





We celebrate over forty years of the Bulletin... ...and then drop the mic!



The future is bright
As our association moves forward – what opportunities lie ahead?



An exploration of the dimensions of chronic pain in dental practice


AS WE CELEBRATE the milestone of our 75th issue of the DHAA Bulletin, I reflect on the incredible journey we’ve had together. This publication has served as a vital platform for sharing knowledge, connecting our community, and amplifying the voices of our members. We’ve seen tremendous growth in both our reach and impact over the years, thanks to the tireless dedication of our editors, contributors, and the unwavering support of all involved with the DHAA.
One of our greatest achievements has been advocating for the improved recognition and inclusion of oral health professionals as independent practitioners. We’ve been successful in many initiatives that have advanced the recognition of our members and the profession as a whole. Together, we’ve made significant strides in raising awareness and creating opportunities for professional development and the Bulletin has been a cornerstone of that effort.
As we transition to the new association with OHAA, I’m excited to introduce Mr Nathan Clarke, who will be leading the charge in this new chapter. Nathan brings a wealth of experience and a vision that aligns perfectly with our shared values and goals. I am confident that under his leadership, we will continue to thrive and grow.
I also want to take a moment to express my deep gratitude to our current DHAA CEO, Bill Suen. Your leadership, dedication, and guidance have been pivotal in navigating our association through times of change and growth. Thank you for your commitment to the DHAA and the profession as a whole.
I am equally grateful to our directors, staff, and members for your unwavering support. It has been a true privilege to serve as your president. Your commitment, passion, and dedication have been integral to our success, and I encourage you to continue contributing to our collective future in the new association.
As we mark the final Destination CPD in Bali and look forward to celebrating 50 Years of Dental Hygiene at the Gala Dinner in Adelaide, I hope to see many of you there. These events will be amazing opportunities to come together, celebrate our achievements, and look ahead to an exciting future.
Please remember to renew your membership and encourage your colleagues and friends to register with the new association. Every voice matters, and now that we are one association, we will be louder than ever, with a stronger collective presence in advancing the profession.
As I transition to a new role on the OHAA Board as one of the directors, I look forward to continuing to work alongside many of you, supporting the next phase of our journey. I now hand over to the OHAA President, Cheryl Dey, whose leadership and vision will guide us into this exciting new chapter. Cheryl’s dedication to advancing the profession and her passion for fostering collaboration within our community will undoubtedly inspire and empower us all.
Thank you, and I look forward to what lies ahead for all of us.
Jinous Eighani-Roushani DHAA President
Contacts



04 In oral health we trust
Announcing the Australian Oral Health Foundation Trust
06 Are you CPD ready?
Get into position to complete the current CPD cycle.
09 Closing in on Congress
Unlock new horizons for 2025 at this landmark event.
12 Ask DHAA
Your questions answered.
16 Get your online CPD fix
Enjoy learning from home.
20 A legacy of innovation
Celebrating 50 years of dental hygiene in Australia.
22 The future is bright
As our association moves forward – what opportunities lie ahead?
24 That's all folks!
Bid farewell to The Bulletin.
28 Pharmacies as partners in oral health
A collaborative and educational approach.
30 Bye-bye Bill
Messages to CEO Bill Suen as he explores pastures new.
34 Stay covered in 2025
Introducing the OHAA Member Insurance Program.
36 Chronic pain in dentistry
An exploration if the dimensions of chronic pain.
40 Living for the now
Finding strength and peace in the present moment.
42 Getting the rinse right
A recommnedation guide..
46 State of the Nation
Our final round-up.

The Dental Hygienists Association of Australia (DHAA) is proud to announce the establishment of The Australian Oral Health Foundation Trust (the Foundation). This initiative celebrates the enduring legacy of the DHAA and honours the contributions of its members to both the association and the broader oral health profession.
Key details
n Purpose
The Foundation will focus on preventive oral health initiatives, reflecting the core mission of the DHAA. Surplus financial assets
accumulated over the operations of the DHAA will be transferred to the Foundation after allocating seed funding for the new Oral Health Association of Australia (OHAA).
n Funding Priorities
The Foundation’s trust deed mandates that funds support activities to improve oral health for all Australians, including:
• Research and education (e.g., scholarships, research grants).
• Community projects promoting oral health awareness.
• Advocacy campaigns to advance preventive care.
n Trustee Responsibilities
OHAA board directors have been appointed as trustees for the Foundation and are required to:
• Manage and grow the Foundation’s assets.
• Invest funds prudently to balance growth and risk.
• Raise awareness of available support.
• Evaluate and approve beneficiary requests.
n Sustainability
The Foundation will operate in perpetuity, using investment income to fund initiatives aligned with its mission.
The Foundation ensures the DHAA’s values and commitment to oral health endure. By channeling resources into prevention, education, and advocacy, we aim to create lasting benefits for Australia’s preventive oral health landscape.
Stay tuned for further updates as we finalise the Foundation’s launch. Members and stakeholders are encouraged to engage with future opportunities for collaboration, applications for support, or contributions to the Foundation’s mission. Together, we look forward to advancing a healthier future through the Australian Oral Health Foundation Trust. n
DHAA President, Jinous Eighani-Roushani, acknowledges the outstanding effort of a few of the many Association stalwarts that have devoted their time and passion to the betterment of all of our professional lives.
As we move forward with the new association, I just want to say a huge thank you to all the staff who’ve worked with us. Your hard work and support have meant so much, and I truly appreciate each of you.
Danielle Gibbens
I’m excited to continue working with Danielle as she transitions into the new association, and I look forward to what we’ll achieve together in this next chapter!
Shida Taheri
A special thank you to Shida, who will be moving on as we transition to the new association. Your work in managing sponsorships and engaging stakeholders and sponsors, especially for the DHAA and OHAA Congress has been outstanding. We are incredibly grateful for everything you’ve done and wish you all the best in your future endeavours!.
Katrina Murphy
As we say goodbye to Katrina, I want to express my deepest appreciation for all the incredible support you've given to the association over the years. Your expertise and dedication in providing industrial relations (IR) advice to our members have been invaluable. You've been a trusted advisor, and your contributions have made a significant impact on the growth and success of our association. Thank you for everything, and we wish you all the best in your future endeavours.
Christina Zerk
Christina, you have been absolutely amazing, and we truly appreciate everything you’ve done for the association and our members. Your dedication, hard work, and unwavering support have not gone unnoticed. I'm personally grateful for your continued support and the positive impact you've had during your time here. We’ll miss you, but we know you’ll continue to do great things. Thank you again for all your efforts, and best wishes for everything ahead.
They may be strangers to most of our readers and members as their names never appear on any official DHAA activities and publications. Kirsty is our finance officer that quietly and consistently making sure all payments and financial reports are made on time with precision - she never missed a beat! Steve is our media production consultant and all the bulletins and advocacy media campaign materials that we enjoy so much are the excellent work of his. We salute them for their tireless work and professionalism that make everything possible towards the seamless operations of the DHAA.

Have you got what you need to complete the current CPD cycle ending on 30 November 2025?
By Elizabeth Milford
The clock is ticking as the current Continuing Professional Development (CPD) cycle for dental professionals approaches its conclusion on 30 November 2025. For many in the dental field, CPD is more than just a regulatory requirement—it is a cornerstone of professional growth, ensuring practitioners remain at the forefront of advancements in technology, research, and clinical practice. But with the deadline looming, are you prepared to meet your CPD obligations and make the most of this opportunity for growth?
Continuing Professional Development plays a pivotal role in maintaining high standards within the dental profession. It allows practitioners to stay updated on emerging technologies, refine their techniques, and adopt evidence-based practices. In an ever-evolving field like dentistry, where new materials, tools, and approaches are constantly being introduced, CPD ensures that professionals can deliver optimal care to their patients.
Over the decades, CPD has undergone significant transformation. Gone are the days when professional development
was limited to attending lectures or reading printed journals. Today’s CPD landscape reflects advancements in technology and modern learning methodologies, offering a diverse range of options tailored to individual learning preferences and professional needs.
One of the most notable changes in CPD is how accessible it has become. Dental professionals now have a wealth of resources at their fingertips:
• Online Journals and Databases: Platforms like Cochrane provide access
to cutting-edge research that can inform clinical decision-making.
• Podcasts: Dental-specific podcasts offer an engaging way to learn on the go, covering topics from clinical case studies to practice management tips.
• Online Lectures: Whether live or asynchronous, online lectures allow practitioners to learn from experts worldwide without leaving their homes.
• In-Person Events: From single-day workshops to multi-day conferences, face-to-face events provide valuable networking opportunities alongside educational content.
The variety of formats ensures that every practitioner can find a mode of learning that suits their schedule and preferences.
While traditional lectures and reading materials remain valuable, there has been a marked increase in hands-on courses within CPD offerings. These practical sessions allow dental professionals to test new skills and techniques in controlled environments before applying them in practice. Whether it’s mastering a new restorative material or refining clinical techniques, hands-on courses bridge the gap between theoretical knowledge and clinical application.
Coaching is emerging as a popular CPD option for those seeking tailored guidance. Unlike traditional courses that focus on delivering information, coaching provides a collaborative space for reflection and problem-solving. It can help practitioners navigate challenging situations—whether they’re unsure about their next steps or need strategies to improve outcomes in specific scenarios. Through coaching, dental professionals can set goals, engage
in guided practice, and gain clarity on how to address complex issues in their practice. This personalised approach not only enhances professional competence but also fosters confidence and resilience.
With so many options available, selecting the right CPD activities can feel overwhelming. To simplify this process, the Dental Board has developed a reflective practice tool. This resource helps practitioners evaluate their current knowledge and skills in relation to their scope of practice. By identifying areas for improvement or growth, the tool enables practitioners to plan their CPD strategically.
Here’s how you can make the most of your CPD planning:
1. Use the Reflective Practice Tool: Regularly reflect on your strengths and areas for development using this resource. Time spent completing the tool can even be claimed as CPD hours
Networking opportunities: Don’t miss out!
CPD is not just about acquiring knowledge—it’s also about building connections within the profession. Face-to-face events like conferences offer unparalleled opportunities for networking with peers and industry leaders. These interactions can spark collaborations, inspire new ideas, and provide insights into best practices from around the world.
One event not to be missed is the upcoming OHAA Conference. Promising an exciting lineup of speakers and topics relevant to oral health professionals, this conference is an excellent opportunity to earn CPD hours while engaging with colleagues from across the country.
As you work toward completing your CPD requirements by 30 November 2025, remember that professional development is not just about
“As you work toward completing your CPD requirements, remember that professional development is not just about meeting regulatory obligations—it’s an investment in yourself and your career”
2. Diversify Your Learning: Aim for a mix of activities—online and face-to-face sessions, participating in coaching, live events, asynchronous learning, reading and hands-on workshops
3. Prioritise Quality: Choose activities grounded in robust research or delivered by reputable organisations
4.Reflect on Your Learning: After completing each activity, take time to consider how it applies to your practice.
5. Integrate New Knowledge: Implement what you’ve learned into your daily work to ensure it has a tangible impact on patient care. Better still, keep a journal or diary of your evolving practice.
meeting regulatory obligations— it’s an investment in yourself and your career. By embracing diverse learning opportunities, reflecting on your progress, and integrating new knowledge into your practice, you can ensure that your efforts translate into meaningful improvements for both you and your patients.
So take stock of where you stand with your CPD hours today. Explore new learning opportunities that excite you or address gaps in your skills. And don’t forget to mark your calendar for key events like the OHAA Congress—it’s shaping up to be an unmissable highlight of this CPD cycle! n
Unlock
Australia’s oral health professionals are invited to the inaugural OHAA National Congress 2025, set against the stunning backdrop of the Gold Coast this spring (16- 18 October 2025). This milestone event promises to elevate professional development, foster collaborations, and shape the future of oral health nationwide. Here’s what attendees can expect:
highlights of the congress
n Professional Growth & CPD Opportunities
The congress offers 20 hours of Continuing Professional Development (CPD). With the current CPD cycle ending on 30 November 2025, this is a timely opportunity for practitioners, students, and industry professionals to meet requirements while engaging in cuttingedge workshops, keynote presentations, and oral research sessions.
“This is a timely opportunity for practitioners, students, and industry professionals to meet requirements while engaging in cuttingedge workshops, keynote presentations, and oral research sessions”
n Diverse Program & Networking Attendees will enjoy a dynamic agenda, including:
• Workshops
• Keynote and invited speaker presentations
• Trade exhibition showcasing the latest innovations
• Social events like the Welcome Cocktail Reception, Gala Dinner, and Breakfast Event
• Exclusive president’s reception (by invitation only)
n Inclusive Destination: Gold Coast Renowned for its accessibility and vibrant atmosphere, the Gold Coast offers inclusive facilities from beaches to accommodations, making it ideal for attendees of all abilities. Participants are encouraged to extend their stay and explore the region’s natural beauty and recreational activities.
n Industry Collaboration & Sponsorship
The event’s theme, “Opening Horizons Across Australia,” underscores its mission to connect professionals nationwide and across the Asia-Pacific. Major sponsors like Platinum Sponsor Piksters/Erskine Dental and Gold Sponsors Colgate and Ozdent are pivotal to delivering this landmark program. Tailored partnership opportunities remain open for organisations aiming to align with this influential audience.
n Early Bird Savings & Registration
Secure discounted rates by registering early! The congress is a one-of-a-kind chance to learn, network, and contribute to advancing oral health practices while enjoying the Gold Coast’s spring bloom.
Shape the Future: Collaborate with peers to drive innovation in oral health. Earn CPD Credits: Fulfil requirements efficiently with high-quality sessions. Network Nationally: Connect with practitioners, mentors, and industry leaders.
Experience the Gold Coast: Combine professional growth with a rejuvenating getaway.
Don’t miss out on this historic event! Early bird tickets are now available, offering savings for those who register soon. Explore sponsorship or exhibition opportunities to showcase your organisation’s role in advancing oral health.
Visit the Congress website for details on registration, the full program, and partnership prospects.
The OHAA National Congress 2025 is poised to be a transformative experience—where expertise meets inspiration, and the future of oral health takes flight. n









