This work is subject to copyright. All rights are reserved by the Publisher, whether the whole or part of the material is concerned, specifcally the rights of translation, reprinting, reuse of illustrations, recitation, broadcasting, reproduction on microflms or in any other physical way, and transmission or information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed. The use of general descriptive names, registered names, trademarks, service marks, etc. in this publication does not imply, even in the absence of a specifc statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use. The publisher, the authors, and the editors are safe to assume that the advice and information in this book are believed to be true and accurate at the date of publication. Neither the publisher nor the authors or the editors give a warranty, expressed or implied, with respect to the material contained herein or for any errors or omissions that may have been made. The publisher remains neutral with regard to jurisdictional claims in published maps and institutional affliations.
This Springer imprint is published by the registered company Springer Nature Switzerland AG The registered company address is: Gewerbestrasse 11, 6330 Cham, Switzerland
Preface
Physical examination techniques have been the basis for medical care for hundreds of years and have been refned over time. Evaluation of the patient and determination of a specifc diagnosis is critical in determining the patient’s condition and need for treatment. We are fortunate to have developed technologies which facilitate the diagnostic process. One may be tempted to rely exclusively on diagnostic studies such as diagnostic imaging, laboratory testing, and/or invasive monitoring to reach a conclusion. The increased use of telemedicine has bolstered reliance on the results of studies instead of physical examination. This reliance on technology would suggest that physical examination of the patient is superfuous.
As technology is not infallible, the goal of this publication is to educate the reader regarding the importance of a well-performed examination during which the practitioner physically examines the patient and evaluates various characteristics of the musculoskeletal system to reach a diagnosis. Many times, there is a discrepancy between physical examination fndings and diagnostic technology results such as from an MRI scan. Having the ability to critically assess the injured body part to determine if the physical fndings are consistent with the MRI results is critical to determine if treatment is necessary. Therefore, we have an obligation to our patients to be able to create a differential diagnosis based on the physical examination.
In this book, we are fortunate to have experts from around the world share their experience in evaluating musculoskeletal injuries and conditions. We hope it will improve the reader’s ability to physically examine the patient in order to render a diagnosis.
San Diego, CA, USA
John G. Lane Milan, Italy Alberto Gobbi Porto, Portugal João Espregueira-Mendes
São Paulo, Brazil Camila Cohen Kaleka Hiroshima, Japan Nobuo Adachi
1 Shoulder Anatomy
Kevin Taniguchi, John G. Lane, and Anshuman Singh
2 Biomechanics of the Glenohumeral, Acromioclavicular, and Sternoclavicular Joints 9 Nahum Rosenberg
3 Evaluation of the Range of Motion of the Glenohumeral Joint
Aaron Martinez-Ulloa, Maria Valencia, and Emilio Calvo
4 Examination of Range of Motion Scapulothoracic, Acromioclavicular, and Scapulothoracic Joints 23
Giovanni Di Giacomo, W. Ben Kibler, Francesco Franceschi, and Aaron Sciascia
5 Clinical Tests for Evaluation of Motor Function of the Shoulder .
Nedal Alkhatib, Catherine M. Coady, and Ivan Wong
6 Evaluation of the Stability and Function of the Sternoclavicular and Acromioclavicular Joint 41
Daniel P. Berthold, Lukas N. Muench, Sebastian Siebenlist, Andreas B. Imhoff, and Augustus D. Mazzocca
7 Evaluation of the Stability and Function of the Glenohumeral Joint 53
Gregory W. Hall, Anthony Kasch, John G. Lane, and Anshuman Singh
8 Evaluation of the Stability and Function of the Scapulothoracic Joint
Maximilian Hinz, Daniel P. Berthold, Lukas N. Muench, and Knut Beitzel
9 Nerve Compressions Around the Shoulder 69
Daniel Adolfo Slullitel, Glasberg Ernesto, Escalante Mateo, and Vega Francisco
Stephen C. Weber, Prashant Meshram, Guillermo Arce, and Edward McFarland
Kyle R. Sochacki and Michael T. Freehill
Nadine Ott and Kilian Wegmann
Carina Cohen, Guilherme Augusto Stirma, Gyoguevara Patriota, and Benno Ejnisman
Carina Cohen, Gyoguevara Patriota, Guilherme Stirma, and Benno Ejnisman 15 Evaluation of Triceps Tendon
