HANDBOOKOFCLINICAL NEUROLOGY
SeriesEditors
VOLUME137
MICHAELJ.AMINOFF,FRANÇOISBOLLER,ANDDICKF.SWAAB
ELSEVIER
Radarweg29,POBox211,1000AEAmsterdam,Netherlands
TheBoulevard,LangfordLane,Kidlington,OxfordOX51GB,UnitedKingdom
50HampshireStreet,5thFloor,Cambridge,MA02139,UnitedStates
©2016ElsevierB.V.Allrightsreserved.
Nopartofthispublicationmaybereproducedortransmittedinanyformorbyanymeans,electronicormechanical, includingphotocopying,recording,oranyinformationstorageandretrievalsystem,withoutpermissioninwriting fromthepublisher.Detailsonhowtoseekpermission,furtherinformationaboutthePublisher ’spermissions policiesandourarrangementswithorganizationssuchastheCopyrightClearanceCenterandtheCopyright LicensingAgency,canbefoundatourwebsite: www.elsevier.com/permissions.
ThisbookandtheindividualcontributionscontainedinitareprotectedundercopyrightbythePublisher(otherthan as may benotedherein).
Notices
Knowledgeandbestpracticeinthisfieldareconstantlychanging.Asnewresearchandexperience broadenourunderstanding,changesinresearchmethods,professionalpractices,ormedicaltreatmentmay becomenecessary.
Practitionersandresearchersmustalwaysrelyontheirownexperienceandknowledgeinevaluatingandusingany information,methods,compounds,orexperimentsdescribedherein.Inusingsuchinformationormethodsthey shouldbemindfuloftheirownsafetyandthesafetyofothers,includingpartiesforwhomtheyhaveaprofessional responsibility.
Withrespecttoanydrugorpharmaceuticalproductsidentified,readersareadvisedtocheckthemostcurrent informationprovided(i)onproceduresfeaturedor(ii)bythemanufacturerofeachproducttobeadministered,to verifytherecommendeddoseorformula,themethodanddurationofadministration,andcontraindications.Itisthe responsibilityofpractitioners,relyingontheirownexperienceandknowledgeoftheirpatients,tomake diagnoses,todeterminedosagesandthebesttreatmentforeachindividualpatient,andtotakeallappropriatesafety precautions.
Tothefullestextentofthelaw,neitherthePublishernortheauthors,contributors,oreditors,assumeanyliability foranyinjuryand/ordamagetopersonsorpropertyasamatterofproductsliability,negligenceorotherwise,or fromanyuseoroperationofanymethods,products,instructions,orideascontainedinthematerialherein.
BritishLibraryCataloguing-in-PublicationData
AcataloguerecordforthisbookisavailablefromtheBritishLibrary
LibraryofCongressCataloging-in-PublicationData
AcatalogrecordforthisbookisavailablefromtheLibraryofCongress
ISBN:978-0-444-63437-5
ForinformationonallElsevierpublications visitourwebsiteat https://www.elsevier.com/
Publisher: ShirleyDecker-lucke
AcquisitionEditor: MaraConner
EditorialProjectManager: KristiAnderson
ProductionProjectManager: SujathaThirugnanaSambandam
CoverDesigner: AlanStudholme
TypesetbySPiGlobal,India
Preface
Vertigoanddizzinessrankamongthemostcommonsymptomsinprimarycare,otolaryngology,andneurology.Causes varyfromharmlessbutbothersomeconditionssuchasbenignparoxysmalpositionalvertigotolife-threateningemergenciessuchasposteriorfossastrokes.Ourunderstandingofdiagnosis,pathophysiologicmechanisms,andeffective treatmentshasincreasedconsiderablyinthelasttwodecades.Newdevelopmentsincludealgorithmsforbedsidedetectionofvestibularstrokes,thedelineationofvestibularmigraineasoneofthemostfrequentcausesofrecurrentvertigo, descriptionofvariantsofbenignparoxysmalpositionalvertigo,devicesfortestingindividualsemicircularcanalsand otolithorgans,andtheadvancementofvestibularrehabilitationasthemostimportanttherapeutictoolinneuro-otology. Thisvolumeofthe HandbookofClinicalNeurology assemblescontributionsfromleadinginternationalauthorsto communicatethecurrentclinicalknowledgeofneuro-otologyandacomprehensivelistofreferences.Chapters1–14 dealwithbasicknowledgeandgeneralprinciplesofneuro-otology,suchasanatomy,physiology,epidemiology, historytaking,examination,andvestibularrehabilitation.Thisisfollowedbythedisease-specificChapters15–28, coveringallcommoncausesofvertigoanddizziness.Thenumeroustablesandfiguresinthisbookmakethefield ofvestibularscienceandmedicineevenmoreaccessible.
JosephM.Furman ThomasLempert
Contributors
A.Alghadir
DepartmentofRehabilitationSciences,Collegeof AppliedMedicalSciences,KingSaudUniversity, Riyadh,SaudiArabia
A.A.Alghwiri
DepartmentofPhysicalTherapy,Facultyof RehabilitationSciences,UniversityofJordan,Amman, Jordan
C.D.Balaban
DepartmentsofOtolaryngology,Neurobiology, CommunicationSciencesandDisorders,and Bioengineering,UniversityofPittsburgh,Pittsburgh, PA,USA
P.Bertholon
DepartmentofOto-Rhino-Laryngology,Centre HospitalierUniversitairedeSaintEtienne,SaintEtienne, France
A.Bisdorff
DepartmentofNeurology,CentreHospitalierEmile Mayrisch,Esch-sur-Alzette,Luxembourg
T.Brandt
GermanCenterforVertigoandBalanceDisordersand InstituteforClinicalNeurosciences,UniversityHospital Munich,CampusGrosshadern,Munich,Germany
A.M.Bronstein
Neuro-otologyUnit,ImperialCollegeLondon,Charing CrossHospitalandNationalHospitalforNeurologyand Neurosurgery,London,UK
C.Chabbert
IntegrativeandAdaptativeNeurosciences,Universityof AixMarseille,Marseille,France
M.Cherchi
DepartmentofNeurology,NorthwesternUniversity FeinbergSchoolofMedicine,Chicago,IL,USA
K.-D.Choi
DepartmentofNeurology,CollegeofMedicine,Pusan NationalUniversityHospital,Busan,Korea
J.G.Colebatch
NeuroscienceResearchAustraliaandDepartment ofNeurology,PrinceofWalesHospitalClinical School,UniversityofNewSouthWales,Sydney, Australia
A.I.Colpak
HacettepeUniversitySchoolofMedicine,Ankara, Turkey
K.E.Cullen
DepartmentofPhysiology,McGillUniversity,Montreal, Quebec,Canada
R.A.Davies
DepartmentofNeuro-otology,NationalHospitalfor NeurologyandNeurosurgery,London,UK
M.Dieterich
GermanCenterforVertigoandBalanceDisordersand DepartmentofNeurology,UniversityHospitalMunich, CampusGrosshadern;andMunichClusterforSystems Neurology(SyNergy),Ludwig-MaximiliansUniversity, Munich,Germany
J.M.Espinosa-Sanchez
OtologyandNeurotologyGroup,Departmentof GenomicMedicine,CentreforGenomicsand OncologicalResearch(GENYO),Pfizer-Universityof Granada-JuntadeAndalucia,GranadaandDepartment ofOtolaryngology,HospitalSanAgustin,Linares,Jaen, Spain
K.Feil
GermanCenterforVertigoandBalanceDisordersand DepartmentofNeurology,UniversityHospitalMunich, CampusGrosshadern,Munich,Germany
HandbookofClinicalNeurology, Vol.137(3rdseries) Neuro-Otology
J.M.FurmanandT.Lempert,Editors http://dx.doi.org/10.1016/B978-0-444-63437-5.00001-7 ©2016ElsevierB.V.Allrightsreserved
Anatomy,physiology,andphysicsoftheperipheral
vestibularsystem
H.KINGMA* ANDR.VANDEBERG
Department ofOto-Rhino-LaryngologyandHeadandNeckSurgery,MaastrichtUniversityMedicalCentre,Maastricht, theNetherlandsandFacultyofPhysics,NationalResearchStateUniversityTomsk,Tomsk,RussianFederation
Abstract
Manymedicaldoctorsconsidervertigoanddizzinessasthemajor,almostobligatorycomplaintsinpatients withvestibulardisorders.Inthischapter,wewillexplainthatvestibulardisordersresultinmuchmore diverseandcomplexcomplaints.Manyoftheseothercomplaintsareunfortunatelyoftenmisinterpreted andincorrectlyclassifiedaspsychogenic.Whenwereallyunderstandthefunctionofthevestibularsystem, itbecomesquiteobviouswhypatientswithvestibulardisorderscomplainaboutalossofvisualacuity, imbalance,fearoffalling,cognitiveandattentionalproblems,fatiguethatpersistsevenwhenthevertigo attacksanddizzinessdecreasesorevendisappears.Anotherinterestingnewaspectinthischapteristhatwe explainwhythefunctionoftheotolithsystemissoimportant,andthatitisamistaketofocusonthefunctionofthesemicircularcanalsonly,especiallywhenwewanttounderstandwhysomepatientsseemto suffermorethanothersfromthelossofcanalfunctionasobjectifiedbyreducedcaloricresponses.
