https://ebookmass.com/product/osborns-brain-imaging-
Instant digital products (PDF, ePub, MOBI) ready for you
Download now and discover formats that fit your needs...
Imaging Anatomy Brain and Spine Anne G. Osborn https://ebookmass.com/product/imaging-anatomy-brain-and-spine-anne-gosborn/
ebookmass.com
Essentials of Osborn's Brain: A Fundamental Guide for Residents and Fellows 1st Edition Anne G. Osborn
https://ebookmass.com/product/essentials-of-osborns-brain-afundamental-guide-for-residents-and-fellows-1st-edition-anne-g-osborn/
ebookmass.com
Notorious (The LA Defiance MC Series Book 1) K E Osborn
https://ebookmass.com/product/notorious-the-la-defiance-mc-seriesbook-1-k-e-osborn/
ebookmass.com
Ceasefire City: Militarism, Capitalism, and Urbanism in Dimapur Dolly Kikon
https://ebookmass.com/product/ceasefire-city-militarism-capitalismand-urbanism-in-dimapur-dolly-kikon/
ebookmass.com
Renewable Hydrogen Production Ibrahim Dincer https://ebookmass.com/product/renewable-hydrogen-production-ibrahimdincer/
ebookmass.com
Principles and Practice of Marketing 8th Edition David Jobber
https://ebookmass.com/product/principles-and-practice-ofmarketing-8th-edition-david-jobber/
ebookmass.com
Fundamentals of Organic Chemistry for the JEE - Vol I (Main and Advanced) Ananya Ganguly
https://ebookmass.com/product/fundamentals-of-organic-chemistry-forthe-jee-vol-i-main-and-advanced-ananya-ganguly/
ebookmass.com
A Viscount’s Stolen Fortune: A Regency Romance: Lost Fortune, Found Love (Book 1) Pearson
https://ebookmass.com/product/a-viscounts-stolen-fortune-a-regencyromance-lost-fortune-found-love-book-1-pearson/
ebookmass.com
Pornography and Public Health Emily F. Rothman
https://ebookmass.com/product/pornography-and-public-health-emily-frothman/
ebookmass.com
https://ebookmass.com/product/critical-care-nursing-diagnosis-andmanagement-8th-edition/
ebookmass.com
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
Trauma Section 1
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
TraumaOverview Trauma is one of the most frequent indications for emergent neuroimaging. Because imaging plays such a key role in patient triage and management, we begin this book by discussing skull and brain trauma.
Westartwithabriefconsiderationofepidemiology.Traumaticbraininjury (TBI)isacriticalpublichealthandsocio-economicproblemthroughoutthe world.Thedirectmedicalcostsofcaringforacutelytraumatizedpatientsare huge.Theindirectcostsoflostproductivityandlong-termcareforTBI survivorsareevenlargerthantheshort-termdirectcosts.
Wethenbrieflydiscusstheetiologyandmechanismsofheadtrauma. Understandingthedifferentwaysinwhichtheskullandbraincanbeinjured providesthecontextforunderstandingthespectrumoffindingsthatcanbe identifiedonimagingstudies.
Introduction EpidemiologyofHeadTrauma https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
Trauma—sometimescalledthe"silentepidemic"—isthemostcommon worldwidecauseofdeathinchildrenandyoungadults.Neurotraumais responsibleforthevastmajorityofthesecases.Atleast10millionpeople worldwidesustainTBIeachyear.IntheUSAalone,twomillionpeople annuallysufferaTBI.Ofthese,500,000requirehospitalcare.
Ofallhead-injuredpatients,approximately10%sustainfatalbraininjury. Lifelongdisabilityiscommoninthosewhosurvive.Between5-10%ofTBI survivorshaveseriouspermanentneurologicdeficits,andanadditional2040%havemoderatedisability.Evenmorehavesubtledeficits("minimalbrain trauma").
EtiologyandMechanismsofInjury https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
Traumacanbecausedbymissileornonmissileinjury.Missileinjuryresults frompenetrationoftheskull,meninges,and/orbrainbyanexternalobject, suchasabullet.Gunshotwoundsaremostcommoninadolescentand youngadultmalepatientsbutrelativelyrareinothergroups.
Nonmissileclosedheadinjury(CHI)isamuchmorecommoncauseof neurotraumathanmissileinjury.Fallshavenowsurpassedroadtraffic incidentsastheleadingcauseofTBI.
So-called"groundlevelfalls"(GLFs)areacommonindicationfor neuroimaginginyoungchildrenandolderadults.Insuchcases,braininjury canbesignificant.WithaGLF,asix-foottalladult'sheadimpactstheground
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
at20mph.Anticoagulatedolderadultsareespeciallyatrisk forintracranialhemorrhages,evenwithminorheadtrauma.
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
Motorvehiclecollisionsoccurringathighspeedexert significantacceleration/decelerationforces,causingthebrain tomovesuddenlywithintheskull.Forcibleimpactionofthe brainagainsttheunyieldingcalvariaandhard,knife-likedura resultsingyralcontusion.Rotationandsuddenchangesin angularmomentummaydeform,stretch,anddamagelong vulnerableaxons,resultinginaxonalinjury.
ClassificationofHeadTrauma Themostwidelyusedclinicalclassificationofbraintrauma, theGlasgowComaScale(GCS),dependsontheassessmentof threefeatures:besteye,verbal,andmotorresponses.With theuseoftheGCS,TBIcanbedesignatedasamild,moderate, orsevereinjury.
generallyineffectivetechniques(e.g.,skullradiographs)to verysensitivebutexpensivestudies(e.g.,MR).Techniques thatarestillrelativelynewincludeCTandMRperfusion, diffusiontensorimaging(DTI),andfunctionalMRI(fMRI).
SkullRadiography Fordecades,skullradiography(whethercalled"plainfilm"or, morerecently,"digitalradiography")wastheonlynoninvasive imagingtechniqueavailablefortheassessmentofheadinjury.
Skullradiographyisreasonablyeffectiveinidentifyingcalvarial fractures.Yetskullx-rayscannotdepictthefarmore importantpresenceofextraaxialhemorrhagesand parenchymalinjuries.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
TBIcanalsobedividedchronologicallyandpathoetiologically intoprimaryandsecondaryinjury,thesystemusedinthistext. Primaryinjuriesoccuratthetimeofinitialtrauma.Skull fractures,epi-andsubduralhematomas,contusions,axonal injury,andbrainlacerationsareexamplesofprimaryinjuries.
Secondaryinjuriesoccurlaterandincludecerebraledema, perfusionalterations,brainherniations,andCSFleaks. Althoughvascularinjurycanbeimmediate(bluntimpact)or secondary(vessellacerationfromfractures,occlusion secondarytobrainherniation),forpurposesofdiscussion,itis includedinthechapteronsecondaryinjuries.
CLASSIFICATIONOFHEADTRAUMA PrimaryEffects
Scalpandskullinjuries
Betweenone-quarterandone-thirdofautopsiedpatientswith fatalbraininjurieshavenoidentifiableskullfracture! Therefore, skullradiographyobtainedsolelyforthepurposeof identifyingthepresenceofaskullfracturehasnoappropriate roleinthecurrentmanagementofthehead-injuredpatient. Withrareexceptions,it'sthebrainthatmatters—notthe skull!
NECT Becauseofitswideavailabilityandrapiddetectionofacute hemorrhage,CTisnowacceptedastheworldwidescreening toolforimagingacuteheadtrauma.Sinceitsintroduction almost40yearsago,CThasgraduallybutcompletelyreplaced skullradiographsasthe"workhorse"ofbraintraumaimaging. Thereasonsaresimple:CTdepictsbothboneandsofttissue injuries.Itisalsowidelyaccessible,fast,effective,and comparativelyinexpensive.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
• Extraaxialhemorrhage/hematomas
• Parenchymalinjuries
•
• Miscellaneousinjuries
SecondaryEffects
• Cerebraledema
Herniationsyndromes
• Cerebralischemia
BothstandardandmultidetectorrowCT(MDCT)areusedin theinitialimagingofpatientswithtraumaticheadinjury. Identifyingabnormalitiesthatmayrequireurgenttreatment tolimitsecondaryinjuries,suchasbrainswellingand herniationsyndromes,isessential.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
• Vascularinjury(canbeprimaryorsecondary)
•
ImagingAcuteHead Trauma Imagingisabsolutelycriticaltothediagnosisand managementofthepatientwithacuteTBI.Thegoalof emergentneuroimagingistwofold:(1)identifytreatable injuries,especiallyemergentones,and(2)detectand delineatethepresenceofsecondaryinjuries,suchas herniationsyndromesandvascularinjury.
HowToImage? Abroadspectrumofimagingmodalitiescanbeusedto evaluatepatientswithTBI.Theserangefromoutdated,
StandardnonenhancedCT(NECT)scans(4or5mmthick) fromjustbelowtheforamenmagnumthroughthevertex shouldbeperformed.Twosetsofimagesshouldbeobtained, oneusingbrainandonewithbonereconstructionalgorithms. Viewingthebrainimageswithawiderwindowwidth(150-200 HU,theso-calledsubduralwindow)shouldbeperformedon PACS(orfilm,ifPACSisnotavailable).Thescoutviewshould alwaysbedisplayedaspartofthestudy(seebelow).
MDCTisnowinwidespreaduse.Coronalandsagittal reformattedimagesusingtheaxialsourcedataareroutinely performedinheadtraumatriageandimprovethedetection rateofacutetraumaticsubduralhematomas.
Three-dimensionalshadedsurfacedisplaysarehelpfulin depictingskullandfacialfractures.IffacialboneCTisalso requested,asingleMDCTacquisitioncanbeobtainedwithout overlappingradiationexposuretotheeyeandlowerhalfof thebrain.
