The business journal for doctors in private practice
In this issue
Difficulties of treating your own
Medico-legal expert Dr Sophie Haroon on the issue of caring for a ‘doctor-patient’ P18
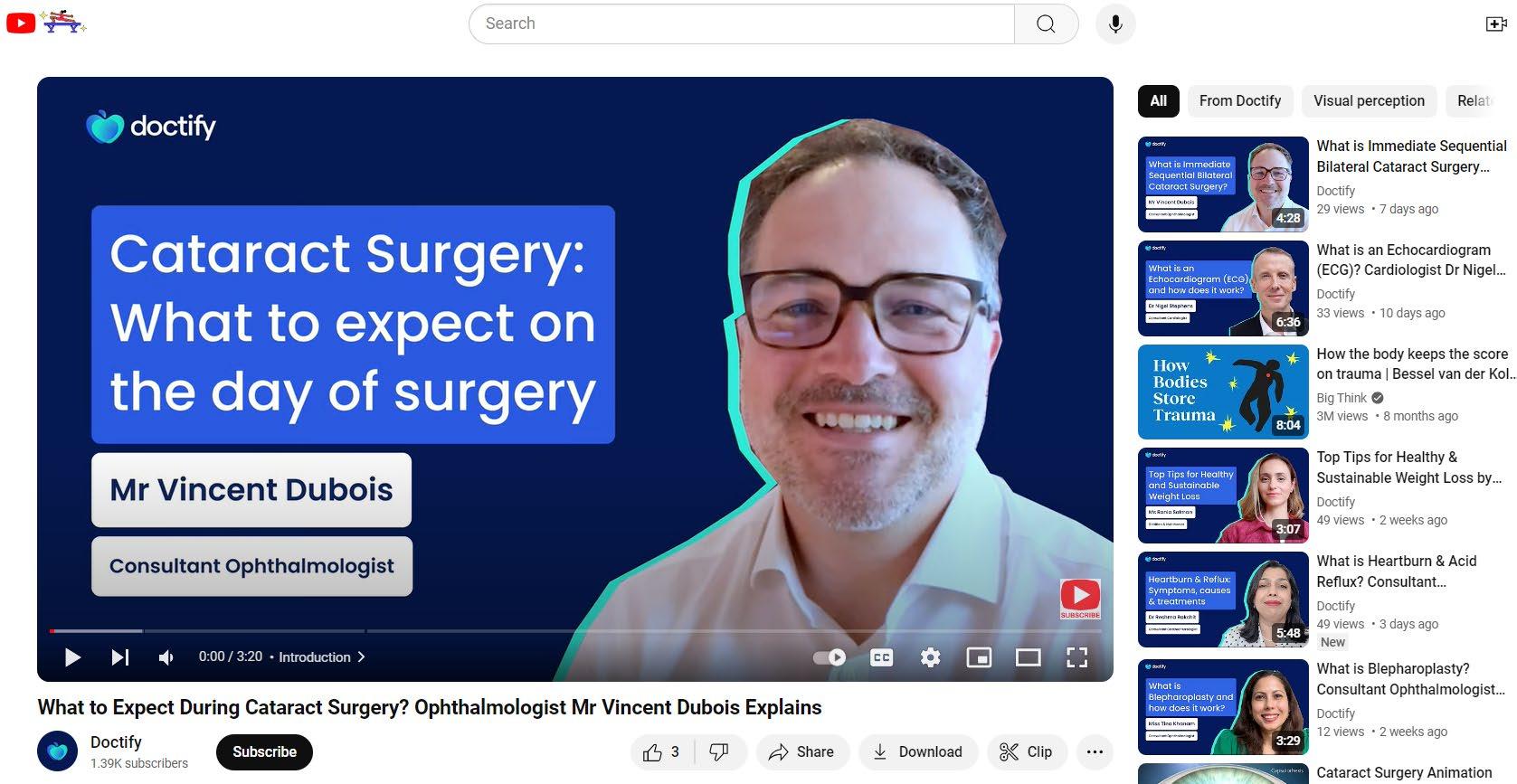
Turn yourself into a medical film star
Making a video for your practice? Make sure you engage your viewers P26
Where the Chancellor will cause you pain
Specialist medical accountant Richard Norbury gives a round-up of the Budget n Page 10
Perils of resigning in the heat of the moment
Legal advice on how to treat your staff fairly in the event of a disagreement P38
Independence declaration
By Robin Stride
Consultants have unveiled their blueprint for a private health market disruptor aimed at giving them greater control over fees and give patients a bigger say over who treats them.
The ambitious move has already received backing from hundreds of specialists and was cheered by doctors at the BMA’s annual private practice conference where the concept was announced.
It is proposed a new unionowned company called ‘BMA Health’ would function as ‘a national super-chambers’ for doctors, providing much of the business back-up they need to practise and it would also administer services for patients.
The plan aims for the first time to unite private doctors into a single corporate entity, legally entitled to collectively negotiate on behalf of its shareholders.
It would have an initial focus on self-payers and new consultants, and provide practice management services such as appointments, diary, letters and billing.
Later it would offer a ‘no exclusions’ comprehensive private medical insurance product, bring in senior consultants and use scale economies to negotiate ‘fairer’ hospital rates for self-payers.
Sports and exercise medicine consultant Dr Leon Creaney, a BMA private practice committee
Our sponsors
member and lead for private medical insurer negotiations, stressed it would not fix prices.
The plan had potential ‘to do a lot of good’ in the private sector with doctors setting their own rates as they thought fit and allowing market forces to decide, he said.
BMA Health would negotiate with insurers on behalf of doctors and patients, who would be offered GP and consultant finder services.
It is hoped consultants will now express widespread interest. Dr Creaney received the day’s biggest applause at the London event, declaring: ‘If we get the feedback from large numbers that this is something the private doctors’ community wants, it’s going to happen – and we are going to fix things not just for doctors but for patients as well.’
If we get the feedback from large numbers that this is something the private doctors’ community wants, it’s going to happen – and we are going to fix things not just for doctors but for patients as well.
DR LEON CREANEY, BMA private practice committee member
tions on what experienced consultants could earn, and consumer inability to shop around.
Patients were experiencing ever increasing premiums for ever decreasing coverage, the reason people went private was being eroded, and now there were private consultant waiting lists.
BMA Health would also negotiate the unbundling of fees for radiologists and pathologists, who would return to setting their own fees with hospitals.
Income would come from doctors paying practice management fees and from patients’ ‘moderate’ subscriptions. It would be a wholly owned subsidiary of the BMA, eventually being 49% owned by doctor-users.
Dr Creaney argued private healthcare is ‘unwell,’ with doctors outsmarted by global corporations employing divide and conquer tactics. ‘Doctors need to show solidarity with each other. It’s up to us to reclaim our territory and mend a broken sector,’ he said.
He listed a variety of consultants’ frustrations including many saying they were not doing private medical insurance-paid work because it was not worth it, restric-
According to a new BMA survey, most private doctors are in the late 40s and 50s age group and there are not the numbers of younger people to replace them, said Dr Creaney. ‘In the next ten years I worry the number of private doctors is going to fall off a cliff.’
Insurance rates are 30-40% less than on the open market and it is becoming more favourable to work in the NHS than privately, he added.
BMA private practice committee chair Dr Jennifer Yell said insurers should allow consultants to charge top-up fees. Doctors wanted fairness all round and she urged delegates to know their worth and not to be afraid of lobbying.
The BMA Health announcement followed a Bupa letter to consultants announcing fee increases. This drew a lukewarm response from the Independent Doctors Federation (IDF) to which the insurer commented to Independent Practitioner Today: ‘We are committed to ensuring the fees we pay balance affordability for customers as well as fairly reimbursing consultants for the services they provide.’
➱ continued on page 13
TELL US YOUR NEWS.
Contact editorial director Robin Stride (right)
Email: robin@ip-today.co.uk
What to do when you open a clinic
Our troubleshooters Sue O’Gorman and Hannah Browning give doctors smart advice to help them make their new venture a long-term success P16
Phone: 07909 997340 @robinstride
ADVERTISE WITH US.
To advertise in the digital journal, on our website or in our business and lifestyle directories, contact Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Email: andrew@spotonmedia.co.uk
Chief sub-editor: Vincent Dawe
Head of design: Jonathan Anstee
Follow Independent Practitioner Today on OUR REGULAR
COLUMNS
Plan your best way to wind down
Approaching retirement can be your most difficult case of all. Circle Group medical director Peter James shares some brilliant advice P22
Merits of private work in NHS units
There are some big advantages for consultants in doing their private practice in NHS private patient units. Andrew Robertson shows why P24
Understand the rules on chaperones
The GMC has updated its guidance on intimate examinations and the role of chaperones. Dr Sally Old of the MDU explains what you need to know P28
What patients seek in a consultant
How do patients choose their consultant? Anne Coyne, of the Private Healthcare Information Network, has the answer P32
What the public think of private care
‘Going private’ is becoming the new normal. David Hare shows why and outlines what private providers are doing to boost public perception P34
Business Dilemmas: Inform GMC about the coroner’s censure
The MDU’s Dr Kathy Leask replies to a cardiologist criticised in an inquest into a patient’s death P44
Start a private practice:
Don’t view accounts as just a big burden
Accountant Richard Norbury explains how accounting systems can help you run a successful business P46
Doctor on the Road:
Tainted image now a distant memory
Our motoring correspondent Dr Tony Rimmer finds the Skoda Octavia beats the opposition for value P48 www.independent-practitioner-today.co.uk
Avoid unpaid invoices
Unpaid invoices can disrupt cash flow, burden admin staff and strain patient relationships. Derek Kelly shows how to boost your clinic’s financial health P40
Avoid the emotion when you invest Investing can be simple in concept but not easy to do well. Samuel Kirton of Cavendish Medical reveals why you need a diligent investment process P42
Remedial pension letters failing to arrive in time
Many private doctors left in limbo awaiting pension tax news
By Edie Bourne
Doctors are still on a waiting list to see if they are owed rebates from tax paid on previous pension savings impacted by the ‘McCloud remedy’.
Every doctor impacted by McCloud should have received ‘remedial service statements’ by 6 October to show the recalculations of their pension growth and therefore their annual allowance positions across the seven years known as the ‘remedy period’. But to the frustration of doctors and their advisers, many of the statements have not yet arrived and there have been significant errors among those that have been received and analysed.
Samuel Kirton, financial planner with specialist financial advisers Cavendish Medical, told Indep endent Practitioner Today : ‘Since we first started talking about “McCloud” several years
ago, the issue has been plagued by complexity.
‘These statements should be putting people’s minds at rest that they can finally unravel the calculations of their pension savings and the tax owed over the last few years. Instead, many doctors are more confused than ever. They may be looking at incorrect figures or they have yet to receive any information at all.
‘To make matters worse, there is a limited time to input their figures into HM Revenue and Custom’s (HMRC’s) new online portal and then submit their selfassessment data as usual before the end of January.
‘We would have expected the deadline for tax submissions to be extended, but this has yet to be confirmed.’
To recap, the ‘McCloud remedy’ aims to recompense NHS Pension Scheme members deemed to have suffered age discrimination when
the 2015 pension scheme was introduced.
Those members now have the option to receive their original benefits from the 1995 or 2008 scheme for the ‘remedy period’ which runs from 2015 when the new pension scheme began to 2022.
Mr Kirton added: ‘Many members will find that their annual allowance position has been reduced over the years, which would lead to a rebate, plus interest, on any erroneous tax paid to
HMRC. For others, the new figures could establish that tax has been underpaid on pension growth –and the treatment of this is not straightforward.
‘We understand that this is an enormous undertaking for NHS Pensions but the fact remains that doctors, already facing challenging and important work, should not need to be chasing their information.’
He said if they contact NHS Pensions to request statements then they are being told there is no time-scale for when their data will be available.
PMI expected to give patients more flexibility
Development of new private medical insurance options to meet the needs of patients wanting more choice and flexibility are among trends independent providers expect to see in the years ahead. These include ‘PMI light’ products for diagnostics and an ability for employers to offer a range of insurance benefits for workers.
Insights from 20 sector leaders and other healthcare experts are highlighted in a new Independent Healthcare Providers Network’s (IHPN) report entitled Tomorrow’s World. They anticipate the sector’s role will continue to grow in importance and become an even more integral part of the UK health system.
The report looks at the next decade for healthcare from the patients, operational and commercial perspectives.
It expects patients to be truly placed at the heart of their care with the future healthcare system built around choice, whether that is choosing how they pay for it, who treats them, where that treatment takes place and what their care pathway looks like.
Central to this is:
Provision of more accessible information including the quality of services;
Strong outcomes data with easyto-navigate platforms to support and empower patients;
More use of digital technology
to bring healthcare into the home as well as at the hospital.
Stronger presence for independent providers in primary and community care is expected to try and meet the growing demand for more preventative healthcare.
Closer integration with NHS services was also cited to ensure a seamless patient pathway – with the potential role for ‘care co-ordinators’ to support the growing numbers of patients who access care in both the NHS and independent sectors.
IHPN chief executive David Hare said: ‘With a new Government and forthcoming ten-year plan for health, it’s the ideal time for the sector to come together and set
out their vision for what the future of healthcare looks like and how they can better support increasing numbers of NHS and private patients.
‘This report sets out just some of the ways that members and sector thought-leaders think healthcare delivery is likely to transform in the years ahead, whether that’s their relationships with the NHS, the way that patients as consumers seek to manage their health in new and emerging ways or the types of care and support the sector provides.’
See the Independent Healthcare Providers Network’s report ‘Tomorrow’s World’ at tinyurl.com/apmpmtxk
Many doctors are more confused than ever
SAMUEL KIRTON (left)
Invoices reveal business is good
Reports by Robin Stride
New figures from the private healthcare’s clearing service reveal healthy double digit growth in the independent market.
Data from Healthcode shows it grew over the year to September 2024 by 11% for private medical insurance cases and overall by 13%.
Private hospitals’ admitted care was up 8.6% and there was a 10.5% rise in outpatient care, its managing director Peter Connor told the conference.
‘We processed 3.7m hospital invoices last year and our forecast is for about 4.2m this year, so the hospital volumes market is up.’
£3.3bn of invoices were processed last year and this had ‘grown massively’ and is predicted to be £3.8bn this year.
Mr Connor – to laughter –added: ‘If you had asked me this time last month, we were predicting £73bn because one provider, who will remain nameless, submitted a £69bn invoice.’
He reported there was no doubt about there being a shift in the private medical insurance provider market space.
As many as nine providers in the
top 50 in 2024 were not there in 2022 and eight of those were nonhospital providers, ‘so we are seeing that side of things growing very, very quickly.’
Dr Rob Findlay, of data management experts Insource, predicted patients would become more accustomed to going to nonhospital settings for treatment and there would be more treatment centres and independent sector
treatment centres, including surgical hubs.
Private medical insurance premiums’ growth had been above the average trend with 7 10% in 2023 and record increases averaging 2040% in 2024.
‘Some moderation’ was expected next year with falling inflation in 2024 and insurers were investing in digital transformation and operation cost reduction programmes.
FUTURE PREDICTED GROWTH
Conference delegates enjoyed adding their opinions to market analyst Ted Townsend’s forecasts for private healthcare:
Claims values grew 20% in 2023 and while volume growth was forecast to slow this year, it remained historically high.
Insurers’ investment in primary care were a means for them to control claims frequency, inflation and reduce referrals into highercosts secondary care, said Dr Findlay.
Self pay expert Liz Heath expected a ‘modest but stable’ growth for the area, adding that this was fuelled by cancelled NHS operations with patients vowing ‘I’m not going through that again’. However, conference chair Ted Townsend, a market analyst and consultant at LaingBuisson, believed self pay had seemingly stalled.
of audience said about right, 34% optimistic, 11%
said optimistic, 32% about right, 23% pessimistic
said about right, 20% pessimistic, 17% optimistic
London
about right, 44% optimistic, 4% pessimistic
about right, 27% optimistic, 21% pessimistic
optimistic, 38% about right, 8% pessimistic
He was ‘pretty bullish’ about private medical insurance growth and thought London’s private patient units had been ‘a bit weak’.
Dr Ian Gargan, chief executive of the Private Healthcare Information Network (PHIN), considered PPUs were ‘really struggling’, although more use of private healthcare was ‘guaranteed’.
PHIN will produce outpatient data from 2026 and NHS data on consultants’ practice too.
Employers getting picky about insurance
Employers are paying increased attention to the health cover they are willing to provide for staff.
