



Hello andwelcometotheAutumn 2025issueofLionMed,HamptonSchool'sveryownhealthsciencesmagazine.
The Lower Sixth MVD Society meets every week to share ideas and talk about the latest advancements within medicine anddentistry.The numberofexciting topicswithinhealthcareis boundless -therearealways interesting news articles to read about the latest health science advancements. And so, we wanted to share our passions for subjectsthatreallyinterestus-fromregenerativedentistrytoresearchintobacteriophages.
However, we could not have created this magazine on our own. We would like to thank Mr Langton, for bringing us all together for stimulating discussions during MVD Society, and reprographics expert Mr Cobb, who helped to put this magazine together. We must also thank the 2024 team of Sixth Form writers for the handing the baton over to us. Finally, I must personally thank all MVD Society members for their hard work and dedication in writing for the magazine.
Joshua Ripon
Contributors:
Editor:JoshuaRipon
Writers:JoshuaRipon,JROzen,EmirAljubouri,IanLeung,IbrahimAmeen,andAzamAhmad
Neurodegenerativediseasereferstoanydiseasewhich cause neuronal loss (the nerve cells which are responsible for transmitting nerve signals). This family ofdiseasesincludeAlzheimer's,MultipleSclerosis,and Parkinson's, but Huntington's Disease has recently beeninthenewsbecauseofapromisingnewdrugtrial.
Dr. George Huntington, an American doctor, first describedthis particularconditionina medicaljournal at just 22yearsold, after he had noticedthat members of the same family exhibited the same characteristic symptoms of a disease, which was later named after Huntington. 1
Research conducted in the last few decades has revealed that it is a mutation of the Huntington gene (HTT)whichcausesthecondition.Inessence,thisgene normally codes for the huntingtin protein which contributes to various processes within the neurons, such as helping to transport other important proteins and neurotransmitters (chemical messengers) to their finaldestinationsinthecell.
However, mutations, which are rare and random changes to the order of the bases (building blocks) of DNA, can occur to this HTT gene. The mutation, in this case, is a repeat of the codon (a set of three bases) which codes for an amino acid called glutamine. As therearemoreglutaminemoleculesbeingcodedforby the gene, the fundamental shape of the overall huntingtinproteinisaltered,andtheabnormalproteins clump together. This clumping is what ultimately causesneurodegeneration. 2

A recent drug trial has provided hope to many su ering with Huntington's Disease.JoshuaRiponinvestigates…
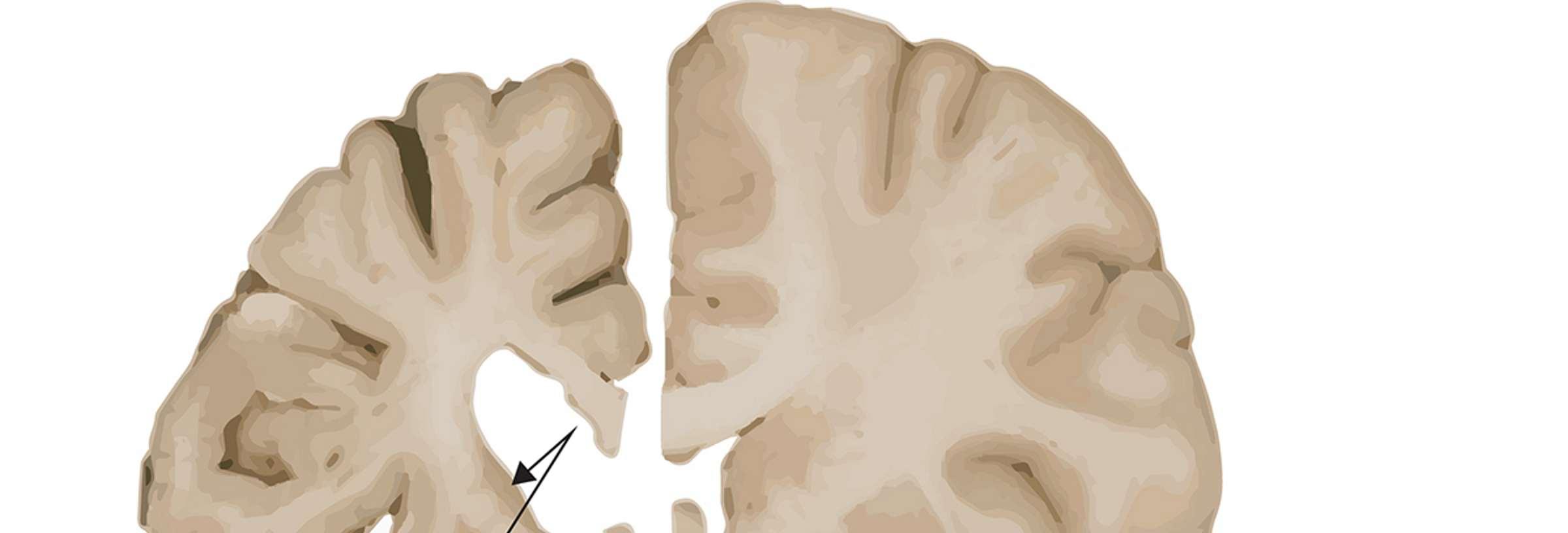
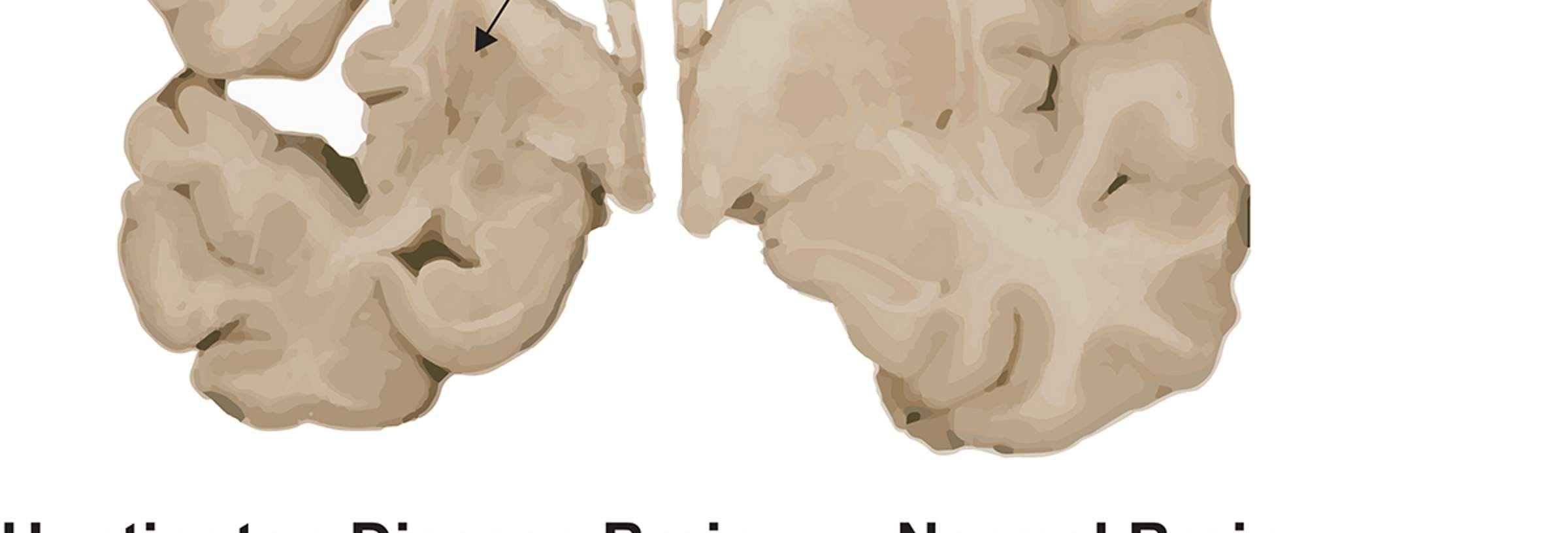
The image on the bottom left shows how the brain of a person who had Huntington's was atrophied (smaller) compared to the non-Huntington's brain. This is evidenceofneuralloss.
