The contribution made by Kalavati Suvarna and Sumathi Nambiar is in public domain. Previous editions copyrighted 2015, 2011, 2007, 2000
No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or any information storage and retrieval system, without permission in writing from the publisher. Details on how to seek permission, further information about the Publisher’s permissions policies and our arrangements with organizations such as the Copyright Clearance Center and the Copyright Licensing Agency, can be found at our website: www.elsevier.com/permissions
This book and the individual contributions contained in it are protected under copyright by the Publisher (other than as may be noted herein).
Notices
Practitioners and researchers must always rely on their own experience and knowledge in evaluating and using any information, methods, compounds or experiments described herein. Because of rapid advances in the medical sciences, in particular, independent verification of diagnoses and drug dosages should be made. To the fullest extent of the law, no responsibility is assumed by Elsevier, authors, editors or contributors for any injury and/or damage to persons or property as a matter of products liability, negligence or otherwise, or from any use or operation of any methods, products, instructions, or ideas contained in the material herein.
Library of Congress Cataloging-in-Publication Data
Names: Mahon, Connie R., editor. | Lehman, Donald C., editor.
Title: Textbook of diagnostic microbiology / [edited by] Connie R. Mahon, Donald C. Lehman.
Description: Sixth edition. | St. Louis, Missouri : Elsevier Saunders, [2019] | Includes bibliographical references and index.
Identifiers: LCCN 2017050818 (print) | LCCN 2017051723 (ebook) | ISBN 9780323482127 (ebook) | ISBN 9780323482189
LC record available at https://lccn.loc.gov/2017050818
Content Strategist: Kellie White
Content Development Manager: Ellen Wurm-Cutter
Content Development Specialist: Alexandra York
Publishing Services Manager: Deepthi Unni
Project Manager: Kamatchi Madhavan
Marketing Manager: Emily Wall
Designer: Margaret Reid
To my husband Dan for his love and continued support and understanding; my son Sean who inspires me; my daughter Kathleen, for showing me courage; and my granddaughters Kelly Amelia, Natalie Page, and Madeline Belle, who have given us so much pleasure.
CRM
To my wife Terri, for her constant support and encouragement, and whose love makes me realize anything is possible, and my grandchildren Shane, Athena, Jordan, and Vincent, who keep me young at heart.
DCL
To George Manuselis, a dedicated microbiologist, educator, and mentor, who inspired all.
Reviewers
Keri Brophy-Martinez, MHA/ED, MT(ASCP) Department Chair/Professor Medical Laboratory Technology Austin Community College Austin, Texas
Delfina C. Domínguez, MT(ASCP), MS, PhD Professor Clinical Laboratory Science/Public Health
Biomedical Laboratory Diagnostics Program Michigan State University East Lansing, Michigan
Joanna Ellis, MS, BS, MLS(ASCP) Clinical Assistant Professor Clinical Coordinator Clinical Laboratory Science Program
Texas State University San Marcos, Texas
Denise Forwick-Whalley, MLT Licensed Funeral Director & Embalmer Microbiology
Northern Alberta Institute of Technology Edmonton, Alberta, Canada
Shawn Froelich, MS, MLS(ASCP)cm Assistant Professor Medical Laboratory Science Allen College – UnityPoint Health Waterloo, Iowa
Julie Gardner, MS, MBA, MLS(ASCP)cm Director of the Medical Laboratory Technician Program Assistant Professor of Biology University of Saint Francis Crown Point, Indiana
Daniel J. Harrigan, MS, MB(ASCP)cm
Professor
MLT Program, Department of Health Sciences Blackhawk Technical College Monroe, Wisconsin
Grace Leu-Burke MSCLS, MT(ASCP)
Assistant Professor
Medical Laboratory Science School of Allied Health University of Alaska Anchorage Anchorage, Alaska
Nicholas M. Moore, MS, MLS(ASCP)cm
Assistant Director, Division of Clinical Microbiology
Assistant Professor
Departments of Pathology and Medical Laboratory Science
Rush University Medical Center Chicago, Illinois
Hamida Nusrat, PhD, PHM(CDPH) Faculty
Clinical Laboratory Science Internship Program
San Francisco State University San Francisco, California
Public Health Microbiologist and Trainer Napa-Solano-Yolo-Marin County Public Health Laboratory Fairfield, California
Susan E. Saullo, RN, MS MT(ASCP) Adjunct Instructor
Nursing
ITT Technical Institute Lake Mary, Florida
Michael Simpson, BA, MS, MT(ASCP) Professor of Clinical Laboratory Science (Full Time)
Laboratory Supervisor (Part Time)
Clinical Laboratory Science College of Southern Nevada (Full Time) Diagnostic Center of Medicine (Part Time) Las Vegas, Nevada
Richard B. States, DHSc, CNMT, RT(N)(ARRT) Chair
Diagnostic Services Department
The University of Findlay Findlay, Ohio
Jane M. Stevens, MS, MT(ASCP)SM
Manager Department of Pathology
Clinical Microbiology Laboratory
Rush University Medical Center Chicago, Illinois
Ronald L. Walker, MBA, CNMT, PET
Assistant Professor
Diagnostic Services Department
The University of Findlay Findlay, Ohio
Dorothy Yvonne Yaschuk, RT, ART, MEd School of Health Sciences College of New Caledonia Prince George, British Columbia
Contributors
Yousif Barzani, MD, MLS(ASCP)CM
Assistant Professor
Department of Integrated Health Sciences School of Medicine and Health Sciences
The George Washington University Washington, DC
Maximo O. Brito, MD, MPH
Associate Professor of Medicine
Division of Infectious Diseases University of Illinois Chicago, Illinois
Chief of Infectious Diseases
Department of Medicine
Jesse Brown VA Medical Center Chicago, Illinois
Nina Clark, MD Professor Department of Medicine Division of Infectious Diseases Director, Transplant Infectious Diseases Loyola University Medical Center Maywood, Illinois
James L. Cook, MD
Clinical Professor of Medicine Division of Infectious Diseases, Department of Medicine Loyola University Medical Center Maywood, Illinois
Staff Physician and Research Scientist Infectious Diseases Section Edward Hines, Jr. VA Hospital Hines, Illinois
Cliff Cymrot, MLS(ASCP), MT(AAB), MT(AMT), MHA
Assistant Professor Medical Laboratory Science
George Washington University Washington, DC
Adjunct Instructor
CAHS School of Social Work Cincinnati, Ohio
Robert C. Fader, PhD, D(ABMM)
Section Chief, Microbiology
Pathology Department
Baylor Scott & White Healthcare Scott & White Medical Center—Temple Temple, Texas
Connie F.C. Gibas, PhD
Clinical Research Project Manager Department of Pathology and Laboratory Medicine University of Texas Health Science Center at San Antonio San Antonio, Texas
Amanda T. Harrington, PhD, D(ABMM) Director, Clinical Microbiology Laboratory Associate Professor, Pathology Loyola University Medical Center Maywood, Illinois
Michelle M. Jackson, PhD Microbiologist
Division of Nonprescription Drug Products Center for Drug Evaluation and Research U.S. Food and Drug Administration Silver Spring, Maryland
Deborah Josko, PhD, SM(ASCP)
Associate Professor and Director—Medical Laboratory Science Program
Clinical Laboratory Sciences
Rutgers, The State University of New Jersey—School of Health Professions Newark, New Jersey
Arun Kumar, PhD
Assistant Professor Nanomedicine Research Laboratory Department of Medical Laboratory Sciences Department of Biomedical Engineering UD Nanofabrication Facility Center for Bioinformatics & Computational Biology (CBCB) College of Health Sciences University of Delaware Newark, Delaware
Steven D. Mahlen, PhD, D(ABMM) Director, Microbiology Affiliated Laboratory, Inc. Bangor, Maine
Frederic J Marsik, PhD Microbiology Consultant New Freedom, Pennsylvania
Kevin McNabb, PhD, MT(ASCP) Director, Microbiology and Immunology New Hanover Regional Medical Center Wilmington, North Carolina
Alfredo J. Mena Lora, MD
Clinical Assistant Professor
Associate Program Director, Infectious Diseases Fellowship Program Division of Infectious Diseases
Department of Medicine
Chicago, Illinois
Sarojini R. Misra, MS, SM(ASCP), SM(AAM) Manager
Microbiology
Christianacare Health Services
Newark, Delaware
Paula C. Mister, MS, MT(ASCP)SM
Educational Coordinator, Medical Microbiology
The Johns Hopkins Hospital
Baltimore, Maryland
Adjunct Faculty
School of Mathematics and Science Community Colleges of Baltimore County Baltimore, Maryland