HeadtraumapatientswithacuteintracraniallesionsonCT haveahigherriskforcervicalspinefracturescomparedwith patientswithaCT-negativeheadinjury.Becauseuptoone-
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
TraumaOverview thirdofpatientswithmoderatetosevereheadinjuryas determinedbytheGCShaveconcomitantspineinjury,MDCT ofthecervicalspineisoftenobtainedtogetherwithbrain imaging.Softtissueandbonealgorithmreconstructionswith multiplanarreformattedimagesofthecervicalspineshould beobtained.
RepeatheadCTscansintraumatransfersfromonehospitalto anotherarecommonandaddtobothradiationdose exposureandcost.Inadequatedatatransferfromthe referringhospital—notpoorimagequality—isthemajor reasonforpotentiallypreventablerepeatheadCTscans.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
Asdelayeddevelopmentorenlargementofbothextra-and intracranialhemorrhagesmayoccurwithin24-36hours followingtheinitialtraumaticevent,repeatCTshouldbe obtainedifthereissuddenunexplainedclinicaldeterioration, regardlessofinitialimagingfindings.
CTA CTangiography(CTA)isoftenobtainedaspartofawholebodytraumaCTprotocol.CraniocervicalCTAshouldalso specificallybeconsidered(1)inthesettingofpenetrating neckinjury,(2)ifafracturedforamentransversariumorfacet subluxationisidentifiedoncervicalspineCT,or(3)ifaskull basefracturetraversesthecarotidcanaloraduralvenous sinus.Arteriallacerationordissection,traumatic pseudoaneurysm,carotid-cavernousfistula,orduralvenous sinusinjuryarenicelydepictedonhigh-resolutionCTA.
Whether—andwhen—toobtainfollow-upimagingintrauma patientsiscontroversial.InalargestudyofchildrenwithGCS scoresof14or15andanormalinitialCTscan,only2%had follow-upCTorMRperformed.Ofthese,only0.05%had abnormalresultsonthefollow-upstudy,andnonerequired surgicalintervention.Thenegativepredictivevaluefor neurosurgicalinterventionforachildwithaninitialGCSof14 or15andnormalCTwas100%.Fromthis,theauthors concludedthatchildrenwithaGCSof14or15andanormal initialheadCTareatverylowriskforsubsequenttraumatic findingsonneuroimagingandextremelylowriskofneeding neurosurgicalintervention.Hospitalizationforneurologic observationofchildrenwithminorheadtraumaafternormal CTscanresultswasdeemedunnecessary.
GLASGOWCOMASCALE BestEyeResponse(Maximum=4)
1=noeyeopening
MR AlthoughMRcandetecttraumaticcomplicationswithout radiationandismoresensitiveforabnormalitiessuchas contusionsandaxonalinjuries,thereisgeneralagreement thatNECTistheprocedureofchoiceintheinitialevaluationof braintrauma.LimitationsofMRincludeacquisitiontime, access,patientmonitoringandinstability,motiondegradation ofimages,andcost.
• 2=eyeopeningtopain
• 3=eyesopentoverbalcommand
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
Withoneimportantexception—suspectedchildabuse—using MRasaroutinescreeningprocedureinthesettingofacute braintraumaisuncommon.StandardMRtogetherwith susceptibility-weightedimagingandDTIismostusefulinthe subacuteandchronicstagesofTBI.Othermodalitiessuchas fMRIareplayinganincreasinglyimportantroleindetecting subtleabnormalities,especiallyinpatientswithmildcognitive deficitsfollowingminorTBI.
WhoandWhenToImage? Whotoimageandwhentodoitareparadoxicallybothwell establishedandcontroversial.PatientswithaGCSscore indicatingmoderate(GCS=9-12)orsevere(GCS≤8) neurologicimpairmentareinvariablyimaged.Therealdebate isabouthowbesttomanagepatientswithGCSscoresof1315.
InanattempttoreduceCToverutilizationinemergency departments,severalorganizationshavedevelopedevidencebasedclinicalcriteriathathelpseparate"high-risk"from"lowrisk"patients.(Severalofthesearedelineatedintheboxes below.)Yettheimpactontheemergencydepartment physicianorderingbehaviorhasbeeninconsistent.Inplaces withhighmalpracticerates,manyemergencyphysicians routinelyorderNECTscansoneverypatientwithheadtrauma regardlessofGCSscoreorclinicalfindings.
• 4=eyesopenspontaneously
•
BestVerbalResponse(Maximum=5)
1=none
• 2=incomprehensiblesounds
• 3=inappropriatewords
• 4=confused
•
• 5=oriented
BestMotorResponse(Maximum=6)
1=none
• 2=extensiontopain
• 3=flexiontopain
• 4=withdrawaltopain
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
• 5=localizingtopain
•
• 6=obediencetocommands
Sum="ComaScore"andClinicalGrading 13-15=mildbraininjury
• 9-12=moderatebraininjury
•
• ≤8=severebraininjury
AppropriatenessCriteria Threemajorandwidelyusedappropriatenesscriteriafor imagingacuteheadtraumahavebeenpublished:The AmericanCollegeofRadiology(ACR)Appropriateness Criteria,theNewOrleansCriteria(NOC),andtheCanadian HeadCTRule(CHCR).
ACRCriteria.EmergentNECTinmild/minorCHIwiththe presenceofafocalneurologicdeficitand/orotherriskfactors isdeemed"veryappropriate,"asisimagingalltraumatized childrenunder2yearsofage.Althoughacknowledgingthat NECTinpatientswithmild/minorCHI(GCS≥13)withoutrisk
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
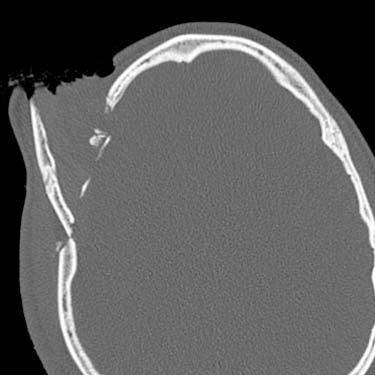
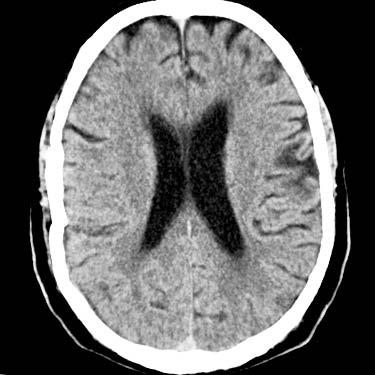
(1-1A)AxialNECTscanofaprisonerimagedforhead
showsnogrossabnormality.(CourtesyJ.A.
factorsorfocalneurologicdeficitis"knowntobelowyield," theACRstillratesitas7outof9inappropriateness.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(1-1B)Scoutviewinthesamecaseshowsaforeignobjectſt(a handcuffkey!)intheprisoner'smouth. Hefakedtheinjuryand wasplanningtoescape,buttheradiologistalertedtheguards andthwartedtheplan.(CourtesyJ.A.Junker,MD.)
aswellasinpatientsover65yearsofage,childrenunderthe ageoftwo,anticoagulatedpatients,andpatientswithlossof consciousnessorfocalneurologicdeficit.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
NOCandCHCR.BoththeNOCandCHCRattempttotriage patientswithminimal/mildheadinjuriesinacost-effective manner.AGCSscoreof15(i.e.,normal)withoutanyofthe NOCindicatorsisahighlysensitivenegativepredictorof clinicallyimportantbraininjuryorneedforsurgical intervention.
NEWORLEANSCRITERIAINMINORHEADINJURY CTindicatedifGCS=15plusanyofthefollowing Headache
• Vomiting
• Patient>60yearsold
• Intoxication(drugs,alcohol)
• Short-termmemorydeficits(anterogradeamnesia)
• Visibletraumaaboveclavicles
• Seizure
Recentstudieshavealsoshownthatcompliancewith establishedimagingguidelinessuchastheCHCRispoor, particularlyinbusyEDsthathandlelargetraumavolumes. Despiteeffortstoeducateurgentcarephysiciansabout limitingpatientexposuretoionizingradiationandusing clinicallybasedriskstratification,nonenhancedheadCTs remainoneofthemostfrequentlyoverutilizedimaging studies.
CTifGCS=13-15andwitnessedLOC,amnesia,or confusion
Highriskforneurosurgicalintervention
GCS<15at2hours
• Suspectedopen/depressedskullfracture
• Clinicalsignsofskullbasefracture
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
• AdaptedfromStiellIGetal:ComparisonoftheCanadianCT headruleandtheNewOrleanscriteriainpatientswithminor headinjury.JAMA294(12):1511-1518,2005
AccordingtotheCHCR,patientswithaGCSscoreof13-15and witnessedlossofconsciousness(LOC),amnesia,orconfusion areimaged,alongwiththosedeemed"highrisk"for neurosurgicalinterventionor"mediumrisk"forbraininjury.
Between6-7%ofpatientswithminorheadinjuryhave positivefindingsonheadCTscans.Mostofthesepatientsalso haveheadache,vomiting,drugoralcoholintoxication,seizure, short-termmemorydeficits,orphysicalevidenceoftrauma abovetheclavicles.CTshouldbeusedliberallyinthesecases,
• ≥2vomitingepisodes
• Age≥65years •
MediumriskforbraininjurydetectedbyheadCT
•
Antegradeamnesia≥30minutes
• "Dangerousmechanism"(i.e.,auto-pedestrian, ejectionfromvehicle,etc.)
AdaptedfromStiellIGetal:ComparisonoftheCanadianCT headruleandtheNewOrleanscriteriainpatientswithminor headinjury.JAMA294(12):1511-1518,2005
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
trauma
Junker,MD.)
