This edition of Travel Medicine is lovingly dedicated to our colleague, our mentor, our friend, Dr. Jay Keystone. One could easily enumerate a list of superlatives for Jay by just reeling off items from his lengthy curriculum vitae – his manuscripts, academic appointments, the many awards he has received, and the immense contributions he has made to travel and tropical medicine in his decades of service. Perhaps the most distinguished of his honors was his induction into the Order of Canada in May, 2016. The Order recognizes individuals who have exhibited lifelong exemplary achievement, service, and have made major contributions to Canada; Queen Elizabeth II is the Sovereign of the Order. This was truly well deserved.
So, if it were the editors’ decision to dedicate this text to Jay just on the basis of his awards and honors, it would be enough.
But many of us who use this text know Jay as a one of the fathers of the practice of clinical tropical medicine and travelers’ health. Jay received his MSc from the London School of Tropical Medicine in 1974 and since then he has cared for countless patients around the world and excelled in judgment and clinical management.
Many of us are students of Jay. Jay received the Ben Kean Medal from the American Society of Tropical Medicine and Hygiene (ASTMH) recognizing his teaching skills. His teaching style connects with students at all levels. Over the decades, he has been on the roster of invited speakers for countless educational conferences that we attend and we are always delighted to see Jay at the podium. His lectures are informative, up to date, and enormously entertaining. In fact, he is one of few who make us all laugh – at ourselves and at the human condition – no matter our background or beliefs.
Some of us know Jay as an early pioneer in travel medicine. He was chosen to speak about malaria at the 1988 travel medicine conference in Zurich, and was one of the founding members of the International Society of Travel Medicine (ISTM). A former president of the Society, Jay sought greater membership from underrepresented countries, and participated in the development of the Certificate in Travel Health examination. During his tenure as ISTM President he created a “Coalition for Healthy Travel” encouraging pharmaceutical industry partners to forgo their own corporate interests and contribute to general education in travel medicine and travelers’ heath. He was the GeoSentinel site director for the Toronto clinic, which was the first GeoSentinel site recruited outside the United States.
And finally, some of us are fortunate enough to know Jay as one of the most caring persons we have ever known. Jay is one of those rare individuals who is always his authentic self. He is equally willing to give his time to advise junior students as senior colleagues. For some of us, his support helped us forge our own careers in travel medicine. As a physician, he is compassionate, understanding the importance of holding the hand of a frightened patient or family member. He will stop at nothing to help his patients, and is incredibly generous with his time in consultations. As a friend, he is always available to lend an ear. He is quick to offer his opinion when asked (and sometimes even when not!). Bright, energetic, fun-loving, realistic, and kindhearted, he embodies those qualities we admire. A loving father of five and grandfather of five, he has found his soulmate, Margaret Mascarenhas, and they cherish the moments they spend together. However, Jay still manages to take time for his patients and for all of us who seek his counsel and rely on his wisdom.
We thank you, Jay, with all our hearts.
Your Editorial Team – Phyllis Kozarsky, Bradley Connor, Hans Nothdurft, Karin Leder, and Marc Mendelson
Travel Medicine
Fourth Edition
Jay S. Keystone CM MD MSc(CTM) FRCPC
Professor of Medicine, University of Toronto
Tropical Disease Unit
Toronto General Hospital
Toronto, ON, Canada
Phyllis E. Kozarsky MD
Professor Emerita
Department of Medicine
Division of Infectious Diseases
Emory University
Bradley A. Connor MD
Clinical Professor of Medicine
Weill Cornell Medical College
The New York Center for Travel and Tropical Medicine
New York, NY, USA
Hans D. Nothdurft MD
Professor
Department of Infectious Diseases and Tropical Medicine
Head, University Travel Clinic University of Munich Munich, Germany
No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or any information storage and retrieval system, without permission in writing from the publisher. Details on how to seek permission, further information about the Publisher’s permissions policies and our arrangements with organizations such as the Copyright Clearance Center and the Copyright Licensing Agency, can be found at our website: www.elsevier.com/permissions
This book and the individual contributions contained in it are protected under copyright by the Publisher (other than as may be noted herein).
Chapter 14: “Malaria: Epidemiology and Risk to the Traveler” by David Lalloo and Alan J. Magill (†) is in Public Domain.
Chapter 20: “Clinical Presentation and Management of Travelers’ Diarrhea” by Mark S. Riddle is in Public Domain.
Chapter 21: “Persistent Gastrointestinal Symptoms in the Ill-Returning Traveler” by Mark S. Riddle is in Public Domain.
Chapter 58: “Eosinophilia” by Amy D. Klion is in Public Domain.
Notices
Practitioners and researchers must always rely on their own experience and knowledge in evaluating and using any information, methods, compounds or experiments described herein. Because of rapid advances in the medical sciences, in particular, independent verification of diagnoses and drug dosages should be made. To the fullest extent of the law, no responsibility is assumed by Elsevier, authors, editors or contributors for any injury and/or damage to persons or property as a matter of products liability, negligence or otherwise, or from any use or operation of any methods, products, instructions, or ideas contained in the material herein.
ISBN: 978-0-323-54696-6
e-ISBN: 978-0-323-54771-0
Content Strategist: Charlotta Kryhl
Content Development Specialist: Nani Clansey
Project Manager: Nayagi Athmanathan
Illustration Manager: Karen Giacomucci
Designer: Amy Buxton
Marketing Manager: Michele Milano
“When you travel, remember that a foreign country is not designed to make you comfortable. It is designed to make its own people comfortable.” Clifton Fadiman
Clifton Fadiman pointed out correctly that travel is not without its challenges. Whether one travels first class or in no class at all, there remain a variety of health issues that may be beyond our control. For example, when it comes to adhering to food and beverage precautions, one can do everything right and become ill, or everything wrong and remain well. Sometimes luck and our body’s immune system are what keep us healthy.
As the scientific base of travel medicine continues to grow, so does the need for synthesizing this material into a formal text. Yes, readers may go online now and research every travel health topic separately to find the most recently published articles, but these may not give the reader sufficient history, perspective, or the various opinions that make up all the features of the topic or this text.
Our aim then has not only been to provide a review of important areas, but to update the previous edition and to include new items that comprise travel health. New information covering immunizations, prophylactic medications, and guidance are all included.
As well, this fourth edition has an expanded editorial team, including representation from other parts of the world: Dr. Marc Mendelson from South Africa and Dr. Karin Leder from Australia. The importance of having a truly global team looking at the text cannot be overstated. We realize that to cover worldwide health issues, we needed to think more globally about inclusion.
On the other hand, there are some things that a text cannot do. We urge all those who need information on a current or new health problem
in a particular country to investigate more widely using WHO or national websites. Certainly, one of the many things we have learned about medicine, and travel medicine in particular, is that health recommendations can change overnight with the emergence or reemergence of disease.
The field’s mandate continues to be the maintenance of health of international travelers. In 1988, the first international meeting of travel medicine experts took place in Switzerland and from that initiative came the International Society of Travel Medicine, now with 3500 members from 94 countries. Since then the world of travel medicine has changed significantly, as is highlighted by changes in our text with each edition. Now the fourth edition includes chapters covering ecotourism, VIP travel, and pretravel considerations in the prevention of non-vaccine preventable infections such as Zika, chikungunya, and MERS viruses. Also, we have provided travel medicine consultants with an approach to the illnesses they might encounter in ill-returned travelers, both the investigations and the management issues. Our outstanding authors are subject matter experts who have comprehensive and authoritative knowledge in their respective fields, individuals who have been selected from a number of countries. We believe that by incorporating both a practical and evidence-based approach, our authors and editors have made this book an essential resource for all travel medicine practitioners.
