No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or any information storage and retrieval system, without permission in writing from the publisher. Details on how to seek permission, further information about the Publisher’s permissions policies and our arrangements with organizations such as the Copyright Clearance Center and the Copyright Licensing Agency, can be found at our website: www.elsevier.com/permissions.
This book and the individual contributions contained in it are protected under copyright by the Publisher (other than as may be noted herein).
Practitioners and researchers must always rely on their own experience and knowledge in evaluating and using any information, methods, compounds or experiments described herein. Because of rapid advances in the medical sciences, in particular, independent verification of diagnoses and drug dosages should be made. To the fullest extent of the law, no responsibility is assumed by Elsevier, authors, editors or contributors for any injury and/or damage to persons or property as a matter of products liability, negligence or otherwise, or from any use or operation of any methods, products, instructions, or ideas contained in the material herein.
Previous editions copyrighted 2012, 2005, 2000, 1992, 1986, and 1983.
Library of Congress Control Number: 2019949237
Content Strategist: Russell Gabbedy
Senior Content Development Specialist: Joanie Milnes
Publishing Services Manager: Catherine Jackson
Senior Project Manager: Claire Kramer
Design Direction: Amy Buxton Printed in Canada Last digit is the print
To Elizabeth, John, Alana, and Daniel for their patience and support. To my sonographers, vascular technologists, and colleagues for always giving their best to our patients.
J. S. P.
To Alex and Jo-Anne.
To my colleague sonographers and vascular technologists. Your work is truly amazing.
J. F. P.
ACKNOWLEDGMENT
I gratefully acknowledge the following individuals who made this edition possible. My co-editor, Joseph Polak, my partner in vascular imaging, for always challenging the status quo and his steadfast dedication to improve patient diagnosis.
All the authors for their excellent contributions to this edition.
My administrative assistant Debbie Kaur, for making a tough job look easy and fun. You’re the best!
My chairs, Jason Naidich and Jesse Chusid, for allowing me the space to develop a world class vascular laboratory with an excellent team to support it.
My colleagues in the Vascular Lab, James Naidich, MD, Catherine D’Agostino, MD, and Brian Burke, MD, for maintaining our high-quality standards.
My vascular technologists, Danielle Berne, RN, RVT; Jane Joo Ah Kim, RVT, RDCS; Bindu Rameshan, RVT; Glenn Prucha, RVT; Maria Sisawang, RVT; Christine Dauber, RVT, RDCS; Athanasios Tziovas, RDMS, RVT; Briana Kresback, RVT; Daniel Hernandez, RDMS, RVT, RDCS; and Floyd Federbush, RVT, for their commitment, diligence, and patience with our research, quality assurance projects, and new technologies.
I would like to thank Adina Haramati, MD, for her excellent illustrations. The folks at Elsevier and Joanie Milnes, in particular, for their support and encouragement. And of course, my family, Elizabeth, John, Alana, Daniel, Peter, and Marie for always being there for me.
John S. Pellerito, MD, FACR, FSRU, FAUM
After thanking John, my co-editor, I cannot resist giving credit to those individuals whose names are not listed on any of the chapter headings of this, the seventh edition of Introduction to Vascular Ultrasonography. Although the title states “Introduction,” John and I have tried to communicate the fact that this edition covers a broad range of experiences and levels of knowledge. The beginner will find the essence of vascular ultrasound, while the advanced will undoubtedly discover pearls.
This edition was built on a foundation of experiences and inputs from those of you who gave feedback, through e-mail, verbally, or in performing a book review. All of your comments were listened to, and every effort was made to address them in this current edition.
As always, I thank my wife, Jo-Anne, for her patience. I also thank my daughter, Alexandra, for understanding that my long hours of work often rolled into work at home. This was motivated by my desire to summarize and explain what it took me so many years to understand.
I give credit to the following sonographers for helping me by providing the high-quality materials that ended up in the chapters I authored and often supplemented materials in other chapters. Foremost, Ms. Jean M. Alessi-Chinetti, RDMS, RVT, for not hesitating to point out questionable interpretations and always submitting studies worthy of publication. I also have to especially thank Gregory Y. Curto, RDMS, with whom I have now worked for years and who was tolerant enough to let me scan even when the schedule was tight. I thank Richard J. Porter, RVT, for asking simple questions that were so difficult to answer. I have to recognize Nicole Wake, RVT who, despite being a great sonographer, decided to invest her career in magnetic resonance imaging. I also thank Andrea L. Ford, RVT, Peter F. Wolstenholme, RVT, Noorjehan M. Tambra, CVS, and, more recently, Julio Perez, RVT, for their questions and feedback.
