Consciences and the Reformation: Scruples over Oaths and Confessions in the Era of Calvin and His Contemporaries (Oxford Studies in Historical Theology) 1st Edition
When we seek to discover the best in others, we somehow bring out the best in ourselves.
–William Arthur Ward
To all the teachers and students: Writing this textbook has been a journey for us that we could not have done alone. The process has enriched our friendship and shaped our teaching and practice. We hope that the information presented will help you on your professional journey and bring out the best in each other and the patients that we serve.
We dedicate this book to our families for their support, patience, and energy during this long and time-intensive process.
To Greg and the Dunleavy, Johnstone, and Smith families.
Kim
To Ken, Miye, and Tyler.
Amy
CONTRIBUTORS
Kim Dunleavy, PT, PhD, MOMT, OCS, FNAP
Board-Certified Orthopedic Clinical Specialist
Director of Community Engagement and Professional Education
Clinical Associate Professor
Department of Physical Therapy
College of Public Health and Health Professions
University of Florida Gainesville, Florida
Krissa Gorman, PT, DPT*
Physical Therapist
UF Health Rehab Center at the Orthopaedic and Sports Medicine Institute Gainesville, Florida
Kevin Lulofs-MacPherson, PT, DPT, FAAOMPT
Board-Certified Orthopedic Clinical Specialist
Clinical Lecturer
Department of Physical Therapy
College of Public Health and Health Professions
University of Florida Gainesville, Florida
* Contributed Case Study 11.3.
William F. McGehee, PT, PhD
DPT Program Director
Department of Physical Therapy
College of Public Health and Health Professions
University of Florida Gainesville, Florida
Jason Roberts, PT, CSCS
Senior Physical Therapist
Rehabilitation Institutes of Michigan Detroit, Michigan
Equilibrium Studio Bloomfield Hills, Michigan
Amy Kubo Slowik, PT, CSCS
Senior Physical Therapist
Rehabilitation Institute of Michigan Detroit, Michigan
Equilibrium Studio Bloomfield Hills, Michigan
Introduction to Therapeutic Exercise for Rehabilitation
Kim Dunleavy
OBJECTIVES
Upon completion of this chapter, the reader will be able to:
1. Describe the role of therapeutic exercise in a patient’s rehabilitation process for promoting maximal functional recovery and preventing further injury.
2. Define the components of the patient management model.
3. Describe the phases of healing.
4. Define and provide examples for the terms precautions and contraindications
USE OF THERAPEUTIC EXERCISE FOR REHABILITATION
Therapeutic exercise is an essential component of any rehabilitation program following injury, deconditioning, or disease. This textbook will emphasize the use of therapeutic exercise for musculoskeletal conditions to promote recovery and restoration of function. Therapeutic exercise is often used in conjunction with other interventions and taught in the clinical setting. After discharge from individual management, patients may continue performing the exercises in the clinic or at home, alone, or in organized groups. While some exercises seem simple, patients often have difficulty learning how to perform them correctly. Exercising using poor form will render less than optimal results, substituting strong muscles for the targeted weak muscle and movement patterns that place continued stress on the injured area. Safe, effective therapeutic exercise requires skilled instruction and teaching strategies.
Prescribing exercise is often a complex process and requires constant monitoring and clinical reasoning. As movement specialists, therapists should select the exercises to meet each individual’s needs and adjust the prescription based on their responses. Some essential aspects of therapeutic exercise prescription include (1) setting individualized goals that are repeatedly adjusted as a patient progresses, (2) selecting appropriate exercises based on foundational concepts, (3) assessing the patient’s ability to perform exercise and choosing appropriate dosage, (4) teaching patients to perform the exercises safely and efficiently, and (5) monitoring and evaluating responses to exercise. The therapist also functions as a coach, encouraging patients to reach their highest potential. There are countless variations of exercises, and therapists have the unique opportunity to create exercise programs that are matched to the patient’s needs rather than only using established exercise protocols. Protocols provide helpful
5. Define SINS (severity, irritability, nature, stage) components and explain how information from subjective complaints, patient history, and diagnoses are used to guide the choice of therapeutic exercise and modify techniques.
6. Define and explain types of exercise.
guidelines and healing time frames, but applying the principles of safe exercise prescription will allow the therapist to prescribe tailored, inspiring exercise programs for their patients. This text is not intended to be an all-inclusive, exhaustive list of exercises and does not include rigid guidelines. Rather, the aim of the content and concepts and their application to case study examples is to provide a framework for the thought processes and decision-making required for exercise prescription, instruction, and evaluation.
