The business journal for doctors in private practice
In this issue
How to defuse disharmony
Jane Braithwaite advises on how to soothe tensions that arise in a group practice P12
Why it’s bad to use WhatsApp
Good reasons for avoiding the use of the messaging app in healthcare P26
Two feature articles on self-pay patients show you how to attract them and how to get paid n Starting on page 18
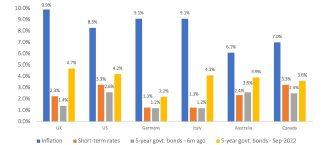
Weathering the storm
Simon Bruce of Cavendish Medical shows how to stay calm when faced with market volatility P32
Crackdown on doctors failing to show prices
By Robin Stride
Consultants face enforcement action if they continue dragging their feet over supplying data about their private work for public scrutiny.
An increasingly tough approach from the competition watchdog will see them publicly ‘named and shamed’ and taken to court if they fail to respond.
The Competition and Markets Authority (CMA) is also warning that some independent hospitals can expect the same fate if they fail to respond.
It warned it would take enforcement action against healthcare providers over concerns that prospective patients were not being given the ‘essential information they need’.
David Stewart, the CMA’s executive director of markets and mergers, argued that patients needed the information to make important and sometimes difficult choices about their private healthcare. He announced the stricter approach to consultants’ representatives, hospital providers and insurers at one of the biggest annual gatherings of the inde
In association with
pendent healthcare sector –LaingBuisson’s Private Acute Healthcare Conference in London.
The CMA says some private operators have failed to supply prospective patients with clear and consistent information that would allow them to compare providers.
This breaches what is known as the Private Healthcare Order of 2014, a legally binding requirement aimed, among other things, at ensuring patients can access ‘clear and consistent information’ on fees and performance from the organisation set up to publish it: the Private Healthcare Information Network (PHIN).
PHIN collates and publicises this data online, allowing prospective patients to compare healthcare
providers by markers such as pricing, customer satisfaction, infection and success rates.
But eight years on, amid some controversy about the requirement and its ability to give patients all the information they might find useful about hospitals and consultants, some providers have not supplied any data and some doctors do not know what PHIN stands for.
Mr Stewart said: ‘We know this isn’t an easy task for hospitals and consultants. However, hundreds of hospitals and thousands of consultants have already supplied the right information to PHIN. We thank them for working hard to meet this requirement.
‘There are still some providers that have failed to make any progress or even attempt it. If they now show a commitment to making the changes needed, we will support them to achieve this, alongside PHIN. However, those that continue to fail to can expect to face enforcement action’.
The CMA’s first step would be to name those in breach of the Order and then, it says, to seek the swiftest possible way of addressing their noncompliance.
‘This could be through voluntary
commitments from the providers, or, if necessary, the CMA could issue legally binding directions or begin court action.’
Mr Stewart gave a message of thanks at the conference to the ‘thousands of consultants’ who have provided information to PHIN. To those ‘trying to get there but not quite there yet’ he said the CMA wanted to work with them to help. He told the meeting that nobody at the CMA wanted to take enforcement action, but a significant proportion of consultants had been ignoring the Order.
Updates on this work can be found on the CMA’s private healthcare market investigation page. The watchdog has approved a new strategic plan proposed by PHIN aimed at ensuring the industry delivers full compliance with the Order.
A letter from the watchdog to the private healthcare sector last month announced it is set to launch enforcement action and the screw is likely to tighten on the unresponsive (see page seven).
n You can check out the CMA’s Private Healthcare Market Investigation Order 2014 at https://tinyurl.com/ms9mrv9p
David Stewart of the Competition and Markets Authority
TELL US YOUR NEWS. Contact editorial director Robin Stride
ADVERTISE WITH US. To advertise in the digital journal, on our website or in our business and lifestyle directories, contact Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT
£90 independent practitioners. £210 organisations. £90 GPs and practice managers (private & NHS).
Save £15 paying by direct debit: individuals £75 (organisations £180).
Time was when some private patients would go to the most expensive consultants because they reasoned the high fees meant they were seeing the best.
But the tough economic climate is bringing in a change of attitude among self-payers.
Private GPs report that cost is an increasingly important factor when they discuss who they think is the best consultant for their patients to see.
The issue was raised at this year’s Private Acute Healthcare Conference, run in London by market analysts LaingBuisson (see news stories on pages 7-9).
Private GP Dr Shaima Villait, GP chairwoman of the Independent Doctors Federation, said patients came to see her because they wanted opinion about whom they should be referred to.
But most important was for there to be transparency about the cost. Everyone, be they consultants or GPs, needed to show
In this issue
in advance how much they would charge.
She told the meeting: ‘With self-pay, the first thing they ask is – before you refer to a consultant now, which they wouldn’t before – is what are their prices.
‘And they may ask you to choose a different consultant according to how expensive they are.’
Independent hospitals increasingly find patients are shopping around, more so in some specialties than others. People are more discerning.
Quality is expected as a given these days, but price is set to be an increasing factor for many patients. With more price visibility in the market, it is important doctors and hospitals make it as easier than many do for patients to find their prices.
Making use of the Private Healthcare Information Network’s resource – even if you have resisted until now – may be a good place to start.
Rehab is the heart of the matter
Cardiologist Dr Ajay Jain argues that cardiac rehabilitation has been left behind in the pursuit of the drive to prevention and treatment P14
A storm brewing in healthcare
As the consequences of the pandemic continue to be felt in the NHS and the private sector, both sides are now more than ever reliant on each other P24
People report improving health
The latest Bupa Wellbeing Index data shows hopeful signs of improvement in our national health, but we must not slacken, says Bupa’s Dr Robin Clark P28
Don’t presume you’re covered
Doctors doing NHS work for private clinics or Waiting List Initiative work should check that they hold indemnity, warns the MPS’s Dr Sophie Haroon P34
Aligning PPUs with private hospitals
The Independent Sector Complaints Adjudication Services plans pilot studies with two NHS units to make it easier for private patients to complain P36
Double jeopardy for doctors
The GMC is set to lose its power to appeal fitness-to-practise proceedings. Hempsons’ solicitor Amie Roadnight reports on the long-running saga P37
PLUS
OUR REGULAR COLUMNS
Business Dilemmas: How you can get rid of an abusive patient
The MDU’s Dr Sissy Frank answers another thorny question from a doctor in our medico-legal series P42
Doctor on the Road: A brand you’re going to hear more of
Motoring correspondent Dr Tony Rimmer drives a premium electric car from a name new to the UK P44
Start a Private Practice:
The tax complexities of saving for old age
Accountant Alec James gives an update on the tax charges and allowances on your pensions P46
Doctors told to demand pension tax statements
The ‘McCloud remedy’ does not mean you can avoid tax issues now
By Edie Bourne
Doctors should urgently request their pension annual allowance statements from the NHS if they have not yet received their copy, say specialist financial planners Cavendish Medical.
Annual pension statements for 2021-22 are now available from the NHS Pensions Agency and are essential to help doctors establish whether they are likely to be paying substantial tax charges on their pension savings.
The NHS Pensions Agency is duty bound to send statements to those believed to be breaching the standard annual allowance of £40,000 but not to those exceeding the ‘tapered’ annual allowance which applies to higher earners and can be as low as just £4,000.
BMA urges Chancellor to fix tax trap on pensions
Chancellor Jeremy Hunt’s priority now must be to rapidly remedy the pension taxation trap, according to the leader of the BMA.
Chairman of council Prof Philip Banfield predicted this would make a material difference in retaining expert and experienced clinical staff.
He said: ‘We urge him to get round the table with us, reform what he said was the national scandal of staff being forced to leave the NHS because of pension arrangements and fix doctors’ pay.’ Mr Hunt is due to make his Autumn statement on 17 November when he is expected to
Patrick Convey, technical director at specialist financial planners Cavendish Medical
Patrick Convey, technical director at Cavendish Medical, said:
‘For this reason, many medics wrongly believe they do not have an excess tax charge to pay on their pension growth, but actually, they just might not have been made aware of the problem.
‘This year, we have the added complication of the McCloud remedy which will offer compensation benefits to those deemed to have suffered age discrimination when moving to the 2015 NHS Pension Scheme.
Former Health Secretary and now Chancellor
announce plans for further changes to Liz Truss’s blueprint for easing the tax take on high earners.
Prof Banfield said Mr Hunt’s role as chairman of the Health and Social Care Committee made him fully aware that the Government must urgently address ‘absurd pension taxation rules and consistent real-term reductions in pay which are driving staff out of the NHS’.
‘While it is true that the judicial ruling may mean the figures for many doctors of the last few years will need to be recalculated, the official legislation is not due until October 2023.
‘For this reason, it is important for doctors to address their pension savings’ tax issues in the normal way with the correct figures now – including paying any tax liable – and then recalculate when their new pension details are known at a later date.’
Those breaching the annual allowance can apply for the NHS to pay the tax charge under Scheme Pays in exchange for reduced future benefits.
The application for Scheme Pays is normally 31 July each year, so for the 2021-22 tax year, this will be 31 July 2023. There are also other
payment options which should be considered.
Mr Convey told Independent Practitioner Today: ‘Many doctors are working long hours and facing another extra busy winter. There is scarce time to spend keeping up to date with the latest tax regulations.
‘This is also the first year that members of the former 1995 and 2008 schemes have been moved to the new 2015 scheme. While you retain your service in the legacy schemes until 1 April 2022, after this date you will accrue benefits in the 2015 scheme – effectively monitoring two sets of pensions and rules.
‘The NHS Pension Scheme gets ever more complex every year and we are here to help you navigate the best path forward.’
Doctors witness rise in private patients
A majority of doctors report they have seen an increase in patients turning to private healthcare over the last five years.
According to a survey of 467 physicians in the UK by information service Medscape UK , 57% have noted the rising trend.
The company said the rise was likely due to long waiting lists for treatment in the NHS.
Nine-in-ten doctors surveyed had seen an increase in patients struggling to access medical healthcare services in the last five years. They ranked access to healthcare as a top concern.
A third of doctors felt the NHS model was the best for the UK, while a third favoured a hybrid model of private and public. Only
3% of those surveyed backed moving to a completely private model. However, the number in favour of a private-only model moved up to 7% among doctors aged under 45.
One survey respondent said: ‘Healthcare access has been severely compromised through the non-evidence-based policies driven by public health authorities and the Government.’
The study found 92% of doctors felt Covid-19 had impacted the overall quality of care. 79% believed the state of healthcare would deteriorate in a post-pandemic world.
For more findings, view the full report on Medscape: www.medscape.com/uk-social-issuesreport-2022.
Jeremy Hunt
Doctors call for menopause help
By Agnes Rose
Female doctors in private healthcare must be better supported through the menopause and feel empowered to take time off to help prevent them leaving the medical profession.
This is the conclusion of a survey of 39 female consultants who do private work, which found that few felt supported by their workplace.
Most did not know where to seek support for their symptoms at work and some said they had considered early retirement due to menopause symptoms and the impact on their well-being.
Survey organisers the Medical Protection Society (MPS) believe those suffering with menopause symptoms would benefit from supportive colleagues and managers who remove barriers to doctors taking time off at short notice.
MPS president Prof Dame Jane Dacre said female doctors who were working in private healthcare were suffering in silence and required more support.
‘Brain fog, forgetfulness, poor
concentration and insomnia can make any job difficult, but particularly so in a complex environment like healthcare.
‘Some female private practitioners also report feeling concerned about their symptoms impacting on their performance, on colleagues’ perceptions of their capability or resulting in medico-legal issues. This causes additional stress.’
Results of the survey of 261 doctors working across different healthcare settings in the UK showed similar concerns.
Prof Dacre called for a shift to a culture which frames doctors’ sick leave as responsible behaviour. This would help female doctors suffering with menopause symptoms continue to perform at their best and thrive longer in their careers.
‘If we do not destigmatise menopause, we may lose many skilled and passionate doctors during a time when the medical profession can ill-afford it.’
An injection of Arthrosamid for knee osteoarthritis is being offered to patients at London’s The Princess Grace Hospital and The Institute of Sport, Exercise and Health (ISEH) under a partnership between HCA Healthcare UK and Contura Orthopaedics Ltd.
The treatment with the polyacrylamide hydrogel, becoming available at other HCA facilities later, is described as a novel one for those who have not responded to standard interventions and are unsuitable for surgery or reluctant to consider it.
Consultant orthopaedic surgeon and ISEH clinical director Prof Fares Haddad said: ‘Early evidence is encouraging and the team at ISEH are therefore undertaking a detailed analysis of its effectiveness and impact on pain and function.’
Contura chief executive Rakesh Tailor reported the company was confident the single-dose treatment, designed to be delivered in outpatient clinics, would ‘completely change the management of osteoarthritic knee pain and delay the need for invasive knee surgery.’
WHAT FEMALE PRIVATE DOCTORS SAY:
‘I could hardly function and knew my decision-making was impaired. As retirement age increases, post-menopausal women need support.’
‘The only matter where a woman can take time off for her reproductive health that is widely accepted is pregnancy – that’s the reality.’
‘I know my clinical performance suffered due to brain fog, but it has now improved again.’
‘I am surprised at times how unsympathetic female colleagues are who are slightly younger than me but have not yet experienced symptoms. I have found much younger colleagues to me more understanding.’
75% of female consultants who have experienced menopause are concerned about their menopause symptoms impacting their work/ performance quality.
62% of female consultants who have experienced menopause said they are concerned about menopause symptoms impacting colleagues’ perception of themselves and their capability.
55% of female consultants who have experienced menopause are concerned about the impact of menopause symptoms resulting in medico-legal issues such as clinical negligence claim, GMC investigation into their practice, disciplinary, involvement in inquest and/or patient complaint.
68% of all consultants surveyed do not know whether their employer/ workplace has a menopause workplace
48% of female consultants who have experienced menopause have considered reducing their hours, 22% have considered early retirement, and 18% have considered stepping back from clinical work to pursue other medical-related projects/jobs.
Doctors at leading private unit train medical students
Cleveland Clinic London consultants are training final-year medical students from Queen Mary University of London’s Faculty of Medicine and Dentistry.
Selected medical students will do a five-week clinical attachment as part of their final year of study, given by medical staff in neuroscience, perioperative medicine and ITU, orthopaedics and musculoskeletal, acute medicine and medical subspecialties, heart and vascular, and digestive diseases.
Fortius becomes top rugby club’s health partner
Fortius Clinic, London, has become a Harlequins official club partner for the 2022-23 season
across the Premiership rugby club’s men’s and women’s teams, formalising a working relationship between the club and orthopaedic and sports medicine specialists. Harlequins members and affiliate clubs will have preferential access to all aspects of Fortius services, including sports injuries, joint replacements, pain management and MRI, X-ray, ultrasound.
Private hopital’s new chief to bring in new products
Innovation is a key aim of HCA’s The Princess Grace Hospital’s new boss Maxine Estop Green. She said she will work with consultants and the company’s teams to also introduce new products and services that are ‘accessible, flexible, and personalised to our patients’.
Prof Dame Jane Dacre
RMOs claim their plight is ‘borderline slavery’
By Douglas Shepherd
Widespread poor conditions, low pay and excessive working hours.
That is the fate of many resident medical officers (RMOs), according to a shock report.
A survey of these doctors, providing services mostly in the independent health sector and most frequently recruited abroad as international medical graduates, describes pay deductions, bullying and multiple instances of racism.
The study, by the BMA and Doctors Association UK (DAUK), found:
Just over a third (34%) reported bullying and harassment;
47% complained of unfair treatment;
31% worked unregulated shifts;
89% reported working over 70-hour weeks, which as the survey organisers point out is in excess of legal limits and advertised contracts.
The BMA and DAUK said terms like ‘borderline slavery’ and ‘sh*ttiest employer anyone could ever have’ were representative of the mass of comments from survey respondents.
Patient safety concerns
Some 92% were recruited by agencies from African countries, which the survey organisers warn raise ‘significant questions about the treatment of international medical graduates by private medical recruiters and by the NHS trusts that employ their services’.
They added: ‘81% had trained in Nigeria, a country where active recruitment by UK firms is prohibited by the Department for Health and Social Care in order to stop the “brain drain” effect that depletes developing countries of their medical workforce.
‘Much of the concern expressed by RMOs in the survey is for patient safety, with fatigue, lack of support and poor mental health
leading to worries that they aren’t able to give patients the care they need.
‘With doctors reporting working for 12-hour shifts for a full week, far beyond the safe limit of what can be expected for medical professionals, the agencies are seen as putting patients in danger with the way they treat their contractors.’
Pay deducted
Many deductions from pay make an already low salary – barely above the living wage in many instances – worse, according to the BMA and DAUK.
