Professor and Associate Chair, Department of Physical Therapy, University of Evansville, Evansville, Indiana
Mary Kessler, PT, MHS
Associate Dean, College of Education and Health Sciences, Director Physical Therapist Assistant Program, Associate Professor, Department of Physical Therapy, University of Evansville, Evansville, Indiana
Table of Contents
Cover image
Title page
Copyright
Contributors
Dedication
Preface
Acknowledgments
Section 1: Foundations
Chapter 1: The Roles of the Physical Therapist and Physical Therapist Assistant in Neurologic Rehabilitation
All rights reserved No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or any information storage and retrieval system, without permission in writing from the publisher Permissions may be sought directly from Elsevier’s Health Sciences Rights Department in Philadelphia, PA, USA: phone: (+ 1) 215 239 3804, fax: (+ 1) 215 239 3805, e-mail: healthpermissions@elsevier com You may also complete your request online via the Elsevier homepage (http://www elsevier com), by selecting ‘Customer Support’ and then ‘Obtaining Permissions ’
Notice
Knowledge and best practice in this field are constantly changing As new research and experience broaden our knowledge, changes in practice, treatment, and drug therapy may become necessary or appropriate. Readers are advised to check the most current information provided (i) on procedures featured or (ii) by the manufacturer of each product to be administered, to verify the recommended dose or formula, the method, and duration of administration, and contraindications It is the responsibility of the practitioner, relying on their own experience and knowledge of the patient, to make diagnoses, to determine dosages and the best treatment for each individual patient, and to take all appropriate safety precautions. To the fullest extent of the law, neither the Publisher nor the Editor assumes any liability for any injury and/or damage to persons or property arising out of or related to any use of the material contained in this book
The Publisher
International Standard Book Number: 978-1-4557-4020-8
Executive Content Strategist: Kathy Falk
Content Development Specialist: Brandi Graham
Publishing Services Manager: Julie Eddy
Senior Project Manager: Richard Barber
Designer: Ryan Cook
Printed in the United States of America
Last digit is the print number: 9 8 7 6 5 4 3 2 1
Contributors
Maghan C Bretz, PT, MPT St Mary’s Rehabilitation Institute, Adjunct Instructor, Department of Physical Therapy, Evansville, Indiana, Evolve videos
To my husband, Terry, who has always been there with love and support, and to my parents who were always supportive of my educational endeavors
Tink
To Craig, my husband, who continues to provide me with love, support, and encouragement to pursue this and all of my other professional goals, and to Kyle and Kaitlyn, who still like to see their photographs in print
A final word of thanks to my parents, John and Judy Oerter, who have always encouraged me to work hard and strive for excellence You have always believed in me and my ability to succeed.
Mary
Preface
Tink Martin Mary Kessler
We are gratified by the very positive responses to the first two editions of the Neurologic Interventions for Physical Therapy text In an effort to make a good reference even better, we have taken the advice of reviewers and our physical therapist and physical therapist assistant students to complete a third edition. The sequence of chapters still reflects a developmental trend with motor development, handling and positioning, and interventions for children coming before the content on adults Chapters on specific pediatric disorders and neurologic conditions seen in adults remain as well as introductory chapters on physical therapy practice and the role of the physical therapist assistant. The review of basic neuroanatomy structure and function and the chapter on proprioceptive neuromuscular facilitation have been updated and continue to provide foundational knowledge The intervention components of each chapter have been enhanced to emphasize function and the use of current best evidence in the physical therapy care of these patients. Concepts related to neuroplasticity and task-specific training are also included. All patient cases have been reworked again to reflect current practice and are formatted in a way to assist students with their documentation skills
We continue to see that the text is used by students in both physical therapist assistant and doctor of physical therapy programs, and this certainly has broad appeal However, as we indicated in our last preface, we continue to be committed to addressing the role of the physical therapist assistant in the treatment of children and adults with neurologic deficits. On the contrary, the use of the textbook by physical therapy students should increase the understanding of and appreciation for the psychomotor and critical-thinking skills needed by all members of the rehabilitation team to maximize the function of patients with neurologic deficits.
