A successful practice is full of happy patients How to improve patients’ experience in the long term P16
The business journal for doctors in private practice
The art of remaining in total obscurity
If you want to know how not to do PR, check out this advice from Tingy Simoes P24
Complaints on the rise
By Robin Stride
The private healthcare complaints watchdog has issued a wake-up call to consultants and healthcare organisations following rising concern at patient grievance levels.
In its annual report published this month, it reveals: ‘How complaints are handled by providers continues to be one of the most frequent concerns raised by patients, in 77% of cases. Complaints about consultant care continue to rise year on year, with 60% of complaints including this element in 2019-20.’
But according to Sally Taber, director of the Independent Sector Complaints Adjudication Service (ISCAS), complaints about consultants have become the top area of dissatisfaction since April.
She said reasons why complaints to ISCAS were upheld include:
Lack of fee transparency by organisations and consultants. Specialists not making patients aware of the requirement to inform them about the costs of procedures and treatments before doing them.
Consultants not providing patients with an outline of the risks and complications with their treatment.
Specialists failing to ensure they include all post-operative instructions in their notes.
Consultants not clearly documenting findings of all examinations and treatments plus failing to clearly record when consent has been obtained.
Organisations and consultants not having guidelines for specialists regarding continuity of care during their absences.
ISCAS said organisations should consider reviewing internal processes to ensure consultants are aware of the GMC and Royal College of Surgeons’ requirements to take account of patients’ vulnerabilities and psychological needs.
It told Independent Practitioner Today it would like to ‘remind’ doctors and independent healthcare organisations of their responsibilities to ensure better complaint handling. ISCAS advice is:
➲ Obtain written statements from all staff involved in complaints at Stage 1, including consultants with practising privileges.
➲ Consultants should not respond to a patient’s complaint directly. One cohesive response should be sent from organisations, incorporating comments from consultants.
➲ Seek an independent clinical
In this issue
Ensure you pass your screen test
How private doctors can reduce the risks associated with remote consultations as a result of Covid See page 20
Outsourcing may be your best bet
Why outsourcing billing and collection has become a common option P28
opinion at Stage 1 rather than relying on the treating consultant’s perspective.
➲ Ensure complaint-handling staff know that complaints can proceed in tandem with a legal claim.
➲ See that consultants know the complaints process so they can direct complainants appropriately.
Mrs Taber said: ‘The specific issues have been communicated to all ISCAS subscribers, which includes the Independent Doctors Federation.’
A total of 509 people complained to ISCAS in the year ending March – up from 314 the year before. But one in five were outside its scope, as their treatment organisation was not among the watchdog’s fast-rising membership of 135 hospitals, clinics and private GP services. They were signposted to other organisations, where possible.
Xxxxx
Of 111 complaints adjudicated
on in the year, there were 348 individual elements of complaint, a rise from 2.6 to 3.1 per application from 2018-19. 62% of ‘complaint heads’ were either ‘upheld’ or ‘partially upheld’.
Baroness Fiona Hodgson, chairwoman of the ISCAS advisory board, said more private patients now had the assurance of access to an independent review of their complaint by an appropriate body. But it was ‘disappointing’ that a large proportion of NHS private patient units – around 90% – did not yet provide access to an appropriate scheme for escalating complaints. Now ISCAS will redouble efforts to engage them and will publish a position statement soon.
It said nursing and discharge are recurring themes in complaints: ‘A change seen in this year has been a large increase in the frequency that ‘accommodation’ was an element of the complaint.
HUGGER-MUGGER: Orthopaedic group Fortius Clinic has formed a partnership with the Rugby Players Association to provide ongoing support for current and former professional rugby players. Full story on page 9
TELL US YOUR NEWS. Contact editorial director Robin Stride
A
more dynamic watchdog
Private hospital groups welcome the Care Quality Commission’s plan to move to a ‘whole systems’ approach to healthcare inspections P12
ADVERTISE WITH US. To advertise in the journal or our website business and lifestyle directories, contact Andrew Schofield at Spot On Media. Email: andrew@spotonmedia.co.uk
Phone: 0161 408 3912
GET A SUBSCRIPTION DISCOUNT
£90 independent practitioners. £210 organisations. £90 GPs and practice managers (private & NHS). Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE
Email karen@marketingcentre.co.uk
Or phone 01752 312140.
Chief sub-editor: Vincent Dawe
Head of design: Jonathan Anstee
Publisher: Gillian Nineham
Email: gillian.nineham@gmail.com
Phone: 07767 353897
EDITORIAL COMMENT
Gripes about complaints
Complaints are not naturally welcomed with open arms, but they can often lead to better service and fewer grievances.
Our pageone story, featuring advice from the Independent Sector Complaints Adjudication Service (ISCAS) in the wake of its annual report, usefully highlights where things go wrong.
As ISCAS says, complaints are an important measure of patient feedback and this was emphasised in the Paterson Inquiry report: ‘Complaints from patients about their care offers hospitals the opportunity to examine the adequacy of the treatment and care their patients receive, to apologise when it has been found wanting and to prevent recurrence.’
ISCAS is probably being polite when it says it would like to ‘remind’ consultants and independent healthcare organisations of their responsibilities to ensure better complaint handling.
There has been a wellreported drive in the private healthcare
sector to improve fee transparency so patients know how much their treatments are likely to cost.
Another area Independent Practitioner Today has alerted readers to has been the requirement to give patients information about treatment risks and complications – but independent adjudicators continue to uphold complaints.
A handful of PPUs have thankfully now signed up to ISCAS, but it is disgraceful that most people treated in private NHS units have been left high and dry if they have a complaint because they are outside The Health Service Ombudsman’s jurisdiction.
The Paterson Inquiry report has recommended that all private patients should have the right to mandatory independent resolution of their complaint.
If the NHS wants to profit from private patients, then surely it at least owes them the courtesy of the ISCAS complaints avenue offered in the private sector.
The future of electronic billing
Healthcode’s boss Peter Connor reacts to criticism of introducing charges and explains why a free electronic billing service is not sustainable P18
Cut drug errors by prescribing safely
Diane Baylis of Medical Protection offers advice for independent practitioners on safe prescribing in a world where litigation is increasing P26
Block out the noise of markets
Investors can be prone to distraction and focusing on past performance. Dr Benjamin Holdsworth shows why caution is needed P34
Gentler view of gripes during Covid
How will the GMC deal with complaints about your practice in the pandemic? Solicitor and doctor Tania Francis examines the latest guidance P36
PPUs victim of NHS pandemic woes
A snapshot survey of NHS private patient units shows their activity was beginning to pick up after the first lockdown earlier in the year P44
PLUS OUR REGULAR COLUMNS
Start a private practice: Communal route to success
Accountant Ian Tongue looks at some of the important factors when considering working with others P40
Doctor on the Road: There’s a buzz about it
If you want to enter the green revolution and have fun too, then the answer could be the Mini Electric P42
Profits Focus: Hard graft is paying off
Orthopaedic surgeons come under the spotlight of our unique benchmarking series on specialists’ finances P47
Don’t pay your tax charge personally, doctors told
By Edie Bourne
Independent practitioners receiving personal pensions statements from the NHS Pensions Agency this month should strongly consider how they will settle any tax charges for 201920, according to specialist financial planners.
Cavendish Medical says this is because the Government has agreed to pay the tax charge of clinicians in England and Wales who breached the pensions savings limits known as the annual allowance – but only if those affected apply for ‘Scheme Pays’.
When individuals elect to use Scheme Pays, the NHS Pension Scheme pays their annual allowance tax bill to HM Revenue and
Customs on their behalf, with the member’s benefits in retirement being reduced accordingly.
Patrick Convey, technical director for Cavendish Medical, told Independent Practitioner Today: ‘You may have recently received a pensions statement which shows an annual allowance breach for the last tax year.
‘You will want to accept the Government’s generous offer of compensation, but to do so, you must elect for Scheme Pays to pay the charge on your behalf.
‘Please do not assume that if you have not received a statement, you do not have a tax charge to pay.
The Pensions Agency is not duty bound to send letters to those breaching the “tapered” annual
allowance, which can mean a yearly limit of just £4,000 for the highest earners.’
The deadline for Scheme Pays 2019 20 is 31 July 2021. To apply, individuals must complete a nomi
Patients ‘need to know their doctor’s employment status’
Patients need to be clearly informed whether the private doctor they are seeing is employed or selfemployed.
During a Zoom meeting between London Consultants’ Association (LCA) members and David Hare, chief executive of the Independent Healthcare Providers Network, it was pointed out that future private healthcare will be less homogenous than in the past.
Previously, it was the hospital providers who varied in the extent of facility provision. But doctors’ representatives said clarity to patients was needed due to the emerging mixed model of employed consultants ‘and those who choose to remain independent and continue to practice with professional autonomy based on their own expert clinical judgement’.
In a wide ranging discussion, concern was also raised about the
need to ensure that specialists whose reputation attracts international interest were not pushed out by the increasing burden and financial overheads of private practice.
Mr Hare agreed that a good relationship between the providers he represents and members of the LCA and its sister organisation, the Federation of Independent Pract itioner Organisations, was essential for good quality care and he acknowledged the important role both bodies play.
Dr
raised concerns about private specialists’ exclusion from the discussions during the NHS contracting process earlier this year, which he said resulted in disenfranchisement, loss of access and ability to deliver patient care.
The LCA warned there was a loss of trust between some doctors and providers they used to work with.
Mr Hare said the nature of the emergency had required agreements to be reached within six days but he concurred that the return of private work after the first lockdown was unnecessarily slow due to uncertainty in NHS decision making to release that capacity.
He said the IHPN was looking at better promotion to international governments of London’s private healthcare to help grow the private sector.
nation form which can be complicated.
Mr Convey continued: ‘The consultation into the remedy benefits for those deemed to have suffered age discrimination when being moved to the 2015 pension scheme has just ended.
‘We await the detail of what this means in practice, but you should not delay in checking your own position nor applying for Scheme Pays in the meantime.
‘Government consultations have a habit of taking a long time to come to fruition and we still await the outcome of the pensions flexibility exercise launched last year.’
The deadline for Scheme Pays 201819 only has been extended to 31 March 2021.
Watchdog’s inspection fees frozen
Care Quality Commission (CQC) fees – a bone of contention for many independent practitioners – are being frozen.
Martha Walker, of CQC Consultancy, said this would be widely appreciated in a year that has seen most independent doctors having to adapt quickly and change their business and consulting models to protect patients, staff and themselves.
The freeze for 202122 is for the third year running. Dawn Hodgkins, of the Independent Healthcare Providers Network, welcomed the move for fees covering registration, monitoring and inspection.
She said: ‘This will provide welcome certainty for independent providers who are making plans and setting budgets in a challenging external environment.’
See ‘A more dynamic CQC’, p12
David Hare, IHPN chief executive
LCA chairman
Mark Vanderpump
Cavendish Medical’s Patrick Convey
Third of doctors suffered abuse due to pandemic
By a staff reporter
Over a third (35%) of doctors say they have suffered verbal or physical abuse from patients or patients’ relatives during the first wave of Covid-19.
According to a survey of 1,250 private and NHS doctors by the Medical Protection Society, a further 7% have experienced verbal or physical abuse from a member of the public outside of a medical setting.
The defence body described its findings as ‘deplorable’ and said the abuse presents yet another source of anxiety for doctors at the worst possible time.
In the same MPS survey, two-infive doctors said their mental wellbeing is worse compared to the start of the pandemic.
Dr Pallavi Bradshaw, its medicolegal lead for risk prevention, called the survey results ‘difficult reading’.
She said: ‘While this is a frustrating and extremely stressful time for the public, it is sad and deplorable to think that one-in-three doctors who go to work every day in the most challenging circumstances, putting patients first, face abuse.
‘One doctor who now works fulltime in private practice told us they had experienced more unpleasantness in six months than in all their previous 50 years working in healthcare and are almost at the point of stopping all clinical practice.
‘Abuse presents yet another source of anxiety for doctors at a time when many have expressed grave concerns about their mental well-being. In our survey, two-in-
five doctors say their mental wellbeing is worse compared to the start of the pandemic’.
She told Independent Practitioner Today : ‘The NHS “people plan” has set out some credible support initiatives, but those working in private healthcare settings must also be supported.
‘In our Breaking the Burnout Cycle report published last year, we recommended that private healthcare settings consider establishing a Wellbeing Guardian role so that everyone has access to someone who is trained to recognise and support them when they are experiencing difficulties.
‘For private practitioners, the well-being concerns include those caused by verbal and physical abuse, but we also know there are an array of other sources of anxiety, such as concern about the huge referral backlog, their patients’ health due to the disruption of care, and the potential for these situations to result in medico-legal disputes, claims and investigations.
‘Without support to address mental well-being concerns, doctors are at risk of becoming disillusioned or will suffer in silence – both of which put the safety of themselves and their patients at risk.’
The survey conducted by MPS ran from 17 September–16 October and had 1,251 responses from members in the UK
WHAT PRIVATE DOCTORS SAID
‘I am now full-time in private practice, and I have had more unpleasantness from patients in the last six months than in all my previous 50 years in healthcare. I am almost at the point of stopping all clinical practice.’
‘We had a five-day backlog of swab results in wave 1 and if we suspected Covid-19, we had to transfer to a query Covid-19 ward. Families were accusing me of killing their vulnerable relative. It was out of my control, but the hate and blame were hard and still haunt me now. So little thanks, just angry, desperate relatives.’
‘I experienced assault partially precipitated by a patient not being able to see his mother, in the context of worry and concern and her being in hospital.’
‘Patients are often much more verbally aggressive about the new ways in which we are working and have a much lower tolerance/patience. The increasingly long waiting times for specialty referrals has led to a huge amount of patient dissatisfaction.’
Covid forces doctors to rethink their working lives
New research shows doctors are radically re-thinking the structure of their working lives following the increased pressures they have experienced during Covid-19.
Over half say they are now more likely to work fewer hours in the next year and taking early retirement is being considered as an increased possibility by more than a quarter.
These are among findings from over 6,500 of doctors in England who responded to a detailed BMA survey.
Asked how they had changed career plans for the next year, 29% reported they were more likely to take a career break, 21% said they were more likely to work in another country and a similar number considered they were more likely to leave the NHS for another career.
Two in three said they were quite or extremely anxious about work in the coming months, over 40% reported their levels of stress, anxiety and emotional distress had worsened since the pandemic began, and 65% were not confident about their own local healthcare service’s ability to cope.
Two in three cited staffing shortages as their most pressing concern and four in ten report that colleagues having to self-isolate was impacting on patient care.
BMA Council chairman Dr Chaand Nagpaul said: ‘Doctors know that this winter is likely be one of the most difficult times of their careers. They are extremely worried about the ability for the NHS to cope and their ability to care for the needs of their patients.’
HCA reveals how virus altered care No let-up for sector over the winter
By Robin Stride
Hospital group HCA is reporting a surge in private work since its release from the Covid-induced NHS national contract.
Its commercial director Andrew Coombs has reported ‘very substantial increases’ in activity levels following its hospitals’ refocus on exclusively private work.
He revealed HCA was running at about 112% against the previous year on inpatient activity, with cancer and cardiac work up by 200%.
Talking via the Hopin platform for the Independent Healthcare Providers Network 2020 Summit, he gave his perspective on the future of the independent healthcare market and how providers could navigate the new postCovid world – which he believed would see ‘alarming’ increases in NHS waiting lists.
Robotics: He said the pandemic had brought robotics to the fore, but this was an area where he believed the UK was lagging behind in several areas on a global basis.
‘Introduction of a far wider use of robotics which are allowing people to spend less time in hospital and more rapid recovery times is an area I hope where we will see technology embraced much further.’
Telemedicine: ‘Fantastic’ progress had been made during the pandemic. ‘We were on the tipping
point of that before we went into the pandemic and it has been massively embraced by the consumers.
‘We’ve done 10,000-20,000 virtual consultations since the beginning of this year. It is about a twenty-fold increase from January and February.’
HCA had been embracing other aspects of technology too, with surgeons checking stitches and wound healing virtually.
Haematology nurses now no longer needed to interact with some of the most vulnerable patients but could work with them virtually.
Algorithms were being used to schedule patient flows through waiting rooms and corridors to minimise patient interaction but maximise throughput.
And HCA also had excellent virtual patient visiting systems allowing patients to ‘visit’ their relatives in the UK and abroad.
Inefficiencies: Mr Coombs summarised some of the areas where hospital operators had seen a rise in inefficiencies as they worked through the Covid-19 pandemic.
These included:
People having to be anaesthetised in the theatre rather than the anaesthetic room;
The use of PPE;
Additional cleaning times;
Theatre teams not allowed to go into theatre until 20 minutes after people were intubated.
He doubted some stakeholders realised the additional cost of delivering this type of safe care on green pathways.
HCA had in recent weeks introduced a formal staff surveillance programme for all its patient-facing staff. ‘That isn’t cheap to do, but it is something you absolutely have to do if you are going to maintain patient safety.’