Bill Suen DHAA CEO
AS WE APPROACH a historic milestone for our profession, I write to you with both nostalgia and optimism. On 1 July 2025, the Dental Hygienists Association of Australia (DHAA) will transition to the Oral Health Association of Australia (OHAA), marking an exciting evolution in our collective journey. This will be the final Bulletin under the DHAA banner, as the next edition – OHAA Connect –will be published by our new, unified association.
Reflecting on the achievements of the DHAA fills me with immense pride. Together, we’ve secured independent practice rights, earned provider number recognition, and laid the groundwork for Medicare access—a critical initiative that the OHAA will continue to advance. These milestones were made possible by the unwavering dedication of our members, volunteers, and partners. The resources and advocacy capacity we’ve built will serve as a strong foundation for the OHAA’s mission to elevate oral health nationwide.
It is my honour to introduce Mr Nathan Clarke, the incoming CEO of the
OHAA. Nathan’s visionary leadership and passion for our profession ensure the DHAA legacy will thrive in this new chapter. I am confident that under his guidance, the OHAA will achieve even greater heights.
As we transition, membership renewals are now open under the OHAA. By renewing, you’ll continue to benefit from education, resources, support, and a united voice for oral health practitioners.
“Every challenge we overcame, every milestone we celebrated, and the camaraderie of our “DHAA family” will stay with me always.
To the DHAA Presidents I have had the privilege to serve alongside— Cheryl Dey, Carol Tran, and our current President, Jinous Eighani-Roushani— thank you for your visionary leadership, wisdom, and steadfast support. Each of you guided the DHAA through pivotal moments, and your contributions have shaped the association’s success.
To the Board Directors, Committee Chairs, volunteers, members, and sponsors: your trust, collaboration, and relentless drive have been the heartbeat
of our progress. A special tribute goes to my incredible staff team—your dedication, creativity, and hard work have been the backbone of every achievement.
Leading the DHAA has been one of the most rewarding experiences of my career. Every challenge we overcame, every milestone we celebrated, and the camaraderie of our “DHAA family” will stay with me always. While my tenure concludes once the DHAA is formally wound up, I depart knowing our work has created a lasting impact.
The future of oral health is bright. The OHAA will champion innovation, inclusivity, and equity in our profession, building on the DHAA legacy. To all members and partners: thank you for allowing me to serve. Keep pushing boundaries, supporting one another, and advocating for the vital role of oral health practitioners in driving the improvement of oral health.
With deepest gratitude and warmest wishes to you all,
Bill Suen Chief Executive Officer
P.S. Stay connected! Renew your membership today and join us in shaping the OHAA’s future. Together, we will continue to make history.

Continue thriving in your career with unmatched support and connecting you to the people, resources, and opportunities that elevate your career
All ADOHTA or DHAA memberships expire on 30 June 2025—renew now to maintain access to essential resources and benefits for the 2025-2026 financial year. Don’t miss out on the tools that keep you ahead in your profession!
Why Renew/Join with OHAA?
Stay Informed: Regular industry updates to navigate changes impacting your work.
Expert Support: Guidance from experienced clinicians for up-to-date advice.
Free Legal Assistance: Industrial relations advice + contract reviews.
CPD Made Easy: 20+ free online webinars + discounted face-to-face events.
Career Growth: Exclusive networking, job boards, and connections.
Optional Insurance: Affordable professional indemnity coverage via BMS (additional fees apply).
Renew/Join Your OHAA-BMS Insurance by 30 June 2025
Your optional member insurance does not renew automatically and lapses if not renewed directly through the BMS Portal (after you have renewed or joined the OHAA membership). Protect yourself from unforeseen claims—act now!
1800 940 762
ohaa@bmsgroup.com
(Formerly Aged Care Chapter)
Exclusively for OHAA members who are working or intending to work in aged care:
• Specialised CPD opportunities
• Business development support
• Purchase the OHAA Aged Care Education Program
Add this option when renewing your OHAA membership!
Don’t Let Your Benefits Expire! Renewing takes minutes, but the rewards last all year.
RENEW NOW
Questions? We’re here to help! admin@ohaa.org.au 0433 022 859
Thank you for your dedication to advancing oral health. We are honoured to support your journey.
Cheryl Dey | OHAA President

Your opportunity to ask the questions, check the rules and share your knowledge
Dear DHAA... I am looking at new professional indemnity insurance for the coming financial year. I know DHAA membership includes the option to purchase PI insurance –what’s the cost? I’m an OHT working just one day a week. The PI insurance price for our members ranges between $195 to $220 per year (depends on the state you are in as stamp duty varies). The risk profile of our policy is so low that the number of hours that you practise is immaterial in calculating the premium, so it is the same rate for all.
Please also note that the premium has not changed since we introduced the PI insurance policy to our members seven years ago, as our risk profile has been steadily low over this period.
Dear DHAA... Just have a question regarding autoclave validation/ calibration. We want to use the 121 degree gentle cycle to sterilise our intra-oral scanner tip as they are plastic and the manufacturer has told us that they will last twice as long on the 121 degree cycle. However, it is extremely expensive to do this validation every year and not really worth it to autoclave one or two tips occasionally. But I have been told that if I use a Class 6 indicator in the 121 degree cycle it will confirm that the cycle was successful and I don’t need to do the yearly validation. Is it OK? Please refer to the Dental Board resource regarding infection control:
The DBA has moved away from prescriptive infection


control guidelines and asks practitioners to ensure safe practice using your professional judgement and relevant published guidelines and evidence.
In terms of validation of your autoclave, each company would make their own recommendations regarding their equipment. You may, based on relevant standards and/or guidelines, decide on the appropriate infection control measures.
The important issue is that you must based on evidencebased standards and/or guidelines as the DBA has explicitly indicated that you will be asked to provide the reference to your infection control practice during a notification investigation. Informal recommendations and verbal comments from other individuals or organisations are not sufficient.
The DHAA is therefore not in the position to make any recommendations on this matter other than referring you to the equipment company, your local health authority and the ADA IPC guidelines. Please also note that cost is not a valid defence for not following established standards and guidelines.
Dear DHAA... I am interested in working for aged care facilities. Could I have guidelines to start with please?
The DHAA has provided its RACF Oral Health Service guidelines and the webinar to explain the guidelines are scheduled for Wednesday 11 June for all members. Please check out the webinar and it will also be made available on the webinar library for future on demand viewing by members. it should provide some useful and practical
information about servicing RACFs. We also have an aged care chapter and education program to prepare and support members. Please check this out: Please note that this will be offered by the new Oral Health Association of Australia (OHAA) as the Aged Care Connect.
Dear DHAA... I’m enquiring as to the process for retirement at the end of this registration period on the 30 November 2025 . If you are seeking permanent cessation of your practice as a dental practitioner, all you need to do is either to let your registration expired and not renew, or inform Ahpra. You should also contact your PI insurer and inform them, so they can organise the appropriate cover post retirement and organise any refund if applicable.
For the DHAA membership and insurance, you should renew them at 30 June this year until you are actually not registered with Ahpra after 1 December 2025 as the CPD and PI Insurance requirements are linked to your Aphra registration. We may wish to transfer your full membership into a retired membership ( a category of affiliate membership) and you will be able to continue enjoying the membership benefits and connect with the association at a much reduced annual subscription.
Dear DHAA... I’m currently on maternity leave and will have had approx 18 months off in June. How long can we have off before it starts to interfere with our registration? I’ve still been registered as a practicing OHT and keeping up with CPD. >>

The recency of practice registration standards currently set the period at five years. You must inform and seek advice from the Board if you have not practised for five years or more.
However, we believe that this standard is currently under review and we will inform members if any changes come through.
Dear DHAA... My employer would like me to complete a nitrous oxide and oral sedation course. It states dentist, OHT and hygienist can attend the course. My question is where do we stand as a dental hygienist and treating patients with nitrous?
Thanks for your query, the DHAA policy on RA, GA and Sedation is available for member access here:
The general principle is that dental hygienists, oral health therapists and dental therapists are not permitted to prescribe, supply or administer relative analgesia (Nitrous Oxide), conscious sedation or general anaesthesia.
In practise the following apply:
1. Dental hygienists, oral health therapists and dental therapists may treat patients under RA, CS or GA provided that the treatment or procedure undertaken is within their scope.
2. Dental hygienists, oral health therapists and dental therapists must be properly trained, proven competent and keeping up to date with the specific skills required to treat and manage patients under RA, CS or GA.
3. The RA, CS or GA is
administered by a qualified practitioner with the appropriate accreditation or endorsement, and that person is taking full responsibility of the patient and is present at all time when the DH, DT or OHT is working on the patient.
You are therefore not allowed to monitor the patient under RA, CS or GA, or to adjust doses at any time - these must be the responsibility for the approved practitioner ( e.g. the dentist with appropriate accreditation as prescribed by local legislations).
You may attend the training to get a better understanding that may help you when you provide oral treatment within your scope for patients under RA, CS or GA, but you can’t handle the anaesthetics or monitor the patient.
Dear DHAA... I’m going on maternity leave on July 1 and will be taking 12 months leave. I’m just wondering what my indemnity insurance obligations are. Please note that your professional indemnity insurance and CPD obligations are linked to your Ahpra registration, regardless of whether you are actually working or not. If you are continuing with your registration, you need to continue with the insurance and CPD.
If you are suspending your registration, or seeking to change your general registration to a nonpractising one, then we can organise a special maternity leave coverage for 12 months (at a smaller cost than the normal insurance), but you still need to continue to be a full member to be able to have
BY
that coverage. So you must continue with the DHAA full membership otherwise your PI insurance with be stopped and no maternity cover can be issued.
As the 2025 renewal will be an invitation to join the new association (OHAA), the best way forward is the renewal your membership as an OHAA member immediately when you receive your renewal notice in May ( check the PI insurance option), and then let us know without clicking
through to renew your PI insurance. We will then organise your maternity cover manually.
Dear DHAA... I’m a newly registered oral health therapist, having recently converted my licence and started working in Australia this year. Is there a way to find out how many CPD hours I need to complete for this registration period, and where I should be recording them?
Thanks for your email. Your
CPD requirements is 60 hours over a three-year period ( From 1 December 2022 to 30 Nov 2025). If you commence your registration in the middle of this three-year cycle, your CPD requirements will be calculated on a pro rata basis. It is a requirement of our AHPRA registration as an oral health practitioner that we maintain records of our CPD activity for five years and provide a logbook of our CPD activities if requested. This means

