This title is a reworked and condensed version of Medicine published by Blackwell, 2004
CRC Press is an imprint of Informa UK Limited
The right of John Axford and Chris O’Callaghan to be identified as the authors of the editorial material, and of the authors for their individual chapters, has been asserted in accordance with sections 77 and 78 of the Copyright, Designs and Patents Act 1988.
This book contains information obtained from authentic and highly regarded sources. While all reasonable efforts have been made to publish reliable data and information, neither the author[s] nor the publisher can accept any legal responsibility or liability for any errors or omissions that may be made. The publishers wish to make clear that any views or opinions expressed in this book by individual editors, authors or contributors are personal to them and do not necessarily reflect the views/opinions of the publishers. The information or guidance contained in this book is intended for use by medical, scientific or health-care professionals and is provided strictly as a supplement to the medical or other professional’s own judgement, their knowledge of the patient’s medical history, relevant manufacturer’s instructions and the appropriate best practice guidelines. Because of the rapid advances in medical science, any information or advice on dosages, procedures or diagnoses should be independently verified. The reader is strongly urged to consult the relevant national drug formulary and the drug companies’ and device or material manufacturers’ printed instructions, and their websites, before administering or utilizing any of the drugs, devices or materials mentioned in this book. This book does not indicate whether a particular treatment is appropriate or suitable for a particular individual. Ultimately it is the sole responsibility of the medical professional to make his or her own professional judgements, so as to advise and treat patients appropriately. The authors and publishers have also attempted to trace the copyright holders of all material reproduced in this publication and apologize to copyright holders if permission to publish in this form has not been obtained. If any copyright material has not been acknowledged please write and let us know so we may rectify in any future reprint.
All rights reserved. No part of this book may be reprinted or reproduced or utilised in any form or by any electronic, mechanical, or other means, now known or hereafter invented, including photocopying and recording, or in any information storage or retrieval system, without permission in writing from the publishers.
For permission to photocopy or use material electronically from this work, access www.copyright.com or contact the Copyright Clearance Center, Inc. (CCC), 222 Rosewood Drive, Danvers, MA 01923, 978-750-8400. For works that are not available on CCC please contact mpkbookspermissions@tandf.co.uk
Trademark notice: Product or corporate names may be trademarks or registered trademarks and are used only for identification and explanation without intent to infringe.
British Library Cataloguing-in-Publication Data
A catalogue record for this book is available from the British Library
ISBN: 978-1-032-04526-9 (hbk)
ISBN: 978-0-367-15059-4 (pbk)
ISBN: 978-1-003-19361-6 (ebk)
DOI: 10.1201/9781003193616
Typeset in Palatino LT Std by KnowledgeWorks Global Ltd.
Instructors can register to gain access to Figures Slides as PowerPoint or PDF. To register, they must request access at the following location: https://routledgetextbooks.com/textbooks/instructor_downloads/
The editors
John Axford is a Consultant in Adult and Paediatric Rheumatology and Emeritus Professor of Clinical Rheumatology at St George’s Hospital, University of London.
After training at University College Hospital he worked at The National Hospital for Neurology, The Hammersmith Hospital, The Royal Brompton Hospital, King’s College Hospital and the New England Medical Center, Boston, Massachusetts, USA.
He has enjoyed teaching medicine throughout his career and pioneered video teaching to developing countries with the Royal Society of Medicine.
He is an author and editor of the textbook UpToDate.
Chris O’Callaghan is Professor of Medicine at the University of Oxford and a Consultant Physician (in Acute General Medicine) and Consultant Nephrologist in the Oxford University Hospitals.
He is Chief Examiner in Medicine for the University of Oxford, runs a research group, teaches medical students, and is a Fellow and former Dean of The Queens’ College, Oxford.
After training and working in Oxford he worked at Guy’s, St Thomas’, Hammersmith, Brompton and Lewisham Hospitals in London, Royal Stoke University Hospital, the University of California, San Francisco, and the California Institute of Technology.
His other books include The Kidney at a Glance and The MRCP Part I: a System Based Tutorial.
Taylor&Francis Group
http://taylorandfrancis.com
Contributors
Rachel L. Allen BSc (Hons) DPhil
Professor & Director of the Institute of Medical and Biomedical Education
St George’s, University of London London, UK
John S. Axford DSc MD FRCP FRCPCH
Emeritus Professor of Clinical Rheumatology
St George’s Hospital University of London London, UK
Kevin C.R. Baynes BA (Oxon) MBBS PhD FRCP
Consultant in Diabetes & Endocrinology
London North West University Healthcare NHS Trust London, UK
Gary Bell BA MB BS FRCPsych
Consultant Psychiatrist Cognacity London, UK
Christopher J. Black MB BS(Hons) PhD MRCP
Consultant Gastroenterologist
Leeds Teaching Hospitals NHS Trust Leeds, UK
Jim Bolton MB BS BSc(Hons) FRCPsych
Consultant Psychiatrist Department of Liaison Psychiatry St Helier Hospital London, UK
Pierre-Marc Bouloux BSc MB BS (Hons) MD FRCP Director and Consultant Endocrinologist Centre for Endocrinology
Royal Free Campus
UCL London, UK
Christopher B. Bunker MA MD FRCP
Consultant Dermatologist and Honorary Professor of Dermatology
UCL and Chelsea & Westminster Hospitals, and University College and Imperial College London, UK
Ruth Corrigan BM BCh PhD Academic Clinical Lecturer in Microbiology and Infectious Diseases
Nuffield Department of Clinical Laboratory Sciences University of Oxford Oxford, UK
Paul I. Dargan MB BS FRCP FEAPCCT FAACT Professor of Clinical Toxicology
Guy’s & St Thomas’ NHS Foundation Trust and King’s College Hospital London, UK
Gareth R. Davies BSc (Hons) MD FRCP Consultant Physician and Gastroenterologist Harrogate District Hospital Harrogate, UK
Maria Dudareva BM BCh PhD MRCP
NIHR Doctoral Research Fellow Bone Infection Unit
Oxford University Hospitals NHS Trust Oxford, UK
Susanna Dunachie BM ChB PhD FRCP FRCPath Professor of Infectious Diseases University of Oxford Oxford, UK
Hanif Esmail MA MBBS MRCP PhD FRCPath
Associate Professor and Honorary Consultant in Infectious Diseases
University College London and Hospital for Tropical Diseases
University College London Hospitals London, UK
Keeley Fairbrass BSc(Hons) MBChB(Hons) MRCP
Gastroenterology Registrar and Clinical Research Fellow
Leeds Teaching Hospitals NHS Trust Leeds, UK
Thomas A. Fox BSc MB ChB MSc MRCP FRCPath Department of Haematology
University College Hospital London, UK
Faye Gishen MB BS BSc FRCP EdD PFHEA
Professor of Medical Education & Palliative Medicine
UCL Medical School London, UK
Harrison Howarth BSc (Hons) MB BS MRCPsych
Core Psychiatry Trainee
Camden and Islington NHS Foundation Trust London, UK
Jeffrey Lee MB BS (Hons) FRCP
Consultant Rheumatologist
Royal Free Hospital London, UK
Alexander Lyon MA BM BCh PhD FRCP FHFA
Senior Lecturer and Honorary Consultant Cardiologist
Imperial College London and Royal Brompton Hospital London, UK
Malcolm R. Macleod BSc(Hons) MB ChB PhD FRCP FRSB
Professor of Neurology and Translational Neurosciences (University of Edinburgh) and Honorary Consultant Neurologist (NHS Forth Valley) Edinburgh, UK
Alison J. Maycock MB BChir (Cantab) MA MRCGP
General Practitioner Partner, Trainer and Appraiser Hollow Way Medical Centre Oxford, UK
Emma C. Morris BA MA MB BChir PhD FRCP
FRCPath FMedSci
Professor of Clinical Cell & Gene Therapy
UCL Division of Infection and Immunity
Hon Consultant Haematologist
University College London Hospitals NHS Foundation Trust and Royal Free London Hospitals NHS Foundation Trust London, UK