Debi O’Donovan, co founder and director of the Rewards and Employee Benefits Association, said they were looking more at what was included and what could be excluded from the level of care and treatments they were buying. Employers were expected to take more responsibility for their
staff’s health than historically, but they were also pushing some of that responsibility onto the employees.
As many as 87% of employers were expecting to take on more responsibility for their staff’s healthcare provision, but they were not thinking of taking on all of it, she told the conference.
‘They are becoming really, really savvy and looking at the health
data and trying to gather more data to look at what exact health interventions they need in their particular workforce to meet their productivity and performance goals.’
Health has become the numberone priority since the pandemic, with individuals and employers now more involved in encouraging people to talk about their health, the meeting heard.
Employee benefit consultant Rachel Western, principal at Aon, was among speakers noting a change in people’s expectations of private medical insurance. She said they were not choosing it just for secondary care. There was now a ‘huge shift’ from NHS GPs to digital private GPs as people took out individual private cover and were referred to private consultants.
Peter Connor of Healthcode
Invite to report safety problems
A former GP at the helm of The Health Services Safety Investigations Body (HSSIB) is keen to hear from Independent Practitioner Today readers who have concerns about raising safety issues at their workplaces.
Set up in 2022, and welcomed by the Independent Healthcare Providers Network (IHPN), its role is to investigate incidents where there are implications for the safety of patients in England, including the private sector.
Chief executive Dr Rosie Benneyworth told this journal she would welcome hearing from those in the private healthcare sector who would like the HSSIB to look into areas they identified as potential risks. She said: ‘If they think it’s a national issue and out of their control to challenge, then they can raise it with us.’
PATIENT SAFETY – ‘EVERYONE’S PRIORITY’
Direct cost of unsafe care accounts for 13% of healthcare budgets
Patient harm slows global economic growth by 0.7% a year
Chance of harm for inpatient care = 1 in 10
Fatal accident rate in aviation is 0.03 million. You need to fly for 103,239 years before being involved in one
237 million medication errors in England annually. Of these, 66 million have potentially clinically significant (cost £98m) and result in 1,708 deaths, 181,626 excess bed days
Source: Health Services Safety Investigations Body
The armslength governmental body was set up under the Health and Social Care Act. It does not attribute blame or liability but takes a system perspective aiming to reduce the likelihood of incidents happening, It is doing around 30 investiga
tions a year, which involve patients, families and healthcare staff.
Resulting report subjects have included retained swabs following invasive procedures, digital tools for online consultation in general practice and the design of the paediatric ward.
Outcomes ‘just an afterthought’
A gulf between how private medical insurers present themselves in promotional wording and their attention to patients’ outcomes posttreatment was highlighted at the private healthcare conference as a speaker called for more transparency.
A post op question might, for example, be about what the patient thought of the hospital’s food, but the speaker complained she did not see much about healthcare outcomes.
Joanne Buckle, principal and consulting actuary at healthcare business consultancy Milliman, said the customer was the patient, although many insurers saw the customer as the hospital or consultant.
Most insurers’ reports to employers paying their staff’s premiums talked of how much they paid out the previous year while giving bosses no sense of the value they were getting for their spend.
Ms Buckle warned the audience that challenges for the sector
included private medical insurance premiums rising 3040% for employers, increasing mental health claims, the high cost of drug inflation and rising mental health claims.
Healthcode boss Peter Connor reported a ‘massive’ rise in mental health PMI claims, possibly the highest growth area his company had seen. He noted that insurers had promoted the facility, so it was hard to pinpoint the real reason for the growth.
Confidence remains for strong growth
A wide range of professionals in private healthcare, including doctors, expressed confidence in strong growth for the private medical insurance market going in to next year.
Dr Susan Alexander of
the IDF
Incentive to stay in NHS is criticised as ‘insane’
The chair and president elect of the Independent Doctors Federation (IDF) has hit out at private medical insurance rules and inducements restricting patients’ access to specialists.
Shoulder surgeon Dr Susan Alexander described one particular incident reported to her by an ‘eminent cardiologist’ the previous week as ‘insane’.
She told the audience: ‘He said patients come in with a huge chest pain; they get treated as a critical patient and on the ward they say they have got private health insurance and they can either choose to go private and have the coronary angiogram that they need within 2448 hours – or if they stay in the NHS they will get £200 a day from their insurance company to stay in the NHS.
‘My reaction is “what the actual ...” For goodness sake, this is insane! It is almost bordering on immoral. How can you justify that?
‘What they don’t explain to the patient is that if they do have an event outside of hours, they are not going to get the same level of care that they would have had if they had gone privately. People’s lives are potentially at risk.’
Dr Alexander also criticised policies disallowing some patients to choose specialists who did not charge within the fee rate.
52% predicting 1013% growth; 33% foresaw 810%; 11% opted for 1315%; 4% thought there would be more than 15%.
An audience survey at the LaingBuisson conference found that for 2024:
For 2025:
39% went for 810% growth;
32% predicted 58%;
23% foresaw 1015%; 3% over 15% and 3% under 5%.
52% expected cash plan growth of between 5%2%+ next year.
And she highlighted another problem of patients not being allowed to have treatment deemed ‘experimental’ despite it being published in a specialty’s top journal years previously and given to hundreds of people.
Boom in insurance allays self-pay dip
By Robin Stride
Record demand is driving continued growth in private healthcare as rising numbers of patients use private medical insurance to fund their treatment.
The total UK market is valued at £12.4bn in 2023, according to market analyst LaingBuisson’s latest annual Private Acute UK Market Report
Private hospitals remain the largest section of the market at £6.8bn –– up nearly £800m since the previous year – but independent clinics and privately practising doctors account for a significant proportion of revenue at £4.9bn.
The remaining market value is made up of NHS PPUs with estimated total revenues of £700m.
Increased revenue from private health insurance is in line with a positive trend in this segment since the pandemic.
LaingBuisson reported: ‘Self-pay volumes have held up more strongly in clinics than in private hospitals, likely reflecting the more accessible lower price points
HIGHLIGHTS OF LAINGBUISSON REPORT
Private medical cover has boomed, with hospital revenue from this source up 17.8% from 2022 to 2023
Overall market value for private acute healthcare is estimated at £12.4bn, with private acute hospitals accounting for around £6.8bn
Private doctors and the private clinic market segment is valued at £4.9bn
NHS private patient revenue is valued at £700m
The five largest operators account for 75% of all private hospital revenue
NHS funding rose from a 10% share in 2003 to an estimated 31% in 2023
Ophthalmology is driving a large volume of all NHS-funded activity. The four largest providers have opened 64 clinics in the last three years.
for services such as outpatient diagnostic tests.’
Report author Tim Read said: ‘Hospital providers are benefiting from the continuing boom in private health insurance and this has offset a slight softening in demand from those paying out of their own pocket for care.
‘For those providers that are more focused on providing additional capacity to the NHS, there remains little sign that there is a lessening of need of independent
sector support and revenue from this segment has remained robust.
‘Continued growth in corporate employers introducing health insurance for staff is helping drive usage of independent sector services – potentially from individuals that have never previously experienced care outside of the NHS – and helps remove some of the traditional price point barriers that may have stopped people paying for their own care in the past.’
Health and social care firms top of growth set
New research has revealed the best growing industries for businesses in the UK, with health and social care at the top.
The sector’s businesses have grown by 8.06% since 2022, meaning 8,540 new ventures have succeeded in this sector.
Health and social care businesses now make up 4.26% of all businesses in the UK and 3.89% of all business births in these two years.
These findings came from MRPeasy, suppliers of material requirement planning (MRP) software for small manufacturers, who collected business birth and death data from the Office for National Statistics to calculate each industry’s success rate from 2022 to 2024.
It then analysed and ranked the best industries for businesses in the UK.
The company’s Karl Heinrich Lauri said: ‘The health and social care industry has emerged as one of the strongest sectors for UK businesses, driven by demand for healthcare services and social support.’
TV doc opens totally overhauled hospital
The newly refurbished Practice Plus Group Hospital, Birmingham, has officially opened its doors at a launch celebration with TV GP Dr Hilary Jones.
Previously known locally as The Edgbaston Hospital, it had a £10m transformation with a new reception, pharmacy, wards, X-ray suite and theatres.
The hospital said NHS patients could ask their GP for a referral and expect to be seen in days and weeks rather than months and years.
It expects to complete up to 8,000 procedures a year when at full capacity.
Dr Jones said many people were unaware they could also go to a
private hospital as an NHS patient, free of charge, and often sooner than waiting for NHS hospitals.
Practice Plus Group boss Jim Easton added: ‘It’s highly unusual, especially in the current climate, to have zero NHS waiting lists and we’re excited to welcome as many people as possible.
‘We are delighted to bring what we do so well elsewhere around the country, helping both NHS and private patients, to the West Midlands. We have an incredible team of specialist consultants, nurses and healthcare professionals, who bring with them a wealth of experience and we have invested heavily in transforming the site into a modern, welcoming hospital.’
Dr Hilary Jones (centre) with chief executive Jim Easton (standing behind Dr Jones) and staff from the new Practice Plus Group Hospital, Birmingham
Private doctors do 20% of all NHS ops
By Agnes Rose
Consultants in private practice continue to deliver record levels of care to NHS patients and so far this year have removed more than one million patients from the health service waiting list.
Specialists in the independent sector now carry out nearly one in five NHS operations (15,000) every week, according to a quarterly analysis from the Independent Healthcare Providers Network (IHPN).
Its chief executive David Hare said: ‘This is a fantastic achievement and one that independent
PPU WATCH
providers are keen to build on even further – including through investing in much-needed new healthcare facilities so that NHS patients can get the care they need at a time when public resources are hugely stretched, as well as ensuring that existing capacity in the sector is fully utilised by the NHS.’
The IHPN says the independent sector consistently delivers 10% of all NHS planned care, equating to 101,000 patient care episodes a week in 2024 – nearly a third up on 2021.
Private providers now deliver 26.3% of all NHS trauma and orthopaedics elective activity and
24.4% of all NHS ophthalmology activity – 26,000 and 22,000 patient episodes every week.
Latest NHS Referral To Treatment (RTT) data also shows waiting times for NHS treatment continue to be shorter in the independent sector. Those seen by private providers had waited an average of just over 11 weeks compared with an average 18 weeks for NHS providers.
The IHPN is urging for all appointment slots made available for the NHS by independent providers to be used. Around one million annually, which could be used for NHS patients, are not taken up.
is a fantastic achievement and one that independent providers are keen to build on even further
Private providers propose to invest £1bn in new healthcare facilities including surgical and diagnostic hubs to help drive down NHS waiting lists.
Innovation on display at PPU summit
Compiled by Philip Housden
NHS Private Patient Service Summit
NHS trusts took the opportunity to share best practice and hear of business innovation at the annual NHS Private Patient Service Summit.
Delegates from 13 NHS trusts heard from a wide range of industry experts and learned from useful breakout sessions about income generation and benchmarking. Experiences when raising income and building an effective business model at Frimley Health’s Parkside brand were passed on by its private patients’ manager Emma Aherne.
And Richard Gregory (right) of Chrysalis Finance outlined payment options for PPUs to attract more self-pay patients.
Trusts also raised key concerns at a Q&A panel session with Bupa,
Axa and Aviva representatives over insurers’ relationships with the NHS and the challenges of achieving tariffs for the often increased complexity of private cases managed in PPUs.
Housden Group’s Luke Minshall highlighted trends and potential for growth in 2025-26 during an update on NHS trusts’ latest private patient performance revealed in their 2023-24 annual accounts.
The conference, organised by SBK Healthcare and sponsored by Streets Heaver Healthcare Computing and Patient Billing, also heard case studies from Mark Bounds, director of private care and his Moorfields Private team, and from the Royal Free London PPU’s Dean Stephen Booth.
Royal Free Private Care focuses on nephrology, HPB and women’s health
A new strategic focus on three services aims to deliver world-leading care at the Royal Free London’s PPU.
Kidney care, hepatobiliary services and women’s health will constitute a core part of the business.
Post-pandemic, the unit has seen a steady flow of patients to its private oncology suites and dialysis unit, and is admitting patients with complex cases including international patients, particularly from the Gulf countries.
By the end of 2023-24, it regained 75% of private patients seen and admitted against the level of patients in 2019-20.
The PPU has three wards, an oncology suite, a dialysis unit, outpatient clinics and private GP services. As part of a teaching hospital, it has a renowned group of consultants and it champions multidisciplinary teams.
The hospital’s private day case facility in Hadley Wood, Barnet, has become the newest women’s health centre in north London, specialising in diagnostics and treatment of non-malignant gynaecological cases.
An ‘excited’ Dean Stephen Booth, director of private and international care, says: ‘By leveraging our existing expertise in these areas plus the embedded patient-centred care, the RFL PPU ensures a consistent and highquality experience for every patient.
‘All profits from the PPU are being used to fund the trust’s NHS services, which means our patients and staff will benefit. We hope to expand our business more in the coming years, so this is an exciting time for the PPU.
In 2023-24 trust accounts, Royal Free reported private patient income of £17.9m, up £3.5m and 24.1% on the previous year and ahead of the London top ten trusts’ average growth of 16.9%.
Philip Housden (right) is director of Housden Group commercial healthcare consultancy
This
DAVID HARE Chief executive, IHPN
CQC urged to hone inspection system
By Olive Carterton
Private doctors have welcomed recommendations to improve the Care Quality Commission (CQC), but continue to be frustrated meanwhile over their treatment at the hands of the organisation
Many still experience a ‘psychological and financial burden’ as they wait for many months to be registered and inspected, according to Dr Laila Kaikavoosi, chair of the Independent Doctors Federation (IDF) regulation committee. She said the CQC assessment framework was often incongruous with the nature and size of practices in the private sector. Providers were expected to adhere to a ‘one size fits all’ framework and adapt their practices accordingly with little advice or support.
‘Many professionals feel that they are constantly under scrutiny and don’t fully understand what is expected of them. Many feel compelled to invest in external consultants or legal advice to navigate the CQC’s complex regulatory environment.
‘Healthcare providers who are preoccupied with passing inspections may prioritise meeting CQC standards over delivering holistic, patient-centred care.
‘This misalignment of priorities ultimately reduces the quality of care received by patients.’
Dr Kaikavoosi said the IDF was happy to see the CQC’s acceptance of the high-level recommendations and its commitment to make the necessary changes to improve the current framework.
Improvement recommendations came in a final report from Dr Penelope Dash, chair of NW London Integrated Care Board.
The IDF expressed commitment to supporting the inspectorate in its quest to get better. It wants a clear and simple regime that fits the service being delivered, plus support for service users and providers.
David Hare, chief executive of the Independent Healthcare Providers Network (IHPN), welcomed the report, saying it rightly set out the importance and urgency of improving the regulator’s performance.
‘This includes not only the need to deliver its fundamental role of carrying out timely inspections of services and the ability to update ratings effectively, but also how to more effectively assess new and innovative service models that are emerging,’ he said.
‘Moreover, with a health system currently under huge strain and in desperate need of new capacity, Dr Dash’s review makes clear that the CQC must urgently prioritise clearing the unacceptable backlog in registrations of new health and care providers – helping enable new resources to be brought to local communities and improve patient access to care.’
He urged the CQC to ‘work at pace’ to implement necessary changes.
‘IHPN looks forward to working with its new leadership team as they seek to turn the organisation around and re-establish the CQC as a regulator that both patients and healthcare providers can have confidence in.’
Kent unit offers ‘game-changing’ injection
Consultants at independent charitable hospital Benenden Hospital are offering a pioneering, nondegradable hydrogel injectable implant to treat patients with pain and discomfort caused by knee osteoarthritis (OA).
Arthrosamid, a polyacrylamide hydrogel developed by Contura Orthopaedics Ltd, treats knee osteoarthritis is reported to offer long-lasting, proven pain relief with a single injection.
Mr Alex Chipperfield, medical
director and consultant orthopaedic surgeon at the hospital in Cranbrook, Kent, said specialists were excited to offer the treatment, as it was an effective alternative to invasive surgery for a debilitating condition, providing rapid onset of pain relief and improved function.
‘It’s truly a game-changing therapy, which could have a huge impact on the quality of life of thousands of people, enabling them to return to the hobbies and pastimes they love.’
Mr Alex Chipperfield
Remote care firms unite to speed up certificates
Remote care companies have united to give a better service for people needing a medical letter or certificate.
Private telehealth services providers Doctor Care Anywhere has partnered with online medical letter provider ZoomDoc to supply sameday medical letters and certificates 24 hours a day, 365 days a year.
Traveling patients are one big target due to the amount of correct documentation needed such as a pregnancy fit-to-fly certificate, chickenpox recovery,or travelling with medication.
