The business journal for doctors in private practice
In this issue
Going the extra mile
Successful practices have to ensure patients’ expectations are exceeded P12
Ways to manage your profile
Tips for private doctors on how to manage their public image P16
Turn to p9 to see what you could be paying
CQC FEES go up AgAIN
Shortfalls
may be cause of downfalls
An accountant explains why fee shortfalls are best avoided P34
Fees fight goes on
By Robin Stride
The Competition and Markets Authority (CMA) has announced its planned timetable for implementing publication of consultants’ fees following the profession’s failed challenge to the appeal court.
Independent doctors’ bodies, given only a few weeks’ notice to react to the ‘consultation’, were working on submitting responses as Independent Practitioner Today went to press.
The Federation of Independent Practitioner Organisations (FIPO), which lost an appeal court challenge on the issue over the summer, said it did not object in principle to the CMA’s ‘fee remedy’.
But chairman Mr Geoffrey Glazer warned it would take ‘some time’ to implement and needed to operate ‘within a genuine and open competitive process, where fees are not controlled or distorted by the insurers’.
Since the appeal rejection, FIPO has informed the CMA of a material change of circumstances following the competition watchdog’s 2014 report.
It said on its website: ‘These are well known to consultants and patients and involve control of fees by the insurer for new and many established consultants and various other restrictions and diversions of
with
patients to alternative consultants, treatments and hospitals.
‘This trend has been increasing since the CMA issued its report and it is on this basis that FIPO has asked for a further review of this matter.’
Independent Doctors Federation (IDF) specialists committee chairman Dr Brian O’Connor told a LaingBuisson private healthcare conference that FIPO’s argument had been: ‘What’s the point in publishing fees if private medical insurers set them?’
As a FIPO board member, he sympathised with that view, although the IDF thought the publication of fees ‘won’t make much difference’ in the short term.
But, in the long term, it could increase fees through patients judging highest fees as evidence of best treatment, he said.
Writing in this issue of Ind ependent Practitioner Today, Dr O’Connor says, on the face of it, the CMA remedy appears reasonable. ‘There is no reason why consultants should not publish and display clearly the cost of their commonly conducted treatment procedures and outpatient fees. Indeed, the vast majority of consultants already provide such information.’
However, he argues the CMA has not taken account of changing circumstances for private specialists
and says the IDF feels the watchdog does not fully understand healthcare and its various nuances.
The IDF would, he writes, strongly endorse the principle of transparency in all doctors’ activities in the independent sector. Therefore, fees publication, cost estimates of procedures and treatments as well as publicity on outcomes, performance and measures of quality delivery are all to be encouraged.
But he warns doctors of an imminent bureaucratic burden. ‘In my own case as an example, as a consultant physician in respiratory medicine and allergy, I could not begin to assess the likely cost of treatment for a patient with cough.
‘The majority of patients would incur very few costs, both in terms of outpatient attendances and investigations.
‘However, a significant minority will have severe disease underlying their cough, such as lung cancer or complex airways disease, and these patients will incur huge and often unpredictable costs over many months.’
Dr O’Connor adds: ‘I have no doubt doctors will rise to the challenge of fulfilling the requirements of the fee remedy.
‘This will mean more transparency on the part of hospitals to inform doctors of the costs of vari-
ThE CMA’S DATElINE
FoR pRIvATE CoNSulTANTS
By 30 June 2017: To regularly give phIN on an online form their outpatient consultation fees information. Can be either a fixed fee or an hourly rate. plus associated standard terms and conditions, exclusions or caveats By 30 June 2018: To similarly supply information on the standard fee for each type of procedure done
FoR pRIvATE hEAlThCARE INFoRMATIoN NETwoRk (phIN) By 30 April 2017: To publish performance information on its website
By 30 September 2017: Information on outpatient consultation fees
By 30 September 2018: Information on standard procedure fees
ous tests and procedures as well as the costs of inpatient hospital care.’
See page 8 and subscribe to Independent Practitioner Today for only £75 on page 20 to stay informed about important fee publication developments and your new responsibilities
a truly integrated cancer care team
Hca’s UK cancer network is the only private one to get official recognition P14
do you rely on a key employee?
What to do if your practice is left in the lurch when a key worker isn’t there P21
connect with gPs to plug your practice networking with colleagues needs to be done correctly to be successful P24
PPU beds help, not hurt, nHS finances How to create strong links with managers to ensure ppUs deliver gains for nHS P30
Balancing act of starting a business a new series examines the legal pitfalls lining up for doctor entrepreneurs P36
Some returns aren’t absolutely fabulous Why promises of ‘absolute returns’ on your investments are hard to keep P38
It all boils down to money
We just can’t escape stories about fees this month.
There’s the Competition and Markets Authority’s preferred timetable for getting consultants’ prices fully out into the public arena (see page one).
Well, ‘they’ might want it, but it looks unlikely they will get it in the time-scale proposed. And we expect a complicated journey before then as consultants and their hospitals try to match up new requirements with onthe-ground reality.
Then there’s NHS England’s bonkers plans to force independent practitioners to publish their private earnings (see
our splash last month and opposite). Well done to all the consultants who have since given their reaction to the consultation about it (now closed).
In this issue, we also reveal more about private hospitals’ controversial plans to put consultants on salaries (p4) and the CQC’s latest costly fee rises (p9).
You might be powerless to do much about all these issues, but there is another fee area worth investigating for many practices. Chasing shortfalls.
Are you spending more to try and retrieve the money than you will ever get back? See page 34 and let us know how you get on.
to advertiSe Contact advertising manager Margaret Floate at margifloate@btinternet.com Phone: 01483 824094 to SUBScriBe lisa@marketingcentre.co.uk Phone 01752 312140
Publisher: Gillian Nineham at gill@ip-today.co.uk Phone: 07767 353897
Head of design: Jonathan Anstee chief sub-editor: Vincent Dawe Circulation figures verified by the Audit Bureau of Circulations
Check you’re not overtaxed on pensions
By leslie Berry
Many doctors who just received letters from the NHS Pensions Agency detailing their annual pension contributions for the tax year 2015-16 have been shocked to find out just how much tax is due on their savings.
Financial advisers say these letters cause significant concern to recipients every year because the figures are often very different to the actual amount of money they believe they have put into their pension pot.
Patrick Convey, technical director at specialist financial planners Cavendish Medical, told Independent Practitioner Today this is because HM Revenue and Customs (HMRC) calculates the contributions for a defined benefit scheme such as the NHS very differently to that of a private pension.
The figures are based on the deemed ‘growth’ of the pension in that year with an allowance made for inflation.
Mr Convey said the calculations were complex and HMRC often got them wrong.
The annual allowance governing the amount that can be contributed to a pension each year
while still receiving tax relief was £40,000 for the 2015-16 tax year.
But if the allowance is breached, the individual can carry forward any unused allowances from the three previous tax years.
If there is still a breach, the excess is added to the individual’s income for the tax year and taxed at their marginal rate of income tax – potentially 45%.
Mr Convey said: ‘It is very easy for busy doctors to unknowingly breach the annual allowance due to NHS scheme membership. Plus, any increase in your pensionable salary because of a statutory pay rise or clinical excellence award, for example, will increase your pension benefits.’
He said there were ways of mitigating tax such as paying any tax charge through self-assessment or possibly using the ‘scheme pays’ route, where the pension scheme pays it on your behalf in exchange for reduced eventual benefits.
‘To make matters worse, from April 2016 onwards for some high earners, the allowance has been reduced to just £10,000 because of the new “tapered annual allowance”. It is now of paramount importance to ensure you are seeking the correct advice in this area.’
Rise in medical cover is likely to be ‘a blip’
Surprise new figures show a 1.8% growth in private medical insurance last year – but the industry has been warned the rise is probably just a blip.
LaingBuisson economist Philip Blackburn said the statistics were ‘great news’ but he added quickly: ‘Unfortunately, they might be a one-off.’
The growth was achieved by demand from corporate customers, which rose 2.6%. Individual demand was down 1.1%.
Mr Blackburn said: ‘The main reason for growth in insurance was a handful of large employers extended their schemes. That had the effect of growing the market.’ See pages 4, 5 and 6
By a staff reporter
Five million people have used Finder – Bupa’s online directory of recognised consultants, therapists and facilities – since it launched four years ago this month.
The insurer said the website (www.finder.bupa.co.uk) had now hit 60,000 visits a week, making it ‘an incredibly powerful free marketing tool for consultants’.
Finder is one of the most comprehensive lists of private consult-
ants in the UK, and is used by Bupa’s customer services advisers and patients as well as GPs and other healthcare professionals.
Following consultant feedback, Bupa has linked Finder to its billing website, Providers Online, to increase security and so consultants only need to remember one password.
used on smartphones and tablets – through which 36% of users now access Finder.
Two-thirds of Buparecognised surgeons have checked their profile is up to date. The insurer said annual verification earned them a blue tick symbol and gave Finder’s users reassurance when choosing a consultant.
The insurer said responsive design meant it could be easily
A spokeswoman said: ‘This is backed up by Bupa’s own research
which shows that consultants who verify their profile is up to date receive 92% more page views than those who don’t. And those who add a photograph of themselves get 27% more views than those without one.’
Bupa has created a template profile to help consultants who are unsure what to include. To view, visit www.finder.bupa.co.uk and put the name ‘Professor Finder Demonstration’ in the search bar ‘name box’.
Bupa directory success Union attacks private work exposure
The Hospital Consultants and Specialists Association (HCSA) has warned NHS England against plans to force hospital doctors to reveal private earnings ( Independent Practitioner Today, October 2016).
The trade union said the plan, not extended to other senior NHS staff, risked exposing individuals to ‘unfair, speculative and unwarranted media and public focus’.
HCSA president Prof Ross Welch said: ‘We remain concerned that this unfair approach of publicly
posting earnings will see a few cases from one section of senior NHS staff being used in a sensationalist manner by the media, but the impact in terms of public perception will be felt by all hospital doctors.
‘It is somewhat bizarre and completely unjustified that, given the wide range of senior NHS staff covered by the consultation,* it is only doctors who will be expected to reveal precise details of their private earnings.
‘Details of private work, albeit
UK’s biggest insurer of health
gets a
Alex Perry has been appointed chief executive of Bupa Insurance, leading the insurer’s regulated insurance business in the UK. He said he was committed to delivering value for money and championing the customers’ corner.
new chief
This included improving their experience, making the case for removing Insurance Premium Tax, which unfairly penalised people who were reducing the NHS’s burden, and getting a better deal for patients from healthcare providers.
GMC specialist register plan panned
Defence body Medical Protection claims doctors will face an extra burden under GMC plans to revamp the List of Registered Medical Practitioners.
not earnings, undertaken on their own time by hospital doctors are already discussed within the annual job planning process and any impact they could potentially have forms part of the annual whole of practice appraisal, disclosed to NHS employers.’
Prof Welch, a consultant in fetomaternal medicine, said the consultants’ contract also enshrined the primacy of the NHS when it came to arranging their workload. ✱ Managing Conflicts of Interest in the NHS: A Consultation
Conference to exhibit best in private health
‘Independents’ Day’ is on its way as the Independent Doctors Feder ation (IDF) prepares for a new London Healthcare Conference on 4 July 2017 to showcase the best in private practice.
and paediatrics.Delegates will include specialists, GPs and other referrers from home and overseas.
IDF president and private GP Dr Peter King-Lewis told Independent Practitioner Today : ‘Apart from showcasing the great medical care in the UK, it is a chance for all clinicians to network with their colleagues at the top of their game.
It voiced concern that increasing information about doctors’ risked the register’s accuracy and dependability.
The clinically-led, multi-specialty conference is designed to highlight all that the capital city and the rest of the UK has to offer in medical innovation and excellence in patient care.
Spokesman Dr Pallavi Bradshaw said it was not the GMC’s job to act as a quasi-advertising platform or replicate information and data available elsewhere.
Expert speakers and clinicians will discuss the latest developments in specialties including orthopaedics, oncology, neuro- surgery and rehab, genetics, diabetes, fertility
‘I have no doubt this conference will become a signature event in the medical calendar.’
More details on the central London conference available by emailing londonhealthcare@bioscientifica.com
HcSa president Prof ross welch
Salaried doctors are ‘the way to go’
By Robin Stride
The chief operating officer at Cleveland Clinic London has revealed more of the company’s plans to ditch the traditional model of consultants’ practising privileges and employ them on a salary instead.
Keith Hague predicted the notfor-profit foundation – awaiting planning permission for a massive restructuring of the building it bought last year at 33 Grosvenor Place – was destined to be ‘a market-changer’.
He told the LaingBuisson Private Acute Healthcare Conference in London it would be ‘a new model for the future of private practice’.
The company bought the premises outright last autumn and plans over three years to remove the roof, gut the building and build a new 205-bed tertiary hospital.
Consultants working there can expect to be paid far more than in the NHS, although Mr Hague would not be drawn on how much this might be at today’s rates.
Quizzed from the audience about the possibility of bonuses, he said the clinic operated on a no-bonus model, but added that there was an annual review tied to performance and patient outcomes, which could be tied to the following year’s salary.
If Cleveland Clinic London consultants follow their physician colleagues in the US, then it is likely that they would be on a oneyear contract, would generally be expected to work full time and be required to wear white coats.
Every sector of the hospital would be under a physician’s leadership.
Mr Hague, former chief execu-
tive of the UK’s largest private hospital at HCA’s The Wellington, expected there would be parttime opportunities for specialists in the capital too.
Salaried doctors would enjoy inhouse medical defence, paid by their employer, and would not be allowed to work in other private independent units.
But asked about consultants being able to work in private patient units in the NHS, he said the Cleveland Clinic was ‘thinking this through – we wouldn’t want to be spiteful’.
In time – at least a decade – the clinic could be training its own doctors.
Patients are expected to come from Europe, north Africa, the Middle East and Mediterranean.
Mr Hague said: ‘My view is this industry needs to change radically. It cannot continue in its present form.’
Outlining Cleveland Clinic’s plans, he questioned a range of issues facing the current UK private healthcare scene. Whether: Consultant clinical outcomes could be correctly monitored and
moRe pRaiSe of SalaRieS
The boss of the company behind another new private hospital in london, due to open next year with salaried consultants, sang the praises of an employment contract for private consultants.
andreas ludowig, managing director at Schön Klinik, Germany, said: ‘That’s the way we’ve been doing it – with great success in Germany.’
The 18-hospital company had attracted and retained ‘the key and most talented senior physicians’ in the country. They also got bonuses – unlike the Cleveland Clinic.
mr ludowig continued: ‘We have data that shows this model can have a very positive effect when it comes to quality.’