CANADIANHEADCTRULEINMINORHEADINJURY
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
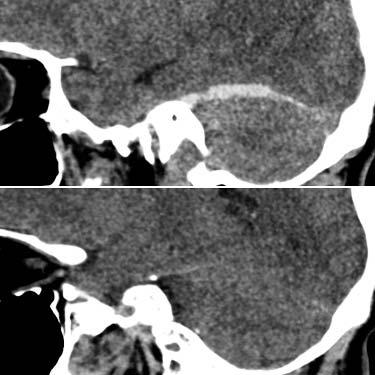
(1-2A)Scoutviewina66ywomanwithaCTheadrequestedto evaluategroundlevelfallshowsaposteriorlyangulatedC1odontoidcomplex
TraumaImaging:Keysto Analysis https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(1-2B)TheheadCTinthesamecase(notshown)wasnormal. CervicalspineCTwasthenperformed.Thesagittalimage reformattedfromtheaxialscandatashowsacomminuted, posteriorlyangulateddensfractureſt.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
Fourcomponentsareessentialtotheaccurateinterpretation ofCTscansinpatientswithheadinjury:thescoutimageplus brain,bone,andsubduralviewsoftheNECTdataset.Critical informationmaybepresentonjustoneofthesefour components.
SuggestionsonhowtoanalyzeNECTimagesinpatientswith acuteheadinjuryaredelineatedbelow.
ScoutImage tSAHinmoderatetosevereTBIapproaches100%.tSAHis usuallyfoundinthesulciadjacenttocorticalcontusions,along thesylvianfissures,andaroundtheanteroinferiorfrontaland temporallobes.ThebestplacetolookforsubtletSAHisthe interpeduncularcistern,wherebloodcollectswhenthe patientissupine.
Anyhypodensitywithinanextraaxialcollectionshouldraise suspicionofrapidhemorrhagewithaccumulationof unclottedbloodor(especiallyinalcoholicsorolderpatients) anunderlyingcoagulopathy.Thisisanurgentfindingthat mandatesimmediatenotificationoftheresponsibleclinician. Lookforintracranialair("pneumocephalus").Intracranialairis alwaysabnormalandindicatesthepresenceofafracturethat traverseseithertheparanasalsinusesormastoid.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
BeforeyoulookattheNECTscan,examinethedigitalscout image!Lookforcervicalspineabnormalitiessuchasfractures ordislocations,jawand/orfacialtrauma,andthepresenceof foreignobjects (1-1).Ifthereisasuggestionofcervicalspine fractureormalalignment,MDCTofthecervicalspineshould beperformedbeforethepatientisremovedfromthescanner (1-2).
BrainWindows Methodicallyandmeticulouslyworkyourwayfromthe outsidein.Firstevaluatethesofttissueimages,beginning withthescalp.Lookforscalpswelling,whichusuallyindicates theimpactpoint.Carefullyexaminetheperiorbitalsoft tissues.
Nextlookforextraaxialblood.Themostcommonextraaxial hemorrhageistraumaticsubarachnoidhemorrhage(tSAH), followedbysub-andepiduralhematomas.Theprevalenceof
Nowmoveontothebrainitself.Carefullyexaminethecortex, especiallythe"high-yield"areasforcorticalcontusions (anteroinferiorfrontalandtemporallobes).Ifthereisascalp hematomaduetoimpact(a"coup"injury),look180°inthe oppositedirectionforaclassic"contre-coup"injury. Hypodenseareasaroundthehyperdensehemorrhagicfoci indicateearlyedemaandseverecontusion.
Moveinwardfromthecortextothesubcorticalwhiteand deepgraymatter.Petechialhemorrhagesoftenaccompany axonalinjury.Ifyouseesubcorticalhemorrhagesontheinitial NECTscan,thisismerelythe"tipoftheiceberg."Thereis usuallyalotmoredamagethanwhatisapparentonthefirst scan.Ageneralrule:thedeeperthelesion,themoresevere theinjury.
Finally,lookinsidetheventriclesforblood-CSFlevelsand hemorrhageduetochoroidplexusshearinginjury.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
Trauma SubduralWindows Lookatthesofttissueimagewithbothnarrow("brain")and intermediate("subdural")windows.Smallsubtlesubdural hematomascansometimesbeoverlookedonstandard narrowwindowwidths(75-100HU)yetarereadilyapparent whenwiderwindows(150-200HU)areused.
temporalbonefractures(withorwithoutossicular dislocation),mandibulardislocation("empty"condylarfossa), andcalvarialfractures.Andremember:nondisplacedlinear skullfracturesthatdon'tcrossvascularstructures(suchasa duralvenoussinusormiddlemeningealartery)areinandof themselvesbasicallymeaningless.Thebrainandbloodvessels arewhatmatter!
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
BoneCT BoneCTreferstobonealgorithmreconstructionviewedwith wide(bone)windows.Ifyoucan'tdobonealgorithm reconstructionfromyourdataset,widenthewindowsanduse anedge-enhancementfeaturetosharpentheimage.Threedimensionalshadedsurfacedisplays(3DSSDs)areespecially helpfulindepictingcomplexorsubtlefractures (1-3)
Eventhoughstandardheadscansare4-5mmthick,itisoften possibletodetectfracturesonboneCT.Lookfor basisphenoidfractureswithinvolvementofthecarotidcanal,
Themostdifficultdilemmaisdecidingwhetheranobserved lucencyisafractureoranormalstructure(e.g.,suturelineor vascularchannel).Keepinmind:itisvirtuallyunheardoffora calvarialfracturetooccurintheabsenceofoverlyingsoft tissueinjury.Ifthereisnoscalp"bump,"itisunlikelythatthe lucencyrepresentsanondisplacedlinearfracture.
BoneCTimagesarealsoveryhelpfulindistinguishinglow densityfromairvs.fat.AlthoughmostPACSstationshavea regionofinterest(ROI)functionthatcanmeasure attenuation,fatfadesawayonboneCTimages,andair remainsveryhypodense.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
(1-3A)AxialNECTinan 18ymanwhofelloffhis skateboardshowsasmall rightepiduralhematoma thatalsocontainsairst. (1-3B)Two-millimeter bonealgorithm reconstructioninthesame caseshowsa nondisplacedlinear fractureofthesquamous temporalboneſt adjacenttotheepidural bloodandairst.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(1-3C)Coronal(left)and sagittal(right)boneCTs reconstructedfromthe axialsourcedatashow thetemporalbone fractureſtiscomminuted andcrossesthemastoid standmiddleear.(13D)BoneCTwithshaded surfacedisplayinthe samecasenicelyshows thesquamous,mastoid aspectsofthe nondisplacedbut comminutedfracture.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
TraumaOverview CTA CTAisgenerallyindicatedif(1)basilarskullfracturescrossthecarotidcanal oraduralvenoussinus (1-4);(2)ifacervicalspinefracture-dislocationis present,especiallyifthetransverseforaminaareinvolved;or(3)ifthe patienthasstroke-likesymptomsorunexplainedclinicaldeterioration.Both thecervicalandintracranialvasculatureshouldbevisualized.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
Althoughitisimportanttoscrutinizeboththearterialandvenoussidesof thecirculation,aCTAisgenerallysufficient.StandardCTAstypicallyshow boththearteriesandtheduralvenoussinuseswell,whereasaCTvenogram (CTV)oftenmissesthearterialphase.
Examinethesourceimagesaswellasthemultiplanarreconstructionsand maximum-intensityprojection(MIP)reformattedscans.Traumatic dissection,vessellacerations,intimalflaps,pseudoaneurysms,carotidcavernousfistulas,andduralsinusocclusionscangenerallybeidentifiedon CTA.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
ScoutImage
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
Evaluatefor
• Cervicalspinefracture-dislocation
○ Jawdislocation,facialfractures
○
○ Foreignobject
BrainWindows
Scalpswelling(impactpoint)
• Extraaxialblood(focalhypodensityinclotsuggestsrapidbleeding)
• Epiduralhematoma
○ Subduralhematoma(SDH)
○ Traumaticsubarachnoidhemorrhage
○ Pneumocephalus
• Corticalcontusion
• Anteroinferiorfrontal,temporallobes
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
○ Oppositescalplaceration/skullfracture
○
Hemorrhagicaxonalinjury
• Intraventricularhemorrhage
• SubduralWindows
• BoneCT
150-200HU(forthinSDHsunderskull)
• Anyfracturescrossavascularchannel?
Bonealgorithmreconstruction>bonewindows
•
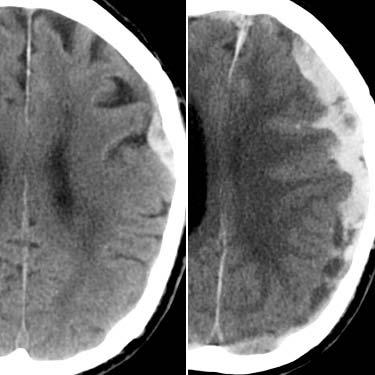
(1-4B)NECTinthesamecaseshowsdiffusebrain swelling,pneumocephalusst,andtraumatic subarachnoidhemorrhage.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(1-4C)CTAinthesamecaseshowsthesigmoid sinusisintactbutdisplacedmedially.Note rapidlyenlargingsubgalealhematomaſt.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
HEADTRAUMA:CTCHECKLIST
(1-4A)NECTshowspneumocephalusst,baseof skullfracturesſtadjacenttoair,whichseemsto outlineadisplacedsigmoidsinus.
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
Trauma https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
SelectedReferences Introduction
EpidemiologyofHeadTrauma
RoozenbeekBetal:Changingpatternsintheepidemiologyof traumaticbraininjury.NatRevNeurol.9(4):231-6,2013
ImagingAcuteHeadTrauma
HowToImage?