In this long road, I thank my friend Irwin. The last few years have been cruel, but participating in “Current Practice of Vascular Ultrasound” taught me much, motivated me, and often helped me keep my sanity.
Joseph F. Polak, MD, MPH, FACR, FAIUM
A bout the editors
John S. Pellerito, MD, FACR, FSRU, FAIUM, is Professor of Radiology at Donald and Barbara Zucker School of Medicine at Hofstra/Northwell. He is Vice Chairman of Education for the Imaging Service Line for Northwell Health, as well as the Program Director for the Radiology Residency Program and Program Director for the Body Imaging Fellowship at North Shore University/Long Island Jewish Hospitals. He continues to serve as the Director of the Peripheral Vascular Laboratory at North Shore University Hospital. He is also the Medical Director for the Molloy College Cardiovascular Technology Program in Rockville Centre, New York. He is the author of many original articles and book chapters, web lectures, and DVD programs
on vascular imaging. His current interests focus on new imaging techniques in cardiovascular and gynecologic diseases. He is an in-demand lecturer and continues to contribute to national and international continuing medical education programs. Dr. Pellerito holds multiple editorial appointments and contributes to many educational programs. He is currently on the Board of the Intersocietal Accreditation Commission for Vascular Testing and serves on the Board of Governors for the American Institute of Ultrasound in Medicine. He is a fellow of the American College of Radiology, American Institute of Ultrasound in Medicine, and Society of Radiologists in Ultrasound. He and his wife, Elizabeth, have three children, John, Alana, and Daniel.
Joseph F. Polak, MD, MPH, FACR, FAIUM, is Professor of Radiology at Tufts University School of Medicine and Chief of Radiology at the Lemuel Shattuck Hospital in Boston. A graduate of McGill University School of Medicine and of the Harvard School of Public Health, his major clinical interests are in the use of ultrasound imaging to detect and follow atherosclerosis. He has co-authored more than 310 peer-reviewed papers and 100 non–peer-reviewed articles and chapters. He has served on the Editorial Board of Radiology and currently serves on the Editorial Boards of the Journal of Neuroimaging, the Journal of Vascular Ultrasound, and the Journal of Ultrasound in Medicine. He is past-president of the Intersocietal Commission for the Accreditation of
Vascular Laboratories, has served on the Board of the American Institute in Ultrasound in Medicine, and is currently serving on the Board of the Society of Vascular Medicine and Intersocietal Accreditation Commission (vascular testing). He has been co-investigator and director of the Ultrasound Reading Center that was funded by the NIH and evaluated many ultrasound markers of atherosclerosis such as carotid artery intimamedia thickness, carotid artery plaque, carotid artery distensibility, brachial artery reactivity, and, currently, brachial artery intima-media thickness. He is working on developing a calibrated methodology that can be used for cardiovascular risk assessment.
The seventh edition of Introduction to Vascular Ultrasonography is a significant update to our previous editions. My co-editor, Joseph F. Polak, and I have pulled together the topics and authors we thought represented the best of vascular ultrasound imaging. Having collaborated together for more than two decades with our vascular course and the sixth edition of this book, we feel that this edition has met our goal to present the definitive text in vascular ultrasound. Jo and I have contributed to 22 of the 35 chapters. Not only have all the chapters in this edition been revised to deliver the newest techniques, protocols, and topics in vascular ultrasound, we also invited several new experts to provide their perspectives and experience in significant areas. For example, the physics section has been completely revamped by Dr. Fred Kremkau, the favored speaker and authority in ultrasound physics. We welcome Heather Gornik, MD, the current president of IAC vascular testing, for her contribution on
credentialing, accreditation, and quality in the vascular laboratory. We also are excited to have several world-renowned experts provide us the state of the art in ultrasound contrast applications for vascular imaging. Of course, we brought back many of our favorite authors who received positive reviews from our previous edition.
In addition to multiple new figures and illustrations, a major enhancement to this version of Introduction to Vascular Ultrasonography is the integration of Practical Tips sections throughout all the chapters. These Tips are intended to focus the reader on major teaching points and pearls for the successful performance and interpretation of vascular studies.
