10 A Year in Review from the American Thoracic Society (ATS) 2025
International Conference
Reid Eggleston
15 Congress Highlights
Congress Features
23 Highlighting Research and Advocacy Efforts on Electronic Nicotine Delivery Systems at the ATS International Conference 2025
Sophia Karandashova
27 Redefining Respiratory Support: Insights from ATS 2025 on the Future of Mechanical Ventilation
Jose A. Meade-Aguilar
Symposium Review
30 Beyond the Lungs: Addressing Cardiopulmonary Risk in COPD
Poster Review
36 Exploring the Clinical and Economic Impact of Non-Cystic Fibrosis
Bronchiectasis
Abstract Reviews
42 Post-sepsis Viral Infection Risk in Patients with COPD
Chuang and Chao
45 Effectiveness of Bronchoscopic Lung Volume Reduction in COPD
Nicholson et al.
48 Invasive Pulmonary Aspergillosis in Lung Transplant Recipients
Patel et al.
50 Impact of Inhaled Tobramycin on Healthcare Utilization and Morbidity
Alabdulkarim et al.
52 Psychosocial and Social Factors in Lung Transplant Survival
Huang et al.
54 A Rare Case of BK Virus Pneumonia
Knight and Katkin
56 Amiodarone and Long-Term Survival After Lung Transplant
Lawson et al.
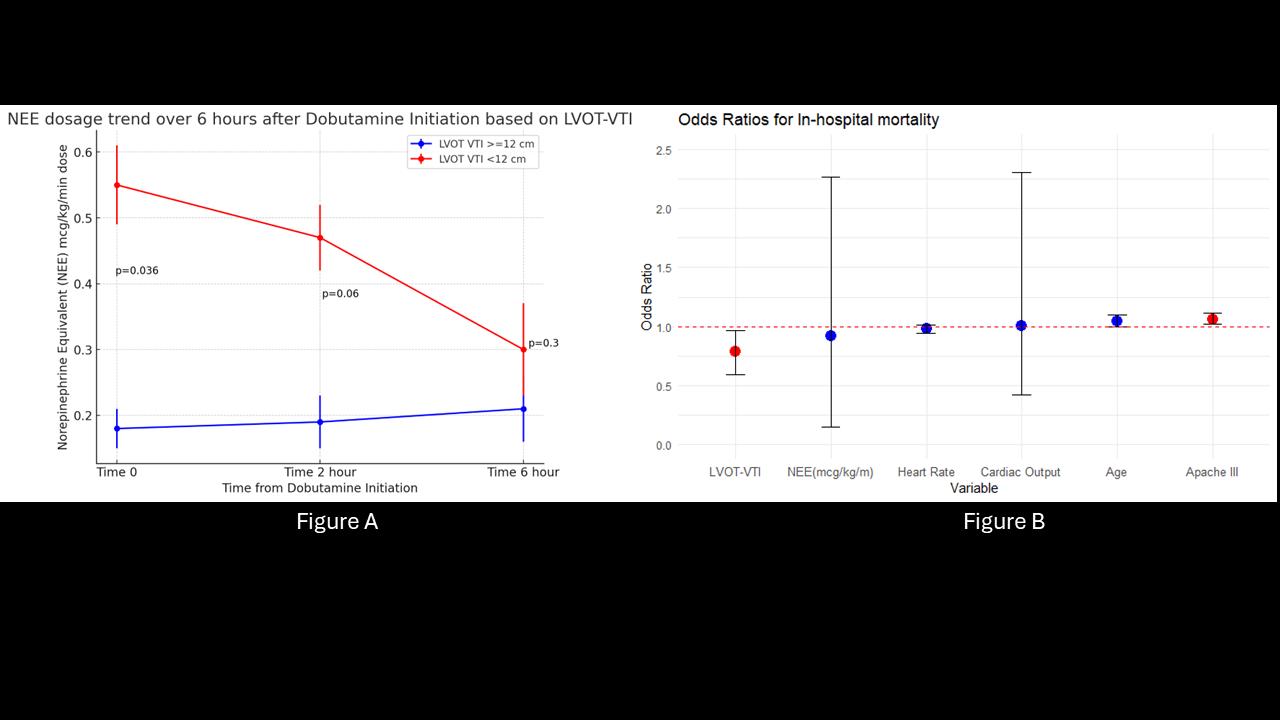
58 Inotropic Agents in Septic Shock
Tarbaghia et al.
60 The Sweet Hour: A Framework for Effective Journal Clubs in Graduate Medical Education
Nanah et al.
62 The Impact of HIV on the Severity of COVID-19 Infection
Arumairaj et al.
65 The Impact of COPD on the Severity of COVID-19 Infection
Arumairaj et al.
68 The Impact of CKD on the Severity of COVID-19 Infection
Arumairaj et al.
71 The Impact of Bronchiectasis on the Severity of COVID-19 Infection
Arumairaj et al.
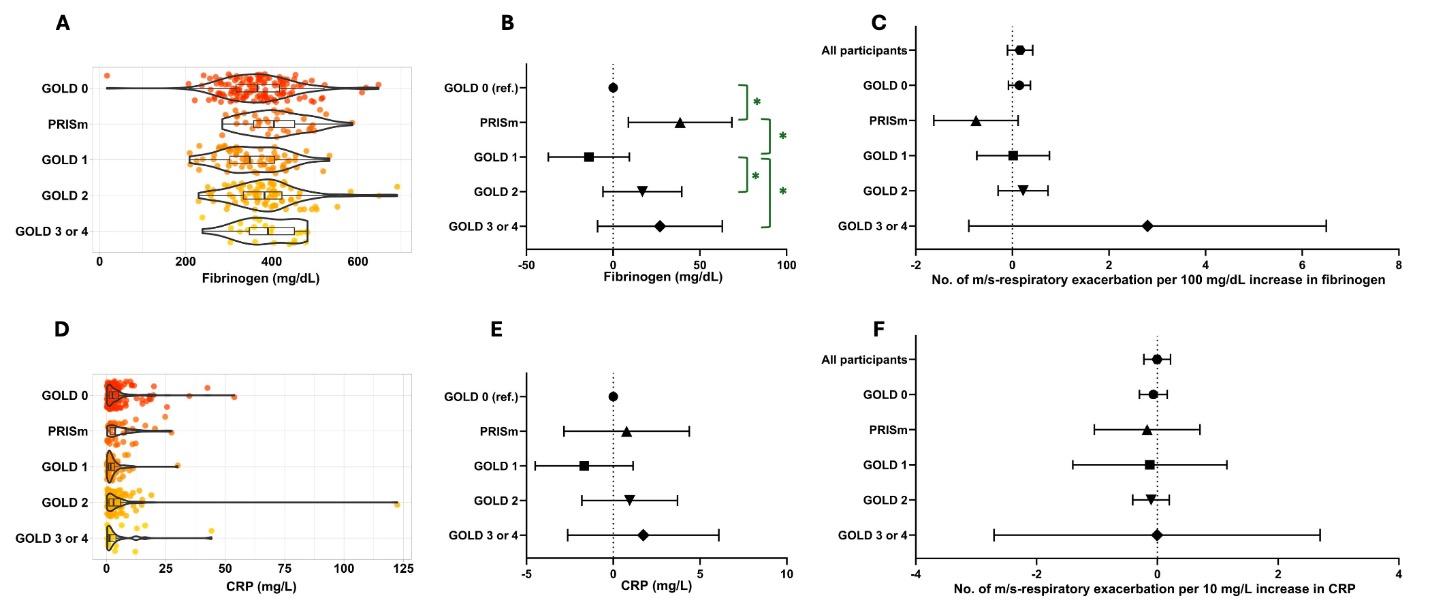
74 Plasma Fibrinogen as a Predictor of Disease Severity and Exacerbation
Abrham et al.
77 Diagnostic Metabolomic Profiling of COPD
Enríquez-Rodríguez et al.
Congress Interviews
80 Raed Dweik
83 Jesse Roman Interviews
86 Jonathan Bernstein
89 Todd Bull Articles
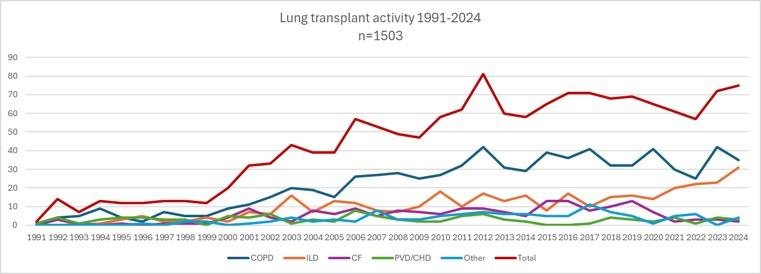
94 The Changing Landscape of Lung Transplantation
De Sadeleer et al.
105 Improving Latent Tuberculosis Screening Amongst Hospitalized Patients Undergoing Initiation of Immunosuppression: A Cross-Sectional Analysis
Ferland et al.
Editorial Board
Dr Kelly Pennington
Mayo Clinic, Minnesota, USA
Prof Laren Tan
Loma Linda University School of Medicine, California, USA
Dr Rohan Thompson
Indiana University, Indiana, USA
Dr Jacques Bouchard
Université Laval, Canada
Dr Jezreel Pantaleón García
The University of Texas MD Anderson Cancer Center, Texas, USA
Prof Michal Senitko
University of Mississippi Medical Centre, Mississippi, USA
Aims and Scope
AMJ Respiratory is an open-access, peer-reviewed eJournal committed to helping elevate the quality of healthcare in respiratory medicine by publishing high quality content on all aspects of lung function and respiratory diseases.
The journal is published annually, 6 weeks after the American Thoracic Society (ATS) International Conference, and features highlights from this congress, alongside interviews with experts in the field, reviews of abstracts presented at the congress, as well as in-depth features on congress sessions. Additionally, this journal covers advances within the clinical and pharmaceutical arenas by publishing sponsored content from congress symposia, which is of high educational value for healthcare professionals. This undergoes rigorous quality control checks by independent experts and the in-house editorial team.
AMJ Respiratory also publishes peer-reviewed research papers, review articles, and case reports in the field. In addition, the journal welcomes the submission of features and opinion pieces intended to create a discussion around key topics in the field and broaden readers’ professional interests. AMJ Respiratory is managed by a dedicated editorial team that adheres to a rigorous double-blind peer-review process, maintains high standards of copy editing, and ensures timely publication.
Our focus is on research that is relevant to all healthcare professionals in pulmonary medicine. We do not publish veterinary science papers or laboratory studies not linked to patient outcomes. We have a particular interest in topical studies that advance research and inform of coming trends affecting clinical practice in the respiratory field.
Editorial Expertise
AMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors are recognised authorities from their respective fields.
• Peer review, which is conducted by AMJ’s Peer Review Panel as well as other experts appointed due to their knowledge of a specific topic.
• An experienced team of editors and technical editors.
Peer Review
On submission, all articles are assessed by the editorial team to determine their suitability for the journal and appropriateness for peer review.
Editorial staff, following consultation with either a member of the Editorial Board or the author(s) if necessary, identify three appropriate reviewers, who are selected based on their specialist knowledge in the relevant area. All peer review is double blind.
Following review, papers are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected. Editorial staff have final discretion over any proposed amendments.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects.
We seek papers with the most current, interesting, and relevant information in each therapeutic area and accept original research, review articles, case reports, and features.
We are always keen to hear from healthcare professionals wishing to discuss potential submissions, please email: editorial@americanmedicaljournal.com
To submit a paper, use our online submission site: www.editorialmanager.com/e-m-j
Submission details can be found through our website: www.emjreviews.com/contributors/authors
Reprints
All articles included in AMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
AMJ is distributed through controlled circulation to healthcare professionals in the relevant fields globally.
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
This Publication Launch Date: 2023 Frequency: Yearly Online ISSN: 2976-7873
AMJ Respiratory is published once a year. For subscription details please visit: www.emjreviews.com
All information obtained by AMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, AMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. AMJ is completely independent of the review event (ATS 2025 International Conference) and the use of the organisations does not constitute endorsement or media partnership in any form whatsoever.
Katrina Thornber, Katie Wright, Aleksandra Zurowska
Creative Director
Tim Uden
Design Manager
Stacey White
Senior Designer
Owen Silcox
Creative Artworker
Dillon Benn Grove
Designers
Shanjok Gurung, Fabio van Paris
Senior Performance & Insight Lead
Darren Brace
Head of Marketing
Stephanie Corbett
Chief Executive Officer
Justin Levett
Chief Commercial Officer
Dan Healy
Founder and Chairman
Spencer Gore
Contact us
Welcome
Dear Readers,
Welcome to the latest issue of AMJ Respiratory. This publication is carefully curated to celebrate the key highlights from the American Thoracic Society (ATS) 2025 International Conference and the important matters in respiratory care right now.
ATS President Irina Petrache welcomed approximately 14,000 attendees to the meeting during the Opening Ceremony. She used an empty chair on stage to make visible the absence of peers who did not attend the meeting due to ongoing cuts to research and healthcare. This felt like a clear, stoic demonstration of leadership in an era of intersecting instability.
This issue covers public health, lung transplant survivorship, determinants of health, and post COVID-19 chronic disease risk patterns, and much more. Abstracts reviews and interviews with thought leaders encourage us to think about larger systemic themes in respiratory care and equity.
The fantastic articles include a review for transplant pulmonologists and readers involved in the care of patients with advanced lung disease. We are extremely proud to publish original research on optimizing latent tuberculosis infection screening in urgent inpatient immunosuppression.
I extend my sincerest thanks to the peer reviewers, Editorial Board, authors, interviewees, and editorial team for their ongoing support and guidance with this publication.
Permissions and copyright: accountsreceivable@emjreviews.com
Anaya Malik Vice President of Content
Reprints: info@emjreviews.com Media enquiries: marketing@emjreviews.com
We provoke conversation around healthcare trends and innovation - we also create engaging educational content for healthcare professionals. Join us for regular conversations with physician & entrepreneur, Jonathan Sackier. Listen Now
Foreword
Dear Colleagues,
I invite you to enjoy the latest issue of AMJ Respiratory, which celebrates this year’s American Thoracic Society (ATS) International Conference and bridges the gap between the live experience held in San Francisco, California, and your post-meeting takeaways.
The Conference provides a valuable opportunity to meet with colleagues from around the world, connect with one another, and learn about the latest literature and research shaping our field. The ATS sets the perfect stage for this each year, with a palpable buzz around the sessions, abstracts, workshops, debates, and numerous other formats organized by the Society. The global community continues to inspire longstanding experts and early-career professionals to drive innovation and progress in respiratory health.
Key themes that emerged this year included AI in respiratory care, lung transplant longevity, targeted gene therapies for cystic fibrosis, and the intersection between climate change and health. You will find each of the major topics from the Conference reflected in this issue’s curated content, which includes abstract reviews, expert-led features, and original articles.
Much like the collaboration of brilliant minds at ATS 2025, I’d like to thank my fellow Editorial Board members, peer reviewers, and contributors for their support in shaping this journal. I hope it offers insights, sparks discussion, and continues the conversation all year round.
You will find each of the major topics from the Conference reflected in this issue’s curated content, which includes abstract reviews, expert-led features, and original articles
Kelly Pennington Division of Pulmonary and Critical Care Medicine, Mayo Clinic,
Rochester, Minnesota, USA
ATS 2025
I think the greatest teachers of all are the patients we have a privilege to care for
Congress Review
A Year in Review from the American Thoracic Society (ATS) 2025 International Conference
Location: San Francisco, California, USA
Date: May 17th–21st 2025
Author: *Reid Eggleston1
1. Mayo Clinic, Rochester, Minnesota, USA
*Correspondence to Eggleston.Reid@mayo.edu
Disclosure: The author has declared no conflicts of interest.
Keywords:
American Thoracic Society (ATS) 2025, antibiotic de-escalation, asthma biologics, critical care trials, EGFR mutation, idiopathic pulmonary fibrosis, lung cancer diagnostics, narrative medicine, non-invasive ventilation, tumor, node, metasisis (TNM) staging.
Citation: Respir AMJ. 2025;3[1]:10-14.
https://doi.org/10.33590/respiramj/RHYT2481
THE American Thoracic Society (ATS) International Conference took place in San Francisco, California, USA, from May 17th–21st, 2025, with over 14,000 attendees from more than 100 countries represented. The conference opened with an address from Kimberly Manning, Grady Hospital, Emory University, Atlanta, Georgia, USA, who is renowned for her contributions to the burgeoning field of narrative medicine. “I think the greatest teachers of all are the patients we have a privilege to care for.” She shared the story of a patient hospitalized for severe pneumonia, who gave a very busy Manning this advice: “One person doing one thing for a person other than themselves goes further than you think.” It was against this backdrop of the impact that pulmonologists and intensivists have on the lives of their patients that ATS commenced. During the conference, several thought-provoking and sometimes practice-changing trials were introduced or reviewed, spanning content ranging from septic shock to lung cancer. Herein, we explore some of the highlights of these discussions.
ASTHMA/COPD
As in prior years, the use of biologic therapies for the treatment of airway disease was a hotly discussed topic.
Sanjay Ramakrishnan, University of Western Australia, Perth, Australia, pointed out that patients receiving treatment for an exacerbation of COPD are more often harmed, rather than helped, by courses of oral corticosteroids. The potential role of biologic therapy for such patients remains unexplored.
In light of this, Ramakrishnan and Lauren Eggert, Stanford University, California, USA, presented findings from ABRA, a multicenter, randomized placebo-controlled trial that assessed the effect of a one-time dose of subcutaneous benralizumab (100 mg) at the time of exacerbation on treatment failure and symptoms, in patients who had an elevated eosinophil count (≥300 cells/µL), compared to patients who received standard exacerbation treatment with prednisolone.1 The study included those with both COPD and asthma. The patients studied had severe airway disease, with a median of four exacerbations in the year prior and a baseline serum eosinophil count of 600 cells/µL. The primary outcome is the proportion of patients with treatment failure within 90 days, which favored patients who received benralizumab (cumulative incidence: 45%) compared to standard of care (cumulative incidence: 74%; hazard ratio: 0.39; 95% CI: 0.25–0.6; p=0.003). Eggert conceded that care should be taken in generalizing results to patients with milder asthma, due to the sample’s baseline disease severity.
Eggert also highlighted the knowledge gap in the treatment of patients who have tried and failed other forms of biologic therapy for asthma. She presented findings from the XALOC-1 observational study, which included a cohort that examined outcomes of patients receiving benralizumab for severe eosinophilic asthma after a transition from an alternate biologic medication.2 Most of the patients in this cohort had previously received mepolizumab, and experienced a 73% relative risk reduction in annualized exacerbation rate when switched to benralizumab.
I
think the greatest teachers of all are the patients we have a privilege to care for
LUNG CANCER
Practice-changing studies that touched on lung cancer included lung nodule diagnostics; a change in tumor, node, metastasis (TNM) staging for lung cancer; and the use of EGFRtargeting therapies for non-small cell lung cancer (NSCLC).
Laura Frye, University of Utah, USA, shared the results of the VERITAS trial, which compared the diagnostic yield of lung nodule biopsy for navigational bronchoscopy to CTguided transthoracic needle biopsy (TTNB).3 This randomized controlled noninferiority trial, conducted across multiple US sites, demonstrated no difference in yield between the two modalities (76% yield in both groups). However, complications were higher among those who underwent TTNB. Pneumothorax occurred in 3% of patients who underwent navigational bronchoscopy compared to 28% of those undergoing TTNB. Frye remarked that navigational bronchoscopy comes with the added benefit of simultaneous mediastinal lymph node staging versus TTNB.
Frye and Nina Thomas, University of Colorado, USA, also discussed a recent change in NSCLC diagnosis by TNM staging. The 9th edition TNM guidelines now specify that the N2 Stage has been split into N2a and N2b, where N2a includes patients with
cancer cells in a single N2 lymph node station, and N2b implicates involvement of multiple lymph node stations. This is important because having N2b disease can upstage a patient from clinical Stage IIB to IIIA, or from IIIA to IIIB, depending on T status. Such upstaging often results in a change in therapeutic strategy. Distant metastasis, represented by the M1c Stage, was also split: M1c1 indicates metastases are located within one organ, and M1c2 refers to metastases in multiple organs.
The use of tyrosine kinase inhibitors for treatment of EGFR mutation-positive lung cancer has revolutionized treatment outcomes for patients who qualify. Osimertinib is one such tyrosine kinase inhibitor with FDA approval for patients with resected Stage III NSCLC. Thomas presented results from the LAURA trial, which investigated the use of osimertinib in patients with unresectable Stage III EGFR+ NSCLC following chemotherapy and radiation.4 This trial showed a dramatic improvement in progression-free survival compared to placebo: 39 months versus 6 months (hazard ratio: 0.16; 95% CI: 0.10–0.24; p<0.001).
Thomas commented: “This highlights the importance of testing for these mutations during diagnostic staging and before the start of treatment.”
Keeping hemoglobin above 9 each day will benefit these patients
CRITICAL CARE
Several studies pertaining to the care of critically ill patients were introduced, of which three were potentially practice-changing.
Patrick Lyons, Oregon Health and Sciences University, Portland, Oregon, USA, presented two such studies. The first addressed hemoglobin transfusion thresholds in patients who are hospitalized with acute brain injury. Restrictive thresholds (transfusion
only when hemoglobin <7 mg/dL) have repeatedly shown benefit, compared to liberal thresholds, in several critically ill populations. However, patients with brain injury have not been well-represented in these studies. In the multicenter RCT, TRAIN, patients with traumatic brain injury, subarachnoid hemorrhage, and intraparenchymal hemorrhage had lower 6-month rates of unfavorable neurologic status by Glasgow Outcome Scale (10% absolute risk reduction; p=0.002), although there was no mortality benefit.5 Lyons’ takeaway: “Keeping hemoglobin above 9 [mg/dL] each day will benefit these patients.”
Lyons also shared the results from the PREOXI trial, which assessed whether pre-oxygenation in anticipation of emergent intubation with non-invasive ventilation (NIV) improved the risk of post-intubation desaturation, compared to pre-oxygenation with a non-rebreather mask.6 The multicenter pragmatic RCT demonstrated a 50% reduction in desaturation with NIV pre-oxygenation (absolute risk reduction: 9%; p<0.001) and no difference in gastric insufflation. Lyons mentioned that he has started using this approach in his clinical practice, as long as he has enough time to safely initiate NIV for a patient.
Lisa Torres, Weill Cornell Medicine, New York, USA, shifted the focus to antibiotic de-escalation in critically ill patients with infection. She summarized the results of the ADAPT-SEPSIS trial, a multicenter RCT that assessed an antibiotic de-escalation protocol based on daily procalcitonin (PCT) measurement initiated at the time of antibiotic commencement, to determine when antibiotics should be discontinued in patients with suspected sepsis.7 The primary outcome, which is the days of exposure to antibiotic, was lower in patients randomized to the PCT-guided protocol, albeit only by one day. There was no difference in mortality. Torres cautioned that this study did not assess the use of PCT to initiate antibiotics and thus, results should not be extrapolated to address that question.
INTERSTITIAL LUNG DISEASE
Ayodeji Adegunsoye, University of Chicago, Illinois, USA, shared several thoughtprovoking studies involving the care of patients with fibrotic lung disease, but perhaps the most anticipated were the FIBRONEER-IPF and FIBRONEER-ILD trials. These trials assessed the treatment effect of the oral PDE4 inhibitor, nerandomilast, in patients with idiopathic pulmonary fibrosis (IPF) and non-IPF progressive pulmonary fibrosis, respectively.8 Both trials included patients receiving antifibrotic therapies. The primary endpoint was change in forced vital capacity at one year, and both studies showed a reduction in forced vital capacity decline with nerandomilast: 69 ml between group difference in FIBRONEERIPF, and 67 ml difference in FIBRONEER-ILD (18 mg twice daily nerandomilast dose). Secondary endpoints also signaled a possible improvement in rate of exacerbation and death in patients receiving nerandomilast.
References
1. Ramakrishnan S et al. Treating eosinophilic exacerbations of asthma and COPD with benralizumab (ABRA): a double-blind, double-dummy, active placebo-controlled randomised trial. Lancet Respir Med. 2025;13(1):59-68.
2. Jackson DJ et al. Benralizumab in severe eosinophilic asthma by previous biologic use and key clinical subgroups: real-world XALOC-1 programme. Eur Respir J. 2024;64(1):2301-521.
BEAR-CAGE
Apart from the opportunity to share recent groundbreaking trial results, ATS also afforded attendees the opportunity to compete in the annual BEAR-cage competition. This event allows participants to pitch their ideas and inventions that are intended to solve a clinical issue pertaining to pulmonary and critical care medicine. This year’s winners, Yi-an Hsieh and Joshua Freedman, presented a prototype incentive spirometer that uses digital and customizable technology to improve patients’ adherence to the use of a spirometry device. For their win, Hsieh and Freedman received funding for their proposal and an additional cash prize.
3. Lentz RJ et al. Navigational bronchoscopy or transthoracic needle biopsy for lung nodules. N Engl J Med. 2025;392(21):2100-12.
4. Lu S et al. Osimertinib after chemoradiotherapy in stage III EGFR-mutated NSCLC. N Engl J Med. 2024;391(7):585-97.
5. Taccone FS et al. Restrictive vs liberal transfusion strategy in patients with acute brain injury: the TRAIN randomized clinical trial. JAMA. 2024;332(19):1623-33.
6. Gibbs KW et al. Noninvasive ventilation for preoxygenation during emergency intubation. N Engl J Med. 2024;390(23): 2165-77.
7. Dark P et al. Biomarker-guided antibiotic duration for hospitalized patients with suspected sepsis: the ADAPTsepsis randomized clinical trial. JAMA. 2025;333(8):682-93.
8. Richeldi L et al. Nerandomilast in patients with idiopathic pulmonary fibrosis. N Engl J Med. 2025;392(22):2193-202.
NEW research presented at the American Thoracic Society (ATS) International Conference, held in San Francisco, California, USA, highlights the rapid advances in respiratory health. The six featured studies provide a snapshot of the research highlights from the extensive meeting, and span a range of topics, including improved outcomes in lung transplant allocation and the long-term effects of air pollution and pediatric pulmonary conditions.
Lung Transplant Waitlist Deaths Halved Under New Allocation System
THE LATEST research presented at the ATS International Conference 2025 revealed that the Composite Allocation Score (CAS) system significantly reduced lung transplant waitlist deaths, particularly among patients who are critically ill.1
Lung donor allocation in the USA has undergone major changes over the past decade, transitioning from a geographically based model to one focused on medical urgency. Following a 2017 lawsuit that led to broader sharing within a 250-nautical-mile radius, the United Network for Organ Sharing (UNOS [Virginia, USA]) implemented the CAS system in March 2023. CAS combines multiple clinical and logistical factors into a single score to prioritize patients more equitably. Researchers conducted a retrospective cohort study of 24,368 patients listed for transplant since February 2015, dividing them into three eras: pre-2017 local allocation, post-2017 regional sharing, and the CAS era.
Results show that 11.2% of waitlisted patients died or were delisted in the pre-2017 era, which declined to 8.4% after the geographic expansion in 2017 and fell sharply to 4.1% following CAS implementation. Patients who were critically ill benefited most: among those in the top 5% of waitlist urgency scores, mortality or delisting dropped from 34.5% before 2017 to just 6.5% under CAS.
Adjusted models confirmed these trends, with pre- and post-2017 patients having a 3.3-fold and 2.1-fold greater risk of death or delisting compared to those in the CAS era, respectively. For the highest-risk group, the risk was up to eight times higher before CAS was introduced. Patients receiving high-flow nasal cannula oxygen at listing also saw significantly improved outcomes under CAS.
CAS combines multiple clinical and logistical factors into a single score to prioritize patients more equitably
These findings confirm that prioritizing medical urgency through CAS is improving survival chances for the most vulnerable patients awaiting lung transplants. Researchers should perform further analysis to determine whether individual components of CAS are driving these improvements and how best to continue refining the system.
