Victoria Wochna Loerzel, PhD, RN, OCN® Associate Professor and Beat M. and Jill L. Kahli Endowed Professor in Oncology Nursing University of Central Florida
Orlando, Florida
Bleeding; Fever With Neutropenia; Fever Without Neutropenia
Heather Thompson Mackey, MSN, RN, ANPBC, AOCN®
Nurse Practitioner, Cancer Prevention and Wellness
Novant Health Derrick L. Davis Regional Cancer Center
Winston-Salem, North Carolina
Cough; Dyspnea
iv Telephone Triage for Oncology Nurses (Third Edition)
Jackie Matthews, RN, MS, APRN-CNS, AOCN®, ACHPN
Oncology and Palliative Clinical Nurse Specialist
Vice President, Palliative and Supportive Care
Innovative Care Solutions
Dayton, Ohio
Dysphagia; Esophagitis; Xerostomia (Dry Mouth)
Deborah Metzkes, RN, BSN, OCN®, MBA
Clinical Educator
IQVIA
Boca Raton, Florida
Anorexia; Menopausal Symptoms
Cynthia Muller, MJ, BSN, RN
Clinical Support Specialist and Educator
Bayer Oncology TKI Division
Whippany, New Jersey
Legal Concerns of Telephone Triage
Mary Murphy, RN, MS, AOCN®, ACHPN
President and Chief Nursing and Care Officer
Ohio’s Hospice of Dayton
Dayton, Ohio
Anxiety; Deep Vein Thrombosis
Tayreez Mushani, BScN, MHS, CON(C), CHPCN(C)
Assistant Professor
Aga Khan University School of Nursing and Midwifery
Nairobi, Kenya
Flu-Like Symptoms
Pamela J. Pearson, RN
Immunotherapy Infusion Registered Nurse
Seattle Cancer Care Alliance
Seattle, Washington
Bone Loss; Nausea and Vomiting
Jody Pelusi, PhD, FNP, AOCNP®
Oncology Nurse Practitioner/Investigator
Phase I Clinical Trials
Honor Health Research Institute
Scottsdale, Arizona
Oral Therapies and Telephone Triage
Mary Ann Plambeck, RN, MSN, NEA-BC, OCN®
Clinical Operations Director
Duke Cancer Center
Durham, North Carolina
Setting Up a Telephone Triage Call Center
Jeanene “Gigi” Robison, MSN, APRN-CNS, AOCN®
Oncology Clinical Nurse Specialist
The Christ Hospital Health Network
Cincinnati, Ohio
Hand-Foot Syndrome; Phlebitis
Sharon Rockwell, BSN, RN, OCN®, CRNI
Immunotherapy Infusion Registered Nurse
Seattle Cancer Care Alliance
Seattle, Washington
Bone Loss
Erin J. Ross, DNP, MS, ANP-BC, CORLN
Nurse Practitioner
Head and Neck Institute
Cleveland Clinic
Cleveland, Ohio
Hemoptysis
Marlon Garzo Saria, PhD, RN, AOCNS®, FAAN
Tarble Foundation Oncology Clinical Nurse Specialist and Nurse Scientist
Assistant Professor of Translational Neurosciences and Neurotherapeutics
Director, Center for Quality and Outcomes
Research
Pacific Neuroscience Institute and John Wayne Cancer Institute at Providence Saint John’s Health Center
Santa Monica, California
Seizures
Gary Shelton, DNP, NP, ANP-BC, AOCNP®, ACHPN
Clinical Program Manager, Hematology and Oncology
Mount Sinai Hospital
New York, New York
Difficulty or Pain With Urination; Hematuria; Pruritus (Itch)
Sharon Steingass, RN, MSN, AOCN®
Nursing Director
The Ohio State University Comprehensive Cancer Center Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Columbus, Ohio
Models of Telephone Triage and Use of Guidelines
Preface
Improved understanding of molecular carcinogenesis and immune therapy has led to considerable strides forward in cancer treatments. Although these new agents bring great promise, they also produce a number of adverse events requiring close monitoring to provide maximal patient benefit. Oncology nurses are challenged to keep abreast of changes in patient management to ensure quality care. Continued nursing research and evidence-based practice guidelines are necessary to enhance patient outcomes related to nursing care.