We are extremely proud to present the seventh edition of Introduction to Vascular Ultrasonography. We hope that this book will provide guidance to students, technologists, sonographers, and all practitioners of vascular ultrasound to improve patient diagnosis and management.
John S. Pellerito, MD, FACR, FSRU, FAIUM
Dennis F. Bandyk, MD
Section Chief
Division of Vascular and Endovascular Surgery
University of California San Diego
San Diego, California
Phillip J. Bendick, PhD
Technical Director
Peripheral Vascular Diagnostic Center
Beaumont Health System
Royal Oak, Michigan
Carol B. Benson, MD
Professor of Radiology
Harvard Medical School
Director of Ultrasound and Co-Director of High Risk Obstetrical Ultrasound
Department of Radiology
Brigham and Women’s Hospital
Boston, Massachusetts
George L. Berdejo, BA, RVT, FSVU
Director, Outpatient Vascular Ultrasound Services
Division of Vascular Surgery
White Plains Hospital
White Plains, New York
Brian J. Burke, MD, RVT, FACR, FAIUM
Assistant Professor
Department of Radiology
Hofstra-Northwell School of Medicine
Uniondale, New York
Attending Radiologist
Department of Radiology
North Shore University Hospital
Manhasset, New York
Corinne Deurdulian, MD
Department of Radiology
University of Southern California
Keck School of Medicine
Los Angeles, California
C ontributors
Heather L. Gornik, MD, RVT, RPVI
President, IAC-Vascular Testing Division
Co-Director, Vascular Center
Harrington Heart and Vascular Institute
University Hospitals
Associate Professor of Medicine
Case Western Reserve University School of Medicine
Cleveland, Ohio
Edward G. Grant, MD
Department of Radiology
University of Southern California
Keck School of Medicine
Los Angeles, California
Ulrike M. Hamper, MD, MBA
Professor of Radiology, Urology, and Pathology
Russell H. Morgan Department of Radiology and Radiological Science
The Johns Hopkins University School of Medicine
Baltimore, Maryland
Jonathan D. Kirsch, MD
Associate Professor of Radiology and Biomedical Imaging and Internal Medicine
Section Chief, Ultrasound
Department of Radiology and Biomedical Imaging
Yale University School of Medicine
New Haven, Connecticut
Frederick W. Kremkau, PhD
Professor of Radiologic Sciences
Center for Experiential and Applied Learning
Wake Forest University School of Medicine
Winston-Salem, North Carolina
Mark E. Lockhart, MD, MPH
Chief, Body Imaging Radiology
University of Alabama at Birmingham
Birmingham, Alabama
Mahan Mathur, MD
Associate Professor of Radiology
Director, Medical Student Education
Associate Director, Diagnostic Radiology
Residency Program
Department of Radiology and Biomedical
Imaging
Yale School of Medicine
New Haven, Connecticut
William D. Middleton, MD
Professor of Radiology
Mallinckrodt Institute of Radiology
Washington University School of Medicine
St. Louis, Missouri
Darius G. Nabavi, MD
Chair, Department of Neurology
Vivantes Klinikum Neukölln Berlin, Germany
Marsha M. Neumyer, BS, RVT, FSVU, FSDMS, FAIUM
International Director
Vascular Diagnostic Educational Services
Harrisburg, Pennsylvania
Daniel C. Oppenheimer, MD
Assistant Professor
Department of Imaging Sciences
University of Rochester Medical Center Rochester, New York
John S. Pellerito, MD, FACR, FSRU, FAIUM
Professor of Radiology
Department of Radiology
Zucker School of Medicine at Hofstra/Northwell
Hempstead, New York
Vice Chairman