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
AmrheinTJetal:Reformattedimagesimprovethedetectionrate ofacutetraumaticsubduralhematomasonbrainCTcompared withaxialimagesalone.EmergRadiol.24(1):39-45,2017
HinzpeterRetal:RepeatedCTscansintraumatransfers:an analysisofindications,radiationdoseexposure,andcosts.EurJ Radiol.88:135-140,2017
RajaASetal:"Choosingwisely"imagingrecommendations:initial implementationinNewEnglandemergencydepartments.WestJ EmergMed.18(3):454-458,2017
ThesleffTetal:Headinjuriesandtheriskofconcurrentcervical spinefractures.ActaNeurochir(Wien).159(5):907-914,2017
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
LolliVetal:MDCTimagingoftraumaticbraininjury.BrJRadiol. 20150849,2016
BodanapallyUKetal:Imagingoftraumaticbraininjury.RadiolClin NorthAm.53(4):695-715,viii,2015
WhoandWhenToImage?
GranataRTetal:SafetyofdeferredCTimagingofintoxicated patientspresentingwithpossibletraumaticbraininjury.AmJ EmergMed.35(1):51-54,2017
SharpALetal:Computedtomographyuseforadultswithhead injury:describinglikelyavoidableemergencydepartmentimaging basedontheCanadianCTheadrule.AcadEmergMed.24(1):2230,2017
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
AtabakiSMetal:Comparisonofpredictionrulesandclinician suspicionforidentifyingchildrenwithclinicallyimportantbrain injuriesafterbluntheadtrauma.AcadEmergMed.23(5):566-75, 2016
BharadwajSetal:Minorheadinjury:limitingpatientexposureto ionizingradiation,riskstratification,andconcussionmanagement. CurrOpinPediatr.28(1):121-31,2016
LolliVetal:MDCTimagingoftraumaticbraininjury.BrJRadiol. 20150849,2016
SadeghRetal:HeadCTscaninIranianminorheadinjurypatients: evaluatingcurrentdecisionrules.EmergRadiol.23(1):9-16,2016
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
ArabAFetal:AccuracyofCanadianCTheadruleinpredicting positivefindingsonCToftheheadofpatientsaftermildhead injuryinalargetraumacentreinSaudiArabia.NeuroradiolJ. 28(6):591-7,2015
BodanapallyUKetal:Imagingoftraumaticbraininjury.RadiolClin NorthAm.53(4):695-715,viii,2015
GunesTatarIetal:AppropriatenessofselectioncriteriaforCT examinationsperformedatanemergencydepartment.Emerg Radiol.21(6):583-8,2014
RyanMEetal:ACRappropriatenesscriteriaheadtrauma--child.J AmCollRadiol.11(10):939-47,2014
StiellIGetal:ComparisonoftheCanadianCTHeadRuleandthe NewOrleansCriteriainpatientswithminorheadinjury.JAMA. 294(12):1511-8,2005
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
PrimaryEffectsofCNSTrauma https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
Primary head injuries are defined as those that occur at the time of initial trauma even though they may not be immediately apparent on initial evaluation.
Headinjurycanbecausedbydirectorindirecttrauma.Directtrauma involvesablowtotheheadandisusuallycausedbyautomobilecollisions, falls,orinjuryinflictedbyanobjectsuchasahammerorbaseballbat.Scalp lacerations,hematomas,andskullfracturesarecommon.Associated intracranialdamagerangesfromnonetosevere.
Significantforcesofacceleration/deceleration,lineartranslation,and rotationalloadingcanbeappliedtothebrainwithoutdirectheadblows. Suchindirecttraumaiscausedbyangularkinematicsandtypicallyoccursin high-speedmotorvehiclecollisions(MVCs).Herethebrainundergoesrapid deformationanddistortion.Dependingonthesiteanddirectionoftheforce applied,significantinjurytothecortex,axons,penetratingbloodvessels,and deepgraynucleimayoccur.Severebraininjurycanoccurintheabsenceof skullfracturesorvisiblescalplesions.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
Webeginourdiscussionwithaconsiderationofscalpandskulllesionsaswe workourwayfromtheoutsidetotheinsideoftheskull.Wethendelineate thespectrumofintracranialtrauma,startingwithextraaxialhemorrhages. Weconcludethischapterwithadetaileddiscussionofinjuriestothebrain parenchyma(e.g.,corticalcontusion,diffuseaxonalinjury,andtheserious deepsubcorticalinjuries).
ScalpandSkullInjuries https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
Scalpandskullinjuriesarecommonmanifestationsofcranialtrauma. Althoughbraininjuryisusuallythemostimmediateconcerninmanaging traumatizedpatients,superficiallesionssuchasscalpswellingandfocal hematomacanbehelpfulinidentifyingthelocationofdirectheadtrauma. Onoccasion,theseinitiallyinnocent-appearing"lumpsandbumps"can becomelife-threatening.Beforeturningourattentiontointracranial traumaticlesions,wethereforebrieflyreviewscalpandskullinjuries, delineatingtheirtypicalimagingfindingsandclinicalsignificance.
ScalpInjuries Scalpinjuriesincludelacerationsandhematomas.Scalplacerationscan occurinbothpenetratingandclosedheadinjuries.Lacerationsmayextend partiallyorentirelythroughallfivelayersofthescalp(skin,subcutaneous fibrofattytissue,galeaaponeurotica,looseareolarconnectivetissue,and periosteum)totheskull (2-1)
Focaldiscontinuity,softtissueswelling,andsubcutaneousairarecommonly identifiedinscalplacerations.Scalplacerations
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-1)Coronalgraphic depictsnormallayersof thescalp.Skin, subcutaneousfibrofatty tissueoverliethegalea aponeurotica,loose areolarconnectivetissue. Thepericraniumisthe periosteumoftheskull andcontinuesintoand throughsuturestomerge withtheperiosteallayer ofthedura.(2-2)NECT showsscalplacerationst, hyperdenseforeignbodies ſt,andsubgalealair.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-3)Graphicshowsthe skullofanewborn, includingtheanterior fontanelle,coronal, metopic,sagittalsutures. Cephalohematomais subperiosteal,limitedby sutures.Subgaleal hematomaisunderthe scalpaponeurosis,not boundedbysutures.(24A)NECTscanina newbornshowsasmall rightſtandalargeleft stparietal cephalohematoma. Neithercrossesthe sagittalsuture.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-4B)Coronalscaninthe samecaseshowsthe smallrightſt,largeleftsidedcephalohematomas st.Theelevated periosteumclearly separatesthetwoblood collections.(2-4C)Sagittal scanreformattedfromthe axialdatashowsthatthe leftparietal cephalohematomast doesnotcrossthecoronal suture.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
PrimaryEffectsofCNSTrauma forthepresenceofanyforeignbodies.Ifnotremovedduring wounddebridement,foreignbodiescanbeapotentialsource ofsubstantialmorbidityandareveryimportanttoidentifyon initialimagingstudies.Woodfragmentsareoftenhypodense, whereasleadedglass,gravel,andmetallicshardsarevariably hyperdense (2-2).
Cephalohematomasaretheextracranialequivalentofan intracranialepiduralhematoma.Cephalohematomasdonot crosssuturelinesandaretypicallyunilateral.Becausetheyare anatomicallyconstrainedbythetoughfibrousperiosteumand itsinsertions,cephalohematomasrarelyattainlargesize.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
Scalplacerationsmayormaynotbeassociatedwithscalp hematomas.Therearetwodistinctlydifferenttypesofscalp hematomas:cephalohematomasandsubgalealhematomas. Theformerareusuallyofnoclinicalsignificance,whereasthe lattercancausehypovolemiaandhypotension.
Cephalohematomasaresubperiostealbloodcollectionsthat lieinthepotentialspacebetweentheoutersurfaceofthe calvariumandthepericranium,whichservesasthe periosteumoftheskull (2-3).Thepericraniumcontinues mediallyintocranialsuturesandisanatomicallycontiguous withtheouter(periosteal)layerofthedura.
Cephalohematomasoccurin1%ofnewbornsandaremore commonfollowinginstrumenteddelivery.Theyareoften diagnosedclinicallybutimagedonlyiftheyareunusually prominentorifintracranialinjuriesaresuspected.NECTscans showasomewhatlens-shapedsofttissuemassthatoverliesa singlebone(usuallytheparietaloroccipitalbone) (2-4).If morethanoneboneisaffected,thetwocollectionsare separatedbytheinterveningsuturelines.
Complicationsfromcephalohematomaarerare,andmost resolvespontaneouslyoverafewdaysorweeks.Occasionally theelevatedperiosteumattheperipheryofachronic cephalohematomaundergoesdystrophiccalcification, creatingafirmpalpablemass.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-5)Autopsyfroma traumatizedinfantshows amassivebiparietal subgalealhematomaſt. Thegaleaaponeurotica hasbeenpartiallyopened toshowlarge biparietalhematomathat crossesthesagittalsuture .(2-6)AxialCECTin3y childshowsmassive subgalealhematomaſt surroundingentire calvarium.Subgaleal hematomascrosssutures, canbecomelifethreatening,while cephalohematomasare anatomicallylimited.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-7)Autopsiedskull showsfataltraumawith exo-(L)andendocranial views(R).Alinear fractureextendsinto thesuperiorsagittal suture,causing diastasisandasubgaleal hematomast.(2-8)Bone CTthroughthetopofthe calvariumshowslinear skullfracturesſt extendingintoand wideningthesagittal suture,causingadiastatic fracture.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
Trauma Subgalealhematomasaresubaponeuroticcollectionsandare commonfindingsintraumatizedpatientsofallages.Here bloodcollectsundertheaponeurosis(the"galea")ofthe occipitofrontalismuscle (2-5).Becauseasubgalealhematoma liesdeeptothescalpmusclesandgaleaaponeuroticabut externaltotheperiosteum,itisnotanatomicallylimitedby suturelines.
Bleedingintothesubgalealspacecanbeveryextensive. Subgalealhematomasareusuallybilaterallesionsthatoften spreaddiffuselyaroundtheentirecalvaria.NECTscansshowa heterogeneouslyhyperdensecrescenticscalpmassthat crossesoneormoresuturelines (2-6).