every registered oral health practitioner should have a CPD log/ logbook that they record their CPD activities in, however DHAA Members do have access to our online CPD logbook to record their CPD.
The entry needs to contain at least the following information for each activity:
• the CPD activity provider’s name
• CPD activity name
• journal name, article name, author (where applicable)
• online content/title, DVD title, CD title (where applicable)
• date, time and location of the CPD activity
• number of CPD hours (excluding breaks), and.
• type of CPD hours (scientific/non-scientific) that are awarded as a result of completing the activity.
You can head to our Member Portal and add any CPD you like your CPD log. You will see there are two areas on the ‘My CPD’ pagethe top for members to self record any CPD you have done and you can use the plus button to add CPD and the pencil to edit.
And the bottom is your DHAA event attendance record which displays CPD from any DHAA run events in this current CPD cycle. This bottom section is not editable by members as it links to our DHAA website events. n
Our regular update on some great reading to improve your skills and top up your CPD hours
Maximise any downtime by studying at home and keep racking up your CPD points.
I this edition we cover a diverse range of areas including; the perils of vaping and support for those looking to quit, the emergence of ChatGPT in diagnosis, advances for indigenous healthcare, and new guidelines relating to sex and gender. Whatever your interest, we strive to include something for everyone.
• Aust Prescriber 2024;47:177-8
• CPD 0.25 hour scientific
Smoking tobacco has well-recognised significant impacts on general and oral health, but data are still emerging on the oral health impacts of vaping compared with smoking. This short article summaries the oral health effects from vaping including oral microbiome

changes, reduced salivary flow, mucosal irritation, injury, and oral cancers.
The oral health care needs of people living in residential aged care, Australia, 2016–20
• Med J Aust 2025; 222 (6): 318-320
• CPD 0.25 non scientific hours
Providing high quality medical care for people living in residential aged care is a national challenge, and oral health care is one area that is inadequate. Despite recent government initiatives to improve the oral health of older Australians, including the National Oral Health Plan 2015–2024,8 current models of care and service delivery in residential aged care are not meeting the needs of residents.
Oral health policy and practice reforms are urgently needed to improve the health and wellbeing of older Australians living in aged care homes.
Therapeutic vapes for smoking cessation and nicotine dependence
• Australian Prescriber, Volume 47: 6: December 2024
• CPD 0.25 hours scientific
The Australian Government has enacted laws restricting the supply of electronic cigarettes (vapes) to people requiring them for smoking cessation or the treatment of nicotine dependence, under the care of a medical practitioner, nurse practitioner or pharmacist.
Currently no vapes are included on the Australian Register of Therapeutic Goods, meaning that the prescription and supply of therapeutic vapes must be through the Special Access Scheme or Authorised Prescriber pathways.
Clinical guidelines state that therapeutic vapes may be considered for supporting people who have been unable to quit smoking using first-line therapies (a combination of behavioural support and registered nicotine

replacement therapies or oral smoking cessation medicines).
Clinical review should occur one week after vape initiation, with additional follow-up according to an individualised management plan, to monitor progress, review adverse effects (e.g. cough, irritated throat, headache or nausea), encourage the use of behavioural smoking cessation supports, and discourage dual use of vapes and conventional cigarettes.
An attempt to wean or stop vaping after 12 weeks is recommended, with a possible transition to registered >>

BY GUSTAVO FRING
smoking cessation medicines if required (in addition to ongoing behavioural support).
The maximum recommended duration of vape use is 12 months.
Appropriate and safe use of chlorhexidine in healthcare settings
• Australian Commission on Safety and Quality in Health Care 2023
• CPD 0.25 scientific hours
Chlorhexidine-containing antiseptic and disinfectant products are widely used in health care, aged care and in the community. There is emerging evidence that some microorganisms have developed tolerance and resistance to chlorhexidine. This may impact the effectiveness of chlorhexidine products that are used as antiseptic or cleaning agents in health care.
National guide to preventive healthcare for Aboriginal and Torres Strait Islander people: Recommendations
• The Royal Australian College of General Practitioners. East Melbourne: RACGP; 2024. p. 324.
• CPD 1 Hour scientific
The National Aboriginal Community Controlled Health Organisation (NACCHO) and The Royal Australian College of General Practitioners (RACGP) recently released the fourth edition of the National guide to preventive healthcare for Aboriginal
and Torres Strait Islander people: Recommendations.
The guide is a practical resource intended for all health professionals delivering primary healthcare to Aboriginal and/or Torres Strait Islander people. Its purpose is to provide GPs and other health professionals with an accessible, user-friendly guide to best practice preventive healthcare for Aboriginal and Torres Strait Islander patients.
Consideration of sex and gender: an analysis of Australian clinical guidelines
• Med J Aust 2025; 222 (4): 205-209. || doi: 10.5694/mja2.52602
• CPD Hours 0.25 non-scientific
Survey of all clinical guidelines published in Australia from 1 January 2014 to 31 April 2024 that employed methods such as Grading of Recommendations,
Assessment, Development, and Evaluations, or were endorsed, approved or acknowledged by the National Health and Medical Research Council or another major national body, or concerned marginalised groups.
The 80 eligible guidelines were from 51 organisations and covered 27 areas of practice. No sex- or gender-related terms were found in 12 of the guidelines. Of the remaining 68 guidelines, most used some of these terms only a few times, with 34 of them using “gender” to mean “sex”. “Sex” and “gender” were defined to some extent in four guidelines. There was no reference to clinical practice concerning sex in 15 of the guidelines. A total of 46 guidelines made no mention of clinical practice concerning gender, only 12 included gender-relevant practice in any detail, and the remaining 22 either implied aspects of gender awareness without stating this or mentioned “psychosocial” or “cultural” considerations.
Guideline development bodies should be encouraged to assess evidence for its treatment of sex and gender, to enable strategies to counter inequity and discrimination.
An urgent need exists for skills to use generative AI

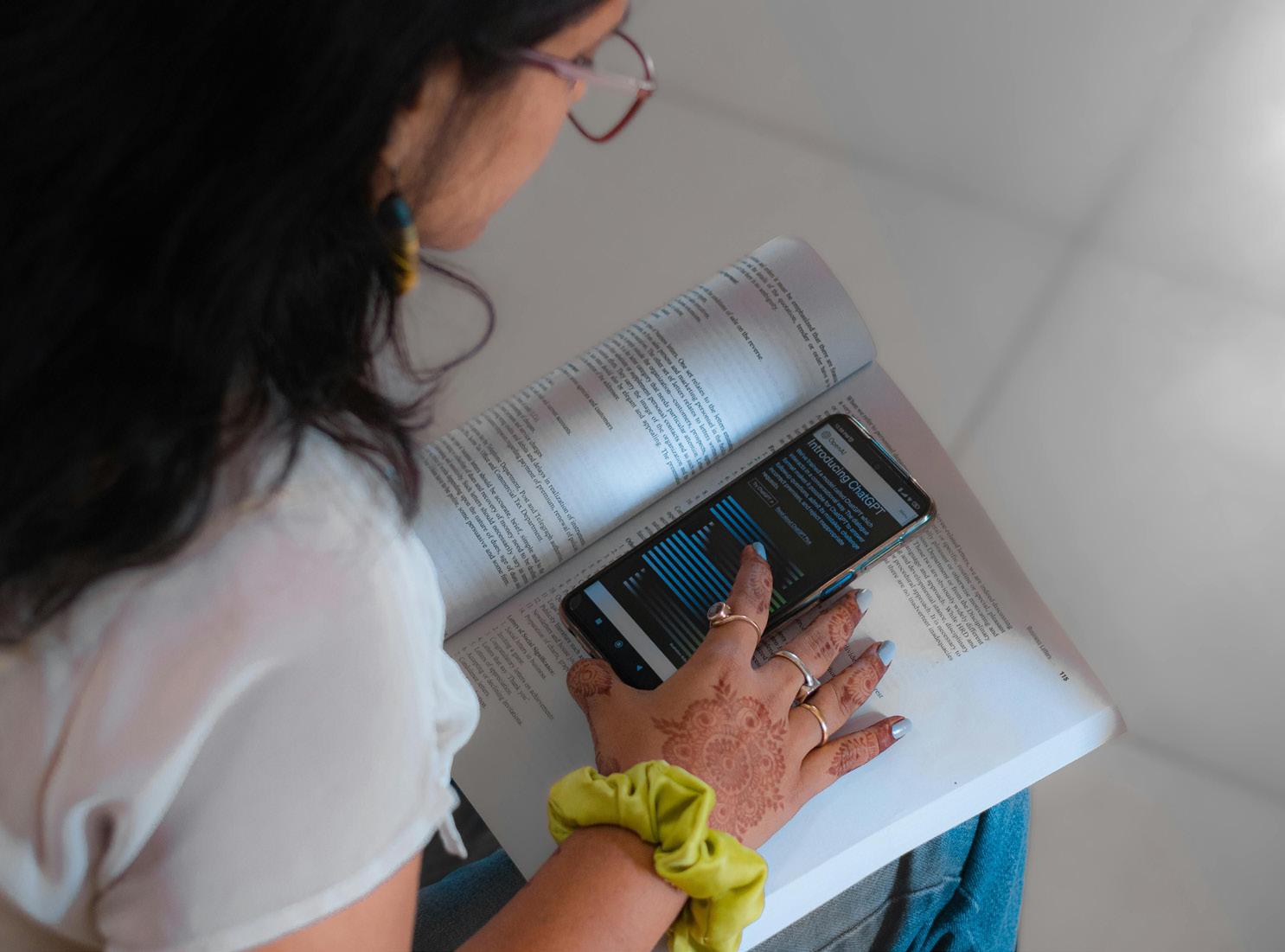
Use of ChatGPT to obtain health information in Australia, 2024: insights from a nationally representative survey
• Med J Aust 2025 || doi: 10.5694/ mja2.52598
• CPD hours 0.25 non-scientific
This project surveyed a nationally representative sample of adults (18 years or older) drawn from the June 2024 wave of the Life in Australia panel. The results shown that 9.9% of Australian adults (about 1.9 million people) asked ChatGPT health-related questions during the six months preceding the June 2024 survey.
The survey also found healthrelated ChatGPT use was higher for groups who face barriers to health care access, including people who were born in non-English speaking countries, do not speak English at home, or whose health literacy is
limited or marginal. The types of health questions that pose a higher risk for the community will change as AI evolves, and identifying them will require further investigation.
There is an urgent need to equip the community with the knowledge and skills to use generative AI tools safely, in order to ensure equity of access and benefit. n

Australia marks a historic milestone in 2025 as the oral health profession celebrates its 50th anniversary of dental hygiene. From humble beginnings in Adelaide to a nationally respected field, dental hygiene has become a cornerstone of preventive oral health care. To honour this golden jubilee, a series of events will reflect on the profession’s achievements and chart its future.
Dental hygiene in Australia began in 1975 when South Australia established the nation’s first training facility, following enabling legislation in 1971. The Dental Hygienists’ Association of South Australia, formed in 1977 by pioneering practitioners and students, laid the groundwork for national collaboration. By 1991, state associations united to create the Dental Hygienists Association of Australia (DHAA), fostering a federated structure that balanced autonomy with collective advocacy. Today, over 5,000 oral health practitioners (OHPs) serve communities nationwide, a testament to decades of legislative progress and educational innovation.
50 Years of Dental Hygiene
Celebration Dinner
When: 26 July 2025
Where: Adelaide Pavilion, Adelaide
Hosted by the newly formed Oral Health Association of Australia (OHAA), this gala dinner commemorates the profession’s origins in Adelaide. Attendees will reflect on milestones such as the DHAA’s founding in 1991 and its evolution into a national voice for OHPs. The evening promises to unite generations of practitioners, featuring speeches, awards, and a retrospective showcase.
Practice – From 1975 to 2030
When: 13 August 2025
Where: Online
This webinar offers a dynamic exploration of the profession’s journey. Founding DHAA President Sue Aldenhoven will outline early challenges, including the transition from state-based practice to national
recognition. OHAA President Cheryl Dey will discuss advancements in education, such as Bachelor of Oral Health programs, while emerging leaders Jesse Kourakis and Courtney Dicken will address future opportunities in preventive care. A live Q&A will engage attendees to further explore dental hygiene’s past and future.
Exhibition at the 2025 OHAA
National Congress
When: 16–18 October 2025
Where: The Star Gold Coast, Qld
Coinciding with the OHAA Congress theme, “Opening Horizons Across Australia,” this exhibition will feature archival contents tracing 50 years of progress.
The past 50 years have shown how collaboration and advocacy can transform a profession. As we enter a new era under the OHAA, our focus remains on expanding access to preventive care and empowering the next generation of practitioners.
Join the celebration
From Adelaide’s historic dinner to the Gold Coast’s forward-looking congress, these events offer opportunities to honour legacy and inspire innovation. For registration and details, visit the OHAA and Congress Websites. n
This milestone not only celebrates Australia’s dental hygiene achievements but also positions the profession as a global leader in oral health innovation.