Huntington'sisanautosomaldominantcondition-this means that a person who has one parent with Huntington's and one without it has a 50% chance of inheritingthecondition.
Huntington’s presents with a wide variety of symptoms fromcognitiveissues,suchasbeingunabletoorganise oneself or becoming more inflexible. Whilst mental health issues, such as depression and mental health issues,aresymptomsofHuntington'sduetodamageto the brain, Huntington's is most commonly associated with chorea. Chorea, which comes from the word χορεία (dance) in Ancient Greek, is characterised by a number of involuntary movements of muscles. This could mean that a person with Huntington's could no longerkeep their balancewhilst walkingormight make abnormal eye movements. In fact, this condition was originally named Huntington's Chorea but was renamedHuntington'sDiseasetoreflecthowvariedthe symptomscan indeedbe.1, 3
Whilst many symptoms of Huntington's could be treated by di erent medications, there was no treatment for Huntington's up until very recently. However, a UCL team has, for the first time, pioneered a new treatment which can slow down the advancement ofHuntington'sbyupto 75%.
This treatment (known as AMT-130) is a type of gene therapy, in which a person's faulty disease-causing genes are altered. It works by surgically inserting a small,harmlessvirus (theadeno-associatedvirus)into the striatum, a part of the brain which is particularly a ected by Huntington's. The virus contains microRNA moleculeswhichbindtomRNAmoleculeswhichmake the huntingtin protein. This binding process is important because it means that the bad mRNA is destroyed by the cell, in a process called autophagy, and so, ultimately, the amount of mutant huntingtin proteinbeingmadeisreduced. 4, 5
An image of the microRNA molecules within the virus (represented by an icosahedron) inhibiting huntingtin productionisshownbelow.
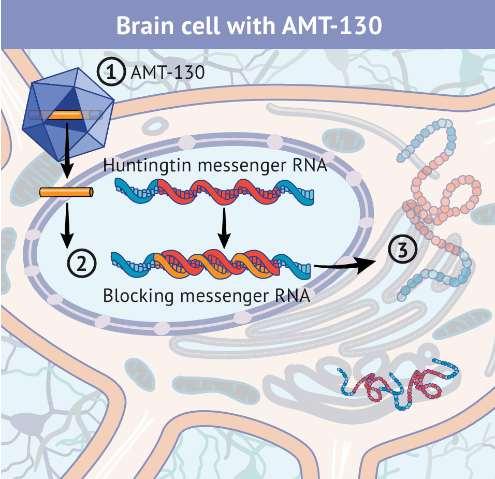
Credit: uniQure
Of course, the development of this treatment is very much in its early stages. Drug trials can take many years, from the moment that research has identified that a particular treatment could be e ective to the moment that that treatment is actually o ered to patients. Only 30 people participated in this initial trial stage, and so we do not really know much about the side e ects of gene therapy and about the complicationsthatcouldpossiblyoccurduetosurgery onthestriatum. 5
The hurdles that this trial has to overcome are numerous, from problems with regulation and funding toproblemswithfindingwillingparticipantstotakepart in the next few rounds of trials. Therefore, it's impossible to say whether this treatment will actually beroutinelyused withintheNHS.
However, on a personal note, I think that the main message, perhaps, of this trial is notthat of the clinical or medical details: it is one of hope. There is hope that treatments will eventually be found for those debilitating conditions which are currently incurable or untreatable. There is hope that trials will progress and that new discoveries will be made. And so, this is a promising medical advancement that we should keep oureyeson.
By Joshua Ripon
Bacteriophages, commonly known as phages, are viruses that infect bacteria. Even though they were discovered over a century ago, Western medicine has largely overlooked them, until now. Today, phages are finally attracting the attention that they deserve. They areneededforourfightagainstinfectionandantibioticresistantbacteria,astheycanbeused tokillbacteria.
Phages are incredibly diverse. Some carry DNA, whilst others carry RNA. However, they all store their nucleic acids in protein shells that, under a microscope, can look like tiny lunar spaceships or intricate geometric puzzles. Additionally, most are extremely specific and only have the capability to target a singular bacterial species or, in some extreme cases, a single strain from aspecies. 1
Phages are everywhere. They are found in oceans, soil, sewage,andevenwithinourownbodysystems.Thegut “phagosome”likelyplaysaroleinkeepingourmicrobial communities balanced, but scientists do not know exactlyhowthisworks.
Phagesattachtothebacteriaviatailfibresorantigens (bindingproteins),whicharecomplementary to the bacteria’sownantigens.
JR Ozen o ers a window into the hidden world of bacteriophages, and theirpotentialuseswithinmedicine…
Bacteria can, though, become resistant to phages by modifying their antigens so that they are no longer complementary tothatofthephages.
Onceattached, thephage, likeotherviruses, injects its genetic material into the bacteria. This means that the viral phage can now reproduce, via either the lytic or lysogeniccycles.