The Evolve site continues to be enhanced as we try to insert additional resources for faculty and students. An instructor Test Bank and PowerPoint slides have been added in this third edition. Also, newly added video clips of interventions as well as gait and proprioceptive neuromuscular facilitation will allow students to increase their understanding of the subject matter and to be better prepared for the neurologic portion of their certification exam
The mark of sophistication of any society is how well it treats the young and old, the most vulnerable segments of the population We hope in some small measure that our continuing efforts will make it easier to unravel the mystery of directing movement, guiding growth and development, and relearning lost functional skills to improve the quality of life for the people we serve
Acknowledgments
I again want to acknowledge the dedication and hard work of my colleague, friend, and co-author, Mary Kessler. Mary’s focus on excellence is evident in the updated adult chapters. Special thanks to Dawn Welborn-Mabrey for her marvelous pediatric insights. Thank you to past contributors, Dr. Pam Ritzline, Mary Kay Solon, Dr Donna Cech, and Terry Chambliss Thank you to the students at the University of Evansville You are really the reason this book happened in the first place and the reason it has evolved into its present form. I want to acknowledge the work of those at Elsevier, especially Brandi Graham, for seeing us through the timely completion of the third edition.
Tink
I must thank my good friend, mentor, colleague, and co-author, Tink Martin Without Tink, none of these editions would have been completed. She has continued to take care of many of the details, always keeping us focused on the end result Tink’s ongoing encouragement and support have been most appreciated
A special thank you to all of the students at the University of Evansville They are the reason that we originally started this project, and they have continued to encourage and motivate us to update and revise the text Additional thanks must be extended to all of the individuals who have assisted us over the last 20 years, including Dr Catherine McGraw, Maghan Bretz, Sara Snelling, Dr Pam Ritzline, Mary Kay Solon, Janet Szczepanski, Terry Chambliss, Suzy Sims, Beth Jankauski, and Amanda Fisher. Every person mentioned has contributed to the overall excellence and success of this text
Mary
SECTION 1 Foundations
CHAPTER 1
The Roles of the Physical Therapist and Physical Therapist Assistant in Neurologic Rehabilitation
Objectives
After reading this chapter, the student will be able to:
The practice of physical therapy in the United States continues to change to meet the increased demands placed on service provision by reimbursement entities and federal regulations The profession has seen an increase in the number of physical therapist assistants (PTAs) providing physical therapy interventions for adults and children with neurologic deficits PTAs are employed in outpatient clinics, inpatient rehabilitation centers, extended-care and pediatric facilities, school systems, and home healthcare agencies. Traditionally, the rehabilitation management of adults and children with neurologic deficits consisted of treatment derived from the knowledge of disease and interventions directed at the amelioration of patient signs, symptoms, and functional impairments Physical therapists and physical therapist assistants help individuals “maintain, restore, and improve movement, activity, and functioning, thereby enhancing health, well-being, and quality of life” (APTA, 2014). Physical therapy is provided across the lifespan to children and adults who “may develop impairments, activity limitations, and participation restrictions” (APTA, 2014) These limitations develop as a consequence of various health conditions and the interaction of personal and environmental factors (APTA, 2014).
Sociologist Saad Nagi developed a model of health status that has been used to describe the relationship between health and function (Nagi, 1991) The four components of the Nagi Disablement Model (disease, impairments, functional limitations, and disability) evolve as the individual loses health. Disease is defined as a pathologic state manifested by the presence of signs and symptoms that disrupt an individual’s homeostasis or internal balance. Impairments are alterations in anatomic, physiologic, or psychological structures or functions Functional limitations occur as a result of impairments and become evident when an individual is unable to perform everyday activities that are considered part of the person’s daily routine. Examples of physical impairments include a loss of strength in the anterior tibialis muscle or a loss of 15 degrees of active shoulder flexion These physical impairments may or may not limit the individual’s ability to perform functional tasks Inability to dorsiflex the ankle may prohibit the patient from achieving toe clearance and heelstrike during ambulation, whereas a 15-degree limitation in shoulder range may have little impact on the person’s ability to perform self-care or dressing tasks.