‘Tremendous’ technologyembracing efficiencies had been taken on board, but Mr Coombs expressed some caution, partially arising from some conversations he had over the previous few days.
He said sometimes talk about digital consultations said these were being driven by cost rather than necessary clinical effectiveness and outcomes.
But he stressed that everyone needed to balance this use of technology to ensure they we giving the best possible patient care, not necessarily the cheapest care.
The private hospital sector has been warned it can expect no letup in the months ahead as providers do their bit for the nation’s healthcare.
According to the boss of their national body – the Independent Healthcare Providers Network – the organisation’s Summit meeting sessions demonstrated only too well that the coming year would be bringing new challenges for all.
Chief executive David Hare told the meeting: ‘So the energy levels, I’m afraid cannot drop. We all collectively need to roll our sleeves up and make sure this innovation and ability that we see inherent in this sector can continue.’
Said Mr Hare: ‘The second wave is upon us; now there’s a potential third wave, there’s a huge job to be done to clear the backlog of NHS and private treatment and maintaining staff morale. Many staff are tired and exhausted.
‘Keeping them moving through what is likely to be a difficult winter is something we all need to keep an eye on. The economic conditions are likely to be some of the most challenging in living memory and we have to continue to adapt services to innovate.’
Private providers had been on a long journey in recent months and seeing how members of the industry body had worked and responded to the unprecedented Covid challenge had been a ‘tremendous privilege’.
For the future, it was important that the Government saw the success of the sector as a priority, he said.
Private GPs launch drive-through Covid test
On-demand GP service GPDQ has launched London’s first private drive-through Covid-19 testing facility.
People experiencing Covid-19 symptoms can book a ten-minute slot at the site in Hadley Wood, Enfield, using the firm’s online system.
If the 24-hour result comes back positive, patients are called by a GP who provides a consultation on how best to manage symptoms and address concerns the patient may have.
Dr Anshumen Bhagat, a GP and co-founder of the company, said: ‘Over the past few weeks, we’ve seen
reports of delays with the UK’s Covid-19 testing system. The situation is becoming increasingly serious; patients are being told to travel miles for a test or, in some circumstances, tests just aren’t available.
‘People have been reduced to staying at home for 14 days with worrying symptoms and no guid-
ance on when a test may be available. We’ve therefore launched this service to support the ever-increasing demand for drive-through testing, especially in the capital, to provide people with peace of mind and the ability to live as normally as possible.’
The fee per test is £139.
Andrew Coombs, commercial director of HCA Healthcare
PRIVATE HEALTHCARE SUMMIT 2020
Tributes paid to private doctors’ Covid reaction
By Robin Stride
Consultants who have fought back from the financially crippling weeks of Covid-19 have been paid a huge tribute by the boss of leading private hospital group HCA Healthcare UK.
Its chief executive and president John Reay told independent healthcare leaders at a major conference that their duty now was to give doctors their strong backing.
He said all healthcare workers had shown ‘true heroism’ in the past year, but he felt sure he was speaking on behalf of the sector in highlighting the action of surgeons in undertaking hours of work in extremely difficult circumstances.
The sector’s anaesthetists, intensivists, radiologists and pathologists had with great determination also ensured the care and safety of patients in both the NHS and private sectors, he reflected.
Talking at LaingBuisson’s Private Healthcare Summit, Mr Reay added: ‘Many of our consultants have faced serious economic damage at times and have shown enormous resolve in returning to rebuild their businesses – and our role is to support them.’
Springboard for change
He told the meeting last month that Covid-19 was a springboard for change and then outlined his thoughts and observations of what his hospital group had been experiencing as more patients returned.
He said the pandemic had brought about massive opportunities for those in the independent sector to rethink how healthcare was provided to patients.
As its second peak approached, it was important to work together as a sector to bring about any necessary changes.
During the pandemic, care continued at HCA hospitals, but what changed for everyone was the way they had to respond ‘with a speed unlike ever before to adapt to a new challenging backdrop for safe care. I know that it took a huge amount of effort across the board to adapt and change so much, so quickly’.
Doors kept open
Mr Reay said: ‘This new way of working, with increased testing, deeper cleaning, higher infection prevention and control standards has led us to raise our already high standards, to deliver the safest possible care for patients. These measures allowed us to keep our doors open and will help us to continue to keep our doors open as we look ahead to the next few months.
‘By having Covid-19-secure “green hospitals” during the peak of the pandemic, it meant we were able to support the NHS to treat thousands of patients both NHS and private, whose care was timecritical.’
In April, May and June, HCA had over 70,000 patient interactions, performed over 4,000 complex surgeries across its network of hospitals – predominantly for patients with cancer or cardiac conditions – and delivered over 200 babies both NHS and privately.
Unlike most independent sector providers, HCA was no longer in a national contract with the NHS, which meant its capacity was not reserved in the same way it was before.
This meant it could continue to provide seamless care for even more private patients who needed it during a second peak, as well as standing ready to support local NHS trusts as and when needed.
‘The message that we’re open, safe and ready to receive patients is
definitely being heard. We have seen rapidly increasing activity in independently funded care since June, when we expanded our care once again to include elective work.
Pent-up demand
‘With waiting lists increasing, we’ve seen a huge pent-up demand as people’s needs outside of immediately urgent care have had to wait.
‘We have already noticed marked increases on last year for private inpatient surgeries – we’re now at 112% against pre-Covid-19 levels.
‘This increase has also been identified across most specialties. For example, in orthopaedics, we are at 115% compared with pre-Covid levels. This is a combination of private medical insurance and self-pay.’
Many patients were on waiting lists and more willing than ever to receive care via an independent provider. For those who wish to access outstanding healthcare fast, HCA was working with the insurers to provide rapid access pathways for patients with cardiac or cancer concerns.
HCA had also noticed that patients were more open to seek-
Many of our consultants have faced serious economic damage at times and have shown enormous resolve in returning to rebuild their businesses – and our role is to support them
JOHN REAY, CHIEF EXECUTIVE HCA HEALTHCARE UK
ing out private care than ever before. Recent consumer research on behalf of Equipsme indicated a 12% rise on last year in the number of people who would consider going private for their care.
Mr Reay said self-pay was a key area of growth for the group. Colorectal was a stand-out specialty area and there had been a 100% plus increase on pre-pandemic levels.
Significant growth
‘We are also seeing significant growth in self-pay at our Neuro Rehabilitation Centre at The Wellington Hospital. We recently launched a Covid-19 rehabilitation programme for those impacted by “long Covid” with knock-on conditions including cardiovascular and musculoskeletal deconditioning, pulmonary embolism, depression, anxiety and post-traumatic stress disorder.’ There was plenty of opportunity for innovation, such as remote consultations and he expressed thanks to the teams at insurers who had worked ‘tirelessly’ to make this happen for patients and helped create a patient journey that worked better for many people.
➱
John Reay: Also praised insurers for being flexible in response to Covid
People undergoing cancer treatment could now get holistic care through patient webinars on physical, emotional and nutritional health, on live exercise classes with specialist oncology physiotherapists and new virtual support groups lead by HCA’s clinical nurse specialists.
For moments of care where physical interaction was unnecessary, it was important these options were provided so patients felt supported.
He said insurers, consultants and hospitals working together could really enhance the private care proposition for patients at a time when people’s attitudes and needs were changing.
Partnerships could work well among competitors too. HCA was working with fellow providers in London to pursue international work. ‘Initially, our international patient occupancy had dropped to a third of prior years.
‘However, the attraction of UK medicine is strong and in the last two months the inquiries have started to come back and every week we are admitting a small but growing number of foreign patients needing complex care. We all stand to benefit by pooling our scarce resources to project Medicine UK overseas.’
Hospitals must push safety to lure custom
A private consultants’ leader has appealed to the independent hospital sector to use its safety record to encourage reluctant patients back.
Dr Sean Preston, specialists committee chairman at the Indepenent Doctors Federation (IDF), reflected that HCA boss John Reay had highlighted at the Summit how safe private hospitals and their facilities were.
But he urged the meeting ‘to get that message back to our patients, because we do have a lot of patients who are reluctant to come to the hospitals at the moment and we need to correct that for many, many reasons.’
Dr Preston, of gastroenterology partnership London Digestive Health, outlined some of the business problems consultants faced leading up to the pandemic.
These included rising costs of rooms, medical indemnity fees that were often prohibitive, and ‘most concerning’ news from
members about being de-recognised by a private medical insurer.
This had often come as a surprise with a letter or email just telling the consultant they were no longer able to see patients, with no explanation or dialogue. Happily, following negotiations, recognition had been regained, but only for some.
Dr Preston continued:‘PostCovid, things have just got more difficult and those concerns have increased the layers of other concerns. You know, I have colleagues who can’t get their patients into private hospitals.
‘We know all about the NHS contract – yes, it’s fewer [patients] than before – but particularly outside London our consultants don’t have the ability to see their patients.’
He said markets had disappeared and in central London a lot of consultants’ practices were dependent on The Gulf and, for obvious reasons, those patients were no longer travelling.
Insurance tax ‘detrimental’
Bupa Insurance chief executive Alex Perry hit out at ‘counter-productive’ Government policy on private health insurance and called for a less hostile policy approach.
He told the Summit that the doubling of insurance premium tax since 2015 meant that, when National Insurance and benefit-inkind factors were taken into account, employers and employees between them faced an effective tax rate on health insurance of between 50% and 72%.
That was ‘punitive’ and Bupa had made the case to Government that it was unfair on businesses and individuals who took out health insurance.
Mr Perry warned it was ultimately
counter-productive ‘as it drives more people out of the market adding further demand on an already massively overstretched NHS’.
He added: ‘Now it is an even more acute issue than ever, as
many businesses are now struggling to stay afloat, never mind pay for health insurance.
‘And we need to be clear that while self-pay has an important role to play in the sector and also in reducing NHS waiting lists, it is really through health insurance that the big savings are made for the NHS.
‘The most vital and expensive courses of treatment can only be provided privately, really at scale, if funded through health insurance – things like cancer and cardiac care.
‘So it’s really in everyone’s interests – the NHS, the Treasury and independent providers – that we have a really thriving health insurance market.’
But there was a flip side to this and he said there had been ‘fantastic’ work from some private medical insurers who had been very supportive of consultants and enabled them to see their patients virtually.
Particularly at the height of the pandemic, almost all his consultations other than emergency endoscopies were done by video.
He paid tribute to Bupa Global and UK Insurance medical director Dr Luke James for getting the message out to patients early so they knew they were not isolated at home and were able to see their doctors virtually.
Dr Preston added that with huge NHS waiting lists, more self-pay patients were coming forward. ‘It may be something as simple as coming to see me for a colonoscopy for rectal bleeding, but equally it may be someone putting in their life savings to access their complex cancer surgery.’
QUALITY IMPROVES
Progress made on quality in the private healthcare sector, and how it is measured needs to be accelerated, Mr Perry told the conference.
Bupa wanted to see more than nine in ten independent hospitals get ‘good’ or ‘outstanding’ Care Quality Commission ratings.
He said the Private Healthcare Information Network had made some good progress but there was still ‘a lot more to do before we can confidently prove our quality across the board is the best that you can get in the UK.’
Mr Perry warned that the Patterson report earlier this year was a timely reminder that the independent sector and the NHS must do more to share information.
Alex Perry, head of Bupa Insurance
PRIVATE HEALTHCARE SUMMIT 2020
Stats reveal scale of bounce-back
By a staff reporter
Consultants have seen a steady rise in insurer-funded work, with activity in September at 93% of the level 12 months earlier.
This is up nearly 20 percentage points compared with August (74%).
Activity levels in parts of the private healthcare sector are now higher than in 2019 as providers deal with pent-up demand, according to the latest snapshot of insurerfunded activity by Healthcode.
The official clearing organisation for the private health sector reported activity for pathology/ haematology was up 28% and radiology 24% higher than the corresponding month last year.
Healthcode managing director Peter Connor said he was impressed by the private sector’s determination to bounce back.
HOSPITAL SPECIALTIES
COUNTRIES AND REGIONS
Operating percentages were up again in all UK countries last month.
England recorded 93% of 2019 level compared with 74% in August;
Scotland was at 84%, up from 61% in August;
Northern Ireland achieved 114% – 88% in August;
Wales reached 71%, up from 54% in August.
Regionally, The East Midlands posted the strongest comeback in September (104% of 2019 activity, up from 89% in August).
London was back to 99% of last year’s activity – compared with 78% in August – and the North-west was at 98% (76% in August). Operating percentages in every English region are above 80% of 2019 levels.
CARE SETTING
Hospital activity in September reached 95% of 2019 levels, compared with 77% in August.
Within hospital settings, outpatient activity was up to 98% of 2019 levels, while admitted care was at 84%. This compares with 79% for outpatient care and 68% for admitted care in August.
Patient numbers in private hospitals were close to pre-Covid levels. Last month, outpatients were 95% and inpatients were 82% of the numbers treated in September 2019. The equivalent in August was 77% and 67% respectively.
Four of the top ten specialties exceeded 2019 activity levels. In September, the year-on-year operating percentage was 128% for pathology/haematology, 124% for radiology, 112% for oncology and 104% for general surgery.
Two hospital specialties hardest hit by lockdown recovered strongly. From an operating percentage of only 12% of 2019 levels in May, orthopaedics was back at 91%.
ENT reached 89% of 2019 activity in September, compared with a low of 10% in May. This also represented significant improvement on August’s operating percentage. Orthopaedics was up 21 percentage points from 70%; ENT was up 25 percentage points from 64%.
Compiled by Philip Housden
NHS PPUs begin re-opening NHS trusts are working hard to make up for millions of pounds lost in private patient income during the Covid pandemic.
As Independent Practitioner Today reported in October, health service private patient income has shrunk by an estimated £35m a month since March as trusts have enforced infection control policies, limited their bed space and received fewer referrals.
The shortfall reached a projected total of £280m at the end of October.
NHS England and Improvement (NHSE/I) told trusts in July to recover private patient income to 2019-20 totals ‘as quickly as possible’ with system funding envelopes for 2020-21 based on this expectation.
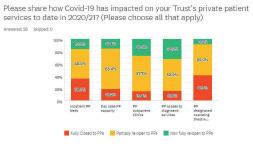
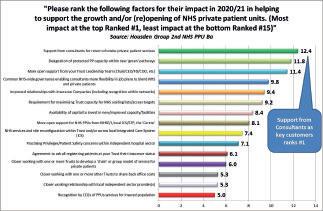
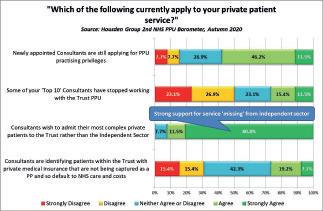
Healthcare consultancy Housden Group has surveyed trusts experiencing this income gap, and its PPU Barometer survey (see page 44) provides detailed evidence that a majority of trusts will do well this year to achieve half of last year’s income by the end of March.
HEALTHCODE WINS INNOVATION PRIZE
Online technology specialist Healthcode has won IT innovator of the year at the HealthInvestor Awards, which celebrate excellence in the independent healthcare sector.
Judges were impressed by The Private Practice Register (The PPR), its online information hub for the independent sector.
Vernon Baxter, HealthInvestor’s managing director, called it a model of best practice among new interoperable platform-based services.
Originally developed to streamline the cumbersome private medical insurance recognition process, the platform connects more than 20,000 practitioners, 300 private hospitals and the major insurers, supporting efficient and secure information-sharing and clinical governance. Healthcode managing director Peter Connor (right) said: ‘The PPR may be Healthcode’s most ambitious project to date, but we will continue to develop innovative solutions in the interests of healthcare providers and their patients.’
The company was also a short-listed finalist in the technology provider of the year category.
NHSE/I has said it will now step in and that ‘NHSE/I regional teams will work with the minority of trusts unable to mitigate the consequences of a material reduction in their non-NHS income’.
Some London trusts have shared with PPU Watch their own progress towards restoring a private patient service.
Robert Thornton, Royal Free’s private patients finance and commercial manager, told us that ‘inpatient services at the Royal Free first re-opened in August, but full capacity is not expected to return until after the end of the financial
year, with capacity still focused on the ongoing Covid response.
‘Hadley Wood, our satellite day care unit, is now growing strongly and was the first area to re-open.’
Paul Goodrich, managing director for private care, Chelsea and Westminster, added: ‘We are reopening our services again at the end of October – although with much less capacity and with the same issue NHS trusts face in meeting Covid-19 guidelines.’
Philip Housden is managing director of Housden Group healthcare consultancy
Fortius tackles rugby players’ health pains Updates on Coronavirus job support
Sport injury orthopaedic group Fortius Clinic hopes for winning ways following an official partnership with the Rugby Players Association (RPA), the collective voice of professionals in the game in England.
It will be supporting members of the organisation through their professional careers and during transition into retirement.
Fortius Clinic was launched in 2009 by a group of consultants who set out to create a centre of excellence in the field of orthopaedic and MSK healthcare.
