David Katz, Amanda Daley, Lennard Lee, and Mariah Stump on bringing
Articles
72 Editor's Pick: Characterising Drug-Associated Nephrolithiasis: Insights from Global Adverse Drug Reaction Database
Baptista et al.
83 Nanomedicine in The Treatment of Diabetes: Emerging Nanotherapeutic Strategies of Novel Drug Delivery Systems
Islam et al.
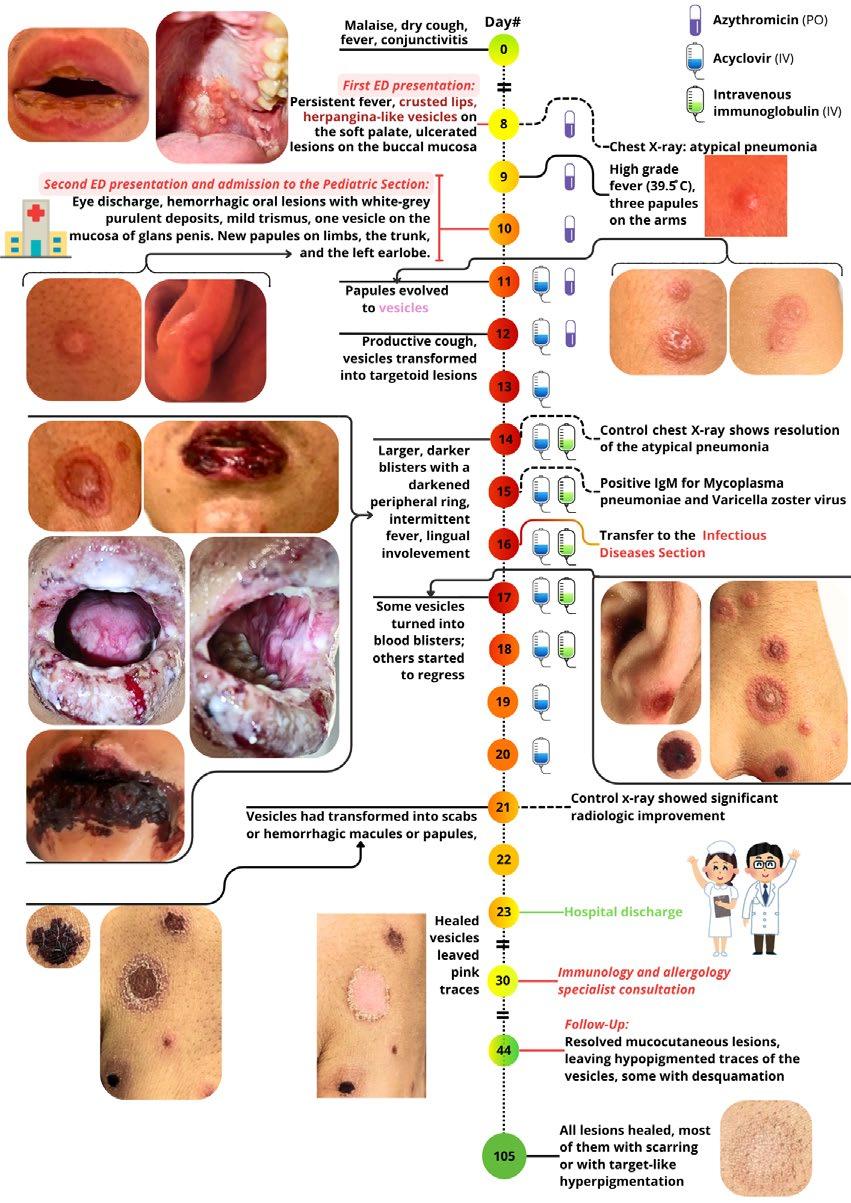
93 Target-Like Lesions with Mucositis in a 13-Year-Old Adolescent Due to Co-Infection with Mycoplasma pneumoniae and Varicella-Zoster Virus: A Case Report and Literature Review
Faludi and Bíró
101 Urinary Tract Infection Turns Out to Be Infective Endocarditis: An Unusual Presentation – A Case Report
Bertlla and Anwar
108 Oesophageal Actinomycosis Masquerading as Squamous Cell Carcinoma
Moinuddin et al.
"I
believe you should be allowed the freedom to think of what the future could be and how it could be better"
Editorial Board
Editor-in-Chief
Prof Markus Peck-Radosavljevic
Klinikum Klagenfurt am Wörthersee, Austria
Current Chairman and Head of the Department of Gastroenterology and Hepatology, Endocrinology, Rheumatology and Nephrology at Klinikum Klagenfurt am Wörthersee, with expertise in portal hypertension, hepatocellular carcinoma, and HIV-HCV coinfection.
Prof Ahmad Awada
Jules Bordet Institute, Belgium
Prof Sorin T. Barbu
“Iuliu Hațieganu” University of Medicine andPharmacy, Romania
Prof Abdullah Erdem Canda
Yildirim Beyazit University, Türkiye
Prof Ian Chikanza
Harley Street Clinic, UK
Prof Lászlo Vécsei
University of Szeged, Hungary
Dr Pierfrancesco Agostoni
St. Antonius Hospital, the Netherlands
Dr Fernando Alfonso
Hospital Universitario de La Princesa, Spain
Dr Emanuele Angelucci
IRCCS Ospedale Policlinico San Martino, Italy
Dr George Anifandis University of Thessaly, Greece
Dr Riccardo Autorino
Virginia Commonwealth University, USA
Dr Mátyás Benyó University of Debrecen, Hungary
Prof Andrew Bush Imperial College London, UK
Dr Hassan Galadari
United Arab Emirates University, United Arab Emirates
Dr Amir Hamzah Abdul Latiff
Pantai Hospital, Malaysia
Dr Lorenz Räber
Bern University Hospital, Switzerland
Aims and Scope
EMJ, the flagship journal of the EMJ portfolio, is an openaccess, peer-reviewed eJournal, committed to elevating the quality of healthcare globally by publishing high-quality medical content across the 18 clinical areas covered in our portfolio. The journal is published quarterly and showcases the latest developments across these clinical areas.
EMJ publishes peer-reviewed research papers, review articles, and case reports across all therapy areas of the EMJ portfolio. In addition, the journal publishes features and opinion pieces create a discussion around key topics in the field and broaden readers’ professional interests. The journal also features interviews with leading experts in various clinical disciplines.
The journal covers advances within the pharmaceutical arena by publishing sponsored content from congress symposia, which is of high educational value for healthcare professionals. This undergoes rigorous quality control checks by independent experts and the in-house editorial team.
EMJ endeavours to increase knowledge, stimulate discussion, and contribute to the delivery of world-class updates in the clinical realm. We do not publish veterinary science papers or laboratory studies that are not linked to patient outcomes. Further details on coverage can be found here: www.emjreviews.com
Editorial Expertise
EMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors who are recognised authorities in their respective fields.
• Peer review, which is conducted by expert reviewers who are invited by the Editorial team and appointed based on their knowledge of a specific topic.
• An experienced team of editors and technical editors.
• A team of internal and independent medical writers.
Peer Review
Every review article, case report, feature, and research article published in EMJ undergoes peer review by at least two independent experts.
On submission, all manuscripts are assessed and undergo a technical check by the EMJ Editorial staff to determine their suitability for the journal and appropriateness for peer review. Editorial staff identify appropriate reviewers who are selected based on their specialist knowledge in the relevant area. All peer review is double-blind.
Following review, manuscripts are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected. Editorial staff are responsible for ensuring that necessary amendments to the manuscript have been made, with input from our Editorial Board or the original reviewers where necessary. The Editor of EMJ has final discretion over any proposed amendments. Manuscripts authored by members of the Editorial Board are subjected to the same double-blind process. Short opinion pieces are published following internal review and publication is at the discretion of the Editor. Congress-associated content authored by the EMJ Editorial staff undergoes internal quality control checks. Congress-related content sponsored or funded by our industry partners undergoes quality control checks independently. Industry-supported content that falls into any of
the categories that are eligible for peer review, undergoes the same peer review process.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects. We seek papers with the most current, interesting, and relevant information in each therapeutic area and accept original research, review articles, case reports, and features.
We are always keen to hear from healthcare professionals wishing to discuss potential submissions, please email: editorial.assistant@emjreviews.com
To submit a paper, use our online submission site: www.editorialmanager.com/e-m-j
Submission details can be found through our website: www.emjreviews.com/contributors/authors
Reprints
All articles included in EMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
EMJ is distributed through controlled circulation to healthcare professionals in the relevant fields globally.
Indexing and Availability
EMJ is indexed on DOAJ, the Royal Society of Medicine, and Google Scholar®.
EMJ is available through the websites of our leading partners and collaborating societies.
EMJ journals are all available via our website: www.emjreviews.com
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
All information obtained by EMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, EMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. EMJ is completely independent of any event reviews in this issue and the use of the organisations does not constitute endorsement or media partnership in any form whatsoever. The cover photo is of Faro, the location of work for the primary author of Editor's Pick.
Speakers: Prof. Dr. Seza Özen & Prof. Dr. Serdal Uğurlu
Episode 4
Targeting IL-1 in RA
Speakers: Prof. Dennis McGonagle & Adjunct Prof. Hugues Allard-Chamard
These podcasts are promotional content funded by Sobi. Prescribing information may vary depending on local approval in each country. For full SmPC for Kineret please visit here. Before prescribing any product, always refer to the local materials such as the prescribing information and/or summary of product characteristics. IL-1, interleukin-1; RA, rheumatoid arthritis.
Katrina Thornber, Katie Wright, Aleksandra Zurowska
Creative Director
Tim Uden
Design Manager
Stacey White
Creative Artworker
Dillon Benn Grove
Designers
Shanjok Gurung, Fabio van Paris, Owen Silcox
Senior Performance & Insight Lead
Darren Brace
Marketing Director
Kristina Mestsaninova
Chief Content Officer
Justin Levett
Chief Commercial Officer
Dan Healy
Founder and Chief
Executive Officer
Spencer Gore
Welcome
Dear Readers,
I am pleased to welcome you to the second issue of the EMJ Flagship Journal for 2025. This issue sheds light on preventive medicine, a topic of increasing importance in the face of population expansion, continued medical advancements, and rising healthcare costs. The proverb ‘prevention is better than cure’ underlines the proactive approach required to avoid certain outcomes, and it is becoming increasingly clear that this approach to healthcare could be transformative.
Our interviews with preventive medicine experts cover how addressing diet and nutrition can impact the risk of chronic disease and mortality; the role of cancer vaccines and early cancer detection through screening; and the value of lifestyle medicine, non-pharmaceutical management strategies, and social prescribing. You will also find an interesting congress feature exploring upcoming European strategies for cancer screening in an effort to tackle the growing cancer crisis, referred to as the ‘silent pandemic’.
This issue also includes a feature addressing the psychological drivers of engagement and social determinants of health, as well as the supporting role that digital health can play, and the need for equity in engagement strategies.
I would like to thank our Editorial Board, contributors, and peer reviewers for their hard work, passion, and insights that have helped bring this journal to life. I hope you enjoy this issue and can take away insights that will help you consider preventive medicine in your day-to-day practice.
Editorial enquiries: editor@emjreviews.com
Sales opportunities: salesadmin@emjreviews.com
Permissions and copyright: accountsreceivable@emjreviews.com
Evgenia Koutsouki Editor
Reprints: info@emjreviews.com Media enquiries: marketing@emjreviews.com
Foreword
Dear Colleagues,
Welcome to the latest issue of the EMJ Flagship Journal for 2025, where we turn our attention to one of the most impactful and increasingly relevant areas in healthcare: preventive medicine. In this issue, we highlight the transformative potential of prevention across a spectrum of medical disciplines, aiming to shift the focus from reactive treatment to proactive care.
Our thoughtfully curated content includes peer-reviewed articles, insightful features, and exclusive interviews with pioneers in the field. Amongst this is a feature that delves into the behavioural and social determinants of health, exploring how digital health tools and equitable strategies can improve engagement with preventive practices.
We are proud to present interviews with leading voices in preventive medicine who are championing change in how we think about health and longevity. They share insights into how early interventions can reduce mortality and enhance quality of life, including the use of food as medicine, the power of snack-sized fitness, the cancer vaccine revolution, and how clinicians can look beyond the prescription pad when treating patients.
As always, I extend my deepest thanks to our Editorial Board, peer reviewers, authors, and interviewees, whose dedication and expertise have brought this issue to life. I hope the insights shared within these pages inspire meaningful reflection and practical application in your daily practice.
We turn our attention to one of the most impactful and increasingly relevant areas in healthcare: preventive medicine
Prof Markus Peck-Radosavljevic
Professor of Medicine and Chairman, Department of Gastroenterology and Hepatology, Endocrinology, Rheumatology and Nephrology, Klinikum Klagenfurt am Wörthersee, Austria
The Silent Pandemic: A European Call to Prevent a Growing Cancer Crisis
“As European doctors, citizens, and possible patients in the future, we need to plan ahead to avoid the silent pandemic of cancer,” implored Milagros Otero-Garcia, University of Vigo, Pontevedra, Spain, who opened the 2025 European Congress of Radiology (ECR) session, entitled ‘New cancer screening programmed: upcoming European strategies’.1
CONTEXTUALISING THE CRISIS AND EXPLORING EU RECOMMENDATIONS
According to Otero-Garcia, in 2020 alone, 2.7 million people across the European Union (EU) were diagnosed with cancer, and 1.3 million lost their lives (including more than 2,000 young people). Projections show that by 2035, cancer cases could rise by 24%, making it the leading cause of death in the EU. Yet, amid these alarming figures lies a powerful opportunity: up to 40% of cancer cases are preventable. This reality highlights the urgent need for proactive, coordinated action to stop a silent pandemic before it grows louder.
According to Regina Beets-Tan, the Netherlands Cancer Institute, Amsterdam, the Netherlands, improved cancer screening is essential to reducing the rising burden of cancer in Europe. As a member of the EU Cancer Mission Board, Beets-Tan emphasised that screening enables cancers to be caught earlier, often before symptoms appear, when treatment is more effective and less costly. The EU’s updated 2022 screening recommendations expand access to breast, cervical, and colorectal cancer screening, with a target of reaching 90%
The EU is focusing on whether digital transformation of AI will help us to reduce the healthcare costs
of eligible citizens by 2025.2 For high-risk groups, the EU is also exploring stepwise approaches to lung, prostate, and gastric cancer screening, she explained.
Investment in digital transformation, particularly AI, is central to this strategy. “The EU is focusing on whether digital transformation of AI will help us to reduce the healthcare costs, and it's also focusing on improving their equitable access to screening and quality of care,” Beets-Tan said.
Additionally, she explained that the “EU is focusing on prevention by projects that will explore the implementation of high-risk screening [and] develop new screening methods”, including programmes such as Horizon Europe and EU4Health.
Ultimately, she emphasised that better screening is not just a clinical tool, it is a cornerstone of more efficient, equitable, and preventive healthcare for all Europeans. With continued support and collaboration, early detection could help shift cancer from a crisis into a manageable condition.
BUILDING A NEXTGENERATION PROSTATE CANCER SCREENING STRATEGY
Efforts to improve prostate cancer screening are evolving rapidly, with MRI emerging as a key tool in the push towards earlier detection, more accurate diagnosis,
and more personalised care. “Prostate cancer is among the most frequent tumours in men, and we are facing an increase in its incidence over the last years,” explained Emmanuel Messina, Department of Radiological Sciences, Oncology and Pathology, Sapienza University of Rome, Italy.
According to Messina, MRI has become a cornerstone in the diagnostic workup of prostate cancer, particularly following development of the MRI-targeted biopsy pathway and the widespread implementation of PI-RADS scoring. “MRI has been introduced as a very strong tool in prostate cancer diagnostic workup, but MRI is still not recommended as an initial tool for prostate cancer screening,” Messina said.
MRI offers high sensitivity for detecting clinically significant tumours and reduces unnecessary biopsies, making it a promising candidate for use in population-level screening programs. However, despite its strengths, MRI as a standalone screening tool faces limitations. These include cost, access, interpretation variability, and the need for further refinement in low-risk
populations. To address these challenges and unlock MRI’s full potential, Messina highlighted that research is increasingly focused on enhancing MRI through integration with AI, computational tools, and molecular biomarkers. “MRI indeed determined a revolution in prostate cancer diagnostic workup in the last decade, proving to be an essential tool in this setting, and non-contrast MRI proved to have a very high accuracy. However, we probably should refine MRI-based score assistance for this specific setting,” he said.
One major advancement is the use of AIbased image analysis, explained Messina. Deep learning models trained on large MRI datasets can now assist radiologists in lesion detection, PI-RADS scoring, and case prioritisation. These systems can improve accuracy, consistency, and reporting speed, particularly in settings with limited radiology expertise or high imaging volumes. AI can also generate synthetic high b-value diffusion-weighted imaging (DWI) images, improving image quality and enabling better lesion characterisation, especially valuable in non-contrast bi-parametric protocols, which are more suitable for mass screening.
In parallel, the integration of molecular biomarkers, especially from liquid biopsies, is proving essential for refining risk stratification. Biomarkers such as prostatespecific antigen (PSA) density, apparent diffusion coefficient (ADC) values, and specific microRNAs (e.g., miR-302, miR367) have been shown to correlate strongly with clinically significant prostate cancer. When used alongside MRI, they enhance the predictive value of imaging and help reduce overdiagnosis and overtreatment.
Computational tools, including multivariate decision models and network-based analyses, further enable the fusion of imaging, and clinical and molecular data. These integrated approaches support the development of personalised screening pathways, where decisions are driven not by a single test, but by a combination of factors tailored to the individual’s risk profile.
Importantly, this convergence of imaging, AI, and biomarker data is scalable and adaptable. It holds great promise for reducing inequalities in access by enabling standardised, high-quality screening protocols that can function even in resource-limited settings, where specialist interpretation or contrast media may not be readily available. To conclude, Messina said: “All of this considered, my final answer is yes, we are indeed on the right track to define the most appropriate prostate cancer screening pathway, and it should indeed include MRI.”
We are indeed on the right track to define the most appropriate prostate cancer screening pathway
AI-POWERED LUNG CANCER SCREENING
Lung cancer remains the leading cause of cancer-related death worldwide, largely due to late-stage diagnosis, explained Carlos F Muñoz-Núñez, La Fe University and Polytechnic Hospital, Valencia, Spain. He went on to say that approximately 75% of patients are diagnosed at Stage III and IV, and the global survival rate is less than 20% at 5 years.
Low-dose CT (LDCT) screening has been proven to reduce mortality in highrisk populations by enabling earlier detection. LDCT uses lower radiation doses than standard CT, making it suitable for repeated use, but it presents challenges such as image noise, false positives, and significant workload for radiologists.
AI offers promising solutions: improving risk-based population selection, enhancing image reconstruction with deep learning techniques, and supporting automated nodule detection and malignancy prediction. “Lung cancer based on risk models are tools designed to estimate an individual’s risk of developing lung cancer based on risk factors, and these models help guide screen decisions, early detection, and personalised prevention strategies,” he explained. AI can also help reduce overdiagnosis by integrating imaging with clinical, genomic, and biomarker data to identify indolent versus aggressive lesions.
However, Muñoz-Núñez continued that there are significant limitations and risks. “There are data biases in a model trained with non-representative data sets, especially if European versus Asian populations are
in these data sets, if the AI models are trained with different kind of data sets, and this affects diagnostic accuracy across diverse populations.” Lack of transparency in AI decision-making can also undermine clinical trust, especially when predictions are not explainable. False positives remain a challenge, and AI-assisted screening can sometimes increase them if sensitivity is prioritised over specificity.
Furthermore, the psychological impact of false alarms, ethical concerns about data privacy, and unequal access to advanced AI tools raise critical questions about implementation. Regulatory oversight and rigorous validation in diverse, real-world settings are essential before wide deployment.
OPTIMISING COLORECTAL CANCER SCREENING ACROSS THE EU
The EU recommends colorectal cancer screening for asymptomatic individuals aged 50–74 years as part of populationbased programmes.2 This strategy addresses a major health burden: colorectal cancer is the second leading cause of cancer death in Europe, with over 300,000 new cases annually. Screening has significantly reduced incidence in countries with established programmes, though uptake varies widely across the EU, from nearly 94% in some areas to under 50% in others, explained Stuart Taylor, University College London, UK.
The cornerstone of the EU approach is the faecal immunochemical test (FIT), a simple, cost-effective, and quantitative assay detecting haemoglobin in stool. FIT has replaced the older guaiac faecal occult blood test (FOBT) due to its higher specificity and better patient compliance,
nd
Colorectal cancer is the second leading cause of cancer death in Europe, with over 300,000 new cases annually
Taylor said. A positive FIT typically leads to colonoscopy, as the likelihood of significant pathology is high. However, the FIT threshold can be adjusted: lower thresholds improve sensitivity (fewer missed cancers) but result in more colonoscopies, impacting healthcare resources. Each country sets thresholds based on capacity. “Colonoscopy is an expensive test, so how you organise your screening program depends on how many resources you have available to you to do multiple colonoscopies,” Taylor explained.
Radiologists contribute primarily through CT colonography (CTC), used when colonoscopy is incomplete or contraindicated, for instance in frail patients or those with complex anatomy. CTC is sensitive for cancers and large polyps, but effectiveness depends heavily on radiologist training and experience.
“The EU needs to make sure we train our radiologists well with appropriate training, looking at the whole spectrum of lesions, how to avoid interpretation pitfalls, and to test ourselves. Unfortunately, we can't assume that we're good just because we've taken a training course. We need to show that we are good and monitor our performance over time,” Taylor said.
How you organise your screening program depends on how many resources you have available to you to do multiple colonoscopies
Although CTC is promising, especially for symptomatic or high-risk individuals, its limited population compliance and cost prevent its widespread use as a primary screening tool. Thus, FIT remains the most effective and economical option in population screening programmes.
A PATIENT PERSPECTIVE
The session was concluded with a talk by Erik Briers, an expert patient advocate and Vice Chairman of Europa Uomo, Antwerp, Belgium, who emphasised the lack of organised prostate cancer screening across
Europe, despite its high incidence and mortality. Unlike breast or cervical cancer, prostate cancer currently lacks a structured, population-wide screening approach.
He highlighted that early detection is crucial when cancers are still curable and treatment is more effective. However, not all cancers can be detected early or prevented. While some cancers like cervical (100% preventable via HPV vaccination) and lung (90% preventable by avoiding smoking) are highly preventable, prostate and brain cancers are considered 0% preventable, with no proven lifestyle or genetic factors to mitigate risk individually.
Prostate cancer also presents no early symptoms, making screening vital. Briers supports risk-based screening, starting with family history and demographic factors (e.g., African ancestry), followed by PSA tests and MRI where needed. The EU has recently supported this direction, funding pilot programmes to explore effective implementation.
References
1. Otero-Garcia et al. New cancer screening programmed: upcoming European strategies. SA 18. ECR, 26 February-2 March, 2025.
Finally, he stressed the importance of distinguishing low-risk prostate cancers that can be monitored with active surveillance, avoiding overtreatment while still detecting and treating highrisk cancers early to reduce mortality.
CONCLUSION
Europe stands at a critical juncture in the fight against cancer. With incidence rising, early detection through organised, riskbased screening programmes is essential to improve outcomes and reduce costs. The EU’s updated strategies, incorporating AI, molecular biomarkers, and improved imaging (particularly in prostate, lung, and colorectal cancer) signal a transformative shift toward personalised, equitable care. Yet, success depends on implementation across all member states, addressing disparities in access and ensuring quality. As patient advocate Briers reminds us, time is of the essence. With coordinated action, Europe can move from crisis management to prevention, ensuring more lives are saved through timely, targeted screening.
2. Council of the European Union. Council Recommendation on strengthening prevention through early detection: a new EU approach on cancer screening
replacing Council Recommendation 2003/878/EC. 2022. Available at: https://data.consilium.europa.eu/doc/ document/ST-14770-2022-INIT/en/ pdf. Last accessed: 5 May 2025.
Advancements in Hydrogel-Based Therapies as Non-surgical Alternatives for Urothelial Carcinoma: Ongoing Research and New Insights
These presentations took place between 26th–27th April 2025, as part of the American Urological Association (AUA) Annual Meeting held in Las Vegas, Nevada, USA.
Speakers: Charles Peyton,1 Brian Hu,2 Neal Shore,3 Sandip Prasad,4 Jay Raman5
1. Department of Urologic Oncology, University of Alabama at Birmingham, USA
2. School of Medicine, Loma Linda University, California, USA
3. Carolina Urologic Research Center, Myrtle Beach, South Carolina, USA
4. Morristown Medical Center; Atlantic Health System, Garden State Urology, New Jersey, USA
5. Department of Urology, Penn State Cancer Institute, Hershey, Pennsylvania, USA
Disclosure: Peyton is a consultant for UroGen Pharma. Hu has received principal investigator funding from UroGen Pharma. Prasad has received principal investigator funding from Janssen, Merk, Pfizer, and UroGen Pharma. Raman has received principal investigator funding from Pacific Edge, Biotechnologies, Steba Biotech, and Urogen Pharma; and has stock in American Kidney Stone Management and United Medical Systems Inc. Clinical trials reported in this article were funded by UroGen Pharma
Acknowledgements: Medical writing assistance provided by Jessica Jinks, EMJ, London, UK.
Disclaimer: JELMYTO (mitomycin) for pyelocalyceal solution is currently approved in the USA and Israel for the treatment of adult patients with lowgrade upper tract urothelial cancer (LG-UTUC). It is not approved for use in the UK, EU, or other jurisdictions unless explicitly stated by local regulatory authorities. Healthcare professionals should refer to their local prescribing information and regulatory guidance for further details. Patients should consult their healthcare provider regarding treatment options suitable for their condition.
Support: The publication of this article was funded by UroGen Pharma.
Erratum: This article was originally published online on 12th June 2025. An erratum has since been issued and can be viewed here
Meeting Summary
Urological cancers are malignancies that affect the organs of the urinary system and male reproductive system. Of these, bladder cancer is the sixth most common cancer in the USA, with 75% of cases being non-muscle invasive bladder cancer (NMIBC). Surgical treatment for urological cancers often lacks durability, requiring multiple procedures due to disease recurrence or progression. New therapies are required to improve treatment prospects, reduce recurrence risk, and maintain patients’ quality of life.
A range of poster presentations took place as part of the American Urological Association (AUA) Annual Meeting 2025. Posters highlighted the potential of reverse thermal gel formulations of anti-cancer agents, including mitomycin as an effective alternative to repetitive surgeries for treating different forms of low-grade urothelial cancers, and zalifrelimab for the treatment of recurrent non-muscle invasive bladder cancer (NMIBC). The posters also considered Patient-Reported Outcomes (PRO) of NMIBC and the effects of hydrogel-based chemotherapy on PROs.
Presenters discussed ongoing research to further evaluate the safety and efficacy of investigational therapies, with the hope of providing an alternative to surgery for patients with NMIBC, as has been demonstrated with low-grade-upper tract urothelial cancers (LG-UTUC).
Introduction
Urological cancers are malignancies that affect the organs of the urinary system and male reproductive system. Of these, bladder cancer is the sixth most common cancer in the USA,1 with 75% of cases being NMIBC.2,3 Despite available treatments, many patients experience disease recurrence or progression, which occurs in 15–30% of high-grade cases and over 50% of intermediate-risk cases.4 New therapies are required to improve treatment prospects, reduce recurrence risk, and maintain patients’ quality of life (QoL).
Current Therapeutic Landscape:
Surgical Interventions
Transurethral resection of bladder tumour (TURBT) surgery is the current standard of care for low-grade intermediate-risk NMIBC (LG-IR-NMIBC).5,6 TURBT is associated with local and systemic side effects including haematuria, urinary tract infection
(UTI), bladder perforation, and transient increase in urination frequency or urgency. Furthermore, TURBT is performed under anaesthesia with associated pre-operative risks.5,6 Recurrence rates of NMIBC after TURBT are high, with patients often requiring multiple procedures. Around 50% of patients with IR-LG-NMIBC experience disease recurrence within 5 years.7
Similarly, LG-UTUC can be treated with endoscopically guided ablation, but recurrence is common, with a 5-year relapse-free survival rate of only 13–54%.8 Patients therefore require lifelong surveillance in the form of repeat ureteroscopy, with 80% of surveyed healthcare professionals (HCP) choosing to perform a repeat procedure 3 months after the initial surgery.9
While immediately effective, surgical ablation is not typically durable, highlighting the clinical urgency for improved, longlasting treatments for bladder cancer.
Symptom Burden and Quality of Life in Patients with Urological Cancers
Symptom burden and health-related QoL are critical concerns for patients with NMIBC, further highlighting the need for ongoing improvements to care. The burden of symptoms for bladder cancer patients includes urinary issues, bloating and flatulence, malaise, intravesical treatment issues, and future worries.10 Loss of sexual function and enjoyment are also key factors, including issues around sexual intimacy and perceived risks of contaminating a sexual partner with treatment-related substances.11 These key themes are captured in the European Organisation for Research and Treatment of Cancer (EORTC) QoL Questionnaire (QLQ) for use in patients with NMIBC 2024 (EORTC QLQNMIBC24).11 With the EORTC QLQ-NMIBC24, patients numerically score their perception of symptom burden, with a recall of 1 week for most items and 4 weeks for sex-related questions. Patients answer questions including: “Was it difficult for you to get enough sleep, because you needed to get up frequently at night to urinate?” with a scale from 1 (not at all) to 4 (very much). Functional and symptom scores are linearly transformed to a 0–100 scale, with higher symptom scores indicating greater symptom burden, and higher functional scores reflecting better functioning or satisfaction.
Validation of EORTC Quality of Life Questionnaire NMIBC24
Charles Peyton, Professor of Urologic Oncology at the University of Alabama, Birmingham, USA, described how this tool has not yet been validated in patients with LG-IR-NMIBC, and presented new data determining the questionnaire’s psychometric properties with LG-IR-NMIBC patients in global trials:12 the ATLAS13 and ENVISION14 studies.
The ATLAS Study
The ATLAS study13 was a Phase III randomised controlled trial assessing the efficacy and safety of intravesical mitomycin
(a reverse thermal hydrogel containing mitomycin) with or without TURBT versus TURBT alone. The trial included patients with newly diagnosed or recurrent LG-IRNMIBC randomised to six once-weekly intravesical instillations of mitomycin with (n=140) or without (n=142) TURBT.
The ENVISION Study
The ENVISION study14 was a multinational, open-label, single-arm Phase III trial evaluating the efficacy and safety of intravesical mitomycin therapy in patients with recurrent LG-IR-NMIBC. In this trial, patients with recurrent LG-IR-NMIBC received six once-weekly intravesical instillations of mitomycin (n=240). For detailed safety and efficacy results from the ENVISION trial, see section: The ENVISION Trial Results and Long-Term Follow-Up.
For the psychometric validation, EORTC QLQ-NMIBC24 data from ATLAS and ENVISION trials administered at baseline, Week 6, and Month 3 were used. Test-retest ability, internal consistency, known group validity, and sensitivity to change were evaluated. The between-group minimal clinically important difference (MCID) was also assessed.
Results presented at AUA 2025 support the utilisation of EORTC QLQ-NMIBC24 to assess health-related QoL in individuals with LG-IR-NMIBC. Peyton reported a moderate-to-high test-retest reliability measured by intraclass correlations, demonstrating stability of the measurement over time. Where symptom areas were covered by multiple questions, the results of these questions were accordant. This internal consistency was measured by Cronbach’s alpha, which measured >0.75 in all multi-question domains except for malaise. The questionnaire was responsive to changes in health over time, specifically reporting sensitivity to change in urinary symptoms, sexual intimacy, and malaise. Results indicate that the EORTC QLQNMIBC24 performed well on known group validity where patients with high scores (>90) on the physical function scale of the QLQ-C30 reported fewer symptoms in NMIBC24 as expected.
MCID data were also presented.12 At Months 3 and 6, between-patient estimates of MCID ranged from 4.37–19.84 and 4.37–19.84, respectively. Importantly, Peyton noted that the MCID estimates reported in these analyses could aid in the clinical interpretation of health-related QoL in patients with LG-IR-NMIBC, thus enabling clinicians to evaluate the impact of different treatment interventions.
PROs are vital when evaluating existing and emerging treatments, alongside safety and efficacy. Peyton highlighted how healthrelated QoL data can inform both patients and HCPs about the impact of treatment on patient QoL, and indicated that QoL questionnaires such as the EORTC QLQNMIBC24 should be used to supplement decision-making both in clinical trials and during patient-HCP discussions.
Considering Patient-Reported Outcomes of Hydrogel-Based Chemotherapy for Non-muscle Invasive Bladder Cancer
With symptom burden and health-related QoL being critical concerns for bladder cancer patients,10 investigating the impact of emerging therapies on QoL is key. At AUA 2025, Peyton presented a poster detailing PROs following treatment of LG-NMIBC with hydrogel-formulated intravesical
mitomycin across three clinical trials: ATLAS (n=142),13 ENVISION (n=240),14 and OPTIMA II (n=63).15,16
The OPTIMA II Study
The OPTIMA II study was an open-label, single-arm, Phase II trial with patients recruited from 20 sites in the USA and Israel after a positive biopsy result for LG-IR-NMIBC.15 A total of 63 patients were treated with six once-weekly instillations of mitomycin intravesical solution (1.33 mg/mL), and 57 patients received all six doses. The primary outcome was complete response (CR), which was defined as visual confirmation and negative wash urine cytology and for-cause biopsy. At the 3-month primary endpoint evaluation, 65% of patients (n=41) patients achieved CR. Of these, 95% (n=39), 73% (n=30), and 61% (n=25) of patients remained disease-free at 6-, 9-, and 12-months post-treatment, respectively. Common adverse events with an incidence of ≥10% included an increase in urinary frequency and urgency, dysuria, haematuria, UTI, and fatigue.
Patient-Reported Outcomes Following Intravesical Mitomycin Treatment
PROs were evaluated using the previously validated12 EORTC-QLQ-NMIBC24 at baseline, 3 months, and 12 months. Peyton highlighted from the ENVISION study that 80% of patients treated with intravesical
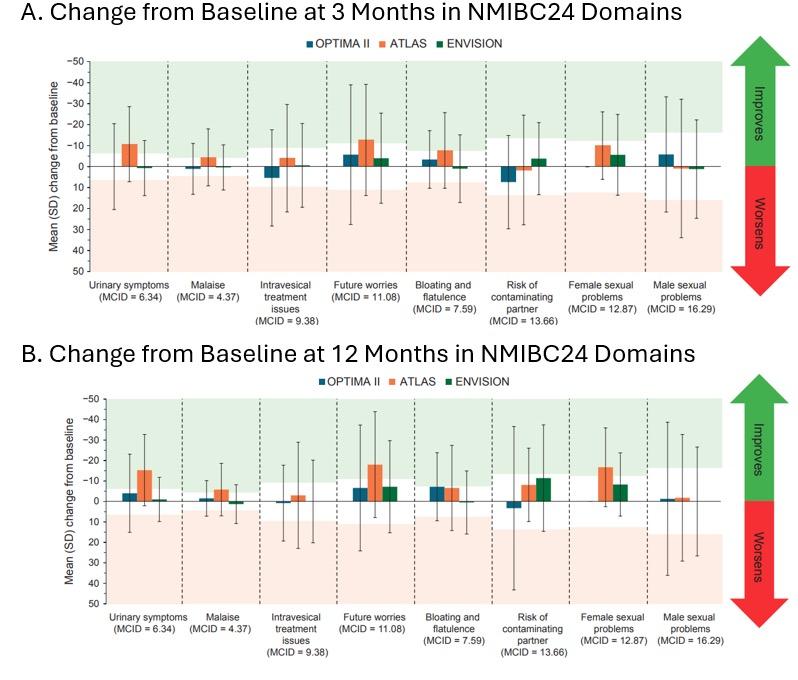
Figure 1:
Figure 1: Change from baseline in patient-reported outcomes following intravesical mitomycin treatment. Continued.
Patients involved in three clinical trials, OPTIMA II (n=63), ENVISION (n=240), and ATLAS (n=142), who had received six once-weekly instillations of intravesical mitomycin were evaluated using the EORTC-QLQ-NMIBC24 to inform patient reported symptom burden at baseline, 3 months, and 12 months after treatment. Outcomes after 3 (Figure 1A) and 12 (Figure 1B) months are presented as mean ± standard deviation. Previous work identified the MCID for each outcome,12 with green and red shaded areas to indicate the MCID threshold for improvement and worsening, respectively, per outcome. Mean PROs did not surpass the ‘worsening’ MCID thresholds for any outcomes.
Figure adapted from Peyton et al.16 2025 MCID: minimal clinically important difference; NMIBC: non-muscle-invasive bladder cancer; SD: standard deviation.
mitomycin achieved a CR at 3 months, with an 82% probability of remaining in response 12 months later.14.16
Patients enrolled in the three studies were predominantly male (65%) and had a median age of 69 years. At baseline, patients reported a high level of functioning and low symptom burden. Peyton explained that treatment with hydrogel-formulated intravesical mitomycin did not result in sustained decrements in functioning and symptom burden. Previous work identified the MCID,12 the difference in scores that would be considered clinically meaningful. Change in scores from baseline can be classified as either ‘improving’ or ‘worsening’ QoL using the MCID. At 3- and 12-months post-treatment, mean PRO scores did not surpass the ‘worsening’ MCID thresholds for any outcomes, as illustrated in Figure 1, indicating that treatment with intravesical mitomycin did not negatively impact QoL.
Peyton described meaningful improvements in urinary symptoms, malaise, and future worries at both 3- and 12-month visits in
the ATLAS trial. At 3 months, meaningful improvements in bloating and flatulence were also observed, whereas at 12 months, improvements to female sexual problems were observed.13 Peyton described that intravesical mitomycin provides a potential non-surgical treatment option that avoids repeat invasive procedures and maintains, and in some cases improves, QoL for patients with LG-IR-NMIBC.
Hydrogel-Based Chemotherapy for Urothelial Carcinomas
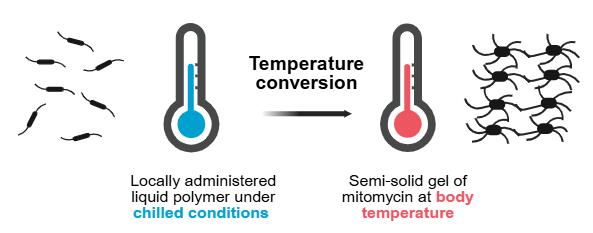
The ATLAS13 and ENVISION14 trials were based on the treatment of LG-IR-NMIBC with a reverse thermal hydrogel containing mitomycin, illustrated in Figure 2. Such nonsurgical treatment alternatives for urological cancers aim to combat many of the adverse effects of surgical treatments, including physiological side effects and patientreported QoL factors, while also improving treatment durability.
