A leading provider of resident medical officers reveals what goes into producing them P14
The business journal for doctors in private practice
Time to take care of your well-being
Bupa’s medical director provides ideas to look after yourself P22
Wealth check needed after tax changes
By Robin Stride
Independent practitioners are advised to seek a wealth check to assess their financial future following last month’s Budget and Spending Review, and earlier announcements.
Accountants warn that, as a result of the Chancellor’s changes, they will see big income changes due to a range of measures including:
n Cost rises due to inflation, a labour supply shortage and supply chain disruption;
n A 1.25% increase in National Insurance for them as employees, and as employers;
n A 1.25% rise on all dividends, even for shareholders with personal allowance basic-rate bands;
n A freeze on tax-free personal allowances – so more is taxed in tandem with the increases.
n A higher corporation tax rate for any business earning over £50,000. Vanessa Sanders, of specialist med ical accountants Stanbridge Associates, gave an example of a consultant with a private practice, paid £100,000 in the NHS with a spouse earning in the doctor’s firm only.
In association with
She told Independent Practitioner
Today : ‘With a turnover of, say, £200,000 with expenses typically at 30% including secretarial costs of £25,000, the result due to all potential increases could mean they find themselves with up to £12,000 less in cash terms.
‘This will hit consultants both in employment and in independent private practice and the costs should be reviewed together with the increase to corporation tax announced for April 2023.’
Other areas she highlighted for the business’s forward planning agenda include:
☛ Income tax basis periods will be reformed, meaning that business profits of sole traders and individual members of partnerships will be assessed to tax in the tax year they arise, regardless of accounting date.
This may mean a review of your accounting date ahead of tax digitisation to ensure no more returns are made than necessary and to spread the costs of bringing the tax liability forward.
For example, if a business has a year-end date of 30 April, tax will
n See page 44
Investment choices have consequences
Dr Benjamin Holdsworth warns against putting all your stocks in one basket P34
be assessed for 23 months in one year to bring the business into alignment.
☛ The Chancellor plans to introduce top-up payments of 20% in respect of contributions made by low-earning individuals saving in a pension scheme under a Net Pay Arrangement. This may be the time to consider pension arrangements for any family member employees on lower salaries.
☛ From 27 October 2021, the deadline for reporting and paying capital gains tax after selling UK residential property extended from 30 days to 60 days after completion.
☛ A hike in the earliest age from which most pension savers can access their pension savings without incurring a tax charge. From April 2028, this goes up from 55 years to 57, affecting those born after 5 April 1973.
☛ Qualifying expenditure for tax relief on research and develop -
JUST WHAT THE DOCTOR ORDERED
A new app from Pharmacierge is easing the prescription admin burden for doctors on the go like Harley Street GP Dr Martin Saweirs. It also includes a delivery service. n See full story on page 9
ment will extend to include data and ‘cloud’ costs. Some doctors developing new ways of working could qualify for relief under the research and development rules. Advice may also be needed on pensions tax and inheritance tax issues.
The main corporation tax rate rises to 25% from April 2023 for businesses with profits above £250,000, but remains at 19% for those with profits under £50,000, and a marginal taper for profits between £50,000 and £250,000.
Mrs Sanders said: ‘For most doctors, running private practices using a company remains an efficient option.
‘This is primarily because of the ability to control the extraction of profits to shareholders and the opportunity to grow the company asset base for use in the future – for example, adding to retirement income when income tax may be paid at lower rates.’
TELL US YOUR NEWS. Contact editorial director Robin Stride
ADVERTISE WITH US. To advertise in the journal or our website business and lifestyle directories, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT
£90 independent practitioners. £210 organisations. £90 GPs and practice managers (private & NHS).
Save £15 paying by direct debit: individuals £75 (organisations £180).
Congratulations to sports medicine consultant Dr Philip Batty for kicking off about climate change issues at this year’s LaingBuisson Private Healthcare Summit.
He was somewhat ahead of the game when, more than two weeks before this month’s COP26 climate change conference in Glasgow, he spoke out to hospital bosses, doctors and other independent sector representatives.
Asked what he would like to change if he was in charge of private healthcare, the presidentelect of the Independent Doctors Federation turned to a subject rarely – if ever – aired alongside the usual recurring topics such as insurers, quality and the state of self-pay: the wider issues affecting that big round ball we all sit on.
‘I think we are all slightly careless,’ he admitted. ‘I’ve worked in many health organisations where the clinical waste bin hap-
pens to have coffee cups in it and things of that nature. And this stuff gets incinerated naturally, there are huge volumes of that. Is it absolutely essential?’
As he says on page 5, sustainability and future of the planet issues are often ignored by those in medicine and they need to be thinking about the plastics and single-use-only items in healthcare.
Where you dispose of your cup or anything else recyclable may not be at the top of your mind during a quick refreshment break – if you can get it – but we can all do more to do our bit.
It so happens that shortly after his remarks, we were pleased to hear over 40 providers across the independent healthcare sector in England had pledged they would aim for net zero emissions by 2035 (page 8).
We look forward to hearing how the 1,500 sites so far affected are taking this forward.
‘Z’ is for Zzzzz...
Accountant Julia Burn reaches the destination in her A to Z of top tips: ‘Z’ is for Zzzzz – don’t sleep through the upcoming tax changes P12
Planning a start in private practice?
Jane Braithwaite uses her insider knowledge to present an essential guide to help bring you success in gaining practising privileges P18
Where private GPs go wrong
Dr Sarah Jarvis of the Medical Defence Union analyses medico-legal files involving private GPs and advises on how to manage risk P20
Keep tabs on your financial situation
Private doctors can use information technology to boost their finances and achieve long-term profitability, explains Kingsley Hollis P26
Embarking on a diplomatic mission?
When expanding your private work to provide services for embassies, there are some essential billing and collection matters you need to be aware of P30
If that fateful GMC missive appears
What should you do if you get a letter from the GMC? Lawyer Dr Tania Francis shares ten tips designed to calm your fears about this dreaded event P36
PLUS OUR REGULAR COLUMNS
Doctor on the Road: Hybrid technology gets even better
Our reviewer Dr Tony Rimmer got 70mpg out of the Toyota Yaris Cross P40
Starting a private practice: Is your practice fit for tax changes?
With so many post-pandemic tax changes on the way, it’s time to see if your trading status is tax-efficient P42
Profits Focus: Covid hits profits hard
Our benchmark survey reveals how the pandemic took its toll on orthopaedic surgeons’ earnings P48
Another NHS pension consultation begins
Proposals change
By Edie Bourne
Independent practitioners who are part of the NHS Pension Scheme have been shocked to discover yet another Government consultation has been launched to alter the contributions they pay.
The changes have been proposed as part of the move for all members who will begin to build up benefits in the 2015 scheme from April 2022. This is a career average revalued earnings (CARE) pension scheme unlike the former finalsalary schemes of 1995 and 2008. If the proposals go ahead, doctors’ contribution rates would be based on pensionable pay rather than their notional whole-time
Budget ‘failed to incentivise health sectors to co-operate’
Private health insurance subsidies should have been introduced in the Autumn Budget to help tackle the current healthcare crisis, according to the Association of Medical Insurers and Intermediaries (AMII).
Executive chairman Dave Middleton said the Chancellor could have done much more to incentivise the NHS and private healthcare sector to work together.
‘The measures he has announced are unlikely to solve the unprecedented issues facing the health service and, while subsidised private health insurance would, without doubt, reduce the burden on the NHS, it is a real shame that there seems to be no appetite within Government to consider this.’
NHS
Pension Scheme contributions for all doctors
equivalent pay. Part-time members would therefore pay reduced pension contribution sums in the future.
The structure of pension saving would also be amended, as the number of different levels of contributions would decrease. The highest contribution tier would be lowered to 12.5% rather than the current 13.5 and 14.5%.
Patrick Convey, technical director at specialist financial planners Cavendish Medical, told Independent Practitioner Today: ‘As ever, the Government changes to doctors’ pensions keep us on our toes.
‘In this instance, the proposals detailed in the consultation could be positive in some respects, but
AMII has campaigned against any increase in the Insurance Premium Tax and Mr Middleton expressed relief this was not increased.
He pledged the association would continue to lobby for lowerrated healthcare products.
‘We will continue to lobby hard that healthcare costs should be zero-rated for IPT purposes in line with other protection and general products, as they make an equally valuable contribution to the health of the nation and the UK economy.’
there is so much confusion among members because of the continuous tinkering that it can be difficult to ascertain your own position.
‘The proposals are meant to ensure that the costs and benefits of the scheme are more evenly shared among members, but with so much uncertainty over the McCloud remedy, which has not yet been fully detailed, we can understand why doctors might be feeling wary.
‘We are not due to receive official McCloud regulations until October 2023. This current proposal suggests restructuring the member contribution tiers over two years from 1 April 2022 with
all final changes made by the following year.’
He said further Government changes to doctors’ benefits could not come at a worse time.
‘As it is, doctors have faced an arduous two years, are concerned by substantial rates of tax on their pensions, are being moved to different pension schemes from April and have a hard winter ahead.’
The McCloud remedy sets out how and when those deemed to have suffered age discrimination by moving to the 2015 NHS pension scheme originally will be compensated.
The current pension contribution consultation closes on 7 January 2022.
GMC head urges more help to tackle burnout
Conversations about doctors’ wellbeing are ‘needed now more than ever’ because the pandemic has heaped such pressure on them, the GMC’s acting chairwoman has warned.
Covid had exacerbated long-standing issues, Prof Dame Carrie MacEwen told an audience at the Royal College of Physicians and Surgeons of Glasgow.
Lengthening NHS waiting lists meant ‘crippling’ uncertainty for patients and were ‘deeply distressing’ for exhausted doctors, she said, leading them to looking at cutting their hours or leaving their posts.
that undermines patient trust and wears doctors down.
‘We know that doctors experiencing severe workload pressures are more likely to consider stepping back from practice.’
Citing new GMC research, she said while issues facing health services were worsened by the pandemic, they were not created by it, ‘This is not new – research shows that doctors who left UK practice between 2004 and 2019 gave dissatisfaction and burnout as two of the main reasons for doing so.
Dame Carrie said: ‘Not being able to give patients what they need has a cumulative effect, one
‘And this was before the start of the pandemic. As this research makes plain, well-being issues are driving doctors out of the service.’ See ‘Time to take care of your own well-being’, page 22
Dave Middleton of the AMII
Prof Dame Carrie MacEwen
PRIVATE ACUTE HEALTHCARE CONFERENCE 2021
Appeal for outcome stats
Robin Stride reports from market analysts’ LaingBuisson’s annual conference at the Royal Society of Medicine, London
Private hospitals have been encouraged to work more with their consultants to develop the benefits of Patient Reported Outcome Measures (PROMS).
The doctor chairman of the Private Hospital Information Network (PHIN) expressed optimism at the potential for the tool to be widely taken up.
But he said it would be difficult and progress over the last few years had not been good.
Dr Andrew Vallance-Owen warned: ‘If it’s searching for bad apples, you are lost.’ PROMS were about improving learning and quality, and finding out what the top people did to get their results.
Trying to get everybody across the private healthcare sector on board was always going to be diffi-
cult, but it was important to build a consensus of what was really important, he said.
A recurring summit theme had been the importance of outcomes,
and PHIN was happy to help move things forward, but it had to be done at hospital and consultant level.
HCA chief medical officer Dr Cliff Bucknall said it was widely thought the PROMS’s beneficiary was the patient. But the patient had not been involved or educated as to what was going to be measured.
He called for meaningful measures. Patients might be told they were part of a programme looking at the five-year outcome of doing hips – but the patient would want to know at six months, so there needed to be feedback much earlier.
Patients needed help to educate providers about: ‘What does good look like?’, he said.
Failure to deal with recognised problems about a doctor’s work has been a recurring historical theme, a defence body medical director warned the summit.
Call for stricter monitoring How private practice has altered over time
Dr Rob Hendry, of Medical Protection, reflected: ‘One of the tragedies I have seen over the years is when things have gone wrong and you go in to speak to individuals and organisations, the number of times people say: “Yeah, we knew it was a disaster waiting to happen”.’
He believed the sector had not been good enough at picking up risk indicators. But now there was very strong research evidence that it was possible to predict those who were going to run into problems before the claims or the regulator came in.
Dr Hendry looked forward to ‘more sophisticated use of data’ and having the indemnity/insurance provider as part of the team looking at this, and subtle indicators that something was not right.
He hoped a positive side-effect of this type of management would
help reduce the cost of premiums alongside risk.
His comments were made during a session entitled ‘Falling between the cracks – regulation and risk in new consultant business models’.
Dr Nigel Acheson, Care Quality Commission (CQC) deputy chief inspector of hospitals, said it was sad as a clinician to see cases where just a bit of forward planning could have helped when a situation deteriorated.
But too often it was like Groundhog Day with time delays
and nobody seeming to know what to do.
He said many doctors naively thought their work was just about running the clinical service and forgot there were regulations and expectations covering the business. The CQC had also found providers who failed to fully understand their obligations.
But he was pleased to see much more openness and transparency between the regulator CQC and stakeholder groups and providers.
Regulatory lawyer Carlton Sadler, of Bevan Brittan, warned that providers would increasingly have ‘to up their game’.
He had seen the CQC telling providers they should have acted after a consultant’s second operation mishap, rather than the third.
There was potential scope for the regulator to say: ‘If you’d been discharging your regulatory responsibilities properly, you would have avoided that third incidence of harm and therefore we are going to hold your hospital accountable for that.’
The number of ‘mega practices’ has declined as doctors seek more of a work-life balance. Some consultants were earning £1m a year in the 1980s and had a ‘very cosy relationship with insurers’.
But, reflecting on the big changes he had seen in private practice, specialist medical accountant Ray Stanbridge said insurers had become more aggressive towards doctors.
The cosiness with private hospitals, now more professionally managed, had gone too.
He noted that the growth in self-pay was increasingly important in London.
Mr Stanbridge added: ‘There are some consultants who are pushing patients away from being insured to being self-pay.’
Dr Andrew Vallance-Owen
Dr Rob Hendry
What three things would you change if you were in charge of private healthcare?
Specialist medical accountant Ray Stanbridge, Stanbridge Associates
Tax breaks on insurance premiums for private healthcare would be top of his list.
He reminded the conference that former Health Secretary Ken Clarke tried this in the 1990s before it was reversed by Labour.
‘The evidence suggested a lot of older people who were a burden on the NHS were taken out of that market and put into the private sector – and it did seem to work.’
Next up, he would encourage the development of group practices. ‘I understand from a number of insurers that the outcome from groups by consultants is better than individuals because, basically, people in groups talk to each other – and they take a second opinion rather than try and do everything themselves, and the outcomes are better.
‘Market evidence suggests that patients like the idea of groups and get a certain amount of comfort and for the figures we have, probably groups have enhanced their members’ incomes by about 15% per year over and above being an individual. So there is an income enhancement and I believe a quality enhancement.’
He also called for basic management skills in training because he had seen many good consultants who were dreadful at business and asked basic questions they should know the answer to.
James Sherwood, Bupa’s director of healthcare management
The biggest challenge is growth, and the decline in the consumer market is a challenge for all, he said.
Mr Sherwood suggested insurers, hospitals and clinicians could work together to further improve the customer journey – which wasn’t always smooth at present.
‘I think we need to look at the way the different players in the healthcare journey share information to create a frictionless customer journey,’ he said.
Mr Sherwood also called for data transparency. Measuring outcomes and experience, and acting on this was crucial. It would help demonstrate the sector’s value, how it differed to the NHS and encourage more people to pay for the service.
Third, he suggested a sectorwide commitment to improve the efficiency of care was needed. ‘We still see high variation in practice and inconsistent management of care pathways. This is something we all need to work together to tackle to further improve the quality of care and slow the rate of cost growth in the health care system.’
He claimed everything on his wish list would be helped by increasing the share of patients seen by consultants with bigger private practices.
A large number of consultants who see very few private patients was not only inefficient, it made it
difficult to identify variation between care pathways, he said.
