Intravascular Ultrasound FromAcquisitiontoAdvanced
QuantitativeAnalysis
EDITEDBY SIMONEBALOCCO
Elsevier
Radarweg29,POBox211,1000AEAmsterdam,Netherlands
TheBoulevard,LangfordLane,Kidlington,OxfordOX51GB,UnitedKingdom 50HampshireStreet,5thFloor,Cambridge,MA02139,UnitedStates
©2020ElsevierLtd.Allrightsreserved.
Nopartofthispublicationmaybereproducedortransmittedinanyformorbyanymeans,electronicormechanical,including photocopying,recording,oranyinformationstorageandretrievalsystem,withoutpermissioninwritingfromthepublisher.Detailsonhow toseekpermission,furtherinformationaboutthePublisher’spermissionspoliciesandourarrangementswithorganizationssuchasthe CopyrightClearanceCenterandtheCopyrightLicensingAgency,canbefoundatourwebsite: www.elsevier.com/permissions.
ThisbookandtheindividualcontributionscontainedinitareprotectedundercopyrightbythePublisher(otherthanasmaybenoted herein).
Notices
Knowledgeandbestpracticeinthisfieldareconstantlychanging.Asnewresearchandexperiencebroadenourunderstanding,changesin researchmethods,professionalpractices,ormedicaltreatmentmaybecomenecessary.
Practitionersandresearchersmustalwaysrelyontheirownexperienceandknowledgeinevaluatingandusinganyinformation,methods, compounds,orexperimentsdescribedherein.Inusingsuchinformationormethodstheyshouldbemindfuloftheirownsafetyandthe safetyofothers,includingpartiesforwhomtheyhaveaprofessionalresponsibility.
Tothefullestextentofthelaw,neitherthePublishernortheauthors,contributors,oreditors,assumeanyliabilityforanyinjuryand/or damagetopersonsorpropertyasamatterofproductsliability,negligenceorotherwise,orfromanyuseoroperationofanymethods, products,instructions,orideascontainedinthematerialherein.
LibraryofCongressCataloging-in-PublicationData AcatalogrecordforthisbookisavailablefromtheLibraryofCongress
BritishLibraryCataloguing-in-PublicationData AcataloguerecordforthisbookisavailablefromtheBritishLibrary
ISBN:978-0-12-818833-0
ForinformationonallElsevierpublications visitourwebsiteat https://www.elsevier.com/books-and-journals
Publisher: MaraConner
AcquisitionsEditor: TimPitts
EditorialProjectManager: FernandaA.Oliveira
ProductionProjectManager: KiruthikaGovindaraju
CoverDesigner: AlanStudholme
TypesetbySPiGlobal,India
Contributors
Theeditorwouldliketoacknowledgeandoffergratefulthanksfortheinputofallcontributors, withoutwhomthisfirsteditionwouldnothavebeenpossible.
SimoneBalocco
DepartmentofMathematicsandInformatics,University ofBarcelona,Barcelona;ComputerVisionCenter, Bellaterra,Spain
R.PawelBanys
DepartmentofRadiology,JohnPaulIIHospital; DepartmentofPhysicsandAppliedInformatics,AGH UniversityofScienceandTechnology,Krakow,Poland
StephaneCarlier
UMONS&CHUAmbroisePare,Mons,Belgium
XavierCarrillo
UniversityHospitalGermansTriasiPujol,Badalona, Spain
MariaElenadeCeglia InspireMD,Tel-Aviv,Israel
ZhiChen
ElectricalandComputerEngineering;IowaInstitutefor BiomedicalImaging,UniversityofIowa,IowaCity,IA, UnitedStates
FrancescoCiompi
DiagnosticImageAnalysisGroup,Pathology Department,RadboudUniversityMedicalCenter, Nijmegen,TheNetherlands
WladyslawDabrowski
JagiellonianUniversity,DepartmentofCardiac& VascularDiseases,DepartmentofRadiology,JohnPaul IIHospital,Krakow,Poland
StamatiaGiannarou
HamlynCenterforRoboticSurgery,ImperialCollege London,London,UnitedKingdom
JoanAntoniGomez-Hospital InterventionalCardiologyUnit,HospitaldeBellvitge, Barcelona,Spain
JosepLluísGómez-Huertas InspireMD,Tel-Aviv,Israel
AkiraIguchi TerumoCorporation,Tokyo,Japan
TomasKovarnik
SecondDepartmentofInternalMedicine,Charles University,Prague,CzechRepublic
Su-LinLee
EPSRCCenterforInterventionalandSurgicalSciences, UniversityCollegeLondon,London,UnitedKingdom
JurgenM.R.Ligthart ErasmusMC,Rotterdam,TheNetherlands
JohnJ.Lopez StritchSchoolofMedicine,LoyolaUniversity, Maywood,IL,UnitedStates
JosepaMauri
UniversityHospitalGermansTriasiPujol,Badalona, Spain
AdamMazurek
JagiellonianUniversity,DepartmentofCardiac& VascularDiseases,JohnPaulIIHospital,Krakow, Poland
PiotrMusialek
JagiellonianUniversity,DepartmentofCardiac& VascularDiseases,JohnPaulIIHospital,Krakow, Poland
RicardoÑanculef
FedericoSantaMaríaTechnicalUniversity,Valparaíso, Chile
EricA.Osborn
CardiovascularDivision,BethIsraelDeaconessMedical Center,HarvardMedicalSchool,Boston,MA, UnitedStates
LukaszPartyka
InspireMD,Tel-Aviv,Israel
PetiaRadeva
DepartmentofMathematicsandInformatics,University ofBarcelona,Barcelona;ComputerVisionCenter, Bellaterra,Spain
FernandoRamos
DepartmentofMathematicsandInformatics,University ofBarcelona,Barcelona,Spain
JosepRigla
DepartmentofMathematicsandInformatics,University ofBarcelona,Barcelona,Spain
JuanRigla
InspireMD,Tel-Aviv,Israel;DepartmentofMathematics andInformatics,UniversityofBarcelona,Barcelona, Spain;InspireMD,Boston,MA,UnitedStates
YukiSakaguchi TerumoCorporation,Tokyo,Japan
EliasSanidas DepartmentofCardiology,LAIKOGeneralHospital, Athens,Greece
YusukeSeki TerumoCorporation,Tokyo,Japan
MilanSonka
ElectricalandComputerEngineering;IowaInstitutefor BiomedicalImaging,UniversityofIowa,IowaCity,IA, UnitedStates
JustynaStefaniak
DataManagementandStatisticalAnalysis(DMSA), Krakow,Poland
LukaszTekieli
JagiellonianUniversity,DepartmentofCardiac& VascularDiseases;DepartmentofInterventional Cardiology,JohnPaulIIHospital,Krakow,Poland
GiovanniJ.Ughi
NewEnglandCenterforStrokeResearch,Departmentof Radiology,UniversityofMassachusettsMedicalSchool, Worcester,MA,UnitedStates
BeatrizVaquerizo
InterventionalCardiologyUnit,HospitaldelMar, Barcelona,Spain
AndreasWahle
ElectricalandComputerEngineering;IowaInstitutefor BiomedicalImaging,UniversityofIowa,IowaCity,IA, UnitedStates
KarenTh.Witberg ErasmusMC,Rotterdam,TheNetherlands
Guang-ZhongYang InstituteofMedicalRobotics,ShanghaiJiaoTong University,Shanghai,China
HonghaiZhang
ElectricalandComputerEngineering;IowaInstitutefor BiomedicalImaging,UniversityofIowa,IowaCity, IA,UnitedStates
LingZhang
ElectricalandComputerEngineering;IowaInstitutefor BiomedicalImaging,UniversityofIowa,IowaCity, IA,UnitedStates
LiangZhao CenterforAutonomousSystems,Universityof TechnologySydney,Ultimo,NSW,Australia
ClinicalUtilityofIntravascular Ultrasound
ELIASSANIDAS a ST EPHANECARLIER b aDepartmentofCardiology,LAIKOGeneralHospital,Athens,Greece, bUMONS&CHUAmbroisePare,
Mons,Belgium
1.INTRODUCTION
Coronaryangiographyremainsthegoldstandardimagingmethodforthedetectionofcoronaryarterydisease (CAD)anditswidespreadclinicalapplicationhas steeredpatientstoahostofbeneficialinterventional medicaltherapies.Nonetheless,thisapproachonlyprovidesatwo-dimensionalimageofthecontrast-filled arteriallumenanddoesnotvisualizethearterialwall wherelargestatheroscleroticplaquesarelocated.Consequently,angiographyoftenunderestimatesthedegree ofintraluminalstenosisanddoesnotgaugethesize oftheplaqueburdenitself.1
Currently,intravascularultrasound(IVUS)provides amoredetailedassessmentofCADandhasemerged asanessentialdiagnostictoolforunderstanding coronarylesionmorphology,deployingstents,and solvingpostpercutaneouscoronaryintervention(PCI) complications.