As our association moves forward – what opportunities lie ahead?
By Associate Professor Melanie Aley
As I sit down to write this final career column for the DHAA Bulletin, I find myself reflecting on how much the profession, and the world, has changed since this publication began. What hasn’t changed, however, is the unwavering passion dental hygienists and oral health therapists bring to their work every day. That passion is what makes me optimistic about the future, not only for the profession, but for the broader field of oral health.
While this is the last issue of this beloved publication, it’s far from the end. With a new oral health association and magazine on the horizon, we’re entering an exciting new chapter - one that reflects the evolving scope and impact of our work.
that oral health practitioners are wellequipped to lead in this space.
One of the most exciting trends is the move toward integrated care models. Oral health practitioners are increasingly collaborating with GPs, nurses, pharmacists, and allied health workers to support patients with chronic conditions, complex needs, or limited access to care.
“This
final column isn’t a farewell. It’s a “see you soon”. A moment to pause and appreciate how far we’ve come, and to look ahead with curiosity, courage, and optimism”
Gone are the days when the role of a dental hygienist and oral health therapist was narrowly defined. Across the globe, we’re seeing expanded scopes of practice, greater autonomy, and recognition of these oral health practitioner’s role as a key player in preventive health.
Many dental hygienists and oral health therapists are now working independently, leading community outreach programs, practicing in aged care and mobile settings, and owning their own clinics. These changes reflect a growing awareness that oral health is inseparable from overall health, and
This opens the door for oral health practitioners to work in settings far beyond the traditional dental chair: hospitals, community health centres, aged care facilities, and even schools. As the link between oral health and systemic health becomes impossible to ignore, opportunities for interprofessional collaboration will only grow.
Technology is transforming how we care for patients, learn, and connect. Digital health records, intraoral scanners, and AI-powered diagnostics are becoming commonplace. For oral health practitioners, this means more efficient workflows, more accurate assessments, and potentially, new career paths in tech, data, and innovation.
Telehealth also offers a glimpse into a more accessible future. Oral health practitioners are now delivering oral health education, triage, and postop follow-up from anywhere. For
rural and remote patients, this can be life-changing. For practitioners, it can mean more flexible work, less geographic limitation, and new ways to deliver impact.
More oral health practitioners are stepping into roles as educators, advocates, researchers, and policy influencers. Whether you’re mentoring students, presenting at conferences, or championing access to care, your voice matters.
As the profession grows, so too does the need for leadership that reflects our diverse, compassionate, and driven community. Don’t wait to be asked - step forward. The next generation of oral health leaders is already among us.
Though we’re saying goodbye to The Bulletin, we’re welcoming something new — a publication that reflects a brand new association, and a broader, more integrated vision for oral health. One that acknowledges the complex challenges we face as a profession, and the even greater opportunities ahead.
This final column isn’t a farewell. It’s a “see you soon”. A moment to pause and appreciate how far we’ve come, and to look ahead with curiosity, courage, and optimism.
To every reader who’s followed this column, shared their story, or taken a leap into a new career path – THANK YOU. You are the reason I believe the future of our profession is bright. n
PHOTO BY KAROLINA GRABOWSKA


Associate Professor Melanie Aley (nee Hayes) is a dental hygienist who has enjoyed a diverse career in clinical practice, teaching, research and management. She has a Masters of Education majoring in Career Development, and after working in multidisciplinary roles, is now an Associate Professor and the Bachelor of Oral Health Program Director at the University of Sydney.
For over forty years, DHAA members have received The Bulletin. Now, in this final issue, we catch up with some of the many volunteers who have been responsible for its success
By Danielle Gibbens
With the beginning of a new chapter on its way, let's take this opportunity to look back over the years in which the Bulletin has been updating our membership on all things DHAA. From announcing new presidents to becoming a national body and who can forget our very first CEO, the Bulletin and its team of hard working volunteers have been tirelessly creating a world class dental magazine every three months for close to two decades now!
Can you remember when the Bulletin was posted to your home? Issue 1-34 were all hard copies printed and diligently posted to each of our members every quarter to keep you up to date with all things DHAA. Hellen
Checker was the president at the time we went digital giving access to our magazine to those near and far. Did you know all of our digital copies are still available online on website to the this day. When you flick through these editions you can see so much has changed but the challenges and triumphs of those before us are really not too dissimilar.
As a past editor of the Bulletin I am aware of the amount of work that goes into producing it - a lot! There are so many wheels in motion to create something people want to read, from our creative and digital guru Steve Moore (eroomcreative.com) who has been with us since the first digital edition who makes every edition look like dental vogue, to our regular contributors like Mel Aley guiding us to a happier work life, Lyn Carmen inspiring us to find the job with love and Ian Epondulan sharing his unwavering passion for oral health promotion. Our Presidents and CEOs who contribute to every edition so that we are on top of what is happening for our profession. Without the support of these people, there is no job for an editor so from all the editors before and after me we thank you all.
I took this opportunity to touch base


with some of our past editors and contributors to find out about their experiences also.
Lesley Denny First Bulletin Editor
I RECALL ONE edition where we featured a photograph on the cover of some young Vietnamese children with the feature article about volunteering at the Long Tan Clinic in the early days of Association's link with AVVRG. Sadly, that project which began with two teams of three going each year, expanded to four or five teams a year, the use of a mobile dental van and expansion into the wider community, came to an abrupt halt when Covid hit the world. To my knowledge it hasn’t started up again.
The biggest change to producing the Bulletin in my time, was using Publisher to compile it and emailing it to the printer! I think before that, we compiled it in MS Word, provided photos to include and put it on a floppy disc, hand delivered to the printer. Times change!
The printer used to deliver them to my home and I packed and mailed them out.About the future, hmmm… I always thought that there should be a scientific element in the Bulletin; also

reflections on what great things we, as professionals, do for the community. There are some clever people in our ranks who have used their training and work as dental hygienists as a steppingstone to further their careers which benefit society in other ways. I would be disappointed if our professional publication went the same way as many, which prioritise articles about how to make more money.
Steve Moore
Publisher & Designer (2013-present)
THE DHAA BULLETIN is not just any old publication. Since the 1980s, it has reported on and celebrated the work of the association, keeping the wider oral health community informed and connected. Its longevity is a testament to the collective passion and creativity of a dedicated team of contributors.
Over the 12 years of my involvement, presidents, editors, and contributors have come and gone — shining bright and then moving on like shooting stars. Others have stayed for longer, like satellites. Contributors like Mel Aley, Lyn Carmen, Danielle Gibbens, Christina Zerk — and the ever-present Shida Taheri, who has expertly shepherded the commercial inclusions — have all played pivotal roles. Not to forget CEO Bill Suen, always keeping a steady hand on the tiller.
I have been constantly amazed by the seemingly endless stream of talented volunteers who generously give their precious time to educate and entertain their peers and colleagues. The Bulletin has been a big part of my professional life, and I will miss the regular interaction with the team. I

hope this momentum carries forward, infusing the new OHAA publication with the same energy and spirit.
Lyn Carmen
Regular Contributor
(2018-present)
THE BULLETIN PROVIDES a wealth of connections, updates and 'need to know' for OHPs, I really enjoy reading about amazing quiet achievers in our community who are doing amazing things for oral health.
Since becoming a regular contributor in 2018 it has been a privilege to share the learnings handed onto me and create a ripple that flows outwards. Its always fun to go back to previous years editions and remember people, events and what was current at the time - its like a time capsule for DHAA in many ways and to be part of that I am truly grateful for.
Marcy Patsanza-Mkonto Bulletin Editor (2019-2020)
AS I REFLECT on my time as Editor, issue 50 (March–April 2019) stands out as my favourite.
Not only was it my first issue in the role, but the process of putting it together was a genuinely enjoyable and collaborative experience. I have fond memories of brainstorming with our contributors and Steve Moore, our talented publisher/designer, where I first proposed the idea of incorporating regular columns within each issue. The suggestion was warmly received, and from that point on, each Bulletin featured consistent dedicated columns on career development and self-development. It was incredibly

rewarding to see this idea brought to life in Issue 50 and to watch it continue in subsequent editions, even after I stepped down.
I hope the new OHAA magazine will incorporate these columns, as they offer valuable support for members’ personal and professional development.
Gibbens Bulletin Editor (2017-2019)
I DO NOT have one favourite edition of the Bulletin I was editor for as I wanted to make sure every edition was very different to one another to be sure it was exciting to read.
During my time I did enjoy the addition of regular columns such as the Rant and Ask DHAA which still features to this day. I saw the importance of these articles as a way for clinicians to connect with one another which as a practitioner who was working remotely at the time felt important. My fondest memory of being editor was the day Steve Moore, our magazine godfather, announced our edition was the most read Bulletin to date - it meant we must have been doing something right!
I want to take this opportunity to thank all of our past editors, along with the presidents and CEOs who stepped into those big shoes when the job was left vacant. Without you and your vision what once was a paper based magazine would not be what it is today. So now we look ahead to the future, OHAA now has the chance to create something even bigger and better than the current Bulletin. Let's welcome the new online publication – OHAA Connect. n
Make friends with your pharmacist and leverage their postion as frontline patient contact
By Dr. Victoria Perchyonok (Oral Health Therapist) and Rachael Starr (Dental Prosthetist)
Pharmacists are among the most accessible and trusted health professionals in the community. With frequent patient contact and established roles in chronic disease management and prevention, pharmacies are uniquely positioned to promote oral health initiatives. This article explores the opportunity for integrating oral health education into pharmacy practice and highlights the benefits of interdisciplinary collaboration between oral health professionals and pharmacists. A preventative, education-based approach in pharmacy settings can enhance health literacy, enable early detection of oral conditions, and improve overall health outcomes.

ORAL HEALTH IS a vital component of overall well-being, closely linked to chronic conditions such as diabetes, cardiovascular disease, and respiratory illness. Yet many people remain unaware of the importance of good oral hygiene or face barriers in accessing regular dental care. Pharmacies, with their extended hours, no-appointment model, and high patient turnover, offer an untapped avenue for delivering oral health education and preventative advice. Incorporating oral health promotion into everyday pharmacy practice— through pharmacist education and collaboration with dental professionals— can help bridge gaps in care, identify oral health concerns early, and empower individuals to make informed decisions about their oral hygiene.

Pharmacists already provide guidance on managing common oral health complaints, such as ulcers, dry mouth, denture discomfort, or tooth sensitivity. However, many pharmacists report limited training in oral health and a desire for further education to confidently advise their clients. Key areas where pharmacists can support oral health include:
• Identifying and advising on oral side effects of medications (e.g. dry mouth, gingival hyperplasia)
• Providing product recommendations for oral hygiene, dry mouth, and denture care
• Educating clients about the oralsystemic health connection
• Encouraging routine dental visits and early intervention
• Supporting patients with chronic diseases that impact oral health (e.g. diabetes, autoimmune disorders)
To build confidence and knowledge, pharmacists can benefit from targeted oral health training that includes:
• Basic oral anatomy and common oral conditions
• The impact of systemic diseases and medications on oral health
• How to conduct brief oral health assessments or triage questions
• Interpreting symptoms such as bleeding gums, halitosis, or tooth mobility
• Effective communication strategies to promote preventative behaviour
• When and how to refer patients to dental professionals
This education can be delivered through Continuing Professional Development (CPD) programs, webinars, collaborative workshops, or in-practice learning with dental professionals.
Oral health professionals—including dental hygienists, dental therapists, oral health therapists and dental prosthetists—can play a key role in supporting pharmacy-based oral health promotion by:
• Conducting outreach sessions for >>
oral screenings and patient education
• Training pharmacy staff on oral health topics and triage
• Providing written materials or digital resources for patients
• Establishing referral pathways between pharmacies and dental clinics
• Collaborating on health promotion campaigns linked to National Smile Month, World Oral Health Day, or diabetes awareness programs
These partnerships enhance the quality and consistency of oral health advice provided in pharmacies and help patients access timely, preventative dental care.
Pharmacy clients represent a broad demographic, many of whom may not visit a dentist regularly. Simple, practical interventions can include:
• Offering oral health checklists at medication reviews
• Displaying educational posters and brochures on oral hygiene and diet
• Providing samples or information on fluoride products, denture cleaners, and interdental aids
• Asking brief oral health questions during consultations for chronic disease
• Encouraging clients to book dental check-ups or follow up on oral symptoms
These small conversations have the potential to shift behaviour and increase awareness of the importance
of oral health as part of general health maintenance.
A collaborative, education-focused model benefits all parties:
• Patients receive timely, accessible advice in a trusted setting
• Pharmacists expand their professional scope and contribute to holistic care
• Dental professionals improve community outreach and early engagement
• Health systems may see reduced burden from preventable oral diseases
By shifting the focus towards prevention and education, community pharmacies can help change the narrative around oral health from reactive treatment to proactive care.
To embed oral health into pharmacy settings, we recommend:
• Developing CPD-accredited oral health training for pharmacy professionals
• Creating interdisciplinary education resources co-designed by dental and pharmacy bodies
• Implementing pilot programmes to evaluate impact and feasibility
• Fostering referral partnerships between local dental teams and community pharmacies
• Advocating for the inclusion of oral health in broader primary care planning and public health policies

