The business journal for doctors in private practice
In this issue
Relieve stress: live with it
Tips for managing stress on the job – without trying to eradicate it P20
The diary of a clinic build
Developing your own premises requires putting on a hard hat P34
Don’t think you can skimp on cover
A legal look at what you need to know about medical indemnity and insurance P40
Tax drive to hit doctors
By Robin Stride
Moves to improve tax compliance could backfire and lead to some doctors cutting their commitment to the private sector, specialist medical accountants warn.
HM Revenue and Customs (HMRC) has announced:
➲ A tightening up of compliance issues for ‘wealthy individuals’. Accountants say most consultants would be regarded as wealthy in the taxman’s eyes;
➲ The introduction of new technology to tackle the ‘hidden economy’ – such as a few consultants who accept cash;
➲ An increasing attack on tax avoidance schemes. HMRC believes doctors and dentists are serial users of these;
➲ New measures from April 2019 to quickly recover tax through PAYE.
‘Hidden print’ in last Autumn’s Budget suggests further trouble for private consultants and GPs who have been less than meticulous with their tax affairs.
But Ray Stanbridge, of Stanbridge Accountants, said: ‘The measures increasingly reflect HMRC’s views that the medical sector is a ripe apple to be squeezed harder and harder. Obviously, in some cases, the proposals are fully justified.
‘However, the vast majority of consultants are honest with
respect to their tax affairs. If such honest consultants are squeezed too hard and unfairly, they respond by withdrawing their labour and increasing their leisure time. The natural result is that there is less tax take – the complete opposite of what was intended.’
He said HMRC’s plan next year to be able to recover tax through PAYE might mean consultants would not be able to plan their monthly net pay if they owed tax. ‘At the very least, this could lead to some individual discomfort.’
The Government is investing a further £155m in additional resources and new technology for HMRC.
The tax authority said this was forecast to help bring in £2.3bn of additional tax revenues by allowing it to:
Transform its approach to tackling the hidden economy through new technology;
Further tackle those who are engaging in marketed tax avoidance schemes;
Enhance efforts to tackle the enablers of tax fraud and hold intermediaries accountable for the services it provides using the Corporate Criminal Offence;
Increase its ability to tackle noncompliance among midsize businesses and wealthy individuals;
Recover greater amounts of tax debt including through a new taskforce to specifically tackle tax debts more than nine months old.
David Redfern, of DSR Tax Claims, said: ‘Although it is important that HMRC is able to collect the tax revenue that they are owed, these new powers have the capacity to throw the finances of hard working taxpayers into chaos.’
HMRC must currently wait until the end of a tax year to recoup any shortfall in tax revenue from any individual taxpayer and is also required to write to inform the taxpayer that their tax code will change due to this underpayment.
He said if new powers gave it the right to deduct extra tax immediately from taxpayers’ salaries if it believed there was an underpayment of tax, then this could lead to taxpayers not knowing how much to expect in their salary each month.
Added Mr Redferm: ‘These new powers will cause major problems for taxpayers, who won’t be able to plan and budget ahead because they will be at the mercy of HMRC.
He doubted tax overpayments would be refunded as efficiently and hoped ‘good sense will prevail at HMRC’ and that the move will be delayed until its full consequences to the taxpayer had been assessed.
ONE OF A KIND: The first private hospital of its type in the UK has opened for business. Read the full story on page 8
get your skates on With the deadline nearing for filing your tax return, we give a few timely tips P14
Full steam ahead for PPUs 2018 is a great time for the nHS to invest in private patient units, an expert says P25
don’t risk your reputation advice on avoiding unforeseen mishaps that can attract the Gmc’s attention P28
when winding down your work plan for retirement by looking to dispose of notes and hand over patients’ care P38
Know your bias when investing your brain could stop you being a good investor. a look at behavioural finance P44
Suspicion of abuse business dilemmas looks at doctors’ ethical duties to domestic violence victims P46
editorial comment
Probe to have big fall-out
As the horrendous detail of the case of rogue surgeon Ian Paterson unfolded, it became clear that a much wider investigation was inevitable.
That is now about to get underway and the only surprise to us is that the Department of Health did not announce it earlier.
The independent nonstatutory inquiry, examining the circumstances and practices of this breast surgeon sentenced in August to 20 years in prison (see story on page 3), begins this New Year and could go on for a year and a half.
It is not expected to report until the summer of 2019 and,
as we went to press, independent practitioners and private hospitals were still awaiting the terms of reference.
We also wait to see how the inquiry, chaired by The Right Revd Graham James, Lord Bishop of Norwich, will be conducted and the extent of the areas it will delve into.
With the inquiry looking at the lessons that can be learned from the case, and how these can improve care, doctors and hospitals can expect no stone to be left unturned.
What emerges is likely to have some big implications for both parties.
tell US yoUr newS Editorial director Robin Stride at robin@ip-today.co.uk
University doctors face pension cut
By edie Bourne
Medical academics who are members of the Universities Superannuation Scheme (USS) are facing considerable changes to their pension following proposals to close the defined benefit section.
Universities UK, which represents 350 university employers, has announced plans to change the scheme to become a full defined contribution fund in a bid to close the reported £13bn fund deficit.
Patrick Convey, technical director of specialist financial planners Cavendish Medical, explained: ‘Consultants who have an academic element to their work and are part of the USS pension scheme could see their estimated annual pension income fall, as well as their pension contributions increase.
‘Employers and members have
been warned they might need to increase contributions by up to 7% to maintain their current benefits.’
The University and College Union (UCU), the trade union for higher education staff, points to actuarial research which suggests that even lecturers who started working in 2007 and have ten years of service will lose out on £131,000, a loss of £6,100 annually. Most academic doctors are much older, so have more to lose.
The research also notes that lecturers would be £385,000 worse off than if they worked in post1992 universities, where pensions are paid by the Teachers’ Pension Scheme rather than USS.
Changes to the scheme were first recommended by employers Universities UK in autumn 2014. The UCU is conducting a ballot to determine whether its members should take industrial action. This will close on 19 January 2018.
Check finances after Budget, doctors told
Private doctors are being advised to check their financial plans are still on the right path in the wake of the autumn’s Budget.
But excess pension savings above this can give a 55% tax charge.
Mr Convey said it was a ‘welcome reprieve’ from the predicted cuts to pension tax relief.
Phone: 07909 997340 @robinstride
to advertiSe Contact advertising manager Margaret Floate at margifloate@btinternet.com Phone: 01483 824094 to SUBScriBe lisa@marketingcentre.co.uk Phone 01752 312140
Publisher: Gillian Nineham at gill@ip-today.co.uk Phone: 07767 353897
Head of design: Jonathan Anstee chief sub-editor: Vincent Dawe Circulation figures verified by the Audit Bureau of Circulations
Cavendish Medical director Patrick Convey said they should enure that they were using all available allowances to minimise tax and would not be penalised for excess pensions’ savings because of their NHS membership.
Good news is that the pensions lifetime allowance, governing the amount which can be saved into a pension while still qualifying for tax relief, rises from £1m to £1.03m in April.
The abolition of Stamp Duty for firsttime buyers purchasing properties worth up to £300,000 is welcome news for parents helping offspring, but Cavendish warned that those buying jointly with their children will be excluded. This highlighted the need for careful planning.
See our round-up of Budget news on page 10
Outcome website ‘a big opportunity’
By robin Stride
An independent doctors’ leader has commended a new online portal as ‘a superb opportunity’ for consultants to showcase their clinical expertise and excellence.
Independent Doctors Federation (IDF) president Dr Brian O’Connor praised the Private Healthcare Information Network (PHIN) for its work providing data about consultant activities and outcomes.
Hundreds of specialists have so far been invited to view their clinical practice data on the secure portal, ordered by the Competition and Markets Authority (CMA) following its lengthy inquiry into private healthcare.
PHIN must publish hospital specialist activities including volumes of procedures, average lengths of hospital stays, infection rates, readmission rates, revision surgery rates, mortality rates and unplanned patient transfers.
It will also show patient feedback and satisfaction, measurement of health improvement
outcomes, frequency of adverse events, and any possible relevant information from clinical registries and audits.
PHIN chief executive Matt James said there had been ‘positive’ comments from over 100 consultants who had viewed their data reports so far and they were using the feedback mechanism to help hospitals improve data quality.
He told Independent Practitioner Today: ‘While some teething issues are inevitable, we are rapidly applying fixes to improve speed and usability.’
Dr O’Connor added: ‘Obviously, the initial data gathered by PHIN
Portal.phin.org.uk provides data about consultants’ activities and outcomes
will have certain flaws and omissions. By the very nature of this new undertaking, the information gathered by hospital providers may not be a true reflection of doctors’ practices.
‘We in the IDF are very happy to work closely with PHIN to encourage our doctors to engage in this process to ensure that the PHIN portal for consultant activity is indeed a true reflection of the activities of doctors within a hospital.’
Most of the data will relate to consultants performing surgery and other procedures where outcomes are very readily measured.
Dr O’Connor said more sophisticated and mature analysis of
data would evolve and there would be better methods of capturing data on patient outcomes, satisfaction and measured improvement in health.
‘The medical profession should be greatly encouraged by this change to a transparent and open declaration of activities and we in the IDF, in conjunction with PHIN and the Federation of Ind ependent Practitioner Organisations of which we are part, will work closely with all stakeholders to ensure that the excellent care delivered in the private sector is available for access to patients.’
PHIN’s portal gives consultants a unique view of their whole practice, private and NHS, and allows them to check data ahead of any information being published. It encouraged all consultants working in private healthcare to log in, check and work with their hospitals to ensure data was complete and correct before publication.
Paterson probe to be wide-reaching
The private healthcare sector has welcomed the widening of a scrutiny into the circumstances and practices surrounding the malpractice of consultant breast surgeon Ian Paterson.
An independent nonstatutory inquiry for the Department of Health is expected to examine a wide range of issues in private care including doctors’ defence cover, providers’ insurers, responsibility for the quality of care, appraisal and ensuring validation of staff.
The scrutiny will also study safety of multidisciplinary working, information sharing, reporting of activity, and raising
concerns between the independent sector and the NHS.
Another aspect will be how data about the scope and volume of work carried out by doctors is shared with the sector.
Health Minister Philip Dunne said: ‘Ian Paterson’s malpractice sent shockwaves across the health system due to the seriousness and extent of his crimes, and I am determined to make sure lessons are learnt from this so that it never happens again in the independent sector or the NHS.’
The Association of Independent Healthcare Organisations said it looked forward to making a constructive contribution to the
inquiry. But chief executive Fiona Booth added: ‘The failings of an individual rogue surgeon such as Ian Paterson do not represent the high quality and compassionate care delivered day in and day out by the multidisciplinary teams working in both independent sector or the NHS.’
The Private Healthcare Information Network said: ‘Informationsharing, activity reporting and raising concerns in the independent sector have been cited as areas of concern in relation to the Ian Paterson case, and we welcome their inclusion as key aspects of the inquiry.
‘Almost all patients in England
who receive some privately funded treatment are also NHS patients for many other elements of their healthcare, and many thousands of consultants practise in both the NHS and private sectors.
‘It is essential that standards are aligned and information effectively shared for the protection of future patients.’
Mr Paterson, who was employed by the Heart of England NHS Trust and had practising privileges at Spire Parkway and Spire Little Aston, was found guilty in April of 17 counts of wounding patients with intent. His 15year sentence was upped in August to 20 years.
dr Brian o’connor, idF president
Eye doctors unite in Harley Street
By Edie Bourne
Arnott Eye Associates has relocated its 22a Harley Street business around the corner to the first floor of Optegra Eye Hospital London at 25 Queen Anne Street.
Director Mr Richard Packard said he chose this new home because he wanted the business to practise in a new, fully equipped facility and develop its compre
hensive ophthalmology services for current and future patients in the UK and abroad.
Around a dozen consultants have transferred to the new premises with a team of orthoptists, optometrists and staff.
The move could now bring new opportunities for other ophthalmologists, according to Optegra managing director Rory Passmore.
The arrangement brings a ready
made referral stream from Arnott, where specialists provided consultation and diagnosis.
Optegra said investing in consultation and diagnostic activity allowed it to broaden the spec
trum of services it provides to patients from its central London base.
It said it wanted to build strong and long lasting relationships with the best ophthalmologists in
THE STORY BEHINd ARNOTT EYE ASSOCIATES
Eric Arnott (1929-2011) was an original pioneer of the ‘no-stitch’ or small incision surgery techniques used to restore loss of vision due to cataracts. He was also instrumental in lens replacement vision correction being developed and recognised across the UK.
Early in his career, he identified that lens implantation was the way forward and brought the technique to Europe. He went on to design many lens implants that have restored sight to millions of people.
In 1969, he met Charles Kelman, an American ophthalmic surgeon who had recently developed phaco-emulsification, a technique which uses ultrasonic waves, making it possible to remove cataracts through a tiny 3mm incision, doing away with the need for stitches.
In 1970, Arnott invited Kelman to make a
presentation at a meeting of the Ophthalmologic Society of the United Kingdom, of which he was secretary, and the following year he became the first non-American physician to take the ‘phaco’ course which Kelman had established in New York.
On returning to the UK, he raised the money to buy the expensive equipment needed and, later the same year, he performed the first phaco-emulsification procedure outside the US, at London’s Charing Cross Hospital.
The new technique encountered strong opposition from old-school ophthalmic surgeons, so, in 1974, Arnott organised the first ‘live’ Ophthalmic Micro-Surgical Symposium, where ten of the world’s top eye surgeons performed surgery. It was relayed live to more than 300 international delegates by the BBC.
the country, and the Arnott Eye reputation, medical and service qualities, was in keeping with this goal, as it was ‘renowned well beyond London and the UK’.
‘This configuration will allow consultants to further develop their practices, and expand the services that can be offered to their patients in fivestar facilities with leading edge technologies wholly dedicated to eye health.’
In 1981, with his senior registrar at Charing Cross, Mr Richard Packard, Arnott was the first to describe the use of a soft lens material which could be folded to go through an unopened phaco-emulsification incision.
Eventually, by showing the excellent results of modern phaco surgery, Arnott succeeded in overcoming resistance in the profession. Today almost all cataract surgery in the developed world is carried out using variations of the techniques which Arnott helped to pioneer.
Lens replacement – ClarivuTM at Optegra – is now a refined and well-regarded vision correction technique, allowing the patient to restore their vision and avoid the need for future cataract surgery by replacing their natural lens with a personally tailored, artificial lens.
Launch of drive to attract self-payers
Two major campaigns aimed at driving more self pay patients towards private healthcare are being launched by the organisation representing independent hospitals.
The Association of Independent Healthcare Organisations (AIHO) is looking at the selfpay market and how it can support its members in raising awareness of the option.
It is also running a patient choice/GP education programme to try and get greater support in
primary care for referrals to private specialists.
AIHO chief executive Fiona Booth said both campaigns aimed to result in sectorwide messaging to raise awareness of selfpay.
She asked members and representatives of other healthcare organisations in the private sector to remind themselves why patients chose to use independent providers.
‘We need to work collectively to protect and enhance our strengths, and band together to improve our
offering where it needs to be strengthened, always ensuring we provide the best level of service and patient outcomes.’
Speaking at a reception in London, she said it was vitally important for the sector to continue to tell the good news of its services, shorter waiting times, its capacity and its excellent standards of care.
Ms Booth added: ‘AIHO will continue to be a strong and effective voice for the sector, but I
implore all of us to continue working together to make sure our standards remain high.’
She urged providers to look for new ways to improve patient experience, work collaboratively to improve patient choice and information, and together provide an effective voice for the sector.
‘We need to demonstrate the value we add to the UK’s health sector and healthcare economy, and emphasise the importance of patient choice.’
Optegra chief Rory Passmore
By Charles King
Doctors’ private practices will be able to operate more effectively using an enhanced version of Healthcode’s online practice management and billing system ePractice manager.
Designers say it will be particularly beneficial for larger practices with multiple locations.
The specialists in IT systems for the private healthcare sector have introduced a host of new features after consulting with users, focusing on the diary and appointments module, document management and reporting.
New and improved features for ePractice manager users include the ability to:
Block time to show when specialists are unavailable or dealing
with administration, as well as clinics and consultations;
Record when patients have arrived for their appointment;
Email appointment confirmations to patients;
Create GP letters from a template which automatically includes GP details and a patient summary;
Personalise letters to patients efficiently with a feature which automatically completes designated fields with the correct patient name and appointment details;
Assign appointments to a cost centre within the organisation;
Record how patients heard about the practice to inform marketing;
Create additional management reports, including ones showing
invoices and aged debt analysis by cost centre.
As ePractice is an online service, ePractice manager subscribers will be able to access the new functions when they log onto Healthcode. They will not have to purchase a new version of the software.
Healthcode’s managing director
Peter Connor said: ‘We know that a growing proportion of Healthcode practices have several specialists who treat patients at multiple locations. The latest version of ePractice manager reflects this growing complexity.
‘As always, our aim is to help expanding practices provide the most efficient service for patients, operate costeffectively and adapt to the latest challenges in private healthcare.’
Leg ulcers are theme at veins conference Healthcode boosted Bupa starts cancer self-referral service
Bupa has launched the UK’s most comprehensive selfreferral cancer service – Cancer Direct Access.
Patients experiencing cancer symptoms need not wait for a GP referral but can call the insurer’s Cancer Direct Access team to have an appointment booked with a specialist consultant.
Bupa said its team of specialist advisers used the latest National Institute for Health and Care Excellence (NICE) guidance to establish whether a customer needed specialist referral.
The launch of Cancer Direct Access builds on the insurer’s direct access service for breast and bowel cancer. Most customers referred to a consultant under the scheme will be seen within a week and, if diagnosed with cancer, would begin their treatment within a month.
Bupa UK medical director Dr Steve Iley said: ‘Oneintwo people in the UK will be diagnosed with cancer during their lifetime, but the good news is that survival rates continue to improve.
‘Early cancer detection can have a significant impact on an individual’s chance of survival and reduces their need for complex and invasive treatment.
‘However, we know that diagnosis and treatment are often delayed as people can’t find the time to book a GP appointment, or worry about wasting the doctor’s time.
‘Cancer Direct Access removes the need for a GP referral and allows customers to access specialist diagnosis services in a way that is easy and convenient for them.
‘In some cases, it offers peace of mind and reassurance that an individual’s symptoms are not cancer or allows them to quickly access the appropriate medical support and treatment for their diagnosis.’
The Direct Access Cancer Service covers the following cases: bladder, breast, colorectal, endometrial, head and neck, lung, oesophageal, oral, pancreatic, renal, skin, stomach and testicular.
www.bupa.co.uk/direct-access
Seniors go extra mile as trainers
Senior doctors are going above and beyond the call of duty in the time they give to helping shape the careers of the next generation of consultants and GPs.