‘Deductions from pay reported by RMOs include those for visas, appraisals, mandatory training
THE BMA AND DAUK ARE CALLING FOR:
Independent operators to publish for patients the main terms and conditions of the doctors which they or third parties working for them are employed on
Both the NHS and the independent sector to take responsibility for the conditions under which people are employed under their roof
Minimum employment standards aligned to NHS terms and conditions
A review of the practices of the agency sector, including their international recruitment practices and the involvement of the UK Government in supporting them
courses and even deductions for being late. Lack of payment for annual leave and sick leave were also flagged by respondents,’ the association said.
BMA council deputy chairman Dr Emma Runswick called the treatment reported by these doctors ‘a disgrace to UK medicine’.
Union recognition
‘Our international colleagues have come a long way to the UK, have left behind families and friends, and deserve to be treated fairly as employees here.
‘What they have found instead are conditions so exploitative that it beggars belief,’ she said.
The BMA is calling for trade union recognition to apply to all
PRIVATE HEALTHCARE SECTOR REACTION
David Hare, chief executive of the Independent Healthcare Providers Network (IHPN), told Independent Practitioner Today: ‘There are a number of different models in the independent healthcare sector of how RMOs are engaged, depending on the services organisations provide and the acuity of patients they treat.
‘Independent sector providers take their responsibilities in this area seriously and both independent providers and other employers must ensure that RMOs have a robust induction to their role, receive regular training and are able to communicate any concerns, including about their workload and health and well-being, with clear action taken if patient safety is put at risk.
‘IHPN have also recently been working with the Royal College of Surgeons of Edinburgh to develop educational resources to support RMOs in their role and ensure they can deliver the highest quality care for patients.’
medical staff in private settings and the NHS, regardless of who their direct employer is.
It can support international doctors new to the country via a contract-checking service and is asking those claiming exploitative behaviour to let it know anonymously through its support channels.
Dr Jenny Vaughan, of the Doctors’ Association UK, said: ‘Bullying, racism, unsafe hours, low pay and threats of withdrawal of visa sponsorship – it is just extraordinary that agencies have been getting away with this behaviour and it is an indictment of the authorities that they let this continue without redress.
‘For agencies to take advantage of British hostile environment policies to push unfavourable conditions on doctors is the very worst of international recruitment practice and brings the entire model into disrepute.
‘The lack of regulation in this area has meant that these practices have become the norm.
‘The reason these agencies think they can get away with this is because many of their doctors don’t have the local knowledge on their rights, so they are ripe for exploitation.
‘This includes foisting on them contracts that nobody would sign if they knew what the NHS standard was. Tired doctors being forced to carry on is in nobody’s interest and is unsafe for patients.’
Insured activity is above 2019 level
By a staff reporter
Insured activity in private hospitals up to the end of September 2022 was 6.7% higher than the same period in 2021 and 12% up on 2019.
Figures unveiled at LaingBuisson’s Private Acute Healthcare Conference from Healthcode, the official clearing organisation for the private healthcare sector, reveal inpatient and outpatient numbers are at or above prepandemic levels.
Private hospitals have bounced back following the severe downturn caused by the pandemic and lockdown in 2020, it reported.
It stated: ‘This recovery could already be seen in 2021 when 3.17m invoices were processed by Healthcode’s Clearing Service; up 40% on 2020, but momentum has continued into 2022 when more insured patients than ever received the specialist care they needed.’
ACTIVITY AT A GLANCE
EPISODE
SETTING
Outpatient care represents 84% of hospital activity, up from 81% in 2019. Billing for these episodes made a strong recovery after the pandemic, although this has levelled out this year and remains consistently above 2019 levels (117% in September 2022).
After a slower recovery, inpatient activity surpassed 2019 in four of the last five months. The long-term trend is for inpatient episodes to become a smaller proportion of hospital activity.
MEDICAL SPECIALTY
Orthopaedics and trauma remains the top hospital specialty by volume, but the level of insured activity has not increased since 2019. In September 2022, the insured bill volume (47k) was slightly down on 2021 (49k) and the average volume for Q3 2022 was also slightly down on pre-pandemic level (98%).
Radiology saw the biggest year-on-year rise in billing volumes (38k in September 2022 compared with 24k in September 2021). Average billing volumes for Q3 were more than double those in 2019 (213%).
Pathology/haematology, which surged in the pandemic, fell back to 20k in September 2022, compared with 22k in September 2021, although billing volumes still far exceeded 2019 (163% in Q3).
In the other major medical specialties, insured billing volumes were slightly higher in September than 2019. The exception was ENT (99%) reflecting a slower rate of recovery in this specialty.
Managing director Peter Connor later paid tribute to the ‘heroes of this story’: the consultants, healthcare professionals and managers in hospitals across the UK who had worked tirelessly to turn things around for patients. He said: ‘In the specialty of radiology, for example, yearonyear billing volumes increased by more than half in September 2022, meaning more patients could learn their diagno
sis or receive essential therapeutic treatment.
‘I have no doubt that demand for safe, highquality private healthcare will continue to increase in the years ahead and Healthcode
COUNTRIES AND REGIONS
England has seen continued steady growth. Volumes in September 2022 were 114% vs 2019 (113% on average in Q3).
By contrast, Wales’s recovery has lagged behind. Volumes for September 2022 were 94% of 2019 (97% for Q3).
In Scotland, volumes were 109% of 2019 in September 2022 (105% in Q3).
North-west England had the strongest showing. Billing volumes in September 2022 were 120% vs 2019 (119% for Q3).
In London, billing volumes vs 2019 were 117% in September 2022 (113% for Q3)
Yorkshire and Humber was static. Billing volumes were unchanged from 2019 in September (102% for Q3).
will do our utmost to support that through the development of online services such as The PPR (Private Practice Register), preauthorisation and real time appointment booking.’
MDU urges Government to adopt its agenda
Support for exhausted doctors and regulatory reform should now be the top healthcare priorities for the Government, according to the Medical Defence Union (MDU).
It has called on re appointed Health and Social Care Secretary Steve Barclay to focus on three key priorities affecting medico legal issues:
1. ‘Support an exhausted workforce: Study after study has demonstrated more doctors are suffering from burnout.
‘This is not good for them nor their patients. The Government
must do more to support doctors and stop fatigue setting in.’
2. ‘Deliver modern healthcare professional regulation: Institute top to bottom reform of GMC regulation, which is too rigid and governed by outdated legislation.
3. ‘Get to grips with runaway clinical negligence costs: The costs of meeting future claims liabilities for the NHS in England now stands at £128bn.
The total budget for the NHS in 202223 is expected to be £155bn. This is not a sustainable situation and legal reform is desperately
needed to rebalance the system.’
MDU chief executive Dr Matthew Lee said: ‘Doctors are working flat out to care for their patients, in many cases to the detriment of their own health and wellbeing.
‘They deserve the support and resources needed to enable them to take regular breaks so that they can care for patients safely.
‘If they then face scrutiny by their regulator, the GMC, it can be truly devastating for them.
‘Doctors deserve a regulatory system that is proportionate, timely
and fair. The legislation needed to modernise regulation was due to be introduced this year and was then delayed – it needs to be a top priority again.
‘Meanwhile, much needed funds could be retained in the NHS through legal reform of the system under which billions of pounds are leaving the NHS in clinical negligence claims.
‘If the Government wants to prove its commitment to the medical profession and to boost morale, we urge them to seriously consider our package of priorities.’
Peter Connor of Healthcode
Reports by Robin Stride
PHIN offers to help doctors show fees
The Private Healthcare Information Network (PHIN) is reprioritising its work to ensure it does all it can to help the independent sector comply with requirements of the Competition and Markets Authority (CMA).
Compliance with the CMA Order compelling fee transparency has not progressed as far or as fast as many would like due to the ‘complexities involved’, according to its new medical doctor boss.
But chief executive Dr Ian Gargan said the organisation was now in a strong position to work together and accelerate the process.
He told the conference that rapid progress was being made, with volumes doubling since May 2021.
The latest figures (September 2022) showed nearly 31,000 patients were visiting the website every month, with 7,000 of them contacting a consultant or hospital directly from the site.
PHIN was also doing more work on its website to help doctors and would continue to train them and hospitals on how to supply information. It aimed to collaborate with hospitals and providers.
The
Dr Ian Gargan, head of the Private Healthcare Information Network
This would only be achieved by hospitals, consultants, and private medical insurers working together across the sector.
Dr Gargan believes the cooperation can make things better for patients by being more transparent and allowing them to make better choices – something patients are asking PHIN to help them with.
He recognised that complying with the CMA Order was sometimes difficult due to patients being a priority, but said PHIN was there to help, offering a range of support through its portal including:
Guides and videos for each process;
Opportunities to attend a virtual session to review each process – which are held biweekly;
Onetoone support where that is easier for the consultant.
Dr Gargan said PHIN was listening to consultants, hospitals and other partners to see how it could help make the process easier and increase compliance even further.
It was working with insurers to involve them in understanding and accessing the measures and how these could be made useful for patients.
Orthopaedic surgeon Susan Alexander said PHIN did not figure high on Google searches and people did not look beyond the second page when searching online.
Doctors were not opposed to information being gathered but it needed to be the right type.
As a patient, she would want to know whether the doctor was going to listen to her and treat her as an individual.
She said she would want someone who made their choices based on what she needed rather than how much they would be remu
ENGAGEMENT WITH PHIN CONSULTANTS
12,390 consultants have episode data, of which:
7,262 (59%) have a profile on the PHIN website
9,330 (75%) have added their consultation fees
7,388 (60%) have included procedure fees
2,905 (23%) have validated their procedures
2,233 (18%) have done all of the above
HOSPITALS
135 healthcare providers covering 458 sites are engaged with PHIN
Data received from just over 98% of hospitals across the UK, most of the care being provided by 55 larger healthcare providers.
The remaining ‘long tail’ of healthcare providers includes most NHS private patient units
Data received from across the UK includes 13 of the 19 sites in Northern Ireland (there are ten providers), eight of 15 sites in Scotland (seven providers), 28 of 31 sites in Wales (13 providers)
nerated and whether the payment was higher from doing one procedure over another – ‘and that is the danger of what people in this room are doing to the private healthcare market’.
➱ more conference stories on page 8
CMA’s letter to private consultants and hospitals
From: David Stewart, executive director, Markets and Mergers. 12 October 2022. (See page 1)
Enforcement action under the Private Healthcare Market Investigation Order 2014
I write to the private healthcare industry nearly three months since PHIN and the industry agreed a new strategic plan to deliver full compliance with Part 4 of the Order by the summer of 2026. The CMA is confident that this plan can keep the sector on track to deliver this valuable information for patients across the UK.
I would specifically like to thank the thousands of private consultants and hundreds of private hospitals who are providing the information required under the Order. Through your hard work, private patients are already seeing benefits.
For those consultants and hospitals that are nearly complaint (sic),
PHIN and the CMA are keen to work with you to achieve full compliance as quickly as possible. To do this, you should log in to the PHIN Portal or speak to PHIN on 020 7307 2862.
There are still some consultants and hospitals who have made little or no effort to comply with their legallybinding obligations. For these organisations and individuals, you should be aware that we are now escalating the public enforcement action against individual consultants and hospitals to ensure all those bound by the Order comply with it. You can expect to see public announcements from the CMA about this enforcement work shortly.
Yours faithfully,
David Stewart
Reports by Robin Stride
CMA attacked for omitting insurers
A prominent consultant orthopaedic surgeon hit out at the Competition and Market Authority’s (CMA’s) failure to include private medical insurers in its drive to improve information for patients.
Ms Susan Alexander, who chairs the Independent Doctors Federation (IDF) education committee, said clinicians generally were not against data being collected, but it had to be a complete picture of the whole health journey.
And this was not happening, she claimed.
She told the conference: ‘The CMA has put up a screen, if you like, and said we are not going to look at that side of the market. But it is not the full picture, because the whole point of healthcare is about safety first from a clinician’s point of view; quality and then choice.
‘But patients are not being offered a proper sense of choice, because what the insurers are doing is they are putting a chokehold on the market.
‘They are driving policies whereby you can see certain consultants who they label as platinum consultants, but the inference there is that the rest of the consultant body are not that good – which is just not right.’
Angry consultants
Ms Alexander warned that the effects of high inflation was getting the consultant body angry and specialists did not know if they could continue sustaining a quality service at the insurance fee offered.
‘In 1999 in my particular field, a procedure would cost £589. Just with inflation costs today that
should be £1,005, but what we are getting remunerated now is £550 –less than last century.’
Addressing insurers, she complained that the market was being driven down so only a few doctors could take part.
‘So you are pricing out the more experienced doctors. There is no reward for experience, no regard for expertise in a particular sector. It is completely unacceptable.
‘You would not have this in another industry. It is like buying holiday insurance and saying “Well, you can only go to certain countries and – oh,by the way – the pilot who is taking you there… year one, should be fine – as long as you don’t have turbulence”. Go figure!
‘It’s not OK. It’s scandalous what’s happening.’
Her comments received the strongest applause of the day.
You are pricing out the more experienced doctors. There is no reward for experience, no regard for expertise in a particular sector. It is completely unacceptable
MS SUSAN ALEXANDER, orthopaedic surgeon
Data-sharing needed to prove value for money
An optimistic speech on the future of the private hospital sector was delivered by the head of Bupa Insurance.
Chief executive Alex Perry said self-pay and private medical insurance subscriptions were growing strongly.
His company’s insurance business had just passed three million subscribers for the first time, driven mostly by the business market and hard work done with consultant partners.
Mr Perry said now, more than ever, value in the sector needed to be proved by providing healthcare that was affordable, easy and quick to access, and delivering better outcomes.
GPs were now digitally handling 10,000 appointments a week for Bupa customers and over 50,000
patients had last year used direct access for musculoskeletal services, cancer or mental health.
The insurer was looking to build more ‘strategic partnerships’ with consultants and hospitals, he said.
But he was critical of ‘glacial’ progress to improve the quality of data available for the sector. This needed to be available much faster.
He believed partnerships would help deliver what customers had come to expect and which other sectors already delivered: Simplifying access to care through digital appointment booking; Creating seamless care pathways by exchanging medical notes and test results between insurers, consultants and hospitals without the customer needing to do the legwork;
Taking the hassle out of claiming through hospitals, and consultants sharing referral and treatment information to enable pre-authorisation of treatment on behalf of customers.
He said: ‘These three changes alone would deliver a radically bet-
ter experience for all those using the private healthcare system. And delivering them will be a team effort.’
While 86% of independent facilities recognised by the insurer were rated good or outstanding by the Care Quality Comission, and 94% of all Bupa members were treated at these facilities, the question remained: ‘But…when will PHIN deliver the data that lets us show our customers are getting the best outcomes?’
Mr Perry also called on the sector to get serious about sustainability. Everyone needed to commit to it. ‘It can be an area where the independent sector leads the healthcare system.’
That would enhance its reputation and attract business with likeminded targets, he said.
Alex Perry, head of Bupa Insurance
Referrals still rely on personal touch
Whose brand matters most in selfpay: the consultant or the hospital?
Conference attendees voted 56% for consultants and 32% for hospitals or clinics, but 12% thought neither. The latter considered patients were only interested in convenience and speed of access.
London Consultants’ Association representative Rosemary Hittinger said that in a straw poll she took of her membership, between 60-80% said they got referrals via personal recommendations.
What’s causing insurance to rise and fall
A LaingBuisson analyst and report author looked into his crystal ball to predict the outlook for private healthcare revenue from medical insurance in the year ahead.
Riko Scandelius gave three reasons why revenue might rise in 2022-23:
The private medical insurance
PPU WATCH
Compiled by Philip Housden
Annual PPU conference returns following Covid Managers from 15 NHS trusts attended the annual NHS Private Patient Services conference. Held online, it was the first since the March 2020 lockdown. Attendees heard from Healthcare UK, Bupa, AXA and Aviva; enjoyed case studies shared by Royal Orthopaedic and Harrogate hospitals and had discussions on best practice and ideas for growth. A face-to-face meeting is planned for next year.
A further 20% were via private GPs – but nobody mentioned anything about branding.
The Private Healthcare Information Network (PHIN) had told her there were four times as many visits to its website consultant page as there were to any hospital page, so she considered the consultant’s reputation, which was hard won and easily lost, was more important than branding.
Private GP Dr Shaima Villait, GP chairwoman of the Independent
market has grown as customer companies have done relatively well;
NHS waiting times are unlikely to improve rapidly;
Medical inflation.
But he also cited a trio of factors which could influence revenue to falter.
These were:
A continued increase in virtual/ digital health engagement;
New and younger subscribers typically claiming less;
Predictions of the UK entering a recession.
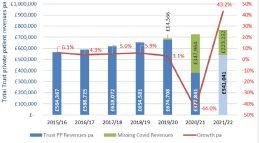
Revenue lost through Covid calculated as £594.8m
Analysis of NHS trusts’ published annual accounts for 2021-22 has shone a light on the lost private patient income caused by the Covid pandemic.
