The business journal for doctors in private practice
In this issue
Answers about insurance
Bupa’s experts answer the questions on PMI that doctors most commonly ask P27
New ethical standards to reflect the real world
n See page 12
The GMC’s Mark Swindells explains changes to Good Medical Practice due to start in January P32 We reveal the results of a survey of people’s views of private healthcare P46 An opportunity to grow private practice
Private care labyrinth
By Robin Stride
Independent practitioners are losing out due to system failures in turning high levels of private healthcare inquiries into bookings.
Although a record year for many in private practice is predicted in 2024, the sector is likely to treat fewer than it could if the patients’ journey was made much easier.
Improving the efficiency of the journey from a phone call to treatment is seen as vital by marketing advisers.
Independent Practitioner Today columnist Sue O’Gorman, of Medici Healthcare Consultancy, advised that the increasing NHS waiting times across many specialties and rising self-pay inquiries meant there had never been a better time for doctors to take a long hard look at their practice.
She advised they should ensure they have a watertight process to capture patients at the point of inquiry.
‘Many patients will be considering the cost, even if insured, and will want to understand up front if the specialist accepts their insurer and if there are any out-of-pocket expenses such as shortfalls.
‘Coupled with easy access to online information, patients increasingly will conduct their own research to identify the specialist with the best reputation, success rates and patient reviews.
‘Patients will often shop around for their specialist for several reasons. For example, they will seek out the most experienced professional for their specific condition, so ensuring your website accurately reflects your clinical expertise will determine the patient’s choice.’
Improve the patient journey
The problem of turning inquiries into bookings was highlighted at this year’s LaingBuisson Private Acute Healthcare Conference which was told that as many as half of inquirers do not become customers.
But the 200-plus audience heard there was a strong potential for providers to improve the various steps
Our sponsors
across the patient journey to make it quicker and nicer.
Market analyst LaingBuisson’s latest annual Private Acute Healthcare UK Market Report values the total UK market at £11.4bn in 2022.
This covers both private hospitals and private clinics/private practising doctors for the first time.
Private hospitals remain the largest section of the market at £6.05bn. But private clinics/doctors account for a significant proportion of revenue at £4.8bn.
Remaining market value comes from NHS private patient units (PPUs) with estimated total revenues of £578m in 2022.
Growth in 2022 and 2023 was positive but decelerated from earlier post-pandemic highs, as the sector returned to a relative stability.
The report says: ‘Self-funder activity volumes appear to have reached a new plateau in the hospital sector – at around 71,000 reported activities per quarter across 2022-23, up from a steady 50,000 activities per quarter reported in 2019.
‘However, this is likely to mask considerable unreported activity in the clinic sector, where it is estimated that almost half of revenues are generated from self-funders’.
Report author Tim Read said the analysis suggested that at a time when people faced unprecedented challenges in accessing NHS ser-
vices, the independent private acute healthcare sector had bounced back from the severe impacts caused by the pandemic.
‘The current strength of the independent market can be seen as income from self-funders and private health insurance has reached record highs, while revenue from NHS-funded care continues to be higher than at any point prior to the pandemic.
‘The surge in the number of people willing to pay for their own care highlights the challenge that many are facing when trying to access services through the NHS.
‘Although they will be seen eventually, it seems clear that people who may not be considered priority cases on the NHS are increasingly considering alternative options in order to have the certainty of a diagnosis or to receive a major quality-of-life improvement, such as by having cataract surgery or undergoing a knee or hip operation.’
He added that with Conservative and Labour parties indicating they saw a role for the independent sector in helping resolve the NHS elective backlog, and as providers played an ever more integrated role in delivery, it was important they fully consider how they could support continuity of care and system interoperability.
n See ‘ Inquirers are not being looked after’, page 4
Sue O'Gorman of Medici Healthcare Consultancy
TELL US YOUR NEWS. Contact editorial director Robin Stride
ADVERTISE WITH US. To advertise in the digital journal, on our website or in our business and lifestyle directories, contact Andrew Schofield at Spot On Media. Phone: 0161 408 3912
George Uglow of specialist financial advisers Cavendish Medical warns investors against short-termism P42
Business Dilemmas: Is the cloud a problem?
Medico-legal experts from the MDU reply to queries on patient data storage and lasting power of attorney P44
Doctor on the Road: Practical EV fails to raise the pulse
The Chinese-made BYD Atto 3 gets a thorough test ride from motoring correspondent Dr Tony Rimmer P50 www.independent-practitioner-today.co.uk
Building your own general practice
Accountant Alec James of Sandison Easson gives advice on a comprehensive list of subjects an aspiring private GP needs to consider when setting up P15
How to make your practice thrive Efficiency is the linchpin of a thriving healthcare clinic. Medserv’s Derek Kelly provides a comprehensive guide to streamlined practice management P18
How doctors see the future Elsevier’s Clinician of the Future 2023 report shows doctors’ readiness to embrace artificial intelligence across the healthcare industry P20
Anaesthesia errors in the spotlight Claims made against MDU anaesthetist members in private practice are looked at by medico-legal experts, who explain how risks can be minimised P24
Avoid being reported to the police Allegations of sexual assault can arise following patient interactions. Dr Emma Davies of Medical Protection shows how to avoid misunderstandings P30
Stop same errors being recycled
Simon Brignall of Civica MBC continues his analysis of the repetitive nature of problems private practices experience with their medical billing P36
Cut staff sick days by managing them Hempsons’ solicitor Henrietta Donnelly examines the updated guidance issued by the arbitration service ACAS on managing sickness absence P38
An eye for excellence
Our ‘PPU Watch’ correspondent Philip Housden takes a look at Moorfields Eye Hospital’s successful and expanding private care business P40
McCloud latest – complex maths to mend tax charge
Online pension tax calculating tool is proving difficult to use
By Edie Bourne
Doctors affected by the ‘McCloud remedy’ – finally introduced last month – have been assessing the impact on their previous annual allowance tax charge payments.
The remedy aims to recompense NHS Pension Scheme members deemed to have suffered age discrimination when the 2015 pension scheme was introduced.
They will now be able to receive their original benefits from the 1995 or 2008 scheme for the seven years of the ‘remedy period’, which runs from 2015 when the new pension scheme began to 2022.
But those who paid annual allowance charges for excess pensions savings growth in that same period must now recalculate their position based on corrected figures.
The annual allowance is the most you can save in your pension pots in a tax year. Once the allowance is exceeded, a pensions tax charge may be payable. Those who have paid charges may now be due a rebate once the figures are recalculated in their legacy scheme.
Patrick Convey, technical director at Cavendish Medical, explained: ‘The “McCloud remedy” is
an incredibly complex area.
Reworking through figures over a number of years – and remember, we may need to go back to the 2010 11 tax year because of the carry forward rules – can be particularly challenging if this is not your day job.
‘The pension scheme is due to provide revised calculations by October next year. It has already said that the 202223 annual statement, which would normally be provided in autumn each year, will be omitted in 2023 while the recalculations take place.
‘However, given the high number of mistakes that we see in normal pension statements and pay slips, I would not advise waiting until late next year to see what your own postMcCloud position might be.
‘We expect that many members will find they have paid too much annual allowance tax and are due a rebate of any overpaid tax, but there is a chance that others will have paid too little. The year that the error has occurred will have a bearing on what steps need to be taken.’
He added that although the new figures are due to be provided by October next year, this leaves little
We expect that many members will find they have paid too much annual allowance tax and are due a rebate of any overpaid tax, but there is a chance that others will have paid too little
PATRICK CONVEY OF CAVENDISH MEDICAL
time to check the calculations, correct any errors and be ready to submit tax positions as normal the following January.
Doctors are advised to get their own standing checked as soon as they receive their figures.
HM Revenue and Customs has launched an online tool to help ‘calculate your public service pension adjustment’.
For the tax years 2015 16 to 201819, members should be able to use the tool to assess rebates for previously overpaid annual allowance charges. If a member has paid too little tax, no repayment will be due.
For the tax years 2019 20 to 202223, members will be able to submit a correction of their previous charges into the online tool plus enter the information for the last tax year. They may have tax owed back to them but will not be asked to pay more.
Mr Convey said: ‘The online tool had a few teething problems, but is hopefully working more efficiently now.
‘One major issue is that users cannot save their progress and return to their work if they do not have the exact information needed to hand. After 15 minutes of inactivity, the service will time out and the member will need to start any calculations again.
‘If using this system, you will need your pension savings statements, your previous self assessment tax returns, P60s and records of other income, plus details of any benefits drawn.
‘This is proving testing for many busy doctors who do not have the time or experience in these calculations.
‘It is very likely many will need specialist help to achieve success when negotiating the remedy. Please do contact us if you require assistance.’
Private sector joins NHS to cut sex harassment
The Independent Healthcare Providers Network (IHPN) has signed an NHS England workplace charter committing to a zero tolerance approach to any unwanted, inappropriate and/or harmful sexual behaviours across the organisation.
Chief executive David Hare said: ‘We are pleased to be one of the early signatories to this charter, to show our commitment on behalf of our own organisation and the wider sector to this subject.
‘It’s important that the healthcare sector speaks with one voice to condemn all forms of sexual harassment and work together to stamp it out.
‘Healthcare providers have a duty of care to the people that work for them, as well as their patients.
‘Organisations across the healthcare system need to work together and individually to tackle unwanted, inappropriate and
harmful sexual behaviour in the workplace.’
IHPN director of regulation, Dawn Hodgkins added: ‘It is very timely that we should be discussing this subject. We heard a few weeks ago with a damning report in the British Journal of Surgery which showed the extent of appalling behaviour towards female surgeons, with six in ten reporting they’d been the target of sexual harassment from colleagues.’
By Robin Stride
Independent practitioners outside of London can expect a continuing surge in both privately insured and self-pay patients, according to market analysts.
LaingBuisson forecasts hospital revenue from private medical insurance will rise 10% next year and 9% in 2025, with a corresponding increase in self-pay of 4% and 3% over the next two years.
Revenues from the NHS are set to increase by 7% in 2024 and 6% the year after, it believes.
Private doctors in central London
could fare even better, with hospital revenues there from insured patients experiencing rises of 12% and 10% in the next couple of years and self-pay rising by 4% and 3% over the same period.
Embassy work in the capital is expected to go up even more, giving 15% and 13% rises in hospital revenues in 2024 and 2025.
All this has to be considered against some outstanding issues for the sector.
threats as consumer confidence, NHS waiting lists (diagnostics, decision to admit and GP appointments), UK politics and a 2024 general election and inflation.
LaingBuisson’s conference director Ted Townsend listed potential
Other influencing factors were the tight labour market, energy and other supply costs, other external shocks involving concerning situations abroad and the threat of Covid.
Mr Townsend asked his audience for their views on his forecasts and from around 100 responses they indicated:
Outside London:
Private medical insurance: about right 63%, optimistic 28%, pessimistic 8%.
Self-pay: about right 49%, optimistic 26%, pessimistic 25%. NHS – about right 52%, optimistic 24%, pessimistic 25%.
Inside London:
Private medical insurance: about right 58%, optimistic 27%, pessimistic 15%.
Self-pay: about right 47%, optimistic 20%, pessimistic 33%. Embassy: about right 42%, optimistic 51%, pessimistic 8%.
Inquirers aren’t being looked after Analysts predict surge from private insurance
Private healthcare providers are losing thousands of potential patients because they fail to turn inquiries about treatment into firm bookings.
But a variety of speakers at the LaingBuisson private acute healthcare conference indicated more could often be done to prevent people from turning away and to transform queries into business.
According to self-pay expert Liz Heath, research by one leading international provider suggested there were potentially up to 16 points in the patient journey where the patient could be ‘lost’, many even before they saw a doctor.
Improving the efficiency of the journey from a phone call to treatment is seen as vital by marketing advisers.
Leander de Laporte, co-founder and chief executive of patient experience researchers Medbelle, told the meeting that for the industry to grow the market, it needed to make information readily available to inquirers.
While a perfect personalised service for every patient was not possible, people could be given various solutions to make bookings and information easily accessible.
It was about making the patient journey ‘extremely smooth’, which meant integrating all the stakeholders and getting information back quickly so that a decision was made to go for private care.
Mr de Laporte revealed Medbelle research showing most inquiries were explorative and had low booking intent. As many as 51% did not subsequently engage.
One in ten were put off by the cost – although once a consultation was booked, the cost factor became a little less relevant.
Four per cent dropped out due to their experience and 5% went with the NHS.
He said there was a strong potential for providers to improve the various steps across the patient journey to make it quicker and nicer.
But Mr de Laporte cautioned that
even with his company’s support, there were still those patients who would not go ahead because they did not consider their experience perfect.
Among the patient experience difficulties cited at the conference was a huge variation in ways to book an appointment. One private hospital group was said to have as many as 84.
Another contributor criticised a ‘disjoint’ between hospitals and consultants, something she had not observed where the doctors were on a salaried contract.
Keith Hague, former boss of The Wellington who helped set up Cleveland Clinic London, said he heard private medical insurers say they wanted to become more of a partner with patients, but added: ‘It’s a long time happening.’
Speaking from the audience, he said: ‘I can tell you, when you are a patient, there’s only one thing that matters and that’s the consultant – the person that’s going to do that complex operation.
‘It’s not so much the hospital; it’s definitely not the insurer; it’s the actual guy that’s going to cut you open.’
The UK’s private health sector was also criticised for failing to do a good enough job of managing patients after they have left hospital.
Medical travel consultant Keith Pollard said people who might be seen here were targeted by providers overseas – including one clinic in Lithuania where 80% of patients having a knee of hip replacement are British.
A patient who had a knee replacement here could be followed up later in case the other knee needed doing.
But he said he had experienced this operation himself and had heard nothing back afterwards from the provider. Now he had yet to decide where he would go for his other knee.
Could private healthcare do more for cancer patients? See page 10
Ted Townsend
LAINGBUISSON PRIVATE ACUTE HEALTHCARE CONFERENCE
Nuffield Parkside Hospital invests in surgical robot
Nuffield Health Parkside Hospital in Wimbledon, London, has become the first of the charity’s 37 UK hospitals to have the robotic da Vinci Xi Surgical System.
Health systems director Kate Farrow said four patients who had prostatectomy surgeries using the robot were recovering well and the equipment would help the hospital increase its capacity and mean more work for consultants.
‘We are proud to be the first Nuffield Health hospital to have the da Vinci Xi Surgical System available and we are looking forward to providing best-in-class outcomes for more people undergoing prostate, kidney and, in time, gynaecological and colorectal cancer surgeries.’
The system enables surgeons to perform with greater precision, with patients likely to experience less pain and faster recoveries.
Nuffield said over 12m procedures have been performed with da Vinci surgical systems on patients worldwide, and more than 34,000 independent studies suggest surgery with a da Vinci Surgical System can offer patients benefits compared with open surgery.
Urologist Mr Hasan Qazi
These can include reduced blood loss; reduced risk of infection; fewer complications; reduced length of stay, and reduced chance of readmission to hospital.
Consultant urologist Mr Hasan Qazi said it transformed the way consultants perform complex surgeries such as prostatectomy, hysterectomy and colorectal cancer surgery.
‘The robotic-assisted system makes it easier to be precise, protecting healthy tissue and enabling faster recovery for my patients. Clinical evidence across the world shows positive outcomes for patients because of the huge advantages the system offers.’
CQC warns of a two-tiered health service
By Olive Carterton
The Care Quality Commission (CQC) and the Parliamentary Health Service Ombudsman have both expressed concerns over a ‘two-tier health service’ increasingly favouring those who can pay privately for their treatment.
Responding to the watchdog’s annual State of Health and Social Care report, Ombudsman Rob Behrens said ‘Our healthcare system can’t keep up with the rising demand for care.
‘With more and more people having to turn to private healthcare, a two-tiered health system has been created where, too often, only those who can afford it are able to be treated quickly.’
He said the report made for ‘extremely difficult reading’ and echoed widespread concerns about people’s access to and experience of healthcare, particularly in maternity and mental health.
CQC chief executive Ian Trenholm said: ‘The combination of the cost-of-living crisis and workforce challenges risks leading to unfair care, with those who can afford to pay for treatment doing so, and those who can’t facing longer waits and reduced access.
‘And the impact of unresolved industrial action on people can’t be ignored. It’s crucial that both parties work towards an agreement so strikes do not continue into the winter, when disruption will have to be managed alongside increased demand for urgent care and staff sickness.’
CQC chairman Ian Dilks added that challenges described in the report were to some degree caused by a lack of joined-up planning, investment and delivery of care.
Now the opportunity needed to be grasped to ensure fairer care for everyone so that people got the
care they needed, not just the care they could afford.
Matthew Taylor, chief executive of the NHS Confederation, said the report laid bare the critical state of the NHS and should provide a salutary warning to political leaders about the abundance of issues facing the health service and the scale of the recovery task ahead.
‘After a decade of underinvestment in staff, buildings and infrastructure, it is no surprise that we are in this position. We now need a credible plan that helps NHS leaders recover services and rebuild public confidence in what has always been one of the UK’s most valued institutions.
‘The report is rightly at pains to point out that there is good work happening across all of the sectors in very tough conditions, particularly around mitigating the risks of staffing shortages, but health leaders will all too readily recognise the many intractable problems outlined within it.’
He highlighted worsening health inequalities, with the report suggesting that those who could afford it were increasingly turning towards private care ‘creating the risk of widening access gaps towards a future two-tier healthcare system’.