Additionally, technologic improvements, such as video telecommunication via smartphones and online communication platforms such as Skype™, have introduced a new dimension to telephone triage. The ability to view a patient during a telephone call can enhance the nurse’s ability to assess the patient’s problem. This combination of video and voice is being used more frequently in the nurse’s triage of patients, so much so that the term telephone triage nursing has evolved into telenursing. A number of updates have been included in this text to address these technologic advances.
This third edition of Telephone Triage for Oncology Nurses has been expanded to address patient needs that may result from the newer cancer treatments— targeted therapies and immunotherapy. Targeted therapies for cancer are commonly small molecules that can be taken orally and managed by the patient and family at home. Although oral therapy supports patient independence, self-management of side effects may be challenging. A section has been added to this edition to address improving nursing management of oral therapies. Immunotherapy may result in adverse effects very different from those with traditional cancer treatments. These effects are addressed throughout the protocols, which discuss some common complaints, as well as in a stand-alone protocol in this text.
This book is a result of efforts by professional nurses from diverse settings and geographic locations who synthesized the most current scientific information related to triaging patient problems. The authors of each protocol have carefully reviewed the literature and updated the content from the second edition. Importantly, both chapters and protocols have been updated to incorporate available evidence-based nursing practice and the latest in nursing policy regarding telenursing and multistate licensure. The information in this text will provide the professional oncology nurse with updated tools to improve patient care through quality telenursing practice.
Margaret Hickey, RN, MSN, MS
Susan Newton, APRN, MS, AOCN®, AOCNS®
Introduction
Margaret Hickey, RN, MSN, MS
Over the past few decades, trends in health care have shifted cancer care delivery from inpatient to outpatient settings. In 2012, the American Academy of Ambulatory Care Nursing reported that more than three million nurses, or 25% of RNs in the United States, cared for patients in ambulatory care settings (Mastal & Levine, 2012). In addition to the large number of nurses working in outpatient settings shown in this survey, a growing number of nurses are also caring for patients using telehealth. A 2015 workforce survey by the National Council of State Boards of Nursing (NCSBN) and the National Forum received responses from 78,700 nurses, or 30% of the U.S. nursing workforce. Nearly half of the respondents said they provided patient care using telehealth (NCSBN, 2016). The results of both surveys made it clear that nursing care is no longer defined within the brick-and-mortar walls of a healthcare setting, further reflecting the demand for nontraditional expertise in professional nursing practice in the ambulatory care setting.
This change to the patient care delivery setting can be a challenge to professional nurses educated in the traditional inpatient model. The inpatient setting continues to be the primary location of basic nursing education, yet many nurses at some point will find themselves practicing outside the inpatient hospital. Nurses transitioning to ambulatory care and other settings often expect to use the same knowledge and skills learned in their acute care practices. Although some competencies may be transferable, the expertise and skills needed in the outpatient setting are unique. An ambulatory nurse is often a coordinator of care rather than a hands-on, direct care provider. A transition to ambulatory nursing requires clinical expertise, leadership, and autonomous critical-thinking skills. Nursing practice can include face-to-face care but also indirect care, such as over the telephone or via computer. Unique assessment and communication skills are required when direct sensory input is not available (Stokowski, 2011).
Since its invention in 1876, the telephone has been used as a tool to seek healthcare assistance. Some accounts of Alexander Graham Bell’s first recorded telephone call claim it was for medical help after he spilled sulfuric acid on himself (WGBH Educational Foundation, n.d.). The telephone, complemented by video or pictures, is an essential and effective means of information sharing and communication, and therefore, it is a vital tool for the ambulatory care nurse. Telephone triage is defined as “an interactive process between the nurse and client that occurs over the telephone and involves identifying the nature and urgency of client health care needs and determining the appropriate disposition” (Rutenberg & Greenberg, 2012, p. 5). Providing telephone triage and telephone advice are essential skills for the ambulatory nurse. Regardless of the nursing specialty (e.g., pediatrics, otolaryngology, oncology), nurses in outpatient clinics often find themselves performing assess-
Oncology nurses from across the United States and as far away as Kenya have contributed these protocols to help other nurses and improve patient care. This text could not have been accomplished without the sharing spirit and collegiality of oncology nurses dedicated to improving the care of patients with cancer.