We hope you enjoy this edition. We believe that all of our authors and editors love to travel, knowing it enhances their careers and lives. Despite travel’s many challenges, one must also consider the alternative and why it is so important to travel, stated so succinctly here:
“If you think adventure is dangerous, try routine, it’s lethal.” Anonymous
LIST OF CONTRIBUTORS
Vernon Ansdell MD FRCP DTM&H
Associate Clinical Professor
University of Hawaii Department of Tropical Medicine
Medical Microbiology and Pharmacology
Honolulu, HI, USA
Olivier Aoun MD MSc
Lieutenant Colonel, French Military Health Service
Chief physician of the 46th Medical Unit 5th Armed Forces Medical Center Strasbourg, Alsace, France
Howard Backer MD MPH FACEP FAWM
Director
California Emergency Medical Services Authority
California State Government Sacramento, CA, USA
Michael Bagshaw MB MRCS FFOM DAvMed
Professor of Aviation Medicine; Army Civilian Consultant Adviser in Aviation Medicine
Centre of Human & Aerospace Physiological Sciences
King’s College London London, UK
J. Kevin Baird PhD FASTMH
Eijkman-Oxford Clinical Research Unit
Eijkman Institute of Molecular Biology Jakarta, Indonesia
Centre for Tropical Medicine & Global Health
Nuffield Department of Medicine University of Oxford Oxford, UK
Roger A. Band MD FACEP
Senior Advisor, Medical, Shoreland-Travax
Vice Chair, Strategic Out of Hospital Initiatives
Director Quality Assurance, Peer Review and Process Improvement
Medical Director Jefferson Enterprise Urgent Care
Department of Emergency Medicine
Thomas Jefferson University Philadelphia, PA, USA
Elizabeth D. Barnett MD
Professor of Pediatrics
Section of Pediatric Infectious Diseases
Boston Medical Center
Boston, MA, USA
Trish Batchelor MD FRACGP MPH
DipCH PG Dip Occ Env Med
Principal Medical Adviser
Australian Department of Foreign Affairs and Trade
Canberra, ACT, Australia
Ronald H. Behrens MD FRCP
Director of Department of Travel Medicine, Hospital for Tropical Diseases
Research Degree Director, Faculty of Infectious and Tropical Diseases, London School of Hygiene and Tropical Medicine
London, UK
Jiří Beran MD
Professor of Medicine
Department for Tropical, Travel Medicine and Immunization, Institute for Postgraduate Medical Education
Prague, Czech Republic
Vaccination and Travel Medicine Centre Hradec Králové, Czech Republic
Sarah Borwein MD
Managing Partner and Physician
Central Health Medical Practice and TravelSafe Hongkong, SAR China
William B. Bunn MD JD MPH Advisor / Consultant
Former VP of Health, Safety, Security & Productivity
Navistar International Corporation Lisle, IL, USA Professor
Medical University of South Carolina Charleston, SC, USA
Gerd D. Burchard MD PhD Professor Department Tropical Medicine / Infectious Diseases
University Medical Center Hamburg Hamburg, Germany
Michael V. Callahan MD DTM&H MSPH Director, Clinical Translation
Vaccine and Immunotherapy Center Division of Infectious Diseases
Massachusetts General Hospital
Harvard Medical School
Boston, MA, USA
Suzanne C. Cannegieter MD PhD
Professor in Clinical Epidemiology
Department of Clinical Epidemiology and Department of Internal Medicine, Thrombosis and Haemostasis
Leiden University Medical Center Leiden, the Netherlands
Eric Caumes MD
Professor
Head of Department Service des Maladies Infectieuses et Tropicales
Groupe Hospitalier Pitié-Salpêtrière Paris, France
Lin H. Chen MD FACP FASTMH FISTM Director, Travel Medicine Center, Mount Auburn Hospital
Associate Professor, Harvard Medical School Division of Infectious Diseases and Travel Medicine
Mount Auburn Hospital Cambridge, MA, USA
Joannes Clerinx MD
Senior Consultant, Department of Clinical Sciences
Institute of Tropical Medicine Antwerp, Belgium
Bradley A. Connor MD
Clinical Professor of Medicine
Weill Cornell Medical College
The New York Center for Travel and Tropical Medicine
New York, NY, USA
Jakob P. Cramer MD PhD Infectious Diseases
Travel Medicine
Tropical Medicine Specialist Hamburg, Germany
Thomas E. Dietz MD
Providence Hood River Memorial Hospital, Emergency Department Portland, OR, USA
Herbert L. DuPont MD
Mary W. Kelsey Chair in Medical Sciences, University of Texas McGovern Medical School, Professor of Infectious Diseases, University of Texas School of Public Health, Clinical Professor, Baylor College of Medicine, President and CEO, Kelsey Research Foundation Houston, TX, USA
Yoram Epstein PhD
Head, Environmental Physiology Branch
Heller Institute of Medical Research
Sheba Medical Center
Tel Hashomer, Israel
Charles D. Ericsson MD
Dr. and Mrs. Carl V. Vartian Professor of Infectious Diseases McGovern Medical School Houston, TX, USA
Philip R. Fischer MD Professor of Pediatrics Mayo Clinic Rochester, MN, USA
Gerard T. Flaherty MB BSc MSc MD FRCPI FFTM RCPS (Glasg) FISTM Professor of Medical Education; Adjunct Professor of Travel Medicine and International Health School of Medicine, National University of Ireland Galway Galway, Ireland
Mark S. Fradin MD
Adjunct Clinical Associate Professor of Dermatology
Department of Dermatology
University of North Carolina at Chapel Hill Chapel Hill, NC, USA
Tifany Frazer MPH Office of Global Health Manager Medical College of Wisconsin Milwaukee, WI, USA
David O. Freedman MD
Professor Emeritus of Infectious Diseases University of Alabama at Birmingham Medical Director, Shoreland Travex Birmingham, AL, USA
Joanna Gaines PhD MPH CHES Senior Epidemiologist Travelers’ Health Branch, Division of Global Migration and Quarantine Centers for Disease Control and Prevention Atlanta, GA, USA
Kenneth Gamble MD FFTM RCPS (Glasg)
President
Missionary Health Institute and International Medical Services Toronto, ON, Canada
Philippe Gautret MD PhD DTM&H
Senior Clinician, Travel and Tropical Medicine
Head of Out-Patients Department, Infectious Diseases and Travel Clinic
Epidemiology, Biostatistics and Prevention Institute
Zürich, Switzerland
Eli Schwartz MD DTM&H
Professor of Medicine
Center for Geographic Medicine and Tropical Diseases
Chaim Sheba Medical Center, Tel Hashomer
Sackler School of Medicine
Tel Aviv University
Tel Aviv, Israel
David R. Shlim MD
Medical Director
Jackson Hole Travel and Tropical Medicine
Jackson Hole, Wyoming
The New York Center for Travel and Tropical Medicine
New York, NY, USA
Frédéric Sorge MD
Consultation Adoption, Enfant Migrant
Département de Pédiatrie
Hôpital Necker Enfants Malades
Paris, France
Mike Starr MBBS FRACP
Pediatrician, Infectious Diseases Physician, Consultant in Emergency Medicine
Honorary Clinical Associate Professor, University of Melbourne
The Royal Children’s Hospital Melbourne, VIC, Australia
Robert Steffen MD
Emeritus Professor
University of Zurich
Epidemiology, Biostatistics and Prevention Institute
WHO Collaborating Centre for Travellers’ Health
Zurich, Switzerland
Adjunct Professor
Division of Epidemiology, Human Genetics & Environmental Sciences
University of Texas School of Public Health
Houston, TX, USA
Kathryn N. Suh MD FRCPC MSc
Division of Infectious Diseases
The Ottawa Hospital
Associate Professor of Medicine
University of Ottawa
Ottawa, ON, Canada
Andrea Summer MD
Professor of Pediatrics
Medical University of South Carolina
Charleston, SC, USA
David N. Taylor MD
Chief Medical Officer
Vaxart, Inc.
South San Francisco, CA, USA
W. Robert Taylor
Mahidol Oxford Tropical Medicine Research Unit
Bangkok 10400, Thailand
Division of Tropical and Humanitarian Medicine
University Hospitals of Geneva Geneva, Switzerland
Shiri Tenenboim MD MSc(MIH)
DTM&H
Medical Doctor
Chaim Sheba Medical Center, Tel Hashomer
Sackler School of Medicine
Tel Aviv University
Tel Aviv, Israel
Joseph Torresi MBBS BMedSci FRACP
PhD
Department of Microbiology and Immunology
The Peter Doherty Institute for Infection and Immunity
The University of Melbourne Melbourne, VIC, Australia
Richard J. Tubb MD
Senior Advisor, Medical, Shoreland-Travax
Brigadier General, USAF (ret)
White House Physician Emeritus Washington, DC, USA
Thomas H. Valk MD MPH
President
VEI, Incorporated
Marshall, VA, USA
Jenny Visser MbChB MTravMed
Senior Lecturer
Department of Primary Health Care and General Practice
University of Otago Wellington, New Zealand
Leo G. Visser MD PhD
Professor of Infectious Disease
Head of Department of Infectious Diseases
Leiden University Medical Center Leiden, the Netherlands
Edward Wasser MD
The Toronto East General Hospital, Sunnybrook Health Sciences Centre, Examiner, Medical Council of Canada
Peer Assessor and Investigator, College of Physicians and Surgeons of Ontario Toronto, ON, Canada
Eric L. Weiss MD DTM&H
Associate Clinical Professor
Department of Emergency Medicine
Stanford University School of Medicine Stanford, CA, USA
Ursula Wiedermann MD PhD
Professor of Vaccinology
Head of Institute of Specific Prophylaxis and Tropical Medicine, Medical University of Vienna Vienna, Austria
Annelies Wilder-Smith MD PhD MIH FAMS FACTM
Professor of Infectious Diseases
Director, Global Health and Vaccinology Programme
Lee Kong Chian School of Medicine
Novena Campus
Singapore
Mary Elizabeth Wilson MD FACP FIDSA FASTMH FISTM
Clinical Professor of Epidemiology and Biostatistics
School of Medicine
University of California San Francisco
San Francisco, CA, USA and
Adjunct Professor
Department of Global Health and Population
Harvard T.H. Chan School of Public Health Boston, MA, USA
Henry M. Wu MD DTM&H
Assistant Professor of Medicine
Division of Infectious Diseases
Emory University School of Medicine Atlanta, GA, USA
The editors of Travel Medicine would like to thank our Elsevier publishing staff for encouraging us to embark on a 4th edition of the Textbook, and for being enthusiastic about moving forward with the addition of our new editors.
We would also like to thank our families, and particularly our partners, for their patience and understanding during the long process of writing and editing.
Introduction to Travel Medicine
Phyllis E. Kozarsky and Jay S. Keystone
Each year the World Tourism Organization (WTO) publishes its statistics revealing staggering numbers of people crisscrossing the globe; indeed, over the last decade there have been double-digit increases in travel. International tourist arrivals reported by the WTO in 2016 grew to 1235 million, 46 million greater than in 2015. Preliminary data show the Asia-Pacific region leading the way with 8% growth, the Americas (primarily South and Central America) with 4% growth, and Europe with 2% growth, primarily in the north. Existing data from Africa show a healthy increase in travel to the sub-Saharan region—8% as well. The Middle East has seen a decrease in about 4%. Despite this continued growth and despite 2017 having been designated by the United Nations as the “International Year of Sustainable Tourism for Development,” challenges continue. Not only were there protests at a recent meeting of the WTO regarding the problem of overtourism and the need for more responsible travel (http://media.unwto.org/press-release/2017-11-08), but also the challenges of safety and security have been reawakened recently with episodes of terror and violence.