The CQC said those who could afford it were increasingly turning to private healthcare. ‘Research by YouGov shows that eight in ten of those who used private health care last year would previously have used the NHS, with separate research showing that 56% of people had tried to use the NHS before using private healthcare.
‘This situation is likely to exacerbate existing heath inequalities and increase the risk of a two-tier system of health care, with people who cannot afford to pay waiting longer for care.’
The da Vinci Xi surgical system
Pharmacierge expands
By Leslie Berry
A 5,500 square-foot expansion in Wimpole Street of Pharmacierge, the e-prescription medtech for private clinicians, is creating central London’s largest robotically-enabled dispensary.
It is equipped with a 30ft dispensing robot projected to improve overall efficiency and enhance rapid availability of the broadest possible pharmacy formulary for a network of over 4,500 GP and consultant users.
The company said acquiring the additional Wimpole Street lease marked a milestone in its mission to be the pharmacy partner of choice to all leading private practices and private hospitals.
Chief executive Edward Ungar said: ‘We’re not just expanding our footprint but creating advanced facilities that offer clinicians and their patients an appreciably better service.
‘Robotics and proprietary software play a core role in our aspiration to set a new benchmark for
pharmacy efficiency; one which will undeniably benefit patient care.’
The brand’s operations parallel to Harley Street will grow to 8,000 square feet – or tenfold the size of its original location in 2015.
Pharmacierge, backed by 80 leading private GPs and consultants spanning all medical specialties, engaged a worldrenowned pharmacy designer to transform two 18th-century Georgian properties into one streamlined clinical space.
Marketing your service to young people well worth it
Marketing to younger patients could reap unexpected rewards, a new survey suggests.
The 18- to 24-year-old age group has raised eyebrows at the Independent Healthcare Providers Network (IHPN) after it discovered they were the most likely to have used the private sector.
Four in ten have already done so. And nearly three-quarters of those under 34 would consider using private healthcare if needed, according to its report Going Private
They are also more generally positive about the independent sector and the most likely group to have accessed private GP services.
The IHPN’s David Furness said: ‘It will probably surprise a lot of people that the age group with the
greatest number of private health care users is 18- to 24-year-olds.
Four in ten have used private healthcare – largely, we believe, for GP appointments, scans and diagnostics.
‘It’s a very interesting finding, showing young people seem to have a very pragmatic view when it comes to accessing the healthcare they need, and there is evidence of clear generational shifts in attitudes and behaviours. Younger people are seemingly more prepared to take immediate steps.’
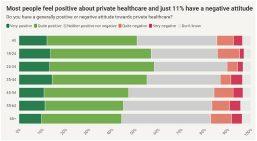
Mr Furness added: ‘I think sometimes there has been a perception that people ‘don’t like’ private healthcare. In fact the majority of people are positive about it, especially those who’ve actually used
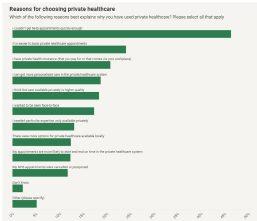
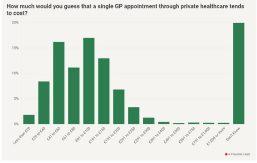
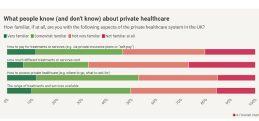
it, and it’s only a minority (11%) who have negative views.’ IHPN research of 2,000 ‘representative people’ found affordability the biggest barrier to people accessing the system – but there is also a lack of awareness and absence of information evident. There could be an opportunity to empower patients by giving them much better information on costs and how to navigate the system.
Mr Furness said people did not always have a good idea about private costs. But 82% of those who paid themselves thought it was worth the money.
Self-pay was more popular with younger people and those from lower social grades.
See page 46
The multi-arm robot, a first in central London, will soon occupy one wing of the new premises, with medication chutes spiralling down through the floor to the spacious modern dispensary below. Plans include dedicated subdivided areas for controlled, refrigerated and biological medications. The development aims to bring the time- and cost-saving benefits of ‘ePrescribing-as-a-service’ to more private practitioners, hospitals and private patient units nationwide.
PHIN grows its database of private consultants
Information on over 10,000 consultants is now available for prospective private patients on the Private Healthcare Information Network (PHIN) website.
The data body is now working with consultant anaesthetists and physicians to begin adding them.
PHIN chief executive Dr Ian Gargan expressed thanks to all the consultants, consisting of the vast majority of surgeons, who have given their details.
He said: ‘We recommend that anyone considering a private procedure visits our unbiased, free website first so that they better understand their options.’
A computer image shows a plan of Pharmacierge’s new 30ft dispensing robot with medication chutes to the dispensary beneath. The reception area is shown in the top right-hand corner
Pharmacierge boss Edward Ungar
Mixed growth for provincial trusts
Compiled by Philip Housden
Analysis of the NHS trust annual accounts now being published for 2022-23 is throwing some light on the mixed growth picture for out-ofLondon private patient earnings.
As the table to the right shows, with eight of the ten highest private patient income trusts now having published, four of these trusts show growth ranging from 37.2% at Frimley Health to 3.5% at Royal Papworth.
Sussex University Hospitals jumped from fifth to third with growth of £1.4m and 17.3%.
However, the other four reported falls in private patient income.
University Hospital Southampton dropped £1.3m and 20.6%, while Robert Jones and Agnes Hunt, Cambridge University and Oxford University Trusts had more modest falls of between 8.3% and 0.8%.
The overall gain was 4.0% over 2021-22, increasing group revenues by £3.2m and this contrasts with the average gain for the top ten London trusts reported by PPU Watch of 22.8%.
This trend further concentrates NHS private patient revenues in the capital.
Opportunity for eye surgeons as Optegra expands
Increasing numbers of consultant ophthalmic surgeons will have practice privilege opportunities as Optegra Eye Health Care expands its clinic network.
Business development director Kathryn Bryant said: ‘The new clinics which we are launching allow us to work even more closely with Integrated Care Boards around the country providing
Agnes
Return of national meeting for private patient units
The annual NHS Private Patient Summit is returning and will be held this year on 13 December, chaired by myself.
The online conference is open to all involved in leading and supporting the growing NHS private patient services sector.
It includes sessions on best practice from across the sector, including case studies from Moorfields Private Healthcare and Buckinghamshire Private Healthcare, a panel discus-
timely cataract care and helping to reduce their cataract waiting lists.
‘For surgeons in these regions this also creates an opportunity for them to individually expand their core NHS or private work and enables them to focus on specialist high-volume cataract surgery.’
Its newest eye clinic in York, opened by Julian Sturdy MP, is purely dedicated to NHS cataract patients.
For each new clinic, such as York, Optegra is appointing one surgeon, with a view to increasing this as demand increases in the future.
UCLH Private Healthcare launches new services
UCLH Private Healthcare, part of University College London Hospitals NHS Foundation Trust, has launched a new paediatric and adolescent allergy service which is available to young people from birth to the age of 25.
The service will provide a comprehensive diagnostic programme to pinpoint specific allergens and tailored treatment plans that address unique needs.
Clinics will take place in University College Hospital’s central London location, alongside UCLH’s highly successful NHS allergy service, which attracts patients from across the UK.
‘Our paediatric allergy service is just one of several new private services we are looking to launch at UCLH,’ said director of private healthcare Kerensa Heffron.
sion with private medical insurers Bupa, AXA and Aviva, and updates and insights to benchmarking, indemnity and contracting.
To find out more, go to www.sbkhealthcare.co.uk/events/nhs-private-patient-service-summit.
Philip Housden (right) is director of Housden Group commercial healthcare consultancy
‘This is a really exciting time for us and we hope to share news of even more new services soon.’
UCLH Private Healthcare is based across eight specialist sites in and around Bloomsbury, central London, and provides a wide range of private services including neurology and neurosurgery, maternity and teenage cancer.
The trust grew private patient income by 12.9% and £950,000 in 2022-23 to reach a total of £8.3m and 0.62% of total income.
Deafness and mental health service
A Harley Street Medical Area clinic has launched a new initiative to help address mental health issues connected to hearing loss.
‘The Well Being by CUBEX’ at 25 New Cavendish Street is a range of health and lifestyle related offerings to support sufferers of cognitive decline or emotional imbalance.
Director and consultant audiologist Adam Shulberg said: ‘Our approach looks at the connection between hearing loss and cognitive function. People with hearing
impairment sometimes retreat from social engagements and can feel quite isolated.
‘This happens because the brain has to work far harder to encode sound, so all cognitive processes are under pressure. It can be mentally exhausting.’
The clinic’s role was to help unlock the ability to function to the patient’s fullest potential ‘in our world of sound, and in all the ways that matter, gracefully and effortlessly’.
UK fertility clinics given thumbs-up
By Agnes Rose
Patients undergoing fertility treatment in UK-licensed clinics can continue to be reassured their care is safe and of a high quality, according to the sector’s independent regulator.
The Human Fertilisation and Embryology Authority’s (HFEA) State of the Fertility Sector 2022-23 report reveals that of nearly 100,000 treatment and storage cycles, over 99% had no incidents.
The annual report summarises HFEA compliance work for 202223, as well as information recorded in incident reports, on its register of fertility treatments and through patient feedback mechanisms.
HFEA chief executive Peter Thompson said: ‘Following each clinic inspection, a report identifying areas of good practice and those which require improvement is published on the HFEA website.
‘We monitor incidents in clinics to make sure that everything is done to understand what went wrong and, crucially, to take steps to ensure it does not happen again.
We also share learning and notify other clinics of potential issues.’
The report found:
Inspections decreased compared to previous years from 105 in 202122 to 85 in 2022-23. There were more inspections due to deferrals during the Covid-19 pandemic.
The HFEA worked with clinics to ensure they do everything possible to prevent and manage ovarian hyperstimulation syndrome (OHSS). In 2022-23, there were 64 cases of severe OHSS reported by UK clinics, occurring in less than 0.1% of cycles.
There were 517 incidents and 89 near misses reported to the HFEA, mostly Grade C (291), followed by Grade B (226 incidents). Both Grade B and C incidents decreased, consistent from previous years.
There were no Grade A incidents from 2020-21 to 2022-23.
Incidents graded as A involve severe harm to one person or major harm to many; B involves serious harm to one person or moderate harm to many; C involves minor harm; Near miss is an event with the potential to cause injury or ill health.
The number of patient complaints decreased from 76 in 202122 to 59.
Of the 107 licensed treatment clinics, 66 (62%) were privately owned, an increase from 62 in 2021-22. Most HFEA-licensed clinics, whether private or NHS, treat both NHS and self-funded patients.
Dr Catherine Hill, interim chief executive of Fertility Network UK, believes the report’s results will be a huge reassurance to fertility patients. But she added: ‘We would like to particularly urge clinics to make a concerted effort to reduce the number of patients affected by OHSS, as we see that the number of women affected by the condition has not dropped demonstrably in recent years.’
The HFEA aims to ensure everyone receives high-quality care in UK fertility clinics by licensing, monitoring and inspecting them. It takes enforcement action where necessary and gives ‘free, clear and impartial information about fertility treatment, clinics and egg, sperm and embryo donation’.
Jamanda Haddock has been appointed chief of staff for Cleveland Clinic London. She joined the hospital as a radiologist and chair of hospital services in 2018. She was previously clinical director for radiology and nuclear medicine at the Royal Free.
Newly launched Bridge Clinic London, in Euston, has announced the appointment of consultant reproductive medicine specialist Dr Ewa Goncikowska to its clinical team.
High-res scanners fitted in Harley St
The Harley Street Clinic has expanded its scanning capabilities after spending £4.5m on two new CT scanners.
It said this includes a first-in-sector high-resolution and high-speed SOMATOM X.ceed CT scanner from Siemens Healthineers.
This offers more precise imaging and will also support clinicians at clinic with time-critical situations, particularly in trauma and brain haemorrhage, as well as cardiac care.
It comes with two unique ‘companions’ to further support clinicians when imaging patients.
myExam Companion is said to push the boundaries of digitisa -
tion. It turns data into built-in expertise to reduce unwarranted variations by unlocking the full potential of the SOMATOM X.ceed automatically.
During CT-guided interventions it offers comprehensive support with integrated lasers to project the needle entry point and insertion angle on to the patient.
Hospital CEO Will Pressley said: ’This investment in our scanning offering reflects our commitment to ensuring we always provide the consultants that we partner with and the patients we care for with fast access to care and the latest in medical innovation.
‘We are proud to be the first in the sector offering this new technology that further supports our delivery of the complex care we are renowned for. By combining the knowledge and expertise of our specialist consultants with the capabilities of the SOMATOM X.ceed, we are also enhancing the care we provide our patients.’
Getting the 2.5-ton scanner into the Grade II listed central London hospital was no mean feat. The HCA UK team worked with local residents and the council to get permission to close the road and bring in a crane to deliver the scanner through the roof.
Dr
Harley Street is closed off while the scanners are craned into position
The London Clinic path lab gets a refit
A £4m two-year refit and design of
The London Clinic’s in-house blood sciences pathology laboratory provides ‘ground-breaking’ technology in the diagnosis of cancer conditions.
It will enable more tests to be processed, around the clock, seven days a week.
The official opening at 120 Harley Street was in partnership with QuidelOrtho, suppliers of the new biochemistry equipment.
Reza Mirza, head of pathology at the hospital, said the development allowed analysis of a larger repertoire of tests in-house and enabled same-day blood results for oncology patients.
‘We can remotely authorise the blood results in situ so that
oncology patients can start their treatments sooner.
‘A further important improvement for oncology clinicians is that we now have Cellavision, a
digital haematology microscopy solution that sends images to their desktops for immediate diagnosis.
‘But this isn’t the end of the story. We are continuing to invest
in a digital improvement journey to ensure all data flows seamlessly to our patients, clients and external users. It’s a case of watch this space.’
The laboratory is also being used for external commercial clients and specialises in the following blood science services:
Biochemistry;
Stem cell – the clinic has the largest stem cell collection in Europe;
Immunology;
Histology and cytology;
Haematology including routine haematology and blood film morphology review;
Blood transfusion;
Microbiology including bacteriology, serology and virology.
Aesthetic op errors rise
By Robin Stride
Aesthetic doctors are reporting a ‘staggering rise’ in complications caused by other practitioners.
Members of The British College of Aesthetic Medicine (BCAM) disclosed they have treated 300 more complications from other practitioners since last year.
The total number has risen to 3,523 from 3,323 since 2022. Of the 357 BCAM members surveyed, 82% said they had handled someone else’s complications.
Most (69%) of the complications had come from treatments performed by beauticians, therapists and podiatrists, which is up from 60% last year.
The remainder were attributed to other aesthetic medicine doctors, surgeons, nurses and pharmacists.
Dermal filler procedures continue to be associated with the biggest number of complications, while adverse events associated with botulinum toxin are not far behind:
Dermal fillers (44%);
Botulinum toxin (30%);
Threads (12%);
Lasers and other energy-based devices (9%).
The BCAM said that due to the lack of the denominator – the number of procedures performed by non-physician practitioners – it was impossible to estimate the relative rate of complications of injectable treatments performed by unregulated practitioners in the UK.
President Catherine Fairris said:
‘We have found that dermal fillers continue to be the treatment with largest number of complications from non-medical practitioners, which confirms how dangerous dermal fillers can be in the wrong hands.
‘Notably, members report that these complications are often more severe and require specialised treatments.
‘We strongly welcome the public consultation for a licensing scheme of aesthetic treatments, which will hopefully reduce the rate of complications and put patient safety first in the coming years.’
The BCAM annual clinical review 2023 states botulinum toxin was again the most fre -
quently performed procedure by BCAM members. More than 283,000 individual botulinum toxin procedures were conducted by 357 individual members, which was down from 315,000 by 331 members last year.
The top five treatments most frequently performed by BCAM members were:
Toxin injections (96% – a decrease of 1%);
HA dermal fillers (93% – a decrease of 1%);
Non-HA dermal filler (53% – an increase of 5%);
Mesotherapy/collagen stimulators (66% – an increase of 4%);
Laser/IPL (36% – an increase of 1%).
BCAM has been collecting data from its members since 2012. It said the data collected in each annual review is used to tailor BCAM’s decisions to best suit the needs of members and improve patient safety.
The results will also be shared with the Department of Health and Social Care ‘to provide insights that inform and help to better co-operate with policies and decision makers’.
BCAM trustee Dr Aggie Zatonska, an aesthetics doctor and former ENT surgeon, co-ordinated the annual clinical review. She said: ‘BCAM will continue to use our survey results to influence its future planning.
‘We look forward to working collaboratively with stakeholders over the next year to further improve patient safety and campaign for better regulation.’
The new-look pathology laboratory at The London Clinic
Dr Aggie Zatonska, the annual clinical review co-ordinator
Private sector ‘should take the lead in cancer’
By Robin Stride
A private hospital group boss has urged the independent healthcare sector to seize the opportunity to be at the forefront of cancer care.
He argued that the private acute sector could be leading the way in innovative and world-class cancer care.
John Reay, president and chief executive of HCA Healthcare UK, challenged providers at LaingBuisson’s Private Acute Healthcare Conference to ‘shape’ healthcare delivery not just follow it.
They should think outside the traditional parameters of the elective private provider model, he said.
For his hospital group, this had meant investing in a system that enabled it to overcome small single-site challenges and achieve the strong governance, innovation and patient-centred care that clients expected.