Historically,thefirstmedicalultrasoundapplication wasdescribedin1953byIngeEdlerandCarlHertz,who introducedtherecordingofthemotionpatternofcardiacstructuresalongasinglesoundbeam.Thistechnique,knownassupersonicreflectoscope,usedshort supersonicsoundpulsesthatweregeneratedbyanelectricallyexcitedquartzcrystalanddeliveredtotheheart. Partofthesoundwasreflectedbacktothequartzcrystal andthetimedifferencebetweentheemanationofthe soundpulseandthereceptionoftheechowasameasureofthedistancebetweenthecrystalandthereflectingmaterial.In1971,thefirsttrueIVUSsystemwas designedbyNicolaasBomandCharlesLanceeinRotterdam.Itwasconceivedasanimprovedtechniqueforthe continuousvisualizationofcardiacchambersandvalves byacatheterwith32elementswithanouterdiameterof
3mm.However,thefirsttransluminalimagesofhuman arterieswererecordedbyPaulYockin1988.2–4 IVUSisconsideredadiagnosticimagingmethodthat deliversreal-time,high-resolutionimagesofthecoronaryarteriesandprovidesaprecisedepictionofthe morphologyofatheroscleroticplaque.5 Itsrolebegins withpre-PCIimagingtargetedto(1)measurethediameterandtheareaofthelesion/referencesegment,(2) measurethelengthofthelesion,(3)evaluatethedistributionofplaqueandpresenceofcalcification,and(4) estimateinvivoplaquecompositionandburden,identifyingplaquecharacteristicsassociatedwithincreased vulnerability.6 Inordertofurtherguidepercutaneous procedures,IVUSwillalsobeperformedpoststenting inorderto(1)evaluatestentexpansion,(2)assessside branchcompromise,(3)assessthepresenceofcoronary dissection,and(4)determinethemechanismorstent restenosisorthrombosis(i.e.,underexpansion).7–9
Notably,2018ESC/EACTSGuidelinesonmyocardialrevascularizationrecommendtheuseofIVUSto detectstent-relatedmechanicalproblemsinleftmain coronaryartery(LMCA)asclassIIawithlevelofevidenceB.10 IVUShasalsobeenshowntobeanadjunctive imagingtechniqueforthecrossingofcoronarychronic totalocclusions(CTO),theperformanceofcomplex aortic,carotid,andperipheralarteryendovascularprocedureswithoutexcludingevenveinintervention.
2.BASICPRINCIPLESOFIMAGING ACQUISITION
Insummary,thefunctionofIVUSisbasedonthefollowinggeneralprinciples:
• conversionofelectricalenergyintosoundwavesvia piezoelectriccrystals;
• transmissionanddetectionofsoundwavesreflected bytissuesusingthesamepiezoelectriccrystals,the transducer,andconvertingbackthereceivedsound wavesintoanelectricalsignal;
• amplificationandprocessingofthiselectricalsignal andconversiontoanimage;
• projectionofthatimageonthedevice’scomputer screenfromwhereitcanbeanalyzedorstored.5
TherearetwotypesofIVUScatheters:themechanicallyrotatedsingle-elementtransducerandthesynthetic steeredphasedarraysystem(Fig.1).Themechanical catheterhasapiezoelectrictransducerplacedattheedge ofaflexibleshaftthatisrotatedandadvancedorwithdrawninordertoscanthearterywithinaprotective sheath.Thesystemsthathavebeenusedlatelyare high-definitiondevicesrunningatfrequenciesbetween 40and60MHz.The20-MHzsyntheticaperturearray catheterhas64tinytransducerspermanentlyembedded aroundthecircumferenceofthecatheteredge.Crosssectionalimagesareproducedusinganelectronically phased-arrayrotatingbeamformingwithoutanynecessarymechanicalrotationofthecatheterwhileadvanced orwithdrawnwithintheartery.11,12 Themainfeatures oftheIVUScathetersaresummarizedin Table1
Agray-scaleIVUSimageisformedfromacodificationofthelevelofechogenicityoftheradiofrequency signalthatisreflectedbythetissues.Signalswithlow echogenicityarecodedasdarkgrayorblack,while highlyechogenicsignalsarecodedaslightgrayorwhite. Thestrongestreflectionofultrasoundcomesfromcollagenandcalcium.Theadventitiaofthecoronaryarteries isveryrichincollagenandappearsasthebrighteststructureinanoncalcifiedsegment.Theexternalelasticlamina(EEL)isliesbetweentheadventitiaandthemedia, mostlymuscular,andtypicallyecholucent(dark).In normal,nonatheroscleroticarteries,thethicknessof themediaistypically200 μm.Theinternalelasticlamina(IEL)separatesthemediafromthemostinnerstructureoftheartery,theintima,coveredbyasinglelayerof endothelialcells.Intimalthicknessincreaseswithage anditistypically200 μmat40yearsofageproducing

FIG.1 TwotypesofIVUSimagingsystems.(A)Mechanical systemwitharotatingelement;(a)cross-sectionalimage providedbyamechanicalsystem(AtlantisSRProCatheter iLabUltrasoundImagingSystem).(B)Electronicsystemwith amultielementarray;(b)cross-sectionalimagegivenbyan electronicsystem(EagleEyeGoldCatheterS5System).
theclassicalthree-layerappearanceofanormalcoronaryarterybyIVUS.Intimalthickeningisthefirstpathophysiologicalchangerelatedtoatherosclerosis.With theaccumulationofplaque,intimaandIELtendto mergeandtheseparationfromthemediaisdifficult toassess.13,14
Thedefinitionsof “referencesegment” alongwiththe mostcommonmeasurementsusingIVUSarepresented in Table2.15
3.IVUSINCLINICALPRACTICE
Atherosclerosis,fromtheGreek ἀθηρα, ath^ era,meaning “gruel” and σκληρωσις,sclerosisor “hardening,” isby essenceadiseaseofthearterialwallwhilethelumenwill onlylatelybecompromised.16–18 Thus,anatheroscleroticlesioncanevolveduringyearswithoutanyclinical symptomorflowlimitation.Previousstudieshave reportedthatacoronaryangiographyperformedweeks beforeanacutemyocardialinfarctionrevealedthatat theculpritlesiontherewasonlyamildtomoderate degreeofstenosisinmorethanhalfofthepatients andassuchanangiogramdoesnotprovideadequate prognosticinformationconcerningfutureischemic events.19 Suchconclusionshavegivenrisetothenotion thatacuteischemicsyndromesaretheresultofhow “vulnerable” anatheroscleroticplaqueistorupture andarelessdependentonthedegreeofluminalstenosis.20 SeveralattemptsofIVUSsignalpostprocessing havebeenreportedtodetectsuchvulnerableplaques21–24;however,itisseldomusednowadaysina clinicalsetting.Ontheotherside,numerousstudies andmetaanalysescomparedtheclinicaloutcomes betweenIVUS-guidedandangiography-guidedstent implantationwiththelatestresultssupportingtheutilityofIVUStoguidecomplexPCIprocedures,yet remainingunderused25 (Table3).
3.1.IVUSinPercutaneousTransluminal CoronaryAngioplasty
IVUScouldimproveangiographicresultsbysafely upsizingthelargestballoonforangioplastyoncevessel remodelingwastakenintoaccount,asdemonstratedin theCLOUTtrial.26 UsingballoonssizedtotheEEL diameter,someadvocatedaggressivepercutaneous transluminalcoronaryangioplasty(PTCA)insteadof systematicstentimplantation.27 Nowadays,withthe adventofDESthatsolvedtheissuesof(1)latelumen losssecondarytonegativeremodelingpostballoon angioplasty,28 and(2)in-stentrestenosisprocess,such provisionalangioplastystrategiesbasedonIVUSor physiologicalmeasurements29 arenomoreconsidered.
TABLE1
MainFeaturesofAvailableIVUSCatheters.
Frequency20MHz20MHz45MHz45MHz40
Workinglength150cm150cm135mm135mm120mm155mm135mm135mm
Wirelumenlength24cm24cm23mm15mm15mm15mm16mm16mm
Maximumguide wire
Maximum pullbackspeed ManualManual1mm/s1mm/s10mm/s1mm/s1mm/s1mm/s
Flushing necessary NoNoYesYesYesYesYesYes
TABLE2
Definitionsof “ReferenceSegment” and MeasurementsbytheUseofIVUS.
Reference segmentDefinitions
Proximal reference
Thesitewiththelargestlumen proximaltothestenosisandwithin thesamesegment
DistalreferenceThesitewiththelargestlumendistal tothestenosisandwithinthesame segment
LargestreferenceThelargestsiteofdistalorproximal reference
Average referencelumen size
Measurements
Theaveragevalueoflumenatdistal andproximalreference
LumenCSATheareaboundedbylumenborder
Minimumlumen diameter
Maximumlumen diameter
Lumenarea stenosis
Plaqueplus mediaCSA
Theshortestdiameterofthelumen
Thelongestdiameterofthelumen
(ReferencelumenCSAminus minimumlumenCSA)/reference lumenCSA
EELCSAminuslumenCSA
PlaqueburdenPlaqueplusmediaCSAdividedby EELCSA
Superficial calcium
Theleadingedgeoftheacoustic shadowingappearswithinthemost shallow50%ofplaqueplusmedia thickness
DeepcalciumTheleadingedgeoftheacoustic shadowingappearswithinthe deepest50%ofplaqueplusmedia thickness
StentCSATheareaboundedbystentborder CSA,cross-sectionalarea; EEL,externalelasticlamina.
Ontheotherside,theimportanceofoptimallesion preparationbeforestenting,usingrotationalatherectomy,cuttingballoons,ornewerdevices,hasbeenidentifiedandIVUSisaveryimportantguidancetoolto assesstheresultsofthesetechniques.30,31
3.2.IVUSintheBareMetalStentEra
Intimalhyperplasiaisthemajorunderlyingmechanism ofbaremetalstent(BMS)restenosis.InBMS,percentage ofintimalhyperplasiavolumeaverages30%ofstent volumeandisconsistentlygreaterindiabeticsthanin nondiabetics.InBMSthatdonotrestenose,initialstudiesshowedthatintimalhyperplasiaremainsstableor regressesslightlyafter6monthsforaperiodofupto 2–3years.Nevertheless,morerecentquantitativeangiographicdataindicateatriphasicBMSluminalresponse characterizedbyearlyrestenosis,intermediate-term neointimaregression(from6monthsto3years),and latere-narrowing(beyond4years).32
MostoftheclinicaltrialsfromtheBMSera(suchas CRUISE,33 TULIP,34 DIPOL,35 AVID36)showedabeneficialeffectofIVUSinBMstenting,mainlybyachieving largeracutelumendimensionswhileavoidingincreased complications.32 TheMUSICtrial37 wasthefirststudy, followedbyasequenceofmanyotherslater,thatestablishedIVUScriteriaforoptimalstentimplantation. AccordingtotheproposedMUSICcriteria,excellent expansionisevidentwhentheminimumlumenarea (MLA)inthestentis >90%oftheaveragereference lumenarea.AlltheproposedcriteriaforIVUSoptimizationusedindifferentstudieshavereliedondistal referenceoronmeanreferencevesselforstentorpostdilatationballoonsizing.However,thisfactreduces thepotentialtooptimallyincreasethelumensizeparticularlyinlonglesionswithoverlappingstentsandinvesselswithdistaltapering.