With 19 trusts still to report, total revenues for all England NHS trusts are projected to be £541m. This is a 43.2% increase on 202021, but still only 82% of 2019-20 financial year.
Prior to the pandemic, NHS trust private patient incomes were growing at a compound rate of 5.3%.
Applying this same rate retrospectively highlights the ‘missing’
Doctors Federation (IDF) and deputy chairwoman of the BMA Private Practice Committee, said patients came to see her because they wanted to ask opinion about who they should be referred to. ‘I would never refer to a brand; I would be referring to a person.’
She said private GPs took a long time to create their individual list of consultants they trusted and who they felt their patients would be happy to see.
‘At no point would I be referring
personally to a specific hospital unless a patient said ‘I’m not going anywhere else apart from this hospital and I need to see someone there’.
Even then she would be researching somebody she considered would be the best person for them to see at that hospital – otherwise it would be going back to the generic open referrals which most private GPs were against. ‘Patients trust you and I don’t feel we should be referring just to a brand.’
e-Prescriptions are saving time
Private clinicians’ practices are saving many thousands of hours of work thanks to e-prescriptions for pharmacy delivery.
Over 90% of 80 practitioners who invested in Pharmacierge considered the service provided by the company was saving their practice five to 15 minutes per prescription.
ket analysts LaingBuisson, by the company’s co-founder and chief executive Edward Ungar.
The figures were given to the conference, organised by mar-
In a straw poll, 80% of those surveyed thought the pandemic had fundamentally altered patient expectations of digital healthcare.
A same proportion said more patients were initiating their treatment online since the pandemic.
expected income that trusts should have achieved.
The calculated ‘missing’ revenues total £585.8m-for the last three years: £14.6m in 2019-20,
£348m in 2020-21 and £232.2m last year.
Philip Housden is a director of Housden Group
Rosemary Hittinger
Edward Ungar
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2012
Investing caution urged
Consultants were being advised to exercise caution with investments in private ventures following a clinic’s collapse just weeks after announcing plans for expansion and ‘innovative partnerships’.
Cash flow problems were cited as Nucleus Healthcare Ltd, trading as Celtic Springs Clinic near Newport, Gwent, went into administration, forcing shocked specialists to revise their business plans.
One unhappy investor told Independent Practitioner Today: ‘This will make a lot of doctors more cautious about investing in the future, and they need to be.
‘The lesson is to get your paperwork tied up at the outset and make sure any commitment is legally binding up-front.
‘When there is an opportunity for
investment in future, consultants won’t be sure now. It’s a case of once bitten, twice shy.’
An administrator urged doctor investors looking at other projects to recognise early on that cash is key to business survival and healthy turnover on its own may not be enough. They should not be over-reliant on one sector or a single revenue stream, he said.
Ready for revalidation
Independent Doctors Federation Responsible Officer Dr Stuart Sanders welcomed Government confirmation of the start of revalidation the following month.
He said: ‘My feeling is that appraisal will improve the standard of care our patients receive and the revalidation process will become second nature to the profession.’
Check clinic credentials, patients told
A new campaign was launched by the cosmetic treatments watchdog to warn patients about the dangers of accepting care from untrained providers.
The campaign from TreatmentsYouCanTrust.org.uk was launched ahead of the December peak period for cosmetic injectable treatments.
It advised people to ‘Always Background Check’ their provider,
to know how to spot and avoid bad practice, and to report bad practice and inappropriate adverts.
Campaigner Dr Hilary Jones said patients were confused about injectable treatments. While Botox and dermal fillers were nonsurgical, they were medical procedures and should only be administered by regulated and appropriately trained doctors, dentists and registered nurses.
NHS fails to utilise the insured
Consultants’ private incomes were taking a hit because the NHS failed to identify thousands of its patients who could be treated under their private medical insurance (PMI) cover.
The problem prevented NHS private patient units increasing their income and meant people were missing out on breakthrough treatments in the independent sector, a private hospital group boss warned.
His comments came after an analysis by health economists found as many as one-in-three privately insured patients in England undergoing hospital treatment had it provided and funded by the NHS – despite being eligible to claim from their policy.
At the same time, emergency and cancer treatment worth hundreds of millions of pounds was being provided on the NHS to people with PMI, said HCA group commercial director Keith Biddlestone.
He said: ‘Private healthcare is about choice and many patients choose to move between private and NHS care – but these figures certainly show just how hard private medical insurers rely on the NHS to maintain profitability.’
Young docs told to prove their quality
Would-be independent practitioners were advised it was increasingly important to compile clinical quality information if they wanted to demonstrate their value to private medical insurers.
Other tips given to doctors at an MDU/Healthcare Performance event included:
Ensure your profile in insurers’ website is up to date;
Get an induction at hospitals giving you practising privileges;
Know your obligations under the Data Protection Act 1998, including registering with the Information Commissioner’s Office as a data controller.
TELL US YOUR NEWS
How about making the news today? Independent Practitioner Today is always keen to hear from doctor entrepreneurs willing to share their stories in private practice – and from independent practitioners embarking on the journey. Contact our editorial director Robin Stride at robin@ip-today. co.uk
Spending too much time on billing instead of patient care?
Let Medical Billing & Collection do the hard work for you.
With 30 years’ experience helping over 1,500 private consultants, groups, clinics and hospitals.
• Dedicated account manager
• Reduce bad debts to less than 0.5%
• Increase net income by up to 25%
• 24/7 online access to your data
• Faster payments through e-billing for insurers and patients
Discover more at medbc.co.uk or 01494 763999
TROUBLESHOOTER: GROUPS
‘It’s good to talk’ to defuse disharmony
Tensions are not uncommon when consultants get together to form groups in private practice in the current financial climate. Our Troubleshooter Jane Braithwaite tackles an appeal for help
‘We have been working in a group for two years now and we are starting to experience tensions between us. How do we manage these tensions without breaking up the group?’
RUNNING A BUSY private practice group can be rewarding but timeconsuming at the best of times. If you are experiencing disagreements with the other members of your group, it can feel overwhelming. Tensions, disagreements or even arguments can be common, especially among the high-performing clinicians that make up your group.
This article will look at how to approach your colleagues to diffuse this tension, how to reduce the chance of divisions going forward and what steps to take if you feel the situation is irretrievable
and the group needs to be dissolved.
There are a number of steps you can take to resolve this situation.
Tensions are common
The nature of a group can lead to building tensions. It is rare that everyone in the group has exactly the same goals, both professionally and personally.
These slight differences in objective can lead to stress, which can manifest in many different ways.
The reasons for these disputes vary from person to person and from group to group. They could
be related to individual financial problems, the clinical direction that the group is moving in, the way work is allocated or how profit is distributed.
Whatever the cause, it will be essential to see the problem from everyone’s point of view in order to come to an amicable solution.
How to start the discussion
The process of understanding the problems within the group and addressing them is key.
One of the best methods is a meeting to talk through all the issues. Everyone must be present,
because if someone feels excluded, it may lead to resentment and the underlying problems cannot get solved.
At the outset, you should set the expectation that these meetings are the forum to talk through all the tensions, with no side discussions or confidential chats that do not involve all members of the group.
This meeting aims to bring up all the problems that people feel are holding the group back, work together to find a solution and decide how it will be implemented.
How to structure the discussion
If you lead or manage the group, you may feel it is natural that you take charge of this meeting.
Depending on what needs to be discussed or what the underlying issues are, the other members may find it more difficult to be open and honest if one person appears to have more sway than the rest.
To ensure that there is no power imbalance in the discussions, you might find that having an independent person to chair the meeting can help things flow a bit better. They can help keep the meeting on topic and make certain that everyone is having their say.
If you have significant problems within the group, it is likely that this meeting will involve a degree of confrontation.
This is never a comfortable position to be in, both for yourself and others. Going into this meeting prepared, either by having thought through what needs to be said or bringing notes with you, will make sure that you can manage to get your point across.
Psychologist Bruce Tuckman described the stages that teams go through when working on a project together. He named these stages ‘forming, storming, norming, performing’.
The ‘storming’ stage is characterised by potential conflict between members as everyone tries to work out individual roles and pushes against boundaries. It may be that, as a group, you have entered the ‘storming’ stage, with its uncomfortable conflicts, and that you need to work through to reach ‘norming’, where everyone resolves their differences, and ‘performing’ where members work together to achieve the group’s goals. If you can push together through this difficult stage, you may find that you have bonded better as a team and can attain greater success in the future.
How could the process go wrong?
Any situation involving confrontation is fraught with pitfalls. If relationships within the group are already fractured, there may be considerable resistance to bring -
ing about the meeting. Sometimes in these circumstances, there is one member of the group who can act as a ‘peacemaker’ and bring the others together.
It can be tempting to phrase all communications about these meetings in hard-nosed business language. By humanising what you say and acknowledging your own and others’ discomfort with the situation, you might find that everyone can open up a bit more about the problems that they see.
Some people may find this level of discomfort and confrontation intolerable and, rather than face the issues, may choose to leave the group.
If there is no way to bring about a meeting between members, then the business relationship, and thus the group itself, may not be salvageable. At this point, the advice of experts such as lawyers and accountants will become invaluable.
How can we improve in the future?
If you have managed to have these discussions, then you have taken a difficult but important step for your business. It would be a shame now to slip back into your old ways and find that the same problems and conflicts are continued. Look back at the contracts and agreements that you had drawn up when you formed the group. Do these still reflect the way the
business is run? You may find that you have altered some of the roles, responsibilities and functions of group members and may wish to put this down in writing in new contracts.
You will need an agreed structure for the future and this should be documented and signed by all members of the group.
If necessary, you should seek advice about drafting these new contracts and agreements to make sure that everyone has clarity about what they can expect of others and what others will expect of them.
Ongoing communication will be essential, perhaps in the form of a monthly group meeting. This will provide a forum for issues to be aired while they are still small and easily solvable and allow them to be dealt with before they become a threat to the group.
What if the group cannot be salvaged?
Sadly, it is not uncommon for disagreements to snowball, ending up with a break-up of the group.
If your founding agreements included provisions for dissolving the group, then this process will be much easier.
If the initial contracts did not cover this, then it will be necessary to negotiate with the other members of the group to find an amicable way to split the assets. This could be complicated and having the advice and input of experts as early as possible is advised.
If you have significant problems within the group, it is likely that this meeting will involve a degree of confrontation
Managing conflicts, tensions and disagreements in a group can be difficult. If you can find a way to bring everyone together as a team, where each individual is empowered to raise problems, you may find that the resulting group functions much better than before.
If you have any specific questions that you would like answered in upcoming editions, please do feel free to get in touch.
Jane Braithwaite (left) is managing director of Desig nated Medical, which offers flexible, experienced support for private practice needs. Its experts offer bespoke support across accountancy, marketing, medical PA, HR and recruitment issues, and can work to suit your requirements, tailored to your practice as and when needed
Rehabilitation is the heart of the matter
Cardiovascular disease is a leading cause of death and disability in the UK and much campaigning has been done to raise awareness of the causes, prevention and treatment. But effective rehabilitation following a cardiac event is often left behind, reflects consultant cardiologist Dr Ajay Jain
THE NHS IS facing another incredibly tough winter, with waiting lists remaining stubbornly high 1 and patients in need of cardiac care are facing a real dilemma.
Once discharged after a cardiac event, many patients are waiting months to begin rehabilitation during what is an undoubtedly critical window.
We must all work together to achieve the best patient outcomes and the independent sector has an incredibly important role to play in this, as well as easing the burden on our national health service.
The benefits of cardiac rehabilitation are well documented and there is a strong evidence base for reducing mortality and morbidity associated with cardiovascular disease.2
Guidelines developed by the National Institute for Health and Care Excellence (NICE) strongly recommend that individuals who have suffered from a heart attack are provided with timely access to comprehensive cardiac rehabilitation, which should include vigorous exercise, high-quality health education and stress management.3
Vital rehabilitation
This is further supported by the British Heart Foundation, which has highlighted that cardiac rehabilitation is vital for a patient’s long-term recovery, considering it as important as taking medicine; with regular exercise being a critical part of this.4
Indeed, for those who have experienced a myocardial infarction and/or coronary revascularisation, attending cardiac rehabilitation provides a 2.8% reduction in cardiovascular mortality, as well as reducing acute hospital re-admissions.5,6,7
Our approach as a sector to cardiac rehabilitation has previously been inconsistent at best, with many patients being discharged from private care back to the NHS to receive their rehabilitation.
This means that while we are helping deal with immediate, often emergency situations, we may be delaying evidence-based rehabilitation interventions which ultimately keep patients out of hospital.
St Bartholomew’s Hospital is
Our approach as a sector to cardiac rehabilitation has previously been inconsistent at best, with many patients being discharged from private care back to the NHS to receive their rehabilitation ➱ continued on page 16
The free digital prescribing platform for all private prescribers.
CloudRx take care of the dispensing, payment and delivery of medicines direct to your patients, wherever in the country they may be, for more convenient access to their medicines.
TRANSFORMATIONAL
Order prescriptions at the touch of a button to support all consultations and add a whole new level of convenience for your patients.
SIMPLE, CONVENIENT AND SECURE
Simple and fast digital prescribing.
Legal paperless prescriptions, repeat prescriptions and controlled drugs.
Prescriber fees can be charged to the patient if requested.
INTEGRATED
Our API enables frictionless integration with healthcare brands & clinical software including Heydoc, MidexPRO, eClinic and YouClinic
“We were struggling to keep up with the admin side of the prescriptions, not to mention storage for medication to cope with a huge increase in prescriptions. CloudRx immediately took away the strain. Since our partnership we have grown by more than 200% in size. We could not have done that without their support.”
– Dr Louise Newson, Newson Health
one of Europe’s leading NHS specialist heart centres and earlier this year the first full-scale independent hospital in the City of London opened its doors on its campus.
Nuffield Health at St Bartholomew’s Hospital has launched a new cardiac rehabilitation programme to support cardiac patients seen at the Nuffield Health’s hospital, a unique offering in the industry.
Driven by Nuffield Health’s approach to building a healthier nation, we are proud to be pioneering an end-to-end programme which takes a preventative look at heart health and provides rehabilitation across the entire patient pathway, including providing support for both mental and physical health.
Empowering patients
Cardiac rehabilitation is more than just undertaking vigorous exercise. There is a deep focus on ensuring that patients are empowered to make the right decisions for their own health in a sustainable and manageable way. At the heart of this is making lifestyle changes. This is underpinned by our approach to connected healthcare, which enables us to provide holistic services to all our patients, helping to make sure they stay fit and healthy throughout their hospital journey and, crucially, throughout their entire lives.
The Nuffield Health team of specialist personal trainers, physiotherapists, emotional well-being counsellors, and nutritionists work in close collaboration between the hospital and nearby Fitness & Wellbeing Centre in Barbican so that we can fully understand a patient’s needs and provide them with personalised care.
As the Covid-19 pandemic begins to gradually recede and our collective attention once again falls towards the wider therapy areas such as cardiovascular care, it is more important than ever that we develop a preventative approach to healthcare that helps stop people requiring hospital services in the first place.
At the core of the NHS Long Term Plan is a commitment to support people keeping healthier for longer through a preventative approach to healthcare.8
Our specialist nurses, physiotherapists and exercise specialists help identify lifestyle changes that would most benefit an individual’s heart health and the eightweek programme combines exercise with education and wellbeing support
The establishment of new initiatives for GPs like Directed Enhanced Services (DES) is an excellent step in better identifying early signs of cardiac issues.9
However, the independent sector has an important role to play in helping the NHS to effectively meet these patient’s needs, and taking a fully connected, preventative approach may mean that fewer patients will be required to go back into the system, relieving the pressures for longer.
Our approach to cardiac rehabilitation is leading the way in this, and we strongly believe that the wider independent sector has an important role to play in supporting the NHS in this difficult time by taking a similar approach.
2. Dalal, H, Doherty, P and Taylor, R, 2015. Cardiac rehabilitation. BMJ, p. h5000.
3. Nice.org.uk. 2022. Recommendations, Acute coronary syndromes, NICE. [online] Available at: www.nice.org.uk/ guidance/ng185/chapter/ Recommendations. [Accessed 15 September 2022].
4. Bhf.org.uk. 2022. Cardiac rehabilitation. [online] Available at: www.bhf.org.uk/informationsupport/ support/practical-support/cardiacrehabilitation. [Accessed 1 September 2022].
We at Nuffield Health at St Bartholomew’s Hospital fully recognise that achieving this goal is a challenge, but one we must aim to achieve.
Our cardiac rehabilitation programme offers support for anyone who has heart disease or is concerned they might be at risk of developing it.
Lifestyle changes
Our specialist nurses, physiotherapists and exercise specialists help identify lifestyle changes that would most benefit an individual’s heart health and the eightweek programme combines exercise with education and wellbeing support.