It is now ‘the largest single group of orthopaedic and MSK consultants in Europe’ with more than 80 leading specialists. They work at three outpatient and diagnostic
clinics in central London, the Fortius Surgical Centre and a Joint Replacement Centre in partnership with Bupa.
Chief executive Jim McAvoy said: ‘Fortius provides extensive medical and surgical care to many professional rugby players and teams and we look forward to developing a long-standing partnership with the RPA through which their members will have access to world-class orthopaedic and musculoskeletal care.’
The RPA’s Gaia Bursell said the physicality of the modern game meant the need for top-class medical support was vital to members, so having access to such a reputable orthopaedic group was key to ensure the longevity of their health.
Dr Haus Dermatology, a specialist skin clinic within the Harley Street Medical Area, has welcomed a new dermatologist to their team: Dr Tatiana Welsch. She also works at the West Middlesex University Hospital.
If you are an employer, then don’t miss out on the Government support available to businesses during Covid-19. The rules have been subject to a number of changes to accommodate the latest lockdown and the financial support has been increased.
If you missed these, check out the latest of what is on offer in the main body of our website news section.
Specialist medical accountant Vanessa Sanders, a partner with Stanbridge Associates, provides a round-up, some useful information and advice – and will keep you updated on www.independentpractitioner-today.co.uk as and when the schemes change again.
‘Zoom boom’ beauty peril
By Douglas Shepherd
Plastic surgeons have warned that unscrupulous cosmetic surgery providers are cashing in on a postpandemic ‘Zoom boom’ by coercing vulnerable patients into panic-buying procedures.
The British Association of Aesthetic Plastic Surgeons (BAAPS) said a post-quarantine plastic surgery boom could see vulnerable patients being taken advantage of by unscrupulous providers. It is warning the public not to fall prey to unethical marketing tactics that attempt to lure them into ‘panic buying’ plastic surgery as a post-lockdown quick fix, highlighting the dangers of virtual cosmetic surgery consultations.
The association, which reported seeing a ‘massive upswing’ (100%) in demand for virtual consultations during lockdown, issued a statement highlighting its concerns following its first Virtual Annual Conference, where it launched a new set of Triple Lock Guidelines to safeguard patients.
While 83% of BAAPS surgeons
said they think virtual consultations are a valuable first step in the process, particularly in the current climate, the association has been concerned to find some clinics are not following safety guidelines.
In a survey of 20 non-BAAPS cosmetic surgery clinics, 75% did not insist on a face-to-face consult with an adequate cooling-off period and 85% did not insist on a cooling-off period at all, despite being a mandatory requirement of the GMC. Some clinics even advocated no face-to-face with a surgeon before surgery.
The association is cautioning the public not to fall prey to marketing deals luring them to ‘panic buy’, as they do not offer the required ‘cooling-off’ period of at least 14 days between a face-to-face consultation and the procedure being done.
Its newly appointed first female president, Miss Mary O’Brien, said: ‘As our world becomes increasingly virtual in this unusual time, we are being proactive in addressing the challenges patients face to make sure high standards are maintained in the delivery of care and information’.
There is also concern that aftercare is being overlooked. She added: ‘There is no such thing as virtual aftercare in the event that intervention is needed. It’s very important when a patient chooses a surgeon that the hospital is accessible so that high-quality postoperative care can be provided. BAAPS has warned against cosmetic surgery tourism for this very reason.
‘The danger of virtual consultations is that the patient may not realise that travelling a long distance for a surgical procedure in the UK can compromise aftercare.’
BAAPS Triple Lock Guidelines
1. A face-to-face consultation involving a thorough clinical and psychological evaluation is essential before you have surgery. Virtual consultations should only be used as an introduction.
2. Time for reflection, or ‘a cooling-off period’, is essential for a minimum of 14 days.
3. Aftercare. Ensure you have made appropriate provision to access your aftercare.
SURVEY OF MEMBERS
☛ 100% saw a rise in virtual consultations over lockdown
☛ 50% did not offer virtual consultations before Covid-19
☛ 66% will continue to offer them
☛ 83% say virtual consultations converts to a face-to-face
☛ 75% of patients then go on to have actual surgery
☛ 33% of members saw an increase in men seeking virtual consultations
☛ 66% said there was an increase in younger women seeking virtual consultations
BAAPS president Miss Mary O’Brien
DOCTOR IN THE HAUS:
A look back through our journal’s archives of ten years ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2010
£££ lost in call fiasco
Consultants’ private practices were losing thousands of pounds because their business support systems were just not up to the job, according to new research.
Doctors were said to be missing potential patients because:
Service was unreliable;
Phones went unanswered;
Responses were made by a machine;
Staff were unfriendly or poorly trained.
The research over four weeks tested the speed of response, efficiency, manners and effectiveness of people answering phones in consultant groups, private hospitals and solo practices.
Rita Livesey, a partner at healthcare management troubleshooters RLG Medical Partners, was ‘stunned’ at the results.
She claimed: ‘Getting through to consultants is a lottery. We were
shocked to discover that 35% of all calls were not answered by a person. As a patient. I would be extremely agitated by such a poor performance.
‘Not only does this make a mockery of private health, it inevitably means that consultants are losing substantial business opportunities.’
The potential loss of business to consultants affected was put at 3-5% of annual practice income.
Bupa starts invoicing online to speed pay
A new online invoice facility from Bupa promised doctors faster and more efficient payments.
Providers Online would give consultants and other providers 24-hour access to transaction details with the insurer and enable them to submit invoices online if they were not already doing so.
GPs ‘should promote PMI’
Most patients believed GPs should do more to encourage people to use their private health insurance, a survey showed.
It found that most people’s family doctors did not even ask if they had private health insurance.
Watchdog wants to hike fees
Proposals for a 15% rise in Care Quality Commission registration fees for private doctors were outlined in a consultation paper.
A spokesperson for the watchdog said: ‘We do not underestimate the impact on providers of paying fees, especially in the current economic climate.’
Bid to boost private care
Leading hospital groups who made up the then H5 Private Hospitals Alliance urged the Government to harness the expertise and resources of private doctors and independent hospitals to help the NHS.
Chief executive Richard Jones said: ‘To meet demand for healthcare in the 21st century, Government must use the expertise and resources of all healthcare providers.’
Surge in referral from NHS ‘likely’
A survey for the UK’s largest private hospital group confirmed Independent Practitioner Today’s advice two months previously to gear up for an NHS bonus.
Independent practitioners could
be in for a surge in referrals from the NHS that winter, the ComRes poll of 1,000 GPs, conducted for BMI Healthcare, revealed. It showed NHS budget and capacity pressures meant 53% of GPs were now more likely to channel patients to the private sector for ‘low priority’ operations, including removal of varicose veins, cataract operations, fertility treatment and knee surgery.
An NHS shake-up will see the responsibility for commissioning and healthcare budgets handed to GPs, with £20bn of savings already being targeted by 2014.
Tax relief cuts are
‘less harsh’
New rules restricting tax relief on pension contributions were at least less draconian than proposed by the previous government.
Accountant Martin Murray, of Sandison Easson, warned the annual allowance would drop from £255,000 to £50,000 from April 2011, with the lifetime allowance reducing from £1.8m to £1.5m from April 2012.
TELL US YOUR NEWS
Share your experience of what has and has not worked in your private practice. Even if it’s bad news, let us know and we can spread the word to prevent other independent practitioners falling into the same pitfalls. Contact editorial director Robin Stride at
A more dynamic CQC
Regulating the recovery – David Hare (right)
explains how the Care Quality Commission is evolving as a result of Covid
AS THE regulator of all health and care services in England, the Care Quality Commission’s (CQC’s) State of Care report assessing the whole of the healthcare system, is always hotly anticipated.
But, this year, its insights have had to evolve and look both at the current state of the healthcare system as well as how it – along with healthcare regulators themselves – can to adapt to the ‘new normal’ environment of living with Covid.
In looking at the state of care pre-Covid, the CQC’s report contains few surprises. While healthcare across England was found to be broadly good, the CQC made clear that improvement was still required in key areas such as NHS urgent and emergency care, maternity and mental health provision.
But, with regards to independent hospitals, there was good news, with the sector continuing on an upward trajectory of improvement and the number of sites receiving good or outstanding ratings increasing from 83% to 87% over the last 12 months.
This is a testimony to the culture of learning and improvement that can undoubtedly be found among the sector and its staff.
Growing backlog
Looking at the broader impact of Covid-19 on the healthcare sector, the CQC’s report rightly recognises the wide-ranging impact the virus has had on the health system.
While health and care staff across all roles and services undoubtedly showed resilience in the health service and adapted quickly to help keep people safe, particularly in terms of the digital transformation in primary care, many patients still struggled to get
the care they need, with an ever growing backlog of elective, diagnostic and cancer care.
The need to address increased waiting lists and, as the CQC put it, ‘finely balance the capacity to provide Covid and non-Covid care, and make sure that people have the confidence to come forward for the treatment they need’ is very much at the forefront of the independent sector’s mind.
Support the NHS
Indeed, ahead of what will be an extremely tough winter, independent hospitals are working hard to ensure they can support both their NHS and private patients and reassure them that the sector is going above and beyond in terms of their approach to infection prevention and control, and that people must seek treatment if they need it.
But what of the role of the CQC itself in a post-Covid world?
For some years now, the regulator has been moving towards taking a more system-wide approach to its inspections, and the ‘whole
systems’ response to the pandemic
– including with staff from both the NHS and independent sector were working hand in hand all across the country – has made this ever more relevant.
Earlier on in the Autumn, the CQC launched its draft strategy for 2021 and beyond, and how it can transform to become a regulator for both single providers and local systems.
Key principles
The strategy sets out four key principles for achieving this –
People – regulating to improve people’s experience so they move easily between different services;
Smart – with the ambition to provide more up-to-date, consistent and accurate snapshots of the quality of care;
Safe – promoting strong safety cultures with the aim of achieving zero avoidable harm;
Improve – playing a much more active role to ensure services improve.
For independent healthcare providers and those working in the sector, we broadly support this more dynamic approach to regulation that the CQC is seeking to take, underpinned by more effective and transparent relationships between regulators, local providers and patients.
As part of this, Independent Healthcare Providers Network welcomes the move to the CQC producing reports and ratings in a more responsive way that presents information about the quality and safety of services in more real-time way.
This can only benefit patients in exercising choice, commissioners in purchasing care, and providers in driving improvement.
With regards the ambition to
For independent healthcare providers and those working in the sector, we broadly support this more dynamic approach to regulation that the CQC is seeking to take
achieve ‘zero harm’, while this absolutely should be the aspiration of all healthcare providers, we must be wary of the potential of this creating a culture where providers and practitioners are discouraged from being open when things go wrong, and continue to emphasise the importance of ‘learning’ rather than ‘blaming’ across the system.
Of course, the devil will be in the detail around how to ensure independent providers, an often forgotten contributor to local systems, are included in these new local approaches and will likely vary for providers across the primary, community and acute sectors.
But the aforementioned principles are the sound basis for bringing regulation into the post-Covid environment and IHPN will be working with our members and those working in the sector to ensure we can help realise them.
David Hare is chief executive of the Independent Healthcare Providers Network (IHPN)
Are you looking to invest responsibly?
WHILE MANY investors have been ethically aware for some time, the past couple of years has seen a dramatic increase in the number of funds which put environmental, social and governance (ESG) issues at their core, alongside aiming to achieve strong financial returns.
In our latest Financial Wellbeing Research,* 49% of respondents felt some responsibility to use their wealth to help improve the environment and society.
Furthermore, our research found that investors of all ages increasingly want a ‘flexitarian’ approach, achieving a balance by allocating a portion of their assets to ESG investments. *
Given the growing demand of investors looking for a more ‘holistic’ return and a more compelling universe of ESG focused funds, we are delighted to have recently launched our Responsible Investing service.
Three-pronged approach
With a growing range of options, we believe it is our duty to ensure a rigorous approach is applied to selecting ESG funds to avoid those simply sprayed ‘green’, while continuing to benefit from the same robust investment process used for our conventional portfolios which have maximum flexibility.
Our three-pronged approach seeks to:
1. Blend responsible strategies to ensure effective diversification; 2. Screen contentious industries; 3. Scrutinise ESG credentials using our in-house scoring system to ensure that our clients are invested in funds which are responsible in more than just name.
As a full-service wealth management firm, individuals who wish
to invest more responsibly will still benefit from our expertise in combining investment and financial planning strategy in a co-ordinated service.
If you wish to invest to achieve both financial and sustainability goals and would like to learn more about our Responsible Investing approach, we would be delighted to hear from you.
*2020 Saunderson House Financial Wellbeing Research
Tom Gerrard, associate director Phone: 0207 315 6588
E: Tom.Gerrard@saundersonhouse. co.uk
Saunderson House is an independent wealth management firm, providing a comprehensive financial planning and investment management service to high-net-worth individuals.
We work with a broad range of clients with complex financial affairs, including private medical professionals, who often have little time to spare. For more information, visit www. saundersonhouse.co.uk/ responsibleinvesting
Investments may go down as well as up, and the relative performance of conventional and responsible mandates may diverge, particularly in the short term and you may not get back the full amount you invested.
We are delighted to have recently launched our Responsible Investing service
Are you looking to invest responsibly?
Responsibility and prudence have always been at the heart of how we do things at Saunderson House, because we recognise the responsibility that comes with managing our clients’ assets.
If you’re looking for strong financial returns that are accompanied with making a positive impact in terms of Environmental, Social and Governance (ESG) outcomes, we’d like to introduce you to Saunderson House’s Responsible Investing.
To learn more about our offering, please visit: www.saundersonhouse.co.uk/responsibleinvesting or you can contact : Ian McNally, Director, ian.mcnally@saundersonhouse.co.uk 020 7315 6513
ACCOUNTANT’S CLINIC: THE BUILDING BLOCKS OF ACCOUNTANCY
to of top tips
is for Personal Tax and Pensions
Our A-Z of top tips continues as Julia Burn turns to the letter P
TAXPAYERS MUST not forget about their personal tax obligations while the Coronavirus pandemic continues. Although the Government has announced it will help taxpayers financially during these difficult times, it is still taxpayers’ responsibility to submit self-assessment tax returns to HM Revenue and Customs (HMRC) by 31 January.
Tax returns due by 31 January 2021, of course, cover the year from 6 April 2019 to 5 April 2020 and income from the NHS, locum engagements as well as private practice must be reported.
Certain expenditure can be claimed against these earnings. This could include professional fees and subscriptions, medical defence premiums, room rental, salaries paid to personal assistants or practice managers and, in certain cases, travelling costs. Speak
to your accountant to decide what can be deducted against your business profits.
Other income
But do not forget that other sources of income you receive must also be reported. This could include rental income, income from savings and investments or pensions. You can claim relief on outgoings, such as pension/superannuation contributions or Gift Aid payments. Ensure your taxation affairs are well organised and copies of invoices and receipts kept safely. HMRC may request these if it checks your tax return. Your tax records should be kept for six years following the end of the tax year they relate to.
Certain sources of income are paid to you net of tax; for example, any income you earn from the
NHS as an employee. The tax withheld on this income is generally correct and it is calculated using your tax code.
But difficulties arise where you have other sources of income or outgoings that HMRC is unaware of, in which case your tax code and the tax withheld at source may be incorrect. Send the tax code calculations you receive from HMRC to your accountant for review.
Unless you are working as an employee, no tax is paid at source on income from private practice and this tax is usually paid by you twice a year under the self-assessment regime.
Usually, you pay your tax in equal instalments by 31 July and 31 January. These are estimated based on your previous year’s liability. The balance, calculated based on your actual liability for the tax year, is due by 31 January together with your tax return.
Deadline extended
Due to the Coronavirus pandemic, the Government initially allowed taxpayers to defer their 31 July 2020 payments on account for the 2019-20 tax year to 31 January 2021. This has now been extended so that the total liability due on 31 January 2021 can be spread over 12 months to 31 January 2022. Please note this is not automatic. A payment plan needs to be arranged with HMRC and only applies if the liability is less than £30,000 and tax return filings are up to date and no other tax liabilities are outstanding.
If you have funds available to pay any deferred payments now, you may wish to consider doing so to help your July 2021 cash flow.
GUIDE TO DELIVERING SUPERIOR PATIENT EXPERIENCE IN PRIVATE PRACTICE
In this month’s sixth and final article of her series, Jane Braithwaite brings together everything we have covered to date and examines how to ensure a continued focus on improving patient experience into the long term
A successful practice is full of happy patients
TO DELIVER a great patient experience, you need to deliver excellence consistently. Every single encounter with your patient makes a difference.
To set the scene, I would like to use the words of the great rock musician Bruce Springsteen: ‘Getting an audience is hard. Sustaining an audience is hard. It demands a consistency of thought or purpose and of action over a long period of time.’
This quote obviously relates to producing music and performing, but his emphasis on ‘consistency of thought or purpose and of action over a long period of time’ is equally true for your focus on your patients.
There is plenty of evidence that a long-term sustained focus on any area leads to improvement and that is what you are aiming to achieve in your own practice, clinic or hospital.