Mr Reay said: ‘At HCA UK, we have run a series of surveys about what our patients most seek in their cancer treatment. It is interesting to discover that, in Britain at least, being treated at known hospitals is “desirable”, but not top of the patients’ list.
‘The key requirement is being treated in a governed and managed system, accompanied in their journey and knowing that the best and latest treatments are available to them.’
He explained that, at HCA hospitals, a clinical nurse specialist accompanies the patient and helps explain their treatment –from supporting their understanding to communicating with doctors, arranging tests and helping schedule appointments.
Medical boards are run for each tumour type across its hospital network, chaired by senior consultants. They oversee best practice, innovation and ensure multidisciplinary teams (MDTs) are reviewed for every patient.
MDTs needed a lot of support, he said, ensuring each meeting had at least two of each specialty to guarantee balanced judgement.
This was easy at site level for common cancers, but for rarer varieties use was made of the group’s network to run a cross-site MDT drawing from 366 cancer specialists.
A key concern for patients was safety. But Mr Reay said the private sector was slowly busting the myth that it could deal with hips or hernias but not cancer.
Part of that safety was having surgical on-call rotas ready to cover an emergency post-op.
Voluntary rotas provided no guarantees, as surgeons had NHS oncall commitments and could not be always on call.
‘Again, using our network of hospitals, HCA UK delivers backup from paid surgical rotas. The cost of these rotas can be carried by our collective group.’
He told the conference consultants were reassured by the presence of a high level of ST5, ST6 trainees and resident doctors.
HCA had 120 critical care beds to guarantee intensive care, if needed, and a 24-hour ambulance service available to move patients when requested.
‘Since 2018, out of over 105,000 inpatient admissions, only 34 or 0.14% have required a transfer out. Conversely, in the past 18 months we have transferred in 461 patients from the NHS.’
Mr Reay said increasingly good Care Quality Commission results were being awarded across the whole private acute care industry and the sector should ensure the message about its quality and safety was much stronger.
Independent providers should embrace opportunities to submit data to national registries and where they could not, to push to be part of them.
‘The divergence that exists between how the NHS and independent sector providers record activity is making it difficult for patients to compare the care being provided. We want to make it easier for patients to make that comparison.
‘We have been lobbying to be able to do more on this and we hope that upcoming changes to the Health and Social Care Act reflect this.’
The hospital chief urged the sector to support the work of the Private Healthcare Information Network (PHIN).
‘Transparency can provide irrefutable evidence of quality care. And transparent outcomes drive improvement. We have introduced patient-recorded outcome measures in multiple specialties, going above and beyond the standard PHIN requirements.’
He said by creating a network of over 800 beds, ‘approximately the size of a large teaching hospital’, HCA UK had provided the infrastructure that enable the type of care that a single-site operation of 50-200 beds would find prohibitive.
The model worked particularly well across London, but the group could also apply elements of this to its location in Manchester and, coming in January 2024, in Birmingham.
John Reay of HCA Healthcare
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2013
Profits are bouncing back
Profits in private practice were on the up as many independent practitioners bounced back from two difficult years.
Accountants reported that 2013’s tax returns, being completed for the 30 January 2014 deadline, were showing a much healthier outlook than 2011 and 2012.
Signs of better times were confirmed most in the accounts of cosmetic surgeons.
Revealing the upturn at an MDU ‘Setting up in private practice’ conference, accountant Vanessa Sanders said their profits had risen by an average of 10%.
Many consultants had been affected in previous years by the decline in the self-pay market, but 2013 returns were showing some
encouraging reversal on that lost ground.
Younger consultants were reported to be seeing a rise in profits more quickly than the more established practitioners.
This was thought to be partly due to the re-arrangement of preferred suppliers of service for private medical insurance companies having an effect.
But younger consultants were also investing in a website to increase their business growth and were paying for courses that would be useful for their private work.
Agree terms before you write for insurers
Doctors asked to do medical reports for which they expected to get paid were being warned to agree terms or risk going unpaid.
The advice came after a disgruntled neurologist told Independent Practitioner Today that an insurer failed to pay his fee for writing a lengthy response to its request for more information.
He explained that he was asked to provide ‘a somewhat in-depth report on a patient with a new chronic condition’.
But when he invoiced the company – ‘as I would anyone requesting a specific undertaking’ – it refused to pay, stating it was not policy to do so and ‘not something they would do with any consultant.’
A billing expert said: ‘Consultants wouldn’t normally charge an insurance company for doing a report unless it was outside of what would be written as part of the normal medical process.
‘If it was and the consultant wanted to charge a fee, then they should agree terms before doing the work, which should always be the process in any commercial transaction.’
Long-term lawsuit peril
Independent practitioners were warned that a claim for clinical negligence could arise at any time and often completely out of the blue.
A Federation of Independent Practitioner Organisations (FIPO) meeting heard that in one case a claim, involving a foreign body, arrived 38 years after the incident occurred.
Private doctors heard that hundreds of claims from doctors working in independent practice were notified more than ten years after an incident occurred.
NHS will boost private earnings
Consultants could expect to continue seeing more of their private income coming through NHS-funded surgical patients for the foreseeable future.
According to analysts Laing & Buisson (now LaingBuisson), independent acute hospital and clinic income from treating NHS patients rose 7.5% in real terms to reach £1.2bn in 2012.
The figure represented 27.5% of total hospital income, up from 26% in 2011, and was projected to grow to nearly 29% in 2013.
Independent hospitals’ private patient business showed no real growth in 2012 from insured patients or self-pay UK residents.
Doctors are more willing to shop colleagues
A rise in the number of doctors being reported by their colleagues in 2012 was welcomed by the GMC. It said this highlighted ‘a welcome change of culture in the medical profession’.
Spire starts fixed-price deals
Spire’s 38 hospitals for the first time fixed prices of 15 procedures to make costs clearer for selfpayers.
The group said it had worked with doctors, who were not all taking part, to ensure the regionally variable prices were fair for all.
SETTING UP A PRIVATE PRACTICE: CONSULTANTS
How to build a solid
specialist practice
LOCATION
Some great practical tips for consultants considering a private practice venture are shared here by Sue O’Gorman (right)
CREDENTIALS
THE OPPORTUNITY to set up in private practice is something most newly appointed substantive consultants will consider.
Whenever the ‘right time’ presents itself, setting up in private practice should involve very careful planning and navigation of multiple fundamental elements and factors.
Following my extensive industry background in supporting consultants across all specialties with practice growth, here are my tips for ensuring a successful practice set up to provide you with the foundations for long term sustainability.
Location, location, location
Chose a facility location accessible to your target market population. This may be in central London or another large city with a critical mass of potential patients likely to utilise your services.
Consider the proximity of the competition. Is the market already
Do not be tempted to gather practising privileges at multiple locations. You will spend more time travelling from A to B to C, for which you are not earning
overprovided for or is there an opportunity to create something new to attract patients to your clinic?
Your second practice location ideally should be one close to home, within your local community perhaps.
Many newly substantive consultants will have young families and today share the responsibilities of all that goes with it, so the benefit of having a clinic close to home should not be underestimated.
Do not be tempted to gather
practising privileges at multiple locations. You will spend more time travelling from A to B to C, for which you are not earning, are likely to run late for clinic and frustrate the hospital staff who may have to pacify agitated patients on your behalf.
Ultimately, you will be treated as a ‘splitter’ rather than someone who is loyal to their facility.
TOP TIP: You may be asked to meet with the facility chief executive ahead of your application, so be prepared to discuss your plans for growth and how you see yourself attracting patients to your clinic.
Discuss your opportunities for cross-referrals to other specialists in the hospital. The hospitals are there to help support your practice, but they will expect a collaborative approach.
Solid credentials
Ensure you have the necessary credentials and documentation
required to support your practising privileges application close to hand.
Many, but not all, private hospitals will only accept applications from consultants who are a minimum of 12 months in a substantive NHS post.
There may sometimes be exceptions to this on a case by case basis. The application process can be an onerous task and one you will need to perform for each hospital you apply to.
TOP TIP: Allow a few hours to complete the application pack and do chase up your referees. Lack of full and complete references is the number-one reason why packs get rejected.
If you have consultant colleagues at your chosen location well known to you, ask them to provide a reference to support your application and act as your ambassador.
➱ continued on page 14
Diagnostic Audiology Including Paediatrics • Tinnitus Rehabilitation • Vestibular Testing • PTA & Tympanometry • Speech Audiometry • Speech In Noise Testing• Specialist Tests Including OAE, VEMP & ASSR • Ear Wax Removal • Independent Hearing Aid Provider
The most successful consultants I have worked with have invested in ensuring their phone is answered promptly, emails are responded to efficiently and the patients are well informed at all times
Prepare to be prepared
It is important from the outset to carve out ‘admin time’ into your schedule, so that you can prepare talks, interview staff, develop a website – or appoint a marketing agency who can – and network with potential referrers and organisations who may be able to direct referrals into your clinic.
The hospital facilities will provide you with opportunities to present to GPs and allied health professionals, so be prepared with those PowerPoint slides and have a selection of topics ready to showcase your expertise.
TOP TIP: Keep information relevant to your audience.
If you are invited to speak at an event, establish who the audience will be. A group of GPs may want to learn more about red flags and when to refer, as opposed to a group of physios who may expect a more interactive and detailed hands-on session.
The money shots
Ensure you register with the private medical insurers as soon as possible.
This can be a lengthy process, so utilise your admin time to do this. A robust Bupa Finder profile will boost your online footprint and serve to better inform the insurers of your areas of specialty and contact details.
Does your specialty lend itself to self-pay work? If so, think about your fee structure and how your services could be packaged to attract greater market share.
Consider how you will bill your patients and the methodology used to collect fees. Some clinicians will do this in-house via their medical secretary, but there are good external agencies who can provide this service too.
TOP TIP: Ensure you verify your Bupa profile annually. Include a professional, high-resolution image of yourself and place semicolons between each of the key specialty words – the Bupa Finder profile works on an algorithm and all of these will help get your profile listed on the first page.
The back office
The success of your practice ultimately will be underpinned by having an efficient back office function, at the helm of which
will be your medical secretary or practice manager.
The most successful consultants I have worked with have understood the value of this from day one and have invested in ensuring their phone is answered promptly, emails are responded to efficiently and the patients are well informed at all times.
In the early stages of practice development, cost is likely to be a consideration, but there are hospitals and agencies who can provide this service remotely and will charge based on hours used. It’s a cost-effective short-term solution until your practice builds.
If you do decide to invest in employing a medical secretary, you will need practice management software to manage all of your patient data, correspondence and billing.
These software solutions are usually operated on a licence basis and there are many providers in the market, so use your admin time to look into what platform will work best for you.
TOP TIP: Make regular time to meet with your medical secretary or practice manager. They are a fountain of knowledge and are the ‘shop window’ to your practice.
Patients often develop a rapport with them, as will the insurers. So their support and feedback will prove invaluable in helping you identify any issues or opportunities early on.
PHIN and the CMA
In 2014, the Competition and Markets Authority (CMA) issued a legally binding Private Healthcare Order requiring providers to submit key data to the Private Healthcare Information Network (PHIN).
As a consultant who will be working in the private sector for the first time, you are required to register with PHIN, a repository of unbiased information on all private hospitals and consultants in the UK for all to access.
TOP TIP: Be aware of Article 22 – a CMA order issued to all consultants six years ago that requires:
Outpatient letters to all patients to include your initial and followup consultation fees – insured and self-pay;
Details of any financial interests you may have in the facilities and equipment used at the hospital;
A list of insurers that recognise you. You can set up your template letters on the practice management software. Adhere to compliance around privacy regulations (GDPR).
Create a roadmap
Private practice is a journey and one that can take several years to become established. It should continue to grow and evolve over the lifetime of the practice.
Having a set of clear goals from the outset will help identify the key elements required to support your vision.
Some initial aspects to consider might include, for example, understanding the demand for your service in your chosen location. Think about ‘niching’ in your clinical specialty to attract the right patients and position yourself as an expert in your field. Include projected costs in the plan, such as operational expenses and revenue projections. Outline time-frames for each of the objectives and note the actions you need to take to achieve them. This will help you have a good understanding of how you see your practice growing, allow you to remain commercially agile throughout the process and keep you on track with your business priorities for continued private practice success.
TOP TIP: Mystery-shop your competitors as part of this process. What do they do well or is there a gap in the market that you can fill? It may be clinical, location or the customer service you provide that sets you apart from others.
This is known as your ‘point of differentiation’ and will be helpful in attracting patients and referrers.
In summary, establishing a private practice requires a comprehensive approach and advice from legal, financial and other business professionals should always be sought, as it will be invaluable during the planning process.
See our next issue for tips to growing your referral network in a competitive climate
Sue O’Gorman of Medici Healthcare Consultancy provides services to help healthcare professionals think and act commercially. Website: www. medicihealthcareconsultancy.co.uk
SETTING UP A PRIVATE PRACTICE: GPs
PRIVATE SURGERY
Building your own general practice
This column often talks about private practice for hospital doctors but rarely those working privately in a primary care setting. Alec James puts that to rights
Read his tips for private GPs overleaf on page 16 ➱
WITH A GROWING demand for private GP appointments, I have been asked to provide some of my top tips for those who are either already working as a private GP or considering the move.
Consider your trading structure
This is one of the most important decisions to make financially.
If you are working independently, you will generally have the options of trading via a limited company or working on a selfemployed basis.
A limited company limits your personal liability exposure and can offer some tax advantages, particularly if you have other sources of income such as a salaried role, but is a lot more involved in terms of compliance.
Working on a self-employed
basis can often be the simplest model.
If you are working collectively with other private GPs, you can either work as a partnership or have a jointly-owned limited company.
A limited company may offer tax advantages for the doctors and it limits your personal liabilities. However, there may be differing financial motives of each doctor.
A company with higher reserves – profits which have not been distributed to the shareholders – can also lead to issues if there are changes to the doctors’ working patterns or where there are incoming or exiting doctors.
A limited liability partnership (LLP) can offer an alternative solution with the flexibilities of a partnership but offering a level of liability protection to the partners.
These discussions should always be held with a specialist medical accountant, as there is not a onesize-fits-all solution.
Face-to-face or virtual appointments
In an increasingly virtual world, you need to consider if your private GP services will be available virtually, face to face or a mixture of the two.
Generally speaking, virtual appointments have the lowest setup and ongoing costs for the doctor, as these costs will be primarily in relation to IT equipment. However, online services generally attract a lower fee from patients for providing the services.
If you are planning to offer faceto-face appointments, these generally attract a higher fee, but depending on where you provide
A limited liability partnership can offer an alternative solution with the flexibilities of a partnership but offering a level of liability protection to the partners the services, could attract significant set-up and ongoing costs.
Rented rooms in an already established private medical setting will have the lowest initial start-up costs, as the rooms are likely to contain the majority of the equipment you need to provide consultations.
As your practice grows, you may find that you need your own premises. This will often have the largest upfront costs and also has additional compliance requirements such as Care Quality Commission registration, but can allow your clinic to grow.
Pricing structure
As a private GP, you need to consider your pricing model.
For those working with an established provider, you will need to negotiate your hourly or sessional rate. For those establishing their own practice, you will need to decide your pricing model. This could be a ‘pay as you go’ or monthly fee model.
An inclusive monthly fee can offer the most financial security in that you will receive a fixed amount per month for each patient registered.
However, there may be ‘winners and losers’ in this model, in that you receive a fixed amount despite the number of appointments offered.
Alternatively, a pay-as-you-go model means you only invoice for the work you have done.
You could also consider a hybrid model where a monthly fee offers a discount against your usual payas-you-go rates.
You will also need to decide on charges for other services such as vaccinations and blood tests.
When first starting out, a cashflow forecast modelling different pricing structures can help you find the right model for you.
Whether you are working with an established provider or operate your own practice, you will need to make sure you regularly review your fees to ensure you are keeping up with inflation.
Another consideration is your future exit strategy because, unlike with NHS patients, a GP practice with private patients can be sold. If you have a consistent and predicable income stream, this will stand you in good stead for maximising the value of your business in the future.
Contracts
When patients are registered to your practice, you will need to ensure you have a contract in place with each patient. This will specify the terms of engagement. It should cover things such as the number of appointments your patients are entitled to in a specified period.
If working collaboratively, a partnership agreement or shareholders agreement is extremely important, as this ensures all parties understand their responsibilities and obligations to the practice.
Having these drafted and reviewed regularly by a solicitor who is specialised in private GP practices will ensure all the important points are covered.
Make sure you are covered
Within the NHS, the majority of your work is covered by the Government-backed indemnity scheme. This does not apply to your private earnings. You should therefore ensure that your private earnings are indemnified.
As a business, you will also need to consider if you have any other areas which may need to be covered. This could include public liability insurance, data protection and, if you employ staff, employer liability insurance.
Financial management
Your business will need to maintain accurate financial records. There are specific clinical software systems which are primarily used by private GPs.
In addition to these, financial book-keeping software will help you keep track of your business’s finances.
Annual accounts will also be
needed. While these are required to ensure your business pays the correct tax, detailed accounts are also a valuable tool to help identify profitable parts of your business and areas you can financially improve your practice.
When considering starting or expanding a practice, it is likely you will also need to prepare financial forecasts to help you ensure your plans will be a financial success.