Supervised exercise at Nuffield Health’s fitness and well-being centres helps to increase physical fitness and confidence, while heart health education helps provide patients with knowledge with how to improve heart health, with the overarching aim of avoiding re-admittance into hospital.
Emotional well-being sessions are also offered, helping to deal with the sometimes-profound after-effects of a heart event, as well as looking at reducing potential lifestyle triggers such as stress.
We fully appreciate the work that the NHS is doing in tackling the backlog and we welcome the NHS and Government’s decision to put cardiac care as a core pillar of healthcare policy.
At Nuffield Health at St Bartholomew’s Hospital we are urging cardiologists and GPs to refer to us those patients who would benefit from our services and ensure that they can receive the comprehensive care and treatment they deserve.
That way, we can help build a healthier nation for all.
Dr Ajay Jain (below) is a consultant cardiologist at the London Chest Hospital, part of Barts Health NHS Trust.
He is the clinical lead for the nationally renowned Heart Attack Centre, among the busiest and most effective centres of its type in the UK.
His clinical interests include chest pain, hypertension and structural heart disease. Dr Jain performs closure of patent foramen ovale and renal sympathetic nerve ablation and acts as proctor for several of these procedures.
He sits on the Guidelines and Standards Committee for the British Cardiovascular Intervention Society and is also a consultant cardiologist at Nuffield Health at St Bartholomew’s Hospital in London.
5. Anderson L, Oldridge N, Thompson DR, Zwisler AD, Rees K, Martin N, Taylor RS. Exercise-based cardiac rehabilitation for coronary heart disease: Cochrane systematic review and meta-analysis. J Am Coll Cardiol. 2016 Jan 5; 67(1): 1-12. doi: 10.1016/j. jacc.2015.10.044. PMID: 26764059.
6. Salzwedel A, Jensen K, Rauch B, Doherty P, Metzendorf M.I, Hackbusch M, Völler H, Schmid J.P, Davos C.H. Effectiveness of comprehensive cardiac rehabilitation in coronary artery disease patients treated according to contemporary evidence-based medicine: Update of the Cardiac Rehabilitation Outcome Study (CROSII). Eur J Prev Cardiol. 2020 Nov; 27(16): 1756-1774.
7. Dalal H.M, Doherty P, McDonagh S.T, Paul K, Taylor R.S. Virtual and in-person cardiac rehabilitation. BMJ 2021; 373: n1270 doi:10.1136/bmj.n1270.
8. Longtermplan.nhs.uk. 2022. [online] Available at: www.longtermplan.nhs. uk/wp-content/uploads/2019/08/nhslong-term-plan-version-1.2.pdf [Accessed 1 September 2022].
9. England.nhs.uk. 2022. [online] Available at: www.england.nhs.uk/ wp-content/uploads/2021/09/B0951-vnetwork-contract-des-20-21-cvdsupplementary-guidance.pdf [Accessed 1 September 2022].
BOOK YOUR DEMO
Are you happy with your current software?
Maybe you're completely happy with the software you use to run your practice. Perhaps you have everything in one place, routine tasks are automated, and reporting is accurate and insightful. If so, stop reading now.
However, if you think the day to day running of your practice could be improved, we'd love the chance to demonstrate e-clinic to you.
The number one choice for private practice
Future-proof your practice and offer everything a modern patient expects:
> iPad compatibility
> Online booking & payments with fully integrated card processing
> Electronic consent & treatment forms
> Integrated drugs database & digital prescribing with direct delivery
> Fast & easy patient communications by email or text BOOK
Spire
Give patients all the info they need
Medical marketing expert Catherine Harriss (right) outlined ways to attract self-payers for Independent Practitioner Today back in August 2014. Eight years on and a global pandemic has impacted us all. Here she revisits the topic to see how private practitioners can improve their self-pay income now
A typical self-pay patient
Value is the main consideration and value can be constructed as this: cost plus availability plus outcome potential, including post-op care = booking
IN JULY 2022, there were a recorded 6.84m people waiting for treatment. 2.67m patients were waiting longer than 18 weeks for treatment, with a staggering 377,689 patients waiting over one year; that’s 356 times more patients than in July 2019.
However, many people now find themselves in a very different financial situation to when I last wrote on the self-pay subject. Russia’s invasion of Ukraine has had profound impacts all around the world, culminating in higher costs for all.
This, combined with long NHS waiting times, can only mean that affordability for private practice is declining. Or does it?
According to the Private Healthcare Information Network (PHIN) – the independent, Governmentmandated source of information on private healthcare in the UK –there has been a 30% increase in people self-funding now compared to 2019, with the 60- to 79-year-old age group being the highest.1
Indeed, there is positive encouragement that people want to selfpay. And there’s more. A recent YouGov poll found that 22% of people said that due to the Covid pandemic, they were more likely to use private healthcare than before.
83% felt that, by having private care, they would be seen more quickly and 62% indicated that the pandemic had made no difference to whether they would consider going private.
Many Independent Practitioner Today readers have started private practice for the first time since 2014. Having run successful private practices simultaneously for over 16 years, my experience in marketing and managing them is considerable.
Today’s self-pay patient will have researched you online, thoroughly. It all depends upon what they find as to whether they decide to contact you.
Having spent years speaking to patients daily, I know that they will travel to see you, that they have been watching you, often for ages, by following you on social media and reading your content.
It is a fallacy that your colleagues’ private practice dictates what is available to you: your actions are entirely responsible for the size of your private practice.
Competition remains high and so it should, as this ensures higher standards. But wins are always found for those who provide greater transparency.
Remember these ten tips:
1 Understand the needs of your new patient
Dr Google is an increasingly frequent companion with new patients and will remain so as long as there is anxiety with whatever issue the patient has, which is bound to be the case.
The first impressions are vital both online and in the clinic. Information should be easily accessible so that you can become the beginning of the answer to their problem.
If your information contradicts Dr Google, then you need to have accessible information on your website that backs up everything you say.
2 Know what you can provide for your patient
Is there a new procedure that will benefit your patients? Is this procedure something that your private hospital could assist with advertising or are they keen to invest to help bring in more patients?
Is it possible for you to start offering this new procedure? Is there training that you need to complete?
Substantial experience with niche procedures over 16 years has identified growing local and national markets when potential customers are presented with information that can be easily understood.
Private patients are willing to travel for the right reasons.2
3
Web presence
With the rise of technology in our lives and the increasing use of smartphones, our attention is waning. In 2000, our attention span lasted 12 seconds. This has now declined to eight seconds; less than a goldfish that has nine!
Perhaps while reading this, even, you have looked at your phone or thought about something else. So this lack of attention is translated to a hastiness that we are all party to.
Research indicates that we make our minds up within 0.05 seconds as to whether we stay on a website. Anyone reading this who has young children will notice the speed at which they seem to move around the web: they scan rather than read everything on the page.
The main reason I explain this is because how you portray yourself online is increasingly important. Your web presence needs to speak to your potential patients, not other doctors.
Visitors will read, at the most, around 28% of the page, so what is it about your website and all of its pages that make your ideal patients linger a little longer and want to read more?
Social media is where people browse. Websites are still where people buy and book. Your website should be for your potential patients, not your colleagues. It should be a good reflection of how you are in practice. You should be easily accessible and procedures need to be simply explained.
4 Add value
In marketing terms, value is perceived by what is on offer.
What is the ‘deal’ that the patient is likely to get and experience? Money is changing hands, so the value is never more important. So is this about ‘how’ you explain the initial consultation, the time to wait, the cost and availability for that all-important first meeting? Is there room for value in caring for the relatives, too, especially if they are coming a long distance?
What information is given out to potential patients and their families – if relevant – so that they have time to read and digest all the implications of the surgery they want or need?
Because of all the patient contact I have had before booking, I know that value is the main consideration and value can be constructed as this: cost plus availability plus outcome potential including postop care = booking.
5 Make your benefits transparent
Unsolicited testimonials are the most powerful measure of your authenticity and credibility. Testimonials sought in the clinic can be identified as being not as genuine and do not have the same currency as those voluntarily given.
This is another reason why you do need to have a central website. I have witnessed on too many occasions, people depending upon large portal websites for their own business. Overnight, an algorithm change by Google or a business failure and many people’s businesses are affected detrimentally.
If all your information and feed-
➱ continued on page 20
back is on a central website that you own and control, then the chances of this happening are minimised.
For every testimonial, it should be printed in full, warts and all, typos included along with the date of receipt.
As long as identifiable information is redacted, these messages from past patients are worth their weight in gold. I have lost count of the number of times that testimonials, in conversations with potential patients, have been quoted back to me.
6
Good first impressions
Family doctors’ receptionists generally get bad press for a very difficult and stressful job. But your private practice is something different and your secretary is possibly your patients’ first contact. Are they kind? Helpful? Convey the information correctly? Portray you positively? Do their job?
I
Respond to emails quickly? Some harsh questions, but all very important. This is a business and your secretary is the ‘face’ of your business being the first point of contact.
The surgeons I have worked for have easily gained patients that had planned treatment with others and then gave up, as they did not get answers to their questions, a date for surgery or even a call-back. I heard this so many times. An easy win for my clients, but only because the others were missing a vital part of their business.
7
Simplify the process
One of my clients was a very early adopter of a booking system for their surgery lists. I developed and tested this after definite theatre slots were agreed upon. It was a game changer.
If you think about your purchasing process for a high-value item, you need to know the cost, how long it will take, when it will happen and how to book. Providing all this information up front helps people make up their minds.
Having all this information available means that the process of the secretary having to contact the surgeon to find a slot was reduced to the secretary booking patients in – and then reduced further to receiving the bookings from the booking system enabling the secretary to do other tasks.
Letting the patient choose when suits them by using an online booking system saves so much time, simplifying it for them.
8 Make pricing clear
Many times, too many times over the past years, I have been contacted by someone who rang one of my surgeons out of frustration, as they had been asking someone else – often very local –for a price for their surgery.
The secretary’s response of ‘I’ll get back to you’ has been too long to wait for them. Why doesn’t your secretary know all the prices?
I then took the opportunity to explain my surgeon’s skill and results and while it is not possible to be found by all potential patients all the time, they frequently then booked with my surgeon after deciding that the information available to them was everything they needed to make a decision.
I like to think this was a positive outcome for both patient and the surgeon.
Do you offer package prices for surgery and care? These should be routine now and except for individuals who need extra care –CPAP postoperatively, for example – these prices should be readily available and preferably on your website.
9 Audit
Being held accountable for your actions is commonplace in the NHS and should be so in pri-
vate surgery too. Patients need to understand your competency, but also they need the transparency of the number of procedures you have undertaken and what the outcomes were along with unexpected events, if any.
Success breeds success and so the more information you can provide, the better informed your patients and you will be about your care. Success percentages matter.
10 Guarantee their aftercare
Many private hospitals have a package of care whereby any unforeseen re-admissions are covered within 30 days of surgery. This is so important and reassuring for any potential patient.
What is your follow-up?
Is this clear on your website?
Is it included in the price?
If not, why not?
Is there anything that can be done if your type of surgery is still causing issues?
Patients naturally will be seeking reassurance that they can trust you to do what you say you can. This element combines value, outcome and success.
Do you know what others are doing in your field? How do they portray their aftercare? Ultimately, you should aim to provide a highquality service that people will want to talk to others about and, in turn, will seek you out. I said this in 2014 and it remains the same today.
Self-payers today are more discerning than ever before, wanting to have all the information that they need available 24/7. Your website is the place where this should be.
Make it easy for your patients to book in with you, over-deliver on information to assist them and your practice will continue to grow as a consequence.
Catherine Harriss is the founder of MultiWorks Marketing, but has a new website: https://attractdreamcustomers.com
The self-pay patient is an increasing component of any successful private practice. Simon Brignall (right) discusses the range of payment pathways you will need to help you reap the benefit
GROWTH IN demand from selfpay patients has been a welldefined trend in private practice over the past decade.
At Medical Billing & Collection (MBC), we partner with over 1,700 consultants, groups, clinics and hospitals across all specialties and our data shows that self-pay was increasing year on year as a percentage of the invoices we raised before the pandemic.
The impact of Covid and the subsequent recovery has only turbo charged this trend. With NHS waiting lists already at a record 6.8m and rising, this will bolster the demand for private healthcare from patients who are not prepared to wait.
Data from the Private Healthcare Information Network (PHIN) for Q1 2022 continues to show a surge in self-pay patients as activity is higher than was seen in 2019 – as reported by Independent Practitioner Today last month.
While London remained the most active self-pay market with 13,800 admissions, the regions saw growth of between 20-114%.
There have been many reasons for the increase in the demand for self-pay over recent years, but I will attempt to outline the key drivers.
NHS
With approximately 10% of the population having private health insurance already, some of the
WHY THIS IS IMPORTANT
Remember, self-pay patients benefit the practice because, whereas the fees for insured patients have remained static or reduced over the past decade, the consultant has complete autonomy in this area.
Consultants can set their fees based on factors such as their experience, the demand for their services and their competition. If you have not updated your fees in a while, this could be a good time to conduct a review of your fee structure to ensure you optimise your income.
remaining 90% of the population impacted by NHS delays have elected to go private.
And with headlines in the press suggesting rising NHS waiting lists, this demand for private healthcare will only continue to increase.
Many self-pay patients who previously were presenting as consultations and second opinions are now converting to treatment.
Wealthy elderly patients
Wealthier elderly patients, many who have benefited from rising house prices, are in a better posi-
➱ continued on page 22
tion to access private healthcare than ever before.
Many now see private healthcare as an option that is for them and, alongside their greater quality-oflife expectations, this means that they are more likely to go private than previous generations.
Increased patient expectations
We have come a long way in the past few decades. Patients no longer feel that healthcare is something that is done to them. Many patients wish to have more choice with regards to their clinical pathway.
This is often where the private sector can excel offering a wide range of clinicians, facilities and treatments.
We may debate the terms that are used from ‘patient’ to ‘consumer’ but the demand for increased choice and higher expectations are here to stay.
International patients
If your practice is based in central London, then international selfpay patients have been a key component, with patients coming from outside of the UK seeking private healthcare.
This area was immediately impacted by travel restrictions imposed at the start of the pandemic, but we have seen increased demand from these patients since 2021.
Best practice
We have shown the value of the self-pay sector and so it is important to make sure these patients are managed effectively both from a billing and collection perspective. However, from our experience, this is often not the case. Practices rarely offer appropriate payment options to allow for simple invoicing and payment collection and the chasing of outstanding debts can be sporadic. This results in practices building a large amount of outstanding debt leading to cash flow difficulties or loss of income.
The reasons for this debt problem is that practices fail to implement robust procedures to effectively manage these patients. Ask yourself these questions: Do you know the percentage of your practice that is self-pay?
MENTAL HEALTH, PRIVATE GPs, AND WALK-IN CLINICS
The mental health sector proved to be more resilient than other specialties during the pandemic, as practitioners were able to quickly transition to remote consultations.
Many practices now offer both remote and in-person clinics to their patients as part of their tool kit.
At MBC, we have seen a growth in private GPs, with many hospitals and clinics choosing to add private GPs to the range of services they offer.
The reason for this is that they find GPs to be a useful referral channel to their other core services. Walk-in clinics, which offer a range of services from same-day access to a GP through to other services such as sexual health screening and vaccinations, are now common in most city centres.
Self-pay typically forms a large proportion of the patient demographic of practices in this field and the ongoing relationship practitioners have with their patients means that the payment pathway needs to be simple and effective.
What type of self-pay patients are they?
Once you have this data, it is vital that your practice has systems in place to deal with each self-pay type.
I will elaborate further on the main types we see at MBC.
UK self-pay
For self-pay patients, it is important that you have a published price list or to have notified the patient of their fee in advance. It is best practice to also confirm the payment options that are available and when payment is due.
At MBC, we have a variety of methods available to offer our clients tailored to the needs of their practice:
Most commonly, we invoice patients after their treatment, offering a range of payment options which includes a link to our payment portal for 24/7 payment collection or via our payments team;
We also offer the option to invoice patients in advance for treatment, where required;
Monies can also be collected on the day via our client self-pay platform.
Remember, when you are invoicing patients post-treatment, you will need to put in place a robust chase process for any outstanding invoices and ensure this is
repeated regularly until payment is collected.
Failure to implement effectively is the most common reason why debt levels increase and can lead to cash flow difficulties.
Overseas patients
If you are going to see a patient who is not a resident of the UK, it is even more important to make sure that your fees, method of payment and payment date are made clear, as once they leave the country it is extremely difficult to collect any money owed.
When we deal with international self-pay patients on behalf of our clients, we routinely collect payment in advance of treatment.
Collection by the hospital or clinic
When we deal with international self-pay patients on behalf of our clients, we routinely collect money in advance of treatment
Many hospitals and clinics collect money on behalf of their clinicians as part of a fixed price package for a procedure where the consultants, anaesthetist and facility fees are combined to show one price to the patient or simply for a consultation.
