OCTOBER 2023 ISSUE CREATED&PUBLISHEDBYFMHCA

2 | InSession- October 2023 | FMHCA.org

May this message find each of you doing well. I hope you all enjoyed a wonderful Summer! Over the summer months, FMHCA hosted its first annual Graduate Student and Registered Mental Health Counselor Intern Summer Bash. Many thanks to our wonderful administrative team for creating, and hosting the Summer Bash, it was a huge success! Please also know in response to the multitude of questions from our FMHCA members and colleagues, we developed and hosted “What
nominations are already being accepted If you are interested in serving on the Board, please do not hesitate to ask me or any of the other board members questions about what we do. We will be electing the positions of President-Elect, Secretary, Treasurer, Regional Directors, and Associate Regional Directors. (Please note that “Associate Regional Director” is not a Board of Directors position.) Here is the link to submit a Board of Directors nomination. Here is the nomination link for Associate Regional Directors.
” We had over 125 attend the live presentation, and it is now available as an on-demand workshop. Speaking of legislation, the FMHCA Government Relations Committee, (GRC), has been hard at work during the summer months preparing for FMHCA’s upcoming Legislative Days (this Fall) and working on our Legislative Agenda for the next Legislative Session. You can read more details in the GRC Committee update column in this edition of InSession magazine.
As my time as your President is coming to a close, please know my goal for FMHCA membership has been achieved ahead of schedule! We are now over 2,000 strong! I have also edited FMHCA’s Leadership Manual so that it is ready to deliver to FMHCA’s 2024 Board of Directors. Please know elections for Board of Director positions will take place soon and

Are you looking to make a mark in the community? Join the 2024 FMHCA Board of Directors and make your mark on the map!

Open positions include: President-Elect, Secretary, NW Regional Director, and NE Regional Director
Candidates must be a FMHCA member in good standing and must be nominated by 10/13/23
Lastly, if you are not a current member of FMHCA, we encourage you to join us There are many benefits of becoming a member. FMHCA is the only organization in Florida devoted solely to the needs of Mental Health Counseling. Increasing our membership allows us to accomplish more in Tallahassee, expand our conference, offer members an ever-increasing number of benefits, and much more! FMHCA is here to serve you and we always welcome your input an organization. It has been a privilege to serv
Page 8
Cultural Competence In Assessment


Page 11
Healing the System from Within: A School-Based Mental Health Approach
Toward Improving Wellness in Schools
Page 14
Depressed Air: Using Breathwork to Improve Depressive Symptoms
Page 17
FMHCA Committee Updates
Page 18
FMHCA's Favorites
Page 20
Ask The Expert- Questions Answered by The Health Law Firm
Page 21
I See You: The Benefits of Visibility in Mental Health
Page 24 (A Conversation with FMHCA Lobbyist, Corinne Mixon) Shaping Mental Health Policy

Page 31
Religious Trauma and the Fear of Hell
Page 33
The Direct/ Inferential Model of Communication
Page 37
A Word With AMHCA
Page 40

Page 44
InSession Magazine is created and published quarterly by The Florida Mental Health Counselors Association (FMHCA)
FMHCA is a 501(c)(3) non for profit organization and chapter of the American Mental Health Counselors Association.
FMHCA is the only organization in the state of Florida that works exclusively towards meeting the needs of Licensed Mental Health Counselors in each season of their profession through intentional and strengthbased advocacy, networking, accessible professional development, and legislative efforts.
Let your voice be heard by becoming a FMHCA Member today!
Click here to view FMHCA's current Bylaws.
CONTRIBUTE:
If you would like to write for InSession magazine or purchase Ad space in the next publication, please email: Naomi Rodriguez at naomi@flmhca org
Naomi Rodriguez- Editor
Victoria Siegel, LMHC- Expert Advisor
There shall be no discrimination against any individual on the basis of ethic group, race, religion, gender, sexual orientation, age, or disability
DISCLAIMER:
Information in InSession Magazine does not represent an official FMHCA policy or position and the acceptance of advertising does not constitute endorsement or approval by FMHCA of any advertised service or product. InSession is crafted based on article submissions received. Articles are categorized between Professional Experience Articles & Professional Resource Articles.
Professional Experience Articles are writer's firstperson pieces about a topic related to their experience as a mental health professional, or an opinion about a trend in the mental health counseling field
Professional Resource Articles are in-depth pieces intended to provide insights for the author's clinical colleagues on how to be more effective with a particular type of client or a client with a particular disorder, or tips for running their practice more efficiently Each article is labeled with their article type

The Florida Mental Health Counselors Association (FMHCA) is the State Chapter of the American Mental Health Counselors Association (AMHCA) FMHCA is the only organization dedicated exclusively to meeting the professional needs of Florida’s Licensed Mental Health Counselors


The mission of the FMHCA is to advance the profession of clinical mental health counseling through intentional and strengthbased advocacy, networking, professional development, legislative efforts, public education, and the promotion of positive mental health for our communities

Its sole purpose is to promote the profession of mental health counseling and the needs of our members as well as:
Provide a system for the exchange of professional information among mental health counselors through newsletters, journals or other scientific, educational and/or professional materials
Provide professional development programs for mental health counselors to update and enhance clinical competencies






Promote legislation that recognizes and advances the profession of mental health counseling

Provide a public forum for mental health counselors to advocate for the social and emotional welfare of clients
Promote positive relations with mental health counselors and other mental health practitioners in all work settings to enhance the profession of mental health counseling

Contribute to the establishment and maintenance of minimum training standards for mental health counselors
Promote scientific research and inquiry into mental health concerns

Provide liaison on the state level with other professional organizations to promote the advancement of the mental health profession
Provide the public with information concerning the competencies and professional services of mental health counselors
Promote equitable licensure standards for mental health counselors through the state legislature


Cultural differences can definitely have an influence on the accuracy and validity of assessments and testing instruments. Especially when they are in relation to the minority populations within society. Cultural factors can have a huge impact on testing instruments that are used for various fields like education, counseling, healthcare, and etc. Most times, there is great emphasis placed on the information being gathered from these assessments and testing instruments Therefore, it is essential that accurate assessments and testing instruments be considered especially when being used to evaluate minority clients
Diller (2011) states that counselors and diagnosis’s can be influenced by an individual’s culture. Diller explains, “According to Gaw (1993), culture shapes and affects the very essence of how clinical work is done,” (p. 102). Yet, the problem is that counselors tend to superimpose their personal beliefs and/or culture when providing a diagnosis Diller continues to state, “Difficulties emerge, however, when practitioners
superimpose their cultural worldviews onto the life experience of culturally diverse clients and then make clinical assumptions or judgments from that perspective,” (p. 102). One such example is the influence of culture on an assessment is given by Dukes and Bjorklund. Dukes and Bjorklund (2011) reveals the biases in the study completed by Perry and Delpit in 1998. Students were asked to reflect on what a man with a suit and briefcase was doing African American students responded he was going to church “Perry and Delpit (1998) reported that the test writers concurred that the correct answer was that he was going to his place of work or business,” (p 293) Perry and Delpit explained that African American children realized on their cultural backgrounds when answering the question. However, Perry and Delpit stated,
From a mainstream cultural perspective, this response is deemed incorrect...for Perry and Delpit, however, marking the African American students’ response incorrect reveals bias toward a knowledge base rooted in North American or mainstream cultural
Professionalvalue system (Dukes & Bjorklund, 2011, p 293)
This is a perfect example of how culture and background can have a significant influence on the accuracy of an assessment. The conventional, generic testing methods and questions cannot address each culture because each individual brings in his/her customs, culture, morals, and family values when completing assessments.
Therefore, appropriate use of assessments and testing instruments for cultural minority clients must be centered on encouraging trainees and therapists to search their personal backgrounds and racial identities. Training must be completed to help counselors see biases in their own behavior and thinking. Diller states they must understand “How microaggressions, especially their own, negatively impact and alienate clients of color,” (Diller, 2011, p. 110). He continues to state counselors must learn to “accept responsibility for becoming aware of and overcoming racial bias,” (p. 110). Sturmer & Gerstein (1997) states one recommendation mental health counselors must understand is the importance of recognizing cultural differences Sturmer & Gerstein state, “Unintended ethnocentric thinking that minimizes cultural differences may lead to erroneous MMPI interpretation,” (p 11)
In conclusion, the value of assessments and testing instruments must be addressed system-wide. It is imperative to do so if we are going to properly care for clients of all cultures. Counselors, educators, and all others involved must become
more aware of the impact of cultural differences. These differences between the client and the counselor may have an impact on the accuracy and reliability of an assessment and testing instrument. It is only when these areas are actively pursued and addressed, can we properly assess, test, diagnose, and help our clients that are in need.
References
Diller, J. (2011). Cultural diversity: A primer for the human services (4th ed.). Belmont, CA: Brooks/Cole Cengage Learning.
Dukes, C., and Bjorklund, D. (2011). Cultural bias in teaching. Psychology of Classroom Learning, 292-296
Poortinga, Y. (1995). Cultural bias in assessment: Historical and thematic issues. European Journal of Psychological Assessment, 1, (3), 140-146.
Sturmer, P. & Gerstein, L. (1997). MMPI profiles of black Americans: Is there a bias? Journal of Mental Health Counseling, 19, (2), 1-21.
Written By: Dr Roydrick V Jones, MS, CRCRoydrick is a substance abuse therapist, certified recovery coach and case manager in a community mental health setting He has experience counseling adolescents, teens, adults, and seniors working to build sobriety from substance misuse
Roydrick has received certifications for Motivational Interviewing, Stages of Change, Forensic Specialist Training, Recovery Coaching, and Recovery Coach Trainer He has received his doctorate in educational leadership Roydrick’s main focus is on assisting colleagues in mitigating burnout and/or compassion fatigue through strong self-care practices



