https://ebookmass.com/product/neurobiology-of-epilepsy-fromgenes-to-networks-1st-edition-elsa-rossignol/
Instant digital products (PDF, ePub, MOBI) ready for you
Download now and discover formats that fit your needs...
Genetics: From Genes to Genomes, 8th Edition Charles Aquadro
https://ebookmass.com/product/genetics-from-genes-to-genomes-8thedition-charles-aquadro/
ebookmass.com
Neurobiology of language 1st Edition Hickok
https://ebookmass.com/product/neurobiology-of-language-1st-editionhickok/
ebookmass.com
The Second Age of Computer Science: From ALGOL Genes to Neural Nets 1st Edition Subrata Dasgupta
https://ebookmass.com/product/the-second-age-of-computer-science-fromalgol-genes-to-neural-nets-1st-edition-subrata-dasgupta/
ebookmass.com
https://ebookmass.com/product/roberts-rules-for-dummies-4th-edition-calan-jennings/
ebookmass.com
https://ebookmass.com/product/girl-sex-101/
ebookmass.com
The Environmental Impact of COVID-19 Deepak Rawtani
https://ebookmass.com/product/the-environmental-impact-ofcovid-19-deepak-rawtani/
ebookmass.com
Age of the Geek: Depictions of Nerds and Geeks in Popular Media 1st Edition Kathryn E. Lane (Eds.)
https://ebookmass.com/product/age-of-the-geek-depictions-of-nerds-andgeeks-in-popular-media-1st-edition-kathryn-e-lane-eds/
ebookmass.com
Handbook of Local Anesthesia – E-Book – Ebook PDF Version
https://ebookmass.com/product/handbook-of-local-anesthesia-e-bookebook-pdf-version/
ebookmass.com
Masked (Abducted Hearts Duet Book 1) Elise Lang
https://ebookmass.com/product/masked-abducted-hearts-duetbook-1-elise-lang/
ebookmass.com
https://ebookmass.com/product/978-1451176742-text-atlas-of-obstetricdermatology/
ebookmass.com
SerialEditor
VincentWalsh InstituteofCognitiveNeuroscience UniversityCollegeLondon 17QueenSquare
LondonWC1N3ARUK
EditorialBoard
MarkBear, Cambridge,USA. Medicine&TranslationalNeuroscience
HamedEkhtiari, Tehran,Iran. Addiction
HajimeHirase, Wako,Japan. NeuronalMicrocircuitry
FredaMiller, Toronto,Canada. DevelopmentalNeurobiology
ShaneO’Mara, Dublin,Ireland. SystemsNeuroscience
SusanRossell, Swinburne,Australia. ClinicalPsychology&Neuropsychiatry
NathalieRouach, Paris,France. Neuroglia
BarbaraSahakian, Cambridge,UK. Cognition&Neuroethics
BettinaStuder, Dusseldorf,Germany. Neurorehabilitation
Xiao-JingWang, NewYork,USA. ComputationalNeuroscience
Elsevier Radarweg29,POBox211,1000AEAmsterdam,Netherlands TheBoulevard,LangfordLane,Kidlington,OxfordOX51GB,UK 50HampshireStreet,5thFloor,Cambridge,MA02139,USA
Firstedition2016
Copyright # 2016ElsevierB.V.Allrightsreserved
Nopartofthispublicationmaybereproducedortransmittedinanyformorbyanymeans, electronicormechanical,includingphotocopying,recording,oranyinformationstorageand retrievalsystem,withoutpermissioninwritingfromthepublisher.Detailsonhowtoseek permission,furtherinformationaboutthePublisher’spermissionspoliciesandour arrangementswithorganizationssuchastheCopyrightClearanceCenterandtheCopyright LicensingAgency,canbefoundatourwebsite: www.elsevier.com/permissions.
Thisbookandtheindividualcontributionscontainedinitareprotectedundercopyrightbythe Publisher(otherthanasmaybenotedherein).
Notices
Knowledgeandbestpracticeinthisfieldareconstantlychanging.Asnewresearchand experiencebroadenourunderstanding,changesinresearchmethods,professionalpractices,or medicaltreatmentmaybecomenecessary.
Practitionersandresearchersmustalwaysrelyontheirownexperienceandknowledgein evaluatingandusinganyinformation,methods,compounds,orexperimentsdescribedherein. Inusingsuchinformationormethodstheyshouldbemindfuloftheirownsafetyandthesafety ofothers,includingpartiesforwhomtheyhaveaprofessionalresponsibility.
Tothefullestextentofthelaw,neitherthePublishernortheauthors,contributors,oreditors, assumeanyliabilityforanyinjuryand/ordamagetopersonsorpropertyasamatterofproducts liability,negligenceorotherwise,orfromanyuseoroperationofanymethods,products, instructions,orideascontainedinthematerialherein.
ISBN:978-0-12-803886-4
ISSN:0079-6123
ForinformationonallElsevierpublications visitourwebsiteat https://www.elsevier.com/
Publisher: ZoeKruze
AcquisitionEditor: KirstenShankland
EditorialProjectManager: HannahColford
ProductionProjectManager: MageshKumarMahalingam
CoverDesigner: GregHarris
TypesetbySPiGlobal,India
Contributors
A.Alexander
StanfordUniversity,Stanford,CA,UnitedStates
S.C.Baraban
EpilepsyResearchLaboratory,UniversityofCalifornia,SanFrancisco,CA,United States
S.Baulac
SorbonneUniversites,UPMCUnivParis06,UM75;INSERM,U1127;CNRS, UMR7225;ICM(InstitutduCerveauetdelaMoelle epinie ` re);AP-HPGroupe hospitalierPitie-Salp^ etrie ` re,Paris,France
D.A.Coulter
PerelmanSchoolofMedicine,UniversityofPennsylvania;TheResearchInstitute oftheChildren’sHospitalofPhiladelphia,Philadelphia,PA,UnitedStates
C.G.Dengler
PerelmanSchoolofMedicine,UniversityofPennsylvania,Philadelphia,PA, UnitedStates
J.Ghaziri
ResearchCentre,Centrehospitalierdel’UniversitedeMontreal,Montreal,QC, Canada
A.Griffin
EpilepsyResearchLaboratory,UniversityofCalifornia,SanFrancisco,CA,United States
F.Gu
EpilepsyResearchLaboratories,StanfordUniversitySchoolofMedicine, Stanford,CA,UnitedStates
A.E.Hernan
UniversityofVermontCollegeofMedicine,Burlington,VT,UnitedStates
G.L.Holmes
UniversityofVermontCollegeofMedicine,Burlington,VT,UnitedStates
X.Jiang
UniversitedeMontreal;CHUSte-JustineResearchCenter,Montreal,QC,Canada
C.Krasniak
EpilepsyResearchLaboratory,UniversityofCalifornia,SanFrancisco,CA,United States
M.Lachance
CHUSte-JustineResearchCenter,Montreal,QC,Canada
M.Maroso
StanfordUniversity,Stanford,CA,UnitedStates
H.C.Mefford
UniversityofWashington,Seattle,WA,UnitedStates
C.T.Myers UniversityofWashington,Seattle,WA,UnitedStates
D.K.Nguyen
ResearchCentre,Centrehospitalierdel’UniversitedeMontreal;CHUM–H^ opital Notre-Dame,Montreal,QC,Canada
I.Parada
EpilepsyResearchLaboratories,StanfordUniversitySchoolofMedicine, Stanford,CA,UnitedStates
D.A.Prince
EpilepsyResearchLaboratories,StanfordUniversitySchoolofMedicine, Stanford,CA,UnitedStates
E.Rossignol UniversitedeMontreal;CHUSte-JustineResearchCenter,Montreal,QC,Canada
I.Soltesz
StanfordUniversity,Stanford,CA,UnitedStates
Y.Zerouali
ResearchCentre,Centrehospitalierdel’UniversitedeMontreal;Ecole PolytechniquedeMontreal,Montreal,QC,Canada
Preface
Thefollowingvolumestemsfromameetingofthesamename“TheNeurobiologyof Epilepsy:FromGenestoNetworks”heldinMontrealonMay4–5,2015,andorganizedbyDrs.L.Carmant,P.Cossette,E.Rossignol,andJ.-C.Lacaille.Theeditors wouldliketoacknowledgethesupportoftheGroupedeRecherchesurleSyste ` me NerveuxCentral,UniversitedeMontreal,fortheorganizationofthemeeting.
Epilepsyisabraindiseasecausedbyabnormalandexcessiveelectricaldischarges ofneurons.Theunderlyingetiologiesaremultiple,butrecentresearchindicatesan importantroleforpathologicalgeneticvariantscausingdysregulationofneuronal networks.Thismeetingbroughttogetheraninternationalgroupofcliniciansand basicscientiststosharenewinformationontheneurobiologicalbasisofepilepsy, includingclinicalaspects,molecularmechanisms,neuronalnetworks,aswellas animalmodelsandnoveltherapies.Bytryingtodiscussthe“neurobiology”of epilepsy,wemeantoaddressthefundamentalmechanismsunderlyingthegenetic basisofepilepsyandhopefullyleadtoanunderstandingofepilepsyatthemolecular, cellular,andnetworklevelsthatwillbetranslatableintoimprovedtreatmentfor patientswithepilepsy.
Thevolumebeginswithsectionscoveringnoveltiesintheclinicalinvestigation ofpatientswithepilepsy.Drs.Zerouali,Ghaziri,andNguyendescribemultimodal imagingtechniquesinvolvedintheinvestigationofepilepticnetworksinpatients, focusingoninsularcortexepilepsy.Drs.MyersandMeffordreviewcurrentknowledgeonthegeneticinvestigationtechniquesusedtoidentifymolecularetiologies inpatientswithepilepticencephalopathies,andprovideanoverviewoftheclinical featuresandbasicmechanismsofrecentlydescribedgeneticepilepticencephalopathies.Dr.Baulacexamineshowgermlineandsomaticmutationsinthegenesofthe GATOR1complex,whichregulatesthemTORpathway,causefocalepilepsieswith variablefoci.
Anunderstandingofthe“neurobiology”ofepilepsymustalsoelucidateseizures atthemicrocircuitlevelandunderstandhowneuronalnetworksareaffectedinepilepsy.Thevolumecontinueswiththreechaptersdiscussingthemolecular,cellular, andnetworkmechanismsinvolvedinthegeneticsofepilepsy.Drs.Jiang,Lachance, andRossignolconsidertheinvolvementofcorticalGABAergicinterneurondisordersingeneticcausesofepilepsy;Drs.Alexander,Maroso,andSolteszdiscusswork ontheorganizationandcontrolofepilepticcircuitsintemporallobeepilepsy;and Drs.DenglerandCoulterreviewthenormalandepilepsy-associatedpathologic functionofthehippocampaldentategyrus.
Amajorjustificationforelucidatingthegenetic,molecular,cellular,andnetwork basisofepilepsiesistodevelopeffectivetreatmenttherapiesforpatients.Thevolumethenmovesintoinvestigationsofanimalmodelsandtherapies.Drs.Hernanand Holmesexamineworkonantiepileptictreatmentstrategiesinneonatalepilepsy,and Drs.Griffin,Krasniak,andBarabandiscussadvancementinepilepsytreatment throughpersonalizedgeneticzebrafishmodels.