In the lytic cycle, the phage hijacks the bacteria’s machinery to make copies of itself, which eventually meansthatthecellburstsopenandreleaseshundreds of new phages.2, 3 The number of viruses produced increasesastonishinglyquickly.
Inthelysogeniccycle,thephageintegratesitsDNAinto the bacterial genome and lies dormant until triggered. However,somelysogenicphagescantransfergenesfor toxinstothesurroundings. 4
Bacteria rarely live isolated from each other. In nature, they form communities called biofilms. They can be very dangerous as they often are resistant to antibiotics. They often appear in chronic wounds, the lungsofcysticfibrosispatients,andinprostheticjoints.
Scientific centres in countries, such as the Eliava Institute in Georgia, are pioneers in phage research. Their early studies, which were originally overlooked, are now being re-examined by scientists who want to usetheir workclinically.
In phage therapy, phages attack the bacterial biofilms by either producing depolymerase enzymes to break down the protective bacterial matrix, or by replicating within thebacterialcluster.
Thereareanumberofsignificantchallengesassociated with phage therapy. Phages do not penetrate into the biofilmuniformly,andsothismeansthatsomebacteria living deep in the biofilm may remain shielded. This is because phages cannot communicate or act in a coordinated manner.
Creating phages for therapy isn’t simple. Scientists must carefully purify the phages, remove any bacterial debris, and screen for harmful genes, such as those that can release harmful toxins. Furthermore, phages constantly evolve and so it is di icult to monitor how thephagechangesgenetically. 5
Theimagebelowshowsthisprocess.
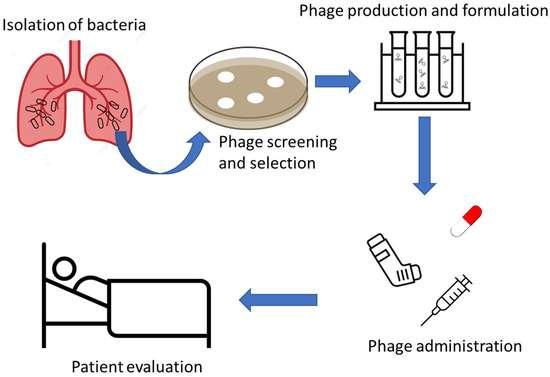
Credit:MDPI
The fact that phages are so specific can be a doubleedged sword. The right phage must match the right bacteriumandsophagetherapyrarelyworkslikeaonesize-fits-alltreatment.
Scientists also need to determine how to introduce a phage into a human body, without it being killed o by the human’s white blood cells, before it even reaches itstargets.
There are an increasing number of bacteria which are becoming resistant to antibiotics and so scientists are racing to find a new treatment to treat these bacterial infections. Therefore, phages are so useful because phages can be engineered in a way to kill o resistant strainsofbacteria.6
A patient with Acinetobacter baumannii managed to recoverafter receivingacustomised phagetreatment.7 This shows that phages could be an important treatment against bacterial biofilms in the future. 8 Whilst promising, more research needs to be conductedto ensurethatthistreatmentisoverallsafe.
Even if phages do not completely replace antibiotics, andonlyactinconjunctionwiththem,phagescouldbe a powerful new treatment. It is, ultimately, incredibly exciting to see what new advancements will be made withinphageresearch.
By JR Ozen
Non-Hodgkin’s Lymphoma (NHL) is the most prevalent adult blood cancer, representing a major challenge in modern oncology. Annually, the UK records around 13,000newcasesofNHL, reputingitself as theUK’s 6th most common cancer. B-cell lymphomas account for about85%ofallNHLdiagnoses. 1
The disease often announces itself quietly: a painless swelling of lymph nodes° typically in the neck, armpits or groin. Other symptoms include persistent fatigue, chest pain, unexplained weight loss, and drenching night sweats. Beneath these symptoms lie a molecular drama involving genetic mutations that transform healthy, normal immune cells into cancerous, malignant clones. 1, 2
In NHL, acquired genetic mutations (spontaneous changes in DNA which develop during a person’s lifetime,whicharenotinherited)disruptthenormalcell cycle of mature B-cell lymphocytes (which produce antibodiesandareinvolvedin humoral immunity°).The neoplasm° of these B-cells cause the uncontrollable divisionoftheseroguecellsformingtumourswithinthe lymphatic system, which is the network of vessels and glands that are involved in producing immune responses. As a result of this, B-cells become defective, and the immune system becomes weakened.3
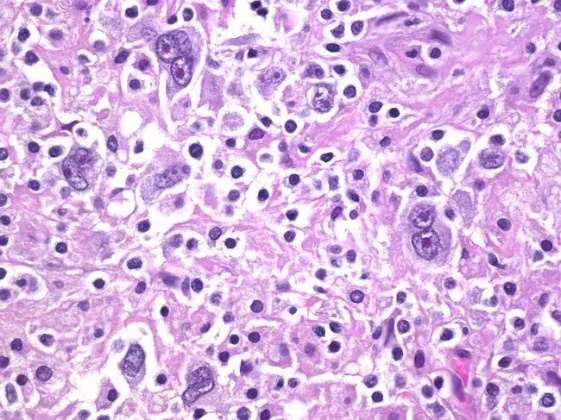
To confirm NHL, a biopsy° of the lymph nodes is taken. Under a microscope, non-Hodgkin’s lymphoma cells areidentifiedbytheirabsenceof Reed-Sternberg cells° (below) which are found in Hodgkin’s lymphoma (a di erenttypeofblood cancer).
Cancer treatments have significantly improvedinthelastfewdecades.Emir Aljubouri examines the use of a promisingnewtreatment…
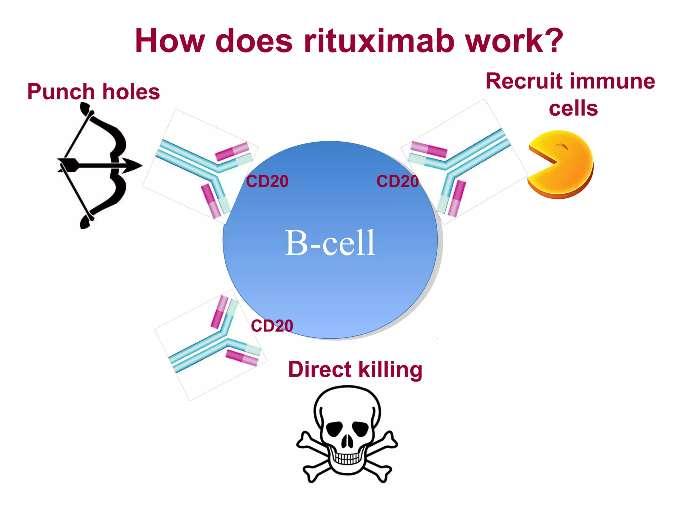
The late 20th century saw quiet yet transformational advancements in cancer treatments: the rise of targeted therapies.Among thesewasRituximab(which is also called Rituxan), the world’s first monoclonal antibody(mAb)therapyapprovedforcancerbytheFDA (theUS’FoodandDrug Administration).
