College of Veterinary Medicine and Biomedical Sciences
Colorado State University
Fort Collins, CO
USA
Booksvets.blogspot.com
1Disorders of the Salivary Gland3
Catriona M. MacPhail
Eric Monnet, Jeffrey J. Runge, and William T.N. Culp
Eric Monnet
Tracy L. Hill, B. Duncan X. Lascelles, and Anthony Blikslager
Elisa M. Mazzaferro and Eric Monnet 8Focal and Linear
Nina Samuel, Barbro Filliquist, and William T.N. Culp 9Mesenteric
Deanna R.
Stewart D. Ryan
Lisa Klopp, Angela J. Marolf, Eric Monnet, and Craig B. Webb 14Liver Lobe Torsion and Abscess171
Daniel A. Degner and Jitender Bhandal 15Liver Tumors and Partial
Daniel A. Degner and Richard Walshaw
Steve J. Mehler and Philipp D. Mayhew
17Extrahepatic Biliary Tract Obstruction
Steve J. Mehler and Philipp D. Mayhew
18Other Surgical Diseases of the Gallbladder and Biliary Tract: Cholecystitis, Neoplasia, Infarct, and Trauma 226
Steve J. Mehler and Philipp D. Mayhew
Panagiotis G. Xenoulis, Jörg M. Steiner, and Eric Monnet
Lori Ludwig
Jennifer Prittie and Lori Ludwig
22Pneumoperitoneum
Jennifer Prittie and Lori Ludwig
23Retroperitoneal
Amelia M. Simpson
24Congenital Abdominal Wall Hernia295
Amelia M. Simpson
25Acquired Abdominal Wall Hernia303
Amelia M. Simpson
26Diaphragmatic and Peritoneopericardial Diaphragmatic Hernias
Janet Kovak McClaran
27Perineal Hernia
F.A. (Tony) Mann and Carlos Henrique de Mello Souza
Raymond K. Kudej
29Surgery of the Thoracic Wall
Julius M. Liptak, Eric Monnet, and Kristin Zersen
30Tumors of the Thoracic Wall
Julius M. Liptak 31Flail
Dennis Olsen and Ronald S. Olsen
Jonathan F. McAnulty
33Pyothorax
Chad Schmiedt
34Pneumothorax
Robert J. Hardie
Naomi Hoyer
36Cleft
Yoav Bar-Am
37Brachycephalic Airway Syndrome438 Dorothee Krainer and Gilles Dupré
Catriona M. MacPhail
41Surgical Diseases of the Lungs486 Eric Monnet Section 7:Urinary Tract
42Pathophysiology of Renal Disease503
Cathy Langston and Serge Chalhoub
43Upper Urinary Tract Obstruction516 Eric Monnet
44Urolithiasis of the Lower Urinary Tract
Eric Monnet
45Ureteral Ectopia and Urinary Incontinence
Philipp D. Mayhew and Allyson Berent
46Treatment Strategies for Urethral Sphincter Mechanism Incompetence 548
Philipp D. Mayhew and Allyson Berent
47Treatment Strategies for Ureteral Ectopia 559
Philipp D. Mayhew and Allyson Berent
48Neoplasia of the Urinary Tract571 Ramesh K. Sivacolundhu and Stephen J. Withrow
49Urinary Tract Trauma
Heidi Phillips
50Urinary Diversion Techniques605 Maureen Griffin, Allyson Berent, Chick Weisse, and William T.N. Culp
51Idiopathic or Benign Essential
Renal Hematuria 627
Allyson Berent and Chick Weisse
52Renal Transplant 635
Chad Schmiedt
Section 8:Reproductive Tract659
53Pyometra 661
Natali Krekeler and Fiona Hollinshead
54Cesarean Section 672
Wendy Baltzer
55Congenital Vaginal Defects 684
Fran Smith
56Ovariectomy and Ovariohysterectomy 690
Thomas J. Smith and Bernard Séguin
57Scrotal and Testicular Trauma and Neoplasia 698
Fran Smith
58Prostatic Disease 704
Michelle Kutzler
59Cryptorchidism 720
Carlos Gradil and Robert McCarthy
60Paraphimosis 726
Michelle Kutzler
61Priapism 730
Michelle Kutzler
62Phimosis 736
Dietrich Volkmann
63Penile and Preputial Trauma and Neoplasia 740
Dawna Voelkl
Section 9:Endocrine 747
64Primary Hyperparathyroidism749
Nicholas J. Bacon
65Feline Hyperthyroidism 767
Marie-Pauline Maurin and Carmel T. Mooney
66Canine Thyroid Neoplasia 779
Deanna R. Worley
67Canine and Feline Insulinoma785
Floryne O. Buishand and Jolle Kirpensteijn
68Adrenal Tumors 798
Pierre Amsellem, Michael Schaer, and James P. Farese
Section 10:Ear Surgery 817
69Anatomy of the Ear 819
Jamie R. Bellah
70Surgery of the Pinna 828
Jamie R. Bellah
71Aural Neoplasia 838
Brad M. Matz and Jamie R. Bellah
72Otitis Externa 846
Robert Kennis
73Feline and Canine Otitis Media851
Dawn Logas
74Surgery of the Vertical Ear Canal857
Anne Sylvestre
75Imaging of the Ear for Surgical Evaluation 864
Robert Cole, Kaitlin Fiske, and John Hathcock
76Total Ear Canal Ablation and Lateral Bulla Osteotomy875
Daniel D. Smeak
77Subtotal Ear Canal Ablation 891
Kyle G. Mathews
78Surgical Diseases of the Middle Ear895
Marije Risselada and Elizabeth M. Hardie
Section 11:Cardiac 905
79Coagulation Disorders and Surgery907
Sara Shropshire and Benjamin Brainard
80Heart Surgery Strategies 917
E. Christopher Orton
81Congenital Cardiac Shunts 924
E. Christopher Orton