James Neuberger DM FRCP
Hon Consultant Physician
The Liver and Hepatobiliary Unit
Queen Elizabeth Hospital Birmingham, UK
Chris A. O’Callaghan BM BCh MA DPhil
DM FHEA FRCP
Professor of Medicine
Fellow of The Queen’s College Nuffield Department of Medicine
University of Oxford
Hon Consultant Physician and Nephrologist
Oxford University Hospitals Oxford, UK
Ian Pavord MA MBBS DM FRCP FERS FMedSci
Professor of Respiratory Medicine
Respiratory Medicine Unit and Oxford Respiratory NIHR BRC Nuffield Department of Clinical Medicine
University of Oxford and John Radcliffe Hospital Oxford, UK
Nayia Petousi MA MB BChir MRCP DPhil
Consultant Respiratory Physician
Oxford University Hospitals NHS Foundation Trust Oxford, UK
Nick Talbot BM BCh MA DPhil MRCP
Departmental Lecturer Department of Physiology, Anatomy and Genetics
University of Oxford Consultant in Respiratory Medicine
Oxford University Hospitals NHS Foundation Trust Oxford, UK
Adrian Tookman MB BS FRCP
Consultant Palliative Medicine
Former Medical Director Marie Curie Hospice London, UK
Richard E. Watchorn MB BCh BAO MD FRCP Consultant Dermatologist
Beaumont Hospital, Dublin and Honorary Consultant Dermatologist
University College London Hospitals NHS Foundation Trust
Honorary Clinical Senior Lecturer
Royal College of Surgeons of Ireland and Imperial College London London, UK
Acknowledgements
All those who contributed to editions of this book’s predecessor, Medicine—this new book builds on their work especially: Stephen H. Gillespie (Chapter 3), Chris Sonnex (Chapter 3), Christopher Carne (Chapter 3), Emma M. Clark (Chapter 5), Jon Tobias (Chapter 5), M.J. Walshaw (Chapter 6), Charles Hind (Chapter 6), C.W. Pumphrey (Chapter 6), J.C. Kingswood (Chapter 8), D.K. Packham (Chapter 8), D.S. Rampton (Chapter 10), D.J. Betteridge (Chapter 11), Felicity Kaplan (Chapter 12), Gerard S. Conway (Chapter 12), C.J. Mumford (Chapter 13), D.H. Bevan (Chapter 15), A.C. Kurowska (Chapter 16), A.K. Fletcher (Chapter 17 ) and F.P. Morris (Chapter 17 ). Peter Saugman was a key supporter from the start.
Jo Koster and Jordan Wearing for superb editorial support with this edition. Nora Naughton for her outstanding and incredibly efficient project management of the production of this book. Becky Freeman and Susan Smyth for their tireless efforts copy-editing and proof-reading respectively.
M. Ali Abbasi, Christine Heron and Andrew Hine for radiology advice. Julia Steed for keeping the text under control.
The following doctors for reviewing the text and providing helpful feedback: Nina Agarwal, Pat Woo Mark Cassar, Vijay Hadela, Marcus Hughes, Simon Lambracos, Brian Lunn, Mike Mendall, Muthana Al Obaidi, Sanjeev Patel, Johnathan Rogers, Malcolm Rustin, Paddy Stone and Malcolm Walker.
Our excellent colleagues for their valued expertise and discussions of medicine.
Taylor&Francis Group
http://taylorandfrancis.com
Introduction
Our focus in this condensed third edition is on helping you to pass your final assessments and examinations with ease and confidence.
Medicine for Finals and Beyond contains all the information that you need to qualify as a doctor. The contributing authors are experts in their respective fields, as well as experienced writers and teachers. The book has been strongly influenced by input from many students and colleagues. Much has changed since the second edition was published and some chapters needed further refinement as the pandemic unfolded.
DESIGNED FOR LEARNING
To pass examinations and to practise medicine well, it is important to understand the basics. There are many textbooks of medicine, but we believe that they are generally not well designed for learning. Some have grown thicker with each edition and include detail that is beyond the needs of students and, indeed, of many qualified doctors. This can make it difficult to see the ‘wood for the trees’ and slows and complicates learning.
Medicine for Finals and Beyond has been carefully crafted to avoid the overwhelming. Each system is presented in an integrated chapter, with sections on the basic structure, function and biology of the system, on clinical presentations, on the approach to the patient and on the diseases affecting that system. There is a clear focus on evidencebased medicine as well as consideration of the social, caring and communicative aspects of practice and the impact of disease and treatment on the lives of patients.
The material in this edition has been arranged to aid learning and recall. The amount of information on each topic has been carefully regulated. Important topics are readily identifiable and deliberately presented in detail if they are very common or are often examined. Illustrations have been used extensively to aid learning.
The book is written for students but will also be of use to doctors and other healthcare workers who are trying to understand or revise medicine, so it will remain useful as you advance beyond your student years.
HOW TO USE THIS BOOK
Chapter 1 provides an overview of the human dimension to clinical medicine and Chapter 2 reviews the basic science. Together, these help you to understand what underpins modern medical practice. The chapters which follow cover systems. Navigation is aided by the coloured page end-tabs that label each chapter. Drugs are referred to by their Recommended International Non-proprietary Name (rINN) although, in a few cases, older names are also provided if they are still in use.
CHAPTER LAYOUT
The system chapters cover structure and function, approach to the patient and diseases and their management. Aids to learning within each chapter highlight important material:
• At a Glance boxes summarize core topics for rapid revision.
• History and Examination boxes outline key features to elicit from the patient.
• Emergency boxes summarize essential information about emergencies.
• Must-know checklists highlight key points. The editors and authors have enjoyed creating this third edition and are confident that students will find it a useful and enjoyable book as they learn medicine and particularly in the pressured run-up to final exams. The editors suggest that you remember:
‘the patient is always right…’ and therefore………. ‘if in doubt, ask the patient.’
Enjoy your career and REMEMBER to have fun outside medicine too.
John Axford and Chris O’ Callaghan
Taylor&Francis Group
http://taylorandfrancis.com
The Human Aspects of Medicine
1
CHRIS O’CALLAGHAN & ALISON MAYCOCK
INTRODUCTION
This chapter considers the context in which the clinical facts and details discussed in the other chapters are gathered and deployed. It is intended to help the student or clinician reflect on how to make the most effective use of the information contained in the other chapters.
The effectiveness of doctors rests not just on their knowledge of clinical facts but also on good communication, clear clinical reasoning and reflective practice. The General Medical Council (GMC), which regulates medical practice in the UK, captures these elements in its guidance ‘Good medical practice’. This is divided into different domains and specifies how doctors should act.
• Knowledge, skills and performance
⚬ Have patient-centred care as their first concern.
⚬ Be competent and up to date.
⚬ Recognize and work within their competence.
• Safety and quality
⚬ Act promptly if patient safety, dignity or comfort is at risk.
⚬ Protect and promote the health of patients and the public.
• Communication partnership and teamwork
⚬ Treat patients politely and considerately.
⚬ Respect patients’ confidentiality.
⚬ Listen to patients and respond to their concerns and preferences.
⚬ Give patients the information they want or need in a form they can understand.
⚬ Respect patients’ right to contribute to decisions about their management.
⚬ Support patients in their self-care.
⚬ Work effectively with colleagues in the patients’ interest.
• Maintaining trust
⚬ Be honest and open and act with integrity.
⚬ Never discriminate unfairly against patients or colleagues.
⚬ Never abuse patient trust or public trust in the profession of medicine. These elements form the basis of doctors’ mandatory annual appraisal and the 5-yearly revalidation of their licence to practise in the UK.