Andrea Celli, Nicoletta Fabio, Duca Vito, and Luigi Adriano Pederzini
Clinical Evaluation of the Distal Biceps Tendon
Deepak N. Bhatia and Gregory I. Bain
17 Evaluation of Elbow Instability with Clinical Testing
Yoav Rosenthal and Mark I. Loebenberg
18 Neurologic Evaluation of the Elbow and Forearm
José Carlos Garcia Jr, Rafael José Zamith Gadioli, and Leandro Sossai Altoé
19 Evaluation of Common Tendinopathies of the Elbow 159
Alessandro Marinelli, Catello Buondonno, Ahmad Al Zoubi, and Enrico Guerra
20 Evaluation of Sports-Related Elbow Instability
Cheli Andrea Filippo, Andrea Celli, and Luigi Adriano Pederzini
21 Compartment Syndrome in the Upper Limb
William N. Yetter and Benjamin R. Graves
22 Evaluation of Pediatric Elbow Conditions
Andrea Celli, Nicoletta Fabio, Duca Vito, and Luigi Adriano Pederzini
24
Christopher M. Stewart and Paul A. Ghareeb
Toshiyasu Nakamura
25 Evaluation of Range of Motion
Esther Ching San Chow
26 Clinical Testing of the Wrist
Toshiyasu Nakamura
27 Evaluation of the Triangular Fibrocartilage Complex
Zhixin Wang and Bo Liu
28 Compartment Syndrome of the Hand
Bernice Heng and Andrew Chin
29 Evaluation of the Neurological Conditions of the Elbow, Forearm and Hand
Margareta Arianni
30 Evaluation of Tendinopathies/Tendon Ruptures/Tendon Instability
Margaret Woon Man Fok
31 Evaluation of Hand Infections
Janus Siu Him Wong and Margaret Woon Man Fok
32 Diagnosis and Evaluation of Fractures of the Hand and Wrist
Lindsey S. Urband, Stephanie Wong, and Dori N. Cage
33 Evaluation of Instability and Joint Dislocations of the Hand
Hassan J. Azimi
34 Rheumatoid and Other Arthritis of the Wrist and Hand
Gregory R. Mack and Dori J. Neill Cage
Part IV Hip/Pelvis Reviewer Dr’s Rath & Hoelmich
35 Hip Anatomy 337
Domenico Potestio
36 Hip Biomechanics 341
Paolo Di Benedetto and Simona Cerulli
37 Evaluation of Dysplasia of the Hip (Children with DDH, Adolescents, and Adults)
Alessandro Aprato and Pietro Persiani
38 Evaluation of Hip Osteoarthritis
Christian Carulli, Lorenzo Ius, and Matteo Innocenti
39 Evaluation of Snapping Hip and Extra-Articular Impingement
Manlio Panascì and Alberto Costantini
40 Evaluation of Athletic Population with Hip/Hamstring/Quad Injuries 363
Paolo Di Benedetto, Giovanni Gorasso, Andrea Zangari, and Nunzio Lassandro
41 Limping Child .
Laura Ruzzini and Daniela Lamberti
42 Evaluation of Chronic Pelvic Pain (Athletic Pubalgia-Sports
373
Hernia and Other Pain Conditions) 377
Bisciotti Gian Nicola
43 Assessment of Outcome Scores of the Hip 385
Filippo Randelli, Gaia Santambrogio, Gennaro Fiorentino, Manuel Giovanni Mazzoleni, Alberto Fioruzzi, and Vittorio Calvisi
Part V Knee Reviewers Dr’s Gobbi, Lane & Espregueira-Mendes
44 Anatomy of the Knee
Fabio Valerio Sciarretta and John G. Lane
393
45 Biomechanics of the Tibiofemoral and Tibiofibular Joints . . . . . 403
Gwenllian Tawy, Alexander Jakubiec, and Leela Biant
46 Evaluation of Range of Motion of the Tibiofemoral Joint . . . . . 411
Laura Ann Lambert and Mike McNicholas
47 Clinical Tests for Evaluation of Motor Function of the Knee 419
Gabriel Ohana Marques Azzini
48 The Stability and Function of the Patellofemoral Joint 433
Laura Ann Lambert and Michael James McNicholas
49 Evaluation of the Stability and Function of the Tibiofemoral and Tibiofibular Joints .
Felipe Galvão Abreu, Renato Andrade, Rogério Pereira, Ricardo Bastos, and João Espregueira-Mendes
50 Evaluation of the Menisci .
Luís Duarte Silva, Philippe Tscholl, Ricardo Bastos, Renato Andrade, and João Espregueira-Mendes
443
459
51 Evaluation of Muscle Injuries 467
Camila Cohen Kaleka, Pedro Henrique C. Andrade, Pedro Debieux, André Fukunishi Yamada, and Moisés Cohen
52 Evaluation of Neuropathies/Nerve Entrapment Around the Knee Joint 473
Dawid Szwedowski, Przemysław Pękala, and Radosław Grabowski
53 Evaluation of Malalignment of the Knee
Ignacio Dallo, John G. Lane, Silvio Villascusa Marin, and Alberto Gobbi
477
54 Evaluation of Bursitis About the Knee 489
Katarzyna Herman, Przemysław Pękala, Dawid Szwedowski, and Jerzy Cholewiński
55 Evaluation of Patellofemoral Knee Pain .
Fabio Valerio Sciarretta and John G. Lane
Part VI Ankle Reviewer Dr Canata
56 Foot and Ankle Anatomy 511
Giovanna Stelitano, Vincenzo Candela, Calogero Di Naro, Carlo Casciaro, Giuseppi Longo, and Vincenzo Denaro
57 Biomechanics of the Ankle Syndesmosis . .
Kenneth J. Hunt
58 Clinical Tests for Assessment of Instability of the Ankle and Syndesmosis 521
Flávio Cruz, Gustavo Vinagre, and Pieter D’Hooghe
59 Evaluation of the Achilles Tendon 539
Niklas Nilsson, Annelie Brorsson, Katarina Nilsson Helander, Jón Karlsson, and Michael Carmont
60 Evaluation of Ankle Impingement . .
Nasef M. N. Abdelatif
61 Stress Syndromes Around the Ankle .
Julie Amendola and Annunziato Amendola
62 Evaluation of Common Injuries of the Ankle and Calf Areas 569
Gian Luigi Canata, Giacomo Zanon, Valentina Casale, Alberto Castelli, and Alberto Polizzi
63 Assessment of Outcome Scores of the Ankle . . .
Cortez L. Brown, Stephen Canton, Lorraine Boakye, and MaCalus V. Hogan
Part VII Foot and Toes Dr Canata
64 Anatomy of the Foot . .
Ivan Saenz, Ignasi Manent, Anna Rubio, and Fernando Conejo
65 The Art of the Musculoskeletal Physical Exam: Foot and Toes Biomechanics of the Foot 607
Masato Takao, Kosui Iwashita, and Yasuyuki Jujo
66 Ankle Joint Range of Motion Evaluation (ROM) Using Smartphone Calculators . .
Marco Quaranta, Francesco Oliva, and Nicola Maffulli
67 Assessment of Instability of the Calcaneus and Lisfranc 623
Ramakanth, Harsh Jalan, and Shanmuganathan Rajasekaran
68 Evaluation of Hindfoot Varus and Valgus Conditions . . . . . . . . . 633
Hamed Mazoochy
69 Hindfoot Tendinopathies . .
Pim A. D. van Dijk
639
70 Examination of Common Heel and Forefoot Conditions . . . . . . 651
Kenneth J. Hunt
71 Evaluation of Stress Fractures
Gustavo Vinagre, Flávio Cruz, and Pieter D’Hooghe
655
72 Clinical Examination: Evaluation of Neurologic Conditions of the Foot (Interdigital Neuromas, Charcot-Marie-Tooth Disease) 671
Giovanna Stelitano, Calogero Di Naro, Vincenzo Candela, Casciaro Carlo, Laura Risi Ambrogioni, Giuseppi Longo, and Vincenzo Denaro
Part I
Shoulder Reviewer John Lane
Shoulder Anatomy
Kevin Taniguchi, John G. Lane, and Anshuman Singh
1.1 Shoulder Anatomy
1.1.1
Osseous
The primary articulation of the shoulder is the glenohumeral joint which is “ball-and-socket” shape with the concave glenoid fossa of the scapula articulating with the slightly ovoid head of the humerus. The glenoid is shallow with a large radius of curvature permitting for a wide arc of motion as it articulates with the humerus [1]. In order to maintain this relationship, however, it requires stabilization by surrounding bones, ligaments, and muscles.