According to a new GMC report, the education and training for young doctors is too reliant on the goodwill and sacrifices made by senior colleagues who act as trainers.
The report, based on its annual survey answered by more than 75,000 doctors, reveals the pressures faced by consultants who provide junior training.
Doctors acting as trainers must try to fit their training roles around daily NHS duties and, in many cases, private work as either consultants or GPs. Nearly half told the GMC that, to do so, they must work beyond their rostered hours each week. Nearly a third do so daily.
Around one in three trainers report that their job plans do not allow them enough time to fulfil their trainer role.
Leg ulcers and pelvic congestion syndrome head the bill at the 2nd international veins meeting being held in London from 1416 March.
A spokesman said: ‘Whether you are new to phlebology or an experienced venous practitioner, there will be something educational for you at the meeting.’
It will be opened by Ellie Lindsay OBE, who set up the Lindsay Leg Clubs spreading through the UK and now abroad. However, these nurseled clinics currently do not look for, nor treat, curable venous leg ulcers due to superficial venous reflux –around half the total.
The meeting aims to provide ‘a perfect amalgamation of nurses and doctors working together to sort out which patients are curable and which need longterm care.’
Judy Holdstock, winner of the first prize at the American College of Phlebology for her work in pelvic venous duplex, will run courses on transvaginal venous duplex.
www.collegeofphlebology. com/meeting2018
GMC chief executive Charlie Massey said trainers were the backbone of medical education, but more needed doing to value them and to give them the support they need.
‘Employers must ensure trainers receive the resources and time they need to meet their education and training responsibilities. Job plans must include adequate provision for senior doctors to provide training.
‘Doctors in training are in a live learning environment, but for that to continue, it has to be made sustainable in the long term. It is not right that there is such a reliance on trainers always somehow finding the time, often their own time, to keep the system going.’
Yet despite the pressures, most doctors in training continue to rate the quality of their training highly. Just over 75% described the quality of teaching in their post as ‘good’ or ‘very good’.
Key findings from the report are available at www.gmcuk.org/keyfindings31410.asp.
By Robin Stride
Doctors who find they are suffering from working under increased pressure are being targeted for help in a new campaign run by a medical charity.
Doctors fail to seek help Medicine fades as a career of choice
According to a Royal Medical Benevolent Fund (RMBF) survey, there is still a stigma among doctors about asking for help and support.
Although more than half (55%) of those responding thought that doctors’ ‘personality type’ makes them particularly resilient when working under increasing pressure, 75% claimed there was a lack of sympathy within the medical profession for doctors seeking help for stress and mental health issues.
The RMBF believes this could be explained by a perceived ‘bravado culture’ among doctors, with 92% of those surveyed thinking that doctors place value on one another’s ability to work under pressure and cope with long hours without complaint.
Chief executive Steve Crone said many doctors felt unable to ask for help when things were not going well for them, either personally or professionally.
But he added: ‘The Royal Medical Benevolent Fund is here to offer confidential support and advice, so I really would urge anyone who needs help to come forward.’
A new RMBF campaign, ‘Together for Doctors’, is highlighting the need to offer vital support to medical professionals working under rising pressure and is urging any doctor in difficulty to reach out.
For help, ring 020 8540 9194 or email help@rmbf.org.
How to cope with burn-out, see page 20
HOW THE RMBF CAn
HELP
The RMBF website and its online resources, such as The Vital Signs, signpost an extensive list of specialist helplines, many of which are available around the clock, every day of the week. These include: BMA Counselling, Sick Doctors Trust, Cruse Bereavement Care and the Samaritans.
The RMBF’s own phone support operates during weekday working hours (9-5pm) and focuses on assisting prospective and existing beneficiaries through the application process for financial support.
It also signposts alternative sources of support for those it is unable to assist directly.
Twothirds of doctors would now not recommend medicine as a career to their children, according to a survey of senior hospital doctors, GPs and trainees.
Nine in ten of those polled by the Royal Medical Benevolent Fund (RMBF) thought UK hospital working conditions had deteriorated in the past decade and were concerned by the number of doctors leaving the profession.
They thought current NHS issues were having a detrimental effect on recruitment, and said hospital doctors were forced into uncomfortable decisions such as discharging patients early to free up beds.
The RMBF annually supports hundreds of doctors and their families who are struggling with financial concerns, ill health or addiction.
The charity also has a free down
loadable online guide for professionals, called The Vital Signs. Authored by Dr Richard Stevens, a coach with Thames Valley Professional Support Unit, the guide highlights key pressure trigger points for doctors and signposts organisations and support networks for those in need of help and advice.
The charity, which relies solely on voluntary donations, is also hoping the campaign will encourage doctors to fundraise for the RMBF and support their colleagues by organising a ‘hospital hopping’ fund raising walk or teaming up for a ‘wear green and purple’ day at work.
To help, visit www.rmbf.org/getinvolved/fundraising or text RMBF17 £5 to 70070 to donate.
1,845 doctors surveyed in July and August 2017 via Survey Monkey
When the team at Spire Bushey Hospital was looking for someone to open their new £11m diagnostic centre, they looked no further than one of their own ‘very satisfied’ patients.
June Thompson has been a regular visitor to the hospital and was treated at the new facility on the first day it was opened to the public.
She said: ‘There have been two
or three times when doctors here saved my husband’s life, so I have spent a fair amount of time at the main hospital.
‘Over the years, you get to know the consultants and nurses; it’s like a great big family – everyone is always so welcoming.’
The centre in Centennial Park, Elstree, Hertfordshire, includes 14 consulting suites and two treatment rooms.
The RMBF’s poster for a campaign offering help to stressed doctors
Blue ribbon event: Patient June Thompson, second right, with consultant dermatologist Dr Hady Bayoumi, hospital director Lisa Trybus and outpatient and cardiac manager Jay Buckley at the official opening
Insurance tax rise hurts
By Leslie Berry
Independent practitioners have lost nearly 200,000 potential patients in the past three years due to the rising taxes on health insurance.
This is the number of customers who have dropped their policies to depend solely on the NHS, according to the first research to assess the impact of insurance premium tax increases on the UK’s health and social care system. Insurance premium tax, added to many insurance policy premiums including private medical health insurance, has doubled since 2015 and currently stands at 12%.
The study was run by the Centre for Economics and Business Research (Cebr) and commissioned by Bupa. It found each percentage point tax increase led to an estimated 21,000 health insurance customers cancelling their policies. The tax avoided a further rise in the Autumn Budget after these figures were revealed.
Summit will unite medic investors and creators
The Paris region is pushing to be known as ‘the world capital of health innovation’.
To add weight to the claim, the Medicen Paris Region competitiveness cluster, the Paris Region and drug firm Sanofi are teaming up to launch MedXperience, which is being billed as the first international summit on the future of healthcare.
It will be held in the French capital on March 15 and 16.
The event aims to bring together doctors, health industries, startup companies, global investors and local stake holders to promote health innovation and its transformation into business processes,
Bupa warned that increasing insurance premium tax again could see even more people cancel their health insurance or reduce their level of cover.
It said this could lead to the unintended consequence that the revenue collected from health insurance fell and NHS demand rose.
The insurer warned the Government that the tax hit hardest on those who most needed it, because older patients with riskier health profiles paid higher premiums and more tax.
Another study last October found that twothirds of people consider health insurance allows others to access NHS treatment earlier and 55% see it as important in relieving NHS pressure. The online research was conducted by Opinium among a nationally representative sample of 2,000 UK adults.
Bupa Insurance chief executive Alex Perry said: ‘The taxes on health insurance are unfair and counterproductive. As insurance
medical practices and economic development.
Organisers said: ‘During two days, international participants will discuss their practices, achievements and ambitions in new therapies and innovative technologies in the healthcare industry.
‘MedXperience is an opportunity for startups and innovative companies to present their solutions to doctors, clinicians, researchers and investors and to meet experts, future partners and health professionals from around the world.
‘Doctors and organisations, both public and private, will discover innovations and their implementation as well as new tools to help them optimise their work.
‘Investors will be able to meet young start ups with proven experience and will be able to get involved in their development.’
Details available from www. medXperience.org
premium tax on health insurance has increased, we’ve seen hundreds of thousands of people who used to pay for their own health insurance drop out of the market to depend solely on the NHS.
‘This means longer waiting times for everyone else for treatments such as cancer care and cataracts, and even more pressure
on overstretched NHS finances.’
Bupa said cost was the main factor for people when choosing to buy health insurance and this explained the high attrition rates for individual policies as taxes have increased.
A third of people questioned in its survey would consider taking out insurance if costs were lower and a similar number would consider cancelling their policy if their premium went up.
Cebr chief economist Oliver Hogan said: ‘The impact of the tax has not been considered by the Government and we hope this research will make for interesting reading for the industry, the Government and the public.
‘As this is a tax that has increased successively over the last three years, and may increase further in the future, research into the financial implications for the NHS and the welfare impact on patients and society is needed.’
See ‘Bid to avert rise in insurance tax’, page 12
MP backs call to alter negligence system
An MP has urged the Government to continue to explore legal reform to tackle rising clinical negligence costs – the underlying problem behind doctors’ rocketing defence subscriptions.
Alex Chalk said those who suffer as a result of clinical negligence must be properly compensated, but affordability should also be considered.
He was speaking to MPs, peers and health leaders at a Parliamentary event organised by the Medical Protection Society (MPS).
TELL uS yOuR STORy
The MPS has put forward a package of legal reforms that it says could control spiralling costs and strike a balance between reasonable and affordable compensation.
These include the introduction of a limit on future care costs based on the realities of providing homebased care, and fixed recoverable costs to stop lawyers charging disproportionate legal fees. Defence bodies also want swift reform to how the discount rate is set to avoid further sudden shocks to the cost of compensation.
Share your experience of what has and has not worked in your private practice. Even if it’s bad news, let us know and we can spread the word to prevent other independent practitioners falling into the same pitfalls.
Contact editorial director Robin Stride at robin@ip-today.co.uk or phone him on 07909 997340
Alex Perry: said taxes on health insurance were counterproductive
First private unit of its kind opens
By Robin Stride
One Healthcare has opened a new 34-bed, private hospital with six operating theatres in Hatfield, Hertfordshire.
Billed as ‘the first private musculoskeletal-centric centre in the UK’, it follows the opening of the company’s first hospital, One Ashford, in Kent in April 2016.
Others are planned over the next few years in the M25 area.
Company founder and chief executive Adrian Stevensen told Independent Practitioner Today that the opening in late November was the culmination of years of engagement with consultants from a wide catchment area and representing a diversity of specialties.
They formed a steering group to work with the company on every aspect of the scheme including:
Optimum site location;
The range of specialties to be offered;
Functional content including the number and type of operating rooms and the design of patient pathways to improve care;
Key personnel to be employed and sitting on interviewing panels for them;
Advising on governance;
Networking with colleagues to create a peer group of leading consultants to act as ‘catalysts and enablers’ to build and sustain specialists’ interest in and commitment to the project.
Around 190 consultants, drawn from central London, Hertfordshire, Essex and Buckinghamshire, have practising privileges, but this is set to rise as Mr Stevensen said the company was ‘always looking for more’.
He said the hospital’s strategy had been led by musculoskeletal
(MSK) consultants and leading private medical insurers, who were keen that One Hatfield had this unique selling point and differentiated its services from traditional private hospitals.
Other specialties represented include anaesthetics and pain management, cardiology, ENT, general surgery, gynaecology, upper- and lower-GI, urology, pathology and radiology.
One Healthcare said its first hospital in Ashford, Kent, had established a strong local presence, was performing well and had been particularly successful in attracting self-pay patients.
Added Mr Stevensen: ‘We set out to change how private healthcare is delivered and to design modern, welcoming hospitals putting our clinical teams, patients and other customers –including medical insurers – at the heart of our plans.
‘We have embarked on a rapid development programme and have a number of schemes in our pipeline to follow Ashford and Hatfield.’
Plans were supported by the major private medical insurers, who shared the company’s vision for modern, safe and efficient private healthcare within the highest-quality surroundings.
One Healthcare said its centres would enable patients requiring elective surgery and diagnostics to access purpose-built, cost-effective and accessible care closer to home and remove the need to be referred to tertiary centres typically in major cities such as London.
This reduced costs and improved outcomes by applying rapid-recovery programmes to enable patients to minimise their time in hospital.
Each hospital is run as a separate local entity rather than adhering to a standard corporate template.
Consultant orthopaedic surgeon Mr Rajeev Sharma, One Hatfield director of consultant development, said: ‘From a consultant perspective, One Hatfield hospital is unique in the UK
regarding the way they prioritise the patient-physician relationship’.
He said the hospital’s Medical Society incorporated both consultants and GPs and introduced a formal governance structure which placed the views of physicians at the top of the management tree.
Mr Stevensen added: ‘The MSK market has grown consistently over recent years, yet private healthcare facilities have been slow to adapt. We believe that One Healthcare offers a new model of MSK-centric services which are attractive to consultants, patients and insurers.
‘The UK private medical insurers have been really supportive of our plans to change the dynamics of MSK delivery in what is the major sector of the UK market.’
Further centres around London and major commuter areas in south-east England will use a similar, MSK-centric template.
Above: One Hatfield’s management team, including chief executive Adrian Stevensen (left) and surgeon Mr Rajeev Sharma (second left)
The atrium of the One Hatfield Hospital, Hertfordshire
Incomes from NHS PPUs go up by 4.6%
By Philip Housden
NHS trusts again achieved record incomes from private patients, an analysis of recently published 2016-17 annual accounts shows.
There are some marked trends apparent from the data compiled by the Housden Group.
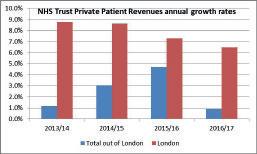
Total revenues were up £26m to a high of £594m for NHS trusts in England (£568m in 2015-16) – an increase of 4.6%.
This growth rate is marginally down on the 6-7% rate achieved in each of the previous four years.
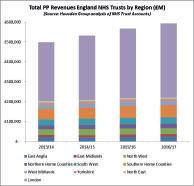
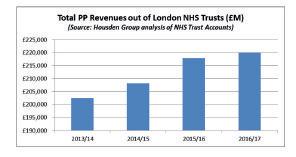
Revenues for trusts in London climbed to £373m, up from £349m the previous year. And this was the main engine of growth, with incomes out of London essentially flat at £220m, up £2m on the year before.
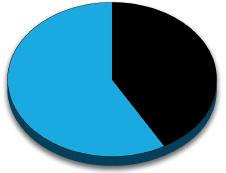
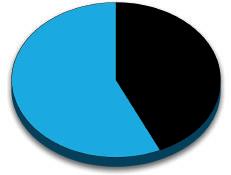
The extent to which growth was skewed is shown in figure 1.
Again, the top ten trusts by revenue were all in the capital, with Royal Marsden at £91.8m and Great Ormond Street Hospitals at £55m, earning 25% of all England NHS trust incomes.
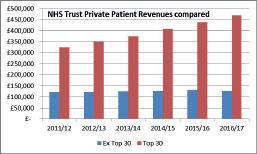
Indeed, the top ten trusts
increased their market share from 57% to over 59% of all private patient earnings.
The top 30 trusts now account for 79% of the total. Indeed, while the top 30 trusts have together grown by 25% in the past three years, overall revenues outside of that group have been flat for some time.
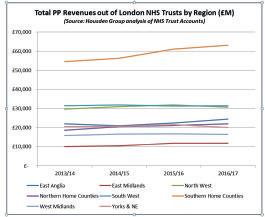
Future articles will analyse NHS private patient performance by region, starting with London in the next issue, discussing present trends and the potential for future growth.
What these trends suggest is that where trusts invest in the development of private patient services and treat the service as a regular part of what the trust does, they then reap the rewards. Even though medical insurance is more prevalent in the Southeast, there are opportunities for growth across the NHS – albeit many unrealised.
Philip Housden (right) is director of Housden Group
What these trends suggest is that where trusts invest in the development of private patient services ... they then reap the rewards
A bright future for PPUs?
So do NHS private patient units have a future given the increasing pressures on daytoday core services?
In the first of two articles, Philip Housden argues they have never been more relevant to the health service than now – and 2018 is a great time for the health service to invest in them.
See page 25
Figure 1
bUdgET RoUnd-Up
What that red box contained
Independent practitioners will be affected by a wide range of changes announced in Chancellor Philip Hammond’s latest Budget. Susan Hutter (right) provides a round-up and some useful tips
pEnsions TAx REliEF
No changes have been announced to the Annual Allowance limits which remain at £40,000 for individuals earning below £150,000.
Those doctors with income of more than £150,000 will be subject to the allowance being tapered by £2 for every £1 of income earned above £150,000, with a minimum allowance available to those earning over £210,000 of £10,000.
The Lifetime Allowance limit will be increased to £1,030,000 – from the £1m first introduced in April 2016 – with effect from April 2018.
Doctors are advised to take specialist advice, especially relevant to those who have an NHS pension as well as a private one.
TAx-FREE AllowAncEs
And TAx bAnds
The Government has announced that the capital gains tax annual exemption for individuals and personal representatives has been increased to £11,700 (from the current £11,300) for 2018-19. The amount available to most trusts and settlements will be £5,850.
The income tax personal allowance will increase to £11,850, from the current £11,500, and the basic rate tax top threshold will go up by £1,350 to £46,350.
The dividend allowance will reduce to £2,000 in accordance with previous announcements.
Make sure that you utilise as many allowances and as much of the lower-rate band as possible. Consider transferring incomeearning assets to a lower-earning spouse.
The ‘residence nil rate band’ limit for inheritance tax purposes will increase to £125,000 with effect from April 2018.
MilEAgE RATEs FoR
UnincoRpoRATEd pRopERTy bUsinEssEs
For those independent practitioners who own investment properties, there is a simplification in
claiming motor expenses and it could work out to be more generous, which is always welcome.
The Government has announced that it will permit the use of mileage rates as an allowable method of calculating the allowable deduction in respect of motoring expenses incurred for the purposes of a property business.
In most cases, mileage rates will not be available in respect of vehicles for which capital allowances have already been claimed or for which expenditure in acquiring the vehicle has been deducted in a business using the cash basis.
However, transitional arrangements will be introduced in these cases.
Currently, the mileage rates are 45p per mile in respect of the first 10,000 business miles and 25p thereafter.
nATionAl insURAncE conTRibUTions (nic)
Class 1 NIC will be payable by employees at 12% on their weekly employment income between £162 and £892 and at 2% thereafter in 2018-19.
The threshold for the employers will increase to £162 per week –above which Class 1 secondary contributions will be due at 13.8%.
The ‘small profits threshold’ for Class 2 NIC purposes will be increased by £180 to £6,205 and the weekly rate of the contributions will go up by 10p to £2.95.
Class 4 NIC will be due at 9% on annual profits between £8,424 and £46,350 and at 2% thereafter.