Dr Philip Batty, sports medicine consultant and Independent Doctors Federation president-elect Sustainability and future of the planet issues are often ignored by those in medicine and they need to be thinking about the plastics and single-use-only items in healthcare, he said.
‘I would be getting some ethic experts and sustainability people to start to engage a conversation –Government as well – in terms of what are the risks of single-use items and how do we dispose of our clinical waste.
‘I think we are all slightly careless. I’ve worked in many health organisations where the clinical waste bin happens to have coffee cups in it and things of that nature. And this stuff gets incinerated naturally, there are huge volumes of that. Is it absolutely essential?’
Another wish concerned benchmarking and transparency. What would be useful would be a comparison of non-surgical outcomes to surgical outcomes, not just the same surgical outcomes among different surgeons, he said.
Dr Batty called for ‘a really holistic approach’. Sometimes doctors were limited to just returning people to daily living or work but ‘we should be thinking more about the well-being and encouraging
The outcome from groups by consultants is better than individuals because, basically, people in groups talk to each other
them to be more physically active and encouraging them to greater activities, and that will involve much more engagement with allied health professionals.’
To contain costs, some of this could be through group sessions as frequently seen in mental health.
HCA commercial director Andrew Coombs called for the sector to be much bolder about its value and capability. It had played the ‘most extraordinary role’ during Covid, treating patients who would have died.
One Healthcare hospital director Claire Armstrong listed data improvements so systems talk to one another, tax breaks for private medical insurance and the need to increase efforts to drive more people into private healthcare Practice Plus Group chief executive Jim Easton highlighted quality issues, reflecting that bad private healthcare performance was very often down to an individual surgeon. The market also needed to offer patients more choice and price certainty.
Ray Stanbridge
James Sherwood
Dr Philip Batty
Andrew Coombs
PRIVATE ACUTE HEALTHCARE CONFERENCE 2021
Evidence of private hospital recovery
Billing volumes for insured hospital treatments have consistently out-performed pre-pandemic levels this year, according to private medical invoice processor Healthcode.
Speaking at LaingBuisson’s Private Acute Healthcare Conference in London, the company’s managing director Peter Connor gave an overview of private medical insurance (PMI) billing trends in 2021.
He revealed that hospital PMI volumes have superseded 2020 levels by 52% over the year to date and were up 6% on 2019.
Before the pandemic struck in early 2020, Healthcode processed around 27,000 medical bills every day on behalf of UK private hospitals and practitioners, carrying out a series of checks and validations before passing it to one of the major insurers for payment.
This billing data meant Healthcode had a unique benchmark to measure the impact of this turbulent period on the private healthcare sector and it has now shared these year-on-year billing trends over the last 18 months to guide and inform industry stakeholders.
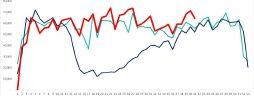
As the graph (right, top) shows, the story of 2021 has been largely positive for private hospitals, particularly from the start of quarter two.
Over the summer, billing volumes even exceeded those in 2019 by a significant margin. In June, for example, they were around 30% higher and in September they were running at 114% of 2019 levels.
Healthcode says the trend suggests that private hospitals – like their NHS equivalents – are dealing with suppressed demand, as well as non-urgent treatments that had to be postponed because of the pandemic.
Regional variations
It has not been a uniform rate of recovery across the sector and, from the beginning of the year, there have been regional differences.
In England, the volume of PMI bills rebounded from 89% of the pre-pandemic level in January to 114% in September, an average of 106% for the year to date.
But the year-on-year trend in London fell behind the rest of the country, with billing volumes dipping below 2019 levels in several months, averaging 104% for the year to date.
After this slow start, billing activity in the capital started to pick up pace again in late summer, reaching 115% of 2019 volumes in September.
In the rest of the UK, Northern Ireland has performed most
strongly, averaging 104% of the 2019 billing volumes in the year to date.
Meanwhile, Scotland has been averaging 101%, while Wales has lagged behind the other home nations with 99%.
Variations
by episode setting
The recovery in hospital billing volumes has been most striking for episodes of outpatient care, but inpatient activity has lagged behind in 2021, even in the best performing hospital groups.
Billing for admitted patients was only 94% of pre-pandemic levels in September, compared with 119% for outpatients. The number of unique insured outpatients in September 2021 was 15% higher than 2019 while the number of unique insured admitted patients was 9% below the 2019 equivalent.
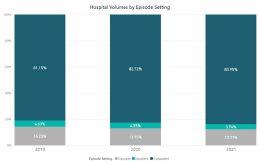
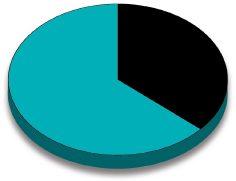
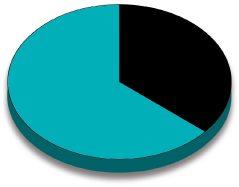
As chart 2 ( left, bottom ) shows, the proportion of outpatient care has increased since the pandemic began. Outpatient care now makes up nearly 84% of billing volumes, compared with just over 81% in 2019.
Meanwhile, inpatient episodes accounted for 14% of billing in 2019, but only 12% in 2021. However, it is too early to say if this trend will continue.
Variations by specialty Orthopaedics continues to account for the bulk of private hospital activity despite the detrimental impact of the pandemic on the specialty.
It was again the top hospital specialty in September 2021 with insured billing volumes of 49,000, double that of the next medical specialty, radiology.
After slumping to just 12% of 2019 billing volumes during the first lockdown, billing volumes in September 2021 were 107% and are now consistently above 2019 levels.
Radiology and pathology/haematology are the medical specialties that have fared best over the course of the pandemic, reflecting demand for diagnostic tests and other investigations.
In September 2021, hospital billing volumes compared with 2019 were 146% and 170% respectively.
Other medical specialties have been consistently above pre-pandemic billing volumes in the second half of 2021 although the rate of recovery has been slower in ENT and urology.
Overall, private hospital billing volumes have largely recovered in recent months, but Healthcode stresses that we cannot be sure this is a long-term trend, amid concerns over the rising infection rate and the possibility of further restrictions.
CHART 1: Billing volumes in UK Private Hospitals – 2021 comparison
Weeks of the year
Peter Connor of Healthcode
CHART 2: Billing volumes in UK Private Hospitals by episode setting
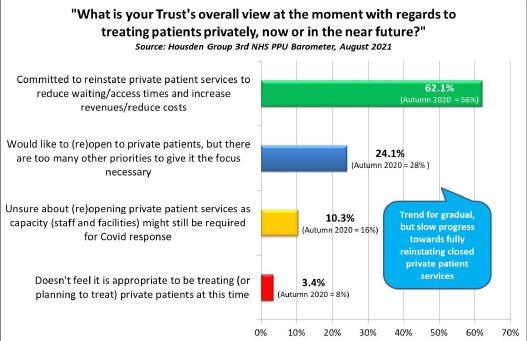
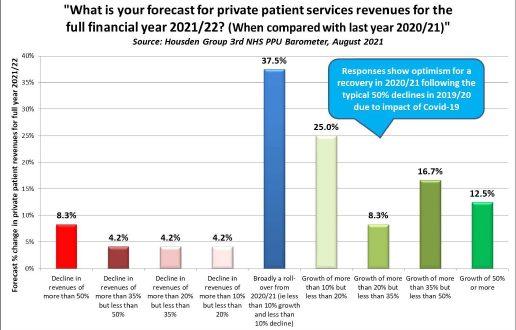
Covid caused a 42% fall in London PPUs’ income
Compiled by Philip Housden
With 130 of the 141 acute NHS trusts having now published their 2020-21 Annual Reports and Accounts, the scale of the Covid-19 pandemic on private patient revenues is becoming clearer.
For several years, the top ten earning NHS trusts have all been in
central London, and these have produced an increasing proportion of total NHS private patient incomes.
This reached a new high of more than 63.4% in 2019-20 when the total was £427.5m.
But, in the last year, a Housden Group analysis reveals the total for this central London top ten
declined by 41.8% and £178.9m to a total of £248.6m.
Top earning trust, as expected, was The Royal Marsden with £102m, down 22.9% from £132.6m last year.
Moorfields best protected its private patient incomes, delivering the lowest fall, with a 21.1% reduction from £30.8m to £24.3m.
The biggest revenue loser was Royal Free, which declined 82.4% to earnings of only £3.6m, down £16.8m from £20.4m in the year to end of March 2020.
A full review of the NHS private patient market as reported in trusts’ 2020-21 annual accounts will feature in a future issue of Independent Practitioner Today.
UCLH’s private arm takes over Queen Square
UCLH Private Healthcare, the private patient arm of University College London Hospitals NHS FT, has taken over the management of the private consulting rooms at 23 Queen Square, London.
This means that both inpatient and outpatient services for private neurosciences patients at the National Hospital for Neurology and Neurosurgery will now be
Bupa
begins menopause helpline for customers
Bupa has extended its women’s health support by launching a new Menopause HealthLine for health insurance customers and Bupa employees.
It offers access to menopausetrained nurses for advice and guidance on managing symptoms.
The insurer’s research found one million women have left their jobs because of the menopause, leaving a huge gap of experience and talent in the workforce and putting an additional strain on household finances up and down the country.
Bupa recently launched a Meno-
managed by a single team, streamlining current administrative processes for private patients.
The current managing organisation, Queen Square Enterprises, will focus on delivering its worldclass diagnostic imaging service at The Queen Square Imaging Centre and its sister site, the Chenies Mews Imaging Centre.
Both UCLH and QSE will con -
Alex Perry, head of Bupa Insurance
tinue to work closely together to offer seamless diagnostic and treatment services for private patients with neurological concerns. Director of private healthcare Kerensa Heffron said: ‘This is an excellent opportunity for us to better integrate our private healthcare service at UCLH. We are also delighted that we will still be working closely with Queen Square
Enterprises, who will continue to provide their superb diagnostics service to our patients.’
The trust’s recently published accounts show private patient revenues was £5.8m for the Covid-hit year of 2020-21, down 73% and £15.9m on £21.7m the previous year.
Philip Housden is a director of Housden Group. See his feature article on the NHS PPU Barometer, page 44
MDU to warn MPs of costs of negligence
pause Plan available through Bupa Health Clinics offering women access to primary care for symptoms through specially trained GPs. It also hosts a free-to-access Women’s Health Hub, which has advice and guidance from resident health experts on topics spanning menopause and endometriosis to periods and fertility.
Bupa Insurance chief executive Alex Perry said: ‘We hope this will help many women continue with their careers and help our business customers retain more of their talent.’
The campaign to reduce spiralling claims payments, which are fuelling doctors’ hefty defence costs, has been taken to an influential parliamentary committee by the Medical Defence Union (MDU).
It warned that the Health and Social Care Levy of 1.25% could be swallowed up by the amounts being paid out each year in NHS clinical negligence claims.
It predicted that the National Insurance tax levy on 8.7m people earning £30,000 and paying an extra £255 annually in tax would be needed to fund the amounts paid out in claims this year alone –money which could otherwise be spent on front-line patient care.
Dr Michael Devlin, head of the defence body’s professional standards and liaison, said: ‘Amounts being paid out in compensation annually are spiralling, increasing nearly 50% in the last five years from £1.48bn to £2.2bn last year.
‘At the same time, funding is urgently needed for front-line patient care to meet the demand for social care and to tackle the elective surgery backlog.
‘With the NHS facing a funding crisis, we simply cannot sit by any longer and ignore numbers like £2.2bn. The Government must reform the system of clinical negligence, so that it is fairer and mirrors society’s ability to pay.’
Private care sets emissions target
By Olive Carterton
Net zero emissions by 2035! That is the ambitious industry-wide pledge from over 40 providers across the independent healthcare sector in England.
Many more are expected to sign up to the aim in the next few months, according to the Independent Healthcare Providers Network (IHPN).
The pledge, announced ahead of the COP26 Climate Change Conference in Glasgow this month, covers 1,500 sites so far.
The commitment from independent healthcare providers builds on the NHS’s own target to achieve net zero by 2040.
To help support independent providers achieve this pan-industry climate change commitment, IHPN said it would continue to
bring members together through its Climate Change group so knowledge and best practice could be shared.
Actions might include procuring electricity from renewable sources, investing in low carbon infrastructure such as LED lighting technology or new higher-efficiency boilers, and having a real focus on data so providers can monitor their carbon and utilities consumption.
IHPN chairman Lord Patel of Bradford said: ‘Climate change is undoubtedly the biggest longterm threat to the health of our nation and indeed the world.
He added: ‘It is therefore vital that healthcare providers not only treat the problems caused by pollution and climate change, but also play their part in tackling the root causes.
‘As a sector which delivers care to millions of patients every year, I’m thrilled that independent providers are uniting to help tackle climate change and their commitment to achieve net zero by 2035 will make an important contribution in responding to this global emergency.’
IHPN chief executive David Hare said: ‘The independent health sector has rightly set an ambitious target to achieve net zero by 2035 and in the coming months and years IHPN will continue to support our members and share best practice –helping to play our part in making the UK a world leader in tackling climate change.’
Dr Nick Watts, NHS chief sustainability officer, said it was ‘fantastic’ to see independent healthcare providers aligning with the NHS target to be net zero.
Call for private and public care sectors to co-operate
Private healthcare providers have welcomed a recommendation by the Healthcare Safety Investigation Branch for new NHS Integrated Care Systems to fully utilise local independent healthcare provision.
Independent Healthcare Providers Network chief executive David Hare said: ‘This is something IHPN have long been calling for and which will ensure the NHS and independent sector can work together to improve patient access to high quality care in the months and years to come.’
Last year’s agreement between both sectors resulted in the independent providers delivering over 3.2m NHS procedures including 160,000 life-saving cancer and cardiology treatments.
The partnership has been praised by NHS England’s chief executive Amanda Pritchard as making a ‘critical’ contribution in ensuring that vital non-Covid NHS treatment went ahead throughout the pandemic.
IHPN says with independent healthcare providers continuing to play a key role in supporting the NHS to clear the elective care backlog, it was vital that the health service and independent sector could continue to work seamlessly together to deliver the safest possible care.
The network has called for NHS hospitals to act urgently on recent NHS England guidance to maximise the use of independent sector capacity.
A spokesman said: ‘With a tough winter just around the corner and a mammoth challenge ahead in recovering NHS services, patients need to be assured that all available staffed capacity – including in the independent sector – is utilised to get them treated.’
Independent charitable hospital King Edward VII has partnered with Chrysalis Finance to offer greater flexibility for self-payers.
Patients will be able to spread the cost of treatment on selected allinclusive fixed-price packages by choosing from a range of payment plans to suit various budgets.
Hospital commercial director Patrick Butterworth said the deal included flexible payment and interest-free options.
A rapid response referral service for patients requiring medical care following a winter sports injury abroad has been opened by HCA Healthcare UK.
The service has partnered with Charles Taylor Assistance – formerly Cega – to arrange international travel for self-pay patients. HCA’s concierge centre will work closely with insurers for those with cover to help navigate this process.
Director Annabelle Neame said rapid response referral aimed to combine this high-quality care with a seamless service at a time when patients or loved-ones needed reassurance, clarity and support in navigating their healthcare.
Cleveland Clinic London and AXA Health have agreed to offer eligible AXA Health members access to the hospital’s medical and surgical services. Earlier agreements have been announced with Bupa and WPA.
Scrip app reduces doctors’ admin
By a staff reporter
A new free app from healthtech company Pharmacierge is giving private medical practices access to easier and time-saving prescription administration.
The iPhone and Androidenabled app called mPrescribe, hailed as the first of its kind in the UK, acts as a portable e-prescription pad so independent practitioner consultants and GPs can prescribe medication on the go. mPrescribe can cut admin by up to 15 minutes per prescription with integrated same-day or nextday delivery, saving time for clinicians, administrative staff and ultimately their patients.
A multidisciplinary team and advisers, including from Google, Babylon Health, HCA and The Doctors Laboratory, were brought together for the platform’s development.
