Cancer survivorship research initiative studies life after diagnosis and treatment.
8 20 14 28
Caring acts
The healing art of theater offers a new avenue for community connection and care.
The resilient brain
Advances in stroke assessment and care are revolutionizing research and recovery.
Health innovation in action
School of Health course explores health equity in the DC area through the Capitol Applied Learning Labs.
From the Archives
3 6 2 36 30 40
Update from Dr. Beauchamp
Announcements
Check Up News & Research On Campus
Alumni Connections
Reflections on Health
Robert Fan, M.D. (G’85, M’89)
The Cadet Nurse Corps (1943–1948) was established to increase nurses’ recruitment and education for practice in civilian and military settings during World War II. Over 1,100 participating schools educated these nurses, including Georgetown’s School of Nursing. Dozens of Georgetown nursing diploma graduates were Cadets, and several later earned the Bachelor of Science in Nursing degree. Today, Georgetown ROTC students in the BSN program are commissioned as military officers upon graduation.
Update from Dr. Beauchamp
Dear Friends,
We continue to hear from so many of you pledging your support for the work at our medical center as we, like all institutions of higher education, face unprecedented changes to the federal funding landscape. I am deeply grateful for your commitment to Georgetown.
Research and education are central to our global mission and values, and we are committed to protecting their vital interplay. The changes in research funding represent a significant threat to advancements in medicine including our basic sciences relevant to biomedical innovation, and to our clinical trials aimed at treating cancer, neurodegenerative diseases, mental health, and many other diseases and maladies. Our education funding is critical as the formation of today’s students yields tomorrow’s changemakers for ensuring future improvements to health, advancing scientific discoveries, and ensuring equitable delivery of care to all.
To meet these complex funding challenges, we are pursuing new strategies in support of our education and research enterprise to ensure we fulfill our shared mission within the broader society to bring hope, health, and healing to the communities we serve throughout our region and across the world.
This is not a “wait and see” moment in our history. Our ability to impact the health of the future requires our action now along with broad support and engagement from our generous community.
In this issue of Georgetown Health, you’ll see so many examples of Georgetown’s contribution to advancing science and medicine, and to the formation of our students who will amplify and carry our mission forward. One of the features highlights the revolutionary work being done at Georgetown to help stroke survivors recover from what some call a “neurological thunderbolt.”
Stroke has touched so many of us, including the Georgetown community last year when then-President DeGioia suffered a stroke. I think we can all be proud of Georgetown’s leadership in this important area and the importance of federal funding for this work.
Sincerely,
Norman J. Beauchamp
Jr., M.D., MHS Executive Vice President for Health Sciences Executive Dean, School of Medicine
At the April 1 Innovation and Research Showcase sponsored by Georgetown’s Office of Technology Commercialization, Beauchamp previewed a new effort to create innovation districts in DC, a geographic area where leading-edge anchor institutions and companies cluster and connect with start-ups, business incubators, and accelerators. Most importantly, the incubators will create economic uplift, and access to education and jobs—all critical in addressing the social determinants of health.
Patti North, Sara Piccini, Natalie Rabner, Karen Teber, Heather Wilpone-Welborn, Lauren Wolkoff (G’13), Kat Zambon
Design Team
Ethan Jeon, Shikha Savdas, Sofia Velasquez
Project Managers
Hilary Koss, Chloë Holman
University Photographer
Phil Humnicky
Georgetown Health Magazine 2115 Wisconsin Ave., NW, Suite 400 Washington, DC 20007-1253
Feedback and story ideas: healthmagazine@georgetown.edu
Address changes: alumnirecords@georgetown.edu
Summer 2025 | Georgetown Health
Georgetown Health is distributed free of charge to alumni, parents, faculty, and staff. The diverse views in the magazine do not necessarily reflect the opinions of the editors or official policies of the university.
Georgetown University provides equal opportunity in employment for all persons, and prohibits unlawful discrimination and harassment in all aspects of employment because of age, color, disability, family responsibilities, gender identity or expression, genetic information, marital status, matriculation, national origin, personal appearance, political affiliation, race, religion, sex, sexual orientation, veteran’s status, or any other factor prohibited by law. Additionally, the university will use good-faith efforts to achieve ethnic and gender diversity throughout the workforce. The university emphasizes recruitment of women, minority members, disabled individuals, and veterans. Inquiries regarding Georgetown University’s nondiscrimination policy may be addressed to the Director of Affirmative Action Programs, Institutional Diversity, Equity & Affirmative Action, 37th and O Sts. NW, Suite M36, Darnall Hall, Georgetown University, Washington, DC 20057, or call 202-687-4798.
Georgetown designated R1 institution for 30th year
n n Earlier this year, Georgetown received the Carnegie Classification of Institutions of Higher Education’s designation as an “R1” institution—the highest classification for research and training—for the 30th year.
Georgetown invests in global, interdisciplinary research across a range of pressing issues, from advancing pancreatic cancer treatment to predicting mass migration patterns. In fiscal year 2023, the university invested more than $337 million in research and development.
in fiscal year 2024 to support a broad continuum of research spanning from behavioral studies to clinical trials and population-level research.
The GUMC community is recognized internationally for its work in the areas of cancer, neuroscience, neurology, health equity, and global health. GUMC is one of few medical centers in the country to hold both a Clinical and Translational Science Award from the National Institutes of Health and a cancer center support grant from the National Cancer Institute.
“To ensure affordable and accessible care for all, we must find new and better ways to sustain health and respond to illness. Basic, applied, and translational research underpins the pathway to improving human health.” —NORMAN J. BEAUCHAMP JR.
Georgetown also trains the next generation of researchers in disciplines ranging from the physical and life sciences to the humanities.
Georgetown University Medical Center (GUMC) is home to the university’s most robust research enterprise, securing approximately $176 million in externally sponsored funding
Georgetown and its academic health system partner, MedStar Health, also collaborate to deliver transformative research from the laboratory to clinical care. Together, GUMC and MedStar Health earned $246 million in extramuralsponsored research in fiscal year 2024.
“To ensure affordable and accessible care for all, we must find new and better ways to sustain health and respond to illness. Basic, applied, and translational research underpins the pathway to improving human health,” says Norman J. Beauchamp Jr., executive vice president for Health Sciences and executive dean for the School of Medicine. n
According to the Carnegie Classification, the R1 category means “Very High Research Spending and Doctorate Production.” There are fewer than 200 R1 institutions in the United States.
$25M gift renames, expands School of Nursing
n n Thanks to a $25 million gift from the Berkley Family Foundation, the School of Nursing will be renamed the Georgetown University Berkley School of Nursing this fall, marking a significant milestone in the university’s 122 years of educating nurses.
The Berkley family’s gift will create opportunities to expand enrollment, reduce financial barriers for students, enhance technology, strengthen faculty, and advance student success and well-being, says Roberta Waite, dean of the School of Nursing.
“This is a transformative gift, and we are very humbled,” Waite shares. “The Berkley family understands the need for graduating more nurses and the impact that nursing has on promoting the health and wellness of individuals, families, and communities.”
A commitment to health
“Two generations of our family have a shared love and appreciation for Georgetown University,” says W. Robert Berkley Jr. (B’95). “We have always maintained an interest in both
education and health care, and the opportunity to support the School of Nursing is a natural intersection of both interests.”
Norman J. Beauchamp Jr., executive vice president for health sciences at Georgetown University Medical Center, says this latest gift will advance the medical center’s mission of cura personalis, or care of the whole person.
“This special family has demonstrated an unwavering commitment to bringing hope and healing to people in need by supporting the growth and diversity of nurse leaders and practitioners,” adds Beauchamp.
Addressing critical nursing vacancies
A cornerstone of the gift is the Berkley Endowed Scholarship Fund, which benefits students who are pursuing a second degree to enter nursing through the Accelerated Bachelor of Science in Nursing (ABSN) program.
“Finances can be an enormous issue for people who might discover their passion for nursing later in their career,” Waite says. “A lot of these individuals are interested in working at
Photo: Rafael Suanes
The Berkley family’s gift supports scholarships for Accelerated Bachelor of Science in Nursing (ABSN) students. Students in this program have often discovered their passion for nursing later in their career.
“Two generations of our family have a shared love and appreciation for Georgetown University. We have always maintained an interest in both education and health care, and the opportunity to support the School of Nursing is a natural intersection of both interests.”
—W. ROBERT BERKLEY JR. (B’95)
the bedside in acute care settings, so if we can create an accessible pathway for them by offsetting and alleviating the burden of the cost of tuition, it’s really a win-win scenario.”
Waite also notes the “ripple effect” in investing in latercareer students.
“What’s so impactful is that we know many of those individuals will go back to live and practice within their own communities,” she adds.
Investing in faculty and technology
Faculty excellence is another pillar of the Berkley family’s gift, which establishes endowed professorship and associate professorship funds.
“Endowed professorships are critical to attracting the highest caliber faculty who are also aligned with our values,” Waite says.
In addition, the gift will invest in technology to advance virtual reality capabilities in the O’Neill Family Foundation Clinical Simulation Center which enables students to practice clinical and communication skills in a controlled, simulated environment.
“Technology is really what will move the needle in terms of enhancing the experience of our in-person students as well as those who are learning virtually or in a hybrid setting,” she explains.
Promoting student well-being and new opportunities
The gift also establishes the Berkley Endowed Student Success and Wellbeing Fund, which will provide resources like tutoring, mentoring, stress management, and resilience skills to support students’ mental health.
“Supporting our students with tools that can help them be proactive in mitigating stress is critical for them to care for themselves and promote their own well-being now and throughout their nursing career,” Waite says.
In addition, students will be able to pursue emerging opportunities through
the Berkley family’s Endowed Dean’s Fund for Strategic Initiatives and Nursing Excellence.
“We’re at a point now where we have a more sophisticated foundation—our structure, our people, our understanding— and there’s real momentum building at the nursing school,” she says. “We’re developing new academic pathways, certificate programs, and refreshing our existing offerings. In this environment of rapid innovation, flexibility becomes essential. The Berkley family’s gift represents a significant recognition of nursing’s importance in health care and in the future. I am most grateful to the Berkley family for their trust in Georgetown and I am genuinely excited for the path ahead.” n
Nursing students get hands-on experience in the O’Neill Family Foundation Clinical Simulation Center. Dean Roberta Waite says “there’s a real momentum building at the nursing school.”
Mapping cancer cells
n n Among the many challenges of effective cancer treatment is the need to monitor the cancer itself. Keeping track of cancer cells as they grow, and hopefully as they die off, may be inexact, too infrequent, and expensive for patients.
A group of GUMC researchers wants to change that. Faculty and students from Biomedical Graduate Education programs, the School of Medicine, and Georgetown University’s Lombardi Comprehensive Cancer Center are developing a new technique that could revolutionize the way cancers are tracked and treated. Instead of invasive surgical biopsies or time-consuming scans, clinicians could use simple blood tests to determine where the cancer is and whether it is responding to treatment.
“From a blood sample, we think you can detect much earlier whether a drug works,” said Anton Wellstein, an oncology and pharmacology professor who is leading the research. “We also see the side effects the drug has at the same time.”