School-based mental health counselors are able to contribute to child and adolescent mental health by, literally, meeting their clients where they are. When structured appropriately, services may be highly effective due to frequency and consistency in treatment. In addition, opportunities for consultation can greatly benefit client outcomes. However, within the scope of school-based mental health, a layer of intervention that is sometimes overlooked, is the promotion of emotional wellness initiatives among faculty and staff members. Having been a school-based mental health counselor and now a counselor educator who has focused on burnout and secondary traumatic stress in helping professionals, I have had the great privilege to work alongside those who directly impact the emotional progress of my client When these individuals are overwhelmed by the extensive demands of their role, students may experience the consequences. Gaps in training can further impede the prosocial functioning of a classroom. Like our young clients, faculty and support staff experience a myriad of barriers which can negatively impact their lives. Therefore, school-based mental health counselors who are actively engaged in a school community can prompt small systemic changes that contribute toward a safe and happy learning environment for all.
Mental health resources can be a life-line to helping professionals who are struggling with work-related distress. One of my goals as a school-based mental health counselor has been to educate teachers and staff on techniques for emotional

self-management. Typically, educators mask their intense feelings, which can exacerbate teacher stress and lead to burnout. Each week, I would send a regularly scheduled email to the entire school discussing a relevant topic aimed at developing adult social-emotion through affirmations, scholarly articles, websites, and worksheets. This can help avoid singling anyone out and possibly missing someone who might be struggling in silence. School-based mental health counselors should frame these messages from a strengths-based lens that reflects compassion and humility The hope is that through acceptance and alternative outlets for expression, there might be a reduction of childhood adverse experiences and an increase in professional longevity
Relationship building is key to improving school climate and preventing burnout Most of the school day is consumed with responsibilities and little breathing room is left for adult socialization School-based mental health counselors can promote collegial relationships by advocating for campus-wide bonding opportunities, such as yoga or mindfulness, at no or low cost They may also facilitate a brief and interactive group activity at the start of faculty meetings. Discussions or activities that require excessive disclosure or explore triggering topics should be highly avoided. Administrators can be provided with psychoeducation on the benefits of relationships among coworkers, as a means to decrease attrition rates and improve morale.
School-based mental health counselors can take the “temperature” of the school’s climate through periodic checkins I would allocate a short window of time each day (30 minutes or less) to focus on stopping into classrooms to say individual hellos to faculty and staff members. This level of engagement models pro-social interactions, fosters rapport with caregivers, and builds a foundation for future referrals. In preparation, make sure that you are aware of testing schedules and other school-wide events. You can prompt your visit with a school-wide email that (a) communicates gratitude for their dedication and energy to their students (b) provides notice of your intention to connect not to assess instructional skills or classroom management (c) offers the opportunity to decline. This invitation can serve as a healthy approach toward relationship building within a model of boundary setting It is critical to consult with school administration and external agency supervisors to gain permission, insight of school culture, and feedback for future interventions
It “takes a village” to support the socio-emotional development
of children While we may be attuned to our client’s primary caregivers’ needs, we may forget that teachers and staff may also need support and encouragement School-based mental health counselors can impact their clients’ mental health by providing those who surround them with empathy, understanding, and professional expertise. By working with all of the stakeholders in a school’s community to expand overall wellness, children can continue to develop outside of our sessions in an environment that is safe and functional.
Written By: Bridget Glass, Ph D , LMHC, ACSDr Bridget Glass serves as the Program Dire and Associate Professor for the Clinical Men

Health Counseling Program at South Univers West Palm Beach Her clinical focus is to help heal the impact of childhood trauma and secondary traumatic stress She hopes to contribute to mental health research through advocacy efforts, writing, teaching, and facilitating training Her self-care consists of cuddles with her two Goldendoodles and travels with her husband


Major depressive disorder is a highly prevalent mental health disorder that has been ranked as the third cause of the burden of disease worldwide by the World Health Organization (WHO). The organization predicts that depression will be the leading cause of burden of disease by 2030 (Bains & Abdijadid, 2023). Since the beginning of the COVID-19 pandemic, both depression and anxiety have seen a substantial rise in the number of Americans experiencing symptoms of either one or both disorders One study found the prevalence of Americans with depression or anxiety increased from nearly 11% in 2019 to approximately 40% from April 2020 to April 2021 (Thomeer, Moody, & Yahirun, 2022) Additionally, a recent Gallup poll conducted from February 21-28, 2023 found 17.8% of respondents currently had or were currently being treated for depression and 29.0% responded as having depression at some point in their lives, both of which were the highest rates recorded since Gallup began measuring depression with the current questions in 2015 (Witters, 2023).
While major depressive disorder is a brain disorder associated with decreased activation in the left hemisphere of the frontal lobe (Meehan, Shaffer, & Zerr, 2022), depression can lead to changes in the autonomic nervous system (ANS), specifically, decreased heart rate variability (HRV) and increased sympathetic tone (Singla, 2017). HRV is a measure of beat-tobeat variations in heart rate and reflects ANS functioning; higher HRV leads to greater vagal tone, which indicates more parasympathetic activity and a greater ability for the ANS to regulate itself (Kopka, 2023) Strategies to increase HRV include breathwork and mindfulness, regular exercise, proper sleep hygiene, healthy diet, sunlight exposure, and avoiding or reducing alcohol and other substance use (WHOOP, 2020); additionally, HRV training is a noninvasive biofeedback training modality that can increase HRV by teaching individuals to engage in diaphragmatic breathing at a consistent respiration rate around six breaths per minute (Kopka, 2023). This article will focus on breathwork as a strategy to improve depression by
Professional Experience ArticleProblems with breathing, particularly variability in respiration patterns such as rapid, shallow breathing from the shoulders and chest instead of deep, abdominal breathing, have been linked to psychological problems including depression (Zamoscik, 2020) This type of breathing can result in increased sympathetic nervous system activity as well as increased posterior cingulate cortex-parahippocampal and default mode network (DMN) connectivity, which are associated with sad mood states (Renner, 2017; Zamoscik, 2020) Fortunately, breathwork has been shown to promote positive physiological changes to areas of the central nervous system (CNS) and ANS that are associated with depressive symptoms (Balban et al., 2023; Kopka, 2023; Meehan, Shaffer, & Zerr, 2022; Thompson & Thompson, 2015; Zamoscik, 2020). For breathwork to be effective, it is important to breathe in slowly through the nose. Unlike breathing in through the mouth, nasal breathing synchronizes activity in the olfactory cortex, amygdala, and hippocampus, which can impact emotional regulation and stress management (Balban et al., 2023). Additionally, breathing from the diaphragm as opposed to the chest and shoulders and extending the exhalation longer than the inhalation can promote increased parasympathetic nervous system activity, whereas shallow breathing with a shorter exhalation can increase sympathetic tone and can lead to anxiety-like symptoms (Khazan, 2022)
One strategy to improve diaphragmatic breathing technique is to encourage clients to “smell the flowers” for 4 seconds by breathing in slowly through their nose and then “blowing the bubbles” for 6 seconds by slowly exhaling through pursed lips as if they are attempting to blow bubbles out of a bubble wand Telling clients to visualize slowly inflating a balloon in their stomachs can help teach breathing from the diaphragm in addition to common practices such as placing one hand on the stomach and one on the chest or a book on the stomach while lying down.
Balban et al. (2023) found that five minutes of daily breathing exercises for 30 days can improve mood, anxiety, and physiological arousal This study also showed that when compared to a mindfulness meditation group, individuals in a breathing exercises group, specifically those focusing on breathing with an extended exhalation, demonstrated greater improvements in mood and physiological arousal. Of note this study did not demonstrate changes in HRV after 30 days. It is generally recommended to engage in breathing exercises for 1020 minutes daily to increase HRV (Khazan, 2022; Kopka, 2023; Meehan, Shaffer, & Zerr, 2022; Thompson & Thompson, 2015);
however, starting out clients out with five minutes of breathwork a day and increasing over time can still be impactful for improving mood and anxiety.
In addition to improved regulation of the ANS and greater parasympathetic tone, increasing HRV through consistent practice of diaphragmatic breathing can also improve communication from the vagus nerve to parts of the brain that influence the affect network (Thompson & Thompson, 2015). Specifically, increased HRV can positively impact areas involved in mood and anxiety, memory formation, and executive functioning such as the amygdala, insula, hippocampus, and prefrontal cortex. Based on improved symptoms in a sad mood challenge following a 4-week breathing exercise program, Zamoscik et al. (2020) recommend breathwork as an important tool for assisting with the treatment of depression.
References
Bains N. & Abdijadid, S. (2023, September 14). Major Depressive Disorder. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK559078/
Balban, M. Y., Neri, E., Kogon, M. M., Weed, L., Nouriani, B., Jo, B., Holl, G., Zeitzer, J. M., Spiegel, D., & Huberman, A. D. (2023, January 17). Brief structured respiration practices enhance mood and reduce physiological arousal. Cell reports. Medicine.
Kazan, I. (2022, July 28). Heart rate variability, mindfulness, and compassion. [Workshop]. International Society for Neuroregulation & Research, Orlando, FL.
Kopka, M. (2023). Heart rate variability biofeedback in the treatment of depression. Biofeedback, 51 (1), 1-6.
Meehan, Z.M., Shaffer, F., & Zerr, C.L. (2022). Depression. Biofeedback, 50 (2), 34-50.
Renner, F.. Siep, N., Arntz, A, Van de Ven, V., Peeters, F.P.M.L., Quaedflieg, C.W.E.M., & Huibers, M.J.H. (2017). Negative mood-induction modulates default mode network resting-state functional connectivity in chronic depression, Journal of Affective Disorders, 208, 590-596.
Singla S, Jhamb S, Singh KD, Kumar A. Depression affects autonomic system of the body? Yes, it does!, Journal of Educational Health Promotion, 9, 217.
Thomeer, M.B., Moody, M.D. & Yahirun, J. (2022) Racial and Ethnic Disparities in Mental Health and Mental Health Care During The COVID-19 Pandemic. J. Racial and Ethnic Health Disparities, 10, 961–976.
Thompson, M. & Thompson, L. (2015). The neurofeedback book: An introduction to basic concepts in applied psychophysiology (2nd ed.). Aurora, CO: AAPB.
Witters, D. (2023, September 14). U.S. depression rates reach new highs. Gallup.com. https://news.gallup.com/poll/505745/depression-rates-reach-new-highs.aspx Whoop. (2020, June 13). 10 ways to increase heart rate variability (HRV). WHOOP. https://www.whoop.com/us/en/thelocker/increase-hrv-heart-rate-variability/ Zamoscik, V., Schmidt, S.N.L., Timm, C., Keuhner, C., & Kirsch, P. (2020). Modulation of respiration pattern variability and its relation to anxiety symptoms in remitted recurrent depression. Heliyon, 6, 1-6.
Written By: Collier Shepard, M.A., M.S., LMHCCollier is a counselor at the University of Florida's Counseling and Wellness Center where he provides brief individual and group therapy to students at the university Collier specializes in neuro- and biofeedback training primarily for anxiety, depression, ADHD, and performance enhancement