Pharmacierge co-founder Robert Ungar said: ‘The healthcare industry faces a number of challenges, not least due to the widespread disruption from Covid-19. Cumbersome and paper-based processes need to be replaced by streamlined apps that are quick and easy, both for the clinician and the patient.
‘A fast and reliable delivery service for prescription medication is therefore a requirement for private clinicians who put patient-centered care at the heart of their practice.’
The streamlined service was launched as Pharmacierge announced it had raised £1.25m in an investement round led by technol-
Clinic gets accolade as data provider for joint ops
ogy angel investors including Cazoo and Zoopla founder Alex Chesterman and Lovefilm cofounder Simon Franks.
Leading doctors have also taken part in the round, including former Independent Doctors Federation presidents Dr Peter KingLewis and Dr Brian O’Connor, plus clinicians at OneWelbeck, the Schoen Clinic, Hormone Health, Physicians Clinic, Cromwell, Wellington, Lister and King Edward VII Hospitals.
The company said it now aimed to expand its footprint throughout the UK and abroad, as well as growing its clinician network.
Co-founder and chief executive Edward Ungar, Robert’s brother, said: ‘Pharmacierge has grown rapidly in the last few years, but to have our users, including many of the UK’s leading independent clinicians, support us through
investment is a great testament to our dispensary and tech teams, and the value we bring to practices and patients.
‘We’ve delivered to a departure lounge and backstage before a rock concert. It all starts with the philosophy of saying “Yes, we can try to do that”.’
Pharmacierge’s formulary contains more than double the range of medicines listed by an average NHS trust, due to the range of specialties it supports.
It said the technology solved all the clinical management problems: combining seamless dispensing with courier delivery and updating doctors and patients on their prescription’s progress.
Pharmacierge said mPrescribe increased accuracy and gave clinicians access to a broader range of medication than an average pharmacy.
BMA decries inaction on pensions
BMA pensions committee chairman Dr Vishal Sharma expressed frustration at the Chancellor’s failure to use the Budget to tackle long-standing pensions tax issues.
He said action was needed to prevent affected doctors from working less for the NHS or leaving due to large, unexpected tax bills for simply doing their normal day job.
The BMA is urging the Government to support hospital trusts to enable doctors to access employers’ pension contributions if they are forced to opt out of the scheme.
Schoen Clinic London is celebrating being named as a National Joint Registry (NJR) Quality Data Provider.
The NJR monitors the performance of hip, knee, ankle, elbow, and shoulder joint replacement operations to improve clinical outcomes.
Orthopaedic data is also collected as evidence to support patient safety, quality care standards and cost-effectiveness in joint replacements.
The Quality Data Provider scheme offers hospitals a blueprint for reaching high standards and rewards hitting registry targets.
NJR medical director Mr Tim Wilton said the award reflected strong departmental efforts and was an important source of evidence for regulators such as the Care Quality Commission to inform judgements about services and a ‘fundamental driver’ to improve quality of care for patients.
Nearly 90% of independent acute services are now rated good or outstanding, according to the Care Quality Commission.
Dawn Hodgkins, director of regulation at the Independent Healthcare Providers Network, said the level demonstrated the sector’s clear commitment to providing the best possible patient care.
The figure was released in the watchdog’s latest State of Care report.
A total of 515 services were rated good (80%) and 51 were outstanding (8%).
But as many as 11% (71) were told they required improvement and four (1%) were found to be inadequate.
Pharmacierge co-founders: brothers Edward and Robert Ungar. Edward is also the firm’s chief executive
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2011
Skimp on PAs and pay the price
Consultants were forfeiting a huge slice of their business potential by directing private patients to phone them at NHS hospitals, we reported.
New research suggested over half the calls made to secretaries who worked for them in the NHS and private went unanswered.
As many as 58% of calls made by private patient mystery shoppers to ‘dual role’ secretaries got nowhere.
When callers did reach a secretary, they were always wrongly assumed to be NHS patients.
The survey covered a dozen calls on different days to consultants who publicised the same phone number for private and NHS work.
Researchers commissioned by health management troubleshooters RLG Medical Partners reported the highest call response rate was just 67%. The lowest was 17%.
Partner Rita Livesey said: ‘When we decided to put NHS secretaries in the spotlight, our expectations were admittedly not very high. To then discover only 42% of our calls were answered was a shock.
‘Consultants cannot avoid losing patients, and therefore business, if only 42% of callers can actually get through. This loss of income will far outweigh any costs saved by using existing NHS resources. It’s a clear false economy.’
Tax shock for seniors retiring
next year
Doctors’ retirement applications might not be processed before significant tax reforms came into place in April 2012, we warned.
This could leave them paying hundreds of thousands of pounds extra in tax and having their retirement plans delayed.
Many doctors had been keen to retire before the Government cut the amount an individual could accumulate tax-free in pension funds from 6 April 2012.
Independent financial planners Cavendish Medical urged doctors to seek professional help to make sense of the complex tax situation.
Give your workers a pension, doctors told
Independent practitioners who employed staff were warned to gear up to contribute a percentage of employees’ salaries to a pension scheme from the following October.
A National Employment Savings Trust (NEST) had to be offered to all employees who were not already enrolled in a ‘Qualifying Pension Scheme’ with benefits equal or better than offered by NEST.
Low earners fuel a rise in self-pay care
A surge in low-income families opting to see private doctors fuelled a 29% rise in self-pay patients at Spire Healthcare.
The increase was reported as a survey announced that one-in-four lower-income families on £21,000£29,000 a year would now consider private healthcare if they could afford it – due to fears over lengthy waiting lists.
A quarter of respondents on below-average salaries of £20,000 said they would pay to go private, even though 87% had no private medical insurance.
Plastic surgeons told to shun pushy ads
Members of the British Association for Plastic, Reconstructive and Aesthetic Surgeons (BAPRAS) were warned they would be investigated if they got involved in media promotions that induced surgery. The alert followed cosmetic surgery promotions in a young women’s magazine.
One offer was for a ‘free boob job’ for a ‘lucky reader’ in exchange for being filmed.
The British Association of Aesthetic Plastic Surgeons also expressed its alarm.
GMC to alter its rules
An updated draft of the GMC’s core guidance Good Medical Practice included new advice to doctors covering behaviour online and use of social networking sites.
TELL US YOUR NEWS
Share your experience of what has and has not worked in your private practice. Even if it’s bad news, let us know and we can spread the word to stop others falling into the same pitfalls.. Contact editorial director Robin Stride at robin@ip-today.co.uk
UpToDate is the premier clinical decision support resource that helps physicians and other medical professionals worldwide drive effective, high-quality patient care.
With UpToDate you can access:
✓ 12,000+ evidence-based topics in over 25 specialties
✓ Relevant “What’s New” and “Practice Changing Updates” to complement NICE guidelines
✓ Reliable clinical content from your computer, mobile device, or tablet with our mobile app and voice-enabled search
“ Well written by experts, succinct but comprehensive, excellent graphics and well referenced.”
ALAN MCGREGOR, MD — UK
ACCOUNTANT’S CLINIC: THE BUILDING BLOCKS OF ACCOUNTANCY
to of top tips
Julia Burn (right) reaches the destination in her A to Z of top tips. Z is for Zzzzzzzzzz
– don’t sleep through the upcoming tax changes
is for Zzzzz . . .
THERE IS no doubt that the last couple of years have had an enormous impact on the economy and finances of our country, but also highlighted where more funding will be required in the future.
As a result, the Government has had to consider how to improve the situation and recover from the pandemic and its consequences. Unfortunately, this is not necessarily good news for some taxpayers.
Below, I have summarised the main changes that are being proposed or are due to be introduced to the current tax system in the near future which may have an impact on you personally or your companies:
INCOME TAX
No changes have been announced to the personal allowance (currently £12,570) and tax rate bands (basic rate limit of £37,700, higher rate limit up to £150,000) as well as annual exemption for capital gains tax purposes (currently £12,300) and these are likely to be frozen up to and including the tax year 202526.
The dividend allowance and savings allowance will remain as £2,000 and £5,000 respectively and there has been no indication that these will change.
However, the Government has proposed an increase to the dividend tax rates by 1.25% with effect from April 2022 to 8.75%, 33.75% and 39.35% for basic, higher and additionalrate taxpayers respectively.
NATIONAL INSURANCE
In line with the increase to the dividend tax rates, the Govern ment has announced that a temporary increase will also be introduced to the National Insurance Contribution (NIC) rates.
All rates will be increased by 1.25% for the tax year 202223 and the rates will return to their current level from 202324 onwards, this includes both employees’ NI and employer’s NI.
However, this is when the
‘health and social care levy’ of 1.25% will be introduced and it will apply to all individuals, including those who are above State Pension age and still working (as employees or self employed) who currently are exempt from paying NIC.
All these revenues will be ringfenced for health and social care.
BENEFITS IN KIND – CAR BENEFITS
The benefit inkind rates for company cars registered after 6 April 2020 have increased by 1%.
This means that even cars which are 100% electric will now be liable to a 1% benefit in kind charge provided that the car was first registered on or after the start of the 202021 tax year. This rate is set to see an additional increase to 2% from the 2021 22 tax year onwards.
CORPORATION TAX
While the current Corporation tax rate of 19% will remain in force until April 2022, increases to Corporation tax are due to come in with effect from April 2023 when the highest rate will be 25% and it will apply to profits in excess of £250,000.
Profits will still be taxed at 19% up to £50,000 and the tax rate will be tiered and gradually increase for profits between £50,000 and £250,000.
No details have, however, been announced yet.
CAPITAL ALLOWANCES
A new superdeduction capital allowance can be used between 1 April 2021 and 31 March 2023 on qualifying new plant and machinery.
This means that companies can claim a deduction of 130% of the qualifying expenditure as a firstyear capital allowance.
In addition, a new 50% firstyear allowance will be in place for companies until 31 March 2023 for
With all of the upcoming changes, it is more important than ever to ensure you review how these changes will affect you
special rate – including long life –assets.
The Annual Investment Allowance which allows a 100% deduction on qualifying plant and machinery has been temporarily increased up to £1m until 31 December 2021. The allowance will be reversed to £200,000 from 1 January 2022.
Review of your tax position
As business owners, when you are discussing your tax affairs with your advisers, you may focus on the effective rate of tax being suffered on the amounts that you are withdrawing from the business.
As you are owners of the business, the overall tax burden is relevant, as everything that is left over in the company is also yours.
This means corporation tax and employers NI suffered by the company need to also be considered alongside income tax and NI paid by the individual – and the new Health and Social Care Levy affecting both the company and the individual.
It will also be good to consider remuneration packages and the most efficient methods for each individual.
As discussed in previous issues of Independent Practitioner Today, to encourage the taxpayers to save for the future, tax relief is available for contributions you make to your pension. This is both at source when you make contributions as well as company pension payments being an allowable deduction for corporation tax purposes. With tax rates increasing on all forms of remuneration, it is likely that pension contributions will increase in popularity, despite the restrictions in place, as these can be made taxefficiently.
With all of the upcoming changes, it is more important than ever to ensure you review how these changes will affect you individually and your practices and to ensure that accounting data is regularly updated so you have realtime information.
This will enable you to update budgets and forecasts regularly and foresee and react to any pinch points early.
Julia Burn is a director at Blick Rothenberg and part of the team that advises medical practitioners
Workhorses of private care deserve nurturing
Leading supplier of RMOs in the independent hospital sector, NES Healthcare UK, has welcomed the GMC’s publication of survey results in Understanding the Role of Resident Medical Officers in the Independent Sector.
But the firm’s medical director Dr Stephen Drotske (below, left) and operations director Justyn Tollyfield (below, right) say an opportunity was missed to provide greater insight into this essential group of doctors
private nurturing
THE AIM of the GMC-commissioned report was to improve its understanding of the role of Resident Medical Officers (RMOs) in the independent sector.
From the survey’s methodology, it is clear that NES, the largest RMO employer in the UK with almost 500 doctors on the designated body, was not invited to participate or to encourage our doctors to engage with the survey.
Both the GMC survey and a Centre for Health and Public Interest (CHPI) 2017 report inferred an inconsistent level of support to the RMOs, yet neither sought clarification on this from RMO employers.
For many years, RMOs have also worked in the NHS, yet this group of clinicians was excluded from the GMC survey and from the CHPI report. It is therefore our view that without the input of a wider range of stakeholders, the results of these exercises are of limited value.
These international graduates fulfil a vital role across the UK healthcare sector
carefully manage their recruitment and introduction to their roles in the UK and that support thereafter is effective.
This article outlines the support provided by NES to its doctors and offers an opportunity for other stakeholders to support us in looking after our RMOs.
Recruitment support
The survey has, however, established some learning opportunities for RMO employers which will help us to enhance the support we already provide for RMOs.
The RMO role is a non-training post and does not have the same supervision or learning opportunities as a training position in the NHS.
Vital role
These limitations ensure that no doctors trained in the UK or established within the NHS are attracted to apply for these positions. It is, however, a vital resource for the independent sector and, increasingly, within NHS trusts looking to address staff shortages.
As with the GMC’s survey sample, the vast majority of NES’s RMOs received their qualifications outside the UK. These international graduates fulfil a vital role across the UK healthcare sector and it is important that employers
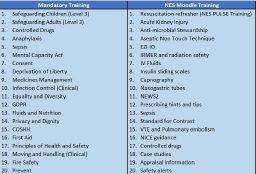
During the recruitment phase, which can take up to six months, doctors are actively supported to learn about the UK healthcare sector. We also start at a very early stage to consider patient safety through online training in life support, blood transfusions and a whole raft of mandatory training.
The table below shows the full list of online training we provide. If this is not completed in full, the doctor will not be cleared to commence their role in the UK.
Training on arrival
Once in the UK, NES doctors complete Intermediate Life Support (ILS), Advanced Life Support (ALS) and European Paediatric Advanced Life Support (EPALS).
The GMC report noted the high level of responsibility an RMO has. To mitigate risk and to enhance care, NES has for many years insisted on training all its doctors in adult and paediatric life support before they commence work.
In addition to this, we provide practical training and support with prescribing and infection prevention.
As part of their introduction to the UK, we support our doctors with opening bank accounts, registering with GPs, resolving occupational health issues and booking their first GMC appraisal. As employees, all NES doctors receive professional indemnity insurance.
Ongoing support
While doctors are working for NES, we regularly offer update training in their role as leader of the resuscitation team. Online workshops also include updates on human factors, new medication and devices. There is also a 24/7 clinical team that is available to offer assurance and or advice to clinicians on duty.
We reported last month the results of an RMO survey
The table below shows the full list of training provided by NES Healthcare
CONSULTANT SUPPORT
NES works closely with the hospitals where our RMOs work to ensure that any issues fed back by the doctors are addressed.
The GMC survey specifically mentioned that the RMOs who contributed had difficulty reaching consultants while on duty. As part of our audit work, NES has been monitoring this for many years and feeding back the audit information for the hospitals to address such issues with their consultants.
Our 2020 audit asked respondents how they rated consultant responsiveness and support at their hospital. The results showed that 86% of calls to consultants were answered immediately, with a further 10% returned after 30 minutes.
This indicates that consultant support is readily available within hospitals supplied by NES. Instances where previous data has identified a lack of responsiveness within the consultant body have been tackled directly with the hospital management.
NES obtains regular feedback from those working in conjunction with our RMOs to further support their individual training needs
NES obtains regular feedback from those working in conjunction with our RMOs to further support their individual training needs. Such feedback can result in case studies or updates for all doctors as part of our ongoing support and learning programme for RMOs.
The GMC survey referenced RMO workload and, for a number of years, NES has been carrying out regular audits to provide data to facilitate the assessment and management of our doctors’ workloads. Each doctor also has a dedicated medical staffing manager who maintains regular contact with them.
As an example, recently a doctor was struggling during his training courses. We learned that he lost his wallet and his luggage following his flight and had no means of support.
We provided him with accommodation and also with food and money for clothes. This doctor is just one of the many who found relocating to the UK to be challenging and benefited from the personal support NES can offer.
Continuity
NES operates safe working rotations for its doctors, with workloads – including night disturbances –and responsibilities closely scrutinised and controlled. The extraordinarily low number of adverse patient outcomes supports the work that we do.