The scapula is a fat, triangular shaped structure that serves as a skeletal strut for the shoulder joint as well as an attachment site for the various soft tissue structures that stabilize the shoulder. The glenoid is located at its lateral aspect and articulates with the humeral head. The acromion is a hook-like structure projecting off the posterolateral border of the scapula. Anteriorly, the acromion articulates with the clavicle, a broad S-shaped bone connecting the scapula to the sternum, together forming the acromioclavicular joint, allowing scapular rota-
K. Taniguchi
US Navy-Balboa Medical Center, San Diego, CA, USA
J. G. Lane · A. Singh (*) University of California at San Diego, San Diego, CA, USA e-mail: jglane@san.rr.com
tion while holding the shoulder out to length [2]. The clavicle articulates with the sternum, or breastbone which is the only connection between the shoulder and the axial skeleton. The coracoid is a bony projection off the anterior-lateral aspect of the scapula and serves as an attachment site of several ligaments: the coracoclavicular ligaments, coracoacromial ligaments, and coracohumeral ligaments. These, along with the acromioclavicular ligaments, form the superior shoulder suspensory complex, a ring of bone and soft tissue that is an important biomechanical structure stabilizing the shoulder joint [3] (Fig. 1.1).
1.1.2 Muscles
The deltoid muscle forms the superior-lateral contour of the shoulder. There are three sets of fbers that form the heads of the deltoid; anterior, intermediate, and posterior. These originate on the anterior aspect of the clavicle, acromion, and scapular spine, respectively [4]. The orientation of these fbers allow for the various functions of the deltoid. The anterior fbers assist in forward fexion of the arm and medial rotation. The intermediate fbers allow for abduction of the arm away from the body in the frontal plane, and the posterior fbers assist in extending the humerus [5]. There are three muscles that originate on the cora-
J. G. Lane et al. (eds.), The Art of the Musculoskeletal Physical Exam, https://doi.org/10.1007/978-3-031-24404-9_1
K. Taniguchi et al.
Fig. 1.1 The shoulder has four articulations: the scapulothoracic, sternoclavicular, glenohumeral, and acromioclavicular. The latter two are visible on this anteroposterior radiograph. Bozkurt, M., & Acar, H. I. (Eds.). (2017). Clinical anatomy of the shoulder: An atlas (1st ed.). Springer International Publishing
coid process of the scapula; the pectoralis minor, coracobrachialis, and short head of the biceps. The pectoralis minor helps to depress and internally rotate the scapula while elevating the ribs aiding with inspiration during breathing; the coracobrachialis and short head of biceps act to fex the arm [6]. The long head of the biceps is a secondary fexor of the arm, its primary function is supination of the forearm. It originates at the supraglenoid tubercle on the scapula and its tendon runs intra-articularly within the glenohumeral joint as it moves distally towards its insertion on the radius of the forearm. The triceps brachii runs opposite the fexors on the posterior aspect of the arm and is an antagonist to the biceps, coracobrachialis, and brachialis muscles, acting to extend the arm at the elbow. It is made up of three heads; the long, medial, and lateral. The long head originates at the infraglenoid tubercle, and since it spans the shoulder joint, contributes to extension and adduction of the shoulder. The medial and lateral heads originate on the posterior humeral shaft, distal to the long head. The three heads converge to a single tendon attaching at the posterior aspect of the olecranon process of the elbow [7].
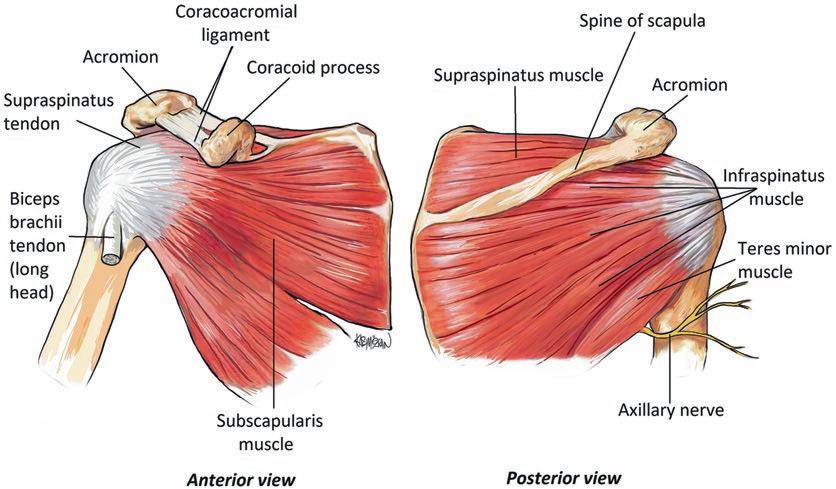
The rotator cuff is a key structure in regard to stability and function of the shoulder joint. It is comprised of four muscles: the supraspinatus, infraspinatus, subscapularis, and teres minor. These muscles function to provide rotatory movement at the shoulder joint and maintain the humeral head centered within the glenoid. The supraspinatus originates on the posterior aspect of the scapula and acts to abduct the shoulder. It has its highest mechanical advantage during the frst 15° of motion, with the deltoid contributing more to abduction at greater degrees of abduction. The infraspinatus is a thick triangular shaped muscle that is located on the posterior aspect of the scapula and separated from the supraspinatus by the bony spine of the scapula. The infraspinatus acts to externally rotate the shoulder when the arm is at the side. The teres minor is the major external rotator with the arm abducted. The supraspinatus, infraspinatus, and teres minor all attach on the greater tuberosity, a bony prominence on the posterior lateral aspect of the proximal humerus. The subscapularis runs along the anterior aspect of the shoulder acting as secondary restraint to anterior translation of the humeral head in addition to performing shoulder adduction and internal rotation [8]. It attaches to the lesser tuberosity of the humerus, located anteromedial to the greater tuberosity (Fig. 1.2).
1.1.3 Ligaments
While the rotator cuff musculature provides dynamic stability with movement of the shoulder, the ligamentous structures act as static stabilizers. These glenohumeral ligaments are capsular thickenings of the shoulder joint that are check reins to excessive rotational or translational movement of the humeral head within the glenoid. They are described as discrete bands, the superior glenohumeral ligament (SGHL), middle glenohumeral ligament (MGHL), and inferior glenohumeral ligament (IGHL) complexes. The IGHL has both an anterior band (aIGHL) and posterior band (pIGHL).