Rituximab binds to the CD20 protein° on B-cell lymphocytes. The monoclonal antibody treatment simply marks out the B-cell lymphocytes to guide the body’simmunesystemtodestroy thecancerous,NHLa ected B-cells as well as being able to destroy these cancerousB-cellsonitsown. 4, 5
Rituximab triggers an immune-mediated cell destruction of malignant NHL cells. This means that Rituximab enables a mechanism called antibodydependent cellular cytotoxicity (ADCC) to occur, in which e ector cells, such as Natural Killer (NK) cells, bind to a receptor in the antibody’s fragment crystallisableregion.ThisultimatelyleadstoNHL-cells dying(cellapoptosis). 6, 7
Although rituximab is generally well-tolerated by its patients, if it is given in combination with chemotherapy,itcanharmhealthy,fast-dividingcellsin the body, like most cancer treatments. Healthy cells a ected include hair follicles, which means that a person might lose their hair temporarily. After treatment, hair follicle cells can repair themselves, but insomecases,damageispermanentand,therefore,so is the hair loss. Other side e ects of Rituximab itself includeaseverelyweakenedimmunesystemduetothe death of B-cells. Rituximab, an immunosuppressant drug, in combination with compromised immune systems from other underlying diseases such as HIV (which causes AIDS) give way for fungal and viral opportunistic infections such as the Epstein Barr Virus (EBV) which infect B-cells. Furthermore, other associated side e ects include nausea, vomiting, dizziness,headachesandfevers. 8, 9
Immunotherapies (treatments that use the body’s own immune system typically to attack cancer) have been circulatinginthemedicalworldforoveracentury.
However, the process of finding e ective antibody therapies has not been a breeze. The first mAbs were produced using hybridoma technology, where Köhler and Milstein immunised mice with sheep red blood cells.
10
This led to a domino e ect in research. The first use of thefirstmAbwasapprovedbytheFDAin1986,whereit was used to treat an acute kidney transplant rejection. Rituximab,achimeric(createdfromtwospecies-mice and humans) antibody, eventually was created by RonaldLevytotargetmalignantB-cellsand,in1982,his first mAb cancer patient was successfully treated with themAb.Furthermore,researchshowedthatRituximab couldkillCD20cellsinvitro.
Since the initial approval of rituximab use in oncology patients in 1997 for a follicular lymphoma° case, outcomes of patients with non-Hodgkin’s lymphoma subtypes have improved substantially. The successful use of the monoclonal antibody has triggered widespread use of CD20 antibodies such as ofatumumab, which are also involved in binding to CD20 proteins on B-cells. mAbs are personalised therapeutics (a medical treatment tailored to an individual’s unique characteristics) which have come asaresultofadvancesinresearch of immunology°.
Credit:Dana-Farber Cancer Institute
A retrospective study on patients with di use large Bcellmalignantlymphoma(DLBCL),whichisatypeofBcell non-Hodgkin’s lymphoma, was carried out to investigate the increase in survival of patients after taking Rituximab. Out of 65 newly-diagnosed patients with DLBCL, 32 were in the pre-rituximab group (with a median follow-up time 60 months) and 33 were in the post-rituximab group (with a median follow-up time of 29 months). Progression-free survival rates increased substantiallyinthepost-rituximabgroup.The18-month progression-free survival rate increased from 59.4% to 81.8% and the overall survival rate at 18 months significantlyincreasedfrom65.5%to81.8%.Thisledto the conclusionthatconventionalCHOP chemotherapy (a combination of chemotherapy with rituximab) resultedinabetterprognosisforpatientswithDLBCL.12
Rheumatoid Arthritis (RA), Multiple Sclerosis (MS) and Systemic Lupus Erythematosus (SLE) are all autoimmune conditions that can also be treated with Rituximab. This demonstrates the wide range of diseasesand conditionsthatRituximabcantreat.
To conclude, Rituximab has o ered an insight into the e ectiveness of the use of monoclonal antibodies in the treatment ofcancer. Since it was introduced, ithas transformed the prognosis of B-cell NHL, especially whencombinedwithchemotherapy.Thishaspavedthe wayformodernimmunochemotherapytreatments.
Moreover, its reduced toxicity compared to cytotoxic treatments like chemotherapy means patients su er less from adverse e ects from treatments of nonHodgkin’s lymphoma. Finally, Rituximab continues to inspire the development of new anti-CD20 antibodies and for this reason, and so it would not come as a surprise if prognosis and survival rates of patients with NHLcontinuedtoimprovesignificantly.
Glossary:
Lymph nodes° – a part of lymphatic system which is composedofsmallareasoftissuethatfilterfluidinyour body for harmful cells which act as a disposal unit for immune cells to get rid of damaged cells and foreign substances.
Humoral immunity° – a part of the immune system whichinvolve antibodies neutralising pathogens.
Neoplasm° –anabnormal growthof tissue.
Biopsy° – taking a small sample of tissue or cells from the body which are then to be examined under a microscope by pathologists.
Reed-Sternberg cells° – large, abnormal cells that look like owleyes.
CD20 Protein° – a glycosylated transmembrane phosphoprotein marker for B-cells; involved in regulating calcium ion concentration and cell cycle progression during B-cellactivation.
Follicular lymphoma° – a type of slow growing nonHodgkin’s lymphoma that develop when malignant Bcellsaccumulatein follicles oflymphnodes.
Immunology° –the studyofthe immunesystem.
By Emir Aljubouri

As I was thinking of what to write for the Hampton MedicalMagazine,athoughtoccurredtome:injuriesin the NBA. I was intrigued by the fact that players in the NBA seemed to su er constantly with injuries despite the advances in injury prevention, medicine, and treatments.