AmetaanalysisofrandomizedtrialscomparingIVUS withangiographic-guidedBMSimplantation(n ¼ 2193 patients)showedthatIVUSguidancewasassociated withasignificantlylowerrateofangiographicrestenosis,repeatrevascularization,andoverallmajoradverse cardiacevents(MACE),buthadnosignificanteffect onmyocardialinfarction.38 Conversely,theresultsof theOPTICUStrialdidnotshowasignificantdifference betweentheangiographic-andIVUS-guidedgroupsnot supportingtheroutineuseofultrasoundguidancefor coronarystenting.39 Likewise,alargemetaanalysisthat includedfiverandomizedtrialsandfourregistrieswitha totalof2972patientsfoundthattheprimaryendpoint (occurrenceofdeathornonfatalmyocardialinfarction) wassimilarforbothstrategiesat6months.Pooleddata ofindividualcardiacendpointsshoweda38%reduced probabilityoftargetlesionrevascularization(TLR)in favorofIVUS-guidedstenting,whiledeath,nonfatal myocardialinfarction,orcoronaryarterybypassgraft wereequallydistributedinbothgroups.40
ClinicalEndPointsofStudiesandMetaanalysesThatComparedIVUSWithAngiographyGuidanceinPCI.
StudyYearPatientsFollow-up
Pariseetal.201121936–30months22%29%.0219%23%.0335%44%.5125%17%.18
Mudraetal.20015506–12months24.5%22.8%.68NANANANANANSNANA.12
Casellaetal.200329726months0.6%1%.215%18.7%.034.1%3.7%.50.6%0.6%1
Zhangetal.201219,61920.7 11.5 months NANA
Hongetal.2015132312monthsNANANA2.9%5.8%.007NANANA0.4%0.7%.48
Steinviletal.201631,2839–48monthsNANA <.001NANA <.001NANA <.001NANA <
Elgendyetal.2016319212–24months0.6%1.3%.046.5%10.3% <
Bavishietal.201732761.4 0.5years0.6%1.3%.156.5%10.5%.00012%2.4%.650.5%1.2%.09
Shinetal.2016117012months0.3%0.5%.320.4%1.2%.0400.4%.020.3%0.7%.134 Witzenbichler etal. 2014858312months0.6%1%.0033.1%4.7%.0022.5%3.7%.0040.8%1.2%.12
Maeharaetal.2018858624months0.55%1.16%.0034.9%7.5%.0033.5%5.6%.00061.7%2.4%.03
Zhangetal.2018144812months1.5%2.9%.072.9%5.4%.021%1.5%.340.71.4.19
NA,nonavailable; NS,nosignificant.
3.3.IVUSintheDrug-ElutingStentEra Drug-elutingstent(DES)implantationiscommonly associatedwithveryfewclinicalevents.IVUSpredictors associatedwithPCIfailuresandincreasedadverseoutcomeswithDESincludestentunderexpansion,nonuniformstrutdistribution,edge-relatedproblemssuchas residualreferencedisease(geographicmiss)anddissections,aswellasacuteand,especially,lateincomplete stentapposition(malapposition).9,41–45
Stentunderexpansionresultsfrompoorexpansion duringimplantationratherthanfromchronicstent recoilandmaybeundetectableangiographicallyin manycases;suspicionmayberaisedinanareaoffluoroscopicallyunderexpandedstentstruts(compared withtherestofstruts)inthecontextofacalcifiedlesion oraninabilitytofullyexpandtheballooninsidethe stent.Nevertheless,theuseofIVUScanbeinstrumental todetectunderexpansion;despitegoodappositionof thestentstrutstothevesselwall,theunderexpandedsite wouldbeevidentbyastentcross-sectionalareasignificantlysmallerthanthevesselcross-sectionalareainthe samesite,smallerthanthestentcross-sectionalareain othersites,andsmallerthanthereferencelumenarea. Accordingtoproposedstrictcriteria,excellentexpansionisevidentwhentheMLAinthestentis 90%of theaveragereferencelumenarea.44
Aconditionthatneedstobedifferentiatedfrom underexpansionisstentmalapposition;unlikeunderexpansion,therearestentstrutsnotapposedtothevessel wall(i.e.,spaceoccupiedbybloodcanbedetected betweenthestentstrutsandthearterialintima).Malappositioncannotbejudgedangiographically(exceptin veryfewextremecases),typicallyoccurswithuseof undersizedstentsorinarteriesthathavesignificanttortuosityandfluctuationsofreferencearteriallumen diameterwithinthetreatedsegmentandisthoughtto predisposetostentthrombosis.However,noassociationwasfoundbetweenearlyorlateincompletestent appositionandstentthrombosisin1580patients enrolledinIVUSsubstudiesofvariousTAXUSclinical trials.Becausebothmalappositionandunderexpansion affectselectedregionsofastent,itisentirelypossible thattheycoexistintwoseparatesitesofthesamestent (i.e.,proximalstrutscanbemalapposedowingtolarge andtortuousproximalreferencesites,whereasthemid stentareaattheoriginallesionsitecanbe underexpanded).44,46
WhetherIVUScomparedtoangiographyguidance reducesstentthrombosisandimprovesclinicaloutcomesassociatedwithDEStreatmenthasbeeninvestigatedovertheyears.Inametaanalysisof11clinical studies(n ¼ 19,619),IVUS-guidedDESimplantation
ascomparedwithangiography-guidancealonewas associatedwithareducedincidenceofdeath,MACE, andstentthrombosis.47 TheIVUS-XPLstudydemonstratedthatIVUS-guidedDESimplantationresultedin lowerrateofMACE(2.8%,HR,0.47[95%CI, 0.27–0.82]; P ¼ .007,perprotocolanalysis)compared toangiography-guidedstentimplantation(5.9%)at 1-yearfollow-upamong1323patientswithlongcoronarylesions,primarilyduetolowerriskofTLR.Inthe posthocanalysisofthepatientsoftheIVUS-guided group,thosewhodidnotmeettheIVUScriteriahada significantlyhigherincidenceofMACEcomparedwith thosemeetingtheIVUScriteriaforstentoptimization (4.6%vs1.5%;HR0.31[95%CI,0.11–0.86], P ¼ .02).ThesedatasupportstronglyIVUSguidancein suchlesions.48
Anupdatedmetaanalysisof7randomizedcontrol trialsand18observationalstudiesconfirmedtheabove dataandfoundthatIVUS-guidedPCIwasassociated withbetterclinicaloutcomesincludingMACE,mortality,stentthrombosis,TLR,andtargetvesselrevascularizationthanangiography-guidedDESimplantation. However,inaseparateanalysisthatincludedonlythe randomizedcontroltrials,theobservedbenefitfor MACEwasdrivenonlybyreducedratesofrevascularizations.49 Similarly,ametaanalysisofsevenrandomized trials(n ¼ 3192)showedthatIVUS-guidedPCIwas notinferiortoangiography-guidedPCIinreducing theriskofMACE(6.5%vs10.3%)mainlyduetothe reductionintheriskofTLR(4.1%vs6.6%).Therisk ofcardiovascularmortality(0.5%vs1.2%)andstent thrombosis(0.6%vs1.3%)werealsolowerinthe IVUS-guidedgroup.50
ADAPT-DESwasaprospective,multicenter, real-worldstudyof8583consecutivepatientsat11internationalcentersundergoingDESimplantationthat investigatedthefrequency,timing,andcorrelation betweenstentthrombosisandadverseclinicaloutcomes post-PCI.Duringtheindexprocedure,IVUSwasusedin 3349patients.IVUSperformanceresultedinlongerstent lengthandlargerstentsizewithoutincreasingperiproceduralmyocardialinfarction.ItwasshownthatIVUSguidanceledtolessstentthrombosis(0.6%vs1%)beginning atthetimeofimplantation,aswellasfewermyocardial infarction(2.5%vs3.7%)withinthefirstyear.51 ThebenefitsofIVUSguidancefurtherincreasedwithlong-term follow-upofupto2years.52
Currently,theULTIMATEtrialthatincluded1448 all-comerpatientswhowererandomlyassigned(1:1 ratio)toeitherIVUSguidanceorangiographyguidance beforeDESimplantationindicatedasignificantreductioninMACEat12-monthfollow-upinIVUS-guided
comparedtoangiography-guidedgroup(2.9%vs5.4%, respectively,HR:0.530;95%CI:0.312–0.901; P ¼ .019).IntheIVUSgroup,TVFwas1.6%forpatients withsuccessfulproceduresversus4.4%inpatientswho failedtoachievealloptimalcriteria(HR:0.349;95%CI: 0.135–0.898; P ¼ .029),namelyMLAinthestentedsegment >5.0mm2 or >90%oftheMLAatthedistalreferencesegments,plaqueburden5mmproximalordistal tothestentedgeis <50%,andnoedgedissection involvingthemediawithalength >3mm.53 Inthe all-comers,open-label,single-armSYNTAXIIstudythat investigatedtheimpactofastate-of-the-artPCIstrategy onclinicaloutcomesinpatientswithtriplevesseldisease,finalminimalstentareameasuredbyIVUSwas availablein819lesionsin367patients(53%oflesions, 81%ofpatients).ThesinglepostproceduralMSAvalue thatbestseparatedlesionswithTLRfromthosewithno TLRwas5.2mm2.54
Alargeregistryofmorethan6000patientsundergoingPCIwithDESforcomplexlesions(definedasbifurcation,chronictotalocclusion,leftmaindisease,long lesion,multivesselPCI,multiplestentimplantation, in-stentrestenosis,orheavilycalcifiedlesion)reported recentlythatIVUSguidanceleadtoasignificantlylower riskofcardiacdeathduring64monthsofmedian follow-up(10.2%vs16.9%withangiography-guided PCI;HR:0.573;95%CI:0.460–0.714; P < .001).55 With IVUS,theimplantedstentshadasignificantlylarger meandiameter(3.2 0.4vs3.0 0.4; P < .001)and weremorefrequentlypostdilatated(49.0%vs17.9%; P < .001).