Unlike most ligaments in the body which impart force through the entire arc of motion, the
Fig. 1.2 The four rotator cuff muscles are critical to shoulder stability and motion. Yılmaz S., Vayısoğlu T., Çolak M.A. (2020) Shoulder Anatomy. In: Huri G.,
glenohumeral ligaments act variably depending on the specifc position of the arm. The SGHL provides restraint to inferior translation when the arm is at the side, the MGHL resists anterior and posterior translation at the midrange of abduction. The IGHL is the most important contributor to stability overall as it acts during the most common position of dislocation, when the shoulder is abducted 45–90°. The aIGHL is important when the arm is externally rotated, and the pIGHL in internal rotation [9, 10]. The coracohumeral ligament (CHL) supplements the function of the SGHL, running from the base of the coracoid process and attaching to the superior aspect of the shoulder capsule. The CHL, MGHL, and SGHL along with the long head of the biceps tendon travel within the rotator interval, which is bordered by the tendons of the supraspinatus and infraspinatus [11, 12].
The glenoid labrum is a fbrocartilaginous structure that serves as an anchor for the glenohumeral ligaments in addition to deepening the socket of the glenoid to enhance stability of the joint. It also serves as an anchor point for the long
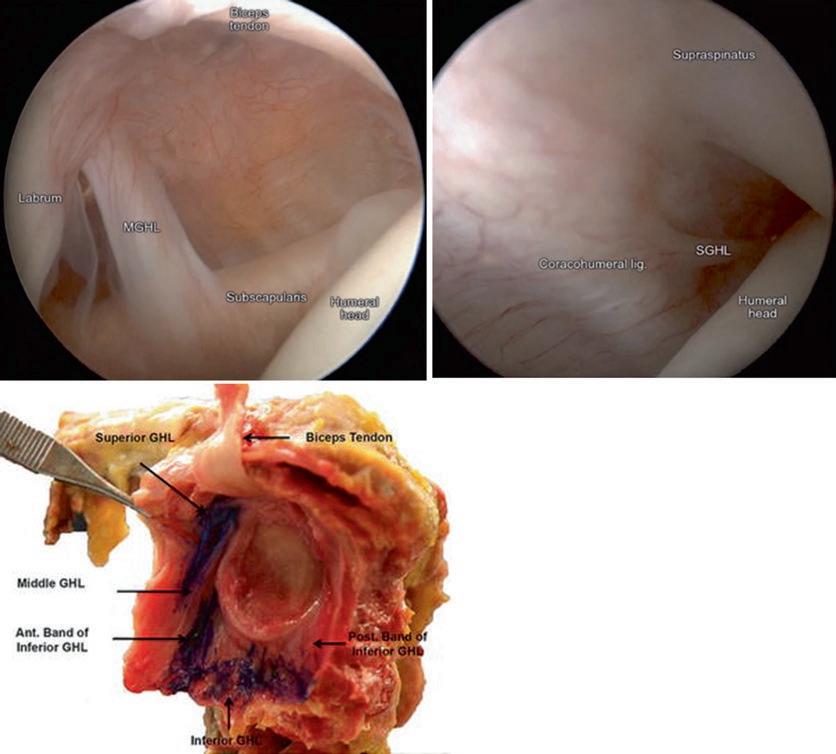
head of the biceps tendon at its most superior position. Injuries to the labrum are common and may manifest as shoulder pain, instability, or both depending on their location and severity [13] (Fig. 1.3).
1.1.4 Nerves
The brachial plexus is made up of a series of nerves that convey sensory and motor function to the upper extremity. They are organized as nerve roots branching off the spinal cord at the C5-T1 levels. These nerve roots initially begin at the neck and are subdivided into trunks, divisions, cords, and branches as they move distally down the arm. The dorsal scapular nerve arises proximally from the C5 nerve root to provide motor function to the rhomboid muscles and levator scapulae, which medialize and elevate the scapula, respectively. The suprascapular nerve arises from the upper trunk formed by the C5 and C6 nerve roots and innervates two muscles of the rotator cuff; the supraspinatus and infraspinatus,
Fig. 1.3 The glenohumeral ligaments are thickenings of the shoulder capsule that serve to as static stabilizers of the shoulder at the end range of motion. (a and b) Arthroscopic images. (c) Anatomic dissection. Apostolakos J. et al.
as well as providing sensory innervation to the glenohumeral joint capsule. Cysts, or abnormal fuid pockets can form at either the suprascapular notch or spinoglenoid notch; fossae about the scapular neck, which can compress the suprascapular nerve causing both supraspinatus and infraspinatus dysfunction if found at the former, or isolated infraspinatus dysfunction if at the latter [14, 15]. The upper and lower subscapular nerves branch off of the posterior cord of the brachial plexus and innervate the subscapularis muscle; the lower subscapular nerve additionally supplies motor function to the teres major muscle. The
(2015) Glenoid Labrum. In: Bain G., Itoi E., Di Giacomo G., Sugaya H. (eds) Normal and Pathological Anatomy of the Shoulder. Springer, Berlin, Heidelberg. https://doi. org/10.1007/978-3-662-45719-1_9
axillary nerve is a large terminal branch of the posterior cord that innervates the deltoid and the teres minor. Its course has been well described as it wraps from posterior to anterior approximately 5 cm distal to the lateral edge of the acromion. It travels through the quadrangular space along with the posterior humeral circumfex artery, this anatomic space is bordered by the humerus laterally, the long head of the triceps medially, teres minor superiorly, and the teres major inferiorly [16]. It gives off a posterior branch to innervate the teres minor and shoulder joint capsule and an anterior branch to innervate the deltoid muscle. The poste-
K. Taniguchi et
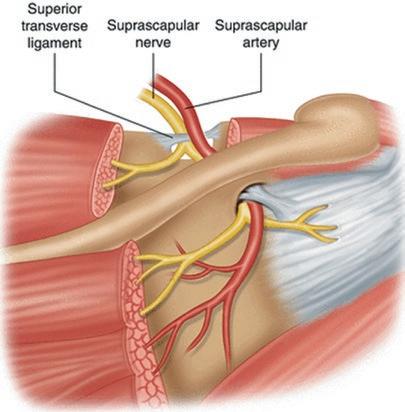
Fig. 1.4 The suprascapular nerve innervates the supraspinatus, infraspinatus and sends branches to the posterior glenohumeral capsule. Martinez, M., Doulatram, G.R. (2018). Suprascapular Nerve Blocks and Neurolysis. In: Manchikanti, L., Kaye, A., Falco, F., Hirsch, J. (eds) Essentials of Interventional Techniques in Managing Chronic Pain. Springer, Cham. https://doi. org/10.1007/978-3-319-60361-2_28
rior branch penetrates the fascia of the deltoid muscle before terminating as the upper lateral cutaneous nerve of the arm which provides sensory innervation to the skin overlying the upper arm [17]. The main terminal branch of the lateral cord is the musculocutaneous nerve which runs in the upper arm, gives off motor innervation to the coracobrachialis prior to piercing its deep surface approximately 6 cm distal to the coracoid process. The musculocutaneous nerve then travels in the anterior arm between the biceps brachii and brachialis, innervating both these muscles. After it exits the interval between these two muscles, it terminates as the lateral antebrachial cutaneous nerve which provides sensation to the lateral forearm [18] (Fig. 1.4).
