
















California Podiatric Physician JULY | AUG | SEPT | 2022 The 2022 WELCOME BACK WESTERN WOWS! – PAGE 14 2 22 WESTERN PICTORIAL EDITION 3 PresidentialInauguralAddress Holly Spohn-Gross, DPM, President 7 CPMAGifted$500KLegacyGrant 9 AnthemBlueCrossBestBillingPractices RegardingL3000-L3030CustomFoot Orthotics 13 EbonieVincent,DPM,MBMS,DABPM, Starof“MyFeetAreKillingMe,” ElectedtoCPMABoardofDirectors 15 FranklinKase,DPM,Receives CPMA’sInauguralLegendAward 17 WaivedCopayments:NoGoodDeedGoes Unpunished. C. Keith Greer, ESQ. 21 Engineering:TheKeytoAchieving QualityinMedicine Jon Hultman, DPM, MBA, CVA 25 TipsforDevelopingorRedeveloping YourTrainingPrograms Tina Del Buono, PMAC 86 OnYOURToes; News YOU Can Use

Visit picagroup.com to learn how we're in your corner!
Dr. Spohn-Gross’ Presidential Inaugural Address
DEAR CPMA HOUSE OF DELEGATES, CPMA BOARD, AND HONORED GUESTS,
Holly Spohn-Gross, DPM CPMA President 2022-23
Good afternoon, Delegates, Alternates, Directors, Distinguished Guests, Esteemed Colleagues, Friends, and Family. Thank you for being here.
I am truly honored to stand before you today as your next president of the California Podiatric Medical Association (CPMA). Isaac Newton wrote, “We all stand on the
HOLLY SPOHN-GROSS, DPM, TAKES OFFICE AS CPMA PRESIDENT
Lake Isabella, podiatric physician and surgeon Holly Spohn-Gross, DPM, was installed as president of the California Podiatric Medical Association (CPMA) during the organization’s 2022 House of Delegates in Anaheim, CA, in June.

Robert Gross, DO, with whom she also practices. Boardcertified in wound care and healing, Dr. Spohn-Gross is affiliated with the Kern Valley Healthcare District, Lake Isabella; Dignity Heath Memorial Hospital, Bakersfield; and Adventist Health Hospital, Bakersfield, CA.
Spohn-Gross, DPM CPMA President 2022-23
In her presidential inaugural address to the over 100 podiatric physicians, residents, students, educators, a variety of stakeholders in The House of Medicine, and guests, Dr. Spohn-Gross (long a champion for the underprivileged) spoke on the need for access to quality, affordable healthcare; recruiting the next generation of podiatric physicians; the importance of mentoring students and residents, the necessity of developing and nurturing relationships, and parity for podiatry and California’s podiatric physicians.
A Michigan native, Dr. Spohn-Gross attended Michigan State University in East Lansing, Michigan, where she was an elite distance runner and received her Bachelor of Science Degree in Biology. Dr. Spohn-Gross received her medical education at the New York College of Podiatric Medicine, from which she earned her Doctorate of Podiatric Medicine Degree. Dr. Spohn-Gross completed her 3-year podiatric medicine and surgery residency at Cornell Medical Center’s Wyckoff Heights Medical Center in Brooklyn, NY; Greater Detroit Hospital in Detroit, Michigan; and Pontiac Osteopathic Hospital in Pontiac, Michigan.
A private practitioner, Dr. Spohn-Gross is the owner and operator of Sienna Podiatry and a Co-Owner of Sienna Wellness Institute with her spouse, Internist, and Hospitalist

A member of the California Podiatric Medical Association (CPMA) since 2002, when she relocated to California, Dr. Spohn-Gross has served on a number of CPMA committees. In 2015 she was elected as a Director-at-Large to the CPMA Board of Directors. After serving two terms in the Director-atLarge position, Dr. Spohn-Gross was elected to the office of Secretary-Treasurer, followed by the offices of Vice President and President-Elect.
Dr. Spohn-Gross is passionate about her philanthropic work and volunteerism. She is active in humanitarian efforts in the underserved community where she practices, and in Rotary International, providing podiatric care to women and children in India through the organizations’ NID Polio Physicians Program, and is a surgical volunteer for LIGA (The Flying Doctors of Mercy). Dr. Spohn-Gross has been active in international programs to educate and protect women and girls in extreme poverty against human trafficking. In addition, she is Chair of the American Association of University Women’s STEM Scholarship Program.
Dr. Spohn-Gross is the recipient of numerous honors and awards, including The American Red Cross Real Heroes Award; the Kern River Valley Chamber of Commerce Woman of the Year Award; Rotary Club of the Kern River Valley Paul Harris Award. And, she has twice been a recipient of the California Podiatric Medical Association’s Humanitarian of the Year Award.
Dr. Spohn-Gross enjoys ultra-trail running, cooking, traveling, and spending time with her husband, three children, and two dogs.
| 3 JULY • AUGUST • SEPTEMBER • 2022
continued
page 4 ▶
Holly
on
shoulders of giants.” This couldn’t be truer.
I would not be here without the support I received over the years from all of you and those that have come before me.
To the board members, delegates, and mentors, I thank you ALL and look forward to working with you.
I would like to extend a special thank you to my family:
To my husband, Dr. Robert Gross, a Hospitalist, colleague, husband, best friend, and life partner! We met 30 years ago as undergrads, and shared our dream of becoming doctors and traveling to underdeveloped countries to deliver medical care. (Little did we know we would do that right here in rural California, providing healthcare to our underserved populations.) You have been a role model for our children and community. You inspire me every day. I am fortunate to have you by myside. Thank you for sharing this dream with me. I love you.
To my Children - my daughter Hannah, son Nate, and my sons Hunter and Rob, who could not be here, you are why I am here today. You are my hearts. Thank you all for your understanding & for your love and support.
To my staff, thank you so much for making it possible for me to do “ALL THIS” when I am away from the office.
I especially want to thank my parents for their love and support and to recognize my father, Dr. Earle Spohn, a general surgeon for over 45 years. He has been my role model and shared with me his passion and love for being a surgeon. He took me on rounds with him after church, and taught me how to tie surgical knots and hold a glass steady. But the real gift was his showing me what it is to be a surgeon threw his eyes, and I am forever grateful.
To my sister Dr. Heidi Jenney - an ER physician who has not one, but two sets of twins - has shown me that anything is possible. I am so fortunate to be able to share the challenges of raising kids while practicing medicine with her. Finally, I would like to point out key influences in my life professionally.
Dr. Lawrence “Larry” Harkless and the late Dr. Oliver “Ollie” Foster, though huge presences in this room, each year found time to ask me how I was doing in Lake Isabella. That amazed me.
Dr. Carolyn McAloon stood before 8 years ago giving her presidential address. Afterward, I asked her how she did it. She looked at me and said, “You can do this - anyone can!” She has been encouraging me ever since.
Dr. Frank Kase - a LEGEND in this Association - believed in me and has been a treasured mentor and friend.
Dr. Peter Bretan has championed our cause. But, it is his story and passion to help those less fortunate that inspires me to keep going.
Dr. Steven Wan, I would not be here if it wasn’t for him. He was the one who asked me to become a delegate. So, you can blame him. He has been a guiding light in my life and has made a difference in our profession.
All these people I have acknowledged - and the many more unmentioned (but not forgotten) - are what I would like to refer to as “Starfish Throwers”. Perhaps some of you have heard this story. I find it helps to be reminded…
One day after a great storm, a man was walking along the beach when he noticed a boy picking something up and gently throwing it into the ocean. Approaching the boy, he asked, “What are you doing?” The youth replied, “Throwing starfish back into the ocean. The surf is up, and the tide is going out. If I don’t throw them back, they’ll die.”
“Son,” the man said, “don’t you realize there are miles and miles of beach and hundreds of starfish? You can’t make a difference!”
After listening politely, the boy bent down, picked up another starfish and threw it back into the surf, and said….” I made a difference for that one.”
This story holds a special meaning for me…not only as a metaphor for medicine and how it has touched our patients’ lives, but it also captures my own experience as a starfish! You see, I was born with a Cleft palate and lip, and I needed immediate medical attention.
My father, a young surgical resident at the time, went to none other than Dr. Dingman (The godfather of cleft surgery) and humbly asked for his help. Dr. Dingman not only agreed to perform the surgery, but he did it for free. That ONE act changed my life forever.
I share this with you all for several reasons. First, as I look out over this audience of experts in the field of foot and ankle surgery, I see doctors that have been sought out over the years for their surgical skills and reputation. It is your gift, your talent, that changed the lives of your patients. You have thrown those starfish back into the ocean not only with new hope, new life, and a second chance.
You have done this with compassion and kindness.This is what makes the real difference. You see, it wasn’t just Dr. Dingmans’ surgical skills that I came to appreciate, but the way he treated me that I remember. Maya Angelou eloquently said, “I’ve learned that people will forget what you said, people will forget what you did, but people will never forget how you made them feel.”
4 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
So, when you agree to perform surgery on a patient with polydactyly or syndactyly, or TEV you are changing that patient’s life forever. So, when you reconstruct a Charcot foot and perform limb preservation surgeries on a diabetic, just remember you are giving them a second chance. That is real HOPE!
But the story of the Starfish Thrower doesn’t end there.
You see, everyone who witnessed the young boy’s dedication and passion for helping save these starfish was touched and inspired to help. It wasn’t just the old man. It was the entire community. They all joined him to save every single one of those starfish.
Again, each one of you has not only made a difference in your patients’ lives, but you have chosen to help our profession by showing up, working hard, and leading the cause. You have mentored others and become role models. You, in this audience, tirelessly use your skills to better our profession. You are the leaders changing the trajectory of Podiatric Medicine.
But still, the story does not end here. What happened to each of the starfish? Yes, you made a difference in their life. Yes, you saved them. But what happened to them?
From the chapter of Luke 12:48 “To whom much is given, much is required.” Having been one of those starfish, I was called to give back. So, like so many of you…I have worked extremely hard to become a Surgeon. I have discovered my purpose. I have learned it’s a true gift. It’s Magic! We all have. We are humbled by it. We are motivated by it. And, we are inspired by it. But there is work to be done. I would like to share my vision.
The struggles in medicine that we are up against are not the ones my father fought. We are faced with limited access to healthcare coupled with a doctor shortage crisis. We must be able to navigate the complexities in billing and insurance regulations, all while trying to provide patient care. We need innovative and motivated thinkers like you to create solutions. These are OUR opportunities….
It is a shared vision that was recognized over 18 years ago… is now coming to fruition. To be classified as Physicians and Surgeons. We do this by maintaining a strong Association to protect our patients and practitioners and by developing strong partnerships with physician and specialty groups. Success comes when groups of people join together and support each other for a common goal. It will take dedication, hard work, and passion to carry this across the finish line, but the time is NOW.
I want PHYSICIAN PARITY! I want a better future for our
residents, students, and young practitioners. And I believe we can. We must do this for the future of our profession. In addition, I want to engage our members and give them more access to what we do as an Association and as a board. We must tell our story, and we have a GREAT story to tell. We need to meet people where they are, and many are on social media. We need to increase our social media presence and highlight CPMA members. After all, aren’t we the bestkept secret in medicine?
So, how will we achieve all this? To begin, I have enhanced our current committees and created new committees to make this happen.
CPMA’s Communications Committee will become the EPICENTER for highlighting the work of the Association, board of directors, and committees.
Furthermore, I’ve created 3 additional committees: Sports Medicine Committee - As an athlete and ultra-runner, I have always felt that there is a missed opportunity to capitalize on what DPMs do for athletes. This committee will highlight DPMs that work directly with athletes, tell their stories, and showcase the athletes they treat. Very exciting!
DEI Committee - Diversity, Equality, and Inclusion. It is vital to the success and well-being of this Association to welcome and support ALL our members. Still, awareness, education, and action are critical components to making impactful changes. This committee will provide a space for those that do this by creating panels to share stories, educate others and support one another. We ARE Stronger Together!
Beginning Practitioners Committee - This committee is designed to help our new practitioners by connecting them to experienced mentors. Provide seminars on practice management to help young members negotiate contracts, network with private practices, etc.
These are just some of the exciting opportunities we will embark upon in the coming year. So, I look forward to knowing all of you better. I am humbled and empowered to be given this opportunity to serve as president of our great Association.
I will conclude with a quote from Goethe, whose words help to set the tone for my presidential year - “Whatever you can do or dream you can, begin it.”
So, let’s begin it!
Thank you!
Holly Sphon-Gross, DPM President, California Podiatric Medical Association
| 5 JULY • AUGUST • SEPTEMBER • 2022
The Premier Provider of Podiatric Diagnostics Services




Onychomycosis

Both PAS and PCR based identification of pathogens provide precise diagnosis, optimizing patient outcomes.
Podiatric Pathology
Wound Care
Histopathologic and histochemical examination of nail, skin, tissue, bone and cytology.
For your premiere podiatric pathology service call your Bach Diagnostics account manager at 800-544-4181, or visit us on-line www.bachdx.com.
Results within 24-48 hours. 3-5x more sensitive than culture. One of the largest organism & resistance gene panels available, providing clinicians a much broader spectrum of antibiotic choices. 800-544-4181
CPMA Gifted $500K LEGACY GRANT
Following the close of the California Podiatric Medical Association’s 2022 House of Delegates on June 22 in Anaheim, CA, the doctor delegates, and alternates joined the newly elected 2022-2023 CPMA Board of Directors, guests, colleagues, family, and friends for an evening of fellowship, camaraderie, reconnecting, and renewing bonds of friendship at the Annual President’s Reception.

