Instant digital products (PDF, ePub, MOBI) ready for you
Download now and discover formats that fit your needs...
Biodiversity Conservation: a Very Short Introduction David W. Macdonald
https://ebookmass.com/product/biodiversity-conservation-a-very-shortintroduction-david-w-macdonald/
ebookmass.com
Cabo do Medo John D. Macdonald [Macdonald
https://ebookmass.com/product/cabo-do-medo-john-d-macdonald-macdonald/
ebookmass.com
Elsevier Weekblad - Week 26 - 2022 Gebruiker
https://ebookmass.com/product/elsevier-weekbladweek-26-2022-gebruiker/ ebookmass.com
Stand Out: A Real World Guide to Get Clear, Find Purpose and Become the Boss of Busy Alison Hill
https://ebookmass.com/product/stand-out-a-real-world-guide-to-getclear-find-purpose-and-become-the-boss-of-busy-alison-hill/ ebookmass.com
The Worlds of John Wick: The Year's Work at the Continental Hotel (The Year's Work: Studies in Fan Culture and Cultural Theory) Caitlin G Watt
https://ebookmass.com/product/the-worlds-of-john-wick-the-years-workat-the-continental-hotel-the-years-work-studies-in-fan-culture-andcultural-theory-caitlin-g-watt/ ebookmass.com
Marriages and Families in the 21st Century: A Bioecological Approach
https://ebookmass.com/product/marriages-and-families-in-the-21stcentury-a-bioecological-approach/
ebookmass.com
Tiroidectomia mediante cervicotomia 1st Edition R.Kania(Professeur Des Universités
https://ebookmass.com/product/tiroidectomia-mediante-cervicotomia-1stedition-r-kaniaprofesseur-des-universites/
ebookmass.com
Developing Solutions for Microsoft Azure Certification Companion: Hands-on Preparation and Practice for Exam AZ-204 Brain L. Gorman
https://ebookmass.com/product/developing-solutions-for-microsoftazure-certification-companion-hands-on-preparation-and-practice-forexam-az-204-brain-l-gorman/ ebookmass.com
NOS4A2 Joe Hill
https://ebookmass.com/product/nos4a2-joe-hill/
ebookmass.com
Beton-Kalender 2023: Schwerpunkte: Wasserundurchlässiger
Beton, Brückenbau (2 Teile) 1st Edition Konrad Bergmeister
https://ebookmass.com/product/beton-kalender-2023-schwerpunktewasserundurchlassiger-beton-bruckenbau-2-teile-1st-edition-konradbergmeister/ ebookmass.com
INTRAOPERATIVENEUROMONITORING
HANDBOOKOFCLINICAL NEUROLOGY
SeriesEditors
MICHAELJ.AMINOFF,FRANÇOISBOLLER,ANDDICKF.SWAAB
VOLUME186
INTRAOPERATIVE NEUROMONITORING
SeriesEditors
MICHAELJ.AMINOFF,FRANÇOISBOLLER,ANDDICKF.SWAAB
VolumeEditors
MARCR.NUWERANDDAVIDB.MACDONALD
VOLUME186
3rdSeries
ELSEVIER
Radarweg29,POBox211,1000AEAmsterdam,Netherlands TheBoulevard,LangfordLane,Kidlington,OxfordOX51GB,UnitedKingdom 50HampshireStreet,5thFloor,Cambridge,MA02139,UnitedStates
Copyright©2022ElsevierB.V.Allrightsreserved.
Nopartofthispublicationmaybereproducedortransmittedinanyformorbyanymeans,electronicor mechanical,includingphotocopying,recording,oranyinformationstorageandretrievalsystem,without permissioninwritingfromthepublisher.Detailsonhowtoseekpermission,furtherinformationaboutthe Publisher’spermissionspoliciesandourarrangementswithorganizationssuchastheCopyrightClearanceCenter andtheCopyrightLicensingAgencycanbefoundatourwebsite: www.elsevier.com/permissions.
ThisbookandtheindividualcontributionscontainedinitareprotectedundercopyrightbythePublisher(other than asmaybenotedherein).
Notices
Knowledgeandbestpracticeinthisfieldareconstantlychanging.Asnewresearchandexperiencebroadenour understanding,changesinresearchmethods,professionalpractices,ormedicaltreatmentmaybecome necessary.
Practitionersandresearchersmustalwaysrelyontheirownexperienceandknowledgeinevaluatingandusingany information,methods,compounds,orexperimentsdescribedherein.Inusingsuchinformationormethodsthey shouldbemindfuloftheirownsafetyandthesafetyofothers,includingpartiesforwhomtheyhaveaprofessional responsibility.
Withrespecttoanydrugorpharmaceuticalproductsidentified,readersareadvisedtocheckthemostcurrent informationprovided(i)onproceduresfeaturedor(ii)bythemanufacturerofeachproducttobeadministered,to verifytherecommendeddoseorformula,themethodanddurationofadministration,andcontraindications.Itis theresponsibilityofpractitioners,relyingontheirownexperienceandknowledgeoftheirpatients,tomake diagnoses,todeterminedosagesandthebesttreatmentforeachindividualpatient,andtotakeallappropriate safetyprecautions.
Tothefullestextentofthelaw,neitherthePublishernortheauthors,contributors,oreditorsassumeanyliability foranyinjuryand/ordamagetopersonsorpropertyasamatterofproductsliability,negligenceorotherwise,or fromanyuseoroperationofanymethods,products,instructions,orideascontainedinthematerialherein.
ISBN:978-0-12-819826-1
ForinformationonallElsevierpublications visitourwebsiteat https://www.elsevier.com/books-and-journals
Publisher: Nikki Levy
EditorialProjectManager: KristiAnderson
ProductionProjectManager: PunithavathyGovindaradjane
CoverDesigner: GregHarris
HandbookofClinicalNeurology3rdSeries
Availabletitles
Vol.79,Thehumanhypothalamus:basicandclinicalaspects,PartI,D.F.Swaab,ed.ISBN9780444513571
Vol.80,Thehumanhypothalamus:basicandclinicalaspects,PartII,D.F.Swaab,ed.ISBN9780444514905
Vol.81,Pain,F.CerveroandT.S.Jensen,eds.ISBN9780444519016
Vol.82,Motorneuronedisordersandrelateddiseases,A.A.EisenandP.J.Shaw,eds.ISBN9780444518941
Vol.83,Parkinson’sdiseaseandrelateddisorders,PartI,W.C.KollerandE.Melamed,eds.ISBN9780444519009
Vol.84,Parkinson’sdiseaseandrelateddisorders,PartII,W.C.KollerandE.Melamed,eds.ISBN9780444528933
Vol.85,HIV/AIDSandthenervoussystem,P.PortegiesandJ.Berger,eds.ISBN9780444520104
Vol.86,Myopathies,F.L.MastagliaandD.HiltonJones,eds.ISBN9780444518996
Vol.87,Malformationsofthenervoussystem,H.B.SarnatandP.Curatolo,eds.ISBN9780444518965
Vol.88,Neuropsychologyandbehaviouralneurology,G.GoldenbergandB.C.Miller,eds.ISBN9780444518972
Vol.89,Dementias,C.DuyckaertsandI.Litvan,eds.ISBN9780444518989
Vol.90,Disordersofconsciousness,G.B.YoungandE.F.M.Wijdicks,eds.ISBN9780444518958