Department of Radiology
Northwell Health System
Manhasset, New York
Joseph F. Polak, MD, MPH, FACR, FAIUM
Professor of Radiology
Department of Radiology
Tufts University School of Medicine
Director
Ultrasound Reading Center
Boston, Massachusetts
Chief of Radiology
Department of Radiology
Lemuel Shattuck Hospital
Jamaica Plain, Massachusetts
Vasileios Rafailidis, MD, MSc, PhD, EDiR
Department of Radiology
AHEPA University General Hospital of Thessaloniki
Thessaloniki, Greece
Margarita V. Revzin, MD, MS, FSRU
Assistant Professor of Diagnostic Radiology
Department of Radiology and Biomedical Imaging
Yale School of Medicine
New Haven, Connecticut
E. Bernd Ringelstein, MD
Medical Faculty Department of Neurology University Hospital Münster Münster, Germany
Martin A. Ritter, MD Consultant Neurologist Chair, Department of Stroke Medicine Clemenshospital Münster Münster, Germany
Michelle L. Robbin, MD, MS Professor of Radiology and Biomedical Engineering
Chief of Ultrasound
Department of Radiology
University of Alabama at Birmingham Birmingham, Alabama
Kathryn A. Robinson, MD
Senior Associate Consultant, Diagnostic Radiology
Assistant Professor of Radiology
Mayo Clinic
Rochester, Minnesota
Deborah J. Rubens, MD
Professor of Imaging Sciences, Oncology, and Biomedical Engineering
Associate Chair for Academic Affairs
Department of Imaging Sciences
University of Rochester Medical Center
Rochester, New York
Leslie M. Scoutt, MD
Professor of Radiology, Surgery, and Cardiology
Vice Chair for Education
Medical Director, Non-Invasive Vascular Laboratory
Yale University School of Medicine
New Haven, Connecticut
Paul Sidhu, BSc, MBBS, MRCP, FRCR, DTM&H
Professor of Imaging Sciences
King’s College Hospital
London, Great Britain
Steven R. Talbot, RVT, FSVU
Co-Editor, Journal for Vascular Ultrasound
Research Associate
Division of Vascular Surgery
Technical Director, Vascular Laboratory
Cardiovascular Services
University of Utah Medical Center
Salt Lake City, Utah
R. Eugene Zierler, MD, RPVI, FACS
Medical Director
D. E. Strandness Jr. Vascular Laboratory
University of Washington Medical Center and Harborview Medical Center
Professor
Department of Surgery
University of Washington School of Medicine
Seattle, Washington
seCtIon 1
Basics
1 tHe HeMoDYnAMICs oF VAsCULAR DIseAse 2
JOSEPH F. POLAK, MD, MPH, AND JOHN S. PELLERITO, MD, FACR, FSRU, FAIUM
2 PRInCIPLes AnD InstRUMents oF ULtRAsonoGRAPHY 23
FREDERICK W. KREMKAU, PhD
3 DoPPLeR FLoW IMAGInG AnD sPeCtRAL AnALYsIs 56
JOHN S. PELLERITO, MD, FACR, FSRU, FAIUM, AND JOSEPH F. POLAK, MD, MPH
seCtIon 2
Cerebral Vessels
4 AnAtoMY oF tHe CeReBRAL stRUCtURe 84
JOSEPH F. POLAK, MD, MPH, AND JOHN S. PELLERITO, MD, FACR, FSRU, FAIUM
5 CARotID sonoGRAPHY: PRotoCoL AnD teCHnICAL ConsIDeRAtIons 96
JOSEPH F. POLAK, MD, MPH, AND JOHN S. PELLERITO, MD, FACR, FSRU, FAIUM
6 eVALUAtInG CARotID PLAQUe AnD CARotID IntIMA-MeDIA tHICKness 110
JOSEPH F. POLAK, MD, MPH
7 ULtRAsoUnD AssessMent oF CARotID stenosIs 139
CORINNE DEURDULIAN, MD, AND EDWARD G. GRANT, MD
8 HoW to Assess DIFFICULt AnD UnCoMMon CARotID CAses 162
JOHN S. PELLERITO, MD, FACR, FSRU, FAIUM, AND JOSEPH F. POLAK, MD, MPH
9
ULtRAsoUnD AssessMent oF tHe VeRteBRAL ARteRIes 183
JOSEPH F. POLAK, MD, MPH
10 ULtRAsoUnD AssessMent oF tHe IntRACRAnIAL ARteRIes 203
DARIUS G. NABAVI, MD, MARTIN A. RITTER, MD, AND E. BERND RINGELSTEIN, MD
