The business journal for doctors in private practice
In this issue
Help is at hand for inspections
A new initiative for private GPs aims to help those struggling with CQC inspections P14
Beating the red tape Advice on how to make your practice comply with the EU’s General Data Protection Regulation P16
Get ahead in the new decade by reading Independent Practitioner Today, bringing you the news and expert advice you need to run a successful private practice
n See page 24 for subscription information
Fiscal resolutions for a new decade Ten New Year resolutions to ensure your practice is ready for the challenges of a new decade P32 Bringing a 20-20 vision to you and your team
Self-pay soars to £1.1bn
By Robin Stride
Independent practitioners are being exhorted to seize new opportunities in 2020 as the market enters a new decade of price transparency and consumer choice.
The advice comes as a new report reveals:
n One in four private patients now self-fund their treatment;
n Self-pay revenue grew an average of 7.4% a year in real terms between 2014 and 2018;
n 21% of independent acute medical hospital revenue in 2018 came from UK-based self-payers, equivalent to a market of £1,105m.
LaingBuisson’s Private Healthcare Self-Pay UK Market Report, second edition, says growth is driven by NHS waiting lists, a more consumerfocused private healthcare sector and demand management by NHS clinical commissioning groups. It finds a ‘buoyant and growing market’ worth £1.1bn for independent hospitals and clinics in 2018 compared to £527m in 2013.
According to report author and LaingBuisson consultant Liz Heath, there is now a greater need than ever for consultants to engage proactively with providers to design and deliver self-pay pathways.
The increasing number of consultants recognising the power of an online and digital presence is seen as an important factor in consumer engagement over the next decade.
Mrs Heath told Independent Practitioner Today : ‘It is vitally important for consultant groups to use their collective strength and bargaining power to work collaboratively with providers to deliver attractive self-pay strategies within local markets.
‘They should use the growing power of social media and patient feedback to promote the affordability and ease of access to self-pay procedures.’
LaingBuisson research shows a greater focus on the consumer in the self-pay market, whether for private and online GP services and diagnostics or promoting affordability of elective procedures like cataract surgery.
But Mrs Heath added: ‘There is, however, progress needed to deliver a truly consumer-centric offer and experience for the self-pay patient in the only true growth sector of the private acute healthcare market.
‘This report provides much greater insight than previously into the market drivers that are fundamental to sustaining and growing the UK self-pay market and the elements of the patient experience that are key to success.’
Growth is evidenced across all specialties and is strong in orthopaedics, ophthalmology, gastroenterology, gynaecology and urology.
Orthopaedics is still the highest volume self-pay elective specialty, but the analysts found welcome
THE PRICE IS RIGHT – OR IS IT?
Self-pay private treatment prices gathered by LaingBuisson researchers for 6,000 procedures in August and September 2019 show huge variation:
n Knee replacements from £8,110 to £15,160 across 171 providers
n Hip replacements from £8,110 to £15,050 across 169 providers
n Cataract surgery in one eye from £1,985 to £3,515 over 155 providers n MRI scan (one body part) from £199 to £570 over 41 providers
growth in specialties such as cardiology, interventional radiology, dermatology and gastroenterology.
The growth in diagnostics is welldocumented, with wider access to CT and MRI scanning and associated competitive pricing strategies driving demand.
Sustained growth in the self-pay sector appears better than might have been expected given modest economic growth and future uncertainty.
Mrs Heath reported little evidence that consumers were actively seeking quality or outcome indicators to influence their decisionmaking.
But feedback via platforms such as Doctify, www.iwantgreatcare.com and GoPrivate.com had increased recently which was ‘encouraging’.
NHS funding restrictions for cancer drugs is fuelling growth in selfpay oncology. There is also growth
in demand for diagnostic ser vices such as MRI scans, CT scans and endoscopy where patients are seeking a more rapid diagnosis than they can obtain under the NHS.
LaingBuisson found demand greatest among the over-60s who had greater disposable income, may have abandoned their private medical insurance and were willing to pay privately rather than wait for NHS treatment.
It said the growth in the number of over-65s would see increasing pressure on NHS services and greater demand for private treatment.
n For more on the report, which shows how and when patients are seeking information about some of the most popular self-pay procedures/diagnostics, go to www. laingbuisson.com
n See ‘Surgery loses faith in beauty therapy’, page 20
TELL US YOUR NEWS Contact editorial director Robin Stride
Surgery loses face in beauty therapy
Market analysts LaingBuission’s first major study into the UK cosmetic enhancement market shows nonsurgical therapies are soaring P20
ADVERTISE WITH US Contact advertising manager Margaret Floate at margifloate@btinternet.com Phone: 01483 824094
GET A SUBSCRIPTION DISCOUNT
£90 independent practitioners.
£90 GPs and practice managers (private & NHS). £210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE – USE SUBSCRIPTION FORM ON PAGE 25
Or email karen@marketingcentre.co.uk Or phone 01752 312140. Or go to the ‘Subscribe’ page of our website www.independent-practitioner-today.co.uk
Chief sub-editor: Vincent Dawe
Head of design: Jonathan Anstee
Publisher: Gillian Nineham at gill@ip-today.co.uk Phone: 07767 353897
EDITORIAL COMMENT
We’ll
give you plenty in ’20
Very best wishes for a new year and the new decade ahead.
Independent Practitioner Today will be doing its best over the next 12 months to provide you with the 20-20 vision that you and your team need to operate your practice business.
As we enter 2020, there is much uncertainty for thousands of consultants – not least those in BMI hospitals (see story opposite) and GPs in private practice.
Doctors and their working environments will be affected on many fronts under the new Tory Government and ‘getting Brexit done’.
We expect a host of changes in coming months and our expert writers will be seeking to help you make the most from future tax changes arising from the upcoming Budget and new laws and regulations affecting you and your business.
Will the powers-that-be finally listen to common sense and ditch
the pensions tax taper? We wait to see, but meanwhile don’t ignore the advice on what to do about the latest official emergency tinkering (see story opposite).
Doctors are booking in pensions advisers, but don’t forget that if you have a large annual allowance tax charges for 201819, you must still pay these in January 2020.
Meanwhile, the recommendations from the Bishop of Norwich’s inquiry following the Paterson case, aimed at improving safety and quality of care in the independent sector and the NHS, are expected soon and could have far-reaching consequences.
All this against a background of more competition from new private hospitals, a contraction in the overall market, the need for many to diversify to grow, and ongoing concerns about defence cover affordability.
We will aim to be the eyes in the back of your head.
How to counter the imitation game
Are they really who they say they are?
Vin Pandha continues her series on fighting fraud in the medical sector, explaining what to watch out for P28
Be a good landlord
Dr Lafina Diamandis continues her series for doctors investing in property. This month, property management and landlord essentials P30
Protection for whistleblowing
A recent employment tribunal case about practising privileges shows that whistleblowing is not just an issue relating to doctors working in NHS P34
Check with family when passing on
Can you talk to loved ones about wealth? Dr Benjamin Holdsworth shows why inheritance planning is about more than just tax P42
Discuss end-of-life care in advance
Dr Ellie Mein explains how patients’ wishes can be respected and upheld when the patient is no longer able to communicate their preferences P48
PLUS OUR REGULAR COLUMNS
Doctor on the Road: Standing out in a crowded market
The second-generation Range Rover Evoque grabs the premium SUV top spot for Dr Tony Rimmer P44
Start a private practice: Visions for a new financial year
Give your private practice 20-20 vision with a new year/ new decade financial review P46
Profits Focus: Costs take the shine off
Our unique benchmarking series looks at the financial fortunes of ophthalmologists P49
Doctors wary of election fix for pension tax woes
By Edie Bourne
Doctors caught out by pension contribution limit changes remain suspicious of a pre-general election promise that the NHS will pay the tax for them – albeit for the current tax year only.
The emergency measure, of no help to doctors’ private pensions, pledged to allow clinical staff to opt for the pension scheme to cover their excess charges resulting from the ‘annual allowance’ –called ‘Scheme Pays’ – for the 2019-20 tax year.
They should then be compensated by the NHS upon their retirement.
The annual allowance limits the amount of tax-free pension savings which can be accrued each year. The standard allowance is £40,000, but 2016 introduced a ‘tapered’ version, reducing the limit on a sliding scale to as little as £10,000 for highest earners.
NHS boss Simon Stevens said the surprise in-year move was necessary because the election and subsequent Budget deferral meant a long-term solution to the tapered annual allowance problems was unlikely before April 2020.
Patrick Convey, technical director at specialist financial planners Cavendish Medical, said the move was completely unprecedented.
‘NHS England expects this surprise announcement to encourage staff to take on extra shifts or additional sessions once more. But many doctors will be apprehensive about trusting a contract
which will not be truly challenged until they retire. For some, this is still several decades away.
‘It would be fair to say that not all our clients have much trust in the ability of any government to keep to their side of the bargain, but NHS England has been forced to explain that the contract will be legally binding.’
He said the temporary measure could help doctors facing punitive tax bills in the short-term, but challenging grey areas remained.
‘For example, the tax will be covered only on charges arising from excess contributions to NHS pensions – not on personal pensions. There are also locally-agreed NHS trust policies which will impact pensions and tax positions at an individual level.’
More details on last summer’s pension flexibility consultation are still awaited. Mr Convey urged doctors to examine their tax position very carefully.
Hospital Consultants and Spec-
ialists Association (HCSA) president Dr Claudia Paoloni said: ‘Hospital doctors remain supremely sceptical about the claim that this facility cannot be reneged upon years down the line.
‘The whole tenor of this quickfix scheme rings alarm bells. It feels half-baked and it has been misrepresented by the Secretary of State as having “abolished” the taper. Will it change doctors’ behaviour? We are doubtful.’
She said doctors faced complicated legwork to access the facility.
As we went to press, there has been no confirmation the one-off tax payment would apply in Wales or Scotland.
The BMA said all doctors needed to understand the details of the reimbursement plan. After taking legal advice, it believed the proposals gave enough detail to bind employers and NHS England to pay, with contractual guarantees that these would be backed by UK government.
The association declared: ‘We are also satisfied that members will not be disadvantaged by any unforeseen tax consequences as a result of using this scheme.
‘Consequently, we believe that clinicians utilising this scheme have a legally binding, contractual entitlement that is backed by UK government, to receive these payments.
‘As such, clinicians will not be financially disadvantaged should they incur an annual allowance tax charge resulting from their NHS pension scheme in 2019-20.’
Call to ditch pension annual allowance
The BMA, HCSA and other bodies quickly pressed the new government to ditch the annual allowance and the taper.
Royal College of Physicians of Edinburgh president Prof Derek Bell advised doctors to get independent advice from a pensions’ adviser.
Andrew Pow, of the Association of Independent Specialist Medical Accountants (AISMA), said the proposals related only to 2019-20 tax payments.
‘Those with large annual allowance tax charges for 2018-19 will still need to pay these in January 2020.
‘It is uncertain if the payment of the 2019-20 tax on retirement may lead to a benefit-in-kind income tax charge. While positive news at first glance, the announcement contains the potential for some form of down-the-line tax charge, which may not lead to the change in behaviour that is intended.
‘Doctors who have already opted out of the NHS Pension Scheme to avoid the annual allowance tax charges should talk to a specialist financial adviser as soon as possible to consider the pros and cons of re-joining the scheme.’
BMI hospitals are getting a new owner
More than 7,000 consultants with practising privileges at 54 BMI hospitals were expecting news of a selloff of the group to Circle as we went to press.
Circle, with private hospitals in Bath and Reading, Berkshire, and one due to open in Birmingham in 2020, was the first private company to run an NHS trust –Hinchingbrooke in Huntingdon, Cambridgeshire.
But it used a contract break clause to withdraw in January 2015, after funding cuts and A&E pressure.
The company has invested heavily in award-winning digital mar-
keting to drive private patient numbers. BMI sold off four of its hospitals earlier in 2019. Check our website www.independent-practitioner-today.co.uk. for updates.
Dr Claudia Paoloni, HCSA president
Shrinking market spurs competition
By Robin Stride
Private hospitals and clinics face a big challenge to stimulate more demand as new hospitals compete with each other on price and quality, especially in London, a market analyst warns.
Philip Blackburn, author of LaingBuisson’s latest Private Acute Healthcare UK Market Report, forecasts nominal revenue growth of around 2-2.5% in the next three years for UK private acute medical care, before taking account of modest economy inflation.
The UK market for private acute medical care in hospitals and clinics was estimated to be worth £5.8bn in 2018, the second year of real-terms decline for the sector which shrank by 1.1% in 2018 and by 2.1% in 2017.
This is blamed on the stalling of key funding streams. NHS spending on independent sector acute services fell for the first time in 2017 and then again in 2018. Medical cover pay-outs were down in real terms and Middle Eastern embassy business fell as governments tried to cut their bills.
Mr Blackburn said: ‘The independent healthcare market has clearly faced challenges, as growth in some traditional revenue streams stalled recently.
‘This has prompted some busy strategising by hospital and clinic providers to best position themselves to meet future demand trends.
‘Generally, providers recognise the need to develop their service offering to attract demand and meet changing healthcare needs of the population, including diversification into new areas for some, targeting new customer segments both here and abroad, and capitalising on healthy interest in what UK private healthcare can offer.
‘There have been more aligned relationships between providers and funders with a shared objective to deliver high-quality healthcare services, but the crucial need is to do so more efficiently to offer affordable private healthcare, both insurance and self-pay.’
e-bills boosting cash flow
Independent practitioners can boost their cash flow and offer a better service by using an online patient e-billing and payment system developed by Healthcode and Patient Zone.
The service gives practices a more efficient way to charge self-pay patients and recharge insurance shortfalls.
In a two-week pilot of Healthcode ePractice users, 29% of 291 patient invoices issued were settled the same day, 43% within three days and 47% within a week. The settlement time for patient invoices was previously typically two weeks.
Jennifer Moore, personal assistant to Glasgow orthopaedic surgeon Mr Andrew Brooksbank, said being able to send bills electronically was far more efficient and had ‘massively’ improved cash flow. ‘I had one patient who paid me just 45 minutes after I sent them the bill.’
The service enables practices to create e-bills and send them to patients securely. Patients are emailed or texted to say they have received a bill which they can pay on the Patient Zone online portal. Practices get an email confirmation when a bill is settled.
There is no need to arrange mer-
chant accounts or pay credit card processing fees. Instead, practices pay a fee to Patient Zone of 2.5% per bill plus VAT to use the service.
Patient Zone boss Richard Shawyer said there was ‘a real appetite’ among doctors and patients for a straightforward billing and payment process.
‘With 29% of e-bills being settled the same day, practices saw a significant boost to their cash flow. Meanwhile, patients had the reassurance of payment confirmation and the reassurance that their financial details were secure.’
See ‘Unified index of doctors’, p8
GMC bid to improve doctors’ well-being
UK health services could be world leaders in creating workplaces that support doctors’ well-being and patient safety if existing good practice was applied more widely, a report for the GMC says.
The council’s document Caring for doctors, Caring for patients identifies a need to address the wellbeing of doctors faced with higher workloads, whose own health impacts on patient care.
Recommendations include compassionate leadership models giving doctors more say over their workplace culture and adopting minimum standards of food and rest facilities.
London’s King Edward VII’s Hospital has introduced the latest da Vinci surgical system, the Xi robot. It gives multi-quadrant anatomical access – increasing the range surgeons can operate in and creating room for more complex and challenging procedures. Its team of urology specialists now includes Prof Caroline Moore – the first woman in the UK to be a professor of urology, Prof Mark Emberton, Mrs Sian Allen and Mr Paul Cathcart.
Boss Lindsey Condron said: ‘Our ambition is to be the leading independent urological centre in the UK.’
Latest robot surgeon for hospital’s urologists Watchdog rates Bupa insurance good all over
Bupa is the first health insurer to receive a Care Quality Commission rating – of ‘good’ across all areas –after registering for inspection.