FacialInjuries Facialfracturesarecommonlyoverlookedoninitialimaging (typicallyheadCTscans).Importantsofttissuemarkerscanbe identifiedthatcorrelatewithfacialfracturesandmaymerita dedicatedCTevaluationofthefacialbones.Theseinclude periorbitalcontusionsandsubconjunctivalhemorrhageaswell aslacerationsofthelips,mouth,andnose.
https://t.me/ebookers
Mostsubgalealhematomasresolvewithouttreatment.In contrasttobenignself-limitedcephalohematomas,however, expandingsubgalealhematomasininfantsandsmallchildren cancausesignificantbloodloss.
Holmgrenetal.(2005)haveproposedthemnemonicLIPS-N (liplaceration,intraorallaceration,periorbitalcontusion, subconjunctivalhemorrhage,andnasallaceration)beusedin conjunctionwithphysicalexamination.Ifanyoftheseis present,atraumatizedpatientshouldhaveadedicatedfacial CTinadditiontothestandardheadCT.
SkullFractures Noticingascalp"bump"orhematomaoninitialimagingin headtraumaisimportant,ascalvarialfracturesrarely—if
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
(2-9)3Dshadedsurface display(SSD)inapatient withmultiplelinear anddiastaticskull fracturesshowsutilityof SSDsindepictingcomplex fractureanatomy.Note slightdepressionof thefracturedparietooccipitalcalvarium.(210A)AxialboneCTina patientwhowashitinthe headwithafallingladder showsanextensively comminuted,depressed skullfracture.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
(2-10B)CoronalboneCT reformattedfromthe axialsourcedatainthe samecaseshowsthatthe depressedskullfracture isnearthemidline, raisingconcernfor superiorsagittalsinus injury.(2-10C)Sagittal boneCTinthesamecase showsthedepressedskull fracture,associated withafocalscalp hematomast.CTV(not shown)demonstratedSSS narrowingwithout occlusionorvenousEDH.
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
PrimaryEffectsofCNSTrauma ever—occurintheabsenceofoverlyingsofttissueswellingor scalplaceration.SkullfracturesarepresentoninitialCTscans inabouttwo-thirdsofpatientswithmoderateheadinjury, although25-35%ofseverelyinjuredpatientshaveno identifiablefractureevenwiththin-sectionbone reconstructions.
LinearSkullFractures Alinearskullfractureisasharplymarginatedlineardefect thattypicallyinvolvesboththeinnerandoutertablesofthe calvaria (2-8).
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
Skullfracturescanbesimpleorcomminuted,closedoropen. Inopenfractures,skinlacerationresultsincommunication betweentheexternalenvironmentandintracranialcavity. Infectionriskishighinthistypeoffracture,asitiswith fracturesthatcrossthemastoidsandparanasalsinuses.
https://t.me/ebookers https://t.me/ebookers
Mostlinearskullfracturesarecausedbyrelativelylow-energy blunttraumathatisdeliveredoverarelativelywidesurface area.Linearskullfracturesthatextendintoandwidenasuture becomediastaticfractures(seebelow).Whenmultiple complexfracturesarepresent,3Dshadedsurfacedisplay (SSD)canbeveryhelpfulindepictingtheiranatomyand relationshipstocranialsutures.
Severaltypesofacuteskullfracturecanbeidentifiedon imagingstudies:linear,depressed,elevated,anddiastatic fractures (2-7).Fracturescaninvolvethecalvaria,skullbase, orboth.Anothertypeofskullfracture,a"growing"skull fracture,isararebutimportantcomplicationofskulltrauma.
Patientswithanisolatedlinearnondisplacedskullfracture (NDSF),nointracranialhemorrhageorpneumocephalus, normalneurologicexamination,andabsenceofotherinjuries areatverylowriskfordelayedhemorrhageorotherlifethreateningcomplication.Hospitalizationisnotnecessaryfor manychildrenwithNDSFs.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-11A)AxialNECTscan showsseverescalp lacerationwitha combinationofelevated st,depressedskull fractures.(2-11B)BoneCT inthesamecaseshows thattheelevatedfracture isliterally"hinged"away fromthecalvaria.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-12A)AxialNECTscan ina20ymanwhohada treefallonhishead showsamassive subgalealhematoma crossingtheanterior aspectofthesagittal sutureſt.Asmall extraaxialhematomast, mostlikelyavenous epiduralhematoma,is present.(2-12B)BoneCT inthesamecaseshowsa diastaticfractureofthe sagittalsutureſt. Nondisplacedlinear fracturesarealso present.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
Trauma https://t.me/ebookers
DepressedSkullFractures https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
Adepressedskullfractureisafractureinwhichthe fragmentsaredisplacedinward (2-9).Comminutionofthe fracturefragmentsstartsatthepointofmaximumimpactand spreadscentrifugally.Depressedfracturesaremostoften causedbyhigh-energydirectblowstoasmallsurfacewitha bluntobject(e.g.,hammer,baseballbat,ormetalpipe) (2-10)
Depressedskullfracturestypicallyteartheunderlyingdura andarachnoidandareassociatedwithcorticalcontusionsand potentialleakageofCSFintothesubduralspace.Fractures extendingtoaduralsinusorthejugularbulbareassociated withvenoussinusthrombosisin40%ofcases.
ElevatedSkullFractures Anelevatedskullfracture—oftencombinedwithdepressed fragments—isuncommon.Elevatedfracturesareusually causedbyalong,sharpobject(suchasamacheteorpropeller)
thatfracturesthecalvaria,simultaneouslyliftingandrotating thefracturefragment (2-11)
DiastaticSkullFractures Adiastaticskullfractureisafracturethatwidens("diastases" or"splitsopen")asutureorsynchondrosis.Diastaticskull fracturesusuallyoccurinassociationwithalinearskull fracturethatextendsintoanadjacentsuture (2-12)
Traumaticdiastasisofthesphenooccipital,petrooccipital, and/oroccipitomastoidsynchondrosesiscommoninchildren withseverelycomminutedcentralskullbasefractures.Asit typicallydoesnotossifycompletelyuntilthemidteens,the sphenooccipitalsynchondrosisisthemostcommonsite.
"Growing"SkullFractures A"growing"skullfracture(GSF),alsoknownas "posttraumaticleptomeningealcyst"or"craniocerebral
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-13A)AxialNECTscan inapatientwith progressiveright hemiparesisfollowing priorheadtraumashows leftparietal encephalomalaciaſt.The overlyingskullappears focallydeformedand thinned.(2-13B)Bone CTinthesamepatient showsawidelucentskull lesionwithrounded, scallopedmargins.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-13C)AxialT2WIinthe samepatientshowsa lobulatedCSFcollection ſtthatextendsintoand almostcompletely throughthecalvarial vault.(2-13D)Coronal T2WIshowsthe intradiploicCSFcollection ſtwithencephalomalacic brainstretchedand tetheredintothelesion .Thisisclassic "growing"skullfracture (leptomeningealcyst).
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
PrimaryEffectsofCNSTrauma erosion,"isararelesionthatoccursinjust0.3-0.5%ofallskullfractures (213).MostpatientswithGSFareunder3yearsofage.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
GSFsdevelopinstagesandslowlywidenovertime.Inthefirst"prephase,"a skullfracture(typicallyalinearorcomminutedfracture)laceratesthedura, andbraintissueorarachnoidmembraneherniatesthroughthetorndura. StageIextendsfromthetimeofinitialinjurytojustbeforethefracture enlarges.EarlyrecognitionandduralrepairofstageIGSFsproducethebest results.
StageIIistheearlyphaseofGSF.StageIIlastsforapproximately2months followinginitialfractureenlargement.Atthisstage,thebonedefectissmall, theskulldeformityisrelativelylimited,andneurologicdeficitsaremild. Nevertheless,theentrappedtissuepreventsnormalfracturehealing.
StageIIIrepresentslate-stageGSFandbegins2monthsaftertheinitial enlargementbegins.Duringthisstage,thebonedefectbecomes significantlylarger.BraintissueandCSFextendbetweenthebonyedgesof thefracturethroughtornduraandarachnoid.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
Patientswithlate-stageGSFsoftenpresentmonthsorevenyearsafterhead trauma.StageIIIGSFscancausepronouncedskulldeformitiesand progressiveneurologicdeficitsifleftuntreated.
Imaging GeneralFeatures.Plainskullradiographshavenoroleinthemodern evaluationoftraumaticheadinjury.One-quarterofpatientswithfatalbrain injurieshavenoskullfractureatautopsy.CTisfast,widelyavailable,sensitive forbothboneandbraininjury,andtheworldwidediagnosticstandardof careforpatientswithheadinjuries.NewgenerationsofmultisliceCT scannersofferveryshortacquisitiontimeswithexcellentspatialresolution.
Bothboneandsofttissuereconstructionalgorithmsshouldbeusedwhen evaluatingpatientswithheadinjuries.Softtissuereconstructionsshouldbe viewedwithbothnarrow("brain")andintermediate("subdural")windows. Coronalandsagittalreformattedimagesobtainedusingtheaxialsource dataarehelpfuladditions.
Three-dimensionalreconstructionandcurvedMIPsoftheskullhavebeen showntoimprovefracturedetectionovertheuseofaxialsectionsalone.
CTFindings.Whilefracturescaninvolveanypartofthecalvariaorskullbase, themiddlecranialfossaismostsusceptiblebecauseofitsthin"squamous" bonesandmultipleforaminaandfissures.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
fracturesofthe skullbasearepresentcrossingthejugular foramenst,bothcarotidcanals.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
NECTscansdemonstratelinearskullfracturesassharplymarginatedlucent lines.Depressedfracturesaretypicallycomminutedandshowinward implosionoffracturefragments (2-10) Elevatedfracturesshowanelevated, rotatedskullsegment (2-11).Diastaticfracturesappearaswidenedsutures orsynchondroses (2-14) (2-15)andareusuallyassociatedwithlinearskull fractures.