Although considerations about health maintenance during travel have probably always been present, as explorers founded new regions, armies overtook others, and nomads wandered with their flocks, travel medicine’s scientific birth can probably be measured in just decades since the first international conference on travel medicine in Zurich in 1988, and the beginning of the International Society of Travel Medicine (ISTM) in 1991.
Much has changed in the last several decades. Conferences and literature still feature the forever lasting topic of malaria chemoprophylaxis punctuated by debates about self-treatment. However, if we quickly scan the most recent news that encompasses our field and engages our constituency, articles in the last several months have included those highlighting tuberculosis in asylum seekers, ceftriaxone-resistant gonorrhea imported into Canada, Zika once again in Miami, and details about the use of CRISPR (gene editing tool) as a diagnostic tool for infectious diseases and the potential use of such new genomics for point-of-care-diagnosis. As well, Brazil is now facing a serious yellow fever outbreak that is challenging public health in that country as well as elsewhere as importations into other countries has occurred. At the same time, the UK Daily Mail featured interactive maps from International SOS highlighting the world’s most dangerous and safest countries by type of risk, labeling Finland, Norway, and Iceland as safest.
Global mobility is now taken for granted, not something unique to any one group, any one company, or any one humanitarian effort, conflict, or migration pattern. Travel health has become the sum of all health maintenance considerations, both physical and emotional, as travelers embark on journeys from days to years for every different reason. In addition, we are now beginning to better understand the concept of One Health, that is, the importance of the interaction and intersection between human and animal health, and how this impacts the spread of emerging and reemerging diseases.
With the fourth edition of the textbook Travel Medicine, the editors needed to be cognizant of the growth of the body of knowledge (www.istm.org) in the field, while respecting the need to focus content on what is most important for the provider to understand practicing pretravel health. In addition, we have tried to include information concerning the more common issues facing travelers at their destinations as well as on return, being sure to capture the most recent developments.
Because travel is no longer just associated with tourism, but often incorporates work, volunteerism, medical care, migration, etc., new content has also been added to assist the provider in caring for specific populations engaging in different types of travel. For example, chapters have been added on ecotourism, military travel, and the VIP traveler. In addition, we have added a section on the pretravel consultation to assist practitioners advising their clients on the prevention of vectorborne diseases such as chikungunya, dengue, and Zika viruses.
Keeping up to date in the field of travel medicine is not easy. It requires a review of travel medicine, infectious disease, tropical medicine, and general medical journals as well as national government and international recommendations. Annual updates and international conferences in these fields may help. This textbook has been designed to bring it all to you, the most recent advances in the field as well as practical information on the management of pretravel and posttravelrelated issues. For example, since the third edition, new vaccines and regimens have been developed to prevent both routine and travel-related infections such as the high dose and adjuvated influenza and herpes zoster vaccines as well as a new oral vaccine from bovine colostrum for the prevention of Enterotoxigenic Escherichia coli, the most frequent cause of travelers’ diarrhea. For the last-minute traveler, both rabies and Japanese encephalitis vaccines now include 1-week accelerated regimens. Newly proposed single-dose antibiotic regimens for selftreatment of travelers’ diarrhea may help to reduce the development of drug-resistant enteric flora that make up our microbiome. In fact, the challenge of increasing antimicrobial resistance has crept into the field, impacting not only the provider but potentially the traveler, and perhaps even the traveler’s contacts on return. This important issue must be addressed not only within the context of travelers’ diarrhea, where new guidelines have been published by the ISTM,1 but also with the use of any antimicrobial agent.
The World Health Organization (www.who.int) and the ISTM (www.istm.org) remain major resources for the provider, as well as various country-specific guidelines for healthy travel. As well, there are many groups and agencies that provide national recommendations and guidance. A goal for those who choose to practice travel medicine should be to join the ISTM and to sit for the ISTM examination that awards the Certificate in Travel Health (CTH), an international standard of care for the practice of travel medicine. As guidance for healthy travel changes, disease outbreaks occur, and science advances, remaining up
to date is critical as it is for any specialty. Although awareness of travel health and the possibility of the global spread of infectious diseases appeared to peak with the Ebola outbreak in West Africa from 2013 to 2016, we are aware of no recent data to support an increasing use of travel health clinics or providers; and with concerns such as vaccine shortages (e.g., yellow fever, hepatitis A), the incidence of even preventable travel-related illnesses will likely not decrease.
Primary providers remain the best to ask the questions whether a person plans travel or has returned from travel. After “thinking travel,” the provider must then determine whether he or she is capable of caring
for the person or whether it is best to refer to someone with more expertise. We hope the material in this text will provide basic information for those who are new to the field, and updates for the veterans. We trust that those providers who choose to care for travelers can count this newest edition as a reliable and “go-to” reference.
REFERENCE
1. Riddle M, et al. Guidelines for the prevention and treatment of travelers’ diarrhea: a graded expert panel report. J Travel Med 2017;24(1):S63–80.
KEY POINTS
Epidemiology: Morbidity and Mortality in Travelers
Sandra Grieve and Robert Steffen
• Travel health risks are dependent on the itinerary, duration and season of travel, purpose of travel, lifestyle, and host characteristics.
• Motor vehicle injuries and drownings are the major causes of preventable deaths in travelers, while malaria remains the most frequent cause of infectious disease deaths.
• Complications of cardiovascular conditions are a major cause of death in travelers, par ticularly when senior citizens spend the winter in southern destinations.
INTRODUCTION
Compared to staying at home, mortality and morbidity are increased in those who travel, especially when their destination is a developing country. Travel health risks vary greatly according to:
Where
• industrialized versus destination in a lower income country
• city or highly developed resort versus off-the-tourist-trail locale
When
• season of travel (e.g., rainy versus dr y, extremes of temperature)
How long
• duration of stay abroad
For what purpose
• tourism versus business versus rural work versus v isiting friends or relatives ( VFR)
• other (militar y, airline crew layover, adoption, medical procedures abroad, etc.)
Style
• hygiene standard expected: high (e.g., multistar hotels) versus low (e.g., low-budget backpackers)
• special activities (high-altitude trekking, diving, hunting, camping, etc.)
Host characteristics
• healthy versus preexisting condition, nonimmune versus semiimmune
• age (e.g., infants, senior travelers)
This chapter w ill concentrate on the available epidemiologic data associated with travel health risks in general ( Tables 2.1 and 2.2); it will only to a limited extent describe the epidemiology of individual diseases at the destinations (Table 2.3). Such data are often unsatisfactory because they are incomplete, old, or were generated in studies that may have been biased.1 Lastly, v isitors often experience far less exposure to pathogens than the native population (e.g., w ith respect to hepatitis B,
• Travelers’ diarrhea ( TD) remains the most frequent illness among travelers; the risk of TD can be divided into three risk categories based on destination.
• Casual sex w ithout the regular use of condom protection continues to be common practice by travelers.
typhoid). Thus, seroepidemiologic data from destination countries are usually of little relevance when assessing the risk in travelers. Among the infectious health risks, only those about which travel-related data have been published w ill be mentioned. The reader should consult current websites and tropical medicine textbooks for information about less common travel-related infections, such as trypanosomiasis.
CORNERSTONES OF TRAVEL HEALTH EPIDEMIOLOGY
Health problems in travelers are frequent. Three of four Swiss or Finnish travelers to developing countries had some health impairment, defined as having taken any therapeutic medication, or having reported being ill.2,3 At first glance, this proportion is alarming, but 50% of short-term travelers who crossed the North Atlantic had health impairments, often constipation.2,3 Acute gastroenteritis, respiratory tract infections, and ear infections were the most frequent.4
A larger follow-up study showed that only a few of these self-reported health problems were severe. Less than 10% of travelers to developing countries consulted a doctor either abroad or after returning home, or were confined to bed due to travel-related illness or an accident; <1% were hospitalized, usually only for a few days.2,3 However, it remains disturbing that >14% of such travelers are incapacitated. The most tragic consequence of travel is death abroad, which occurs in approximately 1/100,000. Sudden cardiac death, defined as an “unexpected, nontraumatic death that occurs w ithin 24h of the onset of symptoms,” has been shown to account for up to 52% of deaths during downhill skiing and 30% of mountain hiking fatalities5 (Fig 2.1).
A study based on medical insurance claims among World Bank staff and consultants demonstrated that business travel may also pose health risks beyond exposure to infectious diseases, and that medical claims are increasing with the increasing frequency of travel.6 Such data illustrate how noninfectious problems also play a significant role.
Abstract
In spite of natural disasters and turmoil in many countries, the number of people travelling abroad continues to increase. Reasons for travel vary with no barrier to age, health status, and proposed activities. Compared to staying at home, the potential for morbidity and mortality increases with travel, especially when people visit exotic or remote destinations in lower income countries. Because disease surveillance may be inadequate at some destinations, predicting the level of individual risk can be difficult and those offering travel health advice will remain uncertain about the risk behaviors of their clients. There are also limited data on people hospitalized abroad with most cases identified by anecdotal reporting on return home.