Inspectors said staff in Manchester, who give clinical advice and support to over 6,000 callers daily, showed kindness, respect and compassion, understood members’ personal, cultural, social and religious needs, and were nonjudgmental.
They also commented on a kindness scheme where staff send a small gift monthly to a customer of their choice. 750 have gone out since May 2018.
Bupa Global and UK Insurance medical director Dr Luke James said insurers, unlike the consultants and hospitals they worked with, had not been regulated.
‘As our specialist support teams offer patients help alongside the care provided by their consultants, we believe it’s important that we demonstrate the quality of the advice and support we’re offering.’
Economist Philip Blackburn
Quiz insurer, patients told
By Olive Carterton
A BMA guide for patients thinking of taking out private medical insurance advises it is crucial they and their GP have free choice of consultant with the right to topup fees if they exceed the insurance reimbursement.
People should also have the option of choosing the hospital where they receive treatment and, if necessary, are able to pay top-up charges, it says.
Drawn up by the BMA Private Practice Committee, the 2,600word document outlines 22 questions to ask insurers.
It tells patients: ‘If the doctor
you want to see is licensed by the GMC and has practising privileges, but is not recognised by one or more private medical insurer, you may want to ask the insurer to provide clarifications as to why he/she is not recognised.
‘In some cases, they may be the best doctor for your particular problem and you should consider pressing the insurer to explain why you cannot see that specialist.
‘Before you buy PMI cover, you may want to ask the insurer for a list of the doctors and hospitals that are covered to help you decide if the insurance cover is right for you.
‘Finally, ask yourself if you are
Cromwell surgical team hails da Vinci robot as masterpiece
Bupa Cromwell Hospital has installed a da Vinci X robot to assist with complex surgery. It can be used in urology, gynaecology, general surgery, hepato-pancreato-biliary (HPB), head, neck and throat surgery and cardiothoracic surgery.
Prof Long Jiao, consultant hepatobiliary and pancreatic surgeon, said consultants and their teams were ‘really excited’ about the installation.
‘Robotic surgery is a highly advanced technological tool, and the da Vinci robot is undoubtedly the most recognised system for robotic surgery in the world, offering huge benefits to both patients and surgeons alike.’
willing to switch insurers if yours isn’t covered?’
The BMA says many policies guarantee no risk of a consultants’ fees shortfall, but the trade-off is that it normally means customers are offered a restricted list of doctors who agree to keep their fees at insurer-dictated levels.
‘This restricts your choice and may mean you are unable to see the doctor who may be most suited to help you with your problem.
The recently introduced restrictions on top-up payments have limited patient choice and reduced consultants’ ability to set their own fees based on the service that they provide.’
Medico-legal experts
‘must have training’
Medical experts should undergo appropriate medico-legal training before appearing as an expert witness, the Royal College of Surgeons of England (RCS) advises in new guidance.
The Surgeon as an Expert Witness –A Guide to Good Practice sets out the role a surgeon should play when acting as an expert witness in civil, criminal and coroners’ cases.
It follows two independent reviews: Prof Sir Norman Williams’s ‘Gross negligence manslaughter in healthcare rapid policy review’ and the ‘Independent review of gross negligence manslaughter and culpable homicide’ led by Mr Leslie Hamilton – highlighting a need to improve the quality and consistency of expert witnesses in gross negligence manslaughter cases.
The Williams Review noted that in the case of the surgeon Mr David Sellu, his conviction for manslaughter by gross negligence was successfully appealed and quashed by the Court of Appeal, ‘in part due to the manner in which expert witness evidence was used during the trial’.
The judgment in the Court of
Appeal noted that the prosecution asked the expert witnesses the leading question: ‘was this gross negligence?’ This was, in fact, a question for the jury to consider.
It stated: ‘…the way in which the issue of gross negligence manslaughter was approached – and, in particular, the consequential direction to the jury – was inadequate. As a result, the conviction is unsafe and is quashed.’
The RCS’s guidance advises surgeons acting as expert witnesses that they should:
Have been a consultant surgeon for at least five years;
Only take on cases they encounter as part of routine practice;
The same applies to subspecialisation. If the case turns on an issue lying within a surgeon’s surgical speciality, but outside their own field of work, they should be wary of accepting instructions;
Not provide medico-legal services after three years from retirement;
Have indemnity – anyone who acts as an expert witness is at risk of litigation.
See ‘The inquest with a sting in the tail’, page 26
The BMA’s advice on insurance
Prof Long Jiao (left) with his surgical team after performing their first operation with the da Vinci X robot
GMC outcomes better if you turn up
New GMC research has found that the outcome of tribunal decisions was consistently linked to doctors’ engagement with hearings rather than their personal characteristics.
The peer-reviewed study published in the journal BMC Medicine found that doctors who did not
Guidance to doctors on prescribing remotely
Good practice guidance covering remote consultations and prescribing has been issued by medical bodies to help protect patient safety and welfare when accessing medication online or by phone.
The ten principles, including prescribing to patients overseas, have been co-authored and agreed by bodies including the Academy of Medical Royal Colleges and the GMC.
attend their hearing or lacked legal representation tended to receive more serious outcomes.
There was no association between the seriousness of tribunal outcomes and a doctor’s age, race, sex or whether they qualified in the UK or abroad.
The study was of 1,049 doctors referred for hearings at the Medical Practitioners Tribunal Service from June 2012 to May 2017. Now the GMC is exploring how to encourage more doctors to engage with hearings. A spokesman said: ‘We are also continuing
Spinal robot is first in UK
By Edie Bourne
HCA Healthcare UK’s London Bridge Hospital is the first in the UK to offer the revolutionary ExcelsiusGPS Robotic Navigation System to patients needing spinal surgery.
our work to tackle the disproportionate representation of some groups of doctors in referrals to a tribunal hearing.
‘We know that doctors who are black and minority ethnic, male, older or non-UK graduates continue to be referred more often.’
HCA starts rapid clinic for prostate cancer
A new Rapid Prostate Clinic at HCA’s The Princess Grace Hospital offers fast testing and diagnosis of conditions for those with an elevated PSA – including a follow-up consultation discussing results and treatment plans.
GMC chief exec utive Charlie Massey said the flexibility of accessing healthcare online can benefit patients, but it was imperative that these services did not impact on their safety, especially when doctors were prescribing high-risk medicines.
‘Doctors working for online services have the same obligations to follow our guidance and to prescribe safely as they would do for face-to-face consultations.
‘These principles will remind all healthcare professionals of the importance of prioritising the safety and welfare of patients when prescribing medication remotely, and will help facilitate a culture where unsafe practice is called out and acted on.’
The guidance is available at: www.gmc-uk.org/ethical-guidance/learning-materials/remoteprescribing-high-level-principles
It said the new technology raised the bar of minimally invasive surgery capabilities to provide improved accuracy, reduced procedure times, significantly shorter recovery periods and lower complication rates.
The robot offers a major advancement in spinal surgery by allowing surgeons to capture images of the spine in 3D and pinpoint exactly the right depth and angle for predetermined screw dimensions that are to be inserted into the vertebra.
It is the first technology to combine a rigid robotic arm and full navigation capabilities for precise trajectory alignment, providing successful screw placement at a rate of 99%.
The improved precision also cuts down on procedure times, reduces exposure to radiation and means shorter recovery periods, earlier hospital discharge and accelerated return to work and sports for patients.
The first UK surgeon to be trained on the technology, consultant orthopaedic surgeon Mr Khai Lam, said: ‘This cutting-edge system is designed to assist in pre-
cise screw placement for a variety of different surgical approaches by eliminating human error and will therefore optimise patient care in those undergoing spinal surgery.
‘Many of these procedures will include screw placements into the posterior cervical, thoracic, lumbar spine and sacroiliac joint, when used to treat spinal disorders.
‘By combining the benefits of navigation, robotics and the expertise of surgeons, this robot has the ability to revolutionise the way we approach spinal surgery, and change lives.’
London Bridge Hospital chief executive Janene Madden said: ‘In the hands of some of the best spinal surgeons in the country, this new technology will offer patients all over the UK – and internationally – more effective treatment.’
It will use the latest ‘gold-standard’ in multi-parametric MRI (mpMRI) scanning for the prostate.
Combining this with blood and urological tests, a complete overview of the patient’s condition can be given on the same day.
HCA said the clinic offers a multidisciplinary approach to patient care, which could include as many as 20 cross-specialism doctors with nutritionists and physiotherapists working together.
See ‘Hospital groups unite to tackle prostate cancer’, page 9
A £12m purpose-built cancer centre opened in 2017, LOC @ Chelsea, has been rated ‘outstanding’ overall by the Care Quality Commission on its first inspection. Run by Leaders in Oncology Care, part of HCA UK, the centre provides a one-stop service for its patients, including: consultation; diagnostic tests; treatment and supportive therapies, all in one location.
The ExcelsiusGPS robot
Charlie Massey
Gastro specialists start big expansion
By Olive Carterton
Up to nine new consultant-funded specialty day case clinics are set to open in 2020 in Welbeck Street, London, at the OneWelbeck Digestive Health site, which opened its doors last Autumn.
Welbeck Health Partners (WHP) has 90 doctors who have invested over £7m of £20m total funding for the venture, with another 60 in the process of partnering.
The company said it was committed to delivering better care at a lower cost than traditional hospitals.
On its eight floors, it will deliver minimally invasive procedures as
day cases ‘rather than with an overnight stay, as other centres would’ for specialties including orthopaedics, women’s health, ENT, general surgery and cardiology.
WHP began as a collaboration between a team from healthcare solutions company AMSURG and a group of senior UK doctors.
Founding partner and medical director, consultant gastroenterologist Prof Julian Teare, said: ‘What started as a small group of four of us looking to do something better has turned into the UK’s largest gastroenterology team with 37 partners.
‘It has been immense fun to
bring together all the best aspects of different gastro clinics from around the world into one place. And I am thoroughly enjoying working with an ambitious team who share my frustration with the existing system and my desire to transform patient care.’
The partnership said clinics were designed on a ‘clean-sheet’ basis with each having the best technology for its specialty.
It said: ‘Our partnership model leads to truly integrated care. Doctors own around half of each clinic and are empowered to put their design and delivery ideas into practice, with the support of their management partners.
‘This collaborative set-up also means that doctors guide their referrals to whichever colleague is the best person for the job, rather than keeping hold of them, as frequently happens elsewhere in the private sector. As a result, OneWelbeck patients always see the right person, first time.’
Old can’t afford insurance any more
Private doctors will see a serious decline in the number of insured older patients coming to them unless rising costs can be pegged.
That is the warning from the head of the organisation representing the salespeople and firms who sell private medical insurance.
Stuart Scullion, chairman of the Association of Medical Insurers and Intermediaries, warned: ‘Unless we can ensure the financial sustainability of private healthcare, I struggle to see how individuals will be able to maintain their cover from retirement in their 70s and beyond.
‘We must find that solution, because to fail to do so will result in an increased reliance on an already overstretched National Health Service.’
He told the association’s annual Health and Wellbeing Summit he believed that two key themes would impact over the next decade.
‘Mental health, particularly workplace mental health, is now receiving the prominence it has long deserved. It cannot be right that any individual feels unable to mention or openly
growth of 10% to £330m – up from £300m in 2018-19.
discuss their mental health with their line manager or employer for fear of being discriminated against or even losing their job.’
Mr Scullion said support from mental health professionals needed to start earlier, ideally at school, to help individuals build resilience to the challenges life threw at them. ‘That alone will not cure the problems of poor mental health, but potentially it will give some a better start.’
The second key theme would be
to deliver effective and financially sustainable social care for Alzheimer’s and dementia. ‘The current system is a lottery,’ he told the meeting.
Prof Willie Hamilton, professor of primary care diagnostics at Exeter University, alluded to the increased importance of private medical insurance being made easily accessible to those aged 70 or above.
He said: ‘PMI among the older generation is becoming more of a topic for discussion due to the fact that we are living longer and the demographics in which cancer is most prevalent.’
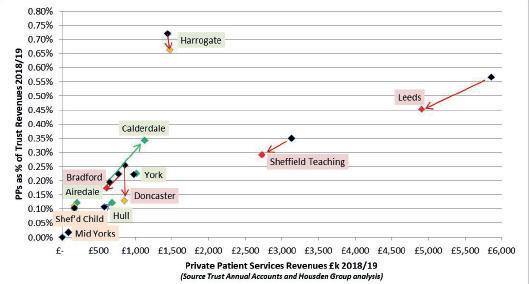
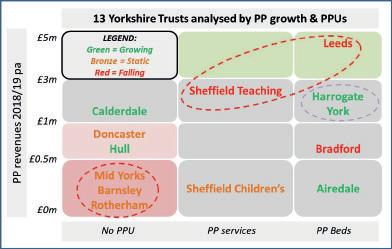
Compiled by Philip Housden
Central London NHS trusts’ PPU income powers ahead Leading NHS private patient units (PPUs) in London are enjoying continued growth.
Analysis of trust board papers reveals that the five largest revenue earners are forecasting combined
The Royal Marsden leads the way, with expected revenues in the region of £137m, up around 13% year on year.
Great Ormond Street forecast lower growth at around 3% to £64m, while reporting this as ‘£5.5m below plan . . . as demand has not emerged in line with plan’.
Imperial’s Trust Board reported
‘significant growth in private income across the trust in the year and income is forecast to be £3m higher this year than in 2018-19’.
This would take the trust to £55m, up more than 5%. Brompton is also reporting ‘over-performance on private patient income’ with an end-of-year total of £43m-£44m looking likely, up around 5%.
Royal Free is growing fast, perhaps 30%, with full-year revenues pro-
jected on October figures reaching over £30m for the first time.
This would take Royal Free up from seventh to fifth in the NHS PPU Top Ten, overtaking Moorfields and Guy’s and St Thomas’, which both are forecasting flat growth this year.
Philip Housden is a director of Housden Group. See his feature article on Yorkshire PPUs on page36
Prof Julian Teare, founding partner of Welbeck Health Partners
Stuart Scullion, AMII chairman
Unified index of doctors
By a staff reporter
All UK independent hospitals will have access to accurate information about their consultants by using what is billed as a groundbreaking online register of independent practitioners.
Medical IT company Healthcode plans to complete its rollout of The Private Practice Register (The PPR) to over 300 independent hospitals and NHS private patient units (PPUs) by early 2020 and will continue to enhance the amount of practitioner information available.
The PPR now has more than 16,000 practitioner profiles which are managed and kept updated by doctors themselves. They pay no fee.
Over 40% of doctors amended their PPR profile in 2019, demonstrating that they recognise the value of ensuring their details are correct when dealing with private medical insurers and now hospitals. All their data is housed securely in a dedicated data warehouse in the UK and access is via encrypted connections.
Healthcode said hospitals will have access to The PPR basic ser
vice, which will enable them to search the database for consultants who have been linked to their organisation.
They can then view basic information from the profiles including their name, specialty registration body and details of their practice at the relevant hospital.
And they will also be able to view profile alerts about GMC warnings, overdue indemnity cover and overdue appraisals for all profiles associated to their site.
Hospitals can also subscribe to The PPR standard service, costing a minimum fee of £250 monthly per hospital site. That includes 125 profiles a month. The fee per additional profile is £2 a month. Prices exclude VAT.
This offers more information and features to support consultant oversight. For example, they will have the ability to view doctors’ full profiles including their NHS and private practice, qualifications, medical secretary details, bank payment details and GMC status.
They will also receive notifications of updates to a clinician’s
profile, including GMC warnings which are available through Healthcode’s GMC republication licence.
Healthcode said the next update of The PPR will augment this with fields showing practitioners’ Resp onsible Officer, designated body, revalidation status, when their GMC fees are due and where else they hold practising privileges.
Hospitals can only correct and update information about a practitioner’s work within their own organisation, such as practice hours and start and end dates of practice. The practitioner is notified when these changes are made.
insurer and hospital each time their details change, while insurers can now save time by automating verification checks for new practitioners.