Linda S. Monson, MS, MT(ASCP) Supervisory Microbiologist (Retired) San Antonio Military Medical Center
Fort Sam Houston, Texas
Sumati Nambiar MD, MPH
Director, Division of Anti-infective Products Center for Drug Evaluation
Food and Drug Administration
Silver Spring, Maryland
Lindsey E. Nielsen, PhD, ASCP(M, MB)
Deputy Chief, Microbiology Laboratories Department of Pathology and Area Laboratories
Brooke Army Medical Center
San Antonio, Texas
Susan M. Pacheco, MD Physician
Medicine
Edward Hines, Jr. VA Hospital Hines, Illinois
Assistant Professor Department of Medicine
Loyola University Medical Center
Maywood, Illinois
Gail E. Reid, MD, MSCTS
Assistant Professor Department of Infectious Diseases
Loyola University Medical Center Maywood, Illinois
St. Joseph’s Hospital & Medical Center Phoenix, Arizona
Linda A. Smith, PhD, MLS(ASCP)CM, BBCM Professor
University of Texas Distinguished Teaching Professor Department of Health Sciences
The University of Texas Health Science Center at San Antonio San Antonio, Texas
Kalavati Suvarna, PhD
Senior Microbiologist
Division of Anti-infective Products, Office of Antimicrobial Products, Center for Drug Evaluation and Research
U.S. Food and Drug Administration Silver Spring, Maryland
Kimberly E. Walker, PhD, MT(ASCP) Manager, Public Affairs
American Society for Microbiology Washington, DC
A. Christian Whelen, PhD, D(ABMM)
State Laboratories Director
Hawaii Department of Health
Pearl City, Hawaii
Adjunct Professor and Graduate Faculty Department of Microbiology and Office of Public Health Studies
University of Hawaii Honolulu, Hawaii
Nathan P. Wiederhold, PharmD
Associate Professor & Director, Fungus Testing Laboratory Department of Pathology and Laboratory Medicine
University of Texas Health Science Center at San Antonio
San Antonio, Texas
Christopher J. Woolverton, BS, MS, PhD
Professor, Environmental Health Sciences Director, Center for Public Health Partnerships and Practice College of Public Health
Kent State University Kent, Ohio
PowerPoint Writer
Elizabeth A. Gockel-Blessing, MLS(ASCP)CM
Associate Dean for Student and Academic Affairs
Associate Professor, Department of Clinical Health Sciences
Doisy College of Health Sciences
Saint Louis University
St. Louis, Missouri
Test Bank Writer
Lorna Ruskin, EdD, MT(ASCP) Assistant Professor Medical Laboratory Sciences Center for Allied Health Programs University of Minnesota Minneapolis, Minnesota
Laboratory Manual Writer
Jimmy L. Boyd, MS, MHS, MLS(ASCP)
Assistant Professor/Program Director
Medical Laboratory Sciences
Arkansas State University-Beebe Beebe, Arkansas
Case Studies Writer
Nicholas M. Moore, MS, MLS(ASCP)CM
Assistant Director, Division of Clinical Microbiology
Assistant Professor
Departments of Pathology and Medical Laboratory Science
Rush University Medical Center Chicago, Illinois
Review Questions Writer
Joanna Ellis, MS, BS, MLS(ASCP)
Clinical Assistant Professor
Clinical Coordinator
Clinical Laboratory Science Program
Texas State University
San Marcos, Texas
Preface
This is the sixth edition of the Textbook of Diagnostic Microbiology. Since the inception and publication of the first edition, the field of diagnostic microbiology has dramatically changed and become more complex. Newly recognized pathogens continue to plague society in epidemic proportion. As examples, Ebola is a virus that produced severe outbreaks in West Africa in 2014–2015. Infection with it is often fatal, if untreated. The primarily mosquito-borne Zika virus is linked to microcephaly, a birth defect. Infection with it has been declared a global public health emergency by the World Health Organization. Highly pathogenic emerging coronaviruses that affect humans, including Middle East respiratory syndrome coronavirus (MERS CoV) and severe acute respiratory syndrome (SARS) virus, cause life-threatening respiratory syndromes. This edition includes discussions on these emerging public health issues.
As in previous editions, this edition maintains the characteristic features of a well-designed and organized textbook. We maintain the building-block approach to learning, critical thinking, and problem solving, attributes that students of clinical laboratory science and clinical laboratory technology, entry-level clinical laboratory scientists, and others have found valuable and effective. The primary goal of the Textbook of Diagnostic Microbiology is to provide a strong foundation for clinical laboratory science students, entry-level practitioners, and other health care professionals; therefore, discussions on organisms are limited to those that are medically important and commonly encountered, as well as new and re-emerging pathogens. The text provides students and other readers with valuable learning tools, such as summary tables, flowcharts, and descriptive illustrations, to help them comprehend the vast amount of information and reinforce learning. In response to our readers’ needs, we continued our efforts to enhance these features that have made this textbook user-friendly.
In this edition, we made considerable changes to show the vital nature and ever-evolving field of diagnostic microbiology. A more in-depth discussion on forensic microbiology has been included in Chapter 30, Agents of Bioterror and Forensic Microbiology. The text has been updated to reflect pathogens newly recognized in the past decade and presents new applications of immunologic and/or molecular approaches to diagnose infections, identify infectious agents, and determine antimicrobial resistance in microorganisms. Despite the progress made and significant advances that have occurred in their control, prevention, and treatment, infectious diseases remain a major threat to human health. The combined effects of rapid demographic, environmental, societal, technologic, and climatic changes, as well as changes in our way of life, have an influence on the incidence of infectious disease. The sixth edition focuses on the continuing spread of infectious diseases and the emerging public health issues associated with them.
Although the identification of etiologic agents through culture remains the gold standard in microbiology for determining the probable cause of an infectious disease, advances in molecular diagnostic techniques and their application in clinical laboratories have increased our capabilities for microbial detection and identification. Extensive biomedical research has focused on nanomedicine—the potential applications of nanotechnology to medicine. We updated Chapter 11 by expanding the discussion on the use of nanomedicine in diagnosing infectious diseases and Chapter 12 by exploring the use and applications of nanotechnology in drug-delivery systems. In addition, a description of the application of matrix-assisted laser desorption–ionization time-of-flight (MALDI-TOF) mass spectrometry in microbial identification has been added to Chapter 11.
Organization
Part I remains the backbone of the textbook, providing important background information; Part II focuses on laboratory identification of etiologic agents; and Part III on the organ system approach—the clinical and laboratory diagnoses of infectious diseases at various body sites.
Part I presents basic principles and concepts of diagnostic microbiology, including quality assurance, providing students with a firm theoretic foundation. Chapters 7 (Microscopic Examination of Materials from Infected Sites) and 8 (Use of Colony Morphology for the Presumptive Identification of Microorganisms) still play a vital role in this text. These two chapters help students and practitioners who may have difficulty recognizing bacterial morphology on direct smear preparations and colony morphology on primary culture plates develop these skills with the use of color photomicrographs of stained direct smears and cultures from clinical samples. These two chapters also illustrate how microscopic and colony morphology of organisms can aid in the initial identification of the bacterial isolate. Chapter 9 introduces the student/ reader to the principles behind various biochemical methods for identification of gram-negative bacteria. This chapter contains several color photographs to help students understand the principles and visualize interpretations of these important tests.