We employ many standby doctors who we can deploy to hospitals in support of clinicians and hospital clients.
This group of doctors allows us to cover those who are unwell or unable to work and safeguards our commitment to provide doctors to hospitals.
As many of the NES doctors were not involved in the survey, it could well be that doctors who responded to the GMC were not aware of this back-up plan available to others.
Conclusion
While welcoming the information gathered by the GMC about RMOs, we are disappointed that no effort was made to engage with RMO employers such as NES. In this way, an opportunity was missed to provide greater insight into this essential group of doctors.
Since 1994, when NES employed its first RMOs, we have invested in the continuity of care for patients as we recognise that regularly seeing the same doctor is hugely beneficial for patient safety and welfare during their hospital stay.
By ensuring high continuity of care by NES doctors, the outcome for patients during the post-operative period is much better. We measure continuity of the ‘same face at the same place’ to support patient care.
To allow for continuing professional development and holidays, we have set 80% as the benchmark for continuity and in 2020 achieved 86.7% across the 1.5m hours of doctor cover we provided.
Employing more RMOs
RMOs who answered the GMC survey suggested that more doctors should be on duty at any one time.
In an ideal world, every hospital has ample doctors and nurses, but reality dictates that there is a shortage of these disciplines in the UK and doctors are currently on the shortage occupation list.
Nevertheless, NES continues to be open to dialogue with the GMC and through this to further improve the support it already offers to its doctors.
Future considerations
The focus of the RMO role is patient care, not on training. Therefore NES, with its robust assessment and selection program, ensures that only welltrained clinicians accept the role. Throughout the Covid pandemic, it has been evident that RMOs played a major role in the UK’s response and they will play a huge part in the future in supporting the private sector to help the NHS clear the millions on the waiting list.
We all therefore need to carefully consider support for this important group of clinicians.
throughout their services; for example, holding quarterly calls with FSUGs across their organisations to provide updates and share best practice, and actively encouraging their Guardians to meet with their local NHS trust counterparts to learn and share from each other’s experiences.
And if anyone has any doubt about the importance of staff at all levels having the confidence to speak out about concerns on safety, quality or how things can be improved, the Paterson inquiry and its ongoing response should once and for all put those to rest.
Appalling actions
Speak up for safety and quality in private healthcare! David Hare (below) reports on progress in the sector
THIS OCTOBER once again saw the start of ‘Speak up Month’ – an initiative set up by the National Guardian’s Office to raise awareness of Freedom to Speak Up Guardians (FSUGs) and the work being done to make speaking up ‘business as usual’ for healthcare providers.
This was originally introduced following Sir Robert Francis’s 2015 review into ‘whistleblowing’ processes within the NHS and aims to develop cultures where safety concerns are identified and addressed at an early stage before people feel the need to ‘blow the whistle’.
All providers of NHS services subject to the NHS Standard Contract must now have in place a FSUG and, in the independent health sector alone, over 100 have already been established.
With ‘Speak up Month’ upon us,
it is therefore a good time to reflect on this issue and why it is important that all parts of the healthcare system – including the independent sector – embrace ‘speaking up’ as a way of improving the safety and quality of care we deliver.
At a time of ever greater pressure on the healthcare system – dealing with the backlog caused by the coronavirus pandemic on top of an ageing population with more complex needs – it is vital that all of us in the sector look at what can be done to drive continuous improvement.
Healthy scepticism
A key part of this – and what FSUGs helps to foster – is embedding culture of ‘healthy scepticism’ in the health system and encouraging a sense of inquisitiveness and curiosity throughout organisations so that problems can be identified with and dealt with at an earlier stage.
Indeed, as the Independent Healthcare Providers Network’s (IHPN’s) recent Medical Practitioners Assurance Framework (MPAF) made clear, staff at all lev-
els are the eyes and ears of any healthcare organisation.
They notice breaches in safety, good and bad behaviours, inappropriate investigations, treatments and interventions. But it is not always easy for staff, regardless of their role, to raise their concerns.
So the MPAF recommended that all independent providers should have effective systems in place to enable staff to speak up and should appoint FSUGs throughout their organisations.
Open dialogue
And I’m pleased to say that the sector has really embraced this agenda.
During the pandemic, many providers produced bespoke ‘Speak Up’ guidance that centred on the management of concerns relating to Covid – encouraging open dialogue and allowing staff to manage issues in a timely manner.
This was complemented by regular reviews of their Speak Up infrastructure to evaluate their systems and processes.
Likewise, providers across the sector have worked hard to embed the importance of ‘Speaking Up’
The Bishop of Norwich’s report made clear the inconsistencies in how concerns were raised by professionals in the NHS and the independent sector with ‘inadequate’ responses in both sectors when professionals did raise concerns, contributing to a climate where Paterson was able to commit such appalling criminal actions.
As many have argued in recent years, healthcare can be a hierarchical business and that is why the ‘Speak up’ movement is so important. FSUGs not only provide a structure for concerns and issues to be raised, but also help develop a culture where employees feel free to contribute ideas, share information and report mistakes and ultimately drive improvements.
As part of Speak Up month, I urge all those working in the independent healthcare sector to raise awareness of FSUGs and encourage many more to be established.
Not only will you be fostering a culture where people can speak up and be confident they will be listened to, it will play a pivotal role in further improving the care provided to millions of patients every year.
David Hare is chief executive of the Independent Healthcare Providers Network (IHPN)
SETTING UP IN PRIVATE PRACTICE
Planning a start in private practice?
One of the most obvious steps for consultants looking to start a private practice is to gain practising privileges. Jane Braithwaite uses her insider knowledge to present an essential guide to help bring you success in this settingup process
THE PROCESS of gaining practising privileges is often viewed as time-consuming and bureaucratic, but there is a lot more to think about than simply filling in a set of forms.
Having an application accepted is not guaranteed and consultants need to consider what they offer the hospital to ensure their application is successful.
For a consultant, practising priv-
Most consultants will need to choose which hospital or clinic they wish to work at and making this decision is complex.
ileges are a licence permitting them to work within a hospital, clinic or independently in private practice. The consultant will be able to make use of the facilities and services provided by the hospital.
Most consultants will be granted
practising privileges within a large organisation operating several locations, but an individual consultant will generally be given access to work from one specific location.
Gaining practising privileges enables a consultant to work in pri-
APPLICATION REQUIREMENTS
The Care Quality Commission (CQC) publishes very clear criteria for service providers to follow to enable practising privileges to be granted.
Here is a summary of the requirements. Full details are available on the CQC website:
Proof of identity including a recent photo
Enhanced criminal records check
Evidence of conduct in previous employment
If an individual has worked previously with children or vulnerable adults, confirmation of the reasons why that employment ended
Documented evidence of qualifications
A full employment history, together with a satisfactory written explanation of any gaps in employment
Information about physical and mental health conditions that may affect an individual capability
vate practice, serving the general public and have the ability to potentially generate a substantial private practice income.
For the healthcare service provider, offering practising privileges to a consultant is also an important decision. The granting of practising privileges is a formal and well-structured process requiring an applicant to pass certain checks and to demonstrate suitable indemnity cover.
A healthcare service provider invests enormously in their facilities, and also its reputation, so it needs to be certain it is granting privileges to consultants who will respect its facilities and uphold its reputation.
Ultimately, though, the private service provider needs consultants to work successfully from its facilities to generate activity and income. So the relationship between the consultant and the service provider is mutually beneficial.
Choosing where to practise
When deciding where to practise there are several key factors to consider. Location is an obvious factor, as it needs to be convenient for the consultant and ideally close to home and their NHS base, if appropriate.
The facilities provided by a service provider and also the reputation of the facilities with patients will be vital.
The demographics of the local area may be relevant to some medi-
A healthcare service provider needs to be certain it is granting privileges to consultants who will respect its facilities and uphold its reputation
feel a consultant is committed to them, looking for a long-term partnership and demonstrating loyalty.
Research the competition
Decisions may also be affected by colleagues and potential competition at a particular hospital.
If there are several very successful consultants in a given specialty at a particular location, it may be hard for a doctor of the same specialty to start a new private practice, unless the existing practices have long waiting lists.
When private consultants first take the leap from solely practising with an NHS contract, they can find themselves in unknown territory when it comes to competitors and self-promotion.
reason, that a practitioner has decided to consult privately. Perhaps it is financial or simply a needed respite from the bureaucracy of the NHS.
Whatever the reason, your patients, their care and treatment should always be at the heart of what you do. Keeping this in mind, makes it easier to promote, support and stay connected in the work that you do.
Every service provider will define their own procedures, incorporating the Care Quality Commission requirements (s ee box, left ) but potentially involving other checks and potentially including interviews with key individuals within their organisation and approval by an advisory committee.
cal specialties and a consultant will need to research whether their ‘target audience’ is well represented in the immediate vicinity.
Less is more
Quite often, when a consultant is starting their private practice, they are tempted to apply for practising privileges with several different service providers.
Their thinking is that they will run clinics at various locations initially, determine which location is most successful for them and then focus on that particular clinic.
Most consultants starting private practices are already busy with demanding schedules and the requirement to manage clinics at several different locations is timeconsuming and onorous, especially in terms of travel, and difficult to manage from an administrative perspective.
This approach often turns out to be a disappointing strategy. The consultant is spread too thinly and the experience of managing numerous clinics at different locations is stressful and ultimately not successful.
This slightly scattered approach is also not welcomed by service providers.
When a service provider grants privileges to a consultant, it will invest time and resources in assisting the new consultant and marketing their practice to its community of GPs and patients.
A service provider will be more highly motivated to do this if they
Never before have they had to look at themselves and their skills as a personal brand that they need to advertise like a business.
They will need to build up a network of contacts as well as considering their online reputation. New consultants would be wise to spend time searching online for their ‘competitors’ to find out the following information to help them plan their own strategy:
How easy are they for patients to find online?
Are their profiles active and up to date?
Do they have their own website?
What is the general sentiment of their online reviews?
Do they use social media and how often do they post online?
Do they use bespoke branding such as logo, brand colours, specific font?
How do they communicate their fees?
How does your own structure compare?
Colleagues not competitors
Though it is important for a new consultant to market their practice and to be aware of competitors in their field and local area, it is also worth them making the effort to network and connect with their peers.
In less specialised areas, private consultants may not have the capacity to treat all patients and there may be a need to hand over cases that require rapid treatment or consultations.
There could be more than one
In the main, service providers are looking for consultants who are safe, reliable and appropriate to practice within their facilities. They are ideally looking for consultants who are committed to them on a long-term basis, demonstrating loyalty and therefore a good investment for the service provider.
See ‘Is your practice fit for tax changes?’, page 42
If you have recently transitioned to private consulting or are in the early stages of considering private practice, my company, Designated Medical, can help. My team has experience in all areas of practice management, so whether you are building your clinic from scratch or are consulting at a larger, more established location, we can aid in the areas of accountancy, marketing and medical PA services.
Please feel free to contact me for more details.
Jane Braithwaite (below) is founder and managing director of Designated Medical, providing bespoke support services for doctors in private practice including accountancy, marketing, human resources, recruitment and medial PA services
Where private GPs go wrong
Dr Sarah Jarvis analyses medico-legal files involving private GPs and advises on how to manage risk
RISK MANAGEMENT ADVICE FOR PRIVATE GPs
Don’t make assumptions about a patient’s knowledge of a procedure or the associated risks. Find out what is relevant to them and explain what they should expect, including possible side-effects such as bruising.
If things go wrong, say sorry, provide an honest and open explanation of what has happened and the likely short- and long-term effects.
Ensure patients are involved in decisions about their treatment and care and supported to make informed decisions if they are able.
Follow the Code of Practice which accompanies the Mental Capacity Act when assessing capacity. Seek advice from your MDO if you are unsure how it applies in specific circumstances.
Remember that a patient who is unable to give informed consent to complex treatment, could still be capable of deciding whether or not to consent to disclosure. Capacity must be carefully assessed based on each patient’s individual presentation and the decision to be made at the time.
If a patient with capacity objects to you sharing information with their NHS GP, you should explain the implications for their care. However, you should respect their wishes if they continue to object, unless disclosure is justified in the public interest – for example, they pose a risk to others.
If a patient lacks capacity, you may need to share information with relatives, friends or carers in their best interests, considering
ONLINE SERVICES such as Livi, Babylon and Push Doctor have increased the profile of private general practice in recent years and it is likely that the pressures of the pandemic on NHS practices may tempt more patients with the disposable income to pay for their GP appointment.
The Medical Defence Union (MDU) recently reviewed files featuring requests for advice and assistance from private GP members over a recent four-year period to see if there were any concerns specific to this group.
Nearly half of these GPs were seeking medico-legal advice to help them manage a particular situation and pre-empt problems.
Just over a third involved patient complaints and 10% concerned the GMC and coroner. There were a handful of claims which are ongoing.
Unsurprisingly, the advice files involving private GPs largely echo the pre-occupations of their NHS colleagues.
For example, we saw a spike in contacts regarding data protection law at the time the General Data Protection Regulations came into effect in 2018 and another in 2020 regarding practice during the pandemic.
We were also struck by the robust clinical governance procedures in evidence. Practices were up-front and transparent in responding to complaints and held regular meetings to discuss the learning points from unusual cases and adverse incidents.
relevant factors such as their health, welfare, and family relationships. You should not disclose information to a third party simply because they are funding the patient’s care and treatment.
Document why you concluded the patient did not have capacity and why you believe disclosing information is justified.
There are no specific retention periods for private clinical records but the GMC’s Confidentiality guidance [paragraph 130] references the relevant Government guidelines to follow ‘whether or not you work in the NHS’.
Ensure old patient records are stored securely and protected from accidental loss, damage or disclosure.
However, we did uncover some themes that were more common among this group of members, which enabled us to put together our top risk management tips for private GPs:
Fewer
complaints about communication
Allegations by patients of poor communication are a relatively common feature of complaints, but we saw a smaller proportion in the private GP files.
It is likely that this was because of the lack of time pressure on private GPs, which allows for longer appointments, and also because patients were able to see the same GP at each visit, which supported continuity of care.
According to a report by the Royal College of General Practitioners in 2019, the number of patients able to see their preferred GP in England fell by 27.5% between 2012 and 2017.
Phlebotomy cases
Requests for help with phlebotomy complaints from NHS GPs are rare but there were more than we expected among private practitioners, including several patients who experienced bruising or soreness after their blood was taken.
This may reflect that private GPs carry out fewer blood tests than NHS services where this task is more commonly done by a dedicated phlebotomist in the practice or local hospital.
Finally, in the MDU’s experience, levels of expectation are likely to be higher in patients who are paying for medical services.
While bruising is a common side-effect of having blood taken, it is possible that the patients who complained did not expect this to happen. It highlights the importance of warning patients about risks when obtaining their consent, so they have realistic expectations.
Mental capacity cases
We saw several cases involving patients whose capacity was in doubt. These included queries about self-neglect in a frail elderly patient, how to assess a patient’s capacity in particular situations, and the authority of someone who had been awarded lasting power of attorney.
Information-sharing with family members was another common aspect to these cases, including whether the GP should still try to obtain consent and what disclosures were in their best interests.
A complicating factor when a family member was paying the bill was that they often expected to be kept informed as a matter of course.
Records and disclosure
There were more general information-sharing concerns too, including patients who objected to certain information being shared with their own GP practice, such
PATIENT CENTRED HEARING CARE
as mental health or addiction problems.
Members sought advice on how to balance their own duty to share information for continuity of care and the need to obtain appropriate consent.
Finally, several files concerned doctors’ responsibility for private patient records, including GPs who were planning to retire and wanted to know how long they needed to retain their clinical records and their responsibilities concerning secure storage and disposal.