The tax-free limit for the ordinary cash/stock and shares ISAs will remain £20,000, of which £4,000 can be saved into a Lifetime ISA. For higher-rate tax payers, this is worth considering, especially as interest rates are on the increase. ➱ p12
THE FIRST 9-VALENT HUMAN PAPILLOMAVIRUS (HPV) VACCINE
GARDASIL® 9 contains 9 HPV types that account for 89% of HPV-related anogenital cancers and 90% of genital warts in Europe.1,2*
* Cervical, vulval, vaginal and anal cancers caused by oncogenic HPV types 16, 18, 31, 33, 45, 52 & 58 genital warts caused by HPV types 6 & 11. Not all cases of anogenital cancer are caused by HPV. The HPV prevalence is: ~100% in cervical cancer; ~88% in anal cancer; ~19% in vulval cancer; ~71% vaginal cancer.2
GARDASIL® 9 is indicated for active immunisation of individuals from the age of 9 years against premalignant lesions and cancers affecting the cervix, vulva, vagina and anus caused by vaccine HPV types and genital warts caused by speci c HPV types. The indication is based on data in males and females aged 9-26 years.
GARDASIL® 9 is not the vaccine offered in the national immunisation programme. The use of HPV vaccines should be in accordance with of cial recommendations.
For information on ef cacy rates and safety considerations, refer to the Summary of Product Characteristics available on the eMC website.
To order please contact AAH on 0844 561 8899.
GARDASIL ® 9 ▼
Human Papillomavirus 9 valent Vaccine (Recombinant, adsorbed))
PRESCRIBING INFORMATION
Refer to Summary of Product Characteristics before prescribing
Adverse events should be reported. Reporting forms and information can be found at www.mhra.gov.uk/yellowcard. Adverse events should also be reported to MSD (Tel: 01992 467272).
PRESENTATION Gardasil 9 is supplied as a single dose pre- lled syringe containing 0.5 millilitre of suspension. Each dose of vaccine contains highly puri ed virus-like particles (VLPs) of the major capsid L1 protein of Human Papillomavirus (HPV). These are type 6 (30 mg), type 11 (40 mg), type 16 (60 mg), type 18 (40 mg), type 31 (20 mg), type 33 (20 mg), type 45 (20 mg), type 52 (20 mg) and type 58 (20 mg). USES Gardasil 9 is a vaccine for use from the age of 9 years for the prevention of premalignant lesions and cancers affecting the cervix, vulva, vagina and anus caused by vaccine HPVtypes and genital warts (condyloma acuminata) caused by speci c HPV types. The indication is based on the demonstration of ef cacy of Gardasil 9 in males and females 16 to 26 years of age and on the demonstration of immunogenicity of Gardasil 9 in children and adolescents aged 9 to 15 years. The use of Gardasil 9 should be in accordance with of cial recommendations. DOSAGE AND ADMINISTRATION Individuals 9 to and including 14 years of age at time of rst injection: Gardasil 9 can be administered according to a 2-dose schedule. The second dose should be administered between 5 and 13 months after the rst dose. If the second vaccine dose is administered earlier than 5 months after the rst dose, a third dose should always be administered. Gardasil 9 can be administered according to a 3-dose (0, 2, 6 months) schedule. The second dose should be administered at least one month after the rst dose and the third dose should be administered at least 3 months after the second dose. All three doses should be given within a 1-year period. Individuals 15 years of age and older at time of rst injection: Gardasil 9 should be administered according to a 3-dose (0, 2, 6 months) schedule. The second dose should be administered at least one month after the rst dose and the third dose should be administered at least 3 months after the second dose. All three doses should be given within a 1-year period. It is recommended that individuals who receive a rst dose of Gardasil 9 complete the vaccination course with Gardasil 9. The need for a booster dose has not been established. Studies using a mixed regimen (interchangeability) of HPV vaccines were not performed for Gardasil 9. Subjects previously vaccinated with a 3-dose regimen of quadrivalent HPV types 6, 11, 16, and 18 vaccine (Gardasil or Silgard), hereafter
referred to as qHPV vaccine, may receive 3 doses of Gardasil 9. The use of Gardasil 9 should be in accordance with of cial recommendations. Paediatric population (children <9 years of age): The safety and ef cacy of Gardasil 9 in children below 9 years of age have not been established. No data are available. Population ≥ 27 years of age: The safety and ef cacy of Gardasil 9 in individuals 27 years of age and older have not been studied. The vaccine should be administered by intramuscular injection. The preferred site is the deltoid area of the upper arm or in the higher anterolateral area of the thigh. Gardasil 9 must not be injected intravascularly, subcutaneously or intradermally. The vaccine should not be mixed in the same syringe with any other vaccines and solution. CONTRAINDICATIONS Hypersensitivity to any component of the vaccine including active substances and/or excipients. Individuals with hypersensitivity after previous administration of Gardasil 9 or Gardasil /Silgard should not receive Gardasil 9. PRECAUTIONS The decision to vaccinate an individual should take into account the risk for previous HPV exposure and potential bene t from vaccination. As with all injectable vaccines, appropriate medical treatment and supervision should always be readily available in case of rare anaphylactic reactions following the administration of the vaccine. The vaccine should be given with caution to individuals with thrombocytopaenia or any coagulation disorder because bleeding may occur following an intramuscular administration in these individuals. Syncope (fainting), sometimes associated with falling, can occur following, or even before, any vaccination, especially in adolescents as a psychogenic response to the needle injection. This can be accompanied by several neurological signs such as transient visual disturbance, paraesthesia, and tonic-clonic limb movements during recovery. Therefore, vaccinees should be observed for approximately 15 minutes after vaccination. It is important that procedures are in place to avoid injury from fainting. Vaccination should be postponed in individuals suffering from an acute severe febrile illness. However, the presence of a minor infection, such as a mild upper respiratory tract infection or lowgrade fever, is not a contraindication for immunisation. As with any vaccine, vaccination with Gardasil 9 may not result in protection in all vaccine recipients. Gardasil 9 will only protect against diseases that are caused by HPV types targeted by the vaccine. Therefore, appropriate precautions against sexually transmitted diseases should continue to be used. The vaccine is for prophylactic use only and has no effect on active HPV infections or established clinical disease. The vaccine has not been shown to have a therapeutic effect and is not indicated for treatment of cervical, vulvar, vaginal and anal cancer, high-grade cervical, vulvar, vaginal and anal dysplastic lesions or genital warts. It is also not intended to prevent progression of other established HPV-related lesions. Gardasil 9 does not prevent lesions due to a vaccine HPV type in
9-VALENT HPV PROTECTION
individuals infected with that HPV type at the time of vaccination. Vaccination is not a substitute for routine cervical screening. There are no data on the use of Gardasil 9 in individuals with impaired immune responsiveness. Safety and immunogenicity of a qHPV vaccine have been assessed in individuals aged from 7 to 12 years who are known to be infected with human immunode ciency virus (HIV). Individuals with impaired immune responsiveness, due to either the use of potent immunosuppressive therapy, a genetic defect, Human Immunode ciency Virus (HIV) infection, or other causes, may not respond to Gardasil 9. Long-term follow-up studies are currently ongoing to determine the duration of protection. There are no safety, immunogenicity or ef cacy data to support interchangeability of Gardasil 9 with bivalent or quadrivalent HPV vaccines. Pregnancy, lactation and fertility: There are insuf cient data to recommend use of Gardasil 9 during pregnancy, therefore vaccination should be postponed until after completion of pregnancy. The vaccine can be given to breastfeeding women. No human data on the effect of Gardasil 9 on fertility are available. SIDE EFFECTS Refer to Summary of Product Characteristics for complete information on side-effects. Very common side effects include: erythema, pain and swelling at the injection site and headache. Common side effects include: pruritus and bruising at the injection site, dizziness, nausea, pyrexia and fatigue. The post-marketing safety experience with qHPV vaccine is relevant to Gardasil 9 since the vaccines contain L1 HPV proteins of 4 of the same HPV types. The following adverse experiences have been spontaneously reported during post-approval use of qHPV vaccine and may also be seen in post-marketing experience with Gardasil 9: urticaria, bronchospasm, idiopathic thrombocytopenic purpura, acute disseminated encephalomyelitis, Guillain-Barré Syndrome and hypersensitivity reactions, including anaphylactic/ anaphylactoid reactions. PACKAGE QUANTITIES AND BASIC NHS
COST Single pack containing one 0.5 millilitre dose pre- lled syringe with two separate needles: £105.00 per dose Marketing
References: 1. GARDASIL® 9 SmPC, 2017. 2. Hartwig S et al
Estimation of the epidemiological burden of HPV‐related anogenital cancers, precancerous lesions, and genital warts in women and men in Europe: potential additional bene t of a nine‐valent second generation HPV vaccine compared to rst generation HPV vaccines. Papillomavirus Res 2015; 1:90–100.
Date of preparation: October 2017 VACC-1231710-0006
➱ continued from page 10
The Junior ISA and Child Trust Fund subscription limits will increase to £4,260. This is effective from April 2018.
Enterprise investment scheme (Eis)
Changes will be introduced to the EIS legislation to encourage investments in knowledge-intensive companies. The changes will apply to shares issued on or after 6 April 2018.
The EIS investment limit will be increased for individuals to £2m – from £1m – provided that any amount over £1m is invested in one or more knowledge-intensive companies.
Many doctors may be interested in this, as a number are involved in start-ups in this field.
stamp duty land Tax (sdlT)
The Government has introduced a new relief for first-time buyers of residential property worth £500,000 or less whereby the first £300,000 of the property costs will be subject to stamp duty at 0% and the following £200,000 at 5%.
The standard SDLT rates will apply to properties costing more than £500,000.
Anti-avoidance rules have been introduced with effect from 22 November 2017 in relation to the 3% stamp duty surcharge where an individual acquires a second residential property.
From 22 November 2017, the relief from the surcharge will only be available where the purchaser of the second residential property disposes the whole of their former main residence to someone other than their spouse.
This new measure now also grants relief where:
A divorce-related court order prevents someone from disposing their interest in a main residence;
A spouse or civil partner buys property from another spouse or civil partner;
A deputy buys a property for a child subject to the Court of Protection;
A purchaser adds to their interest in their current main residence.
Susan Hutter is a partner at Blick Rothenberg and part of the team that advises medical practitioners
Bid to avert rise in insurance tax
By Robin Stride
The independent healthcare sector is being urged to intensify its fight to protect insurance premium tax on private medical insurance from a further increase.
Private consultants, hospitals and insurers breathed a sigh of relief at the end of Chancellor Philip Hammond’s Autumn Budget speech as health cover escaped from suffering yet another tax rise.
But many still fear that private medical insurance could be in for another hit in future with an increase from the current 12% to match the VAT rate of 20%.
A leading voice in the campaign to protect private medical insurance from yet more insurance premium tax increases is the leader of the trade body whose members find the insured customers for consultants and insurers.
Association of Medical Insur ance Intermediaries (AMII) executive chairman, Mr Stuart Scullion, expressed ‘delight’ that the Treasury decided not to impose further increases.
ance products such as life or critical illness.’
But he told 200 members at their Health and Wellbeing Summit in Westminster that the anti-tax lobby must now keep up the pressure.
Mr Scullion continued: ‘We are calling on the Government to commit to stability for insurance premium tax in relation to healthcare during this Parliament, however long that might be, by freezing the rate of insurance premium tax on healthcare spend.
‘Furthermore, we are asking the Government to reappraise how health insurance and cash plans are treated in the fiscal system in line with other zero-rated insur-
Referring to a recent poll for Bupa (see page 7), he added: ‘We know cost is the main factor in the decision to purchase and maintain health insurance cover, with the poll confirming a third (33%) saying they would consider taking out insurance if costs were lower, while 33% of policyholders said they will consider cancelling their policy if their premium goes up.’
Mr Scullion said the research suggested insurance premium tax was contributing to thousands of individuals giving up their policies, resulting in nearly 200,000 customers cancelling their policies in the past three years.
He told the summit: ‘Every 1% increase in insurance premium tax is leading an estimated 31,000 health insurance customers every year to depend solely on the NHS for all of their healthcare.
‘The report reaffirms what I have said previously that insurance premium tax has a greater impact on people who have the most need to keep their health
Every 1% increase in insurance premium tax is leading an estimated 31,000 health insurance customers every year to depend solely on the NHS for all of their healthcare
insurance, such as older individuals with riskier health profiles who pay higher premiums.’
The poll of 2,000 people found 63% said health insurance allows others to access NHS treatment earlier and 55% view it as important in relieving pressure on the NHS.
Mr Scullion said he understood from pre-Budget conversations that the Chancellor had commented on seeing increased commentary and resistance in relation to insurance premium tax.
The AMII had positively contributed to this lobbying, alongside some of its corporate member firms (insurers) and other industry bodies.
He reported that efforts to raise AMII’s profile were working and he was engaged in regular dialogue on healthcare matters, including insurance premium tax, with Craig Tracey MP, chairman of the All-Party Parliamentary Group on Insurance and Financial Services. AMII said it had positive feedback from its first education event about understanding the UK health insurance market, which was run to support employers with members of staff who are new to the industry.
StuaRt SCullioN
PRESCRIBING INFORMATION
AVAXIM®, suspension for injection in a prefi lled syringe.
Hepatitis A vaccine (inactivated, adsorbed). Refer to Summary of Product Characteristics for full product information.
Presentation: Suspension for injection. Available as a 0.5 millilitre single dose prefi lled syringe containing 160 antigen units of inactivated hepatitis A virus. Indications: For primary or booster immunisation against infection caused by hepatitis A virus in susceptible adults and adolescents aged 16 years and above. AVAXIM is to be used on the basis of offi cial recommendations. Dosage and administration: A single 0.5 millilitre dose should be administered by intramuscular injection in the deltoid region. Immediately before use the syringe should be shaken well to obtain an homogenous suspension. To provide long term protection, a booster should be given between 6 and 36 months later. AVAXIM may be used as a booster in subjects from 16 years of age, vaccinated with another inactivated hepatitis A vaccine (monovalent or with purifi ed Vi polysaccharide typhoid) 6 months to 36 months previously. The vaccine is to be injected intramuscularly. AVAXIM may be administered subcutaneously under exceptional circumstances (e.g. in patients with thrombocytopenia or in patients at risk of haemorrhage). Do not inject intravascularly. Also avoid administration into buttocks. Contra-indications: Hypersensitivity to the active substance(s), to any of the excipients or following a previous injection of this vaccine. Known hypersensitivity to neomycin (which may be present in the vaccine in trace amounts). Vaccination should be delayed in subjects with acute severe febrile infections. Warnings and precautions: The effect of AVAXIM on individuals late in the incubation period of hepatitis A has not been documented. Immunogenicity could be impaired in immunosuppressed patients. AVAXIM is unnecessary for individuals raised in areas of high endemicity and/or with a history of jaundice as they may be immune to hepatitis A. Testing for antibodies to hepatitis A prior to a decision on immunisation should be considered in such situations. If not, seropositivity against hepatitis A is not a contraindication. AVAXIM is as well tolerated in seropositive as in seronegative subjects. Caution is advised for the use of AVAXIM in patients with liver disease. No clinical data on concomitant administration of AVAXIM with other inactivated vaccine(s) or recombinant hepatitis B virus vaccine have been generated. AVAXIM can also be given at the same time as immunoglobulin but at different sites, however, antibody titres could be lower than after vaccination with AVAXIM alone. AVAXIM must not be mixed with other vaccines in the same syringe. AVAXIM can be administered at the same time as Vi polysaccharide typhoid vaccine or with a yellow fever vaccine reconstituted with a Vi polysaccharide typhoid vaccine, but at different sites. Syncope (fainting) can occur following, or even before, any vaccination especially in adolescents as a psychogenic response to the needle injection. This can be accompanied by several neurological signs such as transient visual disturbance, paraesthesia and tonic-clonic limb movements during recovery. It is important that procedures are in place to avoid injury from faints. Pregnancy and lactation: AVAXIM should not be used during pregnancy unless clearly necessary and following an assessment of the risks and benefi ts. There are no data on the effect of administration of AVAXIM during lactation. AVAXIM is therefore not recommended during lactation. Undesirable effects: Very common side effects include: asthenia and mild injection site pain. Common side effects include: myalgia/ arthralgia, headache, gastrointestinal tract disorders (nausea, vomiting, decreased appetite, diarrhoea, abdominal pain) and mild fever. In post-marketing experience other adverse reactions have been reported and include vasovagal syncope in response to injection. For a complete list of undesirable effects please refer to the Summary of Product Characteristics. Marketing authorisation holder: Sanofi Pasteur Europe, 2 Avenue Pont Pasteur, 69007 Lyon, France. Further information is available from the Distributor: UK: Sanofi, One Onslow Street, Guildford, Surrey GU1 4YS Tel: 0845 372 7101; Ireland: sanofi -aventis Ireland T/A SANOFI, Citywest Business Campus, Dublin 24, Ireland Tel: 01 403 5600 Package quantities and basic NHS cost: Single dose prefi lled syringes in single packs, basic NHS cost £18.10; packs of 10 single dose prefi lled syringes, basic NHS cost £181.00. Legal category: POM Marketing authorisation number: UK : PL 46602/0001 Ireland: PA 2131/002/001 ® Registered trademark Date of last review:
ACCoUnTAnT’s CliniC: TAx RETURns
Get your skates on
If you haven’t prepared the information for your 2016-17 tax year, you need to get your skates on, as the filing date is 31 January 2018. Susan Hutter (below) gives some top tips about submitting a tidy tax return
Don’t adopt the ostrich approach
With the best will in the world, there are times when administration takes a back seat. Particularly the tax return.
However, I know too many medics who procrastinate and adopt the ostrich approach when it comes to such matters.
Confront your tax affairs now!
Apart from anything else, you will need to know how much tax to pay. The sooner you know what the amount is, the better, as you haven’t much time to get reserves ready so that you can pay your bill at the end of January 2018.
Planning ahead – The paperwork
To those of you who like to plan ahead for your 2017-18 tax return – always advisable – you should start gathering the paperwork as soon as the tax year ends on 5 April 2018.
I know too many medics who procrastinate and adopt the ostrich approach when it comes to such matters. Confront your tax affairs now!
Some information will be supplied by third parties; for example, P60s for salaries (NHS salaries, private pensions, NHS pension if you are drawing on that, and your own salary if also working in the NHS) as well as a P11D if you trade within a company and, for example, you have taxable benefits like a company car.
Your will also need to gather tax certificates received from banks and building societies.
Even though tax is deducted at source, you still need to declare this information on your tax return, as most consultants and private GPs are higher-rate tax payers and only base rate tax is deducted at source.
Sometimes bank and societies need reminding and therefore do chase them if you have not received a certificate three months after the tax year end.
