https://ebookmass.com/product/orthodontics-for-thecraniofacial-surgery-patient-1st-edition-michael-r-
Instant digital products (PDF, ePub, MOBI) ready for you
Download now and discover formats that fit your needs...
Orthodontics for the Oral and Maxillofacial Surgery Patient 1st Edition Michael R.
Markiewicz
https://ebookmass.com/product/orthodontics-for-the-oral-andmaxillofacial-surgery-patient-1st-edition-michael-r-markiewicz/
ebookmass.com
Plastic Surgery-Craniofacial, Head and Neck SurgeryPediatric Plastic Surgery 4th Edition Geoffrey C. Gurtner
https://ebookmass.com/product/plastic-surgery-craniofacial-head-andneck-surgery-pediatric-plastic-surgery-4th-edition-geoffrey-c-gurtner/
ebookmass.com
Alexander’s Care of the Patient in Surgery (Alexanders Care of the Patient in Surgery) 16th Edition – Ebook PDF Version
https://ebookmass.com/product/alexanders-care-of-the-patient-insurgery-alexanders-care-of-the-patient-in-surgery-16th-edition-ebookpdf-version/ ebookmass.com
Cobertu2019s Manual of Drug Safety and Pharmacovigilance 3rd Edition, (Ebook PDF)
https://ebookmass.com/product/coberts-manual-of-drug-safety-andpharmacovigilance-3rd-edition-ebook-pdf/ ebookmass.com
Manual of Cardiovascular Medicine 5th Edition, (Ebook PDF)
https://ebookmass.com/product/manual-of-cardiovascular-medicine-5thedition-ebook-pdf/ ebookmass.com
The Theory and Practice of Change Management, 6th Edition
John Hayes
https://ebookmass.com/product/the-theory-and-practice-of-changemanagement-6th-edition-john-hayes/ ebookmass.com
Reading the Red Book Sanford L. Drob
https://ebookmass.com/product/reading-the-red-book-sanford-l-drob/
ebookmass.com
Membrane-Based Separations in Metallurgy: Principles and Applications 1st Edition Lan Ying Jiang
https://ebookmass.com/product/membrane-based-separations-inmetallurgy-principles-and-applications-1st-edition-lan-ying-jiang/ ebookmass.com
Renegade Anna Schmidt
https://ebookmass.com/product/renegade-anna-schmidt-2/ ebookmass.com
https://ebookmass.com/product/diversity-intelligence-how-to-create-aculture-of-inclusion-for-your-business-1st-edition-heidi-r-andersen/
ebookmass.com
ELSEVIER
1600JohnF.KennedyBoulevard Suite1800 Philadelphia,Pennsylvania,19103-2899
http://www.oralmaxsurgery.theclinics.com
ORALANDMAXILLOFACIALSURGERYCLINICSOFNORTHAMERICAVolume32,Number2 May2020ISSN1042-3699,ISBN-13:978-0-323-69492-6
Editor:JohnVassallo; j.vassallo@elsevier.com
DevelopmentalEditor:LauraFisher
ª 2020ElsevierInc.Allrightsreserved.
ThisperiodicalandtheindividualcontributionscontainedinitareprotectedundercopyrightbyElsevier,andthefollowingterms andconditionsapplytotheiruse:
Photocopying
Singlephotocopiesofsinglearticlesmaybemadeforpersonaluseasallowedbynationalcopyrightlaws.Permissionofthe Publisherandpaymentofafeeisrequiredforallotherphotocopying,includingmultipleorsystematiccopying,copyingfor advertisingorpromotionalpurposes,resale,andallformsofdocumentdelivery.Specialratesareavailableforeducational institutionsthatwishtomakephotocopiesfornon-profiteducationalclassroomuse.Forinformationonhowtoseekpermission visit www.elsevier.com/permissions orcall:(144)1865843830(UK)/(11)2152393804(USA).
DerivativeWorks Subscribersmayreproducetablesofcontentsorpreparelistsofarticlesincludingabstractsforinternalcirculationwithintheir institutions.PermissionofthePublisherisrequiredforresaleordistributionoutsidetheinstitution.PermissionofthePublisheris requiredforallotherderivativeworks,includingcompilationsandtranslations(pleaseconsult www.elsevier.com/permissions).
ElectronicStorageorUsage PermissionofthePublisherisrequiredtostoreoruseelectronicallyanymaterialcontainedinthisperiodical,includinganyarticleor partofanarticle(pleaseconsult www.elsevier.com/permissions).Exceptasoutlinedabove,nopartofthispublicationmaybereproduced,storedinaretrievalsystemortransmittedinanyformorbyanymeans,electronic,mechanical,photocopying,recording orotherwise,withoutpriorwrittenpermissionofthePublisher.
Notice
NoresponsibilityisassumedbythePublisherforanyinjuryand/ordamagetopersonsorpropertyasamatterofproducts liability,negligenceorotherwise,orfromanyuseoroperationofanymethods,products,instructionsorideascontainedin thematerialherein.Becauseofrapidadvancesinthemedicalsciences,inparticular,independentverificationofdiagnoses anddrugdosagesshouldbemade.
Althoughalladvertisingmaterialisexpectedtoconformtoethical(medical)standards,inclusioninthispublicationdoesnot constituteaguaranteeorendorsementofthequalityorvalueofsuchproductoroftheclaimsmadeofitbyitsmanufacturer. OralandMaxillofacialSurgeryClinicsofNorthAmerica (ISSN1042-3699)ispublishedquarterlybyElsevierInc.,360Park AvenueSouth,NewYork,NY10010-1710.MonthsofissueareFebruary,May,August,andNovember.BusinessandEditorial Offices:1600JohnF.KennedyBlvd.,Suite1800,Philadelphia,PA19103-2899.PeriodicalspostagepaidatNewYork,NYand additionalmailingoffices.Subscriptionpricesare$401.00peryearforUSindividuals,$756.00peryearforUSinstitutions, $100.00peryearforUSstudents/residents,$474.00peryearforCanadianindividuals,$906.00peryearforCanadian institutions,$100.00peryearforCanadianstudents/residents,$525.00peryearforinternationalindividuals,$906.00per yearforinternationalinstitutionsand$235.00peryearforinternationalstudents/residents.Toreceivestudent/residentrate, ordersmustbeaccompaniedbynameoraffiliatedinstitution,dateofterm,andthe signature ofprogram/residencycoordinator oninstitutionletterhead.Orderswillbebilledatindividualrateuntilproofofstatusisreceived.Foreignairspeeddeliveryisincludedinall Clinics subscriptionprices.Allpricesaresubjecttochangewithoutnotice. POSTMASTER: Sendaddresschanges to OralandMaxillofacialSurgeryClinicsofNorthAmerica, ElsevierPeriodicals CustomerService,11830WestlineIndustrial Drive,St.Louis,MO63146.Tel:1-800-654-2452(U.S.andCanada);314-447-8871(outsideU.S.andCanada).Fax:314447-8029.E-mail: journalscustomerservice-usa@elsevier.com (forprintsupport); journalsonlinesupport-usa@elsevier. com (foronlinesupport)
Reprints. Forcopiesof100ormore,ofarticlesinthispublication,pleasecontacttheCommercialReprintsDepartment,Elsevier Inc.,360ParkAvenueSouth,NewYork,NY10010-1710.Tel.:212-633-3874;Fax:212-633-3820;Email: reprints@elsevier.com
OralandMaxillofacialSurgeryClinicsofNorthAmerica iscoveredin MEDLINE/PubMed (IndexMedicus), ScienceCitationIndex Expanded(SciSearch ), JournalCitationReports/ScienceEdition,and CurrentContents /ClinicalMedicine PrintedintheUnitedStatesofAmerica.