Registered Intern & Graduate Student Committee Committee Chair: Laura Peddie-Bravo, LMHC, NCC Greetings! The Graduate Student and Registered Mental Health Counselor Intern Committee welcomes Lauren Malone, Registered Mental Health Counselor Intern, as Co-Chair of the committee. Welcome Lauren! Please know If you are a current Graduate Student, we would love to have a Graduate Student Co-Chair as well! Please feel free to contact me if you are interested or would like any additional information.
We will hold two more meetings in 2023 If you are already a member of the committee, please look for a survey about the next meeting day and time. My Co-Chair and I have been brainstorming some new ideas for the committee, and we plan to send out a survey with some of those new ideas for your consideration and feedback, so please look for that as well.
The 1st Annual FMHCA “Summer Bash” went great! We had a fantastic turnout, and this will become an annual event The Summer Bash contained everything a recent graduate/RMHCI needs for licensure: HIV course, Passing the NCMHCE Exam, Florida Laws and Rules, The Do’s and Don’ts of Being a RMHCI, and a free Mixer. All events were virtual, which allows all Graduate Students and Interns across the state of Florida to participate.
Our committee has its own Forum on the FMHCA website. Here you can find recordings of previous meetings, tips, resources, and more! Any committee member is welcome to post in our Forum Examples of posts include Questions for the committee members, information you think would be helpful for Graduate Students and/or Interns, or looking for Qualified Supervisors or placements for pre-masters or post-masters internships
Who may join this committee? Current Graduate Students, Registered Mental Health Counselor Interns, and Qualified Supervisors are all eligible to join. The committee is a part of FMHCA membership. If you would like to join the committee, simply contact the FMHCA office at Office@FLMHCA.org or call 561-228-6129
If you have any questions about this committee or would like to submit any suggestions for topics for us to cover in our upcoming meetings, please feel free to fill out our surveys (which are sent via email) or contact Laura Peddie-Bravo at LauraPeddieBravoLMHC@gmail.com.
Committee Chair: Aaron Norton, PhD, LMHC, LMFT
The Government Relations Committee has been working hard to secure bill sponsors for a bill that would replace the verbiage “registered mental health counselor intern” with “licensed associate mental health counselor,” as well as change similar terminology for marriage and family therapists and clinical social workers. In doing so, we hope to (1) standardize the language used in Florida to be more consistent with terminology used in other states, (2) reduce confusion among legislators, allied healthcare professionals, and the general public about what an “intern” is (i e , “intern” is also used to describe a student who is participating in a college- or university-sponsored practicum or internship); and (3) nullify the statute requiring interns working in private practice settings to have a licensed mental health professional on the premises when providing clinical services, which has been particularly problematic in a telehealth era in which many interns provide telehealth sessions from a home office. We have sponsors for both a House and Senate bill and hope to soon announce that these bills have been filed.
Additionally, the committee is working with our lobbyist and legislators in hopes of updating F S 916 115 to include 491 board licensees among the list of health professionals who can be appointed by the court for evaluations and expert witness testimony on various mental health-related matters for criminal cases, which we view as one of the few remaining statutes that discriminate against 491 board licensees. We have not yet obtained a firm commitment to a bill for this matter but remain optimistic.
Joining a committee is a great way to participate in FMHCA and increase your presence in our community. We have several committees that we would love you to participate in!
Here is a list of all our committees, their purpose, and their chairperson
We invite you to contribute your efforts as there are numerous opportunities for you to get involved and make a difference. For more information on how to participate right away, please contact the chair committee or fill out this form
A Keepsake Puzzle is a great way to capture all of life’s special memories big or small while also making new ones. This puzzle is a great way to celebrate a wedding or a new baby, to commemorate a grad or to honor the memory of a loved one. Create yours here.

Light it easily with just a match or lighter and bring fire's glorious magic to the backyard, beach, or campsite for 3-5 hours Made from recycled materials, this totable firepit burns for hours without smelly smoke or messy cleanup. Get yours here.

A butter board is the next charcuterie board trend. This is just a fun way to have a new appetizer or starter on your table Plus, it’s something your friends can get involved with, it’s way more affordable than a charcuterie board, and it still comes out like a show stopper. Learn how to make your own here.
Want to kick sugar but keep candy? Smart Sweets has developed low sugar gummies and candy that have 92% less sugar than traditional candy. Get yours here.

This brainteasing subscription delivers 6 monthly issues of The Hincks Gazette. Read the lead story, then find and solve hidden puzzles throughout the paper’s sections until you crack the town’s latest off-the-wall conundrum.
Get yours here
This mini coloring book is made for the busy adult. If you get easily overwhelmed by traditional adult coloring books, this was created by A Brighter Year just for you These themed, yet simple designs in these coloring books can be completed in just a few minutes or less Get yours here

Get a new perspective on working from home or relaxing after a long day with a lie-down laptop stand. Laptops weren’t exactly designed with ergonomics in mind, and impossible-to-adjust desk chairs don’t make the situation any more comfortable. Get a new perspective on working from home or streaming your favorite shows after a long day with a lie-down laptop stand made of sustainably sourced birch plywood. It assembles without any tools, and 100 trees are planted with each purchase. Get yours here.

Whether you’ve never tried punch needle crafts or you’re an experienced expert in the genre, this birthday bird kit delivers all you need to craft a cozy pillow for your nest. Choose your birth-month bird or just go with your favorite fowl; from parrots to owls and ravens to robins, there’s a flock of artistic options to help your crafting skills to take flight. Get yours here.


Welcome the Fall season with soups packed with flavor of seasoned Broth Bombs. Drop one of these bombs into your stock pot and watch as it fizzes herbs and spices into your stew, chili, or curry. Simply add veggies and legumes for a complete meal. Each variety pack includes four flavors: Scarborough Fair: A melody of fragrant, familiar herbs
Stone Broke Dharma: A hybrid of garam masala and a classic curry
Speckled Rain: A classic chili seasoned with mild peppers Gesundheit: An anti-inflammatory wellness blend--ginger with turmeric, rosemary, and clove Buy yours here.
Every day brings its own unique stressors and this kit is ready to face them all with a week of self-care treats. Get yours here.

Donut is surprised to discover that therapy isn’t all about talking, but somehow after playing, talking, and drawing through feelings, Donut begins to feel better. Get your own copy here.
Get all the calming benefits of a weighted blanket in a warm, comfy zip-up hoodie. Designed to relieve stress and anxiety to promote a sense of calm. Get yours here.

Sip local while brewing global! Your passport is this international set of ten, single-estate, loose leaf teas. Both a great introduction for the tea novice and a journey off the beaten path for the connoisseur, the assortment offers a taste of the wide variety that tea has to offer. Get yours here.

Enhance your Stanley Tumbler experience with this snack bowl designed to fit seamlessly onto the tumbler's handle Keep your snacks close at hand while on the go The snack ring provides a convenient place to store snacks, freeing up your hands for other activities. Find yours here.

FMHCA Member Questions Answered by President and Managing Partner of The Health Law Firm, George F. Indest, J.D., M.P.A., LL.M.
QAs a Qualified Supervisor, can you bill insurance using your credentials for your supervisees / Registered Mental Health Counselor Interns?
AYes, as long as your contract with the paying insurance company does not state that it is prohibited In the case of a Medicaid managed care insurance company, this is allowed by Medicaid laws and guidelines
It is probably better to have a group provider number, and make sure the intern is signed up as a provider within the health insurance company and with the Medicaid Program, with their provider number re-assigned to the group The group should then bill for the services
QWhen treating a minor child of divorced, separated or never married parents, what type of consent is necessary and from whom? and services.
AUnless there is an order from a court providing otherwise that you are aware of, each parent of a minor child is considered the natural guardian of a minor child Either parent can sign a consent form and authorize any and all care
Mr. Indest is board certified by The Florida Bar in the legal specialty of health law. He is the President and Managing Partner of The Health Law Firm, based in Orlando, Florida. The information provided in this article is for educational and informational purposes only and does not constitute the provision of legal advice.
Want your question featured in the next InSession issue? Submit Here
Must be a FMHCA member to submit Become a FMHCA member by clicking here

Mental health treatment is often stereotyped, inaccessible, and underutilized by marginalized communities, however, in recent years the movement for mental health education and advocacy has grown to towering heights. Organizations, platforms, and foundations are actively searching for ways to increase access and use of mental health services in communities that need it. Despite the influx of these communities reaching out for services, there continues to be a lack of representation in mental health providers Visibility in the mental health field is impactful and powerful for treatment In my personal experience as a masculine gay black woman, finding ways to navigate systems that do not affirm me is a daily burden To see and feel seen by others creates not only a place for me to place down that weight and catch my breath but a sense of connectedness that I am not alone. The relationship between visibility and mental health provides opportunities to provide a sense of understanding and belonging, improve treatment, and create connections through shared experiences. Together this relationship has shown to produce positive outcomes in treatment.
a sense of understanding and belonging unities are more likely to experience tutional racism, homophobia, nce, police involvement, denial of human health services (LGBTQ+ Mental Health es, 2021). They are also more likely to report sion, anxiety, trauma, and suicidal ideation rica, 2020) When looking for mental C and LGBTQIA+ individuals are often ders that look like them or share their In over 1 million mental health bout 4% of therapists are Africantinx, and 12% are LGBTQIA+ (Therapist tatistics, 2011). While racial matching is not esearch has found that clients feel their ipped and competent to understand their he nuances of society, and presenting are a similar background.
Shared experience is the ability to connect and relate to another individual whether it be simple, pleasant, complex, meaningful, or even traumatic. Shared experiences create opportunity for connection, support, and fosters a sense of belonging and not feeling alone. In 2016, The Journal of Black Psychology found in one study that “black therapists and patients reported having a relationship marked by solidarity…. as evidenced by having a better understanding of the context of Black Client’s lives” (Goode-Cross, D.T., 2016).
Through this connection, the relationship between visibility and shared experiences decreases anxiety and depression symptoms. The nature of the therapeutic relationship can be influential in session. When matched with a provider of shared experience, clients were more likely to stay in treatment longer, explore topics that maybe they would stray away from, and need less intensive services.
In the United States, there is a history of poor mental health treatment, misdiagnosis and inappropriate medications. Children of color are less likely to be diagnosed with Attention Deficit Hyperactivity Disorder (ADHD) and more likely have their behavior contributed to other challenges. Left untreated, these children are at an increased risk for other factors as they age including being twice as likely to not complete school, and twice as likely to engage in criminal behavior Black individuals are also more likely to be misdiagnosed with Schizophrenia instead of a mood or trauma disorder as compared to their peers (O’Malley, 2021)
Misdiagnosing can lead to ineffective treatment, inappropriate medications, and in some instances exacerbate other physical and mental health issues Holding acknowledgement and space for cultural nuances, behaviors, and background of an individual, treatment can be appropriately tailored with the whole person in mind.

