Sports Rehabilitation and Injury Prevention 1st Edition by Paul Comfort, Earle Abrahamson ISBN 9780470985632 0470985631 pdf download
https://ebookball.com/product/sports-rehabilitation-and-injuryprevention-1st-edition-by-paul-comfort-earle-abrahamsonisbn-9780470985632-0470985631-312/
Explore and download more ebooks or textbooks at ebookball.com
Sports Rehabilitation and Injury Prevention 1st Edition by Paul Comfort, Earle Abrahamson ISBN 0470985631 9780470985632
https://ebookball.com/product/sports-rehabilitation-and-injuryprevention-1st-edition-by-paul-comfort-earle-abrahamsonisbn-0470985631-9780470985632-2968/
The Anatomy Of Stretching Your Illustrated Overview To Flexibility And Also Injury Rehabilitation 1st edition by Varda Toussaint ISBN B09TMYXBMZ 979-8424930492
https://ebookball.com/product/the-anatomy-of-stretching-yourillustrated-overview-to-flexibility-and-also-injuryrehabilitation-1st-edition-by-varda-toussaintisbn-b09tmyxbmz-979-8424930492-20372/
Get in the Game An Interactive Introduction to Sports Analytics 1st edition by Tim Chartier, Ansley Earle ISBN 022681114X 9780226811147
https://ebookball.com/product/get-in-the-game-an-interactiveintroduction-to-sports-analytics-1st-edition-by-tim-chartieransley-earle-isbn-022681114x-9780226811147-25114/
Biomechanics of Movement The Science of Sports Robotics and Rehabilitation 1st edition by Thomas Uchida, Scott Delp 9780262359191 0262359197
https://ebookball.com/product/biomechanics-of-movement-thescience-of-sports-robotics-and-rehabilitation-1st-edition-bythomas-uchida-scott-delp-9780262359191-0262359197-15122/
Internet Gaming Disorder Theory Assessment Treatment and Prevention 1st edition by Daniel King, Paul Delfabbro 0128129255 9780128129258
https://ebookball.com/product/internet-gaming-disorder-theoryassessment-treatment-and-prevention-1st-edition-by-daniel-kingpaul-delfabbro-0128129255-9780128129258-25214/
Problem Solving in Endodontics Prevention Identification and Management 5th Edition by James Gutmann, Paul Lovdahl ISBN
9780323078016
https://ebookball.com/product/problem-solving-in-endodonticsprevention-identification-and-management-5th-edition-by-jamesgutmann-paul-lovdahl-isbn-032307801x-9780323078016-6974/
Jquery Novice to Ninja 1st Edition by Earle Castledine, Craig Sharkie ISBN 0980576857 9780980576856
https://ebookball.com/product/jquery-novice-to-ninja-1st-editionby-earle-castledine-craig-sharkieisbn-0980576857-9780980576856-10900/
Times Sports 1st edition
https://ebookball.com/product/times-sports-1st-edition-17270/
Oral Cancer Diagnosis Management and Rehabilitation 1st Edition by John W Werning ISBN 1604064854 9781604064858
https://ebookball.com/product/oral-cancer-diagnosis-managementand-rehabilitation-1st-edition-by-john-w-werningisbn-1604064854-9781604064858-7922/
SportsRehabilitation andInjuryPrevention SportsRehabilitation andInjuryPrevention Editedby PaulComfort
SchoolofHealth,Sport&RehabilitationSciences,UniversityofSalford,Salford,UK
EarleAbrahamson
LondonSportInstituteatMiddlesexUniversity,UK
A John Wiley & Sons, Ltd., Thiseditionfirstpublished2010, C 2010JohnWiley&Sons,Ltd
Wiley-BlackwellisanimprintofJohnWiley&Sons,formedbythemergerofWiley’sglobalScientific,TechnicalandMedical businesswithBlackwellPublishing.
RegisteredOffice
JohnWiley&Sons,Ltd,TheAtrium,SouthernGate,Chichester,WestSussex,PO198SQ,UK
OtherEditorialOffices
9600GarsingtonRoad,Oxford,OX42DQ,UK 111RiverStreet,Hoboken,NJ07030-5774,USA
Fordetailsofourglobaleditorialoffices,forcustomerservicesandforinformationabouthowtoapplyforpermissiontoreuse the copyright material in this book please see our website at www.wiley.com/wiley-blackwell
TherightoftheauthortobeidentifiedastheauthorofthisworkhasbeenassertedinaccordancewiththeCopyright,Designs andPatentsAct1988.
Allrightsreserved.Nopartofthispublicationmaybereproduced,storedinaretrievalsystem,ortransmitted,inanyformorby anymeans,electronic,mechanical,photocopying,recordingorotherwise,exceptaspermittedbytheUKCopyright,Designs andPatentsAct1988,withoutthepriorpermissionofthepublisher.
Wileyalsopublishesitsbooksinavarietyofelectronicformats.Somecontentthatappearsinprintmaynotbeavailablein electronicbooks.
Designationsusedbycompaniestodistinguishtheirproductsareoftenclaimedastrademarks.Allbrandnamesandproduct namesusedinthisbookaretradenames,servicemarks,trademarksorregisteredtrademarksoftheirrespectiveowners.The publisherisnotassociatedwithanyproductorvendormentionedinthisbook.Thispublicationisdesignedtoprovideaccurate andauthoritativeinformationinregardtothesubjectmattercovered.Itissoldontheunderstandingthatthepublisherisnot engagedinrenderingprofessionalservices.Ifprofessionaladviceorotherexpertassistanceisrequired,theservicesofa competentprofessionalshouldbesought.
LibraryofCongressCataloging-in-PublicationData
Sportsrehabilitationandinjuryprevention/editedbyPaulComfort,EarleAbrahamson. p.;cm.
Includesbibliographicalreferencesandindex. ISBN978-0-470-98562-5(cloth)
1.Sportsinjuries.I.Comfort,Paul.II.Abrahamson,Earle.
[DNLM:1.AthleticInjuries–prevention&control.2.AthleticInjuries–rehabilitation.QT261S76762010] RD97.S7852010
617.1 027–dc22
ISBN:9780470985625(HB) 9780470985632(PB)
AcataloguerecordforthisbookisavailablefromtheBritishLibrary. Setin10/11.5ptTimesbyAptaraInc.,NewDelhi,India. PrintedinGreatBritainbyAntonyRoweLtd,Chippenham,Wiltshire. 12010
2010005619
Preface Theconceptforthisbookisbasedontheexpanding fieldofsportsrehabilitationandinjuryprevention. Evidenceofthisexpansionincludesanincreasing amountofresearchandpublicationsrelatedtosports rehabilitationandalliedfieldsofpracticesuchas sportstherapy,athletictrainingandsportsphysiotherapy.
Despitethenumberandvolumeofpublications insportsrehabilitation,thereappearstobelimited resourcesthataccuratelyandeffectivelyaccountfor evidence-basedpractices.Whilstsomeresourcesexpandevidence-basedpracticeknowledge,thereis aneedtodevelopacompleteresourcethatfully explainsandarticulatestheseimportantprinciples. Thiscurrenttexthasusedanevidence-basedpractice approachtofullyacknowledgethemanydiverseareas,applicationsandmanagementstrategiesthatare oftenuniquetosportsrehabilitation,butdistinctly differentfromsimilarfieldsofpracticeandstudy.
Fewsportsrehabilitationprogrammescurrently providestudentswiththebreadthofinformationand practicalapplicationrequiredforprofessionalpractice.Thistexthasattemptedtobridgetheknowledge andpracticegap,byconsideringthefunctionaldevelopmentofthesportsrehabilitator’sknowledge andpracticerequirementsforprofessionalcompetency.Thetextprovidesanup-to-datelookatdifferentevidence-basedpracticeprotocolsandinitial assessmentstrategiesforthescreeningofinjuryand pathologicalconditions.
Thefirstfewchaptersintroducethescopeofpracticeforsportsrehabilitation,andthendescribe,explainandevaluatetheinitialassessmentandscreeningproceduresnecessaryfordecisionmakingand clinicalpractice.Thesechaptersfurtherprovide analysisonmusculoskeletalfunctionanddysfunctioninrelationtosystemicorganisation.Thenext
setofchapterscombineausefulintegrationofappliedareasandpracticesofstudyrelevanttosports rehabilitationpractice.Theseinclude,amongstothers,nutritionalanalysis,psychologicalconsiderationsininjurymanagementandprevention,clinical reasoningdevelopment,andstrengthandconditioningprinciples.Thebookconcludeswitharangeof chaptersdevotedtodifferentinjuryconditionsand bodyregions.Thesechaptersdetailthemorecommoninjuriesandpathologiesandargueforbestmanagementstrategiesbasedonresearchandapplied evidence.
Eachchapteralsocontainsseveralpracticalapplicationboxesthatprovideadditionalinformation summarisinguniquechapter-specificinformation. Themajorityofchapterscontainappliedexamples andcasestudiestoillustratetheprocessesanddecisionsnecessaryforclinicalactionandmanagement. Eachcasestudyhasbeencarefullydevelopedtofacilitategroupdiscussionintheclassroom,orforthe cliniciantoconsideraspartofcontinuedprofessionaldevelopment.
Inadditiontoservingasanupperlevelundergraduateorgraduatetextbookforstudentsorclinicians inpractice,thebookisanexcellentresourceguide, filledwithusefulinformationandevidence-based practiceconsiderationsandapplications.Youwill wanttohavethistextbookonyourdeskorbookshelf.Thefeaturesofconsistentorganisation,case studies,discussionquestions,up-to-datereferences, researchevidenceandpracticalapplicationboxesare designedtoprovideinformationrequiredforeffectivestudyaswellasdirectingclinicalpractice.