Contributors CONSULTINGEDITOR RUIP.FERNANDES,MD,DMD,FACS, FRCS(Ed)
ClinicalProfessorandChief,DivisionofHead andNeckSurgery,ProgramDirector,Head andNeckOncologicSurgeryand MicrovascularReconstructionFellowship, DepartmentsofOralandMaxillofacialSurgery, Neurosurgery,andOrthopaedicSurgeryand Rehabilitation,UniversityofFloridaHealth ScienceCenter,UniversityofFloridaCollegeof Medicine,Jacksonville,Florida,USA
EDITORS
MICHAELR.MARKIEWICZ,DDSMPH,MD, FACS
ProfessorandChair,DepartmentofOraland MaxillofacialSurgery,WilliamM.Feagans EndowedChair,AssociateDeanforHospital Affairs,SchoolofDentalMedicine,Clinical Professor,DepartmentofNeurosurgery, DivisionofPediatricSurgery,Departmentof Surgery,JacobsSchoolofMedicineand BiomedicalSciences,UniversityatBuffalo,CoDirector,CraniofacialCenterofWesternNew York,JohnR.OisheiChildren’sHospital, Buffalo,NewYork
AUTHORS
VEERASATHPURUSHALLAREDDY,BDS, PhD
BrodieCraniofacialEndowedChair,Professor andHead,DepartmentofOrthodontics, CollegeofDentistry,TheUniversityofIllinoisat Chicago,Chicago,Illinois
SHAYNAAZOULAY-AVINOAM,DDS Resident,DepartmentofOrthodontics,College ofDentistry,TheUniversityofIllinoisat Chicago,Chicago,Illinois
VEERASATHPURUSHALLAREDDY,BDS, PhD
BrodieCraniofacialEndowedChair,Professor andHead,DepartmentofOrthodontics, CollegeofDentistry,TheUniversityofIllinoisat Chicago,Chicago,Illinois
MICHAELMILORO,DMD,MD,FACS ProfessorandHead,DepartmentofOraland MaxillofacialSurgery,CollegeofDentistry,The UniversityofIllinoisatChicago,Chicago, Illinois
RICHARDBRUUN,DDS
CraniofacialOrthodontist,BostonChildren’s Hospital,CleftLip/PalateandCraniofacial Teams,AssistantProfessorofDevelopmental Biology,Part-Time,HarvardSchoolofDental Medicine,SeniorAssociate,Departmentof Dentistry,BostonChildren’sHospital,Boston, Massachusetts,USA
JENNIFERCAPLIN,DMD,MS AssociateDirectorofPostGraduate Orthodontics,AssistantProfessor,Department
ofOrthodontics,CollegeofDentistry,The UniversityofIllinoisatChicago,Chicago, Illinois
STEPHANIEJ.DREW,DMD,FACS
AssociateProfessor,DepartmentofSurgery, DivisionofOralandMaxillofacialSurgery, EmoryUniversitySchoolofMedicine,Atlanta, Georgia
SEANP.EDWARDS,DDS,MD
Professor,DepartmentofOraland MaxillofacialSurgery,UniversityofMichigan, MottChildren’sHospital,AnnArbor, Michigan
AUSTINGAAL,DDS
FormerCleftandCraniofacialFellow,The UniversityofOklahoma,CollegeofDentistry, DepartmentofOralandMaxillofacialSurgery, OklahomaUniversityChildren’sHospital,JW KeysCleftandCraniofacialClinic,Oklahoma City,Oklahoma,USA;CascadiaOMS, Kirkland,Washington,USA
GHALIE.GHALI,DDS,MD,FACS,FRCS(Ed)
JackW.GambleProfessorandChairman, DepartmentofOralandMaxillofacialSurgery/ HeadandNeckSurgery,Chancellor,Louisiana StateUniversityHealthSciencesCenter, Shreveport,Louisiana
JEFFREYHAMMOUDEH,DDS,MD
AssociateChiefPlasticandMaxillofacial Surgery,AssociateProfessor,University ofSouthernCalifornia,DivisionofOral andMaxillofacialSurgery,Departmentof PlasticandReconstructiveSurgery, Children’sHospitalLosAngeles,LosAngeles, California
RICHARDA.HOPPER,MD,MS
Chief,PediatricPlasticandCraniofacial Surgery,MarlysC.LarsonProfessorof CraniofacialSurgery,UniversityofWashington SchoolofMedicine,CraniofacialCenter, DivisionofPlasticandCraniofacialSurgery, SeattleChildren’sHospital,Seattle, Washington
HITESHKAPADIA,DDS,PhD
Chief,DivisionofCraniofacialOrthodontics, SeattleChildren’sHospital,Craniofacial Center,Seattle,Washington
JAMESMACLAINE,BDS
ClinicalInstructor,Departmentof DevelopmentalBiology,BostonChildren’s Hospital,HarvardSchoolofDentalMedicine, Boston,Massachusetts
ASHLEYE.MANLOVE,DMD,MD
ClinicalInstructor,ProgramDirector,Director ofCarleCleftandCraniofacialTeam, DepartmentofOralandMaxillofacialSurgery, CarleFoundationHospital,Urbana, Illinois
MICHAELR.MARKIEWICZ,DDSMPH,MD, FACS
ProfessorandChair,DepartmentofOraland MaxillofacialSurgery,WilliamM.Feagans EndowedChair,AssociateDeanforHospital Affairs,SchoolofDentalMedicine,Clinical Professor,DepartmentofNeurosurgery, DivisionofPediatricSurgery,Departmentof Surgery,JacobsSchoolofMedicineand BiomedicalSciences,UniversityatBuffalo, Co-Director,CraniofacialCenterofWestern NewYork,JohnR.OisheiChildren’sHospital, Buffalo,NewYork
MARKA.MILLER,MD,DMD
AssistantProfessor,DepartmentsofOraland MaxillofacialSurgery,Neurosurgery,and Pediatrics,UTHealthSanAntonio,San Antonio,Texas
DOUGLASOLSON,DMD,MS
CraniofacialCenterofWesternNewYork, OisheiChildren’sOutpatientCenter,Buffalo, NewYork
BONNIEL.PADWA,DMD,MD
OralSurgeon-in-Chief,SectionofOraland MaxillofacialSurgery,AssociateProfessor, DepartmentofPlasticandOralSurgery, HarvardMedicalSchool,Boston, Massachusetts
VICTORIAPALERMO,MD,DDS
FloridaCraniofacialInstitute,Tampa, Florida
YASSMINPARSAEI,DMD
OrthodonticResident,Divisionof Orthodontics,DepartmentofCraniofacial Sciences,UniversityofConnecticut, Farmington,Connecticut
STAVANY.PATEL,DDS,MD
AssistantProfessorandResidencyProgram Director,DepartmentofOralandMaxillofacial Surgery/HeadandNeckSurgery,Louisiana StateUniversityHealthSciencesCenter, Shreveport,Louisiana
JEFFREYC.POSNICK,DMD,MD
ProfessorEmeritus,PlasticandReconstructive SurgeryandPediatrics,Georgetown University,Washington,DC;Professorof Orthodontics,UniversityofMaryland, BaltimoreCollegeofDentalSurgery, Baltimore,Maryland;ProfessorofOraland MaxillofacialSurgery,HowardUniversity CollegeofDentistry,Washington,DC
CORYM.RESNICK,DMD,MD
AttendingPhysician,OralandMaxillofacial SurgeryProgram,AssistantProfessor, DepartmentofPlasticandOralSurgery, HarvardMedicalSchool,Boston, Massachusetts
PATRICALDE,MD,DDS
Director,FloridaCraniofacialInstitute,St. Joseph’sCleftandCraniofacialCenter, Tampa,Florida
GERARDOROMEO,DDS,MD,MBA
DivisionChiefandProgramDirector,Oral andMaxillofacialSurgery,Departmentsof DentalMedicine,andPediatrics,Northwell Health,MedicalCo-Director,Hagedorn CleftandCraniofacialTeamatCohen Children’sMedicalCenter,Assistant Professor,DonaldandBarbaraZuckerSchool ofMedicineatHofstra/Northwell,LongIsland JewishMedicalCenter,NewHydePark,New York
ELIZABETHROSS,DDS
ClinicalInstructor,Departmentof DevelopmentalBiology,BostonChildren’s Hospital,HarvardSchoolofDentalMedicine, Boston,Massachusetts
RAMONRUIZ,DMD,MD
ArnoldPalmerHospitalforChildren,Orlando, Florida
CURTISD.SCHMIDT,DDS
CleftandCraniofacialSurgeryFellow, DepartmentofOralandMaxillofacialSurgery/
HeadandNeckSurgery,LouisianaState UniversityHealthSciencesCenter,Shreveport, Louisiana
STEPHENSHUSTERMAN,DMD
ClinicalAssociateProfessor,HarvardSchoolof DentalMedicine,Dentist-in-Chief,Emeritus, BostonChildren’sHospital,Boston, Massachusetts
KEVINS.SMITH,DDS,FACS,FACD ProfessorandResident/FellowshipProgram Director,TheUniversityofOklahoma,College ofDentistry,DepartmentofOraland MaxillofacialSurgery,Director,JWKeysCleft andCraniofacialClinic,Children’sHospitalof Oklahoma,UniversityofTulsa,MKChapman CleftandCraniofacialClinic,ProfilesOral FacialSurgeryExperts,OklahomaCity, Oklahoma,USA
DEREKSTEINBACHER,MD,DMD,FACS ChiefofOralandMaxillofacialSurgery, DirectorofCraniofacialSurgery,Associate Professor,SectionofPlasticand ReconstructiveSurgery,YaleSchoolof Medicine,NewHaven,Connecticut
SRINIVASM.SUSARLA,DMD,MD,MPH AssistantProfessorofSurgery(Plastic), UniversityofWashingtonSchoolofMedicine, AssistantProfessorofOral-Maxillofacial Surgery,UniversityofWashingtonSchoolof Dentistry,CraniofacialCenter,Divisionsof CraniofacialandPlasticSurgeryand Oral-MaxillofacialSurgery,Seattle Children’sHospital,Seattle, Washington
TIMOTHYJ.TREMONT,DMD,MS ProfessorandChairman,Departmentof Orthodontics,MedicalUniversityofSouth Carolina,Charleston,SouthCarolina
RAYMONDTSE,MD
SeattleChildren’sHospital,Craniofacial Center,Seattle,Washington
MARKURATA,DDS,MD,FACS
AudreySkirballKenisEndowedChairand Chief,DivisionofPlasticSurgeryand reconstructiveMaxillofacialSurgery,Chair
DivisionofOralandMaxillofacialSurgery, OstrowSchoolofDentistry,Universityof SouthernCalifornia,Children’sHospitalLos Angeles,LosAngeles,California
FLAVIOURIBE,DDS,MDentSc
CharlesBurstoneProfessor,ProgramDirector andInterimChair,DivisionofOrthodontics, DepartmentofCraniofacialSciences, UniversityofConnecticut,Farmington, Connecticut
SHANKARRENGASAMYVENUGOPALAN, DDS,DMSc,CAGE(Ortho),PhD DepartmentofOrthodontics,Associate Professor,TheUniversityofIowa,Collegeof DentistryandDentalClinics,IowaCity, Iowa
JENNIFERE.WOERNER,DMD,MD,FACS AssistantProfessorandFellowshipDirector, CleftandCraniofacialSurgery,Departmentof OralandMaxillofacialSurgery/HeadandNeck Surgery,LouisianaStateUniversityHealth
SciencesCenter,Shreveport, Louisiana
SUMITYADAV,MDS,PhD AssociateProfessor,Departmentof CraniofacialSciences,Universityof ConnecticutSchoolofDentalMedicine, Farmington,Connecticut
DAVIDYATES,DMD,MD,FACS ProgramDirector,EPCHCleftandCraniofacial Fellowship,DivisionChiefofCranialandFacial Surgery,ElPasoChildren’sHospital,Clinical AssistantProfessorofSurgery,TexasTech UniversityHealthSciencesCenterElPaso,Paul L.FosterSchoolofMedicine,Partner,High DesertOral&FacialSurgery,ElPaso,Texas
STEPHENYEN,DMD,PhD DirectorofFellowshipinCraniofacialand SpecialNeedsOrthodontics,Divisionof Dentistry,Children’sHospitalLosAngeles, CenterforCraniofacialMolecularBiology, UniversityofSouthernCalifornia,LosAngeles, California
Contents Preface:OrthodonticsfortheCraniofacialSurgeryPatient
MichaelR.Markiewicz,VeerasathpurushAllareddy,andMichaelMiloro
CraniofacialGrowth:CurrentTheoriesandInfluenceonManagement
AshleyE.Manlove,GerardoRomeo,andShankarRengasamyVenugopalan
Craniofacialdevelopmentisahighlycoordinatedprocessunderatightgeneticcontrolandenvironmentalinfluence.Understandingthecoreconceptsofgrowthand developmentofthecraniofacialskeletonandtheimpactoftreatmentongrowthpotentialisvitaltosuccessfulpatientmanagement.Tomaximizeoutcomesandminimizeiatrogenicconsequences,propersequencingandtimingofinterventionsare critical.Thedevelopmentofthecraniofacialskeletonoccursasaresultofa sequenceofnormaldevelopmentalevents:braingrowthanddevelopment,optic pathwaydevelopment,speechandswallowingdevelopment,airwayandpharyngealdevelopment,muscledevelopment,andtoothdevelopmentanderuption.
xiii
167
AnOverviewofTimelineofInterventionsintheContinuumofCleftLipandPalateCare177
DavidYates,VeerasathpurushAllareddy,JenniferCaplin,SumitYadav, andMichaelR.Markiewicz
Thisarticleprovidesanoverviewoftimelineofinterventionsandthecriticalrole differentprovidershaveinthecontinuumofcleftlipandpalatecare.Theearliest interventionisthepresurgicalinfantorthopedictreatment,whichisinitiatedinthe firstfewweeksoflife.Thisisfollowedbyseveralinterventionsdoneinaphased manner.Theseinclude:liprepair,palaterepair,velopharyngealsurgery,maxillary expansion,maxillarybonegrafting,limitedphaseoforthodontictreatment,comprehensivephaseoforthodontictreatment(with/withoutorthognathicsurgery),and restorativedentistry.
