Series edited by: Nathan R. Selden, MD, PhD, FACS, FAAP
Volume 1: Peripheral Nerve Surgery, Wilson and Yang
Volume 2: Surgical Neuro-Oncology, Lonser and Elder
Volume 3: Spinal Neurosurgery, Harrop and Maulucci
Spinal Neurosurgery
Edited by
James
S.
Harrop, MD, FACS
Professor, Departments of Neurological and Orthopedic Surgery
Director, Division of Spine and Peripheral Nerve Surgery
Neurosurgery Director of Delaware Valley SCI Center
Thomas Jefferson University Philadelphia, Pennsylvania and Christopher M. Maulucci, MD, FACS
Associate Professor of Neurological Surgery
Director of Spine Surgery
Tulane University
New Orleans, Louisiana
Oxford University Press is a department of the University of Oxford. It furthers the University’s objective of excellence in research, scholarship, and education by publishing worldwide. Oxford is a registered trade mark of Oxford University Press in the UK and certain other countries.
Published in the United States of America by Oxford University Press 198 Madison Avenue, New York, NY 10016, United States of America.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, without the prior permission in writing of Oxford University Press, or as expressly permitted by law, by license, or under terms agreed with the appropriate reproduction rights organization. Inquiries concerning reproduction outside the scope of the above should be sent to the Rights Department, Oxford University Press, at the address above.
You must not circulate this work in any other form and you must impose this same condition on any acquirer.
Library of Congress Cataloging-in-Publication Data
Names: Harrop, James S., editor. | Maulucci, Christopher M., editor.
Title: Spinal neurosurgery / edited by James S. Harrop, Christopher M. Maulucci.
Description: New York, NY : Oxford Unversity Press, [2019] | Includes bibliographical references.
Identifiers: LCCN 2018029143 | ISBN 9780190887773 (pbk.)
Subjects: | MESH: Spine—surgery | Spinal Diseases—surgery | Spinal Injuries—surgery | Neurosurgical Procedures—methods Classification: LCC RD533 | NLM WE 727 | DDC 617.4/71059—dc23 LC record available at https://lccn.loc.gov/2018029143
This material is not intended to be, and should not be considered, a substitute for medical or other professional advice. Treatment for the conditions described in this material is highly dependent on the individual circumstances. And, while this material is designed to offer accurate information with respect to the subject matter covered and to be current as of the time it was written, research and knowledge about medical and health issues is constantly evolving and dose schedules for medications are being revised continually, with new side effects recognized and accounted for regularly. Readers must therefore always check the product information and clinical procedures with the most up-to-date published product information and data sheets provided by the manufacturers and the most recent codes of conduct and safety regulation. The publisher and the authors make no representations or warranties to readers, express or implied, as to the accuracy or completeness of this material. Without limiting the foregoing, the publisher and the authors make no representations or warranties as to the accuracy or efficacy of the drug dosages mentioned in the material. The authors and the publisher do not accept, and expressly disclaim, any responsibility for any liability, loss or risk that may be claimed or incurred as a consequence of the use and/or application of any of the contents of this material.
9 8 7 6 5 4 3 2 1
Printed by WebCom, Inc., Canada
Series Editor’s Preface vii
Contributors ix
1. Odontoid Fracture Type II 1
Daniel Tarazona and Alexander R. Vaccaro
2. Cervical Fracture Dislocation 11
Jason Liounakos, G. Damian Brusko, and Michael Y. Wang
3. Occipitocervical Dislocation 21
Alexander B. Dru and Daniel J. Hoh
4. Central Cord Injury 31
Bizhan Aarabi, Charles A. Sansur, David M. Ibrahimi, Mathew Kole, and Harry Mushlin
5. Atlantoaxial Instability 41
Jonathan M. Parish and Domagoj Coric
6. Basilar Invagination and Cranial Settling 49
Benjamin D. Elder and Jean-Paul Wolinsky
7. Cervical Myelopathy: Lordosis 63
Randall J. Hlubek and Nicholas Theodore
8. Cervical Myelopathy: Kyphosis 71
Mario Ganau, So Kato, and Michael G. Fehlings
9. Ossification of the Posterior Longitudinal Ligament: Cervical 81
Todd D. Vogel, Hansen Deng, and Praveen V. Mummaneni
10. Cervical Radiculopathy Due to Central Disc: ACDF/Arthroplasty 93
Michael A. Galgano, Jared Fridley, and Ziya Gokaslan
17. Radiation-Sensitive Spine Tumor 159
Adam M. Robin and Ilya Laufer
18. Cauda Equina Syndrome 175
Emily P. Sieg, Justin R. Davanzo, and John P. Kelleher
19. Lumbar Stenosis 183
Miner N. Ross and Khoi D. Than
20. L4–L5 Degenerative Spondylolisthesis 191
Rani Nasser, Scott Zuckerberg, and Joseph Cheng
21. Isthmic Spondylolisthesis 199
Evan Lewis and Charles A. Sansur
22. Lumbar Degenerative Scoliosis 207
Michael LaBagnara, Durga R. Sure, Christopher I. Shaffrey, and Justin S. Smith
23. Flat Back Deformity 215
Yusef I. Mosley and James S. Harrop
24. Diskitis 225
Jacob R. Joseph, Brandon W. Smith, and Mark E. Oppenlander
25. Epidural Abscess 235
Hector G. Mejia Morales and Manish K. Singh
26. Nonsurgical Spinal Diseases 243
Lahiru Ranasinghe and Aimee M. Aysenne
Index 253
Series Editor’s Preface
I am delighted to introduce this volume of Neurosurgery by Example: Key Cases and Fundamental Principles. Neurosurgical training and practice are based on managing a wide range of complex clinical cases with expert knowledge, sound judgment, and skilled technical execution. Our goal in this series is to present exemplary cases in the manner they are actually encountered in the neurosurgical clinic, hospital emergency department, and operating room.
In this volume, Dr. Jim Harrop, Dr. Christopher Maulucci, and their contributors share their extensive wisdom and experience with all major areas of spinal neurosurgery. Each chapter contains a classic presentation of an important clinical entity, guiding readers through assessment and planning, decision-making, surgical procedure, after care, and complication management. “Pivot points” illuminate the changes required to manage patients in alternate or atypical situations.
Each chapter also presents lists of pearls for the accurate diagnosis, successful treatment, and effective complication management of each clinical problem. These three focus areas will be especially helpful to neurosurgeons preparing to sit for the American Board of Neurological Surgery oral examination, which bases scoring on these three topics.
Finally, each chapter contains focused reviews of medical evidence and expected outcomes, helpful for counseling patients and setting accurate expectations. Rather than exhaustive reference lists, the authors provide lists of high-priority additional reading recommended to deepen understanding.
The resulting volume should provide you with a dynamic tour through the practice of spinal neurosurgery, guided by some of the leading experts in North America. Additional volumes cover each subspecialty area of neurosurgery using the same casebased approach and board review features.
