10 Review of the 62nd European Renal Association (ERA) Congress, 4th–7th June 2025
Congress Features
21 Highlights from the 62nd European Renal Association (ERA) Congress
Geraldo Bezerra da Silva Junior
23 Game Changers in IgA Nephropathy
Aleksandra Zurowska
Abstract Reviews
28 Sleep Habits, Sleep Quality, and Fatigue Among People with Chronic Kidney Disease
Chu et al.
31 Sex Differences in Glomerular Diseases and Their Long-Term Outcomes
Stambolliu et al.
33 The Creatinine Triples After a Whipple: A Case of Chronic Kidney Disease Due to Secondary Oxalate Nephropathy 27 Years PostPancreaticoduodenectomy
Oh and Chong
35 Plan for Hypertensive Disorders in the Puerperium Period: Zero
Vascular and Renal Risk
Gracia-Iguacel et al.
41 Clinical Tools to Stratify Patients on Conservative Kidney Management with Different Care Needs
Teh et al.
43 Burden of Disease and Management of Hyperkalaemia in Patients with Type 2 Diabetes and Chronic Kidney Disease
Managed at Spanish Endocrinology Services
Martínez-Montoro et al.
45 Optimising Phosphate Removal: Is an Extended Dialyser the Answer?
Eftimovska-Otovikj et al.
47 Hyperaldosteronism and Increased IL-6 as Cardiovascular Risk Factors in Haemodialysis Patients and Kidney Transplant Recipients
Maria Smaliakova
49 Desidustat Shows Promising Results in Managing Anaemia in Patients with Chronic Kidney Disease
Ashwinikumar Khandekar
Congress Interview
51 Rainer Oberbauer Interview
53 Patrick Maxwell Articles
58 Lupus Vasculitis, a Rare Diagnosis and a Therapeutic Challenge: A Case Report
Ramos et al.
64 Sarcoidosis Case with Acute Renal Failure, Nephrolithiasis, and Hypercalcaemia After Uncontrolled D3 Vitamin Supplementation
Bakan et al.
"A spotlight was placed on ERA’s continued drive towards greener nephrology, with initiatives aimed at reducing dialysisrelated environmental impact, and promoting climate-resilient solutions"
Editorial Board
Editor-in-Chief
Dr Angela Yee-Moon Wang Duke-NUS Medical School, Singapore
Angela Yee-Moon Wang has a strong and prestigious track record in clinical and academic nephrology, having served at the Department of Medicine, Queen Mary Hospital, the University of Hong Kong, SingHealth Duke-NUS Academic Medical Centre, and the Department of Renal Medicine, Singapore General Hospital. Wang is a world recognised for her research in cardiovascularkidney-metabolic health, trials and innovations in biomarker research for personalised care.
Dr Sanjay Agarwal
Marengo Asia Group of Hospitals, India
Prof Sebastjan Bevc University of Maribor, Slovenia
Prof Harun Ur Rashid
Kidney Foundation Hospital and Research Institute, Dhaka, Bangladesh
Dr Juliette Hadchouel
Hôpital Tenon, Paris, France
Prof Maurizio Salvadori
Careggi University Hospital Florence, Italy
Dr Ankur Shah
Brown University, Providence, Rhode Island, USA
Dr Ahmed Akl Mansoura University, Egypt
Prof Wolfgang Jelkmann University of Lübeck, Germany
Dr Mufti Baleegh
Khyber Medical College and Khyber Teaching Hospital, Peshawar, Pakistan
Prof Djalila Mekahli
University Hospitals Leuven, Belgium
Dr Arjun Sekar
Rochester General Hospital, New York, USA
Aims and Scope
EMJ Nephrology is an open access, peer-reviewed eJournal committed to all aspects of renal function and disease to help elevate the quality of nephrology healthcare.
The journal is published annually, six weeks after the European Renal Association (ERA) Congress, and features highlights from this congress, alongside interviews with experts in the field, reviews of abstracts presented at the congress, as well as in-depth features on congress sessions. EMJ Nephrology also covers advances within the clinical and pharmaceutical arenas by publishing sponsored content from congress symposia, which is of high educational value for healthcare professionals. This undergoes rigorous quality control checks by independent experts and the in-house editorial team.
EMJ Nephrology also publishes peer-reviewed research papers, review articles, and case reports in the field. In addition, the journal welcomes the submission of features and opinion pieces intended to create a discussion around key topics in the field and broaden readers’ professional interests. The journal is managed by a dedicated editorial team that adheres to a rigorous double-blind peer-review process, maintains high standards of copy editing, and ensures timely publication.
EMJ Nephrology endeavours to enhance knowledge, stimulate discussion, and contribute to a better understanding of renal diseases. Our focus is on research that is relevant to all healthcare professionals in the field. We do not publish veterinary science papers or laboratory studies not linked to patient outcomes. We have a particular interest in topical studies that advance knowledge and inform of the coming trends affecting clinical practice in nephrology.
Further details on coverage can be found here: www.emjreviews.com
Editorial Expertise
EMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors who are recognised authorities in their respective fields.
• Peer review, which is conducted by expert reviewers who are invited by the Editorial team and appointed based on their knowledge of a specific topic.
• An experienced team of editors and technical editors.
Peer Review
On submission, all articles are assessed by the editorial team to determine their suitability for the journal and appropriateness for peer review.
Editorial staff, following consultation with either a member of the Editorial Board or the author(s) if necessary, identify three appropriate reviewers, who are selected based on their specialist knowledge in the relevant area.
All peer review is double blind. Following review, papers are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected.
Editorial staff have final discretion over any proposed amendments.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects. We seek papers with the most current, interesting, and relevant information in each therapeutic area and accept original research, review articles, case reports, and features.
We are always keen to hear from healthcare professionals wishing to discuss potential submissions, please email: editorial.assistant@emjreviews.com
To submit a paper, use our online submission site: www.editorialmanager.com/e-m-j
Submission details can be found through our website: www.emjreviews.com/contributors/authors
Reprints
All articles included in EMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
EMJ is distributed through controlled circulation to healthcare professionals in the relevant fields across Europe.
Indexing and Availability
EMJ is indexed on DOAJ, the Royal Society of Medicine, and Google Scholar®; selected articles are indexed in PubMed Central®
EMJ is available through the websites of our leading partners and collaborating societies. EMJ journals are all available via our website: www.emjreviews.com
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
All information obtained by EMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, EMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. EMJ is completely independent of the review event (ERA 2025) and the use of the organisations does not constitute endorsement or media partnership in any form whatsoever. The cover photo is of Vienna, Austria, the location of ERA 2025.
We are delighted to welcome you to the 2025 issue of EMJ Nephrology, which features coverage from this year’s European Renal Association (ERA) Congress, held in Vienna, Austria. Focusing on ‘Game Changers in Nephrology’, the event explored cutting edge innovations across gene therapy, transplantation, vasculitides, acute kidney injury, chronic kidney disease, and both hypertensive and diabetic kidney disease.
Alongside our congress review, you will find a feature summarising key highlights from the event, as well as future perspectives on AI and precision medicine in the field. Additionally, this issue showcases multiple groundbreaking research abstracts presented at ERA 2025, highlighting a plethora of topics that range from sex differences in glomerular diseases and phosphate removal in dialysis, to the impact of sleep and management of anaemia in chronic kidney disease. We also present interviews with experts in the field, who discuss the impact of pioneering translational molecular science research and transplant immunology.
Our peer reviewed content includes fascinating case reports spotlighting what makes lupus vasculitis such a challenging diagnosis in patients with systemic lupus erythematosus, and how exogenous vitamin D3 supplementation caused nephrolithiasis and acute renal failure in a patient with sarcoidosis.
We would like to take this opportunity to thank our Editorial Board, authors, peer reviewers, and interviewees for their support and critical contributions that have helped bring this issue to life. We hope you enjoy reading!
Contact us
Editorial enquiries: editor@emjreviews.com
Sales opportunities: salesadmin@emjreviews.com
Permissions and copyright: accountsreceivable@emjreviews.com
Reprints: info@emjreviews.com Media enquiries: marketing@emjreviews.com
Foreword
Dear Readers,
It is my pleasure to welcome you to the latest issue of EMJ Nephrology. I would like to begin by extending my sincere thanks to the authors, peer reviewers, and Editorial Board members whose dedication has enabled the publication of high-quality, timely, and impactful content in this issue.
This edition includes a curated selection of original, peer-reviewed articles, interviews, and features, alongside comprehensive coverage of the 62nd European Renal Association (ERA) Congress 2025. With the theme of ‘Game Changers in Nephrology’, this year’s Congress highlighted the latest developments poised to redefine clinical practice, from next-generation therapeutics and AI, to a renewed focus on prevention and kidney health.
Held in the historic city of Vienna, Austria, from the 4th–7th June, the Congress set a new benchmark, welcoming over 9,800 participants and receiving a record-breaking 2,800 abstract submissions. Delegates had the opportunity to engage with cuttingedge science across all major areas of nephrology, including acute kidney injury, vasculitis, and glomerular disease.
In addition to our coverage of the Congress, this issue features a curated selection of abstracts from ERA 2025, offering a snapshot of the latest research presented at the meeting. Our expert-led feature explores the key highlights from Vienna, providing commentary on late-breaking trials, clinical developments, and emerging trends. We are also privileged to include exclusive interviews with two leading voices in nephrology: Patrick Maxwell, who reflects on the evolution of translational research; and Rainer Oberbauer, who discusses the future direction of kidney care, as well as the future of ERA.
Thank you for your continued readership and support. We hope this issue of EMJ Nephrology offers valuable insights and practical knowledge to inform your clinical decision-making and inspire new avenues of research and care.
Delegates had the opportunity to engage with cutting-edge science across all major areas of nephrology
Professor
Angela Yee-Moon Wang
Clinical Professor, Medicine Academic Clinical Programme, SingHealth Duke-NUS Academic Medical Centre; Senior Consultant, Department of Renal Medicine, Singapore General Hospital, Singapore.
ERA 2025
This year, the Congress saw its largest attendance to date, with over 9,800 delegates, and the highest ever number of submitted abstracts at 2,800
Review of the 62nd European Renal Association (ERA) Congress Congress Review
Changers in Nephrology' was the theme of the 62nd European Renal Association (ERA) Congress, held in Vienna, Austria, from the 4th–7th of June 2025. Known as the birthplace of modern medicine and a global capital of classical music, Vienna offered an inspiring setting for this year’s advances in renal care.
This year, the Congress saw its largest attendance to date, with over 9,800 delegates, and the highest ever number of submitted abstracts at 2,800, reflecting the growing momentum of innovation in the field. The scientific programme encompassed a wide range of sessions, with the main 12 tracks focusing on game changers in acute kidney injury, kidney vasculitis, chronic kidney disease, IgA nephropathy, and others, in line with the Congress theme.
Opening the ceremony, President Roser Torra addressed the audience with a call to the nephrology community to embrace exciting advances, such as the arrival of new therapeutics, AI, and a shift in focus from kidney failure to kidney health and prevention, all of which will transform patient care. Torra proudly noted her position as the first female president of ERA, inspiring the audience to continue breaking barriers and strive to equality in the "best specialty in the world’’. She emphasised that “at ERA, diversity, equity, and inclusion are not optional. They are mandatory.” In closing, Torra urged delegates to be ambitious in their mission, calling on the nephrology community to "boost nephrology beyond imagination" through innovation, collaboration, and compassion.
Together with Scientific Committee Chair Paola Romagnani, and Michael Rudnicki, President of the Austrian Society of Nephrology, Torra extended thanks to the Austrian Society of Nephrology, the organising committee, and the ERA staff for their invaluable contributions. Together, they encouraged delegates to seize the opportunity to learn, collaborate, and drive progress in nephrology.
The ceremony also celebrated outstanding contributions across clinical care, basic science, research excellence, societal service, sustainability, and the achievements of young investigators, recognising those who are shaping the present and future of nephrology. A spotlight was placed on ERA’s continued drive towards greener nephrology, with initiatives aimed at reducing dialysis-related environmental impact, and promoting climate-resilient solutions.
The ceremony concluded with an invitation to blend science with culture at the Sounds and Science concert, a unique event exploring the connections between music, medicine, and kidney health. The evening concluded with a memorable performance by the same ensemble, offering a taste of Vienna’s enduring role as a city where innovation and the arts go hand in hand.
Limited Renal Transplant Survival Advantage in Older/High-Risk Recipients
INSIGHTFUL findings from a large-scale study presented at the 62nd ERA Congress, which took place in Vienna, Austria, between the 4th–7th of June 2025, challenge the status quo regarding the survival advantage provided through deceased-donor renal transplantation.1
Utilising ERA Registry data from five European countries: Catalonia, Denmark, France, Norway, and the UK, the study reviewed 5-year survival outcome data for 64,013 adult patients who commenced dialysis between 2000–2019 and were on the waiting list for renal transplantation.
The study followed a target trial emulation framework, which imitates the structure of a randomised controlled trial. This allowed the study authors to compare the 5-year survival rates between those who received a renal transplant and those who continued dialysis but did not receive a renal transplant.
The researchers also looked at the survival rates amongst those who received standard-criteria donor kidneys (donors <60 years of age without significant risk factors for poor renal function), and those who received expanded-criteria donor kidneys (donors ≥60 years of age; or 50–59 years of age with at least two of the following: cerebrovascular cause of death, terminal serum creatinine of >133 mmol/L, or a history of hypertension).
The results showed that, for those who received a standard-criteria donor kidney, there was a consistent survival advantage, irrespective of recipient age or comorbidities. For those who did not receive a transplant, but remained on dialysis, the 5-year survival rate was 54%. In contrast, for recipients aged ≥75 years who received an expanded-criteria donor kidney, 5-year survival rates were only marginally higher than in those who didn’t receive a transplant and remained on dialysis, at 57–58%, especially in recipients with cardiovascular disease or kidneys from donors after circulatory death.
The researchers concluded that early post-transplant mortality is higher in those deemed as higher-risk recipients, and that the survival advantage of transplantation plateaus for those who are older or higherrisk, as they are more likely to receive expanded-criteria or circulatory death donor kidneys. They urge clinicians to have transparent conversations with older or higher-risk recipients about the uncertainty of benefit, but stress that the message is not ‘don’t transplant older people’.
Zigakibart Shows Long-Term Promise in IgA Nephropathy Treatment
NEW 100-week data from a Phase I/II trial presented at the 62nd ERA Congress suggest that zigakibart, an investigational anti-A PRoliferation-Inducing Ligand (APRIL) monoclonal antibody, may offer sustained disease control in patients with IgA nephropathy (IgAN), reinforcing its potential as a disease-modifying therapy.2
IgAN is the most common glomerular disease globally, and is a leading cause of chronic kidney disease, with half of affected individuals progressing to kidney failure. The disease is driven by the production of galactose-deficient IgA1 (Gd-IgA1), which triggers inflammation and progressive kidney damage. Zigakibart targets the APRIL pathway to reduce Gd-IgA1 levels and modify disease progression. The ADU-CL-19 trial enrolled 40 adults with biopsy-confirmed IgAN and persistent proteinuria despite optimised supportive care. Patients received intravenous or subcutaneous zigakibart every 2 weeks in addition to renin-angiotensin system inhibitors, unless they were renin-angiotensin system inhibitors-intolerant. The study assessed proteinuria, estimated glomerular filtration rate, serum Ig levels, and safety outcomes over 100 weeks.
By Week 100, proteinuria had decreased by 60% from baseline. More than half of patients (55%) achieved proteinuria <500 mg/24h, and 31% fell <300 mg/24h, indicating clinically meaningful remission. Notably, estimated glomerular filtration rate remained stable across all subgroups, including those with varying levels of proteinuria response. Zigakibart also produced a 74% reduction in IgA and Gd-IgA1, consistent with inhibition of the APRIL pathway.
Safety data were reassuring: most adverse events were mild or moderate, with no treatment-related serious infections or discontinuations reported. Infections were the most frequent adverse events, coinciding with a period of high COVID-19 circulation in trial countries.
This trial represents the longest reported duration of kidney function stabilisation with an anti-APRIL agent in IgAN. These findings support zigakibart’s potential as a cornerstone therapy, with Phase III studies now underway to evaluate efficacy in a broader population, and confirm longterm benefits.
More than half of patients (55%) achieved proteinuria <500 mg/24h, and 31% fell <300 mg/24h
Long-Term Kidney Function Patterns After Acute Kidney Injury
A MAJOR new study from the Netherlands, recently presented at the 62nd ERA Congress, has revealed striking differences in how patients recover kidney function following an episode of acute kidney injury (AKI), a condition that affects up to one in five hospitalised patients and is known to increase the risk of long-term kidney damage and death.3
Researchers at the University Medical Center Utrecht, the Netherlands, analysed health data from 567,527 individuals as part of the NOSTRADAMUS project, identifying 30,150 cases of AKI. Among these, 20,119 patients were followed for at least 1 year after their AKI event.
Using advanced modelling techniques, the team identified eight distinct long-term patterns, or ‘trajectories’ of kidney function: high stable estimated glomerular filtration rate (eGFR), low stable eGFR, rapidly increasing eGFR, moderately increasing eGFR, slowly increasing eGFR, rapidly decreasing eGFR, moderately decreasing eGFR, and slowly decreasing eGFR. The study found that certain patient characteristics, such as age, sex, ICU admission, and the duration and severity of AKI, were closely linked to these different trajectories.
Patients who had been in intensive care, or had prolonged or severe AKI, were more likely to experience declining kidney function. Conversely, younger patients and females were more often found in groups with improving kidney health. The trajectory profiles with the highest risk of death were: rapidly increasing, rapidly decreasing, and moderately decreasing eGFR.