DentofacialOrthopedicsfortheCleftPatient:TheLathamApproach VeerasathpurushAllareddy,StephenShusterman,ElizabethRoss,VictoriaPalermo, andPatRicalde
Presurgicalinfantdentofacialorthopedictreatment(PSIOT)isaprocessbywhich cleftmaxillaryandsofttissuesegmentscanbemovedbeforesurgicalrepairof lip.OneofthePSIOTapproachesusedisthefixedPSIOTusingLathamappliances. Inthisarticle,theauthorsprovideanoverviewofthisapproachandthestep-by-step processofplacingtheseappliancesintraorally.Prospectiverandomizedclinical studiesarenecessarytodefinitivelyanswerconcernssurroundingthelong-termeffectsofPSIOT.
NasoalveolarMoldingforUnilateralandBilateralCleftLipRepair HiteshKapadia,DouglasOlson,RaymondTse,andSrinivasM.Susarla
Nasoalveolarmolding(NAM)isapowerfultoolinthetreatmentofpatientswithunilateralorbilateralcleftlipandpalate.TheprimarygoalofNAMistoimprovealignmentofcriticalanatomicelementsbeforesurgicalrepairoftheunilateralorbilateral cleftlip.Modificationsofthepositionofthealveolarsegmentsandtheirassociated
187
197
lipelements,thelowerlateralcartilages,andthecolumellaachievedwithNAMare helpfulforcreatingasuitableplatformfortension-freeliprepair.
OrthodonticPreparationforSecondaryAlveolarBoneGraftinginPatientswithComplete CleftLipandPalate
VeerasathpurushAllareddy,RichardBruun,JamesMacLaine,MichaelR.Markiewicz, RamonRuiz,andMarkA.Miller
Thisarticleprovidesanoverviewoftheorthodonticpreparationpriortosecondary alveolarbonegraftingofalveolardefectsinthosewithcompletecleftlipandpalate. Useofconebeamcomputedtomographyindiagnosisandtreatmentplanningfor addressingalveolarclefts,therationaleformaxillaryexpansionpriortoalveolar bonegrafting,keystepsindifferentialmaxillaryexpansion,potentialadverseeffects, andoutcomesassociatedwithmaxillaryexpansionareprovidedinthisoverview.
ObturationandTissueTransferforLargeCraniofacialDefects
CurtisD.Schmidt,StavanY.Patel,JenniferE.Woerner,andGhaliE.Ghali
Reconstructionoflargecraniofacialdefectsrequiresseveralfactorstobeconsideredbeforedecidingonthebestreconstructiveoption.Thisarticlediscusses variousfactorstakenintoconsiderationwhendecidingonwhichreconstructiveoptionisidealforagivenpatientanddefect.Forlargecraniofacialdefects,reconstructionusingtissuetransferisconsideredpreferentiallyoverobturation,althoughin selectdefectsobturationusingatraditionaltooth-orimplant-borneprostheticobturatorcanbeconsideredaviableoption.
AnOverviewofCraniosynostosisCraniofacialSyndromesforCombinedOrthodonticand SurgicalManagement
ShaynaAzoulay-Avinoam,RichardBruun,JamesMacLaine,VeerasathpurushAllareddy, CoryM.Resnick,andBonnieL.Padwa
Thisarticleprovidesanoverviewofepidemiology,genetics,andcommonorofacial featuresofthosewithcraniosynostosis.Patientswithcraniosynostosisrequire severalsurgicalproceduresalongwithcontinuumofcare.Theearliestsurgicalinterventionsaredoneduringthefirstfewyearsoflifetorelievethefusedsutures.Midfaceadvancement,limitedphaseoforthodontictreatment,andcombined orthodontics/orthognathicsurgerytreatmentareusuallyrequiredduringlateryears. Thisarticlepresentsseveralexamplesofcaseswithoutcomesassociatedwith theseprocedures.
OrthodonticConsiderationsforCleftOrthognathicSurgery StephenYen,JeffreyHammoudeh,SeanP.Edwards,andMarkUrata
Preparationandplanningfororthognathicsurgeryinlateadolescencedepends onthecomplexityofunresolvedproblemswithwhichthepatientpresents. Differentstrategiesarepresentedtoaddresstheseunresolvedproblemsinthe adultpatientwithcleftlipandpalate.DifferentsurgicalandorthodontictreatmentsarepresentedtocorrecttheclassIIImalocclusioninpatientswithcleft lipandpalateinrangesthatareanalogoustotheenvelopeofdiscrepancy.For complexcases,theprinciplesofachievability,stability,andestheticsshould guidethedecision-makingprocessforplanningthepreparationfororthognathic surgery.
205
219
233
249
StephanieJ.DrewandHiteshKapadia
Thecleftpatientmaypresentwithsignificantmaxillarydeficiencyrequiringmaxillaryadvancementtoestablishbalancedfacialformandfunction.Oftenthese skeletaladvancementsrequiremovementofthemaxillaofmorethan10mm. Thecleftpatientposesspecialchallengesbecauseofdifficultyofmobilizingtissuesonamultiplyoperatedmaxilla,aswellaslong-termstability.Distractionosteogenesisisatechniquethatmaybeappliedtohelpmovethemaxillaovera longdistanceandslowlyexpandthesofttissues.Adiscussionoftheorthodontic andsurgicalconsiderationswhenplanningandexecutingthetechniqueis presented.
OrthodonticandSurgicalPrinciplesforDistractionOsteogenesisinChildrenwithPierreRobinSequence
StephenYen,AustinGaal,andKevinSmith
PatientswithPierre-Robinsequencerecalcitranttononsurgicalinterventionhave historicallyrequiredtracheostomy.Mandibulardistractionprovidesapredictable alternativetreatmenttotracheostomyforimprovingairway.Orthodonticperioperativeinterventionsshouldbeconsidered,includingovercorrection,placementoftemporaryanchoragedevices,elastics,andmoldingtheregenerate.Mandibular distractioncanbetechnicallydifficultandmaycausecomplications.Performed correctly,mandibulardistractionprovidespatientswithabetterqualityoflifethan tracheostomy.
OrthodonticsforUnilateralandBilateralCleftDeformities
YassminParsaei,FlavioUribe,andDerekSteinbacher
Orthodontictreatmentofpatientswithunilateralandbilateralcleftpalaterequiresan extensiveinterdisciplinaryapproachtoachieveoptimalfunctionalandestheticrehabilitation.Interventionisdividedinto3mainstages:earlymixed,latemixed,andpermanentdentition.Treatmentmodalitiescanvaryaccordingtodevelopmentalstage, severityofcleft,andpresenceofotherdentofacialabnormalities.Thisarticledescribestheuseandefficacyofdifferentorthodontic,orthopedic,andsurgicalapproachesateachdevelopmentalstageofunilateralandbilateralclefts,whereby theorthodontistplaysapivotalroleinthedifferentphasesofgrowthanddevelopmentofthecleftlipandthepatient.
Surgical-OrthodonticConsiderationsinSubcranialandFrontofacialDistraction RichardA.Hopper,HiteshKapadia,andSrinivasM.Susarla
Subcranialandfrontofacialdistractionosteogenesishaveemergedaspowerful toolsformanagementofhypoplasiainvo lvingtheuppertwo-thirdsoftheface. Theprimarygoalofsubcranialorfrontofaci aldistractionistoimprovetheorientationoftheupperfaceandmidfacestru ctures(frontalbone,orbitozygomatic complex,maxilla,nasalcomplex)relativetothecranialbase,globes,and mandible.Thevarioustechniquesuseda retailoredformanagementofspecific phenotypicdifferencesinfacialpositi onandmayincludesegmentalosteotomies,differentialvectors,orsynchronousmaxillo mandibularrotation.
297
309
SelectedOrthodonticPrinciplesforManagementofCranio-MaxillofacialDeformities321
TimothyJ.TremontandJeffreyC.Posnick
Anunderstandingoffundamentalorthodonticprinciplesinvolvingdiagnosis,treatmentplanning,andclinicalstrategiesisessentialforachievingsuccessfuloutcomes inthetreatmentofcraniofacialpatients,particularlycleftlip/palate.Thisarticlefocuseson:customizingamandibulardentalarchformusingtheWALAridge;accuratelydiagnosingthemaxillaryskeletaltransversedimension(cusptocusp/fossato fossa);coordinatingtheupperdentalarchwiththelower;usingasmilingprofileand glabellaverticaltoassessanteroposteriorjawposition;andlevelingthemandibular curveofSpeewhileconsideringthelowerone-thirdoftheface.Theseconceptsinfluencetreatmentoutcomestotheextenttheyareused.
ORALANDMAXILLOFACIALSURGERY CLINICSOFNORTHAMERICA FORTHCOMINGISSUES August2020
GlobalOralandMaxillofacialSurgery
ShahidR.Aziz,JoseM.Marchena,andStevenM. Roser, Editors
November2020
DentoalveolarSurgery SomsakSittitavornwong, Editor
February2021
ModernRhinoplastyandtheManagement ofitsComplications
ShahrokhC.Bagheri,HusainAliKhan,and BehnamBohluli, Editors
RECENTISSUES February2020
OrthodonticsfortheOralandMaxillofacial SurgeryPatient
MichaelR.Markiewicz,Veerasathpurush Allareddy,andMichaelMiloro, Editors
November2019
AdvancesinOralandMaxillofacialSurgery
JoseM.Marchena,JonathanW.Shum,and JonathonS.Jundt, Editors
August2019
DentalImplants,PartII:Computer Technology
OleT.Jensen, Editor
SERIESOFRELATEDINTEREST AtlasoftheOralandMaxillofacialSurgeryClinics www.oralmaxsurgeryatlas.theclinics.com
DentalClinics www.dental.theclinics.com
THECLINICSARENOWAVAILABLEONLINE!
Accessyoursubscriptionat: www.theclinics.com
Preface Orthodonticsforthe CraniofacialSurgeryPatient MichaelR.Markiewicz,DDS, MPH,MD,FACS
BDS,PhD
Editors
Thisissueofthe OralandMaxillofacialSurgery ClinicsofNorthAmerica servesasthesecondof a2-partseriesthatemphasizesthecriticalroleof theorthodontistinthemanagementofthecraniofacialsurgerypatient(issue2).Thefirstissue,“OrthodonticsfortheOralandMaxillofacialSurgery Patient”(issue1),reviewed,indetail,common collaborativeproceduresperformedbytheorthodontistandoralandmaxillofacialsurgeonas viewedfromthejointandintegratedperspectives ofbothspecialties.Thisissue,“Orthodonticsfor theCraniofacialSurgeryPatient,”highlightsthe criticalrolethattheorthodontistplaysinthesurgicalproceduresperformedforthecraniofacial patient.