82Valvular Heart Disease 936
E. Christopher Orton
83Cardiac Neoplasia 944
E. Christopher Orton
84Congenital Pericardial Diseases947
Eric Monnet
85Constrictive Pericarditis 950
Eric Monnet
86Pericardial Effusion 953
Eric Monnet
87Pacemaker Therapy 964 Eric Monnet
Section 12:Hematopoietic 981
88Surgical Treatment of Splenic Disease 983
Kyla Walter and William T.N. Culp
89Surgical Treatment of Thymic Disease 997
Erin A. Gibson and William T.N. Culp
List of Contributors
Pierre Amsellem
Veterinary Medical Center University of Minnesota St. Paul, MN, USA
Nicholas J. Bacon
AURA Veterinary Guildford, UK
Wendy Baltzer School of Veterinary Science Massey University Palmerston North, New Zealand
Yoav Bar-Am
Koret School of Veterinary Medicine Hebrew University of Jerusalem Jerusalem, Israel
Jamie R. Bellah Department of Clinical Sciences
Auburn University College of Veterinary Medicine Auburn, AL, USA
Allyson Berent
Interventional Endoscopy/Radiology Animal Medical Center New York, USA
Jitender Bhandal Westbank Animal Care Hospital West Kelowna, BC, Canada
Anthony Blikslager College of Veterinary Medicine North Carolina State University Raleigh, NC, USA
Benjamin Brainard College of Veterinary Medicine University of Georgia Athens, GA, USA
Ronald Bright Retired
Floryne O. Buishand
Royal Veterinary College University of London London, UK
Serge Chalhoub Faculty of Veterinary Medicine University of Calgary Calgary, AB, Canada
Robert Cole
Department of Clinical Sciences
Auburn University College of Veterinary Medicine Auburn, AL, USA
William T.N. Culp School of Veterinary Medicine
University of California–Davis Davis, CA, USA
Daniel A. Degner
Michigan Veterinary Specialists Auburn Hills, MI, USA
Gilles Dupré La Garde, France
James P. Farese
Golden Gate Veterinary Specialists San Rafael, CA, USA
Barbro Filliquist School of Veterinary Medicine University of California–Davis Davis, CA, USA
Kaitlin Fiske
Department of Clinical Sciences
Auburn University College of Veterinary Medicine Auburn, AL, USA
Erin A. Gibson
University of Pennsylvania School of Veterinary Medicine Philadelphia, PA, USA
Carlos Gradil
Department of Veterinary and Animal Sciences University of Massachusetts Amherst Amherst, MA, USA
Maureen Griffin School of Veterinary Medicine University of Pennsylvania Philadelphia, PA, USA
Elizabeth M. Hardie College of Veterinary Medicine North Carolina State University Raleigh, NC, USA
Robert J. Hardie
Department of Surgical Sciences School of Veterinary Medicine University of Wisconsin Madison, WI, USA
John Hathcock
Department of Clinical Sciences
Auburn University College of Veterinary Medicine Auburn, AL, USA
Tracy L. Hill
College of Veterinary Medicine University of Minnesota Minneapolis, MN, USA
Fiona Hollinshead
Department of Clinical Sciences Colorado Sate University Fort Collins, CO, USA
Naomi Hoyer Department of Clinical Sciences Colorado State University Fort Collins, CO, USA
Robert Kennis
Department of Clinical Sciences Auburn University College of Veterinary Medicine Auburn, AL, USA
Jolle Kirpensteijn Hill’s Pet Nutrition Topeka, KS, USA
Lisa Klopp Department of Clinical Sciences Colorado State University Fort Collins, CO, USA
Dorothee Krainer
Department of Small Animal Surgery AniCura Tierklinik Hollabrunn, Austria
Natali Krekeler
Faculty of Veterinary Science University of Melbourne Melbourne, VIC, Australia
Raymond K. Kudej
Cummings School of Veterinary Medicine
Tufts University North Grafton, MA, USA
Michelle Kutzler College of Agricultural Sciences
Oregon State University Corvallis, OR, USA
Cathy Langston
College of Veterinary Medicine Ohio State University Columbus, OH, USA
B.Duncan X. Lascelles College of Veterinary Medicine North Carolina State University Raleigh, NC, USA
Julius M. Liptak
Capital City Small Animal Mobile Surgery Ottawa, ON, Canada
Dawn Logas
Veterinary Dermatology Center Maitland, FL, USA
Lori Ludwig
Sea Island Animal Hospital Beaufort, SC, USA
Catriona M. MacPhail
Department of Clinical Sciences Colorado State University Fort Collins, CO, USA
F.A. (Tony) Mann College of Veterinary Medicine University of Missouri Columbus, MO, USA
Angela J. Marolf
Department of Veterinary Clinical Sciences Columbus, OH, USA
Kyle G. Mathews College of Veterinary Medicine North Caroline State University Raleigh, NC, USA
Brad M. Matz
Department of Clinical Sciences