According to the disablement model, a disability results when functional limitations become so great that the person is unable to meet age-specific expectations within the social or physical environment (Verbrugge and Jette, 1994). Society can erect physical and social barriers that interfere with a person’s ability to perform expected roles. The societal attitudes encountered by a person with a disability can result in the community’s perception that the individual is handicapped Figure 1-1 depicts the Nagi classification system of health status
The second edition of the Guide to Physical Therapist Practice incorporated the Nagi Disablement Model into its conceptual framework of physical therapy practice. The use of this model has directed physical therapists (PTs) to focus on the relationship between impairment and functional limitation and the patient’s ability to perform everyday activities Increased independence in the home and community and improvements in an individual’s quality of life are the expected outcomes of physical therapy interventions (APTA, 2003). However, as our practice has evolved, current practice guidelines recognize the critical roles PTs and PTAs play in providing “rehabilitation and habilitation, performance enhancement, and prevention and risk-reduction services” for patients and the overall population (APTA, 2014)
As physical therapy professionals, it is important that we understand our role in optimizing patient function. The second edition of the Guide to Physical Therapist Practice (APTA, 2003) defined function as “those activities identified by an individual as essential to support physical, social, and psychological well-being and to create a personal sense of meaningful living ” Function is related to
FIGURE1-1 Nagiclassificationsystemofhealthstatus
age-specific roles in a given social context and physical environment and is defined differently for a child of 6 months, an adolescent of 15 years, and a 65-year-old adult Factors that contribute to an individual’s functional performance include personal characteristics, such as physical ability, emotional status, and cognitive ability; the environment in which the adult or child lives and works, such as home, school, or community; and the social expectations placed on the individual by the family, community, or society
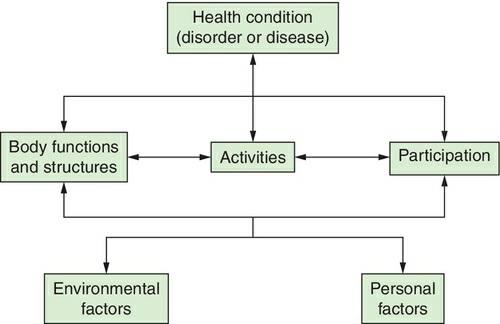
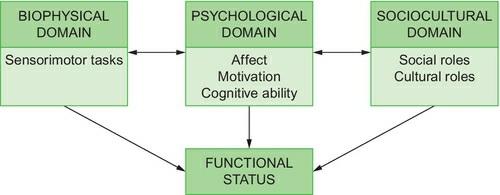
The World Health Organization (WHO) developed the International Classification of Functioning, Disability, and Health (ICF), which has been endorsed by the American Physical Therapy Association (APTA) This system provides a more positive framework and standard language to describe health, function, and disability and has been incorporated into the third edition of the Guide to Physical Therapist Practice. Figure 1-2 illustrates the ICF model. Health is much more than the absence of disease; rather, it is a condition of physical, mental, and social well-being that allows an individual to participate in functional activities and life situations (WHO, 2013; Cech and Martin, 2012). A biopsychosocial model is central to the ICF and defines a person’s health status and functional capabilities by the interactions between one’s biological, psychological, and social domains (Figure 1-3) This conceptual framework recognizes that two individuals with the same diagnosis might have very different functional outcomes and levels of participation based on environmental and personal factors.
FIGURE1-3 Thethreedomainsoffunction biophysical,psychological,sociocultural mustoperate independentlyaswellasinterdependentlyforhumanbeingstoachievetheirbestpossiblefunctionalstatus (From CechD MartinS: Functional movement development across the life span ed3 StLouis 2012 Elsevier)
The ICF also presents functioning and disability in the context of health and organizes the information into two distinct parts. Part 1 addresses the components of functioning and disability as
they relate to the health condition The health condition (disease or disorder) results from the impairments and alterations in an individual’s body structures and functions (physiologic and anatomical processes). Activity limitations present as difficulties performing a task or action and encompass physical as well as cognitive and communication activities Participation restrictions are deficits that an individual may experience when attempting to meet social roles and obligations within the environment Functioning and disability are therefore viewed on a continuum where functioning encompasses performance of activities, and participation and disability implies activity limitations and restrictions in one’s ability to participate in life situations Part 2 of the ICF information recognizes the external environmental and internal personal factors which influence a person’s response to the presence of a disability and the interaction of these factors on one’s ability to participate in meaningful activities (APTA, 2014; WHO, 2013). All factors must be considered to determine their impact on function and participation (O’Sullivan, 2014; Cech and Martin, 2012)
The ICF is similar to the Nagi Model; however, the ICF emphasizes enablement rather than disability (Cech and Martin, 2012). In the ICF model, there is less focus on the cause of the medical condition and more emphasis directed to the impact that activity limitations and participation restrictions have on the individual As individuals experience a decline in health, it is also possible that they may experience some level of disability Thus, the ICF “mainstreams the experience of disability and recognizes it as a universal human experience” (ICF, 2014).