INTRODUCTION
Intheirprefacetothebook, MammalianVestibularPhysiology,publishedin1979,thefamousvestibularscientistsWilsonandMelvillJonesmadeaperceptive statement: “Itiseasytounderratetheimportanceofa sensorysystemwhosereceptorisburieddeepwithin theskullandofwhoseperformanceweareusuallynot aware” (WilsonandMelvillJones,1979).Thisstatement is stilluptodate,asmanydoctorsareunawareoftherelevanceofthevestibularsystemindailylifeandalsothink thatcentralcompensationandsensorysubstitution almostcompletelydealwithvestibularlossandreduce complaintstoaminimum.Also,inunilateralloss,itis oftenstatedthatthehealthylabyrinthwilltakeover. Howabsurdsuchastatementis,becomesclearifwe claimthatlosingoneearoroneeyeisofnoimportance aswecanstillhearwithoneearandseewithoneeye. Losingonevestibularorgan,likelosingoneearoreye, resultsinadisturbingasymmetry.Bilateralvestibular
areflexia(thereisnotevenacommonwordforitinlay language)isamajorhandicaplikedeafnessorblindness. Butapparently,symptomsassociatedwithbilateralvestibularareflexiaareoftennotrecognized,leadingtoadelay ofmanyyearsbeforeacorrectdiagnosisismade(vande Bergetal.,2011;Guinandetal.,2015a;Guyot,2015).The majorreasonisthatthefunctionofthevestibularsystemis poorlyunderstoodbybothdoctorsandpatients.This unawarenessalsoledtoproblemsinobtainingpermission todevelopavestibularimplantforhumans,verydifferent fromthedevelopmentofcochlearimplantsseveral decadesago.Onlyafterpublicationofanumberofscientificarticlesshowingtheimpactandincidenceofsevere bilateralvestibularlosswasaSwiss–Dutchresearchteam allowedtoexecutethefirsthumanvestibularimplantation inAugust2012(Pelizzoneetal.,2014;PerezFornosetal., 2014;Guinandetal.,2015b).
Thisallillustrateshowpoorlythefunctionandrelevanceofthevestibularsystemisunderstoodinclinical practice,andthisiswhathasmotivatedustowritethis
*Correspondenceto:HermanKingma,DepartmentofORLandHeadandNeckSurgery,MaastrichtUniversityMedicalCentre, Maastricht,theNetherlands.E-mail:kingmaherman@gmail.com
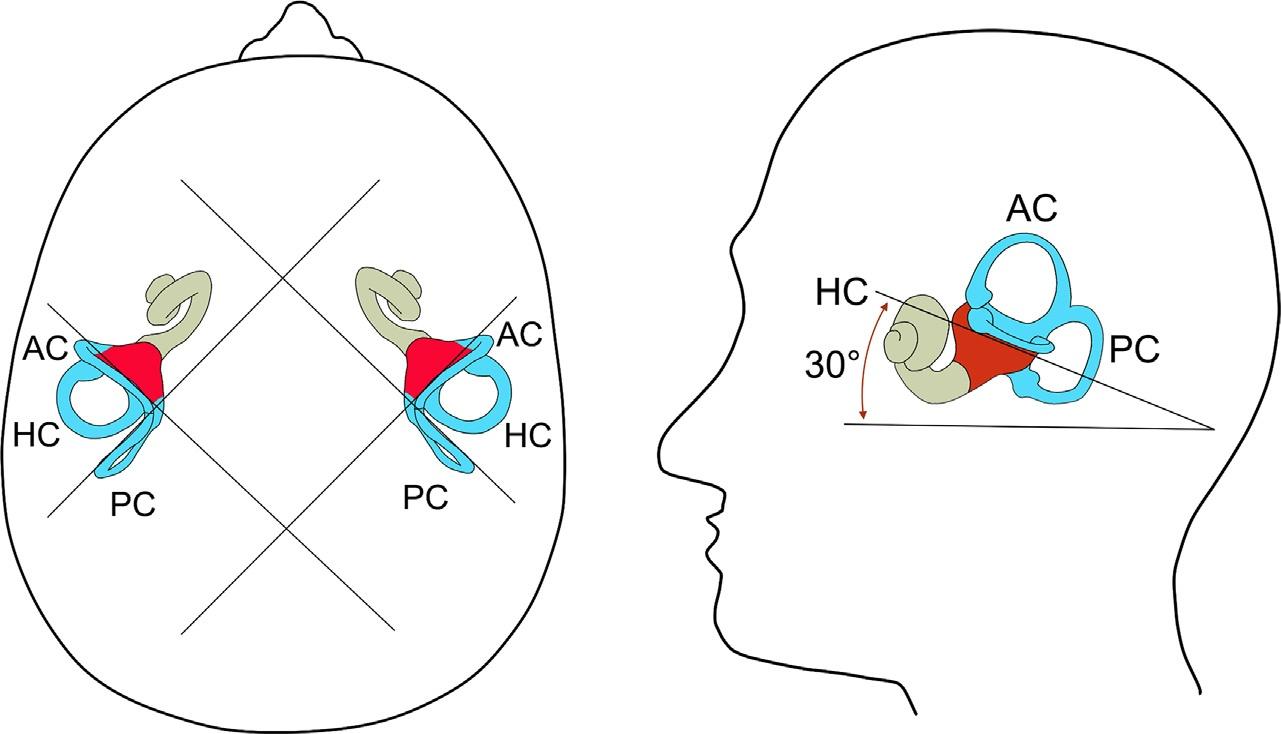
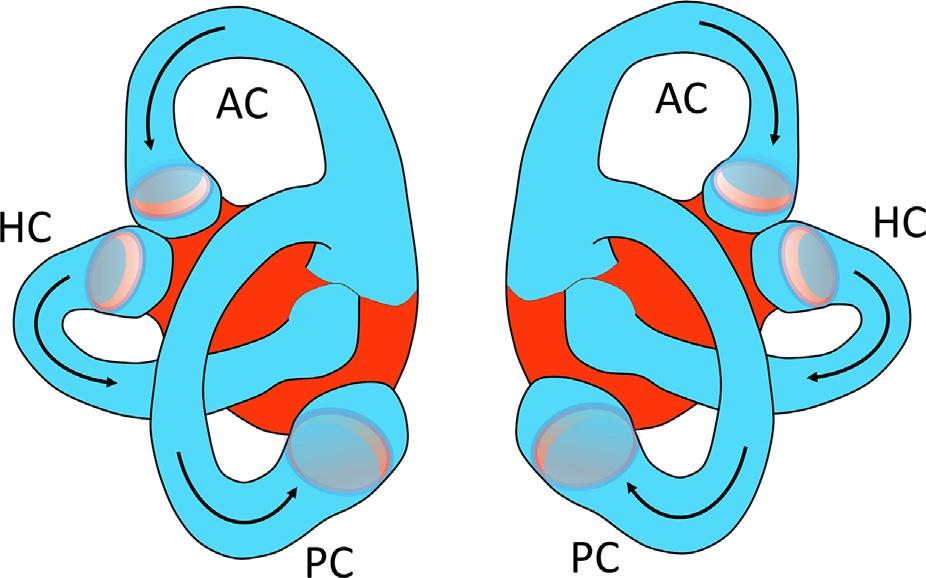
Fig.1.3. Schematicdrawingoftheorientationofthetwolabyrinthsintheskull.HC,horizontal(orlateral)canal;PC,posterior canal;AC,anterior(orsuperior)canal.