OPTIMA II ATLAS ENVISION
The gel has reverse thermal properties: when it is administered as a cooled solution, it is viscous but fluid enough to conform to the urinary tract anatomy. As the gel reaches body temperature, its viscosity increases to become a semi-solid gel which dwells in the ureter and renal pelvis, providing a sustained exposure of mitomycin.20
Figure is based on information from Urogen20 and created with BioRender.com.
A hydrogel-based chemotherapy with mitomycin was approved by the FDA in April 2020 for the treatment of patients with LGUTUC.17, 18 This approval was based on data from the OLYMPUS trial, where mitomycin for pyelocaliceal solution (4 mg/mL) was used as a primary treatment for LG-UTUC, resulting in clinically significant disease eradication.19 Pyelocaliceal solution refers to the administration into the renal pelvis and calyces of the kidney. It is approved for retrograde administration via a ureteral catheter or antegrade administration through a nephrostomy tube.17 The delivery system and reverse thermal properties (Figure 2) of the gel ensure that the mitomycin solution coats the upper urinary tract.
The OLYMPUS Trial
The OLYMPUS trial19 was an open-label, single-arm, Phase III trial that recruited patients from 24 academic sites across the USA and Israel. In total, 71 patients with new or recurrent LG-UTUC were treated with six once-weekly instillations of mitomycin for pyelocaliceal solution (4 mg/mL) via retrograde catheter. Of these patients, 61 received all six instillations. The primary outcome was CR, defined as a negative 3-month ureteroscopic evaluation, negative cytology, and negative for-cause biopsy. Of the enrolled patients, 58% (n=41) had
a CR at the primary endpoint evaluation (around 3 months). Of the patients with a CR, the median follow-up was 11.0 months (interquartile range [IQR]: 5.1–12.4). The most frequently reported all-cause adverse events were ureteric stenosis in 44% (n=31), UTI in 32% (n=23), haematuria in 31% (n=22), flank pain in 30% (n=21), and nausea in 24% (n=17) of 71 patients. Overall, 25% (n=19) of 71 patients had study drug-related or procedure-related serious adverse events (SAE). No deaths were regarded as related to treatment.
Long-Term Durability of Hydrogel Mitomycin for Upper Tract Urothelial Carcinoma
At AUA 2025, Brian Hu, Associate Professor of Urology at Loma Linda University, California, USA, presented a long-term follow-up (LTFU) from patients included in the OLYMPUS trial.21,22 The 41 patients who achieved a CR during the trial, were followed up for 12 months after treatment with optional monthly maintenance doses of mitomycin in the same hydrogel formulation. At 12 months, 23 patients remained in CR and, at 15 months, 20 patients remained at CR and entered the LTFU study. The LTFU was a non-interventional study where
Figure 2: Reverse thermal hydrogel.
Kaplan–Meier estimate of DoR in patients with CR at 3 months
Patients with confirmed LG-UTUC (n=71) were treated with six once-weekly instillations of hydrogel-formulated mitomycin (4 mg/mL) for pyelocaliceal administration. Patients who remained in CR (negative 3-month ureteroscopic evaluation, negative cytology, and negative for-cause biopsy) after 12 months were included in the LTFU study (n=20). Kaplan–Meier survival analysis was conducted, with an estimated DoR of 47.8 months (95% CI: 13.0–NE) for all patients who received CR in the OLYMPUS trial.
supervising physicians provided semiannual updates on each patient’s disease status for 5 years until disease recurrence, progression or death.
For all patients who achieved CR in the OLYMPUS trial (n=41), the median followup was 28.1 months (95% CI: 13.1–57.5), with a Kaplan–Meier estimated duration of response (DoR) of 47.8 months (95% CI: 13.0–not estimable [NE]). Kaplan–Meier survival analysis is illustrated in Figure 3. In patients who entered the LTFU study (n=20), the median follow-up was 53.5 (95% CI: 27.9–65.3) months, with a DoR NE due to the low event rate (95% CI: 43.5–NE). No difference was reported between patients with new onset UTUC at baseline
compared to those who had experienced recurrences before treatment. Of the patients included in the LTFU, 75% had no evidence of recurrence at the last followup, 10% of patients (n=2) experienced UTUC tumour recurrence, and 15% (n=3) of patients died, reported as unrelated to study treatment. These data illustrate a clinically meaningful long-term response in patients treated with hydrogel-formulated mitomycin, which lasted on average nearly 4 years (47.8 months–3.9 years), irrespective of whether the patient enrolled into the OLYMPUS clinical trial with multiple previous recurrences.
Hu explained that, although the study was a post hoc analysis,21 the data presented
Figure 3: Kaplan–Meier estimate of duration of response in patients from the OLYMPUS trial.
give insight into the long-term durability of hydrogel formulation chemotherapies for UTUC. Hu then described an ongoing uTRACT registry23 that will build on the insights from the LTFU study by providing an opportunity to collect and evaluate real-world data in a larger sample, to further inform the use of mitomycin for pyelocaliceal solution in patient with UTUC.
Hydrogel-Based Chemotherapy for Non-muscle Invasive Bladder Cancer: Ongoing Clinical Research
Following the FDA approval of a reverse thermal hydrogel formulation of mitomycin for UTUC, ongoing trials are evaluating the safety and efficacy of an intravesical formulation of mitomycin in reverse thermal hydrogel as a non-surgical treatment option for LG-IR-NMIBC. At AUA 2025, data were presented from a LTFU of the OPTIMA II Phase II study24 and from the ENVISION Phase III study,25 both assessing the intravesical administration of mitomycincontaining reverse thermal hydrogel as a treatment for LG-IR-NMIBC.
Long-Term Durability of Hydrogel Mitomycin for Non-muscle Invasive Bladder Cancer
Neal Shore, Medical Director of the Carolina Urologic Research Center and Doctor of Urology at the Atlantic Urology Clinics, Myrtle Beach, South Carolina, USA, presented results from LTFU of the Optima II trial.24 Twenty-five patients remained in CR at 12 months and 17 of these patients were included in the LTFU study. This non-interventional study followed patients over 4 years or until disease recurrence, progression, or death. Disease status was reported by physicians, who gave semi-annual updates on each patient. In the OPTIMA II study, most patients had recurrent disease at baseline (77.8%) and had undergone multiple TURBT procedures prior to enrolment. Following intravesical mitomycin treatment, the median Kaplan–Meier estimate of DoR was 24.2 months (95% CI: 9.72–47.18), with a median followup time of 33.6 months (95% CI: 10.78–
42.94). Overall, 53.7% (n=22) of patients experienced recurrence, with the majority of these patients (n=20) having low-grade disease. One patient progressed to highgrade disease and one patient died due to a cardiac disorder. At the end of the LTFU, five patients remained disease free. Shore described how these results demonstrate a clinically meaningful long-term response from intravesical mitomycin treatment, and that this treatment may represent a durable and well-tolerated non-surgical alternative to TURBT for patients with LG-IR-NMIBC.
Following the successful completion of the Optima II trial, the ENVISION trial14,26 is now ongoing. It is a single-arm, openlabel, Phase III trial to investigate the safety and efficacy of intravesical mitomycin as treatment for patients with LG-IR-NMIBC.
The ENVISION Trial Results and LongTerm Follow-Up
Following screening and enrolment, 240 patients received six once-weekly intravesical instillations of hydrogel formulation mitomycin (1.33 mg/mL). All patients received at least one of the six planned doses in an outpatient setting and 228/240 patients received all six doses. All patients were assessed for the primary endpoint: CR at around 3 months after the first instillation. CR was defined as negative white light cystoscopy, negative urine cytology and, when required, a negative for-cause biopsy. Patients with a CR at 3 months entered the LTFU period of the study. Patients with a non-CR underwent investigator-designated standard of care treatment of remaining lesions, then entered the LTFU. The LTFU portion of the study is expected to run until 2028, with patients monitored every 3 months until recurrence, progression, death, or end of study at 63 months. Upon first recurrence or progression, patients are offered investigator-designated standard of care treatment of lesions, followed by an end of study evaluation 3 months later.
At AUA 2025, Sandip Prasad, Doctor of Urology at Morristown Medical Center, Atlantic Health System, Garden State Urology, Morristown, New Jersey, USA,
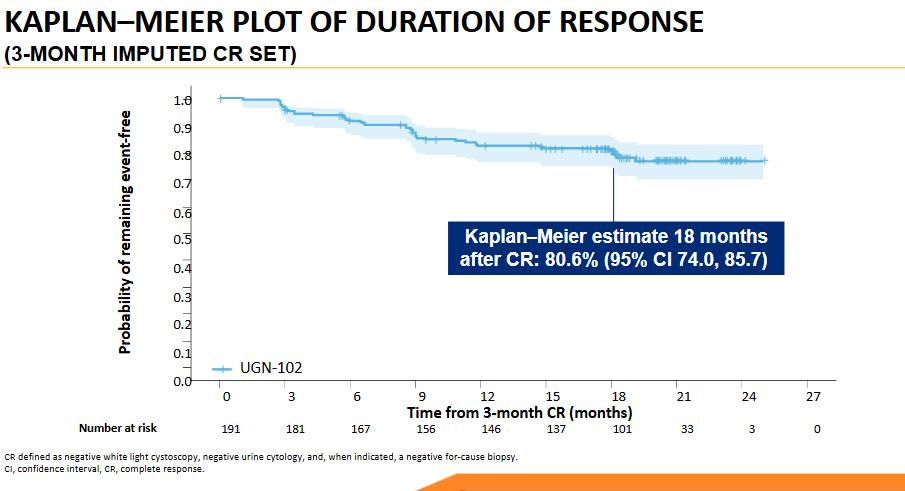
Patients with confirmed LG-IR-NMIBC (n=240) were treated with six weekly instillations of hydrogel-formulated mitomycin (1.33 mg/mL) for intravesical administration. Patients who remained in CR (negative white light cystoscopy, negative urine cytology and, when required, a negative for-cause biopsy) after 3 months were included in the LTFU study (ongoing). Kaplan-Meier survival analysis was conducted on 3-month CR data.24
presented ongoing results from the primary endpoint evaluation of the ENVISION study.24,26 At 3 months, a high proportion (79.6%) of patients had a CR. To inform potential treatment durability, the 3-month CR dataset was used to estimate DoR using Kaplan Meier survival analysis (Figure 4). For patients who achieved CR at 3 months, the probability of remaining event-free 18 months later was estimated at 80.6%.
Prasad described the treatment as welltolerated and provided insight into the side effects reported at the 3-month follow up. Treatment-emergent adverse events (TEAE) were reported as follows: 22.5% (n=54) of patients with dysuria, 8.3% (n=20) with haematuria, 7.1% (n=17) with UTI, 6.7% (n=16) with frequent urination, and 5.4% (n=13) of patients reported fatigue. Two instances of urinary retention and atrial fibrillation were
reported. Single instances of metastatic lung cancer, cerebrovascular accident, and pancreatic adenocarcinoma were reported; however, all were unrelated to treatment as per principal investigator judgment. Three patients died from pneumonia, cardiac failure, or unknown reason, all of which were assessed as unrelated to treatment. Two treatment-relate SAEs were reported: urethral stenosis in one patient (0.4%) and urinary retention in one patient (0.4%), both of which resolved.
Prasad described the CR, durability of response, and benefit-risk profile of intravesical hydrogel-formulated mitomycin as favourable, supporting its further investigation as a non-surgical alternative for LG-IR-NMIBC patients.
Figure 4: Kaplan-Meier estimate of duration of response in patients from the OLYMPUS trial.
Hydrogel-Based Immunotherapy for Non-muscle Invasive Bladder Cancer: Emerging Insights
Immunotherapy is a well-established treatment option for NMIBC. The Bacille Calmette-Guérin (BCG) vaccine is used routinely for preventing or delaying tumour recurrence following high-grade NMIBC resection.4 BCG is administered intravesically to trigger a local immune response within the bladder, activating immune cells including macrophages and T cells to target and destroy cancer cells. Although most patients have an initial response, over 50% of initial responders will experience recurrence or progression,4 illustrating the need for new, more durable treatment options.
Phase I Study: Zalifrelimab for NMIBC
At AUA 2025, Jay Raman, Professor and Chair in the Department of Urology and Department of Surgery at Penn State Cancer Institute, Hershey, Pennsylvania, USA, presented the results from a Phase I, dose-escalation study investigating hydrogel formulated zalifrelimab for the treatment of recurrent NMIBC.27 Zalifrelimab is a monoclonal antibody against cytotoxic T-lymphocyte antigen-4 (CTLA-4) which functions as an immune checkpoint inhibitor, by neutralising the inhibitory effect of CTLA-4 on T cell activation.27
The data reported at AUA 2025 were part of an ongoing, multi-component clinical trial with up to 30 patients included per arm.27 Arm A, reported by Raman at AUA 2025, investigated the safety, efficacy, and pharmacokinetics of intravesically administered, hydrogel-formulated zalifrelimab monotherapy as a dose escalation study.
Arms B and C are currently ongoing (as of April 2025)28 and will investigate a dose escalation of hydrogel formulated zalifrelimab in combination with imiquimod (Arm B), and gemcitabine (Arm C), respectively.28 Imiquimod, a toll-like receptor 7 agonist with immune-stimulating anti-tumour effects, and gemcitabine, a chemotherapy agent, will be administered
intravesically in a non-hydrogel formulation prior to the instillation of reverse thermal hydrogel-formulated zalifrelimab.28,29
In Arm A, key inclusion criteria included patients with recurrent NMIBC with lowgrade disease or high-grade disease (Stages Ta or T1) and/or carcinoma in situ (CIS), who had failed at least one prior course of intravesical therapy. For enrolment, patients were required to have had resection of papillary tumours and obvious areas of CIS fulgurated during screening or within 6 weeks prior to screening.
During the study, patients received six weekly intravesical instillations of hydrogelformulated zalifrelimab across four cohorts: 100 mg (n=3), 300 mg (n=6), 500 mg (n=8), and 700 mg (n=3). A total of 20 patients received at least one dose, and 19 patients received all six doses. Raman reported a favourable safety profile from trial Arm A. The reported TEAEs were mild or moderate in severity except for one severe event, a Grade 3 UTI which was considered related to the procedure, but not the treatment, and did not result in treatment discontinuation. The most common TEAEs were dysuria, haematuria, urinary retention, UTI, headache, and nausea. Raman commented that no dose-dependency of TEAEs or dose-limiting toxicities were observed.
Patients that received at least one treatment dose, and completed the efficacy assessment, were evaluated in this study. Of the evaluated patients, 46.2% (n=6/13) with Ta/T1 disease and 33% (n=3/6) with CIS +/- Ta/T1, respectively, were recurrence free or had a CR at 3 months after initial instillation. During follow-up, one patient in the 100 mg cohort with high-grade Ta disease remained recurrence-free at 9 months; 75% (n=3/5) patients in the 300 mg cohort with Ta/T1 disease remained recurrence-free at 15 months; and 25% (n=1/4) of patients in the 500 mg cohort with Ta/T1 disease remained recurrencefree at 6 months.
Across all dose cohorts, the median duration of detectable zalifrelimab in urine was ≥9.7 hours at Week 1 and Week 6. The maximum concentration in urine (Cmax)
plateaued at 500 mg. Systemic exposure was only detected in one patient who was part of the 700 mg cohort. In this patient, exposure was 50-fold lower than that achieved with systemic administration and was 2,550-fold lower than the urine Cmax. Raman concluded that the intravesical delivery of hydrogel-formulated zalifrelimab allowed sustained exposure of the drug to the target organ, the bladder, while limiting systemic exposure, thus mitigating the risk of systemic immune-related toxicities associated with CTLA-4 inhibition.27
References
1. American Cancer Society (ACS). Cancer facts & figures 2024. Available at: https://www.cancer.org/research/ cancer-facts-statistics/all-cancerfacts-figures/2024-cancer-factsfigures.html. Last accessed: 1 April 2025.
2. Babjuk M et al. European Association of Urology guidelines on non-muscleinvasive bladder cancer (TaT1 and carcinoma in situ) - 2019 update. Eur Urol. 2019;76:639-57.
3. Monteiro LL et al. ICUD-SIU International Consultation on Bladder Cancer 2017: management of nonmuscle invasive bladder cancer. World J Urol. 2019;37:51-60.
4. Lebacle C et al. BCG-unresponsive high-grade non-muscle invasive bladder cancer: what does the practicing urologist need to know?. World J Urol. 2021;39:4037-46.
5. Chang SS et al. Diagnosis and treatment of non-muscle invasive bladder cancer: AUA/SUO guideline. J Urol. 2016;196:1021.
6. National Comprehensive Cancer Network (NCCN). Bladder cancer (version 4.2021). 2021. Available at: https://www.nccn.org/guidelines/ guidelines-detail?category=1&id=1417. Last accessed: 30 September 2021.
7. van Rhijn BWG et al. Prognostic value of the WHO1973 and WHO2004/2016 classification systems for Grade in primary Ta/T1 non-muscle-invasive bladder cancer: a multicenter European Association of Urology Non-muscle-invasive Bladder Cancer Guidelines panel study. Eur Urol Oncol. 2021;4(2):182-91.
8. Cutress ML et al. Ureteroscopic
Conclusion and Outlook
Surgical treatment for urological cancers often lacks durability, requiring multiple procedures due to disease recurrence or progression. These data presented at AUA 2025 highlight the potential of reverse thermal gel formulations of anticancer agents, including mitomycin as an effective alternative to repetitive surgeries for treating different forms of low-grade urothelial cancers, and zalifrelimab for the treatment of recurrent NMIBC. Future work is ongoing to further evaluate the safety and efficacy of these investigational therapies, with the hope of providing an alternative to surgery for patients with NMIBC, as has been demonstrated with LG-UTUC.
and percutaneous management of upper tract urothelial carcinoma (UTUC): systematic review. BJU Int. 2012;110(5):614-28.
9. Shvero A et al. Strategies of endoscopic management of upper tract urothelial carcinoma among endourologists: a global survey. J Pers Med. 2023;13(4):591
10. National Institutes of Health: National Cancer Institute. Bladder Cancer Symptoms. Available at: https://www. cancer.gov/types/bladder/symptoms. Last accessed: 1 April 2025.
11. European Organisation for Research and Treatment of Cancer. EORTC QLQNMIBC24 questionnaire. Available at: https://qol.eortc.org/questionnaire/ qlq-nmibc24/. Last accessed: 31 March 2025.
12. Peyton CP et al. Psychometric validation of a quality of life scale in patients with low-grade intermediaterisk non-muscle invasive bladder cancer. Poster 25-5998. AUA2025, 26-27 April, 2025.
13. Prasad SM et al. Treatment of low-grade intermediate-risk non muscle-invasive bladder cancer with UGN-102 ± transurethral resection of bladder tumor compared to transurethral resection of bladder tumor monotherapy: a randomized, controlled, Phase 3 trial (ATLAS). J Urol. 2023;210(4):619-29.
14. Prasad SM et al. Primary chemoablation of recurrent low-grade intermediaterisk nonmuscle-invasive bladder cancer with UGN-102: a single-arm, openlabel, Phase 3 trial (ENVISION). J Urol. 2025;213(2):205-16.
15. Chevli KK et al. Primary chemoablation of low-grade intermediate-risk
nonmuscle-invasive bladder cancer using UGN-102, a mitomycincontaining reverse thermal gel (Optima II): a Phase 2b, open-label, single-arm trial. J Urol. 2022;207(1):61-9.
16. Peyton CP et al. Patient-reported outcomes following treatment of lowgrade intermediate risk non-muscle invasive bladder cancer with UGN102. Poster 25-2306. AUA2025, 26-27 April, 2025.
17. U.S. Food and Drug Administration. FDA approves mitomycin for lowgrade upper tract urothelial cancer. 2020. Available at: https://www.fda. gov/drugs/resources-informationapproved-drugs/fda-approvesmitomycin-low-grade-upper-tracturothelial-cancer. Last accessed: 1 April 2025.
18. Urogen. Prescribing information: JELMYTO™ (mitomycin) for pyelocalyceal solution. 2020. Available at: https://www.accessdata. fda.gov/drugsatfda_docs/ label/2020/211728s000lbl.pdf. Last accessed: 11 April 2025.
19. Kleinmann N et al. Primary chemoablation of low-grade upper tract urothelial carcinoma using UGN101, a mitomycin-containing reverse thermal gel (OLYMPUS): an openlabel, single-arm, phase 3 trial. Lancet Oncol. 2020;21(6):776-85.
20. UroGen Pharma. RTGel™ technology. Available at: https://www.urogen.com/ our-portfolio/rtgel-technology. Last accessed: 1 April 2025.
21. Hu B et al. Long-term outcomes of primary chemoablation of low-grade upper tract urothelial carcinoma with UGN-101, a mitomycin reverse thermal gel. Poster 25-5939. AUA2025, 26-27 April, 2025.
22. Pierorazio PM et al. Long-term outcomes of primary chemoablation of low-grade upper tract urothelial carcinoma with UGN-101, a mitomycin reverse thermal gel. J Urol. 2025;213(3):313-22.
23. UroGen Pharma. uTRACT Jelmyto Registry: a registry of patients with upper tract urothelial cancer (UTUC) treated with Jelmyto (uTRACT). NCT05874921. https://clinicaltrials. gov/study/NCT05874921.
24. Shore ND et al. Treatment of lowgrade intermediate-risk non-muscle invasive bladder cancer with UGN-102: long-term outcomes of the OPTIMA II study. Poster 25-5953. AUA2025, 2627 April, 2025.
25. Prasad S et al. Treatment of recurrent low-grade intermediate-risk nonmuscle invasive bladder cancer (LGIR-NMIBC) with UGN-102: results from the pivotal Phase 3 trial (ENVISION). PD12-01. AUA2025, 26-27 April, 2025.
26. UroGen Pharma. A Phase 3 singlearm study of UGN-102 for treatment of low-grade intermediate-risk non-muscle invasive bladder cancer (ENVISION). NCT05243550. https:// clinicaltrials.gov/study/NCT05243550.
27. Raman M et al. Treatment of recurrent non-muscle invasive bladder cancer with UGN-301 (zalifrelimab): results of a Phase 1 dose escalation study. Poster 25-2306. AUA2025, 26-27 April, 2025.
28. UroGen Pharma. A Phase 1 doseescalation Study of UGN-301 in patients with recurrent non-muscle invasive bladder cancer (NMIBC). NCT05375903. https://clinicaltrials. gov/study/NCT05375903.
29. Creasy et al. A phase 1 dose-escalation study of UGN-301 (Zalifrelimab) as monotherapy and in combination with other agents in patients with recurrent non-muscle invasive bladder cancer (NMIBC). Poster 206. SUO 2024, 4-6 December, 2024.
Acne Treatment Review and Present Perspectives
Interviewees:
Sandeep Cliff,1 Alison Layton2
1. Surrey and Sussex University Healthcare Trust, Redhill, UK
2. Harrogate and District NHS Foundation Trust, Harrogate, UK
Disclosure: Layton has received sponsorship and/or funding from Almirall, Alliance, Beiersdorf, Galderma, Glenmark, La Roche-Posay, L’Oreal, LEO Pharma, Mylan, Novartis, Sanofi, Viatris, and Vanoka. Cliff has received sponsorship and/or funding from Galderma, LEO Pharma, and Pfizer.
Acknowledgements: Writing assistance was provided by Helen Boreham, HB Medical (UK) Ltd, Wetherby, UK.
Disclaimer:
Prescribing information for WINLEVI▼(clascoterone) can be found here Adverse events reporting information can be found at the bottom of this article.
Winlevi is contraindicated in hypersensitivity to clascoterone or to any of the excipients.
Winlevi is for external use only. Not for ophthalmic, oral or vaginal use. Winlevi should not be applied to cuts, abrasions, eczematous or sunburned skin. Accidental transfer of cream into eyes, mouth or other mucous membranes should be avoided. If contact with mucous membranes occurs, rinse thoroughly with water.
Clascoterone may induce local irritation (oedema, erythema/redness, pruritus, scaling/ dryness, skin atrophy, stinging/burning, striae rubrae, telangiectasia). Concomitant use with other potentially irritating topical products should be limited.
Hypothalamic-pituitary-adrenal HPA axis suppression was observed and may occur during or after treatment with clascoterone. Conditions, which augment systemic absorption, include use over large surfaces areas, prolonged use and the use of occlusive dressings. If HPA axis suppression develops, consider withdrawing the medicinal product.
Elevated potassium levels were observed in some subjects treated with Winlevi or with the vehicle during the clinical trials.
This medicinal product contains excipients including: - 25 mg cetyl alcohol in each gram. Cetyl alcohol may cause local skin reactions (e.g. contact dermatitis).
- 250 mg propylene glycol in each gram. Propylene glycol may cause skin irritation.
Support: The publication of this article was initiated and funded by Glenmark Pharmaceuticals Ltd.
Interview Summary
Acne is a chronic inflammatory skin disease whose visible effects can have a significant psychological impact on patients. A multimodal approach to acne management is vital in order to target the four interlinked pathological processes that underpin this common skin condition. During interviews conducted by EMJ, Sandeep Cliff, Consultant Dermatologist at Surrey and Sussex University Healthcare Trust, and Alison Layton, Consultant Dermatologist from Harrogate and District NHS Foundation Trust, both in the UK, explored the burden, pathophysiology, and current and future landscape of acne treatment. Experts highlighted existing unmet needs in acne care and explained how therapeutic innovations, such as the novel androgen receptor inhibitor clascoterone, may help to reshape acne management in daily clinical practice moving forward.
PATHOPHYSIOLOGY AND BURDEN OF ACNE
Acne is a chronic and inflammatory skin condition characterised by the presence of both comedonal and inflammatory lesions, primarily on the face but also affecting the chest and back.1 “It affects a significant number of patients at some time in their life,” noted Cliff. “Up to 70% of teenagers and young people have acne, but it can also affect older patients as well.”2
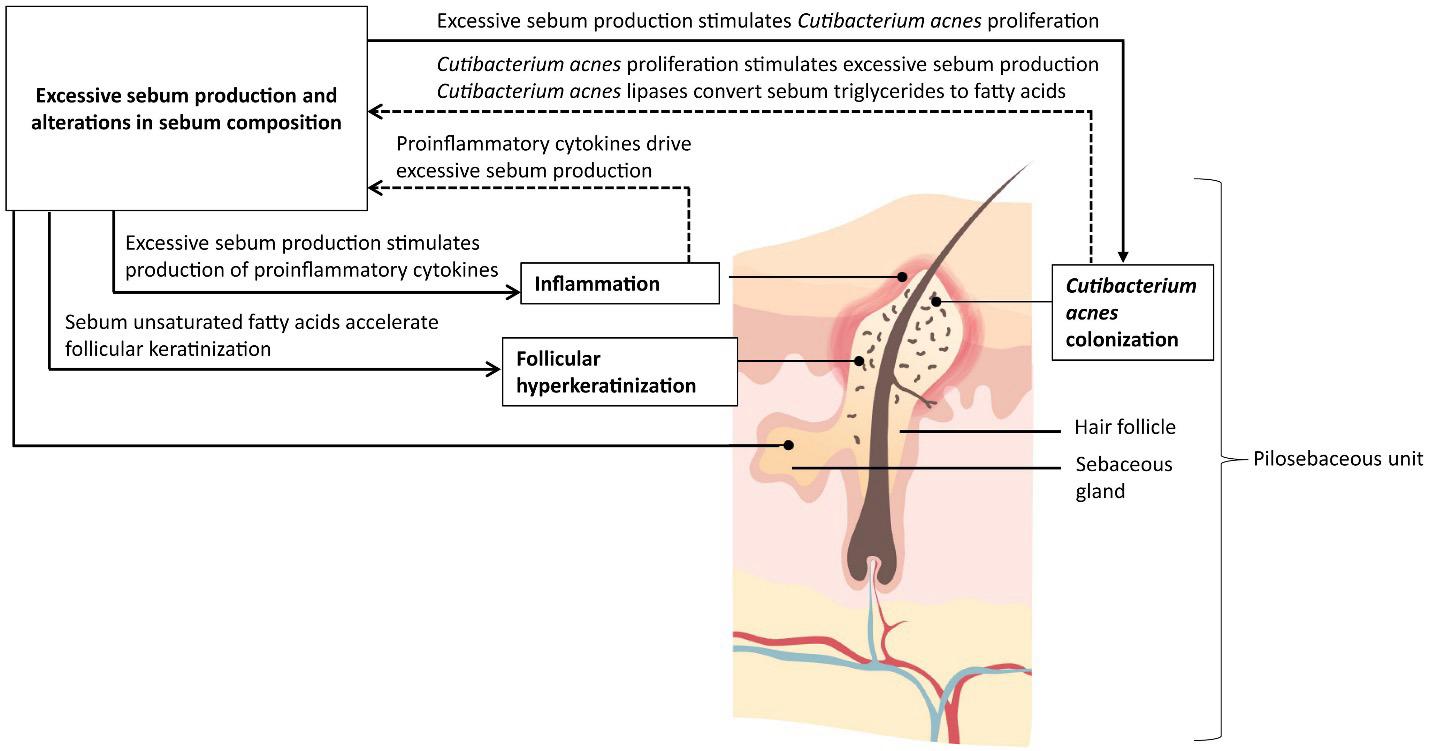
Layton explained that four pathophysiological pillars underpin acne development: excess sebum production, follicular hyperkeratinisation, colonisation and proliferation of Cutibacterium acnes (C. acnes), and inflammation.3 She elaborated: “Dysregulation of the sebaceous gland is very much androgen-mediated and driven by hormones, particularly at puberty.
Those androgens also produce abnormal epithelial proliferation and differentiation of keratinocytes within the intrafollicular duct, and that provides a really favourable milieu for anaerobic Cutibacterium bacteria, which proliferate and colonise. This results in both innate and adaptive immune responses, which lead to the typical inflammatory lesions we see in acne. Many of these are responses triggered by Cutibacterium acnes.”
Both experts emphasised the pivotal role of androgens in acne pathogenesis, with activation of androgen receptors leading to excessive sebum production in the skin (Figure 1).3 “Acne is centred around the pilosebaceous unit, which is responsible for driving the production of sebum onto the skin,” Cliff explained. “The principal problem with acne is that the pilosebaceous unit is producing lots of sebum and this, coupled with other changes, leads to the development of acne.”
Acne is associated with well-documented negative effects on quality of life and may prove emotionally devastating for adolescents at the stage of life when selfimage is paramount.1 “Not only can acne itself have physical effects, it can be inflammatory, sore, painful, and weepy, but it has an impact on mental health as well,” stressed Cliff. “Low self-esteem can affect patients’ ability to function, and they can become depressed and have anxiety. So, it has a dual effect on patients, which I think is sometimes underestimated by many healthcare professionals and society at large.” The damaging psychological sequelae of acne were reiterated by Layton, who pointed to the results of a recent acne impact study that found that acne-related appearance concerns were associated with significant mental health issues, including depression, anxiety, and even suicide in some cases.4
Both experts blamed social media and today’s increasingly ‘cosmetic environment’ for heightening the negative impacts of acne. “For young people, their self-esteem comes from presenting themselves well on a day-to-day basis, which means anything that destroys their appearance can have a negative impact on their mental health,” explained Cliff.
Layton also noted that visible acne could be associated with significant stigmatisation and bias in how those affected are perceived by the wider population. “And, of course, the other big burden is that acne can go on to produce scarring,” Layton stated. “About 90% of patients will get some degree of scarring, and we have very few effective treatments for scarring, and in many cases it is permanent. In some patients, especially with skin of colour, we can see problems with hyperpigmentation, which again produces burden in its own right and is often long-lasting,” she explained.
Figure 1: The contribution of sebum to acne pathophysiology.
TREATMENT LANDSCAPE AND UNMET NEEDS
The main treatment options for acne indicated for use in the UK are topical agents, oral antibiotics, and isotretinoin.5 Layton explained that fixed combination topical products are currently recommended as first-line options in the majority of leading acne guidelines, including the National Institute for Health and Care Excellence (NICE).5,6 “Some of the fixed combination products are actually licensed for moderate-to-severe disease and not just mild-to-moderate, so that’s our starting point, and then if patients are not responding, we would consider adding an oral antibiotic; however, there are concerns about using antibiotics for more than 6 months,” Layton outlined.
In the clinical practice setting, Cliff emphasised the importance of assessing the dominant feature of a patient’s acne and directing treatment according to the principal pathology. “For general management of acne, the idea is to reduce the skin’s oil production. However, if a patient has inflammatory lesions that are probably precipitated or provoked by bacteria, then you want to use antiinflammatory agents, such as an antibiotic, which is given orally or topically,” he explained. “The advantage of that is it’s relatively easy for most patients to take a tablet or to apply a topical preparation. However for many young adults compliance can be a real issue, so effective treatments which have non complicated regimes are favourable in practice.”
For severe acne, experts agreed that isotretinoin is a highly effective therapeutic option. As Cliff described: “It is an oral retinoid that binds to the retinoid receptors in the pilosebaceous units and significantly reduces sebum production in the skin. It also reduces hyperkeratinisation, so it helps to stop the blockage of the pilosebaceous units, and by doing so, it is also thought to have an anti-inflammatory effect on the skin. So, it helps to reduce acne, sometimes definitively, sometimes temporarily.”
However, Cliff cautioned that isotretinoin is also associated with side effects such as teratogenicity and mood and behaviour changes, “some of which have only recently come to the surface”.7 “One should exert a degree of caution, I think, in patients who’ve got issues with mental health, and be careful when instituting isotretinoin. However, more data are coming through showing that isotretinoin itself does not induce depression and that not treating the acne effectively may do more harm than good, so it is important not to deter patients from what is a very effective treatment that is used widely in practice.”
Cliff also noted that, despite clinicians continuing to advocate for the benefits of isotretinoin, patients themselves are now increasingly reluctant to try the drug given the negative media coverage of potential psychological adverse events. “The shoe is on the other foot now because patients, quite rightly, are making decisions about how they wish their care to be delivered,” he remarked. “So a good patient-clinician relationship is needed so that the most effective treatment is offered with the patient being fully informed in the decision-making process.”
Beyond these three key treatment modalities for acne, Cliff mentioned prescription preparations such as oral contraceptives and oral aldosterone antagonists, although he emphasised that these products are not currently licensed for acne in the UK. He also alluded to the range of other nonprescription topical acne products which are available over the counter.
The Importance of a Multimodal Approach
The need to adopt a multimodal approach to acne management in daily dermatology practice was emphasised by both experts. Cliff explained that acne has many different facets, including excess sebum production and inflammatory processes in the skin, which require different strategies to target effectively. “The approach must be multifaceted; otherwise, you will end up treating one component of the acne, not the whole package,” he insisted.
Layton suggested that the reason for isotretinoin’s unparalleled clinical efficacy may lie in its ability to either directly or indirectly impact all four of the main pathophysiological features of acne.
“Isotretinoin has a multimodal mechanism of action in its own right,” she surmised.
“But all these other treatments are just looking at one or two of the pathophysiological factors implicated in acne aetiology. So, in order to actually try and address all of them, we need to be using more than one therapy.”
Current Gaps in Acne Care
Considering the unmet needs that exist with current acne therapies, Cliff highlighted compliance, side effects, and lack of response/breakouts as essential issues. He explained that compliance is a particular challenge given the principally teenage patient population and that side effects of topical agents, such as bleaching with benzoyl peroxide (BPO) and skin drying with topical retinoids, can also further exacerbate this problem. “Patients do not want to use a product that, in their eyes, makes them look worse and feel worse than when they came to see us in the first place, so that’s where there is a definite vacuum that we need to address,” he remarked. Cliff also noted that patients require more effective treatment options to help manage occasional acne breakouts without resorting to ‘aggressive’ therapies such as antibiotics and isotretinoin.
On the subject of isotretinoin, Layton also highlighted the current ‘controversy’ around its positioning for acne treatment in the UK. “The Medicines and Healthcare products Regulatory Agency (MHRA) has reviewed the use of isotretinoin and has reminded prescribers that it is licensed for severe disease, including acne that is at risk of permanent scarring that has not responded to previous and adequate combination therapies,” she expounded.8 “So, there are numerous patients sitting in that moderate disease category that isotretinoin now isn’t licensed for.” The additional measures put in place by the MHRA include the need for two independent prescribers to agree on the initiation of isotretinoin in patients under 18
years, new counselling requirements about potential mental health and sexual function side effects, and assessment of mental health and sexual function before starting treatment, as well as monitoring during treatment.8
“There is also got a big problem with antibiotics,” Layton acknowledged. “As dermatologists, we’re one of the biggest offenders in terms of the number and duration of antibiotics we use. NICE guidance limits use to 6 months, but acne is a chronic disease, and the average duration is probably 6–7 years.5 So, if a patient’s acne deteriorates again when you stop antibiotics and is not controlled on topical therapies, it represents a real unmet need in terms of what we do with those patients.” Cliff also pointed to the increasing problem of antibiotic resistance, which is reducing patients’ responsiveness to antibiotic acne therapies and further underscores the need for novel treatment approaches.
Finally, both experts highlighted the need to address the excess sebum production, which is fundamental to acne pathogenesis. “One of the biggest unmet needs, I think, is that sebum is integral to acne, but until recently there was no topical agent specifically designed to reduce sebum,” Layton pointed out. “For males, we only have oral isotretinoin, which is licensed for severe acne and reduces sebum, but no topical agents. For females, we have things like oral aldosterone antagonists and oral contraceptive pills, but the majority are not licensed in the UK, so, there’s a real unmet need in terms of being able to reduce that sebum, which is so integral to the disease.”
TARGETING THE ANDROGEN RECEPTOR
Clascoterone cream 10 mg/g is a topical androgen receptor inhibitor recently granted a marketing authorisation in the UK for the topical treatment of acne vulgaris in patients aged 12 years and older.9 Although the exact mechanism of action of clascoterone for the topical treatment of acne vulgaris is not fully characterised, in vitro studies suggest that clascoterone binds with high affinity to the
androgen receptor in sebocytes, inhibiting downstream androgen-stimulated gene transcription (in vitro findings may not necessarily reflect in vivo phenomena).10 Both experts described clascoterone’s mode of action as “unique”, being the first topical anti androgen agent that reduces sebum production and thus intervenes early in the acne cascade.
“It’s a really interesting agent because it’s an androgen inhibitor, so it’s acting at the receptor, which means that it prevents the active effects of androgens at the receptor site,” Layton explained. As Cliff elaborated: “Acne is strongly influenced by the male hormone testosterone in both men and women, the byproduct of which is dihydrotestosterone (DHT), which we think binds these androgen receptors and activates the sebum production, which in turn activates the inflammation and activates the keratinisation. The logical thing then is to block the androgen receptors.”
Layton added: “Clascoterone is a competitive inhibitor of the antigen receptor, and there have been some in vitro studies suggesting that it inhibits the downstream signalling of androgen-responsive genes.”10,11 “From a clinical perspective, it’s the only topical agent we’ve got that is specifically developed to reduce sebum,” he continued. Cliff concurred: “This is a different way of looking at acne, a different approach with a topical preparation.”