Theimpetusforthisworkwasinitiatedwiththe goalofdevelopingacomprehensivereference textdescribingthemostcommonlyperformed proceduresinvolvingcraniofacialsurgeonsand craniofacialorthodontistsbyexperiencedauthors inbothspecialties.Theeditorsfeelthatthiswas anoften-overlookedareaintheexistingliterature. Toaddressthisgoal,asinthefirstissueinthisseries,weagainfeelthatwehavebeensofortunate torecruitsomeofthemostnotablecraniofacial surgeonsandcraniofacialorthodontistsinthe worldtowriteontopicsandsharetheir
experiencesforwhichtheyareconsideredauthoritativeexperts.Weareveryproudofthistextand sogratefultothosewhohavecontributedtomakingthisauniquecollaborationofpractitioners.
Asinthefirstissueofthisseries,wechargedauthors(oralandmaxillofacialsurgeonsandorthodontists)withthetaskofcollaborationbased upontheirexpertise,regardlessoftheirinstitution orpriorinteractionsorbiases.Asignificantchallengeinachievingthisgoal,andmajordifficulty fortheseauthors,isthattheymaynothaveever meteachother.Yettheywerestillabletowork togetherandproducequalityarticlesforthistext. Alltheauthors,regardlessofinstitutionalandpreconceivedbiases,agreedtojoinusonthismonumentalendeavor.Eachoftheauthorsproduceda thoughtfulandauthoritativearticleforthetopicfor whichtheywereassigned,andwe,theeditors,are sothankfulforthis.
Finally,thesepatientsdescribedinthisissueare sospecialtous,andwearefortunateenoughto beabletotreatthemandmakemeaningful changesintheirlives.Theyareunique,complex, challenging,andperplexing,oftenrequiringusto “thinkoutsidethebox.”Perhapsmostimportantly, treatingthesepatientsistrulyrewardingandan honorforusall.Wehopethistextwillhelpto
VeerasathpurushAllareddy,
MichaelMiloro,DMD,MD,FACS
contributepositivelytotheircarebyreinforcingthe criticalrelationshipsbetweenspecialistsin achievingsuccessfuloutcomes.
MichaelR.Markiewicz,DDS,MPH,MD,FACS DepartmentofOralandMaxillofacialSurgery SchoolofDentalMedicine
UniversityatBuffalo 3435MainStreet,112SquireHall Buffalo,NY14214,USA
DepartmentofNeurosurgery DivisionofPediatricSurgery DepartmentofSurgery JacobsSchoolofMedicineandBiomedical Sciences
CraniofacialCenterofWesternNewYork JohnR.OisheiChildren’sHospital Buffalo,NY,USA
VeerasathpurushAllareddy,BDS,PhD DepartmentofOrthodontics CollegeofDentistry
UniversityofIllinoisatChicago 801SouthPaulinaStreet 138AD(MC841) Chicago,IL60612-7211,USA
MichaelMiloro,DMD,MD,FACS DepartmentofOralandMaxillofacialSurgery CollegeofDentistry
UniversityofIllinoisatChicago 801SouthPaulinaStreet M/C835 Chicago,IL60612-7211,USA
E-mailaddresses: mrm25@buffalo.edu (M.R.Markiewicz) sath@uic.edu (V.Allareddy) mmiloro@uic.edu (M.Miloro)
CraniofacialGrowth: CurrentTheoriesand InfluenceonManagement AshleyE.Manlove, DMD,MDa,GerardoRomeo, DDS,MD,MBAb,c, ShankarRengasamyVenugopalan, DDS,DMSc,CAGE(Ortho),PhDd,*
KEYWORDS
Craniofacialgrowth Maxillofacialgrowth/development Facialgrowth/development
Dentofacialgrowth/development Craniofacialdevelopment Craniomaxillofacialsurgery
Orthodontics
KEYPOINTS
Tomaximizeoutcomesandminimizeiatrogenicconsequencestogrowth,astrongfoundational knowledgeofcraniofacialgrowthisarequirementofanypractitioner. Thereisacephalo-caudalgradientofgrowthpotentialduringcraniofacialgrowth. Thedevelopmentofthecraniofacialskeletonoccursasaresultofasequenceofnormaldevelopmentalevents.
INTRODUCTION Themanagementofcraniofacialabnormalities andassociatedmalocclusionrequireswellcoordinatedcollaborativeeffortsfromseveral specialists.Theimpactofgrowthofthecraniofacialskeletononsuccessfultreatmentcannotbe understated.Tomaximizeoutcomesandminimize iatrogenicconsequencestogrowth,astrongfoundationalknowledgeofcraniofacialgrowthisa requirementofanypractitioner.Proper sequencingandtimingofinterventionsarecritical inoptimizingoutcomes.Attimes,interventions thatareharmfulareavoideduntilthepreservation ofgrowthallowsforit(ie,secondaryalveolarcleft bonegraftingincontrasttoprimary)andother times,interventionsareusedtomanipulategrowth toeitherincreaseorlimitit(ie,orthodontichead gearandcranialorthotics).
Despitealonghistoryofstudyandstrongsupportiveevidenceforcertaintheories,nosingletheory,todate,appearstocompletelycaptureall aspectsofcraniofacialgrowth.Withvarioustheories inexistence,geneticcontroltheoryandfunctional matrixtheoryarethe2mostpopularandwidely accepted.Itishighlylikelythatsomeamalgamation ofvarioustheorieswouldbeclosetotruedescription oftheconceptsofcraniofacialgrowth.Thisarticle reviewssomebasicterminologiesofgrowthand development,coreconceptsofnormalgrowth, componentsofcraniofacialgrowth,growthby tissuetypesandanatomicsubunits,andgrowth modificationbyorthodonticintervention.
BASICTERMINOLOGY Theterms“development”and“growth”are relatedtooneanotherandtypicallydiscussedin
a DepartmentofOralandMaxillofacialSurgery,CarleCleftandCraniofacialTeam,CarleFoundationHospital, 611W.ParkStreet,Urbana,IL61801,USA; b OralandMaxillofacialSurgery,DepartmentofDentalMedicine, NorthwellHealth,HagedornCleftandCraniofacialTeamatCohenChildren’sMedicalCenter,HofstraNorthwellSchoolofMedicine,LongIslandJewishMedicalCenter,270–0576thAvenue,NewHydePark,NY 11040,USA; c DepartmentofPediatrics,NorthwellHealth,HagedornCleftandCraniofacialTeamatCohen Children’sMedicalCenter,HofstraNorthwellSchoolofMedicine,NewHydePark,NY,USA; d Department ofOrthodontics,TheUniversityofIowa,CollegeofDentistryandDentalClinics,801NewtonRoad,DSB, S232,IowaCity,IA52242,USA
*Correspondingauthor.
E-mailaddress: Shankar-Venugopalan@uiowa.edu
OralMaxillofacialSurgClinNAm - (2020) -–https://doi.org/10.1016/j.coms.2020.01.007 1042-3699/20/ 2020ElsevierInc.Allrightsreserved.
tandemoreveninterchangeably.Conceptually, however,theyaredistinct.Theterm“development”describesformation,differentiation,or specializationoftissues/subunits,usuallybytransitioninginanatomicform.Onthecontrary,the term“growth”referstoincreaseinsizeofanytissue,subunit,orunit.
Craniofacialdevelopmentandgrowthbeginin uteroandcontinuevariablyintoadulthood.Three mainparametersaretypicallyusedtodescribe “growth”intheliterature: magnitude, direction, and velocity.The“magnitude”isusedtocategorizegrowthintermsofsome“relativeamount” foragivendimension(transverse,sagittal,and vertical).The“direction,”however,istypically simplifiedintoavectorrepresentingthe“net” directionalgrowth.Theterm“velocity”refersto therateofgrowthperunittime.
Itiscommontoheartheterm“skeletalmaturity” usedwhenplanninginterventionsamongpractitioners.Oftentimes,skeletalmaturitydetermines whetherornotaninterventionisdeemedtobe indicatedorcontraindicated.Althoughsome wouldmistakenlyassumethat“maturity”iscessationofgrowth,amoreaccurateinterpretationof “maturity”wouldconnotemostofthemagnitude andpeakvelocityofgrowthhasoccurred.
CORECONCEPTSOFNORMALGROWTHAND DEVELOPMENT Concept1
Allindividualsgothroughsimilarstagesofdevelopmentandgrowth,albeitnotalwaystothe sameextentorattheexactsametime.1 Thechronologicage,skeletalage,anddentalagedonotalwayscorrelateinanindividual.Conceptiontobirth averages40weeksandistermedthe“prenatal” period.Developmentandgrowthintermsof magnitudeandvelocityarehighestintheprenatal period.Frombirthto2years(infancy),themagnitudeandvelocityofgrowthanddevelopmentdecreasesuntilitplateausinchildhood.During puberty,themagnitudeandvelocityofgrowthincreasesagain.Followingpubertalgrowth,the magnitudeandvelocityofgrowthsteadily decreases.
Concept2
Notalltissuetypesorpartsofthebodygrowatthe sametimeorthesamerate.Inthecraniofacial subunits,notonlyarevarioustissue typespresent,butthosetissuesarepresentinvariableproportionsatdifferenttimesduringgrowth anddevelopment.Forexample,inagiventime point,thegrowthforneuralorlymphoidtissues
aredifferentinmagnitudeandvelocitythan,say, anysingleboneofthefacialskeleton.
Concept3 Growthpotentialisdrivenbygeneticsandinfluencedbyenvironmentalfactors.“Normalgrowth” occursonaspectrumofwhatwouldbeconsidered“normal.”Therearevaryingdegreesofdeviationfromwhatwouldbeconsideredanormal craniofacialanddentofacialrelationship,which aredeterminedbytheinherentgeneticmakeup. Thosegeneticpredispositions,however,aresubjecttoenvironmentalinfluences.Atthemacro level,growthpotentialofalltissuesandsubunits canonlyberealizedifphysiologyisunimpeded bypathology(ie,propernutritionandabsenceof disease).Atthemicrolevel,introductionofanunfavorablevariable(ie,surgicalscarring)ona growingtissuetypeorsubunitcanalsonegatively impacttheachievementofthegeneticallyprogrammedgrowthpotential.Sometissuesare moresusceptibletoenvironmentalinfluencethan others.