4.IVUSAPPLICATIONS
Gray-scaleIVUSoffersonlyalimitedcharacterizationof theatheroscleroticplaquecompositionandisunableto detectthespecifichistomorphologicalfeaturesthatare associatedwiththeruptureofvulnerableplaques,namely alargeandlipid-richnecroticcore;athinandinflamed fibrouscap,richinmacrophages,thatcoversthenecrotic core;andneovascularization.56,57 Forthesereasons, novelIVUStechniquessuchasintegratedbackscatter IVUS(IB-IVUS),VH-IVUS,iMap-IVUS,near-infrared spectroscopy-IVUS(NIRS-IVUS),andcontrast-enhanced IVUS(CE-IVUS)havebeendeveloped.5,11
4.1.IB-IVUS
Atissueclassificationschemebasedonlyontheanalysis oftheintegratedbackscattered(IB)signal,usingasimplesurfacescanneroncarotidsampleswasprimarily describedin2001.58 Thismethodologywasdeveloped withtheintegrated,rotating,40-MHzIVUScatheter fromBostonScientific(Fremont,California,United
States).IB-IVUSwasappliedto18samplesofcoronary arteryandtheresultswerecomparedwiththecorrespondinghistologicalfindings.TheresultingIB-IVUS valuesweredividedintofivecategoriessothatcoded colormapscouldbeconstructed:thrombus,intimal hyperplasiaorlipidcore,fibroustissue,mixedlesions, andcalcification.TheinitialcomparisonsbetweenangiographyandIB-IVUSshowedthattheangioscopically coloredsurfaceoftheplaquereflectedthethicknessof thefibrouscapmorethanthesizeofthelipidcore.59 InitiallydevelopedwiththeBostonScientificClearview system,IB-IVUS(IB-IVUS,YDCo,Ltd.,Nara,Japan)is nowusedwiththeVISIWAVEplatformfromTerumo (Tokyo,Japan).WiththeViewIT40-MHzcatheter (Terumo,Tokyo,Japan),acomparisonofIB-IVUSwith histopathologyshowsthatthesensitivityintheclassificationofcalcification,fibroustissue,andlipidswas 90%,84%,and90%,whilespecificitywas97%,96%, and86%,respectively.60
4.2.VH-IVUS
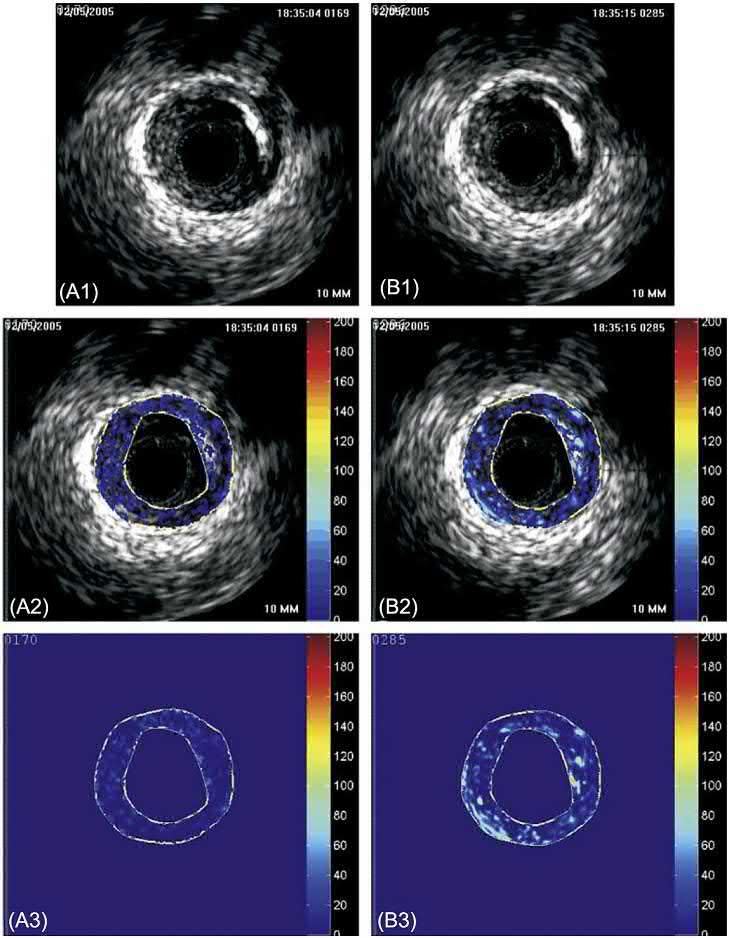
VH-IVUSallowstissuecharacterizationofvascular lesionsandisbasedonthespectralanalysisoftheprimaryrawbackscatteredultrasoundwave (radiofrequency-basedsignal).Thismethodhasanestimatedaxialresolution(basedontheresolutionofthe 20-MHzIVUScatheter)ofapproximately200 μm (Table4).Thespectralsignaturesoffourtissuetypes (fibroustissue,fibrofattytissue,necroticcore,anddense calcium)weredeterminedinvitro.21 Thesesignatures areprogrammedinthesoftwareoftheIVUSconsole oronastand-alonesoftwarepackageforoff-lineanalysisofpatientdata.Radiofrequency-IVUSplaquecomponentsarecolorcodedasdensecalcium(white),necrotic core(red),fibrofatty(lightgreen),andfibroustissue (darkgreen).61,62 Correlationbetweengray-scaleand VH-IVUSimagingisshownin Fig.2
ExvivovalidationofVHimagesdirectlywiththehistopathologysectionsprovidedaccuraciesofupto97%. Independentstudieshavedemonstratedinvivoarelativelyhighlevelofaccuracyandreproducibilityof VH-IVUSinhumanarteriesutilizingdirectionalcoronaryatherectomyspecimens,yieldingpredictiveaccuraciesofupto95%innonacutecoronarysyndrome(ACS) patients.61 Ofnote,suchasequentialassessmentis impactedbypreciseco-registrationofthehistologictissuesampleandtheimaging.Inadultatherosclerosisproneminipigs,nocorrelationwasobservedbetween thesizeofthenecroticcoredeterminedbyVH-IVUS andhistology.63
ThePROSPECTtrialtriedtoassessthenaturalhistory ofatherosclerosisbystudying697patientswithACS
TABLE4
DetectionandTechnicalParametersofIVUS andVH-IVUS.
IVUSVH-IVUS
Detection
Lipid/necroticcore+++
Fibrouscap++++
Thrombus+No
Calcium++++++
Plaquerupture++No
Attenuatedplaque+++No
TCFA(thin-capfibroatheroma)No++
Dissection++No
Stentexpansion/apposition++No
Stentstrutcoverage++
Technicalparameters
Frequency(MHz)20–4520–45
Framerate10–3010–30
Pullbackspeed(mm/s)0.5–10.5–1
Axialresolution(μm)70–20070–200
Tissuepenetration(mm) >5 >5
Easeofuse+++++
NeedforcontrastNoNo
Notes:+:Limitedpossibilitiesonly;++:wellsuited;+++:excellent.
aftersuccessfulPCIofaculpritlesionunderoptimal medicaltherapyusingangiographyplusthree-vessel imagingincludinggrayscaleandVH-IVUS.Inpatients withACS,bothculpritandnonculpritlesionswere equallylikelytospursubsequentadverseeventssuch ascardiacdeath,cardiacarrest,myocardialinfarction, orrehospitalizationduetounstableorprogressive anginaover3years.Independentpredictorsofafuture cardiovasculareventwereplaquesclassifiedas VH-TCFAs(fibroatheromawithoutevidenceofafibrous cap: >10%confluentNCwith >30° NCabuttingthe lumeninatleastthreeconsecutiveframes)withaplaqueburden >70%andanMLA <4mm2 64
Similarly,theVIVAstudywasaprospectiveanalysis of170patientswithstableanginaorACSwhounderwentthree-vesselVH-IVUSbeforeandafterPCI.Ata medianof1.7years,19lesions(13nonculpritand6culprit)resultedinmajoradversecardiacevents(MACE includingdeath,myocardialinfarction,unplanned revascularization).Nonculpritlesionfactorsassociated withnonrestenoticMACEwereVH-IVUSthin-capped fibroatheroma(TCFA),plaqueburden >70%,and MLA <4mm2 suggestingthatVH-IVUScanidentifyplaquesatanincreasedriskofsubsequentevents.65 More recently,afterameanfollow-upof51 6monthsof 86patientswith89intermediatelesionsdefinedas 30%–70%stenosisincoronaryangiography,MACE werefoundtobesignificantlyrelatedtoangiographic diameterstenosis,fibrofattyarea(FFA)butnotnecrotic core,IVUSplaqueburden 70%,andareastenosis
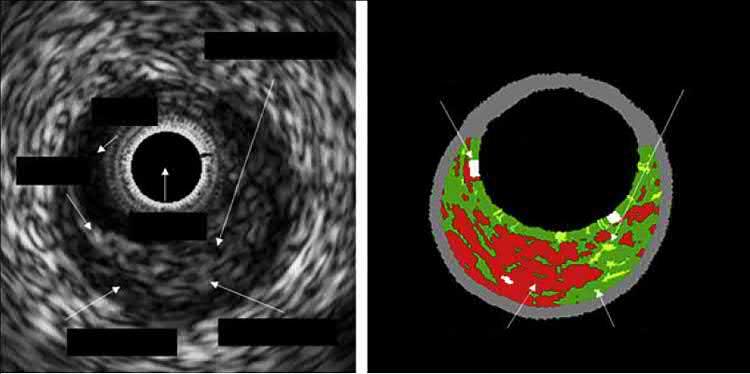
FIG.2 Correlationbetweengray-scaleIVUSandVH-IVUSimaging.Thesetwocross-sectionalframesdepict thesamearteriallocationandallowvisualizationofasignificanteccentricatheroscleroticplaque.Gray-scale IVUS (left) caneasilyidentifylumenandplaqueborders,butVH-IVUS (right) providesadditionalinformation regardingthecompositionalplaquecharacteristics.