Vol.91,Neuromuscularjunctiondisorders,A.G.Engel,ed.ISBN9780444520081 Vol.92,Stroke – PartI:Basicandepidemiologicalaspects,M.Fisher,ed.ISBN9780444520036 Vol.93,Stroke – PartII:Clinicalmanifestationsandpathogenesis,M.Fisher,ed.ISBN9780444520043 Vol.94,Stroke – PartIII:Investigationsandmanagement,M.Fisher,ed.ISBN9780444520050 Vol.95,Historyofneurology,S.Finger,F.BollerandK.L.Tyler,eds.ISBN9780444520081 Vol.96,Bacterialinfectionsofthecentralnervoussystem,K.L.RoosandA.R.Tunkel,eds.ISBN9780444520159 Vol.97,Headache,G.NappiandM.A.Moskowitz,eds.ISBN9780444521392 Vol.98,SleepdisordersPartI,P.MontagnaandS.Chokroverty,eds.ISBN9780444520067 Vol.99,SleepdisordersPartII,P.MontagnaandS.Chokroverty,eds.ISBN9780444520074 Vol.100,Hyperkineticmovementdisorders,W.J.WeinerandE.Tolosa,eds.ISBN9780444520142 Vol.101,Musculardystrophies,A.AmatoandR.C.Griggs,eds.ISBN9780080450315 Vol.102,Neuro-ophthalmology,C.KennardandR.J.Leigh,eds.ISBN9780444529039 Vol.103,Ataxicdisorders,S.H.SubramonyandA.Durr,eds.ISBN9780444518927 Vol.104,Neuro-oncologyPartI,W.GrisoldandR.Sofietti,eds.ISBN9780444521385 Vol.105,Neuro-oncologyPartII,W.GrisoldandR.Sofietti,eds.ISBN9780444535023 Vol.106,Neurobiologyofpsychiatricdisorders,T.SchlaepferandC.B.Nemeroff,eds.ISBN9780444520029 Vol.107,EpilepsyPartI,H.StefanandW.H.Theodore,eds.ISBN9780444528988 Vol.108,EpilepsyPartII,H.StefanandW.H.Theodore,eds.ISBN9780444528995 Vol.109,Spinalcordinjury,J.VerhaagenandJ.W.McDonaldIII,eds.ISBN9780444521378 Vol.110,Neurologicalrehabilitation,M.BarnesandD.C.Good,eds.ISBN9780444529015 Vol.111,PediatricneurologyPartI,O.Dulac,M.LassondeandH.B.Sarnat,eds.ISBN9780444528919 Vol.112,PediatricneurologyPartII,O.Dulac,M.LassondeandH.B.Sarnat,eds.ISBN9780444529107 Vol.113,PediatricneurologyPartIII,O.Dulac,M.LassondeandH.B.Sarnat,eds.ISBN9780444595652 Vol.114,Neuroparasitologyandtropicalneurology,H.H.Garcia,H.B.TanowitzandO.H.DelBrutto,eds. ISBN9780444534903
Vol.115,Peripheralnervedisorders,G.SaidandC.Krarup,eds.ISBN9780444529022 Vol.116,Brainstimulation,A.M.LozanoandM.Hallett,eds.ISBN9780444534972 Vol.117,Autonomicnervoussystem,R.M.BuijsandD.F.Swaab,eds.ISBN9780444534910 Vol.118,Ethicalandlegalissuesinneurology,J.L.BernatandH.R.Beresford,eds.ISBN9780444535016 Vol.119,NeurologicaspectsofsystemicdiseasePartI,J.BillerandJ.M.Ferro,eds.ISBN9780702040863 Vol.120,NeurologicaspectsofsystemicdiseasePartII,J.BillerandJ.M.Ferro,eds.ISBN9780702040870 Vol.121,NeurologicaspectsofsystemicdiseasePartIII,J.BillerandJ.M.Ferro,eds.ISBN9780702040887 Vol.122,Multiplesclerosisandrelateddisorders,D.S.Goodin,ed.ISBN9780444520012 Vol.123,Neurovirology,A.C.TselisandJ.Booss,eds.ISBN9780444534880 Vol.124,Clinicalneuroendocrinology,E.Fliers,M.KorbonitsandJ.A.Romijn,eds.ISBN9780444596024 Vol.125,Alcoholandthenervoussystem,E.V.SullivanandA.Pfefferbaum,eds.ISBN9780444626196 Vol.126,Diabetesandthenervoussystem,D.W.ZochodneandR.A.Malik,eds.ISBN9780444534804 Vol.127,TraumaticbraininjuryPartI,J.H.GrafmanandA.M.Salazar,eds.ISBN9780444528926 Vol.128,TraumaticbraininjuryPartII,J.H.GrafmanandA.M.Salazar,eds.ISBN9780444635211
Vol.129,Thehumanauditorysystem:Fundamentalorganizationandclinicaldisorders,G.G.CelesiaandG.Hickok,eds. ISBN9780444626301
Vol.130,Neurologyofsexualandbladderdisorders,D.B.VodušekandF.Boller,eds.ISBN9780444632470
Vol.131,Occupationalneurology,M.LottiandM.L.Bleecker,eds.ISBN9780444626271
Vol.132,Neurocutaneoussyndromes,M.P.IslamandE.S.Roach,eds.ISBN9780444627025
Vol.133,Autoimmuneneurology,S.J.PittockandA.Vincent,eds.ISBN9780444634320
Vol.134,Gliomas,M.S.BergerandM.Weller,eds.ISBN9780128029978
Vol.135,NeuroimagingPartI,J.C.MasdeuandR.G.González,eds.ISBN9780444534859
Vol.136,NeuroimagingPartII,J.C.MasdeuandR.G.González,eds.ISBN9780444534866
Vol.137,Neuro-otology,J.M.FurmanandT.Lempert,eds.ISBN9780444634375
Vol.138,Neuroepidemiology,C.Rosano,M.A.IkramandM.Ganguli,eds.ISBN9780128029732 Vol.139,Functionalneurologicdisorders,M.Hallett,J.StoneandA.Carson,eds.ISBN9780128017722
Vol.140,CriticalcareneurologyPartI,E.F.M.WijdicksandA.H.Kramer,eds.ISBN9780444636003
Vol.141,CriticalcareneurologyPartII,E.F.M.WijdicksandA.H.Kramer,eds.ISBN9780444635990
Vol.142,Wilsondisease,A.CzłonkowskaandM.L.Schilsky,eds.ISBN9780444636003
Vol.143,Arteriovenousandcavernousmalformations,R.F.Spetzler,K.MoonandR.O.Almefty,eds.ISBN9780444636409
Vol.144,Huntingtondisease,A.S.FeiginandK.E.Anderson,eds.ISBN9780128018934 Vol.145,Neuropathology,G.G.KovacsandI.Alafuzoff,eds.ISBN9780128023952 Vol.146,Cerebrospinalfluidinneurologicdisorders,F.Deisenhammer,C.E.TeunissenandH.Tumani,eds. ISBN9780128042793
Vol.147,NeurogeneticsPartI,D.H.Geschwind,H.L.PaulsonandC.Klein,eds.ISBN9780444632333 Vol.148,NeurogeneticsPartII,D.H.Geschwind,H.L.PaulsonandC.Klein,eds.ISBN9780444640765 Vol.149,Metastaticdiseasesofthenervoussystem,D.SchiffandM.J.vandenBent,eds.ISBN9780128111611 Vol.150,Brainbankinginneurologicandpsychiatricdiseases,I.HuitingaandM.J.Webster,eds.ISBN9780444636393 Vol.151,Theparietallobe,G.VallarandH.B.Coslett,eds.ISBN9780444636225 Vol.152,TheneurologyofHIVinfection,B.J.Brew,ed.ISBN9780444638496 Vol.153,Humanpriondiseases,M.PocchiariandJ.C.Manson,eds.ISBN9780444639455 Vol.154,Thecerebellum:Fromembryologytodiagnosticinvestigations,M.MantoandT.A.G.M.Huisman,eds. ISBN9780444639561 Vol.155,Thecerebellum:Disordersandtreatment,M.MantoandT.A.G.M.Huisman,eds.ISBN9780444641892 Vol.156,Thermoregulation:FrombasicneurosciencetoclinicalneurologyPartI,A.A.Romanovsky,ed.ISBN9780444639127 Vol.157,Thermoregulation:FrombasicneurosciencetoclinicalneurologyPartII,A.A.Romanovsky,ed.ISBN9780444640741
Vol.158,Sportsneurology,B.HainlineandR.A.Stern,eds.ISBN9780444639547
Vol.159,Balance,gait,andfalls,B.L.DayandS.R.Lord,eds.ISBN9780444639165
Vol.160,Clinicalneurophysiology:Basisandtechnicalaspects,K.H.LevinandP.Chauvel,eds.ISBN9780444640321
Vol.161,Clinicalneurophysiology:Diseasesanddisorders,K.H.LevinandP.Chauvel,eds.ISBN9780444641427
Vol.162,Neonatalneurology,L.S.DeVriesandH.C.Glass,eds.ISBN9780444640291
Vol.163,Thefrontallobes,M.D’EspositoandJ.H.Grafman,eds.ISBN9780128042816
Vol.164,Smellandtaste,RichardL.Doty,ed.ISBN9780444638557
Vol.165,Psychopharmacologyofneurologicdisease,V.I.ReusandD.Lindqvist,eds.ISBN9780444640123