The PPR hospital rollout is the latest milestone in Healthcode’s initiative to connect practitioners, insurers and private hospitals using its secure online platform.
It said this provided a central source of accurate information about practitioners offering services in the independent sector which is already benefiting users.
For example, doctors with a PPR profile do not need to update every
Halfway point for City of London’s first private hospital
Building of the City of London’s first independent hospital reached the halfway stage with Nuffield Health chief executive Steve Gray (left) and project manager Peter McStay placing its first Portland stone slab. This will make up the rear facade of the historic building in Giltspur
Street near Smithfield Market, the site of Barts Hospital’s former pathology and residential staff quarters buildings.
Opening in spring 2021, it will have 28 consultation rooms, 48 bedrooms, four operating theatres and specialise in cardiology, cardiac
surgery, oncology, orthopaedics, plus other specialties.
The £65m building, leased from Barts NHS Trust, will also provide physiotherapy, diagnostics, and complement Nuffield Health’s 35 consumer fitness and well-being clubs and 63 corporate gyms.
Healthcode’s Fiona Booth said it was exciting news for hospitals, as they will have access to information and insights to support effective management of their consultants in line with the new Medical Practitioners Assur ance Framework – see our frontpage story in November. She added: ‘In its latest State of Care report, the CQC rated 79% of independent organisations as good or outstanding on the question of leadership and The PPR will be another means of demonstrating to CQC inspectors that a hospital has embedded measures to improve oversight of practising privileges and clinical governance.’
Speaking ahead of the Paterson Inquiry report, she said it was important private healthcare showed it could put its own house in order.
See plans to unify diverse governance systems, page 22
Bid to prevent suicides in anaesthetists
New guidelines in the journal Anaesthesia aim to increase awareness of suicide risk factors among anaesthetists and offer support to doctors, departments and organisations in coping with a suicide. A survey by the Association of Anaesthetists last July highlighted the experiences of almost 1,400 anaesthetists who had lost a colleague through suicide while working in the same department. Past president Dr Samantha Shinde said the guidelines aimed to raise awareness of indicators showing a colleague might be at risk and how they could be supported. See https://doi.org/10.1111/ anae.14890.
Healthcode’s Fiona Booth
Hospital groups unite to tackle prostate cancer
The Rutherford Cancer Centre North East has announced a collaboration with Nuffield Health Newcastle Hospital to aid treatment of prostate cancer radiotherapy patients.
A new oncology pathway for the region introduced by the Rutherford centre for its patients means prostate cancer patients can now have local access to hydrogel spacers which reduce radiation exposure during radiotherapy treatment.
The pathway is designed to meet increasing demand for precision radiotherapy in the region.
After undergoing the hydrogel spacer procedure, patients will typically commence their main treatment – radiotherapy or high energy proton beam therapy – at the Rutherford Cancer Centre in Bedlington.
The SpaceOAR Hydrogel is a soft gel that separates the rectum from the prostate, reducing radiation. The procedures to be carried out at Nuffield Health Newcastle Hosp
ital will be performed by urology consultant Mr Toby Page.
He said: ‘The provision of spacer devices to help minimise the impact of precision therapies on unaffected areas of tissue is a huge leap forward in prostate cancer
treatment. I am pleased to be a part of this collaboration with the Rutherford Cancer Centre as we work together to help transform cancer care across the Northeast.’
Rutherford Centre manager Chris Land said: ‘The North east
has some of the highest incidence of cancer in the UK, and prostate cancer is the most common cancer of them all. We are delighted to bring this crucial oncology pathway to the region which cements its reputation as a fast emerging hub of cutting edge cancer care and precision radiotherapy.
‘Our excellent relationship with Nuffield Newcastle has been key in delivering this and we are confident that it will enhance patient outcomes across the region.’
Matthew Lamb, hospital director at Nuffield Health Newcastle Hospital, said: ‘Being at the forefront of advancements in medical and surgical technologies is a key priority for us, which is why we are delighted to provide the rectal spacer procedure to prostate cancer patients in the region who need it.
‘This is a vital development in cancer care and demonstrates our commitment to working with public and private bodies to ensure the best patient outcomes.’
(Fom left) Chris Land, manager at the Rutherford Cancer Centre North East, Matthew Lamb, hospital director at Nuffield Health Newcastle Hospital and Nuffield Health urology surgeon Mr Toby Page
SP0T THE DOC: 156 members of the Independent Doctors Federation enjoying their study weekend in Malaga, led by their president Dr Neil Haughton
A look back through our journal’s archives of ten years ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2010
Credit card could cure crunch
Independent practitioners were being advised to make 2010 the year they started taking credit cards if they wanted to ensure patients paid up.
Accountant Bobby Lane, of Shelley Stock Hutter, warned that doctors’ billing problems were being exacerbated by the recession as patients inevitably took longer to pay or defaulted on their payments.
He told Independent Practitioner Today: ‘Nobody likes to chase their patients for money, as there are strong relationships that have been built up over a number of years, so anything that can be offered to avoid an uncomfortable situation should be welcomed.
‘Offering payment by credit card is one such opportunity. This offers the benefit for the practice of immediate payment and, for the
Accountant
patient, a way to pay on time but give themselves the benefit of the credit period.’
Mr Lane said many argued that the cost of providing this payment method was high – around 1-2% of income and a few hundred pounds to set up.
But if they considered the cost of their working capital, such as interest on overdrafts or business loans, then the charges for immediate payment could be less than the outstanding debts.
Accountants cited practice in the US where patients got a card on the way in and it activated an alarm on the way out if they haven’t paid. ‘It will happen here sooner or later,’ said one.
(Ed writes: Did it? How will you ensure you get paid in 2020?)
Cosmetic ops ‘in a mess’
British Association of Aesthetic Plastic Surgeons (BAAPS) president Mr Nigel Mercer hit out at the ‘unregulated mess’ in the marketing of cosmetic surgery.
The consultant plastic surgeon said: ‘We have reached a stage where public expectation, driven by media hype and – dare one say – professional greed, has brought us to a ‘perfect storm’ in the cosmetic surgical market.’
In an article in the Royal Society of Medicine’s journal Clinical Risk, he added: ‘There has been a massive increase in “marketing” including discount vouchers, 2-for-1 offers and holidays with surgery.
‘In no other area of medicine is there such an unregulated mess. What is worse is that national governments would not allow it to happen in other areas of medicine. Imagine “2-for-1” adverts for general surgery? That way lies madness!’ Mr Mercer called for tighter regulations in the UK.
NHS wait limits to aid private docs
The private healthcare sector could benefit under NHS constitution proposals to give patients legal rights to maximum waiting times for elective procedures and urgent cancer referrals.
Under the plans, from 1 April, patients would have the legal right to maximum waiting times to start treatment by a consultant within 18 weeks of GP referral and be seen by a cancer specialist within two weeks of GP referrals. We reported that if the NHS could not meet this deadline, it would have to take all reasonable steps to find alternative providers who could.
Company status boon to doctors
All consultants in private practice should look at becoming limited companies in the wake of Chancellor Alistair Darling’s pre-Budget plans, accountants advised.
Specialist medical accountant Ray Stanbridge said: ‘The one piece of good news was that nothing was done to affect the real advantages of incorporation. All consultants should at least consider this option seriously.’
Beware amorous advances
Private doctors were being warned by a defence body not to respond to amorous approaches from patients on social networking sites like Facebook.
The Medical Defence Union said it would be wholly inappropriate to respond to a patient making advances in this way.
SUBSCRIBE TODAY
Don’t miss out on what we report and advise in the future. Sign up for a £75 subscription today –consultants, GPs and practice managers can save £15 with a direct debit.
See page 24
Bobby Lane
ACCOUNTANT’S CLINIC: THE BUILDING BLOCKS OF ACCOUNTANCY
Susan Hutter (right) continues her A-Z guide of essential matters that consultants and GPs need to consider to run their private practices efficiently. This issue, she turns to ‘F’…
to of is for Filing Deadlines
Don’t
FILING DEADLINES apply to your personal tax return and your business. Depending on your trading structure, there are other documents that will also need filing by strict deadline dates.
In all cases, fines are levied if the filing dates are breached.
➤ Your personal tax return for 2018-19, covering the income for the year to 5 April 2019, must be filed by 31 January 2020.
If not, a late filing penalty of £100 will be levied and, if the return is more than three months late, taxpayers are charged £10 for each day. Beyond this, the fines only get worse!
➤ For those who trade as partnerships, either limited liability partnerships or ‘plain’ partnerships, you will also have to file a partnership tax return in addition to the personal tax return. The filing date and penalties are the same as for personal tax returns.
➤ For consultants and GPs who trade as limited companies, the company accounts must be filed at
forget 31 January top tips
Companies House nine months after the financial year end.
For example, if your financial year-end is 31 March 2019, the accounts must be filed at Companies House by 31 December 2019.
The late filing penalty is £100 and this increases to £375 after three months and more after six and 12 months.
The accounts must be filed at HM Revenue and Customs (HMRC) 12 months after the end of the year; in this example, 31 March 2020.
However, the tax must be paid nine months and one day after the end of the year: 1 October 2019. The penalty for late filing with HMRC is £100, which increases after three months to £200. If the tax is paid late, interest, at current rates, runs at 3.25% pa.
There is no point in leaving everything until the last minute, as the unexpected can arise – such as searching for additional documents or getting in touch with previous clients or suppliers.
Aside from that, it leaves you no time to carry out any financial or tax planning.
HMRC will notice those who file late, especially if it happens more than once, and it is not a good idea
to get on the wrong side of the taxmen. Try to provide everything to your accountant as soon as possible and at least three months before the filing deadline date.
is also for Finance Team
IT IS important to ensure your backoffice procedures can cope with modern methods of doing business.
If your administrative procedures are not keeping pace with the growth in the business, then you are likely to encounter serious problems, particularly in areas of patient service and finances, leading to cash flow issues.
Therefore, having a good inhouse team is crucial and, as well as the financial function, it is important to have strong PA/secretarial back-up.
You may need more than one employee in this category depending on the size of your business; for example, a PA and a book-keeper. It is also worth looking at how you use your professional accountant. If you do not need a full-time bookkeeper, many professional accountants will offer a bookkeeping service, say, once a month or once a quarter.
If you use this type of service, you can be sure that your records will be ready for year-end filing purposes.
The best way is to save on a monthly basis, so there are no big surprises when the tax bill lands on your desk
is for Financial Record
IT IS vital to ensure that your records are always up to date and that the source documentation is kept in case your professional accountant or book-keeper needs to look at it.
As well as the bank statements, it is also important to keep third party documents such as credit card statements where you use your credit card for business purposes, and also invoices in respect
of purchases and expenses and copy invoices that you send to your patients and insurance companies.
This documentation should be kept in either hard or soft format for six years.
I normally recommend that clients keep their documents for seven years after the end of the tax year/accounting year to which they relate.
is also for Forecasting
ALL BUSINESSES must ensure that they have enough money to pay the bills. As far as consultants and GPs are concerned, the practice bills usually do not get overlooked, but the taxman sometimes does.
Be careful to set aside enough to pay your personal tax and, if you
‘F’ is also for
trade as a company, your corporation tax as well. If you are unsure as to how much to put aside, ask your accountant for advice.
The best way is to save on a monthly basis, so there are no big surprises when the tax bill lands on your desk.
Family
MANY CLIENTS I work with ask whether they can employ their family, such as spouses and children, in their practice.
This obviously has the effect of mitigating the higher rate of tax that the consultants or GPs themselves must pay, as it reduces their profit. The income is then passed to a lower-earning spouse or child. However, HMRC is obviously
aware of this and if it is a ruse, they will not allow it.
The work carried out by your family must be paid at commercial rates and you must be able to demonstrate the work that they are doing.
Susan Hutter is a partner at Blick Rothenberg and part of the team that advises medical practitioners
Help is at hand for inspections
A new initiative for private GPs aims to help those struggling with Care Quality Commission inspections. Dr Neil Haughton gives the details
Upright Positional MRI Centre inLocations ManchesterLondon&
• Completely open scanner that is well tolerated by claustrophobic patients
• Weight-bearing scans for spine and joints enable a more precise diagnosis
• Patients who are large or cannot lie down can be accommodated
OVER THE past six years, the Independent Doctors Federation (IDF) has developed a close and productive relationship with the Royal College of General Practitioners (RCGP).
What started as meetings over dinner has led to joint ventures and our contribution to college conferences and meetings.
The college – and especially its past chairman Prof Helen StokesLampard – has opened many doors for us and recognised that many of its members work either partly or wholly in private practice and most of our GPs in the IDF are college members.
It introduced us, for example, to the NHS England’s lead on technology and we are in active discussions with them to assist better communication between the NHS and private GPs.
You may already be aware of our ongoing communication with the Care Quality Commission (CQC) and we have advised it for over five years on how to inspect independent primary care.
We are now in the process of being inspected again, this time being rated – at our suggestion – in line with NHS practices. Obviously, inspections are stressful and most of us are being rated as ‘good’ or ‘outstanding’, which is reassuring.
That’s about 95% apparently, which is line with the NHS. But some have struggled to meet expectations and have been rated as ‘inadequate’.
This can be for many reasons, of course, and may or may not be deserved. But the rating is difficult to challenge. The IDF has therefore gone into partnership with the RCGP Development Service in a joint venture to assist ‘inadequate’ practices.
Turn around
It will send in a team of highly experienced primary care professionals who will interview all the staff, look at all protocols and policies, as well as training and governance, eventually coming up with recommendations that should allow the practice to turn around their CQC rating.
There is considerable background to this, of course. Ursula Gallagher, deputy chief inspector of primary care, produced a report last March into the findings of CQC nonrated inspections. She concluded that in practices with problems, there was a ‘limited appreciation of a private practitioner’s responsibilities to the wider healthcare system’ and that areas of improvement included ‘sharing information appro pri
ately, recordkeeping and safe and effective prescribing’.
To the CQC, independent primary care is not just standard practices like my own. They include travel clinics, slimming clinics –which it especially seems to target – functional medicine, circumcision clinics, allergy clinics, psychiatrists working on their own, and even services you might not have realised existed.
These include vitamin infusion clinics and detox tents at festivals where you can have a bag of intravenous saline and paracetamol to cure your hangover; so we are a broad church.
What concerns were highlighted?
➲ The nature of private consultations, which are often episodic and patient driven, sometimes as a oneoff or for a second opinion rather than continuing care linked in with other local healthcare services.
➲ Patients may also not want their NHS GP to know about the problem being presented or there may be cultural or religious reasons. Some patients have never engaged with the NHS at all; others cannot access NHS care due to nationality unless they have an emergency.
➲ Safe and effective prescribing, especially of high risk medicines, opioid analgesics and antibiotics, occasionally when already refused by NHS services, and sometimes unlicensed prescribing or without a strong evidence base.
➲ Patients may not disclose medical information about themselves in order to access medication which may be unsafe and the private provider has no access to NHS records.
➲ Medicines management: how they are stored, packed and supplied.
➲ Clinical records: poor IT systems lacking basic functionality such as audit and no connection to other services or local agencies which might identify safeguarding risks. Some records are kept in foreign languages and even paper records still.
➲ Consent often not recorded or relied on implied consent.
➲ The need to share information between all parties involved in a patient’s care including NHS services, which is a GMC requirement.
➲ Safeguarding, including modern slavery and peopletrafficking where NHS registration is avoided so they can act outside the system. Patient identity was often not requested as well.
➲ Referrals were sometimes made as an open referral letter, leaving the patient to seek out a private consultant themselves, rather than the GP take that responsibility. This is sometimes guided by the insurers where they choose the specialist.
➲ Governance: private practices were criticised for not carrying out adequate clinical audit and often policies and procedures were lacking.
Substantial overlap
Most practices did well and these are not just private practice issues, of course. There is also a huge amount of overlap already between NHS and private GP service requirements, such as policies, training, premises compliance, staff recruitment, infection control, governance and leadership.