Patients who had been in intensive care, or had prolonged or severe AKI, were more likely to experience declining kidney function
These findings offer a vital step toward developing personalised follow-up care and early interventions for patients with AKI, potentially easing the burden on healthcare systems and improving long-term outcomes.
Genetic Variants Influence Blood Pressure Salt Response
A RECENT study, presented at the 62nd ERA Congress, has highlighted the role of genetic variations in influencing blood pressure (BP) response to a low-sodium diet among patients with mild essential hypertension.4 7% of those with the AA genotype were sodium sensitive, compared to just 23% of GG genotype individuals
Sodium sensitivity of blood pressure, a condition in which BP fluctuates in response to sodium intake, affects nearly 30% of the population, and is linked to poorer long-term outcomes. To explore this, 618 untreated patients with hypertension, excluding those with obesity, undertook a 15-day low-sodium diet (<100 mEq/day) to assess compliance and BP variation.
Compliance was determined by a 24-hour urinary sodium excretion reduction of at least 40% from baseline, or a final value under 100 mmol/day. Out of the total cohort, 210 individuals (34%) met the compliance criteria, showing significantly lower sodium excretion than the noncompliant group, as well as greater reductions in systolic, diastolic, and mean BP.
Participants in the compliant group were further classified into three equal subgroups based on BP response: sodium sensitive, sodium resistant, and inverse sodium sensitive. The study investigated
the effects of two specific gene variants, UMOD rs4238595 and NEDD4L rs4149601, known to influence sodium handling in the kidneys. Individuals carrying at least one A allele of the UMOD variant experienced a greater fall in systolic BP, with AA carriers showing the most significant decrease (–11.7 mmHg), compared to GG carriers (–3.5 mmHg). Similarly, A allele carriers of the NEDD4L variant exhibited stronger BP reductions, and 57% of those with the AA genotype were sodium sensitive, compared to just 23% of GG genotype individuals.
These findings suggest that genetic differences contribute to the variation in BP response to sodium restriction, and highlight the potential of using genotyping to tailor dietary interventions in hypertension management. A low sodium diet appears effective in a genetically susceptible subset, underlining the importance of personalised approaches to treatment.
New Data Shows Acute Kidney Injury from Diuresis in Patients with Acute Heart Failure
Often Reversible and Low Risk
A NEW prospective study presented at the 62nd ERA Congress revealed fresh insights into acute kidney injury (AKI) in patients with acute heart failure (AHF) undergoing aggressive diuresis.5 The study aimed to clarify whether AKI observed during decongestive treatment represents true tubular injury, or primarily reflects functional or haemodynamic changes.
The cohort included 100 patients with AHF receiving aggressive diuresis, excluding those requiring inotropic support or dialysis. Serum creatinine and NGAL, a biomarker of tubular injury, were measured at admission and at serial time points over 72 hours. The occurrence of AKI was defined using KDIGO criteria, and patients were followed up at 30 days to assess readmissions and mortality.
AKI was observed in 37% of patients during hospitalisation. Interestingly, while 34% showed a rise in NGAL levels, there was no correlation between changes in NGAL and rising creatinine levels, suggesting minimal tubular injury even among those with AKI. Additionally, baseline NT-proBNP levels were significantly higher in patients who developed AKI (p=0.048), indicating greater heart failure severity in this subgroup.
Importantly, 73% of patients with AKI showed improved kidney function by 30 days post-admission, with lower serum creatinine compared to Day 3 values. Furthermore, the occurrence of AKI did not predict 30-day readmission rates or mortality, underscoring its limited short-term prognostic impact in this context.
In conclusion, this study suggests that AKI in patients with AHF receiving aggressive diuresis is often mild, and predominantly functional or haemodynamic in nature, rather than reflecting true kidney injury. These findings support continuing aggressive decongestive therapy without undue concern for mild AKI in this setting.
73% of patients with AKI showed improved kidney function by 30 days post-admission
Mortality Trends in Self-Reported Chronic Kidney Disease
PRESENTED at the 62nd ERA Congress, a comprehensive national analysis based on the CDC’s NHANES database has revealed critical insights into the outcomes of patients with self-reported chronic kidney disease (CKD) across the USA between 2001–2020.6
Out of 51,743 participants analysed, representing an estimated 195 million USA residents, approximately 2.54% selfreported having CKD. The study, which linked NHANES data to the National Death Index, found a crude mortality rate of 10.3% over a follow-up period of up to 228 months. Notably, the cumulative mortality among patients with CKD reached 26.3% over 20 years, with cardiovascular disease as the leading cause of death, followed by cancer, diabetes, and kidney-specific disorders.
Stratified analysis revealed that mortality was significantly higher among males, non-Hispanic White and Black populations, veterans, USA-born citizens, and individuals of lower socioeconomic status. Education level, marital status, and having Medicare insurance were also linked to poorer survival.
Laboratory analysis using urinary albuminto-creatinine ratio thresholds demonstrated diagnostic accuracies up to 87.6%, suggesting its utility in early detection.
Comorbidities such as heart failure, coronary artery disease, diabetes, hypertension, and COPD were strongly associated with increased mortality risk. These findings underscore the urgent need for public health strategies to address disparities in CKD awareness, prevention, and care, especially given that nearly 90% of individuals with CKD remain unaware of their condition.
Out of 51,743 participants analysed, representing an estimated 195 million USA residents, approximately 2.54% self-reported having CKD
Reducing Unnecessary Referrals: The SCREAM Project
FINDINGS from a retrospective observational study presented at the 62nd ERA Congress highlighted that transitioning to a risk-based model for referring patients with early-stage chronic kidney disease (CKD) to a nephrologist helps reduce unnecessary referrals, without increasing the number of missed cases of progressive kidney disease.7
Given the 2024 Kidney Disease: Improving Global Outcomes (KDIGO) guidelines’ recommendation to use a 5-year kidney failure risk of 3–5% as a criterion for nephrology referral, the study authors aimed to compare this recommendation based on the Kidney Failure Risk Equation (KFRE) with traditional referral models, including the clinical Swedish criteria and the classical 2012 KDIGO criteria.
The researchers analysed data from a healthcare utilisation cohort called the Stockholm CREAtinine Measurements (SCREAM) project. All adults with an estimated glomerular filtration rate <60 mL/ min/1.73m2 who had albuminuria and creatinine measurements on the same date, or within <12 months apart, were included in the evaluation. This yielded a total of 887,388 repeated observations from 192,964 individuals.
The Non-North American 4-variable KFRE, which was recalibrated to better fit the author’s setting, displayed a good prediction performance. Both the Non-North American 4-variable and the SCREAM recalibrated KFREs showed higher specificity and sensitivity than the clinical Swedish and 2012 KDIGO criteria. Moreover, the KRFE-based models for referral exhibited higher positive predictive values, better net reclassification improvement, lower false positive rates, and better performance in decision curve analyses. Overall, the risk-based referral models could potentially reduce the number of unnecessary referrals of non-progressors by 23–25% compared with the traditional referral models.
The authors concluded that, within a large North European healthcare system, the transition to a risk-based referral model would help to reduce unnecessary referral rates, whilst keeping the number of missed cases of progressors low. In a time of increasing healthcare costs and burden on healthcare systems, analysis of referral models could help effectively improve how resources are used.
Better Outlook for Patients with Chronic Kidney Disease as Treatments Improve
NEW research presented at the 62nd ERA Congress shows that the outlook for people newly diagnosed with chronic kidney disease (CKD) in Denmark has improved over the last decade, likely due to the wider use of recommended treatments.8
CKD significantly increases the risk of heart disease, hospitalisation, kidney failure, and death, yet most patients are managed in primary care. Researchers aimed to analyse trends in treatment and outcomes in Danish adults diagnosed with CKD between 2011–2022, using data from national health registers. CKD was defined as two estimated glomerular filtration rate (eGFR) readings <60 mL/min/1.73 m² taken at least 90 days apart. The study excluded those with advanced kidney failure or previous low eGFR. Patients were followed until they reached a key outcome, such as heart attack, kidney failure, or death, or until the end of 2023. Statistical models adjusted for health and demographic factors were used to assess changes in risks and treatment patterns over time.
Among the 315,636 individuals included (median age: 79 years; 45% male), 71% had early-stage CKD with eGFR between 45–59.
Over a median follow-up of 7.6 years, 1-year risks declined modestly for heart failure (p=0.02) and kidney disease progression (p=0.02), while changes in overall mortality, cardiovascular events, and composite outcomes were not statistically significant. Notably, the use of renin-angiotensin system inhibitors and sodium-glucose cotransporter-2 inhibitors, key guidelinebased therapies, rose significantly (p=0.04 and p=0.08, respectively). However, there was no meaningful change in the use of lipid-lowering therapy, kidney biopsy rates, or referrals to specialist nephrology care.
The findings suggest that improvements in prescribing evidence-based therapies may be contributing to better cardio-renal outcomes for people with CKD. However, the authors note that certain aspects of care remain static, and they highlight the need to strengthen pathways for specialist involvement and comprehensive disease management.
Improvements in prescribing evidence-based therapies may be contributing to better cardio-renal outcomes for people with CKD
References
1. Hellemans R et al. Exploring the margins of survival benefit in deceased donor kidney transplantation: an international target trial emulation. ERA Congress, 4-7 June, 2025.
2. Barratt J et al. Sustained long-term efficacy and safety of zigakibart over 100 weeks in patients with Iga nephropathy. ERA Congress, 4-7 June, 2025.
3. Veltkamp DM et al. Identification of heterogenous long-term kidney function trajectories after acute kidney injury reveals subgroups of patients
at higher risk for long-term kidney dysfunc-tion. Abstract 1086. ERA Congress 2025, 4-7 June 2025.
4. Tunesi F et al. Heterogeneity of clinical response to low salt diet in naïve essential hyperten-sive patients. Abstract 2730. ERA Congress 2025, 4-7 June, 2025.
5. Jhajhria A. Acute kidney injury in acute heart failure patients undergoing aggressive diuresis and its impact on short term outcome. Abstract 561. ERA Congress, 4-7 June, 2025.
6. Asghar MS et al. Insights from CDC NHANES survey among self-reported chronic kidney dis-ease patients and
their outcomes: a national database mortality analysis of United States population from 2001-2020. Abstract 1191. ERA Congress, 4-7 June, 2025.
7. Caldinelli A et al. Clinical utility of a risk-based referral model to nephrologist-specialist care; the Stockholm CREAtinine Measurements (SCREAM) project. Abstract 683. ERA Congress, 4-7 June, 2025.
8. Ballegaard EL et al. Guideline-based management of chronic kidney disease and associated risk of cardiorenal outcomes. Abstract 1082. ERA Congress, 4-7 June, 2025.
Highlights from the 62nd European Renal Association (ERA) Congress
Author: *Geraldo Bezerra da Silva Junior1,2
1. School of Medicine, University of Fortaleza, Brazil
2. Federal Institute of Education, Science, and Technology of CearáCeara, Brazil
*Correspondence to geraldobezerrajr@unifor.br
Disclosure: The author has declared no conflicts of interest.
Keywords: Acute kidney injury (AKI), AI, chronic kidney disease, European Renal Association (ERA), kidney transplantation.
THE EUROPEAN Renal Association (ERA) Congress 2025 marked a pivotal moment in nephrology this year, bringing together over 9,000 global experts to explore transformative advancements in kidney disease diagnosis and treatment.
HIGHLIGHTS FROM THE EUROPEAN RENAL ASSOCIATION 2025
A central aspect of this congress that caught our attention was the innovation seen across different areas of nephrology, including novel drugs that are under investigation in several clinical trials, as well as drugs that are already available in clinical practice.
Sessions that explored innovation in kidney transplantation addressed frailty and ageing in kidney transplantation, incorporating advanced assessment techniques and the feasibility of accepting frail patients for transplantation. Further discussions on kidney transplantation included advances in xenotransplantation, along with its social, ethical, and clinical implications.
Another prominent theme in this year’s ERA Congress was diabetic kidney disease and cardiometabolic health, reflecting the growing connection between nephrology, cardiology, and endocrinology. As specialists, we can no longer work in separate clinics. There was an important focus on sodium–glucose cotransporter 2 (SGLT2) inhibitors and glucagon-like
peptide-1 (GLP-1) receptor agonists, as well as promising combination therapies. Insights into the role of aldosterone pathway inhibition, alongside traditional treatments like renin–angiotensin system (RAS) inhibitors, have also been addressed.
Chronic kidney disease remains a key focus of our specialty, with updates this year on metabolic bone disorders and fracture management in patients with chronic kidney disease. There were also discussions regarding personalised therapies for elderly populations and the impact of ageing societies.
Regarding dialysis, we had the opportunity to learn about advancements in home dialysis, and how AI might help drive predictions for dialysis adequacy. A particularly valuable session examined strategies for reducing cardiovascular risk in dialysis recipients.
The theme of AI featured prominent throughout the congress, including its growing role in predicting treatment outcomes and diagnosing conditions, including acute kidney injury (AKI) predictive models. Studies showing the use of AI to predict congenital abnormalities of the
kidney and urinary tract, and showcased the use of generative AI in solving nephrology tests were presented.
The area of genetic and rare kidney diseases has seen interesting advances, with progress made in clustered regularly interspaced short palindromic repeats (CRISPR) and gene therapy research for conditions such as primary hyperoxaluria and cystinosis. Of particular interest were debates on the utility of genetic testing in all patients with autosomal dominant polycystic kidney disease.
As far as AKI discussions are concerned, the congress explored innovations in biomarkers and diagnostic strategies aimed at moving beyond traditional creatinine measurements, as well as discussions on greener approaches to renal replacement therapy for AKI.
The theme of sustainability was also prominent at the congress, highlighted by a session on nephrology and sustainability. This emphasised avenues for reducing the environmental footprint of dialysis and fostering a circular economy within nephrology practices.
Among the presented late-breaking clinical trials were combined therapies with finerenone and empagliflozin, alongside strategies to enhance kidney transplantation outcomes.1
FUTURE PERSPECTIVES
ERA 2025 underscored a shift towards precision medicine, leveraging novel biomarkers, genetic insights, and
AI. Promising drugs and therapeutic approaches are poised to redefine the management of kidney diseases, aiming for better outcomes and sustainability in nephrology. The inclusion of patientcentred care and ethical debates, such as organ donation policies, also highlighted the holistic approach of modern nephrology.
ERA 2025 solidifies the nephrology community's commitment to innovation and collaboration, setting the stage for the next era of kidney disease management.
As a researcher excited about innovation, the author recommends one of their newest publications in this area, a book titled, ‘Innovations in Nephrology’, which brings essential information on technologies that are currently being applied in nephrology and those that can be applied in the future, with real potential to improve the care of kidney diseases.2,3 The book is available in English and German.
Looking forward to seeing the new developments in nephrology at the ERA Congress 2026 in Glasgow!
References
1. Agarwal R et al. Finerenone with empagliflozin in chronic kidney disease and type 2 diabetes. N Engl J Med. 2025;DOI:10.1056/NEJMoa2410659.
2. Da Silva Junior GB, Nangaku M (eds.), Innovations in nephrology: breakthrough technologies in kidney disease care (2022), Switzerland: Springer International Publishing.
3. Da Silva Junior GB, Nangaku M (eds.), Innovationen in der nephrologie - bahnbrechende technologien in der behandlung von nierenerkrankungen (2024), Switzerland: Springer International Publishing.
THE SESSION ‘Game Changers in IgA Nephropathy’, delivered at the European Renal Association (ERA) 2025 Congress, brought together leading experts to spotlight emerging therapies that are reshaping the treatment landscape, from immune modulation to novel approaches addressing structural and inflammatory drivers of disease progression.
B CELL TARGETING THERAPY
Kicking off the session with a talk on B cell targeting therapies, Jonathan Barratt, University of Leicester and John Walls Renal Unit, UK, explained that during that week, two major Phase III trials on B cell directed therapies reported their interim data, which, as Barratt explained, shows just how rapidly things are changing in the IgA nephropathy (IgAN) field.
When considering how to approach this complex, immune-mediated disease, Barratt explained the current focus for treating IgAN in line with the recent Kidney Disease: Improving Global Outcomes (KDIGO) guideline update. Firstly, as IgAN is a complex, immune-mediated glomerular disease, treatment requires specific approaches; symptoms often present late, when patients already have established chronic kidney disease (CKD) complications and, as such, need additional therapies to manage these.
IgAN immunology is characterised by the formation of circulating immune complexes. These can be measured in a laboratory to identify their protein constituents. Barratt noted that these complexes arise due to an overproduction of a particular form of galactose-deficient IgA1 (Gd-IgA1), which is thought to primarily derive from the mucosal immune system. Susceptibility to this is influenced by a complex genetic backdrop. Barratt also explained that multiple
genome-wide association studies have revealed links between genetic risk loci and B cell activation pathways, supporting the rationale for B cell targeted treatments.
Once these immune complexes reach the kidney, they trigger a range of pathological responses. In particular, the mesangium mounts a pro-inflammatory reaction with mononuclear cell infiltration, complement activation, and, in more severe cases, crescent formation and fibrosis. These downstream effects amplify kidney damage and, as patients often present with symptoms late, leading to a late diagnosis, mean they often have significant nephron loss by the time they start treatment.
Barratt then outlined a conceptual framework for therapy, beginning with the need to reduce the formation of circulating immune complexes, followed by mitigating the inflammatory and fibrotic cascade triggered in the glomeruli, and finally, managing the broader complication of CKD. In an ideal world, clinicians would be able to intervene early, halting immune activity before any substantial renal damage is able to occur. However, given the current realities of diagnostics, these strategies often need to be employed concurrently.