Overstretched NHS GPs are regularly asked for these, but people can wait weeks to receive them.
Zoe Sullivan, of Doctor Care Anywhere – which conducts over 60,000 virtual consultations monthly – said: ‘Since partnering with ZoomDoc, our patients can get a guaranteed medical letter the same day, seven days a week, 365 days a year.’
ZoomDoc provides 28 different types of medical documentation.
Dr Kenny Livingstone
Founder GP and chief medical officer Dr Kenny Livingstone said: ‘Once a patient has provided the evidence and information needed to assess them online, our GP reviews and verifies it remotely, before sending the required documentation electronically.
‘A ZoomDoc GP can safely review 15 patients per hour and provide the relevant documents, whereas an NHS or private GP would typically do four or five consultations.
‘By partnering with Doctor Care Anywhere to scale its ability to help more patients with medical certificates, we want to reduce the pressure on their clinicians while providing a simpler and quicker experience for patients.’
Dr Laila Kaikavoosi of the IDF
Innovation hub set for Harley St area
By Douglas Shepherd
A £52m investment in flagship buildings for health innovation and discovery has been announced by Harley Street Health District (HSHD) landlords.
Howard de Walden Estate (HdWE) is partnering with flexible workspace operator Spacemade initially for a project of three buildings with a total of 38,000ft 2 at Hale House, 76-78 Portland Place.
HdWE aims for the street to emerge as a leading London location for healthtech start-ups, investors and venture capital firms.
It says it is committed to working with new companies, policy advisers, capital providers and support services that are shaping better healthcare.
UCLPartners will be the anchor occupier situated on the first floor. It is a leading UK health innovation partnership at the forefront of transforming healthcare through collaboration and patient-focused innovations.
The company also oversees delivery of the NHS Innovation Accelerator, which catalyses growth of small enterprise in the health service.
HdWE’s approach to healthcare has evolved to offer a wider spectrum of ‘whole health services’ encompassing specialist hospitals,
outpatient clinics and state-ofthe-art healthcare facilities in preventative care and aftercare.
Chief executive Mark Kildea said its Hale House project investment and the signing of UCLPartners was hugely complementary to its strategy.
The development will also provide amenity space for the community, including a large roof terrace, 90-person auditorium, café, conferencing and meeting rooms, a dry lab, gym, podcast studio and a content creation room.
UCLPartners chief executive Chris Laing said he was impressed with the estate’s ambitious vision to build a world-leading health innovation cluster in Marylebone.
‘Our new base will help us connect the health technology and life science sectors with healthcare providers, patients and the public, developing novel solutions that will define the healthcare of the future.’
Spacemade co-founder Jonny Rosenblatt explained his mission from the outset was to create the
UK’s most collaborative healthtech cluster and develop a thriving ecosystem where start-ups, investors and supporting services could come together ‘to reshape the future of healthcare for the better’.
He believes industry specific spaces like the Hale House are the future of co-working and the broader office market.
‘With space for over 600 members and facilities to enhance their working activity we want to unite the brightest minds in healthtech under one roof.’
GMC plan to crack down on discrimination
Inequality is embedded in medicine throughout a doctor’s career, from the earliest days of education and training to the leadership positions of latter years, the GMC boss has warned.
Charlie Massey is calling for a cultural upheaval and a focus on longer-term systemic issues across healthcare to eradicate inequalities. His comments came as the regu-
lator gave an update on work to tackle discrimination and inequality in medicine and progress on its drive to eliminate discrimination, disadvantage and unfairness in medical education and training.
The GMC says the past year ‘shows promising signs of progress’. The disparity in fitness-topractise referrals in relation to a doctor’s ethnicity or place of quali-
fication has continued to reduce.
Differences in overall rates of referrals between ethnic minority and white doctors, and between UK-qualified and non-UK qualified doctors, have also fallen.
The GMC has committed to eliminating disproportionality in referrals by 2026. Educational organisations, including medical schools, royal colleges and facul -
ties, must report annually to the council on their actions to address issues.
Mr Massey said: ‘Inclusive and supportive workplaces and training environments are vital to high-quality patient care – a valued and supported doctor performs at their best.
‘When pressure hits our system, this commitment can’t be downgraded.’
An artist’s impressions of the £52m project at 76-78 Portland Place in the Harley Street Health District
Mark Kildea, HdWE chief executive
Where the Chancellor will cause you pain
In the first Budget since 2010 for The Labour Party, Chancellor Rachel Reeves announced £40bn of tax rises, with the majority of this coming from an increase in National Insurance contributions. The Government also announced a pledge of £22.6bn increase in the day-to-day health budget, and £3.1bn increase in the capital budget. Independent Practitioner Today columnist and specialist medical accountant Richard Norbury (right) gives a summary of some of the key changes that may impact you
National Insurance
Employers’ National Insurance will increase from 13.8% to 15% from April 2025, but employees will not pay more directly.
The Government will also lower the threshold when employers’ National Insurance starts to be paid from £9,100 to £5,000. Additionally, the employment allowance – which is the amount that eligible employers can reduce their employers’ National Insurance liability – will increase from £5,000 to £10,500.
In practical terms, the reduction in the employment allowance limit to £5,000 causes an anomaly in the tax system. Currently, eligible employees can be paid up to £533 a month (£6,396 a year) without operating a PAYE scheme, but the new National Insurance rules will effectively reduce this limit.
Private practices will usually be eligible for the employment allowance, but this needs to be checked, as if you do significant work in the public sector, you are unlikely to be entitled to take advantage of this allowance. Businesses with a single employee are not eligible.
Many practitioners will have arranged their affairs to include a salary to family members – and often themselves if operating via a limited company – and this will need to be reviewed following these announcements.
Any practices with a significant number of employees will need to review the additional costs that are not covered in the employment allowance.
The reduction in the band from £9,100 to £5,000 could add up to £615 per employee as an additional cost.
This is in addition to the 1.2% increase in the rate.
If a practice were to employ five members of staff at an average salary of £36,000 per individual, then the additional cost (£5,235) would be covered by the increase in employment allowance of £5,500 – provided the practice is eligible to claim this.
Once these potential increases have been reviewed, a decision can be made whether the practice will absorb any costs or if these can be passed on.
Domicile
The Chancellor confirmed that the current remittance basis of taxation will be abolished for nondoms from 6 April 2025
It will be replaced with a new four-year foreign income and gains system for individuals who become UK tax resident after a period of ten tax years of non-UK residence.
The new regime is essentially as originally announced in March by the previous government.
This can be a complex area and should be discussed with your accountant if this legislation could apply.
The majority of practitioners will pay taxes in the UK on your worldwide income and therefore no change in the way that your earnings are reported.
The Government has pledged to increase the personal tax threshold by inflation, but not until 2028. This is currently set as £12,570, but many practitioners may already lose part or all of this allowance anyway.
Inheritance Tax
Inheritance Tax thresholds have been fixed at their current levels until the tax year 2029-30.
Pension funds which have not already been taken by an individual are currently exempt from IHT on death.
From April 2027, pension funds and death benefits will be included with an individual’s estate and potentially subject to IHT on a taxpayer’s death.
This does not relate to your NHS Pension or other defined benefit pension schemes, as those schemes reduce upon death to a surviving spouse – or dependents – and eventually cease. There are changes to Agricultural Property Relief and Business Property Relief, so any individual owning land and property used for agricultural purposes or business assets including shares in unquoted companies or partnership interests will need to take professional advice on how best to arrange their affairs.
BUDGET REACTION
Capital Gains Tax
Capital Gains Tax will increase, effective immediately. The lower rate, paid by basic-rate taxpayers, will increase from 10% to 18% and the higher rate will increase from 20% to 24%.
But there will be no increase on gains from investment property which remains at 18% and 24%. The annual exemption for capital gains tax remains unaltered at £3,000.
For those assets that qualify for business asset disposal relief (BADR), there will be staged increases from 10% to 14% (effec tive on disposals made after 6 April 2025) and then up to 18% (effec tive from 6 April 2026).
The immediate change in the Capital Gains Tax rates allows no room for planning, but anyone considering selling an asset, or in the latter stages of your private medical practices trading through a limited company that may qualify for BADR, should consider whether this should be expedited to enjoy the lower tax rates.
Furnished holiday lettings
While not an announcement in the recent Budget, changes in the furnished holiday lettings rules will come in to effect from 6 April 2025 to remove so called tax advantages that furnished holiday let landlords have over other residential property landlords.
The main changes will be the removal of the finance cost restriction rules meaning loan/mortgage interest relief is restricted to basic rate for income tax and removing capital allowance rules for new expenditure and allowing replacement of domestic items relief.
Bearing in mind the comments on capital gains tax, property owners who have previously enjoyed the benefit of the furnished holiday letting rules will need to review their affairs to see if there are any other options such as shared ownership or disposal of the property before 5 April 2025 which may crystallise lower capital gains tax rates which may currently qualify for BADR.
As expected, VAT will apply to private school fees from 1 January 2025. This will also apply to boarding services provided by private schools. Any fees paid from 29 July 2024 relating to the term starting in January 2025 onwards will be subject to VAT.
The national living wage for those aged over 21 will increase by 6.7% to £12.21 and 18- to 20-year-olds will see a 16.3% increase to £10. Many practitioners will be paying salaries to their adult children and this increase may well impact on the amount paid per hour.
Stamp Duty Land Tax
The additional dwelling higher rate surcharge will increase from 3% to 5% and is payable by any individual purchasing additional residential properties – other than their principal private residence –or by companies and other nonnatural persons.
There is also an increase from 15% to 17% for any companies and other non-naturalised persons when purchasing residential properties worth more than £500,000
that are not used for commercial purposes.
This is an additional burden for those of you thinking of investing in residential property either personally or via a limited company.
No extension was announced to the temporary increases to Stamp Duty Land Tax (SDLT) reliefs which are effective until 31 March 2025.
Therefore, for anyone moving home, the SDLT liability is likely to be higher from 1April 2025.
Benefits in kind
Many of you will have taken advantage of either the NHS fleet scheme or being provided with an electric vehicle from your own limited company.
The current tax rate of 2% of the list price of the vehicle for fully electric vehicles was already set to increase by 1% per year from 202526 reaching 5% in 2027-28.
The Government has now proposed intentions to further increase the benefit-in-kind rate by 2% from 2028-29 and again by 2% in 2029-30 reaching 9%.
Hybrid and fully petrol/diesel vehicles will also see increased rates which will maintain a gap between fully electric vehicles.
Due to the increase in rates, practitioners who have finance or leases coming to an end should consider if they should take out a new agreement considering that normally they last for three or four years, especially if a hybrid vehicle is currently being provided.
Pensions
It is important to note that there were no changes to:
The pension annual allowance;
The lifetime allowance;
The maximum tax-free lump of £268,275;
Tax relief on pension contributions for individuals or firms.
Many Independent Practitioner Today readers are members of the NHS Pension Scheme and due to the ‘McCloud remedy’ will have recently received a Remediable Pension Saving Statement (RPSS), which is likely to require a review by your accountant before your 2023-24 tax return can be finalised.
The tax-raising measures in the Budget pushed much of the burden onto businesses and those making capital gains rather than directly increasing taxation on an individual’s earned income.
Depending on your circumstances, tax planning opportunities may exist to help mitigate the burden of these additional costs.
Richard Norbury is a partner at Sandison Easson & Co, specialist medical accountants
BMA PRIVATE PRACTICE CONFERENCE
Around 200 consultants and GPs enjoyed the lively BMA private practice conference 2024, both in person and online. Editor Robin Stride (right) reports on the lively proceedings
Doctors want BMA help with business
Consultant members of the BMA have registered staunch support for the association to provide a host of services to help doctors run the business side of their private practice.
It is envisaged that BMA Health (see story on page one) would function as a onestop shop and engage a network of successful independent companies already in the market to deliver competitively priced deals.
A shopping list of what specialists would want to be offered has been drawn up from the responses of 859 association members in a survey organised by the association’s private practice committee.
Top of the list, with support from nearly three quarters (74.30%) of them, is negotiating consultation fees with private medical insurers, while 44.10%
would value negotiating procedure fee splits with hospitals.
Fee setting with self pay patients is popular with 43% of consultants, while more than one in three (36.3%) – apparently not members of the Independent Doctors Federation which provides this service already – would seek an independent appraisal/ revalidation service.
Just over a third are also asking for support around derecognition by private medical insurers, a similar percentage want the service to offer negotiating help for premises charges, and just under a third
think BMA Health should provide billing and collection services.
With the increasing complexities of being an employer, around 30% of consultants also want access to professional HR expertise, support for setting up a new private practice business and private practice privilege applications.
A quarter of responders called for secretarial/patient communications services such as dictation and standard letters, 22% requested debt management know how and 17% asked for appointment booking and scheduling services.
VAT on bills would kill off private practice
Private practice would be killed outright if consultants were forced to charge VAT on all their bills, a BMA private practice committee member warned.
The possibility of VAT being charged in future was raised by a concerned plastic surgeon in the audience during a discussion on outcomes of the new Labour Government’s first Budget.
But Dr Leon Creaney, a BMA private practice committee member, said it would not be worth doctors working privately if VAT was ever imposed.
The tax would prove to be a false economy, as doctors would have to pass on the cost to their patients.
David Hare, chief executive of the Independent Healthcare Providers Network, said he had studied the Budget documents ‘with nervousness’ but private hospitals were pleased to see no increase in insurance premium tax.
There was no suggestion the Government was planning to introduce VAT.
Doctors cite money as top reason for quitting
Money and management problems have been revealed as the top reasons why doctors are quitting private practice.
And while leavers cite relationship problems with private medical insurers and independent hospitals, none blame difficult relationship with their GP colleagues.
These are among the findings of a detailed BMA private practice committee survey of association members.
A total of 90 specialists answering the question ‘Why did you stop undertaking private practice?’ and they were asked to tick all that apply. The results were:
Income from private practices fees was insufficient – 40%;
Administration/management/ bureaucracy associated with private practice too great – 38.9%;
I have a better worklife balance – 32.2%;
Relationship with private medical insurers too difficult – 22.2%;
NHS commitments too great/ have taken on additional NHS work – 22.2%;
Personal reasons/commitments (such as health issues) – 20%;
NHS earnings sufficient for my needs – 20%;
Indemnity costs too high –18.9%;
Availability of private practice opportunities was too limited where I live/work – 16.7%;
Relationship with private hospitals too difficult – 16.7%;
Pension or taxation issues – 11.1%;
Insufficient demand for private practice in my specialty – 7.8%;
Premises/facilities costs too high – 5.6%;
Career break ,such as parental reasons or study leave – 4.4%.
Thousands of consultants experience bad debts and in the worst cases these have reached six figures, according to billing and collection sources. But nobody cited bad debt levels as being a contributory factor to their decision to quit.
David Hare
Private GP’s life is hard but fulfilling
GPs were reminded they would not have the benefit of the NHS pension if they went private nor the ‘security blanket’ they enjoyed when in the health service.
Fulltime private GPs might earn only around the same as they did before and they needed to ensure good credit control so they did not go broke, the conference was told.
But the BMA private practice committee deputy chair told the meeting she would never return to the NHS even though she might miss it.
Dr Shaima Villait, of Chelsea Medics, said she would not want to change the feeling of satisfaction enjoyed at the end of the day knowing she had given patients a good service.
Advising GPs to be transparent
about their charges, she criticised places she knew ‘where you walk in and breathe – they charge you’ and others demanding ‘a ridiculous amount but, in my opinion, they are not very good doctors.’
Dr Villait, who also heads the Independent Doctors Federation GP committee, advised there was enough private GP work opportunity for everyone wanting it. But it was important to have the right location, to know the area and what the GP competition there was doing.
Converts would not have the camaraderie of the NHS, and people did not want to share information – this had to be sought out.
The type of premises used was important and she did not recom
mend working from home like some people did. Options included dedicated consulting rooms or a private hospital with its Care Quality Commission ‘umbrella’.
She recommended doctors considered their legal entity – sole trader, limited liability partnerships, limited company or salaried GP – but she did not advocate being a locum private GP due to lack of benefits and employers not taking anyone on.
Her wealth of tips about going into private general practice included:
Decide what sort of service you will provide: immunisations/ bloods/24hours?
When buying clinical software, try them all at the same time if
Private GPs need pricing model
‘Sort out your pricing model in your business plan’ was the advice of a leading specialist medical accountant who reported increasing numbers of doctors are moving into private sector general practice.
Delegates nodded as Alec James, a partner with Sandison Easson, reflected that GPs could not get what they wanted in the NHS nor give the care they would like.