The Schoen Clinic, in Wigmore Street, london, is due to open in the second half of 2017 with 38 beds, five day-case beds and ten consulting rooms. it plans a ‘one-stop-shop’ for total spine care and ‘multiple innovations’ for spine and orthopaedics.
controlled under the present system of independent consultants; Competition between consultants was best for the patient; The continuing dogfight between doctors and insurers was good for the industry and patient; Insurers should have control over clinical quality and outcomes.
Private care must offer bigger range
Private care’s challenge is not making it more affordable but expanding its offering to entice patients back, according to a hospital boss.
BMI chief executive Jill Watts said: ‘We’ve heard time and again from insurers that private hospitals need to be more affordable in order to re-invigorate the market.
‘But price is not the issue. The issue is how we can attract more people back into private healthcare and offer a broader range of services which will put more balance into the overall system.’
She told the conference that a core part of BMI Healthcare’s strategy was to invest in expanding the range of services on offer, particularly at flagship sites with capability to provide a much broader range of services outside of the traditional surgical model.
And she predicted ‘a real plethora of disruptive innovation’ would hit private healthcare.
Ms Watts said the sector traditionally had a limited offering mainly focused around elective surgical procedures. But now the range of
services did not really match the growing demand for healthcare.
She criticised a rise in ‘narrower insurance products with exclusion clauses’ and continuing incentives for private patients to have their care delivered in the public sector.
‘This just devalues the insurance product and puts additional pressure on the NHS. The reality is that even if you do have access to toplevel private insurance, you are still likely to have to rely on the public sector at some stage to meet your overall health needs.’
However, Ms Watts welcomed instances of closer working together between insurers and hospitals and urged for ‘a more strategic approach to finding ways to alleviate pressure away from the NHS’.
Speaking to the audience of investors, directors, finance executives, insurers and hospital operators, she called for a more active role in positioning the sector to governments as supporting and complementing the NHS, not being in competition with it.
Keith Hague, boss of Cleveland Clinic london
Laingbuisson private acute heaLthcare conference
Who is earning what and where
Compiled by Ray Stanbridge of Stanbridge Accountants and presented to the conference
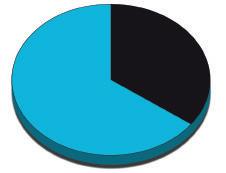
➲ 29.1% of consultants’ private practice fees are earned within five miles of Harley Street. 51.5% are earned between 5.1miles and 40 miles and 19.4% in the rest of the UK.
➲ 200 consultants’ groups generate 20-25% of the market.
➲ The number of consultants entering the market is falling due to the increasing costs arising from Competition and Markets Authority’s requirements – for example, secretarial fees and rooms – and defence costs. They are doing NHS rather than private work.
The following figures, excluding medico-legal and locum income, are provisional estimates:
WHaT’S HoT
Urology, eNT, anaesthetics, ophthalmology
oN THe Way Up
Dermatology, oncology.
WHeRe?
Central london and anywhere with self-pay.
WHo?
any business ‘adding value’; groups
WHaT’S NoT
orthopaedics, general surgery, cardiology, gynaecology
WHaT’S oN THe Way DoWN
Radiology
WHeRe?
Rest of UK where reliance on NHS;
Rest of UK where no private hospital competition.
WHy?
insurer pressure, cost of small practice, sole trader problems
HoT SpoTS
Central london, manchester oN THe Way Up
Bristol, Chelmsford, Guildford, Tunbridge Wells
WHy?
Self-pay, more hospital competition, more innovation
CooleR SpoTS
The North, Wales, Scotland oN THe Way DoWN West midlands, North-west
WHy?
more NHS work, lack of hospital competition, impact of Brexit
pRivaTe pRaCTiCe feeS SHaRe of maRKeT
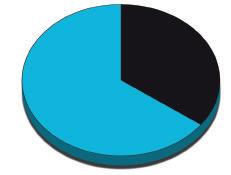
pRivaTe pRaCTiCe iNCome TReNDS
1 incomes holding up – but lower per unit fees
2 profit margins under pressure: ❍ effects of Cma rules ❍ insurance company pressure ❍ indemnity cover premiums
3 Growth in NHS Choose and Book work
The
4 Growth in self-pay patients
Laingbuisson
Poll shows public backs insurance
By Robin Stride
New figures from Bupa suggest a majority of adults would think of buying private medical insurance to escape NHS rationing.
As many as 52% would consider purchasing a policy and 70% of people had a positive view of health insurance, telling a survey for the insurer that those paying for healthcare are relieving NHS pressure.
The figures were released by Bupa Insurance’s new chief executive Alex Perry, who challenged providers to invest in higher-quality, easier to access care and to speak more boldly about the quality and value of independent healthcare.
He urged them to:
Address rising costs;
Keep price rises for health insurance customers below the inflation rate;
Challenge Government on ‘punishing’ insurance premium tax.
The levy was hitting ‘those choosing to pay for a service that’s
Private units slow to send information on quality
Scores of private units have missed the deadline for sending quality data to the Private Health care Information Network, its boss Matt James told the conference.
Only 237 of 531 hospitals providing private healthcare in the UK, including NHS private pat ient units and cosmetic facilities, had provided the information.
Feet-draggers face enforcement proceedings from the Comp -
effectively reducing the burden on an increasingly strained NHS’.
Mr Perry’s comments followed the Association of British Insurers’ figures revealing the 66% rise in insurance premium tax in under a year had seen customers’ health insurance policies rise on average by £52.50.
He said it remained to be seen what the impact would be, but he warned of a ‘real threat’ that it could still rise further to 15 or 20%.
Matt James, PhIn’s chief executive
etition and Markets Auth ority (CMA), could be ‘named and shamed’ and ultimately face jail.
Mr James said the standard of data submitted so far was ‘variable but improving’.
He warned that doctors would expect to see hospitals had done a good job when they checked their data before publication.
He added: ‘The sector also needs to prove that it’s delivering the highest-quality healthcare, showing the general public as well as Government that we can deliver a best-in-class, seamless customer experience.
‘At a time when people are acutely aware of NHS funding constraints, we need to be bolder in our approach to delivery and how we speak about it. Only by demonstrating quality, customer experience and affordability can we make independent healthcare an easier choice for people and their families.’
Bupa said 78% of its customers expected their insurer to pursue value for money on their behalf and 73% agreed health insurers should stop working with a hospital if they believe its charges are unreasonable.
Survey conducted on 28-29 September 2016 by Censuswide through online interviews with 2,002 UK adults aged 16+.
Private income diktat attacked
Bupa Insurance boss Alex Perry warned of a ‘negative force’ operating against the private healthcare sector.
‘A clear sign of hostility’ was how he viewed NHS England’s proposals (see page 3) to force consultants to publish their earnings from independent practice.
Tell uS youR SToRy
Share your experience of what has and has not worked in your private practice.
Contact editorial director Robin Stride at robin@ip-today.co.uk or phone him on 07909 997340
Docklands outpatient unit opens after a refit
HCA Healthcare UK’s outpatients’ centre at Canary Wharf has reopened after renovation and expansion.
Run by London Bridge Hospital, it gives office workers convenient and speedy access to care and treatments.
Services include private GPs, dental care, same day diagnostics, MRI, ultrasound and X-rays.
The 12-year-old centre also caters for sports injuries, including a newly expanded specialist knee unit where patients can see orthopaedic specialists for advice and treatment on knee problems such as meniscal injuries, anterior cruciate ligament (ACL) damage and kneecap instability.
Consultant orthopaedic surgeon Mr Howard Ware, of The Wellington Knee Unit, said he and colleagues Mr Matthew Bartlett, Mr Chinmay Gupte, Mr Rahul Patel and Mr David Sweetnam were delighted to bring their specialist services to patients in the area.
London Bridge Hospital chief operating officer Miranda Dodd said: ‘We are always trying to improve access to our healthcare services, which are designed with our patients in mind.
‘We recognise that people are increasingly time-poor, work long hours and don’t always put their health first, but we are trying to make it easier to combine the two to help improve people’s wellbeing and ensure a healthier workforce for local businesses.’
Laingbuisson private acute heaLthcare conference
Alex Perry, Bupa Insurance’s chief executive, hit out at premium tax
The Canary Wharf outpatient clinic
a cure for cosmetic ills
By edie Bourne
Private surgeons are hailing BREXIT as a great chance to make the cosmetic surgery sector safer.
Worrying data unveiled at the British Association of Aesthetic Plastic Surgeons’ (BAAPS) annual scientific meeting at Olympia, London, showed nine in ten aesthetic plastic surgeons reporting a dramatic rise in patients being dangerously misinformed about procedures.
Members were united in agreeing the impending exit from the EU presents with a unique opportunity to finally clean up a sector long described as the ‘Wild West’.
The association called upon the Government to use a multipronged yet clear-cut approach to ensure the future safety of UK patients.
Two out of five of surgeons have continued to see a rise in problems stemming from cosmetic surgery
abroad, with 60% of those recording an increase by as much as a quarter.
Another new study presented at the BAAPS conference evaluated the resulting cost to a single NHS trust alone to be an average £5,000 per patient.
This excluded imaging, medication or any outpatient appointments –with hospital stays rang ing anywhere from one to 19 days.
could bring about the safe and effective aesthetic plastic surgery the association had battled for.
BAAPS proposes foreign hospitals be invoiced for the necessary reconstructive – and often lifesaving – treatment undertaken by the NHS once these patients come home.
Consultant plastic surgeon and BAAPS president Mr Michael Cadier said Brexit offered ‘a brilliant opportunity’ to implement straightforward changes that
BAAPS’ PlAnS foR BRexIT – duBBed ‘BReASTxIT’ AT The ConfeRenCe
1
european surgeons will no longer have the automatic right to work in the uK, so fly-infly-out surgeons will no longer be as freely contracted by commercial chains, who routinely use them for their lower cost.
2
He added: ‘Our clearcut proposals should be seriously taken into consideration by the Government – at BAAPS we have spent decades doing our best to educate the public and warn them away from unethical offers and procedures performed by untrained practitioners.
‘Yet, as our internal survey has proven, many people are still vulnerable and far from well-informed.
‘Now we have a chance to truly change the landscape of cosmetic surgery in Britain and not only ensure safety for the tens of thousands of patients who seek procedures every year, but also remedy for our health service hospitals treating victims of surgical tourism.’
Bid to stop fierce op sales
The Royal College of Surgeons of England has launched independent information to combat ‘aggressive marketing’ campaigns and ‘ruthless’ sales techniques of some unscrupulous private firms.
Patient resources on the RCS website advise how to choose the right surgeon and hospital, explain the risks of undergoing surgery, and possible complications.
There is a section on questions to ask a surgeon before consenting to an operation, a downloadable checklist, and three short animation films.
The RCS strongly recommends taking at least two weeks between the initial consultation with the operating surgeon and consenting to surgery. It advises patients not
to be afraid to ask questions, or feel pressured into consenting to surgery.
Mr Stephen Cannon, chairman of the RCS Cosmetic Surgery
Interspecialty Committee, said:
‘The cosmetic surgery industry is booming, but due to the aggressive marketing and ruthless sales tactics of some unscrupulous companies, it can be very difficult for patients to find independent, trustworthy information which gives them a clear idea of what an operation would entail.’
The college is also publishing a register of ‘certified surgeons’ in different cosmetic surgical procedures, allowing patients to look for a surgeon by procedure, who has provided evidence to the RCS
that they have the appropriate training, experience and cover to practise in the UK.
It was asked by the Department of Health to produce the patient resources and set up the certification system, following the Keogh Review in 2013 in the wake of the PIP breast implant scandal.
This found there was an urgent need to improve regulation of cosmetic surgical and non-surgical practices in the UK and that some doctors are performing cosmetic surgery even though they had no surgical training.
The new patient resources for people considering cosmetic surgery can be viewed at the college website at www.rcseng.ac.uk/ patient-care/cosmetic-surgery.
With the uK free to set their own required standards of regulation and training, businesses can be forced to meet quality levels and to employ surgeons trained to a uK-defined standard and who are appropriately covered by uK or uK-equivalent indemnity cover.
3
BAAPS calls for dermal fillers – injectables which have historically been unregulated and previously described as ‘the next PIP implant crisis waiting to happen’ – to finally be classed as prescription-only medications (PoM).
4
It calls for nhS hospitals forced to treat patients who have returned from abroad with problems to invoice the foreign providers for the cost of reconstructive or medical care.
Growth plan by One Healthcare
Three new diagnostic, surgery and outpatient centres are in the pipeline from One Healthcare, which opened its first hospital in Ashford, Kent, last April.
A second project in Hatfield, Hertfordshire, is being built and chief executive Adrian Stevensen said another 14 projects are due over the next three years.
BAAPS president Mr Michael Cadier
The roof garden at onehealthcare’s Ashford hospital in Kent
CMA ‘fee remedy’ fails to fix issues
By Dr Brian O’Connor, chairman of the Independent Doctors Federation’s specialist committee
Consultants are required by the Competition and Markets Authority’s (CMA) latest remedy to provide information to patients about cost of consultations and procedures – and total cost of care (see our front page story).
The Private Healthcare Information Network (PHIN) has been charged with receiving this information from consultants, who are obliged to supply it with all relevant information about fees for all treatment, notably frequently conducted treatment procedures.
A lack of fee transparency, and indeed the lack of readily available published information on treatment outcomes, is deemed by the CMA to lead to an adverse effect on competition in the provision of consultant services.
The CMA, which launched its private healthcare investigation over five years ago, feels that patients would be better able to exercise effective choice if they knew the cost of care and if they also had some information about quality of outcomes.
On the face of it, this CMA remedy would appear to be reasonable.
There is no reason why consultants should not publish and display clearly the cost of their commonly conducted treatment procedures and outpatient fees. Indeed, the vast majority of consultants already provide such information.
The CMA’s fee remedy was unsuccessfully opposed by the Federation of Independent Practitioner Organ isations (FIPO), in particular because the basis of the remedy was to improve competition and patient choice.
FIPO’s contention was that the private medical insurance compa
BrIan O’COnnOr:
Full disclosure means full disclosure and should apply not just to privately-funded patients but also to those patients who are insured and who rightly wish to assess whether they are getting true value for money
nies, by virtue of their imposition of restricted fees – particularly on younger consultants – have introduced a fixed fee for private patient consultations and treatment, thereby removing market forces from the equation.
Indeed, the nonlegal minority view of an economist during the CMA appeal totally concurred with FIPO’s view and felt that the influence of insurers totally distorted any potential for a competitive market place for private practice.
Changed circumstances
Notwithstanding all of this, the CMA has, in my view, not taken account of changing circumstances since the original remedy.
The private sector has altered significantly. Private medical insurance companies are imposing severe fee restrictions on doctors, which are preventing the vast majority of new consultants from entering private practice in the traditional way.