Looking closer at immune-directed therapies, Barratt discussed several strategies to target the production of pathogenic antibodies. Budesonide, specifically a gut-targeted steroid
formulation of budenoside, represents a novel way of modifying the mucosal immune environment. After being delivered to the terminal ileum, it suppresses IgA production at the source. Supporting this, Barratt showed data from recent trials, such as the NEFIGAN study,1 which has reported reductions in Gd-IgA1 and corresponding immune complexes without affecting total immunoglobulin levels.
Shifting focus to therapies directly targeting B cells and plasma cells, a key area of interest lies in the role of two cytokines, B cell activating factor (BAFF) and a proliferationinducing ligand (APRIL), both of which are involved in B cell proliferation, survival, and class-switching to IgA. Barratt described numerous clinical studies that have shown that BAFF and APRIL levels are elevated in patients with more severe disease, making them promising therapeutic targets.
Barratt subsequently described a number of agents in development, such as the antiAPRIL monoclonal antibody, sibeprenlimab, which has shown proteinuria reduction in Phase II trials. He also noted the Phase III data from the VISIONARY trial reported at the Congress with similar findings.2 Another
anti-APRIL agent, BION-1301, demonstrated Gd-IgA1 suppression and stable kidney function in 100-week data.3 Dual BAFF/ APRIL inhibitors, such as telitacicept and povetacicept, also showed evidence of reduced proteinuria and slowed estimated glomerular filtration rate decline.4,5
Introducing another novel approach, whereby pathogenic IgA is directly removed from the circulation, Barrat discussed neonatal Fc receptor (FcRn) inhibitors, such as efgartigimod. This is currently used in myasthenia gravis, and may soon be adapted to target IgA. Additionally, new ‘IgA sweepers’ are being developed that bind and clear IgA via hepatic receptors. Although still in early development phases, these new strategies represent a different, cell-sparing approach to disease modification.
Barratt concluded his talk by reflecting on how far the field has come, from highdose systemic immunosuppression to increasingly precise, targeted therapies informed by immunology, genetics, and oncology. He emphasised the need for patient-specific treatment plans, guided by a deeper understanding of disease mechanisms and therapeutic response.
DUAL RENIN-ANGIOTENSIN SYSTEM ENDOTHELIN INHIBITION
Continuing the session, Hiddo J.L Heerspink, University Medical Center Groningen, the Netherlands, took the stage to explore the role of endothelin receptor antagonists in IgAN management. This therapeutic strategy targets the non-immune, progressive drivers of CKD. Heerspink opened his talk with a polling question to gauge the clinical use of ERAs among the audience, none of whom had yet prescribed this treatment for IgAN, emphasising just how novel and underutilised this treatment approach is in routine practice.
Spotlighting the structural drivers of disease, Heerspink explained that, while B cell therapies may reduce inflammation, they are often insufficient alone, as many patients continue to lose nephrons due to glomerular hypertension, fibrosis, and vascular injury. These changes are largely driven by endothelin-1 (ET-1), a potent vasoconstrictor and pro-fibrotic molecule.
ET-1 is upregulated in response to kidney stressors such as aldosterone, angiotensin II, hypoxia, and oxidative stress. Once released, ET-1 binds to endothelin A (ETA) receptors, promoting mesangial expansion, interstitial fibrosis, podocyte injury, and ultimately, glomerulosclerosis. Whilst this has been known since the 1980s, clinical application was limited by side effects, particularly fluid retention and heart failure in patients with diabetes. Now, however, more selective ETA antagonists, lower dosing strategies, and careful patient selection are helping to address these concerns. Importantly, patients with IgAN, who are typically younger with fewer comorbidities, appear at lower risk of ERA-related fluid complications.
Heerspink continued by introducing three endothelin receptor antagonist-based therapies that have shown encouraging data in IgAN treatment: sparsentan, atrasentan, and SC0062. Sparsentan, a dual angiotensin II and ETA receptor antagonist, was tested in the PROTECT trial, where it reduced proteinuria by 43% compared to irbesartan.6 Crucially, this translated into a meaningful slowing of estimated glomerular filtration rate decline over 110 weeks, highlighted by a 9.5 mL/min loss in the irbesartan arm versus 5.8 mL/min in the sparsentan arm. A higher proportion of patients on sparsentan also achieved complete remission, defined as proteinuria below 0.6 g/day.
Atrasentan, a selective ETA antagonist, was studied in the ALIGN trial, which is ongoing but has already released interim data.7 Over 36 weeks, atrasentan achieved a 38% reduction in proteinuria compared to placebo, with effects visible within the first 6 weeks. These rapid changes suggest a strong haemodynamic effect, although, as Heerspink added, longer-term follow-up is needed to understand the full impact on inflammation and fibrosis.
Heerspink went on to note that this effect was consistent regardless of background sodium-glucose co-transporter-2 (SGLT2) inhibitor use, making atrasentan a promising candidate for combination therapy. He then introduced SC0062, a highly selective endothelin receptor antagonist currently in development. In a Phase II dose-finding study, the highest dose (20 mg) reduced proteinuria by 38% compared to placebo, with no signs of fluid retention, as measured by body weight or N-terminal pro B-type natriuretic peptide (NT-proBNP).8
Building on this, Heerspink highlighted the potential of combining endothelin receptor antagonists with SGLT2 inhibitors to maximise benefit while mitigating fluid retention. In the ZENITH trial, zibotentan plus dapagliflozin resulted in a 53% reduction in proteinuria, a statistically significant improvement over dapagliflozin alone.9 Bioimpedance analysis confirmed that dapagliflozin helped counteract the fluid-retentive effects of zibotentan, particularly at lower doses.
Turning briefly to real-world experience, Heerspink described that recent clinical observations from routine practice in Germany have indicated that sparsentan can deliver substantial reductions in proteinuria outside of a trial setting. Around one-third of patients were reported to have achieved complete remission, with most experiencing at least a 30% decline in proteinuria.
He concluded his talk by underlining the importance of considering endothelin receptor antagonists as a viable strategy in IgAN, not only as adjuncts to immunemodulating therapies, but also as standalone options for those with high proteinuria and low inflammation.
COMPLEMENT INHIBITORS
Closing the session, Claudia Seikrit, RWTH Aachen University, Germany, explored complement inhibition in IgAN and the role of complement activation in driving inflammation and progressive kidney injury.
Beginning by looking back at the disease’s history, she noted that Jean Berger’s original description of IgAN in 1968 already
mentioned complement deposits alongside mesangial IgA, something now understood as central to the disease mechanism.
Seikrit explained that complement activation, particularly via the alternative and lectin pathways, contributes to the clinical hallmarks of IgAN, including haematuria, proteinuria, and progressive glomerular damage. Of particular relevance is the alternative pathway, which is continuously active and requires strict regulation. When dysregulated, it can trigger a harmful cycle of complement amplification, driving mesangial and tubulointerstitial inflammation.
Turning to therapeutic targets, Seikrit outlined several points along the cascade currently under investigation: factor b and factor d (early activators), and the central components C3 and C5. She emphasised the importance of balancing efficacy with safety, particularly as the complement system plays a vital role in host defence. As such, prior to initiating any complement-directed therapy, vaccination against encapsulated organisms such as Meningococcus and Pneumococcus is mandatory.
Iptacopan, a selective, oral, factor b inhibitor, featured prominently at the Congress. Data from the Phase III APPLAUSE trial showed a 38% reduction in proteinuria after 9 months, with no significant increase in infections or serious adverse events.10 Seikrit also noted that cemdisiran, an RNA interference therapy that reduces hepatic production of C5, achieved a 37% proteinuria reduction, alongside improvements in haematuria and a favourable safety profile in a recent trial.11
Ravulizumab, a monoclonal antibody targeting C5 that is already in use for other complement-mediated conditions, also showed promise in IgAN. In the SANCTUARY trial, it reduced proteinuria by 30–40% over 26 weeks, and patients switching from placebo to treatment achieved similar benefits, again without major safety concerns.12
In closing, Seikrit underlined that complement inhibition offers a new therapeutic avenue in IgAN, particularly for patients with active inflammation or refractory disease. With several agents now progressing through late-stage trials, she suggested that complement-targeted treatments could soon become part of
References
1. Wimbury D et al. Targeted-release budesonide modifies key pathogenic biomarkers in immunoglobulin a nephropathy: insights from the NEFIGAN trial. Kidney Int. 2024;105(2):381-8.
2. Perkovic V. Sibeprenlimab for patients with IgA nephropathy: results from a prespecified interim analysis of the Phase 3 visionary study. Abstract 98. ERA Congress, 4-7 June, 2025.
3. Barratt J et al. Updated interim results of a phase 1/2 study of BION-1301 in patients with IgA nephropathy. NDT. 2023;38(Suppl 1):gfad063c_4337.
4. Lafayette R et al. A Phase 2b, randomized, double-blind, placebocontrolled, clinical trial of atacicept for treatment of IgA nephropathy. Kidney Int. 2024;105(6):1306-15.
routine care, especially if supported by biomarker-driven patient selection and long-term safety data.
CONCLUSION
Together, these presentations highlighted a rapidly evolving field, with B cell therapies, endothelin receptor antagonists, and complement inhibitors offering promising and increasingly targeted options for managing IgAN.
As more data emerge, the challenge ahead lies in refining patient selection, treatment sequencing, and long-term disease control.
5. Jicheng LV et al. Randomized phase 2 trial of telitacicept in patients with IgA nephropathy with persistent proteinuria. Kidney Int Rep. 2024;8(3):499-506.
6. Rovin BH et al. Efficacy and safety of sparsentan versus irbesartan in patients with IgA nephropathy (PROTECT): 2-year results from a randomised, active-controlled, phase 3 trial. The Lancet. 2023;402(10417):2077-90.
7. Heerspink HJL et al. Atrasentan in patients with IgA nephropathy. N Engl J Med. 2025;392(6):544-54.
8. Heerspink HJL et al. The selective endothelin receptor antagonist SC0062 in IgA nephropathy: a randomized double-blind placebo-controlled clinical trial. J Am Soc Nephrol. 2025;36(4):657-67.
9. Heerspink HJL et al. Zibotentan in combination with dapagliflozin compared with dapagliflozin in patients with chronic kidney disease (ZENITH-CKD): a multicentre, randomised, active-controlled, phase 2b, clinical trial. The Lancet. 2023;402(10416):20040-17.
10. Perkovic V et al. #456 Efficacy and safety of iptacopan in patients with primary IgA nephropathy: interim analysis results of the phase 3 APPLAUSE-IgAN study. NDT. 2024;39(Suppl 1):gfae069-0141-456.
11. Barratt J et al. Cemdisiran phase 2 study investigators and collaborators. Phase 2 trial of cemdisiran in adult patients with IgA nephropathy: a randomized controlled trial. Clin J Am Soc Nephrol. 2024;19(4):452-62.
12. Tumlin J et al. Efficacy and safety of ravulizumab in IgAN: week 50 results from a phase 2 randomized controlled trial: FR-OR60. JASN. 2024;DOI:10.1681/ASN.2024r76pk0r1..
Abstract Reviews
Highlighting key insights from the 62nd European Renal Association (ERA) Congress, the following abstract reviews showcase some of the most exciting developments shaping the future of nephrology.
Sleep Habits, Sleep Quality, and Fatigue Among People with Chronic Kidney Disease
Authors: *Ginger Chu,1,2 Ritin Fernandez,1
Shilpanjali Jesudason,3 Sarah Russo,2 Vasif Abdullatheef,4 Ben Lazarus,5-7 Lisa Matricciani,8
Cassandra Foster,4 Catherine Blackamore,4 Richard LeLeu,3,8 Andrea K Viecelli6
1. School of Nursing and Midwifery, University of Newcastle, Callaghan, Australia
2. Nephrology Department, John Hunter Hospital, New Lambton Heights, New South Wales, Australia
3. Royal Adelaide Hospital, Central Northern Adelaide Renal and Transplantation Service, Adelaide, Australia
4. Gosford Hospital, Gosford, Australia
5. Princess Alexandra Hospital, Department of Kidney and Transplant Services, Brisbane, Australia
6. Australasian Kidney Trials Network, University of Queensland, Brisbane, Australia
7. Faculty of Medicine, University of Queensland, Brisbane, Australia
8. Clinical and Health Sciences, University of South Australia, Adelaide, Australia
*Correspondence to g.chu@newcastle.edu.au
Disclosure: The authors have declared no conflicts of interest.
Healthy sleep habits are highly recommended for individuals with chronic kidney disease (CKD)1 to improve their
quality of life and reduce the decline in kidney function.2 However, there is limited research on the sleep habits of individuals with CKD and how these impact sleep quality and fatigue. This study3 aims to describe sleep habits in the CKD population and identify their correlation with sleep quality and fatigue.
METHODS
A cross-sectional survey was conducted in four nephrology units across three Australian states between 1st August 2024–31st December 2024. Data were collected anonymously from adults with CKD using both paper-based questionnaires and online surveys. Validated instruments, including the Sleep Hygiene Index (SHI), Pittsburgh Sleep Quality Index (PSQI), and Functional Assessment of Chronic Illness TherapyFatigue (FACIT-F), were used to assess self-reported sleep habits, sleep quality, and fatigue, respectively. Spearman’s rank correlation was used to assess the relationship between sleep habits, sleep quality, and fatigue.
RESULTS
A total of 173 surveys were returned. Mean age was 64 years, 70% were male, and participants were predominantly receiving haemodialysis (78%). Overall, sleep hygiene engagement was good (mean SHI: 13.6; SD: 7.9; maximum obtainable: 52, with higher scores indicating poorer sleep hygiene). However, sleep quality was poor across all
participants (median PSQI: 8; interquartile range: 5–12; maximum obtainable: 21, with a score of 5 or greater indicating ‘poor’ sleep). Moderate fatigue was identified (mean FACIT-F: 29.9; SD: 12.8; maximum obtainable: 52, with higher scores indicating a lower level of fatigue). There were a small number of responses from patients receiving conservative management (n=3), those with CKD not requiring kidney replacement therapy (n=7), and postkidney transplant (n=6); therefore, these cohorts are not included in the subgroup comparisons. Sleep hygiene engagement and sleep quality were similar between patients receiving haemodialysis and
peritoneal dialysis. FACIT-F scores showed that patients receiving haemodialysis reported a higher level of fatigue compared to those on peritoneal dialysis. Of all sleep hygiene behaviours, four were most commonly reported: 1) having daytime naps; 2) different bedtime from day-to-day; 3) different wake time from day-to-day; and 4) thinking, planning, or worrying while in bed. Over 50% of participants reported these behaviours as occurring sometimes, frequently, or always (Figure 1). Correlation analysis revealed a weak but statistically significant relationship between sleep habits and sleep quality (r=0.36; p<0.001) and fatigue (r= –0.31; p<0.001).
Do important work before bed (e.g., pay bills)
Sleep in uncomfortable bedroom (e.g., too hot)
Sleep on uncomfortable bed (e.g., poor mattress)
Alcohol, tobacco or caffeine within 4 hours of going to bed
Do something that may wake me up before bed (e.g., play video games)
Go to bed feeling stressed, nervous, upset, or angry
Stay in bed longer than I should
Use bed other things other than sleep or sex (e.g., watching TV
Daytime naps lasted 2 or more hours
Different bedtime
Think, plan, or worry when in bed
Different wake time
CONCLUSION
This study highlights that overall sleep hygiene practices are good among individuals with CKD. Although correlations between sleep habits, sleep quality, and fatigue were weak, they were statistically significant, indicating these relationships are unlikely to be random. These findings suggest that healthy sleep habits are correlated to both fatigue and sleep.
The four most commonly reported sleep hygiene behaviours identified in this study
could serve as targets for interventions to promote sleep hygiene in patients with CKD. However, this study also demonstrates that other factors influencing sleep may not yet have been identified. Therefore, further research is needed to explore these factors to enhance sleep among individuals with CKD. Additionally, future studies should prioritise recruitment efforts targeting people with CKD who are not receiving dialysis to gain a more comprehensive understanding of the impact of sleep on this population.
Figure 1: Self-reported sleep hygiene in people with chronic kidney disease.
References
1. National Kidney Foundation (NKF). 8 self-care ideas for people with kidney disease. 2022. Available at: https://www.kidney.org/news-stories/8-self-careideas-people-kidney-disease. Last accessed: 5 September 2024.
2. Chu G et al. The important role of sleep in CKD prevention and progression. Kidney Int Rep. 2025;10(6):1613-15.
3. Chu G et al. Sleep habits, sleep quality, and fatigue among people with chronic kidney disease. Abstract. ERA Congress, 4-7 June, 2025.
Sex Differences in Glomerular Diseases and Their Long-Term Outcomes
Sex differences in kidney diseases have received limited attention. Research in this area is crucial for developing targeted prevention and intervention strategies that address the unique needs and risk factors of diverse populations. The purpose of this study was to investigate the impact of sex on infection rates and renal survival across different types of glomerulonephritis.1
METHODS
The authors conducted a retrospective, single-centre study at a reference centre for glomerular diseases, located in a tertiary hospital. They evaluated the prevalence of glomerular diseases among males and females in terms of clinical characteristics and long-term outcomes. Logistic regression analysis and time-toevent analyses were employed.