At Georgetown, the researchers are working with the technology of liquid biopsy, which involves examining normal and cancer cell DNA in the bloodstream. They are compiling a “map” of cell types that can be used to tell which organs that cancerous DNA is coming from—providing a clearer picture that can guide rapid, personalized treatment. n
New senior associate dean looks to empower students
n n In January 2025, Khaseem Davis joined the Georgetown School of Medicine as senior associate dean for diversity, equity, inclusion, and belonging, bringing his dedication to advancing equity in education, years of experience empowering students to pursue their career goals, and insight as a first-generation college graduate to his new role.
For his doctoral research, Davis studied the experiences of first-generation, high-achieving students from low-income families as they transitioned to college.
Such students benefited significantly from having access to places or people where they could go when they needed support, including “advisors who looked like them, or advisors who might not have looked like them but were really authentic and were able to see those students for who they were, as a person who deserved to be in that space,” says Davis.
In his new role at Georgetown, Davis hopes to nurture students’ intellectual abilities and ensure that they feel a sense of belonging.
“I’m really looking forward to making an impact with wonderful colleagues and supporting the leadership at Georgetown University School of Medicine,” he says. n
Photos: iStock / Evan Cantwell
Before coming to Georgetown, Khaseem Davis, Ph.D., worked as the executive director of the Early Identification Program (EIP) at George Mason University, the largest public university by student enrollment in Virginia. The EIP serves nearly 1,000 students from historically marginalized populations, including those who are first-generation, lowincome and on nontraditional pathways. The program grew 67% under his leadership.
Event highlights federally funded research
n n Each year Georgetown hosts Hoyas on the Hill, an event to celebrate alumni who serve as members of Congress and work in Congressional offices. This year’s event shined a spotlight on federally funded research endeavors now underway at the university, with projects ranging from cancer to strokes, from health disparities to mental health.
Hoyas in the 119th Congress include 21 representatives and seven U.S. senators who represent 18 states and the District of Columbia and the U.S. Virgin Islands, which have non-voting delegates. They also include faculty and alumni from nearly all of Georgetown’s schools, including 12 faculty and alumni from Georgetown Law and nine alumni from the School of Foreign Service.
At the event, distinguished University Professor Lucile Adams-Campbell, founding director of the Ralph Lauren Center for Cancer Prevention, shared the center’s work, which is focused on a dynamic patient navigation model that supports cancer screening, diagnostic, treatment, and preventative measures as well as solutions for expanding access to clinical trials.
“This research will help patients realize the benefits of clinical trial participation, resulting in longer survival and better quality of life,” said Adams-Campbell.
Hoyas on the Hill speakers also included Matthew Biel, director of the Thrive Center for Children, Families, and Communities, on how his projects support the mental health of military families; Anna Johnson, director of the Context, Development, & Social Policy Lab, on her work on evaluating children’s post-COVID recovery; and Lisa Singh, director of the Massive Data Institute at the McCourt School of Public Policy, on developing technologies that harness modern computing to better understand human behavior and improve decision making. n
Women make up nearly two-thirds of the Class of 2028 in the Georgetown University School of Medicine.
Top: Interim Georgetown University President Bob Groves with Christina Cordell (SFS’25), Andrew Oliver (C’24), and Jaxson Dealy (SFS’24); Bottom: U.S. Senator John Barrasso (R-Wyo.), Senate Majority Whip, addresses the crowd at Hoyas on the Hill.
Photo: Lisa Helfert
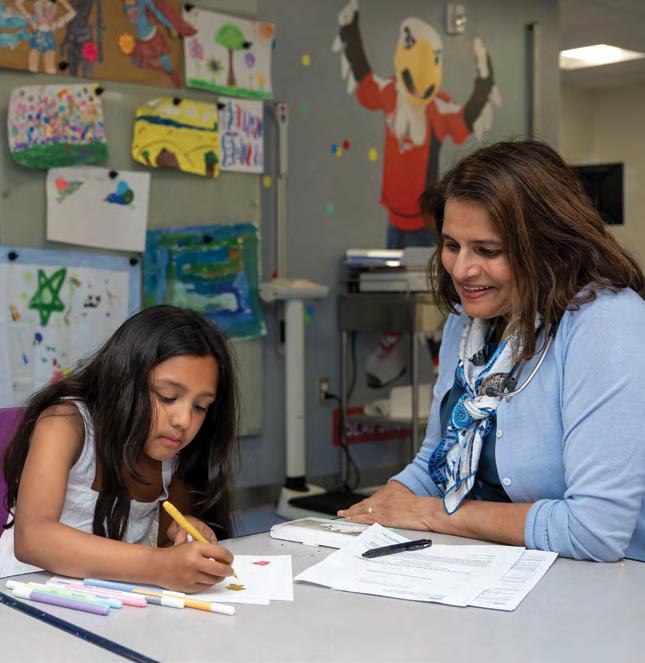
When Georgetown family medicine physician
Sarah Kureshi felt a strange mass in her toddler daughter’s stomach, she suspected something like an intussusception, an intestinal blockage. Two-and-half-year-old Nusayba had vomited once that morning, but was feeling better. Still, to be sure, her mother brought her to the hospital to be evaluated.
“We were in the ultrasound room playing around and the radiologist came in and looked at me and said, ‘I have some really bad news for you,’” Kureshi recalls. “I’ve been on the giving end of that, and it was so hard being on the receiving end. She said, ‘Your daughter has tumors throughout her liver that are pretty diagnostic of hepatoblastoma,’ which is liver cancer. I called Waj.”
Her husband, Wajahat Ali, was so unfamiliar with cancer that he wasn’t sure if stage IV was good news or bad news.
“So many of us don’t know the basic information about cancer,” notes Ali, who is an author and columnist. “Suddenly you’re learning about cancer stages, what it means that it metastasized and that there was a spot on her lung. There were spots all over her liver, so she would need a transplant, from a living donor, with a blood type that matched. Plus chemo.”
There was so much practical information to learn and process, in addition to the emotional and physical toll not only on the patient but on her family as well, including her brother Ibrahim who was four at the time.
The growing field of cancer survivorship
At Georgetown University’s Lombardi Comprehensive Cancer Center, researchers study the long-term care of people living with cancer—how to improve their experiences and minimize any adverse effects of the often intense treatment.
“I define cancer survivorship as optimizing a person’s wellbeing at any point from diagnosis going forward into the future,” says Nina Kadan-Lottick, professor of oncology and pediatrics at Georgetown School of Medicine who leads the Survivorship Research Initiative for Georgetown Lombardi with collaborators at MedStar Health. “We are looking at how to optimize one’s physical, emotional, and family functioning at every point in the cancer journey.”
As a pediatric oncologist, Kadan-Lottick’s interest in survivorship began when she saw patients who were many years past therapy. “I was documenting the kind of medical problems one has later in life, like the risk of new cancers, infertility, osteoporosis, and cognitive difficulties. In caring for patients, I realized those were getting in the way of people living lives the way they wanted. As my career progressed, I began thinking of cancer more like a chronic disease rather than an event.”
Pediatric oncologists pioneered the field of cancer survivorship, she explains, “for the simple reason that we saw high cure rates in people under 20. We saw kids surviving, and we also saw them grow up. We observed things such as cognitive difficulties in people with cranial radiation or chemotherapy with spinal taps. We saw second cancers in girls who had radiation even as pre-pubertal girls. We saw them getting breast cancer in their twenties and thirties. We also saw a lot of infertility.”
Many cancer survivors—young and old—are living with challenging conditions like colostomies, residual swelling in the limbs, and pain in the fingertips and feet. Therapies to treat invasive cancers are intense, and can impact the heart, kidneys, and hearing, as well as affect physical intimacy. Survivorship care includes screenings like cognitive evaluations, or breast MRIs for women who have had chest radiation earlier in life. For younger patients, it may include fertility preservation such as egg and sperm harvesting and storage.
While Kadan-Lottick’s research began with understanding how to measure the late effects of cancer treatment, it has evolved today to include how to prevent or mitigate them earlier in the treatment experience. According to the National Cancer Institute, a part of the National Institutes of Health, today there are more than 18 million cancer survivors in the United States. Currently less than 20% of cancer patients get survivorship care—a figure she hopes to increase.
Importance of social support systems
Kureshi and Ali credit a wide network of people who supported their family— from nurses, physicians, and hospital staff including child life specialists, custodians, and art therapists, to family, friends, colleagues, and people they didn’t even know who signed up to be liver donors.
“A strong social support system is an incredible predictor of well-being,” says Kadan-Lottick. “Not everyone has one, but when you do, leaning into it is really important. Share your needs and let people help you think of what’s possible and what’s not.”
Kadan-Lottick notes that in her experience, the term “cancer survivor” applies not only to the patient but to that person’s caregivers as well.
“Cancer doesn’t affect just the individual. Everyone invested in that person feels emotional distress. Beyond that, there are often opportunities lost that can be disruptive and a financial impact on caregivers. Often caregivers are not taking care of their own health.”
For some cancer patients, the challenge can be asking for and accepting the assistance of their community, she notes.
“Sometimes I see people who do have a support system, but they don’t want to ask for help, and they struggle. It’s not like when you have the flu for a week and you put everything on hold. With cancer you just can’t do it alone for that long. You can’t do it financially, or logistically.”
Her team is researching how to guide people at the time of diagnosis to understand and prepare for the care coordination and practical skills they will need—for example, how to keep track of critical health information, whom to ask for different types of questions, and how to get the most out of visits.
“But this has to be something with a light touch, because these are people who are going through a lot,“ she adds.
Nusayba and her family celebrate the conclusion of her cancer treatment in January 2020.
Photos: Courtesy of the Kureshi family
Kureshi and Ali consider themselves lucky that their relationship grew stronger during the challenging time of Nusayba’s diagnosis and treatment.
“I was in the hospital half the year,” Kureshi recalls. “Couples going through this either grow together or grow apart. We are fortunate that we were on the same wavelength. The other thing is the impact on her older brother. He and I were very close and then, all of a sudden, I’m in the hospital with Nusayba and not home.”
Inspired by medicine
When she was just 11 months old, Grace Bucklin’s parents picked her up from childcare one day and her entire right side was swollen. They brought her into MedStar Georgetown University Hospital, where she was diagnosed with a rare kidney cancer called Wilms tumor.
“I think it was two days later when they took out my entire right kidney, and it was the biggest tumor per body mass that the doctor had seen,” notes Bucklin, now 21 years old.
After surgery, chemo, and radiation, she now marks almost 20 years cancer-free.
“I’ve grown up going to all these different doctors–radiation oncologist, cardiologist, dermatologist. My mom and I added it up and I’ve been to 18 different specialties.”
Her cancer survivorship care at Georgetown has provided critical screening for things like high blood pressure and cognitive function. The support has also helped her family, she says.
“My parents were able to meet with social workers, and my older sister would do all the art therapy. It helped her understand what was going on.”
Bucklin is so comfortable in the medical setting that she’s decided to join the field as a practitioner, beginning her studies in osteopathic medicine next year, specializing in pediatric oncology.
“Two years ago I worked at Georgetown in Dr. Toretsky’s research lab and it was really fun,” she says, referring to pediatric oncologist and researcher Jeffrey Toretsky. “It made me realize that I want to be a doctor and help kids live the life that doctors were able to give to me.”
Making time for cura personalis
“Cancer survivorship care is the embodiment of cura personalis,” says Louis M. Weiner, director of Georgetown Lombardi, noting that care of the whole person means the totality of their needs, including those of their care circle.