REFERENCES
American Hospital Association. (2016). Telehealth: Helping hospitals deliver cost-effective care Retrieved from http://www aha org/content/16/16telehealthissuebrief pdf Car, J., & Sheikh, A. (2003). Telephone consultations. BMJ, 326, 966–969. https://doi org/10 1136/bmj 326 7396 966
Derkx, H.P., Rethans, J.-J.E., Knottnerus, J.A., & Ram, P.M. (2007). Assessing communication skills of clinical call handlers working at an out-of-hours centre: Development of the RICE rating scale. British Journal of General Practice, 57, 383–387.
Lockwood, T. (n.d.). Voice and language. Retrieved from http://www fenman co uk/traineractive/training -activity/voice-and-language html
Mastal, M., & Levine, J. (2012). Perspectives in ambulatory care: A survey. Nursing Economics, 30, 295–304.
National Council of State Boards of Nursing. (2016). Executive summary: The 2015 National Nursing Workforce Survey. Journal of Nursing Regulation, 7(Suppl.), S4–S6.
Rutenberg, C., & Greenberg, M.E. (2012). The art and science of telephone triage: How to practice nursing over the phone. Hot Springs, AR: Telephone Triage Consulting. Stokowski, L.A. (2011). Ambulatory care nursing: Yes, it’s a specialty. Retrieved from https://www medscape com/viewarticle/749906 2
WGBH Educational Foundation. (n.d.). The world’s first phone call happened in Boston. Retrieved from https://www wgbh org/news/2016/03/11/science-and-technology/worlds-first-phone-call -happened-boston
Overview
Margaret Hickey, RN, MSN, MS
Telemedicine describes the provision of medical care across distance using electronic means. Historically, telemedicine centered on consultation or other situations in which a licensed physician is in direct contact with another licensed physician. Telenursing describes nursing services provided via telecommunication channels and is a subset of telemedicine. In 1997, the National Council of State Boards of Nursing (NCSBN) first determined that nursing practice does in fact occur when nurses provide care via telecommunication channels. In 2014, this definition was expanded to include advances in communication technologies: high-speed Internet, wireless, and satellite and televideo communications (NCSBN, 2014). The College of Registered Nurses of Nova Scotia (2017) further defined telenursing as a nursing practice in which nurses “meet the health needs of clients using information, communication, and web-based systems” (p. 1) to deliver, manage, and coordinate care through information and telecommunication technologies.
The most typical example of telenursing is the nurse in direct telephone contact with the patient or caregiver; however, use of video and photographs can augment these calls with additional visual context. Telephone nursing care involves the establishment of a nurse–patient relationship and is facilitated by the nursing process. The nursing process is an interactive problem-solving process used to give organized and individualized patient care. It involves assessment with data collection, identification of the problem, planning, implementation, and evaluation.
Nauright, Moneyham, and Williamson (1999) held two focus groups of nurses involved in telephone triage and consultation. The goals of these focus groups were to examine the evolving role of nurses in telephone triage and consultation, identify and describe issues that affect their practice, and discuss the implications of this emerging role on nursing practice, education, and research. The focus groups included nurses who staffed health maintenance organization (HMO) and hospital call-in advice lines from two states. They were asked to describe what they did in their role as telephone triage nurses. These nurses described the three major activities of telephone triage as educating patients, advocating for patients, and connecting patients with needed resources. These main activities continue yet today. The nurses surveyed did not describe their role in the true sense of triage (i.e., sorting patients into urgency categories based on their injuries or symptoms) but rather as nursing care provided through a new venue—the telephone. The nurses included in these focus groups did not come from oncology offices; however, oncology nurses would most likely describe their role in much the same way.
Telenursing has evolved over the decades. It first came onto the healthcare scene during the 1960s. During that decade and the next, telephone nurses became gate-
last visit. The caller can be the patient or a caregiver. Although both can provide important information, it is recommended that the nurse speak directly with the patient regardless of who initiated the call. This gives the nurse an opportunity to listen to breathing and voice cues, such as slurred speech or signs of confusion.
• Nursing diagnosis: The nurse’s identification of the problem, working diagnosis, or conclusion is derived from the history, telephone interview, and any objective symptoms.
• Identification of expected outcomes or goals: The nurse needs to determine what needs to occur in order to resolve the problem. The goal of care should be realistic and attainable.