Pulmonary Sarcoidosis: Methotrexate Matches
Prednisone Efficacy, with Milder Side Effects
IN THE SEARCH for better-tolerated treatments for pulmonary sarcoidosis, a new study presented at the ATS International Conference 2025 found methotrexate as effective as prednisone, with a potentially more favorable side effect profile.2
Prednisone remains the standard first-line treatment for pulmonary sarcoidosis, but its adverse effects can significantly reduce patient quality of life. Methotrexate, a longstanding immunosuppressant, is considered to have fewer side effects, but it has not previously been studied as an initial therapy for this condition. The PREDMETH trial, a clinician- and patient-designed, randomized non-inferiority study conducted across 17 Dutch hospitals, compared the efficacy and safety of methotrexate to prednisone in treatment-naïve patients. Participants were randomized 1:1 to receive either drug, with forced vital capacity (FVC) at 24 weeks as the primary endpoint. Adverse events (AE) and patient-reported outcomes were monitored throughout.
Out of 138 enrolled patients, 70 were assigned to prednisone (with one exclusion) and 68 to methotrexate. The cohort was predominantly male (73.7%) with a mean age of 46.6 years. Baseline FVC (%) was predicted to be 79.8% (SD: 15.44) in the prednisone group and 74.8% (SD: 12.68) in the methotrexate group. After 24 weeks, methotrexate demonstrated non-
inferiority, with a mean between-group difference in FVC change of –1.8% (90% CI: –4.40–0.76). Protocol adherence was high (83% prednisone, 81% methotrexate). While the total number of AEs was similar between groups, ongoing AEs at 24 weeks were notably fewer in the methotrexate arm (104 versus 171). Prednisone was more often associated with weight gain, insomnia, increased appetite, and cushingoid appearance, whereas methotrexate more frequently caused nausea, fatigue, elevated liver enzymes, abdominal discomfort, and respiratory infections.
While the total number of AEs was similar between groups, ongoing AEs at 24 weeks were notably fewer in the methotrexate arm
The PREDMETH trial is the first to demonstrate that methotrexate is as effective as prednisone as an initial therapy for pulmonary sarcoidosis. The total AEs were comparable; however, their differing profiles, and the fewer persistent side effects with methotrexate, highlight its potential as a viable first-line option.
Maternal Air Pollution Exposure Alters Offspring Asthma Risk
A RECENT study, presented at the ATS International Conference 2025, has shed light on how maternal exposure to particulate air pollution may contribute to increased asthma risk in adult offspring, even when the offspring themselves are never directly exposed.3
RNA sequencing revealed the diffrential expression of over 2,800 genes
The researchers focused on understanding the epigenetic mechanisms that underlie this transgenerational effect using a wellestablished mouse model of allergic airway disease. They exposed female mice to particulate pollution before conception and throughout pregnancy and lactation. The adult offspring of these mice displayed significantly heightened airway hyperreactivity, as confirmed by flexiVent™ (SCIREQ; Montreal, Canada) lung function testing. Interestingly, this was accompanied by a blunted lung transcriptomic response to allergen challenge.
RNA sequencing revealed the differential expression of over 2,800 genes related to pathways such as SMAD and TGFβR, regardless of maternal exposure. However, unique transcriptomic patterns emerged in offspring depending on whether their mothers had been exposed to air pollution (2,792 unique genes in controls and 374 in pollution-exposed progeny). This indicates a divergence in gene expression profiles likely shaped by the maternal environment.
Gene set enrichment analysis further showed a notable loss of pathway activity in offspring of exposed mothers. Whole-genome methylation analysis supported these findings, revealing a reduction and skew toward hypomethylation in differentially methylated DNA regions in the pollution group, particularly in intronic regions and transposons.
The findings suggest that the maternal environment alters epigenetic programming in the lungs of offspring, leading to suppressed gene expression and heightened allergic airway disease. These insights highlight the potential of targeting epigenetic mechanisms to prevent or treat asthma and related respiratory conditions rooted in prenatal environmental exposure.
Two Distinct Recovery Paths for Individuals Impacted by Critical Illness
A NEW study, presented at the ATS International Conference 2025, has identified two distinct recovery trajectories in individuals who have experienced critical illness, shedding light on the long-term challenges faced by many patients and highlighting key risk factors for poor outcomes.4
Researchers analyzed data from 804 adult patients enrolled in the BRAIN-ICU and MIND-ICU prospective cohort studies, all of whom had previously been hospitalized for respiratory failure or shock. The study aimed to better understand how patients recover in the year following discharge from intensive care, with a particular focus on cognitive function and the ability to perform daily activities.
Post-intensive care syndrome is a welldocumented but poorly understood condition affecting a significant proportion of patients coming from the ICU. It encompasses a constellation of long-term impairments in cognitive, physical, and psychological function. However, the patterns of recovery and factors that influence them have remained unclear.
Using advanced statistical modeling techniques, the researchers identified two classes of patients based on recovery trajectories over a 12-month period. Patients in Class 1 (620 individuals; median age: 61.5 years) experienced better cognitive recovery and fewer impairments in basic and instrumental activities of daily living. In contrast, Class 2 (184 individuals; median age: 66.0 years) demonstrated persistently worse cognitive function and increasing dependence on others for daily tasks. These
characteristics are consistent with postintensive care syndrome.
The survival outlook also differed markedly between the two groups. At 12 months, 78.0% of Class 1 patients were still alive, compared with just 51.3% in Class 2.
The study identified older age, worse baseline cognitive function, and greater frailty at the time of ICU admission as significant predictors of Class 2 membership. Interestingly, the severity of illness and the duration of delirium during the ICU stay were not found to be associated with long-term recovery trajectory.
The authors called for the development of a predictive tool to help clinicians identify high-risk patients and explore targeted rehabilitation strategies, including cognitive, physical, and occupational therapies.
The survival outlook also differed markedly between the two groups. At 12 months, 78.0% of Class 1 patients were still alive, compared with just 51.3% in Class 2
Prospective Study Challenges Rarity of Pediatric Pulmonary Embolism
A STEP forward has been made by the BEEPER study, presented at the ATS International Conference 2025, which has offered the first prospective analysis of pulmonary embolism (PE) diagnosis in children, drawing from a large, multicenter cohort.5
PE in children has traditionally been viewed as a rare condition, with existing estimates suggesting it affects fewer than 1 in 100,000 children annually; however, these estimates are primarily based on administrative databases.
Conducted between 2020–2024 at 21 pediatric emergency departments across the US, BEEPER enrolled 4,103 children aged 4–17 years who presented with symptoms warranting a PE workup. Each participant was followed for 45 days, and PE diagnosis was confirmed through a rigorous adjudication process, using imaging criteria for both PE and deep vein thrombosis (DVT).
As of November 1st, 2024, adjudication was complete for 3,663 patients. Among these, 156 children (4.2%) were diagnosed with PE, with 2.1% having isolated PE, 1.1% isolated DVT, and 1.0% both PE and DVT. The mean age of children with confirmed PE was 15 years, slightly older than the overall cohort average of 14 years. Notably, 64.4% of those tested were female, and 57.7% identified as White.
Diagnostic testing showed that D-dimer was used in nearly 80% of cases. CT pulmonary angiography was performed in about one-
third of patients, yielding a 10.4% positive rate. Ventilation-perfusion scans and MRI had a 16.7% positivity rate, while venous ultrasound detected DVT in 17.8% of cases.
This landmark prospective study challenges the long-held assumption of PE rarity in children, revealing rates and diagnostic patterns similar to those observed in adult populations. These findings emphasize the importance of heightened clinical awareness and refined diagnostic strategies in pediatric emergency care.
Ventilation-perfusion scans and MRI had a 16.7% positivity rate, while venous ultrasound detected DVT in 17.8% of cases.
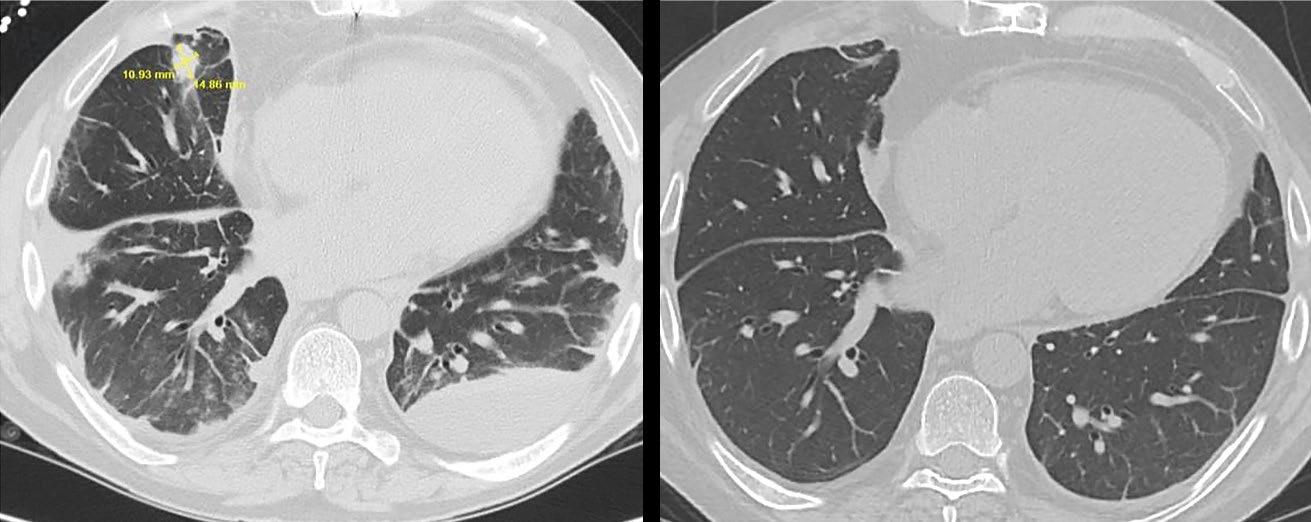
Cilia Analysis Provides New Perspective on Chronic Neonatal Lung Injury
A STUDY presented at the ATS International Conference 2025 revealed new evidence that impaired ciliary motion may play a role in the pathophysiology of bronchopulmonary dysplasia (BPD), particularly in its more severe forms.6
The severity of BPD may be associated with altered ciliary biomechanics, which could impair pulmonary defense and contribute to disease progression
Researchers analyzed nasal cilia dynamics in preterm infants with moderate and severe BPD using high-speed video microscopy and manual image analysis techniques. The study revealed that infants with severe BPD showed significantly reduced net angle and amplitude of ciliary beating compared to those with moderate disease, findings that may indicate disrupted mucociliary clearance in this vulnerable population.
BPD, a chronic lung condition resulting from barotrauma and oxygen toxicity in premature neonates, has traditionally been studied through the lens of lung structure and vascular involvement. However, this investigation shifts the focus toward the functional integrity of the airway epithelium, specifically the respiratory cilia essential for mucus and pathogen clearance.
Using nasal brushings from infants classified by the Jensen criteria (N=9), the team recorded 36 high-speed videos and evaluated multiple ciliary metrics, including length, angle, orientation vector, and bending index. While no significant differences were noted in ciliary length or orientation, reductions in both net angle (p=0.045) and amplitude (p=0.028) were seen in those with severe BPD. These findings suggest that the severity of BPD may be associated with altered ciliary biomechanics, which could impair pulmonary defense and contribute to disease progression.
The authors call for further research with larger cohorts and advanced imaging technologies to validate these findings and explore potential therapeutic targets aimed at improving mucociliary clearance in infants with BPD.
References
1. Raddawi M et al. Improvement in wait list mortality for the most critically ill since the implementation of the CAS. Abstract A1009. ATS International Conference, May 16-21, 2025.
2. Kahlmann V et al. Methotrexate versus prednisone as first-line treatment for pulmonary sarcoidosis: the PREDMETH trial. Abstract A1007. ATS International Conference, May 16-21, 2025.
3. Zakarya R et al. An epigenetic association between heightened airway hyperreactivity and maternal exposure to particulate air pollution. Abstract A5270. ATS International Conference, May 16-21, 2025.
4. Banerdt J et al. Characterizing critical illness recovery trajectories: exploring risk factors for post intensive care syndrome. Abstract A5261. ATS International Conference, May 16-21, 2025.
5. Kline JA et al. High frequency of pulmonary embolism in symptomatic children in the emergency department. Abstract A7102. ATS International Conference, May 16-21, 2025.
6. Yassa D et al. Analyzing respiratory cilia dynamics in relation to bronchopulmonary dysplasia severity. Abstract A3157. ATS International Conference, May 16-21, 2025.
Highlighting Research and Advocacy Efforts on Electronic Nicotine Delivery Systems at the ATS International Conference in 2025
Author: *Sophia Karandashova1
1. Division of Respiratory Medicine, Department of Pediatrics, University of California San Diego, California, USA
*Correspondence to sophia.karandashova@gmail.com
Disclosure: The author has declared no conflicts of interest.
THIS YEAR at the American Thoracic Society (ATS) International Conference, held in San Francisco, California, USA, several abstracts were presented on electronic nicotine delivery systems (ENDS). The popularity of ENDS and the exponential evolution of nicotine products beyond combustible tobacco make researching the effects of e-cigarettes imperative. Emerging clinical data raises concerns regarding the effects of vaping on health. The wide and ever-increasing variety of products available makes basic and translational studies challenging.
EXPLORING THE COMPLEX TOXICOLOGY OF ENDS COMPONENTS
Effah et al.1 exemplified this in their study on the impact of ENDS coil composition, coil resistance, and e-liquid formulation. Their findings showed that both coil composition and e-liquid formulation influenced the reactive oxygen species present in aerosols, and that high coil resistance increased the presence of aluminum, iron, and lead. These findings demonstrate that ENDS components can yield higher toxic exposures; thus, greater adverse effects are anticipated downstream. Nicotine product manufacturers continue to seek ways to bypass regulatory controls. One novel approach involves using
synthetic nicotine analogs, for which there are limited data on toxicity and addictive effects. Using in vitro and in vivo studies, Jordt et al.2 demonstrated that 6-methyl nicotine, for example, is several times more potent than nicotine in rats, and is more cytotoxic to airway epithelial cells. Additionally, they found that product labels were highly inaccurate regarding nicotine analog content.
TRANSLATIONAL STUDIES REVEAL IMMUNOLOGIC CHANGES
Studies in both mice and non-human primates showed evidence of immunomodulation with vaping. Masso-Silva et al.3 demonstrated that
e-cigarette aerosol exposure modulated the activation of neutrophils and macrophages in mice and decreased the presence of lymphocytes in lung-draining lymph nodes. Park et al.4 showed systemic immune system alterations in rhesus macaques after six months of vaping, with decreased expression of TNF superfamily members and increased myeloperoxidase, CXCL2, and brain-derived neurotrophic factor in plasma. They also showed increased inflammation in airways and lung parenchyma, as well as increased collagen deposition in the airways, raising concerns that vaping may increase the risk of pulmonary fibrosis. Noel et al.5 revealed that prenatal exposure to e-cigarette aerosols altered gene expression in the lungs and increased house dust mite-induced inflammation in male mice. Miller et al.6 found that prior exposure to conventional cigarettes led to increased neutrophilic inflammation in mice subsequently exposed to e-cigarette aerosols. Thus, emerging data in animal models foreshadow the magnitude of the effects that vaping will have on human health.
CLINICAL CASES IN E-CIGARETTE OR VAPING-ASSOCIATED LUNG INJURY, ACUTE RESPIRATORY DISTRESS SYNDROME, AND LUNG DISEASE
The Centers for Disease Control and Prevention (CDC) has not collected data on e-cigarette or vaping-associated lung injury (EVALI) since early 2020 due to the COVID-19 pandemic. Nevertheless, EVALI remains a clinical concern, as demonstrated by multiple cases presented at ATS 2025. Case reports showed EVALI presenting concomitantly with infection, as demonstrated by Tangutoori et al.,7 who described a case of EVALI with concurrent Klebsiella pneumonia. A novel presentation described by Othman et al.8 involved EVALI masquerading as an obstructive, necrotic lung mass. Beyond EVALI, concerns persist regarding the link between vaping and both acute lung injury and acute respiratory distress syndrome (ARDS). Jiang et al.9 conducted a retrospective study and reported a fourfold increase in the likelihood of being diagnosed with ARDS among patients who vaped, suggesting that vaping is a risk factor for ARDS and highlighting the need for screening for e-cigarette use in hospitalized patients.
Vaping was strongly associated with severe asthma exacerbations, even more so than smoking
Jiang et al.9 conducted a retrospective study and reported a fourfold increase in the likelihood of being diagnosed with ARDS among patients who vaped.
Clinical researchers are also exploring the deleterious effects of vaping on patients with pre-existing lung diseases. For example, Ramirez et al.10 found that vaping was strongly associated with severe asthma exacerbations, even more so than smoking, and an increased need for mechanical ventilation. Vaping-associated lung disease can manifest in unexpected ways, as illustrated by a case presented by Bhattarai et al.,11 which involved vaping-associated sarcoidosis, with radiologic findings resolving after vaping cessation.
ADVOCACY AND REGULATION: TOWARD A NICOTINE-FREE FUTURE
While the increasing evidence demonstrating the adverse effects of vaping e-cigarettes on pulmonary health is alarming, the advocacy efforts driven by dedicated members of multiple national respiratory societies for a nicotine-free future are encouraging. Bonnie Halpern-Felsher, Stanford Medicine, Stanford University, California, USA, emphasized the insidious effects of promoting flavored nicotine products and the need for a comprehensive ban. There is no evidence that flavored nicotine products help adults with smoking cessation; if e-cigarettes are intended as a means to quit cigarette smoking, there is no reason to produce flavored products at all. She discussed local efforts to broadly ban nicotine-containing products in America, particularly for
adolescents. Some of these efforts, such as the generational tobacco ban passed in Brookline, Massachusetts, in 2020, have been successful. Limited data are available in many countries; however, what is available reveals how critical it is to protect adolescents and young adults. Richard van Zyl-Smit, University of Cape Town, South Africa, described the push to market ENDS in Africa, highlighting the situation in South Africa where no regulation for vaping exists. Data show that between 11–46% of adolescents who are in their final year of public education in South Africa vape. Nurdan Köktürk, Gazi University, Ankara, Türkiye, revealed that in Türkiye, which has a high smoking prevalence in the adult population, the sale of e-cigarettes is banned but the law is poorly enforced, with products remaining widely available. Laura GochicoaRangel, Instituto Nacional de Enfermedades Respiratorias, Mexico City, Mexico, discussed the sweeping ban on e-cigarettes in Mexico, and highlighted the fact that flavored capsule cigarettes, popular with youth, remain unregulated. She also described the merits of a school-based anti-tobacco curriculum. Many of the speakers provided links to free resources for the audience, intended to help listeners build momentum locally as they advocate for change.
CLOSING REMARKS
The above summary highlights a series of snapshots of the variety of cases and basic, translational, and clinical research on the topic of e-cigarettes, as well as the advocacy efforts to combat ENDS presented at ATS 2025. Nicotine products are a resilient, multiheaded hydra; it is important to commit to both research and advocacy, which are the weapons needed to vanquish this beast. For instance, to determine whether vaping does predispose to ARDS, conducting studies using animal models and a variety of clinical insults that lead to ARDS would be enlightening. Alternatively, a prospective trial assessing ARDS in people who vape e-cigarettes may be more informative than the current retrospective data.
References
1. Effah F et al. E-cigarette aerosol toxicity is uniquely dependent on the engineering of the coil, coil resistance, and e-liquid formulation. Am J Respir Crit Care Med. 2025;211:A6842.
2. Jordt SE et al. 6-methyl nicotine in electronic cigarettes: chemical analysis and toxicological properties. Am J Respir Crit Care Med. 2025;211:A7552.
3. Masso-Silva JA et al. E-cigarette modulation of leukocyte activation in lung and airways and T cell numbers in lung-draining lymph nodes in the setting of influenza infection. Am J Respir Crit Care Med. 2025;211:A3561.
4. Park K et al. E-cigarette aerosol inhalation by Rhesus macaques alters
the inflammatory and immune state of the lungs. Am J Respir Crit Care Med. 2025;211:A7447.
5. Noel A et al. Developmental origins of lung disease - prenatal exposures to e-cigarette aerosols exacerbate housedust mite-induced asthma in adult male mice. Am J Respir Crit Care Med. 2025;211:A2875.
6. Miller LA et al. Antecedent conventional tobacco smoke exposure enhances ENDS pulmonary toxicity and inflammation. Am J Respir Crit Care Med. 2025;211:A7563.
7. Tangutoori S et al. Double trouble: vaping-induced lung injury complicated by Klebsiella pneumoniae infection. Am J Respir Crit Care Med. 2025;211:A6371.
8. Othman A et al. EVALI presenting as a lung mass: a diagnostic challenge in a young adult. Am J Respir Crit Care Med. 2025;211:A7575.
9. Jiang X et al. Vaping accentuates risk of acute respiratory distress syndrome. Am J Respir Crit Care Med. 2025;211:A3661.
10. Ramirez CM et al. Unmasking the respiratory risks of vaping in asthma exacerbations. Am J Respir Crit Care Med. 2025;211:A7569.
11. Bhattarai P et al. Vaping-associated sarcoidosis: a case report of recovery following cessation. Am J Respir Crit Care Med. 2025;211:A6113.
Redefining Respiratory Support: Insights from ATS 2025 on the Future of Mechanical Ventilation
Author: *Jose A. Meade-Aguilar1
1. Department of Medicine, Chobanian & Avedisian School of Medicine, Boston University, Massachusetts, USA
*Correspondence to jameade@bu.edu
Disclosure: The author has declared no conflicts of interest.
MECHANICAL ventilation remains one of the most powerful, yet potentially harmful tools in critical care. Despite decades of refinement in ventilator strategies, complications such as ventilator-induced lung injury, oxygen toxicity, and fluid overload continue to impact outcomes in those who are critically ill. At the American Thoracic Society (ATS) International Conference 2025, a series of novel studies pushed the boundaries of our understanding and delivery of respiratory support. Here, three key advances that offer a glimpse into the future of mechanical ventilation are highlighted: quantifying risk with mechanical power and fluid overload, applying machine learning to personalize oxygen targets, and engineering a groundbreaking intravenous oxygenation strategy.
MECHANICAL POWER AND FLUID OVERLOAD: A DEADLY SYNERGY
A large retrospective study from Taichung Veterans General Hospital, Taiwan, analyzed 4,441 patients in the ICU who received continuous mechanical ventilation for over four days.1 Investigators assessed mechanical power (MP), a comprehensive measure of energy transferred to the lungs, and fluid accumulation index (FAI) as predictors of hospital mortality. They found that both MP and FAI were independently and additively associated with increased mortality. Those who survived had consistently lower MP and fluid accumulation across the first four ICU days. Even after adjusting for confounders, both variables remained strong predictors of poor outcomes (hazard ratio for MP: 1.03; hazard ratio for FAI 2.43; both p<0.001).
Implications
This study reinforces the importance of minimizing not only overt ventilator pressures and volumes, but also the total energy delivered to the lungs. MP integrates multiple parameters, including tidal volume, driving pressure, and respiratory rate, into a single meaningful metric that could be incorporated into bedside decision-making. Additionally, the strong association of fluid accumulation with mortality underscores the need for more proactive fluid management strategies. The findings advocate for a dual-pronged approach: mitigating mechanical stress while optimizing volume status early in the ICU stay.
PERSONALIZING OXYGEN TARGETS WITH MACHINE LEARNING: BRIDGING TRIAL DATA AND BEDSIDE CARE
Another innovative study evaluated how current ICU oxygenation practices align with individualized peripheral oxygen saturation (SpO₂) targets predicted by a machine learning model trained on previous randomized trial data.2 Among 619 mechanically ventilated patients, the model predicted that 53% would benefit from higher SpO₂ targets (96–100%) and 47% from lower targets (88–92%). However, real-world SpO₂ values remained strikingly similar across both groups (96.2% versus 95.6%; p=0.18), suggesting a mismatch between personalized optimal targets and standard care. Notably, only patients in shock exhibited differences in oxygen delivery based on predicted benefit.
Implications
These findings highlight a critical gap between evidence-based, individualized targets and clinical practice. Despite growing recognition that "one-size-fits-all" oxygenation may be suboptimal, or even harmful, most patients still receive uniform SpO₂ levels. Machine learning offers an opportunity to tailor oxygen targets in real time, accounting for unique patient phenotypes and risk profiles. Embedding such tools into ICU workflows could bring us closer to precision critical care, improving outcomes by aligning therapy with individualized needs.
INTRAVENOUS OXYGEN MICROBUBBLE THERAPY: A BOLD LEAP BEYOND THE LUNGS
In a striking departure from traditional ventilatory support, researchers introduced a new method for delivering oxygen intravenously via a saline solution infused with nano- and micro-sized oxygen bubbles.3 Generated through high-pressure oxygen saturation and custom-designed cavitation, this milky fluid was infused into an ex vivo desaturated swine blood circuit. The therapy significantly increased both SpO₂ and partial pressure of oxygen (by ~28% and ~26 mmHg, respectively), without the need for lung-based gas exchange. Bubble sizes ranged from ~60 nm (nanobubbles) to ~20 µm (microbubbles).
Implications
This proof-of-concept represents a revolutionary approach to oxygen delivery. In situations of profound hypoxemia where lung mechanics are failing, such as severe acute respiratory distress syndrome or refractory shunt physiology, intravenous oxygenation could act as a rapid bridge to recovery or definitive intervention. While still in early experimental phases, this technology could eventually supplement or even reduce the need for high-pressure ventilation in selected cases. Future research will need to address safety, optimal dosing, and potential complications such as gas embolism, but the foundational work here marks a bold new chapter in respiratory support.
CONCLUSION
The research presented at ATS 2025 reflects a pivotal shift in the landscape of mechanical ventilation. We are moving beyond static parameters and protocolized care, toward a future that is dynamic, personalized, and technologically augmented. Whether it is refining metrics like MP, personalizing oxygen delivery through AI, or bypassing the lungs entirely with intravenous microbubble therapy, the message is clear: innovation in respiratory care is accelerating, and the potential to reshape outcomes has never been greater. For clinicians, researchers, and patients alike, these advances offer not only hope, but a challenge: to rethink how we support the most vulnerable lungs in the ICU.
References
1. Chang YM et al. Synergistic Effects of high mechanical power and fluid accumulation on mortality in mechanically ventilated patients. Am J Respir Crit Care Med. 2025;211:A1495.
2. Seitz KP et al. How do the oxygen saturation values that mechanically ventilated ICU patients experience in clinical care compare to the personalized targets that a machine learning model predicts will result in the best outcomes? Am J Respir Crit Care Med. 2025;211:A1493.
3. Marquez A et al. Intravenous oxygen delivery with free oxygen nano- and microbubbles in saline. Am J Respir Crit Care Med. 2025;211:A1521.
Beyond the Lungs: Addressing Cardiopulmonary Risk in COPD
This presentation was given at the American Thoracic Society (ATS) International Conference, held in San Francisco, California, USA, May 17th−21st, 2025.
Support: The presentation and publication of this article were supported by AstraZeneca.
Speakers: Nicola Hanania,1 Patrick Cambier2,3
1. Baylor College of Medicine, Houston, Texas, USA
2. HCA Florida Trinity Hospital, Trinity, Florida, USA
3. Interventional Cardiology Consultants, Clearwater, Florida, USA
Disclosure: Hanania has received honoraria for serving as a consultant or advisory board member for AstraZeneca, Sanofi, Regeneron, GSK, Genentech, Connect Biopharma, Chiesi, and Verona Pharma; and has received research grant support from AstraZeneca, GSK, Genentech, Chiesi, Sanofi, Regeneron, and Amgen with payments to his institution. Cambier has received honoraria for consultation and promotional activities from Novo Nordisk; consultation honoraria from AstraZeneca and Pfizer; and research protocol support from BMS and Lilly. The author has declared no conflicts of interest related to device design or consulting.
Acknowledgements: Medical writing assistance was provided by Eleanor Roberts, Beeline Science Communications Ltd, London, UK.
Disclaimer: This content is intended for US Healthcare Professionals.
COPD is a growing problem worldwide. Symptoms of COPD may lead to exacerbations, which are associated with an increased incidence of cardiovascular (CV) events. This association is important to recognize as both COPD exacerbations and the presence of cardiovascular disease (CVD) are associated with an early death. At the 2025 American Thoracic Society (ATS) Conference, Nicola Hanania, Baylor College of Medicine, Houston, Texas, USA, and Patrick Cambier, HCA Florida Trinity Hospital, Trinity, Florida, USA; Interventional Cardiology Consultants, Clearwater, Florida, USA, presented the case for examining CV-related issues in all patients with COPD. Studies show that a COPD exacerbation is one of the key symptoms associated with further exacerbations. As such, intervention either prior to any exacerbation, or following the first such incidence, is key to trying to limit both further exacerbations and associated CVD. However, even
PHARMA
at-risk patients with COPD are being undertreated, especially with regard to maintenance therapy. This, the experts posited, may pose a significant health burden. Hanania and Cambier also discussed that the assessment of CVD symptoms in patients with COPD is not routine. They called for cardiologists and pulmonologists to work together and crossrefer patients whenever they present with COPD. This approach can not only reveal CVrelated issues in patients with COPD, but can also lead to more proactive, early treatment of such symptoms to slow disease progression and help prevent death.