Thedesignofthistextcanbecomparedtobuildingahouse,inthateachcomponentofboththetext andhousebuildingcanbemodelledonindividual buildingblocks.Inthecaseofthehousebuilding
theseunitsarerepresentedbythebricks,whereas inthetext,theindividualchaptersaresynonymous withtheseunits.Beforeonecommencesthebuilding process,thereisacarefullyconstructedvisualordiagrammaticplantonavigatetheprocess;sotoodoes thisplanningapplytothedesignandshapingofthis text.Inthebuildingprocess,considerationisgivento thefoundation,intermsofitsshape,depth,form,and length.Thistexthasanumberoffoundationchaptersthatsecurethecontentforfuturedevelopment oftheotherchapters.Themainfoundationknowledgeistheunderstandingofanatomicalapplication, andusingthisknowledgetoguideassessment.This anatomicalfoundationknowledgeinformsthedecisionsnecessaryforclinicalactionintermsofinjury management.Whilstbricksareimportantintermsof informingthestructureofabuilding,itisthecement thatensuresthateachbrickissecuredandarticulates withotherbricksandstructures.Inthistext,thecementisrepresentedbyunderpinningthemes,such asclinicalreasoningskillsandabilities,thattraverse thechaptersandensuresthateachchapteralthough perceptivelydifferent,isabletoarticulatewithother chaptersanddevelopthisconsortiumofknowledge. Aftercompletion,housestakeonanewshapeand design,onewhichmayhavetransformedtheoriginallandscape;howeverthereisalwaysroomfor
change,improvementorrefinement.Thistext,inits finalform,hasorchestratedthejourneyofclinical practicefromconsiderationofthescopeofpractice, throughtotheessentialskillsnecessaryfordecision making,andconcludingwithaconsiderationofhow tomanagearangeofinjuriesandpathologies.The textiscoatedwithanevidence-basedapproachtousingandapplyingknowledge.Thetrueadvantageof developingthetextwithinanevidence-basedcontext isthatitallowsthereadertoconsidertheexisting knowledgeandevidence;challengetheresearch;and movetowardsaskingdifferenttypesofquestionsto considernewwaysofdealingwithclientmanagementissues.Asnewresearchbecomesavailable, clinicalpracticewillbequestioned.Thecontentsof thistextwillevolveandchangetoaccommodateand explorenewideasandadvancesinclinicalresearch. Thisbookprovidesthearchitecturenecessarytoconsidertherealissuescurrenttoclinicalpractices.Itis importanttouseitasamapfornavigatingtheconcepts,principles,challengesanddecisionsofclinical practice.
Wehopethatthisbookisavaluableresourceboth forteachingandasareferenceforsportsrehabilitatorsandclinicians.
PaulComfort EarleAbrahamson
Acknowledgements Thankyoutoalloftheauthorsinvolvedwiththedevelopmentofthistext,includingthosewhoprovided adviceandfeedbackoneachofthemanydrafts. Withouttheexpertise,dedicationandeffortofeach oftheseindividuals,thistextwouldnothavebeen possible.
Thankyoutomyfamily,especiallymychildren, forputtingupwithmy‘absences’andlonghours staringatthelaptop,duringthedevelopmentofthis book.Yoursupportandunderstandinghasbeenmore thanIshouldhaveaskedfor.
PaulComfort
Aspecialthankstothemanycontributorswho workedsodiligently,oftenunderdifficultandpressurisedcircumstances,towritethistextandtothose whoprovidedexpertreviews.Alsotomymany
studentswhotaughtmesomuchabouthowtoarticulateconcepts,theoriesandapplicationsinalearner friendlymanner,whichhelpedshapethelandscape ofthisbook.
Tomywonderfulwife,Emma,andmyadorable son,Benjamin,thanksforputtingupwithmeand providingmuchlove,supportandunderstanding.
Tomyfather,Charles,andmybrother,Michael, thanksforalwaysbelievinginmeandencouraging metosucceedandachieveinlife.
Lastbutnotleast,Iwouldliketodedicatemy contributiontothisbook,tothememoryofmylate mother,Josephine,whosesupport,inspiration,kindnessandgenerosity,willforeverbecherishedand respected.Thankyouforbelievinginmeandsupportingmyacademicandprofessionaldevelopment.
EarleAbrahamson
Abouttheeditors PaulComfort (BSc(Hons),MSc,PGCAP, CSCS*D,ASCC)isaseniorlecturer,programme leaderfortheMScStrengthandConditioningprogrammeattheUniversityofSalford.Paulisalso currentlyHeadofSportsScienceSupportforSalfordCityRedsRugbyLeagueFootballClubandcoordinatestheStrengthandConditioningforEngland Lacrosse(men’ssquad).HeisaCertifiedStrength andConditioningSpecialist(RecertifiedwithDistinction)(CSCS*D)withtheNationalStrengthand ConditioningAssociationandafoundermemberand AccreditedStrengthandConditioningCoachwith theUnitedKingdomStrengthandConditioningAssociation.Heisalsocurrentlycompletingapart-time PhD.
EarleAbrahamson (BPhysEd,BAHons,MA, BPS,BASRaT,FRSM,BRCP,AHPCSA,HPCSA, PsySSA)isaprincipallecturer,teachingfellowand programmeleaderfortheSportsRehabilitationand InjuryPreventionprogrammeatMiddlesexUniversity.Throughhisprogrammeleadershipandteachingfellowshipduties,Earlehasdevelopedaninter-
estinstudentlearningandthinking.Earlespentthe majorityofhislifeinSouthAfrica,studyingand working,andmovedtotheUKin2002.Heisa SouthAfrican-registeredtherapistandpsychologist andhasmembershipandprofessionalregistration withanumberofUKauthorities.Earlehasworked extensivelyasasportsrehabilitatorwithnationaland internationalteams,includingtheworldstrongest manevent.Earlesitsontheexecutivecommittee oftheBritishAssociationofSportsRehabilitators andTrainers(BASRaT),astheirstudentliaisonofficer.Inthisrolehedealswithandpromotesthe BASRaTstudentexperience.EarleistheMiddlesexUniversityrepresentativeforthehighereducationacademy’shospitality,leisure,sportandtourism sector.Heiscurrentlyworkingonaprofessionaldoctorateinvestigatingdifferentlearningapproachesin thedevelopmentofclinicalreasoningskillsonundergraduatesportsrehabilitationprogrammes.
EarleismarriedtoEmmaandhasason,Benjamin. Inhissparetimeheenjoyssportandisanactive cricketerandtennisplayer.Hefurtherenjoysreading andmusic.
Listofcontributors JohnAllen
LeadPhysiotherapist
EnglandAthletics
UK
PhilBarter SeniorLecturerandProgrammeLeader forSportScience
LondonSportInstituteatMiddlesexUniversity, London
UK
StuartButler Physiotherapist
AllenPhysiotherapyRehabilitationandSports Medicine
EnglandAthletics
UK
SarahCatlow
UniversityCollegePlymouthStMark&StJohn, Plymouth UK
NicholasClark
ClinicalDirectorandLowerLimbRehabilitation Consultant
IntegratedPhysiotherapy&ConditioningLtd, London
UK
AngelaClough
SeniorLecturer,ProgrammeLeaderSport Rehabilitation, FellowSocietyofOrthopaedicMedicine UniversityofHull
UK
RhondaCohen Head
LondonSportInstituteatMiddlesexUniversity, London UK
ElezabethFowler Lecturer
UniversityofSalford,GreaterManchester UK
JulianHatcher
SeniorLecturerandProgrammeLeader(Bsc (Hons)SportsRehabilitation)
UniversityofSalford,GreaterManchester UK
LukeHeath GraduateSportsRehabilitator
DrLeeHerrington SeniorLecturerandProgrammeLeader (MScSportsInjuryRehabilitation)
UniversityofSalford,Manchester UK
LeadPhysiotherapistGreatBritainWomens Basketball
SebastianHicks GraduateSportsRehabilitator
IanHorsley
LeadPhysiotherapist
EnglishInstituteofSport UK
VictoriaHyland Lecturer
LondonSportInstitute,MiddlesexUniversity UK
DavidJoyce CharteredSportsPhysiotherapist
BlackburnRoversFC
TheUniversityofBath UK
ChristoKoukoullis GraduateSportRehabilitator
HelenMatthews SeniorLecturerandAssociateDean(Teachingand Learning)
UniversityofSalford,GreaterManchester UK
MartynMatthews SeniorLecturer
UniversityofSalford,GreaterManchester UK
DrSannaM.Nordin ResearchFellow,DanceScience,TrinityLaban
DrStephenPearson SeniorLecturer
UniversityofSalford,GreaterManchester UK
JeffreyA.Russell AssistantProfessorofDanceScience UniversityofCalifornia,Irvine USA
DrorSteiner CharteredOsteopath
Howtousethisbook Thetexthasbeendesignedtoallowthereaderto considerandunderstandimportantthemes,principlesandapplicationsthatinformclinicalpractice. Eachchapterbeginswithanintroductoryparagraph (seebelow)thatidentifiesandoutlinestheaimsand outcomesforthatchapter.
The chapter aims and objectives will be emphasised at the beginning. Use these to confirm your understanding of the chapter content.
Thischapterprovidesanoverview,analysis,andapplicationofclinicalreasoningandproblemsolvingskills inthedevelopmentofprofessionalcompetencieswithinthehealthcareprofessiongenerallyandmore specificallysportsrehabilitation.Thechapterisimportantasitwillhelpyoudevelopyourthinkingskills asyouprogressyourreadingthroughoutthebook.Bytheendofthischapterthereaderwillbeableto locateandexplaintheroleandefficacyofclinicalreasoningskillswithinaprofessionalpracticedomain. Thiswillinformanappreciationforthecomplexnatureofknowledgeconstructioninrelationtoclinical explanationandjudgement.Byconsideringclinicalreasoningasafunctionalskillset,thereaderwillfurther beinapositiontoexplaindifferentmodelsofreasoningandaskstructuredquestionsinanattemptto betterformulateandconstructanswerstoclinicalquestions,issues,anddecisions.Thechapterwillfurther encouragethereadertouseproblemsolvingandclinicalreasoningskillstojustifysubstantially,through researchevidence,professionalpracticeactionsandoutcomes.
Thefirstchapterprovidesanoverviewofthescope ofpracticeforthesportsrehabilitatorand/orallied healthcareprofessional.Withinthischaptercarefulconsiderationhasbeengiventothepositionof thesportsrehabilitatorwithinasportandexercise medicineteam.Thechapterfurtherdealswithissuesaroundmedical,ethicalandlegalconcerns,and
usesaschemadiagramtoillustratehowthesports rehabilitatorworkswithothersportmedicinepractitionerstomanageinjury.Whenreadingthisinitial chapter,considerhowyourscopeofpracticeand professionalidentityisformed.Usethechapterto helpyoureinforceyourcodeofpracticeandreflect onthemedicalethicalandlegalrequirementsfor yourprofession.