Auburn University College of Veterinary Medicine Auburn, AL, USA
Marie-Pauline Maurin
School of Veterinary Medicine University College Dublin Dublin, Ireland
Philipp D. Mayhew School of Veterinary Medicine University of California—Davis Davis, CA, USA
Elisa M. Mazzaferro
Wheat Ridge Animal Hospital Wheat Ridge, CO, USA
Jonathan F. McAnulty
School of Veterinary Medicine University of Wisconsin–Madison Madison, WI, USA
Robert McCarthy School of Veterinary Medicine Tufts University North Grafton, MA, USA
Janet Kovak McClaran London Vet Specialists London, UK
Steve J. Mehler
Hope Veterinary Specialists Malvern, PA, USA
Carlos Henrique de Mello Souza College of Veterinary Medicine University of Missouri Columbus, MO, USA
Eric Monnet
Department of Clinical Sciences
Colorado State University Fort Collins, CO, USA
Carmel T. Mooney School of Veterinary Medicine University College Dublin Dublin, Ireland
Dennis Olsen Veterinary Clinic College of Southern Nevada Las Vegas, NV, USA
Ronald S. Olsen
Virginia–Maryland College of Veterinary Medicine
Blacksburg, VA, USA
E. Christopher Orton
Department of Clinical Sciences
Colorado State University Fort Collins, CO, USA
Heidi Phillips Department of Veterinary Clinical Medicine
University of Illinois Urbana, IL, USA
Jennifer Prittie
Animal Medical Center New York, NY, USA
Marije Risselada Department of Veterinary Clinical Sciences
Purdue University West Lafayette, IN, USA
Jeffrey J. Runge
Soft Tissue & Orthopedic Surgery
Guardian Veterinary Specialists Brewster, NY, USA
Stewart D. Ryan
Department of Veterinary Pathology University of Melbourne Werribee, VIC, Australia
Nina Samuel
School of Veterinary Medicine University of California–Davis Davis, CA, USA
Michael Schaer
Department of Small Animal Clinical Sciences
University of Florida Veterinary Medical Center
Gainesville, FL, USA
Chad Schmiedt
Department of Small Animal Medicine and Surgery University of Georgia Athens, GA, USA
Bernard Séguin
Department of Surgical Oncology
Central Victoria Veterinary Hospital Victoria, BC, Canada
Sara Shropshire
Department of Clinical Sciences
Colorado State University Fort Collins, CO, USA
Amelia M. Simpson
Veterinary Surgical Center of Portland Portland, OR, USA
Ramesh K. Sivacolundhu Balcatta Vet24 Balcatta, WA, Australia
Daniel D. Smeak
College of Veterinary Medicine
Colorado State University Fort Collins, CO, USA
Fran Smith
Smith Veterinary Hospital Burnsville, MN, USA
Thomas J. Smith
School of Veterinary and Biomedical Sciences
James Cook University Townsville, QLD, Australia
Jörg M. Steiner
Gastrointestinal Laboratory Department of Veterinary Small Animal Clinical Sciences
College of Veterinary Medicine and Biomedical Sciences College Station, TX, USA
Anne Sylvestre
Veterinary Referral Surgical Services Kitchener, ON, Canada
Dawna Voelkl
Meadowlands Veterinary Hospital Washington, PA, USA
Dietrich Volkmann
Veterinary Health Center University of Missouri Columbia, MO, USA
Richard Walshaw Animal Surgical Center of Michigan Flint, MI, USA
Kyla Walter School of Veterinary Medicine
Veterinary Medical Teaching Hospital University of California–Davis Davis, CA, USA
Craig B. Webb
Department of Clinical Sciences
Colorado State University Fort Collins, CO, USA
Chick Weisse
Animal Medical Center New York, NY, USA
Stephen J. Withrow
Department of Clinical Sciences
Colorado State University Fort Collins, CO, USA
Deanna R. Worley
Department of Clinical Sciences
Colorado State University Fort Collins, CO, USA
Panagiotis G. Xenoulis
Gastrointestinal Laboratory Department of Veterinary Small Animal Clinical Sciences
College of Veterinary Medicine and Biomedical Sciences College Station, TX, USA
Kristin Zersen
Veterinary Teaching Hospital
Colorado State University Fort Collins, CO, USA
Preface
Claude Bourgelat, Director of the Lyon Academy of Horsemanship, founded the first veterinary school in France in 1761. The main objective was to train veterinarians to protect cattle and horses against diseases. Little did he know about the amazing transformation veterinary science would go through from the time he created the first veterinary school and wrote his book Elements of Horsemanship. A number of specialties have evolved, including internal medicine, dermatology, ophthalmology, cardiology, neurology, oncology, radiology, dentistry, and surgery.