Introduction
It is becoming increasingly recognized that people with COPD have an elevated risk of serious CV events,1 discussed Hanania and Cambier at the ATS 2025 conference. Such CV events can include myocardial infarction, arrhythmia, stroke, heart failure decompensation, and death.1 For example, analysis of 1999–2018 National Health and Nutrition Examination Survey data, representing over 31,500 adults, found that while the prevalence of CVD in people without COPD was around 9%, CVD prevalence in people with COPD (n=2,504) was higher: 17.5% in those with chronic bronchitis, 37.2% in those with emphysema, and 36.1% in those with both.2 “The magnitude of difference speaks to the idea that there is a ‘scarlet letter’ of concurrent pulmonary disease and [shows] why people [with COPD] need to be looked at much more upstream, treated much more aggressively, and watched a little bit more closely,” explained Cambier.
COPD Symptoms as Risk Factors for Exacerbations
Figure 1 shows findings from a retrospective analysis of nearly 60,000 patients with COPD in the UK. Here, increasing dyspnea severity at initial assessment is shown to be related to the risk of having ≥1 moderate-to-severe exacerbations in the following 12 months.3 This is of clinical importance, discussed Hanania, as analysis of nearly 1.5 million patients in the US showed that once a person
has experienced an exacerbation, they are at a 1.5-fold risk of a future exacerbation following a single incidence, and a 2.5-fold risk following multiple exacerbations.4
Occurrence of COPD exacerbations is of importance, as analysis of IQVIA Longitudinal Access and Adjudication Data (LAAD) for this session, which utilized US pharmacy and medical claims information from January− December 2024, reveals that 42% of “at-risk” patients with COPD (defined as ≥2 moderate or ≥1 severe exacerbations in 12 months) attended an emergency room or urgent care center in a 12-month period, with 37% of these patients being hospitalized. Following hospitalization, 30-day readmission rates for all patients with COPD was 20%.5
Also of note, the risk of all-cause mortality is higher following an exacerbation. In a study including almost 436,000 newly diagnosed patients with COPD in the US, compared to patients who had not experienced an exacerbation, the hazard ratio (HR) for mortality within 30 days of the first exacerbation was 1.79 (95% CI: 1.58–2.04), with the risk of death remaining elevated for up to 2 years (HR: 1.15; 95% CI: 1.05–1.25).6
In the IQVIA LAAD analysis of patients atrisk of exacerbations, 30-day mortality was 9% following a hospitalization for COPD.5
In addition, a study utilizing US data from just under 1.3 million hospital admissions for COPD found that, following discharge, 26.2% of patients died within 1 year.7 “To summarize, symptoms drive exacerbation; one exacerbation drives a further exacerbation, and then it’s a vicious cycle,” said Hanania.
Figure 1: Increasing COPD symptoms are associated with an associated risk of exacerbations.3
Proportion of patients with an exacerbation during follow-up
Increasing dyspnea severity
MRC: Medical Research Council dyspnea grade.
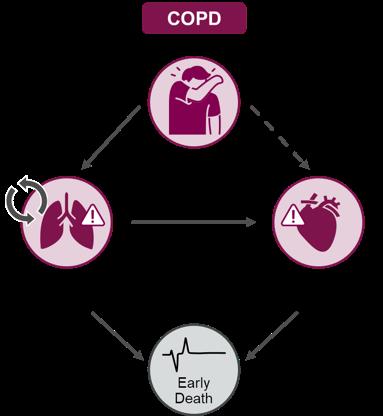
The Relationship Between Cardiovascular Disease and COPD
As can be seen from Figure 2, there is substantial supporting data that COPD exacerbations are associated with CV events, and both are associated with an early death. There are also indications that COPD symptoms alone may be associated with CV events.1 Recognizing these interactions, said Cambier, should encourage pulmonologists and cardiologists to work together, so that “we can […] be more effective in keeping people [with COPD] out of scenarios where they’re coming into the hospital.”
The interrelationship between CVD and COPD is partly due to shared “syndemic” risk factors, such as smoking and aging, as discussed in the 2025 Global Initiative for Chronic Obstructive Lung Disease (GOLD) report.8 Other shared mechanisms for this relationship, Cambier and Hanania suggested, could include air trapping, hyperinflation, and inflammatory pathways.1
COPD Exacerbations as Risk Factors for Cardiovascular Disease
A global assessment of mortality and morbidity in patients with COPD who had CVD, or an increased CVD risk, found that the HR of a CV event in the 30 days following a moderate or severe COPD exacerbation was 3.8 (95% CI: 2.7–5.5). While the risk decreased over time, it remained above 1.0 for around a year (HR: 1.9; 95% CI: 1.5–2.4 at 91−365 days; Figure 3).9 Findings such as this, reported Hanania “have opened [pulmonologists'] eyes to start discussing things with our cardiology colleagues."
However, Cambier relayed that he currently has two patients with COPD in the ICU for an exacerbation, who have never seen a cardiologist or recently undergone CVfocused tests. This highlights, he continued, how such patients are “simply being looked upon as [only having a] COPD exacerbation”. He explained that what potentially happens is that “we get into our track, and we see [a patient’s symptoms] as a singular disease,
when in fact, they have an intimately connected comorbidity." Of course, Hanania added, “we should be worried about the respiratory symptoms during [a COPD] exacerbation […] but we should also be worried about their heart." This shows the need, Cambier reiterated, for “upstream recognition to be aggressive earlier, rather than just tide [patients] over, because the next [exacerbation] could be worse."
Considering Cardiopulmonary Risk When Managing COPD
The evidence regarding the relationship between COPD and CVD, said Cambier, is “why we need to make sure we make adjustments in medications, or at least rethink what we’re treating patients with at [early] stages, because the next day they may have an even more dire outcome." However,
undertreatment is another major issue related to the under-recognition of COPD and CVD comorbidity, explained Hanania. For example, in an analysis of IQVIA LAAD claims data, only 50% of at-risk patients with COPD (≥2 moderate or ≥1 severe exacerbations in 12 months) were receiving maintenance treatment, and only 28% were receiving triple therapy with a long-acting β agonist, long-acting muscarinic antagonist, and inhaled corticosteroid.5 “Undertreatment poses a significant health burden in terms of maintenance,” commented Cambier.
Alongside appropriate drug therapy for both treatment and prevention of CV-related issues, the experts discussed how pulmonary rehabilitation may be useful for patients with comorbid COPD. Treatment, said Cambier, may also involve prompt initiation of proactive drug therapy, for example, lowdensity lipoprotein reduction in a patient with Class I−II heart failure. These patients may
Adapted from Singh D et al.1
Licensed under CC BY-NC 4.0. COPD-associated cardiopulmonary risk.
Figure 2: Associations between COPD and cardiovascular events may lead to early death.1
3: Increased risk of cardiovascular events persisted for up to a year after an exacerbation.9
~4x greater risk of a CV eventd following a moderate or severe COPD exacerbation
CV events included myocardial infarction, stroke, unstable angina, transient ischemic attack, and death.
CV: cardiovascular.
currently, in Cambier’s view, be considered to be in heart failure with only mildly reduced left ventricular function, but downstream this could lead to biventricular failure. At the moment, however, he reported that such patients may be “grossly undertreated” and possibly receiving only low doses of appropriate medication.
The Importance of Early Identification of At-risk Patients
With these figures in mind, Hanania stressed the importance of identifying at-risk patients,10,11 such as those with a recent history of COPD exacerbations,3 and then optimizing management,8,11 to prevent exacerbations, CV complications, and decrease mortality risk.8 CV issues should be investigated, said Cambier, alongside other commonly considered COPD-related diseases, such as diabetes.8 Timing of care is particularly important, and the latest GOLD report highlights how a more proactive
disease management approach with appropriate evidence-based treatments can help improve outcomes.8
Cambier stressed the need to take any opportunity, when a patient with COPD presents, to carry out a range of CVassociated investigations. “Don’t be bashful about ordering CV testing,” he urged, and “look at other signs and symptoms of [for example] right heart failure, such as hepatic congestion, etcetera.” As an example, returning to his patient with COPD in the ICU, Cambier related how relatively high levels of brain natriuretic protein were discovered. Following an echocardiogram, the patient was found to have poor left ventricular function as well.
Cambier recognized that pulmonologists may feel this is more appropriately initiated by the patient’s primary care provider, but advised that pulmonologists can also send patients with COPD to a cardiologist for assessment of their ischemic burden. However, issues can arise, as discussed during open questions and answers, as in some cases, tests such as
Figure
calcium screening and a chest CT scan have to be ordered separately, and the result of one may influence whether or not the next test can be undertaken.
Another query that arose during the discussion concerned which biomarkers should be used to assess COPD over time. This is an “important point, which is an unmet need,” said Hanania. “More strategies [are needed], from both the cardiology societies and lung societies, to come up with a consensus as to what biomarkers to follow.” For example, he said, the U.S. FDA12 have “adopted fibrinogen as the only biomarker
References
1. Singh D et al. Implications of cardiopulmonary risk for the management of COPD: a narrative review. Adv Ther. 2024;41(6):2151-67.
2. Cobb K et al. COPD is associated with increased cardiovascular disease risk independent of phenotype. Respirology. 2024;29(12):1047-57.
3. Müllerová H et al. Risk factors for acute exacerbations of COPD in a primary care population: a retrospective observational cohort study. BMJ Open. 2014;4(12):e006171.
4. Sethi S et al. Relationship of COPD exacerbation severity and frequency on risks for future events and economic burden in the /medicare fee-for-service population. Int J Chron Obstruct Pulmon Dis. 2022;17:593-608.
5. Hanania NA, Cambier PA. Pulmonologist & cardiologist live: a collaborative approach to cardiopulmonary risk in
they believe in for now for COPD, but there are more, and I think we need to work together to find a solution.”
Conclusion
“Certainly, we have to treat patients [with COPD] if they already have CV risk factors,” concluded Hanania; however, he continued, in people with COPD, between the pulmonologist and the cardiologist, “we need to see if, by interacting first and early, we can prevent the late [COPD] events and the CV events."
COPD. ATS International Conference, 1821 May, 2025.
6. Daniels K et al. Risk of death and cardiovascular events following an exacerbation of COPD: The EXACOS-CV US Study. Int J Chron Obstruct Pulmon Dis. 2024;19:225-41.
7. Lindenauer PK et al. Risk trajectories of readmission and death in the first year after hospitalization for chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;197(8):100917.
8. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disesae. 2025. Available at: https:// goldcopd.org/2025-gold-report/. Last accessed: 3 June 2025.
9. Kunisaki KM et al. Exacerbations of chronic obstructive pulmonary disease and cardiac events. A post hoc cohort
analysis from the SUMMIT randomized clinical trial. Am J Respir Crit Care Med. 2018;198(1):51-7.
10. Singh D et al. Overcoming therapeutic inertia to reduce the risk of COPD exacerbations: four action points for healthcare professionals. Int J Chron Obstruct Pulmon Dis. 2021;16:3009-16.
11. Pullen R et al. CONQUEST quality standards: for the collaboration on quality improvement initiative for achieving excellence in standards of COPD Care. Int J Chron Obstruct Pulmon Dis. 2021;16:2301-22.
12. U.S. Food and Drug Administration. Qualification of biomarker plasma fibrinogen in studies examining exacerbations and/or all-cause mortality in patients with chronic obstructive pulmonary disease. Available at: https:// www.fda.gov/media/92782/download. Last accessed: 13 June 2025.
Support:
Exploring the Clinical and Economic Impact of Non-Cystic Fibrosis Bronchiectasis
The studies included herein, and the publication of this article, were developed and funded by Insmed Incorporated. The content of this article reviews two presentations from the American Thoracic Society (ATS) 2025 International Conference that took place in San Francisco, California, USA, between 18th–21st May 2025.
Lead Authors:
Presenters:
Ruxana T. Sadikot,1 Sunjay R. Devarajan2
Ruxana T. Sadikot,1 John Fastenau3
1. College of Medicine, University of Nebraska Medical Center (UNMC), Omaha, USA
2. Baylor College of Medicine (BCM), McNair Campus, Houston, Texas, USA
3. Insmed Incorporated, Bridgewater, New Jersey, USA
Disclosure: Sadikot has received grant funding from Veteran Affairs Merit Review and The National Heart, Lung, and Blood Institute (NIH NHLBI), and honoraria from the American Physician Institute. Devarajan has been a paid consultant for Insmed Incorporated. Fastenau is an employee of Insmed Incorporated.
Acknowledgements: Maitreyee Mohanty, Phani Veeranki, Nnaemeka U. Odo, Melanie Lauterio, Sebastian Fucile, Joseph Feliciano, Guilherme Lopes, Manu Tyagi, Zhun Cao, and John Fastenau were co-authors. Medical writing assistance was provided by Hannah Moir, EMJ, London, UK.
Disclaimer: Insmed Incorporated participated in the study design, research, analysis, data collection, and interpretation of data, as well as review and approval of this article.
Non-cystic fibrosis bronchiectasis (NCFBE) is often under-recognized and misdiagnosed, and is associated with significant clinical and economic burden. This article highlights two presentations from the American Thoracic Society (ATS) 2025 International Conference, which took place in San Francisco, California, USA, between 17th–21st May 2025, highlighting real-world evidence (RWE) data on treatment patterns, complications and healthcare resource utilization (HCRU) associated with NCFBE.
Ruxana T. Sadikot, Professor and Chief of the Pulmonary, Critical Care and Sleep Medicine Division at the University of Nebraska Medical Center (UNMC), Omaha, USA, and Sunjay R. Devarajan, Assistant Professor of Internal Medicine, Pulmonary and Critical Care at Baylor College of Medicine, Houston, Texas, USA, presented realworld evidence of treatment patterns and costs associated with HCRU in NCFBE.
Non-Cystic Fibrosis Bronchiectasis
Bronchiectasis is a chronic and progressive inflammatory lung disease, characterized by permanent and abnormal dilatation of the bronchi and accompanied by cough, sputum production, and recurrent bronchial infection and exacerbations.1,2 Bronchiectasis that is not associated with cystic fibrosis is known as NCFBE.3
The pathophysiology of bronchiectasis has been described as a vicious vortex, driven by inflammation, chronic airway infection, impaired mucociliary clearance, and progressive lung damage.3,4 Neutrophils are the primary inflammatory cells in patients with bronchiectasis and are believed to be key drivers in disease severity and progression.3-8 Bronchiectasis is associated with high disease burden on patients and healthcare systems, presenting with recurrent exacerbations and progressive lung function decline, increased hospitalizations, and worsening health-related quality of life.9-13 International guidelines for bronchiectasis recommend a multi-modal approach focusing on controlling symptoms and infection, reducing exacerbations, enhancing mucociliary clearance, and treatment of etiologies and comorbidities.9,14,15
There are no US guidelines.The primary management goals of bronchiectasis focus on symptom control and reducing exacerbation frequency to improve health-related quality of life.14,15 However, challenges arise due to the clinical heterogeneity and limited treatment options.16 This highlights the need for data on treatment patterns and clinical outcomes to enhance understanding of bronchiectasis management practices. Here, this article focuses on new data presented at the ATS that highlights insights on treatment patterns, complications, and hospitalizations in NCFBE.
Treatment Patterns and Outcomes Among Patients with Non-Cystic Fibrosis Bronchiectasis
Lead
Author/Presenter: Ruxana T. Sadikot
The clinical and economic burden of NCFBE on patients and healthcare systems is significant,16 but not thoroughly understood, especially regarding HCRU.
Findings were presented from a retrospective cohort study using de-identified claims from Optum’s Market Clarity database.16 The study included patients diagnosed with NCFBE in the USA between January 1st, 2017–March 31st, 2020.16 Eligible patients were those ≥12 years old with either ≥2 outpatient claims for bronchiectasis ≥30 days apart or ≥1 inpatient claim, excluding those with cystic fibrosis. Continuous enrollment was required for ≥12 months before (baseline) and ≥24 months after (follow-up) the first bronchiectasis claim.16 The analysis identified 12,018 people with NCFBE (mean age 68.5±13.2 years; 67% female).16
Commonly Prescribed Medications for Patients with Bronchiectasis
During the 2-year follow-up period, the commonly prescribed medications included corticosteroids, short-acting β-agonists antibiotics, and long-acting β-agonists. During the follow-up period, treatment patterns (for any duration), identified that around half of patients received one or more medications (Figure 1).16
Notably, 37.5% were prescribed long-acting bronchodilators for ≥6 months. Injectable corticosteroids were used by 32.6% of the patients, with 28.4% prescribed inhaled corticosteroids/long-acting β-agonist combination inhalers. Bronchodilators were used for a mean duration of 4.5 months.16 Macrolides were the most common firstline antibiotics prescribed (25.7%), with a mean of 7 months.16 Of these patients, 94% discontinued their treatment.17 During
Figure 1: Most common treatments of any duration for bronchiectasis (N=12,018; any time during follow-up using medical and pharmacy claims).16
Oral corticosteroids
SABAs
Injected corticosteroids
Combination ICS/LABAs
Macrolides
Penicillins
Quinolones
Tetracyclines
Nebulizer use*
*General nebulizer-device use, excluding inhalers and distinct from antibiotic or bronchodilator use.
follow-up, nearly half of the patients switched back to a macrolide (49.7%); the remaining were prescribed alternative antibiotics such as penicillin (49.5%), quinolones (62.1%), and cephalosporins (63.0%).16 Long-term use of macrolides (≥6 months) was used in 9.4% of patients, with a mean duration of treatment of 1.2 months, compared to approximately 12 days for other antibiotics.16
Complications and Mortality Associated with Bronchiectasis
Sadikot reported that complications associated with NCFBE included respiratory failure, heart failure, having a lung transplant, and experiencing ≥1 bronchiectasis exacerbation. Approximately one-fifth of patients (22%) experienced respiratory failure over the 2-year follow-up period (Table 1).16
Regarding HRCU, data indicated that 24.3% of patients (n=2,917) experienced respiratoryrelated inpatient hospital stays, and 31.4% (n=3,777) had emergency department visits
(Table 1).16 The all-cause mortality rate during follow-up was 22.5% (n=5,729/25,459).16
Sadikot stated the complexity of treating NCFBE due to its heterogeneity. Frequent switching of antibiotics, reliance on multiple symptom-based therapies and steroids, along with ongoing exacerbations, suggest current approaches often fall short of effectively managing bronchiectasis.16
Hospitalizations Burden and Risk of Readmissions in Non-Cystic Fibrosis Bronchiectasis
Lead Author: Sunjay R. Devarajan
Presenter: John Fastenau
Another RWE study described a retrospective analysis to understand the inpatient journey and readmission risk in patients hospitalized with NCFBE.18
Table 1: Complications and all-cause mortality during follow-up.17
*Continuous enrollment or clinical activity were not required during follow-up.
Using the USA PINC AI™ Healthcare database, 73,656 patients aged ≥12 years (mean [SD] age 71.8±14.7 years; 75.3% White; 58.3% female), hospitalized between January 1st, 2018–June 30th, 2022, with a primary or secondary diagnosis of bronchiectasis were identified (comorbid COPD and asthma were permitted).18 Notably, 92.3% were admitted on an urgent or emergency basis.17 Patients with a primary diagnosis of COPD or asthma, and all those with cystic fibrosis, were excluded from the analysis.18
At index hospitalization, 39.8% of patients had an existing respiratory infection, 29.5% had respiratory failure, and 85.6% had a pulmonary exacerbation.19 The most common treatments during hospitalizations were antibiotics (83.9%), bronchodilators (76.8%), and corticosteroids (68.6%).18 Additionally, 34.6% of patients required mechanical ventilation.19
The average (SD) length of index hospital stay was 7.1±9.4 days, costing on average 22,355±45,160 USD. Approximately 17% required intensive care, averaging 16,375±35,847 USD in costs. Following the index hospitalization, 5.9% of patients died.18
Also, Fastenau reported that post-discharge, most patients had significant post-acute care needs, with over half (53.8%) requiring special discharge plans; 23.3% were discharged to specialized healthcare facilities for long-term, around-the-clock care, and 21.9% received home healthcare.18 Patients were also likely to be readmitted to hospital, resulting in higher healthcare costs; 22.6% were readmitted within 90 days of discharge, for on average 7.9±9.6 days, and costing 24,576±41,189 USD.18
Multivariable logistic regression (Figure 2) indicated that all-cause readmission risk
2: Risk factors for 90-day hospital readmission in patients hospitalized with non-cystic fibrosis bronchiectasis*.18
Sex (ref: male)
Race (ref: White)
Asthma† (ref: no Asthma)
size (ref: <100 beds)
*Multivariate logistic regression modeling was performed. From the total population (N=73,656), 4,380 patients were excluded from modeling because they did not have data available in one or more predictors or died at index hospitalization. Additional variables included in the model that were nonsignificant (CI did not cross 1) were the number of pulmonary exacerbations at baseline, ethnicity, and age.
†Patients with a diagnosis code for COPD or asthma in the secondary position in a claim.
Figure
was associated with prior hospitalizations, a history of COPD or asthma, and longer hospital stays (all p<0.001).18
Fastenau stated that the high healthcare costs associated with NCFBE (hospitalization, readmission, and need for continuous medical care) highlight the need for improved continuity of care postdischarge to reduce readmission rates.18
Conclusion
These presentations highlight considerable variation and suboptimal management strategies for NCFBE. Frequent switching of antibiotics, reliance on multiple symptombased therapies and steroids, along with ongoing exacerbations, suggest current approaches often fall short of effectively managing bronchiectasis. Exacerbations and complications are contributing to high hospital readmission rates and direct medical costs. This review highlights gaps in the current management of NCFBE and underscores the need for more effective approaches to reduce clinical complications and healthcare burden.
3. Dente FL et al. Neutrophilic bronchial inflammation correlates with clinical and functional findings in patients with noncystic fibrosis bronchiectasis. Mediators Inflamm. 2015;2015:642503.
4. Chalmers JD et al. Neutrophilic inflammation in bronchiectasis. Eur Respir Rev. 2025;34(176):240179.
5. Loukides S et al. Exhaled H(2)O(2) in steady-state bronchiectasis: relationship with cellular composition in induced sputum, spirometry, and extent and severity of disease. Chest. 2002;121(1):81-7.
6. Goeminne PC et al. The Sputum Colour Chart as a predictor of lung inflammation, proteolysis and damage in non-cystic fibrosis bronchiectasis: a case-control analysis. Respirology. 2014;19(2):203-10.
7. Watt AP et al. Neutrophil apoptosis, proinflammatory mediators and cell counts in bronchiectasis. Thorax. 2004;59(3):231-6.
8. Tsikrika S et al. The role of noninvasive modalities for assessing inflammation in patients with non-cystic fibrosis bronchiectasis. Cytokine. 2017;99:281-6.
9. Flume PA et al. Advances in bronchiectasis: endotyping, genetics, microbiome, and disease heterogeneity. Lancet. 2018;392:880-90.
10. Chalmers JD et al. Neutrophil elastase activity is associated with exacerbations and lung function decline in bronchiectasis. Am J Respir Crit Care Med. 2017;195:1384-93.
11. Tkacz J et al. Real-world treatment patterns, health care resource utilization, and costs in a US Medicare population with bronchiectasis. J Manag Care Spec Pharm. 2024;30(9):967-77.
12. Shoaib S et al. Real-world disease burden, mortality, and healthcare resource utilization associated with bronchiectasis. Chron Respir Dis. 2025;22:14799731241310897.
13. Chalmers JD et al. Characterization of the “frequent exacerbator phenotype” in bronchiectasis. Am J Respir Crit Care Med. 2018;197(11):1410-20.
14. Polverino E et al. European Respiratory Society guidelines for the management of adult bronchiectasis. Eur Respir J. 2017;50(3):1700629.
15. Flume PA et al. Towards development of evidence to inform recommendations for the evaluation and management of bronchiectasis. Respir Med. 2023;211:107217.
16. Sadikot RT et al. Treatment patterns and outcomes among patients with non-cystic fibrosis bronchiectasis [abstract]. Am J Respir Crit Care Med. 2025;211:A1960.
17. Sadikot RT et al. Treatment patterns and outcomes among patients with non-cystic fibrosis bronchiectasis. Presentation. ATS International Conference, May 16-21, 2025.
18. Devarajan SR et al. Hospitalizations and risk of readmissions in patients with non-cystic fibrosis bronchiectasis [abstract]. Am J Respir Crit Care Med 2025;211:A1950.
19. Devarajan SR et al. . Hospitalizations and risk of readmissions in patients with non-cystic fibrosis bronchiectasis. Presentation. ATS International Conference, May 16-21, 2025.
Abstract Reviews ATS 2025
We are proud to present our selection of abstract reviews, which have been authored by the research teams themselves. They offer firsthand insights into a wide range of pulmonary and critical care topics, from COPD and lung transplantation to COVID-19 outcomes and pediatric care.
The Increased Risk for the Viral Infection after Sepsis in Patients with Chronic Obstructive Pulmonary Disease: A Federated Research Network Study
Authors: Tzu-I Chuang,1 *Wen-Cheng Chao2-4
1. Department of Chest Medicine, Taichung Veterans General Hospital, Taiwan
2. Department of Critical Care Medicine, Taichung Veterans General Hospital, Taiwan
3. Department of Post-Baccalaureate Medicine, College of Medicine, National Chung Hsing University, Taichung, Taiwan
4. Big Data Center, National Chung Hsing University, Taichung, Taiwan
*Correspondence to cwc081@hotmail.com
Disclosure: The authors have declared no conflicts of interest.
Patients with COPD who survive sepsis remain immunocompromised and are at increased risk of subsequent viral infections, including influenza and respiratory syncytial virus (RSV).1-3 However, the risk of viral infections among patients with COPD after sepsis remains unclear.4-5 This real-world data study aimed to investigate the 1-year risk of viral infections among patients with COPD, following sepsis.
MATERIALS AND METHODS
The authors used the TriNetX (Cambridge, Massachusetts, USA) platform, which integrates anonymized clinical data from 92 healthcare organizations, to identify 113,589 patients with COPD and sepsis. The risk of distinct viral infections, including herpes simplex virus (HSV), varicella-zoster virus (VZV), cytomegalovirus (CMV), RSV, and
influenza, within 1-year post-sepsis was analyzed, with 1:1 propensity score matching employed to minimize confounding. The effect of vaccination was also assessed to determine their protective efficacy.
RESULTS
A total of 98,883 patients with COPD and sepsis and 1:1 matched patients with COPD without sepsis were eligible for analyses. Table 1 shows that patients with COPD and sepsis had a consistently higher risk of distinct viral infections within 1-year post-sepsis. Specifically, HSV occurred in 1.36% of the sepsis cohort versus 0.83% of controls (hazard ratio [HR]: 1.936; 95% CI: 1.775–2.112); VZV in 0.34% versus 0.13% (HR: 3.050; 95% CI: 2.489–3.737); CMV in 0.58% versus 0.32% (HR: 2.101; 95% CI: 1.832–2.410); RSV in 7.67% versus 2.86% (HR: 3.297; 95% CI: 3.158–3.443); and influenza in 8.62% versus 3.34% (HR: 3.197; 95% CI: 3.071–3.328). Among the five viral infections, RSV and influenza exhibited the highest absolute and relative risks, representing the greatest viral burden in the post-sepsis setting. Sensitivity analyses revealed that the increased post-sepsis risks for viral infections remained consistent across various sepsis severities, including cases involving bacteremia, vasopressor use, mechanical ventilation, or hemodialysis. Additionally, the authors examined the protective effects of vaccinations in patients with COPD, and found significant risk reduction associated with the VZV glycoprotein E vaccine (HR: 0.724; 95% CI: 0.595–0.882), the RSV prefusion F protein-based vaccine (HR: 0.676; 95% CI: 0.563–0.812), and the influenza vaccine (HR: 0.709; 95% CI: 0.649–0.776).