Nathan R. Selden, MD, PhD Campagna Professor and Chair Department of Neurological Surgery Oregon Health and Science University Portland, Oregon
Contributors
Bizhan Aarabi, MD, FRCSC, FACS
Professor, Neurosurgery
Director of Neurotrauma, R. Adams Cowley Shock Trauma Center Department of Neurosurgery
University of Maryland School of Medicine
Baltimore, Maryland
Aimee M. Aysenne, MD, MPH
Director of Neurocritical Care Department of Clinical Neurosciences
Tulane University, School of Medicine New Orleans, Louisiana
Tej D. Azad, BA
Medical Student Department of Neurosurgery Stanford University School of Medicine Stanford, California
G. Damian Brusko, BS Department of Neurological Surgery The Miami Project to Cure Paralysis University of Miami Miller School of Medicine Miami, Florida
Joseph Cheng, MD, MS Professor of Neurosurgery
Frank H. Mayfield Chair Department of Neurological Surgery University of Cincinnati Health Cincinnati, Ohio
Domagoj Coric, MD
Chief, Department of Neurosurgery Carolinas Medical Center
Carolina Neurosurgery and Spine Associates
Charlotte, North Carolina
Andrew Dailey, MD Professor
Department of Neurosurgery University of Utah Salt Lake City, Utah
Justin R. Davanzo, MD Department of Neurological Surgery Penn State Health Milton S. Hershey Medical Center Pennsylvania, Pennsylvania
Hansen Deng, BS
Medical Student
Department of Neurological Surgery University of California, San Francisco San Francisco, California
Atman Desai, MD
Assistant Professor Department of Neurosurgery
Stanford University School of Medicine Stanford, California
Alexander B. Dru, MD University of Florida Department of Neurosurgery Gainesville, Florida
Benjamin D. Elder, MD, PhD
Assistant Professor of Neurosurgery, Orthopedic Surgery, and Biomedical Engineering
Mayo Clinic School of Medicine
Rochester, Minnesota
Ilyas Eli, MD
Resident
Department of Neurosurgery
University of Utah
Salt Lake City, Utah
Michael G. Fehlings, MD, PhD, FRCSC, FACS
Vice Chair Research
Professor of Neurosurgery
McLaughlin Scholar in Molecular Medicine
Co-Chair Spinal Program
University of Toronto
Gerry and Tootsie Halbert Chair in Neural Repair and Regeneration Head, Spinal Program
Toronto Western Hospital Toronto, Ontario, Canada
Jared Fridley, MD
Assistant Professor of Neurosurgery
Brown University Department of Neurosurgery
Providence, Rhode Island
Michael A. Galgano, MD
Clinical Instructor of Neurosurgery
Brown University Department of Neurosurgery
Providence, Rhode Island
Mario Ganau, MD, PhD, FACS
Spine Fellow
Toronto Western Hospital Toronto, Ontario, Canada
Ziya Gokaslan, MD
Professor and Chair
Brown University Department of Neurosurgery
Providence, Rhode Island
James S. Harrop, MD, FACS
Professor, Departments of Neurological and Orthopedic Surgery
Director, Division of Spine and Peripheral Nerve Surgery
Neurosurgery Director of Delaware Valley SCI Center
Thomas Jefferson University Philadelphia, Pennsylvania
Randall J. Hlubek, MD
Department of Neurosurgery
Barrow Neurological Institute
St. Joseph’s Hospital and Medical Center
Phoenix, Arizona
Daniel J. Hoh, MD
Associate Professor
Dunspaugh-Dalton Endowed Professorship
Department of Neurological Surgery
University of Florida
Gainesville, Florida
David M. Ibrahimi, MD
Assistant Professor Department of Neurosurgery
University of Maryland School of Medicine
Baltimore, Maryland
Rajiv R. Iyer, MD
Department of Neurosurgery
The Johns Hopkins University School of Medicine
Baltimore, Maryland
George I. Jallo, MD
Professor of Neurosurgery, Pediatrics and Oncology
Director, Institute for Brain Protection Sciences
Johns Hopkins All Children’s Hospital
St. Petersburg, Florida
Jacob R. Joseph, MD
Department of Neurosurgery
University of Michigan
Ann Arbor, Michigan
James Kalyvas, MD
Neurosurgeon
Ochsner Clinic Foundation
New Orleans, Louisiana
Michael Karsy, MD, PhD
Resident
Department of Neurosurgery University of Utah Salt Lake City, Utah
So Kato, MD
Spine Fellow Toronto Western Hospital Toronto, Ontario, Canada
John P. Kelleher, MD
Department of Neurological Surgery
Penn State Health Milton S. Hershey Medical Center Pennsylvania, Pennsylvania