It is very important not to overlook this area of self-pay, so make sure that these patients are recorded, reconciled and chased. Hospital administration can vary dramatically between facilities or get impacted by changes to staff. It is very common for payments to be delayed or, worse, missed entirely.
We raise an invoice to the hospital for consultants’ fees, reconcile the payments and chase the relevant finance department when required.
Regular patients
Some practices, due to the nature of their specialty, either regularly treat or form a long-term relationship with the patient and patient’s family.
Mental health practitioners can see patients regularly over a period and a private GP practice may look after an extended family for decades. The fact that these patients will require repeated invoicing makes it even more important that the process is as simple as possible
We provide the ability to settle multiple invoices at the same time as well as provide our clinicians with a payment link that they can add to their website.
As most patients do not review the terms of their insurance policy, they assume that all costs are going to be met by their insurer
Insurance shortfalls
To help control the cost of premiums many private medical insurance companies have amended their policies to include everincreasing elements which are either not covered, have thresholds or require co-payments or excesses.
These patient liabilities still fall on the practice to administer, which means they must have a process in place an ensure that it is routinely followed.
This is always the area that even the most efficient practices find challenging and often makes up most of their aged debt.
As most patients do not review the terms of their insurance policy, they assume that all costs are going to be met by their insurer; so when they receive an invoice for an outstanding balance not covered by their insurance company, this can come as a shock.
From our experience, a lot of patients will ignore the invoice, thinking that it is either a copy of what has been sent to the insurer or that their insurance company is liable. Which means it is important to follow up with the patient directly and explain what it owed.
Some patients will wish to contest this with their insurer because they may believe that the company is liable – which is why it is important to highlight any issues as soon as possible to minimise delays.
Once the patient accepts that the money is owed by them, then steps need to be put in place to chase outstanding balances and take payment.
Moving forward
Self-pay has been the growth sector in private healthcare in recent ears and, combined with the fact that you get to determine your own fees, it is of increasing value too.
It is important that you review how you manage these patients to ensure you offer them the range of functionality they require.
Consultants often find the best solution is to partner with a billing company that offers both the expertise and full range of functionality you need.
Simon Brignall is director of business development at MBC
A storm brewing in
The challenges facing healthcare in the UK today are complex and the consequences of the pandemic will continue to be felt across both the NHS and the private sector. They are now more than ever reliant on each other to meet the health needs of the UK population, says Tim Morris (below)
WE HAVE seen unprecedented challenges over the last two years across healthcare, with resources from both public and private hospitals being used to fight the global Covid-19 pandemic.
The traditional dynamic between the two sectors has become distorted since 2020, and as we emerge into a postpandemic world; both private and public practice are facing significant challenges.
At Elsevier, we want to understand these future challenges better, so we can work with partners across the healthcare sector to meet them head on and continue to improve patient outcomes.
In the UK, there is currently a huge backlog of patients, particularly in oncology. Many patients had their surgeries and treatments postponed throughout the pandemic, as hospitals looked to manage the mass influx of Covid-19 admissions.
Private hospitals, which traditionally are heavily dependent on patients funded by insurance, saw an increase in the number of self-paying patients who perhaps would not have previously considered private practice for everyday ailments.
Most recent data, as I write, from the Private Healthcare Information Network (PHIN) shows the number of UK self-pay admissions between 2019 and 2021 increased by 29%. Now, concerns around delays for referrals and waiting lists for treatment are motivating new patients into the private sector for care.
To support efforts to reduce patients’ wait for routine care,
the NHS again may have to rely on private practice and increase spending on private facilities.
The Government needed the independent hospital sector throughout the pandemic to increase capacity – requiring access to additional beds, staff and equipment to treat patients during the peak of the pandemic. As a result, spending by NHS commissioners on services delivered by the private sector increased by £2.5bn between 2019-20 and 2020-21 to £12.2bn.
The longer-term perspective is that there is a storm brewing across UK health and care services.
Ageing population
We have an ageing population and the proportion of those who are living with long-term chronic conditions is growing, as is the number of younger people presenting with co-morbidities.
The reality is that both public and private healthcare will increasingly be dealing with a significant number of patients requiring more complex and continuous care.
The number of Brits over the age of 85 is predicted to double to 2.6m in the next 25 years and, as such, the population that is dependent on continuous care will also significantly grow.
In addition to this, it is now estimated that a third of middleaged adults in the UK have at least two chronic health issues. And research published in the BMJ has found the risk of middle-aged adults in the UK developing dementia is 2.5 times greater for those that have two or more chronic health issues.
in healthcare
The longer-term perspective is that there is a storm brewing across UK health and care services
There is also a growing number of younger people with comorbidities and obesity-related diseases, as well as the unknown toll of patients suffering from both the physical and mental health impact of Covid-19.
These groups of patients will contribute to the healthcare burden as they age, presenting challenges when planning health and care services for the future.
Critically, these challenges will be coupled with a growing clinician shortage due to persistent burnout and stress.
Global survey
Elsevier Health recently developed the Clinician of the Future report to explore global trends and changes that will impact the future of healthcare.
Through a global survey of nearly 3,000 clinicians from 111 countries, healthcare professionals considered the consequences of the pandemic and provided insights on the challenges and opportunities they expect to face over the next decade.
The data published in the report reveals that 94% of clinicians globally believe the rise of chronic health issues – including heart disease, cancer, chronic obstructive pulmonary disease, and diabetes – will be a key driver of change in healthcare over the next ten years.
Furthermore, 71% of clinicians believe the increase in comorbidities in younger patients will also play a pivotal role in the changing healthcare landscape.
The report suggests a shift to preventive care could potentially reduce the burden of chronic illness and, in the longer term, result in people visiting healthcare facilities less often.
However, findings show that 79% of clinicians believe there is currently not enough being done
on preventive care, and 84% agreed that patients with age-associated diseases will make up the majority of the patient population in ten years’ time.
The Clinician of the Future report highlighted the widespread workforce shortages and staff burnout resulting from sustained work pressure, with 47% of UK clinicians indicating they are considering leaving their current role within the next two to three years.
In addition to this, 86% and 88% believe there will be a shortage of doctors and nurses in the next ten years. Findings suggested those leaving the profession may be doing so due to a general feeling of being undervalued and unappreciated.
Only 18% of UK doctors believe the critical importance of the work they do is fully appreciated by government officials, and only 39% feel appreciated by the public.
The challenges facing healthcare in the UK today are complex, and the consequences of the pandemic will continue to be felt across both the NHS and the private sector. The reality is that the NHS and the private sector are now more than ever reliant on each other to meet the health needs of the UK population.
Only by listening to clinicians and understanding where and how the two systems need to work together effectively, can we begin to manage the scale of the health crisis in the UK.
To find out more on the Clinician of the Future report, visit https://www.elsevier.com/ connect/clinician-of-the-future
Tim Morris is commercial portfolio and partnerships director at medical publisher Elsevier
MESSAGING APPS IN HEALTHCARE
Why it’s bad to use WhatsApp
Despite the popularity of WhatsApp as a platform to converse with family, friends and even colleagues, there is a huge questionmark around its confidentiality.
Simon Hemingway examines the implications of using WhatsApp for communicating in a healthcare environment
IT IS no surprise that Facebook/ Meta-owned WhatsApp is the world’s most popular messaging application; as of 2022, it has around two billion users.
Over time, the convenience, ubiquity and familiarity of the platform has meant that it is becoming increasingly used in a workplace setting, as a way for colleagues to communicate and share information relating to clients or – in a healthcare environment –patients.
However, using WhatsApp in the healthcare sector is ill-advised.
In July, the UK’s Information Commissioner called for a Government review into the risks and areas of improvement around the use of private correspondence channels, in light of a year-long investigation into the use of such channels by ministers and officials at the Department of Health and Social Care during the pandemic.
The investigation revealed that ‘the clear lack of controls and rapid increase in messaging apps and technologies – such as WhatsApp – had the potential to lead to important information around the Government’s response to the pandemic being lost or insecurely handled’.
The rise of WhatsApp among clinical teams
If you search for evidence of WhatsApp being used in a healthcare setting, you would not be hard-pressed to find it, with some articles dating back years.
In 2015, NHS England addressed the use of WhatsApp in the 21st edition of its Information Governance Bulletin , stating: ‘Whatever the other merits of WhatsApp, it should never be used for the sending of information in the professional healthcare environment.
‘WhatsApp is a consumer service, which does not have a servicelevel agreement with users and has no relevant data security certification. There is no valid reason for its use within the NHS. Only apps that have been specifically approved by NHS England should be used.’
Three years later, research published in BMJ Innovations found a widespread use of WhatsApp for communication between healthcare professionals.
According to the study, 97% of
doctors routinely send patient information on instant messenger without consent, despite the fact 68% were concerned about sharing information in this way.
In 2021, a study entitled ‘WhatsApp in Clinical Practice’ was published, with the aim of reviewing the literature on how clinicians who use WhatsApp in clinical practice keep medical records of the content of WhatsApp messages and how they store messages and/or attachments sent via the platform.
In the abstract, it highlights how there is a ‘general lack of awareness or concern about flaunting existing privacy and security legislation’.
More than just a privacy issue
Other than the widespread popularity of WhatsApp, it’s not hard to see why medical professionals would choose to use the platform.
There’s no requirement for a computer, with a possibility of an immediate response being some of the biggest benefits. However, in this case, the cons far outweigh the pros.
Although standard WhatsApp promises end-to-end encryption, it is nowhere near robust enough for internal comms at work.
Consumer-grade messaging apps are long-established and relatively easy targets for malware and other cybercrime, putting confidential patient information at risk.
A report called ‘WhatsApp in Hospital? An Empirical Investigation of Individual and Organisational Determinants To Use’ alluded to WhatsApp in a healthcare setting being an ‘extreme case of back-door adoption’, whereby they are used ‘without formal approval or assessment from top managers about the opportunities and risks that these innovations might bring along with them’.
This can create silos of information known only to members of unofficial and unaccountable messaging groups, with the near impossibility of knowing who is in any given messaging group, as well as the difficulty of ensuring that former staff members have been removed from all groups.
Other dangers include the lack of a coherent audit trail, a lack of
WhatsApp generates unnecessary risk, so should be avoided in the workplace at all cost
THE DANGERS OF WhatsApp
➲ With around two billion users, WhatsApp’s ease of use is leading to it becoming used more and more in healthcare settings
➲ Although NHS England advises against the use of this platform, a study by BMJ Innovations found a widespread use of WhatsApp for communication; 97% of doctors routinely send patient information on instant messenger without consent
➲ One healthcare report states that WhatsApp in a healthcare setting is an ‘extreme case of back-door adoption’ – used without formal approval
➲ The use of WhatsApp is ill-advised for a number of reasons, including:
It does not ensure privacy and is open to cyber attacks
It creates silos of information known only to members of messaging groups, with the near impossibility of knowing who is in any given messaging group, as well as the difficulty of ensuring that former staff members have been removed from all groups
It does not provide an audit trail
It cannot be integrated into existing systems
It blurs the lines between work life and home life
Other communications platforms exist on the market that are GDPR-compliant and are sectorspecific
integration with wider business systems, the transference of patient-identifying information and the illusion that staff need to be available 24/7.
Research from Text Anywhere found 73% of employees are contacted by their manager or colleague about work when they are on annual leave, with experts warning this can lead to greater anxiety and stress.
What is the solution?
Hospitals and other healthcare organisations can empower clinicians, accelerate workflows and reduce operational costs by leveraging mobile technology – if design, deployment and implementation are done right.
WhatsApp, as discussed throughout this article, generates unnecessary risk, so should be avoided in the workplace at all cost.
There are many other other communications platforms available that are designed to be implemented as part of a carefully planned mobility strategy – often
tailored for specific sectors, use cases and devices – which are secure, efficient, compliant with the General Data Protection Regulation and can be integrated with existing software and systems.
A tailor-made platform that offers more value add than just messaging is also a very good productivity investment, while ensuring there are no risks to employees’ physical or mental health, with messages sent outside of office hours, or while on holiday, encouraging them to mix work and pleasure.
Simon Hemingway (below) is healthcare director at technology solutions integrator The Barcode Warehouse
People report improving
The latest Bupa Wellbeing Index data shows encouraging signs of improvement in our national health and well-being. However, we must not take our eyes off the ball, writes Dr Robin Clark (right), medical director for Bupa Global and UK
improving health
AS THE UK approaches its third year of living with Covid-19, we are cautiously optimistic that the worst of the pandemic may now be behind us.
However, as we found in the baseline Bupa Wellbeing Index survey, collected in March and April 2022, there are still barriers to accessing healthcare which the pandemic has only heightened.
Treatment delays and lost appointments continue to be a cause for concern, with the latest figures showing that more than 6.73m people were waiting for treatment for a health condition in June – an all-time high.1
Worryingly, the BMA warns that in addition to current wait times, there is an additional ‘hidden backlog’ of patients who require care but have either not yet presented or who have had referrals cancelled due to the impact of Covid-19.
These are patients who, in normal times, would have been referred for treatment, received elective care and attended outpatient appointments, but who, for a number of reasons relating to the pandemic, have not yet found their way into the health system.
Lower immunity
And the spectre of seasonal influenza is also on the horizon. During the last couple of years, measures put in place to control the spread of Covid-19 meant most of us have had less exposure to illnesses such as flu.
As a result, we have lower natural immunity, resulting in the increased likelihood of becoming unwell with flu this winter.
Infectious disease experts point out that herd immunity is significantly lower than usual, with children under two years of age having no exposure at all and this is compounded by a fall in influenza vaccination rates.
Early signs of improvement
Despite the uncertain backdrop, the findings from the second Bupa Wellbeing Index collected in July to August 2022 show incremental improvements in the nation’s health and well-being since the baseline survey.
The number of respondents who rate their physical health positively has increased slightly since the last survey, with 54% now describing their health as ‘very good’ or ‘somewhat good’ – up from 51%.
Younger adults are particularly upbeat, with 26% describing their physical health as ‘very good’, compared to 18% previously.
A big factor in this is undoubtedly a return to normality. During the pandemic, lockdowns and general uncertainty made it difficult for many people to maintain a consistent exercise regime.
We also know that working from home impacted younger adults more severely and research by the Royal Society for Public Health (RSPH) identified a number of reasons for this.2 This demographic is far more likely to be living in shared households without a dedicated workspace.
The RSPH found that people with multiple housemates were far more likely to report that home working was worse for their health and well-being (41%) compared to those on their own (29%) or who were living with a partner (24%).
A quarter were also working from a sofa or bedroom, which puts them at much greater risk of musculoskeletal problems.
This can also be seen in the Bupa Wellbeing Index, which shows a fall in the number of younger adults identifying back pain and other MSK problems as their primary health concern – compared with their weight, which is the ➱ continued on page 30
mPrescribe® app allows you to prescribe flexibly without a laptop, for same day or next day delivery to your patients nationwide
Secretary Supported
Administrator access reduces workload for practitioners. mPrescribe® facilitates patient entry, status monitoring and preparation of prescriptions for mobile authorisation.
Clinical Governance
Co-founded and co-owned by leading private clinicians, our secure and encrypted technology is compliant with all GPhC, GDPR and e-Prescribing regulations.
“Wonderful, seamless, easy to use service.” Dr Catrin Bevan, London General Practice
“Competitively priced.” Dr Sean White, Consultant in Pain Medicine
“Intuitive and secure.” Dr Tim Wigmore, Consultant Intensivist & Anaesthetist, Schoen Clinic
“Delivered the same day.... Outstanding!” Dr Elisa Astorri, Academic Physician Rheumatologist, Rheumatology
“Go the extra mile.” Dr John O’Donohue, Consultant Gastroenterologist
number-one health concern of that age group and the general population.
Now 11% of 16- to 24-year-olds say MSK is a key concern compared to 13% previously, and 15% of 25- to 34-year-olds compared to 17% previously.
Men are generally more positive about their physical health (55% compared to 51% previously) and 19% now describe their physical health as ‘very good’, compared to 16% previously.
With so many businesses implementing hybrid working for the long-term, it is really important that we encourage patients to address any pain or discomfort they experience when working from home.
Simple changes such not working from beds or beanbags, sitting up with feet planted on the floor, adopting hands-free sets for long phone calls and making time to stretch can go a long way to preventing strain.
IMPROVEMENTS IN MENTAL HEALTH
One of the few positives to come from the pandemic is that it has shone a spotlight on mental health and the help available. It increased the speed of innovation in digital health services, including mental health platforms and these have been promoted by healthcare providers and insurers.
Access to online therapies and digital support from platforms such as Calm has allowed many more people to access evidence-based care for mental health challenges when they need it and in a way which works for them.