CONCLUSION
In this study, the authors used a federated database to identify the increased one-year risk of viral infections, including HSV, VZV, CMV, RSV, and influenza, following sepsis in patients with COPD. Furthermore, the authors demonstrated the protective effect of vaccination against influenza and RSV. The findings underscore the need for heightened
vigilance regarding viral infections in patients with COPD who have survived sepsis and support the prioritization of vaccination in COPD management strategies, particularly among patients with stable disease. Further prospective studies are warranted to validate these findings and to elucidate the postseptic immunological alterations in patients with COPD.
Table 1: One-year risk of distinct viral infections between 98,883 patients with COPD and sepsis, and propensity score-matched patients with COPD without sepsis.
1. Chuang TI, Chao WC. The increased risk for the viral infection after sepsis in patients with chronic obstructive pulmonary disease: a federated research network study. Abstract 13271. ATS International Conference, May 16–21, 2025.
2. Yende S et al. Long-term host immune response trajectories among hospitalized patients with sepsis. JAMA Netw Open. 2019;2(8):e198686.
3. Jensen IJ et al. Sepsis-induced T cell immunoparalysis: the ins and outs of impaired T cell immunity. J Immunol. 2018;200(5):1543-53.
4. Wildenbeest JG et al. Respiratory syncytial virus infections in adults: a narrative review. Lancet Respir Med. 2024;12(10):822-36.
5. van der Slikke EC et al. Exploring the pathophysiology of post-sepsis syndrome to identify therapeutic opportunities. EBioMedicine. 2020;61:103044.
12-Month Effectiveness of Bronchoscopic Lung Volume Reduction in Patients with COPD, with
and without Alpha-1 Antitrypsin Deficiency: A Matched Case-Control Study
Bronchoscopic lung volume reduction (BLVR) with endobronchial valves has established effectiveness in improving lung function in patients with COPD who do not have alpha-1 antitrypsin deficiency (AATD).1,2 However, the effect of BLVR on patients with AATD is less certain. Several small-scale studies have shown a benefit using BLVR in patients with both AATD and COPD.3,4 The authors have previously demonstrated that 6-month BLVR outcomes were similar in patients with COPD, with or without AATD.5 However, there are currently no published studies comparing long-term BLVR outcomes between these two patient groups. This study thus aimed to compare outcomes at 12 months post-BLVR.
METHODS
The authors conducted a retrospective, single-center, matched case-control study involving patients with COPD who underwent BLVR. A thorough chart review was performed for 287 patients who underwent BLVR at the authors’ quaternary care institution between August 2018–April 2024. The chart review revealed 14 patients with severe, homozygous AATD within this group. 14 patients with COPD, but without AATD (nAATD), were selected from the remaining 273 BLVR patients to be matched against the AATD group. Baseline characteristics including demographics, fissure integrity, emphysema destruction score, quantitative computed tomography lobar volume, and baseline pulmonary function testing were recorded. Mean values were compared between groups using an equal variance t-test. Pulmonary function testing data from approximately 12 months following BLVR was then collected. PostBLVR data was compared to baseline data and analyzed using Wilcoxon signed rank test for statistical significance in each group independently. Changes in several variables, including forced expiratory volume in 1 second (FEV1), FEV1 percent change, residual volume (RV), and total lung capacity (TLC), were compared between the two groups using an equal variance t-test.
RESULTS
Baseline characteristics had statistically significant differences in emphysema destruction score (69.92±7.77 versus 61.64±11.62; p=0.04) and modified Medical Research Council score (3.78±0.43 versus 2.85±0.66; p=0.002). There were no other
differences in baseline characteristics. Following BLVR, seven patients (50%) in the AATD group and nine patients (64%) in the nAATD group experienced an increase in FEV1 greater than 15%. The median improvement in FEV1 was 125 mL (interquartile range [IQR]: 0.04–0.24), which equated to 13.94% (IQR: 5.87–30.09), in the AATD group and 155 mL (IQR: -0.07–0.25), which equated to 17.99% (IQR -8.09–29.67), in the nAATD group. Both improvements were statistically significant per Wilcoxon signed-rank test analysis. Statistically significant improvement was also demonstrated in both groups for changes in RV, TLC, and RV/TLC ratio. The improvements in FEV1, FEV1 relative percent change, and TLC were not significantly different between the two groups. However, there was a statistically significant difference
Table 1: Summary of outcomes.
between the groups, in terms of RV and RV/ TLC, which demonstrated more pronounced improvements in the AATD group. A summary of outcomes is illustrated in Table 1
CONCLUSIONS
BLVR may provide significant long-term improvements for patients with both COPD and AATD. These improvements may be similar to those expected for COPD patients without AATD. The lack of airway disease in patients with AATD may allow for more pronounced improvements in certain variables. Further research on a larger scale is warranted to support these findings and investigate the safety profile of this intervention.
*No statistically significant change from baseline. Values are medians with interquartile ranges. Wilcoxon signed rank test performed for each change in baseline. All values except for those marked by an asterisk are statistically significant changes from baseline. All t-tests described as ‘NS’ have p>0.05 indicating no statistically significant difference between group outcomes.
AATD: alpha-1 antitrypsin deficiency; BODE: BMI, airflow obstruction, dyspnea, exercise capacity; FEV1: forced expiratory volume in 1 second; mMRC: modified Medical Research Council; NS: non-significant; post-BD: post-bronchodilator; RV: residual
TLC: total lung
6MWD: the distance walked in 6 min.
References
1. Criner GJ et al. A multicenter randomized controlled trial of Zephyr endobronchial valve treatment in heterogeneous emphysema (LIBERATE). Am J Respir Crit Care Med. 2018;198(9):1151-64.
2. Criner GJ et al. Improving lung function in severe heterogenous emphysema with the spiration valve system (EMPROVE). A multicenter, open-label randomized controlled clinical trial. Am J Respir Crit Care Med. 2019;200(11):1354-62.
3. Everaerts S et al. Bronchoscopic lung volume reduction in patients with emphysema due to alpha-1 antitrypsin deficiency. Respiration. 2023;102(2):134-42.
4. Hogarth DK et al. Efficacy and safety of the Spiration Valve System™ for the treatment of severe emphysema in patients with alpha-1 antitrypsin deficiency (EMPROVE). Respir Med. 2024;224:107565.
5. Nicholson M, Criner GJ. Effectiveness of bronchoscopic lung volume reduction with Zephyr endobronchial valves in alpha-1 antitrypsin deficient chronic obstructive pulmonary disease patients versus chronic obstructive pulmonary disease patients without alpha-1 antitrypsin deficiency: a matched case-control study. Abstract 3794. ATS International Conference, 20-22 May, 2024.
Invasive Pulmonary Aspergillosis in a Lung Transplant Recipient Despite Antifungal Prophylaxis
Authors: Sagar Patel,1 Deepika Razia,1
*Ashwini Arjuna2
1. Creighton University School of Medicine, Phoenix, Arizona, USA
2. Norton Thoracic Institute, Phoenix, Arizona, USA
*Correspondence to ashwini.arjuna@commonspirit.org
Disclosure: The authors have declared no conflicts of interest.
Invasive pulmonary aspergillosis is a potentially life-threatening complication in immunocompromised patients, particularly solid organ transplant recipients.1 Lung transplant patients are at increased risk due to direct airway exposure, prolonged immunosuppressive therapy, and impaired mucociliary clearance. Long-term immunosuppressive therapy, critical for preventing graft rejection, also predisposes patients to opportunistic infections like aspergillosis.1 Although antifungal prophylaxis is routinely employed, breakthrough infections can occur, highlighting the diagnostic and therapeutic challenges involved in maintaining the graft function while treating an active infection.
METHODS
A 60-year-old man, with a history of COPD and previously treated Mycobacterium avium complex infection, underwent a bilateral lung transplantation in July 2024 after completing a thorough evaluation.
The patient was maintained on tacrolimus, prednisone, and mycophenolate mofetil as standard immunosuppression, in addition to itraconazole for fungal prophylaxis per the authors’ center’s protocol.
RESULTS
In September 2024, two months after transplant, the patient developed worsening dyspnea, decreased pulmonary function, and pleural effusions. Chest CT showed bilateral effusions, nodular densities, and compressive atelectasis (Figure 1A). Bronchoalveolar lavage (BAL) confirmed Aspergillus flavus and a high galactomannan antigen level (4.9), necessitating a change in the antifungal prophylaxis to isavuconazonium. His course was complicated by recurrent pleural effusions, requiring chest tube placement, and the persistent growth of Aspergillus in BAL, prompting a change of antifungal therapy to voriconazole along with inhaled amphotericin.2 With combination therapy, careful adjustment of his immunosuppressive regimen to balance infection control and graft function, and adequate monitoring of antifungal levels, he showed remarkable radiological and symptom improvement (Figure 1B).3
CONCLUSION
This case highlights the elevated risk of invasive pulmonary aspergillosis among lung transplant recipients, even when antifungal prophylaxis is implemented, emphasizing the significant risks associated with immunosuppressive therapy and the complexities involved in diagnosing and managing fungal infections in this vulnerable population. The immunosuppressive effects of tacrolimus and prednisone severely impair immune defenses, leading to fungal invasion. The interplay between
A
B
A) Initial CT showing bilateral effusions and nodular densities. B) CT after 3 months of treatment with voriconazole as well as inhaled amphotericin.
immunosuppression, diagnostic uncertainty between infection and rejection, and limitations of standard antifungal prophylaxis with possible antifungal resistance require a multi-disciplinary approach. The use of BAL for direct identification and monitoring of galactomannan levels is essential for an early and accurate diagnosis. Individualized modulation of immunosuppression, in conjunction with combination antifungal therapy, was key to the clinical recovery of the patient.
References
1. Singh N, Husain S. Invasive aspergillosis in solid organ transplant recipients. Am J Transplant. 2009;9(Suppl 4):S180-91.
2. Patterson TF et al. Practice guidelines for the diagnosis and management of aspergillosis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis. 2016;63(4):e1-60.
3. Patel D et al. Invasive pulmonary aspergillosis in a post-lung transplant patient despite antifungal prophylaxis [abstract]. Am J Respir Crit Care Med 2025;211:A6710.
Figure 1: CT before and after treatment.
Impact of Inhaled Tobramycin on Healthcare Utilization and Morbidity in Non-Cystic Fibrosis
Pediatric Tracheostomy Dependent Patients with Pseudomonas Infections
Authors: *Nada Alabdulkarim,1 Kaitlyn Kuntzman,1 Raja Balusu,1 Jonathan Schroeder,2 Jessica Lundeen,3 Maria A. Arroyo1
1. Pediatric Pulmonary Department, Children’s National Hospital, Washington, D.C., USA
2. Pediatric Pulmonary Department, Brooke Army Medical Center, Fort Sam Houston, Texas, USA
3. Department of Pharmacy Services, Children’s National Hospital, Washington, D.C., USA
*Correspondence to nadalkarim.89@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Pediatric patients who are tracheostomy dependent face an increased risk of respiratory infections due to bacterial colonization by Pseudomonas aeruginosa. 1,2 Inhaled antibiotics, such as tobramycin, were developed as targeted treatments to reduce both the infection rates, and the need for systemic antibiotics. However, there is limited research on their use in children who are tracheostomy-dependent, particularly regarding their impact on healthcare utilization and optimal dosing.3,4
METHODS
The authors conducted a retrospective cohort study at Children’s National Hospital in Washington, D.C., including patients who are tracheostomy-dependent aged 0–21 years, from January 1, 2003–June 30, 2023. Patients with cystic fibrosis, bronchiectasis, or primary ciliary dyskinesia were excluded. The primary outcome measured emergency department visits, regular floor admissions, ICU admissions, and systemic antibiotic use 6 months before and after initiating inhaled tobramycin. The secondary outcome assessed changes in Pseudomonas aeruginosa positivity rates.
RESULTS
A total of 42 children were included, with a median age of 2 years; 64.3% were male. Neurologic disorders (45.2%) and bronchopulmonary dysplasia (26.2%) were the most common reasons for tracheostomy. Inhaled tobramycin therapy was associated with reduced regular admissions (p=0.04), ICU admissions (p=0.006), and systemic antibiotic use (p=0.05). Pseudomonas aeruginosa positivity decreased from 40.5% to 30.9% post-treatment (p=0.001; Table 1).
CONCLUSION
This study, the largest involving children with tracheostomies who do not have cystic fibrosis, demonstrates that inhaled tobramycin significantly reduces hospitalizations, ICU admissions, and antibiotic use. Although 40% of patients received doses between 160–300 mg every other month, dose variability did not significantly impact clinical outcomes.
ED: emergency department.
References
1. El Cheikh M et al. Microbiology of tracheal secretions: what to expect with children and adolescents with tracheostomies. Int Arch Otorhinolaryngol. 2018;22(1):50-4.
2. Sanders CD et al. Tracheostomy in children: epidemiology and clinical outcomes. Pediatr Pulmonol. 2018;53(9):1269-75.
3. Vendrell M et al. Evidence of inhaled tobramycin in non-cystic fibrosis bronchiectasis. Open Respir Med J. 2015;9(1):30-6.
4. Langton Hewer SC et al. Antibiotic strategies for eradicating Pseudomonas aeruginosa in people with cystic fibrosis. Cochrane Database Syst Rev. 2023;6(6) CD004197.
5. Alabdulkarim N et al. Impact of inhaled tobramycin on healthcare utilization and morbidity in non-CF pediatric tracheostomy dependent patients with Pseudomonas infections. Am J Respir Crit Care Med 2025;211:A2328.
Table 1: Comparison of healthcare utilization before and after inhaled tobramycin therapy.
A Retrospective Study Identifying Factors Associated with Long-Term Survival in Lung Transplant Recipients: A Focus on Psychosocial Wellbeing and Social Determinants of Health
1. Internal Medicine, Mayo Clinic, Rochester, Minnesota, USA
2. Pulmonary and Critical Care, Mayo Clinic, Rochester, Minnesota, USA
3. Thoracic surgery, Mayo Clinic, Rochester, Minnesota, USA
*Correspondence to huang.eric@mayo.edu
Disclosure: The authors have declared no conflicts of interest.
Keywords: Area Deprivation Index (ADI), housing-based socioeconomic status (HOUSES) index, long-term survival, lung transplant, Psychosocial Assessment of Candidates for Transplantation (PACT) score, psychosocial wellness, social determinants of health.
Long-term survival after lung transplantation remains challenging, with limited research on risk and protective factors. The role of psychosocial wellness and socioeconomic status (SES) are particularly understudied. This study evaluated the impact of pre-transplant surrogate markers of psychosocial health and SES on long-term survival in adult lung transplant recipients.
METHODS
The authors conducted a single-center, retrospective case-control study using the Mayo Clinic lung transplant registry. Cases (survival >6 years) and controls (survival <6 years) were matched by transplant date (±5 years) and indication for transplant, resulting in 190 subjects (63 cases and 127 controls).
Psychosocial health was assessed using the Psychosocial Assessment of Candidates for Transplantation (PACT) score (1–4 scale; ≥2 ultimately required for transplant). Additional variables included proximity to the transplant center, insurance type, marital status, caregiver status, and employment. SES was estimated using two address-based markers: the housing-based SES (HOUSES) index (a novel composite score derived from various housing characteristics where higher scores equal better SES) and the Area Deprivation Index (ADI) at national and state levels (higher scores equal greater deprivation).
Statistical analysis used paired Wilcoxon rank-sum and McNemar’s tests. Results were reported as medians or percentages.
RESULTS
Preliminary data demonstrated that PACT scores and other psychosocial variables had no significant differences between groups. HOUSES index scores were similar (p=0.179), but long-term recipients had significantly higher ADI scores (national: p=0.029; state: p=0.019). Other variables relating to donor and recipient characteristics showed no significant differences (all p>0.05; Table 1).
CONCLUSION
Pre-transplant psychosocial health indicators, including PACT scores, caregiver support, marital status, and proximity to transplant centers, were not linked to long-term survival.
While the HOUSES index was not associated with long-term survival, higher ADI scores correlated with improved survival, suggesting
unique protective factors in socioeconomically disadvantaged populations. These findings highlight the complex role of socioeconomic factors in lung transplant outcomes and underscore the need for further research into how specific socioeconomic and environmental factors influence long-term survival.
Reference
1. Huang E et al. A retrospective study identifying factors associated with long-term survival in lung transplant recipients: a focus on psychosocial wellbeing and social determinants of health. Abstract P1271. ATS International Conference, 18-21 May, 2025.
Table 1: Evaluation of risk factors associated with long-term lung transplant survival.
*p<0.05
ADI: Area Deprivation Index; HOUSES: housing-based socioeconomic status; IQR: interquartile range; PACT: Psychosocial Assessment of Candidates for Transplantation.
A Rare Case of BK Virus Pneumonia
Authors: *Savannah Knight,1 Julie Katkin1
1. Pulmonary Medicine Department, Texas Children’s Hospital, Baylor College of Medicine, Houston, Texas, USA
*Correspondence to savannah.knight@bcm.edu
Disclosure: The authors have declared no conflicts of interest.
Keywords: BK virus, bronchoalveolar lavage (BAL), graft-versus-host disease, hematopoietic stem cell transplant (HSCT), immunodeficient, immunosuppression, opportunistic infection, polyomavirus hominis 1.
BK virus, also known as Polyomavirus hominis 1, is a common virus that infects about 60–90% of the general population during childhood and then remains latent in the kidneys. Reactivation can occur in the setting of immune suppression. Infection with BK virus causing hemorrhagic cystitis has been well documented in patients following hematopoietic stem cell transplantation (HSCT), kidney transplants, and HIV infections.1 However, BK virus causing pneumonia has rarely been reported in the literature. Here the authors present a case of a patient with HSCT complicated by hemorrhagic cystitis and respiratory failure, with concern for BK viral pneumonia.
CASE
A 22-year-old male with a history of B cell acute lymphoblastic leukemia and HSCT was presented to the hospital for graftversus-host disease management. After poor response to initial management, it was recommended to repeat a liver biopsy, which was complicated by right hemothorax and drained by interventional radiology intraoperatively. His course was
then complicated by re-accumulation of the hemothorax with respiratory distress, so he was admitted to the pediatric ICU. His respiratory failure progressed, with new multifocal opacities observed on chest X-ray, and requiring intubation. The chest tube continued to drain copious amounts of blood, so a CT with angiography was obtained to rule out a vascular injury causing hemothorax. The CT revealed multifocal ground-glass opacities and right lower lobe consolidation, representing pulmonary hemorrhage or infection (Figure 1). Due to his immune deficient status, a bronchoscopy with bronchoalveolar lavage (BAL) was obtained to investigate for opportunistic infections.
The patient had a history of BK virus positive urine and developed new hemorrhagic cystitis during his pediatric ICU stay. His BK viral count in the urine was >500,000,000 copies/mL, and he also had significant viremia, prompting BK virus testing in the BAL sample. BAL studies were significant only for a BK viral count of 1,700 copies/ mL. On cytology, the sample was markedly hemorrhagic, with no evidence of fungus on silver stain and 2–4% lipid-laden macrophages. Due to the severity of his graft-versus-host disease, his medical team determined that he was not a candidate for the typical therapy for BK virus, which is the removal of immunosuppressive medications. Unfortunately, the patient continued to decompensate, and he passed away from multiple organ failure.2
DISCUSSION
Per literature review, there have been very few cases reported of suspected BK viral pneumonia, with only three other cases reported where infection was confirmed with BAL.1,3-7 The typical treatment for BK virus nephropathy typically includes withdrawal of immunosuppression, which was not possible in this patient. Other treatments that have
Figure 1: CT with angiography of the chest showing multifocal ground-glass opacities and consolidation in the right lower lobe, that may represent hemorrhage, infection, and/or aspiration.
There was no evidence of vascular injury causing hemothorax or pulmonary hemorrhage.
been attempted for both nephropathy and pneumonia include cidofovir, leflunomide, quinolone antibiotics and intravenous immunoglobin; however, the treatment is not standardized and was used with varying success.1-7 Due to the rarity of cases, it is unclear whether the finding of BK virus in the BAL proves the causality of his pneumonia, or whether it is only a marker of the degree of his immune suppression. In this case, no other infectious etiology was found to explain his clinical symptoms, leading the authors to believe that the BAL was indicative of infection causing disease. Collectively, these cases suggest that the finding of BK virus in the lungs is associated with a high mortality rate.
References
1. Akazawa Y et al. Fatal BK virus pneumonia following stem cell transplantation. Transpl Infect Dis. 2012 Dec;14(6):E142-6.
2. Knight S, Katkin J. A rare case of BK
virus pneumonia. Abstract 11841. American Thoracic Society Conference, 16-21 May 2025.
3. Chaitou A et al. BK virus pneumonia with cmv colitis in a kidney transplant recipient: successful treatment with non-cidofovir based therapy. J Microb Infect Dis. 2021;11(1)36-41.
4. Randhawa P, Brennan DC. BK virus infection in transplant recipient: an overview and update. Am J of Transplant. 2006;6(9):2000-5.
5. Stoner G et al. BK virus regulatory region rearrangements in brain and cerebrospinal fluid from a leukemia patient with tubulointerstitial nephritis and meningoencephalitis. Am J of Kidney D. 2002;39(5):1102-12.
6. Yapa HM et al. Pneumonitis post-haematopoeitic stem cell transplant - cytopathology clinches diagnosis. J of Clin Virol. 2012;55(3):278-81.
7. Yoshimura A et al. BK virus pneumonia following stem cell transplantation against diffuse large B-cell lymphoma. Respirol Case Rep. 2018;6(7):e00348.
Long-term Survival of Lung Transplant Recipients With Early Post-Operative Atrial Fibrillation Treated
with Amiodarone
Authors: *Cameron K. Lawson,1 Isabelle Pokora,1 Edward T. Murphy,1 Gayathri Sathiyamoorthy,1
Sheila Krishnan,1 Ryan Hadley,1 Reda Girgis1
1. Richard DeVos Heart and Lung Transplant Program, Corewell Health, Grand Rapids, Michigan, USA
*Correspondence to Cameron.lawson@corewellhealth.org
Disclosure: The authors have declared no conflicts of interest.
Atrial fibrillation/flutter (AF) is a common early post-operative complication after lung transplantation (LTX) and has been associated with increased morbidity and mortality. Optimal management has not been established. Some studies have suggested increased mortality with the use of amiodarone. The authors’ standard approach is early rhythm control with amiodarone followed by cardioversion if needed. Anticoagulation is withheld if sinus rhythm is restored within 48 hours.
The authors sought to review their experience to determine if the occurrence of AF was associated with increased morbidity and/or mortality, and specifically, if survival was lower with the use of amiodarone.
METHODS
Adult LTX recipients with AF occurring during the index transplant hospital stay were identified. Characteristics of these patients
were compared with a contemporaneous cohort without AF. Wilcoxon rank-sum tests were used to compare length of stay (LOS), duration of mechanical ventilation, and age at time of transplant. Fisher’s exact tests were used to evaluate acute kidney injury and primary graft dysfunction. Post transplant survival was compared with log-rank analysis of Kaplan-Meir estimates.
RESULTS
Between September 2017 and October 2024, 104 out of 294 (35%) LTX recipients developed post-operative AF. The AF group was slightly older (67.7 years versus 64.9 years; p=0.0002), but otherwise similar to the non-AF cohort with respect to gender, comorbidities, underlying disease, and transplant type. Both ICU LOS (median 6.5 days versus 3.5 days; p<0.001), and total hospital LOS (21 days versus 16 days; p<0.001) were longer in the AF group. The AF group had a higher incidence of acute kidney injury of any severity (46% versus 27%; p=0.002) and any grade of primary graft dysfunction (53% versus 42%; p=0.12). Eighty (77%) patients with AF received amiodarone therapy, 16 (15%) underwent cardioversion, and 15 (14%) were anticoagulated. Survival at 1, 3, and 5 years post-transplant was 94%, 86%, and 79%, respectively, in the AF group, compared to 97%, 93%, and 80% in the non-AF cohort (p=0.36). Among subjects treated with amiodarone, survival was 92%, 83%, and 74% at 1, 3, and 5 years, respectively (p=0.19 versus no AF; Figure 1).
CONCLUSION
Early post-transplant AF is associated with longer LOS and higher incidence of acute
kidney injury; however, long-term survival was comparable to recipients without AF. Amiodarone use was not associated with increased mortality. Additional studies are required to determine the optimal approach to the prevention and management of post-operative AF after LTX.
Figure 1: Survival of patients with atrial fibrillation/atrial flutter treated with amiodarone, compared to patients with no atrial fibrillation/atrial flutter.
Product-Limit Survival Estimates
With Number of Subjects at Risk
Time (years)
Atrial Fibrillation/Atrial Flutter and Treated with Amiodarone
References
1. Lawson C et al. Long-term survival of lung tansplant recipients with early post-operative atrial fibrillation treated with amiodarone [abstract]. Am J Respir Crit Care Med. 2025;211:A1740.
2. Isiadinso I et al. Atrial arrhythmias after lung and heart-lung transplant: effects on short-term mortality and the influence of amiodarone. J Heart Lung Transplant. 2011;30(1):37-44.
3. Orrego CM et al. Atrial arrhythmias after lung transplant: underlying mechanisms, risk factors, and prognosis. J Heart Lung Transplant. 2014;33(7):734-40.
4. Waldron NH et al. Adverse outcomes associated with postoperative atrial arrhythmias after lung transplantation: a meta-analysis and systematic review of the literature. Clin Transplant. 2017. doi:10.1111/ctr.12926.
The Surviving Sepsis Campaign Guidelines recommend the use of inotropic agents, such as dobutamine, for patients with septic shock and cardiac dysfunction. However, previous studies have demonstrated that a considerable proportion of these patients do not tolerate dobutamine well. Identifying predictors that indicate a favorable response to dobutamine remains an important yet unclear area of investigation.
METHODS
This single-center, retrospective cohort study (2011–2020) examined adult patients admitted to a quaternary ICU with septic shock, who were started on dobutamine within 72 hours of receiving an echocardiogram.1 Baseline characteristics, echocardiographic data, and serial norepinephrine equivalent (NEE) doses were collected at dobutamine initiation, as well as at 2 and 6 hours post-initiation.
RESULTS
Eighty-two patients met the inclusion criteria, of whom 48% were female. The median age was 66 years (interquartile range [IQR]: 54–75), and the median Acute Physiology, Age, Chronic Health Evaluation (APACHE) III score was 115 (IQR: 97–140). The median lactate level was 5.6 (IQR: 3.1–9.4), with a median fluid balance of 3,634 mL (IQR: 1,645–6,290). The median left ventricular ejection fraction (LVEF) was 35% (IQR: 25–55), and the median left ventricular outflow tract (LVOT) velocity-time integral (VTI) was 12.1 cm (IQR: 9.3–15.0). Of all the patients, 73% were initiated on 2.5 mcg/ min of dobutamine, with a median NEE at dobutamine initiation of 0.24 mcg/kg/min (IQR: 0.15–0.62). In-hospital mortality in all patients was 58.5%. Univariate analysis suggested in-hospital mortality to be higher in patients with a higher admission APACHE III score (101 [IQR: 87–119] versus 131[105, 143]; p<0.001) and a lower LVOT VTI (13.3 [IQR: 10.8–17.5] versus 11.3 [IQR: 8.4–13.9]; p=0.05). LVEF, cardiac output, systematic vascular resistance, and heart rate were not associated with in-hospital mortality. Based on the LVOT VTI groups (LVOT VTI <12 cm versus LVOT VTI ≥12 cm), an assessment of NEE dosage upon dobutamine initiation indicated a trend towards a better response in patients with LVOT VTI <12 cm (Figure 1A). Multivariable-adjusted logistic regression suggested that a lower LVOT VTI at dobutamine initiation was associated with improved outcomes (Figure 1B).
ACONCLUSION
Although guidelines support dobutamine in septic shock with cardiac dysfunction, there is limited guidance on optimal predictors for their use. The authors’ findings suggest a
potential trend for reduced NEE requirements and in-hospital mortality when dobutamine is used in patients with LVOT VTI <12 cm. Larger studies are needed to validate these results and inform indications for inotropic therapy.
A) Norepinephrine equivalent dosage trend over 6 hours after dobutamine initiation based on left ventricular outflow tract velocity-time integral; LVOT-VTI: left ventricular outflow tract velocity-time integral; NEE: norepinephrine equivalent.
Reference 1. Tarbaghia M et al. Dobutamine in septic shock, when and why? Am J Respir Crit Care Med. 2025;211:A3748.