Finally,theconcludingchapterforthevolumeisfromDrs.Prince,Gu,and Parada,describingantiepileptogenicrepairofexcitatoryandinhibitorysynaptic connectivityafterneocorticaltrauma.
ElsaRossignol,LionelCarmant,andJean-ClaudeLacaille Departementdeneurosciences,UniversitedeMontreal,Montreal,Canada
Multimodalinvestigationof epilepticnetworks:Thecase ofinsularcortexepilepsy 1
Y.Zerouali
*,†,J.Ghaziri*,D.K.Nguyen*,{,1
*ResearchCentre,Centrehospitalierdel’UniversitedeMontreal,Montreal,QC,Canada †EcolePolytechniquedeMontreal,Montreal,QC,Canada {CHUM–H ^ opitalNotre-Dame,Montreal,QC,Canada 1Correspondingauthor:Tel.:+1-514-890-8000ext.25070;Fax:+1-514-338-2694, e-mailaddress:d.nguyen@umontreal.ca
Abstract
Theinsulaisadeepcorticalstructuresharingextensivesynapticconnectionswithavarietyof brainregions,includingseveralfrontal,temporal,andparietalstructures.Theidentificationof theinsularconnectivitynetworkisobviouslyvaluableforunderstandinganumberofcognitive processes,butalsoforunderstandingepilepsysinceinsularseizuresinvolveanumberofremotebrainregions.Ultimately,knowledgeofthestructureandcausalrelationshipswithinthe epilepticnetworksassociatedwithinsularcortexepilepsycanofferdeeperinsightsintothis relativelyneglectedtypeofepilepsyenablingtherefiningoftheclinicalapproachinmanaging patientsaffectedbyit.
Inthepresentchapter,wefirstreviewthemultimodalnoninvasivetestsperformedduring thepresurgicalevaluationofepilepticpatientswithdrugrefractoryfocalepilepsy,withparticularemphasisontheirvalueforthedetectionofinsularcortexepilepsy.
Second,wereviewtheemergingmultimodalinvestigationtechniquesinthefieldofepilepsy,thataimto(1)enhancethedetectionofinsularcortexepilepsyand(2)unveilthearchitectureandcausalrelationshipswithinepilepticnetworks.Wesummarizetheresultsofthese approacheswithemphasisonthespecificcaseofinsularcortexepilepsy.
Keywords
Epilepsy,Insula,Connectivity,Networks,Multimodal,Causality,Neuroimaging
1 EPILEPSYASASYSTEMSDISEASE
Formostepilepticpatients( 70%),anticonvulsivedrugsadequatelycontrolseizures.However,amongtherefractorycases,asignificantproportionofpatients areeligibleforsurgicaltreatmentofseizures(Wiebeetal.,2001).Thefundamental
ProgressinBrainResearch,Volume226,ISSN0079-6123, http://dx.doi.org/10.1016/bs.pbr.2016.04.004 © 2016ElsevierB.V.Allrightsreserved.
questioninthosecasesistolocalizethepartofthebrainthatisresponsibleforpatients’seizures,whichconstitutesthecentralthreadofthischapter.Importantadvancesinthesurgicaltreatmentofepilepsyarosefrombothabetterformulation ofthisquestionandthedevelopmentofmethodologicaltoolstoanswerit.Indeed, ournotionofepilepsyhasevolvedfromalocal-basedtonetwork-basedmodel,capitalizingontheabilityofneuroimagingtostudybrainfunctionatincreasinglyhigh spatialandtemporalresolutions.
Earlyinthelastcentury,themeasurementofbrainelectricalpotentialsonthe scalpbyBergerpavedthewayfortheinvestigationoftheneuroelectriccorrelates ofepilepticseizures.Inadditiontoseizures,Bergeralsoreportedtheexistenceof sharpelectricaltransientsthatareobservableontheelectroencephalogram(EEG) ofepilepticpatientsintheabsenceofseizures.These“spikes”areusuallyobserved onelectrodesthatrecordseizuresbutthisisnotalwaysthecase.Thisspatialdistinctionbetweenthegeneratorsofseizuresandspikeswasfurtherelaboratedwiththe adventofintracranialEEGrecordings(icEEG).icEEGallowsexcellentspatialdiscriminationoftheneuralgeneratorsofepilepticactivity,whichledLaufsandRosenowtoproposea“zonal”modeltoexplainthepathophysiologyofepilepsy (Rosenow,2001).The“zonal”modelrecognizesdifferentzonesassociatedwith theclinicalsymptoms(symptomatogeniczone),theinterictalspikes(irritativezone), theinitiationofseizures(seizureonsetzone—SOZ),andthefunctionaldeficitsassociatedwiththeepilepticcondition(functionaldeficitzone).Importantly,theydefinean“epileptogenic”zone(EZ)thatconsistsofthebraintissuethatmustbe surgicallyresectedforseizurestobecured.ThespatiallocationoftheEZisusually estimatedusingmultimodalinvestigationtechniques,aswillbedescribedinthe nextsection,butitstruelocationcanonlybeconfirmedthroughpositivesurgical outcome.
Althoughthezonalconceptofepilepsyhadanimportantimpactontheclinical managementofepilepticpatients,failureratesforepilepsysurgeriesremainrelativelyimportant,ashighas30%fortemporallobe—TLE(Jehaetal.,2006; Wiebeetal.,2001)and50%forfrontallobe—FLE(Jehaetal.,2007;Yunetal., 2006)andparietallobe—PLE(Binderetal.,2009;Kimetal.,2004a)epilepsy.In 2002,Spencerformulatedtheideathatweshouldenvisiongeneratorsofinterictal andictalactivitiesasnetworksofstructuresratherthansinglezones(Spencer, 2002).Sincethetransitionfrominterictaltoictaltopostictalbrainstatesoccurs atthetimescaleofsynapticactivity,thisideahastwocorollaries.First,itimplies thattheneuralmachinerysupportingtheemergenceofepileptogenicnetworks (ENs)ishardwiredintothebrain(Richardson,2012).Thus,epilepsyisasystems disease,thesymptomsofwhichresultfromaberrantconnectivityamongasetof anatomicalhealthystructures(AvanziniandFranceschetti,2003).Someauthorssuggestthatneuralnetworksarebistablesystemsthatcanexhibitbothhealthyandepileptiformactivityforthesamesetofparameters(Breakspearetal.,2006;DaSilva etal.,2003;Martenetal.,2009).Dynamicaltransitionsbetweenthesetwostatesare calledbifurcations,andtheepilepticconditionfacilitatessuchbifurcations.
Thesecondcorollaryisthatthenetworkassemblyisahighlyflexibleprocess;for agivensetofcomponents,therearealargenumberofnetworkarchitectures,allof
whichmaygiverisetodifferentepileptiformactivitiesandclinicalsymptoms.This ideahasdeepimplicationsforcliniciansandneuroscientists,sinceaccuratelocalizationofnetworkcomponentsisinsufficientforfullydescribingthepathophysiologyofepilepsy.Forsuchanendeavor,itisnecessarytostudytime-varyingnetwork dynamics(Hala ´ sz,2010).
Inordertoillustratethenetworksconceptofepilepsyandthecurrenttechniques usedintheirinvestigation,weusetheuniquecaseofinsularcortexepilepsy(ICE). Theinsulaisacorticalstructurelocateddeepinthesylvianfissureandishiddenby thefrontal,temporal,andparietalopercula.Despiteearlyreportsoninsularepileptiformactivity(GuillaumeandMazars,1949;PenfieldandFaulk,1955;Penfieldand Jasper,1954),insulectomywasnotconsideredanefficientsurgicalapproach (Silfveniusetal.,1964)untilthepast15years.Patientseriesfrom Isnardetal. (2004) and RyvlinandKahane(2005) demonstratedthatinsularENsincludetemporal,frontal,andparietalstructuresandthatthesequenceofclinicalsymptomsassociatedwithinsularseizurescanbeexplainedbytheirpatternsofpropagation. Throughoutthischapter,wewillpresentmultimodalinvestigationtechniquesused bothforlocalizingthecomponentsofENsandcharacterizingtheirarchitectures, withemphasisonICE. Section2 presentstheinvestigationtechniquesthatareroutinelyusedinmostepilepsycentersforimagingtheepileptogenicbraintissues. Section3 presentsnewexperimentalinvestigationtechniquesthatpromiseenhanced imagingandunderstandingofENs.
2 INVESTIGATINGTHEEPILEPTICNETWORKS:CLINICAL PRACTICE
2.1 PRESURGICALINVESTIGATIONTECHNIQUES
2.1.1icEEG
Thegoldstandardinthelocalizationoftheanatomicalcomponentsofepileptogenic networksconsistsofdirectrecordingsofneuroelectricactivitythroughelectrodesin contactwithbraintissue.icEEGrecordslocalfieldpotentialsthataregeneratedby neuralpopulationswithina0.5–3mmradiusfromthetipoftheelectrode(Juergens etal.,1999;Mitzdorf,1987);thus,achievingthehighestspatialresolutionamong allneuroimagingtechniquesusedinclinic.Thedownsideofsuchhighresolution isobviouslypoorspatialcoverage,sinceonlyalimitednumberofelectrodescan beusedwithoutriskingcerebralhemorrhageorneurologicaldeficits(Wongetal., 2009).ItisthuspossiblethattheepileptogeniczoneisnotsampledbyicEEG, leadingtothewrongselectionofsurgicaltarget.ICEprovidesanidealillustration ofthisissue.
InsufficientinsularcoverageinpatientswithICEwasassociatedwithasignificant proportionoffailedTLE,FLE,andPLEsurgeries.Initially,suspicionswereraised byastudyonpatientswithTLEwithatypicalclinicalsymptomsthatwereinsteadassociatedwithinsularactivity(Aghakhanietal.,2004).Despitesuccessiveresections (uptofour)ofanteriortemporal,mesiotemporal,andparietotemporalstructures,
patientscontinuedhavingseizures.Unfortunately,noelectrodesampledtheinsulain theirstudyalthoughinsularhyperperfusionwasclearlyshowninonepatient.The potentialbenefitfromicEEGrecordingsintheinsulainTLEwasfurtherdemonstrated,asabout10%ofpatientsdiagnosedwithTLEsufferedfromICE(Isnard etal.,2004).TLE-likesymptomsinthosepatientswereexplainedbysecondarypropagationofictalactivitytosurroundingtemporalstructures.Similarconclusionswere drawnbysomestudiesonPLEandFLE(Roperetal.,1993;Ryvlinetal.,2006).
Basedonthesereports,ourgrouplowereditsdecisionthresholdforinsularimplantationswithdepthelectrodesinpatientswithnonlesionalTLE,FLE,andPLE. Onaseriesof18patientsmeetingthesecriteria,wefoundthat40%patientswho underwenticEEGrecordingshadseizuresoriginatingfromtheinsula.Inaddition, electricalstimulationoftheinsulaprovedthatinsularepilepticdischargesreplicate semiologyofvariousextrainsularepilepsies(Nguyenetal.,2009).Ourfindings, alongwithexistingliteratureonthisissuesuggestthat(1)ICEisprobablymoreprevalentthanpresentlyreported;moreextensivestudiesmustbeconductedtodetermine itsfrequency,(2)despiteextensivepresurgicalworkups,nonlesionalICEisprobably rarelydetected,accountingforasignificantproportionoffailedepilepsysurgeries. Wefurtherreviewthedifferentinvestigationtechniquesusedinpresurgicalworkups anddiscusstheirvaluefordetectingICE.