In my experience, marginalized communities and families at high-risk in Florida benefitted when they had the opportunity to work with a provider that shared their experience and showed cultural competence. People need a sense of connectedness, to feel seen, and to have a space where their perspectives and experiences are valued Bruce Perry said “Belonging and being loved are core to the human experience ” Visibility breaks down the stereotype of therapy and opens the door for mental health treatment as an option Visibility improves mental health outcomes by providing a deeper sense of connection, and a sense of belonging to decrease depressive symptoms and ultimately uplift a community through culture
Written By: Jalia Hurst-Smart, LCSWCalkins, H. (2020, September 1). Increasing the visibility of providers of color. American Psychology Association. https://www.apa.org/monitor/2020/09/increasing-providerscolor
Goode-Cross, D. T., & Grim, K. A. (2016). “An Unspoken Level of Comfort”: Black Therapists’ Experiences Working With Black Clients. Journal of Black Psychology, 42(1), 29–53. https://doi.org/10.1177/0095798414552103
Kim, R. (2022, March 7). Addressing the Lack of Diversity in the Mental Health Field | NAMI: National Alliance on Mental Illness. National Alliance on Mental Illness. https://www.nami.org/Blogs/NAMI-Blog/March-2022/Addressing-the-Lack-ofDiversity -in-the-Mental-Health-Field
LGBTQ+ Mental Health Treatment Disparities. (2021, December). National Alliance on Mental Illness MN. https://namimn.org/wpcontent/uploads/sites/48/2022/01/LGBTQMHTreatmentDisparitie s_LGBTQSpecialty_2021.pdf
Mental Health America. (2020). Black and African American communities and mental health. Mental Health America. https://www.mhanational.org/issues/black-andafrican-american-communities-and-mental -health
O’Malley, L. (2021, November 17). Addressing the Lack of Black Mental Health Professionals. INSIGHT into Diversity. https://www.insightintodiversity.com/addressing-the-lack-of-black-mental-healthprofessi onals/
Therapist Demographics and Statistics [2021]: Number Of Therapists In The US. (2021, January 29). Zippia. https://www.zippia.com/therapist-jobs/demographics/
Jalia Hurst-Smart is a licensed therapist and founder of Soul Priority Counseling and Wellness in Tampa, Florida
Jalia Hurst-Smart specializes in working with youth, young adults and 2SLGBTQIA+ individuals

Corinne is a registered professional lobbyist with 16 years of experience, 15 of them representing FMHCA's state interests.
At Rutledge Ecenia, Corinne represents a broad client base with a particular emphasis on healthcare practitioners, education, and regulated industries and professions She has been instrumental in passing myriad legislation and killing bills that would have negatively impacted her clients
Corinne lobbies across multiple platforms including legislative, executive, and state regulatory boards. Corinne’s professional experience also includes association management, political campaign management, providing continuing education, public speaking, crisis communication, and political action committee management. Corinne was recently named Best Lobbyist (Florida) by Florida Politics.
In this conversation, we go over Corinne’s root passion for advocacy and how her goals align with FMHCA’s mission and vision of Mental Health Policy in Florida.
What led you to become a lobbyist? Was it a career you always saw yourself doing?
I was previously involved with Public Relations. My family did lobbying so I was naturally exposed to the field. What truly led me to make the leap over was my mom being diagnosed with cancer. She was receiving great medical care however it became apparent to me that certain medical professions were not able to perform actions they were qualified to do. This experience led me to develop a passion for healthcare lobbying. A total career shift.
How did your path lead you to FMHCA?
Susan Hanson-Engelhard. She met someone from my firm because the profession had not yet have a lobbyist. At the time the state was going through The Baker Act discussion. Having success with Physicians Assistants, we agreed to meet in
Orlando. We were convinced and have been representing FMHCA ever since.
The way you advocate for FMHCA is almost personal, does this tie back to why you shifted your career?
Yes, it is hard to watch highly qualified people not being able to practice in their full scope of competency. Also, if you like what your clients do, you get involved and it makes the wins personal.
Are there any success stories or significant policy changes that you're particularly proud of achieving through your lobbying efforts?
There are a few but my most recognized win had to have been allowing physician assistants to prescribe controlled substances within 2 years of filing that bill. Mental health-wise, I’d say the requirement of the CECREP accreditation in counseling programs. The profession was not being taken as seriously as it should be so this was a great way to legitimize the profession in future policy conversations.
How do you build relationships with policymakers to effectively advance FMHCA's goals?
I bought a house in downtown Tallahassee right between the Capitol and The Governor's Mansion. I have 5-7 parties each legislative session where we can talk policy and build personal relationships I also like to form relationships with people who are 5-10 years out from running so that when they are finally in office, we already have an established relationship
Mental health awareness has been on the rise in recent years. Have you seen this contribute to FMHCA’s goals at the Capitol?
Yes, there's not a stigma anymore and we are talking about it The shortage created the need for an emergency change which put more focus on the bigger picture This allowed the state to
look at professions that they can give more latitude to
Could you share some specific challenges you've encountered while advocating for mental health policy changes and what we are doing to overcome them?
There are so many associations A legislator only gets 6 bill slots per year and there are hundreds of organizations lobbying Some professions have multiple associations with multiple lobbyists. We have become good at becoming nimble. Showing legislators that they are doing good for the needs of the population, not just the profession. We are able to show we were able to help the public which makes our message strong.
What are some of the key initiatives or policy goals that FMHCA is currently focused on advocating for?
Changing the title of Mental Health Counseling Interns to Associate Mental Health Counselor. Changing this requires a change in statute. The term “intern” sounds like meeting an education requirement when in reality they have met all of their education requirements and are doing legitimate work and it is a misnomer to call them otherwise.
We are also looking at forensic evaluations in our system We want to take out “to the extent possible” so that circuits will want to contract with the profession instead of it being a last resort.
How does FMHCA collaborate with other organizations, both within the mental health sector and beyond, to create a more comprehensive approach to advocacy?
We speak a number of times with professions shared under 491 (LCSWs and LMFTs) and Psychologists to make sure we aren’t stepping on toes. We rather know what we are up against if we put something out there they plan on opposing but oftentimes we are on the same page.
Mental health intersects with various other societal issues. How does FMHCA approach collaboration with groups advocating for related causes, such as healthcare reform, education, or social justice that are sometimes attacked by policy?
It’s good to advocate but we have to keep in mind the political reality. Whatever the policy hot-button policies may be, we have to recognize they are often from the veto-proof majority in our state. We have to message to these leaders when we have concerns- especially when it is consistent with our practice, values, and guidelines It is also important to understand that the voters in our state chose these individuals because of their involvement with these hot-button bills I hate to say it but there is not a lot that we can do which is why we focus so
heavily on items on what we can control This does not mean that we have to be silent but we have to be meaningful in our responses and how we respond to these hot button policies The only thing we can do that is better than what we are doing at FMHCA currently is calling for our members to be active in campaigns and encouraging them to exercise their personal vote.
The legislative process can be slow and challenging. How do you maintain motivation and keep pushing forward during times when progress seems limited?
We only get 60 days to meet each year (how long a legislative session passes). I stay motivated because you can have 3000 bills filled of which 300 may get passed. Looking at that 10% makes each win incredible. It might take a few years but that is a huge win. Even though it seems like a no brainer, it is so rare to be able to move legislature and that's what we get to take back to FMHCA members. It makes for an incredible feeling to show that members dollars are going to change. Another one of my biggest motivations has been watching our presence change the way legislators speak when it becomes to behavioral health The term “psychologist” was the term mostly used when it came to the topic of mental health but now that has been replaced with the term “mental health counselor” and I love that. It’s not just the bills we pass, those are micro changes, seeing the stigma go away and the common terms used change are the macro changes that keep you motivated for decades.
Advocacy often involves addressing misconceptions or lack of understanding. What are some common misconceptions about mental health policies, and how do you work to educate legislators about the realities?
A lot of it is personal stories. Going back to the term “Mental Health Counseling Intern”, because of the way it is written in statute, legislators presume it is part of an educational requirement. What makes real change is a Mental Health Counselor Intern sitting down with a legislator to go over what they actually do. That is all a legislator needs to hear to change their mindset and realize that the current statute does not keep up with reality and a change needs to be made.
Can you elaborate on the importance of a FMHCA membership from your view in the Capitol?
The most important thing a professional can do is join their state organization, I am a member of my own. It is important to be proactive and reactive and that can only be done because we are organized and ready Joining FMHCA has many perks but the most important from this end is the advocacy you receive because remember- If you are not at the table, you are on the menu
A Political Action Committee (PAC) is a term given to a committee organized by like-minded people, like mental health counselors, for the purpose of raising and spending money to elect and defeat candidates PAC money comes from voluntary contributions by members PACs can give to a candidate or committee each election cycle (primary, general, run-off, or special). In Florida, the maximum campaign contribution per statewide candidate is $1,000 In short, PACs give professional associations a legal avenue for financially supporting candidates that will be helpful to their industry
FMHCA was created by LMHC's for LMHC's Our mission is to advance the profession of clinical mental health counseling We are the ONLY organization lobbying for mental health counselors in the State of Florida and we need YOU to join in this upcoming legislative session to promote and advocate for what you stand for
Donate today to take part in the initiatives FMHCA is taking to protect and build our profession!

Engaging minds since 1999! Join us back in Lake Mary for our 2024 Annual FMHCA Conference Return home with up to 29 5* CE credits earned over 3 days of learning! (February 1st-3rd)

The Florida Mental Health Counselors Association (FMHCA) is the leading organization advocating for mental health professionals in the State of Florida. Our objective is to provide education, legislative oversight, and networking opportunities to mental health professionals in our state (and sometimes beyond!)
The FMHCA Annual Conference will be held on February 2nd-3rd with optional pre-conference workshops held on February 1st This is the premier gathering for sharing ideas, discussing challenges, gaining insight, and finding solutions in the mental health field Sessions will tackle the key policy issues impacting the profession today and provide valuable pragmatic advice across the full range of services offered by mental health professionals in both public and private practices
*Attendees have access to up to 21 5 CE credits in General Conference Sessions (2/2-2/3) and up to an additional 8 CE credits in the Pre-Conference Sessions on 2/1 (Additional Fees Apply)
Early Bird Rates End November 1st 2023
Pre Conference Workshops *Separate registration required Not included in general conference registration
EMDR Therapy Refresher Course
We Are Memory Workers- Introducing Neurocise®, EyePointing™ & NeuroPointing™ - Guided Eye Movement Strategies to work with Traumatic Events & Memories
Becoming a Sexually Competent Therapist: Function, Dysfunction, LGTQIA Affirmative Therapy, & Sexual Trauma Required State of Florida Clock Hours for Re-Licensure (Ethics, Medical Errors, Laws & Rules)
The Clinical Mental Health Counselor’s Guide to Psychological Testing
Qualified Supervisor Training (QST)
General Conference Workshops (Friday 2/2)
Healing Emotionally with Self-Compassion and Laughter
Cultural Competence Clinical Intervention
"They Won't Leave Me Alone": An Examination of the Link Between Domestic Violence and Stalking
Cultivating Resilience in Clinical Supervision: Integrating SelfCare Practices to Protect Counselor Well-Being
The Essence of the HEART Model: Gestalt Underpinnings, SelfForgiveness, and Spiritual Awareness Healing Sexual Trauma, A Faith-Based Model
From Birth to Brilliance: Reconnecting with Your Highest Self
An Ethical Approach for Overcoming Trauma and Insecure
Attachment Responses
The Seven Segments of Self-Love: A Practical Approach to Cultivating Self-Love and Mental Wellness
Family Play Therapy
HYPNOTIC EVENING - Taking Care of Trance™
Self-Care is Not an Option: Protecting Against Secondary Trauma and Burnout
Integrating Mindfulness and Creative Expression to Foster Emotional Resilience in Youth
The Great Escape: Domestic Violence and Human Trafficking Exploring Therapeutic Presence and Polyvagal Theory to be a Clinical Super Co-Regulator
EMDR Protocols and Disaster Trauma: Hope for the Disillusionment Dilemma
Awards Luncheon, Annual Membership Meeting, & Legislative Update
Telehealth Update: Using Screen-Sharing to Reach Clients on a Deeper Level
Impact of Generational Trauma on Immigrants, Refugees and Cross-Cultural Families
Uncovering Hidden Gems: Using Psychodrama as a strengthbased tool for Post-Traumatic Growth