These would factor in potential pricing structures, expected patient numbers, set-up and ongoing costs. The forecasts should consider both the profitability and the cash flows of the practice. Both of these documents will be essential if you seek external finance.
Appointing a specialist medical accountant can give you a more detailed insight into where improvements could be made to your business.
Pension
Working privately means you will not have access to the NHS pension scheme on these earnings. With this in mind, you will need to consider your retirement planning, particularly if growing your private earnings leads to a reduction in your NHS income.
Depending on your trading structure, your business may be in a position to pay a pension contribution on your behalf.
Alternatively, you may wish to make personal pension contributions which may attract tax relief on your self-assessment tax return.
From April 2023, the pension savings annual allowance has been increased up to a maximum of £60,000 – depending on your individual tax position.
It is always worth discussing retirement planning with an independent financial adviser to ensure the planning you are doing is the most efficient.
Building your team
As your practice grows, it is likely that you will need to involve either other GPs, healthcare professionals or administrative/management support.
The team you pick can impact the success of your practice and can have different financial implications.
If you are regularly working with someone under your supervision, you may need to consider HM Revenue and Customs’ ‘offpayroll working’ rules and consider whether they need to be paid via a PAYE scheme
As the staff you will be working with have the opportunity to work in the NHS and have access to the NHS Pension Scheme, these employees often demand a higher salary than they would receive in the NHS to compensate for the loss in access to the NHS pension scheme.
Depending on the person you are working with, they are likely to be:
Employed by an external provider;
Work on a self-employed basis or via a limited company;
Employed by your business.
When using staff charged by another provider or self-employed workers, you will be billed monthly for the hours/days the person has supplied or, occasionally, a percentage of your fees.
You should be provided with an invoice detailing the hours they have worked for you and then the amount. For accounting purposes, you should keep either a physical or electronic copy for seven financial years.
Workers paid in this way have no employment rights from your business. This means that if they are sick or on annual leave, they should not be paid or alternatively a replacement should be provided to you.
If you are regularly working with someone under your supervision, you may need to consider HM Revenue and Customs’ (HMRC’s) ‘off-payroll working’ rules and consider whether they need to be paid via a PAYE scheme.
As your practice grows, it is likely that you will need a team that works exclusively for your business. These are more than likely to be considered as employees.
Your employees will be entitled to employment rights such as paid sick leave, holiday pay and parental leave. Your business will have PAYE obligations and you will need to deduct tax and National Insurance from their salary and pay these over to HMRC.
You will also be required to pay employers’ National Insurance and pension contributions. These are often referred to as ‘on costs’.
It is always advisable discussing the potential employment with an accountant so that you are aware of the total cost to your business prior to offering employment. You should also seek the advice of an employment solicitor or HR specialist to have a contract of employment drawn up.
VAT
Generally speaking, healthcare services provided by a GP provider, whether it is in an NHS or private setting, will be exempt from VAT. There is a specific VAT notice which covers healthcare. In order to be exempt from VAT, the work needs to satisfy two conditions:
The services are within the profession in which you are registered to practise;
The primary purpose of the services is the protection, maintenance or restoration of the health of the person concerned.
In instances where both conditions are not met, the supply is likely to be VAT-able. However, it is only if these VAT-able supplies exceed the registration threshold – currently £85,000 – that you would need to register and charge VAT.
For those providing GP services to an established provider, particularly via a limited company, your VAT status needs to be carefully considered.
Working in the private setting of general practice can be an exciting move and very profitable. Hopefully, the above tips will help you consider your obligations when starting or growing your practice.
Coming in our joint December-January issue: accountant Richard Norbury sets out some key ways to reap your rewards
Alec James (right) is a partner at Sandison Easson & Co, specialist medical accountants
FINANCIAL WELLNESS
How to make your practice thrive
Efficiency is the linchpin of a thriving healthcare facility. Derek Kelly (right) provides a comprehensive guide to streamlined medical practice management
EFFICIENT MEDICAL practice
management is the cornerstone of a thriving healthcare facility.
From scheduling patient appointments to managing billing and staff, there are numerous components that demand careful co-ordination.
And in an increasingly complex healthcare landscape, finding ways to streamline operations has never been more critical.
Let’s explore the key strategies and best practices for optimising medical practice management:
1
Prioritise patientcentred care
Efficiency in a medical practice starts with putting patients at the
centre of every decision. Streamlining operations should never come at the expense of patient care.
In fact, a patient-centric approach often enhances efficiency.
Ensure your staff are well-trained in communication, empathy and patient engagement. This leads to smoother patient visits and fosters trust and loyalty.
2 Invest in practice management software
Modern medical practices can no longer rely solely on paper records and manual processes. Practice management software systems offer a centralised solution for scheduling, billing, patient records
and more. These systems can automate repetitive tasks, reduce errors and enhance overall efficiency.
3
Streamline appointment scheduling
Efficient appointment scheduling is a critical aspect of medical practice management. Use scheduling software to minimise appointment gaps and optimise provider availability.
Implement reminder systems to reduce no-shows and late cancellations.
A well-organised appointment system not only improves patient satisfaction but also ensures optimal use of your resources.
4 Optimise staff workflow
Your staff are the backbone of your practice. Ensure their workflow is streamlined by assigning roles and responsibilities clearly.
Encourage collaboration and communication among team members. Implement regular training and performance evaluations to identify areas for improvement. Efficient staff are more likely to provide better patient care.
5 Automate billing and revenue cycle management
Poor billing and revenue cycle management can cause a major bottleneck in medical practice operations. Automate billing processes to reduce errors and speed up re-imbursements.
Regularly review billing claims to identify and resolve any issues promptly. Efficient revenue cycle management ensures a healthy cash flow for your practice.
6 Embrace digital marketing
In today’s digital age, having a strong online presence is essential for attracting and retaining patients.
Invest in digital marketing strategies such as search engine optimisation (SEO), social media marketing and email campaigns. A well-executed digital marketing plan can help you reach a wider
audience and grow your patient base.
7 Ensure GDPR compliance
Complying with the General Data Protection Regulations is nonnegotiable in healthcare. Ensure your practice follows all GDPR rules regarding patient data protection and privacy.
Implement robust cybersecurity measures and educate your staff about the importance of data security.
8
Implement performance metrics
Measuring key performance indicators (KPIs) is essential for monitoring the health of your practice.
Track metrics such as patient satisfaction, appointment wait times, billing claim denials and revenue growth. Regularly review these metrics and make data-driven decisions to improve efficiency.
Regularly solicit feedback from both patients and staff. Use this feedback to identify areas for enhancement and implement changes accordingly
10
Explore outsourcing options
Consider outsourcing certain non-core functions of your practice, such as billing or administrative tasks, to specialised service providers.
This can reduce the workload on your in-house staff and allow them to focus on patient care. Outsourcing can also provide access to expertise and technologies that may not be feasible to maintain in-house.
9 Engage in continuous improvement
Efficient medical practice management is an ongoing process. Encourage a culture of continuous improvement within your practice.
Regularly solicit feedback from both patients and staff. Use this feedback to identify areas for enhancement and implement changes accordingly.
In conclusion, streamlining medical practice operations is an ongoing effort that requires a commitment to efficiency and patient-centred care.
By investing in modern technology, optimising staff workflows and embracing best practices, medical practices can not only improve their operational efficiency but also enhance patient experiences.
Remember that every improve-
ment, no matter how small, can have a significant impact on the overall success of your practice.
Efficient management is not just about cutting costs; it is about delivering better care, increasing patient satisfaction and ensuring the long-term viability of your medical practice in a competitive healthcare environment.
So take the time to evaluate your current operations, identify areas for improvement and implement the strategies mentioned in this guide. With a focus on efficiency, your practice can thrive in the ever-evolving world of healthcare.
Remember, the ultimate goal of streamlining medical practice operations is to create a smoother, more satisfying experience for both patients and providers while ensuring the financial stability of your practice.
Derek Kelly is marketing manager at Medserv
mPrescribe® app allows you to prescribe flexibly without a laptop, for delivery to your patients nationwide
Download the app and register online www.pharmacierge.com/register
Secretary Supported
GP and Consultant Reviews
Administrator access reduces workload for practitioners. mPrescribe® facilitates patient entry, status monitoring and preparation of prescriptions for mobile authorisation.
Clinical Governance
Co-founded and co-owned by leading private clinicians, our secure and encrypted technology is compliant with all GPhC, GDPR and e-Prescribing regulations.
“Wonderful, seamless, easy to use service.” Dr Catrin Bevan, London General Practice
“Intuitive and secure.” Dr Tim Wigmore, Consultant Anaesthetist and Intensivist
“Delivered the same day.... Outstanding!” Dr Elisa Astorri, Academic Physician Rheumatologist
“Go the extra mile.” Dr John O’Donohue, Consultant Gastroenterologist
“Consistent, efficient , friendly and responsive.” Dr Tim Ladbrooke, Courtfield Private Practice
Elsevier’s Clinician of the Future 2023 report shows readiness to embrace generative AI across the global healthcare industry. The company’s Tim Morris answers questions arising from the survey
How doctors see the future
Why did Elsevier Health launch the Clinician of the Future 2023 report and how is it different to the previous one?
Elsevier Health’s Clinician of the Future program, which was launched in 2022 with the original report, serves as a pulse on the state of the global health ecosystem in the eyes of doctors and nurses.
One year later, we have kept our commitment to clinicians and launched the Clinician of the Future 2023 report as the most current pulse on what doctors and nurses think about the challenges and future opportunities in healthcare,
including an additional lens on artificial intelligence (AI).
So this really continues and emphasises our pledge to listen to the voices of healthcare professionals across the globe, which we set out following the launch of the inaugural report.
Role of AI
This new report champions the experiences and voices of 2,607 doctors and nurses worldwide.
While it underscores the gravity of healthcare workforce challenges highlighted in the original survey, like nursing shortages, the latest report puts an additional lens on
the future role of generative AI in healthcare and its implications on patient care and health outcomes. It found almost half of all healthcare professionals are eager for doctors to utilise generative AI in the future to support their clinical decision-making, further affirming the need to drive a technological shift in healthcare.
We conducted this survey of nurses and doctors, including consultants and GPs, to hear their views and to help see the world from their perspective.
Giving a voice to their concerns and their recommendations will help create an industry roadmap
for action, which is especially important as we look to evaluate and understand how AI can positively impact healthcare.
What priorities have doctors and nurses identified that will influence care in the next two to three years?
The first Clinician of the Future report identified that most doctors and nurses anticipated growing staff shortages.
These shortages are now having a significant impact on the frontline workforce in many regions, and, as a result, it has been identified as the number-one concern globally in the 2023 report.
The shortage of nurses ranked top on the list of priorities to be addressed over the next two to three years, as 54% globally selected it as a top priority. But we are now seeing concern grow about shortages of doctors as well.
Forty-five per cent of respondents globally consider the growing shortage of doctors as a top priority to address.
In the UK, the shortage of nurses and doctors were ranked as the top two priorities.
Another top priority for the global healthcare workforce was improving their continuous training, as a total of 49% globally consider this a priority for the next two to three years.
Managing public health was also a prime concern, with 46% highlighting this as a significant area of worry.
Ongoing inequities in the healthcare workforce and the impact it might have on patient care was another priority for many doctors and nurses.
Twenty-four per cent of respondents consider encouraging greater diversity in the healthcare workforce to better represent the local population a pressing issue in the next two to three years.
Generative AI has transformative potential in healthcare. How can this technology be used to support doctors and nurses and what needs to be done to enable adoption? Front-line staff see an imminent need to be experts in using and prescribing digital health technologies.
Over the next two to three years,
Half of all healthcare professionals are eager for doctors to utilise generative AI in the future to support their clinical decision-making
Elsevier’s report encapsulated the views of 2,607 doctors and nurses from around the world
73% said doctors having more expertise in digital health technology will be more desirable.
One promising area of potential for generative AI highlighted in the report was to aid clinical decision-making. While only 11% of today’s clinical decisions are supported by generative AI tools, almost half (48%) of respondents agree that in the next two to three years doctors should use such tools to help make clinical decisions.
Interestingly, China was the most optimistic about generative AI adoption, with 53% expressing doctors using such technologies in the next two to three years is desirable, compared to the US (42%) and the UK (34%).
There is also appetite to understand how AI can aid administrative and time-consuming tasks to support patient care and free up clinician time.
We are excited about how these new technologies can drive further innovation and efficiencies, and ultimately help improve patient outcomes.
We can also see that many doctors and nurses across the world support the notion of utilising AI to train medical and nursing students.
Over half of all doctors and nurses globally welcome the prospect of medical students using generative AI-powered tools as part of their medical education in the next two to three years. However, this is significantly lower in the UK (33%).
What are the key challenges and opportunities facing doctors and nurses in the future?
In this year’s survey, we found that both the UK and US agreed tackling the nursing shortage is a top priority in the next two to three years.
As part of the shortage issue, we also saw an increase in the percentage of respondents considering leaving their roles in the next two to three years compared to our previous report.
➱ continued on page 22
COULD YOUR CLINIC FLY?
Yes! with a better clinic management platform
• Flexible scheduling
• Patient direct booking
• Online payments
• Pleasure to use EMR
• Accurate voice recognition
• Automated clinic notes
• Video consultations
• ePrescribing
• Deliver physical letters if preferred
• Invoice management …and much more
Beautifully designed and easy to use
Of the total 37% who said this, 24% plan to move to another role in healthcare, while 13% plan to leave healthcare altogether, either by moving to a non-healthcarerelated job or retiring.
We also saw a trend towards patient empowerment, as doctors and nurses expect the health literacy and proactive health management of patients to grow in the next five years.
With new technologies like wearables, clinicians are confident patients will take on a larger role in their own health, impacting the expectations and subsequent relationship between doctors and their patients.
Front-line healthcare professionals believe that two in five of their patients are health literate today, but believe this will rise to half of patients by 2028.
Those surveyed also said while only 38% of patients take an active role in the management of their health and 27% use monitoring tools to assess their well-being today, they expect this to rise to 49% and 45% respectively within five years.
What doctor and nurses training needs should be addressed in the next two to three years to truly transform the clinicianpatient relationship?
The Clinician of the Future 2023 report found that the Covid-19 pandemic has had a significant impact on the training of the newly graduated workforce. As a result, newly trained healthcare staff are perceived to be unprepared for clinical practice.
The report found two-thirds of practising healthcare professionals globally believe newly graduated clinicians lack hands-on practical training, as they were not able to physically attend education throughout the pandemic.
Taking into consideration the workforce shortages and the lack of hands-on training, it is vital that steps are taken to support the transition into practice.
As I’ve already mentioned, many of those surveyed recognise the potential of generative AI and large language machine-learning models to support training. But they stress that these technologies should be an adjunct and not a
The report found that the Covid pandemic has had a significant impact on the training of the newly graduated workforce. As a result, newly trained healthcare staff are perceived to be unprepared for clinical practice
THE REPORT IN
SUMMARY
This Clinician of the Future 2023 report champions the views of 2,607 doctors and nurses worldwide and while it underscores the gravity of healthcare workforce challenges highlighted in the original survey, the new findings put an additional lens on the future role of generative AI technologies across the global healthcare industry.
Key data from the report talks about themes including:
THE CURRENT STATE OF HEALTHCARE
78% of UK clinicians believe tackling the shortages of doctors and nurses is a top priority.
replacement for face-to-face learning experiences.
The response to the potential of AI is divergent, with some considering it as a threat to necessary hands-on experience, while others are concerned it may teach inaccurate or erroneous information while hindering critical thinking and decision-making.
As a leader in healthcare technology focused on training the next generation of doctors and nurses, Elsevier feels it is vital that training needs to be elevated at all levels of healthcare to fully engage in innovative technologies meant to alleviate the clinical burden and ultimately improve patient care.
The report revealed doctors and nurses have a positive sentiment towards valuebased care. What do you think is driving this, including considerations around the implications for private practices?
The concept of value-based care is not new, and although it is not yet a broad reality in most countries, some are moving towards it and doctors and nurses generally see this positively.
In the previous report, we outlined how a growing and ageing population was expected to drive change across healthcare systems.
Accelerated population ageing will have an impact on the prevalence of non-communicable and age-related diseases, making a new approach to healthcare even more urgent.
As such, the concept of moving away from a transactional pay-perservice approach to a more holistic, efficient, preventive and patient-centred one is growing.
From this year’s report, we can see that most doctors and nurses expect value-based care to reduce
More than half (54%) of nurses are considering leaving their current role within two to three years.
24% of UK doctors do not enjoy their job and only 56% believe they have a good work-life balance.
39% of UK doctors and 49% of UK nurses believe they have sufficient time to provide good care to their patients.
67% of clinicians from the UK believe newly graduated doctors and nurses lack hands-on practical training which is impacting patient care.
THE FUTURE ROLE OF DIGITAL HEALTH AND GENERATIVE AI
73% of clinicians think doctors need to be experts in the use of digital health technologies in the next two to three years.
Only 11% of today’s clinical decisions are assisted by generative AI tools, but 48% of clinicians say that physicians using generative AI tools to help make clinical decisions will be desirable in two to three years’ time.
China emerges as more optimistic about generative AI adoption, with 53% of clinicians expressing that physician use of generative AI technologies in the next 2-3 years is desirable, compared to those from the US (42%) and the UK (34%).
Over half (51%) of clinicians welcome the prospect of medical students using generative AI-powered tools as part of their medical education in the next two to three years.