PATIENT MANAGEMENT MODEL
Elements of the Patient Management Model described in the American Physical Therapy Association’s Guide to Physical Therapy Practice will be used in this text ( Table 1.1 ), with the major focus on the Intervention category.1 The physical therapist will perform an examination including taking a history, a review of systems, and performing tests and measures to determine the extent of impairments and activity or participation limitations. Some examination techniques are covered in Chapter 4 ; however, because this is not the emphasis of this textbook, the reader is referred to other textbooks such as Magee’s Orthopedic Physical Assessment, 2 Magee and Sueki’s Orthopedic Physical Assessment Atlas and Video,3 Reese and Bandy’s Joint Range of Motion and Muscle Length Tested , 4 and Netter’s Orthopaedic Clinical Examination: An Evidence-Based Approach 5 for details on specific examination techniques. The evaluation process involves interpreting results from the examination while considering pathology to formulate a physical therapy diagnosis. The medical diagnosis is often described using standardized International Classification of Disease (ICD) codes,6 which are now used in all healthcare settings for data records.
BOX 1.1 Impairments, Activity Limitations, and Participation Restrictions7
Impairments: Problems with body functions (physiological) or structure (anatomical)
Participation restrictions: Difficulties an individual has with involvement in life situations (social interaction, work, family, or community activities)
CONTRAINDICATIONS AND PRECAUTIONS
One of the most important tasks is to identify any contraindications (resulting in stopping the examination and referring to other providers) or precautions ( requirements to prevent further or new damage of tissue) (Table 1.2 and Box 1.2 ) . Contraindications and precautions should be determined early in the evaluation process. A thorough review of symptoms and medical history should be used to rule out any serious pathology or reasons for referral to other professionals. 8 Contraindications are elements indicating that severe
TABLE 1.2 Examples of Precautions and Contraindications
Type of
Precautions Diagnosis Precautions
Cardiovascular Contraindications and Precautions
Cardiovascular contraindications
Acute angina
Severe hypertension
Cardiovascular precautions Hypertension (150/90)
Postsurgical Precautions
Total hip replacement precautions
Posterior total hip replacementa
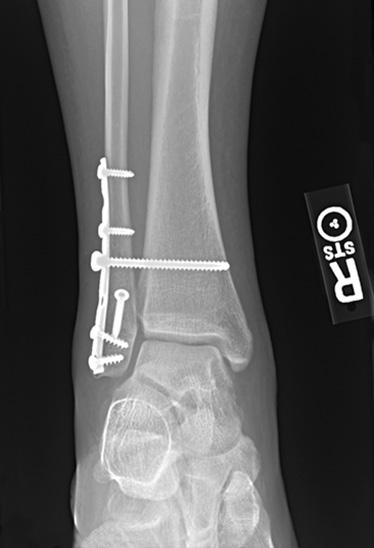
Weight bearing Bi-malleolar fracture treated with internal fixationb
Do not exercise or discontinue exercise with signs of extreme fatigue, sweating, shoulder or chest pain
Exercise is contraindicated if systolic blood pressure is above 200 mm Hg or below 80 mm Hg or if diastolic blood pressure is greater than 100 mm Hg8,9
Discontinue exercise with signs of extreme fatigue, sweating, shoulder or chest pain
Discontinue exercise if blood pressure increases >10 mm Hg
Avoid hip flexion >90 degrees, adduction crossing midline, and internal rotation
Methods/Actions
Do not start to exercise or discontinue; refer for medical attention
Do not start to exercise; refer for medical attention
Monitor cardiovascular responses before, during, and after exercise
Non–weight bearing for 8 weeks, cast boot, and partial weight bearing (50%) after sufficient healing is present at 8 weeks
Choose exercises that do not involve hinging at the hip past 90 degrees
No gluteal or hamstring stretching past 90 degrees of hip flexion or flexion-adduction combinations
Care with functional transitions (sit-to-stand, transfers to the floor)
Exercise equipment settings may require adjustments (raise seat on stationary bike)
See Fig. 1.2
Use scale to ensure amount of force
Use assistive device or parallel bars to reduce and distribute forces
TABLE 1.2 Examples of Precautions and Contraindications—cont’d
Type of
Precautions
Diagnosis
Fall prevention High fall risk after bedrest
Posttrauma Contraindications
Screen for contraindications related to structural damage
Monitor dizziness or lightheadedness during changes in position
Fall prevention precautions
Avoid specific directions of force
Ankle lateral ligament moderate tear
Full examination to rule in or out the possibility of fracture in the presence of swelling, inability to bear weight, extreme pain, or positive screening tests
Possible ligamentous laxity after whiplash
Possible vertebral artery syndrome
Avoid valgus forces during weight-bearing exercises
Methods/Actions
Monitor blood pressure pre-exercise and with transitions
Monitor patient symptoms during transitions or changes in position