Part II highlights methods for the identification of clinically significant isolates. The chapters in Part II present medically important organisms through a taxonomic approach. Although diseases caused by the organisms are discussed, the emphasis is on the characteristics and methods used to isolate and identify each group of organisms. Numerous tables summarize the major features of organisms and use schematic networks to show the relationships and differences among similar or closely related species. Chapters devoted to anaerobic bacterial species, medically
important fungi, parasites, and viruses affirm the significance of these agents. Chapter 29 includes a discussion on Zika virus and other viral pathogens, including SARS virus, the highly pathogenic avian influenza virus, and MERS-CoV. Chapter 31 describes biofilm—an increasingly complex entity. It has become evident that microbial biofilms are involved in the pathogenesis of several human diseases and may be a contributing factor for the failure of antimicrobial therapy.
The organ system approach in Part III has been the foundation of the Textbook of Diagnostic Microbiology and provides an opportunity for students and other readers to “pull things together.”
The chapters in Part III begin with the anatomic considerations of the organ system to be discussed and the role of the usual microbiota found at a particular site in the pathogenesis of a disease. It is important for students to be knowledgeable about the usual inhabitants at a body site before they can appreciate the significance of the opportunistic infectious agents they are most likely to encounter. The case studies included in the chapters in Part III enhance problem-solving and critical-thinking skills and help students apply the knowledge they acquired from Parts I and II. The case studies describe clinical and laboratory findings, providing students with opportunities to correlate these observations with possible etiologic agents. In most cases, the cause of the illness is not disclosed in the case study; rather, it is presented elsewhere in the chapter to give students the opportunity to figure out the explanations independently.
Pedagogic Features
As in previous editions, the “Case in Point” feature introduces the reader to an important pathogen, infectious disease, concept, or principle that is discussed in the chapter text and is used to lead the learner to the main context discussed in the chapter. The Case in Point is followed by “Issues to Consider.” These points are presented in a bulleted format, and learners are asked to think about them as they read the chapter.
“Case Checks,” a feature introduced in the previous edition, aims to reinforce understanding of the content or concept within
the context of the Case in Point at the beginning of the chapter or case study at the beginning of a section within the chapter. The Case Check highlights a specific point in the text and intends to help the learner connect the dots between the points under discussion, as illustrated by the case study.
To further reinforce learning, identification tables, flowcharts, and featured illustrations have been updated, and new ones have been added. Learning objectives and a list of key terms are also provided at the beginning of each chapter. The list of key terms includes abbreviations used in the text so that students can easily find them in the text. At the end of each chapter, readers will find “Points to Remember” and “Learning Assessment Questions,” which help reinforce comprehension and understanding of important concepts. Points to Remember includes a bulleted list of important concepts and highlights what the reader should have learned from the chapter.
The sixth edition of Textbook of Diagnostic Microbiology is enriched by the expertise of contributors and elements to strengthen the learning strategy, such as full-color photographs and photomicrographs, an engaging and easy-to-follow design, learning assessment questions and answers, opening case scenarios, hands-on procedures, and lists of key terms to strengthen the learning strategy.
Ancillaries for Instructors and Students
As in the case of previous editions, we continue to offer a variety of instructor ancillaries specifically geared for this book. For instructors, the Evolve website includes a test bank containing more than 1200 questions. It also includes an electronic image collection and PowerPoint slides. For students, the Evolve website will include a laboratory manual like it always has, but this edition will include new case studies and student review questions.
Connie R. Mahon
Donald C. Lehman
Acknowledgments
We are grateful to all contributing authors, students, instructors, and many other individuals, who have all made invaluable suggestions and comments on ways to improve this edition.
R. Mahon
Donald C. Lehman
Connie
PART I Introduction to Clinical Microbiology
1
Bacterial Cell Structure, Physiology, Metabolism, and Genetics
Connie R. Mahon*, George Manuselis
CHAPTER OUTLINE
■ SIGNIFICANCE
■ OVERVIEW OF THE MICROBIAL WORLD Bacteria
Parasites Fungi Viruses
■ CLASSIFICATION/TAXONOMY
Nomenclature
Classification by Phenotypic and Genotypic Characteristics
Classification by Cellular Type: Prokaryotes, Eukaryotes, and Archaea
■ COMPARISON OF PROKARYOTIC AND EUKARYOTIC CELL STRUCTURE
Prokaryotic Cell Structure
Eukaryotic Cell Structure
Cytoplasmic Structures
■ BACTERIAL MORPHOLOGY
Microscopic Shapes
OBJECTIVES
After reading and studying this chapter, you should be able to:
1. Describe microbial classification (taxonomy), and accurately apply the rules of scientific nomenclature for bacterial names.
2. List and define five methods used by epidemiologists to subdivide bacterial species.
3. Differentiate among archaeal, prokaryotic (bacterial), and eukaryotic cell types.
4. Compare and contrast prokaryotic and eukaryotic cytoplasmic and cell wall structures and functions.
5. Compare and contrast the cell walls of gram-positive and gram-negative bacteria.
6. Compare the acid-fast cell wall with other gram-positive cell walls.
7. Apply the use of the following stains in the diagnostic microbiology laboratory: Gram stain, acid-fast stains (Ziehl-Neelsen, Kinyoun, auramine-rhodamine), acridine orange, methylene blue, calcofluor white, lactophenol cotton blue, and India ink.
8. List the nutritional and environmental requirements for bacterial growth and define the categories of media used for culturing bacteria in the laboratory.
9. Define the atmospheric requirements of obligate aerobes, microaerophiles, facultative anaerobes, obligate anaerobes, and capnophilic bacteria.
10. Define aerotolerant anaerobe.
Common Stains Used for Microscopic Visualization
■ MICROBIAL GROWTH AND NUTRITION
Nutritional Requirements for Growth
Environmental Factors Influencing Growth
Bacterial Growth
■ BACTERIAL BIOCHEMISTRY AND METABOLISM
Metabolism
Fermentation and Respiration
Biochemical Pathways from Glucose to Pyruvic Acid
Anaerobic Utilization of Pyruvic Acid (Fermentation)
Aerobic Utilization of Pyruvate (Oxidation)
Carbohydrate Utilization and Lactose Fermentation
■ BACTERIAL GENETICS
Anatomy of a DNA and RNA Molecule
Terminology
Genetic Elements and Alterations
Mechanisms of Gene Transfer
11. Describe the stages in the growth of bacterial cells
12. Explain the importance of understanding microbial metabolism in clinical microbiology.
13. Differentiate between fermentation and oxidation (respiration).
14. Name and compare three biochemical pathways that bacteria use to convert glucose to pyruvate.
15. Compare the two types of fermentation that explain positive results with the methyl red or Voges-Proskauer tests.
16. Define the following genetic terms: genotype, phenotype, constitutive, inducible, replication, transcription, translation, genome, chromosome, plasmids, insertion sequence element, transposon, point mutations, frameshift mutations, and recombination.
17. Discuss the development and transfer of antimicrobial resistance in bacteria.
18. Differentiate among the mechanisms of transformation, transduction, and conjugation in the transfer of genetic material from one bacterium to another.
19. Define the terms bacteriophage, lytic phage, lysogeny, and temperate phage.
20. Define the term restriction endonuclease enzyme, and explain the use of such enzymes in the clinical microbiology laboratory.
Case in Point
A 4-year-old girl presents with symptoms of redness, burning, and light sensitivity in both eyes. She also complained of her eyelids sticking together because of exudative discharge. A Gram stain of the conjunctival exudates (product of acute inflammation with white blood cells and fluid) showed gram-positive intracellular and extracellular, faint-staining, coccobacillary bacteria. The organisms appeared to have small, clear, nonstaining “halos” surrounding each cell. This clear area was noted to be between the stained organism and the amorphous (no definite form; shapeless) background material. The Gram stain of the quality control organisms Staphylococcus aureus (gram-positive) and Escherichia coli (gram-negative) revealed gram-positive reactions for both organisms.