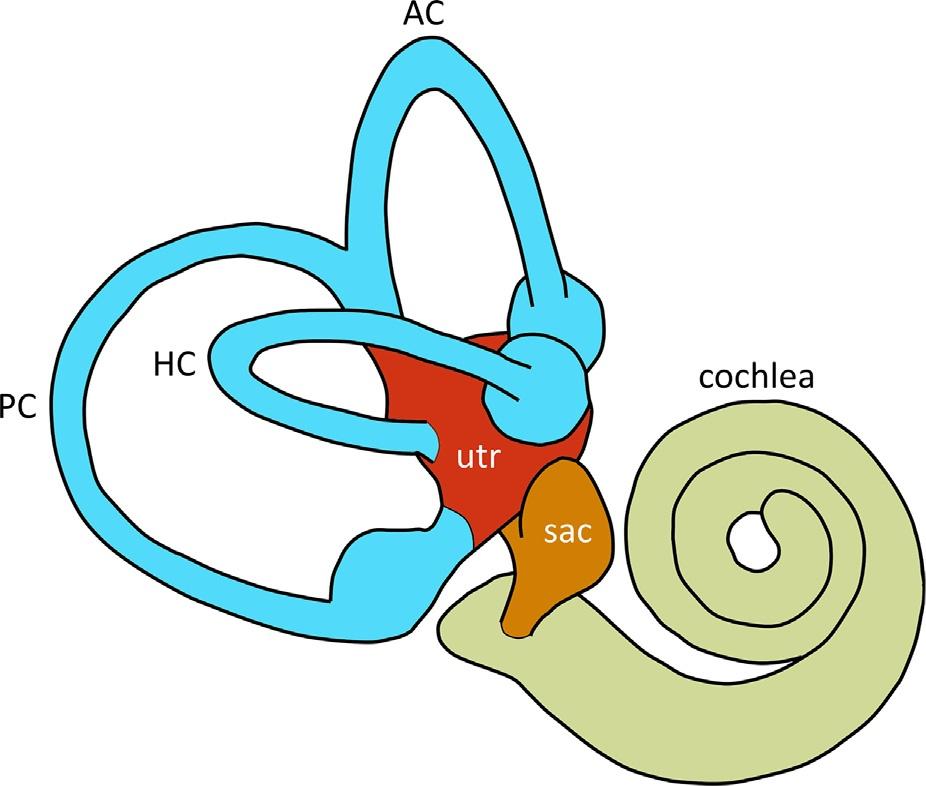
Fig.1.4. Schematicdrawingofthe right membranouslabyrinth:HC,horizontal(orlateral)canal;PC,posteriorcanal; AC,anterior(orsuperior)canal;Utr,utriculus;Sac,sacculus.
Thevestibularhaircells(Fig.1.7)arecomposedof acellbodyandabundleofciliaontopofthem,onaverageabout50stereociliaandonekinocilium(Hudspeth andCorey,1977;frog’ssacculus).Thestereociliaform abundleofciliathatincreaseinlengththecloserthey aretothekinocilium.Ontheirtop,theciliaaremechanicallyinterconnectedbyelastictiplinks.Thetiplinks maketheciliaofonehaircellmovetogetheruponaccelerationsandarealsothoughttomechanicallyopenand closeionchannelspositionedontopofthestereocilia. Thekinociliumisthelongestcilium,thatisdeflected themostbysmallmovementsofthecupulainthe canalsandofthemaculainthevestibule;butthanksto thetiplinks,allciliawillmoveinsynchronywithit andtherebyenhancetotalsensitivity.
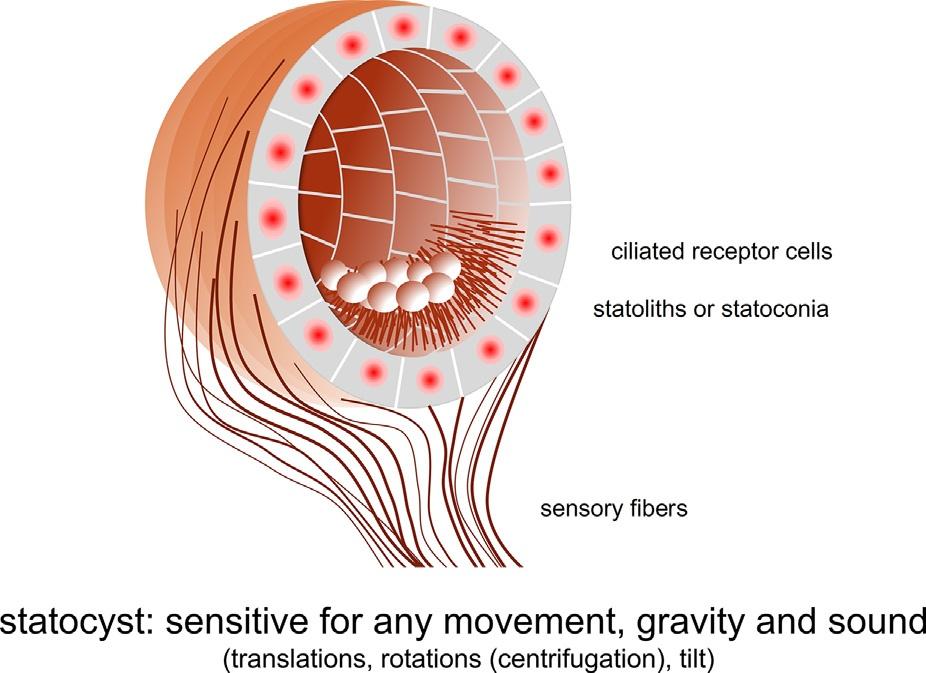
Fig.1.5. Schematicdrawingofthestatocyst:thestatolith organininvertebrates.Thestatocystisamechanoreceptorsystemthatissensitiveforanymovement,tiltandsound.
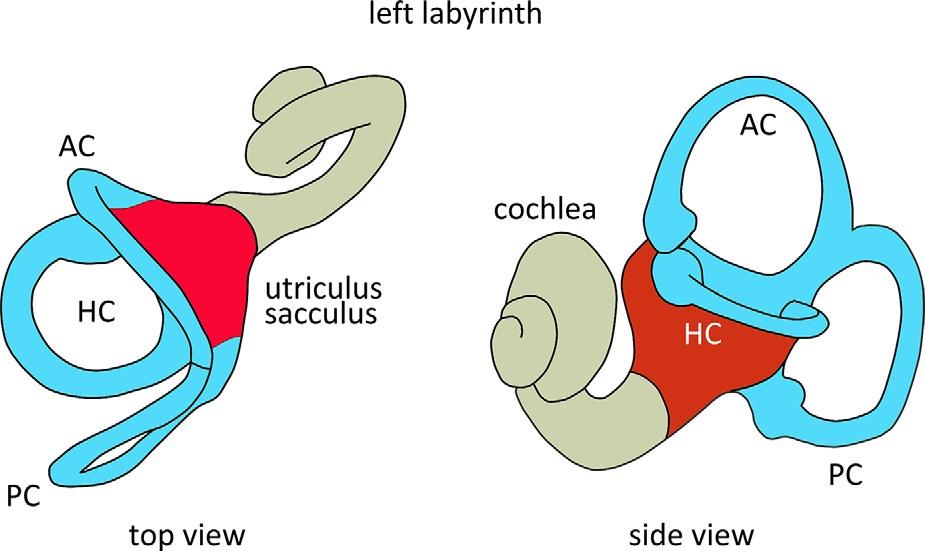
Fig.1.6. Topandsideviewoftheleftlabyrinth.HC,horizontal(orlateral)canal;PC,posteriorcanal;AC,anterior(orsuperior)canal.Thevestibularlabyrinthreachesitsmaturesize between17and19weeksofgestationalage.Adetailedquantitativedescriptionofthedimensionsofthehumanlabyrinthis givenby JefferyandSpoor(2004).