Thefollowingchaptersdealwithissuesaroundinjuryscreeningandperformanceassessment.These chaptersintroduceanddebateissuesconcerning assessmentandscreening,andpresentresearchevidencetovalidateclaims.Itisusefulwhenreading
thesechapterstoconsiderhowscreeningandassessmentworktoaccommodatearangeofathletes fromdifferentsports.Clinicianswhosimplyfollowa setprogrammeorprotocolforassessmentmayfind itdifficulttodefendclinicalactionsanddecisions shouldtheathletenotimprovefollowingtheinterventiondelivered.Itisimportanttobeabletorelate thecontentofthechapteranddecideonhowbestto screenorassessanathletebasedonevidencefrom researchstudies.
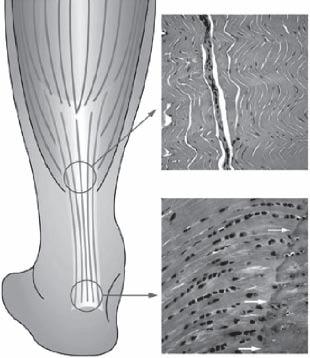
Chapters4–8introduceandevaluatethepathophysiologyofmusculoskeletalcomponents.These chaptersarecrucialwhenconsideringinjurymanagementaswellaspreventionstrategies.Eachof thesechaptersmakesuseofdiagrammaticrepresentationsofthekeymusculoskeletalcomponents(see below)andhighlightsthehealingandrepairstages ofmusculoskeletalinjuries.
(60%
preciatethesportsciencesandhowanunderstanding ofprinciplesofstrengthandconditioning,psychology,nutrition,performanceassessmentandclinical reasoningcouldbeusedtohighlightareasofconcern andmovethepractitionertoamorecompleteevaluationandtreatmentoftheathlete.Thedesignofthese chapters,havebeencarefullyconsideredtoensure thatyou,asreaderandclinician,canuseimportant conceptualapplicationsinthemanagementofthe client.Thethemesexploredwithinthesechapters arenotuniquetothechapterperse,butratherform animportantthreadthroughoutthetext.Exploring thethemeswithinthesechapterswillhopefullyallowthereadertoconceptualisesportsrehabilitation andinjurypreventionasafunctionalongoingand workingoperationthatrequiresthoughtandresearch evidencetofullyappreciatethemeritoftreatment andrehabilitation.
Proteoglycan (0.5% dw) including decorin, versican, lumican
Glycoproteins (5% dw) including tenascin, COMP, elastin
Referencetolaterchaptersandconsiderationof specifictreatmentstrategiessupportedbyresearch isevident.Whenreadingthesepathophysiological chaptersitisusefultoconsidertheprimaryanatomy ofthestructureanditsnormalfunctionalstate.Considerhowthisfunctionalstatechangesorcompensatesmovementasaresultoftraumaorpathology. Usethisknowledgeasaprecursortoinjurymanagementandawaytoshapeclinicaldecisionsand actions.
Thenextsevenchaptersencompassimportant themesnecessaryforeffectiveclinicaldecisionsand managementoptions.Usethesechapterstohelpap-
The pathophysiological chapters make use of diagrams and illustrations to highlight key anatomical landmarks and pathological concerns that could impact healing and prolong recovery.
Thefinalsectionofthetextisdedicatedto joint-specificinjuriesandpathologies.Thesechaptersintroducetheinjuriesandspecificassessment techniquesbyconsideringevidence-basedpractice protocols.Thesechapterstietogethertheimportantconsiderationforinjurypreventionandmanagement.Thechaptersculminateinappliedcasestudies(seebelow)thatareusedtoillustratethethought processandclinicaldecisionmappingnecessaryfor effectiveinjurymanagement.Itisimportanttoconsiderhowdecisionsarereachedandwhatprocesses needtobeexaminedasopposedtosimplyreachinga decision.
Collagen
dw) including type I (III, IV, V, VI, XII, XIV)
Composition Midsubstance
As above, but also includes: collagen type II, IX, XI, aggrecan, biglycan
CaseStudy20.2 A24yearoldmalesprinterwithleftsidedgroindiscomfortsinceaplyometricsessionthreemonthsbefore thisinitialconsultationhadresultedindiscomfortaftereverytrainingsession.
Lowerabdominalandmedialanteriorgroinpainfollowingactivity thatisbecomingprogressivelylongertoimprovewithrest.
Becomesverylowgradeandalmostunnoticeablewithrest.
Thereisirritablepainwhencoughingandsneezing.
Feels‘sore’inthegroinwhensittinguprightforawhile.
Paininthedeepinnergroinwhensqueezingthelegstogether, particularlyinbed.
Painwasdescribedasexerciserelatedandvariablebetween1 and7onthe10pointscale.
Therewereminimalimpingementsignswithhipflexion-ad
Each injury-specific chapter makes use of an applied case study to frame the clinical issues and consider appropriate and evidence-based treatment and rehabilitation programmes. Use these studies to check your own understanding and decide on whether you agree with the clinical management and/or decisions discussed within the study. duction.
Oninvertingthescrotumandplacingthelittlefingerinbothsuperficialinguinalrings,theleftside appearedmoretenderanddilatedthantheright,withacoughimpulse.
Theleftadductorwasrelativelyweakerthantherightandpainfulinresistedadductionlyingwithstraight legs,butnotwithlegsbentinflexion.
Therewasnodiscomfortonstretch.
Storkviewsofthepelvis,standingononelegandthentheotherexcludedpelvicinstability,pubicsymphysis andhippathology.
Thepatientwasreferredtoasurgeonforopinion. Duringsurgerythefollowinggroindisruptionwasidentifiedintheoperativereport: tornexternalobliqueaponeurosis
theconjoinedtendonwastornfrompubictubercle dehiscencebetweenconjoinedtendonandinguinalligament
Eachelementofthisgroindisruptionwasrepairedsurgically.
Treatmentandrehabilitation Normalprotocolforthefirstdaypostoperationincludedstandandwalkingwithgentlestretchingand stabilityexercises.
FivedayspostoperativeultrasoundascertainedcorestabilitytobepoorandTransversusAbdominis activation(Cowan2004)wasachievedwithpractice,usingpatientvisualisationoftheultrasoundreal-time imageforre-education.
Adductorexercises(Figures20.4–5)wereencouragedoneweekpostop,severaltimesperday.
Closedchainexercisesforstability(e.g.,Figures20.6–9)combinedwithslowcontrolledsquatsprogressing tosinglelegsquats,weredevelopedtwoweekspostopwithhydrotherapyforflexibilityandstability.
Swimming,cyclingandcross-trainerellipticalexercisedevelopedinthethirdweek.
Afterfourweekshestartedstraightlinerunningbuildupsalternatedays.
Conclusion
Thisathletereturnedtorelativelyfulltrainingaftertwomonthsandcompetedinternationallysixmonths afterthesurgery.
Discussion
Atwhattimeshouldanathletewithgroindiscomfortbereferredtoasurgeontoconsideroperative intervention.
Shouldalongerperiodofconservativetreatmentandrehabilitationtakeplacebeforereferralforsurgery.
Shouldthepatienthavebeenreferredforotherinvestigations,e.g.ultrasoundscanorMRI.
Whatotherareasofthebodymaycontributetowardsthisathletesinjury.
Insummary,thecontentsofthisbook,aredesignedtoevokeclinicaldecisionsbasedonresearch evidence.Thechaptersaresequencedtoallowthe readertodevelopanappreciationforunderstanding andanalysingclinicalpracticeandactions.Individu-
allythechaptersprovideaframeworkforconceptualisingdifferentscientificapplicationsandpractices, butcollectivelytheyformacompendiumofclinicalknowledge,cementedbyclinicalpracticeand framedwithinanevidence-basedcontext.
Part1 Introductiontosportsrehabilitation 1 Introductiontosportinjury management JeffreyA.Russell
UniversityofCalifornia–Irvine,USA
Introductionandaims Thepopularityofphysicalactivityinallofitsforms continuestosteadilyincrease.Morethanjustthedomainofeliteorprofessionalathletes,thepopulace enjoysavarietyofrecreationalpursuitsfromhiking andrunningtoskiingandsurfing,frombadminton andtennistocricketandhockey.Insuchendeavoursmanyparticipantsfindthatinjuryisinevitable. Unfortunatecircumstancesarenotconfinedtothose engaginginrugbyor“Xgames”,daredevilsports likeParkour,kitesurfingoracrobaticbicyclejumping,althoughclearlythesecarryahighcostinphysicaltrauma(Young2002;SpanjersbergandSchipper 2007;MillerandDemoiny2008).Youngfootballers andseniorgolfersalikearepronetoinjury,asare Olympicperformersand“weekendwarriors”becauseinjurydoesnotdiscriminate(Delaneyetal. 2009;Falveyetal.2009).Likewise,non-traditional athletessuchasdancers(Fitt1996;Stretanski2002; KoutedakisandJamurtas2004)willnotescapeinjury(Bowling1989;GarrickandLewis2001;Bronner,OjofeitimiandSpriggs2003;Laws2005).
Whethertheyarepursuinggoldmedalsorleisure, thosewhoparticipateinphysicalactivityrequire bothproperpreventivetrainingandproperhealthcare;theywillbenefitgreatlyfromexpertswhocan deliverthese.Sportrehabilitatorsandotherallied
healthprofessionalshavemuchtoofferphysically activepeople.Thischapteraimsto:
definetheroleofthesportrehabilitatorasamemberofthesportinjurycareteam;
promoteindividualandorganisationalprofessionalismwithinthefieldofsportrehabilitation;
provideaframeworkforethicalconductofsport rehabilitatorsandrelatedprofessionals;
describelegalparametersthatmustbeconsideredbythoseinsportrehabilitationandrelated fields.