Dr Sarah Jarvis (right), a medicolegal adviser at the MDU, was a GP principal and sat on – and later chaired – the GMC and Medical Practitioner Tribinal Service’s fitness-to-practise panels for ten years
Exceptional audiological care starts with the right referral. At Pindrop Hearing, we understand each case as unique, and our team of expert Audiologists will work with your patients to find the right solution for them
• Specialists in Diagnostic Audiology including Paediatrics and Tinnitus rehabilitation
• Cutting edge on site facilities, including purpose built sound proof rooms and audiovestibular diagnostic services
• Comprehensive range of diagnostic tests including PTA, tympanometry and specialist tests including OAE's and VEMPS
•A wide range of hearing devices, not available on the NHS
• Outstanding aftercare and patient services
• Fully GDPR compliant
• Medico-Legal Audiology service including gold standard objective Audiological testing using Cortical AEP and ASSR
• Full COVID protection measures in all clinics alongside a dedicated online consultant portal
Time to take care of
After more than 20 months of working at an unsustainable intensity, coping with anxious patients, coupled with fears about spreading the Covid virus, it is no surprise so many doctors are feeling the strain both physically and mentally.
Here Dr Robin Clark (left), Bupa UK and Bupa global medical director, gives a gentle reminder for doctors to prioritise their own health and well-being – and provides some ideas to act on
your own well-being
BURNOUT IS when we experience high levels of stress and pressure which we’re not able to manage, causing us to feel emotionally exhausted. As a result, we may lose motivation, feel negatively towards our work and experience lower levels of productivity.
As doctors, we spend a lot of time dispensing well-being advice to our patients, but we don’t always practise what we preach. If we want to avoid burnout, it’s time for that to change.
While you might not be able to lighten your caseload, you can lighten your psychological load by remembering to take charge of your own well-being.
You may feel the demands of your practice don’t allow you to make big changes, so here are some tips to help you focus on small behaviour changes that can incrementally improve your well-being.
Cut down on technology
The constant stream of notifications demanding our attention has implications for our wellbeing. Those who are better able to switch off when they get home tend to sleep better, respond better to stress and have higher life satisfaction.
Technology is a key mediator of this, with those who use the same phone number or laptop for work and home finding it far more difficult to set these boundaries. While the ‘on call’ nature of our roles means we can’t turn off notifications, there are some things we can do to give ourselves a proper break when we’re not working:
➲ Have a phone time-out while you’re eating dinner or watching TV. Try leaving your phone in another room so the effort to go and get it will deter you from checking it.
when we link them to activities or triggers in the environment that already occur in our daily lives.
➲ Get an alarm clock instead of using your phone to wake up – which means it’s the last thing we see at night and the first thing we see in the morning. Using an alarm clock means you can leave your phone switched off all night, reducing your likelihood of being disturbed.
Beware video call fatigue
Video technology has brought us great benefits, particularly in allowing us to connect with patients conveniently in a way that reduces risk of exposure to Covid-19 or brings together multidisciplinary team meetings when we work across different sites.
But a consequence of its increased use is what’s become known as ‘video call fatigue’ – the tiredness, worry or burnout associated with overusing these platforms.
As my colleague Juliet Hodges, senior behavioural insights adviser at Bupa UK, confirms: ‘Processing several different faces and voices on a screen requires a lot of cognitive effort. Our sense of self-awareness is also heightened, as we’re seeing our own faces on the screen too, so we might be concerned about whether we are coming across as we mean to.
‘For some, there will be other worries such as being interrupted by family members or distracting noises. What’s more, if you have lots of back-to-back meetings, there is less of an opportunity to rest your eyes and get away from the screen to stretch your legs. All these factors can lead to video call fatigue.’
She suggests limiting the number of video calls each day and seeing whether you could talk over the phone instead sometimes.
ing video meetings by checking emails. This will help to reduce the additional cognitive load and mean that we are better able to concentrate on the task at hand.
Avoid digital eye strain
Digital devices have become part of everyday life and the pandemic increased our use of them more than ever as we sought to reduce physical contact with other people. We now rely on our smartphones and tablets for work, communication, socialising and entertainment.
The small screens on smartphones and tablets can put particular strain on eye muscles, leading to eye discomfort.
Although mostly temporary and symptoms usually disappear after a break from screen use, digital eye strain can cause frequent and significant discomfort.
Given we often need to use our devices for long periods of time, there are a few steps we can take to protect our eyes:
➤ Make sure the text is in focus and large enough to read comfortably, the screen doesn’t flicker, the brightness is appropriate for the setting and avoid glare. Also select colours that are easy on the eyes –for example, avoid red text on a blue background or vice versa.
➤ Look away into the distance from time to time and blink often.
A good way to remember this is the 20-20-20 rule. For every 20 minutes of screen time, you should look away at something in the distance (about 20 feet away), for 20 seconds.
➤ Break up long spells of screen use with device-free breaks. This is particularly important if working at home, when it can be easy to continue working or sitting at a screen. Short, frequent breaks are better than longer, occasional ones.
➲ Harness existing habits like enjoying your morning coffee completely device-free; try reading a book or journal instead. It’s much easier to form new habits ➱ p24
Other ways to reduce fatigue include turning off your camera when others are presenting and avoiding trying to multi-task dur-
➤ After work, if you’ve had a long stretch at the computer, try to have a break from devices.
Give yourself a break
One-in-three people sit at their desks for too long, and this can cause stiffness and muscle pain. Physiotherapists recommend taking a five to ten-minute break from your desk every hour for to stretch your back, legs and rest your eyes.
A short burst of ten minutes’ brisk walking increases our mental alertness, energy and positive mood. But if you really can’t get away from your desk, try some simple stretches you can do from your desk to avoid stiffness and back pain.
When you are able to take a break during the working day, use it to benefit your well-being. As Juliet says: ‘Try not to scroll through social media or the news during your breaks. Instead, you could try five minutes of mindfulness, listen to music or do some simple stretches to move your body. These practices can boost your mood and leave you feeling re-energised, ready to tackle the rest of the day.’
Set aside time during your evenings and weekends for self care. Do whatever helps you switch off, whether that’s spending time with family and friends, gardening, enjoying creative hobbies or exercising.
As doctors, we’re well aware that the benefits of regular exercise extend far beyond the physical, with the release of cortisol which helps us manage stress. Being physically active also gives your brain something to focus on and can be a positive coping strategy for difficult times.
Juliet has another tip to consider: ‘Aim to spread your annual leave throughout the year to make sure that you get significant chunks of time to switch off – but don’t be tempted to check your emails. Taking time away from your work has a heap of health and wellness benefits.’
Eat for energy
Long working days may mean we’re more inclined to grab the convenient unhealthy snacks rather than a proper meal, but nutritionists tell us that careful food choices can boost our energy as well as our mental well-being.
My colleague Victoria Evans, well-being programme consultant and registered associate nutrition-
Aim to spread your annual leave throughout the year to make sure that you get significant chunks of time to switch off
ist, advises: ‘Aim to snack on fresh fruit, veg sticks or nuts to avoid the post lunch lull.
‘Swapping our foods such as biscuits, chocolates, fizzy drinks and cake for these more nutritious options will help with maintaining your energy levels throughout the day.’
And she recommends opting for lunches that include a mix of the below to keep your energy levels up:
Fruit and vegetables;
Carbohydrates such as quinoa, bread, potatoes, rice or pasta;
Protein such eggs, fish, meat or cheese or dairy alternatives or beans and pulses;
Some healthy fats including nuts, seeds, olive oil or a small avocado.
Victoria also suggests: ‘Homemade soup, chilli, pasta dishes and quinoa salad are all examples of healthy lunches that beat the lunch time lull. If you’re looking for lunchtime recipe inspiration while working from home, try our healthy lunch meal plan.’
If you’re looking for inspiration but are pushed for time to prep, it’s worth checking out some of the popular recipe books focused on quick meals or one-pan dishes.
Using a slow cooker set on a timer can also mean you come home to a healthy home cooked meal, no matter when you finish.
SET YOURSELF UP FOR A GOOD NIGHT’S SLEEP
One-in-three of us suffer from poor sleep, but if you work shifts, sticking to a regular sleep cycle can be tough. You’re working against your body’s natural rhythm because you’re active and alert when you’re used to being asleep.
So what you do before, during and after the shift can make a huge difference to your sleep and your general mood.
Not getting enough, regular sleep can affect our mood, concentration levels and overall health. Being sleep-deprived can also lead to an increase in hormones linked to stress, increase your risk of heart disease and high blood pressure and even affect your immune system.
Fortunately, there are ways to cope with shift work’s impact. Give yourself the best chance of a good night’s sleep by considering the following:
1 Choose your meals carefully. Try avoiding a heavy meal before you start your shift as this can make you sleepy. Instead, lighter meals and snacks are less likely to affect your alertness or cause drowsiness. Fruit and vegetables are good snacks too as their sugar is converted into energy relatively slowly. They also provide vitamins, minerals and fibre. Make sure you’re taking regular breaks too, and keeping the light bright can help you stay alert if you’re feeling tired.
2 Make your bedroom dark, quiet and cool. Light and darkness are powerful cues that tell your body it’s time to rest or get up. Although this can be difficult in the daytime, try to block the light out, because this will help you sleep. Use heavy curtains or blackout blinds to darken your bedroom. Noise can also disrupt your sleep, so try to keep it to a minimum or use earplugs. Adjust your bedroom temperature to a comfortable level, as cool conditions can improve sleep too.
3 Let people know your schedule. Let friends, family and neighbours know your work schedule, so they can be considerate around the times you’re sleeping to avoid your sleep being disturbed.
4
Avoid stimulants before bed. If you can, try to avoid caffeine, energy drinks and other stimulants, as well as big meals a few hours before bedtime, as these can stop you from sleeping.
5 Set a good bedtime routine and unwind before bed. Try to relax by going for a short walk, relaxing with a book or having a hot bath to unwind between work and bedtime. Then put away your electronic devices and dim the lights.
If you’re full of worries when you’re lying in bed, mindfulness can help ease these thoughts. Don’t try to stop these negative thoughts or ignore them. Instead, be aware of them and watch them drift by, as this will help us build awareness of how we think. You may find a mindfulness podcast helpful.
6 Use cognitive behavioural therapy (CBT) techniques to manage stress. CBT can help you manage it by identifying any negative or unhelpful thinking patterns. Note down when you’re feeling distressed, what has triggered this and your mood and thoughts, as this can make it easier to identify your stressors.
You will learn to make sense of your thoughts and actions by breaking them down into smaller areas.
Try creating a sleep diary to share your thoughts before bed; this will help you challenge negative thoughts and explore other ways of dealing with a distressing situation. Visit www.bupa.co.uk/health-information/mental-health/sleeping-well for more tips on dealing with sleep issues.
Keep tabs on your financial situation
Just as technology has a crucial role in driving our national economic recovery, on a smaller scale, independent practitioners can use it to boost their business finances and achieve long-term profitability, explains Kingsley Hollis (right)
AFTER A TURBULENT couple of years, the Government has put its faith in technology to lead the UK economy back to health.
Speaking ahead of the first Treasury Connect Conference ‘to celebrate UK technology and expertise’ and boost investment in the sector, Chan cellor Rishi Sunak said that tech firms ‘have huge economic potential and will play a critical role in our future prosperity.’
The Chancellor was talking on a
macroeconomic level, but the future prosperity of millions of ordinary businesses also depends on how well they utilise technology to operate efficiently, manage their income and seize the new opportunities that arise.
In common with all small to medium sized enterprises, independent practices have faced a financial squeeze as a result of the pandemic, which will be reflected in their latest accounts.
Showed resilience
However, we know they also showed their resilience, with many continuing to hold patient consultations remotely by video or phone, as well as using the enforced pause to focus on business projects such as updating their website and forward planning.
While the pandemic has caused setbacks, there are grounds for optimism compared to the posi
tion of a year ago, particularly the prospects for growth in the selfpay market.
A widely reported survey of more than 4,000 adults by the charity Engage Britain found that one in five had funded their own private treatment rather than face a long wait to be seen by the NHS. In addition, a report by analysts LaingBuisson predicted that the selfpay market would expand by
NHS Pensions & Annual Allowance Tax
Get ready in advance of April 2022 when the proposed changes to the NHS Pensions will allow you to reclaim some or all of any Annual Allowance tax you may have suffered in the past.
With our knowledge and in-house calculators, we will be able to predict in advance and check statements produced by NHS Pensions and Scottish Public Pensions Agency for accuracy for any refunds due.
For further information contact us at aa@semail.co.uk or telephone 01625 527351.
1015% over the next three years, while Spire Healthcare’s latest halfyear report (September 2021) show a 47% surge in selffunded patients from prepandemic levels.
Of course, an expanding market is good news for independent practices, but after a challenging period it is important to ensure that an increased level of activity actually translates into a healthier balance sheet and a positive experience for patients.
In an earlier article in this series, we looked at how technology can help you exceed patient’s expectations. This time, we’ll explain why having the right technology to manage your practice can make the difference between running a profitable business and running yourself into the ground.
Here are just some of the ways that practices can use technology to get financially fit for the future.
Invoice at the click of a button
One of the most common mistakes in business is celebrating an influx of new orders as if they were actually money in the bank.
You may be seeing more patients come through your practice, but if you don’t get paid, then your cash flow will inevitably dry up, leaving you unable to pay your own suppliers.
When it comes to invoicing, it pays to strike while the iron is hot – the longer you delay, the greater the risk the invoice will be rejected, as some insurers have a time limit for submission.
Plus, if a payer has a concern, it’s much easier to resolve it soon after the treatment has taken place
when you are more likely to remember all the details.
An efficient and accurate invoicing operation for insured and selffunded patients is the single most important thing you can do for your practice finances and it almost goes without saying that electronic invoicing is faster, more accurate and secure than oldschool paper invoices.
Healthcode’s technology enables you to create and send invoices to all the major private medical insurers (PMIs), selffunded patients and other payers such as solicitors and embassies: Timesaving shortcuts in ePractice make it quick and easy to create accurate invoices.
For example, if you have treated a patient in a hospital setting, you can search for them on the system and generate an invoice with the correct patient and episode details already completed, thanks to our invoice auto population feature.
All you need to do is add your own fee from your preset schedule of prices.
Clearing services
Healthcode’s Clearing Service means you can submit invoices to all the major PMIs from one place.
Each PMI invoice is automatically checked against the relevant PMI criteria, such as the correct procedure code and description.
Errors and anomalies are instantly flagged so they can be corrected and resubmitted and a status display shows that the invoice has been successfully submitted.
Online Payments via patientzone enables practitioners and clinics who are registered with patient
Having the right technology to manage your practice can make the difference between running a profitable business and running yourself into the ground
problems and even insolvencies, so it is essential to have an effective and efficient system for recording money received so you can focus on collecting outstanding invoices. However, this process is not always straightforward for independent practices, as PMI payments may cover several invoices and there will sometimes be a shortfall amount to be reallocated to the patient.
zone to send electronic invoices to nonPMI payers such as selffunded patients and embassies, and provide the convenience of secure online payment. The latest version means users can also send shortfall letters, details of debt reallocations and payment reminders.
A paper invoicing option is available in ePractice for when it is absolutely necessary. The invoice template ensures that these are clearly laid out and meet industry standards.
Mobile invoicing is available on the ePractice iOS app, enabling you to set up and send an electronic invoice from your phone or tablet while away from the office.
Payment tracking and collection
Bad debt and late payment are perennial problems for UK businesses in every sector causing cashflow
This is where a specialist practice management system can make the difference. It can record and reconcile payments so your accounts receivable are up to date. The payment tracking section of ePractice Lite and Pro makes it easy to find and allocate PMI payments to the correct invoices.
Where PMIs send electronic remittances (Bupa, AXA Health, Aviva, and Cigna), the system analyses the remittance advice and generates a summary that assigns the payment to one or more invoices for the user to then confirm.
For nonPMI payers, online payments via patientzone allows practitioners to set their account to send an email or text confirming an invoice has been paid. Their ePractice account is then automatically updated within 30 minutes so they can keep track of payments. A practice management system can also re allocate debts in the event of a shortfall and create a shortfall letter for the patient which automatically completes the invoice details and outstanding balance. Healthcode users
who are registered with patientzone can send these shortfall letters and payment reminders electronically.
Financial information
Without accurate financial data, it is impossible to manage credit control or to really understand a business’s strengths and weaknesses so you can make informed strategic decisions.