Many observers, including those of us in the Independent Doctors Federation (IDF), are concerned at the lack of presence of
young, talented specialists in the independent sector.
An unintended consequence, I suspect, of the CMA remedy is the emergence of a proposal from hospital providers to enter into a contract with doctors, offering them salary packages to deliver practice in hospitals.
This is a new departure for doctors in private practice and, on the face of it, cannot be good for competition or, for that matter, independent medical practice.
A new young consultant, unable to afford the set up costs of private practice and severely restrained by insurers from charging economic rates for consultations and procedures, may well be encouraged to enter into a contractual relationship with hospital providers.
As a salaried individual, a specialist will effectively have employee status within a provider organisation and may not always act in the best interests of the patient, both clinically and indeed in terms of costs of treatment.
CMA doesn’t understand
These are some of the concerns we have about the remedies. Circumstances have altered. We do not feel that the CMA fully understands healthcare and its various nuances.
But, nonetheless, the IDF would strongly endorse the principle of transparency in all activities undertaken by doctors in the independent sector.
Therefore, publication of fees, estimation of cost of procedures and treatments as well as publication of outcomes, performance and measures of quality delivery are all to be encouraged.
However, there will be a bureaucratic burden. In my own case as an example, as a consultant physician in respiratory medicine and
Our front-page splash this month on the competition watchdog’s plans
allergy, I could not begin to assess the likely cost of treatment for a patient with cough.
The majority of patients would incur very few costs, both in terms of outpatient attendances and investigations.
Unpredicatble costs
However, a significant minority will have severe disease underlying their cough, such as lung cancer or complex airways disease, and these patients will incur huge and often unpredictable costs over many months.
I have no doubt doctors will rise to the challenge of fulfilling the requirements of the fee remedy. This will mean more transparency on the part of hospitals to inform doctors of the costs of various tests and procedures as well as the costs of inpatient hospital care. In that regard, patients might reasonably expect that, even when insured, they will receive full disclosure of the costs incurred during their care. Whether that would be the responsibility of the doctor to provide such information, which is currently not available to doctors – who are actively discouraged from discussing fees with insured patients by their respective insurers – or by the private medical insurers or hospital operators remains to be seen.
Full disclosure means full disclosure and should apply not just to privatelyfunded patients but also to those patients who are insured and who rightly wish to assess whether they are getting true value for money.
Dr
Health watchdog plans 6% inspection fee rise
By Martha Walker Director of CQC Consultancy
Independent doctors registered with the Care Quality Commission (CQC) face a three figure increase in the fees they must pay for 201718.
Last year, the watchdog decided to meet the Government’s requirement to achieve full chargeable cost recovery (FCCR) over a twoyear period instead of four years for most providers, including independent doctors. 201718 is the second year.
In its newly published 2017 fees consultation document, the CQC has announced that in order to achieve this, independent doctors will see a fee increase of 5.9%.
Practically, this will mean an independent doctor with one registered location currently paying £1,763 will see an increase of £104 to £1,867.
note: Independent doctors are part of the community healthcare services and should not be confused with the primary medical services
The CQC says fees will not stand still in future years but will be adjusted according to the ongoing costs of regulating each sector.
Dentists have already reached FCCR and will see a decrease in fees.
But time will tell if, once the new style inspection for independent doctors has been rolled out, this will reduce manpower and workload for the CQC and be reflected in future fee structures.
The fees consultation document can be found in the Guidance for
Providers section of the CQC website: www.cqc.org.uk. Deadline for responses is 11 January 2017. It puts forward three proposals for consultation – set out in the box on the right.
The responses will be used by the CQC when developing the 2018 19 fees structure across all the health and social care sectors and also allows the CQC to reflect the views and opinions of providers to the CQC’s board and the Health Secretary.
Seeking help from defence body won’t raise your subscriptions
A defence body says it is keen to dispel the myth that doctors contacting its advice line will be penalised with higher subscriptions.
The MDDUS said members were encouraged to seek early advice and are not penalised for doing so. Chief executive Chris Kenny
said the union had repeatedly made clear to the BMA that its underwriting and pricing decisions were unaffected by the number of times members sought advice.
He added: ‘Our subscriptions are calculated to reflect likely future costs, including claims which
have occurred but not yet been reported to us, based on our previous claims experience and incorporating expert actuarial and underwriting analysis.
‘We take into account many factors including number of sessions worked as well as doctors’ professional duties and responsibilities.’
CQC’s plans
prOpOsal 1: sets out the CQC’s intention to make changes to fee amounts in the fees scheme for 2017-18 to achieve full chargeable cost recovery (FCCr) across all sectors – including independent doctors – and to continue the trajectory for community social care providers to achieve FCCr by 2019-20.
prOpOsal 2: aims to make a change to a definition in the fees scheme to reclassify providers of substance misuse treatment services.
prOpOsal 3: Is intended to make a change to a definition in the fees scheme to clarify charges for providers of services in minor injuries units and urgent care centres.
Guide to spot signs of stress
A new guide for GPs seeking help with work stress and pressure has been released by the Royal Medical Benevolent Fund (RMBF). It provides practical advice and signposts support and resources for those experiencing stress and difficulty.
Download at www.rmbf.org/ data/files/rmbfthevitalsignsinprimarycare.pdf
Doctors offered customised images
Consultants at King Edward VII’s Hospital, London, now have rapid access to imaging material under a partnership with Vital Images. The hospital claimed a UK first for enabling 2D/3D diagnostic images to be accessible on iPads. It said consultants will now be provided with fast and consistent access to a range of diagnostic data and can easily navigate within images to precisely see and under
stand disease conditions and injuries. Vital’s Vitrea advanced visualisation software also allows doctors to customise the images based on their specific needs.
Hospital imaging manager
Corey Frazer said: ‘The flexibility of the complete Vitrea solution allows us to have full control over patient data. This data is secure, and nothing is shared outside the hospital.’
AccoUnTAnT’s clinic: TAx RETURns
You could miss out
Filing tax returns is something that you may put to the bottom of your ‘to do’ list – but with the 31 January 2017 deadline looming, you will need to make sure you have all the necessary information to hand.
Susan Hutter (below) gives some pointers on making the process as seamless as possible if you are filing online or working with your accountant. These are all areas that independent practitioners often get wrong – so use it as a useful check list
1
If you have had income taxed at source, for example bank or building society interest, make sure you declare this on your tax return.
o nly basic rate is taxed at source. Since most consultants and GPs are higher-rate taxpayers, there may be more tax to pay. Sorry to say this, but this is a common mistake many make when filing their returns.
Also make sure you do not forget to declare any new bank or building society accounts you have either opened or indeed closed during the tax year, as there may be interest accrued on these accounts which your accountant and HMRC will need to know about.
Be warned that HMRC is made aware about all amounts of interest and they pick up on anyone who doesn’t declare interest which could open up a full investigation.
you will also need to declare dividends from private companies or shares.
2 Remember, if your business is a limited company then you can claim extra tax credit on qualifying research and development.
It is quite technical about what can and cannot be claimed, so do make sure you have a record to distinguish what time is spent on this area.
Let’s say you spend £10,000 on R&D-qualifying wages – either you or your staff – then you can claim an extra £13,000 against the company’s profit.
3
Try and regularly keep a record of expenses, as doing this months down the line means you will be wading through mountains of receipts or second guessing what cash you spent on your business.
It may be too late for this tax year,
Some doctors in private practice could be missing out on claiming back hundreds of pounds simply because they were sloppy with administration
but to get into good habits you should ideally be keeping weekly records or monthly at a stretch.
Some doctors in private practice could be missing out on claiming back hundreds of pounds simply because they were sloppy with administration.
your accountant will be able to advise what is claimable, but this includes:
Travel to and from conferences
– but not from home to work and vice versa;
Travel between hospitals and consultancy rooms, professional subscriptions;
IT for work. This includes such things as internet and software packages, use of mobile phone, use of home as an office – provided you can justify this is a separate space and you are not just using your dining room.
Remember, over-claiming can raise HMRC’s eyebrows, so make sure everything you put down is an accurate or fair estimate.
4
Don’t forget to include income from all sources and not just professional income. This may not be just practice work but other areas; for example, if you
get paid to give a lecture or write in a journal.
Keep documentation and, once again, update your records regularly – or advise your secretary/ office manager of what is important to note down.
5
If you have a lower-earning or non-earning spouse, make sure you transfer income – such as dividends from limited companies or interest from bank accounts – to them wherever possible.
Remember, you have to do this at the time, rather than retrospectively. It only counts when you make the transfer.
The same goes for property and rental income. As a rule of thumb, it is better that the property is in both names, as you can reduce tax payments significantly.
By getting more savvy with your tax administration processes and being aware of what you can claim, you will not only find tax deadlines less onerous, but you may even find yourself with more money in your pocket.
Susan Hutter is a specialist medical accountant and a partner at Shelley Stock Hutter
Patient expectations are always changing – what might have been acceptable service ten years ago, probably won’t be today. If a practice is to constantly keep patients satisfied and returning, it has to recognise what these expectations are and ensure they are exceeded.
Stephanie Vaughan-Jones discusses how to provide a service that ticks all the right modern-day
boxes
Where there are patients, there are expectations. Great expectations, in fact.
While the fundamentals of these will always remain roughly the same – people wanting the very best treatment and service –the specifics do change over time as they become accustomed to service being delivered in a particular way.
these can actually catch practices out if they are not acknowledged and met, let alone exceeded.
t here are three important points to consider when making sure your practice, clinic or hospital is delivering for modern needs.
manage instant gratification
Many years ago, when people raised an issue, they might expect a response in a few days. But not anymore.
For the most part, waiting times are a thing of the past and instant
Independent practitioners realise there is much more to a receptionist’s role than simply answering the phone to take bookings
Going the
gratification is the order of the day.
Of course, when running a practice, it is not that straightforward; because of the diverse nature of the patients that you work with, you simply cannot meet everyone’s needs all of the time.
At the intersection between speed and quality, the service you provide could fall down at this point. A patient dealt with too quickly can have much of their actual needs overlooked, whereby if they are made to wait, they may be dissatisfied or even go elsewhere.
the best way around this is to manage the expectations of instant gratification.
People want and expect an immediate response to an inquiry. And this is entirely possible. even if it is just by reassuring the patient that someone will be back in touch shortly.
We at Money penny find that
many private practitioners and GPs appreciate the reassurance that their external contracted receptionist gives their patient when they call – that their inquiry matters and is being dealt with.
Availability is important
A growing number of independent practitioners and clinics are realising that having a receptionist to man the front desk is not enough to meet their patients’ needs.
And they realise there is much more to a receptionist’s role than simply answering the phone to take bookings.
More often than not, receptionists are rushed off their feet tending to the needs of visitors, managing diaries and having a big hand in running the practice. this can leave precious little time to answer the phone and deal with the patients who call.
In a recent analysis of calls to
the extra mile
the healthcare sector, we identified that healthcare practitioners are missing the most calls at the beginning of the week, with their lines busiest at 10am on a Monday – followed by tuesday and Wednesday at 3pm – suggesting clinics are the most under-resourced at these times.
this strongly indicates that, as the high volume of calls are occurring at times when we would expect patients to get in touch – first thing in the morning – many practices are underestimating the number of calls they receive from patients trying to get through to them.
It’s all too easy for a practice to think they have the staff resources to cover busy call times, but many won’t be aware of the number of calls they are missing.
t hese missed calls can have a huge knock-on effect for a practice – not only could this result in lower patient numbers and reve-
nue, but it also reduces the level of service they give to patients.
Over time, this can lead to a poor or even negative reputation. By better understanding needs and behaviour, practices can start to take steps to providing the great patient journey many are striving to achieve.
Liberate your front line
People are used to being given solutions straightaway. t his is understandable: if a patient is being given a service, why should they be left waiting?
But this can wreak havoc if the people that deal with patients the most – people behind the front desk, on the phone and greeting visitors – don’t have the freedom to step up and help.
the employees on the front line are the first faces a patient will see and usually their first point of contact with issues or queries. t heir importance cannot be
Your front-line staff know your patients better than anyone else, and equipping them with the power to make decisions can improve the experience at your clinic
underlined enough. And these days, your patients expect that they have the power to help them when they need it.
With this in mind, giving frontline staff the ability to make decisions off their own bat seems like a no-brainer.
Due to their proximity and level of interaction, your front-line staff know your patients better than anyone else, and equipping them with the power to make decisions can improve the experience at your clinic.
the best way to do this is to listen to them, consider them indispensable and let them go the extra mile for your customers. If a problem requires a simple solution, give them the freedom to do it. It will go to great lengths to delighting patients.
Stephanie Vaughan-Jones (left) is channel manager at telephone answering specialist Moneypenny
A truly integrated
Dr Tobias Arkenau sets out HCA Healthcare UK’s network approach on integrated oncology, palliative care and support services, recently recognised and accredited by the European Society of Medical Oncology (ESMO)
HCA’S CANCER TEAM MEMBERS (Above, left to right) Kelly Grainger, head of dietetics and therapies; Maureen Royston-Lee, lead consultant counselling psychologist; Seraphim Patel, project lead for ESMO; Dr David Feuer, consultant in palliative medicine; Dr Jimmy Kwok, head of oncology service line; Annie James-Woollacott, symptom control clinical nurse specialist; Dr Tobias Arkenau, clinical lead
Patients who have been diagnosed with cancer often face the problem of finding good-quality holistic care, and this may be in the early, curable disease stages or when the cancer is more advanced.
Many cancer services around the country find it is a challenge to deliver this service to a high quality and to patients’ satisfaction, especially in times of financial constraints.
For a long time now, the cancer care team at hCa healthcare has been driving this agenda and particularly focuses on the integration of key elements of care, including palliative care and support services, psychological and survivorship programmes.
a tumour board of dedicated specialists in this field has been established to lead and connect those elements into day-to-day clinical practice.
improved patient experience over the years, hCa healthcare UK’s cancer service line has continued to develop these fundamentally important care programmes and it is anticipated that patients who begin the journey with us will equally feel the direct clinical benefits that, we hope, dramatically improve the overall patient experience.
as a result of continued service improvement and by ensuring that a network-wide approach enables patients and families to access these services, h C a UK’s cancer service line has been accredited by the e uropean s ociety of Medical o ncology (esMo) as a ‘Designated Centre of
cancer care team
integrated oncology and Palliative Care’. it is one of only eight accredited centres in the UK and the only private hospital group to have been recognised.
the scope of this peer-reviewed and independent accreditation programme is to further develop a standardised survivorship and supportive care programme across h C a’s UK cancer service line to ultimately improve patient experience and care.
within our six central London hospitals and outpatient chemotherapy units and services in Manchester, our vision is to establish a unique network of support to ensure all our patients get the same level of access and care in our facilities.
i strongly believe that personalised care and support beyond the individual clinical treatments for cancer will help patients and their families to better cope with the immense stress they undergo, both in the short and long term.