Issues to Consider
After reading the patient’s case history, consider:
■ Role of microscopic morphology in presumptive identification
■ Significance of observable cellular structures
■ Importance of quality control in assessing and interpreting direct smear results
■ Unique characteristics of organisms, such as cellular structures, in initiating infection and disease in hosts
Key Terms
Acid-fast
Aerotolerant anaerobes
Anticodon
Archaea
Autotrophs
Bacteria
Bacteriophage
Capnophilic
Capsule
Codon
Competent
Conjugation
Differential media
Dimorphic
Eukarya
Eukaryotes
Facultative anaerobes
Family
Fermentation
Fimbriae
Flagella
Fusiform
Genotype
Genus
Gram-negative
Gram-positive
Halophiles
Heterotrophs
Hyphae
Krebs cycle
Lysogeny
Mesophiles
Microaerophilic
Minimal medium
Mycelia
Nomenclature
Nutrient media
Obligate aerobes
Obligate anaerobes
Pathogenic bacteria
Phenotype
Phyla
Pili
Plasmids
Pleomorphic
Prokaryotes
Protein expression
Psychrophiles
Respiration (oxidation)
Restriction enzymes
Selective media
Species
Spores
Strains
Taxa
Taxonomy
Temperate
Thermophiles
Transcription
Transduction
Transformation
Translation
Transport medium
Virion
This chapter provides a review of the structure, physiology, metabolism, and genetics of prokaryotic and eukaryotic cells. It also gives examples of common stains used to visualize microorganisms microscopically. Each topic in this chapter emphasizes to clinical microbiologists the inherent importance of their efforts to culture, identify, and characterize the microbes that cause disease in humans.
Significance
Microbial inhabitants have evolved to survive in various ecologic niches (place or location) and habitats (organism’s location and where its resources may be found). Some grow rapidly and some grow slowly. Some can replicate with a minimal number of nutrients present, whereas others require enriched nutrients to survive. Variation exists in atmospheric growth conditions, temperature requirements, and cell structure. This diversity is also found in the microorganisms that inhabit the human body as normal biota (flora), as opportunistic pathogens, or as true pathogens. Each microbe has its own physiology and metabolic pathways that allow it to survive in its particular habitat. One of the main roles of a diagnostic or clinical microbiologist is to isolate, identify, and analyze the bacteria that cause disease in humans. Knowledge of microbial structure and physiology is extremely important to clinical microbiologists in three areas:
• Culture of organisms from patient specimens
• Characterization and identification of organisms after they have been isolated
• Prediction and interpretation of antimicrobial susceptibility patterns
Understanding the growth requirements of a particular bacterium enables the microbiologist to select the correct medium for primary culture and optimize the chance of isolating the pathogen. Determination of staining characteristics, based on differences in cell wall structure, is the first step in bacterial identification. Microscopic characterization is followed by observation of the metabolic biochemical differences among organisms that form the basis for most bacterial identification systems in use today. Recently advances in molecular biology methods, for example, nucleic acid amplification and matrix-assisted laser desorption/ionization, have shifted identification away from biochemical testing. The cell structure and biochemical pathways of an organism also determine its susceptibility to various antimicrobial agents. The ability of microorganisms to change rapidly, acquire new genes, and undergo mutations presents continual challenges to clinical microbiologists as they isolate and characterize the microorganisms associated with humans.
Overview of the Microbial World
The study of microorganisms by the Dutch biologist and lens maker Anton van Leeuwenhoek has evolved immensely from its early historic beginnings. Because of Leeuwenhoek’s discovery of what he affectionately called wee beasties and animalcules in a water droplet in his homemade microscope, the scientific community acknowledged him as the “father of protozoology and bacteriology.” Today, we know that there are enormous numbers of microbes in, on, and around us in our environment. Many of
these microbes do not cause disease. The focus of this textbook is on microbes that are associated with human disease.
Bacteria
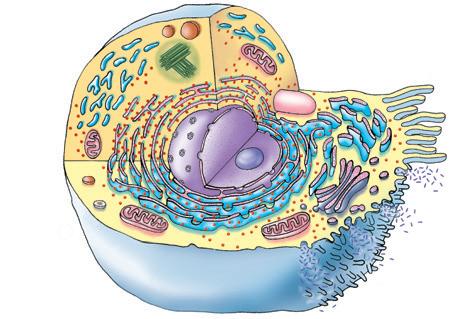
Bacteria are unicellular organisms that lack a nuclear membrane and true nucleus. They are classified as prokaryotes (Greek: before kernel [nucleus]) and lack mitochondria, endoplasmic reticulum (ER), or Golgi bodies. The absence of the preceding bacterial cell structures differentiates them from eukaryotes (Greek eu: well or good; Greek karyon: kernel). Table 1.1 compares prokaryotic and eukaryotic cell organization; Fig. 1.1 shows both types of cells.
Parasites
Certain eukaryotic parasites (organisms that live at the expense of their hosts) exist as unicellular organisms of microscopic size, whereas others are multicellular organisms. Protozoa are unicellular organisms within the kingdom Protista that obtain their nutrition
Characteristic
Typical size
Prokaryote
0.4–2 µm in diameter
through ingestion. Some are capable of locomotion (motile), whereas others are nonmotile. They are categorized by their locomotive structures: flagella (Latin: whiplike), pseudopodia (Greek: false feet), or cilia (Latin: eyelash). Many multicellular parasites (e.g., tapeworms) may be 7 to 10 meters long (see Chapter 28).
Fungi
Fungi are heterotrophic eukaryotes that obtain nutrients through absorption. Yeasts are unicellular fungi that reproduce asexually. “True” yeasts do not form hyphae or mycelia. Most fungi are multicellular, and many can reproduce sexually and asexually. Multicellular fungi are composed of filaments called hyphae that interweave to form mats called mycelia. Molds are filamentous forms that can reproduce asexually and sexually. Certain fungi can assume both morphologies (yeast and hyphae/mycelial forms), growing as yeast at human temperature (37° C) and as the filamentous form at room temperature (22° C). These fungi
Eukaryote
10–100 µm in diameter
0.5–5 µm in length >10 µm in length
Nucleus No nuclear membrane; nucleoid region of the cytosol
Genome
Location In the nucleoid, at the mesosome
Chromosomal DNA
Genome: extrachromosomal circular DNA
Reproduction
Membrane-bound organelles
Golgi bodies
Lysosomes
Endoplasmic reticulum
Mitochondria
Nucleus
Chloroplasts for photosynthesis
Ribosomes: site of protein synthesis (nonmembranous)
Size
Electron transport for energy
Sterols in cytoplasmic membrane
Plasma membrane
Cell wall, if present
Glycocalyx
Cilia
Flagella, if present
Pili and fimbriae
MT, Microtubule.
Circular; complexed with RNA
Plasmids, small circular molecule of DNA containing accessory information; most commonly found in gram-negative bacteria; each carries genes for its own replication; can confer resistance to antibiotics
Asexual (binary fission)
Absent
Absent in all
Absent in all
Absent in all
Absent in all
Absent in all
Absent in all
Present in all
70S consisting of 50S and 30S subunits
In the cell membrane; no mitochondria present
Absent except in Mycoplasmataceae
Lacks carbohydrates
Peptidoglycan in most bacteria
Present in most as an organized capsule or unorganized slime layer
Absent
Simple flagella; composed of polymers of flagellin; movement by rotary action at the base; spirochetes have MTs
Present
Classic membrane-bound nucleus
In the nucleus
Linear; complexed with basic histones and other proteins
In mitochondria and chloroplasts
Sexual and asexual
All
Present in some
Present in some; contain hydrolytic enzymes
Present in all; lipid synthesis, transport
Present in most
Present in all
Present in algae and plants
Present in all
80S consisting of 60S and 40S subunits
In the inner membrane of mitochondria and chloroplasts
Present
Also contains glycolipids and glycoproteins
Cellulose, phenolic polymers, lignin (plants), chitin (fungi), other glycans (algae)
Present; some animal cells
Present; see description of flagella
Complex cilia or flagella; composed of MTs and polymers of tubulin with dynein connecting MTs; movement by coordinated sliding microtubules
Absent
TABLE 1.1 Comparison of Prokaryotic and Eukaryotic Cell Organization
Division septum
Outer membrane
Peptidoglycan layer (Capsule)
Mesosome (Pili)
Inclusion body (Flagellum) Surface proteins
Cytoplasmic membrane
Ribosome Ribosome Chromosome (Capsule)
GRAM-POSITIVE A
GRAM-NEGATIVE
Ribosome s Centrosome Centrioles
Smooth endoplasmic reticulu m
Mitochondrio n Lysosome
Rough endoplasmic reticulu m
Peroxisome
Cytoplasmic membrane
Inclusion body
Peptidoglycan layer
Porin proteins
Periplasmic space
(Flagellum)
Smooth endoplasmi c reticulu m
Fre e ribosome s Cili a
Golg i apparatus
Ve sicle
Nuclear envelope B Nucleus Nucleolus
FIG. 1.1 Comparison of prokaryotic and eukaryotic cell organization and structures. A, Prokaryotic gram-positive and gram-negative bacteria. B, Structure of the generalized eukaryotic cell. (A, From Murray PR, Rosenthal KS, Pfaller MA: Medical microbiology, ed 6, Philadelphia, 2009, Mosby; B, from Thibodeau GA, Patton KT: Anatomy and physiology, ed 6, St Louis, 2007, Mosby.)