Theroleofthesportrehabilitator Preparinganindividualtosuccessfullyparticipate insportrequires,byitsverynature,expertisefrom multiplespecialities.Managingtheinjuriesthat occurtosportparticipantsalsorequiresinputfrom manyspecialists.Thus,atanygivenpointtheathlete maybesurroundedbyateamofprofessionals, includingthecoach,clubmanager,conditioning specialist,biomechanist,physiotherapist,nutritionist,exercisephysiologist,chiropodist,chiropractor,
Table1.1 Thevarietyofsportmedicineteammemberswhoworkwithathletes(seealsoFigure1.1)
MedicalsandsurgeonsPara-medicals
GP
Chiropodist
Sportdentist
Consultants:
Orthopaedicsurgeon
Generalsurgeon
Neurosurgeon
Cardiologist
Radiologist
Physiatrist
Neurologist
Sportrehabilitator
Physiotherapist
Osteopath
Chiropractor
Massagetherapist
Sportoptometrist
Acupuncturist
Firstresponder
Alternativetherapypractitioner
osteopath,sportoptometrist,sportpsychologist, sportdentist,GP,consultantand,indeed,sport rehabilitator(Table1.1andFigure1.1).Depending onthesport,anathlete’slevelinthesportand thevenue,allofthelistedprofessionalsmaynot beinvolvedincare.Further,someprofessionals maybequalifiedtoadministermorethanonecare speciality.However,regardlessofthesituationthe managementofsportinjuryisateamactivity,and thesportrehabilitatorplaysakeyrole.
TheBritishAssociationofSportRehabilitators andTrainers(BASRaT)administerthecredential “GraduateSportRehabilitator,”whichisabbreviated
Figure1.1 Diagramshowingthebreadthofsportinjury management.Notethatinthesituationofanathletewho isaminorchild,theparentsorcarersbecomepartofthe managementscenario.
SportscientistsSporteducators
Biomechanist
Exercise physiologist
Sportpsychologist
Nutritionist
Kinesiologist
Coach
Conditioningspecialist
Physicaleducator
Clubmanager
to“GSR.”Accordingtothisprofessionalsociety, “aGraduateSportRehabilitatorisagraduatelevel autonomoushealthcarepractitionerspecialisingin musculoskeletalmanagement,exercisebasedrehabilitationandfitness”(BritishAssociationofSport RehabilitatorsandTrainers2009b).Further,BASRaToutlinetheskilldomainsofaGraduateSport Rehabilitatorasbeing: professionalresponsibilityanddevelopment prevention recognitionandevaluationoftheindividual managementoftheindividual–therapeuticintervention,rehabilitationandperformanceenhancement immediatecare
Whilstpreventionofinjuryiscertainlydesirable, therealitythatathleteswillbeinjuredispartofsport participation.Thus,thesportrehabilitatormustalwaysbepreparedtoadministerthecareforwhich theyaretrained.Theidealplacetobeginproviding thiscareispitchsideorcourtsidewherethecircumstancessurroundingtheinjuryhavebeenobserved andevaluationoftheinjurycanbeperformedprior totheonsetofcomplicatingfactorssuchasmuscle spasm.Anysportrehabilitatorwhoexpectstooffer thistypeofcaremustpossesstheproperqualification andadditionalcredentialstosupportit.Minimum
Table1.2 ComponentsoftheBritishAssociationofSportRehabilitatorsandTrainers(2009b)skilldomains
SkillDomain Components
Professionalresponsibilityanddevelopment
Prevention
Recognitionandevaluationoftheindividual
Managementoftheindividual–therapeuticintervention, rehabilitationandperformanceenhancement
Recordkeeping
Professionalpractice–conductandethicalissues
Professionalpractice–performanceissues
Riskassessmentandmanagement
Pre-participationscreening
Prophylacticinterventions
Healthandsafety
Risksassociatedwithenvironmentalfactors
Subjectiveevaluation
Neuromusculoskeletalevaluation
Physiologicalandbiomechanicalevaluation
Nutritional,pharmacological,andpsychosocialfactors
Healthandlifestyleevaluation
Clinicaldecisionmaking
Disseminationofassessmentfindings
Therapeuticintervention
Exercisebasedrehabilitation
Performanceenhancement
Factorsaffectingrecoveryandperformance
Monitoring
Healthpromotionandlifestylemanagement
Immediatecare
abilitiesincludecardiopulmonaryresuscitation,first aid,blood-bornepathogensafeguards,strappingand bracing,andpracticalexperience(inaproperclinical educationprogramme)withthevarietyoftraumatic injuriesthataccompanysportparticipation.Furthermore,workingwithcertainsports–suchascricket, icehockeyandNorthAmericanfootball–requires specialisedunderstandingofprotectiveequipment thatincludeshowtoadministercareinemergency situationswhentheinjuredathleteisencumberedby suchequipment.
BASRaT’s(2009b) RoleDelineationoftheSport Rehabilitator documentdetailstheimplementation oftheskilldomainslistedaboveintoascopeof practice.Table1.2outlinesthecomponentsofeach domain;thesearefurthersubdividedintoknowledge componentsandskillcomponentstocreateaframeworkbothfortheeducationofsportrehabilitators andtheextentoftheircapabilitiestoserveashealthcareprofessionals.
Emergencyfirstaid
Evaluation
Initiationofcare
Abriefintroductiontoasimilartypeofsport healthcareproviderintheUnitedStatesofAmericaisusefulhereasacomparison.CertifiedAthleticTrainers(denotedbythequalification“ATC”) are“healthcareprofessionalswhocollaboratewith physicianstooptimizeactivityandparticipation ofpatientsandclients.Athletictrainingencompassestheprevention,diagnosis,andintervention ofemergency,acute,andchronicmedicalconditionsinvolvingimpairment,functionallimitations, anddisabilities”(NationalAthleticTrainers’Association2009b).TheNationalAthleticTrainers’Association,theprofessionalbodyofCertifiedAthleticTrainers,hasexistedsince1950.Standards ofpracticearesetandacertificationexaminationisadministeredbytheBoardofCertification (2009)toensurethattheprofessionisproperly regulated.MostindividualstatesintheUSAalso requirepossessionofalicenceinordertopracticeasanathletictrainer.Comparabletotherole
delineationskilldomainsforsportrehabilitators listedabove,therequisiteskillsofCertifiedAthleticTrainersarecategorisedinto13contentareas (NationalAthleticTrainers’Association2009a):
1.foundationalbehavioursofprofessionalpractice
2.riskmanagementandinjuryprevention
3.pathologyofinjuriesandillnesses
4.orthopaedicclinicalexaminationanddiagnosis
5.medicalconditionsanddisabilities
6.acutecareofinjuriesandillnesses
7.therapeuticmodalities
8.conditioningandrehabilitativeexercise
9.pharmacology
10.psychosocialinterventionandreferral
11.nutritionalaspectsofinjuriesandillnesses
12.healthcareadministration
13.professionaldevelopmentandresponsibility
ThesecontentareasdefinehowCertifiedAthletic TrainersareeducatedandhowtheyretaintheATC credentialviacontinuingprofessionaldevelopment hours(calledcontinuingeducationintheUSA,with theparticipationincrementscalledCEUs,orcontinuingeducationunits).AswithGraduateSportRehabilitators,accountabilitytosuchstandardsisimperativeforsustainingtheintegrityoftheprofession.
Continuingprofessionaldevelopment Thereisnoplacepitchsideforhealthcarepractitionerswhocannotperformtherequireddutiesthat ariseunderthepressureofmanaginginjuryduring sportingcompetition.Therefore,afundamentalresponsibilityofthesportrehabilitator–oranyother healthcarepractitioner–istosecureahighstandardintheireducation.Certainlythisencompasses theundergraduateandpostgraduatecoursesandthe
motivationtoembracediligenceandexcellenceinall requiredmodules,workplacements,internshipsand thelike.Theknowledgerequiredandtasksallowed forspecificprofessionalqualificationsareusually dictatedbyprofessionalorganisations.Asmentioned above,BASRaTholdsportrehabilitatorstoahigh standardofeducation.Onceaqualificationisattained,however,anothereducationalprocessensues: professionalsmustengageincontinuingprofessionaldevelopment(CPD).Theimportanceofthis cannotbeoverstated.CPDhelpsthesportrehabilitatornotonlymaintaintheirskills,butacquirenew onesthatbroadenone’sabilitytoofferhighquality healthcaretoathletes,clientsandpatients.Moreover,knowledgeinsportscienceandsportmedicine isconstantlyevolvingasfurtherbasicandappliedresearchisundertaken.AdequateCPDhelpsthesport rehabilitatorstayabreastofthesedevelopments.
CPDcoursesaffordexcitingopportunitiesforpersonalenrichment.Manytopicsaregermanetothe fieldandaveritablesubcultureexiststoprovideadequatechancesforprofessionalstoenlistintrainingcoursesthatmatcheveryability,needanddesire.Mostprofessionalsocieties,includingBASRaT, advisetheirmembersaboutsuitablecoursesand therequiredquantityofCPDhours.Advancedlife support,manualtherapy,pitchsideemergencycare, strengthtraining,exercisetesting,specialisedjoint examinations,rehabilitativeexerciseandmanagementofnon-orthopaedicinjuriesandconditionsare onlyafewtopicsrepresentativeofthewidegamut ofofferings.
Aqualificationinbasiccardiopulmonaryresuscitationforhealthcareproviders(i.e.BLS/AED–BasicLifeSupport/AutomatedExternalDefibrillation)isconsideredaminimalcredentialthatshould bekeptuptodatebyperiodicskillsretraining.The ResuscitationCouncil(UK)andtheEuropeanResuscitationCouncilpublishtheappropriatestandards forBLSandAEDtraining(EuropeanResuscitation Council2009;ResuscitationCouncil(UK)2009); thelatteralsomaintainsacalendarofmanylifesupportcoursesofferedaroundEurope,includingthe UnitedKingdom.
Knowledge,abilityandwisdom Itisimportantforprofessionalhealthcareproviders todistinguishamongstknowledge,abilityand wisdom.Thesearedistinct,yetinterrelated,
characteristicsthatallsportrehabilitatorsmuststrive forastheyprovidecaretothepublic.Knowledgeis thelearningandunderstandingoffactsthatform thebasisforpractice.Itprovidestheinformation onwhichasuccessfulcareerisbuilt.Abilityisthe applicationofknowledge.Thus,knowledgereally isnotusefuluntilapersonaccomplishesataskby applyingit.