Various functional skills are needed in domestic, vocational, and community environments. Performance of these skills enhances the individual’s physical and psychological well-being Individuals define themselves by what they are able to accomplish and how they are able to participate in the world. Performance of functional tasks not only depends on an individual’s physical abilities and sensorimotor skills but is also affected by the individual’s emotional status (depression, anxiety, self-awareness, self-esteem), cognitive abilities (intellect, motivation, concentration, problem-solving skills), and ability to interact with people and meet social and cultural expectations (Cech and Martin, 2012). Furthermore, individual factors such as congenital disorders and genetic predisposition to disease, demographics (age, sex, level of education, and income), comorbidities, lifestyle choices, health habits, and environmental factors (including access to medical and rehabilitation care and the physical and social environments) may also impact the individual’s function and his or her quality of life (APTA, 2014).
Theroleofthephysicaltherapistinpatientmanagement
As stated earlier, physical therapists are responsible for providing rehabilitation, habilitation, performance enhancement, and preventative services (APTA, 2014) Ultimately, the PT is responsible for performing a review of the patient’s history and systems and for administering appropriate tests and measures in order to determine an individual’s need for physical therapy services If after the examination the PT concludes that the patient will benefit from services, a plan of care is developed that identifies the goals, expected outcomes, and the interventions to be administered to achieve the desired patient outcomes (APTA, 2014).
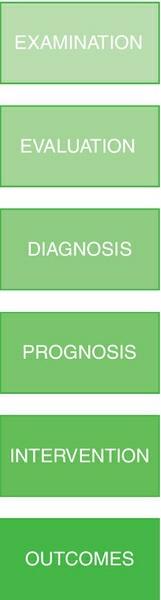
The steps the PT utilizes in patient/client management are outlined in the third edition of the Guide to Physical Therapist Practice and includes examination, evaluation, diagnosis, prognosis, interventions, and outcomes. The PT integrates these elements to optimize the patient’s outcomes, including improving the health or function of the individual or enhancing the performance of healthy individuals Figure 1-4 identifies these elements In the examination, the PT collects data through a review of the patient’s history and a review of systems and then administers appropriate tests and measures. The PT then evaluates the data, interprets the patient’s responses, and makes clinical judgments relative to the chronicity or severity of the patient’s problems. Within the evaluation process, the therapist establishes a physical therapy diagnosis based on the patient’s level of impairment and functional limitations Use of differential diagnosis (a systematic process to classify patients into diagnostic categories) may be used. Once the diagnosis is completed, the PT develops a prognosis, which is the predicted level of improvement and the amount of time that will be needed to achieve those levels Patient goals are also a component of the prognosis aspect of the evaluation The development of the plan of care is the final step in the evaluation process The plan of care includes short- and long-term goals and specific interventions to be administered, as well as the expected outcomes of therapy and the proposed frequency and duration of treatment. Goals and outcomes should be objective, measureable, functionally oriented, and meaningful to the patient Intervention is the element of patient management in which the PT or the PTA interacts with the patient through the administration of “various physical interventions to produce changes in the [patient’s] condition that are consistent with the diagnosis and prognosis” (APTA, 2014).