are called dimorphic. Some systemic fungal diseases in human hosts are caused by dimorphic fungi (see Chapter 27).
Viruses
Viruses are the smallest infectious particles and cannot be seen under an ordinary light microscope. Often, we can see their effects on cell lines grown in the laboratory, such as inclusions, rounding up of cells, and syncytium (fusion of host cells into multinucleated infected forms), where these characteristics become diagnostic for many viral diseases. Viruses are neither prokaryotic nor eukaryotic They are distinguished from living cells by the following characteristics:
• Viruses consist of deoxyribonucleic acid (DNA) or ribonucleic acid (RNA) but rarely both. Their genome may be double-stranded DNA (dsDNA), single-stranded DNA (ssDNA), double-stranded RNA (dsRNA), or single-stranded RNA (ssRNA).
• Viruses are acellular (not composed of cells), lack cytoplasmic membranes, and are surrounded by a protein coat.
• Viruses are obligate intracellular parasites that cannot selfreplicate. They require host cells for replication (increase in number does not involve mitosis, meiosis, or binary fission)
and metabolism. Because they lack enzymes, ribosomes, and other metabolites, they “take over” host cell function using the host cell machinery to reproduce. Growth (increase in size) does not occur in viruses.
Viruses are mostly host or host cell specific. For example, human immunodeficiency virus infects T-helper lymphocytes, not muscle cells, in humans, whereas other viruses, such as the rabies virus, can infect dogs, skunks, bats, and humans. A virus that infects and possibly destroys bacterial cells is known as a bacteriophage (Greek phage: to eat). Viruses are classified and identified by their genome (DNA or RNA), host disease signs and symptoms, chemical makeup, and geographic distribution, the presence or absence of an envelope, their resistance to changes in pH and temperature, their antigenicity (serologic methods), how the virus replicates, and the virion (a complete virus outside a cell).
Classification/Taxonomy
Taxonomy (Greek taxes: arrangement; Greek nomos: law) is the orderly classification and grouping of organisms into taxa (categories). Taxonomy involves three structured, interrelated categories:
Mitochondria
classification/taxonomy, nomenclature, and identification. It is based on similarities and differences in genotype (genetic makeup of an organism, or combinations of forms of one or a few genes in an organism’s genome) and phenotype (observable physical and functional features of an organism expressed by its genotype). Examples of genotypic characteristics include base sequencing of DNA or RNA and DNA base composition ratio to measure the degree of relatedness of two organisms (see later in this chapter and Chapter 11). Examples of phenotypic characteristics include macroscopic (colony morphology on media) and microscopic (size, shape, arrangement into groups or chains of cells) morphology, staining characteristics (gram-positive or gram-negative), nutritional requirements, physiologic and biochemical characteristics, antigenic markers, and susceptibility or resistance to antimicrobial agents or chemicals. See Chapters 7, 8, 9, 12, and 13 for more detailed information.
Taxa (plural of taxon), for example, the levels of classification, are the categories or subsets in taxonomy. The formal levels of bacterial classification in successively smaller taxa or subsets are domain, kingdom, division (or phylum in kingdom Animalia), class, order, family, tribe, genus, species, and subspecies. Below the subspecies level, designations such as serotype or biotype may be given to organisms that share specific minor characteristics. Protists (protozoans) of clinical importance are named similarly to animals; instead of divisions, one uses phyla (plural of phylum), but the names of the others remain the same. Prokaryotes are placed in the domains Bacteria and Archaea (Greek: ancient, origin from the earliest cells), separate from the animals; plants and protists are placed in the domain Eukarya. The domains Bacteria and Archaea include unicellular prokaryotic organisms. Clinical microbiologists traditionally emphasize placement and naming of bacterial species into three (occasionally four or five) categories: the family (similar to a human “clan”), a genus (equivalent to a human last name), and a species (equivalent to a human first name). The plural of genus is genera. For example, there are many genera in the family Enterobacteriaceae. The proper word for the name of a species is an epithet. Although order and tribe may be useful for the classification of plants and animals, these taxa are not always used for the classification of bacteria. For example, Staphylococcus (genus) aureus (species epithet) belongs to the family Staphylococcaceae. In addition, there are usually different strains within a given species of the same species. For example, there are many different strains of S. aureus. If the S. aureus isolated from one patient is resistant to penicillin and another S. aureus from a different patient is susceptible to penicillin, the two isolates are considered to be different strains of the same species. For an additional example, see Corynebacterium diphtheriae in the section on transduction later in this chapter.
Nomenclature
Nomenclature provides naming assignments for each organism in this textbook. The following standard rules for denoting bacterial names are used. The family name is capitalized and has an “-aceae” ending (e.g., Micrococcaceae). The genus name is capitalized and followed by the species epithet, which begins with a lowercase letter; both the genus and the species should be italicized in print but underlined when written in script (e.g., Staphylococcus aureus or Staphylococcus aureus). Often the genus name is abbreviated
by use of the first letter (capitalized) of the genus followed by a period and the species epithet (e.g., S. aureus). The genus name followed by the word species (e.g., Staphylococcus species) may be used to refer to the genus as a whole. Species are abbreviated “sp.” (singular) or “spp.” (plural) when the species is not specified. When bacteria are referred to as a group, their names are neither capitalized nor underlined (e.g., staphylococci).
Classification by Phenotypic and Genotypic Characteristics
The traditional method of placing an organism into a particular genus and species is based on the similarity of all members in numerous phenotypic characteristics. In the diagnostic microbiology laboratory, this classification is accomplished by testing each bacterial culture for various metabolic or molecular characteristics and comparing the results with those listed in established tables or databases. In many rapid identification systems, a numeric taxonomy is used in which phenotypic characteristics are assigned a numeric value and the derived number indicates the genus and species of the bacterium.
Epidemiologists constantly seek means of further subdividing bacterial species to follow the spread of bacterial infections. Species may be subdivided into subspecies (abbreviated “subsp.”), on the basis of phenotypic differences; serovarieties (abbreviated “serovar”), on the basis of serologic differences; or biovarieties (abbreviated “biovar”), on the basis of biochemical test result differences. Phage typing (based on susceptibility to specific bacterial phages) has also been used for this purpose. Current technology has allowed the analysis of genetic relatedness (DNA and RNA structure and homology) for taxonomic purposes. The analysis of ribosomal RNA (rRNA) gene sequencing has proved particularly useful for this purpose. The information obtained from these studies resulted in the reclassification of some bacteria.