Omaditya Khanna, MD
Resident
Thomas Jefferson University Hospital Philadelphia, Pennsylvania
Mathew Kole, MD
Resident in Training Department of Neurosurgery
University of Maryland School of Medicine Baltimore, Maryland
Michael LaBagnara, MD
Assistant Professor of Neurological Surgery
University of Tennessee Semmes-Murphey Clinic
Memphis, Tennessee
Ilya Laufer, MD Department of Neurosurgery
Memorial Sloan Kettering Cancer Center
New York, New York
Evan Lewis, MD
Neurosurgeon
Baptist Medical Group–Neurosurgery Pensacola, Florida
Jason Liounakos, MD
Resident
Department of Neurological Surgery
Univeristy of Miami Miller School of Medicine
Miami, Florida
Christopher M. Maulucci, MD, FACS
Associate Professor of Neurological Surgery
Assistant Residency Program Director School of Medicine
Tulane University
New Orleans, Louisiana
Hector G. Mejia Morales
Medical student
Tulane University School of Medicine New Orleans, Louisiana
Yusef I. Mosley, MD Department of Neurosurgery
Thomas Jefferson University Philadelphia, Pennsylvania
Praveen V. Mummaneni, MD
Joan O’Reilly Endowed Professor Vice Chairman
University of California, San Francisco Neurosurgery
San Francisco, California
Harry Mushlin, MD
Resident in Training Department of Neurosurgery
University of Maryland School of Medicine
Baltimore, Maryland
Rani Nasser, MD
Clinical Instructor of Neurosurgery
University of Cincinnati Health Cincinnati, Ohio
Mark E. Oppenlander, MD
Assistant Professor
Department of Neurosurgery University of Michigan Ann Arbor, Michigan
Jonathan M. Parish, MD
Resident Physician
Carolinas Medical Center Charlotte, North Carolina
Lahiru Ranasinghe, BS Medical Student
Department of Clinical Neuroscience
Tulane University School of Medicine
New Orleans, Louisiana
John K. Ratliff, MD
Professor
Department of Neurosurgery
Stanford University School of Medicine Stanford, California
Adam M. Robin, MD Department of Neurosurgery
Memorial Sloan Kettering Cancer Center
New York, New York
Miner N. Ross, MD, MPH
Resident Physician
Department of Neurological Surgery
Oregon Health and Science University Portland, Oregon
Charles A. Sansur, MD
Associate Professor
Department of Neurosurgery
University of Maryland School of Medicine
Baltimore, Maryland
Christopher I. Shaffrey, MD
John A. Jane Professor of Neurological Surgery
Division Head Spinal Surgery
Professor of Orthopaedic Surgery
University of Virginia Medical Center
Charlottesville, Virginia
Emily P. Sieg, MD
Department of Neurological Surgery
Penn State Health Milton S. Hershey
Medical Center Pennsylvania, Pennsylvania
Manish K. Singh, MD
Assistant Professor of Neurological Surgery
Director of Spine Surgery Program
Tulane University School of Medicine
New Orleans, Louisiana
Brandon W. Smith, MD, MS
Department of Neurosurgery
University of Michigan Ann Arbor, Michigan
Justin S. Smith, MD, PhD
Harrison Distinguished Professor Neurological Surgery
University of Virginia Medical Center
Charlottesville,Virginia
Geoffrey P. Stricsek, MD
Resident
Thomas Jefferson University Philadelphia, Pennsylvania
Durga R. Sure, MD
Department of Neurosurgery
University of Virginia
Charlottesville, Virginia
Daniel Tarazona, MD
Department of Orthopedics
Rothman Institute Philadelphia, Pennsylvania
Khoi D. Than, MD
Assistant Professor
Neurological Surgery
Oregon Health and Science University Portland, Oregon
Nicholas Theodore, MD
Department of Neurosurgery
Barrow Neurological Institute
St. Joseph’s Hospital and Medical Center Phoenix, Arizona
Vincent C. Traynelis, MD
Professor
Department of Neurosurgery
Rush University Medical Centre Chicago, Illinois
Mazda K. Turel, MBBS
Clinical Fellow in Cerebrovascular and Bypass Surgery
Department of Neurosurgery
Rush University Medical Centre Chicago, Illinois
Derrick Umansky, MD
Resident Department of Neurosurgery
Tulane University School of Medicine New Orleans, Louisiana
Alexander R. Vaccaro, MD, PhD, MBA
Department of Orthopedic Surgery
Rothman Institute (President) Philadelphia, Pennsylvania
Anand Veeravagu, MD
Assistant Professor
Department of Neurosurgery
Stanford University School of Medicine Stanford, California
