No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or any information storage and retrieval system, without permission in writing from the publisher. Details on how to seek permission, further information about the Publisher’s permissions policies and our arrangements with organizations such as the Copyright Clearance Center and the Copyright Licensing Agency, can be found at our website: www.elsevier.com/permissions.
This book and the individual contributions contained in it are protected under copyright by the Publisher (other than as may be noted herein).
Notices
Knowledge and best practice in this field are constantly changing. As new research and experience broaden our understanding, changes in research methods, professional practices, or medical treatment may become necessary.
Practitioners and researchers must always rely on their own experience and knowledge in evaluating and using any information, methods, compounds, or experiments described herein. In using such information or methods they should be mindful of their own safety and the safety of others, including parties for whom they have a professional responsibility.
To the fullest extent of the law, neither the Publisher nor the authors, contributors, or editors, assume any liability for any injury and/or damage to persons or property as a matter of products liability, negligence or otherwise, or from any use or operation of any methods, products, instructions, or ideas contained in the material herein.
Library of Congress Cataloging-in-Publication Data
A catalog record for this book is available from the Library of Congress
British Library Cataloguing-in-Publication Data
A catalogue record for this book is available from the British Library
ISBN: 978-0-12-805298-3
For information on all Academic Press publications visit our website at https://www.elsevier.com/
Publisher: Mara Conner
Acquisition Editor: Melanie Tucker
Editorial Project Manager: Halima Williams
Production Project Manager: Edward Taylor
Designer: Matthew Limbert
Typeset by TNQ Books and Journals
13. Assessment, Consequence, and Clinical Implication of Asymmetry
17. Looking Beyond Neurological Impairment in Patients With Multiple Sclerosis During Exercise Intervention: Evidence for Muscular, Cardiac, Pulmonary, and Metabolic Dysfunction Related to Exercise Intolerance and Prognosis
I. WENS AND D. HANSEN
IV
ENVIRONMENTAL FACTORS AND EXERCISE
14. Neuromuscular Taping and Multiple Sclerosis: Reality or Trend?
C. COSTANTINO AND O. LICARI
15. Constraint-Induced Movement Therapy: When Efficacious Motor Therapy Meets Progressive Disease
A. BARGHI, V.W. MARK AND E. TAUB
Multiple Sclerosis: A Progressive Disease That Is Responsive to Constraint-Induced Movement Therapy
Muscular, Pulmonary, Cardiac, and Metabolic Abnormalities
18. Exercise in the Treatment of Multiple Sclerosis: Pragmatic Exercise Intervention in People With Mild to Moderate Multiple Sclerosis—The ExIMS Project
A. CARTER, L. HUMPHREYS AND B. SHARRACK
19. Yoga and Pilates as Methods of Symptom Management in Multiple Sclerosis
R. FRANK, K. EDWARDS AND J. LARIMORE
16. Physical Activity Behavior in Multiple Sclerosis: Definition, Rates, Outcomes, and Safety
R.W. MOTL AND R.E. KLAREN
20. Exercise in Prevention and Treatment of Multiple Sclerosis
R. MARTÍN-VALERO, A.E. GARCÍA-RODRIGUEZ, M.J. CASUSO-HOLGADO AND J.A. ARMENTA-PEINADO
21. Physical Activity and Health Promotion for People With Multiple Sclerosis: Implementing Activities in the Community
M. MACDONALD, A. DIXON-IBARRA AND K. ROGERS
VI
FOODS IN MULTIPLE SCLEROSIS
25. The Role of Natural Products in the Prevention and Treatment of Multiple Sclerosis
A. SHAMSIZADEH, A. ROOHBAKHSH, F. AYOOBI AND A. MOGHADDAMAHMADI