PHARMACIES ARE TRUSTED, approachable, and well-positioned to promote oral health education and early intervention. Empowering pharmacists with knowledge and support from oral health professionals enables the delivery of more holistic care, encourages preventative habits, and helps the public make informed choices about their oral and general health. A collaborative, educational model holds great promise for expanding access to oral health support and improving outcomes across the community. n

References
Australian Institute of Health and Welfare. (2023). Oral health and dental care in Australia. Glick, M., et al. (2016). A new definition for oral health developed by the FDI World Dental Federation. International Dental Journal, 66(6), 322–324.
Durand, R., et al. (2017). Oral health promotion in pharmacy: A Canadian perspective. Canadian Pharmacists Journal, 150(5), 312–317. Tonetti, M. S., et al. (2017). Impact of the global burden of periodontal diseases on health and wellbeing. Journal of Clinical Periodontology, 44(5), 456–462.
World Health Organization. (2022). Global oral health status report.
Victoria Tamara Perchyonok is an Oral Health Therapist with Adult scope, who graduated from the University of Melbourne in 2018 and completed the Adult Restorative Course for Oral Health Therapists.
Victoria Perchyonok also completed an Undergraduate Certificate in Dementia Care from the University of Tasmania as well as numerous short courses in Dental Management of Geriatric and Special Needs Patients as well as Advanced Paediatric Dentistry to provide the best care for our patients of all ages.
Victoria Perchyonok has transitioned into the oral health profession after a successful scientific career both nationally and internationally and completing a PhD in Free Radical Chemistry in 2001 from the University of Melbourne.
Victoria has pursued her passion and
scientific interest in biomaterials for dental and health applications and has published extensively in scientific literature as well as well as acts as Unit Coordinator in Dental Material and lecturer in Geriatric Dentistry as part of Bachelor of Oral Health program at the University of Melbourne.
Victoria combines her passion for delivering evidence-based health care to children and adults. Victoria has been practicing in private practice since graduation and is a passionate advocate for bringing dental care to anyone in need.
In her spare time, Victoria enjoys spending time with her family and her gorgeous miniature poodles Ariel and Shai.
About Rachael Starr
Rachael Starr is a Dental Prosthetist with over 20 years of experience in the dental industry, having graduated from RMIT in 1998. She has a strong clinical focus on
geriatric dentistry and is passionate about providing specialised, compassionate care to aged care residents—ensuring dignity, comfort, and optimal oral health outcomes.
Throughout her career, Rachael has held academic and leadership roles at RMIT University, Holmesglen, and Yorke Institute. She is deeply committed to mentoring, supporting the professional growth of clinical staff, academic staff, and students alike. Her collaborative approach fosters a culture of continuous learning and high-quality care across all settings.
Rachael strongly believes that dental care should be accessible to all, regardless of age or circumstance, and this principle guides both her clinical and professional practice. Outside of dentistry, she enjoys travelling, staying active, and exploring great food and wine.
After
six years at the helm of
the DHAA, CEO Bill Suen has decided to pursue a new challenge. We asked the people who knew him best to say a few words
Margie Steffens
OAM Chair for Special Care in Dentistry SIG
BILL, YOUR ENERGY has enabled the DHAA to bridge some significant gaps in the political arena, driving initiatives such as Mouth Matters. Your support in establishing the various special interest groups and attendance at the many meetings, helping administer webinars and always encouraging.
All the very best wishes where ever your journey takes you.
Shida Taheri Communication & Partnership Officer
BILL HAS BEEN one of the most grounded and supportive leaders I’ve had the pleasure of working with. He leads with trust, never micromanages, and genuinely champions people to grow and pursue their passions. His steady presence and quiet confidence have helped shape not just my own career, but the direction of the DHAA in such a positive way.
I’m incredibly grateful for his encouragement and belief in others. He’s made a real difference, and his leadership will be missed.
Wishing you all the very best for what’s next, Bill — you’ve more than earned it.
Carol Tran Past DHAA President
BILL, IT’S BEEN a privilege to work alongside you. Your leadership, passion, and dedication have left a lasting impact on DHAA and all of us lucky enough to share the journey with you. Thank you for your wisdom and the care you've shown to both the profession and the people within it. Wishing you every happiness and success in this next chapter — you will be greatly missed!
Cheryl Dey OHAA President
BILL, IT’S HARD to put into words the impact you’ve had over the past six years. From the moment I interviewed you, your calm presence, thoughtful approach, and steady leadership stood out. I’ve learned so much from you—your advice was always timely, measured, and exactly what was needed.
During my time as president, you were an invaluable asset, providing unwavering support and insight.
You led our association through the uncertainty of the COVID-19 pandemic with strength and composure, helping to keep us connected and focused when it mattered most.
Your dedication to advocacy and the tireless work you’ve done toward the unification of our professional associations has left a lasting legacy.
Thank you for everything—you will be greatly missed.
Ron Knevel External Director
BILL, I JUST wanted to take a moment to sincerely thank you for your great leadership and dedication since you started with DHAA in 2019. Your guidance has been key in helping the association through some turbulent times, and your efforts to make things more professional have really made a difference.
Your talent for building strong relationships and connecting with different professionals has helped strengthen our community. I especially appreciate your steady support—both personally and professionally—that helped turn our shared goal of a united professional organisation in Australia into reality.
It’s been a true privilege to work with you on this journey. Thank you for being a 'partner in crime' and for your ongoing commitment. Congratulations on everything you’ve accomplished—you’ve made a lasting impact.
Mark Wotherspoon Dentist & Honorary DHAA Member
OVER THE LAST five years I have had the absolute pleasure of working with Bill on a number of projects and within a number of special interest groups. His dedication, professionalism along with his pharmacy background has nurtured new ideas, at the same time as strongly

advocating for, and fiercely supporting, the emerging and expanded role and scope of DHAA members.
The DHAA has no greater friend than Bill Suen and I sincerely wish him all the very best for his future.
Director of Oral Health, The University of Sydney
WORKING WITH BILL during his time as DHAA CEO has been a real privilege. I’ve always appreciated his friendly, calm, and level-headed approach. He brought a steady presence to every meeting and always prioritised collaboration and consultation.
Our conversations, especially about the direction and future of the association, were always thoughtful and engaging. He had a way of listening deeply while also challenging ideas in just the right way to move things forward. I’ve learned a lot from his leadership, and I’ll miss those insightful discussions.
Wishing him all the very best in this next chapter.
McGrath DHAA VIC Director
SINCE ARRIVING IN Australia in 2001, I have been involved with the DHAA and came away from my very first DHAAVB meeting as the Secretary. I was the last DHAAVB President and the first Victoria Committee Chair when DHAA became a ‘single entity’. It has been an absolute pleasure to serve on the DHAA board as the Victorian Director over the last two and-a-half years, and I’m excited to make the transition to a director on the inaugural OHAA board. This is such an auspicious time for us, bringing our three professions and two associations forward as one.
I would like to sincerely thank Bill >>
for his dedication and commitment over the last few years. He has been an unwavering support, and his experience and skills have proven invaluable in advancing the establishment of OHAA. You have definitely earned your retirement.
Cathryn Carboon DHAA VIC Chair
TODAY, WE PROUDLY salute Bill Suen, Chief Executive Officer of the Dental Hygienists Association of Australia (DHAA), for his unwavering leadership, advocacy, and commitment to advancing oral health across the nation.
Bill’s dedication to empowering dental hygienists, oral health therapists and oral health students, has strengthened the DHAA as a national body, advocating for excellence in care and professional recognition. Under his leadership, the DHAA has continued to grow in influence, fostering a more collaborative and prevention-focused future for the dental industry.
With strategic insight and a clear passion for access to care, Bill has guided the organisation through change, innovation, and expansion—ensuring that DHAA members are supported, and that their contributions are recognised within Australia's broader healthcare system.
Bill has been instrumental in leading key reforms within the profession—most notably, his pivotal role in securing provider numbers for dental hygienists, oral health therapists, and dental therapists. This landmark achievement represents a major step forward in the recognition and autonomy of oral health practitioners, enabling them to contribute more directly to patient care and to be more integrated within the broader healthcare system.
Bill has also worked tirelessly to promote and champion the oral health of older Australians in aged care, through the establishment of the DHAA aged


care chapter and a set of ambitious goals to have 50% of Australian Residential Aged Care Facilities with a Dental Hygienist/Oral Health Therapist servicing their residents by June 2026. Through his strategic insight and strong representation of the profession, Bill has strengthened the DHAA’s position as a national voice for its members—supporting practitioners not only in their clinical roles but in their capacity to lead change in oral health delivery. Under his guidance, the DHAA has continued to grow in size and impact, championing high standards of care, education, and continuing professional development.
Here’s to Bill Suen—a true advocate for the profession and a leader of lasting impact, who has achieved significant milestones for the DHAA. As we now begin our journey with the Oral Health Association of Australia, we wish Bill good health and happiness in his retirement.
Marcy Patsanza-Mkonto AdvDipOralHlth(DentHygn), BPsychSc
THANK YOU, Bill, for your unwavering dedication to the growth of the association and your heartfelt commitment to the wellbeing of our members. Your support has enriched us in many ways. As a leader, your
consistent encouragement and belief in members’ potential made a profound impact.
I am grateful for the support you offered me, first as Bulletin Editor and later as a Mental Health First Aid Instructor for the association; where you were a passionate advocate for prioritising this vital resource for all members. Your championing of the Mental Health First Aid course underscored your deep commitment to equipping our community with essential skills for wellbeing.
Despite a demanding workload, your prompt responses and approachable nature never went unnoticed. Your leadership has left a lasting impression on all of us. Thank you for your time, your guidance, and for always creating space for people to be heard.
Wishing you all the very best in what comes next.
Christina Zerk Past Membership Officer
WORKING WITH BILL over the past six years has been an absolute pleasure, and his support and guidance have been instrumental in navigating the challenges (global pandemics included) we've overcome as a team with him steering during that time.
Bill's passion and experience in

advocacy have meant that over the past few years we have always had something to work towards achieving, not just as staff and committees but also helping to drive change for the profession in a positive way.
He always pushed us to work towards our strengths and passions and bring these into our work, letting them shine, and had the utmost faith in the team to get things done to the best of their ability. His trust in the team around him and ability to create opportunities to grow have had a huge influence on my life and career, all while knowing he was a phone call away if support was ever needed.
I will miss working alongside him on a regular basis, but I'm excited to hear about hopefully some well-earned holiday time and future challenges. Wishing you all the best in the future.
Jinous Eighani-Roushani DHAA President
BILL, A HUGE thank you for your incredible leadership and dedication. Under your guidance, our association has achieved great things, and your impact will be felt for years to come.
It’s been a true pleasure working with you, and I wish you all the best in your next chapter. I’m sure you’ll continue to inspire and lead wherever you go.
Carmen Abramich DHAA WA Director
I FIRST MET Bill in June 2019, not long after his appointment as CEO.
I was certainly surprised and curious as to why we had appointed a CEO that was not from the dental sphere. As time went on the reasons became clear. He brought a wealth of association knowledge and significant support for the whole health sphere from his background in Pharmacy.
He also brought with him significant impactful knowledge in association structure and function, successful financial/budgetary guidelines and most importantly his passion for advocacy. Throughout many, many emails, phone calls and meetings, it has been absolutely wonderful to have a national CEO who always made himself available whether it was after business hours, or on weekends to support weekend CPD events or association questions etc.. He would always answer calls or emails and provide direct support through our collective network.
I am very grateful for what he has brought to our profession and the skill set that he has provided to help alongside us, to support the oral health needs of our whole community. His work especially in advocacy is well and truly above and beyond what I've seen
throughout my career and the legacy that will leave will benefit so many in the years and decades to come.
I wish Bill the very best in his future endeavours enjoying his family and other interests and I hope that he feels satisfaction and fulfillment with the work that he has done and knows that he is respected and appreciated.
Thank you, Bill and happy farewell. Wishing you the very best.
Steve Moore
Publisher & Designer - The Bulletin
AFTER SIX YEARS working alongside a string of DHAA Presidents and the first DHAA CEO, Mel Aley, I have to admit to being a touch skeptical of this mild-mannered 'outsider' from the pharmaceutical world. Would he be able to cut it in the world of dental hygiene?
Within minutes of meeting Bill, my skepticism melted. Since then, I have been in awe of his ability to calmly overcome challenges – such as COVID – and steer the Association and the profession toward new pastures.
Quietly confident and always polite, he has been an absolute pleasure to collaborate with.
Bill, I will wish you all the very best in the future – as well as the many beautiful DHAA souls I've had the honour to work with. n