Guarding and gait belt if any symptoms or blood pressure drops with transitions
Choose single-plane motion in sagittal plane to avoid localized forces to the medial structures
Limit tensile forces Achilles tendon partial tear
Avoid full stretch of ligaments (plantarflexion and inversion: the direction of force causing the injury)d
Avoid full stretch of tendon with forces exceeding tissue strength
Ranges and movements that do not stress lateral ligaments (neutral starting position, mid-position, moving into full eversion) with exercise against elastic resistance, avoiding the full stretch of the ligament into inversion and plantarflexion—the position that resulted in the injury (see Clinical Examples 2.1 and 2.2)
Use bracing or taping to assist with limiting movement in full range (see Clinical Examples 2.1 and 2.2)
Limit range to mid-position of the tendon length (see Clinical Example 2.3)
Limit amount of force (see stress-strain curve in Chapter 2)
aFigure from Patton K, Thibodeau G. The Human Body in Health and Disease. 6th ed. St. Louis, MO: Elsevier; 2014, p 193.
bFigure from Rynders SD, Hart JA. Orthopaedics for Physician Assistants. St. Louis, MO: Elsevier Saunders; 2013, Fig 8.15.
cFigure from Manske RC. Fundamental Orthopedic Management for the Physical Therapist Assistant. 4th ed. St. Louis, MO: Mosby; 2016, Fig. 9.1.
dFigure from Manske RC. Fundamental Orthopedic Management for the Physical Therapist Assistant. 4th ed. St. Louis, MO: Mosby; 2016, Fig. 17.1.
Fig. 1.2 Exercises for total hip replacement. (Cameron MH, Monroe LG. Physical Rehabilitation Evidence-based Examination, Evaluation and Intervention. Philadelphia: Saunders; 2007, Fig. 10.5.)
BOX 1.2 Contraindications and Precautions
Contraindication : Direction and degree of motion, extent of force, or other force-related factors that should be completely avoided to prevent further damage and allow structures to heal. Cardiovascular contra indications are used to prevent excessive stress on the cardiovascular system.
Precaution: Direction and degree of motion, amount of force, or other force-related factors that should be limited in order to allow structures to heal. Precautions can also be related to the need to rule out more serious damage or to evaluate responses to exercise. Other precautions are to prevent damage, injury, or adverse event, such as fall prevention.
consequences could result from movement or exercise. As an example, if a patient has symptoms consistent with acute angina or extremely high blood pressure, all exercise would be contraindicated and the patient would be referred for medical attention. If a patient has moderate spinal osteoporosis, spinal flexion against resistance or for long durations is contraindicated, but exercise in supported positions with low resistance may be possible.
Identifying precautions during the subjective history can result in modifying or avoiding examination procedures. An example of a precaution is limiting hip flexion to no more than 90 degrees in patients who recently had a total hip replacement with a posterior surgical approach to avoid stretching the posterior hip capsule. Therefore, the physical therapist would not attempt to measure hip flexion range of motion beyond 90 degrees during this patient’s initial
BOX 1.3 SINS
The acronym SINS is useful for judging the intensity and difficulty of the initial exercise.
• S = Severity (greater severity – use more caution in the choice of exercise)
• I = Irritability (greater irritability – use more caution in the choice of exercise)
• N = Nature (observe precautions and contraindications related to diagnosis and comorbidities, elements of the pathology that influence type of forces allowed or avoided)
• S = Stage (phase of healing – use to determine type of exercise and focus on impairments or functional recovery)
evaluation. The precautions and contraindications are formulated based on subjective information reported by the patient, knowledge of pathology, and the possible identification of additional diagnoses or pathologies derived from the patient’s medical and surgical histories (see Table 1.2 ). There are common precautions that are based on postsurgical healing requirements for incisions, while others are related to the type and extent of tissue damage. Fall and weight-bearing precautions prevent injury (see Table 1.2 ). Contraindications and precautions can also be related to comorbidities (other medical conditions) such as hypertension or cardiac disease. 8,9,10 While most contraindications and precautions are extremely important during the early stages of healing, precautions related to medical comorbidity are followed throughout the rehabilitation process.