22. Interdisciplinary Treatment of Patients With Multiple Sclerosis and Chronic Pain
A.B. SULLIVAN AND S. DOMINGO
V
DRUGS OF ABUSE, ALCOHOL AND TOBACCO, AND DISEASE OF MULTIPLE SCLEROSIS PATIENTS
23. Alcohol and Tobacco in Multiple Sclerosis
M. CARDOSO AND Y.D. FRAGOSO
24. Herbal Oil Supplement
26. Effects of B Vitamins in Patients With Multiple Sclerosis
S.P. KALARN AND RONALD ROSS WATSON
List of Contributors
Y. Arima Hokkaido University, Sapporo, Japan
J.A. Armenta-Peinado University of Málaga, Málaga, Spain
L. Attorri Istituto Superiore di Sanità, Rome, Italy
F. Ayoobi Rafsanjan University of Medical Sciences, Rafsanjan, Iran
A. Barghi Harvard Medical School, Boston, MA, United States
G.S. Cantrell University of Oklahoma, Norman, OK, United States
M. Cardoso Universidade Metropolitana de Santos, Santos, SP, Brazil
A. Carter Sheffield Hallam University, United Kingdom
M.J. Casuso-Holgado University of Seville, Seville, Spain
İ. Coşkun Benlidayı Çukurova University, Adana, Turkey
C. Costantino University of Parma, Parma, Italy
R. Di Benedetto Istituto Superiore di Sanità, Rome, Italy
A. Di Biase Istituto Superiore di Sanità, Rome, Italy
A. Dixon-Ibarra Oregon State University, Corvallis, OR, United States
S. Domingo Mellen Center for Multiple Sclerosis, Cleveland, OH, United States
K. Edwards Precision Performance and Physical Therapy, Atlanta, Georgia
T. Elder Newcastle Community Fire Station, Newcastle Under Lyme, United Kingdom
J.W. Farrell University of Oklahoma, Norman, OK, United States
J. Fitzgerald Fort Lewis College, Durango, CO, United States
Y.D. Fragoso Universidade Metropolitana de Santos, Santos, SP, Brazil
R. Frank Georgia State University, Atlanta, Georgia
A.B. Gaikwad Birla Institute of Technology and Science, Pilani, Pilani, Rajasthan, India
A.E. García-Rodriguez University of Seville, Seville, Spain
M.S. Garud Shobhaben Pratapbhai Patel School of Pharmacy & Technology Management, SVKM’s NMIMS, Mumbai, India
D. Hansen Hasselt University, Diepenbeek, Belgium; Jessa Hospital, Hasselt, Belgium
C.E. Hayes University of Wisconsin–Madison, Madison, WI, United States
K. Higuchi Hokkaido University, Sapporo, Japan
L. Humphreys Sheffield Hallam University, United Kingdom
M. Iridoy Zulet Complejo Hospitalario de Navarra-IdiSNA (Navarra Institute for Health Research), Pamplona, Navarra, Spain
S.P. Kalarn University of Arizona, Tucson, AZ, United States
D. Kamimura Hokkaido University, Sapporo, Japan
J.M. Keppel Hesselink University of Witten/Herdecke, Witten, Germany
W.D.S. Killgore University of Arizona, Tucson, AZ, United States
R.E. Klaren University of Illinois at Urbana-Champaign, Urbana, IL, United States
A. Klimova University of Arizona, Tucson, AZ, United States
D.N. Krementsov University of Vermont, Burlington, VT, United States
Y.A. Kulkarni Shobhaben Pratapbhai Patel School of Pharmacy & Technology Management, SVKM’s NMIMS, Mumbai, India
D.J. Lantis University of Oklahoma, Norman, OK, United States
J. Larimore Agnes Scott College, Decatur, Georgia
R.D. Larson University of Oklahoma, Norman, OK, United States
Epigenetic Changes in DNA Methylation and Environment in Multiple Sclerosis
M. Iridoy Zulet1, M. Mendioroz Iriarte1,2
1Complejo Hospitalario de Navarra-IdiSNA (Navarra Institute for Health Research), Pamplona, Navarra, Spain; 2Neuroepigenetics Laboratory, Navarrabiomed-IdiSNA (Navarra Institute for Health Research), Pamplona, Navarra, Spain
INTRODUCTION
Epigenetic Regulatory Mechanisms
The first time the term epigenetics appeared in literature dates back to mid-20th century (Conrad Waddington, 1905–1975).1 However, it has been only in the last decade that epigenetics has become one of the emerging research fields, as a promising source of knowledge, especially in medicine.