The latest UK Wellbeing Index confirms significant need and demand for this sort of support, with 33% of those with employer-provided health and well-being benefits reporting that they had used some kind of mental health support service in the previous 12 months.
The most common reasons for seeking help were anxiety (11%) and depression (9%) and younger adults were the most likely to seek help, with 55% of 16- to 24-year-olds having used workplace benefits to access a mental health service.
While the duration of the pandemic’s mental health impact is still to be determined, the latest data for mental well-being shows improvements, with 26% of respondents reporting their mental health is ‘very good’ compared to 22% previously.
Overall, 58% now rate their mental health positively, compared to 54% at our barometer baseline and there has been a 10% uplift in the number reporting ‘very good’ mental health: 26%, up from 16% at baseline. Older adults are the most positive, with 62% of 55- to 64-yearolds and 73% of over-65s now feeling good about their mental health.
Reduced anxiety about Covid-19 and a return to relative ‘normality’ are likely to be factors in this improvement, but it is likely to also reflect the fact that more and more people are seeking support now.
This is borne out by our experience at Bupa. We have seen claims for mental health conditions increase by 40% between 2019 and 2021 and this increase is reflective of the national picture.
Between April 2020 and May 2022, the number of people in contact with public mental health services climbed from 1.31m to 1.62m and the number of new referrals rose from 0.21m to 4.2m.
The latest Bupa Wellbeing Index data also confirms improvements in general well-being, with 59% of respondents confirming this – 18% said their well-being is ‘very good’ and 41% ‘somewhat good’ – up from 56%, 16% and 40% respectively.
Fitness levels have risen by 13%, with 43% saying their general fitness is either ‘very good’ (12%) or ‘somewhat good’ (31%). Men continue to rate their fitness more positively than women, with twice the number of males having ‘very good’ levels as women: 16% versus 8% of women.
While the latest data shows that overall health and well-being is improving gradually, it is important to remember there are a broad variety of factors impacting people’s physical and mental health. We should not be complacent about the findings and must continue exploring innovative ways to improve our nation’s health.
Shifting health concerns
WHEN WE delve into more specific concerns, weight continues to be the most common wellbeing worry, with 31% citing it as their number-one concern, down slightly from the 33% reported in our baseline survey.
Back pain and other musculoskeletal problems have now overtaken mental health and physical fitness to be the second most common health concern, with 19% of men and 24% of women identifying these pain problems as their biggest concern.
Women’s health conditions such as menopause, menstrual health and endometriosis are still serious concerns in the baseline data, although these have fallen slightly since the last Index – from seventh to 11th.
Women over the age of 50, the time when women tend to experience menopause, are the fastest growing demographic in the workplace.
So it is no surprise that menopause support has become something that businesses are becoming increasingly aware of, with those who offer support for symptoms seeing greater productivity and performance from their employees.
As well as menopause, organisations are beginning to recognise the need for more support with menstrual health as women’s health continues to creep up the agenda. Supporting women’s health is essential to a resilient workforce during these uncertain times.3
The workplace front line for care and support
IN THE context of an uncertain economic climate and the health legacy of the pandemic, people are increasingly looking to their employer for support with their health.
Not only do employers have a duty of care towards their employees, but attractive well-being packages are an increasingly important benefit to attract and retain talent. And this trend is likely to continue.
The latest Bupa Wellbeing Index findings show that 33% of respondents believe their employers have a responsibility to support their health and well-being, and 53% say they are more likely to choose to work for an organisation which offers good health and wellbeing benefits. One in five has already changed jobs to secure better benefits.
As the economic situation means that real-terms wages are falling at a record rate and pay rises and bonuses may not be on the immediate horizon, knowing that high-quality healthcare is available in times of need eases one area of concern for people.
The Bupa Wellbeing Index
found that health insurance ranked in the top three most sought-after benefits for 39% of employees, following flexible working (53%) and a company pension scheme (46%).
The Wellbeing Index suggests that increased demand is part of a longer-term trend towards staff placing more focus on well-being.
Of those surveyed, 55% said their health is now more important than ever and 41% say the pandemic has pushed health and well-being up their list of priorities.
Health maintenance is particularly important for those entering the workforce, with 33% of 16- to 24-year-olds saying the pandemic has made them more motivated to look after their physical and mental well-being.
This is higher than all demographic groups except the 55- to 64-year-olds, who are approaching retirement and are likely to have become aware of the value of health and well-being benefits (34%).
Conclusion
When our first survey was carried out in March and April, we were in
The Bupa Wellbeing Index found that health insurance ranked in the top three most sought-after benefits for 39% of employees
Bupa’s WELLBEING INDEX
Carried out by Censuswide, this rolling dataset will track five key health and well-being metrics for 8,000 UK adults each quarter, capturing a range of health, well-being, lifestyle and behaviour datapoints to help us and our healthcare partners understand more about the nation’s health.
The survey population is split by demographics including sex, age and geographic location, which enables us to explore key trends and spotlight where there are potential issues so that we can continue to design and deliver healthcare in the most impactful way.
the midst of a spike in Covid-19 infections with uncertainty about rising infection rates and the increased virulence of the Omicron variant.
Now the survey has taken place in more settled circumstances, with normality returning and people able to resume something closer to their usual routine. Consequently, our respondents are beginning to feel improvements, with more rating their physical and mental health positively.
As healthcare providers, we need to encourage our patients to keep up this momentum and build on it, leveraging the motivators identified in the previous survey – the desire to be there for family, to improve life expectancy and head off serious health problems.
In mental health, more people are seeking and getting the care that they need, with many using their employer-provided health and well-being benefits to do so.
However, we must be mindful of the significant pressure this puts on mental health services.
Speed of access may become more of a concern and, as in physical health, it is vital that we understand the barriers to access preventing the ‘hidden backlog’ of patients taking up the care that they need.
With people placing greater emphasis on company health and well-being benefits, this will encourage employers to offer the option of private healthcare to more, enabling faster access to the treatment they may need.
As healthcare providers, it is important we demonstrate the many benefits of private care so that those who are new to the market really appreciate its full value.
The Bupa Wellbeing Index can be read in full at www.bupa.com/ news/press-releases/2022/ demand-for-workplace-benefitssoars
NHS Pensions & Annual Allowance Tax
Get ready in advance of April 2022 when the proposed changes to the NHS Pensions will allow you to reclaim some or all of any Annual Allowance tax you may have suffered in the past.
With our knowledge and in-house calculators, we will be able to predict in advance and check statements produced by NHS Pensions and Scottish Public Pensions Agency for accuracy for any refunds due.
For further information contact us at aa@semail.co.uk or telephone 01625 527351.
When faced with market volatility and alarming headlines, it can be useful to take a new perspective. Simon Bruce (right) gives an upside-down view of currencies and exchange rates
Sterling’s woes or dollar strength? Sterling has been falling against the US dollar for some time, but, turning this upside down, the dollar has been strengthening against Sterling.
In fact, due to its status as a ‘safe-haven’ currency and the Fed’s more aggressive rateraising strategy, which has resulted in more
to 27 September 2022
attractive shorter-term yields, the US dollar has strengthened against most major currencies over the past year, attracting global capital. It is also a major energy exporter, which adds extra support.
The DXY index that tracks the dollar against six major currencies stands today at a 20-year high.
Data: Google
Figure 1: Dollar strength is the key driver of currency ‘weakness’ – one year
storm
As the chart on the left illustrates, Sterling is largely unchanged against the Euro and the Japanese Yen over the past year.
A consequence of the weak pound is importing inflation, as around one third of household consumption is made up of imports, which are now more costly.
From an investor’s perspective, a rising US dollar provides a positive contribution to Sterling-based returns, as US assets are worth more – over 20% more – in the past year. This has helped to shore up portfolio returns for many.
The UK equity market is down only around 3% in the past year, supported by large holdings to sectors such as energy and low holdings to technology. This is combined with the fact that a
majority of earnings are from overseas, benefitting to some degree from these exchange rate movements.
No one really knows where Sterling will go from here and over what time frame.
Hedging fixed income assets remains sensible, as this reduces their volatility, and remaining unhedged – that is to say, exposed to currency movements – in equity assets continues to make good sense and will support portfolio values if Sterling falls further.
Inflation and interest rate rises
Rising interest rates are a global phenomenon as the countries grapple with high inflation caused by a rapid growth in the money supply (quantitative easing), supply side issues caused by Covid and the price pressures on energy and food created by Russia’s war in Ukraine.
The fact that the UK Government needs to borrow more, as a consequence of the energy cost support packages and its unfunded tax cuts, is also contributing to rising yields.
But take a look at inflation, central bank interest rates and bond yields in a number of major economies in the chart above.
It is evident that inflation is universally high. Five-year bond yields are at or near 4% in all but one of these economies and all have risen materially in the past six months.
While that is bad news for mortgage and other borrowers, who have benefited from an extremely low cost of borrowing for many years, it is better news for those
Investors who own globally diversified portfolios of equities and higher-quality shorter-dated bonds should be well-positioned to weather any possible storms
As a consequence, investors’ future liabilities are likely to be more easily funded by their assets.
There is a school of thought, including that of the former chancellor, that the recent support for the supply side of the economy – that is to say, increasing productivity and output – by incentivising companies and entrepreneurs through tax reductions may lead to higher rates of sustainable growth in the future, which will, in turn, help to reduce inflation and allow the Government to bring down debt.
holding cash or investing in bonds.
Despite bond price falls as a consequence of yield rises, long-term investors will be better off, over time, from yields at 4% than at near 0%, which we saw 18 months ago.
In the UK, real (after inflation) yields on index-linked gilts are now in positive territory for the first time since 2010. That is good news for investors.
Obviously, this would take time. The markets currently seem unconvinced. In essence, no one knows how this all plays out exactly.
There is no doubt that there will be uncertainty ahead, but investors who own globally diversified portfolios of equities and higherquality shorter-dated bonds should be well-positioned to weather any possible storms.
Simon Bruce is the chief executive of Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS.
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
Figure 2: Inflation and interest rates on 27 September 2022
Date source: Countries’ central banks. Note that inflation for Germany and Italy is the Eurozone inflation rate
Don’t simply presume
Doctors working for private providers who have been commissioned to provide services to NHS patients, or undertaking extra work through NHS waiting list initiatives, should check that they hold adequate indemnity, warns Dr Sophie Haroon (right)
WE ALL know we need protection for clinical negligence claims when seeing private patients.
And we tend to think that when seeing NHS patients, state-backed indemnity provides the necessary protection in the event of a claim raised by them.
But the NHS is always evolving, and sometimes private providers are commissioned to provide NHS services to NHS patients, and this can complicate things.
It may all look like the NHS, but clinicians working under these arrangements may have an alternative indemnifier for claims, provided by the private provider, or may be required to arrange their own indemnity for claims. It is important to check the arrangements.
Lesson number one: Indemnity for claims arising from treating NHS patients receiving NHS care through private providers may not lie with the state.
Waiting List Initiatives
What about the extra work you may be engaged in through waiting list initiatives (WLIs)? As the NHS ramps up its Covid-19 recovery plan and WLIs run in earnest, who is responsible for providing indemnity in the event of a claim?
The WLI work may be run out of an NHS hospital or the independent sector. The setting may not seem relevant. You are head down, doing the work.
Usually state-backed indemnity would provide protection against claims arising from treating WLI
NHS patients. The provider commissioned to undertake the WLI NHS work can enter into an arrangement for protection for claims from the relevant statebacked clincial negligence scheme.
However, there are a myriad of WLI arrangements across the UK home nations. Sometimes the provider does not obtain state-backed indemnity and then, importantly, clinicians may be required to obtain their own indemnity for seeing WLI patients.
Lesson number two: Statebacked indemnity does not always cover WLI NHS patients.
Check your contract
Doctors should check the indemnity arrangements in their contracts. ‘Contract?’, you ask. ‘What contract?’
How many jobs have you been in where you have had a formal contract outlining all the necessary working arrangements including indemnity arrangements?
For every job, every aspect of your work – substantive, temporary, locum, WLI work – get a contract and get in writing who will protect you in the event of a claim. Make sure you are clear on whether or not you need to arrange your own protection for claims. And do not forget to keep those contracts, because you may need to revert to them many years from now.
Lesson number three: Contracts are important.
For every job, every aspect of your work – substantive, temporary, locum, Waiting List Initiative work – get a contract and get in writing who will protect you in the event of a claim
presume you’re covered
KEY POINTS
Indemnity enables you to request assistance in the event that a claim is brought against you
Be clear on your indemnity arrangements for all aspects of your practice
Ensure you have this in writing in any contracts
Keep your contracts so you can refer to them in years to come
Check the indemnity arrangements before you engage in the work
Obtain support for all medicolegal matters for the entirety of your work – not just claims. The state-backed schemes only provide protection against claims
Sorting out or confirming the indemnity arrangements in place may be the last thing on your mind when setting up a job, shift or some extra work.
But it is important to know where you stand before you start.
The GMC requires all clinicians to have the relevant indemnity or insurance in place to protect the full scope of their work and practice, regardless of who they are seeing and in what setting .
Lesson number four: Ensure you have clarity on your indemnity arrangements prior to engaging in any work.
Get covered
While state-backed indemnity protects against NHS clinical negligence claims, it does not provide assistance with matters such as complaints, disciplinaries, regulatory investigations, inquests and criminal investigations.
These can be challenging to manage and costly to defend. Let your medical defence organisation know about the entirety of your work where you might need to draw on their help, including how many hours, sessions and extra bits you do such as WLI work – even if you have confirmation that there is state-backed protection.
Lesson number five: It is essential to have membership with a medical defence body or insurer so you can request assistance with medico-legal matters not included in state-backed schemes.
Dr Sophie Haroon is a medico-legal consultant at Medical Protection
CASE STUDY
Mr Y undertook regular work in his local private hospital on private patients and had the requisite protection for claims through his medical defence organisation (MDO).
He was then asked by his local NHS trust to undertake some Waiting List Initiative (WLI) work on NHS patients at the same private hospital. Given these were NHS patients whom he would normally have seen at his local NHS trust, he thought that seeing them would be under the same arrangements as his standard consultant contract.
Unfortunately, Mr Y received a claim arising from an operation he had done on one of the WLI NHS patients. He approached the legal team at his local NHS trust who advised him that he needed to have had in place his own protection for claims arising from treating NHS WLI patients. They said the contract they had with the independent sector at the time did not set out that claims relating to this cohort of patients would come under the Clinical Negligence Scheme for Trusts (CNST).
Mr Y approached his medical defence body, but it was unable to assist, as his indemnity only protected against claims relating to his private patients. He had to seek independent legal advice to manage the claim and had to fund it himself.
HANDLING COMPLAINTS IN NHS PRIVATE PATIENT UNITS
Bringing PPUs in line with private hospitals
The Independent Sector Complaints Adjudication Service (ISCAS) is planning to take a pilot study forward with two NHS private patient units to make it easier for private patients to complain. ISCAS director Sally Taber reports
PATIENTS HAVE rights to candour by their healthcare provider and to complain and to escalate a complaint to an external review stage.
For patient complainants treated by the NHS, there is a clear path leading to the Parliamentary Health Services Ombudsman (PHSO) and, for patients in the independent sector, there is the ISCAS Code.
But confusion arises for private patients treated in an NHS hospital private patient unit (PPU).
Patients in NHS PPUs, which are commercial entities, are not allowed to take forward complaints through the PHSO – and this is unlikely to change in the foreseeable future.
The closest equivalent to the PHSO is ISCAS. The majority of larger and small independent hospitals are signed up to ISCAS, which provides independent, third-party arbitration if complaints are not resolved directly with the organisation, as recommended by the Paterson Inquiry in 2020.
Both the NHS and ISCAS incorporate a common complaints standard framework in their complaints code:
Promoting a just and learning culture;
Welcoming complaints in a positive way;
Being thorough and fair;
Giving fair and accountable responses.
Now the long-established ISCAS has made a proposal to the
Department of Health and Social Care to work with two NHS PPUs to trial its Code for Handling Patient Complaints in the PPU environment.
These proposals have been made to the University Hospital Southampton NHS Foundation Trust NHS PPU and the Royal National Orthopaedic Hospital – Private Care, in Stanmore, Middlesex.
Elements of the trial would consist of a review of the documentation used for handling a complaint from a private patient within the trial NHS PPU to see:
How they have included the Complaints Standard Framework within their policy;
How they handle the second stage, which is when the patient cannot agree on resolution and the complaint is passed outside the immediate service provider.
Typically in independent hospitals, this would be to the company head office. In the case of PPUs, it is envisaged that the hospital’s Patient Advice and Liaison Service (PALS) organisation would undertake this stage.
Upon any disagreement at this stage, a complaint goes to an independent adjudicator appointed by ISCAS.