ThisconstantlyfrustratesmeastheteamthatIsupport, the Charlotte Hornets, is repeatedly struggling with injuries every year. The Hornets’ star player, Lamelo Ball, has missed around 40% of his games due to constantly struggling with the same recurring ankle injury. Ankles injuries are the most common, with over 1,800 game-related ankle injuries in an average year. This equates to 14.% of all NBA injuries. Researchers have shown an increase in injury rates ranging from 12.4%to15%withintheNBA.1
KneeinjuriesarethesecondmostcommonintheNBA. Knee injuries usually take the formof Anterior Cruciate Ligament (ACL) or meniscal tears. ACL injuries are usually the most serious, requiring surgery and a long recovery and rehab time. An ACL tear happens when your knee moves or twists more than it naturally can. ThereisahighriskofsustainingACLtearsinbasketball, as itrequires pivotalstop-and-start motions. IntheUS, ACLinjurytreatmentcosts$1billionperyear. 3
NBAmatcheshavecaptivatedmillions ofpeoplearoundtheworld.IanLeung analyses why NBA players seem to su ersomanyinjuries…
League Mismanagement and organisational pressure have increased the number of injuries in the League. The NBA is big business: it generated $12.25 billion in the2024-2025season.Thisseemssmallincomparison to the Premier League which only made $8.29billion in thesame2024-2025season.
Perhaps in attempts to maximise profits, the NBA puts pressure on medical sta to clear players for play too soon, even if they are notin good shape, to attract fans andselloutvenues.
A prominent example of this is when Kevin Durant (KD) su eredaminor calfstrain in 2019duringthe2nd round playo series against the Rockets. Although this strain was later determined to be more serious, just a month into recovery, KD returned to play for Game 5 of the 2019finals.
TheAchillestendon,thelargesttendon inthebody, connectsthe2majorcalfmuscles(thegastrocnemius andthesoleus)totheheelbone.Itislikelythatthe rushedreturnfromhiscalf strain meantthathetore hisAchilles,asaweakcalf canplaceexcessivestress ontheAchillestendon,whichincreasestheriskofan Achillestearorrupture.
This injury wascontroversialassomethink that hewas misdiagnosed in the first place. Dr. David Chao, an orthopaedic surgeon and Team Physician for an NFL team, wrote in the San Diego tribune that Durant’s expression when he sustained the initial injury on May 8th indicatedapossibleAchillestendonrupture,instead of it just being a calf injury. He said that the team specifically avoided the term “calf muscle” and opted for the more ambiguous and broad term “calf,” as an attempt to cover up a more serious injury, so that fans wouldn’t be concerned for his health during the Finals run.
AnultrasoundimageofanAchillestear(notKD’sone)is shownbelow.

Credit:InternationalDayofRadiology
The potential misdiagnoses, along with his rushed return, were perhaps important factors leading to KD’s season ending injury. If KD continued to be sidelined, perhaps he would not have su ered the Achilles rupture.
ThiswaslikelyduetoKDbeingoneofthestarplayersin theteam,andsomanyfanswouldhavewantedtohave seen him play. The team’s competitive nature put pressure on medical sta to clear him so that he could play.4
Thedemandsofthesportitselfcouldbetherootcause ofmanyinjuries, particularlyduetotheriseofAmateur Athletic Union (AAU) sports in the US. Children start playing at a very young age, and often have to play 3+ gameseachdayduringtournaments,whilstundergoing high intensity training sessions, with little time for rest. This can lead to injuries such as patellar tendinitis (jumpersknee)andstressfractures.
Rapid, sudden movements, including abrupt stops, change of directions, and fast movements can place tremendousstressonthejoints,particularlytheankles andknees.
Constant jumping and landing are key in all aspects of basketball: rebounding, dunking, shooting, and in layups. These can cause awkward or hard landings whichcanlead tofreakinjuriessuchasACLtears.
However, given that previous research suggested that NBA players su ered twice as many game-related injuries compared to college basketball players, it is most likely that the NBA training schedules contribute moretoNBAinjuriesthantheactualsportitself.
Intense NBA schedules can also contribute to many recurring injuries. Players have to play 82+ games per season,excludingplayo s.
This, as well as having back-to-back games (playing 2 games on consecutive days), where teams have to travel to other cities, can make it incredibly exhausting for the players. As players have very little time for rest and recovery, fatigue also plays a big part in injury. Research showed that injuries were associated with greater fatigue and game load. Furthermore, studies show that athletes who sleep less than 8 hours a night (which is most NBA players!) are at a much higher risk of sustaining asportrelatedinjury.
This has led to many stars resting in the 2nd game of a back-to-back to reduce the risk of injury, to manage fatigue,and topreparefortheplayo sThiscan then,in turn, mean that people who are specifically wanting to see that star player are disappointed. This can lead to attendancefiguresdropping,aswellasTVratings. 5, 6, 7
In conclusion, despite other contributing factors, such as shortcomings within the League’s organisation and thenatureofthesportitself,itisoverallthedemanding NBA timetable which mainly contributes to the increased number of basketball injuries. This is ultimately because NBA players do not have the time, betweengamesortrainingsessions,toresttheirbodies to ensure that they can play without fatigue. It is, therefore, up to NBA owners to put the wellbeing and health of their players before their financial aims, to ensurethatbasketballisasafersportforall.
By Ian Leung

What is Hypertrophy?
Muscle hypertrophy simply means an increase in the cross-sectional area of skeletal muscle fibres. your body adapts to repeated exercise-induced stress, your muscles grow back stronger and thicker. This is how bodybuilders develop the shape and tone of their muscles. The two types of hypertrophy are myofibrillar hypertrophyandsarcoplasmichypertrophy.
Before we dive into the intricacies of muscle hypertrophy, it is essential to understand how muscles actuallywork.
The sliding filament muscle theory suggests that muscles are composed of small, contractile units. These are called sarcomeres, which each consists of smaller filaments: actin, the thinner filament, and myosin, the thicker filament. During muscle contraction, calcium ions are released, which will bind to proteins on actin. This allows myosin to attach onto actin, forming a cross bridge. This ultimately means thatATP(anenergy-carryingmolecule)helpstopullthe actin filament inwards, to shorten the sarcomere. This repeated pulling action is called a muscle contraction. When our muscles relax, the reverse simply occurs: calcium is pumped away, the cross-bridges release, andthemusclereturnstoitslengthatrest.1
As social media influencers share theiropinionsonhowtobuildmuscle, Ibrahim Ameen turns to science to examinehypertrophy...
Myofibrillar Hypertrophy is the growth of the muscle fibres, actinand myosin. Thiscanbe triggered bylifting heavier weights for less reps, and by doing compound movements,suchasdeadliftsorsquats.Thisproduces stronger, moredense muscles(like theonesthatEddie Hallhas).