2.1.2EEG
EEGisprobablytheoldestandmostwidelyusedimagingmodalityinclinical investigationsofbrainpathologies,includingepilepsy.Overtheyears,epileptologistsdevelopedexpertskillsinreadingandinterpretingEEGseizures,butalso waveformsobservedduringtheinterictalstate,suchasspikes,polyspikes,spikeand-wavecomplexes,sharpwaves,paroxysmalfastactivity(Westmoreland,1998), andhigh-frequencyoscillations(Braginetal.,1999).Advancedbiophysicalmodels andcomputerizedtechniquesallowunprecedentedaccuracyinthelocalizationofthose waveforms,asmostadvancedalgorithmscantheoreticallyreacha10cm2 resolution (Grovaetal.,2006),thusenabling“electricalsourceimaging”(ESI).
ESIreliesonabiophysicalmodelthatrelatesneuralelectricalactivity,modeled asafinitenumberofequivalentcurrentdipoles(ECD),toelectricalpotentials recordedoutsidethehead.WedistinguishtwobroadclassesofESItechniques, accordingtothenumberECDusedformodelingbrainactivity.SingleECDsassumerecordedelectricalpotentialsaregeneratedbyasingle(orafew)neuralpoint source(s).Althoughthisapproachobviouslyoversimplifiesneuralgeneratorsand itsnumericalimplementationrequiresstrongheuristics(numberofdipoles,initialization),itprovedvaluableinepilepsywhencarefulattentionispaidtoitslimitations,asvalidatedbysimultaneousEEGandicEEGrecordings(Boonetal.,2002; Ebersole,1991;Rothetal.,1997).Ingeneral,allstudiesreportusefulnessofsECD forepilepsy,withsensitivityandspecificityexceeding,respectively,80%and60% forthevastmajorityofstudies(see Kaiboriboonetal.,2012,forareview).
Inturn,distributedsourcemodeling(DSM)modelsneuralsourceswithalarge numberofECDshomogenouslydistributedinthebrain.Despitethismathematical challengeimposedbythelargenumberofsources,DSMisincreasinglybeing
validatedintheclinicalmanagementofepilepticpatients,benefitingfromincreased headcoverageofhigh-densityEEGsystemsandincreasedaccuracyofheadmodelingtechniques.Inthestudywiththelargestcohortofpatients,DSMwasshownto accuratelylocalizetheonsetofseizures,withsensitivityandspecificitybothexceeding80%(Brodbecketal.,2011),inlinewithseveralotherreports(Micheletal., 2004;Sperlietal.,2006).InICE,EEGwasfoundtobeinsensitivetospikesgeneratedfromthedeep-seatedinsula;therefore,wedidnotfindanyreportsontheusefulnessofESIforthatkindofepilepsy.
2.1.3MEG
Magnetoencephalography(MEG)isarelativelynewimagingmodalitythatrecords themagneticfieldsgeneratedbyelectricalcurrentsflowinginsideactiveneurons. Despitearelativelyshorthistoryofclinicalinvestigationandhigheroperationcosts thanEEG,MEGhasquicklyestablisheditselfasanimportanttoolinpresurgical evaluationofepilepsy.Owingtotherelativelysimplerphysicsofneuralmagnetic fieldspropagation,MEGissensitivetosmalleractivatedbrainregions( 4cm2 forMEG, Mikunietal.,1997, 10cm2 forEEG, Grovaetal.,2006).SourcelocalizationwithDSMshowedpromisingresultsforthepresurgicalworkupofepilepsy, whichledsomeauthorstosuggestthatitcouldobviateicEEGinvestigationsinsome cases(Fujiwaraetal.,2012).
SeveralstudiesdemonstratedtheusefulnessofsECDmodelingwithMEGon differenttypesofepilepsy.Globally,thereportedaccuracyofsECDisabove 75%forthemajorityofthestudies(Knowlton,2006;Minassianetal.,1999; Stefan,1993).Inaddition,MEGwasalsoshowntobevaluableforappropriately determiningthesubsequenticEEGcoveragezone(Fischeretal.,2005; Knowltonetal.,2009;Mamelaketal.,2002).Unfortunately,onlyafewstudies reportsECDinvestigationofICE.Amongthose,Heersetal.studiedthreepatients withcryptogenicepilepsyandhypermotorseizures(Heersetal.,2012).They showedthatMEGcannotonlyidentifyepilepticfociwhenothermodalitiesfail butisalsoabletolocalizedeep-seatedfocisuchasintheinsula(Parketal., 2012).Werecentlyinvestigated14patientswithinsularseizuresusingMEG. Amongthose,localizationofinterictalspikesshowedclearinsularorperisylvian focusinallbutonepatient.Takentogether,thesestudiessuggestthatMEGisvaluablefordetectingICE.
Inturn,wefoundsubstantiallyfewerreportsofDSM,probablyduetothefactitis morerecentandlessvalidated.Nonetheless,studiesusingDSMadvocateforits moreextensiveuseinpresurgicalworkupssinceitoutperformedsECDinatleast twocomparativestudies(Shiraishietal.,2005;Tanakaetal.,2009).Itwasalso shownthatpatternsofsourceactivityreconstructedwithDSMweregoodpredictors (upto94%)forsubsequentsurgicalresection(Tanakaetal.,2010).
2.1.4MRI
Magneticresonance(MR)scannersexploittheintrinsicmagneticproperties(the spin)ofelectronstoproducehigh-resolutionimagesofbrain(andbody)tissues. Usingasophisticatedcombinationofspinpolarizationandperturbation,MR
imaging(MRI)nowallowsrecoveringthethree-dimensionalpropertiesofthebrain with1mmresolution.MRIisanessentialtoolintheevaluationofpatientswithfocal epilepsy,allowingthevisualdetectionofavarietyofepileptogenicbrainlesions suchasgliosisfromacquiredinsults,tumors,vascularmalformations,ormalformationsofcorticaldevelopment.Globally,thesensitivityofMRIinepilepsysurgery candidatesrangesbetween75%and86%(Bronenetal.,1996;Brooksetal., 1990;Cascinoetal.,1992;Grattan-Smithetal.,1993;Kuznieckyetal.,1993; Lasteretal.,1985;Latacketal.,1986;Ormsonetal.,1986;Scottetal.,1999).
LiteratureonICEprovidescontrastingresultswithrespecttothesensitivityof MRI.Wefoundsixstudiesinwhichallpatients(N ¼ 43)displayedsomeabnormality (Cukiertetal.,1998;Duffauetal.,2002;Heersetal.,2012;Kaidoetal.,2006;Roper etal.,1993;vonLeheetal.,2008),twostudies(N ¼ 23)withbothMRI-positiveand MRI-negativepatients(Malaketal.,2009;Mohamedetal.,2013),andsevenstudies (N ¼ 19)withexclusivelyMRI-negativepatients(Dobesbergeretal.,2008;Isnard etal.,2000,2004;Kriegeletal.,2012;Nguyenetal.,2009;Ryvlinetal.,2006; Zhangetal.,2008).Overall,MRIhadasensitivityof61%,correspondingto87% positivepredictivevaluewhenconsideringtheresultsofsurgery.Overall,ourshort reviewsuggeststhatMRIisahighlyvaluabletoolforinvestigatingICEwithmoderatesensitivitybutexcellentdiagnosticvalue.However,therelativelylargernumberofpatientsdiagnosedwithlesionalratherthannonlesionalICEmightreflectthe factthatnonlesionalICEisapoorlydiagnoseddisease,andthatcurrentlyavailable investigationtoolsotherthanMRIhavelowdiagnosticvalueforthisdisease.
2.1.5PET
Positron-emissiontomography(PET)measurestheconcentrationofaspecific sourceofradiationinthe3Dspace.ThebrainpropertyimagedwithPETthus dependsonthechoiceofanappropriateradioligand,suchthat3Dconcentrations canbeinterpretedintermsofbrainfunction.Inepilepsy,2-[18F]-fluoro-2deoxy-D-glucose(FDG)and[11C]-flumazenil(FLU)aretwocomplimentaryand commonlyusedradioligands,imagingbrainfunction(glucoseconsumption),and structure(neuronalloss),respectively.Theepilepticconditionisassociatedwith neuronallossand,paradoxically,decreasedconcentrationsofFDGinaffectedbrain regions.Althoughthislastobservationislargelyconsensual,theunderlyingneurophysiologicalmechanismsarestillnotunderstood.
StudiescomparingFLU-andFDG-PETforlocalizingthebrainregionsinvolved inepileptogenicnetworksreportsimilarperformanceofbothmoleculesformost groupsofpatients.Globally,thesetwomodalitiesachievesimilarsensitivityand specificity(Ryvlinetal.,1998)andareequallypredictivewithrespecttosurgical outcome(Debetsetal.,1997).Itwasnotedhoweverthattheonlycaseswhere FLU-PETaddednewinformationabovethatofMRIsarewhenFDG-PETisnegative,whichimpliesthatFDG-PETshouldbeperformedfirst,andFLU-PETonly whenFDG-PETisnegative.
Sincetheroleofinsulahasonlygainedrecognitioninthelast10years,earlyPET studiesreportingchangesinmetabolismintheinsuladidnotincludeinsularintracranialelectrodes(Bouilleretetal.,2002;Didelotetal.,2008;Huretal.,2013;Joo,
2005;Wongetal.,2010).Forthisreason,althoughtheyprovidedinterestinginsights intotheinvolvementoftheinsulainthemetabolicchangesassociatedwithTLE, theyareinconclusivewithregardtoICE.WefoundfewreportsofICEwithicEEG andPETdata(Dobesbergeretal.,2008;Heersetal.,2012),includingtwostudies fromourgroup(Nguyenetal.,2009;Surbecketal.,2014).Pooledtogether,these studiessuggestthatFDG-PEThaslowsensitivity(17%)andspecificity(53%) toICE.
2.1.6SPECT
Single-photonemissioncomputerizedtomography(SPECT)consistsinlocalizing thesourceofgamma-rayemissionwithinthebrain.Thesourceconsistsofaradioactivetracer(usuallythe 99mTc-labeledHMPAO—hexamethylpropyleneamineoxime)boundtoamoleculethatfreelycrossestheblood-brainbarrier,suchthatit diffusesintothebrainafterintravenousinjection.SincethetracersusedinSPECT haverelativelylonghalf-lives,theydistributespatiallyinbrainregionswithhigher bloodflowandremainstableforuptoafewhours.PatientscanthusbeEEG-video monitoredandinjectedatthetimeofarelevantbrainactivity(ideallyseizureonset) asseenontheEEGtraces.ItisgenerallyagreedthattheuseofSPECTduringinterictalbrainstateisoflimiteduse(Debetsetal.,1997;Lascanoetal.,2015;Spencer, 1994).Incontrast,SPECTismostlyusefulwhentheradioligandisinjectedatseizure initiation(Jooetal.,2004;Spencer,1994).Inaddition,evenbetterresultscanbe achievedbysubtractinginterictalfromictalSPECTimages,atechniquecalledSISCOM.Suchanoperationisespeciallyusefulincaseswhereictalhyperperfusionis lowinepileptogeniczoneduetosuperpositiononaprecedinghypoperfusedstate (Desaietal.,2013;Neweyetal.,2013;Spencer,1994;vonOertzenetal.,2011).
