owning
more than one property is popular for private doctors and, if chosen wisely, can be both a good source of income and capital growth or be an enjoyable retreat from the pressures of being a consultant. But the rules are changing,
warns Ian Tongue (right)
With house prices continuing to rise and the Government pushing for home ownership for all, a raft of new measures have been introduced which may affect anyone looking to own more than one property.
here are the key changes.
Loan interest deduction
At present, you are able to deduct the loan interest incurred on the mortgage against the rental income received, which can provide a significant tax saving.
From 6 April 2017, changes are proposed to restrict the amount of loan interest that can be deducted against income and these measures are being phased in over four tax years commencing 2017-18.
once fully implemented, loan interest cannot be deducted as an expense against income and a separate allowance of 20% of the loan interest suffered will be given. this does not affect those with no mortgage on a property or basic-rate taxpayers. But for higheror additional-rate taxpayers, this could be a significant shock. t he people most likely to be affected are those higher/additional-rate taxpayers who have a high level of debt relative to the value of the house and/or low rental income relative to value.
For those higher/additional-rate taxpayers where the rent received (after other tax-deductible costs) barely covers the loan interest payable – and hence a largely break-even position from a cash perspective – you will end up paying a tax charge, making the over-
Changes are proposed to restrict the amount of loan interest that can be deducted against income
all cash position being a net loss. see the example in the box above. in the above example, not only has the income tax payable increased by £2,000, but the overall position for the year is costing £900 for the property. this arises from paying £8,000 loan interest and £2,900 income tax with only £10,000 received as rent. this £900 cost may be reasonable if the property is rising in value by an acceptable amount, but if not this represents a longterm cost if the rent cannot be increased to compensate.
Stamp duty
Recently introduced from 1 April 2016 was the increase to stamp duty for second homes. this affects the purchase of any buy-to-let or holiday home but could also catch you out if you already own a property abroad and are buying your first home in the uK.
Also caught are those that decide to retain their existing home and buy a new one. in these circumstances, you are allowed an 18-month window to sell one, but it is expected that you will pay the
additional stamp duty and then have it refunded.
t he additional stamp duty is 3% of the purchase price and so a second home costing £400,000 will cost an additional £12,000 on top of the usual £10,000.
o nly homes under £40,000, houseboats and caravans are exempt.
Wear and tear allowance
For furnished lettings, an allowance of 10% of the rental income was previously allowed as an expense.
From 6 April 2016, the wear and tear allowance was abolished and replaced with a renewals basis for any costs incurred in replacing worn-out or damaged fixtures and fittings. t he first purchase of such items is given no allowances.
t his will likely benefit those landlords in high-value property where the replacement of items will inevitably be more expensive. For those at the cheaper end of the market, this will more than likely result in a higher taxable profit.
come under attack
Limited company ownership
With the changes above potentially hitting landlords hard, the inevitable question arises of whether your property should be transferred into a company. s econd-guessing that people may use the limited company ‘wrapper’ around their property, significant changes were also introduced to discourage the ownership of high-value residential property within a company. h igh value is classified as £500,000, which, for many parts of the country, is not high value
at all. For residential properties enveloped within a limited company, you are hit with a triple whammy:
15% stamp duty to buy the property;
An annual corporation tax charge for owning the property, currently at £3,500 or £7,000 each year depending on value;
28% capital gains tax rate on disposal.
t his ‘hat-trick’ of nasties will certainly discourage the use of a company for holding high-value residential property. it is impor-
tant to note that certain types of property company are excluded from the above and these are mainly where the trade is property-related – e.g. housebuilder. Below the level of £500,000, owning residential property can be beneficial, particularly if you have built up large reserves in the company and are not receiving a good return on the money. however, it is important to note that gifting any residential property that you already own to your company will attract stamp duty. Additionally, upon sale of a
property within a company, a capital gains tax charge will arise and a company does not receive any tax-free capital gains tax allowances. Depending on what happens to the funds, there could be further capital gains tax to pay.
Generally speaking then, owning residential property in a company is unlikely to be the best option for the average person, but, as always, you discuss your circumstances with your accountant. it is clear that property ownership for anything other than your main home is under attack from the taxman. s peak with your accountant to see if there are any tax planning opportunities to help mitigate the raft of measure introduced to target landlords.