1.1.5 Vascular
The subclavian artery and its branches provide the blood supply to the shoulder joint. There are several relevant named arterial branches of the
axillary artery that are clinically important. The suprascapular artery branches off the proximal aspect of the subclavian artery, it then travels over the superior border of the scapula, in most cases over top of the transverse scapular ligament with the suprascapular nerve running underneath the ligament. The suprascapular artery then supplies the supraspinatus and infraspinatus muscles [19]. After passing the frst rib, the subclavian artery changes names to the axillary artery. The axillary artery gives off the anterior and posterior circumfex arteries which supply the deltoid, biceps, coracobrachialis, teres minor, teres major, and triceps muscles. They are however, most important in providing blood supply to the humeral head. The posterior humeral circumfex artery travels with the axillary nerve through the quadrangular space prior to winding around the neck of the humerus to anastomose with the anterior humeral circumfex artery. Based on most recent anatomic studies, the posterior circumfex artery provides the majority of the blood supply to the humeral head [20].
References
1. Bakhsh W, Nicandri G. Anatomy and physical examination of the shoulder. Sports Med Arthrosc Rev. 2018;26(3):e10–22.
3. DeFranco MJ, Patterson BM. The foating shoulder. J Am Acad Orthop Surg. 2006;14(8):499–509.
4. Brown JM, Wickham JB, McAndrew DJ, Huang XF. Muscles within muscles: coordination of 19 muscle segments within three shoulder muscles during isometric motor tasks. J Electromyogr Kinesiol. 2007;17(1):57–73.
5. Gagey O, Hue E. Mechanics of the deltoid muscle. Clin Orthop Relat Res. 2000;375:250–7.
6. Rios CG, Arciero RA, Mazzocca AD. Anatomy of the clavicle and coracoid process for reconstruction of the coracoclavicular ligaments. Am J Sports Med. 2007;35(5):811–7.
7. Casadei K, Kiel J, Freidl M. Triceps tendon injuries. Curr Sports Med Rep. 2020;19(9):367–72.
8. Clark JM, Harryman DT 2nd. Tendons, ligaments, and capsule of the rotator cuff. Gross and microscopic anatomy. J Bone Joint Surg Am. 1992;74(5): 713–25.
9. O’Brien SJ, Neves MC, Arnoczky SP, Rozbruck SR, Dicarlo EF, Warren RF, Wickiewicz TL. The anatomy and histology of the inferior glenohumeral ligament complex of the shoulder. Am J Sports Med. 1990;18(5):449–56.
10. O’Connell PW, Nuber GW, Mileski RA, Lautenschlager E. The contribution of the glenohumeral ligaments to anterior stability of the shoulder joint. Am J Sports Med. 1990;18(6):579–84.
11. Jost B, Koch PP, Gerber CH. Anatomy and functional aspects of the rotator interval. J Shoulder Elb Surg. 2000;9:336–41.
12. Hunt SA, Kwon YW, Zuckerman JD. The rotator interval: anatomy, pathology, and strategies for treatment. J Am Acad Orthop Surg. 2007;15(4):218–27.
13. Burkart AC, Debski RE. Anatomy and function of the glenohumeral ligaments in anterior shoulder instability. Clin Orthopaed Related Res. 2002;400:32–9.
14. Leschinger T, Hackl M, Buess E, et al. The risk of suprascapular and axillary nerve injury in reverse total shoulder arthroplasty: an anatomic study. Injury. 2017;48:2042–9.
15. Westerheide KJ, Dopirak RM, Karzel RP, et al. Suprascapular nerve palsy secondary to spinoglenoid
cysts: results of arthroscopic treatment. Arthroscopy. 2006;22:721–7.
16. Rea P. Chapter 3: Neck. In: Rea P, editor. Essential clinically applied anatomy of the peripheral nervous system in the head and neck. Academic Press; 2016. p. 131–83.
17. Gurushantappa PK, Kuppasad S. Anatomy of axillary nerve and its clinical importance: a cadaveric study. J Clin Diagn Res. 2015;9(3):AC13–7. https://doi. org/10.7860/JCDR/2015/12349.5680.
18. Flatow EL, Bigliani LU, April EW. An anatomic study of the musculocutaneous nerve and its relationship to the coracoid process. Clin Orthop Relat Res. 1989;244:166–71.
19. Singh R. Variations in the origin and course of the suprascapular artery: case report and literature review. J Vasc Bras. 2018;17(1):61–5. https://doi. org/10.1590/1677-5449.008117.
20. Hettrich CM, Boraiah S, Dyke JP, Neviaser A, Helfet DL, Lorich DG. Quantitative assessment of the vascularity of the proximal part of the humerus. J Bone Joint Surg Am. 2010;92(4):943–8.
K. Taniguchi et al.
Biomechanics of the Glenohumeral, Acromioclavicular, and Sternoclavicular Joints
Nahum Rosenberg
“It is the fate of detailed ‘practical’ descriptions to wear the desultory look of curves mapped out with points: each is a series of related but disjoined minutiae—the ‘static snapshots’ which the mind demands before it can proceed to the direction of a complex, uninstinctive act.”