I have already provided training for the RCGP team in how NHS and private practices differ. So if some of our practices fall short of CQC requirements, this IDF/RCGP joint venture will go in
We reported on the IDF’s initiative in November’s issue
and help independent practices in the same way as teams help NHS practices.
Often, it is the culture in a practice that needs to change; there may be challenging personalities, poor leadership and practice, inappropriate facilities, poor staff support and sometimes a lack of engagement.
Our attitude at the IDF has always been to face problems head on. If we must be appraised and revalidated, then we will become a designated body ourselves. If the
CQC has to regulate us, then we will rise to that challenge and do it the best we can.
These are our businesses, which we have built up over many years, nurturing our patients’ needs, and to have that challenged can be incredibly stressful and financially disastrous, which is why investing in this joint venture will be money well spent.
I also want all independent primary care services to have access, whether IDF members or not, which is only fair and equitable, and I’m sure word will get out.
I am therefore delighted that the college has been so receptive to our proposal and look forward to working with them in the future to assist our members.
Dr Neil Haughton (right) is president of the Independent Doctors Federation
Providing first class medical consulting and therapy rooms at prime locations in Central London and Liverpool London www.tenharleystreet.co.uk 020 7467 8300
709 7066
At the heart of medical finance
Untying the red tape
The EU’s General Data Protection Regulation (GDPR) can be confusing. There is conflicting information and numerous myths circulating on the internet and it can be timeconsuming to determine what you need to do to be compliant for your practice or clinic. Jane Braithwaite (above) and Karen Heaton (right) give useful guidance
SOME MISINFORMATION on the data protection regulations can be damaging to a business. Bad advice can mean taking a non-compliant path, create unnecessary work or produce resource-intensive processes.
For independent practitioners, there is a greater emphasis on meeting the data protection standards due to the sensitive medical and child data that is held about your patients, obviously quite necessarily.
However, guidance from the Information Commissioner’s Office (ICO) is clear. Your processes and
procedures need to be reasonable and appropriate to the data you process and the actions you take with it. So, we need to keep things in perspective and consider the appropriate compliance steps for your practice.
Your responsibilities
As a private practice, you decide what systems are implemented to store and manage the data you collect and process so you can provide medical services to your patients. From a GDPR perspective, you are a data controller. The regulator expects you to understand what
personal data you are collecting and how you are handling it. Your systems, your data, your responsibility.
The top five priorities you need to have addressed for your practice are:
1 Do you ‘Know Your Data’ (KYD) – have you mapped the data journey, processes, systems and sub-processors you use?
2
Do you secure your data –using data security techniques like encryption, anti-malware software, and have you tightened up on your physical security?
3
Do you understand your consent requirements – have you used the data and systems maps to ensure consent is obtained at point of collection or onward transfer?
4
Do you have data protection processes in place?
5 Are staff trained and is this training refreshed regularly?
1 Know Your Data
This is the crux of data protection compliance. Without properly mapping out your data, you will struggle to be compliant with many aspects of data protection.
You need to answer basic questions such as:
What type of data do you have? Is it personal data or special category such as sensitive or child data?
Where did the data come from?
Who has access to that data?
Which processing activities do you undertake on that data?
Which lawful basis are you using for processing it?
Which country is it stored in?
Only when you know the answer to these questions can you assess your compliance requirements.
Risks
The impact of this is that you may not be compliant with the core principles of data protection regulations. Breaching these could potentially result in higher-level fines, risk of prosecution, audits by the ICO and restriction of business activities.
As we covered in November’s
article, all actions undertaken by the ICO are made public on their website, so there is the potential for non-trivial reputational damage from any action the ICO might take.
Benefits
There are benefits from mapping your data. You have a dynamic view of your systems and suppliers, which may result in a streamlining of both. You can see which third parties are processing or storing data.
Should you, or they, suffer a breach, you will be able to act quickly and have a better chance of limiting the damage.
Solutions
There are many solutions available and they come in different shapes, sizes and costs.
You can map your data using a spreadsheet or flow chart. These will be low cost in software terms but high cost in terms of time.
There are several more sophisticated software tools on the market which support in-depth data mapping of data flows, systems, subprocessors, security and access controls. These may come with other useful functions such as data breach and management of Subject Access Requests.
These tools will have a higher annual cost than standard desktop software but will save significant amounts of human time and provide a better ongoing solution.
The decision will likely depend on a combination of the capacity and skills of your staff, the levels of data risk in your practice and your budget.
2 Secure your data
As we discussed in the last issue of Independent Practitioner Today, data security and data privacy together equal data protection.
Once you know your data, you can take steps to secure it. Many practices already employ techniques such as cloud storage, antivirus software and physical security for their premises and clinics.
Data security is required for both online and offline data. Storage of physical data is as important as securing your online data.
We would recommend that you
move to a paperless practice if you have not already done so.
For your digital data transfers, you should be looking at how data is transmitted. The most secure way to do this is by encrypted electronic transfer.
Using end-to-end encryption on your email systems, encrypted cloud storage and encrypted transfer will reduce the risk of sensitive data being accessed should you have a breach
We will be looking at common data-handling mistakes and how to avoid them later in this series. However, we recommend that, as part of your overall security regime, you check that any cloudhosting provider or processor you use has provided you with the following information:
☛ The geographical location of the data centres where your data resides;
☛ The safety of that data centre from natural events such as fires, floods, earthquakes and storms; not to forget thieves, who could walk away with your sensitive data;
☛ The security measures in place such as firewalls, anti-virus detection, multifactor user authentication and data encryption, and routine security audits;
☛ Who has access to your data and what controls are in place?
☛ What happens in the event of data loss? How quickly can backups be restored? Who does this and are there additional costs?
There are many software tools on the market to prevent cyberattacks and other malicious malware and it is important is that you ➱ p18
ensure all software is regularly updated.
We also recommend that practices document what their security measures are – both physical and technological – and ensure these are reviewed regularly, at least annually as part of the GDPR audit. If you do not have the skills in house to do this, invest in an external consultancy. Prevention is better – and cheaper – than cure.
3 Understand your consent requirements
Once you have taken steps to map and know your data and have documented your processing activities, this will allow you to walk through each process and determine:
What data is collected and at which point;
What information notice is provided to the individual at the point of data collection;
What is the lawful basis for collecting and using that data;
If you need consent, how that consent is logged and managed;
What you will do if consent is withdrawn.
There are six legal bases for processing data. It is up to you to decide which basis is more appropriate depending on your purpose and relationship with the person whose data you are processing.
For example, consent for processing staff data may be on a different legal basis for processing patient data.
You need to be clear from the outset which legal basis you are using for consent, as it is unlikely to be the same for each processing activity and should not be changed later. For your practice, medical data and child data usually require explicit consent.
The legal bases are:
➫ Consent – the person has given clear consent to process their data for a specific purpose;
➫ Contract – you need to process the data to enter into or due to having a contract with the person;
➫ Legal – data needs to be processed to be legally compliant;
➫ Vital interests – processing the data is necessary to protect someone’s life;
➫ Public task – you need the data to perform your official functions or is in the public interest;
➫ Legitimate interest – processing is necessary for your legitimate business interests or that of a third party.
4
Establish processes for data protection compliance
It is important to have a set of operational procedures and processes in place to enable staff to understand what they need to do to ensure the practice complies with GDPR.
There are a core set of four to six procedures we recommend having in place to address your responsibilities for data protection.
Use standard templates and then involve your staff in customising these procedures and processes to develop them.
Staff benefit from being involved to help them understand what they need to be aware of and why. Consider appointing an owner for each procedure who will be responsible for any updates and training of other staff.
Our experience is that by involving staff in the design and evolu-
tion of a procedure, there is better buy-in to apply it, as well as an insight into what works best alongside their existing work.
Having these procedures develop over time as job roles and responsibilities grow means they do not become outdated and are not treated as a one-off exercise which can then be largely forgotten.
5 Train your staff
Do your staff understand how essential they are to GDPR compliance? Are they aware that they are the ones most likely to cause a data breach? Do they know how to handle data Subject Access Requests or what one may look like?
Your staff are incredibly busy doing their jobs, ensuring that your practice runs smoothly. It is important to ensure that awareness of data protection is part of their everyday activities.
At the end of a long day, they could leave a USB stick on the train by accident. They could lose their bag or their phone, which has
access to work emails. Would they have thought to encrypt the USB stick or anything else carrying the data?
It is possible that poor passwords can become an entry for cybercriminals wishing to sell the data that you hold. Personal information that is freely shared online through social media can be easily hacked if used as part of a password.
By training your staff to be aware of this as part of their everyday routine, you are demonstrating your compliance and you can measure the effectiveness of the training.
There are many ways to continually build training into your operations, through online courses now widely available on the market or lunchtime training sessions from the owners of the data protection procedures you have created. This provides opportunities for knowledge sharing and collaboration. If your practice is unfortunate to suffer a data breach or is subjected to complaints resulting in attention from the ICO, consider holding a ‘lessons learned’ training session with staff to understand what went wrong and the changes that have been put in place to prevent such issues occurring in the future.
Next month, we look at the recent guidance from the ICO on cookies, explain what this means for your existing websites and what solutions are available.
Jane Braithwaite is managing director of Designated Medical, which offers business services for private consultants, including medical secretary support, finance and digital marketing.
Karen Heaton is the founder of Data Protection 4 Business which offers consultancy services to design and implement GDPR-compliant solutions, as well as online training, outsourced Data Protection Officers and specialised software technology to support data protection
Together, Designated Medical and Data Protection 4 Business offer consultancy services and support to help private practices and clinics design and embed a data protection compliance culture into their organisations
New Year, New Solution
Make your life easier by using one of the UK’s leading virtual practice management system.
DGL Practice Manager simplifies your processes and workflows allowing you to manage all areas of the practice or clinic from one location, including:
Appointment Scheduling
Clinical Procedures Electronic Patient Records
Patient Correspondence
Financial Accounting Reporting
DGL Practice Manager offers a cloud-based, safe and secure solution. It saves time and increases efficiencies by helping clinicians and administrative staff run a paperless practice or clinic.
Contact us today for more information:
Web: www.dglpm.co.uk
Email: dglsales@clanwilliamhealth.com
Phone: 01280 824 600
DGL Practice Manager is very user-friendly and provides us with everything we need including a feature-rich accounts package. I have absolutely no hesitation in recommending the system and find all the staff very helpful and pleasant.
Joanne Murray-Brown. Secretary to Mr Sarangi, Orthopaedic Surgeon.
COSMETIC SURGERY MARKET
Surgery loses face in beauty therapy
Market analysts
LaingBuisson’s first major study into the UK cosmetic enhancement market has revealed an interesting new split: near-static growth in the cosmetic surgery sector, pitted against a buoyant market for non-surgical interventions such as Botox and injectable fillers. Report author
Liz Heath gives the details
LAINGBUISSON’S Cosmetic Surgery
UK Market Report, First Edition, estimates that the cosmetic surgery market was valued at around £273m in 2017, with little evidence of realterms growth over the last five years.
The non surgical market in the UK is, however, burgeoning. Although estimates vary, figures suggest it could be worth in excess of £3bn within the next five years.
Overall demand for surgical procedures has softened since the 2008 financial crisis and the PIP scandal of 2012, and the figures
indicate only a marginal growth of 0.5% in real terms in 2017 due to continued consumer caution.
Market data is more difficult to analyse for the highly fragmented nonsurgical market, which is still considered a ‘wild west’ in regulatory quarters. But information provided by Save Face, a national register of accredited practitioners who provide non surgical cosmetic treatments, indicate that the industry was worth £2.3bn in 2010 and could already have reached £3.6bn.
Although precise figures are dif
ficult to pin down, an indicative growth rate of 55% in a decade illustrates the future potential of this market.
Quest for perfection
I believe the growing acceptance of cosmetic procedures has coincided with the rise in social media, which means younger consumers are more confident about seeking advice and treatment, particularly for nonsurgical procedures.
But, unfortunately, this growth comes with well documented issues relating to this younger age
group’s quest for perfection and a perceived ‘selfie’ image.
Cosmetic enhancement is rarely out of the headlines. Stories are often polarised between celebrities or those wishing to promote the positive impact cosmetic treatment has had on them and patients whose horror stories of botched procedures and longterm health impacts create sensationalist headlines.
The use of social media also presents challenges for providers and regulation has unfortunately been slow to keep pace.
With cosmetic surgery, there is already a clear regulatory framework and accountability for individual surgeons.
The framework and processes are also overseen by the Care Quality Commission (CQC), and cosmetic surgery providers themselves have a responsibility to promote themselves in an ethical fashion and not breach guidelines of the Advertising Standards Agency or Committee in Advertising Practice.
There is still a way to go, however, before the cosmetic market as a whole is seen as reputable.
Many cosmetic surgery providers are building strong reputations based on positive customer experiences and now promote surgery in a more balanced way. However, some continue to push the boundaries of social and regulatory acceptability.
Although the traditional surgery market is not currently enjoying the same high levels of growth being experienced in the nonsurgical sector, it is becoming more widely accepted among the 1840 age group.
A feature of the market is the increasing trend for surgeons to offer non surgical interventions themselves or partner with specialist aestheticians who do.
This has the benefit of extending the reach of individual practice and, for the consumer, provides reassurance about treatments being offered in a more balanced, ethical way by properly trained practitioners.
Nonsurgical treatments can act as a gateway to future surgical intervention, so this approach can make business sense, but also retains the patient within a clinical setting where they can have confidence in the skills of the practitioner.
Non-surgical market
The LaingBuisson Cosmetic Surgery UK Market Report found that the nonsurgical market in the UK differs dramatically to that for surgery, with little regulation, patchy oversight and little sanction or redress for consumers.
This market is fragmented and opaque, with many different types of providers, lack of licensing or regulatory framework and frequent evidence of poor training and little or no clinical experience.
In the UK, a 14 day cooling off period is considered good clinical practice for cosmetic surgery, but it is rarely considered in nonsurgical treatments, where immediacy is often the primary driver.
Cosmetic treatments including injections and lasers can be provided in almost any setting with minimal training and oversight, and the attraction of buying cheap treatments from high street beauty salons is clearly influencing consumer choice.
Buyer beware
The report suggests that the consumer, too, must have some responsibility to seek out practitioners of good reputation and ask questions about risk and aftercare.
There is evidence that those seeking cosmetic surgery are more likely to be guided by information they have sought and by personal recommendation and are thus perhaps more likely to make balanced judgements.
But consumers for nonsurgical treatment see cosmetic intervention as simply an extension of a beauty and wellness regime and, in practice, research into the options in this market rarely happens.
The Nuffield Council for Bioethics publishes guidance on all aspects of cosmetic treatment, including controls on practitioners, treatments, premises, products, advertising and marketing and access to procedures.
This is beginning to gain traction in the industry. However, the report notes, it is astonishing that currently there are no statutory controls over access to cosmetic procedures by young people, even though age related controls do exist for tattooing and sunbeds.
Equally, there is no requirement for practitioners to undertake an assessment of the motivations for treatment, which would quickly identify those clients coping with the increasingly common problem of body dysmorphia.
Shifting drivers for demand
Interestingly, the report identified a shift in the underlying drivers of consumer demand as potential patients looked to ‘polish and perfect’ rather than ‘rectify problems’.
This was particularly the case for non surgical interventions, reinforcing the normalisation of nonsurgical intervention as part of an overall health, beauty and wellness regime.
The report also noted a split in consumer behaviour, with the older demographic more likely to undertake substantial research into individual hospitals and clinicians, while younger consumers often wanted to organise treatment as soon as possible.
This split offers an opportunity for providers to ensure their published information meets the needs and expectations of potential clients.
Social media, the Instagram generation and pressures within society to achieve a ‘look’ are frequently cited as influencing factors, particularly among the younger demographic. This group is looking for instant improvement, not longterm rejuvenation.