Epigenetics has been defined as the study of the mechanisms regulating gene expression without changing the sequence of deoxyribonucleic acid (DNA). This discipline has built a bridge between genetic and environmental influences on the development of a phenotype; that is, it provides the means by which genetic material can respond to the diverse environmental conditions not requiring structural changes. Epigenetic changes allow some genes to be expressed or not, depending on the external conditions,
and those changes are essential in cell and tissue differentiation that occurs during embryonic development as well as in adult organisms. Thus, mammalian cells undergo epigenetic changes throughout life. In fact, identical twins with the same genetic background build different epigenetic patterns depending on the environmental factors to which they are subjected, such as smoking, diet, or exercise. 2 In addition, these epigenetics patterns cause observable differences in the phenotype of both twins, either a different behavior or different risk of disease. 3
The main epigenetic mechanisms include DNA methylation, histone modifications, and action of noncoding RNAs. So far, DNA methylation is the best known of these mechanisms. Most studies have been focused on DNA methylation and how it is associated with the development of a disease. Therefore, our review has been focused on DNA methylation and its role in developing multiple sclerosis (MS).
DNA Methylation
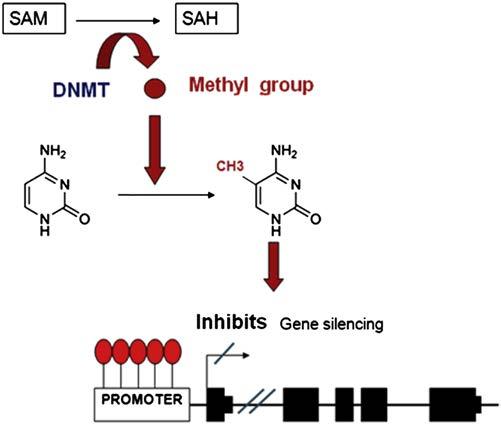
DNA methylation is a biochemical process by which a methyl group is added to a cytosine residue in the DNA nucleotide chain. This binding occurs in cytosine–guanine dinucleotides (CpG), which are clustered in the genome, building the CpG islands. These are especially abundant in the promoter and other regulatory regions of genes. Methylation is performed by DNA methyltransferases (DNMTs) that catalyze the transfer of a methyl group from S-adenosyl-l-methionine (SAM) to carbon 5 of cytosine.4 This process may be carried out following two different models: the occurrence of a “de novo” methylation pattern catalyzed by the DNMT3a and DNMT3b5 enzymes, or by maintaining a methylation pattern in the following cycles of cell replication performed by DNMT1. The latter occurs during DNA replication. Therefore, when a CpG sequence acquires a certain methylation pattern, this modification becomes stable and is inherited as a clonal methylation pattern through subsequent cell divisions.6
Hypermethylation of CpG islands in the promoter region of the gene is typically a mechanism of gene repression as it inhibits transcription. This inhibition is basically performed through two processes: (1) by preventing the binding of transcription factors containing recognition sites for CpGs and (2) by means of adhering protein complexes known as methyl-binding domain (MBD) that are bound to the methylated CpG regions and block access to regulatory proteins or transcription factors.7
As mentioned earlier, the methyl group donor is the SAM molecule which, once it loses the methyl group, becomes S-adenosyl homocysteine (SAH). This molecule is hydrolyzed to homocysteine and then it is remethylated to methionine by 5-methyltetrahydrofolate cofactor (5mTHF). Finally, methionine is transformed back into a SAM molecule by the action of methionine adenosyltransferase (MAT). DNA methylation potential depends on the ratio between SAM level and SAH in blood. The higher the ratio, the more the methylation potential.8 Therefore, it can be inferred that for the process of DNA methylation, proper metabolism of homocysteine and methionine is critical, as well as the metabolism of the various enzymes involved in this metabolic route and of other substances, such as folic acid and vitamin B129 (Fig. 1.1).
Relevance of DNA Methylation in Clinical Practice
Disruption of epigenetic mechanisms involved in human disease has been, for the last few years, an area of emerging research, yielding positive results in various diseases, especially in oncology. The first tumor related to mechanisms of epigenetic regulation was colorectal cancer (CRC). Initially, a loss of overall methylation
FIGURE 1.1 The process of how DNA methylation within gene promoters regulates transcription. SAM, S-adenosyl-l-methionine. SAH, S-adenosyl homocysteine. DNMT, DNA methyltransferases.
was observed in cancer cells of CRC patients compared to healthy controls.10 Also, the promoters of tumor suppressor genes were shown to be hypermethylated, which caused lower expression of those genes.11 These findings supported that hypermethylation of tumor suppressor genes was associated with the occurrence of the disease. However, in other areas of medicine, such as neurological disorders, how disruption of DNA methylation is involved in the disease is not well known yet. In the case of MS, epigenetic changes that might be involved in the pathogenesis of the disease have been identified, which has led to an exciting and new route of research.