Keywords Epidemiology
Morbidity
Mortality
Prevention
Risk Travel Travelers’ health
a Among these travelers, 18% were born outside the United States.
b Among these travelers, 26% were born outside the United States.
c n = 458 (2 missing).
d Other includes volunteers/missionaries, health/medical treatment, research/study, or “other not mentioned.” IQR, Interquartile range; N/A, not available.
TABLE
2.2 Study
Characteristics Used to Determine the Best Estimate of the Number of International Travelers With a Travel-Related Illness (n = 9)
Study Data Source
Chen et al. Boston-Area Travel Medicine Network (BATMN)
Vilkman et al. Travel Clinic of Aava Medical Center
Stoney et al. New Jersey Behavioral Risk Factor Survey (NJBRFS)
Balaban et al. Large American public health agency
Dia et al. Marseille Travel Medicine Centre
Rack et al. Berlin Institute of Tropical Medicine
Hill University of Connecticut Health Center
Steffen et al. Zurich University Travel Clinic
Steffen et al. Returning flights to Switzerland
N/A, Not available.
MORTALITY
Enrollment
Recruited at pretravel consultation
Recruited at pretravel consultation
Random-digit dialing
Recruited at pretravel consultation
Recruited at pretravel consultation
Recruited at pretravel consultation
Recruited at pretravel consultation
Zurich airport
On board airplane by cabin crew
Data Collection Instrument(s)
Extraction from medical record
Weekly diary
Posttravel survey
Pretravel questionnaire
Follow-up questionnaire
At first g lance, data on the primary cause of deaths abroad appear contradictory. While some studies claim that accidents are the leading cause of death, others demonstrate the predominance of cardiovascular events.7
These differences are due primarily to the varied examined populations and destinations as well as to the fact that some see accidents as preventable and cardiovascular events as nonpreventable travel-related deaths. Southern Europe, Florida, Thailand, and parts of the Caribbean are favorite destinations for senior travelers, in whom elevated mortality rates due to a variety of natural causes are to be expected, whereas in developing destinations the risk of fatal accidents is clearly higher. In the 13 years between 1999 and 2011, there were 104 recorded deaths in the GeoSentinel global network, which captures trends in travel-related morbidity; included in these data are those seen at the GeoSentinel clinics who cross an international border, be they tourists, business people, or migrants. Malaria is prominent, along with sepsis, pulmonary syndromes including pneumonia and tuberculosis, and acute encephalitis. Underlying illnesses may also play a significant role, such as cardiovascular disease, AIDS, diabetes mellitus, and cancers (Pauline Han, personal communication, September 2011), as well as cofactors such as substance abuse. One of the limitations of GeoSentinel data is that the providers are generally experts in tropical and travel medicine practicing in tertiary care centers, and thus would not typically be in a position to see patients following trauma or for other ailments unrelated to infectious diseases; thus infectious diseases are overrepresented.
Accidents
Deaths abroad due to injuries are two to three times higher in travelers age 15–44 years than in the same age group in industrialized countries. Fatal accidents are primarily due to motor vehicle injury. There are
Timeframe(s)
At pretravel visit
During travel 2–4 weeks posttravel
At pretravel visit 3 weeks after pretravel visit
NJBRFS Travel Health Module Travel in the previous 12 months
Pretravel survey
Posttravel survey (web-based)
Pretravel questionnaire
Posttravel questionnaire
Extraction from medical record
Posttravel questionnaire
Brief questionnaire (with possible telephone interview)
Standardized questionnaire (phone-based)
Pretravel questionnaire
Retrospective questionnaire
Questionnaire
At pretravel visit N/A
At pretravel visit
Within a week of return
At pretravel visit N/A
Within 2 weeks after travel 2 months after travel
Just prior to boarding a flight 7 months after departure
Flight back to Switzerland
fewer than 20 deaths per 100,000 motor vehicles per annum reported in most Western European countries, compared to 15 in the United States, 20–71 in Eastern Europe, 9–67 in Asia, and 20–118 in Africa.8 Motorbikes are frequently implicated (partly because in many countries there is no obligation to wear a helmet), and alcohol often plays a role. Tourists are reported to be several times more likely than local drivers to be involved in accidents.9
Drowning is also a major cause of death and accounts for 16% of all deaths (due to injuries) among US travelers. Reasons include alcohol intoxication, the presence of unrecognized currents or undertow, and being swept out to sea.
Kidnapping and homicides have been increasing, but these are usually limited to employees of international and nongovernmental organizations. Fatal assaults on tourists and terrorism may occur anywhere, not only in developing countries.
Animals are a relatively uncommon cause of death among travelers. There are now some 50 annual confirmed shark attacks worldwide and the number is rising, possibly due to neoprene wetsuits, which allow the wearer to stay longer in colder water where the risk is greater.10
Among safari tourists in South Africa, three tourists were killed by wild mammals in a 10-year period, two by lions after the individuals left their vehicle to approach them. The number of fatal snakebites is estimated to be 40,000 worldwide (mainly in Nigeria and India), but few v ictims are travelers.
A broad variety of toxins may also be a risk to travelers. Ciguatoxin leading to ciguatera syndrome after the consumption of tropical reef fish is a major risk: The case fatality is 0.1%–12%. “Body-packing” of heroin, cocaine, and other illicit drugs in the gastrointestinal tract or in the vagina may result in the death of travelers when the condoms or other packages break. Fatal toxic reactions and life-threatening neurologic sy mptoms after the inappropriate and frequent application of highly concentrated N,N-diethyl-m-toluamide (DEET, now called
TABLE 2.3 Illnesses Acquired by International Travelers in the Included Studies (n = 9)
Study (No. Ill) Top 5 Illnesses (%)
Chen et al.
(n = 400)
Vilkman et al.
(n = 363)b
Stoney et al.
(n = 48)
Balaban et al.
(n = 33)
Dia et al.
(n = 313)
Rack et al.
(n = 282)
Hill
(n = 501)
Steffen et al.
(n = 1209)
C: Greek/Canary Islands
(n = 178)
Steffen et al. (n = 7906)
C: N. America
(n = 643)
Diarrhea (52)
Headache (26)
Fatigue (25)
Cough (24)
Runny/stuffy nose (24)
Travelers’ diarrheac
problem
tract infection
Diarrhea (21)
Sore throat (11)
Nausea/vomiting (9)
Congestion/runny nose (8)
Coughing (7)
Arthropod bite (62)
Diarrhea (46)
Sunburn (36)
Vomiting (9)
Cough (8)
Gastrointestinal (81)
Respiratory (32)
Fever (15)
Dermatologic (10)
Diarrhea (46)
Respiratory tract symptoms (26)
Skin problem (8)
High-altitude sickness (6)
Motion sickness (5)
Severe diarrhea (56)
Vomiting or abdominal cramps (26)
Common cold (14)
High fever over several days (13)
Dermatosis (8)
Severe diarrhea (43)
Vomiting or abdominal cramps (28)
Common cold (13)
Diarrhea (34)
Constipation (14)
Respiratory infections (12)
Insomnia (11)
Headache (8)
Constipation (20)
Respiratory infection (8)
Headache (8)
N/A (4.3 by M.D., plus 1.0 by nurse) N/A (0.7, some just outpatients)
N/A (0.9 by M.D., plus 0.2 by nurse) N/A (0.2, some just outpatients)
aOne traveler with heart disease and a pulmonary embolism; two others with unspecified chronic medical conditions; one unknown.
bBased upon data available for 459 of the 460 ill travelers in this study.
cDenominator could not be determined from the article.
dOne traveler with malaria and the other with angina.
C, Control group; N/A, not available.
FIG. 2.1 Fatalities among French abroad 2000–2004. (With permission from Jeannel D, Allain-Loos S, Bonmarin I, et al. Bull Epidemiol Hebd 2006;23–24:166–8.)
N,N-diethyl-3-methylbenzamide) in small children have rarely been observed. Lead-glazed ceramics purchased abroad may result in lead poisoning and could remain undetected for a long period of time.
Infectious Diseases
Malaria is the most frequent cause of infectious death among travelers. Between 1989 and 1995, 373 fatalities due to malaria were reported in nine European countries, w ith 25 deaths in the United States.11,12 Most reported malaria cases in Europe were travel related, the overall confirmed case rate in 2014 was 1.24 cases per 100,000 population, which is the highest rate observed during the period 2010–2014.12 This was almost exclusively due to Plasmodium falciparum, the case fatality rate ranging from 0% to 3.6%, depending on the country. The most recent US surveillance data show that there were 1724 cases of imported malaria reported to the Centers for Disease Control and Prevention (CDC) in 2014, numbers indicative of a steady trend upward since 1973. The largest percent were in the VFR population (67%). The number of military cases climbed twofold from 2013 to 2014. Of all cases reported in the United States in 2014, 17% were severe and 1.7% died.
Among deaths due to infectious diseases, HIV previously held a prominent place, although it did not appear in the statistics as it is a late consequence of infection abroad and may not be recognized as having been acquired during travel. With modern treatment options and postexposure prophylaxis, mortality associated with HIV infection abroad has decreased. HIV patients have a higher risk of complications of other infections while traveling, which ultimately may be fatal.13
There is a multitude of other infections that may result in the death of a traveler. There are anecdotal reports about fatal influenza, mainly among older adults par ticipating in cruises. Rabies, if untreated, has a case fatality rate of almost 100%. Overall, however, fatal infections in the traveler can, for the most par t, be effectively prevented. Two cases of West Nile v irus ( WNV) were reported in Dutch travelers returning from Israel14 and one Canadian traveler died of WNV infection after a v isit to the state New York.