Vol.166,Cingulatecortex,B.A.Vogt,ed.ISBN9780444641960
Vol.167,Geriatricneurology,S.T.DeKoskyandS.Asthana,eds.ISBN9780128047668
Vol.168,Brain-computerinterfaces,N.F.RamseyandJ.delR.Millán,eds.ISBN9780444639349
Vol.169,Meningiomas,PartI,M.W.McDermott,ed.ISBN9780128042809
Vol.170,Meningiomas,PartII,M.W.McDermott,ed.ISBN9780128221983
Vol.171,Neurologyandpregnancy:Pathophysiologyandpatientcare,E.A.P.Steegers,M.J.CipollaandE.C.Miller,eds. ISBN9780444642394
Vol.172,Neurologyandpregnancy:Neuro-obstetricdisorders,E.A.P.Steegers,M.J.CipollaandE.C.Miller,eds. ISBN9780444642400
Vol.173,Neurocognitivedevelopment:Normativedevelopment,A.Gallagher,C.Bulteau,D.CohenandJ.L.Michaud,eds. ISBN9780444641502
Vol.174,Neurocognitivedevelopment:Disordersanddisabilities,A.Gallagher,C.Bulteau,D.CohenandJ.L.Michaud,eds. ISBN9780444641489
Vol.175,Sexdifferencesinneurologyandpsychiatry,R.Lanzenberger,G.S.Kranz,andI.Savic,eds.ISBN9780444641236 Vol.176,Interventionalneuroradiology,S.W.HettsandD.L.Cooke,eds.ISBN9780444640345
Vol.177,Heartandneurologicdisease,J.Biller,ed.ISBN9780128198148
Vol.178,Neurologyofvisionandvisualdisorders,J.J.S.BartonandA.Leff,eds.ISBN9780128213773
Vol.179,Thehumanhypothalamus:Anteriorregion,D.F.Swaab,F.Kreier,P.J.Lucassen,A.SalehiandR.M.Buijs,eds. ISBN9780128199756
Vol.180,Thehumanhypothalamus:Middleandposteriorregion,D.F.Swaab,F.Kreier,P.J.Lucassen,A.SalehiandR.M.Buijs, eds.ISBN9780128201077
Vol.181,Thehumanhypothalamus:Neuroendocrinedisorders,D.F.Swaab,R.M.Buijs,P.J.Lucassen,A.SalehiandF.Kreier, eds.ISBN9780128206836
Vol.182,Thehumanhypothalamus:Neuropsychiatricdisorders,D.F.Swaab,R.M.Buijs,F.Kreier,P.J.Lucassen,andA.Salehi, eds.ISBN9780128199732
Vol.183,Disordersofemotioninneurologicdisease,K.M.HeilmanandS.E.Nadeau,eds.ISBN9780128222904
Vol.184,Neuroplasticity:Frombenchtobedside,A.Quartarone,M.F.Ghilardi,andF.Boller,eds.ISBN9780128194102 Vol.185,Aphasia,A.E.HillisandJ.Fridriksson,eds.ISBN9780128233849
Allvolumesinthe3rdSeriesofthe HandbookofClinicalNeurology arepublishedelectronically, onScienceDirect: http://www.sciencedirect.com/science/handbooks/00729752
Foreword
Clinicalneurophysiologyhasprogressedfromthedaysinthe1940sand1950swhenstudieswereperformedby academicsinfar-awaylaboratories,ofteninthehospitalbasement,onpatientswithobscuremaladies.Withthe developmentofnewtechniquessuchastherecordingofevokedpotentials,neurophysiologylaboratoriesflourished inthe1970sand1980stosuchanextentthatclinicalpracticewasdifficulttoimaginewithouttheinformationthat theyprovided.Theirimpactthendeclinedasnewimagingtechniquesbecamewidelyavailabletoaidthediagnostic process.Inthelast30years,however,neurophysiologistshaveassumedanexpandingroleinmonitoringthenervous systemduringsurgicalandotherprocedureswiththeaimofidentifyingandprotectingvulnerableregionsfromdamage.Themainpurposeistowarninterventionalists,surgeons,andanesthesiologistsaboutadversechangesatavery earlystageinordertocorrectthecauseandtherebypreventpostoperativeneurologicdeficits.Thisinvolvestesting neurologicfunctionintheoperatingroomandexploringneurologicfunctionduringsurgeryinordertodetectimpendingneurologicdamageand byleadingtoproceduralchanges preventpermanentdamage.
Intraoperativemonitoringinoneformoranotherhas,infact,beenusedforalmost150years.Thefirstsurgeonto stimulatethehumanbrainelectricallyatoperationwasprobablyVictorHorsleyinLondonin1884,andhewassoon followedbyFedorKrauseinGermany,WilliamKeenintheUnitedStates,andothers.Duringthefirsthalfofthe20th century,WilderPenfieldandhisgroupinMontrealusedfunctionalcorticallocalization(directcorticalstimulationto locatemotorandsensorycortex)duringepilepsysurgeryandthenwentontorecordtheelectricalactivitydirectlyfrom exposedcerebralcortex(electrocorticography)toguidethesurgicalresectionoftheepileptogenicarea.
Thepresentvolumeofthe HandbookofClinicalNeurology isdevotedtointraoperativeneurophysiologicmonitoringandcomplementsVolumes160and161,whichcoveredthemoregeneralaspectsofclinicalneurophysiology. Thevolumecoversboththetechnicalaspectsofvariousneurophysiologicmonitoringproceduresandthespecific approachtomonitoringpatientsundergoingoperativeproceduresondifferentregionsofthebrain;procedureson thespinalcordortocorrectspinaldeformities;surgeryonperipheralandcranialnerves;andsurgeryontheheart, differentregionsoftheaorta,andthecarotidarteries.Intraoperativemonitoringimprovestheoutcomeofvarious butnotallprocedures,andintheyearsahead,itwillbeimportanttoclarifyitsbenefitsinordertoremoveanyambiguity aboutitsindications.
Wecongratulateandaremostgratefultothetwoeditorsofthepresentvolume:MarcR.NuwerisProfessorof NeurologyintheDavidGeffenSchoolofMedicineatUCLAandheadstheDepartmentofClinicalNeurophysiology attheRonaldReaganUCLAMedicalCenterinLosAngeles,California,whileDavidB.MacDonalddirectedthe SectionofClinicalNeurophysiologyattheKingFaisalSpecialistHospital&ResearchCenterinRiyadh,SaudiArabia andnowisScientificDirectorofArkanaForuminEmmendingen,Germany.Together,theyhavebroughttogether agroupofexpertsindifferentaspectsofintraoperativemonitoringtoprovideacomprehensivebutcriticalaccount ofthesubject.
Asserieseditors,wereviewedallthechaptersinthevolumeandmadesuggestionsforimprovement,butthevolume editorsandindividualcontributorsproducedparticularlyscholarlyandthoughtfulaccountsofdifferentaspectsofthe topic,forwhichwearegrateful.Thevolumewillappealtocliniciansandclinicalneurophysiologistsasastate-ofthe-artreference.
Asalways,itisapleasuretothankElsevier,ourpublisher,andinparticularMichaelParkinsoninScotland,Nikki LevyandKristiAndersoninSanDiego,andPunithavathyGovindaradjaneatElsevierGlobalBookProductionin Chennai,fortheirassistanceinthedevelopmentandproductionofthe HandbookofClinicalNeurology.
MichaelJ.Aminoff
Franc ¸ oisBoller
DickF.Swaab
Preface
“Thebestwaytodealwithparaplegiaistopreventitfromhappeninginthefirstplace.” Thegoalofintraoperative monitoring(IOM)istopreventpostoperativeneurologicdeficits.IOMnowincludesavarietyoftechniques appliedtomanystructuresinthenervoussystem.