Good cancer survivorship care involves additional screenings and complicated, nuanced conversations with patients and their caregivers, and among care providers. Whether through a specialist or in the primary care setting, sensitive whole patient care takes training, resources, time, and an effective structure undergirding it all.
“The discipline of cancer survivorship is one where we have to develop the language, tools, and standard operating procedures, and we have to figure out what the right handoffs are,” explains Weiner. “When do they come back to see the oncologist, the surgeon, the radiation oncologist? When do they need to be transitioned back for cancer-related care as opposed to complication-related care?
“We make that happen through our nation’s comprehensive cancer centers, which provide the intellectual framework, and practical knowledge needed, to help drive this process,” he adds. “But people sometimes are coming from great distances to get their treatments. They need to be able to get the care in their
Pediatric oncologist Nina Kadan-Lottick, M.D., MSPH, meets with Nusayba and her mother Sarah Kureshi, M.D., MPH.
communities. We can help by educating community partners so that they understand what they need to do in order to maximize the benefit for their patients.”
When providers are able to offer extra time for cancer survivors and their caregivers, it can make all the difference.
As a physician herself, Kureshi had a strong knowledge base going into the situation with her daughter’s cancer treatment but recalls with gratitude when care providers could fill in the blanks, such as pediatric gastroenterologist and transplant specialist Nada Yazigi at MedStar Georgetown University Hospital.
“I remember Dr. Yazigi, when we were pre-transplant, took me aside and talked to me for an hour and answered all my questions—every single one.”
Kureshi also commends the work of child life specialists, who help children and their families feel more comfortable in hospital and health care settings.
“They were constantly putting games together for the kids. They come to the room and sing with the kids. They offer pet therapy. For her first IV, Nusayba was terrified, and the child life specialist helped calm her by talking about what was happening. They had such an impact on our whole journey.”
A lot of Kadan-Lottick’s research is how to inform primary care providers about cancer survivor screenings and care in a time-efficient, respectful way, so that they can successfully support patients down the road.
“It is more and more challenging,” says Kadan-Lottick. “Often physicians and other providers are very pressured in terms of how much volume they see, forcing them to spend less time with each patient. And insurance companies keep requiring more documentation and test authorizations, so we spend a lot of time on that.”
Financial toxicity
With or without insurance, individuals with a cancer diagnosis often experience financial challenges, which can exacerbate their health concerns. Many people don’t anticipate these added costs, but given uncertainties about insurance coverage it’s critical to consider.
“I did some research and realized we would need an additional $100,000 a year,” says Ali. Even though they had health insurance and both parents earned income, they had to cut back on work to take Nusayba to her appointments and stay with her in the hospital. There were co-pays and deductibles, prescriptions, and other unexpected expenses. They created a GoFundMe and drew support even from strangers who were moved by their story, which helped them avoid going into debt—a problem many American cancer patients and their families struggle with. In fact, 40% of cancer patients deplete their life savings within two years.
“We live in a very complicated world when it comes to the financing of medical care,” says Weiner. “And everybody has
a different set of challenges. Not all medical procedures are going to be covered by insurance, whatever that insurance is.”
When money is tight, cancer survivors and their caregivers end up making difficult choices to make ends meet. They might skip appointments, procedures, or filling prescriptions. And the added stress can compound health issues.
“Dealing with financial toxicity is a real challenge in the cancer survivorship space,” Weiner affirms. “It’s important to have individuals in the health enterprise who can support people through it, including financial counselors and social workers. At Georgetown, we also have the Health Justice Alliance, to help people get access to legal assistance.”
Life-giving research
Today Nusayba is a healthy 8-year-old with little recollection of her time as a toddler with liver cancer. Her parents are grateful not only for the care their family received, but also for the invaluable decades of scientific research that preceded her diagnosis. It saved her life.
“The chemo protocol that she got was incredible,” Kureshi says. “It targeted her tumor, and was extremely effective in getting rid of the tumor in her lung, and all the sites in her liver, while minimizing the chemotoxicity. But in the early 2000s, they did not have that protocol around, so I don’t know if she would have survived then.”
In the future, Kureshi hopes that research will develop immunosuppressants that are gentler on the kidneys, to help people like her daughter minimize the need for a kidney transplant later in life.
Ali notes that Nusayba is down to just two medications, versus 12 different prescriptions at one point. Because she had an organ transplant, she will have lifelong blood draws, Kureshi adds, and she’s had some hearing loss from her treatment. She will also require echocardiograms every two years. Living with a family medicine doctor has of course been a big plus for Nusayba’s survivorship care, but the family plans to enroll in the official program soon.
“I have patients who are part of the cancer survivorship program who appreciate it so much,” Kureshi says. “Once somebody ‘beats the cancer’ then people think it’s done—but this program really takes into account the long-term effects and how to best support people as they continue to live their lives and grow and thrive.”
Kadan-Lottick underscores the ties between this work and cura personalis, at Georgetown and beyond.
“Cancer survivorship aligns with taking care of the whole person, because you are more than your tumor, more than a test result. You are a person experiencing these things, and you’re a person with loved ones who are experiencing this with you.” n
Photo: Lisa Hlefert
Wajahat Ali and Sarah Kureshi with their children (left to right) Nusayba, Ibrahim, and Khadija.
t happens in an instant. One moment, you’re reaching for a coffee mug, preparing breakfast—and the next, everything changes. Your right side feels impossibly heavy, and fingers refuse to respond. Words form in your mind but won’t come out of your mouth. Each passing moment could mean the difference between recovery and life-altering disability.
This is the devastating reality of stroke, a neurological thunderbolt that can erase or severely impair basic human functions in moments.
Every year, stroke hits nearly 800,000 Americans. The aftermath varies dramatically among survivors, with variables such as the type of stroke, the location in the brain, and how long it takes them to receive critical care playing a major role.
The vast majority—about 80%—of strokes are known as ischemic, where blood clots choke off vital circulation to brain tissue. The remaining 20% are hemorrhagic, where a blood vessel ruptures inside the brain and results in bleeding.
Some stroke survivors face one-sided paralysis, aphasia (lost language abilities), partial blindness, or perception issues. Beyond physical disabilities, many survivors struggle with emotional dysregulation and depression.
As America’s leading cause of long-term disability, stroke doesn’t just affect individuals—it overwhelms families and strains the health care system. Its economic aftershocks can include medical bills, rehabilitation costs, lost wages, and the unmeasurable expense of family members becoming caregivers.
Behind the statistics are people and families suddenly thrust into navigating a complex medical system, often with little preparation for the challenging journey ahead.
This can be overwhelming and isolating for patients and families, according to Norman J. Beauchamp Jr., a professor of neurology and radiology who serves as executive vice president for health sciences at Georgetown University Medical Center (GUMC) and executive dean of the School of Medicine.
“You’re going through something and you don’t even know if you’ll survive, let alone get your functions back,” says Beauchamp. “There are just so many unknowns.”
Beauchamp believes the team of elite researchers and clinicians at GUMC and MedStar Health that focus on stroke and related issues has the capacity to shift the narrative for patients and their families.
“We’re bringing together remarkable experts from every field—from skilled clinicians to innovative researchers—all serving a large and diverse patient community,” Beauchamp says. “There is a powerful synergy that enables us to make a real difference for patients who might otherwise feel like they’re walking the road to recovery alone.”
Regaining what stroke has taken Stroke offers a unique model for studying brain plasticity—the brain’s ability to recover and adapt following injury.
“Because we know when and where stroke occurs, and it is not a progressive disorder, we can see exactly where it damages the brain and can better understand how to promote recovery,” says Peter Turkeltaub (M’05, G’05), professor of neurology and rehabilitation medicine at Georgetown’s School of Medicine, who also directs the Cognitive Recovery Lab at Georgetown and the Aphasia Clinic at MedStar National Rehabilitation Network.
By studying patients who exceed recovery expectations, researchers can understand how healthy brain regions compensate for injured areas.
“While your hair, fingernails, and skin can regenerate, your brain doesn’t grow neurons back,” explains Elissa Newport, professor of neurology at Georgetown School of Medicine, and director of the Center for Brain Plasticity and Recovery, a joint enterprise between Georgetown University and MedStar National Rehabilitation Network.
Yet a team of researchers from the center discovered that adults have a critical window of heightened plasticity—approximately 60 to 90
days post-stroke—when the brain demonstrates remarkable rewiring potential.
“The brain essentially returns to early developmental stages like you see in babies, with new synapses and connections sprouting as it attempts to recover,” says Newport.
Newport and colleagues have also found that children who suffer strokes at birth show extraordinary neural adaptation, with language and spatial abilities often developing normally despite significant damage.
Unlike adults who experience brain damage, children effectively recruit the opposite hemisphere to “take over” lost functions. This discovery has prompted Newport and Turkeltaub to try to pinpoint precisely when this neurological flexibility diminishes between infancy and adulthood—potentially unlocking new approaches that could help adult patients tap into similar recovery mechanisms.
“The exciting question is, do these residual abilities exist for adults too but maybe are just underpowered? And how can we tap into them to get better recovery?” Newport says.
Understanding how the brain is wired By studying patients who recover well from stroke, researchers hope to unlock insights applicable to a variety of different neurological conditions such as traumatic brain injury, multiple sclerosis, and neurodegenerative diseases including Parkinson’s and Alzheimer’s.
“Studies of different neurological pathologies cannot be done in silos,” explains Carlo Tornatore (G’82, M’86, R’90), professor and chair of neurology at Georgetown School of Medicine, and regional chief of neurology for MedStar Health.
“People like to put these conditions in their own little containers, but that’s not how nature works— it’s actually a continuum,” he explains.
Discoveries about neural pathway reorganization after stroke have informed new treatments for traumatic brain injury. Similarly, markers identified in stroke patients have provided insights into inflammatory processes in multiple sclerosis. Even research into migraines has yielded insights about the brain’s capacity to heal.
What these crossover insights reveal is that full recovery from stroke is not an impossible dream. In fact, it may be an achievable reality for many patients when we discover the most effective interventions and provide the right support.
“When we talk about return of function, we’ve already done it for some disorders. This is some-
“When we talk about return of function, we’ve already done it for some disorders. This is something we currently know how to do—it’s not something in the distant future.”
Professor
—CARLO TORNATORE (G’82, M’86, R’90)
and chair of neurology at Georgetown School of Medicine and regional chief of neurology for MedStar Health
thing we currently know how to do—it’s not something in the distant future,” Tornatore says.
Even with diseases such as Parkinson’s and Alzheimer’s, which have no cure, patients experience fluctuations in symptoms. These ups and downs are cause for hope for stroke patients.
“The point is that we can see the brain is trying to recover, and the mechanisms exist for it to recover,” Tornatore says. “Our challenge is to keep working to figure out ways to encourage and sustain that recovery.”
In the realm of laboratory science, Georgetown researchers are exploring mechanisms that could transform how stroke is understood and treated— from the circuits neurons use to communicate with each other to the cellular and subcellular levels.
“If we don’t understand the brain’s circuitry— how it functions—then we can’t understand how the brain recovers from an injury such as stroke, or imagine new therapies to help these patients,” explains Kathleen Maguire-Zeiss, professor and chair of the department of neuroscience. “It’s about taking what we learn in the laboratory with the hope of one day applying it to the bedside.”