Intervention are organized into 9 categories: “patient or client instruction (used with every patient); airway clearance techniques, assistive technology, biophysical agents; functional training in selfcare and domestic, work, community, social, and civic life; integumentary repair and protection techniques; manual therapy techniques; motor function training; and therapeutic exercise” (APTA, 2014) Reexamination of the patient includes performance of appropriate tests and measures to determine if the patient is progressing with treatment or if modifications are needed The final component related to patient management is review of patient outcomes. The PT must determine the impact selected interventions have had on the following: disease or disorder, impairments, activity limitations, participation, risk reduction and prevention, health, wellness, and fitness, societal resources, and patient satisfaction (APTA, 2014) Other aspects of patient/client management include the coordination (the working together of all parties), communication, and documentation of services provided
FIGURE1-4 Theelementsofpatient/clientmanagement (FromAmericanPhysicalTherapyAssociation: Guide to Physical Therapist Practice 3 0 Alexandria,VA,2014,APTA)
PTAs assist only with the intervention component of care (Clynch, 2012). All interventions performed by the PTA are directed and supervised by the PT These interventions may include “procedural intervention(s), associated data collection, and communication including written documentation associated with the safe, effective, and efficient completion of the task” (Crosier, 2010). All other tasks remain the sole responsibility of the PT.
There is little debate as to whether PTAs have a role in treating adults with neurologic deficits, as long as the individual needs of the patient are taken into consideration and the PTA follows the plan of care established by the PT Physical therapist assistants are the only healthcare providers who “assist a physical therapist in the provision of selected interventions” (APTA, 2014). The primary PT is still ultimately responsible for the patient, both legally and ethically, and the actions of the PTA relative to patient management (APTA, 2012a) The PT directs and supervises the PTA when the PTA provides interventions selected by the PT The APTA has identified the following responsibilities as those that must be performed exclusively by the PT (APTA, 2012a):
1. Interpretation of referrals when available
2 Initial examination, evaluation, diagnosis, and prognosis
3 Development or modification of the plan of care, which includes the goals and expected outcomes
4. Determination of when the expertise and decision-making capabilities of the PT requires the PT to personally render services and when it is appropriate to utilize a PTA
5 Reexamination of the patient and revision of the plan of care if indicated
6. Establishment of the discharge plan and documentation of the discharge summary
7. Oversight of all documentation for services rendered APTA policy documents also state that interventions that require immediate and continuous examination and evaluation are to be performed exclusively by the PT (APTA, 2012b) Specific examples of these interventions have changed recently. PTs and PTAs are advised to refer to APTA policy documents, their state practice acts, and the Commission on Accreditation in Physical Therapy Education (CAPTE) guidelines for the most up-to-date information regarding interventions that are considered outside the scope of practice for the PTA Practitioners are also encouraged to review individual state practice acts and payer requirements for supervision requirements as they relate to the PT/PTA relationship (Crosier, 2011).
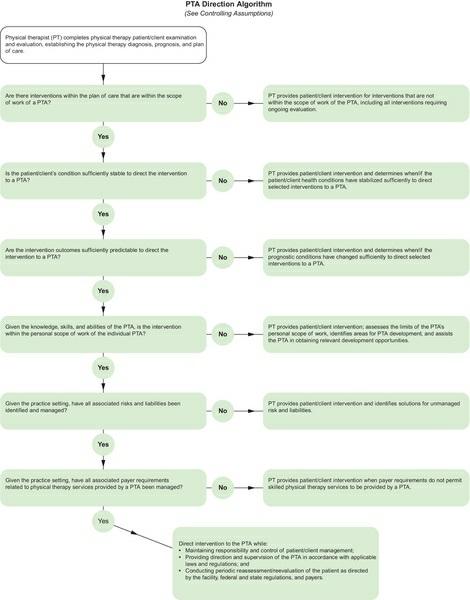
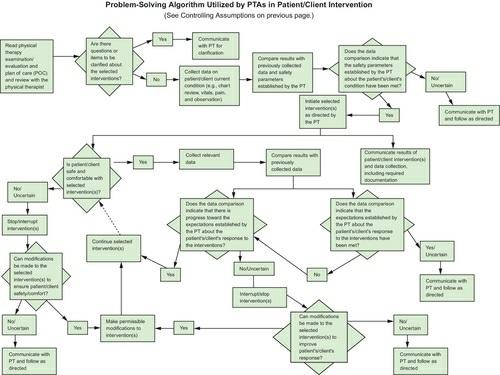