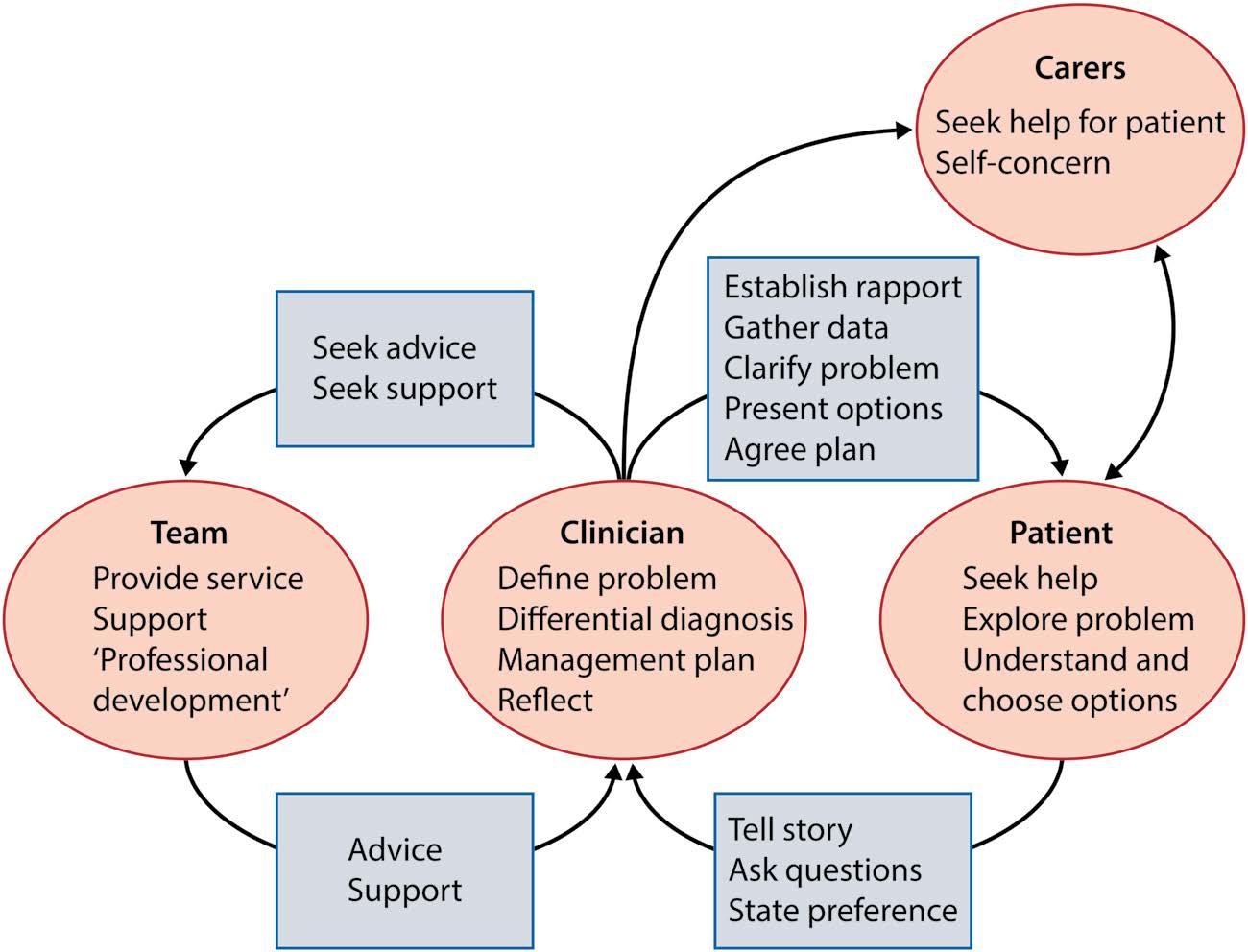
A key element of medical practice is communication and the clinician is involved in a complex communication network ( Figure 1.1).
COMMUNICATION WITH PATIENTS
Being a skilled listener is fundamental to the process of understanding the problems that patients present and their significance for the patient across all aspects of their life. Consultations are usually face-to-face, but increasingly occur via telephone, video, email or even social media, and each medium presents different challenges.
Patient-centredness and shared decision-making should be the defining features of the consultation. The patient’s values and goals should be established by the clinician and incorporated into a negotiated plan of action. Agreeing a plan is important, as the patient has to live with its consequences. A negotiated and agreed plan is much more likely
to be effective than an instruction given by the doctor to the patient. We all engage more fully in plans we have helped devise.
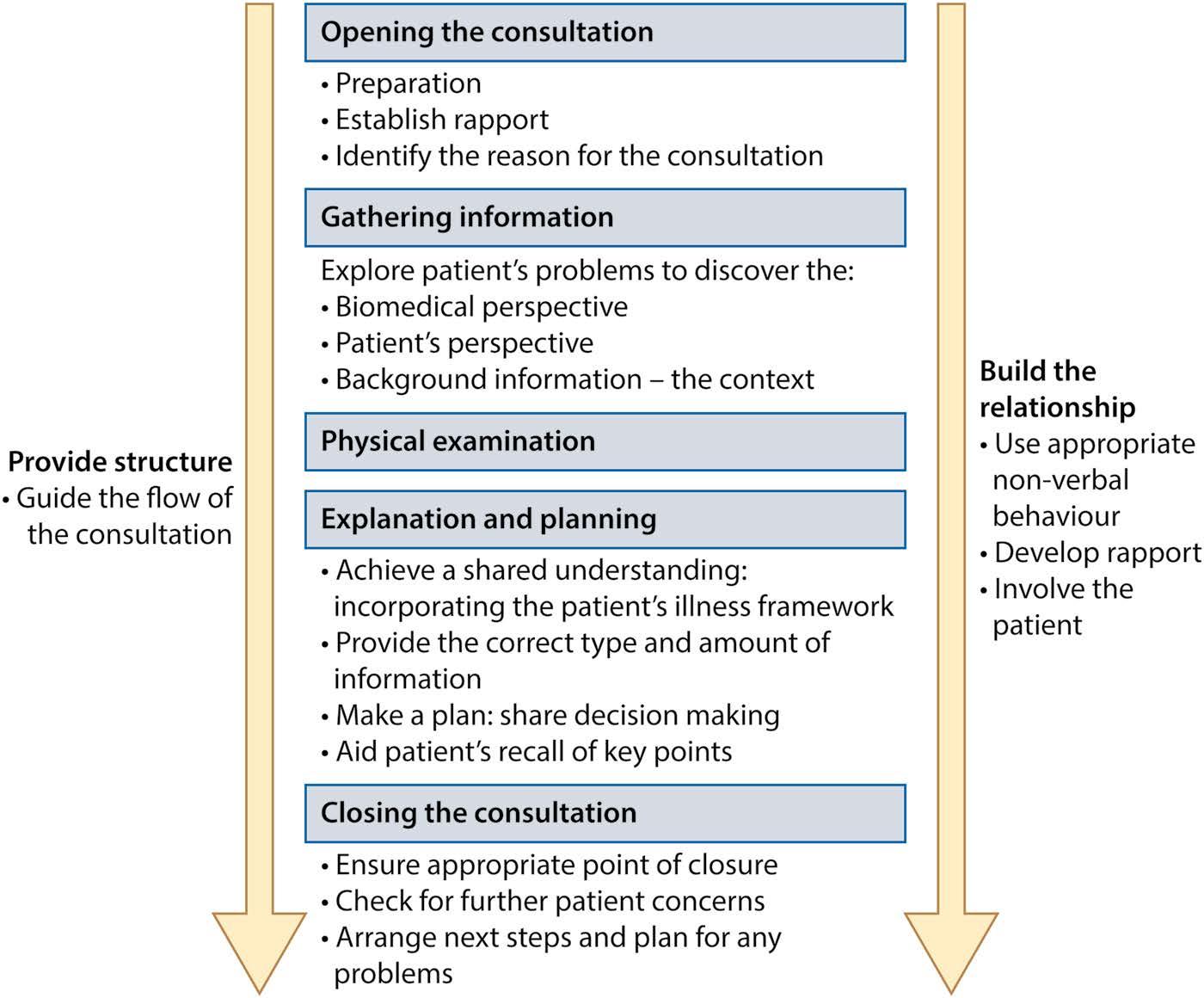
Consider the structure of a consultation, its main phases and tasks ( Figure 1.2).