RESULTS
In total, 232 patients were included in the analysis: 63% were male and 37% were female. The most common glomerular disease in males was IgA nephropathy
(29%), while females most frequently presented with anti-neutrophil cytoplasmic antibody-associated glomerulonephritis (19%) and focal and segmental glomerulosclerosis (19%). Notably, IgG4related nephritis and membranoproliferative glomerulonephritis were observed only in males. At diagnosis, hypertension was more prevalent in males (71% in males versus 56% in females; p=0.035). There were no significant differences in the severity of kidney disease between sexes. The total cohort had a median estimated glomerular filtration rate (eGFR) of 51 mL/min/1.73 m2 (interquartile range [IQR]: 25–85) and a median proteinuria of 3 g/24 hours (IQR: 1–6). During the first year, females had a higher likelihood of infections compared to males (adjusted odds ratio: 3.0; 95% CI: 1.31–7.3; p=0.01) after adjusting for the type of immunosuppressive treatment. Renal recovery at 1 year was similar between the sexes, with males and females showing comparable increases in eGFR (mean±SD: 8±19 versus 11±21 mL/min/1.73 m2; p=0.50) and decreases in proteinuria (median [IQR]: 57% [0–90] versus 55% [0–83]; p=0.35).
Over a median follow-up of 2 years (0.5–4), the 5-year overall survival rate was 90%, with no significant difference between males and females (log-rank: p=0.181). In the total cohort, the 5-year renal survival rate was 86%. However, in the subgroup of patients with baseline eGFR <30 mL/ min/1.73 m2, males tended to have worse renal survival (log-rank: p=0.087) (Figure 1).
CONCLUSION
This study highlights sex differences in glomerular diseases, particularly in infection rates and hypertension prevalence. Despite these differences, long-term renal survival rates, comprising proteinuria and eGFR evolution, were similar between sexes. However, males with severe kidney disease at baseline showed a trend towards worse renal survival.
Figure 1: Renal survival analyses according to sex.
eGFR: estimated glomerular filtration rate.
Reference
1. Stambolliu E et al. Sex Differences in Glomerular Diseases and Their Long-Term Outcomes: Journal of the American Society of Nephrology. 2024;35(10S).
The Creatinine Triples After a Whipple: A Case of Chronic
Kidney Disease Due to Secondary Oxalate
Nephropathy 27 Years Post-Pancreaticoduodenectomy
Authors: *Gayoung Oh,1 Hsu Pheen Chong1
1. West Suffolk Hospital, Bury St Edmunds, UK
*Correspondence to gayoung.oh@wsh.nhs.uk
Disclosure: The authors have declared no conflicts of interest.
Roux-en-Y gastric bypass and chronic pancreatitis are recognised causes of oxalate nephropathy secondary to fat malabsorption.1 Whipple’s procedure is a lesser-known cause of oxalate nephropathy, and there is only one other reported case to this date.2
CASE PRESENTATION
The authors present the case of a 55-year-old female with a background of Type 2 diabetes, hypertension, and Whipple’s procedure performed 27 years prior for a benign pancreatic cyst.3 The patient presented with a 4-week history of abdominal pain, back pain, and weight loss, and an incidental finding of rapidly declining renal function that had been occurring over a period of 1.5 years. Her creatinine levels had increased from 66 μmol/L in February 2023, to 103 μmol/L in November 2023, to 194 μmol/L at the time
of this encounter (Table 1). She denied using nonsteroidal anti-inflammatory drugs. Metformin had been discontinued a month prior by her general practitioner due to impaired renal function.
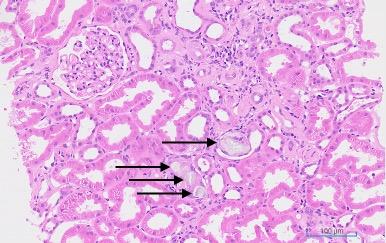
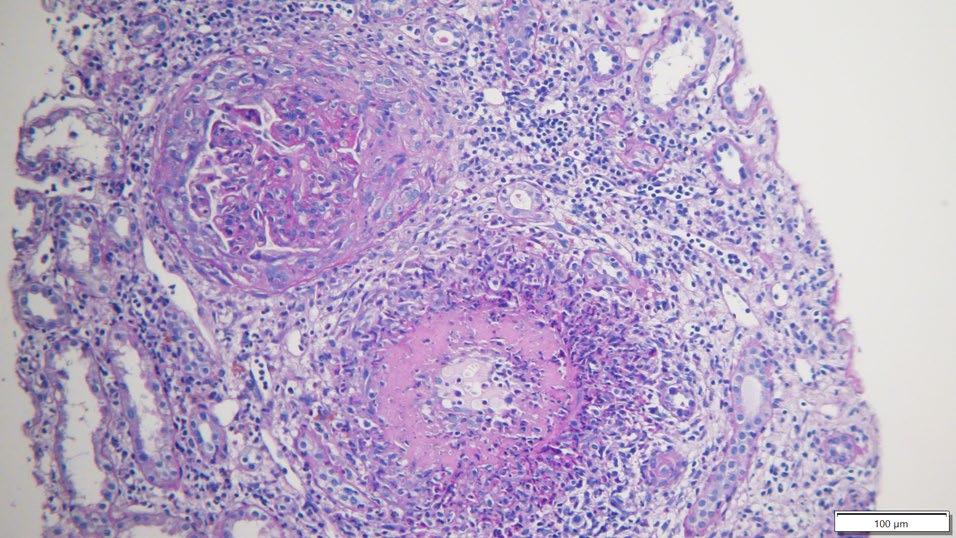
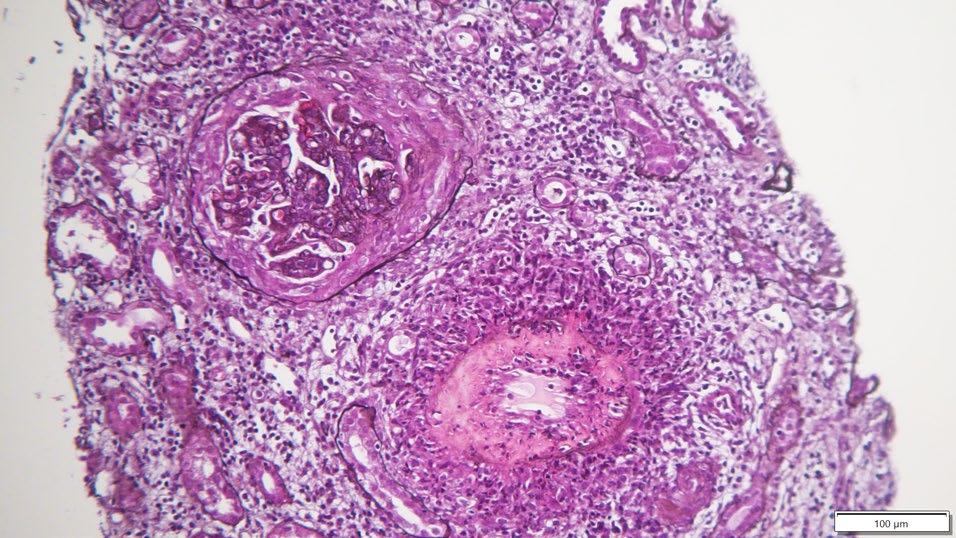
A urine dipstick test was perfomed; the result was unremarkable and revealed no active urinary sediments. The patient’s urine creatinine level was 6.3 mmol/L, her urine albumin was 5.1 mg/L, and the urine albumin to creatinine ratio was 0.8 mg/ mmol. Full myeloma and autoimmune panels were negative. A renal biopsy demonstrated multiple intra-tubular oxalate crystals with moderate tubulointerstitial atrophy and glomerular basement membrane thickening suggestive of diabetic glomerulopathy (Figure 1). Total oxalate excretion over 24 hours was 899 μmol. Faecal elastase was <15 μg/g, indicating severe exocrine pancreatic insufficiency. The patient was diagnosed with chronic kidney disease due to secondary oxalate nephropathy, 27 years after her Whipple’s procedure. She remains under follow-up, with the mainstay of treatment being hydration, pancreatic enzyme replacement therapy, and a low oxalate diet.
CONCLUSION
Through this unusual case, the authors aim to raise awareness of Whipple’s procedure being a cause of oxalate nephropathy and highlight the possibility of chronic kidney disease occurring decades after the operation.
Table 1: Rapid decline in renal function over 1.5 years.
eGFR: estimated glomerular filtration rate.
Figure 1: Renal histology.
The sample shows multiple intra-tubular oxalate crystals (black arrows) with adjacent tubular atrophy.
References
1. Rosenstock JL et al. Oxalate nephropathy: a review. Clin Kidney J. 2021;15(2):194-204.
2. Barani C et al. Oxalate nephropathy after pancreaticoduodenectomy: a case report. BMC Nephrol. 2024;25(1):106.
3. Oh G, Chong HP. The creatinine triples after a Whipple: a case of chronic kidney disease due to secondary oxalate nephropathy 27 years postpancreaticoduodenectomy. Abstract 2394. ERA Congress, 4-7 June, 2025.
Plan for Hypertensive Disorders in the Puerperium Period: Zero Vascular and Renal Risk
Authors: *Carolina Gracia-Iguacel,1,2
M.A Dolores Del Pino Y Pino,2,3 Marta Arias
Guillen,2,4 Itziar Castaño,2,5 Mercedes Salgueira Lazo,2,6 Marco Montomoli,2,7 Iara Dasilva Santos,2,8 Maria Dolores Arenas,2,9 Claudia Yuste Lozano,2,10 Beatriz Fernandez-Fernandez,1,2
1. Renal Medicine, IIS-Fundación Jiménez Díaz
UAM University Hospital, Madrid, Spain
2. Gender and Renal Health Working Group of Spanish Society of Nephrology, Madrid, Spain
3. Virgen de las Nieves University Hospital, Granada, Spain
4. Hospital Clínic of Barcelona, Spain
5. University of Navarra Clinic, Spain
6. Virgen Macarena University Hospital, Sevilla, Spain
7. Clinical University Hospital of Valencia, Spain
8. Germans Trias i Pujol University Hospital, Barcelona, Spain
9. Spanish Renal Foundation Íñigo Álvarez de Toledo, Madrid, Spain
10. 12 de Octubre University Hospital, Madrid, Spain
*Correspondence to cgraciai@quironsalud.es
Disclosure: The authors have declared no conflicts of interest.
Acknowledgements: The authors would like to thank the Spanish Society of Nephrology (SEN) for supporting the Gender and Kidney Health Working Group, Madrid, Spain.
Keywords: Epidemiology, hypertension, hypertension disorders of pregnancy, women.
Hypertensive disorders of pregnancy (HDP) are associated with an increased postpartum risk of cardiovascular disease or kidney failure. In recent years, the profile of pregnant women has changed. Factors such as older age at pregnancy, obesity, diabetes, chronic hypertension, and chronic kidney disease, and the use of assisted reproductive technologies, have become more common. These changes
have contributed to a rise in HDP cases, with the WHO estimating an incidence of 2–10% globally.1-8
However, there is scarce information on current practice regarding follow-up of HDP in diverse healthcare systems, especially in an evolving demographic environment. Spain is one of the Western European countries that does not yet have a national HDP registry.
Recognising this gap, a multidisciplinary group of Spanish healthcare professionals, including nephrologists, primary care physicians, and obstetricians, has proposed a national postpartum care plan. This plan will focus on vascular and kidney health, aiming to improve prevention, health promotion, and longterm monitoring for affected women.
This study9 aimed to analyse, for the first time, the incidence and trends of HDP in Spain between 2016–2022. It also sought to identify regional differences in HDP rates across the country.
METHODS
Researchers used data from the Spanish Ministry of Health’s Registry of Specialized Care Activity (RAE-CMBD). HDP cases were identified using international statistical classification of disease (ICD) codes (ICD9 and ICD-10): pre-existing hypertension complicating pregnancy, childbirth, and the puerperium (010); chronic hypertension with superimposed preeclampsia (O11); gestational (pregnancy-induced) oedema and proteinuria without hypertension (012); and gestational hypertension (O13).
Incidence was calculated by dividing the number of HDP cases by the total number of births and multiplying by 100. To assess trends over time, the incidence in each year was compared to that in 2016. Relative risk (RR) and 95% CIs were used to determine statistical significance. Regional
differences were analysed using Poisson regression models, and adjustments were made for multiple comparisons using the Benjamini-Hochberg method. If the p value for the interaction was <0.05, the temporal evolution differed between the two regions being compared.
RESULTS
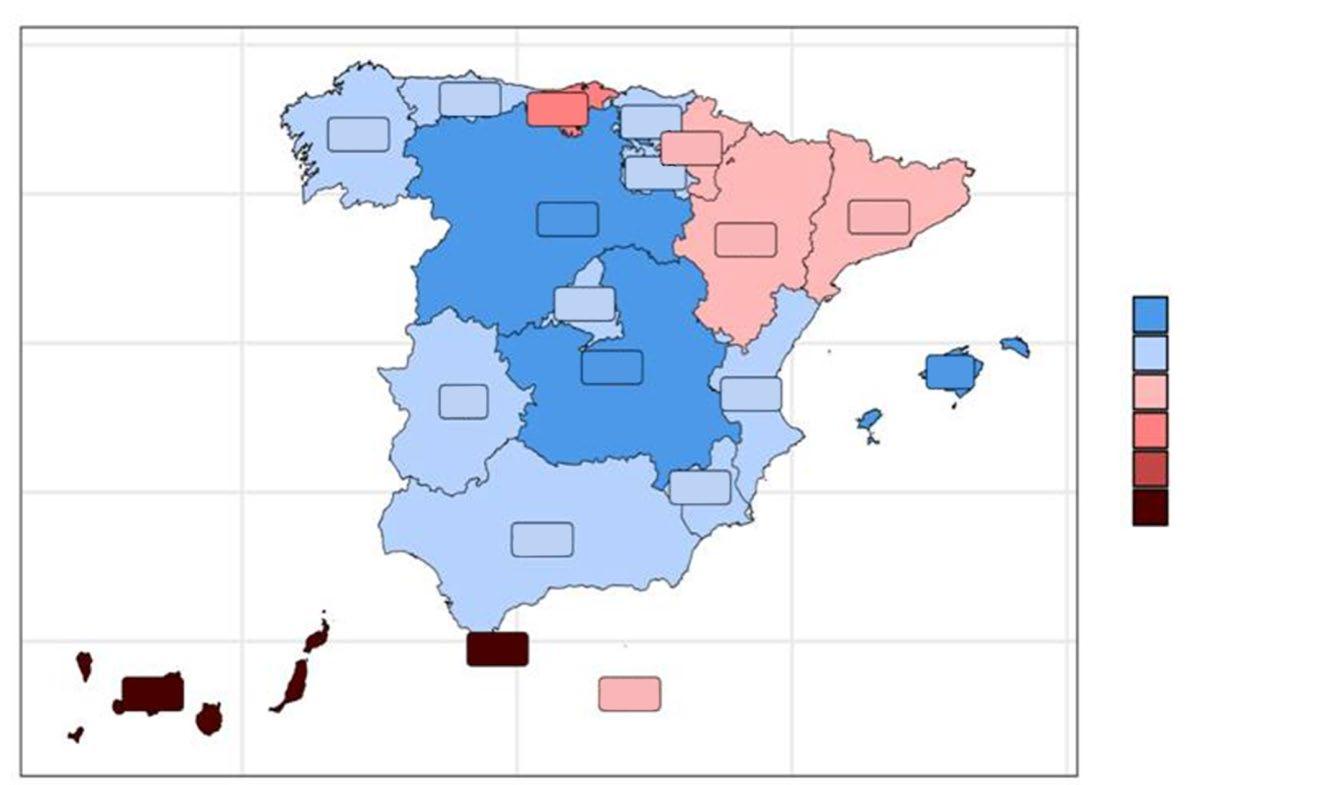
The study found a significant increase in HDP incidence in Spain in 2021 (1.80 versus 1.84; RR: 1.055; 95% CI: 1.033–1.076) and 2022 (1.80 versus 1.90; RR: 1.063; 95% CI: 1.041–1.084), compared to 2016 (Table 1). The regions with the highest rates between 2016–2022 included the Balearic Islands, Canary Islands, Melilla, Aragón, Catalonia, and Ceuta (Figure 1).
Importantly, there were significant differences in HDP incidence across Spain’s regions, suggesting inconsistencies in diagnosis or reporting practices (Table 2). While Spain’s overall HDP incidence
(1.8%) is lower than that of other European countries like France (2.3%), Greece (2.2%), and Norway (4.0%), this may reflect underdiagnosis or gaps in follow-up care.10,11
CONCLUSION
This is the first nationwide study to examine HDP incidence in Spain and its regional variations. A significant increase in incidence was observed over time in Spain from 2016–2022. Most regions in Spain reported an incidence below 1. The relatively low incidence suggests that many cases may go undiagnosed, potentially putting women at risk for future cardiovascular complications. The significant difference in incidence variability between the different regions in Spain points out the need for a homogeneous discharge and hospitalisation followup protocol for primary care. A national registry and coordinated followup system could help ensure better outcomes for mothers and their children.
Bold font means the comparison is significant, where 0.953 is a significantly lower incidence, and
and 1.063 are significantly higher incidences.
Table 1: Incidence of hypertensive disorders of pregnancy according to between 2016–2022.
Figure 1: Incidence rate of hypertensive disorders of pregnancy during 2016–2022 in the different regions of Spain.
Color-coded map illustrating incidence rates, with blue representing regions of lower incidence and red indicating areas of higher incidence. The gradient reflects the range of incidence values observed across the dataset.
Table 2: Comparison of temporal trends across Spanish regions.
Table 2: Comparison of temporal trends across Spanish regions. Continued.