In terms of the type of patient who could benefit from clascoterone’s androgeninhibitory effects, experts highlighted adolescents going through puberty and experiencing the associated testosterone surge that increases sebum levels in the skin. Layton also alluded to its potential utility in “adult female patients with hormonally driven perioral acne”. Cliff suggested that clascoterone could additionally be considered for those patients experiencing acne flare-ups, including both treatment-naïve patients with acne or those previously treated with isotretinoin “who want to target those [breakout] areas with a topical treatment locally to control the acne, rather than treat with oral agents that can upset their stomach”.
Ultimately, however, experts concluded that clascoterone could prove a useful addition to the acne treatment armoury for eligible patients aged 12 years and older. “Sebum is integral to acne, so it should be helpful in most suitable patients,” Layton emphasised.
Clinical Evidence for Clascoterone
Clascoterone was evaluated in two 12week, randomised, vehicle-controlled Phase III trials and a 9-month safety extension study; in the 12-week studies, it demonstrated superior efficacy to vehicle creams.9,12-14 “From the clinical perspective, the big studies are the two pivotal multinational, multicentre studies,” Layton confirmed. “Over 12 weeks, clascoterone showed good efficacy in terms of getting clear, or almost clear, skin in the majority of patients.” These two Phase III trials of clascoterone enrolled a total of 1,440 patients (males and females aged 9 years and older) with moderate or severe facial acne (Table 1).13 At Week 12, the treatment success rate, defined as an Investigator’s Global Assessment (IGA) score of 0 (clear) or 1 (almost clear) and a ≥2-grade improvement from baseline and absolute change from baseline in non-inflammatory and inflammatory lesion counts, was 18.8% with clascoterone versus 8.7% with vehicle in trial 1 and 20.9% with clascoterone versus 6.6% with vehicle in trial 2.9
“The data from the short-term study, compared to vehicle, was significant in terms of the effectiveness and the reduction in inflammatory count or number of acne lesions, both by patient assessment and also by IGA,” remarked Cliff. “Enrolled patients had quite a large number of inflammatory lesions, and the results were significant,” he continued.
Experts also pointed to encouraging results from the open-label, long-term safety extension study that enrolled 609 patients who either continued existing treatment with clascoterone or switched to clascoterone from vehicle. In this study, in which clascoterone was applied twice daily for up to a further 9 months, a low frequency of treatment-emergent adverse events was observed.12
Inflammatory lessons
*IGA success was defined as at least a 2-point reduction in IGA compared to baseline and an IGA score of 0 (clear) or 1 (almost clear).
IGA: Investigator Global Assessment.
“We all worry if the treatment is safe enough to continue in the long term,” Cliff explained. “These data showed clascoterone is generally well tolerated, which is paramount for our patients.”
In terms of clascoterone’s overall safety and tolerability profile in clinical studies, this was viewed favourably by both experts. “Although some patients did get some irritation and a bit of redness, by and large, the side effect profile was low and therefore positive from that angle,” said Cliff. “In all of the studies where clascoterone has been used in Phase III and IV studies, the main side effects have been local skin reactions, dryness, scaling, and redness, very much like you get with a lot of topical agents,” Layton confirmed.
EVOLUTION OF ACNE MANAGEMENT
Clascoterone in Clinical Practice
Based on these Phase III trial findings, experts discussed the potential value of a new product like clascoterone within the existing acne treatment armamentarium. Cliff described the clinical data as “convincing” and sufficient to support “definite benefits” for clascoterone used as a topical cream for patients experiencing acne flare-ups.
“We have here, potentially, a licensed product that blocks the androgen receptor on the pilosebaceous unit, which is where the whole process of acne is going on,”
Cliff elaborated. “This is a different modality of treatment, it’s not a retinoid, not a topical antibiotic, it’s an androgen receptor blocker.”
Layton added that: “One of the major advantages of clascoterone is actually having something you can use in boys as well as girls, and there are reports that have suggested it can be used in all ethnicities and skin of colour.” She also noted the potential utility of clascoterone in people undergoing gender transitioning who may be taking testosterone supplements, which can drive acne development. “Something that might be helpful in terms of reducing the sebum production would be useful in these patients as well,” she elaborated. “So, that’s another clinical area where I think clascoterone could be useful.”
The Future of Acne Care
Looking to the future of acne management, Layton highlighted exciting new advances in microbiome research, modulating the skin’s microbiome to increase the microbial diversity that is lost during acne development, and the potential role of therapeutic and preventative vaccines. She also suggested some interesting avenues for future research, such as the potential impact of early topical treatment on acne evolution.
In terms of acne treatment itself, Cliff acknowledged this has “been pretty flat” for the past 10–12 years and lacks any significant innovation. “While we’ve seen new products like new retinoids come on the market, we haven’t seen any new avenues to address acne through a different modality,” he remarked. “Clascoterone is the first in that respect, so it’s a potential game changer from that perspective.”
Cliff went on to highlight specific areas where clascoterone may fit into the current landscape of acne treatments and help to advance future clinical care. He suggested this new topical agent may be beneficial in treating unpredictable, localised flare-ups of acne that are pustular or comedonal in nature, adding, “particularly for a hormonal flare-up or possibly for patients with polycystic ovaries.”
Cliff also described clascoterone as a potentially useful alternative “for patients who don’t want to take antibiotics because of potential side effects, or who don’t want to take isotretinoin for whatever reason.” However, he cautioned that the availability of this topical anti-androgen would augment, rather than supplant, existing options in the acne toolkit, particularly for severe disease. “If a patient has aggressive, cystic acne that is scarring, no topical agent is going to be effective because they need systemics, they need isotretinoin, and there’s no substitute for that,” he stressed.
Layton reiterated that a move away from antibiotics should be a top priority for acne care going forward. “We definitely need to find new ways of treating people which don’t involve antibiotics because we’ve got patients on antibiotics for years, and we’re often using things like doxycycline, which are important for other diseases,” she stressed. “So, if we’ve got new topicals that can be used as part of a regimen or on their own, that’s really important.”
For female patients of all ages, Layton also emphasised the need for new treatment options. “With earlier menarche, we’re seeing acne earlier, and having welltolerated topical therapies that we could use early on in the onset of acne, I think, is really important,” she stressed. “And then also at the other end of the spectrum for hormonal acne, where we’re seeing adult females with persistent disease.”
“Given the restrictions on isotretinoin, having a topical therapy that can be used as part of a multimodal system is really important,” Layton pointed out. “The fact that clascoterone reduces sebum, and that’s so important in acne, means that all suitable patients potentially could benefit from it. It can be used as monotherapy but also as part of a multimodal treatment regimen as well.”
Cliff concurred that the scope for the use of topical antiandrogen in daily clinical practice could be substantial. “Many patients with mild to moderate acne could benefit from this kind of modality,” he concluded.
Adverse events should be reported. Reporting forms and information can be found at yellowcard.mhra.gov.uk. Adverse events should also be reported to medical_information@glenmarkpharma.com or call 0800 458 0383. Interview
References
1. Costa CS et al. Systemic pharmacological treatments for acne: an overview of systematic reviews (Proto-col). Cochrane Database of Systematic Reviews. 2021;11:CD014917.
2. Collier CN et al. The prevalence of acne in adults 20 years and older. J Am Acad Dermatol. 2008;58(1):56-9.
3. Del Rosso JQ et al. The primary role of sebum in the pathophysiology of acne vulgaris and its ther-apeutic relevance in acne management. J Dermatolog Treat. 2024;35:2296855.
4. Smith H et al. Identifying the Impacts of Acne and the Use of Questionnaires to Detect These Impacts: A Systematic Literature Review. Am J Clin Dermatol. 2021;22(2):159-71.
5. National Institute for Health and Care Excellence (NICE). Acne vulgaris: management. Available at: https:// www.nice.org.uk/guidance/ng198. Last accessed: 6 February 2025.
6. Reynolds R et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2024;90(5):1006. e1-1006.e30.
7. Roaccutane (isotretinoin). Summary of Product Characteristics. Available at: https://www.medicines.org.uk/ emc/product/1114/smpc#gref. Last accessed: 6 February 2025.
8. Medicines and Healthcare products Regulatory Agency (MHRA). Isotretinoin (Roaccutane▼): new safety measures to be introduced in the coming months, including additional oversight on initiation of treat-ment for patients under 18 years. Available at: https:// www.gov.uk/drug-safety-update/ isotretinoin-roaccutanev-new-safetymeasures-to-be-introduced-in-thecoming-months-including-additionaloversight-on-initiation-of-treatmentfor-patients-under-18-years. Last accessed: 6 February 2025.
9. Winlevi 10 mg/g cream. Summary of Product Characteristics. Available at: https://www.medicines.org.uk/emc/ product/100519/smpc. Last accessed: 6 February 2025.
10. Rosette C et al. Cortexolone 17-propionate (clascoterone) is a novel androgen receptor antagonist that inhibits production of lipids and inflammatory cytokines from sebocytes in vitro. J Drugs Der-matol. 2019;18(5):412-18.
11. Ferraboschi P et al. Full conformational characterization of antiandrogen cortexolone-17α-propionate and related compounds through theoretical calculations and nuclear magnetic resonance spectroscopy. MedChemComm. 2014;5:904-14.
12. Eichenfield L et al. Open-label, longterm extension study to evaluate the safety of clascoterone (CB-03-01) cream, 1% twice daily, in patients with acne vulgaris. J Am Acad Dermatol. 2020;83(2):477-8.
13. Hebert A et al. Efficacy and Safety of Topical Clascoterone Cream, 1%, for Treatment in Patients With Facial Acne. JAMA Dermatol. 2020;156: 621-30.
14. Herbert A et al. Efficacy and safety of 1% clascoterone cream in patients aged > 12 years with acne vulgaris. Journal of Drugs in Dermatology. 2023;22(2):174-81.
Job Code: PP-UK-WIN-0008
Date of Prep: June 2025
Selecting the Inhalation Device Most Likely to Benefit Your Patients with COPD: Support Your Choice with the
Interactive Device Selection Tool
Interviewee: Donald A. Mahler1,2
1. Geisel School of Medicine at Dartmouth, Hanover, New Hampshire, USA
2. Valley Regional Hospital, Claremont, New Hampshire, USA
Disclosure: Mahler has royalties or licenses with Johns Hopkins University Press as an author and pharmaceutical companies for the use of the Baseline Dyspnea Index and Transition Dyspnea Index in clinical trials; has received advisory board consulting fees from AstraZeneca, Boehringer Ingelheim, Theravance, Verona, and Viatris; and has other financial or non-financial interests for an educational website for those with COPD and their families.
Acknowledgements: Writing assistance was provided by Nicola Humphry, Nottingham, UK.
Disclaimer: The opinions expressed in this article belong solely to the named interviewee.
COPD is a leading cause of morbidity and mortality worldwide. Inhaled therapies are the mainstay of COPD treatment, including pressurised metered dose inhalers (pMDI), pMDIs with a spacer, soft mist inhalers (SMI), dry powder inhalers (DPI), and nebulisers. Inhalation devices each have distinct advantages and challenges, and selecting the most appropriate device for a patient with COPD is crucial to maximising the benefit of inhaled therapy.
In this expert interview, pulmonologist Donald Mahler, Geisel School of Medicine at Dartmouth, Hanover; and Valley Regional Hospital, Claremont, New Hampshire, USA, offers insights into the nuances of inhaler selection, emphasising how clinical- and patient-specific factors should guide decision-making. He clarifies the roles of different delivery systems, including the role of nebulisers in certain clinical scenarios, and describes how nebuliser efficiency can be objectively measured in terms of the ability to deliver therapeutic doses of medication into the lungs. A case study illustrates the benefits of switching to nebuliser therapy when a patient’s symptoms do not improve with an appropriately used handheld device.
PHARMA
PARTNERSHIP
Mahler also addresses the impact of mucus overproduction in patients with COPD, highlights therapeutic strategies including nebulised agents and positive expiratory pressure (PEP) therapy, and introduces a new interactive COPD Inhalation Device Selection Tool (PARI GmbH, Starnberg, Germany) designed to help healthcare providers (HCP) to make tailored, evidence-informed choices for their patients.
INTRODUCTION
Inhalation therapy is central to the treatment of patients with COPD,1 a condition that affects an estimated 480 million people; roughly 10% of the global population.2 Inhaled therapies deliver medication directly to the lungs, with the benefit of rapid onset of effect and reduced systemic exposure compared with oral or intravenous administration.3
It is critical to ensure that any inhaled drug reaches the site of action in sufficient quantity to exert the desired therapeutic effect.1 To optimise the benefit–risk ratio of inhaled therapy, the most suitable device should be selected.4
To discuss these issues, the European Medical Journal (EMJ) sat down with Mahler, a pulmonologist with extensive experience and expertise in COPD, based at Valley Regional Hospital in Claremont, New Hampshire, USA.
INHALATION DEVICES AND FACTORS AFFECTING SELECTION
Mahler outlined the differences between currently marketed inhalation devices, highlighting patient challenges and how they should inform device selection.
Numerous Publications Have Shown That Not All Inhalation Devices Are Suitable for the Treatment of All COPD Patients. This Can Result in Poor Patient Outcomes. Can You Share Your Perspective on This Issue?
Inhaled therapy in COPD is delivered via four principal device types: pressurised metered dose inhalers (pMDI), dry powder inhalers (DPI), soft mist inhalers (SMI), and nebulisers.5 While drug availability is an
important consideration, effective treatment hinges on aligning the device with individual patient factors.5
For HCPs, selecting the optimal device can be complex;5 with each system presenting unique handling requirements, physiological demands, and logistical considerations. Key distinguishing features are outlined in Table 1
Studies show that up to 87% of patients with COPD make at least one inhaler technique error with pMDIs.7 It is believed that these errors restrict delivery of the inhaled medication into the lower respiratory tract,5,8 resulting in an increased risk of COPD exacerbations, worse health status, overuse of inhaled corticosteroids, and frequent hospitalisation.3,5 In addition, at least half of patients with acutely exacerbated COPD do not reach optimal peak inspiratory flow (PIF) for DPI usage,9,10 which itself may result in worse COPD-related symptom burden, and a greater likelihood of COPD-related hospital readmissions 9,11
What Key Patient-specific Factors
Influence the Choice of an Optimal Inhalation Device? How Can Healthcare Providers Assess and Prioritise These Factors to Ensure Effective Therapy?
HCPs should consider three key questions when selecting an inhalation device to prescribe:
1. Does the patient have sufficient cognitive function to follow instructions and use handheld devices?
2. Does the patient have sufficient manual dexterity to use the handheld device correctly?
3. Does the patient have sufficient PIF to de-aggregate the powder in a DPI?
Inhalation device Key factors
• Deliver medication in aerosol form using a propellant5,6
• Handheld; compact and portable6
• Require coordination between device actuation and slow, steady inhalation6
pMDIs
• The use of holding chambers can help to optimise lung deposition6
• Breath-actuated pMDIs have been developed to provide better drug deposition at low flow rates, but drugs that can be used with them are limited5,6
DPIs
• Deliver dry powdered medication, usually attached to a bulking agent to improve flowability5
• Handheld; compact and portable6
• Do not require coordination between device actuation and inhalation6
• Require strong inspiratory flow to de-aggregate the powder into respirable particles5,6
• Effectiveness can be affected by factors such as ambient humidity6
SMIs
• Deliver a prolonged, fine mist of medication using a spring mechanism5
• Handheld; compact and portable6
• Requires coordination between device actuation and slow, steady inhalation5
Nebulisers
• Deliver a liquid medication as fine aerosol for inhalation through a mask or mouthpiece6
• Do not require coordination between device actuation and inhalation as the patient uses tidal breathing5
• Compared to handheld devices, nebulisers are larger, require a power source and regular maintenance, and may have longer administration time6
• Breath-enhanced and breath-actuated nebulisers have been developed to improve efficiency by delivering more medication during inhalation and minimising waste3,5
The answers to these questions can narrow down the most appropriate inhalation devices for the patient.5,12 For example, nebulisers may be the most suitable devices for patients with impaired cognitive function or poor manual dexterity, and DPIs are unlikely to be suitable for patients with suboptimal PIF.5,12
It is important to teach patients with COPD to use their prescribed inhalation device correctly, and this can include the use of the “teach-back” approach, handouts, and training videos.4
If a patient reports little symptom improvement with the use of their current inhaler, they should be asked to demonstrate their inhaler technique. If they are using their inhaler correctly but not getting any benefit, their HCP should consider switching to a different inhalation device.5
Table 1: Key factors of different types of inhalation device.
THE SPECIFIC CASE OF NEBULISERS
Nebulisers are typically prescribed when patients are unable to use handheld devices correctly, due to impaired cognitive function, poor manual dexterity, or suboptimal PIF, or when a handheld device is not providing the patient with adequate symptom relief.5 Patient preference is also a consideration,13 and Mahler explained that some of his patients choose to use a nebuliser to administer on-demand short-acting bronchodilators, while others use a nebuliser for maintenance medication.
How
Do Different Nebuliser Types
Compare in Terms of Clinical Efficacy and Efficiency for COPD Treatment, and to What Extent Should These Factors Influence Device Selection in Clinical Practice?
Nebulisers can be divided into three main types: jet, ultrasonic, and vibrating mesh, depending on the mechanism by which they generate an aerosol.3 Jet nebuliser systems can be continuous, or more efficient types include breath-actuated (delivery during inhalation only), or breath-enhanced (delivery increased during inspiration and reduced on expiration).14
The selection of a specific nebuliser should be based on the efficiency of the device, in order to optimise medication delivery.15-17 Nebuliser efficiency depends on the respirable dose of medication that reaches the lungs per minute.17 The respirable dose is dependent on both the aerosol output of the nebuliser and the respirable fraction of the aerosol (the proportion of particles <5 µm).17 Therefore, the respirable drug delivery rate (RDDR) can serve as an objective measure to compare the efficiency of different nebulisers in delivering medication to the lower respiratory tract.17,18
There have been a significant number of in vitro studies that demonstrate breathenhanced and breath-actuated nebulisers deliver medication more efficiently than continuous nebulisers.19-23 Comparative data on RDDR is available to help HCPs select the most effective device for their patients.
What Limitations Can Healthcare Providers Face When Selecting the Correct Nebuliser?
In many countries, long-acting beta agonists (LABA), long-acting muscarinic antagonists (LAMA), and inhaled corticosteroids are all available.3,5 The phosphodiesterase (PDE) 3/4 inhibitor, ensifentrine, was only available in the USA as of the time of writing.24 In some countries/regions, there is limited or no access to these COPD medications, which restricts the use of nebulisers to on-demand, rather than maintenance therapy.6,25,26
Could You Share a Case Study from your Clinical Practice Where Nebuliser Therapy Significantly Improved Outcomes for a Patient with COPD?
A 67-year-old patient with moderate COPD (FEV1 58% predicted) was referred for pulmonology consultation following two emergency department visits within three days for acute dyspnoea. Treatment during these visits included short-acting muscarinic antagonist (SAMA) delivered via nebulisation, azithromycin, and a short course of oral prednisone (40 mg/day).
At the time of assessment, the patient reported persistent shortness of breath during minimal exertion (e.g., walking between rooms). Routine testing revealed normal alpha-1-antitrypsin levels and a clear chest X-ray. Maintenance therapy consisted of a LABA/LAMA combination via SMI, and the patient reported frequent reliance (6–8 times daily) on a SABA pMDI, with limited symptom relief.
Based on clinical history and persistent symptom burden, the patient was prescribed a combination SAMA/SABA therapy via jet nebuliser for on-demand use, while continuing their existing maintenance regimen.
At a follow-up visit 3 weeks later, the patient reported marked improvement in symptom control and overall satisfaction with the new inhalation strategy. This case highlights how transitioning select patients to nebulised therapy may enhance bronchodilation and reduce emergency care utilisation.
IMPACT AND OPTIONS FOR EXCESSIVE LUNG SECRETION
How Does Excessive Mucus Production in Patients with COPD Impact Their Respiratory Function, Quality of Life, and Clinical Outcomes?
A subtype of COPD, chronic bronchitis, is characterised by a productive cough caused by excessive mucus production,15 airway obstruction, and inflammation.27 These patients often report feeling that they cannot cough up the mucus in their lungs.
Excessive mucus production is increasingly recognised as an important factor in COPD, though its precise role in the pathogenesis of the disease is not fully understood.28-31 Recent studies have indicated that the presence of mucus plugs on CT scan is associated with increased mortality, higher exacerbation rates, and lung function decline,32-35 demonstrating the importance of their management for optimal patient outcomes.
What Are the Treatment Options for Patients with COPD Who Experience Excessive Mucus Production?
It is important to recommend smoking cessation as a simple and effective way to reduce mucus production among patients with COPD who smoke.4,36 Patients should also drink plenty of water, as this may help to hydrate and thin the mucus.
Although there is a lack of robust clinical studies to support the recommendation of specific interventions for excessive mucus production in COPD, several therapies have been considered.4 For example, the use of mucolytic drugs has been shown to reduce exacerbations,4,31 and nebulised hypertonic saline is sometimes used to assist mucus clearance in patients with COPD.37-40
Another treatment that may improve mucus mobilisation in COPD is oscillatory positive expiratory pressure (OPEP) therapy.4,41,42 OPEP devices generate oscillating intrathoracic pressure in the lungs, reducing the viscoelasticity of bronchial secretions and helping to move mucus plugs towards the central and upper airways.41
THE COPD INHALATION DEVICE SELECTION TOOL
Mahler explained that there are some published tools or instruments available to support HCPs with the choice of inhalation device for their patients.4,12,43,44 He outlined the first interactive, open-access tool that has recently been developed to address this need: the COPD Inhalation Device Selection Tool.45
How
Can
the COPD Inhalation Device
Selection Tool Enhance Clinical Decision-making in Choosing Optimal Inhalation Devices, and in Which Specific Healthcare Settings or Scenarios Might It Be Most Beneficial?
The objective of the COPD Inhalation Device Selection Tool is to support HCPs in the personalised selection of an inhalation device to improve individual patient outcomes. The tool narrows down the suitable options for a patient, simplifying the HCP’s choices (Figure 1).
Upon opening the online interactive tool, the first screen displays a grid with cognitive function and/or manual dexterity on the x-axis and PIF on the y-axis, allowing HCPs to select the grid segment that best represents their patient’s profile. Clicking on the appropriate segment reveals the most suitable delivery system option(s) for that patient. Additional information is supplied in pop-up boxes to provide further guidance, such as the advantages and disadvantages of each device, and why one device might be more appropriate for their patient than another.45
A key advantage of the interactive selection tool is that it can be accessed on a laptop, an electronic tablet, or even a mobile phone. It could be used by a medical assistant to screen a patient and report the recommended devices to the HCP, potentially saving them some face-to-face appointment time. The COPD Inhalation Device Selection Tool is available to all healthcare settings, yet it may be of particular value to primary care, supporting HCPs by simplifying the selection of the most appropriate device(s) for each of their patients.
1: Screenshots from the COPD Inhalation Device Selection Tool.24
The creation of this tool was funded by PARI GmbH and developed in collaboration with EMJ.
Upper image shows the initial screen of the interactive tool, permitting selection of a patient’s cognitive function and/ or manual dexterity from normal to impaired on the x-axis, and their peak inspiratory flow, from optimal to suboptimal, on the y-axis. Lower images show examples of recommendations that are provided on clicking specific areas of the screen (A–B). Further information available to the user is shown in three text boxes (1–3).
Selecting the appropriate inhalation device is complex and highly dependent on patient-specific factors. The COPD Inhalation Device Selection Tool was developed to support HCPs in navigating this complexity, enabling more personalised, effective treatment, and ultimately improving patient outcomes.
References
1. Cazzola M et al. The future of inhalation therapy in chronic obstructive pulmonary disease. Curr Res Pharmacol Drug Discov. 2022;3:100092.
2. Boers E et al. Global burden of chronic obstructive pulmonary disease through 2050. JAMA Netw Open. 2023;6(12):e2346598.
3. Dhand R et al. Recalibrating perceptions and attitudes toward nebulizers versus inhalers for maintenance therapy in COPD: past as prologue. Int J Chron Obstruct Pulmon Dis. 2024;19:2571-86.
4. 2025 GOLD Report. Global Initiative for Chronic Obstructive Lung Disease - GOLD. Available at: https://goldcopd. org/2025-gold-report/. Last accessed: 20 March 2025.
5. Mahler DA, Halpin DMG. Personalizing selection of inhaled delivery systems in chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2023;20(10):1389-96.
6. Izquierdo-Condoy JS et al. Challenges and opportunities in COPD management in latin america: a review of inhalation therapies and advanced drug delivery systems. Pharmaceutics. 2024;16(10):1318.
7. Cho-Reyes S et al. Inhalation technique errors with metered-dose inhalers among patients with obstructive lung diseases: a systematic review and meta-analysis of U.S. studies. Chronic Obstr Pulm Dis. 2019;6(3):267-80.
8. Hindle M et al. Investigations of an optimal inhaler technique with the use of urinary salbutamol excretion as a measure of relative bioavailability to the lung. Thorax. 1993;48(6):607-10.
9. Loh CH et al. Suboptimal inspiratory flow rates are associated with chronic obstructive pulmonary disease and all-cause readmissions. Ann Am Thorac Soc. 2017;14(8):1305-11.
10. Broeders MEAC et al. The course of inhalation profiles during an exacerbation of obstructive lung disease. Respir Med. 2004;98(12):1173-9.
11. Ghosh S et al. Peak inspiratory flow rate in chronic obstructive pulmonary disease: implications for dry powder inhalers. J Aerosol Med Pulm Drug Deliv. 2017;30(6):381-7.
12. Mahler DA. The role of inspiratory flow in selection and use of inhaled therapy for patients with chronic obstructive pulmonary disease. Respir Med. 2020;161:105857.
13. Sharafkhaneh A et al. Perceptions and attitudes toward the use of nebulized therapy for COPD: patient and caregiver perspectives. COPD. 2013;10(4):482-92.
14. Berlinski A. In vitro comparison of different nebulizers delivering 7% hypertonic saline. Respir Care. 2021;66(10):1582-7.
15. NICE. Chronic obstructive pulmonary disease in over 16s: diagnosis and management. Available at: https:// www.nice.org.uk/guidance/ng115. Last accessed: 1 April 2025.
16. Vecellio L et al. Disposable versus reusable jet nebulizers for cystic fibrosis treatment with tobramycin. J Cyst Fibros. 2011;10(2):86-92.
17. EMJ Reviews. Efficiency assessment of 15 nebuliser systems by the respirable drug delivery rate: a comparable quality parameter. EMJ Respir. 2023;11[1]:69-73.
18. Fischer R et al. Efficiency assessment of 15 nebuliser systems by the respirable drug delivery rate. Eur Respir J. 2023;62(Suppl 67):PA4603.
19. Cuevas Brun E et al. Aerodynamic particle size distribution and delivered dose efficiency of a continuousoutput mesh nebuliser and a novel breath-actuated device using terbutaline sulphate. 2021. Available at: https://ddl-conference.com/wpcontent/uploads/2021/10/06.CuevasBrun.pdf. Last accessed: 21 March 2025.
20. Heijerman H et al. Inhaled medication and inhalation devices for lung disease in patients with cystic fibrosis: A European consensus. J Cystic Fibrosis. 2009;8(5):295-315.
21. Arunthari V et al. A prospective, comparative trial of standard and breath-actuated nebulizer: efficacy, safety, and satisfaction. Respir Care. 2012;57(8):1242-7.
22. Sabato K et al. Randomized controlled trial of a breath-actuated nebulizer in pediatric asthma patients in the emergency department. Respir Care. 2011;56(6):761-70.
23. Li J et al. In vitro comparison between inspiration synchronized and continuous vibrating mesh nebulizer during trans-nasal aerosol delivery. Intensive Care Med Exp. 2020;8:6.
24. GlobeNewswire News Room. Verona pharma announces US FDA approval of OhtuvayreTM (ensifentrine). 2024. Available at: https://www. globenewswire.com/newsrelease/2024/06/26/2904839/0/en/ Verona-Pharma-Announces-US-FDAApproval-of-Ohtuvayre-ensifentrine. html. Last accessed: 21 March 2025.
25. Du D et al. The availability of drugs for stable COPD treatment in China: a cross-sectional survey. NPJ Prim Care Respir Med. 2025;35(1):6.
26. Stolbrink M et al. The availability, cost, and affordability of essential medicines for asthma and COPD in low-income and middleincome countries: a systematic review. Lancet Glob Health. 2022;10(10):e1423-42.
27. Widysanto A et al. Chronic Bronchitis. [Internet] (2025) Treasure Island: StatPearls. Available at: http://www. ncbi.nlm.nih.gov/books/NBK482437/. Last accessed 4 March 2025.
28. Cerveri I et al. Revisited role for mucus hypersecretion in the pathogenesis of COPD. Eur Respir Rev. 2010;19(116):109-12.
29. Curran DR et al. Advances in mucous cell metaplasia: a plug for mucus as a therapeutic focus in chronic airway disease. Am J Respir Cell Mol Biol. 2010;42(3):268-75.
30. Shen Y et al. Management of airway mucus hypersecretion in chronic airway inflammatory disease: Chinese expert consensus (English edition). Int J Chron Obstruct Pulmon Dis. 2018;13:399-407.
31. Decramer M et al. Mucoactive therapy in COPD. Eur Respir Rev. 2010;19(116):134-40.
32. Jin KN et al. Mucus plugs as precursors to exacerbation and lung function decline in COPD patients. Arch Bronconeumol. 2025;61(3):138-46.
33. Diaz AA et al. Airway-occluding mucus plugs and mortality in patients with chronic obstructive pulmonary disease. JAMA. 2023;329(21):1832-9.
34. Okajima Y et al. Luminal plugging on chest CT scan: association with lung function, quality of life, and COPD clinical phenotypes. Chest. 2020;158(1):121-30.
35. Dunican EM et al. Mucus plugs and emphysema in the pathophysiology of airflow obstruction and hypoxemia in smokers. Am J Respir Crit Care Med. 2021;203(8):957-68.
36. Shah BK et al. mucus hypersecretion in chronic obstructive pulmonary disease and its treatment. Mediators Inflamm. 2023;2023:8840594.
37. Khan SY et al. Is nebulized saline a placebo in COPD? BMC Pulm Med. 2004;4:9.
38. Cole E et al. Inhaled 7% hypertonic saline is safe to administer in patients with moderate to severe chronic obstructive pulmonary disease (COPD). 2017. Available at: https:// www.atsjournals.org/doi/abs/10.1164/ ajrccm-conference.2017.195.1_ MeetingAbstracts.A5714. Last accessed: 25 March 2025.
39. Taube C et al. Airway response to inhaled hypertonic saline in patients with moderate to severe chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;164(10 Pt 1):1810-5.
40. Valderramas SR et al. Effectiveness and safety of hypertonic saline inhalation combined with exercise training in patients with chronic obstructive pulmonary disease:
a randomized trial. Respir Care. 2009;54(3):327-33.
41. Coppolo DP et al. Non-pharmaceutical techniques for obstructive airway clearance focusing on the role of oscillating positive expiratory pressure (OPEP): a narrative review. Pulm Ther. 2022;8(1):1-41.
42. Alghamdi SM et al. Oscillatory positive expiratory pressure therapy in COPD (O-COPD): a randomised controlled trial. Thorax. 2023;78(2):136-43.
43. Price E et al. Development and evaluation of a tool to optimise inhaler selection prior to hospital discharge following an exacerbation of COPD. ERJ Open Res. 2024;10(2):00010-2024.
44. Voshaar T et al. [Recommendations for the choice of inhalatory systems for drug prescription]. Pneumologie. 2001;55(12):579-86. (In German).
45. EMJ. COPD Device Selection Tool. 2025. Available at: https://www. emjreviews.com/pari-devise-selectiontool/. Last accessed: 2 May 2025.
Interviews
EMJ had the pleasure to speak to four leading experts in preventive health: David Katz, Chief Medical Officer, Tangelo, Intend, and DietID, Detroit, Michigan, USA; Amanda Daley, Centre for Lifestyle Medicine and Behaviour (CLiMB), Loughborough University, UK; Lennard Lee, University of Oxford, UK; and Mariah Stump, Warren Alpert Medical School, Brown University, Providence, Rhode Island, USA. Katz highlights the potential for food to be used as medicine, Daley introduced the concept of snack-sized fitness, Lee explores the ongoing cancer vaccine revolution, and Stump explains how lifestyle medicine can be integrated into everyday practice.
David Katz
Chief Medical Officer, Tangelo, Intend; Founder/CEO, DietID, Detroit, Michigan, USA
What initially sparked your interest in nutrition and preventive health?
I understood how truly wondrous the human body is as a machine and the intricate, elegant choreography that sustains us every day
My interest in food as fuel for a high-performance body began before my commitment to medicine. When I was just 13 years old, for reasons I do not entirely recall, I tried out for the junior high school wrestling team. On Day 1, I was told how many sit-ups and push-ups I ought to be able to do, and I could do nothing remotely close to that many, having never thought about it before. As it turned out, I did not stick with the wrestling team, for various reasons that I will spare you, but the admonition of the coach on what is an acceptable level of fitness stuck with me, and I have worked out, with rare exception, every day of my life since then.
I started getting into other aspects of fitness and thinking about my body as a hardworking machine. The quality of the fuel you put in the tank
of any machine is relevant to its performance, and my body was no different. I started becoming much more interested in my own nutrition. I had grown up with a typical American family's typical American diet, but that started to change. Around the same time, my family had taken a couple of trips where we did horseback riding, and I enjoyed the privilege, the magnificent strength and capabilities of the horse, and the communication with it. Then we did some roundups with cattle and, looking at them, I realised they are not all that different. I cannot form a bond of affection, friendship, and appreciation for this animal and eat that animal. I renounced red meat. At that point, I had established a real interest in many aspects of dietary intake, for personal health, our connection to creatures, and the ethics of our dietary choices.
Ultimately, I wound up choosing medicine, going to medical school, doing internal medicine, and
then doing a second residency in preventive medicine and public health. I carried my interest in nutrition into all of that. Throughout this, I was thinking: ‘This is incredibly important. Food is fuel’. By the time I finished my training in medicine, I understood how truly wondrous the human body is as a machine and the intricate, elegant choreography that sustains us every day. I understood that the importance of fuel for all these different processes is much greater than I ever realised before. You learn how much of your body is being replenished every day. You are turning over hundreds of millions of cells, you are burning through hormones and enzymes. You are depleting your reserves, and you must reconstitute them. The only source of construction material, whether for the growing body of a child or the refurbished body of an adult, is your diet. You only have two places to go: you can cannibalise your own body, taking proteins from here and putting them over there, or you must get what you need from food. The quality of construction material determines the quality of the structure. You would not want to build your house out of rotten wood. Food, uniquely, is both the body’s daily construction material and its fuel; that indicates a staggering influence on overall health, which is exactly what the science indicates. Q2
How did this interest in diet shape the trajectory of your career?
All of that came together, and I finished my training in preventive medicine, my second residency, in 1993. Within a matter of weeks after my graduation and getting my master's in public health, which I got years after my medical degree, a paper was published
titled ‘Actual causes of death in the United States’.1 The two authors, Bill Foege and Mike McGinnis, pointed out that what gets listed on death certificates as the cause of death does not tell us anything about the actual causes of death. If someone dies of cardiogenic shock, secondary to congestive heart failure, secondary to multiple myocardial infarctions, secondary to atherosclerosis, nothing on that causal list tells us what to do. What you really want to know is, what caused the atherosclerosis? What set all of this in motion? McGinnis and Foege looked for that.
The paper was brilliant, and in my opinion, one of the most important in the modern era of biomedical publishing. They enumerated a list of 10 factors that collectively explain nearly all the premature deaths that occur in the USA and, by extension, in the modern world every year. What captured my imagination as a newly minted preventive medicine specialist is that 80% of premature deaths were linked to the poor usage of feet, forks, and fingers. The first one was tobacco use, the second was poor diet quality, and the third was a lack of physical activity. Together, you get 80% of the variance in all-cause mortality and 80% of the variance in chronic disease risk. That is a career right there.
I focus on diet not only because I have a natural interest in it but also because everybody eats. People are more lost and confused about their diets than the other two variables, where it may not be easy to do what you need to do, but there is no lack of clarity about it. For instance, movement is better than sitting all day and not smoking is better than smoking. I need to help people understand that we know what to do regarding diet.
Every health professional should be addressing diet and nutrition. It is the number one single leading predictor variable for all-cause mortality and total risk of chronic disease. If you are ignoring that factor, then I think you are abdicating the primary commitment we made as health professionals, which is to do all we can to advance the human condition, add years to lives and add life to years.
Q3 Could you please tell us a bit about the ways in which you think the public can use food as medicine?
Simple swaps can add up to make a huge difference. One of the reasons is something that I call ‘Taste Bud Rehab’. Taste buds are adaptable. When they cannot be with the foods they are used to loving, they learn to love the foods they are with. If you trade up and think about choosing more nutritious items in every aisle of the supermarket, you are cutting some number of grams of sugar out of your daily diet, you are cutting some number of milligrams of sodium, you are cutting food chemicals, flavourings, texturisers, etc. out of your daily diet. Regarding sugar and salt, we know that the more you get, the more you need. That is called tolerance. It comes from the field of addiction, and there is no question that food has addictive qualities. It is more fundamental than most people realise.
People often ask me if food can really be addictive. Why do you think anything is addictive? Why is it possible for the human nervous system to get addicted? Where does that come from? Did somebody decide we should have an addiction pathway? What purpose could that possibly serve? It is about survival.
Evolutionary biology cares about survival. The reward mechanisms in the human nervous system, and the nervous system of many other species, favour things that support survival, and among those is getting a variety of crucial foods and crucial nutrients.
In a natural world where sugar is hard to get, where you find it in breast milk when you are a newborn, and you find it in honey that you have to wrestle from bees, and you find it in wild fruit, getting sugar is a good thing. There was no concern about excess sugar in the past. Getting sugar, and getting salt, was a good thing. Terrestrial animals will routinely go to a salt lick because it is hard to get enough salt on land. There is an incentive to get salt. The more you get, the more you want. Those are survival mechanisms. It is those reward pathways for survival that were co-opted by drugs and turned into addiction. They are not addiction pathways. They are survival pathways. They exist for food and sex, the two things that are conducive to the survival of the individual and the survival of our genes across generations.
It is not a question of: ‘Can food be addictive?’ Food is the reason anything's addictive. Food is the reason we have these pathways in the nervous system to begin with. Therefore, the more sugar we get, the more sugar we need to feel satisfied, and the more salt we get, the more salt we need to be satisfied. Taste bud rehab says that you can reverse that. If you dial down the sugar, you need less and less to feel satisfied. It is the same with sodium. The goal of this transformation is not just about telling you how you must eat, and you do not have to fix everything all at once. You can get there with one better-
informed choice at a time. The goal is to completely transform your palate so you prefer more wholesome foods. There are many studies that support this. I have 30 years of experience in patient care where I saw this happen innumerable times, but there are published studies that show the same thing: when you transform dietary choices and diet quality incrementally, ultimately leading to a complete overhaul of diet quality, people come to prefer foods they used to dislike, and they become averse to foods they used to prefer. They learn to love foods that love them back, and that is a beautiful place to spend the rest of your life.