Before directing the PTA to perform specific components of the intervention, the PT must critically evaluate the patient’s condition (stability, acuity, criticality, and complexity) consider the practice setting in which the intervention is to be delivered, the type of intervention to be provided, and the predictability of the patient’s probable outcome to the intervention (APTA, 2012a). In addition, the knowledge base of the PTA and his or her level of experience, training, and skill level must be considered when determining which tasks can be directed to the PTA The APTA has developed two algorithms (PTA direction and PTA supervision; Figures 1-5 and 1-6) to assist PTs with the steps that should be considered when a PT decides to direct certain aspects of a patient’s care to a PTA and the subsequent supervision that must occur Even though these algorithms exist, it is important to remember that communication between the PT and PTA must be ongoing to ensure the best possible outcomes for the patient. PTAs are also advised to become familiar with the Problem-Solving Algorithm Utilized by PTAs in Patient/Client Intervention (Figure 1-7) as a guide for the clinical problem-solving skills a PTA should employ before and during patient interventions (APTA, 2007) Unfortunately, in our current healthcare climate, there are times when the decision as to whether a patient may be treated by a PTA is determined by productivity concerns and the patient’s payer source An issue affecting some clinics and PTAs is the denial of payment by some insurance providers for services provided by a PTA Consequently, decisions regarding the utilization of PTAs are sometimes determined by financial remuneration and not by the needs of the patient.
FIGURE1-5 PTAdirectionalgorithm (FromCrosierJ:PTdirectionandsupervisionalgorithms, PT in Motion 2(8):47,2010)
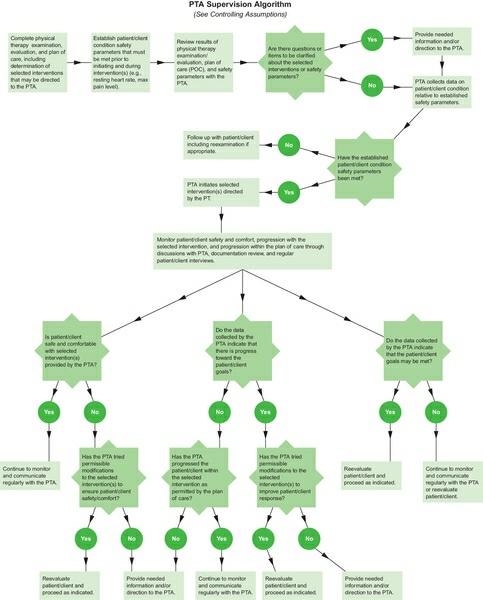
FIGURE1-6 PTAsupervisionalgorithm (FromCrosierJ:PTdirectionandsupervisionalgorithms, PT in Motion 2(8):47,2010)
FIGURE1-7 ProblemsolvingalgorithmutilizedbyPTAsinpatient/clientintervention (FromAmericanPhysicalTherapy Association: A normative model of physical therapist assistant education, Version 2007, Alexandria,VA,2007,APTA,p 85)
Although PTAs work with adults who have had cerebrovascular accidents, spinal cord injuries,
and traumatic brain injuries, some PTs still view pediatrics as a specialty area of practice This narrow perspective is held even though PTAs work with children in hospitals, outpatient clinics, schools, and community settings, including fitness centers and sports-training facilities. Although some areas of pediatric physical therapy are specialized, many areas are well within the scope of practice of the generalist PT and PTA (Miller and Ratliffe, 1998) To assist in resolving this controversy, the Pediatric Section of APTA developed a draft position statement outlining the use of PTAs in various pediatric settings. The original position paper stated that “physical therapist assistants could be appropriately utilized in pediatric settings with the exception of the medically unstable, such as neonates in the ICU” (Section on Pediatrics, APTA, 1995) This document was revised in 1997 and remains available from the Section on Pediatrics The position paper states that “the physical therapist assistant is qualified to assist in the provision of pediatric physical therapy services under the direction and supervision of a physical therapist” (Section on Pediatrics, APTA, 1997) It is recommended that PTAs should not provide services to children who are physiologically unstable (Section on Pediatrics, APTA, 1997). In addition, this position paper also states that “delegation of physical therapy procedures to a PTA should not occur when a child’s condition requires multiple adjustments of sequences and procedures due to rapidly changing physiologic status and/or response to treatment” (Section on Pediatrics, APTA, 1997) The guidelines proposed in this document follow those suggested by Dr. Nancy Watts in her 1971 article on task analysis and division of responsibility in physical therapy (Watts, 1971). This article was written to assist PTs with guidelines for delegating patient care activities to support personnel Although the term delegation is not used today because of the implications of relinquishing patient care responsibilities to another practitioner, the principles of patient/client management, as defined by Watts, can be applied to the provision of present-day physical therapy services. PTs and PTAs unfamiliar with this article are encouraged to review it because the guidelines presented are still appropriate for today’s clinicians and are referenced in APTA documents