seCtIon 3 extremity
Arteries
11 AnAtoMY oF tHe UPPeR AnD LoWeR eXtReMItY ARteRIes 236
JOHN S. PELLERITO, MD, FACR, FSRU, FAIUM, AND JOSEPH F. POLAK, MD, MPH
12
PHYsIoLoGIC testInG oF LoWeR eXtReMItY ARteRIAL DIseAse 250
MARSHA M. NEUMYER, BS, RVT, FSVU, FSDMS, FAIUM
13
AssessMent oF UPPeR eXtReMItY ARteRIAL DIseAse 274
JOSEPH F. POLAK, MD, MPH, AND STEVEN R. TALBOT, RVT, FSVU
14
ULtRAsoUnD eVALUAtIon BeFoRe AnD AFteR HeMoDIALYsIs ACCess 305
MICHELLE L. ROBBIN, MD, MS, AND MARK E. LOCKHART, MD, MPH
15
ULtRAsoUnD AssessMent oF LoWeR eXtReMItY ARteRIes 322
R. EUGENE ZIERLER, MD, RPVI, FACS, AND JOHN S. PELLERITO, MD, FACR, FSRU, FAIUM
16
ULtRAsoUnD AssessMent DURInG AnD AFteR CARotID AnD PeRIPHeRAL InteRVentIons 345
JOSEPH F. POLAK, MD, MPH, AND DENNIS F. BANDYK, MD
17 ULtRAsoUnD In tHe AssessMent AnD MAnAGeMent oF ARteRIAL eMeRGenCIes 370
BRIAN J. BURKE, MD, RVT, FACR, FAIUM
seCtIon 4
extremity Veins
18 eXtReMItY VenoUs AnAtoMY AnD teCHnIQUe FoR
ULtRAsoUnD eXAMInAtIon 390
JOHN S. PELLERITO, MD, FACR, FSRU, FAIUM, AND STEVEN R. TALBOT, RVT, FSVU
19 ULtRAsoUnD DIAGnosIs oF LoWeR eXtReMItY VenoUs tHRoMBosIs 418
JONATHAN D. KIRSCH, MD, ULRIKE M. HAMPER, MD, MBA, AND LESLIE M. SCOUTT, MD
20 RIsK FACtoRs AnD tHe RoLe oF ULtRAsoUnD In tHe MAnAGeMent oF eXtReMItY VenoUs
DIseAse 442
JOSEPH F. POLAK, MD, MPH, AND JOHN S. PELLERITO, MD, FACR, FSRU, FAIUM
21 ULtRAsoUnD DIAGnosIs oF VenoUs
InsUFFICIenCY 461
MARSHA M. NEUMYER, BS, RVT, FSVU, FSDMS, FAIUM
22 nonVAsCULAR FInDInGs enCoUnteReD DURInG
VenoUs sonoGRAPHY 483
JOHN S. PELLERITO, MD, FACR, FSRU, FAIUM
seCtIon 5
Abdomen and Pelvis
23 AnAtoMY AnD noRMAL DoPPLeR sIGnAtURes oF ABDoMInAL VesseLs 496
JOHN S. PELLERITO, MD, FACR, FSRU, FAIUM
24 ULtRAsoUnD AssessMent oF tHe ABDoMInAL AoRtA 509
JOSEPH F. POLAK, MD, MPH
25 ULtRAsoUnD AssessMent FoLLoWInG enDoVAsCULAR AoRtIC AneURYsM RePAIR 529
JOSEPH F. POLAK, MD, MPH, AND GEORGE L. BERDEJO, BA, RVT, FSVU
26 DoPPLeR ULtRAsoUnD oF tHe MesenteRIC VAsCULAtURe 547
MARGARITA V. REVZIN, MD, MS, FSRU, AND JOHN S. PELLERITO, MD, FACR, FSRU, FAIUM
27 ULtRAsoUnD AssessMent oF tHe HePAtIC VAsCULAtURe 582
WILLIAM D. MIDDLETON, MD, AND KATHRYN A. ROBINSON, MD
28
DUPLeX ULtRAsoUnD oF nAtIVe RenAL VAsCULAtURe 615
MARGARITA V. REVZIN, MD, MS, FSRU, AND JOHN S. PELLERITO, MD, FACR, FSRU, FAIUM
29
DUPLeX ULtRAsoUnD eVALUAtIon oF tHe UteRUs AnD oVARIes 654
JOHN S. PELLERITO, MD, FACR, FSRU, FAIUM
30
DUPLeX ULtRAsoUnD eVALUAtIon oF tHe MALe
GenItALIA 678
CAROL B. BENSON, MD
31 eVALUAtIon oF oRGAn tRAnsPLAnts 705
MAHAN MATHUR, MD, DANIEL C. OPPENHEIMER, MD, DEBORAH J. RUBENS, MD, AND LESLIE M. SCOUTT, MD
seCtIon 6 trends in Ultrasound Vascular Imaging
32 CReDentIALInG, ACCReDItAtIon, AnD QUALItY In tHe VAsCULAR LABoRAtoRY 748
HEATHER L. GORNIK, MD, RVT, RPVI
33 ULtRAsoUnD sCReenInG FoR VAsCULAR DIseAse 758
JOSEPH F. POLAK, MD, MPH
34 CoRReLAtIVe IMAGInG 779
JOSEPH F. POLAK, MD, MPH, AND JOHN S. PELLERITO, MD, FACR, FSRU, FAIUM
35 ULtRAsoUnD ContRAst AGents In VAsCULAR
DIseAse 804
VASILEIOS RAFAILIDIS, MD, MSc, PhD, EDiR, PHILLIP J. BENDICK, PhD, AND PAUL SIDHU, BSc, MBBS, MRCP, FRCR, DTM&H
Introduction to Vascular Ultrasonography
1 SECTION BASICS
THE HEMODYNAMICS OF VASCULAR DISEASE
Joseph F. Polak, MD, MPH, and John S. Pellerito, MD, FACR, FSRU, FAIUM
Overview
The human circulatory system is extremely complex. Blood flow is influenced by many factors:
