https://ebookmass.com/product/towards-cleaner-entrepreneurshipbridging-social-consciousness-and-sustainability-ananya-rajagopal/
ebookmass.com
Shared: Powertools: The Shields, Book 6 Jayne Rylon
https://ebookmass.com/product/shared-powertools-the-shieldsbook-6-jayne-rylon/
ebookmass.com
Brenner & Rector's The Kidney 11th Edition Alan S. L. Yu
https://ebookmass.com/product/brenner-rectors-the-kidney-11th-editionalan-s-l-yu/
ebookmass.com
The Complete Ultimate Spanish: Comprehensive First- and Second-Year Course Ronni L. Gordon
https://ebookmass.com/product/the-complete-ultimate-spanishcomprehensive-first-and-second-year-course-ronni-l-gordon/
ebookmass.com
Cybersecurity Law 2nd Edition Jeff Kosseff
https://ebookmass.com/product/cybersecurity-law-2nd-edition-jeffkosseff/
ebookmass.com
https://ebookmass.com/product/the-invention-of-martial-arts-popularculture-between-asia-and-america-bowman/
ebookmass.com
HandbookofClinicalNeurology3rdSeries
Availabletitles
Vol.79,Thehumanhypothalamus:basicandclinicalaspects,PartI,D.F.Swaab,ed.ISBN9780444513571
Vol.80,Thehumanhypothalamus:basicandclinicalaspects,PartII,D.F.Swaab,ed.ISBN9780444514905
Vol.81,Pain,F.CerveroandT.S.Jensen,eds.ISBN9780444519016
Vol.82,Motorneuronedisordersandrelateddiseases,A.A.EisenandP.J.Shaw,eds.ISBN9780444518941
Vol.83,Parkinson’sdiseaseandrelateddisorders,PartI,W.C.KollerandE.Melamed,eds.ISBN9780444519009
Vol.84,Parkinson’sdiseaseandrelateddisorders,PartII,W.C.KollerandE.Melamed,eds.ISBN9780444528933
Vol.85,HIV/AIDSandthenervoussystem,P.PortegiesandJ.Berger,eds.ISBN9780444520104
Vol.86,Myopathies,F.L.MastagliaandD.HiltonJones,eds.ISBN9780444518996
Vol.87,Malformationsofthenervoussystem,H.B.SarnatandP.Curatolo,eds.ISBN9780444518965
Vol.88,Neuropsychologyandbehaviouralneurology,G.GoldenbergandB.C.Miller,eds.ISBN9780444518972
Vol.89,Dementias,C.DuyckaertsandI.Litvan,eds.ISBN9780444518989
Vol.90,Disordersofconsciousness,G.B.YoungandE.F.M.Wijdicks,eds.ISBN9780444518958
Vol.91,Neuromuscularjunctiondisorders,A.G.Engel,ed.ISBN9780444520081
Vol.92,Stroke – PartI:Basicandepidemiologicalaspects,M.Fisher,ed.ISBN9780444520036 Vol.93,Stroke – PartII:Clinicalmanifestationsandpathogenesis,M.Fisher,ed.ISBN9780444520043 Vol.94,Stroke – PartIII:Investigationsandmanagement,M.Fisher,ed.ISBN9780444520050 Vol.95,Historyofneurology,S.Finger,F.BollerandK.L.Tyler,eds.ISBN9780444520081
Vol.96,Bacterialinfectionsofthecentralnervoussystem,K.L.RoosandA.R.Tunkel,eds.ISBN9780444520159 Vol.97,Headache,G.NappiandM.A.Moskowitz,eds.ISBN9780444521392 Vol.98,SleepdisordersPartI,P.MontagnaandS.Chokroverty,eds.ISBN9780444520067
Vol.99,SleepdisordersPartII,P.MontagnaandS.Chokroverty,eds.ISBN9780444520074
Vol.100,Hyperkineticmovementdisorders,W.J.WeinerandE.Tolosa,eds.ISBN9780444520142 Vol.101,Musculardystrophies,A.AmatoandR.C.Griggs,eds.ISBN9780080450315 Vol.102,Neuro-ophthalmology,C.KennardandR.J.Leigh,eds.ISBN9780444529039 Vol.103,Ataxicdisorders,S.H.SubramonyandA.Durr,eds.ISBN9780444518927 Vol.104,Neuro-oncologyPartI,W.GrisoldandR.Sofietti,eds.ISBN9780444521385 Vol.105,Neuro-oncologyPartII,W.GrisoldandR.Sofietti,eds.ISBN9780444535023 Vol.106,Neurobiologyofpsychiatricdisorders,T.SchlaepferandC.B.Nemeroff,eds.ISBN9780444520029
Vol.107,EpilepsyPartI,H.StefanandW.H.Theodore,eds.ISBN9780444528988
Vol.108,EpilepsyPartII,H.StefanandW.H.Theodore,eds.ISBN9780444528995
Vol.109,Spinalcordinjury,J.VerhaagenandJ.W.McDonaldIII,eds.ISBN9780444521378
Vol.110,Neurologicalrehabilitation,M.BarnesandD.C.Good,eds.ISBN9780444529015
Vol.111,PediatricneurologyPartI,O.Dulac,M.LassondeandH.B.Sarnat,eds.ISBN9780444528919
Vol.112,PediatricneurologyPartII,O.Dulac,M.LassondeandH.B.Sarnat,eds.ISBN9780444529107
Vol.113,PediatricneurologyPartIII,O.Dulac,M.LassondeandH.B.Sarnat,eds.ISBN9780444595652
Vol.114,Neuroparasitologyandtropicalneurology,H.H.Garcia,H.B.TanowitzandO.H.DelBrutto,eds. ISBN9780444534903
Vol.115,Peripheralnervedisorders,G.SaidandC.Krarup,eds.ISBN9780444529022 Vol.116,Brainstimulation,A.M.LozanoandM.Hallett,eds.ISBN9780444534972
Vol.117,Autonomicnervoussystem,R.M.BuijsandD.F.Swaab,eds.ISBN9780444534910 Vol.118,Ethicalandlegalissuesinneurology,J.L.BernatandH.R.Beresford,eds.ISBN9780444535016 Vol.119,NeurologicaspectsofsystemicdiseasePartI,J.BillerandJ.M.Ferro,eds.ISBN9780702040863 Vol.120,NeurologicaspectsofsystemicdiseasePartII,J.BillerandJ.M.Ferro,eds.ISBN9780702040870 Vol.121,NeurologicaspectsofsystemicdiseasePartIII,J.BillerandJ.M.Ferro,eds.ISBN9780702040887 Vol.122,Multiplesclerosisandrelateddisorders,D.S.Goodin,ed.ISBN9780444520012 Vol.123,Neurovirology,A.C.TselisandJ.Booss,eds.ISBN9780444534880
Vol.124,Clinicalneuroendocrinology,E.Fliers,M.KorbonitsandJ.A.Romijn,eds.ISBN9780444596024
Vol.125,Alcoholandthenervoussystem,E.V.SullivanandA.Pfefferbaum,eds.ISBN9780444626196
Vol.126,Diabetesandthenervoussystem,D.W.ZochodneandR.A.Malik,eds.ISBN9780444534804
Vol.127,TraumaticbraininjuryPartI,J.H.GrafmanandA.M.Salazar,eds.ISBN9780444528926
Vol.128,TraumaticbraininjuryPartII,J.H.GrafmanandA.M.Salazar,eds.ISBN9780444635211
Vol.129,Thehumanauditorysystem:Fundamentalorganizationandclinicaldisorders,G.G.Celesia andG.Hickok,eds.ISBN9780444626301
Vol.130,Neurologyofsexualandbladderdisorders,D.B.Vodus ˇ ekandF.Boller,eds.ISBN9780444632470
Vol.131,Occupationalneurology,M.LottiandM.L.Bleecker,eds.ISBN9780444626271
Vol.132,Neurocutaneoussyndromes,M.P.IslamandE.S.Roach,eds.ISBN9780444627025
Vol.133,Autoimmuneneurology,S.J.PittockandA.Vincent,eds.ISBN9780444634320
Vol.134,Gliomas,M.S.BergerandM.Weller,eds.ISBN9780128029978
Vol.135,NeuroimagingPartI,J.C.MasdeuandR.G.Gonza ´ lez,eds.ISBN9780444534859
Contributors
F.Agosta
NeuroimagingResearchUnit,InstituteofExperimental Neurology,DivisionofNeuroscience,SanRaffaele ScientificInstitute,Vita-SaluteSanRaffaeleUniversity, Milan,Italy
C.Amlie-Lefond