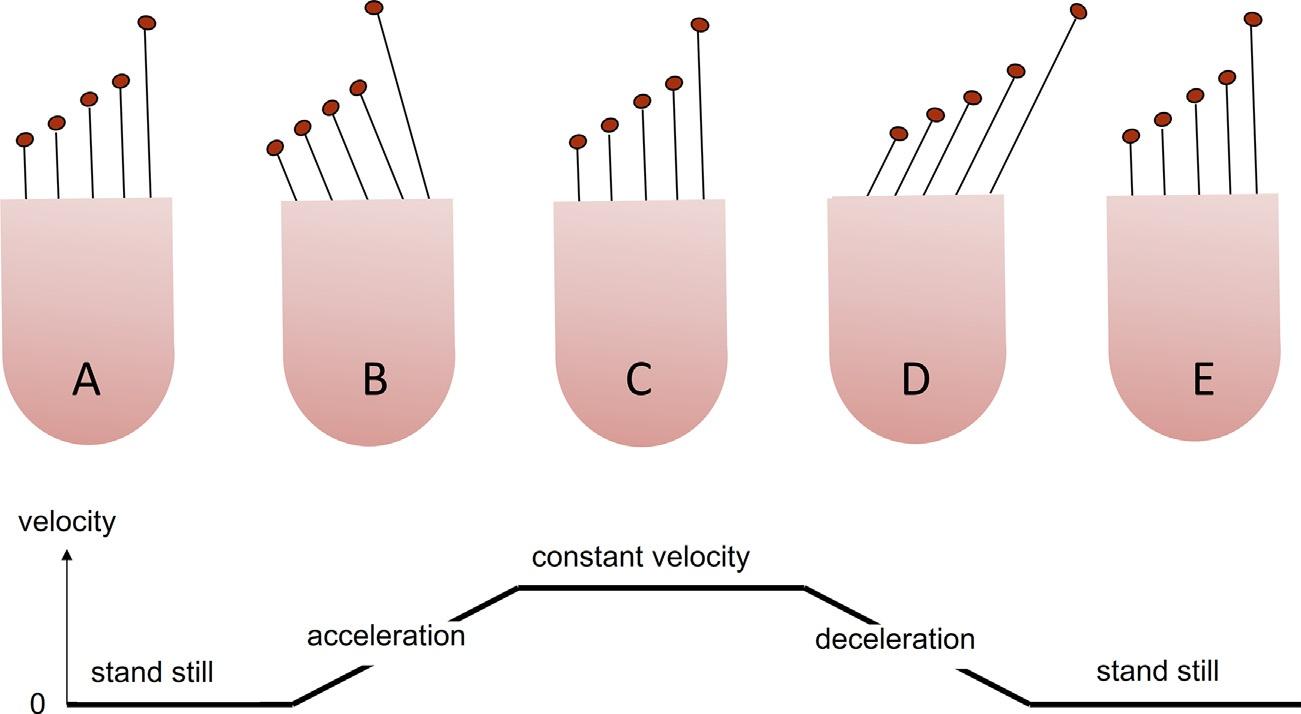
Nowtheerectpositionoftheantennaindicatesconstant velocityorstandstill.Upondecelerationofthecar,dueto theinertiaoftheorange,theantennawillbendforwards. Nowtheinclinationoftheantennaisproportionaltothe deceleration.Duetoitselasticity,theantennawillreturn toitsverticalorientationassoonasthecarstops.When wetiltthecar,theantennawilldeflectinthedirection oftiltoveranangleproportionaltothetiltanglerelative tothegravityvector.Nodistinctionispossiblebetween tiltandtranslation(comparewith Figs.1.11 and 1.12). Also,whenwestarttorotateandholdtheantenna upright,theantennawillstarttobendoutwardsdueto centrifugalforce.
Theotolithsystemissensitivetolinearaccelerations, rotations/centrifugationandtiltthankstotheprincipleof inertiaofmass.Assumethattheheadundergoeslinear acceleration(Fig.1.11).Thelowerpartoftheutricular membraneimmediatelyfollowstheheadmovement, buttheotoconiaonthetopofthemembranewilllag behind,resultinginadeflectionofthecilia.Thisbending causesdepolarizationorhyperpolarizationofthehair cellsdependingonthedirectionofdeflectionofthecilia (Fig.1.7).Thehaircellsofthemaculaarepolarizedinall directions,incontrasttothesemicircularcanals.Atilt relativetothegravityvectororcentrifugationalso inducesashearforceintheplaneoftheotoconial membraneandadeflectionofthecilia.Theotolith organscannotdistinguishbetweenheadtilt,rotation, andheadtranslation(forexample,anaccelerationforwardsleadstoasimilardeflectionoftheciliaasabackwardtiltofthehead: Fig.1.11).Theonlyexceptionto thismaybethattheeccentricityoftheotolithmembranes canbedifferentrelativetotherotationaxis.Thismay resultinadifferenceindirectionand/orstrengthofthe centrifugalforcesactingupontheotolithmembranes. Whetherthisprovidesaphysiologicallyrelevantandsufficientsensitivitytodiscriminatebetweenrotations

Fig.1.12. Schematicdeflectionpatternoftheciliaofthehair cellsintheutriculusandsacculusupontilt.
versustiltortranslationisstillthesubjectofstudy.At constantrotationalheadvelocity,thecanalsarenotstimulated.However,duringbothconstantandchanging rotationalheadvelocitytheotolithsystemisstillstimulatedduetocentrifugalforce,probablyhavingasupportingandregulatoryfunctionforthecanals(seebelow).
THEORETICMODEL
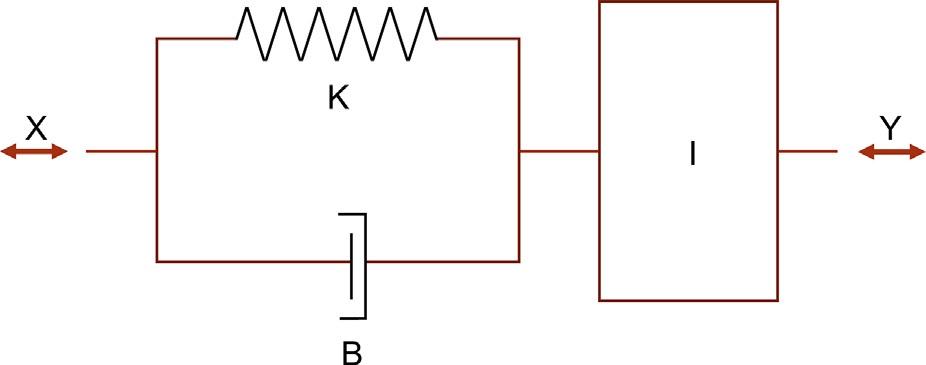
Duringlinearheadacceleration,centrifugation,orhead tilt,theotoconiamassshiftsrelativetothemaculadue tootoconialmassinertia,causingopposingviscousfrictionandanelasticforce.Thereforetheotolithorgan semicircularcanalscanbemodeledsimilarlytothesemicircularcanalswithasimplemechanicanalog,using inertia(I ),viscosity(B),andelasticity(K )asphysical quantities(Fig.1.13).Themomentofinertiaisgiven
Fig.1.11. Schematicdeflectionpatternoftheciliaofthehaircellsintheutriculusandsacculusupontranslation.
Fig.1.13. Mechanicalanalogofthestatolithorgan: I,otoconiamassinertia; B,viscousfriction; K,elasticrestoringforce; x,positionofthehead; y,positionoftheotoconia; □, x y, relativedisplacementoftheotolithmembrane.