ISCAS sees PALS as well suited to this task of resolving a complaint which has been rejected by the provider at operational level. They are already tasked to:
Respond to a patient’s concerns if they are unhappy with an aspect of their health care;
Give advice about the complaints process and deal with problems confidentially;
Listen to suggestions for improving medical services and health care;
Talk to staff on patients’ behalf;
Advise patients on the advocacy services available;
Direct patient to other services or agencies, where appropriate, to address their concerns.
ISCAS believes that most PALS already feed back useful improvement lessons to help management improve performance and would continue to do so for PPUs.
As far as consultants are concerned, we foresee that those using PPUs will have suitable clauses in their practising privileges contracts that require candour and co-operation in resolving complaints.
Costs of adjudicating complaints are expected to be borne by the providing organisation: the PPU. If the adjudicator recommends a financial award to the patient, it
PATERSON INQUIRY –RECOMMENDATION 6
Information about the means to escalate a complaint to an independent body should be communicated more effectively in both the NHS and independent sector. All private patients should have the right to mandatory independent resolution of their complaint.
must be within a ceiling of £5,000 and is paid by the provider. According to Private Healthcare Information Network (PHIN) data, there are 277 PPUs in England that do not have an external review stage. This pilot study will offer a way for PPUs to remedy this unfortunate situation and to fulfil the requirements of the Paterson inquiry. PHIN issues useful guidance on making a complaint as a private patient – see www.phin. org.uk/help/making-a-complaint. Complaints arise in any organisation. Coming from a unique perspective, they provide valuable indication that the service provided may be suboptimal.
So complaints handling should be integral with the management improvement cycle.
A timely and fair settlement of a patient’s concerns avoids disquiet in the community and leads to improved output by the organisation. A good complaints handling system is essential to any organisation.
Double jeopardy faced by doctors
2023 – a year of change at the GMC? The council is set to lose its power to appeal fitness-to-practise proceedings. Amie Roadnight (right) reports on a long-running saga that doctors will be delighted to see is about to be resolved in their favour
EVERY DOCTOR’S worst nightmare is to receive a letter in the post or an email in their inbox from the GMC informing them that their fitness to practise is being investigated.
Once the doctor reaches the end of that process having gone through the stress of a hearing, whatever the outcome, the doctor may think it is all over and they can finally move on with their life. Not necessarily.
Since 31 December 2015, the GMC has been afforded the power to appeal decisions
made by a Medical Practitioners’ Tribunal (MPT) in respect of a doctor’s fitness to practise.
If a decision is made by the MPT that the GMC considers to be too lenient, it is open to the GMC to appeal that decision to the High Court pursuant to s40A of the Medical Act 1983 (as amended) – arguably another bite at the cherry as it were – to secure a more severe sanction on a practitioner’s registration.
➱ continued on page 38
The GMC’s own guidance confirms this is not a decision which should be taken lightly by the GMC and that the GMC will only bring such appeals where it considers the outcome of the MPT hearing is not sufficient to protect the public.
Its guidance makes it clear that the purpose of the power is only to bring appeals where the GMC have reasonable prospects of success.
Fitness to practise
This power has been the subject of controversy and criticism since its introduction.
An MPT hearing takes place before a professional tribunal of three individuals – medically qualified and non-medical members –and a legal assessor who is not involved in the decision-making but provides independent legal advice to the tribunal.
A doctor who is subject to a GMC investigation into his/her fitness to practise goes through a lengthy legal process to defend their position, which, if not disposed of at an earlier stage, culminates in a fitness-to-practise hearing before an MPT panel.
If the GMC has serious concerns about a doctor’s conduct, it can take interim action against the doctor while awaiting the outcome of the MPT hearing.
The tribunal firstly considers the facts of the case, which usually involves hearing witness evidence called on behalf of the GMC and the doctor. The MPT then makes a decision on the facts of the case.
If it finds the facts proved, the MPT goes on to consider whether the doctor’s fitness to practise is impaired by reason of, for example, their misconduct, a criminal conviction, their knowledge of English, their health or a finding of impairment by another health regulatory body.
If a doctor’s fitness to practise is found not to be impaired, the MPT goes on to consider whether issuing the doctor with a warning would be appropriate or whether the case can be closed with no action.
Should the MPT find the doctor’s fitness to practise is impaired, it will then go on to consider an appropriate sanction, which may be:
It has long been argued that such a power by the GMC is excessive and disproportionate, particularly where other healthcare regulatory bodies are not afforded the same power of appeal
THE CASE OF DR HADIZA BAWA-GARBA
A prime example of the controversy associated with the GMC’s power to appeal arose from the well-reported case of Dr Hadiza Bawa-Garba. Without going into the facts of the case here, in brief, Dr Bawa-Garba was convicted of gross negligence manslaughter in November 2015, following the death of a six-year-old boy in 2011.
In June 2017, Dr Bawa-Garba’s fitness to practise was found by the MPT to be impaired and she was suspended from practice for 12 months.
The GMC appealed the decision of the MPT, as it was concerned that the MPT had re-examined the criminal case and arrived at its own, less severe conclusion.
The imposition of conditions;
Suspending the doctor;
Erasing the doctor from the medical register.
In the event a doctor is not satisfied with the outcome of the MPT hearing, there is a statutory right of appeal for the doctor to appeal that decision within 28 days of the outcome of the MPT hearing.
It is also open for the GMC to appeal the MPT’s decision. This is most likely where a registrant is either exonerated or faces a sanction less severe than erasure – such as restricting their licence to practise with conditions or suspension – and the GMC consider the outcome does not sufficiently protect the public or, in other words, it thinks it is too lenient.
Additional stress
The doctor must then deal with another legal process relating to their fitness to practise.
This inevitably comes with the additional stress of further legal proceedings, the prospect of a different outcome being reached at the High Court, as well as further legal costs involved in dealing with the appeal.
It has long been argued that such a power by the GMC is excessive and disproportionate, particularly where other healthcare regulatory bodies, such as the General Dental Council and the Nursing and Midwifery Council, are not afforded the same power of appeal.
In addition, the GMC’s own regulator, the Professional Standards Authority (PSA), has the right to appeal MPT decisions if it considers a determination is too lenient.
A query arises as to why it is necessary for the GMC to have such powers when it can be assured that
The High Court, in January 2018, agreed with the GMC and Dr BawaGarba was erased from the GMC’s register. Dr Bawa-Garba successfully appealed the decision of the High Court and the original 12-month suspension order was re-instated.
Following an outcry over the GMC’s powers after the Bawa-Garba case, independent reviews were commissions by both the GMC (the Marx Review) and the Government (the Williams Review) regarding gross negligence manslaughter charges for doctors.
The Williams Review, which was published on 11 June 2018, recommended that the GMC should be stripped of its right to appeal MPT decisions. Jeremy Hunt, the Health Secretary at the time, confirmed he planned to implement this change.
In 2021, 13 healthcare organisations wrote to Matt Hancock, Health Secretary at the time, to urge the Government to utilise the Health and Social Care Bill to remove the GMC’s power of appeal
its own independent regulator has the power to appeal decisions to ensure the safety and protection of the public is upheld and public confidence in the profession is maintained.
Time for change
Fast forward to the start of 2022 and the GMC’s power to appeal MPT decisions remained firmly in place.
According to information obtained under the Freedom of Information Act by the Medical Protection Society, since June 2018 – that is to say, following the Williams recommendation – the GMC had appealed 23 MPT decisions to the High Court.
It appears that the council takes the view that while the power to appeal remains on the statute book, it must use it where it considers it to be appropriate – even though the power is discretionary.
The Department for Health and Social Care (DHSC) had indicated some 11 years ago that radical reform to health care regulation as part of the Health and Social Care Bill would be incoming. It had been hoped that these changes would include removal of the GMC’s power to appeal.
The changes are yet to be imple-
It appears that the council takes the view that while the power to appeal remains on the statute book, it must use it where it considers it to be appropriate
mented, meaning that the GMC’s power remains in place.
In 2021, 13 healthcare organisations wrote to Matt Hancock, Health Secretary at the time, to urge the Government to utilise the Health and Social Care Bill to remove the GMC’s power of appeal. In a turn of events, the Government announced that rather than including the removal of this power using the Health and Social Care Bill, it would do so using secondary legislation when making a number of other regulatory reforms, which it proposed in its March 2021 consultation concerning the Health and Social Care Bill.
The difficulty, however, is that the response to the March 2021 consultation has not, as I write, yet been published. It therefore seems inevitable that there will be a further period of lengthy delay before the reforms are introduced and the
GMC is stripped of its power to appeal MPT decisions.
The DHSC has more recently updated the likely timetable to implementation of regulatory reform, which will not see legislation implemented until 2024 at the earliest.
However, the DHSC has made a commitment regarding the GMC’s power of appeal that the legislation will be laid next year to remove this power and will not be delayed further.
This will be welcome news to doctors and healthcare organisations who finally, after years of uncertainty, now have the commitment from the DHSC that they have been waiting for.
It remains to be seen whether this commitment will be met, but there can be no doubt that doctors and healthcare organisations will be hot on the heels of the DHSC if this commitment does not come to fruition in 2023.
If you are facing fitness-to-practise proceedings or other proceedings before a regulator, whether that be the GMC, Performers List, or Care Quality Commission investigation, and you require legal advice, do make contact with me.
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation HR/employment
Premises
Regulatory requirements and investigations
Amie Roadnight is a senior solicitor in the professional discipline, regulatory and crime team at Hempsons
Speaking up for an open culture
drive improvements in healthcare
David Hare (right) reflects on the importance for independent practitioners of speaking up in order to report mistakes and
‘SPEAK UP Month’ in October provided an ideal time to reflect on the importance of all parts of the healthcare system – including the independent sector – embracing the ‘speaking up’ agenda as a way of improving the safety and quality of care.
And this year’s theme, ‘Freedom to Speak Up for Everyone’, was a welcome reminder of the need to make speaking up business as usual for everyone in the health service: NHS or private, from consultants to healthcare assistants.
And as an ambitious sector with a strong culture of learning, independent providers and practitioners have much to feel proud of in fostering open, just and learning cultures where speaking up is encouraged.
Indeed, the National Guardian’s annual Freedom to Speak Up survey published earlier this year showed that independent healthcare providers have seen a real improvement in the speaking up culture in their organisation over the last year.
Overall, the report found that almost four-fifths (78%) of respondents from independent healthcare providers said their organisation’s ‘speaking up’ culture had improved over the last 12 months.
Freedom to Speak Up Guardians
in the independent sector were also found to devote more of their time on the ‘proactive’ aspects of their role – such as working within their organisation to tackle barriers to speaking up – than the reactive aspects; for example, supporting workers who speak up to them.
Proactive aspects
Over 70% of Guardians in the independent sector spend at least half of their time focusing on ‘proactive’ aspects, compared with just over 50% of those from NHS Trusts and other parts of the healthcare sector.
While, of course, it is encouraging to see independent healthcare Guardians working so proactively in the sector, there is still much more to do on this agenda to ensure speaking up is fully embraced by independent practitioners all across the country.
To help support the sector on this journey, we were pleased to be joined at the Independent Healthcare Providers Network’s annual Patient Safety Conference this year by the National Guardian for Freedom to Speak Up, Dr Jayne Chidgey Clark, who spoke about how providers can better understand the importance of speaking up at all levels in their organisation.
organisation feel confident and able to speak up is an integral part of this journey.
There is still much more to do on this agenda to ensure speaking up is fully embraced by independent practitioners all across the country
This includes really interrogating and acting on the data that providers collect in their organisations – for example, looking at what the rate of ‘anonymous’ cases are and what this might indicate about an organisation’s speaking up culture.
Equally, understanding what the organisational routes are for speaking up and what barriers there might be in place throughout different parts of the speaking up journey will be vital in encouraging a more open environment.
Getting feedback
Getting feedback from people and groups who have spoken up and ensuring organisations ‘close the feedback loop’ is also key.
And above all, having curiosity about your organisation’s speaking up culture and really reflecting on these issues from the top of the office down so that all parts of the
This is so important in healthcare – a sector which, unfortunately, can be seen as hierarchical and top-down.
Freedom to Speak Up Guardians not only provide a structure for concerns and issues to be raised, but also help develop a culture where employees feel free to contribute ideas, share information, and report mistakes and ultimately drive improvements.
Independent healthcare practitioners know that a key part of improving the care they deliver to patients is to interrogate their performance, to speak up and challenge poor performance wherever it may be.
I urge all those working in the independent healthcare sector to raise awareness of Freedom to Speak Up Guardians and encourage many more to be established.
Not only will you be fostering a culture where people can speak up and be confident they will be listened to, it will play a pivotal role in further improving the care you provide to millions of patients every year.
David Hare is chief executive of the Independent Healthcare Providers Network
LET US HELP YOU GROW YOUR PRIVATE PRACTICE AT WEEKENDS
LONDON MEDICAL, the award-winning outpatient clinic in the Harley Street Medical Area is expanding its weekend opening hours. We are inviting applications for practicing privileges.
We can offer you:
Fully CQC-registered clinic
Nursing support
Appontment-making
Secretarial support
Billing service
In-house pharmacy
For more details
Contact: david.briggs@londonmedical.co.uk
49 Marylebone High Street, London W1U 5HJ
londonmedical.co.uk
Getting the patients in is one thing – but what is it best to do if you wish to remove a patient from your practice?
Dr Sissy Frank (right) answers a doctor’s question
How can you get rid of an abusive patient?
Dilemma 1
How can I strike them off my list?
QI’ve been treating a family in my NHS practice who have been my patients for the last the couple of years. The father has always been difficult to deal with, is very demanding and can be quite intimidating.
On several occasions, he has been verbally abusive and rude to both myself and my receptionists.
He has unrealistic expectations as to what treatments he and his family can or should have and makes unreasonable requests at reception.
I am considering ending my professional relationship with the family due to the ongoing problems we are having. Can you advise how I should go about it?
AYou should only end your professional relationship with a patient when there has been an irrevocable breakdown of trust
Removing a patient is usually the last resort for doctors following a series of incidents, but aggrieved patients who have been de-registered from a practice can make a complaint, contact the press or post their feelings on social media.
Additionally, removing a patient could also lead to criticism by the GMC and the health service Ombudsman. Consequently, it’s important that you’re able to justify your decision.
You should only end your professional relationship with a patient when there has been an
irrevocable breakdown of trust. You must be satisfied your reason for ending the relationship is fair and does not discriminate against the patient.
Justifiable grounds for removing a patient might include:
Violence or aggressive behaviour;
Discriminatory abuse;
Sexual advances;
Theft from the practice, staff or other patients;
Repeated unreasonable or inconsiderate actions;
However, it is more difficult to justify removing a patient based on the following:
They have complained;
Their disruptive behaviour is caused by a medical or psychological condition;
They are related to another patient who is being removed;
You are concerned about the resource implications of their care or treatment;
Their medical condition puts you at risk.
It is important to demonstrate that you have tried to do what you can to restore the professional relationship.
Warn the patient
However, if this is not possible, then prior to removing the patient, you should warn the patient explicitly what aspects of their behaviour are unacceptable and that you will end your professional relationship if they don’t change.
The patient needs to know exactly what they need to stop doing and what will happen if
they don’t. Keep a record of your discussion and follow up the warning in writing.
If you decide to remove the patient, then you will need to tell them of your decision and explain the reasons, in writing if possible, and be clear that they will not be left without medical care.
Remember to record your decision, which should be factual and objective.
The GMC says you ‘should not include anything that could unfairly prejudice the patient’s future treatment’. You should also transfer the patient’s records to their new practice as soon as possible.
However, if a patient has been violent or abusive or has behaved in a threatening way that leaves you or your staff in fear, they can be removed immediately. In this situation, you should report the incident to the police and get an incident number.
Only give the minimum information needed to allow for proper investigation. The patient’s medical details should not usually be required.
Finally, if you have any concerns, it is advisable to contact your medical defence organisation for further advice and guidance.
Dr Sissy Frank discusses what to do if you are asked to help in an emergency
Dilemma 2
Am I covered to give assistance?
QWhen I’m not working as an independent consultant, I enjoy running and have undertaken a number of marathons and half-marathons as a member of my local running club.
Recently, I have been asked whether I am happy to provide medical assistance in case of an emergency during an upcoming half-marathon event.
I would like to help, but am not sure if I am indemnified for this type of work?
ADoctors are often asked to provide medical cover at amateur and charity sporting competitions or other local events. Whether it’s paid or voluntary work, there are a few things you will need to consider.
Firstly, you have an ethical duty and a statutory requirement to ensure you have adequate indemnity or insurance before you offer your services.
Depending on the event, the organising body might provide indemnity for doctors acting in a professional capacity – voluntary or paid – and you should check this before the event.
If the organisers can’t provide you with indemnity, it is important to contact your medical defence organisation in advance of the event to check whether your current membership will indemnify you for this.
Additionally, the GMC’s Good Medical Practice guidance states that ‘you must recognise and work within the limits of your competence’.