Todd D. Vogel, MD
Minimally Invasive and Complex Spine Fellow
Department of Neurological Surgery
University of California, San Francisco San Francisco, California
Michael Y. Wang, MD
Chief of Neurosurgery
University of Miami Hospital Professor
Departments of Neurological Surgery and Rehabilitation Medicine
University of Miami School of Medicine Miami, Florida
Jean-Paul Wolinsky, MD
Department of Neurosurgery and Oncology
Clinical Director of the Johns Hopkins Spine Program
Johns Hopkins University Baltimore, Maryland
Scott Zuckerberg, MD, MPH
Co-Director
Research of the Vanderbilt Sports Concussion Center Research Group
Department of Neurological Surgery
Vanderbilt University Medical Center Nashville, Tennessee
Odontoid Fracture Type II
Daniel Tarazona and Alexander R. Vaccaro
Case Presentation
A 79-year-old woman presents to the emergency department after falling at a nursing home. She denies loss of consciousness. She arrived in a cervical collar placed prior to transfer with a chief complaint of neck pain. She denies any paresthesias or weakness. She is hemodynamically stable and is awake, alert, and oriented. Upon physical examination there is midline cervical spine tenderness without step-offs or deformities. A neurological exam revealed 5/5 motor strength throughout, no sensory deficits, 1+ DTR throughout, and a normal rectal examination.
Questions
1. What is the likely diagnosis?
2. What is the most appropriate imaging modality?
3. How are odontoid fractures classified?
Assessment and Planning
Based on the history and physical exam, the surgeon suspects a cervical spine fracture. The differential diagnosis includes injuries to the upper cervical, subaxial cervical, and upper thoracic spine. Due to the initial concern for a cervical spine injury, spine precautions are maintained and a dedicated computed tomographic (CT) scan of the cervical, thoracic, and lumbar spine is obtained revealing a type II odontoid fracture.
Oral Boards Review: Diagnostic Pearls
1. The Anderson and D’Alonzo classification for odontoid fractures lends prognostic information for risk of nonunion and assists with treatment planning.
2. CT scan is the preferred imaging modality with high inter- and intrarater agreement. It also assists with diagnosis of concomitant spinal injuries.20
3. CT or magnetic resonate (MR) angiography should be considered if vertebral artery injury is clinically suspected.
Initial radiographic evaluation of the cervical spine includes anteroposterior (AP), lateral, and open- mouth odontoid views and CT of the cervical spine. Magnetic
Anderson and D’Alonzo
Type I
Type II
Type III
resonance imaging (MRI) is warranted with neurologic injury or concern for concomitant ligamentous injury. If posterior instrumentation is anticipated, then a CT angiogram may be obtained to evaluate for potential vascular anomalies that would preclude safe C2 pars, C2 pedicle, C1–C2 transarticular, or C1 lateral mass screw placement.
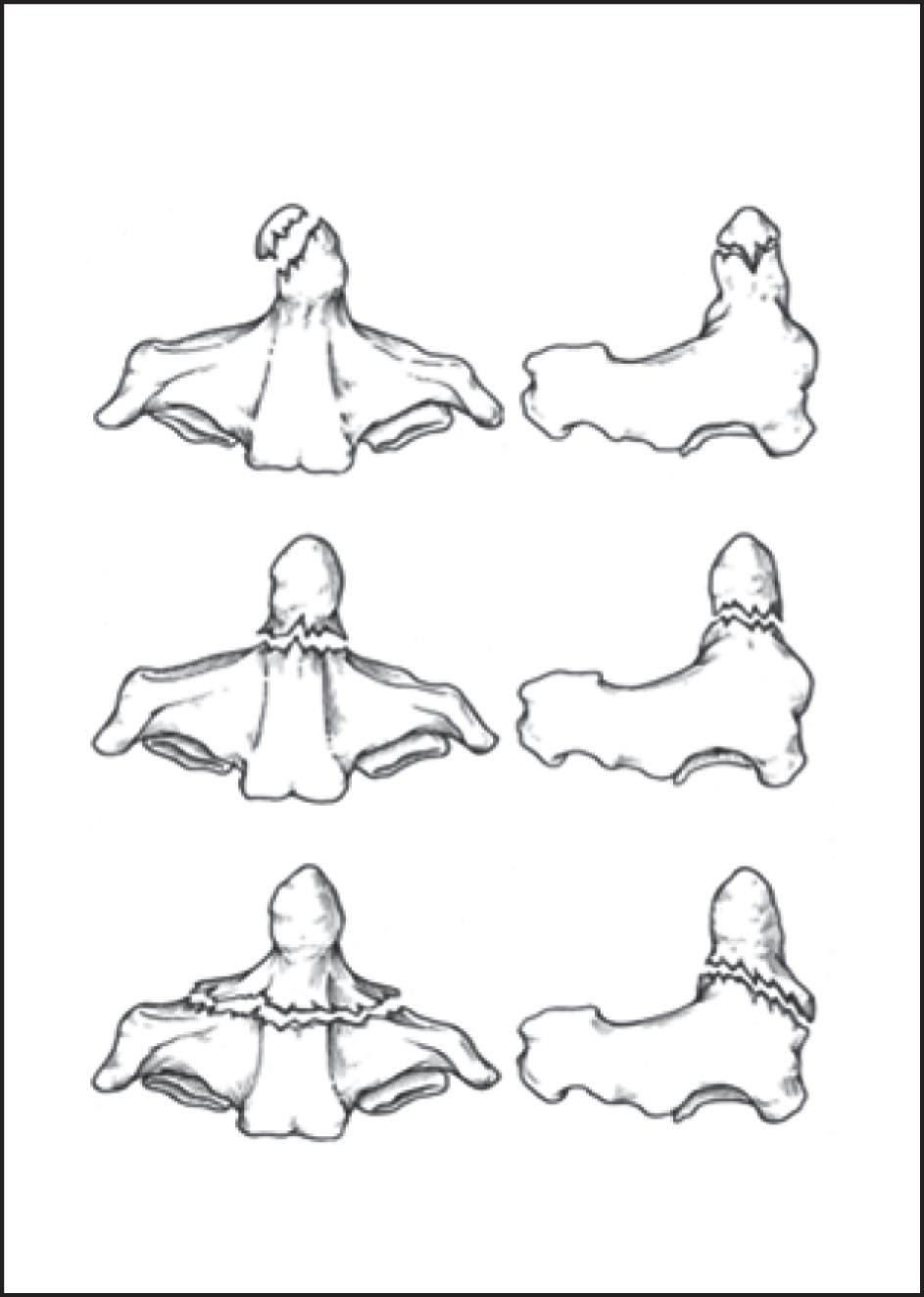
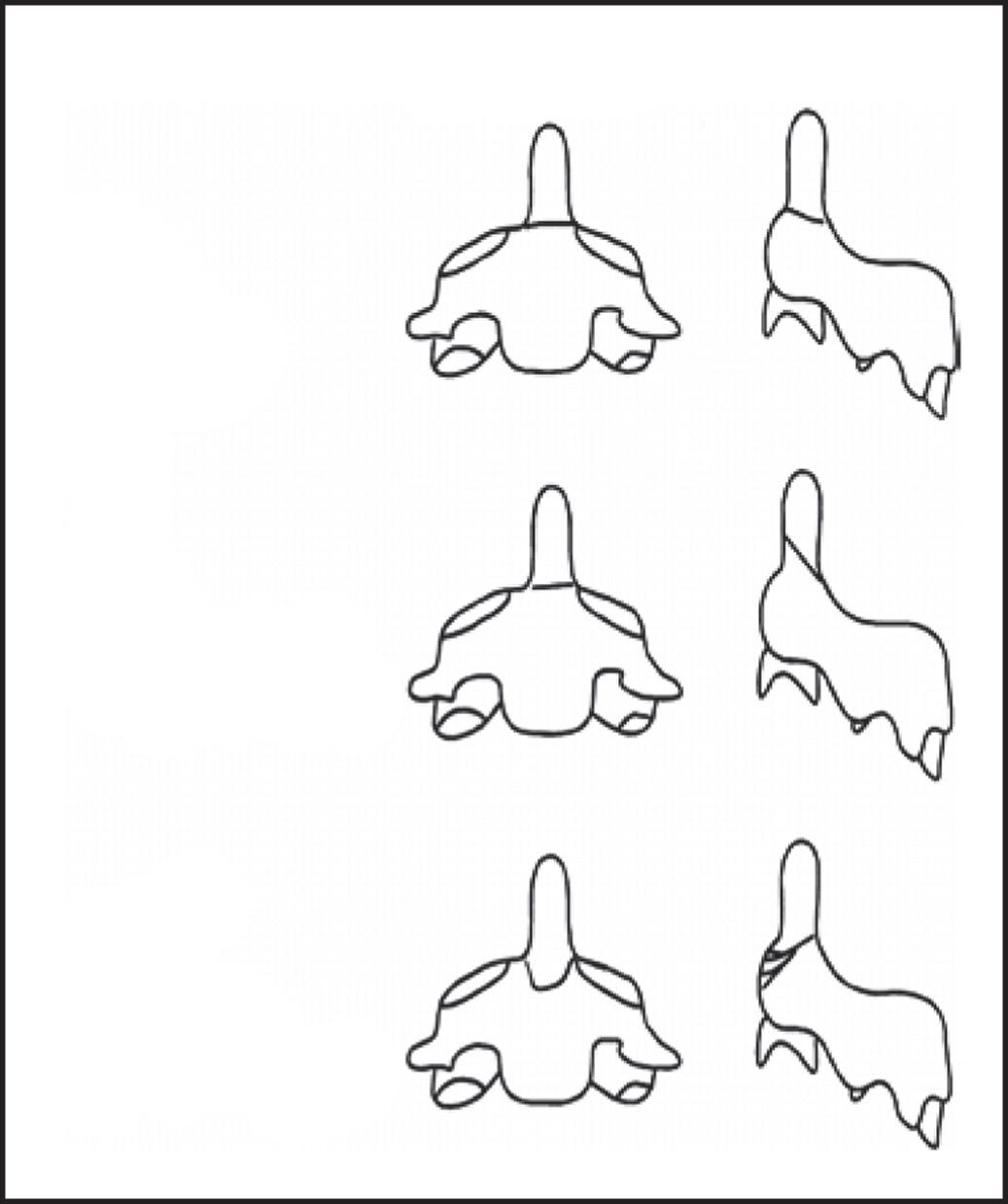
Odontoid fractures can be classified into three types as described by Anderson and D’Alonzo (Figure 1.1).3 Type I odontoid fractures represent an avulsion fracture of the tip of the odontoid through the alar ligament. Type II is the most common C2 fracture pattern and is defined by a fracture line at the base of the odontoid. Type II fractures have the greatest risk of nonunion due to the disruption of the tenuous blood supply.Type III fractures occur through the vertebral body and extend into the superior articular facets. Greater vascularity in the C2 body results in a low nonunion rate with cervical orthosis for this fracture type. Grauer and colleagues proposed subclassifying type II fractures to guide treatment decisions (Figure 1.2).Type IIA are transverse fractures, type IIB are angled anterosuperior to posteroinferior, and type IIC are either angled from anteroinferior to posterosuperior or are comminuted fractures.23 This fracture classification is useful when considering an odontoid screw as patients with a IIC are not appropriate for odontoid screw fixation.