MS is considered the leading cause of severe neurological disease affecting young and middle-aged adults. It is a chronic disease causing inflammatory, demyelinating, and neurodegenerative damage in the central nervous system (CNS). Its etiology is still unknown, although an autoimmune and multifactorial origin has been presumed and several genetic and environmental factors of susceptibility have been described for MS. Given the complexity of the disease and the participation of diverse, both genetic and environmental, etiological mechanisms, it is conceivable that there may be an alteration in the epigenetic regulation involved in its progression.12,13
RISK FACTORS IN MS AND EPIGENETIC CHANGES
Epidemiological and family aggregation studies suggest that there is a genetic predisposition for MS. However, to date, the only locus consistently associated with MS is the major histocompatibility complex (MHC). This predisposition has been associated with DR2
haplotype (HLA-DRB1*1501-DQA1*0102-DQB1*0602), which determines a relative risk of four of having MS.14 Development of new technologies, such as polymorphism arrays, has helped to identify new candidate genes located outside the MHC region. Therefore, MS is considered as a polygenic disease in which each gene shows a different risk score (usually low or moderate).15 Moreover, environmental factors seem essential to the development of MS. For instance, the mismatch rate for disease occurring among monozygotic siblings is 70%, which supports the idea of other variables being involved.16 Indeed, there is a number of environmental factors described to be involved in the etiology of MS, such as vitamin D levels in serum, animal fats in the diet, injuries, and toxic substances17 (smoking, heavy metals, organic solvents, etc.). To date, the most consistent risk factors are smoking, vitamin D deficiency, and infection by Epstein–Barr virus (EBV).18,19
In the following sections, we summarize the three main environmental risk factors described for MS and the effects these factors may have on the various mechanisms of epigenetic regulation, both in MS and in the development of other diseases (Fig. 1.2).
Smoking and Epigenetic Mechanisms
Smoking is one of the environmental factors influencing the development of MS, as shown in different studies.
According to a study conducted by Rodriguez Regal et al., smoking involves an odds ratio (OR) of developing MS of 1.97.20 Cigarette smoke contains hundreds of potentially toxic elements, including nicotine, carbon monoxide, nitric oxide, cyanides, and polycyclic aromatic hydrocarbons, and some studies have suggested that these toxins might cause gene activation responsible for the MS autoimmune pathogenesis.21 In fact, smoking has been associated with an increased relapse frequency and with the number of active lesions in the brain MRI of patients with this disease.22
On the other hand, when the blood of adolescents whose mothers smoked during pregnancy was analyzed, it was observed that prenatal exposure to tobacco is associated with increased methylation of the promoter of the “brainderived neurotrophic factor” (BDNF), which promotes the differentiation and growth of new neurons.23 Likewise, another study conducted by Kjersti Aagaard et al. analyzed the DNA methylation pattern by PCR techniques, in two groups of smokers and nonsmokers. They found changes in DNA methylation in 25 genes in nonsmokers and 438 genes in smokers.24 Interestingly, epigenetic changes associated with smoking have also been found in oncology. In a study conducted in lung cancer patients, hypermethylation of CDKN2A, DAPK, and MGMT tumor suppressor genes was observed in smokers.25 Likewise, in a study conducted on cervical cancer among female smokers aged between 15 and 19, hypermethylation of
EPIGENETICS
GENETIC FACTORS
HLADRB1*1501
Candidate genes
FIGURE 1.2 The interplay between environmental and genetic factors. The interplay is where DNA methylation may play a role to develop multiple sclerosis.
18. Mandia D, Ferraro OE, Nosari G, Montomoli C, Zardini E, Bergamaschi R. Environmental factors and multiple sclerosis severity: a descriptive study. Int J Environ Res Public Health June 19, 2014;11(6):6417–32.
19. Manouchehrinia A, Weston M, Tench CR, Britton J, Constantinescu CS. Tobacco smoking and excess mortality in multiple sclerosis: a cohort study. J Neurol Neurosurg Psychiatry October 2014; 85(10):1091–5
20. Rodríguez Regal A, del Campo Amigo M, Paz-Esquete J, Martínez Feijoo A, Cebrián E, Suárez Gil P, et al. Estudio de casos y controles sobre la influencia del hábito tabáquico en la esclerosis múltiple. Neurología 2009;24(3):177180.