1. The heart influences the strength and amount of ejected blood.
2. The elastic arteries store energy during systole and maintain blood flow during diastole.
3. The muscular arteries maintain tone.
4. The arterioles, capillaries, and the venules supply blood to the different organs.
5. The veins ensure adequate return of blood to the heart.
Introduction
At each level, anatomy and physiology contribute to a steady supply of oxygen by maintaining blood flow. Some of the factors responsible for this coordinated action can be measured and described in reasonably simple terms, but many others are complex and difficult to grasp.
Keeping these limitations in mind, this chapter presents a basic review of the dynamics of blood flow through the circulation, some of the factors that influence blood flow, and the hemodynamic consequences of arterial and venous occlusive disease. These considerations are helpful in understanding the normal physiology of blood circulation and the abnormalities that can occur in the presence of vascular obstruction.
Physiologic Factors Governing Blood Flow and Its Characteristics
Arterial and venous compartments
For blood flow to occur between any two points in the circulatory system, there must be an energy difference between these two points. Usually, this difference in energy levels is due to a blood pressure difference. The circulatory system generally consists of a high-pressure, high kinetic energy
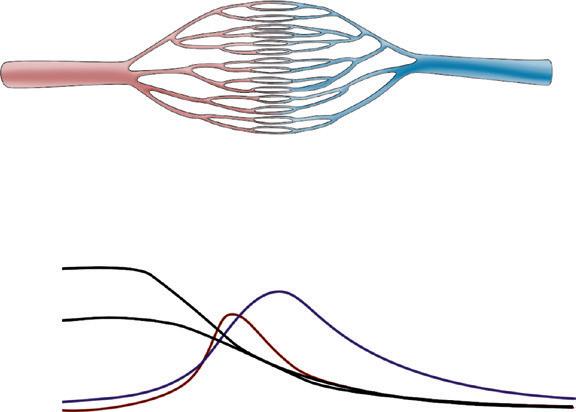
arterial reservoir and a large venous pool with low pressure and low kinetic energy. These reservoirs are connected by a system of distributing branch arteries and the microcirculation, which consist of arterioles and capillaries (Fig. 1.1).
As blood flows through the circulatory system, energy is continuously lost because of the friction between the layers of flowing blood. Both pressure and kinetic energy levels decrease as the red cells transit from the arterial to the venous system. The energy necessary for blood flow is continuously restored by the pumping action of the heart during systole, stored in the elastic wall of the aorta and large arteries, and released during diastole. The generated arterial pressure forces blood to move from the arterial system into the venous system and maintains the arterial pressure and the energy difference needed for blood to keep flowing.
The arterial system has high energy levels as a result of the large volume of rapidly flowing blood and the high pressure in the arterial reservoir. The pumping action of the heart and the mechanical characteristics of arteries work synergistically to maintain adequate volume, flow, and pressure in the arteries. This is in part achieved by maintaining a balance between the amount of blood that enters and leaves the arterial reservoir. The amount that enters the arteries during a cardiac cycle is the stroke volume. The amount that leaves depends on the arterial pressure and on the total peripheral resistance, which is controlled, in turn, by the amount of vasoconstriction in the microcirculation. Both can change from beat to beat.
