2 minute read
COVID

JOURNAL OF THE INDIAN MEDICAL ASSOCIATION, VOL 118, NO 06, JUNE 2020
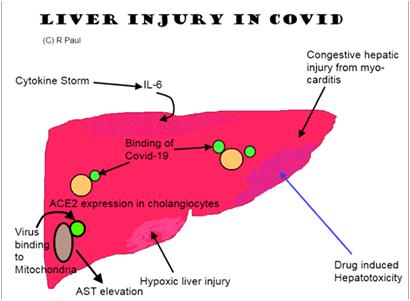
the host response has tipped over from protective immune response to an uncontrolled state of hyperinflammation. These include serum ferritin, CRP, CPK, LDH, IL-1, IL-6, TNF-a, etc.
Advertisement
The ongoing research will reveal whether there is ahierarchical pro-inflammatory cytokine which ushers in the cytokine storm in COVID-19 patients. The existence and understanding of the same will be a potential breakthrough in monitoring and management of COVID-19 patients.
9. How early after admission to start this therapy? Can we have a scoring system with multiple variables or single biomarker value?
The administration of immunomodulators late in the COVID-19 clinical course is unlikely to provide large beneficial effects. Identifying the tipping point when the individual immune response goes into the hyperinflammatory drive is key to take the decision on initiating immunomodulators like tocilizumab. As mentioned above, there is no single known biomarker for identifying the same and we rely on a host of biomarkers in addition to the clinical condition of the patient to take a decision. These need to be built into a scoring system in near future as more data emerge.
10.Since it may aggravate tuberculosis, bacterial or fungal infections; what investigations to precede giving Tocilizumab keeping the time constraint in mind
Active bacterial infection and latent TB should be ruled out prior to administering the drug. The merits and demerits of screening method (TST, IGRA) remains
during the pandemic.
19 unknown in these patients. Close monitoring is warranted in view of recent reports of high secondary infection rates among patients receiving tocilizumab. This is of particular relevance to the Indian ICU settings.
11. What dose modifications (renal, hepatic, pregnancy, elderly, obese) required?
No dose modification is required in patients with pre-existing renal impairment. Tocilizumab is to be avoided in pregnancy. Caution is advised in presence of active hepatitis.
12.When should repeat dose be considered?
The usual dose is 8mg/kg (maximum: 800 mg/ dose); there are various regimens being used in trials. We repeat the dose between 12 to 24 hours later if no improvement is seen after the first dose.
Editorial note : There are ongoing trials of tocilizumab in Covid-19. The data from those trials will further clarify the utility of this drug.
13.What are the contraindications of using this drug or in whom to avoid?
This drug should be avoided in patients with any of the following active infections: viral hepatitis, tuberculosis, HIV, bacterial and/ or fungal and/ or viral infections (other than SARS-CoV-2 infection), neutrophil count < 1000/ mm3, platelet counts <
Dr Soneja, we thank you for the valuable insight into the management of Covid-19 infection. We are sure our readers will benefit a lot from these pearls of knowledge. Please stay safe
50,000/ mm3.