StageI"growing"fracturesaredifficulttodetectoninitialNECTscans,as scalpandcontusedbrainaresimilarindensity.Identifyingtorndurawith herniatedbraintissueissimilarlydifficultalthoughcranialultrasoundcanbe morehelpful.
Later-stageGSFsdemonstrateaprogressivelywideningandunhealing fracture.Alucentskulllesionwithrounded,scallopedmarginsandbeveled edgesistypical (2-13).CSFandsofttissueareentrappedwithinthe expandingfracture.MostGSFsaredirectlyadjacenttoposttraumatic encephalomalacia,sotheunderlyingbrainoftenappearshypodense.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-15B)CTinthesamecaseshowscarotid arteriesſt,sigmoidsinusesarepatent.A smallrightvenousEDHstispresent.
(2-15A)Linearſt,diastatic
(2-14)Autopsyshowsmultipleskullbase fracturesinvolvingclivusſt,carotidcanals, jugularforaminast.(E.T.Hedley-White,MD.)
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
MRFindings.MRisrarelyusedinthesettingofacuteheadtraumabecause ofhighcost,limitedavailability,andlengthytimerequired.Comparedwith CT,bonedetailispooralthoughparenchymalinjuriesarebetterseen. AddingT2*sequences,particularlySWI,isespeciallyhelpfulinidentifying hemorrhagiclesions.
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
Insomecases,MRmaybeindicatedforearlydetectionofpotentially treatablecomplications.Ayoungchildwithneurologicdeficitsorseizures,a fracturelargerthan4millimeters,orasofttissuemassextendingthrough thefractureintothesubgalealspaceisatriskfordevelopingaGSF.MRcan demonstratetheduraltearanddifferentiateherniatedbrainfromcontused, edematousscalp.
Angiography.Ifafracturecrossesthesiteofamajorvascularstructuresuch asthecarotidcanaloraduralvenoussinus (2-14),CTangiographyis recommended.Sagittal,coronal,andMIPreconstructionshelpdelineatethe siteandextentofvascularinjuries.
(2-16)GraphicshowsEDH,depressedskull fracturelaceratingmiddlemeningealartery st.Insetshowsrapidbleeding,"swirl"signſt.
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
Clivalandskullbasefracturesarestronglyassociatedwithneurovascular trauma,andCTAshouldalwaysbeobtainedinthesecases (2-15).Cervical fracturedislocations,distractioninjuries,andpenetratingnecktraumaalso meritfurtherinvestigation.Uncomplicatedasymptomaticsofttissueinjuries oftheneckrarelyresultinsignificantvascularinjury.
SCALPANDSKULLINJURIES ScalpInjuries
Lacerations
• ±Foreignbodies
○ Cephalohematoma
• Usuallyinfants ○ Subperiosteal
○ Small,unilateral(limitedbysutures)
○ Subgalealhematoma
• Betweengalea,periosteumofskull
○ Circumferential,notlimitedbysutures
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-17A)Endocranialviewshowstemporalbone fracturecrossingthemiddlemeningealartery groovest.NotebiconvexmarginsofEDH.
○
○ Canbeverylarge,life-threatening
SkullFractures
Linear
• Sharplucentline
○
○ Depressed
Canbeextensiveandwidespread
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
view
(CourtesyE.T.Hedley-Whyte,MD.)
• Focal
○ Inwardlydisplacedfragments
○
○ Oftenlaceratesdura-arachnoid
• Rare
Elevated
○
Fragmentedrotatedoutward ○ Diastatic
• Typicallyassociatedwithseveretrauma ○ Usuallycausedbylinearfracturethatextendsintosuture
•
○ Widens,spreadsapartsutureorsynchondrosis
○ "Growing"
○
○
Rare
Usuallyinyoungchildren
Fracturelaceratesdura-arachnoid ○
○
Brain/arachnoidherniatesthroughtorndura
Trappedtissuepreventsbonehealing
CT:Roundededges,scallopedmarginsofskull
MR:CSF±brain
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-17B)Dorsal
ofthedura-coveredbrain showsthebiconvexEDHſtontopofthedura.
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
PrimaryEffectsofCNSTrauma ExtraaxialHemorrhages Extraaxialhemorrhagesandhematomasarecommonmanifestationsof headtrauma.Theycanoccurinanyintracranialcompartment,withinany space(potentialoractual),andbetweenanylayersofthecranialmeninges. Onlythesubarachnoidspacesexistnormally;alltheotherspacesare potentialspacesandoccuronlyunderpathologicconditions.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
Epiduralhematomasarisebetweentheinnertableoftheskullandouter (periosteal)layerofthedura.Subduralhematomasarelocatedbetweenthe inner(meningeal)layeroftheduraandthearachnoid.Traumatic subarachnoidhemorrhageisfoundwithinthesulciandsubarachnoid cisterns,betweenthearachnoidandthepia.
Todiscussextraaxialhemorrhages,weworkourwayfromtheoutsideto inside.Wethereforebeginthissectionwithadiscussionofepidural hematomas(bothclassicandvariant),thenmovedeeperinsidethecranium tothemorecommonsubduralhematomas.Weconcludewitha considerationoftraumaticsubarachnoidhemorrhage.
(2-18A)BiconvexaEDHſtisshownwithathin subduralbloodcollectionalongthetentorium, falx,andlefthemispherest.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
ArterialEpiduralHematoma Epiduralhematomas(EDHs)areuncommonbutpotentiallylethal complicationsofheadtrauma.IfanEDHispromptlyrecognizedand appropriatelytreated,mortalityandmorbiditycanbeminimized.
Terminology AnEDHisacollectionofbloodbetweenthecalvariaandouter(periosteal) layerofthedura.
Etiology MostEDHsarisefromdirecttraumatotheskullthatlaceratesanadjacent bloodvessel (2-16).Thevastmajority(90%)arecausedbyarterialinjury, mostcommonlytothemiddlemeningealartery.Approximately10%of EDHsarevenous,usuallysecondarytoafracturethatcrossesaduralvenous sinus(seebelow).
Pathology Location.Over90%ofEDHsareunilateralandsupratentorial.Between9095%arefounddirectlyadjacenttoaskullfracture.Thesquamousportionof thetemporalboneisthemostcommonsite.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-18B)(L)BoneCTshowssubgalealhematoma ,EDHſt.(R)CoronalboneCTdemonstratesa subtlecomminutedfracturest.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
GrossPathology.EDHsarebiconvexinshape (2-17A).Adherenceofthe periostealduratotheinnercalvariaexplainsthistypicalconfiguration.As EDHsexpand,theystriptheduraawayfromtheinnertableoftheskull, formingtheclassiclens-shapedhematoma (2-17B).Becausethedurais especiallytightlyattachedtosutures,EDHsinadultsrarelycrosssuturelines (10%ofEDHsinchildrendocrosssutures,especiallyifafracturetraverses thesutureorsuturaldiastasisispresent).
ThetypicalgrossorintraoperativeappearanceofanacuteEDHisadark purple("currantjelly")lentiformclot.
ClinicalIssues Epidemiology.EDHsaremuchlesscommonthaneithertraumatic subarachnoidhemorrhage(tSAH)orsubduralhematoma.AlthoughEDHs representupto10%offatalinjuriesinautopsyseries,theyarefoundinonly 1-4%ofpatientsimagedforcraniocerebraltrauma.
AxialNECTshowsanactivelybleedingEDH with"swirl"sign,displacedcortex.Afocal cephalohematomaſtispresent.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-19)
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
Trauma https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
Demographics.EDHsareuncommonininfantsandtheelderly.Mostare foundinolderchildrenandyoungadults.TheM:Fratiois4:1.
Presentation.Theprototypical"lucidinterval,"duringwhichatraumatized patienthasaninitialbrieflossofconsciousnessfollowedbyan asymptomaticperiodofvariouslengthpriortoonsetofcomaand/or neurologicdeficit,occursinonly50%ofEDHcases.Headache,nausea, vomiting,symptomsofintracranialmasseffect(e.g.,pupil-involvingthird cranialnervepalsy)followedbysomnolenceandcomaarecommon.
NaturalHistory.Outcomedependsonsizeandlocationofthehematoma, whethertheEDHisarterialorvenous,andwhetherthereisactivebleeding (seebelow).Intheabsenceofotherassociatedtraumaticbraininjuries, overallmortalityratewithpromptrecognitionandappropriatetreatmentis under5%.
(2-20A)Serialimagingdemonstratestemporal evolutionofasmallnonoperatedEDH.Initial NECTscanshowsahyperdensebiconvexEDH.
DelayeddevelopmentorenlargementofanEDHoccursin10-15%ofcases, usuallywithin24-36hoursfollowingtrauma.
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
TreatmentOptions.ManyEDHsarenowtreatedconservatively.Most traumaticEDHsarenotsurgicallesionsatinitialpresentation,andtherateof conversiontosurgeryislow.MostvenousandsmallclassichyperdenseEDHs thatdonotexhibita"swirl"signandhaveminimalornomasseffectare managedconservativelywithcloseclinicalobservationandfollow-up imaging (2-20).SignificantclinicalpredictorsofEDHprogressionrequiring conversiontosurgicaltherapyarecoagulopathyandyoungerage.
Imaging GeneralFeatures.EDHs,especiallyinadults,typicallydonotcrosssutures unlessafracturewithsuturaldiastasisispresent.Inchildren,10%ofEDHs crosssuturelines,usuallythecoronalorsphenosquamoussuture.
Lookforothercomorbidlesionssuchas"contre-coup"injuries,tSAH,and secondarybrainherniations,allofwhicharecommonfindingsinpatients withEDHs.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-20B)Repeatscan10dayslaterrevealsthat densityoftheEDHhasdecreased significantly.