During these processes, the clinician provides a structure to the consultation for the patient to understand, tackles their problem and also builds a relationship with the patient. Let us look in more detail at some of these elements.
OPENING THE CONSULTATION
Preparation
• Gather any data already available (e.g. test results, letters from other clinicians).
• Manage your own feelings and needs (e.g. hunger, tiredness, anxiety or stress).
• Be clear about your own agenda (e.g. you may wish to achieve an audit target or reduce your clinic numbers).
• Choose a comfortable setting.
Establishing rapport
• Make eye contact and smile.
• Identify yourself by name and role.
• Confirm that the patient is ready to talk.
• Ensure the patent is comfortable, appropriately covered and positioned.
• Ensure any other people in the room are appropriate and the patient consents to their presence.
• Put the patient at their ease with a kind and gentle manner.
• Explain any use of computers or other technology as needed.
• Involve the patient and ask questions in a friendly manner. Use non-verbal gestures such as smiling, nodding and allowing silence.
• Acknowledge and respond to each point made by the patient.
• Notice how the patient looks and behaves and draw this into the consultation, if appropriate.
GATHERING INFORMATION
People generally consult doctors because they think that they have a medical problem that should be diagnosed and treated, or because something is adversely affecting them and their coping mechanisms are failing.
Start by asking open and wide questions to capture all the important information from your perspective and the patient’s, such as:
• Why have you come to see me today?
• What outcome are you hoping we will achieve?
• What is it about this problem that worries you?
• What do you think the problem is?
• What next steps do you have in mind?
• Is there anything else that has been bothering you? Follow each of these by an open prompt, such as:
• Can you tell me a bit more about that?
Clarify with open specific questions, such as:
• Do you have a cough?
Pin down your diagnosis by asking increasingly specific closed questions, such as:
• Does anything bring the cough on?
• Does exercise bring the cough on?
Figure 1.1 The network of clinical communication.
Avoid negative leading questions, such as:
• You do not have the cough at night then?
• You don’t get any side effects from these medications?
PHYSICAL EXAMINATION
Tailor your examination according to the history and your differential diagnosis.
EXPLANATION AND PLANNING
Achieve a shared understanding of the problem
• Clarify and summarize what has been said.
• Establish in your own mind your differential diagnosis.
• Use non-specialist language to explain your conclusions.
• Ask for the patient’s opinions, suggestions and preferences.
• Relate explanations to the patient’s own terms or concepts.
• Explicitly check the patient’s understanding.
Provide the correct type and amount of information
• Deliver information in small chunks.
• Provide written material, such as patient information leaflets or web links.
Make a plan
• Agree the forward plan with the patient.
• Empower the patient to manage their own illness and self-care.
• Document key points carefully.
CLOSING THE CONSULTATION
• Check for any outstanding patient concerns.
• Advise whom the patient may contact with further questions.
• Advise what to do in situations that need action and especially those which are a threat to patient safety.
COMMUNICATION WITH RELATIVES AND CARERS
It is important to bear in mind the following, when talking to relatives and/or carers.
• Obtain appropriate consent from the patient for the discussion.
• Establish the identity and role of the carer or relative.
• Be sensitive to the impact of the patient’s illness on the individual carer or relative.
• Establish what they already know and what more they wish to know.
Figure 1.2 The tasks and processes of the consultation.
• Use the skills of the patient consultation, such as active listening, breaking information into small chunks and providing written material, as appropriate.
COMMUNICATION WITH COLLEAGUES
Most doctors work in teams and this can be challenging, rewarding and enjoyable. Good team working requires showing respect and consideration for others. This includes listening to the concerns and points of view of other people and acknowledging and valuing their contributions. Effective communication is needed to optimize efficiency and patient safety.
• Keep accurate and concise records, which are signed and dated or appropriately validated electronically.
• Formulate requests for help as clearly as possible, to obtain the most useful response.
• Be sensitive to the roles and competencies of colleagues.
• Promote a fair and supportive work environment.
• Be willing to help colleagues but realistic about what can be done.
• Obtain patient consent for discussion with outside teams or agencies.
COMMUNICATION IN CHALLENGING CIRCUMSTANCES
Communication with patients or relatives or carers can be especially challenging in certain situations, such as the following:
• The patient and clinician do not speak the same language. An interpreter should be used.
• The patient has impaired hearing. A hearing aid or signing interpreter should be used as appropriate.
• The patient has impaired cognitive skills or lacks capacity. The clinician must establish the level of understanding and the capacity of the patient for each specific decision. Mental capacity is always assumed and is demonstrated for a specific decision when a patient can:
⚬ Understand the information given and the decision required
⚬ Retain the information
⚬ Weigh up the information to make a decision
⚬ Communicate that decision
• The patient displays strong emotions. The clinician should remain calm, speak quietly, acknowledge the emotion displayed and show a willingness to listen further.
• The clinician must break bad news. The clinician should choose a quiet, comfortable place, ask if the patient wants someone else to be present and check what
they already know. It can be helpful to offer a warning along the lines of ‘I am sorry, but I have some difficult information for you…’.
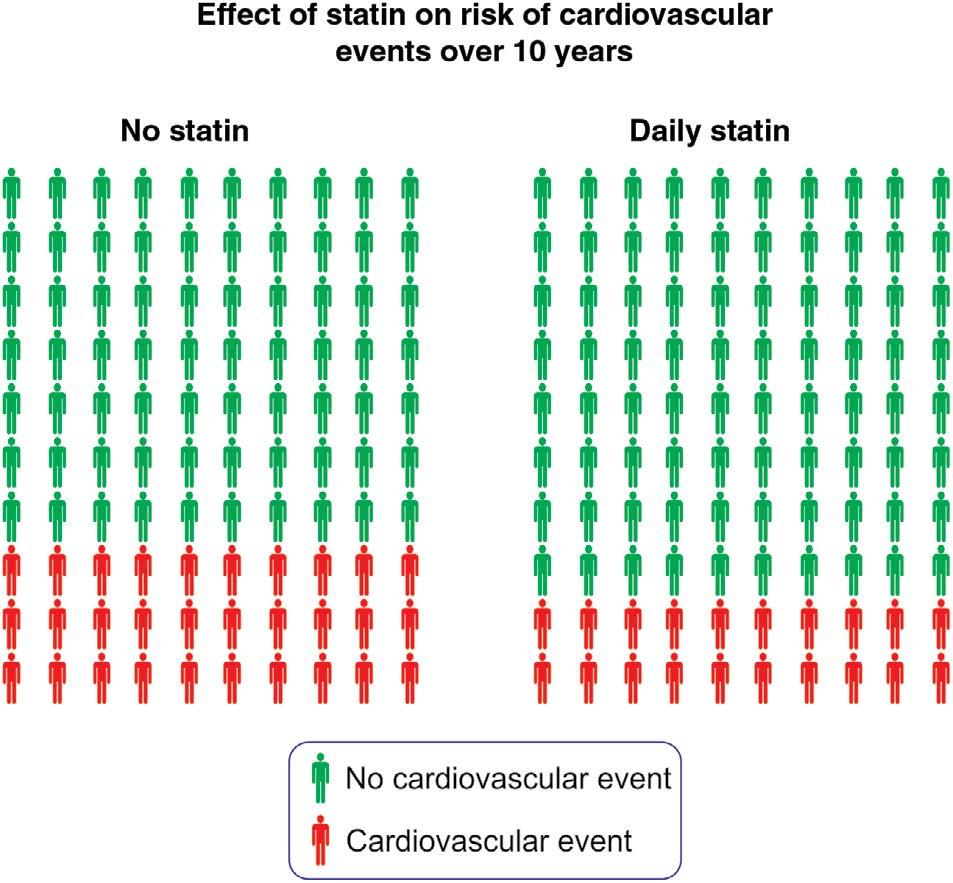
• The clinician is communicating a complex concept such as risk. Advise the patient of absolute risk (not relative). Give numbers not percentages. Use visual decision-making aids if possible (e.g. Figure 1.3, a patient decision-aid chart). Discuss the likelihood of a problem both occuring and not occuring. For example, in the hypothetical situation illustrated in Figure 1.3, if discussing the option of taking a statin with a patient who has a 10-year cardiovascular disease (CVD) risk of 30%, you might say:
‘If there were 100 people like you in the room, over the next 10 years, on average it is likely that 30 of them would have heart pain, a heart attack or stroke and 70 of them would not. If they all take this medicine every day for the next 10 years, then 20 of them would be likely to have a problem and 80 would not. Therefore, 10 people would be likely to avoid the problem.’