Arnold K. Henry
[1]
2.1 General Principles of Shoulder Biomechanics
Normal shoulder mechanics refect the product of compromise between the necessity of maximal range of active movement of the upper limb with the essential need for joint stability. This is achieved by the dynamics of muscles vs. the constraint of bone and the extent of elasticity of tendinous structures. Notably, the “soft” musculotendinous structures, which are responsible for the shoulder’s active movement, also contribute to shoulder stability under the central and local nervous refex control of different muscle groups that act in unison to provide stability of the basically unstable glenohumeral joint [2]. The overall range of shoulder movement reaches almost 30% of imaginary spherical “vol-
N. Rosenberg (*) Specialists Center, National Insurance Institute, Haifa, Israel
ume” when a head humerus is considered the center of rotation [3]. This extensive range of movements occurs primarily through the glenohumeral and scapulothoracic joints with a contribution ratio of 2:1 of movement range, respectively [4]. Two additional joints of the shoulder complex (acromioclavicular and sternoclavicular) have a relatively low contribution to shoulder movement range; their main role is to annex the upper limb to the axial skeleton; therefore, they have stiffer characteristics.
Overall, the torque generated by the shoulder is maximal in the isometric mode [2] and is dependent on muscle size and functional integrity. The maximal isometric strength around the shoulder is higher in the dominant upper extremity (Fig. 2.1) and is found to be higher in men than in women. The dominancy difference also exists in the scapular motion, when a higher range of scapular rotation exists in the dominant limb [5]. The gender difference is not clear enough since even when isometric torque buildup is normalized to a lean body mass, women reach lower maximal torque during isometric force
J. G. Lane et al. (eds.), The Art of the Musculoskeletal Physical Exam, https://doi.org/10.1007/978-3-031-24404-9_2
Fig. 2.1 Example of a profle of isometric force buildup in both shoulders of a 46-yearold man with normal shoulders. Higher magnitude torque is generated in the dominant limb. Measurements were made using a dynamometer (1200 readings/s, resolution 0.04 N; Myometer; Atlantech Medical, Nottingham, UK)
Fig. 2.2 Maximal shoulder torque (normalized to lean body mass) according to age decade. The maximal values in men are in the ffth decade of life and in women in the fourth decade (data from 500 healthy individuals) [4]
generation [6, 7]. The gender difference also exists in the age when maximal shoulder isometric force magnitude is noted in a normal population, i.e., in the ffth age decade in men vs. the fourth age decade in women (Fig. 2.2) [6], indicating that muscle mass is not the only determining factor for the generation of isometric torque around the shoulder axis.
2.2 Glenohumeral Joint
The glenohumeral (GHJ) joint is the main axis of shoulder movement. Its mobility and stability interaction determine most of the shoulder movement. The glenoid concavity depth provides 50%
torque on proximal humerus - 80° of shoulder elevation
of joint stability, and 20% of stability is contributed by the cartilaginous labrum, which increases the glenoid depth by 50% [8]. An additional 30% GHJ stability is generated by the dynamic effect of the rotator cuff (RC) muscles, the long head of biceps (LHB) that cause compression of the humeral head into the central glenoid [8]. GHJ conformity is also a stabilizing factor accompanied by the joint’s capsule components that control humeral head translation during the joint’s passive movements [9]. The maximal reaction force on the glenoid can be as high as 90% of body weight at 90o GHJ abduction [4].
The maximal torque on the GHJ is generated mostly by the external group of large muscles, i.e., latissimus dorsi, serratus anterior, pectoralis
N. Rosenberg
Fig. 2.3 A simplistic representation of force vectors on the humeral head during movement (frontal plane). H humeral head; G glenoid; c center of rotation of the humeral head; m rotational movement direction of the humeral head around the c axis; rc force vector generated by rotator cuff muscles; d force vector generated by external shoulder muscles, mainly by the deltoid muscle. d represents the translational force on the humeral head that is stabilized dynamically by rc into the glenoid fossa; the result is stable rotational movement (m) around the center of rotation c
major, and especially by parts of the deltoid muscle [10]. Subsequently, this group of muscles generates dynamic shearing forces on the GHJ. In order to stabilize this shearing torque dynamically, the RC muscles generate maximal force on the humeral head, which is directed to the center of the glenoid fossa, especially in the midrange of shoulder movement (Fig. 2.3) [11]. Since the humeral head is retroverted by 30o in the threedimensional orientation of the GHJ, the glenoid, which is retroverted on average by 7.4o, provides the main posterior support [4, 10]. The anterior restriction of humeral head translation is based on the static stabilizers that are comprised of the distinct capsular components. The superior and middle glenohumeral ligaments stabilize the GHJ anteriorly and inferiorly when the joint is in adduction. The same effect, but to a lesser extent, is provided by the coracohumeral ligament, and the inferior glenohumeral ligament stabilizes the GHJ when the arm is in abduction and external rotation [4]. These static restrictors prevent a sig-
nifcant magnitude of humeral head translation in the humeral fossa [11], i.e., at shoulder elevation the vertical translation is restricted up to 0.35 mm, while during shoulder fexion the anterior translation is up to 3.8 mm and at extension the posterior translation is up to 4.9 mm [4]. Therefore, the humeral head normally does not translate more than 5 mm in the glenoid fossa. But, since the GHJ is inherently unstable, i.e., the humeral head surface is four times larger than the glenoid fossa surface, dynamic fne-tuning stabilization is essential in addition to static stabilization. This is provided by the RC muscles that fnetune the humeral head stabilization by generating a force vector directed to the center of the glenoid fossa (Fig. 2.3).
An additional stabilizing factor of GHJ, which is neither static nor dynamic, is a negative intraarticular pressure that is especially important for inferiorly directed humeral head stabilization at shoulder adduction and can be compromised when the rotator interval is damaged.
Thus, since the anterior shear force on the glenoid is maximal at 60o of shoulder abduction and reaches 40% of body weight [4], the most important anterior shoulder static stabilizer, as mentioned above, is the inferior glenohumeral ligament.