Other Illness and Mortality
Senior travelers in particular may experience a new illness or complications of a preexisting condition such as cardiovascular problems.15 Evidence has also been generated to support the fact that pulmonary embolism associated with deep vein thrombosis occurs after long-distance air travel, and many of these cases are fatal. Severe sy mptomatic Accidents: Drowning, mountain 18.3%
pulmonary embolism in the period immediately after travel is extremely rare after flights of <8 hours. In flights >12 hours the rate is five per million. Risk factors for this have been clearly identified.16
Aeromedical Evacuation
Accounts on repatriation are instructive, as they are a mirror of serious health problems, many of which are not reported otherwise. Some 50% of aeromedical evacuations are due to accidents, often involving the head and spine, and 50% are due to illness. In the latter group, cardiovascular or cerebrovascular and gastrointestinal problems are the most frequent causes. Psychiatric problems continue to be a cause for evacuation, but their numbers may have decreased. It may be that psychiatric conditions are less likely to be reported as the reason for evacuation or it may be that worldwide communication has improved to the extent that emotional support and assistance from home is more easily accessed.17
MORBIDITY
As mentioned, illness during and following travel is common. Many articles have been w ritten citing a variety of percentages of travelers becoming ill; most recently a review of these data estimated that between 43% and 79% of travelers who v isited developing nations become ill, most frequently w ith diarrhea.1
Men and women present w ith different profiles of travel-related morbidity. Women are proportionately more likely than men to present with urinary tract infection.17
Travelers’ Diarrhea
Classic travelers’ diarrhea ( TD) is defined as three or more unformed stools per 24 hours, w ith at least one accompanying sy mptom, such as fecal urgency, abdominal cramps, nausea, vomiting, or fever. Also milder forms of TD may result in incapacitation.18
TD is usually caused by fecal contamination of food and beverages. The pathogens responsible for TD are described elsewhere in this volume (see Chapters 18 and 20).
There are three levels of risk for TD (Fig 2.2): (1) Low incidence rates (up to 8%) are seen in travelers from industrialized countries who stay for 2 weeks in Canada, the United States, most par ts of Europe, or Australia and New Zealand; (2) intermediate incidence rates (8%–20%) are experienced by travelers to most destinations in the Caribbean, some southern and eastern European countries, Japan, and South Africa; and (3) higher incidence rates (20%–66%) of TD are seen in journeys to developing countries during the first 2 weeks of stay.19 TD is still the most frequent illness among travelers from high to lower income countries, whereas those who live in areas of high endemicity have a lower risk as a result of acquired immunity. Groups at par ticularly high risk of illness include infants, young adults, and persons w ith impaired gastric acid barrier; some have a genetic predisposition. TD often has a par ticularly severe and long-lasting course in small children. If women more often present themselves with acute diarrhea, that may be associated w ith differences in perception.20
Over the first decade of the 21st century the rates of TD have decreased, mainly in emerging economy countries.21 The symptoms of TD in tourists frequently star t early during the stay abroad, though second episodes may occur. Untreated, the mean duration of TD is 4 days (median 2 days), and in 1% the sy mptoms may persist over 1 month. About one in five patients show signs of mucosal invasive or inflammatory disease with fever and/or blood in the stools. In 2.4%–17% of TD patients (and also few without TD symptoms), they will experience a postinfectious irritable bowel syndrome, rarely ar thritis, or other sequelae may develop. There is also concern about the importation of multidrug-resistant enterobacteriaceae.22
Risk:
Low <8%
Intermediate 8%–20%
High 20%–50% No recent data
FIG. 2.2 Incidence rates of travelers’ diarrhea 2006–2008 (n = 2800). (With permission from Pitzurra R. BMC Infect Dis 2010;10:231 and smaller recent studies.)
Malaria
Some 10,000 imported malaria infections are recorded annually by travelers and immigrants to nonendemic countries, but the real number might be six times higher.23 Most reported malaria cases in Europe were travel related; the overall confirmed case rate in 2014 was 1.24 cases per 100,000 population, which is the highest rate observed during the period 2010–2014.24
According to the annually published World Malaria Reports there has been a dramatic decline in the g lobal malaria burden w ith 88% of global cases originating in the World Health Organization ( WHO) African region.25 The risk of infection among tourists has decreased.26 Nevertheless some countries experience an increase of imported cases associated with VFRs and immigrants.27 The risk of malaria transmission also remains high in other parts of tropical Africa, in Papua New Guinea, and on neighboring islands.28
The proportion of P. falciparum infection varies. Depending on the precise destination, patients treated abroad are typically not included in reporting data. If they failed to use appropriate prophylactic medication, malaria would be a frequent diagnosis among travelers to tropical Africa. Using existing surveillance data and the numbers of travelers to the respective destinations, the relative risk of malaria in travelers visiting such countries can be estimated. Such data w ill only indicate a risk per country, not a precise destination.
The annual entomologic inoculation rate clearly demonstrates broad differences w ithin a country. This is illustrated in Kenya, w ith rates from 0 to 416 (at the coast locally exceeding 200), or w ithin a city and its suburbs, such as Kinshasa, 3–612 (equivalent to two infective bites each night).26,29
Risk of infection is influenced not only by destination but also by:
• number of vectors
• Anopheles species (infected vector density)
• population density (infected population density)
• infrastructure condition (housing, water management, mosquito control)
• resistance to insecticides
• seasonality, par ticularly rainfall
• duration of exposure (the cumulative risk of contracting malaria is proportional to the length of stay in the transmission area)
• style of travel (camping versus staying in air-conditioned or wellscreened urban hotel)
• host factors (such as semi-immunity, pregnancy)
These variables illustrate that it is impossible to predict the risk of malaria transmission by more than a rough order of magnitude in any specific traveler. The travel health advisor and even the traveler w ill often ignore at least some of these parameters. Finally, old data may have become obsolete in view of global warming: In Nairobi, for example, in an area previously free of transmission at an elevation of 1700 m, an increasing risk of malaria is reported. Nevertheless, one can at least estimate whether a traveler w ill be at high or low risk.
A more detailed account of malaria epidemiology, w ith maps, is found in Chapter 14, where the adverse events due to prophylactic medication against malaria are discussed.
Vaccine-Preventable Infections
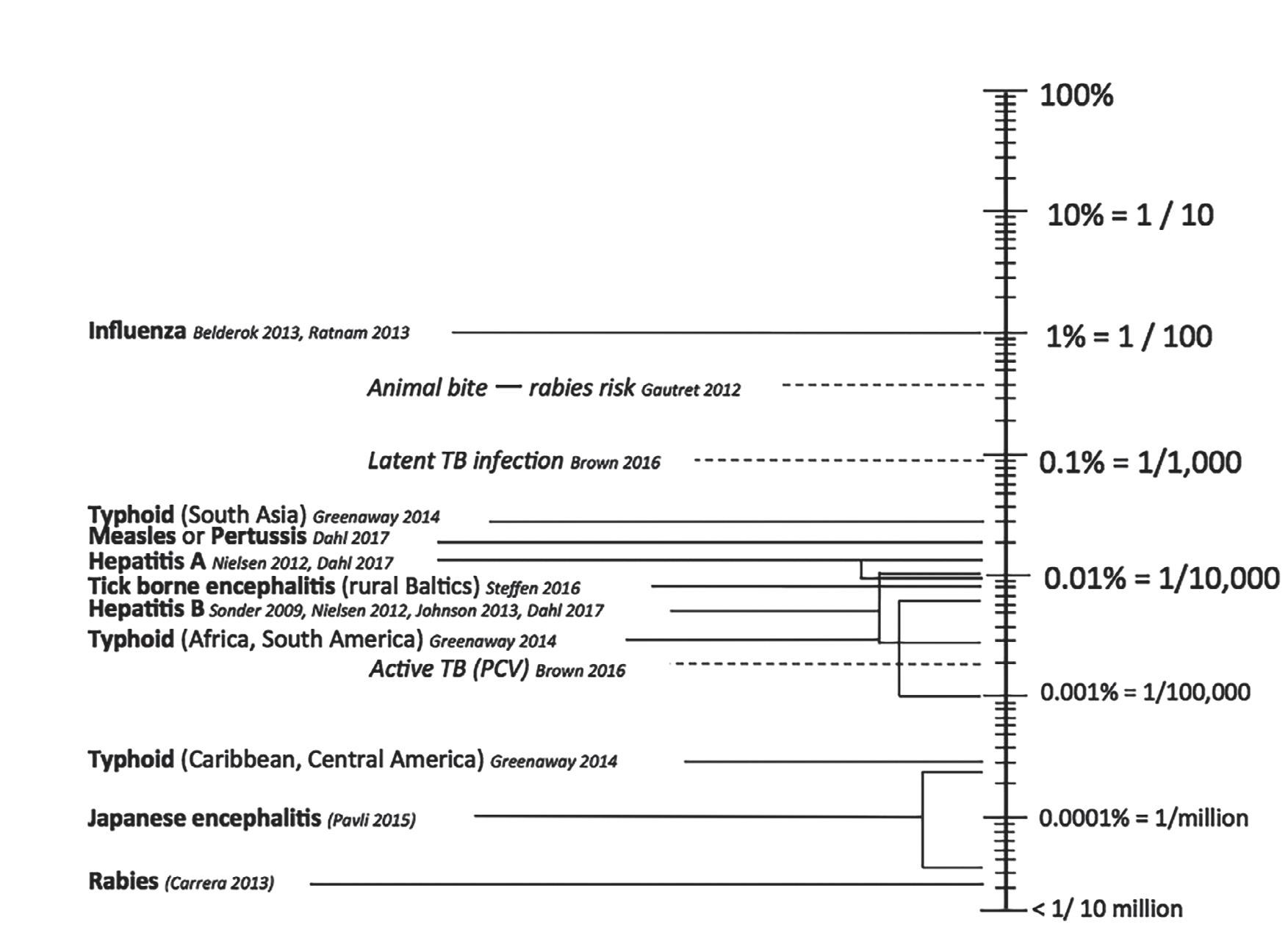
Updated morbidity and mortality data (Fig 2.3) have recently been generated for vaccine-preventable diseases. It is uncertain as to what
Estimated incidence per month of vaccine preventable diseases in lower-income countries among nonimmune Western travelers with most recent references 2017
degree an observed decrease in the risk of hepatitis A is due to improved hygiene conditions at the destinations or to greater immunization rates.21 Travel-related vaccine-preventable diseases are often divided into those that are required, routine, and recommended (see also Chapters 9, 10, 11, 12, and 13). Below is a list of those as well as some of the recent epidemiology relating to the illnesses in travelers.