Religion can be beautifully healing, however, it also has the potential to be incredibly damaging The concept of religious trauma is becoming more widely recognized in communities with the resources to have open discussions about its complexities. Meanwhile, the people who are suffering the most from religious trauma are those who are scared to begin to question if they have experienced it. Questioning harmful religious beliefs often involves confronting the fear of hell or other forms of eternal punishment that are commonly taught in organized religions.
It is important for therapists to recognize the profound impacts of the fear of hell Why would anyone want to question how they are being treated if doing so risks eternal punishment.
Clients grappling with this form of religious trauma often come in with a tension that's almost palpable They are often experiencing existential dread without even realizing it When conversations about religion begin, every thought, question, or doubt may be tinged with the looming fear of being punished by a higher power. The fear of hell is can become a psychological burden that alters one ' s sense of self, disrupts relationships, and infiltrates daily life.
Understanding religious trauma is complex, and there is no one-size-fits-all solution However, as therapists, I believe we can better serve clients by incorporating the following into our practices:
Open the Discussion: Don't wait for a client struggling with religious trauma to tell you they are scared of hell. Facilitate an open-ended conversation in which you can screen for existential concerns. A client struggling with a fear of hell will likely find relief in these conversations and begin to feel secure discussing them.
Offer Validation Before Challenging: Clients struggling with this form of trauma need validation before they can start reframing their beliefs They need to know it's okay to have these fears without feeling shame or judgment A validating environment is the first step in opening them up for deeper therapeutic work.

Be Prepared for Existential Conversations: The fear of hell often brings up big questions about existence, purpose, and the afterlife. Equip yourself with the knowledge and confidence to allow you to navigate these deep waters alongside your client.
The more therapists know about the complexity of religious trauma, the more prepared we can be to help those who are healing from it We cannot underestimate the mental toll that the fear of hell can have on our clients What we may deem as "clearly wrong” By equipping ourselves to effectively manage the complexities of religious trauma, we can provide better care to our clients, allowing them to explore, heal, and eventually find peace.
Written By: Hannah Mayderry, LMHCHannah Mayderry is a Licensed Mental Hea Counselor serving clients in Florida Within private practice, Philosophie Therapy, LLC, Hannah specializes in helping those strugg anxiety, navigating relationship challenges religious trauma She is passionate about h self-empowerment in the midst of an unpr

This relational dynamic model is based on the concept of hypnotic suggestibility, as suggested by John G. Kappas in his book, Professional Hypnotism Manual: Introducing Emotional and Physical Suggestibility and Sexuality (Kappas, 1978).
Kappas posits that we are all hypnotically suggestible to some degree. According to Kappas, “Human behavior has led us to recognize that everyone is suggestible to something; some to sensations, others to emotional stimuli, still others to environmental stimuli; and some, to all three ” (Kappas,1978) For example, when we are listening to another person communicate, we are watching the others’ faces to read thousands of micro-expressions, listening to the tone of their voice and the extra sounds they make when they communicate (paralanguage), rhythm matching, mirroring, as well as watching body language to assist us in interpreting the messages that are being transmitted. Since perception is an active, constructive process, we are then acting upon and building our perception of the signal coming from the other person as we receive it. This is all happening, for the most part, below our conscious awareness and, as it were, at “a thousand
miles per hour ” Communication consists of both transmission and reception And things can go wrong on either end Those of us who work with couples, families or other relationships see that they frequently do just that. When we introduce the concept of suggestibility, it opens up a whole universe of communication possibilities, both positive and negative. Before we speak about attraction and communication in relationships, let us speak for a moment about hypnotic suggestibility.
Kappas posits that each of us has a “suggestibility personality ” This would be a set of dynamics that each of us learned from our parents and our families growing up, most prevalently in the first 6 to 8 years of our lives So, just for a moment, let us apply this to a potential real-world situation.
Most of us that use hypnosis know that anyone can be hypnotized, but to varying degrees, and only if they are willing. We have all had clients who sat there and said, “I cannot be hypnotized ” Some of those can be hypnotized very easily, while some of them are so resistant that they just simply will not allow us to hypnotize them even though they could indeed be hypnotized
The principal here is that a certain percentage of communication is based on the idea of hypnotic suggestibility. In this model, as illustrated above communication may be inferred both in transmission and reception through processes that are below our conscious awareness. This produces the idea or construct of Direct and Inferential communication Thus, in Kappas’ concept, a person would be more Inferential than direct to the extent that they are hypnotically suggestible This is very relevant in working with relationships, especially with couples, since they almost always prevent as their initial problem that they have trouble communicating when they really don't understand what that means in the initial sessions.
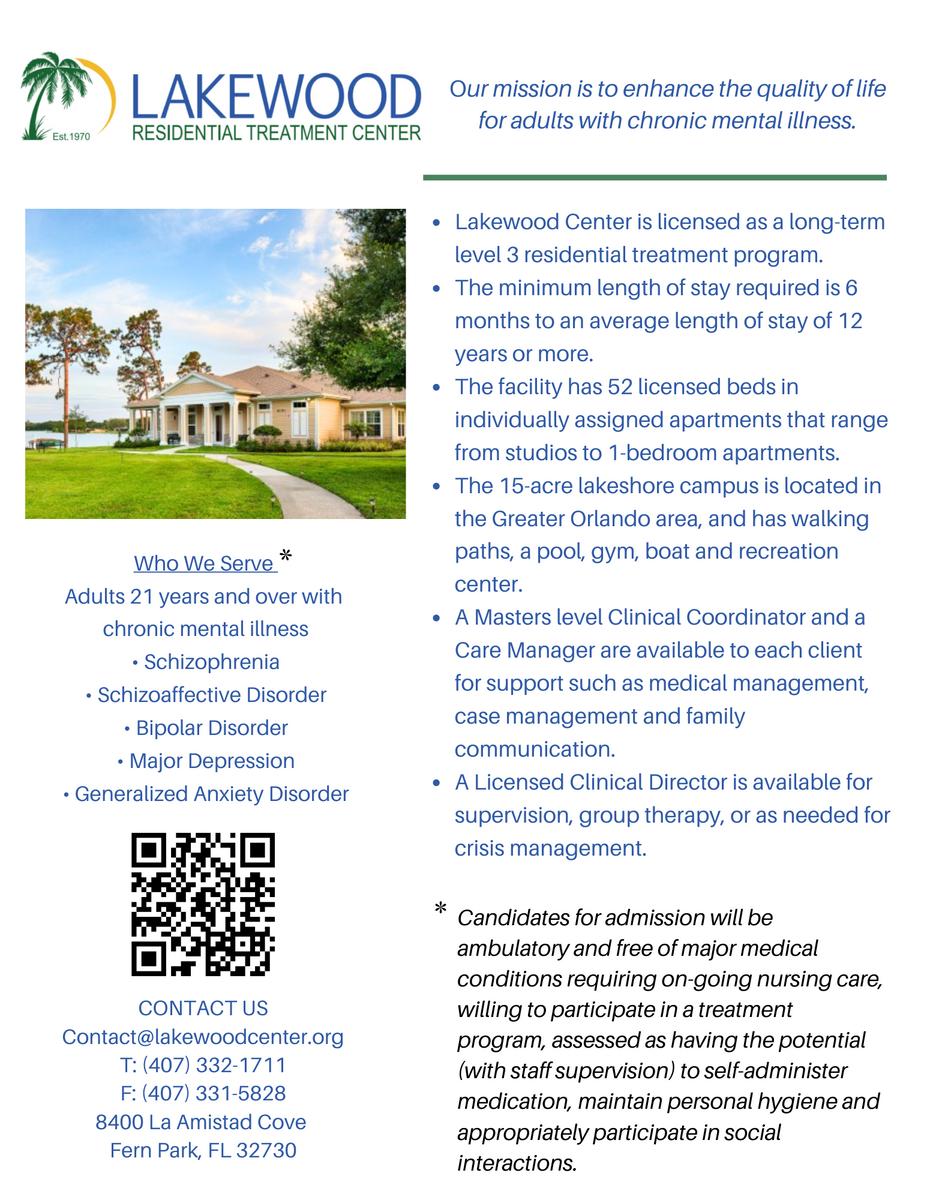
In simply looking at the concepts of Direct/Inferential Communication, we can place this on a simple scale rated 0% to 100%, with 50% in the middle, somewhat like a seesaw. Using Kappas’ test, or, often, simple observations, we can rate people on this scale As a theory, this model can be extremely useful for helping people understand why relational approaches are failing It is also, of note, however, that the author, in his research with James Hoerchler on Direct/Inferential Communication (Hoerchler & Holler, 1987) proved that the phenomenon exists and that in couple-hood, opposites attract and tend to test equidistant from center. While more research needs to be done, there appears to be a strong likelihood, as fits with the anecdotal observations of 36 years of clinical experience, that couples tend to be equidistant from center and opposites on both of these dimensions attract.
We can see that this is a scale with gradations that allow us to see where each person is located on the scale. In our research (Hoerchler & Holler, 1987) we saw that each couple had a direct communicator and an inferential communicator. We expected that result. What we did not expect was that they tended to test equidistant from center. So, we can look at this as a scale. But we can also put a fulcrum in the middle and look at it as a seesaw. The couple tends to space themselves equal distances from center on either side of the fulcrum, essentially balancing the seesaw. But as most of us in the field of psychology know, when we look at scales such as this one, that are both a dichotomy and a scale, functionality or dysfunctionality is not measured by which side of the seesaw we are on, but more often by how far off center we are located
First let us speak to, define, and illustrate the Direct/Inferential Model of Communication, noting, as mentioned above, that a person in this model is theoretically inferential to the extent that they are hypnotically suggestible. Please note that, at first, we will use extreme examples to illustrate the difference, blackand-white examples make for easier understanding of definitions of a phenomenon and then we will illustrate gradients by example It is also of note that we place the Direct (or, as Kappas sometimes calls it, Literal) on the side of the scale marked 100% The reason we are measuring the scale based on Direct Communication is because Direct communicators tend to say exactly what they mean, approaching the heart of the message in a straight line, whereas inferential communicators approach the message in a spiral fashion, inferring and hinting at the message, hoping that they will never actually have to say exactly what they mean. Thus, Inferential communication is measured by what they do not say. Thus, we are measuring “what is.” With the Inferential communicator, we are measuring, “what isn’t.” It is simply much easier to measure what is than what is not.
The Direct Communicator: In the extreme, the Direct Communicator says exactly what they mean, no more, no less They approach the heart of the message by stating it clearly and concisely, leaving no doubt as to what they are trying to say.
(See Direct Communication figure)
The Inferential Communicator: On the other hand, (and the other extreme), the Inferential Communicator approaches the heart of the message in a spiraling manner, hinting and inferring what the message is, and hoping that they will never