Inthepastfourdecades,IOMhasdevelopedintoamajorsubspecialtyofclinicalneurophysiology,onethathas becomewidelyusedandincludesabroadarrayoftechniquesandapplications.Muchofthemethodologyisderived fromcommonoutpatientclinicalneurophysiologytesting,withmodificationstooptimizevalueintheoperatingroom. IOMhasmadeinroadsintomanysurgicalsubspecialties.Thisvolumepresentsthestateofitsartandscience.
IndividualchaptersreviewgeneralissuesofscienceandpracticebehindIOMwithineachofthemajorportionsof thisfield.Theydescribetypicaltechniquesofstimulationandrecording,alongwithinterpretationandalarmcriteria. Drawbacksandproblemsaredescribed,andhowmonitoringteamsmightcopewiththem.Eachchapterreviewsthe relevantIOMliteratureanddiscussesclinicalissuesandanyoutcomestudies.Safetyandanestheticissuesareincluded aswell.
SectionIbeginswithanoverviewofEEG,evokedpotential,andEMGtechniques.Safetyissuesarediscussedforall monitoringmodalities.FurthersectionsdescribeIOMasitappliesindifferentdisordersandanatomicregions. SectionIIincludeschaptersoncommondisordersinwhichIOMisoftenused,namelyintracranialtumors,epilepsy, andmovementdisorders.Thesectioncontinuesbyincludingchaptersonanatomicregions,specificallythebrainstem andcerebellopontineangle.SectionIIIbeginswithachapteronspinaldisorders,specificallyscoliosisandmyelopathy. ItcontinueswithworkdescribingIOMforcertainsurgicalsituations:intracranialandextracranialspinalsurgeries, lumbardecompressionandfusion,caudaequinaandtetheredcordsurgery,andproceduresfortreatingpain. SectionIVcoversboththecranialnervesandtheothersomaticnerverootsandperipheralnerveprocedures. SectionVonIOMduringvascularsurgerycoverscarotidprocedures,intracranialaneurysm,andsurgeryontheascendinganddescendingaorta.Thevariouschaptersinthissectioncovertechniquesaswellasclinicalapplications.
Inthe1920s,WilderPenfieldpioneeredtheroutineuseofneurophysiologyintheoperatingroomtolocalizemotor andsensorycortexwithdirectcorticalstimulation.Onewonderswhetherhehadanyideahowmuchintraoperative neurophysiologywouldgrowoverthenextcentury.
MarcR.Nuwer DavidB.MacDonald
Contributors
J.E.Arle
DepartmentofNeurosurgery,HarvardMedicalSchool andDepartmentofNeurosurgery,BethIsraelDeaconess MedicalCenter,Boston,MA,UnitedStates
L.Bello
DepartmentofOncologyandHemato-Oncology, NeurosurgicalOncologyUnit,UniversitàdegliStudidi Milano,Milan,Italy
B.A.Crum
DepartmentofNeurology,MayoClinic,Rochester,MN, UnitedStates
V.Deletis
DepartmentofNeurosurgery,UniversityHospital Dubrava,Zagreb,Croatia;AlbertEinsteinCollegeof Medicine,NewYork,NY,UnitedStates
C.C.Dong
DepartmentofSurgery,UniversityofBritishColumbia, Vancouver,BC,Canada
I.Fernández-Conejero
UnitofIntraoperativeNeurophysiology,Departmentof Neurology,UniversityHospitalofBellvitge,Barcelona, Spain
G.Galloway
DepartmentofNeurology,WexnerMedicalCenter,Ohio StateUniversityMedicalCenter,Columbus,OH, UnitedStates
J.Gertsch
DepartmentofNeurology,UCSanDiegoHealth, SanDiego,CA,UnitedStates
A.Gonzalez
DepartmentofNeuroscience,UniversityofCalifornia Riverside,Riverside,CA,UnitedStates
Deceased
L.Guo
DepartmentofSurgicalNeuromonitoring,Universityof CaliforniaSanFrancisco,SanFrancisco,CA, UnitedStates
R.N.Holdefer
DepartmentofRehabilitationMedicine,Universityof Washington,Seattle,WA,UnitedStates
A.M.Husain
DepartmentofNeurology,DukeUniversityMedical CenterandNeurodiagnosticCenter,VeteransAffairs MedicalCenter,Durham,NC,UnitedStates
M.J.Jacobs
DepartmentofSurgery,MaastrichtUniversityMedical Center,Maastricht,TheNetherlands
H.L.Journee
DepartmentofNeurosurgery,UniversityMedicalCenter Groningen,UniversityofGroningen,Groningen, TheNetherlands
I.Keselman
DepartmentofNeurology,UniversityofCaliforniaLos Angeles,LosAngeles,CA,UnitedStates
K.Kodama
DepartmentofNeurosurgery,ShinshuUniversitySchool ofMedicine,Matsumoto,Japan
K.F.Kothbauer†
FormerlyDepartmentofNeurosurgery,Universityof BaselandDivisionofNeurosurgery,Luzerner Kantonsspital,Lucerne,Switzerland
A.D.Legatt
DepartmentofNeurology,MontefioreMedicalCenter andAlbertEinsteinCollegeofMedicine,Bronx,NY, UnitedStates
J.R.López
DepartmentofNeurologyandNeurologicalSciences, StanfordUniversitySchoolofMedicine,Stanford,CA, UnitedStates
D.B.MacDonald
ArkanaForum,Emmendingen,Germany
M.Malcharek
DivisionofNeuroanesthesiaandIntraoperative Neuromonitoring,DepartmentofAnesthesia, IntensiveCareandPainTherapy,Klinikum St.Georg,HospitaloftheUniversityofLeipzig,Leipzig, Germany
W.H.Mess
DepartmentofClinicalNeurophysiology, MaastrichtUniversityMedicalCenter,Maastricht, TheNetherlands
M.R.Nuwer
DepartmentsofNeurologyandClinical Neurophysiology,DavidGeffenSchoolofMedicine, UniversityofCaliforniaLosAngeles,andRonald ReaganUCLAMedicalCenter,LosAngeles,CA, UnitedStates
J.Prell
DepartmentofNeurosurgery,UniversityHalleWittenberg,Halle,Germany
F.Sala
SectionofNeurosurgery,DepartmentofNeurosciences, BiomedicineandMovementSciences,University Hospital,Verona,Italy
K.Seidel
DepartmentofNeurosurgery,Inselspital,Bern UniversityHospital,UniversityofBern,Bern, Switzerland
J.L.Shils
DepartmentofAnesthesiology,RushUniversityMedical Center,Chicago,IL,UnitedStates
M.V.Simon
DepartmentofNeurology,MassachusettsGeneral Hospital,Boston,MA,UnitedStates
S.Skinner
DepartmentofIntraoperativeNeurophysiology,Abbott NorthwesternHospital,Minneapolis,MN,UnitedStates
B.Skrap
SectionofNeurosurgery,DepartmentofNeurosciences, BiomedicineandMovementSciences,University Hospital,Verona,Italy
F.Soto
DepartmentofNeurology,ClinicaLasCondes,Santiago, Chile
M.M.Stecker
FresnoInstituteofNeuroscience,Fresno,CA, UnitedStates
J.A.Strommen
DepartmentofNeurophysiology,AbbottNorthwestern Hospital,Minneapolis,MN,UnitedStates
A.Szelenyi
DepartmentofNeurosurgery,UniversityHospital, Ludwig-Maximilians-University(LMU),Munich, Germany
S.Ulkatan
DepartmentofNeurosurgery,MountSinaiHospital, NewYork,NY,UnitedStates
A.Uribe
DepartmentofAnesthesiology,OhioStateUniversity, Columbus,OH,UnitedStates
Contents
Forewordix
Prefacexi
Contributorsxiii
SECTIONIGeneralissues
1.Overviewofintraoperativeneuromonitoring3 M.R.Nuwer,A.M.Husain,andF.Soto(LosAngelesandDurham,UnitedStatesandSantiago,Chile)
2.Electroencephalography,electrocorticography,andcorticalstimulationtechniques11 M.V.Simon,M.R.Nuwer,andA.Szelenyi(BostonandLosAngeles,UnitedStatesandMunich,Germany)
3.Intraoperativeevokedpotentialtechniques39 D.B.MacDonald,C.C.Dong,andA.Uribe(Emmendingen,Germany,Vancouver,Canada,andColumbus, UnitedStates)
4.EMGmonitoring
67 J.PrellandS.Skinner(Halle,GermanyandMinneapolis,UnitedStates)