For practitioners who are simultaneously trying to attend to patients and run their practice, it is even more important to have access to realtime information in a format that enlightens rather than confuses.
Every practice management system should provide a range of realtime financial reporting options, so you can monitor your practice’s vital signs.
Healthcode’s ePractice includes more than 20 types of financial reports, all of which can be exported to other software so they can be anonymised and shared with your business adviser or accountant.
Here are five of the most frequently used:
➤ Aged debt analysis displays outstanding debt by patients and segments the debt by aged bands – for example: 0 30 days, 31 60 days, 6190 days outstanding. It is an essential tool for credit control in any business.
➤ Outstanding invoices by payer shows all invoices with a current outstanding balance by payer type, including or excluding shortfalls. This makes it easy to see who requires a payment reminder.
Without accurate financial data, it is impossible to manage credit control or to really understand a business’s strengths and weaknesses so you can make informed strategic decisions
Transform your practice today.
The new digital prescribing platform that’s free to use for all private prescribers.
CloudRx take care of the dispensing, payment and delivery of medicines direct to your patients – anywhere in the country –it’s a more convenient way for them to get their medication.
➤ Invoice listing by payer provides a summary of invoices, by payer, for a requested date range. A filter allows you to view outstanding or settled invoices.
➤ The payment summary report shows the payments received, by invoice, within a selected date range. This enables you to keep track of what has been paid and the payment method used.
➤ Financial snapshot provides a snapshot for the selected period, including the total number of invoices with values for payments, refunds and debts. It also provides a total of the debt outstanding at the start and end of the period.
Independent practitioners have shown huge reserves of strength, determination and a readiness to adapt when tested during the pandemic.
But they will be keen to nurse their practice finances back to health amid continued uncertainty about infection rates and the imposition of tighter restrictions over winter.
The prospect of growth in the selfpay market is a welcome development, provided practices are able to reap the rewards. And while technology cannot change the weather, it does have an important role in helping to put businesses on a firm financial footing.
By making use of the invoicing, payment tracking and reporting functionality in ePractice, practitioners can ensure they are ready to profit from new opportunities.
Kingsley Hollis is head of business development ePractice, Healthcode
Transformational
The ability to order prescriptions at the touch of a button can transform how you work, supporting the growth in remote consultations and adding a whole new level of ease and convenience to your patients’ experience.
Simple, convenient and secure
Prescribe quickly and easily for everything you need to deliver maximum convenience for you and your patients.
Legal paperless prescriptions, repeat prescriptions and controlled drugs. Prescriber Fees can be charged to the patient if requested
“It’s of significant benefit to both patients and our doctors. CloudRx gives the patient more control, they can see when their delivery is coming and manage it themselves. Doctors can support a customer on the other side of the country over the phone or webcam and have the medication sent to their door.”
Dr Charlotte Norton, Medical Director of The Slimming Clinic
Integrated
Our open and accessible pharmacy API enables fast, frictionless integration with healthcare brands & private practice clinical software including Heydoc, MidexPRO, eClinic and YouClinic.
Embarking on a diplomatic
If you are thinking of expanding your private work to provide services for embassies, then there are some essential billing and collection matters you need to be aware of, suggests Simon Brignall (right)
CONSULTANTS IN private healthcare are often looking to new business opportunities to grow their practice and that can include a wide range of revenue channels.
It certainly makes good sense to review your practice regularly, as there are many areas outside of the traditional private medical insurance (PMI) and self-pay sector where a consultant can operate and generate additional revenue.
It is important for any business to have diverse revenue streams from a variety of sources so that if a particular source of income tails off, the effect on the business is minimised – and private practice is no exception.
The range of options available can depend on where you are located or the type of activity you are prepared to consider.
Revenue channels include:
Medico-legal;
NHS (Choose and Book);
Commercial organisation – this can include billing corporates to treat their staff or consultancy work;
Provision of courses and seminars;
Embassies.
With embassy work having taken a bit of a dive during Covid, let us look at what you need to know from a billing and collection perspective if you are thinking of including this sector as part of your patient mix.
For consultants working in London, international patients make up a significant proportion of the patients they treat.
These are predominantly international self-pay patients, and I
diplomatic mission?
have covered in detail the billing issues that impact this group in my recent article on self-pay, but a significant proportion will be patients that come from the embassies.
The demand from international patients accessing healthcare in the UK saw a significant reduction as the impact of the coronavirus, including lockdowns and travel restrictions, were felt by travelling patients.
This area is starting to recover as the benefits of vaccination programmes in all countries begin to take effect and both confidence and access to international travel returns.
There are over 50 embassies within London; however, most of the patients come from the big four, which are Kuwait Health, Kuwait Military, United Arab Emirates Medical and Qatar. Here are some important things you need to be aware of should you decide to treat this important patient category.
Complex nature of patients
The patients that you will be sent by the embassies often have complex conditions and this is one of the main reasons why they travel to this country. These can include patients whose previous procedures/treatments were unsuccessful or require revisional surgeries.
Extra time required
When you see the patients for their consultation, they will normally be accompanied by an interpreter. This, in combination with the probability of the patient presenting with a complex case, means that the consultation is likely to take longer than normal and so you will need to allow more time in your clinic diary.
Necessary documentation
Before seeing an embassy patient, it is crucial that you obtain a letter of guarantee – referred to as LOG.
Chasing outstanding fees on a continual basis is the hardest part of this whole process, as most practices are not geared up for this specific aspect
that the dates specified in the LOG cover the treatment dates that are on the invoice, as this can often be a reason an invoice is rejected. There is normally a set of terms and conditions covering the LOG and you must always submit this document in conjunction with your invoice to the embassy in a timely manner to ensure the best possible chance of receiving payment.
could have a devastating effect on your cash flow if you haven’t planned accordingly.
Chasing
Even after you have followed all the steps that I have outlined, you will still need a robust system in place to chase for payment that is routinely followed to ensure that your money is collected.
The LOG will authorise treatment for the patient and it is important that is issued in your name. This is a precursor to raising an invoice to an embassy, as, without this vital document, it is unlikely that the invoice will be paid.
Cash flow
Probably the most important point to consider about undertaking embassy activity is that payment often can take a long time. The impact this can have on a practice’s cash flow should be understood and may limit the amount of this type of activity you undertake when compared to other patient groups with faster payment cycles.
Embassy check-list
In our experience, many consultants start seeing embassy patients without having given due consideration to the points that I have highlighted above and so here is simple guide to help you.
Letter of guarantee
It is absolutely vital that a letter of guarantee (LOG) is obtained prior to any treatment that is carried out; this document will vary slightly depending upon the embassy that is issuing it. It will typically specify the patient’s demographic details along with the appointment date(s), the reason for the treatment as well as specifying the consultant and the location.
An important check is to ensure
Some embassies also require a medical report along with the invoice and LOG. If this process is not followed correctly, then you run a much greater risk of treating patients without getting paid.
Fees
How much you want to charge for your treatment needs careful consideration before you start to see patients.
Your fees may consist of a mixture of inpatient and outpatient consultations, inpatient care, procedures and occasionally intensive care.
Procedure pricing should also take into account the level of complexity, especially when it is not accurately described by the Clinical Coding and Schedule Development group (CCSD) code. Your fees may also want to reflect the impact of some of the other factors I have discussed that arise when treating this patient group.
Whatever your decision, it is important that this is communicated clearly to the relevant embassy to avoid any misunderstanding or disputes about payment.
Payment
You will need to be prepared for extended payment cycles and allow for this within your practice cash flow. There are taxation impacts to consider, as you may find yourself paying tax to the HM Revenue and Customs on invoices that have still not be paid. This
The embassies are always busy, particularly the big four, and it is not uncommon for them to have a backlog of invoices waiting to be paid. The reasons for this vary and Covid has only added to the problem, but a major factor is the sheer volume of patients they deal with.
It is vital that you keep a record of when and how your invoices were sent to the relevant embassy and copies of all supplementary documentation provided in case they get misplaced.
It is important to monitor your outstanding debt, and should you continue to have issues collecting payment with a particular embassy, then you need to think long and hard about taking on other cases from them until the problem is addressed.
Chasing outstanding fees on a continual basis is the hardest part of this whole process, as most practices are not geared up for this specific aspect.
This is both time-consuming and requires a specific skill set. It is rare to find a practice which has the time to chase these invoices on a continual basis and maintain adequate records to support this.
It is crucial to get your practice prepared correctly, preferably before engaging with the embassy sector.
Otherwise, you could end up carrying out a lot of work and end up waiting a long time for payment or, worse, not getting paid.
Simon Brignall is director of business development at Medical Billing and Collection
When asked to alter your expert report
Private doctors are increasingly being asked to edit their expert reports in civil claims. Dr Emma Green (below, left) and Angelicka Dom Paul (right) discuss when it is appropriate to do so and warn of the risks of failure to comply with their duty to the court
DOCTORS ACTING as expert witnesses are considered to be experts in their field of medicine.
Guidance from the Academy of Medical Royal Colleges, 1 published in response to a recommendation from the Williams review into gross negligence manslaughter in healthcare, outlines the expectation that experts should be adequately trained for being an expert witness and undertake continuing professional development relevant to both their role as a clinician and as an expert witness.
Although there is no definition of the number of years of practice required to become an expert, it is usually considered that this should be an established consultant with ten years’ experience.2 It is unlikely that an expert with less experience would be instructed by solicitors.
While this article considers expert witnesses acting in civil claims, the general principles of candour and probity apply to those acting as experts in other capacities such as the Family Court or inquests, although the role of an expert in other courts will vary. Experts instructed in civil claims in England and Wales are governed by the Civil Procedure Rules (CPR), with part 35 relating specifically to experts and assessors.
Supplementary information for experts is contained within Practice Directions 35 (PD35). Experts must follow the requirements of the CPR to comply with their duty to the court.
The GMC has published guidance for doctors acting as a witness in legal proceedings3 and outlines to experts that ‘if your instructions are unclear, you should ask those instructing you to explain. If the instructions are still not clear, you should not provide expert advice or opinion’.
When is it appropriate to amend a report?
An expert may be called upon to write a report at any time in the life span of a case from the initial stages, during the course of the pre-action protocol, once proceedings have been issued and mid proceedings.
In turn, an expert may be asked to change their report as the case develops and more evidence emerges.
The whole purpose of an expert report is to assist the court to understand issues that are part of the expert’s area of expertise, and that relate to the issues which the court needs to determine to resolve the case.
When an expert receives any request to amend a report they need to understand why and question in their own mind whether the amendment will in any way mislead the court. This is in accordance with the GMC guidance referenced above.
The Civil Justice Council guidance for experts 4 is clear about amending reports. It considers that there are three scenarios when amending a report may be appropriate:
As a result of an exchange of questions and answers;
Following agreements reached at meetings between experts. Although, in reality, this is rare and experts should ensure that any changes in their opinion are recorded in the agreed note following their discussion, as opposed to amending a report;
Where further evidence or documentation is disclosed; for example, after witness statements are served or even following the service of other expert reports.
The key point within the guidance to experts is that any amendments must not distort the expert’s true opinion.
Solicitors instructing experts often ask experts to change their reports to clarify points, amend the form of the report and may ask the expert to expand upon issues; all of which are permissible, provided that the suggestions don’t change the expert’s true opinion.
Experts may be asked to ensure they are applying the correct test to the factual content of the case, with Bolam, Bolitho and Montgomery being the usual three key cases of relevance in civil medical negligence claims.
Experts acting for defendants are often asked to prepare their reports in response to allegations contained within the Particulars of Claim and those acting for a claimant may be asked to comment upon a defence – both often include a narrative or factual background.
An expert may well find that
Financial remuneration or concerns over being instructed again for future claims should not influence any report that an expert provides
there are relevant elements in the claimant’s history that are inaccurate or missing and feel conflicted on what they can and cannot say within their report.
The overriding duty of the expert is to the court and all aspects of the patient’s medical history that the expert considers relevant should be included.
Risks to doctors
GMC guidance for experts 3 reminds doctors that serious or persistent failures that put the public trust in doctors at risk will jeopardise registration.
Claims and complaints can be, and are, brought against experts. So they need to ensure they obtain appropriate protection for medicolegal work from their indemnity provider.
From October 2020, experts are required to sign a statement of truth; a declaration which has arisen from the case of Liverpool Victoria Insurance Co. Ltd v Zafar [2019].
The expert, Dr Zafar, included information in his report at the request of the instructing solicitors, which directly contradicted his own examination findings.
As such, the Court of Appeal ruled that any expert witness who is found to be either dishonest or reckless as to the truthfulness of their reports would receive a custodial sentence.
Summary
There are some circumstances where it may be reasonable for experts to amend reports.
But it is important to clarify all requests and ensure reports are written for the court, not the lawyers.
Financial remuneration or concerns over being instructed again for future claims should also not influence any report that an expert provides.
Private doctors interested in medico-legal work should not, however, be discouraged from taking on work as an expert witness. It is an important role which can also offer an opportunity to expand your knowledge, challenge yourself and reflect on your own clinical practice.
References
1. Academy of Medical Royal Colleges: Acting as an expert or professional witness: Guidance for healthcare professionals
2. www.bmj.com/content/350/bmj. g7856
3. GMC: Acting as a witness in legal proceedings (2013)
4. Civil Justice Council: Guidance for the instruction of experts in civil claims (2014)
Dr Emma Green is a medico-legal consultant and Angelicka Dom Paul a litigation solicitor at Medical Protection
INVESTMENT STRATEGIES
Choices have consequences
Some investors have strong beliefs and preferences when it comes to picking stocks. Dr Benjamin Holdsworth (right) outlines why taking such a position can have tradeoffs
Owning a portfolio of ‘clean energy’ firms means putting all your eggs in one basket
INVESTING IS all about trade-offs. Each choice made is paired with an implicit decision not to do some alternative: the ‘opportunity cost’.
For example, by investing solely in a basket of UK companies, one accepts the risk of losing out if the UK market struggles relative to the rest of the world, and vice-versa.
An investment portfolio could be constructed to reflect other preferences, such as the appetite to have exposure to certain companies or industries, adopt a specific level of equity or fixed income risk, or attempt to adjust the average fee paid to managers, to name a few.
Choices come with consequences and such trade-offs can be at the detriment to long-term investment returns
Recently, one industry study looked specifically at the preferences of younger investors coming to market. The conclusion stated that ‘The younger generation want things they are passionate about, that they can engage with, that resonate with their particular desires and preferences, whatever those may be.’
The study’s data suggested that younger investors have tended to invest in companies they feel strongly about, a standout theme being the electric car industry at present through firms such as Tesla and NIO.
One industry expert at investment research company Morningstar went on to say: ‘The younger generation will not be happy in a multi-asset balanced 60/40 portfolio, sitting alongside another million other investors that are profiled exactly the same way.’
Concentrated portfolio
The challenge is that preferences naturally come with their own trade-offs. This is crucial to remember.
To avoid a traditional balanced portfolio and instead own a portfolio of ‘clean energy’ firms, perhaps with electric cars, wind turbines and solar energy as themes, one must accept that they own a highly concentrated portfolio of stocks with low levels of diversification, large sector biases and more than likely, with high management costs.
This will probably negatively impact returns in the medium to longer term.
If that fateful GMC missive appears
1
What should you do if you get a letter from the GMC? Dr Tania Francis (left) shares ten tips
Open that ominous letter.
We see cases where doctors have ignored correspondence from the GMC, and it is not a good idea. It might not be bad news; it might be something really simple, such as a reminder about paying your annual registration fee (ARF).
2
Put your ARF onto direct debit, especially if you are moving around a lot.
If your reminder does not get to you, for whatever reason, you may be removed from the register for non-payment, which may lead to you working as a doctor without being registered, which is illegal.
3
Keep your contact details up to date with the GMC.
It may seem counterintuitive, but you are required to do so and if the GMC cannot get hold of you and this delays you receiving any correspondence from it, then that will only make things worse.
If you are moving around a lot, give them your email address so that they can contact you easily if you forget to update your address.
4
The letter might be about something less simple than paying your registration fee –revalidation, for example.