Next month: A recap of the pension annual allowance and new tapering rules
Ian Tongue is a partner with accountants Sandison Easson & Co
PRoFiTs FocUs: URologisTs
Figures too hard to read
Urologists achieved a healthy profits increase in their latest figures, examined here by Ray Stanbridge. But they will have to work harder in the future to maintain income
Sadly, thi S is the last Profits Focus of its kind.
Regular readers have, for some time been aware of the problems we are having in trying to show a consistent basis for our annual comparisons. this has proved to be increasingly difficult in a dynamic market as we wrote in a previous edition of Independent Practitioner Today t he commercial environment in which consultant urologists are working is fast-changing and is making any consistency of comparisons between our figures increasingly difficult.
a s reported in the a pril 2014
edition of Independent Practitioner Today , some consultants have chosen to incorporate – with changes in cost structure; others have focused increasingly on Choose and Book work through private hospitals and have reduced their professional indemnity and other operating costs; yet others have undertaken N h S work at additional Pay E rates rather than private income. in addition, others have added diagnostic and other tests to their range of services and/or have formed themselves into groups. as a result of these continuing factors, we have concluded that it
aveRage INCOMe aND eXPeNDITURe OF a CONSULTaNT UROLOgIST WITH aN eSTaBLISHeD PRIvaTe
is no longer reasonable or helpful to present data in its present form.
We have always argued that readers should exercise caution in interpreting our figures, which are not statistically significant. We advise our readers that our figures are based on a representative sample of consultant urologists who:
have either had an old-style or a new style NhS contract;
have been in a private practice for at least five years;
h ave been earning at least £5,000 a year gross from private practice;
May be trading as a sole practitioner and as a member of a group;
May or may not have incorporated.
Profits up by 5.2%
Expenditure
Year ending 5 April. Figures rounded to nearest £1,000 (percentage is also rounded up)
Source: Stanbridge Associates Ltd.
Subject to what seems to be an ever-extending list of caveats, our view is that average income for urologists in private practice rose by 5.8% between 2013 and 2014, from £120,000 to £127,000.
Costs increased by 7% from £43,000 to £46,000. a s a result, taxable profits went up by about £4,000 (or 5.2%) from £77,000 to £81,000.
For those out in the country, income growth appears to be largely accounted for by additional Choose and Book work,
although there were some signs of small growth in self-pay work. For those in l ondon and the South-east, there seems to have been signs of self-pay growth sup ported by, in certain locations, significant increases in Choose and Book work.
at the same time, many consult ant urologists have been incorpo rating, following the downward pressure on fees. We are seeing an increasing interest among urolo gists in forming groups and, at the time of writing, there are a number of potential groups in serious dis cussions. the trend towards group ing shows no sign of relenting.
cost increases
We have noted a number of changes in costs since 2013 and 2014. Staff costs have shown a slight increase. a s previously reported, there appears to be a cor relation between growth in average staff costs and the growth in the tax-free allowance propounded by the then Coalition Govern t here is evidence of a rise in consulting room hire costs. Our analysis, of course, shows the implications of the Competition and Markets a uthority (CM order ( a pril 2015) and we have evidence from 2015 onwards of even sharper rises in costs of room
hire, secretarial services and even sandwich and tea provision!
Perhaps surprisingly, there has been a slight fall, on average, in professional indemnity costs
One of the effects of the CMa ruling will be to squeeze consultants’ margins even further.
Perhaps surprisingly, there has been a slight fall, on average, in professional indemnity costs. We are aware of new players entering into the market. Some believe that these new providers are cherry-picking and are not in the game for the long term. this may be true, but the evidence is becoming increasingly clear that savings can be made on indemnity insurance premiums for
The squeeze from insurers continues, but at some point, perhaps surprisingly, we expect this to reverse as a shortage in the supply of trained urologists hits the market
those classified as ‘low risk’ and who have a low claims ratio. this market continues to evolve. there has been a slight increase in travel and conference costs. Some urologists, it seems, have started to attend more exotic conference locations following the years of recession.
Finally, ‘other’ costs have shown some increase. a s reported in other sectors, this growth seems to reflect increased expenditure by many doctors on their websites and in taking marketing advice. We expect this to continue.