Georgetown researchers are studying inflammatory responses in the brain, with findings that could help explain why stroke recovery differs with age. Other research focuses on how we can protect neuron function. For example, studies from traumatic brain injury, Alzheimer’s, multiple sclerosis, and Parkinson’s laboratories will add to our understanding of brain plasticity, function, and health.
Neuroscience research is fundamentally interdisciplinary—principals from fields such as neurology, neuroscience, biology, pharmacology, physiology, psychology, and physics are all important to address complex brain recovery challenges, underscoring the notion that discoveries about one condition can affect how we approach and treat others.
“There are overarching themes that are broader than any one disorder, so the data we are generating about inflammation and brain plasticity, for
example, helps us understand how the brain recovers in general,” Maguire-Zeiss says.
A research powerhouse
The Georgetown University and MedStar Health partnership is making great strides in this work.
The collaboration combines Georgetown’s academic research with MedStar Health’s clnical expertise and specialized care—all in close proximity and under the same network umbrella. Researchers, clinicians, and rehabilitation specialists across Georgetown University, MedStar National Rehabilitation Network, MedStar Georgetown University Hospital, and MedStar Washington Hospital Center are able to connect and advance their work.
Strategically positioned at what experts describe as the “buckle of the stroke belt”—a region with high stroke incidence and mortality—the partnership gives researchers access to diverse patients from urban and rural areas. MedStar Health’s broad reach extends from MedStar Washington Hospital Center in the District to hospitals in Maryland including Baltimore, and to urgent care and specialty care facilities throughout DC, Maryland, and Northern Virginia.
The Center for Brain Plasticity and Recovery exemplifies this collaborative approach, with interdisciplinary teams of experts—including linguists, psychologists, computer scientists, neurobiologists, clinical neurologists, and rehabilitation therapists—working together to understand how the brain recovers after injury. The Center for Neuroengineering and the Center for Neural Injury and Recovery also bring together researchers that study recovery of function, ranging from cells to the human experience.
This commitment to advancing stroke research and treatment has earned recognition, with Georgetown’s Department of Rehabilitation Medicine ranking among the top 10 such programs nationwide.
“We’re not just treating symptoms,” Newport explains. “We’re investigating the fundamental mechanisms of brain plasticity. This kind of work demands a wide range of expertise, and there are hardly any other places where you can find what we have here.”
Regional stroke network
At the heart of this collaborative ecosystem between Georgetown and MedStar Health lies the Stroke Central Atlantic Network for Research (SCANR), the leading consortium for stroke clinical trials in the Mid-Atlantic region.
Co-led by Turkeltaub and Amie Hsia, medical director of the MedStar Washington Hospital Center Comprehensive Stroke Center, SCANR covers every stage of stroke care, from emergency treatments like advanced clot removal to better prevention strategies and innovative rehabilitation methods.
“Our population is basically a microcosm of the country’s population of stroke survivors, which greatly benefits our research,” Turkeltaub says.
One of SCANR’s promising initiatives addresses a critical gap—access to specialized rehabilitation services. For many survivors, particularly those in rural areas or with mobility limitations, regularly traveling to rehabilitation facilities can be a significant barrier to recovery.
A new telehealth study looks at occupational therapy for arm recovery that’s delivered remotely. By bringing expert occupational therapy into people’s homes virtually, the research program aims to eliminate geographical and physical barriers that have traditionally limited access to specialized stroke rehabilitation.
“We are not just focused on stroke recovery, but are rethinking how rehabilitation is delivered, particularly to underserved patient populations who might not otherwise have access to critical services,” Turkeltaub says.
Where technology meets brain recovery
New tools and digital platforms are transforming how stroke care is conceptualized, delivered, and personalized.
For example, in January GUMC researchers in collaboration with MedStar Health colleagues launched the Acute Stroke Imaging Database (AStrID), an AI-driven brain imaging platform that helps doctors match patients to clinical trials based on their specific brain damage patterns. By enabling scientists to quickly and effectively group patients with similar stroke characteristics for more targeted clinical trials, the tool will improve treatment options for patients who are most likely to benefit.
“I don’t know of another center that is systematically gathering MRI data, and then using AI to precisely map stroke location and characteristics in this way,” says Turkeltaub, one of the developers of the database.
Turkeltaub and colleagues can set up an alert when a patient is admitted with a stroke affecting a specific brain area, or has a motor deficit in a range that makes them a strong candidate for a particular trial.
“We can even determine if they still have connections between their brain and spinal cord, which helps us sort them into the right clinical trial where the therapy is likely to be successful,” he says.
In another innovative study, Georgetown researchers are exploring advanced neuroimaging techniques to enhance stroke assessment. A new MRI method, developed through collaboration between GUMC, MedStar Health, and the National Institutes of Health, helps doctors better predict how well stroke patients might recover movement in their arms and legs.
This breakthrough, published this past March in the journal Neurology, allows clinicians to better visualize the white matter “wiring” that runs from the brain to the spinal cord, indicating a
“Health care done correctly is about all people feeling cared about and not feeling alone.”
—NORMAN J. BEAUCHAMP JR., M.D., MHS Executive vice president for health sciences at Georgetown University Medical Center and executive dean of the School of Medicine
person’s potential to recover limb function following a stroke.
Complementing these diagnostic advances, Georgetown and MedStar Health are implementing therapeutic innovations such as Vivistim—a device that uses vagus nerve stimulation to help patients recover hand and arm function.
“It’s like a pacemaker, implanted through a very simple operation that stimulates this nerve,” explains Tornatore. “What’s amazing is that people who have had a stroke, even if it was years ago, can still experience a return of some function in their paralyzed arm when stimulation is paired with rehabilitation.”
The treatment protocol is inherently collaborative, requiring neurologists to program the stimulation parameters, physical therapists to guide patients through rehabilitation exercises, and researchers to document and analyze outcomes.
While these cutting-edge treatments offer hope for recovery after stroke, Tornatore emphasizes that prevention remains the ultimate goal— and that technology is the key.
“We have the technology to predict stroke in our hands right now,” he says. “We want to get to the point where we can prevent the disability and have a better understanding of who is at risk years before there is a catastrophic event.”
With its capacity to track measures such as blood pressure, heart rate, and temperature, wearable technology will revolutionize preventative care, Tornatore predicts.
“I am 100% convinced that wearable technologies like your smartwatch will transform stroke prevention,” he says.
Taking it to the community
GUMC and MedStar Health’s approach to stroke care extends beyond the lab and stroke clinic and into the community.
Every Monday evening, a unique gathering takes place via Zoom. What began as a research initiative has evolved into a lifeline for many stroke survivors, especially those experiencing aphasia, a language disorder affecting roughly one-third of stroke patients.
What’s particularly striking about these meetings is the age group. Turkeltaub says there are a surprising number of people in their 30s and 40s who have had a stroke.
“It’s turned into a predominantly young stroke survivor group,” Turkeltaub says.
For these younger survivors, the conversation group offers not just communication practice but also vital community support. It also enables researchers to solicit feedback about planned and ongoing research.
This approach exemplifies Georgetown’s commitment to community-engaged research—where those being studied have a voice in shaping the research itself.
Building on this patient-centered approach, Georgetown’s team is also tackling one of the most overlooked challenges facing stroke survivors: access to mental health care. Depression affects as many as half of all stroke patients, yet finding appropriate care can be particularly difficult for those with communication disorders.
“It can be really difficult to find mental health care when you have aphasia, so we have created a resource guide for people in the region because we want to remove these barriers,” Turkeltaub says.
Teaching the next generation
Sustaining these advances in stroke care depends on preparing future leaders in the field. Recognizing this critical need, GUMC’s interdisciplinary PhD program in neuroscience trains outstanding researchers, and SCANR’s fellowship program cultivates emerging talent across institutions, creating a robust mentorship ecosystem. Each year, SCANR chooses a new fellow from among the participating sites.
“One of SCANR’s concrete goals is to train the next generation of stroke investigators. We also provide an opportunity for newer investigators to take on roles as principal investigators of clinical trials or to participate in working groups at the national level,” Turkeltaub says.
Students and early career faculty also are exposed to the cross-disciplinary experts and resources at Georgetown and MedStar Health, as stroke research and care cuts across so many fields.
This interdisciplinary approach reflects Georgetown’s commitment to cura personalis care for the whole person—where tackling medical challenges addresses not just the condition but the patient’s entire human experience.
At the heart of this philosophy is the recognition that effective health care extends beyond technical interventions to encompass emotional and psychological support.
“Health care done correctly is about all people feeling cared about and not feeling alone,” Beauchamp says.
As a faith-based institution, Georgetown is uniquely able to bring faith and health to bear in ensuring people do not feel isolated.
“This is particularly important for stroke victims, who often face sudden life-changing trauma. For me, a key measure of success is if we have helped them feel less alone along the way,”
Beauchamp says. n
Photo: Chris Banks
As the play The Art of Care opens, ensemble member Susan Rome holds up a deep blue Kintsugi bowl, its mended cracks traced with gold.
Kintsugi is the Japanese art of repairing broken pottery to create a beautiful whole out of imperfect fragments. “It doesn’t hide the scars,” Rome tells the audience.
The bowl provides a visual symbol for the play’s overarching message: that by coming together to care for one another, we can heal in the broken places.
Throughout the play, which is staged on a set resembling a comfortable living room, seven actors share stories—both their own and those of physicians, nurses, and other care providers—in an intimate, theater-inthe-round setting.
These stories are artfully threaded into a tapestry illustrating the myriad ways that care manifests in the world, through relationships between teacher and student, doctor and patient, parent and child, husband and wife, and even two strangers meeting on a dark street at night.
Giving care can mean overcoming fear, as the ensemble demonstrates in stories from the COVID-19 pandemic, including a doctor who protected members of his team who were afraid of bringing the illness home to their families.