Required Immunizations. Yellow fever occurs only in subSaharan Africa, South America, and Trinidad. Usually a few hundred cases are reported to WHO annually, but it is estimated that >100,000 cases occur. Yellow fever has never been transmitted in Asia, although the vectors, Aedes (now Stegomyia) and Haemagogus, have been observed there.28 Yellow fever is extremely rare in travelers, but nevertheless cases in unvaccinated travelers have increasingly been reported in the last few years despite the fact that these travelers should have been immunized.28 In 2016, several cases were imported to China, some of them fatal.30 Even though there is no risk at the destination, sometimes countries w ill require a yellow fever vaccine certificate, because the traveler has just transited a yellow fever zone (even when staying in the aircraft).31 Travel health advisors and travelers alike need to remain vigilant about checking on regulations through the WHO website or national guidelines that are updated frequently. Even so, countries have the capacity to alter their policies as they deem necessary.32
Until the early 2000s, meningococcal disease was frequently observed during or after the hajj or umrah pilgrimage to Mecca (200/100,000), but this problem has been resolved by public health measures issued by the Saudi authorities. The disease is rare even in travelers staying in countries where the infection is highly endemic (0.04/100,000). The case fatality rate among travelers slightly exceeds 20%. Rarely, Neisseria meningitidis may be transmitted during air travel of at least 8-hour duration.33
10% = 1/10
1% = 1/100 0.1% = 1/1,000 0.01% = 1/10,000
0.001% = 1/100,000
= 1/million
million
Proof of polio vaccine for certain populations has also been recently required by the Saudi government for pilgrims to the hajj. Polio immunization is also required for travelers leaving polio-infected countries, such as Pakistan, after a stay exceeding 4 weeks.34
Routine Immunizations. To the authors’ knowledge, a sing le case of tetanus was reported in a traveler several decades ago, but such cases may be hidden in national surveillance data.
As demonstrated by a large epidemic in the former Soviet Union during 1990–1997, diphtheria may flare up under specific circumstances.35 This epidemic resulted in dozens of importations to Western Europe and North America; some travelers died while still in Russia. Far less serious forms of cutaneous diphtheria are occasionally imported, mainly from developing countries.
Poliomyelitis has continued to be a problem in the past few years, mainly in Afghanistan, Pakistan, and Nigeria, from where some cases were exported by travelers.36 In typical travelers, poliomyelitis has in the past decade been observed in a sing le VFR student returning from Pakistan to Australia.37 Thus WHO has developed an interactive map with the countries or areas for which it recommends polio immunization or boosting (http://apps.who.int/ithmap/).
Anecdotal reports exist on pertussis, Haemophilus influenzae B, measles, mumps, and rubella in travelers. European infectious disease surveillance data are available.38 In view of suboptimal compliance with measles vaccination, European, African, and Asian travelers are responsible for outbreaks mainly on the American continent where vaccine uptake is far superior.39,40
Recent reports showed a sharp rise in the number of measles cases reported in European Union/European Economic Area (EU/EEA) countries, five times more than the annual average for the preceding
5 years. These cases may be linked to travel to and from Europe, where unimmunized or nonimmune travelers have come into contact w ith the disease or transported it.41
Pertussis is a reemerging disease in many areas and immunity has waned. New vaccine availability in some areas allows boosting of adults to tetanus, diphtheria, and pertussis in a sing le injection. Hepatitis B, now a routine immunization in most industrialized countries, was mainly a problem for expatriates living close to the local population and for travelers w ith bloodborne or sexual exposures. The estimated incidence in travelers from Amsterdam to HBV-endemic countries is 4.5/100,000 travelers.42 While minute quantities of the virus are sufficient for transmission and the exact mode of transmission may remain undetected in many individuals, clear risk factors (casual unprotected sex, nosocomial transmission, etc.) have often been suspected. Behavioral surveys have shown that 10%–15% of travelers voluntarily or involuntarily expose themselves to blood and body fluids while abroad in high-risk countries. Besides the risk factors mentioned, such persons have also visited dental hygienists, had acupuncture, cosmetic surgery, tattooing, ear piercing, or scarification. Travel specifically for surgical procedures abroad (medical tourism) is increasing and is highlighting the emergence of a new antibiotic resistance mechanism and associated consequences for creating g lobal public health problems.43
Recommended Immunizations. The most frequent vaccinepreventable infection in nonimmune travelers to developing countries is influenza. Various outbreaks on cruise ships have been described (the usual risk groups are at risk of complications). Hepatitis A is now third, with a current average incidence rate of 30/100,000 per month. It is also the case that “luxury” tourists staying at multistar resorts may be at risk of infection.
Typhoid fever is diagnosed with an incidence rate of 30/100,000 per month among travelers to South Asia (Pakistan, Nepal, India); elsewhere (except probably in Central and West Africa), this rate is 10 times lower or even less. Those visiting friends and relatives import a fair proportion of these infections, but tourists originating in industrialized countries are also affected. The case fatality rate among travelers is 0%–1%.44 A paper reviewing the morbidity seen in >37,000 travelers revealed that 580 presented w ith vaccine-preventable diseases. Of those, the most common seen were enteric fever, acute v iral hepatitis, and influenza. Hospitalizations occurred w ith greater frequency in those diagnosed with vaccine preventable diseases, and deaths also occurred.45
The risk of rabies is high in Asia (particularly in India), from where 90% of all human rabies deaths are reported, but there may be underreporting in other par ts of the world. Bat rabies may occur in areas that are thought to be rabies free, such as Australia and Europe. Many among the monthly 0.2%–0.4% who experience an animal bite in developing countries are at risk of rabies. Rabies is a par ticular risk in those who are in close contact w ith indigenous populations over a prolonged time (e.g., missionaries, those traveling by bicycle, those working w ith animals, or those who explore caves) as well as children (because of their attraction to animals and their lack of reporting bites).
Based on post-travel skin tests, the incidence rate of Mycobacterium tuberculosis infection is 3000/100,000 person-months of travel, and 60/100,000 developed active tuberculosis. Transmission during long-haul flights and also during prolonged train and bus rides is rarely reported. Those who travel to work in hospitals, prisons, or orphanages may also be at increased risk. Other transmission can be neglected, except if there is repeated exposure, as may occur particularly among long-term, low-budget travelers or expatriates.46 Migrants and refugees are of even greater concern w ith respect to importation of tuberculosis.47
The risk of cholera was approximately 0.2/100,000 based on older surveys, although asymptomatic and oligosymptomatic infections may
be more frequent, as demonstrated in Japanese travelers. But as a public health issue this is irrelevant, as secondary infections do not occur.48 The case fatality rate among travelers is <2%.
For several potentially vaccine-preventable diseases, the risk of infection is less than one per million. Although a few dozen cases of Japanese encephalitis have been diagnosed in civilian travelers during the last 25 years, the attack rate of sy mptomatic disease in civilians is estimated to be 1 per 400,000–1,000,000. Sixty percent of these cases occurred in tourists, including some short-term travelers to Bali and Thailand.49
Only three international travelers have been diagnosed w ith plague since 1966, the last in 2017 was associated w ith a large outbreak in Madagascar.
Changes in climate and habitation are altering the epidemiology of tickborne encephalitis, and the disease is now being reported from areas previously not known to be endemic. Tickborne encephalitis is a serious health risk par ticularly for those hiking or camping in endemic areas between April and November. Basing on 38 reported cases among international travelers, the attack rate can be extrapolated to be 0.5–1.3 per 100,000 overall in western and central European endemic areas for the exposed at-risk population.50
Other Infections
Only a few selected types of infections will be mentioned in this section. Those about which no more than anecdotal reports have been published will be omitted.