During the celebration, CPMA Life Member Dr. Bruce Lawrence made a momentous announcement noting that he had been moved and inspired by two articles in the current issue of CPMA’s member magazine The California Podiatric Physician. The specific articles were: The Long Path to Parity: Past, Present, and Future by CPMA Executive Director Jon A. Hultman, DPM, MBA, CVA, and the other was The Quest by CPMA President Diane D. Branks, DPM, FACFAS, FACPM, RVT, which he and his spouse Janet felt provided perfect reasons and timing to create and gift the California Podiatric Medical Association with the Legacy Fund. The $500K
endowment is the most significant individual gift the Association has received in its 110-year history.
“This is huge,” said CPMA Executive Director Dr. Jon Hultman. “And the faith and support it shows in CPMA’s leadership and agenda is truly gratifying.”
“Outstanding,” said newly elected CPMA President Holly Spohn-Gross, DPM. “I can’t find the words to express the true magnitude of this honor. It is truly positive reinforcement that we are on the right path.”
Stating that the gift is seed money for a special perpetual fund directed by the CPMA Board of Directors in its ongoing muscular efforts to advance, protect and promote podiatry as it enhances the Legacy of the California Podiatric Medical Association, such as legislative initiatives - e.g. “The Quest.” Dr. Lawrence noted, “we will continue to need other CPMA members to contribute to the Legacy Fund at whatever level they are able and feel comfortable with.”
| 7 JULY • AUGUST • SEPTEMBER • 2022
(l to r) Jon A. Hultman, DPM, MBA, CVA, Executive Director, CPMA and Bruce R. Lawrence, DPM
IS EXCEPTIONAL
Over 1M patients treated.1 25 years of proven bone healing. The choice of 10,000 doctors each year.2 One unique ultrasound technology.

Reference: 1. Bioventus LLC. Data on File, RPT-001321. 2. Bioventus LLC. Data on File, RPT-000965.

Indications for Use: The EXOGEN Ultrasound Bone Healing System is indicated for the non-invasive treatment of established nonunions* excluding skull and vertebra.

• The EXOGEN device has also been reported as effective as an adjunctive non-invasive treatment of established nonunions in patients:
• With internal or external fracture fixation hardware present. EXOGEN cannot penetrate metal and therefore should not be applied directly over hardware.
• Undergoing treatment for infection at the fracture site. EXOGEN is not intended to treat the infection.
• Believed to have diminished bone quality. EXOGEN is not intended to treat diminished bone quality.
In addition, EXOGEN is indicated for accelerating the time to a healed fracture for fresh, closed, posteriorly displaced distal radius fractures and fresh, closed or Grade I open tibial diaphysis fractures in skeletally mature individuals when these fractures are orthopaedically managed by closed reduction and cast immobilization.
There are no known contraindications for the EXOGEN device. Safety and effectiveness have not been established for individuals lacking skeletal maturity; pregnant or nursing women; patients with cardiac pacemakers; on fractures due to bone cancer; or on patients with poor blood circulation or clotting problems. Some patients may be sensitive to the ultrasound gel.
*A nonunion is considered to be established when the fracture site shows no visibly progressive signs of healing.
Full prescribing information can be found in product labeling, at www.exogen.com or by contacting customer service at 1-800-836-4080
Bioventus, the Bioventus logo and EXOGEN are registered trademarks of Bioventus LLC. ©2021 Bioventus LLC. All rights reserved. SMK-003855 06/21
Innovations For Active Healing
Learn more at EXOGEN.com
Anthem Blue Cross Best Billing Practices REGARDING L3000 - L3030 CUSTOM FOOT ORTHOTICS

This article aims to shed light on a few best practices with respect to billing for certain services. It is best practice for providers to work cooperatively with insurers and health plans to resolve billing issues so as to encourage the continued exceptional treatment of patients. We appreciate that sometimes there are billing issues that lack sufficient clarity and may lead to disputes and provide this overview to address common billing issues.
1. Foot Orthotic Unbundling
In a Publication by the American Orthotic and Prosthetic Association (AOPA) and supported by both American Podiatric Medical Association (APMA) and the Pedorthic Footcare Association (PFA) the following components are INCLUDED in the descriptions of each device L3000, L3010, L3020 and L3030. Each code description includes the following passage: HCPCS code(s) L3000, L3010, L3020 and L3030 “includes additions such as postings, padded top covers, soft tissue supplements, balance padding and lesion or structure accommodations. Other additions may be required as well.” https://www.aopanet.org/wp-content/ uploads/2016/06/L-Code-Definition-Clarification-051316.pdf
Thus, some carriers, including Anthem, consider it inappropriate to bill for ADD-ON components in a la carte fashion—including but not limited to L2275, L2280, and L2820—in conjunction with custom foot orthotics (L3000 – L3030).
2. Foot Orthotic Casting (S0395)
The only appropriate billing code to use to represent the impression “casting” service (e.g., plaster slipper cast, foam impression or digital scan) of a patient who will receive custom foot orthotics fabricated by an outside lab (someone other than the one providing the casting service) is HCPCS code S0395. It is advisable to check with individual health
plans and insurers to determine their specific DME or Reimbursement Policy regarding this casting service (S0395).
Anthem considers it inappropriate to bill for Orthopedic casting service codes—including but not limited to CPT code 29515 (application of short leg splint [calf to foot]) and 29799 (Unlisted procedure, casting or strapping) in association with custom foot orthotics as they represent orthopedic casting services and are not specific to the custom orthotic services.
3. Supply Codes for Custom Foot Orthotics
Custom foot orthotic casting (S0395) includes any supplies and/or transport services used to perform this included service. These are not eligible for independent reimbursement. Supply and Transport services include, but are not limited to, 99002, 99070, A4580, A4590, Q4037, Q4038 and Q4050.
Insurers and health plans want physicians, facilities and other health care professionals to submit claims accurately and, to that end, often provide resources to help ensure accurate claim submission. Note also that industry practices are constantly changing, and insurers and health plans review and revise their policies periodically. Thus, it is essential that Providers have a process in place to stay abreast of changes to insurers’ billing guidelines, as they will likely be contractually obligated to follow the current guidelines even if they fail to review them.
| 9 JULY • AUGUST • SEPTEMBER • 2022
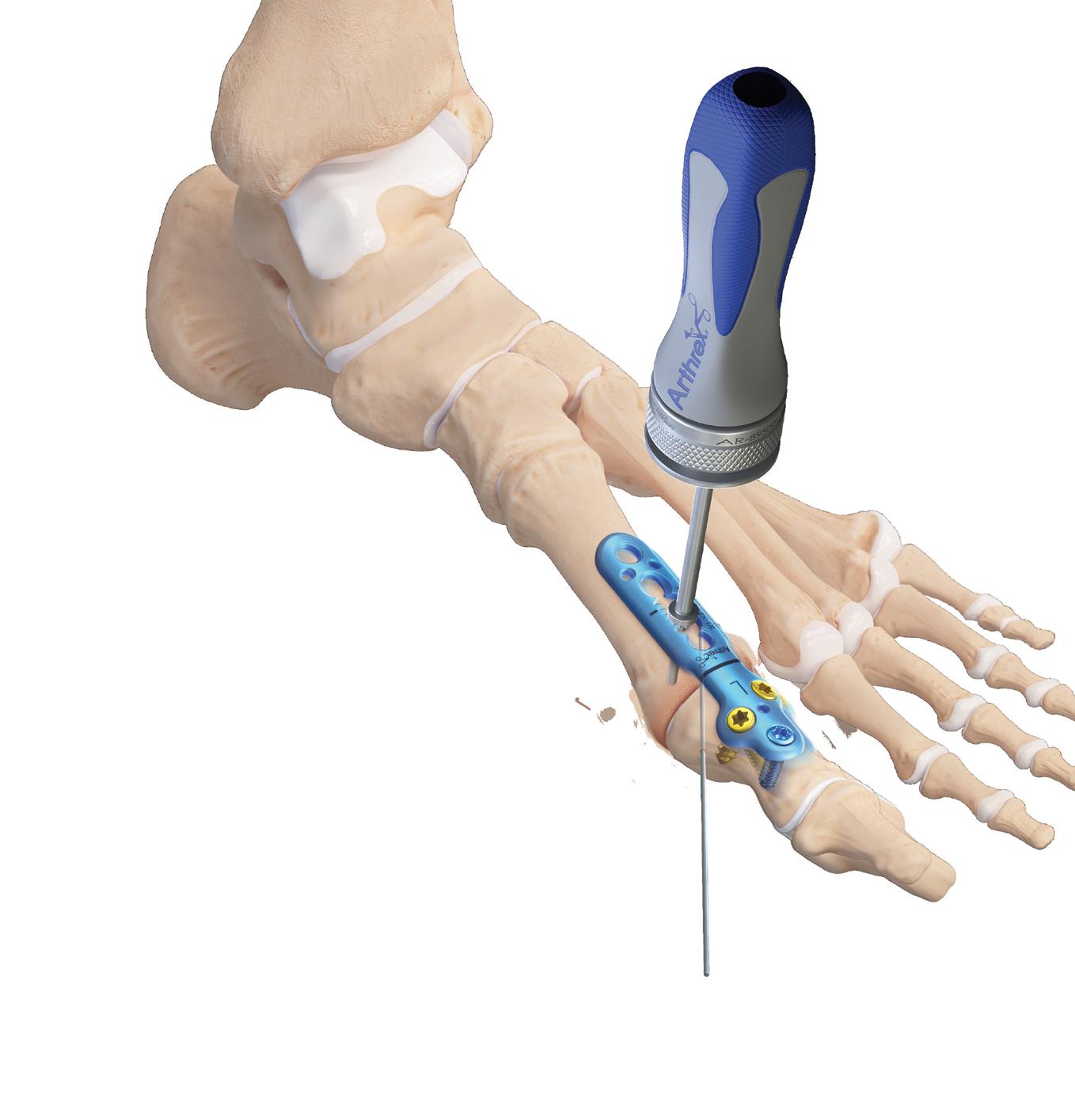
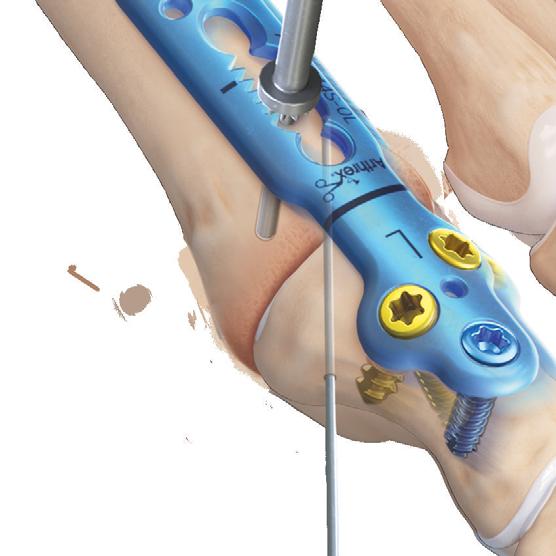

Ad.Arthrex.com/MTP © 2022 Arthrex, Inc. All rights reserved. AD1-000282-en-US_B MaxForce™ MTP Fusion Plates Gear Up for Fusion ■ Patented geared compression mechanism lets you dial in compression ■ New zero-profile, flat-head cortical screws ■ Multiple angle and length options ■ 3.0 mm and 3.0/3.5 mm hybrid screw options for bone density variation ■ Variable-angle locking with a 30° cone of variability Close-up of Geared Compression Mechanism Engage the geared compression mechanism to pull the phalanx and plate towards the metatarsal
CPMA’s House of Delegates Selects Leadership AND SETS GOALS FOR THE COMING YEAR
After an absence of nearly three years due to the COVID-19 Pandemic, the 2022 California Podiatric Medical Association’s House of Delegates (HOD) once again convened at the Disneyland Hotel and Convention Center in Anaheim, CA.