In addition, you will need dividend vouchers if you have shares
in listed companies – and also dividend vouchers if you trade via a company and drew dividends. Your accountant should have the latter, as they probably prepared them on your behalf.
Check list
Use your prior year’s tax return as a check list for the year you are preparing for now.
But make sure you do not follow it blindly – because you could have new sources of income since the last tax return date, such as opening a new bank account or you purchased a rental property.
Don’t forget things such as writing or lecture fees. Talk to your accountant as to how he/she would like the information presented – if presented clearly, it will save on accountancy fees.
Prioritise practice accounts
Make sure your practice accounts are prepared as soon as possible, whether you are a sole trader or a limited company.
Gather the information first, as this is the biggest thing and takes
the longest. If you have a rental property, you need to gather details for all rental income and expenditure.
Also, if you let it through an agent, you will need to provide your agent’s statement, your own bank records and a record of expenses such as for decorating/ cleaner. Your accountant won’t want the receipts for these items, but it is important that you retain them.
Put money in reserve
If you haven’t left your tax return to the last minute – put some money aside for a tax reserve.
Your accountant will point you in the right direction as to how much you will need to reserve, as most independent practitioners know the tax is due in two instalments on 31 January and 31 July each year. This is your chance to get ahead and make sure you always have a tidy tax return.
Avoiding the taxman, see p48
Susan Hutter is a partner at Blick Rothenberg and part of the team that advises medical practitioners
OR RUSHING TO A&E?
Check if your patients need vaccination against rabies before they go:1
PRESCRIBING INFORMATION
Rabies Vaccine BP ≥2.5 IU/ml, Powder and solvent for suspension for injection
Refer to Summary of Product Characteristics for full product information.
• Visiting an area where rabies is common and taking part in higher risk activities e.g. cycling or running?
• Working abroad in close contact with animals?
• Staying in an at-risk area for more than 1 month?
Rabies Vaccine BP from Sanofi Pasteur offers pre- and post-exposure protection against rabies.2
Order at www.vaxishop.co.uk or telephone our Customer Service team on 0800 854 430
Presentation: A single dose vial of powdered vaccine and pre-fi lled syringe of solvent for suspension for injection. After reconstitution, each 1 millilitre dose contains rabies virus (inactivated, strain PM/ WI 38 1503-3M) not less than 2.5 International Units of rabies antigen. Indications: Prophylactic immunisation against rabies and treatment of patients following suspected rabies contact. Dosage and administration: The dose of reconstituted vaccine in all cases is 1 millilitre given by intramuscular injection into the deltoid region. Reconstitute with the solvent supplied and shake carefully to ensure complete reconstitution. Following reconstitution the vaccine will be a pinkish colour and free from particles. Once reconstituted, the vaccine must be used immediately. DOSAGE FOR PROPHYLAXIS: 1 millilitre given on days 0, 7 and 28. For those at regular and continuing risk, a single reinforcing dose of vaccine should be given at 1 year after the primary course has been completed. Further doses should be given at three- to fi ve-year intervals thereafter. For travellers at intermittent risk of exposure, booster doses may be given in line with offi cial recommendations. DOSAGE FOR TREATMENT: For those known to have adequate prophylaxis - 1 millilitre should be given on day 0 and on day 3 following contact with a suspected rabid animal. For those with no, or possibly inadequate prophylaxis - the fi rst injection should be given as soon as possible after suspected contact (day 0) and followed by four further 1 millilitre doses on days 3, 7, 14 and 30 (the earliest that the 5th dose can be given is day 28 as per WHO recommendations). The use of Rabies Immunoglobulin should be considered in unimmunised or incompletely immunised subjects or those with uncertain immune status in accordance with official recommendations and/or expert advice. The treatment schedule may be stopped if the animal concerned is found conclusively to be free of rabies. Subjects with incomplete prophylaxis or unknown history of immunisation should be treated as non- immune. Contra-indications: Pre-exposure: Known systemic hypersensitivity to Rabies Vaccine BP or any of its components; febrile and/or acute disease. Post-exposure: no contra-indications. Warnings and precautions: Appropriate facilities and medicines should be readily available in case of anaphylaxis or hypersensitivity following injection. The vaccine may contain traces of neomycin and betapropiolactone which are used during the manufacturing process. If Rabies Immunoglobulin is indicated in addition to Rabies Vaccine BP, then it must be administered at a different anatomical site to the vaccination site. Rabies Vaccine BP should not be administered to patients with bleeding disorders or to persons on anticoagulant therapy unless the potential benefi t outweighs the risk of administration. The potential risk of apnoea and the need for respiratory monitoring for 48- 72 h should be considered when administering the primary immunisation series to very premature infants (born ≤ 28 weeks of gestation) and particularly for those with a previous history of respiratory immaturity. As the benefi t of vaccination is high in this group of infants, vaccination should not be withheld or delayed. Anxiety-related reactions, including vasovagal reactions (syncope), hyperventilation or stress-related reactions can occur following, or even before, any vaccination as a psychogenic response to the needle injection. This can be accompanied by several neurological signs such as transient visual disturbance and paraesthesia. It is important that procedures are in place to avoid injury from faints. Corticosteroids and immunosuppressive treatments may interfere with antibody production, check antibodies 2 to 4 weeks after course. Pregnancy: The potential risk of administration of Rabies Vaccine BP during pregnancy is unknown. Due to the severity of the disease, pregnancy is not considered to be a contra-indication to post-exposure prophylaxis. If risk of exposure is substantial, pre- exposure prophylaxis may also be indicated. Lactation: It is not known whether the vaccine is excreted in human breast milk. Due to the severity of the disease, breast-feeding is not considered a contraindication. Undesirable effects: Very common side effects include: lymphadenopathy, nausea, diarrhoea, injection site reactions (pain, erythema, pruritus, induration), chills, malaise, headache, arthralgia and myalgia. Common side effects: injection site bruising, dizziness, respiratory manifestations (dyspnoea, wheezing), angioedema, pyrexia, abdominal pain, vomiting and allergic reactions with skin disorders (urticaria, rash, pruritus). Other undesirable effects have been reported, although their frequency is not known. These include serum sickness type reactions, anaphylactic reactions, oedema, encephalitis, convulsion, Guillain-Barré Syndrome, paresis, neuropathy, paraesthesia and asthenia. For a complete list of undesirable effects please refer to the Summary of Product Characteristics. Marketing authorisation holder: Sanofi Pasteur Europe, 2 Avenue Pont Pasteur, 69007 Lyon, France. Further information is available from the Distributor: UK: Sanofi, One Onslow Street, Guildford, Surrey GU1 4YS Tel: 0845 372 7101; Ireland: sanofi -aventis Ireland T/A SANOFI, Citywest Business Campus, Dublin 24, Ireland Tel: 01 403 5600 Package quantities and basic NHS cost: One single dose vial (powder) and one pre-fi lled disposable syringe containing 1 millilitre of solvent with 2 separate needles, basic NHS cost £40.84. Legal category: POM Marketing authorisation number: UK : PL 46602/0004 Ireland: PA 2131/004/001 Date of last review: February 2017
Suspected adverse events should be reported Reporting forms and information can be found at www.mhra.gov.uk/yellowcard and www.hpra.ie
Suspected adverse events should also be reported to Sanofi Tel: 08000 902 314 (for UK) and Tel: 01 403 5600 (for Ireland).
References: 1. Department of Health. Immunisation against infectious disease. Chapter 27: Rabies. Accessed November 2017 2. Rabies Vaccine BP Summary of Product Characteristics SAGB.RABIE.17.10.1326 11/17
ExEcUTivE inFoRmATion
How to figure out what you’re doing
Executive information is increasingly important for private doctors. Jane Braithwaite (below) shows how to analyse your business and make changes based on practice data
All business leaders need executive information to enable them to review and manage their business. And that is equally true of private doctors and clinics.
While patient data is often reviewed, the actual management of the practice is often overlooked. so, this month, i’m taking a look at how independent practitioners can get the most out of non-clinical data.
What is executive information?
The term ‘executive information’ relates to information provided to executive-level employees about what is happening in their business.
i n a private medical practice environment, executive information systems can allow principal
consultants to look at trends and figures extracted from their practice management systems.
These systems could come in the form of a dashboard, providing users with an overview of the figures they consider most important.
Business intelligence and reporting
Dashboards can be constructed to include ‘drill down’ capabilities, so you can dig a little deeper into your information based on the parameters you build in. s ometimes referred to as business intelligence, these systems can also include analytics, forecasting and reporting functions.
Two issues you will need to consider are:
1What do you want to see from your dashboard or executive information system;
2 How do you go about displaying this.
in other words, you are asking ‘which program can i use to extract the data from my practice management system and display it in the format that i want?’
There are many user-friendly programs available that can be used to build dashboards – Tableau or QlikView, for example – and there are online tutorials available that will help you to familiarise yourself with their functions. but creating a dashboard may be something you might prefer to leave to an expert. An expert will also be able to advise you on how best to link your medical practice
management system database to a business intelligence program, which could involve data cleans ing or a knowledge of structured query language (sQl) queries.
They will also be able to advise on the usability, cost and mainte nance of such programs.
Once you have decided on which tool you want to use, you then need to think about what you want to see. You could use your information system to show you:
Attendance rates: Taking an indepth look at this will allow you to co-ordinate clinics to maximise attendance;
Source of referral: by recording in your practice system where a referral has come from – word of
Online videos drive the most internet traffic and naturally engage audiences and increase enquiries
Let us create high-quality videos for you to maximise your potential!
HD and 4K video production
Live clinical review of your content
Animated logos to promote your brand online
Clear calls to action to drive new patient enquiries
Our video clients include:
Improves SEO for your website
Original content for your social media channels
Set-up and management of your YouTube Channel
Fixed price and bespoke packages available for clinics and subscription plans for individual specialists
mouth, through another facility, social media – you can understand where your patients are coming from and focus your marketing accordingly.
You will also need to think about how you wish to display the information. Formatting a report or dashboard in an audience-friendly way will maximise understanding and allow you to make informed decisions.
Reviewing your systems if you do not already have a dashboard or an executive information system, it is worth talking to an iT specialist to get advice about which of the business intelligence programs would be best for you.
Your existing systems will need to ‘speak’ to these programs, feeding them the information that will ultimately be displayed in your dashboard.
Questions you may want to consider are:
Which systems do you use? business intelligence software can speak to most databases. For example, you can easily link Microsoft Access and e xcel to these programs.
Do your current systems have reporting capabilities? s ome medical practice management systems already have reporting capabilities built in. Depending on your requirements, a simple report may be all that you need.
For example, if all you require is a report once a month on the number of patients who attended clinic, it may be that you can easily extract this from your system without the need to build a dashboard.
Does the data need to be cleansed in order to be interpreted easily? s ome data will need to be ‘cleansed’ – that is to say, it needs to be amended into a version that the business intelligence software can understand.
Resources needed
Does your practice manager have a penchant for business analysis? is your secretary keen to develop new skills? if your answer is yes, it sounds like you already have the capability within your team. if they have the time, why not help them develop their skills? Tutorials for business intelligence programs are available online, and there are even classroom training sessions available for those who prefer face-to-face learning. if you are not sure if you want to commit to purchasing business intelligence software, you can try using excel to build a dashboard. This comes as part of Microsoft Office and is therefore likely to be available on office computers. so using excel can be a cost-effective way of getting started with dashboards and, if you need to, you can move on to more dedicated business intelligence software at a later date.
However, it may be that you and your team simply do not have the time to dedicate to setting up and maintaining a business intelligence system. i n this case, you may want to outsource part of or all the work. A data visualisation specialist could help you to set up a dashboard, but you may need help to support you in terms of maintaining the system. This should be considered at the point you think about your requirements. so, to sum up, business intelligence and executive information systems can be a real asset to any business, and private medical practices are no exception.
The data held within your systems is valuable and holds the key to really understanding the way your patients interact with your practice.
Jane Braithwaite is managing director of Designated Medical
Top Tips for execuTive informaTion
Define your requirements – Think about what you need to know, and in what format it needs to be in
Talk to an IT or business intelligence expert – if you are not sure how you can make the most of your information, talk to an expert. They will have great ideas about the different software options out there that will allow you to gain valuable business insights from your practice data
Make the most of your systems – excel has great data visualisation capabilities and many medical practice management programs will allow you to extract data in bulk. Talk to an iT colleague or expert about how this information can be linked to business intelligence software for use in dashboards
Consider all your resourcing options – if time is precious, you could consider outsourcing this work. iT professionals, data specialists and business analysts could all provide valuable input into what needs to be done to set up regular reporting
Make sure you have clear data management/collection policies in place – You should make decisions based on your practice data only if it is accurate and complete. information should be collected and entered into systems fully and as soon as possible after collection. There is no point in assessing how well your practice is managed based on incomplete data
Collect feedback from patients – certain aspects of a practice can be hard to measure in hard data, such as how well staff communicate with patients, how patients feel about the service they receive and so on. so consider collecting feedback from patients – this will give you the chance to understand things on a more personal level
Share your findings with your team – analysing practice data will allow you to see what is working and what isn’t working. sharing information with your team will give you even more insight into the way things work, and your team may have ideas that they are keen to share with you
Improve your processes – By analysing trends against practice procedures, you will be able to see where improvements need to be made. is attendance poor for morning clinics? maybe you could start later or implement a reminder system for 48 hours before the appointment and then review the information again in a month to see if the change makes a difference
Plan for the future – With so much practice data at hand, it should be possible to produce forecasts for different areas of your business. This will help you to plan your resources
Consider cloud-based options – many business intelligence programs and executive information systems are cloud-based, which means that they can be accessed by users on the move. executives can therefore have instant access to business-crucial information, allowing them to make data-driven decisions wherever they are
PROBLEMS WITH THE TAX MAN?
HMRC tax investigations and disputes create difficult and stressful times.
As an award winning firm of tax experts, our highly experienced partners specialise in resolving problems relating to tax investigations and disputes with HMRC.
To find out, in confidence, how we can help call 0800 734 3333.
‘Here to help. Not to judge.’
CoPing wiTh bURn-oUT
Managing stress while you work
Under pressure? In the third of his Independent Practitioner Today series, consultant psychologist Dr Michael Sinclair (left) gives five tips for managing stress on the job – without trying to eradicate it
My last two articles of this series have highlighted the real stressors that come with working as a medical consultant and how suffering in silence is usually not a good idea.
you have also been invited to consider the strategies that you tend to use to cope with stress and to explore whether they work well for you or not.
Now I am keen to introduce you to some interesting and effective alternatives for coping with stress that you might want to try out, especially if you find that the way you have been responding to stress hasn’t been helpful for you, in the longer term, anyway.
I am going to share five strategies here and another five next month.
these strategies are not necessarily focused on the eradication of stress, but more to do with changing our response to it and to be used alongside and in the presence of stress.
When we lessen our preoccupation with trying to eradicate and suppress stress – which is an inevitable part of working as a doctor – we may find that life becomes fuller and that paradoxically stress becomes less of a problem. Here are five ways that you can start to do that:
Practise mindfulness
Research shows how mindfulness can effectively help many difficulties such as work-related stress, depression, anxiety, substance misuse, acute and chronic pain, managing stress related to medical diagnoses such as cancer, relationship problems, to name but a few.
Mindfulness practices take many forms, but essentially all of them share elements of cultivating a disciplined development of present moment awareness – seeing and experiencing the moment just how it is, without attachment or defence.
Mindfulness helps us to notice when we are responding to stress in unhelpful ways. It promotes our psychological flexibility, a skill which enables us to focus on the present moment, so we can respond to thoughts and feelings
in a way which allows us to act in accordance with our chosen goals in any given stressful situation. Use an app and get practising.
Unhook yourself from stressful thoughts
Engaging with the worry, self-criticism and rumination produced by your mind might seem helpful to do, but it’s often stress-inducing and life-narrowing.
take a different perspective by looking at your thoughts as thoughts, rather than looking at your stressful situation through your thoughts.
you might find that repeating any stressful thought and adding these few words before it: ‘I notice that I am having the thought that… (insert stressful thought here)’ helps to gain some perspective and distance from your troublesome mind, freeing up time,
energy and visibility to tackle any situation in a calmer and more composed fashion.
be willing to experience painful emotions you don’t have to like what you feel; you just have to be willing to experience it. Willingness is not about changing how you feel, but about getting better at feeling.
It involves acceptance, which is not about giving up, putting up, or resignation. a cceptance is when you make a choice to stop struggling with your least desirable experiences, such as stress, because you realise you can’t control them – ultimately anyway. and when you persist, well, that doesn’t work too well for you.
When you do this, you start to feel more at ease and, as a result, become more effective on the job and take more enjoyment from life.
accept the guilt that may come from taking some time off work, make some room for the sense of ‘failure’ that may arise if you aren’t coping so well. allow painful feelings to come and go, as they will naturally, and instead focus on what you can control, how you behave, in the service of what matters most to you.
identify what matters most, and act boldly
Research shows us that having a clear sense of direction or meaning and purpose improves our well-being and helps us to cope better with the inevitable challenges throughout our stressful day.
Clarifying what truly matters to you, and the personal qualities you want to demonstrate in and around your work, can help you to make decisions and take action in your preferred direction amid any stressful situation. ask yourself: what matters most to me in this context, at this time – for example, health, work, patient, family? What do I want to stand for in the face of this stressful situation? How do I want to be right now? a caring, kind, compassionate, assertive, self-caring person, maybe?
t hen take bold action aligned with these values. t his might mean that you need to step outside your comfort zone, yet at least you would know that you have moved towards being the kind of person/practitioner that you truly want to be and towards living the life that matters most to you.
Practise soothing rhythm breathing at the risk of teaching a granny to suck eggs, did you know that the way that we breathe is very much connected to our stress levels?
When we feel anxious, panicky or angry, our sympathetic nervous system is activated, leading our breathing rate to increase and become shallower.
By focusing our attention on slowing down our breathing, we activate the parasympathetic nervous system, slowing down the body and mind, helping to loosen the grip that stress has on
us, making space for mindful awareness and a more helpful response to our emotions and troublesome thoughts. try this right now and, if you wish, use it within any given stressful situation:
1. Gently slow down the rate of your breath. Breathe in for five seconds, pause and then breathe out for five seconds. Breathe in 1 – 2 – 3 – 4 – 5, pause for a moment, breathe out 1 – 2 – 3 – 4 – 5.
2. If this feels too slow, begin at a rate that feels comfortable for you and take your time to slow the rate further.
3. Bring your awareness to the sensations of your body and mind slowing down.
t here is no panacea for stress; it’s an inevitable part of work as an independent medical doctor. you can, however, become very skilled at recognising it and the way you respond to it and whether these ‘coping’ strategies are working for you or not.
In remaining aware and in practising some of the techniques described above – and any others that work for you – then you, your practice and your patients are likely to benefit.
Don’t forget to check out next month’s article when I will share another five tips for managing stress without trying to eradicate it.