You need to keep on top of your revalidation submission date and keep up to date with your annual appraisals.
You can lose your licence to practise for failure to revalidate.
You may have strong views about the revalidation system – but so does the GMC.
5
The letter might be about a complaint.
If so, the first letter you will receive is usually at a very early stage and will simply notify you of the complaint and the fact that the GMC is investigating it.
Please resist the temptation to:
A) Ignore it and hope it will go away;
B) Write to the GMC in great detail explaining why the complaint has no merit.
Instead, pick up the phone to your defence organisation/indemnifier/insurer, tell them about it and ask for their advice.
It may be a condition of your cover to notify them and, in any event, they will be able to advise you about whether you should respond.
In the vast majority of cases, you will be advised not to respond, unless the answer to the complaint is extremely straightforward – for instance, the complaint is not about you and you have never met the patient.
It is usually better to wait and let the GMC undertake its initial investigation. It may decide to take it no further, and by writing to it at this stage, you may actually make things worse for yourself.
Believe me – we see it all the time. You won’t have the perspective to realise this because it is about you.
6
Make sure your indemnity/ insurance covers GMC complaints and keep up to date with your renewal premiums.
Put them on direct debit too!
There is only one thing worse than facing a GMC complaint, and that is having to do it without any help or having to pay privately for legal advice.
7
Discuss any complaints –GMC or otherwise – in your annual appraisal and with any mentor you may have access to.
Be willing to consider that things may have gone wrong or at least sub-optimally. Even if the complaint comes to nothing, you can still learn from it.
If you can identify any areas of potential weakness, put together a plan to address these, stick to it and review it regularly. Keep records of what you have done, and of any meetings with a mentor or equivalent.
8
If you get a letter from the GMC informing you that you have been referred to an Interim Orders Tribunal (IOT), act quickly.
These hearings are listed at short notice and it is very difficult indeed to get them postponed, so you will need to get advice and representation for the date of that hearing.
The IOT has the power to suspend you or place conditions on your registration pending the outcome of an investigation, so again – do not ignore it.
Once it has made an order, it is difficult and time-consuming to get it lifted or eased.
9
Remember that GMC complaints are not that common, so do not live in fear.
In 2020, there were 337,717 doctors on the register and the GMC considered 8,468 fitness-to-practise inquiries.
There is only one thing worse than facing a GMC complaint, and that is having to do it without any help or having to pay privately for legal advice
10
Look after yourself. A GMC complaint is horribly distressing to deal with. It will knock your confidence, personally and clinically.
Of these, 1,117 were promoted to investigation. In over half of these cases, the case was concluded with no adverse outcome, and only 276 cases went to a hearing. [Source: GMC Fitness-to-practise statistics 2020. www.gmc-uk.org/-/media/ documents/fitness-to-practisestatistics-report-2020_pdf87198195.pdf]
Discuss it with others, seek support, both professionally and personally. See your GP. Tell your partner about it. You would be surprised how many people do not. You can also get support from the BMA’s doctor support service, aimed specifically at doctors going through GMC fitness-to-practise procedures. You do not have to be a BMA member. Email: doctorsupportservice@bma.org.uk.
Tania Francis is a solicitor and a partner at Hempsons, a specialist healthcare law firm. She is also a qualified doctor. She advises doctors, dentists and other healthcare practitioners and providers, specialising in regulatory law and clinical negligence litigation, including cases where there are related criminal proceedings
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment
Premises
Regulatory requirements and investigations
Michael Rourke
Tania Francis m.rourke@hempsons.co.uk t.francis@hempsons.co.uk
Dilemma 1
Do I report my mistake?
QI am a consultant ophthalmologist and while carrying out cataract surgery on one of my patients, the irrigating cannula accidentally became disengaged from the syringe which resulted in a posterior capsule rupture.
The patient required an anterior vitrectomy and I had to replace their intraocular lens implant. I told the patient what had happened at the time, apologised and explained how I was going to manage the situation.
However, one of my colleagues believes the incident is notifiable under the statutory duty of candour because the patient required additional treatment to prevent sensory impairment. He says the hospital could be fined if we don’t comply. Is this correct?
AYour colleague is right that healthcare organisations which do not comply with the statutory duty of candour can face financial penalties and even prosecution by the Care Quality Commission (CQC).
The first such case was in January 2019 when the CQC issued Bradford Teaching Hospitals NHS Trust with a fixed penalty of £1,250 for failing to notify the parents of a notifiable incident involving their child, and to offer an apology, within a reasonable period of time.
In September 2020, the CQC prosecuted University Hospitals Plymouth NHS Trust for failing to disclose details of a surgical proce
Your duty to own up
Dr Ellie Mein discusses the importance of the statutory duty of candour
dure or apologise, following the death of a 91 year old woman. Magistrates ordered the trust to pay a total of £12,565
And in the first prosecution against a private hospital, Spire was ordered to pay £20,000 in April 2021 after it admitted four counts of non compliance with the duty of candour in relation to potential harm to patients by a surgeon in Leeds.
In this case, you have met your own professional duty to be open and honest by telling the patient what had gone wrong, apologising and explaining how you were going to help them.
But the GMC also requires you to follow your organisation’s policy for reporting adverse incidents and your hospital would certainly expect you to cooperate with its statutory duty of candour procedures if an incident is notifiable.
Notifiable incident
Working out whether this threshold has been triggered can be difficult, as it is possible for an incident to trigger the harm threshold for NHS trusts, but not for other service types.
However, the CQC’s guidance for providers says that an incident is notifiable if it meant your patient then required treatment to prevent a sensory impairment. If in doubt, it’s advisable to discuss this with the manager responsible for duty of candour arrangements rather than risk the hospital being fined and/or prosecuted.
If the threshold has been met, the statutory regulations require an organisation to tell the patient or their representative as soon as possible after the incident, apologise and explain what further inquiries or investigations will take place. The patient must be offered reasonable support.
In addition, the organisation must provide the patient with a copy of a written note of discussions including details of further inquiries and keep copies of all correspondence and meeting notes.
As the treating consultant, it is likely that the hospital would ask you to attend and even be its representative in meetings with the patient and you will certainly be involved in any investigation into what happened so lessons can be learned and shared as necessary.
Kids caught in a divorce
How should a doctor respond to a parental request to change their child’s name on medical records? Dr Ellie Mein gives her judgment
Dilemma 2
Do
I acceed to mum’s request?
QTwo of my patients are currently going through an acrimonious divorce and ,as such, the mother now wants her children, who are also patients, to take her birth name.
She has asked if I can change their medical records, but I’m not sure if I can do this without the consent of the father. What should I do?
AWhile adults are able to change their name as they wish, changing the name of a child is more complicated and requires the consent of all those with parental responsibility or a court order.
As the father was married to the child’s mother, he may have parental responsibility. Parental responsibility is given to the child’s father if he is married to the child’s mother or named on the birth certificate, but this does depend on when and where the child was born.
In England and Wales this applies to any child born on or after 1 December 2003, in Scotland any child born on or after 4 May
2006 and in Northern Ireland any child born on or after 15 April 2002.
Parental reponsibilty
Unmarried fathers who are not named on the birth certificate can also acquire parental responsibility if they obtain a Parental Responsibility Agreement from the mother or a Parental Responsibility Order from the court.
If you’re sure that both the mother and father have parental responsibility, then it may be difficult to fulfil the mother’s request and is likely to lead to a complaint from the father. You could also invite criticism for failing in your ethical duty to ensure that your records are accurate.
You may need to explain to the mother that you are unable to change her children’s names on their medical records. Explain to her the legal reasons why this is not possible and share with her the Government’s guidance for more information.
Dr Ellie Mein (right) is a medico-legal adviser at the Medical Defence Union (MDU)
DOCTOR ON THE ROAD: TOYOTA YARIS CROSS
Hybrid technology gets even better
70mpg! That’s what our tester Dr Tony Rimmer (right) got out of the new Yaris Cross – a good value, fuel-efficient commuter vehicle or small family car
supermini has become a hybridonly car since its last major update in 2020 and combines a 1.5litre three-cylinder petrol engine with a small battery and electric motor.
Now, to compete in the currently popular small SUV sector, Toyota has released the new Yaris Cross, which has the same chassis and powertrain but a more elevated upright body with a bit of an offroader look to it.
The boot is roomy at 395litres but the floor dips down from the entry lip. A raised and flat false floor is available on higher trim levels.
So how does all this latest hybrid technology work on the road? Is it smooth in operation and does it provide decent fuel economy?
The clever electronics ensure that the Yaris runs on pure electric power up to 30mph until the battery runs out or you need extra acceleration
WE HAVE learned that nothing is achieved or improved without hard work and repetition. As the great golfer Gary Player once said: ‘The harder I practice, the luckier I get.’
Manufacturing companies often focus on one aspect of their general operations so that they become expert and gain a certain reputation that attracts clients who have confidence in their products and services.
Motor manufacturers are no different. For example, Porsche is trusted that its cars are all sporty to drive and Skoda is trusted that their cars represent good value.
Hybrid technology
If there is one thing that Toyota is well known and respected for is their knowledge of Hybrid technology. It was the first to launch a mainstream model that combined petrol and electric drive in a model that has become a huge success over several generations since its UK launch in 2000: the Prius.
Toyota has been able to use the advancing knowledge and expertise gained over the years to constantly improve the technology and apply it to a broader range of models.
The highly successful Yaris
The electric motor produces up to 79bhp and the maximum output for petrol and electric combined is 116bhp. The gearbox is an automatic continuously variable transmission (CVT) and drive is through the front wheels.
There will be a four-wheel drive option in due course, but you will pay an extra £2,360 for the benefit. The range offers five levels of trim and equipment: Icon, Design, Excel, Dynamic and Premiere edition.
However, even the base Icon has keyless entry, Apple CarPlay, 16-inch alloy wheels, a rear camera, climate control and adaptive cruise control.
The Design edition, as my test car was specified, adds LED lighting and 20:40:20 folding seats and 17-inch alloys and represents the best value at £24,140. The slightly bigger nine-inch infotainment screen – usually 8” – on my car is a £500 extra.
Looks smart
The Yaris Cross looks smart and the bodywork boasts the usual rugged black-plastic wheel-arch extensions and raised ride height shared with other small SUVs.
Its interior is basically the same as in the latest Yaris hatchback; that means clear, functional, modern with up-to-date technology. Rear space is pretty good for two with average knee room, but would be a push for three.
Well, the clever electronics ensure that the Yaris runs on pure electric power up to 30mph until the battery runs out or you need extra acceleration. It then transfers to hybrid drive and the change is seamless. Engine noise is suppressed and the CVT transmission suits it well.
A dashboard display tells you how much electric driving you are doing and the state of the battery. I found that this encourages a gentler driving style which can only benefit economy.
In fact, despite an officially quoted fuel consumption of 55-60mpg, I managed to get an indicated 70mpg on a particular varied run without too much trouble – impressive stuff.
The handling is pretty good, the steering is sharp, but the ride is a bit firm. This is not a dynamic drive, but it is not designed for that. Buy its fabulous sporty GR Yaris sibling if you want fun and dynamic driving in bucketloads.
So, the new Yaris Cross fills its designed remit successfully. It works as a good value, fuel-efficient commuter car or small family car.
Similar hybrid-drive small SUV competitors include the Kia Niro, Hyundai Kona, Ford Puma and Renault Captur. If you are in the market for a small SUV, you are now spoiled for choice which can only be a good thing.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
The interior is basically the same as in the latest Yaris hatchback; that means clear, functional, modern with up-to-date technology
Is your practice fit for tax changes?
Financial measures put in place during the pandemic made it inevitable the Government would make changes to the tax system to reduce its debt by seeking higher taxes from individuals and companies. With private medicine now seeing a surge in demand, Ian Tongue believes it is a good time to consider whether your current trading structure is still tax-efficient
THE MAIN CHANGES
☛ For individuals
For political reasons, the headline rates of income tax were left alone, but National Insurance (NI) rates for individuals and employers are increasing from 1 April 2022.
Politically, NI is portrayed as money which pays for health and social care, but clearly those services cost more than the NI paid and it is a tax in all but name.
The increased NI will be paid on both employment earnings and the profits of the self-employed. Additionally, an employer also pays more. The increase is 1.25% across the board.
Recognising that many choose to extract funds by way of dividends (investment income) rather than employment or trading income, from 1 April 2022 the income tax rates on dividends also increase by 1.25%.
☛ For companies
The biggest tax changes relate to limited companies, as corporation tax rates will see a significant increase from 1 April 2023.
Instead of there being a flat rate of 19% payable on all earnings, the tax rate payable will be 19% on the first £50,000 of taxable profits increasing to 25% for those earnings more than £250,000.
The jump in these rates creates a zone between £50,000 and £250,000 where the effective tax rate is 26.5%.
This seems excessive, but the principle here is to gradually increase overall tax paid such that you approach a rate of 25% as you near £250,000 of earnings.
For example, earnings of £200,000 would attract £50,000 of tax at 19% and £150,000 at 26.5% which is £49,250 of tax on £200,000 of earnings – an effective rate of 24.6%.
These earning bands are shared between ‘associated’ companies such that if you have two businesses which are associated, the rate would be 19% on the first £25,000 and 25% from £125,000 applicable to both businesses regardless of the size of earnings in each.
Determining whether you have associated companies can be complicated and therefore if you run more than one limited company, you should speak with your accountant.
TAX PLANNING CONSIDERATIONS
Clearly, the tax rate hikes for companies are significant and it may be time to consider changing your strategy of profit extraction from your company or even revert to an alternative structure such as a sole trader or partnership.
For those extracting all their profits from their private practice, it is worth asking your accountant to quantify the additional tax that will be payable from 1 April 2023.
Armed with this, you ask them how this will now compare to other structures that are available to your circumstances.
It may be that partnerships or self-employed businesses are now more appropriate particularly, as the earnings threshold for pension annual allowance tapering has increased to £200,000.
For all companies, the higher tax rates also mean higher tax relief on business expenditures, so as you approach 2023 it may be worth delaying capital expenditure to obtain more tax relief.
This delaying tactic must be balanced against the current higher capital allowances available, which may not be available later.
For those not extracting the funds, you may be building up retained profits. It is important to speak with your accountant regarding the ultimate extraction strategy, as changes to capital gains tax are rumoured and alternative strategies may be required.
Considering your trading status and reviewing matters with your accountant should ensure that you are tax-efficient and not overpaying
The impact of the corporation tax changes depends on the level of profit after tax. The following table provides an indication of the additional tax due at differing levels of earnings:
Less than £50,000: no change
£100,000: + £3,750
£200,000: + £11,250
£250,000: + £15,000 (effectively 6% on £250,000) Thereafter £6,000 more tax per £100,000 when compared to current rates.
IMPACT OF CHANGES
☛ For the self-employed –from 1 April 2022
The impact for the self-employed, whether as a sole trader or in partnership, is straightforward: it is 1.25% more paid on the profits earned.
Where you have employees, the NI rate payable by the employer will increase by 1.25%, but as this additional cost is tax-deductible, the effective increase for a higherrate taxpayer is around 0.73%.
The effective rate of tax including NI for a higher-rate taxpayer becomes 43.25%.
☛ For those trading as a limited company – from 1 April 2022
Where dividends are extracted, the rate of income tax payable increases by 1.25% across the board, ranging from 8.75% to
39.35% depending on your tax rate.
The effective rate of tax to extract profits after the initial £2,000 tax-free dividend allowance is used up becomes 46.4%.
☛ For those trading as a limited company – from 1 April 2023
Due to the increase in corporation tax rates applicable from 1 April 2023, the effective rate of tax payable will increase considerably if you are extracting significant levels of dividends from your firm.
This variation in dividend extraction policy between taxpayers and the proportion of profits extracted from company profits will result in the impact on you personally being unique and therefore is best discussed with your accountant.
However, as an example for a private practice earning £100,000 before tax with the profits fully extracted and all shareholders being higher-rate taxpayers, the following would be payable:
The position now is the company would pay £19,000 and the individual would pay £25,675, assuming that they had their £2,000 dividend tax-free allowance available in full. This would be an effective rate of tax of 44.68%.