That is how I eat, and that is how my family eats. I do not eat food that I dislike. I love the food that is good for me. I do not like the food that is not good for me. I cannot stand it; it is too sweet for me, too salty. I have seen patients who started out one way and ended up the other. Taste bud rehab is a powerful concept, and I think that needs to be folded into the coaching we do. Rather than throwing people into a diet that is radically different from what they are used to, teach them to love food that will love them back. Give them a little bit of time to habituate, and they will have a better life as a result.
Q4‘How to Eat’, the book you co-authored with Mark Bittman, aims to cut through the confusion surrounding food, health, and diet. What do you believe is the biggest misconception people have about nutrition today?
‘How to Eat’ is my most recent book, which I did with Mark Bittman. Mark, among other things, has been a columnist for The New York Times for
many years and is extremely knowledgeable about food systems and food policy. Mark lives on a farm, so we went there, closed the door, and asked one another questions until we ran out of steam. We recorded it all, transcribed it, and then distilled it down to this book. The whole thing is a conversation. The way the book reads is like inviting the readers to just pull up a chair to the coffee table where Mark and I are just chatting. I joke in that book that it ought to be seven words long, and none of them should have been ours. They should be Michael Pollan's “Eat food. Not too much. Mostly plants.” The biggest misconception about diet is that there are misconceptions about diet. It is that simple.
Mark and I talked a lot about this: why are we lost and confused when it is really that simple? We will answer all your questions. What about dairy, and what about yoghurt? What about the microbiome? Can I eat to feed my brain, and can I eat to feed my heart? What about my immune system? Are omega-3s really that good? We broke it down and went into all the particulars, but we agreed on this: eat food, but not too much, mostly plants. Therefore, the main misconception about diet is that there is any real complexity.
For people thinking that it cannot be that simple, think about any other creature. Think about lions or wildebeest. Wildebeest need to eat grass because of the type of animal they are; we would not even think to ask if grass is good for them. Meanwhile, lions must eat wildebeest (or something like them). They cannot eat grass: they are constitutional carnivores. The questions are: what kind of animal are you, and what are you adapted to eat? A big part of
this begins with humility and the recognition that humans are a kind of animal.
Q5With so many conflicting opinions on dietary patterns, how do you define the ‘best’ diet, and what key principles should health care professionals keep in mind when guiding patients?
Optimising diet cannot fix everything. Eating optimally, not smoking, and being physically active give you no guarantee. The way I have always explained it is this: we can be good captains, we can have a good crew, and we can sail the vessel well, but we will only ever be masters of the ship and sails. We will never control the wind and the waves, so anything can happen. No matter how seaworthy your vessel, your body, is, no matter how well cared for or how well crewed it is, there are gales at sea that will cause the best vessels to founder. We get no guarantees, and we ought to be prepared to deal with that. However, it makes no sense to devote all of our resources to the residual 20% of human adversity that we cannot reliably prevent while ignoring the 80% we can. There is a balance to be struck there. Every health professional should be addressing diet and nutrition because it is a critical predictor of everything that matters.
I have a textbook, ‘Nutrition in Clinical Practice’, that is written for healthcare professionals. It is like a peer-reviewed publication, except it is not a single article, and the fourth edition of that textbook has about 20,000 citations. You cannot be biased in your job. If you are going to write a textbook, you must review all the evidence, including the evidence you like and the
evidence you do not, and you must fairly adjudicate all of it and reach a summary judgment. It is perfectly clear that the basic theme of optimal eating for the kind of animal that we are is real food, mostly plants. It is also equally clear that all this nonsense about one superior diet is just confabulated. For instance, we do not have long-term randomised trials comparing an optimal Mediterranean diet, vegan diet, pescetarian diet, and Okinawan diet. We would have no basis to say which of those is the best if we were to match for diet quality, which can be measured objectively.
There is no single, narrowly defined, prescriptive diet for everybody. However, there is one basic theme of healthy eating that makes sense for everybody: eat mostly fruits, vegetables, whole grains, beans, lentils, nuts, and seeds or some combination thereof, and drink mostly plain water when thirsty. If you get that right, you simply cannot go too far wrong. If you get it wrong, it does not matter what else you do; you are not going to get your diet right. It is that simple.
Q6You are the Founder of the True Health Initiative (THI), a global coalition of experts from over 50 countries, united to combat misinformation and disinformation that impact public, personal, and planetary health. How do you ensure a unified, evidence-based consensus on nutrition and lifestyle medicine despite differing cultural and dietary norms?
I have two answers, and they are both actions that I have taken. The first is that we should look beyond any one person's opinion, to a global consensus of diverse experts with passions ranging
from paleo to veganism about the aggregation of scientific evidence and its sensible interpretation. Years ago, when I founded the THI, the innovation there was to start inviting my friends and colleagues, who had very diverse opinions about diet, and explore whether or not we could agree about the fundamentals of a healthy diet. If you have spent your whole life studying one diet, when asked which diet you think is best, you will choose that one. A colleague who has studied a different diet will make a different choice. However, if I ask both what the fundamental principles of a generally healthful diet are, they are likely to agree: real food, mostly plants. I created a pledge that said this is true based on the weight of scientific evidence, and I believe the public deserves to know it is true. While I may have my more narrowly defined specific opinion, I support these general principles. I started asking people to take the pledge and sign up, and it was not long before I had hundreds of colleagues from 50 countries, from paleo to vegan and everything in between, saying ‘we agree’. One thing to do is to look at that kind of evidence, rather than any one person's opinion.
The second thing to do is move past opinion and ideology altogether and do what we do in medicine, which is to adopt an evidence-based approach. We have to be interested in a measure of diet quality that is objective, validated, and correlates with the things that matter most: years in life and life in years. The approach that is most widely used around the world is called the Healthy Eating Index (HEI). The most current version is the HEI 2020, which is an aggregate view of food and nutrient components of the diet that creates a quantitative measure on a 100-point scale.
The higher that number, the lower your risk and probability of dying prematurely from all causes, and the lower your risk and probability of developing any major chronic disease. This has been shown over and over again in massive studies involving hundreds of thousands of people spanning decades. It is epidemiology over ideology. We are scientists. We have signed up to the principle of evidencebased medicine, and that should pertain to nutrition as well. I can't understand why we tolerate fad diets when diet quality, measured objectively, is the single leading predictor of premature death. We should be looking to the evidencebased, sensible interpretation of science, and global expert consensus. The basic theme of optimal feeding for Homo sapiens is not up for debate.
It is perfectly clear that the basic theme of optimal eating for the kind of animal that we are is real food, mostly plants
Q7Can you please tell us a bit more about Diet ID and, given that diet quality is a key predictor of overall health and longevity, how does it help individuals and healthcare providers accurately measure and improve dietary habits at scale?
How do we enable and empower clinicians who are too busy, have too little time, and too many other things to deal with to address nutrition? The answer is twofold. The first method involves innovations, particularly digital delivery, and then community support, and I am involved in both
of these efforts as well. I was in academic medicine for 30-odd years, spent most of my career affiliated with Yale University, both conducting clinical research and seeing patients there. Six years ago, I left academic medicine to become an accidental entrepreneur because I invented something that was too important to neglect, and the only way I could get it to daylight was to start a company. That company is called Diet ID. We invented, developed, widely deployed, patented, published, and validated the first fundamentally new way for conducting comprehensive dietary intake assessments in about 50 years. We can do comprehensive dietary assessments in 60 seconds over any digital interface. Among the data generated instantaneously is an objective measure of overall diet quality using the HEI 2020. We can put that information in front of every clinician, which is a game changer.
It is like the invention of the blood pressure cuff. Diet ID is to diet is what the blood pressure cuff is to blood pressure. Before the blood pressure cuff was invented, you might have asked how we got clinicians to engage with the importance of blood pressure. We all know it is important, but we measured it in no one before we had a scalable means of doing so. Thus, no clinician had that cue to action. Then the blood pressure cuff was invented and socialised, and it democratised access to that crucial information. The next thing we knew, medical education raced to catch up with that information. I am on a mission to make diet quality a vital sign. It deserves to be, and now it can be. We have the means.
The second part of my answer is that every clinician should be looking at an objective measure of
every patient's diet quality. Every patient should also be looking at that information. Everybody who knows their blood pressure should know their diet quality and whether or not it looks healthy. Ideally, we would try to create synergy between clinicians, communities, and culture because when we think about healthy living, it is not a clinical enterprise but a cultural enterprise.
If, for a minute, we look at the world's Blue Zones, those five populations around the world where people routinely live to be 100 and do not get chronic diseases, they are not thanking doctors for those advantages. It happens as a by-product of culture in Ikaria, Greece; Sardinia, Italy; Okinawa, Japan; Loma Linda, California; and the Nicoya Peninsula, Costa Rica. Those five places around the world, where you have the most healthy, vital centenarians with intact minds, are healthy because of their culture, because eating well, being physically active, not smoking, sleeping enough, and not stressing too much are the default. A strong sense of community and social interactions is also the default. We need that.
If we do not have that natively, and most of us do not, then we need to create it, and we need to empower clinicians with awareness of relevant community resources. They need to be empowered with digital resources so they can not only measure your current diet but also help identify an optimised and personalised dietary goal for patients. What we offer allows for all of that. I would like to be able to offer you an app that will coach you every day on how to get from where your diet is to where you want it to be. I would like to be able to point to resources in the community, such
as restaurants, and programmes, that will empower you and make it much easier to get your diet where you want it to be. All of this is in service of adding years to your life, life to your years, and allowing you to love food that loves you back.
If all these elements come together to empower clinicians, I think they will be much more interested in addressing diet. There are several reasons why they do not: they are not trained to do so, they do not have the time to do so, and there is also frustration. Without the right resources, they are basically advising patients to do something that is too hard to achieve. They are also doing it in the dark because they have no real information about the patient's dietary intake or diet quality, so they can only give generic advice: your diet is likely not as good as it should be, and you should probably eat more fruits and vegetables. That is not actionable. We need to measure diet quality and dietary intake in everybody. We need to identify a personalised goal and the difference between where you are and where you want your diet to be, and provide resources to help get there from here. We need to address all the relevant support at the level of community and culture, and create a bridge between clinic and community. That way, we could transform diet quality in the modern world.
Q8As someone who has worked extensively to bridge the gap between science and public action, what steps do you think are necessary to ensure that future healthcare policies and dietary guidelines are both evidence-based and widely accessible?
There is a general way of thinking about cultivating political capital and taking advantage of government systems, which involves thinking in terms of win–win scenarios. You want to do good for the population, but whoever you are talking to is going to immediately convert the conversation to money. Now, as a public health physician, I tend to think that the currency that matters most is the currency of the human condition, but everything must be paid for using another currency, and it is not long before every conversation turns to how you are going to pay for something. We should think about scenarios where everyone wins and try to advance them.
predict the change in risk factors for chronic disease, the change in incident and prevalent chronic disease, and the amount of change in dollars spent. We can project the financial savings for food as a medical intervention.
Diet ID is to diet is what the blood pressure cuff is to blood pressure
For example, we built a return on investment (ROI) calculator for food as medicine interventions. We simply connected the dots. We explained that there is literature showing how changing objectively measured diet quality reliably changes risk factors for chronic disease and the incidence and prevalence of chronic disease. There is literature telling us what the average annual per capita cost is for obesity versus not, or Type 2 diabetes versus not, or coronary artery disease versus not, and we know how we would move the needle with shifts in diet quality. If we connect all that, if we know the population and the baseline epidemiology and are able to improve mean diet quality by a certain number of points on the HEI 2020 scale, we can confidently
What I have tried to do over the course of my career is look for these win–win scenarios, and it all begins with an educated consumer. We have got to activate the public, so they care, because politicians are never going to do anything the public does not care about. Ultimately, politicians are answerable to the populations that put them in power, return them to power, and preserve their power. If we care, they will care. We need to be informed about how we should care, why we should care, what we should care about, and what we are after. We do not want to just cut fat or carbs. We want higher-quality food. If that became political will, and then we offered governments and business leaders the opportunity to do it in a way that saves them money, so there is a financial incentive for them, everybody wins.
Q9 What emerging trends do you find the most promising in the field of nutrition and lifestyle medicine?
I am a big fan of the food-asmedicine movement, and I work in that space now. I think medically tailored meals and food delivery, as both a convenience factor and a way of addressing personalised nutrition, are really important. I think diet quality should be a vital sign. We have that capability, and it would be a monumental advance. It would change everything, just as the blood pressure cuff did.
The one other thing that is clearly a trend, and deserves to be,
is respect for multiculturalism. For far too long, for example, in the United States, a lot of our conversations were about the Dietary Approaches to Stop Hypertension (DASH) diet, or the diet used in the Diabetes Prevention Program, these big NIH-funded studies, where a particular dietary pattern was used. We also tended to talk to people as if there was no other option, no matter who you were or where you were from. That is just wrong. We need to meet people where they are. One of the important innovations in advancing diet quality for all is recognising that we are multicultural societies, and the optimal diet for somebody from a Latin background is not going to be the same as the optimal diet for somebody from East Asia. We should celebrate culinary traditions and acknowledge that we can and must optimise diet quality, using the same high objective standards for measuring diet quality, across this multicultural expanse. If that means developing new tools, we should develop new tools.
Some colleagues and I just published a paper on an adaptation of the HEI. That is the most widely used, robustly validated measure of overall diet quality, but it is related to prevailing nutrition standards
References
1. McGinnis JM, Foege WH. Actual causes of death in the United States. JAMA. 1993;270(18):2207-12.
and dietary guidance in the US and other developed countries. However, if you look around the world, there are some radical differences in how different cultures eat. In East Asia, for example, almost everybody is lactose intolerant, so there is almost no dairy in those diets. There are points for having dairy in your diet in the HEI, and that is not fair, because it would score a Chinese or Japanese diet, no matter how good it was, lower than an American-style diet. That makes no sense, particularly when you consider that Okinawa has one of the world's Blue Zones, so we know that that kind of diet can lead to a longer life.
Hence, we invented something called Adaptive Component Scoring,2 which looks at food groups that come and go with different time-honoured cultural practices and adjusts the scores, so the playing field is level. I think there are a host of related innovations we could use to help people know what their diet is and what it ought to be, to help them understand the divide between where they are and where they want to be, to empower them to get there, to put that information in front of their clinician, who can help them and endorse the journey, to have community-based resources that aid and empower both clinician and patient, and to
2. Katz DL et al. Application of the Healthy Eating Index in a multicultural population: introduc-tion of Adaptive Component Scoring. Front Nutr. 2025;12:1511230.
have financial incentives. We are using behavioural economics and structuring these things in a way where everybody is a financial winner because we are earning back the money that we are spending, and we are saving on the care for chronic disease. We are doing what we set out to do, adding years to life, adding life to years, and saving money.
As I mentioned at the start of all this, the basic theme of feeding Homo sapiens well is real food, mostly plants. There is far too much consumption of meat in the modern world, and that is detrimental, not just to human health but to our fellow creatures, who are often abused horribly in factory farms. It is also devastating to the overall global environment because there is a massive amount of water use, land use, nitrogen use, and greenhouse gas emissions, particularly associated with beef. These shifts in dietary patterns for the sake of human health benefit the planet’s health as well. As I think about where things go from here, it is about a respect for the basic theme of optimal eating. It's also about a respect for the multicultural variance on that theme of optimal eating and doing everything we possibly can to pursue the confluence of human health and planetary health.
Amanda Daley Professor of Behavioural Medicine; Director, Centre for Lifestyle Medicine and Behaviour (CLiMB), Loughborough University, UK
Q1You have dedicated much of your career to investigating the effects of lifestyle interventions on health outcomes. What would you say are the most exciting advancements in this area in recent years?
Lifestyle medicine is a large topic area to cover, but there have been some notable advancements in the areas in which I work that are worth highlighting here.
There has certainly been greater emphasis on empowering health professionals to support patients to prevent, manage, and potentially even reverse chronic diseases, such as diabetes and obesity. We have also seen a lot of developments in how we best deliver lifestyle interventions to the population, whether this be to healthy individuals or those living with a chronic disease.
obesity in the population. It will be interesting to see how this debate plays out in the coming years and whether governments introduce stronger regulations to deter purchasing and consumption.
The rise in the use of new weight-loss drugs, also known as anti-obesity medications, is having a profound effect on how people think about their weight
There is a relationship between the food we eat and the risk of developing chronic illnesses. Much of our food today is processed and/or pre-packaged, and full of sugar and refined white starches. In both the academic literature and the media, there has been a strong interest in the contribution that ultra-processed foods play in causing disease and ill-health, particularly how these types of food may impact the health of children, who, through persuasive marketing strategies, are frequent consumers of these types of foods. While ultraprocessed foods taste nice and are often cheap to buy, there is no doubt that regular consumption contributes to overweight and
While not strictly lifestyle medicine, the rise in the use of new weight-loss drugs, also known as anti-obesity medications, is having a profound effect on how people think about their weight and how they can best achieve significant and lasting weight loss. Unfortunately, minimising weight regain after people stop taking these weightloss drugs has not received the same level of attention. Important questions have been raised about the side effects of these drugs and whether relying on medication is the right approach to reducing obesity in the population. Nevertheless, the evidence to date has shown these drugs to be very effective in helping people lose weight.
Several countries have introduced a soft drinks industry levy, often referred to as a ‘sugar tax’, which applies to soft drinks containing added sugar above a certain threshold. The primary aim of sugar taxes is to incentivise manufacturers of soft drinks to reformulate their products to lower sugar recipes. It has been introduced as part of government initiatives to reduce childhood obesity. Many drinks manufacturers decided to reduce the sugar content in their products to reduce their tax liabilities, although some have opted to pay the tax instead. The sugar tax also aimed to encourage consumers,
particularly young people, to choose cheaper, low-sugar drinks over more expensive, high-sugar options. Not everybody is happy with the sugar tax; however, it is viewed as an overall success in reducing the amount of sugar sold in soft drinks.
An initiative called social prescribing has come a long way in recent years. Social prescribing takes a holistic approach to health by connecting people to community groups for practical and emotional support. Social prescribing recognises that the environment in which we live and our social connections play a critical role in influencing health. Social prescribing refers patients to local, non-clinical services that they select based on their
interests, goals, and needs, and allows health professionals and interprofessional health providers to refer patients to communitybased programmes for support. Examples of the opportunities offered include attending an exercise class, a hiking group, an art group, volunteering, or a community gardening group. Social prescribing aims to empower people to improve their health by developing new skills, participating in meaningful activities, and becoming more connected to their communities. Social prescribing is likely to continue to grow and develop in the coming years, and many ongoing research studies are evaluating the impact that it can have on health.
Q2 Your research focuses on testing lifestyle interventions that can be delivered by healthcare professionals within routine National Health Service (NHS) consultations. Can you elaborate on how you teach healthcare professionals to include these interventions in their consultations?
The Making Every Contact Count (MECC) initiative aims to use the thousands of consultations that take place every day between healthcare professionals and patients to promote healthy behavioural changes. Specifically, MECC seeks to enable and encourage healthcare professionals to capitalise on naturally occurring opportunities in routine practice
to deliver brief health behaviour change interventions to patients. While this may sound straightforward, delivering this at scale within healthcare services is complicated. On a more practical level, healthcare professionals also need to be willing to routinely have conversations about changing health behaviours within consultations each day. Some conversations will be more difficult than others. For example, we know that raising the topic of weight with patients who are living with obesity can be uncomfortable for healthcare professionals who may be concerned about offending patients. However, we also know that it is possible to train healthcare professionals to feel comfortable and be skilled at having these sensitive conversations with patients, and there are now several training resources available to support them. As we strive to live in a more open and inclusive society, MECC is for everyone and may reduce health inequalities because the idea is that all patients receive this support within consultations.
Q3 Are there any key insights in your ongoing research that you think may influence the integration of lifestyle interventions into a clinical setting, and are there any barriers you expect to experience?
One of the key barriers to the integration of lifestyle interventions into clinical settings is the focus of health policies on the treatment of diseases, rather than prevention. Thousands of people die around the world every day from diseases that could be prevented by participation in regular physical activity and weight loss. There must be a fundamental shift in mindsets and health policies towards preventing disease from occurring in the first place.
Without this, we will be constantly swimming against the tide.
Q4
The research you are doing in relation to physical activity calorie equivalent (PACE) food labelling is particularly interesting. Could you describe what this is and how you think this approach could transform public understanding of food choices and ultimately influence behaviour changes on a larger scale?
The public finds calorie labelling difficult to understand, or they do not understand the meaning of the calorie information when it is presented, which is often abstract and can be misleading. Therefore, we need to find other ways to help the public make healthier decisions about what they choose to eat. An alternative or complementary approach to calorie labelling is to provide this information as PACE labelling. The PACE approach to food labelling shows the public how many minutes of physical activity (e.g. walking and running) is equivalent to the calories in food. For example, “the calories in this burger require 120 min of walking to expend.” PACE labelling may catch consumers' attention more than other types of food labelling and may help the public to more easily understand what calories in food means by providing a context in which they can interpret the calorie information. PACE labelling may be particularly useful when displayed on discretionary foods such as cakes, biscuits, and chocolate, which tend to be high in sugar and calories, while offering little nutritional benefits.
Once people have this information, they can then decide if the calories are worth the physical activity required to expend them. PACE labelling has the potential to serve as a regular reminder to the public about the importance of
participating in regular physical activity to maintain good energy balance. We now have some evidence that PACE labelling may be useful in changing the food decisions of the public towards lower calorie options, and several studies have reported that the public (adults and children) support the implementation of PACE labelling to help them make healthier food choices. There have been some concerns that food labelling, such as PACE, might increase the incidence of eating disorders in the population. Whilst we don’t yet have any clear evidence of this happening, it is an important concern that needs to be considered if PACE labelling were to be implemented.
Q5
We are also very interested in the idea of Snacktivity™. Could you describe how the idea for this came around, and any promising results you have seen in your research?
Snacktivity™ is a novel approach to promoting physical activity that focuses on encouraging the public to accumulate at least 150 min of moderate-to-vigorous intensity physical activity per week by promoting short, frequent bouts called ‘activity snacks’. Activity snacks last between 2–5 min and include activities such as leg raises during television adverts, using the stairs and not the lift, and taking the dog for an extra brief walk. Snacktivity™ can be completed throughout the day while also undertaking daily tasks. In line with health guidance, Snacktivity™ also encourages participation in muscle- and strength-based activity twice per week.
There are several reasons why the public may find the Snacktivity™ approach useful for increasing their overall physical activity each day. Small changes are easier for
people to initiate and maintain than large changes. A common barrier to physical activity is a perceived lack of time, and Snacktivity™ addresses this by focusing on completing activity ‘snacks’ that only require a few minutes at a time. Epidemiological and experimental studies have reported associations between brief bouts of physical activity and health outcomes, providing the platform to test effects in randomised control trials which we are doing at the moment in a variety of populations and contexts. Additionally, Snacktivity™ reduces and/or breaks up prolonged time being sedentary each day, which also contributes to health issues.
The Snacktivity™ concept has been well received by the public, who believe it will help them to complete more physical activity each day, and trials are starting to emerge that show Snacktivity™ can help people to integrate more activity into their day. The Snacktivity™ approach has also been designed to allow healthcare professionals to have conversations with patients about integrating Snacktivity™ into their lives. We have also developed a training module for healthcare professionals to have conversations about Snacktivity™ during consultations.
Q6 Given the complexities of public health challenges such as obesity and chronic disease, do you think that current interventions are sufficient, or would you recommend we rethink our approaches to lifestyle interventions, particularly in terms of accessibility and sustainability?
Most of the population is living with overweight or obesity, and most people are not achieving
the recommended amount of participation in aerobic and muscle-strengthening-based physical activity. Furthermore, the health consequences of obesity and physical inactivity are expensive for health services. To me, it seems to be a false economy to help people change their lifestyle and then not offer support to maintain these changes. Tinkering around the edges in helping people change their lifestyles is not a long-term solution. In fact, we have been tinkering around the edges for years, so we already know this approach does not work. The reality is, we need substantial changes to public health policy to support the public in living healthier lifestyles, but this is not always politically popular because it can take a long time to see positive changes in health, so governments shy away from strong and decisive public health policy in this regard. We all know what needs to happen, but delivering on this is another matter.
Q7
Looking back on your journey from being an early-career lecturer to becoming a Professor and Director of the Centre for Lifestyle Medicine and Behaviour (CLiMB), what advice would you offer to healthcare professionals who want to take a more research-oriented path in their careers?
If I were to give advice, I would say to take time to think through your research ideas and talk to as many people as you can about what your vision for the future is. Mentorship is important in a research-oriented career path. You will need people on your side, but you also need people to challenge you and help you think critically about your research. Collaboration with others is critical, and the best science is
team science. We can achieve so much more by working together to improve health. There can be quite a lot of rejections in a research career, whether that be for grants or publications in journals, so it is important to plan for rejection at the outset and have a backup plan of what to do next.
A research career path can be relentless in terms of time and expectations. For example, there can be long hours of writing grant proposals, analysing data, and interpreting research findings. With this level of pressure, it is very important to also look after and protect your own health and wellbeing. It is ironic that in the pursuit of trying to improve the health of others, we often forget to look after ourselves, but there is nothing more important than our own health. I prioritise my own health by making sure that I have time to run five times a week, and if I am struggling to meet this goal, then it is a clear sign my work–life balance is not aligned and something needs to change. I almost always prepare lunch at home, a simple sandwich and some fruit - this stops me needing to buy food on the go. Food prepared outside the home is typically much higher in calories and fat, and doesn’t taste as nice as home-prepared food.
We need to find other ways to help the public make healthier decisions about what they choose to eat
Lennard Lee
Associate Professor, University of Oxford; Chief Medical Officer, Ellison Institute of Technology, Oxford, UK
To start off, we would love to hear about what inspired you to complete so much research alongside your clinical work. Was this always your plan?
I'm a clinical academic, which is quite a rare breed of doctor, because what I'm doing, along with other clinical academics, is being present while maintaining a focus on the future. I treat people with what we know works in 2025, and I also try and bring through anything from the future. Doctors are very good at seeing where the new technology is coming from and bringing it to our patients and our shores. That's why I split my time between research and being an NHS Doctor.
Q2
How would you advise doctors who are currently training to find a balance between clinical work and research?
future with AI, preventative medicines, vaccine technologies, and mRNA. We can put doctors back into the position of feeling empowered about healthcare, so they can bring about change. Healthcare professionals, such as doctors, nurses, and pharmacists, are close enough to see where the issues are and where the solutions are. There's hope that, in the next few years, healthcare professionals can become that agent of change, which will allow the system to become better, much, much better than it is now. You shouldn't have to do the same process repeatedly. I believe you should be allowed the freedom to think of what the future could be and how it could be better. That ownership of the healthcare system is important for the future.
Q3
I believe you should be allowed the freedom to think of what the future could be and how it could be better
It shouldn't be a matter of either/ or. It should be both. Doctors are fantastic because we’re grounded enough to understand the science, and we also see what is needed. I believe a good doctor, a doctor of the future, is one who can understand what the NHS can do right now and envisage the 5–10 years of a patient’s journey. If we don't envisage that, our patients will be stuck in the here and now, will still have complications, and will still die early.
A core part of being a doctor should be seeing that 5-year plan and actively trying to achieve change. That will give patients more hope, because we see where the NHS is at the moment, and yet we can envisage a much brighter
A lot of your work now revolves around COVID-19. How did your work and areas of interest change as a result of the COVID-19 pandemic?
Many of us had to make a choice about what we were going to do and how we would contribute. People did fantastic things: volunteering for Lighthouse Laboratories, knitting, making personal protective equipment, donating to help the NHS, etc. It was absolutely wonderful. My way of contributing was to use my research skills and see how we could use data to inform policy. I sat on the Independent Scientific Advisory Group for Emergencies (Independent SAGE), and in my community, everyone wanted to know if we should continue chemotherapy during the pandemic.
In 2022, everyone said and believed that the safest thing to do was to keep everyone out of the hospital, make everyone stay at home, stop people from getting their treatments, and wait it out for a few months. This caused major problems. Every month, chemotherapy was being stopped for many reasons: patients didn't want it because they thought getting COVID-19 would kill them, hospitals didn't think they were safe, and doctors thought people should just stay at home. We pulled together a national data programme which linked 86 cancer centres, allowing them to share their data for the first time, and we had it published by May 2020. The answer was very clear: it was completely possible to keep people safe. People weren't dying of COVID-19 because they were on chemotherapy; that didn't make any difference at all. The levels of chemotherapy dropped month by month, which was very concerning. People who wanted chemotherapy were getting turned away, but after the evidence came out, no one stopped cancer services without data, because they could say, with confidence, that it was not the chemotherapy that was causing deaths.
The most amazing thing was that the USA was doing something similar. Their consortium was called the COVID-19 and Cancer Consortium (CCC19), while ours was called the UK Coronavirus Cancer Programme (UKCCP), and it showed exactly the same thing. Data changes policy, as it should. Interestingly, the National Institute for Health and Care Excellence (NICE) put out a statement at the start of the pandemic, saying that chemotherapy makes people immunocompromised, which weakens their ability to fight off an infection; therefore, COVID-19 can cause deaths. That type of
statement led to unusual practices in stopping cancer care for many people. I understand why people had to make these statements, and yet the reality is, policy should be guided by data. I was one of the doctors who wanted data to change policy, and we got some change, which was fantastic.
Q4
The development of the COVID-19 vaccine blazed the trail for recent vaccine development. We’ve heard you refer to personalised cancer vaccines as “science fiction”. Can you describe how they work, and why you describe them as such?
Cancer is different. Everyone with cancer has different types, which appear in different locations, and the genetic mutations are all different. On top of that, our immune systems are also different. Some people can fight a cold better than others. Ideally, you’d want to be able to design a vaccine or treatment that is based on what your immune system can recognise and the abnormalities seen in your cancer. That's what we call individualised, or personalised, medicine. It's always had similarities to science fiction. You buy chemotherapy, which is effectively a toxin or poison, and you give it to everyone; it's all the same drug. The current science fiction approach is using AI and designing the treatment specifically for your immune system and your cancer. The first generation of drugs has gone through and completed Phase III testing, so we’re just waiting for the results now.
No one saw this coming. All the investment that went into vaccine development and mRNA meant it could be made cheaper than ever. It can be given across the population, has a low side effect profile, and can be updated as needed. Everyone recognises that it's essentially the same vaccine, but they changed a little bit in the middle when updating the variants. Then people said: ‘Why can't we update that middle bit to target cancer and make a cancer vaccine?’ That’s what’s going on now, and it’s exciting to see so many immune responses against cancer now lasting up to a decade.
These are first-generation products, but they will continue to iterate. As the learning gets better, and as machine AI gets better, I think treatments will continue to get better, but we're now in this science fiction age of N=1, personalised, individualised therapies. That's why I like this field. It's a legacy of everything we've gone through, with major technology spheres coming together: AI, genomics, and mRNA, all combining to make this new field rise.
Q5 You mentioned some limitations, one of which is the task of making cancer vaccines easily accessible to patients, particularly considering how resource-intensive it would be. Can you see any ways in which we can, in the future, make this more accessible?
It's always had similarities to science fiction
The biomedical engineers of the world have perfected the art of making vaccines for millions of people. We have pandemic preparedness, which you can scale up and cover whole countries. However, we now have the opposite problem. Can you scale it down? Can you now make it high throughput while keeping in mind
that N=1, so everyone's going to be different? The greatest minds around the world are thinking about this because it’s the new frontier. It may be a limitation at the moment, but bioengineers are fantastic. Once the first drugs are approved, I think there'll be massive incentives to try and bring these economies of scale and shrink it all down again. I don't think it's an impossible problem. I think many people are currently considering this problem, and though it'll take a bit more research, we will get there.
Q6 You are leading the NHS Cancer Vaccine Launch Pad. Can you describe what this project is, what led to it, and how you planned to achieve its goals?
The first thing we needed to do was to coalesce the idea and keep it simple so that everyone could understand what was happening.
We had three goals that we committed to. We wanted to have 10,000 people through trials by 2030, a big but achievable number, considering about 400,000 people are diagnosed a year. We wanted advances across multiple cancer subtypes and, lastly, we wanted to stimulate a global advance. That's all we had to do. With that in mind, we asked people, ‘Do you agree with that? Do you support it?’ We invited all the leading oncologists, from all the cancer centres, into one room and asked them if this is something they believe in and wanted to champion. That first meeting went very well. Since then, we've had regular meetings and cancer vaccine summits, we write papers together, and we form policy reports. The aim here is to try and get the community to champion it themselves.
What we're seeing now is that together, we have created a community of people who want to see change happen in cancer care. When they open their sites, they let their patients talk to the press about it. This leads to faster opening times, more confidence, more trials, and more input in the UK. More lives are being changed, too.
It was a three-pronged approach: bringing the community together, sustaining the momentum, and maintaining the focus on doing it for our patients. By maintaining those things, we've managed to make it a great success. We're often the top global recruiter, which is quite phenomenal. It's what the UK does, which shouldn't be surprising. In 2020, we gave the world a pandemic vaccine. By 2025, we would have given the world a cancer vaccine.
Q7 Do you see the USA’s ‘war on vaccines’ impacting this work in any way?
We need to be very careful in this space, because two nations gave the world vaccine technology, which changed the world in 2020: the USA and the UK. We had our Vaccine Taskforce, they had Operation Warp Speed. Two of the leading technology providers in the pharmaceutical space worked hard and gave the world this amazing mRNA technology.
I think it’s right that the USA public questions the risks versus the benefits in many age groups. It's good to have dialogue, and yet, like all medicines, it should always be our personal choice at the end of the day. The tricky thing is that signals may be misinterpreted. If an anti-vax response means that cancer therapies are stopped, that's going to cause issues. If that leads USA funders to stop financing research in this space, it may inadvertently be sending signals about cancer therapies. If the market doesn't open, and healthcare systems don't want to engage in this, then it will be a shame. Everything that's been achieved is potentially at risk, including the investment in advancing this field and in bringing together AI and genomics. I don't know whether other nations would have enough headway, as everyone benefits when the whole world comes together to commandeer the charge. The drugs that come out of it, which are so close to being approved and licensed, are going to need the support of the global community. If one part of the world decides not to partake, no matter how effective the drugs may be, it will likely cause major issues. All nations need to stand together, because that's how cancer research is expedited.
Q8The NHS-GALLERI trial is ongoing. What are your expectations for the results of the trial, and how do you predict the rollout of a multicancer early detection tool could impact UK healthcare?
There is a vision that, if people do a blood test every year, you could pick up a cancer from a blood test alone, and it could be an early detection across multiple cancer subtypes. You wouldn’t have to wait until you have symptoms like pain, bleeding, vomiting, or diarrhoea. This could be possible because sequencing is getting cheaper, and the public doesn't mind giving a blood test, because it's an easy thing to do. It uses a similar sort of technology as AI and genomics, but this time, it's using blood tests alone. This trial was one of the world's biggest, with 140,000 people across the NHS, and it's now complete and in the follow-up stage. There are many other trials in this space too. If this is proven effective, and if it's sensitive enough, there is a future where people won't have to have cameras put in their bodies, and they won't need to go through all of these screening methods. It could be much easier, with just a simple blood draw. However, we don't know the results at the moment.
The UK once again led one of the biggest trials, showing our capabilities, opening up space, and showing the strength of the NHS. The results will need to be tested, but this could be a new form of technology. We may be in a world in which blood tests pick up your cancer earlier and, if caught early and cut out, vaccines hopefully stop it from coming back and give you decades of protection. If we ever get to that stage, it would be amazing.
All nations need to stand together, because that's how cancer research is expedited
Brown Physicians, Brown Medicine; Diplomate, American Board of Lifestyle Medicine, American Board of Integrative Health; Medical Acupuncturist; Assistant Professor of Medicine, Clinician Educator, Warren Alpert Medical School, Brown University, Providence, Rhode Island, USA
What initially drew you to preventative health, and was there a particular moment or experience that sparked your passion for this approach to medicine?
Both my parents were in the preventive health field; both were integrated providers, chiropractors, and acupuncturists. My dad has a degree in sports medicine as well, so I grew up with that frame of mind, thinking of prevention, prevention, prevention. This included a lot of healthy, whole food diets, plenty of exercise, and good social connections. I witnessed all those lifestyle medicine pillars from an early age. When I was thinking about the context for providing care to patients in a clinical setting, I drew on that early experience and knew that I wanted something in my work to be prevention-focused.
Q2
In what ways do you integrate lifestyle medicine into your everyday practice to help patients prevent chronic illness before it begins?
to expect that from me. When I meet them, we talk, and if, for example, they have high blood sugar and they are taking diabetes medication, I tell them that this is a reversible condition and we talk about goals and strategies regarding that. No matter what their condition is, we get back to the roots of the pillars, and I find that I actually save time in doing that. I think clinicians expect that it is going to take too much time to counsel patients on sleep, what they are eating, and how much they are moving. However, if you lay that foundation when talking to patients during their annual or preventative visits, I think they really appreciate it, and it saves you time later. You get to know their health goals and what brings them joy in their lives. What do they like doing? What are their hobbies? It creates a holistic picture of them.
Q3 Do you find that patients are quite receptive to integrating those practices into their lives?
If there's one word to summarise taking care of patients in a more lifestyle-focused way, it is connection
I work in a busy primary care practice, and here in the USA, our model should really be restructured. It is a little challenging to incorporate lifestyle medicine in everyday primary care due to time constraints. I focus on women's health, though I treat both men and women, and in our preventative visits, even in follow-ups, I really try to get to the root of the problem with lifestyle measures first. Everyone knows
I do. If there's one word to summarise taking care of patients in a more lifestyle-focused way, it is connection and really figuring out what brings meaning to their life. When you talk about trying to prevent chronic disease, it is about making sure they can do gardening, making sure they can hike that trail they like, or go to their grandson’s game. It is about making sure that they can continue to do the things that bring meaning and quality to their life.
Mariah Stump
Q4
How do modalities like yoga, acupuncture, and mindfulness enhance traditional approaches to preventative care?
All of these are ancient healing tools that we have had for thousands of years. In our Western-centric society, in the USA, we often think that they are not evidence-based enough, or that the trials are not randomised, so they are not scientific enough, and we are hesitant to recommend them. I think that this view is definitely changing: we have an excellent National Center for Complementary and Integrative Health at the National Institutes of Health (NIH), and various other institutes conducting research into these integrative modalities.