21. Hernán MA, Jick SS, Logroscino G, Olek MJ, Ascherio A, Jick H Cigarette smoking and the progression of multiple sclerosis. Brain 2005;128:146165.
22. Healy BC, Ali EN, Guttmann CR, Chitnis T, Glanz BI, Buckle G, et al. Smoking and disease progression in multiple sclerosis. Arch Neurol 2009;66:8.
23. Toledo-Rodriguez M, Lotfipour S, Leonard G, Perron M, Richer L, Veillette S, et al. Maternal smoking during pregnancy is associated with epigenetic modifications of the brain-derived neurotrophic factor-6 exon in adolescent offspring. Am J Med Genet B Neuropsychiat Genet 2010;13B:1350–4.
24. Suter MA, Anders AM, Aagaard KM. Maternal smoking as a model for environmental epigenetic changes affecting birthweight and fetal programming. Mol Hum Reprod January 2013;19(1):1–6.
25. Koturbash I, Beland FA, Pogribny IP. Role of epigenetic events in chemical carcinogenesis—a justification for incorporating epigenetic evaluations in cancer risk assessment. Toxicol Mech Methods 2011;21:289–97.
26. Ma YT, Collins SI, Young LS, Murray PG, Woodman CB. Smoking initiation is followed by the early acquisition of epigenetic change in cervical epithelium: a longitudinal study. Br J Cancer 2011;104:1500–4.
27. Baarnhielm M. Multiple sclerosis is associated with low previous ultraviolet radiation exposure and low levels of current vitamin D: no interaction with HLA complex genes. Mult Scler 2010;16:S7–39.
28. Kimlin MG, Olds WJ, Moore MR. Location and vitamin D synthesis: is the hypothesis validated by geophysical data? J Photochem Photobiol B 2007;86:234–9.
29. Smolders J, Peelen E, Thewissen M, Cohen Tervaert JW, Menheere P, Hupperts R, et al. Safety and T cell modulating effects of high dose vitamin D3 supplementation in multiple sclerosis. PLoS One 2010;5:e15235.
30. Mahon BD, Gordon SA, Cruz J, Cosman F, Cantorna MT. Cytokine profile in patients with multiple sclerosis following vitamin D supplementation. J Neuroimmunol 2003;134:128–32.
31. Joshi S, Pantalena LC, Liu XK, Gaffen SL, Liu H, Rohowsky-Kochan C, et al. 1,25 dihydroxyvitamin D(3) ameliorates Th17 autoimmunity via transcriptional modulation of interleukin-17A. Moll Cell Biol 2011;31:3653–69.
32. Pereira F, Barbáchano A, Singh PK, Campbell MJ, Muñoz A, Larriba MJ. Vitamin D has wide regulatory effects on histone demethylase genes. Cell Cycle 2012;11:1081–9.
33. Sundstrom P. Evidence for virus infections in the presymptomatic stage of MS. Mult Scler 2010;16:S7–39.
34. Handel AE, Williamson AJ, Disanto G, Handunnetthi L, Giovannoni G, Ramagopalan SV. An updated meta-analysis of risk of multiple sclerosis following infectious mononucleosis. PLoS One September 1,2010;5(9)
35. Niller HH, Wolf H, Minarovits J. Epigenetic dysregulation of the host cell genome in Epstein-Barr virus associated neoplasia. Semin Cancer Biol 2009;19:158–64.
36. Tsai CL, Li HP, Lu YJ, Hsueh C, Liang Y, Chen CL, et al. Activation of DNA methyltransferase 1 by EBV LMP1 involves c-Jun NH2terminal kinase signaling. Cancer Res 2006;66:11668–76.
37. Junker A, Krumbholz M, Eisele S, Mohan H, Augstein F, Bittner R, et al. MicroRNA profiling of multiple sclerosis lesions identifies modulators of the regulatory protein CD47. Brain 2009;132:3342–52.
38. Bar-Or A. The immunology of multiple sclerosis. Semin Neurol 2008;28:29–45.
39. Kumagai C, Kalman B, Middleton FA, Vyshkina T, Massa PT. Increased promoter methylation of the immune regulatory gene SHP-1 in leukocytes of multiple sclerosis subjects. J Neuroimmunol 2012;246:51–7.
40. Janson PC, Linton LB, Bergman EA, Marits P, Eberhardson M, Piehl F. Profiling of CD4+ T cells with epigenetic immune lineage analysis. J Immunol 2011;186:92–102.