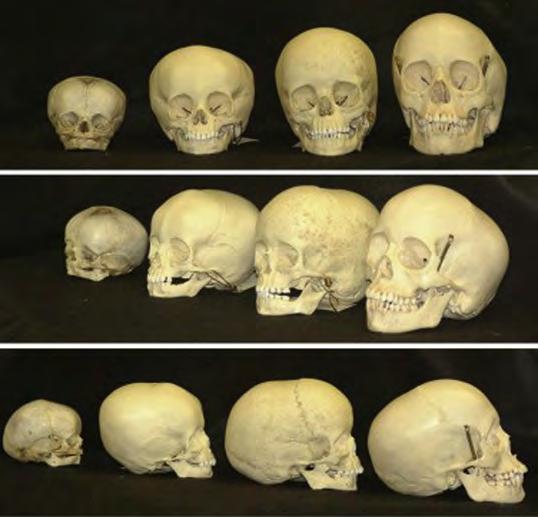
CRANIOFACIALGROWTHBYTISSUETYPE Inthecraniofacialregion,growthofdifferenttissue types,anatomicunits,andfunctionalspaces occurinacoordinatedrelationshiptooneanother atdifferentratesandtimepoints(Fig.1).Itis widelyacceptedthatcomplexsignalingbetween thesetissuetypesandanatomicunitsmustoccur inaprecisefashiontoachievenormalgrowth bothinuteroandthroughoutlife.Themajor componentsofthecraniofacialgrowthareneural tissue,muscle,tonsils/adenoids,cartilage,bone, sutures,andfunctioningspaces.
NeuralTissue Neuraltissuecompletesmuchofitsgrowthearlyin development.Atbirth,theneuraltissueshave achievedapproximately60%to70%ofadult size.Byearlychildhood,neuraltissuesreach 95%ofadultdimensions.Thegrowthofneuraltissues(brainandglobes)drivesthegrowthofthe surroundingboneandmusculoskeletaltissues aroundthem.Functionalmatrixhypothesis,as describedbyMossandSalentijn,2 postulates thatitisthesofttissuegrowth(thebrainandsoft tissueenvelope)thatinducesboneandsutural growthofthecranium.
Muscle Themuscletissueofthecraniofacialregionisless than50%ofadultsizeatbirth.Bythetimeneural tissueshavereachedmaturity,muscletissuehas
reachedonlyapproximately70%ofadultdimensionsinthecraniofacialregion.Muscledimensionsdeveloplaterinchildhoodandadolescence tosupporttheadultdentition,skeletalframe, phonation,anddeglutition.Themusclesare consideredadaptiveinnatureandgrowtosupport function.2
Tonsils/Adenoids Lymphoidtissuesactuallyexceedadultsizein childhood.Thedimensionsofthetonsilsandadenoidsareapproximately125%ofadultsizebyage 5.Thelymphoidtissuesregressinsizeafter5years ofageandareinpartresponsibleforfurtherdevelopmentofthefunctionalpharyngealspace.This involutionoflymphoidtissuemustbetakeninto consideration,particularly,inpatientswithcleft palate,asitcanresultinworseningofvelopharyngealdysfunctionasthechildgetsolder.3
CartilageandChondrogenesis Duringearlydevelopment,thereare2kindsof cartilage:(1)primaryand(2)secondary.Theprimarycartilageisuniqueinthatitgrowsinterstitially,itispressuretolerant(ascomparedwith bone,forexample),andisnonvascularinnature. WorkbyScott4 postulatesthatprimarycartilage isgeneticallydrivenandactsasagrowthcenter drivingmuchofthenetchangeincraniofacial formduringdevelopment.Thecranialbaseand
Fig.1. Multipleviewsofskullsfrominfancythroughadolescenceshowthe progressionofcraniofacialbone growth.Thegeneralprogressionis fromsuperiortoinferiorwithadownwardandforwardgrowthvector. (From CostelloBJ,MooneyMP,Shand JM.Craniomaxillofacialsurgeryinthe pediatricpatient:growthanddevelopmentconsiderations.In:FonsecaRJ, editor.Oralandmaxillofacialsurgery. 3rded.St.Louis:Elsevier;2018.p. 627-44;withpermission.)
nasalseptumarederivedfromprimarycartilage. Thegrowthofthenasomaxillarycomplexis dictatedbythegrowthofthecranialbaseand nasalseptalcartilage.Mostprimarycartilageof thecranialbaseisreplacedbyboneviaendochondralossificationearlyinchildhoodthusprimarycartilageasa“driverofgrowth”ends relativelyearly.4 Onthecontrary,thesecondary cartilageisnotundergeneticcontrolinthesame wayasprimarycartilage.Itisconsideredmore “adaptiveinnature”inthatitdoesgrowandultimatelyossify,butitdoessoinresponsetofunctionandisundersignificantenvironmental influence.Inthecraniofacialskeleton,secondary cartilageisfoundinthecondylarhead,coronoid process,angleofthemandible,andmental protuberance.
BoneandOsteogenesis Boneisacalcifiedtissue,whichishighlyvascular, sensitivetopressure,andissubjectedtoenvironmentalinfluences.5 Theboneformationduring developmentoccursbyeitherintramembranous orendochondralossification.Duringintramembranousossification,themesenchymalcellsdifferentiatedirectlytoosteogeniccells,whereasin endochondralossification,cartilageservesasa template,whichisthenreplacedbybone.Overall bonegrowthdoesnotoccurduetosurfaceappositionofbone.Rather,thebonegrowthoccursby
2majormechanisms:(1)corticaldrift:periosteal depositionofboneandendostealresorptionof bone;and(2)displacement:physicalmovement ofboneduetogrowthoftheadjacentstructure.5 Itmustberememberedthatbonegrowthisnot static,ratherdynamic.Evenafterreachingadult dimensions,boneundergoesnearconstant remodeling.Furthermore,theperiosteumthatsurroundsthebonehasapowerfulinfluenceoverits growthanddevelopment.Therefore,interruption ofthatperiosteumhasthepotentialtoaffectthe growthpotentialofthebone.3
Sutures Thecranialsuturesarefibrousarticulationsformed betweentheapproximatingosteogenicfrontsof thebonesofcranialvault.Ontheexternalsurface ofthesutureliesthefibrouslayerofperiosteum andontheinternalsurfaceliesthefibrouslayer ofduramater.In-betweentheapproximatingosteogenicfrontsofthesutureliesthemesenchyme, whichprovidesasourcefornewosteogeniccells.6 Thesuturesareimportantsitesofcompensatory growthandplayanimportantroleincraniofacial growth.7 Thegrowthatsuturesoccursasanadaptationtothegrowthoftheneuraltissueandsurroundingtissuessuchasprimarycartilageorsoft tissue.Newboneisdepositedincrementally acrossthosesutureswithremodelingand displacementoccurringinaharmoniousphysiologicbalanceundernormalcircumstances8
FunctioningSpaces AsdescribedbyMossandSalentijn,2 thecraniofacialregioncontainsvariousspacesthatsupport function,forexample,respiration,deglutition, vision,olfaction,andcognition/neuralintegration. Thedifferenttissuetypesgrowinsupportofsaid functionsresultingin“functioningspaces.”An examplewouldbethatalthoughneuralintegration isthemostessentialofcraniofacialfunctions, growthofthebrainoccursearlyandquickly.The growthofthebraininturndrivesgrowthofthe cranium.Anotherexamplewouldbethatafter birth,alimentationbecomesahigher-orderfunction,thereforeswallowingandjawmovementdrive thedevelopmentofthefunctioningoralcavityand growthofbone,teeth,andmuscletosupportthat function.Enlowandcolleagues5,9 described2 mainmorphologiceventsthatdirectcraniofacial growth,including(1)growthofthebasalcranium, and(2)developmentofpharyngealandfacial airwaystructures.Accordingtohistheory,remodelingoccursascompensatorychangesoftissueto adapttofunction,asdescribedbythefunctional matrixhypothesisofMossandSalentijn.2
CRANIOFACIALGROWTHBYANATOMIC SUBUNIT Cranium Thecranialvaultandthecranialbasemakeup theentirecranium.Thecranialvaultis composedofintramembranouslyformedbones, wherebonegrowthoccursatthefibroussuture articulations.Thecranialvaultgrowsexponentiallyduringthefirstyearoflife,reachingapproximately86%ofitsadultsizeby1yearofageand 94%ofadultsizeby5yearsofage. 10 Thisreflectsthesignificantneurodevelopmentthatoccursduringthistimeframe.Apractical applicationofthisknowledgeistheorthotic treatmentofpositionalplagiocephalyhas becomemoreprevalentwiththe“backtosleep” campaign.Asparentsareinstructedtoplace theirinfantsontheirbackwhensleeping,this cancauseflatteningoftheocciputandcompensatoryfrontalbossing.Newbornslacktheneuromuscularstrengthandcontrolofneckmuscles duringthisexponentialneurodevelopmentand rapidgrowthoftheircranialvault,whichcan leadtosignificantflatt eninganddysmorphiccranialvaultgrowth.Giventhatmostcranialvault growthoccursduringthefirstyearoflife,cranial orthotictherapyismosteffectivefrom4months ofageuntil1yearofage.
Contrarytothecranialvault,thecranialbaseis composedofbonesthatformbyendochondral ossification.By5yearsofagetheanteriorcranial baseismorematured(w90%ofadultsize) comparedwiththeposteriorcranialbase(80% ofadultsize).Thecranialbasegrowthoccurs interstitiallyatarticulationscalledsynchondroses, amajorgrowthcenterinthecraniofacialskeleton. Thereare3synchondrosesatthecranialbase:(1) intersphenoidalsynchondroses,whichfuseatthe timeofbirth;(2)sphenoethmoidalsynchondroses, whichfuseat w7to8yearsofage;and(3)sphenooccipitalsynchondroses,whichfuseshortlyafterpuberty.Cranialgrowthdiscrepancyalsocan occurfromcraniosynostosis,whichistheprematurefusionofcranialvaultsutures.Single-suture craniosynostosisismostcommonandusually nonsyndromic.11 Multisuturecraniosynostosis canoccurandismorecommoninconditions suchasApert,Pfeiffer,Crouzon,andSaethreChotzensyndromes.Treatmentofcranialgrowth discrepancyfromprematurefusionofcranialsuturesisusuallyperformedatapproximately 10monthsofageascranialgrowthisslowing down,butsurgerywillstillallowforappropriate volumeforbraingrowthtooccur.Cessationofcranialgrowthoccursat14yearsofageforgirlsand 15yearsofageforboys.