DepartmentofNeurology,SeattleChildren’sHospital, Seattle,WA,USA
A.Atri
RayDolbyBrainHealthCenter,CaliforniaPacific MedicalCenterResearchInstitute,SutterHealth, SanFrancisco,CA,USA
J.C.Augustinack
AthinoulaA.MartinosCenterforBiomedicalImaging, DepartmentofRadiology,MassachusettsGeneral Hospital,Charlestown,MA,USA
A.Bali
DepartmentofRadiology,AntwerpUniversityHospital andUniversityofAntwerp,Antwerp,Belgium
A.M.Blitz
Neuro-radiologyDivision,JohnsHopkinsUniversity SchoolofMedicine,Baltimore,MD,USA
N.Bogduk
NewcastleBoneandJointInstitute,Universityof Newcastle,Newcastle,Australia
A.Boon
DepartmentofPhysicalMedicineandRehabilitationand DepartmentofNeurology,MayoClinic,Rochester,MN, USA
B.H.Brinkmann
DivisionofEpilepsy,DepartmentofNeurology,Mayo Clinic,Rochester,MN,USA
H.Brunel
NeuroradiologyService,H^ opitallaTimone,Marseille, France
N.D.Bryant
VanderbiltUniversityInstituteofImagingScienceand theDepartmentofRadiologyandRadiologicalSciences, VanderbiltUniversity,Nashville,TN,USA
P.M.Capone
MedicalImagingandNeurology,WinchesterMedical Center,WinchesterandDepartmentofNeurology, VirginiaCommonwealthUniversity,Richmond,VA,USA
G.D.Cascino
DivisionofEpilepsy,DepartmentofNeurology,Mayo Clinic,Rochester,MN,USA
M.Castillo
DivisionofNeuroradiology,DepartmentofRadiology, UniversityofNorthCarolina,ChapelHill,NC,USA
F.Cendes
UniversityofCampinas,DepartmentofNeurology, Campinas,SP,Brazil
C.T.Chin
DepartmentofRadiology,UniversityofCalifornia, SanFrancisco,CA,USA
H.M.Dahmoush
DepartmentofRadiology,Children’sHospitalof PhiladelphiaandUniversityofPennsylvania, Philadelphia,PA,USA
B.M.Damon
VanderbiltUniversityInstituteofImagingScienceand theDepartmentofRadiologyandRadiologicalSciences, DepartmentsofBiomedicalEngineeringandMolecular PhysiologyandBiophysics,VanderbiltUniversity, Nashville,TN,USA
P.Shankar
DivisionofNeuroradiology,DepartmentofRadiology, UniversityofNorthCarolina,ChapelHill,NC,USA
D.Shaw
DepartmentofRadiology,SeattleChildren’sHospital, Seattle,WA,USA
N.G.Simon
StVincent’sClinicalSchool,UniversityofNewSouth Wales,Sydney,Australia
A.J.Stoessl
PacificParkinson’sResearchCentreandDivisionof Neurology,DjavadMowafaghianCentreforBrain Health,UniversityofBritishColumbiaandVancouver CoastalHealth,Vancouver,BC,Canada
V.Sulc
DepartmentofNeurology,2ndFacultyofMedicine, CharlesUniversityinPragueandMotolUniversity Hospital,CzechRepublic
B.Swearingen
DepartmentofNeurosurgery,MassachusettsGeneral HospitalandHarvardMedicalSchool,Boston,MA,USA
J.Talbott
DepartmentofRadiology,UniversityofCalifornia, SanFrancisco,CA,USA
W.H.Theodore
NationalInstituteofNeurologicalDisordersandStroke, Bethesda,MD,USA
M.M.Thurnher
DepartmentofRadiology,UniversityHospitalVienna, Vienna,Austria
N.A.Tritos
NeuroendocrineUnit,MassachusettsGeneral HospitalandHarvardMedicalSchool,Boston,MA, USA
N.vanAlfen DepartmentofNeurology,RadboudUniversityMedical Center,Nijmegen,TheNetherlands
L.vandenHauwe DepartmentofRadiology,AntwerpUniversityHospital andUniversityofAntwerp,Antwerp,Belgium
A.J.W.vanderKouwe
AthinoulaA.MartinosCenterforBiomedicalImaging, DepartmentofRadiology,MassachusettsGeneral Hospital,Charlestown,MA,USA
J.VanGoethem DepartmentofRadiology,AntwerpUniversityHospital andUniversityofAntwerp,Antwerp,Belgium
A.J.L.VanHoyweghen DepartmentofRadiology,AntwerpUniversityHospital andUniversityofAntwerp,Antwerp,Belgium
A.Vossough DepartmentofRadiology,Children’sHospitalof PhiladelphiaandUniversityofPennsylvania, Philadelphia,PA,USA
C.Zamora DivisionofNeuroradiology,DepartmentofRadiology, UniversityofNorthCarolina,ChapelHill,NC,USA
V.M.Zohrabian DepartmentofDiagnosticRadiology,YaleUniversity SchoolofMedicine,NewHaven,CT,USA
HandbookofClinicalNeurology, Vol.136(3rdseries) Neuroimaging,PartII
J.C.MasdeuandR.G.Gonza ´ lez,Editors © 2016ElsevierB.V.Allrightsreserved
Functionalanatomyofthespine
NIKOLAIBOGDUK* NewcastleBoneandJointInstitute,UniversityofNewcastle,Newcastle,Australia
Abstract
Amongotherimportantfeaturesofthefunctionalanatomyofthespine,describedinthischapter,isthe remarkabledifferencebetweenthedesignandfunctionofthecervicalspineandthatofthelumbarspine. Inthecervicalspine,theatlasservestotransmittheloadoftheheadtothetypicalcervicalvertebrae.The axisadaptsthesuboccipitalregiontothetypicalcervicalspine.Incervicalintervertebrtaldiscstheanulus fibrosusisnotcircumferentialbutiscrescentic,andservesasaninterosseousligamentinthesaddlejoint betweenvertebralbodies.Cervicalvertebraerotateandtranslateinthesagittalplane,androtateinthe mannerofaninvertedcone,acrossanobliquecoronalplane.Thecervicalzygapophysialjointsarethe mostcommonsourceofchronicneckpain.Bycontrast,lumbardiscsarewelldesignedtosustaincompressionloads,butrelyonposteriorelementstolimitaxialrotation.Internaldiscdisruptionisthemost commonbasisforchroniclow-backpain.Spinalmusclesarearrangedsystematicallyinprevertebraland postvertebralgroups.Theintrinsicelementsofthespineareinnervatedbythedorsalramiofthespinal nerves,andbythesinuvertebralnerves.Littlemodernresearchhasbeenconductedintothestructureof thethoracicspine,orthecausesofthoracicspinalpain.
INTRODUCTION
Inwritingachapteronanatomyforneurologiststherisk arisesofbeingarcaneorbanal.Neurologistswillalready befamiliarwiththepreceptsofclassicanatomy,and wouldnotbeinclinedtoreadachapterthatrepeatsboring,undergraduatematerial.Forthesereasons,thepresentchapterhasbeencastinadifferentmanner. Althoughconventionalelementsofanatomyare reprised,theyarepermeatedbyseveralthemes.New factsareprovided,stemmingfrommodernresearchinto thestructureofthespine,alongwithnewperceptions aboutdesignandfunction.Throughout,thefocusis onclinicalrelevance,particularlywithrespecttothe mechanismsofspinalinjuryandspinalpain.Inthat regard,certainstructures – ignoredinconventional undergraduatecurricula – arepromotedtoepidemiologicallysignificant,clinicalimportance.