SarcoplasmicHypertrophyisthegrowthofthefluidand energy-providing substances, such as glycogen and enzymes, in the muscle cells, which is referred to refer to as the sarcoplasm. This can be achieved by lifting less heavy weights less quickly, but more frequently, and with reduced rest periods. Controlled isolation exercises like lateral raises, preacher curls or tricepspushdowns all increase sarcoplasmic hypertrophy, which in turn produces larger, more “full” muscles. However, this will result in a lower direct increase in strength. 1, 2
Myofibrillar hypertrophy can be thought of as the thickening of the actual ropes that pull weights, whereas sarcoplasmic hypertrophy can be likened to addinglayersofpaintorstringtotherope,whichmakes itthicker,butnotnecessarilystronger.
Stimuli for Growth
Mechanicaltension,muscledamage,andmetabolic stressallstimulatemusculargrowth.
MechanicalTension:
When a person lifts a heavy weight slowly (i.e. they are reducing their momentum), they stretch their contracting fibres. This in turn activates sensors in the muscle that triggers mTORs, which regulates muscle protein synthesis. This means that a person can synthesise more muscle when under mechanical tension,leadingtohypertrophy.
Microscopictearstendtoformduring intenseexercise, especially during the eccentric (basically the lowering part)halfofthemovement.Inresponsetothis,thebody activates satellite cells, which are basically muscle stem cells. These fuse to damaged fibres, to repair them. Once repaired these muscle fibres become thicker,andsotheygrow. 2
Metabolic stress is best described as the ‘pump’ or ‘burn’a person feels when working out, especially with highrepexercises,suchaslateralraises.Thisiscaused bylactate,hydrogenionsandlowoxygeninthemuscle, which means that muscle cells swell up, and trigger hormonal signals, that will stimulate growth. The most famous of these hormones is probably testosterone, which enhances protein synthesis and muscle recovery.
A keen athlete would want to maximise hypertrophy during their workout sessions, and there are a number ofdi erentmethodstodothis.Theguidingprinciplesto maximising hypertrophy remain the same for all athletes, whether theyare bodybuilders, rugbyplayers, or goalkeepers.
Muscles will only grow and adapt if they are pushed to theirlimits.Justlikeanythinginlife,apersonwillnotsee progressunlesstheyreallypushthemselves.Toachieve this,apersonneedstoeither liftalittlebitmoreweight or afewmorerepsperweek(asdemonstratedbelow.
When lifting weights, a high degree of intensity is requiredtotriggerhypertrophy.Studiessuggestthatthe idealdegreeofintensityrangesfrom65to85%ofone’s ‘one-rep-max. Doing 6 reps would trigger myofibrillar hypertrophy, and 12 would trigger sarcoplasmic hypertrophy. 3, 4
To improvemusclegrowth,aperson musttrytocontrol their movements, so that the eccentric phase of their exercise lasts for 2 to 4 seconds, depending on the exercise. If the eccentric phase lasts for too long, the muscle will become more fatigued. For example, when one is doing a bicep curl, it is important to lower the weight, straighten the elbow, and slow down the extension to2-4seconds.
There are, though, many di erent things that a person can do at home to continue to maximise muscle hypertrophy,andtoensurethattheyarestayinghealthy.
The one word which is synonymous with muscles is protein. Protein can be found in red meat, eggs, and soya.1.6to2.29gofproteinperkilogramofbodyweight is enough for most people, but this amount can be adjusted to better fit a person’s needs. Proteins makes theaminoacidsweneedforactinandmyosin,whichis neededformusclecontraction.Proteinalsorepairsthe exercise-induced microscopictearsinthemuscle. 5
Many people, including myself, do not get enough sleep,butitisactuallyoneofthemostimportantthings to do to maximise hypertrophy. Most of the muscle proteinsynthesis, whichrepairs muscular microscopic tears,happensduringsleep.Furthermore,70to80%of growth hormone, which helps to repair muscle tissue, isreleasedduring sleep. 6
The science behind hypertrophy is, of course, fascinating. However, perhaps more importantly, these scientific principles can be applied readily whilst exercising. This demonstrates how science is not theoretical, but is actually tangible and applicable to ourpersonaldevelopment.
By Ibrahim Ameen

Dentistry is evolving from repair to regeneration. Insteadofsimplypatchingdamagedteethwithartificial filling,researchersarelearningtocoaxnatureitselfinto rebuilding enamel, dentin, and even pulp. This emerging field - regenerative dentistry - draws heavily on biomimetics, the science of imitating natural structures and processes to engineer materials that behavelikerealtissue.
At the very core of this transformation are biomimetic materials, designed to mimic the mechanical and biochemicalpropertiesoftoothtissues.Recentreviews describe how nanoscale fabrication and smart polymers have accelerated progress in crafting materials that don't just fill, but heal. By integrating calciumphosphate,hydroxyapatite,andbioactiveglass (the same components that form natural enamel and dentin), scientists are creating restorations that can bond seamlesslywiththetoothsurface.1
One striking example is the development of bioactive composites capable of releasing ions that stimulate dentin remineralization and pulp repair. The materials encourage stem cells to regenerate lost or damaged dental tissue, e ectively blending the boundary betweenrestorativeandregenerativedentistry.2, 3
Another innovative approach takes cues from marine organisms.
Innovative technologies in dentistry have been developed to improve patient care. Azam Ahmad finds out more…
Thenacreofseashells(theiridescentinnerlayerknown as mother-of-pearl) has inspired the design of layered composites with remarkable toughness and selfhealing capabilities. By replicating the microstructure of natural materials, these biomimetics systems can endure chewing stresses while facilitating biological repair. 4
Modern regenerative dentistry also explores tissue engineering, combining sca olds, growth factors, and dentalstemcells.Researchershighlightthepotentialof bioactive sca olds that support periodontal and pulp regeneration. These materials provide the 'blueprint' that cells need to rebuild functional dental tissues; that'sabigchangefromtheolddayswhendentistsjust used metal or plastic filling that didn't really fix the tooth,justcovered thedamage.5
However, challenges do still remain. Biocompatibility, long-term stability, and cost all limit clinical adoption. Despite this, optimism is high. The convergence of nanotechnology, biomaterials science, and stem cell researchissettingthestageforaneweraindentalcare, onewheredentistsactlesslikeengineersandmorelike gardenersof tissue,guidingnaturalhealing. 6
The ultimate dream of regenerative dentistry is not just restoringasmile,butrevivingit,makingteeththatgrow, adapt,andendureasliving partsofthehumanbody.