These modalities have been around for centuries. Acupuncture has been around for about 5,000 years, originating in China, but through the centuries it has become more and more well-defined. Now we have about 360–380 acupuncture points, depending on which text you are referring to, and you insert really small filiform needles at specific points in patients’ bodies. The formative clinical trials in acupuncture were around lower back pain and patients suffering from sciatica. Now, there are studies that have been done showing the benefits of acupuncture in reducing pain from diabetic neuropathy pain, knee and hip osteoarthritis, migraines, and fibromyalgia. It is also an evidencebased treatment for anxiety, depression, stress reduction, and many other conditions.
It is also a very effective option to get patients to reduce the dosing of their medicines. For instance, I used to see a lot of pregnant patients who would like to reduce their medications at that time. I also had a patient who was
on higher doses of opioids and narcotic medications for chronic pain, and over a period of about 3 months, while getting acupuncture every week, she was able to reduce her dosage by almost half. Then, in another 3 months, she came off it completely. These are medications she was on for 15–20 years. Things like this happen, and I have not seen these effects with other treatment modalities or when patients are taking medications for pain reduction. Something powerful can be achieved through acupuncture, and it is so important when you are treating patients, so many of whom are dealing with pain and are on medications that are not only inadequately treating their pain, but also often cause unwanted side effects. Acupuncture is a safe and very cost-effective method. I will argue that it should be more cost-effective, meaning insurance should cover more of it, as the actual tool itself is very inexpensive. The needles are around 10 cents. It is not a major injection. It is not a procedure where you are giving your patients medication in their joint or bloodstream with a risk of major infection. The needle is the intervention itself. I hope that we can use it more in the future.
Yoga, similarly, has been around for centuries. It originated in India, but it really has spread around the world. We know there is quite a large body of literature that shows the relationship between yoga and reducing lower back pain, anxiety, and depression, and helping patients with flexibility, balance, and mobility. I use it so much. I have my top five stretches, and I have a handout of those stretches that I give patients with lower back pain. They tell me that physical therapy is great, but that these are the five exercises that
they do every day to keep their back more flexible. I find it to be very much a part of the work that I do. I hope that other providers will also, even if they are not trained in acupuncture or yoga, feel inspired over time to say: these are the benefits of it, I think that you would improve with this, and here is someone doing it in my community. Raising awareness that it is evidence-based is very important. Also, training medical students and doctors-in-training on this evidence is essential.
All of these are ancient healing tools that we have had for thousands of years
Q5With your training in both public health and internal medicine, how do you approach addressing social determinants of health in prevention strategies?
One of the challenges that we face with the structure of our healthcare system in the USA, especially with insurance models that do not always recognise all of these evidence-based complementary modalities, is that when I teach the medical students at Brown University, their number one question is, “While these treatments sound great, how are patients going to pay for it?” I think it is a great question, and that is why we need to do exactly what we are doing, which is raising awareness and advocating for these modalities so that we can get insurance companies to realise that there's already a large body of evidence that exists. In some cases, very little evidence exists for the use of some of the medications we frequently prescribe for pain conditions.
Why are they not covering these less expensive, invasive options with fewer side effects for more patients? Often, patients will come in and they are underinsured, or they are working several jobs to try and support themselves and their family, and it is very challenging because these modalities would surely help them, but they aren’t covered under their insurance.
I often talk about the three free, accessible things that we can do. The first one is walking. A lot of my patients may have limitations and pain, so walking may not be an easy thing for them. For the ones that it does apply to, though, we talk about getting more steps in. Walking is free, easy, and great for their health. The second one is breathing; everyone has breath. I always bring it back to the breath. I have had training in mindfulnessbased attention training and mindfulness-based stress reduction. We focus on teaching patients three breath techniques they can use at any point in their day. It is free, easy, and anyone can learn it. I have even taught it to kids who find it helpful. I think these are things that are accessible always. I tell them, I am going to inspire you today; let us inspire each other by bringing it back to the breath. The third one is their mental state. When we talk about the mind–body interaction, there is so much that we can do in our daily lives. Even though there is a stressor in front of us, like traffic or someone taking forever at the grocery line, or whatever it might be, bringing it back to the breath and changing and creating space between that stressor and our reaction can improve how we respond. Sometimes those things seem really simple, but I tell patients that we can save a lot of money if we practise those three things every day.
Other things we talk about with social determinants of health are diet and access to healthy food. I think we forget that what we put in our bodies is our fuel. Everyone always thinks it is so expensive to eat healthily or that they need supplements, but if you focus on food as medicine, it saves you so much. I think it is easy if you remember that whole foods are plant-based foods from the ground and are often cheaper than buying packaged processed items. Ancient cooking methods, which we have moved away from in our cultures, are affordable if you buy in bulk, eat grains, have legumes, and cook with fruits and vegetables. Those are things that we talk about that cost very little and have an impact on people's lives. I do hope that by spreading awareness of lifestyle medicine, we will get more insurance coverage for all of these things.
Q6
You have led efforts to bring lifestyle medicine into medical education, what are the core lessons you believe all future physicians should learn about prevention?
Medical students all have so much to learn in such a small period of time, relatively speaking, but my core lessons are about bringing it back to the pillars of lifestyle medicine, mainly food as medicine and mental health, which impact physical health. I think we forget that in medicine and talking with patients, we discuss diabetes and heart disease, but some healthcare practitioners do not always ask about the patient’s social or mental state, or the psychological factors that influence those conditions and vice versa. For me, it is about the whole person. When I am teaching my medical students, I always come back to this: I can read in the patient’s chart that they have diabetes, and I understand that
they had a heart attack 5 years ago, but tell me how they are doing. Who do they live with? Who supports them? What do they do in their lives every day? Those factors really impact their habits, their preferences and their general wellbeing; sometimes we medicalise things so much, and we do not get to the heart of what the patients need. That is the movement.
I think lifestyle medicine is a difficult term for people because it somehow implies that you have to have a certain means to achieve these pillars. In fact, it is quite the opposite. It is really about getting back to the basics, the core properties that influence people's health, and how we can reach people. In essence, it is about getting back to the basic principles of how we lived centuries ago and prioritising eating more off the land in sustainable ways for our bodies and communities, and cultivating social connection and meaning in our lives. At the core, it is about connection and making sure that patients feel supported and have the resources they need to optimise their health. In the USA, it is not always equitable, so health equity is a big issue we are dealing with. Making sure that people have the resources they need to be able to make those lifestyle and health behaviour changes is so important, and is the gap we need to close. By educating more physicians and the next generation of physicians, I am hopeful that in 10–20 years, when I am further into my career, I will look back and say, we are really making strides in the USA. That is my hope while doing a lot of this.
Q7What challenges do you face in integrating preventative health concepts into traditional medical training, and how do you navigate them?
For me, it is about the whole person
I work in a very traditional academic medical centre at Brown University; it is the teaching hospital, and it has been like jumping through hoops to be able to practice acupuncture here. I only get half a day a week to do it; I wish I had more time, but I feel grateful for the time that I have. I am trying to do group visits and incorporate lifestyle medicine in the current clinic that I am already in. I envision that, hopefully, in around 10 years, lifestyle medicine will be more integrated into medical school and residency training so that it will just be a part of general primary care. Then enough primary care doctors will be educated in this, and you could go to your doctor, and most of them would know automatically incorporate this perspective when they create your treatment plan. It is just going to take a cultural shift. Right now, it is really hard because I have all these things that I want to do, I have these skills, I have this training, and then I have 15 minutes with the patient in front of me, and sometimes I have 10 topics to cover. The kind of dilemma that a lot of us are facing in this field is this: do we continue to stay in our academic centres where we are educating future physicians and take insurance, or do we go private, where you can set your own time with patients and have patients pay out of pocket for the ability to get more time with their physician. I have decided to stay in the traditional model because I hugely value teaching the next generation, and I want to keep advocating for these modalities to be covered under insurance. The barriers are time and the reimbursement
models that we have here in the USA, which don’t adequately reimburse us for the work that we are doing. I hope that I am doing the right thing because it is definitely not the easiest path, but it is a rewarding one.
Q8
What trends in preventative health do you find most exciting right now, especially as they relate to women’s health or primary care?
There are a lot of things people are asking me about. Everyone wants to be on the glucagon-like peptide-1 (GLP-1) medications for weight management. I do think we are at a crossroads where, in the next 10 years, we may be able to help so many patients with obesity, with their longevity and their health outcomes. I think that is exciting. However, we have to remember to balance initiating these medications with lifestyle changes as well to make the health goals sustainable in the long-term. It is so important to temper our approach with some logic and caution: we can prescribe the medication, but let us also do the walking, and the breathing, and the sleeping, and all the other things, like eating well.
There is also an interesting recent focus on checking hormone levels and treating patients with bioidentical hormones. Many of my patients who are perimenopausal and menopausal are coming to me asking if I can check their hormones as well as initiate hormone therapies. I think we have been seeing, over the past few years, a lot more testing and a lot more research being conducted for the perimenopause and menopause phases of life. Some women really struggle with the menopausal syndrome, and for them, hormone replacement therapy may be the best option.
But, again, the foundation must be laid in lifestyle medicine recommendations at the outset. I do think that patients need to be careful about compounded hormones and need to be able to know and trust the source of the medications. It is often difficult for the public to know the sources of what they read on social media or the internet, as there is quite a market out there for patients and it is confusing for consumers.
Q9If you could change one thing about how the healthcare system approaches prevention, what would it be and why?
In our country, many are very cautious about advocating for a national health insurance plan and a publicly funded healthcare system. While everyone wants the population to be healthy, we are not operating under the ethical principle that healthcare is a human right. We have to find a way to make sure that patients have access to affordable and timely healthcare, and that we have equitable ways of getting resources to them. We need to prioritise medical education and residency training, so that they include content in the curriculum on preventive health, lifestyle medicine, and evidence-based integrative modalities. If I had to pick one thing to change? It would be to restructure the healthcare system in a more equitable way. That way, we can get better reimbursement rates, and that modalities that have evidence behind them, that are helpful for managing chronic disease, are better covered by insurance so that more patients have access to them. Physicians who do this work of lifestyle and integrative medicine would not feel like they have to go private in order to make a decent living because their
hospital systems would recognise the work that they are doing. If we don’t make these changes, the people who need it the most will continue to lack access to appropriate healthcare. I think that is just unethical, and it really needs to be changed. Healthcare is a human right. These are core aspects of people's health that no one should be denied access to.
Disease
Tracking the natural history of Becker Understanding Becker Muscular Dystrophy: Disease Overview
overview1-3
Becker muscular dystrophy (Becker)
Is a serious, rare, neuromuscular disease that can result in irreversible loss of muscle function and can lead to loss of ambulation.
Becker is an X-linked, recessive disorder caused by a gene mutation impacting dystrophin and driven by contraction- induced muscle damage. As muscle damage accumulates, it can be more difficult to perform everyday activities like walking or climbing stairs.
Becker is a multi-system disease that can impact more than just ambulation. For example, patients may develop cardiovascular complications as well.
Muscle loss and functional decline
Can begin at any age in Becker patients. Once decline begins, it continues, so early diagnosis and disease management is crucial to help preserve muscle and overall function.
There are currently no approved treatment options for Becker.
Diagnosing Becker
The NSAA is a functional assessment that measures an individual's ability to perform 17 items that have real-world implications for individuals with Becker.3-6
Real-world implications for individuals with Becker
Measure
Jump, hop, run
Stand on heels
Rise from floor
Climb box steps
Stand on one leg
Gets to sitting
Rise from chair
Walk
Stand
The The
Activity
Playing sports
Walking on uneven ground, cycling, difficulty getting out of a chair, striding, cycling
Getting up after falling, playing on the floor with children
Independent outdoor mobility particularly easy tasks like stairs and sidewalk curbs
Dressing oneself, putting on shoes/socks while standing, reaching high shelves
Sitting up in bed, adjust to falls
Using a toilet independently, getting out of bed, using public transportation to get around
Walking to mailbox to pick up mail, hiking, everyday mobility
Grooming, preparing meals, adapting to mobility device, transferring to chair
The NSAA is a clinically meaningful measure of function
For individuals living with Becker, a 1-point change in NSAA can mean the
From using stairs or steps to requiring assistance from another person or mobility device.
Because Becker is a progressive, irreversible disease, early diagnosis and disease management is important to help preserve muscle and overall function.
Diagnosis of Becker can include:
From using the independently to asking to get up from the
Becker often undiagnosed, misdiagnosed, diagnosed late
Awareness about Becker in the general community remains a challenge and mistaken for Duchenne muscular dystrophy (Duchenne) or referred to as a milder Duchenne. However, Becker is not Duchenne.
Patient assessment of weakness, functional tests, family history of Duchenne or Becker
Lab tests showing elevated biomarkers of muscle injury, such as creatine kinase
Genetic testing with the identification of a pathogenic variant in the DMD (dystrophin) gene
Investigational are currently development treatment
Overview & Natural History
pts 0 pts The NSAA The NSAA consists of 17 items to evaluate motor function.
Hop left leg Hop right leg
Stand on heels
Rise from floor Run Jump
Descend box step (L)
Climb box step (L)
Stand one leg (L)
Descend box step (R)
Climb box step (R)
Stand one leg (R)
Get to sitting
Rise from chair Walk Stand
Each activity is scored on whether it can be completed
pts
Perform normally
Perform with compensation due to weakness
Cannot perform
the loss of independence in one or more activities of daily living. For example:
publication of this Infographic was funded by Edgewise
toilet asking for help the toilet.
From being able to get up from a fall to requiring someone else’s help to get back up.
Key Points
or general healthcare Becker is often dystrophy milder form of Duchenne.
Investigational agents currently in clinical development for the of
Abbreviations:
Becker is a serious, rare, progressive neuromuscular disease that leads to loss of muscle and impaired motor function.
The NSAA is a clinically meaningful assessment of function. Each NSAA item has real-world implications for Becker patients and score changes can represent significant impacts to a patient’s ability to perform activities of daily living.
The NSAA is utilized in muscular dystrophy natural history studies to longitudinally assess function and disease progression.3-6
Persistent decline in Becker muscular dystrophy
of Observation
Studies demonstrate an average decline in NSAA score of
0.9 to 1.7
Slowing or stabilisation of disease progression is a key target for Becker research. points per year.3-6
The NSAA is an assessment used in natural history studies to longitudinally assess disease progression and functional decline in Becker. Current studies demonstrate that individuals with Becker experience an average decline of 0.9–1.7 NSAA points per year.
Research shows that once decline begins in individuals with Becker, it is continuous and irreversible, so early diagnosis and disease management is crucial to help preserve muscle and overall function.
Becker muscular dystrophy; L: left; NSAA: North Star Ambulatory Assessment; Pts: points; R: right.
The Value of Patient Engagement in Preventive Medicine
Authors: *Guendalina Graffigna1
1. EngageMinds HUB, Consumer, Food & Health Engagement Research Center, Department of Psychology, Catholic University of the Sacred Heart, Milan, Italy
*Correspondence to guendalina.graffigna@unicatt.it
Disclosure: Graffigna has received grants from Chiesi Farmaceutici S.p.A, Alexion, Sanofi, and Lundbeck; personal fees from Sanofi, Chiesi, Roche, and Pfizer; and owns intellectual property of the Patient Health Engagement (PHE) model.
Received: 24.04.25
Accepted: 20.05.25
Keywords: Health equity, patient engagement, Patient Health Engagement (PHE) model, preventive medicine, social determinants of health.
In the context of increasing healthcare complexity and chronic disease prevalence, patient engagement is gaining recognition as a key driver of successful preventive strategies. This article explores how patient engagement, defined as a multidimensional psychological process involving emotional, cognitive, and behavioural activation, can enhance the effectiveness and sustainability of preventive medicine. Drawing on recent scientific literature, including the Patient Health Engagement (PHE) model and empirical studies by Graffigna and others, this feature highlights how engaged patients are more likely to adopt healthy behaviours, adhere to preventive guidelines, and develop trust in health systems. It also discusses psychological drivers of engagement, the role of digital health tools, the social determinants of health, and the importance of equity in engagement strategies. The findings support the view that fostering patient engagement is essential to move from passive healthcare consumption to active health citizenship.
AN EVOLVING PARADIGM IN PREVENTIVE MEDICINE
In recent years, the concept of patient engagement has gained increasing attention as a key element in improving healthcare outcomes and sustainability. This is particularly true in the field of preventive medicine, where success often depends not only on clinical efficacy but also on individual behaviours, motivation, and trust in health systems. Patient engagement is defined as the active, informed, and sustained involvement of individuals in their health and healthcare decisions. It is a multidimensional process encompassing emotional, cognitive, and behavioural elements that reflect a person’s psychological readiness and motivation to take part in their own care. An engaged patient is more likely to adopt preventive behaviours, seek timely care, and collaborate with providers. In contrast, disengaged individuals may avoid preventive services, exhibit mistrust toward healthcare systems, or feel unable to influence their health outcomes, often due to social or systemic barriers. A growing body of scientific literature emphasises that involving patients as active partners
in their care can lead to better adherence to preventive protocols, more efficient health services, and, ultimately, healthier populations. For example, engaged individuals are more likely to participate in vaccination campaigns, attend routine screenings, and follow health-promoting recommendations.1,2 These behaviours are fundamental to reducing the incidence of chronic diseases and lowering long-term healthcare costs. Engagement also plays a protective role against misinformation and vaccine hesitancy. Research conducted during the COVID-19 pandemic highlighted how engaged citizens were more willing to adopt public health measures and less susceptible to disinformation.3,4 This indicates that engagement fosters a more resilient and cooperative health culture, especially in times of crisis.
The shift toward patient engagement in preventive medicine reflects a broader transformation in healthcare philosophy, from a paternalistic model to one based on partnership and shared responsibility. Patients are no longer seen merely as recipients of care but as co-creators of their health outcomes. This transformation requires not only behavioural change on the part of patients but also cultural and structural change within healthcare systems. By fostering trust, competence,5 and motivation, engagement becomes one of the essential components of effective prevention. It enables people to see health not just as a clinical goal, but as a personal and social project worth investing in.
As research in this field continues to grow, it becomes increasingly clear that preventive medicine cannot succeed without engaging the people it aims to protect. Promoting patient engagement is not solely the responsibility of individual professionals; it requires system-level change. Training healthcare providers in communication and psychological skills is a first step.6 Equally important is designing care pathways that allow time and space for meaningful patient participation. Health systems that invest in engagement strategies may see long-term benefits in terms of cost-effectiveness, quality of care, and health equity. Preventive care, when combined with high engagement
levels, can reduce the burden of chronic diseases and increase overall population resilience. In this sense, engagement is not an optional add-on but a fundamental component of sustainable healthcare.
PSYCHOLOGICAL FOUNDATIONS OF ENGAGEMENT: THE PATIENT HEALTH ENGAGEMENT MODEL
The development of patient engagement relies on specific psychological conditions. According to the literature, key drivers include self-efficacy,5 perceived autonomy, and relational trust with healthcare providers. These findings align with principles from Self-Determination Theory, suggesting that patients are more likely to adopt preventive behaviours when they feel competent, in control, and supported. Therefore, communication strategies that promote preventive care should not only aim to inform but also to empower. Messaging that resonates with individual values, emotional states, and daily realities is more likely to activate and sustain engagement. This implies a shift from didactic, top-down campaigns to personalised, empathic interactions between systems and citizens. Patient engagement is understood as a multidimensional process, encompassing emotional, cognitive, and behavioural components. It goes beyond mere compliance with medical advice, involving a deeper psychological investment in one’s health management. Several models have been proposed to conceptualise this process. Among them, the PHE model, developed and validated in multiple studies,7,8 offers a structured approach that traces individuals’ emotional and motivational responses as they transition from passive subjects to proactive health agents.
The PHE model describes patient engagement as a progressive journey based on psychological readiness to take an active role in health (Figure 1). It consists of four distinct phases:
• Blackout (emotional shutdown)
• Arousal (heightened awareness with uncertainty)
• Adhesion (early behavioural alignment)
• Eudaimonic Project (full integration and self-realisation)
Each phase is characterised by a different way of coping with health demands and implies varying degrees of support needs.
Blackout
This phase typically arises in moments of psychological vulnerability, such as after a difficult diagnosis, a major health scare, or even a preventive screening result that triggers fear. Individuals feel overwhelmed and disconnected from their ability to take care of themselves. Health behaviours may feel incompatible with one’s lifestyle or identity, leading to inaction, sadness, or denial. These individuals often rely heavily on formal and informal caregivers.
Copyright Graffigna et al.7 2015.
Arousal
Here, individuals begin to acknowledge their health condition or risk. However, their knowledge and skills are still limited, and they may experience anxiety and hypervigilance. Preventive messages can be confusing or overwhelming. Support is needed to help them organise information, build self-efficacy, and develop positive expectations about their ability to act.
Adhesion
People in this phase show good acceptance and awareness of their condition or health risks. They comply with recommendations but still view them as external obligations rather than integrated habits. Health behaviours are not yet part of daily routine, and unusual events may trigger non-adherence. These individuals benefit from structured routines, simple selfmanagement tools, and encouragement to act autonomously.
Figure 1: The PHE-s® model.
Eudaimonic Project
From the Greek εὐδαιμονία (eudaimonia, ‘good spirit’), this phase reflects a full integration of health into one’s identity and purpose. Preventive behaviours become part of the person’s lifestyle and longterm goals. However, even in this phase, setbacks (e.g., new stressors, illness, life changes) may require renewed support and re-engagement. Peer networks, empowerment tools, and continuity of care are key to maintaining engagement.
Although the PHE model was originally developed for patients with chronic illness, it is argued that its principles can also apply to preventive medicine. Even individuals without a diagnosis can move through these psychological stages in response to perceived risk, medical advice, or health communications. For example, someone at high risk of diabetes or cardiovascular disease may initially reject preventive messages (blackout), feel confused about recommendations (arousal), begin adopting changes (adhesion), and eventually internalise a new lifestyle (Eudaimonic Project). Thus, the model offers valuable insight into how people psychologically engage with preventive care.
However, poverty, housing, employment, and education intersect with patient engagement and preventive behaviours. Thus, engagement cannot be considered purely an individual matter but socially mediated. Promoting engagement needs a process-like, systemic vision, in order to enable changes and participation at the micro level (direct care), the meso-level (healthcare organisation and management) and the macro-level (policy making) of the healthcare system.9
IMPLICATIONS FOR HEALTH SYSTEMS AND POLICY
This framework has particular relevance for preventive care, where individuals are often asked to take action in the absence of immediate symptoms. Whether it’s undergoing screenings, adopting healthier lifestyles, or getting vaccinated, these decisions require a degree of engagement that goes beyond information, they require
conviction, trust, and a sense of personal responsibility. Despite its promise, not all individuals engage equally with preventive services. Socioeconomic status, cultural background, health literacy, and past experiences with the healthcare system all influence the degree to which people feel capable and willing to participate. We recognise that engagement is strongly influenced by structural inequalities. Broader social policies are needed to enable universal access, community networks, and workplace protections, which are key to nurturing health engagement and participation. Digital inequality also impacts on the ability to get engaged. There is thus an urgent need for equitable strategies that adapt to diverse needs, particularly among vulnerable or marginalised populations. Inclusive communication strategies, codesign practices, professional training, and integration of digital tools tailored to diverse populations are needed. Examples include the use of multilingual communication, community-based outreach, and inclusive digital solutions designed for people with limited access or digital literacy. Without such considerations, engagement efforts risk widening health disparities rather than closing them. Digital health technologies are increasingly used to support patient engagement in prevention. Mobile apps, wearable trackers, telemedicine, and AIbased decision aids offer opportunities to monitor health behaviours and deliver tailored feedback. However, research emphasises that the effectiveness of these tools depends largely on their design and user experience. If implemented without regard for user engagement, such tools risk being ignored or misused. Scholars argue for a human-centred and co-design approach, involving users early in the development process to ensure the tools align with their motivational and emotional needs.10 Furthermore, digital technologies should be integrated with, not replace, the human aspects of care, such as empathy, continuity, and trust.
CONCLUSION
Patient engagement is increasingly recognised not as a marginal aspect of care, but as a core element of effective
preventive medicine. The evidence suggests that when individuals are supported in becoming emotionally and cognitively involved in their health decisions, their capacity to act preventively increases.
This shift requires a transformation in how healthcare systems communicate, design services, and interact with their populations, moving from information delivery to genuine activation and empowerment.
To make engagement a tangible lever for prevention, health institutions must invest in personalised communication, inclusive technologies, and a culture that values the patient’s voice. Moreover, attention to
References
1. Krist AH et al. Engaging patients in decision-making and behavior change to promote prevention. Information Services & Use. 2017;37(2):105-22.
2. James J. Health Policy Brief: Patient Engagement. 2013. https://www. healthaffairs.org/content/briefs/ patient-engagement. Last Accessed: 17 May 2025
3. Graffigna G et al. Relationship between citizens' health engagement and intention to take the COVID-19 vaccine in Italy: a mediation analysis. Vaccines (Basel). 2020;8(4):576.
4. Palamenghi L et al. Mistrust in biomedical research and vaccine
equity is critical: engagement strategies must reach beyond the “already engaged” and include marginalised groups, reducing barriers to participation.
In a healthcare era increasingly defined by chronic disease, pandemics, and resource constraints, the proactive role of the patient is not optional, it is indispensable. Engagement transforms prevention from a policy goal into a lived, shared responsibility. When patients are seen, and see themselves, as active partners, preventive medicine becomes not only more effective, but more humane and sustainable.
hesitancy: the forefront challenge in the battle against COVID-19 in Italy. Eur J Epidemiol. 2020;35(8):785-88.
5. Bandura A. Self-efficacy: The exercise of control (1997), New York: W. H. Freeman.
6. Garzonis K et al. Improving patient outcomes: effectively training healthcare staff in psychological practice skills: a mixed systematic literature review. Eur J Psychol. 2015;11(3):535-56.
7. Graffigna G et al. Measuring patient engagement: development and psychometric properties of the Patient Health Engagement (PHE) Scale. Front Psychol. 2015;6:274.
8. Barello S et al. Patient engagement as an emerging challenge for healthcare services: mapping the literature. Nurs Res Pract. 2012;2012:905934.
9. Carman, KL et al. Patient and family engagement: a framework for understanding the elements and developing interventions and policies. Health Aff (Millwood). 2013;32(2):223-31.
10. Barello S et al. eHealth for Patient Engagement: A Systematic Review. Front Psychol. 2016;6:2013.
Characterising Drug-Associated Nephrolithiasis: Insights from Global Adverse Drug Reaction Database
Editor's Pick
This insightful review examines drug-associated nephrolithiasis using the VigiBase pharmacovigilance database, identifying medications (some previously unrecognised) linked to kidney stone formation. Highlighting drugs such as indinavir, amoxicillin, and atazanavir, the authors provide valuable data on potential nephrotoxicity, offering important guidance for clinicians and future research.
Markus Peck-Radosavljevic
Klinikum Klagenfurt am Wörthersee, Austria
Authors: *Alexandre Baptista,1,2 Ana Macedo,1,2 Ana Marreiros,1,2 André Coelho3
1. School of Medicine and Biomedical Sciences, Universidade do Algarve (UAlg), Faro, Portugal
2. Algarve Biomedical Centre (ABC), Faro, Portugal
3. Health & Technology Research Center (H&TRC) - Escola Superior de Tecnologia da Saúde de Lisboa, Instituto Politécnico de Lisboa, Lisbon, Portugal
*Correspondence to ambaptista@ualg.pt
Disclosure: The data presented in this study were sourced from VigiBase. The interpretation and reporting of these findings are solely the responsibility of the author(s) and should not be construed as an official policy or interpretation of the Uppsala Monitoring Centre. The authors have declared no conflicts of interest.
Acknowledgements
A very special thanks to the Uppsala Monitoring Centre for allowing access to VigiBase for the completion of this work.
Received: 16.07.24
Accepted: 21.05.25
Keywords: Adverse drug reactions (ADR), drug-associated, nephrolithiasis, pharmacovigilance.
Purpose: Kidney stones are a common condition affecting the urinary system, with 8–12% of the global population experiencing them. Around 1–2% of all kidney stones are adverse drug reactions. VigiBase is a powerful tool to evaluate drug-associated events. However, to the authors knowledge, no study has yet analysed this database to identify the most common drugs associated with nephrolithiasis. The objective of this study was to analyse reports of nephrolithiasis and their associated medications in the VigiBase database.
Methods: The authors conducted a retrospective pharmacovigilance disproportionality analysis using data from VigiBase, covering 1968–2022. They employed the WHO’s IC025 index to identify drugs with significant disproportion in notification frequency. Identified drugs were assessed using a bibliographic score (BS), ranging from 0–5, to determine their previous role as lithogenic agents.
Results: Of the 33,932,051 notifications extracted, 35,008 were related to drugassociated nephrolithiasis. Among all identified drugs, indinavir had the highest disproportionality index (IC025 6.5), followed by amoxicillin (IC025 5.9) and atazanavir (IC025 5.3). The most frequently referenced drugs were adalimumab (n=2,193), infliximab (n=1,300), and etanarcept (n=1,287). Among these drugs, the authors observed a progressive increase in the BS associated with the IC025, with a IC025 of 1.52 for those with a BS=0, and a IC025 of 6.5 for those with a BS=5. Notably, more than 40% of the retrieved and evaluated drugs were not considered lithogenic by the BS evaluation, thus an extensive literature review was conducted to confirm their new potential nephrotoxicity.
Conclusion: Although drug-associated kidney stones were infrequently reported in VigiBase, the authors’ findings suggest potential new lithogenic associations with certain drugs, to be further analysed.
Key Points
1. Drug-induced kidney stones may account for up to 1–2% of all urolithiasis cases, yet are often under-recognised and preventable.
2. A narrative review based on pharmacovigilance data, structured by renal phenotype, focusing on drugassociated nephrolithiasis.
3. Recognising drug-induced stones enables better prevention, especially by reviewing drug histories in high-risk patients.
INTRODUCTION
Kidney stones are the most common condition affecting the urinary system, impacting approximately 8–12% of the global population,1,2 predominantly individuals aged 20–49 years.1 Drug-associated nephrolithiasis accounts for approximately 1–2% of all kidney stones.3 These stones can develop through two pathways: 1) poor solubility of the drug, leading to crystal formation in the urine,3 this model is seen with drugs like atazanavir,4 or other protease inhibitors, and with sulfadiazine;5 2) urinary changes caused by these drugs, particularly modifications in pH and/or changes in the excretion of calcium, phosphate, oxalate, citrate, uric acid, or other purines. Prime examples of this mechanism include dietary supplements containing vitamin D/calcium, or treatment with carbonic anhydrase inhibitors6 or topiramate.7
Pharmacovigilance is an essential tool for monitoring the safety and efficacy of medicines. Studies based on pharmacovigilance databases help identify the main medications associated with specific adverse reactions, providing insights into drugs strongly linked to these reactions. One such database is VigiBase, managed by the Uppsala Monitoring Centre on behalf of the WHO. It collects spontaneous and anonymous reports of adverse drug reactions (ADR) from more than 150 countries worldwide.
To the authors’ knowledge, no study has yet evaluated which drugs are more frequently reported in VigiBase and associated with drug-associated nephrolithiasis.
MATERIALS AND METHODS
The authors performed a retrospective pharmacovigilance descriptive analysis
of the largest global database of ADRs notifications, following approval from the review board. Data for this study were obtained from VigiBase, an extensive database that compiles spontaneous ADR reports from a wide range of participating countries, ensuring full anonymity of the data. Covering the period from 1968–2022, stringent protocols were applied to eliminate duplicate notifications, with each report receiving a unique identification number for accurate referencing. The dataset offers up-to-date information and includes comprehensive details for each notification, such as anonymised patient data, notifier information, the severity of the ADR, the implicated drug, and a description of the identified adverse reaction. Although the data pool was already anonymised, the study underwent ethical review by the Ethics Committee of the Faculty of Medicine and Biomedical Sciences of the University of Algarve, which granted consent for data evaluation.
The compilation of notifications was carried out after filtering for relevant Medical Dictionary for Regulatory Activities (MedDRA) terms, such as ‘nephrolithiasis’, ‘crystalluria’, and related terms. Within these notifications, each drug was recognised by its active ingredient, in accordance with WHODrug nomenclature standards. Moreover, the drugs were classified into pharmacological categories following the WHO’s anatomical Therapeutic Chemical (ATC) classification system. This method enabled a structured analysis of the data, focusing on distinct pharmacological groupings.
In this study, the authors employed disproportionality analysis utilising both the information component (IC025) and the reporting odds ratio (ROR). The IC025 compares the observed frequency of a specific adverse reaction associated with a medication against its expected frequency in the general population. The ROR calculates an odds ratio to evaluate the association between a medication and an adverse event.
An ROR >1 indicates a positive association, suggesting that the medication-induced adverse reaction occurs more frequently than expected. Therefore, while the IC
adjusts observed and expected frequencies using a Bayesian approach, the ROR offers a straightforward measure of association based on odds ratios.
For the main medications evaluated using IC025 and ROR, a bibliographic score was developed to quantitatively determine the degree of nephrotoxicity evidenced in the literature. Each drug was evaluated in five different bibliographic sources regarding its role in the formation of kidney stones (two databases,8,9 one website,10 and two reference books11,12). A bibliographic score (BS) was developed and considered a surrogate for each drug lithogenic role (0: not lithogenic; 1–2: potentially lithogenic; 3–5: lithogenic). The score assigned to each medication corresponded to the total number of sources referencing the adverse event.
RESULTS
Between 1968–2022, VigiBase, the WHO’s global database, accumulated a total of 33,932,051 notifications from numerous contributing countries. Out of these, we extracted 35,008 notifications associated with drug-induced nephrolithiasis, representing 0.1% of all reports during this period. These notifications implicated 3,283 active ingredients or combinations suspected of causing drug-associated nephrolithiasis.
Most notifications of drug-associated nephrolithiasis were reported by consumers (44.1%), followed by physicians (23.9%) and other health professionals (15.6%). The majority of reported cases originated from the USA (72.8%), Canada (7.4%), and the UK (2.8%). Female consumers accounted for the highest proportion of notifications (51.8%), with the most affected age group being 45–64 years old (29%), followed by those aged 18–44 years (16.2%), and the 65–74 years bracket (11.4%).
The MedDRA term ‘nephrolithiasis’ was the most frequently reported, constituting 94.2% of the notifications. ‘Urinary tract infection’ was the most common concurrent condition, noted in 8.3% of the cases (Table 1).
Table 1: Frequencies of either main or concomitant Medical Dictionary for Regulatory Activities terms most frequently reported.
MedDRA: Medical Dictionary for Regulatory Activities
Table 2: Drugs most associated with nephrolithiasis or having a higher disproportionality index and their relationship with the bibliographic score.
Table 2: Drugs most associated with nephrolithiasis or having a higher disproportionality index and their relationship with the bibliographic score. Continued.
ATC: anatomical Therapeutic Chemical; ATC A: alimentary tract and metabolism; ATC H: systemic hormonal preparations (excluding sex hormones and insulins); ATC J: antiinfectives for systemic use; ATC L: antineoplastic and immunomodulating agents; ATC ATC M: musculo-skeletal system, ATC N: nervous system; BS: bibliographical score; IC025: information component; ROR: reporting odds ratio.
Among the pharmacological classes associated with drug-related nephrolithiasis, the ATC Class L: antineoplastic and immunomodulating agents was most prevalent, accounting for 39.3% of the notifications; followed by almost as half of the notifications by ATC Class A: alimentary tract and metabolism (14.8%); and by ATC Class J: antiinfectives of systemic use (14.6%).
In terms of specific drugs, those with the highest disproportionality index, medications reported more frequently in this reaction than expected, included indinavir (IC025: 6.5), amoxicillin (IC025: 5.9), atazanavir (IC025: 5.3), and topiramate (IC025: 4.2). These drugs also had a high average bibliographic score of 3.75, within an interval of 3–5, demonstrating their known nephrotoxicity. Conversely, those most frequently reported (absolute numbers) as adalimumab (n=2,193), infliximab (n=1,300), etanercept (n=1,287), and the COVID-19 vaccine (n=1,140) (tozinameran accounted for 56.8% and elasomeran for 27.0% of the cases), showed a low average bibliographic score of 0.75, with scores ranging from 0–2. These scores suggest the possibility of new nephrotoxins.
Of the medications most frequently reported or with the highest disproportionality, 50%
had no bibliographic references indicating a lithogenic role (BS 0), while 23.3% were considered potential nephrotoxins (BS 1–2), with another 36.7% of those drugs evaluated being considered known nephrotoxins (BS 3–5), as detailed in Table 2
In 77.3% of the notifications for drugassociated nephrolithiasis, the cases were classified as serious, primarily due to the development of medically important conditions, which accounted for 67.4% of these cases and followed by caused or prolonged hospitalisation (42.2%). Within the serious outcomes, the ATC Class A: alimentary tract and metabolism, was most frequently implicated in fatal outcomes, reported in 31.9% of such cases. Sitagliptin emerged as the most frequently reported active ingredient in these notifications, accounting for 10.8%.
DISCUSSION
To the best of the authors’ knowledge, this study is one of the first to compile results from VigiBase, one of the world’s largest databases of spontaneous ADR notifications. It highlights drugs frequently implicated in these notifications, both by reporting frequency and disproportionality index.
Surprisingly, over 70% of the primary drugs reported, or with a high disproportionality index, were found to be non-lithogenic or only potentially lithogenic. Drug-associated nephrolithiasis appears to be a rare condition (or underdiagnosed), which is corroborated by the minimal spontaneous notifications during the study period.
Globally, men are more predisposed to developing kidney stones,13 although recent data suggest a shifting epidemiology, with an increasing incidence among women.14 The authors’ findings reflect this trend, showing a higher reporting frequency among female consumers (51.8%) compared to males (43.6%), although specific epidemiological data on drug-associated nephrolithiasis remain scarce. While differences in reporting patterns between consumers and healthcare professionals may exist, the authors' dataset did not provide sufficient information to allow for definitive conclusions regarding the source of the reports.
In the authors’ analysis and considering the main medications evaluated, half were regarded as potential new nephrotoxins or lithogenic drugs, considering their BS of 0. Overall, the medications evaluated showed moderate to low disproportionality values, except for some medications with BS 3–5. This suggests that the association of these medications with the phenotype in question is not strong.
In these potential new nephrotoxins or lithogenic agents, some stand out. One of these medications is the combination alendronic acid + cholecalciferol (IC025 3.7 and ROR 18.98), which did not reveal bibliographic references obtained through the authors’ BS. However, the absence of this association is curious since deeper research shows associations between cholecalciferol (IC025 2.3 and ROR 6.29) and nephrolithiasis.15 This raises the question of why the combination alendronic acid + cholecalciferol does not have such literature references. One possible reason is that this combination actually represents the association of two medications that are antagonistic to the formation of renal stones. Alendronic acid not only reduces urinary calcium excretion,16 but also inhibits the crystallization of the
calcium-phosphate complex,17 thereby preventing kidney stone formation.