CERVICALSPINE
Thecervicalspineservesasamobilesupportforthesensoryplatformofthehead.Itallowsthesensoryapparatus forvision,hearing,andsmelltobeelevatedordepressed inthesagittalplane,andtoscantheenvironmentinthe horizontalplane.Inordertosubservethesefunctions, thecervicalspinehastobemobile,yetsufficientlystrong tosupporttheweightofthehead.Itsvulnerability,to eitherminorormajorinjuries,liesinbeinglong,slender, andcarryingthelargemassoftheheadatitssummit.
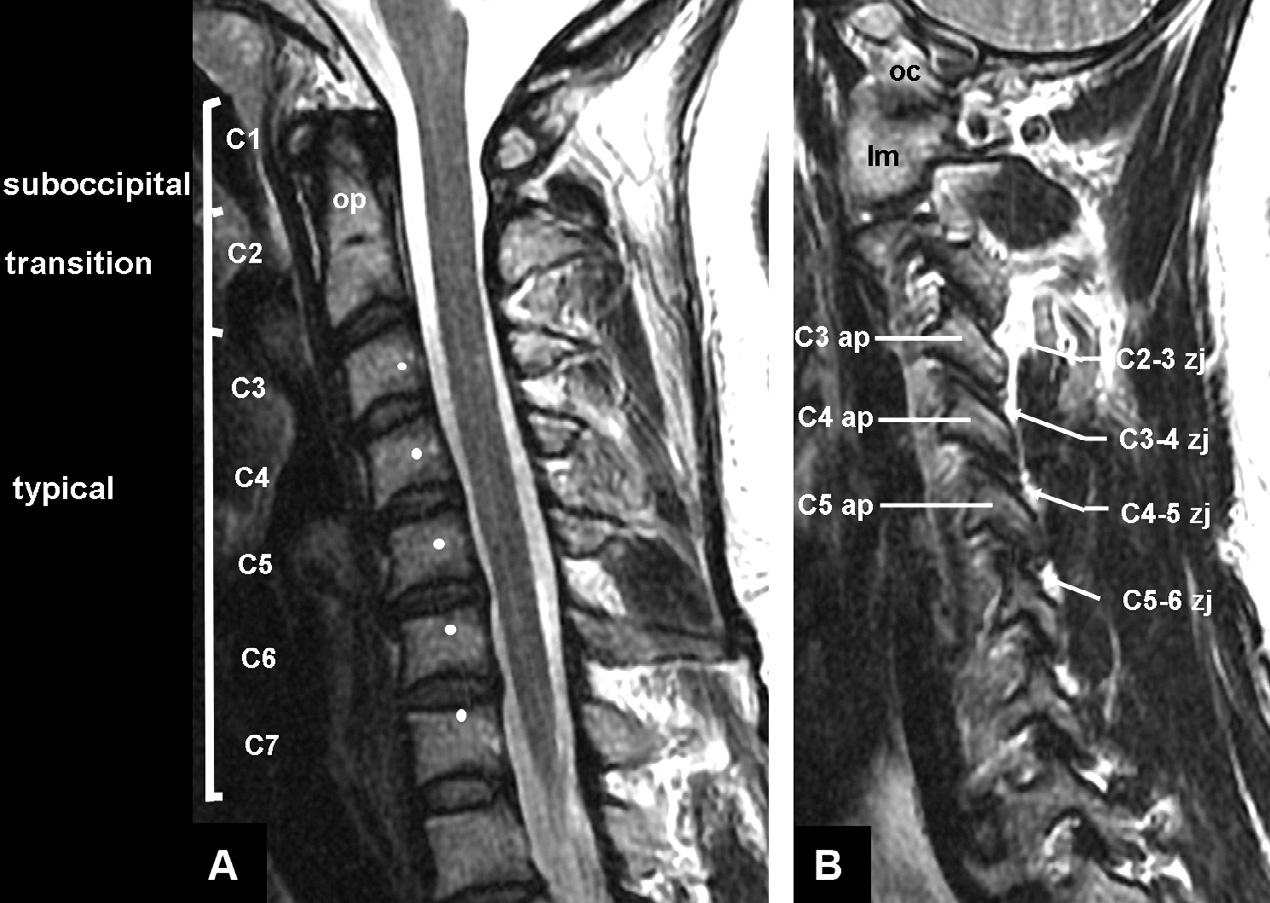
Bothfordescriptivepurposesandfunctionally,the cervicalspinecanbedividedintothreezones:thesuboccipitalzone,centeredontheC1vertebra;atransitional zoneformedbytheC2vertebra;andthetypicalzone, encompassingtheC–7vertebrae(BogdukandMercer, 2000)(Fig.32.1).Thesezonesdifferbothinstructure andinfunction.
*Correspondenceto:NikolaiBogduk,POBox128,TheJunction,NewSouthWales2291,Australia.E-mail:nbogduk@bigpond. net.au
Fig.32.1. Sagittalmagneticresonanceimagesofthecervicalspine,showingitsstructureandzones.(A)Medianscan,showing thevertebralbodiesandinterverterbraldiscs.Thewhitedotsmarkthemeanlocationoftheaxesofrotationforflexion-extensionof thevertebraabove.Theodontoidprocess(op)projectsrostrallyfromthebodyofC2,toliebehindtheanteriorarchoftheatlas(C1). (B)Lateralscan,showingtheoccipitalcondyle(oc),thelateralmass(lm)oftheatlas(C1),thearticularpillars(ap),andthezygapophysialjoints(zj)thattheyform,atthesegmentslabeled.(CourtesyofDr.TimMaus,MayoClinic,Rochester,MN.)
Suboccipitalzone
TheC1vertebra(theatlas)sharesnoneofthefeaturesof typicalcervicalvertebrae,andshouldneverhavebeen consideredcervical.Instructureandinfunctionitis morelikeanoccipitalvertebra.Instructureitresembles theoccipitalbone,ascanbeseeninaxialscans.Infunction,itmorecloselyoperateswiththehead,ratherthan withtheremainderofthecervicalspine.
Theclassicdescriptionoftheatlasasaringvertebra beliesitsdesignandfunction.Thecriticalcomponentsof theatlasareitstwolateralmasses(Fig.32.2).Superiorly, thesepresentsuperiorarticularprocessesthatreceivethe occipitalcondyles,andtherebycradletheskull.Inferiorly,thelateralmassespresentinferiorarticularprocessesthatrestontheC2vertebra,andthereby transmittheloadoftheheadtotheremainderofthecervicalspine.Theanteriorandposteriorarchesoftheatlas servelittlefunctionotherthanholdingthetwolateral massesbothapartandtogether,whilethelatterdothe mechanicalworkoftheatlas.
Uponreceivingtheoccipitalcondylesintotheirdeep sockets,thesuperiorarticularprocessesofeachlateral massformtheatlanto-occipitaljoints(Figs32.2and 32.3).ThesesynovialjointsconstitutetheonlydirectconnectionbetweentheskullandC1.Theyallowasmall rangeofflexion-extension,butthedepthoftheirsockets precludesaxialrotation.Therefore,astheheadrotates (inthetransverseplane)theatlasisobligedtomovewith it.Inthatrespect,theatlasbehaveslikeapassivewasher, betweentheskullandC2.
Uppertransitionzone
TheupperhalfoftheC2vertebra(theaxis)isdesignedto supporttheatlas.Superiorlyandlaterally,itpresents superiorarticularprocessesthatslopecaudallyandlaterally,andactlikeslopingshouldersonwhichthelateral massesoftheatlasrest(Fig.32.2).Theinferiorarticular processesoftheatlashaveareciprocal,caudalandlateralslope.Theapposedarticularprocessesoneachside formthelateralatlantoaxialjoint(Figs32.2and32.3).