• There is uncertainty of diagnosis, prognosis or benefits of intervention options. The doctor should be honest with patients about the limitations of medical certainty and predictability, but should offer reassurance regarding what is known and can be done.
• There are medically unexplained symptoms. Medically unexplained symptoms can be frustrating for both the doctor and patient. The doctor should be explicit about the limitations of current medicine to explain every symptom. It is important to acknowledge that even when no organic illness can be diagnosed, a patient may be significantly affected by their symptoms and
Figure 1.3 Patient decision aid to communicate the benefit of a statin on cardiovascular risk. This hypothetical decision aid could be used to demonstrate how taking a statin might reduce the likely number of cardiovascular events over a 10-year period from 30 to 20 per 100 people.
the doctor can still offer to support the patient in managing their problem.
• The patient is making a complaint. Clinicians have a statutory duty of candour in the UK. This means they must tell patients about any medical errors. Complaints should be handled according to local complaints procedures, which usually involve providing the complainant with:
⚬ A clear written description of what happened
⚬ A clear description of how it was investigated
⚬ An apology for any errors and acknowledgement of the impact on the patient
⚬ An indication of how future problems will be avoided
⚬ An invitation to meet to discuss the matter
• Obtaining informed consent. When obtaining consent for a procedure, the emphasis is now on providing the information which a reasonable patient can be expected to want to know. This includes side effects or consequences which are common and those which are uncommon or rare but which are serious. In the UK, this follows the High Court findings in the case of Montgomery v Lanarkshire. In this situation, a mother sued the hospital trust for not informing her of the risks of a vaginal delivery to her unborn baby. The mother was small and the baby was large. The baby suffered injury during delivery and the court ruled that she should have been informed of this small but important risk.
• The patient has strong cultural or personal values and beliefs which may affect the medical process. This may be refusing certain treatments, such as blood products in the case of some Jehovah’s Witnesses, or gelatin-containing capsules for some Muslims. Clinicians must be sensitive to diversity and avoid making assumptions. They must be alert for cues indicating embarrassment regarding being examined or talking about intimate issues.
• The clinician is working outside their area of competence In this case, the doctor should explain to the patient that this is so and further advice should be sought from a colleague with appropriate expertise.
COMMUNICATION AND CONFIDENTIALITY
Patients’ trust in doctors is, in part, founded on confidentiality. The clinician should not disclose identifiable patient details without consent. Implied consent can be assumed for aspects of direct patient care and local audit as specified in GMC guidance in the UK. All other disclosure requires explicit consent except in the following circumstances:
• Disclosure is in the public interest if it is required to prevent serious crime or communicable disease. For example, clinicians have a duty to inform the
sexual contact of a patient who has HIV infection if the patient is not prepared to prevent the risk of transmitting the infection. A doctor also has a duty in the UK to inform the police or Driver and Vehicle Licensing Agency (DVLA) if a patient is not fit to drive and is continuing to do so.
• The patient lacks capacity and disclosure is in the best interest of the patient.
• A court orders disclosure of information.
In any case of disclosure without consent, the clinician must carefully document the efforts they made to obtain consent and inform the patient of their plans before disclosure or, if this is not possible, as soon as possible thereafter.
Patient confidentiality must be safeguarded when patient information is shared electronically, and any such communication must use systems which are compliant with the appropriate security standards. In the UK, nhs.net accounts currently fulfil these requirements. Outside this facility, clinicians should check the security of the system they are using or remove all patient-identifying data from the communication. When emailing patients, the clinician should make them aware of the potential limitations for security and document the patient’s consent for this type of communication.
In the UK, the British Association of Dermatologists has published GMC-approved guidance on how to take clinical images and email these images for direct patient care. This guidance states that securely configured devices and NHS email or secure data transfer apps must be used. The images must then be deleted immediately after transfer. In any other circumstance, patient data must be completely anonymized.
CLINICAL REASONING OR JUDGEMENT
Clinicians make sense of the information they gather by a process of clinical reasoning, which aims at making a working or differential diagnosis and management plan. Clinical reasoning has several stages which may be reiterated until a best course of action is identified. We have already identified some of the key components of this and a framework for understanding clinical reasoning is summarized in Figure 1.4 .
MAINTAINING PATIENT TRUST
Patients often put enormous trust in the medical profession. When interacting with doctors, patients may feel, and be, very vulnerable. Their health and well-being may be under serious threat. It is unlikely that they are familiar with the concepts and information which form the basis for the decisions they are being asked to make. There is therefore a duty on clinicians to respect and safeguard patient trust by acting honourably and in the patient’s best interests at all times. These requirements are identified by the GMC
Figure 1.4 Stages in clinical reasoning.
as outlined earlier. They contribute to what we think of as professionalism.
REFLECTIVE PRACTICE
In the UK, the ongoing professional development of doctors has been formalized in statutory annual appraisal and a 5-yearly revalidation process. The GMC has recently drawn attention to the key role played by reflection in enabling individuals to develop professionally. In essence, reflection involves taking time to step back and think about a particular event and consider what went well, what could have gone better and how
best to address the learning or other need required to enable better practice in future. The final step is to identify what will confirm that practice has improved.
The professional development of doctors also involves looking after ourselves and building resilience to withstand the demands of the job. We need to have enough time and energy to pursue our interests, both medical and non-medical. We need to nurture ourselves as individuals as well as professionals in order to deal with stress and to avoid burnout. Time for reflection and planning is part of this self-care, as is sharing worries or dilemmas with peers or seniors, forming small peer-support groups or finding a mentor or coach. It is important to remember that doctors are normal people and may, like their patients, need help at times.
PROVIDING LEADERSHIP
As doctors gain in experience and become more senior, they take on more leadership activities, although any doctor may be required to show leadership at any stage. For example, any junior doctor may be asked to organize how the team divides up the tasks they need to do. Being a leader means taking responsibility for the functioning of the team as a whole. Again, the basic skills of communication are key: achieving rapport, listening, clarifying issues and sharing decisions as far as is practical. However, it is the leader of a team who has to take the final decision and, with that, the final responsibility for the actions taken.
LIFE AS A CLINICIAN
The role of the clinician makes enormously varied demands on the individual. These include demands on memory and knowledge, experience, logical reasoning, emotional intelligence, social skills, self-reflection and self-management. Demands are also made on the imagination and creativity of the doctor, as they must help generate a plan with the patient in every circumstance they encounter. It is, however, a role that can reward the individual with a marvellously varied professional life.
MUST-KNOW CHECKLIST
• Effective communication is an essential aspect of clinical medicine.
• If time permits, prepare and plan each consultation.
• Always listen to patients.
• Patient confidentiality is of the utmost importance.