Dozens of doctor delegates and alternates representing CPMA’s eighteen local component societies (from Shasta Region in the North to San Diego in the South) received in-depth briefings from national, state, and local leaders in medicine, management, and education on legislative affairs; the Podiatric Medical Board of California (formally the Board of Podiatric Medicine (BPM)); important healthcare policy issues impacting podiatric physicians, their patients, practices, and specialty; regulatory matters; podiatric medical education, and legal issues affecting the practice medicine and management.
ELECTIONS
Duties of Delegates of the 2022 CPMA House of Delegates include selecting the Association’s leadership for the coming year. The 2022-2023 California Podiatric Medical Association’s elected Board of Directors, as voted by the 2022 CPMA House of Delegates, are as follows: Holly Spohn-Gross, DPM (Lake Isabella), was elevated to President. Diane Koshimune, DPM, FACFAS (San Jose), was elected President-Elect. And, Phong Le, DPM, FACFAS (Sacramento), was elected Secretary-Treasurer. Heather McGuire, DPM (Ventura), was reelected to a second two-year Director-at-Large term. Elected to a one-year Director-at-Large term in 2021, Douglas Taylor, DPM (Walnut Creek), was elected to a new two-year term. Finally, Ebonie Vincent, DPM, MBMS, DABPM (Orange), was elected to the CPMA Board of Directors as a Director-at-Lage for a two-year term.
The 2022 House was also charged with selecting the delegation representing California at the 2023 American Podiatric Medical Association (APMA) House of Delegates (HOD) next spring in Washington, DC. Michael Cornelison, DPM FACFAS (Cupertino) was re-elected as a four-year delegate. Those elected as one-year delegates to the
2023 APMA House of Delegates are Adam Howard, DPM (Cupertino); Jon Hultman, DPM, MBA, CVA (Los Angeles); Holly Spohn-Gross, DPM (Lake Isabella), and Stephen Wan, DPM (Los Angeles). The three Alternates selected to attend APMA’s 2023 HOD are Diane Koshimune, DPM, FACFAS (San Jose); Ronald D. Jensen, DPM (Modesto); and Heather McGuire, DPM (Ventura).
The 2022 CPMA House of Delegates was also the backdrop for the presentation of Awards:
CPMA AWARDS
The 2022 CPMA President’s Award went to California Medical Association (CMA) Immediate Past President Peter Bretan, MD CPMA’s Immediate Past President Adam Howard, DPM, was the recipient of the Executive Director’s Award. Faridi G. Sherieff, DPM, President, San Luis Obispo/Santa Barbara Podiatric Medical Society was named CPMA Local Society President of the Year. Ara Kelekian, DPM, President of the Los Angeles County Podiatric Medical Association, received CPMA’s Step-Up Award for LACPMA’s generous donation to the Clark-Foster-Kaplan Golf Tournament (which raises funds for APMAPAC) and for the society’s assistance in CPMA’s 2021 Membership Campaign. Ebonie Vincent, DPM, star of TLC’s hit show “My Feet Are Killing Me,” was the recipient of CPMA’s 2022 Rising Star Award. Finally, CPMA Past President Franklin Kase, DPM, FACFAS received the Association’s first-ever Legend Award in recognition of his numerous, invaluable contributions to the California Podiatric Medical Association, its members, their patients, and the specialty of podiatric medicine.
CALPPAC AWARDS
The Los Angeles County Podiatric Medical Association received the 2022 CalPPAC Awards for Society with Largest Total Contribution and for Society with the Largest Percentage of Members Contributing. The Santa Clara Valley Podiatric Medical Association received the Honorable Mention Award.
| 11 JULY • AUGUST • SEPTEMBER • 2022
The Law Offices of Greer & Associates
Proudly serving the legal needs of Podiatric Physicians since 1993
We know how much you rely on us. So while you are taking care of your patients, we are taking care of you. That means improving our knowledge and understanding of Podiatric medicine and surgery.





Attorney

It also means honing our litigation and trial skills so that we are ready to go all the way, against the toughest opposition, and win!

Reputations are earned through commitment, experience and results.
We have proudly represented Podiatric Physicians in more than 1,000 malpractice claims, hundreds of Medicare, Medi-Cal and private insurance audits, and more Board of Podiatric Medicine matters than any firm in the state. Aren’t we the type of team you want in your corner in challenging times? When you need legal help:
DEMAND THE BEST, ASK FOR GREER & ASSOCIATES.
Attorney Staci Labovitz performing a plantar fascia release.
Attorney Keith Greer watching Jonathan Labovitz, DPM, demonstrate the intricacies of careful dissection.
Tyler Greer performing an Achilles Tendon lengthening procedure.
Ebonie Vincent DPM, MBMS, DABPM Star of “My Feet Are Killing Me” Elected to CPMA Board of Directors
Dr. Ebonie E. Vincent, a board-certified podiatric foot and ankle specialist, was elected to a twoyear Director position on the California Podiatric Medical Association (CPMA) board of directors during the organization’s Annual House of Delegates held in Anaheim, CA, in June.

Star of TLC’s hit reality tv show “My Feet Are Killing Me,” which deals with extremely challenging and complex foot and ankle diseases and conditions of desperate patients; and the positive transformative effect that the skilled care provided by podiatric foot and ankle specialists can have on patients’ feet and lives. Known for her expertise and compassionate bedside manner, Dr. Vincent is sought out by patients from around the world. “My Feet Are Killing Me” is now in its 4th season and has recently been renewed for a 5th.
A native Californian, Dr. Vincent earned her Bachelor of Science in biology from Hampton University, a historic Black research university founded in 1868 in Hampton, Virginia. She obtained a Masters in Biomedical Science at Philadelphia College of Osteopathic Medicine in Philadelphia, Pennsylvania. Dr. Vincent received her podiatric medical education at Des Moines University College of Podiatric Medicine and Surgery in Des Moines, Iowa, and earned her Doctor of Podiatric Medicine (DPM) degree. And, she completed an intense three-year podiatric medicine and surgical residency program at Inspira Health Network in Vineland, New Jersey. Dr. Vincent has trained under top orthopedic and podiatric physicians in advance treatment for children and adults with upper and lower limb discrepancies, limb deformities, bone defects and
infections, joint contractures, and foot deformities at the Rubin Institute for Advanced Orthopedics in Baltimore, Maryland. She specializes in minimally invasive surgical techniques, corrective and reconstructive foot and ankle surgery, diabetic limb salvage, pediatric foot conditions, and sports medicine.
Dr. Vincent is passionate about podiatry. She notes that she is frequently asked why she chose podiatry as a career, especially since many deem feet the least desirable body part. Dr. Vincent says, “It takes a special heart - and at times a strong stomach - to treat problems with the feet. But to help patients get back on their feet and regain their mobility means that podiatry can literally change peoples’ lives for the better.” Dr. Vincent has appeared on numerous television shows, including E!, ABC, NBC, Fox, Dr. Oz, The Doctors, and The Daily Mail, to talk about the importance of foot health and the vital role podiatry plays in health care.
During her keynote speech at the CPMA House of Delegates, Dr. Vincent quoted poet Maya Angelou in saying, “I’ve learned that you shouldn’t go through life with a catcher’s mitt on both hands. You need to be able to throw something back.” Dr. Vincent strongly believes in giving back to the profession she loves and pays it forward with her affinity for mentoring the next generation of podiatric foot and ankle specialists.
A private practitioner with OC (Orange County) Podiatry Foot and Ankle Specialists (with offices in Orange, Huntington Beach, Irvine, Newport Beach, and Long Beach, California), Dr. Vincent enjoys working out and Broadway musicals. Her favorite daily motto is “Just Do Your Best All the Time.”
| 13 JULY • AUGUST • SEPTEMBER • 2022
The 2022 Welcome Back Western WOWS!

hands-on workshops. In addition, the 2022 Western featured a dynamic, innovative Exhibit Hall where attendees were encouraged to try out the latest tools and technologies in surgery, medicine, and management. Onsite attendees also enjoyed reduced room rates at Disneyland Resort hotels and deep discounts on Disney theme park tickets, where they experienced exciting new rides, shows, and the return of Disney’s dazzling nighttime spectaculars.
To accommodate those desiring a virtual learning experience and those preferring an in-person one, the 2023 Western will also be a hybrid event. The in-person program will again be hosted by the Disneyland Hotel and Convention Center in Anaheim, CA, June 22-25.
This June, over a thousand podiatric physicians, medical assistants, residents, students, faculty, sponsors, exhibitors, and guests gathered in person and online for the 2022 Western Foot and Ankle Conference (The Western) and were Wowed!
The meeting showcased an exciting line-up of inspirational, world-class speakers and leaders in podiatry, surgery, and medicine, presenting cutting-edge lectures, courses, and
2023 will be the 100th Anniversary of Disney Studios! The Disneyland Resort and theme parks will unveil new rides, parades, shows, nighttime spectaculars, and other surprises to celebrate the big event. And, Western attendees will be able to experience the Magic with significant savings on tickets to the theme parks, as well as reduced hotel room rates at Disneyland Resort hotels.
2023 Western Advance Registration is Now OPEN at TheWestern.org
Become A Leader!
The California Podiatric Medical Association’s (CPMA) Board of Directors comprises members of the Association who are selected and elected to help lead and shape the profession’s future. Serving on the CPMA Board of Directors or as a member of the California Caucus to the APMA House of Delegates is one of the many ways you can invest in your Profession, Association, and YOURSELF! CPMA’s success in its efforts on behalf of California’s podiatric physicians, their patients, practices, and medical specialty depends on a diverse group of leaders from a variety of backgrounds and consisting of young, mid-career, and senior podiatrists who:




• Are open to the ideas and opinions of others

• Participate in thoughtful discussions










• Work well with a variety of other volunteers and staff








• Are committed to meeting attendance (both in-person and remotely)
• Follow through on commitments and assignments Recognize yourself in the above? If so, then CPMA wants YOU!
If you would like to be considered for a seat on the CPMA Board of Directors, and or as a member of the California Caucus to the 2024 American Podiatric Medical Association’s House of Delegates, please fax your Letter of Interest/ Intent (LOI) and CV/Resume to Diane Branks, DPM, Chair, CPMA Nominating Committee at 916-448-0258 by March 10, 2023.
14 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
Franklin Kase, DPM, Receives
CPMA’S INAUGURAL LEGEND AWARD
CPMA’s Past President and Health Policy Chair Franklin Kase, DPM, FACFAS, was honored with the California Podiatric Medical Association’s first-ever Legend Award during the organization’s 2022 House of Delegates.
“Frank has received just about every CPMA Award,” said CPMA Executive Director Jon Hultman, DPM, MBA, CVA, “Including the Distinguished Service Award, Meritorious Service Award, President’s Award, Executive Director Award, Award of Excellence, Lifetime Achievement Award and Pinnacle Award.
“He has played a pivotal role in the advancement of podiatric medicine in the state. For example, he was indispensable in the Association’s successful effort to pass CPMA’s bill AB932, which codified the right of California’s podiatric physicians (due to their rigorous medical education and training) to perform amputations within their scope. And, of course, he is affectionately known as ‘The Bulldog’ when fighting payor discrimination in reimbursement for services provided by podiatric physicians.”
The Legend Award was presented to Dr. Kase virtually
(who was joined by his wife Beth, and daughter Alison). The presentation was made by his longtime dear friend and colleague CPMA Past President and APMA Immediate Past President Dr. Jeffrey DeSantis, who read aloud the Award’s inscription:
“In Recognition of His Innumerable and Invaluable Achievements and Efforts on Behalf of Podiatric Physicians, Their Patients, and the Healing Art of Podiatric Medicine…The California Podiatric Medical Association’s 2022 Legend Award is Presented to Franklin Kase, DPM -
“True Stars Rise to the Top Not by Chance but Through Purpose and Passion.”
A visibly moved Dr. Kase thanked the CPMA Board of Directors, Society Presidents, Committee Chairs, Delegates, and Alternates for their great honor and continuing support, thoughts, and prayers. After which, the entire House rose and gave Dr. Kase an exuberant, extended standing ovation.
THANK YOU, DR. KASE!
| 15 JULY • AUGUST • SEPTEMBER • 2022

Consider EPIFIX® and EPICORD® as part of your treatment protocols for acute and chronic wounds ©2021 MiMedx Group, Inc. All Rights Reserved. SB823.001 Dehydrated Human Umbilical Cord Allograft Dehydrated Human Amnion/Chorion Allograft ADVANCED TREATMENT OPTIONS mimedx.com
Waived Copayments:
NO GOOD DEED GOES UNPUNISHED.
By C. Keith Greer, Esq

In these tough financial times, Dr. Thoughtful decides to help his community by advertising that the practice will accept insurance payments as payment in full for all professional services. The community appreciates the offer and Dr. Thoughtful’s gift to the community is reciprocated as the practice flourishes. However, Dr. Lostbizness isn’t so happy, and notifies CMS/Medicare of what’s going on down the street. Is Dr. Thoughtful in trouble? Short answer: yes.
Dr. Thoughtful’s kind gesture is problematic because routine waiver of deductibles and copayments violates the federal Anti-Kickback Statute. Moreover, because it results in Medicare paying more than it should, it also violates the False Claims Act. Penalties include repayment demands, treble damages, civil monetary penalties, and potential imprisonment.
Under these laws, copayment waiver occurs whenever a health care provider is paid by an insurer but chooses not to collect a copayment. This includes: billing but not collecting a
copayment; writing-off copayment amounts; and routine use of “financial hardship” forms which state that the beneficiary is unable to pay the coinsurance/deductible (i.e., there is no good faith attempt to determine the beneficiary’s actual financial condition).
Although it is not illegal to write off a patient’s copay balance, in order to legally do so the provider must make a good faith individualized determination that the patient has a “demonstrable financial hardship.” In making the financial hardship determination, the provider should consider the following factors: “(i) the local cost of living; (ii) a patient’s income, assets, and expenses; (iii) a patient’s family size; and (iv) the scope and extent of a patient’s medical bills.”
The reason copayment waiver results in a false claim is that Medicare typically pays 80% of a provider’s actual charge. So, when a provider performs a $100 service, it reports the $100 and bills Medicare $80. When the copayment is collected, the patient pays $20, Medicare pays $80, and the actual charge

| 17 JULY • AUGUST • SEPTEMBER • 2022
continued on page 19 ▶
Dedicated to the Foot & Ankle surgeon