Dr Michael Sinclair is a consultant counselling psychologist. He is the clinical director of City Psychology Group in London, with clinics in Liverpool Street, Harley Street and Canary Wharf.
He is the author of a range of self-help books, including Mindfulness for Busy People, Working with Mindfulness, The Little ACT Workbook, The Little CBT Workbook, and Fear and SelfLoathing in the City.
He provides effective, evidencebased psychological interventions to individuals of all ages, couples and families experiencing a range of psychological problems such as stress, anxiety and depression and adjustment to physical health conditions. He provides training to medical and other health practitioners, consultation to a growing number of corporate occupational health departments and delivers psychological interventions to large firms to improve employees’ health and performance
Dear Reader,
Subscribing to Independent Practitioner Today is the only way you can be sure you will see every issue and have the option of reading us online using our special page-turnable edition. Don’t risk missing out. Our personal subscription for doctors and managers is only £90 a year and £210 for organisations. But you can cut this to just £75 and £180 respectively if you pay by direct debit. So take advantage of this offer now for our unique business journal dedicated to supporting you in your private practice. We’re confident your subscription will repay itself many times over!
Editorial director
ApplicATion FoR sUbscRipTion
r
i enclose a cheque for £ ........... made payable to the independent practitioner Ltd please debit my mastercard/Visa/amex/diners
no
manager* r * indicates this item must be filled in Doctors, please give GMC No. (See rates listed above)
I encose a cheque made payable to The Independent Practitioner Ltd
Please debit my Mastercard/Visa/
i would like to pay by direct debit (please complete all details in box below). Don’t forget, it’s £15 cheaper to pay by direct debit; £30 less for organisations.
the manager
Instructions to your Bank or Building Society to pay Direct Debits Name and full address of your bank/Building Society
Name(s) of account holders
name(s) of account holders branch sort code
banks and building Societies may not accept direct debit instructions for some types of account
post your application (no postage required – uK only) to: independent practitioner today Subscriptions department, FreepoSt, po box 36, plymouth, pL1 1br
Please post to: Proact Ltd Subscriptions Dept., 12 Mary Seacole Road, The Millfields, PLYMOUTH PL1 3JY Or email to: jackie@marketingcentre.co.uk Or fax
Banks and Building Societies may not accept Direct Debit instructions for some types of
Signature(s) date ___________ phone: 01752 312140 Fax: 01752 313162 email: lisa@marketingcentre.co.uk or subscribe online at www.independent-practitioner-today.co.uk if you want to pay by card
Debit at any time, by writing to your Bank or Building Society. Please also send a copy of your letter to us.
Full steam ahead for PPUs
So do NHS private patient units (PPUs) have a future given the increasing pressures on day to day core services?
In the first of two articles, Philip Housden argues they have never been more relevant to the health service than now – and 2018 is a great time for the health service to invest in them
The NhS PPU sector is characterised by having a few big players –essentially in London– and many individual and local smaller providers.
This market feature means that, particularly for the area outside the capital, the PPU sector is rarely considered as a whole and for what it is: a billion-pound-ayear opportunity.
So what could and should be done by trusts, the NhS at large and individual consultants?
My analysis of recently published NhS trust 2016-17 annual reports and accounts shows that the long-term trend in the growth
of private patient earnings continues.
The big trends are there from previous years. The top ten highest-grossing trusts are all in London. The fastest regional growth is in the capital.
A majority and growing proportion of total earnings is made by the London trusts and, taken together, total private patients still represent well under 1% of all N h S patient episodes and total revenues.
Nothing new there then. But the emphasis every year seems to be on the 60% of NhS private
patient earnings in the city and I think it is time more effort is spent on the 40% outside London.
What is happening outside of the M25? Let’s examine the new data and consider the megatrends at work, taken from my analysis of 131 NhS acute trusts outside Greater London.
ppU trends
1Growth is up again but lower than in recent years. NhS PPU revenues were £220m, up only £2m on 2015-16 (0.9%).
For these same trusts, private patient earnings grew by 4.7% the previous year and 2.8% the year before. This £220m represents 0.5% of total trust patient care activities revenues for the year (see Figure 1).
2Growth remains patchy and shows regional variation.
It was highest in the southern home Counties of Kent, Sussex, Surrey and hampshire (up £2m to £63m and 3.3%) and in e ast Anglia (up £2m to £24.5m and 9.4%).
But patient revenues fell by 7% in Yorkshire and the North-east from £21.6m to £20m and also fell by £1.2m to £30.6m in the North-west (3.4%) (see Figure 2).
3earnings are up where there is a PPU, but not all trusts have one.
In the southern h ome Counties, where 13 out of 19 trusts have a PPU, trusts’ private patient revenues were 0.95% of total income, while only 0.24% of total incomes in Yorkshire and the North-east, where only six of 20 trusts have a PPU.
These proportions of total revenues have remained largely static for some years and in each region.
What can we learn from these big three trends?
The slower 2016-17 growth is likely to be a response to the activity pressures the NhS is experiencing now throughout the year. The currency of a PPU is the bed, and beds everywhere are at a premium.
‘Front-door’ non-elective admissions are impacting on NhS trust elective surgery programmes, and as the majority of PPU activity is elective surgery, this has restricted growth.
In the face of the above, some PPUs have not managed to protect their bed capacity for private patients and this can be seen in year-on-year decline in a few trusts.
But I think it is time to turn this thinking on its head. NhS PPUs are not a problem; they are an opportunity.
Private patient capacity and services are not part of the problem. They are and can be very much part of the answer to the sustained need to transform NhS services and performance.
Let’s remind ourselves what private patient services are for. They are there to provide a financial surplus to underpin the core NhS service.
They do this by providing a premium return on marginal use of already invested expensive resources: principally, built infrastructure, expensive equipment and specialist skills.
The private patient ‘tail’ should never wag the NhS ‘dog’ and so the range of non-financial benefits are best achieved when private patient services are very clearly aligned with wider trust strategies.
Figure 1
Delivering what the private sector doesn’t
This applies to any PPU, but particularly to those outside the largest conurbations, regardless of region.
On the ground, this means the typical NhS PPUs deliver the services the independent sector does not.
If the local independent hospital cannot or will not look after the highest-risk patients with co-morbidities or those requiring very complex cancer surgery or those that develop complications or those needing specialist regional care, then the NhS trust will. What happens to those patients the local independent sector provider screens out or on occasion transfers into the trust? Well, that depends on whether a trust has a PPU or not.
In the absence of a PPU, these patients default to the NhS. They join the queue and cost the NhS money. But, in a trust with a PPU, the patient and their consultant have an additional choice.
Many advantages
By choosing the PPU, a number of advantages are accessed. A charge can be made to the insurer and that delivers a surplus.
If a trust is over-performing against contract or works within a local healthcare economy fixed ‘envelope’ of funding, the marginal costs impact are also saved. Targets are eased, as the patient is out of the 18-week pathway or
N h S bed. And, for the patient, they have received a benefit from the insurance premiums they or their funder has paid for and would otherwise not enjoy.
While the above example is principally described in elective admission terms, the same is basically true for patients that need a non-elective admission to a bed or a service.
The insurer should pay, subject to certain requirement that the trust’s private practice business office will manage the process, although often it does not contact the insurer to do this.
Why? Because the patient or their relative does not know there is a PPU or because the trust does not ask or help to make them aware of their choices.
What consultants need to know is that a NhS PPU does not cannibalise the local private patient market and neither does it simply split consultant practice and make practitioners’ working lives more complex.
On the contrary, extended capacity and choice for patients and for insurers is also the experience of consultants too. These still underdeveloped, elective and non-elective service niches represent presently untapped fee income that is ‘lost’ from the provider system, remaining with the funders of care.
inadvertent subsidy
Also, these issues apply in the North and Midlands in the same
nHs PPus are not a problem; they are an opportunity
way as they do in the South –although insured populations are smaller, the need to access the NhS for patient safety is the same.
It is not known what the present cost of this inadvertent subsidy by the N h S of the private medical insurance system is, but it was estimated at £1bn a year in 2012 by Laing & Buisson – as named then – with £359m on patients with insurance that were not charged and £659m the estimated value of non-elective care for those with insurance.
Perhaps this is £1.2bn a year now, and maybe 20-25% of this is picked up by the extensive private sector infrastructure in London.
But if so, it still remains a £1bna-year opportunity for the rest of england’s NhS.
next month: a five-point action plan for ppUs
Philip Housden (right) is a director of Housden Group
Figure 2
Don’t risk your reputation
Doctors are expected to meet the highest standards of conduct in their work and in their personal lives – but sometimes it can go horribly wrong and put your private practice and reputation at risk.
Dr Nicola Lennard shows how a misjudgement can easily cast doubt on your character and attract attention from the GMC
A doctor’s first duty is to their patients, but, beyond this, they also have a responsibility to justify the public’s trust in the medical profession.
the GMc expects doctors to be honest and trustworthy in everything they do and will investigate allegations that cast doubt on a clinician’s integrity.
in our experience, such cases do not necessarily involve a deliberate attempt to mislead. More often, the doctor concerned has acted hastily, paid insufficient attention or simply failed to think through the consequences of their actions.
t he following scenarios illustrate the type of mistake which could put your private practice and reputation at risk – and also some advice on how to deal with these situations.
Misleading marketing
After several years working at an NHs trust, where he focused on coronary angioplasty procedures, a cardiologist was persuaded to join a private chambers which had been set up by several of his medical school contemporaries.
Asked to supply a profile for the website, the doctor provided a short biography and left the rest to the marketing team.
He thought no more of it until he was warned that another doctor had made a complaint to the GM c after the website text was amended to imply he was experienced in a range of interventional procedures he had little experience of.
mdU advice:
When advertising your services, the GM c expects you to make sure the material is factual and accurate.
Even if a third party is acting on your behalf, you remain accountable for material which is published in your name, so it is important to manage the process. As other people’s perceptions are important, it may also be helpful to ask a colleague to review material before it is published to ensure nothing can be misconstrued.
The doctor was shocked to be told some time later that she was being investigated by the GMC for failing to declare a criminal conviction
Most software includes tools which enable you to cite your sources on presentation slides or documents.
Even if you are under pressure to meet a deadline, try to make time to double-check a presentation or written paper.
Being overcommitted
A gynaecologist agreed to cover for an NH s colleague who was signed-off sick for two weeks.
When he looked at the rota for the following week, he saw that the doctor was on call on an evening when he held a regular private clinic in another town.
Not wanting to inconvenience these private patients, the gynaecologist went ahead with the clinic, but he was interrupted by a call from the registrar who was struggling to manage a patient with an ectopic emergency.
The perils of copying and pasting
A consultant was invited to give a presentation to the annual meeting of her specialist society. While researching online, she found a sentence in a published paper which neatly encapsulated a point she wanted to make.
in a hurry to finish the presentation – as she was being chased by the organisers – the consultant copied and pasted the quote into her presentation, but forgot to go back and reference the source.
c oincidentally, one of the authors of the original paper happened to be in the audience for the presentation and later complained to the society that the consultant was passing off the work as her own. the matter was also reported to the GMc
mdU advice:
Given the growing sensitivity about the issue of plagiarism –and the availability of plagiarismchecking software, it makes sense to make a note of references and citations as you go rather than trust yourself to spot them later.
Speeding into trouble
A consultant was driving back from a conference when she was recorded driving well over the speed limit on the motorway. instead of a fixed penalty notice, the doctor received a court summons.
the doctor pleaded guilty, but already had points on her licence and was disqualified from driving. the doctor was shocked to be told some time later that she was being investigated by the GMc for failing to declare a criminal conviction.
mdU advice:
the threshold for reporting criminal or disciplinary matters to the GMc is set out in ‘reporting criminal and regulatory proceedings within and outside the UK’.3
By the time the gynaecologist made it back to the hospital, the patient was already in surgery.
Although she recovered, her family complained that her treatment had been delayed because the consultant on call had not been available and later reported him to the GMc
mdU advice:
When on duty, the GMc expects you to be ‘readily accessible to patients and colleagues seeking information, advice or support’.1
According to the department of Health’s c ode of c onduct for Private Practice, 2 consultants should ensure that ‘private commitments do not prevent them from being able to attend a NHs emergency while they are on call for the NHs, including any emergency cover that they agree to provide for NHs colleagues.
‘in particular, private commitments that prevent an immediate response should not be undertaken at these times.’
to help avoid clashes, it makes sense to inform NHs employers about regular private commitments. in this instance, the hospital may have been able to arrange alternative cover if the consultant had given them enough notice.
While you do not have to inform the GM c about a fixed penalty notice for a road traffic offence, you are obliged to report any criminal conviction, regardless of where in the world it was incurred.
contact your medical defence organisation for advice if you are unsure whether to report something.
References
1. Paragraph 34, Good Medical Practice; GMC, 2013.
2. A Code of Conduct for Private Practice; Department of Health, January 2004. www.nhsemployers.org/~/media/ Employers/Documents/Pay%20and%20 reward/DH_085195.pdf.
3. Reporting criminal and regulatory proceedings within and outside the UK; GMC, updated November 2014. www.gmc-uk.org/guidance/ethical_guidance/21184.asp#Homeoffice
Dr Nicola Lennard (below) is a medico-legal adviser at the MDU
REviEw oF ThE yEAR
The news we brought you in 2017
December 2016-January 2017
➤ The Independent Doctors Federation (IDF) announced ambitious New Year plans to beef up services to members and become a stronger voice in 2017.
It revealed plans to better represent independent practitioners by taking a more proactive approach and relationship with the many stakeholders, such as insurers, who influence private medical practice.
It also announced plans to boost its membership of private consultants and GPs from the then level of around 1,200 doctors.
The IDF told Independent Practitioner Today it wanted to now ‘harness the strength’ of new doctor entrants to the independent sector and develop the range of services it could offer them.
Chief executive Sue Smith said IDF members should benefit from improvements being made to the IT infrastructure. These would give the organisation a more dynamic website and tool for both
members and the organisation’s administrative team.
She added: ‘But key to the future is to implement an active recruitment programme to harness the strength of new doctor entrants to the independent sector and develop the services that can be offered.
‘This includes a more proactive approach to and relationship with the many stakeholders that influence private medical practice, such as the private medical insurers.’
Ms Smith said a recurring theme during her review of the organisation was that in order to be a voice and to be heard, there needed to be sustained feedback on issues affecting the membership.
➤ The Government should support, not penalise, people with private medical insurance because they relieve the burden on a struggling NHS, according to an insurance boss.
Bupa Insurance chief executive Alex Perry warned that the latest rise in insurance premium tax made ‘no sense’.
He said: ‘The Government has announced three rises in less than two years on what is a completely misguided tax when it comes to health insurance.
‘It punishes those who take responsibility for protecting their health. Health insurance should be zero-rated like it is in many other countries and like life or critical illness insurance in the UK.’
The Chancellor’s Autumn statement bid to hit private patients yet again came despite new Bupa UK research showing that 58% of people believe health insurance should be tax-free just like life or critical illness cover.
Bupa said 50% of the general public thought it is unfair that people choosing to pay for health insurance were taxed on top of the taxes they pay to fund the NHS.
February
➤ The target date for official publication of consultant-level performance measures was scrapped following the failure of some smaller private hospitals to hand over all their data.
Instead, the Private Healthcare Information Network (PHIN) planned to publish hospital performance measures only in April 2017.
Consultant-level performance figures, which around 14,000
independent practitioners had been told would be issued at the same time, would be delayed until next year.
PHIN confirmed that many private hospitals – including all the larger national groups and a number of NHS private patient units –had begun submitting data to it in line with the requirements of the Competition and Markets Authority’s (CMA) Private Healthcare Market Investigation Order 2014. The network would start publishing hospital-level performance measures from 30 April 2017.
March
➤ The future of potentially thousands of consultants and GPs in private practice was under threat from a shock rise in indemnity costs.
Independent Practitioner Today warned that defence subscriptions would rise dramatically due to Lord Chancellor Liz Truss changing the controversial formula courts use to adjust large compensation payments to take account of future investment returns.
Lawyers said the ‘discount rate’ switch could see some multi-million-pound damages bills rocketing by 30% to 50%.
The Medical Defence Union warned lowering the discount rate from 2.5% to minus 0.75% would mean ‘a dramatic increase’ in the cost of indemnifying members.
It warned compensation award costs would go up immediately for known claims and also those arising from future incidents. And it would apply retrospectively to claims for past negligent incidents where no claim has yet been made but will be at some future date.
Chief executive Dr Christine Tomkins said: ‘We need a longterm solution to the inflationbusting rises we are seeing in clinical negligence compensation payments. Personal injury law needs root and branch reform.
‘The impact on our members and the provision of healthcare is calamitous and a solution is needed urgently.’
➤ ‘Surprising numbers’ of independent practitioners are putting themselves at risk because they have not caught up with new duties for obtaining consent to treatment, we revealed.
Solicitor Paul Sankey said doctors across the specialties seemed to have missed a law change two years previously.
The landmark Montgomery v Lanarkshire Health Board case redefined the legal doctor-patient relationship and placed a higher obligation on specialists to warn of treatment risks.
But Foot Anstey LLP partner Mr Sankey said: ‘Many seem to know little or nothing of the change. The continued use of standardised consent forms suggests practice has not sufficiently changed. Standard forms are unlikely to record the sort of patient-centred advice and discussion the law expects.’
➤ Consultants and Independent Practitioner Today won their campaign to halt NHS England plans to force them to reveal private practice earnings.
They had labelled the proposals, issued the previous Autumn, pointless, unworkable and ludicrous.
We warned the idea did not add up, calling it ‘bonkers’ – and all the leading consultants’ bodies joined in the criticism.
So NHS England had a re-think, although concerns remained about possible attempts by trusts to control consultants’ activities.
April
➤ Independent practitioners were urged to sign a petition aimed at protecting private patients from further increases in the insurance premium tax they pay on health cover.
Supporters of a new campaign, launched by the professional body representing companies who sell an estimated 70% of the UK’s private medical insurance, feared the tax element on policies could otherwise be the same as VAT.
But they warned thousands of policyholders could not afford a 20% tax level and would cancel their cover, leading to more pressures on an already overloaded NHS.
May
➤ Independent practitioners were being cautious about chasing more overseas business following a fall in the number of acute patients coming to central London from abroad.
New figures for the area showed the self-pay market dipped 15% between 2014-15 – a drop in value from £261m to £222m.
According to LaingBuisson’s report entitled Private Acute
Medical Care in Central London, the fall in international self-pay dragged down a general growing trend in UK self-pay.
Embassy patients held up overall, rising 1% from £320m to £323m, and were helped by an improved NHS PPU performance, although many independents suffered declines.
The UK private medical insurance contribution rose 11% from £782m to £870m, representing 61% of the funding.