The minimum wage rise was hitting NHS practices as well as private surgeries, but doctors were enjoying the independent option’s greater flexibility without Government interference and not having to hit Quality and Outcomes Framework (QOF) targets.
They also had longer appointments to care for their patients and better job satisfaction, he said. Independent Practitioner Today columnist Mr James advised doctors to research how much they would charge by using websites or calling other private GPs and to always cater for inflation.
AVOID HMRC PROBES
Hot topics for tax officials are:
Under-declared income
High-risk tax schemes
Motor and travel claims
Annual allowance tax charges
Lifetime protection schemes
Late filing of returns
Source: Sandison Easson
Accountant Alec James and his advice on how to avoid HMRC inquiries
They also needed to work out their pricing model, such as: Pay as you go (PAYG);
Monthly;
Monthly plus reduced PAYG;
Discounts for family;
Additional services, online or face to face; The premium for out of hours work.
He urged doctors to take advice about charging VAT in private practice.
possible and get one with drug interactions;
Ensure every patient who comes to see you has a contract with you and copy of a complaints procedure;
With medical indemnity so expensive, research who you want to use. There are increasing options;
A website is essential – they are the way people find you;
Networking is important with other doctors you might refer to;
Patients have higher expectations of your service because they are paying, so make sure they are not going away unhappy.
Bupa offers fee increases
➱ continued from front page
Bupa’s letter promised more fee transparency to ‘make it easier for you to work with us’, more input from clinicians, 10 28% rises for anaesthetic procedures and 523% for surgical procedures depending on the complexity rating, all from 1 November 2024.
While healthcare is generally exempt, the work must satisfy two conditions:
1. These services are within the profession you are registered to practice in;
2. The primary purpose of the services is the protection, maintenance or restoration of the health of the person concerned.
If income from VAT able supplies is over £90,000 then doctors must register and charge VAT.
Bupa wrote it would review fees regularly using an improved model, ‘continue our helpful dialogue with consultant representative bodies’ and was committed to maintaining an ongoing dialogue with individual consultants.
The IDF called the fee rise a ‘positive step’ towards addressing issues with remuneration but warned these fell short of reflecting consultants’ rising costs.
It said most fees were currently 20 30% from where they should be and, while it appreciated the setting up of a consultant panel, it called for this to represent all consultants working in private practice bound by fee constraints.
Dr Shaima Villait of Chelsea Medics
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2014
Patients need more data on prices
Independent practitioners agreed that patients should have access to information about fees – and quality and outcomes – to help them make informed choices about their treatment.
Online private healthcare solutions provider Healthcode surveyed a customer sample to gauge awareness of the Competition and Markets Authority’s (CMA) final report and support for its remedies.
Eight-five per cent thought it right that patients could research private providers’ fees and 94% favoured publication of consultants’ performance data.
Consultants said this would
bring the private sector into line with the NHS and increase the private sector’s credibility.
One specialist commented that healthcare providers should be like ‘any other industry or service, otherwise it is like getting a menu at a restaurant with no prices listed and being expected to order a meal’.
But there were fears statistics might be misleading without careful explanation and could lead some to practise more conservatively and avoid difficult cases.
Healthcode managing director Peter Connor said the survey showed most consultants recognised that data transparency was essential for the private health sector’s success.
Patients use EU law to get free private care abroad
More than 600 NHS patients who had surgery in other European countries had reclaimed their medical costs from the health service under a new law introduced the previous year.
Under the EU Directive on CrossBorder Healthcare, UK patients could receive treatment anywhere in Europe.
This effectively meant that UK patients awaiting treatment could choose to have an operation at a private hospital in Europe and reclaim the cost, provided the
treatment was medically necessary and would cost no more than in an NHS hospital.
855 patients had submitted claims with 621 successful. They reclaimed a total of £833,491 – an average of £1,432 per claim.
Huge hospital planned
Top independent practitioners were set to be given practising privileges in a palatial multimillion-pound international hospital destined for London.
We revealed early plans for the development, which would aim to be a beacon for high-net-worth self-pay patients from overseas.
The development, said to have United States connections, was welcomed by commentators who voiced concern at a huge drop-off in the number of overseas patients coming for treatment in the UK.
Many were going instead to newer and more modern hospitals outside of the UK, which had been marketing themselves strongly around the world.
Screening offers criticised
A GPs’ leader called for action to protect patients from companies promoting ‘inappropriate health screening when, in fact, the
evidence of benefit is often lacking’.
Responding to the House of Commons’ Science and Technology Committee’s report into health screening programmes, Dr Richard Vautrey, deputy chairman of the BMA’s GP Committee, said many doctors should share MPs’ concerns.
He said: ‘As the BMA has repeatedly warned, it is vitally important that people being invited for screening fully understand the pros and cons of the procedure.
‘Patients must also be aware that there is a risk that false positive results could lead to unnecessary and potentially harmful further investigations.’
GMC probes boost stress
Private doctors facing GMC investigations were likely to experience mounting stress, we reported.
A defence body survey of 180 doctors investigated by the organisation in the previous five years found nearly three-quarters of them thought their experience harmed their mental and/or physical health.
Respondents’ involvement in GMC investigations impacted on their stress/anxiety (93%), personal life (76%), health and well-being (74%), confidence (69%) and professional reputation (52%), the MPS found.
Seventy per cent said the GMC should offer more support to doctors facing an investigation.
Are you a clinician looking to start or grow your medico-legal career?
TMLEP offers you a unique opportunity to not only enhance your income but also drive real change in healthcare standards.
By partnering with TMLEP, you will contribute expert medico-legal opinions that help healthcare providers learn from incidents, improve patient safety, and enhance clinical practice.
Shape the Future of Healthcare and Medico-Legal Standards.
Join our community of over 2,600 independent healthcare professionals across all specialties who are making a significant impact on patient safety and clinical excellence. Whether you’re an established expert or looking to start your journey in medico-legal work, TMLEP offers the support, resources, and opportunities to succeed.
To get involved, contact Charlee Keen Charlee.keen@tmlep.com / 02033559796 or visit www.tmlep.com
TROUBLESHOOTERS: GROWING YOUR PRACTICE
What to do when you open a clinic
Our troubleshooters Sue O’Gorman and Hannah Browning give more doctors some smart advice to help make their new venture a long-term success
Being able to delegate tasks and set projects for your team at an early stage will help you to manage your workload better but also add interest for them
QWe have just opened a new clinic. What are the key areas we now need to focus on to ensure we develop sustainable revenue growth?
AYou have spent months, possibly even years, in bringing to life your vision of setting up a new healthcare facility.
The last few weeks will have been especially hectic as you push towards the opening date.
The clinic is now open and you can breathe again . . . not quite!
The hard work now starts in making your clinic or hospital financially viable.
How to start?
It would be much easier if there was a logical order and single priorities at a time, but in the real world of business, this isn’t the case.
This, therefore, means that you will need to focus on multiple areas and it will be dependent on your own set-up to understand which needs prioritising first.
One of the benefits of starting out is that you will hopefully have some team members that are not yet fully utilised. It is important to understand their skill sets, even if they don’t relate to their main role.
Being able to delegate tasks and set projects for your team at this early stage will help you to manage your workload better but also add interest for them when patient numbers are low.
Patient journey
Starting out as you mean to go on is one of the main benefits of a new organisation. There are no pre-existing behaviours or expectations: you get to the write the rule book.
Being able to survive in the competitive world of private healthcare means that your patient experience must be excellent. It is worth spending time in the first few weeks going through all the various patient journeys. This is down to:
The details of the forms a consultant may use to request a test;
How much the test will be and how payment is made;
How this is logged on the computer system and patient record;
How does the referer get the
Things will inevitably go wrong at the start. However, use these errors to learn and improve so that everyone sees you are serious about providing excellent customer service
ants on board and there needs to be an understanding that the clinic will generate patients and not just rely on consultants moving business to them.
Digital marketing
Your marketing efforts should have started prior to opening with a brand, website and social media all in place.
results and what happens if there is an urgent diagnosis.
Going through the journey to this level of detail will help to iron out any issues and ensure that the experience for the clinicians is equally as good as for the patients.
Clinician engagement
Consultants are cautious with change and take time to commit to a new practice location. So it is important that you have a strong consultant engagement strategy if you are to bring doctors on board. Be clear on what the offer is for consultants and why they should want to work at your clinic.
Consultants generally look for three things when considering a practice:
1. It needs to be safe for them and their patients;
2. You need to be easy to work with;
3. It needs to be financially rewarding.
Having robust clinical processes and an experienced and confident team will help to reassure consultants on the safety of the practice.
Working hard on your processes will make it easier for the consultant, medical secretary and patients to deal with your facility.
Things will inevitably go wrong at the start. However, use these errors to learn and improve so that everyone sees you are serious about providing excellent customer service.
If your business plan expects consultants to move their whole practice to your location, then, unfortunately, you may have a problem.
Consultants will rarely move all their practice to a new hospital, with most treading cautiously to see first whether it works for them and their patients.
It will take time to bring consult-
Work with your marketing company to create a plan for the next three months that has a clear budget with an expectation on return.
This needs to be realistic both in terms of what you can invest but also how much it will generate and how quickly.
No one has a magic wand, and it does take time to build a new brand and generate patients from it.
Relationship management
A valuable project is to get your brand out directly into the local market. Look at who your potential referrers are and create a plan to engage with them.
This may involve going to see them and taking some information, inviting them to an event or holding an education evening. Bringing people on site is a great way of them seeing the facility and gives you an opportunity to show them your vision.
Expanding this to patient events will not only give you content for social media feeds but also create a positive word-of-mouth reputation.
Depending on the space you have available, offering a meeting room to local groups also gives you an excuse to engage with a new audience and helps you to embed into the community.
Depending on the space you have available, offering a meeting room to local groups gives you an excuse to engage with a new audience and helps you to embed into the community
Team-building and culture
The delivery of the patient experience will only be as good as the people you have. So it is critical that you spend time with your team to build positive relationships and to start creating a culture that puts excellent patient care in the centre.
Train your team to understand how the whole patient journey works and how their part is dependent on others and vice versa. This should prevent silo working and give you greater flexibility if you have a team that can cover multiple roles.
This is not something that will ever be ticked off your ‘to do’ list and needs continued commitment to ensure the positive culture is embedded and clear to everyone who has contact with the clinic.
Sue O’Gorman is director of Medici Healthcare Consultancy. Website: www.medicihealthcareconsultancy. co.uk. Email: sue@medicihealthcareconsultancy.co.uk.
Hannah Browning is director of Beyond Excellence Healthcare Consultancy. Website: https:// beyondexcellenceconsultancy.co.uk. Email: info@beyondexcellenceconsultancy.co.uk.
Sue O’Gorman and Hannah Browning
DOCTORS AS PATIENTS
The difficulties of treating one of your own
Dr Sophie Haroon (right) reflects on the sometimes complicated doctor-‘doctor-patient’ relationship and ways to manage it
A WHILE AGO , a friend told me this story. Her father, a retired paediatrician, had a nasty infection. He was prescribed ciprofloxacin. He was checked for allergies but not counselled about side-effects. Within 24 hours of the first dose, he developed Achilles tendinitis and went on to rupture his left Achilles tendon, a known risk he later found out.
As an avid runner, this was not a risk he would have entertained. When he told his doctor what had happened, their response was that it was assumed he would have known about ciprofloxacin’s sideeffects because he was a doctor. In fact, being a paediatrician, he only knew it was not an antibiotic to be used in children because of the risk of juvenile arthropathy, and that it caused problems in weight-bearing joints in lab rats.
Making assumptions
This scenario, of doctors being drawn into their own management and assumptions being made about their medical knowledge, is not uncommon.
➱ continued on page 20
Don’t miss our special December-January issue
To commemorate 17 years of informing private doctors and 168 editions, Independent Practitioner Today is publishing a special issue with 168 tips from top experts in the field on how to make your practice even more successful
And it does not stop there. A former colleague once described how an eminent surgeon had left her to counsel her mother about three surgical options for a gynaecological condition.
As an experienced GP, she knew a lot, but having never undertaken any of the procedures, her counsel of risks and benefits was naturally limited.
A different relationship?
The doctor-patient relationship has evolved from paternalism to one of patient-centredness and a collaborative dynamic. However, throw in a patient who is also a doctor and the relational boundaries become blurred.
Yet, in Good Medical Practice, the GMC is clear: doctors should not treat themselves and should seek independent professional advice rather than relying on their own judgement.
At some point, a doctor is going to have to seek medical attention. In navigating the doctor-‘doctorpatient’ relationship, it is useful to look at both perspectives.
Doctors as ‘doctor-patients’
Studies have shown that despite GMC advice about not seeking medical care from family members or colleagues, doctors do utilise these avenues through formal and informal consultations. The latter tend to be ‘corridor’ consultations.
Again, despite GMC advice, others go on to self-treat, especially if they are GPs compared to specialists. A range of barriers – patient, provider or system-related – can facilitate this behaviour.
Patient elements include embarrassment of exposing oneself to peers, feeling a failure for not coping with illness, being worried about imposing on another busy doctor, shame and stigma especially around mental illness, and loss of control/professional identity as the illness drives a wedge between the healthy doctors and the now sick ‘doctor-patients’.
Provider elements include confidentiality concerns and doctors not being related to as patients in consultations, but instead as doctors.
System elements include lack of time, the culture in the medical profession to be healthy and
TAKE-HOME ADVICE
Taking the factors in this article into account, what can doctors do when consulting with ‘doctor-patients’? Here are some pointers:
1
Speak up if a colleague is unwell. They may not be able to see it themselves.
2 See the ‘doctor-patient’ as a person. Get to know them beyond their medical identity and their illness.
3
Strive for continuity of care rather than the structured disruption of it which simply deforms who ‘doctor-patients’ and doctors can be to, and for, each other.
4
Acknowledge medical care’s limitations. Interestingly, doctors tend to choose less intensive treatment than they recommend to their patients.
5 Do not be led into ‘corridor’ consultations. ‘Doctor-patients’ should use the proper healthcare channels available to the general population, be they through primary care or emergency medicine and then on to secondary care, with the choice to go private like for anyone else.
6 Do not avoid difficult questions. A history is a history. If that involves probing about mental health, alcohol and drug use, the treating doctor only does a disservice to the ‘doctor-patient’ by omitting this.
7
Negotiate the language to be used so the dialogue is based on a shared understanding of terminology.
8 Find out what the ‘doctor-patient’ knows about their diagnosis, investigation and management so there is a common platform from which to discuss further and information is not lost or assumed to be already known.
uncomplaining, self-treatment being perceived as ‘OK’, and presenteeism being an expected phenomenon.
Doctors as treating doctors
Doctors can find managing ‘doctor-patients’ anxiety-provoking. For the treating doctor, there can be awkwardness, intimidation and feeling less able to form independent judgements about the best treatment options.
Over-investigation can prevail in a bid to demonstrate competency of the treating doctor and reduce the likelihood of errors.
Histories may be less interrogated for fear of embarrassing or upsetting the ‘doctor-patient’.
9
Investigation, treatment and follow-up should be like that for any patient.
10
Determine with the ‘doctor-patient’ whether they are a patient, a critical analyst studying themselves being a patient, an observant doctor assessing how other doctors work, a researcher processing and analysing the healthcare structures and procedures affecting them as patients, or all four?
Note that the proportions of what a ‘doctorpatient’ is will vary over time – some becoming more passive and dislocating from the doctor role, others engaging further.
11
Be aware of concerns around confidentiality and access to medical records. Be open and honest when information needs to be shared, seek appropriate consent to disclose and have in place safeguards to protect it.
Only in exceptional cases can any patient’s confidentiality be breached. But disclosure may be needed if the ‘doctor-patient’ puts others at risk.
12
Consider out-of-area referrals if there is further concern about a ‘doctor-patient’ being treated by colleagues and this is negatively impacting them.
13
Drop the ‘super doctor’ culture. Promoting presenteeism is no good for the doctor, their colleagues or patients.
14
15
Avoid using doctors as proxies for managing patients who are their family.
If you are concerned about treating a doctor, and have a choice, do not see them but ensure their care is provided by an alternative doctor and they are not negatively impacted
Just as the ‘doctor-patient’ can find it difficult to relinquish authority, the treating doctor may hand over treatment decisions and abdicate their responsibility for fear of scrutiny or because of deference to the ‘doctor-patient’s’ perceived superior medical knowledge.
Boundary issues and role ambiguity are recurrent themes. Some treating doctors may over-identify with ‘doctor-patients’ to improve rapport and empathy.