What then of the future? there are those who say that Choose and Book work has peaked and is unlikely to exhibit future growth. the evidence is mixed here. there certainly seems to be a growth in self-pay at the expense of insurance fees.
the squeeze from insurers continues, but at some point, perhaps surprisingly, we expect this to reverse as a shortage in the supply of trained urologists hits the market. Costs, not growth, will continue, we believe, in the broad term shown in 2013-14.
Overall, we feel that urologists in private practice will, on average, continue to prosper – although they may have to work harder to achieve the same income levels as their elders did and are doing.
Stanbridge runs an accountancy, finance and tax
service specialising in the medical profession
years ending 5 april
Source: Stanbridge Associates Ltd
what’S coMing in oUr MaY iSSUe
Make sure you don’t miss our next issue, published on 19 May. Only subscribers to the journal are guaranteed to receive every copy and we don’t think anybody who is serious about continuing private practice in the future, when there is so much happening that will affect them, can afford to miss any issue.
Coming up next month:
What now for your pension?
The right staff are critical to your success. Pam Underdown explains why the team you surround yourself with can make or break your business, how to find the right team players and how to ensure they produce a consistent experience for your patients every time they visit
Defending doctors under suspicion – behind the scenes of a medical crime lawyer
Prof Keyoumars ashkan, of the London Neurosurgery Partnership, comments on developments in neurosurgery including The Harley Street Clinic’s latest acquisition – the ROSa Robot
With prescribing issues being one of the top three things doctors ask for help on, a medico-legal doctor gives some timely advice
Branding to succeed. Our Practice Builder series shows how it needs to offer an emotional connection between the practice and patients, from the visit to the website/app or brochure to the first phone call, to the initial visit and to the consultation.
Latest news from the Independent Doctors Federation
Winning Ways with your PPU. Knowing what your local unit is up to will stimulate business ideas and opportunities for you
eDITORIaL INqUIRIeS
gary Nials presents a self-pay billing and collection analysis and suggests how to increase your market share
The clinical negligence expert witness is most frequently asked to write a liability and causation report. Our series helps you get it right
accountant’s Clinic looks at winding down the business
In a crowded market space, it’s often the little things that have the biggest impact. So if you want to stand out from your competitors, a focus on client service could be the key differentiator.
Hempsons lawyers consider a Court of appeal decision that impacts upon the requirement for employers to make reasonable adjustments for certain members of staff to avoid a discrimination claim being made
Our motoring correspondent Dr Tony Rimmer tests the Land Rover Discovery Sport
What should you do if you discover your secretary takes work home on a memory stick
aDveRTISeRS: The deadline for booking advertising for our
Robin Stride, editorial director
Email: robin@ip-today.co.uk
Tel: 07909 997340
aDveRTISINg INqUIRIeS
Margaret Floate, advertising manager
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution.
Printed by Pepper Communications Ltd Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
£90 GPs and practice managers (private & NHS). £210 organisations.
But if you pay by direct debit, individuals pay only £75, and organisations £180 Call Proact Ltd on 01752 312140
Email: lisa@marketingcentre.co.uk
To guarantee your copy of Independent Practitioner Today by taking out a subscription (at the rates shown on the left), phone 01752 312140 or send off a subscription form on page 22 or email lisa@marketingcentre.co.uk or go to the ‘about’ page of our website www.independent-practitioner-today.co.uk
If you pay by direct debit, individuals pay only £75 for a subscription. Just fill in the form on page 22 and send it to the Freepost address shown at the bottom of the form.
BaCK ISSUeS: £12.50 including post & packaging CHaNgINg aDDReSS OR SUBSCRIPTION DeTaILS?
Phone 01752 312140 or email lisa@marketingcentre.co.uk
The status page is the best feature of ePractice because I can see the outstanding payments at a glance. The system makes it simple and cost effective to manage billing and collections in house.
”
Maxine Mealey, Medical Secretary
Securely manage your payment tracking and financial reporting
Client management and financial control is core for any enterprise. The latest Healthcode online ePractice management tool enables you to streamline your financial tasks. Using ePractice you can ensure you are paid for the services you provide and gives you access to real time financial reports at your fingertips.