ElEmEnTs oF cARE
supportive care and psychological support supportive care and psychological support is open to all h C a UK cancer patients.
i t focuses on each cancer patient’s emotional stress as a result of living with the diagnosis of cancer and its treatment, fear of recurrence and the distress imposed by living with the dayto-day physical problems. this can create new, or worsen pre-existing, psychological distress for people living with cancer, their families and other caregivers.
o ne key element of h C a healthcare UK cancer services is to support cancer patients who are undergoing physical and psychological impairments, which may lead to substantial social problems, such as the inability to
At the heart of the day-to-day care, the focus is to ensure that people’s physical, practical, emotional, spiritual and social needs are met in a timely and appropriate way
work or fulfil other normative social roles.
importantly, and at the heart of the day-to-day care, the focus is to ensure that people’s physical, practical, emotional, spiritual and social needs are met in a timely and appropriate way, and that resources are targeted to those who need them most. t his includes the assessment of needs via specialised tools, counselling or further psychological interventions.
Palliative and end-of-life care i t is widely acknowledged that when caring for someone at the end of their life, we have but one chance to get that care right. Failing to do so can not only deprive our patients of the best end-of-life care, but leave a devastating legacy for the bereaved.
we recognise we have a duty to deliver end-of-life care of the highest quality to our patients, promoting excellence in all elements of the patient’s treatment and care, and that such duty extends to the care of the relatives and care-givers.
when inadequately controlled symptoms are identified, oncologists and specialist nurses
work collaboratively to evaluate symptoms and plan treatments accordingly. this may be either in an outpatient setting or wardbased.
treatment plans are regularly reviewed for symptom control, including review by community palliative care teams as needed.
survivorship – living Well Programme the Living well Programme’s aim is to anticipate and address any effects of cancer and its treatments; above all, focusing on living well.
Patients have access to this programme via an hCa-wide referral network and the focus here is, once patients have finished their active treatment, to alleviate any physical, psychological or practical problems which arose during treatment.
Dr Tobias Arkenau (right) is medical director of Sarah Cannon Research Institute UK and clinical lead for HCA Healthcare UK’s cancer service line
TAx ADviCE AND PLANNiNG FOR DOCTORS
• Tax consultancy
• Self-employed and company accounts
• Property investment structuring
• Payroll and vAT services
Contact: Nick Brecker. Tel: 020 7253 0030
Email: nbrecker@caldwellandbraham.co.uk
Web: www.caldwellandbraham.co.uk
Ways you can manage
profile
Our monthly series by Jane Braithwaite (right) gives some vital tips to help independent practitioners manage their public image
What do i know about you?
Have you evaluated the image you portray to prospective patients? Your personal information is easily accessible, including your social media profile and Companies House business records. But how can you manage your profile proactively?
Why is this relevant?
The most reliable form of marketing is undoubtedly word of mouth. Contented patients will recommend you to their families, friends and colleagues, establishing an initial element of trust and setting high expectations about your expertise for prospective patients.
Previously, a patient might have looked up your practice in a directory and called your secretary to make a booking; but this no longer applies. Inevitably, a patient is going to do some online research prior to making an appointment.
What will a patient find when they google your name?
Ideally, the information listed will consolidate their positive expectations, leading to a booking.
Your website should appear high up in the search results, followed by your Linked In profile. This is an optimal result, as your patients would see the image you would like to portray.
But the reality may be somewhat different...
In a not uncommon scenario, your name may be shared by multiple people, leading to a convoluted wild goose chase by the prospective patient – and a negative result.
So here’s what to look out for: Directorships: If you have been a director or owned a limited company, you will be listed on Companies House. There are numerous agencies offering information about your financial performance for a small fee.
Your home address may be
listed if it has been utilised at any point as your registered address.
Patients will also be able to view your business associates and collaborators. If you are involved in a family business, your patients will be able to see personal details you may wish to keep private.
Social media platforms: These set your profile as ‘public’ by default; if you are a Facebook, Twitter or Instagram user, you need to go to rigorous lengths to keep your posts private.
It’s common practice for people to check you out on Facebook. If the result portrays you drinking beer in the Caribbean, the prospective patient may opt to go elsewhere.
Website listings: Often doctors are listed on numerous hospital websites; this can be confusing for prospective patients. Where do you actually work? Why are you working across five different locations?
Online directories: Private healthcare directories are a thriving business and you may find you have been listed on several of these without your knowledge or consent.
Directories amass their data in a random fashion and it’s often out of date. It would be fairly offputting for a prospective patient to be referred to an obsolete address. Patient reviews: Increasingly, services are being evaluated online by clients, and patients will find opportunities to leave reviews and comments on the service you provide. This phenomenon is only going to grow.
This could be excellent for your practice if the reviews are positive; however, negative reviews are clearly undesirable. Assessment is always subjective and this is a factor to consider. Mumsnet is a good example of a very active site which is often used by patients to evaluate doctors and post and share reviews.
manage your
Celebrity endorsements: It’s possible you may be linked to a famous patient via an article in the press. This can be invaluable if your name is associated with positive accolades, but how does one deal with potentially negative comments?
privacy
At this stage, you may be strongly considering a rigorous privacy policy, excluding any mention of yourself or your family from potential internet searches. Whether this is possible or advisable is open to question.
It would take concerted time and effort to remove all personal data and would require dedicated, meticulous attention. There is a compelling argument for managing your profile proactively and taking control.
You can ensure that positive comments and endorsements are easily found – this is technically achievable.
Recommendations
Taking control of your profile will entail an initial investment of time, as well as ongoing, regular maintenance, by means of the following: Your website: The creation and management of a professional website is a separate issue. But, in summary, check that your website is smart, functional and contemporary, including updated contact details.
If you don’t already have a website, we would strongly encourage you to create one. A one page website including a professional photograph, relevant contact details and a succinct welcome message about your services would be sufficient to start with. LinkedIn profile: Currently, most professionals use LinkedIn and your patients will fully expect to find you listed on this service. It’s fundamental to include a professional photograph and a good introduction.
The free service is adequate, there’s no need to upgrade to a premium facility. LinkedIn invests heavily in ensuring its results are prioritised; you will miss out if you are not listed accordingly.
Social media: The vast majority of the global populace use social media; it is feasible to participate while managing and retaining your privacy. Platforms periodically change their privacy setting and conditions and you need to check these regularly. Ask someone to look you up and see what they find.
Other websites: Check the websites on which you are listed. Are they appropriate? If this isn’t the case, instigate removal of your details. If the websites are relevant, ensure listings are correct and consistent with your website and LinkedIn profiles.
Directories: Directories can easily be contacted to update your details, upload a photo and so on. Services will try to upgrade you to a premium package, which is unnecessary in most cases.
Google alerts: These are technically inspired. It’s possible to set up free, daily alerts and notifications on specific topics featured on the internet. You can set up your contact preferences and receive an email each time something relevant comes online.
Regular reviews of your online profile: This is an ongoing consideration. You need to evaluate and monitor your profile periodically to ensure there are no unpleasant surprises. In most cases, a brief monthly check will suffice, especially if using Google Alerts effectively.
We are happy to assist with any aspect of the above. Meanwhile, enjoy exploring and taking control.
Next time: check out Jane’s choice of the top 10 apps for you
Jane Braithwaite is managing director at Designated Medical
How to analyse others’ reports
Take steps to see you will be paid before taking on any extra work arising from your medical report, advises Michael r. young in his ongoing series for clinical negligence expert witnesses
Be ReAdY for solicitors to return with some follow-up questions after you have submitted your medical report.
This is more likely to happen if:
You have not expressed yourself clearly in the report;
You have not answered the solicitor’s questions;
You have left something out;
There are inconsistencies in your reasoning;
The report is not compliant with paragraph 35 of the Criminal Prosectution Rules when it needs to be.
Meticulous editing and redrafting of all reports before submission should help keep the number of follow-up questions to a minimum.
However, if after every report you submit, you repeatedly receive a vast number of followup questions, then you should seriously re-appraise your analytical and writing skills.
If you keep repeating the same mistakes, then solicitors will stop sending you work.
The solicitor may send you further evidence – more clinical records, X-rays, factual evidence – as the case progresses. This will all have to be evaluated and incorporated into your overall analysis, and it may mean you having to amend your report.
The other side may also put written questions to you, asking for clarification of your opinion(s).
At this stage, the solicitor might ask you to review another expert’s report: not only ones from the other side but also sometimes from experts working on your side.
The solicitor may ask questions about specific aspects of the report or s/he may just want you general comments. So where to begin?
Before undertaking any of the work discussed here, and indeed for any other additional pieces of work, confirm in writing with the solicitor that you will be paid and sent a new Terms of Business setting out the fee.
balanced and objective d o not be too excoriating with your assessment of the other side’s arguments. Attacking the other side’s expert because that is what you think you are being paid to do might be seen as hostile and even unprofessional. Criticise the report where criticism is justified, but do it in a balanced and objective way. And always support your arguments with good evidence.
Critically appraising a piece of written work is a skill that, as a clinician, you may not have had to develop. As an expert, this skill is essential. The tips in the box on the right will help you.
The ability to closely read and critically analyse a piece of written work will come with practice.
Make notes about the report on a separate sheet of paper or in a notebook, not on the report.
The solicitor will have already read the report and formed his or her own opinions and conclusions before sending it on to you.
Your critical explanation and interpretation should show you have carefully and critically read the report. Be prepared to say where you agree with the other side’s arguments or their conclusions.
Next issue: the case conference and the barrister
Adapted from The Effective and Efficient Clinical Negligence Expert Witness , by Michael R. Young, price £60 from Otmoor Publishing
special offer! Buy The Book and save £20
The book costs £60, but independent practitioner Today has secured discount of a third off for readers, so you pay only £40.
listen to the audio content which accompanies the book at this website: www.otmoorpublishing.com/audio. for more information and to order, email stephen.bonner@ otmoorpublishing.com, quoting reference ‘young/ipT’.
Tips for criTicising anoTher docTor’s reporT
read it through once without making any notes
read it again and make a note of any spelling or syntactical mistakes
closely examine the clinical issues under investigation
next, focus on the arguments. apply the peach (point, evidence, analysis, conclusion, highlight) method to see whether or not the points they raise are, in fact, supported by the evidence. is it the same evidence as you found, but a different interpretation? different evidence that you perhaps overlooked or missed altogether?
does the expert’s incorrect use of language introduce ambiguity into his or her arguments?
are there any non sequitur conclusions?
www.theportlandhospital.com/childrensdoc
Dear Reader,
subscribe to Get every issue aNd read us oNliNe
Subscribing to Independent Practitioner Today is the only way you can be sure you will see every issue and have the option of reading us online using our special page-turnable edition. Don’t risk missing out. Our personal subscription for doctors and managers is only £90 a year and £210 for organisations. But you can cut this to just £75 and £180 respectively if you pay by direct debit. So take advantage of this offer now for our unique business journal dedicated to supporting you in your private practice. We’re confident your subscription will repay itself many times over!
Editorial director
(See rates listed above)
I encose a cheque made payable to The Independent Practitioner Ltd
Please debit my Mastercard/Visa/ Amex/Diners
* indicates this item must be filled in Doctors, please give GMC No.
Instructions to your Bank or Building Society to pay Direct Debits
Name and full address of your bank/Building Society
Society
Name(s) of account holders
sort code
No
banks and building Societies may not accept direct debit instructions for some types of account
Banks and Building Societies may not accept Direct Debit instructions for some types of account To: The Manager
post your application (no postage required – UK only) to: independent practitioner today Subscriptions department, FreepoSt, po box 36, plymouth, pL1 1br
Please post to: Proact Ltd Subscriptions Dept., 12 Mary Seacole Road, The Millfields, PLYMOUTH PL1 3JY Or email to: jackie@marketingcentre.co.uk Or
phone: 01752 312140 Fax: 01752 313162 email: lisa@marketingcentre.co.uk or subscribe online at www.independent-practitioner-today.co.uk if you want to pay by card
payment dates change, The Independent Practitioner Limited will notify you 10 working days in advance of your account being debited or as otherwise agreed.
If an error is made by The Independent Practitioner Limited or your Bank or Building Society, you are guaranteed a full and immediate refund from your branch of the amount paid.
You can cancel a Direct Debit at any time, by writing to your
Do you rely on a key employee?
For all the financial benefits of running your own business as a doctor in private practice, there is one big potential risk that you could be exposed to.
a nd that is the business’s dependence on you or another member of staff like a practice manager or secretary as the main cog in the wheel.
You may have started small, but as your practice evolves and grows, this key person dependency may begin to hold you back and it can especially become a problem when it comes to cash flow.
To determine if your business
has ‘key person dependency’, ask yourself these two questions:
1 Is there one person solely responsible for any or every task/decision-making process in my practice?
2 If I were to take a couple of weeks – or more – out of my business, will it run as efficiently as it does with me or another per son there?
What is ‘key person dependency’?
Key person dependency is when you or one of your team members is solely responsible for something
Finance for the Independent Healthcare Sector
and there is no back-up plan for their absence.
This could mean the techie stuff, the accounts or something else and there is no one in the business to call upon to do the same skills.
So, if that key person disappears, your business would struggle, to say the least.
We have consultants join us where their practice and the billing and collection is in various
states of distress. a common problem is the practice has grown and the admin support has not kept up with the growth. Problems have also arisen where the secretary has become ill and no one was put in place to cover the billing and collection. The consultant managed to handle the day-to-day correspondence on his own for a period of time,
teach someone else in your business how to carry out the same tasks and, at the same time, create a systems manual detailing each step of the process
as well as the very important job of managing patients, even if there is a job-sharing arrangement in place.
So although it is good to train staff in the various skills required that they can cover, another solution is to identify outsourcers who are specifically trained in your key-person area.
This is becoming increasingly common with dictation, answering the phones or managing your billing and collection.
3 systematise affairs one of the best risk management tools is also the simplest. It is called having a system.
So this means getting your key person to systematise as they go along. Whatever they are doing, get them to make notes along the way and then record these notes in a central systems manual where everyone can access it. If you are a sole practitioner, then it makes good sense to start compiling this systems manual immediately.
but this still did not remove the problem.
Here are three risk management strategies to combat key person dependency in your practice:
1 systems and training
Teach someone else in your business how to carry out the same tasks and, at the same time, create a systems manual detailing each step of the process.
The manual will be useful for holiday leave or any other cover requirement or if your key person suddenly disappears.
This is also known as succession planning.
Succession planning is basically making sure you have a contingency plan if you or one of your key people should get run over by a bus tomorrow.