As DHAA transitions to the newly unified Oral Health Association
Australia (OHAA), the commitment to provide you, our members, with a value packed membership, advocacy and benefits is more important than ever. Comprehensive and competitively priced insurance is a key benefit that will continue to be offered under OHAA. DHAA is excited to announce that BMS will be the insurance partner under OHAA. This means when you renew your DHAA membership (as a new OHAA member), you can continue to access comprehensive Professional Indemnity Insurance – all at a member exclusive price!
Why the OHAA Member Insurance Program?
The Program is carefully reviewed annually by OHAA with BMS to
ensure the offering remains relevant, comprehensive and competitively priced for our members.
The Professional Indemnity Insurance meets the Ahpra registration requirements with additional support through the dedicated OHAA Clinical Support Advisor.
Professional Indemnity Insurance Policy includes:
• $20M Professional Indemnity#
• Run-off cover
• Retroactive cover
• Worldwide cover (except USA)
• Risk mitigation resources
• Additional support via the OHAA Clinical Support Advisor
• Option to add Public Liability Insurance
Plus, complimentary cover for students – simply opt-in!
Support when you need it most
The OHAA member insurance is more
than just great cover, it is an extra layer of support when you need it most.
OHAA Clinical Support Advisor
Not just a support hotline, the Advisor is a qualified and practising oral health practitioner, with deep understanding of the day-to-day challenges you might face in your work. Armed with this expertise, the Advisor is there to support you from a clinical perspective but can also assist throughout the claims process.
Risk mitigation resources
Mitigating risk is your first line of defence when avoiding a potential claim. Access webinars and a growing library of risk mitigation resources via the OHAA Member Insurance Program.
More cover, all in one place
As you progress through your career your insurance needs might change.
The OHAA Member Insurance

Program takes the hassle out of finding professional insurance with plenty of additional cover available via our insurance partners’ insurance portal. This includes:
Cover for breaches of security or data, or network related software, programming, and systems.
Business
Covers various general elements of
business risk from property, stock and contents damage, to business interruption and operations.
Cover for your practice’s liability exposure, in the event it is named in an action due to injury, negligence, error, omission, malpractice, or breach of professional duty.
Simply log in to the BMS Portal to get a quote for cover. n
Not yet insured? Now is a great time to join. Register for an account in the BMS Portal and get covered in 2025, ohaa.bmsgroup.com
Already an insured member? Keep an eye on your inbox. BMS will contact you at the time of your policy expiry to renew your policy so you can enjoy continued coverage.
For more information, speak to BMS at ohaa@bmsgroup.com or call 1800 940 762
Policy features are current for policies incepted from 30 June 2025. #Professional Indemnity Insurance limits up to $20M per claim.
You must be a current Oral Health Association of Australia (OHAA) member to be eligible to register for the OHAA Member Insurance Program. You must be part of the OHAA Member Insurance program in order to access additional cover. If your membership ceases you will not be offered renewal when your policy expires. In offering this insurance to our members OHAA is a distributor of BMS Risk Solutions Pty Ltd (BMS) AFSL 461594, ABN 45161187980. The insurance is issued by BMS under binder with Certain Underwriters at Lloyds. When acting under a binder BMS acts as agent for the insurer and not as your agent. This is general advice only and BMS has not considered whether it was suitable for your personal circumstances, current objectives, needs or financial situation. Please read the Policy Wording and the BMS Terms of Engagement which contains the Financial Services Guide before making a decision about purchasing this policy. As a distributor, OHAA may receive a percentage of the commission paid to BMS by the insurer and/or a fee per policy in offering this insurance to members.


From
An exploration of the biological, emotional, and professional dimensions of chronic pain in dental practice
By The DHAA Special Care Dentistry SIG
Chronic pain is a significant, persistent challenge in modern healthcare, affecting individuals on both personal and professional levels. Within dentistry, this challenge is uniquely dual in nature— impacting both patients who seek relief and the clinicians who provide care. This article offers a comprehensive overview of chronic pain in dental settings, examining its biological mechanisms, daily implications, medication impacts, and strategies to support patients and practitioners alike. It underscores the importance of empathy, communication, and systemic support in managing chronic pain to promote better health outcomes and sustainable dental practice.
The diagram below illustrates the dual impact of chronic pain in dentistry,
highlighting the experiences of both patients and clinicians. Understanding these perspectives is crucial for developing effective strategies to manage chronic pain and improve overall care delivery in dental practice.
Chronic pain is a complex public health issue affecting over 1.5 billion people globally. In the dental field, it takes on a uniquely dual role—affecting both the patients who seek care and the clinicians who provide it. While patients may present with orofacial pain, temporomandibular joint dysfunction, or post-surgical discomfort, dental professionals themselves are often silently burdened by occupational pain conditions such as musculoskeletal strain, migraines, or neuropathic pain.
This dual impact is often overlooked. Chronic pain in dental patients may result in fear, care avoidance, and poorer health outcomes. Meanwhile, pain in clinicians can affect concentration, manual dexterity, and emotional well-being, compromising the quality and longevity of their careers. In this article, we examine chronic pain in dentistry from both perspectives—clinician and patient—by exploring its biological basis, its daily consequences, and its management through medical, ergonomic, and psychological strategies.
Chronic pain is defined as pain that persists beyond the normal tissue healing time, typically over three to six months. Unlike acute pain, which is a protective biological signal indicating tissue damage, chronic pain often becomes a condition in and of itself. It involves significant changes to the
nervous system and may persist even in the absence of ongoing tissue damage.
Neurobiological mechanisms
Chronic pain is driven by several neurophysiological processes:
n Peripheral Sensitisation occurs when prolonged inflammation or nerve injury increases the sensitivity of peripheral nociceptors. This results in heightened responses to stimuli that would not normally cause pain.
n Central Sensitisation reflects changes in the spinal cord and brain where neurons become more responsive to pain signals, leading to amplified pain experiences. This explains why chronic pain sufferers often feel pain out of proportion to their injury.
n Neuroplasticity involves the rewiring of pain pathways, which may lead to allodynia (pain in response to non-painful stimuli) and hyperalgesia (increased pain response).
n Psychosocial Factors, such as anxiety, depression, and trauma, also feed into chronic pain syndromes. These conditions may alter how pain is perceived and can affect how individuals cope with it.
In dentistry, understanding these mechanisms is crucial. Orofacial pain may stem from neuropathic, musculoskeletal, or idiopathic origins, and clinicians must consider the full biopsychosocial picture when diagnosing and treating patients.
Dental professionals are uniquely prone to chronic pain due to the physical and emotional demands of the profession.

“Dental professionals are uniquely prone to chronic pain due to the physical and emotional demands of the profession. ”

Maintaining awkward positions for prolonged periods, repetitive wrist and hand movements, and sustained static postures contribute to musculoskeletal disorders. Emotional stress from patient care and administrative pressures further exacerbates physical symptoms.
• Neck and shoulder myalgia from poor ergonomics
• Chronic lower back pain from prolonged chairside positions
• Carpal tunnel syndrome from repetitive hand instrumentation
• Chronic tension headaches due to postural strain and stress
For many dental professionals, these conditions lead to reduced clinical hours, frequent absenteeism, and in some cases, early retirement. The psychological toll is significant. Living with pain can lead to irritability, decreased concentration, and emotional exhaustion—components of professional burnout. Many clinicians underreport or ignore symptoms, fearing judgment or loss of income, which worsens long-term outcomes.
Clinicians living with chronic pain may rely on pharmacological therapies to function. While medications may enable them to continue working, they also introduce side effects that can impair safety and performance.
n NSAIDs (e.g., ibuprofen, naproxen): Provide pain relief but may lead to gastrointestinal issues and increased cardiovascular risk with long-term use. n Muscle Relaxants (e.g., cyclobenzaprine): Help relieve musculoskeletal pain but may cause drowsiness, impairing motor coordination.
n Antidepressants (e.g., amitriptyline, duloxetine): Used for neuropathic pain, they may cause sedation and dry mouth. n Anticonvulsants (e.g., gabapentin, pregabalin): Used for nerve pain, often cause brain fog and fatigue.
Impact on clinical function
Medication side effects such as drowsiness, dizziness, and reduced alertness can impair clinical decisionmaking and manual dexterity. Chronic fatigue and cognitive dulling may lead to diagnostic errors or difficulty performing intricate procedures.
Clinicians may need to adjust work schedules or reduce clinical loads to accommodate their health. In some cases, regulatory bodies must be informed if medications compromise safe practice. Transparency and regular medical assessments are vital.
• Investing in ergonomic equipment (e.g., loupes, saddle chairs)
• Incorporating stretching and posture breaks
• Seeking multidisciplinary pain management (e.g., physiotherapy, psychology)
• Participating in peer support groups or mentorship programs
Dental patients experiencing chronic pain face unique barriers to care. Many live with overlapping pain syndromes—such as fibromyalgia, migraines, or arthritis—which can influence how they perceive and respond to dental treatment. Orofacial pain conditions, such as burning mouth syndrome, atypical facial pain, or temporomandibular disorders (TMD), are particularly challenging to diagnose and manage.
Clinical challenges in managing patients living with pain
• Misinterpretation of pain behaviours:
“For many dental professionals, these conditions lead to reduced clinical hours, frequent absenteeism, and in some cases, early retirement”
Dentists may mistake chronic pain symptoms as anxiety or noncompliance.
• Avoidance of care: Fear of triggering pain can lead to poor attendance and worsening dental issues.
• Limited treatment options: Some patients are unable to tolerate procedures under local anaesthetic alone, requiring sedation or staged care.
Empathy and communication are critical in building trust. Acknowledging the patient’s lived experience of pain fosters a collaborative relationship and enhances treatment outcomes.
For both patients and clinicians, chronic pain management often involves medications. While they may offer relief, they also carry oral and systemic side effects that impact dental care.
n NSAIDs May cause mucosal irritation or ulcers and contribute to xerostomia (dry mouth).
n Opioids: Associated with sedation, dry mouth, constipation, and risk of dependency.
n Antidepressants: Commonly lead to dry mouth and altered taste.
n Anticonvulsants ( e.g. gabapentin): May contribute to sluggishness, cognitive dulling, and weight changes.
Xerostomia increases the risk of caries, candidiasis, and periodontal disease. Some medications may delay wound healing post-extraction or interfere with local anesthetic efficacy. Furthermore,
patients on long-term opioids or medication such as gabapentin may have reduced pain thresholds or complex analgesic needs.
It is important to tailor treatment plans based on the patient’s full medical profile and collaborate with other healthcare providers where appropriate.
A multidisciplinary approach offers the most benefit. Collaboration with pain specialists, physiotherapists, and psychologists enhances outcomes. Clinicians should adapt procedures to minimise discomfort, employ desensitising techniques, and use adjunctive therapies like topical anaesthetics or TENS (transcutaneous electrical nerve stimulation). Oral appliances, such as occlusal splints, may help in cases of TMD or bruxism.
Maintaining career longevity requires proactive management. Ergonomic assessments, flexible scheduling, and regular physical therapy may prevent escalation of symptoms. Institutions should support clinicians through access to occupational health services, mental health support, and policies that prioritise practitioner well-being.
Ongoing professional education in pain neuroscience, trauma-informed care, and communication skills enhances the ability to manage patients and self-care effectively.
Chronic pain, regardless of origin, is deeply intertwined with oral health. Pain can disrupt sleep, reduce motivation for self-care, and affect diet—all of which influence oral disease risk. Conversely, dental issues—such as chronic pulpitis or abscesses—can contribute to systemic inflammation and prolonged pain.
Examples of the pain-oral health
n Bruxism, often stress-induced, can cause or worsen TMD and lead to tooth wear or fracture.
n Nutritional Deficiencies from tooth loss or pain during eating may worsen inflammatory conditions.
n Poor Oral Hygiene in chronic pain sufferers leads to rapid progression of periodontal disease or caries.
Breaking this cycle requires an integrative approach that acknowledges pain as both a symptom and a driver of disease.
CHRONIC PAIN IS a pervasive issue that affects both patients and clinicians in dentistry. It impacts the delivery of care, professional performance, and personal quality of life. By understanding the neurobiology of pain, recognising medication implications, and implementing systemic support strategies, dental professionals can improve outcomes for patients and safeguard their own health. Promoting empathy, open dialogue, and holistic treatment planning is essential. Institutions and individuals must collaborate to address chronic pain as a legitimate and ongoing challenge in dental practice. Only then can we create sustainable, resilient care environments that honour the needs of both those who heal and those who suffer. n
References
Woolf CJ. Central sensitisation: Implications for the diagnosis and treatment of pain. Pain. 2011;152(3 Suppl):S2–S15.
Gatchel RJ, et al. The biopsychosocial approach to chronic pain: Scientific advances and future directions. Psychol Bull. 2007;133(4):581–624.
Greene CS. Diagnosis and treatment of temporomandibular disorders: Emergence of a new care guideline. J Am Dent Assoc. 2010;141(9):1086–1088.
Durham J, et al. Orofacial pain and psychological distress: A review. Br Dent J. 2011;211(11):451–455.
Okeson JP. Management of Temporomandibular Disorders and Occlusion. 8th ed. Elsevier; 2020.
International Association for the Study of Pain (IASP). www. iasp-pain.org
National Institute of Dental and Craniofacial Research. www. nidcr.nih.gov