Calcium
Fibro-fatty tissue
Lumen
Necrotic core
Fibrous tissue
Necrotic core
Catheter
Calcium
Lumen
Fibro-fatty tissue
Fibrous tissue
50%.Inamultivariableanalysis,onlyFFAwasindependentlyassociatedwiththeoccurrenceofMACE (HR1.36,95%CI1.05–1.77, P ¼ .019).66 ThedifferentialpredictivevalueoftheIVUS-VH-derivednecrotic coreorfibrofattycomponentsamongdifferentstudies illustratesthechallengesofIVUS-derivedtissuecharacterization,fromthereliabilityofthetrainingdatasetto thecomplexityoftherecognitionalgorithms67 with underestimatedissuesinitiallysuchasthelackof enoughultrasoundsignalforanyspectralanalysis behindcalcifiedlesions.68
4.3.iMap-IVUS
Withthissoftware,resultsarepresentedinawaysimilar totheVH-IVUSsystem.However,therearedifferences: itisbasedonafullspectrumanalysisandtheapplied colorschemeshows(i)fibroustissueinlightgreen, (ii)lipidtissueinyellow,(iii)necroticcoreinpink, and(iv)calciuminblue.23 Furthermore,theapplied IVUScatheterisa40-MHzrotatingsingle-elementcatheterinsteadofthe20-MHzmechanicaloneusedin VH-IVUS.Exvivovalidationdemonstratedaccuracies atthehighestlevelofconfidence(97%,98%,95%, and98%fornecrotic,lipid,fibrotic,andcalcified regions,respectively).69,70 Inastudyof87patients, iMapanalysisshowedthattheACSlesionshadlarger lipidicandnecroticcomponentscomparedtononACSlesions.71 Among63patientswithST-segment myocardialinfarction(STEMI),iMap-IVUSdetecteda higherpercentageofnecrotictissueinculpritlesions thatremainedhighafter10monthswhereastheproportionoflipidictissuedecreased.72 Itcanalsopredictslow flow,aseriouscomplicationofPCIthatiscorrelated withpoorprognosis.73 Finally,iMapevaluatesthe neointimaltissueafterstentplacementprovidingadditionalinsights.74
4.4.NIRS-IVUS
Infraredregionisthemostreliableforthedocumentationofcomplexmoleculesbecauseeachbondvibration contributestoafingerprintofthemolecule.Identificationofalipidcoreplaque(LCP)isbasedonthedistinctionofcholesterolspectralfeaturesdifferentiating cholesterolfromtheotherchemicalspresentandespeciallycollagen.TheNIRS-IVUSsystemprovidesrealtimechemicalmeasurementsinthecoronaries.It includesaconsole,apullbackmotorunit,arotation device,andacatheterthatautomaticallyscanstheartery likeIVUS.Spectraareprocessedbyaspecificalgorithm trainedinvitro75 anddisplayedasachemicalimageof lipid-richplaqueprobability(calledthe “chemogram”), whichisdepictedasyellow(Fig.3).Thesystemacquires
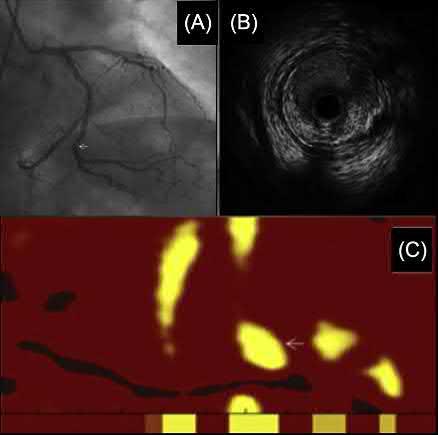
Multimodalityassessmentinthecatheterization laboratory.Anintermediateangiographiclesionlocatedatthe distalLCX(A).TheMLAmeasuredbyIVUSwas4.0mm2 and theplaqueburden63%(B).Therelatedchemogramshows yellowareas indicatinglipidcoreplaque(C).Physiologic lesionassessmentafterintravenousadministrationof adenosinedemonstratedafractionalflowreserve(FFR)of 0.80.Thelesionwasfinallytreatedwithadrug-elutingstent (DES).
1000measurements/12.5mmandeachmeasurement interrogates1–2mm2 oflumen.TheavailableLipiScan IVUS(InfraReDx,Inc.,Burlington,Massachusetts, UnitedStates)combinesa40-MHzrotationalIVUS imagingsystemalongwiththeNIRSadvancedtechnology.Thisallowsacompletevisualizationofcoronary structureandplaquemorphologytogetherwitha detailedchemicalmapofthevesselforthesimultaneousdetectionandlocalizationofLCP.61
NIRS-IVUSishighlyaccurateindetectingLCPin humancoronaryarteriesandshowtheexistenceand distributionofnecroticcore,butnottheamountor thefibrouscapthickness.Increasingevidenceislinking LCPtovulnerableplaque,lesionsatriskforembolization,andstentthrombosis.Aspartofacontinuinggoal tounderstandthelinkagebetweenNIRsignalsindicatingthepresenceofalipid-richplaqueandsubsequent coronaryevents,theCOLORregistryshowedthatthe absenceofalipid-richplaqueisassociatedwithgood prognosis.Inparticular,PCIperformedinlesionswith largelipidcorewascorrelatedwitha50%riskofperiproceduralmyocardialinfarctioncomparedwithonly a4.2%riskinlesionswithoutlargelipidcore.76
FIG.3
TheCANARYstudyaimedtoevaluatecriteriafor definingLCPthatisathighriskofrupturingduring standard-of-caretherapyandcausingintraprocedural complicationssuchasdistalembolization.According tothisstudy,plaquesresponsibleforperiprocedural myonecrosiswerelipidrichandhadalargeplaqueburdenandasmallMLA.However,nonlipidrichplaques couldevokeasubstantialproportionofmyocardial infarction.77
Finally,theLRPstudyisaprospective,multicenter trialthatwasdesignedtoinvestigatethecorrelation betweenLCPandtheoccurrenceofMACE.Itincluded 1563patientswithsuspectedCAD(46.3%stable angina)thatunderwentangiographyandpossiblyPCI foranindexevent.Allthepatientswereevaluatedwith IVUS-NIRStoassessthevesselstructureandtheplaque compositionandwerefollowedfor2years.Accordingto thistrial,theriskforanonculpritorunstentedMACE eventwas18%higherwitheach100unitincreasein maxLCBI4mm(maximumlipidburdeninany4mm subsegment).However,theriskincaseofavulnerable coronarysegmentwas45%higherwitheach100unit increaseinmaxLCBI4mm.Ofnote,theriskinacoronarysegmentwithamaxLCBI4mm >400was422% higherthanasegmentwithalessermaxLCBI4mm.78
4.5.Contrast-EnhancedIVUS
Neovascularizationinanatheroscleroticplaquehas beenlinkedtoplaquegrowthandinstabilityand contrast-enhancedIVUS(CE-IVUS)isaproposed methodforthedetectionofvasavasorum(VV),the microvesselsthatnourishthevesselwalls.CE-IVUSis basedontheinfusionofcontrastmicrobubbles,which cancauseanincreaseintheechogenicityofselected regionsontheIVUSimagesthatincludeatheromatous plaques.Itisabletorecordqualitativelyandquantitativelytheflow(presence)ofmicrobubblesinhuman atheroscleroticplaques,mainlywithinthemicrovessels andneovasculatureusingspeciallydevelopedsoftware forthispurpose(Fig.4).79–82
Theperivascularnetworkwasexaminedusing CE-IVUSinananimalstudythataimedtodetectblood flowintothecoronarylumenandperivascularflow. Astatisticallysignificantenhancementwasfoundin theechogenicityofthetotalperivascularspace(adventitialregionandperivascularvessels),asindicatedbyan increaseingraylevelintensityaftermicrobubbleinjection.83 Arecentlypublishedstudyalsoshowedthat CE-IVUSimagescoulddetectaorticwallneovascularizationinrabbitsbeinginagreementwithhistological data.84
TheimplementationofthismethodinACSpatients demonstratedthatCE-IVUSimagescouldshedlighton theneovascularizationoftheadventitiaandwithinthe atheroscleroticplaqueregion.Hence,CE-IVUScanprovideimportantinformationconcerningthepresenceof avulnerableplaqueandcardiovascularrisk stratification.81
5.IVUSASSESSMENTOFPLAQUE PROGRESSION
UltrasoundwavesfromIVUScatheterscantraveldeep enoughtoimagecompletelythethickenedatheroscleroticvesselwallandstudyatherosclerosisprogression.1 SeveralstudieshaveindicatedthevalueofIVUSinevaluatingplaquevolumeregressionovertimeusingdifferenttreatment.TheIVUS-derivedrateofprogressionof atheroscleroticburdenisasurrogateendpointthat couldreflectthebeneficialclinicalimpactoftheinvestigatedtherapies.