Clinicians from the UK and the US are more reserved about generative AI technologies supporting medical students, as only 33% in the UK and 40% in the US find this desirable.
Realising systemic cost savings will require overcoming initial growing pains as new models are implemented the burden on secondary care, as 73% expect most patients to be managed in primary care settings.
We also see that they believe this shift will improve the patient experience, with 69% expecting hospital stays to be shorter as a result, while only 51% said valuebased care would save costs.
The fact that nearly half did not expect cost reductions demonstrates the challenges in achieving this outcome across all patient populations at scale.
Realising systemic cost savings will require overcoming initial growing pains as new models are implemented.
While doctors and nurses recognise the importance of this shift, they ultimately think there is still a journey ahead – 74% think more should be done in preventive care, while 40% consider personalised treatment approaches a top priority.
This indicates many providers see room for improvement in how
holistic, proactive care is delivered and funded.
What actions does the wider healthcare sector need to take to help address the challenges facing doctors and nurses of the future?
This report paints a dynamic picture of the current state of healthcare, and as new doctors and nurses enter the workforce, the landscape will continue to shift. The wider sector should con -
tinue to listen to front-line healthcare professionals, including those on their way to qualification, to hear their views and to see the world from their perspectives.
With those insights, we can continue to develop solutions that help them deliver the best possible care for their communities.
We have played a role in healthcare at Elsevier by supporting doctors and nurses for more than a century.
We recognise the challenges they face, their concerns for the future and we also see the opportunities there are to support as they navigate them.
And we have actively supported healthcare professionals for more than a century. We recognise the challenges they face, their concerns for tomorrow and the role we can play in helping them to navigate the opportunities of the future.
We are excited about new tech-
nologies like generative AI and large language machine-learning models, as they can drive further innovation and efficiency to help future-proof healthcare systems. By combining our industry-specific human expertise, in-depth trusted content and high-quality data and generative AI technologies, we can work with healthcare professionals to help enhance patient care.
Tim Morris (below) is a former A&E nurse and vice-president of clinical solutions at Elsevier Health
BOOK YOUR DEMO Are you happy with your current
software?
Maybe you're completely happy with the software you use to run your practice. Perhaps you have everything in one place, routine tasks are automated, and reporting is accurate and insightful. If so, stop reading now.
However, if you think the day to day running of your practice could be improved, we'd love the chance to demonstrate e-clinic to you.
The number one choice for private practice
Future-proof your practice and offer everything a modern patient expects:
> iPad compatibility
> Online booking & payments with fully integrated card processing
> Electronic consent & treatment forms
> Integrated drugs database & digital prescribing with direct delivery
> Fast & easy patient communications by email or text
ANALYSIS OF MEDICO-LEGAL CLAIMS
Anaesthetic errors under the spotlight
Claims made against MDU anaesthetist members in private practice are examined here by Dr Claire Wratten and Peter Renwick (below) and they explain how risks can be minimised
REASONS FOR CLAIMS
Dental damage
Drug reaction and error
45 (23%)
32 (17%)
Brain damage or death 21 (11%)
Nerve damage 19 (10%)
Patient awareness 15 (8%)
Needle misplacement 13 (7%)
Positioning 13 (7%)
Airway damage 6 (3%)
Other/Miscellaneous
In 78% of cases, the claim was successfully defended without any payment of damages or claimant legal costs
28 (14%)
FACING A CLAIM can be very upsetting. The MDU’s expert claims handlers and medico-legal advisers understand how stressful this can be and are available to provide advice and support should the need arise.
This article is based on an analysis of almost 200 clinical negligence claims made against MDU anaesthetist members working in private practice.
Common causes of claims included dental damage, drug errors or adverse reactions, needle misplacement and anaesthetic awareness.
There were also claims relating to significant brain damage or death of the patient and in those cases, damages claimed can be substantial (see box on page 26).
But in 78% of cases reviewed, the claim was successfully defended without any payment of damages or claimant legal costs.
Dental damage
Twenty-three per cent of all anaesthetic claims related to damage to teeth and/or dental work during intubation, with damage to crowns, bridges and veneers being very common.
The risk of damage when using a metal laryngoscope is well known. Claims also arose due to the use of endotracheal tubes and laryngeal mask airways.
The risk may also be greater in the case of a difficult intubation, either for anatomical reasons or because of circumstances.
Difficult intubations cannot always be anticipated and, in an emergency setting, securing the airway as quickly as possible will be the priority even at the expense of damage to teeth.
Dental damage is not necessarily negligent and, in 89% of these cases, we were able to defend the actions of our members without making any compensation payments.
Of those claims that were settled, the majority were settled for a modest amount, though two cases were settled for over £20,000 due to the need for extensive dental remedial work or dental implants. However, these figures are for damages only and the MDU would have also paid claimant costs.
Medical records can be critical to the successful defence of a claim, which might be brought months or years after the incident.
When an assessment has been made of the upper airway, dentition and other factors, this should be clearly documented, along with a record of any warning of possible complications given to the patient.
Drug-related concerns
Drug-related concerns accounted for almost 17% of cases.
The most common issue was an allergic or adverse drug reaction, with the most common culprit being antibiotics.
Other claims arose following acute kidney injury, allegedly consequent on either prescription of non-steroidal anti-inflammatories or failure to stop ACE inhibitors.
Claims were also made following alleged prescription errors. The most common concern was excessive prescription of drugs, in particular opioids, but other claims including excessive doses of prophylactic anticoagulation resulting in bleeding.
Two claims were brought following allegedly inadequate postoperative pain relief.
Twenty-seven per cent of claims in this category were settled on behalf of the MDU members, with the damages paid ranging from a few thousand pounds to almost £300,000 in a case in which the claimant developed chronic fatigue following an allergic reaction during anaesthesia.
While in some cases the reaction was unexpected, in others a careful history would have identified the potential for an adverse or allergic drug reaction and the issues could have been avoided.
Brain damage or death
Almost 11% of the claims notified to the MDU during the review period related to patients who had suffered brain damage or died during or shortly after an anaesthetic.
The cause of death in the claims reviewed was generally hypoxic brain injury; for example, following oesophageal intubation or cardiorespiratory arrest during the procedure.
Other causes including bleeding due to coagulopathy and drugrelated complications including anaphylaxis.
In some cases, it was alleged that the pre-operative anaesthetic assessment was inadequate, resulting in complications during the operation, or that there was a lack of appropriate intra-operative monitoring.
Most of these cases arose following a general anaesthetic, but two were following an epidural and in two cases the patient became hypoxic during sedation. Claims arose following anaesthesia in adults and children, and for medical and dental procedures.
If a patient is left with a significant disability, they will have considerable care needs. This means not only that damages paid are substantial but also high costs are incurred by both the claimant and the defendant.
The costs mount up due to instructing medical experts and obtaining legal advice on what those care needs are and how they are best met, with the aim of returning the patient as far as possible to the position they would have been in but for the alleged negligence.
Claims following brain damage or death had a higher rate of settlement compared to other claims against anaesthetists, with over 50% of the claims being settled. Also, these injuries resulted in the highest sums being paid by the MDU in damages and claimant costs.
The range of damages payments was from just over £40,000 up to several million pounds and with payment of claimant costs ranging from £12,000 up to over £400,000.
Nerve damage and spinal cord injury
Almost 10% of claims analysed arose following nerve damage, ➱ continued on page 26
ranging in severity from paraesthesia in the fingers to significant paralysis. The anaesthetic implicated was in most cases either an epidural – over 30% of claims – or a local nerve block, particularly a scalene block.
Local nerve damage was also alleged in some cases, allegedly causing issues such as foot drop and numbness and loss of arm function.
Although only 21% of these notified claims were settled by the MDU, again some of the highest damages payments arose from these claims in cases where the patient had suffered a spinal cord injury resulting in paralysis following an epidural or spinal anaesthetic.
This emphasises the importance of discussing this rare but potentially life-changing complication with patients pre-operatively, as well as ensuring that discussion includes any alternative methods of anaesthesia that could be used.
Patient awareness
The concept of ‘awareness’ covers a whole range of experiences, from vague but painless recollections to the extremely rare cases where patients are paralysed but not anaesthetised.
Awareness only factored in a small number of notified claims in our analysis, and the majority of cases were successfully defended. Causes included instances of alleged failures with equipment such as machinery or tubing and inadequate levels of anaesthetic or sedation.
Of the claims that were settled, in the majority the damages paid ranged from £10,000 to £33,000, but in one case a six-figure compensation payment was made because the claimant developed post-traumatic stress disorder following a period of awareness during a laparoscopic procedure.
Positioning
The risks to anaesthetised patients of sustaining pressure damage or nerve palsies as a result of positioning on the operating table are well-known.
Nearly 7% of claims reviewed were due to problems arising following positioning during or following a general anaesthetic or conscious sedation. Claims related
Almost 10% of claims analysed arose following nerve damage, ranging in severity from paraesthesia in the fingers to significant paralysis
MANAGE THE RISK TO CUT CLAIMS
Claims involving anaesthetists can arise for a wide range of reasons and very few cases result in compensation being paid.
Nonetheless, there are steps you can take to manage common risk factors and reduce the risk of misunderstandings which can lead to a claim:
Ensure the patient has given informed consent before being anesthetised. For example, patients should understand why the anaesthetic is necessary, the risks involved and any alternatives. This discussion should be documented in the notes.
to anaesthesia or sedation for both medical and dental procedures.
The skin of various areas of the body was affected in different cases, ranging from the face – for example, pressure areas on the chin during prone positioning – to damage to the heels.
Some injuries arising in these cases were relatively minor – such as a small burn from radiofrequency ablation – to more serious injuries, including alleged nerve damage due to compression. Thirty per cent of claims in this category were settled on behalf of the MDU anaesthetist, with damages up to £50,000.
Needle misplacement
There were 13 claims in relation to needles allegedly being misplaced. These ranged from alleged incorrect insertion of cannulas, causing phlebitis and areas of necrosis at the site of injections, to incorrect administration of cervical epidural injections.
Three of these claims were settled for sums ranging from around £5,000, where the patient suffered a pneumothorax, up to £500,000, where the patient unfortunately suffered paralysis.
Airway damage
The potential for instrumental damage is not confined to the teeth and to dental work – the soft tissue structures of the oropharynx, nasopharynx and trachea may also sustain injury, though rarely.
A handful of claims were reported following alleged airway damage, only one of which was settled for a modest sum.
Dr Claire Wratten is claims team manager and Peter Renwick, lead claims handler at the Medical Defence Union (MDU)
Record any warnings given pre-operatively, such as risk of a sore throat postoperatively or of some awareness during sedation.
If there are additional risk factors for a particular patient, such as the risk of dental damage, you should discuss these and document them in the records. This will show that you were aware of the increased risk at the time you undertook the procedure and that you communicated this to the patient.
It is important that patients are not given the impression that the cost of repairing dental damage will automatically be met.
Develop a regular routine for pre- and postoperative assessments and stick to it. Make a note of your assessments in the records.
Check the past medical history, known allergies and concurrent medication before prescribing any drug.
Document that you have checked pressure points and ensure those assisting you are aware of the risks to pressure points.
Make sure procedures are in place to eliminate the risk of ‘wrong side’ errors, such as checking the patient’s clinical record and consent form and confirming details with the patient.
Consider your professional duty of candour. If something goes wrong, apologise and notify the patient and any necessary parties as soon as possible. If something does go wrong, do seek early advice from your medical defence organisation, consider shared learning from errors and ensure protocols and procedures are up to date.
AN EXPENSIVE BUSINESS
Damages in clinical negligence claims reflect the injury suffered by the patient rather than the magnitude of the clinical error. Compensation payments aim to return the claimant to the position they would have been in had they not suffered an injury.
Therefore, if the claimant is unable to work, they will be entitled to claim for a loss of earnings for the period when they cannot work, and if they need additional care with activities of daily living, then the costs of this can also be claimed from the compensating party. Damages claimed for both of these can be substantial.
If a claim is settled, then the compensator also pays the costs incurred by the claimant’s legal team in bringing the claim.
The MDU can also incur considerable legal costs in defending or negotiating settlement of a claim, particularly if the claimant has suffered a significant injury.
These claims can be complex to investigate and can require instruction of many different disciplines of experts to establish what the claimant’s ongoing needs are in terms of care, occupational therapy, physiotherapy and accommodation.
Questions on medical insurance answered
The world of health insurance can seem like a mysterious place to consultants who are new to private practice – and even those who aren’t. Bupa’s experts answer the questions doctors most commonly ask
How do I begin treating insured patients?
Kris Martindale, Bupa’s head of clinician strategy, says: ‘You’ll need to apply for what we call “recognition”. This means that you can claim payment for treating the insurers’ customers.
‘Most insurers will ask consultants for details of their training and qualifications, and proof that they hold appropriate indemnity insurance. You’ll need to take out separate indemnity insurance for your private work, as this isn’t covered by your NHS indemnity.’
How can I promote my new private practice?
‘Aside from making the most of networking opportunities with local GPs, I’d recommend making the most of online directories,’ advises Mr Martindale.
‘At Bupa, our directory Finder receives more than 100,000 visits a week, so it’s a great place to showcase your practice.
‘We encourage our customers to take a look at consultants’ Finder profiles before deciding who to see. We know that profiles with a photo get more visits than those without, and the more information you can share about your skills and expertise the better.’
How do I invoice for delivering private care?
Mr Martindale says: ‘We want to make sure the consultants we work with are paid quickly, correctly and efficiently, so we ask them to invoice us electronically within
six months of carrying out any consultations, tests or treatment.
‘Like most insurers, we offer a number of ways to do this. One way is using our free Providers Online website.
‘We create a consultant’s own Providers Online account when they become Bupa recognised and they can also use this to view preauthorisations, pre-populate invoice details and track the progress of their accounts and when they will be paid.’
Find out more on page 20 of the Bupa Consultant Guide.
Why do I have to invoice for my patient’s care within a specific time-frame?
Mr Martindale responds: ‘At Bupa we expect doctors to invoice us within six months of delivering care. This is important because it gives us an up-to-date picture of their patients’ claims, so we can let them know their available allowances when they call about further treatment.
‘It also means we can calculate renewal prices accurately, customers aren’t surprised by unexpected bills and consultants get paid quickly for treating them.’
What does health insurance cover?
Dr Robin Clark, medical director for Bupa Global and UK Insurance, says: ‘Health insurance is designed to cover the cost of acute conditions. The Association of British Insurers (ABI) defines an acute ➱ continued on page 28
condition as a disease, illness or injury that is expected to respond quickly to treatment which aims to return the patient to their previous state of health.
‘Health insurance covers the cost of medically necessary, planned private consultations, tests and treatment for these conditions.’
What about chronic conditions?
Dr Tim Woodman, Bupa’s medical director, policy and cancer services, told Independent Practitioner Today : ‘Most health insurance doesn’t usually cover treatment and care of chronic or long-term conditions. We use the ABI definition of chronic conditions.
‘This is a disease, illness or injury which has one or more of the following characteristics:
It needs ongoing or long-term monitoring through consultations, examinations, check-ups and/or tests;
It needs ongoing or long-term control or relief of symptoms;
It requires rehabilitation or for you to be specially trained to cope with it;
It continues indefinitely;
It has no known cure;
It comes back or is likely to come back.
‘Bupa patients may have cover for diagnosis and some tests if they’re unwell. However, once a chronic condition is diagnosed,
cover for it is no longer available. They’ll need to be referred to their GP and the NHS for the ongoing management, screening and monitoring of the condition. Or they may decide to self-pay for private treatment.
‘If a Bupa patient has an unexpected acute flare-up of a chronic condition, a short course of treatment that can modify or cure the symptoms may be covered.
‘Treatment is covered when the condition is likely to respond quickly and the treatment aims to restore them to their previous level of health immediately before the acute flare-up.
‘After this, the patient would need to be referred to the NHS for the ongoing management of their condition, as health insurance cover isn’t available for this, or they may decide to self-pay for private treatment.’
What is an outpatient allowance ?
Dr Woodman explains: ‘An outpatient allowance covers tests like X-rays, consultations with a specialist surgeon or doctor and therapies like physiotherapy.
‘Patients can choose to have outpatient allowances of £500, £750 or £1,000 to help reduce their monthly premiums. Once patients have used their outpatient allowance, they need to pay for further private appointments themselves.’
How do insurers’ hospital networks work?
Mr Martindale says: ‘Most health insurance policies cover patients to be treated at hospitals and clinics in their chosen hospital network by healthcare professionals recognised by their insurer.
‘Bupa offers patients a range of hospital networks. For example, depending on where they live, they may choose a smaller network or to exclude central London hospitals if they’re looking to reduce their premium.
‘We also have specific hospital networks for some services that are covered by our health insurance policies, such as cataract treatment, MRI and CT scans, to make sure that they meet our quality standards for these services.
‘The agreements we have with hospitals and clinics offering these services are separate to our main agreement.’
How do I know what the insurer is covering for my patient?
‘Patients should call their health insurer to authorise any consultants’ tests or treatment before they begin,’ advises Dr Woodman.
‘Pre-authorisation lets the patient, and you, know that the care the patient needs is covered by their health insurance policy. This is especially important if the patient’s policy doesn’t cover a specific condition the patient may
Mr Kris Martindale
Dr Robin Clark
Dr Tim Woodman
have; for example, a pre-existing condition that their insurer is unable to cover.