5.Safetyissuesduringsurgicalmonitoring83 H.L.JourneeandJ.L.Shils(Groningen,TheNetherlandsandChicago,UnitedStates)
SECTIONIIIntracranialsurgery
6.Neurophysiologyduringepilepsysurgery103 D.B.MacDonald,M.V.Simon,andM.R.Nuwer(Emmendingen,Germany;BostonandLosAngeles, UnitedStates)
7.Neurophysiologyduringmovementdisordersurgery123 J.L.Shils,J.E.Arle,andA.Gonzalez(Chicago,Boston,andRiverside,UnitedStates)
8.Intraoperativemappingandmonitoringduringbraintumorsurgeries133 K.Seidel,A.Szelenyi,andL.Bello(Bern,Switzerland,Munich,Germany,andMilan,Italy)
9.Mappingandmonitoringofbrainstemsurgery151 K.Kodama,K.F.Kothbauer,andV.Deletis(Matsumoto,Japan,Lucerne,Switzerland,Zagreb, Croatia,andNewYork,UnitedStates)
10.Monitoringcerebellopontineangleandskullbasesurgeries163 I.Fernández-Conejero,S.Ulkatan,andV.Deletis(Barcelona,Spain,NewYork,UnitedStates,and Zagreb,Croatia)
SECTIONIIISpinalsurgery
11.Monitoringscoliosisandotherspinaldeformitysurgeries179 M.R.Nuwer,D.B.MacDonald,andJ.Gertsch(LosAngelesandSanDiego,UnitedStatesand Emmendingen,Germany)
12.Intraoperativeneuromonitoringduringsurgeryforlumbarstenosis
205 S.SkinnerandL.Guo(MinneapolisandSanFrancisco,UnitedStates)
13.Intraoperativeneurophysiologyinintramedullaryspinalcordtumorsurgery
229 F.Sala,B.Skrap,K.F.Kothbauer,andV.Deletis(Verona,Italy,Lucerne,Switzerland,Zagreb, Croatia,andNewYork,UnitedStates)
14.Monitoringspinalsurgeryforextramedullarytumorsandfractures
245 L.Guo,R.N.Holdefer,andK.F.Kothbauer(SanFranciscoandSeattle,UnitedStatesandLucerne, Switzerland)
15.Mappingandmonitoringoftetheredcordandcaudaequinasurgeries
257 G.GallowayandF.Sala(Columbus,UnitedStatesandVerona,Italy)
16.Dorsalrootentryzoneprocedureandothersurgeriesforpain
271 A.M.Husain(Durham,UnitedStates)
SECTIONIVPeripheralnervesurgery
17.Neurophysiologyduringperipheralnervesurgery
295 J.A.Strommen,S.Skinner,andB.A.Crum(MinneapolisandRochester,UnitedStates)
18.Monitoringsurgeryaroundthecranialnerves
319 J.R.LópezandA.D.Legatt(StanfordandBronx,UnitedStates)
SECTIONVVascularsurgery
19.Monitoringincarotidendarterectomy
355 M.V.Simon,M.Malcharek,andS.Ulkatan(BostonandNewYork,UnitedStatesandLeipzig,Germany)
20.Surgeryandintraoperativeneurophysiologicmonitoringforaneurysmclipping
375 A.Szelenyi,I.Fernández-Conejero,andK.Kodama(Munich,Germany,Barcelona,Spain,andMatsumoto, Japan)
21.Monitoringcardiacandascendingaorticprocedures
395 M.M.SteckerandI.Keselman(FresnoandLosAngeles,UnitedStates)
22.Neuromonitoringduringdescendingaortaprocedures
407 M.V.Simon,C.C.Dong,M.J.Jacobs,andW.H.Mess(Boston,UnitedStates,Vancouver,Canadaand Maastricht,TheNetherlands)
SectionI Generalissues
HandbookofClinicalNeurology, Vol.186(3rdseries) IntraoperativeNeuromonitoring M.R.NuwerandD.B.MacDonald,Editors https://doi.org/10.1016/B978-0-12-819826-1.00011-9 Copyright©2022ElsevierB.V.Allrightsreserved
Overviewofintraoperativeneuromonitoring
MARCR.NUWER1*,AATIFM.HUSAIN2,ANDFRANCISCOSOTO3
1DepartmentsofNeurologyandClinicalNeurophysiology,DavidGeffenSchoolofMedicine,UniversityofCaliforniaLosAngeles, andRonaldReaganUCLAMedicalCenter,LosAngeles,CA,UnitedStates
2DepartmentofNeurology,DukeUniversityMedicalCenterandNeurodiagnosticCenter,VeteransAffairsMedicalCenter, Durham,NC,UnitedStates
3DepartmentofNeurology,ClinicaLasCondes,Santiago,Chile
Abstract
Intraoperativeneuromonitoring(IONM)isusedwidelytoreduceneurologicadversepostoperative outcomes.Avarietyoftechniquesareused.Initialtechniqueswereusedasfarbackasthe1930s,and thevarietyofmethodsexpandedgreatlysincethe1980s.Manymethodsmonitorbaselinefindingsover time.Othermethodstestforneurologicfunctiontoidentifynervesoreloquentcortex.Physicianstrainedin neurophysiologyarekeyforinterpretationoffindings,supervisionofstaff,andmakingmedicalrecommendationstothesurgeonoranesthesiologist.Someneurophysiologistsprovidetheservicespersonally, andinothercircumstanceswell-trainedtechnologiststaffhelpwiththetechniques.MuchIONMis providedbytheneurophysiologyphysicianintheoperatingroom,whereasinothercases,thephysician maybeon-lineinrealtimefromaremotesite.Whenmonitoringidentifieschanges,theIONMteammust giveaclear,timely,andcompellingmessagetothesurgeonandanesthesiologist.
Intraoperativeneuromonitoring(IONM)isusedwidely topreventneurologicadversepostoperativeoutcomes. MostIONMmethodsarecommonclinicalneurophysiologyoutpatienttechniques,suchaselectroencephalography(EEG),electromyography(EMG),evokedpotentials (EPs),andnerveconductionstudies.OtherIONM methodsareusedsolelyintheoperatingroom,suchas directcorticalstimulation,electrocorticography,and epiduralspinalcordrecording.
ThemainaimofIONMistowarnthesurgeonand anesthesiologistaboutadversechangesintimetocorrect thecause,therebypreventingpostoperativeneurologic deficits.Also,IONMmayidentifysomesystemicproblems.Byfollowingapatient’sneurologicstatus,asurgeon mayproceedmoreconfidentlytoprovideamorethorough procedureoroperateonahigh-riskpatient.Inaddition, IONMprovidespatientsandfamiliesadegreeofcomfort
knowingthatneurologicrisksarebeingassessedand respondedtoduringsurgery.
Intraoperativetestingormappingalsoisapartofthis IONMdiscipline. Monitoring establishesbaselinefindingsandmonitorsforchangeacrossthewholetimeof thecase,whereas testing assessesandinterpretsfindings onceorduringalimitedportionofsurgery.Testingmay seeksuchlocationsasthesiteofpathology,functional tissue,eloquentcortex,orthespinalcordposterior midline.
Surgeonsaretrainedtorecognizeanatomiclandmarks duringyearsofpracticeandstudy.Theygoin-depthinto anatomy,firstindiagramsandthree-dimensionalstructures,andthenincadavericspecimensandfinallyin patients.Theyaretrainedtoseethelimitsbetween normalandpathologictissueusingtheireyesorwith thehelpoftheaugmentedrealityofthemicroscope.
*Correspondenceto:Dr.MarcR.Nuwer,M.D.,Ph.D.,DepartmentHead,ClinicalNeurophysiology,ReedResearchBuilding, Room1-194,710WestwoodPlaza,LosAngeles,CA90095-6987,UnitedStates.Tel:+1-310-206-3093,Fax:+1-310-267-1157, E-mail:mnuwer@mednet.ucla.edu
Neuro-Navigationincreasedthesurgeon’sabilitytosee inrealtime,tocompareasurgicalinstrument’slocation tothepatient’sanatomyandimagedpathology.Moreand more,themorphologyofcomplexbiologicsystemsis betterexploredinthesurgicalfield.However,thesame well-trainedsurgeonsneedhelpseeingthatwhichis invisibletothemostcapablevisualsystem,theneurologicfunctionofthetissuesbeforethem.Toshowneurologicfunctioninrealtimeintheoperatingroomis anessentialroleofIONM,toexploreneurologicfunction duringsurgery,todetectimpendingneurologicdamage, andtotrytopreventit.