2 identify outsourcers
Depending on the size of your practice, you might not want to employ more than one or two members of staff to manage the admin side of the practice. and often the secretary(ies) will have many different roles to fulfill
Start by making a list of tasks you do in your practice this week, then make some time to go back and compose a ‘How To’ guide for each task – clearly stating where it fits into each process.
Then repeat this list on a weekly basis until you have recorded the details of every process and related task in your practice.
Store your systems manual where it can be accessed easily by a couple of trusted people around you – for example, your partner or parents. Then, if the situation ever does arise that requires you to take time out, any necessary handover process can be carried out efficiently.
r isk management is one of those processes a practice tends to ignore until it’s too late. So to avoid risk in your practice, make time this week to implement the above strategies to minimise your key person dependency. and remember, outsourcing is an option. Especially for the all important cash flow which is crucial to any business so it might be an idea to start there.
Gary Nials (right) is the managing director of Medical Billing and Collection
Break the code – not your firm
IS BIG BuSINESS, SO lET code buster! kEEP yOu IN ThE kNOW
Every month, the Clinical Coding and Schedule Development Group (CCSD) reviews its 2,000-plus procedure codes, and more than 3,000-plus diagnostic codes, that form the basis of private medical insurance. It is crucial for independent practitioners and their practices to know these codes, so they bill correctly. If they don’t, then it could cost them money
cHaNGes to Note tHis moNtH Specialties recently affected include bones, joints and connective tissue/tendon muscle (Code W); ear, nose and throat (Code D); urology (Code M); spine (Code V); interventional radiology (X r ); endoscopic gastro-intestinal tract procedures (Code H); skin (Code S); spine (Code a ) and vascular (Code l).
advanced notice of new codes and inactivations, with effect from 24 November 2016 are:
New codes
W4214 – Customised unicompartmental knee replacement; W4218 – Customised total prosthetic replacement of knee joint; W4216 – Customised bicompartmental knee replacement. One inactivation: W4211 – Customised knee arthroplasty.
There are seven narrative changes: W9170, D0702, W8300, W8380, W8600, W8620 and W8680 ; seven unacceptable combinations (also known as unbundling): M0910 with M2920, M0910 with M2930, M6533 and M4430, V4280 with 22026, V4280 with 22027, XR450 with H2502, H2502 with H5101; and one declined/withdrawn request for U1290 for a narrative change to ‘Invasive urodynamic assessment including pressure/ flow measurement using fluoro-
scopy’, as additional supporting information was not received from the requester.
a special note this month relates to an advanced notice where Bupa will no longer fund follow-up consultations carried out on the same day as planned procedures.
This will apply to the following codes with effect from 21 November 2016:
S0602 – Primary excision of malignant lesion – head and neck;
S0603 – Primary excision of malignant lesion – trunk and limbs; S0604 – Secondary excision of malignant lesion – head and neck; S0605 – Secondary excision of mal ignant lesion – trunk and limbs;
Please remember, however, that codes are not mandatory by insurers. In other words, the inclusion of procedure codes within the CCSD Schedule does not indicate the automatic agreement of individual insurers to provide benefit for this procedure.
You need to contact each insurer directly to find out whether benefit is provided.
Connect with GPs to plug your practice
Networking with colleagues needs to be done correctly to be successful. Mr Dev Lall (right) shares his tips
To succeed in private practice, I would argue that you need a constant stream of new patients coming in through the door of your clinic. The question, of course, is how to create that.
The time-honoured approach many consultants take is to network with those people most likely to send them patients –GPs. And the traditional way of doing that is by holding educational meetings.
This allows the consultant to meet GPs and offer latest updates
and insights on the conditions they treat. By getting to know their colleagues in primary care, the idea is that when patients request referral for private care, the GP will remember the consultant who held the meeting and gave the talk and refer the patient accordingly.
The trouble is that, unless planned and executed with care, holding educational meetings for GPs can turn into a poorly attended and rather awkward affair, failing both to generate
patients in the future but also creating a bad impression among GP colleagues along the way. We’ve all experienced meetings like that in the past.
so what is the best way of planning your event so it is enjoyable, well attended and most likely to generate private patients in the future?
Warning number one
Holding educational or networking meetings with GPs can be a great way to grow your private
practice. If you are warm and a ‘people person’ who enjoys meeting new people and networking, then this could work very well for you.
on the other hand, not everyone is like that. We don’t all want to speak in public or flit about a room full of strangers introducing ourselves, ‘pressing the flesh’ and making small talk.
If that’s you, then you might be better advised not to bother holding these types of events at all. You will be uncomfortable, your audience will likely be uncomfortable too and it could even be counterproductive. The good news, though, is that there are very many other ways you can grow your private practice – so save yourself the stress and try one or more of those instead.
Warning number two
My second warning is that while networking done well can be a good way to build a private prac-
tice, it is not a fast way to build a practice. Meetings such as these take time to generate patients, so networking should be only a part of your practice marketing strategy. Furthermore, you need to hold them regularly so you get to know people – one-off meetings are not enough.
Getting started
The first thing to remember is that GPs, like specialists, are under enormous pressure. They too are busy and short-staffed. They too have demanding and often difficult patients to look after – but without the back-up of a team of juniors. And remember that, unlike us, they are generalists without easy access to advice from other specialists.
This understanding is crucial to organising a successful event. It means you need to organise it well in advance. It means you need to choose a time and date that is ➱ p26
least likely to clash with their other commitments. so an evening may well be a better bet than in the middle of the day.
And as with any talk, you have got to make it relevant to your audience and of interest to them. s o, when planning your event, don’t make the mistake of just talking about latest developments in your field. Worse still, don’t just talk about rare and unusual cases either. Generally speaking, these things are only of interest to other experts in your specialty.
Far better to put yourself in the GPs’ shoes. What sorts of issues do they have to deal with daily? Where are their pain points? For example, a gastro-enterologist might talk about how to deal with the patient with non-organic or recurrent abdominal pain, a neurologist about the primary care management of simple headaches or how to differentiate sinister headaches from the benign.
Always ask yourself how you can help them deal with the clinical problems they regularly face. Not sure what those problems and issues might be? Then ask them. Asking GPs what they want you to talk about is a great way of building those relationships and improving attendance at the talk.
promoting your meeting
Whatever the topic you choose to talk about, it’s all going to be for naught if no one turns up, so you have to think about promoting it. Your hospital – private or NHs –may well be able to help with this, but you can’t just leave it to them, so get out there and plug the talk yourself.
You could easily email local GPs, write to them yourself or even create a press release and send that out to the local newspapers in the area. This will serve the dual purpose of encouraging GPs to attend as well as getting your
name out in the wider community as an expert in the field.
The talk itself
Practise, practise then practise some more. You should aim to make your presentation using a small stack of cards as an aide memoire only. under no circumstances read from a sheaf of notes, and avoid at all costs the infamous death by PowerPoint. secondly, you have got to avoid boring the pants off your audience. Inject a bit of humour if you can. Involve them, start a discussion perhaps. Make it lively, make it interesting.
Your goal is to have attendees learn something of real value and have a great time meeting you and other people there. That way they are more likely to attend future events you hold and to think of you favourably when patients request a private referral in your specialty.
Maximising the value of your presentation
I recommend that you have the event recorded on video. This need not be expensive and is definitely worthwhile.
You can then use the content in multiple ways; for example, you could send the dVd to attenders as a thank-you or send it to GPs who were unable to attend the first time. You could upload it to your website for people to see there or as a YouTube video linking back to your website. depending upon the topic and nature of the talk, you could even give the recording to patients or have the content transcribed for use elsewhere.
Follow up
It is critical you collect the contact details of everyone who attends your meeting – at the very least their name and email address, and ideally phone number as well.
Because, with all networking, the critical step is follow-up. I cannot overemphasise how important following up on those who attended your talk really is. It serves several purposes:
It provides valuable feedback. You can find out whether your talk really was of interest; was it useful, did it address their needs?
This matters because even if you were wide of the mark, it means next time you hold a meeting, you will do a much better job;
It reinforces your name, specialty and expertise in their minds;
It reminds them of you and your talk. GPs attend numerous meetings, both clinical and nonclinical and anything that helps you stand out is a good thing;
It helps to differentiate yourself from your colleagues – who largely won’t bother with follow-up at all. It shows you have a genuine interest in them and their needs.
I recommend you follow up a
week after your talk. Any later and your talk will have become a distant memory. Furthermore, you should follow up more than once. Leave it perhaps a further month or six weeks and call again to ask how they are getting on and if there is anything you can do for them. Then call again maybe another month down the line to invite them to your next talk. It might sound an odd thing to do, but remember what you are trying to achieve here: to form a relationship and to be ‘front of mind’ in your specialty.
Final thoughts
Marketing your private practice is all about building relationships, both with potential patients – so they go on to become actual patients – and with colleagues who can refer patients to you. Holding talks for GPs in the hope that they will send you private patients is something very
many consultants already do and, to many, the planning, promoting and following up I’ve described will seem strange and a lot of work.
And, yes, it is far more work than just putting a talk together about the latest advances in your field, letting your hospital promote the talk and hoping people come along. But hope is no way to run a private practice.
The more effort you put in, the better results you will get. You will have greater recognition and visibility among local GPs and, over time, you will get more private referrals.
If you’re a warm and fuzzy people person, educational or networking meetings can be a great and fun way to grow your private practice – if you’re willing to put in the effort.
Mr Dev Lall is an upper-GI surgeon who runs a specialist private practice consultancy www.privatepracticeexpert.co.uk
mEdicAl TAlEs
Doctor detested rich patients
TV doctor and full-time writer
Dr Michael O’Donnell (right) continues his series with the 1798 tale of the private surgeon who had a dislike of operating
John Abernethy, an eighteenth-century surgeon, was notorious for his brusqueness when dealing with wealthy patients. one of them, the duke of somewhere or other, was so angered by what he perceived as the surgeon’s rudeness that he barked: ‘I will make you eat your words, Sir,’ only for Abernethy to respond: ‘It will be of no use, for they will be sure to come up again.’
yet, despite his abrasive attitude to private patients, Abernethy was always kind to those under his care in charity hospitals. once when he was leaving to do a hospital round and a wealthy patient tried to detain him, he explained that the man would have to call another day. ‘Private patients, if they do not like me, can go elsewhere; but the poor devils in the hospital I am bound to take care of.’
h is selective brusqueness was rarely calculated, more often an instinctive reaction to pomposity. When he was after a job as surgeon at St b artholomew’s h ospital, he called on each of the
governors in turn to make himself known to them.
During his visit to one palatial home, the governor, a wealthy grocer, said rather loftily: ‘I presume you are after my vote at this important point in your career.’
‘no, I am not,’ said Abernethy. ‘I want a pennyworth of figs. Look sharp and wrap them up – I want to be off.’
Abernethy had two great dislikes. the first, strange for a man
celebrated as ‘a daring surgeon’, was of operating. An assistant described how he once found him ‘in the retiring room, after a severe operation, with big tears in his eyes, lamenting the possible failure of what he had just been compelled to do by dire necessity and surgical rule’.
his second great dislike was of what he called ‘idle chatter’. one evening, after visiting a woman he’d been treating for some weeks, he spoke to the daughter who’d been nursing her. ‘I have witnessed your devotion and kindness to your mother. I am in need of a wife and I think you are the very person who would suit me.
‘My time is incessantly occupied, and I have therefore no leisure for courting. reflect upon this matter until Monday.’ She did and they got married. t heir subsequent harmonious relationship confirmed he had made a shrewd diagnosis.
John Abernethy earned a place in countless anthologies on the afternoon he told a melancholic
‘Go and see the clown Grimaldi,’ he said, only for the patient to reply: ‘I am Grimaldi’
Advertisers in Independent Practitioner
Today are attracted by our ability to reach 14,000 doctors with a private practice and their managers/administrators every month in print and online. Let your advert be seen 24 hours a day, every day of the year when you advertise with us.
Email Margaret Floate at margifloate@btinternet.com or phone her on 01483 824094 www.independent-practitioner-today.co.uk
patient that he needed to get out more and learn to laugh. ‘Go and see the clown Grimaldi,’ he said, only for the patient to reply, ‘I am Grimaldi.’
he earns a place in this collection of strange cases with his account of the ideal consultation for a hater of ‘idle chatter’.
A young woman entered his consulting room and, without a word, held out an injured finger for examination. Abernethy dressed the wound in silence.
the woman returned a few days later.
‘better?’ asked Abernethy.
‘better,’ said the patient.
Subsequent visits were conducted in much the same way. on her last visit, the woman held out her finger, now healed.
‘Well?’ asked Abernethy.
‘Well,’ she replied.
‘Upon my word, Madam,’ said Abernethy, ‘you are the most rational woman I have ever met.’
Medicine’s Strangest Cases, recommended price £7.99, ISBN 9781910232941. Published by Portico, an imprint of Pavilion Books
Independent Practitioner Today is your vital resource!
To see previous editions as well as the articles featured in this month’s journal, sign up today to become a subscriber.
Subscriptions cost only £75 if you use direct debit for our annual ten issues a year – and you will then have access to a library of useful articles to help you. You will find many of the answers to the questions you are asking are just waiting to be read!
Fully serviced cQc-registered consulting rooms
Air conditioned
Full nurse And secretAriAl suPPort
UK Top 20 accountants specialising in the healthcare sector
National firm of the Year 2013
AISMA member (Maidstone and Leicester offices) 12 offices including London City
Tax Structures for Hospital Consultants - dispelling myths
Surgeon groups and consortia
• GP Practices including mergers and federations
Solvent liquidations (for companies at the end of their lives)
For more information please contact:
South East
James Gransby FCA
E: james.gransby@mhllp.co.uk
T: +44 (0)1622 754033
M: +44 (0)7712321899
East Midlands
Robert Nelson DChA FCA
E: robert.nelson@mhllp.co.uk
T: +44 (0)1162 894289
M: +44 (0)7814009160
General email: healthcare@mhllp.co.uk www.macintyrehudson.co.uk
PUTTing ThE cAsE FoR yoUR
PPU beds hurt, NHS
Philip Housden (right) shows how best to build on strong relationships between the consultant and management to ensure the private patient unit (PPU) delivers commercial and service gains for the NHS trust
help, not finances
If your NHS trust has not yet begun to hit the buffers of bed pressures, then it soon will. It may be late autumn outside, but inside it’s likely to be winter.
o ne of the major operational challenges for a trust in supporting a PPu is to protect access to a number of beds.
‘Impossible to do,’ many say, or I often hear said: ‘That’s oK until things get difficult.’
But what I have learned is that it really is possible to find a win-win that supports the trust operational objectives while also enabling a PPu to flourish. The result is beneficial not just financially but in many other ways too.
PROBLEMS WITH THE TAX MAN?