The limits of surgery have been extended with the development of new diagnostic tools, better understanding of pathophysiology, and new imaging techniques such as ultrasound, magnetic resonance imaging, computed tomography, and nuclear medicine. Cardiopulmonary bypass has become available to small animal surgeons. Oncologic surgery has expanded in the last 30 years because of the development of imaging technology and a better understanding of the pathophysiology of different tumors. Minimally invasive surgery and interventional radiology have emerged and have expanded exponentially in the last decade. As a consequence, veterinary surgery is becoming more specialized, with a general division between orthopedic surgery and soft tissue surgery. Thus a textbook of small animal soft tissue surgery is required.
In this second edition of this textbook, all the chapters have been revised and edited, and some new chapters have been added. This second edition of this textbook, like the first, has four goals. First, it had to be based as much as possible on evidence. Therefore, authors were selected who were known for the most recent contributions to the field. Each author was asked to perform a thorough review of the literature and to present evidence-based information. Since soft tissue surgery requires the interaction of several specialties (internal medicine, imaging, and critical care), most chapters have several authors. Each author was responsible for a specific aspect of the chapter (i.e., internal medicine, radiology, surgery, and critical care).
Second, since the textbook is strictly focused on soft tissue surgery, general chapters on surgical biology and
on anesthesia and pain management are not included. Similarly, I did not include chapters on wound management or neurosurgery, since excellent textbooks on these topics are already available.
Third, I wanted the textbook to provide good documentation and illustrations. Surgery cannot be understood and performed without good illustrations. With this in mind, I selected one of the best medical illustrators, Dennis Giddings, who was the illustrator of An Atlas of Surgical Approaches to the Bones and Joints of the Dog and Cat, edited by Piermattei and Johnson. The illustrations went back and forth several times between the illustrator, authors, editor, and publisher to ensure the best results. Also, a website with excellent color intraoperative pictures and videos about the procedures is included with the textbook. The videos describe each surgical procedure step by step. This website is a work in progress and will be expanded with future editions.
Lastly, this textbook is intended for a wide audience, from private practitioners to specialists, including residents studying for boards. Because the most recent literature has been reviewed, the book should be of great help to residents.
The book is divided into systems, and each system subdivided into diseases or syndromes. This has allowed a thorough discussion of each important topic. The anatomy or physiology related to a certain condition is only briefly reviewed when needed. Readers are referred to specific textbooks that specialize on the topic. Knowledge of each topic is becoming so important that each chapter focuses specifically on the pathophysiology, diagnosis, and treatment of each disease or syndrome.
I would like to thank all the authors and section editors who helped me during the long process of creating the second edition of this textbook. This book will be updated as often as needed in order to stay up to date with progress in the veterinary surgery of small animals.
Eric Monnet Professor, Small Animal Surgery, Colorado State University
About the Companion Website
This book is accompanied by a companion website:
www.wiley.com/go/monnet/small
The website includes:
• Videos Booksvets.blogspot.com
Password (case sensitive): Sliding
Section 1
Gastrointestinal Surgery
Disorders of the Salivary Gland
Catriona M. MacPhail
Salivary glands can be affected by inflammation, trauma, calculus formation, and neoplasia, resulting in abscessation, rupture of the duct or gland, and formation of a salivary mucocele, obstruction, or pain on palpation or opening of the mouth. The mode of therapy is generally dictated by the type of lesion present (abscess, mucocele, neoplasia).
Anatomy
There are four paired salivary glands in the dog and cat: parotid, mandibular, sublingual, and zygomatic glands. The cat also has paired molar glands, which lie in the lower lip at the angle of the mouth. In addition, there are numerous buccal glands present in the soft palate, lips, tongue, and cheeks. The salivary glands most commonly injured or involved in pathologic processes (calculi, neoplasia, trauma) are the mandibular and sublingual salivary glands.