The Sweet Hour: A Framework for Effective Journal Clubs in Graduate Medical Education
Authors: *Abdelrahman Nanah,1 Marwa Tarbaghia,1 Noor Ramahi , 1 Walaa Abu Alya,1 San Kim,1 Divyajot Sadana,2 Sudhir Dudekonda,2 Mohammed Jaghbeer,3 Megan McGervey1
1. Department of Internal Medicine, Cleveland Clinic Foundation, Ohio, USA
2. Department of Pulmonary and Critical Care Medicine, Cleveland Clinic Foundation, Ohio, USA
3. Department of Pulmonary and Critical Care Medicine, King Hussein Cancer Center, Amman, Jordan *Correspondence to NANAHA@ccf.org
Disclosure: The authors have declared no conflicts of interest.
Keywords: Journal club, medical education, quality improvement (QI).
Quality improvement (QI) has proven instrumental in identifying and addressing systemic changes in healthcare, yet its application in medical education remains limited. The authors hypothesize that QI interventions can be effectively adapted to enhance didactic medical education. Here, they describe their experience applying QI strategies to improve an extracurricular journal club known as the "Sweet Hour Journal Club". This was a monthly extracurricular session led by a volunteer resident or faculty member, discussing a publication of interest in pulmonary and critical care. Held after hours (5:15 p.m.–6:00 p.m.) in the residency lounge, prereadings were distributed via email the week prior, and both faculty and residents were invited to attend optionally. Desserts were provided per the presenter's request.
METHODS
The authors employed QI methodologies, including process mapping, plan-dostudy-act (PDSA) cycles, and run charts, to strengthen the extracurricular Journal Club didactic series.
Process mapping revealed that the after-hours timing and the requirement of prereadings likely contributed to decreased attendance and engagement rates. Additionally, qualitative interviews with attendees and volunteer presenters identified residents’ intimidation in discussing methodology and statistical analysis as a barrier to presenting at the club.
During the first PDSA cycle, the Sweet Hour Journal Club was rescheduled to a bimonthly optional session held during the noon break (12:00 p.m.–1:00 p.m.). In the second cycle, prereadings were eliminated, and guest speakers were invited to act as study critics, facilitating discussions on study methodology and result generalizability. In the final PDSA cycle, a critical appraisal worksheet was integrated into each session, enabling learners to actively document their thoughts on study randomization, internal and external validity, and result interpretation (e.g., number needed to treat, number needed to harm, and statistical and clinical significance).
RESULTS
Following these interventions, the authors’ run chart (Figure 1) indicated a trend toward higher attendance rates with each successive PDSA cycle.
Cycle 1
PDSA: plan-do-study-act.
CONCLUSION
QI methodologies can enhance curricular design and didactic medical education. Further studies are needed to determine if such interventions lead to higher knowledge retention and learner engagement compared to traditional didactic methods.
Cycle 2 PDSA Cycle 3
Reference
1. Nanah ER et al. Leveraging quality improvement in medical education: The sweet spot. Am J Respir Crit Care Med. 2025;211:A1450.
Figure 1: Attendance per “Sweet Hour Journal Club” session.
PDSA
Determining the Impact of HIV on the Severity of COVID-19 Infection: 2020–2021 Nationwide Analysis
Authors: *Antony Arumairaj,1 Phool Iqbal,1 Joseph Mattana,2 Shobhana Chaudhari,2 Fnu Samaksh,1 Thomas Newman1
1. New York Medical College/Metropolitan Hospital Center, New York, USA
2. Department of Medicine, New York Medical College/Metropolitan Hospital Center, New York USA
*Correspondence to antojack99@gmail.com
Disclosure: The authors have declared no conflicts of interest.
HIV causes immunodepression, which can lead to severe outcomes of COVID-19 infection. However, clinical studies have shown conflicting reports regarding outcomes of COVID-19 infection in patients with HIV. This National Inpatient Sample (NIS) study aimed to determine the impact of HIV on the severity of outcomes in patients with COVID-19 infection.1-3
METHODS
The authors identified patients hospitalized with COVID-19 infection who had a history of HIV using the 2020–2021 NIS database. STATA/MP 17.0 software (StataCorp, College Station, Texas, USA) was used for statistical analysis. Multivariate logistic regression analysis was performed.
RESULTS
There were 818,011 patients hospitalized with COVID-19 infection, and 36,232 patients hospitalized with a history of HIV. The patients with COVID-19 infection were stratified based on their HIV status. There were 815,979 patients with COVID-19 who did not have HIV, and 2,032 patients who had both COVID-19 and HIV (Table 1).
White people constituted the largest ethnic group in the category of COVID-19 infection without HIV, while African American people constituted the largest ethnic group in the category of COVID-19 infection with HIV. Hispanic people constituted the second largest group in both categories. Patients in the lowest national income quartile and those with Medicaid insurance constituted the largest group among the national income quartile and insurance groups, respectively. The length of hospital stay among patients with COVID-19 and HIV was 10.4 days. For those without HIV, it was 8.2 days, with a p value of <0.001. The mortality rate was 13.1% among patients with COVID-19 but without HIV. For those with HIV, it was 13.3%, with a p value of 0.72. The unadjusted odds ratio (OR) of mortality in patients with COVID-19 and HIV was 1.02. The adjusted OR of mortality, after adjustment for age, sex, race, Charlson Comorbidity Index (CCI), national income quartile, and insurance, was 0.53, with a p value of <0.001. This indicated that the mortality rate among patients with COVID-19 and HIV was significantly lower than those without HIV (Table 2). The unadjusted OR of invasive ventilation in patients with COVID-19 and HIV was 1.26, while the adjusted OR was 0.50, with a p value of <0.001. This indicated that the need for invasive ventilation among patients with COVID-19 and HIV was significantly lower compared to those without HIV.
CONCLUSION
The authors’ analysis of the NIS database suggests that HIV was not a major risk factor for severe COVID-19 infection.
Patients with COVID-19 infection and HIV had longer lengths of stay. However, they had a lower need for invasive ventilation and a lower mortality rate than those without HIV.
Table 1: Demographic and clinical characteristics, 2020–2021 National Inpatient Sample database.
LOS: length of stay.
Table 2: Outcomes-adjusted odds ratio.
References
1. Danwang C et al. Outcomes of patients with HIV and COVID-19 co-infection: a system-atic review and meta-analysis. AIDS Res Ther. 2022;19(1):3.
2. Del Amo J et al. Incidence and severity of COVID-19 in HIV-positive persons receiving an-tiretroviral therapy. Ann Intern Med. 2021;174(4):581-2.
3. Arumairaj A et al. Determining the Impact of Human Immunodeficiency Virus (HIV) on the Severity of COVID-19 Infection: 2020-2021 Nationwide Analysis. Abstract 6618. ATS International Conference, May 16-21, 2025.
Determining the Impact of COPD on the Severity of COVID-19 Infection: 2020-2021 Nationwide Analysis
Clinical studies have shown conflicting reports regarding the impact COPD on the outcomes of patients with COVID-19 infection, with few studies reporting worse outcomes and some studies showing better outcomes. This National Inpatient Sample study aimed to determine the impact of COPD on the severity of outcomes in patients with COVID-19 infection.1-4
METHODS
The authors identified patients hospitalized with COVID-19 infection and a history of COPD from the 2020–2021 National Inpatient Sample database. STATA/MP 17.0 (StataCorp LLC, College Station, Texas, USA) software was used for statistical analysis. Multivariate logistic regression analysis was then performed.
RESULTS
There was a total of 818,011 patients hospitalized with COVID-19 infection and 908,337 patients with a history of COPD (Tables 1 and 2). The patients with COVID-19 infection were stratified based on their
COPD status. Among them, 788,284 patients had COVID-19 infection without COPD, while 29,727 patients had both COVID-19 infection and COPD. The mean age was 61.3 years for patients with COVID-19 infection without COPD, compared to 71.7 years for those with COPD. People who are White constituted the largest ethnic group in both categories. Patients in the lowest national income quartile, and those with Medicaid insurance, constituted the largest group among the national income quartile and insurance groups, respectively, in both categories. The length of hospital stay was 8.2 days for patients with COVID-19 infection without COPD and 7.5 days for those with COPD (p<0.001). The mortality rate was 13.1% among patients with COVID-19 infection without COPD and 12.9% for those with COPD (p=0.54). The unadjusted odds ratio (OR) of mortality in patients with COVID-19 infection with COPD was 0.99. After adjustment for age, sex, race, Charlson comorbid index, national income quartile, and insurance, the adjusted OR of mortality was 0.62 (p<0.001), indicating that the mortality rate was significantly lower among patients with COVID-19 infection with COPD, compared to those without COPD. The unadjusted OR for invasive ventilation in patients with COVID-19 infection with COPD was 0.67, and the adjusted OR was 0.56 (p<0.001), indicating that the need for invasive ventilation was significantly lower in patients with COPD compared to those without COPD.
CONCLUSION
The authors’ analysis of the National Inpatient Sample database suggests that COPD was not a major risk factor for severe COVID-19 infection. Patients with both COVID-19 infection and COPD had shorter lengths of stay, a lesser need for invasive ventilation, and a lower mortality rate compared to those without COPD.
Table 1: Demographic and clinical characteristics from the 2020–2021 National Inpatient Sample database.
LOS: length of stay.
Table 2: Outcomes and adjusted odds ratio.
References
1. Singh D et al. Chronic obstructive pulmonary disease and COVID-19: interrelationships. Curr Opin Pulm Med. 2022;28(2):76-83.
2. Gerayeli FV et al. COPD and the risk of poor outcomes in COVID-19: A systematic review and meta-analysis. EClinicalMedicine. 2021;33:100789.
3. Leung JM et al. COVID-19 and COPD. Eur Respir J. 2020;56(2):2002108.
4. Arumairaj A et al. Determining the impact of chronic obstructive pulmonary disease (COPD) on the severity of COVID-19 infection: 2020-2021 nationwide analysis. Am J Respir Crit Care Med 2025;211:A1082-A7905.
Determining the Impact of Chronic Kidney Disease on the Severity of COVID-19 Infection: 2020-2021
Nationwide Analysis
Authors: *Antony Arumairaj,1 Phool Iqbal,1 Natoushka Trenard,1 Shobhana Chaudhari,1 Fnu Samaksh,1 Joseph Mattana1 1. New York Medical College/Metropolitan Hospital Center, New York, USA *Correspondence to antojack99@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Keywords: Chronic kidney disease (CKD), COVID-19 infection, length of stay, mortality rate, need for invasive ventilation.
Clinical studies have reported that patients with chronic kidney disease (CKD) with COVID-19 infection have higher hospitalization, ICU admission, and higher mortality compared to patients without CKD. This National Inpatient Sample study aimed to determine the impact of CKD on the severity of outcomes with COVID-19 infection.1-3
METHODS
The authors identified patients hospitalized with COVID-19 infection and a history of CKD from the 2020–2021 National Inpatient Sample database. STATA/MP 17.0 software (StataCorp LLC., Texas, USA)was used for statistical analysis. Multivariate logistic regression analysis was then performed.
RESULTS
There was a total of 818,011 patients hospitalized with COVID-19 infection and 407,312 patients with a history of CKD (Tables 1 and 2). The patients with COVID-19 infection
were stratified based on their CKD status. Among them, 787,351 patients had COVID-19 infection without CKD, while 30,660 patients had both COVID-19 infection and CKD. The mean age was 61.2 years for patients with COVID-19 infection without CKD, compared to 73.2 years for those with CKD. People who are White constituted the largest ethnic group in both categories. Patients, in the lowest income quartile and those with Medicaid insurance, constituted the largest group among patients constituted the largest group among the national income quartile and insurance groups, respectively, in both categories. The length of hospital stay was 9.3 days for patients with COVID-19 infection without CKD and 8.2 days for those with CKD (p<0.001). The mortality rate was 12.7% among patients with COVID-19 infection without CKD and 22.5% for those with CKD (p<0.001). The unadjusted odds ratio (OR) of mortality in patients with COVID-19 infection with CKD was 1.99. After adjustment for age, sex, race, Charlson comorbid index, national income quartile, and insurance, the adjusted OR of mortality was 1.03 (p<0.001), indicating that the mortality rate was significantly higher among patients with COVID-19 infection with CKD, compared to those without CKD. The unadjusted OR for invasive ventilation in patients with COVID-19 infection with bronchiectasis was 1.26, and the adjusted OR was 0.89 (p<0.001), indicating that the need for invasive ventilation was significantly lower in patients with CKD.
CONCLUSION
The authors’ analysis of the National Inpatient Sample database suggests that CKD was a significant risk factor for severe COVID-19 infection. Patients with both COVID-19 infection and CKD had longer lengths of stay, a lower need for invasive ventilation, and a higher mortality rate compared to those without CKD.
Table 1: Demographic and clinical characteristics from the 2020-2021 National Inpatient Sample database.
LOS: length of stay.
Table 2: Outcomes and adjusted odds ratio.
References
1. Jdiaa SS et al. COVID-19 and chronic kidney disease: an updated overview of reviews. J Nephrol. 2022;35(1):69-85.
2. Ajaimy M, Melamed ML. COVID-19 in patients with kidney disease. Clin J Am Soc Nephrol. 2020;15(8):1087-9.
3. Arumairaj A et al. Determining the impact of chronic kidney disease (CKD) on the severity of COVID-19 infection: 2020-2021 nationwide analysis. Abstract 6876. ATS International Conference, May 16-21, 2025.
Determining the Impact of Bronchiectasis on the Severity of COVID-19 Infection: 2020–2021
Nationwide Analysis
Authors: *Antony Arumairaj,1 Phool Iqbal,1 Fnu
Samaksh,1 Vikas Yadav,1 Joseph Mattana,1 Shobhana Chaudhari,1 Natoushka Trenard1 1. New York Medical College/Metropolitan Hospital Center, New York, USA *Correspondence to antojack99@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Keywords: Bronchiectasis, COVID-19 infection, length of stay, mortality rate, need for invasive ventilation.
The impact of bronchiectasis on the severity of COVID-19 infection has been contradictory. Some studies report that bronchiectasis is a risk factor for severe COVID-19 infection, whereas others have found no relationship between bronchiectasis and the severity of COVID-19 infection. This National Inpatient Sample study aimed to determine the impact of bronchiectasis on the severity of COVID-19 infection.1-3
METHODS
The authors identified patients hospitalized with COVID-19 infection and a history of bronchiectasis from the 2020–2021 National Inpatient Sample database (Tables 1 and 2). STATA/MP 17.0 (StataCorp LLC, College Station, Texas, USA) software was used for statistical analysis. Multivariate logistic regression analysis was then performed.
RESULTS
There was a total of 818,011 patients hospitalized with COVID-19 infection and 31,439 patients with a history of bronchiectasis. The patients with COVID-19 infection were stratified based on their bronchiectasis status. Among them, 815,213 patients had COVID-19 infection without bronchiectasis, while 2,798 patients had both COVID-19 infection and bronchiectasis. The mean age was 61.6 years for patients with COVID-19 infection without bronchiectasis, compared to 69.7 years for those with bronchiectasis. People who are White constituted the largest ethnic group, and patients with Medicaid insurance constituted the largest insurance group in both categories. Patients in the lowest income quartile constituted the largest group among patients with COVID-19 infection without bronchiectasis, whereas those with bronchiectasis mostly belonged to the second highest income quartile. The length of hospital was 8.2 days for patients with COVID-19 infection without bronchiectasis and 16.7 days for those with bronchiectasis (p<0.001). The mortality rate was 13.0% among patients with COVID-19 infection without bronchiectasis and 21.5% for those with bronchiectasis (p<0.001). The unadjusted odds ratio (OR) of mortality in patients with COVID-19 infection with bronchiectasis was 1.82. After adjustment for age, sex, race, Charlson comorbid index, national income quartile, and insurance, the adjusted OR of mortality was 1.37 (p<0.001), indicating that the mortality rate was significantly higher among patients with COVID-19 infection with bronchiectasis, compared to those without bronchiectasis. The unadjusted OR for invasive ventilation in patients with COVID-19 infection with bronchiectasis was 2.12, and the adjusted OR was 1.89 (p<0.001), indicating that the need for invasive ventilation was significantly higher in patients with bronchiectasis.
Table 1: Demographic and clinical characteristics from the 2020-2021 National Inpatient Sample database.
Variables
LOS: length of stay.
Table 2: Outcomes and adjusted odds ratio.
CONCLUSION
The authors’ analysis of the National Inpatient Sample database suggests that bronchiectasis is a major risk factor for severe COVID-19 infection. Patients with both COVID-19 infection and bronchiectasis had longer lengths of stay, a higher need for invasive ventilation, and a higher mortality rate compared to those without bronchiectasis.
References
1. Seo C et al. Bronchiectasis and COVID-19: for better or for worse? Ann Am Thorac Soc. 2024; 21(2):208-10.
2. Oscullo G et al. Bronchiectasis and COVID-19 infection: a two-way street. Chin Med J (Engl). 2022; 135(20):2398-2404.
3. Arumairaj A et al. Determining the impact of bronchiectasis on the severity of COVID-19 infection: 2020-2021 nationwide analysis. Am J Respir Crit Care Med 2025;211:A4546.
Plasma Fibrinogen as a Predictor of Disease Severity and Exacerbation: Insights Across the Pre-COPD and COPD Continuum
Plasma fibrinogen and C-reactive protein (CRP) are acute phase reactants that are increasingly being investigated as potential biomarkers for COPD severity, progression, and exacerbation risk.1,2 However, their roles across the full spectrum of spirometric disease severity, especially in pre-COPD, remain poorly understood. Emerging data suggest that the pre-COPD population, such as those in Global Initiative for Chronic Obstructive Lung Disease (GOLD) Stage 0 and preserved ratio impaired spirometry (PRISm), represent a heterogenous mix of individuals. Some individuals progress to develop milder disease (GOLD 1), while others progress to develop a more severe disease (GOLD 2–4) within the same timeframe.3 Yet, how fibrinogen or CRP levels vary across this continuum, particularly in pre-COPD, which is a stage marked by distinct progression patterns, remains unclear.
OBJECTIVE
The authors’ objective was to determine the distribution of plasma fibrinogen and CRP levels across the spirometric spectrum of pre-COPD and COPD.
METHODS
The authors conducted pulmonary function testing and respiratory health surveys among U.S. Veterans with a smoking history, with or without a COPD diagnosis, who were undergoing lung cancer screening at the San Francisco Veterans Affairs Health Care System.4 Blood samples obtained at the time of survey completion were tested for fibrinogen (using the Clauss method) and C-reactive protein (CRP; via high-sensitivity immunoturbidimetric assay). The authors examined fibrinogen and CRP distributions across GOLD stages and analysed their associations with respiratory exacerbation frequency using regression modeling, adjusting for age, sex, height, weight, and smoking status (current versus former) as well as smoking burden (pack-years).
RESULTS
Among 312 participants (96% male, mean age 70 years) with stable disease (no exacerbation for ≥6 weeks prior), 40% had GOLD 0, 11% had PRISm, 20% had GOLD 1, 23% had GOLD 2, and 7% had GOLD 3 or 4. As previously reported,4 the frequency of moderate/severe exacerbations increased with advancing spirometric disease.
Fibrinogen levels were 367±83, 407±72, 354±73, 386±83, and 391±68 mg/dL for GOLD 0, PRISm, GOLD 1, GOLD 2, and GOLD 3/4, respectively. Participants with PRISm had
higher fibrinogen levels compared to GOLD 0 and GOLD 1 (Figure 1A and 1B). In severe COPD (GOLD 3 and 4), higher fibrinogen trended toward more frequent exacerbations, while in participants with PRISm, higher fibrinogen showed a trend toward fewer exacerbations (p=0.08; Figure 1C). CRP levels were 5.0±7.7, 6.3±6.9, 3.0±4.1, 5.5±13.9, and 5.3±9.8 mg/dL for GOLD 0, PRISm, GOLD 1, GOLD 2, and GOLD 3/4, respectively, with no significant differences observed (Figure 1D–F). CRP levels did not show a significant trend with exacerbation risk. Notably, both fibrinogen and CRP appeared lowest in GOLD 1, although these differences were not statistically significant.
CONCLUSION
Fibrinogen and CRP levels do not follow a linear trend across the COPD severity spectrum, possibly reflecting the underlying heterogeneity of pre-COPD and COPD. The lower levels of fibrinogen and CRP levels in GOLD 1 align with recent data suggesting that individuals who develop mild COPD (GOLD 1) may follow a different disease trajectory than those progressing to moderate or severe disease (GOLD 2–4).5
The higher fibrinogen level observed in PRISm, along with its inverse association with the exacerbation frequency, may reflect a systemic inflammatory phenotype that is not
primarily driven by airway obstruction. This could represent underlying comorbidities such as obesity, metabolic syndrome, or cardiovascular disease, conditions that are more common in PRISm and contribute to systemic inflammation.6,7 Alternatively, it may indicate a distinct pathobiological pathway in PRISm, in which extrapulmonary factors such as vascular remodeling or restrictive physiology, play a greater role than classic airflow obstruction.
The lower levels of fibrinogen and CRP levels in GOLD 1 align with recent data suggesting that individuals who develop mild COPD (GOLD 1) may follow a different disease trajectory than those progressing to moderate or severe disease (GOLD 2–4).5
The higher fibrinogen level observed in PRISm, along with its inverse association with the exacerbation frequency, may reflect a systemic inflammatory phenotype that is not primarily driven by airway obstruction. This could represent underlying comorbidities such as obesity, metabolic syndrome, or cardiovascular disease, conditions that are more common in PRISm and contribute to systemic inflammation.6,7 Alternatively, it may indicate a distinct pathobiological pathway in PRISm, in which extrapulmonary factors such as vascular remodeling or restrictive physiology, play a greater role than classic airflow obstruction.
A and D: Distribution of fibrinogen (A) and CRP (D) levels across the pre-COPD and COPD disease spectrum. B and E: Covariate-adjusted values of fibrinogen (B) and CRP (E). Values are presented as mean±95% CI. * and brackets indicate significant (p<0.05) comparisons. C and F: Associations between the number of moderate to very severe (m/s) respiratory exacerbations and levels of fibrinogen (C) or CRP (F) for each pre-COPD and COPD categories. Each line on Y-axis represents a separate regression. Values are presented as parameter estimate±95% CI.
CRP: C-reactive protein.
References
1. Agustí A et al. Evaluation of COPD longitudinally to identify predictive surrogate endpoints (ECLIPSE) investigators. Persistent systemic inflammation is associated with poor clinical outcomes in COPD: a novel phenotype. PLoS One. 2012;7(5):e37483.
2. Mannino DM et al. Plasma fibrinogen as a biomarker for mortality and hospitalized exacerbations in people with COPD. Chronic Obstr Pulm Dis. 2015;2(1):23-34.
3. Wan ES et al. COPDGene Investigators. Longitudinal phenotypes and mortality in preserved ratio impaired spirometry in the COPDGene Study. Am J Respir Crit Care Med. 2018;198(11):1397-405.
4. Abrham Y et al. Self-report underestimates the frequency of the acute respiratory exacerbations of
COPD but is associated with BAL neutrophilia and lymphocytosis: an observational study. BMC Pulm Med. 2024;24(1):433.
5. Arjomandi M et al. Phenotypes and trajectories of tobacco-exposed persons with preserved spirometry: insights from lung volumes. Ann Am Thorac Soc. 2025;22(4):494-505.
6. Guerra S et al. Morbidity and mortality associated with the restrictive spirometric pattern: a longitudinal study. Thorax. 2010;65(6):499-504.
7. YD Abrham et al. Plasma fibrinogen as a predictor of disease severity and exacerbation: insights across the pre-COPD and COPD continuum. Am J Respir Crit Care Med 2025;211:A1349.
Table 1: Acute inflammatory markers in COPD spectrum.
Diagnostic Metabolomic Profiling of COPD as Potential Biomarkers in Older and Younger Patients
3. Centro de Investigación Biomédica en Red, Área de Enfermedades Respiratorias (CIBERES), Instituto de Investigación Carlos III (ISCiii), Madrid, Spain
4. The Ruth and Bruce Rappaport Faculty of Medicine, Technion, Israel Institute of Technology, Haifa, Israel
*Correspondence to cesarjesse.enriquez01@alumni.upf.edu
Disclosure: The authors have declared no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results. This research was co-funded by the Spanish Ministerio de Economía y Competitividad and the European Union (project SAF201454371), the Instituto de Salud Carlos III (ISCIII) and European Union (projects PI17/00369, PI18/01008, PI21/00785 and M-BAE BA22/00009), SEPAR Grants (2015, 2016, and 2019), a FUCAP Grant (2014); a SOCAP Grant (2020), and Menarini Spain (unrestricted Grant 2015–19). Enríquez Rodríguez is a recipient of a Predoctoral Grant PFIS (ref. FI22/00003) and a Mobility of Research Personnel Grant (M-AES MV23/00012) from ISCIII and co-funded by the European Union.
Acknowledgements: This was written on behalf of BIOMEPOC and EARLY-COPD groups. The authors would like to thank Eyal Gottlieb for facilitating the material and human infrastructure of his laboratory at the Rappaport Family Institute for Research in Medical Sciences (Technion, Israel Institute of Technology). The authors would also like to thank Alia Ghrayeb and Natan Weissman for their help with the study, as well as all their collaborators, including the patients and nurses that have participated in the BIOMEPOC and Early-COPD studies.
COPD is a highly prevalent condition, but it often remains underdiagnosed due to its nonspecific clinical presentation and reliance on technically demanding spirometry.1 Blood-based biomarkers could help in identifying individuals at risk and offer insights into disease pathophysiology.2 This study aimed to identify metabolic alterations associated with COPD and to develop a biological signature potentially useful for screening purposes.
METHODS
A case-control study design was used, including 182 fasting plasma samples from 91 patients with COPD and 91 controls (individuals who either formerly smoked or currently smoke, without airflow limitation), drawn from the BIOMEPOC3 and EARLY-COPD4 multicenter Spanish cohorts. Patients underwent extensive clinical characterization to match both groups for age, sex, BMI, and smoking history. Metabolomic profiling was performed using a combination of semi-targeted and untargeted liquid chromatography-tandem mass spectrometry, providing broad metabolite coverage and improving identification accuracy. Only metabolites detected in ≥80% of samples were included in the analysis. Data processing and statistical analyses were carried out using MetaboAnalyst 6.0.5 Differentially abundant metabolites were identified through comparative analysis adjusted for multiple comparisons (false discovery rate <0.1). These were further examined using multiple regression analysis controlling for confounding variables, including age, sex, BMI, and plasma cotinine levels (as a marker of recent smoking). Pathway enrichment analyses were conducted using the Human Metabolome Database and the Kyoto Encyclopedia of
Genes and Genomes database. For biomarker discovery, support vector machine models were applied with 100 Monte Carlo crossvalidation iterations to derive a minimal 10-metabolite panel, excluding xenobiotics to enhance endogenous biological relevance.
RESULTS
Both the COPD and control groups included adults predominantly in their 40s to 60s, with a balanced sex distribution (52% male) and a mean BMI within the overweight range (26 kg/m2). Patients with COPD exhibited impaired respiratory function characterized by airflow obstruction and reduced diffusing capacity for carbon monoxide, with most classified (using the Global Initiative for Chronic Obstructive Lung Disease [GOLD] classification) as GOLD 2, followed by GOLD 3 and GOLD 1.6,7
Out of 360 quantifiable metabolites, 74 differed significantly between COPD and controls, with 56 remaining significant after adjustment for confounders. The main endogenous changes were related to lipid metabolism, including both over- and underrepresentation of specific fatty acids and acylcarnitines, as well as alterations in amino acid and carbohydrate metabolism. Notably, the largest group of differentially abundant metabolites consisted of xenobiotics. These non-endogenous compounds likely reflect environmental or microbiota-derived exposures, and were therefore excluded from the final diagnostic model to preserve biological relevance.6,7
The final 10-metabolite endogenous panel comprised of N-methylglutamate, diethanolamine, and gluconic acid (increased), as well as leucic acid, palmitic acid, 14-methylhexadecanoic acid, 2-hydroxymyristic acid, glyceric acid, 2-aminonicotinic acid, and urocanate (decreased). It achieved high discriminatory power (area under the curve: 0.916; 90.1% sensitivity; 89% specificity; Figure 1). Pathway analysis highlighted disruptions in fatty acid β-oxidation, amino acid catabolism, and the pentose phosphate pathway.6,7
CONCLUSION
The exclusive use of endogenous metabolites reinforces both biological plausibility and clinical translatability. The identified metabolic profile provides novel insights into energy metabolism, inflammation, and redox balance in young and old COPD. This may aid in screening individuals at high-risk. Nonetheless, further mechanistic research and long-term external validation are required to confirm causality. Despite this, the proposed signature marks a step forward in precision diagnostics for COPD.