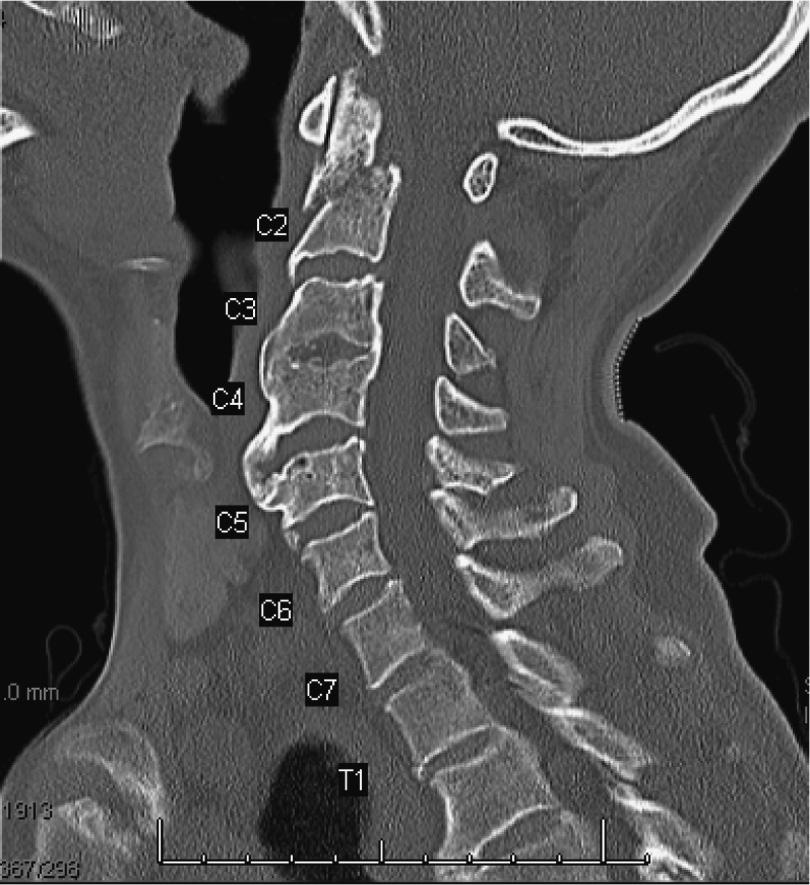
In the present case, CT of the spine demonstrates a displaced type II odontoid fracture with type IIC obliquity (Image 1) and a C3 right transverse process fracture. There is no apparent cord compression. A CT angiogram does not reveal any vascular insult or anomalies (Figure 1.3).
Figure 1.1 Anderson and D’Alonzo.
Grauer
Type II
Subclass A (Nondisplaced)
Type II
Subclass B (Displaced transverse or ant superior to post inferior)
Type II
Subclass C (Comminuted or ant inferior to post superior)
Figure 1.2 Grauer classification.
Figure 1.3 Sagittal view of cervical spine showing type IIC odontoid fracture.
Questions
1. What are risk factors for nonunion?
2. How should management be approached in a patient of advanced age?
3. How do these clinical and radiological findings influence surgical planning?
Decision-Making
No uniform treatment algorithm has been established for odontoid fractures. Instead, each case should be tailored with special considerations for comorbidities, concomitant injuries, prior functional status, neurological status, and fracture morphology. Treatment options are also based on the risk of nonunion, favoring surgical intervention for patients with a higher risk of nonunion. Known risk factors for nonunion include age 50 years or greater, comminution, greater than 5 mm of posterior displacement, fracture gap of more than 1 mm, more than 4 days between injury and treatment, and greater than 10 degrees of angulation. Furthermore, there is extensive literature demonstrating a decrease in mortality with operative fixation and an improvement in health-related quality of life outcomes in type II fractures in the geriatric population.18,19,24
Adults with a type II fracture without nonunion risk factors can be managed in a hard collar or a halo vest to prevent subsequent displacement. Most commonly, adults with risk factors for nonunion or geriatric patients who may safely undergo anesthesia are treated with a posterior C1–C2 fusion. In the properly selected patient, an odontoid screw may be beneficial, but this has been demonstrated to lead to a high risk of dysphagia in the elderly as well as screw pull-out in the setting of osteopenia/osteoporosis.16,26
The management of type II odontoid fractures in the elderly has changed in the past decade. Historically, acceptable outcomes with asymptomatic stable fibrous nonunions in the elderly have been reported.4 More recent literature supports operative management for patients 65 years or older, reporting improved functional outcomes and union rates, no difference in complications, and a trend toward improved mortality.19 However, an increased risk of complications can be seen in surgically treated patients 80 years or older.24 Rigid external immobilization (halo vest) is contraindicated in the elderly due to high morbidity and mortality rates.5 They generally have lower overall functional reserve and decreased pulmonary function, so prolonged immobilization could have morbid implications. Consequently, more surgeons are advocates for early surgical intervention, and there is a growing body of evidence to support this as well.18–20,22,24
There are multiple surgical treatments for odontoid fractures with the most commonly used being segmental fixation consisting of C1 lateral mass with either C2 pedicle or pars screws. Other options included an anterior odontoid osteosynthesis and C1–C2 transarticular screw fixation. While posterior instrumentation demonstrated greater rates of osseous union, anterior odontoid osteosynthesis avoids fusion of the C1–C2 articulation, which is responsible for 50% of cervical rotation. Each option has unique advantages and disadvantages which should be balanced with the fracture pattern, body habitus, and patient expectations.
In this case, due to the displacement and instability of the odontoid fracture, as well as the potential serious complications of immobilization, the surgeon opted
for surgical fixation. The surgeon elected for C1–C2 posterior instrumented fusion. Anterior screw osteosynthesis is often not indicated because of the patient’s age and potential for fixation failure due to poor screw purchase with osteoporosis, as well as the fact that lag screw fixation would result in translation and displacement with a type IIC fracture. Body habitus is also an important consideration as this patient’s obesity makes anterior odontoid osteosynthesis technically challenging to place a screw due to the trajectory.
Surgical Procedure
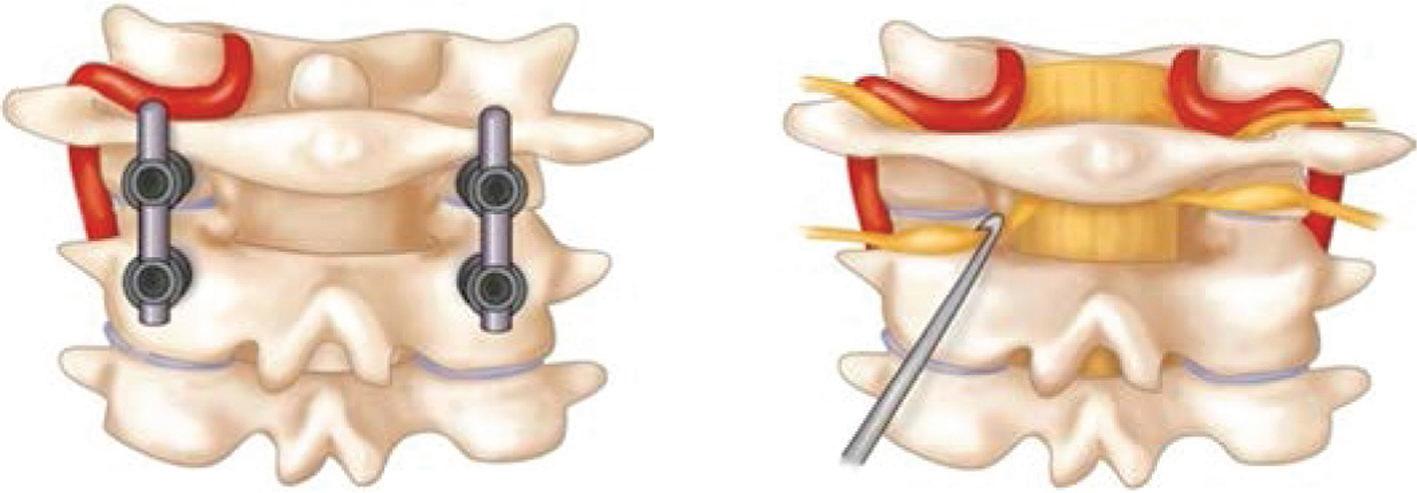
As previously mentioned, there are multiple surgical options for type II odontoid fracture but here the focus will be on segmental C1–C2 instrumentation and fusion (C1 lateral mass technique, Figure 1.4).