Thecaudolateralslopeofthelateralatlantoaxialjoint helpsstabilizetheatlasinthecoronalplane,butalso underliesthemechanismofJeffersonfractures.Severe axialloads,appliedtotheskull,willdrivetheatlascaudally,butitslateralmasseswillalsospreadlaterally downthelateralslopeofthelateralatlantoaxialjoints, resultinginburstfracturesoftheanteriorandposterior arches.
Centrally,theaxispresentsalongodontoidprocess (thedens)thatprojectsbehindtheanteriorarchofthe atlas,withwhichitformsthemedianatlantoaxialjoint (Figs32.1,32.3,and32.4).Theanteriorarchisheldagainst theodontoidprocessbythetransverseligament,which spanslikeabeltbetweenthetwolateralmassesofthe atlas,behindtheodontoidprocess(Figs32.4and32.5).
Posteriordisplacementoftheatlasispreventedby impactionoftheanteriorarchagainsttheodontoidprocess,atthemedianatlantoaxialjoint.Anteriordisplacementispreventedbytensioninthetransverseligament (Fieldingetal.,1974).Theligamentallowsupto3mm normalrangeofseparationbetweentheodontoid
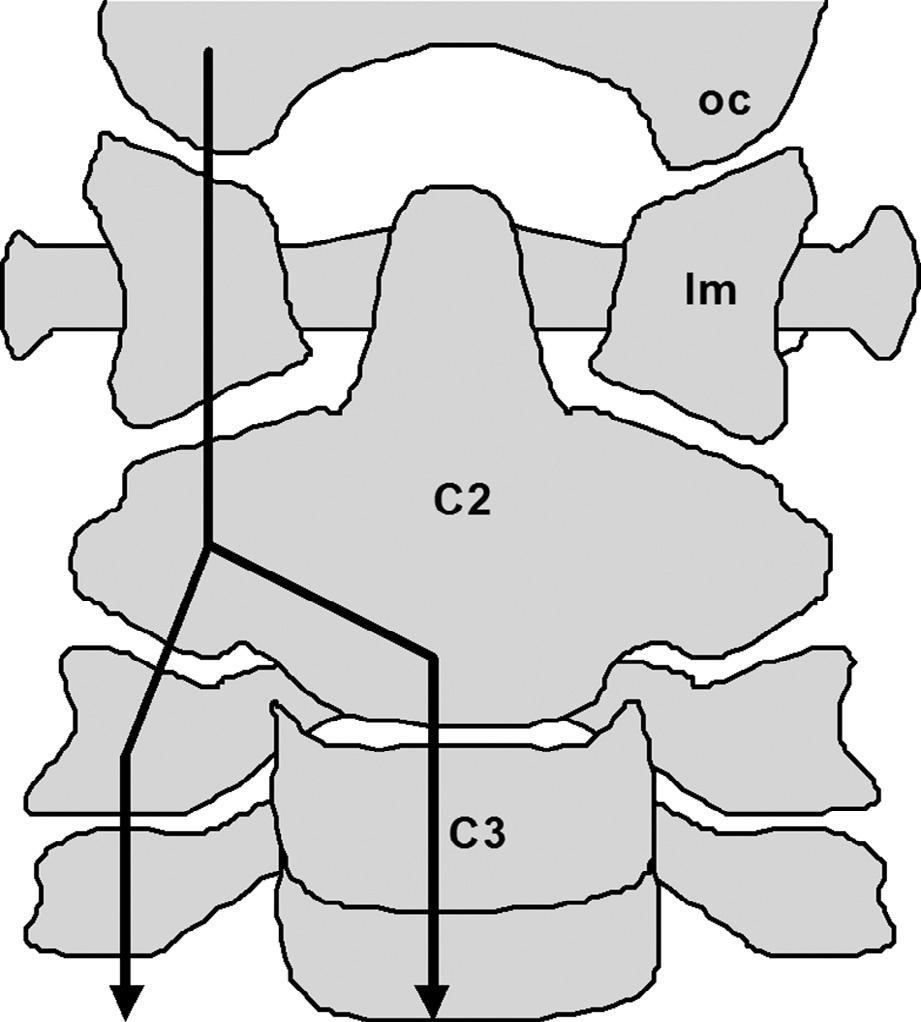
Fig.32.6. Asketchofacoronalviewofhowforcesfromthe headaretransmittedintothecervicalspine.Oneachside,the weightoftheheadpassesthroughtheoccipitalcondyle(oc), intothelateralmass(lm)oftheatlas,andintotheaxis (C2)throughthelateralatlantoaxialjoint.Fromthere,theforces diverge,partlyintotheposteriorcolumnofzygapophysial joints,andpartlyintotheanteriorcolumnofvertebralbodies anddiscs.Halftheloadpassesanteriorlyandhalfposteriorly.
Increasinginteresthasbeenfocusedonthelateral atlantoaxialjointsasapossiblesourceofcervicogenic headache.Thiscontentioncanbetestedbycontrolled, intra-articular,diagnosticblocksoftheputativelypainfuljoint(BogdukandBartsch,2008;Bogdukand Govind,2009;Bogduk,2014).
Lowertransitionzone
ThelowerhalfoftheC2vertebrahasthestructureofa typicalcervicalvertebra(Figs32.1and32.2).Centrallyit presentsavertebralbody,andlaterallyitpresentspaired inferiorarticularprocesses.Havingreceivedthelateral massesoftheatlas,theaxistransmitstheloadofthe headalongananteriorchannel,throughitsvertebral bodytothevertebralbodiesbelow,andalongpairedposteriorchannels,throughthezygapophysialjoints (Fig.32.6).Approximatelyhalfoftheaxialloadistransmittedthroughtheanteriorchannel,andhalfthroughthe twoposteriorchannels.
Typicalcervicalvertebrae
Thecardinalelementsofatypicalcervicalvertebraare itsvertebralbodyandtwoarticularpillars(Figs32.1
and32.2).Secondarily,transverseprocessesprojectlaterallyfromthearticularpillars,andposteriorlythetwo pillarsareunitedbyapairoflaminae,whichsupporta midlinespinousprocessattheirjunction.Thetransverse processesandspinousprocessesserveasleversupon whichactthemusclesthatcontrolthepositionofthecervicalvertebrae.Alongitssuperior,posterolateralmargin oneachside,eachvertebralbodybearsuncinateprocesses.Previouslyenigmatic,theuncinateprocesses underliethenatureofthejointsbetweenthecervicalvertebralbodiesandhowtheyoperate.
Consecutivearticularpillarsareunitedbythezygapophysialjoints(Figs32.1and32.2),whicharesynovial jointsformedbytheinferiorarticularprocessofthe vertebraaboveandthesuperiorarticularprocessof thevertebrabelow.Fibroadiposemeniscoidsintervene betweenthearticularcartilagesofthesejoints(Mercer andBogduk,1993).Thezygapophysialjointsareplanar, andattypicalcervicallevelsareorientedatabout40° to thecoronalandtransverseplanes,sothattheyfacebackwardsandupwards(Nowitzkeetal.,1994).AttheC2–3 level,however,thejointsalsofacemedially,suchthatthe pairofjointsdepictanellipsoidsocketintowhichnestles theweightoftheaxis,andtheloadthatitcarriesfrom thehead(Figs32.2and32.6).
Consecutivevertebralbodiesareunitedbyintervertebraldiscs,andbytheanteriorandposteriorlongitudinalligaments(MercerandBogduk,1999).Theanteriorligament connectsonlythetypicalcervicalvertebrae,fromC2caudally.Theposteriorlongitudinalligamentformsa carpetalongthefloorofthevertebralcanalattypicalcervicallevels,butexpandsintothemembranatectoriato coverthebackoftheatlantoaxialregion.Indoingso, theligamentseparatestheduralsacandspinalcordfrom themechanicsofthemedianatlantoaxialjoint.