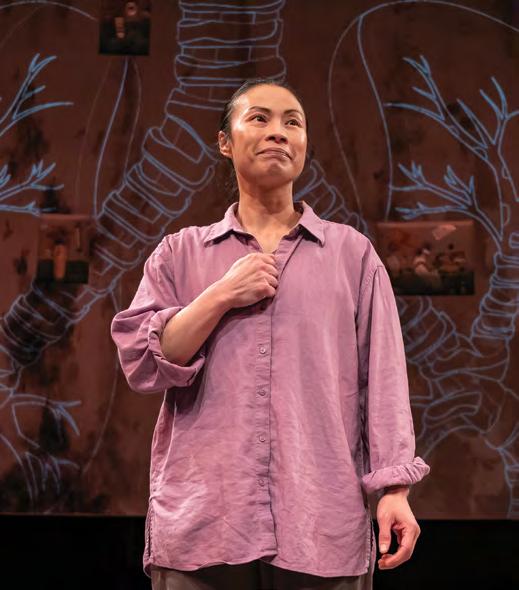
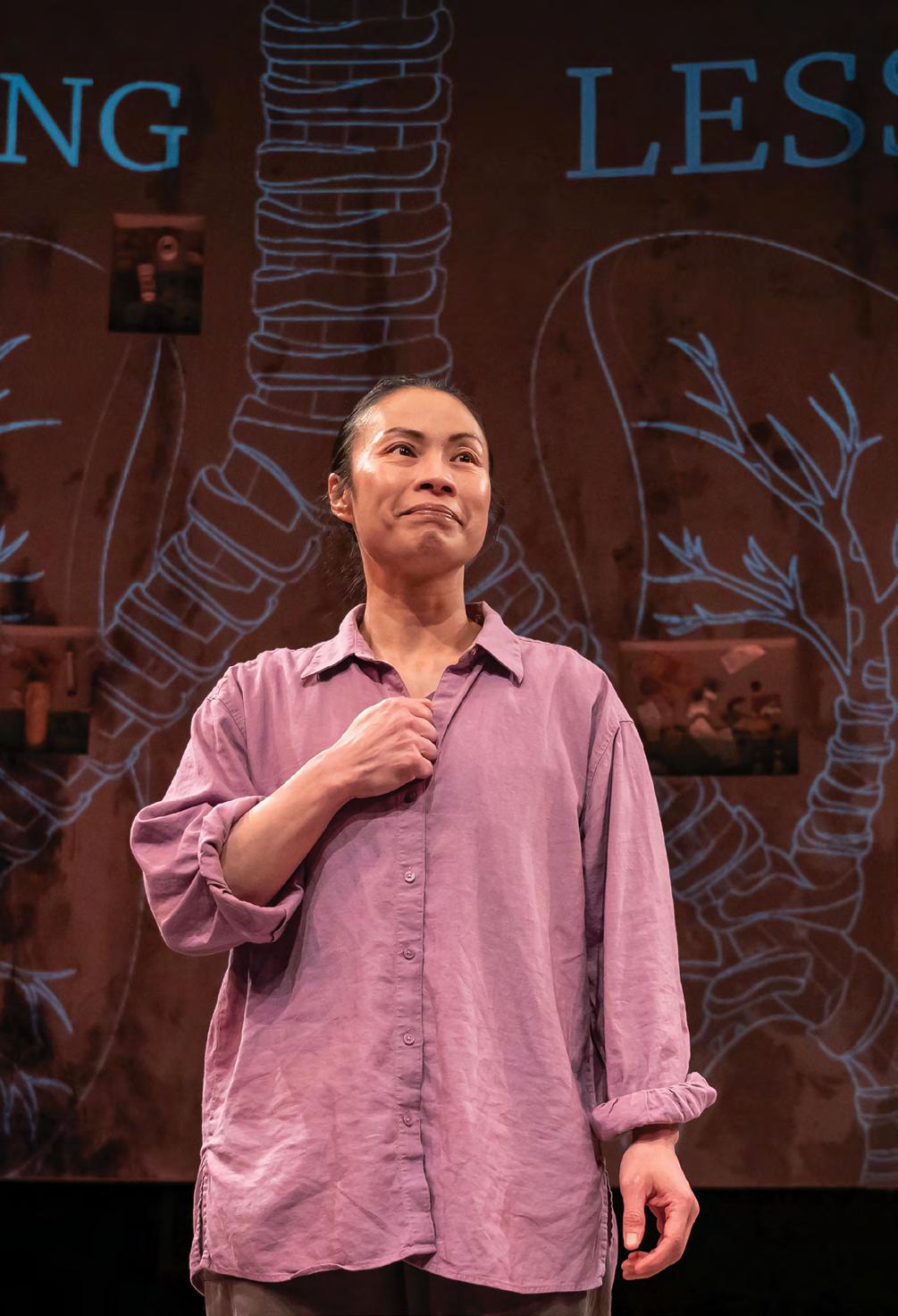
Ensemble member Tuyết Thị Phạm tells of her family’s escape by boat from Vietnam and her mother’s courage as she climbs aboard a U.S. Navy ship while clinging to Tuyết, then just 6 months old.
There is also heroism in small acts of care—the woman who drives 80 miles round trip to paint the nails of her friend with cancer, the man who accepts a bandage for a bleeding knee from a physically imposing stranger.
“An openhearted ensemble has collaboratively created an extraordinary experience of communal connection,” wrote DC Theater Arts critic John Stoltenberg of The Art of Care
Left: Professional percussionist Jabari Exum’s performance on the djembe throughout the play provided the underlying heartbeat for The Art of Care; Right: Reginald Douglas (C’09), artistic director of Mosaic Theater Company. In 2024, Douglas was honored with Georgetown’s John Thompson Jr. Legacy of a Dream Award.
The play is woven through with humor as well as tears. It’s punctuated by music, most notably in the djembe drumming of ensemble member Jabari Exum, a professional percussionist.
Exum’s own story exemplifies the healing power of art. When he was mastering the djembe, he spent hours practicing each day. “I had these little sacred spaces all through Rock Creek Park,” he says. When his godsister began struggling with depression, he would take her with him and she’d sit for hours listening to the drumming and the sound of the water, the trees, the insects. She always came away with a lightened mood.
“What became clear in that process,” Exum says to the audience, “is that the human being is actually electricity, and with art and care, we can plug a person back in.”
STARTING BY LISTENING
The genesis of The Art of Care is itself a story of community and collaboration. In 2020, Georgetown theater professor Derek Goldman began teaching the class Performance and Pandemic. Working with colleagues involved with the Medical Humanities Initiative, he designed the course to help students process their wide-ranging emotions as they coped with COVID-19’s shutdown of campus.
“That kind of manifestation of personal narratives around health laid a foundation for what would become the Art of Care project,” says Goldman, who holds a joint appointment in the School of Foreign Service.
Using the innovative In Your Shoes method, Goldman initiated a series of intimate conversations about care with a wide range of partners. In Your
Shoes, a signature program created by Goldman and other members of Georgetown’s Laboratory for Global Performance and Politics, promotes empathetic listening to build trust. Goldman, The Lab’s co-founder, currently serves as its executive and artistic director.
Christopher King, dean of the School of the Health, became an early supporter of the project.
“When I learned about what Derek was doing, I said, ‘This is exactly what our mission aspires to,’” King says.
“Our graduates must be empowered with skill sets that enable them to communicate health information in various ways,” he continues.
“We teach them highly sophisticated research methods, and they get an output. But how do they share the findings? You can’t just say, ‘Read my report.’ That’s not likely to be the most effective way to enlighten minds and influence policy. We must meet people where they are. Storytelling helps humanize the data.”
King began collaborating with Goldman at a time when King was caring for his elderly mother, who passed away in January 2025. “I was grappling with my mom’s condition, and so it was a very emotional time in my life. I shared that with Derek and the team. Through sharing my story, I think it helped them imagine what this might look like in performance.”
SEEKING ATTUNEMENT
As the script for The Art of Care began to take shape, Goldman connected with a former student, Reginald Douglas (C’09), the artistic director of Mosaic Theater Company in Washington, DC. Douglas recognized the special nature of the project and signed on to present the play.
“Derek directed Mosaic’s first production 10 years ago, so it’s very full circle to have his relationship with the company grow in this way,” Douglas says. “The topic of the play embodies both our missions, as well as our vision about how theater can activate a community.”
The company’s performers committed themselves to a long process of development through workshops and conversations with health care providers, whose stories were incorporated into the script. For example, the actors visited Georgetown
“What became clear in that process is that the human being is actually electricity, and with art and care, we can plug a person back in.” JABARI EXUM
“We need to go beyond the traditional biomedical approach and take a bio/psycho/social approach to how we care for populations. Wonnie wanted that health care degree, but she also realized the power of art.”
University’s Lombardi Comprehensive Cancer Center and spoke with Julia Langley, director of Lombardi’s Arts and Humanities program. Her story of caregivers performing unique songs by each patient’s bedside is featured in The Art of Care.
Another health care narrative came from an oncology nurse, a sister of one of the actors. “She talked a lot about how she thinks of her role as a kind of artist,” Goldman says. “Although on the surface she and her sister’s roles are different, both have this deep attentiveness at the core.
“‘Attunement’ is the word that she used, which is a beautiful word, and the core animating presence of the piece.”
As time went on, the ensemble members themselves began to shape the nature of the play. “The actors were originally hired to take on other people’s stories,” Douglas notes. “But as they were doing their interviews through the In Your Shoes method, they started to become more vulnerable and courageous in talking about their own moments of care. And those stories very naturally came to top.
“They really had to push their craft, because you have to find a way to tell your personal story—some of which has great trauma—multiple times a week to a group of strangers,” he continues.
“For them, it was terrifying at times, it was joyful at times. And it was a moment of great confidence and pride for them to stand firm and tell their story to strangers.”
A ‘THEATER KID’ FINDS HER PLACE
In the spring of her junior year, Wonnie Kim (H’25) learned about Goldman’s work with The Art of Care from one of her professors, John Kraemer, associate professor and chair of the Department of Health Management and Policy in the School of Health.
“The project seemed like the answer to the internal turmoil in my mind. I’m a health care major and I’m also very passionate about theater, and the two don’t seem to mesh,” Kim says. But she was still hesitant to reach out.
During the summer, Kim finally took the plunge and sent an email to Goldman, offering her help as a student volunteer. To her great surprise, Goldman responded within several hours. The two struck up
a dialogue over email and phone. “We realized how my interests academically and professionally were very aligned with what he was doing with this project. Everything just clicked.”
Goldman ultimately invited Kim to become assistant director of The Art of Care, a high honor for her. In addition to her work during rehearsals performing a variety of tasks, from stage blocking to impromptu guitar lessons, Kim helped translate scientific information into the artful language for the script. She attended 25 to 30 hours of rehearsals each week while maintaining a full-time academic schedule.
“During tech week, I was watching the run of the show and making notes of my own, like, ‘I think Raghad should pause a little before saying this line,’ Kim says. “I had felt insecure at first, being a young member of the team, but I could see my changes being implemented day after day,” Kim says. “Derek took my opinions seriously.”
At the same time Kim was involved with The Art of Care production, she was conducting research for her senior thesis, which also deals with the intersection of art and health. “It felt very meta,” she says with a laugh.
CHRISTOPHER KING, P h .D., MHS c , FACHE
Left: Professor Derek Goldman, writer and director of The Art of Care, greets a Mosaic Theater board member. Right: Ensemble member Tuyết Thị Phạm speaks eloquently of her mother’s care as the family fled from war-torn Vietnam.
“This is one of the rare projects where I felt that power of connection across culture, generations, and educational backgrounds.” DEREK GOLDMAN
Working with advisor Jennifer Natalya Fink, a professor of English and disability studies in the College of Arts and Sciences, Kim is drawing parallels between theatrical and public health responses to the U.S. AIDS epidemic and, more recently, COVID.
Christopher King calls Kim’s career aspiration a “perfect example” of what he means by reconceptualizing what health care looks like. “We must go beyond the traditional biomedical approach and normalize a bio/psycho/social approach to how we care for populations,” he says.
“Wonnie wanted that health care degree, but she also realized the power of art,” he continues.
“The fact that she has been able to carve out her own pathway—I’m so excited about her future.”
BREATHING WITH THE ENSEMBLE
When The Art of Care had its world premiere in November 2024, the response from theater critics—a notoriously tough crowd—was overwhelming with praise.
Calling the play “a tremendously heartfelt treatise on the power of human connection,” Washington Post theater critic Naveen Kumar wrote: “The show is almost entirely crafted from the perspectives of its seven-member ensemble, whose
radical vulnerability is its marvelous lifeblood. There’s a lot of pain dug up here, but just as much transformative generosity and healing.” The Washington Post named it one of the top productions of the year.
Most gratifying for Goldman and the ensemble, however, was the audience response. “The intensity of the emotional connection for the audience was beyond our wildest imaginings,” he said. “It was a piece where people ended up feeling they were really in community and breathing as one with the ensemble.