Falsealarmsoccurrarelyinthehandsofexperienced monitoringteams.Inspinalcordmonitoring,thefalse alarm(falsepositive)ratehasbeenmeasuredas1% (Nuweretal.,1995).Someactuallyaretruepositive events inwhichanalarm-triggeredinterventionsuccessfullypreventedapostoperativeneurologicadverseoutcome,butitisimpossibletoclearlyseparatesuccessful truepositivealarmsfromtechnique-relatedfalsealarms. Technicalfailuresmaycausedifficultyobtaininggood qualitytracings.Anestheticchangesmayconfusecomparisonstobaselinerecordings.Raisinganalarmdoes notnecessarilypreventdeficits.Apatientrarelyhasa postoperativeneurologicinjurynotpredictedbyIONM (false-negativecases).Someareduetodeteriorationafter surgery.Someinjuriesareinpathwaysthatwerenot monitored.Rarefalse-negativecasesareduetoerrors bytheIONMteam,whofailedtorecognizeandcommunicateclearlytheadversechanges.Forthelatterreason, theskills,knowledge,training,andexperienceofthe IONMteamareimportant.
HISTORYOFMONITORING
EarlyuseofIONMdatestothefirsthalfofthe20th century.Penfield(PenfieldandBoldrey,1937)used functionalcorticallocalizationinsurgeryforpatients withepilepsy.Theyuseddirectcorticalstimulationto locatemotorandsensorycortex.Jasperjoinedthatteam torecordEEGdirectlyfromexposedcerebralcortex,a techniquehecalledelectrocorticography.Thisguided thesurgeontoresectregionsofepilepticdischarges, slowing,orlackoffastactivity(Jasper,1949; Marshall and Walker1949).Thesetechniquesarestillused. RoutinescalpEEG-monitoredcarotidendarterectomysurgerystartedinthe1970s(Sharbroughetal., 1973).TheEEGmeasuredcerebralischemiafrom carotidclamping(Sundtetal.,1974).Intraoperative EEG replacedassessmentwithawakeneurologicexaminationduringcarotidendarterectomyorotherischemia testingtechniques,andstillservesasasafeguardduring carotidendarterectomy.
Inthe1970s,Japaneseinvestigatorsevaluated spinalcordIONMusingepi duralspinalstimulation andrecording( Shimojietal.,1971 ; Imai,1976 ; Tamakietal.,1972,1981 )(Japanesefigure).Inthe United Kingdom, Jonesetal.(1982) continuedwith e piduralspinalrecordingsbutchangedthestimulus totheposteriortibialnervesatthepoplitealfossae.This avoidedsafetyconcernsaboutrepeatedspinalepidural electricstimulation.Theben efitofthesedevelopments wastoreplacetheStagnarawake-uptest( Vauzelle e tal.,1973 )duringthecorrection of scoliosisandother spinaldeformities.
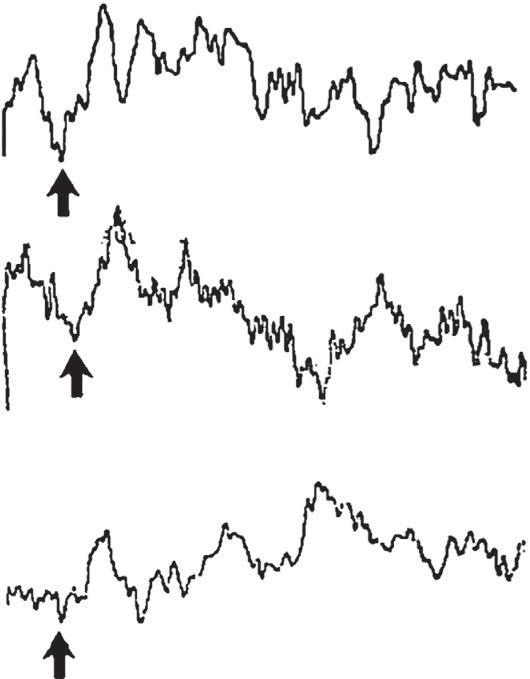
Anklestimulationwithscalprecordingwasproposed bytheClevelandgroupandtheirfollowers(Nashand Brodkey,1977; Nashetal.,1974,1977; Engleretal., 1978; Speilholzetal.,1979).Thispreliminarygeneration ofsomatosensoryevokedpotential(SEP)cortical IONMtechniquesused1–100Hzfilterstorecord middle-andlong-latency50–200mscorticalpotentials. Fig.1.1 showsanexampleoftheseearlycorticalSEP peaks (Spetzleretal.,1979).Thesewerenoisy,variable, and toosensitivetoanesthesia.Signalsoftenwerejudged aseitherthepresenceorabsenceofanypeaksinthe 200msrecording. Grundy(1982) wentontocontrol variability ofanestheticeffects,anddescribedthealert criterionof50%decreaseinamplitude.
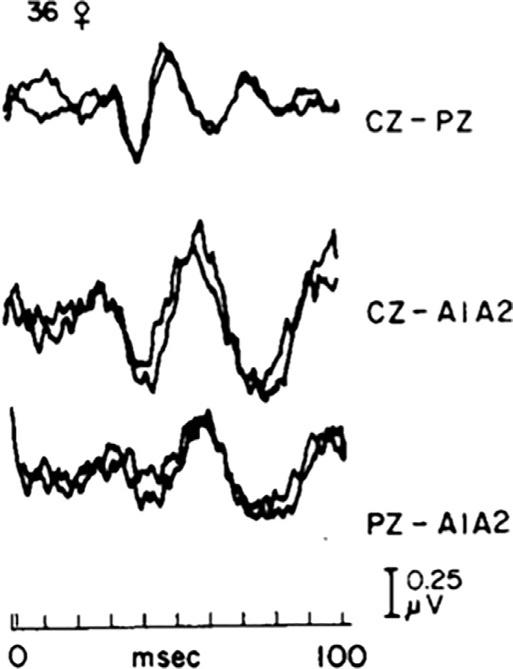
SpinalcordIONMwithscalpSEPsremained problematicintheearlydaysbecausethosepreliminary techniqueshadexcessivenoiseandirreproducible backgroundvariability( Fig.1.1 ).Beginninginthelate 1970s, NuwerandDawson(1984) studiedthevariability problem,anddeterminedthatshort-latencySEP techniques,recordedwithrestrictedfiltersandother technicalmodifications,substantiallyreducedvariabilityandestablishedmodernreliableSEPmonitoring. Fig.1.2 .showsreproduciblepeaksusingthesenew methods. ThislatterSEPmethodbecamewidely adoptedforspinalcordIONM.
SomatosensoryspinalcordIONMwasthetechnique ofchoiceforthenexttwodecades,eventhoughSEPsare sensorywhereasthemostfearedpostoperativeproblems weremotor.Rarefalse-negativeSEPmonitoringcases werereported.Burkeextendedmonitoringtothemotor pathwaysasshownin Fig.1.3,popularizingtranscranial electric stimulation(Hicksetal.,1991; Burkeetal., 1992).Thetechniquehasdevelopedsincethenwith changes inelectrodelocationsandstimulationtrains.
MethodsforauditoryEPandfacialnerveEMG IONMweredevelopedinthe1980s.Thesewereused forposteriorfossaprocedures,initiallymicrovascular decompressionandacousticneuromaresection(Moller and Moller,1985).Subsequently,EMGtechniqueswere developedformonitoringothercranialnervesandthe limbs(Beattyetal.,1995; Harper,2004).Theapplication
SYMPTOMATIC SIDE–IMPROVEMENT IN LATENCY
Fig.1.1. EarlymethodsforintraoperativecorticalSEPrecordingduringuppercervicalsurgery.Theauthorsnoteimproved latency(shiftofarrowtotheleft)onthesymptomaticsideatthetimeofdecompression.FromSpetzler,R.F.,Selman,W.R., Nash,C.L.,Brown,R.H.,1979.Transoralmicrosurgicalodontoidresectionandspinalcordmonitoring.Spine6,506–510.
spreadtoIONMasusedinbrainandcerebellopontine angletumors,intracranialandthoracicvascularpathology,tetheredcordandintramedullarytumors,andmany otherapplications.