In your work with patient experience, you started by defining your patient experience strategy, setting out your vision, which forms your guiding map of what
you want your practice to be and setting your objectives to achieve in order to have this vision.
In last month’s article, we focused on measuring patient experience, discussing the various methods of doing so, including surveys and focus groups, and the importance of capturing and presenting the data in a format that can be easily understood and used.
Identify what patients are telling you
The next step in the process is to reflect on the findings from the measurement activities to fully understand what your patients are telling you.
Identify the highlights and lowlights. You will celebrate the highlights with your team, as these show the respects in which you are delivering a very positive experience for your patients.
The lowlights are where you will need to focus more attention, as these are the identified areas for improvement.
Even if all your results are good, I would encourage you to focus on the lowlights. The results may not seem to be disappointing, but there is always room for improvement and focusing on consistent improvement is what you are aiming to achieve.
I would suggest choosing three lowlights and create an improvement plan for each of these.
The time-scales can vary, but a quarterly plan with monthly review points would allow enough time to deliver and measure improvement, while the monthly reviews will ensure you and your team retain a focus on following up the actions and improving patient experience.
The monthly reviews will come around very quickly.
Take ownership
Agree who will take ownership of the improvement plans and who will develop them and manage their progress.
I would suggest the overall owner is a senior individual within the team to ensure the right level of focus is given and that actions can be delegated with authority. But you may want to choose a team member to create the actual improvement plans and own the management of the process.
Often middle managers are tasked with making the business more efficient and more profitable and this does not lead to a focus on improving patient experience
In an open culture, you will receive lots of suggestions and you will need to consolidate on a few actions which you all agree will deliver the best results.
For those who are unable to take part in these early discussions, ensure you invest time in communicating your plans with them and giving them the opportunity to contribute.
Your improvement plans are basically action plans describing what actions will be taken, by whom and by when. They should be short, very clear and easy to review. Many of you will be familiar with the SMART methodology – Specific, Measurable, Actionable, Realistic, Time-scales – and this would be a good tool to use.
Your success will be measured when you next review your patients using the measurement strategies you implemented previously.
If you are running ongoing surveys, you will be able to review the results monthly. If you are running one-off surveys from time to time, your implementation plan should include an action to run a new survey to measure improvement in the key focus areas, ideally quarterly.
improvement on a regular basis, ideally quarterly. Every three months, you can review your highlights and lowlights and change the focus of the improvement plans, if appropriate.
Once each year, you can invest time with your team reviewing your patient experience strategy. Is your vision still relevant? Are your objectives and your measurement criteria still correct or do they need refining?
Patient expectations do evolve over time
The experience of living through 2020 has taught us many things, but one important lesson is that change is inevitable and can be drastic.
The growth in telemedicine has been phenomenal and is a good example of how delivery of the patient experience can alter, and very quickly. Not so long ago, our patients would regularly pay their invoices in person by cheque and we would do a weekly bank visit to pay them in, and then BACS transfers became more popular.
How will your improvement plans be developed?
Every individual who interacts with your patients, from your marketing manager through to the receptionist at the hospital where you operate, is a member of your own patient experience team.
But it may not be possible to involve every individual in the development of the improvement plans, although, ideally, you want to involve as many as possible. Involving people at the creation stage is more likely to result in their buy in to the process.
The best method might be to set up a 30-minute team video call, but, prior to the meeting, circulate the results of your survey, highlight the three lowlights you are going to focus on and ask everyone to come to the meeting prepared to suggest ways to improve.
During the meeting, everyone should be encouraged to contribute their thoughts and ideas, and this is more likely to occur in an open culture where individuals know that their input is valued and will be considered seriously.
Barriers to improvement
There is much research to show that middle managers can be a barrier to the improvement of patient experience, and the reason for this relates to their objectives not being aligned.
The leaders and senior members of organisations are committed to improvement and intrinsically believe that it is vital. The frontline staff are engaging with patients every day and they want to deliver the best experience possible.
But often middle managers are tasked with making the business more efficient and more profitable and this does not lead to a focus on improving patient experience. To engage middle managers fully, their objectives and key performance indicators need to include goals for improvement in patient experience.
Embedding an improvement culture
If you follow this plan, you will be reviewing the progress of your actions in your improvement plans monthly and measuring for
Nowadays, it is common for patients to receive a text message containing a link to a payment page where they pay by credit card.
I believe that online appointment booking will become increasingly popular over coming months and we will make greater use of video in a broader range of applications. While we cannot predict everything that will happen as we adapt to new ways of working, we can ensure we deliver a positive patient experience.
This process described here, of continual review, will ensure that the focus on improving patient experience is embedded in your team culture and happy patients will equate to the ongoing success of your practice.
Jane Braithwaite (right) is managing director of Designated Medical, which offers business services for private consultants, including medical secretary support, book-keeping and digital marketing
CHARGES FOR ONLINE BILLING
Securing the future of electronic billing
Healthcode’s managing director Peter Connor (right) reacts to doctors who have criticised the introduction of charges for its electronic bill Clearing Service and explains why a free service is no longer sustainable
LAST MONTH, I had to make a difficult announcement to the independent practitioners who submit electronic bills to private medical insurers through Healthcode’s online Clearing Service.
After nearly 20 years, it has become necessary to charge for this service to secure its future.
Of course, I was fully aware that this news would disappoint practitioners that have an account with us. There is never a good time to introduce fees. And we held back from making the change as long as possible in recognition of the impact of Covid-19. But we had reached the point when further delay would have been irresponsible.
Only by putting the Clearing Service on a firm commercial footing can we prevent it becoming a victim of its own success.
Let me explain. Healthcode was established to develop an electronic billing solution for the private healthcare sector, but we recognised the need for something more sophisticated than a simple online postal service.
Alternative to paper
The electronic bill Clearing Service we launched in 2002 fulfilled our ambition to provide an accurate, efficient, secure and cost-effective alternative to traditional paper invoicing or sending invoices by email.
The Clearing Service eliminates the printing, postage and manpower costs associated with paper
Only by putting the Clearing Service on a firm commercial footing can we prevent it becoming a victim of its own success
We are asking independent practitioners to pay £6.99 per month to subscribe to the Clearing Service, plus a transaction fee of 25p per cleared invoice. These charges apply to those using Healthcode’s ePractice software and those who access our service using third party practice management software
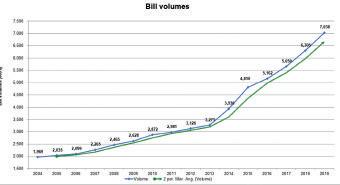
Back then, I could not have predicted that we would be processing and clearing more than three million electronic bills each year by 2012 or that this would have doubled to over seven million by 2019, accounting for more than £3.3bn revenue for the sector.
While volumes fell during the pandemic, we are already seeing a significant recovery since lockdown restrictions were eased and we expect this to continue.
billing. But, beyond this, it gives independent practitioners access to a convenient one-stop shop from where they can submit electronic bills to all the leading private medical insurers.
For each submitted invoice, Healthcode automatically carries out a series of checks on the information in accordance with the relevant insurer’s own validation rules and anomalies are flagged immediately.
Benefiting cash flow
The whole process is designed to ensure the invoice is ready for processing on receipt, minimising the likelihood of insurers’ queries and expediting payment. Invoices can be paid as soon as one week after submission, which benefits practitioners’ cash flow.
A bill status display gives practitioners the reassurance of knowing when their electronic bill has been received by the insurer. They also have the comfort of knowing that their electronic bills are encrypted to internet banking standards to protect sensitive financial and patient data. Considerable technology and processing power are required to maintain this vital link between practitioners and insurers, as well as ensuring the platform is compliant with the latest information security standards.
Historically, Healthcode has been able to absorb these costs, but this ‘hand to mouth’ approach is not responsible given the pace of technological change and accelerating demand for the Clearing Service.
The graph on the left shows the long-term upward trend in electronic bill volumes since 2004.
In the beginning, the growth in electronic bills was driven by hospitals. But in 2018 the number of bills from non-hospital providers –including independent practitioners – overtook those from hospitals, showing that electronic billing had become standard practice across the sector. Some 22,000 practitioners and 300 hospitals currently have a Healthcode account.
Secure servers
I am proud that Healthcode has facilitated the private healthcare sector’s transition to electronic billing, but if we are to continue to provide a viable clearing service that meets demand, we need to invest in technical expertise, reliable and secure servers and customer support. This is impossible with the current free business model.
We are asking independent practitioners to pay £6.99 per month to subscribe to the Clearing Service, plus a transaction fee of 25p per cleared invoice. These charges apply to those using Healthcode’s ePractice software and those who access our service using third party practice management software.
All payments will be re-invested into the Clearing Service and not be taken as profits or dividends by Healthcode’s shareholders.
At the same time, Healthcode has made every effort to ensure that electronic billing remains the best value option for practitioners, as well as being the most efficient and secure.
The Clearing Service charges cover:
Validation of electronic invoices to private medical insurers and other healthcare payers based on their specific rules;
Positive confirmation that invoices have been collected by healthcare payers;
Flagging invoice content which does not meet the validation rules;
The ability to view and print remittances, where the insurer has made this information available.
The table below gives a breakdown of charges, depending on the number of invoices. For example, a consultant who sends 50 electronic bills in a month would pay £19.49 (£6.99 subscription and £12.50 transaction charge) which equates to 39p per bill.
This is significantly less than the
We reported on Healthcode’s move to introduce charges on our website last month
alternatives when you take into account:
a) The administrative time required to generate, check, print and post the invoice – or chase the insurer to confirm it has been received and cleared;
b) Printing and stationery costs;
c) Postage.
In addition, as these costs are directly associated with running a private practice, they are allowable as a business expense, thereby reducing the amount on which practitioners pay tax.
At the beginning of this article, I said that this has been a tough decision. However, I am equally sure it is the right one for Healthcode’s long-term future and for those we serve in the private healthcare sector who want to spend time with patients rather than on paperwork.
By acting now, we can continue to provide a high-quality Clearing Service and ensure the business benefits of electronic billing are accessible and affordable to all.
Bills validated and cleared per month
Ensure you pass your screen test
The Coronavirus pandemic has resulted in a significant increase in online consultations.
While these may be convenient and ease time pressures, Dr Sharmala Pranklin (below) discusses how private practitioners can reduce the risks associated with remote consultations
ONLINE CONSULTATIONS are at the forefront of a digital transformation in medicine which has only intensified since the Coronavirus pandemic.
It seems inevitable that online consultations will remain more routine in medicine over the coming months and it is likely that many patients and practitioners will continue to take advantage of this option when the pandemic is over.
It is hoped that such technology will help ease some of the time pressures on doctors and will provide greater convenience to patients.
While online consultations do have clear benefits, concerns persist about the medico-legal risks and limitations of interacting with patients remotely online, rather than during a traditional face-toface consultation where it is possible to examine the patient and may be easier to communicate.
A Care Quality Commission
report on the state of care in online primary care services described six common concerns identified during inspections of online providers:
Safe prescribing, particularly of antibiotics and opioid-based medicine (see page 26);
Safeguarding;
Verifying patient identity;
Assessing mental capacity;
Obtaining consent;
Communicating with patients’ GPs.
Limited access
Furthermore, responding to the increase in online consultations due to the Coronavirus outbreak, the Royal College of General Practitioners’ chairman commented that it was a sensible measure but added: ‘These consultations have their limits and not all patients will feel confident about communicating with their doctor in this way –or have access to the technology to
make it happen – and we must ensure that they are not disadvantaged as a result.’
Additionally, the GMC has created an ‘ethical hub’ of relevant guidance on remote consultations as an area that doctors often ask about or find challenging.
The resource includes a flowchart to help doctors determine whether a remote consultation is appropriate in a given situation.
Also, the GMC’s basic good practice principles apply as much to remote consultations as to any other type. Doctors must:
Obtain adequate patient consent;
Ensure patient confidentiality;
Keep contemporaneous notes;
Make an appropriate assessment of the patient’s symptoms;
Communicate with other doctors to ensure continuity of care, especially when seeing people who may be registered with another GP; Have appropriate indemnity.
Obtain adequate patient consent
Any online exchange with or about a patient should take place only with the patient’s full agreement. Before conducting an online consultation, you should outline the limitations of making a clinical assessment without carrying out an examination to the patient. It is important also to make an assessment of the patient’s capacity to make decisions about any treatment proposed.
Ensure patient confidentiality
It is important to have suitable security arrangements in place when personal information is stored, sent or received electronically.
In its Confidentiality guidance, the GMC says that you should make use of professional expertise when selecting and developing systems to record, access and send electronic data (para 128) and be satisfied that any members of staff you manage are trained and understand their information governance responsibilities (para 123).
Before the online consultation, it may be worth advising the patient to be somewhere quiet and private where details of the consultation cannot be overheard or seen by someone else.
Keep contemporaneous notes
Detail the online consultation as well as your assessment and management plan.
If you decide to record the consultation, then you must inform the patient beforehand and obtain their consent. You should tell the patient the reasons why you are recording the consultation, how it will be stored and for how long. Remember to record details of the patient’s consent in their records alongside the recording and that it will form part of the patient’s medical record, and consequently should be treated in the same way as other medical records.
Make an appropriate assessment of the symptoms
In some instances, you may need to consult with a patient remotely, as it may be in their best interests; for example, in the interests of their safety and welfare. However, in undertaking an online consultation, certain
Any online exchange with or about a patient should take place only with the patient’s full agreement
aspects of communication such as non-verbal cues will be lost which could lead to misunderstandings by the patient or healthcare professional.
As with all consultations, the importance of careful clinical assessment, communication and documentation cannot be underestimated.
This is particularly true if you are working for a digital provider of medical services when you have not previously seen the patient face to face and do not have access to their medical records.
Ensure continuity of care
If you have not treated the patient before, the GMC says you should ensure continuity of care by asking ‘the patient for consent to get information and a history from their GP and to send details of any treatment you’ve arranged’.
Explain to the patient why this is necessary and if they have concerns, discuss these and the possible consequences. If they continue to refuse, you should consider whether treatment is safe and make a record of your decision.
Have the appropriate indemnity
Before undertaking online consultations, it is important to make sure you have appropriate and adequate indemnity. Some digital health providers provide insurance cover for the work that is carried out for them, but it is best to check with the organisation concerned and understand the terms.
When undertaking online consultations outside of an NHS contract, it is also worth contacting your defence organisation, as they should be able to provide further advice and guidance as well as indemnity.
Dr
Sharmala Pranklin is deputy head of underwriting at the Medical Defence Union
THE FUTURE OF HEALTHCARE
IMPROVING SYSTEMS FOR A SUSTAINABLE FUTURE
Telehealth and consultations by video are here to stay
SURVEY
OF 700 HEALTHCARE PROFESSIONALS
The Future of Healthcare webinar series was a fiveweek programme featuring a line-up of healthcare practitioners from around the Asia Pacific and Europe, the Middle East and Africa regions. Tim Morris (below) reports
In a recent survey by Elsevier to understand how Covid-19 has impacted the work of over 700 healthcare professionals, the majority of the doctors noted that telemedicine had become the norm, especially for general practitioners, who have been conducting remote consultations from their homes
PRESENTERS FROM across the globe have been outlining how their countries and hospitals rose to the challenges presented by Covid-19.
Discussions at the Elsevierhosted event focused on understanding the role of technological innovations and digital disruption, while outlining the importance of healthcare quality and safety. Essentially, how to improve the healthcare systems for a sustainable future.
In the wake of the Covid-19 pandemic, the UK has needed to revaluate the healthcare system, redesign models of care delivery and refresh the healthcare workforce in the light of the experience gained in recent months.
My report summarises the key take-aways from the webinar sessions and discusses how a knowledge-driven care framework will be the beacon in navigating this new reality for consultants and GPs in private practice in the UK.
Putting patients at the heart of healthcare
Digital health and medical technologies, including healthcare personalisation delivery via smartphones and online consultation, are seemingly shifting the perception from disease to healthy lifestyle management.
Despite this, it is important to note that telehealth consultations are not a new phenomenon in the UK. In fact, clinicians were describing the phone as having become as much a part of standard medical equipment as the stethoscope from as far back as the 1970s.
Covid-19 and the recent lockdown has, however, altered the patient’s perspective on what a healthcare consultation with their clinician should entail.
In this country, patients have become accustomed to experiencing significant wait times when booking routine appointments. Increased access to online consultation has somewhat curbed this trend by adding a quicker way of receiving medical advice, which in many cases is just as effective as the traditional process.
One of the big advantages – to all – of the increase in virtual consultations is the actual or potential efficiency gains, enabling doctors and patients to be connected
There has been a dramatic rise in the number of people considering paying for private treatment or insurance since the increase in pandemic rates –despite its impact on personal finances
27% after the outbreak of Covid19.
Additionally, over recent years, the UK has seen a significant uptake in the growth of services like Babylon Health, Push Dr, AttendAnywhere and AcuuRxand that offer both support for the NHS and private consultations to patients over the phone and through video consultation.
These services have seen a steady increase in use through lockdown as online services become more accepted by patients. The growth in ‘virtual’ consultations are ‘just the start’ of digital healthcare’s possibilities.