Posteriorligamentsarelackinginthecervicalspine. Interspinousligamentsarerepresentedbyonlyasagittal layeroffascia(MercerandBogduk,2003).Theligamentumnuchaelacksthestructureofaligament.Itconsists largelyofanarrow,coronalraphe,anchoredtotheC7 spinousprocess,andformedbyinterlacingtendonsof thespleniusmusclesandtrapezius(Mercerand Bogduk,2003).
Theintrinsicstructureofthecervicalintervertebral discsisunlikethatoflumbardiscs,anddifferswith age(Odaetal.,1988;MercerandBogduk,1999).The nucleuspulposusofcervicaldiscsisgelatinousonlyin childrenandyoungadults.Bytheageof30itdries outtoformafibrocartilaginousplate(Odaetal., 1988).Moreover,thenucleusisnotsurroundedbyconcentriclamellaeoftheanulusfibrosus(Mercerand Bogduk,1999).Theanulusfibrosusislargelydeficient posteriorly,andconsistsofathin,paramedianbandof collagenfibersthatrunlongitudinallybetweenthe

Fig.32.7. Sketchesofvariousviewsoftheinternalstructure ofthecervicaldisc.Inafrontview,allfibersoftheanterior anulusfibrosuspasstowardsapointontheinferioranterior surfaceofthevertebralbodyabove.Inatopview,theanulus fibrosus(af)iscrescenticinshape,thickanteriorlybuttapering attheuncinateprocesses(u).Thenucleuspulposus(np)isa fibrocartilaginousplate.Posteriorlytheanulusisrestricted toasmallbundleofparamedian,longitudinalfibers.Aside viewshowsthefibersoftheanulusfibrosuspassingupwards andforwards.Atransversecleftrunsfromoneuncinateprocesstotheother.
vertebralbodies(Fig.32.7).Posterolaterally,thenucleus iscoveredbytheposteriorlongitudinalligament,rather thanbyanulusfibrosus.Anteriorly,theanulusfibrosus iscrescenticinshape,thinposteriorlyneartheuncinate processes,butthickeranteriorlytowardsthemidline.All ofitscollagenfiberspassinasimilardirection,effectivelyaimingtoamedianpointontheloweranteriorsurfaceofthevertebralbodyabove.Thisconfiguration endowstheanulusfibrosuswiththestructureofathick interosseousligamentthatbindstheanterioredgesof consecutivevertebralbodies.
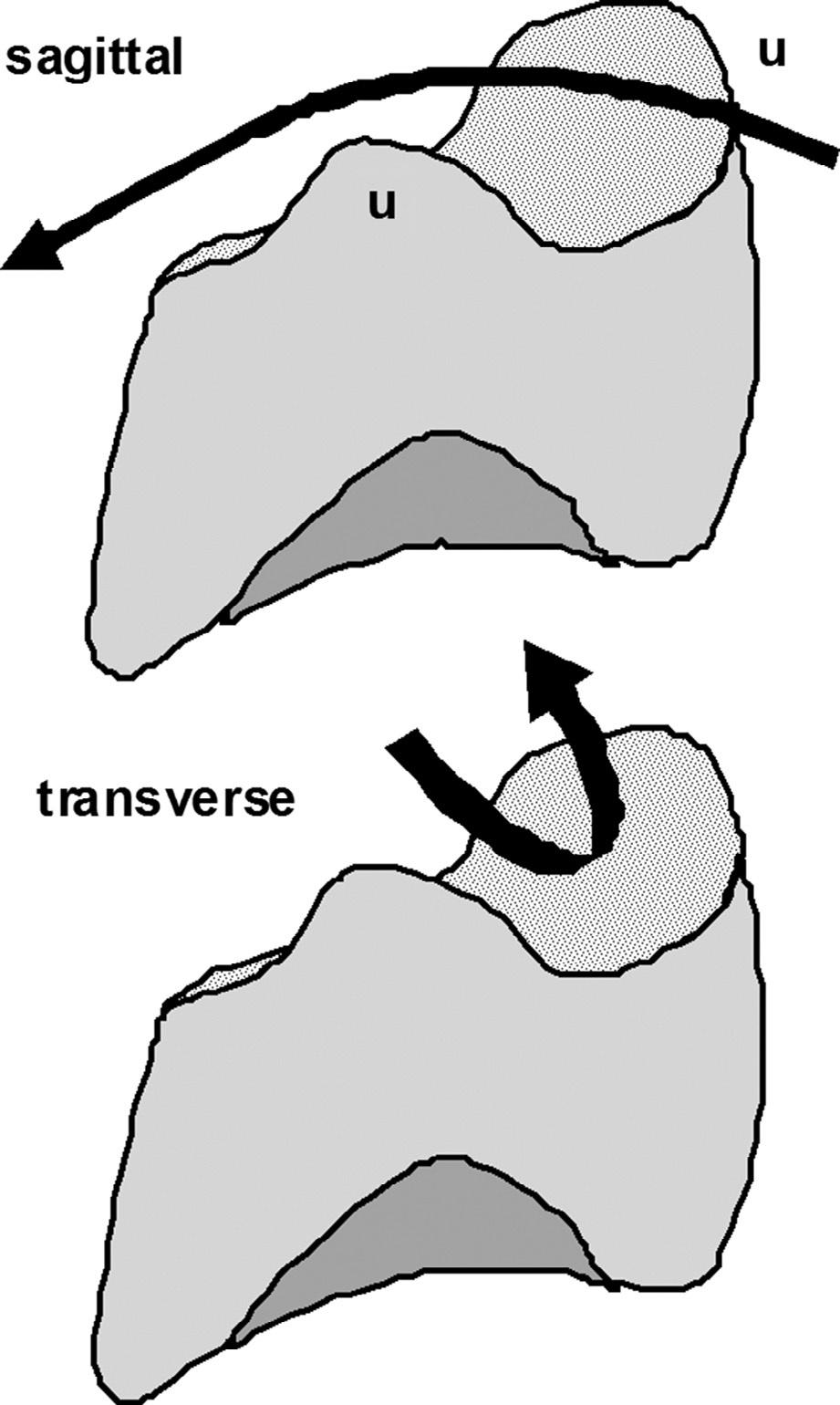
Thesuperiorsurfaceofeachcervicalvertebralbody presentstwocurvatures:aslightconvexcurvaturealong thesagittalplane,andadeepconcavecurvaturetransverselybetweentheuncinateprocesses(Fig.32.8).These curvaturesendowthevertebralbodywiththeconfigurationofasaddlejoint(BogdukandMercer,2000).Consequently,thecervicalinterbodyjointsoperatelikea saddlejoint,withmotionrestrictedtotwoplanes:the sagittalplaneandanobliquecoronalplane.
Inthesagittalplane,thevertebralbodiescanrockand slide(rotateandtranslate),toprovideforflexionand extensionoftheneck.Fromabovedownwards,thetypicalcervicalvertebraeexhibitprogressivelylesstranslationforeachdegreeofrotation,duringflexionor extension.Thisisreflectedbythedifferentlocations oftheiraxesofmovement.Athigherlevelstheaxes
Fig.32.8. Sketchesofaposterolateralviewofatypicalcervicalvertebralbody,showingthetwocurvaturesofitssuperior surface:adownwardconcavityalongthesagittalplane,anda secondconcavity,facingupwardsandforwards,betweenthe uncinateprocesses(u).Thesetwoconcavitiesendowtheintervertebraldiscwiththefeaturesofasaddlejoint.
lieinthevertebralbodybelowthemovingvertebra, butareprogressivelyclosertotheirintervertebraldisc atlowerlevels(Amevoetal.,1991)(Fig.32.1).Thesedifferencescorrelatestronglywiththeheightofthearticularpillarateachsegment(Nowitzkeetal.,1994).Taller pillarsprovidelessspaceintowhichthevertebracan translateonceithascommencedsagittalrotation.Conversely,atsegmentswithshorterpillars,sagittalrotation liftstheinferiorarticularprocessesofthemovingvertebraoffthesupportingarticularpillar,andprovidesa greatergapintowhichitcantranslate(Nowitzke etal.,1994).