Report author Ted Townsend told Independent Practitioner Today: ‘While it is hard to tell if the downturn in overseas patients is a hiccup or a new longer-term trend, it would appear that many practitioners are becoming wary of overcommitting time and energy to this historically lucrative market.’
He said a drop in the oil price hit the amount of money available to overseas patients, while new competition plus a desire to keep patients at home had affected overseas revenues in London ‘and apparently continues to do so’.
The issue for many private practice businesses was how much time and effort they should now invest in overseas patients if the trend was going away from them ‘although it is still a big “if”’.
His report for market analysts LaingBuisson said NHS PPUs overall have a higher dependence on embassy earnings than the independent sector, suggesting there was still demand out there. They were thought to have suffered less of a down-turn in 2015 than private hospitals.
➤ HCA Healthcare UK unveiled a £50m investment in cutting-edge
cancer care with two state-of-the-art centres – the £38.2m London Bridge Hospital, Private Care at Guy’s and the newly-built £12m HCA at Sydney Street, an outpatients and diagnostics centre in Chelsea.
June
➤ Independent practitioners were alerted to gear up for far bigger tax payments than expected from January 2018 following new pension rules.
Changes in the pension savings annual allowance rules in the 2016-17 tax year meant many would face an additional hit of £11,000 – and some nearly double that.
And specialist medical accountants warned more consultants, and some private GPs, will be caught by the revised regulations in future years.
One accountant told Independent Practitioner Today: ‘Our concern is that, for many consultants, this problem is off their radar and many will be unprepared for the potential problem.
‘We would therefore recommend they take action early and speak to their accountants and independent financial advisers.
‘This is further compounded by the fact that, in many cases, NHS Pensions will not be providing information to enable an accurate assessment of this at an early stage.’
July-August
➤ The whole private health sector was urged to commit to breaking down barriers preventing patients from easily accessing consultants and treatment information.
Fiona Booth, chief executive of the Association of Independent Healthcare Organisations (AIHO), revealed patients’ frustration at a ‘double whammy’ facing them when they tried to access private care.
New research from the organisation found the two least satisfactory aspects of a patient’s
experience when receiving independent healthcare was the information given to enable their choice, and the referral process.
She said: ‘We asked patients what sources of information they used to decide about receiving treatment at an independent hospital and how they rated this information out of ten.
‘Most people said their GP’s recommendation guided their choice of provider. And sadly, they only rated the quality of this information two out of ten. Some patients found their GP could not offer them comprehensive information.
‘This should concern all of us, as GPs are the first point of call and tend to be the main channel for patients seeking treatment.’
Ms Booth said AIHO’s research also uncovered mixed reviews on the information received from insurers, with patients complaining the information did not provide treatment costs or clear explanations on what their package covered.
Patients criticised the referral process both from the NHS and insurers.
She warned the audience at the Private Healthcare Summit 2017 that it would be ‘foolish’ if independent hospitals ignored these findings.
September
➤ A £1bn self-pay acute market is now seen as a potential reality in the UK within the next four years – and business-minded consultants were being advised to gear-up to take advantage of it.
The rise and rise of self-pay patients was a key feature of a new report out this month which
found observers and commentators agree this market growth is between 10% and 20% a year.
According to the Private Healthcare UK Selfpay Market Report 2017, the growth rate is as much as 25% a year in London. But if a straight-line growth of around 15% a year was assumed for the next three years, the self-pay market non-cosmetic spend could rise from its current level at around £623m to around £948m by 2020.
A document highlighting key themes of the report, researched and written by chief executive Keith Pollard and his team at www. privatehealth.co.uk, stressed the role and visibility of consultants is changing and there is now a greater need than ever for them to collaborate with providers to design and deliver self-pay pathways.
It recognised a growing trend for consultants to establish a strong personal online and digital presence and said this would have an important future role in influencing patient choice.
➤ Hopes were high that private doctors would find the medical revalidation experience far more useful in future.
The independent sector backed a GMC plan to improve it by making it a more meaningful experience for private practitioners and responsible officers.
october
➤ Mounting numbers of independent practitioners are being helped to reduce stress levels brought on by rising pressures in private practice.
Psychologists at one City practice said tension factors included financial concerns arising from
higher expenses on indemnity cover, rooms and secretaries. They were also losing out due to static income from private medical insurers, having to work harder to match previous year’s profits, and fears about being selected for a costly tax probe.
Increased administrative paperwork and red tape from newer requirements – including CQC inspections, revalidation and appraisal – was also taking its toll.
Consultant counselling psychologist Dr Michael Sinclair told Independent Practitioner Today : ‘I am seeing increased stress among doctors in private practice, consultants and GPs.’
November
➤ Doctors’ expressions of interest in working on a salaried basis in a new flagship private hospital have gone through the four-figure mark, said its chief operating officer.
Mr Keith Hague said London’s Cleveland Clinic, due to open in two-and-a-half years’ time with an initial 200 beds (29 ITU), had sparked interest from ‘thousands’.
His remarks came in response to a challenge from a representative of the Independent Doctors Federation (IDF), whose members have voiced opposition to a private salaried service model.
IDF president-elect Dr Neil Haughton, chairman of the group’s GP Committee, warned him private doctors liked being self-employed, adding: ‘I wonder where you are going to get all the doctors from.’
Don’t be without us in 2018 sign up for a subscription by direct debit today and save £15. see page 24
Diary of a clinic
Developing your own clinical premises requires grasping the nettle and putting on a hard hat. But for those bold enough to do it, there are plenty of rewards, says Maurice Citron. Dr Ian Drever, a consultant psychiatrist, has successfully risen to the challenge and is the entrepreneurial spirit behind Esher Groves, a new psychiatric day clinic in Surrey
Us I n G Esh E r Groves as a case study, here and for the next three issues of Independent Practitioner Today, I will sketch out some of the important issues and processes you will need to consider if you decide to acquire, develop and trade from your own clinical property.
Location, location, location
Esher Groves acquired 17 Church street in May 2014. The property is in a secondary retail position off the main h igh s treet in the affluent s urrey market town of Esher.
The location is interesting in
that it is a good example of how healthcare practices are able to take advantage of the uncertainty evident across many retail locations up and down the country.
Online retail shopping as well as the effects of the 2007 downturn has put a strain on the high street.
Commercial rents and investment valuations have either dropped or remained stagnant because of falling demand on the occupier side as well as the investor side.
This has given alternative use occupiers, such as private healthcare practices, an opportunity to competitively set up shop on or be just beside the high street.
Chartered surveyors classify retail units as primary, secondary or tertiary. The classification essentially differentiates locations by the amount of footfall they receive.
s ince private healthcare is a planned event, not an impulsive buy, it suits practices to have secondary locations, which offer good value for money.
Transport connectivity and parking require careful consideration. Parking can potentially be the most problematic part of a client’s booking decision-making process.
Local and accessible private
healthcare is an attractive proposition as long as the anxiety of finding parking doesn’t negatively impact the client’s experience.
Esher Groves is a 15-minute walk from the local train station. There is a large council car park within a five-minute walk and full day permits are available at relatively competitive prices.
Land rights and restrictions
In legal terms, when a property is purchased, an interest in the land is acquired and this is usually a freehold or leasehold.
A freehold interest provides for the exclusive right to possess the land forever without any superior interest. In the case of a leasehold, interest in the exclusive possession will be defined by a number of years and the land is held by agreement with a superior landlord.
A freehold interest affords the greatest freedom on the land, but there may still be restrictions on the land and these can come in a variety of forms.
seek legal advice
It is important to seek legal advice on the interest you are considering purchasing and what restrictions, if any, exist, particularly if you intend to develop the land or extend the property. A simple
The front and back of the esher property are shown before building work began
Dr Drever’s DreaM
Dr Ian Drever is a consultant psychiatrist with an interest in the treatment of depression and anxiety, and has practised full time in the private sector for the past ten years.
During this time, he has become very proficient in the treatment of high-functioning individuals, often from the corporate world, who have developed a range of illness features.
The project at esher Groves brings to life a long-held dream of providing top-quality clinical care within a unique, purpose-built environment.
example would be in the case where a property is located in a conservation area.
The property in Esher was subject to an issue of acquired rights or easement. An easement is a right to use or restrict the use of the land of another person in some way or other.
A neighbour had used the rear of the property to park their cars for several years. Although the freehold was subject to an existing pedestrian right of way on the land established in 1920, the neighbours claimed a right to park their car because of the length of time they had done so. In law, the principle is called ‘prescription’ and relies on a continuous use for at least 20 years.
Esher Groves successfully defended the claim by referencing an email the previous landlord sent to the neighbours.
In it, the landlord advised them the use of his land to park their car would end after he had sold his interest.
This is a good example of how interests in land can be complex, historical and contentious. Care should be taken to ensure you are buying a property that will allow you to achieve the clinical premises you want.
property finance
There are plenty of commercial real estate lenders keen to support private healthcare practices for the simple reason that the healthcare sector has a good trackrecord.
What will lenders look for? Lenders will consider the debt requirements in relation to the value of the property, but since the purchaser will invariably occupy the property, lenders will want to see that the trading busi-
ness can generate enough earnings to service the debt required. servicing includes interest payments and capital repayments with a certain amount of additional capacity to protect against interest rate volatility.
Earnings before interest, tax depreciation and amortisation (EBITDA) is the performance measurement used to appraise the financial strength of the business. An application will have a good chance of success if the clinical business can present a resilient and predictable earnings trackrecord over the last three years. Bear in mind that lenders are amenable to include other assets and income streams in support of an application. This strategy was successfully used by Esher Groves, who were able to support debt servicing from other clinical incomes.
This was particularly useful, since Esher Groves intended to conduct major extensions to the property before trading started. Other clients of mine have also been able to provide additional security using their buy-to-let investment properties and on their principal place of residence. next month, we will look at the planning process and development preliminaries.
Following successful acquisition, Esher Groves set out to secure planning consent to extend and completely refurbish the property.
An act of god will illustrate why it is very important to ensure due attention is given to getting your buildings insurance right.
Maurice Citron (left) is director of Citron Singer Finance, a commercial property finance broker specialising in the health-care sector
Dr Ian Drever pictured on site during building work
Maurice Citron
How outsourcing can fit your bills
The ‘Big Five’ common questions private consultants are asking about medical billing and collection are answered here by Findlay Fyfe (right)
Five big questions seem to dominate when consultants ask me about medical billing and collection.
These queries kept arising when my company exhibited at two conferences recently in Liverpool: the annual congresses of the b ritish Orthopaedic Association and the Association of Anaesthetists of g reat b ritain and ireland.
And they cropped up again when Medical b illing and Collection presented at two seminars for doctors setting up in private practice.
So i thought i ’d share the answers with a wider audience.
1
What is the set-up process?
We use a software package which has been designed specifically for our business where we create the practice by name and structure and set up the appropriate rules applied to that practice. We have a contract and a set of forms to notify the insurance companies that we act as the billing provider for the practice.
The AXA process now involves online registration; however, with the correct information to hand, it can be done fairly quickly.
Once our contract and forms are
signed, we can start working on behalf of the practice. How long this can take is mainly down to the practice, but can be as short as a few days.
Once the practice is ready, then an account manager is assigned to the practice who will be responsible for all aspects of the billing and collection.
This means that they get to understand the business of the practice, ensuring both continuity and good communication between all parties.
2 Will you chase any backlog?
Almost all of the individual consultants and group practices, clinics or hospitals that join us have a backlog of debts owed, so we are very experienced at dealing with them. And we are proving very successful in collecting the outstanding amounts.
We have an established process in place to deal with all the outstanding invoices and chasing them in an appropriate and sensitive manner.
For example, we have taken on many clients in the past with several hundreds of thousands of pounds worth of unpaid bills. And that’s something we are very comfortable taking on.
3
How does the billing and collection process work?
The billing information can be sent to us by a variety of ways: these include Dropbox or scanned and emailed with preferably encrypted password or posted, as well as pictures of patients’ details taken and emailed, with any additional information added.
We raise the invoice the same day that we receive the billing information or certainly within 24 hours.
e ach payment company –insurer, embassy, solicitor, selfpayer, sponsor, hospital group – has different payment terms, which are preset in our bespoke medical billing software. i n turn, this means that we can chase any late payment of the money as quickly as possible.
The pricing is again preset into the software per payment company as per the instructions of the practice, so that it is priced correctly.
Any billing information which cannot be converted into an invoice for any reason is stored on our software until we receive the correct information. This ensures nothing is missed.
We aim to get all insurance payments made directly to the practice bank account by automatic bank transfer ( b ACS) with the remittance advice being sent to us, where it is reconciled on our software.
Any cheques we receive made out to the practice from any payment company or selfpayer are accurately recorded before sending the money direct to the client or their bank account.
Any money we collect on behalf of the client (credit/debit card payments) will be transferred electronically to the practice bank account on a Monday morning. We will always consult with the practice on a case by case basis before sending anything to the debt collectors or writing an amount off. Using debt collectors is included in our fees and does not cost the practice any more.
4
So what reports do I get?
Our practice management module allows the client to have online access to a wide range of
financial and management data relating to the practice.
This includes:
Aged debt information;
b ank reconciliation information;
billing and payment analysis;
Patient activity data;
Referral analysis;
Location breakdown:
insurance breakdown;
Fee analysis.
This data can be viewed online as well as downloaded into a spreadsheet. And some reports can even be set up to be sent directly to you by text (SMS) and/ or email on a weekly basis.
5 What other services do I get from MBC?
With over 25 years’ experience, we are in a position to offer advice on all commercial aspects of the practice as well as the billing process, including medico legal terms, patient registration forms and many other aspects.
We send out periodic emails to keep our clients up to date with what is happening within the private medical market as well as providing one to one advice as required.
Findlay Fyfe is managing director at Medical Billing and Collection
Chasing the money: many doctor clients have had several hundreds of thousands of pounds-worth of unpaid bills
When winding down your work
Whether you are counting down the days or feeling somewhat sad about leaving the medical world, retirement needs to be well planned for. And that is especially true for those with a private practice.
Thought needs to be given to the ongoing management of medical records, and ensuring the safe hand-over of patients can be a lengthy process.
Dr Lucy Hanington looks at the rules and practicalities a retiring doctor may need to consider
CHENIES MEWS IMAGING CENTRE
SPECIALIST MRI IN THE HEART OF LONDON
• Advanced Cardiac MRI
• 3T Neuro MRI
• MRI for patients with cardiac pacemakers
T: 0203 887 0566
E: referrals@cheniesmews.com
W: www.cheniesmews.com
medical records
The GMC’s Confidentiality guidance states at paragraph 128:1
‘If you are responsible for managing patient records or other patient information, you must make sure the records you are responsible for are made, stored, transferred, protected and disposed of in line with data protection law and other relevant laws.
‘You should make use of professional expertise when selecting and developing systems to record, access and send electronic data.’
It may be necessary to make alternative arrangements for the secure storage of records on retirement, if you are unable to keep them in their current location.
While there are no specific guidelines dealing with how long private records need to be kept for, paragraph 130 of the above GMC guidance states:
‘The UK health departments publish guidance on how long health records should be kept and how they should be disposed of. You should follow the guidance, even if you do not work in the NHS.’
Review records
Details of the guidance for each country can be found in the table on the opposite page. A summary of recommendations has been included, but it will be important to review the guidance in each case, as there are a number of exceptions to the rules.
It is advisable to review records towards the end of the retention period, as if there has been an adverse incident or there is poten-
tial for a claim, it may be sensible to keep them for longer.
Defending yourself as a doctor is much harder in the absence of records. However, you should bear in mind the Data Protection Act 1988, which states:
‘Personal data processed for any purpose or purposes shall not be kept longer than is necessary for that purpose or those purposes.’ If you are planning to retain records beyond the recommended period, it is worth recording the reason for doing so.
If you have decided that records should be destroyed, you will need to ensure that this is done in an appropriate manner.
For example, you may wish to incinerate paper records, shred them using a cross-cut shredder or approach an appropriately accredited commercial company who can assist with this process on your behalf. Such companies will also issue a certificate of destruction for your own records, which testifies your compliance with the Data Protection legislation.
Given your ongoing obligations in relation to your private patient records, you may wish to consider registering with the Office of the Information Commissioner as a Data Controller, if you have not done so already.
Handover of patients
If patients are likely to require ongoing care, it will be necessary to discuss future arrangements with them. It will also be important to ensure that you follow the
GMC’s Good Medical Practice 2 in handing patients over.
This guidance states that you must:
‘Check, where practical, that a named clinician or team has taken over responsibility when your role in providing a patient’s care has ended. This may be particularly important for patients with impaired capacity or who are vulnerable for other reasons.’
Ask the patient
You will need to ask each patient whether they wish to continue with private care or return to the NHS.
Private patients may well have a view as to which practitioner they would prefer to see in future. The doctor you are to hand over to should be someone who ‘has the appropriate qualifications, skills and experience to provide safe care for the patient’.
Identifying an individual who will take over your private practice on your retirement can significantly ease the administrative burden.
Dealing with medical records and the hand-over of patients are likely to be the most burdensome retirement-related tasks.
Other issues to consider include your GMC registration status and your indemnity/insurance arrangements (see page 40), as well as the potential for ongoing involvement in cases if you have carried out expert work.
You may wish to seek specific advice from your medical defence organisation regarding these matters.
Dr Lucy Hanington (below) is a medico-legal adviser at Medical Protection
the minimum retention times for various types of records are set out in appendix 3.
For adult patients, in cases where the notes do not relate to oncology, maternity or mental health conditions, this time is usually eight years.
t he notes of paediatric patients should be kept until the 25th birthday unless the patient was 17 at the time treatment ended, in which case they should be kept until the 26th birthday.
maternity notes should be retained for 25 years.
For GP records, the retention period is ten years after death (exceptions exist).
Wales
Welsh Health Circular (2000) 71: For the record (the national assembly for Wales, 2000) – appendix B
www.wales.nhs.uk/sites3/ d ocuments/ 950/WHC_2000_71.pdf
Scotland
records management: nHS Code of Practice (Scotland) (Scottish Government, 2008)
www.gov.scot/Publications/2008/ 07/01082955/0
See a nnex d – t he m anagement, r etention and d isposal of Personal Health records
r equirements for adult, child, maternity and GP records similar to those for england set out above.
Northern Ireland Good management, Good records; d epartment of Health, Social Services and Public Safety, 2005
records of adult patients (not relating to maternity or oncology) should usually be kept for six years after last date of entry – or three years after death, if earlier.
Children – as for england; if a child dies, records to be kept for three years after death.
m aternity notes should be retained for 25 years after the birth of the last child.
GP records should usually be kept for the lifetime of the patient and for three years after death. there are specific provisions for electronic patient records.
adult records (not included in another category) should be kept for eight years.
Children – records should be kept until the patient’s 25th birthday or 26th if young person was 17 at conclusion of treatment or eight years after last entry, if longer. if the child dies, keep for eight years after death. Consider keeping for longer if relevant to adult condition or there are genetic implications.
maternity – 25 years.