Earlyreportshavedescribedareductioninthelipoid componentsandanincreaseinfibroustissueafterstatin therapy.85 TheREVERSALtrialwasthefirstdoubleblindrandomizedmulticenterstudythatdemonstrated adifferenceintheeffectsoftwostatins(atorvastatinvs pravastatin)administeredfor18months.86 TheIVUSderivedchangeinatheromavolumeshowedasignificantlylowercoronaryplaqueprogressionrateinthe atorvastatingroup.TheESTABLISHtrialthatincluded ACSpatientsshowedthataggressivelipid-loweringatorvastatintherapydecreasedsignificantlytheplaquevolumeafter6-monthfollow-up,positivelycorrelated withtheLDLlevel.87 Themostimportantchangesin IVUSmeasurements(progressionandregression)were seenintheASTEROIDtrial.Amongpatientswithan ACSorstableCADwhoreceivedintensivetherapywith rosuvastatin,LDLleveldecreasedby53%whilemean percentageatheromavolumefortheentirevesselwas lowerby1% 3%.88
IVUSplaqueregressionhasbeenalsoinvestigated withothertherapiessuchasezetimibeandPCSK9 inhibitors.ThePRECISE-IVUSstudyrevealedagreater plaqueregressioncombiningezetimibewithstatins probablyduetothemostaggressivelipid-lowering effectbecauseoftheinhibitionofcholesterolabsorptionbyezetimibe.89
Additionally,theGLAGOVtrialshowedthatamong 868patientswithCAD,theadditionofevolocumabto statintherapyresultedinasignificantdecreaseinLDL-C levels(93.0vs36.6mg/dL)andtheprimaryefficacy parameter,thenominalchangeinpercentatheroma
FIG.4 CE-IVUS.AnalysisofanimageobtainedbyIVUSusingtheACESsystem,before(A)andafter(B)the infusionofcontrastmicrobubbles.(1)InitialIVUSimage;(2)IVUSimagefromtheregionoftheplaqueunder analysis;and(3)resultofprocessingwithouttheoriginalimage.
volume(PAV),increased0.05%withplaceboand decreased0.95%withevolocumab(difference, 1.0% [95%CI, 1.8%to 0.64%]; P < .001).ThisPCSK9 inhibitorbyfurtherreducingLDLcholesterolinduced plaqueregressioninagreaterpercentageofpatients thanplacebo(64%vs47%; P < .001forPAV).90
Nevertheless,intheGLAGOVRF-IVUSsubstudy,there wasnosignificantchangeinplaquecompositionsuch ascalcium,fibrous,fibrofatty,ornecroticcoretissues betweenthetwogroups.91 Lastbutnotleast,theODYSSEYJ-IVUSisanongoingprojectthatwasdesignedto investigatetheeffectofalirocumabcomparedtostatin
monotherapyoncoronaryatheroscleroticplaquevolumeinJapanesepatientswitharecentACSand hypercholesterolemia.92
6.IVUSINCOMPLEXCORONARYLESIONS
Sincetheintroductionofthesecond-generationDES, therateofPCIfailurehasmarkedlydecreased.Nevertheless,theissueofadequatestentimplantation becomesevenmoreimportant,especiallyinregardto complexcoronarylesionssuchasLMCAdisease,multivesseldisease,longlesions,coronarycalcification,and CTO.61
Inpatientswithcomplexlesions(i.e.,bifurcations, longlesions,CTOs,orsmallvessels),treatedexclusively withDES,theuseofIVUSintheAVIOtrialdemonstratedabenefitinMLAafterstentingwhencompared toangiographyalone.Nevertheless,nostatisticallysignificantdifferencewasfoundinMACEupto 24months.93 TheefficacyandsafetyofIVUS-guided PCIinpatientswithcomplexcoronarylesions,treated withDES,wasalsoinvestigatedinanothermetaanalysis ofeightrandomizedtrials(n ¼ 3276)thatindicatedthe superiorityofIVUS-guidedinterventions.Patients undergoingIVUS-guidedPCIhadsignificantlylower riskforMACE,TLR,andtargetvesselrevascularization. Nonetheless,therewerenosignificantdifferencesfor stentthrombosis,cardiovasculardeath,orall-cause mortalitybetweenthetwogroups.94 Ametaanalysisof threerandomizedtrialsincluded2345patientswith longlesionsorCTOsalsodemonstratedthatinayear postprocedureMACEhadoccurredin0.4%ofthe patientswhounderwentIVUS-guidednewgeneration DESimplantationcomparedto1.2%ofthosewho underwentangiography-guidedimplantation.95
Arecentlypublishedstudythatincluded6005 patientswithatleastonecomplexlesion(bifurcation, CTO,LMCAdisease,longlesion,multivesselPCI,multiplestentimplantation,in-stentrestenosis,orheavily calcifiedlesion)confirmedthebeneficialeffectsof IVUS-guidedPCIcomparedwithangiography-guided PCI.PatientswithIVUSguidancehadasignificantly largermeanstentdiameter,longerstentlength,and morefrequentuseofpostdilatationcomparedtothose withangiographyguidance.Moreover,inIVUS-guided group,theriskofall-causemortality,myocardialinfarction,stentthrombosis,andMACEwassignificantly lower.Ofnote,thegreatestbenefitofIVUSguidance wasobservedinpatientswithLMCAdisease,although favorableoutcomeswereidentifiedinmostcomplex coronarylesions.55
6.1.LeftMainCoronaryArteryLesions
Leftmaincoronaryartery(LMCA)lesionshaveproven tobenotoriouslydifficulttobeaccuratelyevaluated byangiographyalone.Angiographicappraisalofleft maindiseasecorrelatesverypoorlywithIVUSandfractionalflowreserve(FFR)determinationsoflesionseverity.Thisisrelatedtohighintra-andinterobserver variabilityaswellastheangiographicunderestimation ofleftmaindimensions.Moreover,theextentofleft mainbifurcationplaqueburdenbyIVUSinfluences PCIoutcomeand,ingeneral,PCIofdistalleftmain bifurcationlesionsarerelatedtopoorerprognosis.IVUS isveryusefulindistinguishingsignificantfrominsignificantleftmaindisease,depictingthedistributionofplaqueandplanningtheappropriatetreatmentstrategy.61 Indeed,among115patientswithangiographically intermediateLMCAstenosis,fewerthanhalfhadsignificantstenosesinIVUSevaluation,especiallyforlesions locatedattheleftmainostium.96
Severalstudieshavedifferedovertheyearsregarding thecutoffvalueoftheIVUS-derivedMLAthatissuggestiveofasignificantLMCAstenosis.Among121patients withangiographicallynormalLMCAsthatwereevaluatedwithIVUS,thedeferralofrevascularizationincase ofanMLA 7.5mm2 seemedtobesafe.Furthermore, basedonclinicallong-termoutcomes,thebestcutoff oftheMLAforperformingordeferringrevascularization was9.6mm2 97 Anotherstudyof55patientswithan angiographicallyambiguousLMCAstenosisshowed thatanMLAof5.9mm2 had93%sensitivityand95% specificityfordeterminingasignificantLMCAstenosis asdefinedbyafractionalflowreserve(FFR) <0.75.98 KoreanauthorshavesuggestedthatinisolatedLMdisease,anIVUS-derivedMLA <4.5–4.8mm2 intheir populationswasusefulforpredictinganFFR <0.80.99,100 However,differencesbasedonethnicity mustbetakenintoaccount:astudycomparedcoronary LMlesionsbetween99whiteNorthAmericanand 99Asianpatientsmatchedonbasisofage,gender, anddiabetesmellitusanddemonstratedthatAsian patientshadasignificantlysmallerLM-MLA (5.2 1.8mm2 vs6.2 1.4mm2; P < .0001).101
GiventheuniqueprognosticimplicationsofLMCA disease,theEuropeanBifurcationClubrecommends usingathresholdMLAcutoffof6mm2 toindicatean LMCAlesionthatshouldbetreatedwithrevascularizationinaEuropeanpopulation.102 Datafrompatients withintermediateLMCAlesionshowedsimilarlongtermresultswhenFFR > 0.8orMLA > 6mm2 wereused todeferrevascularizationcomparedtopatientswith FFR < 0.8treatedwithrevascularization.103
In2011,themulticentricLITROstudyvalidatedthe MLAin354patientsincludedin22centers.LMCA lesionwasrevascularizedin91%(152of168)ofthem withMLA < 6mm2 whileitwasdeferredin96%(179of 186)withMLA 6mm2.After2-yearfollow-up,cardiac death-freesurvivalratewas95%intherevascularized groupversus98%inthedeferredgroupwhereas event-freesurvivalratewas81%versus87%, respectively.104
IntheMAIN-COMPAREregistry,975patientsunderwentunprotectedleftmainstenting;ofthose,756had IVUSguidanceand219didnot.Inparticular,thecomparisonbetween145equivalentmatchedgroupsof patientswhoreceivedDESshowedthatIVUSguidance inleftmainPCIwasassociatedwithreducedlong-term myocardialinfarctionandmortality.Accordingtothe samedata,theoptimalminimumstentareainleftmain lesionstopreventTLRwas8.7mm2.105
IntheEXCELIVUSsubstudy,thepost-PCIminimum stentareawas9.9 2.3mm2 andwasstronglycorrelated withadverseeventssuchasdeath,myocardialinfarction,andstentthrombosisduringthe3-yearfollowup. 106 IVUSwasalsoperformedpre-PCIin270(47%) andpost-PCIin430(74%)of580PCI-treatedpatients withLMCAlesionsintheNOBLEtrialwhichsuggested thatcoronaryarterybypassgrafting(CABG)mightbe betterthanPCIforthetreatmentofLMCAdisease.107 However,therearenumerousongoingtrialsthatare expectedtoshedlightonthemanagementofpatients withLMCA.108
6.2.OtherCoronaryLesions