Thesecondplaneofmovementoftypicalcervical vertebraeissetat40° forwardsofthecoronalplane, andliesparalleltotheplaneofthezygapophysialjoints
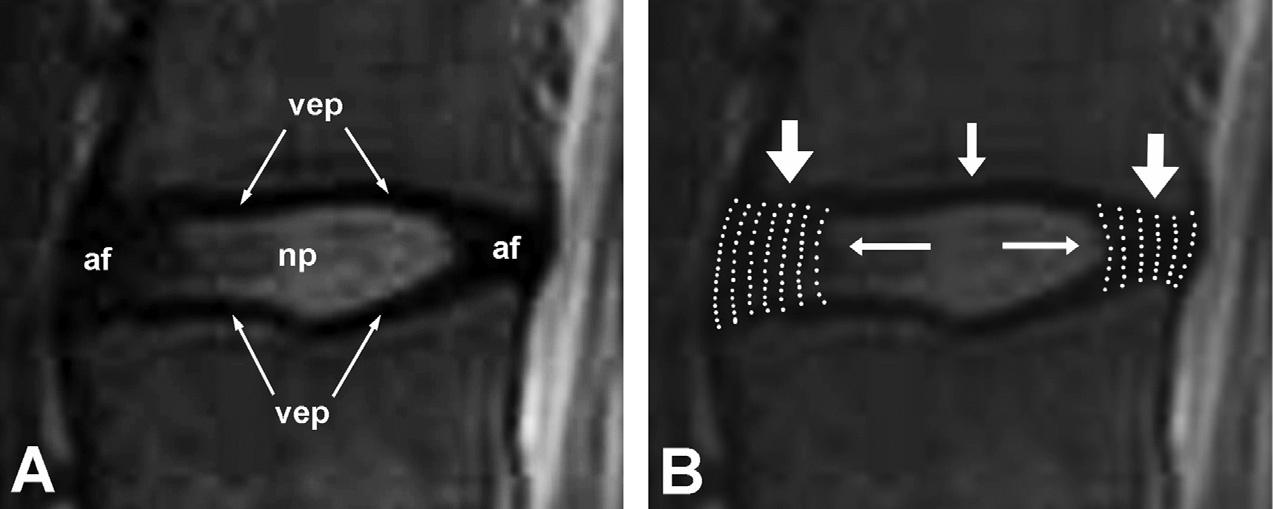
Fig.32.12. Close-upviewsofasagittalmagneticresonanceimageofanL3–4intervertebraldisc.(A)Thecomponentsofthedisc. np,nucleuspulposus;af,anulusfibrosus;vep,vertebralendplate.(B)Themechanicsofthedisc.Axialcompressionloadsare primarilybornebythelamellaeofcollagenintheanulusfibrosus.Whencompressed,thenucleuspulposusexertsradialpressure tobracetheanulus,andpreventitfrombucklingunderload.
movementoccursiscompressedslightly,whiletheanulus ontheoppositesideisstretched(Bogduk,2012a).
Whilestronglydesignedtoresistcompression,the lumbardiscsarepoorlydesignedtoresistaxialrotation. Becausethecollagenfibersoftheanulusfibrosusalternateindirectioninsuccessivelayers,onlyhalfareavailabletoresistaxialrotationinonedirectionortheother. Forstabilityinaxialrotation,thelumbarvertebralbodies andintervertebraldiscsrelyontheposteriorelementsof thelumbarvertebrae(Bogduk,2012a).
Theposteriorelementsarebasedonanarch(Bogduk, 2012a)(Fig.32.13).Thearchissupportedbystoutpediclesthatemanatefromtheupperposteriorsurfaceof eachvertebralbody.Thepediclesservetotransmit forcesfromthesucceedingposteriorelementstothevertebralbodies,whichcontrolthepositionormovements ofthevertebralbodies.Thearchiscompletedbyleft andrightlaminaethatjoininthemidline.Fromthejunctionofthetwolaminaespringsalargespinousprocess, andfromthejunctionbetweenthepedicleandlaminaon eachsidearisesalongtransverseprocess.Theseprocessesserveasleverstowhichattachthemusclesthat controlthemovementsofthelumbarvertebrae.
Atitssuperiorandinferiorlateralcornersrespectively,eachlaminabearsasuperiorandinferiorarticular process.Likelargemittens,thepairedsuperiorarticular processesreachcraniallytograsptheinferiorarticular processesofthevertebraabove,andformthezygapophysialjoints.Theplaneofthesejointsisparallelto thelongitudinalaxisofthelumbarspine.Consequently, duringflexionofthevertebralbodies,theinferiorarticularprocessesglidefreelyoutofthesocketsformedby thesuperiorarticularprocesses,untilmovementis arrestedbytensioninthejointcapsules(Bogduk, 2012a).Theaxisofthismovementtypicallyliesinthe discbelowthemovingvertebra(PearcyandBogduk, 1988)(Fig.32.11A),whichindicatesonlyasmallamount oftranslationforeverydegreeofrotationofthemoving
vertebra.Astheinferiorarticularprocessesmove,they liftawayfromthesuperiorarticularprocess,tantamounttopartiallysubluxatingthejoint.Fibroadipose meniscoidsprotecttheexposedsurfacesofthearticular cartilagesduringthisdisplacement(EngelandBogduk, 1982;BogdukandEngel,1984).
Inaxialviews,thelumbarzygapophysialjointsvariouslypresentflat,C-shaped,orJ-shapedappearances, whichcorrespondtotheprimaryfunctionsofthese joints(HorwitzandSmith,1940).Flatjointsessentially facemediallyandposteriorly.C-shapedjointshavean anteriorendthatfacesposteriorly,andaposteriorend thatfacesmedially.J-shapedjointshaveasmallanterior lipfacingposteriorly,andalargersurfacefacingmedially.Themediallyfacingsurfacesservetoresistaxial rotationofthevertebrae.Attemptedaxialrotation swingstheinferiorarticularprocesslaterally,butthis movementisarrestedbytheopposingsuperiorarticular process.Therangeofmotionislimitedtoabout2° orless persegment(PearcyandTibrewal,1984),andisaccommodatedonlybycompressionofthearticularcartilage. Thesurfacesthatfaceposteriorlyservetoresistforward displacement(listhesis)ofthevertebra.
Impactionofaninferiorarticularprocessagainstits superiorarticularprocesstendstoforcetheinferiorprocessbackwards,andliftthelaminafromwhichitarises (likeopeningahatchback).Inturnthistendencystresses thejunctionbetweenthelaminaanditspedicle.Repeated impactions – particularlyduringrepeatedaxial rotation – cancausestressfracturesatthispoint,resultinginparsinterarticularisdefects.
Thelumbarzygapophysialjointscanbeasourceof low-backpain,butitsprevalenceisuncertain.Itappears tobeuncommonorrareininjuredworkers,butiscommoninelderlypatients(Bogduk,2008,2012b).
Themostcommoncauseofchroniclow-backpainis internaldiscdisruption(Bogduketal.,2013).Thisconditionischaracterizedbydegradationofthenucleus
Fig.32.14. Sagittalmagneticresonanceimagesofthethoracic spine.(A)Mediansection,throughthevertebralbodies,spinal cord(sc),andspinousprocesses(sp)cord.(B)Paramediansectionthroughthezygapophysialjoints(zj).Intervertebraldiscs (ivd)areevidenceinbothsections.(CourtesyofDr.TimMaus, MayoClinic,RochesterMN.)
communicans.Eachpassesbackintotheintervertebral foramentosupplytheduralsac,theposteriorlongitudinalligament,andtheposterioranulusfibrosus(Bogduk etal.,1981b;Bogduk,1983).Thesenervesprovidethe sensorypathwayforlumbardiscogenicpain.