Another medication considered a potential new nephrotoxin is the antiviral combination of emtricitabine + tenofovir disoproxil (IC025 2.8 and ROR 8.07), to which no literature references associating this dual combination with the development of nephrolithiasis could be found, even after extensive research, including exploration within HIV medication literature. IFN-β1a is another potential new lithogenic drug (IC025 2.1 and ROR 4.7), in which thorough literature evaluation failed to uncover any references that even remotely support this association. The same with natalizumab (ROR 3.57), nor was there in the evaluation of biosimilars.18
Ibandronic acid has been reported as a therapeutic solution for reducing kidney stone formation, noted as one of the most potent inhibitors of crystallisation.19 However, the authors found 83 notifications associating this medication with this phenotype. Upon further evaluation of these notifications, only five of them co-reported other lithogenic drugs as a concomitant medication, suggesting a potential bias in attributing the association between nephrolithiasis and ibandronic acid. Similar reasoning can be applied when evaluating the association between zoledronic acid and nephrolithiasis. However, among those medications for which the authors’ BS was null, there are some in which they were able, in a deeper literature search, to find associations with nephrolithiasis. One of those examples was omeprazole and pantoprazol, both known for their association with nephrolithiasis in a dose-dependent manner.20 Tofacitinib, despite having a BS of 0, is already known for its association with nephrolithiasis,21 albeit showing a low association with an IC025 of 1.49 and an ROR of 2.85. The same occurred with sodium oxybate, which has also seen nephrolithiasis reported as an ADR in other references.22
In the description of the results of drugassociated nephrolithiasis, the authors found that certain medications were reported much more significantly than
others. Among these, adalimumab (IC025 1.7 e ROR 3.44) stands out (6.3% of the notifications), which showed an BS of 2, indicating that it is already a medication with some evidence of nephrotoxicity. This medication is a monoclonal antibody that blocks TNF-α,23 used in the treatment of diseases such as Crohn’s disease and ankylosing spondylitis, with literature references associating it with this phenotype.24 However, as nephrolithiasis is an apparent extra-articular manifestation of the disease25 and adalimumab is used to treat these conditions, it is plausible that there may be biases associated with the incidence of nephrolithiasis associated with the use of adalimumab. In fact, recently, in a study evaluating the odds ratio of biological treatments and nephrolithiasis, adalimumab showed an odds ratio of 1.1 without statistical significance (p<0.05).26
Similarly to adalimumab, infliximab (IC025 2.7 and ROR 6.96) is a monoclonal antiTNF-alpha antibody,27 which was also described in the reported spontaneous notifications (3.7%). Indeed, prevalence studies of renal stone disease in patients treated with anti-TNF have demonstrated a significant association between this class of drugs and increased risk of nephrolithiasis, and recently this association was widely described in a Danish population-based study, which reported an increased risk of nephrolithiasis in patients under this type of medication.28
Finally, etanercept, a fusion protein of the p75FC receptor of human tumour necrosis factor obtained by DNA recombinant technology, used in the treatment of rheumatoid arthritis, juvenile idiopathic arthritis, psoriatic arthritis, ankylosing spondylitis, etc.,29 was the third most reported medication in notifications of renal stone disease associated with medication use, being involved in 3.7% of the notifications obtained. Its association with the nephrolithiasis phenotype, according to our results, was considered very weak, with an IC025 of 1.1 and ROR of 2.26. However, there may be some pathophysiological substrate for this association since etanercept has been associated with the
development of hypercalcemia,30 which is a strong risk factor for the development of kidney stones.
Among the medications showing a stronger association with nephrolithiasis (due to their high disproportionality index), indinavir stands out. This medication exhibited the highest IC025 among the highlighted drugs, with an IC025 of 6.5 and ROR 111.98, indicating a significantly higher disproportionality index concerning nephrolithiasis. In other words, it is involved in nephrolithiasis notifications much more frequently than expected in the general population. This aligns with extensive literature documenting the association between indinavir and nephrolithiasis. In fact, it is estimated that approximately 20% of patients taking this medication present some type of urinary crystallisation or even the presence of kidney stones,31 with isolated kidney stone formation estimated to have an incidence between 4–13%.32 The formation of kidney stones results from the excretion of indinavir in the urine, which has low urinary solubility, leading to crystal formation,33 causing up to 67% of patients treated with Indinavir to present with asymptomatic crystalluria, with symptoms in 8% and nephrolithiasis in 3%.34
Another medication strongly linked to this phenotype is amoxicillin (IC025 5.9). In fact, the association of amoxicillin with kidney stones is well known, especially when used in high intravenous doses.35 Despite this lithogenic effect, it also appears that this association is a characteristic of its pharmacological class, largely associated with the elimination of colonisation by Oxalobacter formigenes,36 leading to reduced fecal degradation of oxalate. Oxalobacter formigenes, by degrading oxalate in the intestine, results in lower urinary oxalate concentration, thus providing protection against calcium oxalate stone formation.
Similarly, atazanavir, another medication for HIV infection treatment, showed a strong link to nephrolithiasis (IC025 5.3 and ROR 47.34), often used in conjunction with other antivirals, notably ritonavir.37 Although its label states that nephrolithiasis
associated with atazanavir is “rare”,37 this association has been reported in post-marketing contexts.37 Specifically, atazanavir significantly increases the risk of nephrolithiasis more than other regimens involving other protease inhibitors.38 Atazanavir, by reaching high urinary concentrations, triggers the formation of atazanavir crystals,4 but only after long periods of exposure to the medication,39 which is the mechanism of its association with nephrolithiasis. Indeed, switching from atazanavir to other antivirals is recommended in patients who have developed kidney stones.40
Finally, topiramate, a medication indicated for migraine prophylaxis, was another medication that showed a strong association with this phenotype (IC025 4.2 and ROR 21.16). One of the earliest references to the association between topiramate and nephrolithiasis was in the year 2000,41 and since then, publications have been made about the various changes caused by topiramate, both in paediatric ages and in the underlying urinary pathophysiological mechanisms of kidney stone formation,42 where kidney stone formation results from the development of hypocitraturia and elevated urinary pH, leading to high formation of calcium phosphate stones. It is estimated that patients taking an average dose of 300 mg/day and with an average treatment duration of 48 months have a prevalence of symptomatic nephrolithiasis of 10.7%,43 although this association is disputed by some authors.44
Although pharmacovigilance studies do not provide definitive conclusions, they offer insights for further discussion and confirmation in dedicated studies. Identifying medications with high IC025 values should lead to several implications, particularly in terms of surveillance.45 A medication with a high IC025 value should undergo more rigorous and frequent monitoring by healthcare professionals and regulatory agencies (EMA, FDA, Brazilian Health Regulatory Agency [Anvisa]), which may conduct a more detailed safety review. This could involve additional data analysis, epidemiological studies, or even clinical
trials to confirm the association between the medication and the adverse reaction.46 In essence, a high IC025 serves as a potential alert signal that can trigger a series of actions aimed at ensuring patient safety and maintaining the medication’s continued effectiveness, while balancing the benefits and risks of treatment.47
Population-based or cohort studies published about drug-associated nephrolithiasis are scarce. One study that utilised a pharmacovigilance database specifically evaluated acute kidney injury in the context of nephrolithiasis but exclusively in patients using SGLT2 inhibitors.48 Other studies that also assessed pharmacovigilance databases for the adverse reaction ‘nephrolithiasis’ did so exclusively for specific medications or classes such as proton pump inhibitors49 and SGLT2 inhibitors.50 Another populationbased study only reflects a significant increase in the annual incidence of nephrolithiasis, at an average rate of 1%, in both children and adults, to which medications available on the market may have also contributed.51 Delving into the existing literature, the authors' data support medications such as topiramate, sulfadiazine, indinavir, atazanavir, and antibiotics, among other frequently implicated medications,52,53 while also putting into perspective the possibility of new lithogenic agents.
Research on nephrolithiasis associated with medication use also involves advancing our understanding of the mechanisms associated with the development of nephrolithiasis, whether they are metabolic risk factors related to receptors, promoters, and inhibitors, or through the evaluation of the roles of the immune system, microbiome, or sex hormones.54 In addition to this pathway, the discovery of new medications, or new treatment or prevention pathways for nephrolithiasis,55 may also help identify new solutions to reduce or prevent the development of nephrolithiasis associated with medication use. The exploration of new biomarkers and the use of AI will certainly provide more answers to the countless questions currently being asked. Pharmacovigilance-based
studies, in the future, whether through the development of connectable networks between various databases or through the introduction of deep learning, will improve the identification of signals and enhance the post-marketing knowledge of newly introduced medications.56
This study boasts several strengths, beginning with the generalisability of its results. Drawing from VigiBase, a database aggregating data from over a hundred countries, ensures the findings can be generalised across diverse populations. Another significant advantage is the standardised approach to data collection mandated by VigiBase, employing both the MedDRA dictionary and WHODrug. This standardisation minimises biases in data manipulation, enhancing the reliability of the study. Additionally, the study’s ability to identify signals is noteworthy. Leveraging such a comprehensive data source facilitates the detection of drugs associated with specific adverse reactions, potentially uncovering new signals. Furthermore, the integration of the IC025 disproportionality index into VigiBase facilitates the analysis process, reducing the likelihood of calculation errors or biases that may occur with other disproportionality methods. However, the detection of signals through disproportionality analysis does not establish a causal relationship, nor does it confirm that the clinical event is more frequently associated with the drug in question. It merely suggests that this adverse drug reaction is reported more frequently for this drug compared to others.
However, this study is subject to certain limitations. Firstly, as this study relies on spontaneous reports of ADRs, the available data lack both clinical narratives and information on the temporal relationship between drug administration and the adverse reaction. Moreover, causality assessment may be biased due to inherent limitations of spontaneous reporting systems. Secondly, the authors' classification of lithogenic roles based on five bibliographic references may not be as precise as direct evidence linking drugs to kidney lithiasis. Moreover, the results of our study may also be influenced by several
biases inherent in pharmacovigilance studies. Among these biases, they highlight underreporting bias, which can lead to an underestimation of the frequency of adverse events, making a medication appear safer than it actually is. Additionally, there is the bias of selective reporting, where there is a tendency to report newer adverse reactions (Weber effect), more severe reactions, or those associated with well-known medications, creating a false perception of higher risk for these drugs. Furthermore, since the majority of notifications assessed involve more than one medication, we must also consider recall or information bias, where clinical information obtained may inadvertently be distorted (incorrect information regarding occurrence, severity, or medications involved) or significant parts of information may be missing, leading to conclusions that are not based on all actual facts. This could even lead to wrongly attributing causality to a different medication.57
Despite these caveats, the study provides valuable insights into medications most commonly associated with nephrolithiasis, highlighting several drugs with potential new lithogenic roles. However, further studies are required to confirm these findings.
CONCLUSION
Pharmacovigilance studies enable direct data collection from clinical settings, and their analysis can pinpoint medications most frequently associated with specific phenotypes. This underscores the need for heightened scrutiny of these drugs and emphasises the importance of enhanced surveillance to improve patient safety.
Reports of drug-associated kidney stones in VigiBase are infrequent. The authors’ data highlights some of the medications most linked to nephrolithiasis, identifying those with a strong association through disproportionality indices (IC025 and ROR). Additionally, this study employed a BS developed by the authors to identify potential new nephrotoxins. These findings necessitate targeted studies to evaluate the lithogenic potential of these medications.
Nevertheless, clinicians should remain vigilant when prescribing these drugs, monitoring patients for the development of kidney stones, and minimising potential iatrogenic effects. The authors urge every clinic to actively report any adverse drug reactions encountered in clinical practice.
References
1. Nojaba L, Guzman N. Nephrolithiasis (Kidney Stones) (Archived) [Internet] (2023) Treasure Island (FL): StatPearls Publishing. Available at: https://www. ncbi.nlm.nih.gov/books/NBK559227/. Last accessed: 21 January 2024
2. Stamatelou K, Goldfarb DS. Epidemiology of kidney stones. Healthcare (Basel). 2023;11(3):424.
3. Daudon M et al. Drug-induced kidney stones and crystalline nephropathy: pathophysiology, prevention and treatment. Drugs. 2018;78(2):163-201.
4. Hara M et al. Atazanavir nephrotoxicity. Clin Kidney J. 2015;8(2):137-42.
5. Dong BJ et al. Sulfadiazine-induced crystalluria and renal failure in a patient with AIDS. J Am Board Fam Pract. 1999;12(3):243-8.
6. Go T. Effect of antiepileptic drug polytherapy on crystalluria. Pediatr Neurol. 2005;32(2):113-5.
7. Paul E et al. Urolithiasis on the ketogenic diet with concurrent topiramate or zonisamide therapy. Epilepsy Res. 2010;90(1-2):151-6.
8. European Medicines Agency. Summary of product characteristics. 2025. Available from: https://www.ema. europa.eu/en/glossary/summaryproduct-characteristics. Last accessed: 21 January 2024
9. UpToDate. UpToDate. 2025. Available at: https://www.wolterskluwer.com/engb/solutions/uptodate. Last accessed: 21 January 2024
10. Drugs.com. Find Drugs & Conditions. 2025. Available at: https://www.drugs. com/. Last accessed: 21 January 2024
11. James ET, Douglas AM (eds.). Drug-induced diseases: prevention, detection, and management (2018) 3rd ed, Bethesda: American Society of Health-System Pharmacists.
12. Ray SD (ed.), Side Effects of Drugs Annual 38 - A worldwide yearly survey of new data in adverse drug reactions (2016), Amsterdam: Elsevier.
DATA AVAILABILITY STATEMENT
The data will be available for consultation if deemed necessary.
13. Ferraro PM et al. Factors associated with sex differences in the risk of kidney stones. Nephrol Dial Transplant. 2023;38(1):177-83.
14. Gillams K et al. Gender differences in kidney stone disease (KSD): findings from a systematic review. Curr Urol Rep. 2021;22(10):50.
15. Letavernier E, Daudon M. Vitamin D, hypercalciuria and kidney stones. Nutrients. 2018;10(3):366.
16. Sakhaee K et al. Nephrolithiasisassociated bone disease: pathogenesis and treatment options. Kidney Int. 2011;79(4):393-403
17. Yasui T et al. Alendronate reduces the excretion of risk factors for calcium phosphate stone formation in postmenopausal women with osteoporosis. Urol Int. 2009;83(2):2269.
18. Wessels H et al. Pharmacokinetic and pharmacodynamic similarity of biosimilar natalizumab (PB006) to its reference medicine: a randomized controlled trial. Expert Opin Biol Ther. 2023;23(12):1287-97
19. Prochaska M. Bisphosphonates and management of kidney stones and bone disease. Curr Opin Nephrol Hypertens. 2021;30(2):184-9.
20. Simonov M et al. Use of proton pump inhibitors increases risk of incident kidney stones. Clinical Gastroenterology and Hepatology. 2021;19(1):72-79.e21.
21. Song YK et al. Potential adverse events reported with the janus kinase inhibitors approved for the treatment of rheumatoid arthritis using spontaneous reports and online patient reviews. Front Pharmacol. 2022;12:792877.
22. Thorpy MJ et al. Efficacy and safety of lower-sodium oxybate in an open-label titration period of a phase 3 clinical study in adults with idiopathic hypersomnia. Nat Sci Sleep. 2022;14:1901-17.
23. Abbott Laboratories. Humira Summary of Product Characteristics. 2003. Available at: https://ec.europa.eu/
health/documents/communityregister/2009/2009082865869/ anx_65869_en.pdf. Last accessed: 25 May 2025
24. Adam A. Bilateral obstructive ureteral stones after using a dose of frozen adalimumab in a patient with Crohn’s disease. Am J Gastroenterol. 2018;113:S1651.
25. Jakobsen AK et al. Is nephrolithiasis an unrecognized extra-articular manifestation in ankylosing spondylitis? A prospective populationbased Swedish national cohort study with matched general population comparator subjects. PLoS One. 2014;9(11):e113602.
26. Alameddine Z et al. Risk of nephrolithiasis in patients with inflammatory bowel disease receiving biologic treatment. J Clin Med. 2023;12(19):6114.
27. European Medicines Agency. Remicade (infliximab). 2012. Available at: https:// www.ema.europa.eu/en/documents/ overview/remicade-epar-summarypublic_en.pdf. Last accessed: 21 January 2024
28. Dimke H et al. Risk of urolithiasis in patients with inflammatory bowel disease: a nationwide Danish cohort study 1977–2018. Clin Gastroenterol Hepatol. 2021;19(12):2532-2540.e2.
29. WyethLerderle. Etanercept - Resumo das Características do Medicamento. 2000. Available at: https://www.ema. europa.eu/en/documents/overview/ enbrel-epar-summary-public_en.pdf. Last accessed: 25 May 2025
30. Tsevi YM et al. [Life-threatening hypercalcemia and acute kidney injury induced by etanercept]. Nephrol Ther. 2018;14(6):478-82. (In French)
31. Schwartz BF et al. Imaging characteristics of indinavir calculi. J Urol. 1999;161(4):1085-7.
32. Saltel E et al. Increased prevalence and analysis of risk factors for indinavir nephrolithiasis. J Urol. 2000;164(6):1895-7.
33. Gagnon RF et al. Indinavir crystalluria. Kidney Int. 2006;70(12):2047.
34. Fogo AB et al. AJKD atlas of renal pathology: indinavir nephrotoxicity. Am J Kidney Dis. 2017;69(1):e3.
35. Garnier AS et al. High incidence of amoxicillin-induced crystal nephropathy in patients receiving high dose of intravenous amoxicillin. J Clin Med. 2020;9(7):2022.
36. Joshi S, Goldfarb DS. The use of antibiotics and risk of kidney stones. Curr Opin Nephrol Hypertens. 2019;28(4):311-5.
37. KRKA. Atazanavir - Summary of Product Characteristics. 2019. Available at: https://www.ema.europa. eu/en/documents/product-information/ atazanavir-krka-epar-productinformation_en.pdf. Last accessed: 25 May 2025
38. Grant MT et al. Ureteral obstruction due to radiolucent atazanavir ureteral stones. J Endourol Case Rep. 2017;3(1):152-4.
39. de Lastours V et al. High levels of atazanavir and darunavir in urine and crystalluria in asymptomatic patients. J Antimicrob Chemother. 2013;68(8):1850-6.
40. Hamada Y et al. High incidence of renal stones among HIV-infected patients on ritonavir-boosted atazanavir than in those receiving other protease inhibitor-containing antiretroviral therapy. Clin Infect Dis. 2012;55(9):1262-9.
41. Takhar J, Manchanda R. Nephrolithiasis on topiramate therapy. Can J Psychiatry. 2000;45(5):491-3.
42. Pelzman DL et al. Urinary metabolic disturbances during topiramate use and their reversibility following drug cessation. Urology. 2022;165:139-43.
43. Maalouf NM et al. Nephrolithiasis in topiramate users. Urol Res. 2011;39(4):303-7.
44. Shen AL et al. Topiramate may not increase risk of urolithiasis: a nationwide population-based cohort study. Seizure. 2015;29:86-9.
45. Cutroneo PM et al. Conducting and interpreting disproportionality analyses derived from spontaneous reporting systems. Front Drug Saf Regul. 2024;3:1323057.
46. European Medicines Agency. Medicines under additional monitoring. 2023. Available at: https://www.ema. europa.eu/en/human-regulatoryoverview/post-authorisation/ pharmacovigilance-post-authorisation/ medicines-under-additionalmonitoring. Last accessed: 21 January 2024
47. Harpaz R et al. Performance of pharmacovigilance signal-detection algorithms for the FDA Adverse Event Reporting System. Clin Pharmacol Ther. 2013;93(6):539-46.
48. Frent I et al. A description of acute renal failure and nephrolithiasis associated with sodium–glucose co-transporter 2 inhibitor use: a VigiBase study. Front Pharmacol. 2022;13:925805.
49. Makunts T et al. Analysis of postmarketing safety data for protonpump inhibitors reveals increased propensity for renal injury, electrolyte abnormalities, and nephrolithiasis. Sci Rep. 2019;9(1):2282.
50. Alshehri BJ, Shalabi HS. SGLT-2 inhibitors and their correlation with kidney stones. a systematic review. Journal of Health and Rehabilitation Research. 2024;4(2):282-90.
51. Tasian GE et al. Annual incidence of nephrolithiasis among children and adults in South Carolina from 1997 to 2012. Clin J Am Soc Nephrol. 2016;11(3):488-96.
53. Daudon M t al. Drug-induced kidney stones and crystalline nephropathy: pathophysiology, prevention and treatment. Drugs. 2018;78(2):163-201.
54. Wang Z et al. Recent advances on the mechanisms of kidney stone formation (Review). Int J Mol Med. 2021;48(2):149.
55. Khan SR, Canales BK. Proposal for pathogenesis-based treatment options to reduce calcium oxalate stone recurrence. Asian J Urol. 2023;10(3):246-57.
56. Trifirò G, Crisafulli S. A new era of pharmacovigilance: future challenges and opportunities. Front Drug Saf Regul. 2022;2:866898.
Diabetes is a chronic metabolic disorder characterised by insulin resistance and impaired insulin secretion. Effective management of diabetes requires sustained blood glucose control, often necessitating long-term medication adherence. Traditional drug delivery systems, while effective, often face challenges such as poor bioavailability, patient noncompliance, and undesirable side effects. This paper explores the advancements in novel drug delivery systems specifically tailored for antidiabetic drugs. Different nanoparticles such as polymeric nanoparticles, nanocarriers, liposomes, and lipid nanoparticles are used in the novel drug delivery systems for antidiabetic drugs. These systems showed potential in enhancing drug efficacy, improving pharmacokinetics, and reducing side effects. The integration of nanotechnology and personalised medicine is also discussed for these delivery systems, providing insights into their role in achieving better glycaemic control. The review concludes with a discussion on the current challenges and future prospects of novel drug delivery systems in diabetes.
Key Points
1. Diabetes is a global health challenge, with millions of patients struggling to achieve effective and sustained glycaemic control. Traditional treatments are often limited by poor bioavailability, suboptimal pharmacokinetics, and side effects. This article addresses how novel, nanomedicine-based drug delivery systems could make diabetes treatment more effective, targeted, and patient-friendly.
2. This article comprehensively covers various nanotherapeutic strategies employed in the treatment of diabetes. It also explores the role of various nanoparticles, including polymeric nanoparticles, nanocarriers, liposomes, and lipid-based nanoparticles, in enhancing the delivery and efficacy of antidiabetic drugs.
3. Nanomedicine represents a breakthrough approach in diabetes management by enabling smarter, more targeted drug delivery systems. These novel nanotherapeutic systems could lead to safer, more effective, and more patient-friendly diabetes management.
INTRODUCTION
Diabetes is a chronic metabolic disorder characterised by persistently high blood sugar levels (hyperglycaemia) caused by deficiencies in either insulin secretion, insulin action, or both. The impaired glucose metabolism can lead to long-term complications that affect various organs. Millions of people worldwide live with diabetes and require constant blood glucose control, which makes care particularly challenging. Traditional drug delivery methods, such as oral tablets and injectable formulations, have consistently been the main therapeutic options for diabetes treatment. However, these approaches come with significant drawbacks, such as suboptimal bioavailability, frequent dosing requirements, inefficient drug absorption, issues with patient compliance, and unwanted side effects. These limitations often result in reduced therapeutic effectiveness and patient discomfort. Consequently, there is a growing demand for advanced drug delivery systems that can boost the efficacy of treatments, decrease the frequency of doses, and minimise adverse reactions.
Recently, innovative drug delivery methods have surfaced as alternatives to traditional approaches, offering more effective treatments for diabetes. These cuttingedge systems, including nanoparticles, microneedles, transdermal patches, and smart drug delivery mechanisms, have demonstrated the ability to enhance drug stability, target specific tissues, and provide controlled drug release. These advancements enhance the pharmacokinetic and pharmacodynamic profiles of antidiabetic drugs and offer the potential for personalised treatment strategies.
This paper explores the latest advancements in these innovative delivery systems, focusing on how nanoparticles, such as polymeric nanoparticles, liposomes, and lipid-based carriers, are being synthesised and developed to optimise the delivery of antidiabetic medications. Studies of these methods showed improvements in drug efficacy and pharmacokinetics, as well as reduced side effects.
The integration of nanotechnology and personalised medicine lays the groundwork for improved glycaemic control in future diabetes treatment. The paper examines various drug delivery methods, including their mechanisms, advantages, and limitations, as well as their potential to improve patient outcomes.
NANOMATERIALS USED IN THE MANAGEMENT OF DIABETES
Polymeric Nanoparticles
Polymeric nanoparticles (PNP) are made from polymers and typically measure between 1 and 1,000 nanometres. These tiny particles come in two forms: nanospheres, which are solid, and nano-capsules, which have a polymeric outer layer surrounding a liquid or solid core.1 PNPs possess remarkable characteristics, such as an exceptionally high ratio of surface area to volume, tuneable dimensions, and the capacity to envelope various therapeutic agents. These properties make PNPs suitable in drug delivery, medical imaging, and other biomedical applications.2,3
The structure of PNPs is significantly influenced by their synthesis methods, which can include solvent evaporation, coacervation, and self-assembly techniques. When amphiphilic block copolymers go through self-assembly, they can form structures called micelles or vesicles, which can play a crucial role in drug delivery.4 PNPs can be designed to incorporate stimuliresponsive agents for controlled drug release, triggered by environmental changes such as temperature or pH fluctuations.5,6 This adaptability enhances their effectiveness in targeting specific tissues while minimising side effects.
The surface modification of PNPs can be done through various chemical strategies in order to improve their biocompatibility and targeting capabilities.2,7 These nanoparticles are special because of their unique structural properties and ability to be engineered for different applications. Advances in the application of PNPs could unlock new therapeutic approaches to the treatment of diabetes and other diseases.2,3
Polymeric Nanocapsules
Polymeric nanocapsules are nanostructures that consist of a core-shell architecture, where the liquid or solid core is encapsulated by a polymeric shell. This unique structure distinguishes them from polymeric nanospheres, which are composed of a solid polymeric matrix without a core.8 The core of polymeric nanocapsules can be composed of various materials, including oils, drugs, or other active compounds, while the shell is generally made from biocompatible polymers such as poly(lactic-co-glycolic acid) and poly(alkylcyanoacrylate).9 The choice of materials for both the core and shell is crucial, as it influences the release kinetics, the nanocapsule’s stability, and the overall functionality in different applications.10
Nanocapsules can be synthesised through various methods, including miniemulsion polymerisation, interfacial polymerisation, and layer-by-layer assembly.11,12 Miniemulsion polymerisation allows for the formation of nanocapsules with controlled sizes, typically below 100 nm, which is essential for biomedical applications.13 In the controlled drug delivery systems, the polymeric shell can act as a diffusion barrier for the release of the encapsulated core material, which is particularly beneficial.10 Nanocapsule properties can be tailored through chemical modifications by using different polymer blends to enhance their performance.14,15
The structural characteristics of polymeric nanocapsules play a vital role in their functionality by providing a protective environment for the encapsulated materials. This can enable the responsive systems to release their contents in response to specific stimuli, such as pH or temperature changes.16,17 This responsiveness is particularly advantageous in targeted drug delivery, where the release of therapeutic agents can be controlled according to the physiological conditions of the target sites.9,10 Their properties can also be modified to improve biocompatibility and targeting capabilities for better therapeutic efficacy.18,19
Liposomes
Liposomes are spherical vesicles composed of lipid bilayers used in drug delivery and other biomedical applications. The structure of these nanoparticles is defined by lipid composition, which influences their physicochemical properties such as size, charge, fluidity, and stability. The lipid bilayer typically consists of phospholipids, which are often modified with various components to enhance their function. A recent study shows significant effects on membrane fluidity and permeability by incorporating cholesterol into liposomes, impacting drug release rates.20
Liposomes are synthesised through a self-assembly process, wherein lipids are organised into bilayers in an aqueous environment. This process can be affected by various factors, such as lipid concentration, temperature, and the presence of other additives. Certain techniques, such as micromixing in acoustic fluids, have recently shown precise control over liposome sizes and shapes, allowing them to be specifically tailored for targeted drug delivery.21,22 The interaction of liposomes with biological systems is also critical for their design. When biological fluids enter them, liposomes form a protein corona and alter their biodistribution. The corona is influenced by the liposomes’ surface charge, hydrophobicity, and surrounding proteins.23-25 Cationic liposomes attract negatively charged proteins, which can allow or inhibit cellular uptake depending on the specific interactions with the target cells.26
In studies, these nanoparticles are incorporated into liposomal structures, which have proven to enhance their functionality. They can be embedded within the liposomal bilayer, which provides additional properties like magnetic or photothermal responsiveness. For example, magnetoliposomes have been prepared to target drug delivery and imaging applications, where the magnetic properties can provide controlled transport of the liposomes.27,28 The structure of liposome nanoparticles is complex, with lipid composition, size, and surface collectively influencing their efficacy as drug delivery vehicles.
Lipid Nanoparticles
Lipid nanoparticles (LNP) are known as adaptable vehicles for delivering drugs, especially genetic material and therapeutic compounds. LNPs are similar to liposomes in structure, but are distinct due to their single phospholipid layer, unlike the multilayered structure of liposomes.29 LNPs feature reversed micelles within their core, which is comprised of a lipid centre surrounded by a lipid bilayer. This structure can be modified to boost stability, encapsulation efficiency, and bioavailability of enclosed drugs. The core-shell design is vital for the function of these nanoparticles, influencing their interaction with biological systems and the efficacy of drug delivery.30 The lipid bilayer of LNPs consists of various lipids, including phospholipids, cholesterol, and ionisable lipids, each serving a specific purpose in the formation and stability of nanoparticles. Ionisable lipids are crucial for binding mRNA, creating a central structure that is subsequently wrapped by helper lipids, such as phospholipids and cholesterol. These helper lipids strengthen the nanoparticle and help it enter cells more easily.31 Research also indicates that adjusting the crosslinking density of the hydrogel core can alter the elasticity of nanoparticle cores, which in turn can attract proteins from the biological surroundings.32 The physical characteristics of LNPs, such as their flexibility and dimensions, play a crucial role in determining their circulation lifetime and how they interact with biological barriers.
GLUCOSE-SENSITIVE DRUG DELIVERY
The glucose-sensitive drug delivery systems gained a significant advancement in diabetes management, particularly for insulin delivery. These systems are designed to respond dynamically to changes in blood glucose levels, which can mimic the natural insulin secretion by the pancreas. The use of phenylboronic acid (PBA) as a glucose-sensitive component, which binds with glucose by forming reversible covalent bonds, allows changes in the hydrophilicity of the drug delivery vehicle. The disassembly or swelling of the delivery system facilitates
the release of drugs in response to elevated glucose levels.33-35 For instance, PBA-based micelles have demonstrated enhanced glucose-responsiveness at physiological pH, making them suitable for insulin delivery.36,37 The integration of PBA into polymeric structures has also demonstrated the ability to create self-regulating systems that can efficiently manage insulin release with minimal patient involvement.38
The incorporation of glucose oxidase in the drug delivery systems has also been promising. Glucose oxidase catalyses the oxidation of glucose and produces hydrogen peroxide. This lowers the local pH, which can trigger the release of drugs by pH-sensitive carriers.39,40 This is a dual-responsive system for glucose-triggered insulin release that can enhance the therapeutic efficacy of the treatment.41 The combination of glucose oxidase with other materials, such as PBA, also demonstrated a multifunctional system that can effectively integrate glucose sensing and drug release functions.42
The application of nanotechnology has been crucial in advancing glucose-sensitive drug delivery systems. The development of nanocarriers, such as supramolecular vesicles and hybrid nanogels, has allowed for higher drug loading and better release under normal physiologic conditions.43 In a recent study, glucose-responsive supramolecular vesicles were engineered to release insulin in a controlled manner, showing great promise for practical use in diabetes treatment. These systems can be designed to work with specific body triggers, making them more effective and reducing the need of frequent injections.34,44 The nanocarriers can hold and transport genetic material, such as small interfering RNA, which could be a new approach in tackling the underlying causes of Type 2 diabetes, including problems with insulin response and pancreatic β-cell dysfunction.45,46 Biogenic synthesis of nanoparticles has also gained recognition as a safe and effective approach for creating antidiabetic agents in recent studies. This innovative method significantly broadens the therapeutic options available for combating diabetes.47,48
Various nanoscale materials have been utilised in glucose-sensitive drug delivery and improving insulin sensitivity using various methods markers.49,50,47
DRUG DELIVERY USING NANOPARTICLES IN ORAL ADMINISTRATION
Oral administration of insulin is generally challenging due to instability in the gastrointestinal tract and poor absorption. Recent advancements in nanotechnology showed promising solutions, using various nanoparticles to protect insulin, enhance absorption, and improve pharmacokinetics. These advancements aim to increase the bioavailability of orally administered insulin.
Chitosan (a natural polysaccharide that is biocompatible, biodegradable, and hydrophilic) nanoparticle-based systems have been widely explored regarding oral insulin delivery. These nanoparticles have shown promise in controlling blood sugar in diabetes studies. Research has found that chitosan-pentasodium tripolyphosphate nanoparticles can keep blood glucose levels steady for up to 11 hours after giving insulin at a dose of 100 IU/kg.51 Researchers have also investigated using other natural polymers, like hyaluronic acid and alginate, to boost insulin’s stability and uptake. For instance, chitosan nanoparticles coated with hyaluronic acid have demonstrated enhanced transcellular insulin delivery, which can effectively overcome the obstacles posed by the intestinal mucosa.52 Nanoparticles that are pH-responsive also offer a novel method for oral insulin delivery. Scientists have created poly(ester amide) microspheres, and their biodegradability and hydrophobic nature proved to interact with intestinal epithelium. This interaction prolongs insulin’s presence in the gut and can improve its absorption.53 An approach with self-assembled lecithin/ chitosan nanoparticles has shown improved functionality and enhanced delivery effectiveness in oral insulin administration.54
Understanding mucus barriers when designing nanoparticles is crucial, as they can penetrate these barriers and
become trapped. Research has shown that hydrophilic and electroneutral nanoparticles can be used to overcome this through better absorption.55 Nanoparticles functionalised with zwitterions have been tested for oral bioavailability against absorption barriers, showing even more improvements.56 Zinc oxide nanoparticles have also shown the ability to traverse biological membranes, making them suitable for antidiabetic oral drug delivery.57
Oral nanoparticle drug delivery systems have shown great promise in improving bioavailability and efficacy.32,58 Research on these nano-formulations reveals that nano-encapsulated insulin has a much higher oral bioavailability than free insulin, demonstrating the enhanced effectiveness of nanoparticles in insulin delivery.59 Studies have shown that insulin-loaded nanoparticles can produce long-lasting blood sugar-lowering effects in diabetic animal models, suggesting their potential for practical use in humans.60
GENE THERAPY USING NANOSCALE MATERIALS
In diabetes treatment, the application of nanoparticles in gene therapy has been explored, and in many studies, they have emerged as a pivotal technology. Gene therapy aims to either fix faulty genes or replace them with healthy ones so that the body is capable of fighting off the disease. It is promising as a treatment for a wide range of diseases, including diabetes. The application of nanoparticles in gene therapy offers several advantages, including enhanced delivery efficiency, reduced toxicity, and the ability to target specific tissues or cells. Researchers have utilised several types of nanoparticles in antidiabetic gene therapies for their unique therapeutic potentials.
The advantage of using nanoparticles in gene delivery is that they are capable of encapsulating genetic material like small interfering RNA and plasmid DNA, which can alter specific gene expression linked to diabetes. Lipid nanoparticles have shown potential in suppressing tumour necrosis
factor α, which is a protein involved in diabetic wound healing.61 A significant improvement in the efficacy of gene therapy was reported using engineered chitosan nanoparticles for targeted gene transfer functions.54 These modified nanoparticles can improve targeting and biocompatibility in patients with diabetes. Research also shows that glucose metabolism can be regulated by therapeutic genes delivered effectively using nanoparticles. Insulin plasmid-loaded nanoparticles were administered orally in diabetic mice, which sustained therapeutic gene expression and reduced hyperglycaemia significantly.62 This method addresses the challenges faced by traditional insulin injections and improves patient compliance as it can provide a noninvasive alternative.63 Biologic nanoparticles derived from a specific medicinal plant (Momordica Charantia) extract have been studied for their ability to influence gene expression involved in lipid metabolism and nephrotoxicity in diabetes models, offering potential therapeutic applications.64
Lipid-based nanocarriers were also investigated for their encapsulating capabilities and utilised in gene therapy to combat inflammatory cytokines in the chronic wound healing process in patients with diabetes.65 The application of geneactivated collagen scaffolds, functionalised with polyplex nanoparticles carrying specific genes, has also shown potential in enhancing the regenerative capabilities of human adipose-derived stem cells in patients with diabetes.66 In a recent study, silver nanoparticles have also been recognised for their therapeutic potential in diabetes treatment. Their distinct physical and biochemical properties have been observed in response to inflammation, as well as in boosting insulin sensitivity.67 Combining these nanoparticles with traditional antidiabetic therapies improved outcomes in preclinical studies, although the combined impact requires further study.68 These innovative approaches could potentially revolutionise the gene therapy methods in various aspects of diabetes management.
NANOPARTICLES IN STEM CELL THERAPY
Cell therapy represents a promising frontier in the treatment of diabetes. Stem cell therapy is primarily used to restore and increase the function of β-cells responsible for insulin production, reduce complications, and improve the wound healing process in diabetes patients. These insulin-producing β-cells can be regenerated by using stem cell therapy. Studies indicated that the successful differentiation of mesenchymal stem cells into insulin secreting cells has been shown. These mesenchymal stem cells, derived from tissues such as bone marrow and adipose tissue, can offer a potential cure for diabetes.69,70 The regenerative abilities of mesenchymal stem cells are especially significant in Type 1 diabetes, as β-cell destruction is caused by autoimmune responses. Stem cell therapy can also promote neovascularisation along with β-cell regeneration, which is critical in improving insulin production and glycaemic control.71-73 A recent clinical trial showed significant improvements in diabetic wound healing associated with chronic ulcers.74-76 Despite these promising results, there are significant concerns regarding the impairment of stem cells, which could potentially alter their functionality in patients with diabetes and limit their therapeutic capabilities.77,78 In the case of patients with autoimmune diabetes, studies showed risks of rejection caused by immunogenicity of transplanted cells.79
To further enhance stem cell therapies and reduce risks, nanoparticles have been combined with stem cells to improve cellular response and delivery in recent studies. The unique properties of the nanoparticles can also allow for enhanced delivery and tracking of stem cells. Magnetic nanoparticles have been used to transport stem cells to specific tissue sites, such as post-surgical myocardium for regeneration, especially in patients with both diabetes and cardiovascular conditions.80,81 Nanoparticles improve cell culture by utilising 3D nanofiber scaffolds and enhancing cardiomyocyte growth. Gold nanoparticles and poly(lacticco-glycolic acid)-derived microparticles also promote stem cell survival.82 The use
of polymeric nanoparticles in stem cell therapies can influence their biological behaviours by altering differentiation pathways, which is beneficial under the cellular stress that is common in diabetes.83 The research on stem cell therapies for diabetes using different nanoparticles has opened the door to better treatment options.