The mandibular salivary gland is a mixed gland (serous and mucous secretion) located in the junction of the maxillary (internal maxillary) vein and lingual facial (external maxillary) vein as they form the jugular vein. It is adherent cranially to the darker monostomatic portion of the sublingual gland, and shares a common heavy fibrous capsule with that gland. The mandibular duct leaves the medial portion of the gland near the sublingual gland and runs craniomedially, medial to the caudal sublingual gland, between the masseter muscle and mandible laterally and the digastricus muscle medially, to empty in the sublingual papilla lateral to the cranial frenulum of the tongue.
The sublingual duct originates at the caudal portion of the gland and joins the mandibular duct. The secretions
of the separate lobes of the monostomatic portion of the sublingual gland drain through four to six short excretory ducts into the sublingual duct. The polystomatic portion of the sublingual gland lies under the mucosa of the tongue and secretes directly into the oral cavity rather than through the main sublingual duct.
Diseases of the parotid and zygomatic salivary glands occur infrequently in the dog and cat. The parotid gland is triangular in shape and is located at the base of the horizontal ear canal. The parotid duct runs rostrally along the lateral surface of the masseter muscle and opens into the oral cavity at the level of the second to fourth premolars. The zygomatic gland is located deep and medial to the zygomatic arch, dorsolateral to the medial pterygoid muscle. The major zygomatic duct opens into the oral cavity opposite the last upper molar.
Pathophysiology
Disorders of the salivary glands are generally uncommon in the dog and cat. Salivary gland problems most often manifest as submandibular swelling, which can either be painful or nonpainful depending on the underlying cause. Differential diagnoses for submandibular swelling include inflammation, abscess formation, lymphadenopathy, neoplasia, or salivary mucocele. Submandibular abscessation is usually secondary to bite wounds or oropharyngeal foreign body penetration. These abscesses are rarely associated with the salivary glands. Fine-needle aspiration and cytology facilitate definitive diagnosis, although diagnostic imaging may also be indicated. Both the ultrasonographic and computed tomographic appearance of sialoceles have been
will determine the affected side. This procedure is timeconsuming and can be technically difficult to perform. If the affected side is unable to be determined or if the mucocele appears to be bilateral, bilateral resection of the mandibular and sublingual glands can be performed without any consequences to saliva production.
Removal of the mandibular and sublingual salivary glands is performed by first positioning the dog in lateral recumbency with the affected side facing up. The neck and jaw should be positioned slightly obliquely and towels or sandbags placed under the neck to elevate the surgical site for better visualization of the bifurcation of the jugular vein.
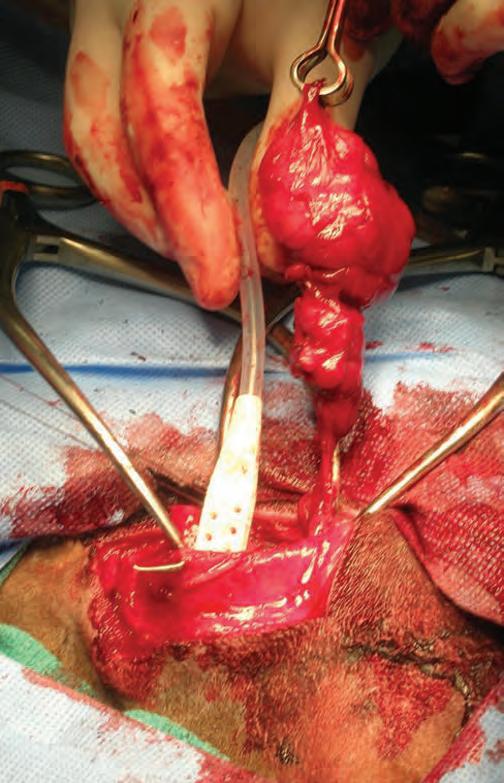
The incision is made from the ramus of the mandible cranially to the bifurcation of the jugular vein caudally; occlusion of the jugular vein prior to incision will facilitate visualization of landmarks. Dissection is carried into the capsule of the mandibular and sublingual salivary glands. An intracapsular dissection of the glands is performed and the ducts of the mandibular and sublingual salivary glands are followed craniomedially to the mandible. The ducts are followed as far cranially as possible and ligated or stripped out to complete the resection. Tunneling under the digastricus muscles may improve the completeness of the salivary duct excision (Marsh & Adin 2013). A small active drain can be placed in the cervical mucocele to allow drainage of the remaining saliva and accumulated fluid (Figure 1.2). The drain is typically removed 3–5days postoperatively. If the salivary glandular tissue has an unusual appearance at the time of resection, it should be submitted for histopathologic evaluation. Closure of the incision includes apposition of muscle, subcutaneous tissues, and skin with simple interrupted or simple continuous sutures. Alternatively, a ventral approach can be considered (Ritter et al. 2006). An incision is made from the level of the linguofacial vein to the rostral intermandibular space. The mandibular gland is located at the caudal aspect of this incision. An intracapsular dissection is performed as already described with dissection of the salivary chain rostrally to the level of the digastricus muscle. The digastricus muscle is then undermined from a cranial direction in order to follow the ducts as they course rostrally under the mylohyoideus muscle. This muscle is incised to gain access to residual sublingual salivary glandular tissue.