Classification by Cellular Type: Prokaryotes, Eukaryotes, and Archaea
Another method of classifying organisms is by cell organization. Organisms fall into three distinct groups based on type of cell organization and function: prokaryotes, eukaryotes, and archaea. Taxonomists have placed all organisms into three domains that have replaced some kingdoms: Bacteria, Archaea, and Eukarya. These three domains are the largest and most inclusive taxa. Each domain is divided into kingdoms on the basis of the similarities of RNA, DNA, and protein sequences. The group prokaryotes includes the domains Archaea and Bacteria (Eubacteria), whereas fungi, algae, protozoa, animals, and plants are eukaryotic in nature and are placed in the domain Eukarya.
The domain Archaea (formerly Archaeobacteria) cell type appears to be more closely related to eukaryotic cells than to prokaryotic cells and is found in microorganisms that grow under extreme environmental conditions. Archaeal cell walls lack peptidoglycan, a major reason they are placed in a domain separate from bacteria. These microbes share some common characteristics with bacteria; they too can stain gram-positive or gram-negative. Gram-positive archaea have a thick wall and stain purple. Gramnegative archaeal cells, in contrast to the typical gram-negative bacterial lipid membrane, have a layer of protein covering the cell wall and stain pink. See the Gram stain discussion later in this chapter.
The structure of the cell envelope and enzymes of archaea allows them to survive under stressful or extreme (extremophiles; lovers of the extreme) conditions. Examples include halophiles (salt-loving cells) in Utah’s Great Salt Lake, thermophiles (heat-loving cells) in hot springs and deep ocean vents, and the anaerobic methanogens that give off swamp gas and inhabit the intestinal tracts of animals. Because archaea are not encountered in clinical microbiology, they are not discussed further in this textbook.
In general, the interior organization of eukaryotic cells is more complex than that of prokaryotic cells (see Fig. 1.1). The eukaryotic cell is usually larger and contains membrane-encased organelles (“little organs”) or compartments that serve specific functions, whereas the prokaryotic cell is noncompartmentalized. Various structures are unique to prokaryotic cells (see Fig. 1.1). Differences also exist in the processes of DNA synthesis, protein synthesis, and cell wall synthesis and structure. Table 1.1 compares the major characteristics of eukaryotic and prokaryotic cells.
Pathogenic (disease-causing) bacteria are prokaryotic cells that infect eukaryotic hosts. Targeting antimicrobial action against unique prokaryotic structures and functions inhibits bacterial growth without harming eukaryotic host cells. This is one reason that pharmaceutical companies have been successful in developing effective antimicrobial agents against bacterial pathogens, but they have been less successful in finding drugs effective against parasites and fungi, which are eukaryotic and similar to their human hosts, and viruses, which use host cells for replication.
Comparison of Prokaryotic and Eukaryotic Cell Structure
Prokaryotic
Cell Structure
Cytoplasmic Structures
Bacteria do not contain a membrane-bound nucleus. Their genome consists of a single circular chromosome. This appears as a diffuse nucleoid or chromatin body (nuclear body) that is attached to a mesosome, a saclike structure in the cell membrane.
Bacterial ribosomes, consisting of RNA and protein, are found free in the cytoplasm and attached to the cytoplasmic membrane. They are the site of protein synthesis. They are 70S in size and dissociate into two subunits: 50S and 30S (see Table 1.1). The S stands for Svedberg units, which refer to sedimentation rates (unit of time) during high-speed centrifugation. The Svedberg unit is named for Theodor Svedberg, Nobel Prize winner and inventor of the ultracentrifuge. Larger particles have higher S values. The S value is not additive. When the previously mentioned two subunits 50S and 30S bind together, there is a loss of surface area and the two subunits produce a complex 70S in size. The same occurs in the eukaryotic cell, where the two subunits 60S and 40S combine to form an 80S complex.
Stained bacteria sometimes reveal the presence of granules in the cytoplasm (cytoplasmic granules). These granules are storage deposits and may consist of polysaccharides such as glycogen, lipids such as poly β-hydroxybutyrate, or polyphosphates.
Certain genera, such as Bacillus and Clostridium, produce endospores in response to harsh environmental conditions. Endospores are small, dormant (inactive), asexual spores that develop inside the bacterial cell as a means of survival. Endospores are not a means of reproduction. Their thick protein coat
makes them highly resistant to chemical agents, temperature change, starvation, dehydration, ultraviolet and gamma radiation, and desiccation. Under harsh conditions, each vegetative cell (active, capable of growing and dividing) produces internally one endospore (inactive) that germinates under favorable environmental conditions into one vegetative cell. Endospores should not be confused with the reproductive spores of fungi (see Chapter 27).
Spores appear as highly refractile bodies in the cell. Spores are visualized microscopically as unstained areas in a cell with the use of traditional bacterial stains (Gram) or with the use of specific spore stains. Schaeffer-Fulton stain is the most commonly used endospore stain. The size, shape, and interior location of the spore, for example, at one end (terminal), subterminal, or central, can be used as identifying characteristics. For instance, the terminal spore of Clostridium tetani, the etiologic (causative) agent of tetanus, gives the organism a characteristic tennis racquet–shaped or lollipop-shaped appearance.
Cell Envelope Structures
The cell envelope consists of the membrane and structures surrounding the cytoplasm. In bacteria, these are the plasma membrane and the cell wall. Some species also produce capsules and slime layers.
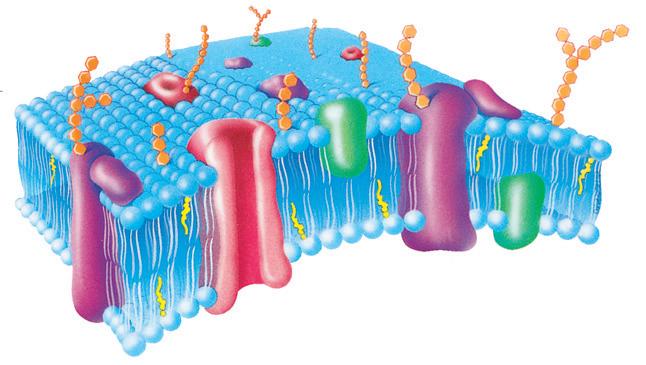
Plasma (Cell) Membrane. The plasma membrane is a phospholipid bilayer with embedded proteins that surrounds the cytoplasm. The prokaryotic plasma membrane (except for those of members of the Mycoplasmataceae, which do contain sterols) is made of phospholipids and proteins and does not contain sterols. This is in contrast to eukaryotic plasma membranes, which do contain sterols. The plasma membrane acts as an osmotic barrier (prokaryotes have a high osmotic pressure inside the cell) and is the location of the electron transport chain, where energy is generated. The general functions of the prokaryotic plasma membrane are identical to functions in eukaryotes (Fig. 1.2).
Cell Wall. The cell wall of prokaryotes is a rigid structure that maintains the shape of the cell and prevents bursting of the cell from the high osmotic pressure inside it. The different types of cell walls in bacteria have traditionally been categorized according to their staining characteristics. The two major types of cell walls are gram-positive and gram-negative (see Fig. 1.1A). Although they stain poorly gram-positive, mycobacteria have a modified cell wall called an acid-fast cell wall, while mycoplasmas are bacteria that have no cell wall and therefore do not Gram stain.
Gram-Positive Cell Wall. The gram-positive cell wall is composed of a very thick protective peptidoglycan (murein) layer. Because the peptidoglycan layer is the principal component of the gram-positive cell wall, many antimicrobial agents are effective against gram-positive organisms (e.g., penicillin) by preventing synthesis of peptidoglycan. Gram-negative bacteria, which have a thinner layer of peptidoglycan and a different cell wall structure, are less affected by these agents.
The peptidoglycan or murein layer consists of glycan (polysaccharide) chains of alternating N-acetyl-D-glucosamine (NAG) and N-acetyl-D-muramic acid (NAM) (Fig. 1.3). Short peptides, each consisting of four amino acid residues, are attached to a carboxyl group on each NAM residue. The chains are then cross-linked to form a thick network via a peptide bridge (differing in number of peptides) connected to the tetrapeptides on the NAM.
Carbohydrate chains
External membrane surface
Phospholipid bilayer
Internal membrane surface Membrane channel protein
Glycolipid
Polar region of phospholipid
region of phospholipid
FIG. 1.2 Structure of the plasma membrane. (From Thibodeau GA, Patton KT: Anatomy and physiology, ed 6, St Louis, 2007, Mosby.)