Galicia
Islas
Baleares La Rioja
Melilla
Table 2: Comparison of temporal trends across Spanish regions. Continued.
Poisson regression models applied to analyse the temporal evolution in different regions. The models include an interaction term between time and Spanish region, allowing for the assessment of differences in temporal trends across regions.
References
1. Bell MJ. A historical overview of preeclampsia-eclampsia. J Obstet Gynecol Neonatal Nurs. 2010;39(5):510-8.
2. Rana S et al. Angiogenic factors and the risk of adverse outcomes in women with suspected preeclampsia. Circulation. 2012;125(7):911-9.
3. Chappell LC et al. Diagnostic accuracy of placental growth factor in women with suspected preeclampsia: a prospective multicenter study. Circulation. 2013;128(19):2121-31.
4. Zeisler H et al. Predictive value of the sFlt-1:PlGF ratio in women with suspected preeclampsia. N Engl J Med. 2016;374(1):13-22.
5. ACOG Committee on Obstetric Practice. ACOG practice bulletin. Diagnosis and management of preeclampsia and eclampsia. American College of Obstetricians and Gynecologists. Int J Gynaecol Obstet. 2002;77(1):67-75.
6. Kedziora SM et al. Kidney injury caused by preeclamptic pregnancy recovers postpartum in a transgenic rat model. Int J Mol Sci. 2021;22(7):3762.
7. Butler MJ et al. The pathological relevance of increased endothelial glycocalyx permeability. Am J Pathol. 2020;190(4):742-51.
8. Vikse BE et al. Preeclampsia and the risk of end-stage renal disease. N Engl J Med. 2008;359(8):800-9.
9. Gracia-Iguacel C et al. Spanish plan for hypertensive disorders in the puerperium: zero vascular and renal risk. Abstract 1002. ERA Congress, 4-7 June, 2025.
10. Abalos E et al. Global and regional estimates of preeclampsia and eclampsia: a systematic review. Eur J Obstet Gynecol Reprod Biol. 2013;170(1):1-7.
11. Gracia-Iguacel C et al. Increasing incidence of hypertensive disorders of pregnancy and association with decreased GFR and albuminuria: The need for post-partum follow-up. Placenta. 2025;165:42-9.
Murcia
Navarra
Pais
Clinical Tools to Stratify Patients on Conservative Kidney Management with Different Care Needs
Authors: *Swee Ping Teh,1 Sye Nee Tan,1 Ivan Wei Zhen Lee,1 Shashidhar Baikunje,1 Lee Ying Yeoh1
1. Department of Renal Medicine, Sengkang General Hospital, Singapore *Correspondence to teh.swee.ping@singhealth.com.sg
Disclosure: Teh has received support for attending meetings and/or travel from Fresenius Medical Care and AstraZeneca Singapore Pte Ltd., with payments to the institution. The other authors have declared no conflicts of interest.
Acknowledgements: The authors would like to thank the participants and family members, for their willingness to participate in this pilot project, and the unwavering support from the Tzu-Chi Foundation, Singapore.
Personalised care in conservative kidney management (CKM) provides personcentred care for patients who have opted for non-dialytic therapy. However, the illness trajectory of patients with chronic kidney disease (CKD) G5 on CKM can be unpredictable. A previous study suggested a sharp increase in symptom distress and health-related concerns in the 2 months before death.1 The aims of this study were to identify clinical tools associated with mortality in patients on CKM, and to evaluate the concordance between preferred and actual place of death.2
METHOD
This was a single-centre cohort study including 109 patients with CKD G5 who opted for CKM from April 2021–September 2024. Baseline demographic, clinical data, laboratory data, Clinical Frailty Score (CFS), Edmonton Symptom Assessment System Revised: Renal (ESAS-r: Renal) score,3
Resources Utilisation Group-Activities of Daily Living (RUG-ADL) score,4 Palliative Performance Score (PPS),5 and Karnofsky Performance Score (KPS) were collected. Logistic regression and survival analysis were performed.
RESULTS
The mean±SD age of the patients was 79.8±7.3 years, 64.2% were female, and 82.6% were Chinese. The primary cause of CKD G5 was diabetes (69.7%). Baseline mean estimated glomerular filtration rate CKD-epidemiology collaboration (eGFRCKD-EPI) was 10.3 mL/min, with a Charlson comorbidity index of 8.5, a CFS of 4.6, and a KPS of 67.3. The median total ESASr-Renal score was 1, the RUG-ADL score was 4, PPS was 60, serum albumin was 38 g/L, and haemoglobin was 9.6 g/ dL. Sixty-two patients (56.9%) became deceased during follow-up, with a median survival of 11.9 months. After adjusting for variables, baseline eGFRCKD-EPI remained the only significant predictor of mortality (Figure 1A). Patients with eGFRCKD-EPI ≤5 mL/min had a median survival of 4 months. A PPS of <50 showed a clear correlation with poorer survival estimates (Figure 1B). The advance care planning completion rate in this cohort was 60.5%. There was a moderate concordance between preferred and actual place of death, with 35.5% of the deceased patients passing away at home.
CONCLUSION
Baseline eGFRCKD-EPI is a significant predictor of mortality in patients on CKM. PPS demonstrated utility in estimating survival and may aid in timely transitions to hospice care. While ‘home’ remains the preferred place for end-of-life care for most, fulfilling this preference remains challenging. This study highlighted the importance of early identification of patients at-risk, as well as the need for personalised care plans in CKM. Recognition of these
A B
Figure 1: Duration of survival for patients who opted for conservative kidney management. Independent-Samples
eGFR_grp
eGFR >10
eGFR 6–10
eGFR ≤5
eGFR >10-censored
eGFR 6–10-censored
eGFR ≤5-censored
A) Duration of survival for patients on CKM of varying eGFR. B) Duration of survival based on PPS.
poor prognostic values may facilitate timely referrals to hospice service.
References
1. Murtagh FE et al. Trajectories of illness in stage 5 chronic kidney disease: a longitudinal study of patient symptoms and concerns in the last year of life. Clin J Am Soc Nephrol. 2011;6(7):1580-90.
2. Teh SP. Clinical tools to stratify conservative kidney management patients with different care needs. Abstract 459. ERA Congress, 4-7 June, 2025.
3. Kidney Supportive Care Research Group.
Edmonton Symptom Assessment System Revised: Renal (ESAS-r: Renal). 2022. Available at: https://www.ckmcare.com/Resources/ Details/62. Last accessed: 10 August 2024.
4. Mlinac ME, Feng MC. Assessment of activities of daily living, self-care, and independence. Arch Clin Neuropsychol. 2016;31(6):506-16.
5. Wainright W, Downing GM (eds.), medical care of the dying (2006) 4th ed, Victoria: Victoria Hospice Society.
Burden of Disease and Management of Hyperkalaemia in Patients with Type 2 Diabetes and Chronic Kidney Disease Managed at Spanish Endocrinology Services
Authors: *José Ignacio Martínez-Montoro,1,2
Belen Pimentel,3 Ana Roncero Martín,3 Miren
Sequera Mutiozabal,3 Mónica Juárez Campo,3
José Carlos Fernández-García2,4
1. Department of Endocrinology and Nutrition, Hospital Universitario Virgen de la Victoria, Málaga, Spain
2. Instituto de Investigación Biomédica de Málaga (IBIMA), Spain
4. Department of Endocrinology and Nutrition, Regional University Hospital of Málaga, Spain
*Correspondence to joseimartinezmontoro@gmail.com
Disclosure: Roncero Martín, Pimentel, Juárez Campo, and Sequera Mutiozabal are employees of AstraZeneca. Fernández-García has received sponsorship and consultancy fees from AstraZeneca. Martínez-Montoro has received sponsorship and consultancy fees of 3,000 EUR from AstraZeneca.
Acknowledgements: This study has been sponsored and funded by AstraZeneca. The authors would like to thank Telómera S.L.U (TELOTRON Database) for descriptive analyses, and Coral Berriochoa Hausmann from AstraZeneca’s Patient Safety function for her contribution to the revision of safety data gaps.
Keywords: Chronic kidney disease (CKD), hyperkalaemia, Type 2 diabetes (T2D).
Chronic kidney disease (CKD) is a global public health problem with a high impact on morbidity and mortality.1 Diabetes is one of the leading causes of CKD, and up to 40% of patients with Type 2 diabetes (T2D) have CKD.2 Although patients with metabolic diseases are primarily managed by endocrinology units, there are currently no studies describing the burden associated with the loss of kidney function and the risk of developing hyperkalaemia in these
patients. The ENDO-CKD study aimed to describe and characterise the prevalence, associated burden, and management of hyperkalaemia in patients with T2D and CKD managed by endocrinologists in Spain.3
METHODS
This was a retrospective observational study using data from the TELOTRON database in Spain. Adult patients with T2D (as per diagnosis code, at least one HbA1c value of ≥6.5%, or prescription of any antidiabetic drug) and CKD (as per diagnosis code or lab criteria for CKD diagnosis [one estimated glomerular filtration rate of <60 mL/min/1.73 m2 and/ or one urine albumin-to-creatinine ratio of ≥30 mg/g]) with at least one visit to the endocrinology services between January 2013–November 2023 were included. Hyperkalaemia was defined as per diagnosis code and/or with potassium laboratory values >5 mmol/L. Baseline characteristics, treatments, and hyperkalaemia management were analysed.
RESULTS
A total of 8,017 patients were identified. The mean age was 70.7 years (SD: 11.8 years), 45.2% were female, the mean BMI was 31.8 kg/m² (SD: 6.5), the mean estimated glomerular filtration rate was 61.9 mL/ min/1.73 m² (SD: 24.6), the median urine albumin-to-creatinine ratio was 53.5 mg/g (interquartile range: 25.0–146.2), and the median Charlson Comorbidity Index (CCI) score was 4.0 (interquartile range: 2.0–5.0). These patients were highly comorbid (81.6% hypertension; 77.8% hyperlipidaemia; 45.6% obesity; 21.4% heart failure) and had a high use of drugs (96.1% glucoselowering; 83.5% lipid-lowering; 80.6% renin–angiotensin–aldosterone system inhibitors; 63.7% sodium-glucose cotransporter v2
(SGLT2) inhibitors; 43.1% β-blockers). Among them, 26.4% (2,116) had an event of hyperkalaemia, yet only 29.7% (628) were formally diagnosed and 12.6% (267) received treatment with potassium binders (Table 1).
CONCLUSION
Hyperkalaemia is a prevalent condition, but it remains underdiagnosed
and undertreated in patients with CKD and T2D managed by Spanish endocrinology services, despite guideline recommendations for achieving optimal cardio-renal-metabolic therapy. Over 70% of hyperkalaemia cases are not formally identified, and more than 85% of patients do not receive appropriate treatment. The authors’ findings underscore the need for early detection and management of hyperkalaemia in high-risk patients.
Table 1: Management of hyperkalaemia in patients with Type 2 diabetes and chronic kidney disease managed by endocrinology services in Spain.
Severity of hyperkalaemia
Mild (>5.0–5.4 mmol/L)
Moderate (5.5–5.9 mmol/L)
Severe (≥6.0 mmol/L)
Patients with a hyperkalaemic event (N=2,116)
n (%)
1,599 (75.6%)
447 (21.1%)
70 (3.3%)
Treatment of hyperkalaemia n (%)
Potassium binders
New potassium binders
Resins
Identification of hyperkalaemia
Patients with diagnosed hyperkalaemia (diagnosis code ICD-10 E87.5 and potassium values >5 mmol/L)
- Treated with potassium binders
Patients with unidentified hyperkalaemia (only potassium values >5 mmol/L)
267 (12.6%)
118 (5.6%)
194 (9.2%)
n (%)
628 (29.7%)
198 (31.5%)
1,488 (70.3%)
ICD-10: International Classification of Diseases, Tenth Revision
References
1. Xie Y et al. Analysis of the Global Burden of Disease study highlights the global, regional, and national trends of chronic kidney disease epidemiology from 1990 to 2016. Kidney Int. 2018;94(3):567-81.
2. Wu B et al. Understanding CKD among patients with T2DM: prevalence, temporal trends, and treatment patterns-NHANES 2007-2012. BMJ Open Diabetes Res Care. 2016;4(1):e000154.
3. Martínez JI et al. Burden of disease and management of hyperkalemia in patients with type 2 diabetes mellitus and chronic kidney disease managed at Spanish endocrinology services. Abstract 2422. ERA Congress, 4-7 June, 2025.
Optimising Phosphate Removal: Is an Extended Dialyser the Answer?
Hyperphosphataemia is a significant contributor to morbidity and mortality in patients undergoing haemodialysis.1,2 While dietary phosphate restriction and the use of phosphate binders remain foundational in management, effective phosphate removal through dialysis is equally essential.3-6 This study aimed to investigate the key factors influencing phosphate elimination, with a focus on dialyser membrane type and surface area, session duration, serum phosphate levels, and purified blood volume.7
MATERIALS AND METHODS
Eight patients on chronic haemodialysis (3 females and 5 males) with pre-dialysis serum phosphate levels ≥2.0 mmol/L were enrolled. Each patient underwent two midweek bicarbonate dialysis sessions: one using a high-flux polysulfone membrane (ultrafiltration coefficient: 55 mL/h/mmHg) with surface areas of 1.8 m² or 2.1 m² (n=4 per group), and a subsequent session using an extended haemodialysis setup with a medium-permeability polyarylethersulfone membrane (ultrafiltration coefficient: 59 mL/h/mmHg) with surface areas of 1.8 m² or 2.0 m². Each patient served as their own
control. The average treatment time was 263.12±23.97 minutes, with a dialysate flow of 550 mL/min. All patients had an arteriovenous fistula as vascular access.
Phosphate removal (MPO4) was calculated based on dialysate and blood phosphate concentrations, session duration, and total phosphate cleared using the formula for estimating MPO4 during haemodialysis. The formula is as follows: MPO4=0.1·t17+50·Cds60 +11·Cb60, where ‘t’ is treatment time in minutes, Cds60 and Cb60 are dialysate and plasma phosphate concentrations at 60 minutes in mg/dL, respectively, and MPO4 is the estimated amount of phosphate removed in mg/ treatment.8 Statistical analysis assessed the relationship between MPO4 and key variables, including plasma phosphorus levels, dialyser membrane and surface area, blood volume processed, and session length.
RESULTS
The results demonstrated a strong positive correlation between phosphate removal and both pre-haemodialysis serum phosphate levels and purified blood volume (p=0.001). However, no significant association was found with dialyser membrane type (high-flux: 32.67±9.5 mmol/session versus extended mediumflux: 34.94±10.01 mmol/session; p=0.29), surface area (p=0.67), or treatment time (p=0.15). Multivariate regression analysis confirmed that only pre-dialysis phosphate levels and blood volume processed were independent predictors of MPO4.
CONCLUSION
Pre-dialysis serum phosphate levels and purified blood volume are the main determinants of phosphate clearance in haemodialysis. Dialyser type, membrane surface area, and session duration appear to have minimal impact, suggesting that
enhancing blood volume processed may provide greater benefit in managing hyperphosphataemia than using extended or alternative dialyser designs alone.
References
1. Suki WN. Phosphorus balance and CKD: what have we learned? Clin J Am Soc Nephrol. 2007;2(Suppl 2):S118-123.
2. Hung KY et al. Effect of dialysis membrane and treatment time on phosphate removal in hemodialysis patients. Nephrol Dial Transplant. 2001;16(2):278-82.
3. Kuhlmann MK et al. Phosphate removal during hemodialysis: a comparison of four dialyzers. Kidney Int. 2007;71(9):918-23.
4. Daugirdas JT. Removal of phosphorus by hemodialysis. Semin Dial. 2015;28(6):620-3.
5. Daugirdas JT et al. Handbook of Dialysis (2015) 5ᵗʰ edition, Philadelphia: Wolters Kluwer Health.
6. Ketteler M et al. KDIGO 2017 clinical practice guideline update for the diagnosis, evaluation, prevention, and treatment of CKD–MBD. Kidney Int Suppl. 2017;7(1):1-59.
7. Eftimovska-Otovikj N et al. Optimizing phosphate removal: is an extended dialyzer the answer? Abstract 1858. ERA Congress, 4-7 June, 2025.
8. Gutzwiller JP et al. Estimating phosphate removal in haemodialysis: an additional tool to quantify dialysis dose. Nephrol Dial Transplant. 2002;17(6):1037-44.
Hyperaldosteronism and Increased IL-6 as Cardiovascular Risk Factors in Haemodialysis Patients and Kidney Transplant Recipients
Author: *Maria Smaliakova1
1. Minsk Scientific and Practical Center for Surgery, Transplantology and Hematology, Minsk, Belarus
*Correspondence to dr.smaliakova@gmail.com
Disclosure: The author has declared no conflicts of interest.
Acknowledgements: The author is grateful to the team of Minsk Scientific and Practical Center for Surgery, Transplantology, and Hematology.
Renal replacement therapy prolongs life in patients with Stage 5 chronic kidney disease. Сardiovascular diseases are the main cause of death in this group of patients. Identifying and correcting cardiovascular risk factors can improve the quality of life, and increase the life expectancy of patients receiving renal replacement therapy. The aim of the study was to assess the blood levels of aldosterone and IL-6 in these patients and assess their association with adverse cardiovascular events.1,2
METHODS
The study included 52 patients with Stage 5 chronic kidney disease receiving dialysis. In which, 46.2% (n=24) were men, and the average age was 54.6±5.2 years. Fifty percentage (n=26) of patients underwent donor kidney transplantation, while the remaining continued haemodialysis treatment 12 hours a week. The study groups were comparable in gender, age, and traditional cardiovascular risk factors (smoking, family history, obesity, hypertension, hyperglycaemia, and hypercholesterolaemia).