Providing quality care and ensuring safety
sooner, based on the doctor’s specialty or the patient’s ailment.
The growth of interest in private healthcare
The NHS remains free at the point of care and all consultations, whether via face to face or by phone, are available and accessible to all. Covid-19 has resulted in a shift in priorities with increased levels of the public placing more value on their health and wellbeing.
There has been a dramatic rise in the number of people considering paying for private treatment or insurance since the increase in pandemic rates – despite its impact on personal finances.
A nationwide survey of 1,049 by Consumer Intelligence for health insurance provider Equipsme, shows that 15% said they were likely to have considered paying for private treatment or insurance before the pandemic.
The figure has nearly doubled to
post-event survey highlighted that 85% of the attendees indicated that a safety and health management system needs to be established to ensure clinical safety in hospitals, post Covid-19.
Effective collaboration and co-ordination for better care
One of the crucial elements to success in containing the pandemic was the effective collaboration and co-ordination between public and private stakeholders.
As we look towards using new technology solutions during a pandemic, we must not lose sight of the importance of providing quality care to ensure patient safety and the best possible care. In all situations, having access to current evidence-based clinical information should not be underestimated.
Approximately 90% of clinical decision-making is based on the quality and accuracy of the recorded medical history, with the remaining 10% based on a combination of examination, tests, individual experience and knowledge of similar situations.
Clinicians have to learn how to effectively capture and interpret the medical records to accurately make further decisions on what tests and examinations may be required.
New tools could support clinicians in presenting clinical problems, such as high-quality video for orthopaedic surgeons to explain surgical procedures or videos for cardiologists to explain disease progression.
All such resources becoming available will enhance delivery of care and revolutionise future consultations.
While these new solutions and technologies hold incredible promise, there are potential quality and safety considerations that need to be thoroughly examined.
It is equally important to consider the impact and optimisation of the user experience, for both clinicians and patients.
The Future of Healthcare series
Countries who were successful in curbing and controlling the pandemic broke down barriers of information flow to enable realtime transfer of information across disciplines and healthcare systems, which allowed for more efficient decision-making processes.
In times like these, research needs to be combined with realworld evidence to allow the knowledge lag and the degree of knowledge variability to be minimised for health care professionals.
It is important that trusted evidence-based knowledge partners are available for healthcare professionals to seek information and corroborate clinical data with academic research to enable better quality and safety of patient care.
There has never been a better time to boost the potential of sharing information between the Government and healthcare systems – which as we know can ultimately shape governmental responses to a healthcare crisis and inform the development of potential treatments.
This collaborative effort is helped by the presence of the right data being shared to produce the relevant information and right knowledge, which can guide both broad public health decisions and actions in co-ordination with local patient care by healthcare systems.
Ultimately, all institutions must work together to cultivate a culture of cross-sharing to tackle any future global health crises.
As commercial portfolio and partnerships director at Elsevier, Tim Morris focuses on world-class clinical decision support tools and evidencedbased content, helping healthcare professionals integrate them into their workflows
The art of remaining in total obscurit y
There are ways for independent practitioners to do PR – but if you really want to crash and burn, check out the advice from Tingy Simoes (right)
THERE ARE many ‘How to succeed in PR’ books out there – I should know, I’ve written one myself! But what if – and hear me out – you wanted to know the secrets of failure? And not just trip over in your publicity efforts, but do so spectacularly?
For you, your prayers have been answered. I am here for those who want to know exactly what NOT to do and succeed in not publicising your practice favourably; how to achieve media obscurity and alienate
journalists; how to produce stories that will not only not gain attention, but actively earn press disdain. I am here to reveal the closely guarded mysteries of those who you probably won’t ever hear from.
So, let’s get instantly down to business. Some who have read me before or have listened to me speak at events may have heard
me mention the healthcare public relations ‘Holy Trinity’; the ingredients to the secret sauce of publicity victory, if you will. I like to summarise them as Science, Numbers and People.
Shall we begin with science, one of the key tenets? To achieve abject disappointment in your marketing endeavours: ignore it. Ensure that you do not have any particular breakthrough – clinical or medically interesting – to announce.
Little relevance
Make sure to have a development that has very little, if any, scientific relevance. For example, you could use a news release to reveal your waiting room has been redecorated or you hired a new office manager. Or – be still, my beating heart – that you’re offering a sales promotion because it’s Valentine’s Day or Diwali.
Do not, under any circumstances, announce an actual clinical improvement, a refinement of a technique or a new approach to a procedure that reduces pain, expense or recovery time.
Avoid anything that might have a novelty factor, like a treatment that you have pioneered or that only your clinic offers. The last thing news outlets want is news.
If you are sadly cursed with having something medically interesting to promote, make absolutely sure that you present it to mainstream media as if you were writing for a peer-reviewed journal.
Use incomprehensible jargon wherever possible, no diagrams, ideally graphic photos and anonymous case histories – more on that later.
Do not link it to anything remotely topical that regular people reading their Sunday newspapers or a woman’s magazine could possibly relate to.
Now we can move on to statistics: the ‘numbers’. A lot of the times, we advise those heathens who do look for favourable publicity – yet are blessed enough not to have an interesting development to report – to focus on trends.
For example, are they seeing more teachers, young men, older women, petrol station attendants having teeth whitening or lip enhancement? Is there a seasonal rise in bankers and boardroom execs looking for acid reflux relief when it’s annual report time? Stay out of it. Do not look for fascinating spikes that normal people – particularly your potential patients –would find interesting.
Popular culture
If at all possible, remain in your Olympian heights and look down your nose at popular culture and the latest topics people talk about while hopefully socially-distancing at the pub, if it’s open. You don’t need no stinkin’ stats.
As with the science, if you find yourself in the tragic circumstances of having a vaguely exciting trend to unveil, make a concerted effort to make the numbers murky and use sweeping generalisations as much as possible. Never show the real data!
Journalists love to take time from their 317th deadline of the day to try and work out what in Woodward and Bernstein’s name you’re going on about.
In the best-case scenario, try to have no proof of anything at all. If you can make sure to annoy journalists and frustrate their editors with a strong premise but no back-up, congratulations! You’re well on your way to securing that tantalising place at the bottom of the pile.
Finally – and this is the most important bit – let’s talk about ‘People’. It’s an odd phenomenon, how ‘people’, can relate to people. I don’t understand it myself, but I know it to be true, and therefore in achieving roughly 90% success rate in my own PR campaigns I have had to – ugh – involve actual human beings. Case histories, patient ambassadors, relatable citizens. Individuals with – I hope you’re sitting down – actual names and face photos. I know!
But not you, my lucky reader on your way to media oblivion. You will not bow down to this
absurdity. You will hopefully have no case studies to prove your claims, or if you’re stuck with one, they will be anonymous and refuse to have their face shown.
Or, if you’re really stuck, only have gross medical photography that no regular outlet could use or a hilarious before-and-after where no one can tell the difference without a jeweller’s loupe.
To those of you about to embark on this ground-breaking mission: I salute you. Or I would, if I could see you
Tingy Simoes is an award-winning publicist with over 20 years’ experience. She is founder and managing director of Wavelength Marketing Communications (www.wavelengthgroup. com) and author of the first-ever PR manual for the plastic surgeons and aesthetic professionals: How to Cut it in the Media
Cut drug errors by prescribing safely
Diane Baylis (below) offers advice for independent practitioners in a world where complaints and litigation are increasing
THE SHEER number of prescriptions processed means errors will occur with potential harm to patients.
While many mistakes fortunately do not result in patient harm, you will have seen the headlines when a medication error results in serious harm or a patient’s death.
Given the challenging claims and complaints environment for private doctors and the various studies highlighting the frequency of medication errors, 1,2 now is a good time to look at how you can enhance patient safety and reduce your risk in managing medicines.
So, what is ‘good’ prescribing? It is in fact poorly defined. Depending on your perspective, there are several values and behaviours involved in the prescribing process. For example, it should be evidencebased, appropriate, minimise harm, involve good communication and involve the patient. It should achieve concordance and be costeffective.
Writing prescriptions
When writing prescriptions, it is important to consider some fundamental points which may seem
obvious, but in a busy clinical setting can be easily overlooked.
You should only prescribe drugs to meet the identified needs of the patient and which will be in their best interest.
Remember that the person who signs the prescription is the one who will be held accountable should something go wrong.
Correct dose
If you prescribe at the recommendation of another healthcare professional who does not have prescribing rights, you must be personally satisfied that the prescription is appropriate for the patient concerned and that you exercised sound clinical judgement.
You should check that you are prescribing the correct dose of the medicine; this includes checking the strength, frequency and route. This is especially important in prescribing for children.
You need to ensure the patient:
Is not allergic to the proposed medication;
Is not taking any medication –prescription, overthecounter or alternative medicine – which may interact with the proposed medication;
Does not have an illness that may be exacerbated by the medication.
You should clearly communicate the medication and dosage instructions to the patient and check their understanding.
You may, on occasion, be asked to continue prescribing a medication started in another care setting or if the patient obtained the medication in another country. Make sure that you obtain adequate information before you agree to prescribe the drug. The clinician involved with the original prescription must provide enough relevant information to enable you to prescribe safely. It is important to be clear who will be undertaking any required monitoring and review of the medication.
Computer generated prescriptions are now common, but unfortunately errors can still occur. You should therefore be aware of the risk of accidentally clicking on the wrong drug in a dropdown menu or confusion between similarsounding drug names.
These are common mistakes that, in our experience, happen frequently.
Informed consent
The principle of informed consent applies as much to the prescribing of medication as it does to the performance of a surgical procedure. Patients should be fully informed about the reason for recommending the proposed medication, what they can expect in terms of improvement, the need for any monitoring and review, and sideeffects that may occur – including interactions with other drugs, such as over the counter medicines and alcohol.
It may be appropriate to warn the patient of potential adverse effects; for example, if the drug could cause drowsiness affecting driving or handling dangerous machinery.
You should agree with the patient the appropriate arrangements for followup and monitoring. Patients need to know under what circumstances they need to come back and the potential consequences of failing to attend for review.
Medication errors
Every year, more drugs are being prescribed with greater potential to cause harm through errors, interactions, sideeffects and lack of monitoring. So perhaps you will not be surprised to hear that medication errors make up 20% of Medical Protection claims. Many of these are preventable.
Medical Protection data shows
CASE EXAMPLES
INCORRECT DOSE
An elderly man was started on MST (morphine) 60mg, twice a day, for chronic back pain as an initial dose. Before this, he was taking tramadol 50mg, three times a day, for analgesia. After taking four doses of MST, he was confused, hallucinating and drowsy. The patient was admitted to hospital, where he received naloxone.
WRONG DRUG
A patient with chronic obstructive pulmonary disease received the wrong inhaler when the doctor misinterpreted an abbreviation on a letter for a ‘LAMA’ inhaler and prescribed a salmeterol inhaler (a longacting beta agonist: a LABA) instead of a tiotropium inhaler (a longacting muscarinic antagonist: a LAMA).
DRUG INTERACTIONS
The patient had a cardiac arrest and was admitted to intensive care. A digoxin blood level was taken, as the patient was on a high dose while on clarithromycin. Results showed digoxin toxicity. A review of past prescriptions show that the patient has been receiving in total the equivalent of several loading doses of digoxin, which ultimately led to this toxic level.
DRUG MONITORING
An 80-year-old patient receiving long-term ACE inhibitors and a loop diuretic to treat hypertension did not receive any urea and electrolyte monitoring in the previous 15 months and developed impaired kidney function.
You will not be surprised to hear that medication errors make up 20% of Medical Protection claims. Many of these are preventable
that the most common prescribing errors involved a contraindicated drug or an incorrect drug – most commonly antibiotics – followed by prescribing the wrong dose, then selecting the incorrect dose of the correct drug, most commonly opiates.
Other common prescribing errors are:
A failure to warn about or recognise drug sideeffects;
A problem associated with an injection;
Not checking for interactions.
Research shows that only seven drugs or classes of drug account for nearly half of all serious medication errors.1 These are:
Methotrexate;
Warfarin;
Aspirin;
NSAIDs;
Digoxin; Opioids;
B blockers.
And four classes of drug are responsible for 50% of admissions to hospital:2 These are antiplatelets, anticoagulants, NSAIDs and diuretics.
You will see the two lists are similar. These medicines frequently cause serious harm, warranting special care and rigorous monitoring. Therefore, concentrating on a small number of drug classes
could significantly reduce errors, admissions and fatalities.
Ensure that you have a robust recall system for the blood monitoring of patients who are taking high risk medication. Drugs including digoxin, methotrexate, loop diuretics and angiotensinconverting enzyme inhibitors require regular blood monitoring.
In order to reduce the risk from NSAIDs, avoid their use in older people and those at higher risk by prescribing an alternative, whenever possible. For those patients on long term NSAIDs, more frequent review and monitoring for adverse effects is advised.3
Issues relating to medication errors can result in serious harm to patients. By considering some of these points and issues, you can reduce your risk in relation to how you manage medicines and enhance patient safety.
If you would like some more information on this subject, take a look at our eLearning platform: prism.medicalprotection.org.
References
1. Saedder et al, Identifying high-risk medication: a systematic literature review. Eur J Clin Pharmacol, 2014 Jun; 70(6): 637-45.
doi: 10.1007/s00228-014-1668-z. Epub 2014 Mar 27. www.ncbi.nlm.nih.gov/ pubmed/24671697
2. Avery et al, Research into Practice; Safer Prescribing. British Journal of General Practic3e, 2014; 64: 259-61. http://bjgp.org/content/64/622/259
3. National Institute for Health and Care Excellence. Clinical Knowledge Summaries: NSAIDs – prescribing issues.
Diane Baylis is clinical risk educator in the Risk Prevention department at Medical Protection
BILLING AND COLLECTION
Outsourcing may be your best bet
The billing and especially chasing side of private practice is not something medical secretaries enjoy, and they are often happy to relinquish responsibility for this task
Outsourcing
private practice medical billing and collection has become an increasingly common option for consultants. Simon Brignall discusses some of the most common reasons why this is the case
OVER THE past decade, there has been three distinct trends in private healthcare:
1
2
The rise and rise of the selfpay patient;
An increase in the number of consultants working in groups;
3
A growth in outsourcing the medical billing and collection side of the practice.
As I have covered the first two trends in previous articles this year (August and April), I turn to the third, highlighting the main reasons why consultants, groups and clinics are choosing to outsource this key role.
Splitting the practice into clinical care and finance
Probably the most important, and often overlooked, benefit from outsourcing is that your medical secretary can maintain a clinical relationship with the patient that is not hampered by the business side of the practice.
Remember that your medical secretary is the first point of contact for your practice and is a vital part in the patient journey.
Outsourcing allows this relationship to remain warm and engaging by compartmentalising the two sides of the practice, leaving the billing company to focus on the business side and those difficult conversations about money.
This improves the patient experience and benefits the practice, as the secretary can focus on responding to new and existing patient inquiries.
Experts in their field
Consultants spend years in education and training to become experts in their specialty, but when they start out in private practice, running a business often presents challenges that they are not prepared for.
Even busy practices that have been running for many years still can find this difficult. Procedures often are not as robust as they should be or, more importantly, seldom routinely followed.
I still come across consultants that do their own billing – not a valuable use of their time or experience.
If you are going spend time billing, surely it is better to use that time more productively by seeing
If you are going spend time billing, surely it is better to use that time more productively by seeing patients and leaving the billing to experts
Poor practice financial data – no visibility of the scale of the problem;
Limited payment options for the patient.
I often meet with practices that are writing off 5-10% in bad debts a year because they find it difficult to stay on top of this side of the practice. A professional medical billing company that specialises only on this role will have robust procedures in place to resolve these issues and provide you with a range of payment pathways. This will all help to keep your bad debts to a minimum.
At MBC, our bad debt level is less than 0.5% across the firm.
Billing complexity
patients and leaving the billing to experts.
Most billing companies’ fees are calculated against received income, so their business model means that they are incentivised to ensure that they always bill the optimal amount on your behalf and that these invoices are settled as soon as possible.
Cash flow/bad debts
The most common inquiry we receive are from practices that have problems with their cash flow due to issues with outstanding debt. This can be the result of a range of issues such as:
Delays in raising invoices;
Delays in the reconciliation of payments;
Outstanding invoices not being chased effectively;
Medical billing is a complex process and some countries require you to have medical billing qualifications to carry out this task. There are over 2,000+ Clinical Coding and Schedule Development codes as well as diagnostic codes to consider and each insurance company has its own price list and rules in relation to how these codes can be billed.
These are updated monthly, so keeping on top of this can be challenging. Failure to do so can mean the practice loses out on income or, worse, result in issues with the insurers from incorrect billing. I still come across practices that are not billing what they could be due to errors in this key role.
Chasing outstanding debt requires a specific skill set and, for many medical secretaries, this is a task they do not relish, which can often mean that it gets put off. A
At the heart of medical finance
medical billing company provides a wealth of experience in this task as it is core to what they do.