Positioning and Preparation
The patient should undergo intubation with in-line cervical immobilization to prevent excessive neck hyperextension. This may be done with a GlideScope or as a fiber-optic intubation.The Mayfield clamp is applied after intubation. Neuromonitoring is routinely utilized, and preintubation and prepositioning somatosensory and transcranial motor evoked potentials (SSEPs and tcMEPs) are recorded. The patient is then positioned prone with the neck in a slightly flexed position followed by repeat SSEPs and tcMEPs. The cervical spine is prepped and draped in sterile fashion. If iliac crest bone graft harvesting is required, then the posterior iliac crest should also be prepped and draped.
Approach
A midline longitudinal incision is utilized. Intraoperative radiographs should be taken to confirm spinal levels. Particular care should be taken to stay in the midline and follow the midline raphe for an avascular approach. Subperiosteal dissection of the posterior elements of C2 and inferior arch of C1 is performed. Avoid sharp dissection lateral to the C1 lateral masses and cephalad to the C1 ring to reduce risk of injuring the vertebral artery. As dissection extends from the base of the C1 arch to the C1 lateral masses, significant bleeding from the venous plexus in this region may be encountered.
Figure 1.4 (A) C1 lateral mass technique. (B) Retraction of C2 nerve root and exposure of lateral mass.
Procedure
Fluoroscopy is initially used to confirm adequate position of C1 relative to C2. Next, the starting point of the C2 pars screw is determined. A pilot hole is made approximately 2–3 mm proximal to the C2–C3 facet joint and slightly laterally (2–3 mm) to the palpated medial border of the C2 isthmus. The drill is angled cephalad and slightly medial along the path of the C2 isthmus and advanced to the predetermined unicortical depth. Next, a probe is used to confirm the absence of bony breach, the tract is tapped, and the screw is placed.
Following placement of C2 pars screw, fluoroscopy is then used to help identify the starting point and trajectory of the C1 lateral mass screw. Prior to screw placement, the C2 nerve root must be gently retracted inferiorly, exposing the bony anatomy (Figure 1.5). The entry point is identified 5 mm lateral to the medial aspect of the lateral mass and just caudal to the C1 posterior arch. A drill can be used to cannulate the lateral mass, aimed approximately 10 degrees medial with fluoroscopy guiding a cephalad parallel trajectory to the midpoint of the C1 anterior arch. Depth gauge measurements can then confirm the screw length and size prior to its insertion into the lateral mass. This is repeated for the contralateral C1 lateral mass. Screw positions are checked under lateral fluoroscopy and rods are placed. The C2 lateral masses and inferior arch of C1 is decorticated and a structural graft is placed in the C1–C2 interspace. Final x-rays are then taken to confirm hardware positioning.
Oral Boards: Management Pearls
1. Evaluation of vertebral artery anatomy with preoperative imaging, minimizing sharp dissection around the cephalad edge of the atlas, and using a superomedial trajectory of C1 lateral mass screw trajectory will reduce the risk of injury to the vertebral artery.
2. Suboptimal lateral fluoroscopic imaging for C1–C2 instrumentation can result in improper screw placement and neurologic or vascular injury.
3. C1–C2 polyaxial screw and rod fixation does not require direct odontoid anatomic reduction, and intraoperative reduction by manipulation can be achieved using direct manipulation of the C1 posterior arch.
Pivot Points
1. If an aberrant vertebral artery is present, then an alternative operative technique, such as a C2 laminar screw, should be considered. C1–C2 transarticular screw and C2 pedicle screw placement should be avoided with aberrant anatomy.
2. Although the lateral mass screw placement may initially appear to be without complication, if the screw tip is in close proximity to the vertebral artery, normal pulsatile flow may result in delayed damage to the vessel. Any concern for excessive screw length should prompt screw removal, with a shorter screw subsequently inserted.
Aftercare
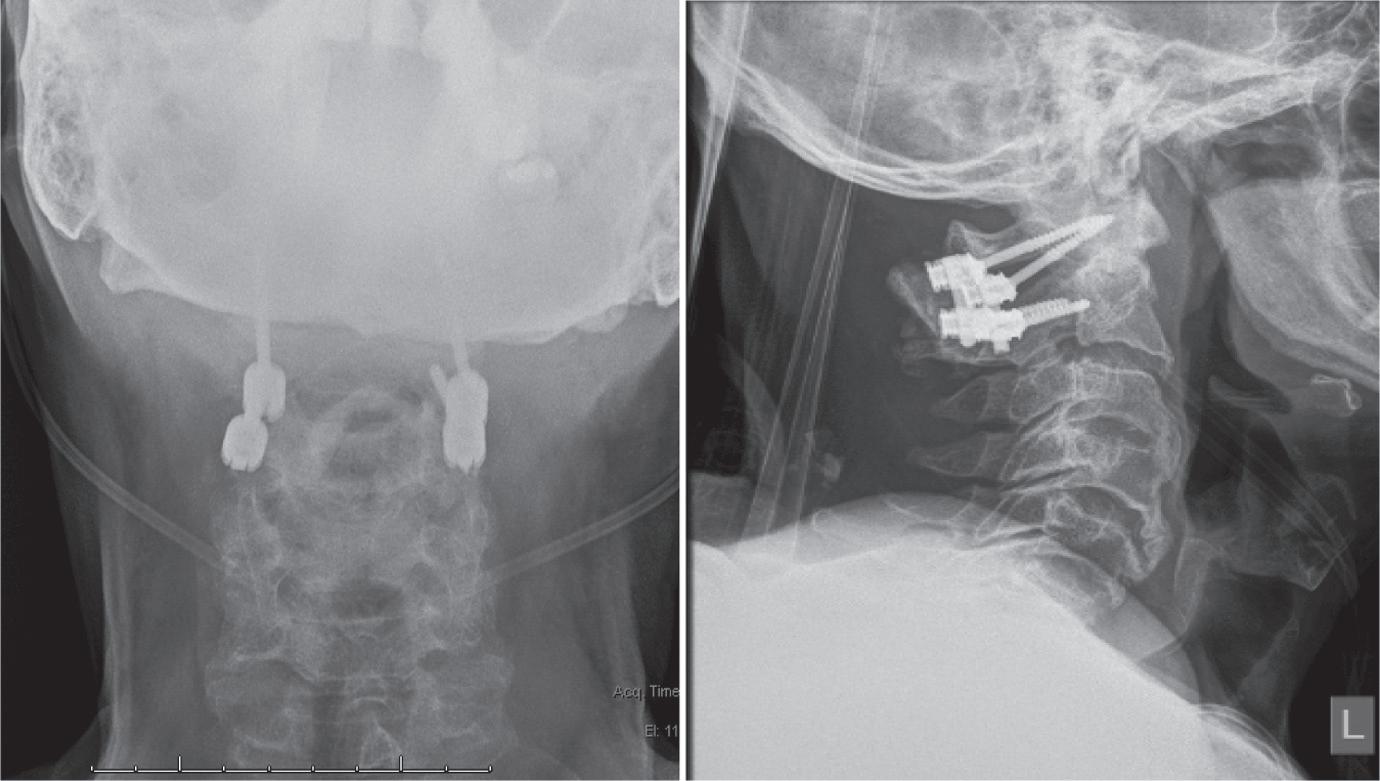
It is recommended that patients undergoing fixation of type II odontoid type fractures be placed in a cervical orthosis and admitted for close monitoring of potential postoperative complications. In geriatric patients, a soft collar is used, but in high-energy injuries a hard collar is used. The patient can be mobilized immediately after surgery. Follow-up imaging should be obtained at 2 weeks and 6–8 weeks to ensure there is no early hardware failure (Figure 1.5). Also, functional radiographs in flexion and extension can be obtained to evaluate stability 3–6 months after surgery. Once initial healing and maintenance of stability is established, the patient may be weaned from the cervical orthosis.