‘Once a test or treatment is authorised, Bupa will give the patient a pre-authorisation number, which you should use when invoicing for that test or treatment.’
Consultants treating Bupa patients can use Bupa’s Providers Online website to check what has been pre-authorised for their patients. More details on how to do this can be found on page 12 of the Bupa Consultant Guide.
What does ‘fee assured’ or ‘fee approved’ mean?
‘It is what some insurers call consultants who charge within their benefit limits’, says Mr Martindale. ‘It’s important because it means we can reassure Bupa patients won’t receive extra bills for their treatment, as long as it’s covered by their policy.’
What happens if a patient’s surgery is more complicated than originally expected and takes longer than usual?
Dr Woodman says: ‘Most insurers have a list of industry standard surgical and medical services that’s updated monthly, However this can’t address every potential medical situation for all patients so that’s where our surgical fee uplift process comes in.
‘Consultants can request an uplift where a procedure is more
complex and may take significantly longer than indicated in the Bupa Schedule of Procedures or more than one consultant operates on a patient during the same theatre session – known as two-handed or multiple-handed surgery.’
To find out more about Bupa’s surgical fee uplift process, visit page 16 of the Bupa Consultant Guide.
Where do you stand on experimental medicine?
Dr Woodman answers: ‘Our policies cover treatments that are consistent with generally accepted standards of medical practice, clinically appropriate in terms of type, frequency, extent, duration and the hospital, clinic or location where the services are provided; and demonstrated through scientific evidence to be effective in improving health outcomes.
‘We want to give our customers with cancer fast access to breakthrough drugs and treatment. Our policies cover chemotherapy and advanced therapies – for example, gene therapy medicines, somaticcell therapy medicines and tissueengineered medicines.
‘They may cover cancer drugs or treatment if there is good evidence to support their use, even if the treatment does not have NHS approval.
‘We welcome consultants calling us to find out if the cancer drug therapy they’re proposing to use is covered by the patient’s policy.’
The free and integrated digital prescribing platform for all private prescribers.
CloudRx take care of the dispensing, payment and delivery of medicines direct to your patients, wherever in the country they may be, for more convenient access to their medicines.
TRANSFORMATIONAL
Order prescriptions at the touch of a button to add a whole new level of convenience for your patients.
SIMPLE, CONVENIENT AND SECURE
Simple and fast digital prescribing.
Legal paperless prescriptions, repeat prescriptions and controlled drugs.
Prescriber fees can be charged to the patient if required.
INTEGRATED
Our API enables frictionless integration with healthcare brands & clinical software including Semble, WriteUpp, MidexPRO, eClinic, Pabau and ClinicYou.
“We were struggling to keep up with the admin side of the prescriptions, not to mention storage for medication to cope with a huge increase in prescriptions. CloudRx immediately took away the strain. Since our partnership we have grown by more than 200% in size. We could not have achieved this seamless scalablity without them.”
– Dr Louise Newson, Newson Health
Avoid being reported
Allegations of criminal activity can arise following patient interactions. Dr Emma Davies sets out steps to mitigate any misunderstandings or miscommunications
THERE ARE about 30 cases a year in the UK where our teams assist doctors facing allegations of criminal activity arising from their dayto-day work.
While allegations of gross negligence manslaughter are brought against doctors, thankfully this is rare. More common, however, are allegations of sexual assault/misconduct or physical assault arising from patient encounters.
The term sexual assault refers to sexual contact or behaviour that occurs without explicit consent of the victim.
Sexual misconduct is uninvited or unwelcome behaviour of a sexual nature, or which can reasonably be interpreted as sexual, that causes offence, embarrassment, harm, humiliation or intimidation. Sexual misconduct includes causing offence by what we say as well as what we do.
Physical assault beyond the obvious can include physically restraining another person. As the need for physical restraint is uncommon in the context of private practice, I will focus on sexual assault/misconduct.
Complaints and allegations of this nature may be made directly to the clinic or doctor, to the police or to the regulator. If made to your clinic, they should always be taken seriously and investigated robustly. Allegations can come from patients of all ages, gender and sexuality.
Understanding how unfounded sexual assault allegations come about can help reduce the risk of it happening to you. Even the most experienced practitioners can find themselves at the centre of an allegation of this nature following a patient interaction.
reported to the police
Communication
and adequate consent
What we may think of as routine or necessary may not be apparent to the patient. For example, a patient may not understand why a presentation of painful calves when walking could indicate the need for palpation of a femoral pulse or listening to their heart. Both are intimate areas of the body and are not the place where the pain is.
Taking time to explain your thought process, rationale for examination and what the examination will involve is an essential part of consent.
Offering a chaperone
Patients will differ in what they deem to be an intimate examination and, for some, just being touched or having to be in close proximity to the doctor may be very difficult, especially for vulnerable people.
There may also be cultural reasons why a patient may find an examination distressing. For all intimate examinations and for examinations where your patient appears particularly nervous or embarrassed, you should offer a chaperone.
The chaperone should be suitably trained, familiar with the examination and be able to see what the doctor is doing, if practical.
If a patient declines a chaperone but you feel uncomfortable in proceeding and the examination is not time-critical, you could defer the examination to someone else. You should make clear notes about the discussion around chaperones and the presence of a chaperone in the consulting room.
Understanding of dignity
Patients should be offered a space to be able to undress in private and have something available to keep them covered as much as possible. You should not remove a
Understanding how unfounded sexual assault allegations come about can help reduce the risk of it happening to you
patient’s clothing or start helping them undress unless you have their specific permission to do so.
Behaviour and attitude
Patients need to know that they can trust their doctor; maintaining a professional attitude and taking into account any sensitivities the patient may have is essential. Making personal remarks or going ‘off topic’ can lead to patients misinterpreting intentions. While humour can sometimes help to put patients at ease, the timing may not always be appropriate and it is advisable to think twice and read the situation carefully before considering making a light-hearted remark.
It is important to maintain awareness of the power dynamic between doctor and patient. If a patient asks you to stop during an examination, you should abide by their wishes.
You should also be alert to nonverbal communication, which may indicate that the patient does not want to continue with the examination.
If you receive an allegation of criminal activity following a patient consultation, always contact your medical defence organisation as soon as possible for advice and support.
Dr Emma Davies (below) is a medico-legal consultant at Medical Protection
CASE STUDY
FAILURE TO USE A CHAPERONE
Miss B wrote a letter of complaint to the private healthcare provider and the police following a consultation with Dr A.
She stated that Dr A had asked her to take off her top and go behind the curtain. When Dr A listened to her chest at the back, it took a long time and she had to hold her discarded clothing to cover herself.
Dr A then told her to stand up and face him so he could listen to the front. Miss B said she was shaking, as she felt very vulnerable and uncomfortable and alleged that Dr A’s behaviour was sexually motivated.
Dr A contacted Medical Protection and we instructed a solicitor, who assisted in preparing a detailed statement for the police investigation and advised and accompanied Dr A when being interviewed by the police.
The police did not charge Dr A, but they did refer the matter to the GMC and, in turn, Dr A was advised to consider the need to inform their Responsible Officer (RO) and/or the medical director of the private hospital.
Our medico-legal consultant worked with Dr A to reflect on what happened and why, as well as supporting Dr A through what was a very stressful and emotionally difficult time.
Dr A reviewed the relevant GMC guidance and undertook some targeted continuing professional development in professional boundaries.
He identified changes to practice he had made, which included ensuring an appropriately trained chaperone was available for any examination that may be perceived as intimate or may be distressing or feel personal to patients. He also reflected on how he communicated with patients and how he may be perceived by patients.
The GMC was satisfied that Dr A’s actions were not sexually motivated. It was also satisfied that Dr A had provided evidence of remediation, had fully reflected on the incident and had made changes to practice. The GMC closed the case with no further action.
New standards to reflect real world
The GMC’s Good Medical Practice 2024 updates professional standards for doctors and sets out the principles of care and professional behaviour expected of all doctors in the UK.
Mark Swindells (right), the council’s assistant director of standards and guidance, sets out what independent practitioners can expect ahead of it coming into effect next year
The diverse views we heard during our consultation have also helped to make sure the updated standards are reasonable to deliver in high-pressure environments
WE’VE PUBLISHED an updated version of Good Medical Practice , which sets out the standards of care and professional behaviour expected of all doctors in the UK.
This is the first major revision of the standards for a decade and it has taken a huge amount of thought, investigation, listening and learning over the last two years to get to this point.
To give doctors plenty of time to become familiar with the updated standards, they won’t come into effect until 30 January 2024.
While many of the duties from the 2013 version are the same, we’re conscious that they will need time to familiarise themselves with the new structure and some new duties.
So we’d urge all doctors to read and get to know more about the updated standards as soon as they can, as they will govern every aspect of practitioners’ future interactions with patients and colleagues.
It’s important for independent practitioners to continue to be open and honest with patients about any interests they have that may affect the way they propose, provide or prescribe treatments or refer patients
What is Good Medical Practice 2024?
The updated standards are a supportive framework to guide doctors when caring for patients and working with colleagues. They will underpin the care we all receive throughout our lives, so it’s vital they reflect the experiences of those who use and are affected by them. The standards are also at the core of medical education and training, appraisals and revalidation.
To develop the updated standards, we’ve listened to and acted on feedback from thousands of medical professionals, patients and others supporting the UK’s health services, including organisations and individuals from the independent sector.
We also reviewed the findings of public inquiries and reviews when things have gone wrong in healthcare recently. This means they are a shared agreement of what good practice looks like, for patients and doctors.
How does Good Medical Practice 2024 affect independent practitioners?
The updated Good Medical Practice places greater emphasis on listening to patients.
It’s important for independent practitioners to continue to be open and honest with patients about any interests they have that may affect – or could be seen to
affect – the way they propose, provide or prescribe treatments or refer patients. There is also a stronger emphasis on caring for the whole patient and ensuring continuity of care.
This is because recurrent themes of recent public inquiries sadly include a lack of candour when things go wrong, poor collaboration or communication and the failure to raise or act on patient safety concerns.
The standards will apply to all doctors on our register, in all four countries of the UK, at all stages of their career, whatever their specialty or field of practice and whether they work in the NHS, an independent care setting or both.
Why have the standards been updated?
We last reviewed Good Medical Practice in 2013. Since then, the way we all access care has changed.
➱ continued on page 34
CHECK OUT OUR BUSINESS DIRECTORY
Independent Practitioner Today now features an online advertising directory to complement our journal and website.
Split into ‘business’ and ‘lifestyle’ directories, they list the services independent practitioners need to run their practices or spend their well-earned money on.
Demand and pressures on healthcare in the UK have continued to grow and the pandemic accelerated the use of new technologies and saw medical professionals continually adapting to new challenges.
An extensive public consultation, the largest we’ve ever undertaken, allowed us to carefully explore the collective impact of the updated standards on doctors, the UK’s health services and patient care.
We have also been guided by findings from public inquiries, our own and others’ research and data, and other developments in healthcare.
These diverse sources highlighted a range of emerging issues that are increasingly relevant to patient care, medical practice and professional behaviour today.
In particular, there was widespread support for Good Medical Practice being an opportunity to emphasise the importance of respectful, fair, inclusive, compassionate workplaces and cultures.
These types of environments enable good teamwork, they make everyone feel safe to speak up, they support doctors’ well-being and they empower them to provide good patient care.
Our role is also evolving. Regulatory reform means not only will the updated standards eventually apply to physician assistants and anaesthesia associates, but will also allow us to become a more effective regulator.
So, given all these developments over the last decade – both in medical practice and broader changes in UK society as a whole – it’s vital that all the medical professionals registered with us, now and in the future, are supported by standards that can enable them to deliver good quality, compassionate, safe patient care.
What has changed?
Doctors on the register will already be familiar with the broad principles in Good Medical Practice , including working in partnership with patients, keeping their knowledge and skills up to date and acting promptly if patient safety risks arise.
However, the standards have been updated in five key areas to help doctors to:
1. Create respectful, fair and compassionate workplaces for colleagues and patients;
2. Promote patient-centred care;
3. Tackle discrimination;
4. Champion fair and inclusive leadership;
5. Support continuity of care and safe delegation;
We’ve also made it easier for busy medical professionals to find the information they’re looking for.
We’ve restructured the standards and made sure each sectionor domain – more clearly reflects the content.
The new domains are:
➲ Knowledge, skills and development;
➲ Patients, partnership and communication;
➲ Colleagues, culture and safety; ➲ Trust and professionalism.
The feedback we had during the consultation strongly supported the continuing use of ‘musts’ and ‘shoulds’ in Good Medical Practice 2024 as a well-understood signal about the expectations for each specific duty.
We have, however, taken the opportunity to improve our description of what those expectations are, as follows.
We use the terms ‘you must’ and ‘you should’ in the following ways:
‘You must’ is used for a legal or ethical duty you are expected to meet – or be able to justify why you didn’t;
‘You should’ is used for duties or principles that either may not apply to you or to the situation you’re currently in, or you may not
ual circumstances and consider any relevant factors known to us, such as:
☛ How serious the concern is. This includes looking at the extent of the doctor’s departure from the standards, whether the behaviour is premeditated, whether the concern involves abuse of power and whether the behaviour or concern relates to an isolated incident or has been repeated;
☛ Systems and interpersonal factors in the doctor’s working environment and their role and level of experience;
☛ How the doctor responded to the concern, including whether they’ve shown insight and if there is evidence of remediation.
be able to comply with because of factors outside your control.
Have we considered the impact of these changes?
Yes, and we are fully aware of the pressure doctors across the UK are under. We’ve considered every paragraph of the updated Good Medical Practice 2024 in that context.
The diverse views we heard during our consultation have also helped to make sure the updated standards are reasonable to deliver in high-pressure environments.
The updated version will help doctors navigate the changes in medicine, working practices and UK society that have emerged since Good Medical Practice was last reviewed in 2013.
We have also given doctors five months to familiarise themselves with the updated standards before they formally come into effect on 30 January.
What happens if a doctor doesn’t meet the updated standards?
The updated standards describe the principles of good practice, but they aren’t a set of rules. You should apply them using your professional judgement, in the specific circumstances you face.
In response to feedback in our consultation, the updated Good Medical Practice also includes a detailed explanation about how the standards relate to our fitnessto-practise procedures.
If a concern is raised with us, we will always consider the individ-
What’s next?
Our outreach, standards and strategic engagement teams are busy working with doctors, employers, healthcare leaders, royal colleges, medical defence organisations and other partners to ensure they are familiar with the updated standards before they come into effect. At the same time, we’ll also be updating our more detailed guidance, building on the general principles contained in Good Medical Practice 2024 and providing more specific support on a range of areas:
Ending a professional relationship with a patient;
Delegation and referral;
Acting as a witness;
Conflicts of interest;
Social media;
Good practice in research;
Maintaining personal and professional boundaries;
Intimate examinations and chaperones.
While the updated standards come into effect on 30 January, that will not be the end of our work.
As we saw during the decade since they were last updated, we can’t predict what the next ten years or so may bring, in medical practice or in wider society. That’s why we’ll continue working to ensure the standards are relevant, achievable and support and enable the best outcomes, both for the professions we regulate and for patients.
See www.gmc-uk.org/ethicalguidance/good-medicalpractice-2024/get-to-knowgood-medical-practice-2024
The new Good Medical Practice emphasises the importance of respectful, fair, inclusive, compassionate workplaces and cultures
With you every step
Protection that’s by your side
For over 130 years, we’ve supported our members with discretionary indemnity that covers a wide range of occurrences and claims.
Never feel restricted by your protection again.
BILLING AND COLLECTION
Stop same errors being recycled
Simon Brignall continues his analysis of the repetitive nature of the problems private practices experience with their medical billing
IN MY article last month, I cited the example of Bill Murray’s character Phil Connors in the 1993 film Groundhog Day and how he repeats the same day over and over until he learns from the error of his ways.
To save you from the various missteps of taking this journey in your private practice business, I detailed just some of the common problems I hear when consultants outline their medical billing challenges.
Now let’s look at more of the issues that just keep cropping up again and again.
Failure to reconcile payments
For many practices, the inability to reconcile payments is one of the most common problems and is often allied with their failure to deliver a robust chase process.
All successful businesses need to know the total of how much money they are currently owed.
This is even more important for medical practices, because the allocation of payments from insurance companies often results in the requirement to raise a separate invoice to the patient for the outstanding balance when the original invoice amount is not settled in full.
These outstanding balances can occur when there is either a shortfall or an excess. A shortfall is when the balance of the invoice is not settled in full by the insurer for a variety of reasons such as:
The rate of fees charged;
The policy is exhausted from a previous claim;
The claim is not covered under the policy’s terms and conditions.
Problems arise when invoices are not reconciled in a timely manner because the outstanding funds negatively impact the cash flow for the practice.
It is important to note that any delay in raising these invoices to the patient not only makes the practice look unprofessional, but also often leads to the patient choosing to defer payment.
One of my first meetings I had was with a dermatologist who had an aged debt going back several years. The total amount outstanding was more than his annual turnover.
Payments had not been consistently allocated to invoices and, to make matters worse, many remittances from insurance companies had been lost because they had been sent to the wrong address.
This meant that, despite some of the funds having been received, shortfall invoices had not been raised and outstanding payments with the insurers had not been followed up.
Because the consultant was embarrassed about the state that the practice finances had sunk to, he had chosen to write off some of the money owed rather than tackle the problem.
One of the first steps in our onboarding process is to make sure
all the private medical insurers are notified that we are the billing provider and the new contact point for this information.