NANOPARTICLES IN DIABETIC WOUND HEALING
Wound healing in patients with diabetes is a continuous, programmed process of events. In diabetic wound healing, nanoparticles and nanocomposites improve the repair process by delivering growth factors or antimicrobials to the wound site. They reduce inflammation, prevent infection, and promote tissue regeneration, which speeds up recovery. Some nanoparticles have shown intrinsic antibacterial properties that are crucial for infection prevention in diabetic wounds. For instance, significant antibacterial activity was reported from zinc-based nanoparticles against common pathogens such as Escherichia coli and Staphylococcus Aureus, which are the main causes of wound infections in patients with diabetes.84 Cerium oxide nanoparticles, which are inorganic compounds, were used in several formulations to progress wound healing by promoting their antioxidant properties and reducing oxidative stress.85,86 The incorporation of such nanoparticles into wound dressings could effectively facilitate a more conducive healing environment and reduce the infection.
The application of nanoparticles extends to their ability to modulate the wound healing process. Gallocatechin-silver nanoparticles embedded in cotton gauze have been used to accelerate diabetic wound healing in rats by inhibiting apoptosis with the Wnt/βcatenin signalling pathway and promoting cell proliferation.87 Lipid-based nanocarriers have been studied for their capacity to deliver growth factors and anti-inflammatory drugs to facilitate an accelerated healing response.65,88 Utilising these targeted delivery methods can significantly improve the bioavailability of drugs.
Thermosensitive hydrogels with nanoparticles can remove reactive oxygen species, which obstruct the healing process, and provide a moist environment to aid in healing. In a recent study, Prussian blue nanoparticles were incorporated into hydrogels, which promoted angiogenesis and restored mitochondrial function in the diabetic healing process.89 The dual action of reactive oxygen species removal and modulation of cellular functions is critical in managing the oxidative stress observed in diabetic wounds. The use of microneedle patches and multifunctional nanocomposite scaffolds has been developed to further enhance diabetic wound healing. These innovative delivery systems can provide controlled drug release while facilitating the regeneration of tissue.90,91 Moreover, chitosan-coated nanoparticles have recently been shown to act on cytokine profiles in diabetic models, which can play a role in modulating immune response and reducing inflammation in diabetes.92
CONCLUSION
The use of nanotechnologies shows great promise in the advancement of innovative treatment approaches and offers significant potential to transform diabetes treatment. This review has explored the use of various nanomaterials, including polymeric nanoparticles, liposomes, lipid nanoparticles, and their variations, which have demonstrated key benefits. These include targeted drug delivery, controlled drug release, improved drug absorption, enhanced diabetic wound healing, and immune modulation. These advantages address many limitations of conventional diabetes therapies, particularly by ensuring better precision and efficacy.
Incorporating glucose-responsive mechanisms into nanomaterials has opened doors for adaptive drug delivery systems that respond to blood sugar fluctuations. These systems improve drug discharge, minimising the risks of hypoglycaemia or hyperglycaemia. Nanoformulations can also protect insulin from degradation, enhancing its bioavailability and absorption, which could overcome current challenges
in oral insulin delivery. Using nanoparticles in oral therapies could reduce the need for invasive delivery methods, improving patient adherence. The combination of nanotechnology with gene and stem cell therapies is particularly promising, offering opportunities to regenerate damaged tissues, which can also enhance insulin production and address the underlying causes of diabetes.
However, there are some challenges to overcome. Large-scale nanoparticle manufacturing remains complex and costly, with concerns regarding toxicity, immune reactions, and long-term effects. Some nanoparticles may have a related risk of toxicity, and they can accumulate in different organ tissues. Nanomaterials can also trigger immune reactions with long-
References
1. Zielińska A et al. Polymeric nanoparticles: production, characterization, toxicology and ecotoxicology. Molecules. 2020;25(16):3731.
2. Sivadasan D et al. Polymeric lipid hybrid nanoparticles (PLNs) as emerging drug delivery platform - a comprehensive review of their properties, preparation methods, and therapeutic applications. Pharmaceutics. 2021;13(8):1291.
3. Elmowafy M et al. Polymeric Nanoparticles for Delivery of Natural Bioactive Agents: Recent Advances and Challenges. Polymers (Basel). 2023; 15(5):1123.
4. Perumal S. Polymer Nanoparticles: Synthesis and Applications. Polymers (Basel). 2022;14(24):5449.
5. Tamminana M, Kumar BVVR. Formulation design and characterization of nilotinib polymeric nanoparticles by nanoprecipitation technique for the improved drug solubility and dissolution rate. Curr Nanomaterial. 2025;9(3):252-65.
6. Li Z et al. Mesoporous silica nanoparticles in biomedical applications. Chem Soc Rev. 2012;41(7):2590-605.
7. Stella S et al. Structure of the Cpf1 endonuclease R-loop complex after target DNA cleavage. Nature. 2017;546(7659):559-63. Erratum in: Nature. 2017;547(7664):476.
8. Deng S et al. Polymeric nanocapsules as nanotechnological alternative for drug delivery system: current status, challenges and opportunities. Nanomaterial (Basel). 2020;10(5):847.
term use, which may affect their efficacy and needs better understanding through clinical trials. These issues contribute to delays in regulatory approval. These novel approaches are still experimental and have not received FDA approval for clinical use just yet. Ongoing research and clinical trials are crucial to improving the safety, biocompatibility, and cost-efficiency of these therapies. Despite the hurdles, the potential of nanotechnology to advance diabetes care is immense. With continued progress in clinical trials and manufacturing processes, nanomedicine could offer groundbreaking therapies, which will improve patient outcomes and quality of life. The integration of nanotechnologies may reshape the future of diabetes management and provide long-term solutions for millions of patients worldwide.
9. Frank L et al. Improving drug biological effects by encapsulation into polymeric nanocapsules. Wiley Interdiscip Rev Nanomed Nanobiotechnology. 2015;7(5):623-39.
10. Chen C et al. Biodegradable cationic polymeric nanocapsules for overcoming multidrug resistance and enabling drug–gene co-delivery to cancer cells. Nanoscale. 2014;6(3):1567-72.
11. Ashkenazi S et al. Study of PEGb-PLA/eudragit s100 blends on the nanoencapsulation of indigo carmine dye and application in controlled release. ACS Omega. 2024;9(11):13382-90.
12. Sunoqrot S et al. Development of a thymoquinone polymeric anticancer nanomedicine through optimization of polymer molecular weight and nanoparticle architecture. Pharmaceutics. 2020;12(9):811.
13. Shirin‐Abadi A et al. New approach for the elucidation of PCM nanocapsules through miniemulsion polymerization with an acrylic shell. Macromolecules. 2011;44(18):7405-14.
14. Zhou Y et al. Further improvement based on traditional nanocapsule preparation methods: a review. Nanomaterials. 2023;13(24):3125.
15. Hu J et al. Synthesis and characterization of polybutylcyanoacrylate‐encapsulated rose fragrance nanocapsule. Flavour Frag J. 2011;26(3):162-73.
16. Lee B et al. Polymeric nanocapsules containing methylcyclohexane for improving thermally induced debonding of thin adhesive films. App Pol Sci J. 2018;135(31):46586.
17. Huang X et al. Synthesis of welldefined photo-cross-linked polymeric nanocapsules by surface-initiated raft polymerization. Macromolecules. 2011;44(21):8351-60.
18. Ali S et al. Vesicle-templated pHresponsive polymeric nanocapsules. Soft Matter. 2011;7(11):5382.
19. Hajebi S et al. Stimulus-responsive polymeric nanogels as smart drug delivery systems. Acta Biomaterialia. 2019;92:1-18.
20. LaMastro V et al. Antifungal liposomes: lipid saturation and cholesterol concentration impact interaction with fungal and mammalian cells. J Biomed Mater Res A. 2023;111(5):644-59.
21. Hong J et al. Microfluidic directed self-assembly of liposome−hydrogel hybrid nanoparticles. Langmuir. 2010;26(13):11581-8.
22. Vardin AP, Yesıloz Gurkan. Nanoscale liposome synthesis for drug delivery applications via ultrafast acoustofluidic micromixing. HJSE. 2023;10(3):237-41.
23. Pozzi D et al. Surface chemistry and serum type both determine the nanoparticle–protein corona. J Proteomic. 2015;119:209-17.
24. Pozzi D et al. The biomolecular corona of nanoparticles in circulating biological media. Nanoscale. 2015;7(33):1395866.
25. Francia V et al. Corona composition can affect the mechanisms cells use to internalize nanoparticles. Acs Nano. 2019;13(10):11107-21.
26. Dietz L et al. Uptake of extracellular vesicles into immune cells is
enhanced by the protein corona. JVE. 2023;12(12):e12399.
27. Barreto G et al. Magnetoliposomes as model for signal transmission. R Soc Open Sci. 2019;6(1):181108.
28. Lizoňová D et al. Multilobed magnetic liposomes enable remotely controlled collection, transport, and delivery of membrane-soluble cargos to vesicles and cells. Acs App Bio Material.2021;4(6):4833-40.
29. Kulkarni JA et al. Lipid nanoparticles enabling gene therapies: from concepts to clinical utility. Nucleic Acid Ther. 2018;28(3):146-57.
30. Leung AK et al. Microfluidic mixing: a general method for encapsulating macromolecules in lipid nanoparticle systems. J Phys Chem B. 2015;119(28):8698-706.
31. Eygeris Y et al. Deconvoluting lipid nanoparticle structure for messenger RNA delivery. Nano Letters. 2020;20(6):4543-9.
32. Li M et al. Nanoparticle elasticity affects systemic circulation lifetime by modulating adsorption of apolipoprotein A-I in corona formation. Nat Commun. 2020;13(1):4137.
33. Cui G. Synthesis and characterization of phenylboronic acid-containing polymer for glucose-triggered drug delivery. Sci Technol Adc Mater. 2019;21(1):1-10.
34. Li Z et al. Boronic acid as glucosesensitive agent regulates drug delivery for diabetes treatment. Materials. 2017;10(2):170.
35. Ma Q et al. Bioresponsive functional phenylboronic acid-based delivery system as an emerging platform for diabetic therapy. Int J Nanomed. 2021;16:297-314.
36. Ma R et al. Phenylboronic acidbased complex micelles with enhanced glucose-responsiveness at physiological pH by complexation with glycopolymer. Biomacromolecules. 2012;13(10):3409-17.
37. Yuan Y et al. Glucose-responsive hydrogels based on phenylboronic acid. MSF. 2018;913:714-21.
38. Wang C et al. Recent advances in phenylboronic acid-based gels with potential for self-regulated drug delivery. Molecules. 2019;24(6):1089.
39. Li Z et al. Glucose-sensitive polymer nanoparticles for self-regulated drug delivery. Chem Commun. 2016;52(49):7633-52.
40. Hu X et al. H2O2-responsive vesicles integrated with transcutaneous patches for glucose-mediated insulin delivery. Acs Nano. 2017;11(1):613-20.
41. Yu J et al. Hypoxia and H2O2 dualsensitive vesicles for enhanced glucose-responsive insulin delivery.
Nano Letters. 2017;17(2):733-9.
42. Wu W et al. Multifunctional hybrid nanogel for integration of optical glucose sensing and self-regulated insulin release at physiological pH. Acs Nano. 2010;4(8):4831-9.
43. Gao L et al. Glucose‐responsive supramolecular vesicles based on water‐soluble pillar[5]arene and pyridylboronic acid derivatives for controlled insulin delivery. ChemEur J. 2017;23(27):6605-14.
44. Lin Y et al. Glucose- and pH-responsive supramolecular polymer vesicles based on host–guest interaction for transcutaneous delivery of insulin. Acs Applied Bio Materials. 2020;3(9):637683.
45. Neumann K et al. Responsive polymeric nanoparticles for controlled drug delivery. Polymer Int. 2017;66(12):175665.
46. Liu Y et al. Emerging theranostic nanomaterials in diabetes and its complications. Advance Sci. 2021;9(3):2102466.
47. Wahab M, Janaswamy S. A Review on Biogenic Silver Nanoparticles as Efficient and Effective Antidiabetic Agents. ASFFBC. 2023;3(7):93-107.
48. Alamri ES, El Rabey HA. The Protective effects of vanillic acid and vanillic acidcoated silver nanoparticles (AgNPs) in streptozotocin-induced diabetic rats. J Diabetes Res. 2024;2024:4873544.
49. Gutiérrez-Pérez IA et al. Outcome predictors in COVID-19: An analysis of emergent systemic inflammation indices in Mexican population. Front Med (Lausanne). 2022;9:1000147.
50. Abdulmalek S, Balbaa M. Synergistic effect of nano-selenium and metformin on type 2 diabetic rat model: diabetic complications alleviation through insulin sensitivity, oxidative mediators and inflammatory markers. Plos One. 2019;14(8):e0220779.
51. Bahman F et al. Oral insulin delivery using poly (styrene co-maleic acid) micelles in a diabetic mouse model. Pharmaceutics. 2020;12(11):1026.
52. Wu H et al. Hyaluronic‐acid‐coated chitosan nanoparticles for insulin oral delivery: fabrication, characterization, and hypoglycemic ability. Macromol Biosci. 2022;22(7):2100493.
53. He P et al. Novel biodegradable and pH‐sensitive poly(ester amide) microspheres for oral insulin delivery. Macromol Biosci. 2012;12(4):547-56.
54. Liu L et al. Self-assembled lecithin/ chitosan nanoparticles for oral insulin delivery: preparation and functional evaluation. Inte J Nanomed. 2016;2016:761-69.
55. Tan X et al. Hydrophilic and electroneutral nanoparticles to
overcome mucus trapping and enhance oral delivery of insulin. Molecular Pharmaceutics. 2020;17(9):3177-91.
56. Shan W. Enhanced oral delivery of protein drugs using zwitterionfunctionalized nanoparticles to overcome both the diffusion and absorption barriers. Acs App Materi & Interface. 2016;8(38):25444-53.
57. Kamel M et al. Therapeutic efficacy of zinc oxide nanoparticles in diabetic rats. Slov Vet Res. 2019;56(Suppl 22): https://doi.org/10.26873/SVR-7562019.
58. Nie X et al. Oral nano drug delivery systems for the treatment of type 2 diabetes mellitus: an available administration strategy for antidiabetic phytocompounds. Int J Nanomedicine. 2020;15:10215-40.
59. Gündoğdu E, Yurdasiper A. Drug transport mechanism of oral antidiabetic nanomedicines. Int J Endocrinol Metab. 2014;12(1):e8984.
60. Mukhopadhyay P et al. Oral insulin delivery by self-assembled chitosan nanoparticles: in vitro and in vivo studies in diabetic animal model. Mater Sci Eng C. 2013;33(1):376-82.
61. Kasiewicz L, Whitehead K. Lipid nanoparticles silence tumor necrosis factor α to improve wound healing in diabetic mice. Bioeng Transl Med. 2018;4(1):75-82.
62. Lin P et al. Oral nonviral gene delivery for chronic protein replacement therapy. Adv Sci. 2018;5(8):1701079.
63. Mohammed SR et al. De novo fabrication of oral insulin-loaded chitosan/dextrin/pectin nanospheres and their antidiabetic efficacy in streptozotocin-induced diabetic rats. Journal of Optoelectronic and Biomedical Materials. 2024;16(2):73-87.
64. Elekofehinti O, Akinjiyan M. Effects of momordica charantia silver nanoparticles on the expressions of genes associated with lipid metabolism and nephrotoxicity in streptozotocininduced rats. Niger J Biotechnol. 2021;37(2):126-33.
65. Kandregula B et al. Exploration of lipid-based nanocarriers as drug delivery systems in diabetic foot ulcer. Molecular Pharmaceutics. 2022;19(7):1977-98.
66. Laiva A et al. SDF-1α gene-activated collagen scaffold restores proangiogenic wound healing features in human diabetic adipose-derived stem cells. Biomedicines. 2021;9(2):160.
67. Paul S et al. Silver nanoparticles in diabetes mellitus: therapeutic potential and mechanistic insights. Bulletin of the National Research Centre. 2024;48(1):33.
68. Wahab M et al. Evaluation of antidiabetic activity of biogenic
silver nanoparticles using thymus serpyllum on streptozotocin-induced diabetic BALB/c mice. Polymers. 2022;14(15):3138.
69. Purwati P et al. Adipose-derived mesenchymal stem cells for treatment tertiary failure diabetes mellitus type 2. JBBBE. 2017;31:91-5.
70. Firoz S et al. A review on stem cellstherapyis a new era in type 2 diabetes. World Journal of Current Medical and Pharmaceutical Research. 2020;2(2):206-10.
71. Nasli-Esfahani E et al. Transitional meningioma after fetal liver-derived cell suspension allotransplant: a case report. Experimental and Clinical Transplantation. 2017;15(2):231-34.
72. Lavoie J et al. Brief report: elastin microfibril interface 1 and integrinlinked protein kinase are novel markers of islet regenerative function in human multipotent mesenchymal stromal cells. Stem Cells. 2016;34(8):2249-55.
73. Seewoodhary J, Evans P. Diabetes and stem cells: endogenous effects and reparative mechanisms. BJD. 2013;13(5-6):224-8.
74. Huang Y et al. Radially electrospun fibrous membrane incorporated with copper peroxide nanodots capable of self-catalyzed chemodynamic therapy for angiogenesis and healing acceleration of diabetic wounds. Acs Applied Materials & Interfaces. 2023;15(30):35986-98.
75. Xu Z et al. Progress and expectation of stem cell therapy for diabetic wound healing. World J Clin Cases. 2023;11(3):506-13.
76. Shi H et al. Research progress and challenges in stem cell therapy for diabetic foot: bibliometric analysis and perspectives. World J Stem Cells. 2024;16(1):33-53.
77. Yang M et al. Stem cell therapy for lower extremity diabetic ulcers: where do we stand? Biomed Res Int. 2013;2013:462179.
78. Almasoudi L et al. Awareness of stem cell therapy for diabetes among type II diabetic patients in makkah: a cross-sectional study. Cureus. 2023;15(6):e40981.
79. Yang X et al. Immunogenicity of insulin-producing cells derived from human umbilical cord mesenchymal stem cells. Exper Therapeut Med. 2017;13(4):1456-64.
80. Cores J et al. Magnetically targeted stem cell delivery for regenerative medicine. J Funct Biomater. 2015;6(3):526-46.
81. Moysidis S et al. Magnetic field-guided cell delivery with nanoparticle-loaded human corneal endothelial cells. NBM. 2015;11(3):499-509.
82. Oyelaja O et al. Applications of nanotechnology in the field of cardiology. Cureus. 2024;16(4):e58059
83. Brüstle I et al. Hematopoietic and mesenchymal stem cells: polymeric nanoparticle uptake and lineage differentiation. BJON. 2015;6:383-95.
84. Zhang J et al. Nanomaterials for diabetic wound healing: visualization and bibliometric analysis from 2011 to 2021. Front Endocrinol (Lausanne). 2023;14:1124027.
85. Zhang X et al. Self-powered enzymelinked microneedle patch for scar-
prevention healing of diabetic wounds. Sci Adv. 2023;9(28):eadh1415.
86. Augustine R et al. Cerium oxide nanoparticle-loaded gelatin methacryloyl hydrogel wound-healing patch with free radical scavenging activity. ACS Biomater Sci Eng. 2020;7(1):279-90.
87. Reddy V et al. Gallocatechinsilver nanoparticles embedded in cotton gauze patches accelerated wound healing in diabetic rats by promoting proliferation and inhibiting apoptosis through the Wnt/βcatenin signaling pathway. Plos One. 2022;17(6):e0268505.
88. Pandey S et al. Leveraging potential of nanotherapeutics in management of diabetic foot ulcer. Exp Clin Endocrinol Diabetes. 2022;130(10): 678-86.
89. Zhao X et al. Thermosensitive hydrogel incorporating Prussian blue nanoparticles promotes diabetic wound healing via ROS scavenging and mitochondrial function restoration. Acs Applied Materials & Interfaces. 2022;14(12):14059-71.
90. Zhao E et al. Separable microneedles with photosynthesis-driven oxygen manufactory for diabetic wound healing. ACS App Material Interfaces. 2023;15(6):7725-34.
91. Renuka R et al. Diverse nanocomposites as a potential dressing for diabetic wound healing. Front Endocrinol (Lausanne). 2023;13:1074568.
92. Muchtaromah B et al. Effect of pegagan (Centella asiatica) nanoparticle coated with chitosan on the cytokine profile of chronic diabetic mice. Narra J. 2024;4(1):e697.
Target-Like Lesions with Mucositis in a
13-Year-Old Adolescent Due to CoInfection with Mycoplasma pneumoniae and Varicella-Zoster Virus: A Case
Report and Literature Review
Authors: *Norbert Faludi,1 Judit Bíró2
1. Spitalul Clinic Județean Mureș, Târgu Mureș, Romania
2. Department of Infectious Diseases, Spitalul Municipal Odorheiu Secuiesc, Odorheiu Secuiesc, Romania
*Correspondence to faludinorbert1996@gmail.com
Disclosure: AI technologies were used for language refinement, grammar correction, and structural organisation of the manuscript. It is important to note that the AI was used under strict human supervision, ensuring that all content generated was thoroughly reviewed and edited by the authors to maintain accuracy and coherence. They were not involved in the generation of original research ideas or conclusions. The authors have declared no conflicts of interest.
Acknowledgements Written consent was obtained by the participant’s legal representative in this case report.
Received: 16.01.25
Accepted: 27.05.25
Keywords: Mycoplasma pneumoniae, Mycoplasma pneumoniae-induced rush and mucositis, reactive infectious mucocutaneous eruption (RIME), target-like lesions with mucositis, varicella-zoster virus.
The case concerns a 13-year-old male patient admitted to the authors’ department, presenting with the following symptoms: malaise, fever, cough, and scattered vesicular and targetoid skin eruptions on his limbs, earlobe, and trunk, sparing the scalp, palms, and soles. Furthermore, mucositis was observed at three mucosal sites: ocular, oral, and urogenital. The mucosal involvements included bilateral conjunctivitis, stomatitis, initial herpanginalike eruptions on the buccal mucosa and the soft palate, and lip crusts. These subsequently progressed to severe mucositis and ulcerative lesions of the glans penis. Serological testing yielded positive results for IgM antibodies to Mycoplasma pneumoniae and varicella-zoster virus. The chest X-ray indicated atypical pneumonia. The diagnosis was made based on the patient's medical history, clinical presentation, paraclinical investigations, and serological findings. The treatment regimen was symptomatic, localised, and etiological (oral azithromycin for 5 days, intravenous Ig for 5 days and intravenous acyclovir for 10 days). The patient's clinical evolution was prolonged, with full recovery taking several weeks.
Key Points
1. Community-acquired pneumonia is the leading cause of hospitalisation and infection-related death, with the most frequent bacterial aetiology being Mycoplasma pneumoniae
2. This case report presents a reactive infectious mucocutaneous eruption triggered by M. pneumoniae and varicella-zoster Virus, including images, clinical, and paraclinical examinations in chronological order.
3. Reactive infectious mucocutaneous eruption, including M. pneumoniae-induced rash and mucositis, shares a common immune-mediated pathomechanism.
INTRODUCTION
Cases involving co-infections with Mycoplasma pneumoniae and varicellazoster virus (VZV) are exceedingly rare in medical literature.
M. pneumoniae infections are characterised by a long incubation period (2–4 weeks) and asymptomatic carriage for weeks following infection. Most frequently, it causes upper respiratory tract infections, bronchitis, community-acquired pneumonia (10–30%), and extrapulmonary complications (40%), including mucocutaneous diseases such as erythematous maculopapular/vesicular rashes, urticaria, M. pneumoniae-induced rush and mucositis (MIRM), erythema multiforme, and Stevens-Johnson syndrome. Encephalitis, haemolytic anaemia, and carditis are rare and are associated with respiratory infection.1-4
Extrapulmonary manifestations of M. pneumoniae infection are categorised into direct, indirect, and vascular occlusion mechanisms. The theories suggest MIRM is caused by both direct bacterial effects and indirect immune-mediated processes. The indirect mechanisms include immune modulation via autoimmunity or formation of immune complexes. While M. pneumoniae typically doesn’t infect squamous epithelia, its isolation from blister fluid suggests hematogenous dissemination. The pathogenesis of M. pneumoniae includes multiple mechanisms:1 1) the CommunityAcquired Respiratory Distress Syndrome toxin targets NLRP3 inflammasome, resulting in increased production of the proinflammatory cytokine IL-1β and enhancing the host innate immune response;
2) hydrogen peroxide and nuclease production of M. pneumoniae also contribute to cellular damage; 3) inflammatory response mechanisms include TLR2 recognition of M. pneumoniae lipoproteins, autophagy-mediated signalling, and activation of inflammasomes, and the cytadherence properties of M. pneumoniae; 4) molecular mimicry between the M. pneumoniae P1 adhesin protein and keratinocyte antigens leads to crossreacting autoantibodies against mucosal antigens; 5) immune complexes deposited in mucosa and skin can activate the complement system or phagocytic cells; 6) polyclonal activation of B cells and plasma cells at sites of infection leads to altered responses to other unrelated antigens or infections; 7) genetic susceptibility; and 8) combination of infection and medication can trigger mucosal lesions, where interferon and other cytokines downregulate cytochrome P450 enzyme expression, thereby lowering the threshold for a medication to cause a drug reaction.
MIRM is a relatively new entity (introduced in 2015) used to describe mucosal with or without dermal reaction triggered by M. pneumoniae infection.4,5 Ramien et al.6 proposed to the term reactive infectious mucocutaneous eruption (RIME) to unify the terminology for MIRM and other clinically similar mucosal-predominant parainfectious eruptions. MIRM is essentially a subtype of RIME caused by M. pneumoniae. Therefore, in the following sections, the authors will focus on the characterisation of RIME.
RIME represents a broader category of mucocutaneous reactions with an infectious aetiology (including non-M. pneumoniae
and viral causes), but it does not encompass toxic or iatrogenic aetiologies. Diagnosis of RIME requires evidence of an infectious trigger, including a preceding history (7–10 days) of cough, fever, malaise, or arthralgia, supported by clinical examination or investigations confirming a respiratory infection. Diagnostic evaluations include chest radiography and laboratory testing for acute infections caused by respiratory viruses, M. pneumoniae, or Chlamydophila pneumoniae. These assessments may involve culture or PCR analysis of nasopharyngeal/oropharyngeal samples, or serological testing for IgM and acute/convalescent IgG. Confirmation of RIME requires at least two of the following criteria: a non-contributory medication history; erosive mucositis affecting two or more sites; and vesiculobullous lesions or atypical (often bullous) target lesions covering <10% of the body surface area. Supporting features include prodromal symptoms and histological findings excluding alternative diagnoses.7
PATIENT INFORMATION
A 13-year-old male with an unremarkable medical history except for a negative history for chicken pox, no prior vaccination for VZV, and a four-year history of athletic activity. The patient was unable to recall any contact with an ill individual within the past month.
The patient’s first presentation at the emergency department was on the 8th day post-onset of an acute illness. The patient exhibited symptoms of malaise, nonproductive cough, bilateral conjunctivitis (without chemosis), stinging ocular pain, crusted lips, herpangina-like eruptions on the buccopharyngeal mucosa (Figure 1). The lung auscultation revealed diffuse crackles sounds; and a chest X-ray was performed, which indicated atypical pneumonia (right middle lung field cuffing; Figure 2A).
The patient was discharged with the following prescription: azithromycin 500 mg orally once daily for 5 days; Anaftin spray (Ketof, Salutas Pharma GMBH, Germany; 15 mL, three puffs four times/day) contains
polyvinylpyrrolidone and hyaluronic acid; salbutamol sulphate inhaler; an expectorant; an antitussive; ibuprofen and paracetamol in case of fever.
Following a 2-day interval, the patient re-presented to the emergency department and was subsequently admitted to the paediatric section with a presumptive diagnosis of Stevens-Johnson syndrome, induced by the non-steroidal antiinflammatory drug (ibuprofen).
Clinical Findings at Admission
Physical examination revealed high-grade, refractory fever (39.5 °C/ 103.1 °F), scattered papulovesicular eruptions with erythematous halos on the arms and trunk, sparing the scalp, palms, and soles. Furthermore, a vesicle was observed on the glans penis. On the swollen lips and buccopharyngeal mucosa, haemorrhagic and buccal ulcers with white-grey purulent deposits were noted, accompanied by mild trismus due to pain. Notably, there was an absence of arthralgia, hepatosplenomegaly, and lymphadenopathy.
TIMELINE
On the 11th day of the disease’s progression, the generalised exanthem extended to the left auricle and evolved into vesicles resembling those seen in varicella. The vesicles were slightly larger, reducing the likelihood of Stevens-Johnson syndrome. Intravenous acyclovir therapy was initiated.
On the 12th day, the vesicles transformed into targetoid lesions; their contents were clear. The lip lesions became haemorrhagic and crusted. The patient developed a productive cough with pink sputum, intermittent fever (a diffuse, generalised dermal erythema developed while the fever was present). The conjunctivitis resolved.
On the 13th day, suspicion was raised for Kawasaki disease. However, as not all criteria for Kawasaki disease were present, intravenous Ig therapy was started the next day.
On the 14th day, some vesicles evolved into larger, darker blisters with a darkened peripheral ring. The oral mucosa became extremely painful due to the oral ulcers, haemorrhagic crusting, and the patient could not feed. The control X-ray described right-sided accentuated hilar and perihilar prominence, and resolution of opacity in the right upper lobe (Figure 2B).
On the 15th day, serological testing (chemiluminescence immunoassay) yielded positive results for IgM antibodies to M. pneumoniae and VZV. The herpes simplex virus 1+2 IgM antibodies were negative.
On the 16th day, the patient was transferred to the infectious disease section. He was afebrile. Aspirin was stopped, as it can lead to Reye’s syndrome in varicella.
On the 17th day, some vesicles turned into blood blisters, while others started to regress. A paediatric cardiology consultation ruled out the cardiac complications associated with Kawasaki disease. Consequently, intravenous Ig therapy was stopped after a total of 5 days of treatment.
On the 21st day, most vesicles had transformed into scabs or haemorrhagic macules or papules. Some vesicles healed, leaving pink traces. The control X-ray showed significant radiological improvement, with mild bilateral prominence of the hilar, perihilar, and infrahilar regions (Figure 2C).
2A) Day 8: pulmonary radiography described right middle lung field cuffing and bilateral hilar prominence. 2B) Day 14: control radiography described right-sided accentuated hilar and perihilar prominence, with resolution of the opacity in the right upper lobe. 2C) Day 21: control radiography showed significant radiologic improvement, with mild bilateral hilar, perihilar, and infrahilar prominence.
On the 23rd day, due to the extent of healing of the oral, urogenital mucosa, and the skin lesions, and as the patient no longer had a fever, he was discharged from the hospital with symptomatic treatment.
DIAGNOSTIC ASSESSMENT
The diagnosis of RIME due to coinfection with M. pneumoniae and VZV was established based on the integration of clinical presentation, laboratory findings, and imaging results. The illness began with
Figure 2: The patient's X-ray results from Day 8, 14, and 21.
a prodromal phase, characterised by high fever and cough, subsequently progressing to atypical pneumonia. Physical examination identified a rash that evolved into papules, vesicles, target-like eruptions affecting <10% body surface area, with involvement of three mucosal sites: conjunctival, oral, and urogenital. Laboratory results indicated the presence of leucocytosis, neutrophilia, lymphocytopenia, and elevated acute phase protein levels. Serological tests were positive for IgM antibodies to M. pneumoniae and VZV, therefore the authors think RIME is a more accurate diagnosis than MIRM with VZV co-infection.
The diagnostic process was complicated by the parents’ refusal to consent to vesicle sampling or skin biopsy; the serology results took too long to arrive, and the unavailability of PCR testing as a diagnostic tool further delayed the establishment of the diagnosis.
TREATMENT
Etiologic treatment:
• Azithromycin 500 mg orally once daily for 5 days
• Acyclovir 250 mg intravenous (100 mL/ min) four times daily for 10 days
• Privigen (intravenous Ig, CSL Behring GMBH, Germany) 2.5 g intravenous (25 mL/h) once daily for 5 days.
Local agents:
• Oral mucosa: Anaftin spray (15 mL, three puffs four times/day); mouthwash preparation containing borax glycerine, nystatin, anestezine, metronidazole, vitamin A; chlorhexidine digluconate mouthwash (three times/day); bathing with sage tea.
• Conjunctival mucosa: netilmicin+dexamethasone eye drops (four times/day) and artificial tear in both eyes.
Supportive therapy: Paracetamol 1 g intravenous three times/day; aspirin 500 mg orally four times/day; salbutamol sulphate inhaler; expectorant; an antitussive (Ketof); multivitamins; inosine pranobex 500 mg orally twice/day for 10 days.
FOLLOW-UP AND OUTCOMES
An allergology and immunology consultation was conducted, and laboratory tests were performed. All results were within normal range except where indicated in bold (see Supplementary Table 1): complete blood count, AST, ALT, serum albumin, ALP, urea, creatinine, total IgA, IgM, IgG, CRP, complement C3c, C4, IL-6, circulating immune complexes, ANA screen, anticardiolipin IgG Ab, ACA IgG Ab, anti dsDNA IgG, anti Jo-1 IgG, anti MPO-ANCA IgG, anti nRNP or Sm IgG, anti SCL-70 IgG, Anti Sm IgG, Anti SS-A IgG, Anti SS-B IgG, B2 glycoprotein 1 IgG, anti HSV-1 and 2 IgM and IgG, anti VZV IgM and IgG, anti SARSCoV2 IgM, and anti M. pneumoniae IgM and IgG.
Re-evaluation by the infectious diseases unit showed favourable progression, as evidenced by the resolution of cutaneous lesions with residual mild hypopigmentation. The oral and urogenital mucosa were clear, with minimal hyperaemia. Laboratory investigations revealed eosinophilia and absence of inflammatory markers.
DISCUSSION
Strengths
The strengths of the case presentation lie in its well-photodocumented, chronologically structured format, which encompasses comprehensive clinical and paraclinical examinations, along with interprofessional consultations in dermatology, ophthalmology, paediatric cardiology, aimed at excluding other diseases. This method ensures a systematic and evidence-based approach, facilitating diagnostic accuracy and enhancing the clarity of findings.
Limitations
Although PCR testing for viral DNA is the recommended method for diagnosing varicella, limited availability restricts diagnostic options. In the authors’ case, despite the unavailability of PCR testing, serological analysis conducted at two distinct time points confirmed a recent varicella infection. The initial serological result was positive for varicella-specific IgM antibodies but negative for IgG. An additional limiting factor was the absence of parental consent for obtaining vesicular fluid samples for further analysis. It’s important to note that PCR is a more sensitive diagnostic method compared to serological testing, meaning that enzyme immunoassay tests with lower sensitivity may yield false-negative results. Park et al.8 reported that the sensitivity and specificity of PCR analysis of salivary DNA for detecting VZV were 88% and 100%, respectively.8 Kombe Kombe et al.9 found that the sensitivity of chemiluminescence immunoassay-based detection for IgM and IgG antibodies in varicella was 93.6% and 69.4%, respectively, while the specificity was 98% and 99.8%, respectively.9
The diagnostic process for RIME was notably complex due to the overlapping clinical features with VZV infection. Although VZV can cause RIME or erythema multiforme, it is a rare occurrence compared to herpes simplex virus. M. pneumoniae is known to cause both erythema multiforme and MIRM.1,10,11
Comprehensive examinations excluded other conditions such as Kawasaki disease, Stevens-Johnson syndrome, toxic epidermal necrolysis, co-infections (HIV, syphilis), and autoimmune diseases (lupus, rheumatoid arthritis, scleroderma, antiphospholipid syndrome, systemic sclerosis, polymyositis, dermatomyositis, vasculitis, mixed connective tissue disease, Sjögren’s syndrome). All tests returned negative results.
CONCLUSION
This case presentation aligns with recent academic studies on RIME, particularly regarding symptom manifestation, clinical and paraclinical findings. In an adolescent male patient, following a prodromal phase of general symptoms, lesions appeared on three mucosal surfaces: oral, ocular, and urogenital, accompanied by maculopapular vesicular skin eruptions. These later evolved into target-like lesions, which were sparsely distributed across the skin while sparing the face, scalp, palms, and soles.
Although PCR is the gold standard for determining the aetiology of VZV, both PCR and serology are recommended for diagnosing M. pneumoniae in paediatric patients.1 English-language medical literature contains limited studies on VZV-induced RIME. However, two documented cases describe VZV reactivation following SARSCoV-2 coinfection with influenza A and coronavirus NL63 co-infection with group A Streptococcus. In both cases, mucosal involvement was reported; however, only the paediatric patient exhibited rash affecting 40–50% of the body surface area, later progressing to 70%. The VZV DNA PCR test was positive, confirming viral presence in multiple erosions.12,13 The fact that RIME can be triggered by a diverse range of infectious agents supports the theory that VZV induces RIME through an indirect rather than a direct mechanism. While antiviral therapy for VZV might be necessary to treat an underlying infection, immunomodulatory agents are likely crucial for controlling the mucocutaneous eruption itself.
Future studies are warranted to better understand the pathophysiology and optimal treatment strategies for MIRM, RIME, and similar conditions.
1. Ramien ML. Reactive infectious mucocutaneous eruption: Mycoplasma pneumoniae-induced rash and mucositis and other parainfectious eruptions. Clin Exp Dermatol. 2021;46(3):420-29.
2. Alawad S et al. Reactive infectious mucocutaneous eruption (RIME) in an adult male with mycoplasma pneumoniae: A case report. Cureus. 2025;17(1):e78301.
3. Abdulhadi B, Kiel J. Mycoplasma Pneumonia [Internet] (2023) Treasure Island: StatPearls Publishing. Available at: https://www.ncbi.nlm.nih.gov/ books/NBK430780/. Last accessed: 26 May 2025
4. Frantz GF, McAninch SA. Mycoplasma pneumoniae–Induced Rash and Mucositis (MIRM) [Internet] (2024) Treasure Island: StatPearls Publishing. Available at: https://www.ncbi.nlm. nih.gov/books/NBK525960/. Last accessed: 26 May 2025.
5. Mathes E, Kittler NW, "Reactive infectious mucocutaneous eruption (RIME)," Levy ML, Corona R (eds.), UpToDate [Internet] (2024), Waltham, MA: UpToDate, Inc.
Available at: https://www. uptodate.com/contents/reactiveinfectious-mucocutaneouseruption-rime?search=Reactive%20 infectious%20mucocutaneous%20 eruption%20(RIME)&source=search_ result&selectedTitle=1~9&usage_ type=default&display_rank=1. Last accessed: 26 May 2025.