By Lyn Carman

In our sometimes turbulent world of oral healthcare and the complexities of our personal lives, it’s easy to get caught in the undertow of what was or what might be. Yet, amongst this constant pull between yesterday’s should-haves and tomorrow’s whatifs, lies a profound opportunity for grounding and strength - the present moment. This isn’t about ignoring our experiences or aspirations; it’s about recognising where our true power resides: in the right here and now moment. By consciously shifting our focus
to the present, we can release the burdens of past ruminations and the anxieties of future projections, setting ourselves up for a more resilient, engaged, and ultimately, more fulfilling experience of our professional and personal journeys. Think of it like this… what we choose to think and do right now directly shapes our very next moment, just as planting a seed determines the plant that will grow. This understanding becomes crucial when considering the illusion of the past and the future, which we often get stuck on.
Our minds are incredible storytellers, often replaying scenes from yesterday or writing narratives for tomorrow. While reflection and planning have their place, getting stuck in repetitive loops of past regrets or future worries can drain our energy and diminish our experience of the present. Mindfulness teacher Sam Harris, says true awareness lies in “a vivid awareness of whatever is appearing in one’s mind or body... without grasping at the pleasant or recoiling from the unpleasant.” When we’re lost in rumination, we miss the richness of the moment, the one reality we can influence.
The present, where life unfolds
‘Living’ in its truest form appears in the present moment. The warmth of the sun, the sound of a friend’s voice, and the focused attention on a patient are the real things. Positive psychology reminds us to savour these moments; they are the building blocks of joy and contentment. When we are fully present, we engage more effectively, connect more deeply, and life feels brighter. The Resilience Project’s emphasis on mindfulness encourages us to intentionally bring our attention to the now, noticing our breath, sensations, and surroundings without judgment, because what we choose and do right now creates what happens next.
Our minds love to replay old stories, especially when things didn’t go as planned. These memories can feel heavy, making it hard to focus on what’s happening now. As Cognitive Behavioural Therapy (CBT) reminds us, how we think about past events strongly affects how we feel in the present. Try this…when thoughts about the past come up, simply notice them, like clouds moving across the sky. That’s mindfulness creating space. The past is done, and our real power is in how we relate to it now. We often bring old reactions to new situations where they don’t belong without realising it. Think about it… a past negative experience with a critical colleague might make you automatically guarded with a new colleague offering feedback, even if their intention is positive. That reaction is borrowed from the past. In such moments, gently ask: “Does this old reaction belong here?” Just as researcher
“Taking a mindful pause – a conscious breath –before engaging with a patient allows for clearer communication and improved focus, ultimately leading to more effective care and preventing burnout”
clearly, instead of getting lost in what might happen. The Resilience Project’s GEM (Gratitude, Empathy, Mindfulness) framework also supports this shift away from future anxieties towards the positive present.
Kristin Neff suggests, treating ourselves with kindness when reflecting on past missteps, recognising these outdated reactions with mindful awareness, allows us to choose a more appropriate and compassionate way to engage with the present moment and the people in it, moving forward with greater ease.
Worrying about what might happen often takes away the joy of the present. While planning is useful, excessive future anxiety can be paralysing. Mindfulness helps us recognise these thoughts as mental projections, not necessarily reality. Think about it… enjoying a lovely walk, a thought pops in about a challenging patient tomorrow. If you get caught in that worry, you’ll likely miss the beauty and peace of your walk. You can reclaim the present by becoming aware and noticing what’s around you – what you see, hear, and feel, like the sun on your skin or birds singing on your walk. Anchoring yourself in these small moments helps you handle today’s tasks
Whether it’s working through a busy appointment schedule or savouring precious personal moments, the ability to be fully present is invaluable. Taking a mindful pause – a conscious breath – before engaging with a patient allows for clearer communication and improved focus, ultimately leading to more effective care and preventing burnout. This same intentional presence transforms personal experiences, allowing you to truly appreciate the warmth of connection or the simple beauty of being alive. By consciously anchoring yourself in the “right here and now,” you enrich professional interactions, build resilience against workplace stress, create a deeper appreciation for everyday joys, and nurture inner peace.
Ultimately, the past is gone, and the future isn’t here yet. All we truly have is this breath, this moment. By gently bringing our attention to what’s happening right now – the feeling of your feet on the floor, the air coming in and out – we tap into a quiet strength within. It’s in these small moments of presence, inspired by simple wisdom and practical ideas on finding inner stillness passed down through millennia, that we find our footing. Choose to be here, now. That’s where your power lies… to navigate anything life brings, one peaceful moment at a time. n
BY
The use and selection of mouthrinses or mouthwashes is one of the more common queries patients ask of their dental professional. There are many options available on the shelves of supermarkets and pharmacies which can be quite overwhelming not just for patients, but also for us clinicians. The following article may serve as a guide to better help you understand which mouthrinse you can recommend to your patients to support their oral health.
Mouthrinses are generally divided into two main categories - cosmetic and medicinal. Cosmetic mouthrinses can remove oral debris, temporarily suppress bad breath, reduce bacteria in the mouth and refresh the mouth with a pleasant taste. Mouthrinses classified as medicinal, on the other hand may have the benefits associated with a cosmetic rinse, but also have other therapeutic efficacy benefits. These mouthrinses contain active agents which have a
therapeutic effect on the mouth, such as antiseptic or high levels of anti-cavity ingredients. These can help patients with caries risk management as well as gingivitis, and periodontitis.
While the majority of mouthrinses can be bought over the counter, instructions for use are always recommended so patients get the best out of the product to support their oral health.
Clinicians and patients may be aware that some mouthrinses contain alcohol whilst others are alcohol free. Some mouthrinses can contain anywhere between 5-27% alcoholic concentrations. Alcohol in mouthrinses is used for several reasons for example, as a solubiliser, stabiliser, preservative, anti-plaque efficacy enhancer and provides a distinctive flavour. Some patients may be concerned about the risks of alcohol containing mouthrinses being a risk of future oral

cancer. However, studies show there is insufficient evidence to confirm that alcohol containing mouthrinses represent an independent risk factor for the development of head and neck cancer.1 Importantly, it is recommended that alcohol containing mouthrinses should be avoided for certain patient groups including young children, pregnant and nursing women, and those who suffer from dry mouth. For these demographics, an alcohol free mouthrinse is ideal.
Preprocedural rinsing is considered to be one key infection control strategy that can be adopted by dental practices to reduce the extent of contamination to the dental team who are working in the contamination zone. The oral cavity is colonised by various oral microorganisms which become aerosolised during certain dental procedures. Preprocedural rinsing is undertaken to decrease the number of microorganisms in the dental aerosol.2,3

Patients with periodontal disease:
Given periodontal disease is one the most common diseases that the global population suffers, the use of a mouthrinse can be effective to promote healthy periodontal tissues in conjunction with periodontal treatment. Gingivitis occurs after two to three weeks of undisturbed plaque accumulation alongside a shift in composition of subgingival bacteria from gram-positive to gram-negative species. Chlorhexidine Gluconate has a biocidal action that is more effective against gram-negative bacteria given their cells have a larger negative charge.4 Following a course of periodontal treatment for patients with active periodontal disease, a chlorhexidine mouthrinse, containing 0.2% Chlorhexidine Gluconate, can be prescribed as a mouthrinse (10mL undiluted for 30 seconds twice daily for two weeks). Patients should also be advised that they may experience superficial staining from the prolonged
use of Chlorhexidine mouthrinses, and patients should be assured that the stain can be removed.
If patients are looking for a daily mouthrinse to support their oral hygiene routines and promote healthy periodontium, clinicians can recommend the use of an anti-plaque mouthrinse such as Colgate Total Plaque Release Mouthwash. Colgate® Total Plaque Release Mouthwash is boosted with Zinc, a powerful mineral. It helps eliminate the bacteria that causes plaque and keeps working after rinsing to reduce heavy plaque build up 3X better**. Clinicians should instruct patients to rinse 20mL (fill to the cap line) for 30 seconds twice daily before spitting out.
For patients who suffer from a chronic dry mouth due to reduced salivary flow
(xerostomia), a mouthrinse can help to increase the moisture of the oral cavity providing some temporary relief. Specially formulated mouthrinses have been created with active moisturising agents which help to relieve mouth dryness. Aside from this, you can also recommend an alcohol free mouthrinse.
Patients who suffer from sensitive teeth because of exposed root surfaces from gingival recession or loss of enamel from tooth abrasion, abfraction or acid erosion will usually be already using some therapeutic agent to manage their sensitivity. For patients looking to use a mouthrinse to add to their sensitive toothpaste management, clinicians can recommend a mouthwash that helps to gently clean the mouth and gums. For example, Colgate Sensi Pro Mouthwash is formulated for use in sensitive mouths and can be used for 30 seconds after brushing and flossing twice daily. >>

Patients undergoing teeth whitening:
Long term management of tooth discolouration either after or during any tooth whitening treatment is an important consideration for patients. Patients wishing to use a mouthrinse which will help promote a whiter smile, can use mouthrinses with active agents that are designed to remove surface stains and whiten teeth. These surface stains generally are caused by highly pigmented foods and drinks including coffee and wine. These mouthrinses provide a barrier on the surface of the enamel which reduces the chances of surface stains from forming. Colgate Optic White Mouthwash can be
recommended to patients which uses a unique formula with an optic brightener that activates as it is swished to reflect light, leaving the teeth looking white instantly. Patients should rinse 20mL of mouthrinse for 30 seconds twice daily for best effects.
Patients with ulcers or postextraction wounds:
There are occasions where patients will present with ulcers intraorally either from stress, dehydration or from a traumatic injury of the soft tissues. Trauma can be experienced from hot foods or drinks or from biting the cheek, lip or tongue. Although oral ulcers are generally self-limiting
to 10 days of when it initially formed, clinicians can suggest an antiseptic rinse such as Colgate Savacol Antiseptic Mouth & Throat Rinse* which may relieve the discomfort of mouth ulcers. As previously mentioned, be sure to warn patients of prolonged use of chlorhexidine mouthrinses beyond the two-week period which can lead to extrinsic staining of teeth. For ulcers, Colgate Savacol Antiseptic Mouth & Throat Rinse* can be used three times daily during the period of the ulcer. For patients who have recently undergone a dental extraction, promoting good healing of the postextraction socket and wound is pivotal to the post-operative experience of a