How can this be true? Is there not an almost inexhaustible demand for the finite supply of bed capacity?
My experience when working with many trusts up and down the country suggests that there are three reasons to identify and protect private beds.
Each of these initiatives justifies a PPu and, in turn, reduces NHS bed pressures. But, taken together, they deliver a strong case for identifying and holding onto private patient bed capacity in every NHS trust.
The first is that, as any surgeon will confirm, there are limits to the range of treatments and the ➱ p32
HMRC tax investigations and disputes create difficult and stressful times.
As an award winning firm of tax experts, our highly experienced partners specialise in resolving problems relating to tax investigations and disputes with HMRC.
To find out, in confidence, how we can help call 0800 734 3333.
‘Here to help. Not to judge.’
level of clinical risk that the typical private sector hospitals will treat.
Patients with complex needs, co-morbidities and the rare and the difficult conditions are often inappropriate for independent hospitals.
Limited range of course, there are some exceptions, but generally a non-metropolitan private hospital does not have critical care cover, is some distance away from the local NHS trust and is really set up for fast throughput of a limited range of procedures and treatments.
The patient safety risk is assessed by the clinician and increasingly I see a trend for surgeons and anaesthetists feeling more comfortable when they have the 24/7 backing of the trust infrastructure.
So, what happens if the local trust does not have a PPu? In this situation, the patients, insured or not, most probably default to the NHS.
of course, holding private medical insurance does not impact on the eligibility of the patient to access the NHS, but when there is a private bed available on the NHS trust site, then this is an option that the patient and their surgeon can choose.
Making that choice both saves the NHS costs while also increasing revenue for re-investment in core NHS services. of course, not
making that choice achieves the reverse.
The second – and in a way linked – area relates again to insured patients and their choice of treatment, but this time is better understood when thinking about the ‘hospital front door’.
Average take-up of private medical insurance remains at just over 10% of the population and across most of England. At least, this is a typical figure – with some ‘hot spot’ areas considerably higher and others, of course, a lot lower.
This is despite the falls in individual subscription since the last recession and the further impact of recent insurance tax increases. So, that means that one in ten of the catchment of most trusts holds insurance and, in addition of course, many more people are prepared to consider the selffunding of private care.
often these patients do not know they can use their insurance, do not know how to use it or are not even sure they can use it if they attend the nHs
What this means is that a significant proportion of patients attending the trust actually have insurance or would consider paying for treatment.
I don’t mean sometimes or some days more than others or perhaps. I mean every day, in every trust, patients arrive for both planned and unplanned treatment and care who are insured.
ignorant of insurance often these patients do not know they can use their insurance, do not know how to use it or are not even sure they can use it if they attend the NHS.
How do we know this happens? Surveys carried out with consultants in several trusts have repeatedly evidenced that it is a regular occurrence for that clinician to
i believe in PPus
Following my 2014 independent Practitioner today series on PPus, i have continued to work with many nHs trusts to help develop and grow profitable private patient services.
this has enabled a real insight into the day-to-day challenges of delivering a private service within a public sector environment.
i am passionate about how PPus can be part of the answer to the strategic and financial challenges that the nHs faces and so, in these articles, i plan to share learned, practical insights and also comment on how PPus can best respond to changing policy issues and healthcare current affairs.
the net result is that not accessing a patient’s insurance cover . . . represents lost potential income to the trust
see patients on the NHS with insurance, but often have no way of admitting them privately.
The overall net result is that not accessing a patient’s insurance cover means insurers achieve higher profit margins while the same represents lost potential income to the trust.
If a trust has a PP u and those beds are protected so they can ‘take’ admissions, then asking patients at registration about their insurance status will increase private patient activity.
Every patient taken out of the four-hour queue is one less potential ‘breacher’, and every patient admitted to the PP u from the ‘front door’ would have been admitted to the trust anyway. So when a trust holds protected PPu beds, it really does not reduce NHS capacity. Instead, what is achieved is some demand is shifted back to the right funder and away from the NHS cost base.
‘Topping up’
But what about managing the inevitable peaks and troughs of patient activity? How can empty PPu beds be justified on a ‘just-incase’ basis?
The answer lies in the third approach to achieve the best management of a successful PPu Through forward planning of admissions and close working relationships with the rest of the trust operational teams, it is perfectly possible to aim for the PPu occupancy to be ‘topped-up’ with NHS patients ‘pulled-in’ to the ward, and to achieve close to 100% occupancy.
next time: Thoughts on how PPUs can best create a high-quality patient experience without losing the very best that an nhs trust campus provides for private patients
This works especially well with identified pathways for short-stay, high-turnover patients. Again, this maximises the benefit to the NHS while still enabling the benefits of private care to productively and symbiotically co-exist within the heart of the trust. opening or defending a PPu is not part of the problem of bed capacity pressures of the trust – it is a key part of the solution to those pressures. It is time for NHS PPus to become a full part of winter bed planning for the NHS.
Philip Housden is a director of Housden Group, a management consultancy specialising in commercial support in the healthcare sector
Shortfalls: a sign of financial virility or financial folly? Ray Stanbridge gives his views on one of the biggest practical problems facing consultants in private practice
Shortfalls may be cause of downfalls
The righT of any professional to set his or her fees at the rate considered appropriate has long been an accepted practice.
Patients and customers have the right to accept the fee levels quoted or to shop around. h owever, the commonly accepted practice has obviously been challenged by insurers in the medical sector in a number of ways.
Firstly, newly appointed con -
sultants have to accept, by and large, fee levels proposed by insurers. i f they do not accept them, then they are denied registration rights.
Sadly, the fee levels are pretty much standardised across the whole country even though there is very strong evidence that it costs much more to practise in London and the South-east.
Secondly, pressures are sometimes put on those consultants
who seek to charge outside of the insurers’ advisory ranges. Such pressure can include suspension, threat of audit, moral pressure –
‘Your fees are much higher than most of your contemporaries’ –and diversion of work.
Worrying factors
All of these factors are worrying to an economist interested in ordinary free markets. it is a pity that the Competition and Market
Authority (CMA) has not fully considered the strong argument put forward by the Federation of independent Practitioner Organis ations (F i PO) in defence of an open market for consultant fees. however, we are where we are, and insurers still finance a significant proportion of the private sector medical market.
Consultants, therefore, have to manage insurers’ behaviour as best they can, and deal with issues
appropriately. it is here that the micro-economics may differ significantly from the macro-economics, in so far as they affect an individual’s taxable profit.
Some consultants continue to charge the fees they believe are justifiable. This then creates the problem of shortfalls in payment, as insurers frequently will not meet the full cost of treatment. it goes without saying that consultants who do wish to charge their own pre-determined level of fees should advise patients in writing in advance of treatment.
Enforceable contract
There are some consultants who make things crystal clear to patients with excellent information sheets. i f they do, and patients accept the terms, they have a legal contract which is enforceable.
if they have not advised patients appropriately, the validity of any contract may be in doubt and patients may not have to pay any shortfalls. if, as a consultant, you are charging outside of insurer cover rates, then this clear documentation is essential.
But what happens when consultants do create a situation where shortfalls are frequent? There are often a number of consequences.
Firstly, there is a potential problem of payment. Patients – generally wrongly – automatically assume they are fully covered and are reluctant to pay what are generally small shortfall fees.
Secondly, if a consultant decides to pursue a claim, there is an administrative cost in pursuing it – several letters may be required, for example. Phone calls may also be necessary.
Despite such debt collection pressure, some patients still do not pay. At this point, a consultant has to consider taking the matter to a small claims court. i f this happens, there are County Court fees to pay up front. Currently, these are £35 for a paper form fee for a claim up to £300 and £25 for an online claim form.
Again, the issue of a writ sometimes works. in others, it does not and a consultant may be compelled to attend court.
At the very least, this can be
Taking patients to court can be extremely timeconsuming and the real opportunity cost to the consultant will far exceed the potential recovery benefit
extremely time-consuming and the real opportunity cost to the consultant will far exceed the potential recovery benefit.
i n some cases, the judge may rule that there is no formal contract in place and may rule in favour of a defendant. Yet more time lost.
Thirdly, what a large number of consultants seem to do in the event of unpaid shortfalls is effectively to adopt a ‘do nothing’ strategy.
This can create further tax problems. hM revenue and Customs has now adopted a policy of differentiating debtors between ‘slow payers’ and ‘bad debts’.
Bad debts – where, in the opinion of the consultant, the debt is never likely to be paid – is deductible. But claims cannot be made for slow payers.
ironically, there have been cases where h M r C has not allowed unpaid shortfall claims because they have not been pursued despite the costs. i n such a scenario, a consultant has the worst of all worlds:
Unpaid bills;
Disgruntled patients;
Possibly upset insurers;
A tax bill.
Additional costs
Finally, there is the question of additional accounting costs as accountants struggle through schedules of relatively small unpaid items.
A straw poll – non-statistical –suggests that for those consultants who have a higher shortfall rate as a result of their fee policy, accounting costs may increase by £200-£300 a year over those who stick to insurance company rates.
While obviously the exception proves the rule, evidence suggests that for many consultants who create a large number of small shortfalls, the administrative costs of chasing them are actually greater than the potential benefit.
Some secretaries are spending 10% of their time chasing up shortfalls and, in many cases, this is just not effective.
Conversations i have had with some insurers suggest that they face similar problems.
One of the major causes of patient complaints, we understand, is shortfalls. Obviously,
For those consultants who have a higher shortfall rate as a result of their fee policy, accounting costs may increase by £200-£300 a year over those who stick to insurance company rates
insurers have to staff up to deal with these problems, which, in turn, leads to higher premiums. The true market cost of shortfalls can therefore really be significant.
so what can consultants do? Firstly, if they wish to charge their own fee levels, they should ensure that their patient communication is perfect to avoid problems described above.
Secondly, as an industry – and this can only be undertaken by representative bodies such as FiPO and the independent Doctors Federation (iDF) – ongoing dialogue should continue with insurers over the problems faced.
There is a strong case, for example, for a London/South-east premium on fees, as costs are higher. And there is also a strong economic case for higher fees where there is a preponderance of difficult second-opinion cases.
There is also a case to be argued whereby, as with home, motor and other insurance protection, insurers make it clear to their members that they will only fund for a certain level and will follow a policy of ‘averaging’. Some loose insurer or broker promises do not help in this respect.
Finally, if consultants really do not like what they perceive to be blacklists placed on their business by insurers, there is the self-pay, NhS and overseas markets to pursue. As mentioned above, insurers only currently account for about 50% of the market spend.
While the macro-economics are barely evidence of a competitive market system, on a micro level there can be real net cost to a consultant in charging fees outside insurers’ recommendations.
in my view, individuals on their own are fairly powerless to combat insurers. Their professional bodies, appropriately prepared, can make a difference to the macro-environment.
This, to my mind, is the longterm solution to a shortfall problem, which is costly to deal with, frustrating and a major source of angst to all.
Ray Stanbridge (left) is a partner with Stanbridge Associates, an accountancy, finance and tax advisory service specialising in the medical profession
LEgAL
The balancing act of starting a business
New legal pitfalls are lining up for doctor entrepreneurs. Jamie Foster and Simon Lee give an introduction to a vital new series for Independent Practitioner Today aimed at ensuring you don’t trip up
IT WAs ever thus, but the speed of change in recent years as a result of technological advances has been immense.
Just by way of example, around the turn of the century – not that long ago, at least in our eyes –having one internet-connected computer on each floor of the office and barely using email was normal.
That seems almost incomprehensible by current standards and children these days probably wouldn’t believe us if we told them.
In the same way, we are seeing a shift in the way our clients want to set up new healthcare businesses.
While this isn’t by any means limited to doctors, we are increasingly seeing doctors and other medical practitioners who approach us for advice, wanting to engage in private business in a different way.
With increasing use of smart phones and apps in recent years, doctors are among the innovators. In many ways, the technology is liberating, allowing doctors both to work and to win work in new ways.
Other recent events, such as the junior doctors’ contract challenges, have made some think that they would prefer to use their medical skills outside the traditional routes.
However, ‘the law is an ass’ and there can be legal pitfalls for those who are not wary.
what’s to come
For this reason, within this article – the first of an important new series – we are simply highlighting some of the legal issues that can arise in the new world of technology innovation and the ‘gig economy’ to help those who are interested in reaping the potential rewards through development of new healthcare businesses.
We hope these initial observations will set the scene for what is to follow in future editions, when each of these scenarios will be analysed in greater depth:
☞ In resourcing a new business, what is the line between offering someone work when they want it and employing them, with all the obligations that entails? The recent Employment Tribunal ruling against Uber highlights the need for clarity on this complex area of law.
☞ One of the first things you will do will be to set up a website for the new business, but are you clear about whether you own and control the website?
This can be something of a minefield, but there are
some simple tips that can protect you as you develop the website.
☞ How can you possibly guard your hard-earned intellectual property in the age of Google and file-sharing? Protecting your ideas is an important way of protecting both your brand and your earning power from it.
☞ What on earth does the Consumer Rights Act have to do with doctors? The act covers a wide range of areas, including digital services, and it is important to be aware of what can and cannot go in your contracts.
☞ Were you aware that certain apps – such as those designed to help a person monitor or control their health – might count as ‘medical devices’ and therefore need to comply with the Medical Devices Regulations?
This is a technical area, but clearly it is essential to stay on the right side of the law.
☞ Did you realise that by taking
Did you realise that by taking advantage of cloud computing, you might be in breach of the Data Protection Act?
advantage of cloud computing, you might be in breach of the Data Protection Act?
These days, computer servers can be almost anywhere and anything based outside the European Economic Area might land you in hot water, so understanding data law in the digital age is key.
☞ How do you develop online terms and conditions, and how do they differ for websites and apps? Being aware of issues such as privacy and cookies policies is essential if you’re running an online business.
☞ Can you prescribe medication online or via an app and what are the pitfalls? This is a complex area, so it’s as well to know what’s what.
The kinds of legal issues set out above are in addition to the usual issues one has to consider when starting any new business, which include:
What is the right legal structure?
How do you develop online terms and conditions, and how do they differ for websites and apps?
What are appropriate governance structures?
What is needed to get contracts in place with customers, staff and suppliers alike?
Of course, there are also nonlegal matters too, such as:
Crunching the numbers on the business plan,
Mulling over insurance policies;
Getting creative with branding and logos.
However, in this series, we will be concentrating on the issues which are more novel – and our colleagues with specialisms in the areas identified above will be sharing their experiences to help get your new businesses from the drawing board to the board room without falling foul of the law.
Jamie Foster (far left) is a partner and Simon Lee (left) an associate in the commercial team at Hempsons Solicitors
Free legal advice for Independent Practitioner Today readers IPT
Independent Practitioner Today has joined forces with leading niche healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
call Hempsons on 020 7839 0278 between 9am and 5pm monday to Friday for your ten minutes’ of free legal advice.