Under normal conditions, blood flow to all the body tissues is adjusted according to the tissues’ particular needs at a given time. This adjustment is accomplished by local alterations in the level of arteriolar vasoconstriction within a given organ. Maintenance of normal volume and pressure in the arteries thus ensures the distribution of blood flow, and therefore oxygen delivery, to all parts of the body and helps regulate cardiac output.
Arterioles Arteries
Capillaries
Venules
Veins
FIG. 1.1 This diagram is a simplified representation of the relative differences in pressure, effective resistance, and overall vessel cross-luminal area at the different levels of the circulation. The curves on the bottom correspond to the respective levels of the circulation shown above. For example, the effective area of the circulation is greatest at the capillary level, whereas the resistance peaks in the small arteries and arterioles.
Potential and kinetic energy
The physical factors that govern how blood once ejected from the heart dissipates energy as it transits through the circulation are related to friction, resistance, and the influences of laminar and turbulent flow. The basic relationships between flow, pressure, and resistance as summarized by Bernoulli’s equation, Poiseuille’s law, and Poiseuille’s equation are discussed. The connecting vascular channels have intrinsic resistances that connect either in parallel or in series. These interconnections modulate how blood flows through the circulation.
The main form of energy stored in flowing blood is the potential energy due to the pressure distending the vessels. This is created by the pumping action of the heart. However, some of the energy stored in blood is kinetic and a direct function of its velocity. Usually, the kinetic energy component is small compared with the pressure energy, and under normal resting conditions, it is equivalent to only a few millimeters of mercury or less. The kinetic energy of blood is proportional to its density (which is stable in normal circumstances) and to the square of its velocity. In essence, over relatively straight arterial segments, the sum of kinetic (blood flow) and potential (blood
pressure) energy is constant. The equation that summarizes this relationship is Bernoulli’s equation (Fig. 1.2). If the artery lumen increases, kinetic energy is converted back into pressure (potential energy) as velocity decreases. Conversely, if the artery lumen narrows, the potential energy is converted into kinetic energy. Therefore within certain limits, important increases in kinetic energy occur in the systemic circulation when blood flow is high (e.g., during exercise) and in mildly stenotic lesions where luminal narrowing leads to increases in blood flood velocities. The effects of gravity due to differences in height of the blood vessel (the term ρgz in the equation) are normally neglected over short arterial segments especially if they are oriented along the horizontal plane.
Energy differences related to differences in the levels of body parts
There is a large variation in the potential energy of blood due to differences in posture. For example, in the standing position the pressure in the feet is increased by an amount that is proportional to the height of the column of blood resting on the blood in the legs. This hydrostatic pressure increases the transmural pressure and the distention of the vessels. Gravitational potential energy (potential for doing work related to the effect of
Vena cava
AB
FIG. 1.3 Blood flow velocity profiles across an arterial lumen. (A) This parabolic profile is typical of normal laminar flow. The velocity is maximal in the center of the artery and lowest near the artery wall and decreases toward the artery wall according to Eq. 1.1. (B) Flattened profile with a central core of relatively uniform velocity encountered at the site of a maximal stenosis. This flow profile is also maintained in the velocity jet before it dissipates. It is an idealized representation of blood flow because viscous forces will always impair the motion of red blood cells so that they are not moving at the same velocity.
Energy differences due to laminar flow
IDEALIZED STENOSIS
Energy of flowing blood is constant.
Bernoulli’s equation:
P + ½ ρV2 + ρgz = constant
P = Pressure
ρ = Density of blood
g = Acceleration due to gravity
z = Relative height of column of blood
V = Average blood flow velocity ––
FIG. 1.2 This diagram represents the complementary changes in potential and kinetic energy taking place at an idealized stenosis. Bernoulli’s equation indicates that as velocity increases the potential energy (pressure) of blood decreases. This idealized representation is not to scale and neglects viscous and inertial forces.
gravity on a free-falling body), however, is reduced in the dependent parts of the body by the same amount as the increase resulting from hydrostatic pressure. Therefore differences in the level of the body parts do not usually lead to changes in the driving pressure along the vascular tree unless the column of blood is interrupted, as may be the case when the venous valves close. Changes in energy and pressure associated with differences in height are noticeable with changes in posture or with activation of the calf pump muscles during walking.