Whatever event you are helping with, you should have the appro-
Giving medical aid at a fun run
You have an ethical duty and a statutory requirement to ensure you have adequate indemnity or insurance before you offer your services
priate skills, experience, equipment and support. For example, if you are volunteering at a local running event, you may need to be expert in areas such as cardiopulmonary resuscitation, airway maintenance and spinal fracture immobilisation.
If you are unsure what experience or training you might need, check with the event organiser or relevant sporting organisation.
Should a medical problem occur during the event, your ethical responsibilities – such as the need to obtain consent and maintain confidentiality – remain the same as in your regular medical practice. Finally, keep detailed notes of any incidents that arise and the medical care you provided, in case you are later asked about the treatment you gave.
Dr Sissy Frank is a medico-legal adviser at the Medical Defence Union
INTRODUCING A NEW CLASS OF INJECTABLE THERAPY TO TREAT KNEE OA iPAAG — SAFE AND SUSTAINED PAIN RELIEF WITH A SINGLE INJECTION2
For more information, read the IFU for full details about Warnings and Precautions. The IFU is also available from https://www.arthrosamid.com or info@arthrosamid.com.
References: 1 Bliddal H, Beier J, Hartkopp A, Conaghan PG, et al. (2022) A Prospective Study of Polyacrylamide Hydrogel Injection for Knee Osteoarthritis: Results From 2 Years After Treatment. Poster presented at OARSI 2022; 2. Bliddal H, Overgaard A, Hartkopp A, Beier J, Conaghan PG, et al. (2021) Polyacrylamide Hydrogel Injection for Knee Osteoarthritis: A 6 Months Prospective Study. J Orthop Res Ther 6: 1188. OUS/ARTHRO/NOV2022/114
DOCTOR ON THE ROAD: GENESIS GV60 SPORT
A brand you’re going to hear more of
WHEN LOOKING for a new car, we like to be able to trust the brand.
And you probably haven’t heard of the Genesis brand, but that is no great surprise; they are still a rare sight on our roads.
It is the luxury branch of the Korean Hyundai/Kia group, which launched its first car in 2017 and only came to the UK in 2021.
The first cars to come here were conventional premium petrol and diesel models and sales have been slow. But now we have a car that could do great things for the brand: the all-electric GV60.
In the same way that Lexus is the luxury brand of Toyota and uses Toyota tech, Genesis uses the same all-electric floorplan used for the Hyundai Ioniq 5 and the Kia EV6.
Fortunately, these are well sorted and impressive medium-sized electric vehicle (EV) cross-overs, so the Genesis is off to a good start. Like those cars, the GV60 is a mediumsized SUV, so its practicality will appeal to the urban medic with a growing family.
Luxury features
There are three model options: the £47,005 226bhp rear-wheel drive Premium, the £53,605 314bhp allwheel drive Sport and the £65,405 458bhp all-wheel drive Sport Plus.
All use a battery of 77.4 kWh and claimed ranges are 321, 292 and 289 miles respectively. As with Lexus cars, the Genesis is extensively equipped with many luxury features as standard, so you are
unlikely to spend a lot more on options, which is a welcome relief compared to its German competitors from Audi, Mercedes and BMW.
The styling is very rounded and neatly proportioned but, to my eye, suits darker colours than the pale metallic blue or white finishes available. The Genesis signature horizontally split headlights give it a futuristic look that fits well with this all-electric car.
There are no unnecessary aerodynamic addenda either and this is also welcome. The interior is like a modern, welcoming lounge. Plenty of leather trim and the lack of hard plastics make this a plush place to spend time while travelling.
The gear selector is a crystal
The gear selector is a crystal sphere that rotates into place when you turn the car on
trolled by physical buttons which makes life a lot easier.
Physical buttons
Out on the road, the first impression is that this is a smooth, quiet, solid quality car sphere that rotates into place when you turn the car on – dramatic but a bit glitzy for my taste. The plastic that is made to look like metal that surrounds the selector also feels a little overdone.
Apart from these minor niggles, the driving seat is very comfortable and the electronic dashboard is large and really clear.
Thankfully, the infotainment and ventilation systems are con -
Rear space benefits from the dedicated EV platform, so there is more legroom and headroom than you would expect, the seats can actually recline and the lack of transmission tunnel helps the middle rear-seat passenger get comfortable.
Boot space is pretty good, but the floor is high to accommodate the batteries and motor. Charging the EV60 should be easy, as it
accepts the public network’s fast chargers although they are not as numerous as Tesla’s supercharger.
Real-world range from the 77.4kWh battery in the Sport model is likely to be around 230 miles, but the less powerful Premium rear-wheel drive model should break the 250 mile barrier.
Out on the road, the first impression is that this is a smooth, quiet, solid quality car. It definitely feels like a premium step up from its Hyundai and Kia siblings, just as it should.
Smooth and supple
Performance is swift in the Premium model, fast in the Sport model and super-fast like a Tesla Performance model in the Sport Plus. The ride is smooth and supple and the handling is pretty good for a heavy electric car.
The steering is nicely direct but lacks a degree of feedback that would be appreciated by keen drivers.
My overall reaction is that it drives like a swift but not overtly sporty luxury hatchback and this is exactly how it is promoted.
I think that the Premium model would fit the bill for most of us, but the mid-range Sport has more dynamism.
The GV60 will appeal to an EV-buying medic who wants a premium car but not from the obvious brands and not a ubiquitous Tesla either.
It is very well built, benefits from all the positive elements that the Hyundai/Kia group can deliver and is overall, a really good package. You can embrace the new Genesis badge with confidence.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
GENESIS GV60 SPORT
Body: Five-seat, five-door hatchback cross-over
Engine: Two electric motors. All-wheel drive
Power: 321bhp
Torque: 605Nm
Top speed: 146mph
Acceleration: 0-62mph in 4.0 seconds
Claimed range (WLTP): 289 miles
CO2 emissions: 0g/km
On-the-road price: £53,605
Tax complexities of
Annual allowance – don’t you just hate the restrictions?
Alec James (right) gives an update on the tax charges on your pensions
of saving for old age
The annual allowance growth is determined by the value of the pension at the start compared to the end of the year, adjusted by certain arithmetical factors and the Consumer Price Index
MANY READERS may not be aware that when the pension savings annual allowance was first introduced in April 2006, the allowance was £215,000 rising in successive years to £255,000.
This meant that considering the annual allowance position was rarely an issue for doctors.
However, when the markets took a downturn in 2008, it was seen by successive governments as a mechanism to generate more tax by reductions in the allowance. The allowance is now normally £40,000, but can decrease down to £4,000 if tapering is applied.
In this article is a summary of the rules and the upcoming changes.
A recap on pension savings
The annual allowance for each taxpayer is currently £40,000. The type of pension scheme you are contributing to determines what amounts are assessed against the annual allowance.
For defined contribution schemes – such as private pension schemes and many employment schemes – the annual allowance is applied to the total contributions from both the taxpayer and employer contributions made during the year.
For defined benefit schemes, such as the NHS Pension Scheme, the taxpayer is assessed not on the contributions paid during the tax year, but instead by how much the pension pot has grown by. This makes annual allowance tax planning much more complicated.
If you are an active member of the NHS scheme and you contribute to a private pension or you also contribute to a non-NHS workplace pension scheme, you have to consider the combined implication of all the pension schemes.
NHS Pension Schemes
Many Independent Practitioner
Today readers will have been members of either the 1995 or the 2008
scheme – now often referred to as the ‘legacy schemes’ – and the 2015 scheme.
It is the combined growth across the schemes that will be assessed against the annual allowance each year.
Although what is known as the McCloud remedy may eventually alter the growth figures, legislation dictates that the figures up to 2021-22 will be assessed on the current rules.
As you would expect with different schemes, the legacy and 2015 schemes all grow at different rates. This is due to the way the pension is calculated in each of the schemes:
The 1995 scheme is based on the best pensionable earnings of the last three years prior to your retirement;
The 2008 scheme is based on the best average consecutive three years pensionable earnings out of the last ten years prior to your retirement;
The 2015 Scheme is a Career Average Revalued Earnings (or CARE) scheme.
In the CARE scheme, each year your historic earnings are revalued by the Consumer Price Index (CPI) to bring them in line with current monetary values. The CPI rate used for the 2015 scheme is from September within the tax year.
As an active member of the NHS Pension Scheme, you are also given a 1.5% inflationary increase.
The 1995 and 2008 schemes as detailed above are linked one way or another to final salary and that is an important distinction between these two schemes and the 2015 scheme.
In the three schemes, the annual allowance growth is determined by the value of the pension at the start compared to the end of the year, adjusted by certain arithmetical factors and the CPI.
In determining growth for annual allowance purposes, infla-
➱ continued on page 48
tionary influences were intended to be discounted in calculating any annual allowance growth.
This is done by using the CPI figure of the September preceding the tax year that it relates to. For example, in calculating the annual allowance growth for 2021-22, HM Revenue and Customs (HMRC) would use the September 2020 CPI figure.
In some years, the CPI can have the opposite effect to that which it was intended.
Former Health and Social Services Secretary Thérèse Coffey has highlighted the impact the difference in the CPI rates used by NHS Pensions, and HMRC is looking to correct the rules.
At the time of writing this article, there has been no further updates, but hopefully there will be more formal announcements in the near future.
In addition, although you are not actively contributing to the legacy schemes, they are subject to growth when there is a change to your pensionable pay.
This could include:
Pay increments;
Any inflationary pay;
National Clinical Excellence Awards;
Salary sacrifice scheme such as a NHS Fleet Car.
National Clinical Impact Awards (NCIA)
From April 2022, the historic National Clinical Excellence Award (NCEA) scheme was replaced by the NCIA. With the change in name comes a change to the level of funding available and also a change in the pension status.
The NCIA is now non-pensionable, whereas the NCEA was pensionable. This means that if you were to have been granted a bronze award or similar, you would likely have seen a significant growth in your legacy scheme as a result of the award.
Similarly, if you cease to be in receipt of a NCEA, you may well see a reduction in your legacy scheme’s pension pot.
It is possible to protect the pension benefit of the award and any other additional pensionable pay over and above the normal ten pensionable programmed activities.
The annual allowance is a complex area for doctors and careful planning should be taken if your circumstances within the NHS are changing
If a loss of this income arises or is anticipated to occur, then advice must be sought.
Going forwards, any NCIA received will not impact your annual allowance growth. It may, however, cause tapering of annual allowance issues.
Tapering of annual allowance
As stated at the beginning of this article, each taxpayer is currently entitled to a £40,000 annual allowance.
This allowance is reduced if the following limits are exceeded:
If your threshold income is more than £200,000;
If your threshold income together with your pension savings are more than £240,000.
Your threshold income is effectively your total taxable income in the year and is not limited to your NHS income.
If both limits are exceeded, you will be subject to a tapering of annual allowance. This means that for every £2 your adjusted income goes over £240,000, your annual allowance for the current tax year reduces by £1.
The minimum reduced annual
allowance you can have in the current tax year is £4,000. If you have self-employed income, you may wish to consider incorporating the self-employed business into a separate legal entity such as a limited company, even if the income levels are modest.
Annual allowance tax charges
If you believe you may have an annual allowance tax charge or you have received a statement from NHS Pensions, you should always seek the advice of a specialist medical accountant.
It is important to identify the assessable annual allowance growth. It may be possible for you to utilise unused relief from previous years against growth in the current year, if this is in excess of £40,000. This could either reduce or remove an annual allowance tax charge.
If you do have a liability, this can either be paid personally or by opting for a Scheme Pays Election or a mixture of the two options. If you opt to pay the tax personally, it follows the usual tax system and is included on your personal tax return.
A Scheme Pays Election is effectively asking your pension pot to pay the tax liability on your behalf. The tax paid is treated like a loan secured against your pension pot and is therefore subject to interest and charges by NHS Pensions.
On retirement, the Scheme Pays Elections are crystalised before your pension is calculated. There are deadlines for submitting these forms.
Whichever option you choose, disclosures will need to be included on your personal tax return and, if necessary, a Scheme Pays Election needs to be submitted. An incorrect disclosure can prove to be very costly.
Salary sacrifices
Many consultants have opted for an NHS fleet car over the past few years, particularly since the benefit-in-kind rates on electric cars have been low.
Salary sacrifices are deducted from your pensionable pay and therefore can have an impact on either the pension you receive when you come to retire or cause
significant pension growth when you return the vehicle. There can be tax-planning opportunities in respect of the timing of taking out and returning an NHS fleet car and this should be discussed with a specialist medical accountant prior to making any decisions.
McCloud remedy
Your annual allowance positions for 2021-22 will be based on being in the two pension schemes.
As part of the remedy, for the purpose of assessment of your annual allowance position and depending on when you joined the NHS Pension Schemes, the seven-year period covering 1 April 2015 to 31 March 2022 is likely to be recalculated as if the transition to 2015 scheme had never taken place.
This means that the annual allowance positions for 2015-16 onwards will be recalculated in the legacy scheme relevant to you. This will mean that the annual allowance positions in these years will change, which could result in tax refunds or a tax liability. When you come to retire, you will be given a choice as to which scheme benefits you wish to receive. This is known as the Deferred Choice Underpin (DCU). If you are due to retire before 1 October 2023 or are already in receipt of your NHS pension and you will be party to the McCloud remedy, you will continue to receive benefits based on both the legacy scheme and the 2015 scheme, but you will be given the option of making a retrospective choice.
The annual allowance is a complex area for doctors and careful planning should be taken if your circumstances within the NHS are changing.
Many of you will have received a letter from NHS Pensions in the last few months. If you have received statements, you should seek the advice of a medical specialist accountant to review whether you have any hidden tax liabilities.
Next issue: Keeping pace with inflation
Alec James is a partner at Sandison Easson & Co, specialist medical accountants
Coming in our December-January issue, published on 3 January 2023:
Fasten your seatbelts and stow your tray tables – there may be turbulence ahead in 2023 for independent practitioners’ finances, warns Simon Brignall of Medical Billing & Collection
Keeping pace with inflation will be a massive challenge for private doctors’ businesses in the months ahead. Don’t miss the views of specialist medical accountant Richard Norbury, of Sandison Easson
That was the year that was: highlights of some of the big stories we brought you in 2022 that you need to know about in 2023
Chancellor Jeremy Hunt’s plans – what doctors can expect and do now. A specialist medical accountant reports
Are you burying your head in the sand? Check out Cavendish Medical’s round-up of the financial issues you cannot ignore any longer
Make sure patients can find you. There is still so much that you can do to be found by potential patients. Catherine Harriss presents a check list to help doctors who need to increase their reach or are just starting out in private practice
In case you missed it – news from the BMA’s annual private practice conference
Working in groups: our Troubleshooter Jane Braithwaite, of Designated Medical, tackles a consultant’s problems arising from working in a group with two other partners who have both dropped the bombshell that they are aiming to retire soon
INDEPENDENT PRACTITIONER TODAY
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution. Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Registered office: 7 Lindum Terrace, Lincoln LN2 5RP
Claims arising after retirement: Even long after retirement, doctors can be subject to a clinical negligence claim, so it’s important to act quickly and get the right advice and support from your defence organisation. A claim can arise many years after a doctor’s involvement in a patient’s care. Among other things, a claim can relate to a delayed diagnosis, surgical errors and poor communication. Dr Claire Wratten, senior medical claims handler at the MDU, gives her advice
Hempsons’ solicitors provide a quick guide to disclosure and medical records, from the perspective of clinical negligence lawyers, to help you in your daily work
Handling undercover investigations: media interest in a patient’s care or treatment is a daunting prospect for any doctor, but being the subject of an undercover investigation can be even more challenging. Dr Caroline Osborne-White, of Medical Protection, explains how these situations can be handled
Ray Stanbridge’s Profits Focus article analyses the recent financial results for cardiologists in private practice
Our motoring correspondent Dr Tony Rimmer reports on the VW Taigo
Business Dilemmas: More questions answered by Medical Defence Union medico-legal adviser Dr Kathryn Leask
Plus our other regular columns and all the latest news and views
And don’t forget to check out our additional news updates every week online
ADVERTISERS: The deadline for booking adverts in our December-January issue is 25 November
Write to Independent Practitioner Today
7 Lindum Terrace, Lincoln LN2 5RP
CHANGING ADDRESS, EMAIL ADDRESS OR SUBSCRIPTION DETAILS?
Phone 01752 312140 or email karen@marketingcentre.co.uk
TELL US YOUR NEWS
Robin Stride, editorial director
Email:
robin@ip-today.co.uk
Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the digital journal, on our website or in our business directory, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912 Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners.
£90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE
Email karen@marketingcentre.co.uk or phone 01752 312140
Publisher Gillian Nineham
Phone: 07767 353897.
Email: gillian.nineham@gmail.com
SAVE £15 WITH DIRECT DEBIT!
Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.