The reverse is true of the older age group, who take a longerterm view of cosmetic surgery as part of a wider wellbeing mindset.
This demographic is also likely to be repeat clients for hospitals and surgeons and is more likely to want to develop a longer term clinical relationship, with perhaps more invasive surgical interventions interspersed with nonsurgical enhancements. This demographic is also less likely to be driven by treatment price.
New research reveals patterns of consumer behaviour
One of the key features of the report is the new research undertaken to understand how, when and where potential patients are seeking information on the top ten cosmetic procedures.
For example, around 76% of searches for information on breast enlargement were carried out using a mobile phone: the advent of the smartphone has clearly been a gamechanger in terms of how consumers search for and access cosmetic surgery and nonsurgical treatments.
The research also shows the geographic spread across the UK of searches and the times of year people are most likely to be seeking information – invaluable for clinics and surgeons to tailor their
marketing and promotional activities.
Future view
Looking ahead, the overall surgical market is expected to remain fairly static, although the picture could vary significantly between different procedures and different geographies, with demand for popular procedures such as breast augmentation likely to increase and areas such as London and the Northwest continuing to be cosmetic surgery hotspots.
The report predicts that the biggest changes are likely to be in the nonsurgical market, where laser techniques are rapidly evolving and becoming common, even in a small clinic setting.
The concept of non surgical treatment being seen very much as part of a normal beauty and wellness regime is also likely to drive increased activity.
Greater oversight
Self regulation and greater oversight are beginning to have an impact and the Department of Health has confirmed it is reviewing the current market.
Prospects for cosmetic surgery are dependent on consumer economic confidence and confidence in cosmetic treatments, and currently there are vulnerabilities to both these factors.
Future economic prosperity in the UK remains uncertain. And while confidence in cosmetic surgery treatments has been improving since demand took a knock from the PIP scandal several years ago, this market may be impacted by the popularity of and increasing variety in nonsurgical cosmetics.
The report concludes, however, that while interest in nonsurgical solutions is likely to remain high, outcomes delivered by surgical procedures will still be a cornerstone of the market and important in patient decisionmaking.
Visit www.laingbuisson.com/shop/ cosmetic-surgery-uk-market-report/ to see the report’s contents pages
Liz Heath (right) is a consultant with LaingBuisson and author of the cosmetic report
GOVERNANCE OF PRIVATE DOCTORS
Single point of control
Coming your way in 2020 – the Medical Practitioners Assurance Framework. David Hare (right) tells more about plans to unify diverse systems of reporting
AS INDEPENDENT Practitioner
Today reported last month, we at the Independent Healthcare Providers Network (IHPN) are progressing a major package of work to improve the independent sector’s consistency in safety and medical governance.
Indeed, with 1.9m acute patient journeys and rising across the independent sector every year, it is vital that both providers and clinicians are working together to do all they can to ensure patients receive the safest, highest quality of care and to drive forward continuous improvement.
As part of this work, we asked former NHS England national medical director Sir Bruce Keogh to support us in designing a framework that would aid improvement and consistency in medical governance in the independent sector.
The Care Quality Commission (CQC) believes this is a key area for improvement and the forthcoming Paterson Inquiry is likely to raise issues around how medical practitioners work with independent healthcare providers and how performance and scope of practice can be more effectively monitored.
Expected practice
Our Medical Practitioners Assurance Framework (MPAF) launched after almost a year of consultation with independent sector providers, royal colleges, the Federation of Independent Practitioner Organisations and the Indepen dent Doctors Federation.
It identifies expected practice across several key areas including: clinical governance structures; patient safety, clinical quality and continuous improvement; supporting annual wholepractice appraisal; and raising and responding to concerns from staff and patients.
It sets out a clear view of how providers and medical practitioners can work together to improve the assurance around clinicians working in both the NHS and independent sectors
The launch of the framework was our top story in November
information about the practice of medical practitioners working in the sector.
The system will set out the principles of what/when and with whom information is shared, with a key aim being to reduce the burden on practitioners in reporting different information sets to multiple organisations, a complaint we hear often in discussions with consultants.
CQC backing
IHPN is, of course, not a regulator and while adherence to the MPAF is not mandatory, we are pleased that all our acute hospital members and many other service providers have signed up to implement its principles.
Critically, it sets out a clear view of how providers and medical practitioners can work together to improve the assurance around clinicians working in both the NHS and independent sectors.
Most providers already have robust clinical governance structures in place, so we are clear that the framework is not about reinventing the wheel, but about codifying systems already in place.
The MPAF takes a principlesbased approach to medical governance, avoiding creating any new bureaucracy or making the system more complicated.
Medical advisory committees
For example, on the role of medical advisory committees (MACs), we make clear that these can provide organisations with a vital resource around medical advice on professional and clinical issues.
However, their constitution and functions vary in different organisations, sometimes creating a lack of clarity around expectations from both independent providers and committee members.
The framework therefore makes
clear that the role of MACs – or equivalent body – in clinical medical practitioners’ governance should be clearly defined and understood by the independent provider, committee members and doctors practising in the organisation.
In particular, if the committee is to have a role in advising the independent provider on the granting, extension, renewal and suspension or restrictions of practising privileges, this should be transparent and conflicts of interest clearly declared and managed.
Share information
The framework also contains a longerterm, and arguably transformational, aspiration around developing a single reliable and definitive view of any given doctor’s scope of practice, activity, outcomes and performance.
In the absence of any current system around this, IHPN and its members are overseeing the development of a secure system for use by independent providers – and other stakeholders, such as NHS Responsible Officers – to share
We are working closely with the CQC. It has committed to considering the effective and robust implementation of the framework’s principles as evidence of good governance, which will inform judgements it makes about how wellled a service is.
The framework is also designed to be iterative with an inbuilt review process and should be viewed as a starting point for the sector to build on.
There have been significant changes in the healthcare system and regulation over the last few years and it is a real achievement that in just the last year the proportion of independent acute hospitals rated good or outstanding has risen from 70% to 77%.
But there is always more to do and we believe the MPAF can play a critical role in helping providers and practitioners work together to raise the bar in medical leadership across the independent sector so that all patients can be confident of receiving the safe, highquality care they deserve.
David Hare is IHPN’s chief executive
SUBSCRIBE TODAY TO GET EVERY ISSUE IN 2020 AND READ US ONLINE
Dear Reader,
Subscribing to Independent Practitioner Today is the only way you can be sure you will see every issue and have the option of reading us online using our special page-turnable edition. Don’t risk missing out. Our personal subscription for doctors and managers is only £90 a year and £210 for organisations. But you can cut this to just £75 and £180 respectively if you pay by direct debit.
So take advantage of this offer now for our unique business journal dedicated to supporting you in your private practice. We’re confident your subscription will repay itself many times over!
Editorial director
APPLICATION FOR SUBSCRIPTION
Instructions to your Bank or Building Society to pay Direct Debits
Name and full address of your bank/Building Society
To: The Manager Bank/Building Society
Address
Banks and Building Societies may not accept Direct Debit instructions for some types of account
Building Society. Please also send a copy of your letter to us.
ON TRIAL FOR MANSLAUGHTER
The inquest with a sting in the tail
Surgeon Mr David Sellu (right), convicted for gross negligence manslaughter of a patient – overturned on appeal after a 30-month prison sentence, continues his story from last month
The Clementine Churchill Hospital, June 2010
The internal investigation, conducted by the now defunct company Healthcare Performance Ltd, was asked by BMI’s group medical director Prof Duncan Empey to also investigate all my work over the previous years to see where I might have made mistakes.
Put any surgeon’s work under such close scrutiny and they will have cases that went badly – we are all human and we do not always make perfect decisions. And if I had mismanaged patients, the matter should have been dealt with then and there, not years later.
The role of the hospital and any failings in its systems were unknown at this stage. As we found out later, these findings were suppressed throughout my subsequent case. And the training and qualification of the investigators to carry out such an inquiry were unknown and never questioned.
Hard-hitting criticisms
A critical report into my handling of the index case, referred to unofficially as the Empey report, followed but suppressed the Root Cause Analysis (RCA) carried out by the hospital’s own quality manager.
The RCA was frank and hardhitting in its criticism of many of the hospital’s procedures and personnel, including the nurses and the ITU outreach team. But this document only came to light after my incarceration, following Subject Access requests and from an investigation by the Mail on Sunday (reported on 26 July 2015).
It was not produced at the inquest, in contravention of a statutory requirement, and was not alluded to at my trial.
October 2010
I was summoned to the GMC –one of 12 times – where the prosecuting barrister read out the charges, taken almost verbatim from the Empey report. He did not then read the patient’s case notes to get more accurate and first-hand information of the events leading to my patient’s death.
Another failing was the lack of an emergency anaesthetic rota, something I argued was a necessity, without which a hospital could not be deemed compliant in its duty to implement an effective breakthrough procedure. I continued working at the Clementine Churchill Hospital until September 2010, when my practising privileges were suspended a month before the inquest.
He closed by saying: ‘We conclude by declaring that Mr Sellu’s treatment of patient JH fell below the standards expected of a consultant colorectal surgeon to a serious degree, particularly in regard to his operative care.’
I was in shock. I had never been criticised as a doctor. Over my career, I had always been praised as a caring surgeon, a skilled operator and a good teacher by those with whom I had worked.
Even the Empey report had not criticised my operative care; on the contrary, the way I performed the patient’s operation was declared faultless.
My barrister spoke for nearly an hour, saying I’d saved many lives, seen around 4,500 private patients at the Clementine and there had been no previous concerns or complaints either there or about my NHS practice in Ealing.
The panel concluded that, having heard all the evidence and weighing it up carefully, I had ‘no case to answer’ and ‘no conditions’ would be placed on my practice. They would review this after the following week’s inquest.
18 October 2010
I was due to give my inquest evidence on the third day according to the Coroner’s Office schedule. I planned to spend two days preparing. But after lunch on the first day the Coroner changed his mind about the order of proceedings. I was required to give evidence next.
I was not prepared for this. My barrister told me to give it my best. I came out in a cold sweat and my heart pounded. Shaking off a feeling of paralysis, I took the stand, where I was sworn in. Then commenced a series of quick-fire questions to which I hardly had time to give answers.
The coroner frequently interrupted me to ask questions before I had time to finish answering the previous one and I was then interrogated by the family’s barrister. During this, the coroner interrupted to ask for me to be taken out, as he needed to discuss a matter with counsel.
It was as if I’d told a patient who was suffering from cancer, whom I was about to operate on, to leave the consulting room so I could relay his diagnosis and treatment
to his family and to the people in the waiting room.
The next 40 minutes seemed like a lifetime. I was surprised when people I had seen in the courtroom now began to walk past me to the front door. They walked as close to the far wall as possible, as if trying to avoid me, turning to steal a brief look in my direction but avoiding making eye contact.
A senior manager from the Clementine Churchill Hospital walked past me with a mobile phone. I greeted her: ‘Hello…’, but she ignored me. What the hell is going on? I said to myself.
Crime committed
My barrister asked me to follow her into a small room. ‘I am afraid the inquest has been adjourned. The coroner is going to refer this case to the police, as he suspects a crime has been committed.’
‘What crime and by whom?’ I said, stunned. My mind went into overdrive. Was it the hospital? My mind flashed back to the lack of an anaesthetic rota and my inability to operate when the elective procedure being performed that evening overran.
Employing a single doctor to cover a busy hospital with over 100 patients and making him work seven days in a stretch. Was it the RMO? Was it the nurses?
I had become aware of the patient’s frustration to get the nurses and the RMO to understand his concerns and in desperation he had phoned his consultant’s secretary. Was it the anaesthetist, who had seen the patient and yet scheduled an elective operation before what was an emergency procedure for my patient?
Hang on. Was it me? ‘The allegation is manslaughter, against you,’ my barrister responded.
‘Surely I did not kill Mr Hughes,’ I protested.
‘I am afraid that is the law. The coroner is entitled to adjourn the inquest if he suspects a crime has been committed. You have not been charged . . .’, she paused, ‘yet.’
Adapted from Did He Save Lives?
A Surgeon’s Story, £9.99, Sweetcroft Publishing ISBN 9781912892327 from Amazon. His story continues in Independent Practitioner Today next month
Learn how to counter the
imitation game
computers using malicious software. This may not be due to a vulnerability in the computer system used by the practice, but often the fraudsters hack into systems of others that the practice communicates with via email, thus enabling the fraudsters to organise a very convincing attack.
The fraudulent email, when it’s received, will be made to look like it’s been sent by the genuine supplier or practice manager.
It may even come from their email account if they’ve been hacked and the content of the email will look genuine, containing previous email exchanges and attachments.
It will often be timed so that it falls in line with expected payment dates. Everything could look genuine apart from the account number which will be altered to a fraudulent one.
Are they really who they say they are? Impersonation frauds are targeting medical practices. Vin Pandha (right) continues her series on fighting fraud in the medical sector, explaining what to watch out for and what you can do
IMPERSONATION FRAUD techniques are used by criminals attempting to trick private doctors’ practices and surgeries into making payments to fraudulent accounts.
Let’s look at the methods of deception used, which can make these scams very convincing.
Impersonation fraud, as the name suggests, is where a fraudster impersonates a genuine person or business and makes a request for
their target victim to make a payment to what they do not realise is a fraudulent bank account.
Fraudsters will impersonate anyone whom they think staff within the practice will trust to be genuine.
From the practice manager to regular medical suppliers or government bodies, their aim is to make the payment request seem as genuine as possible so that funds are sent without a second thought.
COMMON TYPES OF IMPERSONATION FRAUD
Business email compromise (BEC)
This is the method by which the vast majority of impersonation frauds occur. Fraudsters will usually prepare for this type of attack by monitoring existing genuine email traffic between medical practices and their suppliers, contractors and employees. They do this by hacking into
Of course, an email attack could also be supported by advance phone calls from the fraudster trying to gather important information from staff at the practice. Or they might set the scene for a fraudulent email by impersonating the supplier on the phone, saying to expect an email or otherwise priming staff for the email attack.
CEO fraud
This is called CEO because this is a fraud which impersonates a senior person within an organisation. This is a specific type of BEC which has been prevalent in recent times. Within the medical sector, this might be someone like a senior GP, the practice manager or a health trust finance director; anyone whom fraudsters think will fool staff into acting on a payment request believing it to be genuine.
The request will often state that
the payment needs to be made urgently and be labelled as strictly confidential and therefore not to be shared with any other staff due to the sensitivity of the transaction.
If the fraudster has done some research on the individual they are impersonating, they will likely send the request when the genuine person is not available due to holiday or meetings. Of course, this is all intended to deter the member of staff from questioning the payment or to rush things.
Invoice fraud
This refers to a fraudulent payment which a victim makes in the belief that it’s a payment being made to a usual or genuine beneficiary – one which the practice intended to pay.
However, in reality, the fraudsters have tricked a member of staff into making the payment to a fraudulent account number.
A common way in which this happens is where fraudsters
impersonate a supplier or contractor and provide fraudulent account details on an invoice or email communication.
If the accounts details are not checked before the invoice is paid, the funds will be lost.
Payroll fraud
This is a fraud which combines aspects of both CEO and invoice fraud; it is a fake request from a senior member of staff to change the account number for their next salary payment.
If the person responsible for payroll does not check whether the request is genuine, then the next salary payment is sent to the fraudulent account.
Other types of impersonation fraud include phishing (email) and vishing (voice phishing), which we’ve covered in more detail in last month’s article.
Vin Pandha is commercial fraud manager at Lloyds Banking Group
TOP TIPS TO ENABLE YOUR PRACTICE TO GUARD AGAINST IMPERSONATION FRAUD
Don’t rely on the email address appearing to be legitimate or the wording to be familiar when it comes to making payments. staff need to understand that email is not a secure method of communication
Don’t assume that because you’ve confirmed aspects of an email to be genuine previously, the recent bank account number or contact phone number supplied in that same email trail is also genuine.
Independently verify all requests to change bank account details or changes to contact details by calling on a number known to be correct for the genuine payment recipient.