This study identifies a xenobiotic-free 10-metabolite plasma panel that allows for high-accuracy COPD diagnosis and sheds light on the disease’s underlying metabolic disturbances. Plasma metabolomics reveals a distinct, physiologically relevant COPD profile. Future studies should validate its clinical utility and investigate therapeutic strategies targeting altered metabolic pathways.
1: Receiver operating characteristic curve from the best model (which included 10 metabolites).
References
1. Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for Prevention, Diagnosis and Management of COPD: 2025 Report. 2025. Available at: https://goldcopd.org/2025-gold-report/. Last accessed: 30 May 2025.
2. Gea J et al. Metabolomics in COPD. Arch Bronconeumol. 2023;59(5):311-21.
3. Gea J et al.; BIOMEPOC. The BIOMEPOC project: personalized biomarkers and clinical profiles in chronic obstructive pulmonary disease. Arch Bronconeumol. 2019;55(2):93-9.
4. Borràs-Santos A et al. EARLY COPD: determinantes de la aparición y progresión de la enfermedad pulmonar obstructiva crónica en adultos jóvenes. Protocolo de un estudio caso-control con seguimiento. Arch Bronconeumol. 2019;55(6):312-8.
82.1-95.4 80.7-94.6 83.7-93.3
5. Pang Z et al. MetaboAnalyst 6.0: towards a unified platform for metabolomics data processing, analysis and interpretation. Nucleic Acids Res. 2024;52(W1):W398-406.
6. Enríquez-Rodríguez CJ et al. Diagnostic metabolomic profiling of COPD as potential biomarkers in older and younger patients. Am J Respir Crit Care Med. 2025;211(Abstracts):A2503.
7. Casadevall C et al.; EARLY COPD and BIOMEPOC Groups. Metabolomic plasma profile of chronic obstructive pulmonary disease patients. Int J Mol Sci. 2025;26(10):4526.
Figure
Congress Interviews
AMJ speaks with two influential leaders about their work with the American Thoracic Society (ATS), reflecting on the current landscape of pulmonary medicine and the global community behind it. We had the honor of speaking with Raed Dweik, incoming President of ATS, who shared his clinical insights and vision for the year ahead. Jesse Roman, esteemed ATS member since 1988 and incoming President for 2027–2028, reflects on decades of research, leadership, and innovation in respiratory care.
Featuring: Raed Dweik and Jesse Roman
Raed Dweik
President, American Thoracic Society (ATS), Professor and Inaugural Chief, Integrated Hospital Care Institute (IHI), Cleveland Clinic, Ohio, USA
Your work in pulmonary vascular diseases has been groundbreaking. What initially drew you to this area of medicine?
Q2
What are some of the most promising advances in pulmonary medicine this year that you're most excited by?
The public’s eroding trust in science and scientists is a major challenge
As a physician-scientist, studying the pulmonary circulation has given me the opportunity to align my clinical practice in pulmonary hypertension clinic with my research interest in nitric oxide biology. This has also allowed me to build a world-class destination program in pulmonary vascular disease; a program that provides exceptional care for patients while performing cutting-edge basic, translational, and clinical research. Our Pulmonary Hypertension Educational Summit draws attendees from across the county, including clinicians, researchers, patients, and families.
We are on the cusp of many advances in so many areas, from big data and artificial intelligence, to genomics, genetics, and epigenetics, to advances in diagnostics, therapeutics, and precision medicine. Some examples include advances in lung cancer screening and diagnostics, biologics for asthma and COPD, immunotherapy for lung cancer, antifibrotic medications for idiopathic pulmonary fibrosis, disease-modifying drugs for pulmonary hypertension, and bronchoscopy interventions for airway diseases, among others.
Q3 Are there any major clinical challenges in the field you are particularly focused on right now?
The public’s eroding trust in science and scientists is a major challenge. Regulatory challenges and uncertainty regarding funding for research and clinical care are also major challenges. The burden of chronic lung diseases remains very high, as does the impact of occupational and environmental exposures.
Q4 As the incoming ATS President, what are your top priorities for the organization over the next year?
Our long-term strategic plan for ATS includes transforming patient care, leading scientific discoveries, impacting global health, and advancing professional development, all while we strengthen our ATS community. My focus will be on maintaining the premier status of the society and ensuring that ATS is a large
tent for all including clinicians, researchers, educators, and innovators; a place for both U.S and international members; a space for trainees, junior faculty, seasoned professionals, patients, and families.
Q5 This year's ATS conference brought together thousands of experts from around the world. What were your standout moments from the Conference – a talk, presentation, or discovery?
One of the most valuable aspects of the ATS International Conference is the opportunity to connect with colleagues and leaders from across the U.S and around the world. The keynote lectures are always highlights: thought-provoking, insightful, and inspiring. The yearin-review sessions are a great way to catch up on the latest literature in our fields.
The assembly business meetings also stand out as both informative and enjoyable, offering a great
mix of updates, networking, and community building.
My favorite part, however, is walking through the poster halls, seeing the latest research up close and engaging with the incredible early career professionals who are driving innovation in our field.
It’s also deeply gratifying to walk through the convention center and witness the vibrant networking and collaboration happening among peers from every corner of the globe. The exhibition hall is another highlight, showcasing the latest advancements in respiratory care. Attendees get access to cutting-edge technologies, tools, and solutions that are shaping the future of our field.
Q6 How do you envision ATS continuing to foster global collaboration across the respiratory community?
ATS continues to foster global collaboration by actively partnering with respiratory societies around
the world. Our members and leaders regularly engage in each other’s conferences, creating valuable opportunities for shared learning and collaboration.
ATS thrives on empowering others and fostering inclusive leadership
ATS thrives on empowering others and fostering inclusive leadership. These efforts reflect our ongoing commitment to strengthening global partnerships across the respiratory community, and we will continue to build on this foundation moving forward.
A cornerstone of our global efforts is the long-standing Methods in Epidemiologic, Clinical, and Operations Research (MECOR) program, which has evolved into a globally connected research
and education community. With increasingly structured and regionally tailored courses, the MECOR program now operates in Africa, Southeast Asia, China, India, Latin America, and Türkiye, empowering both students and faculty to drive advances in respiratory health.
Q7What would you say to your peers who are considering attending ATS International Conference 2026?
The ATS International Conference is returning to Orlando, Florida in 2026 for the first time in many years, and it's the perfect opportunity to be part of something special. It is a great place for clinicians, researchers, educators, and innovators to connect and collaborate. I encourage everyone to begin planning now by submitting an abstract. ATS recognizes outstanding work through assembly awards and the
international trainee scholarship program, which supports the best abstracts submitted by international participants.
Beyond the scientific program, the conference offers rich opportunities for global engagement and networking. The International Participants Center and the ATS Global Community provide welcoming spaces to connect with colleagues from around the world, share experiences, and build lasting collaborations.
Whether you're presenting research, seeking inspiration, or growing your professional network, ATS 2026 in Orlando is the place to be. Don’t miss it!
Jesse Roman
Secretary, American Thoracic Society (ATS); Ludwig A. Kind Professor of Medicine, Thomas Jefferson University; CEO, Jane & Leonard Korman Respiratory Institute; Philadelphia, Pennsylvania
In my view,
the best patient care enterprises are those that efficiently integrate research and education
Q1As CEO of the Jane & Leonard Korman Respiratory Institute of Jefferson Health and National Jewish Health, Philadelphia, Pennsylvania, how do you approach integrating academic, clinical, and translational goals within a large health system?
In my view, the best patient care enterprises are those that efficiently integrate research and education. In following the Flexnerian Model, academic centers can provide multidisciplinary, patient-centered care while educating the next generation of providers and partnering with patients to engage in clinical or translational research. Over the years, more and more attention has been given to the clinical enterprise, which may dilute other missions, especially in large and complex healthcare systems. Nevertheless, many centers continue to excel across all missions through clear vision and leadership alignment. This, paired with the recruitment of faculty who are committed to the broader vision and excited about participating in diverse activities, fosters such an environment.
Consequently, my approach is to integrate these goals by: ensuring that leadership and faculty are aligned in their commitment to all three missions of the academic model (patient care, education, and research); developing specialized clinical programs that incorporate all three missions; and establishing partnerships both inside and
outside the organization to advance the mission. Such efforts require careful consideration of space requirements, laboratory utilization, and other resources.
Q2
How have your leadership positions at such institutions shaped your approach to patient care and research?
I have been involved in patient care, education, and basic and clinical research since very early on in my career. This has given me an insight into the benefits of integrating patient care, education, and research in the same setting. The opportunity to observe how mentors and other leaders approached challenges has been invaluable, and every post I have served in has added skills to my toolbox.
I am most proud of having been able to do this work at private and public organizations in different states. This suggests that partnering with leadership, patients, and other stakeholders to establish effective programs is possible in all types of organizations, as long as there is a united vision, resources, and will.
A unified vision, careful planning, and frequent communication at all levels are important.
Q3
Your work in lung tissue remodeling has spanned decades. What advances are you most focused on right now?
Nearly every lung disease that we treat is associated with tissue remodeling. For example, emphysema is characterized by destruction of the alveolar walls, while pulmonary fibrosis is associated with aberrant deposition of excess connective tissue matrices. These are only two examples of several disorders that are characterized by erosion of the normal lung architecture leading to the loss of lung function. My work has focused on the factors that trigger fibroblast activation and uncontrolled expression of connective tissue matrices (e.g., fibronectin, collagens, etc.) in various settings. We have also worked on how cells recognize these newly deposited matrices through integrin receptors capable of signal transduction. These studies have emphasized the importance of such interactions and how they might drive disease progression.
Many of these efforts have been directed at defining the pathways leading to lung disorders; however, most patients do not develop lung disease. This suggests that there
are counter regulatory mechanisms that prevent disease development, and such mechanisms need to be better delineated and utilized for the development of preventive strategies. In addition, we should take advantage of knowledge about tissue remodeling to generate useful biomarkers capable of predicting disease progression and therapy response. These biomarkers should help reduce the cost and duration of clinical trials. Finally, we need to identify novel targets for intervention that help halt, and potentially reverse, disease progression. Learning more about the aging process and the interactions between immunity and remodeling, as well as taking advantage of new basic science and AI techniques, should drive progress in the field.
Q4
Having been a member of the American Thoracic Society (ATS) since 1988, what have been the biggest changes you’ve seen in the Society during this time?
The ATS remains the premier international society focusing on respiratory health, sleep medicine, and critical care. I have seen the organization grow in members and mission over the past 37 years. Not only does the organization
address the needs of Americans, but it also engages in addressing global challenges related to climate change, pollution, and infectious diseases such as tuberculosis. It has also invested in enhancing the infrastructure for research in low- and middle-income countries through its Methods in Epidemiologic, Clinical, and Operations Research (MECOR) program. The organization’s involvement in discovery through research is also evident, having invested over 20 million USD in the past two decades to fund early career researchers, with a great return on investment based on discoveries, publications, and faculty development. Finally, I am most proud of its efforts in advocacy.
Each of these efforts was limited in scale early on, but they have grown significantly. The ATS has expanded its missions, which has led to greater complexity and the need for more resources. Importantly, this growth has attracted volunteers and members to the organization which, in turn, have found ways to channel their talents to advance our goals.
Q5 What were your standout moments at this year’s ATS International Conference?
As I get older, I tend to enjoy lectures that describe new medical knowledge alongside personal or historical information. The Amberson Lecture was very moving, as were those delivered at the Diversity and Women’s Forums. The panel presentations on homelessness and air pollution were also terrific.
Moreover, the international conference is known for providing a platform for the announcement of new discoveries. Presentations related to novel interventions approaching clinical application for the management of COPD, bronchiectasis, asthma, and pulmonary fibrosis, among others, were truly exciting. The lectures given by this year’s Research Recognition Awardees gave us a window into the enormous talent of our investigators and how they continue to shape our understanding of the lungs. Finally, my favorite aspect of the ATS International Conference has always been meeting with colleagues, friends, and global leaders focused on the same goals. I have known these people for years, and witnessing their evolution as providers, educators, investigators, and leaders has been a source of great learning and satisfaction.
Q6 How can early career professionals make the most out of large meetings like the ATS International Conference?
The ATS places major emphasis on early career professionals, as demonstrated by the research funding it provides, the travel support for trainees, and the
countless opportunities to participate in committees, poster presentations, and oral presentations at the international conference. The conference may seem daunting to newcomers, as hundreds of presentations and activities are held; thus, I recommend that early career professionals identify a conference “mentor”, someone who has participated in the conference and can ensure that they have an enjoyable and productive meeting. I also recommend that early career professionals start by joining one of the several ATS Assemblies. There, they can meet people with similar interests, learn about the activities, and identify opportunities for engagement.
Q7
Looking ahead to your upcoming presidency in 2027–2028, what does this role mean to you, and what impact do you hope to have?
The ATS became my professional home early on in my career. I owe much of my career to this organization and the ATS members who provided me with invaluable support. I will be working with my colleagues on the Executive Committee and the Board to further expand our mission by enhancing our research portfolio, advancing educational opportunities, expanding the reach of our journals, and developing alliances with likeminded organizations and patient advocacy groups. Importantly, we must continue to support advocacy efforts, both locally and nationally, during this time of uncertainty. Finally, it is safe to say that the strength of the ATS lies in its diverse and talented membership. We must continue to find new ways to tap into that talent, as it provides the energy that fuels our efforts.
Interviews
Two leading experts at the forefront of respiratory medicine, Jonathan Bernstein and Todd Bull, share insights from their extensive and celebrated careers in the following interviews. Perspectives from a lifetime dedicated to severe asthma care, holistic patient management, pulmonary vascular disease, and pulmonary hypertension are detailed, as well as the most exciting ongoing trials in respiratory research.
Featuring:
Jonathan Bernstein and Todd Bull
Jonathan Bernstein
Professor of Clinical Medicine, Department of Internal Medicine, Division of Rheumatology, Allergy and Immunology, University of Cincinnati College of Medicine, Ohio, USA
First of all, what led you down the path of asthma, allergy, and clinical immunology?
I grew up in a family of allergists and immunologists. My father was an allergist and immunologist, and Past President of the American Academy of Allergy, Asthma, and Immunology (AAAAI) in 1982. So, environment was an influence, and as a both a teenager and a college student I had many laboratory and clinical experiences in allergy and immunology. As a medical resident, I enjoyed my allergy and immunology rotations, especially the clinical immunology aspects. I liked the broad spectrum of pathology we saw as clinicians, and that allergy and immunology is a Conjoint Board that allowed me to see both children and adults.
Failure to treat chronic rhinitis in patients with asthma and COPD results in increased 30-day hospital readmission rates
Q2 Given your extensive experience in both clinical practice and research, how has your approach to diagnosing and managing severe asthma evolved over the years?
Major advancements in diagnosis, assessment of asthma control, and treatment outcomes with patient reported outcome measures and therapeutics have made severe cases of asthma manageable. Our biggest challenge is with patient adherence to medications and office visits. Prior to advanced therapeutics beyond inhaled corticosteroids and long-acting β2-agonists, we had oral corticosteroids or offlabel use of therapies such as methotrexate or oral gold, which had marginal benefits at best. A better understanding of asthma pathogenesis has allowed the development of novel therapeutics, including anti-IL-4 receptor alpha, anti-IgE, anti-IL-5/IL-5 receptor, and anti-thymic stromal lymphopoietin
agents that treat different asthma phenotypes/endotypes. Currently we are working on a longer acting anti-IL5 antagonist for asthma.
Q3
Your research includes the health effects of both home and occupational environmental exposures in patients with asthma. What are some of the most significant findings you’ve encountered in this area?
Our findings confirm the importance of obtaining an indoor environmental history to assess indoor air quality; specifically allergen exposures for patients with IgE-mediated asthma, but also other irritant/ chemical triggers in cleaning agents, potpourris, secondary smoke exposure, mold, or other outdoor air pollutants that become indoor pollutants when windows are left open. We have looked at many environmental interventions to mitigate these exposures with success. The workplace is an extension of the home, but often more difficult to access and implement avoidance measures. For example, we demonstrated that immunosurveillance programs implemented in industries where
high or low molecular weight antigen can induce asthma, are effective at preventing exposure and the development of occupational asthma and rhinitis symptoms.1 A more recent study investigating the use of an ultraviolet irradiation air cleaning device installed in the central furnace duct of asthmatic children’s homes compared to a sham unit, found significant improvement in many asthma variables for children where the home had an active unit after one year.2
Q4
You emphasize looking at the ‘whole patient’ rather than just the primary complaint. Can you share an example where addressing comorbid conditions significantly improved a respiratory disorder?
We see many patients presenting with asthma who also have chronic rhinitis which is untreated. However, when you address the upper respiratory tract, their asthma symptoms are overall better controlled. We showed that failure to treat chronic rhinitis in patients with asthma and COPD results in increased 30-day hospital readmission rates.3
We also see many patients presenting with mast cell activation syndrome, and many also have symptoms of dysautonomia. Treatment of these patients holistically improves their overall condition.4 Thus, it is essential to get a comprehensive history to develop a management plan that will improve the patient’s outcomes.
Q5
Hereditary angioedema (HAE) can have significant respiratory complications. How do you differentiate between hereditary and other forms of angioedema in clinical practice, and what are the latest advancements in treatment?
HAE is due to a genetic mutation resulting in a gene that doesn’t produce C1INH (85% of cases [Type 1 HAE]), or a gene that makes C1INH that doesn’t work (15% of cases; [Type 2 HAE]). The swelling episodes can involve the upper airways, tongue and lips, abdomen, genitalia, or extremities, and does not respond to H1-antihistamines or other medications used to treat histaminergic angioedema. These patients have a low C4 level, low C1INH functional level, and depending on the HAE subtype,
a low C1INH for Type 1 HAE or a high or normal C1INH for Type 2 HAE. We now have on-demand treatments that can be used to treat an acute attack. These target kallikrein, the molecule important for regulating bradykinin production. For example, icatibant, which is a molecule that blocks bradykinin 2 receptors, or C1INH plasma or recombinant replacement therapy. These all work well when used early on after the onset of an attack. For patients with more frequent attacks, involving the throat or abdomen, prophylactic treatment with a longacting kallikrein inhibitor called lanadelumab, dosed every 2 weeks subcutaneously, or intravenous/subcutaneous C1INH replacement therapy dosed every 3–4 days can be given. These are major advances compared to what we had previously, which were androgens, fresh frozen plasma, and tranexamic acid.
Q6
What role do allergic and non-allergic rhinitis play in exacerbating respiratory conditions like asthma, and how do you tailor treatments for patients dealing with both?
It is extremely important to diagnose chronic rhinitis subtypes correctly, as treatment differs.
References
1. Ghosh D et al. The utility of monitoring trimellitic anhydride (TMA)-specific IgG to predict IgE-mediated sensitization in an immunosurveillance program. Allergy. 2018;73(5):1075-83.
As discussed above, proper management of chronic rhinitis can significantly improve asthma control. Untreated rhinitis contributes to significant morbidity, associated with worsening asthma and recurrent sinus disease.
Proper management of chronic rhinitis can significantly improve asthma control
Q7 With your longstanding contributions to medical education, what key lessons do you emphasize to your students and fellows about diagnosing and managing complex respiratory disorders?
The most important lesson is to characterize the patient: what is the allergic status, what are their triggers (infectious, exercise, allergens, pollutants, etc.), and what is the nature of their environments at home and work or school?
Confirm a diagnosis of asthma by history and objective testing with spirometry, and if available, exhaled nitric oxide. Assess for
chronic rhinitis subtypes and other comorbid conditions, such as gastroesophageal reflux disease, obstructive sleep apnea, chronic sinusitis, and vocal cord issues. Provide patients with a way to assess their asthma control with patient reported outcome measures. Be familiar with the American Thoracic Society (ATS) and Global Initiative for Asthma (GINA) guidelines. Start medications based on asthma severity per guidelines, and schedule follow-up visits to assess response to treatment and control; peak expiratory flow rate meter readings should be obtained at each visit, and spirometry should be obtained once the patient is stable, at least once per year. With the resources we have today to manage asthma, we should not be seeing asthma hospitalizations or asthma-related deaths.
With the resources we have today to manage asthma, we should not be seeing asthma hospitalizations or asthma-related deaths
2. Bernstein JA et al. Randomized trial of ultraviolet irradiation units installed in homes of children and adolescents with asthma. J Allergy Clin Immunol Glob. 2025;4(2):100427.
3. Singh U et al. Chronic rhinitis is a highrisk comorbidity for 30-day hospital readmission of patients with asthma and chronic obstructive pulmonary disease. J Allergy Clin Immunol Pract. 2019;7(1):279-85.
4. Conway AE et al. Beyond confirmed mast cell activation syndrome: approaching patients with dysautonomia and related conditions. J Allergy Clin Immunol Pract. 2024;12(7):1738-50.
Todd Bull Professor of Medicine, Division of Pulmonary Sciences & Critical Care Medicine, University of
Firstly, what led you to specialize in the field of pulmonary and critical care medicine?
I love physiology, and even during medical school I thought pulmonary and critical care would be a potential career path. My experience in the medical intensive care unit as a house officer helped solidify this interest. In the intensive care unit, having an understanding of the physiology of health and disease allows you to make the correct decisions quickly to help your patients. Pulmonary vascular disease similarly requires a deep understanding of the physiology. The interaction of the heart and lungs in health and disease is complex and fascinating. If you understand this physiology you can make adjustments to help your patient.
Q2 Your research and clinical work focus on pulmonary vascular diseases, particularly pulmonary hypertension (PH). What are the key priorities and challenges when diagnosing PH, especially regarding PH categorization?
The key priorities in terms of diagnosis are identifying the underlying cause and then appropriately assessing severity; this allows the correct therapeutic decisions. Deciding which WHO group the patient belongs to is an important first step. Right heart catheterization is an essential part of this evaluation. The importance of following non-invasive studies and biomarkers, and continually assessing patient risk and making adjustments to therapy based on risk is also becoming better understood.
Q3
There is currently no cure for PH, but the University of Colorado has one of the only designated PH Care Centers in the region and one of the largest programs, overseeing numerous clinical trials in this area. What are the current options for PH management, and are there any recent advancements in treatment that you are particularly excited about?
It is a very exciting time in the management of PH. We have gone from no specific or effective treatments in the 1980s to a few options in the 1990s, to now five classes of medication and more than 15 different therapeutics available. We are also learning how to use these classes of medications effectively in combination, and have medications to use in Class III and IV PH. The area that many of us in the field are most excited about, is the development of an entirely new class of medications that bind activins and impact the TGF-β pathway. This pathway is integral to the development of pulmonary arterial hypertension (PAH), and as such, targeting this represents an exciting new direction moving forward.
Q4
Pulmonary hypertension associated with COPD has been a significant area of study, including your work on the PERFECT study. What insights have emerged regarding the role of inhaled treprostinil, and how do you see this shaping future management strategies?
Inhaled treprostinil is a proven, effective treatment for interstitial lung disease-related PH, which was a huge step forward. Unfortunately, it was not found
efficacious for COPD-PH and the PERFECT trial was stopped early.1 COPD-associated PH is a tricky entity. I think a major issue we have in finding a treatment is the existence of multiple phenotypes in COPD-associated PH. We need to better understand how to identify these phenotypes, and then study the impact of treatment on them individually.
A major issue we have in finding a treatment is the existence of multiple phenotypes in COPD-associated PH
Q5 You recently co-authored a case report highlighting a heritable risk and overlapping features of pulmonary venoocclusive disease and PH. How should clinicians approach genetic considerations in pulmonary vascular disease, and what implications might this have for screening and treatment?
We have known for many years that there are heritable forms of PH. It is this recognition and the identification of the BMPRII mutations that has led to the development of our newest therapy for PAH. There are also genetic mutations associated with pulmonary veno-occlusive disease. Evaluation for these mutations is becoming much more commonplace in the assessment of PAH, though it is important that such evaluations are also coupled with genetic counseling, as not all patients with mutations will go on to develop disease (variable penetrance).
Q6
Pulmonary embolism (PE) affects around 900,000 people every year in the USA. How are advanced therapies in PE, such as catheter-directed thrombolysis or novel anticoagulants, improving patient outcomes?
There is a lot of excitement around the evolving management of acute PE. Certainly, catheter-directed therapies are gaining a much bigger foothold in the management of acute PE. However, we need clinical trials to better inform us on the appropriate use of these devices. Thankfully, these trials are underway, and we should be learning a lot about their role in the optimal management of acute PE in the next few years. There are also ongoing studies of novel anticoagulants under investigation, which appear efficacious in the treatment of thrombosis, while decreasing bleeding risk.
Q7 With your extensive experience in pulmonary vascular disease, what excites you most about the future of pulmonary medicine? Are there any emerging trends that you believe will significantly change the field in the next decade?
As I mentioned earlier, for PAH treatment, the move away from simply targeting vasodilation to targeting the potential causes of cellular proliferation in the precapillary pulmonary vasculature is very exciting. I am also very excited to see the rapidly developing evidence base in the treatment of acute PE, as well as the improvement in treatment of chronic PE/chronic thromboembolic pulmonary hypertension; especially as it relates to balloon pulmonary angioplasty. I think we have a lot
to learn about balloon pulmonary angioplasty and its application in chronic thromboembolic pulmonary hypertension. There is also a lot of exciting work in the area of imaging of the pulmonary vasculature, which I think will help us further refine our ability to select and then modify therapies. It is a very exciting time to be involved in the management of patients with pulmonary vascular disease.
Reference
1. United Therapeutics. A phase 3 adaptive study to evaluate the safety and efficacy of inhaled treprostinil in participants with pulmonary hypertension (PH) due to chronic obstructive pulmonary disease (COPD) (PERFECT). NCT03496623. https:// clinicaltrials.gov/study/NCT03496623.
It is a very exciting time to be involved in the management of patients with pulmonary vascular disease
The Role of IL-5 in Inflammatory Diseases
The Role of IL-5 on Eosinophils Has Been Well Established as Central to Its Development, Maturation, and Activation1,2
‡Found in airway tissue. Support:
New evidence has shown that the IL-5 receptor is present and active on multiple cell types in sinus and airway tissue*,3-5
Ciliated epithelial cells†
Fibroblasts‡
Neutrophils‡
*18,036 surgically excised sinus tissue cells from patients with AERD (n=3), CRSsNP (n=5), and CRSwNP (n=3).
†Found in sinus tissue.
Effects of IL-5 on eosinophils and other cell types6
Airway epithelium
Columnar ciliated epithelial cells
Basal epithelial cells
hypersecretion
Evolving Evidence Suggests Lead to Epithelial Barrier
plugs
• Impaired epithelial barrier
• Susceptibility to injury from viruses, allergens, pollutants
• Epithelial activation
• Persistent repair response
signalling and airways remodelling
Smooth muscle
Downregulates genes to tight junctions barrier function in epithelial cells3,7
Enhances proliferation and activation of fibroblasts4
Is responsible for differentiation, proliferation, and survival of eosinophils, 2 contributing to increased eosinophil protein signaling and downstream airway remodeling effects8
Promotes epithelial barrier dysfunction and fibrosis3,4,7
Stimulates expression of functional IL-5Rα on plasma cells3,9
Mediates T reg cell production10
Mediates ILC2 activity11
Leads to airway remodeling12 and disease progression14
Plays a role in immune responses2,3,8-11 and formation of mucus plugs13
The relative contributions of IL-5 beyond eosinophils to disease pathology have yet to be quantified and require further studies to understand the impact of each contributing factor in the disease processes of patients with IL-5-mediated conditions.
This information is scientific and non-promotional in nature and is not intended for further distribution.