SEVERITY, IRRITABILITY, NATURE, STAGE
The acronym SINS (Box 1.3) can be used to help determine the intensity and difficulty of the initial choice of exercise. In the subjective interview, the therapist collects information from the patient, including medical history, relevant medical tests, symptoms, and the relationships with movement. The therapist will use the interview findings as well as intake forms and validated tools to supplement the patient interview and determine an initial hypothesis to help plan further examination. The SINS acronym can assist with an early clinical judgment of whether the examination needs to be cautious or can be somewhat more aggressive.
Severity
Severity is usually determined by the amount of pain reported, but it can also be based on the extent of physical damage. The greater the severity of the symptoms or damage, the more cautious the initial exercise choice should be and the slower the exercise progression (Clinical Example 1.1). For example, a patient who is recovering after a fracture that required surgical fixation will be progressed cautiously, taking into account the amount of bone healing. A patient with a mild ankle sprain can be progressed faster than a patient with a moderate ankle ligament tear.
CLINICAL EXAMPLE 1.3 Nature of Problem: Influence of Diagnosis and Extent of Pathology on Exercise Choices—cont’d
Patient B
A 53-year-old administrative assistant was referred to the clinic for management of pain in her hands. She has been diagnosed with osteoarthritis.
Precautions
Forces that increase the angulation of the index or fifth fingers would be adjusted in this patient. Excessive force is limited for the proximal and distal interphalangeal joints.
Exercise Implications
Active or passive movement may be limited by bony changes. Functional movement and exercise would need to be evaluated, keeping in mind the need to distribute forces and avoid excessive angulation.
Comparison of Patients A and B
The amount of force applied to both patients would need to be monitored, but Patient A’s inflammatory disease condition requires very strict precautions and extremely limited loads. Patient B might be able to start with functional movement reeducation and with exercises at a slightly higher level than Patient A. Both patients will need to be monitored for joint effusion and exacerbation of symptoms, but the expectation for the speed of exercise progression would be higher for Patient B.
3
Radiograph showing osteoarthritic changes similar to Patient B. There is generalized osteopenia with joint space narrowing at the proximal and distal interphalangeal joints and osteophytic changes. While range of motion at the second and third proximal interphalangeal joints and distal fifth interphalangeal joint may be restricted, there is less need for caution here than with Patient A, and exercise would be progressed as tolerated. (From Eisenberg R. Comprehensive Radiographic Pathlogy 5th ed. St. Louis: Mosby; 2012, Fig. 4.23.)
through stages varies. This chapter will briefly summarize each phase. Chapter 2 will cover the goals for each phase, the characteristics of various tissue types, and how these characteristics impact exercise prescription.
Phase I: Inflammation (Immediately to Approximately 10 Days)
Inflammation is the normal initial response to injury and is necessary for healing; it is typified by redness, swelling, increased warmth, and pain. Resolving the inflammation as soon as possible can help prevent the ill effects of prolonged immobility and disuse. The forces that the tissue is normally designed to withstand may need to be decreased to allow resolution of the inflammatory process. Exercises during this phase can be used to reduce inflammatory by-products while avoiding increasing the inflammatory responses. Chronic inflammation related to inflammatory arthritis, infection, or connective tissue disorders may continue for longer than 10 days, and there are occasions where aggravation of a chronic condition results in low-grade chronic inflammation for longer periods.
Phase II: Tissue Repair (10 Days to
According to Tissue Type)
3 Months, Variable
Fibroblasts lay down tissue to repair the injured site and macrophages remove waste tissue. The new tissue is organized in response to stresses placed on it by a slow progression of either stress or strain (usually separately). Too much stress can reinitiate the inflammatory process and result in damage to the newly formed tissue. Exercises during this phase should address impairments.
Phase III: Functional Recovery (6 Weeks to 2 Years, Variable by Tissue Type)
Mature tissue is able to withstand the demands of functional activities. Exercises during this phase help restore the patient’s functional deficits, or activity and participation limitations.
TYPES OF EXERCISE
The types of exercise are characterized by the amount of muscle activation and by the assistance provided for movement or the specificity of exercise to address impairments while providing optimal support for healing (Box 1.4).