The PTA functions as a member of the rehabilitation team in all treatment settings. Members of this team include the primary PT; the physician; speech, occupational, and recreation therapists; nursing personnel; the psychologist; case manager; and the social worker However, the two most important members of this team are the patient and his or her family. In a rehabilitation setting, the PTA is expected to provide interventions to improve the patient’s functional independence. Relearning motor activities, such as bed mobility, transfers, ambulation skills, stair climbing, and wheelchair negotiation, if appropriate, are emphasized to enhance the patient’s functional mobility In addition, the PTA participates in patient and family education and is expected to provide input into the patient’s discharge plan. Patient and family instruction includes providing information, education, and the actual training of patients, families, significant others, or caregivers and is a part of every patient’s plan of care (APTA, 2014; APTA, 2003) As is the case in all team activities, open and honest communication among all team members is crucial to maximize the patient’s participation and achievement of an optimal functional outcome.
The rehabilitation team working with a child with a neurologic deficit usually consists of the child; his or her parents; the various physicians involved in the child’s management and other healthcare professionals, such as an audiologist and physical and occupational therapists; a speech language pathologist; and the child’s classroom teacher. The PTA is expected to bring certain skills to the team and to the child, including knowledge of positioning and handling, use of adaptive equipment, management of abnormal muscle tone, knowledge of developmental activities that foster acquisition of functional motor skills and movement transitions, knowledge of familycentered care and the role of physical therapy in an educational environment. Additionally, interpersonal communication and advocacy skills are beneficial as the PTA works with the child and the family, as well as others Family teaching and instruction are expected within a familycentered approach to the delivery of various interventions embedded into the child’s daily routine. Because the PTA may be providing services to the child in his or her home or school, the assistant may be the first to observe additional problems or be told of a parent’s concern These observations or concerns should be communicated immediately to the supervising PT Due to the complexity of patient’s problems and the interpersonal skill set needed to work with the pediatric population and their families, most clinics require prior work experience before employing PTAs and PTs in these treatment settings (Clynch, 2012)
PTs and PTAs are valuable members of a patient’s health-care team To optimize the relationship between the two and to maximize patient outcomes, each practitioner must understand the educational preparation and experiential background of the other. The preferred relationship between PTs and PTAs is one characterized by trust, understanding, mutual respect, effective communication, and an appreciation for individual similarities and differences (Clynch, 2012) This relationship involves direction, including determination of the tasks that can be directed to the PTA, supervision because the PT is responsible for supervising the assistant to whom tasks or interventions have been directed and accepted, communication, and the demonstration of ethical and legal behaviors Positive benefits that can be derived from this preferred relationship include more clearly defined identities for both PTs and PTAs and a more unified approach to the delivery of high-quality, cost-effective physical therapy services
Chapter summary
Changes in physical therapy practice have led to an increase in the number of PTAs and greater variety in the types of patients treated by these clinicians. PTAs are actively involved in the treatment of adults and children with neurologic deficits After a thorough examination and evaluation of the patient’s status, the primary PT may determine that the patient’s intervention or a portion of the intervention may be safely performed by an assistant. The PTA functions as a member of the patient’s rehabilitation team and works with the patient to maximize his or her ability to participate in meaningful activities Improved function in the home, school, or community remains as the primary goal of our physical therapy interventions