actually have to directly say it The extreme of this side of the communication can be totally nonverbal (See Inferential Communication figure)
Since this scale is both a dichotomy and a graduated scale, let us illustrate through some examples of communication how this works, starting from the extreme of Direct to the extreme of Inferential (The reader will please note several things First, these examples are much easier to demonstrate visually, especially as we approach the inferential side Second when we listen to what is stated “Literally,” they become more wordy, less parsimonious, and, sometimes, comical ) The example we usually use has to do with the notion that it is hot in this room We would like the person nearest the door to open the door, because it is cooler outside, and, thus, that would cool down the room. Let us give the person next to the door the name of Steve.
So, starting at 100% direct, I look at Steve and say, “Steve, open the door.” While this is the most parsimonious way to say this, as well as the clearest way to say this, many people would find it insulting, as it sounds like I just barked an order Graduating down the scale I could then say, “Steve would you please open the door?” Notice that I am becoming slightly “more wordy ” A little further down the scale, I could say, “Steve, could you please open the door?” If we listen to this in a completely literal manner, it sounds as if I am now beginning to question Steve’s “ability” to open the door – “could you.” Moving a little further down the scale, “Steve, is there any possibility that you could open the door?” I am now literally questioning the “possibility” that the door can be opened by Steve. Things are becoming absurd. The implications become much larger. Am I questioning the possibility that the door can be opened? Am I questioning the possibility that Steve could open, or is even capable of opening the door? Moving a little further down the line, “Steve, is there any way that you could see your way clear to opening the door?” Now it sounds as if I am questioning whether there is something between Steve and the door that is hindering his visibility of the door, or questioning his vision, as if he might
Inferential Communication Figure Direct Communication Figureneed glasses
We are now below 50%, whereupon I could ask, “Steve, are you warm? Because if the door were open, it would be cooler in here ” Most people who speak like this would swear that they simply asked Steve if he would open the door.
Moving a little further down: “Steve, are you warm? Because, you know, if the door were open…” Moving a little further: “Steve are you warm?” (Moving my eyes back and forth between Steve and the door”) – to “Whew!” (Mopping my brow and looking back and forth between Steve and the door )
We can see from the extremes of what is and what is not said that couples who are equidistant from center, but way far out on the ends of the scale, are balancing the seesaw but having huge problems communicating with each other. Simply put on this dynamic, functionality or dysfunctionality is not determined by which side of the scale one is on, but by how far off center they are. In the research we did with couples, as previously mentioned, we found that they were generally equidistant from the center on the scale. But one of the implications for clinicians here is that the information as to how far they are separated can be very useful to the clinician, as well as to the couple I believe that psychoeducation is extremely helpful in this venue for the couple, as it allows them to see the exact nature of what their problem is and, therefore, the beginnings of how to start to solve it.
Real-world example: In my relationship, I am the Direct, and my wife is the Inferential. She cannot comfortably tell me that she is hungry. If she is hungry, she will ask me if I am hungry. Knowing what I know, I tend to ask her if her questioning whether I am hungry is her way of saying that she is hungry She will then cast her eyes at the floor, look horribly uncomfortable, and say, “Well, I was just asking if you were hungry ” No matter how much I question whether she is hungry, she will generally avoid telling me that she is hungry It is almost painful for her to say, “I am hungry, and I would like to eat.”
But imagine if the couple does not understand, or is unaware of any of this. This can turn into a big fight over nothing.
If we look at Kappas’ model of suggestibility, with the presumption that all children start out as Direct communicators, our findings indicate that about 50% of us become Inferential, when we were all originally Direct. However, people who are Direct have always been Direct and, thus, have never been Inferential. The principle here is that all Inferential people were, at one time, Direct. The implication is that Inferential people have some capability of functioning in a Direct mode, even if it is difficult for them. However, Direct people, having never been Inferential, are really bad at trying to
There are four points to remember here:
1.
2.
3.
4.
We can receive Directly
We can transmit Inferentially
We can receive Inferentially.
We also must keep in mind the emotional load that can occur with communication. For example, I could say to you, “You look great today!” You could reply, “Oh fine! So, I looked like crap yesterday?” inferring more than what I said, but in a negative manner. Remember, perception is an active constructive process.
So, we need to understand that Direct communicators experience Inferential communicators as, “Vague, wordy, confusing, obtuse, manipulative, sneaky and underhanded ” Inferential communicators experience Direct communicators as, “Rude, crude, abrupt, uncaring, unempathic, insensitive, ‘bull-in-a-china-shop,’ ‘machine gun,’ and ‘bulldozer’.” Direct communicators experience other Direct communicators as, “Clear, concise, straightforward, ‘cards-on-the-table,’ refreshing, and honest.” Inferential communicators experience other Inferential communicators as, “Considerate, empathic, sensitive, caring, intuitive and diplomatic.” It all depends on from whose perception we view it.
Since Direct communicators tend to say exactly what they mean and Inferential communicators often place their messages between the lines, there are several implications to this In relating to each other, Inferential communicators put messages between the lines, and, on the receiving end, tend to read messages between the lines. The problem with this situation, if the Direct communicator is the transmitter, is that the Direct communicator doesn’t put anything in between the lines. But this never seems to stop the Inferential communicator from reading something there. In point of fact, the blank space between the lines in the transmission from the Direct communicator serves as a blank slate onto which one can project anything they want. And we humans tend to project negative things into those spaces. For example, if you are sitting in a restaurant and notice that there is a person across the room who has been staring at you for a long time with an unbroken stare, you don’t tend to think, “I must be really good-looking today ” You are more likely to think, “That person means me harm,” or, “Do I have food on my shirt?” or something like that
Inevitably, when you teach a client this concept, the first thing they will ask is, “What do I do about this?” Regardless of whether they are Inferential or Direct, we can suggest that they use “Active Listening.” Active Listening (as opposed to passive
listening, which is where you just hear the words) can take several forms, but the primary form is to say back in your own words what you thought the person just said to you and ask if that is correct. Inferential communicators tend to get more Direct when they are asked a direct question. Thus, with Inferential communicators, we will need to coach them to refrain from insisting that their interpretation is correct, even when the Direct communicator has told them that they are incorrect. With the Direct communicator, we may have to teach them how to consider options about what could be in the spaces, and/or ask questions about what is in the spaces.
Listening Inferentially requires some use of deductive reasoning
Written By: Michael G. Holler, MA, NCC, CFMHE, CCCE, CCMHC, LMHC
Michael, current Parliamentarian of FMHCA, has a private practice in Tavernier in the Florida Keys Michael has been working with individuals, familie couples and organizations for over 36 years Michael is also a published author of the book, Structured Relationship Theory: Nothing Less Would Have Sufficed

As I have completed my tenure as AMHCA president, I would like to formally acknowledge and thank the wonderful members from the FMHCA chapter During my presidency, I was very blessed to collaborate with various FMHCA members to assist other states with passing the Counseling Compact, advocate for counselors to receive Medicare reimbursement, and protect the integrity of our profession by assuring CMHCs in all states have diagnostic privileges while promoting appropriate requirements to indicate the expertise we provide to all those who receive our services I can't thank FMHCA enough for having a strong national voice, for your willingness to support the national office, and for your willingness to support CMHCs across the country and internationally It is with full humility that I thank everyone for their support for myself and our profession It is with great pride that I hand over the reins as AMHCA president to Florida resident, FMHCA member, and former Florida Mental Health Counselors Association and Suncoast Mental Health Counselors Association President Dr. Deirdra SanderBurnett. Dr. Sanders-Burnett is forward focused, collaborative, and has the tools needed to help amplify our voices and improve the profession. We are all in good hands. I sincerely thank FMHCA for all you do!
With full appreciation:
Fredrick Dombrowski, PhD (he, him, his)
LMHC, CASAC, LPC, LADC, NCC, CCMHC, MAC, ACS, BC-TMH, HS-BCP, ICADC, DCMHS Past President of the American Mental Health Counselors Association
Greetings,
I am honored to serve you as the American Mental Health Counselors Association’s 47th President and continue to serve in the position of Florida Mental Health Counselors Association’s Immediate Past President. I am grateful for the unwavering support that I have received from the Florida Mental Health Counselors Association’s and the Suncoast Mental Health Counselors Association’s members during my tenure as President at the regional, state, and now national level. As I transition into President of the AMHCA I am blessed to continue receiving support from AMHCA’s leaders, staff, and members. AMHCA’s Interim CEO/ED Dr. Beverly Smith and AMHCA’s Past President Dr. Fredrick Dombrowski continue to provide me with mentorship and support as they remain strategically focused on advancing the vision and mission of AMHCA. We welcome AMHCA’s new President-Elect Dr. Yoon Suh Moh.
I commend FMHCA’s President, ED, Board of Directors, Staff, committee members, and members for their dedication and service to the mental health profession and those they serve. FMHCA has a strong presence and is highly respected at the national level. I am grateful to work beside several of FMHCA’s leaders at both the state and the national level. I am appreciative to FMHCA’s leadership who continues to meet the needs of its members, expand the scope of practice of Clinical Licensed Mental Health Professionals, and provide services to clients.
AMHCA continues to partner with other organizations to provide quality care for the clients we serve AMHCA has partnered with Anna Lieber, LCMHC, NCC/CCMHC, DE of the American Association of Suicidology to provide a Suicidality Certification Course
AMHCA is a member of the Medicare Mental Health Workforce Coalition Dr Beverly Smith AMHCA’s Interim CEO/ED is an exofficial member of the Counseling Compact
I remain Strategically focused on advancing the visions and missions of the American Mental Health Counselors Association and the Florida Mental Health Counselors Association. During the first three months of my tenure as AMHCA’s President, I have worked collaboratively with AMHCA’s Interim CEO/ED, Executive Committee, Board of Directors, Staff, and Committees to implement my goals as President for the 2023-2024 year.
Build Capacity to do the work of AMHCA: AMHCA has strengthened the internal structure of AMHCA to ensure collaboration between all stakeholders and better serve our state chapters and members by upgrading the infrastructure and expanding the
capacity of staff and committees AMHCA is currently expanding its partnerships, visibility, and social media presence Committees and task forces are actively engaged in implementing the objectives and goals of AMHCA’s Strategic Plan Increase Membership Recruitment, Retention, and Reclamation: I have actualized a membership committee designed to recruit, retain, and reclaim members as we strive to increase AMHCA’s membership by 10 percent. I am asking each state to assist by encouraging at least 15 members to join AMHCA and become actively involved in the work of AMHCA by serving on a committee or task force.
Develop Leaders and Support Succession Planning: During my tenure as AMHCA’s President, I will launch a Leadership Institute designed for emerging AMHCA leaders. The prospective leaders will attend quarterly training sessions designed to equip current members and emerging clinical mental health professionals to serve in AMHCA’s leadership positions.
I welcome you to join us in advancing the vision and mission of AMHCA with C A R E E (Collaboration, Advocacy, Research, Ethical Practice, Education, Training, and Professional Development) I encourage you to invite 15 mental health professionals to join FMHCA and AMHCA and become actively involved by joining a committee or task force Identify and inspire 15 current members and emerging leaders to apply for the AMHCA Leadership Institute when it opens Submit an article to the Advocate Magazine and/or a manuscript for the Journal of Mental Health Counselors. Submit a proposal for a webinar. Stay informed of the implementation of Medicare Part B coverage of MFTs and Counselors by attending the Medicare 501 Webinar on October 5, 2023, at 12:00 p.m. EDT. Please join us at the AMHCA Virtual Fall Summit on November 8-9, 2023. Thank you for your dedication to FMHCA, AMHCA, our members, and the people we serve.
With gratitude,