Passive
Passive movement is performed by someone other than the patient (Video 1.1), by a mechanical device, or using gravity. Patients can also perform passive movement using another limb, without active muscle contraction of the affected area. Passive range of motion exercises are used to maintain range of motion in two instances: if a patient is unable to actively move the body part or if muscle activity at the time is likely to cause further damage.
Active-Assisted
Active-assisted exercise is conducted by the patient using some assistance from the other limb (Video 1.2), another person, mechanical devices, or gravity (Video 1.3). Active-assisted exercise may be used to help the patient achieve full range of motion when weakness or pain is limiting the range of motion or as a progression during the recovery when limited muscle force on structures is preferable.
Review of Foundational Concepts
Kim Dunleavy
OBJECTIVES
Upon completion of this chapter, the reader will be able to:
1. Compare the causes, signs, and symptoms of traumatic versus repetitive strain injuries.
2. Describe the implications of the history of the damage on the examination and treatment using exercise.
3. List and describe the phases of tissue repair and recovery and factors for promotion of optimal recovery.
TISSUE DAMAGE: TRAUMATIC VERSUS REPETITIVE STRAIN INJURIES
Musculoskeletal injuries can be categorized as either traumatic or repetitive strain injuries (Box 2.1 and Table 2.1). Traumatic injuries occur when major forces are applied beyond the body part’s capacity to withstand (Fig. 2.1). The individual can identify a specific incident when the injury occurred and often complains of immediate functional difficulty. Signs include inflammation (swelling, pain, redness) and inability to use the region. The sooner the symptoms appear, the greater the likelihood of major damage. Examples of traumatic injuries are fractures, cartilage tears, tendon ruptures, or complete muscle tears. Traumatic injuries are related to excessive load (stress), excessive tensile force (strain), or combinations of both types of forces. These injuries often occur with high-speed, uncontrolled movements, or when the individual is unable to avoid or withstand external force (Fig. 2.1A). Another possible mechanism of injury is when a patient attempts to move one body part in one direction while stabilizing another body part, such as when the foot is firmly planted and the individual attempts to turn or move the body in another direction (Fig. 2.1B).
BOX 2.1 Traumatic Versus Repetitive Strain Injury
• Traumatic injury: An injury resulting from a major force in a single, identifiable event.
• Repetitive strain injury: An injury occurring over time, from the cumulative effect of repeated minor trauma to an area.
4. Describe how tissue healing concepts for bone, muscle, tendon, ligament, and cartilage influence goals for exercise therapy.
5. Describe the forces that should be limited or applied through exercise therapy to allow optimal tissue recovery.
6. Describe the biomechanical concepts that will influence functional movement and therapeutic exercise techniques during exercise therapy rehabilitation.
TABLE 2.1 Traumatic Versus Repetitive Strain Injury
Traumatic Injury (or Resultant Surgery)
Extent of forces causing damage
Major forces (speed, torque, localized direction)
History Sudden onset: History of an identifiable incident
Signs of inflammation Signs of inflammation (redness, heat, swelling, pain) appear immediately or shortly after incident, constant pain and limited function
Implications for evaluation
Need to identify extent of tissue damage (for possible referral) and to identify precautions and contraindications
After surgical management, evaluation may need to be adjusted based on surgical technique and postoperative contraindications and precautions
Repetitive Strain Injuries
Minor forces (repeated, concentrated)
Gradual onset: slow build up and multiple minor incidents, OR patient is not able to identify an incident
Low-grade inflammation or no visible redness, heat, swelling; pain experienced with movement, specific positions, or after onset of movement not constant, symptoms can be due to fibrosis
Need to identify extent of damage and possible contributing factors
in microfailure, while macrofailure is a complete tissue tear. Microfailure can occur after the yield point when the loads reach the plastic region of the stress-strain curve and tissue is unable to return to the initial length after the force is removed. Application of repeated forces without sufficient time for the tissue to recover and mild damage after a traumatic incident can both result in failure of some fibers and are both described as microfailure. Macrofailure occurs when the failure point is reached and permanent rupture of collagen occurs.1,2
Ligament, tendon, and muscle tears are often classified according to the extent of damage, such as Grade I (mild), Grade II (moderate), and Grade III (complete disruption) (Box 2.3).4,5 Grade I damage is the result of microfailure. More fibers reach the failure point in Grade II. In Grade III, complete macrofailure and disruption occurs.4 The greater the tissue damage, the greater the inflammatory response and the risk of further structural damage to the affected or nearby tissues.