THORACICSPINE
Therehavebeennosubstantialadvancesinthedescriptionoftheanatomyofthethoracicspinesinceeditions ofanatomytextbooksofthe19thand18thcentury.In parallel,therehasbeenlittleadvanceintheunderstandingofthoracicspinalpainanditssources,letalone causes.Nodiagnosticortreatmentprocedureshavebeen validated.Thoracicspinalpainessentiallyremainsa mystery.
Likecervicalandlumbarvertebrae,thethoracicvertebraehavevertebralbodiesthatareconnectedbyintervertebraldiscsandlongitudinalligaments,andposterior elementsthatareconnectedbyzygapophysialjoints (Fig.32.14).Thedistinctionofthethoracicspineisthat itsuspendstheribs.Attypicalthoraciclevels,thehead oftheribarticulateswiththeintervertebraldiscand demifacetsontheedgesofthevertebraethatbindthat disc,andthearticulartubercleoftheribarticulateswith thetransverseprocessoftheupperofthetwovertebrae
Fig.32.15. Axialmagneticresonanceimageofatypicalthoracicspinalsegment.vb,vertebralbody;zj,zygapophysial joint;sp,spinousprocess;cvj,costovertebraljoint;ctj, costotransversejoint.(CourtesyofDr.TimMaus,Mayo Clinic,Rochester,MN.)
(Fig.32.15).ExceptionstothisarrangementoccuratT1 andatT11andT12,wheretheheadoftheribfullyarticulateswiththelike-numberedvertebrae.
Fewstudieshaveexploredtheinnervationofthethoracicspine(Bogduk,2002).Thethoracicsinuvertebral nervesareassumedtobehomologoustothoseatcervical orlumbarlevels.Thecoursesofthethoracicdorsalrami appeartodifferfromthoseatcervicalandlumbarlevels, butareneverthelesshomologous(ChuaandBogduk, 1995).Whereasthemedialbranchesatcervicalandlumbarlevelswindaroundthebaseofthesuperiorarticular processateachsegmentallevel,atthoraciclevelsthe dorsalramusstretchestothetipofthetransverseprocessbeforedividingintomedialandlateralbranches. Thisdifferenceisreconciledonceitisrealizedthatwhat arecalledthetransverseprocessesatcervicalandlumbar levelsareembryologicallycostalelements(rudimentary ribs),whereastheembryologictransverseelements(or truetransverseprocesses)areabsorbedintothebase ofthesuperiorarticularprocess.Consequently,atcervicalandlumbarlevels,themedialbranchescrossthe superiorarticularprocessbecausethetruetransverse processesalsoliethere.Thisdistinctionbecomespertinentforminimallyinvasive,diagnostic,andtreatment proceduresthattargetthoracicmedialbranches.Thetargetliesonthetransverseprocess,notonthesuperior articularprocess(ChuaandBogduk,1995).
Apersistingcuriositypertainstothestructureofthoracicintervertebraldiscs.Cervicaldiscsdiffergreatly fromlumbardiscs,butundiscoveredisthetransition
zone.Arethoracicdiscslikecervicaldiscs,ordotheyhave thestructureoflumbardiscs?Giventhatcervicaluncinate processesarehomologoustotheheadsoftheribs,unpublishedobservationssuggestthatdiscschangetheirstructurewhereuncinateprocessesortheirribequivalent cease.ThoracicdiscsbecomelumbarinnatureatT11, wheretheribnolongerarticulateswiththedisc.
REFERENCES
AmevoB,WorthD,BogdukN(1991).Instantaneousaxesof rotationofthetypicalcervicalmotionsegments:astudyin normalvolunteers.ClinBiomech 6:111–117.
BastideG,ZadehJ,LefebvreD(1989).Arethe‘littlemuscles’ whatwethinktheyare?SurgRadiolAnat 11:255–256.
BogdukN(1982).Theclinicalanatomyofthecervicaldorsal rami.Spine 7:319–330.
BogdukN(1983).Theinnervationofthelumbarspine.Spine 8:286–293.
BogdukN(2002).Innervationandpainpatternsofthethoracic spine.In:RGrant(Ed.),PhysicaltherapyoftheCervical andThoracicSpine,3rdedn.ChurchillLivingstone,New York,pp.73–81.
BogdukN(2006).Whiplashinjury.In:FCervero,TSJensen (Eds.),HandbookofClinicalNeurologyVol.81:Pain, Elsevier,Amsterdam,pp.791–801.
BogdukN(2008).Evidence-informedmanagementofchronic backpainwithfacetinjectionsandradiofrequencyneurotomy.SpineJ 8:56–64.
BogdukN(2011).Oncervicalzygapophysialjointpainafter whiplash.Spine 36:S194–S199.
BogdukN(2012a).ClinicalAnatomyoftheLumbarSpineand Sacrum,5thedn.Elsevier,Edinburgh.
BogdukN(2012b).Lumbarmedialbranchneurotomy.In: SDagenais,SHaldeman(Eds.),Evidence-Based ManagementofLowBackPain,Elsevier,StLouis, pp.351–363.
BogdukN(2014).Theneckandheadaches.NeurolClin 32: 471–487.
BogdukN,BartschT(2008).Cervicogenicheadache.In: SDSilberstein,RBLipton,DWDodick(Eds.),Wolff’s Headache,8thedn.OxfordUniversityPress,NewYork, pp.551–570.
BogdukN,EngelR(1984).Themenisciofthelumbarzygapophysealjoints.Areviewoftheiranatomyandclinical significance.Spine 9:454–460.
BogdukN,GovindJ(2009).Cervicogenicheadache:an assessmentoftheevidenceonclinicaldiagnosis,invasive tests,andtreatment.LancetNeurol 8:959–968. BogdukN,MercerSR(2000).Biomechanicsofthecervicalspine.I:NormalKinematics.ClinBiomech 15: 633–648.
BogdukN,YoganandanN(2001).BiomechanicsofthecervicalspinePart3:minorinjuries.ClinBiomech 16:267–275.
BogdukN,LambertG,DuckworthJW(1981a).Theanatomy andphysiologyofthevertebralnerveinrelationtocervical migraine.Cephalalgia 1:11–24.
BogdukN,TynanW,WilsonAS(1981b).Thenervesupplyto thehumanlumbarintervertebraldiscs.JAnat 132:39–56.
BogdukN,WilsonAS,TynanW(1982).Thehumanlumbar dorsalrami.JAnat 134:383–397.
BogdukN,WindsorM,InglisA(1988).Theinnervationofthe cervicalintervertebraldiscs.Spine 13:2–8.
BogdukN,PearcyM,HadfieldG(1992).Anatomyandbiomechanicsofpsoasmajor.ClinBiomech 7:109–119. BogdukN,JohnsonG,SpaldingD(1998).Themorphology andbiomechanicsoflatissimusdorsi.ClinBiomech 13: 377–385.
BogdukN,AprillC,DerbyR(2013).Lumbardiscogenicpain: state-of-the-artreview.PainMed 14:813–836. ChuaWH,BogdukN(1995).Thesurgicalanatomyofthoracic facetdenervation.ActaNeurochir 136:140–144.
CuratoloM,BogdukN,IvancicPCetal.(2011).Theroleof tissuedamageinwhiplash-associateddisorders.Spine 36: S309–S315.
DvorakJ,HayekJ,ZehnderR(1987).CT-functionaldiagnosticsoftherotatoryinstabilityoftheuppercervicalspine part2.Anevaluationonhealthyadultsandpatientswith suspectedinstability.Spine 12:726–731. EngelR,BogdukN(1982).Themenisciofthelumbarzygapophysialjoints.JAnat 135:795–809.
FieldingJW,CochranGvanB,LawsingJFetal.(1974).Tears ofthetransverseligamentoftheatlas.JBoneJointSurg 56A:1683–1691.
HickeyDS,HukinsDWL(1980).Relationbetweenthestructureoftheanulusfibrosusandthefunctionandfailureof theintervertebraldisc.Spine 5:100–116.
HorwitzT,SmithRM(1940).Ananatomical,pathological androentgenologicalstudyoftheintervertebraljoints ofthelumbarspineandofthesacroiliacjoints.Am JRoentgenol 43:173–186.