For a moment, I want you to imagine your life and what it would look like if you had to prepare every day for a potential hurricane or natural disaster. Take a moment to think about what goes into the preparation. What happens emotionally when you must prepare for the worst? What happens when you’re in the middle of the storm or even after? Now how do you feel?
Hold on to that feeling and think of people with chronic illness
That heavy feeling that you might be experiencing after reading this, is comparable to what people with a chronic illness may feel. Chronic Illness is like preparing for a storm every single day. With chronic illness, you never know what to expect, what you’re going to feel, or how bad your symptoms will be. Every day can lead to something different. Individuals with chronic illness prepare for their “storm” by focusing on managing their symptoms, the different treatment options available, managing
their stress and emotional wellbeing, as well as working through any changes in functioning they may go through.
From my own personal experience dealing with a chronic illness, it can be physically exhausting and emotionally overwhelming; the daily preparation for my own “storm”, experiencing painful symptoms, the unwelcoming and intrusive thoughts that pop up when experiencing pain, the hopelessness, the hurt, feeling alone as if no one understands, and the lack of support.
When I work with clients who experience chronic illness, one of the first things we do is process their feelings Often clients come to me because they feel shut down They feel that family or friends don’t understand what they are experiencing Chronic illness is considered an “invisible disease” meaning it is not outwardly visible to others. A person can’t just look at
Professional Experience Articlesomeone and see that they are experiencing a chronic illness This makes it hard for others to understand and develop compassion for those experiencing a chronic illness
When my clients process their feelings with me, I often hear them tell me that their symptoms are minimized and even dismissed This makes them feel shut down and alone Someone experiencing a chronic illness wants to be heard, wants to feel validated, and wants to feel that they are supported As mental health clinicians, we can provide this much needed support We can offer them compassion and empathy, we can validate their feelings and symptoms, we can instill hope, and build resilience.
There may be a time that your client who has a chronic illness experiences hopelessness When you are in pain and there is little relief, you begin to experience intrusive and unwanted thoughts Thoughts that may look like “things will never get better”, or “I can’t take this pain anymore” Helping your client to find hope on tough days is critical in their treatment Finding hope can look like “what are things you can look forward to on days that you’re not in pain”, or “what are things that bring you enjoyment on good or bad days”. Helping your client identify things they are grateful for or identifying positive things in life can help instill hope. Implementing Cognitive Behavioral Therapy can be useful as well as it teaches clients to identify irrational thoughts and replace with helpful and hopeful thoughts.
Also, helping your client build resilience can help them manage their chronic illness Our physical, emotional, and psychological states are interconnected It is important that your client work on their physical health as well as build resilience to manage and support their mental health. You can help your clients build resilience by encouraging them to identify their strengths. Focusing on your client’s strengths can help them move through intense emotions and challenges. Also, helping your client to engage in self-reflection can help build resilience. Journaling can help clients become more self-aware by helping them understand their thoughts, experiences, and even manage pain. Lastly, encouraging your client to connect with others, such as joining support groups where others can share their experiences, will foster resilience During challenging times staying connected can reduce depression, anxiety, stress and improve wellness
Written By: Amanda Walch, LMHC
Amanda is a Licensed Mental Health Counselo and owner of Healing Words Therapy She wor with individuals, couples, and families Amand has years of experience in private practice, inp psychiatric units, and community mental heal specializes in chronic illness, depression, anxi Amanda can be reached at info@healingwordstherapy com or her website www healingwordstherapy com