Others distance themselves to maintain objectivity or because the ‘doctor-patient’ represents a mirrored reflection of their own unconscious fears about illness, the myth of doctor invulnerability being usurped. This can lead to the
negative outcome of ‘doctorpatients’ being less supported than non-medical patients.
Unintended consequences
The use of medical terminology can have unintended consequences. While the ‘doctorpatient’ deploys it to exercise greater control in treatment decisions and the treating doctor uses it out of respectfulness of the ‘doctor-patient’s’ knowledge and status, it can result in inadequate information being imparted because of the assumption that the ‘doctor-patient’ has sufficient knowledge. Furthermore, sometimes medical knowledge may not be consen-
Do not be led into ‘corridor’ consultations. ‘Doctor-patients’ should use the proper healthcare channels available to the general population
sually understood and the ‘doctor-patient’ may feel unable to question this, so leading to poorly informed consent.
Additionally, the treating doctor can mistakenly accept the ‘doctorpatient’s’ opinion about their illness and management.
Confidentiality can be a huge concern for treating doctors just as it can be for ‘doctor-patients’. Seeking a second opinion is accepted practice, but for the treating doctor, they may be concerned that this questions their competence.
For the ‘doctor-patient’, this may mean more peers know of their illness – for better or worse.
Medical culture and socialisation strongly influence how treating doctors either underestimate or over-manage the ‘doctor-patient’.
Dr Sophie Haroon is a medico-legal consultant at Medical Protection
Diagnostic Audiology Including Paediatrics • Tinnitus Rehabilitation • Vestibular Testing • PTA & Tympanometry • Speech Audiometry • Speech In Noise Testing• Specialist Tests Including OAE, VEMP & ASSR • Ear Wax Removal • Independent Hearing Aid Provider
THE ROUTE TO RETIREMENT
Plan your best way to wind down
Approaching retirement can be your most difficult case of all – but it doesn’t have to be that way.
Mr Peter James (below), group medical director at Circle Health Group, shares some brilliant advice
AMERICAN FOOTBALL sports coach Vince Lombardi famously said ‘the harder you work, the harder it is to surrender’. Consultants know this feeling all too well.
Having endured one of the longest periods of training of any profession – with many gruelling years of shift work, rotating round the country and endless examinations to become a specialist – giving it all up can be psychologically difficult to contemplate or plan.
Accepting we are getting older can also be challenging. Perhaps thinking of it as stages in ‘the journey of life’ is more palatable, but however you approach it, proper planning is the key to making a success of the twilight days of your career and ensuring your transition into the sunset goes smoothly.
The most important practical consideration is winding down your surgical workload. This process is likely to take six to 12 months, so my advice is to select a date by which you would definitely hope to be retired and work backwards from there.
Taking the time to meet with management teams at the hospitals you practise in will make the process much smoother.
As with so many other areas of life, communication is key. Consider all the stakeholders in your career and devise a plan to
communicate your decision and the time scales effectively with each of them: your patients, your hospital, your colleagues and then your wider professional network.
There will be no worse feeling as you approach your finish date than being inundated with questions and queries about aspects of your practice. Trust me when I say that you will be thanked, and you will thank yourself by arranging this well in advance.
Regular catch-ups
As previously stated, it can be hard saying goodbye to a practice you have spent many years nurturing. Being actively involved with the process will be extremely beneficial on a personal level.
In my role as Circle Health Group’s Responsible Officer, I always make a point of ensuring that retiring doctors also have regular catchups and planning sessions with the hospitals they work at.
We all like feeling in control. Being on top of the details is what makes us great practitioners. Just as you would not transfer the care of a patient without briefing your colleagues, avoid heading into retirement without including your hospital provider in the planning stage.
In terms of stopping surgery, it is a largely mathematical process.
Firstly, estimate the number of patients midtreatment cycle; secondly, assess the requirements to complete their treatments and, thirdly, set a date to stop new patients being seen, with a timescale to run down follow up patients.
This staged approach – closing your practice to new patients, completing your surgical lists, and then following up on your final lists in recovery and outpatients – will give you the time and space to prepare mentally and plan practically for retirement.
Carefully select the colleague you wish to hand over to. We all care deeply about our patients; they deserve the best and your legacy and reputation will be preserved by handing over to someone with the highest standards on clinical outcomes and patient satisfaction.
Defence subscriptions
On a more technical level, it is critically important to keep on top of your defence or insurance subscriptions and investigate what policy will cover past surgeries once you have retired.
Medical defence organisations offer a different level of cover to commercial insurance. Read up on this carefully and be certain you are covered for several years post
retirement so that you have peace of mind should a delayed claim come your way.
Be honest with yourself and your close family that the psychological process whereby an eminent and highly respected consultant becomes a seemingly anonymous member of the public may not always be entirely smooth or easy.
It rarely works well to leave with no plan or pastimes. Before you hang up your scrubs, consider revisiting old hobbies, developing new ones or getting involved with mentoring and charitable projects that combine passion and purpose.
Charitable projects
I witnessed Massoud Fouladi, Circle’s co founder and former medical director, gradually wind down his responsibilities from full time Circle board executive and consultant ophthalmologist to a parttime role setting up clinical chairs in Circle sites across the country.
He spent his final working months in employment organising an inspirational charitable project to deliver over £3m or 300 tonnes worth of medical supplies to wartorn hospitals in Ukraine. Now he spends his retirement working on charitable projects to
support refugees and help immigrant doctors work towards GMC accreditation.
This for me is the definition of a medical career that ended well, and then transitioned seamlessly to projects that combine passion and purpose in retirement – and you will struggle to meet a more contented or fulfilled retired consultant.
The lesson for me is the importance of being proactive in mentoring younger colleagues, developing interests and maintaining connections.
Giving back
Work hard at staying in contact with colleagues and professional bodies so it all does not just stop on a Tuesday afternoon; there is no need to sever all ties. This is a practical way of ensuring that all your expertise is not lost when you leave.
You have spent decades getting to know every aspect of your trade, and your expertise and experience will remain invaluable for many years after your retirement should you choose to share it, so give yourself a legacy by giving something back.
Finally, know when it is time to go. As they say in showbiz, it is always better to leave the audience wanting more. Picking the right
However you approach it, proper planning is the key to making a success of the twilight days of your career and ensuring your transition into the sunset goes smoothly
time to go is vitally important to ending well.
Do not leave when you are forced to or because you can no longer keep up with the pace. As clinicians, we understand the biological fact that motor skills and stamina deteriorate over time.
Undertake introspection
It is so easy to become less tolerant and more impatient as we progress in life, so undertake some introspection and challenge yourself as to whether you are still giving your patients your best.
Practically, keep an eye on your patient satisfaction statistics, patient reported outcome measures and registry data. Retire at the top of your game and do not wait until you are an outlier.
We all feel deeply the extraordinary privilege and pleasure that comes from a long career in medicine. Cicero said ‘in nothing do men more nearly approach the gods than in giving health to men’.
A vocation as rewarding and worthwhile as medicine is very hard to part with, but knowing when to step back will give you the legacy you deserve.
Consultant orthopaedic surgeon Mr Peter James is Circle Health Group’s group medical director and responsible officer
NHS PRIVATE PATIENT UNITS
Merits of private work in NHS units
There are some big advantages for consultants in doing their private practice in NHS private patient units (PPUs). Andrew Robertson (right) shows why
WHEN I MANAGED my first private surgical hospital some 25 years ago, a patient, funded by the NHS, arrived for his elective surgery and immediately ordered a bottle of champagne, thinking it would be on the house.
I mention this by way of an example as to what people thought when ‘going private’ –the smart environment, one’s own room with en suite bathroom, a fine selection of food and drink.
Speed of access to treatment and one’s own consultant were also considerations. But quality of treatment, safety and outcomes were not necessarily at the forefront of a patient’s mind.
Thankfully, this has changed over the years with patients far more focused on the quality of their care and the performance of both surgeon and hospital.
Environment and experience do, of course, matter – we all enjoy a little luxury – but they are not the most important elements of restoration to good health.
The range and complexity of treatments offered in any hospital will depend upon its facilities, equipment and resources, particularly the training and expertise of its staff.
Safety net
NHS hospitals in general have large departments focused on specific specialties, with those departments having specialist staff including consultants, nurses, radiographers and therapists.
In addition, there is always a range of medical and clinical staff onsite as well as oncall. They will have intensive care units that support the more complex surgery
and provide a safety net to any adverse events.
Although some will say that all those staff and facilities are there for NHS patients, all patients, whether on a public or private pathway, are trust patients and will of course be cared for, irrespective of this, should the need arise.
Many private hospitals, particularly the smaller ones, have more limited facilities and staffing structures and therefore have a limit on what treatments they can offer. That does not mean to say that the care is substandard; far from it
Many will concentrate on more routine, elective surgery with only those with higher dependency or intensive care units able to offer more complex surgery.
Consultants who choose to develop their private practices in any hospital should think about
whether that hospital will support and even enhance their reputation.
They will want their patients to be grateful that their consultant chose to take them to that hospital because they had an excellent outcome and felt safe and well looked after. The overall experience is very important, but the outcome the highest priority.
Mix of facilities
There is a real mix of facilities offered by trusts specifically for private patients. These range from dedicated private patient wards, theatres and consulting rooms comparable to any smart private hospital, to the use of side rooms and little differentiation between NHS and private pathways.
For the less complex surgery where risk is much lower, perhaps
the quality of facilities may be more important to some, but the more complex the surgery the importance surely diminishes.
While I would argue that it is worth trusts investing in private patient facilities, even those that are still considering it have much to offer consultants that complement the quality of care for their private patients.
Key factors include convenience and familiarity. If the trust enables the development of private practices, then why waste time travelling elsewhere when it’s on your doorstep and one can see inpatients more easily?
Familiarity a bonus
Familiarity of the environment and facilities is an advantage, as well as with the staff one is used to working with and trust. If specialist NHS staff who regularly work with consultants can be involved in the treatment of private pat ients, it gives consultants confidence in the delivery of excellent care.
Few would argue that multidisciplinary healthcare is not optimal; something the NHS is very good at. Having one’s consultant colleagues available to discuss difficult cases is something not always available at another hospital and provides an extra level to the quality of care.
Trusts that support and develop private patient services will want their consultants to practise with them rather than go to the local private hospital. This provides consultants with the opportunity to organise their job plans to accommodate both their NHS and private work.
There is no doubt that certain days of the
week and times of the day are more popular with private patients, so being available at those times will help facilitate the growth of a practice.
If the commitment is to see and treat private patients at the trust, then it is in the trust’s interests to look at how job plans can be arranged to suit the demands of both the NHS and private patients.
Support the NHS
During my time at Moorfields
Private, the message that resonated most with potential referrers was that all monies generated from private patients in the trust went towards all patient care, education and research. GPs, optometrists, physiotherapists and other referrers generally want to support the NHS and the work it does.
Referring their private patients to the trust is one way of doing this. It is also another reason for consultants to base their private practices where they are employed.
But to get this message out there, it’s important there are resources and mechanisms to do so. Setting up private patient services is one thing, but having the right staffing to deliver and promote the services is essential if they are to prove successful and give consultants the confidence that seeing and treating private patients at their trust will be beneficial.
There are distinct advantages in having a private patient service within NHS trusts, both for the patients in terms of their care but also for the consultants. But if the opportunity is to be realised, there needs to be the right investment both in facilities and staffing.
Andrew Robertson has spent his career managing private hospitals, for the last five years as director of private care at Moorfields Eye Hospital. He is now keen to support the development of other PPUs. Contact him at andrew@
MARKETING YOUR PRACTICE
Making a video for your practice? Communications specialist David Johnson (left) unveils five tips for clinicians to ensure their creation engages the viewer
Turn yourself into a medical film star
IN TODAY’S digital age, wherever you look, people are lost in their smartphones, swiping through social media feeds, consuming content and seeking answers online.
This trend extends to healthcare, where an increasing number rely on the internet for advice.
In fact, around 7% of Google’s daily searches are health-related. That is approximately 70,000 searches every minute on various health topics, spanning from conditions and medications to symptoms and insurance queries.
But the high volume of medical queries is not experienced just by
Google. YouTube, the second largest search engine, also reports a surge in demand for health-related videos, with a staggering total of three billion views in the UK and 110 billion globally in 2022.
As patients are six times more likely to make an inquiry with a consultant who has video content
on their Doctify profile than those who do not, here are our top five tips for creating engaging healthcare videos.
1
Find your why
Start by defining your audience’s demographics and interests. Clarify your mission as a clinician
on YouTube: whom you want to reach and what value you can offer.
Establish your unique perspective and expertise to create engaging, hard-to-replicate videos tailored to your niche.
By differentiating yourself through specialised knowledge, you ensure that those seeking your insights can easily find and benefit from your content.
2
Experiment with different formats
Exploring various video formats can enhance engagement and attract diverse audiences on YouTube.
Especially in the early stages of your YouTube journey, consider embracing formats that online audiences are familiar with and find engaging.
Here are some ideas and examples:
☛ Day-in-the-life videos: Showcasing a typical day in your practice or specialty area can offer insights into your professional life.
☛ Reaction videos: React to trending health topics, medical breakthroughs or patient stories while providing expert insights.
☛ Medical news updates: Keep your audience informed with timely updates on medical research, health news or public health issues.
☛ Collaborations: Collaborate with other clinician creators, healthcare organisations or media outlets to bring diverse perspectives and expertise.
☛ Explainer videos: Simplify complex medical concepts, procedures or conditions to educate your audience effectively.
☛ Interviews: Conduct interviews with fellow experts or patients to share insights and experiences.
☛ Q&A sessions: Engage directly with your audience by answering common health questions or addressing specific concerns they may have.
☛ Myth-busting videos: Address common myths or misconceptions about health conditions, treatments or lifestyle choices with evidence-based information.
☛ Discuss expected recovery times: Explain factors that influ-
A good example of a thumbnail image: the ‘headline’ for your video, which should have clear graphics to stand out
ence recovery and offer practical tips for patients to support their recovery process.
☛ Animated content: Use animations to visually explain medical topics, making them easier to understand and engaging for viewers.
3 Embrace authenticity
Creating compelling video content does not require high production values such as an expensive camera, professional lighting, or advanced editing software.
Authenticity is key – it is your content’s ‘bedside manner’.
Recognise that some viewers seek your content due to personal health issues, so treat them as you would patients.
Do not worry too much about polish; showing your personality or sharing personal connections humanises your content. By acknowledging viewers’ concerns and showing empathy, you build rapport and trust.
Professionalism is important, but it is not about choosing one over the other – authenticity also resonates and fosters meaningful connections with your audience.
4 Keep viewers engaged
In today’s fast-paced world, capturing and maintaining viewers’ attention is crucial.
Short attention spans require strategies to keep viewers engaged effectively.
Here are some practical tips to achieve this:
Utilise props to enhance visual
interest and effectively illustrate key points.
Get straight to the point by skipping introductions that don’t provide new information.
Keep your video focused and ensure your content relates to your video’s title and thumbnail.
High-quality audio is vital; while video quality can be forgiven, viewers have little patience for poor audio.
Consider using chapters for longer videos. It will help viewers navigate longer content and find the information they are looking for.
Maintain eye contact by facing the camera, establishing a personal connection with your audience.
These tactics not only enhance engagement but also ensure that your content remains compelling and valuable to your audience.
5
Bonus tip: make your thumbnails stand out!
Thumbnails are the first impression your video makes and are crucial for attracting clicks.
Think of your thumbnail as your personal billboard – if it is not eyecatching, viewers may pass over your content, no matter how good your video is.
Here are my tips to create compelling thumbnails:
➲ Using contrasting colours, such as yellow text on a black background or black text on yellow, can grab attention.
➲ Utilise large, short text that is easy to read on small screens to ensure viewers quickly understand your video’s content.
➲ The inclusion of engaging images can significantly boost engagement and make your content more personal. Don’t be afraid to use your face.
➲ Ensure your thumbnail accurately reflects the content of your video to meet viewer expectations and avoid misleading clicks.
Did you know? Software company Canva offers free thumbnail templates, making it easy to create eye-catching thumbnails without design expertise.
Position yourself as the expert patients seek
Now that you’re equipped with all the best practices to create engaging healthcare videos, it is time to put your knowledge into action. While YouTube serves as the second-largest search engine, offering a direct pathway to patients seeking answers to their pressing health questions, do not limit yourself to this platform alone.
To expand your reach, you can repurpose the content you create for YouTube and adapt it for other social media platforms such as LinkedIn, Instagram, TikTok and even Doctify.