“Some people tended to stay in the lobby for long periods afterwards waiting for the cast, wanting to continue the dialogue.”
Working with Georgetown, Mosaic Theater scheduled a series of special events during the play’s run. These included a conversation for caregivers featuring physicians Lakshmi Krishnan, founding director of the Georgetown Medical Humanities program, and Katie Ryder of Kaiser Permanente, a family medicine doctor whose insights were featured in the production, as well as “Arts and Health,” a program focusing on nationwide initiatives at the intersection of art and care.
One of Mosaic’s innovations is an intergenerational matinee program, and The Art of Care proved to be a perfect vehicle for bringing those age groups together. “Teenagers and
With its universal message of care, the play bridged generations and backgrounds. At left, Raghad Makhlouf, whose performance included memories of her experience as a Syrian refugee, engages with audience members. Below: Wonnie Kim (H’25), center, bridges her dual interests in health care and theater through her work with the Art of Care Initiative at The Lab.
seniors enjoying the same experience, talking to one another and learning from each other, beautifully connected to the themes of community and care,” says Douglas.
Goldman found the embrace of the play by the Georgetown community especially moving. “They literally came by the busloads. Some saw it four or five times,” he says. “I underestimated the degree to which a process that foregrounded care—not just as a topic, but manifested in a very specific way—would reach students and young people, that they would feel seen by that.
“There were nights when we had a big multigenerational reunion of an African American family from DC who were viewing it from a different lens than, say, the Global Health Institute team, but they were moved by the same experience,” he continues.
“In some way that for me is the legacy of this project, how this topic of care and this way of approaching is a connecting force. This is one of the rare projects where I felt that power of connection across culture, generations, and educational backgrounds.”
A MOVEMENT OF ENERGY
From the start of developing The Art of Care, as Goldman explains, he and his colleagues envisioned the stage play as part of a larger whole. “The work we were experiencing in so many spaces with community members allowed us to imagine a larger initiative about the role that narrative storytelling could play around care. We saw the theater production as a first catalytic phase.”
As an initial step, The Art of Care ensemble devised a novel method of engaging audience members beyond the life of the play. “At the end of each show, we distributed these little prescription bottles with fun things like the recipe for peach
cobbler mentioned during the show,” Kim says. The bottles also had a QR code inviting interested people to sign up for an Art of Care workshop.
“We thought we’d get a few stray people, but in fact the demand was beyond our capacity,” Goldman says.
Over the course of the following months, Goldman partnered with King and other colleagues across the university to further develop the Art of Care Initiative, officially launched in May. The initiative’s interrelated activities include expansion of In Your Shoes collaborations and theatrical performances on and beyond campus. In addition, a new interdisciplinary Art of Care course will be offered beginning in spring 2026 for undergraduate students pursuing both liberal arts and health studies.
Kim, who is continuing her involvement as associate director of the Art of Care Initiative at The Lab, will be focusing on another key element—convenings at the intersection of art and health with partners from across the country as well as internationally to share best practices. “One of our goals is to make this initiative tangible and practical, so people really understand it.”
King is also working on plans for outreach programs to take advantage of the School of Health’s presence at the new Georgetown Capitol Campus.
“We’re going to be downtown, so we’re exploring ways to deepen our impact into the community,” King says. “For example, how can we use the performing arts to amplify our research—much of it focused on health care disparities, especially in lower income populations in DC? We’ll be partnering with schools and units across Georgetown to heighten awareness and inspire change in policy and practice—all for the sake of advancing health and well-being.”
Both King and Douglas are now serving on the advisory board for the Georgetown–Howard Center for Medical Humanities and Health Justice, further aligning the Art of Care initiative with efforts to improve health care delivery and outcomes in the DC community.
“This partnership is changing the way that we as theater artists think about the role of health care, and vice versa— the health care community celebrating live storytelling performance can be a really impactful way to make a difference,” Douglas says.
For Goldman, the Art of Care initiative gives voice to the Georgetown mission of cura personalis. “I feel like this project is just a small element of a much broader movement of energy around the connection between art and health and social cohesion and well-being,” he says. “Part of the hope is to become a meaningful cohering factor for networks of people who are often working in relative isolation to gather strength from each other.
“With Georgetown’s values in this area, I love the idea that we can be one kind of hub to amplify this work.” n
HEALTH INNOVATION IN ACTION
CALL course explores health equity outside the classroom
By
Health Innovation for the Common Good, a course offered on Georgetown’s Capitol Campus through the Capitol Applied Learning Labs (CALL) program, is getting undergraduates out of the classroom to explore health equity from different angles.
“Health affects everything, everywhere,” says Brian Floyd, assistant dean of academic affairs at the School of Health.
Floyd envisioned and designed the one-credit course during the COVID-19 pandemic so that students could see how health inequities translated outside of classroom theory.
Using Georgetown’s Capitol Campus as a home base, the sixweek course meets once a week at different locations throughout the city.
He believes the course’s varied sites show the dynamic circumstances of where and how health care is delivered.
Locations from previous semesters include the Martin Luther King Jr. Memorial Library, a community health center called Mary’s Center, founded by Maria Gomez (NHS’77), and the offices of the National Association of County and City Health Officials.
Photo: Lisa Helfert
Gabrielle Barone and Heather Wilpone-Welborn | Design by Shikha Savdas
The sites and learning objectives change from semester to semester to provide students with the fullest understanding possible of social determinants of health. To do that, “we’re thinking about lots of different levels of interaction,” Floyd says, from research to policy, education, and housing. He particularly enjoys visits to community-based organizations, where the “actual direct service” happens.
Nursing student Francyne Diola (N’27) was searching for these kinds of real-life interactions when she chose the course. “Most of my courses have been focused on the clinical setting,” says Diola, “so it was great to have the opportunity to learn about health equity and what drives social determinants of health.”
Before each onsite visit, students prepare with readings and academic work. The class is designed to be small, with 9–12 students, to allow for more engagement and easier movement around onsite locations. The interdisciplinary course invites participants from any major and counts toward minors in medical humanities, disability studies, and justice and peace studies. Past students have gone on to medical school, local public health work, and master’s degrees in policy.
For their final class project, groups envision ways to improve a health equity issue—for example, expanding health care coverage, improving procedure protocols, and addressing barriers to reproductive care.
In future semesters, Floyd hopes to host organizational leaders as audience members during final presentations. n
or major requirements, and have access to a variety of professional development workshops. In Fall 2025, the
In addition to Health Innovation for the Common Good, there are CALL courses that range from urban ecology to political philosophy, digital news, and feminist thought. CALL students complete a part-time, for-credit internship while taking experiential learning courses to fulfill core
CALL program will be one of many programs moving to 111 Massachusetts Ave., NW.
The ‘GI cancer powerhouse’ celebrates 15 years
By Kat Zambon
Since its establishment in September 2009, the Otto J. Ruesch Center for the Cure of Gastrointestinal (GI) Cancers at Georgetown University’s Lombardi Comprehensive Cancer Center has been dedicated to advancing transformative research to save lives.
“I’ve had the privilege of getting to know [founding donor] Jeanne Ruesch over the years,” said Louis Weiner, director of Georgetown Lombardi. “Her visionary investment in the Ruesch Center for the Cure of Gastrointestinal Cancers transformed—and continues to transform—the work we do at Georgetown.”
John Marshall, director of the Ruesch Center, professor of oncology and medicine at Georgetown, and clinical director of oncology and chief of the division of hematology/oncology at MedStar Georgetown University Hospital, met Jeanne Ruesch in 2003 when her husband, Otto, a prominent Washington, DC-area businessman and philanthropist, was diagnosed with pancreatic cancer.
Otto fought cancer for 14 months before his death in October 2004. Over that time, the Rueschs were shocked to learn about the bleak prognosis for many GI cancers.
“When I started, the average survival of patients with metastatic colon cancer was around 11 months; pancreatic cancer was about four months,” Weiner said. “It was horrible.”
The Rueschs saw the need for research and advocacy funding to treat GI cancer. In Otto’s memory, Jeanne
established the Ruesch Center with Marshall as its director, encouraging him to focus on high-risk, high-reward research to make significant strides in the fight against GI cancers.
“Without [Jeanne’s] guidance and future focus, I think we wouldn’t be having a 15th anniversary of the Ruesch Center,” says Marshall.
Standard chemotherapy regimens are ineffective for the majority of GI cancer patients. Over the last 15 years, Ruesch Center researchers have improved their understanding of the genetic mutations that drive the development of cancer and identified targeted treatments for specific tumor types. Recently, its researchers led a clinical trial combining immunotherapy with an immune activator to treat pancreatic cancer, with patients experiencing reductions in a biomarker that indicates the presence of pancreatic cancer.
The Ruesch Center gives patients access to the latest therapies from innovative clinical trials with experienced nurses. Additionally, the student summer program helps train future cancer research leaders.
“I am so lucky to work in what has become a GI cancer powerhouse,” Marshall says. “Everywhere I look, I’ve got people thinking about, caring about, spending their energy on how we make the outcomes for GI cancer patients better. The future has never looked brighter for GI cancers.” n
Photos: Donna Parry
Left: Jeanne Ruesch and John Marshall, M.D. Right: Winners of the Luminary Awards in GI Cancers celebrate the 15th anniversary of the Ruesch Center for the Cure of Gastrointestinal Cancers.
SOM students team up with local barbers
By Nowshin Chowdhury
A year after five Georgetown School of Medicine students won a scholarship prize at the Georgetown Public Policy Challenge, they are implementing their “Trimming the Risk” proposal to improve heart health in Washington, DC, through barbershops.
According to the Centers for Disease Control (CDC), heart disease is the leading cause of death in the District, and hypertension is the number one risk factor for heart disease, which can lead to heart attack, stroke, and death. Ryan Braun (M’26), Evan Czulada (M’25), Stefan Prvulovic (M’27), Holly Shan (M’26), and Mana Sheykhsoltan (M’25) proposed setting up regular blood pressure screenings at barbershops where patrons may be at high risk.
Historically, barbershops, particularly those in Black and brown communities, have played a role in educating and leading community health care. The students felt that individuals visiting a barbershop would be more receptive to preventive health care ideas.
“We have these amazing hospitals in DC, but they’re typically only accessed by the sickest of patients,” says Braun. “We want to reach people earlier, before they come to us at the hospital.”
After winning the McCourt prize in April 2024, the team secured more funding through one of Georgetown’s RADIANCE (Respect, Advocacy, Diversity, Inclusion, Anti-racism, Collaboration, and Equity) grants. The award monies cover the cost of blood pressure cuffs, as well as small incentives.
Volunteers have started training barbers at three local barbershops on how to take blood pressure readings.
“We thought that it might be difficult to get community buy-in, but that has not been the case,” says Braun. “The barbers are willing to take time away from their families to stay after work and learn about blood pressure from us. Their dedication shows how invested they are in their community.”
As two of the students from the team graduate this year, the younger students will take over the efforts, partnering with LaTasha Seliby Perkins, assistant professor of medicine at the School of Medicine, and a local organization called Black Men in White Coats, which provides underrepresented minority youth with exposure to the medical field.