Stryker Foot & Ankle @strykerfoot.ankle footankle.stryker.com
Ankle Forefoot
Midfoot Hindfoot
is $100. Thus, Medicare was correctly charged. But when the copayment is waived, the patient pays $0, Medicare pays $80, and the “actual charge” is $80. Thus, in this scenario Medicare was overcharged $16 (i.e., 20% of the $80.00 “actual charge”). While the individual amount is small, over the course of four-year period the waived payments can push six figures.
Application of the Federal Anti-Kickback Statute:
The federal Anti‐Kickback Statute prohibits knowingly and willfully offering, paying, soliciting, or receiving remuneration to or from any person to induce such person to order or receive any items or service for which payment may be made under a federal healthcare program, unless the arrangement falls within a regulatory safe harbor. (42 USC 1390a‐7b(b)). Violations may result in up to a five-year prison term, $25,000 criminal penalties per incident, $50,000 in administrative penalties, treble damages, and exclusion from Medicare and Medicaid. (Id.; 42 CFR 1003.102).
The Office of Inspector General (“OIG”) has interpreted the Anti‐Kickback Statute to apply to waiving patient cost‐sharing amounts if “one purpose” of the waiver is to induce or reward federal program business, which is a difficult standard to defend against. In short, when a provider regularly waives copays in order to make his services seem cheaper to potential customers, he is offering a thing of value and violates the Anti-Kickback Statute.
Application of the False Claims Act:
Under the False Claims Act (“FCA”), a provider is liable for three times the damages plus False Claims Act penalties of up to $25,000 per violation, exclusion from Medicare, and up to 5 years imprisonment. In addition, OIG may also initiate administrative proceedings to exclude a person from Federal health care programs. Similarly, under the federal Civil Monetary Penalties Law (“CMPL”), a provider can be liable for penalties of $10,000 per item or service provided, treble damages, repayment of amounts paid, and exclusion from federal programs. (42 CFR 1003.102). The CMPL specifically defines “remuneration” to include waivers of copays and deductibles. (42 USC 1320a‐7a(i)).
CONCLUSION
While it seems like waiving copays is good for patients, CMS takes a different view. Routinely waiving copays can violate the Anti-Kickback Statute and the False Claims Act. Accordingly, doctors should: (1) never publish a policy of waiving copayments; (2) not have a policy of routinely waiving copayments; (3) assess any potential exposure for previously waived copayments; and (4) if potential liability is identified, consider speaking with a healthcare attorney about potential self-disclosure to CMS.
If you have questions about this article, or any other legal issue affecting your practice, please feel free to contact CPMA at 1(800)794-8988.

| 19 JULY • AUGUST • SEPTEMBER • 2022
YOU’VE COME A LONG WAY, DOCTOR
You’ve Come A Long WAY, DoCtor !
A Single Stroke of the Legislative Pen Can Write Podiatry into - Or Out Of - the Law
What you can do in your practice, how you get reimbursed, and the role podiatric medicine plays in - and will play in - California’s health care deliver y system all depends on the decisions made by lawmakers
What can do in your how you get reimbursed, and the role in - California’s health care delivery all depends on the decisions made lawmakers.
What you can do in your practice, how you get reimbursed, and the role podiatric medicine plays in - and will play in - California’s health care delivery system all depends on the decisions made by lawmakers.
Did you ever wonder how California’s podiatric physicians obtained the right to treat ankles along with feet, perform surgery and amputations, treat lower leg wounds, prescribe and administer medications? It did not just magically happen overnight. It has taken years of arduous work, hard-fought fights, lots of sweat, and some tears. And, the key to these victories (and many more) were Team CPMA/CalPPAC and the ability and resources needed to gain and maintain access to legislators in order to tell our story. We have an excellent story to tell, and in doing so, we have successfully removed many of the barriers to podiatric physicians’ ability to provide treatment and care.

Did you ever wonder how California’s podiatric physicians obtained the right to treat ank les along with feet, per form surger y and amputations, treat lower leg wounds, prescribe and administer medications? I t did not just magically
lots of sweat, and some tears. And, the key to these victories (and many more) were Team CPMA/CalPPAC and the ability and resources needed to gain and maintain access to legislators in order to tell our stor y We have an excellent stor y to tell, and in doing so, we have successfully removed many of the barriers to podiatric physicians’ ability to provide treatment and care.
Did you ever wonder how obtained to treat ankles along perform surgery treat lower and administer medications? It not magically happen overnight. It has taken years of arduous work, hard-fought fights, lots of sweat, and some tears. And, the key to these victories (and many more) were Team CPMA/CalPPAC and the ability and resources needed to to in order to tell our story. We have an excellent story to tell, so, we have removed barriers to treatment and care.
CPMA’s political action committee, the California Podiatric Political Action Committee (CalPPAC), is a bipartisan organization run by - and for - podiatric physicians to give podiatry the ability to identify, help elect and support lawmakers who understand, value, and fight to protect the podiatric medical profession, its physicians, and their patients.
CPMA’s political action committee, the California Podiatric Political Action Committee (CalPPAC), is a bipartisan organization run by - and for - podiatric physicians to give podiatry the ability to identify, help elect and support lawmakers who understand, value, and fight to protect the podiatric medical profession, its physicians, and their patients.

Today more than ever before, podiatric physicians must fight and advocate to keep the clinical care of their patients in their well-trained hands. However, successful legislative advocacy is contingent upon an integrated approach consisting of lobbying, grassroots activity, and political action through CPMA and the financial resources provided by CalPPAC for legislative advocacy.
Today more than ever before, podiatric physicians must fight and advocate to keep the clinical care of their patients in their well-trained hands. However, successful legislative advocacy is contingent upon an integrated approach consisting of lobbying, grassroots activity, and political action through CPMA and the financial resources provided by CalPPAC for legislative advocacy.
Making contributions to CalPPAC is a way to ensure that podiatric medicine continues to have a seat at the decision-making table and that podiatry’s voice is heard when and where it counts!
CPMA’s political action committee, the California Podiatric Political Action Committee (CalPPAC ), is a bipar tisan organization run by - and protect the podiatric medical profession, its physicians, and their patients hands. However, successful legislative advocac y is contingent upon an integrated approach consisting of lobbying, grassroots activity, Mak ing contributions to CalPPAC is a way to ensure that podiatric medicine continues to have a seat at the decision-mak ing table and that podiatr y ’s voice is heard when and where it counts!
Making contributions to CalPPAC is a way to ensure that podiatric medicine continues to have a seat at the decision-making table and that podiatry’s voice is heard when and where it counts!
Team CPMA/CalPPAC has been behind ever y pro -podiatric medicine bill that has become California law! And, this dynamic duo has STOPPED many bills that would have hur t podiatric physicians, their patients and profession.

Team CPMA/CalPPAC has been behind every pro-podiatric medicine bill that has become California law! And, this dynamic duo has STOPPED many bills that would have hurt podiatric physicians, their patients and profession.
Team CPMA/CalPPAC has been behind every pro-podiatric medicine bill that has become California law! And, this dynamic duo has STOPPED many bills that would have hurt podiatric physicians, their patients and profession.
A Single Stroke of the Legislative Pen can write Podiatry into - or out
of - the Law.
Please make your CalPPAC contribution TODAY!
Please make your CalPPAC contribution TODAY!
Please make your CalPPAC contribution TODAY!
Scan (securely) the QR Code below with your cellphone camera; or log onto calppac.square.site, or send your check - made payable to CalPPAC and mail to 7311 Greenhaven Drive, Suite 208, Sacramento, CA 95831

Scan (securely) the QR Code below with your cellphone camera; or log onto calppac.square.site, or send your check - made payable to CalPPAC and mail to 7311 Greenhaven Drive, Suite 208, Sacramento, CA 95831
Scan (securely) the QR Code below with your cellphone camera; or log onto calppac.square.site, or send your check - made payable to CalPPAC and mail to 7311 Greenhaven Drive, Suite 208, Sacramento, CA 95831

Thank you for your time, consideration and support,
Thank you for your time, consideration and suppor t,
Thomas Elardo, DPM Chair, CalPPAC
Thomas CalPPAC
!
If You Don’t Have a Seat at the Table, You’re On The Menu!
Thomas Elardo, DPM Chair, CalPPAC
Thank you for your time, support,
A Single Stroke of the Legislative Pen Can Write Podiatry into - Or Out Of - the Law
By Jon A. Hultman, DPM, MBA, CVA

Engineering: THE KEY TO ACHIEVING QUALITY IN MEDICINE
Agoal consistently mentioned by everyone proposing change in healthcare delivery is quality; yet, few physicians understand the definition of this term as it is applied to the practice of medicine by employers and third party payers. Some physicians argue that they provide a superior quality of care and, therefore, should be paid more for the care they give; however, these doctors are usually unable to demonstrate what it is that sets their care apart as being “of higher quality” – why it should be considered to be worth more. John M. Burns, former Vice President and Medical Director for Honeywell, Inc., summed up what large purchasers of health care products define as quality: “Quality in health care should be defined in the same way that all services and products are acquired, on the basis of the specifications of the purchaser.”
For a period of time, Americans considered Japanese autos as inferior to ours. When higher quality cars at affordable prices began arriving from Japan in the United
States, opinions changed because people could “see” the difference. The quality of a service, however, is less easily “seen” than the quality of a product, and quality is especially difficult to “see” in medicine. As stated above by John Burns, in highly competitive businesses, the customer is the one who defines “quality.” The same will be true for medicine. This means that quality will be defined by all of medicine’s “customers”: patients, employers, government, and other third-party payers.
At one time, quality was defined as the absence of defects. In today’s more competitive markets, quality has become the basis of competition, with its achievement requiring more than this simple “absence of defects”. In their 1991 book, Quality or Else, authors Lloyd Dobyns and Clare Crawford-Mason define quality as, “a better way of producing goods and services, a way that eliminates waste, gives employees pride in their work, and keeps the customer coming back for more. As you produce quality, productivity automatically goes up and
| 21 JULY • AUGUST • SEPTEMBER • 2022
continued on page 22 ▶
costs automatically go down.” This definition is equally useful as it pertains to the delivery of health care, especially since doctors “compete” in the arenas of both quality and price.
Both doctors and patients perceive good treatment outcomes as quality, and this is not in conflict with the use of statistical measurement. Once a majority of doctors are able to agree upon a desired outcome, that outcome can be quantified in terms of how consistently, and at what price, it is achieved by each doctor. Quality treatment becomes defined as that which consistently achieves the desired outcome at the minimum cost. The fact that a “world renowned surgeon” performs a procedure at a “world class hospital,” is irrelevant if a “lesser known” doctor at a competing institution can achieve the same, or better, outcome consistently and at a lower cost.
The key to improving consistency, and thus raising quality, is standardization of the process tasks utilized by a practice. The McDonalds Corporation is a useful example of effective process standardization. While McDonalds may not deliver your idea of the best hamburger in the world, the company has determined the quality level of the hamburger it wants to achieve and has implemented standardized processes that consistently deliver this pre-defined quality. Jet Blue is another company that has been well served by its use of standardization. When the company was a startup, its goal was to do a better and cheaper job than its competitors. To
achieve this goal, Jet Blue focused on standardization. One of its strategies was to fly the same model of plane for all its routes, thus making it possible for pilots and crews to handle any flight, for maintenance to be expedited, and for errors to be kept to a minimum. Creating this type of standardization which achieves consistent, superior outcomes in both clinical and business processes, can also help a medical practitioner achieve better results while lowering costs.
The term “customer focus” is often used when defining quality in medicine. Doctors believe that customer focus simply means that they should have compassion for their patients, delivering the best level of care they are capable of. This, however, is merely expected doctor behavior. Any doctor who participates in a contract or network is expected to be well trained and render compassionate, high-quality care; this is the entry level qualification necessary just to “play the game.” True quality care is also customer focused. In today’s medicine, customer focus is not simply defined by these expected, entry-level attributes; rather, it is a desired outcome that can be measured statistically by cycle time (the total time a patient spends in the treatment facility). Patients value their time, and when they encounter a medical facility that in addition to providing quality treatment, recognizes the value of their time, they perceive that the practice is offering them total quality care. The primary patient complaints

22 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
regarding HMOs have not been about the quality of the treatment received, but about the poor access to that care and the length of time spent in facilities after arriving at an appointed time. Several years ago, when national news agencies were focusing on “bad quality” at VA hospitals, the focus was not on the actual care that patients received, but rather, on how long it took patients to access that care and how long they waited to be seen after arrival at the facility.
Doctors who are able to reduce their patients’ total cycle time will be supplying the most efficient care – the kind of high quality and cost-effective care that is valued by patients. The first step to achieving this higher level of quality is to identify inefficiencies in a practice’s business processes.
Procedures are constantly changing in medicine, and doctors understand the need to “keep up.” Today, some treatment procedures learned in medical school ten or twenty years ago might even be considered malpractice! Doctors must be aware that what is true for the medical procedures performed by their practices is also true for its business components; business processes too must be continuously monitored, updated, and made more efficient. Fortunately, the same basic sciences that doctors have studied in their premedical training can be applied to evaluate business processes as well.
In a medical practice, treatment procedures, unlike business processes, are under the direct supervision of the physician throughout regular business hours. For this reason, they are easy for him/her to manage and/ or change and are generally of high quality. On the other hand, managing business processes is difficult for many. The typical practitioner has received little business training

in medical school, and compounding this obstacle is the fact that a practice’s business processes are usually “out of the doctor’s sight” during normal business hours, with him/ her being unaware of their progress. Because of this, s/ he experiences difficulty in supervising or changing these processes, and they easily become more lengthy, complex, and inefficient. It is important for a doctor to understand and become more involved in monitoring these constant, underlying business processes. With effective process monitoring, an efficient, well-run practice will allow a doctor more “patient time” – a win-win outcome that increases both physician productivity and patient satisfaction.
In spite of the fact that doctors are well versed in scientific laws that can be applied to create efficient workflow in a medical practice, they often create business processes unscientifically – ones that often defy the laws of physics. Because the high cost of practice overhead is due in large part to the inefficiencies that are created in processes that are spiraling out of control, streamlining these processes is the most important thing doctors can do to increase the quality of their patient care, raise levels of patient satisfaction, lower overall costs, and increase the profit of their medical practices. As they have done with medical treatment, doctors must learn to apply scientific laws to the business processes in their practices, keeping in mind that these laws remain “relatively fixed” in spite of the constantly changing economic environment. Laws of physics that can be applied to accomplish the kind of quality that matters to doctors, patients, and payers will be covered in my next article in the California Podiatric Physician.
| 23 JULY • AUGUST • SEPTEMBER • 2022


The most accurate diagnostic method for infectious dermatitis, combined with ease of use and rapid results. Web Space PCR Testing ERYTHRASMA, TINEA CANDIDAL INTERTRIGO? only available at BakoDx The BakoDx Web Space PCR Assay tests for: • Corynebacterium minutissimum • Gram-negative bacteria • Staphylococcus aureus* *If positive, reflex to mecA (methicillin resistance) BACTERIA • Dermatophytes • Candida spp FUNGI All results should be utilized in context with clinical presentation. Currently unavailable in NY. Bako Diagnostics | 855-933-1305 | bakodx.com/webspace SCAN ME
Tips for Developing or REDEVELOPING YOUR TRAINING PROGRAMS
 By Tina Del Buono, PMAC
By Tina Del Buono, PMAC









































The year 2020 brought about more changes than any of us could have imagined. Not only in our personal lives, but in the medical practice as well. We have had to adjust with how we work together and serve our patients.