When comparing the lateral to the ventral approach, the ventral paramedian approach was associated with a lower risk of recurrence but higher rate of surgical wound complications (Cinti et al. 2021); long-term outcomes appear to be comparable between the two techniques (Swieton et al. 2022).
Complications associated with salivary gland resection are few, but may include inadvertent lymph node removal, operation on the incorrect side, incisional
infection, submandibular seroma, and recurrence due to incomplete removal. Prognosis following surgery is generally good to excellent, with very low recurrence rates. This is in contrast to a 42% recurrence rate associated with surgical drainage alone (Bellenger & Simpson 1992). Radiation therapy has been shown to be effective in resolving cervical sialoceles refractory to surgical management (Poirier et al. 2018).
Ranula
A ranula is a thin-walled linear swelling that results from ruptured sublingual or mandibular salivary ducts below the oral mucosa next to the tongue. It may also occur due to rupture of the polystomatic portion of the sublingual gland. Diagnosis is based on history, oral examination, palpation, and aspiration of the mass. Blood-tinged saliva on aspiration is diagnostic.
The treatment of choice is marsupialization of the ranula. Marsupialization is performed by incising into
Figure 1.2 Intraoperative view of mandibular and sublingual salivary gland removal with active drain placement into the cervical mucocele.
the swelling and resecting an elliptical segment of the overlying sublingual mucosa. The cut edges of the remaining mucosa are sutured to adjacent tissues in a simple continuous pattern with rapidly absorbable suture, thereby creating a pouch that allows saliva to drain into the oral cavity.
If there is recurrence or the ranula is associated with a cervical mucocele, the mandibular and sublingual salivary glands on the affected side should be removed.
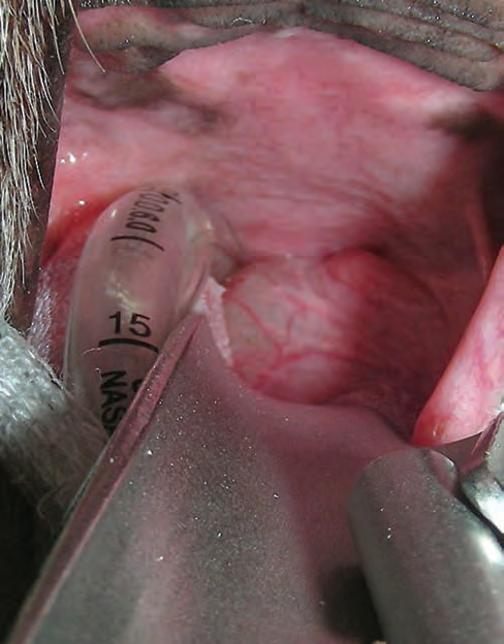
Pharyngeal mucocele
Patients with pharyngeal mucocele may present with signs related to upper airway obstruction, since the swelling eventually becomes large enough to occlude the laryngeal orifice (Figure 1.3). Affected patients may have a history of noisy respiration progressing to intermittent dyspnea, cyanosis, and syncope in severe cases.
A presumptive diagnosis can be made by careful oral examination. The pharyngeal mucocele appears as a fluctuant, smooth, dome-shaped swelling in the lateral pharyngeal wall. Aspiration of blood-tinged saliva is diagnostic, and is generally performed when the patient is under anesthesia to avoid unnecessary stress.
Pharyngeal mucoceles are treated by marsupialization. The swelling is incised and drained by partially excising the overlying pharyngeal mucosa and suturing
the cut edges of the mucosa to the adjacent pharyngeal wall. An alternative technique is to dissect the mucocele free from the surrounding tissue and remove it en bloc. The pharyngeal wall is allowed to heal by granulation. Either procedure generally gives rewarding results. Recurrence is rare, but unilateral mandibular and sublingual salivary gland resection should be done if recurrence does occur or to avoid the potential for recurrence, due to the life-threatening clinical signs associated with this condition.