After diagnosis of the location and degree of damage, appropriate medical or surgical management should follow.
Precautions or contraindications are determined based on the extent of damage and the need to protect healing structures. The process of orthopedic physical therapy examination and diagnosis is described extensively in other texts.4–6 The extent of the damage is considered when determining the severity of the injury (Clinical Example 2.1; see Chapter 1), which guides the aggressiveness of the exercise choices and progression. If tissue is partially torn, the amount of stress or strain that will result in further damage is less than for intact tissue. The anatomical plane and tissue type are used to establish precautions related to which directions of movement and forces are safe and promote optimal healing (see Box 2.1 and Clinical Example 2.1; Videos 2.3 and 2.4).
BOX 2.3 Classifications of Tissue Damage
• Grade I: Mild tear (microfailure)
• Grade II: Moderate tear
• Grade III: Complete disruption (macrofailure)
CLINICAL EXAMPLE 2.1 precautions During healing after Grades I–III ankle Sprain
The types of precautions will depend on the structure and function of the damaged tissue. The degree and length of time required for precautions increase based on the extent of tissue damage (see the following figures).
Grade I Ankle Sprain:
Stress and strain need to be limited more for Grade III tears. (Image on left from Mansfield P, Neumann D. Essentials of Kinesiology for the Physical Therapist Assistant 2nd ed. St. Louis, MO: Mosby; 2014.)
• Brace or taping is used to limit inversion for 6 weeks for walking, up to 3 months or longer for running and sports.
• Avoid placing the anterolateral ligaments in the fully stretched position (full combined plantarflexion and inversion). Midrange plantarflexion and dorsiflexion or isometrics are used to assist with resolution of the inflammatory by-products.
• While the ligament heals, full stretch of the ligaments in plantarflexion and inversion and outer range of the peronei is avoided, especially with high forces in weight-bearing positions. Often the position and direction of force of the injury is the same as the directions that need to be avoided.
TABLE 2.2 Goals of Exercise During phase I (acute Inflammation)
Goals
Protect injured structures
Increase circulation to region
Assist with removal of edema and effusion
Maintain muscle activation without excessive stress on injured structures
Exercise Choices
Avoid placing excessive load (stress or strain) on injured tissue where microfailure or macrofailure is likely to occur (see stress-strain curve)
Additional protection may be provided by use of assistive devices, bracing, or taping
Active low-intensity exercise of other joints around the injured region
Alternating active muscle contraction within available range (low intensity)
Isometric muscle contraction for short durations followed by relaxation
Generalized movement of the affected limb or trunk as well as localized muscle contractions listed above will help with motion of edema and effusion
Small-range active movement without stress on injured structures to maintain range or assist with removal of effusion. Decreasing effusion helps restore range if caused by increased intraarticular volume or pain at the end of range
Elements to Consider
Motion without strain may be possible in planes other than the plane controlled by the injured tissue
Muscle activity will assist with venous return, particularly if the limb is elevated
Only used if likelihood of bleeding is small
Active contractions are likely to provide mechanical “pumping” actions for circulation as well as promote movement of extracellular edema or intraarticular effusion
Motion of proximal or distal joint or other areas of the body can increase overall circulatory flow and challenge
Motion may increase immediately if effusion is the cause of limited range
Minimize effects of lack of activity or immobilization
Minimizing muscle atrophy and cardiovascular effects of immobility for the uninvolved regions and general body systems; may need to be adapted to follow precautions and allow adequate healing of the affected structure
Stimulation of nociceptive pathways occurs with the tissue damage and continues with the release of inflammatory mediators such as histamine and bradykinin (Fig. 2.6). Inflammatory responses also include a secondary vasoconstriction to reduce bleeding and muscle spasm to avoid further motion and damage. The inflammatory cycle is intended to restrict further damage and is completed by the removal of the damaged cellular debris and stimulation of fibroblastic activity. Scar tissue is formed to repair the structures.
Allow movement in other regions and joints, include equipment and unloaded exercise such as bike, aquatic therapy, upper body ergometer, upper body and trunk exercise, or resistance exercise with uninvolved body regions
During Phase I, the primary rehabilitation goals are to limit excessive forces to protect the damaged area and assist with resolution of inflammatory by-products (Table 2.2). Exercises can target the injured area or uninvolved areas and can assist with promoting circulation to the area, limiting pain, and assisting with resolution of edema.