Complications and Management
The different complications of surgery are largely dependent on the approach and technique used.These complications can be further categorized into intraoperative and postoperative complications.
Intraoperative Complications
Neurovascular injuries are the most concerning intraoperative complications. With a posterior approach, one of the feared complications is injury to the vertebral artery with screw malposition. An anomalous vertebral artery further increases the risk of injury, especially with C1–C2 transarticular or C2 pedicle screw placement. Preoperative imaging should be closely evaluated for aberrant vessels. Careful intraoperative technique, avoiding C2 pedicle screws with aberrant vertebral artery anatomy, and directing the C1 lateral mass screw superomedially is essential to avoid vertebral artery damage.13 Damage to a single vertebral artery may be asymptomatic with intact contralateral supply, but bilateral injury can be catastrophic. With an anterior approach, careful retraction and dissection should be used to avoid injury to the internal carotid and esophagus. Other potential rare complications
Figure 1.5 (A,B) Anteroposterior and lateral view of cervical spine with posterior C1–C2 fusion.
include neurologic injury from past-point drilling or excessive depth of the anterior odontoid screw.
Postoperative Complications
Following a posterior cervical approach, occipital neuralgia is a common complaint. To minimize the risk, the C2 nerve root should be gently retracted downward and protected with a Penfield dissector during lateral mass screw placement. Additionally, partially threaded screws are used at C1. Wound complications are also more common with a posterior approach.17 Sterile technique, antibiotics, and proper wound irrigation help reduce the risk of infection. Surgical site infections with any concern for deep extension should be addressed with surgical debridement.
Following an anterior approach, dysphagia can be common and may necessitate the use of a feeding tube.27 This approach can be further complicated by aspiration pneumonia, which should be promptly treated with antibiotics.11,27 Hoarseness or vocal cord paralysis may ensue from neurapraxia or ischemic injury to the superior laryngeal and recurrent laryngeal nerves, respectively. Patients should also be closely monitored for signs of respiratory distress as this may be a sign of a retropharyngeal hematoma, which should be emergently surgically evacuated.
Failure of instrumentation and pseudarthrosis can complicate the postoperative recovery. Routine follow-up radiographs are scrutinized for evidence of union. CT scans can be utilized if the surgeon is concerned for nonunion.
Oral Boards Review: Complications Pearls
1. If there is an inadvertent injury to the vertebral artery, bleeding should be immediately controlled with primary vascular repair, temporary insertion of screw into the drilled hole, or by occlusion with a hemostatic agent or bone wax. If hemorrhage control is not possible and ligation is planned, intraoperative angiography should be performed.28 Contralateral screw placement should not be attempted to avoid bilateral injury.
2. C2 neuralgia can be a result of C1 lateral mass screw placement or excessive traction during exposure of lateral mass.
3. Bicortical fixation of lateral mass screw could place the internal carotid artery at risk for injury.10
4. The congenital arcuate foramen can be confused with the C1 lamina and must be identified to avoid vertebral artery injury
Evidence and Outcomes
The optimal surgical technique for type II odontoid fractures remains a matter of debate, with both anterior odontoid screw fixation and posterior cervical atlantoaxial fusion being acceptable choices.16,24 However, a posterior approach is especially indicated in geriatric patients and when anterior approaches are contraindicated in cases such as type IIC odontoid fracture, associated C1–C2 injury, nonreducible fractures, nonunion, large body habitus with a barrel chest, severe kyphosis, and severe osteoporosis.16 Posterior
C1–C2 fusions may also be used for salvage of an anterior fixation failure. Overall, posterior atlantoaxial fixation has been associated with a high rate of fusion, approaching 100%, with a low complication rate thus making it a very effective treatment option for type II odontoid fractures.12 When appropriately indicated, anterior screw fixation can provide similar clinical results.24
Another previous area of uncertainty was the optimal management of elderly patients; however, there has been a significant amount of research in the past decade demonstrating the superiority of surgery. Vaccaro et al. conducted a multicenter, prospective cohort study comparing operative and nonoperative treatments for patients 65 years of age or older. The study revealed better outcomes, lower nonunion rates, no difference in complication rates, and a nonsignificant trend toward lower mortality.19 Schroeder et al. performed a systematic review that found a decrease in both short- and long-term mortality in patients treated surgically. However, there is likely an upper age to surgery.24 Schoenfeld et al. conducted a retrospective study, and, although patients between 65 and 74 years old who underwent surgery had lower mortality rates, there was no difference when patients approached 85 years of age.22
References and Further Readings
1. Boos N, Aebi M, eds. Spinal Disorders: Fundamentals of Diagnosis and Treatment. Berlin: Springer-Verlag; 2008.
2. Keller S, Bieck K, Karul M, et al. Lateralized odontoid in plain film radiography: Sign of fractures?—A comparison study with MDCT. RöFo—Fortschritte Auf Dem Geb Röntgenstrahlen Bildgeb Verfahr. 2015;187(09):801–807. doi:10.1055/s-0035-1553237.
3. Anderson LD, D’Alonzo RT. Fractures of the odontoid process of the axis. J Bone Joint Surg Am. 1974;56(8):1663–1674.
4. Pal D, Sell P, Grevitt M.Type II odontoid fractures in the elderly: An evidence-based narrative review of management. Eur Spine J. 2011;20(2):195–204. doi:10.1007/s00586-010-1507-6.