by I y,themomentofviscousfrictionby B _ d,and themomentofelasticityby K d,whichwouldlead toasecond-orderdifferentialequationsimilartothe semicircularcanals.Inthecaseoftheotolithorgan,however,sincetheotoconialmassisimmersedinendolymph fluidofdensity re,anylinearaccelerationwillgeneratea buoyancyforceactingaccordingtoArchimedes’ principleinthedirectionofimposedaccelerationandequalto re =ro ðÞ I x,with ro thedensityoftheotoconialmass. Therefore,thesecond-orderdifferentialequationofthe otolithorganis:
1 re ro I x ¼ I d + B d + K d
with € x linearheadacceleration, € y linearotoconiaacceleration,and d relativedisplacementoftheotolithicmembrane,using d ¼ x y (MelvillJones,1979;Kingmaand Janssen,2013).Thetransferfunctioncanbewrittenas:
€ x s ðÞ¼ 1 re ro I I s2 + B s + K
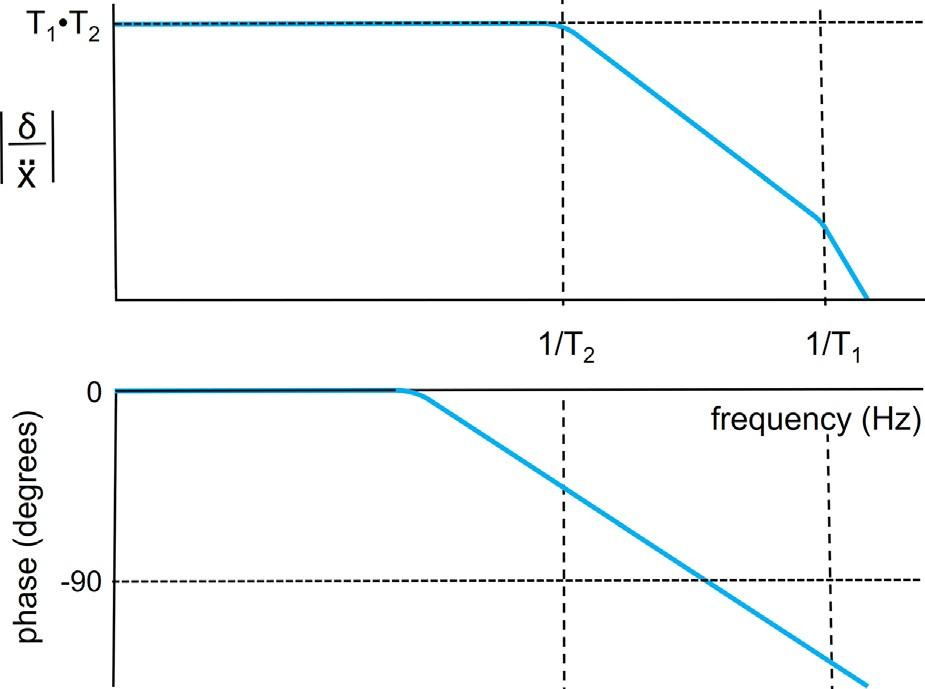
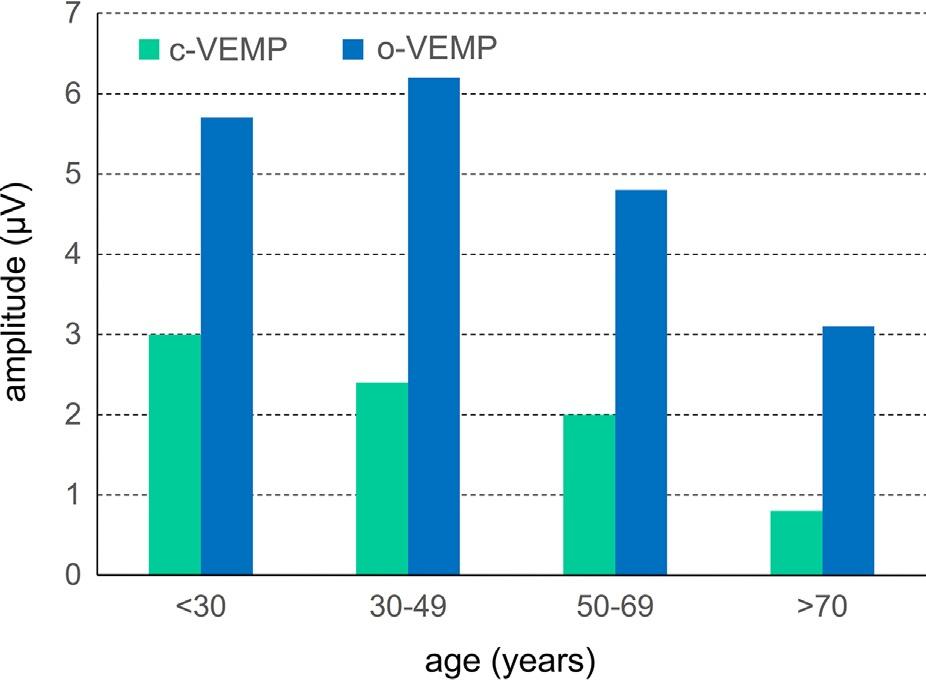
withlinearheadacceleration x asinputandrelativeotolithicmembranedisplacement d asoutput.Theformof thistransferfunctionisshownin Figure1.14A,using thefactthat I/B (T1 0.1s)issmallerthan B/K (T2 1s). Theotolithorganissensitiveforconstant(0Hz)and low-frequencylinearaccelerations.Becauseagravitationalaccelerationandacorrespondinglinearacceleration ofthesystemarephysicallyequivalent(Einstein’sequivalenceprinciple),theotolithorganscannotdistinguish betweenpureheadtranslations,headtilts,androtations, unlesstheymakeuseofaspecificarrangementofthe direction-sensitivehaircellsinthesensoryepithelium. Therelativeotolithmembranedisplacement d inresponse toconstantlinearaccelerationissimilartothecupuladisplacementinresponsetoangularacceleration,asshownin Figure1.12. Agrawaletal.(2012) foundadecreasein amplitudeofthecervicalandocularvestibular-evoked myogenicpotentialswithage,suggestinganage-related declineofthestatolithsystem(Fig.1.14B).
SEMICIRCULARCANALS
Asshownin Figure1.4,threesemicircularcanalscanbe identifiedinthevestibularlabyrinth:thelateral,posterior,andanteriorcanalthatslightlydifferinsize:thelateralcanalhasadiameterofabout2.3mm(SD 0.21),the posteriorcanal3.1mm(SD 0.30),andtheanteriorcanal 3.2mm(SD 0.24).Thecanalsareorientedmoreorless orthogonallytoeachother(Fig.1.4);theorientationof allcanalsvariesamonghealthysubjects(SD between 4.1° and5.4°).Theinnerdiameterofthecanalsisestimatedtovarybetween0.2and0.3mm(see Melvill Jones,1979).
Fig.1.14. (A)Bodeplotofthefrequencyresponseofthetransferfunctionequation4,representingthedynamicresponseofthe mechanicalanalogoftheotolithorgan.Uppertrace:amplitudespectrum(gain ¼ sensitivity).Lowertrace:phaseasafunctionof frequency.(B)Responseamplitudesofc-VEMP(asummedtoreflectsaccularfunction)ando-VEMP(assumedtoreflectutricular function)asafunctionofage(afterAgrawaletal.).
Fig.1.15. Schematicpresentationofthesemicircularcanalswiththecupulaholdingthehaircells.Duetothesimilarorientationof allhaircellsinthecupula,theasymmetricsensitivityofthehaircellsresultsinanasymmetricsensitivityofthesemicircularcanals.
Fig.1.16. Backviewofthetwovestibularlabyrinths.Thearrowsindicatethepreferred(maximumsensitivity)rotationdirection ineachcanal.HC,horizontalcanal;PC,posteriorcanal;AC,anteriorcanal.Notethatthedirectionofthesensitivityofthecanalsis oppositefortheHCcomparedtothatoftheACandPC(oppositeorientationofthehaircellsinthecupulae).
Thehaircellsofthecanalsarelocatedinthebasalpart ofagelatinousmass,thecupula,thatextendsthroughthe ampullaofeachcanalandformsaflapthatclosesthe semicircularcanal,preventingendolymphfrompassing theampulla(Fig.1.15).Theciliaextendintothecupula.
Asindicatedabove,thehaircellshavethehighestsensitivityfordeflectionstothekinocilium:thepolarization direction.Inthecupulaallhaircellsarearrangedwiththe samedirectionofpolarization.Asaconsequence,the receptorpotentialofallhaircellsinacupuladecreases orincreasesinsynchronyuponacupuladeflection. Butagain,asthemaximumsensitivityisinthepolarizationdirection,thereisalsoapreferreddirectionofa cupuladeflection,explainingtheasymmetricsensitivity ofeachsemicircularcanal:actually,eachcanalismost sensitiveforrotationsinthedirectionofthatspecific canal(Fig.1.16).
Thepolarizationdirectionofthehaircellsinthecupula ofthehorizontalcanalissuchthatthecanalismoresensitiveforacupuladeflectiontowardstheampulla(ampullopetal),whichcorrespondstoaheadrotationinthe oppositedirection(arrow;seeexplanationbelowrelated tothephysicsofcupuladeflection).Thepolarization directionofthehaircellsinthecupulaofthevertical canalsissuchthatthecanalismoresensitiveforacupula deflectionawayfromtheampulla(ampullofugal),which againcorrespondstoaheadrotationintheoppositedirection(arrow).Asaruleofthumb,eachcanalismaximally sensitiveforrotationsinthedirectionofthatcanalabout anaxisorthogonaltotheplaneofthatcanal.