“I came to Georgetown wanting to leave something past my time here,” says Braun. “This program is sustainable, has community buy-in, and positively impacts the local residents. It helps Georgetown medical students get out into the community and helps increase interactions that will ultimately save lives.” n
Holly Shan (M’26), Ryan Braun (M’26), Evan Czulada (M’25), Stefan Prvulovic (M’27), and Mana Sheykhsoltan (M’25) won the Georgetown Public Policy Challenge with their “Trimming the Risk” proposal in 2024. ON CAMPUS
A teacher with a ‘healing touch’
By Nowshin Chowdhury
Earlier this year, the School of Medicine community mourned the loss of beloved physician-educator Donald M. Knowlan (R’60, W’82, HON’04), who joined the faculty in 1961. He served as the director of the Federal Aviation Agency Cardiac Research Institute at Georgetown.
More recent medical school graduates remember Knowlan from the Pellegrino Lecture he delivered from 2008 until 2017 at the School of Medicine’s White Coat Ceremony. In it, he inspired doctors-in-training to focus on “the patient, the patient, the patient” above all else.
“Knowlan always taught with cura personalis in mind, reminding his students to treat the whole person,” says Joe Panarelli (B’03, M’07), who helped launch the Donald M. Knowlan, M.D. Scholarship at Georgetown in 2019.
“When I was on the Medical Alumni Board and we were looking to start a scholarship based on an alumnus who’s had an impact across generations, I suggested Dr. Knowlan and his name resonated with everyone,” says Panarelli.
Panarelli recalls that Knowlan could hear things with his stethoscope during clinical exams that others couldn’t—things that would later be confirmed with an echocardiogram.
Panarelli shares that Knowlan’s key message to students was, “learn how to be a really good doctor by listening to people, learning how to do a clinical exam, and knowing how to talk to patients.”
Stephen Ray Mitchell (W’86, MBA’13, Parent’15), dean emeritus for medical education at the School of Medicine, says that upon Knowlan’s retirement, Georgetown commissioned a painting of him that still hangs in the School of Medicine lobby.
“The portrait has become symbolic of the strength of Georgetown,” says Mitchell. “It shows ‘the healing touch.’”
Rather than a portrait in a white coat, Knowlan wanted the painting to be based on a photograph of him working with students.
“There are two students [Eric Vallone (C’90, M’97, R’00) and Katie Burgess (M’01)] with him in the painting,” says Mitchell. “Katie is examining the patient’s abdomen and Don is looking into Katie’s eyes. He told me he wanted to see her eyebrows raise when she felt the spleen. He said, ‘that’s what I spent my career doing: looking for the eyebrows.’”
An inspiration to many alumni—and to current students who are part of the Knowlan Learning Society—Knowlan will continue to be remembered through the Donald M. Knowlan, M.D. Scholarship and the Donald M. Knowlan, M.D. Award, given to a graduating medical student who shows excellence in internal medicine. n
Photo: Leslie Kossoff
Donald M. Knowlan, M.D., MACP (1929–2025), professor emeritus of medicine, won so many Golden Apple teaching awards that he became the first recipient of Georgetown’s coveted Golden Orchard.
Nurse executives pay it forward to the next generation
By Karen Teber and Racquel Nassor
In 2025, Georgetown University School of Nursing launched the Nurse Executives in Residence program as part of its growing focus on leadership development, enhancing the Post-Master’s Executive Doctor of Nursing Practice (DNP) in Health Systems Leadership and Policy degree program.
“We are proud to welcome national thought leaders in nursing executive leadership and governance as Georgetown Nurse Executives in Residence,” says School of Nursing Dean Roberta Waite.
“Our unique program gives Executive DNP students exclusive access to some of the foremost nursing leaders,” explains Waite. “We have created an opportunity for them to learn directly from executives who have made significant contributions to the nursing profession and to health care delivery.”
The seven inaugural Nurse Executives in Residence provide their expertise through lectures for Executive DNP courses, exclusive talks for the broader DNP learning community (including faculty, preceptors, and alumni), and focused mentoring for exceptional Executive DNP students.
“The Nurse Executives in Residence serve in a special faculty capacity, bringing a wealth of knowledge and experience
“Nurse Executives in Residence help us reach a broader audience to share the transformative power of a Georgetown education.”
—DEAN ROBERTA WAITE
to the Executive DNP program,” says Stephan Davis, executive director of leadership, policy, and DNP education at the School of Nursing. “Along with our core DNP expert faculty, Nurse Executives in Residence will enhance Executive DNP education through the integration of theory and practice, preparing our graduates to contribute to the future of nursing leadership and health care transformation.”
The Executive DNP program is designed for nurses who hold a relevant graduate degree, are currently practicing in an advanced nursing role, and aim to advance their careers in nursing leadership, policy, and advocacy. Additionally, the program features executive coaching to enhance leadership development and interpersonal effectiveness.
“Nurse Executives in Residence help us reach a broader audience to share the transformative power of a Georgetown education,” Davis says.
Recently, Georgetown School of Nursing held a breakfast at the American Organization for Nursing Leadership (AONL) Conference in Boston with four Nurse Executives in Residence, launching the DNP program’s collaboration with the organization.
“Executive DNP students can now participate in the AONL Advocacy Academy in DC where they learn and network with nurse leaders, and interact with congressional staffers, and legislators,” says Davis. “It is my vision that Georgetown’s Executive Doctor of Nursing Practice in Health Systems Leadership and Policy will be the program of choice for nurses who aspire to lead transformational change in practice and health care systems and through shaping health policy.” n
Nurse executives in residence came together at Georgetown School of Nursing’s inaugural breakfast at the AONL Conference in Boston.
GUMC Advancement VP Jackie Wood supports ‘hope, health, and care’
By Racquel Nassor
In March 2025, Jackie Wood was appointed the new vice president for advancement for the Georgetown University Medical Center (GUMC). Georgetown Health sat down with Wood to talk about her new role as she envisions Georgetown’s future.
Tell me about your background. What experiences have led you to your work at Georgetown?
I grew up in small towns in Tennessee and Virginia with a dad who was a radiologist and a mom who was a nurse—and later a nurse practitioner. From a young age, I went with my dad to the hospital when my mom was at nursing school and watched him engage with patients in our community. I saw
that communities need to have access to care in order to be vibrant.
I didn’t follow a clinical care path, but quickly learned the advancement field has a unique opportunity to assist alumni, patients, and community members who want to help our educators, physicians, and researchers train the next generation and develop better tools to support healthier communities. I have spent several years at Vanderbilt, University of Alabama at Birmingham, and George Washington University at this intersection between philanthropy and health.
Where are you focusing to help facilitate the university’s work in health care research, education, and clinical care?
We’ve identified five pillars of excellence: cancer, return to function after a neurologic event, global health, health equity, and the creation of innovation districts. With a strategic investment in each of these areas, we can leverage our expertise alongside our academic health system partner MedStar Health. Our deep talent across medicine, nursing, health, law, policy, and business is positioned to support healthier communities through improved access to care and better outcomes.
What are you looking forward to in your work at Georgetown?
I’m excited about engaging with alumni and friends to learn about their foundational Georgetown experiences. Understanding the depth and breadth of the work that we do here is the biggest part of my first several months.
In my short time here, I’ve been inspired by our commitment to Jesuit values, our alumni and friends’ deep enthusiasm for Georgetown, and the momentum with the arrival of Norman Beauchamp, GUMC’s new executive vice president for health sciences. We have a powerful story to tell about the work that we do here. By partnering with our community, we can provide hope, health, and care with energy and enthusiasm. I am humbled and thrilled to be part of this team. n
Photo: Phil Humnicky
In her new role as GUMC’s vice president for advancement, Jackie Wood looks forward to sharing the “powerful story” of the work being done at Georgetown.
Group therapy helps students with body dysmorphia
By Nowshin Chowdhury
Last fall, two counselors at Georgetown’s Counseling and Psychiatric Services (CAPS) launched the Body Image and Eating Concerns support group for undergraduate and graduate students.
The group explores cognitive and behavioral aspects of food and body dysmorphia, and helps students overcome their fears through exposure therapy and other resources.
“Eating disorders are a disease that affects you cognitively, behaviorally, and physically,” says Jessica Kuszelewicz, who founded the group with Shanice Anderson and serves as one of the facilitators. “It’s important to cover as many aspects that we can in order to create a comprehensive level of support for those we serve.”
The group creates a welcoming atmosphere for students of all backgrounds.
“Eating disorders do not discriminate,” says Kuszelewicz. “We encourage community because eating disorders thrive in secrecy and isolation.”
“Universities can be seen as a ‘red zone’ for eating disorders,” says Anderson, who also serves as a facilitator for the group. “It’s a time where either pre-existing or new symptoms present in many college-aged students. We have a unique opportunity to intervene before it gets too far or to provide support before they have to put their life on hold in order to receive services.”
During the sessions, students state their personal beliefs that affect how they see themselves or what they eat. Kuszelewicz and Anderson, both of whom have a background working with eating disorder patients, meet after each session to devise a challenge to identify and overcome those obstacles in the following session. Then, the students take home the behavioral experiments, which may include journaling or avoiding checking their weight, and record their results and observations for discussion at the next session.
“This support group really helps to create community around something that can feel taboo—almost like a dirty secret,” says Anderson. “It allows students to know they’re not alone in this fight—that not only do they have us as clinicians, but they also have peers who have similar difficulties or challenges, who are looking for community and connection.”
With more funding, Kuszelewicz and Anderson would like to do food exposures with the group to encourage healthy eating habits, overcome fears of eating in public, and create a safe space.
“This group has helped me realize that I’m not alone in my struggles,” shares a nursing student. “I want to be healthy to provide the best care to my patients as a nurse.” n
ALUMNI CONNECTIONS
One alumna’s ‘Why not me?’ approach to making a difference
By Racquel Nassor
Courtney Pladsen (G’11,’17) made history as the first nurse practitioner (NP) to serve as the Medicaid medical director in the state of Maine.
A graduate of Georgetown’s masters in nursing and Doctor of Nursing Practice (DNP) programs, Pladsen also works as a family medicine NP with a clinical focus on substance use treatment and harm reduction for people experiencing homelessness. Her work with Health Care for the Homeless for the past 13 years gives her particular insight into current challenges with harm reduction care.
“After a Jesuit education, I feel an ethical obligation to develop a health care system that meets everyone’s needs, especially the most marginalized,” she says.
As the state’s Medicaid medical director, Pladsen provides clinical leadership, informing the development of policy and addressing systemic challenges. “It’s a big job. My goal is to ensure all Mainers have access to high-quality health care,” she says.
Maine’s Medicaid program covers a third of the state, half of all children and deliveries, and two-thirds of seniors in long-term care facilities or nursing homes. As one of five states without managed care, Maine directly runs its Medicaid office within the Department of Health and Human Services. Pladsen leverages Medicaid to provide innovative pilot programs like the Food is Medicine initiative and traditional healing therapies for the Wabanaki Nations.
Designing personalized health systems
Pladsen’s early experiences influenced her career, motivating her research at Georgetown screening and addressing social determinants of health in primary care, and later, her projects improving the health care safety net though MaineCare.
“I grew up in poverty and experienced homelessness, so I know what it’s like to be a Medicaid recipient and have to navigate it,” she says. “I remember a year when the state legislature didn’t have funding, and they cut dental benefits. I remember the indignity of living at the whim of those benefits.”
Courtney Pladsen, DNP, FNP, R.N. (G’11,’17) is the Medicaid medical director for the state of Maine. Formerly the clinical director at the National Health Care for the Homeless Council, she developed Maine’s first medical respite program. She continues to use expertise in harm reduction care to help design programs that benefit individual’s lives.