Sexually Transmitted Diseases. According to most surveys, casual sex, in almost 50% of cases w ithout regular condom protection, is practiced by 4%–19% of travelers while they are abroad, resulting in HIV infection and other sexually transmitted diseases (STDs).51 In Switzerland it is estimated that 10% of HIV infections are acquired abroad. In the United Kingdom, the risk of acquiring HIV is considered to be 300 times higher while abroad, compared to staying at home. A third of heterosexuals acquired their infection in the United Kingdom; the remaining two-thirds are thought to have been acquired in subSaharan Africa.52,53
The WHO estimates that 75% of all HIV infections worldwide are sexually transmitted, and that the efficiency of transmission per sexual contact ranges from 0.1% to 1%. The transmission probability of HIV is greatly enhanced by the presence of other STD and genital lesions, as is often the case in female commercial sex workers and other infected persons in developing countries. Typically, 14%–25% of cases of gonorrhea and sy philis diagnosed in Europe were imported from abroad.54 Only 14% of cases reported in 2013 were among young people between 15 and 24 years of age; the majority of cases were reported in people 25 years and older. More than half (58%) of the sy philis cases were reported in men who have sex w ith men (MSM). Young adults and MSM remain the key vulnerable groups for STDs in the EU/EEA.55 The first campaign targeting those over 50 years of age was launched to highlight rising STDs and poor sexual health in this age group, many of whom indulge in casual sexual activity abroad.56,57
Upper Respiratory Tract Infection (URTI). This is one of the most frequent health problems, w ith attack rates varying from 8% to 34% in Finnish short-term travelers.3,4 From interviews in Chinese hospitals, there is anecdotal evidence that lower respiratory tract infections occur particularly often in this country.
Other Arboviral Infections: Dengue, Chikungunya, Zika. In Southeast Asia and other endemic areas, the seroconversion rate of dengue in travelers is quite impressive. In Thailand the daily risk of
dengue infections per 100,000 travelers has been estimated to be 2.14 and 7.03 for low and high dengue seasons, respectively.58 Similarly, chikungunya endemicity has expanded mainly to the Americas, to a limited degree also to Southern Europe. Many travelers have been affected; the main problems associated w ith this infection are ar thritis and arthralgias.59
Most recently, a Zika epidemic mainly in Latin America and the Caribbean has caused concern not only among the local population, but also among travelers. Transmission occurs not only through Aedes mosquitoes, but also through sex, blood transfusion, or rarely laboratory exposure. The main fear is that intrauterine infection may result in microcephaly of the newborn. Additionally, some patients subsequently may suffer Guillain-Barré syndrome.60
Legionella. The rate of Legionella infections reported to European surveillance is on a plateau with some 5000 cases having been reported both in 2009 and 2010; 20% were associated with travel.61 In the United States, about 6000 cases were reported in 2015, though this is probably an underestimate because the disease is underdiagnosed. Legionnaires disease is waterborne and typically transmitted from air-conditioning and heating units, hot tubs, fountains, and water features. Common contributing factors include inadequate disinfection, maintenance, and monitoring; water stagnation; poor temperature control; and poor ventilation. Interestingly, some outbreaks repeatedly occurred on the same site.62
Leishmaniasis. Cutaneous disease has frequently been described in travelers, w ith those infected w ith HIV being at par ticularly high risk, but to the authors’ knowledge no systematic review with data has been published.
Schistosomiasis. Using newer serologic tests, there are data to suggest that schistosomiasis is an infection that both long-term and short-term travelers, but particularly missionaries and volunteers, acquire in endemic areas.63 Some returning travelers have symptoms, but many are diagnosed by serology alone. It is currently unknown whether or not most exposed travelers would ever develop typical signs and sy mptoms of chronic disease.
Trypanosomiasis. Trypanosomiasis, in its African form, was reported in only 29 cases in the United States in the 20th century, but the risk seems to be increasing.
Noninfectious Health Problems
This covers a broad variety of problems, accidents, and illnesses, which can be divided into environmental or host factors.
Environmental. Travel may result in stress, par ticularly fear of flying—most prominent during take-off, landing, and turbulence—and flight delays, which are frequent causes for anxiety.64 Motion sickness may affect up to 80% of passengers in small vessels in rough seas, but also affects passengers (albeit fewer) on jet flights. In-flight emergencies occur in 1/11,000 passengers, the most frequent ones being gastrointestinal, cardiac, neurologic, vasovagal, and respiratory. Changes in climate and altitude also create problems. In par ticular, high-altitude sickness (described in Chapter 42) w ill affect every hiker if ascent to high altitudes is rapid.
Health impairments related to diving are described in Chapter 43. Other environmental issues occasionally come into play. For example, consideration should be given to long-term travelers or expatriates with chronic hear t or lung disease planning on staying in regions where there is excessive air pollution.
In addition to the accidents described in the mortality section, small bruises acquired while swimming, and other marine hazards or lacerations due to sporting activities, may take longer to heal in view of suprainfection. Sprained ankles and other sports injuries are frequent, particularly among senior travelers who tend to fall, for example, in dimly lit hotels and on stairs.
Host. Persons w ith pre-existing medical conditions may experience exacerbations. This is particularly common in those with immunosuppressive illnesses, chronic constipation, diarrhea, or other gastrointestinal ailments, whereas others, such as dermatologic conditions or degenerative joint pain, may improve in a sunny, warm climate.65
CONCLUSION AND PRIORITIZATION
In conclusion, health professionals who advise travelers must keep the described epidemiologic facts in mind when determining what preventive measures are needed. Ultimately, the decision regarding to what degree one wishes to protect future travelers is an arbitrary one; no one should give the illusion that “complete protection” is possible. Prioritization (e.g., with respect to vaccines) is possible, but one ought to have concrete goals to reduce morbidity. However, even when prioritization is necessary, consideration should be given to the specific individual, his or her medical history, and travel circumstances. For travelers to malaria-intense regions, despite financial limitations and unwillingness to continuously use medication, chemoprophylaxis should still be strongly encouraged. Advisors should keep in mind that TD is the most frequent health problem and counsel accordingly, particularly including self-treatment abroad.
Despite the need for prioritization, educational needs do not change and efforts to provide as much information as possible are always imperative. Although these measures can certainly mitigate health problems, travel will always have some inherent additional risks compared to staying at home.
REFERENCES
1. Angelo KM, Kozarsky PE, Ryan ET, et al. What proportion of international travelers acquire a travel-related illness? A review of the literature. J Travel Med 2017;24:tax046.
2. Steffen R, DeBernardis C, Banos A. Travel epidemiology—a global perspective. Int J Antimicrob Agents 2003;21:89–95.
3. Vilkman K, Pakkanen SH, Lääveri T, et al. Travelers’ health problems and behavior: prospective study w ith post-travel follow-up. BMC Infect Dis 2016;16:328.
4. Siikamäki H, Kivela P, Fotopoulos M, et al. A closer look at travellers’ infections abroad: finnish nationwide data w ith incidences, 2010-2012. Travel Med Infect Dis 2016;ii, S1477.
5. Windsor JS, Fir th PG, Grocott MP, et al. Mountain mortality: a review of deaths that occur during recreational activities in the mountains. Postgrad Med J 2009;85:316–21.
6. Liese B, Mundt KA, Dell LD, et al. Medical insurance claims associated w ith international business travel. Occup Environ Med 1997;54:499–503.
7. Pawun V, Visrutaratna S, Ungchusak K, et al. Mortality among foreign nationals in Chiang Mai City, Thailand, 2010 to 2011. J Travel Med 2012;19(6):334–51.
8. Kopits E, Croper M. Traffic fatalities and economic growth. Accid Anal Prev 2005;37:169–78.
9. Sleet DA, Ederer DJ, Ballesteros MF Safety and Security Injury Prevention in Centers for Disease Control and Prevention. CDC Health Information for International Travel 2016. Oxford University Press; 2016. Chap 2. Available at: https://wwwnc.cdc.gov/travel/yellowbook/2016/the-pre-travel -consultation/injury-prevention
10. Ricci JA, et al. Shark attack-related injuries: epidemiology and implications for plastic surgeons. J Plast Reconstr Aesthet Surg 2016;69(1):108–14.
11. Leder K, Black J, O’Brien D, et al. Malaria in travelers: a review of the GeoSentinel surveillance network. Clin Infect Dis 2004;39(8):1104–12.
12. European Centre for Disease Prevention and Control. Annual Epidemiological Report 2016—Malaria. Stockholm: ECDC; 2016. Available at: http://ecdc.europa.eu/en/healthtopics/malaria/Pages/ Annual-epidemiological-report-2016.aspx
13. Furrer H, Chan P, Weber R, et al. Increased risk of wasting syndrome in HIV-infected travelers: prospective multicentre study. Trans R Soc Trop Med Hyg 2001;95:484–6.
14. Aboutaleb N, Beersma M, Wunderink H, et al. Case report: west Nile virus infection in two Dutch travellers returning from Israel. Euro Surveill 2010;15(34):art4.
15. Gautret P, Gaudar t J, Leder K, et al. Travel-associated illness in older adults (>60 y). J Travel Med 2012;19(3):169–77. doi:10.1111/j.1708-8305.2 012.00613.x. Available at: http://jtm.oxfordjournals.org/content/jtm/19/ 3/169.full.pdf
16. Watson HG, Baglin TP Guidelines on travel-related venous thrombosis. Br J Haematol 2010;152:31–4. Available at: http://www .bcshguidelines.com/documents/travel_related_vte_bjh_2011.pdf
17. Foreign and Commonwealth Office. Foreign travel advice for people w ith mental health needs. UK FCO 2016 Oct. Available at: https://www.gov.uk/ government/uploads/system/uploads/attachment_data/file/466424/FCO _MentalHealth_DL_071015web.pdf.