RESULTS
Over 3 years of observation, 44.2% (n=23) of patients had adverse cardiovascular events, such as acute coronary syndrome, acute heart failure, or life-threatening rhythm disturbance. These cardiovascular complications were more common in patients on haemodialysis (57.7%; n=15) compared to kidney transplant recipients (30.8%; n=8), p<0.05.
Among dialysis patients, those with adverse cardiovascular events more often had episodes of hypotension (40.0%; n=6 versus 9.1%; n=1), increased blood levels of aldosterone (73.3%; n=11 versus 36.6%; n=4), and IL-6 (26.7%; n=4 versus 0.0), all p<0.05, at the time of inclusion, compared to patients without adverse cardiovascular events.
Conversely, kidney transplant recipients did not have such differences. Six months after kidney transplantation, the aldosterone blood level in recipients (122 [73–240] pg/mL) was lower than the preoperative level (465 [197–1,000] pg/mL; p<0.05).
The incidence of hyperaldosteronism also decreased from 65.4% (n=17) to 15.4% (n=4), p<0.05. An elevated IL-6 level was diagnosed in 7.8% (n=2) patients in the preoperative period and in 3.8% (n=1) 6 months after transplantation, p>0.05.
CONCLUSION
Based on this study, it was found that the incidence of adverse cardiovascular events in patients receiving renal replacement therapy is high. Patients with adverse cardiovascular events, on haemodialysis, have a higher preceding incidence of hypotension and elevated blood levels of aldosterone and IL-6, compared to patients without these complications. Kidney transplantation has a positive effect on eliminating these cardiovascular risk factors.
References
1. Smaliakova MV et al. Hyperaldosteronemia and increased interleukin-6 as a cardiovascular risk factors in hemodialysis patients and kidney transplant recipients. Abstract 631. ERA Congress, 4-7 June, 2025.
2. Smaliakova MV et al. Факторы
2020;4(1): 846-52.
Desidustat Shows Promising Results in Managing Anaemia in Patients with Chronic Kidney Disease
Author: *Ashwinikumar Khandekar1
1. KIMS-Kingsway Hospital, Nagpur, India
*Correspondence to aakhandekar@gmail.com
Disclosure: The author has declared no conflicts of interest.
Chronic kidney disease (CKD)-related anaemia is a common and debilitating complication, primarily due to a relative deficiency in endogenous erythropoietin production, resulting from a declining renal function. This anaemia contributes significantly to fatigue and increased cardiovascular risk in patients with CKD. Currently, erythropoiesis-stimulating agents (ESA) represent the standard of therapy. However, ESA require parenteral (subcutaneous) administration and cold chain maintenance, posing logistical challenges, especially in tropical countries. Moreover, there are risk about cardiovascular safety and hypo-responsiveness to ESA therapy in patients with CKD.
Desidustat, an orally administered hypoxiainducible factor prolyl hydroxylase inhibitor, represents a novel therapeutic class that stimulates endogenous erythropoietin production by mimicking the body’s natural response to hypoxia. Notably, desidustat was indigenously developed in India. Its oral formulation eliminates the need for injections and cold storage, offering a practical and patient-friendly alternative to ESA.
METHODS
Retrospective data from a single-centre study, presented at European Renal Association (ERA) Congress 2025 by the author, evaluated the real-world
effectiveness and safety of desidustat in 116 patients with CKD-related anaemia.1 The cohort included 66.4% of patients on predialysis, 28.5% of patients receiving dialysis, and 5.2% of post-transplant recipients. Among them, 59.5% were initiated on desidustat de novo, while 40.5% were switched from ESA therapy. Haemoglobin (Hb) and serum potassium levels were monitored from baseline through five followup visits.
RESULTS
Efficacy Outcomes
The overall mean Hb increased significantly from 9.65 g/dL at baseline to 11.13 g/dL at 5th day follow-up visit (p<0.05), with a mean absolute rise of 1.47 g/dL. Patients on pre-dialysis demonstrated the most robust response, with an increase of 1.74 g/dL. Patients receiving dialysis showed a delayed but meaningful improvement, with Hb rising by 0.78 g/dL. Post-transplant recipients also responded positively, with Hb increasing from 9.2 g/dL to 10.3 g/dL.
Comparison with ESA Therapy
Both patients de novo and those switched from ESA therapy exhibited comparable improvements in Hb levels, with no statistically significant difference between the groups (p>0.05), suggesting desidustat’s consistent efficacy regardless of prior treatment history.
Safety Profile
Serum potassium levels remained stable throughout the treatment period across all subgroups, indicating a favourable safety profile with no significant electrolyte disturbances (p>0.05). Adverse events were observed in 11 patients, including arteriovenous fistula failures (n=4), left ventricular failure (n=2), arterial thrombosis (n=1), deep vein thrombosis
(n=2), acute pancreatitis and transamintis (n=1), and haemorrhagic stroke (n=1).
CONCLUSION
This real-world analysis supports desidustat as a safe and effective alternative to traditional ESA therapy for managing anaemia in patients with CKD. The most pronounced benefits were observed in patients on pre-dialysis, with
consistent Hb improvements and stable potassium levels across the cohort. These findings reinforce the potential role of desidustat in the evolving therapeutic landscape of renal anaemia, particularly in settings where cold chain logistics and injection-based therapies pose challenges.
Reference
1. Kandhekar A. Retrospective single center analysis of desidustat in CKD anemia. Abstract 3024. ERA Congress, 4-7 June, 2025.
Congress Interview
The following interview offers expert insights into the standout themes and scientific momentum of the 62nd European Renal Association (ERA) Congress, held in Vienna, Austria, from the 4th–7th of June, 2025. We spoke with Rainer Oberbauer, who shared his reflections on this year’s record-breaking meeting, the evolving role of nephrologists in driving innovation, and ERA’s commitment to sustainability, equity, and education.
This conversation forms part of our wider congress coverage, which includes selected abstracts from ERA 2025, an expert-led congress highlights feature, and exclusive interviews with thought leaders shaping the future of renal care.
Rainer Oberbauer Professor of Medicine and Chair of the Department of Nephrology and Dialysis at the Medical University of Vienna, Austria
Moreover, it offered me the chance to help people who would otherwise face a life on dialysis, by giving them a new lease of life
You’ve been a key figure in advancing kidney transplantation, particularly in biomarker research and individualised immunosuppression. What first drew you to this field, and how has your research focus shifted over the years?
I’ve been in the field for almost 30 years now. I started by chance after my postdoctoral training. I became interested in kidney transplantation because, at that time, it was very innovative and the cutting edge of science. Moreover, it offered me the chance to help people who would otherwise face a life on dialysis, by giving them a new lease of life. That’s how my journey in the field began.
Q2
At the European Renal Association (ERA) 2025, you're presenting on both genome-wide non-HLA versus HLA alloimmunity and regulatory T cell therapy with donor bone marrow infusion. What are the main messages you hope to share through these sessions?
Regarding non-HLA, our HLA system is highly polymorphic, and therefore, the match between donor and recipient is important. However, it doesn’t explain all the causes of graft attrition, because it covers only 0.1% of the entire human genome. There’s still a lot of variability in the remaining 99.9% of the genome, and that’s what it’s all about. HLA makes sense, and we have standardised tools to measure antibodies against donor HLA antigens. However, in our paper from 2019, we showed that the same applies to non-HLA mismatches.
As for the cell-based therapy, this is more of a Phase I/IIa study. We’re trying to induce chimerism without toxic or immunosuppressive induction therapy, and without body irradiation. There are three other centres also trying this: Stanford, Boston, and Northwestern in Chicago, USA.
Q3
How close are we to implementing precision medicine routinely in kidney transplantation, for example, using biomarkers to guide immunosuppressive therapy?
The term ‘personalised medicine’ or ‘precision medicine’ is, in my opinion, misused because whatever we do as physicians, surgeons, or researchers is personal. We’re not working in a company managing stocks or portfolios; we take care of one patient at a time, even when following guidelines. In transplantation, we have several immune markers, including biopsies, MRIs, and other tests. These markers help guide treatment, but it’s not as if we have HLA antigen-specific CAR-T regulatory cells that are used for each donor–recipient pair, at least not yet.
Q4
What do you see as the main barriers to translating biomarker research into clinical practice, and how might the field overcome them?
There’s a very good paper, an article by Graham Lord, who is now the MRC head at King’s College London, UK, which describes why the process is so complicated and why it is unlikely that we will have new biomarkers solely for diagnosis or prognosis. Many researchers have funding and access to patient samples, thus, the early steps of research are relatively straightforward. However, the challenge lies in conducting multinational validation, which requires funding. It is essential to ensure biomarker specificity. A critical distinction exists between prognostic and predictive markers; prognostic markers estimate outcomes such as life expectancy or graft halflife, while predictive markers predict a response to therapy. It is the latter that is needed, a biomarker that indicates whether a specific treatment will be effective. Unfortunately, such predictive biomarkers are not yet available and probably will not be in the near future.
Q5
For those particularly interested in transplant immunology and personalised medicine, are there any other ERA 2025 sessions you’d recommend attending or watching after the congress ends?
Yes, for example, we have a session on transplantation, autoimmunity, and spatial phenotyping. There’s also a late-breaking session at the ERA meeting in The Square meeting hall about combined bone marrow and kidney transplant.
Moreover, I am giving a session on paired donation in kidney transplantation. This is where, for example, I want to donate a kidney to someone, but we are not a match. Another donor–recipient pair faces a similar problem, so the donors are swapped. This process works better in larger catchment areas. Smaller countries, such as Austria or the Czech Republic, need to pool together internationally to find good pairs.
Interview
Patrick Maxwell, Regius Professor of Physic and Head of the School of Clinical Medicine at the University of Cambridge, UK took us through a fascinating exploration of his career in renal medicine and translational research. Maxwell reflected on how early discoveries in oxygen sensing and hypoxia-inducible factors have transformed our understanding of kidney disease, laying the groundwork for new therapeutic avenues. He also shared his perspective on the importance of embedding research into clinical settings and building cross-disciplinary teams to drive innovation that directly benefits patients.
Patrick Maxwell
Regius Professor of Physic and Head of the School of Clinical Medicine, University of Cambridge, UK
Nephrology continues to evolve rapidly, from molecular discoveries to new therapies. In your view, what makes this field so exciting and important today?
The implications of the discoveries made go far beyond nephrology
It has completely changed from when I started in nephrology, which was back in 1987. A much greater proportion of nephrology then was focused on acute renal failure. An attractive aspect compared to many medical specialties was that you could make an accurate diagnosis quickly, with blood tests, imaging, and renal biopsy. At that time, we had rather limited options to alter the course of disease. For example, when treating autoimmune conditions, we only had a few immunosuppressive therapies available. We often gave large doses, which caused major side effects, and often didn’t work very well. Even if we couldn’t reverse kidney damage, we had replacement therapies (dialysis and transplantation). We were mainly seeing younger people, and we could often help them quickly.
One change is that we now support a much wider population with chronic kidney disease (CKD), including many elderly patients and those with comorbidities. Some argue that this makes the specialty less interesting, but I find it more rewarding. There are so many more people we can help now. Over my career, nephrology has become more inclusive, and also more effective.
A second difference is that we are now much better at slowing the progression of CKD. Back then, we mostly just watched kidney function deteriorate and planned for dialysis. Today, we can slow progression in many people with CKD, and that’s improving all the time.
A third change is that knowledge about kidney diseases, especially autoimmune and genetic diseases, has increased enormously. This is leading to better approaches to diagnosis and treatment.
However, there is still a huge amount to do! For example, we still
don’t really know how to improve recovery after acute kidney injury, and we still have a serious shortage of transplant organs. I believe that both of those issues will be solved in the coming years. I anticipate that we will learn how to stimulate the kidneys’ ability to repair and regenerate.
Q2Your pioneering research on hypoxiainducible factors (HIF) has shaped our understanding of oxygen sensing. How did your interest in this area begin, and what do you see as its most significant impact on nephrology?
My first nephrology training post was in 1987 at Hammersmith Hospital in London, UK. At that time, they were doing the first human studies with recombinant erythropoietin (EPO). Kidney patients were often anaemic and needed regular blood transfusions, which carried all kinds of risks, such as infection and immune sensitisation, which makes transplantation more difficult. Most patients were chronically anaemic and tired.
EPO had been identified as a kidney-produced hormone that was relatively deficient in people with kidney disease. So, it was produced as a recombinant drug. Strikingly, in these early studies, it worked. Patients felt better, and as long as the haemoglobin wasn’t increased too rapidly, it was safe and well tolerated.
Emerging knowledge about EPO raised fascinating questions. If you are very anaemic, then your kidneys can increase EPO production by 10,000-fold. So, which cells are producing it? How do they know how much oxygen is reaching them? And why does this process go wrong in kidney disease?
I joined Peter Ratcliffe’s group in the Institute of Molecular Medicine at the University of Oxford, UK, to work on this in 1991. We set out to find the cells that produce EPO, and how they sense oxygen. Over the next 11 years, we solved those problems. At the time, HIF hadn’t yet been identified. My early experiments showed that oxygen sensing happens in every cell we
tested, which suggested that it had functions beyond regulating EPO. We now know that the underlying system, HIF, regulates thousands of genes and is active in every cell all the time.
We also discovered that fibroblasts in the kidney produce EPO. These were not the cells that people had expected. It was surprising because fibroblasts were thought to be quite boring, but from a design perspective, they are well placed to be reliable monitors, situated between the capillaries that are supplying the oxygen and the tubular cells that are using it.
We found that these cells are still present in people with CKD and can still produce EPO, though aspects of the disease processes alter that ability.
The implications of the discoveries made go far beyond nephrology. HIF research has been especially important in cancer. Tumours often grow in low-oxygen environments, and the HIF pathway is critical in how they behave. It is particularly
important in adapting their metabolism and driving signals for new blood vessel growth.
In nephrology specifically, we later discovered that HIF-2 activation is the key genetic event in the most common form of kidney cancer, clear cell renal carcinoma. That was completely unexpected. It involves different cells (tubular epithelial cells rather than fibroblasts) and reveals something fundamental about how kidney cells behave under low oxygen.
Clinically, the research led to new treatments for anaemia in kidney disease. Instead of injecting EPO, we can now give tablets that stimulate its production. There are about six such drugs in patients globally now. They’re cheaper, easier to administer, and, in some cases, may be even better than EPO.
Q3
The discovery of prolyl hydroxylase domain (PHD) enzymes opened up new therapeutic avenues. How do you reflect on the journey from that basic science discovery to the development of HIF stabilisers that are now used clinically?
A first reflection is that it’s impressive how quickly this went from discovery to therapy. We identified the enzymes in 2002, and within a decade, companies developed drugs that could be used in patients. These were
compared to EPO and found to be as effective, sometimes safer, sometimes not, depending on the drug and the setting.
A second reflection is that, although using these drugs has superficial similarity to using EPO, in that they boost red blood cell production, they’re completely different. EPO is specific and acts on a cognate receptor. With PHD inhibitors, you’re activating a whole system that affects thousands of genes. That complexity has pros and cons. On the positive side, because HIF activation helps cells survive low oxygen, they could reduce the severity of heart attacks or strokes in patients, but it might also increase the risk of cancer or speed up tumour progression.
A third reflection is that we learned a lot from studying humans with natural mutations in this pathway. People with certain HIF or PHD variants resulting in mild HIF activation have higher red blood cell counts but no major problems, suggesting that activating the pathway is relatively safe. In contrast, in von Hippel Lindau (VHL) disease, both copies of the VHL gene are affected in occasional cells throughout the body. This results in genetic HIF activation in those cells, with serious consequences, including a very high lifetime risk of kidney cancer; thus, dosage and targeting matter.
What I find slightly disappointing is that these drugs have mainly been tested as EPO replacements. Their real potential may be in treating conditions such as acute kidney injury, stroke, or heart attack. In animal studies, they look very promising, but we still lack good clinical trials in those areas.
Currently approved HIF stabilisers inhibit all three PHD enzymes. Over time, it may be attractive to selectively inhibit one of them, like PHD3 but not PHD2, which could be more beneficial in certain diseases. That’s still an open question.
Q4 Are there any novel biomarkers or targets emerging from the hypoxia pathway that you believe could change how we monitor or manage kidney disease?
Not at the moment, but I think there’s a lot of potential, particularly in the area of kidney repair and regeneration. We don’t yet have markers that can show us how well the kidneys are repairing themselves.
It would be fantastic if we could take a urine sample and assess the regenerative state of the kidney cells. That would give us a whole new window into what’s happening and how to intervene earlier or more effectively.
Q5 Beyond hypoxia, what other molecular pathways or mechanisms excite you the most in the context of kidney disease research today?
I’m very interested in the complement system. We studied families with kidney disease and discovered a mutation in a complement factor H-related protein. This mutation is very common among Cypriots, and can cause kidney disease by subtly altering the complement pathway.
It looks very similar to IgA nephropathy, which is a common condition. Until recently, there weren’t many effective treatments for IgA nephropathy, but now new therapies are emerging that target IgA deposition and the complement response. More broadly, complement activation plays a role in many kidney diseases and transplant rejection. We now understand this pathway well enough to develop targeted interventions, and I think that’s incredibly exciting.
Another area is immune responses to kidney proteins. In minimal change nephropathy, for example, it looks like we might now know
which protein is being targeted by the immune system. That could revolutionise how we treat it. Back in the 1980s, we just gave high-dose steroids to everyone because we didn’t know who would respond. It usually worked, but the side effects and dealing with recurrences made it very challenging for many patients. With more understanding, we can do much better.