Throughthisorientationwearesuppliedwiththree pairsofcanalswithacomplementaryandopposingoptimalsensitivity(Fig.1.16):(1)theleftandrighthorizontalcanal;(2)theleftanteriorandrightposteriorcanal;
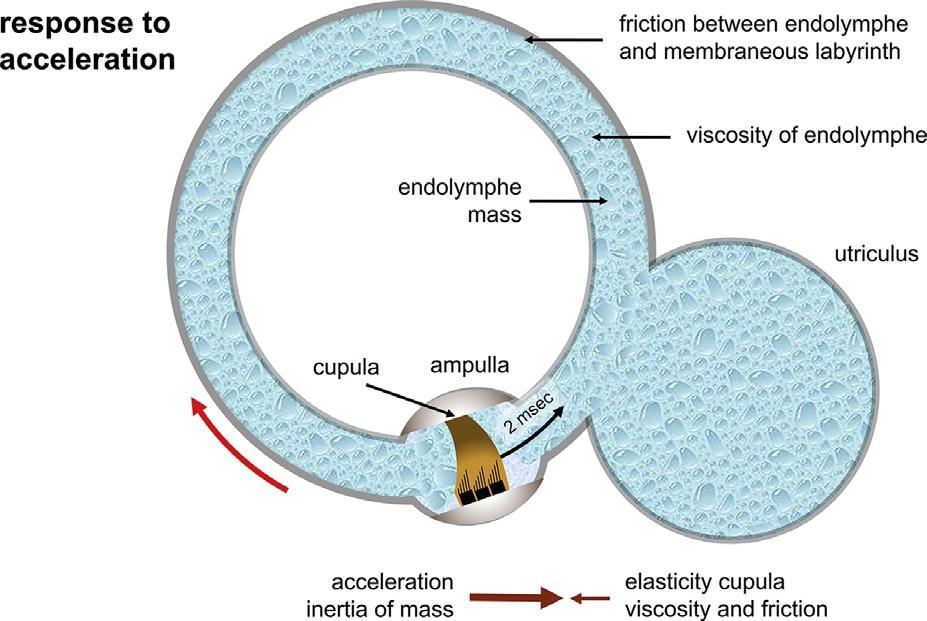
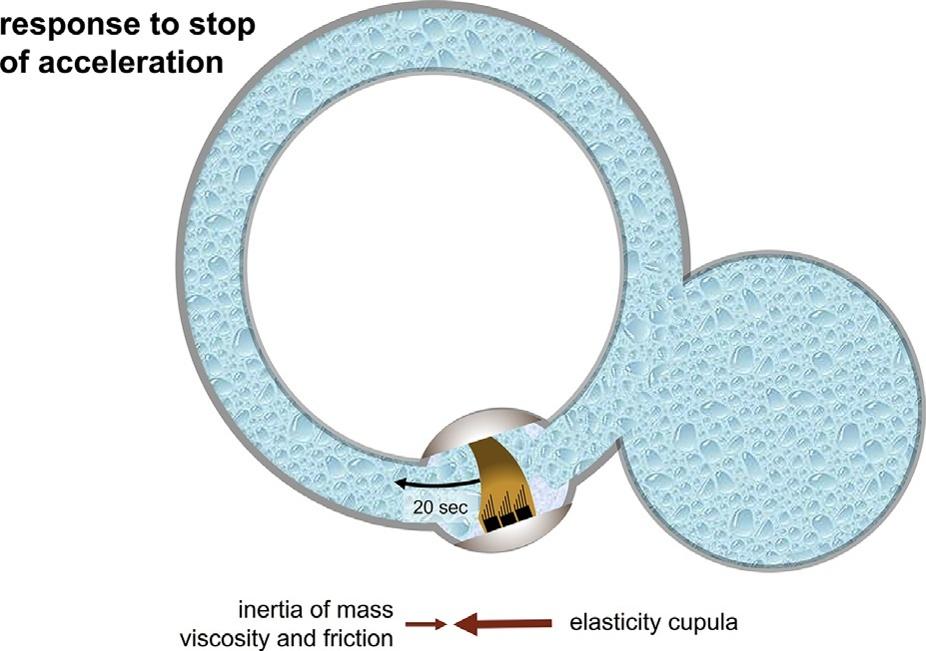
Fig.1.17. (A)Clockwiseangularaccelerationofthecanalsleadstoaampullopetalendolymphaticflowandadeflectionofthe cupulaandhaircellsthatallhavethesamepolarisation.Clockwiseangularaccelerationleadstocupuladeflectionintheopposite direction.(B)Whenrotationvelocitybecomesconstant,thecupulastartstomovebacktotheoriginal(resting)position,which takesabout20secondsonaverage(timeconstantabout6seconds).Thisimpliesthatitisnotpossibletodistinghuishonthebasisof canalinputtothebrainbetweenstandstillandconstantrotation.
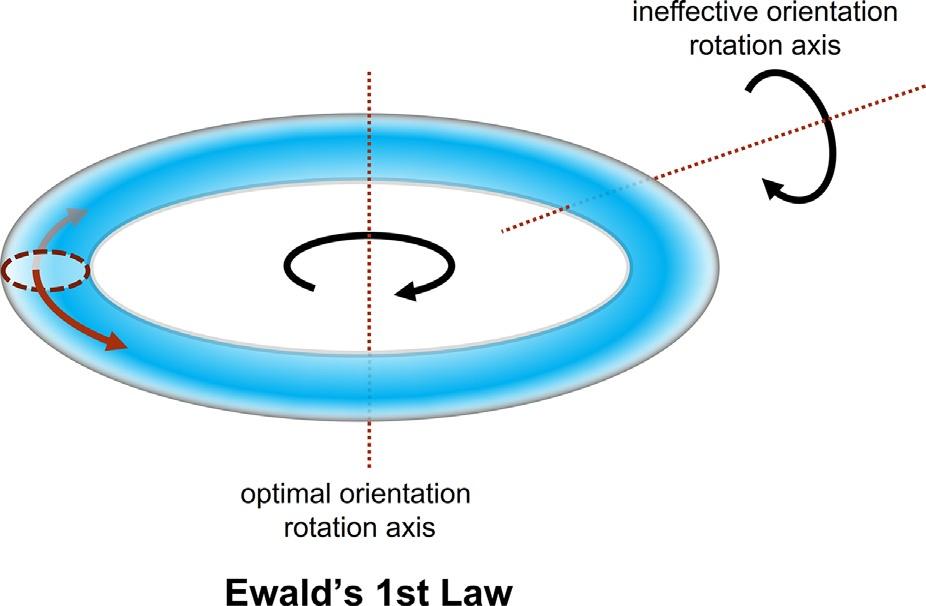
Fig.1.18. FirstlawofEwald:cupuladeflectionwillbemaximalforrotationsaroundanaxisorthogonaltotheplaneinwhich thecanalissituated;cupuladeflectionwillbeminimalforrotationsaroundanaxisintheplaneinwhichthecanalissituated.
and(3)therightanteriorandleftposteriorcanal.Thesensitivity(gain)ofthesemicircularcanalissuchthatitgeneratescloseto1spike/sper °/sat0.5Hzintheafferent nervefibers(YangandHullar,2007).
Whentheheadisrotated,theendolymphfluidlags behindduetomassinertiaandexertsaforceagainst thecupula(Fig.1.17A),causingthecupulatobend. Whenconstantrotationisreached(Fig.1.17B)andaccelerationbecomesnil,thedrivinginertialforcewillbecome niltoo(Newton ’slaw:force ¼ mass acceleration).Now thecupulawillbendbacktoitsoriginalposition,driven bythecupulaelasticityagainsttheviscosityoftheendolymphandthefrictionbetweenendolymphandmembranouslabyrinth.Theendolymphwillmovemaximally whentherotationaxisisorthogonaltotheplaneinwhich thecanalisoriented(Fig.1.18;theendolymphandcupula
willnotmovewhentherotationaxisisintheplaneofthe canal:Ewald’sfirstlaw).Asmentionedalready(Fig.1.1), theimpactofrotationonanindividualcanaldoes notdependonthedistancebetweentheaxisofrotation andthecenterofthecanal – parallelaxistheorem (Feynman,2011).Incontrast,thecentrifugalcomponent relatedtorotationdependsonthelocationofthelabyrinth relativetotherotationaxis.
Thebrainreceivesoppositesignalsfromthetwolabyrinthsanddetectsthedifferencebetweenbothofthem, whichinengineeringtermsisconsideredasworkingasa differentialamplifier.Theredundancyinasystemwith twolabyrinths(similartohearingandvision)makesit lessvulnerableforunilaterallossoffunction.But,also, detectingthedifferencebetweenthetwooppositely sensitivelabyrinthsenhancesthesensitivitytwofold, whereasacommondisturbancefromoutsideissubtracted(common-moderejection).