Advice is available on: Business structures: Commercial contracts: Ian Hempseed Faisal Dhalla
Disputes: Hilary King
Fiona McLellan Lynne Abbess
Some returns aren’t absolutely fabulous
The combinaT ion of shortterm market uncertainty, human nature and an immediately attractive-sounding moniker is a marketing man’s dream.
i n the past, the investment industry has been masterful at constructing and selling such products, not least ‘absolute return’ products.
We know that markets are always uncertain and that shortterm market losses are a normal part of investing. a nd we also know from behavioural finance research that human beings feel twice as much pain from losses than they feel pleasure from upside gains.
i n some older investors, this emotional asymmetry can be even more pronounced. This deep-seated behavioural trait has a tendency to result in investors overpaying for both downside protection, such as insurance, and gambling-like activities.
The promise of ‘absolute returns’ on your investments is easy to make but hard to keep. Patrick Convey explains why all is not what it seems with such a strategy
it is perhaps worth remembering that a 35-year-old man who buys a lottery ticket on a monday has more chance of dying during the week than winning the lottery. Products that put the two together – such as structured products and absolute return funds – tend to sell like expensive hot cakes.
There are no risk-free returns to be conveniently collected above the so-called ‘risk-free rate of return’ delivered by cash – and even that bears inflation risk and the risk of the bank failing. a ny such returns would be quickly pocketed by the vast number of extremely bright and hardworking professional investors.
so what are ‘absolute return’ strategies?
a bsolute return funds employ active management strategies that seek to deliver positive (absolute) returns in any market conditions – up, down or sideways.
by way of background, in June 2016, net inflow into these funds was £221m, whereas equity funds suffered withdrawals of around £2.8bn in the month. in eight out of the 12 months to July 2016, the sector had the highest monthly net retail inflows in response to the poor start to the year by equity markets and brexit worries.
The i nvestment a ssociation ( ia ), which represents the fund management industry in the UK, sets a three-year horizon over which returns should be expected to always be positive in order to qualify for its absolute return badge.
however, it is worth noting that the ia itself states that it ‘recognises that there is a wide expectation among consumers and advisers that funds in the Targeted absolute Return sector will aim to produce positive returns after 12-month periods’.
Yet the reality of being able to deliver on this promise is far from convincing because:
Strategies are varied, complex and hard to compare;
Fees are high, relative to sensible alternatives;
correlations to underlying assets – such as equities and bonds – are higher than might be expected.
Reviewing short-term outcomes
We do not normally review shortterm performance data, as it constitutes noise. but, in this case, we wanted to do so to make a point: market timing is exceptionally difficult, as markets move on the release of new information, which, by definition, is random.
This year (2016) started badly, with equity market falls driven by panic over the perceived slowdown of the c hinese economy. The Times, for example, had this scaremongering headline on 16 January: ‘ m arkets suffer their worst start to the year since Great Depression’.
From December 2015 to a pril 2016, Targeted a bsolute Return funds were the best-selling funds
Trying
to respond to past market events or to second-guess the market’s response to future events is extremely difficult
of any ia sector. b y m arch, the headlines had changed; an example from USA Today on 6 m arch read as follows: ‘Stock storyline shifts from “worst start to year” to “not too bad…”.’
Prior to the brexit referendum in the UK, doom and gloom returned and subsequent to the vote, according to The Guardian on 24 June: ‘brexit panic wipes $2 trillion off world markets’.
it then changed its sentiment a month later with the headline on 11 July: ‘US stock market closes at record high, rebounding from losses after brexit vote’.
The point to be made is that trying to respond to past market events or to second-guess the market’s response to future events is extremely difficult and investors risk being whip-sawed by market noise and media hyperbole.
an investor with a long investment horizon can afford and should be determined to stay the course and to simply remain invested; rebalancing his or her portfolio back to its original strategy when needed, thereby avoiding needless timing decisions and considerable transaction costs.
With all the freedom of absolute return funds comes the dangers of excess activity and emotionallydriven decisions.
Where are the economies of scale?
a quick analysis of the funds in the ia sector reveals that the average o ngoing c harges Figure ( oc F) of these funds is around 1.2% a year. o ne of the major constituents of the sector has assets of over £26bn. i ts lowest cost share class has an oc F of 0.72% and, on this basis, the fund management company extracts around £190m of investors’ money for itself each year. at this size of fund, some of the economies of scale should be passed to investors. They are not. as we know in investing, you get what you don’t pay for.
Academic research
a recent piece of research on absolute return funds in the US reveals that most active managers add nothing to performance over and above the known market returns. The research also showed that
As ever, the siren songs of the investment industry can draw the naïve onto the rocks
equity-related strategies exhibit significant exposure to the equity markets and bond strategies exhibit significant exposure to bond markets, despite the freedom and flexibility to mitigate such exposures. a s such, losses should be expected from these portfolios when markets get tough.
Fees were high, too, with expense ratios ranging from 1% to 2% depending on the strategy.
The long and short of the research is that the absolute return fund industry has not really covered itself in glory. There may be a small number of funds managed with truly exceptional skill. The trouble lies in identifying them, which requires long track records and the ability to distinguish between skill and luck.
as ever, the siren songs of the investment industry can draw the naïve onto the rocks. There is little evidence at the sector level that suggests that absolute return funds really do add something different to traditional portfolios. With exposure to market risks –and thus potential losses – high fees and esoteric and complex strategies, most longer-term investors are better off sticking with their traditional, systematically managed portfolios.
Short-term market losses are part and parcel of investing and are not uncommon. Those with the fortitude to stay invested and stay the course should be well rewarded. Patience, discipline and fortitude are the values that lead to success in this game.
Patrick Convey (left) is technical director of Cavendish Medical, specialist financial planners helping senior consultants in private practice and the NHS.
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
• how to start in private practice
• how to maximise private practice income
• computer software
An independent firm offering one to one meetings anywhere in the UK giving advice and help with:
• tax and financial advice re: car purchases
• how to start in private practice
• ways to reduce tax payments
• computer software
• how to maximise private practice income
• setting up in Chambers/Groups
• ways to reduce tax payments
• limited companies and LLP’s
• setting up in Chambers/Groups
• financial planning
• record keeping
• limited companies and LLP’s
• tax and financial advice re: car purchases
• pensions: NHS, personal and employee schemes
• pensions: NHS, personal and employee schemes
• purchase of consulting rooms and surgeries
• inheritance tax and capital gains tax planning
• purchase of consulting rooms and surgeries
• VAT
• inheritance tax and capital gains tax planning
For more information please contact us by:
• VAT
Wilmslow
For more information please contact us by:
Phone: 01625 527351
Wilmslow
Fax: 01625 539315 Harley Street
Phone: 01625 527351
Phone: 020 7307 8759
Harley Street
Fax: 01625 539315
Phone: 020 7307 8759
Email: info@sandisoneasson.co.uk
Fax: 01625 539315
Fax: 01625 539315
Website: www.sandisoneasson.co.uk
Email: info@sandisoneasson.co.uk
Website: www.sandisoneasson.co.uk
Answers to your ethical puzzles
Dilemma 1 What do I do with testy colleague?
QI am a consultant surgeon and have become increasingly concerned about the behaviour of a consultant gastroenterology colleague of mine, whom I work with regularly.
She seems to be becoming increasingly irritable and somewhat distracted.
I’ve also overheard endoscopy staff commenting on her unpredictability and she recently made a prescribing error for a patient whom we were both treating under a shared-care arrangement. What should I do?
AAs a colleague and a clinician, you have the dual concerns of the welfare of your colleague and the safety of patients. The GMC reminds us in Good Medical Practice that we must support colleagues who have problems with their health, but we must put patient safety first at all times.1
There may be variability in each individual’s performance from time to time and it can be difficult to know when concerns should be raised. Irritability and errors may be the first signs of stress or other health concerns.
Encouraging your colleague to get help and support at this early stage could help to prevent matters from deteriorating. It could help to protect them from disciplinary or regulatory investigation and to prevent patients from coming to harm.
The concerns about this colleague’s performance appear to be progressive and other individuals have also noted a difference in her behaviour. There has also been a patient incident.
The threshold for raising concerns is relatively low. The GMC indicates that you must ask for advice from a colleague or from your medical defence organisation if you have concerns that a colleague may not be fit to practise and may be putting patients at risk.
As a friend and a colleague, you might wish to discuss your concerns with her first and explore any reasons she may have for the change in her behaviour and the clinical error.
If appropriate, you should encourage her to seek support either from her own GP or occupational health department, should that facility be available. You may wish to help her reflect on the prescribing error and put systems in place to prevent a recurrence.
Each organisation will have its own policy on how concerns should be raised and you should follow that policy.
In the case of clinical concerns, these matters should usually be discussed with the clinical or medical director. You should keep a record of what steps you have taken to deal with the matter.
Dilemma 2
She bars
I am a cosmetic surgeon working in a private clinic and a 37-year-old woman recently self-referred requesting an abdominoplasty. She attended the clinic unaccompanied. When taking her history, the patient indicated that she suffers from asthma so severe that she has required admission to intensive care in the past with a period of ventilation.
I’m concerned about the sever-
Ultimately, if you believe that the intervention will not be of overall benefit to the patient or that you cannot adequately assess the potential risks of the procedure without further discussion with her GP, you must discuss this with the patient and explain your reasoning.
If, after that discussion, you still believe that the intervention will not be of benefit, you must not go ahead with the treatment. You should document the discussion carefully in the notes and respect the patient’s right to seek a second opinion.
References
1. Paragraph 43, Good Medical Practice, www.gmc-uk.org/guidance/good_medical_practice/teaching_training.asp
Dr Nicola Lennard is a medico-legal adviser at the MDU
ity of her asthma and the potential for complications to arise following a general anaesthetic. I told her I would like to liaise with her GP and, if necessary, her respiratory physician, but she has objected. What should I do?
AYou have a duty to give clear and accurate information to the patient about the risks of the proposed intervention in a manner that the patient can understand.
This information should be individualised for the patient and should include her potential risk of side-effects, complications and outcome of the procedure she can expect.
You also have a duty to talk about the potential adverse physical and psychological impact of the intervention going wrong or failing to meet the patient’s expectations.
You should also explore the other treatment options that are available to the patient, including less invasive options and noninterventional methods.
In order to assess this patient’s individual risk, you will need to consider the patient’s general health and any other circumstances that may affect the likelihood of an adverse outcome occurring.
These could include the environment where the procedure is taking place and any trigger factors that might be relevant to the patient’s asthma, as well as the availability of additional medical support such as facilities for intensive care, should they be required.
Given the potentially significant nature of this patient’s comorbidity, you would want to seek further information regarding her asthma and its current management.
The GMC’s guidance on cosmetic interventions indicates that you must consider whether it is necessary to consult the patient’s GP to discuss the benefits and risks of surgery. However, the guidance indicates that you should seek the patient’s consent prior to consulting with their GP.
As the patient has declined consent for you to have this discussion, you will need to explore with her the reasons behind this as well as explaining your reasons for wanting to have such a discussion.
If your patient remains determined that she does not want you to contact her GP, this information must be recorded in the medical record and you will then need to consider how this affects the balance of risk of the procedure.
Upright Positional MRI
• Completely open scanner that is well tolerated by claustrophobic patients
• Weight-bearing scans for spine and joints enable a more precise diagnosis
• Patients who are large or cannot lie down can be accommodated
For more information go online at: www.mri-london.com or call 020 7370 6003 Medserena Upright MRI Centre 114a Cromwell Road, Kensington, London, SW7 4ES
Protect your pension
Some doctors reading this could be saving up to £125,000 in tax – so there is no time to waste if you could be eligible. Ian Tongue reports
Much is being said about pension protection at the moment and the clock may be ticking for private consultants and GPs to save a fortune in tax by having their circumstances reviewed.
As always, each person is in a different position and it is important that you obtain professional advice from your independent financial adviser and accountant before applying for pension protection.
What is it all about?
Despite a push many years ago by the Government to encourage you
to save large sums in a pension scheme, austerity and general meddling around pensions has seen successive back-tracking on this policy.
The lifetime allowance is the maximum your pension pots can reach before attracting a tax charge. i t was as high as £1.8m, but it fell to £1.5m in 2012, then £1.25m in 2014 and is now £1m from 6 April 2016.
To be fair, at each of these reduction points, pension protection has been available for those whose pension pot(s) exceed the new lower threshold.
if you are entitled to a form of protection and do not apply for it, you could be throwing away significant amounts of your hardearned pension.
What are the different types?
There have been many different types of protection in the past and several cannot be applied for now.
The most common protection that a doctor is likely to have if they are still paying into the Nhs Pension scheme – or any other – is enhanced protection.
This is complicated and through earnings increases from the date
applied for up to retirement, it is likely that a consultant will lose this protection. Therefore, it is important to consider whether you are eligible for alternative protections that can sit alongside what you may already have.
Fixed protection
Fixed protection was available in 2012, 2014 and 2016 and protected your lifetime allowance at the appropriate level before reduction – that is to say, £1.8m, £1.5m and £1.25m respectively. crucially, for those applying for this protection, they effectively
pension from tax
This allows you to retain a bespoke lifetime allowance based on the value of your pension as at that date.
For example, if your pension fund(s) were worth £1.35m as at 5 April 2014, you would lock in your lifetime allowance at this level.
With individual protection, you are able to continue contributing into pension schemes but will face a lifetime allowance charge at 25% of the excess over your individual lifetime allowance.
A good yardstick for your annual N hs Pension accrued to date is your ‘total reward statement’ which shows a snapshot of your pension accrued.
it is important to note the date on which the statement is valuing your annual pension, as there is often a significant time lag for the latest information to be received and processed by Nhs Pensions.
Nhs Pensions has set up a dedicated website to obtain your total reward statement which is www. totalrewardstatements.nhs.uk.
Once a high-level review has been performed and eligibility considered, you will need to apply to Nhs Pensions requesting a valuation of your pension as at 5 April 2014 or 5 April 2016.
the time of writing) and therefore you will need to prepare the application yourself, but with some help from your adviser. At the time of writing, there is no portal for agents, but hopefully this will be rectified in the months to come.
How much could this save me?
if you are eligible for individual protection 2014 and the current level stays at £1m, you could be saving up to £125,000 in tax, so there is no time to waste if you could be eligible.
I have already retired. Should I consider individual protection?
For individual protection 2014, you only have until 5 April 2017 to apply. As the information can take some time to obtain, you have no time to lose if you are eligible for this protection
Individual protection 2016
This protection is available for those individuals who had a pension fund(s) value of between £1m and £1.25m as at 5 April 2016.