For example, on Instagram, TikTok and YouTube Shorts, you could create 30- to 60-second video clips featuring key insights, quick tips or snippets from your fulllength YouTube content, leveraging popular sounds and hashtags to increase visibility.
David Johnson is head of business development at doctify.com
Understand rules on chaperones
The GMC has updated its guidance on intimate examinations and the role of chaperones. Dr Sally Old (right) explains what you need to know
TRUST IS central to the relationship between you and your patients and never more so than when you need to carry out an intimate examination.
These situations leave many people feeling uncomfortable and vulnerable. It is your responsibility to ensure the patient understands why the examination is necessary, that it does not cause them unnecessary pain or discomfort and that they are treated with respect throughout.
If you get it wrong, you could undermine your patient’s confidence in you and the wider profession.
It could also lead to a GMC complaint, which is likely to be stressful and has the potential to cause long term damage to the reputation of your practice and your live-
lihood. In the worst-case scenario, you might even be accused of sexual assault.
Unsurprisingly, the MDU regularly receives calls for medico-legal advice on this subject from concerned practitioners.
Common queries include whether a relative can act as a chaperone, whether a chaperone is necessary for non-intimate examinations and whether the doctor can insist on the presence of a chaperone when a patient doesn’t want one.
These points are covered in the GMC’s new version of Intimate examinations and chaperones which emphasises the importance of patients feeling ‘as safe and as in control of the situation as possible’.
CloudRx take care of the dispensing, payment and delivery of medicines direct to your patients for more convenient access their medicines.
Prescribe within your chosen clinical system via our frictionless integration with Semble, WriteUpp, MidexPRO, eClinic, Pabau, Jelly Software, and ClinicYou.
Alternatively, simply register for free and prescribe directly at www.cloudrx.co.uk.
Repeat prescriptions and controlled drugs.
Prescriber fees can be charged if desired.
Easy access to medicines not normally stocked by most pharmacies at great prices.
“We were struggling to keep up with the admin side of the prescriptions, not to mention storage for medication to cope with a huge increase in prescriptions. CloudRx immediately took away the strain. Since our partnership we have grown by over 200% in size. We could not have done that without their support. It has allowed for seamless scalability...”
– Dr Louise Newson, Newson Health
Defining an intimate examination
These are generally considered to relate to the breast, genitalia and rectum, but the GMC says that they could include any examination ‘where it is necessary to touch, examine intimate parts of the patient’s body’ or ‘be close to the patient’.
Be aware that some patients have concerns about undressing or exposing parts of their body but are hesitant to speak. For example, patients who have suffered abuse or who are vulnerable for other reasons may need a chaperone in any situation where it is necessary to touch or be close to them.
The GMC also notes that an intimate examination can ‘take place in a variety of settings, including inperson and remote consultations, such as by video-link or other digital technology’ (paragraphs 3-6).
Before the examination
Clear and effective communication is essential when getting consent for an intimate examination, taking into account any barriers that might affect the patient’s understanding.
The GMC says before the examination you should explain:
Why a particular examination is necessary;
What it entails in a way the patient understands so they know what to expect, including possible pain or discomfort;
That they can ask for the examination to stop at any time;
The offer of a chaperone and what their role is.
In rare cases where you believe a patient lacks capacity, the GMC has guidance on decision-making and consent and treating patients aged 0-18 years.
Ensure patients’ privacy and dignity when they are undressing for an examination – and dressing afterwards – by using screens and gowns. Do not help the patient remove clothing unless they ask you to or you have checked if they want your help (paragraphs 7-12).
During the examination
When carrying out the examination, you need to:
➲ Explain what you are going to do before you do it;
➲ Explain if the examination will differ from what you have told the
patient beforehand and get their permission;
➲ Be alert to the patient showing signs of discomfort or distress;
➲ Stop the examination if the patient asks you to. Consent to a procedure can be withdrawn at any time and for a number of reasons, and you must respect and comply with this as soon as you become aware;
➲ Keep comments professional and avoid personal remarks (paragraph 13).
The MDU advises you to invite the patient to tell you if they feel uncomfortable, rather than assume that they will. If this happens, stop the examination to check whether the patient has questions, wants to stop the examination permanently or agrees for the examination to continue.
The purpose of a chaperone
A chaperone is there to be an ‘impartial observer’ during intimate examinations and patients should be offered this option ‘wherever possible’.
The guidance explains that chaperones need to be:
➤ Sensitive and respect the patient’s dignity and confidentiality;
➤ Alert to the patient showing signs of distress or discomfort;
➤ Aware of the most appropriate route to raise concerns and do so if they are concerned about the medical professional’s behaviour or actions;
➤ Trained for the role they are undertaking – they should usually be a health professional;
➤ Familiar with the procedure/ examination or briefed in advance and given chance to ask questions;
➤ Able to stay for the whole examination and to see what you are doing, as much as practical, without obstructing the examination or interfering with the patient’s dignity.
While a relative or friend would not meet these criteria, a patient can still ask for someone like this to be there to support them, alongside a chaperone (paragraphs 16-20).
Examinations without a chaperone
If no suitable chaperone is available, you can suggest delaying the appointment, provided this
BENEFITS OF A CHAPERONE
In the MDU’s experience, the presence of a chaperone can be beneficial in many ways during an intimate examination.
They can reassure the patient, help with communication and discourage unfounded allegations of inappropriate behaviour.
We recommend every practice has a chaperone policy to define what happens when a patient refuses a chaperone or prefers a samesex chaperone. This can help manage expectations and encourage patients to make their wishes known at an early stage.
It is important to familiarise yourself with the new GMC guidance and contact the MDU or your own medical defence organisation if you have specific concerns.
The MDU website has further advice on chaperones: www.themdu. com/guidance-and-advice/guides/guide-to-chaperones
If no suitable chaperone is available, you can suggest delaying the appointment, provided this wouldn’t adversely affect the patient’s health
wouldn’t adversely affect the patient’s health. Try to avoid putting pressure on the patient to proceed without a chaperone and reassure them they are not inconveniencing you.
If a patient wants to proceed with an intimate examination without a chaperone but you are unwilling, you should explain why you would prefer to have one present. If the patient remains adamant and you are uncomfortable, the GMC says you may consider referring them to another doctor if the patient’s health won’t be adversely affected.
All discussions about intimate examinations and chaperones should be documented in the patient’s record, including the identity and role of any chaperone who was present or if the offer was made and declined (paragraphs 21- 23).
Dr Sally Old is a medico-legal adviser at the Medical Defence Union (MDU)
What patients look for in a consultant
How do patients choose their consultants? Anne Coyne, consultant services manager at the Private Healthcare Information Network, has the
answer
AT the Private Healthcare Information Network (PHIN), we exist to help patients make more informed private healthcare decisions. Over the past few months, we have worked to better understand their healthcare journeys, information needs and priorities, expectations and experiences. Building on past efforts by PHIN and other industry stakeholders, we have conducted new research – which includes qualitative focus groups and a quantitative UKwide survey – engaging directly with patients who have used or would consider using private treatment. We published the highlights of this research in our new publication, Patient Perspectives, which is available on our website.
While not everything in the report is a surprise to those working in healthcare, the research provides evidence to back up feelings and experience. In this article, we take a closer look at the data relevant to consultants and share some more detailed information.
Key factors in choosing a consultant
Reinforcing the importance of consultants completing their fee information on PHIN’s website, ‘Cost and payment options’ came out as the top factor influencing patients’ choice of consultant in our quantitative research, with 47% of the 2,036 respondents choosing this option. However, this was very closely followed by the ‘Consultant’s qualifications’ and ‘Patient reviews/recommendations from
family and friends’, which were both selected by 46% of respondents. ‘Clinical outcomes’ were also an important factor at 44%.
The full breakdown of responses for all respondents is in the box below.
Now let’s take a look in more detail at the key factors and break the findings down into different groups. We think this information could help consultants to know the areas to focus on when targeting and talking with potential patients.
Cost and payment options
These were important factors in our focus groups: ‘Very first thing I looked at was cost. It was just like either this is totally prohibitive or this is possible, because I’ve no idea how much it would cost.’ (Woman from London who received cosmetic surgery).
‘The most important part would be prices, so are they transparent about the prices? So I know I’m prepared for the cost and that there are no hidden fees.’ (Middleaged private patient from the West Midlands).
In our quantitative survey, ‘Cost and payment options’ were slightly more important to female respondents (48%) than male ones (46%), but there was not a significant difference.
There was more variety in age groups, with 35 to 44 year olds most likely to consider it important (53%) and those over 55 least likely to consider it important (41%).
When looking at percentages by working status, retired respond
ents were most likely to consider it important (40%), and those who were unemployed are least likely to consider it important (60%).
Respondents who had never married were much more likely to select ‘Cost and payment options’ (54%) than those who are widowed (29%).
There was very little difference in terms of demographic classification. Fortyseven per cent of those in the ABC1 category (higher and intermediate managerial, administrative and professional occupations and supervisory, clerical, and junior managerial, administrative and professional occupations) selected this factor and a similar 48% among those in the C2DE category (skilled manual workers, semiskilled and unskilled manual workers, state pensioners, casual and lowest grade workers, unemployed with state benefits only).
Cost and payment options were most likely to be selected as important by patients in the East Midlands (55%) and least likely in Wales (38%).
Consultant’s qualifications
The ‘consultant’s qualifications’ category can also include providing information on the volume of procedures performed by consultants, research behaviour and interest in certain procedures/ conditions, and scientific research as well as medical qualifications.
These qualification were significantly more important to female respondents surveyed (50%) than male ones (41%) when choosing their consultant.
They also became increasingly
important depending on the respondent’s age, starting at 40% for 18 to 24yearolds and rising to 48% for ages 4554, 47% for 5564, 48% for 6574 and 52% for those aged 75+.
They were also significantly more important for those in the ABC1 category (48%) than the C2DE category (43%).
Qualifications were more likely to be seen as important in southwest England (53%) and least likely in Wales (31%).
Those who were not working valued ‘The consultant’s qualifications’ the most (52%), with fulltime students much less likely to select it as important (36%). It is quite possible that someone out of work may need surgery and a good outcome in order to return to work.
Patient reviews and recommendations from family and friends
Reviews and recommendations are the joint second most important factor influencing the choice of consultant.
Patients value feedback from other people like them who have experience with a consultant. This is why we publish patient satisfaction feedback on the PHIN website.
The ability to get a ‘feel’ for the manner of the consultant came out as a major reason for wanting word of mouth/reviews in the focus groups too.
The breakdown of the quantitative figures provides more insight into who values reviews and recommendations the most.
Female respondents (51%) val
FACTORS FOR CHOOSING A CONSULTANT ALL
ued this factor significantly more highly than males (40%).
Reviews and recommendations were selected as important by a higher proportion of 45 to 54year olds and 65 to 74 year olds (49%) than 35 to 44 year olds (41%) or the 75+ group (39%).
Those in the higher socio economic category placed more value (48%) on reviews and recommendations than those on the lower category (44%).
They had the highest selection among respondents from East Midlands (54%) and the lowest were those from Wales (30%).
One focus group attendee told us: ‘Independent reviews of everything you go through from previous patients is crucial as far as I’m concerned.’ ( Middle-aged NHS chemotherapy patient).
How PHIN can help
Consultants have a legal duty to submit their fee information to PHIN, but the research shows that beyond that obligation, making information about fees available is a key factor in patient choice. Patients want to know about the experience a consultant has had in performing a particular procedure. This is why we ask consultants to review their data so that we can share this information on our website and patients have an accurate view of a consultant’s activity. In addition, consultants can add profile details which cover many of the other factors patients use to select their consultant, and hospitals supply patient feedback information.
Providing a more complete profile and pointing patients in the direction of PHIN’s website is an opportunity for consultants to appeal to a range of patient choice factors that could benefit their business.
You can read our Patient Perspectives report by downloading it from https://www.phin.org.uk/ news/patientprioritiesreport. All figures, unless otherwise stated, are from YouGov Plc. Total sample size was 2,036 adults. Fieldwork was undertaken between 30 April-7 May 2024. The survey was carried out online. The figures have been weighted and are representative of all UK adults (aged 18+).
Base:
See ‘What the public think of private healthcare’, page 34
Public is changing its view of private care
‘Going private’ for healthcare is becoming the new normal. David Hare (right) shows why and outlines what the Independent Healthcare Providers Network is doing to improve the public’s understanding of the sector
INDEPENDENT PRACTITIONER
Today readers will know that much is written about private healthcare in this country. But, more often than not, it is done so in a sensationalised manner.
Articles look at whether it is leading to a ‘two tier’ healthcare system, whether the sector is ‘stealing doctors’ or ‘undermining the NHS’ in pursuit of an American-style system of care.
But given that we have a £10bn+ industry which serves millions of people every year, surprisingly little is actually known about what private patients, and indeed the public, think of private healthcare.
The Independent Healthcare Providers Network (IHPN) has therefore decided to commission annual research into attitudes around private healthcare:
What people think about it;
What services do they use;
What do they understand about it.
This is not only to help us understand more about the market trends and why more people are choosing private healthcare, but also to help the sector to continue to improve the service it offers to patients and consumers, particularly in terms of helping people understand and navigate the system.
This autumn we were therefore delighted to launch Going Private 2024 – the second in our series –which contained some interesting results.
The new normal What came across most in the results is that paying for healthcare is very much becoming ‘the new normal’, with a majority of the public – almost seven in ten –saying they would consider using private healthcare.
Looking at people’s more immediate needs, over one-third of the public (34%) said they would pay for treatment in the next 12 months if they needed it, which rises to almost half (44%) of 25- to 34-year-olds who expect to use private healthcare in the coming year.
This openness to using private healthcare among young people is a theme that was apparent in our 2023 report and shows no sign of waning.
What came across most in the results is that paying for healthcare is very much becoming ‘the new normal’, with a majority of the public saying they would consider using private healthcare
think that the care available privately is higher quality.
Interestingly, one-in-five people said that they used private healthcare because they have private health insurance, either paid for by themselves or through their work. And this was backed up by the significant rise in the proportion of people using private medical insurance (PMI).
Of those that have used private healthcare, six in ten (58%) said they paid through private medical insurance, compared with under half (49%) in 2023.
Regardless of whether they used insurance or self-pay, the vast majority (88%) of people who have used private healthcare considered it worth the expense
Our results found that younger people between 18 and 34 years of age are generally more positive about the private health sector; more willing to consider using it; more likely to have used the sector; and more likely to have accessed private GP services.
Indeed, while overall, 27% of those who have used private healthcare said they had used it for an appointment with a private GP, this rate increased even more dramatically in the younger age groups.
In 2024, more than half (54%) of all 18- to 24-year-olds who had used private healthcare had accessed GP appointments privately, with the rate of usage dropping off as the age of respondents goes up – with 10% of those aged 65 or more having used private GPs.
Desire for convenience
There is likely to be many reasons for this, but young people’s general desire for convenience undoubtedly extends to health services, so it’s not surprising that quick and flexible access to private GP services – both virtually and in person – and which have a relatively low price point are seen as key drivers.
Looking more broadly at why people use private healthcare, the most common single reason remains the difficulty with accessing NHS care – nearly half of people (45%) cited this as a factor in their decision to use private healthcare.
Others choose private healthcare because they think that the quality of care may be higher. Almost one in five (19%) say that they can get more personalised care in the private healthcare system, with 18% saying that they
Perhaps not surprisingly, 55% of respondents indicated that they would be somewhat or much more likely to apply for a job if it came with private health cover.
Affordability factor
Affordability is, of course, a key issue when it comes to using private healthcare, and although most people (67%) would consider paying for treatment, we asked people who said they would not consider using private healthcare to tell us why (17% of the public gave this answer).
By far the most common reason is affordability. Sixty-four per cent of people said that they ‘could never afford it’, rising to above 71% among DE social grades and those on the lowest incomes.
But delving into this issue more closely, we found that the availability of payment plans – allowing self-pay patients to spread the cost of treatment – would also make people more likely to consider accessing private healthcare if they had previously assumed they could not afford it.
Some 42% of respondents said they would be more likely to consider using private healthcare if they could spread the cost of treatments.
Of course, this will come as no surprise to readers of Independent Practitioner Today and those working in the sector, but, overall, people are very positive about the private healthcare sector.
Regardless of whether they used insurance or self-pay, the vast majority (88%) of people who have used private healthcare considered it worth the expense. Sixin-ten people (59%) feel very or quite positive about private healthcare – up from 51% last year
– with only 8% having a negative attitude.
This positive sentiment increases significantly among people who have used private healthcare, with 78% of people who have used private healthcare feeling positive about the sector.