Zygomatic mucocele
Sialoceles associated with the zygomatic glands are rare. Dogs may present with a variety of clinical signs, the most common being ventral periorbital swelling. Other signs included exophthalmos, periocular pain, chemosis, and nictitating membrane protrusion. The typical location of the swelling is similar to that seen with maxillary carnassial tooth root abscesses. These conditions are differentiated by fine-needle aspiration. Advanced imaging (computed tomography [CT] or magnetic resonance imaging [MRI]) may also be beneficial in diagnosis, particularly in investigating other causes of exophthalmos. Treatment of choice is excision of the zygomatic gland, most often requiring resection of the zygomatic arch for best exposure and access. However, a ventral nonostectomy approach has been described in cadavers, allowing for complete zygomatic gland excision (Dörner et al. 2021). Intracanalicular injection of 10% N-acetylcysteine has also been reported with good success for resolution (Ortillés et al. 2020).
Parotid mucocele
Sialoceles associated with the parotid glands are also very uncommon. Dogs present with a fluctuant nonpainful swelling over the area of the parotid gland on the lateral side of the face. Advanced imaging (e.g., sialography, CT, MRI) is often required for diagnosis. Treatment is complete parotidectomy, which can be a difficult procedure due to the regional anatomy (e.g., facial nerve) and as the capsule is tightly adhered to the gland. Alternatively, the parotid duct can be ligated as close as possible to the gland to cause atrophy.
Neoplasia
Salivary gland neoplasia is a rare condition, but when it does occur it is usually adenocarcinoma of the mandibular or parotid salivary gland. Salivary gland adenocarcinoma is locally invasive and is typically associated with concurrent lymph node metastasis. Other reported salivary gland neoplasms include squamous cell carcinoma, basal cell adenocarcinoma, and mast cell tumor. Siamese cats appear to be overrepresented, although there is no
Figure 1.3 Intraoral view of a pharyngeal mucocele.
breed association in dogs. Recommended treatment is aggressive surgical resection, with or without adjunctive radiation therapy. The most recent reported median survival times for dogs and cats with salivary gland neoplasia are 550 and 516days, respectively (Hammer et al. 2001).
Sialolithiasis
Salivary calculus formation is very uncommon in the dog and cat. When it does occur, salivary stones can obstruct salivary ducts, causing an acute painful swelling or rupture of the affected gland. Most stones are composed of calcium phosphate or calcium carbonate and have been reported to occur mostly in the parotid gland, although sialolithiasis associated with cervical and pharyngeal sialoceles has been reported (Han et al. 2016). Diagnosis is made using skull radiographs with or without sialography, although advanced imaging may also be beneficial. Surgical removal of the calculus is the treatment of choice. This is followed by cannulation and lavage of the affected salivary duct. If this is not possible due to fibrosis, inflammation, or a concurrent sialocele, surgical excision of the affected gland and duct will also be curative.
Sialoadenitis
Salivary gland inflammation (sialoadenitis) is uncommon, but has been reported in the zygomatic, mandibular, and parotid salivary glands of dogs. Causes are numerous, including blunt trauma, iatrogenic trauma, penetrating bite wounds, foreign body migration, tumor infiltration, and systemic viral infection. Severe inflammation can progress to abscess formation and require surgical intervention. Otherwise, treatment of the underlying cause may help resolve this condition.
Necrotizing Sialometaplasia
Necrotizing sialometaplasia is a benign, ischemic, and inflammatory disease of the mandibular glands, although a case involving the parotid gland has been reported (Kim et al . 2010). This condition is manifested by severe retropharyngeal pain, gagging, nausea, ptyalism, and dysphagia. Surgical excision of the mandibular glands tends not to resolve clinical signs, although transient administration of anticonvulsants has resulted in marked improvement (Brooks et al. 1995).
References
Bellenger, C. and Simpson, D.J. (1992). Canine sialoceles: 60 clinical cases. Journal of Small Animal Practice 33: 376–380.
Brooks, D., Hottinger, H.A., and Dunstan, R.W. (1995). Canine necrotizing sialometaplasia: a case report and review of the literature. Journal of the American Animal Hospital Association 31: 21–25.
Cinti, F., Rossanese, M., Buracco, P. et al. (2021). Complications between ventral and lateral approach for mandibular and sublingual sialoadenectomy in dogs with sialocele. Veterinary Surgery 50: 579–587.
De Lorenzi, D., Bertoncello, D., Mantovani, C., and Bottero, E. (2018). Nasopharyngeal sialoceles in 11 brachycephalic dogs. Veterinary Surgery 47: 431–438.
Dörner, J., Oberbacher, S., and Dupré, G. (2021). Comparison of three surgical approaches for zygomatic sialoadenectomy in canine cadavers. Veterinary Surgery 50: 564–570.
Hammer, A., Getzy, D., Ogilvie, G. et al. (2001). Salivary gland neoplasia in the dog and cat: survival times and prognostic factors. Journal of the American Animal Hospital Association 37: 478–482.
Han, H., Mann, F.A., and Park, J.Y. (2016). Canine sialolithiasis: two case reports with breed, gender, and age distribution of 29 cases (1964–2010). Journal of the American Animal Hospital Association 52: 22–26.