AsforPET,thereareonlyafewstudiesthatreportedonthevalueofSPECTin ICE.WefoundfewreportsofICEwithicEEGandPETdata(Dobesbergeretal., 2008;Heersetal.,2012),includingtwostudiesfromourgroup(Nguyenetal., 2009;Surbecketal.,2014).Pooledtogether,thesestudiessuggestthatSPECT haslowsensitivity(23%)andspecificity(48%)toICE.
2.2 ILLUSTRATIVECASE
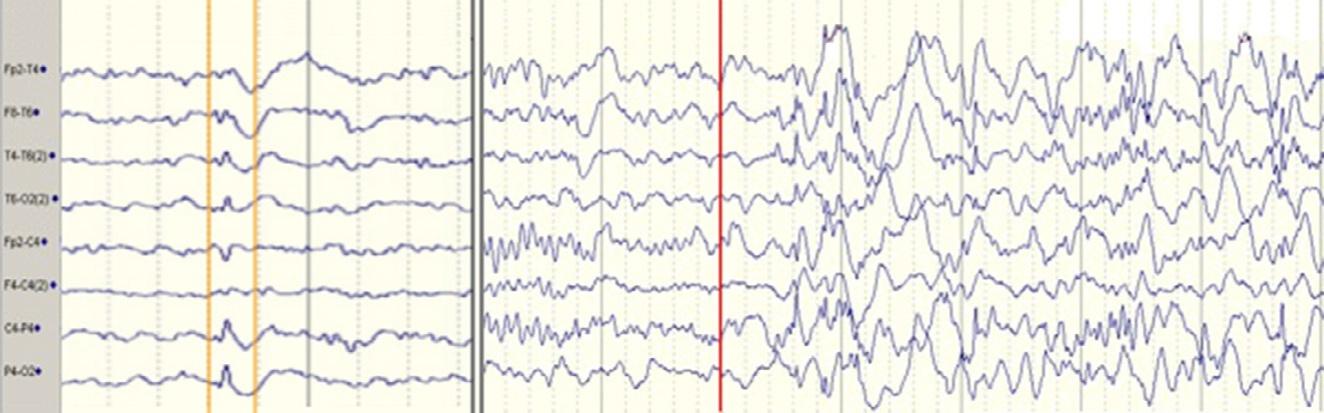
A10-year-oldambidextrousgirlwithmildlanguagedelaystartedhavingseizuresat theageof4yearscharacterizedbyanunpleasanttinglingsensationinthelowerback, rightarm,andbothlegsfollowedbyfearandcomplexmotorbehaviors.Seizures becamepredominantlynocturnalafterafewweeksandhaveremainedsosince,recurringinclustersof4or5(upto15)every2–3days.Afterfailingsixadequateantiepilepticdrugtrials,thepatientwasreferredforepilepsysurgery.Whiletheclinical historymighthavesuggestedafrontallobefocus,video-EEGmonitoringrevealed righttemporal,central,orcentro-temporaldischargesinterictallyandrightcentrotemporalrhythmicactivityatseizureonset(Fig.1).High-resolution3Tbrain MRIandvolumetricstudiesfailedtodiscloseanepileptogeniclesion.Interictal FDG-PETwasnormalbutictalSPECTshowedincreasedcerebralbloodflowover therightinsularregion(Fig.2).Sourcelocalizationofinterictalepileptiform
FIG.1
EEGrecordingsoftheepilepticactivityfromtheillustrativepatient.Thetimeaxis(horizontal) isdiscontinuousasshownbythe doubleverticalblacklines.Interictalandictalactivity aredisplayed,respectively,totheleftandrightofthe blacklines.Acleartemporo-central spikeisdisplayedbetweenthetwo verticalorange (lightgray intheprintversion) lines. Aseizurestartsrightafterthe verticalred (gray intheprintversion) bar.Fromthosetraces, EEGdoesnotallowthedetectionoftheinsularfocus.
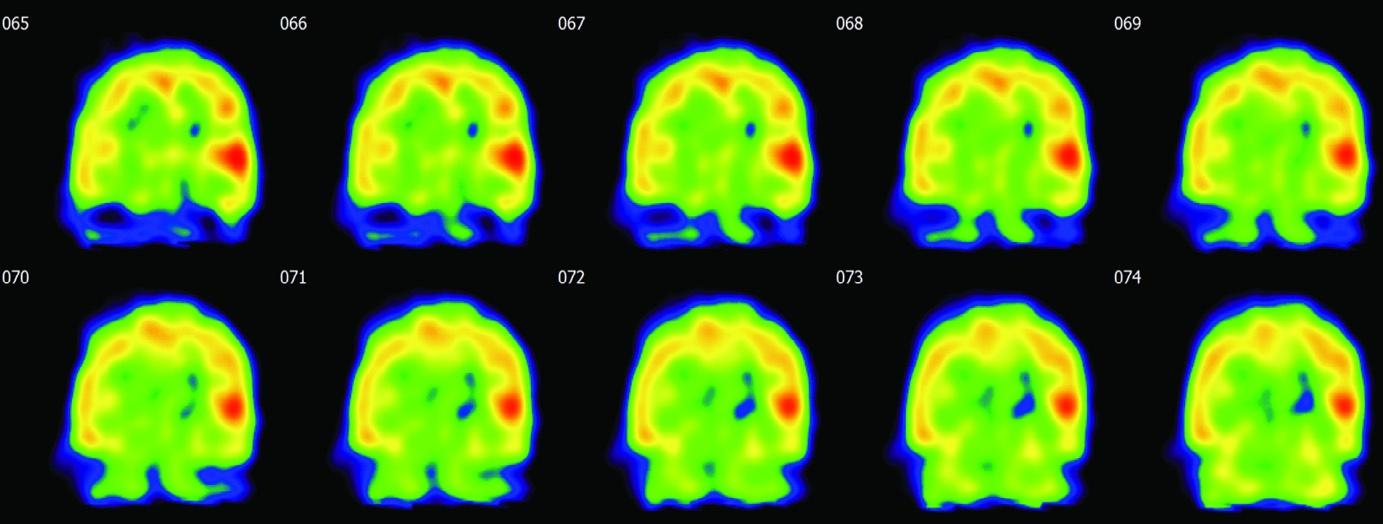
FIG.2
IctalSPECTimagesfromtheillustrativepatient.Theselectedcoronalslicesaredisplayed intheneurologicalconvention(righthemisphere attheright)andspantheantero-posterior axisoftheinsula.Thesesliceshowclearasymmetryinbloodperfusion,therightinsula showingclearhyperperfusionascomparedtotheleftside.
dischargesrecordedduringMEG(CTF275-sensorysystem,Canada)usinganelectricalcurrentdipolemodelrevealedaconcordanttightclusterattheveryposterior endoftherightSylvianfissure(posteriorinsulaandparietalmorethantemporal opercula—Fig.3).Duringspikes,combinedEEG–fMRIrecordingsshowed(blood oxygenlevel-dependent,BOLD)activationsovertherightposteriorinsula,theoverlyingperisylviancortexbutalsoincentralregionsandthecingulategyrus(Fig.4). FunctionalMRIforlanguagesuggestedleft-hemispheredominance.Basedonthis multimodalnoninvasiveevaluation,epilepsysurgerywasrecommended.Withthe removaloftherightparietaloperculum,temporaloperculum,andposteriorinsula, seizure-freedomwasattained(follow-up2years).
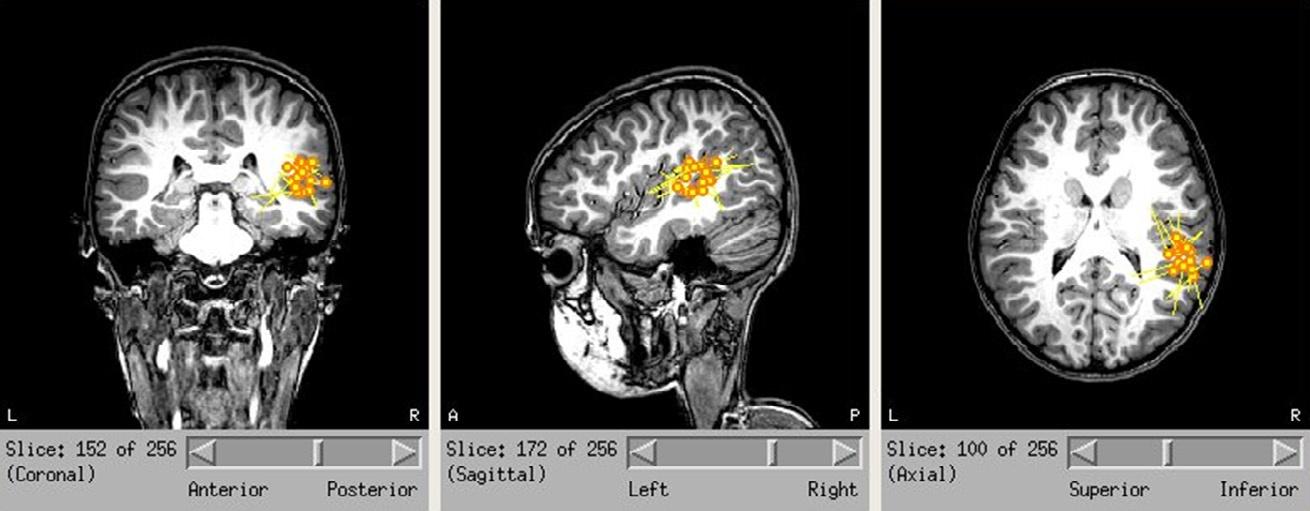
FIG.3
Single-dipolemodelingoftheinterictalspikesrecordedfromtheillustrativepatientusing MEG,eachdipolecorrespondingtoasinglespike.Localizeddipolesclearlyclusterinthe posteriorportionoftheinsulaandinthecentro-parietalopercula.