GP records – see guidance, as provisions are detailed.
KEEp iT lEGAl: indEMniTy & insURAnCE
Don’t think you can skimp on your cover
All doctors and other healthcare professionals should, of course, be aware of the need for insurance or indemnity cover.
But, from time to time, I am referred a client who, for one reason or another, doesn’t have cover for a case – be it civil litigation, regulatory (GMc) proceedings or a criminal investigation.
this can be a disaster for many reasons.
For a start, there is the expense. lawyers aren’t cheap, and however painful it may feel to pay your indemnity/insurance fee or premium every year, a lawyer’s invoice is not something you want to spend your hard-earned cash on.
Paying for legal advice and representation is just the beginning. If you are being sued for clinical negligence and/or breach of contract and you lose or make an offer of settlement, you will also have to pay compensation/damages to the patient and the patient’s legal fees.
Even if you win, you will probably still be liable for your own lawyers’ fees, as the other side will only be ordered to pay your costs in very limited circumstances since the introduction of qualified one-way cost shifting – and they will never pay 100%.
then there is the stress. lawyers
may not have the best bedside manner, but they are at least a source of advice. Your insurer/ indemnifier may also provide you with support and advice.
GMC sanction
Another potential, and serious, consequence is that you may face GMc proceedings. You are professionally obliged to have adequate insurance/indemnity cover in place and the GM c has been known to erase doctors who do not.
An example is the recent High court case in which a consultant obstetrician unsuccessfully appealed against a finding by the GMc’s Medical Practitioners tribunal service (MPts) panel to erase his name from the register because he had practised privately for nearly five years without professional indemnity cover.
the reason you are required to have cover is to protect your patients. You are required to have cover that enables your patients to be paid compensation if you are liable for loss or damage they have suffered as a result of your acts or omissions.
You are not allowed to selfinsure – that is, to work on the basis that you will pay compensa-
➱ 42
With mounting claims and defence costs hitting private doctors hard in the pocket and purse, Hempsons’ Tania Francis (right) takes a legal look at what every independent practitioner needs to know
Reasons why docToRs aRe
noT coveRed:
sometimes it’s deliberate, believe it or not, perhaps because of the cost
sometimes healthcare professionals don’t realise that they need indemnity cover – perhaps believing that they will be covered by the nhs
sometimes it’s an administrative error – not opening your renewal notice or not giving your insurer or indemnifier your new address so that you don’t receive it. direct debit helps to avoid this scenario
There are also times when a doctor has not told their insurer or indemnifier of a change in their scope of work or earnings/turnover. This can lead to refusal of cover/assistance
tion out of your own pocket if you are sued, perhaps because you think you are at a low risk of being sued or that any claim is unlikely to be for a sum you can’t afford.
Even if you were allowed to, I wouldn’t recommend it. Even in a low-risk specialty, the value of claims plus legal fees can be high.
Crown indemnity
You don’t need cover if your patients are protected in some other way. If you work exclusively as an employed doctor in NH s secondary care, you will be covered by NH s – or ‘ c rown’ –indemnity. Your employing NHs trust will be liable for any claim made by a patient treated by you.
In practice, the patient will sue the trust rather than you personally. However, NH s indemnity will not cover your private practice or assist with a GMc or criminal complaint.
In addition, if you are called to give evidence at an inquest, and there is some conflict between you and your employer, you may also require your own independent legal advice, which may not be funded by your employer.
Gps not covered
As you will be well aware, NH s GPs are not covered by NH s indemnity – a topical bone of contention – and must therefore have their own cover, although recently the Health secretary has announced a new state scheme is being considered.
If you have a private practice, insurance/indemnity is essential. You should discuss your needs carefully with your insurer or indemnifier.
You must have insurance/ indemnity cover for your entire scope of work. If you employ staff, you are vicariously liable for their acts and omissions, and you must therefore ensure that you have cover that includes your employees.
And if you are treating NH s patients in the private sector, you need to check the indemnity arrangements so that you know whether the NH s is providing indemnity or whether you will be personally liable.
If the latter, make sure you are covered by your own policy for what you are about to do, and
If you start doing something in the private sector that you used only to do in the nhs, discuss it with your insurer/indemnifier
check whether you will be increasing your profit/turnover as a result of taking on the work. the reasons for lack of cover are many.
s ometimes it’s deliberate, believe it or not, perhaps because of the cost. sometimes healthcare professionals don’t realise that they need cover – perhaps believing that they will be covered by the NHs s ometimes it’s an administrative error – not opening your renewal notice or not giving your insurer or indemnifier your new address so that you don’t receive it. direct debit helps to avoid this scenario.
t here are also times when a doctor has not told their insurer or indemnifier of a change in their scope of work or earnings/ turnover.
t his can lead to refusal of cover/assistance. It’s important to review the information provided to your insurer or indemnifier at each renewal date and when any changes occur during the year.
Check your turnover
When you prepare/approve your tax return, think to check whether your income/turnover has increased since the previous year.
Equally, if you start doing something in the private sector that you used only to do in the NHs, discuss it with your insurer/ indemnifier.
You must also be aware of what your policy/membership does and does not cover. Your professional obligation is only to have cover for your liabilities to patients. However, you may also want cover for GMc complaints and criminal proceedings and possibly inquests.
Although patients cannot
recover damages via these means, you will need legal assistance and representation, and that can be costly, especially if the proceedings go all the way to an MP ts hearing, or a crown court trial. It happens…
Changing provider
If you change your indemnity/ insurance provider, there are some issues you should be aware of.
You need to know what your current and prospective providers will cover and ensure that there are no gaps and no double cover. It is important to report any claims or potential claims you become aware of, both to your insurance company/indemnifier at the time, and to any future provider. this is to ensure that liability is accepted by the appropriate company and cover is not refused or your policy invalidated. When you are shopping around,
once you’ve had a claim or GMc complaint, it is harder and more expensive to get cover – without which you cannot work. so prevention really is better than cure
you for a claim made – and reported – during the period of cover, even if the alleged negligence took place years previously, as long as it took place after the retroactive date. so it’s very important to have the correct retroactive date in your policy.
make sure you are comparing like with like. look at what they will cover you for, check the exclusions and excesses, the limits of liability and what sort of advice/ support they will offer you. take advice if you need it. there are basically two ways in which claims/complaints can be covered. these are on a:
‘claims made’ basis; ‘claims/losses occurrence’ basis. A ‘claims made’ policy will cover
A ‘claims occurring’ policy will cover you for a claim relating to negligence that occurred during the period of cover, even if the claim is made some time later – by which time you may not be with that company any more or may have retired. s o make sure you keep details of all old policies for that reason.
Whenever you cancel cover or allow it to lapse, you need to think about run-off cover, especially for ‘claims made’ policies. similarly, when you retire, before you cancel anything, think about run-off cover.
You should ensure that you have cover for any claims that
may be made after cancellation of your policies, relating to treatment provided during your entire previous career, as claims can be made many years after the allegedly negligent treatment for a variety of reasons.
this may all sound like a lot of hard work, but it’s worth getting it right. once you have had a claim or GM c complaint, it is harder and more expensive to get cover –without which you cannot work. so prevention really is better than cure.
Tania Francis is a solicitor and a partner specialist healthcare law firm Hempsons. She is also a qualified doctor. Tania advises doctors, dentists and other healthcare practitioners and providers. She specialises in regulatory law and clinical negligence and healthcare-related contractual disputes, including cases where there are related criminal proceedings
Free legal advice for independent practitioner Today readers IPt
independent practitioner Today has joined forces with leading niche healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
call Hempsons on 020 7839 0278 between 9am and 5pm monday to Friday for your ten minutes’ of free legal advice.
contracts: ian Hempseed Faisal dhalla
Hilary King HR/employment: premises: Fiona Mclellan lynne Abbess
Know your bias when investing
Your brain could stop you being a good investor. Dr Benjamin Holdsworth (right) shows why behavioural finance should be important to you
I have been interested in the field of behavioural finance and the implications for our financial decision-making for a long time.
news that one of the most wellknown behaviour finance experts, Prof Richard Thaler, has scooped this year’s n obel Prize for economics is welcome.
You may question why a lauded economics authority is important to you on a day-to-day level, but his work on why and how we make decisions can impact your own financial outcomes.
Richard Thaler created the concept of ‘nudge theory’ – the notion that small prompts can change our behaviour. his book of the same name continues to feature as a best-seller.
Thaler has applied ‘nudging’ to a wide range of everyday challenges. he worked with Schiphol International a irport to reduce the unpleasant effects that thousands of travellers’ bad aim can have in toilets. he found that putting an image of a black fly into the male urinals reduced spillage by some 80%.
Under David Cameron, Thaler created the ‘behavioural Insights Team’ – often referred to as the ‘ n udge Unit’. h e realised that millions of elderly people would
be inclined to heat their homes if the Government named the financial pay-out a ‘winter fuel payment’ despite there being no restrictions on how they could actually spend the cash.
The nudge Unit was created to focus on public health issues such as organ donation – the results were an impressive 100,000 extra donations a year – but it grew to cover pensions and taxes too.
Thaler rewrote hMRC’s letter to wealthy tax-avoiders detailing the local community facilities which would miss out should they continue to evade their liabilities. The
result? The collection of an extra £200m in income tax.
In south London, Thaler reduced vandalism on shops by asking graffiti artists to paint babies’ faces on the shutters. The list goes on, and soon we realise we too have probably been ‘nudged’ at some time.
In the wider area of behaviour finance, Thaler promotes that once we understand why and how people make decisions, we can shape their future judgements to be more logical.
Conventional financial theory dictates that people are rational ‘wealth maximisers’ – that is, they are generally well informed, consistent and make decisions in their best interests. but the evidence to the contrary is vast: the dot-com bubble, the financial crisis and backing ‘sure thing’ investments such as Tesco, which recently suffered the worse downturn in UK retail history.
h umans have evolved mental ‘short cuts’ to allow us to make day-to-day decisions quickly. h owever, as a result of our own processing limitations, in complex situations these short cuts lead to ‘biases’ – a systematic pattern of deviation from rational thinking.
b iases can affect every type of
decision, but have substantial implications when assessing financial choices. how we process information and the preferences that lie within our psyche can be detrimental to our long-term aims and objectives.
There are several different biases which include:
overconfidence
Savers hold too much confidence in their ability to predict the outcome of their investment decisions. They often place ‘too many eggs in one basket’, resulting in high-risk, under-diversified portfolio.
Representativeness
Investors believe that a good company will be a good stock. See the previous note on Tesco. virgin is another name which tends to be cast in a good light despite historically poor balance sheets.
loss aversion
We feel the pain of loss more acutely than we feel the pleasure of gain. If there is a part of our financial commitments which is not working effectively, we are hesitant to change it to bring it in line with the rest of our investment profile.
Economist Prof Richard Thaler, inventor of ‘nudge theory’
Often people will stick with the status quo, even if it is costing money, rather than admit their mistake.
Mental accounting
Individuals often allocate wealth to separate mental compartments and ignore the relationship between these ‘pots’, focusing simply on the behaviour of individual assets. assets are inherently part of a portfolio and should be considered as such.
For example, for most, the nhS pension is by far their most valuable asset, but doctors can happily receive investment ‘advice’ which ignores it.
Frame dependence and anchoring
The manner in which information is presented to us affects our decision-making process and leads us to concentrate on irrelevant factors. For example, an item
‘reduced’ from £75 to £50 appears as better value than a full-price item at £50. a lthough biases cannot be cured, once recognised, it becomes easier to avoid the pitfalls they can cause.
The study of behaviour finance has subsequently led to the notion of ‘behaviour coaching’. a good financial adviser should be a constant source of guidance, helping investors to avoid knee-jerk reactions and to maintain a long-term perspective.
although each investor is different, human nature means that most of us will display emotionally-led behaviour while investing.
Your financial adviser should work with you to assess your own objectives, your attitude to risk and the biases that you are inclined to reference when considering important options. a s investment guru b enjamin
Graham famously stated: ‘The investor’s chief problem – and even his worst enemy – is likely to be himself.’
Dr Benjamin Holdsworth is a practising medic and business development director of Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
For most, the NHS pension is by far their most valuable asset, but doctors can happily receive investment ‘advice’ which ignores it
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
EXPERT ADVICE YOU CAN TRUST
EXPERT ADVICE YOU CAN TRUST
Since starting in the mid 1970’s Sandison Easson has continued to grow and is one of the largest independent medical specialist accountants in the UK.
Since starting in the mid 1970’s Sandison Easson has continued to grow and is one of the largest independent medical specialist accountants in the UK.
Since starting in the mid 1970’s Sandison Easson has continued to grow and is one of the largest independent medical specialist accountants in the UK.
Sandison Easson acts for medical professionals throughout all stages of their career and has clients in almost every town in England, Scotland and Wales.
Sandison Easson acts for medical professionals throughout all stages of their career and has clients in almost every town in England, Scotland and Wales.
Sandison Easson acts for medical professionals throughout all stages of their career and has clients in almost every town in England, Scotland and Wales.
We provide the usual services you would expect from an accountant such as preparation of your accounts and tax declarations but offer so much more including advice on:
We provide the usual services you would expect from an accountant such as preparation of your accounts and tax declarations but offer so much more including advice on:
We provide the usual services you would expect from an accountant such as preparation of your accounts and tax declarations but offer so much more including advice on:
• Setting up in Private Practice
• Setting up in Private Practice
• Setting up in Private Practice
• Developing your Private Practice
• Developing your Private Practice
• Developing your Private Practice
• Tapering of the Annual Allowance
• Tapering of the Annual Allowance
• Tapering of the Annual Allowance
• Lifetime Allowance planning
• Lifetime Allowance planning
• Lifetime Allowance planning
• Personal Allowance planning
• Personal Allowance planning
• Personal Allowance planning
• Reviewing your PAYE Coding Notices SPECIALIST
• Expenses that you can claim and those you cannot
• Expenses that you can claim and those you cannot
• Expenses that you can claim and those you cannot
• Minimising your tax bills
• Minimising your tax bills
• Minimising your tax bills
• Reviewing your PAYE Coding Notices
• Reviewing your PAYE Coding Notices
T 01625 527 351 E info@sandisoneasson.co.uk
Suspicion of abuse
Dr Ellie Mein (right), medico-legal adviser at the MDU, explores medical professionals’ legal and ethical duties to patients who may be experiencing domestic violence
Dilemma 1 My patient may be abuse victim
QI am a private GP and recently one of my patients came to me complaining of headaches, feeling tired all the time and having palpitations. She was tearful and admitted to feeling anxious and having a low mood.
She confided that she went to the accident and emergency department for a fractured zygoma following a fall down the stairs two weeks ago, and when I took her blood pressure I noticed bruises on her wrists.
How can I establish whether everything is OK within the home?
AIt is estimated that one-infour women in the UK will experience domestic violence. Medical professionals are often in a position to spot the signs, so it is important to be alert to the possibility of domestic abuse, aware of your duty to safeguard patients and to maintain confidentiality in such cases.
Safeguarding patients is especially important, as while GPs may pick up on signs of possible domestic abuse, patients may well be reluctant to confirm this.
In 2012, the Royal College of General Practitioners (RCGP) issued guidance on the development of a practice policy for managing cases of domestic abuse. The guidance recommends electing a senior person within the practice to identify and engage with local domestic violence support services and establishing a care pathway for people to access these services.
Also, remember that all members of the healthcare team have a duty to be alert to the symptoms of possible domestic abuse. Training should be provided to staff on how they should investigate the situation sensitively with patients and the steps that need to be taken in response to a disclosure. It is important that careful records of such consultations are made, and that information should only be shared with the consent of the patient, unless there are safeguarding and/or child protection concerns. Although cases should be treated on a case-by-case basis, the advice below is a good starting point:
Be alert to the possibility of domestic abuse in any patient;
Be aware of and follow local and national guidance on the identification and management of patients presenting with signs of possible domestic abuse;
Ensure that you have a clear protocol in place for dealing with domestic abuse;
Liaise with local services who offer support for victims of domestic abuse;
Consider the family as a whole if abuse is, or may be, present in the household;
Be mindful of your duty of confidentiality and seek consent for disclosure unless there is a compelling reason not to do so;
Seek advice if considering disclosure without or contrary to a patient’s consent.
Dr Edward Farnan, medico-legal adviser at the MDU, looks at how to deal with a negative
online review
Dilemma 2
They have made false allegations
QI work as a cosmetic sur-
geon. Yesterday, I discovered that a patient had published a critical post on an online review site.
In the review, the patient made a number of false statements against me and my colleagues. What can I do?
APatients are increasingly using social media and online rating sites as a tool to provide feedback about their medical care, which may include negative comments or complaints.
Some of this feedback may seem unjustified, misleading and, on occasion, may be offensive or abusive.
It is worth contacting your defence organisation for advice before considering how to respond.
Remember, should you choose to respond, it is important to do so positively and professionally to the post in a manner which does not breach patient confidentiality. If you believe your reputation has been damaged online, your options include:
Responding to the comment;
Flagging the comment to the website and/or asking for the offending information to be removed;
Using the ‘right to be forgotten online’ to remove the page from search results.
However, all these approaches can be risky and it is imperative that you do not overlook patient confidentiality.
Responding to critical comments or attempting to have
When reviews are not true
them removed can often be risky, counterproductive and add fuel to the fire.
In Confidentiality: responding to criticism in the media (2017) , the GMC acknowledges that it can be frustrating for doctors to see inaccurate or misleading information about their diagnosis, treatment or behaviour, but says this ‘does not relieve you of your duty to respect your patient’s confidentiality’.
Instead, you should respond positively by thanking patients for their comments, apologising if they are not happy with their treatment and asking the person to get in touch directly to raise concerns, while respecting patient confidentiality.
This approach is in line with the NHS complaints procedure, which emphasises the need to be open and honest with complainants and to learn lessons from complaints.
Attempting to have a post removed may inflame the situation and could prompt the person to re-post their comments on another site.
The GMC states: ‘Disputes between patients and doctors conducted in public can also prolong or intensify conflict and may undermine public confidence in the profession, even if they do not involve the disclosure of personal information without consent.’
It is important that colleagues seek to balance an occasional negative comment against positive feedback received.
A helpful response, acknowledging a patient’s concerns and inviting the patient to contact the practice, so that these may be addressed, presents a positive opportunity for the practice to demonstrate its professional approach to patient satisfaction.
• Completely open scanner that is well tolerated by claustrophobic patients
• Weight-bearing scans for spine and joints enable a more precise diagnosis
• Patients who are large or cannot lie down can be accommodated Upright
Stop the taxman visiting
For many consultants, there is a clear angst that HM Revenue and Customs may come calling with an unexpected tax bill or inquiry. Ian Tongue (right) explores some common areas of risk and the steps that can be taken to minimise the risk of the taxman ringing your doorbell
Phew! ThANKFULLY, it is actually quite rare to have a representative from h M Revenue and Customs (hMRC) literally turn up at your door.