18. Steffen R, et al. Travelers’ diarrhea: a clinical review. JAMA 2015;313:71–80.
19. Pitzurra R, Fried M, Rogler G, et al. Irritable bowel syndrome among a cohort of European travelers to resource-limited destinations. J Travel Med 2011;18(4):250–6.
20. Schlagenhauf P, Chen LH, Wilson ME, et al. Sex and gender differences in travel-associated disease. Clin Infect Dis 2010;50:826–32.
21. Baaten GG, Sonder GJB, Schim Van Der Loeff MF, et al. Fecal-orally transmitted diseases among travelers are decreasing due to better hygienic standards at travel destination. J Travel Med 2010;17(5):322–8.
22. Riddle MS, Connor BA, Beeching NJ, et al. Guidelines for the prevention and treatment of travelers’ diarrhea: a graded expert panel report. J Travel Med 2017;24(suppl 1):S57–S74.
23. Tatem AJ, et al. The geography of imported malaria to non-endemic countries: a meta-analysis of nationally reported statistics. Lancet Infect Dis 2016;doi:10.1016/S1473-3099(16)30326-7.
24. European Centre for Disease Prevention and Control. Annual Epidemiological Report 2016—Malaria. Stockholm: ECDC; 2016. Available at: http://ecdc.europa.eu/en/healthtopics/malaria/Pages/ Annual-epidemiological-report-2016.aspx
25. World Malaria Report 2016. Geneva: World Health Organization; 2016. Licence: CC BY-NC-SA 3.0 IGO
26. Behrens RH, Carroll B, Hellgren U, et al. The incidence of malaria in travellers to South-East Asia: is local malaria transmission a useful risk indicator? Malar J 2010;9:266.
27. Public Health England. Malaria imported into the UK: 2015: implications for those advising travellers. Health Protection Report 2016;10(24):table4.
28. Cullen KA, et al. Malaria surveillance—United States, 2013. MMWR Surveill Summ 2016;65(S2):1–22.
29. Hay SI, Rogers DJ, Toomer JF, et al. Annual Plasmodium falciparum entomological inoculation rates (EIR) across Africa: literature survey, internet access and review. Trans R Soc Trop Med Hyg 2000;94:113–27.
30. Chen Z, Liu L, Lv Y, et al. A fatal yellow fever virus infection in China: description and lessons. Emerg Microbes Infect 2016;5(7):e69. doi:10.1038/emi.2016.89.
31. Schönenberger S, Hatz C, Bühler S. Unpredictable checks of yellow fever vaccination certificates upon arrival in Tanzania. J Travel Med 2016;23(5).
32. World Health Organization. WHO International Travel and Health Amendment to IHR Annex 7 Yellow Fever. July 2016 Countries w ith Risk of Yellow Fever Transmission and Countries Requiring Yellow Fever Vaccination. Available at: http://www.who.int/ith/2016-ith -annex1.pdf?ua=1
33. Steffen R. The risk of meningococcal disease in travelers and current recommendations for prevention. J Travel Med 2010;17:S9–17.
34. WHO Fact Sheet Poliomyelitis. Available at: http://www.who.int/ mediacentre/factsheets/fs114/en/.
35. Cameron C, White J, Power D, et al. Diphtheria boosters for adults: balancing risks. Travel Med Infect Dis 2007;5(1):35–9.
36. WHO Global Polio Eradication Initiative (GPEI). Available at: http:// polioeradication.org/where-we-work/.
37. Stewardson AJ, et al. Imported case of poliomyelitis, Melbourne, Australia, 2007. Emerg Infect Dis 2009;15:63–5.
38. European Centre for Disease Prevention and Control (ECDC). Surveillance Atlas of Infectious Diseases. Available at: http:// ecdc.europa.eu/en/data-tools/atlas/pages/atlas.aspx.
39. Lochlainn NL, Mandal S, de Sousa R, et al. A unique measles B3 cluster in the United Kingdom and the Netherlands linked to air travel and transit at a large international airport, February to April 2014. Euro Surveill 2016;21(13):doi:10.2807/1560-7917.ES.2016.21.13.30177.
40. Bednarczyk RA, Rebolledo PA, Omer SB Assessment of the role of international travel and unauthorized immigration on measles importation to the United States. J Travel Med 2016;23(3):ii, taw019.
41. European Centre for Disease Prevention and Control. Measles and rubella monitoring, July 2016—Disease surveillance data: 1 July 2015 – 30 June 2016. Stockholm: ECDC; 2016. Available at: http://ecdc.europa.eu/en/ publications/Publications/measles-rubella-monitoring-july-2016.pdf
42. Sonder GJ, Van Rijckevorsel GG, Van Den Hoek A. Risk of hepatitis B for travelers: is vaccination for all travelers really necessary? J Travel Med 2009;16:18–22. doi:10.1111/j.1708 – 8305.2008.00268.x.
43. Hanefeld J, Smith R, Horsfall D, et al. What do we know about medical tourism? A review of the literature w ith discussion of its implications for the UK National Health Service as an example of a public health care system. J Travel Med 2014;21(6):410–17.
44. Greenaway C, Schofield S, Henteleff A, et al. Summary of the Statement on International Travellers and Typhoid by the Committee to Advise on Tropical Medicine and Travel CATMAT. CCDR 40-4 2014. Available at: http://www.phac-aspc.gc.ca/publicat/ccdr-rmtc/14vol40/dr-rm40-04/ dr-rm40-04-tropmed-eng.php
45. Boggild AK, Castelli F, Gautret P, et al. GeoSentinel Surveillance Network. Vaccine preventable diseases in returned international travelers: results from the GeoSentinel Surveillance Network. Vaccine 2010;28(46): 7389–95.
46. Brown ML, Henderson SJ, Ferguson RW, et al. Revisiting tuberculosis risk in Peace Corps volunteers, 2006-13. J Travel Med 2015;23(1):doi:10.1093/ jtm/tav005.
47. Pareek M, Greenaway C, Noori T, et al. The impact of migration on tuberculosis epidemiology and control in high-income countries: a review. BMC Med 2016;14:48. doi:10.1186/s12916-016-0595-5.
48. Steffen R, Connor B Vaccines in travel health: from risk assessment to priorities. J Travel Med 2005;12:26–35.
49. Pavli A, Maltezou HC. Travel-acquired Japanese encephalitis and vaccination considerations. J Infect Dev Ctries 2015;9(9):917–24.
50. Steffen R. Epidemiology of tick-borne encephalitis ( TBE) in international travellers to Western/Central Europe and conclusions on vaccination recommendations. J Travel Med 2016;23(4):ii, taw018.
51. Richen J Sexually transmitted infections and HIV among travellers: a review. Travel Med Infect Dis 2006;4:184–95.
52. Skingsley A, Yin Z, Kirwan P, et al. HIV in the UK—Situation Report 2015: Data to End 2014. Public Health England; 2015 Nov. Available at: https://www.gov.uk/government/uploads/system/uploads/attachment_ data/file/477702/HIV_in_the_UK_2015_report.pdf
53. Sexually Transmitted Infections (STIs): Surveillance, Data, Screening and Management. The Surveillance and Epidemiology of STIs. Data Collection, Public Health England; 2016. Available at: https://www.gov.uk/ government/collections/sexually-transmitted-infections-stis-surveillance -data-screening-and-management
54. Tanton C, Johnson AM, Macdowall W, et al. Forming new sex partnerships while overseas: findings from the third British National Survey of Sexual Attitudes & Lifestyles (Natsal-3). Sex Transm Infect 2016;92(6):415–23. doi:10.1136/sextrans-2015-052459.
55. European Centre for Disease Prevention and Control. Sexually Transmitted Infections in Europe 2013. ECDC; 2015. Available at: http:// ecdc.europa.eu/en/publications/publications/sexual-transmitted-infectionseurope-surveillance-report-2013.pdf.
56. Family Planning Association (FPA) warns of rising STIs and poor sexual health in the over 50s. Available at: http://www.fpa.org.uk/news/fpawarns-rising-stis-and-poor-sexual-health-over-50s
57. Rice B, Gilbar t VL, Lawrence J, et al. Safe travels? HIV transmission among Britons travelling abroad. HIV Med 2012;13(5):315–17.
58. Polwiang S. Estimation of dengue infection for travelers in Thailand. Travel Med Infect Dis 2016;14(4):398–406.
60. Hamer DH, Barbre KA, Chen LH, et al. GeoSentinel Surveillance Network. Travel-associated Zika virus disease acquired in the Americas through February 2016: a GeoSentinel analysis. Ann Intern Med 2016.
61. Beauté J, Zucs P, de Jong B European Legionnaires’ Disease Surveillance Network. Legionnaires disease in Europe, 2009-2010. Euro Surveill 2013;18(10):20417.
62. Mouchtouri VA, Rudge JW. Legionnaires’ disease in hotels and passenger ships: a systematic review of evidence, sources, and contributing factors. J Travel Med 2015;22(5):325–37.
63. Nicolls DJ, Weld LH, Schwartz E, et al. GeoSentinel Surveillance Network. Characteristics of schistosomiasis in travelers reported to the GeoSentinel Surveillance Network 1997–2008. Am J Trop Med Hyg 2008;79(5):729–34.
64. Oakes M, Bor R. The psychology of fear of flying (par t I): a critical evaluation of current perspectives on the nature, prevalence and etiology of fear of flying. Travel Med Infect Dis 2010;8(6):327–38.
65. Carroll B, Daniel A, Behrens RH. Travel health par t 1: preparing the tropical traveler. Br J Nursing 2008;17(16):1046–51.