Staffing issues
Outsourcing often provides a simple yet effective solution to a range of staffing issues. We often get inquiries from consultants where a long-valued medical secretary has retired and their replacement is not as proficient on the billing and collection side.
A well-resourced billing company means that the financial side of the practice is no longer impacted when the secretary is on holiday, as they will continue to provide continuity in service.
This can be beneficial with growing practices or groups where sometimes binary decisions about staffing need to be made when workload increases or decreases. Outsourcing means you have the capacity of the billing firm available to meet your requirements.
The Coronavirus pandemic has highlighted the need to have adequate disaster-recovery planning, which can be difficult to manage.
At MBC, all our systems, including our phones, are web-based, which meant we adapted a remote working model swiftly with no drop in our service levels. Our staff have now been back in the office since July and we are prepared to react to events accordingly.
Practice financial data
A common complaint I receive from consultants is that they do not have easy access to up-to-date and accurate financial data on their practice. All practices rely on this information as the first step in
the chase process, otherwise the whole process is flawed.
At MBC we provide our clients with access to a full array of reporting tools to review their practice data via our software. Clients can access this information 24/7 allowing them to view reports detailing: How much they have invoiced and collected based on a range of criteria including patient type, payment company and location; What codes they are billing; Aged debt.
Access to a range of practice data allows consultants to make informed decisions about their practice. Billing companies can also provide end-of-year reports that can be sent directly to their accountant.
New functionality
Outsourcing can provide a range of payment pathways that were pre-
and allow the partnership to flourish.
Another concern I hear from consultants is that they do not want to upset their secretary. In my experience, the billing and especially chasing side of private practice is not something medical secretaries enjoy, and they are often happy to relinquish responsibility for this task.
Building a partnership
It is important to make sure that you understand how the billing company operates, its workflow and who will be responsible for your practice, as this will ensure a smooth transition.
viously unavailable to the practice or difficult to implement.
Many of these not only improve the patient journey but benefit the cash flow to the practice. Here are some examples of what billing companies can offer:
E-billing of private medical insurers and patients;
Ability to collect 24/7 card payments via our card portal linked to each invoice;
Collection up front of monies when required;
Collection on the day via our client self-pay platform.
Billing companies’ costs
Most billing companies work on a cost structure that is calculated against received income, not on what you invoice.
It is always good business practice to have a cost structure that is correlated to the monies you receive. This has been highlighted this year when income has been less predictable.
As I have presented an in-depth examination of why outsourcing has been proved to be a popular choice for many practices, I think it would be useful to discuss some of the concerns that are raised.
The most common concern is around a perception that the practice is giving up control. This is best addressed through transparency. It is important that you know what the billing company is doing for you, therefore access to practice data is key so you can review its performance. Only then will you be able to establish trust
Establishing a good foundation to build a partnership with the practice is key. Our onboarding process, which is called ‘intensive care’, is managed by a senior dedicated personal account manager who establishes a good working relationship with the secretary so that this takes place.
By removing the billing and chasing side of the practice, this leaves the secretary to focus on the higher-value side such as patient engagement and can often lead to increases in revenue.
In summary, the outsourcing of the medical billing and collection role to billing companies is a trend that is well established and I expect will continue. Should you feel that is something that may benefit your practice, then why not contact a professional medical billing and collection company.
At MBC, we have over 28 years of experience in this sector and, as such, have a wealth of knowledge, making us ideally positioned to offer advice and guidance.
Simon Brignall (below) is director of business development at Medical Billing and Collection
Expertly different Protection as unique as you are
With the world’s largest medicolegal team and the greatest reserves of any defence organisation, we’re here to protect both your finances and reputation.
Medical Protection membership benefits include:
• Discretionary support that has the flexibility to ask, ‘How can we help?’
• Support in GMC investigations and representation at hearings
• The right to request assistance with criminal investigations
• Access to a free counselling service as part of your membership for stress or anxiety that you feel could impact your practice
• Free access to the Croner advice line which provides support with tax and VAT, company law and health and safety support
IMPRISONED FOR MANSLAUGHTER
Surgeon Mr David Sellu (right), convicted for gross negligence manslaughter of a patient –overturned on appeal after a 30-month prison sentence –continues his story from last month
My long drawn-out
release
AFTER NINE months behind bars, I was allowed home on temporary leave. This meant getting clearance from my probation officer, who was tasked with visiting the house to make sure there was no reason not to go back there.
There were rules to obey:
➲ I was to be picked up at 8.30am and brought back at 3.30pm on the day of return. I was allowed only two nights at home the first time and then three nights on subsequent visits, subject to my complying with all regulations.
➲ I was permitted to take out small items such as a toothbrush and shaving gear and a restricted number of items of clothing, all of which I had to declare before I left.
➲ I was to return with the exact articles and each item would be checked to make sure it tallied with the leaving inventory. I was to get clearance from the health centre that I was fit to travel out and, soon after return, I was to report there to be verified free of illness.
➲ I had to report to my probation officer on the day I came home to inform him that I had made it to the designated location and I had to spend all my nights in that location until I returned to prison. I
was to refrain from logging on to the internet and from engaging in all social media activities.
➲ I was not allowed to drink alcohol. It was possible the probation officer could call on me any time, day or night, to ensure I was in full compliance and any deviation from the rules could see me forcibly returned behind bars and with penalties.
I could see my car on the drive as we drove up. The battery had died, as the car hadn’t been driven but had been declared off road with the DVLA and the insurance suspended.
Interestingly, the car insurance company did not have any problem with the fact that I was serving a prison sentence and were happy for me to resume my policy once I was out and ready to have the car back on the road.
Worried about neighbours
I worried about what to say to the neighbours. We knew they were aware of the problems we were going through because the case had been reported in the newspapers. They knew I was a surgeon and that, typically, I left home early and came back late.
‘I will get out of the car when
there is no one around and go straight into the house,’ I told Catherine. ‘I cannot see anyone around,’ she said. I dashed straight into the house. There were decorations and balloons hanging up and messages welcoming me home. It was an emotional occasion and we were all aware this was a shortlived visit.
This was the first time in over four years since the start of this case that I had seen anyone in my household smile. We hugged and wiped tears from our eyes.
I rang my friends Ian Franklin and Paul Shapira who had been in constant touch with me in prison and always offered words of support. Ian was a consultant vascular surgeon whom I had met for the first time when I needed specialist help during an operation.
The patient had cancer and, unexpectedly during operating, I had found the cancer was stuck to a major blood vessel. At the time, Ian was on call for our hospital from Charing Cross Hospital several miles away in another part of London and I asked him to come over.
I waited with the patient on the table while he travelled to my theatre. His technical skills were exemplary and the patient made a good recovery from the operation. Ian later paid for and set up a website for my appeal.
Paul, now sadly deceased, was an ex-patient who had become a great friend. We used to drink together in a pub in Ealing near his home.
Catherine and I were optimistic that I would be out of prison soon. I tried to encourage her by telling her it was only six months, but I knew that even one more day in prison was a form of hell. It was wonderful to be home and to sleep in my own bed. The hours passed quickly.
In prison, I had no internet access and it was difficult for me to use the phone. But I was keen to contact the BMA to ask for advice on how to access the information held on me by BMI, the parent organisation that owned and ran the Clementine Churchill Hospital, in case we sought to appeal my conviction in the future. I knew they had a legal department that doctors I was acquainted with had used. I rang from home and someone
at the BMA in London answered the phone. ‘How can I help you?’
‘My name is David Sellu and I am a paid-up member of the BMA.’
I went on to inform him that I was a consultant surgeon and related my case. I told him I had just come home on temporary release from prison and I explained the reasons I was ringing.
‘You said you have been convicted of a crime and were in prison?’ he asked brusquely.
‘If you want to put it like that. I have explained the background,’ I replied.
‘Hang on, just for a minute. I will put you through to Subscriptions who will cancel your name from our list. Our policy is to remove all those who have been convicted of a crime from our books.’
I hung up.
I had supported the BMA for nearly 40 years, yet now, when I needed them most, they were going to ditch me. Had it not been for intervention from one of their top officials to whom a dear colleague later complained, this would indeed have been the case.
My next home visit the next month, in September, was less awkward. We were now better prepared and knew the drill. My probation officer did not need to see me and I had an extra day at home.
Jenny Vaughan and her husband, Matt, both friends and staunch supporters, came to our home for dinner. Jenny was a consultant neurologist with whom I had worked at Ealing Hospital. Matt was a specialist registrar in colorectal surgery.
Planning my appeal
We had a pleasant meal together and my friends assured me that they would lead my appeal. Jenny had read through my case and was by this time more familiar with the fine details than anyone else, probably even my legal team. Jenny was an ardent campaigner for justice. She had led the successful fight to stop the closure of the breast surgery unit some years earlier. She was incensed at what she saw as injustice in the hospital investigation, the charges, the trial and the prison sentence. I warned her that the task she was taking on, free of charge, was going to be time consuming and difficult.
Matt said: ‘Ever since I have known Jenny, she has been a crusader and has always got a cause to campaign for. Yours is going to be her biggest challenge. Don’t worry about me and the family. We are all behind her and you.’
Jenny added: ‘David, when I read the judge’s sentencing remarks on your case, I did not recognise the colleague I know that he was talking about. This fired me up enough to take on this case.
‘Also, if we do not reverse this conviction, it will set a bad precedent for medicine. We do not want to work in this atmosphere of fear. We do not want to be above the law, but this is a bad law and this conviction has been a travesty.’
3 February 2015: My last day There were several formalities to complete and I wanted to be sure that all the paperwork for my discharge would be completed so my leaving would not be delayed by some bureaucratic bungle.
I had been informed they did not write routinely to outside GPs to inform them of any medical episodes I had sustained nor the medication I was supposed to continue to take after I left.
The administrator in charge made me doubt my ability to handle my own records. She asked me whether I understood the value of the records and whether she could trust me to hand them over to my GP. If they got lost, the prison would not give duplicates and they would be absolved of responsibility.
Given her ignorance of my medical qualification, I felt now was not the time to inform her. I simply affirmed that I was legally entitled to the notes. I had to sign to say that I was responsible for the safe delivery of these records to my outside GP. I was also dispensed a twoweek supply of my blood pressure medications with instructions to see my own GP for a check-up for continuation of my treatment.
I got up at about 5.30am on my final day and finished all my packing. I was going to give the room a last thorough clean. At 6am, most of the people on the corridor were already up waiting to say their goodbyes. This was a touching gesture.
I would definitely not miss prison, but had got to know some of the inmates well.
It was strange using the word
friends to describe some of my fellow inmates, but I got to like a few of them and we did confide in one another. Prison would have been a lonelier place without someone to share problems with. I refrained from judging them and felt sorry for them when I left.
For the next 15 months, I would need to see my probation officer at regular intervals and would not be allowed to travel outside the UK.
I had survived
My discharge home was the moment my family and I had dreamed about, the moment we had talked about. It had seemed so far away and yet now here it was. It was the end of prison; I had made it and survived.
There were times when I had felt I would not survive. I had endured long nights and difficult days on my own. Now we could share them and lighten the pain.
I could eat what I wanted and, more importantly, not eat if I did not feel like it and not be suspected of going on a hunger strike. I could phone whomever I wanted to phone, although I was aware the authorities could use my phone records in any way they chose.
I could get out of the house and go shopping, to the gym, drive my car and take long walks. I was no longer in a regimented environment with someone else telling me when to go to bed, eat, take exercise, wake up or attend a roll call. Without a salary and having to pay for food, utilities and clothes I was now watching every penny I spent.
Our house insurance provider, if our policy was to remain valid, had to be informed of any significant change to our circumstances, including criminal convictions. When told about my prison sentence, we were given two weeks to find alternative cover. Companies that were prepared to take us on increased the premiums by more than 200%.
Next issue, last of the series: My conviction is quashed
Adapted from Did He Save Lives? A Surgeon’s Story, £9.99, Sweetcroft Publishing ISBN 9781912892327 from Amazon
INVESTING APPROACHES
Block out the noise of markets
Investors can be prone to distraction and focusing on past performance. Dr Benjamin Holdsworth (right) shows why caution is needed
IN MOST industrial settings, health and safety rules demand that the right protective gear be worn, including donning ear defenders in high-decibel environments.
Yet, when it comes to our investing in health and safety, we have little by the way of regulatory guidance except the obligatory phrase ‘Past performance is no guide to future performance’ to protect ourselves from the noise of market outcomes.
Investing in markets is a very noisy business and some form of ear defence may be required.
Given that markets do a pretty good job incorporating information into prices, they tend to move randomly on the release of new information.
Many investors are probably wondering today what returns will be like from equities in the final months of 2020 and perhaps next year too. However, nobody knows – and do not believe anyone who claims to know.
The only defence that we have is behavioural. We must keep our true investment horizons – 20 to 30 years or more, in many cases – at the forefront of our minds, accept that investing is a ‘two steps forward and one step back’ process and not look at our investment portfolios too frequently.
Rear-view mirror
Similarly, if we could invest by simply looking at what has done well in the recent past – and by that we mean the past few years, not just months – then life would be so much simpler.
Unfortunately, rear-view mirror investing is not the best way to build portfolios for the future, which is where our spending and intergenerational transfers will take place.
If we take the past three years or so, looking through our rear-view lens, we certainly would not want to have too large a position in the UK or emerging equity markets or
Rear-view mirror investing is not the best way to build portfolios for the future, which is where our spending and intergenerational transfers will take place
global commercial property or value or smaller company stocks, which fared poorly on a relative rather than an absolute basis, compared to large companies in overseas developed markets.
The latter, in turn, lagged the broad US market, which, in turn, lagged the growth-oriented stocks, particularly technology companies.
In an extreme rear-view mirror scenario, a hindsight investor would invest heavily in US growth stocks going forward. That would be a very concentrated bet and would ignore the fact that all future growth expectations are captured in today’s prices. These companies need to perform better than these expectations for prices to rise.
At the end of the 2000s, the rearview mirror investor would have avoided the broad US and World developed markets, yet in the 2010s they were exceptionally
strong performers and emerging markets and value stocks suffered relative to the US, and the UK was a laggard.
To want to place all your investment eggs in one basket – and in particular the one that has just performed best – seems a little naïve.
No one knows what the 2020s will bring and diversification is a key tool in mitigating the unknown.
As such, we take a highly diversified approach when building our clients’ portfolios.
Delivering returns
We also believe that limited exposure to more risky parts of the markets, including companies in emerging countries, smaller companies and relatively cheaper companies provide the opportunity – although never the guarantee – of delivering returns a little above the broad markets.
It can take some time for them to shine through. If an extra return
were guaranteed, there would be no risk to picking up the return –and it would not exist.
In an environment when cash delivers a negative return after inflation, and the expected returns for both bonds and equities are reduced as a consequence, these incremental returns are not to be sniffed at.
They happen to be all the things that have not done as well, in a relative sense, in the past few years, although they have still delivered strong absolute returns to investors.
Rear-view investors would avoid them to their detriment. More fool them.
Do not look back and wish you had owned a different portfolio, but take comfort from the fact that your highly diversified and soundly structured portfolio gives you every chance of a successful outcome in an unknown, forwardlooking world.
Dr Benjamin Holdsworth is director of Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS.
The content of this article is for information only and must not be considered as financial advice.
Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor.
The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
Cavendish Medical Ltd is authorised and regulated by the Financial Conduct Authority to provide independent financial advice to individuals and businesses.
For more information, please visit www.cavendishmedical.com
YOUR NHS ANNUAL ALLOWANCE
KEEP IT LEGAL: COMPLAINTS
A gentler attitude to gripes in pandemic
How will the GMC deal with complaints about your practice during the pandemic?
Solicitor and doctor
Tania Francis (below) examines the latest guidance
THE GMC issues guidance to its decision-makers which they should follow when making decisions about how complaints about doctors should be dealt with. For example, there is guidance about how to deal with concerns about a doctor’s health or doctors who self-prescribe or doctors who have criminal convictions or cautions.
It has now published guidance for decision-makers on how to assess the risk posed by a doctor in relation to allegations of impaired fitness to practise in a clinical setting during the Covid-19 pandemic. See www.gmc-uk.org/-/ media/documents/dc13028-guidance-for-decision-makers-oncovid-19--external-version-_pdf83985701.pdf
In early March 2020, a number of the health regulators – including the GMC – issued a joint statement about regulation in the pandemic.
In this statement, they recognised that professionals might need to depart from established procedures and sought to reassure registrants that concerns would always be considered on the specific facts of the case, taking into accounts the environment in which they were working and any relevant information about resources, guidelines or protocols in place at the time.
The GMC and the chief medical officers went on to emphasise that all doctors are expected to follow GMC guidance and use their judgement in applying the principles to the situations they face, including the very abnormal emergency situation of the pandemic. They stated that a ‘rational approach to varying practice in an emergency is part of that professional response’.
Mitigating cirumstances
GMC guidance for decision-makers gives more detail about how they will assess allegations arising out of the Covid-19 pandemic, taking into account the circumstances and how they impacted on the systems in which doctors worked –and continue to work.