Questions and answers to test your understanding of Chapter 1 can be found by clicking ‘Support Material’ at the following link: https://www.routledge.com/Medicinefor-Finals-and-Beyond/Axford-OCallaghan/p/book / 9780367150594
2
The Scientific Basis of Medicine
CHRIS O’CALLAGHAN & RACHEL ALLEN
In this chapter, we outline some of the scientific foundations of modern medicine, highlighting how scientific advances have opened up the potential for new therapies and diagnostic tests.
BIOLOGICAL MACROMOLECULES
NUCLEIC ACIDS
Genetic information is stored and transferred in the form of the nucleic acids deoxyribonucleic acid (DNA) and ribonucleic acid (RNA). These molecules provide the necessary information for protein production. Like many biological molecules, nucleic acids are multimers of smaller units; which in this case are known as nucleotides. A set of four nucleotide components is used to generate DNA or RNA. Adenine (A), guanine (G ) and cytosine (C ) are common to both DNA and RNA. Thymine (T ) is found in DNA but absent from RNA, with uracil (U ) present in its place.
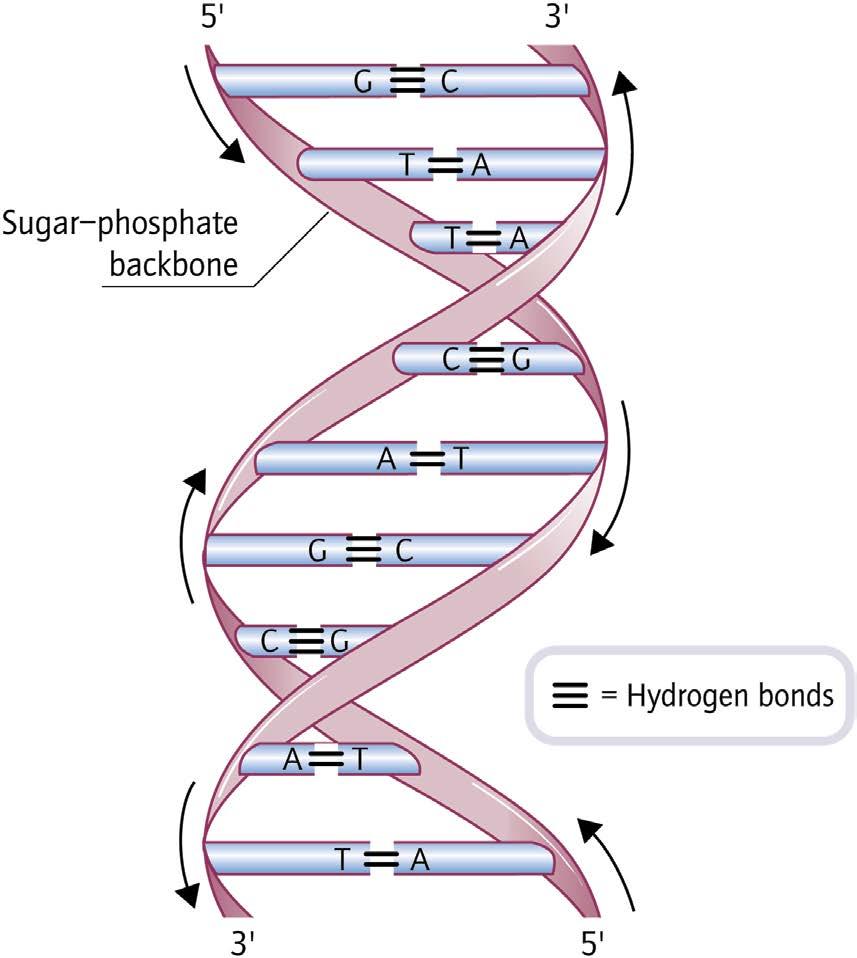
DNA strands consist of nucleotides joined by phosphodiester bonds linking the sugar of one nucleotide to the phosphate group of the next. DNA coils into a double helix of two antiparallel strands ( Figure 2.1). Complementary base pairing of adenine with thymine and guanine with cytosine ensures the fidelity of DNA transcription and replication. When DNA is copied, each parental strand acts as a template for replication: incoming nucleotides form hydrogen bonds with an appropriate base on the template strand. Base mispairing, induced by damage or mutation, introduces structural alterations which can be detected and/or removed by DNA repair proteins.
RNA differs from DNA in its sugar content and usually exists as a single strand. RNA is a versatile molecule that is fundamental to protein synthesis; information from a DNA strand is copied (transcribed) into a new strand of
RNA, which acts as a template for protein production. Some viruses use RNA as their hereditary material; retroviruses such as human immunodeficiency virus (HIV) encode their genome on a single strand of RNA, which is reverse transcribed into DNA upon infection of a host cell.
PROTEINS
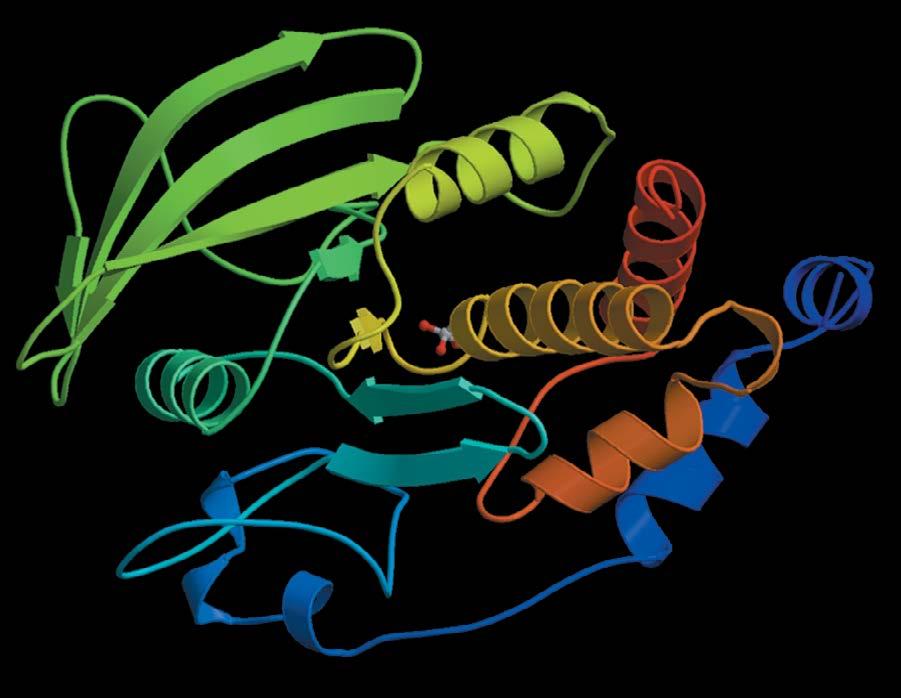
Proteins are long chains of amino acids held together by peptide bonds. Each amino acid is composed of an amino group, a carboxyl group and the particular side chain that defines their chemical nature. Individual proteins are constructed from a library of 20 amino acids, which may be subgrouped according to the acidic, basic, uncharged polar or non-polar character of their side chains ( Figure 2.2). Like all large molecules, proteins adopt a conformation that confers the most stability. Protein modifications can result from the addition of other substances, such as metal ions (e.g. iron in haemoglobin), lipids (lipoproteins) or carbohydrates (glycoproteins).
CARBOHYDRATES
Carbohydrates are composed of carbon, hydrogen and oxygen with a general formula Cx(H 2O) y. They range from simple monosaccharides of three to six carbons to large complex polysaccharides ( Figure 2.3). Glycoproteins are usually generated by covalent attachment of carbohydrate groups to the amino acids asparagine, threonine or serine. Some diseases, such as cancers and arthritis, may have characteristic glycosylation patterns, which can be useful for diagnosis and for predicting prognosis.