41. Liggett T, Melnikov A, Tilwalli S, Yi Q, Chen H, Replogle C, et al. Methylation patterns of cell-free plasma DNA in relapsing-remitting multiple sclerosis. J Neurol Sci Mar15, 2010;290(1–2):16–21.
42. Koch MW, Metz LM, Kovalchuk O. Epigenetic changes in patients with multiple sclerosis. Nat Rev Neurol January 2013;9(1):35–43
43. Mastronardi FG, Noor A, Wood DD, Paton T, Moscarello MA Peptidyl arginine deiminase 2 CpG island in multiple sclerosis white matter is hypomethylated. J Neurosci Res 2007;85:2006–16.
44. Graves M, Benton M, Lea R, Boyle M, Tajouri L, Macartney-Coxson D, et al. Methylation differences at the HLA-DRB1 locus in CD4+ T-Cells are associated with multiple sclerosis. Mult Scler December 12, 2013;20(8):1033–41.
45. Huynh JL, Garg P, Thin TH, Yoo S, Dutta R, Trapp BD, et al. Epigenome-wide differences in pathology-free regions of multiple sclerosis-affected brains. Nat Neurosci January 2014;17(1):121–30.
46. Maltby VE, Graves MC, Lea RA, Benton MC, Sanders KA, Tajouri L, et al. Genome-wide DNA methylation profiling of CD8+ T cells shows a distinct epigenetic signature to CD4+ cells in multiple sclerosis patients. Clin Epigenetics November 5, 2015;7:118.
47. Chestnut BA, Chang Q, Price A, Lesuisse C, Wong M, Martin LJ. Epigenetic regulation of motor neuron cell death through DNA methylation. J Neurosci 2011;31:16619–36.
48. Zhou Y, Simpson Jr S, Holloway AF, Charlesworth J, Van der Mei I, Taylor BV. Potential role of epigenetic modifications in the heritability of multiple sclerosis. Mult Scler February 2014;20(2):135–40.
49. Huynh JL, Casaccia P. Epigenetic mechanisms in multiple sclerosis: implications for pathogenesis and treatment. Lancet Neurol February 2013;12(2):195–206.
2
EBV Infection and Vitamin D in Multiple Sclerosis Patients
Sayed Mahdi Marashi1, Zabihollah Shoja2
1Virology Department, School of Public Health, Tehran University of Medical Sciences (TUMS), Tehran, Iran; 2Virology Department, Pasteur Institute of Iran (IPI), Tehran, Iran
MULTIPLE SCLEROSIS AND ENVIRONMENTAL FACTORS
Multiple sclerosis (MS) is a chronic, inflammatory, and debilitating autoimmune disease of the central nervous system (CNS) with unknown etiology. The inflammatory phenotype of MS is expressed as a relapsing–remitting course of neurological dysfunction, although the clinical symptoms vary between individuals.1 MS mostly occurs in young adults, although MS risk appears to decline largely after the age of 50.2,3
As documented for a variety of autoimmune diseases, MS is more prevalent in females.4,5 The female to male ratio ranges from 2:1 to 3:1 based on region,6 and it is tempting to speculate that the female bias in immune complex diseases such as MS might be a consequence of sex hormones. However, it is not clear whether sexrelated factors potentially exert deleterious effect or protective effect, although results from animal models remain conflicted, with some research showing no effect7 and other findings indicating a slight worsening of clinical experimental autoimmune encephalomyelitis (EAE) following ovariectomy.8 A number of MS-related genetic
variations have also been reported,9 highlighting the potential role of gene–environment interaction as well as the epigenetic phenomenon for female predominance.10 Indeed, the female to male ratio for MS susceptibility is shown to be higher in individuals with certain human leukocyte antigen (HLA) haplotypes. In addition, the female to male ratio is higher in MS patients with HLADRB1*15 haplotypes than those who are negative for DRB1*15. 9
Both infectious and noninfectious factors have been implicated in MS development.11,12. Rather than a sole trigger, the initiation of MS disease seems to be reliant on the elaborate interactions between infectious or noninfectious environmental risk factors with shared susceptibility genes.13
MS AND INFECTIONS
Infectious agents are considered an important environmental risk factor for autoimmune diseases. In this regard, viruses have long been considered as possible etiological agents of MS.14 As far back as 1946, the rabies