1. Travers J et al. Mucosal Immunol. 2015;8(3):464-75. 2. Pelaia C et al. Front Physiol. 2019;10:1514. 3. Buchheit KM et al. J Allergy Clin Immunol. 2021;148(2):574-84. 4. Bajbouj K et al. Allergy. 2023;78(3):882-5. 5. Gorski SA et al. PLoS ONE. 2019;14:1-13. 6. Buchheit KM et al. Allergy. 2024;79(10):2662-79. 7. Barretto KT et al. Allergy. 2020;75(8):2127-30. 8. Siddiqui S et al. J Allergy Clin Immunol. 2023;152(4):841-57. 9. Buchheit KM et al. J Allergy Clin Immunol. 2020;145(6):1574-84. 10. Bergantini L et al. Scand J Immunol. 2021;94(1):e13031. 11. Malik B et al. Respirology. 2023;28(8):758-66. 12. Domvri K et al. J Allergy Clin Immunol. 2025;155(2):425-35. 13. Dunican EM et al. J Clin Invest. 2018;128(3):997-1009. 14. Huang Y et al. Ann Transl Med. 2022;10(18):1023.
The Changing Landscape of Lung Transplantation
Authors: Laurens J De Sadeleer,1,2 Laurent Godinas,1,2 Lieven J Dupont,1,2 Laurens J Ceulemans,2,3 Robin Vos,1,2 *Saskia Bos1,2
1. Department of Respiratory Diseases, University Hospitals Leuven, Belgium
2. Laboratory of Respiratory Diseases and Thoracic Surgery (BREATHE), Department of Chronic Diseases, Metabolism and Ageing (CHROMETA), KU Leuven, Belgium
3. Department of Thoracic Surgery, University Hospitals Leuven, Belgium
*Correspondence to saskia.bos@uzleuven.be
Disclosure: The authors have declared no conflicts of interest. Vos is supported as a Senior Clinical Research Fellow by the Research Foundation-Flanders (1803521N).
Ceulemans has received a grant from Medtronic, paid to their institution.
Lung transplantation is increasingly used as a last resort treatment for end-stage chronic lung diseases. In the last decade, important improvements have been noted in terms of surgical techniques and perioperative and postoperative management, as well as greater acceptance of older recipients. However, the most drastic changes are observed in recipient and donor profiles due to advances in the treatment of chronic lung diseases. Such advances include novel patient stratification systems, such as the concept of progressive fibrosing interstitial lung diseases in pulmonary fibrosis; novel findings regarding etiology of disease, such as telomere length in pulmonary fibrosis; novel pharmaceutical treatment options, such as CFTR modulators in cystic fibrosis; and novel interventions, such as lung volume reduction in chronic obstructive pulmonary disease, and endarterectomy and balloon angioplasty in chronic thromboembolic pulmonary hypertension. In this review, the authors discuss the latest developments in the management of chronic lung diseases and how this affects recipient profiles and lung transplant management. Finally, the authors point out the uncertainties and knowledge gaps in these developments regarding transplant management.
Key Points
1. Lung transplantation is a valuable treatment option for patients with end-stage chronic lung disease. Recipient and donor profiles have changed significantly over the years due to advances in the treatment of chronic lung diseases, such as novel patient stratification systems, novel findings regarding disease etiology, novel pharmaceutical treatment options, and novel interventions.
2. Pulmonary fibrosis is now the most common indication for lung transplantation worldwide. The impact of telomeropathies on post-transplant outcomes needs to be further assessed. This should include adequate risk assessments for post-transplant complications related to the type of underlying telomeropathy, as well as guidance on how immunosuppressive regimens should be optimized in these patients.
3. Chronic obstructive pulmonary disease also remains a common indication for lung transplantation. As the role of lung volume reduction in the treatment of emphysema continues to expand, further studies assessing the peri-transplant risks and benefits of prior lung volume reduction, as well as its use as a bridge to transplant, should be conducted.
INTRODUCTION
It is clear that the landscape of clinical lung transplantation has noticeably changed since its introduction in the 1960s. Surgical techniques, as well as perioperative and postoperative patient care, have improved significantly, contributing to better shortand long-term outcomes.1 Changes are also evident in the patient population. Parallel to that of the general population, the average age of both lung donors and recipients continues to rise globally. In Europe, donors over the age of 65 are becoming increasingly common, while in the United States, the number of lung transplants in recipients over 65 has doubled over the past decade, now accounting for over 30% of transplant activity.2-4
The profile of lung transplant patients is not only changing in terms of age, but in other factors as well. The advancement of various medical therapies (e.g., antifibrotic agents) and surgical interventions (e.g., lung volume reduction) has influenced the need and timing of lung transplantation. In addition, more patients with comorbidities and technically complex cases, such as those with prior interventions, are now being considered for transplantation. Still, substantial variation remains in clinical practices across transplant centers and regions worldwide.
In this review, the authors focus on changes in the patient population and timing of lung transplantation from a disease-specific perspective for the major transplant indication groups. Rarer indications for lung
transplantation, including acute respiratory distress syndrome,5 pulmonary chronic graftversus-host disease,6 and re-transplantation,7 are described elsewhere.
LUNG TRANSPLANTATION FOR PULMONARY FIBROSIS
Pulmonary fibrosis comprises a group of chronic fibrotic interstitial lung diseases (ILD) that carry a substantial risk of progressive respiratory failure and death, despite optimal medical treatment.8
Main Indication for Lung Transplantation
Indications for lung transplantation have evolved, and ILD has surpassed chronic obstructive pulmonary disease (COPD) as the leading indication for lung transplantation worldwide.3 In addition to increased awareness and diagnosis of ILDs, this is also due to the implementation of the Lung Allocation Score (LAS), a numerical score that prioritizes patients based on medical urgency and likelihood of successful transplant outcomes.9 Since the implementation of LAS, more high-priority patients have received transplants, leading to changes in recipient profiles. As reflected by LAS values, disease severity has increased and waiting times have decreased for patients with ILD.9 The same prioritization principles apply under the newer Composite Allocation Score (CAS) system in the US.
Moreover, the tendency to transplant older candidates has shifted transplant indications
Impact of Antifibrotic Agents on the Need and Timing of Lung Transplantation
Two antifibrotic agents, pirfenidone and nintedanib, are currently used in patients with pulmonary fibrosis. Their availability has altered the previously known clinical disease course by attenuating functional decline and disease progression and potentially increasing survival.14,22-26 Despite these positive findings, however, antifibrotics merely slow down the disease and do not stabilize or improve pulmonary function.22,24 Hence, progressive and ultimately fatal disease remains the long-term outcome for both IPF and PPF cases, for which lung transplantation remains the only definitive treatment option in well-selected patients. As such, the use of antifibrotic agents may postpone the need for a transplant. This could lead to a greater demand for transplants at older ages, which could present societal and ethical challenges while placing pressure on centers that apply strict age limits.
IPF has been associated with cardiovascular and other comorbidities,27,28 and aging further increases these risks. Age remains a controversial selection criterion for lung transplantation. Nevertheless, the recipient population is aging, partly due to an increasing number of older patients with pulmonary fibrosis receiving transplants. Frailty assessment is essential, especially in older patients, to distinguish chronological age from biological and functional age.
Importantly, most studies show that antifibrotics are generally safe up to the time of transplant, with no significant effect on suture complications, bleeding, or reintervention rates.29
When To Transplant: Risk of Exacerbation
The ISHLT has established disease-specific recommendations to help determine the appropriate timing for referral and listing of patients with pulmonary fibrosis.30 In general, two-thirds of both PPF and IPF
cases experience a forced vital capacity decline of >5% in one year, and almost half of patients experience a >10% decline.12,31 Still, the clinical course of pulmonary fibrosis is variable. Some patients remain stable for extended periods, while others deteriorate rapidly or incrementally. As such, determining the ideal time to place a patient on the waiting list and proceed with the transplant is not easy and largely depends on the individual’s disease trajectory. Other risk factors, such as secondary pulmonary hypertension and concurrent emphysema, should also be taken into account.32 In patients with combined pulmonary fibrosis and emphysema, diffusion capacity is typically severely impaired, whereas airflow rates and lung volumes are relatively preserved. The latter may contribute to underestimation of disease severity and complicate monitoring of disease trajectory by lung function, as changes in forced vital capacity are not reliable indicators of disease progression in this patient group.33
The unpredictable nature and potentially severe consequences of ILD exacerbations must be recognized, and in some cases, patients who were not previously considered or fully assessed for lung transplantation may need to be urgently evaluated.14
Unique Features Related to Pulmonary Fibrosis
Several unique characteristics in patients with pulmonary fibrosis may influence lung transplant candidacy, as well as pre- and post-transplant risks and management strategies. For instance, the importance of telomere biology disorders, extrapulmonary disease manifestations, and allosensitization in patients with connective tissue disease should be considered.14,34
Historically, patients with connective tissue disease-related ILD were considered suboptimal candidates for lung transplantation due to multi-organ disease manifestations and surgical risk. Severe esophageal dysmotility and gastroesophageal
as well, as ILDs tend to occur later in life than COPD. According to 2017 registry data from the International Society for Heart and Lung Transplantation (ISHLT), ILD accounted for 40% of transplant indications, followed by COPD (26%), and cystic fibrosis (CF) at 13%.3 The number of transplants for idiopathic pulmonary fibrosis (IPF) has risen substantially in recent years, particularly in the US.10
At the authors’ large-volume center, which has performed >1,500 lung transplants since the introduction of its program in 1991, transplant indications have similarly shifted. While the center continues to primarily transplant patients with COPD, there has been a noticeable rise in the number of ILD transplants, whereas CF transplant activity has dropped to nearly zero in recent years (see Figure 1).
The Concept of Progressive Fibrosing ILD
The most fundamental paradigm shift in fibrosing ILD management is the advent of the progressive fibrosing ILD (PF-ILD) concept, acknowledging that subgroups of patients with a non-IPF fibrosing ILD diagnosis behave similarly compared to IPF in terms of pulmonary function decline,11 survival,12 and treatment response to antifibrotics.13 IPF remains the most common type of ILD for lung transplantation, but other PF-ILDs, such as fibrotic hypersensitivity pneumonitis and idiopathic non-specific interstitial pneumonia, have increased as indications for transplantation.3,14 Interestingly, the PF-ILD criteria are already woven into the ISHLT guidelines on transplant candidacy for referral and listing. Patients with IPF and patients with progressive pulmonary fibrosis (PPF) are both recommended to be referred for lung transplantation intake and evaluation.
Overview of lung transplant activity at the Leuven lung transplant program, a high-volume center that has performed over 1,500 transplants from the introduction of its program in 1991 to 2024. Although the transplant activity for COPD has remained relatively stable, a clear increase in the number of ILD transplants has been observed, while CF lung transplant activity has almost completely decreased to zero in recent years.
Currently, it is recognized that genetic variants linked to short telomeres are prevalent in patients with pulmonary fibrosis, even among those without a known family history of ILD. Besides pulmonary fibrosis, telomere shortening and related genetic mutations are associated with disorders in other organ systems, including myelodysplasia, cirrhosis, and hematological and solid organ malignancies.8 Short telomere length (<10th percentile), often caused by specific telomere-related mutations (e.g., TERC or TERT), has also been connected to worse post-transplant outcomes and
may increase the risk of hematological complications, cytomegalovirus-related complications, and malignancy. Studies on the impact of short telomere length and chronic lung allograft dysfunction have shown conflicting results.15-20 Routine pretransplant testing for telomere length and/ or associated mutations is performed in candidates with ILD in some centers. Currently, there is no consensus on the posttransplant (immunosuppressive) management of patients with telomere disorders, but an ISHLT consensus document is being developed (Table 1).
Table 1: Uncertainties and knowledge gaps in (pre-)lung transplant management due to advances in chronic lung disease care.
Disease Innovation
PF Telomeropathy as a cause of PF
COPD ELVR LVRS
CF CFTR modulators
Knowledge gap
Adequate risk assessment for post-transplant complications related to the type of underlying telomeropathy.
How can immunosuppressive regimens in patients with PF and a telomeropathy be optimized? How to improve post-transplant outcomes in these patients?
Are specific selection criteria needed for patients with COPD who have undergone ELVR/LVRS? When is the ideal time for transplantation in these cases? What is the impact of prior LVRS on perioperative transplant management?
Should current referral and listing criteria be updated to better reflect the effect of CFTR modulator therapies, especially in patients with already advanced lung disease? Will the use of CFTR modulators lead to transplantation in older CF cases? Will comorbidities in these patients have an impact on lung transplant eligibility? Should CFTR modulators be continued post-transplant?
Pulmonary vascular disease Combination therapy in PAH
Should risk stratification tools such as REVEAL and LAS include current treatment to better assess ideal timing and urgency for transplantation in patients with PAH? Understanding sotatercept use in the perioperative period of lung transplantation.
Medical therapy of pulmonary fibrosis is based on the specific underlying diagnosis and disease behavior, and may include immunosuppression in nonIPF entities. Any potential benefit of ongoing immunosuppression at a fibrotic disease stage must be weighed carefully against its risks.8 While deleterious effects of immunosuppression have been acknowledged for years in IPF, evidence
is emerging that this treatment in patients with non-IPF fibrotic ILD and short telomere length portends worse survival,21 and its use should be stringently evaluated. In general, it is best to limit immunosuppressants to the lowest effective dose while a patient is listed for transplantation. In particular, chronic, high-dose corticosteroids may increase the risk of wound healing complications and anastomotic dehiscence, and should be avoided if possible.14
reflux are of particular concern, along with the need for cardiovascular evaluation and assessment of gastrointestinal, renal, musculoskeletal, and other organ systems.8,34 Importantly, no difference in survival or allograft function was noted in carefully selected patients compared with patients transplanted for other indications.8,14 In the context of extrapulmonary disease manifestations, it is also necessary to be vigilant for the possibility of cardiac involvement in sarcoidosis.
Given that several post-transplant complications are unique to this patient population, multidisciplinary management by experts familiar with telomere disorders and infectious, hematological, oncological, and cardiac complications may be necessary to increase the likelihood of better outcomes.8,14
LUNG TRANSPLANTATION FOR COPD
COPD has historically been the most common indication for lung transplantation. Although ILD has surpassed COPD as the most common indication globally, COPD remains an important indication too, despite medical and surgical advancements in its treatment.3
Impact of Lung Volume Reduction Techniques on the Need for Lung Transplantation
Endoscopic and surgical lung volume reduction (ELVR and LVRS) are increasingly used therapeutic options for well-selected patients with emphysema who have not yet progressed to end-stage lung disease.35 LVRS, in which diseased areas of lung parenchyma are resected, may lead to improved exercise capacity, quality of life, and survival in carefully selected patients.36,37 Insertion of endobronchial valves is the most common technique for ELVR, and has positive effects on lung function, exercise tolerance, and quality of life.38 Despite these clinical benefits, pulmonary function may decline further in some of these patients, ultimately requiring a lung transplant.39 Both
LVRS and ELVR can be considered bridging strategies, as they do not prohibit future lung transplantation.35 Indeed, some centers are now using LVRS to delay the need for transplantation, which could potentially improve overall survival, or to stabilize and enhance a candidate’s pulmonary and general status prior to transplantation.
Impact of Prior LVRS on Transplant Outcomes
LVRS before lung transplantation has long been controversial, with outcomes still not entirely understood. Single-center studies have reported conflicting results.39 Some of them observed increased perioperative risks, such as graft failure, increased need for blood transfusion, extracorporeal membrane oxygenation, and empyema, as well as longer hospital stays after LVRS and higher wound infection rates following ELVR.39,40 However, neither short- nor long-term survival was negatively affected.40
These risks may stem from the technical challenges of transplanting patients who have previously undergone LVRS, including pleural adhesions, which can increase operative time, bleeding complications, phrenic nerve injury, and transfusion needs.39,40 Interestingly, the multicenter study by Krishnan et al.39 noted that the proportion of lung transplants with prior LVRS ranged from 0–11% per center, suggesting that outcomes may benefit from specialized expertise and institutional volume, other technically complex procedures. Theoretically, it could also be the case that patients requiring lung transplantation after LVRS represent a more severe phenotype of COPD.39
Thus, while LVRS prior to lung transplantation does not seem to affect post-transplant survival, it may increase perioperative risk.39,40 Therefore, such patients require thorough pre-transplant evaluation.39 As the role of lung volume reduction in the treatment of COPD continues to expand, further studies assessing the risks and benefits of prior LVRS/ELVR and their use as a bridge to
transplant should be conducted (Table 1). ELVR is a less invasive approach and has the potential to reduce some of the risks associated with LVRS that could complicate subsequent lung transplantation.39
Impact of Targeting Type 2 Inflammation in COPD
It is known that COPD is a heterogeneous disease, and that Type 2 inflammation occurs in 20–40% of COPD cases.41 In such cases, targeting Type 2 inflammation can reduce acute exacerbation rates by up to 30%.42,43 As these treatment options have not yet been routinely used, their impact on pulmonary function decline, transplant indication, and timing is not yet fully elucidated. However, it is clear that these therapies, which significantly lower COPD exacerbation rates, will have a profound impact on the COPD transplant landscape.
LUNG TRANSPLANTATION FOR CYSTIC FIBROSIS
CF is the most common autosomal recessive disorder in White people, and it is caused by biallelic mutations in the gene encoding for the CFTR protein.44 Until recently, it was the third most common indication for lung transplantation.3 Nowadays, the number of patients referred for and transplanted due to CF continues to decline drastically as a result of multifaceted symptomatic management and new disease-modifying drugs, with favorable pre-transplant evolution and increased life expectancy.44
Impact of CFTR Modulators on the Need for Lung Transplantation
CF is a multisystem disorder, with CF lung disease causing the majority of morbidity and mortality. Lung transplantation is the ultimate treatment option for patients with progressive, advanced lung disease, with superior long-term survival outcomes compared with other primary underlying diseases, which is associated in part with younger age at the time of transplant.3,45
However, the introduction of CFTR modulators, which target the underlying defect, has profoundly transformed CF management. These modulators have substantially impacted the disease course of many patients with CF by significantly improving lung function, quality of life, and predicted survival rates.44
These drugs are highly effective and, as a result, there has been a marked reduction in the number of patients referred for and transplanted due to CF in recent years.2,46 Although an increasing amount of data confirms the long-term efficacy of these drugs, patients with already advanced lung disease might still need a lung transplant later in the course of their disease.47-52 This may also affect the patient profile, with a potentially increased perioperative risk profile due to age-related comorbidities (cardiovascular, renal disease) or CF-related liver disease.53
With CFTR modulators now being introduced at a younger age, CF lung disease will likely be prevented in the majority of patients. There remains a small subgroup of patients with CF who have rare CFTR mutations and are currently ineligible for or demonstrate a heterogeneous response to CFTR modulator therapy.54 Although generally well tolerated, there is also a small group of patients with CF who have to discontinue their CFTR modulators due to side effects.55 However, as the CF drug discovery pipeline continues to expand with various nucleic-acid-based strategies in Phase I and II clinical studies,56 it seems reasonable to expect that CF will become an increasingly rarer indication for lung transplantation.
Lung transplant referral and listing recommendations have not yet incorporated the impact of the new CFTR therapeutics. Currently recommended thresholds for transplant referral and listing require reassessment, especially as more data become available on the long-term effects of CFTR modulators and disease progression in patients with advanced lung disease.30,44
Is There a Role for CFTR Modulators After Lung Transplantation?
Patients with CF who are undergoing lung transplantation require specialized posttransplant care due to the multisystem nature of CF and its unique comorbidities. The Cystic Fibrosis Foundation (Maryland, USA) consensus statement provides guidance for post-transplant management.57 Because CFTR modulators can also have a positive effect on other tissues and organs where CFTR is expressed, interest is emerging in the continuation or initiation of CFTR modulators after lung transplantation.
Infections remain a significant issue posttransplant and are attributed to chronic immunosuppression as well as pre-transplant colonization with typical CF pathogens, including the colonization of the upper respiratory tract in individuals with CFrelated sinus disease. Organisms such as Pseudomonas aeruginosa, along with gastroesophageal reflux disease and (micro) aspiration, are associated with higher chronic lung allograft dysfunction (CLAD) risk. These factors provide some justification for the post-transplant use of CFTR modulators to mitigate extrapulmonary inflammation, which could influence CLAD development and/or progression, and improve quality of life.58
Although post-transplant data are scarce, CFTR modulators have shown benefits regarding extrapulmonary disease manifestations in non-transplant patients, improving chronic rhinosinusitis, gastrointestinal disease, diabetes, and possibly BMI and bone health.44,58 A Dutch multicenter study on lung transplant recipients with CF found that elexacaftor/ tezacaftor/ivacaftor improved healthrelated quality of life, chronic rhinosinusitis, and gastrointestinal symptoms, though not BMI or HbA1c.59 Post-transplant drug monitoring is needed given the potential drug–drug interactions that can occur (e.g., increased calcineurin inhibitor levels), as CFTR modulators are metabolized through cytochrome P450 enzymes.44,58
There is a potential role for CFTR modulators after lung transplantation, as extrapulmonary CF comorbidities remain a considerable issue in some individuals.44 This was also supported by a patient survey, which showed that over 80% of respondents prioritized treating extrapulmonary symptoms, and 90% wanted more information on the posttransplant use of CFTR modulators. However, their high cost warrants further studies to better assess their risks, benefits, and potential impact on key outcomes such as quality of life and CLAD.58
LUNG TRANSPLANTATION FOR PULMONARY VASCULAR DISEASE
Patients with pulmonary vascular disease, mainly consisting of group 1 pulmonary arterial hypertension (PAH), group 4 chronic thromboembolic pulmonary hypertension (CTEPH), and group 5 pulmonary hypertension with unclear and/ or multifactorial mechanisms, comprise approximately 5% of all lung transplants. 3 Therapeutic advances, including medical therapies and interventions such as pulmonary endarterectomy and pulmonary artery balloon angioplasty, have greatly improved the prognostic implications of pulmonary hypertension and led to a marked change in timing for referral and listing of patients.32,60 Additionally, improved cardiovascular surgical approaches in patients with congenital heart defects have drastically reduced the prevalence of Eisenmenger’s syndrome later in life as an indication for (heart-)lung transplantation.
Impact of Medical Treatment for PAH on the Need for a Transplant
Several types of drugs are available for the treatment of PAH, depending on the presence or absence of vasoreactivity and the results of risk stratification. Importantly, all of these drugs act in a non-permanent manner by inducing temporary vasodilation and reduction in pulmonary vascular resistance.
As such, these drugs must be continued to maintain a beneficial effect on disease progression.61,62
Despite these medical options, survival remains poor, and lung transplantation remains the definitive treatment for selected patients with disease that is refractory to, or progressing despite, optimal therapy. Although revisions to the LAS have attempted to appropriately reflect disease severity and have improved the likelihood of transplantation for listed patients with PAH, it still does not fully reflect waitlist mortality, thus disadvantaging this population.30 Many patients with severe PAH receive a lung transplant after high-urgency listing due to life-threatening clinical deterioration.63 This also illustrates the difficulty in predicting clinical decline in patients with PAH.61
Lung transplantation for PAH is a complex procedure that requires a highly experienced team and access to circulatory support to achieve good post-transplant outcomes. Among lung transplant patients, patients with PAH have the highest perioperative mortality rate, although a favorable evolution has been observed due to improved surgical techniques; intraoperative management, with the implementation of extracorporeal membrane oxygenation; and prevention and management of primary graft dysfunction.60
Finally, more data are needed on posttransplant outcomes and timing of drug cessation regarding the recently approved PAH drug, sotatercept, a growth differentiation factor inhibitor that has been associated with increased risk of bleeding.64
Impact of Surgical Treatment for CTEPH: Is There Still Room for Transplantation?
CTEPH is characterized by the obstruction of proximal pulmonary arteries by fibrothrombotic material, along with
microvasculopathy similar to that seen in PAH. In addition to lifelong anticoagulation, treatment options for CTEPH vary based on the patient’s profile and include: pulmonary endarterectomy; balloon pulmonary angioplasty, which is used for inoperable patients and patients with residual disease after pulmonary endarterectomy; and/or medical therapy.61 Due to these advancements in medical and surgical treatments, as well as the use of a multimodal approach,65,66 lung transplantation is now seldom considered for this patient group.3,61 Nevertheless, it may still be considered in well-selected patients with persistent or recurrent pulmonary hypertension, or in patients with very distal disease not amenable to other treatments.67 Notably, due to the welldeveloped bronchial collateral circulation, lung transplantation in these patients can be technically difficult and may carry a substantial risk of bleeding complications.61
CONCLUSION
The demographic profile of lung transplant candidates is shifting, with an increasing number of older patients and patients with complex comorbidities being considered for transplantation. Pulmonary fibrosis and COPD continue to be important transplant indications, although the role of new therapies, such as antifibrotic agents in pulmonary fibrosis, lung volume reduction techniques in COPD, CFTR modulators in CF, and multimodal vascular management in PAH, is reshaping the timing and need for transplants. Overall, the evolving landscape of lung transplantation presents both challenges and opportunities, requiring continued refinement of patient selection, timing, and management strategies to ensure optimal outcomes.
References
1. Bos S et al. Survival in adult lung transplantation: where are we in 2020? Curr Opin Organ Transplant. 2020;25(3):268-73.
2. Valapour M et al. OPTN/SRTR 2023 annual data report: lung. Am J Transplant. 2025;25(2s1):S422-89.
3. Chambers DC et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: thirty-sixth adult lung and heart-lung transplantation report-2019; Focus theme: donor and recipient size match. J Heart Lung Transplant. 2019;38(10):1042-55.
4. Yusen RD et al. The Registry of the International Society for Heart and Lung Transplantation: thirtieth adult lung and heart-lung transplant report-2013; Focus theme: age. J Heart Lung Transplant. 2013;32(10):965-78.
5. Hoetzenecker K et al. Lung transplantation for acute respiratory distress syndrome. J Thorac Cardiovasc Surg. 2023;165(4):1596-601.
6. Zajacova A et al. Lung transplantation for pulmonary chronic graft-versus-host disease: a missed opportunity? JHLT Open. 2025;7:100209.
7. Rucker AJ et al. Lung retransplantation in the modern era. J Thorac Dis. 2021;13(11):6587-93.
8. Durheim M et al. “Pulmonary fibrosis,” Perch M et al. (eds.), Lung Transplantation (ERS Monograph) (2024), Sheffield: European Respiratory Society, pp.24-37.
9. Egan TM, Edwards LB. Effect of the lung allocation score on lung transplantation in the United States. J Heart Lung Transplant. 2016;35(4):433-9.
10. Perch M et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: thirty-ninth adult lung transplantation report-2022; Focus on lung transplant recipients with chronic obstructive pulmonary disease. J Heart Lung Transplant. 2022;41(10):1335-47.
11. Brown KK et al. The natural history of progressive fibrosing interstitial lung diseases. Eur Respir J. 2020;55(6):2000085.
12. Nasser M et al. Progressive fibrosing interstitial lung disease: a clinical cohort (the PROGRESS study). Eur Respir J. 2021;57(2):2002718.
13. Flaherty KR et al. Nintedanib in progressive fibrosing interstitial
lung diseases. N Engl J Med. 2019;381(18):1718-27.
14. Kapnadak SG, Raghu G. Lung transplantation for interstitial lung disease. Eur Respir Rev. 2021;30(161):210017.
15. Tokman S et al. Clinical outcomes of lung transplant recipients with telomerase mutations. J Heart Lung Transplant. 2015;34(10):1318-24.
16. Courtwright AM et al. Shorter telomere length following lung transplantation is associated with clinically significant leukopenia and decreased chronic lung allograft dysfunction-free survival. ERJ Open Res. 2020;6(2):00003-2020.
17. Newton CA et al. Telomere length in patients with pulmonary fibrosis associated with chronic lung allograft dysfunction and post-lung transplantation survival. J Heart Lung Transplant. 2017;36(8):845-53.
18. Popescu I et al. Impaired cytomegalovirus immunity in idiopathic pulmonary fibrosis lung transplant recipients with short telomeres. Am J Respir Crit Care Med. 2019;199(3):36276.
19. Silhan LL et al. Lung transplantation in telomerase mutation carriers with pulmonary fibrosis. Eur Respir J. 2014;44(1):178-87.
20. Borie R et al. Severe hematologic complications after lung transplantation in patients with telomerase complex mutations. J Heart Lung Transplant. 2015;34(4):538-46.
21. Zhang D et al. Telomere length and immunosuppression in nonidiopathic pulmonary fibrosis interstitial lung disease. Eur Respir J. 2023;62(5):2300441.
22. Noble PW et al. Pirfenidone in patients with idiopathic pulmonary fibrosis (CAPACITY): two randomised trials. Lancet. 2011;377(9779):1760-9.