Professional Resource Article
In the vast landscape of mental health, certain topics emerge with pressing urgency, demanding attention, understanding, and action. One such topic is the concept of moral injury, a psychological construct that delves into the deep-seated internal conflicts individuals face when their moral beliefs are challenged or violated While moral injury can affect anyone, its manifestation within the LGBTQIA community is particularly poignant, given the unique societal, familial, and internal pressures they often encounter
The LGBTQIA community, celebrated for its diversity and resilience, has long navigated a complex web of challenges. The path is rarely straightforward, from the struggle for rights and acceptance to the personal journey of self-discovery and affirmation Intertwined with these challenges is the shadow of moral injury, casting its influence on the mental well-being of many within the community For mental health professionals, understanding this intricate interplay is not just a professional obligation but a moral imperative
This article aims to shed light on the multifaceted nature of
moral injury within the LGBTQIA community, exploring its origins, manifestations, and implications. By delving into key points such as defining moral injury, its relevance to mental health counselors, and the broader societal context, we hope to provide a comprehensive overview that informs, educates, and inspires action. As we embark on this exploration, it's essential to approach the topic with empathy, openness, and a commitment to fostering a more inclusive and understanding world for all
Moral injury, a term that has been increasingly recognized in the mental health lexicon, is a complex and multifaceted psychological construct. At its essence, moral injury arises when individuals are exposed to events or make decisions that deeply violate their internal moral compass or ethical beliefs. This violation can stem from one ' s actions or inactions or from bearing witness to acts contradicting deeply held moral beliefs.
Historically, the concept of moral injury has been strongly
associated with war veterans who, upon reflection, grapple with the moral implications of their actions or decisions made during combat However, its application has expanded beyond the military context, shedding light on various populations, including the LGBTQIA community.
Moral injury is not characterized by specific symptoms or diagnostic criteria, unlike traditional psychiatric disorders. Instead, it represents a profound existential crisis, a deepseated feeling of guilt, shame, and a sense of betrayal from one ' s values It's a rupture in the moral foundation that often forms the core of an individual's identity
The LGBTQIA community, with its rich tapestry of identities and experiences, faces a unique set of challenges in the realm of mental health For mental health professionals, understanding the specific nuances of these challenges is not just beneficial it's essential. Among these challenges, the concept of moral injury stands out as particularly salient, and its relevance to counselors working with the LGBTQIA population cannot be overstated.
Unique Moral Dilemmas: Many LGBTQIA individuals grow up in environments where their identities are not accepted or actively condemned This can lead to situations where they might feel compelled to hide or deny their true selves to gain societal or familial acceptance Such experiences can lead to profound internal conflicts, where individuals feel they betray their authentic selves, resulting in moral injury
Societal and Cultural Pressures: The societal expectation to conform to heteronormative or CIS normative standards can be a significant source of distress. When LGBTQIA individuals internalize these societal prejudices, it can lead to guilt, shame, and a sense of moral wrongdoing, even when they merely seek to live authentically
Religious and Familial Conflicts: Many LGBTQIA individuals come from religious or cultural backgrounds that may not affirm or accept diverse sexual orientations or gender identities. Navigating the tension between one ' s faith or family's beliefs and one ' s identity can lead to moral injury, especially if they feel they are betraying their faith or family by being true to themselves.
Therapeutic Implications: For mental health counselors, understanding the concept of moral injury within the LGBTQIA context is crucial for effective therapeutic intervention. Recognizing the signs of moral injury allows for a more tailored approach, addressing the root causes of distress and facilitating
Affirmative Therapy: Counselors need to adopt an affirmative approach, validating and affirming the identities and experiences of LGBTQIA individuals. This helps address moral injury and fosters a therapeutic environment where clients feel seen, heard, and understood.
Intersectionality: It's also essential for counselors to recognize the intersectional challenges faced by LGBTQIA individuals. For instance, a queer person of color might face compounded discrimination, intensifying their experience of moral injury. Understanding these layered experiences is crucial for providing holistic care.
Continued Education and Training: The landscape of LGBTQIA identities and experiences continually evolves As such, mental health professionals must commit to ongoing education and training to stay informed and provide the best care possible
The relevance of understanding moral injury for mental health professionals working with the LGBTQIA population is profound. It offers a lens through which counselors can better comprehend this community's unique moral dilemmas and challenges. By integrating this understanding into their therapeutic approach, professionals can more effectively support and guide their LGBTQIA clients toward healing and self-acceptance
The experience of moral injury, while universal in its potential to affect any individual, manifests uniquely within the LGBTQIA community Given the societal, familial, and internal pressures many LGBTQIA individuals face, the risk of experiencing moral injury is heightened For mental health professionals, recognizing the signs and nuances of moral injury within this population is paramount to providing effective care.
Internalized Homophobia and Transphobia: One of the most significant indicators of moral injury in the LGBTQIA community is the internalization of societal prejudices. When individuals absorb negative beliefs about their identities, it can lead to feelings of shame, guilt, and a profound sense of moral wrongdoing This internal conflict, where one ' s authentic self is at odds with internalized societal beliefs, is a clear manifestation of moral injury
Concealment and Dual Lives: Many LGBTQIA individuals hide their identities to fit into societal norms or protect themselves from potential harm. Living a dual life, where one ' s public persona is at odds with their private self, can lead to feelings of betrayal and moral distress.
Religious Conflicts: For those coming from religious backgrounds that may not be affirming LGBTQIA identities, there can be a deep-seated moral conflict The tension between religious beliefs and one ' s true self can be a significant source of moral injury, especially if individuals feel they are betraying their faith.
Rejection and Isolation: Experiencing rejection from family, friends, or community due to one ' s LGBTQIA identity can lead to feelings of moral isolation The pain of being ostracized, combined with the internal belief that one might be morally wrong for being true to oneself, amplifies the experience of moral injury
Navigating Relationships: LGBTQIA individuals might sometimes enter heterosexual relationships or deny their gender identity to align with societal expectations. The moral distress of not being authentic in intimate relationships can be a potent source of moral injury.
Intersectional Identities: LGBTQIA individuals who also identify with other marginalized groups, such as racial or ethnic minorities, may experience compounded moral dilemmas. The layered experiences of discrimination and prejudice can intensify feelings of moral distress and injury.
Physical and Mental Health Manifestations: Moral injury, while primarily a psychological construct, can also manifest in physical and mental health symptoms This might include anxiety, depression, sleep disturbances, substance abuse, and somatic symptoms like unexplained aches and pains.
Seeking Affirmation: A continuous search for validation and affirmation, often from external sources, can indicate underlying moral injury This might manifest as seeking constant reassurance or validation of one ' s worth or moral standing
Recognizing moral injury within the LGBTQIA population requires a deep understanding of this community's unique challenges and experiences. It's not just about identifying symptoms but understanding the root causes and the intricate interplay of societal, personal, and internal factors contributing to moral distress. By recognizing and addressing moral injury, mental health professionals can pave the way for healing, acceptance, and holistic well-being for their LGBTQIA clients
Several elements play into the development of moral injury. Moral injury, while a universal concept, is deeply influenced by many factors that vary across individuals and communities. Within the LGBTQIA community, the experience of moral injury
is shaped by a unique set of circumstances and pressures Multifaceted factors contributing to its onset and persistence:
Societal Norms and Expectations: At the forefront of factors contributing to moral injury is the weight of societal norms. Many societies uphold heteronormative and cisnormative standards, which can exert immense pressure on LGBTQIA individuals to conform. The constant push to fit into these molds can lead to internal conflicts, where individuals feel they're betraying their authentic selves
Family Dynamics: The family unit plays a pivotal role in shaping an individual's moral framework. For LGBTQIA individuals, familial rejection, or the expectation to uphold family honor can be a significant source of moral distress. The pain of feeling morally wrong in the eyes of one ' s family can intensify feelings of guilt and shame.
Religious and Cultural Beliefs: Many religious and cultural doctrines have explicit stances on LGBTQIA identities Navigating the tension between one ' s faith or cultural beliefs and one ' s true self can be a profound source of moral injury. The internal struggle of reconciling personal identity with deeply held religious or cultural values can lead to intense moral dilemmas.
Internalized Prejudices: Over time, continuous exposure to societal prejudices can lead to their internalization When LGBTQIA individuals absorb and believe these negative messages about their identities, it can result in self-loathing, guilt, and a profound sense of moral wrongdoing
Experiences of Discrimination and Violence: Direct experiences of discrimination, hate crimes, or violence because of one ' s LGBTQIA identity can lead to feelings of moral isolation. The trauma of such experiences and internal beliefs of deserving such treatment can amplify moral injury.
Intersectional Challenges: LGBTQIA individuals who also belong to other marginalized groups, such as racial or ethnic minorities, face compounded moral challenges. The layered experiences of discrimination, prejudice, and societal expectations can intensify feelings of moral distress.
Relationship Dynamics: Engaging in relationships where one ' s true identity is hidden or suppressed can potentiate moral injury The emotional toll of not being authentic, especially with intimate partners, can lead to feelings of betrayal and moral conflict
Media Representation: The portrayal of LGBTQIA identities in the media can influence perceptions of morality. Negative or stereotypical representations can reinforce societal prejudices, leading to heightened feelings of moral distress among
Legislative and Institutional Factors: Laws and institutional policies that discriminate against or do not affirm LGBTQIA identities can contribute to societal prejudices. Living in environments where one ' s identity is legally marginalized can be a significant source of moral injury.
Mental Health Stigma: Within many communities, seeking mental health support is stigmatized. For LGBTQIA individuals grappling with moral injury, this added layer of stigma can exacerbate feelings of isolation and moral wrongdoing.
The factors contributing to moral injury within the LGBTQIA community are intricate and interwoven Recognizing and understanding these factors is mental health professionals' first step in providing holistic care By addressing the root causes and providing a safe space for exploration and healing, professionals can support LGBTQIA individuals in navigating the complexities of moral injury and pave the way for emotional and psychological well-being.
While the importance of addressing moral injury within the LGBTQIA community is evident, mental health professionals often encounter several barriers to providing effective therapy and support. These obstacles, if not recognized and addressed, can hinder the therapeutic process, and even exacerbate the distress experienced by LGBTQIA individuals.
Stigma and Discrimination: One of the most significant barriers is the pervasive stigma associated with LGBTQIA identities. Many individuals have faced discrimination in various settings, including healthcare. This history can make them wary of seeking therapy, fearing further discrimination, or misunderstanding.
Lack of Cultural Competence: Not all therapists are equipped with the knowledge or training to address LGBTQIA-specific issues A lack of cultural competence can lead to misinterpretations, unintentional microaggressions, or even reinforcement of harmful stereotypes, all of which can hinder the therapeutic process
Therapist Biases: Regardless of training, every therapist brings their biases into the therapeutic space. Unaddressed biases related to sexuality, gender identity, or even moral injury itself can impede the therapeutic relationship and the healing process.
Limited Access to LGBTQIA-Affirming Resources: In many regions, there's a dearth of LGBTQIA-affirming resources, be it therapists specializing in LGBTQIA issues, support groups, or
educational materials This lack can limit the options available for individuals seeking support
Financial Constraints: Quality mental health care can be expensive, and not all LGBTQIA individuals have the means or insurance coverage to access the support they need. This economic barrier can deter many from seeking therapy.
Confidentiality Concerns: Given the potential repercussions of being "outed," many LGBTQIA individuals are concerned about confidentiality in therapy. They might fear that their identities or experiences will be disclosed, leading to further discrimination or harm.
Legislative and Policy Barriers: In some regions, laws and policies can actively discourage or even criminalize LGBTQIAaffirming therapy For instance, laws prohibiting discussions about LGBTQIA topics in schools or therapy can severely limit the support available to individuals
Lack of Interdisciplinary Collaboration: Addressing moral injury often requires a holistic approach, involving medical professionals, social workers, and community support. A lack of collaboration between these entities can lead to fragmented care
Overemphasis on Pathologization: Some therapeutic approaches might pathologize LGBTQIA identities, viewing them as disorders rather than natural variations of human experience. This perspective can be harmful and counterproductive in addressing moral injury.
Limited Research: While our understanding of moral injury and its implications for the LGBTQIA community has grown, there's still limited research in this area. This gap can make it challenging for therapists to rely on evidence-based practices tailored to this community's needs.
While the need for effective therapy and support for the LGBTQIA community grappling with moral injury is pressing, several barriers stand in the way Recognizing these obstacles is the first step Mental health professionals, institutions, and policymakers must collaborate to overcome these challenges, ensuring that every LGBTQIA individual has access to the compassionate, informed, and affirming care they deserve
While dedicated to supporting and healing others, mental health practitioners often face intense emotional and psychological demands in their line of work. When working with marginalized communities, such as the LGBTQIA population, these demands can be even more pronounced due
to the unique challenges and traumas these individuals face As such, emphasizing the importance of self-care for practitioners is not just beneficial it's essential for sustaining their wellbeing and ensuring they can provide the best care to their clients.
The Emotional Toll of the Profession:
Vicarious Trauma: Therapists often hear deeply traumatic stories and experiences from their clients. Over time, this can lead to vicarious trauma, where practitioners begin to experience symptoms similar to those of their clients.
Compassion Fatigue: Continuously offering empathy and support can sometimes lead to compassion fatigue, where therapists feel emotionally drained and find it challenging to empathize with their clients
Burnout: The cumulative stress of the profession, combined with personal life stresses, can lead to burnout, characterized by emotional exhaustion, reduced performance, and detachment.
Self-Care Strategies:
Regular Supervision: Seeking regular supervision provides therapists with a space to discuss challenging cases, receive feedback, and process their emotions.
Mindfulness and Meditation: Engaging in mindfulness practices can help therapists stay present, reduce stress, and cultivate emotional balance
Physical Activity: Regular exercise can relieve stress, enhancing mood and overall well-being.
Boundaries: Setting clear professional boundaries ensures that therapists don't overextend themselves, preserving their emotional and psychological resources
Hobbies and Interests: Engaging in activities outside of work can provide a necessary distraction, allowing therapists to recharge.
The Role of Peer Support:
Peer Supervision: Engaging in peer supervision groups can offer therapists a supportive environment to discuss challenges, share strategies, and receive validation.
Professional Networks: Being part of professional associations or networks can provide therapists with resources, training opportunities, and a sense of community.
Continuous Learning and Training:
Skill Enhancement: Regularly updating and enhancing therapeutic skills can instill confidence in practitioners,
Self-Care Workshops: Attending workshops focused on selfcare can equip therapists with tools and strategies to prioritize their well-being.
Recognizing the Signs: Therapists must be attuned to the signs of burnout, compassion fatigue, or vicarious trauma in themselves Early recognition allows for timely intervention, ensuring that they seek support before their well-being is severely compromised.
Prioritizing Mental Health: Just as they advocate for their clients' mental health, therapists must prioritize their own. This might involve seeking therapy themselves, engaging in relaxation techniques, or even taking necessary breaks from work
While mental health practitioners play a pivotal role in supporting and healing others, they must not neglect their own well-being. The nature of their work, especially when working with marginalized communities, underscores the importance of self-care. By prioritizing their mental, emotional, and physical health, therapists can ensure they are best equipped to support their clients while also leading fulfilling, balanced lives.
The journey of understanding and addressing moral injury within the LGBTQIA community is both intricate and deeply significant. As society continues to evolve in its acceptance and understanding of diverse identities, the challenges faced by the LGBTQIA population remain multifaceted The emotional and psychological toll can be profound, from the internal struggles stemming from societal pressures to the external challenges of discrimination and prejudice However, with awareness comes the power to instigate change
Mental health professionals stand at the forefront of this transformative journey. Their role is not just to heal but to empower, validate, and affirm the experiences of LGBTQIA individuals. They can make a lasting impact by recognizing the nuances of moral injury, implementing evidence-based interventions, and prioritizing their clients' and their own wellbeing The emphasis on resilience, self-care, and continuous learning underscores the dynamic nature of the therapeutic process
Furthermore, the broader community, including policymakers, educators, and families, plays a crucial role in shaping a more inclusive, understanding, and supportive environment. The collective effort to address and mitigate the effects of moral injury can pave the way for a society where every individual, regardless of their sexual orientation or gender identity, can live
authentically, free from the burdens of moral distress
The exploration of moral injury within the LGBTQIA community is a poignant reminder of the human spirit's resilience and the transformative power of empathy, understanding, and informed action. As we move forward, let us do so with a commitment to fostering a world where every individual feels seen, heard, and valued.
 Written By: Maria Giuliana, LMHC, FMHCA NE Regional Director
Written By: Maria Giuliana, LMHC, FMHCA NE Regional Director
Maria (she/her) is a 20-year Retired N Veteran and founder of Beyond The M Counseling and Consulting Services LL provides virtual services in Florida an supporting Military Veterans and their addressing the unique concerns of th Maria creates an inclusive and safe sp

Join in on one of our upcoming webinars! Topics include: Bioregulation Therapy, Trauma Informed Care, Workplace Trauma, & More!
Register Now