CTFindings.NECTscanistheprocedureofchoiceforinitialimagingin patientswithheadinjury.Bothsofttissueandbonereconstruction algorithmsshouldbeobtained.Multiplanarreconstructionsareespecially usefulinidentifyingvertexEDHs,whichmaybedifficulttodetectifonlyaxial imagesareobtained.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
(2-20C)Repeatstudy6weeksaftertrauma revealsthattheEDHhasresolvedcompletely.
Theclassicimagingappearanceofclassic(arterial)EDHsisahyperdense (60-90HU)biconvexextraaxialcollection (2-18).Presenceofahypodense component("swirl"sign)isseeninaboutone-thirdofcasesandindicates active,rapidbleedingwithunretractedclot (2-16) (2-19).
EDHscompresstheunderlyingsubarachnoidspaceanddisplacethecortex medially,"buckling"thegray-whitematterinterfaceinward.
AirinanEDHoccursinapproximately20%ofcasesandisusually—butnot invariably—associatedwithasinusormastoidfracture.
Patientswithmixed-densityEDHstendtopresentearlierthanpatientswith hyperdensehematomasandhavelowerGlasgowComaScores(GCSs),larger hematomavolumes,andpoorerprognosis.
Imagingfindingsassociatedwithadverseclinicaloutcomearethickness>1.5 cm,volume>30mL,pterional(lateralaspectofthemiddlecranialfossa) location,midlineshift>5mm,andpresenceofa"swirlsign"withinthe hematomaonimaging.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
PrimaryEffectsofCNSTrauma MRFindings.AcuteEDHsaretypicallyisointensewithunderlyingbrain, especiallyonT1WI.Thedisplacedduracanbeidentifiedasadisplaced"black line"betweenthehematomaandthebrain.
Angiography.DSAmayshowalaceratedmiddlemeningealarterywith "tram-track"fistulizationofcontrastfromthemiddlemeningealarteryinto thepairedmiddlemeningealveins.Masseffectwithdisplacedcortical arteriesandveinsisseen.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
CLASSICACUTEEPIDURALHEMATOMA Terminology
• Etiology
EDH=bloodbetweenskull,dura
• Arterial90%
Associatedskullfracturein90-95%
• Mostoftenmiddlemeningealartery
○ Venous10%
• Pathology
Unilateral,supratentorial(>90%)
Graphic
basilarskullfracture withtransversesinusocclusionandposterior fossavenousEDHst.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
• Durastrippedawayfromskull→biconvexhematoma
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
• Usuallydoesnotcrosssutures(exception=children,10%)
• Doescrosssitesofduralattachment
• Clinical
Rare(1-4%ofheadtrauma)
• Olderchildren,youngadultsmostcommon
• M:F=4:1
• Classic"lucidinterval"inonly50%
• Delayeddeteriorationcommon
• Lowmortalityifrecognized,treated
• SmallEDHs
• Ifminimalmass,no"swirlsign"oftenmanagedconservatively
○
Imaging
Hyperdenselens-shaped
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
•
• "Swirlsign"(hypodensity)=rapidbleeding
VenousEpiduralHematoma https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
NotallEDHsarethesame!!VenousEDHsareoftensmaller,areunderlower pressure,anddevelopmoreslowlythantheirarterialcounterparts.Most venousEDHsarecausedbyaskullfracturethatcrossesaduralvenoussinus andthereforeoccurintheposteriorfossaneartheskullbase (transverse/sigmoidsinus) (2-21)orthevertexofthebrain(superiorsagittal sinus).Incontrasttotheirarterialcounterparts,venousEDHscan"straddle" intracranialcompartments,crossingbothsuturesandlinesofdural attachment (2-22)andcompressingoroccludingtheadjacentvenous sinuses.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
VenousEDHscanbesubtleandeasilyoverlooked.Coronalandsagittal reformattedimagesarekeytothediagnosisanddelineationofthesevariant EDHs (2-23).SeveralanatomicsubtypesofvenousEDHs,eachwithdifferent treatmentimplicationsandprognosis,arerecognized.
https://t.me/ebookers
VertexEDH "Vertex"EDHsarerare.Usuallycausedbyalinearordiastaticfracturethat crossesthesuperiorsagittalsinus,theyoftenaccumulateoverhoursoreven dayswithslow,subtleonsetofsymptoms (2-24)."Vertex"hematomascan besubtleandareeasilyoverlookedunlesscoronalandsagittalreformatted imagesareobtained.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-23)(L)Coronal,(R)sagittalCTVshowsvenous EDHstraddlingthetentoriumſt,elevating thelefttransversesinusst.
(2-22)AutopsyshowsthatvenousEDHcaused bytransversesinusinjury"straddles"the tentoriumſt.(CourtesyR.Hewlett,MD.)
(2-21)
shows
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
Trauma https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
AnteriorTemporalEDH https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
AnteriortemporalEDHsareauniquesubgroupofhematomasthatoccurin theanteriortipofthemiddlecranialfossa.AnteriortemporalEDHsare causedeitherbyanisolatedfractureoftheadjacentgreatersphenoidwing orbyanisolatedzygomaticomaxillarycomplex("tripod")facialfracture.The sphenoparietalduralvenoussinusisinjuredasitcurvesmediallyalongthe undersurfaceofthelessersphenoidwing,extravasatingbloodintothe epiduralspace.Limitedanatomicallybythesphenotemporalsuturelaterally andtheorbitalfissuremedially,anteriortemporalEDHsremainstableinsize anddonotrequiresurgicalevacuation (2-25) (2-26)
ClivalEDH (2-24A)BoneCTina57ymanshowsalinearskull fractureſtthatcrossesthemidline.Noother abnormalitieswerepresent.
ClivalEDHsusuallydevelopafterahyperflexionorhyperextensioninjuryto theneckandarepossiblycausedbystrippingofthetectorialmembrane fromattachmentstotheclivus.Lesscommonly,theyhavebeenassociated withbasilarskullfracturesthatlaceratetheclivalduralvenousplexus.
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
ClivalEDHsmostoftenoccurinchildrenandpresentwithmultiplecranial neuropathies.Theabducensnerveisthemostcommonlyaffected,followed bytheglossopharyngealandhypoglossalnerves.Theyaretypicallylimitedin sizebythetightattachmentoftheduratothebasisphenoidandtectorial membrane (2-27)
VENOUSEPIDURALHEMATOMA
NotallEDHsarethesame!
• Prognosis,treatmentvary
Differentetiologiesindifferentanatomiclocations
• VenousEDHs=10%ofallEDHs
• Cancrosssutures,duralattachments
Skullfracturecrossesduralvenoussinus
○ Oftensubtle,easilyoverlooked
• Coronal,sagittalreformattedimageskeytodiagnosis
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
○ Usuallyaccumulateslowly
• Canbelimitedinsize;oftentreatedconservatively
• Subtypes
(2-24B)CTvenogramafterthepatient deterioratedshowsalargevenousEDH.The middleSSSiscompressedandthrombosedst.
•
VertexEDH
○ SSScanbelacerated,compressed,thrombosed
Skullfracturecrossessuperiorsagittalsinus(SSS)
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
○ Hematomaunderlowpressure,developsgradually
○ Slowonsetofsymptoms
(2-24C)CoronalscanshowsavertexvenousEDH crossingthemidline.ThethrombosedSSSst, corticalveinsaredisplacedinferiorlyſt.
https://t.me/ebookers
○
○ Maybecomelarge,causesignificantmasseffect
AnteriortemporalEDH
• Sphenoidwingorzygomaticomaxillaryfracture
○
○
○
○
○
Injuressphenoparietalvenoussinus
Hematomaaccumulatesatanteriortipofmiddlecranialfossa
Limitedanatomically(laterallybysphenotemporalsuture, mediallybyorbitalfissure)
Benignclinicalcourse
ClivalEDH
• Mostcommon=childwithneckinjury
○
○
○
○
○
Maycausemultiplecranialneuropathies(CNVImostcommon)
Hyperdensecollectionunderclivaldura
Limitedbytightattachmentofduratobasisphenoid,tectorial membrane
Usuallybenigncourse,resolvesspontaneously
ManagementofaclivalEDHisdictatedbyseverityandprogressionofthe neurologicdeficitsandstabilityoftheatlantoaxialjoint.Inpatientswith
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
PrimaryEffectsofCNSTrauma https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-25)Graphicdepicts benignanteriortemporal epiduralhematoma. Fractureſtdisruptsthe sphenoparietalsinus. Low-pressurevenousEDH isanatomicallylimited, mediallybytheorbital fissurestandlaterallyby thesphenotemporal suture.(2-26A)Axial NECTina33ymanwith headtraumashowsa biconvexanterior temporalacuteepidural hematoma. https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-26B)AxialboneCTin thesamecaseshowsa fracturethroughtheright greatersphenoidwingſt. (2-26C)CTvenogramin thesamecaseshowsa displaced,lacerated sphenoparietalsinuswith contrastextravasation ("spotsign")st.Notethe EDHislimitedmediallyby theorbitalfissure.The patientwastreated nonsurgically.TheEDH showednofurther enlargementandresolved completely.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
(2-27A)AxialCTAina childwithcraniovertebral junctiontraumashowsa smallclivalEDH.There wasnoevidencefor vascularinjury.(2-27B) SagittalCTAreformatted fromtheaxialsourcedate nicelydemonstratesthe clivalepiduralhematoma .
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-28)Graphicdepictscrescent-shapedacuteSDH stwithcontusionsand"contre-coup"injuries, diffuseaxonalinjuries.
minorcranialnerveinvolvement,theclinicalcourseisusuallybenign,and treatmentwithacervicalcollaristypical.