With the many changes our offices have encountered it has been easy to get derailed from some of the critical fundamentals of running a successful medical practice. One of these important areas has been training and continued improvement of staff skills which is necessary to keep our practices running efficiently and profitably. For reasons that are understandable training and continuing education for staff has been a struggle for practices to keep up and improve on.

I have heard from many offices that lost valuable staff members and have had difficulty replacing them, even two years later. This has caused the need to adjust positions, job tasks, and schedules and many things that we use to do have been put on hold.













Whenever there is any type of change, we must look at and possibly re-invent systems to stay efficient, there is no better time than now to begin to evaluate what would be necessary

to create a great onboarding and continued training program for the practice.
It is not that we do not know the necessity and value of training and continued education for our practices, because this is how they will grow and have a more positive impact in our communities. Assistants play an important role in the advancement of the profession of Podiatry and in improving patient care.
When physicians take the time to train their assistants providing ongoing education, they are not only creating value for the office, but they are creating value for their medical staff. It is a known fact that when staff members learn new skills it increases their motivation to learn more, creates engagement with the practice and the quality of patient care goes up.
All physicians and their managers want to have great training and continuing education for their staff. At this point it is more of knowing how one develops and implements these training programs along with keeping the rest of the office running during this, “recovery time”
Most reasons training doesn’t happen is the mindset that think it takes hours of time and there just isn’t that kind of
| 25 JULY • AUGUST • SEPTEMBER • 2022
continued on page 27 ▶
2022 WESTERN SPONSORS
www.picagroup.com www.ArizeClinical.com
DIAMOND GOLD SILVER
www.stryker.com www.treace.com www.paragon28.com www.mimedx.com www.organogenesis.com
https://bakodx.com www.extremitymedical.com
BRONZE PROGRAM
https://thepodiatry.foundation/ https://sealexfx.com www.integralife.com www.averitaspharma.com www.hfxforpdn.com/healthcare-providers www.pangealab.com www.sanfordhealth.org


www.tricemedical.com

WESTERN FOOT AND ANKLE CONFERENCE 2022 5
time during the day to set aside. When in reality people learn better with bit-sized training sessions. They can retain what was taught and then have time to practice it.
First, decide on a task that needs to be trained on. Write a simple protocol for it by bullet-pointing all the steps, simply and clearly to get the result. Then set aside 15-20 minutes a week that training will happen. If you have a new employee this will be more as training will happen throughout the day for the first couple of months, but that is where a training mentor comes in.
Have tasks that are to be trained/re-trained in written form (protocols) and visual/audio form (recorded video). This way they can be reviewed easier without having to ask someone physically to show them again. Make a Dropbox folder that houses all your training protocols and videos for easy access.
Here are a few more ideas that may help your practice to redevelop its training program.
• Know what each person is to accomplish each day. (Job description with job tasks)
• Have clear protocols for the defined job tasks of each position/person.
• Employees need to know what they will be taught and can read the protocols and watch other staff members do the tasks visually prior to be taught themselves.
• Establish routines to ensure what is expected from each staff member can be accomplished each day.
• Create a training timeline for various tasks and the time allotted for when the training will occur so the trainee will know what to expect.
• Assign a Training Mentor to staff who are learning various tasks for the first time, so they have one person to go to for help and explanation.
• When possible, involve the physician in trainings. Teaching staff allows for the physician to have the opportunity to give praise, which is a motivator
• When you invest in staff members it creates environment of trust, where employees are not afraid to ask questions.
• Physicians will learn staff member’s individual motivators which will allow them to understand each staff member better.
• Continued training offers opportunities for learning and advancement.
• When you implement a good, continued training program staff do not get bored with their job.
• When staff train together, they develop connections with each other which can create better team relationships. Staff that learn together become more self-motivated, loyal, and dedicated to their employers. It is a fact that businesses that have self-motivated employees have less turnover and overall higher profits. The more motivated your staff is the higher your office productivity will be and the better-quality patient care that will be given. Investing in your staff’s education is essential to having a successful practice.
If you would like more information on developing training programs for your practice, just email me at Tina@ toppractices.
Tina Del Buono, PMAC, CPC Director/Performance Consultant and Coach: Top Practices Virtual Practice Management Institute
Author: Truths from the Trenches, The Complete Guide to Creating a High-Performing Medical Team
| 27 JULY • AUGUST • SEPTEMBER • 2022
Credentialing & Breaks 2 22 HOD









28 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
Bakodx Representative Jenn Watson
Credentialing & Breaks









| 29 JULY • AUGUST • SEPTEMBER • 2022
Credentialing & Breaks










30 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
House of Delegates 2 22









| 31 JULY • AUGUST • SEPTEMBER • 2022
Naleen L. Prasad, DPM, President, Delegate, Alameda/ Contra Costa Podiatric Medical Association
2022 House of Delegates











32 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
Peter Bretan, MD, Immediate Past President, California Medical Association
Derick Ball, DPM, Delegate, Los Angeles County Podiatric Medical Association
Laura Pickard, DPM, President, American Podiatric Medical Association
2022 House of Delegates








| 33 JULY • AUGUST • SEPTEMBER • 2022
Newly elected members of the 2022-2023 CPMA Board of Directors: Ebonie Vincent, DPM, Director-at-Large; Heather McGuire, DPM, Director-at-Large; Holly Spohn-Gross, DPM, President; Diane Koshimune, DPM, President-Elect
Ebonie Vincent, DPM, Delegate, Orange County Podiatric Medical Association
Michael Cornelison, DPM, FACFAS, President, American College of Foot and Ankle Surgeons
James Christina, DPM, Executive Director, American Podiatric Medical Association.
Robin Farias-Eisner, MD, PhD, MBA, President, Western University of Health Sciences
2022 House of Delegates









34 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
C. Keith Greer, JD, General Counsel, California Podiatric Medical Association
Kathleen Satterfield, DPM, Dean, College of Podiatric Medicine, Western University of Health Sciences
Diane Koshimune, DPM, FACFAS President-Elect
2022 House of Delegates









| 35 JULY • AUGUST • SEPTEMBER • 2022
Jon Hultman, DPM, MBA, CVA, Executive Director, California Podiatric Medical Association
Student Delegates/Alternates/Representatives – Harsh Varshney (WesternU); Christopher Overton (CSPM); Andrew Attia (CSPM); CPMA President Holly Spohn-Gross, DPM; Michael Ogbonna (CSPM), and Robert Erickson(WesternU)
2022 House of Delegates










36 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
Ching-Hua Wang, MD, PhD, President, Samuel Merritt University
Ryan Spencer, Legislative Counsel, California Podiatric Medical Association
Eric Stamps, DPM, Dean, California School of Podiatric Medicine at Samuel Merritt University
Carolyn McAloon, DPM, Member, Podiatric Medical Board of California; Past President, California Podiatric Medical Association
2022 House of Delegates









| 37 JULY • AUGUST • SEPTEMBER • 2022
2022-2023 CPMA Board of Directors: Arman Kirakosian, DPM, Director-at-Large; Ronald Jensen, DPM, Parliamentarian; Ebonie Vincent, DPM, Director-at-Large; Heather McGuire, DPM, Director-at-Large; Holly Spohn-Gross, DPM, President; Jon Hultman, DPM, MBA, CVA, Executive Director; Diane Koshimune, DPM, President-Elect; Phong Le, DPM, SecretaryTreasurer; Douglas Taylor, DPM, Director-at-Large; Alan Sue, DPM, Director-at-Large. Not pictured Diane Branks, DPM, Immediate Past President
2022 House of Delegates









38 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
Adam Howard, DPM, Immediate Past President
Neil Mansdorf, DPM, Chair, Credentials Committee and Delegate, Orange County Podiatric Medical Association.








| 39 JULY • AUGUST • SEPTEMBER • 2022
Thomas Elardo, DPM, Chair, CalPPAC, Past President, Delegate, Santa Clara Valley Podiatric Medical Association
Ross Taubman, DPM, President, PICA
2022 House of Delegates
2022 House of Delegates







40 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
Patrick (PJ) Andrus, MBA, CAE, Executive Director, American College of Foot and Ankle Surgeons
2 22 AWARDS




| 41 JULY • AUGUST • SEPTEMBER • 2022
(l to r) Jeffrey DeSantis, DPM, Past President, American Podiatric Medical Association and California Podiatric Medical Association, and Jon Hultman, DPM, MBA, CVA, Executive Director and Past President, California Podiatric Medical Association announcing that Dr. Franklin Kase is the first-ever recipient of CPMA’s Legend Award
Thomas Elardo, DPM, Chair, CalPPAC and CPMA Past President (r) presented the 2022 CalPPAC Award for Society with Largest Total Contribution and the 2022 CalPPAC Award for Society with Largest Percentage of Members Contributing to Ara Kelekian, DPM, President, Delegate, Los Angeles County Podiatric Medical Association
Thomas Elardo, DPM, Chair, CalPPAC, (r) presented the CalPPAC Honorable Mention Award to Jisun Julia Lee, DPM, Delegate, Santa Clara Valley Podiatric Medical Association
(l to r) CPMA Executive Director Jon Hultman, DPM, MBA, CVA, presented the Executive Director Award to CPMA Immediate Past President Adam Howard, DPM





42 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
Holly Spohn-Gross, DPM, President-Elect, presented Ara Kelekian, DPM, President, Delegate, Los Angeles County Podiatric Medical Association with CPMA’s Step Up Award
Holly Spohn-Gross, DPM, President-Elect ( r) presented Faridi Sherieff, DPM, President, Delegate, San Luis Obispo/Santa Barbara Podiatric Medical Society with CPMA’s 2022 Local Society President of the Year Award
CPMA and APMA Past President Jeffrey DeSantis, DPM presenting CPMA’s Inaugural Legend Award to CPMA Past President, Health Committee, Chair and PIAC Representative Franklin Kase, DPM, FACFAS
Holly Spohn-Gross, DPM, President-Elect, presented Peter Bretan, MD, Immediate Past President, California Medical Association with CPMA’s President Award on behalf of CPMA President Diane Branks, DPM, FACFAS, who was unable to attend
Holly Spohn-Gross, DPM, President-Elect, presented Ebonie Vincent, DPM (l) with CPMA’s Rising Star of the Year Award
22


HOD LUNCH






| 43 JULY • AUGUST • SEPTEMBER • 2022
2
2022 HOD Lunch









44 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
Holly Spohn-Gross, DPM, President-Elect











| 45 JULY • AUGUST • SEPTEMBER • 2022 2022 HOD Lunch
2022 HOD Lunch










46 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION







| 47 JULY • AUGUST • SEPTEMBER • 2022
2022 HOD Lunch
William P. Scherer, DPM, MS, DABFAS, BakoDx Senior Podiatric Medical Advisor
THANKS FOR ITS GENEROUS SUPPORT bakodx.com
2022-2023 CPMA BOARD OF DIRECTORS











| 49 JULY • AUGUST • SEPTEMBER • 2022
Diane D. Branks, DPM Immediate Past President Ontario, CA 91761
Phong H. Le, DPM Secretary-Treasurer Sacramento, CA 95828
Arman A. Kirakosian, DPM Director-at-Large San Francisco, CA 94121
Holly Spohn-Gross, DPM President Lake Isabella, CA 93240
Diane M. Koshimune, DPM President-Elect San Jose, CA 95119
Heather R. McGuire, DPM Director-at-Large Ventura, CA 93003
Alan W. Sue, DPM Director-at-Large Mountain View, CA 94040
Douglas M. Taylor, DPM Director-at-Large Walnut Creek, CA 94596
Jon A. Hultman, DPM, MBA, CVA Executive Director Sacramento, CA 95831 (916) 448-0248 / (800) 794-8988
Ronald D. Jensen, DPM Parliamentarian Modesto, CA 95355
Ebonie E. Vincent, DPM Director-at-Large Long Beach, CA 90813
President’s Reception 2 22







50 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
President’s Reception












| 51 JULY • AUGUST • SEPTEMBER • 2022
President’s Reception










52 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
President’s Reception











| 53 JULY • AUGUST • SEPTEMBER • 2022
President’s Reception












54 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
President’s Reception










| 55 JULY • AUGUST • SEPTEMBER • 2022
2 22
CPMA VISION Leadership Lunch








56 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION









| 57 JULY • AUGUST • SEPTEMBER • 2022
CPMA VISION Leadership Lunch







58 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
Dylan Bach MD, MBA, Bach Diagnostics Founder & President, Director, Clinical Pathology
CPMA VISION Leadership Lunch









| 59 JULY • AUGUST • SEPTEMBER • 2022
Adam Howard, DPM, Past President, Chair, Corporate Relations Committee Arman Kirakosian, DPM, Director-at-Large
CPMA VISION Leadership Lunch