It says it will take account of a number of factors – see box on the right.
So, what does this actually mean? How will it take these issues into account?
The truth is, of course, that we won’t know until complaints start being made to the GMC about doctors’ actions during the pandemic, and we can see how the GMC deal with these. There are likely to be some difficult cases which go to a hearing before a Medical Practitioners Tribunal because the GMC
MAKING ALLOWANCE
The GMC says it will take account of:
The availability of resources and the changes due to social distancing guidance
The uncertainty and rapidly evolving evidence-base about treating Covid-19
The disproportionate impact of Covid-19 on black and minority ethnic groups
Availability of PPE
Staff shortages due to illness or self-isolation
Working outside of normal practice and in unfamiliar roles
Rapidly changing and sometimes conflicting guidance and protocols
is unable to reach a decision to close the case or resolve it at an earlier stage.
Even if the tribunal then decides that the allegations do not amount to impaired fitness to practice, that doctor will have been through months or years of stress and uncertainty.
The GMC has given some examples of allegations which are unlikely to be pursued – such as:
Undertaking remote consultations rather than seeing the patient face to face;
Delay for non-Covid-19 treatment where access to treatment or diagnostic services was limited or unavailable;
Using PPE outside of the norm
– for instance, re-using PPE because of diminishing stocks –where this was an agreed response and concerns had been raised. They have also given examples of cases which might seem serious, but which would be unlikely to raise a question of impaired fitness to practise because they were reasonable in the circumstances –such as:
➤ Where a doctor’s actions may have led to harm or risk of harm to a patient but the doctor was required to work outside their usual area of practice with limited or no support and guidance.
➤ A doctor denied access to treatment, but this was a reasonable
It is well worth keeping careful records of current resources, guidance and protocols during the pandemic, especially as these can change so rapidly decision in the circumstances of the pandemic at that time.
➤ A doctor did not treat a patient due to a lack of PPE, but the doctor was at higher risk of infection and had raised concerns or tried to make alternative arrangements for the patient.
You can see that these examples are carefully nuanced and caveated and very fact-specific – thus, the defence of a doctor facing such allegations would rely on the evidence of the circumstances being
available, months or even years down the line.
There is little we can do to prevent or limit how far such complaints proceed, but it is well worth keeping careful records of current resources, guidance and protocols during the pandemic, especially as these can change so rapidly.
Records should be carefully dated and stored securely. You could consider keeping a diary of:
➲ Your commitments while you are not working in your usual role;
➲ A note of why you were assigned to that ward/clinic/list –perhaps because the usual doctors had themselves been redeployed elsewher, or were ill;
➲ Whom you worked with. Were you supervised if you required supervision in an area which was not your usual area of practice?
➲ Whether there were sufficient medical and nursing staff on duty. You should, as always, keep full, accurate and contemporaneous
clinical records in the patient’s notes including, if possible, the reasons for treatment decisions, and whether and with whom you have discussed these with.
Of course, the very nature of the circumstances we find ourselves in means that you may have limited time to carefully file all the guidance and keep perfect notes, when you barely have time to eat and drink and have not had any annual leave for months.
It is to be hoped that our digital world will make it possible to turn the clock back and remember what the situation was like, if we ever get to a time when it has been forgotten.
Tania Francis is a solicitor and a partner at specialist healthcare law firm Hempsons and she is also a qualified doctor. She specialises in regulatory law and clinical negligence litigation, including cases where there are related criminal proceedings
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes’ of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment
Premises
Regulatory requirements and investigations
Michael Rourke Tania Francis m.rourke@hempsons.co.uk t.francis@hempsons.co.uk
Any advice about my online inquest?
Remote hearings throw up some concerns for this consultant when asked to give evidence. Dr Kathryn Leask responds with some useful advice
Dilemma 1 I’m edgy about remote inquest
QI am a private psychiatrist and have been asked to attend an inquest remotely, using video. I have given evidence at an inquest before, in person, and have been carrying out video consultations with my patients, but I feel a bit uneasy about giving evidence to a court by this route.
Do you have any advice you could give me?
ADue to the coronavirus pandemic, tribunal and court hearings have either been put on hold or those that could not wait have taken place remotely.
It is possible hearings will continue in this format for some time. You should be sent all the information you need prior to the hearing taking place. If you feel anything is missing, let the court know in plenty of time and make sure you have downloaded the necessary app to allow you to join the meeting.
If there is any documentation that you need, ask for this to be emailed to a secure email address, preferably in an encrypted form. If possible, use an electronic device that is associated with your work, rather than a personal one.
On the day of the hearing, ensure your device is fully charged and you have your charger and an electric socket close by. Make sure your mobile phone is turned off and you have a suitable background.
If you are in your office, make sure there is no confidential information visible and dress smartly. You never know whether you may have to stand up or move, so consider your entire outfit, not just the top. If you are required to –or prefer to – stand, make sure
your camera can accommodate this.
Make sure the room you are in is not affected by external noise and, if necessary, close and lock the door to prevent interruptions.
Log on early and make sure you have all the necessary documents with you. This will give you time to flag up problems and ensure you are ready to start. If you know you are going to have to speak and not just listen, have a glass of water handy. If the hearing is a lengthy one, there will be breaks, but it is worth making sure you have all you need before your start, and use the toilet.
During the hearing itself, unless you are speaking, mute your microphone to prevent feedback or unwanted noise. You may be asked to turn off your video if you are not giving evidence, so make sure you know how to turn it off, and back on again when it is your turn to speak. When your video is on, be aware of your posture and body language.
Make sure you are central within the frame. Behave in a way that you would if you were in the courtroom in person.
Like any hearing, when it is your turn to give evidence, follow the instructions you are given and make sure you have understood the question and if you are not sure, ask.
This will inevitably be necessary if there is any interference and non-verbal cues will be more difficult to interpret. Speak clearly while looking at the camera.
Have any documents or notes you need to rely on in front of you and any relevant pages marked for ease of reference. Let the court know if you are having to refer to your notes so they understand why you may be looking away. At the end, do not leave until you are told to do so and follow any other instructions. If you are asked to take any other action once the hearing is over, make sure you do this as soon as possible.
A
‘notifiable safety incident’ is one where there is an unintended or unexpected outcome that, in the reasonable opinion of a health care professional, appears to have resulted in:
The patient’s death – not relating to natural progression of the illness or condition;
Impairment of sensory, motor or intellectual function, lasting or likely to last for 28 days;
Issues surrounding duty of candour rise to the surface in this query from a private GP. Dr Kathryn Leask (right) gives her response
You owe it to your patient
Dilemma 2 How do I make things right?
QI am a private GP and have recently been informed by the daughter of a patient that she intends to make a complaint following her mother being admitted to hospital.
The patient had several comorbidities including type 2 diabetes, hypertension and ischaemic heart disease and was also being seen by a private nurse who was dressing varicose leg ulcers.
As I was concerned about peripheral vascular disease, I also had specifically asked the nurse to monitor the patient’s anklebrachial pressure index (ABPI). The nurse carried out the measurement and rang to let me know that the ABPI was reduced and needed to be actioned.
Unfortunately, I was not in clinic that day, so the receptionist took a message which she said she would pass on to me when I returned. However, she did not record the conversation. Regrettably, due to sick leave, I did not return for another three weeks and the message about the
reduced measurement was not passed on to another doctor.
During my absence, the patient developed rest pain and the nurse was concerned about discolouration of the patient’s foot. Unfortunately, the patient had developed an acutely ischaemic foot that had to be amputated.
As a clinic, we have carried out a significant event analysis, which identified where system failures had occurred, and had reminded all staff of the protocols in place to ensure this does not happen again.
However, what actions do I need to take with regards to duty of candour?
ADoctors have an ethical duty to tell patients when things have gone wrong, to apologise and, if possible, put things right. This is reflected in the GMC’s Good Medical Practice guidance.
In addition to this, all care providers registered with the Care Quality Commission (CQC) also have a statutory duty of candour which applies to organisations rather than individuals and has a higher threshold than the ethical duty. But individuals are expected to co-operate with the organisation dealing with the incident.
Changes to the structure of the body – for example, an amputation;
Prolonged pain or psychological harm – defined as experienced or likely to be experienced for at least 28 days;
Shortening of life expectancy;
The need for treatment to prevent death or the above adverse outcomes.
The patient should be informed that a notifiable safety incident has taken place as soon as possible after the event. They should receive an explanation of what has
happened and be told what information is known to date and be advised of any further inquiries that might need to be made.
An apology should be offered and a written record of the notification to the patient must be made. If necessary, the patient should be provided with any support they need during this time.
The patient should receive written documentation and not simply a phone call. You may wish to seek the advice of your medical defence organisation about the wording.
In addition, the CQC needs to be notified of an incident meeting the criteria. The necessary forms are available from the CQC. It is important to be aware that failure to do so by, or on behalf of, the organisation’s registered person could be a criminal offence.
Dr Kathryn Leask is a medico-legal adviser at the MDU
NOW OPEN ON SATURDAYS
New sessions are available for independent private practice on Saturdays.
Fully CQC-registered clinic Nursing support
Appontment-making
Billing service
Secretarial support
In-house pharmacy
We are a leading private outpatient clinic and we are inviting new applications for practising privileges for our extended opening hours on Saturdays.
A PRIVATE PRACTICE – Our series for doctors embarking on the independent journey
More than one way of working together
With the current unusual environment, we are seeing more consultants considering working privately with colleagues whether that be in a loose association or more formally in a group.
Ian Tongue (right) looks at
some of the important factors when considering working with others
WORKING WITH colleagues can take many forms and these can have different commitment levels.
When deciding to join with one or more as a group, it is important to ensure that everyone has the same common goals and objectives.
The timing and method of achieving these goals may differ between each member.
This is usually not a problem, as a road map can easily be agreed, but is it important to establish those that are committed from those that are perhaps curious of the arrangement.
Common goals and objectives can simply be a cost or expensesharing agreement or it could be running a commercial business together.
It is important to establish these matters early on, as this usually determines the accounting and tax structure of the group.
Expense sharing
Under this type of arrangement, you are trying to achieve the financial term ‘economies of scale’. Put simply, the goal is to lower costs by the combined operations having lower costs that the collective individual businesses would have.
This is how barristers have operated for a long time and, as a result, is commonly referred to as a chambers arrangement.
The most common types of expenses shared are secretarial and room rental expenses. Each member contributes to the shared expense in a predetermined basis, usually activity-driven.
This is the simplest of all the options when working with colleagues.
Running a business together
Beyond simply sharing costs is working together in a relationship that requires a new business to be formed. These businesses will usually take one of the three forms:
A partnership;
A limited company;
A limited liability partnership (LLP).
Partnership
This is traditionally the choice of professionals such as solicitors and accountants and still the most common trading structure for GP practices.
In this type of arrangement, income and expenses are shared on an agreed basis with either a written or verbal agreement. Partnership accounts and a partnership tax return are required.
This structure is not common among consultant groups, because apart from sharing income, each member is sharing risk, as they are jointly and severally liable for the actions of other members.
Limited company
Many of you will already trade as a limited company for your private practice and will be familiar with the concept of a legally separate trading entity from yourself personally.
A limited company, unlike partnership structures, is subject to corporation tax, which is currently at a lower rate than income tax, making it attractive in a variety of tax planning applications. The company can shield profits from income tax which only becomes taxable when monies are extracted from the company.
In the vast majority of scenarios, the liability of the directors and shareholders is limited to the initial share capital, which is usually a modest sum.
Annually, the company prepares two sets of accounts, one of which is filed with the registrar of companies and is available to view publicly. But this version is usually a filleted version of the accounts with much less information than the main accounts prepared for the directors/shareholders and HM Revenue and Customs. These accounts have to be prepared in line with company law and accounting principles and the tax return in line with corporate tax law. This has now become the favoured structure among consultants for their private practices and is also popular for group structures.
Limited liability partnership
A limited liability partnership (LLP) can be seen as a hybrid of a partnership and a limited company. It carries the tax treatment of the partnership, so it follows the partner/member but has the
limited liability concept of the limited company.
As the name suggests, the limited liability partnership limits the liability of the partners to the capital they have in the LLP. With most LLP arrangements paying out the profits, this is usually a relatively low amount, but could be higher if the business required more significant day-to-day funding.
As with a conventional partnership, a tax return and accounts are required, but the partnership itself does not pay tax. The public filing of accounts and accounting principles largely mirror that of a limited company.
Combination of structures
There are certain taxation pitfalls to avoid, but there is no reason why a combination of structures cannot exist, commonly the LLP and limited company structure. These arrangements are more complex, but can be more tax-efficient for the members and perhaps allow greater scope for extracting value for founder members, which can often be a consideration.
Aside from any restrictive agreements entered into, there is also no reason why a consultant could not be part of more than one arrangement to work with colleagues or perhaps keep their private practice completely separate.
Where your businesses do overlap, it is important that you have measures in place to avoid breaching any regulations in relation to free market completion. The Competition and Markets Authority has been keeping a keen eye on the medical sector and has fined consultants in ophthalmic groups.
The members rulebook
Simple cost-sharing agreements rarely need anything too formal, but working in business together requires a rulebook of how the business will operate and provide prescriptive policy on a whole host of areas that you may come across.
For a limited company, this starts with the articles of association, but these are often largely generic between companies and therefore a shareholders’ agreement is where the nitty gritty rules and regulations of how the business will operate is covered.
For LLPs, the equivalent document to the shareholders agree -
ment is the members’ agreement and it serves exactly the same purpose.
Agreeing these terms and conditions will take a lot of time, so ensure that you have scheduled enough meetings to cover this. No doubt, many policies and procedures will be easy to agree, so focus on the harder ones, as it is easier to agree up front than when you are already trading.
Sharing profits
This can often be a contentious area, as the financial or practical contribution to the business of the member may be different. This imbalance in contribution could arise on an ongoing basis or perhaps at the outset of the arrangement if it is being driven by certain consultants and they want something extra to be built into the arrangement for set-up and ongoing management.
Frequently, profits are shared on the basis of what you generate; an ‘eat what you kill’ basis with costs weighted in a ratio of activity. This is particularly important if existing private practices of differing sizes are being brought together.
Ventures set up to target new income are often on an equal basis, but in the longer term these founding members may be given preferential treatment to new members or associates.
It is important to understand the tax implications of the structure adopted, as, depending on the trading structure, you may pay income tax, corporation tax or both on your share of the profits.
This is an area where a specialist medical accountant can really help, as they understand the nuances of the medical profession and the nature of the arrangement itself.
As services restart in the private hospitals post-Covid, there are likely to be opportunities to work with colleagues.
It is important to involve a specialist medical accountant in these discussions to ensure that any proposed arrangement is viable and set up efficiently for tax. If you are considering such arrangements, speak with an accountant without delay.
Ian
Tongue is a partner with Sandison Easson accountants
A digital prescription platform to allow convenient prescribing from home
CloudRx is a digital prescription system that allows prescribers to create and send an electronic prescription to our fully licensed pharmacy for fast delivery direct to your patient. It can be used from home by doctors working away from their practices.
No cost to prescribers
Simple and quick prescription creation.
Legal paperless prescriptions, including repeat prescriptions and controlled drugs.
Patients receive text and email requesting secure payment. Alternatively, we can invoice the prescriber or clinic each month.
Prescriber Fees can be added if requested
Medicines are dispensed and dispatched by a variety of delivery options
Fully integrated into Midex Pro
“We have worked with CloudRX to maintain a cold chain for the medication and direct delivery to patients at home.”
Dr Charlotte Norton, Medical Director of The Slimming Clinic, the UK’s largest chain of private doctor-led weight loss clinics
DOCTOR ON THE ROAD: MINI ELECTRIC
There’s a buzz about it
If you want to enter the green revolution and have some fun too, then Dr Tony Rimmer (right) believes he’s found the answer
WE ARE all being encouraged to climb on board the green transport policies being promoted by Governments across the world. As medics, we tend to have a decent awareness and care about the serious issues involved.
So, is now the time to dip our toes in the electric car pool? What about starting with a smaller or second car replacement?
If you get the chance to drive any one of the fully electric cars presently available, I can guarantee that you will be smitten.
The instant acceleration and the silent powertrain will take you back to days of riding dodgems at the fairground. The rekindling of this sense of fun is immediate and addictive. The fact that this is the greenest way to travel by road and contributes no ongoing burden to CO2 release and global warming is the icing on the cake.
It is only when considering the practicalities of running such a vehicle as regular work and family transport that certain shortcomings make themselves apparent. The two factors that tend to put people off is concern about the ease of re-charging and the potential range available.
Stumbling block
There is no doubt that if you live in a house or flat with no designated off-road parking space, then relying on public charging alone is a significant stumbling block.
The infrastructure – apart from Tesla with its dedicated network –is just not yet up to the job. If you do have your own space at home and can therefore charge regularly from a designated 7.4Kw charger, then the only thing that will deter you is the car’s range.