Long-term complications associated with diabetes can result from hyperglycaemia. In a non-enzymatic process, glucose attaches to the amino group of proteins such as collagen (e.g. in blood cell walls). Consequent chemical
rearrangements irreversibly generate advanced glycosylation end products (AGE). AGE have a range of pathological effects including peptide cross-linking.
LIPIDS
The structural units of lipids are fatty acids, containing long chains of 4–24 carbon atoms joined to a carboxylic acid group ( Figure 2.4). Fatty acids may be saturated or nonsaturated depending on the presence of double bonds within their hydrocarbon tail. Polyunsaturated fatty acids contain multiple double bonds. One of the most important in vivo functions performed by lipids is the formation of cellular membranes. Phospholipids contain a hydrophilic phosphate group, linked by glycerol to a hydrophobic fatty acid tail. The amphipathic nature of phospholipids allows them to form a sealed membrane bilayer in aqueous solution. Another physiologically important group of lipids are the cholesterol derivatives (steroids). These molecules contain four hydrocarbon rings, one of which carries a hydroxyl group which gives the molecule an amphipathic nature.
CELL BIOLOGY
CELL STRUCTURE
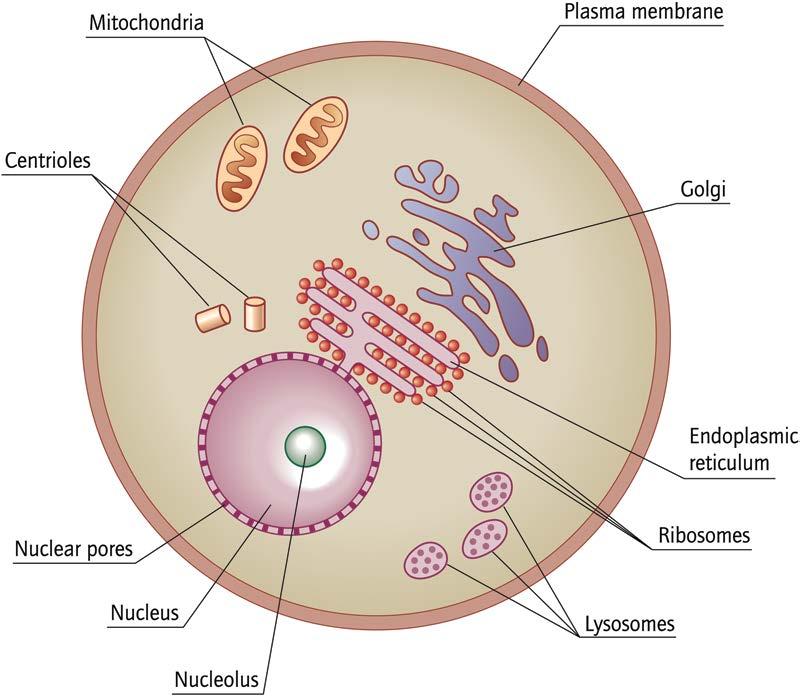
Cells are the basic structural unit of all living organisms. Each cell has the means to maintain itself within the organism and interact with other cells and body systems. Subcellular organelles compartmentalize processes such as respiration or digestion ( Figure 2.5).
An example of an α-helix is shown in red and an example of a β -sheet is shown in green.
The fluid nature of the outer phospholipid membrane that surrounds the cell allows proteins to move around its surface. The cytosol is the site of many cellular reactions and contains all the necessary machinery for protein synthesis. A cytoskeleton of microfilaments, intermediate filaments and microtubules provides physical support for the various organelles and forms transport routes between them.
The membrane-bound nucleus acts as a store for genetic information. Nuclear pores facilitate exchange of protein and RNA between the nucleus and the rest of the cell. Newly formed proteins destined for transport to lysosomes or the cell surface are inserted into the endoplasmic reticulum (ER), a system of folded membranes. Initial protein glycosylation may also occur within the ER. From the ER, proteins progress through a related system of compartments known as the Golgi complex, where further modifications take place. The Golgi complex sorts macromolecules for onward transport and, on leaving it, proteins progress through a system of vesicles until they reach their ultimate location.
Endocytosed proteins and other materials are degraded within membrane-bound lysosomes, which store the hydrolytic enzymes required for such degradation. Deficiency of a lysosomal enzyme causes the neurological condition Tay–Sachs disease in which gangliosides accumulate in the brain causing neural degeneration and early death.
Figure 2.2 (a) Amino acid side chains (designated by a black box) may be acidic, basic or hydrophobic in nature. (b) Amino acids join to form a polypeptide chain. (c) Protein secondary structure is composed of α-helices and β -sheets, both of which can be seen in the structure of human tyrosine phosphatase 1B.
Figure 2.1 The DNA double helix.
Figure 2.3 Carbohydrate structures. Most common monosaccharides adopt a ring conformation in aqueous solution. (a) Fructose and (b) glucose are examples of 5-carbon (pentose) and 6-carbon (hexose) monosaccharides, respectively. (c) Lactose is a disaccharide formed from galactose and glucose subunits. (d) Heparin is a polysaccharide.
Mitochondria are the powerhouses of the cell. These maternally inherited organelles carry their own small genome encoding various components of the respiratory process.
CELL DIVISION
Mitosis
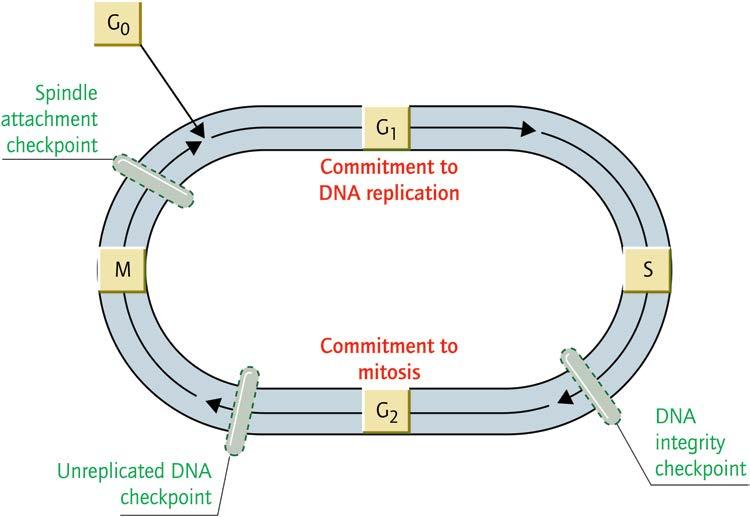
In order to divide successfully, a cell must copy its DNA so that each daughter cell receives its full set of chromosomes. This is achieved by a tightly regulated mitosis following the cell cycle pathway ( Figure 2.6). Passage through the cell cycle is controlled by cyclin proteins, in a cascade of phosphorylation events. Each cyclin acts as a catalytic subunit in partnership with a cyclin-dependent kinase (CDK). Upon cyclin binding, CDKs phosphorylate target proteins that are required for cell-cycle progression. CDK-specific inhibitors (CDKIs) bind cyclin–CDK complexes to regulate their activity and can themselves be regulated by other proteins. During mitosis, one member of each chromosome pair becomes attached to a centriole. Centrioles move to opposite ends of the cell, taking the chromosomes with them. In order to prevent inappropriate proliferation of cells, mitosis is tightly controlled, with various checkpoints to ensure
that every part of the mitotic process is completed correctly before the next stage begins. Because uncontrolled proliferation is a hallmark of cancer, the cell cycle provides an obvious target for therapy. CDKIs often act as tumour suppressors and are potentially useful anticancer agents.
Meiosis
A more specialized form of cell division generates gametes bearing a single set of chromosomes. Meiosis requires two rounds of cell division, with DNA replication occurring during the first round of division. The second division results in each daughter cell inheriting a single set of chromosomes.