60 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
Holly Spohn-Gross, DPM, President, CPMA; Dylan Back MD, MBA, President, Bach Diagnostics
CPMA VISION Leadership Lunch









| 61 JULY • AUGUST • SEPTEMBER • 2022
Ebonie Vincent, DPM, Director-at-Large and Phong Le, DPM, Secretary-Treasurer
Alan Sue, DPM, Director-at-Large
Holly Spohn-Gross, DPM, President, California Podiatric Medical Association
Thomas Elardo, DPM, Past President, Chair, CalPPAC
Naleen L. Prasad, DPM, President, Alameda/Contra Costa Podiatric Medical Association
THANKS FOR ITS GENEROUS SUPPORT bachdx.com










| 63 JULY • AUGUST • SEPTEMBER • 2022
Sponsor/CPMA Corporate Member
22 RECEPTION
Western
2
Western Sponsor & CPMA Corporate Member Reception










64 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
Western Sponsor & CPMA Corporate Member Reception












| 65 JULY • AUGUST • SEPTEMBER • 2022









66 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
Western Sponsor & CPMA Corporate Member Reception









| 67 JULY • AUGUST • SEPTEMBER • 2022
Western Sponsor & CPMA Corporate Member Reception








68 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
2022 Western In the Hall









| 69 JULY • AUGUST • SEPTEMBER • 2022
2022 Western In the Hall










70 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
2022 Western In the Hall











| 71 JULY • AUGUST • SEPTEMBER • 2022
2022 Western In the Hall










72 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
Spotlight on Education






| 73 JULY • AUGUST • SEPTEMBER • 2022
Western Keynote Speaker Gary Hall, Jr, Olympic and World Swimming Champion
Edward Barnes, MD Timothy Dutra, DPM, MS
Kevin Rosenbloom, CPed
Spotlight on Education










74 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
Kevin Kirby, DPM
Jesus C. Vazquez, PMAC
Daniel C. Fulmer, DPM
Richard Blake, DPM
Spotlight on Education










| 75 JULY • AUGUST • SEPTEMBER • 2022
Timothy P. Shea, DPM, DABFAS
Jay Spector, DPM, FAAPSM
Doug Richie, DPM, FACFAS
Western Workshop Crew: Caitlyn Lo, Tiffany Duarte, Brian Wong, Jennifer Mansdorf, and Neil Mansdorf, DPM, Director, Western Workshops.
Spotlight on Education











76 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
Bruce Dobbs, DPM and Anjali Dayal, ESQ.
Jarrod Shapiro, DPM, FACFAS, FACPM
Spotlight on Education









| 77 JULY • AUGUST • SEPTEMBER • 2022
Martina Randall, DPM
Tiffany Facile, MHA, BS, RN
Stephen Wan, DPM, FACFAS
Joseph Park, DPM, FACFAS
Spotlight on Education






78 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
William Tettelbach, MD
Roya Mirmiran, DPM, FACFAS
Gabriel Halperin, DPM, DABFAS
Spotlight on Education







| 79 JULY • AUGUST • SEPTEMBER • 2022
Bhanu Sud, MD
James Collen, MD
Jonathan Labovitz, DPM, FACFAS, CHCQM
Ross E. Taubman, DPM, FACFAS
OUT & ABOUT











80 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION











| 81 JULY • AUGUST • SEPTEMBER • 2022
Devon Glazer, DPM, FACFAS, Western Education Chair; Gary Hall, Jr, Olympic and World Swimming Champion, Western Keynote Speaker; Jonathan Labovitz, DPM, FACFAS, CHCQM, Western General Chair.
OUT & ABOUT
2022 Western Sponsors



82 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
Bakodx: Tom Sager; Devon Glazer, DPM, Chair, Western Education Committee; Holly Spohn-Gross, DPM, President, California Podiatric Medical Association; Jenn Watson; Jonathan Labovitz, DPM, Chair, Western Foot & Ankle Conference
Paragon28: Ben Snider; Dylan Tartz; Isabella Roldan; Mindy Goodrich; Holly Spohn-Gross, DPM; Jonathan Labovitz, DPM, and Devon Glazer, DPM
Arize: Jonathan Labovitz, DPM; Mark Sabory; Steven Whisler; Irina Roulin; Melanie Shelton; Holly Spohn-Gross, DPM; Ron Verrilla; Brian Jung, and Devon Glazer, DPM



| 83 JULY • AUGUST • SEPTEMBER • 2022
PICA: Jonathan Labovitz, DPM, Chair, Western Foot & Ankle Conference; James Gray; Brian Cesario; Holly Spohn-Gross, DPM, President, California Podiatric Medical Association; Devon Glazer, DPM, Chair, Western Education Committee; Ross Taubman, DPM, President, PICA
Extremity Medical: Devon Glazer, DPM; Lindsay Reynolds; Holly Spohn-Gross, DPM; Ira Benson; Jonathan Labovitz, DPM
Treace: Jonathan Labovitz, DPM; Hala Yim; Heather Dwyer; Holly Spohn-Gross, DPM; Devon Glazer, DPM
2022 Western Sponsors



84 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
Stryker: Devon Glazer, DPM, Chair, Western Education Committee; Lindsey Luke; Kevin McGuire; Holly Spohn-Gross, DPM, President, California Podiatric Medical Association; Ovi Muresan; Shannon McGuire; Jonathan Labovitz, DPM, Chair, Western Foot & Ankle Conference
Organogenesis: Devon Glazer, DPM; Jonathan Labovitz, DPM; Nick Stellings; William Shiebler, and Holly Spohn-Gross, DPM
Bach Diagnostics: Jonathan Labovitz, DPM; Keith McFatridge; Amber McComb; Holly Spohn-Gross, DPM; Devon Glazer, DPM





| 85 JULY • AUGUST • SEPTEMBER • 2022
Arthrex: Jonathan Labovitz, DPM; Roman Ledman; Amy Whirlow; Ryan Yoshida; Josh Heinold; Holly Spohn-Gross, DPM, and Devon Glazer, DPM
Pangea Lab: Shelly Sarain; Abigail Kang; Maria Burton; Holly Spohn-Gross, DPM; Jonathan Labovitz, DPM, and Devon Glazer, DPM
Averitas Pharma: Devon Glazer, DPM; Jonathan Labovitz, DPM; Dana Brown; Mike Lippman; Holly Spohn-Gross, DPM
Nevro: Jonathan Labovitz, DPM; Brian Hall; Daniel Stabile; Holly Spohn-Gross, DPM; Devon Glazer, DPM
THANK YOU FOR YOUR SUPPORT THE WESTER N Foot and Ankle Conference
MiMedx: Jonathan Labovitz, DPM; Jerem Sutherland; Mark Garcia; Stephen Stafford; Holly Spohn-Gross, DPM, and Devon Glazer, DPM
ON YOUR TOES
GOVERNOR SIGNS CPMA BILL TO ADDRESS
PODIATRIC X-RAY TECHNICIAN SHORTAGE
California Governor Gavin Newsom has signed Assembly Bill 1704, sponsored by the California Podiatric Medical Association (CPMA) and authored by Assemblymember Phillip Chen, to address the chronic shortage of podiatric x-ray technicians.
AB 1704 will help alleviate the existing barriers to education and to accommodate the specialized podiatric setting by providing a simplified pathway (which is more accessible, flexible, and cost-effective) that will enable podiatric medical assistants to take the state-limited permit exam, so they may assist podiatrists in taking in-office x-rays.
“CPMA thanks Governor Newsom for signing AB 1704, which will help to ensure that podiatric physicians will be able to provide necessary care to their patients in a timely manner, which can often make all the difference in the world,” said CPMA President Holly Spohn-Gross, DPM.
CPMA Working for YOU!
CIGNA HITS PAUSE TO REEVALUATE BURDENSOME MODIFIER 25 POLICY IN THE FACE OF FIERCE CPMA ADVOCACY
Cigna has delayed the August 13, 2022, implementation of its recently announced policy to require the submission of medical records with all Evaluation and Management (E/M) claims with CPT 99212-99215 and modifier 25 when a minor procedure is billed.
CPMA had serious concerns with Cigna’s policy change as it would result in significant, unnecessary administrative burden and compliance cost to physician practices, would delay patient care, and would create duplicate requests thus wasting health care dollars. The policy also lacks clarity on the product types impacted, is inconsistent with industry standards and CMS guidance, and appears to violate California law.
CPMA, the California Medical Association (CMA), and other stakeholders reached out to Cigna regarding these serious concerns and urged the payor to rescind the policy. Due to this advocacy, Cigna has delayed implementation and the policy is under additional review.
CPMA believes a more collaborative approach to identify alternative policies and methods for cost containment— including provider education on proper coding practices that do not bluntly penalize physicians using the modifier appropriately—will prove more effective and less costly in the
long term. The Association will continue to work with Cigna to address our concerns and will provide updates as more information becomes available.
CPMA Working for YOU!
REPORTING FOR PROVIDER RELIEF FUND PAYMENTS RECEIVED IN PERIOD 4 BEGINS JANUARY 1, 2023
Reporting for period 4 ― for Provider Relief Funds (PRF) payments exceeding $10,000 received July 1-Dec. 31, 2021 ― will open January 1, 2023. Recipients of period-4 payments must use their funds on eligible pandemic-related expenses by December 31, 2022.
Allowable Expenses
Under the Provider Relief Fund, allowable expenses are those used to prevent, prepare for and respond to the coronavirus and may include healthcare related expenses or general and administrative-related expenses. All recipients of PRF payments are subject to auditing.
Examples of eligible expenses common for practices include:
• N95s, surgical masks, temperature-monitoring devices, and other infection-control supplies
• Ventilators, improved filtration systems, and other infection-control equipment
• Mortgage or rent on practice office
• Employee health insurance, hiring bonuses, recruitment and retention payments to expand or maintain patient care capacity, and other fringe benefits.
Providers should read the HRSA’s explanation of allowable expenses for additional guidance, https://www.hrsa.gov/ provider-relief/reporting-auditing
HHS will look very closely at how funds are used, so it is important to be precise in reporting. Funds must have been used for healthcare-related expenses before they can be applied to lost revenue.
Providers should maintain records related to their reporting for a minimum of five years.
Reporting requirements
HRSA has a “How to Report” webpage with instructions broken into three main steps: registering to use the portal, reading the reporting requirements notice, and completing and submitting the report at https://www.hrsa.gov/ provider-relief/reporting-auditing
86 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
When registering to use the portal, providers will want to have certain information on hand, such as their tax ID or employer identification number and PRF payment information. Providers who submitted a PRF report during a prior reporting period do not need to re-register.
The reporting requirements notice provides details on how to report on the use of the funds and lists the required reporting data categories.
Most COVID-19 relief programs have stringent requirements that funds from multiple sources not be used to cover the same expenses. The best way to avoid having expenses disallowed in a follow-up audit is to maintain good records of which expenses were covered by specific programs, whether EIDL, Paycheck Protection Program or HHS’s Provider Relief Fund.
Again, the portal for providers to begin reporting the use of those funds begins January 1, 2023, if the payments exceeded $10,000. Providers will report the use of their period-4 funds through the U.S. Health Resources & Services Administration’s PRF reporting portal at https://www.hrsa.gov/ provider-relief/reporting-auditing
(Source: CDA 6/8/2022)
2023 MINIMUM WAGE HIKE BRINGS CHANGES FOR CALIFORNIA EMPLOYERS
California doesn’t have just one minimum wage—it has many.
California has several minimum wage laws that can often be confusing and overwhelming for businesses. In California, the minimum wage is determined by a law that links it to the cost of living. Additionally, many cities and counties across the state have legislated their own minimum wage laws that are even higher than federal or state minimum wage.
Current California Minimum Wage
The minimum wage in California for 2022 for employers with 25 or fewer employees is $14 an hour. Employers with 26 or more employees pay $15 per hour.
The minimum wage in California was set to increase yearly until it reached $15/hour in 2022. However, on July 27, 2022, a new minimum wage of $15.50 was set to go into effect on January 1, 2023, due to the high inflation rate in the past year. This is for all sizes of employers!
Local regulations add yet another layer of complexity to California’s labor laws. If you operate in more than one location, you could be subject to multiple different minimum wage levels in a single day. Employers should check the city websites where their practices are located.
How should small business owners prepare for minimum wage increases?
While minimum wage increases may pose a challenge for small businesses, there are ways to stay ahead of the curve. Small business owners can avoid being caught off guard by keeping up to date on changes to the minimum wage and adjusting prices and compensation as necessary.
If a minimum wage increase is on the horizon, it’s important to look at your budget and financial records, such as operational costs, in preparation for the change.
(Paycor 10/18/2022)
CALIFORNIA LAW CREATES