6. Ramien ML et al. Redefining severe cutaneous reactions in children. Society for pediatric dermatology 43rd annual meeting poster presentations July 2018, 2018.
7. Ramien ML et al. Blistering severe cutaneous adverse reactions in children: proposal for paediatricfocused clinical criteria. Br J Dermatol. 2021;185(2):447-9.
8. Park SY et al. Diagnostic usefulness of varicella-zoster virus real-time polymerase chain reaction analysis of DNA in saliva and plasma specimens from patients with herpes zoster. J Infect Dis. 2017;217(1):51-7.
9. Kombe Kombe AJ et al. Detection of circulating VZV-glycoprotein e-specific antibodies by chemiluminescent immunoassay (CLIA) for varicellazoster diagnosis. Pathogens. 2022;11(1):66.
10. Wetter DA, "Erythema multiforme: Pathogenesis, clinical features, and diagnosis," Callen JP, Ofori AO (eds.), UpToDate [Internet] (2023), Waltham, MA: UpToDate, Inc. Available at: https://www.uptodate. com/contents/erythema-multiformepathogenesis-clinical-features-anddiagnosis?search=Erythema%20 multiforme:%20Pathogenesis%2C%20 clinical%20features%2C%20 and%20diagnosis&source=search_ result&selectedTitle=1~92&usage_ type=default&display_rank=1. Last accessed: 26 May 2025.
11. Mahon C. Mycoplasma pneumoniae infection. 2022. Available at: https:// dermnetnz.org/topics/mycoplasmapneumoniae-infection. Last accessed: 30 August 2024.
12. Moshayedi A et al. Reactive infectious mucocutaneous eruption secondary to SARS‐CoV‐2 and influenza A coinfection with varicella zoster virus reactivation. JEADV Clinical Practice. 2023;2(3):617-20.
13. Rodriguez I et al. A severe case of reactive infectious mucocutaneous eruption associated with two possible triggers: Coronavirus and group A streptococcus. Pediatr Dermatol. 2025;42(1):150-3.
Authors:
Urinary Tract Infection Turns Out to Be Infective Endocarditis: An Unusual Presentation – A Case Report
David Bertlla,1 Muhammad Usman Anwar1 1. Department of Internal Medicine, Midland Regional Hospital Tullamore, Ireland
*Correspondence to davidsamwell@yahoo.com
Disclosure: The authors have declared no conflicts of interest.
This case highlights an unusual presentation for infective endocarditis (IE). The patient was initially admitted with symptoms indicative of a urinary tract infection, with a concerning and unexplained symptom of significant weight loss. As per local hospital protocol, intravenous antibiotics were initiated to treat the urinary tract infection. However, due to the patient’s persistent and unexplained weight loss, further investigations were recommended, including a CT scan of the thorax, abdomen, and pelvis to rule out malignancy or deep-seated infections. The CT scan revealed splenic infarction, prompting an echocardiogram, which subsequently showed vegetation on the aortic and mitral valves, confirming IE.
Treatment for IE was promptly initiated, and a transoesophageal echocardiogram was performed. The patient underwent open-heart surgery to replace the aortic valve and repair the mitral valve. Post-surgery, the patient made an excellent recovery.
Key takeaway: this case underscores the importance of maintaining a high index of suspicion, as the symptoms of IE are often nonspecific, vary widely, and can develop insidiously. Endocarditis should be considered as a differential diagnosis, particularly in patients with fever and no obvious source of infection. This case illustrates how a rare and unusual presentation of IE can be diagnosed with timely intervention, leading to a favourable outcome.
Key Points
1. The clinical manifestations of infective endocarditis can vary widely, and often present with subtle or nonspecific symptoms.
2. A high index of suspicion is essential for the accurate diagnosis of infective endocarditis.
3. Early diagnosis and prompt management are crucial, as they significantly improve prognosis and patient outcomes.
INTRODUCTION
Infective endocarditis (IE) often presents in an unusual and vague manner, especially in its early stages, where symptoms can be nonspecific. This case was initially presented as a urinary tract infection (UTI), but later revealed underlying IE.
In the case presented in this article, the key concerning symptom during presentation was unexplained weight loss, which prompted further investigation. The vague and unclear history raised suspicions, ultimately leading to a more thorough workup and the correct diagnosis of IE.
This case emphasises the importance of considering a broader differential diagnosis, particularly when the clinical presentation is ambiguous.
PATIENT INFORMATION
A 65-year-old White male patient, who had resided in Ireland for over 10 years and lived with his teenage son. His immediate family remain in his home country, and his next of kin is a close friend. The patient was not employed at the time of admission, and had a history of alcohol abuse, with a daily consumption of a bottle of vodka.
CLINICAL FINDINGS
A 65-year-old male patient presented to the emergency department after being bought in by an ambulance from home. He reported a history of nonspecific symptoms, including generalised weakness, fatigue, and low energy. He denied any recent flu-like symptoms, cough, shortness of breath, cardiac symptoms, gastrointestinal complaints, or neurological issues. The patient did note increased urinary frequency and dysuria. He had experienced intermittent fever for the past 2 days, along with occasional night sweats and unquantified weight loss, as he had not weighed himself. His symptoms had started 3 months prior to presentation, but had worsened in the preceding 2 weeks.
Notably, the patient did not have a general practitioner and had not had any recent or prior hospital visits.
Upon presentation, the patient’s vital signs were recorded as follows: blood pressure of 144/72 mmHg, pulse of 124 bpm, respiratory rate of 28 breaths/min, oxygen saturation of 96% on room air, temperature of 37.8°C, and a Glasgow Coma Scale (GCS) score of 15/15.
Physical examination revealed an elevated jugular venous pressure, but otherwise, the head and neck were unremarkable. The chest examination revealed no abnormalities, and the cardiac examination was normal, with no murmurs detected. The abdominal examination was also normal, with no tenderness or organomegaly. The general examination revealed no limb oedema, changes in fingers or toes, or palpable lymph nodes.
TIMELINE
Day 1:
The patient was admitted to the emergency department with a suspicion of UTI based on his symptoms and investigation findings. His weight loss, along with his history of alcohol abuse, raised concerns. Intravenous antibiotics were started as per hospital protocol, and further investigations were planned.
Day 2:
The patient was reassessed by the admitting team, and daily blood tests were scheduled to monitor his inflammatory markers and trace his urine culture results.
A CT scan (thorax-abdomen-pelvis) was advised to investigate the cause of his weight loss, particularly to rule out malignancy or deep-seated infection.
Day 3:
The CT scan revealed a splenic infarction, prompting further investigations. An urgent echocardiogram (ECHO) was ordered, which revealed large vegetations on both the aortic and mitral valves. Infective
endocarditis was diagnosed, and the patient was started on intravenous vancomycin and gentamicin. The case was discussed with the cardiology and microbiology teams, who confirmed the management plan. The patient was also observed to have a new soft diastolic murmur and macular rashes on his trunk and left foot, which were not present initially. His poor dental hygiene was noted as a potential source of infection. A CT brain was urgently performed, revealing subacute infarction in the left cerebellum, which added urgency to his management.
Day 4:
The patient underwent a transoesophageal echocardiogram (TOE), which confirmed severe aortic and mitral regurgitation, and large vegetations on both valves. He started on telemetry for monitoring. During the night, the patient developed a broad complex tachycardia, which was managed with intravenous magnesium sulfate.
The case was urgently discussed with the cardiothoracic team, and the patient was accepted for immediate surgery. Blood was cross-matched, and a full blood workup was performed. The patient was transferred to the operating theater for urgent aortic valve replacement and mitral valve repair.
DIAGNOSTIC ASSESSMENT
Blood Cultures
Both bottles of blood cultures flagged positive within 1 day: bottle A flagged positive for Gram-positive cocci in chains resembling Streptococcus spp., and in clusters resembling Staphylococcus spp., while bottle B flagged positive for Gram-positive cocci in chains resembling Streptococcus spp.
Culture Results
Both Staphylococcus hominis and Streptococcus oralis were sensitive to ceftriaxone and vancomycin.
Urine Analysis and Culture (Emergency Department)
• Red cells: >200/µL
• White cells: 27/µL
• Culture: No growth
Full Blood Count on Presentation
• Leukocytic Count: 14.89x109/L (high)
• Neutrophils: 12.63x109/L (high)
• Platelets: 72x109/L (low)
• Haemoglobin: 9.7 g/dL (low)
Biochemistry Results on Presentation
• Urea: 5 mmol/L
• Creatinine: 65 µmol/L
• C-reactive protein: 65.7 mg/L (high)
• Aspartate aminotransferase: 47 U/L (high)
• Alanine Aminotransferase: 18 U/L
• Lactate Dehydrogenase: 427 U/L (high)
• Corrected Calcium: 2.25 mmol/L
• Phosphorus: 1 mmol/L
• Magnesium: 0.78 mmol/L
CT Scan (Thorax, Abdomen, and Pelvis)
There was no evidence of malignancy. Wedge-shaped low attenuation areas were noted in the anterior and posterior aspects of the spleen, indicative of splenic infarcts. Dilatation of both ureters to the vesicoureteral junctions was seen, as well as bilateral prominence of the renal calyces.
CT
Brain
Multiple cortico-subcortical hypoattenuating foci in the left cerebellum were identified, suggesting acute to subacute infarcts. No space-occupying lesions, bleeding, or other abnormalities were seen.
Initial Echocardiogram Report
Study Indications: Referred for evaluation of bacterial endocarditis.
There was a sinus rhythm on the ECG, and the patient’s heart rate was 99 bpm.
Study Quality
This was a technically difficult study with suboptimal views.
Left ventricle and right ventricle
The left ventricle was markedly dilated, and mild septal hypertrophy was noted. The overall left ventricular systolic function was normal, with an ejection fraction of >55%, and diastolic dysfunction was indeterminate. The right ventricle was normal in size and function.
Left atrium and right atrium
The left and right atrium were normal in size and function.
Aortic valve
The aortic valve appeared tri-leaflet and was mildly thickened. There was at least moderate aortic regurgitation with turbulent flow, as well as mild aortic stenosis with a peak/mean pressure gradient of 46.00 mmHg/25.38 mmHg. The aortic valve area had a large vegetation.
Mitral valve
Mitral inflow was unable to be measured due to turbulent mitral regurgitation. Moderate mitral regurgitation (a posteriorly directed jet) was present. Evidence of a medium-sized mobile mass (a vegetation) attached to the anterior mitral valve leaflet.
Tricuspid valve
There was mild tricuspid regurgitation. The right ventricular systolic pressure, as measured by Doppler, was 32 mmHg + right atrial pressure.
Pulmonary valve
The pulmonary valve was not well visualised.
Pericardium
Trivial pericardial effusion was present, and there was no evidence of cardiac tamponade.
Aorta
The aortic root and ascending aorta were notably dilated, measuring up to 4.7 cm.
Inferior vena cava/hepatic veins
The inferior vena cava was normal.
Report summary
The report was relied upon immediately by the treating consultant.
Post-Operative Echocardiogram Findings
There was a sinus rhythm on the ECG. The study was technically adequate.
Left ventricle and right ventricle
The left ventricle size was normal, but there was mild concentric left ventricular hypertrophy. The overall left ventricular systolic function was normal, with an ejection fraction of >55%, and the diastolic filling pattern indicated impaired relaxation. The right ventricle was normal in size and the right ventricular systolic function was normal.
Left atrium and right atrium
The right atrium was normal in size and function, and the left atrium was dilated.
Aortic valve
There was no evidence of aortic regurgitation, and the maximum pressure gradient across the aortic valve was 17.16 mmHg. Aortic valve replacement appeared well seated. Turbulent flow was noted at the left ventricular outflow tract, and there was no evidence of paravalvular leaks.
Mitral valve
The mitral valve was thickened with myxomatous degeneration, and the anterior leaflet appeared calcified. Turbulent flow was noted; however, no significant mitral regurgitation was observed.
Tricuspid valve
The tricuspid valve appeared structurally normal. There was trace/mild (physiologic) tricuspid regurgitation.
Aorta
The ascending aorta was dilated, measuring up to 4.4 cm. An aortic aneurysm was noted at the aortic arch.
Cardiac physiologist observations
All findings need to be clinically correlated.
THERAPEUTIC INTERVENTION
Initial management of the patient was admission on intravenous antibiotics and intravenous fluids. As the findings of IE came to the surface, the patient was started on intravenous vancomycin and gentamicin. Open-heart surgery to replace the aortic valve and repair the mitral valve was the main intervention this patient received. Antibiotic treatment (ceftriaxone) was continued for 6 weeks as per cardiothoracic advice.
FOLLOW-UP AND OUTCOMES (1 MONTH AFTER SURGERY)
The patient was discharged and transferred back to the authors' local hospital following his surgery. He made an excellent recovery, with his surgical wounds fully healed. He was on intravenous antibiotics for 6 weeks as per the cardiothoracic and microbiology teams’ recommendations. Upon discharge, he was seen by the cardiology team for a follow-up, and future appointments were scheduled for echocardiography and routine check-ups. The patient’s weight stabilised, and the rashes and murmur resolved. His cognitive function remained intact, and he was able to resume a more normal routine following a period of rehabilitation.
DISCUSSION
IE is an uncommon but potentially lifethreatening condition that can present with a wide range of nonspecific symptoms. The clinical manifestations
of IE vary from rapidly progressive acute infections to subacute or chronic forms with mild, constitutional symptoms.1 Early diagnosis requires a high level of suspicion, particularly when the presentation is vague, as was the case with the author's patient. Due to the nonspecific nature of the symptoms, it is important to consider several differential diagnoses that can mimic the clinical features of IE.2 Major conditions to consider include systemic infections such as sepsis, bacterial pneumonia, or deep tissue abscesses, which can present with fever, weight loss, and vague systemic signs. Systemic lupus erythematosus can also present with similar symptoms and valvular lesions (Libman-Sacks endocarditis), but it is distinguished by the absence of positive blood cultures and the presence of autoantibodies. Rheumatic fever can present with carditis, but the history of a recent streptococcal throat infection and migratory arthritis can help to differentiate it. Malignancy, especially metastatic disease to the spleen, can cause weight loss, fever, and organ dysfunction, but it is not associated with positive blood cultures or vegetations. Pulmonary embolism can present with shortness of breath or chest pain, but it lacks typical echocardiographic findings. Lastly, splenic infarction from conditions like sickle cell disease or vasculitis may look similar, but positive blood cultures and echocardiographic findings of vegetations help confirm the diagnosis of IE.
In many cases, IE is associated with a primary source of infection such as dental and skin infections, or intravenous drug use. Interestingly, Aerococcus urinae, a rare pathogen typically associated with UTIs, can also cause IE, particularly in elderly patients with comorbid conditions such as diabetes or alcohol abuse. A study by Melnick et al.3 highlights A. urinae as an uncommon, yet important pathogen in the aetiology of IE, emphasising its unexpected role in UTI cases that progress to endocarditis.8 This finding underscores the importance of considering rare microorganisms when managing patients with UTI symptoms and unexplained complications.
The author's case further supports the notion that a high index of suspicion is critical when diagnosing IE, especially in patients who exhibit nonspecific symptoms. In this case, the patient’s unexplained weight loss prompted further investigation and resulted in the discovery of splenic infarction, which led to a TOE that revealed significant vegetations on both the aortic and mitral valves. This was highlighted in another case report of a middle-aged male who presented to the emergency department with complaints of excessive weight loss.4 An additional learning point from the author's case is the importance of conducting a thorough cardiac examination. Although the patient had no murmurs, 85% of cases will have a new or changing cardiac murmur.1 Previous case reports, such as a 51-year-old male who presented with confusion as a sign of IE,5 and a 52-yearold male who presented with weight loss,4 have highlighted the atypical presentations of this condition. In these cases, confusion and weight loss were key symptoms that led to the eventual diagnosis. These cases, along with the author's case, demonstrate that endocarditis can often present with subtle or unusual symptoms, making early recognition crucial for optimal outcomes.
Interestingly, in the author's case, the patient’s poor oral hygiene was identified as a possible source of the infection. As noted in previous literature, dental infections are a well-known risk factor for IE, and patients with poor oral hygiene are at a higher risk.6 In this case, the patient’s dental health was addressed by the maxillofacial team, who extracted all of the patient’s teeth to help prevent further complications.
The role of echocardiography in diagnosing IE is paramount. As outlined in the 2023 Duke-International Society for Cardiovascular Infectious Diseases (ISCVID) criteria for endocarditis, echocardiographies and blood cultures are key diagnostic tools.7 The criteria incorporate major components such as positive blood cultures and echocardiographic evidence of vegetations or abscesses, along with minor criteria like predisposing conditions, fever, and vascular or immunologic phenomena. TOE is particularly useful in detecting vegetations in
cases where the diagnosis is not immediately apparent from initial examinations.
In the author's case, TOE confirmed the presence of large vegetations on both the aortic and mitral valves, which contributed to the diagnosis under the Duke criteria, ultimately leading to urgent surgical intervention. The criteria can be easily calculated using online medical calculators, such as those on MDCalc (New York, USA),7 enhancing diagnostic accuracy.
Literature reviews, such as the one by Kang et al.,8 support the idea that early detection and intervention, including surgical valve replacement, when necessary, can significantly improve patient outcomes. The management of IE typically involves a combination of prompt antimicrobial therapy and, in many cases, surgical intervention.9 For the author’s patient, the decision to proceed with urgent open-heart surgery to replace the aortic valve and repair the mitral valve proved to be lifesaving. Postoperative recovery was excellent, and the patient was discharged with continued antibiotic therapy for 6 weeks.
Additionally, the brain and spleen are common sites for emboli in left-sided IE. In this case, the patient’s splenic infarction was the first major clue that suggested the presence of IE, prompting further investigation. Studies like those by Monteiro et al.10 emphasise the importance of considering embolic events as part of the diagnostic workup for IE, especially in patients with unexplained organ dysfunction.
A skin rash can also be an unusual presentation of IE, and is separate from the well-known Janeway lesions and Osler’s nodes. For example, in the case described by Peterson et al., there was a 37-yearold male who presented with a painful, petechial rash on his torso and extremities.11
One of the key strengths in the authors’ approach to this case was maintaining a high level of suspicion for a possible sinister cause right from the start, particularly given the patient’s significant weight loss and nonspecific symptoms. This suspicion led the team to perform
a CT scan of the abdomen and pelvis, which, although initially considered for a deep-seated infection or malignancy, revealed a splenic infarction. This finding prompted further investigations, including a CT scan of the brain and an ECHO, which initially showed signs of vegetations. These findings were later confirmed with a TOE, ultimately leading to the correct diagnosis of IE.
However, a potential limitation was the broad approach to diagnosis, which might have caused some delays in identifying the exact cause. While these delays didn’t affect the final outcome, they emphasised the need to balance a detailed evaluation with timely decision making. Still, the early imaging and further investigations were crucial in confirming the diagnosis and guiding further treatment, resulting in a positive outcome for the patient.
In summary, the key takeaway from this case is the critical importance of maintaining a high level of suspicion for IE, particularly in patients with nonspecific
References
1. Chu VH, Wang A. Clinical manifestations and evaluation of adults with suspected left-sided native valve endocarditis. 2024. Available at: https://www.uptodate.com/ contents/clinical-manifestations-andevaluation-of-adults-with-suspectedleft-sided-native-valve-endocarditis. Last accessed 14 September 2024.
2. Yallowitz AW, Decker LC, Infectious Endocarditis [Internet] (2023) Treasure Island: StatPearls. Available at: https://www.ncbi.nlm.nih.gov/books/ NBK557641/. Last accessed: 8 April 2025.
3. Melnick S et al. Aerococcus urinae, a rare cause of infective endocarditis. BMJ Case Rep. 2016:bcr2016215421.
4. Rahman A et al. A case report of subacute infective endocarditis presenting with extreme weight loss, aortic regurgitation, and splenic infarct. Cureus. 2024;16(5): e59866.
or unusual symptoms like weight loss, confusion, or splenic infarction. Early diagnosis, appropriate antimicrobial therapy, and timely surgical intervention are crucial for achieving favourable outcomes.
PATIENT PERSPECTIVE AND INFORMED CONSENT
During the patient’s admission, the authors had the opportunity to discuss the possibility of publishing his case for educational purposes. He was fully supportive and expressed that he was pleased his unique presentation could provide valuable learning for other healthcare professionals and potentially help save other patients’ lives. The patient’s positive response and eagerness to contribute to medical knowledge made the authors even more motivated to publish his case. He provided informed consent for the publication of his case report. When the authors saw him again during his follow-up visit, he asked eagerly whether his case report had been published yet, showing his continued interest in contributing to medical knowledge.
5. Dabbous M et al. Confusion as an unusual presentation of infective endocarditis. Cureus. 2021;13(12):e20809.
6. Bumm CV, Folwaczny M. Infective endocarditis and oral health-a narrative review. Cardiovasc Diagn Ther. 2021;11(6):1403-15.
7. Fowler VG. 2023 Duke-International Society for Cardiovascular Infectious Diseases (ISCVID) criteria: diagnostic criteria for endocarditis. 2024. Available at: https://www.mdcalc.com/ calc/10564/2023-duke-internationalsociety-cardiovascularinfectiousdiseases-iscvid-criteria. Last accessed: 8 April 2025.
8. Kang DH et al. Early surgery versus conventional treatment for infective endocarditis. N Engl J Med. 2012;366(26):2466-73.
9. Wang A, Holland TL. Overview of management of infective endocarditis
in adults. 2024. Available at: https:// www.uptodate.com/contents/ overview-of-managementof-infective-endocarditis-inadults?search=infective%20 endocarditis%20 treatment&source=search_ result&selectedTitle=2~150&usage_ type=default&display_rank=.%20 Last%20accessed%2014%20 September%202024. Last accessed: 14 September 2024.
10. Monteiro TS et al. Asymptomatic and symptomatic embolic events in infective endocarditis: associated factors and clinical impact. Braz J Infect Dis. 2017;21(3):240-7.
11. Peterson EJ et al. An unusual presentation of infective endocarditis. HCA Healthc J Med. 2023;4(4):297-301.
Oesophageal Actinomycosis Masquerading as Squamous Cell Carcinoma
Authors: Sultan Moinuddin,1 *Ashwini Patil,1 Samvid Kotia,2 Padma Badhe2
1. Department of Radiology, Vedantaa Institute of Medical Sciences, Maharashtra, India
2. Department of Radiology, Seth GSMC and KEM Hospital, Maharashtra, India
*Correspondence to patilashwini799@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Acknowledgements Written informed consent was obtained from the patient.
Actinomycosis is an uncommon, chronic, and slowly developing granulomatous infection observed in individuals who are immunocompromised and those who are immunocompetent. Thoracic actinomycosis is particularly challenging to diagnose due to its varying presentations, which can mimic bronchogenic carcinoma, pneumonitis, or tuberculosislike infections. In some cases, bronchopleural fistulas have been reported. The authors report a case of a 38-year-old male presenting with dysphagia and weight loss. A series of radiological assessments were conducted. The chest X-ray revealed fine reticular opacities, while a high-resolution CT of the thorax showed centrilobular nodules affecting both lungs. A contrast-enhanced CT of the thorax identified a mass in the lower oesophagus, as well as circumferential wall thickening in the lower third of the oesophagus and the gastrooesophageal junction. Oral contrast imaging demonstrated a fistulous tract originating at the gastro-oesophageal junction and extending superolaterally to the right lower bronchus. Despite initial concerns for oesophageal carcinoma, a biopsy confirmed an infection caused by Actinomyces. The nonspecific clinical presentation and radiological findings can make diagnosing pulmonary actinomycosis difficult, but they remain valuable for clinicians when considering differential diagnoses.
Key Points
1. Oesophageal actinomycosis is a rare cause of dysphagia and can be mistaken for cancer. This case report underscores the importance of taking notice of underlying local factors in a patient who is otherwise immunocompetent.
2. Imaging and clinical findings of oesophageal actinomycosis closely resemble those of squamous cell carcinoma. The diagnosis of oesophageal actinomycosis involves imaging studies, endoscopic biopsy, and tissue sampling for histopathological analysis.
3. Timely and accurate diagnosis is very important, as surgery is indicated for oesophageal actinomycosis complications. Successful management depends on thorough patient education and counselling, owing to a long-term antimicrobial regimen.
INTRODUCTION
The Actinomyces family includes 47 different species. Actinomycosis infections are characterised by abscess formation, granulation, dense fibrotic tissue development, and cutaneous sinuses that discharge ‘yellow sulfur’ granules. In some cases involving the lungs, cavitations can form and may eventually lead to sinus tracts opening to the skin. Gastrointestinal infections may result in fistula formation, while bone involvement often leads to permeative bone destruction.1
The most frequently encountered form of Actinomyces infection is cervicofacial actinomycosis, which accounts for 50% of all cases. Thoracic actinomycosis represents 15–20% of cases, while abdominopelvic involvement occurs in approximately 20%. Less commonly, Actinomyces can infect the central nervous system, bones, muscles, and prosthetic joints.2
A functional immune response plays a key role in controlling actinomycosis. Factors that suppress this response, such as chemotherapy, HIV infection, organ transplants (e.g., lung or renal), or the use of steroids, can increase the risk of developing an infection. Additional risk factors include being male, aged 20–60 years, having poor oral hygiene, diabetes, alcohol use, trauma, recent surgery, or radiation exposure.3
Diagnostic imaging, including barium swallows, oral contrast CTs, and contrastenhanced CTs, is vital for differentiating actinomycosis from conditions like oesophageal tuberculosis or neoplasms.4 On CT and PET/CT scans, pulmonary actinomycosis often appears as a slowly progressing mass, which can be mistaken for a malignancy.5,6 Clinicians should be aware of the unusual presentation of oesophageal actinomycosis and its tendency to mimic cancer before surgery.
In this report, the authors present a rare case of oesophageal actinomycosis in a patient who is immunocompetent and has experienced symptoms including chronic cough, chest pain, dysphagia, and weight loss, closely resembling a malignancy.
CASE REPORT
A 38-year-old man presented with chronic cough, chest pain, dysphagia, weight loss, odynophagia, and vomiting that had all been going on for 9 months. The patient had dysphagia to both solids and liquids (more severe with solids than liquids), and had frequent episodes of vomiting that usually occurred after meals. These symptoms were accompanied by coughing fits with sputum production and intermittent exacerbations. The patient had lost 20 kg over 1 year and had a history of chronic alcoholism and tooth extraction with poor oral hygiene.
Upon physical examination, the patient appeared with symptoms of paleness, cachexia, and hypotension. Laboratory investigations showed anaemia, leukocytosis, and a negative serology for HIV. Chest radiographs showed fine reticular opacities in the left perihilar region (Figure 1A). A highresolution CT chest showed centrilobular nodules involving both lungs. Cavitatory subsegmental consolidation was seen in the posterobasal segment of the right lower lobe (Figure 1B).
Further imaging showed dilation of the thoracic oesophagus, with circumferential wall thickening in the lower third of the oesophagus and the gastro-oesophageal (GO) junction. There was an extension into the stomach, with a maximum wall thickness of 20 mm and a loss of distensibility. Fat planes adjacent to the liver were lost. Multiple peripherally enhancing mass lesions were seen in the subdiaphragmatic and subhepatic spaces, as well as in the left lobe of the liver (Figure 2A).
A) Chest radiograph showed fine reticular opacities in the left perihilar region. B) High-resolution CT thorax showed centrilobular nodules (blue arrows) involving both lungs. Cavitatory subsegmental consolidation (red arrows) is seen in the posterobasal segment of the right lower lobe.
2: Contrast-enhanced CT thorax and oral contrast CT.
A) Contrast-enhanced CT thorax showed circumferential wall thickening (blue arrows) at gastro-oesophageal junction. Multiple peripherally enhancing mass lesions (yellow arrows) are seen along liver surfaces, with loss of fat plane as well as stomach distensibility (red arrows). B) Oral contrast CT showed fistulous communication at the gastro-oesophageal junction, which was coursing superolaterally up to the right lower bronchus (blue arrows).
Figure 1: Chest radiograph and high-resolution CT thorax.
Figure
A B
A CT scan with oral contrast showed fistulous communication originating at the GO junction and coursing superolaterally up to the right lower bronchus (Figure 2B).
A barium swallow confirmed the CT findings: a concentric irregular narrowing involving the retrocardiac and epiphrenic oesophagus, with proximal barium hold-up (Figure 3A). The endoscopy of the patient was attended. During the endoscopy, upon reaching the lower oesophagus, two openings were encountered: one was the GO junction, and the other was the broncho-oesophageal fistula.
The oesophageal mucosa is nodular with areas of ulceration in the epiphrenic segment. Serpiginous tracts and monstrous ulceration were also observed along the lesser curvature of the stomach. At the GO junction, there were whitish exudates that could not be washed off.
A fistulous communication was seen just adjacent to the GO junction (at a level of 39 cm; Figure 3B)
The differential diagnosis included tuberculosis, neoplasms, and actinomycosis. Biopsies taken from the oesophagus revealed discrete sulfur granules consistent with an Actinomyces infection, and this was confirmed upon a histopathological examination (Figure 3C). The patient subsequently received a high dose of intravenous penicillin for 4 weeks. The patient improved after this, and was changed to oral penicillin. Following medical treatment, the patient improved clinically, and at 10 weeks, a follow-up ultrasonography revealed no left lobe liver lesions. Following therapy, the patient subsequently recovered, and no additional invasive testing or imaging was required.
A B C
A) Barium swallow confirmed the CT findings of a concentric irregular narrowing (blue arrow) involving the retrocardiac and epiphrenic oesophagus, with proximal barium hold-up. B) Endoscopy revealed that oesophageal mucosa is nodular, with areas of ulceration in the epiphrenic segment (red arrows). Serpiginous tracts and monstrous ulceration were also observed along the lesser curvature of the stomach. At the gastro-oesophageal junction, there were whitish exudates with fistulous communication (red arrow) seen just adjacent to the gastro-oesophageal junction (at a level of 39 cm). C) Biopsies taken from the oesophagus revealed discrete sulfur granules (yellow arrows) consistent with Actinomyces infection, which was confirmed upon histopathological examination.
Figure 3: Barium swallow, endoscopy, and biopsy results.
DISCUSSION
Actinomyces is an anaerobic, gram-positive bacillus commonly found in the normal flora of the gastrointestinal and genitourinary tracts. These organisms are slow-growing and of low virulence, often taking months to develop into infections. Therefore, they are frequently mistaken for malignancies or other diseases such as tuberculosis, candidiasis, herpes simplex virus, or cytomegalovirus.4
Actinomycosis seldom stands alone, often involving additional pathogens such as Actinobacillus, Eikenella, Enterobacteriaceae, Fusobacterium, Streptococcus, and Candida Isolation of Actinomyces from Nocardia, using the acid-fast stain, is pivotal. In this case, only the microorganism Actinomyces, which produces sulfur granules (frequently with club-shaped ends), was present.4,7 However, sulfur granules are only present in about half of cases; hence, the absence of sulfur granules does not rule out an actinomycosis infection.7
Pulmonary actinomycosis is rarely encountered in thoracic surgery. As it were, 13 cases of pulmonary actinomycosis were distinguished among 2,247 patients with radiological pulmonary opacities, aligning with the Rizzi et al.8 study. Actinomyces israelii, a commensal organism of the oropharyngeal flora, typically causes infection following disruption to the mucosal barrier. Pulmonary involvement typically results from aspiration, particularly in individuals with poor oral hygiene, and accounts for approximately 15% of all actinomycosis cases.9 Aspiration of oropharyngeal or gastrointestinal secretions is a key mechanism of transmission to the respiratory tract.10
Fever, productive cough, dyspnoea, haemoptysis, pleuritic chest pain, weight loss, anaemia, and leukocytosis are the most common clinical symptoms of pulmonary actinomycosis.11-13 Due to these nonspecific symptoms, pulmonary actinomycosis is frequently misdiagnosed as a malignancy or another serious infection.10 Actinomycosis is found worldwide and may affect any age group. This pathogen is normally found in the oral cavity and gastrointestinal tract of healthy individuals.
In this case, the key indicators prompting the consideration of actinomycosis are poor oral hygiene, odynophagia, and weight loss.9,10 Although Actinomyces typically causes infections in the cervicofacial region, it can also affect the thorax, abdomen, and pelvis.7 Radiological findings in actinomycosis include mucosal abnormalities, such as ulcers or fistulas, on oesophagogram, while a CT scan shows oesophageal wall thickening in numerous cases.13 The gold standard for opinion is the discerning of filamentous bacteria and sulfur granules by histology or culture. However, recent antibiotic use, coinfections, or improper specimen handling may hinder culture results.13-15 Thoracic actinomycosis is particularly rare and may mimic conditions such as tuberculosis or lung cancer, both primary and metastatic.16-18 Other pathologies can also accompany actinomycosis in some cases. Lung, pleura, mediastinal, or chest wall infections may result from direct spread from a cervicofacial infection, oesophageal perforation, aspiration, or even hematogenous dissemination from a distant site.16
During radiographic examinations, pulmonary actinomycosis can appear as infiltrates, cavitary lesions, or tumour-like masses.19-22 Bone changes and pleural involvement may also be observed, though these findings are not specific to actinomycosis.22,23 The lack of distinctive clinical or imaging findings makes diagnosing actinomycosis particularly challenging. With oesophageal involvement, a barium swallow may show deep ulcers, fistulas, or sinus tracts.24,25 However, they can also reveal more common mucosal irregularities, ulcers, or strictures similar to those seen in infections like candidiasis, herpes simplex virus, or cytomegalovirus.26 CT imaging typically shows oesophageal wall thickening in the early stages of infection, potentially progressing to sinus tract formation.24
Ultimately, despite the value of radiologic findings, a definitive diagnosis requires a bacterial culture or histopathological examination of biopsy specimens, where filamentous bacteria and sulfur granules are identified.27
Based on inference, actinomycosis is a rare infection. Due to its ability to mimic
other infections or malignancies, such as tuberculosis or adenocarcinoma, it is often misrecognised, particularly in young adults.4 These infections typically occur after an insult to the oesophageal mucosa, such as prior surgery or instrumentation, trauma, or infection.14 They can present as submucosal masses, ulcers, fistulas, abscesses, strictures, or draining sinus tracts.7 Thoracic actinomycosis has an excellent prognosis with early recognition and appropriate treatment, which underscores the importance of considering actinomycosis in cases that initially appear to be tuberculosis or neoplasms.28 Early diagnosis may prevent severe complications and unnecessary surgery.
CONCLUSION
Actinomyces is a slow-growing anaerobic bacterium that can cause hidden infections, leading to complications such as fistulas, abscesses, and strictures.
References
1. Könönen E, Wade WG. Actinomyces and related organisms in human infections. Clin Microbiol Rev. 2015;28(2):419-42.
2. Wong VK et al. Actinomycosis. BMJ. 2011;343:d6099.
3. Brook I. Actinomycosis: diagnosis and management. South Med J. 2008;101(10):1019-23.
4. Pillappa R et al. Esophageal actinomycoses mimicking malignancy. Ann Thorac Surg. 2016;101(5):1967-70.
5. Andreani A et al. Unexpected positron emission tomographypositive actinomyces-related mass of the bronchial stump. Can Respir J. 2012;19(2):77-9.
6. Qiu L et al. Pulmonary actinomycosis imitating lung cancer on (18)F-FDG PET/ CT: a case report and literature review. Korean J Radiol. 2015;16(6):1262-5.
7. Zhang AN et al: Esophageal stricture caused by actinomyces in a patient with no apparent predisposing factors. Case Rep Gastrointest Med. 2019:2019:7182976.
8. Rizzi A et al. Pulmonary actinomycosis: surgical considerations. Monaldi Arch Chest Dis. 1996;51(5):369-72.
9. KAY EB. Actinomyces in chronic bronchopulmonary infections. Am Rev Tuberc. 1948;57(4):322-9.
This case highlights the importance of distinguishing actinomycosis from malignancy, as a misdiagnosis can lead to unnecessary and invasive procedures.
Clinicians should consider actinomycosis as part of the differential diagnosis, especially when clinical findings do not align with more common conditions such as tuberculosis or neoplasms. Oesophageal actinomycosis is a rare but important cause of oesophageal pathology, particularly in patients who are immunocompromised. Radiologic findings in actinomycosis, including oesophageal wall thickening on CT and potential sinus tracts and mucosal irregularity/ulceration on a double-contrast oesophagogram, can be suggestive of the entity but are nonspecific. A biopsy with culture and histopathology should always be performed to confirm the diagnosis and avoid surgical interventions. Early recognition and an accurate diagnosis of actinomycosis can prevent serious complications and ensure effective, conservative treatment with antibiotics.
10. Russo TA. Agents of actinomycosis. Principles and practice of infectious disease, Elsevier (1995) 5th edition, Philadelphia: Churchill Livingstone, pp.2645-54.
11. Hsieh MJ et al. Thoracic actinomycosis. Chest. 1993;104(2):366-70.
12. McQuarrie DG, Hall WH. Actinomycosis of the lung and chest wall. Surgery. 1968;64(5):905-11.
14. Welling RD et al. Esophageal actinomycosis: a case report and review of radiographic findings. J Radiol Case Rep. 2009;3(12):44-8
15. Ossorio MA, et al. Thoracic actinomycosis and human immunodeficiency virus infection. South Med J. 1997;90(11):1136-8.
16. Smego RA Jr, Foglia G. Actinomycosis. Clin Infect Dis. 1998;26(6):1255-61.
17. Lee IJ et al. Abdominopelvic actinomycosis involving the gastrointestinal tract: CT features. Radiology. 2001;220(1):76-80.
18. Wu S, Qin Z. Pulmonary actinomycosis misdiagnosed as lung cancer: a case report. J Int Med Res. 2024;52(9):3000605241275375.
19. Kuijper EJ et al. Disseminated actinomycosis due to Actinomyces meyeri and Actinobacillus actinomycetemcomitans. Scand J Infect Dis. 1992;24(5):667-72.
20. Frank P, Strickland B. Pulmonary actinomycosis. Br J Radiol. 1974;47(559):373-8.
21. Tomm KE et al. Thoracic actinomycosis. Am J Surg. 1972;124(1):46-8.
22. Wand A et al. MRI of thoracic actinomycosis. J Comput Assist Tomogr. 1996;20(5):770-2.
23. Datta JS, Raff MJ. Actinomycotic pleuropericarditis. Am Rev Respir Dis. 1974;110(3):338-41.
24. Spencer GM et al. Actinomycosis of the esophagus in a patient with AIDS: findings on barium esophagograms. AJR Am J Roentgenol. 1993;161(4):795-6.
25. Ng FH et al. Esophageal actinomycosis: a case report. Endoscopy. 1997;29(2):133.
26. Levine MS, Rubesin SE. Diseases of the esophagus: diagnosis with esophagography. Radiology. 2005;237(2):414-27.
27. Taştepe AI et al. Thoracic actinomycosis. Eur J Cardiothorac Surg. 1998;14(6):578-83.