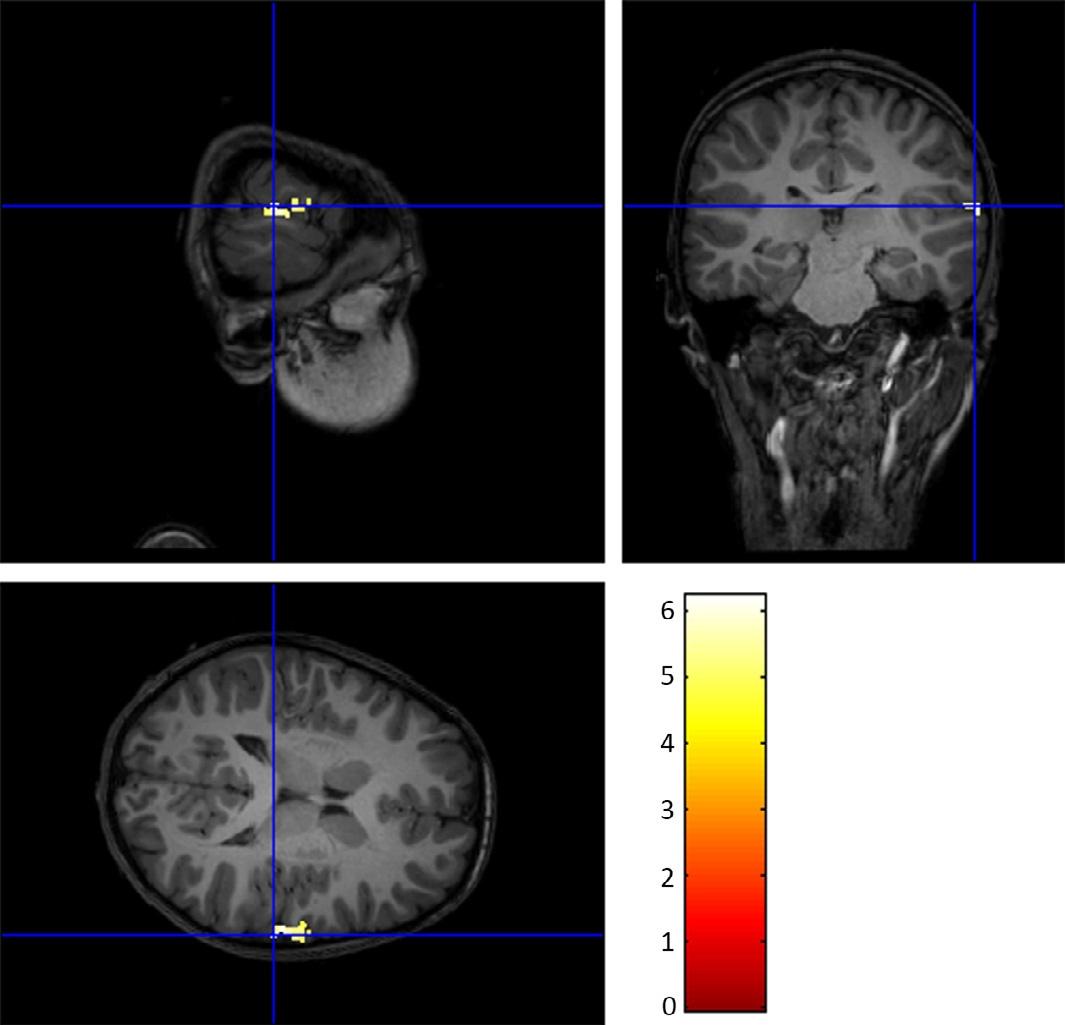
FIG.4
CombinedEEG–fMRIrecordingsofinterictalspikesfromonepatientofourcohortof insularcortexepilepsy.GenerallinearmodelrevealsasingleBOLDactivationclusterinthe posteriorportionoftherightinsulaalongwiththeoverlyingcentraloperculum.Althoughthey werefoundinotherpatients,activationofotherstructures,suchasthecingulategyrusdidnot reachsignificance.
3
INVESTIGATINGTHEEPILEPTICNETWORKS: PERSPECTIVES
3.1 ADVANCEDLOCALIZATIONTECHNIQUES
3.1.1EEG/MEGfusion
BothEEGandMEGdirectlyaddressneuronalactivitybyrecordingdifferencesin electricalpotentialsandmagneticfields,respectively,outsidethehead.Although bothmodalitiesrecordactivityfromthewholebrain,theyarepreferentiallysensitive todifferentpopulationsofneurons.Indeed,EEGismainlysensitivetoradiallyorientedsourceslyingoncorticalgyrisincetheyareclosertothesensorswhilethemagneticfieldsgeneratedbythosesourcesvanishduetothequasi-sphericalheadshape. Inturn,MEGismainlysensitivetotangentialsourcelyingalongthesulciwalls (Ahlforsetal.,2010;Sharonetal.,2007).Thusacorticalregionparticipatingin anENwouldonlybepartiallyrecoveredbyEEGandMEGifitextendsspatially fromthetopofagyrustoacorticalfold.Somestudiesfurtherobservednoticeable epileptogenicactivityononemodalitybutnottheother(BarkleyandBaumgartner, 2003;Iwasakietal.,2005),highlightingtheneedforsimultaneousEEG–MEGrecordings.Importantly,itwasshownthatEEGandMEGacquiredsimultaneously aresuperadditive,ie,theyprovidemoreinformationrelevanttosourcelocalization thanthesumofunimodalinformation(Pfliegeretal.,2000).
SimultaneousEEG/MEG(MEEG)recordingswereintroducedinepilepsywith theaimtobetterdelineatethelocationandspatialextentofcorticalsourcesparticipatinginepileptogenicnetworks.Usingsimulationsofrealisticepilepticspikes, Chowdhuryetal.showedthatMEEGprovidesbetterlocalizationthanEEGor MEGalone,regardlessoftheinversionschemeused(Chowdhuryetal.,2015).However,contrarytowhatiscommonlybelievedtheyshowedthatthemaximumentropy onthemeanframework(Amblardetal.,2004)notonlyprovidesthemostaccurate localizationofthesimulatedsourcesbutisalsoabletorecovertheirspatialextent (Chowdhuryetal.,2013;EbersoleandEbersole,2010).Inaddition,inthesame studyontwopatientswithfrontallobeepilepsy,MEEGwasabletotrackinterictal spikepropagationpatternswhileindividualmodalitieswereinsensitivetospatiotemporaldynamicsofthespikes.Similarconclusionsweredrawnfromarecentstudy comparingunimodalandmultimodalMEEGsourcelocalizationswithintracranially recordedEEGonapatientwithmultifocalrefractoryepilepsy.Theauthorsshowthat MEEGisabletorecovermostoftheregionsparticipatinginthegenerationofspikes, evenwhennosinglemodalitywasabletorecoverthem(Aydinetal.,2015).This studyillustratesthesupraadditivenatureofMEEGanditspotentialtorecovermore componentsofENs.
WerecentlystartedexploringthepotentialofMEEGsourceimagingofepileptic spikestodetectinsularactivationsinICE.Extendingthepreviouslycitedreports,we foundthatEEGandMEGareeachabletodetectinsularactivationsonsubsetsbut notallspikes.However,MEEGsourceimagingprovidedmorerobustresultsand coulddetectinsularactivationsincaseswhereonlyasinglemodalitywaspositive (see Fig.5A)andevenwhenbothmodalitieswerenegative(Fig.5B).These
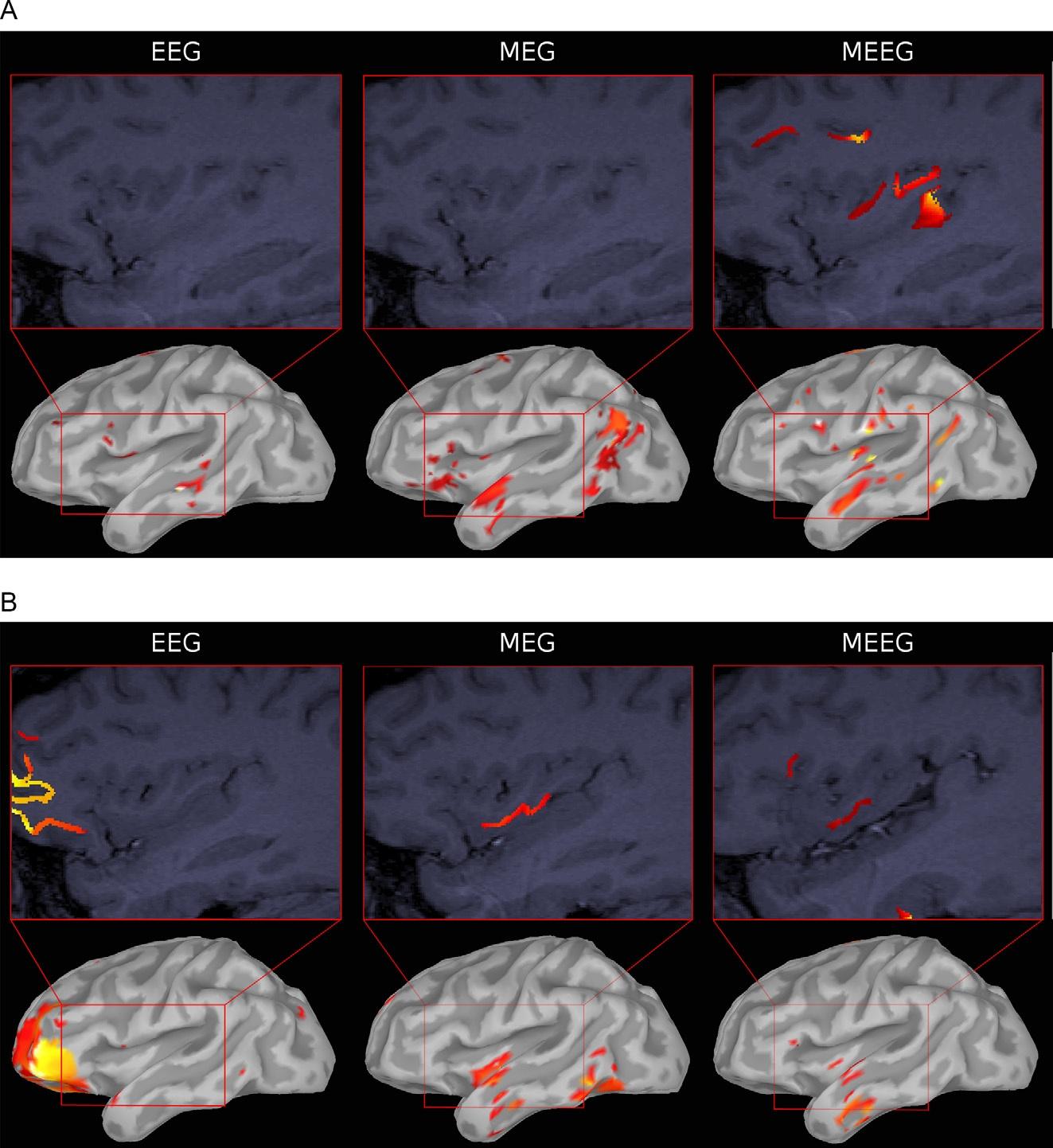
FIG.5
CombinedEEG–MEGsourcereconstructionoftwoepilepticspikesfromonepatientwithICE. (A)Forthisspike,theEEGwasunabletodetecttheinsularactivationandrevealsmainly activityintheorbitofrontalcortex.Inturn,bothMEGandMEEGcoulddetectactivationinthe ventralregionoftheinsula.(B)Forthisspike,neitherEEGnorMEGcoulddetectinsular activationwhileMEEGclearlydisplaysmaximaofpowerintheventralandposteriorinsular regions.
preliminaryresultssuggestthatMEEGsourceimagingofepilepticspikesisapromisingavenueforthecomputer-assisteddetectionofICE.