ThefirstreportshowingthatanIVUS-derivedminimal lumenarea(MLA) >4mm2 wascorrelatedwithacoronaryflowreserve 2waspublishedin1998.109 After 1year,anMLA < 4mm2 wasfoundtobeassociatedwith ischemiaonscintigraphy.110 Currently,availabledata indicatethattheMLAthresholdsuggestiveofmyocardialischemiarangefrom2.1to4.4mm2.Nevertheless, thisindexhashighnegativepredictivevalueandpositivepredictivevalueindicatingthatitissurelysafeto defertheinterventionofalesionwithMLA > 4mm2. However,usingthecutoffofMLA < 4mm2 toperform aPCIcouldleadtotreatmentof50%oflesionswithout ischemia.111 Among300patientswithadeferredrevascularization,becauseMLA > 4mm2,theMACEratewas only4.4%andtheTLRratewas2.8%at1-yearfollowup. 112
Ontheotherhand,theFFR,whichisaninvasive physiologicalindexthatpredictscoronarystenosisinducedischemia,hasbeenextensivelyvalidated againstnoninvasiveischemiatestinganddiscriminates
ischemicandnonischemiclesionswithanaccuracyof 95%.61 AccordingtoastudythatevaluatedeitherFFR orMLAin167consecutivepatientswithintermediate coronarylesions,atotalof94lesionsweredetectedin theIVUSguidancearmwhile83lesionsintheFFR group.TheIVUS-guidedgroupunderwentrevascularizationtherapysignificantlymoreoften,butat1-year follow-up,nosignificantdifferencewasfoundinMACE ratesbetweenthetwogroups.113
Moreover,inatotalof692consecutivepatientswith 784coronarylesionsthatwereevaluatedbyIVUSand FFRbeforeintervention,thebestcutoffvalueofMLA forpredictingFFR < 0.8was2.4mm2 withsensitivity 84%andspecificity63%.Inthesubgroupanalysis, theMLAcutoffwas2.4mm2 fortheleftanteriordescendingcoronaryartery,1.6mm2 fortheleftcircumflex coronaryartery,and2.4mm2 fortherightcoronary artery.114
TheFLAVORstudyisaninternational,multicenter, prospectiverandomizedongoingclinicaltrialwherea totalof1700patientswithintermediatecoronaryartery stenosiswillberandomized1:1toreceiveeitherFFRguidedorIVUS-guidedstenting.Thisstudyhasbeen designedtoevaluatethesafetyandtheefficacyoftwo strategiescomparingtherateofall-causemortality, myocardialinfarction,andrevascularizationafter 24-monthfollow-up.115
6.3.CalcifiedLesions
Calciumisapowerfulreflectorofultrasoundsincelittlebeampenetratescalciumand,thus,itcastsa shadowoverdeeperarterialstructures.Bytheuseof IVUS,calciumisillustratedasechodenseplaquethat isbrighterthanthereferenceadventitiawithshadowing.Additionally,multiplereflectionsareproducedby theoscillationofultras oundbetweenthetransducer andcalciumcausingconcentricarcsatreproducible distances.Calciumcanbeassessed(1)quantitatively bymeasuringthearcindegreesandthelength;(2) semiquantitativelyclassifyingcalciumasabsentor subtending1,2,3,or4quadrants;and(3)qualitativelybasedonitslocation(lesionvsreferenceor superficialvsdeep).Notably,IVUSisconsideredmore accuratecomparedtoangiographyalonefordetecting thecoronarycalcification.Inastudyof1155native vesseltargetlesions,IVUSdetectedcalciumin73% oflesions,significantlymoreoftenthanstandard angiography(38%).7,116,117 Coronarycalciumisassociatedwithatheroscleroticplaquegrowth.In101 IVUS-detectedrupturedplaquescomparedto101 computer-matchedcontrolplaqueswithoutrupture, therewasquantitativelylesscalcium,especially
superficialcalcium,butalargernumberofsmallcalciumdeposits,mainlydeepcalciumdeposits.118 The ruptureofathinfibrouscapatheromamightalso berelatedtominute(10- μm-diameter)cellular-level microcalcificationsinthecap,ahypothesisexperimentallyconfirmedonautopsyspecimensusing invitroimagingtechniqueswitharesolutionexceedingintravascularultrasoundandopticalcoherence tomography.119 AtheromathatareactivelyundergoingcalcificationaremostlikelytocauseMACE. Recently,molecularPET/CTimagingwithionic18F fluoridehasbeendevelopedtoidentifysuch lesions.120
6.4.CoronaryChronicTotalOcclusion
Incoronarychronictotalocclusion(CTO)PCI,IVUS playsanimportantroleinguidingtherecanalization oftheCTOandforstentoptimization.121 Initial reportsofIVUSguidanceafterCTOlesioncrossingto provideinformationaboutlesionlengthandmorphologyandidentifyasafeintraluminallandingzonefor stentingaremorethan20yearsold,122 yetthis approachremainsconsideredasanicheindicationperformedbyveryfewinterventionalistsandonlymasteredbyourJapanesecolleagues.123,124 Anintramural hematomawasoftenobservedinacarefulreviewin ourcorelabof67CTOproceduresfrom4Japanesecenters,suggestingthattheguidewirefrequentlyentered themedialspaceduringsuccessfulrecanalization.125 CTOlengthasmeasuredwithangiographywasshorter thantheIVUSlength.Inareportof219patientswith successfullyrecanalizedCTOfollowedbyIVUS,subintimaltrackingwasdetectedin52%ofcases,moreoften whenusingdissectionreentrythanwireescalation (87%vs28%,respectively).Inthesubintimaltracking group,therewasahigherrateofMACE,mostlydriven byperiproceduralmyocardialinfarctionandtherewas asignificantlygreaterincidenceofangiographicdye staining/extravasation,andbranchocclusion.126 After stenting,strutsexpansionandappositioncanbe optimizedwithIVUSassessment,improvingclinical outcomes.Among201propensity-scorematchedpairs includedintheKorean-CTORegistry,IVUS-guidedPCI wascorrelatedwithalowertrendofmyocardialinfarctionandlessstentthrombosiscomparedto angiography-guidedprocedureduringa2-year follow-up.127 Inthefirstrandomizedstudycomparing IVUS-guidedwithconventionalangiography-guided CTOinterventionusingnew-generationDES,402 patientsafterwirecrossingoftheCTOswererandomizedtotheIVUS-guidedgrouportheangiographyguidedgroup.128 At12-monthfollow-up,therewasa lowerrateofMACEratesintheIVUS-guidedgroup
(2.6%vs7.1%; P ¼ .035;HR:0.35;95%CI: 0.13–0.97).TheAIR-CTOstudyalsofoundthattherate ofdefiniteand/orprobablestentthrombosisat2-year follow-upwassignificantlyloweramongpatientswith IVUSguidance.129 Asoftenhappensininterventional cardiology,subsequenttowell-conductedrandomized trialsdemonstratingalong-termbeneficialimpactof IVUSguidance,themulticentricPROGRESSCTOregistrydidnotfind,in619CTOPCIswhereIVUSwasused in38%ofthe606patients,adifferenceincrossingor inproceduralsuccess,norin-hospitalMACE,130 so manyinterventionalistsarenotconvincedthatIVUS guidanceisusefulinthissubsetofpatients,whilea positionpaperfromexpertsrecommendsitsuse.8
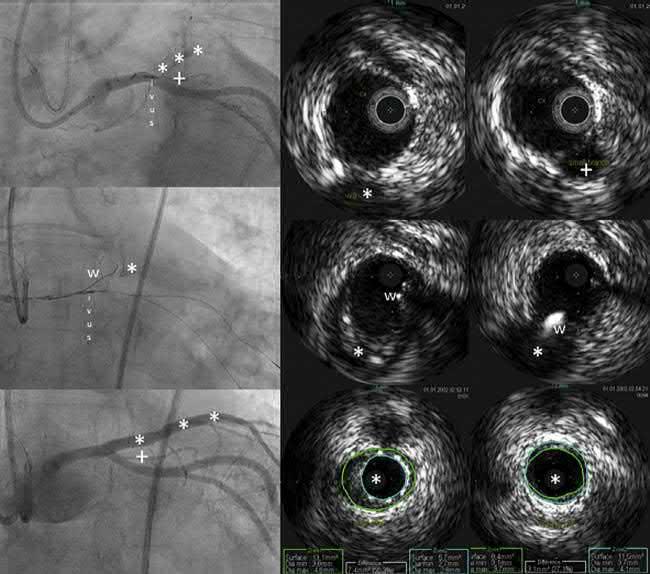
Asillustratedin Fig.5,IVUScanalsobeusedto resolveproximalcapambiguityandguidethepuncture ofstumplesslesionsbyimagingthroughasidebranch adjacenttotheocclusion.Ingeneral,afterlesioncrossing,IVUSwillconfirmthepresenceofthewireinthe distaltruelumen.Itmightalsobehelpfultonavigate theguidewirebackinthetruelumenincaseofadissectionandsubintimaltracking,usingtheIVUScatheterinthesubintimalspacetoguideantegradereentry inthetruelumen.Thishighlycomplexmethodisonly recommendedasalaststepinthelatestalgorithmproposedtotreatCTO,131 recommendingcarefulselection foraretrogradestrategyinwhichIVUSisalsoveryuseful.Thepreferredretrograderecanalizationstrategyis basedonthe(reverse)controlledantegradeandretrogradesubintimaltracking(CART)techniqueforwire reentryinthetrueproximallumen.IVUScanshow (i)therespectivepositionoftheantegradeandretrogradewireintraplaqueorinthesubintimalspace, (ii)thesizeofthevesselforoptimalballoonselection fortheCART,and(iii)thebestlocationformakingthe connectionofthewires.132,133
However,theuseofIVUSinCTOPCIhasseverallimitations.Firstly,thepresenceofcalciumobscuresthe positionoftheocclusionstumporimpairsthedetection ofthecollapsedtruelumen.Furthermore,theprobeis side-looking,sothatthecathetermustbeinsertedinto theocclusiontoimageit.Newcathetersareunderdevelopmentwithforward-lookingdesignthatmightoffer newrecanalizationstrategies.134,135
7.IVUSPITFALLS
DespitetheprofoundadvantagesofIVUSintheassessmentofatherosclerosisinvivo,themajorlimitationis mainlyrelatedtothefactthatitisinvasive.Inorder toprovideitsuniqueinformation,itismandatoryto beheldinacatheterizationlaboratoryunderexperiencedandwell-trainedoperatorsandstaff.Prolonged radiationexposureandincreasedcontrastusageshould
FIG.5 IVUSperformedduringaCTOPCIprocedure.Atotallyoccludedleftanteriordescending(LAD)arteryat theleveloftheostiumispointedontheangiogramonthe topleft by *** Topright,onthecorrespondingIVUS crosssectionobtainedjustdistallytotheoriginoftheLAD,withthecatheterintheleftcircumflexartery(Cx),a smallsidebranchismarkedby+,alsovisibleontheangiogram.TheIVUScrosssectioninthemiddlejustmore proximallyshowstheoriginoftheLAD(*). Middlepanel,left,showstheangiogramduringthefunctionofthe proximalcapoftheLADwithawire(w)thatcanalsobefollowedontheIVUSimagesinrealtime.The lowerpanel showsthestentedLADandtheIVUSassessmentofstentexpansionintheLAD (middlepanel) anditsdistal reference.