Looking ahead, while there is much to be positive about, the research does show there is huge scope to better inform the public about private healthcare.
Educating the public
More than four-in-ten people (42%) said they are not very familiar or not familiar at all with the range of treatments and services available, with likewise 43% saying they are not very familiar or not familiar at all with how to access private healthcare.
Again, half of people (49%) are not familiar with how to pay for private healthcare, such as through insurance or self-pay.
And even of those people who would be open to using private healthcare but have not used it in the past only around half (48%) said they would know where to go for more information.
Educating the public on how private healthcare works is something IHPN will be looking to work on in the coming months and years – helping to further normalise private healthcare so growing numbers can benefit from the high-quality, accessible care the sector provides.
We hope you find these insights helpful. The full results can be found at www.ihpn.org.uk/goingprivate-2024-introduction.
David Hare is the chief executive of the Independent Healthcare Providers Network
How private sector is boosting safety
Patient Safety Specialists
are on the march. David Hare explains what you need to know
PATIENT SAFETY is undoubtedly everyone’s business.
We know from a range of metrics – whether it is the Care Quality Commission’s (CQC’s) scores or national audits – that independent providers and practitioners take the issue of safety and quality very seriously and perform well when compared with the wider healthcare system.
But with so many initiatives currently in place to foster a safe culture – from Duty of Candour to Freedom to Speak up Guardians, as well as the new Patient Safety Incident Framework (PSIRF) and the change in reporting safety events to Learning from Patient Safety Events (LFPSE) – taking a more co-ordinated approach to safety and quality is essential.
As part of the National Patient Safety Strategy, which calls for a ‘whole systems’ approach to safety and quality where all parts of the healthcare ecosystem play their part, the NHS therefore introduced the requirement to establish Patient Safety Specialists (PSSs) in all providers delivering NHS-funded care, which will include most independent sector providers.
At its heart, the role is designed to be a focal point for patient
safety activities and ‘provide dynamic senior patient safety leadership’. This includes helping to drive a culture of safety, learning from incidents and ensuring consistent improvements in care.
Share ideas
With the role still relatively new, this autumn the Independent Healthcare Providers Network (IHPN) was pleased to hold our first ever event to support patient safety specialists working in the sector.
It provided a great opportunity to hear from experts from academia and NHS England, patient safety partners, and for PSSs to network and share ideas on how to gain maximum benefit from the role.
The theme of the day was to ‘innovate, collaborate and elevate patient safety specialist leadership’. This was reflected in the agenda where we brought together a diverse range of speakers from both the NHS and independent sector to talk about PSSs.
We also looked at wider patient safety initiatives, including medical examiners and the implementation of PSIRF and LFPSE.
Looking at the practicalities of the role first, PSSs have a wide remit. It covers everything from embedding PSIRF, transitioning to LFPSE and supporting uptake of the patient safety syllabus.
And it has to lead on involving patients in the patient safety framework, ensuring a robust system for responding to National
Patient Safety Alerts; as well as supporting relevant national patient safety improvement programmes – including Martha’s rule.
Key role
Given the importance of fostering a culture of safety and improvement, PSSs should have direct access to an organisation’s board, and will play a key role in interacting with the various legal frameworks, regulatory bodies like the CQC and external agencies such as the Health and Safety Executive. This to-do list, which will be on top of the specialists’ day job, may well sound intimidating and so was great to hear from The Healthcare Improvement Studies (THIS) Institute at the event, who have been conducting an evaluation
into the PSS role in both the NHS and independent sector.
Overall, it found that while there is real enthusiasm for the role, PSSs were undoubtedly concerned about the feasibility of delivering it and the managing the competing priorities of having both an operational and strategic role in a healthcare provider.
We were therefore delighted to be joined by Bill Savage, who is a patient safety partner (PSP) – one of the eight priorities of a PSS – and Julie Watkinson from Nuffield Health, who were able to talk about their journey in developing the patient safety partner and what they learnt on the way.
Engaging with patients
While the ‘innate ability to understand complex information and not be terrified’ is definitely top of the list for the partner role, as well as ‘embracing acceptance of the corporate independence’ that comes with being a PSP, what really came across from their presentations was the importance of engaging with patients and their families throughout the process.
In particular, calling out the ‘roulette of acronyms’ often used in healthcare was highlighted, with a timely reminder that many of our patients and families do not speak in our ‘code’.
The importance of culture in delivering safe care was a key theme throughout the day and was really brought to life by the NHS’s head of patient safety policy, Hester Wain, who provided invaluable insights into what we mean by safety culture and how we can continue to turn the dial.
For all the patient safety initiatives that currently exist in our health system, developing a culture of safety is not just about documents or procedures – as important as they are.
It is about creating an environment where everyone from staff, patients, and families can thrive to ensure safe, high-quality care.
Hester identified the three key elements you need to achieve this:
‘fluffy’ to those working in the sector who are highly skilled, highly trained technical clinicians, a safe and open culture can really make a substantive difference in reducing patient harm.
Study after study shows that a poor safety culture can lead to higher re-admission rates, increased patient safety incidents and complication rates.
Safe cultures
Fostering positive safe cultures is not easy, but ultimately it is about both practitioners and organisations challenging their own actions and really putting patients at the centre. Or as Hester sagely put it: ‘Anyone can do an investigation, but does it make a difference?’
Bringing the conversation back to the here and now, we were also pleased to be joined by a number of experts who were on hand to talk about some of the specific priorities for PSSs.
Dr Suzy Lishman, an independent mortality adviser for Spire Healthcare and a NHS medical examiner, spoke about the new
National Medical Examiner system and death certification reforms.
Wendy Halliburton, a patient safety specialist at North Tees & Hartlepool NHS Foundation Trust, discussed her involvement in implementing the new Patient Safety Incident Response Framework (PSIRF) and Mandy Williams set out her experiences in improving the quality of patient safety incident reporting and supporting transition to the Learning from Patient Safety events (LFPSE) as a patient safety reporting lead and user researcher.
These sessions provided much food for thought for attendees with some fantastic discussion and Q&As afterwards.
With over 25 Patient Safety Specialists currently working in IHPN members alone, we were delighted to play our part in supporting the development of this important new role and work they do. We hope to build on this event and host further events in the coming years.
David Hare is chief executive of the IHPN
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes of free legal advice.
Advice is available on: Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment
Premises
Regulatory requirements and investigations
A recent Employment Appeal Tribunal (EAT) case dealt with the problems caused by an employee who resigned verbally, but retracted his words later. Employment law specialist Markus Schober outlines the key take-aways for independent practitioners to ensure your staff are treated fairly and professionally in the event of a disagreement
Perils of resigning the heat of the moment
in moment
A notice of resignation or dismissal, once given, cannot be unilaterally retracted. The giver of the notice cannot change their mind unless the other party agrees
A RECENT EMPLOYMENT
Appeal Tribunal (EAT) case serves as a reminder for doctors who employ staff to handle verbal resignations with caution.
It highlights the importance of not accepting verbal resignations immediately, especially when they occur in the heat of the moment.
What happened
The claimant in the case of Omar v Epping Forest District Citizens Advice resigned verbally in the heat of the moment following an altercation with his manager. On the two previous occasions when the claimant had resigned, he had been talked back into his job.
This time, the claimant wished to retract his resignation and continue in his role – but the claimant’s manager no longer wanted to work with him and decided his resignation would stand.
The claimant brought claims for unfair dismissal and wrongful dismissal on the basis that he had not officially resigned. He argued that the situation fell within the ‘special circumstances exception’.
The Employment Tribunal concluded that the claimant had brought his employment to an end with his verbal resignation and dismissed the claims. The claimant appealed to the EAT.
It held that the question of whether an employee has resigned is to be determined objectively from the perspective of the reasonable bystander viewing the matter from the employer’s perspective.
The EAT concluded that the tribunal had not considered the factual question of whether the resignation was intended, and the appeal was therefore successful and it remitted the case to a fresh employment tribunal for a full rehearing.
There is likely to be a fine line
TAKE-AWAY POINTS FOR INDEPENDENT HEALTHCARE PROVIDERS TO CONSIDER
➤ This case sets out helpful guidance on resignation and dismissals, as the EAT conducted a full review of the key principles to consider when there are heat-of-the-moment resignations.
➤ There is no such thing as the ‘special circumstances exception’. The same rules apply in all cases where notice of dismissal or resignation is given in the employment context.
➤ A notice of resignation or dismissal, once given, cannot be unilaterally retracted. The giver of the notice cannot change their mind unless the other party agrees.
➤ Words of dismissal or resignation, or words that potentially constitute words of dismissal or resignation, must be construed objectively in all the circumstances of the case.
➤ The circumstances that may be considered include ‘absolutely anything’ that was ‘reasonably available’ to the parties ‘that would have affected the way in which the language used would have been understood by a reasonable bystander’.
➤ The perspective from which the words used are to be judged is that of the reasonable bystander in the position of the recipient of the words used.
Where the employee resigns, the relevant perspective is that of the employer who hears the words of resignation; where the employer dismisses, the relevant perspective is that of the employee.
➤ What must be apparent to the reasonable bystander in that position, objectively, is that the dismissal or resignation was ‘seriously meant’ or ‘really intended’ or ‘conscious and rational’.
This means that the speaker of the words genuinely intended to resign – or dismiss – and was ‘in their right mind’ when doing so. It does not mean that it needs to be a rationally thought through or sensible decision.
between cases where resignation was not ‘really intended’ and cases where there had been a change of mind. The EAT acknowledged that this would be a question of fact for the tribunal to consider in each case.
‘Really intended’
In most cases where words are used that objectively constitute words of dismissal or resignation, there will be no doubt that they were ‘really intended’ and the analysis will stop there.
An Employment Tribunal will not err if it only considers the objective meaning of the words and does not go on to consider whether they were ‘really intended’, unless one of the parties has expressly raised a case to that effect to the tribunal or the circumstances of the case are such that fairness requires the tribunal to raise the issue of its own motion.
Evidence as to what happened afterwards is admissible insofar as it is relevant and casts light, objectively, on whether the resignation/dismissal was ‘really intended’ at the time.
Finally, the same rules apply to written notices of resignation or dismissal as to oral ones, except that a notice given in writing will usually indicate a degree of thought and care that will make it less likely that there are circumstances which, objectively, would lead the reasonable bystander to conclude that the notice was not ‘really intended’.
Markus Schober is an associate solicitor at specialist healthcare law firm Hempsons. For more information, please email M.Schober@ hempsons.co.uk
BILLING AND COLLECTION
invoices Avoid unpaid
Unpaid invoices can disrupt cash flow, burden administrative staff, and strain patient relationships for independent healthcare practices.
Here are some ways unpaid invoices negatively impact practices:
➤ Disrupted cash flow: Unpaid invoices make it harder to cover essential expenses, such as payroll, equipment and day-to-day operational costs.
Expert companies use structured, patient-friendly follow-up procedures to ensure outstanding balances are collected without damaging patient relationships
Derek Kelly (below) shows how to boost the practice’s financial health
INDEPENDENT PRACTITIONERS
face a constant balancing act between providing excellent patient care and managing the financial health of their practice. And one of the most significant challenges is handling unpaid invoices.
Delayed payments can have a serious impact on cash flow, causing stress, operational disruption and administrative overload.
So it is essential to address unpaid invoices quickly and efficiently to keep your practice financially stable.
Many private practices find that outsourcing their billing and invoicing processes to a professional medical billing company is the key to staying on top of their cash flow.
By introducing streamlined invoicing procedures, proactive follow-ups and live reporting systems, medical billing companies can significantly improve collection rates and provide greater financial transparency.
The hidden cost of unpaid invoices
Unpaid invoices create more than just cash flow issues. They add administrative strain, divert resources and risk damaging patient relationships if handled poorly.
➤ Increased administrative burden: Chasing late payments is time-consuming. Practice staff often do not have the necessary resources or expertise to follow up on unpaid invoices effectively. This can divert focus from patient care and create inefficiencies.
➤ Strained patient relationships: Handling overdue payments can be sensitive and aggressive follow-ups or unclear communication can alienate patients.
Striking a balance between financial diligence and maintaining positive patient relations is difficult but necessary.
Invoice management is critical to financial health. Invoices issued promptly, monitored and followed up with consistency can dramatically improve cash flow.
But many practices find themselves bogged down by manual processes, resulting in missed or delayed follow-ups, incomplete records and inefficiencies that affect overall collections.
Outsourcing advantages
Outsourcing invoicing and billing processes to a professional company like Medserv provides several important advantages.
They not only handle every aspect of the invoicing process but also offer live reporting, giving practitioners real-time visibility into the status of every invoice.
➲ Comprehensive billing services
They manage the entire invoice life cycle; from the moment a patient receives care to the point the invoice is settled. This includes issuing invoices, tracking payments and following up on any unpaid amounts.
With a dedicated team handling the process, your practice can focus on what truly matters: delivering quality care.
➲
Proactive pursuit of unpaid invoices
One of the biggest challenges in managing unpaid invoices is
ensuring timely and consistent follow-up.
Expert companies use structured, patient-friendly follow-up procedures to ensure outstanding balances are collected without damaging patient relationships. This reduces the time invoices remain unpaid and helps practices recover funds faster.
➲ Advanced technology with live reporting
Perhaps one of the most valuable tools is live reporting systems. They give practices real-time updates on the status of every invoice, providing transparency and control over your financials. You will always know which invoices have been paid, what is still pending or overdue and the exact stage of the follow-up process for unpaid invoices.
Transparency allows for quicker decision-making, better cash flow planning and fewer financial surprises.
With a live reporting dashboard, you can track your practice’s financial health in real time and stay informed without having to chase down status updates.
Live reporting ensures invoices are paid more promptly and, in turn, improves cash flow stability, ensuring you can cover operational costs without disruption and doctors find it gives them the data they need to act with confidence.
More healthcare providers are choosing this option. Every practice is different and outsourcing companies can offer customised solutions catering for a practice’s specific needs.
Unpaid invoices are a common problem for many independent practices, but they do not have to be a drain on your resources.
Derek Kelly is marketing manager at Medserv
Ditch the emotion when you invest
Investing can be simple in concept but not easy to do well. Samuel Kirton (below) reveals why you need a diligent investment process and a good adviser
IT IS a simple statement that the decision to invest in the first place provides an opportunity to protect hard-earned savings from inflation and perhaps grow further. But it is not easy to have the foresight, as well as the discipline, to deny oneself spending today for the opportunity of a better tomorrow. And it is also not simple to work out how much one might want, need and be able to invest in stock markets to help fund future spending goals. Getting this right is key and where good financial advisers can add value.
Stock markets, of course, act as a core driver of returns in an investor’s portfolio and bonds act as a protection from economic turmoil and help to smooth returns. But it’s hard to know what evidence to look for to gain an understanding about what types of long-term investments typically improve a portfolio’s structure. This comes with the need to build an understanding of the risks one wants to be exposed to.
Insurance policy
It is also not straightforward to decide which bonds are deemed to be defensive ‘enough’ to be considered an insurance policy against the uncertainty inherent in stock markets.
Finally, it is a simple concept that a low-cost fund structured to capture the target strategy gives investors a better chance of achieving their investing goals relative to a high-cost one. It is a big challenge to regularly screen for which funds might be best positioned to capture the returns of each part of the market, and to understand the trade-off
between the management costs of a fund and the opportunity cost –what could have been – of omitting an investment.
And it is harder still to implement a thorough and regular investment oversight process, which is required to maintain confidence in the approach.
We also need to consider one of the great challenges all investors face: that there is no easy or quick way to investment success.
Hold on
Aesop’s fable of the tortoise and the hare is a useful metaphor. You must use the time on your side –which could be over multiple decades – to capture the returns of the markets effectively, but slowly.
Market returns can be disappointing in the short-term. The longer you can hold for, the more likely the returns you receive will be at worst survivable, and hopefully far more palatable.
Time allows small returns to compound into large differences in outcome for the patient investor. The reality is that markets go up and down with regular monotony.
One of the best-known investors, Warren Buffett, called the stock market a device for transferring money from the impatient to the patient.
Be patient if you want to be a good investor. On your investing journey, you will spend a lot of time going backwards, recovering from the set-back and then surging forwards again, often in short, sharp bursts of upward market movement.
You just need to stick with it. Remember, you have to be in the markets to capture their returns. Impatient investors tend to lose faith in their investments too quickly, with painful consequences.
There are no certainties in investing, but investors can give themselves the best chance of achieving their expectations by allowing the passage of time to let short-term uncertainty be overwhelmed by long-term expected outcomes.