2.3 Acromioclavicular Joint
The acromioclavicular joint (ACJ) is also basically non-congruent. In most individuals (about 50%), it has an “overriding” confguration when the distal clavicle overrides the acromion, and the less common confgurations are either parallel articular surfaces in 27% of the population, or the acromion overrides the distal clavicle, i.e., “under-riding” the ACJ [12]. Naturally, all these osseous confgurations of ACJ are unstable, and ACJ stability is primarily based on static support of the articular capsule and adjacent ligaments, as well as on some dynamic stabilization by the deltoid and trapezius muscles anteriorly and posteriorly, respectively. Since these stabilizing structures are not solid, some degree of axial rotation (up to 8o of 45o of maximal clavicle axial 2 Biomechanics of the Glenohumeral,
rotation) in the ACJ is possible. The acromioclavicular ligament can constrain joint displacement in the range of 50% anteriorly and 90% posteriorly [13]. In the vertical direction, ACJ can withstand up to 635 N [14] when most of the stabilizing resistance is provided by the acromioclavicular ligaments. The coracoclavicular ligament also plays an important stabilizing role when the conoid component acts as an anterior and superior constraint, and the trapezoid component mainly resists axial compression on the ACJ [12]. ACJ is primarily stabilized by the coracoclavicular ligament in the vertical plane and by the acromioclavicular ligaments in the horizontal plane [15]. Due to the high grade of stability, ACJ contributes less to shoulder range movement, and rather behaves as a stable axial fulcrum for combined GH and scapular movement since its semistiff structure is crucial for the mechanically reliable suspension of the upper limb [16].
2.4 Sternoclavicular Joint
The sternoclavicular joint (SCJ) is also unstable in its osseous confguration. This joint is the only articulation of the shoulder to the axial skeleton. Its stability is mainly due to solid restriction caused by the “saddle shaped” articulation of the diarthrodial components (medial clavicle articulation with upper sternum and superior surface of the frst rib). The congruity of the SCJ is partly achieved by an intra-articular disc that provides some medial stability of the joint [12]. Additional stabilization is provided by the sternoclavicular ligament. Still, some range of movement exists in the horizontal and frontal planes and around the clavicular axis. The movement does not exceed 50o in all planes [17]. This movement occurs at a shoulder elevation of up to 90o with a 2:5 ratio of SCJ movement to shoulder elevation [18]. The main static posterior stabilization of the SCJ is provided by the posterior joint capsule and is controlled by the dynamic stabilization of the trapezius muscle.
The joints at both ends of the clavicle (ACJ and SCJ) “compromise” to some extent their stability primarily to allow the rotational movement
N. Rosenberg
of the clavicle along its long axis with high stability in other planes of potential movements, aiming at providing reliable anchorage for effective scapulothoracic rhythm that is controlled and interrelated by glenohumeral and scapulothoracic movements essential for optimal shoulder mobility.
References
1. Henry AK. Extensile exposure. 3rd ed. Edinburgh, London, New York: Churchill Livingstone; 1995. p. 308.
2. Morrey BF, Itoi E, An KN. Biomechanics of the shoulder. In: Rockwood CA, Matsen FA, editors. The shoulder. 2nd ed. Philadelphia, London, Toronto, Montreal, Sydney, Tokyo: W.B. Saunders Company; 1998. p. 233–76.
3. Harryman DT II, Lazarus MD, Rozencwaig R. Chapter 20: The stiff shoulder. In: Rockwood CA, Matsen FA, editors. The shoulder. 2nd ed. Philadelphia, London, Toronto, Montreal, Sydney, Tokyo: W.B. Saunders Company; 1998. p. 1067–8.
4. Halder AM, Itoi E, An KN. Anatomy and biomechanics of the shoulder. Orthop Clin North Am. 2000;31(2):159–76.
5. Matsuki K, Matsuki KO, Mu S, Yamaguch SI, Ochiai N, Sasho T, Sugaya H, Toyone T, Wada Y, Takahashi K, Banks SA. In vivo 3-dimensional analysis of scapular kinematics: comparison of dominant and nondominant shoulders. Shoulder Elbow Surg. 2011;20(4):659–65.
6. Schezar A, Berkovitch Y, Haddad M, Soudry M, Rosenberg N. Normal isometric strength of rotator cuff muscles in adults. Bone Joint Res. 2013;2:214–9.
7. Rosenberg N. Rotator cuff isometric strength across the life span in normal population and in patients with rotator cuff pathology. Chapter 2. In: Imhoff A, Savoie F, editors. Rotator cuff across the life span. Berlin: Springer Nature; 2019. p. 11–7.
8. Lippitt S, Matsen F. Mechanisms of glenohumeral joint stability. Clin Orthop Rel Res. 1993 Jun;291:20–8.
9. Karduna AR, Williams GR, Iannotti JP, Williams JL. Kinematics of the glenohumeral joint: infuences of muscle forces, ligamentous constraints, and articular geometry. J Orthop Res. 1996;14:986–93.
10. Lugo R, Kung P, Ma CB. Shoulder biomechanics. Eur J Radiol. 2008;68(1):16–24.
11. Bigliani LU, Kelkar R, Flatow EL, Pollock RG, Mow VC, Glenohumeral stability. Biomechanical properties of passive and active stabilizers. Clin Orthop Relat Res. 1996;330:13–30.
12. Renfree KJ, Wright TW. Anatomy and biomechanics of the acromioclavicular and sternoclavicular joints. Clin Sports Med. 2003;22(2):219–37.
2 Biomechanics of the Glenohumeral,
13. Stine IA, Vangsness CT. Analysis of the capsule and ligament insertions about the acromioclavicular joint: a cadaveric study. J Arthroscop Relat Surg. 2009;25:968–74.
14. Abat F, Sarasquete J, Natera LG, Calvo A, PérezEspaña M, Zurita N, Ferrer J, del Real JC, Paz-Jimenez E, Forriol F. Biomechanical analysis of acromioclavicular joint dislocation repair using coracoclavicular suspension devices in two different confgurations. J Orthop Traumatol. 2015;16(3):215–9.
15. Saccomanno MF, Ieso DE, C, Milano G. Acromioclavicular joint instability: anatomy,
biomechanics and evaluation. Joints. 2014;2(2): 87–92.
16. Abbott LC, Lucas DB. The function of the clavicle. Ann Surg. 1954;146:583–99.
17. Dhawan R, Singh RA, Tins B, Hay SM. Sternoclavicular joint. Shoulder Elbow. 2018;10(4): 296–305.
18. Rockwood CA, Williams GR, Yong DC. Disorders of the acromioclavicular joint. In: Rockwood CA, Matsen FA, editors. The Shoulder. 2nd ed. Philadelphia, London, Toronto, Montreal, Sydney, Tokyo: W.B. Saunders Company; 1998. p. 483–553.
Evaluation of the Range of Motion of the Glenohumeral Joint
Aaron Martinez-Ulloa, Maria Valencia, and Emilio Calvo
3.1 Anatomy
The shoulder complex is made up of three main joints: acromioclavicular, scapulothoracic, and glenohumeral joint; and four less contributing joints: sternoclavicular, costomanubrial, costosternal, and costovertebral [1].