3.1.2CombinedEEGandfMRI
Aclinical-gradeMRmagnetisprobablyamongthemosthostileenvironmentsfor recordingscalppotentialswithEEG.Indeed,evensmallmovementsoftheEEG electrodesinsidethescannerasaresultofsmallheadmovementsor
ballistocardiographiceffects,translateintocurrentinductioninelectrodes.Inaddition,theon/offswitchingoftheradiofrequencyantennascreatesevenlargerartifacts ontheEEG,twoorders-of-magnitudelargerthantheactivityofinterest.Nonetheless,modernsignalprocessingtechniquesallowforapropercleaningofEEGdata suchthatEEG–fMRIcanbeusedforrelatinghemodynamicandneuroelectricbrain activity.Giventhedeterministicnatureofthegradientartifact,waveformaveraging wasintroduced(Allenetal.,2000)andvalidated(Gonc ¸alvesetal.,2007;SalekHaddadietal.,2002)tosubtracttheartifactfromtheEEG.Otherfilteringtechniques, applicabletotheballistocardiographiceffect,werealsoproposedbasedonspectral domainfiltering(Sijbersetal.,1999),waveletfiltering(Kimetal.,2004b),spatial Laplacianfiltering,PCA(Niazyetal.,2005),andICA(Mantinietal.,2007; Srivastavaetal.,2005).
Inthecontextofepilepsy,oneofthemostwidelyusedEEG–fMRIparadigmsis toanalyzetheBOLDsignalinanevent-relateddesignwheretheeventsareEEGmarkedinterictalspikes.Afterpreprocessing,spikesaremarkedontheEEGby expertepileptologists.TheEEGsignalisthenbinarizedaccordingtothespikemarking,downsampledtomatchfMRItimeresolution,andconvolvedwithamodelof thehemodynamicresponsefunctionthatisthencastasaregressorinthegeneral linearmodel.Themostcommonmodelisthecanonicalhemodynamicresponse function(HRF),whichaccountsforlocalelasticdeformationofbloodcapillaries andtheresultanttransientincreaseinlocalbloodoxygenationinresponsetoneuronalactivity—alsotermedneurovascularcoupling(Buxtonetal.,1998).However, itwasshownthattheshapeandonsetoftheHRcanvarysignificantlyamongsubjects(Aguirreetal.,1998;Lindquistetal.,2009),withrespectto:subjectsage (D’Espositoetal.,1999;Jacobsetal.,2008),brainregions(Handwerkeretal., 2004)andbrainlesionsincludingepileptogeniclesions(Lemieuxetal.,2008; Mastertonetal.,2010).SeveralalternatemodelsoftheHRFwereproposedtoaccountforsuchvariability,includinggeneralnonlinearfitsoftheHRF,multiple HRFswithvaryingonsetandpeaktimes,HRFalongwithitstimederivatives (Fristonetal.,1998),generalbasisfunctionssets(JosephsandHenson,1999), andthesuperpositionofthreeinverselogitfunctions(Lindquistetal.,2009).These modelsarethenintegratedinagenerallinearmodeltoinfertheresponseofeach voxeltotheepilepticactivity(Friston,1995).Irrespectiveofthechosenmodel,usefulnessofEEG–fMRItoimagingepilepticnetworkshasbeendemonstratedinseveralstudies.
First,itwasshownthattheBOLDsignalprovidesusefulinformationforconfirmingthelocationofthesuspectedepilepticfocus.Dependingonthestudy,proportions ofpatientswhodisplayIED-relatedchangesintheBOLDsignalrangedfrom67%to 83%(Kobayashietal.,2006;Salek-Haddadietal.,2006).Themostclinicallyuseful BOLDchangesareactivations,sinceidentificationofasingleactivationclusterwas foundtobeconcordantwithelectro-clinicalsymptomsinover80%ofcases (Krakow,1999;Salek-Haddadietal.,2006;Thorntonetal.,2010)andaregoodpredictorsofpositivesurgicaloutcome(Anetal.,2013).Importantly,anumberofstudiesshowedthatEEG–fMRIhasthepotentialtorevealthecomponentsofENs. Indeed,inmesialTLE,BOLDoccasionallydisplayssignificantactivationclusters
inthecontralateraltemporalandextratemporalregions(Avesanietal.,2014; Kobayashietal.,2006;Tousseynetal.,2014).Thoseclusterswereconsideredas patternsofspikepropagationsincesurgicaloutcomesaregooddespitesparingthose clusters.Similarly,inpatientswithintractablegeneralizedepilepsywhoseinterictal activityischaracterizedbysharpspike-wavebursts,BOLDchangesshowsignificant activationofthethalamuswhileEEGdoesnot(Aghakhani,2004).
WerecentlyconductedanEEG–fMRIstudyaimedatrevealingtheENassociated withICE(unpublishedresults).Werecruited13ICEpatients,asconfirmedbysurgicaloutcomeafterinsulectomy.WewereabletodetectIEDsin62%ofpatients, similarlytowhathasbeenreportedinstudiesonotherkindsofepilepsies.Wefound ipsilateralinsularandorperisylvianBOLDactivationsinsixpatientswhilethe remainingtwodisplayedsignificantBOLDactivationinthecontralateralinsula (datafromonepatientisshownin Fig.4).Inadditiontoinsularandperisylvianactivations,significantBOLDclusterswerefoundinthepostcentralgyrus,superior parietallobule,middleorsuperiorfrontalgyri,andanteriorcingulateormedialfrontalgyri,allofwhichwerepreviouslyshowntosharestructuralconnectivitywiththe insula(Augustine,1996;Nieuwenhuys,2012).WethusthinkthatEEG–fMRIisa promisingtoolforrevealingcomplexENsinICE.
3.1.3QuantifiedicEEG
Inprinciple,icEEGrecordingsarethegoldstandardinepilepsyastheyallowfor directsamplingofepileptogenicbrainregions,assumingcoverageisappropriate. Localizationoftheseizureonsetzonethusamountstoidentifyingthefirstcontact displayingepileptiformactivityatseizureinitiation.However,suchactivityoften appearsnearlysimultaneouslyonanumberofcontactsandvisualidentification ofrelevantnodesoftheENisachallengingtask.Thus,somestrategieswereproposedforautomaticallylabelingthemostimportantcontactsatseizureinitiation.
Bycombiningspectralandtemporalinformationatseizureonset,Bartolomei etal.introducedanempiricalindexthatmeasuresthepropensityofeachnodetoinitiateseizures(Bartolomeietal.,2008).Morespecifically,theycomputedaratioof energyofhighfrequencies(betaandgamma)overlowerfrequencybands(delta, theta,andalpha)ateachtimebinofthetime-frequencydecompositionofEEGsignals.Thisratioisthennormalizedandcumulatedovertimeinwhatiscalledthe “energyratio”function.Whenaseizureisrecorded,thisfunctioncontainsalocal maximumatseizureonset,andtheamplitudeandlatencyofthatmaximumareused todefinetheso-calledepileptogenicindex(EI),whichmeasurestheinvolvementin seizureinitiation.
TheEIprovedusefulforthestudyonepileptogenicnetworks,especiallyinmesialTLE.Indeed,thenumberonnodeswithhighEIwashigherforpatientswith identifiedlesionsthanforpatientswithnormalMRI,whichwasanimportantpredictorofsurgicaloutcome(Bartolomeietal.,2008).Inaddition,theEIcaptures somesubtletiesintheclinicalsymptomatologyofpatients,sinceitcanbeusedto classifypatientswithclinicalsubtypesofmesialTLE(Bartolomeietal.,2010) anddiscriminatepatientswithmesialMTLEfromthosesufferingfromothertypes ofTLE(Vaugieretal.,2009).
3.1.4Neuroimagingbrainnetworks
Networkscanbeschematizedasasetofnodesconnectedtoeachotherthroughspecificlinkscallededges.Nodesandedgesaretheworkhorseofalargeresearchcommunitystudyingnetworks,rangingfromairtraffic,powerplantstobrainnetworks. Inneuroscience,networkanalysesanswertwobroadcategoriesofquestions:(1)how doesedgestrengthbetweenagivennodeandasetofothernodesevolvewithrespect toexperimentalparadigmand(2)howdotheglobalfeaturesofnetworksevolvewith respecttoexperimentalparadigm?
Themainchallengeshereconsistindefiningrelevantnodesandedges.Many approacheswereproposedfordesigningnodesencompassingrandom,data-driven andatlas-basedstrategies.Wenotethatatlas-basedstrategiesprovideregionsof interest(ROIs)thataremoreeasilyinterpretableintermsofneurophysiologyas theyallowfortheunderstandingofneuralsystemsintermsofassociationsof broadlyspecializedfunctionalunits.Edgesrepresentthestrengthoftheconnectivitybetweentwonodes,andtheirinterpretationdependsontheimagingmodality. Briefly,wedistinguishthreetypesofconnectivity:functional,effective,andstructural.Functionalandeffectiveconnectivityaremeasuresofundirectedanddirected statisticalcouplingamongsignals,respectively,andmustbeestimatedusing multivariatetimeseries(EEG,MEG,andfMRI).Inturn,structuralconnectivity isdefinedintermsofanatomicalassociationbetweenROIssuchasfibertracts densityandisusuallyestimatedthroughdiffusionimaging.Onecananalyzethe valuesofedgeslinkingaspecificsetofnodes,alsocalled“seeds.”Thoseseedbasedanalyseswerecarriedoutinawidevarietyofepilepsytypes,encompassing “focal”and“generalized”types.Inthoseanalyses,variationsinedgevaluesare assessedwithrespecttoexperimentalparadigms,allowingtheinterpretationof pathophysiologyandclinicalsymptomsintermsofbrainconnectivity.Asample ofthosestudiesisdescribedinthefollowingsectionswithrespecttoimaging modalities.
Thecompletegraphofconnectionsbetweenallavailablenodesiscalleda “connectome”andanalysesofsuchgrapharethustermed“connectomics.”This fieldofmathematicswasoriginallyframedintotheso-calledgraphtheory,which recentlyraisedspectacularinterestinneuroscienceingeneral,andepilepsyinparticular.Graphtheoryprovidesavarietyofmetricsthatdescribeinterpretablefeaturesofconnectomes,suchastheclusteringcoefficient,whichindexesthe tendencyofnodestoform“cliques”withdenseinternalconnections,andtheaveragepathlength,whichmeasurestheaveragenumberofrelayswhiletryingtogo fromonenodetoanother.Strikingly,manynetworks,includingbrainnetworks, werefoundtohaverelativelyhighclusteringcoefficientandlowaveragepath length.Those“small-world”networkssharefastprocessingofinformationwithin functionalunitsthroughdenselocalconnectionsandtheabilitytoparallelizeinformationprocessingthroughsparsebutefficientlong-rangeconnections(Wattsand Strogatz,1998).Inepilepsy,metricssuchas“small-worldness,”efficiency,and modularityshednewlightonthelarge-scaleneurophysiologicalmechanismsatplay duringinterictalandictalstates.