Wisdom,though,islikethegluethatholdsaprofessionalcareertogether.Itisthemostdifficult–butalsothemostsignificant–ofthethreetogarner becauseitisgainedovertimeasonematuresandis exposedtoanever-wideningvarietyofexperiences. Wisdomconsidersboththeavailableknowledgeand ability,mixingthemintherightproportiontoelicit thebestresultwithinagivensetofpresentcircumstances.Whilstthismayseemsomewhatesoteric, thethreecharacteristicsarefundamentaltosuccess andallhealthcareprofessionalsdrawoneachofthem everyday.
Ethicalconsiderations Ethicsreferstoasetofconcepts,principlesandlaws thatinformpeople’smoralobligationtobehavewith decency.Partofthisisthenecessitytoprotectpeoplewhoareinarelativelyvulnerableposition,such asapatientorclientinahealthcaresetting.Similar tootherprofessionals,eachsportrehabilitatormust considerthemselvesahealthcarepractitionerand, therefore,underanethicalobligationforinscrutable professionalconduct.Sportmedicinepresentschallengingparameterswithinwhichtoapplyanethical framework(Dunn etal. 2007;Salkeld2008),due largelytothehighpublicvisibilityofsportitself. Thisisperhapsanevenmoresignificantreasonfor thesportrehabilitatortoardentlyensurethattheir practicefallsunderappropriateaccountability.
Unfortunatelyethicaldilemmasdonotalways lendthemselvestoclear,objectivedispensation; thus,governingbodiescodifyguidingprinciplesfor conduct.TheCodeofEthicsoftheBritishAssociationofSportRehabilitatorsandTrainers,shownin Table1.3,isanexampleofguidelinesthatpromote properbehaviour.
Inhealthcarethefieldofethicssetsappropriate andacceptablestandardstoprotectthepublicfrom damagesincurredatthehandsofunscrupulousor incompetentpractitionersandthedeleteriouseffects ofunwarrantedordangerousdiagnosticortherapeu-
ticinterventions.Respectforthedignityofhumans isplacedforemostandhealthcarepracticemustaccommodatetothishighstandard.Thereareanumber ofcircumstancesthatoccurinsportthatcanstrain thetypicalapplicationofethics;areaswheredifficultiesariseinclude:
decisionsaboutreturntosportactivitywithapersistinginjury
pharmaceuticaltherapiestoassistparticipation participationofchildren,especiallyinhigh-risk sport
sharingofconfidentialathletemedicalinformationamongstpractitioners,orbetweenpractitionersandpublicrepresentatives,suchasthepress ergogenicaids,suchasanabolicsteroidsandblood “doping.”
Ofthese,treatinganathlete’smedicalinformationwithconfidentialityislikelytobethemostdifficultandfrequentlycompromised,particularlyin thepitchsideenvironment(Salkeld2008).Salkeld suggeststhatseveralcompetingchallengesandpressurescollidepitchsidetocreateethicaldilemmas:the closeproximityofaninjuredplayertootherplayersandcoacheswhenbeingexamined,thepublic visibilityofaninjury,theinterestsofthesporting clubandthedesireofthecoachingstafftoreceive informationabouttheinjurycoupledwiththeconcomitantdesireoftheplayertoshieldthisinformationfromthecoaches.Additionalareasofcontemporaryethicalchallengesforpractitionerscaring forathletesincludeinformedconsentforcare,drug prescriptionanduseofinnovativeoremergingtechnologies(Dunn etal. 2007).
Themostappropriatewayforthesportrehabilitatortomanagepotentiallydifficultethicalpredicamentsistopractisediligentlyunderanapproved ethicalcode,suchasthatoftheBritishAssociationforSportRehabilitatorsandTrainers,andtodecidehowindividualethicalquandarieswillbehandled prior tobeingconfrontedbythem.Theconsequencesofinfractionsaresevereandhaveresulted inrevokedprofessionallicences,registrationsand certifications,andhaveendedcareersinparticularly egregiouscases.
Table1.3 TheCodeofEthicsoftheBritishAssociationofSportRehabilitatorsandTrainers(2009a)
PRINCIPLE1:Membersshallacceptresponsibilityfortheirscopeofpractice
1.1Membersshallnotmisrepresentinanymanner,eitherdirectlyorindirectly,theirskills,training,professional credentials,identityorservices
1.2Membersshallprovideonlythoseservicesofassessment,analysisandmanagementforwhichtheyarequalified andbypertinentlegalregulatoryprocess
1.3Membershaveaprofessionalresponsibilitytomaintainandmanageaccuratemedicalrecords
1.4Membersshouldcommunicateeffectivelywithotherhealthcareprofessionalsandrelevantoutsideagenciesin ordertoprovideaneffectiveandefficientservicetotheclient SupportingLegislation:DataProtectionAct1998;HumanRightsAct1998
PRINCIPLE2:Membersshallcomplywiththelawsandregulationsgoverningthepracticeofmusculoskeletal managementinsportandrelatedoccupationalsettings
2.1Membersshallcomplywithallrelevantlegislation
2.2MembersshallbefamiliarwithandadheretoallBritishAssociationofSportRehabilitatorsandTrainers’ GuidelinesandCodeofEthics
2.3Membersarerequiredtoreportillegalorunethicalpracticedetrimentaltomusculoskeletalmanagementinsport andrelatedoccupationalsettings
PRINCIPLE3:Membersshallrespecttherights,welfareanddignityofallindividuals
3.1Membersshallneitherpracticenorcondonediscriminationonthebasisofrace,creed,nationalorigin,sex,age, handicap,diseaseentity,socialstatus,financialstatusorreligiousaffiliation.Membersshallcomplyatalltimes withrelevantanti-discriminatorylegislation
3.2Membersshallbecommittedtoprovidingcompetentcareconsistentwithboththerequirementsandlimitationsof theirprofession
3.3Membersshallpreservetheconfidentialityofprivilegedinformationandshallnotreleasesuchinformationtoa thirdpartynotinvolvedintheclient’scareunlessthepersonconsentstosuchreleaseorreleaseispermittedor requiredbylaw
PRINCIPLE4:Membersshallmaintainandpromotehighstandardsintheprovisionofservices
4.1Membersshallrecognisetheneedforcontinuingeducationandparticipationinvarioustypesofeducational activitiesthatenhancetheirskillsandknowledge
4.2Membersshalleducatethosewhomtheysuperviseinthepracticeofmusculoskeletalmanagementinsportand relatedoccupationalsettingswithregardtothecodeofethicsandencouragetheiradherencetoit
4.3Wheneverpossible,membersareencouragedtoparticipateandsupportothersintheconductandcommunication ofresearchandeducationalactivities,thatmaycontributetoimprovedclientcare,clientorstudenteducationand thegrowthofevidence-basedpracticeinmusculoskeletalmanagementinsportandrelatedoccupationalsettings
4.4Whenmembersareresearchersoreducators,theyareresponsibleformaintainingandpromotingethicalconduct inresearchandeducation
PRINCIPLE5:Membersshallnotengageinanyformofconductthatconstitutesaconflictofinterestorthat adverselyreflectsontheprofession
5.1Theprivateconductofthememberisapersonalmattertothesamedegreeasisanyotherperson’s,exceptwhen suchconductcompromisesthefulfillmentofprofessionalresponsibilities
5.2Membersshallnotplacefinancialgainabovethewelfareoftheclientbeingtreatedandshallnotparticipatein anyarrangementthatexploitstheclient
5.3Membersmayseekremunerationfortheirservicesthatiscommensuratewiththeirservicesandincompliance withapplicablelaw
Legalconsiderations Anadditionalconcernwhenprovidingcaretoathletesistheincreasinglylitigiousaurathatpervades muchofWesternsociety.Sportrehabilitatorsand otherpractitionersofsportinjurycarearesubject tolawsuitsbroughtbyathletesandtheirrepresentatives(e.g.parents,carers).Aspreviouslymentioned, consistentlyfollowinganappropriatecodeofethics andcontinuallyeducatingyourselfviaCPDaretwo waystoamelioratetherisk.Itisalsocrucialthat sportinjuryprofessionalsmaintainmalpracticeand liabilityinsurancecover,acaveatforwhichBASRaT ensurescomplianceofitsmemberGraduateSport Rehabilitators.
Thediscussionoflegalliabilityfirstneedsadirectivecitingtheproperwayofactingthatisacknowledgedbycourtswhenderivingjudgments.“Theman ontheClaphamomnibus”isacommonphrasein Englishlawthatdenotesapersonwhoactstruly andfairly(GlynnandMurphy1996)withallfacultiesthatwouldbeexpectedunderthecircumstances. (AnAmericanequivalentis“areasonableandprudentperson.”)Astructureofaccountabilityisfundamentaltoapplicationofthisconcept.Withinagiven contextitmaybemodifiedappropriately;healthcare isonlyonerealmtowhichitpertains(Glynnand Murphy1996).Whilstbeingafraidofthepotentialforlitigationinasporthealthcareenvironment wouldunnecessarilyconstrainawell-qualifiedprofessional,undeniablysportrehabilitatorsandother healthcarepractitionersmustbecognisantoftheinherentriskofbeingsuedforwrongactions(acts ofcommission)orforinactionwhenactioniswarranted(actsofomission).Insteadofbeingintimidated,oneshouldtakeallnecessarystepstoreduce thelikelihoodofalawsuitasmuchaspossible.
Thetenetofa“publicrighttoexpertise”wasproposedforthesportandphysicaleducationfields morethan25yearsago(Baker1980,1981).The generalconceptstatesthatmembersofthepublic havetherighttoexpectthatthosewhoofferthemselvesasprofessionalsinagivenfieldofendeavourarequalifiedasexpertsinthatfield.Inthecontextofsportrehabilitation,affordingthepublicthis rightisparamountbecauseofthepotentialforsevereconsequenceswhenhealthcareprovidersare inadequatelyskilledormakeerrorsinpracticeor judgement(Goodman2001).
Countlesslegalcasestranscendrecentdecades (Appenzeller2005)asplaintiffs(peoplefilingalawsuit)persistinclaimingnegligencebydefendants (peoplebeingsued)suchashealthcareproviders, coachesandinstitutions.Generallyanegligence claimmustshowthefollowing(Champion2005):
thereisaverifiablestandardofcaretowhichthe defendantshouldbeheld
thedefendanthadadutytocarefortheplaintiff thedefendantbreachedtheirduty theplaintiffsustaineddamagesorinjury
thedamagesorinjurywerecausedbythedefendant’sbreachoftheduty.