5. Majercik S, Tashjian RZ, Biffl WL, Harrington DT, Cioffi WG. Halo vest immobilization in the elderly: A death sentence? J Trauma. 2005;59(2), 350–358.
6. Goel A. Treatment of odontoid fractures. Neurol India. 2015;63(1):7. doi:10.4103/ 0028-3886.152657.
7. Robinson Y, Robinson A-L, Olerud C. Systematic review on surgical and nonsurgical treatment of type II odontoid fractures in the elderly. BioMed Res Int. 2014;2014. doi:10.1155/ 2014/231948.
9. Bodon G, Patonay L, Baksa G, Olerud C. Applied anatomy of a minimally invasive musclesplitting approach to posterior C1–C2 fusion: An anatomical feasibility study. Surg Radiol Anat SRA. 2014;36(10):1063–1069. doi:10.1007/s00276-014-1274-x.
10. Seal C, Zarro C, Gelb D, Ludwig S. C1 lateral mass anatomy: Proper placement of lateral mass screws. J Spinal Disord Tech. 2009;22(7):516–523. doi:10.1097/BSD.0b013e31818aa719.
11. Dailey AT, Hart D, Finn MA, Schmidt MH, Apfelbaum RI. Anterior fixation of odontoid fractures in an elderly population: Clinical article. J Neurosurg. 2010;12(1):1–8.
12. Harms J, Melcher RP. Posterior C1–C2 fusion with polyaxial screw and rod fixation. Spine 2001;26(22):2467–2471.
13. Gautschi OP, Payer M, Corniola MV, Smoll NR, Schaller K, Tessitore E. Clinically relevant complications related to posterior atlanto-axial fixation in atlanto-axial instability and their management. Clin Neurol Neurosurg. 2014;123:131–135. doi:10.1016/j.clineuro.2014.05.020.
14. Spine Surgery Basics, Springer. http://link.springer.com.ezproxy.rowan.edu/book/ 10.1007%2F978-3-642-34126-7. Accessed May 1, 2016.
15. Wang L, Liu C, Zhao Q-H, Tian J-W. Outcomes of surgery for unstable odontoid fractures combined with instability of adjacent segments. J Orthop Surg. 2014;9:64. doi:10.1186/ s13018-014-0064-9.
16. Joaquim A, Patel A. Surgical treatment of type II odontoid fractures: Anterior odontoid screw fixation or posterior cervical instrumentation fusion. Am Assoc Neurosurg. 2015:38(4):E11.
17. Harel R, Stylianou P, Knoller N. Cervical spine surgery: Approach-related complications. World Neurosurg. 2016;94:1–5.
18. Chapman J, Smith JS, Kopjar B, et al. The AOSpine North America Geriatric Odontoid Fracture Mortality Study: A retrospective review of mortality outcomes for operative versus nonoperative treatment of 322 patients with long-term follow-up. Spine 2013;38(13):1098–1104.
19. Vaccaro AR, Kepler CK, Kopjar B, et al. Functional and quality-of-life outcomes in geriatric patients with type-II dens fracture. J Bone Joint Surg. 2013;95(8):729–735.
20. Barker L, Anderson J, Chesnut R, Nesbit G, Tjauw T, Hart R. Reliability and reproducibility of dens fracture classification with use of plain radiography and reformatted computer-aided tomography. J Bone Joint Surg (Am). 2006;88(1):106–112.
21. Koivikko MP, Kiuru MJ, Koskinen SK, Myllynen P, Santavarita S, Kivisaari L. Factors associated with non-union in conservatively treated type II fractures of the odontoid process. J Bone Joint Surg (Br). 2004;86-B:1146–1151.
22. Schoenfeld AJ, Bono CM, Reichmann WM, et al. Type II odontoid fractures of the cervical spine: Do treatment type and medical comorbidities affect mortality in elderly patients? Spine. 2011;36(11):879–885.
23. Grauer JN, Shafi B, Hilibrand AS, et al. Proposal of a modified, treatment-oriented classification of odontoid fractures. Spine J. 2005;5(2):123–129.
24. Schroeder GD, Kepler CK, Kurd M, et al. A systematic review of the treatment of geriatric type II odontoid fractures. Neurosurgery 2015;77:S6–S14.
25. Smith HE, Kerr SM, Maltenfort M, et al. Early complications of surgical versus conservative treatment of isolated type II odontoid fractures in octogenarians: A retrospective cohort study. J Spinal Disord Tech. 2008;21(8):535–539.
26. Andersson S, Rodrigues M, Olerud C. Odontoid fractures: High complication rate associated with anterior screw fixation in the elderly. Eur Spine J. 2000;9(1):56–59.
27. Vasudevan K, Grossberg JA, Spader HS, Torabi R, Oyelese AA. Age increases the risk of immediate postoperative dysphagia and pneumonia after odontoid screw fixation. Clin Neurol Neurosurg. 2014;126:185–189.
28. Peng CW, Chou BT, Bendo JA, Spivak JM. Vertebral artery injury in cervical spine surgery: Anatomical considerations, management, and preventive measures. Spine J 2009;9(1):70–76.
Cervical Fracture Dislocation
Jason Liounakos, G. Damian Brusko, and Michael Y. Wang
Case Presentation
A 30-year-old man was transferred to a local level 1 trauma center by emergency medical services (EMS) 3 hours after diving into a shallow pond head first. He presents with a Glasgow Coma Scale (GCS) score of 15, without loss of consciousness, and states that immediately after the dive he was unable to move his arms or legs. He also complains of an intermittent burning sensation in his arms and neck pain. He is rigidly immobilized on a backboard with strict spine precautions. His blood pressure is 90/60 mm Hg with a heart rate of 55 bpm. Detailed physical examination is significant for 5/5 strength in deltoids, 4+/5 in biceps, and 0/5 distally. He has absent rectal tone. Biceps reflexes are 2+ bilaterally. Brachioradialis, triceps, patellar, and achilles reflexes are absent bilaterally. Hoffman sign is negative, and no clonus or plantar response is equivocal. Sensation to pin prick and light touch is preserved throughout, including the perianal region.
Questions
1. What is the most likely diagnosis?
2. At what level is the suspected injury?
3. What is the international standardized classification system used for spinal cord injury?
4. What imaging examinations are most appropriate to accurately diagnosis the injury?
5. Describe common fracture patterns associated with cervical facet dislocations.
Assessment and Planning
Given the acute onset of symptoms in an otherwise healthy patient sustained after an obvious traumatic injury, the on-call neurosurgeon suspects a traumatic spinal cord injury. Spinal cord injuries in the cervical spine are frequently associated with cervical fracture dislocation. An initial complete trauma evaluation is necessary to rule out other injuries, particularly in the setting of neurogenic shock where hypotension may be related to hemorrhagic shock rather than to a loss of sympathetic tone secondary to the spinal cord injury. Until the injury has been identified and stabilized, strict spine precautions are necessary, particularly in the setting of an incomplete spinal cord injury (as in this case). Instability due to a fracture predisposes the patient to further injury