EXEMPTION FOR PRESCRIBERS MEETING SPECIFIC CRITERIA
Under a law that takes effect in 2023, California prescribers can request an exemption from the current requirement to electronically prescribe all medications if they register with the California State Board of Pharmacy and state that they meet one or more specified criteria. Although the law takes effect January 1, 2023, the Board of Pharmacy is responsible for creating the prescriber registration and currently does not expect to have it ready by the first of the year. The new law also authorizes a pharmacy to decline to dispense an electronic prescription submitted via software that fails to meet any specified criteria.
Healthcare practitioners in California who issue 100 or fewer prescriptions in a calendar year could receive an exemption from the state’s existing law requiring practitioners to electronically prescribe all medications.
| 87 JULY • AUGUST • SEPTEMBER • 2022
NEW
E-PRESCRIBING
BUT the exemption is not automatic. Authored by Assemblymember Jim Wood (D-Santa Rosa), and signed into law by Governor Gavin Newsom in late September, AB 852 requires that prescribers meet designated criteria and take specified action at a date to be determined after the law takes effect in January 2023.
The exemption will be available to prescribers who register with the California State Board of Pharmacy and state that they meet one or more of the following:
• They issue 100 or fewer prescriptions per calendar year.
• Their practice is in the area of an emergency disaster declared by a federal, state, or local government.
• They are unable to issue electronic data transmission prescriptions due to circumstances beyond their control.
Prescriber registration with the Board of Pharmacy will be enabled in 2023.
Again, while the law takes effect January 1, the Board of Pharmacy does not expect to have it ready by the first of the year. CPMA is in contact with the board to help make the registration process goes as smoothly as possible and will keep members updated about its availability. The board has confirmed the registration will be online and annual, with email reminders sent to registered prescribers.
Prescribers who wish to be exempted from the electronic prescribing requirement should carefully evaluate and forecast their prescribing numbers to confidently determine whether they will fall below the threshold of 100 or fewer prescriptions per calendar year. Prescribers should do this before they register with the Board of Pharmacy. Until successful registration with the board, and for all prescribers who issue more than 100 prescriptions annually, electronic prescribing for all medications remains the law.
A few other exemptions for the existing e-prescribing requirements already exist, such as due to a temporary service interruption or technological failure.
E-prescriptions submitted via non-compliant software can be declined
The new law also authorizes a pharmacy, pharmacist, or other authorized practitioners to decline to dispense or furnish an electronic prescription submitted via software that fails to meet any one of the specified criteria, including compliance with the federal Health Insurance Portability and Accountability Act of 1996.
While CPMA does not endorse any particular electronic prescribing system, there are a few recommendations for doctors in the market for an e-prescribing platform. First and foremost, if the practice does any prescribing of controlled substances, the system MUST have the ability to do EPCS and query the CURES database. Not all commercially available systems can do both, so practices should ask prospective vendors before investing in a system. And, get it in writing.
CPMA suggests that members checkout SureScripts site https://surescripts.com/network-connections/eprescribingprescriber-software. It is the largest electronic prescribing network in the country. Vendors on their certified product list will give doctors and patients the largest number of pharmacies from which to choose.
Another site to checkout is the software review/rating site Capterra, which also offers live chat with software experts https://www.capterra.com/eprescribing-software/
Please note that the listing of Capterra and SureScripts is for informational purposes only and does not denote CPMA endorsement of the sites or products listed on these sites.
HHS EXTENDS COVID PUBLIC HEALTH EMERGENCY TO JANUARY 2023
The Biden Administration extended the COVID-19 public health emergency for an additional 90 days. As the U.S. braces for a spike in cases this winter, the public health emergency (PHE) will continue through at least January 11, 2023.
When a decision is made to terminate the declaration or let it expire, HHS has said the agency will provide 60 days notice prior to termination.
During the COVID-19 pandemic, through California Podiatric Medical Association (CPMA) and other stakeholders’ advocacy, both public and private health plans expanded their coverage and reimbursement for services provided via telehealth. As long as the nation continues to be in a public health emergency, these policies remain in effect.
Congress also recently extended the current COVID-19 pandemic telehealth waivers for five months beyond the end of the public health emergency.
NEW ICD-10 CODE SET EFFECTIVE OCTOBER
1, 2022
Providers must use the “2023 ICD-10-CM” code set for services provided on or after October 1. There are changes to the new code set that impact podiatric medicine and surgery. There are ICD-10 code changes pertinent to social determinants of health, diabetes, alcohol use, noncompliance, and use of immunosuppressive drugs.
New ICD-10-CM Code Set Takes Effect October 1:
• Z79.85 Long-term (current) use of injectable non-insulin antidiabetic drugs
• Z59.82 Transportation insecurity
• Z59.86 Financial insecurity
• Z79.620 Long-term (current) use of immunosuppressive biologic
• Z91.190 Patient’s noncompliance with other medical treatments and regimen due to financial hardship
88 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
New ICD-10-CM Codes can be found at https://www.cms.gov/medicare/icd-10/2023-icd-10-cm
APMA will host a webinar covering podiatry-relevant coding changes on December 14. Register now at https://tinyurl. com/4jr5vw5n
(Source: APMA 10/17/2022)
PHYSICIANS ARE NOW REQUIRED TO UPDATE PRACTICE DEMOGRAPHIC INFO EVERY 90 DAYS
Since 2016, California health plans and insurers have been required to comply with uniform standards and provide timely updates for their provider directories, as required by SB 137. As part of the requirements, plans/insurers must regularly contact contracting providers to advise them of the information the payor has about them in the directory.
While under state law the interval for these communications had been either every 180 days or annually, depending on the size of the practice, a new federal law took effect in January 2022 that now requires health plans/insurers to verify the accuracy of their contracting providers’ demographic information every 90 days. Providers should have received notification from payors.
Providers who fail to comply with the verification requests risk payment delays and removal from the provider directory. Health plans or insurers may also terminate a contract with a provider for a pattern or repeated failure to update the required information.
In addition to reviewing/updating you practice information at least every 90 days, practices should also note that if the practice is moving, adding or losing providers, changing the practice name and/or TIN, closing a practice or changing specialties, it’s important to inform payors with at least 90 days advance notice to prevent payment issues.
Under SB 137, health plans/insurers operating in California are also required to offer an electronic method to allow providers to verify or submit changes to their directory information.
Major California Insurance Payer sites to check/ change provider demographics:
Anthem Blue Cross https://tinyurl.com/2p8fzeww

United Healthcare https://tinyurl.com/3zmey759
Aetna https://tinyurl.com/45bn6zwu
Cigna https://tinyurl.com/59wpyjpa Blue Shield https://tinyurl.com/3zmey759
Kaiser – South https://tinyurl.com/bdhkrcsn
Kaiser – North https://tinyurl.com/bdhkrcsn
(Source: CMA 7/5/2022)
DMEPOS ENROLLMENT CONTRACTORS CHANGE
REMINDER; November 6 is the final day the National Supplier Clearinghouse (NSC) will process Medicare enrollment applications for DMEPOS suppliers. Starting November 7, two new contractors will process Medicare enrollment applications for DMEPOS suppliers:
• Novitas Solutions (NPEAST DMEPOS): Alabama, Connecticut, Delaware, Florida, Georgia, Illinois, Indiana, Kentucky, Maine, Maryland, Massachusetts, Michigan, Mississippi, New Hampshire, New Jersey, New York, North Carolina, Ohio, Pennsylvania, Rhode Island, South Carolina, Tennessee, Vermont, Virginia, West Virginia, Wisconsin, District of Columbia, Puerto Rico, US Virgin Islands
• Palmetto GBA (NPE WEST): Alaska, Arizona, Arkansas, California, Colorado, Hawaii, Idaho, Iowa, Kansas, Louisiana, Minnesota, Missouri, Montana, Nebraska, Nevada, New Mexico, North Dakota, Oklahoma, Oregon, South Dakota, Texas, Utah, Washington, Wyoming, American Samoa, Guam, Northern Mariana Islands
For more information, take advantage of APMA’s DME Resources for members at apma. org/dme
(Source: APMA 10/17/2022)
| 89 JULY • AUGUST • SEPTEMBER • 2022
CALIFORNIA PAID FAMILY LEAVE GRANTS AVAILABLE TO ELIGIBLE BUSINESSES
Eligible small businesses in California may now apply for grants up to $2,000 per employee utilizing California’s Paid Family Leave program (PFL).
These grants, funded by the California Employment Training Panel and California Labor and Workforce Development Agency, are geared toward helping small businesses offset the increased costs that may arise when an employee is out on leave, such as cross-training existing staff, and hiring and training new and/or temporary employees.
California’s PFL program provides eligible employees with up to eight weeks of wage replacement benefits when the employee is off work for certain qualifying reasons, such as to bond with a new child or to care for a seriously ill family member.
$2,000 and $1,000 Grants are Available
Grants are available in the following amounts:
• Businesses with 51–100 employees may receive up to $1,000 per employee utilizing Paid Family Leave.
• Businesses with one to 50 employees may receive up to $2,000 per employee utilizing Paid Family Leave.
To qualify, businesses must:
• Employ between one and 100 employees;
• Be registered to do business in the State of California;
• Be in an active status with the office of the California Secretary of State; and
• Have an active California Employer Account Number under which employees are listed for payroll
For more information or to apply for a grant, visit CaliforniaPFL.com, including their Frequently Asked Questions. After reviewing the eligibility requirements
and collecting the necessary information to apply, it will take businesses approximately 10 to 15 minutes to fill out the online application.
The grant period is June 1, 2022, to May 31, 2024, or until funds run out.
(Source: Calchamber 8/23/2022)
LIDOCAINE SHORTAGE INFORMATION AND RESOURCES