Riskofexposuretolegalliabilityrelatedtohealthcareinsportusuallyoccursinfourmainareas,the firstthreeofwhicharerelatedtooneanother(Kane andWhite2009):
1.Pre-participationphysicalexamination–A screeningprocesstoevaluatetheathlete’sphysicalandmentalstatuspriortoengaginginsport shouldbeafundamentalrequirementbeforesuch engagementoccurs.
2.Determinationofanathlete’sabilityto participate–Whetherconfrontedwithsignsand symptomspitchside,courtside,inafirstaidfacility,inapolyclinic,orelsewhere,properdecision makingaboutanathlete’sfitnesstoparticipate mustbemadeinaccordancewithcurrenthealthcarepractice.
3.Evaluationandcareofsignificantinjuriesonthe pitchorcourt–Healthcareprofessionalsnotonly mustbewell-qualified,theymustdelivercarethat isappropriateforagivensituation.Concussions, spinalcordinjuriesandhyperthermiaarethree examplesofinjuriesrequiringurgent,specialised diagnosticandtreatmentprocedures.Asponsoringclub,university,schoolororganisationmust ensurethataplanisinplacetoadequatelyrespond toemergencysituationsthatmayariseinsport.
Table1.4 Someexamplesofnegligencethatcanleadtoinjurylitigationinsport
Areaofpotential negligence Examples
Facilitysafety
Warningof (orunnecessary)risk ordanger
Poorconditionofthesurfaceofthepitch,court,track,etc.(e.g.holes,unevensurfaces)
Unsafeequipment(e.g.exposedsharpedges,brokenorrustedparts)
Unsafepractices(e.g.reducedvisibilityiflightsarenotusedwhentrainingheldatnight)
Impedingobjectsthatarenotpartofthesportactivity
Failuretoteachsafetechniquesforthesport
Failuretodisclosepotentialinjuryconsequencesofplayingandofnotplayingusingsafe techniques
Failuretointervenewhenplayersdonotusesafetechniques
Mismatchedplayers(e.g.adultplayersparticipatingtogetherwithyoungplayers)
ProtectiveequipmentFailuretoprovideproperprotectiveequipment
Failuretorequireuseofprotectiveequipment
Improperfitofprotectiveequipment
DocumentationofinjuryFailuretomaintaininjuryrecords
Failuretomaintaintreatmentandrehabilitationrecords
Failuretomaintainconfidentialityofrecords
Falsifyingoralteringmedicalrecords
Appropriatecare
Failuretofollowpropercareprotocols
Failuretoreferinjuredplayertohealthcareprofessionalofgreaterexperienceorhigher qualification
Failuretoremoveinjuredplayerfromparticipation
4.Disclosureofpersonalmedicalrecordinformation–Confidentialityisafundamentalrightand expectationofallpatientsandclients,including athletes.Thesportrehabilitatormusttakecare tonotconvey–evenunwittingly–information aboutanathlete’scasetootherswithouttheathlete’spermission.
Additionalconcernsforthesportrehabilitator thatrelatetopotentialinjurycircumstancesinthese generalcategoriesareaccumulatedinTable1.4 (Anderson2002;Champion2005;KaneandWhite 2009).
Followingareviewofpertinentlegalcases,Goodman(2001)corroboratedthatthosewhosupervise teamscouldbeliableiftheyortheirsporthealthcare providersfailedtoperformproperlyinanyofthese specificareas:
Provideappropriatetraininginstruction.
Maintainorpurchasesafeequipment.
Hireorsupervisecompetentandresponsiblepersonnel.
Giveadequatewarningtoparticipantsconcerning dangersinherentinasport.
Providepromptandpropermedicalcare.
Preventtheinjuredathletefromfurthercompetitionthatcouldaggravateaninjury(Goodman 2001,p.449).
Finally,KoninandFrederick(2005,p.38)identifiedsixcommonmistakessporthealthcareproviders makeincaringforathletes;theseareshownbelow andprovidekeyareasforattentionbysportrehabilitators:
1.Notestablishingbaseline(i.e.“normal”uninjured)datawithrespecttoapatient/athlete
2.Accidentallyverballybreachingapatient’sprivacy
3.Notknowingrulesandregulationsrelatedtoconfidentialityofpatientinformationandmedical records
4.Makingdecisionsbasedonexperienceandinstinctsratherthanseekingappropriateauthoritativeadvice
5.Noteducatingapatient/athleteaboutatherapeutic modalityintervention
6.Underestimatingtheamountofdocumentationrequiredwithcatastrophicinjuryevents
Inshort,sadlytherearevirtuallynolimitstowhat onecanbesuedforwithrespecttomanagingsport injury.Thisshouldbesosoberingthattheprudent sportrehabilitatorwillprepareaccordinglytoreduce asmuchaspossiblethelikelihoodofthisoccurring.
Conclusion Thesportrehabilitatorisakeymemberofthesport injurymanagementteam.Assuch,youmustadhere toseveralimportantprofessional,practical,ethical andlegalprinciples.Properlyequippingyourselfto administeracuteinjurymanagementinthevenues wherepracticewillbeundertaken–whetherpitchside,courtside,trackside,inaclinicorelsewhere–isvitallyimportant.However,simplybeingprepared todelivercarerequiredbysportparticipantsdoesnot sufficientlyqualifyasportrehabilitator,oranyother sporthealthprofessionalforthatmatter.Properethicalandlegalframeworksareintegraltosuccess,as well.Withouttheseunderpinningsthemostskillful healthcareworkerwillnotbeabletosustaintheir practiceundertheguidelinesdeemedappropriateby civilisedsocieties.
Insummary,thisentiretextbookisdevotedtoensuringthereader’ssuccessinsportrehabilitationor arelatedfield.Itisawelcomeinstructionalresource tothestudent,butitisavaluableinformationalreferencetotheclinician,too.Thereisawealthof materialpresentedwheretheauthorsofferinsights fromtheirknowledge,abilitiesandwisdominorder toequipthereaderforexcellenceintheircareerpost.
References
Anderson,M.K.(2002) FundamentalsofSportsInjury Management.Philadelphia,PA:LippincottWilliams andWilkins. Appenzeller,H.(2005)Riskmanagementinsport.InAppenzeller,H.(Ed.) RiskManagementinSport:Issues
andStrategies,2ndedn.Durham,NC:CarolinaAcademicPress,pp.5–10.
Baker,B.B.(1980)Thepublicrighttoexpertise(part1). InterscholasticAthleticAdministration, 7 (2),21–23. Baker,B.B.(1981)Thepublicrighttoexpertise(part2). InterscholasticAthleticAdministration, 7 (3),22–25.
BoardofCertification(2009) WhatistheBOC? Omaha, NE:BoardofCertification(accessed14thAugust 2009), <http://bocatc.org/index.php?option=com content&task=view&id=27&Itemid=29> Bowling,A.(1989)Injuriestodancers:prevalence,treatmentandperceptionofcauses. BritishMedicalJournal, 298,731–734.
BritishAssociationofSportRehabilitatorsandTrainers (2009a) RoleDelineationandDefinitionofGraduate SportRehabilitator(GSR).Salford:BritishAssociationforSportRehabilitatorsandTrainers(accessed 27thJuly2009) <http://www.basrat.org/role.asp> BritishAssociationofSportRehabilitatorsandTrainers(2009b) RoleDelineationoftheSportRehabilitator.Salford:BritishAssociationforSportRehabilitatorsandTrainers(accessed14thAugust2009) <http://basrat.org/docs/basrat role delineation.pdf> Bronner,S.,Ojofeitimi,S.andSpriggs,J.(2003)Occupationalmusculoskeletaldisordersindancers. Physical TherapyReviews, 8,57–68.
Champion,W.T.,Jr.(2005) SportsLawinaNutshell.St. Paul,MN:Thomson/West.
Delaney,R.A.,Falvey,E.,Kalimuthu,S.,Molloy,M.G. andFleming,P.(2009)Orthopaedicadmissionsdueto sportsandrecreationinjuries. IrishMedicalJournal, 102 (2),40–42.
Dunn,W.R.,George,M.S.,Churchill,L.andSpindler,K.P. (2007)Ethicsinsportsmedicine. AmericanJournalof SportsMedicine, 35 (5),840–844. EuropeanResuscitationCouncil(2009) EuropeanResuscitationCouncil.Edegem,Belgium:European ResuscitationCouncil(accessed27thJuly2009) <https://www.erc.edu/new/>
Falvey,E.C.,Eustace,J.,Whelan,B.,Molloy,M.S.,Cusack,S.P.,Shanahan,F.andMolloy,M.G.(2009)Sport andrecreation-relatedinjuriesandfractureoccurrence amongemergencydepartmentattendees:implications forexerciseprescriptionandinjuryprevention. EmergencyMedicineJournal, 26 (8),590–595.
Fitt,S.S.(1996) DanceKinesiology.NewYork:Schirmer Books.
Garrick,J.G.andLewis,S.L.(2001)Careerhazardsfor thedancer. OccupationalMedicine, 16 (4),609–618. Glynn,J.J.andMurphy,M.P.(1996)Failingaccountabilitiesandfailingperformancereview. InternationalJournalofPublicSectorManagement, 9 (5/6),125–137.
Goodman,R.S.(2001)Sportsmedicine.InSanbar,S.S., Gibofsky,A.,Firestone,M.H.,LeBlang,T.R.,Liang, B.A.andSnyder,J.W.(Eds) LegalMedicine,5thedn. St.Louis:Mosby,pp.448–450. Kane,S.M.andWhite,R.A.(2009)Medicalmalpracticeandthesportsmedicineclinician. ClinicalOrthopaedicsandRelatedResearch, 467 (2),412–419. Konin,J.G.andFrederick,M.A.(2005) Documentation forAthleticTraining.Thorofare,NJ:Slack. Koutedakis,Y.andJamurtas,A.(2004)Thedancerasa performingathlete. SportsMedicine, 34 (10),651–661. Laws,H.(2005) FittoDance2.London:DanceUK. Miller,J.R.&Demoiny,S.G.(2008)Parkour:anewextremesportandacasestudy. JournalofFootandAnkle Surgery, 47 (1),63–65.