23. King TE Jr. et al. A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. N Engl J Med. 2014;370(22):2083-92
24. Richeldi L et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N Engl J Med. 2014;370(22):2071-82.
25. Distler O et al. Nintedanib for systemic sclerosis-associated interstitial lung disease. N Engl J Med. 2019;380(26):2518-28.
26. Petnak T et al. Impact of antifibrotic
therapy on mortality and acute exacerbation in idiopathic pulmonary fibrosis: a systematic review and metaanalysis. Chest. 2021;160(5):1751-63.
27. Nathan SD et al. Prevalence and impact of coronary artery disease in idiopathic pulmonary fibrosis. Respir Med. 2010;104(7):1035-41.
28. Kreuter M et al. Impact of comorbidities on mortality in patients with idiopathic pulmonary fibrosis. PLoS One. 2016;11(3):e0151425.
29. Bos S et al. Antifibrotic drugs in lung transplantation and chronic lung allograft dysfunction: a review. Eur Respir Rev. 2021;30(160):210050.
30. Leard LE et al. Consensus document for the selection of lung transplant candidates: An update from the International Society for Heart and Lung Transplantation. J Heart Lung Transplant. 2021;40(11):1349-79.
31. Paterniti MO et al. Acute exacerbation and decline in forced vital capacity are associated with increased mortality in idiopathic pulmonary fibrosis. Ann Am Thorac Soc. 2017;14(9):1395-402.
32. Weill D et al. A consensus document for the selection of lung transplant candidates: 2014: an update from the Pulmonary Transplantation Council of the International Society for Heart and Lung Transplantation. J Heart Lung Transplant. 2015;34(1):1-15.
33. Cottin V et al. Syndrome of combined pulmonary fibrosis and emphysema: an official ATS/ERS/JRS/ALAT research statement. Am J Respir Crit Care Med. 2022;206(4):e7-e41.
34. Crespo MM et al. ISHLT consensus document on lung transplantation in patients with connective tissue disease: Part I: Epidemiology, assessment of extrapulmonary conditions, candidate evaluation, selection criteria, and pathology statements. J Heart Lung Transplant. 2021;40(11):1251-66.
35. Esendagli D et al. “Chronic obstructive pulmonary disease,” Perch M et al. (eds.), Lung Transplantation (ERS Monograph) (2024), Sheffield: European Respiratory Society, pp.11-23.
36. Criner GJ, Sternberg AL. National Emphysema Treatment Trial: the major outcomes of lung volume reduction surgery in severe emphysema. Proc Am Thorac Soc. 2008;5(4):393-405.
37. van Agteren JE et al. Lung volume reduction surgery for diffuse emphysema. Cochrane Database Syst Rev. 2016;10(10):Cd001001.
38. Criner GJ et al. Improving lung function in severe heterogenous emphysema with the spiration valve system (EMPROVE). A multicenter, openlabel randomized controlled clinical trial. Am J Respir Crit Care Med. 2019;200(11):1354-62.
39. Krishnan A et al. Lung volume reduction surgery before lung transplantation: a propensity-matched analysis. Ann Thorac Surg. 2022;113(2):491-7.
40. Slama A et al. Lung volume reduction followed by lung transplantation in emphysema-a multicenter matched analysis. Transpl Int. 2022;35:10048.
41. Rabe KF et al. Targeting type 2 inflammation and epithelial alarmins in chronic obstructive pulmonary disease: a biologics outlook. Am J Respir Crit Care Med. 2023;208(4):395-405.
42. Bhatt SP et al. Dupilumab for COPD with type 2 inflammation indicated by eosinophil counts. N Engl J Med. 2023;389(3):205-14.
43. Bhatt SP et al. Dupilumab for COPD with blood eosinophil evidence of type 2 inflammation. N Engl J Med. 2024;390(24):2274-83.
44. Benden C, Schwarz C. CFTR modulator therapy and its impact on lung transplantation in cystic fibrosis. Pulm Ther. 2021;7(2):377-93.
45. Ramos KJ et al. Lung transplant referral for individuals with cystic fibrosis: Cystic Fibrosis Foundation consensus guidelines. J Cyst Fibros. 2019;18(3):321-33.
46. Martin C et al. Major decrease in lung transplantation for patients with cystic fibrosis in France. Am J Respir Crit Care Med. 2022;205(5):584-6.
47. Salvatore D et al. Effectivenesss of ivacaftor in severe cystic fibrosis patients and non-G551D gating mutations. Pediatr Pulmonol. 2019;54(9):1398-403.
48. Elborn JS et al. Efficacy and safety of lumacaftor/ivacaftor combination therapy in patients with cystic fibrosis homozygous for Phe508del CFTR by pulmonary function subgroup: a pooled analysis. Lancet Respir Med. 2016;4(8):617-26.
49. Ejiofor LCK et al. Patients with cystic fibrosis and advanced lung disease benefit from lumacaftor/ ivacaftor treatment. Pediatr Pulmonol. 2020;55(12):3364-70.
50. Hubert D et al. Real-life initiation of lumacaftor/ivacaftor combination in adults with cystic fibrosis homozygous for the Phe508del CFTR mutation and severe lung disease. J Cyst Fibros. 2017;16(3):388-91.
51. Daines CL et al. Long-term safety and efficacy of elexacaftor/tezacaftor/ ivacaftor in adults and adolescents with cystic fibrosis and at least one F508del allele: a phase 3, open-label extension study. Am J Respir Crit Care Med. 2025; DOI: 10.1164/rccm.202411-2231OC.
52. Perrotta N et al. Improved clinical outcomes with elexacaftor/tezacaftor/ ivacaftor in patients with cystic fibrosis and advanced lung disease: real-world evidence from an Italian single-center study. Pharmacol Res Perspect. 2025;13(2):e70083.
53. Riddell P et al. “Cystic fibrosis,” Perch M et al. (eds.), Lung Transplantation (ERS Monograph) (2024), Sheffield: European Respiratory Society, pp.38-49.
54. Burgel PR et al. The French compassionate programme of elexacaftor/tezacaftor/ivacaftor in people with cystic fibrosis with advanced lung disease and no F508del CFTR variant. Eur Respir J. 2023;61(5):2202437.
55. Dagenais RVE et al. Real-world safety of CFTR modulators in the treatment of cystic fibrosis: a systematic review. J Clin Med. 2020;10(1):23.
56. Terlizzi V et al. Cystic fibrosis: new challenges and perspectives beyond elexacaftor/tezacaftor/ ivacaftor. Ther Adv Respir Dis. 2025;19:17534666251323194.
57. Shah P et al. Cystic fibrosis foundation consensus statements for the care of cystic fibrosis lung transplant recipients. J Heart Lung Transplant. 2021;40(7):539-56.
58. Kapnadak SG, Ramos KJ. Elexacaftortezacaftor-ivacaftor use after solid organ transplant. Curr Opin Pulm Med. 2024;30(6):660-6.
59. van Gemert JP et al. Evaluation of elexacafor/tezacaftor/ivacaftor therapy after lung transplantation in cystic fibrosis: the Dutch national KOALA study. JHLT Open. 2025;7:100210.
60. Hwalek A et al. Lung transplantation for pulmonary hypertension. J Thorac Dis. 2021;13(11):6708-16.
61. Delcroix M et al. “Pulmonary hypertension,” Perch M et al. (eds.), Lung Transplantation (ERS Monograph) (2024), Sheffield: European Respiratory Society, pp.50-64.
62. Humbert M et al. Treatment of pulmonary arterial hypertension: recent progress and a look to the future. Lancet Respir Med. 2023;11(9):804-19.
63. Pradère P et al. Outcomes of listing for lung and heart-lung transplantation in pulmonary hypertension: comparative experience in France and the UK. ERJ Open Res. 2024;10(1):00521-2023.
64. Hoeper MM et al. Phase 3 trial of sotatercept for treatment of pulmonary arterial hypertension. N Engl J Med. 2023;388(16):1478-90.
65. Delcroix M et al. ERS statement on chronic thromboembolic pulmonary hypertension. Eur Respir J. 2021;57(6):2002828.
Background: Latent tuberculosis testing prior to immunosuppression is recommended by national and international guidelines. However, no structured process currently exists for testing adult patients at tertiary care hospitals in Calgary, Alberta, Canada. Additionally, there is limited data describing interferon-γ release assay, QuantiFERON® (QFT; QIAGEN, Hilden, Germany) among inpatients. In 2021, a QFT order set was implemented for hospitalized patients with the aim to facilitate rapid testing prior to immunosuppression. This study aimed to compare the proportion of in-hospital immunosuppression started prior to QFT collection before and after QFT order set implementation, and to assess variables associated with indeterminate test results.
Methods: The authors performed a retrospective chart review of adult inpatients who underwent QFT at four acute care hospitals from 2020–2022. The Z-test was used to compare the proportion of pre-immunosuppression QFT testing pre- and post- order set implementation. Associations were analyzed using logistic regression.
Results: A total of 639 inpatients had QFT testing. The most common indication for QFT testing was immunosuppression. The proportion of patients who began immunosuppression prior to QFT decreased following order set implementation (54% versus 45%; p=0.0388). Indeterminate QFT results were associated with immunosuppression initiation before QFT (p<0.005). In multivariable analysis, the odds of an indeterminate QFT increased for patients with low lymphocyte counts (adjusted odds ratio [OR]: 3.45; 95% CI: 1.49–7.69) or those who received prednisone ≥50 mg (adjusted OR: 1.84; 95% CI: 1.0–3.39).
Conclusion: QFT should be performed before immunosuppression and, if possible, prior to hospitalization. Despite implementation of a QFT order set, immunosuppression was still frequently started before QFT collection. Further work is needed to identify barriers to early testing and evaluate strategies to optimize screening.
Key Points
1. Latent tuberculosis infection (LTBI) testing prior to immunosuppression is recommended by both national and international guidelines. Many hospitalized patients require urgent immunosuppression, however there is limited published data regarding LTBI testing in this population.
2. In this cohort of adult patients hospitalized at four tertiary acute care hospitals, immunosuppression was the most common reason for LTBI testing.
3. Starting immunosuppression before LTBI testing using QuantiFERON® was associated with an increased rate of indeterminate results. Despite this, many patients in the authors’ cohort received high-dose immunosuppression prior to QuantiFERON. More work is required to optimize inpatient LTBI testing.
INTRODUCTION
Latent tuberculosis infection (LTBI) affects up to one quarter of the worlds’ population.1 Although Canada is a lowincidence nation, the majority of incoming migrants originate from endemic areas, and it is estimated that over 1.5 million people carry the infection.2 Patients with LTBI who require immunosuppression are high risk for tuberculosis (TB) reactivation. Both the WHO and Canadian Tuberculosis Standards (CTS; 2022) recommend systematic testing and treatment of patients initiating immunosuppressive drugs associated with high risk for TB reactivation.3,4 Despite these recommendations, there is no structured process in Calgary, Alberta, Canada, to ensure LTBI screening is performed before the initiation of immunosuppression in hospitalized patients.
LTBI testing can be performed with a tuberculin skin test (TST) or an interferon (IFN)-γ release assay (IGRA). QuantiFERON® (QFT) is the IGRA test that is used in Alberta. Locally, there has been a shift to QFTbased testing for inpatients due to several advantages, including single blood draw collection, improved specificity, and more objective results.4 However, there is limited
published data describing the results of QFT among inpatients and none, to the authors’ knowledge, in a Canadian setting.5,6
Until 2021, ordering an inpatient QFT in Alberta required approval from a TB physician. This may have delayed testing, and anecdotally, LTBI testing was delayed by days to weeks after immunosuppression initiation. Immunosuppression prior to LTBI testing is associated with an increased rate of indeterminate results, thereby reducing the clinical utility of the test.6-8 In order to streamline the ordering process, a QFT order set was implemented in 2021 for inpatients at all acute care hospitals in Calgary. This allowed providers to order a QFT for patients requiring immunosuppression without TB physician approval, facilitating rapid testing prior to immunosuppression.
The objectives of this study were:
1. To compare the proportion of in-hospital immunosuppression started prior to QFT collection before and after QFT order set implementation; and
2. To assess patient variables associated with indeterminate test results among hospitalized patients.
METHODS
The authors performed a cross-sectional study using retrospective chart review data from all adult inpatients who underwent a QFT at any of the four acute care hospitals in Calgary, between January 1st–October 31st 2020 (prior to QFT order set implementation), and January 1st–December 31st 2021 (post QFT order set implementation). Calgary, has four publicly funded acute care hospitals for adults, and the general population is able to access any center. Demographics between hospitals were not expected to differ significantly, except based on geographic location. The QFT order set was implemented in November 2020; thus, the period from November 1st–December 31st 2020, was excluded from data collection to allow for roll-out/awareness of the order set. The study cohort was identified from the Alberta Precision Laboratories Public Health database, which performs all QFT testing in Alberta.
Inclusion criteria were: age 18 years or older at the time of QFT collection; acute care inpatient at time of testing; and a valid QFT result (positive, negative, or indeterminate). Electronic charts were manually reviewed, and data was abstracted using a structured form. The first ten charts were reviewed by two reviewers (Julien Ferland, McGill University, Montreal, Canada, and Leila Barss, University of Calgary, Canada) for consistency in data abstraction. For patients with duplicate testing, the result from only the first test was used for analysis.
Demographic variables including age, sex, co-morbid conditions, and home immunosuppression medications were collected. Ethnicity was collected if noted in admission documentation. Details of immunosuppression medication administered in hospital were recorded, including medication type, dose, and the timing of first administration. New immunosuppression was defined as any new immunosuppressive drug started or escalation in the home medication dose, between hospital admission and QFT collection. The indication for
immunosuppression and QFT testing was collected by chart review for all patients. The QFT order set allowed providers to indicate if the QFT was for immunosuppression or ‘other (e.g. recent close contact or recent immigration)’. For ‘other’, TB physician approval was required. This information was also collected for all patients who underwent a QFT in the ‘post order set implementation’ period and used to assess the appropriate use of the order set; specifically whether providers were using it to bypass TB physician review when ordering QFTs for indications other than immunosuppression. Lymphocyte count, C-reactive protein (CRP), and albumin results were collected if available within 72 hours of QFT collection. QFT results, including mitogen and nil results, were collected from the Alberta Precision Laboratories Public Health Laboratory database.
QFT testing was done using QuantiFERONTB® Gold Plus (QFT-Plus; QIAGEN, Hilden, Germany) for all patients. Incubation was performed according to manufacturer’s guidelines, and results were classified as positive, negative, or indeterminate.9 Blood samples were collected by trained phlebotomists for all hospitalized patients, except for patients admitted to the ICU, where either a bedside nurse or phlebotomist collected samples.
The primary outcome of this study was the proportion of patients who began immunosuppressive treatment prior to QFT collection in the pre- versus post-order set periods. Secondary outcomes included the number of patients with indeterminate QFT results and an examined association of five a priori factors for association.
Baseline characteristics among patients who underwent a QFT for immunosuppression screening were compared among the pre- versus post-order set implementation period using Pearson’s chi-square tests. Because the two groups were independent, a two-proportion Z-test was used to assess proportions of pre-immunosuppression QFT
testing. To identify variables associated with indeterminate results, a univariate and multivariable binary logistic regression was performed on the entire cohort. The variables tested were age, sex, year of study, hospital site, and factors known to possibly influence the QFT result: timing of immunosuppression, autoimmune disease, prednisone dosage, albumin level, CRP level, and lymphocyte count below the lower limit of normal. All analyses were performed using Stata version 16.1 (StataCorp LP, College Station, Texas, USA).
This study was approved by the University of Calgary Conjoint Health Research Ethics Board (REB 22-0365). Patient informed consent was waived due to the retrospective nature of the study.
RESULTS
Patient Characteristics and QuantiFERON Test Results
Between January 1st–October 31st 2020, and January 1st–December 31st 2021, 643 QFT results were reported from hospitalized patients at the four adult acute care hospitals in Calgary. Four results were duplicate tests and were excluded from analysis. Of the 639 patients included in analysis, there were 224 QFT results in the pre-order set implementation period (2020) and 415 QFT results in the post-order set implementation period (2021).
The most common indication for QFT testing was immunosuppression in both periods (85% in pre-order and 83% in post-order; Supplementary Table 1). Characteristics for patients undergoing testing due to immunosuppression are shown in Table 1. There was no significant difference in the proportion of patients taking home immunosuppressive medications prior to hospitalization (26% pre- versus 21% post-order; p=0.16). In the pre-order set period, vasculitis was the most common diagnosis associated with
immunosuppression testing (20%), whereas inflammatory bowel disease (25%) was most common in the post-order set period.
Among the entire cohort of 639 patients, QFT results were positive in 34 (5%), negative in 497 (78%), and indeterminate in 108 (17%). Among the cohort of 534 patients undergoing testing for immunosuppression, QFT results were positive in 23 (4%), negative in 415 (78%), and indeterminate in 96 (18%). There was no significant difference in indeterminate results between pre- versus post-order set periods (21% versus 16%; p=0.18).
Immunosuppression
Order Set Implementation
There was a significant decrease in the initiation of inpatient immunosuppression prior to collection of QFT following implementation of the order set (103/191 [54%] versus 153/343 [45%]) in the preorder set versus the post-order set period, respectively (p=0.0388). Steroids were the most common immunosuppressive medication started prior to QFT collection, administered in 99/151 (52%) patients in the pre-order set period and in 146/343 (43%) of patients in the post-order set period (Supplementary Table 2).
The immunosuppression order set was appropriately used in 313/343 (77%) patients. This included cases where QFT testing was due to ‘immunosuppression’ and ‘immunosuppression’ was selected, or QFT was done for an 'other' indication and ‘immunosuppression’ was not selected. Incorrect order set use was due to provider selection of ‘immunosuppression’ on the order set for non-immunosuppression testing (e.g. test was performed as part of active TB work up) in 26/343 (6%) of patients, and due to 'immunosuppression' not being selected on the order set for immunosuppressive QFT (based on chart review) in 69/343 (17%) of patients.
Table 1: Baseline characteristics among population undergoing QuantiFERON® for immunosuppression screening.
*Ethnicity not mentioned in admission documentation
**Defined according to admission date: steroid within 2 weeks; chemotherapy, immunotherapy, or biologic within 6 weeks; rituximab within 6 months
Table 2: Univariate and multivariable logistic regression analyses of factors associated with indeterminate QuantiFERON® result.
Table 2: Continued.
*Defined as either new start of immunosuppression and/or increased home dose administered before QFT collection. There was no difference in the rate of IND results among patients started on new immunosuppression versus those who had escalation of their home immunosuppression (Supplementary Table 3).
**Vasculitis, neurologic, inflammatory bowel disease, or connective tissue disease
An indeterminate QFT result was associated with immunosuppression initiation before QFT collection (Chi-square [1; n=639]: 20.55; p<0.005). Results of the univariate and multivariable analyses are presented in Table 2 and Supplementary Table 3 The multivariable analysis included timing of new immunosuppression prior to QFT, prednisone dosing, autoimmune disease, albumin, CRP, and lymphocyte count. In the multivariable analysis, the odds of an indeterminate QFT were significantly increased if patients had an abnormally low lymphocyte count (adjusted odds ratio [OR]: 3.45; 95% CI: 1.49–7.69) or received daily prednisone dosed at ≥50 mg (adjusted OR: 1.84; 95% CI: 1.0–3.39). Steroids started before QFT in 96% of those receiving immunosuppression, with 56% receiving high-dose steroids. The frequency of
other immunosuppressive medications were too low to analyze individually in association with QFT results.
Elevated CRP, lower lymphocyte counts, and the use of immunosuppression in hospital was associated with lower IFN-γ responses (p<0.005, p=0.008, and p<0.005, respectively). Indeterminate results were due to a low mitogen response in all except one patient.
DISCUSSION
Inpatient latent TB screening is often required urgently to prevent iatrogenic TB reactivation in the face of impending immunosuppression for acute illness. To the authors’ knowledge, this is the largest retrospective study assessing indications
for QFT use among hospitalized patients and the relationship between test timing and inpatient immunosuppression medication. Among the authors’ cohort of hospitalized adult patients in Calgary, over 80% of QFTs performed in hospital were for the indication of immunosuppression medication initiation/ escalation. Immunosuppression was frequently started before QFT collection, despite the potential adverse impact on test sensitivity. Several studies have determined that immunosuppressive medications can result in higher rates of indeterminate and even falsely negative results.10-12 Similarly, this study found that immunosuppression initiated in hospital prior to QFT collection was associated with an indeterminate result. In the multivariable analysis, the timing of initiation relative to QFT (e.g. started <24 hours prior to the test versus started >72 hours prior to the test) was not associated with an indeterminate result, but dosing of steroids (>50 mg prednisone equivalent) did significantly increase the odds of an indeterminate result (adjusted OR: 1.84; 95% CI: 1.0–3.39).
The implementation of an electronic QFT order set may have reduced the proportion of patients who had delayed QFT testing. The electronic order set streamlined ordering by reducing the time needed to speak with a TB physician prior to ordering every test, and also reduced the need for laboratory staff to confirm the test was approved. However, there was still a large proportion of patients started on immunosuppression prior to QFT collection (reduced from 54% to 45%). The order set was also used incorrectly in almost a quarter of patients, indicating that a lack of clinician education/awareness around the ordering process may be a contributor to suboptimal screening. We found that 11% of QFTs were ordered as part of the work-up for active TB, which is generally not recommended due to inadequate specificity and sensitivity (possibility of anergic response in active disease).13 Bouton et al.14 showed that almost two-thirds of QFTs done in their regional health network were ordered for the purposes of ruling out
active TB, demonstrating that this may be an ongoing knowledge gap. Other strategies to optimize screening practices for TB infection, particularly before immunosuppression is initiated, are needed considering the rising frequency of immunosuppressive conditions and medication use among the general population.15 An accurate and timely TB infection diagnosis is essential for providing effective TB preventative therapy among immunosuppressed patients. Indeterminate results may delay initiation of immunosuppressive treatment and/or lead to inappropriate LTBI treatment choices, due to lack of an accurate diagnostic test. The importance of this cannot be understated, as preventative therapy has been shown to be up to 90% effective in reducing the incidence of reactivation TB, which carries significant morbidity and mortality.16
Interestingly, the indeterminate QFT frequency of 17% among the author's entire cohort was much higher than reported among both immunocompetent (1.9%) and immunocompromised (5.7%) populations in a recent meta-analysis.8 While immunosuppressive medications in the author's cohort was a factor, the indeterminate rate was still high (10%) among inpatients with no immunosuppression at the time of testing. Three previous studies also reported a high frequency of indeterminate results (20–27%) among hospitalized patients.5,6,14 One study found that being an inpatient had an OR of 8.6, compared to outpatients.6 Another study found that inpatients were 11 times more likely to have an indeterminate result compared to outpatients.14 A few of these studies surmised that this phenomenon could be related to collection factors (residents/bedside nurses versus trained phlebotomists). However, in the author's cohort, all testing, except patients from the ICU, was performed by trained phlebotomists. Therefore, there are likely additional host factors associated with acute illness and hospitalization that contribute to the high indeterminate rate among the author's cohort.17
One such host characteristic is lymphocyte count, as a low lymphocyte count was associated with an indeterminate result in the author's study. Insufficient lymphocytes or an inability of the patient’s lymphocytes to generate IFN-γ can result in an indeterminate assay result, due to a low IFN-γ response to mitogen.18 Previous studies have also reported an association between low albumin and lymphocytes with increased frequency of indeterminate QFT results.5,19 Both can be related to the severity of illness among acutely unwell patients, suggesting that disease severity and consequent immune function may affect QFT results.17,20
A limitation to this study includes the absence of standardized LTBI testing criteria for hospitalized patients (physician discretion of whom to test and when). Disease severity was not assessed, it is possible that more severe inflammatory disease may be associated with higher rates of indeterminate QFT results. These patients may be more likely to start on early immunosuppression (prior to QFT collection), which could impact the results. Finally, due to the retrospective nature of this study, the authors were not able to collect data on provider awareness of the QFT order set and the impact this may have had on QFT ordering patterns.
References
1. Cohen A et al. The global prevalence of latent tuberculosis: a systematic review and meta-analysis. Eur Respir J. 2019;54(3):1900655.
2. Essue BM et al. Better data to drive more effective care for people with latent tuberculosis infection in Canada. CMAJ. 2018;190(23):E700-1.
3. World Health Organization (WHO). Latent tuberculosis infection: updated and consolidated guidelines for programmatic management. 2018. Available at: https://www.who.int/ publications/i/item/9789241550239. Last accessed: 6 January 2025.
4. Campbell JR et al. Chapter 4: diagnosis of tuberculosis infection. Can J Respir Crit Care Sleep Med. 2022;6(Suppl 1):49-65.
An important strength of this study is that a detailed chart review was undertaken to determine accurate indications for QFT orders and other patient characteristics, rather than reliance on administrative data like International Classification of Diseases (ICD) codes, to facilitate an exploratory analysis of risk factors for an indeterminate result.
CONCLUSION
Initiation of immunosuppression medication was the most common reason for QFT use among the cohort of hospitalized patients. QFT should be performed before immunosuppression initiation, and if possible, prior to hospitalization to obtain an accurate TB infection status and facilitate appropriate TB preventative therapy among this high-risk population. Implementation of an inpatient QFT order set reduced delayed testing in this cohort. However, immunosuppression was still started before QFT collection in a large proportion of patients. Further work is needed to identify barriers to early inpatient testing and evaluate strategies to optimize screening among hospitalized patients.
5. Fabre V et al. High proportion of indeterminate QuantiFERON-TB Gold In-Tube results in an inpatient population is related to host factors and preanalytical steps. Open Forum Infect Dis. 2014;1(2):ofu088.
6. Osakabe Y et al. In-hospital blood collection increases the rate of indeterminate results in interferongamma release assays. Ther Adv Respir Dis. 2022;16:17534666221077817.
7. Park CH et al. Impact of immunosuppressive therapy on the performance of latent tuberculosis screening tests in patients with inflammatory bowel disease: a systematic review and meta-analysis. J Pers Med. 2022;12(3):507.
8. Zhou G et al. Indeterminate results of interferon gamma release assays in the screening of latent tuberculosis
infection: a systematic review and meta-analysis. Front Immunol. 2023;14:1170579.
9. QIAGEN. QuantiFERON®-TB Gold Plus (QFT®-Plus) Package Insert. 2023. Available at : https://www. qiagen.com/us/resources/download. aspx?id=ac068fc7-a994-4443ac7c-dda43ce2bc5e&lang=en. Last accessed: 18 February 2025.
10. Belliere J, Blancher A. QuantiFERON test interpretation in patients receiving immunosuppressive agents: an alert. Eur Respir J. 2017;49(4):1602102.
11. Calabrese C et al. Evaluating indeterminate interferon-gammarelease assay results in patients with chronic inflammatory diseases receiving immunosuppressive therapy. Arthritis Care Res (Hoboken). 2015;67(8):1063-9.
12. Jung HJ et al. Analysis of predictors influencing indeterminate whole-blood interferon-gamma release assay results in patients with rheumatic diseases. Rheumatol Int. 2014;34(12):1711-20.
13. World Health Organization (WHO). Use of tuberculosis interferongamma release assays (IGRAs) in low- and middle-income countries : policy statement. 2011. Available at: https://www.who.int/publications/i/ item/9789241502672. Last accessed: 18 February 2025.
14. Bouton TC et al. High rates of indeterminate TB tests among hospitalized patients: can we optimize
use of gamma interferon release assays in tuberculosis? R I Med J (2013). 2019;102(6):27-30.
15. Martinson ML, Lapham J. Prevalence of immunosuppression among US adults. JAMA. 2024;331(10):880-2.
16. Comstock GW. How much isoniazid is needed for prevention of tuberculosis among immunocompetent adults? Int J Tuberc Lung Dis. 1999;3(10):847-50.
17. Huang CT et al. Effects of acute critical illnesses on the performance of interferon-gamma release assay. Sci Rep. 2016;6:19972.
18. Komiya K et al. Impact of peripheral lymphocyte count on the sensitivity of 2 IFN-gamma release assays, QFT-G and ELISPOT, in patients with pulmonary tuberculosis. Intern Med. 2010;49(17):1849-55.
19. Kaur M et al. Factors that contribute to indeterminate results from the QuantiFERON-TB Gold In-Tube test in patients with inflammatory bowel disease. Clin Gastroenterol Hepatol. 2018;16(10):1616-21.e1.
20. Andreu-Ballester JC et al. Lymphopenia in hospitalized patients and its relationship with severity of illness and mortality. PLoS One. 2021;16(8):e0256205.