That approach is mainly for onthe-spot record-keeping checks or if it thinks you have done something really bad.
The norm is to receive the brown envelope with hMRC saying that it is inquiring into your affairs. The natural reaction is to hit the panic button. But don’t. Contact your accountant and discuss the reasons for the inquiry. There are two main types of inquiry that you would potentially have: an ‘aspect’ inquiry or a ‘full’ inquiry.
The aspect inquiry is just that: one or a small number of aspects
are being queried; for example, salary or bank interest disclosure.
hMRC has long been the recipient of certain information that allows them to compare information on your tax return to theirs.
Increased chances of inquiry with the push to digital disclosure of information, h MRC has never had so much information to use, which inevitably will increase the chance of an inquiry if you fail to disclose something or record a figure inaccurately.
A full inquiry usually asks for all of your records and after a review or reconstruction of certain figures, they will ask questions.
This type of inquiry is less common for consultants engaging in private work.
w here h MRC discovers that additional tax is due, it allows it to open earlier year tax returns on the basis that they could be inaccurate as well.
In addition to any underpaid tax, interest and penalties are charged on a percentage scale based on various factors but usually carrying a minimum of 20-30% of the tax underpaid.
Therefore, it is really important to ensure that your financial circumstances are managed to reduce your risk of financial loss.
Record-keeping
Keeping adequate records is a requirement of running any business and hMRC actually has powers to fine a business for not keeping adequate records.
It doesn’t actually define what is adequate, but it can generically be seen as a system that records and is able to report information which is complete and accurate.
The use of software can significantly help here, as it should ensure that more focus is placed on the accounting system, making it more robust. when submitting your records each year, ask your accountant if there are any areas of deficiency in your systems or recommendations. This reduces your risk of inaccuracies and can help reduce costs.
Choice of accountant
Unlike the medical profession, calling yourself an accountant can take many forms.
Costs are obviously an important consideration and it is easy to simplify the role of an accountant. If you go with the cheapest option, you are likely to receive a scaledback service and ultimately it is you, not them, that are responsible for your tax submissions. It is always sensible to go with an accountant who is regulated, and one who has medical experience is essential, in my opinion, as a general accountant is unlikely to understand the nuances of the medical profession.
Full disclosure
with the influx of doctors from other countries, it is really important that you provide full disclosure to your accountant when preparing your tax returns.
A number of years ago, there were significant changes for those who are tax resident in the UK but are not domiciled in the UK.
It used to be the case that many countries did not share information with h MRC, but nowadays there are few countries that don’t supply hMRC with information. There have been various amnesties to own up to assets/income from abroad, so anyone not disclosing their worldwide income and capital gains are likely to be hit hard.
It goes without saying that you should disclose everything to your accountant and they will be able decide what should be included on your tax return based on your individual circumstances.
Aggressive tax planning
Tax planning can take different forms and many structures are low risk and have tax cases that support their use; for example, a husband-and-wife-owned limited company. h owever, there are many structures and products that are higher risk and, in some cases, asking for trouble.
hMRC has been extremely successful with its drive to challenge the abuse of products such as film partnerships and offshore planning.
In recent years, hMRC has been given more powers to target aggressive arrangements and to also target those promoting such schemes. This new power is called GAAR, which stands for general anti-abuse rule.
For those who are in such arrangements, get a second opinion, as the promoter almost always will say the scheme is compliant with all regulations – but they would, wouldn’t they. Often the businesses promoting the most aggressive schemes are limited companies and it is easy for them to walk away from advice given with little or no recourse on them.
As with many things in life, if something looks too good to be true, then it probably is. A lot of higher-risk tax planning falls into this category.
Annual allowance
This is an area where more inquiries are likely over the coming years due to an unworkable system. The
It used to be the case that many countries did not share information with HMRC, but nowadays there are few countries that don’t supply HMRC with information
suspect they knew the timetable was too ambitious.
It remains to be seen how this will impact on businesses and your accountant should keep you informed over the coming years to ensure you are best placed for the inevitable new digital reporting.
VAT registration
Most medics are not VATregistered, as medical services are exempt from VAT. But for those carrying out medico-legal or other non-medical services, it is important that you understand the additional requirements of being VAT-registered.
Government made changes to the amount you can save into a pension, which reduces the headline figure of £40,000 per year to just £10,000 for those earning more than £210,000.
NhS Pensions is only under an obligation to issue a pension growth statement when you have exceeded the limit if your growth is over £40k.
Therefore, someone who has a limit less than £40,000 and, importantly, a tax charge won’t receive a statement to calculate the figures. It is a fundamentally flawed and unfair system that will require close contact with your accountant to manage your obligations.
The future: Making Tax Digital (MTD)
There is an argument to say that MTD, as it is known by h MRC, should be rebadged as ‘making tax difficult’. It requires taxpayers to report to h MRC quarterly, which is a significant burden to small businesses and the cynic in me believes this is part of a wider agenda to provide taxpayers with less scope for tax planning and to accelerate tax payments.
It has been parked for now, having previously had an April 2018 implementation for some. Brexit was the excuse, but seeing as hMRC’s digital links for 2016-17 tax returns are still not functioning fully at the time of writing, I
Unlike the general tax inspector, the VAT inspectors will periodically inspect the records and this will happen on a cycle; for example, every three or four years. h aving robust systems is essential, as you are acting as a collector of tax for h MRC and there is no tolerance for inaccuracies when it comes to VAT.
Common areas for tax return inaccuracies
These include:
Omission of bank interest;
Salary details incorrect;
Overclaim of costs against salaried earnings;
Gains/income from investments omitted;
Child Benefit not repaid when not entitled;
Student loan inaccuracies;
Property income omitted or not reflective of true ownership;
excess pension savings.
Keeping yourself protected from the long arm of the taxman is important and it is always best to get things right from day one rather than having to remediate your systems later on.
Speak to your accountant to ensure that you understand your affairs in detail, particularly if you are engaging in tax-efficient structures or products.
Choose an accountant wisely and you should find that this alone helps shield you from unwanted attention from the taxman.
Next month: Property taxes explained
Ian Tongue is a partner with Sandison Easson accountants
DocToR on ThE RoAD: FIAT 500
Cheeky car puts a smile on your face
We’ve reviewed some big cars in recent issues. But here’s one Dr Tony Rimmer (below) finds will be easier for getting into the doctors’ car park and running around the city. Even in Italy…
Life as an independent practitioner is always busy and often stressful. We all have different ways of relieving these pressures outside of work: by playing sports or indulging in favourite pastimes or hobbies.
To this end, those of us who consider ourselves to be car enthusiasts will enjoy driving any vehicle that gives us a sense of well-being.
True petrolheads will know that a car does not have to be expensive or fast to deliver this positivity, it just has to put a smile on your face.
One such car is the f iat 500 which, like BMW’s MiNi, took all of the classic attributes of the original 1950s’ car and reiterated them in a bang up-to-date package with masses of appeal.
The original 500 Nuova was
True petrolheads will know that a car does not have to be expensive or fast to deliver this positivity, it just has to put a smile on your face
launched in 1957 and, over a 17year lifespan, gave four-wheeled mobility to thousands of lessaffluent owners who were mostly from its native italy.
The new 500 was launched in 2007 and has only had one significant update since then. i n 2015, subtle styling changes and some necessary refinement of the suspension took place.
Appealing qualities
Like its rival the M i N i , it has spawned other bigger models such as the five-door 500L and the small s UV 500X. But again, like the MiNi, it is the three-door model that retains most closely the appealing qualities of the original.
There are three trim levels; Pop, Popstar and Lounge. The base model does without air-condi -
FIaT 500
Body: Three-door hatchback
Engine: 1.2 litre four-cylinder petrol
Transmission: Continuously variable automatic
Power: 69bhp
Torque: 102Nm
acceleration: 0-62mph in 12.9 secs
Top speed: 99mph
Fuel economy: Combined 60.1mpg
On-the-road price: £13,365
tioning and has steel wheels. The top-of-the-range Lounge model has extra driving lights, a sunroof and a more sophisticated infotainment system.
engine options include the base 1.2litre petrol engine with 69bhp and a 1.3litre diesel engine with 94bhp, but it is the 875cc twocylinder turbo-petrol Twin- a ir models that most suit the car’s character.
Italian job available in 84bhp or 104bhp versions, these high-revving but punchy units need a lot of work to deliver their best but they do so in a satisfying and sporty way. What better way to test this small fiat but on the roads of rural i taly. a nd i have been lucky enough to spend some time
The 500 is not exactly roomy: it only just about accepts a driver and passenger of modern six-foot proportions
The ride is very firm, despite the improvements of 2015 and the steering and brakes lack the directness and power to induce full confidence on twisty B roads.
I found that the innate cheerful and cheeky nature of the car as a whole was more than enough to compensate for average driving dynamics
exploring the magnificent Umbrian countryside peppered with hilltop medieval towns in a bright red Lounge model, albeit with the 1.2 litre petrol engine.
Like most things i talian, the new 500 is all about the styling and design. from the cheery frontal aspect through to the recognisable stumpy tail, it cuts a dash in any environment, but looks particularly at home in a town or city.
Park one next to a 1950s’ 500 and you will be amazed how small the original car was. The new car is not exactly roomy; it only just about accepts a driver and passenger of modern six-foot proportions and the rear seats are definitely limited to small teenagers. The body-coloured dash is a nod to the original and cheers up the driving environment.
The driving position itself is not ideal but all the controls are clear and light to use. The full-length but fixed sunroof on my car brightened up the interior and for those who want more of a convertible experience, fiat offer the 500C which has a full-length retractable fabric sunroof.
The boot is tiny, even smaller than the MiNi, but it is amazing how few problems this causes given the ease of expanding the useable space with the flip-down rear seats.
Driving experience
Driving the 500 is a bit of a mixed bag. it is great around town – its natural environment – but get it on a few open roads and certain deficiencies make themselves apparent.
s omehow, though, this does not matter very much. i found that the innate cheerful and cheeky nature of the car as a whole was more than enough to compensate for average driving dynamics.
as long as you do not buy this little fiat as a sports car, you will not be disappointed. They do, in fact, sell the a barth models as sporty alternatives and these variants are great for the single driver on smooth roads but a challenge for passengers.
You cannot fail to fall in love with the new 500 and you do not have to be in italy to enjoy the driving. it has something that is lacking in most new cars; character and a bit of quirkiness.
if most of your commuting is in a city or urban environment, i can guarantee that you arrive at your destination feeling cheerier than when you left.
i am sure that we could all benefit from an injection of italian flair.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
The original 1950s’ model of the Fiat 500 was much smaller
All you need to know about accountancy for private practitioners
Eye specialists blink
Ophthalmologists are still flourishing in private practice, but are having to contend with a lot of change, Ray Stanbridge reports on our latest benchmark survey
Back in our December 2016January 2017 issue, i reported in Independent Practitioner Today: ‘ a preliminary look at early 2016 figures suggests that ophthalmologists have done quite well. choose and Book work seems to have still been fairly strong.
‘We are also seeing an increase in self-pay work as opposed to insured work. On top of this, the growth of groups and organisations such as Optegra continued to have a positive effect on those involved.
‘ i t looks as if ophthalmology private practice still flourishes –but we will see next year.’
Well, 12 months on and i believe these comments are still valid, although profits for a typical practice have shown a small fall.
Our headline figures show that between 2015 and 2016, average gross incomes of ophthalmologists in private practice have reduced by about 1.5% from £129,000 to £127,000.
costs have increased slowly by 1.8% from £54,000 to £55,000. as
aveRage INCOMe aND eXPeNDITURe
Expenditure
a result, taxable profits have fallen by about 5.3% from £75,000 to £72,000.
What are the reasons for the income changes? i have reported before that ophthalmologists are particularly vulnerable to changes in choose and Book referrals, and it is some decrease in this work that seems to have been the major cause or factor for the slight decrease in gross incomes.
Fee squeezes
i n addition, i am noticing that some insurance company fee squeezes are starting to bite for those heavily reliant on insurers. Others, as previously reported, have sought to develop the selfpay market.
What then of cost changes?
Firstly, there seems to have been a modest increase in staff costs. again, i have commented in the past that there appears to be a correlation between staff costs and growth in the personal allowance, particularly where family members are employed in the practice.
Secondly, consulting room hire costs have shown a small but noticeable increase as the effect of the c ompetition and Markets authority order starts to bite.
On the other hand, there seems to have been a modest decrease
I am noticing that some insurance company fee squeezes are starting to bite for those heavily reliant on insurers
on average, for professional indemnity/insurance costs. as a current feature of the market, there are an increasing number of consultants shopping around for cover. a nd there are some highly competitive quotes available, although in some cases it is not always immediately obvious to me as to exactly what is covered.
Attractive option
Most other costs seem to have been broadly unchanged. Ophthalmologists are continuing to spend on marketing and i expect that this trend will continue.
What of the future? My view is that ophthalmology continues to be an attractive option in private practice, although it is subject to the vagaries of choose and Book
Year ending 5 April. Figures rounded to nearest £1,000 (percentage is also rounded up)
Source: Stanbridge Associates Ltd.
13-14 March, London, Olympia
Future Healthcare 2018 brings together the world’s leading organisations and experts at London’s Olympia, 13-14 March to showcase the latest healthcare products, services and innovations on a global scale.
International exhibition where you can source highly effective and efficient solutions to future-proof your organisation – free to attend.
Future Healthcare Conference addressing disruptive innovations, integration and collaborative patient experience – stay ahead of the curve so that you compete on a global-scale (limited free 2-day conference passes available for NHS/public sector)
Invest in Health Theatre presentations focusing on cutting edge technologies that are still in development – free to attend funding opportunities available for investors.
HealthTech Theatre case studies of existing technologies in practice – free to attend.
VIP Hosted Buyer Programme – available for purchasers looking for specific introductions and meetings with suppliers.
Speakers include:
Organised in association with
James Caan, Investor & Entrepreneur
João Bocas, Top 100 Global Digital Health Influencer
Lord James O’Shaughnessy, Department of Health
Dr Bertalan Mesko, Healthcare Futurist
Mariano Gonzalez, Moorfields Eye Hospital Dubai
Sangita Reddy, Apollo Hospitals India
Professor Arne Björnberg, Health Consumer Powerhouse
Keith Hague, Cleveland Clinic London
and other nHS contracts when we are looking at national figures.
a s a trend, we are seeing an increasing volume of self-pay and this perhaps is the way forward for those looking for a sustainable and flourishing private practice. i t must be stressed that it is
increasingly difficult to provide meaningful comparison on a year by year basis. Some consultants have incorporated and others have chosen to enter into group arrangements.
Other eye specialists have chosen to do more choose and Book
work as employees in an n HStype environment rather than as an independent consultant in a private hospital.
These problems make for increasingly difficult comparisons. So i stress that, as a result, this survey can in no way be deemed to be statistically significant. Rather it is a measure of the incomes and costs of ‘typical’ private ophthalmology practices.
The definitions of our survey membership remain as before. consultants who are included in the survey are those who:
a re not in full-time private practice;
Have at least five years private practice experience;
are seriously interested in private practice as a business;
Earn at least £5,000 gross in the private sector;
Hold either an ‘old-style’ or ‘new-style’ nHS contract;
May or may not be a member of a group or have incorporated.
Next issue: gynaecologists
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists, Stanbridge Associates
years ending 5 april Source:
what’S coming in our februarY iSSue
Make sure you don’t miss our next issue, published on 15 February. you may not receive every issue if you have not yet subscribed to the journal. Don’t risk missing out on vital topics we tackle next time, including:
Free! If you buy goods or services in your private practice, check out the people who can help you in our Product guide 2018
Self pay: how do your ensure your practice gets its fair share of these new private patients? Dawn Cremin sets out some practical tactics you should consider when planning to increase the number of patients choosing to pay for their own treatment
Ten tips for managing stress on the job without trying to eradicate it
Looking for a better investment experience? Simon Bruce of Cavendish Medical reveals the key principles to improve your odds of success
Increasing numbers of Independent Practitioner Today readers are doctor entrepreneurs. Jane Braithwaite looks at some success stories, what it takes to be an entrepreneur, and what support is out there to help doctors bring their innovative ideas to market
Tips on starting an aesthetic practice – by Dr Rajveer Thethi,who has just done it and set up Skinradiance Clinics, Leeds, gives some advice
When a patient refuses treatment
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution.
Printed by Pepper Communications Ltd
Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Registered office: 7 Lindum Terrace, Lincoln LN2 5RP
to
a private gP’s dilemma when a patient requests dental treatment
Tackling poor performance and misconduct. Lucy Miles, of hempsons solicitors, looks at two common employment scenarios and gives guidance on how best to manage them successfully
Our motoring correspondent Dr Tony Rimmer finds the new volvo XC60 is the right match for medical professionals who appreciate a quality product but do not want to be too flashy
Dr karen ellison of Medical Protection answers the questions young consultants moving to the private sector often ask
PPUs: Philip housden gives his five-point action plan for growth
There are common billing and collection issues whether you work as an individual or a group, or whether you are working in a clinic or hospital. Findlay Fyfe, of Medical Billing and Collection, looks at the scale of the problem
The second in our new series learning from the experience of a consultants who has just built his private practice premises
Profits Focus: gynaecologists,
Plus all the latest news and views
aDveRTISeRS: The deadline for booking advertising for our February issue falls on 19 January
£90 GPs and practice managers (private & NHS). £210 organisations.
But if you pay by direct debit, individuals pay only £75, and organisations £180
Call Proact Ltd on 01752 312140
Email: lisa@marketingcentre.co.uk
Save £15 WITh DIReCT DeBIT!
guarantee you get the next copy of Independent Practitioner Today. Take out a subscription (at the rates shown on the left) by phoning 01752 312140 or by sending off a subscription form on page 24 or by emailing us at lisa@marketingcentre.co.uk. Or go to the ‘Subscribe’ page of our website www.independent-practitioner-today.co.uk
If you subscribe by direct debit, individuals pay only £75. Just fill in the form on page 24 and send it to the Freepost address shown at the bottom of the form.
Robin Stride, editorial director @robinstride
BaCk ISSUeS: £12.50 including post & packaging ChaNgINg aDDReSS OR SUBSCRIPTION DeTaILS?
Phone 01752 312140 or email lisa@marketingcentre.co.uk
Circulation figures verified by the Audit Bureau of
• Submit electronic invoices and reach the insurer’s payment cycle quicker
• Real-time online checks for patient membership number • Online system – access from any place, any time
is encrypted • Pre-populated invoices
Access to your
• Automated prompts (raise invoice on completed appointment, shortfall and reminder letters)
• 24/7 data back up and disaster recovery • Logins are role-based access controls