NationalAthleticTrainers’Association.(2009a) Competencies.[online].Dallas,TX,USA:NationalAthletic Trainers’Association.[accessed14thAugust2009]. <http://www.nata.org/education/competencies.htm>
NationalAthleticTrainers’Association.(2009b) What isanAthleticTrainer? Dallas,TX:NationalAthleticTrainers’Assocation(accessed14thAugust2009) <http://www.nata.org/about AT/whatisat.htm> ResuscitationCouncil(UK)(2009) Guidelines,medicalinformationandreports.London:ResuscitationCouncil(UK)(accessed27thJuly2009) <http://www.resus.org.uk/pages/mediMain.htm> Salkeld,L.R.(2008)Ethicsandthepitchsidephysician. JournalofMedicalEthics, 34 (6),456–457. Spanjersberg,W.R.andSchipper,I.B.(2007)Kitesurfing: whenfunturnstotrauma–thedangersofanewextreme sport. JournalofTrauma, 63 (3),E76–E80. Stretanski,M.F.(2002)Classicalballet:thefullcontact sport. AmericanJournalofPhysicalMedicineandRehabilitation, 81 (5),392–393. Young,C.C.(2002)Extremesports:injuriesandmedicalcoverage. CurrentSportsMedicineReports, 1 (5), 306–311.
Part2 Injuryscreeningandassessment ofperformance 2 Injurypreventionandscreening PhilBarter
LondonSportInstituteatMiddlesexUniversity,London,UK
Introduction
Themainaimsofthischapteraretointroduce musculoskeletalscreeningandoutlinetheavailable methodsandtherelatedreliabilityandvalidityissues.Thischapterwillallowthereadertogainan understandingofmusculoskeletalscreeningandits roleininjuryprevention,identifythemusculoskeletalscreeningmethodsavailableincludingadiscussionofthevalidityandreliabilityofscreeningmethods.Thechapterwillfinallyrecommendascreening procedureforinjuryriskidentification.
Pre-habilitationcanoftenbeoverlookedinthe makeupofasportssupportteam,whichcanoften leadtoproblemsbeingoverlookedandtheteamor individualnotperformingtotheirpotentialthroughouttheirseasonduetoinjury.Incontrastsome professionalclubsspendtoomuchtimeonremediallevelpre-habilitationandnotenoughtimeon highintensitytrainingthatmeetsthedemandsof thesport.Proceduresneedtobeimplementedtoensuretheamountoftrainingdaysandcompetitive sessionsmissedareminimised.Practitionersneedto beproactivewiththeirtreatmentsplansandnotrely onthetraditionalreactiveplans.Inorderforthis tobethecasepractitionersneedtobefullyaware ofthelatestresearchandmethodsintheareaof needthroughcontinuedprofessionaldevelopment. Theseplansoftencommenceduringtheoffseason ortheearlypartofpre-season.Duringthisperiod theathletecanbeassessedwithoutthedemandsof competition,whichwillenablethepractitionerto gaintheknowledgeneededtoplanfortheupcoming season.
Screeningcanbecompletedthroughavarietyof testsincludingphysicalactivitytests,functionalassessmentandquestionnaires.Theseallhavevarying strengthsandweaknessesandarealsodependenton thepractitionerwhoiscarryingoutthescreening.
Withtheneedforathletestoplayaneverincreasingnumberoffixtures,theenforcedbreaks duetoinjuryneedtobedecreased.Severalapproachescanbetakentoensurethattheathleteis trainedandpreparedsothatanypossibleproblems areeitherdealtwithbeforetheyariseormeasures areinplacesothattreatmentcanbeadministered rapidlyuponinjury.Injurypreventionisaprocess wherebytheathleteisscreenedthroughavariety ofteststoidentifyanypotentialproblemswith theirmusculoskeletalcomposition.Theseproblems canthenbeidentifiedandtrainingpracticesputin placetoeithereradicatetheseproblemsorreduce theirpossibleimpact.Severalproceduresareused bysportspractitionerswithvaryingdegreesof successastheneedforonecommonprocedure formusculoskeletalscreeningbecomesapparent. Severalresearchershaveattemptedtoidentify whichmethodsofferthehighestdegreeofaccuracy andvalidity(Gabbeetal.2004;MillerandCallister 2009;McCleanetal.2005).
Regardlessofthemethodchosentheaimistoidentifyaseriesofriskfactorsthatwillenableanypotentialproblemstobeidentifiedanddiagnosed.The findingsoftheathletescreeningcanbeassessedfor riskofinjurysothatplanscanbemadetoreducethe levelofriskfortheathlete.
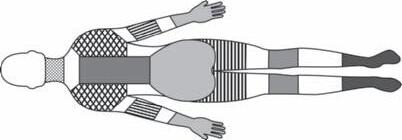
Screeningmethods Theapproachtakenbytheleisureindustryasa wholetowardsinjurypreventionisonethatinvolved ahealthscreeningquestionnaire.Thequestionnaire canoftenbemodifiedtoincludeafewgeneral musculoskeletalquestionswhich,ifanswerednegatively,canthenresultintheathletebeingreferred totheirGP.ThemethodofscreeningwhichincludesthisGPreferralapproachisverygeneraland mainlyfocusesonreducedliabilityoftheadministeringfacilityorpractitioner.Althoughthisapproach wouldnotberecommendedwhenworkingwithathletesinsportrehabilitation,theuseofaquestionnaireisoftenoverlooked,eventhoughresearchhas shownittobeausefulscreeningtool.Researchby Dawsonetal.(2009)suggeststhatthroughtheuse oftheExtendedNordicMusculoskeletalQuestionnaire(NMQ-E)(seeFigure2.1)potentialpainareas andconsequentialproblemscanbeidentified.The questionnaireneedstobeadministeredbyasuitable practitionerandnottheathleteinvolved,ensuringthe resultsarevalid.Researchsuggestedthatinconjunctionwithrelevantfunctionalassessmentsthisquestionnairewasausefulstartingpointinthescreening process.Theresultsfoundthatprevalenceofmusculoskeletalproblemscouldbecorrectlydiagnosed andtreatedeffectively.Thereliabilityofthequestionnaireusedwastestedoveraseriesoftrialswith thesameresultsshown,indicatingthevalidityand repeatability(Dawsonetal.2009).Figure2.1clearly showstheimportantareasofthebodysotheathlete knowswhichpartthequestionsarerelatedtoand thenfollowsalogicalorderthroughtheareaidentifyingthedegreeofanypossiblepain.Thequestions thenfollowalogicalorderdownthebodycovering allthegeneralpointsofthebody.Theresultscan thenbepassedontoasportsrehabilitationpractitionerforfurtherfocusedfunctionalassessmentof theidentifiedproblemareas(Dawsonetal.2009).
Assessmentbythemeansofquestionnaireisnot, ofcourse,anewmethodology,buttheintegration withfunctionalandphysicalteststoformaholistic processis.Thewayinwhichthescreeningelements
areintegratedintotheinjurypreventionprocesscan havealargeimpactontheathletesinvolved.Ifathletesfeelpartofthisprocessthentheycouldtake ownershipandreallyfullycommittothemeasure thatisultimatelyproposed.Ifathletesareinsufficientlyinvolvedthentheymightseetheprocessand resultantprogrammeasunnecessaryandtherefore notworthyofexpendingtoomuchenergyon.The othersituationiswheretheathletecouldlearntoo muchandbecomede-motivatedabouttheirlongtermfutureinthesportandasaresultnotcommit. Thelattertwoscenarioswillmeanthatthepractitionersplansmayfailandtheproblemsidentified willprobablyarisewithanegativeeffectonperformance.
Amoresimplisticapproachtoquestionnairescan alsoproducegoodresultsinreducingtheamount ofteststhatanathleteneedstoperform.Thereductionoftestingtimeisimportantinlargesquads astheamountoftimethepractitionerspendswith theathletereducestheamountoftimethecoach canspendworkingonsport-specifictraining.Therefore,theneedtodevelopausefultooltoidentifythe membersofthesquadwhodonotneedanyfurther testingorthosewhocanbedealtwithinareduced fashionisimportant.TheprocessshowninFigure 2.2indicatesasimplepathwaytogroupthesquad intodifferentlevelsoftestingthroughasimplesetof questions.Thishasbeenshowntobereliableinidentifyingconditionsandmoreimportantlynotmissing anyproblems.Thequestionnaireagainneedstobe administeredbyapractitionertoinsurethevalidity oftheanswers(Berg-Riceetal.2007).
WhenthescreeningquestionsshowninFigure 2.2werecompletedbyapractitionerthepotential injurieswerecorrectlyfoundin92%ofathletes screened.Whenthesameprocesswascompleted byanon-practitioneronly80%ofcaseswherepositivelyscreened.Althoughtheresultsofthescreening processshowthatitneedstobeconductedbytherelevantpractitioner,theoverallimpactontheaverage numberofdayslostthroughinjurywasstillsimilar 23(non-screened)versus21days.Thissuggeststhat stringentfollow-uptestsarestillneededtoensure thatproblemsaredealtwitheffectively(Berg-Rice etal.2007).
Theinitialquestionnaireusedforscreeningcan alsoaccesstheathlete’spsychologicalstatetowards injuryandthesocialfactorsthatcouldaffecttheir ownapproachtoproblems.TheOrebroMusculoskeletalPainScreeningQuestionnaire(OMPSQ)
How to answer the questionnaire:
During the best 12 months have you at an ytime: been preverted from doing your normal work (at home or away from home) because of the trouble? seen a doctor, physio- therapist, chiropractor or other such person because of the trouble? taken medication because of the trouble? taken sick leave from work/studies because of the trouble?
Have you had trouble (ache, pain, discomfort) today?
Have you had trouble (ache, pain, discomfort) at anytime during the last month (4 weeks)?
If ‘No’, go on to the next body region. If ‘Yes’, please continue
Have you had trouble (ache, pain, discomfort) at anytime during the best 12 months?
Have you ever had to change jobs or duties (even temporarly) because of the trouble?
Have you ever been hospitalised because of the trouble?
At the time of initial onset of the trouble, what was your age?
Have you ever had trouble (ache, pain or discomfort) in: If ‘No’, go on to the next body region. If ‘Yes’, please continue
Please answer by putting a cross in the appropriate boxone cross for each question. Answer every question, even if you have never had trouble in any part of your body. Please answer questions from left to right before going down to the next body region. This picture shows how the body has been divided. Limits are not sharply defined and certain parts overlap. You should decide for yourself which part (if any) is or has been affected.