Remember that emails can be intercepted between staff within your own practice. Checking new payment instructions or changes to account details received in internal emails can be just as important.
Have a robust policy in place for running software and operating system updates, avoiding unnecessary delays to minimise any time you are running out-of-date versions. Fraudsters often identify and target practices who are slow to act.
Undertake regular staff training on how to spot and prevent fraud scams, such as BEC, and consider running a phishing email simulation exercise to test their ability to detect and report suspicious emails.
Create a culture whereby staff feel comfortable reporting instances where they believe they may have clicked on a link or attachment in a rogue email. Urgent action taken in these circumstances can limit the extent of damage caused by malicious software.
INVESTING IN PROPERTY
Be a good landlord
Dr Lafina Diamandis continues her series for doctors investing in properties. This month: property management and landlord essentials
ONE ASPECT of property investment that puts some people off is the idea of being a landlord and having to manage issues like maintenance, repairs and tenant disputes.
This is a valid concern, but there are ways to address this. The first is to put measures in place, so your experience of being a landlord is as stress-free as possible.
There are five key areas to consider.
1 Get educated
Learning as much as you can about being a landlord and your responsibilities is imperative. Even if you’re a landlord already, I recommend the one-day landlord accreditation course run by the National Landlords Association (NLA).
It costs about £100 and is a great way of learning about the most important aspects of being a landlord and becoming an accredited landlord.
If you join the NLA – also approximately £100 per year – you can become an accredited landlord for free by completing their online
course modules at your own pace.
The NLA also runs other useful courses on subjects such as tenant eviction and portable appliance testing for landlords.
2
Outsource tasks you don’t want to do
Make a list of all the tasks you can think of pertaining to preparing, letting and managing your property.
Identifying those you can’t or don’t want to do means you can find ways to delegate and outsource them, if this is affordable, and avoid doing things you hate or are too time-consuming.
However, it’s always useful to do a task at least once, as it might give you valuable experience, particularly when it comes to training other staff members.
You can outsource anything these days, such as: putting furniture together, painting and decorating, cleaning, creating tenant adverts, doing viewings, processing credit and reference checks and much more.
Remember that the time you spend doing low-value activities
may come at the cost of missing out on high-value opportunities.
3
Focus on one strategy at a time, if possible
One benefit of focusing on just one or two strategies is the expertise you can quickly build up in that area and the economy of scale that comes with managing a portfolio of the same type of property.
By sticking to the same strategy, you can more easily and effectively source new properties of the same kind, find tenants, manage the property, fix maintenance issues and find staff who can easily work across different properties, for example.
This is true for any strategy, but particularly for houses in multiple occupation mortgages (HMOs), which generally require higher maintenance and resources, but, due to the strong cash flow, are considered higher reward and worthwhile.
4 Communication skills
Ensure that communication between yourself, the tenants and any others involved – for example,
property manager – is optimum from the start and is invaluable. This includes clearly communicating house rules or important parts of the rental agreement to the tenant from the start and ensuring important conversations – for example, about damage to the property or giving notice to terminate the contract – are documented.
Communication also ensures that everyone clearly understands the responsibilities of the tenant or landlord; for example, gardening costs.
Clear and regular communication can prevent problems arising throughout a tenancy or misunderstandings occurring.
5
Systemising and outsourcing your property business
Busy doctors are often time-poor, so it’s important to put in place some systems to ensure important things don’t get forgotten and you fulfil your obligations as a landlord.
This includes registering your tenant’s deposit in a timely man-
ner or returning it to them, paying utility bills, managing a broken boiler quickly or making plans for viewings when a tenant’s tenancy ends and they move out.
There are many ways to deal with this using landlord software with built in reminders, apps, virtual assistants and property managers to ensure your experience of being a landlord or managing your properties is smooth and straightforward.
Ensuring you set time aside each month to review your property or portfolio is a good way to stay on track.
Dr Lafina Diamandis is co-founder of Eurekadoc, a start-up helping doctors to realise their full potential through diverse medical education and careers curation and is passionate about helping doctors to become financially independent through property even with limited time, funds or experience
LETTING A PROPERTY – WHAT’S INVOLVED
Thinking about what is involved in your own property investment will help you identify any group tasks and create systems for those tasks. For example, the following are the different parts involved in letting a property:
PREPARATION FOR LETTING: Cleaning; furnishing; photography; agent valuations or price research; advertising.
FILLING PROPERTY: Finding tenants or a lettings agent; carrying out viewings; reference-checking tenants; signing rental agreements; collecting and transferring deposits and rent; doing tenant checkins or check-outs.
CLEANING AND MAINTENANCE: Cleaning, maintenance checks – for example, gutters or regular inspections every three to six months; problems and repairs troubleshooting; monitoring annual service dates for gas or electrical appliances.
FINANCES: Rent collection; payment of utilities and service charges; payment of other expenses – for example, insurance; maintenance; repairs; management; monitoring upcoming tenancy expiration dates and communicating with tenants.
You might be someone who really doesn’t want to deal with tenants. If so, fear not, as there are strategies you can use.
1
You could pay for your properties to be let and fully managed by agents, which puts tenants and management issues at arm’s length. Bear in mind you will still be contacted by agents about issues and any decisions regarding repairs.
2
You may enter into a joint venture project where your partner deals with all matters to do with tenants and maintenance while you take responsibility for some other aspect – for example, refurb or funding.
3
4
5
You could go into property development and build houses to be sold rather than rented.
You could source great property projects and sell them on to developers or investors for a fee.
Or, like one tech savvy doctor I know has done, you could set up an entire business to outsource every single task so that you only have to oversee the systems and staff managing the tasks.
Fiscal resolutions for a new decade
Setting the correct New Year’s resolutions for your business could ensure your practice is ready for the challenges a new decade may bring. Simon Brignall (below) suggests ten for independent practitioners to consider
A NEW YEAR, and especially one heralding a fresh decade, is a good time to reflect on oneself and what you have achieved as well as to introduce changes and set personal goals. Here are ten to follow:
1
I will review the way my work is being billed to ensure I am compliant with the rules and regulations communicated monthly from the Clinical Coding and Schedule Development group (CCSD). Keep abreast of the CCSD’s monthly changes and establish if they affect your specialty and possibly your income.
Practices commonly make billing errors through being unaware of the changes. Also establish what rules each insurer adopts, because they can choose their own variants.
2
I will ensure I regularly review my procedure fees.
This is important if you bill to insurance guidelines, because these constantly change and are not often communicated clearly. You could be charging less than you could or more than you should. Practices still make wrong assumptions, leading to issues with insurance companies or revenue losses.
3
I will make sure my work is invoiced as soon as possible.
Some major insurers now enforce time limits for submitting invoices and if you miss the deadline, they will not pay.
Late invoices are also poor service to patients and a major contributor to their dissatisfaction and bad debts. Knowledge of any shortfall is
delayed and patients assume the invoice has been settled, so there is then a bone of contention.
Late invoices sent direct to patients can be ignored if they think you are not serious about wanting payment.
4
I will make sure that my price structure/policy is clear and that my patients are made aware of it before commencing treatment. A clearly defined, well documented and communicated patient registration form is vital in the modern practice. It will ensure no room for ambiguity when it comes to settlement.
Fee and payment terms transparency is of paramount importance and also a key requirement of the Competition and Markets Authority (CMA).
5
I will ensure my practice has a robust process for chasing outstanding invoices on a consistent and continual basis until they are fully paid.
Failures in this important area mean continued high levels of bad debt. Almost every practice that joins Medical Billing and Collection (MBC) has an outstanding invoice backlog, with some going back years.
Debt levels are typically over 20% of turnover and sometimes have reached 50% of annual turnover. On average, we achieve bad debts of less than 0.5%. This is a huge difference.
6
I will make myself aware of any bad payers so I can decide if I want to continue seeing them while they have outstanding invoices. If you don’t do this, you will end up regularly throwing money away. Visibility around this key area means you can take steps to police this more effectively.
When we take on a backlog of outstanding invoices, there are often patients who have built up debt over years. Practices continued to see them despite never being paid.
7
I will ensure I have key management information on my practice to allow me to make informed decisions for the future. This vital area is mostly overlooked and can mean weekly losses. All practices should know where patients are being referred from, which insurers they are dealing with, how much income is self pay and the most common procedure codes carried out.
Consultants should know financially what is happening to revenue generated each month in their practice, the same for payments received and what is happening with outstanding invoices. Without this data, it is difficult to understand which direction your practice is going, as it is very easy to come to the wrong conclusions without real time accurate data.
At MBC, we provide all the above data online 24/7 to assist you in running your practice.
Take stock and consider what elements of your practice could be outsourced – enabling you to generate more revenue
8
I will make sure I spend as much time as possible focusing on my core skill set – treating and looking after the patient. Running a private practice is not easy and many tasks do not fall naturally into a consultant’s skill set.
If you and your secretary focus on the medical side of the practice, this will, in turn, make you more money, because you are focused on what you do best rather than spending time on tasks that can be delegated.
Take stock and consider what elements of your practice could be outsourced – enabling you to generate more revenue.
9
I will ensure I have a robust secure IT infrastructure in place to deal with my practice’s administration.
This can be a common weakness in many practices and is often only highlighted when it’s too late.
Enjoy the peace of mind that your business is on a secure platform and your data cannot be lost. A wide range of options can facilitate this, so it should not be difficult to implement.
10 I will consider whether I should join thousands of other doctors who have outsourced this crucial element to a professional billing company. For most consultants, the billing and collection is very difficult to manage and when done wrongly it often results in consistent financial losses.
Outsourcing could be the best decision you make this year to guarantee your practice is futureproofed for what lies ahead.
Simon Brignall is director of business development at Medical Billing and Collection
PROBLEMS WITH THE TAX MAN?
HMRC tax investigations and disputes create difficult and stressful times.
As an award winning firm of tax experts, our highly experienced partners specialise in resolving problems relating to tax investigations and disputes with HMRC.
To find out, in confidence, how we can help call 0800 734 3333.
‘Here to help. Not to judge.’
KEEP IT LEGAL
What has whistleblowing got to do with doctors working in private practice? Isn’t that an issue relating to doctors in employment only? The recent employment tribunal case of Shoukrey v BMI Healthcare Limited shows this is not the case, warns Paul Spencer (right)
Protection for whistleblowing
MR MAMDOUH Shoukrey is a consultant surgeon and he is employed by Dorset County Hospital NHS Foundation Trust. He also worked at BMI Healthcare Limited, where he had admitting rights. He raised a complaint in a report to the Care Quality Commission against a well established colleague concerning an operation the colleague performed on a private patient of Mr Shoukrey at BMI Healthcare Ltd without notifying Mr Shoukrey.
Mr Shoukrey considered that the procedure employed by his colleague was unsafe and that his actions in operating without telling Mr Shoukrey were unprofessional.
This report became a substantial dispute between Mr Shoukrey and his colleague. The colleague complained about Mr Shoukrey and, as a result, BMI Healthcare withdrew his admitting rights.
Mr Shoukrey was successful in his claim against BMI Healthcare and the employment tribunal was satisfied that he had been subjected to detriments because of his whistleblowing, and the detri
ments included the decision to suspend him, ignoring his legitimate concerns and withdrawing his practising privileges.
Although the practising privileges were later restored, Mr Shoukrey subsequently resigned in response to the way in which he had been treated by BMI Healthcare.
Substantial compensation
As this was a long running case, only the remedy decision – relating to the award of compensation – is available online and not the decision where BMI Healthcare were found liable and the basis for that.
The tribunal awarded substantial compensation to Mr Shoukrey – £920,302 – albeit not as much as claimed, which was in excess of £3.2m.
Contrary to expectations, there is no single or consistent definition of ‘employee’ or ‘worker’
This means a doctor in private practice should have the same level of protection if he or she whistleblows about standards in a private hospital as they have if concerns are raised about treatment in the NHS which applies across UK employment legislation.
‘Workers’ are protected by whistleblowing legislation. A person who makes ‘a protected disclosure’ – the technical name for whistleblowing – may not be dismissed or subjected to a detriment because of the fact he or she has made a protected disclosure.
A worker who has been treated in this way may pursue a claim in the employment tribunal and there is
no limit to the amount of compensation that may be awarded, unlike unfair dismissal claims.
So, how does the granting of admitting rights bring a doctor within the scope of whistleblowing protection?
The definition of worker includes an individual who works under a contract whereby the individual undertakes to do or perform personally any work or services for another party to the contract.
That other party must not be a client or customer of the individual’s business. The contract may be express or implied and – if it is express – whether oral or in writing.
It seems clear that the employment tribunal has accepted that the relationship between a doctor and a private hospital which grants admitting rights meets this definition.
Crucially, this means that a doctor in private practice should have the same level of protection if he
or she whistleblows about standards in a private hospital as they have if concerns are raised about treatment in the NHS.
Nevertheless, what should be a straightforward area of law to encourage best practice is notoriously complex and contains many loopholes.
It is recommended that advice is sought before taking action if there is any uncertainty.
There are a number of charities which offer guidance to whistleblowers such as Protect, formerly Public Concern at Work. They can be contacted via https://protectadvice.org.uk/contactus/.
Read the full Employment Tribunal judgment, published on 20 June 2019, here: www.gov.uk/ employmenttribunaldecisions/ m shoukrey v bmi healthcareltd14015052015
Paul Spencer is Hempsons employment partner
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes’ of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment Premises
Regulatory requirements and investigations
Michael Rourke
Tania Francis m.rourke@hempsons.co.uk t.francis@hempsons.co.uk
Stiff competition lies in the cities
Private patient revenue growth for 13 NHS acute trusts across the county of Yorkshire is put under the spotlight here by Philip Housden (right)
THE FIGURES used here are from the most recently published 201819 annual accounts. However, two trusts, Mid Yorkshire and Sheffield Children’s, had not published private patient revenues at the time of writing and so the 2017-18 figures have been used.
For this group of trusts, the data reveals that total private patient
revenues fell back in 2018-19 after a year of growth in 2017-18.
Below average
Total revenues are estimated at £13.8m, down approximately 6% from £14.7m last year. This level of income represents 0.25% (down from 0.27%) of these trusts’ total revenues. This remains below the
combined national average outside of London of 0.5%.
These 13 acute trusts vary significantly by private patient revenues. For the following analysis, they have been grouped together, where relevant, according to whether they have a dedicated private patient unit (PPU) or not and present turnover.
➱ p38
Total revenues are estimated at £13.8m, down approximately 6% from £14.7m last year
TAX-SAVING EXPERTS
Having served healthcare professionals since its inception in 1993, Tax-Link, chartered tax advisers and accountants in Wimbledon, has built a wealth of knowledge and experience in dealing with taxation issues faced by doctors in private practice. Our focus is on tax planning and compliance.
l Tax structuring to suit personal circumstances (LLP, limited companies)
l Solvent liquidations
l Consultant groups and consortia
l Assessment of pension contributions in light of tapering annual allowances
l Ad hoc assistance with HMRC investigations and reviews.
more information and tax-efficient advice, please:
020 8540 1920
rakesh@tax-link.com
The
Figure 3
The regional top earner remains Leeds Teaching Hospital Trust at £4.9m, but this fell £950,000 (16.2%) last year from £5.85m. This is a reduction from 0.57% to 0.45% of trust revenues.
Leeds holds a partnership with Nova Healthcare, part of Aspen Healthcare, located within St James’s Institute of Oncology in the Leeds Cancer Centre in Bexley Wing.
The service offers the full range of cancer treatment including radiotherapy, gamma knife and robotic surgery and chemotherapy. There is also access to private beds within the Bexley Wing for patients requiring inpatient admission.
Sheffield hospitals
Sheffield Teaching Trust has no specific private patient services, but instead offers a range of treatments privately across its five hospitals.
Incomes have fallen back after a period of growth, dropping £403,000 or 12.9% last year at 0.29% of turnover, down from 0.35%.