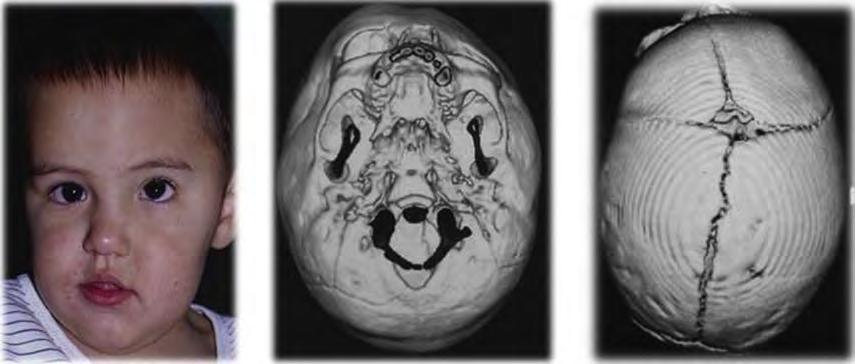
Orbits Theorbitiscomposedofbonesfromthenasomaxillarycomplex(palatine,maxillary,zygomatic bones),aswellasfromthecranialvault(frontal, ethmoid,sphenoid,lacrimalbones).Thegrowth inthisregionoccursatthesuturesbetweenthese bones.Orbitalgrowthoccursrapidlyinthefirst yearoflifeinassociationwiththegrowthofthe cranialbase,vault,andglobes.Mostorbital bonegrowthiscompleteatapproximately5years ofage.12,13 Intercanthalwidthiscompleteat 8yearsofageingirlsand11yearsofagein boys.Orbitalheightgrowthismoregradual whencomparedwithorbitalvolume,whichultimatelycontributestomidfacialheight.Disruption ofnormalorbitalgrowthisseeninunicoronalcraniosynostosis(Fig.2),aswellasinTessierclefts (Fig.3)thatinvolveanyofthebonesthat constructtheorbit.
Nose Aninfant’snosehasmorecartilagethanbone whencomparedwithanadultnose.Thereare2 mainperiodsofgrowthofthenose:2to5years ofageandthenduringpuberty.Theseptalcartilageisthoughttobeamajorgrowthcenterand drivingforceinmidfacegrowthearlyindevelopment.Theperpendicularplatearisesfromendochondralossificationalongtheskullbaseand eventuallymeetswiththevomeratapproximately 6to8yearsofagethroughcartilagegrowthand ossification.14 Inaddition,wherethevomerand premaxillameetisanimportantgrowthcenter. Thissuturelineisabnormalincleftpatientsand maycontributetoasymmetricnasalgrowthin thecleftpopulation.15
Zygoma Thezygomaticbonesalsogrowquicklyduringthe firstyearoflifewithcessationofgrowthatapproximately5to7yearsofage.By5yearsofagethe bizygomaticwidthis83%ofadultwidthandthe widthofthefaceismatureat13yearsofagein girlsand15yearsofageinboys.12,13 Zygomatic deformitiescanbeseenfollowingtraumaaswell asincongenitaldisorderssuchasTreacherCollins andcraniofacialdysostosis.
Maxilla Themaxilladevelopsbyintramembranousossification.Thegrowthatthecranialbaseexertsamajorinfluenceonmaxillarygrowth,resultingina downwardandforwarddisplacement.Ina compensatoryfashiontothisdisplacement,bone isdepositedatthecircumaxillaryandintermaxillarysutures,andresorbedfromtheanteriorsurfaceofthemaxilla.Inaddition,maxillarygrowth isalsodependentonearlynasalseptalgrowth. Intheantero-posteriordirection,boneisdepositedinthemaxillarytuberosityregion,whichcontributestothelengtheningofthemaxillato accommodatedevelopingdentition.Furthermore, asthemaxilladescendsduringgrowth,boneis resorbedfromthenasalflooranddepositedin thepalatalvault.
Thepremaxillary/maxillarysuturefusesat approximately3to5yearsofage,themidpalatal suturefusesatapproximately15to18yearsof age,andthetranspalatalsuturefusesatapproximately20to25yearsofage.16–18 Thevertical heightofthemaxillareachesitsmaximumgrowth atapproximately12yearsofageingirlsand 15yearsofageinboys.12,13 Theanteriorprojectionofthemaxillareachesskeletalmaturityat
Fig.2. Leftunicoronalcraniosynostosiscausingfacialandorbitalasymmetry.
13yearsofageingirlsand14yearsofageinboys. Growthanddevelopmentofthemaxillaparallels growthandpneumatizationofthemaxillarysinus. Midfacehypoplasiaisaclinicalphenotypeinpatientswithachondroplasia,craniofacialdysostosis syndromes,asaniatrogeniceffectinpatientswith cleftlip/palate,andasaresultoftraumainmidface andnasalfractures.19
Mandible Thebodyofthemandibledevelopsbyintramembranousossificationandthecondyleby endochondralossification.Inthecraniofacial complex,themandiblehas thegreatestpostnatal growthpotential.Withreferencetothecranial base,themandibleisdisplaceddownwardand forward;however,thedirectionofgrowthatthe condyle,amajorcontributorofpostnatalgrowth, isupwardandbackward.Duringgrowth,increaseinthecorpuslengthisachievedby resorptionalongtheanteriorsurfaceoftheramus anddepositionalongtheposteriorsurfaceofthe ramus.Furthermore,themandibularwidth increasesbybonedepositionalongthebuccal surface.Therefore,growthofthemandibleoccursinallregions,includingthecondyles,rami, andbodythroughdisplacementand remodeling.5 , 20
Mandibularwidthisnearlycompleteat5years ofage.Mandibularheightreachesmaturityat 12yearsingirlsand15yearsinboys.Mandibular anteriorprojectiongrowthiscompleteat13years ofageingirlsand15yearsofageinboys.12,13 Mandibularhypoplasiaiscommonlyseen inPierreRobinsequence,craniofacial microsomia,TreacherCollinssyndrome,Nager syndrome,condylartrauma,andidiopathic condylarresorption,amongothercauses. Mandibularhyperplasiacanbegeneticandis alsoseeninacromegaly.
Fig.3. Tessierorbitalcleft9to10in conjunctionwithleftunicoronalcraniosynostosiscausingsignificantdysmorphiaandfacialasymmetry.
ToothFormationandEruption Theprocessoftoothformationisundertightgeneticcontrolandtakesplacebyreciprocalinteractionbetweenthedentalepitheliumandneural crestderivedmesenchyme.21 Thedevelopment anderuptionofthedentitioniscloselyintertwined withgrowthanddevelopmentofthemaxillaand mandible.Developmentoftheprimarydentition isinitiatedbythesixthweekofgestation,and thepermanentdentitionisinitiatedatapproximatelythe10thto13thweek.21 Inanormalgrowingpatient,allprimaryteethareeruptedin themaxillaandmandibleby2to2.5yearsof age.Allpermanentteethexceptthirdmolarserupt by12to13yearsofage.Thisisroutinelydelayed inpatientswithcleft.Forteethtoerupt,dentalfolliclesinitiateresorptionofbonealongthepathof eruptionandboneisdepositedontheopposite end.22 Mostteethemergewhenhalftotwothirdsofrootisformedandtherootformationis fullycompleteby2to4yearsaftereruption.There isthereforeanetincreaseinthebonethatsupportsteeththatisassociatedwitheruption.
Tootheruptionisratheradynamicprocessand therateoferuptionparallelstherateofjawgrowth. Duringadolescence,themaxillaryandmandibular molarsdriftmesiallyby w0.6mmperyearand w0.5mmperyear,respectively,23 whereasthe maxillaryandmandibularincisors,duringadolescence,driftmesiallyby w0.3mmperyear.23 In theverticaldimension,themaxillarymolars (w1.2mm/y)andincisors(w1mm/y)eruptslightly morethanthemandibularmolars(w0.9mm/y)and incisors(w0.9mm/y).23 Therefore,asthejawsare displaceddownwardandforwardduringgrowth, teetherupttofillthespaceandtomaintainthe functionalocclusion.Thiseruptionofteethcontributesgreatlytotheverticaldentoalveolar growthinthemaxillaandmandible.23 Thefinalpositionofteethwithinthejawsareinfluencedbythe
balanceestablishedbythepressurefromthe tongue,lips,andcheekmusculature.
GROWTHMODIFICATION Thedentofacialorthopedicintervention,byan orthodontist,isanattempttomodifygrowthto correctthedevelopingskeletaldiscrepancies.In routineorthodonticdiagnosis,thediscrepancies ingrowthareanalyzedin3dimensions:(1)transverse,(2)sagittal,and(3)verticalplanesofspace. Thewidespreadconsensus,albeitthereareindividualvariations,isthattransversegrowthis completedfirst,thenthesagittalgrowth,and finally,theverticalgrowth.
TransverseDimension Skeletaldiscrepanciesinthetransversedimension manifestas(1)constrictedorwidemaxilla,and/or (2)constrictedorwidemandible.Thegrowth modificationofconstrictedmaxillaisoften achievedwithpalatalexpansion.Inchildrenat theagegroupof8or9yearsofage,expansion ofthemidpalatalsutureiseasilyachievedwithlittleforceusingtooth-supportedappliances,such asW-archorQuadHelix.24 However,children whoare10yearsorolderrequireheavierforces toopentheinterdigitatedmidpalatalsuture. Therefore,correctionofmaxillaryconstrictionat w10yearsofageoftenrequiresjackscrewdevicestocreatemicro-fracturestoopenthemidpalatalsuture.24 Althoughthegoalofexpansionisto produceskeletalchanges,itisnotalwaysthe case.Thetooth-supportedpalatalexpansiondevicesproduceapproximately50%dentaland 50%skeletalexpansion.24
Theuncorrectedmaxillaryconstrictionat adolescentagegrouppresentsamajorchallenge inopeningthemidpalatalsuturewithtoothsupportedjackscrewdevices.Thisisbecause theheavierforcesdeliveredwithsuchdevices oftenfailtoopenthesutureandwillcausedental tippingandinsomecasesmaycausebuccal bonefracture.Theadventofminiscrewsinorthodontictreatmentallowsdeliveringforcesdirectly tothemidpalatalsutureinachievingtruesutural split.25 Theminiscrew-assistedrapidpalatal expanderisausefulmodalitytocorrectmaxillary constrictioninyoungadultswhomightotherwise requiresurgery.
Unlikethemaxilla,expansionoftheconstricted mandibleispossibleonlywithsurgicalapproach, suchasdistractionosteogenesisduetoearlyossificationofthemidlinemandibularcartilage.24 Currently,therearenoviablegrowthmodification modalitiestocorrectexcessivetransverse
maxillaryormandibulargrowth,andsurgeryis theonlytreatmentofchoice.