CPMA is aware of the ongoing shortages of lidocaine and the significant impact these shortages have on members’ practices. While the causes of the shortage and potential solutions are complex and multifactorial, CPMA/APMA has compiled the following resources for those members facing lidocaine shortages.
These resources provide information on the drug supply chain and shortage issues. The last listed link, ASHP Shortage List, is a searchable database. This database provides anticipated release dates for products. Note that the release date is when the product is available to distributors. Where your practice falls within the distributor’s allocation process will determine when you receive the product.
In terms of immediate options, CPMA/ APMA suggests the following:
• Establish relationships with multiple distributors
• Consider alternate local anesthetics when medically appropriate
• Look to non-traditional sources such as dental suppliers
• Draw up only the required amount of local anesthesia needed rather than filling the entire syringe when the syringe holds more than what is necessary for the procedure
CPMA will continue monitoring this concern and investigating solutions with policymakers and other impacted stakeholders.
Additional Resources
• FDA Drug Shortages Information Web Page https://tinyurl.com/sxk3kk4u
90 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
• FDA Drug Shortages Database
https://www.accessdata.fda.gov/scripts/drugshortages/
• ASHP Current Drug Shortages List
https://www.ashp.org/drug-shortages/current-shortages ?loginreturnUrl=SSOCheckOnly
PAY SCALE MUST BE INCLUDED IN JOB POSTINGS
BY
CALIFORNIA EMPLOYERS
EMPLOYEES
WITH 15 OR MORE
Beginning January 1, 2023, California employers with 15 or more employees will be required to (1) disclose a position’s pay scale in any job posting or advertisement and (2) provide the pay scale to any third party used by the employer to announce, post, publish or otherwise advertise a job. The third party, in turn, will be required to include the pay scale in the job posting. Also under the new law, employers with 15 or more employees are required to provide to an employee, upon the employee’s request, the pay scale for the position in which the employee is currently employed.
Pay scale for positions must be included in all job postings
California employers of all sizes are already required under a state law that took effect in 2019 to provide a position’s pay scale to any applicant applying for that position upon the applicant’s “reasonable request.” As defined by existing law and SB 1162, pay scale means the salary or hourly wage range that the employer reasonably expects to pay for the position.
That requirement will continue, but the requirements of SB 1162 are intended to further ensure that employers do not rely on an applicant’s salary history information when determining whether to offer employment to an applicant or what salary to offer.
Effective January 1, 2023, SB 1162 will require employers with 15 or more employees to:
Disclose a position’s pay scale in any job posting or advertisement.
Provide the pay scale to any third party used by the employer to announce, post, publish, or otherwise advertise a job. The third party, in turn, will be required to include the pay scale in the job posting.
Companies based outside of California and hiring for positions or work to be done in California will be required to disclose pay scales in job postings in compliance with the new law.
The law increases wage transparency for currently employed
Also under the new law, employers with 15 or more employees are required to provide to an employee, upon the employee’s request, the pay scale for the position in which the employee is currently employed.
Maintenance of job title, and wage rate history required
Employers of all sizes will be required to maintain job title and wage rate history records for all their employees for the duration of the employment plus three years after the end of the employment.
The Labor Commissioner is authorized to inspect the employer’s records, and the specified time frame allows the Labor Commissioner to determine if a pattern of wage discrepancy exists.
Employers can be ordered to pay a civil penalty between $100 and $10,000 per violation.
An individual can file a written complaint with the Labor Commissioner alleging an employer has violated the pay-scale disclosure requirements within one year of learning about the violation.
The Labor Commissioner is required under the law to “promptly investigate” such complaints and, if a violation is found, can order the employer to pay a civil penalty of between $100 and $10,000 per violation with the exception of a first-time violation if the employer demonstrates that all job postings for open positions have been updated to include the required pay scales.
Individuals themselves can also bring a civil action against the employer for appropriate relief.
(Source: CDA 11/1/2022)
EMPLOYEE FINAL PAYCHECK: FAQS AND ANSWERS
CPMA has received several inquiries from members regarding employees’ final checks. The following is from the California Chamber of Commerce on the issue:
When an employee quits without any notice at all, you have 72 hours to cut a final paycheck and have it ready for them to pick up. If an employee gives less than 72 hours’ notice, you have 72 hours from the time notice is given to have the check ready. The 72 hours runs regardless of business hours. It generally is the responsibility of the employee to return to pick up their check or request that it be mailed.
Some of the most common questions about final paychecks in this situation are:
Where should the check be for the employee to pick up? A final paycheck must be available for them to pick up “at the office of the employer within the county in which the work was performed,” according to California Labor Code Section 202.
So, for example, an employee who works at a Northern California branch of your company could not be required to travel to your Southern California branch where your payroll is done to pick up a final paycheck. You would need to make sure it was available for the employee to pick up at the Northern California branch by the 72-hour deadline.
| 91 JULY • AUGUST • SEPTEMBER • 2022
What if my payroll is done out of state, and I can’t get a check in time?
Unfortunately, there is no exception to the 72-hour rule based on where your payroll is done, so if the check is late, you would be subject to waiting time penalties of a day’s wages for every day it is late up to 30 calendar days.
What if an employee doesn’t come to pick up their final paycheck?
Often an employee will not return to pick up a check, in which case an employer might wonder if they need to eventually mail it to the employee.
California law is clear that the final paycheck should be mailed to an employee who quits only if the employee specifically requests that it be mailed and also designates a mailing address.
If the employee does not come in to pick up their final paycheck and never requests that it be mailed, should I mail it anyway just to be sure they get their wages?
No. If you drop it in the mail and then the employee comes in to pick up the check before it arrives at the employee’s home, you will be liable for penalties for late wages for every day the employee then has to wait for the check to arrive.
In addition, if you don’t have a current address on file, the check may go to the wrong address and cause even further penalties to accrue.
If an employee requests that I mail the check, does it have to arrive at the employee’s home within 72 hours?
No. The date of the mailing is considered the date of payment for purposes of the requirement to provide payment within 72 hours of the notice of quitting. So as long as the check is mailed on time, there is no legal violation even though it may take several days in the mail to reach the employee’s home.
First-class mail is considered sufficient for mailing, although some employers may choose to use a form of delivery that provides proof of receipt.
What if an employee is working remotely from their home in another county?
The law on final paychecks simply says the check must be available at the office of the employer within the county in which the work was performed — and does not address remote workers.
If an employee is working from home in a different county than the one where the employer is located, it’s unclear where the final check would need to be. However, an employer could ask the employee if they would simply like the check mailed to avoid any issues.
What if the employee has given more than 72 hours’ notice, or if we have terminated them or laid them off?
Note that the above mailing rules do not apply when an employee quits with more than 72 hours’ notice, in which
case the wages are due on the last day of work. These rules also do not apply when an employee is terminated or laid off, in which case the wages are due at the time and place of termination or layoff.
(Ellen
Savage, J.D., HR Adviser, CalChamber 10/11/2022)
BEREAVEMENT LEAVE PROTECTED BY CALIFORNIA LAW BEGINNING JANUARY 2023
California employers with five or more employees will be required beginning Jan. 1 to provide up to five days of protected bereavement leave to employees for the death of a family member, including a domestic partner or extended family member. A second law that takes effect Jan. 1 adds “designated person” to the list of persons an employee is allowed to take unpaid and paid off time to care for, respectively, under the California Family Rights Act and Paid Sick Leave laws.
Amendments to the California Family Rights Act and Healthy Workplaces, Healthy Families Act, expand employees’ leave rights and take effect January 1, 2023.
The changes, brought by two pieces of legislation signed into law in September by Gov. Gavin Newsom, require covered employers to provide protected bereavement leave, and they add “designated person” to the list of persons an employee is allowed to take time off to care for under both CFRA and Paid Sick Leave laws.
Up to five days of bereavement leave protected
Many California employers already provide some form of bereavement leave to employees as a benefit, and some California cities and counties enforce local bereavement laws, but bereavement leave will be defined and protected for all covered employees across the state beginning in January.
Employers with five or more employees will be required by Assembly Bill 1949, which amends the California Family Rights Act, to provide up to five days of bereavement leave to employees for the death of a family member, including a domestic partner or extended family member.
Employees are eligible for the leave if they have been employed for at least 30 days before their leave begins. Employers cannot lawfully refuse to grant a request for bereavement leave by any eligible employee.
Bereavement leave may be unpaid as specified
Specifically, under the new law:
• “Family member” means a spouse, child, parent, sibling, grandparent, grandchild, domestic partner, or parent-in-law.
• Employees are not required to take bereavement leave on consecutive days.
• The leave is considered unpaid unless the employer already has a paid bereavement leave policy in place.
92 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION
• Employees must complete their leave within three months of the family member’s death.
• Employees can elect to use accrued vacation, sick time, or other paid time for the leave but are not required to do so.
• Employers can request documentation of the death of the family member, such as a death certificate or published obituary.
• Employers must maintain the confidentiality of any employee who requests the leave. Practices may want to create a bereavement policy or should update their existing policy before the law takes effect and communicate the change to employees.
• CFRA and Paid Sick Leave can be used to care for ‘designated person’
California employers with five or more employees are already required under CFRA to provide up to 12 weeks of unpaid protected leave to employees who request it to care for a child, parent, parent-in-law, grandparent, grandchild, sibling, spouse or domestic partner with a serious health condition.
Existing state law also requires employers of every size to provide eligible employees working in California a set amount of paid sick leave to all eligible employees for qualified reasons for themselves or a “family member.”
Starting January 1, under Assembly Bill 1041, employees can also take protected CFRA leave and Paid Sick Leave to care for a designated person.
DESIGNATED PERSON DEFINED DIFFERENTLY FOR CFRA, PAID SICK LEAVE
For the purpose of CFRA leave, the law defines designated person as “any individual related by blood or whose association with the employee is the equivalent of a family relationship,” whereas designated person is completely undefined under the Healthy Workplaces, Healthy Families Act for the purpose of Paid Sick Leave.
Because the law does not explicitly define “designated person” practices should avoid defining designated person in their Paid Sick Leave policy. Unless the law further defines designated person, employers should allow the employee to define their designated person when they request their Paid Sick Leave or consult with their legal counsel.
Specifically, the law:
Allows the employee to identify the designated person at the time they request CFRA leave or the Paid Sick Leave days.
Authorizes the employer to limit an employee to one designated person per 12-month period.
The law does not change the amount of allowable leave or other terms of CFRA.
(Source: CDA 10/25/2022)
THE LAST DAY TO CHANGE YOUR MEDICARE PARTICIPATION STATUS FOR 2023 IS DECEMBER 31, 2022
It’s that time of year again—time for physicians to decide if they want to make changes to their Medicare participation status https://tinyurl.com/yck7u3kt
Physicians have until December 31,2022 to make changes https://tinyurl.com/4rjp2css for the 2023 participation year. The effective date for any changes made will be January 1, 2023.
In making the decision for the 2023 participation year, clinicians should be aware that the Centers for Medicare and Medicaid Services (CMS) recently released the final rule and policies https://tinyurl.com/2p86njsb for next year. The fee schedule has not been released yet.
As always, physicians have three choices regarding Medicare: Be a participating provider; be a non-participating provider; or opt-out of Medicare entirely. Details on each of the three participations options are as follows:
A participating physician must accept Medicare-allowed charges as payment in full for all Medicare patients. A participating provider receives 5% more reimbursement than a non-participating provider.
A non-participating provider can make assignment decisions on a case-by-case basis and bill patients for more than the Medicare allowance for unassigned claims. Nonparticipating physician fees are 95% of participating physician fees. If you choose not to accept assignment, you can charge the patient 9.25% more than the amounts allowed in the participating physician fee schedule (which equates to 15% of the non-participating fees).
Physicians who opt out of Medicare are bound only by their private contracts with their patients. Medicare’s limiting charges do not apply to these contracts, but Medicare does specify that these contracts contain certain terms. When a physician enters into a private contract with a Medicare beneficiary, both the physician and patient agree not to bill Medicare for services provided under the contract. As a result of the Medicare Access and CHIP Reauthorization Action of 2015 (MACRA), validated opt-out affidavits signed on or after June 16, 2015, will automatically renew two years after the effective date.
Physicians who want to change their participation status for 2023 must submit a signed Medicare Participating Physician or Supplier Agreement (CMS-460) to Noridian, California’s Medicare contractor, postmarked by December 31, 2022. The participation agreement will automatically renew each year. However, if there is a name or EIN (tax identification number) change, you will need to complete a new participation agreement.
For more information on open enrollment can be found on the Noridian website.
| 93 JULY • AUGUST • SEPTEMBER • 2022
PRESIDENT Holly Spohn-Gross, DPM Lake Isabella, CA 93240
PRESIDENT-ELECT Diane M. Koshimune, DPM San Jose, CA 95119
IMMEDIATE PAST PRESIDENT Diane D. Branks, DPM Pomona, CA 91766

SECRETARY/TREASURER
Phong H. Le, DPM Sacramento, CA 95828
2022/2023 BOARD OF DIRECTORS
DIRECTORS
Arman A. Kirakosian, DPM San Francisco, CA 94121
Heather R. McGuire, DPM Ventura, CA 93003
Alan W. Sue, DPM Mountain View, CA 94040
Douglas M. Taylor, DPM Walnut Creek, CA 94596
Ebonie E. Vincent, DPM Long Beach, CA 90813
PARLIAMENTARIAN
Ronald D. Jensen, DPM Modesto, CA 95355
EXECUTIVE DIRECTOR
Jon A. Hultman, DPM, MBA, CVA
7311 Greenhaven Drive, Suite 208 Sacramento, CA 95831
P: (916) 448-0248/(800) 794-8988
GENERAL COUNSEL
C. Keith Greer, Esq. San Diego, CA 92128
GOVERNMENTAL REPRESENTATIVES
Ryan Spencer Sacramento, CA 95814
STUDENT REPRESENTATIVES
Nida Ahmed (CSPM@SMU)
Harsh Varshney (CPM@WesternU)
2022/2023 CPMA SOCIETY PRESIDENTS
ALAMEDA/CONTRA COSTA
Naleen Prasad, DPM Castro Valley, CA 94546
P: (510) 517-2721
CENTRAL VALLEY
Jack A. Harvey, DPM Modesto, CA 95336 P: (209) 823-2700
COACHELLA VALLEY
Steven L. Ginex, DPM Palm Desert, CA 92260 P: (760) 340-3232
INLAND Jan Tepper, DPM Upland, CA 91786 P: (909) 920-0884
LOS ANGELES COUNTY
Ara O. Kelekian , DPM Montebello, CA 90640 P: (323) 346-0996
MID-STATE Richard Motos, DPM Visalia, CA 93292 P: (559) 734-1171
MONTEREY BAY AREA
Bobby Yee, DPM Monterey, CA 93940 yeedoc@sbcglobal.net
N. CALIFORNIA KAISER Christy King, DPM Oakland, CA 94611 P: (510) 752-6905
ORANGE COUNTY Thomas Rambacher, DPM Mission Viejo, CA 92692 P: (949) 916-0077
REDWOOD EMPIRE Rachel A. Hoyal, DPM Santa Rosa, CA 95404 P: (707) 546-2107
SACRAMENTO VALLEY Eunice Cho, DPM Rocklin, CA 95677 P: (916) 435-5000
SAN DIEGO Brittany Rice, DPM San Diego, CA 92108 P: (619) 291-0777
SAN FRANCISCO/SAN MATEO
Jasper Lee, DPM San Francisco, CA 94123 P: (415) 731-6700
SAN LUIS OBISPO/SANTA BARBARA Faridi G. Sherieff, DPM Lompoc, CA 93436 P: (805) 736-8818
SANTA CLARA VALLEY Kevin Ragothaman, DPM Cupertino, CA 95014 (408) 358-6234
SHASTA REGION
Michael L. Wilson, DPM Chico, CA 95928 P: (530) 895-3668
SOUTHERN CALIFORNIA HMO Suzette Lee, DPM Los Angeles, CA 90066 sleedpm@aol.com
VENTURA COUNTY
Anh Nguyen, DPM Oxnard, CA 93030 P: (805) 983-0222
The California Podiatric Physician is the official publication of the California Podiatric Medical Association. CPMA and the California Podiatric Physician assume no responsibility for the statements, opinions and/ or treatments appearing in the articles under an authors’ name. For editorial or business information and advertising, contact California Podiatric Medical Association, 7311 Greenhaven Drive, Suite 208 Sacramento, CA 95831; Telephone, (916) 448-0248; Facsimile; (916) 448-0258; E-mail; cpma@calpma.org.
94 | CPMA • CALIFORNIA PODIATRIC MEDICAL ASSOCIATION


FACE-TO-FACE IS BACK! For those craving to meet and visit exhibits again in person, we will have limited space available, so be sure to register early We can’t wait to see you! For those wanting to watch the live sessions from home, we will have unlimited tickets available. VIRTUAL OPTION* Simply choose your option when registering! their PICA Renewal Premiums by attending the risk management sessions DPMS GET 15% OFF Live General Sessions Offering 25 CECH for DPMs Radiology and Fluoroscopy CECH Risk Management Program for PICA discount Hands-On Workshops 3 Days of In-Person Exhibits Combined Clinical and Administrative Assistants Program Full Featured Web and Mobile App Discounted Hotel Rates for In-person Attendees ‘Easy to Get to’ from Anywhere – and Everywhere! TheWestern.org /WesternFootandAnkleConference @TheWesternFAC (800) 794-8988 7311 Greenhaven Dr Ste 208, Sacramento, CA 95831 STAY CONNECTED REGISTER NOW AND SAVE THROUGH MARCH 29 No code required! 20 2 3 Assistants will only have the face-to-face option. Clinical and Administrative sessions will be combined into one program. AND ONLINE DISNEYLAND ® HOTEL & CONVENTION CENTER ANAHEIM, CA JUNE 22-25 Registration for the virtual meeting will not grant access to the onsite event, and registration for the onsite event will not grant access to the virtual sessions. Virtual attendees wishing to visit the exhibit hall may purchase an Exhibit Hall Pass onsite. Confirm your selection before paying for registration. PLEASE NOTE:

PRESORT STANDARD US POSTAGE PAID CPS WHEN SELECTING SERVICES & SUPPLIES FOR YOUR PRACTICE… SUPPORT THE COMPANIES THAT SUPPORT YOU!
the companies
our Corporate Member Family, and their
to excellence in
to learn more about their products, services and efforts to promote quality foot health.
California Podiatric Medical Association 7311 Greenhaven Drive, Suite 208 Sacramento, CA 95831
CPMA gratefully acknowledges the generous support of
in
commitment
the podiatric medical community. Please visit their websites