Also in Sheffield is the specialist Children’s Hospital Trust, one of only four such specialist trusts in the NHS – the others being Great Ormond Street, Birmingham Children’s and Alder Hey.
The trust has a private patients business manager and work is underway to think through the opportunities for developing overseas markets, to grow the last
reported private patient revenues of £165,000, which are only 0.1% of turnover.
Harrogate and York, by contrast, both have private patient units and are in relative regional hot spots for private medical insurance take-up. Both are reporting growth.
Harrogate’s ten-bed Harlow Suite is branded the Harrogate Harlow Private Healthcare Service and delivered growth of 2.3% last year to £1,470k.
The unit has access to dedicated space within endoscopy in addition to the ward. Harrogate achieves 0.66% of trust turnover as private income, the highest in the region, and the only one in Yorkshire ahead of the out-of-London national average.
York hospitals
York Hospitals offers private patient services at York, Bridlington and at Scarborough. These are for a range of surgical, ambulatory and diagnostic services.
The group service is not collectively branded and this could be an opportunity to develop another local ‘chain’ approach.
Revenues were up 3.4% in 201819 to just over £1m for the first time for five years, now reaching 0.23% of turnover.
A third trust increasing private activity is Airedale. Airedale Hospital similarly has a PPU, with Ward 19 having 11 bedrooms and two private consulting rooms. Last
year, the trust grew £35,000 and 21% from £166,000 to £210,000 private patient revenues at 0.12% of total trust incomes.
Bradford also has an inpatient PPU, having invested in recent years in refurbishing the 12-bed The York Suite located on Level 4 of the Duke of York Wing at the Bradford Royal Infirmary.
This offers a range of medical care and surgical interventions from outpatient consultations, diagnostic scanning, minor daycase treatments to complex surgery.
The trust reported a disappointing 21% drop in private patient incomes from £768,000 to £604,000, which is now the fifth consecutive year of decline from a high point from £1.34m in 201314.
Of the remaining trusts, these can be split into two groups, none of which have a dedicated private patient ward. The first comprises Calderdale, Doncaster and Hull, each of which has a material private patient revenue stream but, as yet, without inpatient facilities.
Significant mover
Calderdale and Huddersfield is a significant mover with an increase in 2018-19 of £479,000 and 74% to £1.1m.
Over the past two years, the trust has more than doubled revenues and taken income from 0.15% to 0.34% of trust revenues.
Doncaster has remained static in 2018-19 at £848,000 and 0.24% of
The regional top earner remains Leeds Teaching Hospital Trust at £4.9m, but this fell £950,000 (16.2%) last year from £5.85m
turnover and Hull grew 19% to £682,000 from £574,000. In all three trusts, these results have been achieved without dedicated private patient facilities.
The final group has very little private patient incomes and apparently little appetite to offer private services.
Mid Yorkshire, Rotherham and Barnsley together reported well under £100,000 private patient revenues with no change year on year.
Across the Yorkshire region, there is no single discernible trend with regards to private patient revenues. However, some themes may be emerging.
The trusts in the biggest cities of Leeds and Sheffield must compete with the largest private hospitals, which have significant infrastructure and protected capacity. Here the independent sector appears to be taking market share.
In smaller markets, such as Calderdale, Harrogate, Hull, York and Airedale, where there is higher than average insurance and/or self-pay take-up and smaller independent hospitals, the NHS is developing brands that are growing the market and/or taking share.
Future reviews will examine these themes further to identify any wider trends.
Next month: North-west PPUs
Philip Housden is a director of Housden Group
BUSINESS DILEMMAS
27-30 January 2020
• Hands-on workshops
• Multidisciplinary lectures
• Satellite and joint sessions
• Bedside ultrasound course
• Contribution from allied specialities
•
Indemnity on the run
Am I covered? It’s a question doctors often phone their defence bodies about. Dr Ellie Mein (right) answers a private consultant’s query
Dilemma 1 Am I insured for volunteer work?
QOutside of my work as an independent consultant, I enjoy running and have done marathons and half-marathons as a member of my local running club.
Every year, there is a marathon hosted in my home city and this year I have been asked if I would like to volunteer to provide med-
ical support on the day of the event. I would like to help but am unsure if I am indemnified for this type of work?
AAs the GMC states, ‘you must make sure you have adequate insurance or indemnity cover so that your patients will not be disadvantaged’ ( Good medical practice: paragraph 63, 2013) when taking on additional clinical responsibilities, regardless of whether these are voluntary or paid.
Additionally, in its document on
Before agreeing to provide assistance, it is important to check whether or not the event organisers will be providing indemnity for doctors acting in a professional capacity
Getting consent to treat a child
Insurance, indemnity and medicolegal support, the GMC advises doctors who wish to volunteer to provide medical assistance at an event.
‘Good neighbour acts include helping out, in your professional capacity, at a local sports club or similar planned voluntary work.
‘You are providing professional medical services whether they are paid or unpaid. If adequate and appropriate insurance or indemnity cover is not given by the organisation for which you are providing this service, you must make your own arrangements to cover yourself.’
Appropriate skills
Before agreeing to provide assistance, it is important to check whether or not the event organisers will be providing indemnity for doctors acting in a professional capacity. If they don’t have any arrangements in place, then you must contact your medical defence organisation to see if your current indemnity will cover you for the voluntary work you would like to undertake.
If your indemnity enables you to volunteer, it is important you consider whether you have the appropriate skills and experience, before accepting. Do not practise outside of your area of expertise.
In Good Medical Practice , the GMC states that ‘you must recognise and work within the limits of your competence’. (GMC, Good Medical Practice : paragraph 14, 2013).
As with all the care you provide, you should keep detailed records. It is also important to make sure that you have adequate equipment and support to perform your duties.
Dr Ellie Mein is a medico-legal adviser for the MDU
Consent for treating a minor is the substance of a private GP’s inquiry. Dr Ellie Mein gives her view
Dilemma 2
How do I ensure I have consent?
QI recently saw a young child who had attended my practice along with their stepfather. The child was epileptic and her stepfather wanted to discuss her regular medication. The mother had died and the stepfather, who had been married to the child’s mother, had been caring for the girl since her death.
The child was not Gillick competent and her biological father had been estranged from the family for many years. However, during the consultation, it emerged that the stepfather did not have parental responsibility for the child.
How can I ensure that I have the appropriate consent for the continuing treatment of this child in the absence of an individual with parental responsi bility?
AIn the short-term, if urgent treatment was needed, you should do what is considered to be in the best interests of the child. However, for non-urgent treat ment, you would need the consent of one person with parental responsibility to treat the child. In time, you will need to estab
lish who has parental responsibility, as the biological father of the child may have parental responsibility.
The stepfather may be able to acquire parental responsibility for the child either through an agreement with the biological father or through the courts.
If the biological father retains parental responsibility, he could also authorise the stepfather to attend any appointments with the child in his place.
However, this may not be con -
sidered sufficient if any contentious or important issues arose that required parental consent.
It may also be appropriate to refer the family to social services, with the stepfather’s consent, to help him sort out the issue of parental responsibility.
This may also provide the family with some additional support during a difficult time, given that the stepfather is dealing on his own with a young child with long-term health needs, as well as dealing with his wife’s death.
PRACTISING PRIVILEGES NOW AVAILABLE
Check with family when passing on
Can you talk to loved ones about wealth? Dr Benjamin Holdsworth (above) shows why inheritance planning is about more than just tax
SUCCESSFUL PROFESSIONALS
like doctors are often fully aware of the need to consider how best to pass on their wealth to future generations.
You may have already made detailed plans to transfer assets by setting up tools such as trusts, partnerships or charitable donations.
Yet, many financial planners have seen that wealth transition can fail – not because of poor planning, but poor communication with loved ones.
Often the head of the family will have paid attention to the logistics of preparing assets to be passed down, but spent little time preparing heirs for their future inheritance.
Family members can be illequipped to shoulder new-found responsibility and surprise postdeath gestures can generate negative standpoints based on a lack of trust.
Ingrained beliefs
Money remains a difficult subject to broach – particularly in Britain – as there is a sense of secrecy and people can be influenced by experiences and beliefs that may have been ingrained since childhood.
Some of the trickiest conversations can be between generations, where there can be widely different understandings of the value of money and how it should be spent.
Yet, without clear discussion on the current position and future progression of wealth within the family, estate-holders are simply storing up trouble for the next generation to discover after their death.
At this time, those who have inherited wealth may be too emotional to contemplate significant life decisions.
Consider how you might pass on a family business. Your heirs would expect to be well prepared to move into the organisation and the chances of failure would be high without such education. There is little difference when inheriting other assets.
Inheritance problems will be
exasperated in the coming years. Research by the Centre for Economics and Business Research estimates that ‘intergenerational financial transfers’ worth in the region of £5.5trillion will occur in the UK over the next 30 years.
Wealthiest generation
It is the ‘Baby Boomers’ – often cited as the wealthiest generation with final-salary pension schemes and property value success behind them – who are now planning how best to help the next generation.
According to the Office for National Statistics, 20% of over-65s in the UK are millionaires compared with just 7% a decade ago.
Individuals over 65 are the age group to have experienced the greatest increase in their household wealth in the last ten years with a rise of 96% – ten times the increase enjoyed by those aged between 25-54.
Individuals aged between 35 and
44, known as ‘generation X’, watched their proportion of UK household wealth fall by 5% in the same period. Millennials, aged between 25 and 34, faced a 2% fall.
If it is the younger generation most in need of financial support, they cannot afford for inheritance transfers to be poorly handled.
With life expectancy rising, we might spend three decades in retirement. This means that the transfer of wealth might not happen until beneficiaries are in their 50s and 60s.
This may not be the ideal time to receive inheritance, but, understandably, people can be unwilling to give away money or assets they might still need.
However, with careful consideration, there should be sufficient funds to enjoy the type of retirement you had envisaged while ensuring you can help your children and grandchildren at the same time.
And you may also discover that you can help them with key milestones now, when you are still around to see them enjoy it.
You may be concerned that children could become negatively affected by the idea that there is wealth in place and therefore little need to work hard to achieve it.
Discuss intentions
Worse still is the notion that the family’s assets will be squandered once received. Nevertheless, these scenarios can only be improved by educating future generations and establishing clear lines of communication to discuss possible intentions and likely outcomes.
We have helped hundreds of medical families to see the value in having a structured review of each person’s assets. In doing so, and in being as honest as you can be with each other, we can normally create a clear path ahead which allows the older generation to continue to
live their life to the full while younger members get the kickstart they need.
Talking about inheritance is your first step to helping your offspring and acting sooner rather than later can pay dividends.
Dr Benjamin Holdsworth is director of Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS.
The content of this article is for information only and must not be considered as financial advice.
Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
CALCULATE YOUR NHS ANNUAL ALLOWANCE
DOCTOR ON THE ROAD: RANGE ROVER EVOQUE
Standing out in a crowded market
The second-generation Range Rover Evoque grabs the premium SUV top spot for Dr Tony Rimmer (right) on the drive to his medical school reunion
I HAVE MENTIONED before how important the image and reputation of a clinic or, indeed, an individual practitioner can be for the continuing success of the business.
This reputation must to be nurtured so that any new developments keep to established high standards.
This holds true for the successful car brands too. There are few car makers as successful as Jaguar Land Rover and its premium brand Range Rover. When the smaller Evoque was revealed as a concept vehicle in 2008, it received such interest it was given the go-ahead for production and went on sale in 2011.
This stylish compact SUV was launched to huge fanfare and celebrity endorsements followed; notably by Victoria Beckham.
This, I am sure, has contributed to a general impression that the Evoque has been more popular with female owners. Certainly, its styling was more important than functionality. The rear seating was a bit tight and the hatched boot space was not generous.
So now, after eight years, we have the second-generation Evoque. It
RANGE ROVER EVOQUE
p200 se r-dynamic
Body: Five-seat SUV
Engine: 2.0 litre four-cylinder petrol
Power: 200bhp
Torque: 320Nm
Top speed: 134mph
Acceleration: 0-60mph in 8.0 seconds
WLTP combined economy: 28.6–30.7mpg
CO2 emissions: 176g/km
On-the-road price: £44,100
enters a marketplace that has caught up very quickly and there are excellent rivals out there such as the Audi Q3, the BMW X1 and Volvo’s brilliant XC40. Can the new Evoque regain ground and still retain its individual style?
Well, my test car was a petrolpowered P200 SE R-Dynamic model with all-wheel drive and a nine-speed automatic gearbox. At £44,100 before options, it is right in the middle of the range and represents the best compromise of equipment and value.
Totally new
Although the looks have been retained, particularly at the front, the car is totally new. The floor pan is designed to take electric-hybrid and even full electric powertrains in the future.
There are six engine options. Three are from a 2.0 litre four-cylinder petrol unit producing 200, 250 or 300bhp, depending on the state of tune. Another three are from a 2.0 litre diesel unit with 150, 180 or 240bhp output. Trim options range from the base model through S, SE and
HSE. All are available with the R-Dynamic upgrade, which gains some cabin extras and some neat external styling features in satin and copper finish. These improve the appearance of what should be a car of special style.
Energy from braking
Standard on all models is a smart 48-volt mild-hybrid system. This stores energy from braking and can redeploy it briefly on hard acceleration. Also standard is a ten-inch infotainment screen, rear parking camera and digital driver’s dials on SE models and above. A clever option is the ClearSight interior rear-view mirror which can give a wide rear camera’s view of following traffic.
Externally, the new car’s proportions are, to my eyes, much better balanced and I love the new ‘Teslamimicking’ retracting door handles. Inside, the new Evoque feels right up to date.
The clear digital dials and central infotainment screen work as well as in any competitor and Apple Play/Android Auto is now standard. The interior is crisp and
cleanly designed and the dashboard materials feel of high quality. Thanks to a longer wheelbase, rear passengers have a much roomier cabin and the boot is also significantly bigger.
All passengers are treated well on the move, too. The Evoque is a quiet and refined cruiser. The ride, although a bit firm at low speeds, does a good job of controlling body roll and allies with the reasonably direct steering to provide some zest for the keen driver behind the wheel.
Although the 200bhp petrol engine of my test car was quiet and smooth, I would have preferred more power. The engine doesn’t struggle, but it is obviously working hard to travel at a decent pace.
The nine-speed, automatic gearbox also seems to be spoiled for choice with so many ratios to choose from and can be slow to respond.
Over the course of a few hundred miles to attend my medical school reunion, the Evoque grew on me. It also impressed my medical colleagues who enjoyed the ride.
It was going to take a lot to challenge the impressive Volvo XC40 as the compact premium SUV to beat, but I think that the new Evoque might have done it.
The only concern I have is for JLR itself. The Range Rover Velar is an almost identical but slightly bigger product and the Jaguar E-Pace and Land Rover Discovery Sport compete directly in the same sector. There are only so many buyers out there for this type of car.
That is good for us medic buyers, though. You might be able to assess and compare all of them in a single showroom. It is worth keeping an eye out for the new Evoque.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
Thanks to a longer wheelbase, passengers have a much roomier cabin and the boot is bigger
A PRIVATE PRACTICE – Our series for doctors embarking on the independent journey
Visions for new financial
THE NEW YEAR can be viewed as a fresh start to look at your business even if you are not at your normal financial year-end.
Give your private practice 20-20 vision with a new year, new decade financial review, says Ian Tongue (right)
Periodic review of your circumstances is the best way to ensure you are optimised for tax and managing taxation around your pension, which has become a particularly difficult aspect of a doctor’s financial affairs. Here are some of the common areas that you should be considering.
Trading structure
Usually, the most effective change to your tax burden is to consider your trading structure, particularly
if you have a large self-employed private practice.
Your individual circumstances are important, as one-size-fits-all planning doesn’t work for doctors. The key variables to determine the optimum structure are going to be your spouse’s financial circumstances and whether you need all the money generated from your private practice at this point or whether you could live with accessing it later on.