APOPTOSIS
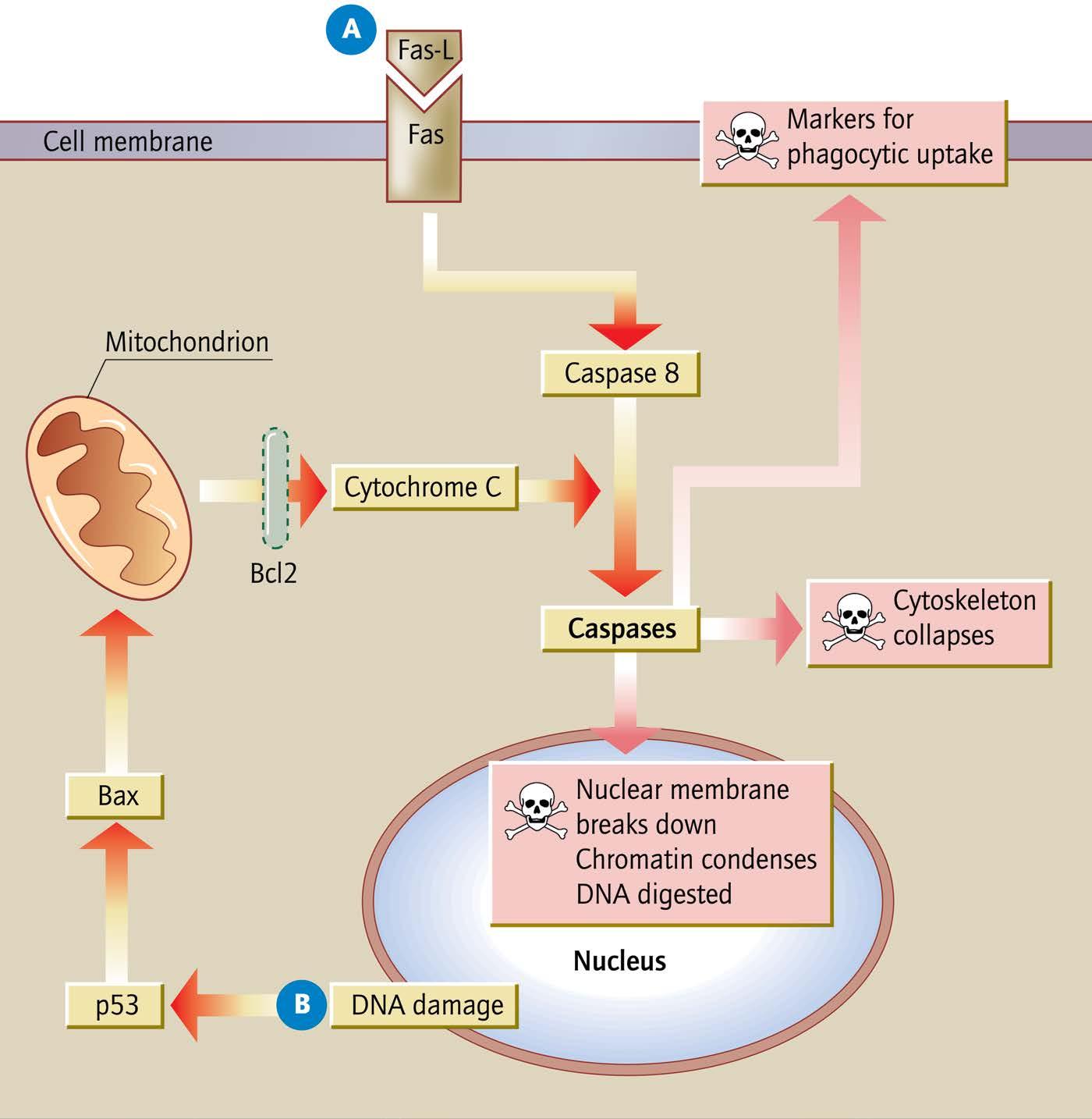
An effective mechanism is required to remove cells that are damaged or no longer necessary. This programmed cell death is generally known as apoptosis ( Figure 2.7 ), and follows a carefully controlled series of events allowing the cell to condense its cytoskeleton and fragment its DNA. Apoptosis is driven by members of the caspase protein family. Bcl proteins regulate caspase activity. Programmed cell
Figure 2.4 Lipids. (a) Saturated and (b) unsaturated fatty acids are termed according to the presence of double bonds within their hydrocarbon tail. (c) Steroid molecules such as cholesterol are based on a skeleton of four carbon rings. (d) Phospholipids are amphipathic molecules with two hydrophobic (green) hydrocarbon tails attached to a hydrophilic polar head group (blue). (e) In aqueous solution, phospholipids form a bilayer with a hydrophobic interior. This arrangement forms the basis for eukaryotic cellular membranes.
death can be triggered in response to stimuli such as cell surface signals or mitochondrial stress. Following ligand binding, cell-surface death receptors such as Fas recruit adaptor
proteins to trigger procaspase activation, and thus elicit apoptosis. Mitochondria can initiate an alternative apoptotic pathway in response to DNA damage or intracellular oxidative stress. A dying cell will show membrane blebbing, cell shrinkage and protein fragmentation as it collapses in upon itself. Within the nucleus, chromatin condensation and DNA degradation occur. Finally, the cell is flagged for uptake by phagocytic cells.
CELLULAR HOMOEOSTASIS AND COMMUNICATION
The human body maintains a stable environment for its cells and tissues through a combination of physiological and biochemical processes. Cell membranes form a barrier to large molecules, allowing the cell to maintain a constant internal environment. Specific transport mechanisms are therefore required to transfer material in and out of the cell. Membranes contain many different proteins that actively or passively facilitate the movement of ions or molecules across
Figure 2.6 The cell cycle. Cells resting between divisions are held indefinitely in the quiescent (G 0) phase. Upon appropriate stimulation (e.g. exposure to growth factors) cells enter ‘gap 1’ (G1), the first stage of the cell cycle, during which various RNAs and proteins are synthesized. The cell then enters a period of DNA synthesis termed the ‘S-phase’. Once each chromosome has been replicated, a second ‘gap’ phase, G 2 takes place. When the cell is ready to divide, mitosis begins (M phase). During mitosis, chromosomes condense and the nuclear envelope breaks down, allowing paired chromosomes to attach to centrioles by a microtubule spindle. Chromosome pairs separate and are moved to opposite ends of the cell preceding cytoplasmic division (cytokinesis). Positive and negative control points operate throughout the cell cycle. Various commitment points and regulatory checkpoints are marked in red and green, respectively. Cell cycle control proteins include p21, p53 and Rb (the retinoblastoma protein).
membranes. Three major classes of transport protein are membrane channels, pumps and transporters.
Cells can use extracellular molecules to communicate with one another. Signal transduction pathways translate these stimuli into an appropriate cellular response, usually through a series of phosphorylation reactions leading to novel gene transcription in the nucleus. Signalling pathways play a role in the development of many cancers.
MOLECULAR BIOLOGY
CHROMOSOMES
The human genome organises our entire genetic information into a set of 46 chromosomes, which segregate our DNA for storage or transcription. Humans have 23 pairs of chromosomes, with one set inherited from each parent. These include 22 pairs of standard chromosomes and one pair of sex chromosomes (XX in females, XY in males). In the absence of transcription or replication, DNA is packed into chromosomes as chromatin with DNA wrapped tightly around very many nucleosome cores. The most densely packed form, heterochromatin, has a closed structure to maintain genes in a transcriptionally inactive state. In
Figure 2.7 Apoptosis. There are two major pathways of apoptosis. (A) Death signals from cell surface receptors such as Fas (CD95) trigger activation of caspase 8 to initiate a signalling cascade through downstream enzymes. Mitochondria host a range of pro-apoptotic factors including cytochrome C, which is necessary for downstream caspase activation. A second apoptotic pathway (B) operates through these organelles. Triggers such as DNA damage (signalled through p53 and Bax) initiate the release of pro-apoptotic factors from mitochondria. Bcl2 acts as an anti-apoptotic regulator of this