This form is called an AW295 and is available on Nhs Pensions website. i t is highly recommended that this process takes place through an adviser to ensure the correct valuation is requested.
Due to the volume of requests, Nhs Pensions has recently started introducing a fee of £120 for the valuation.
Definitely! i f you have retired since 6 April 2014 and have not retained enhanced protection or another form of protection, speak with your individual financial adviser or accountant without delay, as you can still apply for the protection despite being in receipt of pension benefits.
needed to cease contributing to all pension schemes by the 5 April of the appropriate year.
As you can no longer apply for this protection, i will not consider this further within this article. however, if you hold any form of fixed protection, you should consider whether you still meet the criteria to retain this fixed protection. This is because, should your fixed protection be lost, individual protection may be available. speak to your adviser if you are in this position.
Individual protection
individual protection is split into two types and these are a hot topic of conversation for medics at present:
individual protection 2014;
individual protection 2016.
Individual protection
2014
This protection is available for those individuals who had a pension fund(s) value of between £1.25m and £1.5m as at 5 April 2014.
Again, this protection allows you to retain a bespoke lifetime allowance based on the value of your pension as at that date. As with individual protection 2014, you are able to continue contributing into pension schemes but will face a lifetime allowance charge.
Time limits to application –tick tock!
For individual protection 2014, you only have until 5 April 2017 to apply. As the information can take some time to obtain, you have no time to lose if you are eligible for this protection. Your independent financial adviser or accountant should be able to advise you further.
individual protection 2016 does not carry a time limit and therefore the pressure is off, but it is always good to get matters reviewed at the earliest opportunity to ensure that things are dealt with and don’t get forgotten later on.
Valuation of pensions
First, you will need to decide on which of the individual protections apply to you and you should seek advice on this.
For anyone with personal pensions, these will also need to be valued at 5 April 2014 or 5 April 2016 as appropriate.
Applying for the protection
Once the eligibility has been confirmed and valuations obtained, you need to apply through h MR c ’s dedicated pension protection portal.
u nlike most administration with hMRc, your agent – usually accountant – is not presently able to apply for this on your behalf (at
Pension protection is a complex area and it is important that you get things right, as potential tax saved is huge. s peak with your independent financial adviser or accountant and ask them to review your position.
Next month: Things to consider before the end of the tax year
Ian Tongue (right) is a partner with Sandison Easson accountants
Get online for faster invoice payment and quicker cash collection!
Forget billing and collection agencies, forget phone payments and forget cheques!
JAY WEB MEDICAL SERVICES will build you your own secure online payment website where patients can settle their account using just their invoice number and a major credit or debit card
Your own personalised website 100% of funds in your bank account in 4 working days
Receipt emailed to the patient and doctor upon successful transaction Log in to your website for a full report of payments
Contact us now to for a free no obligation consultation www.jaywebservices.co.uk info@jaywebservices.co.uk 07795488186
The best of both
The doctors’ longtime favourite could always be bought with an electrifying performance version. This one really is. Independent Practitioner Today’s tester Dr Tony Rimmer (right) reports
Ad VA n CES I n technology have always heavily influenced the world of medicine. Many ideas formulated by medical research departments find their way into our day-to-day practice.
However, there is usually a delay while we all wait for initial promises to materialise. Rigorous trials and testing inevitably takes time and cost-effectiveness issues need to be ironed out.
Independent practitioners cannot afford to lose out on the latest advanced equipment and techniques, but early adopters risk subsequent updates being more efficient and better value for money.
It is much the same story in the world of motoring. The rising concerns of increased fuel costs and global warming have triggered massive investment by the car makers looking at alternative drivetrains and fuels.’
Totally electric propulsion is an obvious solution to tackle both
issues, but there are still problems with regard to limited battery storage, therefore range, and an inadequate infrastructure for recharging. Hybrid vehicles would seem to be a logical and transitional alternative.
The hybrid market
Toyota was the first brave manufacturer to release a petrol-electric hybrid model onto the new car market when it launched the Prius in 1997.
Since then, over a period of nearly 20 years, the hybrid market has changed enormously and we now have most major brands offering a petrol/electric model with plug-in recharging capability.
For example, Mercedes has the e350 C-class, BMW has the 330e 3-series and Audi has its eTron A3 and Q7. So does that mean that the hybrid versions of the popular cars that we know and love are now developed well enough to be a real option?
As I have indicated in past reviews, the Volkswagen Golf, particularly the GTI version, has always had great appeal as a brilliant all-rounder. The keen driving medic can enjoy a quality product that has plenty of room for the family and still entertains on the way back from clinic.
Best of both worlds
But what if you do most of your driving in an urban or city environment and support green and eco-friendly policies? Well, you might be able to experience the best of both worlds with Volkswagen’s new Golf GTE.
This plug-in hybrid has a 1.4litre turbo petrol engine producing 150bhp, linked to a lithium-ion battery-powered electric motor to bring the total power up to 201bhp.
This is the same output as the 2.0litre turbo petrol GTI, although the GTE weighs 230kg more.
both worlds
There are five operating modes that include E-mode, BatteryHold, Battery-Charge, GTE mode and Hybrid-Auto. In pure electric mode, it can travel up to 31 miles on a full charge and up to 81mph.
Very satisfying
So what it is like in the real world? d oes the technology work smoothly and efficiently? does it really drive like a GTI?
I spent a week with the car and drove it on short local trips as well
as long motorway trips. There is something very satisfying about setting off on any journey using silent pure-electric power.
If you select E-mode, it won’t start the petrol engine at all –unless you really floor the throttle – and this is perfect for short urban trips. The standard sixspeed direct-shift gearbox ensures smooth progress and the power delivery benefits from the usual electric motor attribute of maximum torque from rest.
There is something very satisfying about setting off on any journey using silent pureelectric power
VW golf gTE
Body: five-seat hatchback
Engine: 1.4 litre four-cylinder turbo petrol
Electric motor power: Combined output 201bhp
Torque: 250Nm
Acceleration: 0-62mph in 7.6 secs
Claimed economy: Up to 166mpg
Read-world economy: 45-50mpg
on-the-road price: £33,320 (including £2,500 government grant)
On the motorway, the BatteryHold mode uses the petrol engine alone and although adequate, it does not have the oomph of the GTI. However, if you are cruising, it doesn’t really matter.
If you want to charge the battery at the same time in BatteryCharge mode, the engine has to work a bit harder and economy suffers. GTE mode is for when you are on back roads and want to put your foot down.
Extra weight
The car then uses petrol and electric power together and you can really travel swiftly. Unfortunately, the extra weight of the drivetrain makes the GTE less agile and the driving experience is not as satisfying as in the GTI.
Overall, you are better off leaving the clever computers to choose the most suitable drive combination in Hybrid-Auto mode.
The general equipment levels in
the GTE are excellent and, being a Mark 7 Golf, quality levels are high.
Boot space is a bit reduced by the under-floor batteries and the ride is firm, although optional adaptive dampers should help. Charging from a standard wallplug takes less than four hours and less from a more powerful public supply.
I am really intrigued and impressed by the growing number of hybrid cars available and the technology is progressing in leaps and bounds.
This hybrid Golf is a mature petrol/electric vehicle and a wonderful example of how far things have come. For the eco-friendly independent practitioner whose driving is mainly urban with occasional long trips, the GTE could be just the car that ticks all the boxes.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
Spaced-out: The boot space is a bit reduced by the under-floor batteries
Bright spark: the general equipment levels in the gTE are excellent and, being a Mark 7 golf, quality levels are high
A steady performance
Independent Practitioner Today’s latest earnings survey of orthopaedic surgeons reveals more profit growth despite rising costs. Ray Stanbridge reports
Private Practice gross incomes for orthopaedic surgeons in the UK have risen by around 2.8% from £180,000 to £185,000 between 2014 and 2015.
c osts have gone up by about 3.2% on average, from £63,000 to £65,000.
as a result, taxable profits have increased by about 2.6% in the year from £117,000 to £120,000. all in all, it has been a steady performance and one consistent with our predictions when we looked at this specialty last year.
t here has continued to be a
growth in choose and Book work for many and this, in our view, is the primary explanation for the growth in average earnings. For some, there is also a modest increase in self-pay income.
i nsured work appears to have shown little growth and, in a number of cases, there is evidence of fee pressure – meaning orthopaedic consultants are having to work harder to earn the same money.
there have been some interesting changes in costs noticed during the year.
aveRage INCOMe aND eXPeNDITURe
Following a period of recession, it seems that orthopaedic surgeons have again started to attend more expensive courses abroad
a verage salary costs have increased. Mostly, this reflects the impact, on average, of the continuing rise in the personal allowances reflected in salaries paid to family members.
t here has also been some increase in average salaries paid to secretaries – and some early evidence of an increase in hospital charges made to consultants for these services.
Unknown impact
Similarly, there has been a small rise in consulting room hire costs. again, the full impact of increases will not be shown until the 201516 year, following the c ompetition and Markets a uth ority (cMa) order effective from april 2015.
We have also noticed a small increase in ‘courses and conferences’ expenditure on average. Following a period of recession, it seems that orthopaedic surgeons have again started to attend more expensive conferences abroad.
t here seems to have been a slight fall, on average, in professional indemnity costs, and that has come as a relief to many specialists.
We have seen, for a number of years, a steady growth in increasing defence costs.
Source: Stanbridge Associates Ltd.
If you plan to sell, retire or move away – or grow bigger – why not advertise with us and reach over 14,000+ consultant and gP colleagues working in private practice?
If you plan to sell, retire or move away –or grow bigger – then why not advertise with us and reach 13,000 consultant colleagues working in private practice?
For full details of how we can help contact Mararet Floate on 01483 824094. Email: margifloate@ btinternet.com
For full details of how we can help, contact Margaret Floate by phone on 01483 824094 or email her at: margifloate@btinternet.com
there has also been a growth in recent years in the number of alternative providers – not necessarily providing the same extent of cover, but cheaper than traditional providers. Some consultants with good claims records have chosen to transfer their business to cheaper providers.
t he long-term impact of this move has yet to be seen, but, in the short term, there appears to
have been some cost savings for a number of consultants.
We have also noticed some reduction, on average, on car expenses claims. this seems to be purely as a result of the now allowable claims for motor travel following the Samadian tax case (January 2014). a ctual expenditure incurred is pretty well much the same.
Other costs seem to be broadly
similar – again we notice the increasing expenditure on average on marketing costs.
higher secretarial costs
What then of the future? initial figures suggest orthopods’ incomes will continue ‘steady as she goes’. We will expect to see higher secretarial and room hire costs from april 2015 as the full effect of the cMa charges become apparent.
We also expect to see more pressure on fees where patients have medical cover. Nonetheless, we would expect orthopaedic surgeons to retain their pre-eminence as the top earners in the medical sector, on average.
Note that, as in previous years, our sample consists of those who:
earn at least £5,000 a year gross from private practice;
Have at least five years’ private practice experience;
are seriously interested in private practice as a business;
a re on either an old-style or new-style NHS contract;
May or may not work through a group or a limited liability company.
next time: ophthalmologists
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists Stanbridge Associates
Use
compare your
performance with others
years ending 5 april
Source: Stanbridge Associates Ltd
ORThOPaeDIC SURgeONS’ RaTIO OF PROFITS aND eXPeNSeS ReMaINeD STaBLe
what’S coming in oUr december-JanUarY
Make sure you don’t miss our next issue, published on 5 January 2017. you may not receive every issue if you have not yet subscribed to the journal. Don’t risk missing out on vital topics we tackle next time, including:
Make sense of your monthly management account. ebert hyman, a chartered global management accountant and general manager at London Urology group, shows how
Ten top New year resolutions for your business/practice
Code Buster! Medical Billing and Collection gives an update on the latest codes to help prevent you losing money
Which apps are you using to make your working life easier? Don’t miss Jane Braithwaite’s guide
Can you discuss your wealth with your family? Cavendish Medical’s Simon Bruce explains why it’s good for grandparents to ‘talk money’
Three key issues you need to consider when using the services of doctors in your new healthcare business
Starting a private practice: things to consider before the end of the tax year
What is that physical patient journey and customer experience like in your private patients unit and how could it be improved?
Business Dilemmas answers your questions about backdating fit notes and the issue of disputed parental responsibility for a child patient
eDITORIaL INqUIRIeS
Published by The Independent Practitioner Ltd. Independent Practitioner
Today is editorially independent and thanks Bupa for its assistance with distribution.
Printed by Pepper Communications Ltd Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Registered office: 7 Lindum Terrace, Lincoln LN2 5RP
Write to Independent Practitioner Today PO Box 198, Cranleigh GU6 9BB
iSSUe
For petrolhead medics, our ‘Doctor on the road’ Dr Tony Rimmer gets behind the wheel of the latest Porsche 911 turbo
Medicine’s Strangest Cases
a doctor’s experience aboard state-of-the-art ship africa Mercy, run by international charity Mercy Ships, deliverers of free healthcare and education, specialising in a wide range of medical needs
Why gPs should consider a medical admissions service for their patients
get protection from those nasty computer viruses. Caroline Corrigan reports
Breaking into medico-legal work
Profits Focus: ophthalmologists – plus all the latest news and views
Thanks for all your support in 2016 – see you in print and online again on 5 January
aDveRTISeRS: The deadline for booking advertising for our December-January issue falls on 19 December
£90 GPs and practice managers (private & NHS). £210 organisations.
But if you pay by direct debit, individuals pay only £75, and organisations £180
Call Proact Ltd on 01752 312140
Email: lisa@marketingcentre.co.uk
To guarantee your copy of Independent Practitioner Today by taking out a subscription (at the rates shown on the left), phone 01752 312140 or send off a subscription form on page 20 or email lisa@marketingcentre.co.uk or go to the ‘about’ page of our website www.independent-practitioner-today.co.uk
If you pay by direct debit, individuals pay only £75 for a subscription. Just fill in the form on page 20 and send it to the Freepost address shown at the bottom of the form.
Robin Stride, editorial director @robinstride
BaCk ISSUeS: £12.50 including post & packaging ChaNgINg aDDReSS OR SUBSCRIPTION DeTaILS?
Phone 01752 312140 or email lisa@marketingcentre.co.uk
Membership enquiry is one of my favourite features and a real time-saver. By quickly checking patients’ insurance details online, I can ensure my invoices are correct and avoid delays.
Kate Wilkinson, Medical Secretary
Securely confirm your patients’ membership details online
Healthcode’s ePractice solution allows you to verify patient’s insurer membership and demographic details quickly and securely online. You are able to ensure the information you hold against an insured patient is correct and accurate.
Using Membership Enquiry within ePractice, you can:
• Confirm a patient’s membership details
• Confirm if a patient’s policy is active*
• Increase first time pass rates
• Ensure bills submitted are accurate and eliminate payment delays