It'scrazytothinkhowscienceandnaturearestartingto mix together, as if technology is learning to grow teeth back,bitbybit.
Glossary:
Dentin-Thehardlayer beneaththe enamelthatmakes up most of the tooth. It protects the pulp and carries tinytubesthatsenseheatandpressure.
Pulp - The soft inner part of the tooth that contains nervesand bloodvessels.Itkeepsthetooth alive.
Bioactive-Amaterialthatcaninteractwithlivingtissue to help it heal or grow, instead of just sitting there passively.
Remineralization - The natural process where minerals like calcium and phosphate are added back into the toothtorepairearlydamage.
Biocompatibility-Howsafelyamaterialcanexistinside thebodywithoutcausingharmorrejection.
By Azam Ahmad
1) BhattacharyyaKB.ThestoryofGeorgeHuntingtonandhisdisease. Annals ofIndian AcademyNeurology. [Online].2016Jan-Mar;19(1):25-8.[Accessed 5October2025]. Availablefrom:https://pubmed.ncbi.nlm.nih.gov/27011624/
2) NationalInstituteofNeurologicalDisordersandStroke.Huntington'sDisease.[Online] [Accessed7October2025].Availablefrom:https://www.ninds.nih.gov/healthinformation/disorders/huntingtons-disease
3) MayoClinic.Huntington'sDisease.[Online][Accessed9October2025].Availablefrom: https://www.mayoclinic.org/diseases-conditions/huntingtons-disease/symptomscauses/syc-20356117
4) UCL.GenetherapyappearstoslowHuntington’sdiseaseprogression.24September 2025.[Online][Accessed20October 2025].Availablefrom: https://www.ucl.ac.uk/news/2025/sep/gene-therapy-appears-slow-huntingtonsdisease-progression
1) HymanPandAbedonST.(2010)Bacteriophagehost rangeandbacterialresistance. Advances inApplied Microbiology. [Online].2010;70:217-48.[Accessed21November 2025].Availablefrom:https://pubmed.ncbi.nlm.nih.gov/20359459/
2) Abedon STetal.Phagetreatmentofhumaninfections. Bacteriophage. [Online]. 2011;Mar;1(2):66-85.[Accessed21November2025].Availablefrom: https://pubmed.ncbi.nlm.nih.gov/22334863/
3) ChanBKetal.Phagecocktailsandthefutureofphagetherapy. FutureMicrobiology. [Online].8(6),pp.769–783.[Accessed 21November2025].Availablefrom: https://pubmed.ncbi.nlm.nih.gov/23701332/
4) EmenchetaSCetal.TheRoleofBacteriophagesintheGutMicrobiota:Implicationsfor HumanHealth. Pharmaceutics. [Online].2023Oct3;15(10):2416.[Accessed22 November2025].Availablefrom:https://pmc.ncbi.nlm.nih.gov/articles/PMC10609668/
5) PirnayJPetal.Thephagetherapyparadigm:ascientificandregulatorychallenge. JournalofAntimicrobialChemotherapy. [Online].70(4),pp.1155–1164.[Accessed22 November2025].Availablefrom:https://pubmed.ncbi.nlm.nih.gov/21063753/
6) GuLiuCetal.Phage–antibioticsynergy:mechanismsand clinicalimplications. Current OpinioninMicrobiology.[Online].2020Aug 4;11(4):e01462-20.[Accessed21November 2025].Availablefrom:https://pubmed.ncbi.nlm.nih.gov/32753497/
7) Schooley RTetal.Developmentanduseofpersonalisedphagetherapytotreatapatient withmultidrug-resistantAcinetobacter baumanniiinfection. AntimicrobialAgentsand
Chemotherapy.[Online].2017Sep 22;61(10):e00954-17.[Accessed 22November 2025].Availablefrom:https://pubmed.ncbi.nlm.nih.gov/28807909/
8) DedrickRMetal.Engineeredphagesfortreatmentofapatientwithadrug-resistant Mycobacteriumabscessusinfection. Nature Medicine. 2019May;25(5):730-733.Epub 2019May 8.[Accessed 21November 2025].Availablefrom: https://pubmed.ncbi.nlm.nih.gov/31068712/
1) BowzykAl-Naeeb A.Non-Hodgkin lymphoma. BMJ. [Online].2018Aug 22;362:k3204.[Accessed9November 2025].Availablefrom: https://pubmed.ncbi.nlm.nih.gov/30135071/
2) ClevelandClinic.Unknown. Non-Hodgkin lymphoma. [Online].[Accessed9November 2025].Availablefrom:my.clevelandclinic.org
3) SapkotaS.2023.Non-HodgkinLymphoma. StatPearls. [Online].2023Feb 24.[Accessed 9November 2025].Availablefrom:https://www.ncbi.nlm.nih.gov/books/NBK559328/
4) TavarozziR.2023.ChangingTrendsinB-CellNon-Hodgkin Lymphoma Treatment:The RoleofNovelMonoclonalAntibodiesinClinicalPractice. Cancers(Basel). [Online]. 2023Nov13;15(22):5397.[Accessed9November2025].Availablefrom: https://pmc.ncbi.nlm.nih.gov/articles/PMC10670523/
5) PloskerGL.Rituximab:areviewofitsuseinnon-Hodgkin’slymphomaandchronic lymphocyticleukaemia. Drugs. [Online].2003;63(8):803-43.[Accessed 9November 2025].Availablefrom:https://pubmed.ncbi.nlm.nih.gov/12662126/
6) HarrisonAM.RituximabforNon-Hodgkin’sLymphoma:AStoryof RapidSuccessin Translation. Clinicaland Translational Science. [Online].2014Feb;7(1):82-6.[Accessed 9November 2025].Availablefrom:https://pmc.ncbi.nlm.nih.gov/articles/PMC4264563/
7) NationalCancerInstitute(NIH).UsingtheImmuneSystemin theFightAgainstCancer: DiscoveryofRituximab.[Online].2014.[Accessed9November 2025].Availablefrom: https://www.cancer.gov/research/progress/discovery/blood-cancer
8) Mohammed R.Howthediscoveryofrituximabimpacted thetreatmentofB-cellnonHodgkin’slymphomas. Journal ofBlood Medicine. [Online].2019Feb27;10:71-84. [Accessed9November2025].Availablefrom: https://pubmed.ncbi.nlm.nih.gov/30881167/
9) PierpointTM.Past,Present,andFutureofRituximab–TheWorld’sFirstOncology MonoclonalAntibody Therapy. Frontiers in Oncology. [Online].2018Jun4;8:163. [Accessed9November2025].Availablefrom: https://pubmed.ncbi.nlm.nih.gov/29915719/