3.1.5EEG/MEGconnectivity
DefinitionofnodesandedgesinEEGandMEGisusuallydoneinthesourcesspace sinceeachEEGelectrodeandMEGsensorrecordsmixturesofneuralsignalsfroma largeportionofthebrain,whichimpliesthatconnectivityinthesensorsspaceshas littleinterpretabilitywithrespecttounderlyingneuralgenerators(butsee Holmes etal.,2010;Horstmannetal.,2010;vanMierloetal.,2014 forinterestingreports onfunctionalconnectivityonthesensors).Inthemajorityofstudies,DSMisdone usingthousands( 10k)ofECDsandconnectivityanalysesatsuchresolutionisimpracticablefortworeasons:(1)thecomputationalcostincreasesexponentiallywith thenumberofsourcesand(2)thespatialresolutionofESI/MSIismuchlowerthan thatoftheheadmodel,whichimpliesthatneighboringsourcesareheavilycrosscontaminated.Themostcommonstrategytoaddressthesetwoissuesistoperform spacereductionbypooling(Hillebrandetal.,2012;Tanaetal.,2012)sourcesignals intoROIs,whicharethentakenasthenodesoftheconnectome.Connectivityamong ROIscanthenbeevaluatedusingvariousmetrics,allofwhichhavespecific strengthsandweaknessesandtheyalldisplayacceptableperformanceinthemajority ofcases(Wendlingetal.,2009).
Whenanalyzinginterictaldischarges,fewstudiesshowedthatfunctionalconnectivityprovidesusefuldiagnosticinformationabouttheepilepticnetworksofpatients andevenforsurgicaloutcomeprediction.UsingESIofinterictalspikesandatimevaryingfrequency-resolvedeffectiveconnectivitymetric,Coitoetal.founddissociationinthepatternofconnectivitybetweenpatientswithleftandrightTLE(Coito etal.,2015).Indeed,thelatterexhibitedincreasedcontralateralconnectivity,inline withcontralateralfrontalfunctionaldeficitsinrightTLE.Inaddition,effectiveconnectivityonMEGdatashowedthatsurgicalresectionofthemaindrivingnodesof ENscouldpredictfavorableoutcomein9/10patients(Daietal.,2012;Jinetal., 2013).However,definiteconclusionsaboutoutcomepredictionarelimitedbythe factthatthosestudiesdidnotincludecaseswithnegativesurgicaloutcome.Similarly,Malinowskaetal.showedthatMEG-identifiednetworkdriversshowedgood concordancebothwithdriversidentifiedfromicEEGandwithresectedareas (Malinowskaetal.,2014).
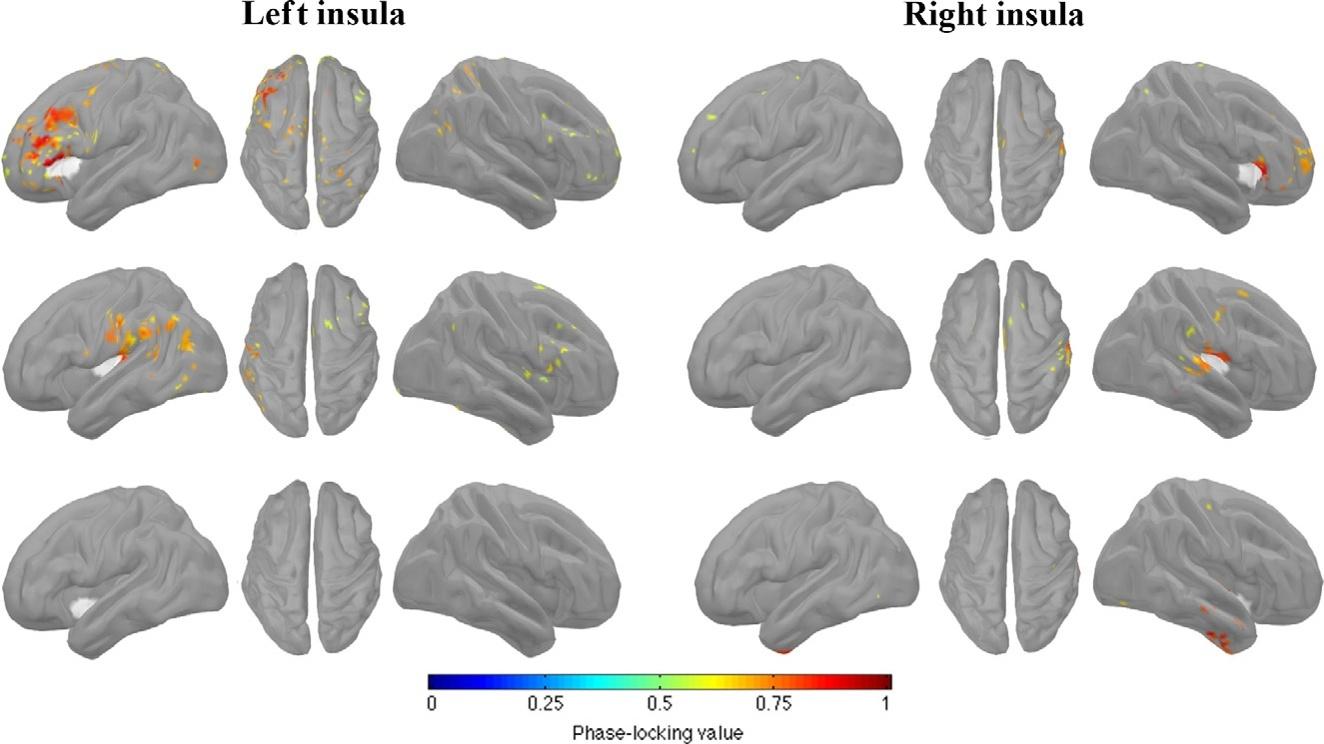
OurgrouprecentlyconductedaMEGstudyaimedatstudyingfunctionalconnectivitynetworksatplayduringinterictalinsularspikes(Zeroualietal.,accepted).We computedtheconnectomesofinsularspikesusingMSIbasedonthemaximumentropyonthemeanalgorithmandphasesynchronizationmeasuresandconducted seed-basedconnectivityanalyses.Weshowedthatanteriorandposteriorpartsof theinsulaarecharacterizedbymarkedlydistinctconnectivitynetworks,withtheformerconnectedmainlytoanteriorstructureswhilethelatterismainlyconnectedto parietalandoccipitalstructures(Fig.6).Inthisstudy,weshowedthatMEGisableto establisharobustsignatureofICEbasedonfunctionalconnectivitymeasures,which couldopenimportantavenuesintheautomaticdetectionofICE.
Otherstudiesanalyzingseizuresshowedthattransitionsbetweenbrainstatesdisplaydeepmodificationsinconnectivity.UsingEEGandGrangercausality,Coben etal.showedhyperconnectivityatthetransitionbetweenictalandpostictalstates
FIG.6
FunctionalconnectivityofinsularsubregionsduringinterictalspikesrecordedwithMEGand quantifiedusingthephase-lockingvalueofnarrowband-filteredsignal(betaband, 12–30Hz).Eachinsularsubregionisrepresentedinthreepanels(left,top,andrightviews), withinsularseedsappearingin white Toprow, anteriorsubregion; middlerow, posterior subregion; bottomrow, inferiorsubregion.The color (grayshades intheprintversion) scale encodesthestrengthofcouplinginsularseedsandtherestofthecortex,afterstatistical thresholding.
(CobenandMohammad-Rezazadeh,2015).Inaddition,accordingtoElshoffetal., thepatternofconnectivityatseizureinitiationisentirelydrivenbyasinglenodethen becomescirculararoundthemiddleofseizures(Elshoffetal.,2013).Theyalso showedthatsurgicalresectionofthemaindrivingnodeatseizureinitiationyielded apositiveoutcome(8/8)whiletheoppositeyieldedanegativeoutcome(3/3)forpatients.Interestingly,topologicalfeatureswerealsoshowntovaryatthosetransitions. Usingfrequency-resolvedconnectivity,Guptaetal.showedthattransitionfrom preictaltoictalstatesdisplaynetworkswithincreased“small-worldness,”which suggestsseizureinitiationnecessitatesmoreorderednetworkstructure(Gupta etal.,2011).
3.1.6fMRIconnectivity
Earlyseed-basedconnectivitystudiesusingfMRIwereconductedduringrestsessions,wherehealthysubjectsareinstructedtoavoidfocusingonanyparticular thoughts.Usingsuchparadigm,Biswaletal.showedthatbilateralmotorcortices arenotsilentbutratherexhibitstrongconnectivityatrest,whichsuggeststhatthese regionscontinuesharingandprocessinginformationoffline(Biswaletal.,1995, 1997).Later,otherstudiesshowedthatlarge-scalebrainconnectivityatrestisrather thenormthantheexception,andanumberofnetworkswerefoundtobehighly
consistentacrosssubjectsandexperiments(see FoxandRaichle,2007,forareview). Theseresting-statenetworksarenowwellestablishedasrobustsignaturesofhealthy brainfunctioning.
Seed-basedanalysiswasappliedtostudythefunctionalconnectivityofthehumaninsula,revealingtwomaininsularclusters,oneanteriorandoneposterior.The anteriorportionoftheinsula(aI)wasfoundtobeconnectedtotheanteriorcingulate cortex,theanteriorandposteriorpartsofthemiddlecingulatecortex(MCC)while theposteriorportionoftheinsula(pI)wasfoundtobeconnectedonlytotheposterior MCC(Tayloretal.,2009).Inaddition,theaIisfunctionallyconnectedtothemiddle andinferiorfrontalcortexwhilethepIisconnectedtotheprimaryandsecondary somatosensoryandthesupplementarymotorareas(Caudaetal.,2011).Somestudies refinedthisparcellation,showingthataIcanbesubdividedintoventralanddorsalaI, eachhavingspecificpatternsoffunctionalconnectivitywiththecortex(Deenetal., 2011).Inaddition,thistripartiteparcellationissupportedbythedistinctinvolvement ofthosethreeregionsintospecificcognitivetasks(Changetal.,2013).However,to ourknowledge,nostudyhaslinkedthesespecificconnectivitynetworkstoepileptic activityinICE.Suchstudiesareneededtoshedsomenewlightonthepathophysiologicalmechanismsofthatdisease,aswasdoneforotherkindsofepilepsies.
3.1.7Structuralconnectivity
Theanatomicalconnectionslinkingneuralpopulationscanbestudiedinvivousing diffusionweightedimaging.Thismodalityexploitsinformationaboutthediffusivity ofmolecules(mostlywater)inthebraintissue.Mathematicalmodelswereproposed totranslatethisinformationinto3Dimagesofwhitefibertracts.Ingeneral,these modelsassumethatwaterdiffusivityinthebrainisconstrainedbycellularstructural elementssuchthatithaspreferentialdirections,whichcanbeestimatedintheform offractionalanisotropy(FA).Forinstance,waterdiffusesmuchmorefreelyalong thanacrosstheaxon,thusavoxelcrossedbyanaxonalbundlewouldhaveahighFA. Importantly,bytrackingtheFAalongconsecutivevoxels,therebyperformingtractography,itispossibletoreconstructthemajorwhitefibertractsofthebrain(Jbabdi andJohansen-Berg,2011;LeBihan,2003;Morietal.,2002).