The dermatology practice also catered for a large proportion of self-pay patients who were offered the ability to pay via a variety of payment methods, including bank transfer, cheque, cash and card payments.
Unfortunately, as these payments were not uniquely identified and allocated against the relevant invoice when they were received, patients were frequently chased for payment by mistake when, in fact, they had paid. So the practice looked unprofessional despite the excellent clinical care it had provided and it often received negative reviews.
When I meet with a consultant to discuss their practice, the figure that I am generally quoted for their aged debt ranges between 10-20%. But we find this is often an underestimate of the actual figure we take on when we take the practice on board.
We define ‘backlog’ as any outstanding invoices that were previously raised by the practice. The average ‘backlog’ our company has taken on during its ‘intensive care process’ for consultants we have partnered with this year is 19%.
The backlog figure we were discussing at a recent meeting trebled in size as talks progressed. This was because the consultant initially
felt too embarrassed to declare the actual amount outstanding. It helped when I was able to put things in perspective and explain that we have had practices with hundreds of thousands of pounds outstanding, as well as clinics where the amounts were into seven figures. Facing up to the extent of the problem is an important first step, but you still need to implement an effective reconciliation process supported by a robust chase procedure.
Challenges around chasing
Without exception, chasing is the area we find gives most practices the biggest operational headache and is the task most often deferred. Many practices find conversations that mix medicine and money challenging and consider they detract from the patient’s experience of the care they receive. In our experience, all invoices need to be routinely chased, including invoices sent to insurance companies.
Reasons for a delay in the processing of invoices can be:
Non-receipt of the invoice due to Electronic Data Interchange (EDI) issues or postal problems;
Treatment that was not preauthorised;
Incorrect membership numbers or lapsed policy details provided by the patient.
For a robust chase process to be effective, it must be clearly defined
Many practices find conversations that mix medicine and money challenging and consider they detract from the patient’s experience of the care they receive
and routinely applied. There needs to be clear understanding who is responsible for this role so there can be direct accountability for this activity.
Once the chasing process has begun, it needs to be followed up or the patient will think you are not being serious. This will reflect on the professionalism of the practice and will give the patient permission to withhold or delay payment. The process should allow for a mixture of communication methods used to contact the patient as well as the sending of formal letters. All this needs to be recorded alongside a complete log of any action taken.
Debt decisions
Once all the avenues in the chasing process have been exhausted, the practice needs to decide whether to send the patient to debt collection.
What you do will typically depend upon the patient, the circumstances involved in the treatment and the associated costs.
If you decide not to send the patient to the debt collectors, then the practice should consider writing the amount off as a bad debt, because it is unlikely the patient will choose to pay the outstanding amount in the future.
You may choose to consult your accountant, who will know the individual circumstances of the practice and will be in the best position to offer the correct advice.
It is not uncommon for the practices I meet with to have a bad debt rate of 5%, but we have a bad debt rate of less than 0.5% and in some instances this is as low as 0.19%.
Visibility
To analyse and make informed decisions about your practice and have confidence in the billing pro-
cess, as well as monitor its effectiveness, it is important to have access to accurate, real-time financial data.
I am constantly amazed how many consultants do not have access to current financial information about their practice. This means their ability to review and manage their practice is impaired.
At Civica, we provide our consultants with real-time access to their practice information and offer a range of tools in our reporting dashboard to analyse this data.
Additionally, I often meet with consultants for review meetings to discuss their practice, where we examine a range of financial and activity data – often extremely illuminating .
This typically includes the total value of work invoiced, where this work was done, the patient types seen, types of procedures carried out and aged debt.
This ensures each consultant has a good overview of their practice and allows them to focus on areas of interest and make informed decisions when required.
As you can see from issues I have covered over these two articles, it is very easy to have billing and collection difficulties and often these problems result in unnecessary losses of income.
If you review your practice and feel it is weak in any of the areas I have outlined, then you really do need to take time to put adequate steps in place to address this.
One option may be to consider outsourcing this vital element of your practice to a medical billing and collection company instead.
Simon Brignall (right) is director of business development at Civica Medical Billing and Collection
Cut staff sick days by managing them
What’s new in employment law? Solicitor Henrietta Donnelly examines the updated guidance issued by the arbitration service ACAS on managing sickness absence
AS INDEPENDENT practitioners expand their services and start growing support teams, the challenges of being an employer become increasingly important to understand and manage.
An essential resource for all employers are the guidance and documents produced by ACAS –the Advisory, Conciliation and Arbitration Service. These are regularly updated and reflect the lessons learnt and best practice from the large number of issues it manages daily.
One of the most recent documents updates its guidance on managing sickness absence. This is very helpful because it aims to try and reduce the impact of sickness absence on both employers and employees.
Best practice
The new guidance recommends that employers review their sickness absence policies and procedures in order to ensure they are up to date and show best practice.
The updated guidance covers:
Holiday entitlement and sick pay;
Proof of sickness and fit notes;
Covid advice;
Time needed off for parents and or dependants;
Time off work for bereavement;
Supporting disabled people at work;
Returning to work after an absence;
Producing absence policies;
Keeping records and reducing sickness absence;
Absence trigger points.
Below are some elements of the new guidance in further detail that we feel are of particular interest to independent practitioners.
Recording and monitoring sickness absence
Most employers will likely already have processes in place to record employee sickness absences. The last day of sickness is the day the employee returns to work rather than the day before. It is worth noting that sickness absence is viewed as continuous and so
weekends and bank holidays factor into the calculation of how many days are taken.
It is essential that records recording sickness absence are accurate and up to date. This information can help employers keep track of different types of sickness absence, rather than simply looking at collated statistics, which can be misleading.
This also assists in avoiding errors such as noting pregnancy absence as sickness absence, which would be discriminatory.
Accurate records also assist with establishing whether an employee has an underlying medical condition which could be the cause of repeated absences.
This will enable the practice to try to work with the employee to try and reduce periods of absence and encourage a return to work where possible.
Fit notes and self-certification
Employees might need a fit note when they are off sick. A fit note is an official statement from a registered healthcare professional giving their medical opinion on a person’s fitness for work.
If someone is off sick for seven calendar days or less – including weekends – they do not need a fit note. They can tell their employer they are not well enough to work. They do not need to provide medical evidence. This is called ‘selfcertifying’ their sick leave.
If an employee is off sick for more than seven calendar days, they should get a fit note from a registered healthcare professional. This is the case even if the employee was not supposed to be at work for some of the seven calendar days.
Certification can be managed well with efficient processes and communication with staff so that they understand the requirement to provide certification on the eighth day of sickness absence.
It is important to make clear that weekends, bank holidays and nonworking days need to factor into the calculation of when medical certification is needed.
Long-term sickness absence
Long-term sickness can be a complex issue and it is a key area to handle appropriately and with sensitivity.
The key theme of the ACAS updated guidance is to encourage employers to use sickness absence information to help manage employee leave effectively and ensure best practice is followed
a trade union representative or a colleague and a human resources representative should also be involved throughout this process. While an employee is absent due to sickness it is important to keep them informed of any significant developments in the practice to ensure they feel included.
This can include promotions and job opportunities as well as any restructures and it is important that the employee knows that they are able to engage with any changes that may affect them.
Return to work meeting
Regardless of the length of a sickness absence, when an employee returns to work, it is important to have a return-to-work meeting with them. It can be an informal discussion between an employee and their line manager.
This is important as part of your duty of care to the employee in ensuring that they feel ready to return to work and any required adjustments have been noted and actioned.
It is important to carefully review each employee’s individual situation when reviewing sickness absences. For example, an employee with a disability that requires absences for appointments is likely to reach an absence review point more quickly.
Being mindful about an employee’s circumstances when reviewing absences and showing flexibility are simple ways of managing absences affectively and sensitively and avoiding allegations of discrimination.
Sickness and absence because of long Covid
A legacy of the pandemic has been the emergence of ‘long Covid’, which can cause fluctuating symptoms that last for a long time after the infection. As this is a condition which is still being understood, it is important that employers are aware that the effects of long Covid can come and go and sickness absence can fluctuate.
It can be a high-risk area for employment tribunal claims if mismanaged, and it is always best to seek the appropriate advice when managing long-term sickness absence.
When an employee has been on sickness absence for longer than 21 days, it is helpful for the relevant manager to liaise with the employee about keeping in touch on a regular basis. It is recommended this is done every fortnight and either via a phone call or by email.
Furthermore, it is important for there to be a more formal meeting, either online or via phone, once a month in addition to the regular keeping in touch.
This meeting will review the sickness absence and look at how to help enable the employee to return to work.
For these meetings, it would be useful to refer the employee to occupational health services in order to get the best possible advice and recommendations on what adjustments can be made to help support and facilitate a return to work.
The employee may be accompanied to these meetings with either
It can also be helpful to see if there are any general ways to help reduce sickness absence by reminding the employee of any relevant well-being initiatives that are available and seeing whether any personal targets can be implemented.
Absence trigger points
The guidance also explores the issue of absence trigger points for when an employee has taken a large amount of sick days or there is a high number of ‘random’ sick days. The guidance recommends using a review points system that looks at the number of absences within a certain period of time and the length of these absences.
If an employer does choose to use this system, it needs to be carefully set out in their sickness absence policy so that employees are aware of it.
The guidance stresses that absence trigger points should not be used to automatically punish employees and that it is important to communicate and work with the employees to try and find the best solution and way forward.
Absence reviews are recommended as a way of looking at the cause of the absences as well as checking in with an employee.
It vital that employers communicate with the employee in question and engage properly with occupational health to assist with arrangements to help enable support for the employee and facilitate their return to work.
The key theme of the ACAS updated guidance is to encourage employers to use sickness absence information to help manage employee leave effectively and ensure best practice is followed.
There is also an emphasis on the need for effective communication and flexibility when managing sickness absence. It is also important to take advice from occupational health and employment law specialists, when necessary to avoid any potentially discriminatory conduct.
If you would like any further advice or support for your practice on any of the issues raised in this article, Hempsons employment team would be more than happy to assist.
Henrietta Donnelly
(right) is a solicitor at Hempsons. Email her at H.Donnelly@ hempsons.co.uk
An eye for excellence
Moorfields Private opened its doors of its new clinic in New Cavendish Street, in the heart of London’s medical district, a year ago. Philip Housden (right) takes a look at how it enhances the hospital’s private offering
THIS IMPRESSIVE new facility in New Cavendish Street adds to Moorfields Private’s established presence in Old Street as part of the main Moorfields City Road campus.
For nearly 20 years, thousands of patients have been receiving comprehensive and innovative eye care at the City Road campus.
The facility offers the highestquality eye treatment, from the most complex eye conditions to the latest laser and implantable contact lens treatments for vision correction and also cosmetic eye procedures.
Moorfields Private’s financial surplus is invested back into Moorfields Eye Hospital NHS Trust to advance excellence in eye care.
In 2022-23, the trust reported private patient revenues of £40.8m, up £3.65m (9.8%) on the previous year.
This is 15.4% of total trust revenues, up from 14.7% in 2021-2 and the highest it has achieved. Moorfields ranks second only to The Royal Marsden in the percentage of trust income earned from private patients.
Since 1805, Moorfields has pioneered research, employed the brightest minds and delivered exceptional eye care, and it continues to set international standards in ophthalmology and trains surgeons from all over the world.
Today, together with the UCL Institute of Ophthalmology, Moorfields forms the only biomedical research centre dedicated to vision research that advances the use of artificial intelligence in diagnostics, robotic surgery, gene therapies and sight restorative technology.
Nearly 90 Moorfields Private consultants, all of whom are accredited at Moorfields Eye
Hospital NHS Foundation Trust, lead on international research projects, are members of national and international professional ophthalmology bodies and regularly present at international conferences and symposiums.
Complex cases
All of the nurses and allied health professionals at Moorfields Private are specialists in ophthalmology and the team’s expertise means that they take on complex cases, which often require treatment unavailable anywhere else in the world.
Moorfields Private, the UK’s largest private hospital site for cataract surgery, delivers over 3,000 private cataract procedures each year achieving high success rates.
Patients interested in vision cor-
rection can choose from laser eye surgery, refractive lens exchange and implantable contact lenses. These are all performed using the most advanced refractive laser techniques and high-tech equipment, which is regularly updated to provide high accuracy, reduced operation time and better results.
The hospital’s oculoplastic surgeons offer a variety of cosmetic procedures treating areas around the eyes for functional and aesthetic purposes.
All of them are both cosmetic surgery specialists and consultant ophthalmologists, which ensures the best advice and treatment available for the patients.
Opened two years ago, Moorfields Private Rapid Access and Urgent Care Clinic offers sameday and next-day appointments
with A&E ophthalmologists for adult patients with acute or undiagnosed symptoms and can be self-referred by patients.
Paediatric patients are cared for at the Richard Desmond Children’s Eye Centre, one of the world’s largest specialist children’s ophthalmology centres.
Dedicated pharmacy
At the City Road location, a standalone private outpatient centre is adjacent to the main hospital and offers patients a relaxed and welcoming atmosphere. It is set over four floors, where each floor has its own consulting rooms, diagnostic rooms and waiting area, where patients can relax prior to their appointment or while they wait for their diagnostic test results.
Moorfields Private Eye Centre in New Cavendish Street, central London
The outpatient centre also has a dedicated pharmacy and offers 15 consulting rooms for adult patients, two dedicated consulting rooms for paediatric patients and three private in-patient areas with 19 rooms for overnight stays and cabins for day patients. There is a dedicated private pat-
ient’s refractive suite, situated on the fourth floor of the main hospital. Laser eye surgery equipment, including excimer and femtosecond lasers, is upgraded every three years.
The New Cavendish Street clinic is equipped with 11 consulting rooms, a refractive laser suite, operating theatre and two minor proce-
The New Cavendish Street clinic is equipped with 11 consulting rooms, a refractive laser suite, operating theatre and two minor procedure rooms for consultations, diagnostic and day treatments
tioners to continue to deliver a high standard of care for the whole patient pathway.
Andrew Robertson, director of private care, explains: ‘We work closely with primary care providers, optometrists and GPs, taking on board their needs – whether it’s learning more about ophthalmic red flags and when to refer or getting support with complex cases or learning about the latest treatments and research.
dure rooms for consultations, diagnostic and day treatments. Patients see the same consultant throughout their patient journey to ensure continuity of their care and high patient satisfaction. Moorfields Private is also providing educational and professional support to primary care practi -
‘We run regular free webinars accredited for continuing education and training and continuing professional development accredited webinars, courses, seminars, in-practice talks and other face-to-face events where participants can receive the most recent information and advice directly from our leading consultants.’
Philip Housden is director of Housden Group commercial healthcare consultancy
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment
Premises Regulatory requirements and investigations
Michael Rourke
Tania Francis m.rourke@hempsons.co.uk
for the returns
Long-term goals, short-term emotions. George Uglow (right) looks at the tension which often exists between investor goals and market movements
THERE IS always a dynamic tension that exists between the sensible, well thought-out, long-term financial goals that investors set in place – often with the help of their financial adviser – and the emotions that they are likely to experience in the moment, as markets respond to new information and portfolio values are impacted.
This tension can sometimes be most acutely felt by both the investor and their adviser in the early stages of their relationship when a portfolio either goes down or sideways in the first year or so.
However, as much as one would like to start one’s investing experience with markets rising, the reality is obviously not always the case, as newer investors have recently experienced.
From the investor’s point of view, an aversion to loss, the feeling of loss of control and disappointment at seeing hard-earned money falling in value can feel unsettling.
From the adviser’s perspective, it can also be a challenging time, knowing that, however sound the financial plan, however sensible the portfolio asset allocation and however much time they have spent providing insight into the up-and-down journey a client will experience, emotions often trump logic when a portfolio shows a fall in value.
At such times, it can be useful to reflect on several things:
1Cash is the only investment that avoids losses, but only before inflation.
And cash’s low, long-term, afterinflation returns are unlikely to allow most investors to meet their financial goals, hence the need to add equities and bonds into the asset allocation.
Cash does play an important part in a well-constructed financial plan, especially for liquidity, contingency and short-term goals. But when considering the longer term, keep your faith in the markets.
Do not be fooled by today’s high cash interest rates relative to recent years.They are a chimera for long-term investors and are not a substitute for a sensibly structured long-term portfolio designed to meet long-term goals.
2It is the very uncertainty of the shorter-term outcomes of equities and bonds that delivers the longer-term, higher afterinflation returns that most investors need to meet these goals.
The longer-term expected returns from a sensibly structured investment portfolio are far higher than those of cash.
3 Returns come from markets, not advisers, at least those employing a systematic approach to investing that aims to capture market returns.
Blame should not be apportioned to an adviser because a portfolio has not gone up in value in the same way that praise should not be heaped on them if it has risen spectacularly. Markets are not predictable in the short term.
4
Falls in portfolio values are not losses and, while there are no guarantees, have every likelihood of recovering in time.
Patience allows the longer-term expected returns to be realised. Avoid emotionally driven investment decisions that might impact these longer returns.
If we look at historic data depicting the likelihood of gains in purchasing power over the last 30 years, we gain a useful insight into the proportion of times that investors in a 60% equity, 40% balanced portfolio have suffered falls in value over different time horizons.
While falls in purchasing power – that is to say, after inflation – and even nominal value over two years are common, over five years –which is only a fraction of the time horizon of most investors – the chances of a fall decreases materially.