patient. Especially in areas which can be difficult to keep clean post-operatively such as the posterior area following third molar extraction, an antiseptic rinse such a Savacol* can be prescribed for two weeks, instructing the patient to rinse for 30 seconds after meals. Reducing the bacterial load around the extraction socket and wounds can help promote good healing and reduce postoperative pain.3
Patients undergoing dental implant treatment:
To aid healing and manage any postoperative infection following implant surgery, use of an antiseptic rinse for 7-14 days after surgery is advised. 6
In the 2015 NHS England Guidelines, there was a recommendation to prescribe a Chlorhexidine Gluconate mouthrinse, twice daily in the week before extractions and then post operatively for up to two months to facilitate healing. However, NHS England guidelines have since been superseded by Scottish guidelines, advising not to use Chlorhexidine Gluconate mouthwashes prior to extraction in patients categorised as either low or high risk of MRONJ, stating that there is insufficient evidence to support the use. Importantly, for patients that do develop MRONJ, the American Association of Oral and Maxillofacial Surgeons advise to use a Chlorhexidine Gluconate mouthrinse in the early phases of managing these conditions.6
A frequent question from patients who are parents of children may ask if their child can use a mouthrinse. Children or adolescents with a higher caries risk or increased susceptibility to dental caries during orthodontic treatment can be prescribed a fluoride mouthrinse to prevent dental caries. Studies show the use of a fluoride mouthrinse twice daily, can reduce caries approximately 26% when used regularly. Importantly, only children above the age of six years should be recommended the use of a mouthrinse.9
This recommendation guide aims to simplify and demystify mouthrinses for clinicians so that you make the appropriate suggestions and prescriptions for your patients to help promote good oral health. Mouthrinses are a great adjunctive to include as part of a patient’s oral hygiene routines so they can continue to experience healthier teeth and gums. n
References
1. Ustrell-Borràs M, Traboulsi-Garet B, Gay-Escoda C. Alcoholbased mouthwash as a risk factor of oral cancer: A systematic review. Med Oral Patol Oral Cir Bucal. 2020;25(1):e1-e12. Published 2020 Jan 1. doi:10.4317/medoral.23085
2. Rautemaa R, Nordberg A, Wuolijoki-Saaristo K, Meurman JH. Bacterial aerosols in dental practice - a potential hospital infection problem? J Hosp Infect. 2006 Sep;64(1):76-81. doi: 10.1016/j.jhin.2006.04.011. Epub 2006 Jul 3. PMID: 16820249; PMCID: PMC7114873.
3. Vanessa Costa Marui, Maria Luisa Silveira Souto, Emanuel Silva Rovai, Giuseppe Alexandre Romito, Leandro Chambrone, Claudio Mendes Pannuti,Efficacy of preprocedural mouthrinses in the reduction of microorganisms in aerosol: A systematic review, The Journal of the American Dental Association, Volume 150, Issue 12, 2019, Pages 1015-1026. e1,ISSN 0002-8177,https://doi.org/10.1016/j.adaj.2019.06.024
4. Poppolo Deus F, Ouanounou A. Chlorhexidine in Dentistry: Pharmacology, Uses, and Adverse Effects. Int Dent J. 2022;72(3):269-277. doi:10.1016/j.identj.2022.01.005
5. Kolahi J, Soolari A. Rinsing with chlorhexidine gluconate solution after brushing and flossing teeth: a systematic review of effectiveness. Quintessence Int. 2006;37(8):605-612
6. Llewelyn, J. A double-blind crossover trial on the effect of cetylpyridinium chloride 0.05 per cent (Merocet) on plaque accumulation. Br Dent J 148, 103–104 (1980). https://doi. org/10.1038/sj.bdj.4804396
7. Brookes ZLS, Bescos R, Belfield LA, Ali K, Roberts A. Current uses of chlorhexidine for management of oral disease: a narrative review. J Dent. 2020;103:103497. doi:10.1016/j. jdent.2020.103497
8. Marinho VC, Higgins JP, Sheiham A, Logan S. Fluoride toothpastes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2003;2003(1):CD002278. doi:10.1002/14651858.CD002278
9. How does mouthwash work?: Types and benefits. Colgate. com. Published November 24, 2022. Accessed October 31, 2023. https://www.colgate.com/en-gb/oral-health/selectingdental-products/how-does-mouthwash-work
10. Should you use a fluoride mouthwash? Com.au. Published January 18, 2023. Accessed October 31, 2023. https://www. colgate.com.au/oral-health/fluoride/who-should-use-afluoride-mouth-rinse-and-why
11. Rama S. Lord of the rinse: Choosing the right mouthwash for you. The Dental Room. Published June 20, 2017. Accessed October 31, 2023. https://www.thedentalroom.com.au/lordrinse-choosing-right-mouthwash/

About the author Dr Kaejenn Tchia is a member of the Colgate Advocates for Oral Health, a group of dental and oral health professionals dedicated to promoting preventive oral health practices. He is a recent graduate working in a corporate private practice in Darwin, Northern Territory and is the current President of the Australian Dental Association NT Branch Inc. He has also served leadership positions for Bupa Dental Corporation including the Clinical Advisory Panel, Clinical Procurement Committee, Graduate Committee and the recently revamped Dental Advisory Panel. He is passionate about helping and collaborating with fellow dental colleagues, recently embarking on a new journey to help recent graduates eliminate burnout through a 6-step B.E.L.I.E.F System. As a Colgate Advocate for Oral Health, Kaejenn aims to inspire clinicians to have practical tools and guides to help them create the fulfilling dental career of their dreams.
Republished with permission from Colgate Advocate’s for Oral Health colgateprofessional.com.au/Advocates

full state-by-state run-down of Association happenings around
ACT contacts:
Director Amy McDermott directoract@dhaa.info
Chair Kate Spain chairact@dhaa.info
n The next ACT event is going to be a full day seminar on Saturday 16 August, to be held at the Verity Lane - Juliet Room, Northbound Avenue in Civic. The program features Dietitian Lisa Donaldson, Periodontist Dr Lakshami Boyapati, GP Dr Ian Chan, Pharmacist Dr Belinda Mackenzie covering a variety of clinical topics on perio and impacts, skin cancer, menopause and pharmacology update.
“ This keynote will leave you inspired to reflect, empowered to act, and reminded that you don’t need permission to lead — just the courage to begin ”
Entrepreneur of the Year
Award Recipient 2025 and Elevative founder Mariana Marcano Franco will provide a keynote presentation on Empowered self-leadership through personal transformation to navigate changes. With authenticity, humour, and warmth, Mariana doesn’t offer quick fixes — she plants a seed. A spark of curiosity. A call to take just one small step toward leading more intentionally. This keynote will leave you inspired to reflect, empowered to act, and reminded that you don’t need permission to lead — just the courage to begin.
Please check this out and register ASAP to secure your place. Registration has opened on the new OHAA website: REGISTER
NSW contacts: Director Jinous Eighani-Roushani directornsw@dhaa.info
Chair. Belinda Hines chairnsw@dhaa.info
Deputy Chair Angelee Murdock contactnsw@dhaa.info
n The next NSW event will be the last DHAA event before transitioning to
“ The program is designed to foster learning, innovation, and collaboration to shape the future of oral health and patient care management”
the new OHAA. It will be held on Saturday 21 June at Rydges North Sydney. The program is designed to foster learning, innovation, and collaboration to shape the future of oral health and patient care management. Discussions will span from paediatric care to oncology management, wellbeing and AI technology, offering valuable insights for professionals dedicated to improving oral and overall health. Expert speaker included our TV celebrity A/ Prof Matthew Hopcraft, Oral Medicine Specialist Dr David Joe, Paediatric Dentist Dr Yvonne Chau, Periodontist Dr Wesley Wong and our fellow OHT Patrick Westhoff
Registration through the DHAA website: REGISTER
Qld Contacts:
Director Carol Tran. directorqld@dhaa.info
Chair Gabby Williamson chairqld@dhaa.info
Deputy Chair Courtney Dicken contactqld@dhaa.info
n After cancelling the half day event in March due to severe weather, the seminar was eventually moved to Saturday 3 May. Fortunately both A/Prof Michael Stubbs and Dr Devan Naidu were able to attend the rescheduled day and delivered their lectures in Toowoomba. The Queensland Committee is now running a Stainless Steel Crown hands-on workshop on Saturday 19 July at the ADA Queensland dental Simlab.
This education day provides an opportunity to join paediatric dentistry specialist Dr Alex Mogilevski for an in-depth lecture series followed by a practical hands-on workshop focused on two essential aspects of modern pediatric dentistry: stainless steel
For all the latest info on DHAA events please visit www.dhaa.info/events
crowns/pulpotomies and the management of the hypomineralised dentition.
This interactive session is structured to provide both theoretical knowledge and real-world application. After the lecture series, participants will engage in a hands-on workshop, allowing them to practice and refine their skills in a supportive environment.
Please note: This is a hands-on course in the ADAQ Simlab which means we have to cap our participants at a maximum of 20. Please register early to avoid disappointment:
REGISTER
A reminder that the 2025 Oral Health Congress will be held at the Star Gold Coast, 16-18 October. The full program offering 20 CPD hours is now available on the website so please check it out and register ASAP to make use of the early bird discount: REGISTER
Thanks to Chris Henderson who represented both ADOHTA and DHAA at the Griffith University Dentistry and Oral Health Professional Advisory Group meeting to oversee its academic program on dental hygiene.
SASA Contacts: Director Cheryl Dey cheryl.dey@dhaa.info
Chair Courtney Rutjens chairsa@dhaa.info
Deputy Chair Jesse Kourakis contactsa@dhaa.info
n The SA 2025 destination event was held on Saturday 29 March at the Mount Lofty Retreat. The event was attended by 60 delegates, some travelled from interstate to experience a full day of wellness exercises, Qi Gong, breathing exercises, Yoga, complementary medicines and reliance building. The day was completed with drinks and canapés to celebrate the success of of the SA Committee as this was the last SA event under the DHAA banner.
SA is the host for the Gala Dinner to celebrate 50 years of dental hygiene on Saturday 26 July at the Adelaide Pavilion. This event is hosted by the new Oral Health Association of Australia to reflect on the achievements of our colleagues over the past half century, and to celebrate the new era and opportunities

in dental hygiene moving forward for OHPs. Join us to be part of this momentous event to honour the past, celebrate the present and embrace the future of dental hygiene for our profession.
REGISTER
SA will also run a full day seminar at the Adelaide Pavilion on the same day as the Gala Dinner. The program include periodontist A/Prof Andre Bendyk presenting on managing Periimplantitis, dentist Dr Mark Wotherspoon on Healthy ageing - oral health related quality of life researcher Prof Toby Hughes on genetic risk for oral disease; Paediatric dentist Dr Emilija Jensen on Communication and Collaboration Across the Dental Team; and endocrinologist Dr Lachlan Angus on transgender health and implications for oral health practice. REGISTER
Congratulations to the Rural and Remote SIG Chair Lyn Carman who represented the DHAA on the language project Katiti Wiru
(Healthy Teeth) Closing the Gap through Oral Hygiene and Language in Remote SA. The project was run by the University of Adelaide mobile language team. The project led to the development of oral health resources in Aboriginal languages which will be made available for members to support their oral health practice. Lyn also represented DHAA on the SA Oral Health Plan Monitoring Group in overseeing the implementation of the current SA Oral Health Plan 2019-2026.
TAS Contacts: Staff Bill Suen bill.suen@dhaa.info
n TAS hosted a joint full day event held at the Tailrace Centre in Launceston on Saturday 17 May. The day seminar featured orthodontist Dr Derek Mohanoy on orthodontic >>


treatments for children; dentist Dr Chris Sanzaro on clinical photography, special needs dentist Dr Helen McInnes on medical history taking and working with people with special needs, and dental therapist Julie Barker on value adding at dental check-ups.
VicVic Contacts
Director Roisin McGrath
directorvic@dhaa.info
Chair Cathryn Carboon chairvic@dhaa.info
Deputy Chair Sarah Laing contactvic@dhaa.info
n Congratulations to Emily Sporle for being awarded the DHAA 2025 La Trobe University Oral Health Student Prize at the La Trobe University. Victorian DHAA
Chair Cathryn Carboon presented her with the award on Tuesday 15 April at the Bendigo Student Awards and Prizes ceremony.
Congratulations also to Melbourne University’s Jessica Fry who have received the DHAA Award from Cathryn Carboon on Thursday 15 May at the 2025 Melbourne Dental School Awards Ceremony.
Victoria hosted the first OHAA face-to-face board meeting on 3-4 May with OHAA CEO elect Nathan Clarke meeting the full OHAA Board for the first time. The Board dinner was attended by ADAVB CEO Ilsa Hampton, President Dr Heredia and ADC CEO Johnathon Kruger.
Victoria’s next full day seminar is scheduled fro Saturday 16 August at the Courtyard by Marriott at Flagstaff Gardens. The program features pharmacist Jarrod McMaugh on quit smoking, OHT Aisha Mansfield on cultural safety and special needs dentist A/Prof Warren Shnider on fluoride and caries risks.
Registration now open at: REGISTER
WA Contacts
Director Carmen Abramich directorwa@dhaa.info
Chair: Michelle Wright contactwa@dhaa.info
Staff: Bill Suen bill.suen@dhaa.info
n WA ran an afterwork evening session on Wednesday 19 March with clinical psychologist Lan Chen delivered a presentation on
Understanding and Managing Burnout and Other Occupational Stressors at the ADA House in West Perth.
On Saturday 5 April, a full day seminar at Aloft Perth with oral medicine specialist Dr Amanda Phoon Nguyen, Periodontist A/ Prof Leticia Algarves Miranda, Radiologist Dr Mary Lam, Periodontal Therapist Jennine Bywaters and OHT Chelsea Rohekar covering a wide range of interesting topics that provided six hours of quality CPD to attendees. Thanks to WA Director Carmen Abramich and Chair Michelle Wright who joined their ADOHTA counterparts at the Australian Dental Congress in Perth on 8-10 May. They staffed the OHAA stand to promote OHAA membership and inform delegates the commencement of the OHAA from July this year. n

www.dhaa.info