bealsotakenintoconsideration.Fromatechnicalpoint ofview,theneedtocatheterizeeachvesselindividually isalsoamatteroftimeandconcernandreliesalwayson theexperienceandskillsoftheinterventionalcardiologist.Anatomicallyspeaking,anotherrestrictionis relatedtolimitedcapabilitiesofimagingsmall-diameter vesselsandaorto-ostiallesions.61
Aswithanyvisualizationmodality,certainartifacts mayoccursuchasringdown,geometricdistortion effect,bloodspeckle,nonuniformrotationaldistortion, orevenbrokencathetersanddevices.Thedrawbackof high-frequencyIVUSsystemsisthattheintensityof thebloodspeckleincreasestothefourthpowerofthe transducerfrequencysothattheechodensityofblood mightbecomeashighastheplaque,ifnothigherin thepresenceofbloodstasiswithrouleaured-cellformation.Electronicfilteringandimageprocessingmight reducethisphenomenon.136 Moreover,intravascular
imagingsequencesrecordedinvivosufferfrommotion artifactsmainlyrelatedtothebeatingheart.Attempts havebeenmadetoacquireelectrocardiogram(ECG) gatedframeswithdedicatedpullbackdevices.Frames arecollectedatthepointsintimeassociatedwithaparticularfractionofthecardiaccycle.However,thereare difficultiestodeterminetheoptimalfractionatwhich togate,subsequenttotheratherbulkyspecificpullback devicetouse.Tocircumventthisproblem,frame-gating methodsforIVUSpullbacksthatmimicECGgating(i.e., thatselectonlyoneframepercardiaccycle)havebeen developed.Thealgorithmautomaticallyselectsthefractionofthecyclethatrendersthemoststablegatedframe set.137 Finally,calcificationsproduceastrongreflection oftheultrasoundbeamhamperingtheevaluationof deeperatherosclerosis.68
Anothermajorconcernisthatimageanalysisshould alwaysbeperformedbywell-trainedexpertswith
thoroughunderstandingofthisimagingfield,otherwise itmightleadtoinaccuratemeasurementsandmislead interpretation.Thehighcostandtheoccasionallylimitedavailabilityduetoapprovalordistributionissues remainarestrictiontoitsworldwidespread.61
8.IVUSCOMPLICATIONS
IVUSshouldbeprecededbytheadministrationofanticoagulantsandintravenousnitratesinordertoavoid vasospasm.ClinicalstudieshaveshownthatIVUScan beperformedsafelywithalowincidenceofsideeffects (mainlylocalvasospasm),oftheorderof1%.Inamulticenterreportofmorethan2000patients,common complicationswerevasospasm,acuteocclusion,embolism,dissection,andthrombusformationwithsome patientspresentingmajoreventssuchasmyocardial infarctionoremergencycoronaryarterybypasssurgery. ThecomplicationratewashigherincaseofACS (2.1%)ascomparedwithpatientswithstableanginapectoris(0.8%)andasymptomaticpatients(0.4%).138,139 In thePROSPECTtrial,1.6%ofevents(10coronarydissectionsand1perforation)wererecordedamong697ACS patients.64 In103STEMIsubjectswhounderwentthreevesselcoronaryimagingduringPCIfortheIBIS-4 study,140 imagingofthenoninfarct-relatedvesselswas successfulinapproximately90%ofthemwithoutimpact oncardiovasculareventsatlong-termfollow-up.Another recentreportinabout2500IVUSprocedureswaseven morereassuring,withanIVUS-relatedcomplicationsrate of0.5%.Complicationswereself-limitingafterthe retrievaloftheimagingcatheteroreasilytreatablein thecatheterizationlaboratorywithoutMACE.141
9.FUTUREPERSPECTIVES
Forthefuture,hybridintravascularimagingbasedon theuseofbothOCTandIVUShasbeenrecentlyproposedtobettercharacterizelesioncomponentsandprovideadetailedevaluationoftheatheroscleroticplaque biology.Thistechniqueusingmultimodalcathetersis expectedtoconstituteaninterestingapproachforthe studyofatherosclerosis.142 Additionaleffortsmay includethedevelopmentofamagneticresonance catheter-basedsystemthatcanidentifylipid-richtissue orevenimagingcathetersabletomeasurethermalgradientsassociatedwithinflammationinthecoronary arteries.Anidealfuturisticconceptinvolvesthepotentialuseofasinglecatheterandpullbackwiththefusion ofNIRS-IVUSin3D.Finally,molecularimagingagents mayenhancetheidentificationofspecificmolecular processeswithintheplaques.
DISCLOSURES
SCisaconsultantforBostonScientificandTerumo.
REFERENCES
1. TopolEJ,NissenSE.Ourpreoccupationwithcoronary luminology.Thedissociationbetweenclinicaland angiographicfindingsinischemicheartdisease. Circulation.1995;92:2333–2342.
2. YockPG,FitzgeraldPJ,LinkerDT,AngelsenBA. Intravascularultrasoundguidanceforcatheter-based coronaryinterventions. JAmCollCardiol.1991; 17:39B–45B.
3. BomN,LanceeCT,VanEgmondFC.Anultrasonic intracardiacscanner. Ultrasonics.1972;10:72–76.
4. EdlerI,HertzCH.Theuseofultrasonicreflectoscopefor thecontinuousrecordingofthemovementsofheart walls.1954. ClinPhysiolFunctImaging.2004;24:118–136.
5. SanidasEA,VavuranakisM,PapaioannouTG,etal.Study ofatheromatousplaqueusingintravascularultrasound. HellJCardiol.2008;49:415–421.
6. JohnsonTW,RaberL,diMarioC,etal.Clinicaluseof intracoronaryimaging.Part2:acutecoronary syndromes,ambiguouscoronaryangiographyfindings, andguidinginterventionaldecision-making:anexpert consensusdocumentoftheEuropeanAssociationof PercutaneousCardiovascularInterventions. EurHeartJ 2019;40:2566–2584.
7. SongHG,KangSJ,MintzGS.Valueofintravascular ultrasoundinguidingcoronaryinterventions. Echocardiography.2018;35:520–533.
AvailabledataunderlinetheevidencethatIVUSisan excellentdiagnosticimagingtoolandwiththelatest DESmultipleobservationalandrandomizedclinicaltrialsdemonstratedthepotentialofIVUSguidanceto improvePCIoutcomes.IVUSguidanceforPCIremains recommendedonlyin “selected” patients,withaclass IIarecommendationforassessingtheseverityofaLMCA stenosisorforunderstandingstent-relatedmechanical problemsleadingtorestenosis.IthasalsoaclassIIa inselectedpatientstooptimizestentimplantation,specificallyleftmainlesions.10 Itisforsureanadditional burdenanditincreasesproceduraltimeandmightbe difficulttoimplementforallproceduresinabusycatheterizationlaboratorywithoutanyreimbursement,as quotedbyCarloDiMarioinhiseditorialaboutthe ULTIMATEtrial, “inviewofthetotalityofRCTevidence, thereisnoquestionthattheuseofIVUSguidanceto optimizePCIdoesimprovepatientprognosis.Against thisbackground,thereisnoscientificjustificationfor theobservedinertiainintegratinganimaging-guided strategymorebroadlyinclinicalpractice.”25