SagittalDimension Inthesagittaldimension,theskeletaldiscrepanciesmanifestas(1)ClassIIskeletalrelationship duetoprognathicmaxillaand/orretrognathic mandible,and(2)ClassIIIskeletalrelationship duetoretrognathicmaxillaand/orprognathic mandible.The2majorgrowthmodificationmodalitiesforClassIIgrowthpatternare(1)tractionwith extraoralforces,suchasheadgear;and(2)functionalappliances,suchasTwinBlock,Bionator, andHerbstappliances.InClassIIskeletaldiscrepancyduetoexcessivemaxillarygrowth,orinsome situationswithnormalmaxillaandretrognathic mandible,extraoraltractionwithheadgearisa reasonabletreatmentmodality.24 Theheadgear therapybeforeorduringadolescencedelivers compressiveforcestothecircumaxillarysutures inrestrainingtheforwardmaxillarygrowthandallowsthemandibletocatchuptoitsinherent geneticallydeterminedgrowthpotential.Thesecondtreatmentmodalityoffunctionalappliance therapyhasbeensurroundedwithmuchcontroversyintheorthodonticliterature.Increasingevidencesupportsthenotionthat,onashort-term basis,functionalappliancetherapybeforeorduringadolescenceacceleratesforwardmandibular growth,but not anymorethantheinherentlydeterminedgeneticpotential.Generally,thefunctional appliancestendtohavesomerestrainingeffect onthemaxilla,withasignificantpartoftheClass IIcorrectionachievedthroughdentoalveolarrather thanskeletalchanges.24,26,27 Thecurrent consensus,basedonmultipleclinicaltrials,with regardtoClassIIgrowthmodificationisthat2phasetreatmentduringadolescenceisnotany moreeffectivethan1-phasetreatmentduring adolescence.24 Therefore,earlytreatmentisindicatedwhenpsycho-socialburdenisamajor concern.
Thecurrentlyavailabletreatmentapproaches forgrowthmodificationinClassIIIgrowthpattern arefacemask(ReversePullHeadgear),chin-cup, andClassIIIelasticsaffixedtoskeletalanchorage. Inpatientswithdeficientmaxillarygrowth,facemasktherapyisindicated,andthegoalofthe interventionistobringthemaxillaforwardand downward.Duringfacemasktherapy,protraction forcesareappliedtothemaxillawithelastics attachedfromafixedintraoralappliancetoan extraoralfacemask.Thefacemasktherapyis effectivebefore8to10yearsofageinproducing improvedskeletalanddentalchanges.24,28 During facemasktherapy,inadditiontomaxillary
protraction,itisnotuncommontofindbackward rotationofmandible.
InthecontinuumofClassIIIskeletaldiscrepancy,excessivemandibulargrowthisontheother endofthespectrum.Inthesepatients,thegoalis toattempttorestrainmandibulargrowthwithchincuptherapy.Thistherapyinvolvesacuporcapon thechinwithanattachmenttothebackofthe head.TheClassIIIpatientswithashortface benefitthemostbychin-cuptherapy.24 Although thegoalofthistherapyistorestrainmandibular growth,italmostalwaysresultsinreductionof chinprojectionbyredirectionofcondylargrowth; backwardrotationofthemandiblewithminimal ornorestraintintheactuallengthofthemandible. Therefore,chin-cuptherapymayactuallyworsen theprofileinindividualswithalong-faceClassIII growthpattern.Chin-cuptherapyiseffectiveat anearlyage;however,thecircumpubertalgrowth ofthemandiblemayreversetheeffectsofearly chin-cuptherapy.28
Theusageofelasticstoboneanchorplatesis growinginpopularity.Theminiplatesareinserted intheinfrazygomaticcrestandinthemandibular canineregion,andClassIIIelasticsareworn fromthemaxillarytothemandibularminiplates tocorrecttheClassIIIskeletalgrowth.Thesuitabletimingofinterventionforthismodalityis w11yearsorolder,asthiswouldallowforstable anchorageintheinfrazygomaticcrestandavoidanceoftoothbuds.Thistherapyappearseffective inproducingmaxillaryprotractionwhileminimizing sideeffectslikedentoalveolarchangesandbackwardrotationofthemandible.24
VerticalDimension Themanifestationofskeletaldiscrepanciesinthe verticaldimensionare(1)short-faceand(2)longfaceproblems.Oftentimes,theseproblemsmay manifestalongwithskeletalClassIIorIIIgrowth pattern.Inindividualswithshort-faceproblems, typicallythelowerfacialthirdissmallerthanthe upperandthemiddlefacialthirds.Theshort-face individualswillpresentwithlongramus,acute gonialangle,andhypodivergentmandibularplane angle.24 Theaimofgrowthmodificationinthese individualsistoallowfortheverticaldentoalveolar changesbyeruptionofposteriorteeth.Appliances suchasactivatororbionatorwithpalatalacrylic contactingthemandibularincisorsandinterocclusalclearanceintheposteriorregionwould alloweruptionofmaxillaryandmandibularmolars. Suchverticaldentoalveolarchangescould improvetheshortfaceheight.
Contrarytotheshort-facephenotype,isindividualswithlargelowerfacialthird,shortramus,
obtusegonialangle,andsteepmandibularplane angle.Thegrowthmodificationinlong-faceindividualsisratherchallenginganddifficult.Theoretically,growthmodificationingrowinglong-face individualscouldbeachievedwithhigh-pullhead geartorestraindownwardmaxillarygrowthwith posteriorbiteblocktoimpedetheeruptionofteeth andauto-rotatethemandibleintheforwarddirection.24 However,suchagrowthmodification approachnotalwaysproducesthedesiredskeletalchangespredictablyinthelong-faceindividuals.Interestingly,miniscrewimplantsprovidea uniqueopportunityforinterventioninadolescents withlongface.Availablelimiteddatasuggest that,ingrowinghyperdivergentpatients,miniscrewimplantsinthepalateandmandiblewithrigid attachmenttointrudetheupperandlowerposteriorteethcouldpreventtheeruptionofteeth, improvechinprojection,decreasemandibular planeangle,andimprovefacialconvexity.29
SUMMARY Thedevelopmentofthecraniofacialskeleton occursasaresultofasequenceofnormaldevelopmentalevents:(1)braingrowthanddevelopment,(2)opticpathwaydevelopment,(3)speech andswallowingdevelopment,(4)airwayand pharyngealdevelopment,(5)muscledevelopment,and(6)toothdevelopmentanderuption. Asanorthodontistorsurgeon,itisimportanttounderstandthegrowthanddevelopmentofeach subunitofthefacesotreatmentcaneitherharness andmanipulategrowthoristimedappropriately soastominimizenegativeimpact.Orthopedicappliancescanoftenbeusedduringgrowthphases toattempttomanipulategrowthfavorably.In contrast,itisoftenidealifelectivesurgicalinterventionsaretimedwhenmostgrowthanddevelopmentiscompletesoastonotinterferewith growthpotential.
DISCLOSURE Theauthorshavenothingtodisclose.
REFERENCES 1. ValadianI,PorterD.Physicalgrowthanddevelopment:fromconceptiontomaturity.Boston:John Wright-PSG;1977
2. MossML,SalentijnL.Theprimaryroleoffunctional matricesinfacialgrowth.AmJOrthod1969;55(6): 566–77
3. FergusonDJ,McDonaldRE,AveryDR.Dentistryfor thechildandadolescent.7thedition.Philadelphia: Mosby;2000
4. ScottJH.Thecartilageofthenasalseptum:acontribution tothestudyoffacialgrowth.BrDentJ1953;95:37–43
5. EnlowDH,HansM.Essentialsoffacialgrowth.Philadelphia:Saunders;1996
6. LentonKA,NacamuliRP,WanDC,etal.Cranialsuturebiology.CurrTopDevBiol2005;66:287–328
7. BaumeLJ.Principlesofcephalofacialdevelopment revealedbyexperimentalbiology.AmJOrthod 1961;47(12):881–901
8. KoskiK.Cranialgrowthcenters:factsorfallacies? AmJOrthod1968;54(8):566–83
9. EnlowDH,KurodaT,LewisAB.Themorphological andmorphogeneticbasisforcraniofacialformand pattern.AngleOrthod1971;41(3):161–88
10. FarkasLG,PosnickJC,HreczkoTM.Anthropometricgrowthstudyofthehead.CleftPalateCraniofacJ1992;29(4):303–8
11. AdamoMA,PollackIF.Currentmanagementofcraniosynostosis.NeurosurgQ2009;19(2):82–7
12. WaitzmanAA,PosnickJC,ArmstrongDC,etal. Craniofacialskeletalmeasurementsbasedon computedtomography:PartI.Accuracyandreproducibility.CleftPalateCraniofacJ1992;29(2):112–7
13. WaitzmanAA,PosnickJC,ArmstrongDC,etal.Craniofacialskeletalmeasurementsbasedoncomputedtomography:PartII.Normalvaluesandgrowthtrends. CleftPalateCraniofacJ1992;29(2):118–28
14. FunamuraJL,SykesJM.Pediatricseptorhinoplasty. FacialPlastSurgClinNorthAm2014;22(4):503–8
15. JohnsonMD.Managementofpediatricnasalsurgery(rhinoplasty).FacialPlastSurgClinNorthAm 2017;25(2):211–21
16. BehrentsRG,HarrisEF.Thepremaxillary-maxillary sutureandorthodonticmechanotherapy.AmJOrthodDentofacialOrthop1991;99(1):1–6
17. MelsenB.Palatalgrowthstudiedonhumanautopsy material.Ahistologicmicroradiographicstudy.AmJ Orthod1975;68(1):42–54
18. PerssonM,ThilanderB.Palatalsutureclosurein manfrom15to35yearsofage.AmJOrthod 1977;72(1):42–52
19. PreciousDS,DelaireJ,HoffmanCD.Theeffects ofnasomaxillaryinjuryonfuturefacialgrowth. OralSurgOralMedOralPathol1988;66(5): 525–30
20. CostelloBJ,RiveraRD,ShandJ,etal.Growthand developmentconsiderationsforcraniomaxillofacial surgery.OralMaxillofacSurgClinNorthAm2012; 24(3):377–96
21. JuuriE,BalicA.Thebiologyunderlyingabnormalitiesoftoothnumberinhumans.JDentRes2017; 96(11):1248–56
22. MarksSCJ,SchroederHE.Tootheruption:theories andfacts.AnatRec1996;245(2):374–93
23. BuschangPH,RoldanSI,TadlockLP.Guidelines forassessingthegrowthanddevelopmentoforthodonticpatients.SeminOrthod2017;23(4): 321–35
24. DeClerckHJ,ProffitWR.Growthmodificationofthe face:acurrentperspectivewithemphasisonClass IIItreatment.AmJOrthodDentofacialOrthop2015; 148(1):37–46
25. LeeKJ,ChoiS-H,ChoiT-H,etal.Maxillarytransverseexpansioninadults:rationale,appliance design,andtreatmentoutcomes.SeminOrthod 2018;24(1):52–65
26. Vaid NR,DoshiVM,VandekarMJ.ClassIItreatment withfunctionalappliances:ameta-analysisofshorttermtreatmenteffects.SeminOrthod2014;20(4): 324–38
27. D’Anto ` V,BucciR,FranchiL,etal.ClassIIfunctionalorthopaedictreatment:asystematicreview ofsystematicreviews.JOralRehabil2015;42(8): 624–42
28. WoonSC,ThiruvenkatachariB.Earlyorthodontic treatmentforClassIIImalocclusion:asystematicreviewandmeta-analysis.AmJOrthodDentofacial Orthop2017;151(1):28–52
29. BuschangPH,CarrilloR,RossouwPE.Orthopedic correctionofgrowinghyperdivergent,retrognathic patientswithminiscrewimplants.JOralMaxillofac Surg2011;69(3):754–62
AnOverviewofTimelineof Interventionsinthe ContinuumofCleftLipand PalateCare DavidYates, DMD,MDa,VeerasathpurushAllareddy, BDS,PhDb,*, JenniferCaplin, DMD,MSb,SumitYadav, MDS,PhDc, MichaelR.Markiewicz, DDS,MPH,MDd,e,f,g
KEYWORDS
Cleftlipandpalate Timelineofinterventions Orthognathicsurgery Liprepair Palaterepair Alveolarbonegrafting Cleftmaxilla
KEYPOINTS
Manyhealthcareprovidersareinvolvedinthecontinuumofcleftlipandpalatecare. Communicationbetweenprovidersispivotaltorealizegoodend-of-treatmentoutcomes. Treatmentphilosophiesvaryacrosscraniofacialteams.