Photo: Flynn Larsen
“I also have a sibling who has been incarcerated and spent time in federal prison. I want to make sure that whoever’s moving through these systems gets the care that they need and deserve to be their healthiest selves,” she adds.
“When I’m designing a system that works for everybody, I think of a system that I would want for my own family. It’s not an abstraction; it’s real and close,” she says.
Building Maine’s reentry program for prisoners
For the last year and a half, Pladsen has also led the development of Maine’s 1115 waiver. This re-entry program for prisoners gives Maine permission to use Medicaid to pay for services for people who are incarcerated 90 days prior to release.
“When I’m designing a system that works for everybody, I think of a system that I would want for my own family. It’s not an abstraction; it’s real and close.” —COURTNEY PLADSEN
“The health outcomes of individuals in the two weeks following release from jail or prison are poor, with high rates of overdose deaths, hospitalizations, and all-cause mortality,” she says. “Having a plan for that first day upon release and having that safety net built in to build a continuum of healthcare.”
Pladsen will work with the Department of Corrections and the Centers for Medicare and Medicaid Services to design the program to expand services for people in jails and prison, with the goal of implementing it in 2027.
“To build the program, I systematically toured every jail and prison, meeting with sheriffs, jail administrators, people working in partnership with the Maine Reentry Network and the Maine Prisoner Advocacy Coalition, and people who’ve been imprisoned,” she says.
“We have rural counties with 30-person jails, and densely populated counties with 300-person jails. They require different resources and services,” says Pladsen. “We’re working with each county to design services that best fit their needs.”
Three months before people leave jails and prisons, the program will develop their plan of care, scheduling appointments with psychiatric, substance use treatment, or primary care providers; identifying their housing options; and connecting them to jobs. It will also secure their access to treatment and medicine before they leave.
“This is a massive transformation of our entire system,” says Pladsen. “This is the first time Medicaid will be paying for services for people in jails and prisons, the first time carceral health care providers will have a role in Medicaid. I can’t overstate how transformative this
could be, because right now we have no window into the care being provided in jails and prisons.”
With the reentry waiver program, MaineCare will have quality assurance reviews to ensure people in prisons and jails are receiving high-quality behavioral health, substance use treatment, and primary health care. Pladsen hopes raising the standard of care will reduce overdose deaths, all-cause mortality, and ER utilization and hospitalization, improving their health outcomes.
“It’s a big project, many years in the making, and it will be transformative across our entire state. I’m feeling really hopeful about the positive outcomes that will come from it,” Pladsen says.
Using the DNP’s transferable
skills
Pladsen credits her Georgetown support network for her success today. She is still in touch with her doctoral mentor, Edilma Yearwood, and her DNP cohort peer, Danielle McCamey (G’11, ’17). McCamey and Pladsen were recently inducted as fellows in the American Academy of Nurse Practitioners.
“I’m immensely grateful to Georgetown that my path crossed with Yearwood and McCamey,” she says. “They have been unbelievably supportive of me personally and professionally.”
Ultimately, she believes the DNP gave her essential tools, transferable to many leadership roles—including her role as a leader in state government. “Nurses need to think about how transferable nursing skills are,” Pladsen says. “We just have to say, ‘Why not me? I have the skill set for those jobs.’” n
Tools of the Trade
Interview by Nowshin Chowdhury
Mechem Frashier, MBA, BSN., R.N. (NHS’01), a member of Navajo Nation, is the nursing director for children’s programs at Presbyterian Healthcare in New Mexico.
Mechem Frashier serves on the boards of the National Coalition of Ethnic Minority Nurse Associations and National Alaska Native American Indian Nurses Association. Frashier won the Scholars for Change Award from the American Nurses Foundation in 2024.
“One of my proudest accomplishments is being able to provide health care services to my fellow tribal communities and being an advocate for their care,” says Frashier.
Frashier carries Georgetown’s value of servant leadership into her career of over 20 years.
“At Georgetown, I learned that we are created to serve others who are in need and to be grateful for what we are blessed with,” says Frashier. “I make it a mission in my career and my life to make sure I help those around me.”
During the COVID-19 pandemic, Frashier was asked to lead mobile testing in the greater Albuquerque area. Then the local Pueblo and Native American community asked for help.
“We jumped at the chance, using our mobile clinic (bus) to drive out to tribal reservations and provide testing seven days
a week,” says Frashier. “We were their only option for testing. To provide this service for almost two years, we partnered with the Indian Health Service and the New Mexico Department of Health.”
Frashier says the lack of minority nurse leaders has been challenging for her as she navigates her career, but Bette Keltner, former dean of the Georgetown School of Nursing and former president of the National Alaska Native American Indian Nurses Association, has been a great mentor and guide to her.
The tools of her trade are:
1. Phone: to communicate
2. Notebook: to take notes on rounds
3. Kids’ toys (jacks and ball): a reminder of her humble beginnings
4. Picture of family and Navajo rug in office: a reminder of who supports her and the tribal communities she serves
5. Bible app: a daily reminder of servant leadership n
Photos: Courtesy of Mechem Frashier / iStock
Alumna finds her calling in repurposing medical supplies
By Nowshin Chowdhury
Three years ago, Tammy Kenney Bevins (N’83) was working at a rehab and long-term care nursing facility where she would always try to repurpose extra supplies. A nurse recommended she join Partners for World Health (PWH), a nonprofit organization based in Portland, Maine, that does the same thing on a broader spectrum.
Unused items like syringes and dressing supplies can’t be used past their expiration dates in the U.S., but are still considered usable in other countries.
“At the nursing facility, I had to take these items out of circulation and pay a fee to dispose of them,” says Kenney Bevins. “When we donate those supplies, there’s cost savings for the organization.”
Kenney Bevins says that when the care facility where she worked upgraded from manual crank beds to electric adjustable beds, the crank beds were shipped to Bangladesh through PWH. A charitable or government organization then distributed them to those in need.
Volunteering with PWH gives Kenney Bevins an opportunity to see those items get used overseas. Since 2023, she has been to Kenya, Senegal, and Uganda as co-leader for the medical service trips.
In addition to the large-scale shipments, volunteers bring additional duffel bags full of medical supplies to set up clinics.
“We hold clinics in different villages—sometimes in the mountains, sometimes by the shores of Lake Victoria, and often in places where they’ve never had a medical clinic,” says Kenney Bevins. “You’re just under a tent with chairs, kind of making it happen. People visit with various medical issues since we provide primary care.”
PWH seeks out pregnant women to educate them about what is and isn’t a concerning side effect of pregnancy. Pregnant patients receive free birthing kits to bring to the clinic or hospital for their child’s birth and are instructed on how to use them in case of emergency. Kenney Bevins and her fellow volunteers also work with the local health care providers and the country’s leaders to enhance the health and well-being of their citizens.
“My relationship Partners for World Health ticks a lot of boxes, but the reduce/reuse aspect—the effort at sustainability—really speaks to me,” says Kenney Bevins. “There are copious amounts of waste in our medical system across the board.” n
Since 2023, Tammy Kenney Bevins R.N., BSN (N’83) has visited Kenya, Senegal, and Uganda as co-leader for the medical service trips on behalf of Partners for World Health. Pictured from the top is a boat she used for transportation on Lake Victoria to Kimi Island in Uganda; Kenney Bevins at a Kenya pharmacy; and later at Sirongo Village Clinic in Kenya.
Reflections
on Health with Robert Fan,
M.D. (G’85, M’89), Orthopedics in Salem, Oregon
I was born in London, England. My father was a surgeon with the National Health Service. When I was six, we moved to New York and then New Jersey where he worked at Hackensack University Medical Center. In high school I worked summer jobs there.
For college I went to Cornell and then applied to medical school but didn’t have the GPA to get in. I enrolled in Georgetown’s Special Master’s in Physiology—a great decision. It got my foot in the door for medical school.
I chose orthopedics because the people I met during rotations were even-keeled, personable, and enjoyed life. It’s no coin cidence that many friends also went into orthopedics. I like to analyze a problem, fix it, see results, and understand how it happened. I enjoy being in the oper ating room. It’s great to get to know my patients and see them get better.
At our med school orientation they asked us to always remember the excitement of that moment, the butterflies. As your career goes on, you want to keep being excited about what you do, and be willing to learn.
I grew up playing lacrosse. Played in college and all through med school and I still play, but now it’s in slow motion. It’s a tight community. I do it for the social aspect.
Today I focus on the shoulder—arthroscopic surgery and replacements, often seeing athletes. We are fragile. A bad injury can be a life-changer. Lower extremity strength and balance is hugely important for longevity. I encourage patients to keep up exercise, even if it’s just walking.
Orthopedics has changed a lot. There’s no procedure I learned in medical school, residency, or fellowship that I continue to do. My career has been one of early adoption of new techniques. You have to innovate, because medicine evolves, like the use of robotics in hip and knee replacement surgery.
For shoulder replacement surgery, we are developing the use of mapping using virtual reality goggles to implement a preop plan in real time. With arthroscopic surgery, video technology and instrumentation has evolved quite a bit.
Today medicine suffers without a collective political voice to advocate for patients. We see Medicare cuts year after year, and millions of dollars going to health insurance executives that should be going to patient care.
Last year I was playing in a tourna ment in Colorado, and someone ran from the other field asking for a doctor. When I got there a player was down, pulseless and not breathing. I helped do CPR and he ended up surviving. He was transported to Denver for an open-heart bypass. I later learned he was my Cornell teammate who I hadn’t seen in 42 years. We’ve since met up—it was pretty incredible.
I reflect on success as a combination of hard work, good luck, and a strong foundation of family support. It’s true about the spouse standing next to you.
Thrive Center opens to support children and families in the community
Since its opening last fall, the Thrive Center for Children, Families, and Communities, a multidisciplinary academic center launched by Georgetown University and MedStar Health, has focused on child and family mental health, disabilities, health equity, and digital health.
Its programs are designed to rapidly advance equitable systems of care and support that enable children, families, and communities.
“Our goal is to look at the entire spectrum of what helps people thrive across the lifespan, beginning in childhood,” explains Matthew Biel, the center’s director.
As the Marriott Chair of Child, Adolescent, and Family Mental Health, Biel serves as professor of psychiatry and pediatrics at Georgetown University School of Medicine, and chief of the division of child and adolescent psychiatry at MedStar Georgetown University Hospital, which developed the center in partnership with the Center for Child and Human Development.
Major donors include the A. James & Alice B. Clark Foundation, Shelley and Allan Holt, the J. Willard and Alice S. Marriott Foundation, and the Gerard B. Lambert Foundation.
Read more about the Thrive Center and its focus on cura personalis, or care of the whole person.
The Innovation Hub at the Thrive Center, which offers 12-week fall and spring fellowships, held an inaugural Solutions Fair highlighting the work of its Spring 2025 fellows. Here, a diagram at the Hand in Hand Parenting display explains the program’s structural model to support parents and caregivers.
Eric Woods (B’91) (center) was honored with a 2025 John Carroll Award for his distinctive volunteer service to Georgetown, including his work in building a team of BellRinger Riders who, together, rode over 500 miles to raise over $18,000 for critical cancer research at Georgetown University’s Lombardi Comprehensive Cancer Center. To learn more about the fundraiser, visit bellringer.org