PHYSICSOFTHECANALS
Ananalogofacanalwithoutcupulaisaclosedbottle completelyfilledwithwater(withoutanyairontop) fixedonaturntable.Assoonastheturntablestartsto rotate,thebottlewillfollowtherotationimmediately. However,duetotheinertiaofmass,thewaterwilllag behindandonlyafterawhile – duetotheadhesionof thewatertothebottlewallandtheinternalcohesionof thewatermolecules – willthewaterstarttorotateand thenrotatewiththesameangularvelocityasthebottle andturntable.Withoutthisfriction(adhesion)andviscosity(cohesion),thewaterwouldnotmoveatall;with morefrictionandviscositythewaterwillfollowthebottlemovementfaster.Besidesfrictionandviscosity,the
totalmassandspecificmassofthefluidorinertiaplaya crucialrole:thegreaterthefluidmass,themoreforce (acceleration)isneededinordertomovethewater.Friction,viscosity,mass,andaccelerationalldeterminehow muchthewaterlagsbehindthebottlemovementand overwhichangleitwillbedisplaceduntilthewater hasreachedthesameangularvelocityasthebottle.As longastheturntable,bottle,andwaterrotateataconstant velocity,nofurtherchangewilloccur.Theangleover whichthewaterisrotatedcomparedtothebottleisproportionaltotheappliedangularaccelerationofthebottle. Assoonastheturntablestops,thebottlewillstopaswell, butthewaterwillstillrotateinsidethebottle.Thevelocityofthewaterwilldecreaseovertimeduetothefriction betweenbottleandwaterandultimatelythewaterwill cometoacompletestandstill.Ifthedecelerationisthe sameastheacceleration,thesametimewillbeneeded forthewatertocometoastandstillandthewaterwill haverotatedtoexactlythesamepositionasinthebeginningoftheexperiment:nonetrelativeangulardisplacementisleft.Infact,decelerationandaccelerationneed notbethesame:thesamepositionisalwaysreached whenthestepsinvelocityduringaccelerationanddecelerationareoppositebuthavethesamemagnitude.For example,thevelocitystepisthesamebutopposite (120°/sand –120°/s)whenweacceleratein12seconds with10°/s2 to120°/s,andthebottlestopswhenwedeceleratein2secondsby60°/s2 from120°/stostandstill. Sotherelativedisplacementisproportionaltothevelocitystep: ¼ acceleration Tacceleration.Thishasadirect clinicalapplication:velocitystepsareusedwidelyin vestibulardiagnosticsusingrotatorychairs.
Whenweputaverylightfluidorgas(lowspecific mass)inthebottle(decreasingthemassinertia)oravery viscousfluidthathasastrongadherence(highfriction)to thebottlewall,thedisplacementofthecontentrelativeto thebottlewillbealmostnegligible.
So,therelativedisplacementincreaseswithmass, decreaseswithfriction(adhesionandcohesion),and increaseswiththemagnitudeofthestepinvelocity. Anytranslationoftheturntableandbottleontopwill notleadtoanymovementofthewaterasthewatercannot becompressed.Thewaterwillonlystarttomoveby rotation.
Thesituationisslightlymorecomplexinthesemicircularcanal:herethecupulapreventstheendolymphfrom rotatingfreelyinthecanal(Fig.1.15).Thecupulacanbe consideredasanelasticmembranethatcanslightlybend inbothdirections.Assoonasthecanalstartsrotating,the endolymphlagsbehindduetoitsinertiaofmass.Again, thelessfrictionandthemoreendolymphmassarein thecanal,themorethefluidwilltendtolagbehind andthestrongerwillbetheforceactinguponthecupula. Thestiffnessofthecupulawill,however,preventalarge
deflection:withinmillisecondsanequilibriumwillbe reachedbetweentheinertialforceactinguponthecupula andtheelasticforcefromthecupula.Aslongasthe accelerationcontinues,thisequilibriumwillremain, resultinginapersistentdeflectionthatstimulatesthehair cellsinthecupula.Thestrongertheacceleration,the morethecupulawillbend:theconstantdeflectionof thecupulawillbeproportionaltotheacceleration. Lowcupulastiffness(highelasticity),highendolymph mass,andlowfrictionwillallresultinalargercupula deflection(highersensitivity).Whenconstantangular velocityisreached,thecupulawillstarttobendback toitsneutralpositionasthereisnodrivingforce(acceleration)anymoretomaintainthecupuladeflection. However,thereturnlastsquitelong,asnowtheelastic forceofthecupulaalonewillhavetomovetheendolymphmassagainstfriction.Alowcupulastiffness(high elasticity ¼ smallelasticforce),ahighendolymphmass, andstrongfrictionwillresultinaslowerreturnofthe cupulatoitsneutralposition.Inpathologyandaging, endolymphviscosity(friction)andcupulastiffnesscan change;inbenignparoxysmalpositionalvertigo (BPPV)thespecificmassoftheendolymphcanbe assumedtoincrease.Insummary:
1.increaseofcupulastiffnessorincreaseofendolymphviscosity:lowercanalsensitivityand shorterpostrotatorysensations
2.increaseofabsoluteendolymphmass:higher canalsensitivityandlongerpostrotatory sensations
3.changeofendolymphspecificmasscompared tothatofthecupula:sensitivityofthecanals forgravityandlinearaccelerationsisinduced.
Acanalisphysiologicallyinsensitiveto(coincidental) linearaccelerations(MelvillJones,1979)becausethe cupula andendolymphhavethesamedensity.Ifdifferencesindensitiesoccur,thecanaldynamicswillbe morecomplex,andwouldleadtoadependencyonthe orientationofboththegravityvectorrelativetothecanal planeandtheaxisofrotation,aswellasonthedistance betweentheaxisofrotationandthecenterofthesemicircularcanal(Kondrachuketal.,2008).Thiseffectisa familiar experienceafteralcoholintake,resultinginthe sensationofrotationwhenlyinginbed,andcaneven induceeyemovementsknownaspositionalalcohol nystagmus(Goldberg,1966).Thisisalsotheeffectexperienced inthecommonvestibulardisorderBPPV.In BPPV,otoconiaarepresentinthesemicircularcanals. Theseparticlesmakethesemicircularcanalsystemsensitivetotheorientationofgravityandcanadheretothe cupula – cupulolithiasis(Schuknecht,1962) – or remain free-floating,whichiscalledcanalithiasis(Rajguruetal., 2004, 2005).
Manyattemptshavebeenmadetodevelophighfrequencytests(vestibularautorotationtest,head shakers,high-frequency(hydraulic)torsionswingchair tests).Noneoftheseobtainedawidespreadapplication comparabletothecalorictestduetomanypractical limitations,andlimitedsensitivityandreproducibility. Passiveheadimpulsetests,fastsmall-amplitudehighvelocityheadrotations,canbeconsideredasevaluating thehigh-frequencyfunctionofthecanals,allowing quantificationofthegain,butnotbothtimeconstants. Thankstothedevelopmentofvideoeye-trackingdevices thatallowquantificationofheadandeyevelocityduring theseheadimpulses,headimpulsetestinghasbecome thefirstchoiceforquantificationofcanalfunctionathigh frequencies.Thecaloricteststillremainsavaluabletool toquantifythelow-frequencypartofcanalfunction.As canbeeasilyunderstoodfromthephysicsofthecanals, low-,middle-,andhigh-frequencylosscanoccur,bothin isolationandindifferentcombinations.
MULTISENSORYASPECTS
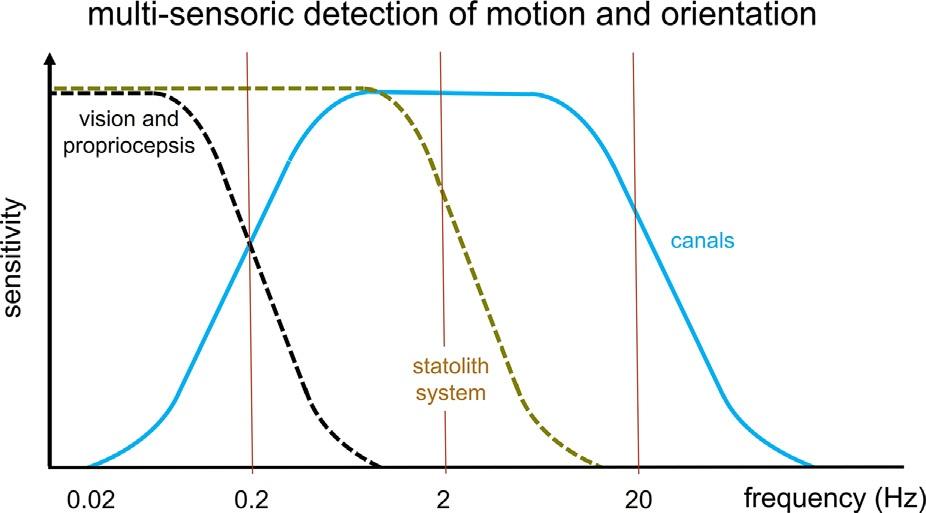
Canals,maculae,vision,andproprioceptionallcontributetomotionandtiltperception.Boththevisualand somatosensorysystemcanonlyprocessrelativelyslow bodymovements,andcanbemodeledwithalow-pass transferfunction,withacutofffrequencyofabout 0.2Hz.Theotolithorgansdetectlow-frequencylinear accelerations(translationsandtilt)uptoabout1Hz, whereasthesemicircularcanals(semicircularcanals) detectangularvelocitybetween0.1and10Hz.Based onthephysicsdescribedabovewecanestimatethefrequencydependenceofhumancanalsandstatolithorgans asdepictedin Figure1.21,butthereadershouldrealize thatthisisspeculationratherthanestimation.Atpresent
Fig.1.21. Graphicpresentationofthefrequencydependence ofcanalandstatolithfunction,incombinationwithpropriocepsionandvision.Motionsicknessisknowntooccuroften atmovementfrequenciesaround0.2Hz,wherethetransition occursfromdominanceofvisual-proprioceptiveinputversus thatofcanalinput.