Phase I exercises directed toward the injured joint should avoid excessive loads (stress) or stretching (strain), or the inflammatory phase can reinitiated. Movement in directions
Fig. 2.6 Secondary responses to traumatic injury.1
Phase II: Tissue Repair and Early Tissue Regeneration (5–10 Days to 3 Months, Depending on Tissue Type)
The primary mechanism for tissue repair occurs through fibrous tissue bridging the gap in damaged tissue. The amount of fibrous tissue is proportional to the amount of damage and the length of time that fibroblasts remain active. Phase II normally begins around 5–10 days after injury and can last through 3 months, depending on the tissue type (Box 2.7 and Table 2.3). The rate of production of new collagen fibers is greatest between 7 and 14 days post injury.1 The repair phase will overlap with the removal of inflammatory products.
The ability to monitor and evaluate a patient’s tolerance to load is an essential skill for therapists. Therapists should verify that there is adequate distribution of forces, graded load, and activity, and monitor responses to exercise (delayed-onset pain, edema, effusion, or other abnormal symptoms). Adverse responses warrant constant reevaluation and reduction of exercise load. If excessive load or tension is placed on tissue during Phase II, damage to the immature collagen or regenerated tissue results in inflammation and increased fibrosis. The subsequent edema and pain can also result in the patient
• Address impairments
• Provide optimal stimulus for tissue regeneration
• Minimize the effects of inactivity or immobilization
• Protect injured structures
• Improve muscle function without placing undue stress on injured tissues
TABLE 2.3 Goals for healing in phase II
Goals Exercise Choices
avoiding use of the region and compensating with other movement strategies. This can cause muscle atrophy, weaker connective tissue, and, ironically, further stresses on the damaged region. If additional stress occurs and damage of the immature collagen or the injured tissue ensues, the inflammatory cycle is reinitiated (see Phase I, Fig. 2.8).
The organization and strength of fibrous tissue is remodeled in response to stress applied to the structures during Phases II and III.1–3 Phase II exercises should promote tissue repair with targeted, smaller loads specific to the tissue type and function without reaching the ultimate failure point of the tissue. In addition, impairments such as muscle atrophy, joint restrictions, muscle tightness, pain, and compensatory mechanisms should be addressed during this phase (see Fig. 2.8 and Clinical Example 2.2). Exercises may target the impairments that are in the primary, injured area or in secondary regions that are contributing to biomechanical accumulation of forces.
Phase III: Tissue Maturation and Remodeling (6 Weeks to 2 Years, Depending on Tissue Type)
Phase III involves maturation and remodeling of the involved tissue as well as removal of excessive fibrotic tissue (Table 2.4 and Box 2.8). Tissue is remodeled by organizing the direction of collagen fibers to promote tissue capable of withstanding the forces needed for function. This process occurs in response to the appropriate type and direction of force for a particular tissue (see the section “Factors Influencing Healing: Tissue Characteristics”). The entire process may take up to 2 years, depending on the type of tissue.1–3 If necessary, Phase III treatment should
Protect injured structures Avoid placing excessive load on injured tissue or stretching to lengths where microfailure or macrofailure is likely to occur (see stress-strain curve).
Load (stress) is increased slowly in planes of movement of the injured structures, and range is limited to avoid maximum tension (strain).
Improve muscle function without excessive stress on injured structures
Minimize effects of inactivity or immobilization
Address specific impairments
Provide optimal stimulus for regeneration
Target other joints around the injured region with active, moderate-intensity exercise to assist with overall aerobic conditioning, improving muscle function and distributing forces.
Mobility, strength, specific muscular endurance, aerobic conditioning, coordination, or balance exercise
Elements to Consider
Load can be increased using isometric contractions or contractions in the inner or mid-range of injured structures to avoid extreme strain.
Midrange is determined by available range and not necessarily by normative values.
Other diagnoses, comorbidities, and higher severity or irritability are indications for stricter monitoring and extending periods of contraindications and precautions.
Positioning and choice of exercise can be adjusted to avoid excessive stress on injured structure with slow reapplication of stress.
Allow and progress movement in other regions and joints.
Tissue will regenerate in response to appropriate loads and strains placed on the structure. Initial loads should be light and directed in a way that places little stress on the healing tissue.
Monitor for adverse responses (delayed-onset muscle soreness, pain, effusion, or regression of improvements).