10) Köhler G,MilsteinC.Continuousculturesoffused cellssecretingantibodyofpredefined specificity. Nature. [Online].1975Jun26;256,495–497.Availablefrom: https://www.nature.com/articles/256495a0#citeas
11) Rodenburg EM.ImprovedsurvivalforpatientswithlargeB-celllymphomaafter introduction of rituximab. The NetherlandsJournalofMedicine. [Online].2009 Sep;67(8):355-8.[Accessed 9November2025].Availablefrom: https://pubmed.ncbi.nlm.nih.gov/19767667/
1) MooreMLetal.Management ofankleinjuriesinprofessionalbasketballplayers: Prevalenceandrehabilitation. Orthopaedic Review. [Online].2021Mar31;13(1):9108. [Accessed18November2025].Availablefrom: https://pmc.ncbi.nlm.nih.gov/articles/PMC8077287/
2) DrakosMCetal.Injuryinthenationalbasketballassociation:a17-yearoverview. SportsHealth. [Online].2010;2:284-90.[Accessed18November2025].Availablefrom: https://pubmed.ncbi.nlm.nih.gov/23015949/
3) Alentorn-GeliEetal.Prevention ofnon-contactanterior cruciateligamentinjuriesin sports.Part II:systematicreviewofthee ectivenessofpreventionprogrammesinmale athletes. Knee surgery,sports traumatology, arthroscopy. [Online].2014Jan;22(1):16-25. [Accessed18November2025].Availablefrom: https://pubmed.ncbi.nlm.nih.gov/24162718/
4) Associated Press.Warriors'KevinDurant undergoessurgeryforrupturedachilles tendon. The Guardian. [Online].2019Jun13.[Accessed 18November2025].Available from:https://www.theguardian.com/sport/2019/jun/12/kevin-durant-achilles-injurynba-finals
5) TeramotoM.GameinjuriesinrelationtogameschedulesintheNationalBasketball Association. Journal of ScienceandMedicine in Sport. [Online].2017Mar;20(3):230235.[Accessed 19November2025].Availablefrom: https://pubmed.ncbi.nlm.nih.gov/27622705/
6) LewisM.It'saHard-KnockLife:GameLoad,Fatigue,andInjuryRiskintheNational BasketballAssociation. Journal ofAthleticTraining. [Online].2018May;53(5):503-509. [Accessed19November2025].Availablefrom: https://pubmed.ncbi.nlm.nih.gov/29771139/
7) StarkeyC.Injuriesand illnessesinthenationalbasketballassociation:a10-year perspective. Journalof AthleticTraining. [Online].2000Apr;35(2):161-7.[Accessed 19 November2025].Availablefrom:https://pmc.ncbi.nlm.nih.gov/articles/PMC1323413/
1) HallJEandHallME.2020.GuytonandHallTextbookofMedicalPhysiology.14th edn. Philadelphia:Elsevier.
2) SchoenfeldBJ.Themechanismsof musclehypertrophyandtheirapplicationto resistancetraining. Journal of Strength and Conditioning Research. [Online].2010 Oct;24(10):2857-72.[Accessed 8November2025].Availablefrom: https://pubmed.ncbi.nlm.nih.gov/20847704/
3) PhillipsSMand WinettRA.Uncomplicatedresistancetrainingandhealth-related outcomes:evidenceforapublichealth mandate. Current SportsMedicineReports. [Online].2010Jul-Aug;9(4):208-13.[Accessed 9November2025].Availablefrom: https://pmc.ncbi.nlm.nih.gov/articles/PMC4086449/
4) PhillipsSM.Abriefreviewofcriticalprocessesinexercise-inducedmuscular hypertrophy. Sports Medicine.[Online].2014May;44Suppl1(Suppl1):S71-7.[Accessed 8November 2025].Availablefrom:https://pubmed.ncbi.nlm.nih.gov/24791918/
5) MortonRW.Asystematicreview,meta-analysisandmeta-regressionofthee ectof proteinsupplementationonresistancetraining–inducedgainsinmusclemassand
strengthinhealthyadults. British Journal ofSportsMedicine. [Online].2018 Mar;52(6):376-384.[Accessed 8November2025].Availablefrom: https://pubmed.ncbi.nlm.nih.gov/28698222/
6) VanCauter Eetal.Growthhormonereleaseduringsleep. The Journalof Clinical Investigation. [Online].1996May;128(5Pt2):S32-7.[Accessed8November2025]. Availablefrom:https://pubmed.ncbi.nlm.nih.gov/8627466/
1) Zafaretal.BiomimeticAspectsof RestorativeDentistryBiomaterials. Biomimetics (Basel). [Online].2020Jul15;5(3):34.[Accessed 29October2025].Availablefrom: https://pubmed.ncbi.nlm.nih.gov/32679703/
2) SingerLetal.Biomimeticapproachesand materialsinrestorativeandregenerative dentistry:reviewarticle. BMC Oral Health. [Online].2023Feb16;23(1):105.[Accessed1 November2025].Availablefrom:https://pubmed.ncbi.nlm.nih.gov/36797710/
3) AlsolaihimANetal.BiomimeticRegenerativeMaterialsinRestorativeDentistryand Endodontics. Journalof InternationalHealth. [Online].2023Jun 15(3):p250-256. [Accessed1November2025].Availablefrom: https://journals.lww.com/jioh/fulltext/2023/15030/biomimetic_regenerative_materials_i n_restorative.5.aspx
4) Green DWetal.Osteogenicpotencyofnacreonhumanmesenchymalstemcells. Moleculesand Cells. [Online].2015Mar;38(3):267-72.[Accessed 1November2025]. Availablefrom:https://pmc.ncbi.nlm.nih.gov/articles/PMC4363727/
5) Luo Xetal.Researchprogressofbiomimeticmaterialsinoralmedicine. Journal of BiologicalMedicine. [Online].2023Nov23.17,72.[Accessed 1November2025]. Availablefrom:https://link.springer.com/article/10.1186/s13036-023-00382-4#citeas
6) ParyaniMetal.EvolutionofBiomimeticApproachesforRegenerativeandRestorative Dentistry. Cureus. [Online].2023Jan18;15(1):e33936.[Accessed1November2025]. Availablefrom:https://pubmed.ncbi.nlm.nih.gov/36819376/