KaneokaK,OnoK,InamiSetal.(1999).Motionanalysisof cervicalvertebraeduringwhiplashloading.Spine 24: 763–770.
KimmelDL(1960).Innervationofthespinalduramaterand duramateroftheposteriorcranialfossa.Neurology 10: 800–809.
KoebkeJ,BradeH(1982).Morphologicalandfunctionalstudiesonthelateraljointsofthefirstandsecondcervicalvertebraeinman.AnatEmbryol 164:265–275.
LambertGA,DuckworthJW,BogdukNetal.(1984).Low pharmacologicalresponsivenessofthevertebro-basilarcirculationin Macacanemestrina monkeys.EurJPharmacol 102:451–458.
LazorthesG,GaubertJ(1956).L’innervationdesarticulations interapophysairevertebrales.ComptesRenduesde l’AssociationdesAnatomistes 43:488–494.
MacintoshJE,BogdukN,GracovetskyS(1987).Thebiomechanicsofthethoracolumbarfascia.ClinBiomech 2: 78–83.
MarkolfKL,MorrisJM(1974).Thestructuralcomponents oftheintervertebraldisc.JBoneJointSurg 56A: 675–687.
MercerS,BogdukN(1993).Intra-articularinclusionsofthe cervicalsynovialjoints.BrJRheumatol 32:705–710.
MercerS,BogdukN(1999).Theligamentsandanulusfibrosusofhumanadultcervicalintervertebraldiscs.Spine 24: 619–626.
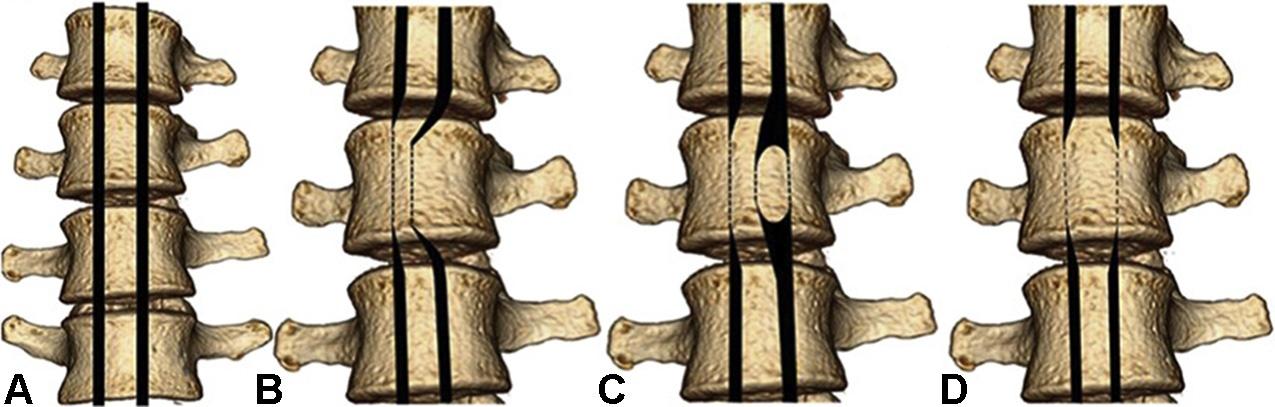
Fig.33.1. Historicclassificationofspinetumorsbasedoncomputedtomographymyelography.(A)Normal,(B)extraduralextramedullary,(C)intraduralextramedullary,and(D)intraduralintramedullary.From MechtlerandNandigam(2013).
(ShahandSalzman,2011).Metastaticdiseaseofthevertebralcolumnismorefrequentthanprimaryneoplastic diseases.Approximatelytwo-thirdsofcancerpatients willdevelopbonemetastasisandsymptomaticspinal metastasiswilloccurinalmost10%ofcancerpatients. Themostcommonprimarysitesaretheprostate,breast, kidney,lung,andthyroid.Theincidenceofskeletal metastasesaccordingtotheprimarytumorisasfollows; breast73%(47–85%),prostate68%(33–85%),thyroid 42%(28–60%),lung36%(30–55%),kidney35% (33–40%),esophageal6%(5–7%),andgastrointestinal 5%(3–11%)(Maccauroetal.,2011)Themostcommon causeofmetastaticspinediseaseisbreastcancerin women;however,inmen,prostatecancerismostcommon.Thethoracicspineisthemostcommonlyinvolved. Themajorityofthelesionsareextraduralinlocation, consistingoflesionswhicharelocalizedtotheepidural spaceandthosewhicharenestedinthevertebralbody. Prostate,breast,andlungcancerareagaintheleading causeofspinalcordcompression,eachaccountingfor about15–20%ofthecases.Theremainingcancersstem fromrenalcell,non-Hodgkin’slymphoma,multiple myeloma,colorectalcancers,sarcomas,andunknown tumors.Pain,themostcommoninitialfeature,occurs in95%ofadultsand80%ofchildren.Painisusually localizedtothesiteofmetastasisandiscausedby stretchingthepain-sensitivebonyperiosteum.Radicular painislessfrequentbutisalsolocalizing.Nocturnalpain uponlyingdownistypical.
Threetypesofbonemetastasisaredistinguished: osteolytic,osteoblastic,andmixed;71%areosteolytic, 8%areosteoblastic,and21%aremixed.
Osteolyticmetastasestypicallydevelopincancers ofthebreast,lung,kidney,thyroid,oropharyngealcancers(ShahandSalzman,2011)andinmelanoma(Sun etal.,2013).Thisisaresultofosteoclastactivation,rather thanadirectinvasionofbonetissuebytumorcells.
Inosteoblasticmetastasesthebalanceofbonemetabolismisshiftedtothebenefitofboneproductionas aresultofpathologicactivationofosteoblasts.Osteoblasticlesionsusuallyoccurinprostate,bladderand
nasopharyngealcancer,medulloblastoma,neuroblastomas,andbronchialcarcinoid(Longetal.,2010).
Imagingofvertebralmetastases
Intoday’sclinicalpracticeMRIisthemostimportant modalityinimagingofmetastaticspinedisease.Plain filmisnolongertheroutinediagnostictoolbardueto itslowsensitivityandspecificity(Salvoetal.,2009; ShahandSalzman,2011).Nuclearmedicinestudieshave awell-definedroleinmetastasisimaging.Bonescans havebeenusedforscreening,sincethetraceraccumulatesinmetastaticsiteswithhighsensitivity,thusreflectingtheincreasedboneturnover.Thesensitivityand specificityofbonescanswereimprovedwithsinglephotonemissioncomputedtomography(SPECT)scans (RyanandFogelman,1995).Flurodeoxyglucose(F18FDG)positronemissiontomography(PET)aloneand PETCTcandiscoverspinalmetastaseswithasensitivity of74%and98%,respectively(Metseretal.,2004).F18FDGPEThasbeenreportedtobemoresensitivein detectingosteolyticmetastases(CookandFogelman, 2000).CThasalowersensitivityindetectingosseous metastasesandaninferiordiagnosticaccuracycomparedtoMRI(BuhmannKirchhoffetal.,2009).Infact, CTislessaccurateindetectingparaspinalsofttissue, boneedema,andbonemetastasesthatmaybemissed ifdestructionisnotpresent(ShahandSalzman,2011). Therefore,CThasarathercomplementaryrolein first-lineimagingofspinalmetastasesandownspriority onlyinthosecaseswhentheintegrityandfinestructure ofthetrabecularandcorticalboneareaquestion,preoperativeplanningisrequired,orwhenMRIiscontraindicated.MRIissuperiortoCTinallothercases.
Metastaticlesionsaremostcommonlyfocalormultifocalandthediffuseinvolvementofthevertebralbodies islesscommon.Focalabnormalitiesarehypointense onT1andhyperintenseonT2andshorttauinversion recovery(STIR)sequences.Ingeneral,metastaseswill enhancewithcontrast,althoughitisimportanttoalways acquireanoncontraststudyforcomparison.Thediffuse