Investing using a well thoughtout, evidence-based and systematic investment process helps to reduce the emotional pressures involved and delivers investors
with the highest probability of a successful investment outcome.
It does not guarantee the outcome will always be favourable; it can’t, given the uncertainty of the markets. What it does do is to help us make strong, rational decisions and to avoid the silly mistakes that prove to be so costly, so often.
Avoid latest fads
In particular, make sure you avoid chasing markets and managers in search of market-beating returns and being sucked into the latest investment fad by recent trends, plausible marketing stories and press coverage. Bad process, or a lack of process, has an upside outcome that is down to luck rather than judgment.
We can reflect on these wise words written by Charles D. Ellis in his excellent book Winning the Loser’s Game (Ellis, 2002):
‘The hardest work in investing is not intellectual, it’s emotional. Being rational in an emotional environment is not easy. The hardest work is not figuring out the optimal investment policy; it’s sustaining a long-term focus at
EXPERT TAX AND ACCOUNTANCY ADVICE YOU CAN TRUST
Sandison Easson is a firm of truly specialist medical accountants who provide personal and tailored advice to clients.
We act for medical professionals throughout all stages of their career with clients in almost every town in England, Scotland and Wales.
We cut through the complicated jargon and deliver practical, easy to understand advice. Call us today to organise your FREE no obligation consultation.
•
market highs or market lows and staying committed to a sound investment policy.
‘Holding on to sound investment policy at market highs and market lows in notoriously hard and important work, particularly when Mr Market always tries to trick you into making changes.’
Simple but not easy. A systematic process and a guiding hand from your adviser are the keys to success.
Samuel Kirton is a financial planner with Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
WE PROVIDE THE USUAL SERVICES YOU WOULD EXPECT FROM AN ACCOUNTANT SUCH AS PREPARATION OF YOUR ACCOUNTS AND TAX DECLARATIONS BUT OFFER SO MUCH MORE INCLUDING ADVICE ON:
• SETTING UP A NEW PRIVATE PRACTICE
• BUILDING AN EXISTING PRIVATE PRACTICE
• BUSINESS STRUCTURES TO PROTECT WEALTH
• BUSINESS STRUCTURES TO MAXIMISE TAX EFFICIENCY
• CLAIMING TAX REFUNDS INCLUDING OVERPAID ANNUAL ALLOWANCE TAX
• REMUNERATION PLANNING FOR YOU AND YOUR
Should this cardiologist self-refer to the GMC following an inquest? Dr Kathryn Leask (right) gives her advice
Dilemma 1
Do I need to inform the GMC?
QI am a private cardiology consultant who has recently attended a coroner’s inquest regarding the death of a patient I was treating.
He was undergoing investigations at the time of his death, and I was asked to write a report and attend the inquest hearing.
The patient’s family had raised concerns about the care I provided after the patient was admitted as an emergency to their local district general hospital, where he sadly died following a cardiac arrest.
During the coroner’s summing up and conclusion at the hearing, he was critical of some of the aspects of the care I’d provided.
The coroner provided a narrative conclusion which specifically mentions the care I provided and the coroner’s concerns.
One of my colleagues has told me that under these circum -
Inform GMC about coronor’s censure
stances I need to inform the GMC about this.
Is that correct and, if I do, what is likely to happen?
AIt is understandably stressful attending a coroner’s inquest and having to answer questions put to you by the coroner and the family or their legal representative.
Usually, when a doctor is likely to be criticised, they will be given ‘interested person’ status by the coroner, which allows them to have access to all of the documents the coroner will be relying on and to have their own legal representation.
We would always encourage doctors to contact their medical defence organisation for advice and support if they are involved in an inquest, whether or not they are likely to be criticised.
Your colleague is correct in that
the GMC states that you must tell them without delay if, anywhere in the world, you have been criticised by an official inquiry. A coroner’s inquest would fall under that definition (GMC Good medical practice, paragraph 99d).
Additional information
You should, therefore, contact your defence organisation for advice. They can assist you in informing the GMC that you have attended an inquest at which you have been criticised by the coroner. If you have a copy of the coroner’s conclusion, you could include this.
Your defence organisation can also advise you on whether it would be helpful to include additional information with your selfreferral. If you have already changed your practice in response to the coroner’s criticisms, then it may be helpful to reassure
the GMC about this at the outset. Sometimes it may also be helpful to share your reflections and learning arising from the case with the GMC. If the coroner or family instructed an expert for the inquest and a report is available, you could consider any concerns raised in that.
It may also be helpful to discuss the clinical care with a trusted colleague and engage in relevant continuing professional development.
The GMC will value evidence that you have taken the concerns seriously and proactively taken the opportunity to learn from this incident.
Even though you need to inform the GMC of this case, it may be possible to reassure it that they do not need to investigate the matter further.
Kathryn Leask is a medico-legal adviser at the Medical Defence Union
A parent requests access to their child’s clinical records – Dr Kathryn Leask gives her opinion on what to do
Dilemma 2
Do I have to give the data to dad?
QI am a private GP. I have been consulting with a 13-year-old girl who has been accompanied to appointments by her mother.
As well as some physical health complaints, we have also discussed the child’s mental health and the stress she is under due to her parents’ separation. She is currently living with her mother but sees her father, reluctantly, at weekends. Her parents are still married and her father’s name is on her birth certificate.
The father is aware that his daughter has been seen by me and has contacted me directly asking for a copy of her recent clinical records. He has mentioned that fact that he has parental responsibility and, therefore, has a right to her records, as she is under 16 years of age.
Am I legally obliged to provide him with the information he has requested?
AMothers and married fathers automatically have parental responsibility, as do unmarried fathers who are registered on the child’s birth certificate.
Parents do not lose parental responsibility if they divorce. From the information you have provided, therefore, this father does have parental responsibility for his daughter.
Even where parental responsibility has been established, this does not automatically mean that parents can make decisions on behalf of the child or young person.
Father wants his daughter’s notes
Where a young person is competent to make their own decisions, they should be consulted about a request for the disclosure of personal information about them
Where a young person is competent to make their own decisions, they should be consulted about a request for the disclosure of personal information about them.
You should explain to the father that you will need to speak to his daughter about his request. As such, it would be helpful to know why he has requested the information.
If, after speaking to her, you decide that she is able to understand the nature of the request and what information will be disclosed to her father and objects to this, you should respect her wishes.
Even where a young person does not have the capacity to make such a decision themselves, it is important to consider what is in their best interests rather than simply disclose information.
This might involve a discussion with the patient’s mother to establish whether she has any concerns about the information being disclosed to the father.
The GMC provides specific guidance for doctors in relation to patients aged 0-18 and notes that capacity to consent to a decision depends more on a young person’s ability to understand rather than on their age and, therefore, the fact that she is under 16 is not relevant.
If you need further advice, your medical defence organisation will be able to help you.
A PRIVATE PRACTICE: ACCOUNTING SYSTEMS
Don’t view accounts as just a big burden
Businesses are required to keep accounting records that include the financial information and calculations needed to prepare their accounts and tax return submissions.
But robust systems can offer much more than that and can help you to run a
successful business.
Systems will vary between businesses and as your private practice grows, you may need to evolve the function as you go along, advises Richard Norbury
SOFTWARE
When discussing accounting systems, often our minds will automatically think of accounting software, which is a good place to begin.
For those starting out in private practice, it may be sufficient to operate spreadsheets, which can be really useful and a powerful tool.
Often these are maintained by the consultant themselves or a family member and the level of transactions are relatively low. As such, you have a high level of control.
For established businesses or as private practice grows, it may be the case that a software package is more suitable. Consultants will often utilise clinical management software packages which have accounting functions built in.
As you would expect, these packages tend not to have the same functionality of a full accounting system, but this may not always be necessary. Some clinical management software will allow links to full accounting systems which may be more suited to larger, more complex businesses.
The important thing is that the system can accurately record financial information in an efficient manner that not only fulfils the requirements demanded by HM Revenue and Customers (HMRC) but also allows you to make important business decisions to ensure you run your business as efficiently as possible.
INVOICING
It is vital that fees are raised in a timely manner and you are able to track payment of invoices and identify slow payers so your team
can chase payment if necessary. Fees raised should be in a chronological order and have sequential invoice numbers.
Modern software will allow for invoices to be generated directly from the program and it is important that you have systems in place to ensure a fee note is raised for all work done.
It is surprising how many times we come across a client saying they – or their secretary – did not bill something and they ultimately miss out. If this aspect of your business is not working effectively, you could end up working for free or even at a loss when taking into account costs.
It is common for medico-legal work to be paid months or sometimes years in arrears of actually performing the work, so it is important that a robust system is in place to ensure you are able to track these invoices.
For those of you who operate via a limited company, you will need to declare income based on when the work is undertaken. As the invoice is often raised a few days after the surgery or clinic, you should record the date of the work to allow your accountant to do a review at the year end.
FEES OWING AND BAD DEBTS
Regardless of which method you choose to record your income, reports should be available to allow you to check how much the business is owed at a point in time. These reports will usually show each patient or client and have a further summary allowing you to see how long these fees have remained outstanding.
It is good practice to review them regularly to ensure timely payment and so the team can identify slow payers and bad debts.
Payment of invoices in private practice can sometimes be complicated and may well be received from more than one source, meaning some fees will be ‘part paid’, which makes it more important that accurate record-keeping is in place.
Bad debts should be kept to a minimum, but if they do exist, then be sure to identify them to your accountant. Review the ‘older than six months’ column on your reports.
If identified, you will be able to claim tax relief on specific bad debts. HMRC does expect evidence of the debt being chased to allow you to claim relief, so keep notes and correspondence to support these claims.
This is even more important if you are VAT-registered because you may be able to claim back VAT previously paid over to HMRC. Of course, some of the older debts may not be bad debts at all and simply need following up for payment.
The fees owed or ‘aged debtors’ report is also used by your accountant to reconcile the overall income received in your bank account and, when used properly, can help identify errors or problems early on so they can be rectified quickly.
It is not uncommon to encounter payments in advance in private practice. These payments often show as negative amounts on your aged debtors report, as you have received the cash but not yet raised an invoice.
Identifying these payments or having a separate system in place for recording such transactions may well be useful so that they are deferred into the correct tax yearend so you do not inadvertently pay tax earlier than needed.
VAT
If you are a VAT-registered business, such as a medico-legal practice, your systems will need to be able to cope with analysing the different aspects of VAT on income and expenditure and produce the relevant reports that you can rely upon to submit returns to HMRC. There are various different VAT schemes available and you should consult with an accountant to choose the best options for your business.
Often, due to the amount of time it takes for a case to be settled and thus the amount of time it takes for you to be paid, you will pay VAT only when you receive payment of an invoice. This is known as ‘cash accounting’. In these cases, it is important that the system can accurately record the dates and amounts received.
If you are reporting VAT under the traditional method, then you may be able to claim some VAT back from amounts suffered on your expenses.
This makes recording such expenses even more important, as not only are you claiming the tax relief on the expense, you are able to claim back VAT. Ensure you include all expenses including any expense that you may not have paid directly from the limited company bank account.
OUTSOURCING
Many consultants now outsource their finance function, which can prove efficient and save time.
If you decide to go down this route, bear in mind that these companies will use particular software across all of their clients, so you should ensure that the reports and function is compatible to your needs.
You should still review older debts, as the people processing the data will not have your intimate knowledge of the cases.
SECURITY
The security of your financial affairs is obviously very important. Software and systems are now more sophisticated and will allow different functions such as remote access and multiple users, so you should ensure that your passwords are secure and changed
Accounting systems are often seen as a necessary evil to allow you to send annual reports to your accountant, but in reality they can also be a really useful management tool to ensure you make your business as successful as possible
regularly and your IT systems are sufficiently protected.
If you have staff members who are able to pay for items on behalf of the business, then this puts you at a higher risk. Consider having additional systems in place to help protect your business such as a maximum amount per transaction and approval of invoices before payment is allowed.
MAKING TAX DIGITAL
For most businesses, Making Tax Digital (MTD) will be an administration and financial burden, so careful planning should be considered.
This includes planning to ensure that adequate systems and software are in place for you to meet the requirements as and when MTD becomes mandatory, so any implementations you make now should incorporate a review to ensure that is the case.
Accounting systems are often seen as a necessary evil to allow you to send annual reports to your accountant, but in reality they can also be a really useful management tool to ensure you make your business as successful as possible.
Richard Norbury (right) is a partner at Sandison Easson & Co, specialist medical accountants
DOCTOR ON THE ROAD: SKODA OCTAVIA
Tainted image now a distant memory
Now you can get a good-looking well-appointed and well-built family car for under £30k. Dr Tony Rimmer (right) says it beats most of the opposition for value for money – and hurrah, it’s not a SUV!
I HAVE TALKED before about brand image and the positive power of a good reputation when it comes to attracting clients. There is a place for good solid dependable performance that also provides excellent value for money.
Our practices will continue to prosper if we are reliable and consistent in the quality of our services.
In the automotive world, this approach is exemplified by the Czech car maker Skoda. Its medium-sized family car, the Octavia, forms the bedrock on the back of which all other Skoda models have shared their success.
Now refreshed, this fourth-generation Octavia has a lot to live up to. It would be a mistake to mess with the attributes that have made it so popular over the last 28 years, so the changes are subtle.
Recent changes
As the engines and chassis are shared directly with the VW Golf, every update to the Golf model inevitably finds its way to being applied to the Octavia.
The driver-focused ten-inch ‘Virtual Cockpit’, once the preserve of premium Audi products, is now standard in every Octavia model
The current VW hatchback is now sold in version 8.5 and it is the recent changes, mainly to the interior and infotainment system, that have found their way to the latest Octavia.
A noticeable progression by each successive generation of every Skoda throughout its whole model range has been that of increased material quality of the interiors. I was interested to find out if this improvement has continued in this revised edition.
Even roomier
As a five-door hatchback, the Octavia is a direct competitor to the Golf, but is roomier, particularly in its useful luggage space. This has made it popular with families who rarely need to opt for the even roomier estate version or the bigger Superb model.
You can choose petrol or diesel variants but, to keep things simple, there is no hybrid or plug-in hybrid version available.
The fuel economy of the diesel variants may be slightly better, giving a real-world 60mpg or more, but as the 1.5litre petrol engine
models give a reliable 50mpg or above, then the smoother and quieter power plants are the ones to go for.
Available with either 114bhp or 148bhp, I have been testing the perfectly adequate base engine and had no complaints.
Feels sportier
The latest Skodas all look modern and stylish and this new Octavia is no exception. I have to say that it is quite refreshing to test a family car that does not follow the usual SUV playbook.
Sitting lower to the road makes it feel somehow sportier although this is definitely no sports car. The revised interior is smart and does indeed use higher-quality materials; the gap to the supposedly more upmarket Volkswagen models is very slim nowadays.
The newest 13-inch VW group infotainment touch screen is clear and easy to use and the driverfocused ten-inch ‘Virtual Cockpit’, once the preserve of premium Audi products, is now standard in every Octavia model.
Skoda’s ‘Simply Clever’ features include an umbrella mounted in the driver’s door and an icescraper/tyre-tread depth gauge packaged in the fuel filler cap; useful and clever indeed.
Although the base Octavia models come with a manual gearbox, my test car had the optional 7-speed DSG automatic gearbox. This is, as ever, a refined unit that takes the effort out of any journey that involves lots of traffic stop starts and is smooth on long motorway trips too.
Passengers’ car
Performance is not electrifying but is perfectly adequate, helped by a high torque output from the 1.5 litre turbo-petrol engine.
This Skoda is a great car for passengers – a supple suspension gives an excellent ride quality and most road irregularities are damped away effectively. Together with the interior roominess, this cements its position as a fantastically pragmatic family car.
As I mentioned before, this is not a sporty car, but you can always consider the Golf GTI engined vRS model if you want to up the performance stakes.
So this latest updated Octavia picks up where its predecessor left off. For under £30k you get a goodlooking, well-appointed and wellbuilt family car that has most of the opposition beaten regarding value for money. The old, tainted brand image is now a distant memory and rightly so.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
CHECK OUT OUR BUSINESS DIRECTORY
Independent Practitioner Today features an online advertising directory to complement our journal and
Split into ‘business’ and ‘lifestyle’ directories, they list the services private doctors need to run their practices or spend their well-earned money on.
ADVERTISERS: The deadline for booking adverts in our December-January issue is 29 November
or for reprints, we would be happy to discuss licensing the copyright to you.
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent.
Material is governed by copyright.
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites
Robin Stride, editorial director Email: robin@ip-today.co.uk Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the digital journal, on our website or in our business directory, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912