Essentially, the bigger the battery, the greater the range. But the bigger the battery, the greater the weight and, with it, the reduction of driving agility. Electric cars are at their best in an urban environment and what you need from a city car is that agility. So when MINI decided to do an all-electric version of their iconic small runabout, they could only keep the famed go-kart handling intact by having a smaller battery.
The 32kWh battery allows a claimed range of up to 141 miles, which, in real use, will be more like 105. Now this is much less of a
problem than you might think. Most urban commutes are less than 20 miles and that leaves plenty of reserve for unexpected detours. True, if you plan to do lots of longer trips, the MINI will not suit, but most will be bought for urban use or as a second car.
There are three trim levels to choose from and all have the same 181bhp electric motor and 32kWh battery and therefore performance.
Level 1 is pretty well specified but the Level 2 additions of keyless operation, heated seats and rearview camera are worthwhile extras.
Level 3 gives you a panoramic sunroof and matrix-LED lights among other things but is significantly more expensive.
Stylish elements
So how does it compare to a petrol powered MINI and what is it like to drive? Well, externally, the MINI Electric looks just like any other MINI. Unless you specify modelspecific wheels and bright yellow trim, you would not know the difference. It even has ‘Cooper S’ badging on the boot.
It is a similar story as far as the interior goes too. This policy ensures that all the attractive and stylish elements of the MINI’s
design are there to enjoy and it should also attract previous owners.
The controls are familiar and the central gearshift is there to engage the single-speed forward or reverse ratios. The driving position is sporty and there is plenty of comfort and gadgets for the driver and front-seat passenger to enjoy. The materials used and the general build quality is, as usual, up to high and impressive levels.
Driving experience
As with all MINIs, rear passenger room has restrictive access, but is surprisingly comfortable for two adults once in place. The boot, although small, is not compromised by the electric drivetrain and there is underfloor storage for the charging cables.
With all MINIs, it is the sporty driving experience that marks them out compared to rivals. Thank fully, I can report that the MINI Electric fulfils that promise and, with its direct steering, compact dimensions, nippy handling and instant torque, feels closer to a go-cart around town than anything else on the road. It is great fun.
These positive attributes continue on the open road, but you do notice a drop off in performance
As a car for use in the environment it has been designed for, it is rewarding for the keen driver and brilliant fun
over 50mph and you also become aware of the associated range drop of higher speeds. As a car for use in the environment it has been designed for, it is rewarding for the keen driver and, as I have said before, brilliant fun.
New electric cars are being released thick and fast and the MINI has strong competition from the Honda E, the Peugeot e-208 and the Vauxhall Corsa-e. The well-established Renault Zoe also makes a strong case for itself ,especially with its latest 135bhp motor and 52kWh battery giving a real range of around 200 miles.
However, nothing drives like a MINI and if you are like me and put a high value on driving pleasure and your lifestyle can accommodate the restrictive range, then you will not regret owning a MINI Electric as your entry into the green transport revolution.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
MINI ELECTRIC
Body: Four-seat hatchback
Engine: Single electric motor.
Front-wheel drive
Power: 181bhp
Torque: 270Nm
Top speed: 93mph
Acceleration: 0-62mph in 7.3 secs
Claimed range (WLTP): 141 miles
CO2 emissions: 0g/km
On-the-road price: £27,900
The MINI’s 32kWh battery allows a claimed range of up to 141 miles
There are plenty of gadgets for the driver and front-seat passenger to enjoy
NHS PRIVATE PATIENTS’ BAROMETER
PPUs victim of NHS pandemic pressure
This report on the second NHS PPU Barometer provides an exclusive snapshot of performance and provides valuable insights into the sector following the impact of Covid-19. Philip Housden (right) gives the highlights
• Completely open scanner that is well tolerated by claustrophobic patients
• Weight-bearing scans for spine and joints enable a more precise diagnosis
• Patients who are large or cannot lie down can be accommodated
THE NHS PPU Barometer is a unique measure of trading performance and of the confidence levels of the management teams of NHS trusts’ private patient services. It was completed as an online survey by 26 trusts in September 2020.
These trusts accounted for approximately £341m revenue in 2019-20, which is 50% of the total NHS PPU market. Both these values are up from £219m of revenues and 33.4% of the market in Housden Group’s first survey.
The 26 trusts delivered growth of £10m and 3.0% last year, slightly down on the overall market growth estimated at 3.4% and lower than the average in recent years of 5%, the reduction due to the impact of Covid-19 in early 2020.
Given the dramatic impact of the pandemic on the NHS and its capacity, the Barometer first asked: ‘What is your trust’s overall view at the moment with regards to treating patients privately, now or in the near future?’
Chart 1
Results show:
53% of responding trusts agreed with the statement that their trust was ‘Committed to re-instate private patient services to reduce waiting/access times and increase revenues/reduce costs’.
TOPICAL PPU ISSUES TO WATCH
Private patient service managers in trusts were also asked four topical questions and to score these for application to their own PPU.
The first two questions dealt with consultant relationships. In the first, 57.7% agreed with the statement ‘Newly appointed consultants are still applying for PPU practising privileges’, while only 16% disagreed.
For the second question, 50% disagreed with the statement ‘Some of your top ten consultants have stopped working with the trust PPU’, and 37% agreed. So it seems that consultants have not lost confidence in their PPUs re-opening to private patients.
In contrast, 8.3% of responders preferred the statement choice for their trust that it ‘Doesn’t feel it is appropriate to be treating – or planning to treat – private patients at this time’.
Trusts have reported struggling with two main factors that have driven reduced private patient income.
The first is that while theatre capacity has recovered in recent weeks, it was very constrained at the beginning of the Covid recovery phase and continues to be under pressure due to lower efficiency and throughput with the extra infection control measures, coupled with extra demand from the NHS backlog.
Several trusts reported that it has not felt appropriate to prioritise private work in these circumstances, although some volume has been possible.
The second is that, in many clinical services, side rooms are required for Covid pathways; for example, the isolation of patients with Covid or those awaiting test results or those who are most vulnerable.
This has made it much more difficult in many trusts to guarantee a single room for private patients, and therefore more difficult to offer a private service at all.
Although the Barometer was completed before the NHS contracts and payment guidance October 2020-March 2021 telling NHS trusts to ‘recover income as quickly as possible’, many trusts were already hopeful, if not confident, of restoring a service for private patients.
As one NHS PPU manager completing the Barometer survey put it: ‘Although the service is suspended, I am asked almost daily by clinicians when services might resume. Support remains but there is understanding of the current situation.’
The Barometer then asked: ‘How has your trust private patient services performed so far in the current financial year 2020-21?’ The purpose of this question was to learn of the present impact of private patient capacity closures.
Chart 2
Not surprisingly, trusts shared that they are experiencing significant reductions in income, with over 90% reporting drops of more than
25% and nearly half (48%) seeing a reduction of more than 75% by September.
In London, six of the top ten highest-earning NHS trusts responded to the Barometer. In the capital, predictions are less severe, with most seeing a fall between 50% and 75%.
To put this in context, 2019-20 total NHS income is expected to be circa £690m – a provisional figure pending remaining trusts’ annual accounts – equating to £55-60m a month. So the Barometer evidence
points to a fall of around £35-40m a month since April.
Chart 3
Are trusts delivering a service?
The Barometer asked for details of the changes to capacity in terms of inpatient and day case beds, outpatient clinics, diagnostic services and operating theatres. Were these presently fully closed to private patients or partly or fully open within the trust?
Chart 1
Chart 2
Chart 3
Responses show that, for each category, more than 50% of trusts are at least partially re-open for private patients.
Access to diagnostic services fares best, with 84% either fully or partly open to private patients. But access to operating theatres remains most restricted, with 43% sharing that their facilities remain closed to insured and self-pay patients while only 8% are full open.
However, experience across trusts varies widely. Consider these three summaries from managers in different trusts:
1. ‘Until NHS backlog is under control and we have excess capacity we will not be undertaking any PP work.’
2. ‘Private patient services have only just started to be restored. We are opening services up in a controlled manner and are looking to restore more services over the coming period, subject to the pandemic situation.’
3. ‘Our private clinic is now fully open and is extremely busy. The inpatient and day case beds are scheduled to open at the end of September. We have limited access to diagnostics and these are being triaged depending on clinical priority.’
Chart 4
What would help trusts most now?
The survey asked for a ranking of the factors most likely to help deliver the re-opening of presently closed or restricted NHS private patient services.
Those with the most impact ranked #1, the least impactful ranked #15.
The average scores out of 15 show that support from consultants for return of onsite private patient services ranks highest, followed by designation of ‘protected green pathways’ for private patients.
These were two new categories in this Barometer survey. The previously highest-scoring option from the first Barometer survey, ‘more open support from your trust leadership team (chairman/ CEO/FD/COO, etc)’, ranked third this time round, re-inforcing previous research undertaken by Housden Group across many trust Consultant Surveys in recent years.
The responding trusts remain positive that the second half of the financial year will begin to see the return of private patient services within NHS trusts –albeit at a modest and restricted level
Chart 5
The final questions were interested in consultant practice. A striking majority of 93% agreed with the statement that ‘Consultants wish to admit their most complex private patients to the trust rather than the independent sector’, up a little from 87% in the first Barometer survey.
This is in line with patient safety and governance-driven trends and is the issue most highlighted in survey comments because the highest complexity patients cannot typically be treated within most independent sector hospitals.
As one PPU manager stated: ‘Access to facilities continues to be a problem, but there is increased enthusiasm to use PPU services, as the NHS brand is enhanced by Covid and the independent sector
is also disrupted, giving an opportunity to approach consultants previously embedded at [the private provider].’
However, there was much less consensus over the final statement: ‘Consultants are identifying patients within the trust with private medical insurance that are not being captured as a private patient and so default to NHS care and costs’. Twenty-seven per cent agreed and 31% disagreed on this.
This second Barometer survey has gained the support of NHS private patient units, as they are keen to share and then learn how their own service compares with the market.
In these challenging times, the responding trusts remain positive that the second half of the financial year will begin to see the return of private patient services within
NHS trusts – albeit at a modest and restricted level.
There is no doubt one of the impacts of Covid on the NHS has been a dramatic loss of income in 2020-21. The NHS PPU management community have shared through the Barometer how they are working to re-instate services before the end of the financial year. However, with the independent sector now re-open and with reports of self-pay private activity growing fast, fuelled by public fears of Covid within the NHS and restrictions on NHS capacity, it remains to be seen whether the NHS PPU sector will recover and at what speed.
Philip Housden is managing director of Housden Group commercial healthcare consultancy
Chart 4
Chart 5
Hard graft is paying off
Consultants in this specialty have achieved a 5.5% rise in profits – but the inability of many to work normally during Covid-19 is set to hit hard. Ray Stanbridge reports
FOR 2019, we have made a major change in our criteria for selection to our sample. For over ten years, we have required participants to earn at least £5,000 a year from private practice.
This year we have upped this requirement to £10,000. To qualify for our non-statistically valid survey, each surgeon must:
Have earned at least £10,000 per annum gross from private practice in the year to 5 April 2019;
Have at least five years’ private practice experience;
Be seriously interested in the business of private practice;
Have either an old-style or newstyle NHS contract.
They may or may not have worked through a group, a limited liability partnership or a limited liability company.
The change in earnings criteria has resulted in a slight upward bias in our figures.
Structural changes
In addition, there are ongoing structural changes in the market that have affected our figures, and in particular the ability to make year-on-year comparisons.
Insurance companies are chang-
Groups are developing in the orthopaedic sector and these generally generate higher income for their members than singletons are able to achieve
ing the ways in which they do business. They are looking, in theory, to reward those who are efficient in the delivery of services. However, we would say that the theory here is better developed than the practice. Groups are developing in the orthopaedic sector and these generally generate higher income for their members than singletons are able to achieve.
Some consultants have chosen to incorporate and effectively divert income to others or delay receiving income. Yet others have chosen to pursue a full or hybrid employment model. All these factors have affected the comparability of our data on a year to year basis.
5.5% profits rise
Having made a long list of caveats, what then has happened in the marketplace?
Gross incomes for orthopods have increased by 5.1% from £193,000 on average in 2018 to £203,000 in 2019.
Of course, costs have also risen, on average, by 4.6% from £65,000 in 2018 to £68,000 in 2019. As a result, taxable profits have increased by about 5.5% from £128,000 to £135,000.
Year ending 5 April. Figures rounded to nearest £1,000 (percentage is
What then are the principal explanations for these trends?
Gross fees continue to rise. Again, we are noticing a growth in self-pay for minor procedures, particularly in London and in some rural areas. This growth has helped to offset insurance company pressure on fees.
Costs, by and large, have remained fairly constant between 2018 and 2019. Staff costs have increased very modestly. Professional indemnity costs have also
increased a little – this is because some specialties, such as spinal surgery, have had to take out more expensive insurance than they did from traditional providers in the past.
Conference costs have increased a little. It does appear that orthopaedic surgeons do enjoy exotic venues for their professional gath erings!
Other costs, primarily market ing, have fallen a little. As with other disciplines those consult ants who wish to acquire websites have generally already done so.
All in all, it was a satisfactory year for orthopaedic surgeons. Having a quick look at 2019-20 fig ures, it looks as if this trend has continued.
However, figures so far since the outbreak of the Covid-19 pandemic from about March 2020 show there has been a very dramatic effect on many orthopaedic practices.
Next time: Ophthalmologists
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists, Stanbridge Associates Limited
Years ending 5 April
Source: Stanbridge Associates Ltd
Innovative industry online solutions at the heart of the healthcare community
By industry for industry, Healthcode are the experts in information technology focussing solely on solutions for the healthcare sector. Trusted by leading hospitals, independent practitioners and insurers to deliver high quality, secure, cost effective IT systems that connect key stakeholders to seamlessly enable transparency within the sector and enhance patient safety.
• Circa 20k clinician accounts
• Over 300 private hospitals
• All major private medical insurers
• Process and clear an average of 28k bills daily worth £3bn
22k practitioner accounts £3.3bn
Coming in our December-January issue, published in the New Year:
Competition rules in private practice –what you need to know: Louise Banér is the Competition and Markets Authority director who earlier this year led an investigation into price fixing in the private ophthalmology sector. She gives some useful advice to Independent Practitioner Today readers to help them stay out of trouble
Social media is, by nature, social – and like any social gathering, there are not only rules dictating acceptable conduct, but also ‘unwritten rules’ that encourage – or discourage – success. We focus on two classic faux pas in the online self-promotion of private doctors.
Remote handovers with colleagues: reducing the risks:
Communication between clinicians during patient handovers is a known point of medico-legal risk. Dr Sarah Coope, of the MPS, looks at the gaps in information, misunderstandings and assumptions that can increase the risk of errors, conflict and complaints
Matters related to driving can be emotive, so Dr Sissy Frank advises a consultant cardiologist to keep detailed notes of the discussions with the patient so he can explain his approach in the event of a problem.
A consultant cardiologist with a small private practice is due to retire in six months’ time. He has handed over his active private patients to other colleagues, with the patient’s consent. So how long does he need to retain the records for those whom he has now discharged? The MDU’s Dr Kathryn Leask gives her response in our Business Dilemmas series
INDEPENDENT PRACTITIONER
TODAY
The
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution. Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Write to Independent Practitioner Today 7 Lindum Terrace, Lincoln LN2 5RP
CHANGING ADDRESS, EMAIL ADDRESS OR SUBSCRIPTION DETAILS? Phone 01752 312140 or email karen@marketingcentre.co.uk
The Royal Institution of Chartered Surveyors recently published an updated Code for Leasing Business Premises, which private doctors will need to be aware of when negotiating leases as a landlord or as a tenant. Myles Evans, a senior solicitor at Hempsons, reports
An update on the GMC’s new consent guidance. ‘Decision-making and Consent’ came into effect from 9 November and is intended to support doctors in having a meaningful discussion with their patients. A medico-legal expert and doctor summarises the essential points for independent practitioners
In a new HR series for doctors in private practice, Jane Braithwaite explores topics that range from the responsibilities for employers through to work-life balance, working remotely and motivation
Ray Stanbridge takes a detailed look at opthalmologists’ latest income, expenses and profits figures
Simon Brignall of Medical Billing and Collection spells out some billing rules
The financial impact of changes to pension tax charges
Motoring writer Dr Tony Rimmer tests the Hyundai Kona Electric
In the last of his series, surgeon Mr David Sellu writes of the day his conviction for manslaughter of a patient was finally quashed
Plus all the latest news and views
Don’t forget to check our website home, news and features section every week for breaking news and information
ADVERTISERS: The deadline for booking adverts in our December-January issue is 27 November
TELL US YOUR NEWS
Robin Stride, editorial director
Email: robin@ip-today.co.uk
Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the journal or our website business and lifestyle directories, contact Andrew Schofield at Spot On Media
£90 independent practitioners. £90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE
Email karen@marketingcentre.co.uk or phone 01752 312140
Publisher Gillian Nineham
Phone: 07767 353897.
Email: gillian.nineham@gmail.com
SAVE £15 WITH DIRECT DEBIT!
Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.
BACK ISSUES: £12.50 including post & packaging Sponsors