BACKGROUND Cleftlipand/orpalate(CL/P)isthemostcommon congenitalcraniofacialanomaly,withaprevalence of1in700livebirths.1–3 AccordingtotheUSCentersforDiseaseControlandPrevention,eachyear 2650babiesarebornwithacleftpalate,and4440 babiesarebornwithacleftlipwithorwithoutacleft palateintheUnitedStates.2,3 Cleftscanbeunilateralorbilateral,completeorincompleteandinvolve thealveolus,lip,and/orpalateinvarious combinations.ThehighestratesofCL/ParereportedinAsianpopulations(0.8–3.7casesper 1000individuals),whilethelowestratesarereported
inAfricans(0.2–1.7casesper1000individuals).4,5 Bothgeneticandenvironmentalfactorshavebeen associatedwiththedevelopmentofCL/P.Some oftheenvironmentalfactorsimplicatedinclude maternalsmokingandalcoholconsumption,poor nutrition,andviralinfections.6 Over350genesand 300syndromeshavebeenassociatedwithCL/P.7 GenesassociatedwithnonsyndromicCL/Pinclude IRF6,8q24,WNT3,10q25,andRFC1.8–11 Inadditiontotraditionalpolymorphisms,certainmethylationpatternshavealsobeenassociatedwithan increaseriskinCL/.12,13 AchildbornwithCL/Pis typicallyfollowedatacleft/craniofacialcenterwhere
a EPCHCleftandCraniofacialFellowship,ElPasoChildren’sHospital,TTUHSC,ElPaso–PaulFosterSchoolof Medicine,HighDesertOral&FacialSurgery,601SunlandParkDrive,bldg2,suite2,ElPaso,TX79912,USA; b DepartmentofOrthodontics,CollegeofDentistry,UniversityofIllinoisatChicago,801SouthPaulinaStreet, 138AD(MC841),Chicago,IL60612-7211,USA; c DepartmentofCraniofacialSciences,UniversityofConnecticut SchoolofDentalMedicine,263FarmingtonAvenue,Farmington,CT06030,USA; d DepartmentofOraland MaxillofacialSurgery,SchoolofDentalMedicine,UniversityatBuffalo,3435MainStreet119SquireHallBuffalo,NY14214,USA; e DepartmentofNeurosurgery,JacobsSchoolofMedicineandBiomedicalSciences,Buffalo,NY,USA; f DivisonofPediatricSurgery,DepartmentofSurgery,JacobsSchoolofMedicineandBiomedical Sciences,Buffalo,NY,USA; g CraniofacialCenterofWesternNewYork,JohnOisheiChildren’sHospital,Buffalo,NY,USA
*Correspondingauthor. E-mailaddress: sath@uic.edu
OralMaxillofacialSurgClinNAm - (2020) -–https://doi.org/10.1016/j.coms.2020.01.001 1042-3699/20/ 2020ElsevierInc.Allrightsreserved.
manyspecialistsareinvolvedinthecontinuumof care.Theobjectiveofthisarticleistoprovidean overviewofmajordentalandsurgicalinterventions thatareperformedinpatientswithCL/P. Ifnottreatedappropriatelyinatimelymanner, thosewithCL/Pcanexperiencecatastrophic eventssuchasprematuredeathandlife-longdifficultiesinfeeding,speaking,hearing,self-esteem, andpsychosocialrelationships.14–16 Theearliest interventioninthosewithCL/Pstartsduringthe firstfewweeksoflife(infantorthopedictreatment
Table1
performedbyapediatricdentistororthodontist inpreparationforrepairofthelip),andthefinal phaseoftreatmentiscomprehensiveorthodontic treatment(with/withoutorthognathicsurgery)that isusuallyperformedinthelateteenyears.Dentists playacrucialroleinthecontinuumofcleftlipand palatecare(Table1);thereforeitbecomescritical thatdentistsareknowledgeableofthetreatment protocolsandtiming.17 Anoverviewofthe timelineofinterventionsfortheCL/Ppatientispresentedin Table1.
Overviewofthetimelineofinterventionsinpatientswithcleftlip/palateandtheprovidersinvolvedat eachstage
Chronologic Age Dental DevelopmentInterventionsProviders
By6moPredentitionInfantorthopedictreatmentOrthodontistand/orpediatric dentist LiprepairCleftandcraniofacialsurgeon
10–24moPrimarydentitionPalaterepair Cleftandcraniofacialsurgeon
1–2yPrimarydentitionEstablishmentofdentalhome (andfollowevery6mo)
2.5–3yPrimarydentitionSpeechassessmentand velopharyngealsurgery(if indicated)
5–10yPrimarydentition andmixed dentition
9–12yEarlytolate mixeddentition
Assesstimingofmaxillary (alveolar)bonegrafting
Maxillaryexpansiontoestablish archformsandcorrect posteriorcross-bites
Pediatricdentist
Cleft/craniofacialsurgeon
Orthodontist/pediatricdentist/ cleftandcraniofacialsurgeon
Orthodontist
Maxillary(alveolar)bonegraftingCleftandcraniofacialsurgeon
Limitedorthodontictreatment followingmaxillary(alveolar) bonegrafting
Orthopedictreatmentusingface mask/reversepullheadgear
12–14yPermanent dentition
>14yPermanent dentition
Boneplate-supportedclass3 elasticstocorrectmaxillary/ mandibularantero-posterior discrepancies
Maxillarydistraction osteogenesis(ifthereislarge maxillary/mandibularanteroposteriordiscrepancy)
Comprehensivephaseof orthodontictreatment(if determinedthattherewillnot beaneedfororthognathic surgery)
Comprehensiveorthodontic treatment(withorwithout orthognathicsurgery)
Orthognathicsurgery(following completionofgrowth)
Orthodontist
Orthodontist
Orthodontistandcleft/ craniofacialsurgeon
Orthodontistandcleft/ craniofacialsurgeon
Orthodontist
Orthodontist
Cleft/craniofacialsurgeon
FinalrestorativetreatmentPeriodontist/prosthodontist/ primarycaredentist
PRESURGICALINFANTORTHOPEDIC TREATMENT Presurgicalinfantorthopedictreatment(PSIOT)is oftenthefirstmajorclinicalinterventionthatisperformedonpatientswithCL/P.PSIOTisinitiated withinthefirstfewweeksoflife,beforesurgical repairofthelip.PSIOTispurportedtorestorethe skeletal,cartilaginous,andsofttissueanatomic relationshippriortoliprepairandconsequently enhancethesurgicaloutcomes.18,19 Facialtapes, Lathamappliances,andNasoalveolar molding(NAM)techniquehavebeenwidelyused forPSIOT(Figs.1). NasoalveolarMoldingfor UnilateralandBilateralCleftLipRepair byKapadia andcolleaguesinthisissueprovideanoverview oftheNAMapproachand Dentofacial OrthopedicsfortheCleftPatient:TheLatham Approach byAllareddyandcolleaguesinthisissue provideanoverviewofLathamapproachforPSIOT. CertaincraniofacialcenterselecttoperformPSIOT onlyifthereisalargedefect,whileseveralothersdo notperformanytypeofPSIOT.20 Therehasbeen considerablecontroversyregardingthelong-term efficacyofPSIOTanditsandadverseimpacton maxillarygrowth.21 StudiesoriginatingfromEurope haveshownthatPSIOTisnotaneffectiveinterventionandrecommendagainstit.22,23 However, severalcraniofacialcentersintheUnitedStates electtoperformPSIOTwithvaryingdegreesofsuccess.ArecentsurveysuggestedthathalfofcraniofacialteamsreportedofferingPSIOT,withtheNAM techniquebeingthemostpopular.20 Graysonand
colleagues24–26 havedemonstratedthatuseof NAMisassociatedwithimprovementsinnasal angleandincreasesofnostrilwidth,columellar height,andcolumellarwidth.27
LIPREPAIR Primarycleftliprepairisthefirstsurgicalprocedurethatisundertakenbythesurgicalteam (Fig.2).Therepairisgenerallyperformedbetween theagesof3and6monthswiththepurposeof establishinglipcompetencebytheunificationof theunderlyingorbicularisorismuscle.28 Lip competenceisessentialforfeeding,speech,and controloforalsecretions.Therearemultiple differenttechniquesforclosureoftheunilateral cleftlipdefect,withthemostpopularincluding theMillardtechnique,theFisherunilateralcleft liptechnique,andMohlertechnique.Alltechniquesshareincommontheneedtoincreaselip heightontheaffectedsidebyregionalgeometric flaps;however,eachtechniqueapproachesthis problemdifferently.29 Thesurgicaltechniquefor abilateralcleftliprepairisgenerallyapproached inamorestandardfashionacrossallcenters. Theneedforprimaryrhinoplastyatthetimeoflip surgeryhasbeenfiercelydebatedthroughoutthe years.Mostsurgeonshaveincorporatedatleast aminimalnasaldissectionatthetimeoftheprimarylipsurgery,convincedthatitleadstobetter nasaloutcomesanddoesnotsignificantlyincreasetheriskofnasalstenosis.30 Itisessential thatpriortotakingthechildtotheoperating
Fig.1. NAMperformedbyDrLizbethHolguin.Defectsizepre-NAM24mm;post-NAM4mm.(Courtesyof Lizbeth Holguin,DDS,ElPaso,TX.)