Q6
Translating scientific discoveries into therapies is not very straightforward. What do you see as the biggest challenges and opportunities in bringing cutting-edge kidney research to the bedside?
First, you need a solid understanding of the disease and the pathways involved. Then, you need measurable indicators, ideally things you can track reliably and repeatedly.
A challenge in nephrology is that, by the time kidney function is measurably reduced, a lot of irreversible damage has already occurred. We need earlier markers to tell whether our interventions are making a difference before serious harm has occurred.
Another challenge is infrastructure. Most clinical settings are good at patient care but lack the time and resources for research, taking extra samples, running additional tests, or explaining studies to patients.
We also need a workforce trained in research. I was fortunate to get a Medical Research Council fellowship to do my PhD in Oxford, UK, and that gave me proper scientific training and changed my career.
Here at our medical school, every student does the equivalent of an intercalated science degree. That gives them a strong foundation for understanding research over the course of their career.
A challenge in nephrology is that, by the time kidney function is measurably reduced, a lot of irreversible damage has already occurred
And finally, reflecting on your journey so far, what factors do you think have been essential to driving impactful research in nephrology?
I think there are three things. First, where I worked, I had the privilege of training in units where research was happening and where people were changing the future of nephrology. That environment is vital.
Second, inspiring individuals. These included Stuart Cameron (Guy’s Medical School, now part of King's College London, UK), Chris Winearls (Hammersmith and Royal Postgraduate Medical School, now part of Imperial College London, UK), and Peter Ratcliffe (University of Oxford, UK), who all made major contributions to the field and inspired me personally. Science is a team effort, but individuals can have a huge impact.
Third, the patients. Most kidney patients stay with us for life. You build long-term relationships with them, and that creates a real partnership. Patients with VHL, complement factor H-related protein 5 (CFHR5) nephropathy, and polycystic kidney disease have all inspired me and helped drive my research. That shared understanding makes the doctor–patient relationship stronger and makes research more impactful.
My final point is this: nephrology is a specialty where I believe the NHS approach works well. There’s very little private medicine in nephrology. We can’t have long waiting lists because kidney function can decline quickly, and renal failure is an emergency. In general, care is delivered equally and promptly, which I think is a huge strength of the specialty.
Authors:
Lupus Vasculitis, a Rare Diagnosis and a Therapeutic Challenge: A Case Report
1. Nephrology Department, Centro Hospitalar Médio Tejo, Torres Novas, Portugal
*Correspondence to anaritap.ramos1996@gmail.com
Disclosure: The authors declared no conflicts of interest.
Acknowledgements: The authors would like to express their gratitude to the Renal Morphology department of Centro Hospitalar de Lisboa Central for providing the Figures.
Background: More than 50% of patients have renal involvement in systemic lupus erythematosus (SLE) and may present different patterns according to glomerular, tubulointerstitial, and vascular involvement. Lupus vasculitis (LV), the least frequent renal vascular lesion encountered in SLE, is a serious clinicopathological entity rarely described, and its therapeutic guidelines are not formally defined.
Case presentation: The authors present a case of a 44-year-old woman with SLE admitted to the hospital with a history of general tiredness, worsening of polyarthralgia, hypertension, oedema, and chest pain with new kidney failure, hematuria, and proteinuria. A kidney biopsy was performed, establishing the diagnosis of Class IV lupus nephritis associated with LV, and intravenous cyclophosphamide was started according to the CYCLOPS protocol. She developed orthopnoea associated to peripheral oedema, leading to a diagnosis of lupus myocarditis, and the treatment was adjusted to mycophenolate mofetil with rituximab, resulting in the resolution of symptoms.
Conclusion: LV is a rare condition, and there are no consensus or protocol guidelines for the treatment of this pathology, whose severity requires an emerging diagnostic and therapeutic approach.
Key Points
1. Lupus vasculitis (LV) is a rare but severe manifestation of systemic lupus erythematosus, significantly influencing prognosis and requiring urgent diagnostic and therapeutic interventions.
2. This case report presents a 44-year-old patient with Class IV lupus nephritis and associated LV, managed with cyclophosphamide, rituximab, and mycophenolate mofetil.
3. Recognising and managing LV is critical, as it poses unique diagnostic and therapeutic challenges, necessitating tailored, multidisciplinary approaches to improve patient outcomes.
INTRODUCTION
More than 50% of patients with systemic lupus erythematosus (SLE) develop lupus nephritis (LN) during the disease, which may manifest with various patterns involving the glomerular, tubulointerstitial, and vascular involvement. It is estimated that around 10–40% of patients with LN present vascular lesions on renal biopsy, which often serve as a marker of poor prognosis.1-3
Despite several morphological patterns that have been identified, LV is characterised by the rarity of the histological pattern found, limited descriptions in the literature, and its severity, which requires an urgent diagnostic and therapeutic approach. LV is marked by an inflammatory infiltrate of neutrophils and mononuclear leukocytes of the intima and media of the vessels, with fibrinoid necrosis and rupture of the elastic lamellae on optical microscopy. In immunofluorescence there is strong staining for antigens related to fibrin in the vascular wall, with weak and variable staining for immunoglobulins and complement.1,2,4 The treatment of LN depends on the histological class identified in the renal biopsy and is primarily focused on addressing glomerular pathology. However, there is no consensus regarding the therapeutic approach to LV.1,4
CASE REPORT
The authors present a 44-year-old woman with a personal history of SLE diagnosed in 2018 with joint, skin, haematological, and serous involvement usually medicated with prednisolone (5 mg daily) and hydroxychloroquine (400 mg daily), without kidney function changes (serum creatinine: 0.8–1 mg/dL) or in the urine test.
She presented to the hospital in January 2023 due to general fatigue, worsening of polyarthralgia, hypertension, generalised morning oedema, and chest pain with pleuritic characteristics that had been ongoing for a month. On physical examination, she was hypertensive, tachycardic, exhibited marked peripheral oedema, and had decreased breath sounds at the lung bases. Laboratory findings indicated anaemia (haemoglobin: 7.7 g/ dL), worsening of kidney function (urea: 108 mg/dL; serum creatinine: 3.2 mg/dL), and urine analysis revealed haematuria and proteinuria, with urinary sediment showing 39 erythrocytes/field with dysmorphic erythrocytes and 24 leukocytes/field, proteinuria 4.9 g/24h, and albuminuria 3 g/24h. Immunological studies highlighted complement consumption (C3: 25.8 mg/ dL; C4: 2.7 mg/dL; C1q: 2.6 mg/dL), positive antinuclear antibodies (1/1280), positive anti-dsDNA antibodies (576.25 IU/mL), and negative antineutrophil cytoplasmic antibodies, as shown in Table 1
The kidney ultrasound revealed no significant changes, while the chest CT and echocardiogram showed bilateral pleural effusion and pericardial effusion with preserved systolic function, respectively.
LN was assumed to be probable, and intravenous methylprednisolone pulses (500 mg for 3 consecutive days) were administered, followed by prednisolone (1 mg/kg/day). After achieving clinical and analytical stabilisation, a kidney biopsy was performed (Figures 1 and 2), revealing the following:
• Optic microscopy with nine glomeruli, of which two with global sclerosis, six with crescents (five cellular and one fibrocellular), with rupture of the capsule, carriorexis, endocapillary
Table 1: The patient's laboratory results at admission.
Peripheral blood smear
White blood cell count, red blood cell count, and platelets were normal. Schistocyte screening was negative.
2: Fibrinoid necrosis and transmural inflammatory infiltrate in lupus vasculitis.
Silver staining, 50x magnification.
Figure
proliferation with polymorphonuclear cells, and subendothelial deposits (wire loops). Interstitium with intense global infiltrate and a band of interstitial haemorrhage. Two medium-sized arteries, one with fibrinoid necrosis of the wall and intense transmural inflammatory infiltrate with abundant polymorphonuclear cells surrounding the artery, and the other with mononuclear infiltrate.
• Immunofluorescence with mesangioparietal glomerular deposits of IgG++, IgM++, C3++, C1q+, Kappa++, and Lambda++. Circumferential fibrinogen deposition in the wall of a medium-sized artery. Test for negative amyloid substance.
A diagnosis of Class IV LN was established, with an activity index of 21/24 and chronicity index of 1/12 associated with LV. Intravenous cyclophosphamide (CYC) treatment, adjusted to the patient’s age and kidney function (12.5 mg/kg), was initiated following CYCLOPS protocol. However, there was a progression of kidney damage (urea: 157 mg/dL; creatinine: 4 mg/dL) despite improvement in proteinuria (7.2 g/24h), resolution of anaemia, decrease in anti-dsDNA (108 IU/mL), and increase in complement (C3: 50.7 mg/dL; C4: 12.8 mg/ dL; C1q: 22.4). After completing the fourth cycle of CYC (cumulative dose of CYC: 2,750 mg), the patient began to experience new generalised fatigue, orthopnoea, and worsening of peripheral oedema. An echocardiogram was performed, which revealed new-onset impaired global systolic function with an estimated left ventricular ejection fraction of 43% along with elevated levels of B-type natriuretic peptide (>10,000 pg/mL). A CT angiography was performed, excluding acute coronary syndrome. Subsequently, cardiac magnetic resonance and PET scans were conducted, both highly suggestive of lupus myocarditis, leading to the decision to omit myocardial biopsy. After a multidisciplinary discussion, immunossupressive treatment was adjusted to mycophenolate mofetil (3 g/day) and rituximab (1 g, two administrations at 15-day intervals). Nine months after presentation, patient reassessement exhibited resolution
of symptoms, improvement in kidney function (serum creatinine: 2.9 mg/dL, proteinuria: 2g/24h), and cardiac imaging and laboratory tests also showed significant improvement of cardiac dysfunction.
DISCUSSION
LN can present various histological patterns depending on disease activity and kidney involvement, which influence the clinical presentation and dictate the appropriate therapeutic approach. Thus, kidney biopsy plays a crucial role in characterising the disease and defining therapeutic and prognostic criteria.5
Given the predominant vascular involvement with marked disease activity, and the absence of consensus guidelines or randomised studies regarding the treatment of LV, considering the severity of the disease, it was decided to initiate immunosuppression with higher doses of CYC, in accordance with the protocol CYCLOPS, rather than following the treatment recommended for LN Class III/IV according to the EuroLupus protocol.5,6 It’s important to note that, in this case, drawing any conclusions regarding the effectiveness of the chosen treatment is challenging due to the necessity of changing therapy given the course of the disease.
It is worth emphasising that the measurement of antineutrophil cytoplasmic antibodies was negative. Although these antibodies are mainly associated with primary vasculitis, they can also be associated with vasculitis secondary to systemic connective tissue diseases. It is crucial to consider these overlapping conditions to avoid misdiagnosis.6
During treatment with CYC, the patient developed heart failure, prompting consideration of various aetiologies. Among the differential diagnoses, cyclophosphamide toxicity was deemed unlikely due to the cumulative dose being below the cardiotoxic range. Additionally, the temporal association between the worsening of left ventricular dysfunction and the renal disease flare
suggested a different underlying cause. The imaging findings were not indicative of cyclophosphamide toxicity, as there was no restrictive pattern observed, and the left ventricular function appeared to normalise within 1 week under immunosuppressive therapy. Ischaemic heart disease was also considered; however, coronary angiography did not reveal any abnormalities consistent with thisa etiology. The findings documented on cardiac MRI fulfilled the modified Lake Louise criteria, further supported by evident myocardial inflammation observed
References
1. Kaul A et al. Vasculitis and vasculopathy in lupus nephritis: clinical variability, outcome, and new insight into treatment. Saudi J Kidney Dis Transpl. 2017;28(2):415-24.
2. Descombes E et al. Renal vascular lesions in lupus nephritis. Medicine (Baltimore). 1997;76(5):355-68.
3. Appel GB et al. Renal vascular complications of systemic lupus
on PET imaging, rendering myocardial biopsy unnecessary. In this context, treatment with mycophenolate mofetil was initiated in combination with rituximab, which according to guidelines should be considered in patients with persistent active disease or consecutive flares.7
Therefore, it is imperative to recognise the vascular component of lupus in clinical practice and to encourage further research into the therapeutical management of this serious and rare clinical entity.
erythematosus. J Am Soc Nephrol. 1994;4(8):1499-515.
4. Kidney Disease: Improving Global Outcomes (KDIGO) Lupus Nephritis Work Group. KDIGO 2024 Clinical Practice Guideline for the management of lupus nephritis. Kidney Int. 2024;105(1S):S1-69.
5. de Groot K et al., European Vasculitis Study Group (EUVAS). Pulse versus daily oral cyclophosphamide for
induction of remission in antineutrophil cytoplasmic antibody-associated vasculitis: a randomized trial. Ann Intern Med. 2009;150(10):670-80.
6. Leone P et al. Lupus vasculitis: an overview. Biomedicines. 2021;9(11):1626.
7. Urzua F et al. Cardiac imaging in myocarditis: current evidence and future directions. Can Assoc Radiol J. 2023;74:147-59.
Sarcoidosis Case with Acute Renal Failure, Nephrolithiasis, and Hypercalcaemia After Uncontrolled D3 Vitamin Supplementation
Authors: Ali Bakan,1 *Hatice Zeynep Ceylan,1 Ali Fuad Durusoy,2 Sina Ercan2
1. Department of Internal Medicine, Yeditepe University Hospital, Tesvikiye, Türkiye
2. Department of Thoracic Surgery, Yeditepe University Hospital, Tesvikiye, Türkiye
*Correspondence to zeynep.ceylan@yeditepe.edu.tr
Disclosure: The authors have declared no conflicts of interest.
Sarcoidosis is a multisystemic disorder of unknown aetiology, characterised by fibrosis and non-necrotising granuloma deposition. Typical presentation includes bilateral hilar adenopathy, skin, eye and articular lesions, pulmonary nodules, serum hypercalcemia, and nephrolithiasis. The authors’ case presented with hypercalcaemia and kidney stones after exogenous vitamin D use, who subsequently was diagnosed with sarcoidosis. Granulomatous diseases like sarcoidosis account for less than 10% of all hypercalcemia cases, and 10–20% of all sarcoidosis patients present with nephrolithiasis. The mechanism of nephrocalcinosis is related to vitamin D and calcium metabolism. Interferon gamma (IF-γ) and IL-2 are released from macrophages activated by T cells. Extrarenal 1-alpha hydroxylation occurs in granulomas, leading to elevation of active 1,25(OH) vitamin D. This causes increased intestinal calcium absorption and osteoclast activity, while tubular reabsorption of calcium decreases due to secondary parathyroid hormone suppression. Vitamin D replacement in this group is a controversial issue. Patients with multisystemic sarcoidosis are usually treated with intravenous methylprednisolone, which increases the risk of bone fractures. However, supplying vitamin D may also worsen hypercalcaemia in patients with sarcoidosis. Previous research indicates vitamin D supplementation may be given in select cases, if the 25-OH levels are low and sarcoidosis is in remission. In conclusion, serum calcium, 24-hour calcium, vitamin D levels, and disease activity should be monitored in patients with sarcoidosis who receive vitamin D supplementation.
Key Points
1. The case describes a patient who presented with severe hypercalcaemia and acute kidney injury. She was on exogenous vitamin D supplements. The patient was diagnosed with sarcoidosis. Haemodialysis was initiated, and steroid therapy was commenced. Nine months into therapy, her calcium and kidney function markers were in their normal range.
2. Sarcoidosis that presents with hypercalcaemia may worsen with Vitamin D supplementation. Therefore, Vitamin D supplements should not be prescribed without a clear deficiency.
3. In some cases, vitamin D may be prescribed to patients with sarcoidosis, especially those receiving steroid treatment. However, 24-hour calcium and parathyroid hormone levels must also be monitored in these patients.
INTRODUCTION
Sarcoidosis is a multisystemic disorder, characterised by fibrosis and nonnecrotising granuloma deposition of unknown aetiology. The worldwide incidence is approximately 60/100,000, and this number is estimated to be 4/100,000 in Türkiye.1,2 The female/male ratio of incidence in systemic sarcoidosis is estimated to be 2:1.1,2 The cases are more frequent between 2–6 years of age, half of the cases being above the age of 40 years. Typical findings include bilateral hilar adenopathy; skin, eye, and articular lesions; and pulmonary nodular opacities. Hypercalcaemia and kidney stones related to granulomatosis are frequently encountered. The authors’ case is a sarcoidosis patient who presented with severe hypercalcaemia and acute kidney injury (AKI). She had been using vitamin D3 supplements for 3 years during the COVID-19 pandemic. This case presentation hopes to add to the existing evidence on the effect of vitamin D3 supplementation on sarcoidosis-related hypercalcaemia, as well as arguing against uncontrolled use of vitamin supplements.
CASE PRESENTATION
Initial Presentation
A 63-year-old woman presented to the authors’ nephrology outpatient clinic with nausea, vomiting, and weight loss of 24 kg over 2 years. She was on amlodipin 10 mg/ day for essential hypertension, and her blood pressure was within normal range. She had also been using sublingual Vitamin D3-K2 10 puffs/day during and after the COVID-19 pandemic.
Diagnostic Workup
Biochemical studies revealed a creatinine level of 4.7 mg/dL, glomerular filtration rate (GFR) of 10 mL/min/1.73 m2, a serum calcium (Ca) of 14.6 mL/dL, serum phosphorus (PO4) of 3.3 mg/dL, parathyroid hormone (PTH) of 14.59 pg/mL, and 25-hydroxy vitamin D (25(OH)D) level of 52.95 ng/mL. Her initial laboratory studies (Table 1) were significant for AKI and severe hypercalcaemia (Table 1), the calcium level in 24-hour urine was measured as 539 mg/ day (reference: 100–320 mg/day), and urine total protein was measured as 479 mg/day.