Kim, H.Y., Woo, G.H., Bae, Y.C. et al. (2010). Necrotizing sialometaplasia of the parotid gland in the dog. Journal of Veterinary Diagnostic Investigation 22: 975–977.
Marsh, A. and Adin, C. (2013). Tunneling under the digastricus muscle increases salivary duct exposure and completeness of excision in mandibular and sublingual sialoadenectomy in dogs. Veterinary Surgery 42: 238–242.
Oetelaar, G.S., Heng, H.G., Lim, C.K., and Randall, E. (2022). Computed tomographic appearance of sialoceles in 12 dogs. Veterinary Radiology & Ultrasound 63: 30–37.
Ortillés, Á., Leiva, M., Allgoewer, I., and Peña, M.T. (2020). Intracanalicular injection of N-acetylcysteine as adjunctive treatment for sialoceles in dogs: 25 cases (2000–2017). Journal of the American Veterinary Medical Association 257: 826–832.
Poirier, V.J., Mayer-Stankeová, S., Buchholz, J. et al. (2018). Efficacy of radiation therapy for the treatment of sialocele in dogs. Journal of Veterinary Internal Medicine 32: 107–110.
Ritter, M.J., von Pfeil, D.J., Stanley, B.J. et al. (2006). Mandibular and sublingual sialoceles in the dog: a retrospective evaluation of 41 cases, using the ventral approach for treatment. New Zealand Veterinary Journal 54: 333–337.
Swieton, N., Oblak, M.L., Brisson, B.A. et al. (2022). Multi-institutional study of long-term outcomes of a ventral versus lateral approach for mandibular and sublingual sialoadenectomy in dogs with a unilateral sialocele: 46 cases (1999–2019). Journal of the American Veterinary Medical Association 260: 634–642.
Torad, F.A. and Hassan, E.A. (2013). Clinical and ultrasonographic characteristics of salivary mucoceles in 13 dogs. Veterinary Radiology & Ultrasound 54: 293–298.
Surgical Treatment of Esophageal Disease
Eric Monnet, Jeffrey J. Runge, and William T.N. Culp
In comparison to other portions of the alimentary tract, surgery of the esophagus is associated with a greater percentage of postsurgical complications (Moore & Goldstein 1959; Bouayad et al. 1992). A multitude of factors have been theorized to contribute to the difficulty in achieving successful esophageal surgery. The absence of a serosal layer may prevent the formation of a quick seal as seen in other regions of the intestinal tract after a surgical incision is made (Parker & Caywood 1987; Orton 1995). Allowing tissue to rest after being incised is one of the basic requirements for wound healing; however, the esophagus is under constant motion from the head, neck, heart, diaphragm, and peristalsis and this may prevent normal wound healing (Parker & Caywood 1987; Orton 1995). Also saliva is constantly passing in the esophagus. Another concern is that the esophageal wall poorly tolerates tension, and a mortality rate as high as 33% has been reported after resection of up to one-third of the thoracic esophagus (Parker et al. 1989). Passage of food boluses and saliva over an anastomotic site results in delayed epithelial migration and later ultimate healing (Parker & Caywood 1987). It was once believed that the esophagus had a segmental blood supply, and that damage to these regions resulted in ischemia and poor healing; however, a rich plexus of intramural vessels exists within the submucosa, and these vessels have been shown to support segments of the esophagus that have had blood supply compromised by experimental segmental vessel ligation (Macmanus et al. 1950; Shamir et al. 1999). The mechanical problems associated with
motion from swallowing and respiration, the relatively fixed anatomic position, and the lack of a mobile omentum-like structure to help seal wounds are all factors that contribute to the susceptibility of the esophagus to various surgical complications (Orton 1995).
Prior to surgery, nutritional deficiencies associated with esophageal disease should be considered. Delaying surgery and correcting malnourishment through the use of parenteral solutions, or feeding via pharyngostomy, gastrostomy, or jejunosotomy tubes, may be indicated (Parker & Caywood 1987; Han 2004). Studies have shown that humans and animals that are nutritionally depleted have poorer recovery from surgery, decreased immune function, longer hospitalization, and increased risk of morbidity and mortality compared with wellnourished patients (Dionigi et al. 1977; Dempsey et al. 1988). The location of the esophagus allows the extension of infectious microorganisms into the mediastinum as well as other tissues within the thorax that are inherently difficult to treat (Parker & Caywood 1987). Reports have indicated that improved surgical healing is evident when infection is minimized through the prophylactic use of antibiotics in esophageal surgery (Borgstrom & Lundh 1959).
Surgical principles
The major complications associated with esophageal surgery are dehiscence, leakage, and stenosis (Parker & Caywood 1987; Flanders 1989). Many of these complications can be overcome by careful surgical technique