(NAM)
(NAG)
Meso-diaminopimelate HC CH3
D-Alanine
L-Alanine
D-Glutamate
Meso-diaminopimelate
D-Alanine
FIG. 1.3 The structure of the peptidoglycan layer in the cell wall of Escherichia coli. The amino acids in the cross-linking tetrapeptides may differ among species. NAG, N-acetyl-D-glucosamine; NAM, N-acetyl-D-muramic acid. (From Neidhardt FC, Ingraham M, Schaechter M: Physiology of bacterial cell: a molecular approach, Sunderland, MA, 1990, Sinauer Associates.)
Other components of the gram-positive cell wall that penetrate to the exterior of the cell are teichoic acid (anchored to the peptidoglycan) and lipoteichoic acid (anchored to the plasma membrane). These two components are unique to the gram-positive cell wall. Other antigenic polysaccharides may be present on the surface of the peptidoglycan layer.
Gram-Negative Cell Wall. The cell wall of gram-negative bacteria comprises two layers: the inner peptidoglycan layer, which is much thinner than in gram-positive cell walls, and an additional outer membrane unique to the gram-negative cell wall. The outer membrane contains proteins, phospholipids, and lipopolysaccharide (LPS). LPS contains three regions: an antigenic O–specific polysaccharide, a core polysaccharide, and an inner lipid A (also called endotoxin). The lipid A moiety is responsible for producing
fever and shock conditions in patients infected with gram-negative bacteria. The outer membrane functions in the following ways:
• It acts as a barrier to hydrophobic compounds and harmful substances.
• It acts as a sieve, allowing water-soluble molecules to enter through protein-lined channels called porins.
• It provides attachment sites that enhance attachment to host cells.
Between the outer membrane and the inner membrane and encompassing the thin peptidoglycan layer is an area referred to as the periplasmic space. Within the periplasmic space is a gel-like matrix containing nutrient-binding proteins and degradative and detoxifying enzymes. The periplasmic space is absent in grampositive bacteria.
Case
Check 1.1
The differential ability of the Gram stain makes it useful in classifying a bacterium as gram-positive or gram-negative. As in the Case in Point at the beginning of the chapter, correct interpretation and assessment of the Gram-stained smear results are critical in the presumptive identification of the organism present. See also Procedure 9 in Appendix C. The use of quality control organisms with known Gram stain reactions ensures that the Gram stain procedure is performed correctly. Bacteria with thick cell walls containing teichoic acid retain the crystal violet–iodine dye complex after decolorization and appear deep blue; they are gram-positive (e.g., S. aureus). Bacteria with thinner walls containing lipopolysaccharides do not retain the dye complex; they are gram-negative (e.g., E. coli). The alcohol-acetone decolorizer damages these thin lipid walls and allows the stain complex to wash out. All unstained elements, such as Gram-negative bacteria and products of inflammation, are subsequently counterstained red by safranin dye.
Acid-Fast Cell Wall. Certain genera, such as Mycobacterium and Nocardia, have a gram-positive cell wall structure that also contain a waxy layer of glycolipids and fatty acids (mycolic acid) bound to the exterior of the cell wall. More than 60% of the cell wall is lipid, and the major lipid component is mycolic acid, which is a strong hydrophobic molecule that forms a lipid shell around the organism and affects its permeability. This makes Mycobacterium spp. difficult to stain with the Gram stain. Mycobacteria are best stained with an acid-fast stain, in which the bacteria are stained with carbolfuchsin, followed by acid-alcohol as a decolorizer. Other bacteria are decolorized by acid-alcohol, whereas mycobacteria and nocardiae retain the stain. Therefore these bacteria have been designated acid-fast bacteria. The nocardiae are generally considered partially acid-fast and can more easily be decolorized with the acid-fast stain. In addition, the norcardiae will appear a darker blue in the Gram stain compared with the faint blue for the mycobacteria.
Absence of Cell Wall. Prokaryotes that belong to the genera Acholeplasma, Mycoplasma and Ureaplasma are unique in that they lack a cell wall and contain sterols in their plasma membranes. Because they lack the rigidity of the cell wall, they are seen in various shapes microscopically referred to as being pleomorphic Some gram-positive and gram-negative cells can lose their cell walls and grow as L-forms in media supplemented with serum or sugar to prevent osmotic rupture of the cell membrane.
Surface Polymers
Various pathogenic bacteria produce a discrete organized covering termed a capsule. Capsules are usually made of polysaccharide polymers, although they may also be made of polypeptides. Capsules act as virulence factors in helping the pathogen evade phagocytosis. During identification of certain bacteria by serologic typing, capsules sometimes must be removed to detect the somatic (cell wall) antigens present underneath them. Capsule removal is accomplished by boiling a suspension of the microorganism. Salmonella Typhi must have its capsular (Vi) antigen removed for the laboratory scientist to observe agglutination with Salmonella somatic (O) antisera. The capsule does not ordinarily stain with use of common laboratory stains, such as Gram stain or India ink. Instead, it appears as a clear area (“halo-like”) between or surrounding the stained organism and the stained amorphous background material in a direct smear from a clinical specimen.
Slime layers or a glycocalyx are similar to capsules but are more diffuse layers surrounding the cell. They also are made of polysaccharides and serve either to inhibit phagocytosis or, in some cases, to aid in adherence to host tissue or synthetic implants. Glycocalyx production can be the first step in the formation of a biofilm; see Chapter 31.
Case Check 1.2
The most common mechanism for evading phagocytosis used by many microorganisms is having a polysaccharide capsule on the surface. Microorganisms possessing a capsule are generally highly virulent (as in the Case in Point at the beginning of the chapter) until removal of the capsule, at which point virulence becomes extremely low. Encapsulated strains of S. pneumoniae and H. influenzae are associated with highly invasive infections and are known to be more virulent than nonencapsulated strains. See also the section on ability to resist phagocytosis in Chapter 2. Antibodies produced against the capsule often lead to phagocytosis and immunity against that bacterial strain.
Cell Appendages. The flagellum is the organ of locomotion. Flagella are exterior protein filaments that rotate and cause bacteria to be motile. Bacterial species differ in their possession of flagella from none (nonmotile) to many (Fig. 1.4). Flagella that extend from one end of the bacterial cell are polar. Polar flagella may occur singly at one end (monotrichous) or both ends (amphitrichous) or multiply in tufts at one end termed lophotrichous. Flagella that occur all around the bacterium are peritrichous. The number and arrangement of flagella are sometimes used for identification purposes. Flagella can be visualized microscopically with special flagellum stains.
Pili (plural of pilus) and fimbriae (plural of fimbria) are nonflagellar, proteinaceous, hairlike appendages that adhere some bacterial cells to one another and to host cells. Conjugation pili are protein tubes that connect two bacterial cells and mediate DNA exchange.
Eukaryotic Cell Structure
The following structures are associated with eukaryotic cells (see Table 1.1 and Fig. 1.1). In the diagnostic microbiology laboratory, the eukaryotic cell type occurs in medically important fungi and in parasites.
FIG. 1.4
Three flagellar arrangements that occur in bacteria. Other variations can occur.
Cytoplasmic Structures
The nucleus of the eukaryotic cell contains the DNA of the cell in the form of discrete chromosomes (structures in the nucleus that carry genetic information; the genes). They are covered with basic proteins called histones. The number of chromosomes in the nucleus differs according to the particular organism. A rounded, refractile body called a nucleolus is also located within the nucleus. The nucleolus is the site of rRNA synthesis. The nucleus is bounded by a bilayered lipoprotein nuclear membrane.
The ER is a system of membranes that occur throughout the cytoplasm. It is found in two forms. The “rough” ER is covered with ribosomes, the site of protein synthesis. The ribosomes give the ER the rough appearance. The smooth ER does not have ribosomes on the outer surface of its membrane—hence the smooth appearance. Smooth ER does not synthesize proteins, but it does synthesize phospholipids. The major function of the Golgi apparatus or complex is to modify and package proteins sent to it by the rough ER, depending on the protein’s final destination.