NECTscansshowahyperdensecollectionbetweentheclivusandtectorial membrane.SagittalMRofthecraniocervicaljunctionshowsthehematoma elevatingtheclivalduraandextendinginferiorlybetweenthebasisphenoid andtectorialmembraneanteriortothemedulla.
AcuteSubduralHematoma Acutesubduralhematomas(aSDHs)areoneoftheleadingcausesofdeath anddisabilityinpatientswithseveretraumaticbraininjury.SDHsaremuch morecommonthanEDHs.Mostdonotoccurasisolatedinjuries;thevast majorityofSDHsareassociatedwithtraumaticsubarachnoidhemorrhage (tSAH)aswellassignificantparenchymalinjuriessuchascorticalcontusions, brainlacerations,anddiffuseaxonalinjuries.
Terminology AnaSDHisacollectionofacutebloodproductsthatliesinorbetweenthe innerbordercelllayeroftheduraandthearachnoid (2-28)
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
Etiology TraumaisthemostcommoncauseofaSDH.Bothdirectblowstothehead andnonimpactinjuriesmayresultinformationofanaSDH.Tearingof bridgingcorticalveinsastheycrossthesubduralspacetoenteradural venoussinus(usuallythesuperiorsagittalsinus)isthemostcommon etiology.Corticalveinlacerationscanoccurwitheitheraskullfractureorthe suddenchangesinvelocityandbrainrotationthatoccurduringnonimpact closedheadinjury.
Bloodfromrupturedvesselsspreadsquicklythroughthepotentialspace betweentheduraandthearachnoid.LargeSDHsmayspreadoveranentire hemisphere,extendingintotheinterhemisphericfissureandalongthe tentorium.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-29)AcuteSDHspreadsoverlefthemisphere ſt,alongtentorium,intointerhemispheric fissurestbutdoesnotcrossmidline.
TearingofcorticalarteriesfromaskullfracturemayalsogiverisetoanaSDH. Thearachnoiditselfmayalsotear,creatingapathwayforleakageofCSFinto thesubduralspace,resultinginadmixtureofbothbloodandCSF.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-30)NECTscanshowsthatsmallSDHſtis easiertoseewithwider(R)comparedwith standard(L)windows.
LesscommoncausesofaSDHincludeaneurysmrupture,skull/duraarachnoidmetastasesfromvascularextracranialprimaryneoplasms,and spontaneoushemorrhageinpatientswithseverecoagulopathy.
Rarely,anacutespontaneousSDHofarterialoriginoccursinsomeone withoutanytraumatichistoryorvascularanomaly.Thesepatientsusually havesuddenseriousdisturbanceofconsciousnessandhaveapooroutcome unlesstheaSDHisrecognizedandtreatedpromptly.
Pathology GrossPathology.ThegrossappearanceofanaSDHisthatofasoft,purplish, "currantjelly"clotbeneathatensebulgingdura.Morethan95%are supratentorial.MostaSDHsspreaddiffuselyovertheaffectedhemisphere andarethereforetypicallycrescent-shaped.
ClinicalIssues Epidemiology.AnaSDHisthesecondmostcommonextraaxialhematoma, exceededonlybytSAH.AnaSDHisfoundin10-20%ofallpatientswithhead injuryandisobservedin30%ofautopsiedfatalinjuries.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
PrimaryEffectsofCNSTrauma Demographics.AnaSDHmayoccuratanyagefrominfancytotheelderly. Thereisnosexpredilection.
Presentation.Evenrelativelyminorheadtrauma,especiallyinelderly patientswhoareoftenanticoagulated,mayresultinanaSDH.Insuch patients,adefinitehistoryoftraumamaybelacking.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
Clinicalfindingsvaryfromnonetolossofconsciousnessandcoma.Most patientswithaSDHshavelowGCSsonadmission.Delayeddeterioration, especiallyinelderlyanticoagulatedpatients,iscommon.
NaturalHistory.AnaSDHmayremainstable,growslowly,orrapidly increaseinsize,causingmasseffectandsecondarybrainherniations. Prognosisvarieswithhematomathickness,midlineshift,andthepresenceof associatedparenchymalinjuries.AnaSDHthatisthickerthan2centimeters correlateswithpooroutcome(35-90%mortality).AnaSDHthatoccupies morethan10%ofthetotalavailableintracranialvolumeisusuallylethal.
TreatmentOptions.ThemajorityofpatientswithsmallSDHsareinitially treatedconservativelywithcloseclinicalobservationandfollow-upimaging. Approximately6-7%ofthesedemonstrateanincreaseinSDHsizeovertime andeventuallyrequiresurgicalintervention.
CoronalgraphicdepictsthinaSDHlayering alongthetentoriumandinferiorfalxcerebri.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
PatientswithlargerSDHs,alesionlocatedattheconvexity,alcoholabuse, andrepetitivefallsareatthegreatestriskfordeterioration.Surveillancewith follow-upCTscansisrecommendeduntiltheSDHresolvesoratleastupto5 weeksfollowingtheinitialtrauma.
Imaging GeneralFeatures.TheclassicfindingofanaSDHisasupratentorialcrescentshapedextraaxialcollectionthatdisplacesthegray-whitematterinterface medially.SDHsaretypicallymoreextensivethanEDHs,easilyspreading alongthefalx,tentorium,andaroundtheanteriorandmiddlefossafloors (2-29).SDHsmaycrosssuturelinesbutgenerallydonotcrossdural attachments.BilateralSDHsoccurin15%ofcases."Contre-coup"injuries suchascontusionofthecontralateralhemispherearecommon.
Bothstandardsofttissueandintermediate("subdural")windowsaswellas bonealgorithmreconstructionsshouldbeusedinalltraumapatients,as small,subtleaSDHscanbeobscuredbythedensityoftheoverlyingcalvaria (2-30).Coronalandsagittalreformattedimagesusingtheaxialsourcedate areespeciallyhelpfulinvisualizingsmall("smear")peritentorialand parafalcineaSDHs (2-31) (2-32)
CTFindings
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
NECT.Approximately60%ofaSDHsarehyperdenseonNECTscans (2-29). Mixed-attenuationlesionsarefoundin40%ofcases.Pocketsofhypodensity withinalargerhyperdenseaSDHusuallyindicaterapidbleeding (2-33) (234)."Dots"or"lines"ofCSFtrappedwithincompressed,displacedsulciare oftenseenunderlyinganaSDH.
MasseffectwithanaSDHiscommonandexpected.Subfalcineherniation shouldbeproportionatetothesizeofthesubduralcollection.However,if thedifferencebetweenthemidlineshiftandthicknessofthehematoma is3mmormore,thenmortalityisveryhigh.Thisdiscrepancyoccurswhen underlyingcerebraledemaistriggeredbythetraumaticevent.Early recognitionandaggressivetreatmentforpotentiallycatastrophicbrain swellingareessential (2-35)
Inothercases,especiallyinpatientswithrepeatedheadinjury,severebrain swellingwithunilateralhemispherevascularengorgementoccursvery
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers
(2-32B)Sagittalscansinthesamecaseshowthe rightperitentorialaSDH(top)withnormalleft sagittaldura(bottom)forcomparison.
(2-32A)ReformattedcoronalNECTscanusingthe axialsourcedateshowsasmallright peritentorialaSDHſt.
(2-31)
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
Trauma https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
quickly.Herethemasseffectisgreatlydisproportionatetothe sizeoftheSDH,whichmayberelativelysmall.
Occasionally,anaSDHisnearlyisodensewiththeunderlying cortex.Thisunusualappearanceisfoundinextremelyanemic patients(Hgbunder8-10g/dL) (2-36)andsometimesoccurs inpatientswithcoagulopathy.Inrarecases,CSFleakage throughatornarachnoidmaymixwith—anddilute—the acutebloodthatcollectsinthesubduralspace.
CECT.CECTscansarehelpfulindetectingsmallisodense aSDHs.Thenormallyenhancingcorticalveinsaredisplaced inwardbytheextraaxialfluidcollection.
PerfusionCT.CTorxenonperfusionscansmaydemonstrate decreasedcerebralbloodflow(CBF)andlowperfusion pressure,whichisoneofthereasonsforthehighmortality rateofpatientswithaSDHs.Thecortexunderlyingan evacuatedaSDHmayshowhyperemicchangeswithelevated
rCBFvalues.Persistinghyperemiahasbeenassociatedwith pooroutcome.
MRFindings.MRscansarerarelyobtainedinacutelybraininjuredpatients.Insuchcases,aSDHsappearisointenseon T1WIandhypointenseonT2WI.SignalintensityonFLAIR scansisusuallyiso-tohyperintensecomparedwithCSFbut hypointensecomparedwiththeadjacentbrain.aSDHsare hypointenseonT2*scans.
DWIshowsheterogeneoussignalwithinthehematomabut mayshowpatchyfociofrestricteddiffusioninthecortex underlyingtheaSDH.
Angiography.CTAmaybeusefulinvisualizingacorticalvessel thatisactivelybleedingintothesubduralspace.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-33)(L)InitialNECTin ananticoagulatedmale patientshowsasmall mixed-densitySDH.(R) Scan6hourslatershows expanding,actively bleedingaSDH.(2-34) NECTscanshowsa55y manwithanactively hemorrhagingaSDH. Someclottedbloodis presentſt,butmuchof thehematomaconsistsof isodenseunclotted hemorrhage.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
(2-35)NECTshowsa mixed-density12-mm aSDHwitha disproportionatelylarge subfalcineherniationof thelateralventricles(17 mm),indicatingthat diffuseholohemispheric brainswellingispresent. Subfalcineherniation≥3 mmportendsapoor prognosis.(2-36)NECT scaninaveryanemic patientshowsanisodense aSDH.TheaSDHis almostexactlythesame densityastheunderlying cortex.Thegray-white interfaceisdisplaced inward.
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers https://t.me/ebookers
https://t.me/ebookers
https://t.me/ebookers https://t.me/ebookers