itisnotpossibletoverifythesecurvesindetaildueto limitsofthediagnostictests,especiallybecauseitisstill notpossibletostimulateanyoneofthefivevestibular sensorsperlabyrinthseparately.Also,themagnitude ofthevestibularresponsesdependsonmanyfactors, includingcognitivefactors(alertness,instruction)and theprecisestimulusconditions(indarknessversusin thelight).Thevisualandsomatosensorysystemssupport theotolithorgansinthedetectionofconstantlinear accelerations(Vaugoyeauetal.,2008)andtiltperception atlowfrequencies,whereasthesemicircularcanalssupporttheotolithorganstodistinguishtruebodytiltfrom translationsatfrequenciesabove0.1Hz(Greenetal., 2005;Merfeldetal.,2005).Ifdifferentsensorysystems giveconflictingorinsufficientinformation,hindering thedeterminationofthedirectionofgravityordistinguishingcorrectlybetweenenvironmentalandselfmotion,motionsicknessisquitecommon(Blesetal., 1998),especiallyinindividualswithaneasilyactivated autonomicnervoussystem(neurovegetativesensitivity). Wealsoaddedthehypotheticfrequencysensitivityof proprioceptionandvision,whichcontributetomotion perceptionandorientationinthelow-frequencyrange.
PATHOLOGY
Losingsensorsformotionandtiltdetectionunavoidably leadstoalossoffunctionalityandcannotbecompensatedforbyothersensorysystemsthatdonothavesufficientsensitivityforthehigherfrequencies(Fig.1.15). Indeed,apermanentunilateralorbilateralperipheralloss leadstoapermanentreductionofautomaticimagestabilizationduringheadmovement(oscillopsia,reductionof dynamicvisualacuity),apermanentlossofautomatic balance(“nomoretalkingwhilewalking”)andapermanentlossofautomationofspatialorientation(feeling insecureinsituationswithstrongoptokineticstimuli,like busytrafficandsupermarkets).Thecontinuousand intenseextracognitiveloadneededforvision,balance, andorientationleadstofastfatigue,whichisamajor probleminpatientswithpermanentvestibulardeficits.
Adecreaseinvestibularsensitivitywithaging,presbyovestibulopathy,similartoperceptivehearingloss (presbyacusis)isamajorcauseofadecreaseofdynamic visualacuity,reducedbalance,andhighincidenceoffalls intheelderly.Besideshaircelldegeneration,agingmight alsoaffecttissuestiffnessandhydration,andthusalso affectsthevestibularphysicalquantitiesofboththesemicircularcanalsandotolithorgans:
1.anincreasingstiffness K increasesthelower cutofffrequency(K/B)anddecreasesthegain (I/K)belowthiscutofffrequency
2.anincreasingviscosity B decreasesthehigher cutofffrequency(B/I)anddecreasesthegain (I/B)belowthiscutofffrequency.
Theseeffectsareschematicallyshownin Figures1.16 and 1.17.Thevestibularsystemasawholeisthus affected aswell,reducingthedistinctionbetweentilt andtranslation,becausetheoptimalrangeofthesemicircularcanalsshiftstohigherfrequencies.Thisisparticularlyunfortunatebecausewithagebodymovements becomeslowerduetostifferbodymechanics.
CONSIDERATIONSCLINICALLY RELEVANTTOTHEIMPACTOF LABYRINTHINEFUNCTIONLOSS
Thevestibularlabyrinthsactasverysensitivesensorsof headaccelerationandtilt.Asexplainedabove,theutriculusandsacculuscanbeconsideredasveryrudimentary sensors,sensitiveforallmotionsandtilts,butnotableto discriminatebetweenthedifferenttypesofmotion. Dependingontheprecisemotionpattern,additional informationfromcanalsallowsdiscriminationbetween translations,centrifugations,andtilts.
Whenwelosecanalfunction,asmonitoredbythe calorictest,rotationaltest,andheadimpulsetests,we canstilldetectallmotionwiththestatolithsystem, althoughwithalowersensitivity,especiallyathigher frequencies.Whenwelosestatolithfunction,thefast intuitivedetectionofgravityandthesensitivityfortranslationswillbeimpaired,butrotationalsensitivitywillbe preserved.Oftenadistinctionismucheasierwhenadditionalvisualandproprioceptiveinformationisavailable. Adistinctionbetweenslowtiltsandtranslationsexplicitlyrequiresforeknowledgeaboutthetypeofmovement oradditionalinformationfromvisionand/orproprioception.Forexample,diversindarkwaterandpeoplecoveredbyanavalancheareunabletosensetheirorientation towardsgravity:thissuggeststhatthebrainisunableto detecttheorientationrelativetogravitywhencompletely deprivedofvisualorproprioceptiveinput,whichmaybe duetothisambiguityinthestatolithsystem.
Motionsicknessisconsideredtooccurespeciallyin conditionswhereweexperienceconflictsbetweenthe motion-sensitiveinputsignalstothebrainand/orwhen theperceivedverticaldiffersfromtheexpectedvertical. Subjectswithoutlabyrinthinefunctiondonotsufferfrom motionsickness.Interestingly,motionsicknesscanbe causedbystimulithatdonotactivatethelabyrinth,such asvisualillusionofmotion.Thiscanbeexplainedbythe factthatthecentralvestibularsystemisalwaysinvolved intheperceptionofself-motionandthedetectionofgravity, eveniftheinformationissuppliedbythevisualsystem.
Tosummarize,themajorfunctionsofthevestibular systeminrelationtoclinicalsymptomsare:
● Maintainingvisualacuityduringheadmotions: dynamicvisualacuitybymeansofthe vestibulo-ocularreflex.Vestibularfunctionloss mayleadtoapermanentlossofvisualacuityand oscillopsiaduringwalkingandheadmotion (oscillopsiaistheperceptionthattheimageis unstableontheretina).Especiallyduringwalking,verticalheadmovementsrequirecompensatoryeyemovements.Itisasyetunclearwhatthe precisecontributionofthestatolithandcanal systemsisforimagestabilizationasthehead movementsarecomposedoftranslational,rotational,andtiltcomponents.Thissuggeststhat thecorrelationbetweenalossofdynamicvisual acuitydependsonmanyfactors.Theoverall impactofa(frequency-dependent)labyrinthine lossforimagestabilizationneedsmoreresearch: patientsmightcompensateforthelossofimage stabilization(thevestibulo-ocularreflex)partly bysmallsaccades,so-calledcovertsaccades,or byimprovingtheabilityofthevisualsystemto analyzetheinformationpresentinmoving imagesontheretina,similartowhathasbeen suggestedincongenitalnystagmus.
● Allowingfastbalanceandposturalcorrectionsby anintuitiveperceptionofthegravityvectorand fastvestibulospinalreflexes.Sothespecificcontributionofthelabyrinthtobalancecontrolseems tobespeed.Severelabyrinthinelossmaythereforeleadtopermanentimbalance(walkinglike adrunkensailor),fearoffalling,andfalls.The impactofafunctionlossofthestatolithsystem maybeofgreaterrelevancethanlossofcanal function.However,weshouldstillbeawarethat thebrainneedsthecanalorothersensoryinputin additiontotheinherentlyambiguousotolithinput toallowareliabledetectionofthegravityvector.
● Spatialorientation:discriminationbetweenselfmotionandenvironmentalmotionandorientation relativetothegravityvector.Thelossoflabyrinthinefunctionmaythereforeleadtouncertainty. Thetrivialsensorysubstitutionthatisobserved inmanypatients,particularlywithregardto vision,canhaveadverseconsequencesasitmay leadtovisualdependenceandsometimesintolerancetomovingvisualstimuliorrepetitivepatterns withhighcontrasts(optokineticstimuli):oneof thepresentationsofso-calledvisualvertigo.
Asecondaryimpactofvestibularlossisalossofautomaticimagestabilization,balancecontrol,andspatial