From 1 April 2022, the same example would give rise to a further 1.25% of tax on the dividends, making the effective rate of tax 45.66%.
From 1 April 2022, the corporation tax rates also increase and this will increase the marginal rate of tax to 48.8% in this example.
Additional to the above rates of tax, factors such as lost personal allowances and pension annual allowance charges also come into play.
It was inevitable that tax rates would be reviewed following the Covid financial measures undertaken by the government.
Increased taxes will be payable by most, but considering your trading status and reviewing matters with your accountant should ensure that you are tax-efficient and not overpaying.
Next issue: Understanding your financial accounts
Ian Tongue (left) is a director of Sandison Easson accountants
NHS PRIVATE PATIENTS’ BAROMETER
Covid halves trusts’ private earnings
The third annual NHS PPU Barometer provides a snapshot of performance and valuable insights into the impact of Covid-19 on the sector. Its author Philip Housden reports
THE NHS PPU Barometer is a unique measure of trading performance and of the confidence levels of the management teams of trusts’ private patient services.
Completed as an online survey by 28 trusts during August 2021, all regions are represented with the exception of the North-west.
The highest number of returns came from London and south-west regions with seven and there were
CHART 1
five responses from trusts in the southern Home Counties.
The 28 trusts accounted for approximately £336m revenue in 2019-20, which was 50% of the total NHS PPU market that year of £673m.
Both these values are comparable with the £349m of revenues and 53.3% of the market in last year’s second Barometer.
Individual comments from trust
managers confirmed that this significant reduction from the longterm average was due to the prolonged and ongoing impact of Covid-19 throughout the year. Given the dramatic impact of the pandemic on the NHS and its capacity, the Barometer first asked: ‘What is your trust’s overall position at the moment with regards to treating patients privately, now or in the near future?’
CHART 1
Results show that 62.1% of responding trusts agreed with the statement that their trust was ‘Committed to re-instate private patient services to reduce waiting/ access times and increase revenues/reduce costs’ and this was a 6.1% points increase from the 56% agreement in 2020.
Only 3.4% of responding trusts in contrast preferred the state -
ment choice for their trust that it ‘Doesn’t feel it is appropriate to be treating – or planning to treat – private patients at this time’, and this is a decrease from the 8% reported last year.
Trust managers reported two main factors linked to Covid-19 as the principal causes of reduced private patient income.
The first is clinical priority-setting: private patient activity was possible through the pandemic in many/most trusts, but only in so far as clinical urgency allowed within NHS priority guidance.
As one manager put it: ‘We reduced all PP activity in line with national NHS priority guidance, so were still able to operate on patients deemed urgent enough. This did reduce our activity significantly.’
The second is capacity constraints: in many trusts, physical capacity for private patients has been redirected towards the NHS’s efforts to increase volume throughput recognising the lengthening waiting times and waiting lists.
An example of this is one trust reporting: ‘We have access to NHS
beds for procedures, but the PP unit is still in use by the NHS currently. No timeline to re-instate dedicated PP beds until pandemic truly under control.’
The Barometer asked for details of the changes to capacity in terms of inpatient and day-case beds, outpatient clinics, diagnostic services and operating theatres. And it asked whether these were presently fully closed to private patients or partly or fully open within the trust.
CHART 2
As can be seen from chart 2, trusts’ responses this year show that, for each category, more than 67% of trusts report being partially or fully re-open for private patients – up from 65% last time.
Access to diagnostic services fares best with 96.4% (was 84%) either fully or partly open to private patients.
However, access to inpatient beds remains most restricted, with 32.1% of trusts sharing that their facilities remain closed to insured and self-pay patients while only 17.9% are fully open.
Experience varies widely; consider these summaries from managers in different trusts:
☛ ‘PPU beds were repurposed as part of the Covid response. A new PPU ward will be made available December 2021 with just a small inpatient offering to start. It will likely be closer to February when capacity more fully resumes.’
☛ ‘The PPU was scheduled to reopen Sept/Oct 2021. However, winter pressures may mean it will not be operational until Spring 2022.’
☛ ‘Only offering PP theatre procedures at weekends and with limited capacity since Spring 2021.’
☛ ‘Currently no plans to re-open services and any decision is likely to be months away.’
CHART 3 (overleaf)
The Barometer then asked: ‘What is your forecast for private patient services revenues for the full financial year 2021-22 when compared with last year 2020-21?’
The purpose of this question was to gain an insight into how present restrictions on private patient capacity are likely to impact the future recovery of revenues.
Although many trusts shared that they were expecting increases this year, this needs to be put into context given the significant reductions in income delivered in 2020-21.
As can be seen from the chart, over one-third (37.5%) expect outturn for this year to be a broadly roll-over position, with a further 25% predicting growth of between 10% and 20%, and the most bullish commenting that their trust was ‘looking to restore 95% of 2019-20 activity – keeping alignment with NHS restoration targets.’
In contrast, 20.9% predict further private patient income reductions of more than 10%, with nearly half of these expecting a 50% or more fall.
One manager stated: ‘The capacity pressures imposed by the recovery of elective care and the growing waiting lists will have a reducing impact on the growth of private patient activity.
‘The anticipation of a third wave of the pandemic and ensuing winter pressures on capacity will also
➱ p47
CHART 4
impinge on the rate of recovery or private patient activity.’
35% growth
In London, five of the top ten highest-earning NHS trusts responded to the Barometer – six in 2020. There is a marked spread of forecasts for 2021-22: three of these five predict growth of over 20%, with one of the three suggesting greater than 35% growth. The other two shared their views that income would fall; in one case by between 10-20% and the other over 50%.
CHART 4
The survey also again asked for a ranking of 15 factors identified as
SUMMARY
potentially most likely to help deliver the re-opening of presently closed or restricted NHS private patient services.
Those with the most impact ranked #1, the least impactful ranked #15, with the weighted average scores shown in chart 4.
The three highest average weighted scores for 2021 were the same as last year. The importance of trust executive support has been further emphasised with a rise from third to first, chiming with the similar results consistently reported from consultant user surveys.
Open support from consultants for return of onsite private patient services ranks second, followed by
This third Barometer survey has continued to build on the support of NHS trusts’ private patient services, as they are keen to share and then learn how their own service compares with the market.
In these challenging times, the responding trusts remain positive that there will be an increasing trend to re-instate private patient services within NHS trusts – albeit with recognition of the over-arching need to support the wider NHS core priorities to tackle growing waiting lists and times and in the context of the coming winter and potential future waves of the pandemic.
The NHS PPU management community has shared how they are working hard to
designation of ‘protected green pathways’ for private patients. Unsurprisingly, the requirement for maximising trust capacity rose from 5th to 4th place.
Flexible job plans
Noticeable decliners were common NHS-wide governance enabling consultants more flexibility in job plans to blend NHS and private patients – down to 7th from 4th – and reducing concerns over practising privileges/patient safety concerns with the independent sector – down to 11th from 9th.
CHART 5
Private patient service managers in trusts were also asked a set of topi-
re-instate services, but are realistic as to the extent and speed of recovery.
But it is clear that the lasting impact of Covid for NHS trusts has been the dramatic loss of private patient income in 2020-21 and into 2021-22.
This needs to be set alongside the significant positive contribution that PPU capacity, both beds and workforce, has made throughout the pandemic period to the wider NHS effort.
Not all trusts have yet published 2020-21 annual accounts, but, from those that have at the time of writing, we estimate the total NHS private patient revenues for 2020-21 will be in the range £325m to £350m.
cal questions related to the management of patient complaints raised because of the recent highlighting of this in the Paterson Report.
In the first, 20 of 26 trusts answered ‘yes’ to the statement ‘Private patient complaints are managed and resolved following the NHS patient processes’.
The second question asked whether private patient complaints were resolved using alternative processes. Nine trusts, approximately one-third, said they were. As one manager put it: ‘We follow NHS PALS complaints process with the right to appeal to ISCAS at stage 3 if unresolved.’
Third, a clear majority of 16 of 26 trusts confirmed that their trust private patient service did not use the Independent Sector Complaints Adjudication Service (ISCAS), but one trust shared that ‘the trust is aware of ISCAS and is updating processes to include this as services resume.’
Finally, 20 trusts responded to the question regarding their lack of awareness of ISCAS with 11 (30.4%) saying they would be keen to know more or subscribe to ISCAS in the future.
Next month: We return to our regional reviews to consider developments in the Northwest.
Philip Housden (right) is managing director at Housden Group commercial healthcare consultancy
This is a year-on-year drop of approximately 50% and a fall of around £25-30m a month private patient income since April 2020 to the NHS in England.
A further fall may well be reported in due course for the present financial year, but that will not become clear until 2021-22 accounts are published in autumn next year.
This multi-year impact should be seen in the context of the average annual growth of private patient revenues for the six-year period 2013-19 for all NHS trusts in England being 5.8%.
Housden Group plans to continue the annual survey to help trusts build a picture of the sector’s emerging key trends.
All you need to know about accountancy
FOCUS: ORTHOPAEDIC SURGEONS
Covid hits profits hard
It only took a few weeks of the Covid-19 pandemic to take its toll on orthopaedic surgeons’ profits. For the first time since we started this benchmarking series 13 years ago, they made a loss. Ray Stanbridge reports
IN MY report this time last year, I wrote about this specialty’s 2019 figures and commented: ‘All in all, this was a satisfactory year for orthopaedic surgeons. Having a quick look at 2019-20, it does look as if this trend has continued.
‘However, the outbreak of the Covid-19 pandemic from about March 2020 does appear to have had a very dramatic effect on many orthopaedic practices.’
Well, as things have turned out, orthopaedic surgeons were one of
the earliest-hit victims of the pandemic from about February 2020.
Our benchmarking survey this time round shows that, on average, a consultant orthopaedic practitioner’s private income fell by 5.9%, dropping from £203,000 in 2019 to £191,000 in 2020.
Decline in income
On average, costs fell by 10.3%, falling from £68,000 to £61,000 in the year. The end result was that
gross margins fell by 3.7%, sliding from £135,000 to £130,000.
In our view, the decline in income is virtually all accounted for by the effects of the first few weeks of the Covid crisis and subsequent lockdown. Consultants’ incomes had continued to do well up until then.
Some consultants took immediate steps to reduce their costs when the pandemic hit. But we did notice a slight increase in staff costs, representing cost pressure trends on secretarial fees prior to the pandemic.
As might be expected, there was a slight reduction in consulting room costs, reflecting reduced use in February and March 2020.
Attractive deals
There was also a slight fall in professional indemnity/insurance costs, reflecting the ability of some consultants to negotiate attractive deals in the marketplace.
There was a noticeable reduction in travel costs, partially explained by the early cancellation of some face-to-face courses and conferences.
Other costs also showed some reduction. We cannot uniquely specify which of these costs on
The decline in income is virtually all accounted for by the effects of the first few weeks of the Covid crisis and subsequent lockdown. Consultants’ incomes had continued to do well up until then average fell, but there does seem to be some evidence of general belttightening later in the financial year.
What then of the future?
We have noticed that, for the first six months or so of 2020-21, some orthopaedic surgeons’ earning figures, to be frank, look dire. However, there does seem to have been some improvement in the latter half of 2021, but it looks as if this year will seem to have been a poor one for many orthopaedic consultants.
In 2019, we listed the required requirements for entry to our survey. Those who qualify for our non-statistically-valid survey each year must:
Have earned at least £10,000 a
Year ending 5 April. Figures rounded to nearest £1,000 (percentage
year gross from private practice in the year to 5 April 2020;
Have at least five years’ private practice experience;
Either have held an old-style or
hold a new-style NHS contract. We exclude full-time private practice consultants from our survey; Be seriously interested in the business of private practice;
They may or may not have worked through a group, a limited liability partnership or a limited liability company.
As reported previously, structural changes in the market have affected our figures and increased difficulties in making realistic year to year comparisons. The growth of groups, for example, has taken business away from sole practitioners.
Indemnity and insurance company pressures on fees have been offset in part by the large growth in self-pay over the past few years.
We have now started to see the impact of the employment model on some consultants’ earnings. It seems that for some, certainly in the short term, the employed model generates more take-home pay than the self-employed model.
However, it is still much too early to judge the longer-term effects of this trend.
Next time: Ophthalmologists
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists Stanbridge Associates Limited
HOW ARE YOU DOING?
Use
ONLINE SOLUTIONS
INNOVATIVE ONLINE SOLUTIONS AT THE HEART OF THE HEALTHCARE SECTOR.
Our Online Solutions
Trusted by leading hospitals, independent practitioners and insurers to deliver high quality, secure and cost-effective IT systems. Seamlessly connect key stakeholders to support transparency within the sector and enhance patient safety.
Healthcode is the UK’s official medical bill clearing company and has provided secure and encrypted systems to healthcare professionals since 2000. Pre-pandemic we processed around 27,000 electronic medical bills to insurers daily.
To find out more about our solutions visit our website www.healthcode.co.uk
Coming in our December-January issue, published on 4 January.
Make a new start in 2022:
Get back on track! Jane Braithwaite gives advice covering a useful check-list of a range of private practice business issues you may have forgotten or overlooked during the pandemic
New Year’s resolutions for your business could really boost your income in 2022. Medical Billing and Collection’s Simon Brignall suggests ten for independent practitioners and their PAs or managers to consider
Clinical negligence claims against psychiatrists come under the spotlight and Dr Shabbir Choudhury, of the Medical Defence Union, offers tips on managing commonly encountered risks in this specialty
Investments: Good outcomes are the result of a sensible process. Cavendish Medical demonstrates that focusing on structure and risk exposures, rather than performance, leads to positive outcomes
Many of the most pressing healthcare challenges today are social or behavioural in nature rather than purely medical. Understanding how people behave in the real world, rather than how we expect or want them to behave, is key to designing effective healthcare interventions. Bupa’s Dr Caroline Wood explains how behavioural insights benefit healthcare
Keep it Legal: Should I incorporate and, if so, which corporate entity should I use? Justin Cumberlege, a partner in Hempsons’ healthcare team, explains what should be considered when forming a group.
INDEPENDENT PRACTITIONER
TODAY
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution. Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
So what’s the Private Healthcare Information Network (PHIN) all about? Anne Coyne highlights six things about it that consultants really need to know
Business Dilemmas: Dr Kathryn Leask, medico-legal adviser at the Medical Defence Union, discusses when a private GP can and cannot provide a fit note for a patient, while her colleague Dr Ellie Mein advises how to respond to a breach of confidential data
If you work in a private patients unit in the north-west of England, then don’t miss Philip Housden’s analysis of their latest results
The increasing use of social media and prevalence of online review or comparison sites has given patients various platforms to comment on the care or treatment they have received at a private clinic. We like to see positive comments from patients, but negative comments can be challenging. Dr Bobby Nicholas, of Medical Protection, discusses how best to handle these.
Our motoring correspondent Dr Tony Rimmer is lucky to meet up with a bit of an Italian beast – the Alfa Romeo Giulia Quadrifoglio (fourleaf clover)
Trouble understanding your financial accounts? Accountant Ian Tongue guides you through the maze in his ongoing series: Start A Private Practice
And don’t forget to check out our additional news updates every week online
ADVERTISERS: The deadline for booking adverts in our December-January issue is 3 December
Write to Independent Practitioner Today 7 Lindum Terrace, Lincoln LN2 5RP
CHANGING ADDRESS, EMAIL ADDRESS OR SUBSCRIPTION DETAILS?
Phone 01752 312140 or email karen@marketingcentre.co.uk
TELL US YOUR NEWS
Robin Stride, editorial director Email: robin@ip-today.co.uk Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the journal or our website business and lifestyle directories, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912 Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners.
£90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180). TO SUBSCRIBE
Email karen@marketingcentre.co.uk or phone 01752 312140
Publisher Gillian Nineham Phone: 07767 353897.
Email: gillian.nineham@gmail.com
SAVE £15 WITH DIRECT DEBIT!
Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.
BACK ISSUES: £12.50 including post & packaging Follow Independent Practitioner Today on