Toourknowledge,onlythreestudiesusedtractographytoinvestigatethestructuralconnectivityoftheinsula.Theyreportcomparableconnectivityprofilesshowingthattheanteriorinsularcortexhasconnectionsmostlywithfrontalandtemporal (inferiorandsuperiorgyri,amygdala)structures.Themiddleinsularcortexhasconnectionswithfrontal(superior,inferior,andprecentral),parietal(postcentraland supramarginal),andtemporal(inferiorandsuperior)gyri.Finally,theposteriorinsularcortexhasconnectionswithfrontal(superior,inferior,andprecentral),parietal (postcentral),andtemporal(inferiorandsuperior)gyriandwiththeputamen (Cerlianietal.,2012;Cloutmanetal.,2012;Jakabetal.,2012).Theseresults areinaccordancewithtract-tracingstudiesbutsomeconnectionsinprimates werenotfoundinhumans.Usingstate-of-the-arttractography,ourgroupfurther investigatedthestructuralconnectivityofthehumaninsulaandfoundmanypreviouslymissedconnections,suchasthosewiththecingulate,parahippocampal,
supramarginal,angular,andlingualgyriaswellastheprecuneus,cuneus,andoccipitalcortex(Ghazirietal.,2015).
Tractographycanalsobeusedtostudywhitematterinsultsinrelationtoepilepsy (forareview,see Anastasopoulosetal.,2014;Ciccarellietal.,2008;Winston,2015). StudiesgenerallyreportaFAdecreaseandameandiffusivityincreaseinpathways neartheepileptogenictemporallobe(eg,opticradiations,uncinateandarcuatefasciculi,cingulum,fornix,andexternalcapsule),whichreflectsreducedaxonaldensity inTLE.WhitematterinsultsinTLEaremostlyipsilateraltotheSOZandtracts closelyconnectedtotheaffectedtemporallobearethemostdisturbed.Furthermore, fibertractsremotefromthetemporallobearealsoaffected,whichsupportstheview ofepilepsyasabrainnetworkdisease(Conchaetal.,2012;Gross,2011;Otteetal., 2012;Rodrı´guez-CrucesandConcha,2015).Tofollow-uponourstudyonhealthy controls,weperformedtractographyonpatientswithICE.Usingnonparametricstatisticaltests,weassessedthedifferencesbetweeneachpatientandcontrolsinfiber tractdensitylinkingtheinsulatotheremainingcortex.Althoughpreliminary,our resultssuggestthatanterior,posterior,andinferiorICEdifferentiallyaffectsthe whitefibertracts,whichcouldopennewperspectivesinthediagnosisofthiskind ofepilepsy.
3.1.8icEEGconnectivity
ThemainspecificityoficEEGascomparedtoEEG/MEGconnectivityisthesparse samplingofneuralgenerators,andcoverageextentisdeterminedbybalancingthe amountofdiagnosticinformationandhealthrisksforpatients.Forthatreason,itis usuallyagreedthaticEEGconnectivityonlyallowspartialassessmentofthebrain connectome.However,judiciouschoiceofepilepticcasesinconjunctionwiththe optimizedplacementofelectrodesallowsforcharacterizingthemostrelevantaspectsofENs.Indeed,mostofthestudieswedescribebelowareconductedonpatientswithfocalseizureonsetsandlimitedpropagation,suchthattheENcan mostlybesampledwithintracranialelectrodes.
Sincetheintroductionofthenetworkconceptofepilepsyintheearly2000s,a largeresearcheffortwasdevotedtocharacterizingneuralsynchronizationrelated totheepilepsy.Theunequivocalfindingsofsuchresearcharethat(1)fromastatic pointofview,theepilepticconditionischaracterizedbydeepimpactsonlarge-scale neuralsynchronizationand(2)themostspectacularchangesinneuralsynchronizationarerelatedtobraindynamics,ie,occurattransitionsbetweenconsecutivebrain statesbefore,during,andafterseizures.Inthefollowing,wediscusstheliterature relativetothosetwofindingsseparately.
3.1.8.1Staticnetworkproperties
Inordertostudytheimpactoftheepilepticconditiononbrainnetworks,themost commonparadigmconsistsinusingartifact-freerestEEGdata.Usingsuchdata,two independentstudiesshowedthatpatternsofneuralsynchronizationcharacterizedistinctgroupsofepilepticpatients.Ortegaetal.analyzedECoGdatafrom29patients withTLEandcomputedthreesynchronizationmeasuresinashorttimeframesliding
overcontinuousrecordings(Ortegaetal.,2008).Theyshowedthatsynchronized ECoGcontactscaneitherspreadoverthewholelateraltemporallobeorcluster tightlyinspecificsubregions.Importantly,theyfoundthatthepredictivevaluewith respecttoseizure-freedomaftersurgery(EngelIa)wasveryhighandverylowfor tightanddiffusesynchronizationclusters,respectively.Thissuggeststhatsynchronizationpatternscanbeusedtoidentifyregionsparticipatinginseizures.
Inadditiontospatialpatterns,synchronizationstrengthwasalsoshowntopredict surgicaloutcome.Inaseriesof29patientswithTLE,Antonyetal.assessedsynchronizationstrengthsamongEEGsignalsrecordedwithintracerebralelectrodesatrest. Theyshowedthatpatientswithlowconnectivitystrengthhadbettersurgicaloutcomethanpatientswithhighconnectivitystrength,andthatthelinearclassifier wasabletoaccuratelyclassifythosetwogroupsofpatientsbasedontheaverage andstandarddeviationofglobalsynchronization(Antonyetal.,2013).Theideathat decreasedlevelsofsynchronizationmightbecharacteristicoftheepilepticcondition receivedfurthersupportwhen Warrenetal.(2010) comparedsynchronyatrestbetweenepilepticpatientsandcontrolswithintracranialelectrodesimplantedfortreatingintractablefacialpain.Controllingforintercontactdistance,synchronylevels betweenpatientsandcontrolswereeitherdecreasedorincreaseddependingon thefrequencybandanalyzed.However,fineranalysisrevealedthatsynchronybetweentheSOZandotherbrainregionsissignificantlyweakerthanincontrols,while synchronyeitherwithinSOZoroutsideSOZwasunchanged(Warrenetal.,2010). Furtherinsightsintotheroleofsynchronyinepilepsywereprovidedbystudiesof seizuredynamics.
3.1.8.2Networkdynamics:Synchrony
Inordertostudytemporalevolutionofsynchronylevels,Wendlingetal.recorded seizureswithicEEGin10patientswithfocalepilepsy.Comparingglobalsynchrony levels(asmeasuredwithalinearcorrelationcoefficient),theyshowedthatseizure initiationdisplayslargedecreasesinsynchronyascomparedtopreictalandpostictal states(Wendling,2003).InanotherstudyonpatientswithmedialTLE,Mormann etal.showedthatsynchronylevelsbetweenbilateralhippocampiaremarkedlydecreasedbeforeseizureonsetandreturngraduallytobaselinelevelsasseizureunfolds (Mormannetal.,2003).Interestingly,in8outof10patients,theywereabletoaccuratelypredictseizuresbydetectingpreseizurestatebasedonreportedlowersynchronizationvalues.
Inaddition,someauthorstrackedsynchronylevelsinepilepticnetworksalong seizures.UsingicEEGrecordingsfrom11patientswithfocalepilepsy,Kramer etal.performedtemporalnormalizationforaligningseizuresfromdifferentpatients into10consecutivewindows(eachcovering10%oftheseizure).Incontradiction tothetwopreviousstudies,theyfoundasteepincreaseinsynchronylevelsinthe firstandlastwindowsduringseizures(Krameretal.,2010).However,theyalso foundthatseizureswerecharacterizedbynetworkswithconstantnodaldegree andsmall-worldtopology,whilethetransitionfromictaltopostictalstatewascharacterizedbyhighlyincreasednodaldegreeandrandomness.Furtherrefiningthis
strategy,Burnsetal.usedadata-drivenapproachtorepresentnetworkdynamics withafinitesetofrepresentativenetworks.Theirmainresultisthatforsomepatients,thereexiststwostatesduringwhichtheSOZisspecificallydisconnected(isolatedfocus,IF,state)andoverconnected(connectedfocus—CF),respectively.When present,theIFstateoccurredatseizureinitiationandlastedforaboutthefirsthalfof seizures.Importantly,patientsforwhomIFstatecouldbedetectedhadsignificantly bettersurgicaloutcomethanpatientsforwhomIFstatewasnotdetected(Burns etal.,2014).Thisimportantstudyshowsthattheepilepticzonesthatspecifically detachfromtheENatseizureinitiationaregoodcandidatesforsurgicalresection. Furtherrefinementofthesynchronyanalysesreviewedhereispossiblebyconsideringthedirectionalityofconnectionsthroughtheassessmentofeffective connectivity.
3.1.8.3Networkdynamics:Directionality
Formaldistinctionbetweencontributionsofoutgoingandincomingconnectionsin ENanalysiswasprovidedbyVarottoetal.whocomparedtheconnectivityofintracranialelectrodecontactsin10patientswithlesionalepilepsy.Theydividedcontacts intothreegroups:withinthelesion(LES),involvedintheseizurebutoutsidethe lesion(INV),andnotinvolvedinseizures(NINV)andshowedthatoutgoingconnectionsofLESandINVcontactsincreasesignificantlyatseizureonset.Interestingly,whileoutgoingLESconnectionsweredirectedtowardtheINVgroup, outgoingconnectionsoftheINVgroupwerediffuse.Incontrast,incomingconnectionsdidnotshowsignificantdifferencesbetweenthethreegroups(Varottoetal., 2012).Inthesamevein,itwasshownthatblindidentificationoftheelectrodecontact withthehighestnumberofoutgoingconnectionsatseizureinitiationlocalizedthe surgicallydefinedSOZintwopatientseries(8/8, vanMierloetal.,2013;11/11, Wilkeetal.,2010).Finally,therewasalsoagoodcorrelationbetweenthepercentage ofconnectionsexitingnodeslocalizedwithinSOZandpercentageofseizurereductionaftersurgery(Wilkeetal.,2010).
3.1.8.4Networkdynamics:ThecaseofICE
Sincetheearly2000s,ourgroupstartedsamplinginsularregionswithintracranial electrodessystematicallywhenpatientsweresuspectedofeitherfrontal,temporal, orparietallobeepilepsywithinconsistentclinicalsemiology.Wethusconstituted alargedatabaseofICEcasesincludingicEEGrecordingsandrecentlystartedanalyzingnetworkdynamicsandtopology.Wefoundthatmostsignificantchangesin effectiveconnectivitywerefoundinthegammaband(Fig.7),morespecificallyat seizureinitiation,electrographicshift,andtermination(Fig.8).Inaddition,insular contactswerecharacterizedbyanincreaseinoutgoingconnectionsatseizureinitiation,followedbydisconnection.Theseresultsareinagreementwiththosereported by Burnsetal.(2014),whichsuggeststhatanIFstateispresentinpatientswithICE. ThisinterpretationissupportedbythefactthatmostofourICEcaseswereseizure freeafterinsulectomy.