As a hemodynamic approximation, blood flow is said to be laminar because blood flows in concentric layers or laminae. Each infinitesimal layer flows with a different velocity. In theory, a thin layer of blood is held stationary next to the vessel wall at zero velocity because of an adhesive force between the blood and the inner surface of the vessel. The next layer flows with low velocity, but its movement is delayed by the stationary layer because of friction between the layers, generated by the viscous properties of the fluid. The second layer, in turn, delays the next layer, which flows at a greater velocity. The layers in the middle of the vessel flow with the highest velocity and the basic physics underlying this effect are such that the mean velocity averaged across the vessel is half of the maximal velocity measured in the center. Because the rate of change of velocity is greatest near the walls and decreases toward the center of the vessel, a velocity profile in the shape of a parabola exists along the vessel diameter, and this type of blood flow is typically referred to as laminar flow (Fig. 1.3A).
Loss of energy during blood flow occurs because of friction, and the amount of friction and energy loss is largely determined by the dimensions of the vessels. In a small diameter vessel, especially in the microcirculation, even the layers in the middle of the lumen are relatively close to the wall and are thus delayed considerably, resulting in a significant opposition or resistance to flow
in that vessel segment. In contrast, the central core of blood is far from the walls in large arteries, and the frictional energy losses are less important. As indicated later, friction and energy losses increase if laminar flow is disturbed.
In a cylinder tube model of radius, R, the linear velocity, v, of blood flow in a given lamina located at a given radial distance, r, from the center is directly proportional to the pressure difference, ΔP, between the ends of the tube and the square of the radius and is inversely proportional to the length of the tube and the viscosity of the fluid. This is summarized by Poiseuille’s equation for velocity:
difference, ΔP, and the volume blood flow, Q, can be measured, and the resistance can thus be calculated as a systemic vascular resistance. Because resistance is equal to the pressure difference divided by the volume flow (the pressure difference per unit flow), it can be thought of as the pressure difference needed to produce one unit of flow and therefore can be considered as an index of the difficulty in forcing blood through vessels.
For volume flow, the equation can be integrated showing that volume flow, Q, is proportional to the fourth power of the vessel radius:
where Q is the volume flow; ΔP is the pressure difference between the proximal and distal ends of the tube; r and L are the radius and length of the tube, respectively; and η is the viscosity of the fluid.
Because volume flow is proportional to the fourth power of the radius, even small changes in radius can result in large changes in volume flow. For example, a decrease in radius of 10% would decrease volume flow in a tube model by about 35% and a decrease of 50% would lead to a 95% decrease in volume flow. Because the length of the vessels and the viscosity of blood do not change much in the cardiovascular system, alterations in volume blood flow occur mainly as a result of changes in the radius of the vessels and in the difference in the pressure energy level available for blood flow.
Poiseuille’s equation can be rewritten as follows:
Vessel Branching and Energy Dissipation. Poiseuille’s law applies to constant laminar flow of a simple Newtonian fluid (such as water) in a rigid tube of uniform diameter. In the blood circulation, these conditions are not fully met because blood is a nonnewtonian fluid and most vessels do not stay straight without branching. Instead, the resistance is influenced by the presence of numerous branch vessels with a combined effect similar to that observed in electrical circuits. In the case of vessels in series, the overall resistance is equal to the sum of the resistances of the individual vessels, whereas in the case of parallel vessels, the reciprocal of the total resistance equals the sum of the reciprocals of the individual vessel resistances. Thus, the contribution of any single vessel to the total resistance of a vascular bed, or the effect of a change in the dimension of a vessel, depends on the presence and relative size of the other vessels linked in series or in parallel.
In addition, deviations from the conditions to which Poiseuille’s law applies also occur in relation to changes in blood viscosity, which in turn is affected by hematocrit, temperature, vessel diameter, and rate of blood flow.
The resistance term, R, depends on the viscous properties of the blood and on the dimensions of the vessels. Although these parameters cannot be measured in a complex system, the pressure
Loss of Laminar Flow Patterns. Various degrees of deviation from orderly laminar flow occur in the human circulation. Minor factors responsible for these deviations include changes in blood flow velocity during the cardiac cycle as a result of acceleration during early systole and deceleration in late systole and diastole and alterations of the lines of flow due to small changes in the diameter of the vessel. Alterations in the blood flow profiles occur at curves (Fig. 1.4), at bifurcations (Fig. 1.5), at any branch point, and at stenotic lesions. Once altered, the laminar (parabolic) velocity profile is often not reestablished for a considerable distance. Instead, the velocity distributions can remain flattened within and just distal to stenotic lesions as plug flow (Fig. 1.3B), be skewed after