• Planning: Once the problem is identified, the urgency of the problem and the appropriate disposition are determined. The most effective decision makers consider the whole situation and not just the symptoms. Other factors such as age, gender, illness, recent treatment, and distance from care must be considered. The process needs to be interactive so that the nurse can determine the patient’s willingness and ability to comply with advice. For example, a nurse identifies a 32-year-old woman’s complaint of severe abdominal pain as requiring urgent care and recommends that the patient go to the nearest ED. The nurse failed to elicit that the woman has a three-year-old child at home, and no one is available to care for the child. Subsequently, the patient disregards the advice.
• Implementation: Once the urgency is determined and a referral is made, the nurse needs to work with the patient to set an appointment and arrange appropriate transportation, if necessary, for medical evaluation. The nurse must provide instructions to the patient, regardless of whether the problem requires the patient to be seen today or to monitor symptoms at home.
• Evaluation: Before the call has ended, the nurse should review the plan with the patient and evaluate the caller’s understanding of the instructions and the patient’s intended compliance with the advice. For example, the nurse should ask the patient to repeat back the plan and also ask the patient if there is any reason that he or she cannot or will not follow through with it. If it is deemed necessary, the nurse should schedule a follow-up call to evaluate the patient’s status.
Multiple authors, nursing organizations such as the American Nurses Association, and state boards of nursing repeatedly emphasize the importance of using guidelines or protocols for telephone triage. Standard protocols provide written guidance of questions that best elicit information from patients, as well as advice and disposition instructions for the patients.
This text provides examples of protocols designed to address common complaints of patients with oncologic conditions. Protocols do not stand alone; rather, they complement and support established policies and procedures. These protocols are designed to be a guide and should be closely reviewed by the experts in the department, including the RNs, nurse practitioners, and medical team responsible for the practice, and edited as needed to meet the needs of the patients seen in the oncology ambulatory center.
Required policies include telephone call processing and instruction in directing patients’ calls. Appropriate documentation of the calls needs to be outlined,
and documentation forms or electronic medical record templates should be developed to streamline the process and ensure that the needed information is captured. Policies and procedures need to be written to outline the actions to be taken by the nurse and physician and should include the communication process between the two. Finally, policies must ensure that patient confidentiality is maintained. See Appendix A for an example of a policy guideline.
Protocols and policies improve the telephone nursing process. However, they do not guarantee quality telephone triage and improved patient outcomes. Telephone protocols are only as good as the nurses who use them. These protocols will never replace sound clinical judgment and critical-thinking skills. It is essential that while assessing a patient and the patient’s situation, nurses gather adequate information from the patient’s medical record, the patient, and other resources as needed. Telephone protocols serve as guidelines for nurses, especially less-experienced oncology nurses, to aid them in the nursing process and decision making.
Telenursing has evolved over the years, and it will continue to change with the explosion of communication technology. The scope of telenursing is multifaceted, addressing triage, health advice, and information. The number of nurses practicing telenursing is increasing annually, as is the number of patients using the services available.
REFERENCES
American Academy of Ambulatory Care Nursing. (2016). The role of the registered nurse in ambulatory care: Position statement. Retrieved from https://www aaacn org/sites/default/files/documents /PositionStatementRN pdf
American Academy of Ambulatory Care Nursing. (2017). Scope and standards of practice for professional ambulatory care nursing (9th ed.). Pitman, NJ: Author.
American Academy of Ambulatory Care Nursing. (2018). Scope and standards of practice for professional telehealth nursing (6th ed.). Pitman, NJ: Author.
College of Registered Nurses of Nova Scotia. (2017). Practice guidelines: Telenursing. Retrieved from https://crnns ca/wp-content/uploads/2017/09/Telenursing pdf
National Council of State Boards of Nursing. (2014, April). The National Council of State Boards (NCSBN®) position paper on telehealth nursing practice. Retrieved from https://www ncsbn org /14 Telehealth pdf
NATO Standardization Office. (2017). NATO glossary of terms and definitions (English and French). Retrieved from https://nso nato int/nso/terminology Public html
Nauright, L.P., Moneyham, L., & Williamson, J. (1999). Telephone triage and consultation: An emerging role for nurses. Nursing Outlook, 47, 219–226. https://doi.org/10.1016/S0029-6554(99)90054-4
provide a context to support training, develop competencies, define scope of practice, and measure and improve outcomes.