NECK
TheExtendedNordicMusculoskeletalQuestionnaire(NMQ-E)(Da wsonetal.2009).Reproduced,withpermission,fromDawson,A.P. ,Steele,E.J., Hodges,P.W.,&Stewart,S.(2009).DevelopmentandTest-Retest reliablityofanextendedversionofthenordicmusculoskeletalquestionnaire (NMQ -E):AScreening instrumentformusculoskeletalpain.ThejournalofPain,10(5), 517–526
Figure2.1
Do you plan to take the diagnostic APFT?
Are you presently on Profile?
Yes
For what?
Do you presently have an injury or are you experiencing pain in your arms, legs, back, neck or hip? Where?
Do you want a referral to the TMC?
Yes Yes Yes No No No
Yes No No
Have you had an injury within the last 6 months?
Does the injury still bother you?
Yes No
Do you want a referral to the TMC?
Do you feel that you can safely take the diagnostic APFT?
Yes No No
Perform the Complete Screen
Yes
Refer to TMC (If athlete is already on profile, TMC referral is discretional)
Figure2.2 Initialscreeningquestions(Berg-Riceetal.2007).Reproduced,withpermission,fromBerg-Rice,V.J., Conolly,V.L.,Pritchard,A.,Bergeron,A.,&Mays,M.Z.(2007).Effectivenessofascreeningtooltodetectinjuriesfuring armyhealthcarespecialisttraining.Work,29,117–188, © 2007IOSPress.
hasbeenusedinresearchtolookatpotentialproblemsandthesubject’spainavoidance.Theathlete’s injuryhistorywillhaveaneffectontheirability todealwithinjuryandhowtheyratetheircurrent musculoskeletalstate.TheOMPSQfactorsintothe score:fearavoidance;howwellthepersonperceives theycandealwithpain;howdistressedtheyhave beeninthepastaboutinjuries;andtheathlete’sown ratingoftheirfunction.Thesescoreswerethencombinedandfactorsgiventotheratingtoproducethree predictingfactorsofhowmanydaystheathletewill missonaverageayear.Thefirstpredictingfactorwas thefunctiongroupofquestions,whichsignificantly (p = 0.001),predictedtheamountof‘Sick’daysthe athletewouldhaveoverthecourseofathree-year
period(Westmanetal.2008).Thefunctionalassessmentquestionslookedintohowathletesperceived theinjuryaffectedthemandtheirabilitytoperform. Thesecondfactorthatsignificantlypredictedthe amountofthemissedtrainingdaysduetoproblems wasthepainfactor.Theathletes’painandinjuryhistorywasfactoredintothispredictortosignificantly predicttheamountofdaystheathletewouldmiss duringthenextthreeyears,(p = 0.0026)(Westman etal.2008).Thefinalfactorinthisquestionnaire, whichwaslabelledfear-avoidanceandwasthepain thattheathletehadexperienced,didnotsignificantly predicttheamountofmissedtrainingdays.The lastfactorincludedtheathlete’sfearoftrainingdue theperceivedaffectitwouldhaveonaninjuryand
elicitedbynonpainfulstimulationoftheskin’)”
Figure2.3 VAScharacteristics(Laslettetal.2004).Reproduced,withpermission,fromLitcher-Kelly,L.,Martion, S.A.,Broderick,J.E.,&Stone,A.A.(2007).Asystematicreviewofmeasuresusedtoassesschronicmusculoskeletal paininclinicalandrandomizedcontrolledclinicaltrials.Thejournalofpain,8(12),906–913, © 2007Elsevier.
thereforethelengthoftimeawayfromcompetition (Westmanetal.2008).
Thescalebywhichathletesareoftenaskedto reportpaincanbevariedbutthemostreliableand mostcommonistheVisualAnalogScale(VAS).The characteristicsoftheVAScanbeseeninFigure2.3. Thescalecanhaveavarietyofanchorpointsand reportingperiods.Thewayinwhichitcategorises paincanalsobevariedwithglobal,intenseandgeneralterms,allbeingusedtointeractwiththepatient tohelpthemidentifytheirpain.Thereisaneedfor a‘goldenmeasure’ofassessmentofpatientpain, andtheVASseemstobethemostcommonlyused methodatpresent(Litcher-Kellyetal.2007).
Functionalassessmentscanfollowascreening questionnaireorbetheinjurypreventionprocessin itsentirety.Thetestusedtofunctionallyassessan athletecanbevariedanddifferdependinguponthe areaofthebodyandtheactivitytheathletecom-
petesin.Thebackandkneearetwoofthemajor areasthatthescreeningprocessneedstoassessdue totheirimportancetolocomotionandthereforethe resultantsportingperformance.Theflexibilityand posturecanbegovernedextensivelybythebackand inparticularthelowerbackstrengthoftheathlete. Iftheathletessufferfromlowerbackpain(LBP) thentheycanoftenmisstrainingsessionsdueto thelackofmobilityorworkatareducedlevel.The importancetoscreenthisareaofthebodyproperly andplanforanypotentialproblemsisessentialinan athlete’ssportinglife.
Revelsmodelcanbeusedasscreeningtestfor LBP,withnospecificconditions.AthleteswithspecificLBPwouldneedtobefurtherscreenedtoassessthefullextentoftheirproblems.Thesefindings wereshowninresearchtobeapplicablefor11% ofthepopulation,asthetestingprocedurelacked specificity(Laslettetal.2004).TheRevelstesting
Figure2.4 TheRevelsmodelphysicalexamination (Laslettetal.2004).ReproducedfromLaslett,M.,Oberg, B.,Aprill,C.N.,&McDonald,B.(2004).Zygapophysial jointblocksinchronicelowbackpain:Atestofrevel’s modelasascreeningtest.BMCMusculoskeletalDisorders,5(43),1–6,publicdomaininformationcourtesyof BioMedCentralLtd.
procedureinvolvesthepatientbeingaskedtoassess thebackpaincurrentlyexperiencedusingaVAS, thenthehighestamountofpainandthenthelowestamountofpainexperienced.Subjectswerethen askedtocompletetheexercisesshowninFigure2.4. Oncompletionoftheexercisesthesubjectswere thenaskedtore-evaluatetheirpainscoresonthe VAS.UsingtheRevelsmodelthesubjectswerecategorisedintogroupsthathadmetthecriteriaand thosethathadnot.Thegroupsthathadmetthecriteriahadafurtherassessmentonthelowerbackjoints. Aspreviouslystatedthisonlyproducedapositive resultinthosesubjectswithverygeneralproblems, butwassignificantlylinked(p = 0.04)tothepatients amountof‘sickdays’,i.e.thosewithapositiveRevelstesthadagreaternumberof‘sickdays’(Laslett etal.2004).
ThesafetyoftestsliketheRevelsmodelhasbeen questionedduetothedangerimposedbypossible furtherdamagetoexistinginjuries.Theconditionof mostconcernisvertebralarterydissection(VAD). Whenassessingtheback,practitionersmustensure thatthepatient’shistoryisfullyrecordedbefore examination,rulingoutanysymptomsforVAD. Thepatientshouldbeassessedinitiallybymeans ofnon-provocativemanipulation.Iftheareaof thecervicalspineneedstobemanipulatedthen thepractitionershouldensurethatallsymptoms forVADhavebeeneliminatedanddecidewhether theprovocativemanipulationresultsarenecessary orconclusionscanbedrawnthroughothermeans (ThielandRix2005).
Anotherareaonthebodythatisofparamount importancetothepractitioneristheknee.Aninjury
totheanteriorcruciate(ACL)isoneofthemost seriousproblemsthatcanhappentoanathleteand haveaseriouseffectontheircareer(Bonci,1999). ThepreventionofinjurytotheACLandthekneeis veryimportantandisdependentonidentifyingaseriesofriskfactors.Themajorriskfactorsassociated withACLinjuriesincludelowerextremitymalalignments,ligamentouslaxity,lowerextremitymuscular strengthconsiderations,neuromuscularcontrol,hormonalinfluences,intercondylarnotchwidthandthe biomechanicsoftheathletes’sportingtechniques (Bonci,1999).Therehabilitatorcanonlyimprove andmodifythestrengthandneuromuscularcontrol riskfactors,whichiswhythesearekeyareasofa screeningprocess(Bonci,1999).Themisalignment ofthebodycanincreaseriskofinjury,particularly inthebackandknee.andthisisveryimportantin thelowerlimbsinathletes.Thelocomotionpartof anysporttechniquemeansthatanyproblemwiththe lowerlimbwillbesubjectedtoextremeforces.The kneeinparticularcanonlyabsorbacertainamountof theseforcesandthroughthenatureofsporttheathletewillatsomepointsufferinjuryasaresult.The degreesofmisalignmentthatwillcausesufficient risktocausepotentialkneeproblemsisvaried,dependingonseveralassessments(Bonci1999).(For greaterdetailregardingACLinjuriesseeChapter21, TheKnee.)Inordertogainafullassessmentofthese risks,theathlete’sfootpronation,kneerecurvatum, tibialtorsionandpostureneedtobemeasured.Neuromuscularcontroltestsforthelowerlimboften involveavarietyofmovementsbutwithcommon goals:toobtainanobjectiveassessmentoffunction andtochallengedynamickneestabilityduringlandinganddeceleration(Bonci1999).Arangeoftests canbeusedtoachievethesegoals,withthesingleleghop,one-legverticaljump,timedhop,figureof eightrunning,sidesteppingandstairrunningbeing afewofthecommonlyusedones(Lephartetal. 1991).Thesetestscanalsobecombinedwithisokinetictestingtogivearoundedpictureoftheknee (Barberetal.1990;Lephartetal.1991).Theway theathlete’sfootlandsduringtheirgaithasalarge impactonthedistributionoftheforcecreated.If thelevelofpronationistoohighthenoneofthe body’snaturalshockabsorbers,theheel,willbeunabletopreventforcefromtravellinguptotheknee. Thecontactphaseiswherethelevelofpronationin thefootiscritical.Ifthecorrectamountispresentthe movementwillbeinefficientandshockabsorption willnotoccuradequatelyintheheel.