BeforecommercialIONMequipmentbecameavailablearound1981,clinicalneurophysiologistshadto adaptresearchequipmentforIONM.Earlycustomized equipmentwasadaptedtospecificapplicationsor surgicalteams.ThefirstgeneralIONMclinicalservice, setupatUCLAin1979,offeredanarrayoftechniques toanyhospitalsurgeonfromanysurgicaldiscipline. Academicneurophysiologyandsurgerysocietymeetingsinthe1980sbegantoincludeIONMresearch reports.DedicatedsymposiataughtIONMtoclinical neurophysiologists,surgeons,andtechnologistsstarting inthe1980s.ThosemeetingsbroughtIONMtoamuch wideraudience.TwoearlyIONMtextbooks(Nuwer, 1986; Møller,1988)providedteachingdetailtothis growingaudience.Bythelate1980s,IONMhadbecome establishedasatechniqueingeneraluse.
TECHNOLOGISTSTAFFING ANDSUPERVISION
ThetwokindsofIONMaremonitoringandtesting. Monitoring identifiesadversechangesfrombaseline
signals,usedasasignofinjury,andwiththegoalof raisinganalarmwhenkeychangesoccur. Testing identifiesneurologicstructuressuchaseloquentorpathologiccortex.Monitoringoccursovertimelooking foranychangethatoccurs.Testingisataspecifictime toanswerapendingquestionduringthecase.The twoarereferredtotogetheras intraoperativeneuromonitoring (IONM).Sometimesothertermsareused: intraoperativemonitoring,surgicalneurophysiology,or neurophysiologicintraoperativemonitoring.
Monitoringneedssufficientexpertiseandgoodcommunicationfromtheteamprovidingtheservice.Each IONMteamincludesafewroles.Atechnologistmay serveasin-roomstafftohookupelectrodes,runsoftware,andassistthephysician.Mostimportant,aphysicianneurophysiologistservestosupervisetheservice, makesmedicaldecisionstointerpretthefindings,and recommendsinterventionstothesurgeonandanesthesiologist.SometimesanadditionalphysicianornonphysicianmayserveasanexpertinIONMtechnologyand application.
Thephysicianneurophysiologistmonitorsinthe operatingroominrealtime,orsometimesmonitorsin realtimeremotelyfromoutsidetheoperatingroom.If remote,theneurophysiologyphysiciancommunicates withthein-roomtechnologistbyphone,audio-video,
PRE OP DURING ANESTHESIA
EXPOSING VERTEBRA
Fig.1.2. Methodsweredevelopedtoproducebetter,reproducibleSEPs.Bipolarrecordingsshownhereonthetopline werelessnoisyandmorereproduciblethanreferentialrecordings.Stimulationherewasposteriortibialnerveandrecording useda30Hzlowfrequencyfilter.FromNuwer,M.R., Dawson,E.C.,1984.Intraoperativeevokedpotentialmonitoringofthespinalcord:enhancedstabilityofcorticalrecordings. ElectroencephalogrClinNeurophysiol59,318–327.
ortext.Themonitoringphysicianmustbeonthemedical staffofthehospitalinwhichthesurgeryoccurs,privilegedbythemedicalstafffortheneurophysiology proceduresperformed,andlicensedtopracticemedicine inthatregion.TheIONMteamconceptdescribesmonitoringrolesandexpertise,whilepreservingthetraditionalhealthcareoversightrolesofhospitalandpublic agencies.
Thephysicianclinicalneurophysiologistnotonly monitorsbutalsotestsneurologicstructures,suchas forlocalizationoflanguageormotorcortex.Professional physicianjudgmentisrequiredtorecommendwhat cortextoresect,whattospare,andwhattotestfurther.
Thephysicianclinicalneurophysiologistshouldbein theoperatingroomtointerprettherecordingsanddiscuss withthesurgeontherecommendationsbasedontesting. Thisin-roomparticipationisreferredtoas personal supervision.
Thephysicianneurophysiologistmusthaveawellgroundedneurophysiologicbackground,in-depthneuroanatomicknowledge,andbeabletointerpretquickly thephysiologicchangesthatoccurduringsurgery. Knowledgeofmedicationeffectsarekeytodiscussions withtheanesthesiologistforplanningandforinterventionsduringthecase.Thephysicianneurophysiologist
supervisorisinthebestpositiontoofferadviceabout changesduringthecase,includingchangesrelatedto anesthesia,bloodpressure,andsurgicaltactics.
Someclinicalneurophysiologistsprovidedirect supervisionformorethanonecasesimultaneously. TheliteratureshowsgoodoutcomeforIONMbased onmonitoring1or2oroccasionally3patientssimultaneously(Nuweretal.,1995).Thereisinsufficientliteraturetosupportmonitoringmoresimultaneouscases duetotheeffectsofdividedattention.Whenthemonitoringphysiciandivideshisorherattentionamongalarge numberofcases,signalchangesinonecasemaybe missedandthephysicianmaybeslowtorecognized deteriorationinsignalsfromoneofmanycases.When acuteclinicalproblemshappeninoneofthesimultaneouscases,thephysicianneurophysiologistmayneed tofocusundividedattentionsolelyonthatoneproblem case.Whenmonitoringsimultaneouscases,aplanis neededtocoveranyothersimultaneouscaseswhen onecaseneedsundividedattention.
Atechnologistgenerallylackssufficientskills, knowledge,abilities,training,andexperiencetoprovide theIONMserviceswithoutsupervisionbyaphysician neurophysiologist.Technologistsneedtoknowthetechnicalrequirements,supplies,machinesettings,troubleshooting,andtheymustfollowtheneurophysiologic signalsduringtheprocedure.Technologistshowever lackthemedicalknowledgeandauthoritytoadvisea surgeonaboutclinicaloptionstochooseorconsider whenadversechangesoccur.
InstitutionsrequirephysiciansupervisionandinterpretationofmedicalproceduresincludingCT,MRI, andIONM.TheIONMteamshouldbeappropriatelycredentialedinthehospital,state,andcountryinwhichthe serviceisbeingprovided.Thephysicianmustbetrained inclinicalneurophysiologybytheusualstandardsfor thatspecialty.
ForatechnologisttoserveasakeypartoftheIONM team,theyneedsufficientexperienceinneurophysiologictesting,techniques,basicsciences,andrelevant clinicalsciences.Usually,technologisttrainingand experienceincludesseveralyearsofregularinpatient andoutpatientexperienceconductingEEGandevoked potentials.Thatexperienceisanimportantbasisfor knowingwhatsignalslooklike,identifyingchanges andabnormalities,anddealingwithtechnicalproblems. SometimesanindividualistraineddirectlyinIONM duringaseveralyearprocessofeducationandapprenticeshipwithaskilledtechnologistwhohasmastered thefield.Eachtechnologistshouldbeproctoredand givenprogressivelyreducedsupervisionwhenintroducedtoIONM.Thetechnologist’strainingandprivilegingshouldbespecifictoindividualtechniques.Adegree ofsupervisionandprogressivelyreducedimmediate

Fig.1.3. Anearlycombinedsomatosensoryandmotorevokedpotentialtechnique.(A)Thetechniqueusedforrecordingsimultaneouslydescendingcorticospinalvolleysinresponsetoanodalelectricstimulationofthemotorcortex,andascendingsomatosensoryvolleysinresponsetostimulationofthetibialnervesinthepoplitealfossae.Thestimuliweredeliveredsimultaneously, andtheevokedvolleyswererecordedattwolevelsfromthespinalcord,asshowninthelowertraces.Thedescendingcorticospinal volleyhadashorterlatencyandpropagateddownthespinalcord,whiletheascendingsomatosensoryvolleyhadalongerlatency andpropagatedupthespinalcord.(B)Thetracesareduplicateaveragesof10sweeps.Negativityforthecorticospinalvolleyis shownasanupwarddeflection,andnegativityforthesomatosensoryvolleyisshownasadownwarddeflectionreflectingthefact thatthevolleysapproachthebipolarrecordingelectrodesfromoppositedirections.FromBurke,D.,Hicks,R.,Stephen,J.,etal., 1992.Assessmentofcorticospinalandsomatosensoryconductionsimultaneouslyduringscoliosissurgery.Electroencephalogr ClinNeurophysiol85,388–396.
supervisionisneededtoqualifyatechnologistforIONM proceduresnewtohimorher.