It is common to start off with one type of structure and change this later, as your private practice and circumstances evolve. Historically, it was common to
year
start your private practice as a selfemployed individual and, as it grew, consider either a limited company or partnership with your spouse later on.
With the pension annual allowance charge affecting almost all doctors who are working for the NHS and are active members of the pension scheme, these choices are often made earlier nowadays.
Limited company
For most, the limited company structure for trading is the preferred option, as it provides more flexibility and, where a spouse can be involved, can derive significant
tax savings even with a modest private practice due to the pension annual allowance charge.
As always, your individual circumstances will determine your best trading structure, so speak with your accountant to ensure you are best placed for the year ahead.
Pension annual allowance
The pension annual allowance charge has caught many doctors off guard, particularly those with small or no private practice who didn’t think it applied to them. Not so!
The standard allowance for pension saving is £40,000, but for those earning over £110,000 from all sources, this allowance may be less, possibly as low as £10,000.
The temptation can often be to look at how much your pension contributions are and conclude that you are within the limits.
But a very important part of the calculations is that your actual contributions are set aside and it is your actual pension growth that is relevant.
Calculating the growth can be difficult and confusing and your accountant or independent financial adviser are best placed to help you manage your individual position. For those who want to obtain an indication of their position, you can use tools such as www. nhsannualallowance.co.uk to assist.
Ultimately, you need professional help managing your pension annual allowance position and it has become almost essential to have a specialist medical accountant.
While a general accountant should understand the concept of the annual allowance charge, few understand the nuances of what factors affect pension growth and can proactively help you manage and mitigate your annual allowance charges.
Due to the mechanics of the pension annual allowance charge calculations, it can be a disincentive to work and this has resulted in waiting lists getting ever longer.
NHS Pensions and the Government are starting to listen (see page 3) and, at the time of writing, more flexible pension options and the abolishment of annual allowance tapering are being considered.
It is the latter that would be the solution to not penalising doctors for working harder with this very unfair and ill thought-out tax charge.
If you have not had an annual allowance review, the New Year is prime time to address this to avoid any nasty surprises later on.
Personal circumstances
Over your career life cycle, you will go through various stages where your financial circumstances change. In the early years with marriage and a family, your ability to generate income is often the key factor and, later on, generating wealth for retirement becomes the focus.
The best strategies ultimately involve the two from the outset and this is where a good independent financial adviser (IFA) comes in.
Some people may have been burnt in the past with financial advisers, as it used to be a market with less financial regulation. But in order to best manage your affairs, having an IFA that you know and trust should be seen as an essential part of the process.
If you do not have one or have not had a review for some time, get in touch with them for a pension and general review.
If you do not have an IFA or yours is not a medical specialist, ask your accountant for a recommendation, as no doubt they will work with a number of trusted IFAs.
Expansion
Despite the pension annual allowance, most consultants still want their private practices to grow, albeit with less exposure to the annual allowance charge.
It is common for doctors to want to try and do too much themselves and there comes a point where the extra time spent dealing with the admin around your practice is best spent earning more money and employing someone to do the admin.
Larger private practices have secretaries and other employees to help run the business. Depending on the role, it may be that you need to employ that person and this will lead to maintaining a PAYE payroll scheme.
Your accountant will no doubt have a department that can offer this service. For those that engage
Your individual circumstances are important, as one-size-fits-all planning doesn’t work for doctors
self-employed secretaries, review the position annually to see if this status is still appropriate, because the tax status of an individual may change. The individual cannot simply choose to be self-employed.
Accounting systems
A new year can be a good time to review your accounting systems well in advance of the new tax year commencing on 6 April 2020.
Significant change is proposed in the coming years in relation to reporting your tax information to HM Revenue and Customs (HMRC) and this is known as Making Tax Digital.
The process requires more frequent reporting to HMRC and the system is already in place for VATregistered businesses.
While many will not be affected just yet, it is important that any decisions on your practice management or accounting software are made with one eye on the changes ahead to avoid disruption and surprises later on.
Speak to your software provider and accountant to understand whether you are on track to be compliant when the new regime becomes mandatory for almost all self-employed individuals and companies.
Treating the new calendar year as a time to reflect and consider your circumstances will almost certainly bring financial benefits for the year ahead. Working closely with your medical accountant and IFA will ensure you are set up efficiently for tax and your wealth generation strategy for the future is on track.
Next issue: A detailed look at trading structures
Ian Tongue is a partner with Sandison Easson accountants
Discuss end-of-life care in advance
How patients’ wishes can be respected and upheld when the patient is no longer able to communicate their preferences is explained by Dr Ellie Mein
OFTEN, IT can often be difficult to broach the subject of end-of-life care with a patient who has a lifelimiting or terminal illness.
Patients may want to discuss the progress of their condition and the limits of available treatments.
But even if they don’t raise the subject, if the patient’s condition makes it likely that they could lose consciousness or mental capacity, then it makes sense to gently initiate a conversation.
This can be as part of a wider discussion about their wishes regarding future care, so they have time to make an informed advanced decision about their treatment.
These conversations can be challenging, but it is a good opportunity to talk about the realities of end-of-life care and find out what the patient wants.
When it comes to invasive lifesustaining treatment such as cardio pulmonary resuscitation (CPR), this can make the difference between a dignified death and one which is traumatic for the patient and their family.
Quite often, the decision not to carry out CPR – known as a DNACPR order – are made after the patient has been admitted to hospital.
However, the GMC states in its Treatment and care towards the end of life: good practice in decision making : ‘If a patient has an existing condition that makes cardiac or respiratory arrest likely, establishing a management plan in advance will help to ensure that
the patient’s wishes and preferences about treatment can be taken into account and that, if appropriate, a DNACPR (do not attempt CPR) decision is made and recorded.’
Risks of CPR
The risks associated with CPR interventions should be communicated during your conversation with the patient. The question of whether these risks would outweigh the benefits of CPR should also be discussed at this time.
This can be very upsetting and doctors should respect the wishes of patients who do not want to know details about their condition or treatment while making it clear that they can change their mind at any time.
If a patient decides they do not want to receive CPR, document this and seek their consent to share this information with those
close to them to support their continued treatment and care.
However, some patients will want CPR, even if it has a small chance of success. In these cases, the GMC says ‘you should make sure that they have accurate information about the nature of possible CPR interventions [and] should explore the reasons for their request and try to reach agreement.
‘When the benefits, burdens and risks are finely balanced, the patient’s request will usually be the deciding factor. If, after discussion, you still consider that CPR would not be clinically appropriate, you are not obliged to agree to attempt it in the circumstances envisaged.
‘You should explain your reasons and any other options that may be available to the patient, including seeking a second opinion.’
Making an advance decision
An advance decision is when an individual with capacity who is 18 years old or over can refuse specific medical treatment for a time in the future when they lack capacity. Advance decisions are provided for on a statutory basis by the Mental Capacity Act 2005.
An advance decision can be made either in writing or verbally. However, if it relates to the refusal of life-sustaining treatment, the decision needs to be in writing, signed and witnessed.
While there is no specific
requirement to discuss an advance decision with a healthcare professional, if a patient does ask for help it is important to be satisfied they have capacity and understand the limitations of any decision they make.
Such limitations may include where treating clinicians, in an emergency, may be unaware of the advance decision and provide treatment which they see to be in the patient’s best interest.
Alternatively, an advance decision would become invalid if the patient later appointed a power of attorney to decide on their behalf.
Most importantly, while clinicians are legally bound to respect valid advance decisions to refuse treatment, patients have no legal right to demand specific treatment.
And as with CPR, clinicians are not obliged to provide treatment that is thought to be futile or not of overall benefit to the patient.
Remember, if you are asked to discuss or witness a written advance decision, ensure you keep a record of the advance decision or a record of the discussion in the patient’s notes.
It is important to encourage the patient to carry the decision with them in the event of an emergency and tell family members or close friends so they can inform healthcare professionals if they are admitted to hospital.
Dr Ellie Mein is a medico-legal adviser at the Medical Defence Union
Costs take the shine off
Despite a drop in indemnity charges due to increased competition, ophthalmologists’ 6.6% rise in costs has dented their profits, as Ray Stanbridge’s analysis shows
HEADLINE FIGURES show that average gross income has risen by 5.3% between 2017 and 2018, from £132,000 to £139,000.
Costs have increased sharply by 6.6%, from £57,000 to £61,000. As a result, taxable profits have increased by 4% from £75,000 to £78,000 with a slight fall in margins from 56.8% to 56%.
What are the reasons then for the changes between 2017 and 2018? Income has risen and it seems to a large extent that this has been through Choose and Book work –on average – rather than any growth in self-pay or insured work.
The lack of growth in self-pay work in this period is a little surprising, considering the growth elsewhere in the medical sector.
Large cost rises Costs have shown quite a large increase over the year in a number of areas.
There has been a slight increase in the costs of medical assistants over the year. Staff costs have also risen a little. This is often the function of adjusting family salaries to changes in the tax-free personal allowance and, in a number of cases, this is what has happened.
AVERAGE INCOME AND EXPENDITURE OF A CONSULTANT OPHTHALMOLOGIST WITH AN ESTABLISHED PRIVATE PRACTICE
There has been a slight increase in the costs of medical assistants over the year. Staff costs have also risen a little
There have been small falls in the cost of room hire. Some consultants have negotiated better deals, based on volume, with the hospitals, which are still compliant with Competition and Markets Authority rulings.
Professional indemnity costs have also fallen slightly and this, almost certainly, is a function of increased competition in the market.
We still do not know if the new insurers are offering full retrospective cover. Time will tell.
Use of home and office costs have risen slightly, primarily the result of inflationary pressures. Similarly, accounting/legal costs have been subject to inflationary pressures.
Other costs have broadly remained the same.
What then of the future?
As we have recorded in previous articles, the Choose and Book market is highly volatile and, for a number of ophthalmologists, particularly in the country, it is a case of feast or famine.
We would have expected to see greater growth in self-pay than we have done, and hopefully this will materialise in 2019-20. Preliminary reviews for this year suggest that there may be some growth here.
Year ending 5 April. Figures rounded to nearest £1,000 (percentage is also
OPHTHALMOLOGISTS
Costs have shown some readjustment and we would not expect to see any large growth in 2019-20. All in all, it is a case of ‘steady as she goes’.
As established readers will know,
our survey is not statistically significant; rather, it is an attempt to measure what is actually happening in the private ophthalmology market in the UK.
We have commented in previous
services on the difficulties of effecting consistent and fair comparisons on a year-on-year basis.
Consultants now trade in a variety of ways; for example, limited liability partnerships and companies, which complicates the collection of data. In many areas, Choose and Book – at lower real margins – is a very important, though volatile, source of income.
Having made the necessary caveats, our survey has been conducted on the same basis as in the past. Consultants included in our survey are those who:
Are not in full-time private practice;
Have at least five years of private practice experience;
Are seriously interested in pri
vate practice as a business;
Earn at least £5,000 gross in the private sector;
May or may not be a member of a group or have incorporated.
Next issue: Gynaecologists
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists, Stanbridge Associates Limited
HOW ARE YOU DOING?
Use
benchmarks to compare your financial performance with others
Urologists
Years ending 5 April
HAVE A 20-20 VISION FOR YOUR PRACTICE
Subscribing for just £75 direct debit to Independent Practitioner Today – and it’s tax deductible! – will keep you abreast of all the big private practice changes affecting you in 2020 and help the business side of your practice to stay ahead of the curve. See subscription information below. Coming in our February issue, published on 13 February:
Setting up a private GP practice has been the most rewarding time since Dr Sibel Peck qualified. ‘I have been able to enjoy a good work-life balance. I have been able to offer clinical care that is patient-centred. I have been able to assert more of my ideas when it comes to our business development.’ Read her story
How practices are targeted with fraud by their own employees! We look at the methods used to obtain the practice’s money. Plus essential prevention tips
When planning a website, it can be easy to overlook whether it is compliant with data protection regulations. In fact, it is often an afterthought once the site is up and running or not considered at all. A key consideration for all website owners is their cookie policy. Karen Heaton and Jane Braithwaite give their advice
Expert witness work – it should be for trainee doctors too, claims a consultant psychiatrist
Growth and goodwill – specialist medical accountant Susan Hutter on selling and buying a practice
INDEPENDENT PRACTITIONER
TELL US YOUR NEWS
Robin Stride, editorial director
Email: robin@ip-today.co.uk
Phone: 07909 997340
Published by The Independent Practitioner Ltd. Independent Practitioner
Today is editorially independent and thanks Bupa for its assistance with distribution. Printed by Pepper Communications Ltd Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Registered office: 7 Lindum Terrace, Lincoln LN2 5RP
Write to Independent Practitioner Today PO Box 198, Cranleigh GU6 9BB
Are you considering taking on staff? Should you opt for a freelancer or offer an employment contract? Julia Gray addresses the most common questions about employment status, with particular focus on the risks and benefits of self-employment.
‘Up like a rocket, down like a stick!’ is a commonly-used expression in the investment industry. Cavendish Medical’s Dr Benjamin Holdsworth explains why taking a more pragmatic approach will lead to a better investment experience
Our unique income analysis feature, Profits Focus, examines the accounts of gynaecologists
Private consultants in the North-west – check out what is happening to private patient units in your area
Key person dependency – it’s a big risk to many practices, warns Medical Billing and Collection’s Simon Brignall
Our ‘Start A Private Practice’ series presents a detailed look at trading structures
Electrifying? Our Doctor On The Road Dr Tony Rimmer gets to grips with the Tesla Model 3
The pains and pitfalls of property investing and how to avoid them
PLUS – our news pages are your eyes and ears, bringing you more on the new decade’s big issues affecting you and your business
ADVERTISERS: The deadline for booking adverts in our February issue is 17 January
ADVERTISE WITH US
Margaret Floate, advertising manager Email: margifloate@btinternet.com Phone: 01483 824094
GET A SUBSCRIPTION DISCOUNT! £90 independent practitioners. £90 GPs and practice managers (private & NHS). £210 organisations. Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE – USE SUBSCRIPTION FORM ON PAGE 25 or EMAIL: karen@marketingcentre.co.uk or phone 01752 312140 or go to the ‘Subscribe’ page of our website www. independent-practitioner-today.co.uk
Publisher Gillian Nineham
Phone: 07767 353897. Email: gill@ip-today.co.uk
SAVE £15 WITH DIRECT DEBIT!
Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left. BACK ISSUES: £12.50 including post & packaging
Giving voice to the private sector
INDEPENDENT PRACTITIONER
Thanks to Healthcode for helping us to reduce the use of plastic
The new president of the Independent Doctors Federation, private GP Dr Neil Haughton, reveals his plans and hopes for the organisation in the years ahead n See page 18
business journal for doctors in private practice
Make access to self-pay easy
The private healthcare sector needs to do much more to make it easier for patients to access. And clearing up price confusion would be a good place to start, argues Keith Pollard n See page 21
What are you doing to attract patients
ADDRESS LABEL
Jane Braithwaite shows you how to choose the right marketing strategy to attract new patients and grow your practice
n See page 26
If undelivered, please return to: The Marketing Centre, 12 Mary Seacole Road, The Millfields, Plymouth, PL1 3JY
What are you doing sector
Integrated online solutions on one platform built to give customers time efficiency, compliance, robust data security and ability to connect seamlessly
Your financial and practice management on one secure platform
Improve:
• cash flow
• operational efficiency
Peace of mind knowing:
• your data is held securely and backed up
• your data is hosted in the UK
• no additional back office costs
A cost-effective integrated toolkit on one platform that:
• is scalable
return to: The Marketing Centre, 12 Mary Seacole Road, The Millfields, Plymouth, PL1 3JY
• includes key tools to manage both your financial and administrative tasks and processes
• allows you to manage your practice bookings for one or multiple locations
• maintains and manages your patient records and their associated transactions
• gives you the ability to communicate securely with other organisations such as hospitals and insurers
For more information and a demo of the system: ( 01784 263 150