The nursing process is a systematic method commonly used by nurses to plan, provide, and evaluate nursing care. AAACN (2017) defines the nursing process through six steps: assessment, nursing diagnosis, identification of expected outcomes or goals, planning, implementation, and evaluation. This same framework can be seen in the earliest model of telephone nursing, the Data to Wisdom Continuum, first described by Englebardt and Nelson in 2002. The authors defined telephone nursing as the study of how health data, information, and knowledge are collected, stored, processed, communicated, and used to support the process of healthcare delivery to clients, providers, administrations, and organizations involved in healthcare delivery. The Data to Wisdom Continuum describes the elements of telephone nursing performed daily: nurses collect and organize data and draw conclusions; use their knowledge, expertise, and wisdom; and act on and communicate the data and conclusions across the continuum of care. Although this model describes some of the major steps that a nurse takes during the telephone interaction, it does not completely describe how the work is accomplished.
In 2004, with the evolution of evidence-based practice, a new model of telephone nursing emerged, the Decision-Making Triad (Greenberg & Pyle, 2004). In this model, Greenberg and Pyle illustrated how telephone nurses use three primary sources of information to make decisions: knowledge, clinical context, and patient preference. The Decision-Making Triad expands on the data collected in the Data to Wisdom Continuum, acknowledging the clinical context that influences collected data. The patient’s current health or disease issues, treatment plans, and settings are important aspects of the data and thus may influence the judgment or decision making of the telephone nurse (Greenberg & Pyle, 2004). For example, fever in a postchemotherapy neutropenic patient may be treated very differently than a transient fever as the result of an upper respiratory condition in a patient with cancer no longer undergoing active treatment. Although the fever symptom is consistent in these examples, the clinical context will drive the telephone nurse to think differently as data are collected and interpreted. The addition of evidence-based knowledge and practice is also critical to this model. As oncology nurses continue to learn about new treatments, the management of side effects may again require different interventions and actions. Consider the various types of skin reactions that patients may report via the telephone. Understanding the treatment plan and the potential cause of a skin reaction is critical when conducting an assessment over the phone, as it will allow the patient to receive the correct plan of care and the most appropriate advice. The Decision-Making Triad also takes into consideration patient preferences, ensuring that patients/callers receive information consistent with their current learning and communication styles. Nurses must continually learn and adapt to the diverse ethnic and generational communication and care needs of an ever-changing patient population.
As telephone nursing continued to evolve through the early 2000s, the need for a more formal model of nursing care delivery emerged to provide a comprehensive description of the process of care used by telephone nurses. Building on the Data to Wisdom Continuum and the Decision-Making Triad, Rutenberg and Greenberg
(2012) created a telephone nursing model that describes and defines the processes used in a telephone nursing encounter, as well as the structure of a call.
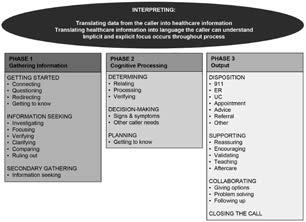
The Greenberg Model of Care Delivery in Telephone Nursing Practice (see Figure 1) has four distinct components: interpreting, information gathering, cognitive processing, and output. Interpreting occurs throughout the telephone encounter, as the nurse continuously listens and translates the information conveyed by the caller. During phase 1, or the information gathering phase, the nurse does most of the data gathering by connecting with the caller, seeking information on the nature and urgency of the call, and putting the call into context. This is when the telephone nurse uses his or her knowledge to gather information about the call and begins to establish a viable plan of care for the caller. Questioning and redirecting are strategies that elicit the caller’s story and allow the nurse to manage the call to ensure all pertinent information is collected. The information gathering phase will be more comprehensively described in the assessment section of this chapter. In phase 2, or the cognitive processing phase, the nurse verifies the information obtained and begins the decisionmaking process. Based on the urgency of the call, some cognitive planning may begin early in the information gathering phase. In the output phase, the nurse recommends a disposition for the call and gives specific advice or information that will be important for the caller based on the established plan of care. It is important for the nurse to validate that the caller has understood all instructions and the plan of care during
Note. Copyright 2005 by M. Elizabeth Greenberg, RNC, PhD. Used with permission.
Figure 1. Greenberg Model of Care Delivery in Telephone Nursing Practice