If you are a new investor, keep the faith and remain invested for the long term, because that is what is required to give yourself a chance of meeting your long-term goals.
If you have been investing for some time and been through one or more cycles of market falls and recoveries, hopefully the tension between longer-term goals and
short-term emotions will be greatly tempered.
As Charlie Munger, vice-chairman of US holding company Berkshire Hathaway, once said: ‘The big money is . . . in the waiting’.
George Uglow is a chartered financial planner with Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions. Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount.
Annual Allowance Tax
Is the cloud a problem?
Storing information on a data cloud? Dr Sally Old (right) advises on what independent practitioners need to consider
Dilemma 1
Can I put patient data on ‘cloud’?
QI am a consultant gynaecologist and am thinking of updating my IT systems so that, moving forwards, patient data will be stored on a data cloud system. What issues do I need to consider when using cloud computing services?
AA data cloud or a cloud computing service enables data to be stored on a virtual, offsite server run by a third party.
One of the main benefits of this is that you and your team can, providing there is a legitimate reason to do so, access the data from any computer with an internet connection.
For example, the Information Commissioners Office’s (ICO’s) guidance on cloud computing advises that anyone planning to use cloud computing to store patient data should consider whether the ‘processing of certain types of personal data could have a greater impact on individuals’ privacy’.
Before using the cloud as a data storage method, the ICO recommends considering the following points:
Will data be encrypted when in transit?
What are the deletion and retention time-scales and will the data be deleted securely if you withdraw from the cloud?
What audit trails are in place so
you can monitor who is accessing the data?
In which countries does the provider process data? The UK General Data Protection Regul ation restricts the transfer of personal data outside the UK.
Will there be a digital contract in place that includes confidentiality clauses?
Data controllers also need to review all personal data that they process and decide whether there is any data that shouldn’t be put in the cloud. This might be the case if specific assurances were given when the data was collected.
Even though you are a private practitioner, it is worth adhering to the same levels of security as those implemented by the NHS. In England, NHS Digital’s good practice guide to cloud security suggests a four-step process to using cloud services:
1. Understand the data you’re dealing with;
2. Assess the associated risks with the data;
3. Implement appropriate controls;
4. Monitor the implementation and ongoing risks.
The Scottish Government has produced public-sector cloud computing guidance here, which contains advice on security considerations and suggested risk assessment considerations and questions.
The NHS Wales Shared Services Partnership has also published guidance on cloud-based platforms, including specialist advice on cyber security.
There is currently no guidance on using cloud-based platforms in Northern Ireland, but the ICO retains oversight.
If you do decide to use a cloud
computing service, it is vital that you take appropriate steps to inform your patients of the arrangements and to be as open and transparent as possible.
Data protection law requires that personal data should only be handled in ways people would reasonably expect.
It’s unlikely patients would expect their sensitive medical information to be held in an offsite storage facility not under the direct control of their doctor. Consequently, it’s advisable to seek patient consent if you or your organisation is storing patients’ personal data in this way, making them aware of any risks involved and, as far as possible, in which countries the data will be stored.
Dr Sally Old is a medico-legal adviser with the Medical Defence Union (MDU)
A
consultant seeks guidance after being asked to be a certificate provider
for Lasting Power of Attorney. Dr Kathryn
Leask gives her response
Dilemma 2
Should I sign the LPA certificate?
QI am a private cardiologist and have been asked by one of my patient’s daughters to be a certificate provider for a Lasting Power of Attorney (LPA) for health and welfare.
The patient has been under my care for some time and has now been admitted very unwell. I am aware that they were discussing setting up an LPA, but they hadn’t got round to completing all the forms.
The patient had signed the form and this has been witnessed by a neighbour. The daughter has assured me that her mother wanted her to be an attorney, as evidenced from the forms, and has asked me to be a certificate provider.
I understand that this carries more responsibility than simply witnessing the signatures. Would it be appropriate for me to do this?
AThe certificate provider is an independent person whose role it is to confirm or certify that the donor, in this case the patient, is making the LPA of their own free will and without any pressure from anyone else.
To do this, the certificate provider must discuss the LPA with the donor to ensure that they understand the implications of it and that they have the mental capacity to make this decision. This should involve talking to the donor in private, away from the attorney(s). The certificate is
Is it right for me to sign this LPA?
The certificate provider must discuss the Lasting Power of Attorney with the donor to ensure that they understand the implications of it and that they have the mental capacity to make this decision
not valid if an attorney is present during the discussion.
The certificate provider role provides one of the main safeguards in the LPA process. If anyone were to object to the LPA when it is being registered, the certificate provider may need to justify their decision-making and explain the reasons why they felt the donor had the capacity to create the LPA.
This could be some time in the future, so it can be helpful to make a record of the reasons for your decisions.
In this case, you are not able to speak privately with the donor, and you cannot, therefore, fulfil your role as a certificate provider.
If the patient recovers sufficiently for you to be satisfied that she has capacity to create the LPA, you could have a private discussion with her then.
Dr Kathryn Leask (below) is a medico-legal adviser at the Medical Defence Union Providing first class medical consulting and therapy rooms at prime locations in
7467 8300
709 7066
PEOPLE’S VIEW OF PRIVATE CARE
An opportunity to grow private care
Going Private 2023 is a major new report on people’s perceptions of private healthcare from the Independent Healthcare Providers Network. Its director of policy, David Furness, picks out the key highlights and potential implications for the sector
It is clear that independent practitioners would be well advised to be really visible, readily available and provide a swift, straightforward service –these are things which patients are particularly looking for
WE COMMISSIONED the research which informed Going Private 2023 to understand more fully the reasons behind some of the trends we have seen regarding people’s usage of and feelings about private healthcare, particularly during and since the pandemic.
While we know lots about the numbers of patients being seen in the independent sector, and often what they are being seen for, what we know less about is how they feel and think about the sector, about why they are going private and whether different groups of people feel or think differently.
The research identified many things, but three overarching headlines are worth highlighting:
1
Demand for private healthcare is being strongly driven by challenges within the NHS. 46% of people who have used private healthcare said being unable to get an NHS appointment was a factor in their decision.
2
Most people feel positive about private healthcare –particularly if they have actually used it. 51% of people feel very or quite positive about private healthcare. That goes up to over seven-in-ten people who have used it.
3
There is evidence of a significant generational shift in the attitudes and usage of younger people. Surprisingly, younger people are more likely to have used, or be prepared to use, the private healthcare sector and are more positive about it.
Most people feel positive about private healthcare
you have a generally positive or negative attitude towards private healthcare?
Why are people going private?
We asked people to explain why they chose to go private, and the most common answer was the difficulty of accessing NHS care, with nearly half of people (46%) citing this as a factor in their decision.
The next most popular answer was ‘It is easier to book private healthcare appointments’, with 24% of respondents.
All of the drivers to private healthcare are consistent across different demographics, social grades and geographic regions. While there are minor differences, people have remarkably consistent reasons for going private.
When we asked people what they like about private healthcare, over half of people spoke of how you can be treated at short notice, with the second most popular answer being the quality of care.
The third most popular answer was that people are seen on time. This is further proof that patients believe the private sector sees peo-
ple quickly, especially in comparison to the NHS.
We see further proof that wait times are a key driver towards private care through the number of people that first try to be treated by the NHS. 56% of people had tried to use the NHS before using private healthcare, while 42% had gone straight to the private system.
Younger people (63%) and those from DE social grades (63%) were more likely to have tried to use the NHS first before using the private system.
We also asked people to tell us about all the times they had used private healthcare – not just the most recent – and whether they had tried to use the NHS first.
Here the numbers are different – only around one-in-five (21%) people say they usually or always go straight to the private system, while 78% say that they usually or always try to go to the NHS first.
REASONS FOR CHOOSING PRIVATE HEALTHCARE
Which of the following reason explains why you have used private healthcare
I couldn’t get NHS appointments quickly enough
It’s easier to book private healthcare appointments
I have private health insurance (that you pay for or that comes via your workplace)
I can get more personalised care in the private healthcare system
I think the care available privately is higher quality
I want to be seen face to face
I needed particular expertise, only available privately
There were more options for private healthcare available locally
My appointments are more likely to start and end on time in the private healthcare system
My NHS appointments were cancelled or postponed
Don’t know
Others (please specify)
Essentially, more people have gone straight to the private system for their most recent episode of care, but these people may typically have tried to use the NHS first.
The inferences we can make from this data is that people tend to try and be treated through the NHS, but then choose to go private.
We can see this through the amount of people citing the NHS waiting times as a driver in their decision, coupled with patient perception that appointments within private healthcare are easier to book and it is quicker to be seen.
In terms of opportunities, it is clear then that, at the moment, independent practitioners would be well advised to be really visible, ➱ continued on page 48
Young people are key for the private healthcare industry: 18-24 and 25-34 are the two groups with the largest positivity for the sector, the group that uses it the most and the group with the most amount of people willing to use private healthcare
How much would you guess that a single GP appointment through private healthcare tends to cost?
readily available and provide a swift, straightforward service –these are things which patients are particularly looking for.
Positive views
One of the narratives which has sometimes had traction in recent times is that people ‘don’t like’ private healthcare – that there is a negative reaction to it.
Our research showed that while there are some concerns, actually, a large proportion of people feel positive about going private and would consider doing so.
51% of people feel very or quite positive about private healthcare, and only 11% have a negative attitude.
Positive sentiment increases significantly among people who’ve used private healthcare. 73% of people who have used private healthcare say they have a positive attitude towards it, with just seven per cent having a negative attitude, and over eight-in-ten people who paid themselves said they thought it was worth the money.
GET CRACKING!
What people know (and don’t know) about private healthcare
How familiar, if at all, are you with the following aspects of the private system in the UK?
Once they are there and they have used it, they are happy with the experience and are more likely to use it again. This is a promising position for the industry to be in, where more young people are using them and more likely to continue to once they have.
Access to information
The data tells us that people do not use private healthcare because they think they could not afford it. But it also shows us that patients lack knowledge about the costs.
Very familiar Somewhat familiar Not very familiar Not familiar at all
How to pay for treatments or services (e.g. via private insurance plans or self-pay)
How much different treatments or services cost
How to access private healthcare (e.g. where to go, what to ask for)
The range of treatments and services available
Get ‘em young
So where might there be opportunities to grow and take advantage of these opportunities?
For starters, it might make sense to think about targeting younger potential patients. While nearly two-thirds of people are open to using private health care, this goes up to nearly three-quarters of respondents aged 25-34 (74% of 25-34 and 73% of 18-24 year olds).
The 18- to 24-year-old age group has the largest number of private health care users, with 40% of them having used private healthcare – largely, we believe, for GP appointments, scans and diagnostics.
There are a variety of ways that the industry can increase general understanding and awareness of private healthcare, which could also reduce the perception of unaffordability.
Here are some:
Increasing the transparency of the costs of appointments and procedures
Improving websites to become more patientfriendly
Incorporating functionality for easier booking or appointment movement
Thinking more about marketing and promotion to potential customers who may not be your ‘traditional’ clientele
Young people are key for the private healthcare industry: 18-24 and 25-34 are the two groups with the largest positivity for the sector, the group that uses it the most and the group with the most amount of people willing to use private healthcare.
From the data, we are able to see that NHS waiting lists for straightforward interactions such as GP visits, scans and mental health support are driving young people towards the private healthcare sector.
When we asked people why they do not use the independent healthcare sector, 63% of people said they could never afford it, with 70% among DE social grades and those on the lowest incomes citing this reason.
But a vast majority of people also feel like they do not have good knowledge of how much private healthcare costs, with 67% of people saying that they were not very familiar or not at all familiar with how much different treatments or services cost.
We also gave people some information about the costs of different appointments and treatments to see if that made any difference to whether they thought they could afford it. The responses differed depending on the total cost.
36% of people said that they thought they could not afford private healthcare. But after telling them the accurate price of a GP appointment, a fifth of those respondents then said that they actually could afford it.
The point is that it is probably the case that better information and transparency around price –especially for lower cost appointments and treatments – would help tackle perceived affordability barriers and potentially bring more people to think about private care.
As you can see from the graphs above, there are lots of aspects of the private healthcare system which people are not so familiar with. This presents an opportunity for the industry.
David Furness (right) is director of policy at the Independent Health care Providers Network (IHPN)
Spending too much time on billing instead of patient care?
Let the UK’s number 1 provider, Civica Medical Billing & Collection do the hard work for you.
• Reduce bad debts to less than 0.5%
• Increase net income by up to 25%
• 24/7 online access to your data
• Enable faster payments through e-billing for insurers and patients
• Focus on your practice whilst our account managers manage it all for you
DOCTOR ON THE ROAD: BYD ATTO 3
Practical EV fails to raise the pulse
A solid buy for any medic looking for an entry family-sized electric SUV. That’s the verdict of our motoring correspondent, Dr Tony Rimmer, (right) on a new offering from China
BYD ATTO 3
Body: Five-seat SUV hatchback
Engine: Single electric motor.
Front-wheel drive
Power: 201bhp
Top speed: 99mph
Acceleration: 0-60mph in 7.3 secs
WLTP range: 260 miles
CO2: 0g/kms
On-the-road price: £38,990
WE HAVE been using equipment with Chinese-made components for some years without really realising it in both our medical work and our personal lives.
The contents of many of our phones, computers and the electronic diagnostic equipment we use are sourced from China. And this is also true for the cars we drive.
Globally, the US has the greatest reliance on car parts made in China, but most of the European manufacturers, particularly German ones, also rely on the supply chain from this vast industrial base.
With the advent of electric vehicles (EVs), the need for specialised electronics and batteries has only increased. This has put the established Chinese manufacturers of EVs, which it has been selling in its home market, in pole position to start exporting to other countries including the UK.
This has already happened with brands we recognise such as MG and Polestar, whose cars are all made in China. But now there is a new wave of Chinese cars arriving from brands that we have never heard of before. They promise great value in products that will rattle the established market leaders such as Tesla, VW and Kia/Hyundai.
Bigger than Tesla
One important new Chinese entry to the UK electric vehicle marketplace is BYD, which stands for ‘Build Your Dreams’. It has actually been around since 2003, making everything from lorries and buses to cars and, in 2022, was the biggest producer of EVs in the world – even bigger than Tesla, which is saying something.
It has launched the Atto 3, a medium-sized SUV to compete with the VW iD4 and the Kia Niro among others. It has an up-to-date second-generation EV platform, a 60.5kWh battery and a 201bhp electric motor driving the front wheels.
It has a claimed range of 260 miles and costs from £36,490. There are three trim levels – Active, Comfort and Design.
Party trick
I have been testing the top-of-therange Design model, which gets a bigger 15.6-inch tablet-style touchscreen that has a party trick: it can rotate 90° from landscape to portrait mode with the touch of a button – impressive, but not really very useful.
The exterior of the Atto 3 is pretty unremarkable and it could be mistaken for any other mediumsized SUV on the market. The interior, however, is a different kettle of fish.
BYD has been adventurous with some unusual design features such as the elasticated ‘guitar strings’ used in the side pockets to secure different items. The sweeping dashboard is impressive and although the centre infotainment
screen is vast, clear and fast-functioning, the driver’s display is a little small and simple.
There is plenty of room for passengers in the rear, although three adults abreast is a bit of a squeeze. The boot is as roomy as in all its rivals and you can store the cover under the boot floor when not needed – a welcome feature.
Interior trim feels solid and the plastics are soft, giving it a more premium feel than the VW EVs. So, what is it like to drive?
Good ride quality
Well, if you are looking for a sporty drive like the MG4 or the Cupra Born, you will be disappointed. The steering is a bit numb and the handling is underwhelming. What is good, though, is the ride.
In many EVs the ride is too stiff and harsh – take note, Tesla Model Y – but the Atto 3 glides around town with great smoothness.
Unfortunately, it does get unsettled at speed and wind noise intrudes more than it should, but, generally, you travel in comfort. Performance is in line with all its rivals and it never feels lacking.
In many ways, this BYD is a very capable ‘white goods’ vehicle with some interesting interior design features and an excellent ride in the urban environment.
It offers great value as an alternative to the usual EV players and it bodes well for future models. It would be a solid buy for any medic looking for an entry family-sized electric SUV.
The range, at around 200 miles in the real world, is long enough for most needs and its practicality and useability is spot on. Just don’t expect to get excited behind the wheel if you are a keen driver.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
The exterior could be mistaken for any other medium-sized SUV
This BYD is a very capable ‘white goods’ vehicle with some interesting interior design features and an excellent ride in the urban environment
The centre infotainment screen is vast, clear and fast-functioning
To
contact Andrew Schofield at Spot On Media
ADVERTISERS: The deadline for booking adverts in our December-January issue is 24 November
INDEPENDENT PRACTITIONER
TODAY The business journal for doctors in private practice
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent.
Material is governed by copyright.
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Registered office: 7 Lindum Terrace, Lincoln LN2 5RP
Write to Independent Practitioner Today 7 Lindum Terrace, Lincoln LN2 5RP
CHANGING ADDRESS, EMAIL
ADDRESS OR SUBSCRIPTION DETAILS?
Phone 01752 312140 or email karen@marketingcentre.co.uk
TELL US YOUR NEWS
Robin Stride, editorial director
Email: robin@ip-today.co.uk
Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the digital journal, on our website or in our business directory, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners.
£90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE
Email karen@marketingcentre.co.uk or phone 01752 312140