The glenohumeral joint is formed by the glenoid cavity and the humeral head, stablishing a spheroid joint. By having the greatest range of motion, covering 65% of a sphere, it lacks the stability other joints such as the hip has. Its stability is provided mainly by active muscle control, with a minor role of the glenohumeral capsule, labrum, and ligaments [2]. The following stabilizers have been defned: [3].
The musculature of the shoulder can be divided into deep and superfcial layers. The deep one, consisting mainly of the rotator cuff which, enhanced by the biceps, stabilizes the humeral head within the glenoid giving an effective fulcrum for the superfcial layers to create a stable motion. Superfcial layers, being part of it deltoid, trapezius and pectoralis mayor; act as power and controller of the arm motion once the joint has been stabilized [1].
Glenohumeral ligaments are disposed in a multi-directional fashion, providing stability to the joint. Coracohumeral and superior glenohumeral ligament (GHL) act as inferior stabilizers in adduction and external rotation. Middle GHL restrains external rotation and provides anterosuperior stability. Finally, the inferior GHL complex is the most important stabilizer against anteroinferior translation [4].
Each of the restraints and stabilizers of the shoulder joint portraits a particular function. We should be able to examine every single structure individually to identify the issue and localize the possible sources of pain.
A. Martinez-Ulloa · M. Valencia · E. Calvo (*) Shoulder and Elbow Reconstructive Surgery Unit, Department of Orthopedic Surgery and Traumatology, Fundacion Jimenez Diaz, Universidad Autonoma, Madrid, Spain
When joints are examined passively higher range of motion is observed, whereas in active positioning muscles tend to limit humeral head translation, specially rotational range, keeping the humeral head centered in the glenoid (Karduna et al., 1996).
J. G. Lane et al. (eds.), The Art of the Musculoskeletal Physical Exam, https://doi.org/10.1007/978-3-031-24404-9_3
15
3.2 Evaluation of the Shoulder Joint
Shoulder pain makes up for a great number of visits in our daily practice, some articles estimating its annual incidence close to 15/1000 in a GP consultation [5]; but that does not mean we can consider it an easy pathology. The wide spectrum of possible etiologies makes it hard to achieve a proper diagnosis without the use of complementary test. That is one step we can avoid in many cases, especially for soft tissue disorders, by performing a meticulous and thorough physical examination.
We must take into account that pain around the shoulder girdle is poorly localized, where the patient refers its origin is rarely the location of the lesion. The typical pattern for shoulder intrinsic diseases is one that radiates down the arm and stops at the elbow. Whereas ache of cervical origin radiates from the base of the ear towards the scapula. The two branches in which we can sort out shoulder pain are rotator cuff disorders and instability due to osteoarthritis. Some particular occupations and sport activities have a higher risk of suffering shoulder disorders. Other complaints that may arrive at our daily practice are loss of motion, stiffness, neurologic dysfunction, or scapular dyskinesia. Here, a proper clinical evaluation will help us differentiate issues of the shoulder itself or referred symptoms with its origin on the neck. The scapulothoracic and acromioclavicular joints should always be specifcally examined.
Examination can be performed in a seating position when the patient has trouble standing up, although it is preferred to evaluate and assess the joint in a standing position. It should always be performed bilaterally from the front and from the back in order to detect any muscular atrophy or scapular dyskinesia.
It is also paramount to examine both active and passive range of motion. When joints are examined passively, higher range of motion is observed, whereas in active positioning muscles tend to limit humeral head translation, especially rotational range, keeping the humeral head centered in the glenoid. By testing joint motion pas-
sively, we can stablish the maximum allowance of the soft tissues (ligaments and capsule), somehow ignoring the possible restraint of muscles. On the other hand, active range of movement can be limited not only by soft tissue disorders but by pain which should be addressed. If we have limitation in both active and passive we most likely be looking at shoulder stiffness, the primary reason being adhesive capsulitis or primary osteoarthritis [6].
The angle obtained during evaluation of ROM can be measured using traditional methods, such as employing a goniometer, using angle paintings on the wall and asking the patient to step in front of it. However, more advanced systems that use laser and high-resolution cameras to track the motion performed by the patient have recently been advocated. It has been found that using these new options, we can achieve, higher accuracy than compared to the goniometer or anatomical references such as in the Constant classifcation [7].
Different scoring systems to evaluate shoulder function are available in the literature, being the Oxford shoulder score and the Constant score the ones being used by most surgeons [8]. Most of them include range of motion as one of the most relevant sections of the test. The Oxford shoulder score is patient assessed, answering 12 questions regarding the ability to perform daily living activities and pain derived from doing them [9]. The Constant score is considered the gold standard in Europe, assessing pain reported by the patient, activities of daily living, ROM, and strength determined by examiner, with a maximum of 100 points. It was designed in 1987 based on four parameters to assess shoulder performance [1]. These parameters are pain (0–15 points), activities of daily living (0–20), range of motion (0–40), and power (0–25) making up to a sum of a hundred points. Several measurements are taken in each, such as forward and lateral elevation, external/internal rotation, or degree of activity level.
Once we have calculated the score we can sort patients as very good function (86–100 points), good (71–85), fair (56–70), and poor (<56). The minimum our patients should be able to do by
A. Martinez-Ulloa et al.
themselves are the daily living tasks such as perineal care task, comb their hair, washing their axilla, and eat with a spoon [10]. If these goals are not met, surgical treatment should be an option.
3.2.1 Resting Position
Posture in which the soft tissue surrounding the glenohumeral joint are in its most relaxed state and the capsule achieve its greatest laxity. The articular surface is minimally congruent. Owing to all these circumstances, the joint allows maximum mobility in passive manipulation.
We should be looking for 40° of abduction or 45% of the maximum abduction, neutral rotation and 30° of anteversion, within the plane of the scapula [11]. It should be noted that this position varies depending on factors such as hyper or
hypomobility, and thus the degrees of abduction should be adapted to the maximum range of motion, looking for 45% of the maximal abduction range (Fig. 3.1).
3.2.2 Abduction
Motion of the humerus when elevated in the coronal plane towards the head with a straight arm extended laterally. Normal range goes from 0° to 180° [12]. Since the normal anteversion of the shoulder joint is 30° [3], abduction can be tested maintaining the anatomical forward angulation in order to keep posterior and anterior soft tissues relaxed. Examination looking for an absolutely straight lateral abduction increases the stress on anterior structures, thus giving abnormal results (Fig. 3.2).