Whenchangesoccur,communicationsarevery important.Thepersoninchargemustgiveaclear,timely, andcompellingmessagetothesurgeonandanesthesiologist.Theclearunderstandingofthismessageistheonly chanceofpreventingdamagetothenervoussystem. Effectivecommunicationrequirestrustandcredibility.
Forthisreason,theIONMphysicianneurophysiologist needssufficientknowledge,training,andexperience (Skinneretal.,2017).
CONCLUSIONS
IONMincludesmanyusefultechniquesappliedto varioussurgicalprocedures.Suitabletechnologist,and
neurophysiologyphysiciantrainingandprivileging servewellforstaffingIONMprocedures.Thegoalis toimprovepatientcare,avoidpostoperativeneurologic deficits,encouragemorecompleteprocedures,andopen theopportunityforproceduresonhigherriskpatients,by givingfeedbackaboutcircumstancesthatcouldinjure thenervoussystem.ThefutureofIONMispromising. Thenewgenerationofsurgeonshastrainedandlearned theirsurgicalskillsusingIONM,whichiswhytheyare demandingtoseetheanatomywithincreasingdetailsas welltoseetheneurologicfunctionusingintraoperative neurophysiology.Theynowknowthatitissaferfor patients.Thereisachangeofparadigm;newsurgeons arethinkingintermsofmorphologyandfunction.
Newmethodologiesaredevelopingeveryyear,such asbrainstemreflexes(Sinclairetal.,2017)mappingof the corticospinaltractinsidethespinalcord,mapping andmonitoringthecomplexcircuitsandfasciclesthat connectdifferentareasofthebrain,andthegradual knowledgeofthebrainconnectomeduringsurgery. EvidencewillshowthatIONMmakesadifferencein theoutcomeofsomespecificpathologieswherethis disciplinewillbeastandardofcare,whileinothersurgicalprocedures,itwilldemonstratenoaddedbenefit, makingcleartheindicationsofintraoperativeneurophysiology.Newdirectionsandtrainingopportunities arebringingimprovedIONMpatientcaretopatients worldwide.
REFERENCES
BeattyRM,McGuireP,MoroneyJMetal.(1995).Continuous intraoperativeelectromyographicrecordingduringspinal surgery.JNeurosurg 82:401–405.
BurkeD,HicksR,StephenJetal.(1992).Assessmentofcorticospinalandsomatosensoryconductionsimultaneously duringscoliosissurgery.ElectroencephalogrClinNeurophysiol 85:388–396.
EnglerGL,SpeilholzNI,BernhardWNetal.(1978). SomatosensoryevokedpotentialsduringHarrington instrumentationforscoliosis.JBoneJointSurg(Am) 60: 528–532.
GrundyBL(1982).Monitoringofsensoryevokedpotentials duringneurosurgicaloperations:methodsandapplications. Neurosurgery 11:556–575. HarperCM(2004).Intraoperativecranialnervemonitoring. MuscleNerve 29:339–351. HicksRG,BurkeDJ,StephenJP(1991).Monitoringspinal cordfunctionduringscoliosissurgerywithCotrelDuboussetinstrumentation.MedJAust 154:82–86. ImaiT(1976).Humanelectrospinogramevokedbydirect stimulationonthespinalcordthroughepiduralspace. JJapaneseOrthoAssoc 50:1037–1056.
JasperHH(1949).Electrocorticogramsinman.ElectroencephalogrClinNeurophysiol 2:16–29.
JonesSJ,EdgarMA,RansfordAO(1982).Sensorynerve conductioninthehumanspinalcord:epiduralrecordings
madeduringscoliosissurgery.JNeurolNeurosurg Psychiatr 45:446–451.
MarshallC,WalkerAE(1949).Electrocorticography.Bull JohnsHopkinsHosp 85:344–359.
MøllerAR(1988).Evokedpotentialsinintraoperativemonitoring,Williams&Wilkins,Baltimore,224pp.
MollerMB,MollerAR(1985).Lossofauditoryfunctioninmicrovasculardecompressionforhemifacial spasm.Resultsin143consecutivecases.JNeurosurg 63: 17–20.
NashJrCL,BrodkeyJS(1977).Clinicalapplicationofspinal cordmonitoringforoperativetreatmentofspinaldisease, CaseWesternReserveUniversity,Cleveland140.
NashJrCL,SchatzingerL,LorigR(1974).Intraoperative monitoringofspinalcordfunctionduringscoliosisspine surgery.JBoneJointSurg(Am) 56:1765.
NashJrCL,LorigRA,SchatzingerLAetal.(1977).Spinal cordmonitoringduringoperativetreatmentofthespine. ClinOrtho 126:100–105.
NuwerMR(1986).Evokedpotentialmonitoringintheoperatingroom,RavenPress,NewYork,246pp.
NuwerMR,DawsonEC(1984).Intraoperativeevokedpotentialmonitoringofthespinalcord:enhancedstabilityof corticalrecordings.ElectroencephalogrClinNeurophysiol 59:318–327.
NuwerMR,DawsonEG,CarlsonLCetal.(1995). Somatosensoryevokedpotentialspinalcordmonitoring reducesneurologicdeficitsafterscoliosissurgery:results ofalargemulticentersurvey.ElectroencephalogrClin Neurophysiol 96:6–11.
PenfieldW,BoldreyE(1937).Somaticmotorandsensory representationinthecerebralcortexofmanasstudiedby electricalstimulation.Brain 37:389–443.
Sharbrough FW,MessickJrJM,SundtJrTM(1973). Correlationofcontinuouselectroencephalogramswith cerebralbloodflowmeasurementsduringcarotidendarterectomy.Stroke 4:674–683.
ShimojiK,HigashiH,KanoT(1971).Epiduralrecordingof spinalelectrograminman.ElectroencephalogrClin Neurophysiol 30:236–239.
SinclairC,TellezM,TapiaOetal.(2017).Anovelmethodologyforassessinglaryngealandvagusnerveintegrityin patientsundergeneralanesthesia.ClinNeurophysiol 128: 1399–1405.
SkinnerS,HoldeferR,McAuliffeJetal.(2017).Medicalerror avoidanceinintraoperativeneurophysiologicalmonitoring:thecommunicationimperative.JClinNeurophysiol 34:477–483.
SpeilholzNI,BenjaminMV,EnglerGLetal.(1979). Somatosensoryevokedpotentialsduringdecompression andstabilizationofthespine:methodsandfindings. Spine 4:500–505.
SpetzlerRF,SelmanWR,NashCLetal.(1979).Transoral microsurgicalodontoidresectionandspinalcordmonitoring.Spine 6:506–510.
SundtJrTM,SharbroughFW,AndersonREetal.(1974). Cerebralbloodflowmeasurementsandelectroencephalogramsduringcarotidendarterectomy.JNeurosurg 41: 310–320.
TamakiT,YamashitaT,KobayashiHetal.(1972).Spinal cordmonitoring.JJpnElectroencephalogrElectromyogr 1:196.
TamakiT,TsujiH,InoueSetal.(1981).Thepreventionof iatrogenicspinalcordinjuryutilizingtheevokedspinal cordpotential.IntOrthop 4:313–317. VauzelleC,StagnaraP,JouvinrouxP(1973).Functionalmonitoringofspinalcordactivityduringspinalsurgery.Clin Orthop 93:173–178.
FURTHERREADING
BurkeD,HicksRG(1998).Corticospinalvolleysevoked bytranscranialelectricalandmagneticstimulation.In: EStalbergHSSharma,YOlsson(Eds.),Spinalcord monitoring.Springer,Vienna,NewYork,pp.445–461. NuwerJM,NuwerMR(1997).Neurophysiologicsurgical monitoringstaffingpatternsintheUSA.ElectroencephalogrClinNeurophysiol 103:616–620.