Eukaryotic ribosomes, where protein synthesis occurs, are 80S in size and dissociate into two subunits: 60S and 40S. They are attached to the rough ER. Eukaryotic cells contain several membrane-enclosed organelles. Mitochondria are the main site of energy production. They contain DNA and the electron transport system that produces energy in the form of adenosine triphosphate (ATP). Lysosomes contain hydrolytic enzymes for degradation of macromolecules and microorganisms within the cell. Peroxisomes contain protective enzymes that break down hydrogen peroxide and other peroxides generated within the cell. Chloroplasts, found in plant cells, are the sites of photosynthesis. Chloroplasts are the sites where light energy is converted into chemical energy (ATP). Photosynthesis produces oxygen from carbon dioxide and water. Fungi are not plants and have no chloroplasts.
Cell Envelope Structures
Plasma Membrane. The plasma membrane (see Fig. 1.2) is a phospholipid bilayer with embedded proteins that envelops the cytoplasm and regulates transport of macromolecules into and out of the cell. A substantial amount of cholesterol is found in the plasma membrane of animals. Cholesterol has a stabilizing effect and helps keep the membrane fluid. The polar heads of the phospholipids are hydrophilic (water loving) and lie on both the intracellular and the extracellular fluids; their nonpolar tails are hydrophobic (water hating) and avoid water by lining up in the center of the plasma membrane “tail to tail.” This type of hydrophobic makeup of the interior of the plasma membrane makes it potentially impermeable to water-soluble molecules. Proteins perform several important functions of the membrane. They may act as enzymes, hormone receptors, pore channels, and carriers.
Cell Wall. The function of a cell wall is to provide rigidity and strength to the exterior of the cell. Most eukaryotic cells do not have cell walls. However, fungi have cell walls principally made of polysaccharides, such as chitin, mannan, and glucan. Chitin is a distinct component of fungal cell walls.
Motility Organelles. Cilia are short projections (3 to 10 µm), usually numerous, that extend from the cell surface and are used for locomotion. They are found in certain protozoa and in ciliated epithelial cells of the respiratory tract. Flagella are longer projections (>150 µm) used for locomotion by cells such as spermatozoa.
The basal body, or kinetosome, is a small structure located at the base of cilia or flagella, where microtubule proteins involved in movement originate.
Bacterial Morphology
Microscopic Shapes
The largest bacterium known, Thiomargarita namibiensis, is found in ocean sediment and generally has a diameter of 0.1 to 0.3 mm. Most bacteria range in size from 0.4 to 2 µm. They occur in three basic shapes (Fig. 1.5):
• Cocci (spherical)
• Bacilli (rod-shaped)
• Spirochetes (spiral)
Individual bacteria may form characteristic groupings. Cocci (plural of coccus) may occur singly, in pairs (diplococci), in chains (streptococci), or in clusters (staphylococci). Bacilli (plural of bacillus) vary greatly in size and length from very short coccobacilli to long filamentous rods. The ends may be square or rounded. Bacilli with tapered, pointed ends are termed fusiform. Some bacilli are curved. When a species differs in size and shape within a pure culture, the bacterium is termed pleomorphic. Bacilli may occur as single rods or in chains or may align themselves side
Microscopic Morphology of Bacteria
COCCI
In clusters
In chains
In pairs
In tetrads
Coccobacilli
Bacilli of various sizes
Fusiform bacilli
Palisading
SPIROCHETES
1.5 The microscopic shapes and arrangements of bacteria.
BACILLI
FIG.
by side (palisades). Spirochetes vary in length and in the number of helical turns (not all helical bacteria are called spirochetes).
Common Stains Used for Microscopic Visualization
Stains that impart color or fluorescence are needed to visualize bacteria under the microscope. The microscopic staining characteristics, shapes, and groupings are used in the classification of microorganisms (Fig. 1.6).
Gram Stain
The Gram stain is the most commonly used stain in the clinical microbiology laboratory. It places bacteria into one of two main groups: gram-positive (blue to purple) or gram-negative (pink; see Fig. 1.6A–B). Some organisms are gram-variable or do not stain at all. As mentioned previously, the cell wall structure determines the Gram-staining characteristics of a species. The Gram stain consists of gentle heat fixing (methyl alcohol may be used instead for fixation) of the smear and the addition of four sequential components: crystal violet (the primary stain, 1 minute), iodine (the mordant or fixative, 1 minute), alcohol or an alcoholacetone solution (the decolorizer, on and quick rinse), and safranin (the counterstain, 30 seconds). The time frames listed are not exact and vary with the organism; rinsing with water between
each step is important. The bacteria are initially stained purple by the crystal violet that is bound to the cell wall with the aid of iodine. When the decolorizer is applied to bacteria with a gramnegative cell wall, the crystal violet washes out of the cells, which then take up the pink counterstain, safranin. For this reason, gram-negative bacteria appear pink under the light microscope. Bacteria with a gram-positive cell wall retain the primary crystal violet stain during the decolorizing treatment and appear purple. Cells in a direct smear from a patient specimen, such as epithelial cells, white blood cells, red blood cells, and amorphous background material, should appear pink (gram-negative) if the Gram stain procedure was performed correctly.
Case Check 1.3
Review of quality control slides is important in the detection of errors in the performance of the Gram stain procedure and in interpretation of results. As illustrated in the Case in Point at the beginning of the chapter, the gram-positive control organism, S. aureus, stained gram-positive, which is an acceptable result. However, the gram-negative control organism, E. coli, also appeared gram-positive, which is an unacceptable result and indicative of an error in performing the Gram stain procedure. When such an error occurs, the results may not be reported until the discrepancy is resolved and the procedure is repeated with acceptable quality control results.
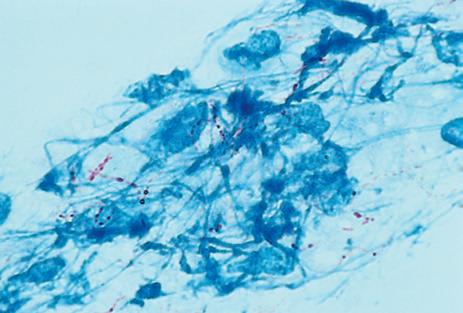
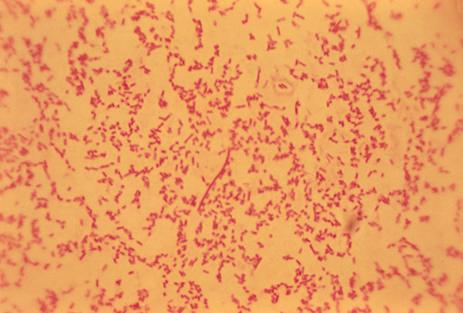
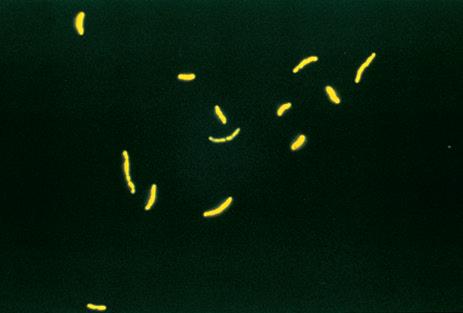
FIG. 1.6 A, Gram stain of Lactobacillus species illustrating gram-positive bacilli, singly and in chains. A few gram-negative–staining bacilli are also present. B, Gram stain of Escherichia coli illustrating short gram-negative bacilli. C, Acid-fast stain, Carbol fuchsin-based. Sputum smear demonstrating the presence of acid-fast Mycobacterium species (arrow) stained by the Kinyoun or Ziehl-Neelsen carbol fuchsin method. D, Acid-fast stain, fluorochrome-based. Mycobacterium species stained with the acid-fast fluorescent auramine-rhodamine stain. This stain is useful for screening for the presence of acid-fast bacteria in clinical specimens. Continued