A urinary system ultrasonography was ordered. Both kidneys were normal in size. In the right kidney, on the level of the right renal pelvis, there was a 13 mm calculous image with a hyperechogenic acoustic shadow. In the right kidney, the renal pelvis revealed Grade 1–2 ectasia, the anteroposterior diameter being 16 mm (Figure 1). In her abdominal CT, Grade 1–2 hydronephrosis in her right kidney was demonstrated. Kidney stones up to 15 mm in her renal pelvis were noted (Figure 1).
Hospitalisation
The patient was promptly admitted to the hospital due to acute kidney injury and severe hypercalcaemia. Her Vitamin D supplement was immediately discontinued due to kidney stones and hypercalcaemia, which did not respond to hydration and furosemide therapy. Haemodialysis with a temporary jugular venous catheter was initiated.
Further Studies
Several studies were performed to screen for a malignancy considering high calcium in the setting of low parathyroid hormone. Results for antinuclear antibody (ANA), antineutrophil cytoplasmic antibody (ANCA), complement,
Table 1: The biochemical parameters at presentation.
thyroid-stimulating hormone (TSH), and angiotensin-converting enzyme (ACE) were all found to be within normal limits (Table 1). In the serum immune electrophoresis, the IgA was 347 mg/dL, IgM was 115 mg/dL, IgG was 960 mg/dL, serum free Kappa light chain level was 58 mg/L, and serum free Lambda light chain level was 102 mg/L (Figure 2). No plasma cell dyscrasia was found in the bone marrow biopsy. The overall findings were not found to be significant for monoclonal gammopathies.
The laboratory testing for multiple myeloma, HIV, and hepatitis all came back negative.
In her PET/CT and posteroanterior chest X-ray, enlarged lymph nodes, the largest being 23x14 mm in the mediastinum, paravascular, bilateral paratracheal, and bilateral hilar spaces were observed (Figure 3). The X-ray also revealed diffuse reticulonodular opacities at this time. A mediastinoscopic lymph node biopsy was performed by thoracic surgery. Diffuse fibrosis with non-necrotising granulomatous inflammation was observed. Occasional CD20+ lymphoid follicules, CD3+ lymphocytes, and CD68+ histiocytes
were present; Ki-67 was 5%. No malignant involvement was found, and the findings were reported to be consistent with sarcoidosis.
Treatment and Follow-Up
Methylprednisolone 1 mg/kg was initiated, then gradually tapered down to 5 mg/day over a 1-month period. In the follow-up of 9 months after her treatment was initiated, serum creatinine level was 1.9 mg/dL, e-GFR was 26 mL/min/1.73 m2, BUN was 36 mg/ dL, the serum calcium level was 10.4 mg/dL, PO4 level was 3.3 mg/dL, PTH was 55.61 pg/mL, and proteinuria of 30 mg/day (Table 2). The hilar adenopathy was no longer observed on the chest X-ray (Figure 4).
DISCUSSION
Sarcoidosis was first discovered in 1877 as a granulomatous disorder affecting multiple systems, the cause of which was unknown. The characteristic marking was the presence of noncaseating granulomas, observed most frequently in the lungs and the hilar lymph nodes.
Figure 2: Serum immunoelectrophoresis.
Alpha 1 Alpha 2
Beta 1 Beta 2 Gamma
Albumin
Figure 1: Urinary ultrasonography at presentation.
3: PET/CT before treatment, showcasing bilateral hilar lymphadenopathy.
Figure
Figure 4: Chest X-Ray before (left) and after (right) treatment.
Table 2: Biochemical parameters after 9 months of treatment.
In sarcoidosis, direct renal involvement is seen rarely, but progression can lead to irreversible end-stage renal failure. Since epidemiology data come from small case series with up to 60 patients, the exact incidence of renal sarcoidosis remains unknown.7,11 It has a wide spectrum of presentation, including abnormal calcium metabolism, nephrolithiasis, nephrocalcinosis, and acute tubulointerstitial nephritis with or without granulomas.9,16 Non-granulomatous tubulointerstitial nephritis is the most common histological entity (44%), followed by granulomatous interstitial nephritis (30%), IgA-GN (26%), and nephrocalcinosis (11%).17 Some of the rare manifestations include amyloid A amyloidosis, urinary tract obstruction with renal masses, and glomerular diseases such as membranous nephropathy, IgA nephropathy, minimal change disease, proliferative or crescentic glomerulonephritis, and focal segmental glomerulosclerosis. The presentation of renal sarcoidosis would vary according to the underlying pathology.18-20 Sarcoid-related interstitial nephritis is usually identified as
the initial presentation of sarcoidosis and rarely develops among patients who have a longstanding diagnosis of sarcoidosis.13
Kidney stones occur in 10–20% of patients with chronic sarcoidosis. Other studies report an incidence between 6–12%. Kidney stones are thought to peak in Caucasian men between the ages of 40–60 years. Kidney stones are the first finding in 1% of patients with sarcoidosis, and nephrolithiasis is asymptomatic in 2–7% of patients diagnosed with sarcoidosis. However, the risk of progressive kidney damage is increased in sarcoidosis patients with nephrocalcinosis.5 Hypercalcaemia occurs in about 10–20% of patients with sarcoidosis,21,22 while hypercalciuria is more frequent.23-25 The over production of 1,25-(OH)2D depends on the activity of the enzyme 1-alpha hydroxylase, which is expressed in pulmonary alveolar macrophages trapped in granulomatous inflammation and is stimulated by IFNgamma.22,26 As a result, 1,25-(OH)2D levels in sarcoidosis are directly related to the availability of its substrate, 25-hydroxy vitamin D. 1,25-(OH)2D vitamin D stimulates
bone reabsorption by increasing osteoclast activity, augments calcium absorption in the gastrointestinal tract, and increases renal tubular calcium reabsorption.23,27 Since the activity of 1-alpha hydroxylase is refractory to normal negative feedback mechanisms,20 this leads to a progressive increase of calcium in plasma. The consequent suppression of PTH by direct and indirect mechanisms, coupled with an increased renal calcium load, results in the development of hypercalciuria.23,28 Hypercalcaemia causes reduction of GFR and enhances sodium excretion through the inhibition of sodium–potassium ATP-ase, with consequent depletion of total body water, leading to increased bicarbonate reabsorption and metabolic alkalosis.29,30 As a result, calcium reabsorption in the distal nephron increases, aggravating the hypercalcaemia.29 Moreover, hypercalcaemia may be responsible for tubular dysfunction and damage, and for AKI caused by vasoconstriction of afferent arterioles.28,29 In the acute phase, the consequences of hypercalcaemia and hypercalciuria are reversible.27 Nephrocalcinosis, a diffuse calcification of the kidney parenchyma, is the result of prolonged hypercalciuria and is less frequent than nephrolithiasis, the presence of calcium-rich kidney stones.24-32 Renal biopsy can reveal nephrocalcinosis in the initial stages, showing calcium deposits of either calcium phosphate or calcium oxalate.35Severe hypercalcaemia is defined as a calcium level of 14 mg/dL, or 3.5 mmol/L and higher, and an ionised calcium level of 10 mg/dL or 2.5 mmol/L or higher. Primary hyperparathyroidism and malignancy constitute 90% of all hypercalcaemia cases. In the differential diagnosis, granulomatous diseases, including sarcoidosis, tuberculosis, or cat-scratch disease; endocrine disorders like hyperthyroidism; genetic diseases; immobilisation; use of thiazide diuretics; and exogenous use of calcium, vitamin D, or vitamin A supplements should be evaluated. SGLT-2 inhibitors, immune checkpoint inhibitors, discontinuation of RANKL inhibitors such as denosumab, ketogenic diet, SARS-CoV-2 infection, and excessive exercise cause less than 1% of all hypercalcaemia cases. PTH is the first consideration in the differential diagnosis of hypercalcaemia. A high or normal level
indicates primary hyperparathyroidism, and a lower level of PTH (<20 pg/mL) indicates a different etiology.36
The mechanism of nephrocalcinosis appears to be linked with vitamin D and calcium metabolism. In granulomatous diseases, interferon-γ (IF-γ) and IL-2 are released from macrophages activated by T cells. Extrarenal 1-alpha hydroxylation occurs in granulomas, leading to elevation of active 1,25(OH)2D. Increased levels of calcitriol cause increased intestinal calcium absorption and osteoclast activity. While calcium filtration increases at the glomerular level, tubular reabsorption of calcium decreases due to PTH suppression.37
Vitamin D is a fat-soluble hormone that has endocrine, paracrine, and autocrine functions. Consumption of vitamin D-supplemented food and drugs has increased significantly since the COVID-19 pandemic. Despite such wide use of artificial vitamin D supplements, the serum level of 25-hydroxyvitamin D does not always reflect the amount of uptake. In contrast to the safe sunlight exposure, prolonged and disproportionate consumption of vitamin D supplements may lead to vitamin D intoxication, even without developing hypervitaminosis D. The reason why vitamin D supplementation is believed to be safe is that even repeated intravenous ingestion of extremely high doses of synthetic vitamin D analogs raise serum vitamin D levels to the toxic range. However, prolonged consumption of vitamin D supplementation may induce hypercalcaemia, hypercalciuria, and hyperphosphatemia, which are considered to be the initial signs of vitamin D intoxication. It is likely that calcium and phosphorus dysregulation, induced by exogenous vitamin D supplementation, leads to tissue and organ damage, even without developing hypervitaminosis.38 Vitamin D replacement remains a controversial issue. In a cohort study conducted with 104 patients, the risk of hypercalcaemia was found to be higher in the patient group not given vitamin D supplementation.39 However, since glucocorticoids are frequently used in patients with sarcoidosis, there is also a risk of skeletal fractures. Administration of exogenous inactive vitamin D supplements
is advised to prevent the risk of fractures in patients using glucocorticoids. In a study conducted on 142 patients, 23.5% of the patients had at least one fracture, and the mean age was 51 years. In addition to glucocorticoid exposure, low calcium consumption and 25(OH)D levels higher than 20 ng/mL and lower than 10 ng/mL were found to be risk factors for fractures. Other studies have found that calcium replacement causes a greater increase in serum calcium in patients with sarcoidosis. It was concluded that vitamin D supplementation can be administered if the 25(OH)D levels were low and sarcoidosis was in remission.39
References
1. Arkema EV, Cozier YC. Sarcoidosis epidemiology: recent estimates of incidence, prevalence and risk factors. Curr Opin Pulm Med. 2020;26(5):527-34.
2. Demirel K, Korkmaz M. Sarkoidoz ve Amiloidozda Moleküler Görüntüleme. Nucl Med Semin 2018;4:133-44.
3. Walker MD, Shane E. Hypercalcaemia: A Review. JAMA. 2022;328(16):1624-36.
4. Zia Z et al. A rare case of renal sarcoidosis. Cureus. 2021;13(6):e15494.
5. Mio K et al. Hypercalcaemia worsened after vitamin D supplementation in a sarcoidosis patient: A case report. Medicine (Baltimore). 2022;101(40):e30883.
6. Osman O et al. Case report: Disease mechanisms and medical management of calcium nephrolithiasis in rheumatologic diseases.BMC Urology. 2023;DOI: 10.1186/s12894023-01203-y.
7. Statement on sarcoidosis. Joint Statement of the American Thoracic Society (ATS), the European Respiratory Society (ERS) and the World Association of Sarcoidosis and Other Granulomatous Disorders (WASOG) adopted by the ATS Board of Directors and by the ERS Executive Committee, February 1999. Am J Respir Crit Care Med. 1999;160:736-55.
8. Baughman RP et al.: Clinical characteristics of patients in a case control study of sarcoidosis. Am J Respir Crit Care Med. 2001, 164:1885-19.
CONCLUSION
The aetiology of the hypercalcaemia in the authors’ patient appears to be the increased rate of conversion of the exogenous inactive 25(OH)D vitamin supplement into the active 1,25(OH)2D, due to increased activity of the 1-alpha-hydroxylase enzyme as a result of granulomatous disease. Moreover, clinicians and patients must be aware that inactive vitamin D serum levels may not always reflect adverse effects of excessive vitamin D use. Therefore, if exogenous vitamin D is supplemented in a patient with sarcoidosis for any reason, disease activity, serum calcium levels, and 24hour urinary calcium levels need to be closely monitored, as opposed to simply monitoring 25(OH)D levels alone.
9. Casella FJ, Allon M. The kidney in sarcoidosis. J Am Soc Nephrol. 1993;3:1555-62.
10. Dahl K et al. A 56-year-old woman with sarcoidosis and acute renal failure. Kidney Int. 2008;74:81721.
11. Goldszer RC et al. Glomerulonephritis in a patient with sarcoidosis. report of a case and review of the literature. Arch Pathol Lab Med. 1981;105:478-81.
12. Mahévas M et al. Renal sarcoidosis: clinical, laboratory, and histologic presentation and outcome in 47 patients. Medicine. 2009;88:98-106.
13. Singer DR, Evans DJ: Renal impairment in sarcoidosis: granulomatous nephritis as an isolated cause (two case reports and review of the literature). Clin Nephrol. 1986;26:250-6.
14. Bergner R et al. Frequency of kidney disease in chronic sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 2003;20:126-32.
15. Baughman RP et al. Clinical characteristics of patients in a case control study ofsarcoidosis. Am J Respir Crit Care Med. 2001;164:1885-9.
16. Löffler C et al. Renal sarcoidosis: epidemiological and follow-up data in a cohort of27 patients. Sarcoidosis Vasc Diffuse Lung Dis. 2015;31:306-15.
17. Casella FJ, Allon M. The kidney in sarcoidosis . J Am Soc Nephrol. 1993;3:1555-62.
18. Dahl K et al. A 56-year-old woman with sarcoidosis and acute renalfailure. Kidney Int. 2008;74:817-21.
19. Goldszer RC et al. Glomerulonephritis
in a patient with sarcoidosis. Report of a case and review of the literature. Arch Pathol Lab Med. 1981;105:478-81.
20. Lower EE and Baughman RP, “The calcium–kidney–bone axis in sarcoidosis,” Baughman RP, Lower EE (eds.), Sarcoidosis (2022) 1st edition, Sheffield: European Respiratory Society, pp.193–205.
21. O.P. Sharma. Hypercalcaemia in granulomatous disorders: a clinical review. Curr Opin Pulm Med. 2000;5(5):442-7.
22. Baughman RP, Papanikolaou I. Current concepts regarding calcium metabolism and bone health in sarcoidosis. Curr Opin Pulm Med. 2017;23(5):476-81.
23. Cameli P et al. Hypercalciuria in sarcoidosis: a specific biomarker with clinical utility. Front Med. 2020;7:568020.
24. Cameli P et al. The role of urinary calcium and chitotriosidase in a cohort of chronic sarcoidosis patients. Respiration. 2020;99(3):207-12.
25. Monkawa T et al. Identification of 25-hydroxyvitamin D3 1alphahydroxylase gene expression in macrophages. Kidney Int. 2000;58(2):559-68.
26. Hilderson I et al. Treatment of renal sarcoidosis: is there a guideline? Overview of the different treatment options. Nephrol Dial Transplant. 2014;29(10)1841-7.
27. Berliner AR et al. Sarcoidosis: the nephrologist’s perspective. Am J Kidney Dis. 2006;48(5):856-70.
28. Felsenfeld AJ, Levine BS. Milk alkali syndrome and the dynamics of calcium homeostasis. Clin J Am Soc. Nephrol. 2006;1(4):641-54.
29. Aghsaeifard Z, Alizadeh R. Two-way road of kidney and hypercalcaemia: a narrative review, Cardiovasc Hematol Disord Drug Targets. 2023;22(4):200-6.
30. Calatroni M et al. Renal sarcoidosis. J Nephrol. 2023;36(1):5-15.
31. Bergner R, Loffler C. Renal sarcoidosis: approach to diagnosis and management. Curr Opin Pulm Med. 2018;24(5):513-20.
32. Wachtell K et al. Nephrocalcinosis and urolithiasis as primary symptoms in
Boeck’s sarcoidosis. Ugeskr Laeger. 1996;158 (12):1685-6. (In Danish).
33. Rizzato G, Colombo P. Nephrolithiasis as a presenting feature of chronic sarcoidosis: a prospective study. Sarcoidosis Vasc Diffuse Lung Dis. 1996;13(2):167-72.
34. Correia F et al. Renal manifestations of sarcoidosis: from accurate diagnosis to specific treatment. Int Braz J Urol. 2020;46 (1):15-25.
35. Walker MD, Shane E. Hypercalcaemia: a review. JAMA. 2022;328(16):1624-36.
36. Mio K et al. Hypercalcaemia worsened after vitamin D supplementation
in a sarcoidosis patient: A case report. Medicine (Baltimore). 2022;101(40):e30883.
37. Mohammed S Razzaque. Can adverse effects of excessive vitamin D supplementation occur without developing hypervitaminosis D?. Review. J Steroid Biochem Mol Biol. 2018;180:81-6.
38. Kamphuis LS et al. Calcium and vitamin D in sarcoidosis: is supplementation safe?. J Bone Miner Res. 2014;29(11):2498-503.
39. Saidenberg-Kermana N et al. Vitamin D supplementation in patients treated for sarcoidosis: controversy or consensus?. Joint Bone Spine. 2017;84(5):521-3.